Geriatric Population. Geriatric Palliative and End-of-Life Care.
Jul 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Place of death
Preference:
Majority want to die at home
Reality:
Minority will die at home
Most institutional deaths could occur at home
Societal and clinician lack of familiarity with dying

Large Gap Reality vs. Desire
Fears
Die on machine
Die in discomfort
Be a burden
Die in institution
Desires
Die NOT on
ventilator
Die IN comfort
Die WITH family
Die at HOME
Place of death
Our health care system is oriented toward providing
life-sustaining treatment, unless a patient actively
chooses against it.
More interventions and life-sustaining treatments are
associated with poorer patient quality of life and
higher family distress.
Bernacki RE, Block SD, for the American College of Physicians High Value Care Task Force. Communication About Serious
Illness Care Goals: A Review and Synthesis of Best Practices. JAMA Intern Med. 2014;174(12):1994-2003.
Place of death
In the absence of conversations about prognosis, goals,
and outcomes of treatment, patients do not have the
opportunity to express their values and preferences.
Leading clinicians to assume that patients want
additional interventions, even late in the illness.
Bernacki RE, Block SD, for the American College of Physicians High Value Care Task Force. Communication
About Serious Illness Care Goals: A Review and Synthesis of Best Practices. JAMA Intern Med.
2014;174(12):1994-2003.


The relief you need when you are experiencing serious medical illness
PALLIATIVE CARE
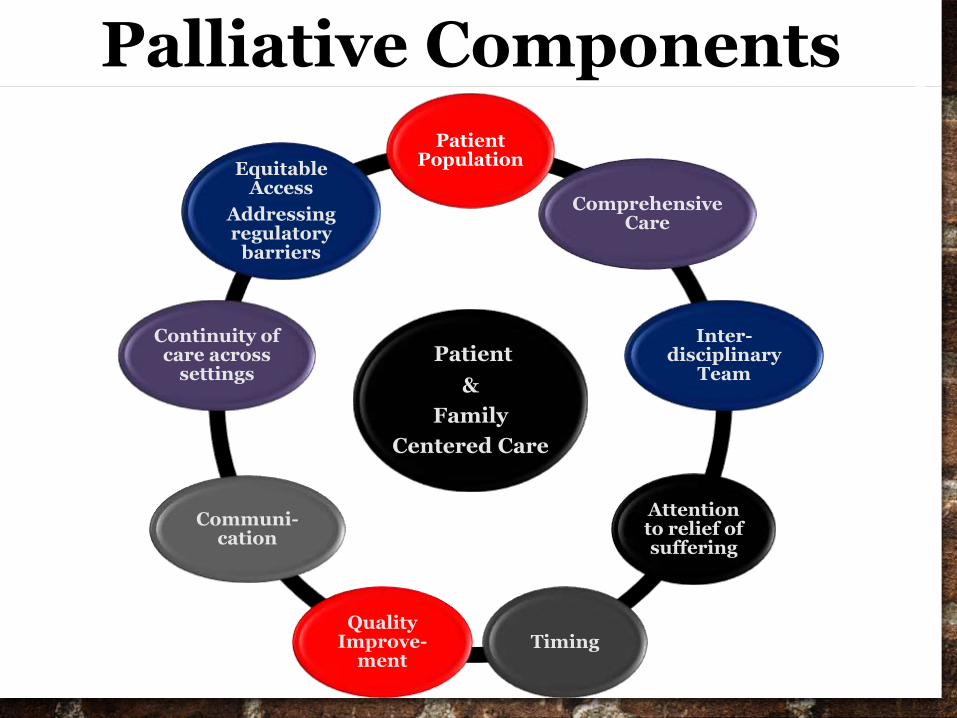
Patient
&
Family
Centered Care
Patient Population
Comprehensive Care
Inter-disciplinary
Team
Attention to relief of suffering
TimingQuality
Improve-ment
Communi-cation
Continuity of care across
settings
Equitable Access
Addressing regulatory
barriers
Palliative Components

Palliative Care Team
Clinical Team:
Physician
Nurse Practitioner
Physician Assistant
Nurse
Therapists, Dietician
Pharmacist
Psychosocial Team:
Social Worker
Case Manager
Psychologist
Chaplain
Grief Counselor
Child Life Specialist

Who Uses Palliative Care?
People of all ages…
Life threatening
illness
Limiting injuries
from accidents or
other trauma
Congenital injuries
Dependent on life-sustaining treatments
Serious, life-threatening illness
Progressive chronic conditions
Palliative Care Indications
Uncontrolled
symptoms
Goals of care
Cardiac arrest
Advanced cancer
Multi-organ failure
Ventilation support
Hospice eligibility
Prolonged
hospitalization
Multiple
hospitalizations
Family distress

Reduce physical/emotional symptoms
Improve function and reduce disability
Integrating complimentary therapies
Coordinate with specialists, resources
Assist in making informed decisions
Palliation of suffering along with
continued treatment (no requirement
to give up curative)
What are the goals of Palliative Care?

Pain and symptom control
Avoid inappropriate prolongation of the
dying process
Achieve a sense of control
Relieve burdens on family
Strengthen relationships with loved ones
Singer, et al. JAMA 1999;281(2):163-168.
The Patient’s PerspectiveWhat Do Palliative Care
patients want?

Who is eligible for hospice?
Advanced disease
with life expectancy
of “six months or
less” given natural
course of disease
(may be longer if
patient meets
criteria)
Who is eligible for hospice?
Poor functional/nutritional
status
High morbidity/mortality
markers
Patient/surrogate decision
maker consent
Payment sources

Hospice Care
Physician services
Nursing services
Health aide,
homemaker
services, volunteers
Spiritual support
and social work
Hospice Care
Medical equipment, supplies
Medications
PT/OT, speech therapy, dietary counseling
Bereavement counseling, support services
Where is Hospice?
Home: primary or family
residence, nursing home,
group home, assisted living
facility; mandated to be
>80% of delivered care of
any hospice’s services
Where is Hospice?
Inpatient facility:
Short term, 3-5 days
Continuous care at
home: Highly
regulated, typically
24 hours
Respite care

Hospice Access IssuesCulture, Race
Religious Diversity
Insurance Issues
Geography
Healthcare Staff
Median survival in Hospice care is 2-
3 weeks, primarily due to late
physician referrals

Last Hours of Life
Semicomatose State
Impaired Heart & Renal Function
Respiratory Dysfunction
Neurologic Dysfunction

Semicomatose State
Eyes become
sunken and glazed
Senses are
generally dulled
Hearing may not
be lost, light
sensitivity
Ability to move
decreases
Beginning in the legs
and then the arms
Body becomes stiff,
joints painful if moved
Medicate symptoms

Impaired Heart, Renal Decrease
cardiac output
peripheral and
renal perfusion
blood pressure
Pulse rate first
increases, then
weakens, irregular
Peripheral cooling,
bluish, skin
mottling
May perspire, may
have peripheral
swelling
Body temperature
may increase

Respiratory Dysfunction
Breathing may become
shallow or labored
Respiration rate
fluctuations
Secretions may increase
Breathlessness feeling
may increase
Death “rattle”
Terminal
congestion occurs
due to changes in
respiratory rate and
inability to clear
secretions
Is distressing to
family

Neurologic Dysfunction
Multiple nonreversible factors:
Metabolic imbalances
Acidosis
Kidney failure
Infection
Reduce blood flow to brain
THE “USUAL ROAD”
Decreasing level of consciousness
Sleepy
Lethargic
Semicomatose
Comatose
Death

THE “DIFFICULT ROAD”
Nervous system agitation prior to
semicomatose state
Restlessness, Confusion, Tremors
Hallucinations, Mumbling Delirium
Muscle jerking, Seizures
Semicomatose
Comatose
Death

Large amount of research evidence shows….
Early discussions of serious illness care goals
are associated with:
♛ beneficial outcomes for patients,
♛ no harmful adverse effects, and
♛ potential cost savings.
Bernacki RE, Block SD, for the American College of Physicians High Value Care Task Force. Communication About Serious
Illness Care Goals: A Review and Synthesis of Best Practices. JAMA Intern Med. 2014;174(12):1994-2003.

To die differently you must prevent dying badly…
Bet on Luck or
Take Control

Take Control…
Dreams are only dreams until you write them down. When you write them down then dreams
become goals.
How do YOU take control?
Do ♛ The Conversation Project a collaboration with the Institute for Healthcare Improvement.
http://theconversationproject.org/starter-kit/intro/
Do your conversation kit now and make your loved ones aware of your wishes.

Related Documents