AIDS Education and Prevention, 27(1), 84–101, 2015 © 2015 The Guilford Press 84 Jeffrey S. Crowley is affiliated with the O’Neill Institute for National and Global Health Law, George- town Law/Georgetown University, Washington, D.C. Shari Feirman and David R. Holtgrave are affiliated with the Department of Health, Behavior & Society, Johns Hopkins Bloomberg, School of Public Health, Baltimore, Maryland. Chris Collins is affiliated with the Community Mobilization Division, UNAIDS, Geneva, Switzerland and Formerly with amfAR, the Foundation for AIDS Research, Washington, D.C. The views or opinions expressed in this paper are those of the authors and not of UNAIDS. This manuscript was prepared using grants from amfAR to Georgetown and Johns Hopkins Universities, funded by a grant to amfAR from the Elton John AIDS Foundation. Address correspondence to Jeffrey S. Crowley, MPH, Distinguished Scholar, Program Director, National HIV/AIDS Initiative, O’Neill Institute for National and Global Health Law, Georgetown Law, 600 New Jersey Ave., NW, Washington, DC 20001. E-mail: [email protected] EXPLAINING DECLINING HIV INFECTION CROWLEY ET AL. GENERATING HYPOTHESES TO EXPLAIN DECLINING HIV INFECTION IN FOUR U.S. JURISDICTIONS Jeffrey S. Crowley, Shari Feirman, Chris Collins, and David R. Holtgrave The aims of this study were (1) to generate hypotheses to explain declines in HIV incidence in Massachusetts, North Carolina, San Francisco, and Se- attle, and (2) based on lessons learned from these jurisdictions, to offer rec- ommendations for implementation elsewhere. Through in-depth interviews, we identified policies and practices that stakeholders across jurisdictions believe are important to achieving successful outcomes. The most unify- ing observation was that leadership within health departments is critical to achieving success. With this consideration, we developed a list of tools for public health officials to assert leadership to address challenges posed by HIV: extending access to health insurance, using an array of approaches to increase knowledge of serostatus, investing in services to retain people in care, collecting and using better data, translating data into policy change and public health practice, developing targeted programming for vulnerable populations, minimizing administrative policies that attenuate program suc- cess, and diversifying funding sources. A December 2013 interim report on implementation of the U.S. National HIV/AIDS Strategy pointed out that progress on the domestic HIV/AIDS epidemic requires leadership at the local and state levels, as well as nationally (White House Office of National AIDS Policy, 2013). The most recent estimates of HIV incidence in the U.S. suggest that the annual number of new HIV infections remains relatively flat, with increasing incidence among young gay men of all races, but particularly young Black gay men offsetting stable or declining incidence in virtually all other population groups (Centers for Disease Control and Prevention, 2012). Stable HIV incidence, however, is not seen everywhere in the country. Several jurisdictions have reported evidence that the number of annual new HIV infections is falling, in some cases sig-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

AIDS Education and Prevention, 27(1), 84–101, 2015 © 2015 The Guilford Press
84
Jeffrey S. Crowley is affiliated with the O’Neill Institute for National and Global Health Law, George-town Law/Georgetown University, Washington, D.C. Shari Feirman and David R. Holtgrave are affiliated with the Department of Health, Behavior & Society, Johns Hopkins Bloomberg, School of Public Health, Baltimore, Maryland. Chris Collins is affiliated with the Community Mobilization Division, UNAIDS, Geneva, Switzerland and Formerly with amfAR, the Foundation for AIDS Research, Washington, D.C. The views or opinions expressed in this paper are those of the authors and not of UNAIDS.This manuscript was prepared using grants from amfAR to Georgetown and Johns Hopkins Universities, funded by a grant to amfAR from the Elton John AIDS Foundation. Address correspondence to Jeffrey S. Crowley, MPH, Distinguished Scholar, Program Director, National HIV/AIDS Initiative, O’Neill Institute for National and Global Health Law, Georgetown Law, 600 New Jersey Ave., NW, Washington, DC 20001. E-mail: [email protected]
EXPLAINING DECLINING HIV INFECTIONCROWLEY ET AL.
GENERATING HYPOTHESES TO EXPLAIN DECLINING HIV INFECTION IN FOUR U.S. JURISDICTIONS Jeffrey S. Crowley, Shari Feirman, Chris Collins, and David R. Holtgrave
The aims of this study were (1) to generate hypotheses to explain declines in HIV incidence in Massachusetts, North Carolina, San Francisco, and Se-attle, and (2) based on lessons learned from these jurisdictions, to offer rec-ommendations for implementation elsewhere. Through in-depth interviews, we identified policies and practices that stakeholders across jurisdictions believe are important to achieving successful outcomes. The most unify-ing observation was that leadership within health departments is critical to achieving success. With this consideration, we developed a list of tools for public health officials to assert leadership to address challenges posed by HIV: extending access to health insurance, using an array of approaches to increase knowledge of serostatus, investing in services to retain people in care, collecting and using better data, translating data into policy change and public health practice, developing targeted programming for vulnerable populations, minimizing administrative policies that attenuate program suc-cess, and diversifying funding sources.
A December 2013 interim report on implementation of the U.S. National HIV/AIDS Strategy pointed out that progress on the domestic HIV/AIDS epidemic requires leadership at the local and state levels, as well as nationally (White House Office of National AIDS Policy, 2013). The most recent estimates of HIV incidence in the U.S. suggest that the annual number of new HIV infections remains relatively flat, with increasing incidence among young gay men of all races, but particularly young Black gay men offsetting stable or declining incidence in virtually all other population groups (Centers for Disease Control and Prevention, 2012). Stable HIV incidence, however, is not seen everywhere in the country. Several jurisdictions have reported evidence that the number of annual new HIV infections is falling, in some cases sig-

EXPLAINING DECLINING HIV INFECTION 85
nificantly. For example, in San Francisco, HIV incidence is estimated to have fallen from 2.6% in 2004 to 1% in 2011 (Raymond et al., 2013). In Massachusetts, new HIV diagnoses declined by 25% between 2006 and 2009 (Greenwald, 2012).
Each of these jurisdictions is clearly unique, with differing HIV epidemic pro-files and different programmatic and policy approaches to tackling HIV. Until now, however, no systematic assessment has been made of common factors that may be contributing to falling HIV incidence in some metropolitan areas and states. A fuller understanding of the elements of success in reducing HIV incidence could be particu-larly useful at this stage in the domestic HIV epidemic.
This is a time of critical advances in our understanding of how to achieve popu-lation level impact at reducing HIV infections in the United States and in better sup-porting people living with HIV to sustain effective antiretroviral therapy (ART) and maintain their health. Federal policy through the National HIV/AIDS Strategy pro-vides a framework for coordinated action and supports evidence-based and strategic approaches focused on achieving specific public health outcomes. Implementation of the Affordable Care Act (ACA) provides the opportunity to broaden a base of stable insurance coverage through Medicaid and private health insurance plans that can help to expand the reach of HIV prevention and treatment services.
Further, the HPTN 052 study has provided critical evidence of the benefits of early versus delayed initiation of ART. This has led the NIH to update the HHS ART Treatment Guidelines that form the standard of HIV care in the United States and now recommend immediate offering of ART on diagnosis (Panel on Antiretro-viral Guidelines for Adults and Adolescents, 2014). The Centers for Disease Control and Prevention (CDC) also has updated its guidance to health departments and other grantees through its implementation of High Impact Prevention, encouraging greater integration of biomedical and behavioral interventions to improve impact, while also preserving flexibility to respond to local conditions. The U.S. Preventive Services Task Force (USPSTF) has updated its evidence-based recommendation for HIV screening giving it its highest rating, making such screening available for no cost-sharing in ACA marketplace health plans (U.S. Preventive Services Task Force, 2013). Additionally, President Obama issued an Executive Order in 2013 establish-ing an HIV Care Continuum Initiative designed to enhance coordination among federal agencies and state and local stakeholders to improve population-level perfor-mance along the care continuum (Executive Order, 2013).
Amid all of this rapid policy change, local and state public health officials, as well as others concerned about the domestic epidemic, could benefit from under-standing what has gone right in jurisdictions with a reduced burden of HIV inci-dence. In order to identify common factors that may have contributed to the decline in HIV incidence in Massachusetts (MA), North Carolina (NC), San Francisco, Cali-fornia (SF), and Seattle, Washington (SE), we conducted interviews with key infor-mants in those jurisdictions. Recognizing that this is a small sample of jurisdictions, these locations are geographically diverse and they offer snapshots of both state and local efforts. The aim of this qualitative study was to generate hypotheses to explain the decline in HIV incidence in these areas, and based on our findings, to develop policy and programmatic recommendations for other jurisdictions.
86 CROWLEY ET AL.
METHODS
Phone interviews were conducted with participants from MA, NC, SF, and SE. Inter-views took place from August to November 2013.
We selected jurisdictions that offer some evidence suggestive of success at pre-venting new infections from different parts of the country with differing health care systems and political and legislative contexts. We do not represent these jurisdictions as the most successful jurisdictions. Rather, we looked for diverse jurisdictions in dif-ferent parts of the country that appeared to have some measure of success in lowering HIV incidence and/or diagnoses. The evidence for declining HIV incidence is fairly strong in San Francisco and Massachusetts. As stated, it has been estimated that HIV incidence has fallen in San Francisco from 2.6% in 2004 to 1% in 2011 (Raymond et al., 2013; San Francisco Department of Public Health, 2013).Massachusetts has reported consistent declines in HIV diagnoses and deaths among people with HIV from 2002 to 2011 (with a negligible increase from 2010 to 2011; Massachusetts Executive Office of Health and Human Services, 2013). Similarly, Seattle reported a trend of declining HIV diagnoses and deaths over 1993 –2012, although there were slight upticks from 2011 to 2012 (Washington State/Seattle-King County, 2013). While less conclusive, there is some evidence of success in reducing HIV infections in North Carolina (North Carolina Department of Health and Human Services, 2014). State reports of HIV diagnoses from 1992 to 2012 shows two periods of declines fol-lowed by increases in diagnoses, with 2012 representing the lowest number of new diagnoses reported following its recent peak in 2008. The state believes that changes in reporting practices contributed to the first peak in 2002 and believes that the most recent peak in 2008 could be tied to the success of a campaign begun in 2007 to increase testing for HIV and other STDs, increase access to care, and keep people in care, known as the “Get Real. Get Tested. Get Treated” campaign.
SAMPLE SELECTION
In each jurisdiction, the authors spoke with at least one individual who could pro-vide information from the perspective of (1) a health department, (2) an academic institution, (3) health system staff and/or medical provider, (4) a community-based organization, and (5) consumer advocates. The authors of this study have worked extensively in the field of HIV/AIDS and, thus, they developed an initial list of in-formants based on their knowledge of individuals working in each of these juris-dictions. This list was supplemented by asking interviewees for additional key in-formants. The authors aimed to ensure that the informants list was racially and ethnically diverse. Interviews were conducted until we reached data saturation.
DATA COLLECTION
One author (JC) served as the lead interviewer and note-taker for all interviews; however, at least one other author was present on every phone call to assist in these tasks. Interviews lasted for approximately one hour. The interview tool was divided into the following sections: (1) health care coverage environment, (2) strength of HIV prevention and surveillance systems, (3) engagement of public health with key actors, (4) access to supportive and affirming environments for diverse populations, (5) funding environment, and (6) other topics. While the investigators addressed each topic area in every interview, the specific questions asked varied slightly de-

EXPLAINING DECLINING HIV INFECTION 87
pending on the flow of the conversation to that point; while it was important to keep the topical areas constant, it was also important to keep experts in the field engaged in a meaningful conversation so consistency and flow were both taken into account. The complete survey instrument can be found in the Appendix. Notes were tran-scribed and checked by at least two investigators for each interview. The majority of informants were interviewed individually; two pairs of individuals were interviewed together. This project did not collect individually identifiable protected health infor-mation.As such, it is exempt from review by the authors’ institutional review boards. This determination was made in consultation with relevant staff at the Georgetown University Law Center and a determination that this research was not human sub-jects research by the Johns Hopkins University Institutional Review staff.
DATA ANALYSIS
This study was designed as a hypothesis-generating project, and the data analysis process reflects this goal. Once the interview notes were fully transcribed, the authors identified themes that emerged from the data. All investigators reflected upon those themes until a consensus was reached. The authors then identified policy recommen-dations and barriers associated with each theme. While the themes were developed based on data obtained from the interviews, the recommendations and barriers were based on the interview data, as well as the authors’ experiences working in the field.
ROLE OF THE RESEARCHERS
The authors of this study have extensive experience working in the HIV/AIDS arena. They have diverse training and work experiences, and currently are affiliated with different institutions. One author (JC) has worked in HIV advocacy and policy for many years with an emphasis on health care financing and also served as President Obama’s lead HIV policy advisor from 2009 to 2011; one author (SF) is a graduate research assistant who has two years of experience working on international HIV issues; one author (CC) has broad policy and legislative experience and has been the senior policy and advocacy representative for a leading national HIV research organization; and one author (DH) has worked in academia on HIV issues for many years and also served in senior positions at the US Centers for Disease Control and Prevention from 1991 to 1995 and 1997 to 2001.The authors acknowledge that their experiences working in this field may have contributed both to the robustness and limitations of this study.
The survey instrument used to guide the key informant interviews was designed to encourage participants to expand upon important topics that they felt had not been emphasized through the questions. However, the authors of this study both developed the survey instrument and conducted the interviews. Thus, the authors’ biases may have influenced the direction of the interviews.
The authors inevitably had existing relationships with some of the interview-ees. This may have made some participants feel more or less comfortable than they would have felt with unfamiliar interviewers. The authors made an effort to create an environment that allowed participants to speak freely.
The authors’ experiences doing HIV/AIDS-related work may have contributed to the high response rate. Nearly all participants who were contacted for this study accepted their invitation, although scheduling conflicts led to two substitutions for the interview subjects that were originally contacted.

88 CROWLEY ET AL.
RESULTS
A total of 25 participants were interviewed. Table 1 contains a description of key informants by jurisdiction.
The results of this study can be found in the Key Themes (Results) column of Table 2. Each key theme, along with a brief explanation, was developed based upon data obtained from the interviews. These themes represent successful elements of HIV prevention, care and treatment across jurisdictions.
The Major Barriers and Policy Recommendations in the remaining two col-umns of Table 2 incorporate insights from both participants and the authors of the study. These columns are included to aid readers in translating the successes of MA, NC, SF, and SE to other jurisdictions. The Major Barriers column describes challenges that may arise in this translation process, as the ability and willingness to implement practices and policies described in the Key Themes column may vary by region or state. The Policy Recommendations column provides suggestions for implementing the lessons learned from this study, taking potential barriers into con-sideration. These themes and recommendations are explored in more depth in the Discussion section below.
Illustrative quotes are presented in Table 3, in which participants note strengths and challenges of HIV prevention and care in their jurisdictions. While these quotes are presented according to state, in many cases, these sentiments were expressed across jurisdictions.
DISCUSSION
This study is constrained by the limitations of conducting qualitative research in four divergent jurisdictions. Given the small number of persons interviewed within each of these categories, the potential for individual bias is a limitation of this study. Other jurisdictions could have been selected and could have provided other lessons of success and jurisdictions that are either struggling to lower HIV incidence or that present less clear evidence of progress may have unique factors constraining them. We sought to identify both states and cities that are geographically diverse and with differing epidemic profiles that appeared to have some measure of success in lower-ing HIV incidence and/or diagnoses. Our hope is that by identifying common ap-proaches to responding to the HIV epidemics in these states and communities we can offer hypotheses for future research and potential lessons for other jurisdictions who are making policy decisions in the absence of fully validated approaches to operating maximally effective prevention and care programs. While we have not evaluated or validated any specific strategies, by querying a diversity of voices within a commu-nity and learning where there is agreement across stakeholders on the importance of
TABLE 1. Number of Key Informants by Jurisdiction
Jurisdiction Number of Interviews
Massachusetts 9
North Carolina 5
San Francisco 5
Seattle 5

EXPLAINING DECLINING HIV INFECTION 89
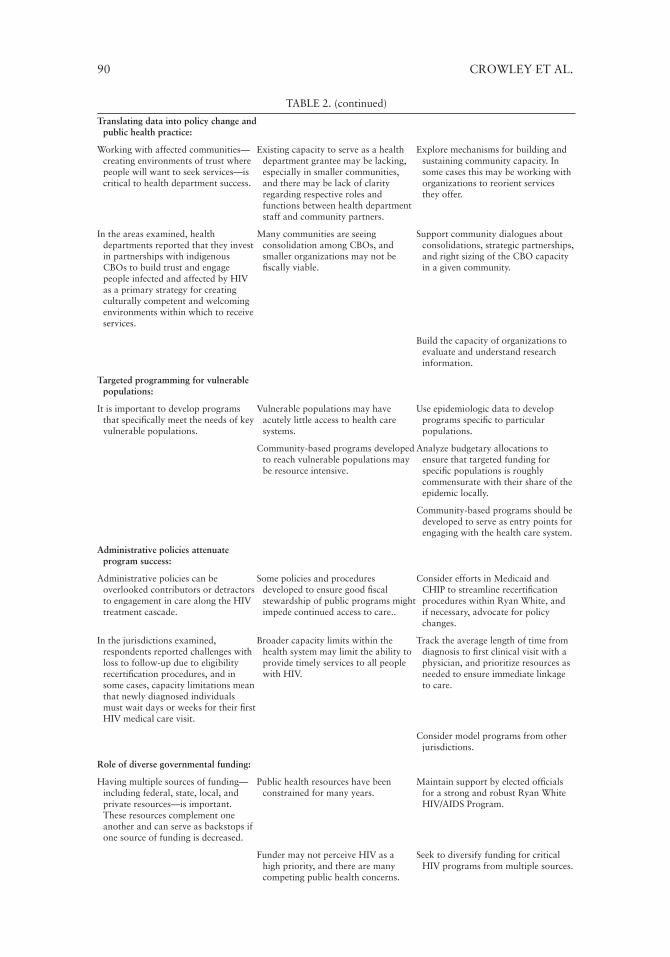
TABLE 2. Key Themes, Barriers, and Policy Recommendations
Key Themes (Results) Major Barriers Policy Recommendations
Extending access to health insurance:
Health care access is critically important.
There may not be a willingness to expand access to care in some jurisdictions.
Review and learn from other jurisdictions that have bridged a patchwork of federal, state, and local programs to effectively ensure access to quality HIV care.
With Medicaid expansion in Massachusetts, Healthy San Francisco and Ryan White funds to fill in gaps, individuals in the jurisdictions studied are able to access care easily.
While health care is available to individuals living in rural areas, they may have difficulty utilizing services if transportation is not accessible.
Explore mechanisms for expanding access to care in jurisdictions where it is not easily accessible.
Using an array of tools and approaches to increase knowledge of serostatus:
Broad accessibility to testing is critical; a mix of different approaches to testing is needed (i.e., clinic-based, community-based).
Barriers might include a lack of: available resources, provider prioritization.
Consider the mix of testing providers, venues, and types of testing offered in a community and within specific high-risk populations.
Community perceptions that testing is needed.
Leverage the USPSTF A rating for HIV screening to push for greater reutilization of non-risk-based HIV screening in clinical settings.
Prioritize resources for community testing initiatives based on local epidemiological information about trends in new infections and populations at greatest risk.
Ensure that all entities receiving public funds for HIV testing have fully integrated HIV testing with linkage programs.
Investing in services to retain people in care:
Retention in care is an important public health service in its own right.
Having client-centered services to enhance retention in care can be both time consuming and resource intensive.
Develop comprehensive strategic plans for retaining people in care that recognize some people may need intensive supports, but many may not want such support.
Holding health care providers accountable for outcomes such as retention in care and viral suppression can be an effective way to employ data to achieve results.
Conduct ongoing evaluation of retention in care and require programs and grantees to implement specific policies to support retention in care.
In the areas studied, intensive programs to keep clients in care were central, and rates of retention in care were high.
Examine clinical leadership, staffing, and physical environment to ensure that programs are welcoming, respectful, and culturally competent.
Collecting and using better data:A commitment to the evidence base—
rapidly translating epidemiologic and other types of data into practice—is needed.
In resource-constrained health departments, analytical capacity is often underfunded.
Establish formal partnerships with academic institutions.
In the areas examined, public health-academic partnerships facilitated the quick implementation of research into practice.
There can be so much information collected that it is difficult to set priorities for monitoring key outcomes.
- Consider joint appointments for university faculty as health department staff
There may be resistance among CBOs or other organizations to change longstanding practices. Such organizations may also not have the capacity to alter their activities.
-Work with university faculty to extend the analytical and research capacity of the health department
-Permit university programs to serve as independent, trusted community stakeholders to gather public input and explore complex policy issues.
90 CROWLEY ET AL.
TABLE 2. (continued)
Translating data into policy change and public health practice:
Working with affected communities—creating environments of trust where people will want to seek services—is critical to health department success.
Existing capacity to serve as a health department grantee may be lacking, especially in smaller communities, and there may be lack of clarity regarding respective roles and functions between health department staff and community partners.
Explore mechanisms for building and sustaining community capacity. In some cases this may be working with organizations to reorient services they offer.
In the areas examined, health departments reported that they invest in partnerships with indigenous CBOs to build trust and engage people infected and affected by HIV as a primary strategy for creating culturally competent and welcoming environments within which to receive services.
Many communities are seeing consolidation among CBOs, and smaller organizations may not be fiscally viable.
Support community dialogues about consolidations, strategic partnerships, and right sizing of the CBO capacity in a given community.
Build the capacity of organizations to evaluate and understand research information.
Targeted programming for vulnerable populations:
It is important to develop programs that specifically meet the needs of key vulnerable populations.
Vulnerable populations may have acutely little access to health care systems.
Use epidemiologic data to develop programs specific to particular populations.
Community-based programs developed to reach vulnerable populations may be resource intensive.
Analyze budgetary allocations to ensure that targeted funding for specific populations is roughly commensurate with their share of the epidemic locally.
Community-based programs should be developed to serve as entry points for engaging with the health care system.
Administrative policies attenuate program success:
Administrative policies can be overlooked contributors or detractors to engagement in care along the HIV treatment cascade.
Some policies and procedures developed to ensure good fiscal stewardship of public programs might impede continued access to care..
Consider efforts in Medicaid and CHIP to streamline recertification procedures within Ryan White, and if necessary, advocate for policy changes.
In the jurisdictions examined, respondents reported challenges with loss to follow-up due to eligibility recertification procedures, and in some cases, capacity limitations mean that newly diagnosed individuals must wait days or weeks for their first HIV medical care visit.
Broader capacity limits within the health system may limit the ability to provide timely services to all people with HIV.
Track the average length of time from diagnosis to first clinical visit with a physician, and prioritize resources as needed to ensure immediate linkage to care.
Consider model programs from other jurisdictions.
Role of diverse governmental funding:
Having multiple sources of funding—including federal, state, local, and private resources—is important. These resources complement one another and can serve as backstops if one source of funding is decreased.
Public health resources have been constrained for many years.
Maintain support by elected officials for a strong and robust Ryan White HIV/AIDS Program.
Funder may not perceive HIV as a high priority, and there are many competing public health concerns.
Seek to diversify funding for critical HIV programs from multiple sources.

EXPLAINING DECLINING HIV INFECTION 91
a policy or practice, we believe we can identify tools for public health officials that merit further empirical attention.
Perhaps the most unifying observation from this study is that state and local leadership within health departments is critical to achieving programmatic success. Health departments may wish to consider how they can monitor and quantify steps they are taking to implement new research and adapt their programs to match their own epidemics and better incorporate best practices from other jurisdictions. While this may seem intangible, we believe that these actions are an important form of leadership and we were struck that each of these jurisdictions was intent on not just going through the motions of operating prevention and care programs. In some critical areas, public health officials in each of these jurisdictions see themselves as leading their field and pushing their agencies and communities to test and adopt new approaches to HIV prevention and engagement in care. Other local and state juris-dictions may want to consider how to incentivize public health leaders to use data, evidence and different resource streams to be innovative and focused on improved HIV-related outcomes.
Leadership can take many forms and is exercised not only by government of-ficials. Further, jurisdictions have different types of resources upon which to draw. Importantly, while we find that financial resources from state and local governments has a larger impact than the mere level of funding provided, this leadership was not contingent upon financing. The following are potential tools for public health of-ficials to assert leadership to improve their response to the public health challenges posed by HIV in their communities:
EXTENDING ACCESS TO HEALTH INSURANCE
At this time when there is an increased focus on diagnosing people with HIV and getting them engaged in care and on ART as soon as possible, we found agreement that access to insurance coverage is critically important. Most respondents in three of the jurisdictions examined felt that access to care for people with HIV was largely available. In the jurisdiction with the biggest access challenges (North Carolina), observations of many respondents were consistent with the other jurisdictions when considering access available to people who were enrolled as patients within the ma-jor academic medical institutions in the state. Further, even though states such as Massachusetts and North Carolina differ greatly in the resources expended and the programs available to ensure access to care, both states identified ongoing challenges of ensuring appropriate access to high quality and culturally sensitive HIV care out-side of major urban areas, thus highlighting that insurance coverage, on its own, does not ensure capacity to deliver HIV and other specialty care throughout a state.
Several respondents in Massachusetts reported that the game changer for their response to HIV came when they initially received a Medicaid waiver in the early 2000s to extend Medicaid coverage to nondisabled people with HIV, which first enabled them to offer a promise of coverage for people seeking HIV testing and on diagnosis coming forward for care. Even in San Francisco, which operates the Healthy San Francisco program to provide health services for uninsured residents of the city, respondents noted the importance of insurance that comes with a promise of coverage for a defined set of medically-necessary services.
In the current environment, stakeholders in these jurisdictions suggest that broad-based efforts to extend health insurance coverage is one of the most effective ways to get more people with HIV engaged in care, bolstering efforts to encourage

92 CROWLEY ET AL.
TABLE 3. Illustrative Quotes From Key Informants.
Massachusetts
“Getting easy community testing with health care reimbursement is important.”
“HIV health care is pretty accessible. It is very clearly better in larger cities than in rural or bedroom communities. There is a hub and wheel model of HIV expertise. It was challenging, but it has improved. There is a density of excellent HIV providers in Boston.”
“It has taken us too long to integrate our HIV and STD data. There are huge opportunities to operate surveillance driven programs.”
“Our biggest struggle is linking up clinical and non-clinical providers. We believe peer support is important, but figuring out how to use it in smart ways is a challenge...We have shifted to supporting full-time staff that must meet a level of qualification for their role and they must have a concrete set of responsibilities.”
“We get attention by focusing on the idea that, by reducing disease burden, we could save money.”
“We were fortunate in setting up a formative data collection process. It gave us longitudinal data...the data allows you to read your [epidemiological] profile and redirect resources. It would have been impossible to do the things we did without that data in place.”
“The people who need to get tested are the people who are least likely to walk through the door easily. The populations we are trying to find are the hardest to reach. It’s hard to reach the people who aren’t accessing health care.”
“We need to simplify the health system. It is too burdensome and too much documentation. Eligibility recertifications twice a year are problematic. In disenfranchised populations, people cycle on and off. Lives are complicated, yet the system is too complicated.”
“There is a strong commitment of all providers around state money. All agree that it will be provided across the state to fund a spectrum of services from prevention to care, and there will be no line items for specific organizations.”
“No single agency could work with all of our key populations...what do the demographics of the epidemic in a region look like? We take a surgical approach.”
“A real barrier is trust. In rural communities and among recent immigrants, people in these communities know what will work. For fisherman, if you are not on the docks, you will miss them. Our efforts need to match the cycle of their pay...You need to find the right target populations, then you need targeted approaches.”
“State funds meant that we could always do the next thing. And, it was always more flexible than federal resources.”
“State money is also symbolic. It shows that the legislature recognizes that HIV is a problem and they need to deal with it.”
“State funding has been absolutely critical. When I have a big group of federal auditors, to be able to say, no, the state paid for that, it is absolutely critical.”
“We need to focus on the bottom line: what is the most effective use of resources?”
North Carolina
“We recognized the need to pay attention to data. We are using it to visualize how people are doing on the continuum. We are becoming more outcomes driven.”
“For me the strength of NC has been collaboration between public health and the university. This has allowed us to develop innovative programs that may be funded by other streams with support of the state allows a way to engage the community who may not be otherwise engaged to think about other interventions.”
“Our biggest population is young black gay men. Stigma is still an issue. The state has tried to respond a little under the radar. I would prefer to make a bigger marketing play, but we just can’t in this environment.”
“I would put testing in the ERs with money, but also put in these bridge counselor sort of people. It needs to be active. There needs to be phone calls and home visits to get people into care. There are a number of areas where I think testing needs to increase in our more rural areas. Not just testing, but that old-fashioned health educator...Of course you would need to hire people who are trustworthy or reflective of that community. It has to be a passion, it can’t just be people working 9 to 5.”
“We need to do more on immediate linkage to care to shorten the time to get people into care. And, we need to invest money in working with newly diagnosed people in those first six months outside of the clinic environment.”
“We recognized the need to pay attention to data. We are becoming more outcomes driven and looking at viral suppression. It is important because that’s a good message to share with our legislature. This is what you get for putting money into that [specific program].”
“We hold providers accountable for aggregate viral load. We compare networks across the state. We have been serious about this for 2–3 years, and most of the time, our providers are on board. If you look along the cascade and you can’t clearly see that your program has a place on the cascade in terms of making a difference, then we shouldn’t be funding you.”

EXPLAINING DECLINING HIV INFECTION 93
San Francisco
“We are well resourced for access to care and medication.”
“We need real time prevention. We need to keep up with technology and social media. We need to be looking at sexual decision making and higher ed choices...kids who think they can’t make it in college go, ‘why not have sex?’. We can’t be focused solely on HIV as the motivator for people to change behaviors.”
“Ryan White is extremely important. The single best-resourced clinics have been the Ryan White-funded clinics.”
“We need a database system to routinely notify providers of people missing appointments or personnel so they can respond if they know.”
“We are seeing that the small culturally competent clinics get defunded because the large multi-service clinic gets the money. It has been sad to not see collaboration in a way that most benefits the client.”
“After the [National HIV/AIDS] Strategy, there was more direction from the health department on de-siloeing. When requests for proposals come out, there really has to be collaboration with other entities in the community. It has started to gel organically and now we talk to each other more.”
“One challenge of engaging and retaining is the administrative burden of re-certification. People become viremic because they forget to re-certify...it happens on your birthday.”
“People have forgotten that as a DPH physician, we do real time observation. People always talk about how you have to wait for the research to come out. But in our case, we have so much robust data…We use local data to make decisions with our population.”
Seattle
“Scheduling the first appointment before they leave is important.We also follow-up with no shows.”
“Access is excellent for people in and around Seattle. The question is access in outlying areas of King County. Anyone with HIV can get their care and meds paid for. We have a very good system of coverage. Medicaid is widely available. Ryan White is used extensively for insurance continuation.”
“When everyone has coverage, disease control looks different.”
“Starting in 1999, we implemented HIV reporting. Then, we decided to hire someone to help us find people who had fallen out of care using lab results. We looked for people without a recent viral load or cell count. This was supported by the planning council. We found people who had moved or died and this allowed us to target our resources on the remaining people.”
“A barrier for engagement and retention is the recertification requirement every six months. There are two tiers of coverage: Full coverage and limited labs. If a patient doesn’t pick up their meds on time or fill out their paperwork, they are bumped down to the second tier of coverage and they are penalized for a full year.”
“Most people love commercial insurance, but we can’t survive on their reimbursement. If you add up the cost of salary, you can’t pay your costs. Patients need 30 minutes, not 15. Our patients are not the worried well. It’s expensive to take care of them. You can’t do 40 patients a day.”
all states to take advantage of the Affordable Care Act’s Medicaid eligibility expan-sion. Health departments may consider the role that they can play in providing data to policymakers and the public about the lack of insurance among people with HIV and how this impacts efforts to promote diagnosis and retention in care. Health departments in states that have expanded Medicaid through the ACA may wish to consider analytical studies to assess the clinical outcomes of new coverage and the fiscal impact on state HIV programs. For states that have not expanded Medicaid, they may consider analytical work to assess the fiscal impact on HIV programs and the impact on relative outcomes of people with HIV in their own state and those in states that have expanded Medicaid. All respondents interviewed believe that the Ryan White HIV/AIDS Program will remain critically important to the nation’s response to the care and treatment needs of people with HIV. As Massachusetts dem-onstrates, however, this program can become more effective if its primary role is not as a stand alone care system, but as a strategic supplement for health care services delivered through both public and private insurance, while retaining the capacity to provide comprehensive HIV services for those with no others sources of coverage.

94 CROWLEY ET AL.
USING AN ARRAY OF TOOLS AND APPROACHES TO INCREASE KNOWLEDGE OF SEROSTATUS
There is broad agreement among interview subjects that increasing knowledge of serostatus among people living with HIV as soon as possible after infection is a criti-cally important to preventing HIV transmission and improving engagement in care. All jurisdictions examined in this study already invest heavily in HIV testing and screening. Because promoting HIV screening involves multiple overlapping strate-gies, when asked how to build on current efforts to increase knowledge of serosta-tus, no single strategy was identified as uniquely important. Rather, respondents stressed differing needs for different contexts.
Health departments may wish to sharpen the focus of community testing pro-grams on the communities at greatest risk to ensure the greatest possible yield of new HIV positive individuals identified. Health department respondents often spoke of the need to support testing in a variety of venues and using a mix of trusted com-munity partners. Some respondents expressed the view that some communities may have maxed out the benefits of community based testing and suggested maintaining these investments, but expanding efforts in other settings such as health centers and emergency departments at major hospitals. Given that the USPSTF now gives an A rating for population-based HIV screening, this could facilitate reimbursement for HIV screening from insurers when clinical sites (such as provider offices, health centers, and emergency departments) adopt routine screening programs that do not depend on an identification of a risk basis for testing. Some respondents recommend prioritizing diagnosis of cases of acute HIV infection. It should be noted that more than a decade ago, Pilcher and colleagues published a study on the use of pooled specimen nucleic acid testing for the diagnosis of acute HIV infection (Pilcer et al., 2002).Three of the four jurisdictions examined have deployed this technology. While it is beyond the scope of this paper, both wider adoption of pooled testing and the strategic deployment of fourth-generation HIV testing may offer opportunities to strengthen current HIV testing strategies in a given jurisdiction. How to deploy such technologies and how best to make financial and other investments with scarce re-sources merits further consideration.
INVESTING IN SERVICES TO RETAIN PEOPLE IN CARE
As highlighted by the launch of the President’s HIV Care Continuum Initiative, there is a current emphasis on improving engagement in care along the care continuum. Estimates of engagement in care show that some of the largest drop-offs along the care continuum occur after people have been linked to HIV medical care, but be-fore they have been retained into ongoing clinical care. The interviews conducted in this study suggest a need to reconceptualize linkage and retention from merely out-come measures to increase the prioritization given to specific services that support engagement in care. Health departments may consider developing plans to ensure that adequate clinical and nonclinical workforce capacity exists to deliver services that assist with retention and that they are appropriately targeted. Further, such a plan may need to consider staging strategies such that services are delivered only to those desiring and requiring such services. This also may include formalized require-ments for programs and contractors to monitor and report on how funded activities support retention and engagement in care. In the jurisdictions examined, we also learned that the physical settings in which services are received, the composition
EXPLAINING DECLINING HIV INFECTION 95
and outlook of clinical and other staff, and other factors could dramatically impact whether individuals will feel comfortable accessing services.
COLLECTING AND USING DATA MORE EFFECTIVELY
Collecting and analyzing data and reporting to federal public health authorities is a central function of all HIV prevention and care programs. One notable aspect of the jurisdictions examined is that they all extend the capacity of the health de-partment by leveraging the expertise of local academic institutions and individual clinicians and researchers to enable them to collect and use data more effectively. They also report that they base programming on the latest evidence. Where the expertise exists within a state, health departments may consider establishing formal partnerships with university HIV programs. In three of the jurisdictions examined, this consisted of joint appointments where university faculty also was employed by the health department. Other types of partnerships could include data sharing agreements, formally or informally tasking universities to convene stakeholders and experts to grapple with pressing policy issues, or using university faculty to conduct evidence-based Grand Rounds for health department staff. The National Institutes of Health (NIH) also operates its HIV research network through the Centers for AIDS Research (CFARs) which exist in academic institutions in several communities across the country. CFARs could be enjoined to assist health departments in various capacities.
TRANSLATING DATA INTO POLICY CHANGE AND PUBLIC HEALTH PRACTICE
One of the resounding messages from the interviews conducted was that commu-nity-based organizations (CBOs) have a central role in helping health departments to be successful at accomplishing their missions. Nonetheless, this is a period of unrelenting pressure on many HIV-focused CBOs as public and private funding may be diminishing and as changes in evidence and national policy priorities are upend-ing, in some cases, what has been the primary focus on many CBOs. Respondents in some of the jurisdictions felt that they had already lived through a painful period of consolidation of CBOs and now were right sized to sustain the existing organiza-tions into the future. More commonly, however, respondents noted that they had seen organizations close and were worried that more closures were coming. Con-currently, some respondents lamented the absence of strong CBOs serving specific geographic communities or specific populations. This study suggests that CBOs per-form functions and have credibility in some communities that cannot be replicated easily by health department staff. Further research may be needed to better elucidate those functions or activities that are optimally performed by CBOs in place of health departments. Additionally, respondents suggested that health departments may need to consider ways to bolster existing community capacity and build new capacity based on epidemiological trends within specific communities. This could involve facilitating further dialogue with community stakeholders, providing clear guidance on how the health department views the role of CBOs evolving, and offering techni-cal assistance services to assist organizations to adapt to new roles. Similarly, just as health departments benefit when they build their internal capacity to evaluate and use research findings, health departments may wish to consider ways to build the capacity of community partners to evaluate and use research data.
96 CROWLEY ET AL.
TARGETED PROGRAMMING FOR VULNERABLE POPULATIONS
Across the country, appropriately targeting resources to the communities at highest risk for HIV infection remains surprisingly challenging. Some respondents in the four jurisdictions examined highlighted the educational and political barriers that can impede effective resource allocation, but also identified specific populations that they perceive as being especially needy of expanded prevention and care resources. In North Carolina, we heard of the need to do more to serve gay men and Black gay men in particular, but we were told of challenges in generating the political will or support to overtly target these populations. Given that many states and com-munities have historically underfunded services for gay men and young gay men are the only population in the United States experiencing rising HIV incidence, health departments may consider specifically evaluating the extent to which they are ad-equately targeting their programs and making funding allocations to serve gay men, including young gay men and gay men of color. In the jurisdictions examined, we also heard concern over the need to target more services to immigrants, including sub-populations, such as African immigrants. In San Francisco and Seattle, which have smaller populations of people of color than many other major urban areas, we were told that there is a need to do more to ensure culturally appropriate services in the most affected geographic communities. In all four jurisdictions, we consistently heard that investing in CBOs within affected communities to act as a bridge to larger institutions and formal systems of care was perhaps the most effective strategy to effectively serving these communities.
ADMINISTRATIVE POLICIES CAN IMPACT ENGAGEMENT IN CARE
An examination of the care continuum shows that there are numerous factors that cause people with HIV to fall out of care. Some administrative policies and practices can serve as overlooked barriers to engagement in care and conversely, can facilitate continued engagement in care. This study does not purport to systematically iden-tify all administrative policies that impose barriers to engagement in care or even to identify the most important ones. The following examples were cited by interview subjects and may illustrate that a narrow focus on policy could inadvertently over-look factors related to the translation of policy into practice that either facilitate or impede successful implementation of policy: A common issue identified was that persons that have been successfully engaged in care fall out of care because of Ryan White requirements to re-certify eligibility every six months. Health departments may consider working with HRSA on ways to minimize barriers to care caused by this policy and potentially moving to a 12-month eligibility period. Further, this type of policy dialogue may be enhanced by a review of the research literature and policy work that has been done in the Medicaid and Children’s Health Insurance Program (CHIP) programs and was incorporated in the Affordable Care Act to establish 12 months of continuous eligibility as a strategy for mitigating interruptions in care. Another administrative issue that interrupts access to care is that capacity limita-tions in some jurisdictions may cause newly diagnosed individuals to wait days or weeks from receiving an HIV diagnosis until a medical provider for specialized HIV care sees them. Health departments may wish to explore model programs for active and immediate linkage, for which several successful models exist across the country. Additionally, few HIV prevention interventions have a more solid evidence base supporting their effectiveness than the provisioning of sterile syringes to people who

EXPLAINING DECLINING HIV INFECTION 97
inject drugs. Three of the four jurisdictions examined provide funding for syringe services. Across the range of stakeholders interviewed in these jurisdictions, they cited access to sterile syringes as among the singular policy changes most directly responsible for observable declines in HIV transmission. Health departments may consider ways to sustain and bolster support for these programs. In addition to funding for syringe services, respondents also highlighted the value of other policy changes such as changing state laws to provide for nonprescription access to sterile syringes in retail pharmacies, a policy change with benefits beyond HIV prevention, such as for people with diabetes and other health conditions.
ROLE OF DIVERSE GOVERNMENTAL FUNDING
All of the jurisdictions examined receive important supplemental funding either from the state (WA, MA, and NC) or the local government (SF). Respondents noted that these resources often carry an outsize role in their response to HIV. While the presence of additional funds (or in some cases, back filled funds to mitigate the im-pact of federal cuts) is important for increasing the resources available, these funds were also valuable for giving jurisdictions greater flexibility to be innovative. Several respondents said that the ability to do things on the cutting edge and not be con-strained by federal funding limitations enabled them to be creative and make correc-tions in programing as lessons were learned. At a time of continuing fiscal challenges at all levels of government, health departments may consider ways to sustain and/or obtain state or local support for HIV programs.
CONCLUSIONS
As researchers and policymakers strategically address ongoing challenges in respond-ing to the domestic HIV epidemic, it is important to be mindful of and learn from our successes. The jurisdictions examined here provide important snapshots into challenges facing individuals living with HIV, their communities, and public health officials tasked with responding to HIV. We hope that the commonalities of experi-ence provide useful suggestions for further inquiry by other jurisdictions seeking to optimize the impact of prevention and care resources dedicated to fighting the HIV epidemic in the United States. At a minimum, we hope this project has allowed for the surfacing of key hypotheses about what best contributes to success in lowering HIV incidence in jurisdictions, and that these hypotheses can be discussed, debated, and evaluated in other jurisdictions.
APPENDIX
Survey InstrumentHealth Care Coverage Environment1. How accessible is HIV health care in your state or community?Is Medicaid considered to be widely available and accessible to people with HIV? Are there other programs available to assist individuals with HIV? How big of a problem is it for people who seek HIV care to be turned away? Which groups are most likely to fall through the cracks? Have any access expansions been imple-
98 CROWLEY ET AL.
mented in recent years? Have any access restrictions, such as waiting lists for services, been imposed in recent years?2. Have state or local policy makers been proactive about seeking to expand access to insurance coverage?Has expanding insurance coverage been a policy priority in your state or commu-nity? Do your elected officials see themselves as being leaders on this topic? What has been the nature of the policy debate…and has HIV featured prominently in the discussion?3. What has been the history of coverage policy in your state or community?Have there been health reforms enacted over time that have made a difference? Which policies have had the biggest impact on people with HIV?4. Currently, which coverage policies or programs are having the biggest impact on enabling people with HIV to be retained and engaged in care?5. Currently, which coverage policies or programs are the biggest barriers to retain-ing and engaging people with HIV in care?6. How strong is the clinical care capacity in your state or community?Is there an extensive network of health centers? Are there many Ryan White Part C and D clinics? If people have coverage, how adequate is the network of medical providers?7. How strong is the HIV community-based support services capacity?Are there a sufficient number of services providers? Are they financially strong? Do they have widespread community support? Do they provide high quality and evidence-based services?8. What can other jurisdictions learn from yours? Strength of HIV Prevention and Surveillance Systems1. How would you rate the strength of your state or community’s HIV prevention system?Compared to other jurisdictions, do you think that your state and local health de-partments are effective? Are there areas in which they have been national leaders? Are there critical HIV prevention programs or interventions that you believe have been innovative or especially important? What do you see as their biggest deficien-cies?Compared with other jurisdictions, are the community-based organizations in your jurisdiction effective in HIV prevention? In linkage to care? Are there major chal-lenges confronting the local CBOs at this time?2. How would you rate the strength of your state’s HIV surveillance system?Do you feel that your surveillance system is as robust as necessary for program planning, targeting, and evaluation purposes? Are there any gaps in the surveil-lance system you think need to be addressed in your jurisdiction? How pro-active is your health department in using surveillance data to increase linkage and reten-tion? Are there any innovative activities to highlight? Is surveillance information key to reducing HIV incidence in your jurisdiction? If so, how is it used?3. How accessible is HIV testing and screening?How aggressive has your state or community been about promoting HIV screen-ing? What have they done? Are routine and targeted testing both utilized, or is one emphasized much more than the other? Are many or most ERs routinely screening for HIV? Which populations is the health department targeting for more intensive testing? What strategies are they using? Have they been successful? What have
EXPLAINING DECLINING HIV INFECTION 99
been the biggest challenges?4. How do partner services fit into your jurisdiction’s approach to HIV prevention?Partner services have been controversial in some communities, but many public health officials view such services as critical to an effective HIV prevention pro-gram. How has your health department approached partner services? Have they worked with community groups on these issues? Are these services widely accepted within your state or community? Are there any partner services successes? What have been the biggest challenges?5. How have other prevention interventions (such as syringe exchange, certain be-havioral interventions, or social marketing campaigns) contributed (or not) in your reduction in HIV incidence? If so, which ones have been most useful?6. What can other jurisdictions learn from yours? Engagement of Public Health with Key Actors1. One potential ingredient of a successful HIV prevention program relates to meaningful collaboration with other key public officials or agencies and private stakeholders. Has your health department’s HIV prevention staff established mean-ingful partnerships?How has your health department worked with other actors? What have been key successes? What have been the biggest challenges? Are there specific initiatives or types of issues that are most meaningfully tackled through external collaboration?How has your health department worked with the following?
a. HIV community stakeholdersb. HIV prevention and/or Ryan White planning councilsc. Medicaid and/or Ryan Whited. Health Department’s STD programe. Medical provider community f. Academic researchersg. Other partners (please specify)
2. What have been some of your biggest successes with respect to coordination and collaboration with these other entities?3. What are the biggest challenges with respect to coordination and collaboration with these other entities?4. How is HIV prevention planning being orchestrated in your jurisdiction? Is this body blended in with the care planning council?5. What can other jurisdictions learn from yours?
Access to Supportive and Affirming Environments for Diverse Populations1. How would you rate the access to welcoming and culturally competent medical care and support services for vulnerable populations?How welcoming and affirming are most clinical environments to diverse HIV com-munities? How accessible are welcoming and affirming social services for diverse HIV communities? If one of the following individuals presented for services, can you readily identify medical and support providers that you know are equipped to provide competent and quality care?
• Active substance users• Gay youth• Women of color• Transgender women of all races• Sex workers
100 CROWLEY ET AL.
• People who are homeless• Other key communities (please specify)
2. Has your health department made specific investments to ensure cultural compe-tency?What has been done to provide welcoming and affirming environments for diverse populations? Have investments been made in staff training? If so, training for which type of staff? Have investments been prioritized for agencies that service specific communities? Which communities have been prioritized? How do these decisions get made? Are there lessons from your experience that could be applied elsewhere?3. What do you see as the biggest successes in your community or state with regard to creating welcoming and affirming environments in which people can receive HIV-related services? 4. What can other jurisdictions learn from yours? Funding Environment1. How committed has your state been to funding HIV services?To what extent does your state or city fund HIV services in addition to federal resources or in addition to meeting minimum federal requirements? Has this fund-ing increased or decreased over time? What do state resources fund? What are the most important activities or functions that would not be possible without these funds?2. Does your local community fund its own HIV services?Does your local community (or do local communities in your state) supplement federal and state funding with local funds for HIV services? If so, how much fund-ing is provided? What is the history behind this funding? Does this funding play a major or minor role in your jurisdiction’s HIV response? 3. How active has the private sector been in supporting HIV prevention and care programs?Do local charities, corporations, churches, or other private sector entities support HIV programs? What do they support? Is a significant level of resources provided? Do these resources serve any larger strategic purpose, through either funding things that public money cannot support or to leverage increased public support?4. How important are non-federal resources?Are these resources nice, but still a small part of overall funding? Or, do these resources make important activities possible that could not be undertaken without them? Do these resources supplement existing funding or do they support different types of activities?5. Do you think your state or jurisdiction will meet the HIV incidence goal of the National HIV/AIDS Strategy by reducing HIV incidence by 25% from 2010–2015?How many incident cases were there in 2010? If you do not believe you will meet this goal, why not? What are the most significant barriers you face to meeting this goal?6. Are there lessons for other jurisdictions with respect to garnering and maintain-ing support for funding HIV services? Other Topics1. We are trying to identify common factors to successful HIV prevention pro-grams that can be used to maximize the implementation of the ACA and make progress throughout the country at reducing HIV incidence. Are there other topics
EXPLAINING DECLINING HIV INFECTION 101
we should have asked you about that you believe are important?2. Do any of the following issues seem important and worth exploring as policies or issues that are critically important to success?
a. Targeting of prevention servicesb. Strength of school-based and/or out-of-school prevention and care programs for youthc. Broader environmental factors, i.e., role of faith community in public life, etc.d. Federal or state policies with respect to syringe services programs
3. Is there anything else that you would like to recommend being tried in other jurisdictions attempting to reduce HIV incidence in their local area?
REFERENCES
Centers for Disease Control and Prevention. (2012). Estimated HIV incidence in the United States, 2007-2010. HIV Surveillance Supplemental Report, 17, 2–26 . Retrieved June 10, 2014, from http://www.cdc.gov/hiv/pdf/statistics_hssr_vol_17_no_4.pdf
Executive Order—HIV Care Continuum Initia-tive, issued by President Barack Obama. (2013, July 15). Retrieved June 10, 2014, from http://www.whitehouse.gov/the-press-office/2013/07/15/executive-order-hiv-care-continuum-initiative
Greenwald, R. (2012). Health care reform update: Initiatives to address the care and treatment needs of people living with HIV. Retrieved June 10, 2014, from http://www.gih.org/files/3 Greenwald Presentation.pdf
Massachusetts Executive Office of Health and Hu-man Services. (2013). Regional HIV/AIDS epidemiologic profile of Massachusetts: 2013. Retrieved June 10, 2014, from http://www.mass.gov/eohhs/docs/dph/aids/2013-profiles/mass-total.pdf
North Carolina Department of Health and Human Services. (2014). 2012 HIV/STD surveil-lance: Addendum (March 2014). Retrieved June 10, 2014, from http://epi.publichealth.nc.gov/cd/stds/figures/std12rpt_addendum.pdf
Panel on Antiretroviral Guidelines for Adults and Adolescents. (2014). Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. Retrieved June 10, 2014, from http://aidsinfo.nih.gov/con-tentfiles/lvguidelines/adultandadolescentgl.pdf
Pilcher, C. D., McPherson, J. T., Leone, P. A., Smurzynski, M., Owen-O’Dowd, J., Peace-Brewer, A. L., et al. (2002). Real-time, uni-versal screening for acute HIV infection in a routine HIV counseling and testing popula-tion. Journal of the American Medical As-sociation, 288(2), 216–221.
Raymond, H., Chen, Y., Ick, T., Scheer, S., Ber-nstein, K., Liska, S., et al. (2013). A new trend in the HIV epidemic among men who have sex with men, San Francisco, 2004–2011. Journal of Acquired Immune Defi-ciency Syndromes, 62(5), 584–589.
San Francisco Department of Public Health. (2013). San Francisco semi-annual HIV surveillance report (December 2013). Re-trieved June 10, 2014, from http://www.sfdph.org/dph/files/reports/RptsHIVAIDS/HIV-SemiAnnualReport2013.pdf
U.S. Preventive Services Task Force. (2013). Hu-man immunodeficiency virus (HIV) infec-tion: Screening. Retrieved August 15, 2014, from http://www.uspreventiveservicestask-force.org/uspstf/uspshivi.htm
Washington State/Seattle-King County. (2013). HIV/AIDS epidemiology report (first half of 2013). Retrieved June 10, 2014, from http://www.kingcounty.gov/healthservices/health/communicable/hiv/epi/reports.aspx
White House Office of National AIDS Policy. (2013). National HIV/AIDS Strategy, Im-proving outcomes: Accelerating progress along the HIV care continuum. Retrieved June 10, 2014, from http://www.white-house.gov/sites/default/files/onap_nhas_im-proving_outcomes_dec_2013.pdf
Related Documents











