Targeted therapies in renal cell carcinoma Geriatric Oncology: Cancer in Senior Adults Geriatric Oncology: Cancer in Senior Adults Stéphane OUDARD Stéphane OUDARD, Service de Cancérologie Médicale Hôpital Georges Pompidou, Paris Université René Descartes, Paris 5, France

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Targeted therapies in renal cell carcinomaGeriatric Oncology: Cancer in Senior AdultsGeriatric Oncology: Cancer in Senior Adults
Stéphane OUDARDStéphane OUDARD, Service de Cancérologie MédicaleHôpital Georges Pompidou, Paris
Université René Descartes, Paris 5, France

IntroductionIntroduction
• Renal cancer occurs mostly between age 62 andRenal cancer occurs mostly between age 62 and67 in Europe (IARC 2007).
• Metastatic renal cancer is observed in 25% of these patients and median age is slightly higherpatients and median age is slightly higher.
• mRCC patients are often > 65 and 1/3 to ½ are >• mRCC patients are often > 65 and 1/3 to ½ are > 70.

Efficacy of targeted agents, lt f d i d t i lresults of randomized trials
Agent Nber Range of benefit Median age Patients > 70 years, pts (∆ PFS results) (years) %
Sunitinib1 750 6 62 [27-87] NR[ ]
Sorafenib2 903 2.7 59 [19-86] 16
Bevacizumab 649 & 4.8 61 [30-82] NRBevacizumaband IFN3,4
649 & 732
4.83.3
61 [30 82]61 [56-70]
NR
Temsirolimus5 626 2.4* 58 [32-81] NR
Everolimus6 410 2.1 61 [27-85] NR
Pazopanib7 435 5 59 [25-85] 35 (> 65y)
1 Motzer RJ, et al. New Engl J Med 2007; 2 Escudier B, et al. New Engl J Med 2007; 3 Escudier B et al, Lancet 2007 ; 4 Rini B et al, J Clin Oncol 2008
5 Hudes G et al, New Engl J Med6 Motzer B et al, Lancet 2008
7 Sternberg C et al, J Clin Oncol 2010
Not reported

Prospective clinical trials : inclusion of older patients?
P ti t ld th 70 t l• Patients older than 70 represent only a limited subgroup in Phase III trials.I f ti th ti t i li it dInformation on these patients is limited.
• Subgroup analyses as well as results of compassionate programs seem to indicate th f ffi i ld l dthe same range of efficacy in elderly and younger patients1
Stadler Cancer 2010, Gore Lancet 2009, Eisen T et al, JNCI 2008, vol 100:1454-63

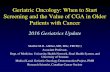
Efficacy of different targeted therapies based on the pivotal trials in metastatic renal cell carcinoma of ≥
65 ld ti t65-year-old patients<65 years sunitinib>65 years sunitinib
<65 years sorafenib>65 years sorafenib
<65 years bevacizumab + IFN
<65 years temsirolimus
<65 years bevacizumab + IFN>65 years bevacizumab + IFN
>65 years temsirolimus
>65 years everolimus<65 years everolimus>65 years everolimus
<65 years pazopanib>65 years pazopanib
0.1 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8
Targeted therapy better Alternative therapy better

Analysis of sorafenib in older population f th TARGET t i lfrom the TARGET trial
Retrospective analysis from TARGET trialSafety and efficacy of sorafenibsorafenibN= 115 > 70 years old vs 787 younger pts < 70 PFS : 26 3 weeks older pts vsPFS : 26.3 weeks older pts vs 23.9 younger ptsClinical benefit = 84.3 % vs 83.5%Maintenance of health status PS: 121 d vs 85 daysy
Eisen T et al, JNCI 2008, vol 100:1454-63

Analysis of sorafenib in older population from the TARGET trialfrom the TARGET trial
Time to self-reported health status deterioration (FACT–G PWB)*
1 00 1 00Patients > 70 years
func
tion
0.75
1.00
0.75
func
tion
1.00Patients < 70 years
al d
istr
ibut
ion
0.50
al d
istr
ibut
ion
0.50
Surv
iva
0.25
0
Surv
iva
0.25
0
Eisen T et al, JNCI 2008, vol 100:1454-63PlaceboSorafenib Censored data
Time (days)
0 400300200100 0
Time (days)
400300200100 500
, ,
*Physical Well-Being domain of the Functional Assessment of Cancer Therapy–General Eisen T et al, JNCI 2008, vol 100:1454-63

Toxic effects of targeted agents in older ti t di t b lpatients according to subgroup analyses:
S iti ib f t f ti• Sunitinib : more frequent fatigue • Beva/IFN : more grade ¾ events (66 vs 58%)• Sorafenib : no difference in trialSorafenib : no difference in trial
Fatigue and cutaneous symptoms more frequent in Access program
• Temsirolimus :• Everolimus : No major differences
But !Most comorbidities were exclusion criteria in controlled trials.Toxicity in older patients may be underestimated

Which toxicities are you waiting for in the era of antiangiogenic drugs?era of antiangiogenic drugs?
Bellmunt J et al, Critical Rev Oncol Hematol 2009 vol 69:64-72

Main toxicities of antiangiogenic therapies that i k f ld irepresent risks for older patients
• # 1 cardio-vascular effects +++• # 1 cardio-vascular effects +++- Hypertension- Edema with a certain degree of water
retention- Arterial thrombosis (heart infarct)- Venous thrombo-embolismVenous thrombo embolism- Cardiac failure
Cardiac rhythm troubles- Cardiac rhythm troubles.

Main toxicities of antiangiogenic therapies that i k f ld irepresent risks for older patients
• # 2 renal effects +++Renal insuffisiency- Renal insuffisiency
- Hypertension- Glomerular thrombotic microangiopathy- Anemia (decrease secretion EPO)( )
Launay Vacher V et al, Anti-Cancer Drugs 2009, 20:81–82

Main toxicities of antiangiogenic therapies that i k f ld irepresent risks for older patients
• # 3 Digestive symptoms:# 3 Digestive symptoms:- Nausea-vomiting
M iti- Mucositis- Diarrhea
Decreased food intake
# 4 General symptoms:- Fatigue
Hand and foot syndrome Decreased mobility- Hand and foot syndrome

Main toxicities of antiangiogenic therapies that i k f ld irepresent risks for older patients
• # 5 Biologic disturbances:• # 5 Biologic disturbances:
- Hyperglycemia- Hypercholesterolemiayp- Anemia
Neutropenia- Neutropenia- Thrombopenia- Hypothyroidism

Factors to consider in the ederly mRCC populationpopulation
Bellmunt J et al, Critical Rev Oncol Hematol 2009 vol 69:64-72

Absorption and Metabolism change in the elderly populationelderly population
Physiological Changes from Aging: Consequence on Drug Absorption:Decreased gastric motilityDecreased secretionsDecreased absorptive surface
May lead to slower absorption and delayed onset of effect
Ph i l i l Ch f A i Consequence on Drug Metabolism:Physiological Changes from Aging:
Decreased Liver Size (Between 18‐44%)
Consequence on Drug Metabolism:
Antiangiogenic drugs that undergo “Ph 1Decreased Hepatic Blood Flow “Phase 1
Metabolism” will result in higher concentrations from decreased
metabolism

How can we manage potential risks in the i t i l ti ?geriatric population?
Geriatric appraisalpp
To help making a decision on whether to treat cancer in ederly patients
• Geriatric assessment scores based on:treat cancer in ederly patients
- Functionality (self ability)- Cognitive status and moodCognitive status and mood- Social situation (familial help?)
C biditi d th i t t t- Comorbidities and their treatments.

To help making a decision on whether to treat i ld l icancer in elderly patients
• Geriatric algorithm (Balducci-Extermann)g ( )3 categories
Healthy Frail Too sick
E al ate life LimitedTreat as usual
Evaluate life expectancy without cancer versus with
Limited interventions, supportive
treated cancer (onco-geriatric assessment)
care

Survival probability correlates with individual h l hhealth status
IndependentIndependent
Vulnerable
val r
atio
FragileHigher vulnerability and
frailty are associated with increased risk of death
Surv
i
IndependentIncontinent
g increased risk of death
Survival (months)
Incontinent Vulnerable*Frail** 5 years
Survival (months)
Rockwood K et al. Lancet 1999, 353, 205-206

Incidence of comorbidities in « frail » elderly patients (>70) in France (2006)elderly patients (>70) in France (2006)
Type of comorbity %CardiovascularCardiovascular
Cardiac failure 29Coronaropathy 22
Hypertension 47Cardiac rhythm 23
Thrombo-embolism 15Thrombo embolism 15Digestive system 18Denutrition 10Osteoarticular syndrome with impact on mobility 43Metabolic disturbances
Diabetes 12Diabetes 12Dehydration 9
Thyroid disease 9

Toxic effects of treatments targeted therapies for mRCC in patients with comorbidities
Type of comorbity Treatment ToxicityCardiovascular HTA Cardiovascular HTA, ….Digestive system Digestive symptomsDenutrition Weight lossgOsteoarticular with mobility impact Hand and foot Syndome, fatigueMetabolic disturbances hypothyroidismRenal insufficiency MAT, proteinuriaDiabetes Normalization of glycemia (SU)1
1Billemont B and Medioni J et al, Br J Cancer. 2008 Nov 4;99(9):1380-2

Example from our institution regarding ld ti t t t d ith TKIolder patients treated with TKI
• Clinical Case of a women, 78 years oldKidney cancer, lung metastasisHTA, well controlled with 3 medicationsSunitinib given at 37 5 mg 4w/6Sunitinib given at 37.5 mg 4w/6
• After 1 cycle, PRES syndome y , ywith coma, ocular vision disturbance, epilepsia and HTA
iti ib t- sunitinib stop- complete recovery in 7 days- need to manage HTA especially in g p y
ederly populationMedioni J et al, Targeted Oncol 2007

Example from our institution regarding older patients treated with TKIolder patients treated with TKI
• Clinical Case of a man, 70 years oldL ft h t l ll i F 4Left nephrectomy, clear cell carcinoma, F gr 4residual GFR = 41 ml/minlung metastasislung metastasisBevacizumab (B) & IFN
Aft d i j ti (B) HTA• After second injection (B) HTA, nephrotic syndrom, haemolytic-uraemic syndromehaemolytic-uraemic syndrome- B stop- biopsy: glomerular thrombotic microangiopathy- Response: normalization blood pressure, return to
renal function to previous baseline levelsFrangie C et al. Lancet Oncol 2007, 8:177-78

If an elderly patient appears to be a candidate for targeted therapiescandidate for targeted therapies
• Consider situations at risk:- Comorbidities >2 = risk ++- Polypharmacy >3 = risk ++yp y- Familial status (alone or with an elderly spouse)
Think that these risks have potential synergisticeffects:comorbidities x polypharmacy x familial status =
Very high risk of complications !

Adjusting targeted therapies in elderly ti tpatients means
Estimate the risk of complications• Estimate the risk of complications• Reinforce information to general practitioner
d f iland family• Close management with frequent visits & calls
Hold or decrease treatment doses before f t i iti !!!!occurrence of severe toxicities !!!!
Related Documents