Getting to Goals: Practical Approach Heart Failure Management Presented by: Sandra Oliver-McNeil DNP, ACNP Wayne State University, College of Nursing

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Getting to Goals: Practical Approach Heart Failure Management
Presented by: Sandra Oliver-McNeil DNP, ACNP
Wayne State University, College of Nursing

Course Speaker Disclosure Information
Sandra Oliver-McNeil DNP, ACNP-BC, CHFN, AACC
Disclosures
None

Audience Response Question
• According to the ACC/AHA Guidelines for management of HFrEF, which of the following medication combination should patients be on to reduce mortality?
• a. Ace-inhibitor, betablocker, and loop diuretic
• b. Ace-Inhibitor, betablocker, aldosterone antagonist.
• c. Betablocker and loop diuretic only
• d. Digoxin, Ace-Inhibitor, and loop diuretic

Audience Response Question
• According to CHAMP-HF study, what is the average percentage of patients who are on target GDMT for HFrEF?
• a. 50%
• b. 75%
• c. 20%
• d. 30%

Case Study
• George is a 56-year-old black male who presents to the emergency department with symptoms of shortness of breath and 5 lb. weight gain over the last 2 weeks. He was discharged two weeks prior with new diagnosis HFrEF.

• PMH:• Hypertension• OSA• Obesity BMI 40
• PSH:• T&A• Heart Cath 2 weeks ago
• Social History:
• Married for 30 years
• 5 children
• Employed as a mechanic but has not returned to work
• Hx alcohol abuse
• Denies cocaine, heroin or opioid use
• Smokes marijuana

• Medications:• Coreg 3.125 mg twice daily
• Enalapril 5 mg daily
• Furosemide 40 mg daily
• Data:
• Echo: LVEF 25%, minimal mitral regurgitation, RVSP 35 mmHg, Mild LV enlargement
• Cath: Coronary angiogram: “Normal”, no right heart cath.
• Chest x-ray: Mild pulmonary vascular congestion, no effusion
• Labs:
• CBC WNL
• Na 135, K+4.0, BUN 25, Creatinine 1.8

• Physical exam
• VS: BP 135/80 HR 83, RR 20 Temp 37.0C
• Regular rate and rhythm, no additional heart sounds, +JVD, +2 peripheral edema bilaterally, + hepatic jugular reflex
• LS rales in bases, no respiratory distress O2 sat on room air 90%
• Abdomen round, obese.
• No neuro deficits

CHAMP-HF Registry
• Overall, 3,518 patients• 150 primary care and cardiology practices were included.
• Mean age was 66 ± 13 years
• Female: 29%
• Mean EF was 29 ± 8%.
• Greene, S. J. et.al. Medical Therapy for Heart Failure With Reduced Ejection Fraction.
JACC (7/2018). 72 (4), 351-366.

CHAMP-HF continue
• Among eligible patients, • 27%, 33%, and 67% were not prescribed ACEI/ARB/ARNI, beta-blocker, and
MRA therapy, respectively.
• When medications were prescribed, few patients were receiving target doses of ACEI/ARB (17%), ARNI (14%), and beta-blocker (28%), whereas most patients were receiving target doses of MRA therapy (77%).
• Among patients eligible for all classes of medication, 1% were simultaneously receiving target doses of ACE/ARB/ARNI, beta-blocker, and MRA.

CHAMP-HF (continue)
• Lower medication utilization or dose in adjusted models:
• Older age
• Lower blood pressure
• More severe functional class
• Renal insufficiency
• Recent HF hospitalization
• Social and economic characteristics were not independently associated with medication use or dose.


Pathophysiology


2017 ACC Expert Consensus Decision Pathway
• Yancy, Clyde W. 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction. JACC (01/2018). 71 (2), 201-230. DOI: 10.1016/j.jacc.2017.11.025


Starting dose Target dose
Beta Blockers
Bisoprolol 1.25 mg once daily 10 mg once daily
Carvedilol 3.125 mg twice daily 25 mg twice daily for weight <85 kg and 50 mg twice daily for
weight ≥85 kg
Metoprolol succinate 12.5–25 mg/d 200 mg daily
ARNI
Sacubitril/valsartan 24/26 mg–49/51 mg twice daily
97/103 mg twice daily
ACEI
Captopril 6.25 mg 3× daily 50 mg 3x daily
Enalapril 2.5 mg twice daily 10–20 mg twice daily
Lisinopril 2.5–5 mg daily 20–40 mg daily
Ramipril 1.25 mg daily 10 mg daily
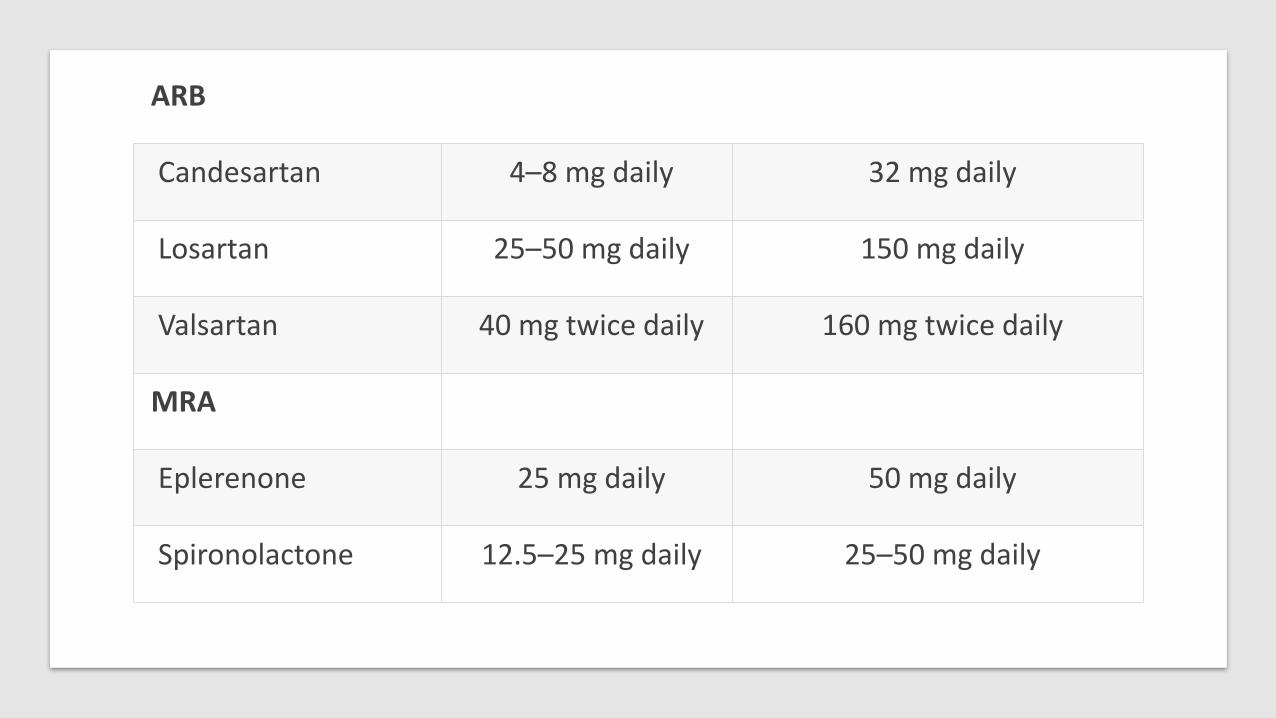
ARB
Candesartan 4–8 mg daily 32 mg daily
Losartan 25–50 mg daily 150 mg daily
Valsartan 40 mg twice daily 160 mg twice daily
MRA
Eplerenone 25 mg daily 50 mg daily
Spironolactone 12.5–25 mg daily 25–50 mg daily

Vasodilators
Hydralazine 25 mg 3× daily 75 mg 3× daily
Isosorbide dinitrate 20 mg 3× daily 40 mg 3× daily
Fixed-dose combination isosorbide dinitrate/hydralazine
20 mg/37.5 mg (one tab) 3× daily
2 tabs 3× daily
Ivabradine
Ivabradine 2.5–5 mg twice daily Titrate to heart rate 50–60 bpm. Maximum dose
7.5 mg twice daily

Additional points
• Digoxin remains indicated for HFrEF, but there are no contemporary data to warrant additional comment in this document. The reader is referred to already available guideline statements.
• Isosorbide mononitrate is not recommended by the ACC/AHA/HFSA guideline.
• The ACC/AHA/HFSA guideline considers either the fixed dose combination or the separate combination of isosorbide dinitrate and hydralazine as appropriate guideline directed therapy for HF.

Conclusion
• GDMT is imperative to treatment of HFrEF
• As per the CHAMP-HF registry Medications are underutilized
• Recommended dose for GDMT is 50% of target dose for each classification.
Related Documents











