The Safety and Efficacy of Daclizumab HYP in Relapsing-Remitting Multiple Sclerosis in the SELECTION Extension Study: Primary Results Dr Gavin Giovannoni, MBBCh, PhD, FRCP, FRCPath March 19, 2013 Gavin Giovannoni 1 , Ralf Gold 2 , Krzysztof Selmaj 3 , Eva Havrdova 4 , Xavier Montalban 5 , Ernst-Wilhelm Radue 6 , Dusan Stefoski 7 , Manjit McNeill 8 , Jitesh Rana 8 , Jacob Elkins 8 , and Gilmore O’Neill 8 1 Queen Mary University of London, Barts and The London School of Medicine and Dentistry, London, UK; 2 St. Josef-Hospital/Ruhr-University Bochum, Bochum, Germany; 3 Medical University of Lodz, Lodz, Poland; 4 Charles University in Prague, Prague, Czech Republic; 5 Hospital Vall d'Hebron University, Barcelona, Spain; 6 University Hospital Basel, Basel, Switzerland. 7 Rush University Medical Center, Chicago, IL. USA; 8 Biogen Idec, Cambridge, MA, USA American Academy of Neurology 65th Annual Meeting San Diego, California

Giovannoni aan selection main 3 18-2013- final
Jul 03, 2015
My platform presentation at the AAN 2013 in San Diego
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Safety and Efficacy of Daclizumab HYP in Relapsing-Remitting Multiple Sclerosis in the SELECTION Extension Study: Primary Results
Dr Gavin Giovannoni, MBBCh, PhD, FRCP, FRCPath
March 19, 2013
Gavin Giovannoni1, Ralf Gold2, Krzysztof Selmaj3, Eva Havrdova4,
Xavier Montalban5, Ernst-Wilhelm Radue6, Dusan Stefoski7,
Manjit McNeill8, Jitesh Rana8, Jacob Elkins8, and Gilmore O’Neill8
1Queen Mary University of London, Barts and The London School of Medicine and
Dentistry, London, UK; 2St. Josef-Hospital/Ruhr-University Bochum, Bochum,
Germany; 3Medical University of Lodz, Lodz, Poland; 4Charles University in Prague,
Prague, Czech Republic; 5Hospital Vall d'Hebron University, Barcelona, Spain; 6University Hospital Basel, Basel, Switzerland. 7Rush University Medical Center,
Chicago, IL. USA; 8Biogen Idec, Cambridge, MA, USA
American Academy of Neurology
65th Annual Meeting
San Diego, California

Disclosures
2
This study was supported by Biogen Idec and AbbVie Biotherapeutics.
Gavin Giovannoni: Has received research grant support from Bayer Schering Healthcare, Biogen Idec, GW Pharma, Merck Serono, Merz, Novartis, Teva and sanofi-aventis. Dr Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design, trial steering committees and data and safety monitoring committees from: Bayer Schering Healthcare, Biogen Idec, Eisai, Elan, Five Prime Therapeutics, Genzyme, Genentech, GSK, Ironwood Pharma, Merck Serono, Novartis, Pfizer, Roche, sanofi-aventis, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals.
Ralf Gold: Has received speakers’ honoraria and research grant support from Bayer Schering Healthcare, Biogen Idec, Merck Serono, Merz, Novartis, Teva and sanofi-aventis. Dr Gold has received compensation for Advisory Board activities from Biogen Idec, Merck Serono, Novartis and TEVA
Krzysztof Selmaj: Has received speaker’s honoraria from Novartis, Merck Serono, Gedeon Richter, ONO Pharma, and Biogen Idec. Dr Selmaj has received personal compensation for participation in Advisory Boards and steering committees from Biogen Idec, Roche, Genzyme, ONO Pharma, Merck Serono, and Novartis.
Eva Havrdova: Has received speakers’ honoraria and research grant support from Bayer Schering Healthcare, Biogen Idec, Genzyme, Merck Serono, Novartis, and Teva. Dr Havrdova has received compensation for Advisory Board activities from Biogen Idec, Genzyme, Merck Serono, Novartis and TEVA.
Xavier Montalban: Has received speaking honoraria and travel expenses for speaking and scientific meetings, has been a steering committee member of clinical trials or participated in advisory boards of clinical trials in the past years with Bayer Schering Pharma, Biogen Idec, EMD Merck Serono, Genentech, Genzyme, Novartis, sanofi-aventis, Teva Pharmaceuticals, Almirall and BTG.
Ernst-Wilhelm Radue: Has received research support (mainly for MS projects) and lecture fees from: Actelion, Basilea, Bayer Schering, Biogen Idec, Merck Serono, Novartis and others. Lecture fees have been mainly used for research funding at the Medical Image Analysis Center (former MS MRI Evaluation Center), University Hospital Basel
Dusan Stefoski: Has received research funding and support, and speaker bureau honoraria from: Biogen Idec, EMD Serono, Teva, Pfizer, Elan, and Novartis.
Manjit McNeill, Jitesh Rana, Jacob Elkins, and Gilmore O’Neill: Full-time employees of Biogen Idec.

Hypothesized Immunomodulatory
Effect of Daclizumab Treatment
3 1. Bielekova B, et al. Proc Natl Acad Sci USA 2006;103: 5941–5946. 2. Martin J, et al. J Immunol 2010;185:1311–1320.
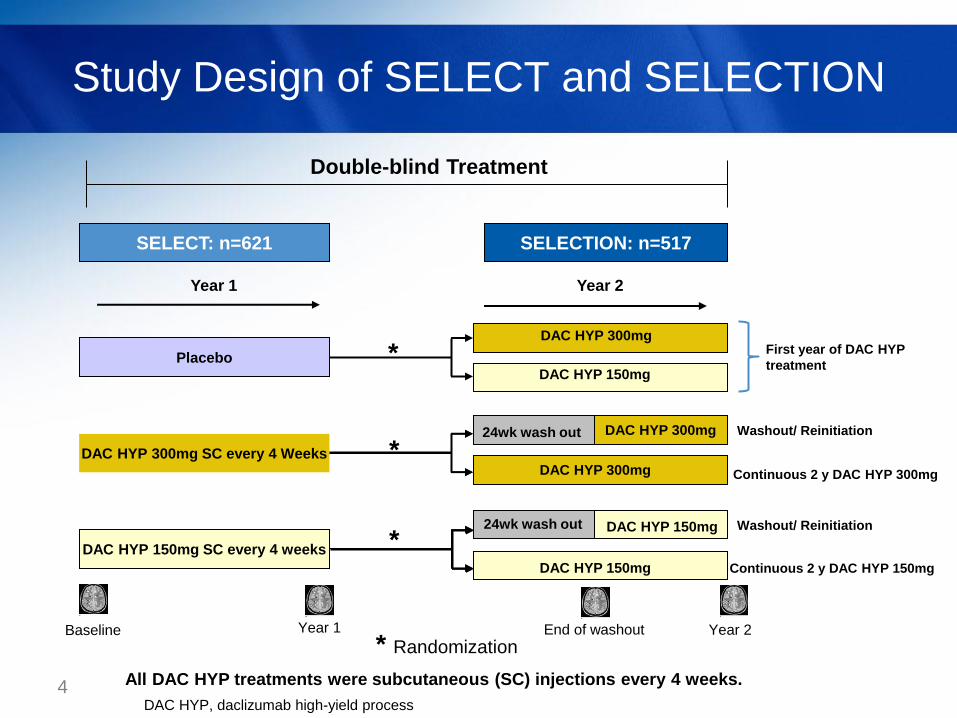
Study Design of SELECT and SELECTION
4 All DAC HYP treatments were subcutaneous (SC) injections every 4 weeks.
SELECT: n=621 SELECTION: n=517
Placebo
DAC HYP 150mg SC every 4 weeks
DAC HYP 300mg SC every 4 Weeks
Year 1
DAC HYP 150mg
DAC HYP 300mg
DAC HYP 150mg
DAC HYP 300mg
DAC HYP 150mg
Year 2
DAC HYP 300mg 24wk wash out
24wk wash out
Double-blind Treatment
*
*
*
* Randomization
Continuous 2 y DAC HYP 150mg
First year of DAC HYP
treatment
Continuous 2 y DAC HYP 300mg
Washout/ Reinitiation
Washout/ Reinitiation
Year 1 Year 2 Baseline End of washout
DAC HYP, daclizumab high-yield process
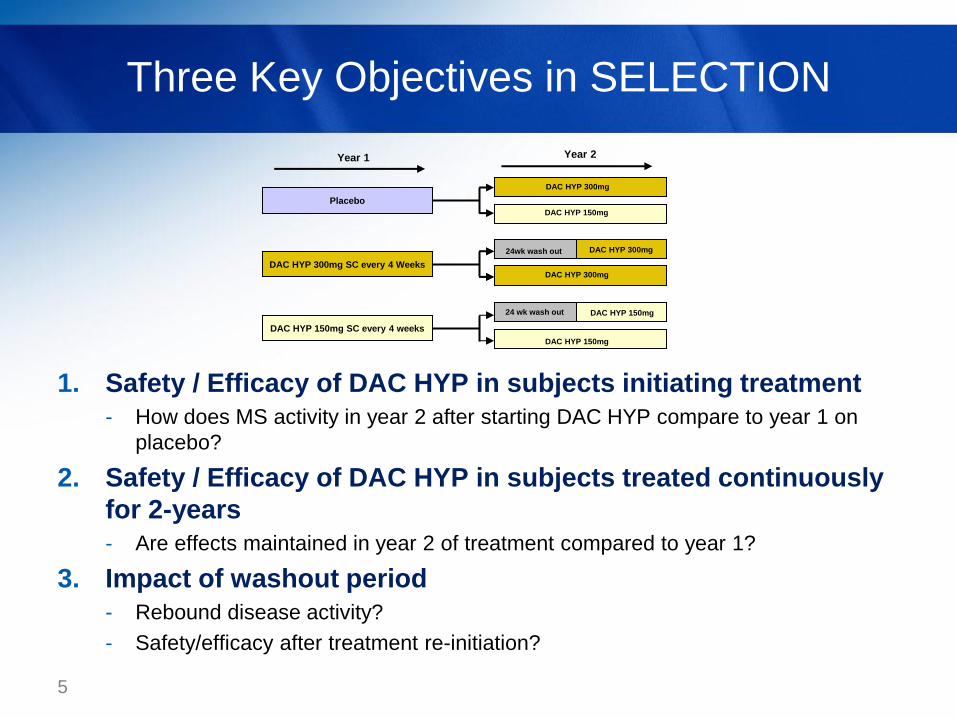
Three Key Objectives in SELECTION
5
1. Safety / Efficacy of DAC HYP in subjects initiating treatment
- How does MS activity in year 2 after starting DAC HYP compare to year 1 on
placebo?
2. Safety / Efficacy of DAC HYP in subjects treated continuously
for 2-years
- Are effects maintained in year 2 of treatment compared to year 1?
3. Impact of washout period
- Rebound disease activity?
- Safety/efficacy after treatment re-initiation?
Placebo
DAC HYP 150mg SC every 4 weeks
DAC HYP 300mg SC every 4 Weeks
Year 1
DAC HYP 150mg
DAC HYP 300mg
DAC HYP 150mg
DAC HYP 300mg
DAC HYP 150mg
Year 2
DAC HYP 300mg 24wk wash out
24 wk wash out
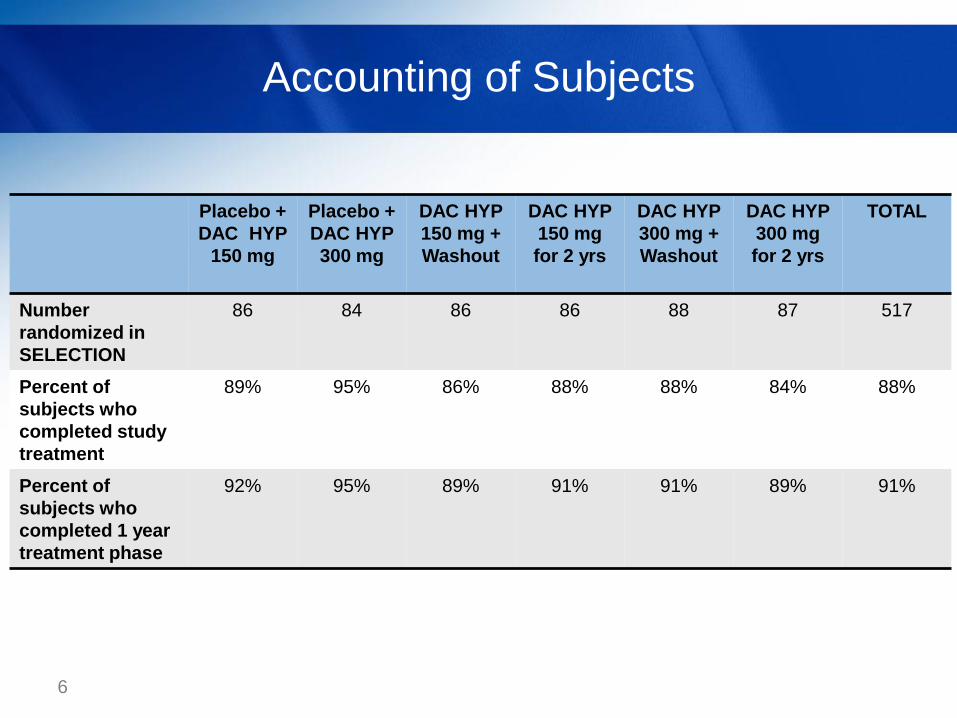
Accounting of Subjects
6
Placebo +
DAC HYP
150 mg
Placebo +
DAC HYP
300 mg
DAC HYP
150 mg +
Washout
DAC HYP
150 mg
for 2 yrs
DAC HYP
300 mg +
Washout
DAC HYP
300 mg
for 2 yrs
TOTAL
Number
randomized in
SELECTION
86 84
86
86
88
87
517
Percent of
subjects who
completed study
treatment
89% 95% 86% 88% 88% 84% 88%
Percent of
subjects who
completed 1 year
treatment phase
92% 95% 89% 91% 91% 89% 91%

Efficacy of DAC HYP in Subjects Initiating
Treatment
7
SELECT SELECTION
Placebo
DAC HYP 150mg SC every 4 weeks
DAC HYP 300mg SC every 4 Weeks
Weeks 0-52
DAC HYP 150mg SC every 4 weeks
DAC HYP 300mg SC every 4 weeks
DAC HYP 150mg
DAC HYP 300mg
DAC HYP 150mg
Weeks 0-52
DAC HYP 300mg Wash Out
Wash Out

Reduced Annualized Relapse Rate
after 1-year of DAC HYP
8
Year 1 Year 2 Placebo
n=163
DAC HYP
n=163
ARR Reduction = 59%
P<0.001
ARR=0.434 (0.347,0. 544)
ARR=0.179 (0.123, 0.261)
ARR, annualized relapse rate
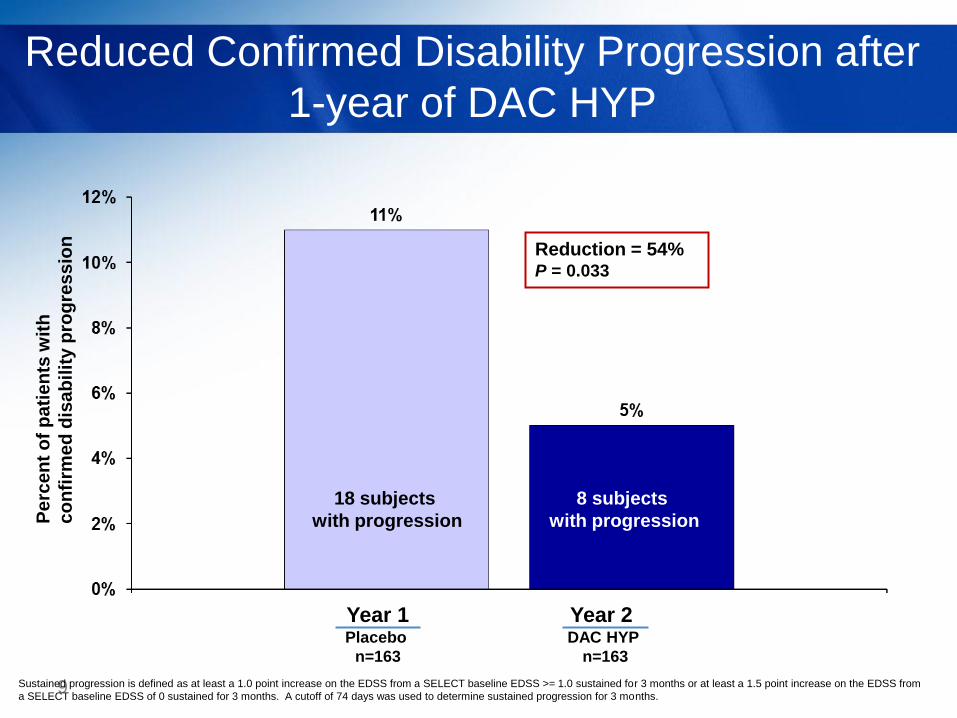
Reduced Confirmed Disability Progression after
1-year of DAC HYP
9
Reduction = 54% P = 0.033
18 subjects
with progression
Year 1 Year 2
8 subjects
with progression
Placebo
n=163
DAC HYP
n=163
Pe
rce
nt
of
pa
tie
nts
wit
h
co
nfi
rme
d d
isa
bilit
y p
rog
res
sio
n
Sustained progression is defined as at least a 1.0 point increase on the EDSS from a SELECT baseline EDSS >= 1.0 sustained for 3 months or at least a 1.5 point increase on the EDSS from
a SELECT baseline EDSS of 0 sustained for 3 months. A cutoff of 74 days was used to determine sustained progression for 3 months.
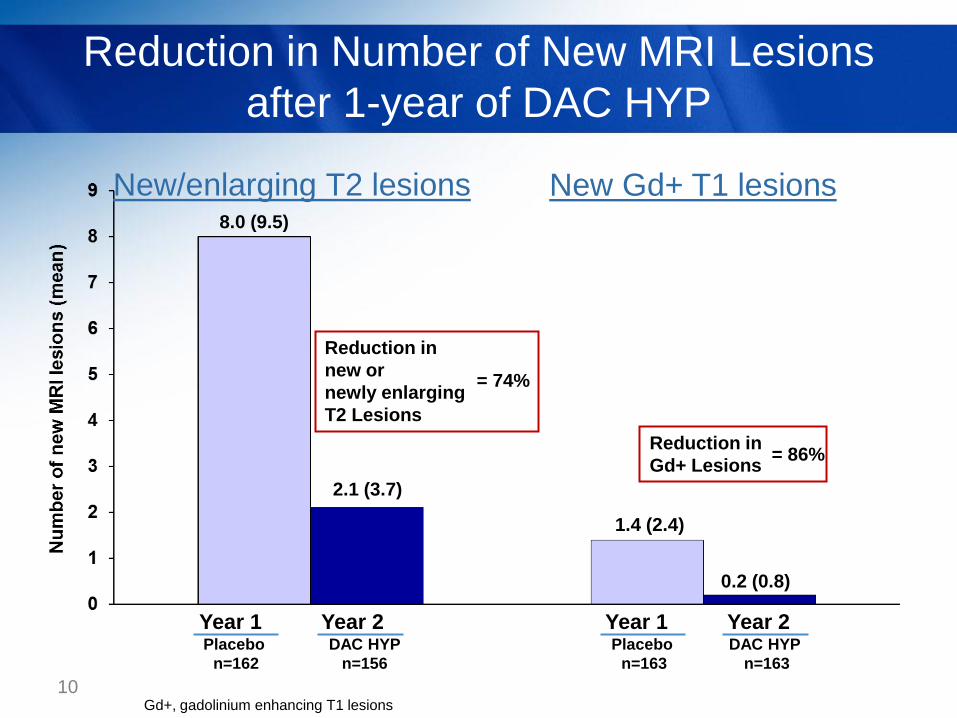
Reduction in Number of New MRI Lesions
after 1-year of DAC HYP
10
1.4 (2.4)
2.1 (3.7)
8.0 (9.5)
0.2 (0.8)
Year 1 Year 2 Year 1 Year 2 Placebo
n=162
DAC HYP
n=156
Placebo
n=163
DAC HYP
n=163
New/enlarging T2 lesions New Gd+ T1 lesions
Reduction in
Gd+ Lesions = 86%
Gd+, gadolinium enhancing T1 lesions
Reduction in
new or
newly enlarging
T2 Lesions
= 74%
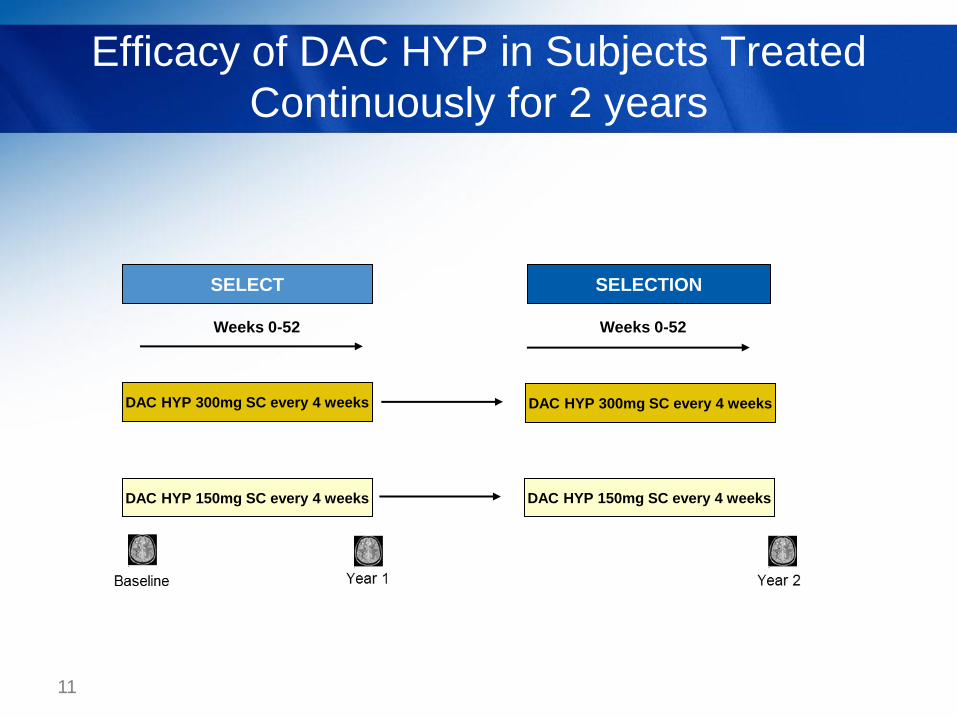
Efficacy of DAC HYP in Subjects Treated
Continuously for 2 years
11
SELECT SELECTION
DAC HYP 150mg SC every 4 weeks
DAC HYP 300mg SC every 4 weeks
Weeks 0-52 Weeks 0-52
DAC HYP 300mg SC every 4 weeks
DAC HYP 150mg SC every 4 weeks

Reduction in ARR was Sustained during
Year 2 of DAC HYP Treatment
12
0.434 (0.347, 0.544)
Year 2 of DAC HYP
62% reduction vs.
SELECT placebo
Year 1 of DAC HYP
66% reduction vs.
SELECT placebo
0.148 (0.096, 0.229)
Placebo
n=163
Year 1 Year 1 Year 2 DAC HYP
n=129
DAC HYP
n=129
An
nu
ali
ze
d R
ela
ps
e R
ate
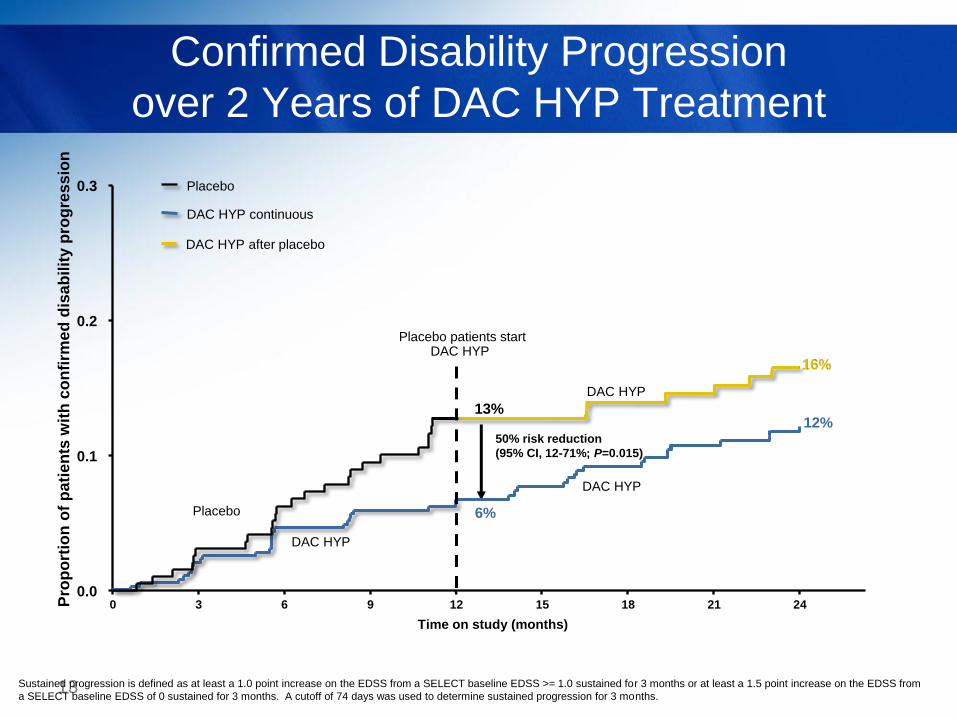
Confirmed Disability Progression
over 2 Years of DAC HYP Treatment
13
50% risk reduction
(95% CI, 12-71%; P=0.015)
0.0
0.1
0.2
0.3
DAC HYP continuous
0 12 24 6 3 9 15 18 21
DAC HYP
Placebo
Placebo
16%
12%
DAC HYP
DAC HYP after placebo
6%
13%
Placebo patients start DAC HYP
Time on study (months)
Pro
po
rtio
n o
f p
ati
en
ts w
ith
co
nfi
rme
d d
isa
bilit
y p
rog
res
sio
n
DAC HYP
Sustained progression is defined as at least a 1.0 point increase on the EDSS from a SELECT baseline EDSS >= 1.0 sustained for 3 months or at least a 1.5 point increase on the EDSS from
a SELECT baseline EDSS of 0 sustained for 3 months. A cutoff of 74 days was used to determine sustained progression for 3 months.
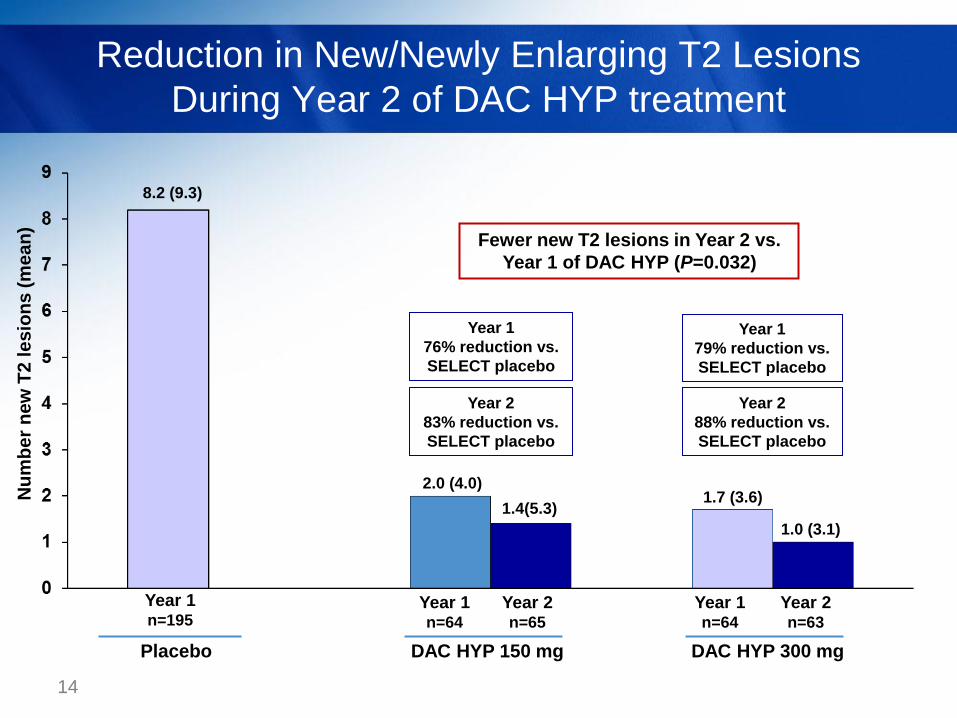
Reduction in New/Newly Enlarging T2 Lesions
During Year 2 of DAC HYP treatment
14
2.0 (4.0) 1.7 (3.6)
1.4(5.3)
1.0 (3.1)
8.2 (9.3)
Year 1
76% reduction vs.
SELECT placebo
Year 2
83% reduction vs.
SELECT placebo
Year 1
79% reduction vs.
SELECT placebo
Year 2
88% reduction vs.
SELECT placebo
Fewer new T2 lesions in Year 2 vs.
Year 1 of DAC HYP (P=0.032)
DAC HYP 150 mg
Year 1 n=195
Year 1 n=64
Year 2 n=63
Year 1 n=64
Year 2 n=65
Placebo DAC HYP 300 mg
Nu
mb
er
ne
w T
2 le
sio
ns
(m
ea
n)
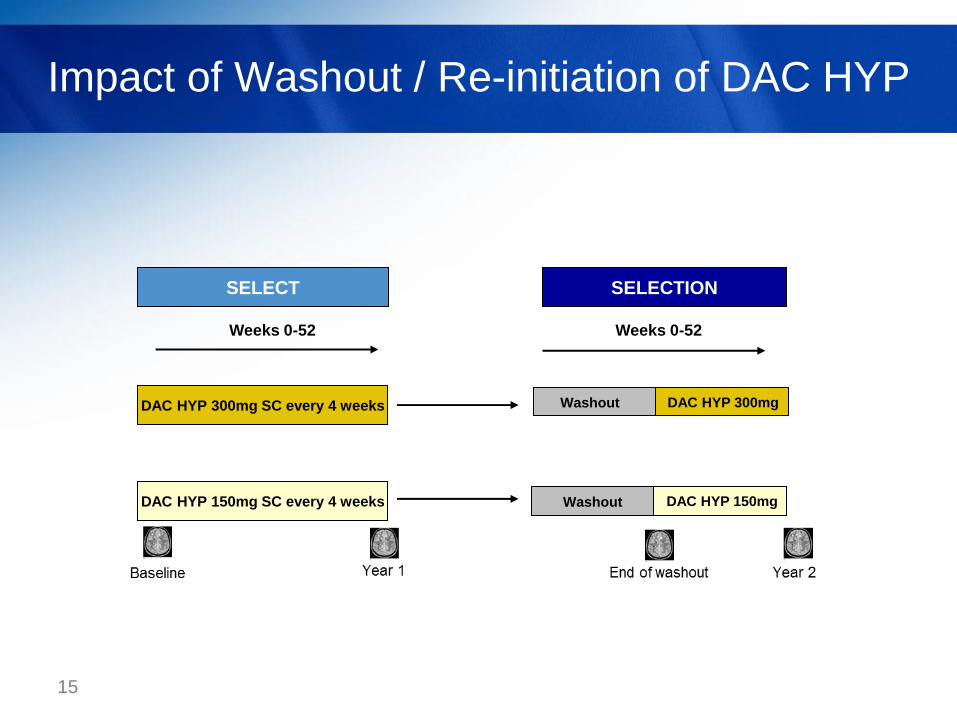
Impact of Washout / Re-initiation of DAC HYP
15
SELECT SELECTION
DAC HYP 150mg SC every 4 weeks
DAC HYP 300mg SC every 4 weeks
Weeks 0-52 Weeks 0-52
DAC HYP 150mg Washout
DAC HYP 300mg Washout
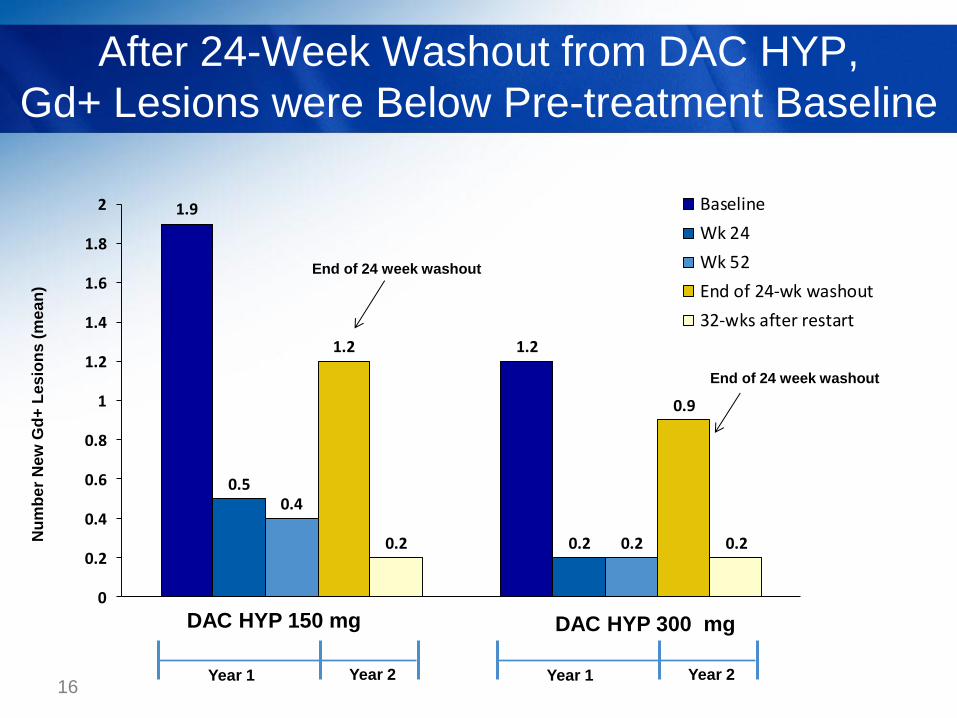
After 24-Week Washout from DAC HYP,
Gd+ Lesions were Below Pre-treatment Baseline
16
1.9
1.2
0.5
0.2
0.4
0.2
1.2
0.9
0.2 0.2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2 Baseline
Wk 24
Wk 52
End of 24-wk washout
32-wks after restart
DAC HYP 300 mg DAC HYP 150 mg
End of 24 week washout
End of 24 week washout
Nu
mb
er
Ne
w G
d+
Les
ion
s (
me
an
)
Year 1 Year 2 Year 1 Year 2
Safety Results
17
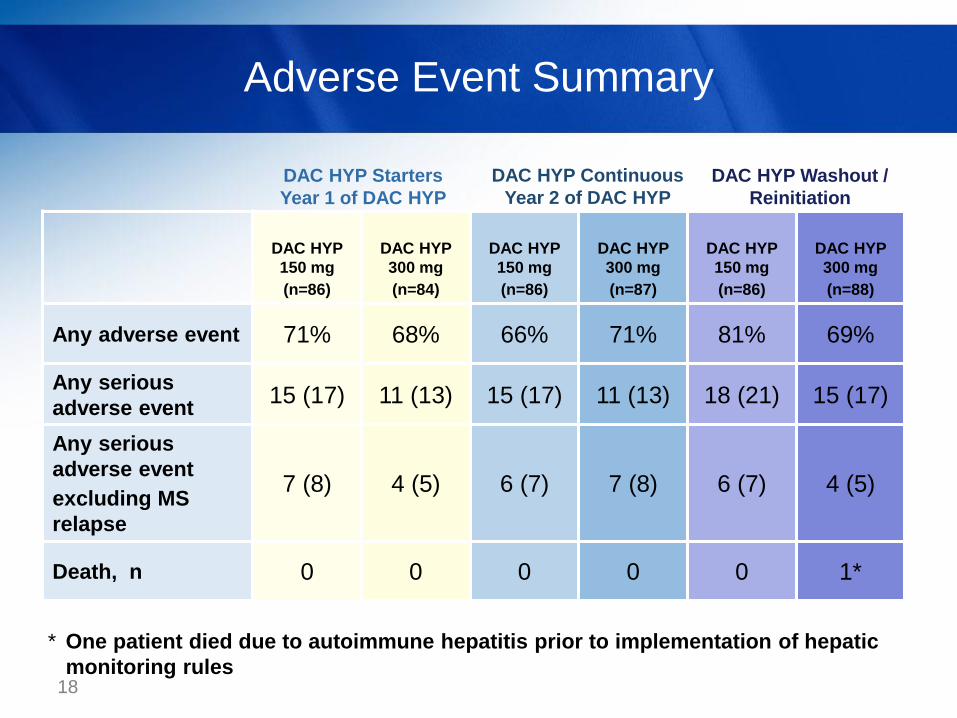
Adverse Event Summary
18
DAC HYP
150 mg
(n=86)
DAC HYP
300 mg
(n=84)
DAC HYP
150 mg
(n=86)
DAC HYP
300 mg
(n=87)
DAC HYP
150 mg
(n=86)
DAC HYP
300 mg
(n=88)
Any adverse event 71% 68% 66% 71% 81% 69%
Any serious
adverse event 15 (17) 11 (13) 15 (17) 11 (13) 18 (21) 15 (17)
Any serious
adverse event
excluding MS
relapse
7 (8) 4 (5) 6 (7) 7 (8) 6 (7) 4 (5)
Death, n 0 0 0 0 0 1*
* One patient died due to autoimmune hepatitis prior to implementation of hepatic
monitoring rules
DAC HYP Starters
Year 1 of DAC HYP
DAC HYP Continuous
Year 2 of DAC HYP
DAC HYP Washout /
Reinitiation

Adverse Events of Interest
19
DAC HYP
150 mg
(n=86)
DAC HYP
300 mg
(n=84)
DAC HYP
150 mg
(n=86)
DAC HYP
300 mg
(n=87)
DAC HYP
150 mg
(n=86)
DAC HYP
300 mg
(n=88)
Serious Infections, n 3 1 2 2 3 2
Serious Cutaneous
Events, n 2 0 0 3 1 0
ALT/AST > 5x ULN, n 1 1 0 2 1 3
Other Serious
Immune-Mediated
Adverse Events, n 0 0 0 2 0 1
Malignancy, n 0 1 0 0 0 0
DAC HYP Starters
Year 1 of DAC HYP
DAC HYP Continuous
Year 2 of DAC HYP
DAC HYP Washout /
Reinitiation
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ULN, upper limit of normal

PD Results
20

CD56bright NK Cell Counts During Washout and
Continuous DAC HYP treatment
21 NK, natural killer
0 8 16 24 32 40 48 56 64 72 80 88 96 104 0
20
40
60
80
100 2-Year Continuous Treatment
With 24-Week Washout
Time (Weeks)
Med
ian
(25 th
-75 th
perc
en
tile
s)
CD
56 b
rig
ht N
K c
ell
co
un
t (c
ells/m
m 3
)
Summary (1)
Evidence for high efficacy in subjects initiating DAC HYP
59% reduction in ARR after treatment start vs. year 1 placebo phase
(P<0.001)
54% reduction in EDSS progression after treatment start vs. year 1
placebo phase (P=0.033)
Evidence for sustained efficacy in subjects continuing on DAC
HYP for 2 years
In subjects randomized to DAC HYP for 2 years
• ARR (0.15 in year 1; 0.17 in year 2)
• New T2 lesions at 52 weeks (1.9 in year 1 reduced to 1.2 in year 2,
P=0.03)
No evidence for disease rebound during DAC washout
22
Summary (2)
Pharmacodynamic changes plateau by second year of treatment
and are reversible over 24-week washout
Safety profile was similar in year 2 compared to year 1
SELECTION vs. SELECT
• Serious infections: 2% vs. 2%
• Serious cutaneous events: 1.1% vs. 1.0%
• New LFT abnormalities >5x ULN: 1.5% vs. 4%
• No LFT elevations > 5x ULN or serious cutaneous events in year 2
of DAC HYP 150mg continuous treatment group
23

Acknowledgements
SELECTION Study Investigators
• Czech Republic: Prof. Zdeněk Ambler, Prof. Ivan Rektor, Dr. Radomir Talab, Prof. Petr Kanovsky, Dr. Pavel Stourac, Dr. Denisa Zimova, Dr. Marta Vachova
• Germany: Prof. Dr. Bernd C. Kieseier, Dr. Björn Tackenberg, Prof. Dr. Heinz Wiendl, Prof. Dr. Reinhard Hohlfeld, PD Dr. Klemens Angstwurm, Prof. Dr. Judith Haas, Prof. Dr. Uwe Zettl, Prof. Dr. Florian Stögbauer, Dr. Ralf Linker, Prof. Dr. Andrew Chan, Prof. Dr. Patrick Oschmann
• Hungary: Dr. Attila Csányi, Dr. Péter Diószeghy, Dr. János Nikl, Dr. Gyula Pánczel, Dr. Béla Clemens, Dr. Etelka Jófejű, Dr. Attila Valikovics, Dr. István Kondákor, Dr. Dániel Bereczki, Dr. Zsuzsanna Lohner, Prof. Lászlo Csiba, Dr. András Folyovich, Dr . Péter Harcos, Dr. Gabriella Kovács, Dr. Mária Sátori
• India: Dr. Rajaram Agarwal, Dr. Pahari Ghosh, Dr. Sangeeta Ravat, Dr. Subhash Mukherjee, Dr. Rustom Wadia, Prof. Kolichana Venkateswarlu, Dr. Meenakshisundaram Umaiorubahan, Prof. Medasari Padma, Dr. Thomas, Dr. A K Meena, Dr. Suresh Kumar
• Poland: Dr. Wieslaw Drozdowski, Dr. Waldemar Fryze, Dr. Jan Kochanowicz, Prof. Anna Kaminska, Dr. Krzysztof Selmaj, Dr. Andrzej Szczudlik, Dr. Andrzej Wajgt, Dr. Anna Czlonkowska, Dr. Zbigniew Stelmasiak, Dr. Gabriela Klodowska-Duda, Dr. Janusz Zbrojkiewicz
• Romania: Dr. Ovidiu Bajenaru, Dr. Dafin Fior Muresanu, Dr. Mihaela Simu
• Russia: Dr. Olga Vorobyeva, Dr. Leonid Zaslavsky, Dr. Sergey Shvarkov, Dr. Miroslav Odinak, Dr. Anna Belova, Dr. Irina Sokolova, Dr. Farit Khabirov, Dr. Natalia Nikolaevna Maslova, Dr. Irina Poverennova, Dr. Nikolay Spirin, Dr. Nadezhda Malkova, Dr. Semen Prokopenko, Dr. Alexey Rozhdestvensky, Dr. Alexei Boiko, Dr. Rim Magzhanov
• Turkey: Prof. Sabahattin Saip, Prof. Omer Faruk Turan, Ass. Prof. Serhat Ozkan, Prof. Ayse Sagduyu Kocaman
• Ukraine: Dr. Natalia Buchakchyys'ka, Dr. Natalia Lytvynenko, Dr. Borys Palamar, Dr. Tatyana Nehrych, Dr. Natalia Voloshina, Dr. Larisa Sokolova, Prof. Olexandr Kozyolkin, Dr. Olena Moroz, Prof. Valeriy Pashkovskyy, Dr. Elena Statinova, Dr. Tetjana Kobys, Dr. Igor Pasyura
• United Kingdom: Dr. Clive Hawkins, Dr. Basil Sharrack, Dr. Cris Constantinescu, Dr. John Zajicek, Dr. David Bates, Dr. Eli Silber
Data Safety Monitoring Board: Dr. Volker Limmroth (Chair), Dr. Richard Furie, Dr. Daniel McQuillen, Dr. Raymond Chung, Dr. Richard Kay
Relapse Adjudication Committee: Dr. Chris Polman, Dr. Ted Phillips, Dr. Paul O’Connor, Dr. Ari Green, Dr. Oliver Lyon-Caen
24
This study was supported by Biogen Idec and AbbVie Biotherapeutics. Ed Parr of UBC Scientific
Solutions provided editorial support to the authors in the development of this presentation, which
was funded by Biogen Idec and AbbVie Biotherapeutics.
Related Documents











