© The Children's Mercy Hospital, 2014. 11/14 Center for Genomic Medicine Center for Genomic Medicine Joshua E. Petrikin, MD Joshua E. Petrikin, MD Director of Neonatal Genomics Director of Neonatal Genomics Genomic Medicine in the NICU Genomic Medicine in the NICU

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
© The Children's Mercy Hospital, 2014. 11/14
Center for Genomic Medicine Center for Genomic Medicine
Joshua E. Petrikin, MDJoshua E. Petrikin, MD
Director of Neonatal GenomicsDirector of Neonatal Genomics
Genomic Medicine in the NICUGenomic Medicine in the NICU

© The Children's Mercy Hospital, 2014. 03/14
2
© The Children's Mercy Hospital, 2014. 11/14
DisclosuresDisclosures
• I have no conflicts of interest to disclose
• I will not be discussing off label medication uses

© The Children's Mercy Hospital, 2014. 03/14
3
© The Children's Mercy Hospital, 2014. 11/14
OverviewOverview
• Discuss past and current genetic testing
• Define Genomic Medicine
• Speculate on future directions for genomics
• Elucidate some ethical considerations in Neonatal genomic testing

© The Children's Mercy Hospital, 2014. 03/14
4
© The Children's Mercy Hospital, 2014. 11/14
Genetic TestingGenetic Testing
• The analysis of human DNA, RNA, chromosomes, proteins, and certain metabolites in order to detect heritable disease-related genotypes, mutations, phenotypes or karyotypes for clinical purposes.
• Prenatal, newborn, and carrier screening included.

© The Children's Mercy Hospital, 2014. 03/14
5
© The Children's Mercy Hospital, 2014. 11/14
http://www.indiana.edu/~oso/lessons/Genetics/MyFamily2.html

© The Children's Mercy Hospital, 2014. 03/14
6
© The Children's Mercy Hospital, 2014. 11/14
Genetic Testing:Genetic Testing:Chromosome KaryotypeChromosome Karyotype

© The Children's Mercy Hospital, 2014. 03/14
7
© The Children's Mercy Hospital, 2014. 11/14
ExampleExamplePatient #1 is a 10 year old girl with short stature and a broad neckPatient #1 is a 10 year old girl with short stature and a broad neck

© The Children's Mercy Hospital, 2014. 03/14
8
© The Children's Mercy Hospital, 2014. 11/14
Microarrays aka “CHIPS”
• Short oligos are attached to a solid support (microarray).
• Hybridize with fluorescently labeled PCR products containing SNP of interest.
• Can analyze many mutations at once
• Currently > 740k SNP per chip

© The Children's Mercy Hospital, 2014. 03/14
9
© The Children's Mercy Hospital, 2014. 11/14
Array-CGH (comparative genomic hybridization)

© The Children's Mercy Hospital, 2014. 03/14
10
© The Children's Mercy Hospital, 2014. 11/14
Deletion on array
Muscular Dystrophy
• Since 65-85% of cases are due to deletions, start with deletion testing.
• The lab we use for dystrophin deletion testing uses an “exon array” with high density probes spanning entire dystrophin gene.
• Case 4 patient has a deletion including exons 44-48 (not shown here).
• If no deletion detectable, sequence entire DMD gene (79 exons!).

© The Children's Mercy Hospital, 2014. 03/14
11
© The Children's Mercy Hospital, 2014. 11/14
Genomic MedicineGenomic Medicine
• A structured approach to disease diagnosis & management that prominently features genome sequence information.
• Decoding Genomes to diagnose diseases better and help choose the best treatments

© The Children's Mercy Hospital, 2014. 03/14
12
© The Children's Mercy Hospital, 2014. 11/14
Monogenic DiseasesMonogenic Diseases
J Clin Invest. 2008;118:1590-1605. doi:10.1172/JCI34772.
© The Children's Mercy Hospital, 2014. 03/14
13
© The Children's Mercy Hospital, 2014. 11/14
7,700 monogenic diseases7,700 monogenic diseases
• 4,174 causal genes known• Affect 4% of children• Cause 20% of infant deaths• Cause 17% of pediatric hospitalizations
• Genome Variants determine phenotype• Genome variants = individual changes in the DNA
sequence from “normal”• Proving ground for genomic medicine
• 20 year experience with sequence-based diagnosis • 1-gene-at-a-time• Slow (months – years)• Expensive ($2500 - $10,000)• Requires right gene to be nominated
© The Children's Mercy Hospital, 2014. 03/14
14
© The Children's Mercy Hospital, 2014. 11/14
Neonatal Intensive CareNeonatal Intensive Care
• 4.1 million babies born in US / year• 1 in 20 admitted to NICU
• 220,000 (5.4%) NICU admissions/year• 30% due to congenital abnormalities
• 19,000 neonatal deaths/year• 6.8/1000 • 22% due to congenital abnormalities
• $3,000 - $8,000 per day
© The Children's Mercy Hospital, 2014. 03/14
15
© The Children's Mercy Hospital, 2014. 11/14
Neonatal Diseases are UniqueNeonatal Diseases are Unique
• Emergencies• Rapid results can guide management
• Largely stereotyped presentation• Broad differential diagnosis workups
• Considerable genetic heterogeneity• Molecular diagnoses almost never made

© The Children's Mercy Hospital, 2014. 03/14
16
© The Children's Mercy Hospital, 2014. 11/14
Neonatal Genomic Medicine
NICU
$3,000 - $8,000 per day
Rapid Genome Sequence• Test for things too rare and/or
heterogeneous to be considered• Identification of genotype before
phenotype fully manifests• Diagnose or rule out known
mutations• Reduce unnecessary tests &
empiric therapies• Improve prognostic assessment,
genetic counseling
• Unique opportunity to intervene before irreversible disease processes manifests with irreversible symptoms

© The Children's Mercy Hospital, 2014. 03/14
17
© The Children's Mercy Hospital, 2014. 11/14
Genomic Sequencing – Sanger
© The Children's Mercy Hospital, 2014. 03/14
18
© The Children's Mercy Hospital, 2014. 11/14
Human GenomeHuman Genome
3.2 billion base pairs, 6.4 billion ntEqual to typing 60 words/min x 8hrs/day x 50 years
20,000 genes (just 2% of genome) which encode 100,000 proteins
7700 Monogenic diseases

© The Children's Mercy Hospital, 2014. 03/14
19
© The Children's Mercy Hospital, 2014. 11/14
© The Children's Mercy Hospital, 2014. 03/14
20
© The Children's Mercy Hospital, 2014. 11/14
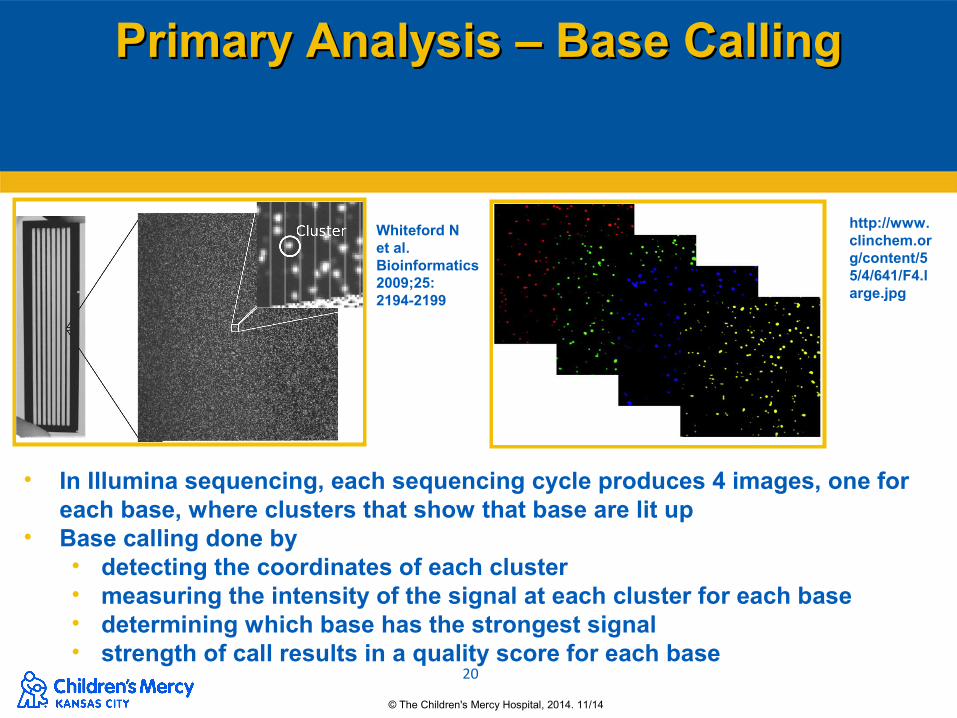
Primary Analysis – Base CallingPrimary Analysis – Base Calling
• In Illumina sequencing, each sequencing cycle produces 4 images, one for each base, where clusters that show that base are lit up
• Base calling done by• detecting the coordinates of each cluster• measuring the intensity of the signal at each cluster for each base• determining which base has the strongest signal• strength of call results in a quality score for each base
Whiteford N et al. Bioinformatics 2009;25:2194-2199
http://www.clinchem.org/content/55/4/641/F4.large.jpg
© The Children's Mercy Hospital, 2014. 03/14
21
© The Children's Mercy Hospital, 2014. 11/14
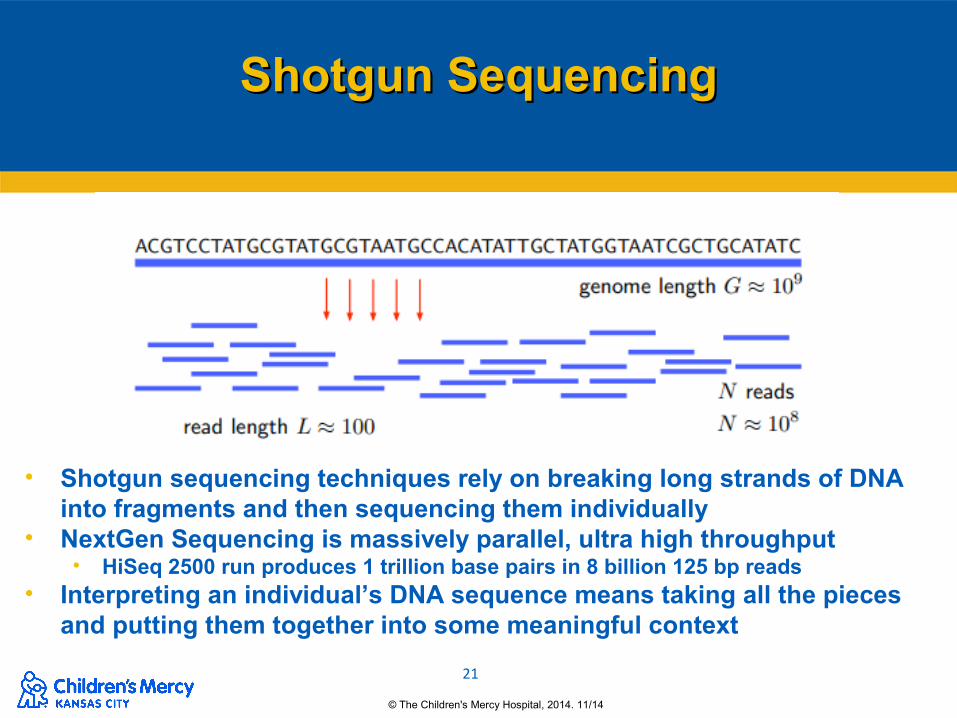
Shotgun SequencingShotgun Sequencing
• Shotgun sequencing techniques rely on breaking long strands of DNA into fragments and then sequencing them individually
• NextGen Sequencing is massively parallel, ultra high throughput• HiSeq 2500 run produces 1 trillion base pairs in 8 billion 125 bp reads
• Interpreting an individual’s DNA sequence means taking all the pieces and putting them together into some meaningful context
© The Children's Mercy Hospital, 2014. 03/14
22
© The Children's Mercy Hospital, 2014. 11/14
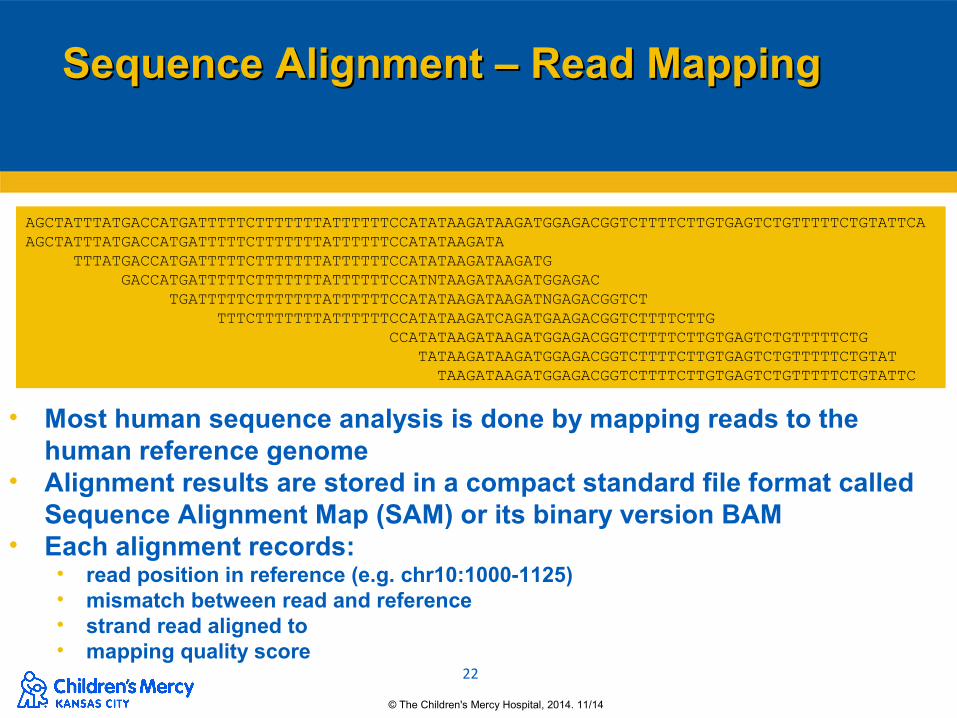
Sequence Alignment – Read MappingSequence Alignment – Read Mapping
AGCTATTTATGACCATGATTTTTCTTTTTTTATTTTTTCCATATAAGATAAGATGGAGACGGTCTTTTCTTGTGAGTCTGTTTTTCTGTATTCAAGCTATTTATGACCATGATTTTTCTTTTTTTATTTTTTCCATATAAGATA TTTATGACCATGATTTTTCTTTTTTTATTTTTTCCATATAAGATAAGATG
GACCATGATTTTTCTTTTTTTATTTTTTCCATNTAAGATAAGATGGAGAC TGATTTTTCTTTTTTTATTTTTTCCATATAAGATAAGATNGAGACGGTCT TTTCTTTTTTTATTTTTTCCATATAAGATCAGATGAAGACGGTCTTTTCTTG CCATATAAGATAAGATGGAGACGGTCTTTTCTTGTGAGTCTGTTTTTCTG TATAAGATAAGATGGAGACGGTCTTTTCTTGTGAGTCTGTTTTTCTGTAT TAAGATAAGATGGAGACGGTCTTTTCTTGTGAGTCTGTTTTTCTGTATTC
• Most human sequence analysis is done by mapping reads to the human reference genome
• Alignment results are stored in a compact standard file format called Sequence Alignment Map (SAM) or its binary version BAM
• Each alignment records:• read position in reference (e.g. chr10:1000-1125)• mismatch between read and reference• strand read aligned to• mapping quality score
© The Children's Mercy Hospital, 2014. 03/14
23
© The Children's Mercy Hospital, 2014. 11/14
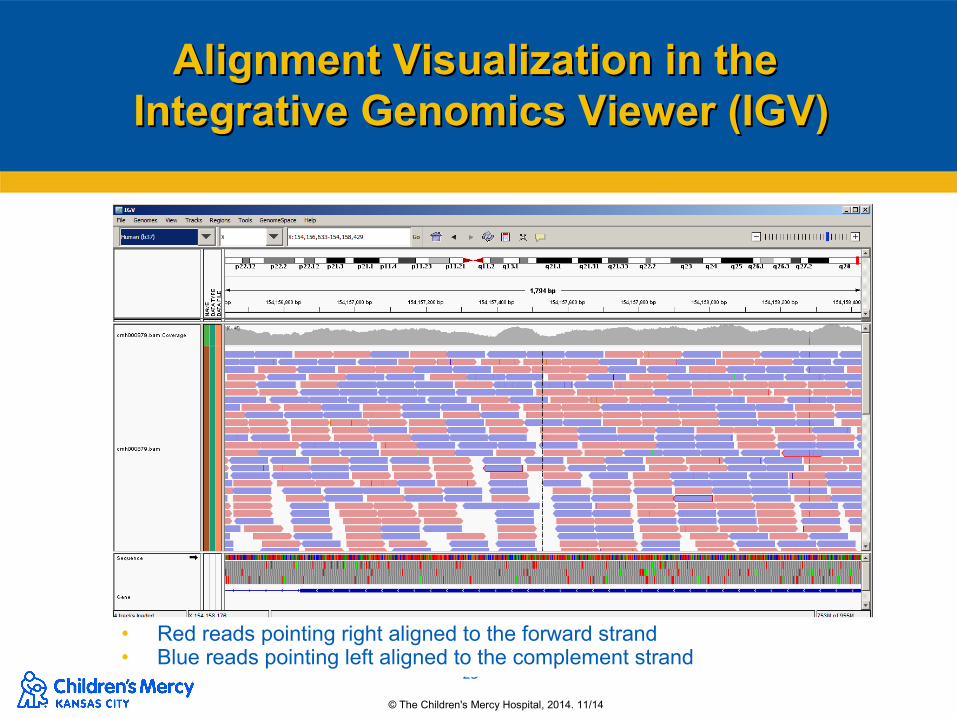
Alignment Visualization in the Alignment Visualization in the Integrative Genomics Viewer (IGV)Integrative Genomics Viewer (IGV)
• Red reads pointing right aligned to the forward strand• Blue reads pointing left aligned to the complement strand

© The Children's Mercy Hospital, 2014. 03/14
24
© The Children's Mercy Hospital, 2014. 11/14
SubstitutionsSubstitutions

© The Children's Mercy Hospital, 2014. 03/14
25
© The Children's Mercy Hospital, 2014. 11/14
DeletionsDeletions

© The Children's Mercy Hospital, 2014. 03/14
26
© The Children's Mercy Hospital, 2014. 11/14
Infant CMH487
Diagnosis!
Bioinformatic Filter 5

© The Children's Mercy Hospital, 2014. 03/14
27
© The Children's Mercy Hospital, 2014. 11/14
Newborn TestingNewborn Testing
• ““If medical or psychosocial benefits of genetic test will not accrue until adulthood, as in case of carrier status or adult-onset diseases, genetic testing should be deferred…”
• Guides gene analysis/interpretation• Do not analyze newborns for carrier status or
adult conditions or off-target diseases

© The Children's Mercy Hospital, 2014. 03/14
28
© The Children's Mercy Hospital, 2014. 11/14
Secondary Secondary Findings
• Also called incidental or unanticipated findings
• Highly likely, if not inevitable, whenever WGS/WES is performed
• Examples include:• finding of a previously unsuspected high risk of
future disease • discovery of a disorder in an asymptomatic
individual• detection of carrier status

© The Children's Mercy Hospital, 2014. 03/14
29
© The Children's Mercy Hospital, 2014. 11/14
Incidental Findings in Incidental Findings in Neonates?Neonates?
• Mandate to avoid violating a child’s right to an open future?
• Considerations• Parents of critically-ill children “just tell me where
to sign”• Feasibility of reporting secondary findings -
accuracy, expectations, defining the scope• Impacts:
• Test design (SSAGA)• Consent• Communication of results

© The Children's Mercy Hospital, 2014. 03/14
30
© The Children's Mercy Hospital, 2014. 11/14
Francis Collins, Director of the NIH, Francis Collins, Director of the NIH, Wall Street Journal, July 8, 2014
"Over the course of the next few decades, the availability of cheap, efficient DNA sequencing technology will lead to a medical landscape in which each baby's genome is sequenced, and that information is used to shape a lifetime of personalized strategies for disease prevention, detection and treatment."

© The Children's Mercy Hospital, 2014. 03/14
31
© The Children's Mercy Hospital, 2014. 11/14
Not quite inexpensive enough for generalized newborn screening—but right up there for diagnosis of ill infants in the NICU

© The Children's Mercy Hospital, 2014. 03/14
32
© The Children's Mercy Hospital, 2014. 11/14
Adapted from Sir George Poste, circa1999

© The Children's Mercy Hospital, 2014. 03/14
33
© The Children's Mercy Hospital, 2014. 11/14
Take Home PointsTake Home Points
• Genomic Medicine hold promise, but is not the final answer• Proteinomics, metabolomics, epigenetics
• WGS compares most of a patient’s genome against a reference genome• Deletions, insertions, triplet repeats
centrimeric anomalies undetected• The focus on care will shift from disease
centered to patientcentered

© The Children's Mercy Hospital, 2014. 03/14
34
© The Children's Mercy Hospital, 2014. 11/14
Take Home PointsTake Home Points
• Whole genome sequencing is not ready for prime time use for newborn screening
• Don’t invest in WGS equipment and bioinformatics tools yet
• Ethical questions arise as to the use of WGS for NBS
• Adult onset disorders
• Variants of unknown significance
• Paternity
© The Children's Mercy Hospital, 2014. 03/14
35
© The Children's Mercy Hospital, 2014. 11/14
Children’s Mercy HospitalCenter for Pediatric Genomic Medicine
Supported ByClements
FoundationMarion Merrell Dow
FoundationNational Institutes of
HealthWT Kemper FoundationPatton Trust
Director Dr. Stephen Kingsmore
Related Documents











