Journal of Social Research & Policy, Vol. 5, Issue 1, July 2014 Ghana’s Family Planning Program: A Neglected Policy Initiative? ABDULAI KUYINI MOHAMMED 1 Department of Political Science University of Ghana Abstract Ghana’s Family Planning Program (FPP), maternal mortality intervention, and HIV/AIDS control program are all health policy priorities, which are supposed to be complementary to achieve desirable reproductive health outcomes. However, it appears disproportionately less attention is being paid to the former compared to the latter two, which are relatively new health policies. This may have implications not only for the effectiveness of the FPP and the other two policies, but more broadly reproductive health outcomes. This study investigates this claim and finds that the FPP has policy merits and that its relegation to the background has led to a marginally little incentive to space births, and a marginally positive incentive to increase fecund level, with attendant negative developmental consequences. It then concludes that despite the alarming rate of maternal mortality and loss of lives through HIV/AIDS, Ghana’s population is still growing at a dangerous pace, making the FPP as relevant as ever. Keywords: Family Planning Program (FPP); Optimum population size; Development; Maternal health; Free Medical Care for Pregnant Women (FMCPW); Policy synergy. Introduction The world’s population in 2002 was estimated to be 6.2 billion; expected to be growing by 75 million per annum, with 97 percent of this increase occurring in developing countries (Goldstein & Whitworth, 2005). A disproportionate share of developing countries’ contribution to this rise is accounted for by the faster growth rate in Sub-Saharan African nations. This has raised fears of the inevitability of overpopulation in the sub region with its attendant negative consequences such as scarcity of productive resources, stress and strain on social infrastructure, environmental degradation etc. The concern about population size has also been expressed in Ghana over the years. The country’s population increased from 6 million at independence in 1957 to nearly 18 million in 1996 with a projected estimate of 27 million by 2020 (Arjun, 1996; GMHS, 2007). With the current growth rate of 2.7 percent, the population may reach 32 million by 2040. The past rapid growth of Ghana’s population was an outcome of high fertility, which until recently remained fairly constant, and declining mortality (Arjun, 1996; PPAG, 2009). Even though life expectancy at birth is low at 57.7 years and infant mortality is high at 71 per 1000 births (UNDP, 2007), this has not prevented the population from growing above annual desirable rate. This has raised fears of an imminent overpopulation, with the government responding by introducing the Family Planning Program (FPP) in 1970. The FPP was strengthened by the launching of the Road Map for Repositioning Family Planning – 2006 to 2010 in 2006 (PPAG, 2009). Despite the fact that the FPP has been running for many years in Ghana it has failed to impact population in a meaningful way. The failure is attributed to factors such as dwindling government commitment in terms of advocacy and resourcing, gap 1 Postal Address: University of Ghana, Department of Political Science, P. O. BOX LG 69, Legon, Accra Ghana. E- mail Address: [email protected], [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Social Research & Policy, Vol. 5, Issue 1, July 2014
Ghana’s Family Planning Program: A Neglected Policy Initiative?
ABDULAI KUYINI MOHAMMED1
Department of Political Science University of Ghana
Abstract
Ghana’s Family Planning Program (FPP), maternal mortality intervention, and HIV/AIDS control program are all
health policy priorities, which are supposed to be complementary to achieve desirable reproductive health outcomes.
However, it appears disproportionately less attention is being paid to the former compared to the latter two, which are
relatively new health policies. This may have implications not only for the effectiveness of the FPP and the other two
policies, but more broadly reproductive health outcomes. This study investigates this claim and finds that the FPP has
policy merits and that its relegation to the background has led to a marginally little incentive to space births, and a
marginally positive incentive to increase fecund level, with attendant negative developmental consequences. It then
concludes that despite the alarming rate of maternal mortality and loss of lives through HIV/AIDS, Ghana’s
population is still growing at a dangerous pace, making the FPP as relevant as ever. Keywords: Family Planning Program (FPP); Optimum population size; Development; Maternal health; Free Medical
Care for Pregnant Women (FMCPW); Policy synergy.
Introduction
The world’s population in 2002 was estimated to be 6.2 billion; expected to be growing by 75
million per annum, with 97 percent of this increase occurring in developing countries (Goldstein
& Whitworth, 2005). A disproportionate share of developing countries’ contribution to this rise is
accounted for by the faster growth rate in Sub-Saharan African nations. This has raised fears of
the inevitability of overpopulation in the sub region with its attendant negative consequences such
as scarcity of productive resources, stress and strain on social infrastructure, environmental
degradation etc. The concern about population size has also been expressed in Ghana over the
years. The country’s population increased from 6 million at independence in 1957 to nearly 18 million in 1996 with a projected estimate of 27 million by 2020 (Arjun, 1996; GMHS, 2007).
With the current growth rate of 2.7 percent, the population may reach 32 million by 2040. The
past rapid growth of Ghana’s population was an outcome of high fertility, which until recently
remained fairly constant, and declining mortality (Arjun, 1996; PPAG, 2009).
Even though life expectancy at birth is low at 57.7 years and infant mortality is high at 71
per 1000 births (UNDP, 2007), this has not prevented the population from growing above
annual desirable rate. This has raised fears of an imminent overpopulation, with the
government responding by introducing the Family Planning Program (FPP) in 1970. The FPP
was strengthened by the launching of the Road Map for Repositioning Family Planning – 2006
to 2010 in 2006 (PPAG, 2009). Despite the fact that the FPP has been running for many years
in Ghana it has failed to impact population in a meaningful way. The failure is attributed to factors such as dwindling government commitment in terms of advocacy and resourcing, gap
1 Postal Address: University of Ghana, Department of Political Science, P. O. BOX LG 69, Legon, Accra Ghana. E-
mail Address: [email protected], [email protected]
2 | JSRP Abdulai Kuyini Mohammed
between knowledge of family planning and use of contraceptives, unpredictability of donor
funding, and high unmet need (PPAG, 2009; GMHS, 2007).
Meanwhile, a seemingly conflicting initiative to the FPP, an exemptions policy for delivery
fees for pregnant women was introduced in 2004 (MoH, 2004). This was gradually phased out and was replaced by health insurance in 2008 (popularly referred to as the Free Medical Care
for Pregnant Women - FMCPW). The exemptions policy has an objective of addressing some
of the challenges hindering the attainment of one of the Millennium Development Goals
(MDG), which focuses on improving maternal health of women by 2015 (Osabutey, 2008). In
other words, the policy is meant to curb the high rate of maternal and baby deaths.
From the above exposition, it appears the FPP with its emphasis on limiting the number of
children per woman, has an anti-natal intent (reducing fertility), while the FMCPW, which
focuses on safe delivery, has a pro-natal motive. However, the government has prioritized the
unacceptable level of maternal deaths as a national emergency and has diverted much attention
and resources to dealing with the problem. The questions that then arise are: Has the
prioritizing of the FMCPW left the FPP unattended to? What are the implications of this
apparent neglect of the FPP for population growth and development of Ghana? These questions can be answered by providing responses to three further questions:
1. Does Ghana need a Family Planning Program?
2. Will the Family Planning Program reduce fertility?
3. Is the FPP a neglected policy initiative?
Methodology
Data for the study was obtained from both primary and secondary sources. The primary
information was obtained by interviewing 21 key personnel from relevant organizations including
the Ghana Health Service, hospitals, and the Planned Parenthood Association of Ghana (PPAG). These respondents were originally identified because of their role connected directly to the
development and implementation of the FPP and FMCPW policies. The secondary information
was derived from content analysis of published works on both policy initiatives.
Theoretical Framework
It seems to be the case that, policy-makers in developing countries believe that
overconcentration on getting the content and administration of public policies right is most
critical in exacting desirable outcomes. In so doing, they totally neglect or pay little attention to
ensuring that synergy exists between related public projects and programs that are trying to
achieve the same macro level objectives. Yet the literature demonstrates that complementarities of efforts (cooperation, collaboration and coordination as well as mutual reinforcement of
related initiatives) of change agents whose separate program of activities ultimately lead to the
same endpoint, is extremely crucial in not only achieving the objectives of the individual
projects concerned, but also the ends of the bigger whole to which they all contribute their
quota (Brislin, 1981; Pressman & Wildavsky, 1984). As Walt & Gilson observe (1994), the
traditional focus on the content of policy neglects the other dimensions of process, actors and
context which can make the difference between effective and ineffective policy choice and
implementation (Walt & Gilson, 1994). Thomas & Gilson (2004) and Cassels (1995) make
similar comments in relation to the apparent neglect of these other dimensions of reality of
policy making in the Third World.
Grindle & Thomas’ (1991) research on the political economy of reform in developing countries has been cited by many scholars. Grindle & Thomas (1991) based their analysis of
policy and organizational reform in recent decades from several developing countries to
propose a multivariate framework for understanding the emergence, discussion,
implementation and sustainability of policy reform in developing countries. They placed
premium on the role of policy elites in shaping policy agendas, weighting policy options and
3 | JSRP Ghana’s Family Planning Program: A Neglected Policy Initiative?
managing political and bureaucratic challenges of policy reform. They define policy elites as
those who have official positions in government and whose responsibilities include making or
participating in making and implementing authoritative decisions for society. The main factors
in their framework are environmental context of reform, the agenda setting circumstances, and international context, as well as policy characteristics. A fifth factor that also affects policy
success or failure, but that has not been mentioned by Grindle & Thomas (1991) is synergy
between related public social projects and programs. The first three of their factors together
with synergy are adopted here and discussed in turn below.
Elements of the environmental context include the individual characteristics of policy elites
such as their ideological predispositions, professional expertise and training, experiences of
similar policy situations, position and power, political and institutional commitments, loyalties,
and personal attributes and goals. It also enfolds the context of policy choice such as societal
pressures, historical and economic context.
The agenda setting circumstances embrace whether there is a perception of a crisis situation
or not. According to Grindle & Thomas (1991), in a perceived crisis situation there is strong
pressure for reform and immediate action, the stakes are considered high, change is seen as innovative and high level decision-makers are involved in the reform process. The behavior of
policy stakeholders is different in situations that are perceived as non crisis. In non crisis
scenarios the agenda setting circumstances are “politics as usual”. Policy makers, without
pressure and without extreme limit on their time, select the agenda items. The stakes are seen
as low and decisions are often left to middle level decision-makers; incremental change is
acceptable and there is flexibility in timing. Decision-making in perceived crisis situations
tends to be dominated by concerns about macro political relationships whereas in politics as
usual, decision-making tends to be preoccupied by concerns about political and bureaucratic
relationships (Grindle & Thomas, 1991, Bridgman & Davis, 2004).
The international context or environment refers to the forces that surround and influence the
life and development of domestic policies from outside the borders of a country. An increasing body of literature contends that states are increasingly constrained and shaped by global forces
(Ohmae, 1995; Falk, 1997). Recognition of the international system’s influences on public
policy has opened up an interesting field of studies in the policy discipline. The international
system, not only affects policy sectors that are clearly international – examples, trade and
defense – but also sectors with no immediately apparent international connection, such as
health care. The influence comes from the overall structure of the international system, and a
country’s place in it (Howlett & Ramesh, 2003).
The influence of the international system is probably not a novel phenomenon, what
distinguishes the current movement is that its scope and intensity have greatly increased. This
has resulted in what is generally referred to as globalization or, more precisely,
internationalization (Hirst & Thomson, 1996). Although originally, internationalization was
thought of as a somewhat simple concept, the recent policy literature acknowledges its highly complex nature, the different forms it takes across space and time, and the varying impacts it
has on different policy sectors and states (Bernstein & Cashore, 2000; Bennett, 1997; Brenner,
1999). This recognition has prompted scholars to research more curiously into the means,
manner, and mechanisms through which domestic policy processes are connected to the
international system (Coleman & Perl, 1999; Finnemore & Sikkink, 1998; Bridgman & Davis,
2004). Thus, it could be argued that the domestic healthcare system and policies in Ghana are
more international than can be assumed because a proportion of the health budget is funded by
donor agencies such as USAID, DANIDA, and the World Bank. These donors dictate health
projects and programs that may not fit neatly into the domestic healthcare agenda.
Synergy in policy development and implementation
Another issue that determines the success or failure of public policies is synergy between
related public social projects and programs. According to Brislin (1981), synergy is a behavior
of whole systems that cannot be predicted by the behavior of any parts taken separately. In
4 | JSRP Abdulai Kuyini Mohammed
order to really understand what is going on, the individual parts should be examined in their
relationships to the other components as well as the whole system.
In their book entitled “Managing Cultural Synergy”, Moran and Harris reflect that ‘the very
differences in the world’s people can lead to mutual growth and accomplishment that is more than the single contribution of each party to the intercultural transaction’ (Moran & Harris, 1981, p. 3).
In terms of the FPP and FMCPW, one can infer from Brislin, Moran & Harris’ thoughts on
cultural synergy that both policies are part of a system or a bigger whole called reproductive
health of women. So in order to improve reproductive health of women we cannot start by
working separately on the FPP and FMCPW as this approach will not give us the opportunity to
determine their effects on each other and their implications for the broader goal of improving
women’s reproductive health. Rather we must act on them as a joint project in order to ensure
they are mutually supportive and generate consistent reproductive health outcomes. If they are
managed as a joint project it will lead to mutual growth and realization of not only their
respective objectives, but also the broader goal of attaining a high standard of reproductive health.
I argue that policy synergy, as an approach to designing, implementing and managing the
diverse major social policies and programs in developing countries should involve a process in which policy makers and administrators form organizational strategies, structures and practices
based on, but not limited to, the workings of individual policies. They need to create linkages
between related policies and programs to ensure that their activities are mutually reinforcing.
Synergetic policy organizations create new forms of management and transactions that
transcend the distinct operations of individual policies to align and harmonize with related
initiatives. The harmonization will contribute to the achievement of not only the respective
objectives of the individual programs but also the ends of a broader policy domain to which
they all belong. This approach recognizes both the similarities and differences between the
policies and suggests that we neither ignore, nor minimize the dissimilarities, but that we view
them as a resource in designing organizational systems that engender complementarities of
efforts across individual policies so that we achieve system-wide objectives. Literature on the technical and political challenges of implementing health policies in
developing countries exists and is growing (examples, Carrin, 2003; Carrin & James, 2004;
Preker, 2002; Adjei & Agyeapong, 2008). However, work on the challenges of creating synergy
between related public social policies and programs, is scanty or non-existent. This article is a
modest contribution toward filling this gap in the literature by examining the problem of lack of
synergy between the FPP and the FMCPW in Ghana. It also looks at the difficulty of managing
the environmental, agenda setting, and international contexts in the development and
implementation of the two initiatives. I do this by using some of the elements of Grindle &
Thomas’ (1991) framework as well as ideas from Brislin, Moran & Harris’ thoughts on cultural
synergy in the analysis. Further, I evaluate the outcomes of the implementation of the FPP based
on what some scholars refer to as the six criteria of evaluation (Ayee, 2000; Dunn, 1994; Howlett
& Ramesh, 2003). These criteria are efficiency, effectiveness, adequacy, equity, responsiveness and appropriateness. These six criteria of evaluation have been adopted without consenting that
they are yardsticks on which all stakeholders in policy making agree. They are criteria from the
policy analyst’s perspective rather than those which take into account the various interested
individuals and groups who also evaluate public policies and programs. Nevertheless, they
provide a useful starting point for examining the facets of policy success and failure. Lessons are
then drawn that will be useful for policy reform.
Is an FPP policy necessary?
A legitimate question to ask about the FPP is: Is it an appropriate policy? Appropriateness refers to the value or worth of a program’s objectives and the tenability of assumptions underlying these
objectives (Ayee, 2000; Dunn, 1994). In relation to the FPP, the policy could be justified on the
grounds that Ghana’s population is rising rapidly due to high fertility rate and immigration. The
fertility rate is said to be rising perhaps at above replacement level and there is a foreseeable
chance of Ghana’s population actually increasing. An above replacement fertility means a rising
5 | JSRP Ghana’s Family Planning Program: A Neglected Policy Initiative?
population level in Ghana because a natural increase is augmented by the uncontrolled migrant
arrivals. Even when we consider the situation with the lowest fertility rate (4.4 in 1998 compared
with the current 4.6) and the lowest migration level (75,843 in 1999 compared with the current
estimate of 3 million), Ghana’s population will rise by 2020 to 26,516 million because the natural increase will be augmented by an appreciable immigration to Ghana, mostly other Africans who
are undocumented (Nigerians, Ivoirians, Burkinabe, etc.), for example, there are an estimated 1
million Malians and 26, 0000 Liberians in Ghana (RIPS, 2009).
Granting that there is a foreseeable risk of Ghana’s population overgrowing we must find
reasons for FPP policies. Government interference in the private decisions of individuals, and one
cannot get more private than the decision to have a child, has to be made on grounds of market
failure. In other words, it has to be demonstrated that the private decisions lead to sub-optimal
outcomes from the point of view of society. In the context of FPP policy then, the question that
easily comes to mind is: What is the optimum population size of Ghana? We might also ask: Are
the unfettered choices of parents likely to put us on a path to the optimum population?
It certainly is an elusive exercise to search for the optimum population size. Unlike The
Hitchhikker’s Guide to the Galaxy where the answer to the ultimate question was revealed as 42 (Guest, 2007), there is no undisputable figure for a country’s optimum population size. There are
no certainties and there are many unresolved ethical issues. The Jones Report on Australia’s
population carrying capacity put the difficulty this way: ‘they search for a magic figure (for
optimum population) or a Rubicon between safety and danger’ (Australian Parliament, 1994, p.
129). In a similar fashion, McDonald & Kippen (1999), contend that it is not sensible to specify
particular population targets because of uncertainty about fertility, mortality rates, environmental
issues and other circumstances. They posit that in any case our choices of a population target
would be very limited due to demographic realities of past fertility rates and achievable future
rates, and of a limited range of immigration levels that would be both desirable and achievable.
On the basis of the above analysis it will be contentious to state an exact figure for Ghana’s
optimum population size. However, what cannot be disputed is that the current high level of population growth rate of 2.7 percent clearly puts the country on an inappropriate demographic
path. This argument wins favor from the Planned Parenthood Association of Ghana (PPAG)
which estimates that Ghana’s current population growth rate of 2.7 percent is not optimal for the
country’s income per capita (PPAG, 2009). It is reasonable to suggest that the optimum rate of
growth of Ghana’s population should be below that of Australia, which has almost the same
population size as Ghana (24 million), but which boasts of a bigger land size (compare Ghana’s
land area of 238,537 sq km to Australia’s 7,617,930 sq km). Moreover, Australia has a bigger per
capita income than Ghana ($28,900 as against $584) and is technologically more advanced than
Ghana – an advantage which can enable it to better deal with the challenges to higher productivity
associated with finite land size. Neville (1990) reveals that the optimum rate of growth of
Australia’s population is equal to 1.3 percent per annum but that anywhere in the range of 1.1
percent to 1.6 percent would be close to the optimum that is, it generates close to the optimum growth of income per capita. This implies that Ghana with a smaller per capita income and land
area should have an optimum population growth rate far lower than that of Australia, rather than
the current alarming rate of 2.7 percent. To further understand the dangerous demographic path
Ghana is walking, we need to examine, even if briefly, the merits of a policy aimed at reducing
the fertility rate. This area of analysis is known as population economics.
The starting point to an economic analysis of optimum population is to understand the
principle that optimum population size must balance two dramatically opposed forces: those
that bring advantages to size and those that yield disadvantages to size (Guest, 2007; Galor &
Zang, 1997). Advantages that accrue to economies of scale include those issuing from public
goods (such as national defense and public order and safety) where the total cost of the good is
not affected by an increase in population up to a point, thereby permitting a higher population to reduce the cost per capita. It is also argued that a larger market can compel innovation in the
sense of making it more profitable. A bigger population would also mean greater probability of
knowledge breakthroughs which produce multiplier effects on productivity (a process of so-
called endogenous growth) (Guest, 2007; PPAG, 2009).
6 | JSRP Abdulai Kuyini Mohammed
There are disadvantages to a bigger population size which derive from the exhaustible supply of
natural resources (land for example), which lead to congestion and environmental costs and
diminishing marginal productivity of labor. A large population size can also mean cheaper labor
which can discourage innovation in labor saving technology (Guest, 2007). There is growing evidence that productivity and fertility are negatively correlated, and perhaps in both directions
(Becker & Barro, 1998; Galor & Zang, 1997; Gillespie et al., 2009; Guest & Swift, 2006). One of
the determinants of this is a situation, where parents with more children spend less on education per
child. This suggests that population growth compelled by high fertility may lower productivity.
Weighing the advantages against the disadvantages of bigger populations in order to ascertain
the net effect is an indeterminate or unresolved issue, both in theory and in practice. A point
emphasized in the seminal work of Cutler et al. (1990). But for a country like Ghana, with an
alarming population growth rate of 2.7 percent and low technology to mitigate the challenges to
productivity increases, the specter of overpopulation looms high. If this fear materializes then
foreseeable variations in population size are going to impact productivity significantly. Majority
of the respondents agree, arguing that the population size is a concern and if it is not controlled it
will not only lead to productivity decline but also reduction in quality of life. It would be an incomplete exercise if an analysis of optimum population considers only
population size (or its growth) to the neglect of dependency. Analysis should take account of
the consumption needs of dependent young and dependent old people and the fact that the
proportions of young and old in the population are changing (Guest, 2007; RIPS, 2009). Two
points have to be questioned here.
First, a movement to a path of higher fertility rate necessarily reduces consumption per capita
for a number of decades. This will come about because the youth dependency rate increases while
it takes some decades for this to be offset by a fall in the old dependency rate. When the old age
dependency rate eventually falls, consumption per capita recovers (Gillespie et al., 2009; Guest,
2007; Well, 1999).
Second, once the population has become stable at a higher fertility rate after many decades, the total dependency rate (youth plus old age) is likely to be higher than a lower fertility stable
population. Thus, the difference in living standards would be much different. Hence we suffer
the consequences of an increase in population size for many decades which may not be
reversible without government intervention, since private decisions are yielding sub-optimal
outcomes (Guest, 2007; Well, 1999). However, examining the dependency effects on living
standards only provides us with half of the picture.
A further consideration is that a transition to a higher fertility path has implications for
intergenerational equity because of productivity growth overtime. The continuous effects of
productivity growth through technological growth and technological transfer will mean that
living standards will continue to grow irrespective of the fertility rate (Guest & McDonald,
2002; Productivity Commission, 2005). However, this analysis is truer for a developed country
than a developing nation. This is because the creation and/or transfer, and application of new technology to improve productivity, are at lower levels in developing countries to bring about
the enhanced standard living.
It has already been explained in the preceding sections that an increase in fertility would
impose a cost on people alive now and in the near future, which will be reversed in several
decades later, boosting the living standards of people who would in any case have been
probably twice as well off as people today (Productivity Commission, 2005). But this is a
description of the scenario in advanced industrial countries like the US, UK and Germany or
Australia, whose standards of living are expected to be nearly double their current levels
(Productivity Commission, 2005). For developing nations, where the creation of new
technology is at a lower level, it is unlikely that their people will enjoy standards of living
comparable to the developed world. This means that a transition to a higher fertility rate in Ghana would yield an enhanced standard of living for neither present, nor future generations.
One of the respondents, the Director of the Family Health Division of the Ghana Health
Service agrees, when she asserts that the ‘FPP brings benefits to the family, benefits to the
society and benefits to the country and the world at large’. She adds that, ‘Without FPP Ghana
cannot attain the entire 8 Millennium Development Goals’.
7 | JSRP Ghana’s Family Planning Program: A Neglected Policy Initiative?
Will the FPP reduce fertility?
Effectiveness is the degree to which a policy or program attains its objectives. It is concerned
about whether the valued outcome of a policy has been achieved (Ayee, 2000; Dunn, 1994; Howlett & Ramesh, 2003). It has already been demonstrated at length that Ghana does need the
FPP. The next question to pose is: will this initiative work? In other words, will it achieve its
objectives? Findings internationally indicate that public policies do reduce fertility, albeit part
of the calculated effect may be traced to the timing impact where mothers delay childbirth in
their lifecycle rather than decrease or increase the number of children they prefer to have over
their lifetimes (Gillespie et al., 2009; Guest, 2007). Evidence from China shows that its “One
Child Policy” has reduced fertility rate drastically. Rwanda, one of the poorest, most densely
populated countries in the world, demonstrates the potential for family planning success in
Africa. The country documented one of the most rapid increases in contraceptive use ever
recorded, from 10 percent to 27 percent of women of reproductive age (Gillespie et al., 2009).
Between 1965 and 2005, use of family planning by women of reproductive age in the
developing world (excluding China) rose from less than 10 percent to 53 percent. The actual numbers grew from 30 million users in 2008, a dramatic increase. The result: a significant
decline in the average number of children born to each woman during her lifetime, from more
than six children to just over three (Gillespie et al., 2009).
In Ghana efforts at promoting family planning have yielded modest, but significant results.
Knowledge of family planning is almost universal, annual population growth rate has slowed
down from a peak of 3 percent in the 1970s to the current 2.7 percent (DHS, 2008; PPAG,
2009). The number of women using modern methods of family planning rose steadily from 6
percent in 1988 to 19 percent in 2003, but reduced to 17 percent in 2008. Total fertility rate
consequently reduced from 6.4 in 1988 and stagnated at 4.4 in 2003, and then decreased to 4.0
percent in 2008 (DHS, 2008).
However, caution should be exercised in reading too much into these statistics, because the total fertility rate does jump around a bit. For example, the Ghana Maternal Health Survey
recorded an increase in the total fertility rate from 4.4 in 2003 to 4.6 in 2008 (PPAG, 2009).
The Ghana Health Service (GHS) notes that the average Ghanaian woman marries at the age of
19 years, has her first child a year later and has an average of 4.5 children in her lifetime.
Moreover, there are regional variations in total fertility rate, ranging from 3 in Greater Accra
Region to about 7 children in the Northern region (DHS, 2003; GMHS, 2007). In addition,
there has been a slowing of the pace of decline in fertility rate, with little change demonstrated
in the past ten year period. Furthermore, there is the element of an announcement effect of
family planning programs. Barberis & Harvey (2001) contend that after the first few years of
the implementation of family planning programs the birth rate decreases somewhat, but rises
many years later. There is evidence that parents respond to advertisements in making family
planning decisions. But when these advertisements are scaled down or are withdrawn altogether a lapse in incentive to stay the course occurs.
The general consensus among experts in the 1960s when organized family planning
programs were introduced in Africa was that population growth in excess of 2 percent per year
is among the structural factors inhibiting the achievement of a wide range of development
objectives (PPAG, 2009). This implies that the current rate of growth of Ghana’s population of
2.7 percent is above the standard, and therefore sub-optimal from a developmental standpoint.
The analysis implies that the family planning program even though has achieved modest, but
significant gains, has failed to drastically reduce the total fertility rate to a level deemed
optimal from a developmental point of view. In other words, the adequacy of the FPP is
questionable. Adequacy refers to the extent to which a given level of effectiveness satisfies the
needs, values, or opportunities that gave rise to a problem. As a summary, it can be stated that on the basis of international evidence, family planning programs reduce fertility, but the Ghana
results are mixed or indeterminate.
8 | JSRP Abdulai Kuyini Mohammed
Expensive policy
From a policy evaluation perspective it is not sufficient to ask whether the FPP will reduce
fertility rate. Like any public spending program the FPP must be ultimately financed by taxation, which imposes a deadweight loss on society by distorting private choices, in
particular the work/leisure choice. Hence, public spending programs should be delivered as
efficiently and effectively as possible, meaning with minimum deadweight loss for a given
outcome. This coincides with Howlett & Ramash’s (2003) view that public policy should
achieve the public interest by the best possible means. In other words, public policy has to
achieve its goals and do so in a way that yields the greatest possible benefit at the least possible
cost (Curtain, 2000). Put in another way, we need to determine whether the FPP is an efficient
policy. Efficiency refers to the relationship between inputs and outputs. It asks whether we
have accomplished more with little.
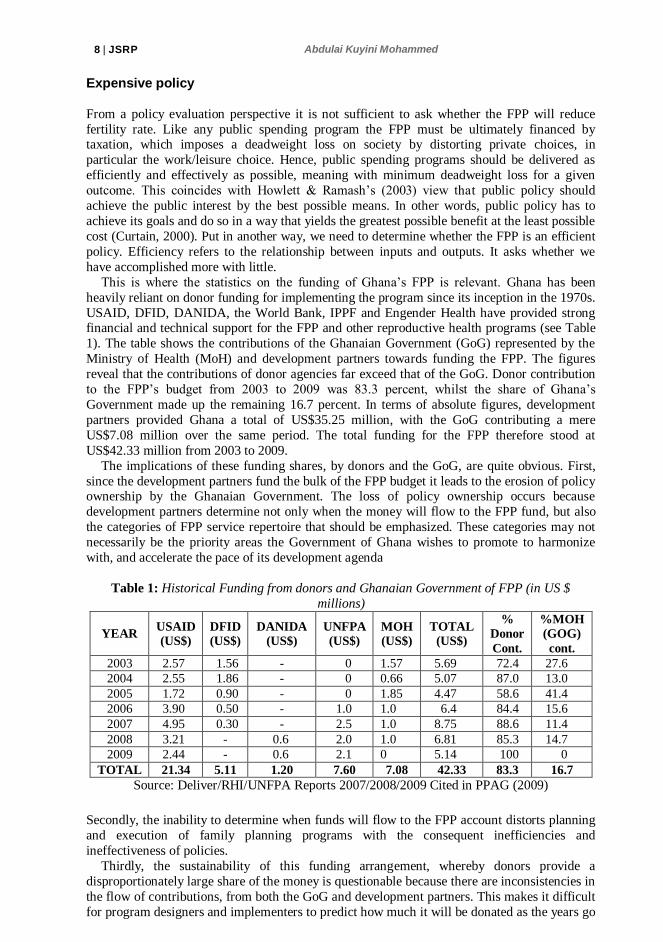
This is where the statistics on the funding of Ghana’s FPP is relevant. Ghana has been
heavily reliant on donor funding for implementing the program since its inception in the 1970s.
USAID, DFID, DANIDA, the World Bank, IPPF and Engender Health have provided strong financial and technical support for the FPP and other reproductive health programs (see Table
1). The table shows the contributions of the Ghanaian Government (GoG) represented by the
Ministry of Health (MoH) and development partners towards funding the FPP. The figures
reveal that the contributions of donor agencies far exceed that of the GoG. Donor contribution
to the FPP’s budget from 2003 to 2009 was 83.3 percent, whilst the share of Ghana’s
Government made up the remaining 16.7 percent. In terms of absolute figures, development
partners provided Ghana a total of US$35.25 million, with the GoG contributing a mere
US$7.08 million over the same period. The total funding for the FPP therefore stood at
US$42.33 million from 2003 to 2009.
The implications of these funding shares, by donors and the GoG, are quite obvious. First,
since the development partners fund the bulk of the FPP budget it leads to the erosion of policy ownership by the Ghanaian Government. The loss of policy ownership occurs because
development partners determine not only when the money will flow to the FPP fund, but also
the categories of FPP service repertoire that should be emphasized. These categories may not
necessarily be the priority areas the Government of Ghana wishes to promote to harmonize
with, and accelerate the pace of its development agenda
Table 1: Historical Funding from donors and Ghanaian Government of FPP (in US $
millions)
YEAR USAID
(US$)
DFID
(US$)
DANIDA
(US$)
UNFPA
(US$)
MOH
(US$)
TOTAL
(US$)
%
Donor
Cont.
%MOH
(GOG)
cont.
2003 2.57 1.56 - 0 1.57 5.69 72.4 27.6
2004 2.55 1.86 - 0 0.66 5.07 87.0 13.0
2005 1.72 0.90 - 0 1.85 4.47 58.6 41.4
2006 3.90 0.50 - 1.0 1.0 6.4 84.4 15.6
2007 4.95 0.30 - 2.5 1.0 8.75 88.6 11.4
2008 3.21 - 0.6 2.0 1.0 6.81 85.3 14.7
2009 2.44 - 0.6 2.1 0 5.14 100 0
TOTAL 21.34 5.11 1.20 7.60 7.08 42.33 83.3 16.7
Source: Deliver/RHI/UNFPA Reports 2007/2008/2009 Cited in PPAG (2009)
Secondly, the inability to determine when funds will flow to the FPP account distorts planning
and execution of family planning programs with the consequent inefficiencies and
ineffectiveness of policies.
Thirdly, the sustainability of this funding arrangement, whereby donors provide a
disproportionately large share of the money is questionable because there are inconsistencies in
the flow of contributions, from both the GoG and development partners. This makes it difficult
for program designers and implementers to predict how much it will be donated as the years go
9 | JSRP Ghana’s Family Planning Program: A Neglected Policy Initiative?
by. Added to this is the specter of default in contributions by all or any of the development
partners. And indeed, as Table 1 indicates, UNFPA for three consecutive years from 2003 to
2005 did not donate to the program. The GoG also could not contribute to the FPP in 2009. The
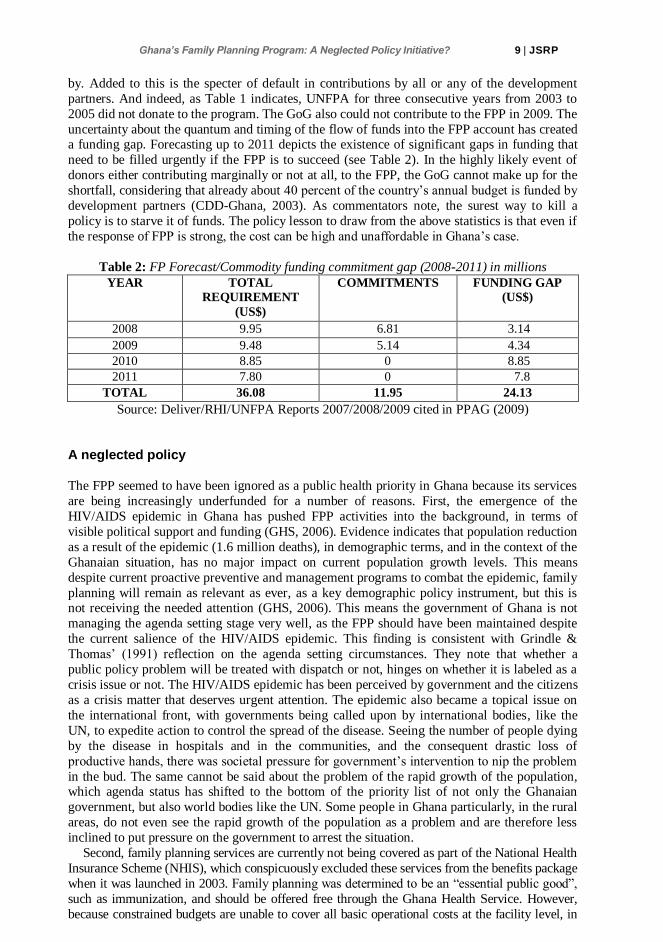
uncertainty about the quantum and timing of the flow of funds into the FPP account has created a funding gap. Forecasting up to 2011 depicts the existence of significant gaps in funding that
need to be filled urgently if the FPP is to succeed (see Table 2). In the highly likely event of
donors either contributing marginally or not at all, to the FPP, the GoG cannot make up for the
shortfall, considering that already about 40 percent of the country’s annual budget is funded by
development partners (CDD-Ghana, 2003). As commentators note, the surest way to kill a
policy is to starve it of funds. The policy lesson to draw from the above statistics is that even if
the response of FPP is strong, the cost can be high and unaffordable in Ghana’s case.
Table 2: FP Forecast/Commodity funding commitment gap (2008-2011) in millions
YEAR TOTAL
REQUIREMENT
(US$)
COMMITMENTS FUNDING GAP
(US$)
2008 9.95 6.81 3.14
2009 9.48 5.14 4.34
2010 8.85 0 8.85
2011 7.80 0 7.8
TOTAL 36.08 11.95 24.13
Source: Deliver/RHI/UNFPA Reports 2007/2008/2009 cited in PPAG (2009)
A neglected policy
The FPP seemed to have been ignored as a public health priority in Ghana because its services
are being increasingly underfunded for a number of reasons. First, the emergence of the
HIV/AIDS epidemic in Ghana has pushed FPP activities into the background, in terms of
visible political support and funding (GHS, 2006). Evidence indicates that population reduction
as a result of the epidemic (1.6 million deaths), in demographic terms, and in the context of the
Ghanaian situation, has no major impact on current population growth levels. This means
despite current proactive preventive and management programs to combat the epidemic, family
planning will remain as relevant as ever, as a key demographic policy instrument, but this is not receiving the needed attention (GHS, 2006). This means the government of Ghana is not
managing the agenda setting stage very well, as the FPP should have been maintained despite
the current salience of the HIV/AIDS epidemic. This finding is consistent with Grindle &
Thomas’ (1991) reflection on the agenda setting circumstances. They note that whether a
public policy problem will be treated with dispatch or not, hinges on whether it is labeled as a
crisis issue or not. The HIV/AIDS epidemic has been perceived by government and the citizens
as a crisis matter that deserves urgent attention. The epidemic also became a topical issue on
the international front, with governments being called upon by international bodies, like the
UN, to expedite action to control the spread of the disease. Seeing the number of people dying
by the disease in hospitals and in the communities, and the consequent drastic loss of
productive hands, there was societal pressure for government’s intervention to nip the problem
in the bud. The same cannot be said about the problem of the rapid growth of the population, which agenda status has shifted to the bottom of the priority list of not only the Ghanaian
government, but also world bodies like the UN. Some people in Ghana particularly, in the rural
areas, do not even see the rapid growth of the population as a problem and are therefore less
inclined to put pressure on the government to arrest the situation.
Second, family planning services are currently not being covered as part of the National Health
Insurance Scheme (NHIS), which conspicuously excluded these services from the benefits package
when it was launched in 2003. Family planning was determined to be an “essential public good”,
such as immunization, and should be offered free through the Ghana Health Service. However,
because constrained budgets are unable to cover all basic operational costs at the facility level, in
10 | JSRP Abdulai Kuyini Mohammed
actual practice, almost every public facility and all private facilities charge fees for family planning
services (PPAG, 2009). This evidence conflicts with Brislin (1981), Moran and Harris’ thoughts
on synergetic policy making, which calls for linkages and mutual support for related social policies
and programs. By excluding the FPP from the funding arrangement we are literally saying that: “deliver free of charge at any facility, but pay at the same facility to control your births:” In other
words, government is creating marginal incentives for women to have more children and marginal
disincentive to space their births. This scenario will not augur well for the reproductive health of
women, which is the broader goal of government.
A cost-benefit analysis of adding coverage of long term and permanent contraceptives, as well
as injectables, to the NHIS benefits package revealed that including family planning would cause
a decrease in fertility and would avert births that would otherwise have cost the NHIS
considerable expenditures. Adding this benefit would lead to an annual savings to the NHIS that
would increase over time. The size of the net savings depends on a number of variables, which
may change over time. According to the consultant’s assumptions, if family planning had been
covered in 2009, by 2011 the NHIS will realize almost GH₡ 11 million in net savings in that year
alone. This increases to over GH₡ 18 million in 2017 (USAID/Banking on Health, 2008). In
other words, excluding the FPP from the NHIS has generated significant inefficiencies.
In contrast, funding is increasingly being made available to support the FMCPW as part of
an international effort to improve progress towards the Millennium Development Goals
(MDGs). Achieving the MDGs is an international policy agenda that was mooted by the UN
and subscribed to by all member nations, including Ghana. Advanced industrialized countries
are promoting the agenda by supplying funds to developing countries and monitoring their
performance in achieving these goals. Ghana has accordingly included the achievement of the
MDGs as part of its domestic policy agenda, with a priority tag attached to it, but has relegated
the FPP to the background. This confirms Ohmae (1995) and Falk’s (1997) assertion that
nations are increasingly constrained and shaped by global forces. Out of pocket spending for family planning services and commodities is roughly estimated
to be $2 million per year. The replacement of these in the light of stagnating donor support and
government funding, despite recent increases in need, is woefully inadequate (PPAG, 2009). In
2008, forecast demand for family planning products exceeded the amount allocated in the
health budget for family planning by $7 million (PPAG, 2009). Counseling for family planning
is free, but reproductive health supply has to be paid for.
This findings corroborate the views of Brislin (1981), Moran & Harris (1981) that we are
developing and implementing the FPP and FMCPW in Ghana as separate programs; that
instead of working on the policies as a joint initiative, we are treating them as separate parts
and privileging the former over the latter, and that handling them this way will not bring
mutual growth and accomplishment of their respective objectives and the broader goal of achieving a high standard of reproductive health of women. In other words, there is no synergy
between the FPP and FMCPW.
Policies at odds with each other
While FPP is not covered under the National Health Insurance Scheme (NHIS) the FMCPW is
well placed on it. The question that arises is: Are the FPP and FMCPW at odds with each
other? In answer, it does appear financial incentives now favor more, rather than fewer births.
Expanded NHIS coverage for pregnant women makes the medical care costs of additional
births zero for women, which provides a marginal incentive to increase average total fertility
per woman. Lack of NHIS coverage for family planning services disadvantageous in delaying or limiting births, providing a marginally negative incentive to delay or limit births (PPAG,
2009). This point of view, however, does not win favor from Ghana’s Eastern Regional
Population Officer. He contends that rather than increasing the fertility rate, the FMCPW could
result in a decrease in birth rates as it focuses on comprehensive management of pregnancies
that include mother and child survival, promotion of family planning and health practices. He
added that uptake of education opportunities by girls and women, and the lengthening of their
11 | JSRP Ghana’s Family Planning Program: A Neglected Policy Initiative?
time in educating up to the tertiary level has reduced fecund level or the number of children
born per woman during her lifetime to 2, although the Eastern Region’s average is still above
four (Abinah, 2008).
His assessment should be treated with caution since the fertility rate has not dropped for the past several years. It should also be noted that the FPP has a yawning funding gap, and there is
a potential for donor support to dwindle and dry up in the future. In contrast, funding for the
FMCPW is assured for many years to come, this implies there is a real danger of the FPP being
crowded out of government priorities.
The consequences of this lack of synergy between the programs is that family planning
services and commodities have become more costly to access since parents will have to fully
finance these services and products out of their pocket. On the other hand, couples who would
have been reluctant to have more children due to the cost of antenatal and post-natal medical
care would have an incentive to have them. Perhaps the only way to make the FMCPW cost-
effective is to limit it to expectant mothers who will be having their first, second or third
children. Then from the fourth child onwards a co-contribution from government and couples
will apply. The contribution from parents should be means tested where progressively those in the lower income bracket pay less. The idea is that if parents bear part of the cost it will
influence their decisions in favor of fewer children.
However, majority of the respondents do not agree with the above point that the FPP and
FMCPW are conflicting. On the contrary, they think they are complementary. However,
minority views put these initiatives at odds with each other. One of these respondents alludes
that ‘If you say free maternal care, then the woman should also come for free family planning
of her choice’. She adds, ‘Without free family planning, the message seems to be that the
government will pay for you to have a baby, but will ask you to pay from your pocket to
practice family planning’. She concludes by implying that, ‘the Slogan is: you are encouraged
to have more babies but discouraged to limit your birthrate’.
Discussion
Based on the analytical framework of Grindle & Thomas (1991), the agenda setting
circumstances of Ghana’s FMCPW initiative were such that there was a strong perception of a
crisis and a need for action among political, as well as technical and bureaucratic actors and
civil society. There was strong pressure for change from a “Cash and Carry” system to a
national health insurance scheme (NHIS), which would enfold the FMCPW, to make health
care costs less burdensome for the masses. The stakes for reform were therefore high. High
level decision makers, including the president, were concerned about getting national health
insurance and the FMCPW in particular to work in Ghana and made this clear in public
statements. The then National Patriotic Party (NPP) government was keenly interested in materializing NHIS and the FMCPW to pride itself that it had delivered on an election promise
so as to bolster its electoral advantages in the next elections. For the then opposition National
Democratic Congress (NDC) – which sees itself as a social democratic party, it did not want to
be seen as opposing a major policy reform that would support the underprivileged and the
vulnerable and therefore approved of the policy, but with reservations. These reservations
compelled the party to continue to criticize the government on implementation bottlenecks.
Thus, the policy decision making focus seemed to have been centered on concerns about
political relationships and stability.
The priority tag the government attached to the FMCPW was prompted by international
bodies like the UN, which had already declared maternal mortality as an international health
crisis, and adopted MDG Goal 5 to stem it. As a member of this world body, Ghana accordingly conformed by also placing it high on its policy agenda. Unlike the FMCPW, the
FPP has been running in Ghana since the 1970s and even though it was repositioned in 2006 to
achieve its goals, it was not perceived as a crisis issue, both internationally and domestically,
the stakes were therefore low, and incremental decision making by low and middle level policy
makers was acceptable. This confirms Grindle & Thomas’ (1991) contention that the crisis or

12 | JSRP Abdulai Kuyini Mohammed
non crisis nature of an issue, and whether the problem is topical or otherwise on the
international scene, would determine whether or not it would have placement on a
government’s policy agenda.
Conclusion The study set out to determine whether the FPP has policy merits and whether it is a neglected
government priority. This question has been answered through responses to three further
questions. The first question related to whether Ghana needs an FPP. In other words, is the FPP
an appropriate policy? The answer to this question is, yes. It is clear from the study that there is a
need for it because we are already on or close to an inappropriate or even dangerous demographic
track. I have also demonstrated that a higher population growth rate will increase total
dependency in the long run and along the transition path. The consequences will be suffered by
the present and future generations. Issues about the net effect of economies versus diseconomies
of bigger populations are salient to mention, but they remain indeterminate. Yet we cannot ignore
them when they are considered against the current demographic trends in Ghana. It thus appears in the Ghanaian situation that the diseconomies of population size are weighing more than the
advantages and intervention is certainly needed to at least, restore a balance.
The second question demanded an answer as to whether the FPP is efficacious in reducing
fertility. The evidence shows that even though the FPP has made modest, but significant gains, it
has failed to drastically reduce the total fertility rate to a level deemed optimal from a
developmental point of view. Looking at it from another side, the FPP is not adequate because the
given level of effectiveness from it has not significantly tamed the rapid rate of growth of
Ghana’s population. In terms of equity, both the rich and the poor pay the same amounts to
procure family planning products, meaning there is no equity in the provision of family services.
The third question probed about whether the FPP is a neglected policy. The answer is in the
affirmative, because the salience of the HIV/AIDS epidemic and the FMCPW has pushed the FPP to the background. The evidence shows that unless family planning services and
commodities are included for funding under the NHIS, there will be a cost for delaying or
limiting births, providing little incentive to delay or limit births. And that the current free
maternal health care without a family planning component is serving as an incentive to reduce
birth spacing and increase pregnancies, thereby undermining the impact of family planning. In
other words there is no synergy between the FPP and FMCPW. A situation appalled by Brislin,
Moran and Harris as not engendering mutual growth and accomplishment of broader overall
objectives. The FPP appears to be a neglected government policy.
References
1. Abinah, K. (2008). Free Medical Care for Pregnant Women Would not Lead to
population Explosion. Modern Ghana, Retrieved 30 July, 2010, from
www.modernghana.com/news/167603/1/free-medical-care-for-pregnant-women-
would-not-lea.html.
2. Adjei, S., & Agyeapong, I. K. (2008). Public Social Policy Development and
Implementation: A Case Study of the Ghana National Health Insurance Scheme,
Health policy and Plannning, 23, pp. 150-160.
3. Arjun, A. (1996). Population Trends: Ghana, United States Department of Commerce.
4. Australian Commonwealth Parliament (1994). The Jones Report on Australia’s
population Carrying Capacity: One Nation Two Ecologies, report by the House of
Representatives Standing Committee on Long Term Strategies, Canberra: Australian Government Publishing Service.
13 | JSRP Ghana’s Family Planning Program: A Neglected Policy Initiative?
5. Ayee, J. R. A. (2000). Saints, Wizards, Demons and Systems: Explaining the Success
or Failure of Public Policies and Programmes. Accra: Ghana Universities Press.
6. Barberis, M., & Harvey, P. D. (2001). Costs of Family Planning Programmes in
Fourteen Developing Countries. Cambridge: Cambridge University Press.
7. Becker, G., & Barro, R. (1998). A Reformulation of the Economic Theory of Fertility.
The Quarterly Journal of Economics, 103(412), pp. 1-25
8. Bennett, C.J. (1997). Understanding Ripple Effects: The Cross-National Adoption of
Policy Instruments for Bureaucratic Accountability. Governance, 10(3), pp. 313-33.
http://dx.doi.org/10.1111/0952-1895.401997040
9. Berstein, S., & Cahoe, B. (2000). Globalization, Four Paths of Internalisation and
Domestic Change: The Case of EcoForestry in British Colombia, Canada. Canadian
Journal of Political Science, 33(1), pp. 67-100.
10. Brenner, N. (1999). Beyond State Centrism? Space Territoriality and Geographical
Scale in Globalisation Studies. Theory and Society, 28(1), pp. 39-78.
http://dx.doi.org/10.1023/A:1006996806674
11. Bridgman, P., & Davis, G. (2004). The Australian Policy Handbook. 3rd edition. Crow’s Nest NSW: Allen and Unwin.
12. Brislin, R. W. (1981). Cross Cultural Encounters. New York: Pergamon.
13. Ghana Centre for Democratic Development (CDD-Ghana) (2003). The Funding of
Key Governance Institutions in Ghana, Report of a Diagnostic Study (Accra: National Governance Program).
14. Carrin, G. (2003). Community Based Health Insurance Scheme in Developing
Countries: facts, problems and perspectives. Discussion Paper No. 1, Geneva, World
Health Organization.
15. Carrin, G., & James, C. (2004). Reshaping Universal Coverage via Social Health
Insurance: Key Design Features in the Transition Period. Discussion Paper No. 2,
EIP/FER/DP 042, Geneva, World Health Organization.
16. Cassells, A. (1995). Health Sector Reform: Key Issues in Less Developed Countries.
Forum on Health Sector Reform, Discussion paper No. 1 (WHO: SHS/NHP/954).
Geneva, World Health Organization.
17. Coleman, M. M., & Perl, A. (1999). Internationalized Policy Environment and Policy
Network Analysis. Political Studies, 47(4), pp. 691-709.
http://dx.doi.org/10.1111/1467-9248.00225
18. Curtain, R. (2000). Good Policy Making: How Australia Fares? Agenda, 8(1), pp. 33-46.
19. Cutler, D., Poterba, J., Sheiner, l., & Summers, L. (1990). An Aging Society:
Opportunity or Challenge? Brookings Papers in Economic Activity, Spring, pp. 1-74.
20. Dunn, J. E. (1994). A Systems Analysis of political Life. New York: Wiley.
21. Falk, R. (1997). State of Seige: Will Globalization win out? International Affairs,
73(1), pp. 124-36. http://dx.doi.org/10.2307/2623553
14 | JSRP Abdulai Kuyini Mohammed
22. Finnemore, M., & Sikkink, K. (1998). International Norm Dynamics and Political
Change. International Organization, 52(4), pp. 887-917.
http://dx.doi.org/10.1162/002081898550789
23. Galor, O., & Zang, H. (1997). Fertility, Income Distribution, and Economic Growth:
Theory and Cross-Country Evidence. Japan and World Economy, 9(2), pp. 197-229.
http://dx.doi.org/10.1016/S0922-1425(96)00245-9
24. Ghana Health Service (DHS) (2008). Ghana Demographic and Health Survey Report.
25. Ghana Health Service (DHS) (2003). Ghana Demographic and Health Survey Report.
26. Ghana Maternal Health Study (GMHS) (2007). Report, Ghana Health Service.
27. GHS (2006). A Road Map for Repositioning Family Planning in Ghana (2006-2010).
Accra: Duke and Duke Inc.
28. Goldstein, J. S., & Whitworth, S. (2005). International Relations, Canadian ed.
Toronto: Pearson Longman.
29. Gillespie, D., Maguire, E., Neuse, M., Sinding, S., & Speidel, J. J. (2009). Making the
Case for US International Family Planning Assistance. The Bill and Melinda Gates
Institute for Population and Reproductive Health. Baltimore, MD
30. Grindle, M. S., & Thomas, J. W. (1991). Public Choice and Policy Change: The
Political Economy of Reform in Developing Countries, Baltimore, MD: John Hopkins
University Press.
31. Guest, R. (2007). The Baby Bonus: A Dubious Policy Initiative. Policy, 23(1), pp. 11-15.
32. Guest, R., & McDonald, I. (2002). Would a Decrease in Fertility be a Threat to Living
Standards in Australia? Australian Economic Review, 35(1), pp. 29-44.
http://dx.doi.org/10.1111/1467-8462.00221
33. Guest, R., & Swift, R. (2006). Fertility, Income Inequality and Labour Productivity,
Brisbane: Griffith University.
34. Hirst, P., & Thompson, G. (1996). Globalization in Question, Oxford: Polity Press.
35. Howlett, M. & Ramesh, M. (2003). Studying Public Policy: Policy Cycles and Policy
Systems. UK: Oxford University Press.
36. McDonald, P., & Kippen, R. (1999). Population Futures for Australia: the Policy
Alternatives, Parliament of Australia, research paper No. 5, Canberra: APH. October
12. Retrieved June 20, 2009, from http://www.aph.gov.au/library/pubs/rp/1999-2000/2000rp05.htm
37. Ministry of Health (MoH) (2004). Guidelines for Implementing the Exemption Policy
on Maternal Deliveries, Accra, Ministry of Health. Report No: MoH/policy, planning,
Monitoring and Evaluation 59.
38. Moran, R. T., & Harris, P. R. (1981). Managing Cultural Synergy, Houston, Tex: Gulf
Publishing Company.
39. Ohmae, K. (1995). The End of the Nation State, London: Harper-Collins.
15 | JSRP Ghana’s Family Planning Program: A Neglected Policy Initiative?
40. Planned Parenthood Association of Ghana (PPAG) (2009). The Case for Adding
Family Planning on the National Health Insurance Scheme. Position Paper.
41. Productivity Commission (2005). Economic Implications of an Aging Australia,
Canberra: PC, April.
42. Neville, J, (1990). The Effect of immigration on Australian Living Standards, Bureau
of Immigration Research, South Carlton: Commonwealth of Australia
43. Osabutey, P. D. (2008). Ghana: Achieving MDG5 through Free Medical care for
Pregnant Women, The Chronicle, July 25.
44. RHI/UNFPA Reports (2007, 2008, 2009). Cited in Planned Parenthood Association of
Ghana (PPAG) (2009). The Case for Adding Family Planning on the National Health
Insurance Scheme. Position Paper.
45. Preker, A. S. (Ed.) (2002). Health Care Financing for Rural and Low Income
Populations: The Role of Communities in Resource Mobilization and Risk Sharing.
Washington DC: IBRD/World Bank.
46. Pressman, J., & Wildavsky (1984). Implementation, 3rd ed., Berkeley: California
University Press.
47. Productivity Commission (2005). Economic Implications of an Aging Australia,
Canberra: PC, April.
48. Regional Institute for Population Studies (RIPS) (2009). Measuring Economic and
Social Impact of Migration in Ghana, Mid-Grant Presentation to CDN/JPPR.
49. Thomas, S., & Gilson, L. (2004). Actor Management in the Development of Health
Financing Reform: Health Insurance in South Africa, 1994-1999. Health Policy and
Planning, 19(5), pp. 279-291. http://dx.doi.org/10.1093/heapol/czh033
50. UNDP (2007). Ghana Human Development Report, United Nations Development
Programme, Ghana. Retrieved 13 May, 2014, from
www.undp.org/sites/default/files/nhdr_2007_ghana.pdf.
51. USAID/Banking on Health (2008). An Analysis of the Costs and Benefits to the
National Health Insurance Scheme in Adding Family planning Products and Services
to the Coverage Package.
52. Walt, G., & Gilson, L. (1994). Reforming the Health Sector in Developing Countries:
The Central Role of Policy Analysis. Health Policy and Planning, 9, pp. 353-370.
http://dx.doi.org/10.1093/heapol/9.4.353
53. Well, D, (1999). Population Growth, Dependency and Consumption. American
Economic Review, 89(2), pp. 251-255 (Papers and proceedings).
http://dx.doi.org/10.1257/aer.89.2.251
Related Documents











