June 2012 VOL. 39 NO. 6 www.medicalprogress.com Volume 39 Number 6 Colorectal Cancer In Focus: Peer-reviewed CME Journal Get your copy of today and earn JPOG and Medical Progress SKP IDI 1 SKP CME ACCREDITED BY IDI The Ravages of Bed Rest Low Back Pain Management: Approaches to Treatment Global Summaries Clinical Review A Middle-aged Woman With Morbid Obesity – How to Treat? In Focus Colorectal Cancer: Prevention & Early Diagnosis Colorectal Cancer: Features & Investigation Can Metastatic Colorectal Cancer Be Cured? Continuing Medical Education

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

June 2012 VOL. 39 NO. 6
Med
ica
l Pr
og
ress • JU
Ne 2012
www.medicalprogress.com
Volume 39 N
umber 6
Colorectal CancerIn Focus:
Peer-reviewed C
ME Jo
urnal
P i s H
MissN
1015-4256
Get your copy of today and earnJPOG and Medical Progress SKP IDI
1 SKP
CME ACCREDITED BY IDI
The Ravages of Bed Rest
Low Back Pain Management: Approaches to Treatment
Global Summaries
Clinical Review
A Middle-aged Woman With Morbid Obesity – How to Treat?
In Focus
Colorectal Cancer: Prevention & Early Diagnosis
Colorectal Cancer: Features & Investigation
Can Metastatic Colorectal Cancer Be Cured?
Continuing MedicalEducation
MP 0612-CVR_01.indd 4 25/07/2012 11:15 AM


Medical Progress June 2012 i
June 2012 VOL. 39 NO. 6Anaesthesia & Intensive Care Medicine
Prof Gavin JOYNTThe Chinese University of Hong Kong, HKSAR, China
Andrology
Prof Wimpie PANGKAHILAUdayana University, Indonesia
Cardiology
Emeritus Prof Ramon F ABARQUEZUniversity of the Philippines, Philippines
Prof Boon-Lock CHIANational University of Singapore, Singapore
Dr Anna Maria CHOYNinewells Hospital and Medical School, UK
Prof Harmani KALIMUniversity of Indonesia, Indonesia
Dr Anwar SANTOSOUdayana University, Indonesia
Clinical Pharmacology
Prof Bernard CHEUNGUniversity of Hong Kong, HKSAR, China
Prof Chay-Hoon TANNational University of Singapore, Singapore
Dermatology
Dr Adrian YP FUNGPrivate Practice, HKSAR, China
Dr Yoke Chin GIAMNational Skin Centre, Singapore
Endocrinology
Dr Norman CHANPrivate Practice, HKSAR, China
Prof Siew-Pheng CHANUniversity of Malaya, Malaysia
Dr Ma Teresa P QUEPhilippine Diabetes Association, Philippines
Prof Sidartawan SOEGONDOUniversity of Indonesia, Indonesia
Family Medicine
Prof Cindy LK LAMThe University of Hong Kong, HKSAR, China
Gastroenterology & Hepatology
Prof Khean-Lee GOHUniversity of Malaya, Malaysia
Prof George KK LAUThe University of Hong Kong, HKSAR, China
Prof HA Aziz RANIUniversity of Indonesia, Indonesia
Prof Benjamin CY WONGThe University of Hong Kong, HKSAR, China
Geriatric Medicine
Dr Leung-Wing CHU The University of Hong Kong, HKSAR, China
Haematology & Oncology
Prof Raymond LIANGThe University of Hong Kong, HKSAR, China
Dr Raymond WONGPrince of Wales Hospital, HKSAR, China
Infectious Disease
Dr Christopher LEEHospital Sungai Buluh, Malaysia
Prof Amorn LEELARASAMEESiriraj Hospital, Thailand
Prof Ron HH NELWANUniversity of Indonesia, Indonesia
Nephrology
Prof Philip KT LI Prince of Wales Hospital, HKSAR, China
Prof Wiguno PRODJOSUDJADIThe University of Indonesia, Indonesia
Neurology
Prof Raymond TF CHEUNG The University of Hong Kong, HKSAR, China
Dr Gardian CY FONG The University of Hong Kong, HKSAR, China
Dr Chen-Ya HUANGThe University of Hong Kong, HKSAR, China
Dr Venketasubramanian RAMANINational University Hospital, Singapore
Prof Hasan SJAHRIRUniversitas Sumatera Utara, Indonesia
Prof Lawrence KS WONG The Chinese University of Hong Kong, HKSAR, China
Occupation Medicine & Public Health
Prof David KOHNational University of Singapore, Singapore
Dr Judy SNGNational University of Singapore, Singapore
Ophthalmology
Dr Michael SH LAWPrivate Practice, Malaysia
Orthopaedics & Orthopaedic Surgery
Prof David SK CHOONUniversity Malaya Medical Centre, Malaysia
Dr Daniel KH YIPPrivate Practice, HKSAR, China
Adj Asst Prof Eugene WONGPerdana University Graduate School of Medicine, Malaysia
Otorhinolaryngology
Prof Dato’ Balwant Singh GENDEHThe National University Hospital Malaysia, Malaysia
Prof William I WEI Queen Mary Hospital, HKSAR, China
Pharmacy
Prof Vincent HL LEEThe Chinese University of Hong Kong, HKSAR, China
Psychiatry
Dr Eric YH CHENThe University of Hong Kong, HKSAR, China
Dr M Parameshvara DEVAKPJ Selangor Specialist Hospital, Malaysia
Respiratory & Critical Care Medicine
Prof Menaldi RASMINUniversity of Indonesia, Indonesia
Assoc Prof Dessmon YH TAITan Tock Seng Hospital, Singapore
Dr Kenneth WT TSANGPrivate Practice, HKSAR, China
Rheumatology & Immunology
Prof Handono KALIMBrawijaya University, Indonesia
Dr Swan-Sim YEAPPrivate Practice, Malaysia
261-264 Global Summaries261 Cardiology •Rivaroxabanafteracutecoronarysyndrome
•Vorapaxarinacutecoronarysyndromes
•Strokeriskwithsub-clinicalatrialfibrillation
Diabetes •Diabetesriskmodelsandscores
262 •Intensiveglucosecontroltopreserverenalfunction
Gastroenterology •NewdrugsforchronicHCVgenotype1
General Medicine •GenetherapyforhaemophiliaB
263 •Catheter-directedthrombolysisforacuteileofemoralDVT
•Managementofdiabetesandhypertensionbyruralhealth-
careworkersinIran
264 Oncology •Genechangesandresistanceofcolorectalcancerto
chemotherapy
•Denosumabforprostatecancer
•Prostatecancergenemutation
265-268 Clinical Review GENERAL MEDICINE
A Middle-aged Woman With Morbid Obesity – How to Treat?
Sharon Marks
Director:
Assoc Prof Gerald KOH, National University of Singapore, Singapore
Deputy Director:
Dr Adrian WU, Private Practice, HKSAR, China
ContentS
eDItoRIAL BoARD
264262

Untitled-1 1 6/11/2012 2:01:11 PM

Medical Progress June 2012 ii
June 2012 VOL. 39 NO. 6
ContentS
ChinaYang Xuan Tel: (86 21) 6157 3888 Email: [email protected]
Hong KongKristina Lo-Kurtz, Jacqueline Cheung, Marisa Lam, Miranda Wong Tel: (852) 2559 5888 Email: [email protected]
IndiaMonica Bhatia Tel: (91 080) 4346 4500 Email: [email protected]
IndonesiaSri Damayanti, Hafta Hasibuan, Ritta Pamolango Tel: (62 21) 729 2662 Email: [email protected]
JapanMamoru Takagi Tel: (81 3) 5562 6961 Email: [email protected]
KoreaKevin Yi, Tel: (82 2) 3019 9350 Email: [email protected]
MalaysiaLee Pek Lian, Irene Lee,Grace Yeoh, Sumitra PakryTel: (60 3) 7954 2910Email: [email protected]
PhilippinesPhilip KatipunanTel: (63 2) 886 0333Email: [email protected]
SingaporeJason Bernstein, Carrie Ong, Elijah Lee, Reem Soliman Tel: (65) 6223 3788 Email: [email protected]
ThailandWipa Sriwijitchok Tel: (66 2) 741 5354 Email: [email protected]
VietnamNguyen Thi Lan Huong, Nguyen Thi My Dung Tel: (84 8) 3829 7923 Email: [email protected]
Europe/USAKristina Lo-Kurtz, Tel: (852) 2116 4352 Email: [email protected]
PUBLISHeR: Medical Progress is published 12 times a year by UBM Medica, a division of United Business Media.
CIRCULATION: Medical Progress is on controlled circulation to medical practitioners in Asia. It is also available on subscription to members of allied professions.
SUBSCRIPTION: The price per annum is US$60 (surface mail, students US$30) and US$72 (overseas airmail, students US$36); back issues US$6 per copy.
eDITORIAL MATTeR published herein has been prepared by professional editorial staff and by honorary specialist consultants from all fields of medicine. Views expressed are not necessarily those of UBM Medica. Although great effort has been made in compiling and checking the information given in this publication to ensure that it is accurate, the authors, the publisher and their servants or agents shall not be responsible or in any way liable for the continued currency of the information or for any errors, omissions or inaccuracies in this publication whether arising from negligence or otherwise howsoever, or for any consequences arising therefrom. The inclusion or exclusion of any product does not mean that the publisher advocates or rejects its use either generally or in any particular field or fields. The information contained within should not be relied upon solely for final treatment decisions.
COPYRIGHT © 2012 UBM Medica. All rights reserved. No part of this publication may be reproduced in any language, stored in or introduced into a retrieval system, or transmitted, in any form or by any means (electronic, mechanical, photocopying, recording or otherwise), without the written consent of the copyright owner. Permission to reprint must be obtained from the publisher.
ADVeRTISeMeNTS are subject to editorial acceptance and have no influence on editorial content or presentation. UBM Medica does not guarantee, directly or indirectly, the quality or efficacy of any product or service described in the advertisements or other material which is commercial in nature.
Philippine edition: entered as second-class mail at the Makati Central Post Office under Permit No. PS-326-01 NCR, dated 9 Feb 2001. Printed by Fortune Printing International Ltd, 3rd Floor, Chung On Industrial Building, 28 Lee Chung Street, Chai Wan, Hong Kong.
enQUIRIeS AnD CoRReSPonDenCe
Published by: UBM Medica Pacific Limited27th Floor, OTB Building, 160 Gloucester Road, Wan Chai, Hong Kong
email: [email protected]
269-293 In Focus: Colorectal Cancer
270 Colorectal Cancer: Prevention and Early Diagnosis
Robert Dennis, Samson Tou, Richard Miller
278 Colorectal Cancer: Features and Investigation
Nigel Hall
283 Can Metastatic Colorectal Cancer Be Cured?
David L Bartlett, edward Chu
293-296 Drug Profile
293 Roflumilast—Last But Not Least?
Tan Tze Lee, Ong Kian Chung
Publisher
Publication Manager
Deputy Managing editor
Associate editor
Advertising Coordinator
Design Manager
Designer
Production
Circulation
Accounting Manager
Ben Yeo
Marisa Lam
Greg Town
Grace Ling
Jenny Lim
Rowena Sim
Mark Foo
edwin Yu, Ho Wai Hung,
Jasmine Chay
Christine Chok
Minty Kwan
270
283279

Formulir Berlangganan
Beri tanda √ pada buku/majalah yang Anda pesan
Penawaran Spesial !*selama persediaan masih ada
ONGKOS KIRIM: Untuk pesanan di Pulau Jawa: Rp 10.000,-/edisi & luar pulau Jawa Rp 15.000,-/edisi.*Harga khusus berlangganan (Bila dihitung berdasarkan harga satuan nilai paket = Rp 530.000,-).
Nama (dr/Apotek/RS) : _______
__________________________
__________________________
__________________________
Alamat : ___________________
__________________________
__________________________
__________________________
__________________________
__________________________
Tel : ______________________
Fax : _____________________
Email : ____________________
No. Langganan : ____________
Type of Practice :
GP Dentist
Pharmacist Nurse
Spesialist
(Please specify) ________________
Pembayaran melalui transfer ke Rek.
UBM Medica Asia Pte LtdNo. Acc 050-0675-29-001 (IDR)
HSBC IndonesiaWorld Trade Centre
Jl Jend. Sudirman Kav.29-31, Jakarta Indonesia
Sebagai tanda pemesanan mohon formulir diisi & kirim atau fax kembali ke
PT Medidata Indonesia disertai bukti pembayaran.
MIMS/MT/JPOG 2012 Jml Harga Berlangganan Harga Satuan
*Ongkos kirim
TOTAL
PAKET SPESIALMIMS 3 edisi +MIMS Annual Rp 375.000,-*
MIMS Regular/Edisi - Rp 130.000,-
MIMS Annual - Rp 140.000,-
MSE - Internal Medicine - Rp 115.000,-
MSE - Rheumatology, - Rp 115.000,- Allergy, & Immunology
MSE - Pediatric - Rp 125.000,-
MSE - Cardiovascular - Rp 115.000,- Risk Management
Medical Tribune Rp 180.000,-/12 edisi Rp 20.000,-/edisi
JPOG Rp 150.000,-/6 edisi Rp 30.000,-/edisi
Jumlah
Dokter yang terhormat,
Dalam mendukung upaya peningkatan kesehatan, khususnya dalam mengoptimalkan kemanan pemberian obat dan penyediaan layanan keprofesian berkelanjutan, maka dengan ini kami menyediakan MIMS. Saat ini selain dalam bentuk cetak, juga telah tersedia MIMS dalam bentuk online. JPOG berisi artikel CME yang telah diakreditasi untuk mendapatkan nilai SKP IDI.
Dapatkan MIMS, JPOG dan Medical Tribune dengan mengisi formulir berlangganan!
Subs+Mims Online_JUNE 2012_JPOG 20,5x27,5 Size.indd 1 6/1/2012 2:46:44 PM
iii Medical Progress June 2012
June 2012 VOL. 39 NO. 6
The Cover: Colorectal Cancer
Rowena Sim, Art Director
Mark Foo, Illustrator
ContentS297-312 Continuing Medical education297 The Ravages of Bed Rest: Rehabilitation After
Prolonged Immobility
Shari Parker, Robert Rollinson, Michelle Gilad, Kate Holmes, Nicky Sygall,
Steven Faux
305 Low Back Pain Management: Approaches to Treatment
Gerard A Malanga, Kevin R Dunn
Com
ing
nex
t...
◆ In Focus ◆
Poisoning• AssessmentandDiagnosisofthePoisonedPatient
• Low-toxicityIngestions
• ManagementofPoisoning:InitialManagementandNeedfor Admission
and more!
Coming in the July 2012 Issue of Medical Progress
Medical Progress contains articles under license from UBM Medica LLC. The articles appearing on pages 283–293 and 305–311 are from Oncology and The Journal of Musculoskeletal Medicine, respectively. Copyright © 2010, 2012 UBM Medica LLC.
1 SKP

Medical Progress June 2012 261
Global Summaries Synopses of major trials from leading international journals
Peer Reviewed
CARDIOLOGY
Rivaroxaban after acute coronary syndromeRivaroxaban is a direct, selective inhibitor
of factor Xa. A preliminary trial showed
that rivaroxaban therapy reduced the risk
of death, myocardial infarction, or stroke
in patients who had recently had an acute
coronary syndrome. Now, a phase III trial
has been reported.
At 766 sites in 44 countries, a total of
15,526 patients were randomized, within
7 days of hospital admission for myocardial
infarction (ST-segment elevation or non-ST-
segment elevation) or unstable angina, to
rivaroxaban 2.5 mg twice daily, rivaroxaban
5 mg twice daily, or placebo, for up to 31
months (mean, 13 months). The rate of the
primary efficacy end point (cardiovascular
death, myocardial infarction, or stroke)
was 9.1% (2.5 mg dose), 8.8% (5 mg
dose), and 10.7% (placebo), a significant
reduction at either dose compared with
placebo. The lower dose, but not the higher
dose, reduced all-cause and cardiovascular
mortality. Rivaroxaban was associated
with significantly increased rates of non-
coronary-artery-bypass-grafting-associated
major bleeding (2.1% vs 0.6%) and intrac-
ranial haemorrhage (0.6% vs 0.2%), but
not of fatal bleeding (0.3% vs 0.2%). There
were fewer fatal bleeds with the lower dose
(0.1%) than the higher dose (0.4%).
Rivaroxaban reduced the cardiovascular
risk but increased the risk of major bleeding
but not of fatal bleeding.
Mega JL et al. Rivaroxaban in patients with a recent acute coronary syndrome. NEJM 2012; 366: 9–19; Roe MT, Ohman EM. A new era in secondary prevention after acute coronary syndrome. Ibid: 85–87 (editorial).
Vorapaxar in acute coronary syndromesVorapaxar is an oral drug that inhibits
thrombin-induced platelet aggregation by
acting as an antagonist of protease-
activated receptor 1, an activator of such
platelet aggregation. It has been compared
with placebo in patients with acute non-ST-
segment-elevation coronary syndromes in a
multinational trial.
A total of 12,944 patients with a
non-ST-segment-elevation acute coronary
syndrome were randomized at 818 sites in
37 countries to vorapaxar (40 mg loading
dose, then 2.5 mg daily) or placebo, in
addition to standard therapy. The trial was
stopped early after a safety review. After an
average follow-up of 502 days, the rate of
the primary end point (cardiovascular death,
myocardial infarction, stroke, rehospitali-
zation for recurrent ischaemia, or urgent
coronary revascularization) was 1,031/6,473
(16%) in the vorapaxar group and
1,102/6,471 (17%) in the placebo group,
with Kaplan–Meier 2-year rates of 18.5%
vs 19.9%, a non-significant difference.
The composite outcome of cardiovascular
death, myocardial infarction, or stroke
occurred in 14.7% vs 16.4%, a significant
11% reduction in the vorapaxar group.
There was a highly significant increase
of 35% in moderate or severe bleeding
in the vorapaxar group compared with
the placebo group. There was a 3.4-fold
increase in risk of intracranial haemorrhage
in the vorapaxar group.
The addition of vorapaxar to standard
therapy increased the risk of major bleeding
and did not reduce the rate of the primary
end point significantly.
Tricoci P et al. Thrombin-receptor antagonist vorapaxar in acute coronary syndromes. NEJM 2012;
366: 20–33.
Stroke risk with sub-clinical atrial fibrillationAbout 15% of strokes are attributed to
known atrial fibrillation (AF), but AF may
be asymptomatic and undetected. In about
25% of cases of ischaemic stroke, the cause
remains unknown. The results of a multina-
tional study have suggested that in some of
these cases, the cause may be undetected AF.
The study, in 23 countries, included
2,580 patients aged 65 years or older with
hypertension and no history of AF. They
had all recently received an implanted
pacemaker or defibrillator. Patients were
monitored for 3 months for episodes of
subclinical atrial tachyarrhythmia (atrial rate
>190 beats per minute for > 6 minutes)
indicative of AF. Mean follow-up was for
2.5 years. At 3 months, subclinical atrial
tachycardia had occurred in 261 patients
(10%). The occurrence of subclinical atrial
tachyarrhythmia was associated with a
5.6-fold increase in risk of clinical AF and a
2.5-fold increase in risk of ischaemic stroke
or systemic embolism. Fifty-one patients had
an ischaemic stroke or systemic embolism,
and 11 of them had had subclinical atrial
tachyarrhythmia on monitoring in the first
3 months. None had had clinical AF during
that time. The population attributable risk of
stroke or systemic embolism associated with
subclinical atrial tachyarrhythmia was 13%.
Subclinical AF may explain many strokes
of which the cause is not apparent.
Healey JS et al. Subclinical atrial fibrillation and the risk of stroke. NEJM 2012; 366: 120–129; Lamas G. How much atrial fibrillation is too much atrial fibrillation? Ibid: 178–180 (editorial).
DIABETES
Diabetes risk models and scoresA systematic review has assessed risk
models and scores for the prediction of risk
of type 2 diabetes.
262 Medical Progress June 2012
Global Summaries
and ribavirin for 12 weeks. Randomization
was to daclatasvir plus asunaprevir with
(DAPR) or without (DA) peginterferon
plus ribavirin. In the DA group, four of 11
patients achieved a sustained virological
response at 12 and 24 weeks after
treatment. In the DAPR group, all 10
patients had a sustained virological response
at 12 weeks and nine at 24 weeks. In the
DA group, six patients had viral break-
through on treatment, and in all six cases
there were resistance mutations to both
daclatasvir and asunaprevir. Diarrhoea was
common in both groups, and six patients
had transient rises in alanine aminotrans-
ferase levels.
Adding daclatasvir and asunaprevir
to peginterferon and ribavirin achieved
sustained virological response in patients
who had not responded initially to peginter-
feron and ribavirin alone.
Lok AS et al. Preliminary study of two antiviral agents for hepatitis C genotype 1. NEJM 2012; 366: 216–224; Chung RT. A watershed moment in the treatment of hepatitis C. Ibid: 273–275 (editorial).
GENERAL MEDICINE
Gene therapy for haemophilia BHaemophilia B (Christmas disease)
results from a mutation in the gene for
coagulation factor IX (FIX). In severe
haemophilia B, functional FIX levels are <
1% of normal. Current therapy with FIX
protein concentrate is not curative, and it is
associated with inhibitor formation as well
as being expensive. Gene therapy offers
the prospect of a cure. Researchers in the
UK and the USA have assessed a new gene
therapy—a serotype-8-pseudotyped, self-
complementary adenovirus-associated virus
(AAV) vector expressing a codon-optimized
human factor IX (FIX) transgene (sc AAV2/8-
LP1-hFIXco) given intravenously.
Six patients with severe haemophilia B
received a single gene therapy dose via a
peripheral vein: two given a high dose, two
(intensive group) versus 46 (conventional
group), a significant 50% risk reduction with
intensive therapy. End-stage renal disease
occurred in eight patients vs 16. Intensive
therapy slowed the rate of decrease in eGFR.
The effect on eGFR was fully explained
by the control of diabetes (glycated
haemoglobin levels) and of proteinuria.
Intensive glucose control preserves renal
function in type 1 diabetes.
The DCCT/EDIC research group. Intensive diabetes therapy and glomerular filtration rate in type 1 diabetes. NEJM 2011; 365: 2366–2376.
GASTROENTEROLOGY
New drugs for chronic HCV genotype 1
Treatment of chronic hepatitis C virus
(HCV) infection with pegylated interferon
(peginterferon) alpha and ribavirin for 48
weeks achieves a sustained virological
response at 24 weeks after stopping
treatment in 40–50% of patients. Adding
a protease inhibitor to treatment for non-
responders after 12 weeks of treatment
produces a sustained virological response in
14–33%. Now, a multicentre phase II study
in the USA has shown that the use of two
new antiviral agents may improve results.
Daclatasvir is an HCVNS5A replication
complex inhibitor and asunaprevir is an HCV
NS3 protease inhibitor.
The trial included 21 patients with
chronic HCV genotype 1 infection unre-
sponsive to treatment with peginterferon
Global Summaries
The review included 43 papers with
details of the development and/or validation
of 145 models and scores, of which 94 were
assessed in detail. They had been based
on data from almost 7 million people with
follow-up for up to 28 years. Meta-analysis
was not possible because of the hetero-
geneity of the data. The mean number of
components per score was 8 (3–14), and
some, but not all, models and scores were
statistically robust and had been externally
validated on a different population. Seven
risk scores were chosen as having a high
potential for use in practice, and ten
mechanisms were outlined whereby the
assessment of risk of type 2 diabetes might
lead to improvement in outcomes.
There are many risk scores for the
development of type 2 diabetes, but
few are used routinely. Seven risk scores
were considered to be highly suitable for
clinical use.
Noble D et al. Risk models and scores for type 2 diabetes: systematic review. BMJ 2011; 343: 1243 (d7163).
Intensive glucose control to preserve renal functionAn impaired glomerular filtration rate
(GFR) increases the risk of end-stage renal
disease in patients with diabetes. Intensive
blood glucose control reduced the risk of
developing both microalbuminuria and
macroalbuminuria in patients with type
1 diabetes in the Diabetes Control and
Complications Trial (DCCT) reported in
1993. Now, 22-year follow-up data from
that trial have been used to assess the effect
of intensive glucose control on glomerular
filtration rate deterioration.
A total of 1,441 patients aged 13–39
with type 1 diabetes were randomized in the
DCCT to intensive diabetes therapy (target
glycated haemoglobin, < 6.05%) or conven-
tional therapy for 6.5 years. Over a median
of 22 years, impaired GFR (estimated
GFR [eGFR] < 60 mL·min/1.73 m2 on two
successive visits) occurred in 24 patients

Medical Progress June 2012 263
an intermediate dose, and two a low dose.
Follow-up was for 6–16 months. All patients
benefitted: the two given the low dose
were able to increase the intervals between
injections of FIX and the other four were
able to stop FIX prophylaxis and remained
free of spontaneous bleeding. One
patient who received the high dose had a
transient asymptomatic increase in serum
aminotransferase levels with detection of
AAV8-capsid-specific T cells in peripheral
blood. The other high-dose patient had a
transient increase in aminotransferase. Both
had normal aminotransferase levels after
a course of steroids. Their FIX levels were
3–11% of normal values.
This gene therapy at intermediate or high
dosage was successful in raising FIX levels
sufficiently to stop spontaneous bleeding
without prophylactic FIX. The investigators
express concern about immune-mediated
clearance of AAV-transduced hepatocytes
but point out that the process can be
controlled with a short course of steroid
without loss of transgene expression.
Nathwani AC et al. Adenovirus-associated virus vector-mediated gene transfer in haemophilia B. NEJM 2011; 365: 2357–2365; Ponder KP. Merry Christmas for patients with haemophilia B. Ibid: 2424–2425 (editorial).
Catheter-directed thrombolysis for acute ileofemoral DVTThe incidence of acute deep vein
thrombosis (DVT) in the legs is about 1
in 1,000 people per year. Anticoagulant
therapy prevents extension of the thrombus,
recurrence and pulmonary embolism, and
reduces mortality. It does not, however,
dissolve the clot, and patients may develop
post-thrombotic syndrome (PTS) with pain,
swelling, a feeling of heaviness, oedema,
skin pigmentation, and, in severe cases,
venous ulcers. In most cases of symptomatic
DVT, the thrombus is in the popliteal and
more proximal veins. The risk of PTS can
be halved by daily use of compression
stockings, but more effective initial
treatment is needed. Systemic thrombolysis
is effective but associated with a high risk
of bleeding. A multicentre trial in Norway
has shown that local delivery of the throm-
bolytic agent into the clot via a catheter is
effective with less risk.
At 20 hospitals in southeast Norway, a
total of 209 patients aged 18–75 with a first
iliofemoral DVT were randomized within
21 days of symptom onset to conventional
treatment with or without catheter-directed
thrombolysis (CDT). Data were analysed
from 189 patients. At 24 months, PTS had
occurred in 41% (CDT) vs 56% (controls),
a significant difference with an absolute
reduction in risk of PTS of 14% and a
number-needed-to-treat of seven. After 6
months, the rate of iliofemoral patency was
66% vs 47%. Among the 90 patients in the
CDT group, there were 20 bleeding compli-
cations related to the CDT, with three major
and five clinically relevant bleeds.
These researchers conclude that
additional CDT should be considered in
patients with a high proximal DVT and low
risk of bleeding.
Enden T et al. Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVen T study): a randomised controlled trial. Lancet 2012; 379: 31–38; The Lancet; ibid: 1 (editorial); Hofmann LV, Kuo WT. Catheter-directed thrombolysis for acute DVT. Ibid: 3–4 (comment).
Management of diabetes and hypertension by rural health-care workers in IranIn high-income countries, the incidence
of cardiovascular and some other non-
communicable diseases has decreased after
population ageing has been accounted for.
Dietary and lifestyle interventions, decrease
in smoking, and better control of blood
pressure and cholesterol levels may have
played a considerable part. The prevalence
of cardiovascular risk factors has changed
little, however, in low- and middle-income
countries. Little is known about optimal
method of providing primary care, especially
in rural areas, and its influence on non-
communicable disease in poorer countries.
A rural primary care system in Iran, the
Behvarz system, has been assessed.
In the Behvarz system, rural primary care
is provided by community health workers,
who are community members who, having
been educated to at least a primary level,
are given 2 years of medical education after
passing an entrance examination. Survey and
census data for 2005 and 2006 were used to
assess the contribution of Behvarz workers
(BWs) to diabetes and hypertension control.
From the Non-communicable Disease
Surveillance Survey (NCDSS) of 2005,
data for systolic blood pressure (SBP)
were available for 64,694 adults (11,521
in rural areas) and for fasting plasma
glucose (FPG) for 50,202 (9,337 in rural
areas). Overall, 39% of people with
diabetes and 36% with hypertension
were receiving treatment (more likely in
women and in urban areas). On average,
treatment in rural areas lowered FPG by
1.34 mmol/L and SBP by 2.5 mm Hg. In
urban areas, the corresponding reductions
were 0.21 mmol/L and 3.8 mm Hg. A
single additional BW per 1,000 adults was
associated with a significant 0.09 mmol/L
lowering of district-level average FPG but
did not reduce SBP significantly.
These researchers conclude that primary
care systems with trained community
health-care workers and well-established
guidelines can be effective in non-communi-
cable disease prevention and management.
Farzadfar F et al. Effectiveness of diabetes and

264 Medical Progress June 2012
Global Summaries
hypertension management by rural primary health-care workers (Behvarz workers) in Iran: a nationally representative observational study. Lancet 2012; 379: 45–54; Habibzadeh F. The control of non-communicable diseases in Iran. Ibid: 6–7 (comment).
ONCOLOGY
Gene changes and resistance of colorectal cancer to chemotherapy
Gene alterations, both genomic and
epigenetic, are common in human cancers,
and some of them may affect response to
chemotherapy. Researchers in Germany
have concentrated on the gene encoding
transcription factor AP-2 epsilon (TFAP2E)
and its potential downstream target, DKK4,
the gene encoding Dickkopf homologue
4 protein. Tumour samples were obtained
from 74 patients treated for colorectal
cancer and, later, another four cohorts
(total, 220 patients) undergoing chemo-
therapy with or without radiotherapy. The
expression, methylation, and function of
TFAP2E was analysed in colorectal cancer
cell lines in vitro and in patients with
colorectal cancer. The gene was hypermeth-
ylated in 38 of the initial 74 samples, and
this was associated with decreased gene
expression. Cancer cell lines with overex-
pression of DKK4 had increased resistance
to fluorouracil but not to irinotecan or
oxaliplatin. In the four later cohorts, hyper-
methylation of TFAP2E was significantly
associated with resistance to chemo-
therapy. Hypomethylation was associated
with a sixfold increase in likelihood of
chemotherapy responsiveness. Epigenetic
alterations in TFAP2E were independent
of key regulatory cancer gene mutations,
microsatellite instability, and other genes
affecting fluorouracil metabolism.
Hypermethylation of TFAP2E is
associated with chemotherapy resistance
in patients with colorectal cancer, and
this resistance is mediated through DKK4.
Targeting of DKK4 could potentially reverse
this resistance.
Ebert MPA et al. TFAP2E-DKK4 and chemoresistance in colorectal cancer. NEJM 2012; 366: 44–53.
Denosumab for prostate cancerBone metastases are common in prostate
cancer. Tumour cells in bone secrete growth
factors that induce RANKL production by
stromal cells and osteoblasts, and RANKL
induces osteoclastic activity. Such activity
is suspected to promote the establishment
of metastases. Prostate cancer cells might
themselves express RANKL and that too
might increase the likelihood of metastases
in bone. Denosumab is a human monoclonal
antibody that inactivates RANKL. It has been
shown to be better than zoledronic acid in
the prevention of bony metastases in breast
or prostate cancer. Now, a multinational
trial has shown that denosumab delays the
development of bone metastases in men
with prostate cancer.
At 319 centres in 30 countries, a total
of 1,432 men with castration-resistant
prostate cancer but without, though at high
risk of, bone metastases were randomized
to subcutaneous denosumab 120 mg, or
placebo, every 4 weeks. Median bone-
metastasis-free survival was 29.5 months
(denosumab) vs 25.2 months (placebo), a
significant difference. Time to first bone
metastasis was 33.2 vs 29.5 months. There
was no significant difference in overall
survival (43.9 vs 44.8 months). Osteonecrosis
of the jaw occurred in 33 patients (5%) in
the denosumab group but in none of the
placebo group. Hypocalcaemia occurred in
12 (2%) vs 2 (< 1%).
Denosumab may delay the development
of bone metastases in men with high-risk
prostate cancer. The optimal clinical use of
denosumab has yet to be determined.
Smith MR et al. Denosumab and bone-metastasis-free survival in men with castration-resistant prostate cancer: results of a phase 3, randomised, placebo-controlled trial. Lancet 2012; 379: 39–46; Logothetis CJ. Treatment of prostate cancer metastases: more than semantics. Ibid: 4–6 (comment).
Prostate cancer gene mutationProstate cancer may be familial, but the
genetic basis is unclear. Genome-wide
association studies have identified > 30
single nucleotide polymorphisms associated
with increased risk, but the increase in
risk from each of them has been low.
An intensely studied locus has been at
chromosome 17q21-22. Now, a US study
has identified a new variant in the gene
HOXB13 that is associated with increased
risk of hereditary prostate cancer.
More than 200 genes in the 17q21-22
region were screened by sequencing
germline DNA from 94 unrelated patients
with prostate cancer from families with
familial prostate cancer linked to the
17q21-22 region. Four of these subjects
had a mutation (G84E) in HOXB13
(rs138213197), a homeobox tran-
scription factor gene important in prostate
development. In these four families, there
were 18 men with prostate cancer and
available DNA, and all of them carried the
mutation. This mutation was present in
72 of 5,083 unrelated men of European
descent with prostate cancer (1.4%) and 1
of 1,401 controls without prostate cancer
(0.1%), a highly significant difference. It
was significantly more common in men with
early-onset, familial prostate cancer (3.1%)
than in men with late-onset non-familial
prostate cancer (0.6%).
The new variant accounts for a small
proportion of prostate cancers but may
provide increased understanding of
the disease.
Ewing CM et al. Germline mutations in HOXB13 and prostate-cancer risk. NEJM 2012; 366: 141–149.
Medical Progress June 2012 265
General MedicinePeer Reviewed
An individual approach should be taken when treating morbidly obese patients, with
multidisciplinary input.
A Middle-aged Woman With Morbid Obesity – How to Treat?Sharon Marks, MB BS, FRACP
Case Scenario
Shirley is 41 years of age and has presented in despair about her huge weight gain since the birth of her sixth child, who is now 10 years old. She is 165 cm tall
and weighs 179 kg. She is dyspnoeic on even minimal exertion, has painful knees and has recently developed a large inguinal hernia. She reports that she is uncomfortable in bed at night and sleeps poorly.
A full blood check finds no major problems, although she reports a very strong family history of diabetes (she is of South Sea Island descent).
Shirley enjoys all the cooking she does for her large extended family and reports eating fre-quently and voraciously.
What strategies or treatments would have the best chance of success for a patient with this level of morbid obesity?
Commentary
This level of obesity (body mass index [BMI] of 65.7 kg/m2) is referred to as extreme morbid obesity or super obese (BMI of more than 50 kg/m2) and is difficult to treat. In most cases, specialist intervention is required because
Extreme morbid obesity is difficult to treat and requires specialist intervention.

266 Medical Progress June 2012
General Medicine
many GP offices are not adequately equipped. Many patients (and their GPs) are unable to find scales to give an accurate weight, and hospital clinics need industrial type scales. (Some patients use weighbridges to weigh themselves.) Waiting room chairs as well as examination couches need to be able to support extremes of body weight.
The problems for this particular patient are not so much the metabolic disorders that are usually connected with obesity, but more the physical effects of her extreme body weight hindering mobility through breath-lessness and joint problems. However, Shirley’s family history suggests an increased risk of diabetes. She needs initial rapid and substantial weight loss prior to the initiation of an exercise routine. Starting exercise too early can lead to further joint damage and thus limit ongoing weight maintenance.
It is important to exclude any other factors that may be contributing to immobility, such as obstructive sleep apnoea, which is commonly seen in this group of patients. A sleep study is essential, particularly if excessive tiredness limits weight loss attempts or increases snacking behaviour. Nightly use of a continuous positive airway pressure pump should be considered if the patient has periods of hypoxaemia overnight or if the obstructive sleep apnoea is considered to be moderate to severe.
Another issue to consider is the medications the patient is taking. Diabetic medications such as insulin, sulfonylureas and glitazones can con-tribute to increasing body weight and may need to be altered or ceased. Other medications, particularly high-dose corticosteroids and some of the antipsy-chotic and antiepileptic treatments, can markedly increase appetite. Although the patient in this scenario is taking no
medications, she is the exception rather than the rule.
Patients should also be assessed for depression and obsessive–com-pulsive behaviour as these conditions can contribute to increased snacking behaviour.
TreatmentThe energy required for initial weight loss in this situation usually needs to be achieved by calorie restriction rather than by increasing physical activity. More substantial weight loss can be achieved and maintained by intro-ducing a very-low-calorie diet. Once weight loss (even a small amount) has occurred, increased incidental activity such as walking can help potentiate further weight loss. Surgical inter-vention may give the best outcome for patients who have little chance of long-term maintenance.
MedicationsSome of the selective serotonin reuptake inhibitors (SSRIs; eg, fluoxetine and sertraline) and some of the serotonin and noradrenaline reuptake inhibitors (SNRIs; eg, duloxetine and reboxetine) used to treat depressive and obsessive–compulsive disorders have effects on satiety. The balance between increased satiety and overstimulation (insomnia and anxiety) needs to be found. These medications are not weight-loss drugs in their own right (and are not Therapeutic Goods Administration [TGA]-approved for the management of obesity), but they can be helpful if a patient is demotivated and struggling with frustration about their weight. It should also be noted that many patients find long-term diets to be very depriving and actually show signs of depression and anger if food is restricted. These patients benefit from being ‘primed’ prior to altering their food intake.
Until recently, it was possible to use sibutramine to induce satiety and help patients eat smaller portions while maintaining a higher metabolic rate. However, sibutramine was withdrawn from sale in mid-October 2010 and is no longer an option. The recently published SCOUT study showed an increased risk of non-fatal cardiac events in high-risk patients, most of whom were treated ‘off-licence’.1 Most of the patients recruited had type 2 diabetes and had known cardio-vascular disease with either a previous myocardial infarction or episodes of angina and so were at high risk of recurrent cardiac events. The weight loss achieved in the study group did not meet the minimum (5% of initial body weight) set by the Food and Drug Administration for a weight loss product. However, sibutramine’s efficacy and safety in a low-risk popu-lation was not evaluated.
In some individuals, sibutramine was an effective medication that enabled greater adherence to a long-term diet, and in patients with morbid obesity it was possible to see significant weight losses in ‘responders’, although not in all cases. There is very little to use in its place as, apart from orlistat (discussed later), the only other drug approved by the TGA for the management of obesity is phentermine. This medication has been around for many years and has not undergone a similar rigorous study to prove efficacy and safety in this group of patients. It is approved only for short-term weight loss (less than 3 months) and has a very limited role in the management of extreme morbid obesity, which requires a long-term approach.
Orlistat is a lipase inhibitor that may be of some benefit in producing a weight loss effect as it reduces the absorption of about 30% of ingested dietary fat. In the ‘diet-naïve’ patient,

Medical Progress June 2012 267
General Medicine
who may not have a good compre-hension of the fat content of food, it can help identify high-fat foods. The medication causes diarrhoea, abdominal pain and oil incontinence if a high-fat diet is consumed, thus encouraging adherence to a low-fat diet.
Orlistat may help commence the weight loss process but is unlikely to cause substantial weight loss (ie, of more than 12 to 20 kg) in this group of patients. It may also have a place in the ongoing management of obesity because it can be used inter-mittently and has few side effects other than the effect of the drug to cause fat malabsorption. Supplemen-tation with fat-soluble vitamins is not usually required unless the patient has a nutrient-poor diet overall. The cost of this over-the-counter treatment, about A$120 for a packet of 84 capsules (1 month’s supply) or A$70 for 42 capsules, needs to be placed in per-spective with the outcome of the intervention. It is not available on the Pharmaceutical Benefits Scheme but is available on the Repatriation Pharma-ceutical Benefits Scheme on authority for a once per lifetime treatment of obesity (BMI of 30 kg/m2 or greater with specified comorbidities, including type 2 diabetes, or BMI of 35 kg/m2 or greater without associated problems).
DietIn patients with extreme morbid obesity, an energy-restricted diet should be used in the first instance. Some patients do respond to a well-balanced, low-fat, calorie-reduced diet, particularly if satiety is increased. Thus, initial substantial weight loss can be seen with the use of low glycaemic foods and regular meal times plus the altering of other factors such as tiredness (related to obstructive sleep apnoea) or medications causing
increased appetite. The assistance of a qualified dietitian can be of great benefit, and weight losses of up to about 20 kg can occur fairly rapidly using a food-based dietary approach.
In patients who are unable to modify their food intake because of excessive appetite or uncontrollable snacking behaviour, a very-low-calorie diet (VLCD) programme can achieve an energy deficit even in those with extreme immobility. Once weight loss has occurred, the patient can become more mobile as joint pain and obstructive sleep apnoea benefit greatly from relatively small weight losses. A VLCD programme (a diet of 800 calories [about 3,350 kJ] per day or less) can be expected to achieve a weight loss of 15 to 30 kg in the first 3 months, with ongoing weight loss if the intensive programme is continued.
Patients need blood tests including liver and renal function testing as well as a lipid profile and diabetes screening before starting a ketogenic programme. Other investigations should include thyroid function test and a full blood count as well as iron studies. Medi-cations such as insulin, sulfonylureas and glitazones may need to be adjusted or ceased during the weight loss phase to avoid episodes of hypogly-caemia, which may prevent the patient adhering to the strict ketone-inducing
regimen. Blood pressure medications may also need to be reduced to avoid hypotension. If a diuretic is being used, electrolytes should be monitored on a regular basis as weight loss occurs.
I encourage all patients to follow the intensive regimen using the VLCD as a complete three-meal per day replacement for at least the first 2 weeks. During this initial phase, only a large bowl of steamed low-starch vegetables is allowed in addition to the three meal replacements. Once ketone bodies are produced, appetite usually reduces dramatically, which enables the continuation of the intensive programme (ie, three meals per day) for at least 3 months. Some people are able to continue further, particularly if motivated by initial weight loss.
A gradual reintroduction of a low-fat and carbohydrate-reduced diet together with increasing exercise tolerance helps with ongoing weight maintenance. It is not unusual to see some weight regain when normal meals are introduced as the low carbohydrate content of the intensive phase contributes to an early diuresis. It is almost inevitable that some fluid regain will occur, and so it helps if the patient is prewarned. Weight maintenance needs to be encouraged although there should be a low threshold to returning to the intensive phase (replacing three meals
An energy-restricted diet should be used in the first instance for patients with extreme morbid obesity.

268 Medical Progress June 2012
General Medicine
a day) if needed. Patients need to be encouraged to be proactive with regard to weight regain and not see it as a failure of a particular programme.
Regular follow-up is essential during the VLCD programme. Other health professionals, such as clinical psychologists, dietitians and exercise physiologists, can help lighten the load as it is fairly time-intensive to monitor these patients. A multidisciplinary team approach is of great value with regard to goal setting and provides useful feedback as many patients with extreme morbid obesity cannot weigh themselves at home or be weighed at the local doctor’s surgery.
SurgeryFor some patients, the task of initiating and then continuing weight loss is overwhelming. Those with severe sleep apnoea (and associated tiredness) as well as those with debilitating joint disease may achieve initial weight loss but have little chance of maintaining the loss in the long term. A surgical intervention may give the best outcome in these patients.
Laparoscopic gastric banding has become the most common bariatric surgery procedure in Australia as it is relatively non-invasive and adjustable and provides a long-term weight main-tenance strategy. Other options include the gastric sleeve procedure and the Roux-en-Y gastric bypass. These pro-cedures have their own complications, including risk of nutritional inadequacy and wound breakdown, but their suit-ability must be assessed in the light of the severity of the obesity and its com-plications. For instance, a patient with an insatiable appetite or a ‘sweet tooth’ may be a poor candidate for a lap band, which requires food restriction. These patients may take in excess energy in the form of frequent small portions or by drinking high-calorie drinks that
About the AuthorDr Marks is a Consultant Physician in Clinical Nutrition at Monash Medical Centre, Melbourne, Victoria, Australia.
may pass around the band. Gastric bypass, which causes malabsorption by reducing the absorptive area of the small bowel, may be the best option to achieve significant weight loss even though life-long monitoring of nutri-tional indices is required.
Generally, any intervention will be most successful if it reduces appetite and increases satiety. The gastric sleeve procedure is thought to achieve this by removing the portion of the stomach that produces ghrelin, the hormone that stimulates appetite. Long-term data is not yet available for this procedure. With the lap band, however, weight losses of more than 50% of excess body weight have been maintained over a 5-year period. Again, patients who have had lap bands need lifelong monitoring to ensure ongoing com-pliance and weight maintenance.
SummarySuccessful treatment of patients with extreme morbid obesity is very complex. Patients vary greatly in their expectations and in their physical ability. It is imperative that an indi-vidual approach is taken with as much input from a multidisciplinary team as possible. Often the simple problem of weighing a patient who is more than 150 kg means that the treatment cannot be undertaken by the local doctor alone. Access to public hospital bariatric clinics is severely limited, with waiting lists of up to 12 months for initial assessment. The opportunity to obtain a lap band or gastric bypass procedure is similarly problematic, with even longer waiting lists. Those patients with private health insurance fare better although the out-of pocket expenses are sometimes prohibitive. Although there is much discussion about the obesity epidemic and the need for better bariatric assessment clinics with greater access to surgery,
very little has changed in this regard over the past 10 years.
For the individual patient pre-senting at this level of obesity, the first interaction with a doctor will often dictate the long-term outcome. First attempts at long-term weight loss and maintenance are often unsuc-cessful, and the doctor needs to avoid expressing disappointment because it will only confirm the patient’s belief that the problem is insurmountable. A positive approach, balanced by a clear understanding of the physical and emotional barriers inherent in patients with extreme morbid obesity, will at least facilitate compliance. Obviously, the prevention of weight gain in at-risk patients is a vital component as it is easier to treat obesity in a mobile patient than in one unable to be active due to osteoarthritis, breath-lessness or obstructive sleep apnoea.
Declaration of InterestsDr Marks has been a member of medical advisory boards
for Optifast, sibutramine and orlistat and has been involved
in clinical trials of these products. She has also received
honoraria from Nestle, Abbott and Roche for talks on obesity
management.
Reference1. James WPT, Caterson ID, Coutinho W, et al.; for the
SCOUT Investigators. Effect of sibutramine on cardiovascular
outcomes in overweight and obese subjects. N Engl J Med
2010;363:905–917.
© 2010 Medicine Today Pty Ltd. Initially published
in Medicine Today November 2010;11(11):74–76.
Reprinted with permission.

Medical Progress June 2012 269
In focus
Colorectal cancer is one of
the most common cancers
worldwide and is a disease of
‘Westernized’ populations.
With early detection, diagnosis
and treatment, the morbidity
and mortality associated with
this cancer can be prevented.
Colorectal CancerReviews
• Colorectal Cancer: Prevention and Early Diagnosis
• Colorectal Cancer: Features and Investigation
• Can Metastatic Colorectal Cancer Be Cured?
True False
1. It is estimated that among those with colorectal polyps, 95% will develop invasive ■ ■
colorectal cancer (CRC).
2. Central obesity is a risk factor for CRC. ■ ■
3. Colonoscopy is the gold standard investigation for CRC and polyps. ■ ■
4. The liver is the most common metastatic site. ■ ■
5. Metastatic CRC is potentially incurable, even when limited to a specific organ site. ■ ■
How much do you know about colorectal cancer?
See page 292 for answers
270 Medical Progress June 2012
In focusPeer Reviewed
Colorectal Cancer:Prevention and Early DiagnosisRobert Dennis, MSc, FRCS; Samson Tou, MSc, FRCS; Richard Miller, MSc, FRCS
Colorectal cancer (CRC) is a curable disease; over 90% of patients who have surgical
resection of a Dukes’ A tumour will still be alive after 5 years. This is direct evidence
that an early diagnosis will reduce mortality from CRC. Despite this, CRC is the
second most common cause of cancer-related death in the UK. The discrepancy
suggests that outcomes can be improved by a better understanding of the causes of
the disease and its early detection and treatment. In this article, prevention and early
diagnosis are discussed.
Colorectal cancer (CRC) is a major cause of cancer morbidity in the UK, and in 2006 there were more than 37,500 new cases and 16,000 deaths
from the disease. After lung cancer, it is the second most common cause of cancer-related death.1
Pathogenesis
The pathogenesis of the majority of CRC is well understood in terms of the ‘adenoma–carcinoma sequence’. This describes the progression of CRC as an accumulation of mutations in key genes, for example, tumour suppressor genes, such as the adenomatous polyposis coli (APC) and TP53 genes, and in proto-oncogenes such as K-ras. In macroscopic terms, these molecular changes contribute to the development of polypoid lesions and, later, invasive carcinoma. In polyps, the normal architecture of colonic crypts is disrupted by disturbances in the sequence of basal proliferation, migration, and differen-tiation. Many individuals have polyps, but it is
Many individuals have colorectal polyps, but it is estimated that only 5% will develop invasive cancer.
In focus
Medical Progress June 2012 271
estimated that only 5% will develop invasive cancer. Prevention of colorectal cancer, therefore, depends on early elimination of these polyps and/or the factors that predispose the colonic epi-thelium to become transformed.
Aetiology
Eighty-five percent of CRC cases fall into the category of ‘sporadic’ disease, where the primary cause of polyp formation is unknown. The remaining 15% of cases are accounted for by less common causes of CRC, for example familial CRC (ie, where one first-degree relative aged < 45 years old is affected by CRC or there are two affected first-degree relatives), dominantly inherited CRC syndromes and inflammatory bowel disease (IBD). In the latter two groups, the molecular events of polyp formation are understood. The hereditary CRC syndromes (eg, hereditary non-pol-yposis colorectal cancer (HNPCC), familial adenomatous polyposis (FAP),
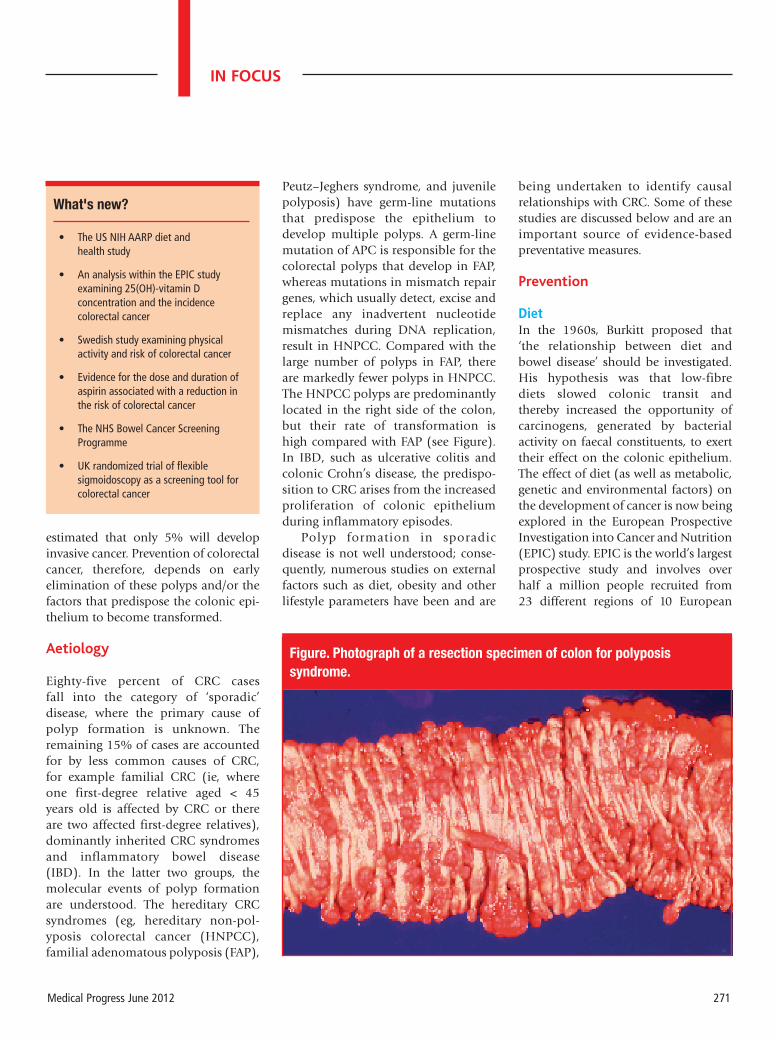
Peutz–Jeghers syndrome, and juvenile polyposis) have germ-line mutations that predispose the epithelium to develop multiple polyps. A germ-line mutation of APC is responsible for the colorectal polyps that develop in FAP, whereas mutations in mismatch repair genes, which usually detect, excise and replace any inadvertent nucleotide mismatches during DNA replication, result in HNPCC. Compared with the large number of polyps in FAP, there are markedly fewer polyps in HNPCC. The HNPCC polyps are predominantly located in the right side of the colon, but their rate of transformation is high compared with FAP (see Figure). In IBD, such as ulcerative colitis and colonic Crohn’s disease, the predispo-sition to CRC arises from the increased proliferation of colonic epithelium during inflammatory episodes.
Polyp formation in sporadic disease is not well understood; conse-quently, numerous studies on external factors such as diet, obesity and other lifestyle parameters have been and are
being undertaken to identify causal relationships with CRC. Some of these studies are discussed below and are an important source of evidence-based preventative measures.
Prevention
DietIn the 1960s, Burkitt proposed that ‘the relationship between diet and bowel disease’ should be investigated. His hypothesis was that low-fibre diets slowed colonic transit and thereby increased the opportunity of carcinogens, generated by bacterial activity on faecal constituents, to exert their effect on the colonic epithelium. The effect of diet (as well as metabolic, genetic and environmental factors) on the development of cancer is now being explored in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. EPIC is the world’s largest prospective study and involves over half a million people recruited from 23 different regions of 10 European
Figure. Photograph of a resection specimen of colon for polyposis syndrome.
What's new?
• TheUSNIHAARPdietand health study
• AnanalysiswithintheEPICstudyexamining25(OH)-vitaminDconcentration and the incidence colorectal cancer
• Swedishstudyexaminingphysicalactivity and risk of colorectal cancer
• Evidenceforthedoseanddurationofaspirin associated with a reduction in the risk of colorectal cancer
• TheNHSBowelCancerScreeningProgramme
• UKrandomizedtrialofflexiblesigmoidoscopy as a screening tool for colorectal cancer

272 Medical Progress June 2012
In focus
countries. The advantage of obtaining data from multiple regions is that a clearer relationship between different dietary habits and the development of cancer may be seen.2
The first completed data sets from the ongoing EPIC study have now been analysed; these show that dietary patterns are regional and that diet does have an impact on the development of CRC. For example, it has been dem-onstrated that dietary fibre is likely to be protective against colorectal cancer; comparison between the lowest daily fibre intake of 12 g and the highest intake of 30 g showed a 40% reduction in the risk for CRC after cali-bration.3 The source of fibre was not significant.3 As a result, it has been suggested that about eight portions of fruit and vegetables and the equivalent of five slices of wholemeal bread should be eaten daily if the benefits of dietary fibre are to be realized.2
Linked studies have also shown that a high intake of red or processed meat is associated with a 35% increase in
colorectal cancer if more than 160 g are consumed per day (two or more portions) when compared to less than one portion per week.4 In contrast, a high fish consumption of 80 g or more is protective.4 The increased risk of CRC with a high consumption of red and processed meat may be related to the association of these foodstuffs with increased amounts of N-nitrosocompounds in the faeces. These compounds bind to the epithelial DNA and may act as mutagens to initiate the adenoma–carcinoma sequence.
The US prospective National Institutes of Health–AARP Diet and Health Study5 analysed 293,615 men and 198,767 women aged 50–71 years with self-administered food-frequency questionnaire at baseline in 1995–1996 and then 5 years of follow-up. Men with high scores on the fruit and vegetable factor were at decreased risk of colorectal cancer (relative risk, RR, 0.81; 95% con-fidence interval, CI, 0.70–0.93; P for
trend = 0.004). High scores on the red meat factor were associated with increased risk (RR, 1.17; 95% CI, 1.02–1.35; P for trend = 0.14 for men; and RR, 1.48; 95% CI, 1.20–1.83; P for trend = 0.0002 for women).
Not all studies have demonstrated that a high-fibre diet reduces the risk of CRC. A pooled analysis of 13 pro-spective cohort studies6 found that dietary fibre was not associated with a reduced risk of colorectal cancer after adjusting for other dietary risk factors. A Cochrane collaboration systematic review7 has analysed five studies of over 4,000 subjects for the effect of intervention with soluble and insoluble dietary fibre or a com-prehensive dietary intervention with high-fibre whole food sources. Over the 2- to 4-year period of the studies, combined data showed no outcome difference between the intervention and control groups in the number of subjects with at least one adenoma or a new diagnosis of colorectal cancer.
A more recent analysis within the EPIC study has shown a possible relationship between pre-diagnostic, serum 25(OH)-vitamin D concen-tration and risk of colorectal cancer.8 After correcting for dietary and other possible confounding factors, serum 25(OH)-vitamin D concentration showed a strong inverse linear dose- response association with risk of colorectal cancer (P for trend < 0.001), although subgroup analyses showed this association for colon but not rectal cancer (P for heterogeneity = 0.048). Greater dietary intake of calcium was also associated with a lower colorectal cancer risk. The authors noted that further ran-domized trials are needed to assess whether increases in circulating serum 25(OH)-vitamin D concentration can effectively decrease the risk of colorectal cancer.
Not all studies have demonstrated that a high-fibre diet reduces the risk of colorectal cancer.
In focus
Medical Progress June 2012 273
Obesity and ExerciseThere is accumulating epidemiological evidence that central obesity is a risk factor for CRC. The biological mech-anisms still need to be elucidated, but hyperinsulinaemia appears to play a role. With further research, it may emerge that weight loss is an important preventative measure against CRC, as it is against endometrial cancer, heart disease, and type 2 diabetes mellitus.
Regular exercise also protects against CRC.9,10 Furthermore, there is evidence that CRC patients have an absolute improvement of 14% in their 5-year survival if they had active lifestyles before presenting with symptoms of CRC.9 An active patient is defined as someone who exercises vig-orously for 20 minutes at least once a week or participates in weekly general health and fitness.9 The Swedish study showed differing distributions of colon cancer between the sexes, and no asso-ciation between physical activity and rectal cancer.10
Alcohol and SmokingThe link between alcohol and CRC remains equivocal. Some evidence suggests that there is a dose–risk rela-tionship that is particularly pertinent to rectal cancer. The evidence for tobacco is slightly stronger in rectal cancer, with a relationship to smoking even after adjustment for alcohol.11 This epide-miological evidence is also supported by other studies that have shown that smokers have a higher incidence of colorectal polyps.
Chemoprevention
Non-steroidal anti-inflammatory drugs may inhibit progression and devel-opment of CRC. A recent Cochrane meta-analysis analysed four ran-domized controlled trials that compared aspirin with a placebo in
‘average’-risk populations.12 No sig-nificant reduction in the incidence of adenomas was noted in the primary prevention trial, but data from the three secondary prevention trials showed a statistically significant reduction in the recurrence of sporadic adenomas in the ‘treatment’ groups. The overall results (which included trials treating FAP patients with aspirin) showed a trend in favour of treating with aspirin to prevent colorectal adenomas.12 However, this may be a type I error, since the subgroup taking 325 mg of aspirin did not see the benefit of the subgroup receiving 81 mg.13
A prospective study of 47,363 male health professionals aged 40–75 years followed up for 18 years showed that men who regularly used aspirin (≥ 2 times/week) had a multivariate RR for colorectal cancer of 0.79 (95% CI, 0.69–0.90), compared with non-regular users.14 However, this potential benefit necessitates at least 6 years of consistent use with maximal risk reduction at doses greater than 14 tablets/week. As noted by the authors, the risks of gastrointestinal bleeding and haemorrhagic stroke must be weighed against the benefit of treatment.
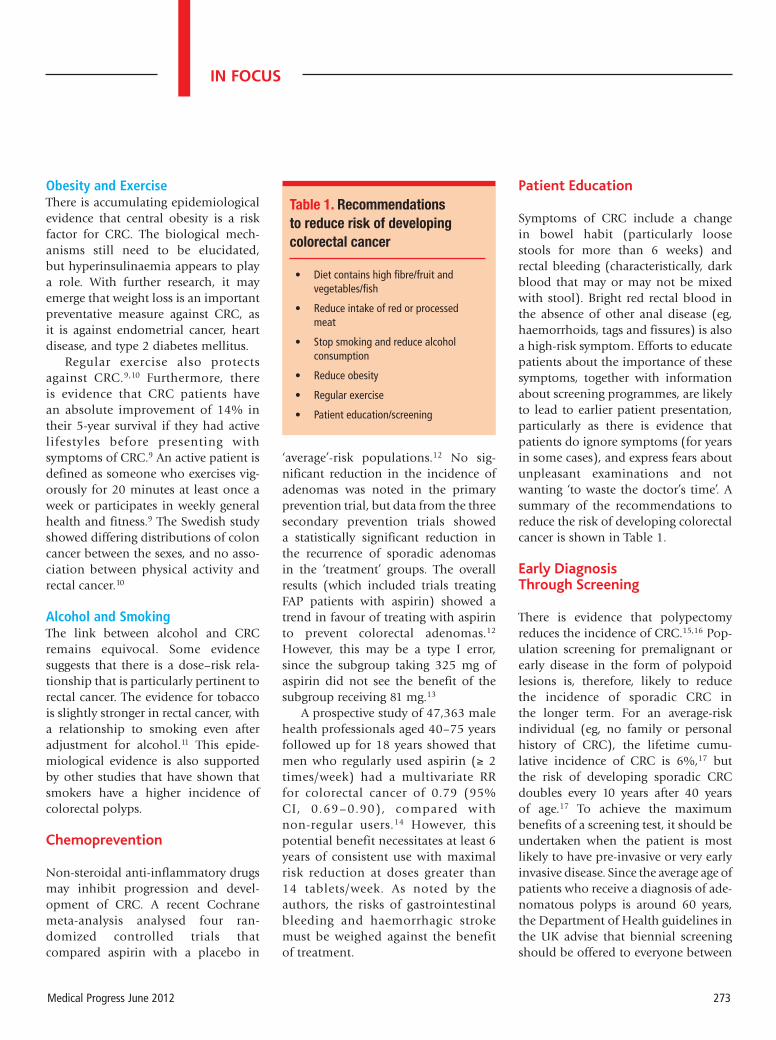
Table 1. Recommendations to reduce risk of developing colorectal cancer
• Dietcontainshighfibre/fruitandvegetables/fish
• Reduceintakeofredorprocessedmeat
• Stopsmokingandreducealcoholconsumption
• Reduceobesity
• Regularexercise
• Patienteducation/screening
Patient Education
Symptoms of CRC include a change in bowel habit (particularly loose stools for more than 6 weeks) and rectal bleeding (characteristically, dark blood that may or may not be mixed with stool). Bright red rectal blood in the absence of other anal disease (eg, haemorrhoids, tags and fissures) is also a high-risk symptom. Efforts to educate patients about the importance of these symptoms, together with information about screening programmes, are likely to lead to earlier patient presentation, particularly as there is evidence that patients do ignore symptoms (for years in some cases), and express fears about unpleasant examinations and not wanting ‘to waste the doctor’s time’. A summary of the recommendations to reduce the risk of developing colorectal cancer is shown in Table 1.
Early Diagnosis Through Screening
There is evidence that polypectomy reduces the incidence of CRC.15,16 Pop-ulation screening for premalignant or early disease in the form of polypoid lesions is, therefore, likely to reduce the incidence of sporadic CRC in the longer term. For an average-risk individual (eg, no family or personal history of CRC), the lifetime cumu-lative incidence of CRC is 6%,17 but the risk of developing sporadic CRC doubles every 10 years after 40 years of age.17 To achieve the maximum benefits of a screening test, it should be undertaken when the patient is most likely to have pre-invasive or very early invasive disease. Since the average age of patients who receive a diagnosis of ade-nomatous polyps is around 60 years, the Department of Health guidelines in the UK advise that biennial screening should be offered to everyone between
274 Medical Progress June 2012
In focus
respectively (see Table 2 for defi-nitions). Estimates of the sensitivity for CRC range from 12.9%19 to 50%,20 and for large adenomas are as low as 12%.19 The English Bowel Cancer Screening Pilot invited 480,250 individuals to take part in FOBT screening. There was a 56.8% uptake with an overall positive test rate of 1.9%. The cancer detection rate was 1.62/1,000 individuals screened. This gave a positive predictive value of 10.9% for cancer and 35.0% for adenomas.16 It is predicted that for every 1,000 individuals screened in the National Health Service (NHS) Bowel Cancer Screening programme, approxi-mately 20 will be offered colonoscopy, 16 of whom will take up the offer. Half of these colonoscopies are expected to be normal, six are expected to detect adenomas, and two to detect cancer. The normal colonoscopies are the most significant cost to screening. They impose a financial burden to patients and the health service as well as the associated morbidity and mortality rates of the procedure, even though these are low.21
Despite the criticisms, FOBT
60 and 69 years of age and extended to 75 years from 2010 (http://www.cancer screening.nhs.uk/bowel/index.html). Initial screening is performed using the faecal occult blood test (FOBT). Patients with positive tests are offered colonoscopy in quality-assured centres. Using this test fits the World Health Organization criteria for screening: ‘a screening test should be inexpensive, rapid, and simple, and is not intended to be diagnostic; those with positive tests require further evaluation’.18
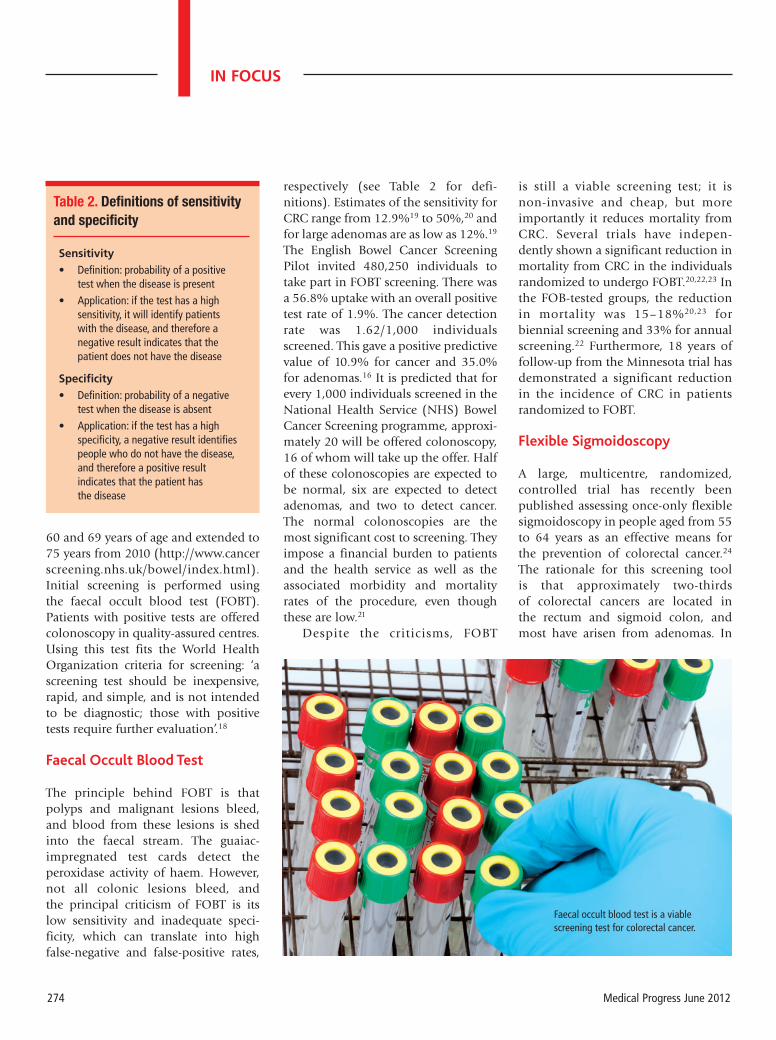
Faecal Occult Blood Test The principle behind FOBT is that polyps and malignant lesions bleed, and blood from these lesions is shed into the faecal stream. The guaiac-impregnated test cards detect the peroxidase activity of haem. However, not all colonic lesions bleed, and the principal criticism of FOBT is its low sensitivity and inadequate speci-ficity, which can translate into high false-negative and false-positive rates,
is still a viable screening test; it is non-invasive and cheap, but more importantly it reduces mortality from CRC. Several trials have indepen-dently shown a significant reduction in mortality from CRC in the individuals randomized to undergo FOBT.20,22,23 In the FOB-tested groups, the reduction in mortality was 15–18%20,23 for biennial screening and 33% for annual screening.22 Furthermore, 18 years of follow-up from the Minnesota trial has demonstrated a significant reduction in the incidence of CRC in patients randomized to FOBT.
Flexible Sigmoidoscopy
A large, multicentre, randomized, controlled trial has recently been published assessing once-only flexible sigmoidoscopy in people aged from 55 to 64 years as an effective means for the prevention of colorectal cancer.24 The rationale for this screening tool is that approximately two-thirds of colorectal cancers are located in the rectum and sigmoid colon, and most have arisen from adenomas. In
Table 2. Definitions of sensitivity and specificity
sensitivity
• Definition:probabilityofapositivetest when the disease is present
• Application:ifthetesthasahighsensitivity, it will identify patients with the disease, and therefore a negative result indicates that the patient does not have the disease
specificity
• Definition:probabilityofanegativetest when the disease is absent
• Application:ifthetesthasahighspecificity, a negative result identifies people who do not have the disease, and therefore a positive result indicates that the patient has the disease
Faecal occult blood test is a viable screening test for colorectal cancer.
In focus
Medical Progress June 2012 275
the majority of cases, people who develop a distal colon cancer will have developed an adenoma by 60 years of age, so removal of adenomas by sig-moidoscopy would provide long-term protection against the development of distal colorectal cancer.
Recruitment and screening were
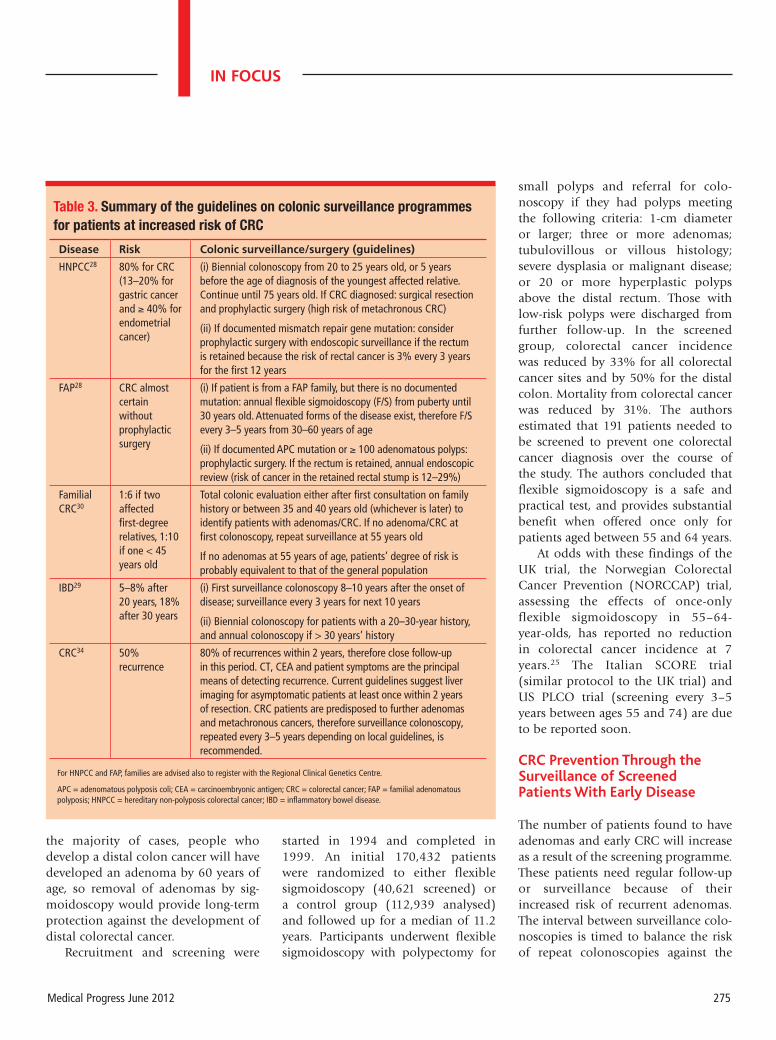
Table 3. Summary of the guidelines on colonic surveillance programmes for patients at increased risk of CRC
Disease Risk colonic surveillance/surgery (guidelines)
HNPCC28 80% for CRC (13–20% for gastric cancer and ≥ 40% for endometrial cancer)
(i) Biennial colonoscopy from 20 to 25 years old, or 5 years before the age of diagnosis of the youngest affected relative. Continueuntil75yearsold.IfCRCdiagnosed:surgicalresectionand prophylactic surgery (high risk of metachronous CRC)
(ii)Ifdocumentedmismatchrepairgenemutation:considerprophylactic surgery with endoscopic surveillance if the rectum is retained because the risk of rectal cancer is 3% every 3 years for the first 12 years
FAP28 CRC almost certain without prophylactic surgery
(i) If patient is from a FAP family, but there is no documented mutation:annualflexiblesigmoidoscopy(F/S)frompubertyuntil30yearsold.Attenuatedformsofthediseaseexist,thereforeF/Severy 3–5 years from 30–60 years of age
(ii) If documented APC mutation or ≥100adenomatouspolyps:prophylactic surgery. If the rectum is retained, annual endoscopic review (risk of cancer in the retained rectal stump is 12–29%)
Familial CRC30
1:6iftwoaffected first-degree relatives,1:10if one < 45 years old
Total colonic evaluation either after first consultation on family history or between 35 and 40 years old (whichever is later) to identifypatientswithadenomas/CRC.Ifnoadenoma/CRCatfirst colonoscopy, repeat surveillance at 55 years old
If no adenomas at 55 years of age, patients’ degree of risk is probably equivalent to that of the general population
IBD29 5–8% after 20 years, 18% after 30 years
(i) First surveillance colonoscopy 8–10 years after the onset of disease; surveillance every 3 years for next 10 years
(ii) Biennial colonoscopy for patients with a 20–30-year history, and annual colonoscopy if > 30 years’ history
CRC34 50% recurrence
80% of recurrences within 2 years, therefore close follow-up in this period. CT, CEA and patient symptoms are the principal means of detecting recurrence. Current guidelines suggest liver imaging for asymptomatic patients at least once within 2 years of resection. CRC patients are predisposed to further adenomas and metachronous cancers, therefore surveillance colonoscopy, repeated every 3–5 years depending on local guidelines, is recommended.
ForHNPCCandFAP,familiesareadvisedalsotoregisterwiththeRegionalClinicalGeneticsCentre.
APC = adenomatous polyposis coli; CEA = carcinoembryonic antigen; CRC = colorectal cancer; FAP = familial adenomatous polyposis;HNPCC=hereditarynon-polyposiscolorectalcancer;IBD=inflammatoryboweldisease.
started in 1994 and completed in 1999. An initial 170,432 patients were randomized to either flexible sigmoidoscopy (40,621 screened) or a control group (112,939 analysed) and followed up for a median of 11.2 years. Participants underwent flexible sigmoidoscopy with polypectomy for
small polyps and referral for colo-noscopy if they had polyps meeting the following criteria: 1-cm diameter or larger; three or more adenomas; tubulovillous or villous histology; severe dysplasia or malignant disease; or 20 or more hyperplastic polyps above the distal rectum. Those with low-risk polyps were discharged from further follow-up. In the screened group, colorectal cancer incidence was reduced by 33% for all colorectal cancer sites and by 50% for the distal colon. Mortality from colorectal cancer was reduced by 31%. The authors estimated that 191 patients needed to be screened to prevent one colorectal cancer diagnosis over the course of the study. The authors concluded that flexible sigmoidoscopy is a safe and practical test, and provides substantial benefit when offered once only for patients aged between 55 and 64 years.
At odds with these findings of the UK trial, the Norwegian Colorectal Cancer Prevention (NORCCAP) trial, assessing the effects of once-only flexible sigmoidoscopy in 55–64-year-olds, has reported no reduction in colorectal cancer incidence at 7 years.25 The Italian SCORE trial (similar protocol to the UK trial) and US PLCO trial (screening every 3–5 years between ages 55 and 74) are due to be reported soon.
CRC Prevention Through the Surveillance of Screened Patients With Early Disease
The number of patients found to have adenomas and early CRC will increase as a result of the screening programme. These patients need regular follow-up or surveillance because of their increased risk of recurrent adenomas. The interval between surveillance colo-noscopies is timed to balance the risk of repeat colonoscopies against the

276 Medical Progress June 2012
In focus
for patients with ‘at risk’ symptoms/signs, but delays still exist where, for example, the doctor gets ‘locked’ into the wrong diagnosis or makes a routine referral because TWR criteria are either not met or not included.32 In practice, therefore, it may be necessary for all patients with suspicious symptoms, not just those who meet TWR criteria, to have rapid investigation. This could be via GP direct-access colonoscopy or the ‘direct to test’ approach, where a consultant receives a referral and arranges investigation before a clinic visit. Clearly, this would require a sig-nificant improvement in colonoscopy services, especially since hospital waiting times, particularly for colo-noscopy and computed tomographic scans, are significant in many units. The common factor to improve the efficiency of the TWR is rapid access to high-quality colonoscopy, the current gold-standard investigation.
Prevention and EarlyDiagnosis – The Future
Screening promises to improve the detection of early CRC and ulti-mately contribute to its prevention. The value of FOBT as a single test is currently limited because of its low sensitivity and inadequate specificity, but if FOBT were complemented by another non-invasive test, sensitivity could be significantly improved. Various potential ‘complementary’ non-invasive tests are currently being developed, such as faecal DNA tests and molecular tests on isolated colo-nocytes.33 However, the availability of these tests for clinical investigation is still in the future. Consequently, continuing patient education about lifestyle, symptoms of CRC and screening, as well as promoting and funding initiatives to expedite diagnosis, staging and treatment of
CRC27 associated with this syndrome. Furthermore, surveillance frequency for HNPCC is based on the early age of presentation with the disease (median age, 40–45 years) and the likelihood that progression from adenoma to invasive carcinoma is more rapid than sporadic CRC – sometimes within 3 years of a clear colonoscopy. In contrast to HNPCC, the disease profiles and risks for FAP, IBD and familial CRC are all different, and so different sur-veillance guidelines are required.28–30 These guidelines are summarized in Table 3, but they remain flexible and practice standards will evolve as new data are published.
Prevention and EarlyDiagnosis Through UK Government Initiatives
The ‘NHS Cancer Plan’, introduced to reform cancer services, directed that by 2005, the time from GP referral to treatment for all cancers should be a maximum of 62 days. The ini-tiative introduced the 2-week wait rule (TWR) and the ‘two-week wait clinics’. An implicit benefit of the rule is the earlier diagnosis and treatment of CRC and, therefore, better survival rates for patients. However, although 99.5% of patients referred via the TWR are seen within the specified time, a recent study has shown that less than 25% of CRC cases were diagnosed through these clinics.31 Most CRC patients still present through the emergency services and other routes (eg, general medical or surgical outpatients). This suggests that for most CRC patients the TWR has had little impact. To optimize the benefits of the TWR, factors that inhibit its effi-ciency need to be explored. The reasons for delays are multiple and include patient and primary and secondary care factors. In the primary care setting, early referral via the TWR is available
need to diagnose and treat any further neoplasia and/or CRC before it causes significant morbidity. Initially, a 3-year interval was proposed based on the data from the US National Polyp Study, but further studies have modified this recommendation. It has been shown that if adenomas are found, the number and size of the adenomas often predict the polyp findings at sub-sequent follow-up colonoscopies. As a result, patients can be risk-stratified according to the number and size of the adenomas found at initial colo-noscopy.26 At the next follow-up, the patient is re-stratified according to the new colonoscopic findings.
Prevention Through Surveillance of Patients at Above-average Risk of CRC
For patients with a higher risk of CRC compared with the general popu-lation (eg, inherited CRC syndromes and IBD), early detection of CRC depends on appropriate surveillance programmes. Strong evidence (level II) has shown that surveillance of HNPCC patients reduces both the incidence of CRC and the risk of mortality from
"The number and size of the adenomas often
predict the polypfindings at subsequent
follow-up colonoscopies"

In focus
Medical Progress June 2012 277
About the AuthorsRobert Dennis is a Specialist Registrar at the CambridgeColorectalUnit,Addenbrooke’sHospital,Cambridge University Hospitals NHS FoundationTrust, Cambridge, UK. SamsonTou is LaparoscopicColorectal Fellow,The Queen Elizabeth Hospital,Australia. Richard Miller is a Consultant Colorectal Surgeon at the Cambridge Colorectal Unit,Addenbrooke’s Hospital, Cambridge UniversityHospitalsNHSFoundationTrust,Cambridge,UK.
© 2011 Elsevier Ltd. Initially published in Medicine
2011;39(5):243–249.
CRC, are vital to help prevent the mortality and morbidity associated with the disease.
Declaration of InterestsNone.
References1. Cancer Research UK. UK bowel cancer statistics. Available
at: http://info.cancerresearchuk.org/cancerstats/types/bowel/
(accessed 16 Jul 2010).
2. Bingham S, Riboli E. Diet and cancer – the European
Prospective Investigation into Cancer and Nutrition. Nat Rev
Cancer 2004;4:206–215.
3. Bingham SA, Day NE, Luben R, et al. Dietary fibre in food
and protection against colorectal cancer in the European
Prospective Investigation into Cancer and Nutrition (EPIC): an
observational study. Lancet 2003;361:1496–1501.
4. Norat T, Bingham S, Ferrari P, et al. Meat, fish, and colorec-
tal cancer risk: the European Prospective Investigation into
cancer and nutrition. J Natl Cancer Inst 2005;97:906–916.
5. Flood A, Rastogi T, Wirfält E, et al. Dietary patterns as
identified by factor analysis and colorectal cancer among
middle aged. Americans Am J Clin Nutr 2008;88:176–184.
6. Park Y, Hunter DJ, Spiegelman D, et al. Dietary fiber intake
and risk of colorectal cancer: a pooled analysis of prospective
cohort studies. JAMA 2005;294:2849–2857.
7. Asano T, McLeod RS. Dietary fibre for the prevention of
colorectal adenomas and carcinomas. Cochrane Database
Syst Rev 2002;(2):CD003430.
8. Jenab M, Bueno-de-Mesquita HB, Ferrari P. Association
between prediagnostic circulating vitamin D concentration
and risk of colorectal cancer in European populations: a
nested case-control study. BMJ 2010;340:b5500.
9. Haydon AM, Macinnis RJ, English DR, Giles GG. Effect of
physical activity and body size on survival after diagnosis
with colorectal cancer. Gut 2006;55:62–67.
10. Moradi T, Gridley G, Björk J, et al. Occupational physi-
cal activity and risk for cancer of the colon and rectum in
Sweden among men and women by anatomic subsite. Eur
J Cancer Prev 2008;17:201–208.
11. Doll R, Peto R, Boreham J, Sutherland I. Mortality from
cancer in relation to smoking: 50 years observations on
British doctors. Br J Cancer 2005;92:426–429.
12. Asano TK, McLeod RS. Non steroidal anti-inflamma-
tory drugs (NSAID) and aspirin for preventing colorectal
adenomas and carcinomas. Cochrane Database Syst Rev
2004;(2):CD004079.
13. Baron JA, Cole BF, Sandler RS, et al. A randomized trial
of aspirin to prevent colorectal adenomas. N Engl J Med
2003;348:891–899.
14. Chan AT, Giovannucci EL, Meyerhardt JA. Aspirin dose
and duration of use and risk of colorectal cancer. Gastroen-
terology 2008;134:21–28.
15. Atkin WS, Morson BC, Cuzick J. Long-term risk of colorec-
tal cancer after excision of rectosigmoid adenomas. N Engl J
Med 1992;326:658–662.
16. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of
colorectal cancer by colonoscopic polypectomy. The National
Polyp Study Workgroup. N Engl J Med 1993;329:1977–1981.
17. Nicholson FB, Barro JL, AtkinW, et al. Review article:
population screening for colorectal cancer. Aliment Pharma-
col Ther 2005;22:1069–1077.
18. Wilson JMG, Jungner G. Principles and Practice of Screen-
ing for Disease. Public Health Papers No. 34. Geneva: World
Health Organization; 1968.
19. Imperiale TF, Ransohoff DF, Itzkowitz SH, Turnbull BA,
Ross ME. Fecal DNA versus fecal occult blood for colorectal-
cancer screening in an average-risk population. N Engl J Med
2004;351:2704–2714.
20. Hardcastle JD, Chamberlain JO, Robinson MH, et al. Ran-
domised controlled trial of faecal-occult-blood screening for
colorectal cancer. Lancet 1996;348:1472–1477.
21. NHS Bowel Cancer Screening Programme. Evaluation
of English Bowel Screening Pilot. Available at: http://www
.cancerscreening.nhs.uk/bowel/pilot-2nd-round-evaluation
.pdf (accessed 16 Jul 2010).
22. Mandel JS, Bond JH, Church TR, et al. Reducing mortality
from colorectal cancer by screening for fecal occult blood.
Minnesota Colon Cancer Control Study. N Engl J Med
1993;328:1365–1371.
23. Kronborg O, Fenger C, Olsen J, Jorgensen OD, Sonder-
gaard O. Randomised study of screening for colorectal cancer
with faecal-occult-blood test. Lancet 1996;348:1467–1471.
24. Atkin WS, Edwards R, Kralj-Hans I, et al. Once-only
flexible sigmoidoscopy screening in prevention of colorectal
cancer: a multicentre randomised controlled trial. Lancet
2010;375:1624–1633.
25. Hoff Geir, Grotmol Tom, Skovlund Eva, Bretthauer
Michael; Norwegian Colorectal Cancer Prevention Study
Group. Risk of colorectal cancer seven years after flexible
sigmoidoscopy screening: randomized controlled trial. BMJ
2009;338:b1846.
26. Atkin WS, Saunders BP. Surveillance guidelines
after removal of colorectal adenomatous polyps. Gut
2002;51(suppl 5):V6– V9.
27. Jarvinen HJ, Aarnio M, Mustonen H, et al. Controlled
15-year trial on screening for colorectal cancer in families
with hereditary non-polyposis colorectal cancer. Gastroenter-
ology 2000;118:829–834.
28. Dunlop MG. Guidance on gastrointestinal surveillance for
hereditary non-polyposis colorectal cancer, familial adeno-
matous polypolis, juvenile polyposis, and Peutz–Jeghers
syndrome. Gut 2002;51(suppl 5):V21–V27.
29. Eaden JA, Mayberry JF. Guidelines for screening and sur-
veillance of asymptomatic colorectal cancer in patients with
inflammatory bowel disease. Gut 2002;51(suppl 5):V10–
V12.
30. Dunlop MG. Guidance on large bowel surveillance for
people with two first degree relatives with colorectal cancer
or one first degree relative diagnosed with colorectal cancer
under 45 years. Gut 2002;51(suppl 5):V17– V20.
31. Thorne K, Hutchings HA, Elwyn G. The effects of the Two-
Week Rule on NHS colorectal cancer diagnostic services: a
systematic literature review. BMC Health Serv Res 2006;6:43.
32. Flashman K, O’Leary DP, Senapati A, Thompson MR. The
Department of Health’s “two week standard” for bowel
cancer: is it working? Gut 2004;53:387–391.
33. Davies RJ, Freeman A, Morris LS, et al. Analysis of
minichromosome maintenance proteins as a novel
method for detection of colorectal cancer in stool. Lancet
2002;359:1917–1919.
34. Scholefield JH, Steele RJ. Guidelines for follow up after
resection of colorectal cancer. Gut 2002;51(suppl 5):V3– V5.
Further ReadingCappell M. Colon cancer screening, surveillance, prevention
and treatment: conventional and novel technologies. Med
Clin N Am 2005;89:1–217.
Steele RJC. Module 14 – Disorders of the colon and rectum.
In: Cuschieri A, Steele RJC, Moosa AR, eds. Essential Surgi
cal Practice: Higher Surgical Training in General Surgery.
4th ed. London: Arnold; 2002.
National bowel cancer audit 2009. http://www.ic.nhs
.uk/webfiles/Services/NCASP/audits%20and%20reports
/National%20Bowel%20Cancer%20Audit%202009%20
Interactive%20for%20web.pdf
278 Medical Progress June 2012
In focusPeer Reviewed
Colorectal Cancer: Features and InvestigationNigelHall,BA, DM, FRCS
Colorectal cancer, also known as bowel cancer, is a common malignancy and is common
in ‘Westernized’ populations, owing largely to dietary factors. Bowel cancers are thought
to arise through a combination of hereditary predisposition, exposure to environmental
agents (eg, diet), lifestyle, and chance.
Colorectal cancer, often known simply as bowel cancer, is a common solid organ malignancy affecting 35,000 patients a year in the UK,1 about half
of whom will die from it. At all ages, it is more common in males (especially rectal cancer), but because of the greater longevity of women the overall sex distribution is equal. It is generally a disease of advancing years, with a peak age at diagnosis of 70 years; the lifetime risk by the age of 80 years is about 5–10%.
Epidemiology
Colorectal cancer is common in ‘Westernized’ populations, probably owing largely to dietary
Colorectal cancer is generally a disease of advancing age.
factors. Europe, the USA and Japan have high rates compared with Africa and Asia. Bowel cancers are thought to arise through a combi-nation of hereditary predisposition, exposure to environmental agents (eg, diet), lifestyle, and chance. Dominantly inherited strongly penetrant syndromes, such as familial ade-nomatous polyposis (FAP) and hereditary non-polyposis colorectal cancer (Lynch syndrome), are responsible for a small per-centage of colorectal cancers, often developing before the age of 40 years.2 A much greater pro-portion may be the result of weakly penetrant but more common susceptibility genes, which are yet to be identified.3 Other known risk factors include diets high in red meat and low in
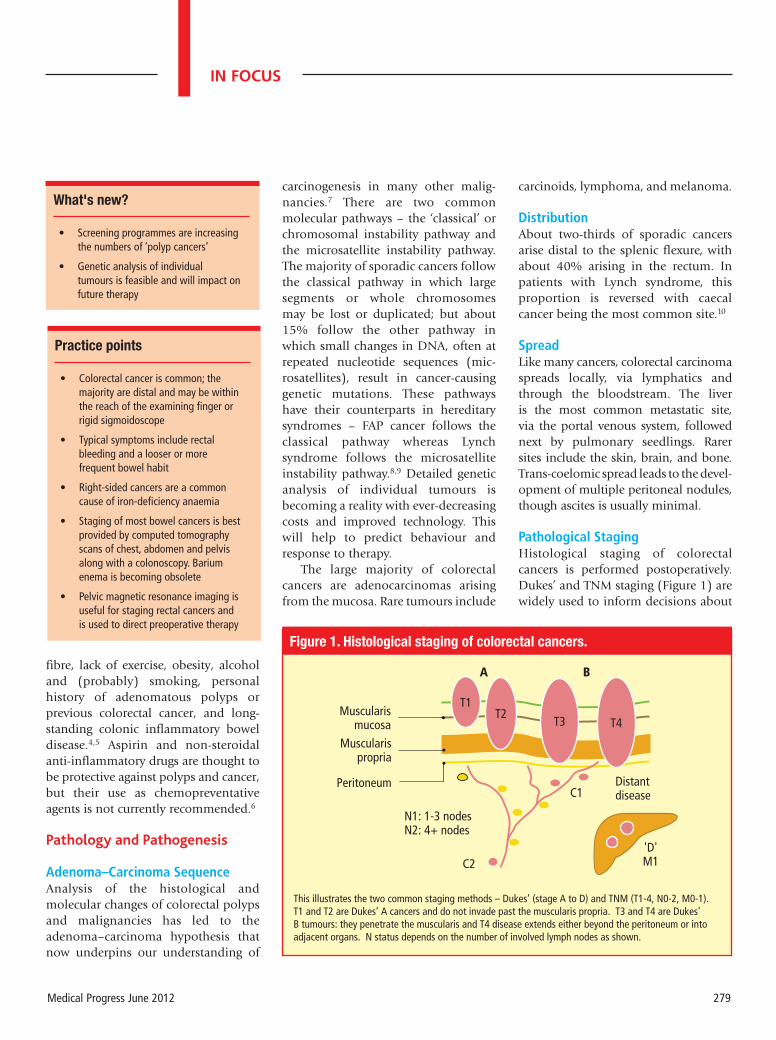
In focus
Medical Progress June 2012 279
fibre, lack of exercise, obesity, alcohol and (probably) smoking, personal history of adenomatous polyps or previous colorectal cancer, and long-standing colonic inflammatory bowel disease.4,5 Aspirin and non-steroidal anti-inflammatory drugs are thought to be protective against polyps and cancer, but their use as chemopreventative agents is not currently recommended.6
Pathology and Pathogenesis
Adenoma–Carcinoma SequenceAnalysis of the histological and molecular changes of colorectal polyps and malignancies has led to the adenoma–carcinoma hypothesis that now underpins our understanding of
carcinogenesis in many other malig-nancies.7 There are two common molecular pathways – the ‘classical’ or chromosomal instability pathway and the microsatellite instability pathway. The majority of sporadic cancers follow the classical pathway in which large segments or whole chromosomes may be lost or duplicated; but about 15% follow the other pathway in which small changes in DNA, often at repeated nucleotide sequences (mic-rosatellites), result in cancer-causing genetic mutations. These pathways have their counterparts in hereditary syndromes – FAP cancer follows the classical pathway whereas Lynch syndrome follows the microsatellite instability pathway.8,9 Detailed genetic analysis of individual tumours is becoming a reality with ever-decreasing costs and improved technology. This will help to predict behaviour and response to therapy.
The large majority of colorectal cancers are adenocarcinomas arising from the mucosa. Rare tumours include
carcinoids, lymphoma, and melanoma.
DistributionAbout two-thirds of sporadic cancers arise distal to the splenic flexure, with about 40% arising in the rectum. In patients with Lynch syndrome, this proportion is reversed with caecal cancer being the most common site.10
SpreadLike many cancers, colorectal carcinoma spreads locally, via lymphatics and through the bloodstream. The liver is the most common metastatic site, via the portal venous system, followed next by pulmonary seedlings. Rarer sites include the skin, brain, and bone. Trans-coelomic spread leads to the devel-opment of multiple peritoneal nodules, though ascites is usually minimal.
Pathological StagingHistological staging of colorectal cancers is performed postoperatively. Dukes’ and TNM staging (Figure 1) are widely used to inform decisions about
What's new?
• Screeningprogrammesareincreasingthe numbers of ‘polyp cancers’
• Geneticanalysisofindividualtumours is feasible and will impact on future therapy
Figure 1. Histological staging of colorectal cancers.
This illustrates the two common staging methods – Dukes’ (stage A to D) and TNM (T1-4, N0-2, M0-1). T1 and T2 are Dukes’ A cancers and do not invade past the muscularis propria. T3 and T4 are Dukes’ Btumours:theypenetratethemuscularisandT4diseaseextendseitherbeyondtheperitoneumorintoadjacent organs. N status depends on the number of involved lymph nodes as shown.
A B
T1T2
T3 T4
C1Distant disease
Muscularis mucosa
Muscularis propria
N1:1-3nodes N2:4+nodes
Peritoneum
'D' M1C2
Practice points
• Colorectalcanceriscommon;themajority are distal and may be within the reach of the examining finger or rigid sigmoidoscope
• Typicalsymptomsincluderectalbleeding and a looser or more frequent bowel habit
• Right-sidedcancersareacommoncause of iron-deficiency anaemia
• Stagingofmostbowelcancersisbestprovided by computed tomography scans of chest, abdomen and pelvis along with a colonoscopy. Barium enema is becoming obsolete
• Pelvicmagneticresonanceimagingisuseful for staging rectal cancers and is used to direct preoperative therapy

280 Medical Progress June 2012
In focus
adjuvant therapy.Dukes’ staging: node-negative
tumours are staged A if they have not penetrated the muscularis propria, B if they have. If there is lymph node spread, the tumour is automatically a Dukes’ C.11 A C2 tumour is one in which there is lymphatic invasion at the node furthest away from the tumour – at the ‘high tie’. Although not described by Dukes, it is now conventional to label any metastatic spread as stage D.
TNM staging is more precise than Dukes’ staging but clinically less useful because there are so many subgroups.
Malignant polyps: with the advent of screening programmes, earlier detection of cancers has led to an increased detection of ‘polyp cancers’, which are T1 lesions. Many of these are cured by polypectomy alone. Use of other staging methods that take into account the depth of penetration, such as the Haggitt12 and Kikuchi13
classifications, is helpful in judging the risk of lymph node metastasis and thus in deciding whether a formal resection is indicated.
Circumferential margin: for surgery to be potentially curative, espe-cially for rectal cancers, it is important to remove a margin of normal tissue around a cancer. Measurement of whether the circumferential resection margin is involved with cancer can be a very useful predictor of local and even distant recurrence.14,15
Diagnosis
SymptomsGastrointestinal symptoms are common, even in the absence of pathology, and there is a wide overlap of symptomatology for malignant and benign causes. Based on a large clinical database in Portsmouth, referral criteria have been developed that identify patients with colorectal cancer most reliably (Table 1),16 but only about 10–14% of patients meeting such criteria harbour a malignancy.
Obstructive symptoms: as tumours enlarge, they tend to narrow the bowel lumen. This commonly leads to a looser more frequent stool rather than constipation, although any persistent change in bowel habit should be inves-tigated. Distal tumours are more likely than proximal tumours to lead to an alteration in bowel habit, as the stool consistency is more solid. Proximal tumours may produce no symptoms at all until they obstruct completely. In the rectum, the mass effect of a cancer leads to tenesmus (a feeling of incomplete evacuation).
Bleeding: rectal bleeding, espe-cially if associated with a change in bowel habit, is a worrying symptom. Low rectal tumours can bleed bright blood just like haemorrhoids; bleeding from left-sided tumours may be darker
red and mixed in with the stool. Although right-sided tumours bleed, this is not visible in the stools, and so these cancers classically present with iron-deficiency anaemia because there is no warning sign to the patient.
Symptoms not usually associated with colorectal malignancy: bowel cancers are biologically inert and do not display paraneoplastic features. Weight loss and anorexia are very uncommon unless there is widespread metastatic disease. Pain is also unusual unless a tumour is so advanced that it is nearly obstructing the bowel lumen or invading bone or nerves.
Acute presentation: about 20% of patients with colorectal cancer present as emergencies – usually with obstruction but occasionally with per-foration or abscess formation. Most of these will require emergency surgery.
SignsPatients with symptoms suggestive of colorectal pathology should undergo abdominal examination, rectal exami-nation and a rigid sigmoidoscopy in the clinic.
Palpable mass: many colorectal cancers are palpable – typically, a right colon cancer gives rise to a firm mass in the right iliac fossa. Rectal cancers can often be felt on digital examination, and a rolled edge or circumferential nature can easily be appreciated. If a tumour is found, the surgeon will be greatly helped by information about the height of tumour from the anal verge, whether it is mobile, tethered, or fixed, and which quadrants are involved.
Sigmoidoscopic findings: a rigid sigmoidoscope will be able to examine most of the rectum and sometimes the distal sigmoid, so it can easily identify rectal tumours in the clinic. Equally important, it may reveal bleeding and inflamed mucosa from inflammatory
Table 1. Criteria for referral tofast track colorectal clinic
• Achangeinbowelhabit(looserand/or more frequent stools) persisting > 6 weeks without rectal bleeding in a person aged 60 years or older
• Rectalbleedingpersisting>6weekswithout a change in bowel habit and without anal symptoms, in a person aged 60 years or older
• Rectalbleedingwithachangeofbowel habit towards looser stools and/orincreasedstoolfrequencypersisting for 6 weeks or more, in a person aged 40 years or older
• Apalpablerightlowerabdominalmass or a palpable rectal mass (intraluminal and not pelvic)
• Iron-deficiencyanaemiawithahaemoglobinof11g/dLorlessinaman,orof10g/dLorlessinanon-menstruating woman

In focus
Medical Progress June 2012 281
bowel disease as an alternative expla-nation of the patient’s symptoms. The presence of streaks of blood in the lumen of the rectum is strongly indicative of pathology in the sigmoid above the reach of the rigid scope – usually a large polyp or cancer.
Differential DiagnosisThere is a wide differential diagnosis: alteration in bowel habit may be caused by irritable bowel syndrome, diverticular disease, infections, thyroid dysfunction, coeliac disease or inflam-matory bowel disease; rectal bleeding may be caused by haemorrhoids, anal fissure, inflammatory bowel disease or polyps; iron-deficiency anaemia may be caused by gastric or small bowel pathology, poor diet, celiac disease or bleeding from other organ systems (eg, renal or genital tract).
Investigations
DiagnosisBiochemical tests: no blood test will confirm or refute the diagnosis of colorectal cancer. A full blood count is useful to detect anaemia. Although car-
cinoembryonic antigen is commonly assayed, its value is more in follow-up than diagnosis. Faecal occult blood testing is a screening tool and is not indicated in persons with colorectal symptoms – such individuals need full colonic evaluation as described below.
Colonoscopy: it is the gold standard investigation for colorectal cancer and polyps. Completion rates
should be over 90% in good centres with a perforation rate less than 0.1%. Colonoscopy will identify cancers and enable biopsy, and has thera-peutic potential for removing polyps distant from the cancer to prevent metachronous malignancy developing during follow-up. A tattoo can be placed to allow the site of a tumour to be recognized at subsequent lapa-
Figure 2.
Figure 3. Magnetic resonance imaging of a locally advanced rectal cancer.
a, b. This polyp in the descending colon was removed by endoscopic mucosal excision after raising it off the muscularis propria by injecting succinylated gelatin and methylene blueinthesubmucosalplane.c.Thesiteofthepolypwasmarkedwithablacktattooinkoneithersideofthepolyp.Histologicalanalysisrevealedittobeamalignantpolyp,and the patient subsequently underwent a laparoscopic colectomy; the tattoo was essential for the surgeon to know exactly which part of the colon to remove.
This transverse section clearly demonstrates the mesorectal fascial envelope, which is the boundary of surgical excision. The tumour is extending through the full thickness of the bowel wall and is very close to the edge of the mesorectum. One of many enlarged lymph nodes is shown on this image. This patient had preoperative chemoradiotherapy to downstage the tumour and then underwent a potentially curative resection of his rectal carcinoma.
Mesorectal fascia
Rectal tumour encroaching mesorectal fascia
Bladder
Lumenof rectum
Lymphnode
Sacrum
a b c

282 Medical Progress June 2012
In focus
About the AuthorsNigel Hall is Consultant Colorectal Surgeon atAd-denbrooke’sHospital,Cambridge,UK.
roscopic resection (Figure 2). Even if a rectal cancer is diagnosed in the clinic, luminal imaging is still required to rule out synchronous disease. Barium enema is rapidly and rightly becoming obsolete because it is inaccurate and consistently both over-diagnoses and misses cancers.17
Computed tomography (CT) scans: particularly for elderly patients, a CT of the abdomen and pelvis is a useful diagnostic tool and is non-invasive.18 Occasionally, spasm on the right side of the abdomen can mimic the appearances of cancer on CT: if there is no clinically palpable mass in this situation, a colonoscopy is required to visualize the right colon and corroborate the CT findings.
CT colography: with multislice volume acquisition CT, excellent views can be obtained by insufflating air into a prepared colon. CT colonography is almost as accurate as colonoscopy and can visualize bowel proximal to an obstructing tumour.19
Biopsy: all rectal cancers require biopsy proof of malignancy before treatment is decided. For colonic disease, this is less important as the endoscopic appearances usually indicate the need for surgery.
Pre-operative Clinical StagingOnce a colorectal cancer has been diagnosed, clinical staging investi-gations should be performed to detect synchronous polyps and cancer, local spread, and metastatic disease. CT of the chest, abdomen and pelvis is used for all patients to detect distant spread. Rectal cancers should be discussed at a multidisciplinary meeting before surgery; all tumours are discussed postoperatively.
Rectal cancer: the extent of local spread determines pre-operative therapy, and so pelvic imaging is very important. Transrectal ultrasound
can accurately stage bowel wall invasion but is less good at detecting lymph node involvement.20 Magnetic resonance imaging is probably the most useful method for determining tumour invasion and nodal status (Figure 3). More importantly, it is the best way of assessing whether the tumour is close to the edge of the mesorectal envelope: this has impli-cations for the surgeon and informs decisions regarding pre-operative chemoradiotherapy.21
Declaration of InterestNone.
References1. Toms JR, ed. CancerStats monograph 2004. London: Can-
cer Research UK; 2004.
2. Fearnhead NS, Wilding JL, Bodmer WF. Genetics of colorec-
tal cancer: hereditary aspects and overview of colorectal
tumorigenesis. Br Med Bull 2002;64:27–43.
3. Bodmer WF. Cancer genetics: colorectal cancer as a model.
J Hum Genet 2006;51:391–396.
4. Bingham SA, Day NE, Luben R, et al. Dietary fibre in food
and protection against colorectal cancer in the European
Prospective Investigation into Cancer and Nutrition (EPIC): an
observational study. Lancet 2003;361:1496–1501.
5. Boyle P, Langman JS. ABC of colorectal cancer: epidemiol-
ogy. Br Med J 2000;321:805–808.
6. Elwood PC, Gallagher AM, Duthie GG, Mur LA, Morgan
G. Aspirin, salicylates, and cancer. Lancet 2009;373:1301–
1309.
7. Fearon ER, Vogelstein B. A genetic model for colorectal
tumorigenesis. Cell 1990;61:759–767.
8. Hall NR, Madoff RD. Genetics and the polyp-cancer
sequence. In: Edelstein PS, ed. Colon and Rectal Cancer.
Wilmington, DE: Wiley-Liss, 2000.
9. Hardy RG, Meltzer SJ, Jankowski JA. ABC of colorec-
tal cancer: molecular basis for risk factors. Br Med J
2000;321:886–889.
10. Lynch HT, Lynch PM, Lanspa SJ, Snyder CL, Lynch JF,
Boland CR. Review of the Lynch syndrome: history, molecular
genetics, screening, differential diagnosis, and medicolegal
ramifications. Clin Genet 2009;76:1–18.
11. Dukes CE. The classification of cancer of the rectum. J
Pathol Bacteriol 1932;35:323–332.
12. Haggitt RC, Glotzbach RE, Soffer EE, Wruble LD. Prog-
nostic factors in colorectal carcinomas arising in adenomas:
implications for lesions removed by endoscopic polypectomy.
Gastroenterology 1985;89:328–336.
13. Kikuchi R, Takano M, Takagi K, et al. Management of
early invasive colorectal cancer. Risk of recurrence and clinical
guidelines. Dis Colon Rectum 1995;38:1286–1295.
14. Adam IJ, Mohamdee MO, Martin IG, et al. Role of circum-
ferential margin involvement in the local recurrence of rectal
cancer. Lancet 1994;344:707–711.
15. West NP, Hohenberger W, Weber K, Perrakis A, Finan PJ,
Quirke P. Complete mesocolic excision with central vascular
ligation produces an oncologically superior specimen com-
pared with standard surgery for carcinoma of the colon. J
Clin Oncol 2010;28:272–278.
16. Thompson MR. Referral guidelines for colorectal cancer.
Colorectal Dis 2002;4:287–297.
17. Winawer SJ, Stewart ET, Zauber AG, et al. A comparison of
colonoscopy and double-contrast barium enema for surveil-
lance after polypectomy. National Polyp Study Work Group.
N Eng J Med 2000;342:1766–1772.
18. Fink M, Freeman AH, Dixon AK, et al. Computed tomogra-
phy of the colon in elderly people. Br Med J 1994;308:1018.
19. Halligan S, Altman DG, Taylor SA, et al. CT colonography
in the detection of colorectal polyps and cancer: systematic
review, meta-analysis, and proposed minimum data set for
study level reporting. Radiology 2005;237:893–904.
20. Brown G, Davies S, Williams GT, et al. Effectiveness of pre-
operative staging in rectal cancer: digital rectal examination,
endoluminal ultrasound or magnetic resonance imaging? Br
J Cancer 2004;91:23–29.
21. Brown G, Radcliffe AG, Newcombe RG, Dallimore NS,
Bourne MW, Williams GT. Preoperative assessment of prog-
nostic factors in rectal cancer using high resolution magnetic
resonance imaging. Br J Surg 2003;90:355–364.
Further ReadingCunningham D, Atkin W, Lenz HJ, et al. Colorectal cancer.
Lancet 2010;375:1030–1047.
National Institute for Health and Clinical Excellence. Guid
ance on Cancer Services: Improving Outcomes in
Colorectal Cancers – Manual Update. London:NICE;
2004.
© 2011 Elsevier Ltd. Initially published in Medicine
2011;39(5):250-253
In focus
Medical Progress June 2012 283
Peer Reviewed
Can Metastatic Colorectal Cancer Be Cured?DavidLBartlett, MD; Edward Chu, MD
Significant advances have been made in the treatment of metastatic colorectal cancer.
Development of the targeted biologic agents and their integration with cytotoxic
chemotherapy regimens has led to improvements in clinical efficacy. A multimodality
team-based approach involving medical oncologists, surgical oncologists, radiologists,
and other health-care providers is absolutely critical for the success of this therapeutic
approach. This article reviews the main issues that must be considered from the surgical
oncology and medical oncology perspectives, respectively.
Introduction
In 2012, colorectal cancer (CRC) continues to be a major public health problem. In the United States this year, there will be an estimated 147,000 new cases diagnosed
and nearly 50,000 deaths resulting from this disease.1 Worldwide, approximately 1 million new cases of CRC are diagnosed each year, with nearly 500,000 deaths attributed to this disease annually. About 25% of patients present
with metastatic disease, and of this group, 50% to 75% will have disease confined to the liver.2–4 In patients who present initially with early-stage disease, up to 50% will eventually develop metastatic disease, with the liver being the most common site. Another 10% to 20% of patients will present with disease involving the lung and other less common sites of meta-static involvement, including the peritoneum, ovaries, adrenal glands, bone, and brain.5,6
When metastatic disease is limited to an
In patients who present initially with early-stage colorectal cancer, up to 50% will eventually develop metastatic disease.
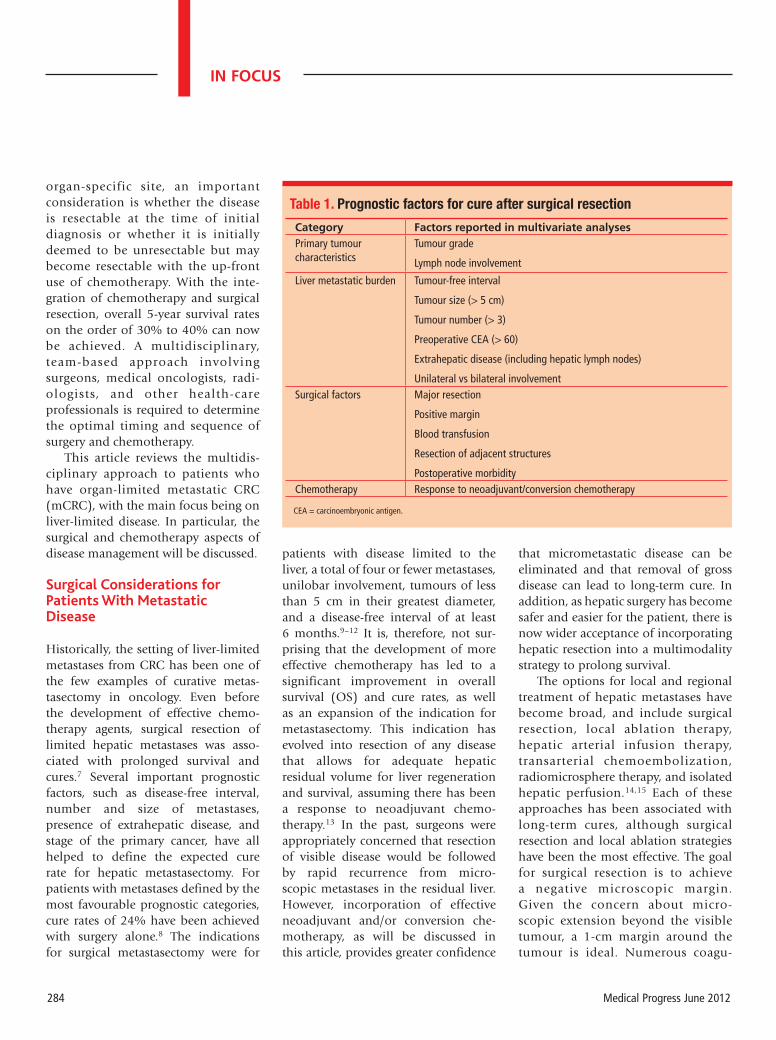
284 Medical Progress June 2012
In focus
organ-specific site, an important consideration is whether the disease is resectable at the time of initial diagnosis or whether it is initially deemed to be unresectable but may become resectable with the up-front use of chemotherapy. With the inte-gration of chemotherapy and surgical resection, overall 5-year survival rates on the order of 30% to 40% can now be achieved. A multidisciplinary, team-based approach involving surgeons, medical oncologists, radi-ologists, and other health-care professionals is required to determine the optimal timing and sequence of surgery and chemotherapy.
This article reviews the multidis-ciplinary approach to patients who have organ-limited metastatic CRC (mCRC), with the main focus being on liver-limited disease. In particular, the surgical and chemotherapy aspects of disease management will be discussed.
Surgical Considerations for Patients With Metastatic Disease
Historically, the setting of liver-limited metastases from CRC has been one of the few examples of curative metas-tasectomy in oncology. Even before the development of effective chemo-therapy agents, surgical resection of limited hepatic metastases was asso-ciated with prolonged survival and cures.7 Several important prognostic factors, such as disease-free interval, number and size of metastases, presence of extrahepatic disease, and stage of the primary cancer, have all helped to define the expected cure rate for hepatic metastasectomy. For patients with metastases defined by the most favourable prognostic categories, cure rates of 24% have been achieved with surgery alone.8 The indications for surgical metastasectomy were for
patients with disease limited to the liver, a total of four or fewer metastases, unilobar involvement, tumours of less than 5 cm in their greatest diameter, and a disease-free interval of at least 6 months.9–12 It is, therefore, not sur-prising that the development of more effective chemotherapy has led to a significant improvement in overall survival (OS) and cure rates, as well as an expansion of the indication for metastasectomy. This indication has evolved into resection of any disease that allows for adequate hepatic residual volume for liver regeneration and survival, assuming there has been a response to neoadjuvant chemo-therapy.13 In the past, surgeons were appropriately concerned that resection of visible disease would be followed by rapid recurrence from micro-scopic metastases in the residual liver. However, incorporation of effective neoadjuvant and/or conversion che-motherapy, as will be discussed in this article, provides greater confidence
that micrometastatic disease can be eliminated and that removal of gross disease can lead to long-term cure. In addition, as hepatic surgery has become safer and easier for the patient, there is now wider acceptance of incorporating hepatic resection into a multimodality strategy to prolong survival.
The options for local and regional treatment of hepatic metastases have become broad, and include surgical resection, local ablation therapy, hepatic arterial infusion therapy, transarterial chemoembolization, radiomicrosphere therapy, and isolated hepatic perfusion.14,15 Each of these approaches has been associated with long-term cures, although surgical resection and local ablation strategies have been the most effective. The goal for surgical resection is to achieve a negative microscopic margin. Given the concern about micro-scopic extension beyond the visible tumour, a 1-cm margin around the tumour is ideal. Numerous coagu-
Table 1. Prognostic factors for cure after surgical resection
category factors reported in multivariate analyses Primary tumour characteristics
Tumour grade
Lymphnodeinvolvement
Livermetastaticburden Tumour-free interval
Tumoursize(>5cm)
Tumour number (> 3)
Preoperative CEA (> 60)
Extrahepatic disease (including hepatic lymph nodes)
UnilateralvsbilateralinvolvementSurgical factors Major resection
Positive margin
Blood transfusion
Resection of adjacent structures
Postoperative morbidityChemotherapy Responsetoneoadjuvant/conversionchemotherapy
CEA = carcinoembryonic antigen.

In focus
Medical Progress June 2012 285
lation devices exist to enhance the safety of parenchymal transection by limiting blood loss. Minimally invasive approaches, such as lapa-roscopic and robotic assistance, have become commonplace, and they are associated with reduced blood loss, shortened hospital stay, and decreased narcotic usage postoperatively.16,17 For patients undergoing multimodality therapies, minimally invasive surgery may also improve quality of life during treatment and decrease the recovery time necessary before adjuvant che-motherapy is administered. The options for resection include extended lobectomy, lobectomy, segmentec-tomies, and non-anatomic wedge resections. Many surgeons remove the least amount of liver tissue feasible to preserve the anatomy for future resections, if necessary, while others prefer formal anatomic resections in order to provide the best chance of a negative margin. These two approaches have not been directly compared in a randomized trial; however, retro-spective data suggest that the ability to achieve a negative margin, as opposed to the specific type of resection, determines long-term prognosis.18
Local ablative approaches have provided an alternative to surgical resection for patients with mCRC. These approaches include radiofre-quency ablation (RFA), microwave ablation, cryotherapy, and focused radiotherapy (eg , us ing the CyberKnife). RFA is a reliable technique to ablate metastases up to 5 cm in size. However, it has limited efficacy in centrally located tumours in which proximity to the main portal triads or hepatic veins may cause bile duct injury, extensive hepatic necrosis, or inadequate tumour cell death adjacent to the vessels. The potential advantages of these local strategies over surgical resection include enhanced safety,
outpatient percutaneous treatment options, and the ability to preserve hepatic parenchyma. The local recurrence rate after local ablative pro-cedures is clearly higher than with surgical resection, with rates as high as 34% having been reported.19 The local recurrence rate at the site of ablation is influenced by the size and location of the metastatic lesions, as well as the use of percutaneous vs lap-aroscopic approaches. Although local recurrence can often be salvaged with repeat ablation or resection, for patients with limited comorbidities in whom the goal is curative intent, surgical resection is the preferred and most reliable method for actual cure. A meta-analysis of non-randomized studies comparing RFA with surgical resection demonstrated an improvement in 5-year survival for patients treated with hepatic resection.20
The curative potential of surgical resection for hepatic metastases from CRC varies depending on a number of important prognostic factors (Table 1). Nomograms for predicting cancer-related survival have been
developed and may be helpful when considering the utility of resection.21 A patient’s risk for morbidity and mortality also plays a significant role in defining the eventual treatment strategy. Surgical resection is still associated with a defined mortality rate of 2.8% (0% to 6.6%), which is influenced, in large part, by the health of the background liver.22,23 Liver failure is the most common cause of death after hepatectomy, and as discussed below, this compli-cation is influenced by the specific type and cumulative dose of chemo-therapy received. The indications for surgical resection are currently based on feasibility and safety in patients who have responded to chemo-therapy. It is critically important for the surgical resection to leave 20% to 25% of functioning liver volume (future liver remnant) in patients with a normal background liver, and 40% of liver volume in patients whose background liver is diseased from previous chemotherapy.24 Preoperative planning computed tomography scans, including residual volume calcu-lations, are essential when planning an extended or bilobar resection.25
To date, more than 750 series of hepatic metastasectomy for meta-static CRC have been reported in the literature. The actuarial 5-year survival rate for patients who underwent R0 resections (negative margins) was 30% when combining 16 well-reported series of more than 100 patients with follow-up greater than 2 years (15% to 67%).22 While 5-year survival was historically considered a cure for this disease, because of advances in systemic chemotherapy an increasing number of patients are now living with their disease beyond 5 years. A single-institution study of 455 patients revealed a median OS of 33 months, with 5- and 10-year actuarial survival
“A patient’s risk for morbidity and mortality also plays a significant
role in defining the eventual treatment
strategy”

286 Medical Progress June 2012
In focusPeer Reviewed
rates of 34% and 25%, respectively.26 In that study, 124 patients were iden-tified as actual 5-year survivors (27%), and of this group 59 were found to be 10-year survivors. This finding suggests ongoing disease-related mortality beyond the 5-year time-frame, with actual cure rates of 10% to 15%. Randomized clinical data suggest an improvement in disease-free survival (DFS) when systemic che-motherapy is incorporated as part of a combined neoadjuvant and postop-erative adjuvant approach, as will be discussed in detail in this article.
With the extended indications for hepatic metastasectomy in the presence of active systemic chemotherapy, larger resections can now be safely and effec-tively performed. Commonly used techniques include staged resections for bilobar disease and preoperative portal vein occlusion to achieve com-pensatory hypertrophy and safer extended resections.27,28 While there appear to be impressive actuarial 5-year survival rates in these series of extensive surgical resections, it is expected that the true cure rate will be much lower. When looking at patients with initially unresectable colorectal liver metastases who were treated with chemotherapy and then resected, 16% of this group were considered cured, with a disease-free interval of more than 5 years after metastasectomy.29 On multivariate analysis, the main predictors of cure included maximum size less than 3 cm, no more than three metastatic lesions, and complete pathologic response.
Systemic Chemotherapy
Long-term cures are exceedingly rare when patients with organ-limited mCRC are treated with chemotherapy alone. In a retrospective review of 2,751
patients with metastatic CRC, during a median follow-up of 10.3 years, only six (0.24%) were found to be free of disease after having received chemotherapy alone.30 It is now well established that a multimodality strategy results in a much higher chance of long-term cure. In patients with organ-limited disease, chemotherapy is administered in three main settings, which include neoad-juvant therapy, conversion therapy, and adjuvant therapy. Neoadjuvant therapy refers to chemotherapy given to patients with potentially resectable disease, while conversion therapy refers to chemotherapy given to patients deemed to have initially unresectable disease. Adjuvant chemotherapy is use of chemotherapy following an R0 surgical resection, with the intent of preventing disease recurrence.
Neoadjuvant Chemotherapy
Up to 20% to 30% of patients with liver-limited mCRC may have poten-tially resectable disease at the time of initial presentation. However, because a large proportion of patients expe-rience recurrence of their disease either in the liver or systemically, chemo-therapy has been integrated in their up-front care to improve upon the potential benefit of surgery.
Several cl inical tr ials have specifically evaluated the role of neo-adjuvant therapy for patients with potentially resectable liver metastases. In a single-arm trial involving 20 patients, neoadjuvant therapy with a weekly administration of FOLFOX (fluorouracil [5-FU], leucovorin/folinic acid [LV], and oxaliplatin) resulted in a partial or complete response in all patients enrolled.31 A total of 16 patients underwent a potentially curative resection, with seven developing recurrence during the median follow-up period
of 23 months. A phase II trial of neoadjuvant therapy investigated bev-acizumab plus the combination of capecitabine and oxaliplatin.32 In this study, 56 patients received six cycles of therapy prior to surgical resection, and a remarkably high objective response rate of 73% was observed. A total of 52 of the 56 patients were able to undergo an R0 resection, with complete pathologic response occurring in nearly 10% of patients. Given concerns over the potential risks of bleeding or wound-healing complications, bevacizumab was not given with the last cycle of chemo-therapy prior to surgery. This study is important as it showed that beva-cizumab could be safely administered to patients with no increased risk of intraoperative bleeding or wound-healing complications. Moreover, it was estimated that normal liver regen-eration occurred in all but one patient.
The European Organisation for Research and Treatment of Cancer (EORTC) randomized phase III trial 40983 investigated use of periop-erative FOLFOX4 chemotherapy in patients with up to four resectable liver metastases. In this study, patients were randomized to surgery alone or to receive six cycles of FOLFOX4 before surgery and six cycles of FOLFOX4 after surgery.33 The overall response rate was 43% in patients receiving chemotherapy. Of note, surgery was performed in 83% of patients ran-domized to chemotherapy and in 84% of patients randomized to surgery alone, providing evidence that use of initial chemotherapy did not com-promise the ability of patients to undergo surgical resection. While there was an increased risk of post-operative complications in patients receiving neoadjuvant chemotherapy, these events were reversible and not associated with an increased risk of
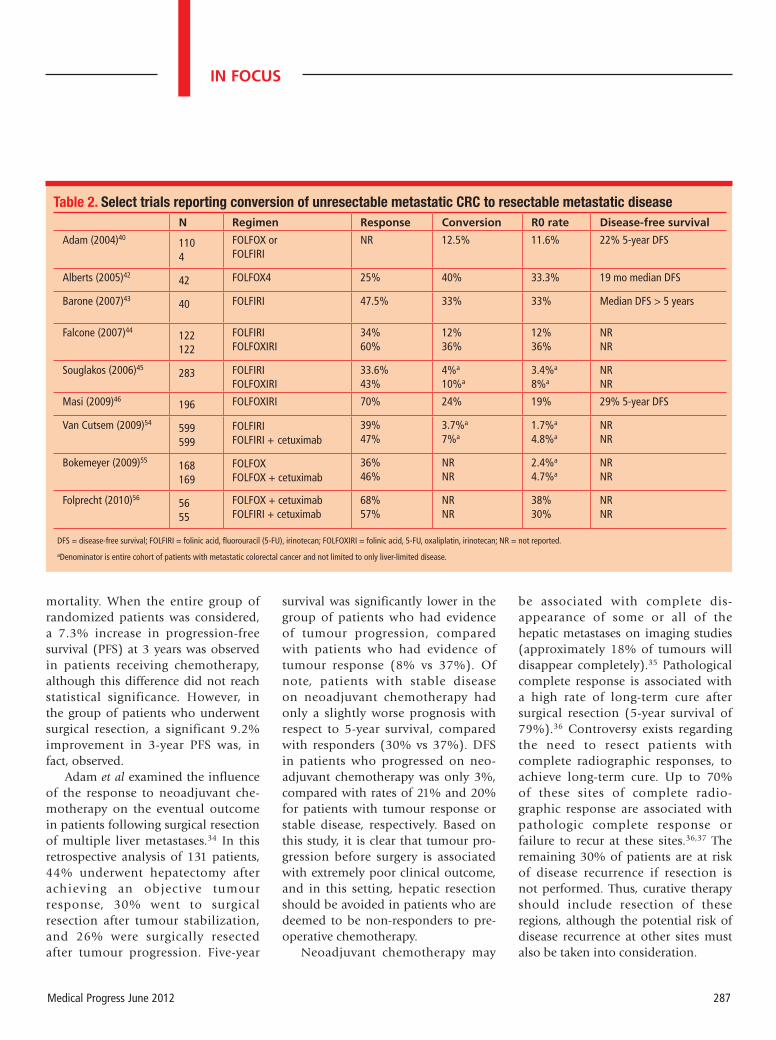
In focus
Medical Progress June 2012 287
mortality. When the entire group of randomized patients was considered, a 7.3% increase in progression-free survival (PFS) at 3 years was observed in patients receiving chemotherapy, although this difference did not reach statistical significance. However, in the group of patients who underwent surgical resection, a significant 9.2% improvement in 3-year PFS was, in fact, observed.
Adam et al examined the influence of the response to neoadjuvant che-motherapy on the eventual outcome in patients following surgical resection of multiple liver metastases.34 In this retrospective analysis of 131 patients, 44% underwent hepatectomy after achieving an objective tumour response, 30% went to surgical resection after tumour stabilization, and 26% were surgically resected after tumour progression. Five-year
survival was significantly lower in the group of patients who had evidence of tumour progression, compared with patients who had evidence of tumour response (8% vs 37%). Of note, patients with stable disease on neoadjuvant chemotherapy had only a slightly worse prognosis with respect to 5-year survival, compared with responders (30% vs 37%). DFS in patients who progressed on neo-adjuvant chemotherapy was only 3%, compared with rates of 21% and 20% for patients with tumour response or stable disease, respectively. Based on this study, it is clear that tumour pro-gression before surgery is associated with extremely poor clinical outcome, and in this setting, hepatic resection should be avoided in patients who are deemed to be non-responders to pre-operative chemotherapy.
Neoadjuvant chemotherapy may
be associated with complete dis-appearance of some or all of the hepatic metastases on imaging studies (approximately 18% of tumours will disappear completely).35 Pathological complete response is associated with a high rate of long-term cure after surgical resection (5-year survival of 79%).36 Controversy exists regarding the need to resect patients with complete radiographic responses, to achieve long-term cure. Up to 70% of these sites of complete radio-graphic response are associated with pathologic complete response or failure to recur at these sites.36,37 The remaining 30% of patients are at risk of disease recurrence if resection is not performed. Thus, curative therapy should include resection of these regions, although the potential risk of disease recurrence at other sites must also be taken into consideration.
Table 2. Select trials reporting conversion of unresectable metastatic CRC to resectable metastatic disease n Regimen Response conversion R0 rate Disease-free survival
Adam (2004)40110 4
FOLFOXor FOLFIRI
NR 12.5% 11.6% 22% 5-year DFS
Alberts (2005)42 42 FOLFOX4 25% 40% 33.3% 19 mo median DFS
Barone (2007)4340 FOLFIRI 47.5% 33% 33% Median DFS > 5 years
Falcone (2007)44 122 122
FOLFIRI FOLFOXIRI
34% 60%
12% 36%
12% 36%
NR NR
Souglakos (2006)45283 FOLFIRI
FOLFOXIRI33.6% 43%
4%a
10%a3.4%a
8%aNR NR
Masi (2009)46196 FOLFOXIRI 70% 24% 19% 29% 5-year DFS
Van Cutsem (2009)54599 599
FOLFIRIFOLFIRI+ cetuximab
39% 47%
3.7%a
7%a1.7%a
4.8%aNR NR
Bokemeyer (2009)55168 169
FOLFOXFOLFOX+cetuximab
36% 46%
NR NR
2.4%a
4.7%aNR NR
Folprecht (2010)5656 55
FOLFOX+cetuximab FOLFIRI+cetuximab
68% 57%
NR NR
38% 30%
NR NR
DFS=disease-freesurvival;FOLFIRI=folinicacid,fluorouracil(5-FU),irinotecan;FOLFOXIRI=folinicacid,5-FU,oxaliplatin,irinotecan;NR=notreported.
aDenominator is entire cohort of patients with metastatic colorectal cancer and not limited to only liver-limited disease.

288 Medical Progress June 2012
In focus
Conversion Therapy
The majority of patients will present with liver metastases from CRC that are unresectable or not optimally resectable based on their size, number, or location at the time of initial assessment. In this setting, conversion therapy is used in appropriately selected patients. The primary focus, therefore, is on achieving downsizing of the meta-static disease that is sufficient to allow surgical resection to be performed, but not with the goal of achieving a complete or even maximal response.
Adam and colleagues in France have had the largest experience in this area to date, and their work has provided important insights into the potential role of conversion therapy.38–40 In their original series of 701 patients with initially unresectable liver metastases, treatment with oxali-platin-based chemotherapy resulted in downsizing in nearly 15% of patients, and subsequent surgery. Based on 5-year follow-up after surgery, 22% of
patients had no evidence of residual or recurrent disease. When stratified according to the underlying reasons for initial unresectability, the 5-year OS rates were 60% for patients with large tumours, 49% for those with poorly located tumours, and 34% for patients with multinodular tumours. In an expanded series of 1,439 patients treated with a broader range of cytotoxic chemotherapy, the con-version rate was 12.5%, with a 5-year survival rate of 33%.
Folprecht and col leagues 41 conducted an interesting analysis of all published/presented clinical trials and retrospective studies of the rate of objective response and the subsequent rate of resection of initially unre-sectable metastases. They observed a strong correlation (r = 0.96) between response rates and the subsequent resection rate in patients with isolated liver disease. Moreover, their analysis confirmed that patient selection and efficacy of preoperative chemotherapy were strong predictors of potential
resectability of liver metastases. Since this analysis, several prospective clinical trials incorporating systemic chemotherapy plus surgery have been performed. In these studies, use of oxaliplatin- vs irinotecan-based che-motherapy has shown similar clinical outcomes.42,43 Of note, approximately 20% to 30% of patients were able to undergo R0 surgical resection. Two trials have directly compared the clinical efficacy of FOLFOX plus iri-notecan (FOLFOXIRI), an aggressive regimen that incorporates the three active cytotoxic agents, against that of FOLFIRI (5-FU, LV, irinotecan). Falcone et al randomized patients with mCRC to receive either FOLFOXIRI or FOLFIRI, and they reported a sig-nificant increase in R0 resection for the subgroup of patients with liver-only metastases who were ran-domized to the FOLFOXIRI arm.44 The R0 resection rate was 36% in the FOLFOXIRI arm vs 12% in the FOLFIRI arm (P = 0.017). Despite the increased clinical activity of FOLFOXIRI, patients receiving this regimen experienced a significantly higher incidence of grade 3/4 toxicity in the form of myelosuppression and neurotoxicity. In contrast to the positive findings of the Falcone study, Souglakos et al observed a non-sig-nificant increase in overall response rate (43% vs 33.6%), conversion rate (10% vs 3.4%), and R0 resection rate (8.8% vs 3.4%).45 A pooled analysis of the Falcone phase III study and two phase II studies reported an overall response rate of 70% with the FOLFOXIRI regimen and a 19% R0 resection rate. The 5-year DFS and OS were 29% and 42%, respectively.46
Is there an optimal cytotoxic che-motherapy regimen for conversion therapy? To date, there has been a sig-nificant absence of randomized trials directly comparing the various che-
Metastatic colorectal cancer is potentially curable when it is limited to a specific organ site.

In focus
Medical Progress June 2012 289
motherapy regimens in patients with liver-limited disease. In reviewing the literature, it appears that irinotecan- and oxaliplatin-based regimens yield approximately the same rate of con-version, on the order of 20% to 30%. While FOLFOXIRI appears to result in higher conversion rates in the 40% to 60% range and higher R0 surgical resections, this treatment regimen is clearly associated with increased toxicity and should be used only in certain select patient populations. Upon review of the recent National Comprehensive Cancer Institute (NCCN) guidelines, several regimens are currently recommended, and they include FOLFIRI, FOLFOX, the combi-nation of capecitabine and oxaliplatin, and FOLFOXIRI.47
The introduction of targeted therapies with either the anti-angiogenic agent bevacizumab or the epidermal growth factor receptor (EGFR) inhibitors cetuximab and panitumumab has improved the clinical efficacy of chemotherapy in patients with mCRC. As a result, com-bination regimens incorporating these agents have now been evaluated in clinical trials for patients with liver-limited metastases.
The addition of the anti–vascular endothelial growth factor (VEGF) antibody bevacizumab to either FOLFOX or to capecitabine and oxali-platin vs the cytotoxic chemotherapy regimens alone was investigated in a randomized phase III trial in advanced mCRC.48 Unfortunately, there was only a slightly higher incidence of R0 surgical resection with bevacizumab (8.4%) vs chemotherapy alone (6.1%).
The ant i -EGFR ant ibodies cetuximab and panitumumab have been approved for use in patients with mCRC.49 Subsequent studies have shown that these agents are active only in patients with wild-type KRAS
tumours. KRAS mutations occur in up to 30% to 40% of patients with CRC, and they typically involve codon 12 or 13. In general, KRAS mutations lead to resistance to antibody therapy. However, recent studies have suggested that the G13D mutation in codon 13 may still allow for sensitivity to anti-EGFR antibody therapy, in sharp contrast to mutations in codon 12.
Retrospective analyses of clinical trials in mCRC have provided insights into the potential role of cetuximab in the treatment of liver-limited disease. In a phase II trial of FOLFOX plus cetuximab, 37 of the 43 patients enrolled had liver involvement, and in 17 of these patients, the liver was the only site of metastatic disease.50 An objective response was seen in 34 of the 37 patients; 10 of these patients underwent surgical resection of their metastases, including eight patients with liver metastases. In a series of 151 patients with unresectable mCRC liver metastases refractory to systemic che-motherapy, the addition of cetuximab to combination chemotherapy allowed 27 patients to undergo surgical resection, and of this group, 25 underwent potentially curative hepatectomy.51 Of note, this group included a majority of patients who were deemed to have either technically unresectable or marginally resectable disease. Moreover, the incorporation of cetuximab with chemotherapy conferred significant clinical benefit, with median PFS and OS of 13 and 20 months, respectively.
Several single-arm phase II trials have investigated the combination of cetuximab with either irinotecan- or oxaliplatin-based regimens. Min et al reported a radiologic response rate of 39%, with 30% of patients treated with FOLFIRI plus cetuximab able to undergo resection of their liver metastases.52 Nearly identical results
were observed with the combination of FOLFOX and cetuximab, which yielded an R0 resection rate of 29%.53
Two recent randomized studies have investigated the safety and efficacy of cetuximab in combi-nation with either FOLFIRI54 or FOLFOX.55 The addition of cetuximab to FOLFIRI significantly increased the overall response rate (59% vs 43%; P = 0.004) in patients with wild-type KRAS when compared with FOLFIRI alone, and this resulted in a higher number of patients able to undergo R0 surgical resection (4.3% vs 1.5%). An exploratory analysis revealed a twofold higher rate of R0 surgical resection in patients with liver-limited disease (9.8% vs 4.5%).54 Similar findings were reported by Bokemeyer et al55
with the combination of cetuximab plus FOLFOX4. The overall response rate increased from 37% to 61% in patients with wild-type KRAS and in those treated with the combination vs FOLFOX4 alone. This improvement in response rate in patients treated with the combination was associated with an increase in the R0 resection rate from 2.4% to 4.7%.
A trial of 114 patients with initially non-resectable liver-limited metastases randomized patients to receive cetuximab in combination with either FOLFOX6 or FOLFIRI. R0 resection rates of 38% and 30% were observed, respectively, with an overall R0 resection rate of 34%.56 In a retrospective analysis of response according to KRAS status with the two arms of the trial combined, the clinical response rate in patients with wild-type KRAS was 70% compared with 41% for those with mutant KRAS. This study provides further evidence of the strong association between high tumour response rate and increased rate of liver metastasectomy.
PRIME ( the Pani tumumab

290 Medical Progress June 2012
In focus
Randomized Trial in Combination With Chemotherapy for Metastatic Colorectal Cancer to Determine Efficacy) was designed to evaluate the efficacy and safety of pani-tumumab plus FOLFOX4 vs FOLFOX4 alone as initial treatment for mCRC. The addition of panitumumab to FOLFOX4 chemotherapy significantly improved the overall response rate (57% vs 48%; P = 0.02) and median PFS in patients with wild-type KRAS tumours (9.6 vs 8.0 months; P = 0.01), which translated into a non-significant increase in median OS from 19.7 to 23.9 months.
In terms of surgical resection, metastasectomy of any site was attempted in 10.5% of patients treated with the combination regimen as opposed to 9.4% of patients treated with chemotherapy alone. However, the R0 resection rate was higher in patients with wild-type KRAS tumours and liver-limited disease (28% vs 18%) who were treated with pani-tumumab plus FOLFOX4. At the time of the most recent analysis, median OS had not been reached in patients who underwent R0 liver resection, in contrast to a median OS of 23.6 months in those who were unable to undergo complete surgical resection.57
Adjuvant Chemotherapy
To date, only a limited number of clinical trials have investigated the role of adjuvant chemotherapy following surgical resection of organ-limited metastases. Two randomized phase III trials were conducted to determine the potential role of adjuvant che-motherapy with 5-FU/ LV vs surgery alone.58,59 Both trials showed a non-significant trend for improvement in DFS. Unfortunately, both studies closed prematurely due to slow patient enrolment. As a result, neither study
had sufficient statistical power to dem-onstrate the predefined difference in OS. A pooled analysis of the individual data from these two trials was subse-quently conducted by Mitry et al to improve the statistical power of the survival analysis. This analysis showed a marginally significant trend toward improved PFS for patients receiving chemotherapy (27.9 vs 18.8 months).60 This study is important as it provides proof of concept for the potential role of adjuvant chemotherapy in patients who have undergone curative resection of liver or lung metastatic disease. Unfortunately, a randomized phase III trial was unable to document the benefit of the FOLFIRI regimen as adjuvant therapy following surgical resection of liver metastases when compared with infusional 5-FU/LV.61
What should the recommen-dations be for adjuvant chemotherapy following surgical resection? Although definitive clinical data are lacking, the current approach would be to offer adjuvant therapy with an oxaliplatin-based regimen, whether it be FOLFOX or XELOX, for a defined 3- to 4-month period. As is the case for the adjuvant treatment of early-stage colon cancer, there is presently no role for a biologic agent, such as bevacizumab or the anti-EGFR antibodies cetuximab and panitumumab, in oxaliplatin-based chemotherapy. Further support for this approach comes from the recently published NCCN clinical practice guidelines for adjuvant therapy of resected metastatic disease, which recommend a shortened course of cytotoxic chemotherapy, as would be offered for patients with resected stage III colon cancer.47
Limitations of Chemotherapy
The role of chemotherapy is to enhance the outcomes of surgery and/or permit
potentially curative resection to be performed. Unfortunately, chemo-therapy has potential disadvantages, which relate to direct toxic effects on the liver, leading to an increased risk of potential postoperative complications. There is now a large body of evidence showing that systemic chemotherapy can result in non-alcoholic fatty liver disease and sinusoidal injury. The chemotherapy-associated liver disease ranges from steatosis to steatohepatitis (CASH).62 Steatosis resulting from che-motherapy and/or any other etiology has been shown to lead to a higher rate of complications following hepatic resection. However, the development of CASH appears to hold greater signif-icance.63 Of note, CASH appears to be more closely associated with the use of irinotecan-based chemotherapy and to occur more commonly in patients with higher body mass index.64 The devel-opment of CASH has been associated with a higher postoperative mortality rate related primarily to postoperative liver failure. In one series, the 90-day
“There is now a largebody of evidence
showing that systemic chemotherapy can
result in non-alcoholic fatty liver disease and
sinusoidal injury”
In focus
Medical Progress June 2012 291
mortality rate in patients with steato-hepatitis was 14.7% vs 1.6% for those who did not have steatohepatitis.65 In contrast to treatment with irinotecan, oxaliplatin-based chemotherapy has been typically associated with liver sinusoidal injury.62,65,66 In more severe cases, perisinusoidal fibrosis, sinusoidal obstruction, and portal hypertension have been observed. In contrast to CASH, the development of sinusoidal dilation has not been associated with an increased risk of perioperative morbidity and mortality.67,68
Peritoneal Carcinomatosis
While this review has focused on liver-limited metastatic disease, cures have also been reported after pulmonary metastasectomy, isolated nodal recur-rences, and ovarian metastases.69–71 While these are highly selected cases, they are worthy of consideration for patients with favourable tumour biology and/or for those who are responsive to chemotherapy. A growing field of interest has been the surgical man-agement of peritoneal metastases from CRC, using cytoreductive surgery and intraoperative chemoperfusion with mitomycin C or oxaliplatin, combined with hyperthermia (HIPEC).72,73 This interest stems from early randomized trials with this treatment strategy in gastric cancer and a randomized trial in mCRC from the Netherlands.74,75 This mCRC carcinomatosis trial dem-onstrated an improvement in median survival in patients receiving intraop-erative HIPEC, compared with systemic 5-FU/LV (22.3 months vs 12.6 months). Patients whose tumours could be com-pletely resected from the peritoneum followed by HIPEC had an actuarial 3-year survival of 95%. A follow-up report on this trial demonstrated an overall actual 5-year survival of 45% in the HIPEC arm for patients with
all disease resected.76 A recent report from France noted a 5-year survival of 26% in patients receiving HIPEC with oxaliplatin for colorectal peri-toneal carcinomatosis.77 A number of series have compared surgical cyto-reduction and HIPEC for peritoneal carcinomatosis vs surgical resection of hepatic metastases from mCRC, dem-onstrating similar survival curves.78–80 This finding suggests that an aggressive combined-modality approach for peritoneal carcinomatosis may have a defined cure rate. Presently, most centres combine surgical cytoreduction and HIPEC with neoadjuvant and postoperative adjuvant systemic che-motherapy, such as has been described for liver-limited metastatic disease.
Conclusions
When limited to a specific organ site, mCRC is potentially curable. To date, nearly all of the clinical studies have focused on liver-limited disease, but similar results are now being reported for patients with disease limited to the lungs, ovaries, and peritoneum. It is clear that a multidisciplinary team-based approach is required for the optimal care of this particular subset of patients. The development of an individual treatment plan comes from a careful discussion and ongoing communication among a multidisci-plinary team of specialists, including surgeons, medical oncologists, and radiologists. With the appropriate integration of chemotherapy plus biological agents and surgery, up to 30% to 40% of patients with organ-limited metastatic disease can be cured. While the costs of the three biological agents—cetuximab, pani-tumumab, and bevacizumab—are not insignificant, the clinical evidence is now well-established that their incorporation with cytotoxic chemo-
therapy regimens in the neoadjuvant and conversion settings has greatly facilitated curative resection of liver-limited metastatic disease. However, further improvements are needed to enhance the clinical outcome of the remaining 60% to 70% of patients. Further refinements in whole-body and hepatic imaging should provide for a more accurate selection of the subset of patients who would benefit most from resection and would identify the presence of minimal residual disease following surgery. Finally, clinical trials are needed to develop novel cytotoxic agents and biologic/targeted agents that can be used in both the preoperative and postoperative settings to reduce the risk of local and systemic recurrence.
Declaration of InterestNone.
References1. Siegel R, Ward E, Brawley O, Jemal A. Cancer Statistics,
2011. Ca Cancer J Clin 2011;61:212–236.
2. Weiss L, Grundmann E, Torhorst J, et al. Haematogenous
metastatic patterns in colonic carcinoma: an analysis of
1541 necropsies. J Pathol 1986;150:195–203.
3. Manfredi S, Bouvier AM, Lepage C, et al. Incidence
and patterns of recurrence after resection for cure of
colonic cancer in a well defined population. Br J Surg
2006;93:1115–1122.
4. Manfredi S, Lepage C, Hatem C, et al. Epidemiology and
management of liver metastases from colorectal cancer.
Ann Surg 2006;244:254–259.
5. Labianca R, Beretta GD, Kildani B, et al. Colon cancer.
Crit Rev Oncol Hematol 2010;74:106–133.
6. Sundermeyer ML, Meropol NJ, Rogatko A, et al. Chang-
ing patterns of bone and brain metastases in patients with
colorectal cancer. Clin Colorectal Cancer 2005;5:108–113.
7. Wagner JS, Adson MA, Van Heerden JA, et al. The
natural history of hepatic metastases from colorectal
cancer. A comparison with resective treatment. Ann Surg
1984;199:502–508.
8. Scheele J, Stang R, Tendorf-Hofmann A, Paul M.
Resection of colorectal liver metastases. World J Surg
1995;19:59–71.
9. van Ooijen B, Wiggers T, Meijer S et al. Hepatic resec-

292 Medical Progress June 2012
In focus
tions for colorectal metastases in the Netherlands. A
multiinstitutional 10-year study. Cancer 1992;70:28–34.
10. Fortner JG, Silva JS, Golbey RB, et al. Multivariate
analysis of a personal series of 247 consecutive patients
with liver metastases from colorectal cancer. I. Treatment
by hepatic resection. Ann Surg 1984;199:306–316.
11. Hugh TJ, Kinsella AR, Poston GJ. Management strate-
gies for colorectal liver metastases—Part I. Surg Oncol
1997;6:19–30.
12. Ekberg H, Tranberg KG, Andersson R et al. Determi-
nants of survival in liver resection for colorectal secondar-
ies. Br J Surg 1986;73:727–731.
13. Charnsangavej C, Clary B, Fong Y, et al. Selection
of patients for resection of hepatic colorectal metas-
tases: expert consensus statement. Ann Surg Oncol
2006;13:1261–1268.
14. Pwint TP, Midgley R, Kerr DJ. Regional hepatic chemo-
therapies in the treatment of colorectal cancer metastases
to the liver. Semin Oncol 2010;37:149–159.
15. Alexander HR, Jr, Bartlett DL, Libutti SK, et al.
Analysis of factors associated with outcome in patients
undergoing isolated hepatic perfusion for unresectable
liver metastases from colorectal center. Ann Surg Oncol
2009;16:1852–1859.
16. Idrees K, Bartlett DL. Robotic liver surgery. Surg Clin
North Am 2010;90:761–774.
17. Nguyen KT, Gamblin TC, Geller DA. World review of
laparoscopic liver resection 2,804 patients. Ann Surg
2009;250:831–841.
18. Sarpel U, Bonavia AS, Grucela A, et al. Does anatomic
versus nonanatomic resection affect recurrence and sur-
vival in patients undergoing surgery for colorectal liver
metastasis? Ann Surg Oncol 2009;16:379–384.
19. Berber E, Siperstein A. Local recurrence after laparo-
scopic radiofrequency ablation of liver tumors: an analysis
of 1032 tumors. Ann Surg Oncol 2008;15:2757–2764.
20. Wu YZ, Li B, Wang T, et al. Radiofrequency ablation vs
hepatic resection for solitary colorectal liver metastasis:
a meta-analysis. World J Gastroenterol 2011;17:4143–
4148.
21. Gomez D, Cameron IC. Prognostic scores for colorectal
liver metastasis: clinically important or an academic exer-
cise? HPB (Oxford) 2010;12:227–238.
22. Simmonds PC, Primrose JN, Colquitt JL, et al. Surgical
resection of hepatic metastases from colorectal cancer:
a systematic review of published studies. Br J Cancer
2006;94:982–999.
23. Rees M, Tekkis PP, Welsh FK, et al. Evaluation of
long-term survival after hepatic resection for metastatic
colorectal cancer: a multifactorial model of 929 patients.
Ann Surg 2008;247:125–135.
24. Charnsangavej C, Clary B, Fong Y, et al. Selection
of patients for resection of hepatic colorectal metas-
tases: expert consensus statement. Ann Surg Oncol
2006;13:1261–1268.
25. Shoup M, Gonen M, DAngelica M, et al. Volu-
metric analysis predicts hepatic dysfunction in patients
undergoing major liver resection. J Gastrointest Surg
2003;7:325–330.
26. Chua TC, Saxena A, Chu F, et al. Predictors of cure
after hepatic resection of colorectal liver metastases: an
analysis of actual 5- and 10-year survivors. J Surg Oncol
2011;103:796–800.
27. Hemming AW, Reed AI, Howard RJ, et al. Preoperative
portal vein embolization for extended hepatectomy. Ann
Surg 2003;237:686–691.
28. Adam R, Laurent A, Azoulay D, et al. Two-stage
hepatectomy: a planned strategy to treat irresectable liver
tumors. Ann Surg 2000;232:777–785.
29. Adam R, Wicherts DA, de Haas RJ, et al. Patients with
initially unresectable colorectal liver metastases: is there
a possibility of cure? J Clin Oncol 2009;27:1829–1835.
30. Ferrarotto R, Pathak P, Maru D, et al. Durable complete
responses in metastatic colorectal cancer treated with che-
motherapy alone. Clin Colorectal Cancer 2011;10:178–
182.
31. Wein A, Riedel C, Bruckl W, et al. Neoadjuvant treat-
ment with weekly high-dose 5-fluorouracil as 24-hour
infusion, folinic acid, and oxaliplatin in patients with
primary resectable liver metastases of colorectal cancer.
Oncology 2003;64:131–138.
32. Gruenberger B, Tamandl D, Schueller J, et al. Beva-
cizumab, capecitabine, and oxaliplatin as neoadjuvant
therapy for patients with potentially curable metastatic
colorectal cancer. J Clin Oncol 2008;26:1830–1835.
33. Nordlinger B, Sorbye H, Glimelius B, et al: Perioperative
chemotherapy with FOLFOX4 and surgery versus surgery
alone for resectable liver metastases from colorectal
cancer (EORTC Intergroup trial 40983): a randomised
controlled trial. Lancet 2008;371:1007–1016.
34. Adam R, Pascal G, Castaing D, et al. Tumor progres-
sion while on chemotherapy: a contraindication to liver
resection for multiple colorectal metastases? Ann Surg
2004;240:1052–1061.
35. Tanaka K, Takakura H, Takeda K, et al. Importance of
complete pathologic response to prehepatectomy chemo-
therapy in treating colorectal cancer metastases. Ann Surg
2009;250:935–942.
36. Adam R, Wicherts DA, de Haas RJ, et al. Complete
pathologic response after preoperative chemotherapy for
colorectal liver metastases: myth or reality? J Clin Oncol
2008;26:1635–1641.
37. Auer RC, White RR, Kemeny NE et al. Predictors of a
true complete response among disappearing liver metas-
tases from colorectal cancer after chemotherapy. Cancer
2010;116:1502–1509.
38. Bismuth H, Adam R, Levi F, et al. Resection of non-
resectable liver metastases from colorectal cancer after
neoadjuvant chemotherapy. Ann Surg 1996;224:509–520.
39. Adam R, Avisar E, Ariche A, et al. Five-year survival
following hepatic resection after neoadjuvant therapy for
nonresectable colorectal. Ann Surg Oncol 2001;8:347–
353.
40. Adam R, Delvart V, Pascal G, et al. Rescue surgery for
unresectable colorectal liver metastases downstaged by
chemotherapy: a model to predict long-term survival. Ann
Surg 2004;240:644–657.
41. Folprecht G, Grothey A, Alberts S, et al. Neoadjuvant
treatment of unresectable colorectal liver metastases:
correlation between tumour response rate and resections
rates. Ann Oncol 2005;16:1311–1319.
42. Alberts SR, Horvath WL, Sternfeld WC, et al. Oxalipla-
tin, fluorouracil, and leucovorin for patients with unresect-
able liver-only metastases from colorectal cancer: a North
Central Cancer Treatment Group phase II study. J Clin
Oncol 2005;23:9243–9249.
43. Barone C, Nuzzo G, Cassano A, et al. Neoadjuvant
treatment of unresectable liver disease with irinotecan and
5-fluorouracil plus folinic acid in colorectal cancer patients.
Br J Cancer 2007;97:1035–1039.
About the AuthorsDavid LBartlett is chief of theDivisionof SurgicalOncology, Department of Surgery, and staff inves-tigator of the Molecular Therapeutics and Drug Discovery Research Program, University of Pitts-burgh Cancer Institute, University of PittsburghSchool of Medicine, Pittsburgh. Edward Chu is chief of the Division of Hematology-Oncology, Depart-ment of Medicine and Pharmacology & Chemical Biology, and leader of the Molecular Therapeutics andDrugDiscoveryResearchProgram,UniversityofPittsburghCancerInstitute,UniversityofPittsburghSchoolofMedicine,Pittsburgh,Pennsylvania,USA.
© 2012 UBM Medica LLC. Initially published in
Oncology 2012;26(3):266–275. Reprinted with
permission.
Answers to questions on page 269: 1. F, 2. T, 3. T, 4. T, 5. F
A complete list of references can be obtained upon
request from the editor.

DRuG Profile
Medical Progress June 2012 293
Peer Reviewed
Roflumilast, a novel phosphodiesterase-4 inhibitor, has demonstrated efficacy in improving lung function in
severe chronic obstructive pulmonary disease (COPD). Its anti-inflammatory properties appear to address
COPD’s underlying chronic inflammatory process, and it has been shown to improve the forced expiratory
volume in the first second of expiration and quality of life, and reduce exacerbations, especially in the chronic
bronchitis subgroup.
Roflumilast—Last But Not Least? TanTzeLee,MBChB(Edin),MRCP(UK),FRCP(Edin);OngKianChung,MBBS,MRCP(UK),FRCP(Edin),FCCP(USA)
Introduction
Chronic obstructive pulmonary disease (COPD) is an increasing problem in the world today, with an
estimated 64 million having moderate to severe disease in 2004.1 By 2020, it is estimated to be ranked fifth worldwide in terms of burden of disease based on a World Bank/World Health Organization study, and is expected to become the third ranked cause of death by then.2 The predominant cause is cigarette smoking, although exposure to biomass and occupational pollution also play a role, in some cases significantly.3
This chronic inflammatory disease of the lungs and airways is a major cause of morbidity and mortality.4 It is well recognized to be a progressive chronic inflammatory disease, and early detection, smoking cessation and therapeutic intervention are key to optimizing COPD management.5
Until recently, there has been no available treatment that alter the progression of COPD, and current therapies have, to date, focused on symptom relief and improvement of quality of life (QOL).6 Inhaled short-acting β2-agonists, long-acting
β2-agonists (LABA), short-acting muscarinic antagonists (SAMA), long-acting muscarinic antagonists, and LABA–inhaled corticosteroids (ICS) combinations have all been used to manage COPD.
Theophylline has been used for
Chronic obstructive pulmonary disease is an increasing health problem, the predominant cause of which is cigarette smoking.

DRuG Profile
294 Medical Progress June 2012
over 100 years in clinical practice. Concerns about its narrow therapeutic window and drug interactions can limit its use in COPD.7 A weak bron-chodilator, it nevertheless remains popular because it is inexpensive and widely available.
Background
Cyclic adenosine monophosphate (cAMP) plays an important part in regulating inflammatory cell activity and is degraded by the phosphodies-terase enzymes. The phosphodiesterase 4 (PDE4) enzyme is the main cAMP-metabolizing enzyme in inflammatory cells, and its inhibition leads to accu-mulation of cAMP levels in the cell, which reduces the cell’s inflammatory activity.
Pharmacology
PDE4 is a primary regulator in most inflammatory and immune cells. By inhibiting PDE4, various pro-inflam-matory processes are suppressed, and this have shown, in some studies, to benefit animal models of pulmonary inflammation.8–11
PDE4 inhibitors have demon-strated many anti-inflammatory properties, including inhibition of inflammatory mediators and immune cell activation.12 Roflumilast, together with its active metabolite roflumilast N-oxide, is a potent PDE4 inhibitor (Figure).8
In both animal models and patients with COPD, roflumilast has been shown to suppress inflammatory mediator release, reduce airway inflam-mation, and reduce the neutrophil and eosinophil counts. These outcomes are very promising but did not always correlate with good clinical outcomes for all COPD patients. It would appear that the chronic bronchitis phenotypic group of COPD patients would tend to benefit the most.13
Roflumilast is active orally and has been approved for the treatment of moderate to severe COPD. It is given orally, is highly bioavailable (f = 0.79), bounds extensively to plasma proteins (98.9%), achieves a steady state in 4 days (daily dosing regime), has an elimination half-life of 7 to 25 hours, and is subject to negligible first-past hepatic metabolism. The pharmacokinetic profile is linear and predictable over the dose ranges of 250 to 1,000 µg.
The major metabolite is roflumilast N-oxide by the N-oxidation pathway. This is primarily by the cytochrome P450 isozymes CYP3A4 and CYP1A2. The half-life of roflumilast N-oxide is considerably longer than that of its parent, at approximately 27 hours. This suggests that the pharmacological ability of roflumilast to produce a long-lasting, competitive, 24-hour inhibition of PDE4 is in fact through its metabolite.14–18 Roflumilast N-oxide is finally deactivated and excreted via the renal pathway.
There are no specific contrain-dications except for specific allergy
to roflumilast or its excipients. Care should be taken in patients with moderate to severe hepatic impairment (Child-Pugh B or C) in view of the cytochrome P450 pathways. Data suggest that roflumilast has little adverse interaction with erythromycin, ketoconazole, monte-lukast, digoxin, warfarin, sildenafil, midazolam, and inhaled salbutamol, formoterol and budenoside. Oral magnesium hydroxide was also found not to affect the pharmacokinetics of roflumilast.19–26
Inducers of the cytochrome P450, such as rifampicin, have been shown to significantly affect the efficacy of roflumilast.17 Strong inducers, such as carbamazepine, phenytoin and phe-nobarbital, could potentially limit the efficacy of roflumilast.
The Evidence
The early studies used forced expiratory volume in the first second of expiration (FEV1) and QOL as end points. Rabe et al and Calverley et al found roflumilast to be effective in moderate to severe
Cl
O
F O
O
Cl
NH
N
F
3-(cyclopropylmethoxy)-N-(3,5-dichloropyridin-4-yl)-4-(difluoromethoxy)benzamide;C
17H
14Cl
2F
2N
2O
3; M
r = 403.2
Figure. Chemical structure of roflumilast.

Medical Progress June 2012 295
COPD (M2-107 trial) and severe COPD (M2-112 trial), respectively.27,28
In the former study conducted over a treatment period of 24 weeks, significant improvements in post-bronchodilator FEV1 were found in subjects taking roflumilast 250 or 500 µg as compared with placebo (dif-ference, 74 mL for 250 µg, and 97 mL for 500 µg; P < 0.0001). QOL using the St George’s Respiratory Questionnaire total score was also found to be improved as compared with placebo (-1.6 for 250 µg, and -1.7 for 500 µg).
The latter trial focused on subjects with severe COPD and studied the effect of roflumilast 500 µg daily in these patients for a year. Concomitant ICS were permitted (60% of subjects). The results found improvements in post-bronchodilator FEV1 (39 mL; P = 0.001) and a non-significant reduction of moderate to severe exacerbations.
Subsequent post hoc analysis of M2-112 and its replicate M2-111 demonstrated a significantly reduced exacerbation rate (14.3%; P = 0.026), with the following subgroup of patients benefitting the most: patients with chronic bronchitis (26.2%, P = 0.001), or with high cough (20.9%, P = 0.006) or sputum scores (17.8%, P = 0.03) prior to randomization, or patients receiving concomitant ICS or SAMAs (18.8%, P = 0.014). The finding that roflumilast preferen-tially reduced exacerbations in COPD patients who had characteristics of chronic bronchitis, with or without ICS, led the investigators to craft the design of the subsequent phase III studies to examine the effect of roflumilast on acute exacerbations of COPD.13
Two 12-month studies, M2-124 and M2-125, were pivotal in estab-lishing the therapeutic benefits of roflumilast in severe COPD cases. They were of identical design and compared roflumilast 500 µg daily with placebo, and were different
only in their study population ethnic composition. The subjects were not allowed ICS, and only half used long-acting bronchodilators. There was improvement in pre-bronchodilator FEV1 of 48 mL (P < 0.0001) as well as post-bronchodilator FEV1 of 55 mL (P < 0.0001). There was also a relative risk reduction of 17% in rate of exac-erbations (P = 0.0003), which was greatest in moderate exacerbations. The pooled analyses of M2-124 and M2-125 by Calverley et al revealed that the mean rate of moderate and severe exacerbations were significantly lower in patients receiving roflumilast as compared with placebo, be it with concomitant inhaled LABA (20.7%, P = 0.011), SAMA (13.1%, P = 0.0458), or previous ICS (19.3%, P = 0.0038).29
Two further 6-month studies provided the evidence for roflumilast use as an add-on to long-acting bron-chodilator therapy. M2-127 studied the concomitant use with salmeterol and M2-128 with tiotropium. The tiotropium subjects recruited were more symptomatic, and in both studies the subjects were randomized to roflumilast 500 µg or placebo added on to inhaled salmeterol or tiotropium. The salmeterol group showed improved pre- and post-bronchodilator FEV1 of 49 mL and 60 mL (both P < 0.0001), respec-tively, whereas the tiotropium group similarly showed improvement for both pre- and post-bronchodilator FEV1 of 80 mL and 81 mL (both P < 0.0001), respectively.30
Safety
The most common adverse effects encountered with roflumilast are gas-trointestinal, with diarrhoea (9%) being the most common, followed by nausea (5%) and decreased appetite (3%). Weight loss (12%) was also commonly reported. The rates of car-diovascular events were similar in both
the treatment and placebo groups in pooled safety studies, and there were 6% of roflumilast subjects exhibiting psychiatric disorders compared with 3% in those receiving placebo. There remain concerns about the incidence of completed suicides in the COPD safety pool, although none have been iden-tified as being related to roflumilast.
Conclusion
COPD is a multiorgan and multisystem disease. It not only involves the airways and lung parenchyma but also has effects far removed from its origins in the respiratory system. The inflam-matory process that accompanies COPD often progresses even when smoking has ceased, and therapies in the past were unable to address this.
Historically, the drugs used to manage COPD have primarily been bronchodilators and, in cases of recurrent exacerbations, ICS. Prior to the arrival of roflumilast, these therapies did not adequately address the issue of inflammatory processes in
"The mainstay ofthe benefits from
roflumilast use in COPDis through its unique
anti-inflammatoryeffect"

DRuG Profile
296 Medical Progress June 2012
COPD. The mainstay of the benefits from roflumilast use in COPD is through its unique anti-inflammatory effect. Even though it does not have a direct bronchodilator effect, studies have shown that FEV1 improves following regular administration of roflumilast.
Many questions remain unan-swered. Long-term survival studies are needed to address whether or not the benefits of roflumilast are only confined to the severe-stage chronic bronchitis phenotype cohort, or whether it extends to other phenotypes and severity stage and under what conditions.
Would roflumilast be the panacea for COPD, by suppressing inflam-mation and reducing mortality as well as the rate of decline of FEV1, ie, lung function? Only time will tell.
References1. World Health Organization. The Global Burden of Disease:
2004 Update. Geneva: World Health Organization; 2008.
2. Murray CJL, Lopez AD. The Global Burden of Disease.
Cambridge, MA: Harvard University Press; 1996.
3. Salvi S, Barnes PJ. Is exposure to biomass smoke the big-
gest risk factor for COPD globally? Chest 2010;138;3–6.
4. Global Initiative for Chronic Obstructive Lung Disease.
Global strategy for the diagnosis, management and pre-
vention of chronic obstructive pulmonary disease. http://
www.goldcopd.org/Guidelines/guidelines-resources.html.
Accessed 30 March 2012.
5. Price D, Freeman D, Cleland J, Kaplan A, Cerasoli F. Earlier
diagnosis of COPD in primary care and earlier treatment.
Prim Care Resp J 2011;20:15–22.
6. National Clinical Guideline Centre. (2010) Chronic
obstructive pulmonary disease: management of chronic
obstructive pulmonary disease in adults in primary care
and secondary care. London: National Clinical Guideline
Centre. Available from: http://guidance.nice.org.uk/CG101
/Guidance/pdf/English.
7. Ramsdell J. Use of theophylline in the treatment of COPD.
Chest 1995;107(5 Suppl):206S–209S.
8. Hatzelmann A, Schudt C. Anti-inflammatory and immuno-
modulatory potential of the novel PDE4 inhibitor roflumilast
in vitro. J Pharmacol Exp Ther 2001;297:267–279.
9. Bundschuh DS, Eltze M, Barsig J, Wollin L, Hatzelmann
A, Beume R. In vivo efficacy in airway disease models of
roflumilast, a novel orally active PDE4 inhibitor. J Pharmacol
Exp Ther 2001;297:280–290.
10. Martorana PA, Beume R, Lucattelli M, Wollin L, Lun-
garella G. Roflumilast fully prevents emphysema in mice
chronically exposed to cigarette smoke. Am J Respir Crit Care
Med 2005;172:848–853.
11. Grootendorst DC, Gauw SA, Verhoosel RM, et al. Reduc-
tion in sputum neutrophil and eosinophil numbers by the
PDE4 inhibitor roflumilast in patients with COPD. Thorax
2007;62:1081–1087.
12. Lipworth BJ. Phosphodiesterase-4 inhibitors for
asthma and chronic obstructive pulmonary disease. Lancet
2005;365:167–275.
13. Rennard SI, Caverley PM, Goehring UM, Bredenbröker D,
Martinez FJ. Reduction of exacerbations by the PDE4 inhibi-
tor roflumilast – the importance of defining different subsets
of patients with COPD. Respir Res 2011;12:18.
14. Bethke TD, Böhmer GM, Hermann R, et al. Dose-propor-
tional intraindividual single- and repeated-dose pharmacoki-
netics of roflumilast, an oral, once-daily phosphodiesterase 4
inhibitor. J Clin Pharmacol 2007;47:26–36.
15. Hauns B, Hermann R, Hünnemeyer A, et al. Investigation
of a potential food effect on the pharmacokinetics of roflu-
milast, an oral, once-daily phospho-diesterase 4 inhibitor,
in healthy subjects. J Clin Pharmacol 2006;46:1146–1153.
16. Neville KA, Szefler SJ, Abdel-Rahman SM, et al. Single-
dose pharmacokinetics of roflumilast in children and adoles-
cents. J Clin Pharmacol 2008;48:978–985.
17. Nassr N, Hüennemeyer A, Herzog R, et al. Effects
of rifampicin on the pharmacokinetics of roflumilast and
roflumilast N-oxide in healthy subjects. Br J Clin Pharmacol
2009;68:580–587.
18. David M, Zech K, Seiberling M, Weimar C, Bethke
TD. Roflumilast, a novel, oral, selective PDE4 inhibitor,
shows high absolute bioavailability. J Allergy Clin Immunol
2004;113:S220–S221
19. Lahu G, Hüennemeyer A, von Richter O, et al. Effect of
single and repeated doses of ketoconazole on the phar-
macokinetics of roflumilast and roflumilast N-oxide. J Clin
Pharmacol 2008;48:1339–1349.
20. Nassr N, Lahu G, Hünnemeyer A, et al. Magnesium
hydroxide/aluminium hydroxide-containing antacid does
not affect the pharmacokinetics of the targeted phos-
phodiesterase 4 inhibitor roflumilast. J Clin Pharmacol
2007;47:660–666.
21. Nassr N, Lahu G, von Richter O, et al. Lack of a phar-
macokinetic interaction between steady-state roflumilast
and single-dose midazolam in healthy subjects. Br J Clin
Pharmacol 2007;63:365–370.
22. Bethke TD, Giessmann T, Westphal K, et al. Roflumilast, a
once-daily oral phosphodiesterase 4 inhibitor, lacks relevant
pharmacokinetic interactions with inhaled salbutamol when
co-administered in healthy subjects. Int J Clin Pharmacol Ther
2006;44:572–579.
23. Böhmer GM, Nassr N, Wenger M, et al. The targeted oral,
once-daily phosphodiesterase 4 inhibitor roflumilast and the
leukotriene receptor antagonist montelukast do not exhibit
significant pharmacokinetic interactions. J Clin Pharmacol
2009;49:389–397.
24. Hermann R, Siegmund W, Giessmann T, et al. The
oral, once-daily phosphodiesterase 4 inhibitor roflumilast
lacks relevant pharmacokinetic interactions with inhaled
budesonide. J Clin Pharmacol 2007;47:1005–1013.
25. Lahu G, Hüennemeyer A, Herzog R, et al. Effect of
repeated dose of erythromycin on the pharmacokinetics of
roflumilast and roflumilast N-oxide. Int J Clin Pharmacol Ther
2009;47:236–245.
26. von Richter O, Lahu G, Hüennemeyer A, Herzog R, Zech
K, Hermann R. Effect of fluvoxamine on the pharmacokinetics
of roflumilast and roflumilast N-oxide. Clin Pharmacokinet
2007;46:613–622.
27. Rabe KF, Bateman ED, O’Donnell D, Witte S, Bredenbro-
ker D, Bethke TD. Roflumilast—an oral anti-inflammatory
treatment for chronic obstructive pulmonary disease: a ran-
domised controlled trial. Lancet 2005;366:563–571.
28. Calverley PM, Sanchez-Toril F, McIvor A, Teichmann P,
Bredenbroeker D, Fabbri LM. Effect of 1-year treatment with
roflumilast in severe chronic obstructive pulmonary disease.
Am J Respir Crit Care Med 2007;176:154–161.
29. Calverley PMA, Rabe KF, Goehring U-M, et al; M2-124
and M2-125 study groups. Roflumilast in symptomatic
chronic obstructive pulmonary disease: two randomised clini-
cal trials. Lancet 2009;374:685–694.
30. Fabbri LM, Calverley PMA, Izquierdo-Alonso JL, et al;
M2-127 and M2-128 study groups. Roflumilast in moderate-
to-severe chronic obstructive pulmonary disease treated with
long-acting bronchodilators: two randomised clinical trials.
Lancet 2009;374:695–703.
About the AuthorsDrTanisGeneralPractitionerandPrincipalPartnerof a private practice; HonoraryTreasurer of theCollege of Family Physicians Singapore; Visiting Consultant to the Department of Medicine at the National University Hospital; Vice-President ofthe Chronic Obstructive Pulmonary Disease As-sociation (Singapore); and Clinical Preceptor and Adjunct Assistant Professor at the Duke-NUSGraduate Medical School, Singapore. Dr Ongis Specialist in respiratory medicine in private practice at the Mount Elizabeth Medical Centre;President of the Chronic Obstructive Pulmonary Disease Association (Singapore); and National Leader in Singapore of the Global Initiative forChronicObstructiveLungDisease.

Medical Progress June 2012 297
Continuing Medical Education Take the challenge, test your knowledge
1 SKP
Continuing Medical Education Take the challenge, test your knowledge
The Ravages of Bed Rest: Rehabilitation After
Prolonged ImmobilityShari Parker, BSc (Med) Hons, MBBS (Hons), FAFRM (RACP); Robert Rollinson, BSW; Michelle Gilad, MSW; Kate Holmes, BApplSc Physio;
Nicky Sygall, BA (Hons), M Clin Psych, MAPS, MAACBT; Steven Faux, MBBS, BA, FRACGP, FAFRM, FFPMANZCA
The patient complains of weakness and the relative’s and the
GP’s intuition is that the patient is not the same as before their
hospitalization. Is recovery just a matter of time or will the
changes be permanent? Is there something that can be done?
Debility, also called ‘deconditioning’, is caused by prolonged immobility or bed rest and is the third most common reason for admission of patients to Australian rehabilitation units, after fractured femur and stroke. Nationally, over 5,000 patients per year are treated in rehabilitation hospitals for debility;1 however, far more in the community will be seen by GPs.
This article reviews the physiological effects of bed rest, the approaches of allied health professionals to recondi-tioning and how GPs can coordinate rehabilitation in the community using the ‘Team Care Arrangements’ in the Medicare Schedule.
Physiological Effects of bed Rest
A variety of conditions can lead to hos-pitalisation, bed rest and immobility (Table 1) and physiological changes can start to occur after as little as two days of being in bed. Common patient complaints following a period of hos-pitalization are shown in Table 2; these ‘side effects’ of prolonged immobility occur in up to 40% of elderly hospi-talised people.2
Long after they have recovered from the original cause of admission, patients can continue to experience symptoms of deconditioning and functional decline. They may never return to their premorbid level of functioning.
Musculoskeletal Effects
Muscle WastingWith complete bed rest, up to 1.5% of muscle strength is lost per day. After one week of bed rest, up to 20% of strength is lost. This loss is greatest during the first week and peaks at 40% with prolonged bed rest. The loss of strength is associated with wasting of the muscles. Weight-bearing muscles of the legs are particularly affected.
It can take up to three times as long to regain strength as it took to lose it.
Contractures During periods of bed rest, contractures can develop in the joints and limit their motion. During immobility, the number of collagen crosslinks increases in the connective tissue around joints and the muscles shorten. This process
Peer-Reviewed
Table 1. Common causes of prolonged bed rest*Pulmonary infectionExacerbation of COPDConfusion following sepsisFalls with fracture or soft tissue injuryArrhythmiasCellulitisUrinary tract infectionCardiac failureOsteomyelitisValvular repairAbdominal surgery with complicationsUrological surgery with complicationsENT surgery with complicationsEndoscopic procedures with complicationsSkin ulcer and skin graftingPulmonary surgeryKidney failureOverdose or poisoning
*Associated with hospital stays in excess of five days in patients over the age of 60 years.
Table 2. Common symptoms of deconditioningFatigueDizzinessBreathlessnessDepressionConfusionFallingNot eatingIncontinence Poor coping with usual lifestyle

298 Medical Progress June 2012
Continuing Medical EducationContinuing Medical Education
can start to occur after a week, and is eventually irreversible. Typically, joint flexion contractures occur at the hip, knee and shoulder, and affect walking and activities of daily living.
OsteoporosisBed rest and the absence of weight-bearing increases the risk of osteoporosis and fracture. After 12 weeks of bed rest, bone density is reduced by up to 45%.3 Bisphosphonates are the drugs of choice to both prevent and treat this condition.
Cardiovascular Effects
Postural HypotensionPostural hypotension can occur within three days of bed rest and can lead to falls. On standing from a lying position, blood pools in the legs. Normally this is compensated for by vasoconstriction and a rise in heart rate and in systolic blood pressure, but following bed rest, these compensations are lost.
TachycardiaWith immobility the patient’s resting heart rate increases by about one beat per minute every two days for up to four weeks. Resting stroke volume declines, mainly due to a reduction in blood volume caused by bed rest. With submaximal exercise fol lowing
bed rest, the heart rate response is increased, and the cardiac output and maximum oxygen uptake are reduced. This results in poorer aerobic fitness and the patient fatigues more easily with exertion.
DVT and PEWith bed rest, the patient’s plasma volume decrea ses and there is a relative increase in haematocrit and blood viscosity. As such, the bedridden person is at risk of deep vein thrombosis (DVT) and pulmonary embolism (PE). The use of fractionated heparin, compression stockings and bed exercises are the mainstay of prevention for DVT and PE.
Respiratory Effects
There is also an increased risk of pneumonia and atelectasis. Lying flat, it is harder to expand the lungs because of the mech anical disadvantage, so further blood pools in the thorax, leading to decreased lung volume. Cough is impaired due to weak abdominal muscles, so secretions pool in the back part of the lungs and the front segments become relatively dry. This results in ineffective mucociliary clearing mechanisms.
Dermatological Effects
Immobility leads to an increase in capillary pressure over bony prominences like the heels, sacrum, occiput and greater troch anters. This leads to a risk of decubitus ulcers and subcutaneous bursitis. This risk is even greater when combined with intrinsic factors like sensory impairment, confusion, malnutrition, incontinence and being underweight. Immobility also leads to dependent oedema, with an increased risk of cellulitis.
Metabolic and Endocrine Effects
While the patient’s overall weight may remain static, immobility causes a relative reduction in lean mass and a relative increase in body fat. Urinary nitrogen and calcium loss occurs and parallels muscle and bone loss; while potassium, chloride and zinc loss also occur.3 Sodium loss is associated with a diuresis, especially in the elderly, which can contribute to incontinence.
Diabetes may become apparent in the immobile person. Impaired glucose tolerance occurs with bed rest due to reduced insulin sensitivity in peripheral muscle.2
Genitourinary Effects
Urinary stasis, which leads to infection, occurs with bed rest because it is harder to fully empty the bladder when lying flat. Further, increased excretion of urinary calcium increases the risk of bladder and renal calculi.
Incontinence due to bed rest is also common, particularly in the elderly hospitalized patient. The incontinence is often multifactorial as disorientation, confusion and decreased mobility can all contribute.
Gastrointestinal Effects
Constipation is often seen in bedridden patients. This is due to a combination of factors including decreased mobility, decreased fluid intake, decreased peristalsis and incomplete bowel evac-uation as a result of being in bed.
Neurological Effects
Pressure neuropathies, particularly of the ulnar and peroneal nerve, can occur with bed rest, as can critical illness polyneuromyopathy (CINM). CINM
”Constipation is often seen in bedridden
patients“
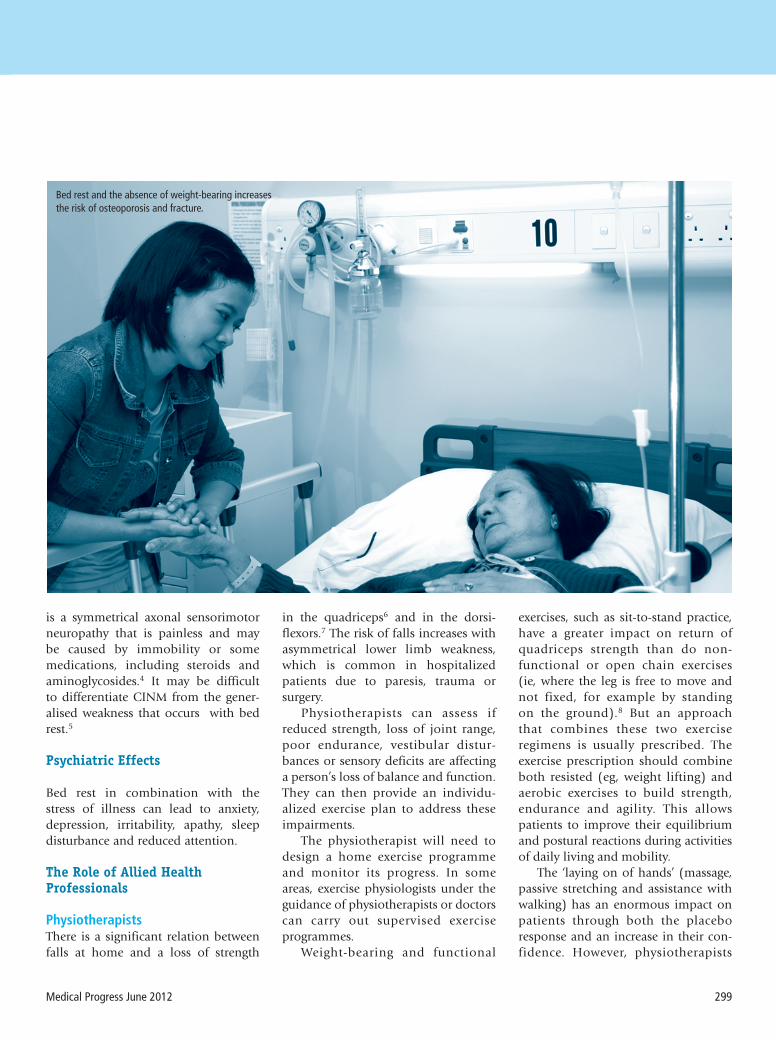
Medical Progress June 2012 299
is a symmetrical axonal sensorimotor neuropathy that is painless and may be caused by immobility or some medications, including steroids and aminoglycosides.4 It may be difficult to differentiate CINM from the gener-alised weakness that occurs with bed rest.5
Psychiatric Effects
Bed rest in combination with the stress of illness can lead to anxiety, depression, irritability, apathy, sleep disturbance and reduced attention.
The Role of Allied Health Professionals
PhysiotherapistsThere is a significant relation between falls at home and a loss of strength
in the quadriceps6 and in the dorsi-flexors.7 The risk of falls increases with asymmetrical lower limb weakness, which is common in hospitalized patients due to paresis, trauma or surgery.
Physiotherapists can assess if reduced strength, loss of joint range, poor endurance, vestibular distur-bances or sensory deficits are affecting a person’s loss of balance and function. They can then provide an individu-alized exercise plan to address these impairments.
The physiotherapist will need to design a home exercise programme and monitor its progress. In some areas, exercise physiologists under the guidance of physiotherapists or doctors can carry out supervised exercise programmes.
Weight-bearing and functional
exercises, such as sit-to-stand practice, have a greater impact on return of quadriceps strength than do non-functional or open chain exercises (ie, where the leg is free to move and not fixed, for example by standing on the ground).8 But an approach that combines these two exercise regimens is usually prescribed. The exercise prescription should combine both resisted (eg, weight lifting) and aerobic exercises to build strength, endurance and agility. This allows patients to improve their equilibrium and postural reactions during activities of daily living and mobility.
The ‘laying on of hands’ (massage, passive stretching and assistance with walking) has an enormous impact on patients through both the placebo response and an increase in their con-fidence. However, physiotherapists
Bed rest and the absence of weight-bearing increases the risk of osteoporosis and fracture.

300 Medical Progress June 2012
Continuing Medical EducationContinuing Medical Education
will often caution that overuse of the ‘hands-on’ approach may encourage dependence on passive therapies and discourage exercise, which is the mainstay of treatment for post-immo-bility reconditioning.
Occupational Therapists
The occupational therapist (OT) focuses on functional return and will teach safe
transfers from bed to chair, chair to chair and toilet, and in and out of a car seat. Repetition of activities of daily living are the mainstay of therapy and OTs will also undertake a home visit to identify whether the installation of rails and other home modifications can make the home safer and more accessible and minimize falls.
The OT will also often accompany patients to assess whether they are safe
to take public transport, go shopping or cook for themselves. This is often important for those with cognitive impairment who live in less than ideal settings (eg, cluttered homes, caravans, homes in disrepair) or who have had difficulties in leaving the home. OTs can also advise carers on safe manual handling techniques; for example, for transfers or showering.
If a patient has an upper limb injury or reduced dexterity of the hands, OTs can design exercise programmes for the hand and also offer assistive devices (eg, tap turners, modified cutlery and kitchen implements) which can allow the patient to be independent in many activities of daily living.
The interaction between the phys-iotherapist and the OT can make a signi ficant difference to the efficacy of both therapies. Co-ordination is the key to successful rehabilitation.
PsychologistsCognitive behavioural therapy as undertaken by a trained psychologist (with a Masters Degree in Clinical Psychology) can have a significant impact in minimizing falls and treating depression and anxiety. Also, collabo-ration with the physiotherapists can assist patients who have become fearful of exercising.
”Co-ordination is the key to successful
rehabilitation“
The occupational therapist (OT) focuses on functional return and will teach safe transfers
from bed to chair, chair to chair and toilet, and in and out of a car seat.
Medical Progress June 2012 301
Fear of Falling Since most falls leading to fracture occur outdoors, it is understandable that people who fear falling may avoid outdoor activity. Fear of falling limits functional recovery after surgery for hip fracture perhaps more than pain or depression. It is a predictor of falls themselves9 and is associated with lower life satisfaction and depressed mood.
Education about falls risk may not be sufficient to reduce anxiety and the rate of falls. Psychological treatment should emphasize the value of a realistic and adaptive approach to activities of daily living and community participation.10 Graduated exposure covering a broad domain of activities, supported by cognitive behavioural therapy, will address anxiety and depression. Low levels of optimism and perceived control con-tribute to the fear of falls, and focusing on these feelings may be helpful.
Treatment for DepressionThe rate of depression among older people who have recently experienced significant illness requiring hospitali-sation is about 38%, and the depression can persist for a significant period. Effective psychological treatments can include revers ing depressive thinking habits, improving coping skills, rein-troducing rewarding activities and improving relationships.11
Social Workers
Following hospitalization some pat- ients may require permanent support with aspects of their personal care, domestic duties or managing their med-ication. There are frequently financial, emotional and social concerns that social workers are trained to address with families.
Services for CarersCarers run the risk of exhausting them-selves by attempting to provide care without adequate assistance. The gov-ernment is committed to assisting older people to stay in their own homes and currently fund programmes such as Home Care and Community Aged Care Packages (CACP), and services such as Meals on Wheels. These services can relieve some of the pressure on carers.
Home Care services may be provided in the person’s house up to three times a week to assist with a variety of tasks including daily chores, personal care, meal preparation, laundry and/or domestic assistance.
Community Aged Care Packages offer a planned and managed package of ser vices that are designed to meet the individual needs of the person. Community Aged Care Packages are coordinated by a specialist and provide assistance with physiotherapy, occupa-tional therapy and nursing, as well as personal and domestic care.
Respite care offers the opportunity for the carer and the person being cared for to have a break. This may be for a few hours, a day or a few weeks. Day care respite is often provided at day care centres, community centres
and some residential aged care homes. In some cases a Transition Care
Programme is organized by the hospital on discharge to provide reha-bilitation in the patient’s home. The programme usually lasts for 12 weeks, but may be able to be extended for a further six weeks in some cases. To be eligible, patients must be over 65 years of age, an inpatient of a hospital and have an assessment by an Aged Care Assessment Team.
Social IsolationSocially isolated patients, unlike other patients, do not have family members or many social supports on which to rely. They may need to be connected to transport services, such as community transport and/or day care centres, which may promote social activities. The culture and background of a person is important to keep in mind and many ethnic communities offer support services for isolated members.
The GP’s Role
Patients affected by deconditioning after a period of bed rest may present with a relative, a carer or alone, com-plaining of fatigue, falls, pain or simply a loss of independence. ‘I can’t do as much as I used to’, ‘I won’t drive yet’ and ‘I haven’t been able to leave the house since I left hospital’ are common complaints from patients. The carer or relative might say that the patient needs to do more for him or herself or that the patient is sleeping excessively, is not his or her old self or has become fearful of being alone.
As a GP, you are in a position to rule out any intercurrent illnesses, including depression and anxiety, which of course will require a full history, examination and appropriate tests. It is important to note that many patients suffer silent illnesses during
”Respite care offers the opportunity for the carer and the person
being cared for to have a break“

302 Medical Progress June 2012
Continuing Medical Education
necessary. However, if the psychologist feels the patient needs cognitive behavioural therapy for anxiety or depression, or fall anxiety, a Mental Health Care Plan may need to be activated.
Mid-programme ReviewIt is wise to review the patient in your rooms about four to six weeks into the programme to assess whether the goals are being met, and if the patient is being compliant. This community case conference can occur again through a phone link up, with or without the patient in the room.
In some cases, the patient may not be responding due to a hitherto concealed or indolent disease. In this case the patient will need to be re-examined and investigated. However, in most cases the patient will have been progressing well and therapists are able to offer rich and detailed infor-mation on progress and assessment. It is at this stage that a Mental Health Care Plan may need to be activated. Documentation needs to be reviewed, and in some cases the intensity of therapy may need to be increased. If significant problems arise, such as the patient fails to attend, therapy
bed rest, such as stroke, heart disease and infection.
However, in cases where you do not find any obvious cause for the symptoms, you may want to put patients through a rehabilitation programme in the community. In this way you will be able to treat their deconditioning and monitor their pro-gress, clinically and through regular review by therapists and/or in your rooms.
Co-ordinating Rehabilitation in the CommunityRehabilitation is a coordinated multi-disciplinary treatment programme that is goal-oriented. This means that you need to make a plan with the patient and your local allied health profes-sionals about what you want to achieve (Table 3) and in what time frame.
It is important that patients agree to participate, the allied health profes-sionals agree the goals are realistic, and the carers understand that they will be doing less for the patients as they attempt to do more for themselves.
GP Management Plan and Team Care ArrangementWhile the GP may have access to a reh a bi litation physician or geriatrician for inpatient or outpatient rehabili-tation, many may chose to undertake the rehab ilitation in the community using both the GP Management Plan (GPMP) and Team Care Arrangement (TCA) provisions of the Medicare Schedule (item numbers 721 to 731). These items are part of the Enhanced Primary Care Programme, which provides a Medicare rebate for five allied health visits per year. If anxiety or depression is the major component of the patient’s presentation, GPs may decide to add in a Mental Health Care Plan to provide up to 12 episodes of psychological treatment over and
above the original five that could be funded by the Enhanced Primary Care Programme.
Case ConferenceOnce you have decided to start a community based rehabili-tation programme via a Team Care Arrangement, a case conference is needed (Medicare item numbers 740 to 765). This can be via a phone link up with or without the patient in the room. At the case conference the patient’s goals and treatment will be discussed, and the number and type of funded sessions will be decided upon. (For veterans, there is separate and more generous funding for allied health services.) This community case conference forms the beginning of the Team Care Arrangement.
In most cases, three sessions with a physiotherapist, one with an OT and one with a psychologist will be
Table 3. Common goals for rehabilitation after deconditioning• Independentmobilityandstairclimbing• Independenceinactivitiesofdailyliving
(eg, toileting, dressing, showering, cooking, cleaning, driving, shopping, gardening)
• Improvementsinfatigue(usingavisualanalogue scale)
• Improvementsinmood,fearandavoidance behaviour and anxiety*
• Decreaseddependenceonhomeservicesor carers
• Improvedlevelsofparticipation(beingable to leave the home regularly and engage in community or family activities)
• Decreasedfallsrisk• Minimizedcarerstress
* Using the Depression Anxiety and Stress Scale (DASS) of Lovibond et al. Available online: www2.psy.unsw.edu.au/groups/dass
”Rehabilitation is a coordinated
multi disciplinary treatment programme that is goal-oriented“

Medical Progress June 2012 303
About the AuthorDr Parker is a Consultant in Rehabilitation Medicine at Sacred Heart Rehabilitation Service, St Vincent’s Hospital, Sydney, and at Griffith Base Hospital. Mr Rollinson is a Senior Social Worker at Sacred Heart Rehabilitation Service, St Vincent’s Hospital, Sydney. Ms Gilad is a Social Worker at Sacred Heart Rehabilitation Service, St Vincent’s Hospital, Sydney. Ms Holmes is a Senior Physiotherapist at Sacred Heart Rehabilitation Service, St Vincent’s Hospital, Sydney. Ms Sygall is a Clinical Psychologist at the Sacred Heart Rehabilitation Service, St Vincent’s Hospital, Sydney. Dr Faux is a Rehabilitation and Pain Physician and Director of Sacred Heart Rehabilitation Service and St Vincent’s Pain Service, St Vincent’s Hospital, Sydney, NSW.
assessment reveals hidden problems (eg, a home visit may reveal dangerous living conditions, squalor or significant cognitive impairment) or therapists feel the patient cannot manage at home and is unlikely to respond to the treatment, inpatient treatment may be required in a rehabilitation unit.
Mostly, however, the patient is responding, the therapists are opti-mistic and the goals look achievable but might need to be fine-tuned. For example, independent mobility as a goal may need to be changed to inde-pendent mobility with a walking stick.
Final ReviewIn the final case conference, held at 10 to 12 weeks, the same phone link- up occurs and the goals are reviewed. Hopefully they have all been achieved and the patient is set up to continue exercises in the home or is linked up with ongoing community services. In some instances the patient will wish to continue the therapy beyond this time; however, the only way this can be undertaken is by self-funding or referral to public outpatient pro-grammes through the local geriatric or rehabilitation service.
In any case, patients who have undertaken a rehabilitation programme in the com munity should ideally be followed up three to six months later to ensure that they have maintained their achieved goals. It is at this stage that the Team Care Arrangement and GP Management Plan can be reviewed (Medicare items 725 and 727).
Conclusion
The future of hospital care is in flux; over the next 10 years there are likely to be an assortment of programmes to minimize bed rest and hospital length of stay and almost all of these programmes will include an element of
rehabilitation in the community. GPs are poised to be at the helm of these innovations. Medicare support is in place, hospitals are groaning with the current demand and certainly evidence points to the facts that patients are safer being treated at home by well supported care teams.
Teach us to live that we may dread,
Unnecessary time in bed.
Get people up and we may save,
Our patients from an early grave.
— Dr Richard Asher 1965.
References1. Simmonds F, Stevermuer T. The AROC annual report: the
state of rehabilitation in Australia 2006. Aust Health Rev
2008;32(1):85–110.
2. Gillick MR, Serrell NA, Gillick LS. Adverse consequences
of hospitalization in the elderly.
Soc Sci Med 1982;16:1033–1038.
3. Chobanian AV, Lille RD, Tercyak A, et al. The metabolic
and hemodynamic effects of prolonged bed rest in normal
subjects. Circulation 1974;49:551–559.
4. Jarrett SR, Mogelof JS. Critical illness neuropathy:
diagnosis and management. Arch Phys Med Rehabil
1995;76:688–691.
5. Foster CB, Gorga D, Padial C, et al. The develop ment and
validation of a screening instrument to identify hospitalized
medical patient in need of early functional rehabilitation
assessment. Qual Life Res 2004;13:1099–1108.
6. Asakawa Y, Ikezoe T, Hazaki K, Kawano I, Irie S, Kanzaki
H, Aoki N. Relationship between falls and knee extension
strength in the elderly. J Phys Ther Sci 1996;8:45–48.
7. Skelton DA, Kennedy J, Rutherford OM. Explosive power
and asymmetry in leg muscle function in frequent fallers and
non-fallers aged over 65. Age Ageing 2002;31:119–125.
8. Olivetti L, Schurr K, Sherringon C, et al. A novel weight-
bearing strengthening program during rehabilitation of older
people is feasible and improves standing up more than a
non-weight-bearing strengthening program: a randomised
trial. Aust J Physiother 2007; 53:147–153.
9. Friedman S, Munoz B, West SK, Rubin GS, Fried LP. Falls
and fear of falling: which comes first? A longitudinal predic-
tion model suggests strategies for primary and secondary
prevention. J Am Geriatr Soc 2002; 50:1329–1335.
10. Zijlstra GA, van Haastregt JC, van Rossum E, van Eijk JT,
Yardley L, Kempen GI. Interventions to reduce fear of falling
in community-living older people: a systematic review. J Am
Geriatr Soc 2007;55:603–615.
11. Australian Psychological Society 2008. Available online:
http://www.psychology.org.au (accessed July 2008).
© 2009 Medicine Today Pty Ltd. Initially published
in Medicine Today August 2009: 9(8);36–44.
Reprinted with permission.
”Patients who have undertaken a rehabilitation
programme in the com munity should ideally be followed up three to
six months later to ensure that they have maintained
their achieved goals“

This continuing medical education service is brought to you by the Medical Progress Institute, an institute dedicated to CME learning. Read the article ’The Ravages of Bed Rest: Rehabilitation After Prolonged Immobility’ and answer the following questions. Answers are shown at the bottom of this page.
Please answer True or False to the questions below. True False
304 Medical Progress June 2012
CME Questions
CME Article:The Ravages of Bed Rest: Rehabilitation After Prolonged Immobility
1. Physiological changes (deconditioning) can start as soon as two weeks of being restricted to ❏ ❏
bed rest.
2. After one week of bed rest, up to 25% of strength is lost, due to wasting of the muscles. ❏ ❏
3. Postural hypotension can occur within three days of bed rest, and can lead to falls. ❏ ❏
4. Many patients suffer from silent illnesses such as deep vein thrombosis or osteoporosis during ❏ ❏
bed rest.
5. Critical illness polyneuromyopathy (CINM) is a symmetrical axonal sensorimotor neuropathy that is ❏ ❏
painless and may be caused by immobility, and it may be difficult to differentiate CINM from the generalized weakness that results from bed rest.
6. The risk of falls increases with asymmetrical lower-limb weakness, which is common in hospitalized ❏ ❏
patients due to paresis, trauma or surgery.
7. Overuse of the ‘laying on of hands’ approach in physiotherapy may discourage exercise.
8. The rate of depression among older people who have recently experienced significant illness ❏ ❏
requiring hospitalization is about 48%, and the depression can persist for a significant period.
9. Fear of falling is a predictor of falls, and is associated with lower life satisfaction and depressed ❏ ❏
mood.
10. There is increasing evidence that patients are safer being treated at home by well-supported care ❏ ❏
teams than in long-term hospital stays.
Answers: 1. F; 2. F; 3. T; 4. T; 5. T; 6. T; 7. T; 8. F; 9. T; 10. T
Medical Progress June 2012 305
Continuing Medical Education Take the challenge, test your knowledge
Peer-Reviewed
Continuing Medical Education Take the challenge, test your knowledge
Low Back Pain Management:
Approaches to TreatmentGerard A Malanga, MD; Kevin R Dunn, MD
Management of low back pain includes a variety of approaches.
These approaches include remaining active, use of lumbar traction
and bracing, and treatment with acetaminophen, NSAIDs, muscle
relaxants, opioid analgesics and oral corticosteroids.
Management of low back pain (LBP) involves a multifaceted approach with the goals of relieving the patient’s pain and restoring normal function. With a detailed evaluation, clinicians may establish an appro-priate diagnosis and formulate a targeted treatment plan. Approaches to treatment include lifestyle modifi-cation, medications, physical therapy and various modalities, psychological counseling and, where appropriate, interventional procedures.
In this article, we provide an update on approaches to LBP man-agement and explore the treatment options.
Lifestyle Modification
EducationAfter a thorough history, physical examination, and review of diagnostic testing, the clinician should involve the patient in the discussion of the treatment plan. This is the appropriate time to review the pertinent anatomy, biomechanics, and underlying pain generators of the spine.
Discussion of the treatment plan should include a description and rationale for additional diagnostic testing, if necessary, and medications, therapeutic exercises, or interven-tional procedures (Figure). The patient should be encouraged to become an active participant in his or her treatment. The clinician can engage the patient in the discussion with a review of proper posture, spine biomechanics in activities of daily living, and simple methods to minimize symptoms.
Bed RestHistorically, bed rest was the treatment for patients with LBP. Although some benefits may be gained from reducing intradiskal pressure while the patient is prone, bed rest has many deleterious effects on bone, connective tissue, muscle, and cardiovascular fitness. The proactive approach emphasizes activity modification rather than strictly bed rest.
Remaining active is more effective than bed rest for patients who have acute or subacute LBP.1,2 The patient should be instructed to avoid activities
that increase intradiskal pressure, such as sitting, bending, and lifting.
Traction
Lumbar traction has long been a preferred method for managing lumbar disk problems. About 1.5 times a patient’s body weight is required to develop distraction of the vertebral bodies. In a recent literature review, there was no evidence to support lumbar traction as a treatment.3 In fact, there was the suggestion that sustained traction might cause more harm than good. However, a randomized con-trolled trial conducted by Fritz and associates4 showed that there may be a subgroup of patients who may benefit from traction in the short term. This subgroup is characterized by the presence of leg symptoms, signs of nerve root compression, and either peripher-alization with extension movements or a positive crossed straight-leg raising test result.
Lumbar Bracing
Braces have been used prophylactically to prevent injury to the lumbosacral spine, and they purportedly help manage existing pathology. The use of lumbar bracing has not demonstrated efficacy as a means to prevent LBP in the workplace.5
Lumbar supports are not more effective than other marginal therapies in reducing LBP, and there is minimal

306 Medical Progress June 2012
Continuing Medical EducationContinuing Medical Education
evidence to support their use.6 Lumbar bracing may help prevent reinjury by serving as a kinesthetic reminder for using proper biomechanics when lifting or bending, although this has not been demonstrated in the literature.
Exercise
There is no good scientific evidence to support therapeutic exercise in acute LBP. In subacute back pain, however, an intensive interdisciplinary reha-bilitation programme that includes physician consultation with psycho-logical, physical therapy, and social/vocational intervention has been shown to be moderately effective.7 In patients with chronic LBP, programmes that incorporate tailoring to individual needs, supervision, stretching, and strengthening are associated with the best outcomes.8
The overall goals of exercise pro-grammes for LBP are to reduce pain, restore normal motion, and develop muscular strength of the trunk and spine sufficient to diminish stress to the intervertebral disk and static sta-bilizers of the spine.9 In addition, therapy should be directed to the patient who demonstrates reasonable understanding of his pain and good technique in performing the exercises on his own and to implementation of an appropriate home exercise programme.
Manipulation
There is conflicting evidence about spinal manipulation and manual mobilization in the management of LBP, although recent clinical guidelines suggest that spinal manipulation in the hands of trained professionals provides a small to moderate short-term benefit in relieving pain.10 Moderate evidence
Figure. Low back pain diagnosis and treatment algorithm
Low back pain
Perform detailed history and physical examination
• Assurance• Patienteducationonpathophysiology,biomechanics• Encouragepatienttoremainactiveandcontinue normal activities• Educationonself-care/homeexercises,superficialheat/ice• Avoidbedrest• ConsidershortcourseofNSAIDsvsacetaminophen• Ifindicated,considermusclerelaxant• Considerspinalmanipulation• Initiatephysicaltherapy
Rule out ‘red flags’• Fevers/chills:infectiousaetiology• Nightsweats,nightpain,weightloss: metastatic process•Bowel/bladderdysfunction,saddleanaesthesia: cauda equina syndrome
Requires immediate workup; if indicated,
consider surgical consultation
Limitedimprovement;signs/symptomsofradiculopathy or spinal stenosis?
Considerreferraltolowback pain specialist vs obtaining diagnostic imaging•Radiography•MRI
Concordantnerverootimpingement or stenosis• Referforevaluationand consideration of interventional procedure
Consider:• Imaging• Additionalpharmacologicaltherapy (eg, tramadol, opioid analgesics, tricyclic antidepressants, anticonvulsants)• Referralformultidisciplinarytreatment approach• Additionaltherapy(eg,physicaltherapy, massage, manipulation, acupuncture, yoga, cognitive behavioural therapy, relaxation)
Pain resolved, nofunctionaldeficits
Followupafter 4 weeks, assess
response to treatment
Continuehomeexerciseprogramme
Reassess risk factors,
symptoms, diagnosis
Followupafter4–6weeks
Yes No

Medical Progress June 2012 307
suggests that the effect of manipulation in combination with strengthening exercise is similar to the effect of pre-scription NSAIDs with exercise in both the short and long terms.11
Spinal manipulation has not been found to be more effective than other treatments, such as analgesics, exercise, and physical therapy. However, there appears to be a subgroup of patients with LBP for whom spinal manipulation results in significant reductions in pain and disability.12–14
Manipulation should be performed in conjunction with and to facilitate an active physical therapy programme.
Medications
Patients with LBP have been treated with medications in a number of classes, including acetaminophen, NSAIDs, muscle relaxants, opioid anal-gesics, and oral corticosteroids. Each agent has unique trade-offs between risk and anticipated benefits. Therefore, before prescribing a medication, the clinician should be aware of its contra-indications, common adverse effects, and mechanism of action.
AcetaminophenThis para-aminophen derivative has analgesic and antipyretic effects equal to those of aspirin, but it has weak anti-inflammatory effects. Acetaminophen is relatively inexpensive and is available without a prescription. It is effective for mild to moderate pain but lacks other desirable effects on inflammation and muscle spasm. In acute LBP, studies have shown no difference between acetaminophen and no treatment,15 and no clear difference was seen in pain relief between acetaminophen and NSAIDs.16,17
Acetaminophen generally is not a first-line medication for LBP unless
there are contraindications to other medications. Prolonged use is contra-indicated because of the potential for liver toxicity.
NSAIDsThese agents are a reasonable first-line treatment for acute LBP because of their combined analgesic and anti-inflam-matory effects. Non-selective NSAIDs have been shown to be more effective for pain relief than acetaminophen.17 The dose needed to produce anti-inflammatory effects differs substantially from that for analgesic effects. These medications often are taken intermittently, and a significant level is not sustained to take advantage of the anti-inflammatory properties. Patients should be advised to take the medications at regular intervals to maximize both the analgesic and the anti-inflammatory effects.
Not one NSAID has been shown to be more effective than the others in terms of pain relief for patients with LBP. In a systematic review, the selective cyclooxygenase-2 inhibitors showed fewer adverse effects than the traditional NSAIDs.18 The major adverse reactions to NSAIDs include gastrointestinal bleeding and reno-vascular damage. NSAIDs also have been shown to slow bone and tissue healing.19 Prolonged use should be avoided to minimize the associated risks. The lowest effective dose is rec-ommended for the shortest duration that is necessary.20
AntidepressantsThere is good evidence to support the analgesic effect of tricyclic antide-pressants in the treatment of patients with LBP. In a systematic review, tricyclic antidepressants were more effective than placebo in controlling pain.21 Other antidepressants in the selective
serotonin reuptake inhibitor class and trazodone have been shown to be no more effective than placebo.22,23
Antidepressants typically take up to 4 weeks to achieve effect, but whether the same time is required to achieve pain relief is unknown.23 Of note, depression is a common problem in patients with chronic LBP, and it should be addressed appropriately.24
Muscle Relaxants
These often are prescribed in the management of acute LBP to relieve pain, improve range of motion, and interrupt the pain-spasm-pain cycle. They have been shown to be more effective when they are used in con-junction with NSAIDs.25
Tizanidine has been shown to be effective in the management of acute LBP.26 Other studies have not determined superiority for any par-ticular muscle relaxant in terms of benefit or adverse effects. The most frequently reported effect of muscle relaxants is sedation; they usually are prescribed at bedtime to take advantage of this property.
Opioid AnalgesicsThe use of opioid analgesics in the management of LBP should be limited to pain that is unresponsive to other treatments or when other medications are contraindicated. A careful risk-benefit analysis should be considered before starting these medications because of the potential risk of aberrant drug-related behaviours with long-term use in patients who have a history of or predilection to addiction or abuse. There is no evidence to support the use of one opioid versus another.27 Prolonged or repeated use of opioids is not necessary for most patients who have acute LBP.

308 Medical Progress June 2012
Continuing Medical Education
TramadolThis centrally acting analgesic has a combined mechanism of binding to μ receptors and a mixed serotonin/norepinephrine reuptake inhibitor. Although no studies have compared tramadol with acetaminophen, NSAIDs, or opioid analgesic mono-therapy, there is evidence to suggest that tramadol is effective for short-term pain relief and improved function.28
Antiseizure MedicationsGabapentin, an antiepileptic medi-cation widely used in the management of neuropathic pain, has been shown to provide short-term benefit in patients with radicular pain.29,30 The most frequently noted adverse effects include drowsiness, loss of energy, and dizziness. There is insufficient evidence for or against other antiepileptic medi-cations in the management of LBP with or without radiculopathy.20
Oral CorticosteroidsThe use of oral corticosteroids in the management of LBP is unsupported in the literature, especially when there are radicular symptoms, because these agents have not been shown to be
more effective than placebo.20,31-34 In a double-blind placebo-controlled trial, Holve and Barkan35 demonstrated that patients treated with a tapering course of prednisone have a more rapid return to baseline in pain, mental well-being, and disability scores and require fewer subsequent epidural injections. There was no difference in physical exami-nation findings, the use of NSAIDs or other pain medications, or return to work. Better studies clearly are needed to determine the role and effectiveness of oral corticosteroids in LBP, partic-ularly for lumbar radiculopathy.
Modalities
Modalities offer an adjunct to evidence-based treatment in patients with LBP. However, the evidence to support their use is generally poor, despite their widespread use.
Transcutaneous Electrical Nerve Stimulation (TENS)TENS, the use of electrical impulses over surface electrodes to provide symptomatic relief by modifying pain perception, has not been shown to be effective for chronic LBP.20 In recently published American Academy of Neurology guidelines, TENS is not recommended for chronic LBP because it has not been shown to be more effective than placebo.36
Electrical StimulationHigh-voltage pulsed galvanic stimu-lation has been used to reduce muscle spasm and oedema in patients with acute LBP. The use of electrical stimu-lation typically is limited to the initial stages of treatment to allow patients to progress to more active treatments in restoring normal range of motion and strength. There is insufficient sci-entific evidence for or against its use in patients who have LBP.37
UltrasonographyThis deep-heating modality has been shown to improve the distensibility of connective tissue and facilitate stretching.38 Ultrasonography is con-traindicated in acute inflammatory conditions because it may exacerbate the inflammatory response. In addition, this modality is contraindicated over a previous laminectomy site.
There is insufficient evidence for or against the use of ultrasonography in LBP.37 It may be best used to improve segmental limitations in range of motion by facilitating soft tissue mobi-lization and stretching with a skilled physical therapist.25
Superficial HeatThis modality produces effects to a depth of 1 to 2 cm and has been shown to reduce muscle spasm and pain. Heat packs often are used in combination with electrical stimulation therapy. Heat wrap therapy has been shown to be more effective than placebo in short-term pain relief and functional status.39 These effects typically last for less than 1 week and are not more effective than exercise.
Therapeutic Injections
Trigger Point InjectionsMyofascial trigger points are thought to be hyperirritable foci within muscles and fasciae that are associated with taut muscle bands. Trigger points are iden-tified on palpation, which produces a focal twitch response and referred pain distal to the site of muscle irri-tability. Palpation examinations have poor inter-rater reliability.40 In an assessment of intra-rater reliability, local twitch response and referred pain varied from one session to the next; taut bands, tender points, and ’jump sign’ remained consistent.41
”The proactive approach emphasizes activity
modification rather than strictly bed rest“

Medical Progress June 2012 309
Trigger points are managed initially with stretching; restoration of normal posture and biomechanics; and modalities, such as superficial heat or cryotherapy. Muscle relaxants also may be useful.
Trigger point injections may be considered when more conser-vative measures have not succeeded. However, there is no evidence that injections of normal saline with cor-ticosteroids are more effective than normal saline alone. The benefit may result from needling alone or from placebo or nonspecific effects.
In one study, there was no dif-ference among dry needling, injection with lidocaine, lidocaine with corti-costeroid, and vasocoolant spray with acupressure.42,43 As a result, the type of injections, appropriate dosage, and interval are not known.
Trigger point injections remain an option for myofascial-related LBP resistant to conservative treatments. They should be limited and used in
conjunction with an appropriate func-tional rehabilitation programme.
Epidural Corticosteroid InjectionsThese injections are a frequently performed interventional procedure aimed at reducing pain and inflam-mation resulting from disk herniation and subsequent nerve root irritation. The effectiveness of these injections is increased if they are used in the first weeks after the onset of pain and followed with an active exercise programme. Even though they are used widely, good scientific evidence for their use in the management of LBP is limited. In a multicenter randomized controlled trial, epidural corticosteroid injections offered transient benefit in symptoms at 3 weeks in patients with sciatica but no sustained benefits in terms of pain, function, or the need for surgery.44
Epidural injections should be used when clinical evidence based on the history and physical examination
correlates well with radiographic evidence. To minimize the risks, they should be performed with fluo-roscopic guidance and contrast enhancement. There is no indication for performing injections in ’series’. Typically, one or two injections are suf-ficient to improve the radicular pain symptoms and facilitate a successful course of rehabilitation.
Facet InjectionsAlthough lumbar facet joints are a potential source of LBP, there is a poor correlation between history and physical examination findings and true facet-mediated LBP. In addition, diagnostic imaging is unreliable for identifying underlying facet joint pathology. In spite of various attempts reported in the literature, an identifying clinical feature of facet-mediated pain has yet to be found. Thus, the only means of diagnosis is through facet joint blocks.
Facet joint injections with cor-ticosteroids have not been shown to be more effective than placebo in controlling pain.45,46 Therefore, lumbar medial branch blocks or radiofrequency neurotomies remain a potential treatment, given an appro-priate patient response to diagnostic blockade.46
Sacroiliac Joint InjectionsThe sacroiliac joint is a potential pain generator in the lumbar spine, with an overlapping referral pain pattern around the posterosuperior iliac spine. Sacroiliac joint–mediated pain should be considered in patients for whom a comprehensive rehabilitation programme and a trial of NSAIDs, ice/heat, and mobilization or manipu-lation have not succeeded. Injection should be considered for both diag-nostic and therapeutic purposes; if the results are positive, it should
Proliferation therapy involves injection of solution into the tendons and ligaments to promote healing.

310 Medical Progress June 2012
Continuing Medical Education
be followed with an active physical therapy programme.
ProlotherapyThis therapy involves injection of solution to promote healing of loose tissue, ligaments, tendons, and joint capsules. Prolotherapy remains poorly studied and validated in spite of a long history of use to manage various conditions thought to be the result of ligamentous instability.
In the management of LBP, prolo-therapy has been shown to be effective in combination with spinal manipu-lation therapy.47,48 It has yet to be studied as a single treatment without co-interventions.
Acupuncture
This modality has been used to manage various conditions for more than 2,000 years. Evidence for the use of acu-puncture in the management of acute LBP is sparse,49 but it has been shown to be effective in the management of chronic LBP.50,51 The literature on acu-puncture is not of high quality.49
Psychological Counselling
Cognitive-behavioural therapy is an effective component in the treatment of patients who have chronic pain.52
However, it needs to be combined with other therapeutic components, such as physical therapy, to deal with physical deconditioning issues. Currently, there are no studies that directly address what combination of components might provide the best therapeutic outcomes for what type of chronic pain syndrome.52
Spinal Cord Stimulation
With this modality, an implantable device is used primarily to manage
failed back surgery syndrome, complex regional pain syndrome, and chronic back pain. As the number of low back surgeries increases, so do the number and the use of spinal cord stimulation therapies.53
In a recent systematic review, Frey and associates53 found strong evidence for the clinical use of spinal cord stimulation in failed back surgery syndrome in terms of pain relief and cost-effectiveness. Spinal cord stimulation does involve risk, which is estimated to exist in up to 43% of patients. The most common complications include electrode or lead problems, infection, generator problems, extension cable problems, and cerebrospinal fluid leakage.53
Conclusions
LBP is a frequently encountered complaint associated with great costs that continue to increase. Most patients improve with time if they remain active. Physicians need to have a clear understanding of the pertinent anatomy and physiology of the spine and correlate this with their findings in the history and on physical exami-nation to develop a good differential diagnosis and a proper treatment plan. The literature may help guide the decision-making process, but much of the evidence is not well validated. The best evidence is for a short course of NSAIDs, active exercise and, as soon as possible, a return to normal activities. Physical therapy, injections, and other approaches to treatment may help in properly selected patients.
References1. Hagen KB, Hilde G, Jamtvedt G, Winnem M. Bed rest for
acute low back pain and sciatica. Cochrane Database Sys
Rev 2004;(4):CD001254. Article withdrawn June 16, 2010.
2. Hilde G, Hagen KB, Jamtvedt G, Winnem M. WITH-
DRAWN: advice to stay active as a single treatment for
low-back pain and sciatica. Cochrane Database Syst Rev
2007;(2):CD003632.
3. Gay RE, Brault JS. Evidence-informed management
of chronic low back pain with traction therapy. Spine J
2008;8:234–242.
4. Fritz JM, Delitto A, Erhard RE. Comparison of classification
based physical therapy with therapy based on clinical practice
guidelines for patients with acute low back pain: a random-
ized clinical trial. Spine (Phila Pa 1976) 2003;28:1363–1372.
5. Woodhouse ML, McCoy RW, Redondo DR, Shall LM. Effects
of back support on intra-abdominal pressure and lumbar
kinetics during heavy lifting. Hum Factors 1995;37:582–590.
6. Jellema P, van Tulder MW, van Poppel MN, et al. Lumbar
supports for prevention and treatment of low back pain: a
systematic review within the framework of the Cochrane
Back Review Group. Spine (Phila Pa 1976) 2001;26:377–
386.
7. Karjalainen K, Malmivaara A, van Tulder M, et al. Multi-
disciplinary biopsychosocial rehabilitation for subacute low
back pain in working-age adults: a systematic review within
the framework of the Cochrane Collaboration Back Review
Group. Spine (Phila Pa 1976) 2001;26:262–269.
8. Hayden JA, van Tulder MW, Tomlinson G. Systematic review:
strategies for using exercise therapy to improve outcomes in
chronic low back pain. Ann Intern Med 2005;142:776–785.
9. Saal JA. Dynamic muscular stabilization in the nonop-
erative treatment of lumbar pain syndromes. Orthop Rev
1990;19:691–700.
10. Assendelft WJ, Morton SC, Yu EI, et al. Spinal manip-
ulative therapy for low back pain: a meta-analysis of
effectiveness relative to other therapies. Ann Intern Med
2003;138:871–881.
11. Bronfort G, Haas M, Evans R, et al. Evidence-informed
management of chronic low back pain with spinal manipula-
tion and mobilization. Spine J 2008;8:213–225.
12. Flynn T, Fritz J, Whitman J, et al. A clinical prediction rule
for classifying patients with low back pain who demonstrate
short-term improvement with spinal manipulation. Spine
(Phila Pa 1976) 2002;27:2835–2843.
13. Childs JD, Fritz JM, Flynn TW, et al. A clinical prediction
rule to identify patients with low back pain most likely to
benefit from spinal manipulation: a validation study. Ann
Intern Med 2004;141:920–928.
14. Cleland JA, Fritz JM, Kulig K, et al. Comparison of the
effectiveness of three manual physical therapy techniques in
a subgroup of patients with low back pain who satisfy a clini-
cal prediction rule: a randomized clinical trial. Spine (Phila Pa
1976) 2009;34:2720–2729.
15. Milgrom C, Finestone A, Lev B, et al. Overexertional
lumbar and thoracic back pain among recruits: a prospective
study of risk factors and treatment regimens. J Spinal Disord

Medical Progress June 2012 311
1993;6:187–193.
16. van Tulder MW, Scholten RJ, Koes BW, Deyo RA.
Non-steroidal anti-inflammatory drugs for low back pain
[published updates appear in Cochrane Database Syst Rev
2008;(1):CD000396 and 2006;(2):CD000396]. Cochrane
Database Syst Rev 2000;(2):CD000396.
17. van Tulder MW, Scholten RJ, Koes BW, Deyo RA. Non-
steroidal anti-inflammatory drugs for low back pain: a
systematic review within the framework of the Cochrane
Collaboration Back Review Group. Spine (Phila Pa 1976)
2000;25:2501–2513.
18. Roelofs PD, Deyo RA, Koes BW, et al. Non-steroidal anti-
inflammatory drugs for low back pain: an updated Cochrane
review. Spine (Phila Pa 1976) 2008;33:1766–1774.
19. Riew KD, Long J, Rhee J, et al. Time-dependent inhibitory
effects of indomethacin on spinal fusion. J Bone Joint Surg
2003;85A:632–634.
20. Chou R, Qaseem A, Snow V, et al; Clinical Efficacy Assess-
ment Subcommittee of the American College of Physicians;
American College of Physicians; American Pain Society
Low Back Pain Guidelines Panel. Diagnosis and treatment
of low back pain: a joint clinical practice guideline from
the American College of Physicians and the American Pain
Society [published correction appears in Ann Intern Med
2008;148:247-248]. Ann Intern Med 2007;147:478–491.
21. Staiger TO, Gaster B, Sullivan MD, Deyo RA. Systematic
review of antidepressants in the treatment of chronic low
back pain. Spine (Phila Pa 1976) 2003;28:2540–2545.
22. Salerno SM, Browning R, Jackson JL. The effect of anti-
depressant treatment on chronic back pain: a meta-analysis.
Arch Intern Med 2002;162:19–24.
23. Malanga GA, Dennis RL. Use of medications in the
treatment of acute low back pain. Clin Occup Environ Med
2006;5:643–653, vii.
24. Bair MJ, Robinson RL, Katon W, Kroenke K. Depression
and pain comorbidity: a literature review. Arch Intern Med
2003;163:2433–2445.
25. Malanga GA, Nadler SF. Nonoperative treatment of low
back pain. Mayo Clin Proc 1999;74:1135–1148.
26. van Tulder MW, Touray T, Furlan AD, et al; Cochrane
Back Review Group. Muscle relaxants for nonspecific low
back pain: a systematic review within the framework
of the cochrane collaboration. Spine (Phila Pa 1976)
2003;28:1978–1992.
27. Chou R, Clark E, Helfand M. Comparative efficacy
and safety of long-acting oral opioids for chronic non-
cancer pain: a systematic review. J Pain Symptom Manage
2003;26:1026–1048.
28. Schnitzer TJ, Gray WL, Paster RZ, Kamin M. Efficacy of
tramadol in treatment of chronic low back pain. J Rheumatol
2000;27:772–778.
29. McCleane GJ. Does gabapentin have an analgesic
effect on background, movement and referred pain? A ran-
domised, double-blind, placebo controlled study. Pain Clinic
2001;13:103–107.
30. Yildirim K, Sisecioglu M, Karatay S, et al. The effectiveness
of gabapentin in patients with chronic radiculopathy. Pain
Clinic 2003;15:213–218.
31. Finckh A, Zufferey P, Schurch MA, et al. Short-term effi-
cacy of intravenous pulse glucocorticoids in acute discogenic
sciatica: a randomized controlled trial. Spine (Phila Pa 1976)
2006;31:377–381.
32. Friedman BW, Holden L, Esses D, et al. Parenteral cor-
ticosteroids for Emergency Department patients with non-
radicular low back pain. J Emerg Med 2006;31:365–370.
33. Haimovic IC, Beresford HR. Dexamethasone is not
superior to placebo for treating lumbosacral radicular pain.
Neurology 1986;36:1593–1594.
34. Porsman O, Friis H. Prolapsed lumbar disc treated with
intramuscularly administered dexamethasonephosphate: a
prospectively planned, double-blind, controlled clinical trial in
52 patients. Scand J Rheumatol 1979;8:142–144.
35. Holve RL, Barkan H. Oral steroids in initial treatment
of acute sciatica. J Am Board Fam Med 2008;21:469–474.
36. Dubinsky RM, Miyasaki J. Assessment: efficacy of trans-
cutaneous electric nerve stimulation in the treatment of pain
in neurologic disorders (an evidence-based review): report
of the Therapeutics and Technology Assessment Subcom-
mittee of the American Academy of Neurology. Neurology
2010;74:173–176.
37. Poitras S, Brosseau L. Evidence-informed management
of chronic low back pain with transcutaneous electrical
nerve stimulation, interferential current, electrical mus-
cle stimulation, ultrasound, and thermotherapy. Spine J
2008;8:226–233.
38. Lehmann JF, Masock AJ, Warren CG, Koblanski JN. Effect
of therapeutic temperatures on tissue extensibility. Arch Phys
Med Rehabil 1970;51:481–487.
39. French SD, Cameron M, Walker BF, et al. Superficial heat
or cold for low back pain. Cochrane Database Syst Rev
2006;(1):CD004750.
40. Nice DA, Riddle DL, Lamb RL, et al. Intertester reliability of
judgments of the presence of trigger points in patients with
low back pain. Arch Phys Med Rehabil 1992;73:893–898.
41. Al-Shenqiti AM, Oldham JA. Test-retest reliability of myo-
fascial trigger point detection in patients with rotator cuff
tendonitis. Clin Rehabil 2005;19:482–487.
42. Malanga G, Wolff E. Evidence-informed management of
chronic low back pain with trigger point injections. Spine J
2008;8:243–252.
43. Garvey TA, Marks MR, Wiesel SW. A prospective, ran-
domized, double-blind evaluation of trigger-point injec-
About the AuthorsDr Malanga is director of the PM&R SportsMedicineFellowshipandDrDunnisaPM&Rsportsmedicine fellow at Atlantic Health System inSummit, New Jersey. Dr Malanga also is directorof pain management at Overlook Hospital, also in Summit.
© 2010 UBM Medica LLC. Initially published
in The Journal of Musculoskeletal Medicine
2010;27(8):305–315. Reprinted with permission.
tion therapy for low back pain. Spine (Phila Pa 1976)
1989;14:962–964.
44. Arden NK, Price C, Reading I, et al; WEST Study Group.
A multicentre randomized controlled trial of epidural cortico-
steroid injections for sciatica: the WEST study. Rheumatology
(Oxford) 2005;44:1399–1406.
45. Ogsbury JS 3rd, Simon RH, Lehman RA. Facet denervatio-
nin the treatment of low back syndrome. Pain 1977;3:257–
263.
46. Bogduk N. Evidence-informed management of chronic
low back pain with facet injections and radiofrequency
neurotomy. Spine J 2008;8:56–64.
47. Ongley MJ, Klein RG, Dorman TA, et al. A new
approach to the treatment of chronic low back pain. Lancet
1987;2:143–146.
48. Klein RG, Eek BC, DeLong WB, Mooney V. A randomized
double-blind trial of dextrose-glycerin-phenol injections for
chronic, low back pain. J Spinal Disord 1993;6:23–33.
49. Ammendolia C, Furlan AD, Imamura M, et al. Evidence-
informed management of chronic low back pain with needle
acupuncture. Spine J 2008;8:160–172.
50. Furlan AD, van Tulder M, Cherkin D, et al. Acupuncture
and dry-needling for low back pain: an updated systematic
review within the framework of the cochrane collaboration.
Spine (Phila Pa 1976) 2005;30:944–963.
51. Manheimer E, White A, Berman B, et al. Meta-anal-
ysis: acupuncture for low back pain. Ann Intern Med
2005;142:651–663.
52. Gatchel RJ, Rollings KH. Evidence-informed management
of chronic low back pain with cognitive behavioral therapy.
Spine J 2008;8:40–44.
53. Frey ME, Manchikanti L, Benyamin RM, et al. Spinal cord
stimulation for patients with failed back surgery syndrome: a
systematic review. Pain Physician 2009;12:379–397.
312 Medical Progress June 2012
CME Questions
ThiscontinuingmedicaleducationserviceisbroughttoyoubytheMedicalProgressInstitute,aninstitutededicatedtoCMElearning.Readthearticle’LowBackPainManagement:ApproachestoTreatment’andanswer the following questions. Answers are shown at the bottom of this page.
PleaseanswerTrueorFalsetothequestionsbelow. True False
CME Questions
1. Bed rest used to be the treatment of choice for low back pain (LBP).
2. Lumbar bracing is effective in preventing LBP.
3. The goals of exercise programmes for LBP patients are to decrease pain, restore normal motion, and develop muscular strength of the trunk and spine.
4. Spinal manipulation has been demonstrated to be more effective than other treatments such as analgesics, exercise and physical therapy in the management of LBP.
5. The analgesic and antipyretic effects of acetaminophen are superior to those of aspirin.
6. Gastrointestinal bleeding, renovascular damage, and slow bone and tissue healing are some of the major adverse reactions to NSAIDs.
7. Studies have shown that tricyclic antidepressants are less effective than placebo in controlling LBP.
8. Tizanidine has not been demonstrated to be effective in the management of acute LBP.
9. Electrical stimulation reduces muscle spasm and oedema and restores normal range of motion and strength in patients with acute LBP.
10. One or two epidural corticosteroid injections are usually not sufficient to improve radicular pain symptoms.
❏ ❏
❏ ❏
❏ ❏
❏ ❏
❏ ❏
❏ ❏
❏ ❏
❏ ❏
❏ ❏
❏ ❏
CME Article:Low Back Pain Management: Approaches to Treatment
Answers: 1. T; 2. F; 3. T; 4. F; 5. F; 6. T; 7. F; 8. F; 9. T; 10. F
Related Documents











