4/27/2016 1 Genetic Counseling & the Woman’s Health Patient MCW Women’s Health Conference Morgan Depas, MS, CGC Samantha Stachowiak, MS, CGC At the conclusion of this presentation, participants should understand the following: • How to recognize patients and families who may benefits from a prenatal or cancer genetics consult • Understand how a patient’s family history may impact cancer screening recommendations • Understand the benefits and limitations of cell free DNA testing 2 Family History is Important • 5 – 10 % of all cancers are HEREDITARY • 15‐20% of cancers are FAMILIAL • 70‐80% of cancers are SPORADIC • Family history tailors cancer screening recommendations and reduces cancer risks 3 Frezzo et al. 2003; Guttmacher et al. 2004; Yoon et al. 2002; Nagy et al. 2004. Hereditary Familial Sporadic 70‐80% 15‐20% 5‐10% “The identification of at‐risk individuals can facilitate individualized preventative care and surveillance, which could impact disease morbidity and mortality” Owens et al, 2011

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

4/27/2016
1
Genetic Counseling & the Woman’s Health Patient
MCW Women’s Health Conference
Morgan Depas, MS, CGC
Samantha Stachowiak, MS, CGC
At the conclusion of this presentation, participants should understand the following:
• How to recognize patients and families who may benefits from a prenatal or cancer genetics consult
• Understand how a patient’s family history may impact cancer screening recommendations
• Understand the benefits and limitations of cell free DNA testing
2
Family History is Important
• 5 – 10 % of all cancers are HEREDITARY
• 15‐20% of cancers are FAMILIAL
• 70‐80% of cancers are SPORADIC
• Family history tailors cancer screening recommendations and reduces cancer risks
3Frezzo et al. 2003; Guttmacher et al. 2004; Yoon et al. 2002; Nagy et al. 2004.
Hereditary Familial
Sporadic
70‐80%
15‐20%
5‐10%
“The identification of at‐risk individuals can facilitate individualized preventative care and surveillance, which could impact disease morbidity and mortality”
Owens et al, 2011

4/27/2016
2
Family History: The Basics
• Who?– Mom, dad, siblings, aunts, uncles, nieces, nephews, children,
grandchildren, grandparents, and cousins
– Maternal and paternal relatives
• What?– Cancer type
– Age of diagnosis
– Unusual pathological features
– Multiple primaries
• “Are there other cancers?”
• Ancestry?
4
Who Should Be Referred?
Red Flags for Hereditary Cancer: EMR
Early age at cancers diagnosis (personal or family history)
– Pre‐menopausal breast cancer
– Colorectal cancer diagnosed <50 years of age
Multiple
– Individuals with multiple primary cancers• Women with breast and ovarian cancer
• Individual with two separate colorectal cancers
– Clusters of the same or related types of cancer
– Breast & ovarian cancer or colon & endometrial cancer
Rare
– Rare cancers present in patient and/or family history• Ovarian cancer
• Male breast cancer
4/27/2016
3
What is Genetic Counseling?
• Process of helping people understand and adapt to the medical, psychological and familial implications of genetic contributions to disease
• Genetic Counselors are specially trained Advanced Practice Providers
7
What is the Role of a Cancer Genetic Counselor?
• Provide risk assessment based on family history
• Evaluate for possible hereditary cancer syndromes
• Determine appropriate genetic test and testing strategy
– Genetic counseling does not always include genetic testing
• Aid in test interpretation
8
9
Maternal grandfather
Maternalgrandmother
Aunt Uncle
Brother
2 2 2 2
Proband
1
1 1 22
3
Sister First cousin
(female)
MotherFather
1
Paternal grandfather
Paternal grandmother
22
NephewNiece
1 1
Son Daughter
22
GrandsonGrand‐daughter
3
Great aunt
Great uncle
3

4/27/2016
4
What is the Role of a Cancer Genetic Counselor?
• Explore the psychological impact of genetic testing
• Work closely with insurance companies
• Address genetic discrimination concerns
• Introduce medical management options
• Talk about implications for family members
• Discuss the option of DNA banking
• Acts as a resource for the patient and family
10
d. 56 y OvCa dx 46 y
d. 45 y BrCa
BrCa
d. 53 y OvCa
Laboratories offering genetic testing for hereditary cancer
…and many more.

4/27/2016
5
Genetic Testing is Multifaceted
• Multiple genes for a syndrome• Different testing methods
– Tumor testing– Genetic testing
• Single site analysis• Multisite analysis• Sequencing• Deletion/duplication testing• NextGeneration sequencing technologies
• New genes become available for testing• Determine most informative family member for testing• Challenges in test interpretation and variants of uncertain
significance
13
Movement away from single gene testing and toward Next Generation Sequencing (NGS)
multi‐gene panels
Why?• Efficient sequencing of multiple
genes• Many genes implicated in each
cancer– Testing multiple genes
simultaneously can be more time efficient and more cost effective
• Overlapping clinical presentation among different hereditary cancer syndromes
– Approximately 9‐10% of BRCA‐negative patients have a causative gene mutation identified via panel testing (Ambry Genetics data)
Genes Associate with Hereditary Breast and Ovarian Cancer
Courtesy of
4/27/2016
6
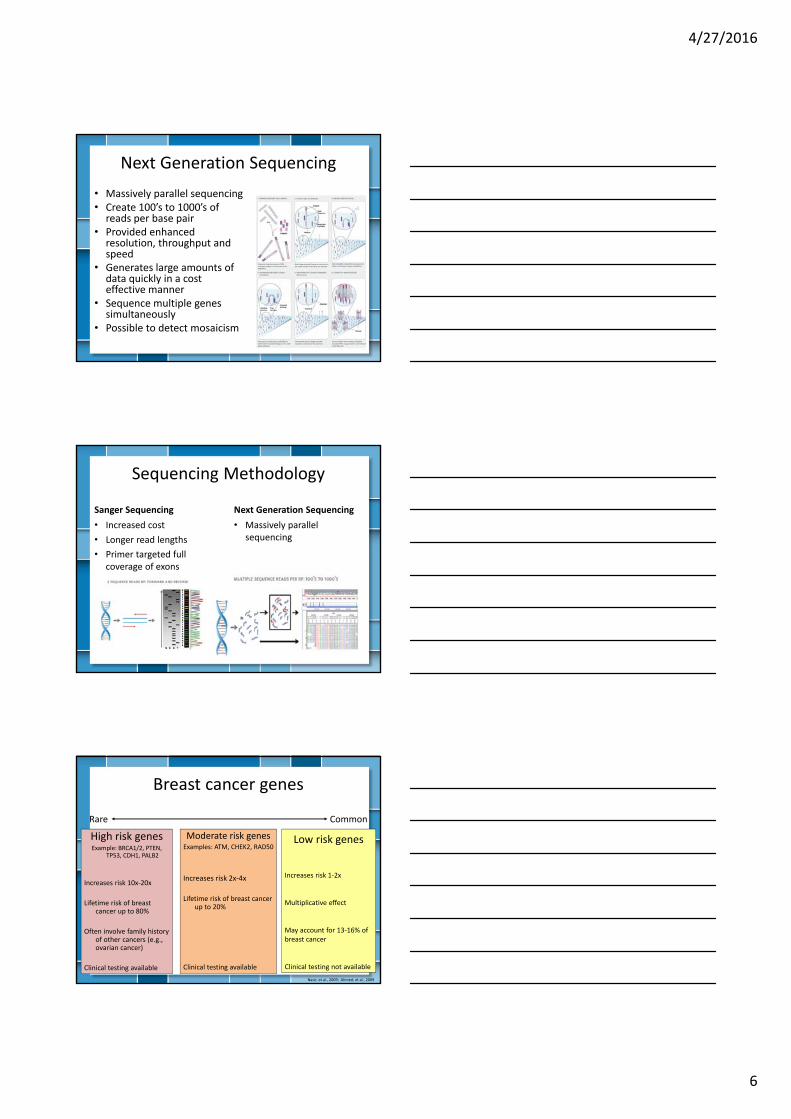
Next Generation Sequencing
• Massively parallel sequencing• Create 100’s to 1000’s of reads per base pair
• Provided enhanced resolution, throughput and speed
• Generates large amounts of data quickly in a cost effective manner
• Sequence multiple genes simultaneously
• Possible to detect mosaicism
Sequencing Methodology
Sanger Sequencing
• Increased cost
• Longer read lengths
• Primer targeted full coverage of exons
Next Generation Sequencing
• Massively parallel sequencing
Breast cancer genes
High risk genesExample: BRCA1/2, PTEN,
TP53, CDH1, PALB2
Increases risk 10x‐20x
Lifetime risk of breast cancer up to 80%
Often involve family history of other cancers (e.g., ovarian cancer)
Clinical testing available
Moderate risk genesExamples: ATM, CHEK2, RAD50
Increases risk 2x‐4x
Lifetime risk of breast cancer up to 20%
Clinical testing available
Low risk genes
Increases risk 1‐2x
Multiplicative effect
May account for 13‐16% of breast cancer
Clinical testing not available
Nasir, et al., 2009; Ahmed, et al., 2009
Rare Common
4/27/2016
7
Genetic Testing
• Benefits– Provides more accurate risk of cancer moving forward for individuals
and families– Provides information useful for medical management– Leads to cancer PREVENTION and EARLY detection of cancer– May actually relieve anxiety
• Risks– Emotional (increased fear/anxiety)– Insurance Discrimination
• State and Federal Laws
• Limitations– Genetic testing is not able to detect all causes of hereditary cancer– Continued risk for sporadic cancers– Some management strategies not proven effective
19
Genetic Information Nondiscrimination Act (GINA)
• GINA is a federal law passed in 2008 that protects individuals from genetic discrimination in health insurance and employment
– GINA prohibits employers from discriminating against employees and applicants based on genetic tests and genetic information and prohibits health insurers from restricting enrollment or adjusting premiums for health insurance on the basis of genetic information
• For additional information: http://ginahelp.org/
20
Breast Cancer
21American Cancer Society Breast Cancer Facts & Figures 2011‐2012
Most commonly diagnosed cancer in women
2nd leading cause of cancer death in women
Risk Factors
Age
Risk increases with age
Median age at diagnosis is 61 years
Hormonal factors
Early menarche/Late menopause
Nulliparity
Hormone replacement therapy
Lifestyle
Alcohol consumption
Physical inactivity
Obesity
4/27/2016
8
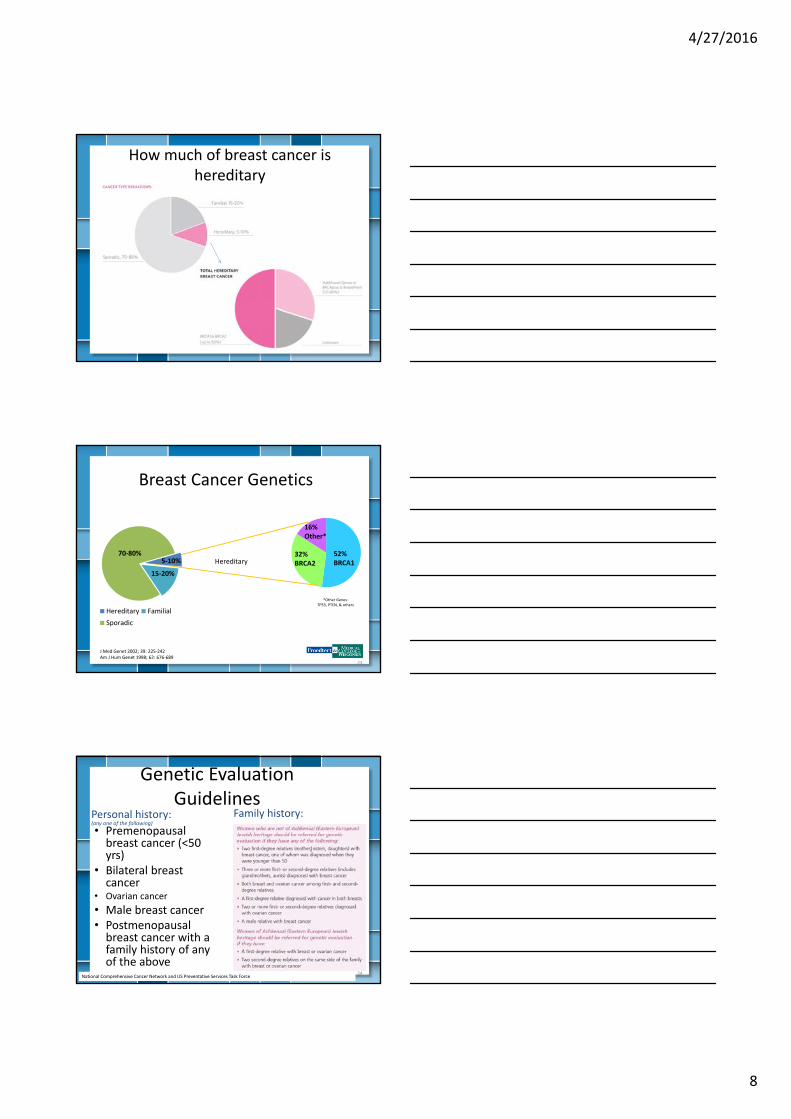
How much of breast cancer is hereditary
Breast Cancer Genetics
23
52%BRCA1
32%BRCA2
16%Other*
*Other Genes:TP53, PTEN, & others
J Med Genet 2002; 39: 225‐242Am J Hum Genet 1998; 62: 676‐689
Hereditary Familial
Sporadic
70‐80%
15‐20%
5‐10% Hereditary
Genetic Evaluation Guidelines
• Premenopausal breast cancer (<50 yrs)
• Bilateral breast cancer
• Ovarian cancer
• Male breast cancer• Postmenopausal breast cancer with a family history of any of the above
24National Comprehensive Cancer Network and US Preventative Services Task Force
Family history:Personal history: (any one of the following)

4/27/2016
9
Breast Cancer Risk Models
• Risk assessment models can aid in patient management
• Chance of developing breast cancer– Gail model– Claus tables– BRCAPRO– Tyrer‐Cuzick (IBIS)– BOADICEA
• Chance of having BRCA gene mutation– BRCAPRO – Tyrer‐Cuzick (IBIS)– BOADICEA
25Saslow et al, Ca Cancer J Clinic 2007;57:75‐89 Bellcross Oncology Genetics 2009; 6(8): 373‐382
Hereditary Breast and Ovarian Cancer (HBOC) Syndrome
• BRCA1 & BRCA2 gene mutations• Autosomal dominant inheritance• Breast cancer
– 45‐85% lifetime risk– Risk for a 2nd primary breast cancer
• Ovarian cancer– 15‐45% lifetime risk
• Other increased cancer risk– Prostate, male breast, pancreatic, melanoma, ocular melanoma
26
AJHG. 2003:1117‐1130 Science. 2003:643‐646 J Clin Oncol. 2007:1329‐33
HBOC Medical Management
• Change in screening recommendations – National Comprehensive Cancer Network– American Cancer Society– US Preventive Services Task Force– American College of Obstetrics and Gynecology
• High risk surveillance – Annual mammogram and breast MRI
• Starting at age 25
– Semi‐annual transvaginal ultrasound and CA‐125 • Starting at age 30
• Risk reduction options– Tamoxifen for chemoprevention of breast cancer– Prophylactic mastectomy– Oral contraceptive use for chemoprevention of ovarian cancer– Prophylactic salpingo‐oophorectomy
• Decision Tool from Women with BRCA Mutation, http://brcatool.stanford.edu/brca.html
• Information for family members
27
4/27/2016
10
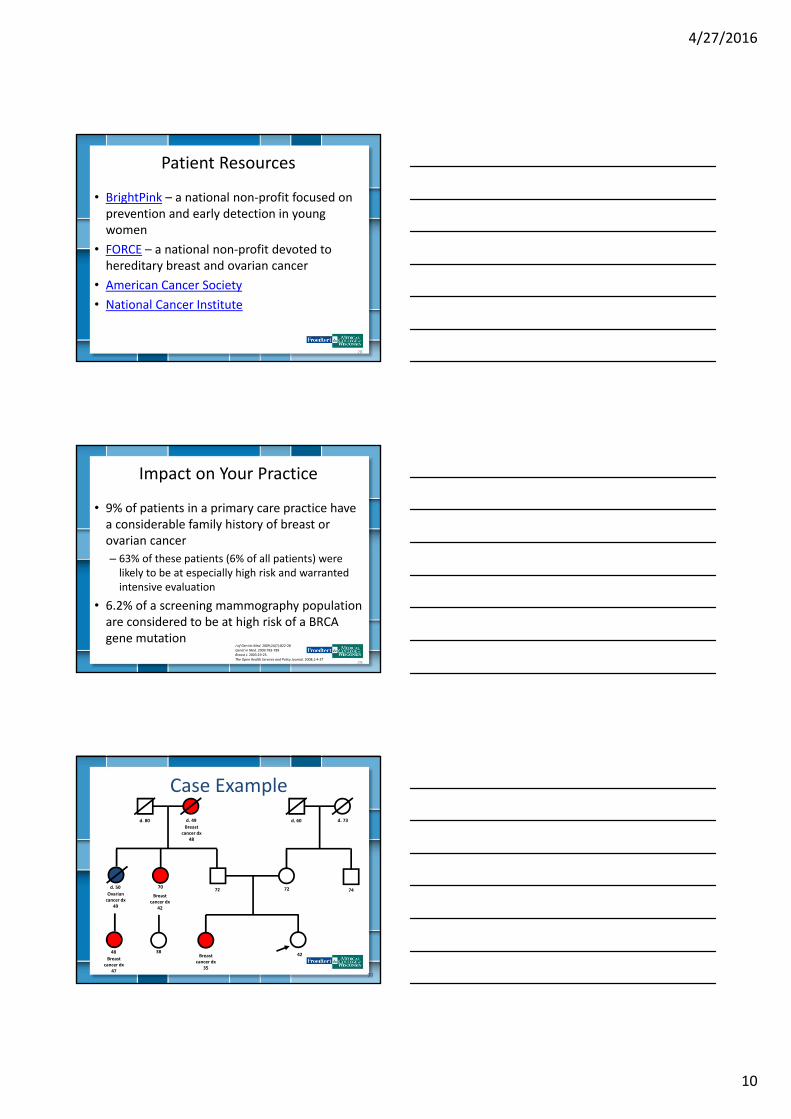
Patient Resources
• BrightPink – a national non‐profit focused on prevention and early detection in young women
• FORCE – a national non‐profit devoted to hereditary breast and ovarian cancer
• American Cancer Society
• National Cancer Institute
28
Impact on Your Practice
• 9% of patients in a primary care practice have a considerable family history of breast or ovarian cancer
– 63% of these patients (6% of all patients) were likely to be at especially high risk and warranted intensive evaluation
• 6.2% of a screening mammography population are considered to be at high risk of a BRCA gene mutation
29
J of Gen Int Med. 2009;24(7):822‐28Genet in Med. 2009:783‐789 Breast J. 2003:19‐25.The Open Health Services and Policy Journal. 2008;1:4‐37
30
42
7272
3848Breast
cancer dx 35
Breast cancer dx
47
70d. 50
Ovarian cancer dx
49
Breast cancer dx
42
d. 49
Breast cancer dx
48
d. 80
74
d. 73d. 60
Case Example

4/27/2016
11
Case Example
• Lifetime risk of developing breast cancer
– 26% based on BRCAPRO Model
– 35% based on Tyrer‐Cuzick Model
• Include annual breast MRI in medical management recommendations
31
32
42
7272
3848Breast
cancer dx 35
Breast cancer dx
47
70d. 50
Ovarian cancer dx
49
Breast cancer dx
42
d. 49
Breast cancer dx
48
d. 80
74
d. 73d. 60
Case Example
BRCA1 Mutation POSITIVE
+
BRCA1 Mutation NEGATIVE
‐
• Patient is now a TRUE NEGATIVE
• No increased risk for breast or ovarian cancer
• Medical management should include only annual mammogram
Prenatal Genetics
Samantha Stachowiak, MS, CGC

4/27/2016
12
Who should be referred for prenatal genetic counseling?
Indications
• Advanced maternal age• 35 years or older at delivery
for singleton pregnancy• 33 years or older for multiples
• Fetal ultrasound findings indicating an increased risk for aneuploidy
• Positive screening result for aneuploidy
• Pregnancy history• Multiple miscarriages• Prior pregnancy with a
trisomy
• Personal history• Carrier of genetic condition• Translocation carrier
• Family history• Genetic condition• Congenital anomaly
• Ancestry/Ethnicity• Carrier screening
Benefits of Seeing A Prenatal Genetic Counselor
• Assess individual risk of having a child with birth defects or a genetic condition– Learn more about birth defect or genetic condition
• Have a conversation about testing options
• What to expect and to prepare for the birth of a child with special needs and/or genetic condition
• Discuss pregnancy options, such as continuation of pregnancy, termination or adoption
4/27/2016
13
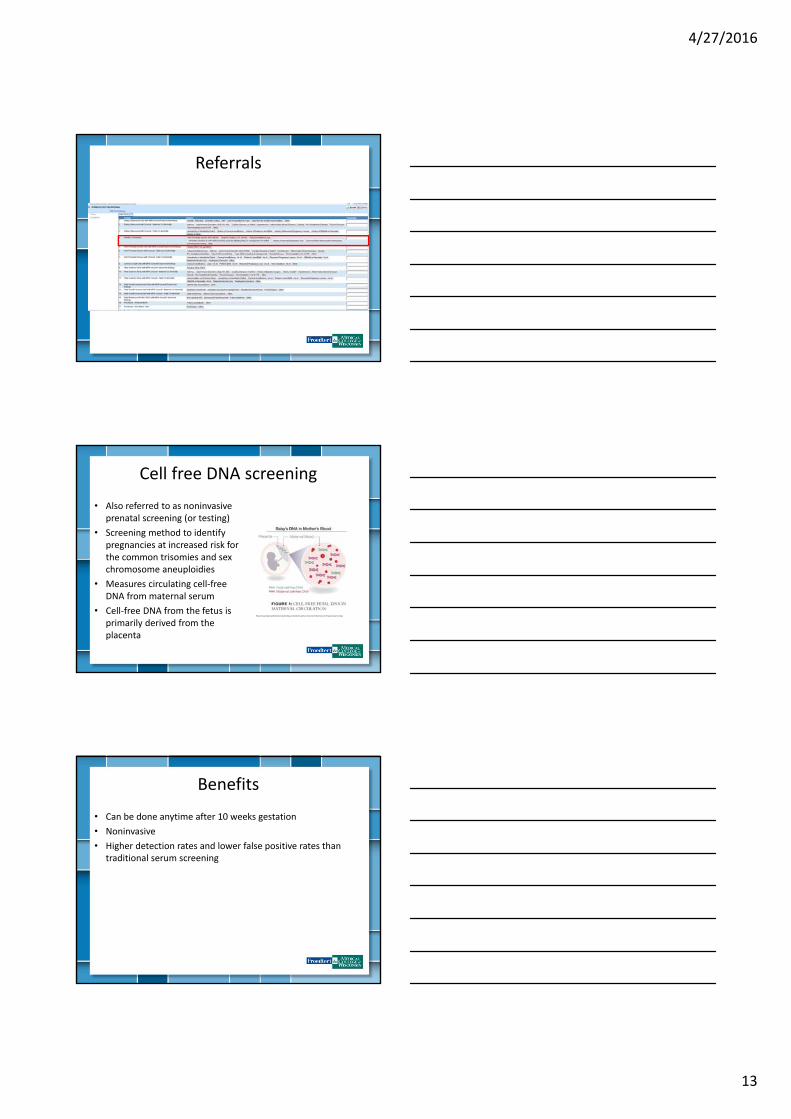
Referrals
Cell free DNA screening
• Also referred to as noninvasive prenatal screening (or testing)
• Screening method to identify pregnancies at increased risk for the common trisomies and sex chromosome aneuploidies
• Measures circulating cell‐free DNA from maternal serum
• Cell‐free DNA from the fetus is primarily derived from the placenta
http://www.downsyndromeprenataltesting.com/what‐exactly‐is‐maternit21‐harmony‐verifi‐panorama‐testing/
Benefits
• Can be done anytime after 10 weeks gestation
• Noninvasive
• Higher detection rates and lower false positive rates than traditional serum screening
4/27/2016
14
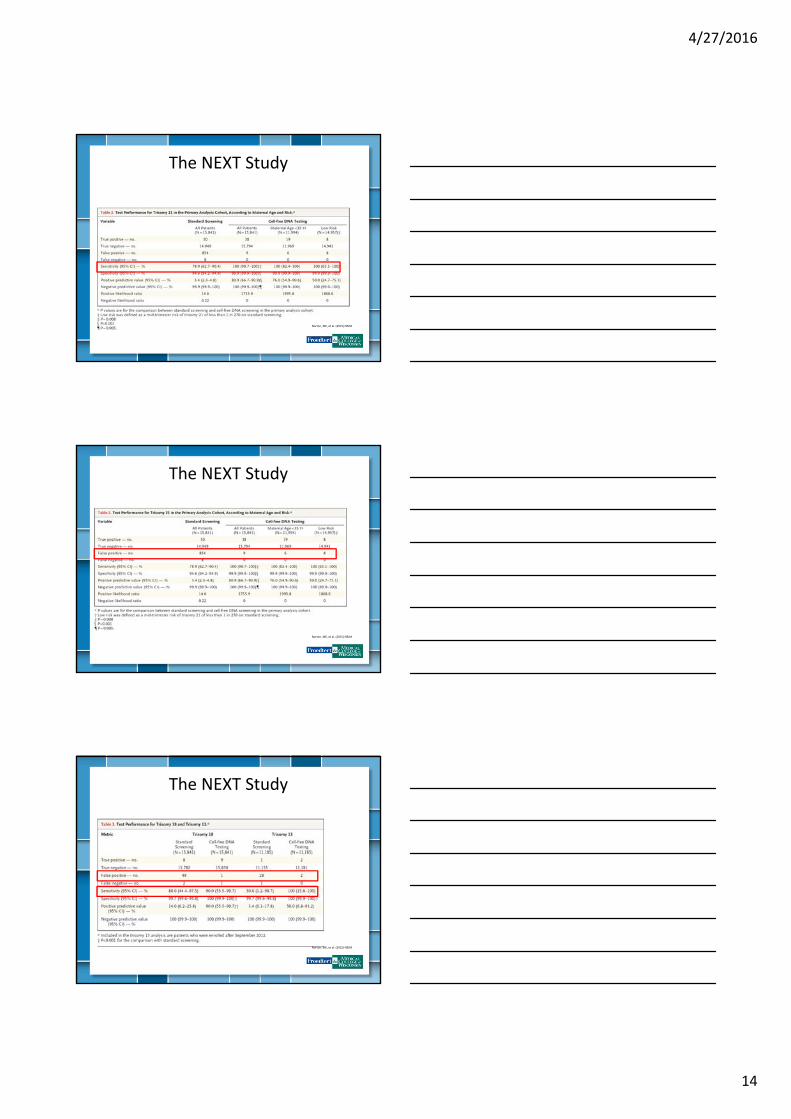
The NEXT Study
Norton, ME, et al. (2015) NEJM
The NEXT Study
Norton, ME, et al. (2015) NEJM
Norton, ME, et al. (2015) NEJM
The NEXT Study

4/27/2016
15
Limitations
• Non‐reportable results
• False positives
– Positive Predictive Value (PPV)
https://quizlet.com/8226119/blk‐8c‐genetics‐flash‐cards/
ACOG Committee Opinion 640
The NEXT Study
Norton, ME, et al. (2015) NEJM

4/27/2016
16
Updates in cell free DNA screening
Timeline of cell free DNA screening
Norton, ME. (2015) Am J Obstet Gynecol.
68%10%
22%
Chromosome Abnormalities
Common trisomies(T21, T18, T13)
Sex chromosomeaneuplodies
Other
Oct. 2011 Cell free DNA screening for T21 available
Feb. 2012T18 & T13 are added
Feb. 2013SCAs available
July 2015MaterniTGenome launches
Oct. 2013Microdeletions available
Microdeletion syndromes
• Missing piece of chromosome
• Common deletions screened:
– 22q11.2 deletion syndrome (DiGeorge)
– 1p36 deletion syndrome
– Cri‐du‐chat syndrome
– Prader‐Willi/Angelmansyndrome
– Wolf‐Hirschhorn syndrome
• Often have wide range of symptoms
• Rare in general population
• Most occur sporadically
4/27/2016
17
MaterniT Genome
• Most advanced information available from NIPT
• Looking at all chromosomes
• Identifies > 95% of genome‐wide deletions or duplications ≥ 7 Mb– Resolution of a karyotype
© 2015 Sequenom
Who should get this testing?
• ACOG and SMFM do not recommend routine screening for deletions or duplications
• Clinical validation needed
Carrier screening
4/27/2016
18
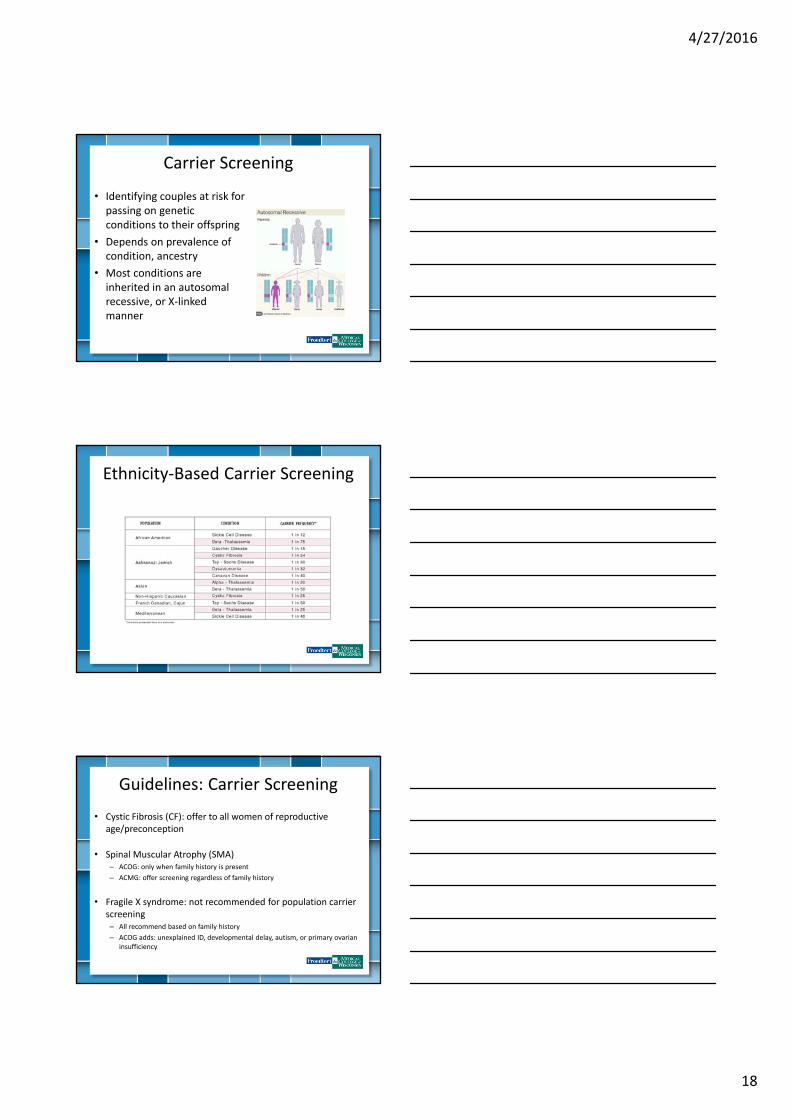
Carrier Screening
• Identifying couples at risk for passing on genetic conditions to their offspring
• Depends on prevalence of condition, ancestry
• Most conditions are inherited in an autosomal recessive, or X‐linked manner
Ethnicity‐Based Carrier Screening
Guidelines: Carrier Screening
• Cystic Fibrosis (CF): offer to all women of reproductive age/preconception
• Spinal Muscular Atrophy (SMA)– ACOG: only when family history is present
– ACMG: offer screening regardless of family history
• Fragile X syndrome: not recommended for population carrier screening– All recommend based on family history
– ACOG adds: unexplained ID, developmental delay, autism, or primary ovarian insufficiency

4/27/2016
19
Guidelines: Carrier Screening
– Hemoglobinopathies
• ACOG: African‐American, Mediterranean, Southeast Asian
– Ashkenazi Jewish:
• ACOG: Tay‐Sachs disease, CF, Canavan disease, familial dysautonomia
• ACMG: same as ACOG as well as Niemann‐Pick disease (type A), Bloom syndrome, Fanconi anemia group C, Mucolipidosis IV, and Gaucherdisease
– French Canadian/ Cajun: offer screening for Tay‐Sachs disease(ACOG)
Expanded Carrier Screening
• More comprehensive screening
– Advancements in technology allows screening of a large number conditions simultaneously
• Same conditions offered to everyone (regardless of race or ethnicity)
• Ideally should be offered before conception
– Provides couples with information for reproductive decision‐making
Expanded Carrier Screening
• In a study of 23,453 people, 24% were found to be a carrier of at least one non‐mild condition– 5.2% were found to be carriers of two or more conditions
– 127 “carrier couples” were identified
Lazarin GA, et al. (2013)Genet Med

4/27/2016
20
Expanded Carrier Screening
• Take away points from this study:– ACOG & ACMG guidelines would have missed 70% of carriers that were identified
– Several severe diseases had higher carrier frequencies than expected• Smith Lemli‐Opitz syndrome carrier frequency was 1 in 68 vs 1 in 123
– Several conditions were present outside their characteristic ethnic group• 26.3% of familial dysautonomia carriers did not report Jewish ancestry
Limitations/Considerations
• Conditions screened for range in severity
• Many are rare• Screen negative results
reduce likelihood of being a carrier but does not eliminate it
• MANY labs to choose from– Different conditions– Detection rates
• Genotyping vs Sequencing
How to Find Us
• Main GC phone line: 414‐955‐5899– Morgan Depas: 414‐805‐9036, [email protected]
• Email: [email protected]• Website: http://www.mcw.edu/Human‐and‐Molecular‐Genetics‐
Center‐HMGC/Genetic‐Counseling.htm
4/27/2016
21
How to Find a Genetic Counselor
• The National Society of Genetic Counselors website: http://www.nsgc.org/
• The Wisconsin Genetics Website: http://www.slh.wisc.edu/genetics/index.dot
• Contact State Genetic Coordinator– 608‐267‐7148
– Contact Us tab of Wisconsin Genetics Website
61
References
• American College of Obstetricians and Gynecologists. Committee Opinion No. 640: Cell‐free DNA Screening for fetal aneuploidy. Obstet Gynecol. 2015;126:e31‐7.
• Edwards JG, Feldman G, Goldberg J, Gregg AR, Norton ME, Rose NC, Schneider A, et al. Expanded carrier screening in reproductive medicine—points to consider: a joint statement of the American College of Medical Genetics and Genomics, American College of Obstetricians and Gynecologists, National Society of Genetic Counselors, Perinatal Quality Foundation, and Society for Maternal–Fetal Medicine. Obstet Gynecol. 2015;125:653–62.
• Lazarin GA, Haque IS, Nazareth S, Lori K, Patterson AS, Jacobson JL, Marshall JR, et al. An empirical estimate of carrier frequencies for 400+ causal Mendelian variants: results from an ethnically diverse clinical sample of 23,453 individuals. Genet Med. 2013 Mar;15(3):178‐86.
• Norton ME, Baer RJ, Wapner AJ, Kuppermann M, Jelliffe‐Powlowski LJ, Currier RJ. Cell‐free DNA vs sequential screening for the detection of fetal chromosomal abnormalities. Am J Obstet Gynecol. 2015 Dec 18.
• Norton, ME, Jacobsson, B, Swamy, GK, Laurent, LC, Ranzini, AC, Brar, H, Tomlinson, MW, et al. Cell‐free DNA analysis for noninvasive examination of trisomy. New England Journal of Medicine. 2015; 372(17), 1589–1597.
• Tomita‐Mitchell A, Mahnke DK, Larson JM, Ghanta S, Feng Y, Simpson PM, Broeckel U, et al. Multiplexed quantitative real‐time PCR to detect 22q11.2 deletion in patients with congenital heart disease. Physiol Genomics. 2010 Sep;42A(1):52‐60.
• Yaron Y, Jani J, Schmid M, Oepkes D. Current Status of Testing for Microdeletion Syndromes and Rare Autosomal Trisomies Using Cell‐Free DNA Technology. Obstet Gynecol. 2015 Nov;126(5):1095‐9
• Zhang H, Gao Y, Jiang F, Fu M, Yuan Y, Guo Y, & Wang W. Non‐invasive prenatal testing for trisomies 21, 18 and 13: clinical experience from 146,958 pregnancies. Ultrasound in Obstetrics & Gynecology. 2015; 45(5), 530–538.
Acknowledgements
• Wisconsin Cancer Risk Program Network (WiCRPN)
Related Documents











