Sot. Sci. Med. Vol. 36, No. 1, pp. 21-32, 1993 Printed in Great Britain. All rights reserved 0277-9536/93 $5.00 + 0.00 Copyright0 1993 Pergamon PressLtd GENDER INEQUALITIES IN HEALTH: SOCIAL POSITION, AFFECTIVE DISORDERS AND MINOR PHYSICAL MORBIDITY JENNIE POPAY,’ MEL BARTLEY’ and CHARLIE OWEN) ‘Public Health Research and Resource Centre, Bolton, Salford, Trafford and Wigan Health Authorities, Salford Royal Hospital, Chapel Street, Salford M60 9EP, U.K., 2King’s Fund Institute, 126 Albert Street, London NW1 7NF, U.K. and ‘Thomas Coram Research Unit, Institute of Education, Gordon Square, London, U.K. Abstract-Research has consistently reported a female excess of minor physical morbidity and affective disorders compared to men. Using data from a national cross sectional survey of British women and men aged 18-59, this paper explores three prominent explanations for these patterns: that the female excess is due to problems associated with menstruation and the menopause; that it is ‘caused’ by the social positions which women occupy in contemporary western societies; and that the excess of affective disorders is ‘caused’ by women’s social positions but that their higher rate of physical illness is psychosomatic in origin. The analysis presented here suggests that problems with menstruation and the menopause cannot explain gender inequalities in minor illness. Similarly the argument that the female excess of minor physical illness is psychosomatic is not supported, indeed, there is evidence that women’s experience of minor physical illness may ‘cause’ their higher rates of affective disorders. Finally, with a few exceptions, the relationship between minor illness and four dimensions of social positions-marital status, employment status, social class and income-were broadly the same for women and men but in each social position category, women report higher rates of both types of ill health than men. It is concluded that present measures of these social positions do not capture the differing experiences of women and men and that more gender sensitive measures are needed if gender inequalities in minor illness are to be understood. Key words-sex differences, health, minor illness, social position, psychosomatic illness INTRODUCTION Amongst the most consistent of the research findings on the social patterning of health and illness is the excess of both affective disorders and minor physical morbidity reported amongst women compared to men. The literature contains a somewhat confusing array of possible explanations for this pattern, but there are two particularly prominent themes. First there is the argument that the female excess of ill health is caused by the social positions they occupy in contemporary society. Second, it is argued that whilst women’s experience of affective disorders is linked to their social positions, it is these affective disorders that lead to an excess reporting of minor physical morbidity. Additionally, there is the argu- ment that women’s experience of both affective dis- orders and minor physical morbidity is the result of problems associated with menstruation and the menopause. In this paper we use data from a national sample of British women and men aged 18-59 to consider the possible contribution each of these ex- planatory modes might make to the overall female excess of minor morbidity. In the first part of the paper we provide a brief review of the background literature. Next, we de- scribe the data sources we have used and discuss some methodological questions raised by our work. We then move on to discuss our findings considering in turn the three explanations for gender inequalities in health listed above. Finally, we discuss the impli- cations of our findings for future research. BACKGROUND Research concerned with sex difference in the experience of affective disorders commonly reports a female excess, though this is not invariably the case. There are those working in this field who would argue that this excess is entirely or at least primarily the result of hormonal or genetic factors [ 11.One variant of this biological approach is the argument that much, if not all, of the female excess of both minor physical and psychological ill health is associated with menstruation and the menopause. Within the social sciences two particularly promi- nent explanatory models can be identified. The first focuses on the nature of and interactions between the social positions and roles characteristic of women and men in western societies. In this model, women’s higher rates of affective disorders are causally linked to their experiences of domestic labour, motherhood, marriage, paid employment, etc. [see for example 2-41. In support of this argument, where groups of women and men carefully matched along social and economic dimensions have been compared, the fe- male excess has disappeared, or in some instances a male excess has been reported [see for example 51. A female excess in minor physical morbidity is also commonly reported in the literature and once again, albeit perhaps to a more limited extent than is the case with affective disorders, this is linked to women’s social roles/positions [6-l 11. However, more fre- quently women’s experience of minor physical mor- bidity is argued to be psychosomatic in origin. 21

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Sot. Sci. Med. Vol. 36, No. 1, pp. 21-32, 1993 Printed in Great Britain. All rights reserved
0277-9536/93 $5.00 + 0.00 Copyright 0 1993 Pergamon Press Ltd
GENDER INEQUALITIES IN HEALTH: SOCIAL POSITION, AFFECTIVE DISORDERS AND MINOR PHYSICAL
MORBIDITY
JENNIE POPAY,’ MEL BARTLEY’ and CHARLIE OWEN)
‘Public Health Research and Resource Centre, Bolton, Salford, Trafford and Wigan Health Authorities, Salford Royal Hospital, Chapel Street, Salford M60 9EP, U.K., 2King’s Fund Institute, 126 Albert Street, London NW1 7NF, U.K. and ‘Thomas Coram Research Unit, Institute of Education, Gordon Square,
London, U.K.
Abstract-Research has consistently reported a female excess of minor physical morbidity and affective disorders compared to men. Using data from a national cross sectional survey of British women and men aged 18-59, this paper explores three prominent explanations for these patterns: that the female excess is due to problems associated with menstruation and the menopause; that it is ‘caused’ by the social positions which women occupy in contemporary western societies; and that the excess of affective disorders is ‘caused’ by women’s social positions but that their higher rate of physical illness is psychosomatic in origin. The analysis presented here suggests that problems with menstruation and the menopause cannot explain gender inequalities in minor illness. Similarly the argument that the female excess of minor physical illness is psychosomatic is not supported, indeed, there is evidence that women’s experience of minor physical illness may ‘cause’ their higher rates of affective disorders. Finally, with a few exceptions, the relationship between minor illness and four dimensions of social positions-marital status, employment status, social class and income-were broadly the same for women and men but in each social position category, women report higher rates of both types of ill health than men. It is concluded that present measures of these social positions do not capture the differing experiences of women and men and that more gender sensitive measures are needed if gender inequalities in minor illness are to be understood.
Key words-sex differences, health, minor illness, social position, psychosomatic illness
INTRODUCTION
Amongst the most consistent of the research findings on the social patterning of health and illness is the excess of both affective disorders and minor physical morbidity reported amongst women compared to men. The literature contains a somewhat confusing array of possible explanations for this pattern, but there are two particularly prominent themes. First there is the argument that the female excess of ill health is caused by the social positions they occupy in contemporary society. Second, it is argued that whilst women’s experience of affective disorders is linked to their social positions, it is these affective disorders that lead to an excess reporting of minor physical morbidity. Additionally, there is the argu- ment that women’s experience of both affective dis- orders and minor physical morbidity is the result of problems associated with menstruation and the menopause. In this paper we use data from a national sample of British women and men aged 18-59 to consider the possible contribution each of these ex- planatory modes might make to the overall female excess of minor morbidity.
In the first part of the paper we provide a brief review of the background literature. Next, we de- scribe the data sources we have used and discuss some methodological questions raised by our work. We then move on to discuss our findings considering in turn the three explanations for gender inequalities in health listed above. Finally, we discuss the impli- cations of our findings for future research.
BACKGROUND
Research concerned with sex difference in the experience of affective disorders commonly reports a female excess, though this is not invariably the case. There are those working in this field who would argue that this excess is entirely or at least primarily the result of hormonal or genetic factors [ 11. One variant of this biological approach is the argument that much, if not all, of the female excess of both minor physical and psychological ill health is associated with menstruation and the menopause.
Within the social sciences two particularly promi- nent explanatory models can be identified. The first focuses on the nature of and interactions between the social positions and roles characteristic of women and men in western societies. In this model, women’s higher rates of affective disorders are causally linked to their experiences of domestic labour, motherhood, marriage, paid employment, etc. [see for example 2-41. In support of this argument, where groups of women and men carefully matched along social and economic dimensions have been compared, the fe- male excess has disappeared, or in some instances a male excess has been reported [see for example 51.
A female excess in minor physical morbidity is also commonly reported in the literature and once again, albeit perhaps to a more limited extent than is the case with affective disorders, this is linked to women’s social roles/positions [6-l 11. However, more fre- quently women’s experience of minor physical mor- bidity is argued to be psychosomatic in origin.
21
22 JENNIE POPAY et al
According to this argument, at least some part, if not all, of the excess is caused by women’s higher rates of affective disorders [2, 12-181. In their important paper spelling out the nurturant role hypothesis, for example, Gove and Hughes [6] argue that whilst some part of the female excess of somatic illness is caused by the physical demands of their caring roles in the family:
In general, most of these illnesses would seem to be prime candidates for the categories of physical disorders that are reactive to psychological distress [6].
Similarly, in a recent paper, Verbrugge argues that women and men are exposed to a range of acquired risks over the lifetime which threaten their physical health. However, whilst the health risks associated with work and leisure are argued to disadvantage men, those associated with psychological distress are argued to disadvantage women [17].
Despite the widespread consensus that at least some part of women’s higher rates of minor physical morbidity is psychosomatic in origin, there seems to be relatively little empirical evidence to support this hypothesis. It has been convincingly argued that there is a strong positive association between physical and psychiatric disorders [19]. Psychiatric disorders also appear to be more strongly associated with non- organic or functional physical illness than with organic physical illness [4]. However, evidence for sex differences in these relationships is patchy and confused.
Women have been reported to be more likely than men to have functional physical disorders and as already noted, these are more strongly linked to psychiatric disorders than organic physical illness (see for example [20-221). It has to be said, however, that the distinction between organic and non-organic physical illness is problematic, as the controversy over the aetiology of chronic fatigue illustrates [23].
A few researchers have directly addressed the question of sex differences in the relationship between physical and psychiatric illness. Barguero and col- leagues [24], for instance, reported that in their Spanish sample there was no significant difference in the rates of physical illness amongst women and men with a neurotic disturbance. In contrast amongst those with a physical illness, women were more likely than men to have a neurotic disorder as well [24]. Eastwood and Trevelyan [19] also found no sex difference in the rates of major physical illness amongst women and men with psychiatric disorders, though interestingly, they reported higher rates of minor physical illness amongst the men [19]. The relationship between depression and subsequent mor- tality has also been reported to be stronger for men than for women [25].
Finally, the direction of causality in the relation- ship between psychiatric and physical illness appears to be very much an open question. Most researchers take a somewhat guarded position on this difficult
issue. Eastwood and Trevelyan [19], for instance, argue that their findings do not support the idea of physical illness leading to psychiatric illness, but neither do they conclude the opposite. Rather they suggest that:
some people in the general population, for unknown reasons, are vulnerable to illness of all kinds [19].
Murphy and Brown 1221, in contrast, argue that their data on women do suppbrt the argument that psychi- atric disorders, brought about by severe life events, lead to organic physical disorders [22]. However, they also note that there were a few instances in their sample where affective disorders followed organic illness, even though the study design mitigated against such findings because the women were inter- viewed shortly after the onset of an organic physical illness.
In summary then this brief review of some of the social science literature in this complex field has highlighted two dominant approaches to explaining the female excess of both affective disorders and minor physical morbidity. On the one hand there is the argument that women’s higher rates of both are caused by the social positions they occupy in contem- porary industrial societies. On the other hand it is argued that whilst the female excess of affective disorders is causally linked to their social positions, at least some part, if not all of their higher rates of minor physical morbidity is a somatization of their psychological distress. Additionally reference was made earlier to the more biologically oriented argument that links the female excess of minor morbidity to the experience of menstruation and/or the menopause-to what might be termed ‘women’s problems’.
There are a number of difficulties with these expla- nations. Research has rarely looked explicitly at the possibility that problems associated with menstrua- tion and the menopause underlie the female excess of ill health. More importantly though ostensibly con- cerned with sex differences in morbidity, in reality much research ignores men’s experience of affective disorders or minor physical morbidity and the re- lationship, if any, with the social positions and roles they occupy. We therefore do not know whether, and in what ways, the relationship between different social positions and the experience of ill health differs for women and men. Nor do we know whether any variations that do exist could contribute to the overall female morbidity excess.
Finally, it is not clear from the literature whether the relationship between affective state and minor physical illness is being conceptualized as different in kind, or simply in scale, for women and men.
In this paper we therefore consider these three explanations for sex differences in the experience of minor illness in some detail. First, however, we describe the data and methods we have used and how we constructed our key variables.

Gender inequalities in health 23
DATA, MEASUREMENT AND METHODS
The data used in the analysis presented here have been taken from the Health and Lifestyles Survey (HALS). This was a nationwide interview based survey of attitudes and behaviour covering 9003 men and women aged over 18, in England, Wales and Scotland and carried out between 1984-85. Details of sampling, response rates and method for the survey are available elsewhere [26,271. A subsample was constructed including women and men aged between 18-59, who were either economically active or ‘housewives’ and who could be allocated to a Regis- trar-General’s social class. Married women were allo- cated on the basis of their husband’s occupation, unmarried women on the basis of their present or most recent occupation and members of the armed forces are excluded. Additionally a small number of men in part-time employment were excluded. This gave a total of 3589 women and 2643 men.
For part of the analysis a further 1602 people were excluded because no data were available with which to measure affect state. These non responders were people who did not return the self-completion booklet containing a version of the General Health Questionnaire, which was left behind after the inter- view. They do not differ significantly from those who returned the booklet in terms of sex or age, nor in terms of the rate of minor physical morbidity re- ported. However, there are some significant differ- ences in the social characteristics of the non responders which should be noted.
Amongst younger men the non responders were somewhat more likely to be from skilled and semi or unskilled social classes and to be unemployed. The younger female non responders were more likely to be single and to be in the clerical class, whilst the older female non responders were more likely to be in the skilled and the semi/unskilled classes.
Measurement of ill-health was undertaken along three dimensions. Firstly, there is the question of how best to measure minor physical illness or health state. The term health state, as defined by Blaxter, refers to health in the present ‘how am I now? and very recent past [28].
In HALS, health state is measured by a check list of symptoms. Respondents were asked whether they had, in the past month ‘suffered from any problems with . . . ’ one of these symptoms. The check list was divided into 16 ‘physical’ symptoms, such as joint pain, fainting, kidney or bladder trouble and hay fever, and 8 ‘malaise’ symptoms, such as difficulty sleeping, nerves and worry. However, assigning indi- vidual symptoms to either the physical or malaise list is not unproblematic.
A symptom checklist, in various forms, is widely used in social and medical research and has a number of strengths as a measure of morbidity. Unlike measures of consultation or activity limitation, for example, responses are unlikely to be heavily con-
taminated by the local availability or perceived acces- sibility of medical care, or by any of the disputed factors held to influence whether or not a person sees it as either necessary or possible to limit activity in response to a symptom. A weakness of the symptom check list is that asymptomatic conditions, such as high blood pressure, will not be picked up, but this consideration is not relevant to the present analysis. A more important weakness, is that it has been shown that any symptom is more likely to be recalled if it appears on a list than if the respondent is asked an open ended question on what symptoms have been experienced. What is included in the list may there- fore affect the social patterning of the responses obtained, biasing them towards women, for example, or towards a particular social class or age group. Care therefore needs to be exercised in deciding what to include in a checklist, or, in secondary analysis, what to include in the analysis.
In the analysis presented here, an attempt has been made to address these problems by constructing a list of symptoms from the fuller original list chosen to reflect the theoretical and empirical purposes of the paper. The items included are shown in Scheme 1 and they are:
a. symptoms which were not similar to any of the General Health Questionnaire items and there- fore could be argued to more clearly reflect physical morbidity
b. symptoms which more clearly discriminate be- tween women and men by satisfying the cri- terion that they should have a sex ration of more than 1 (i.e. 1:l).
Headache, Hay fever, eye trouble, ear trouble, fainting, kidney or bladder trouble, palpitations or breathlessness, sinus trouble or catarrh, constipation, foot trouble, tiredness.
Scheme 1. Items included in physical health state symptom list
Perhaps the most controversial of these is the in- clusion of tiredness as a physical symptom. It is common practice to include this along with sleep problems as a malaise or psychological symptom. However, there is rarely any justification for doing so. We would argue that tiredness could equally well be included as a physical symptom. It is certainly associ- ated with some physiological signs of ill health, such as anaemia, or it could be associated with a heavy burden of physical labour. We have therefore in- cluded it in the physical symptom list. We have, however, removed sleep problems as there is a great deal of evidence to link these with affective disorders. The resulting variable had a range between 0 and 11. In the analysis we have used a cut-off point of 3 or more symptoms to indicate the presence of minor physical morbidity.
The second dimension of health needing to be measured was ufictioe state. In the Health and

24 JENNIE POPAY et al.
Lifestyle Survey the best available measure of this dimension is the General Health Questionnaire (GHQ) as described by Goldberg [29]. There are several versions of this instrument, and ways of scoring it. In the HALS, the 30 item version was used, scored in the usual dichotomous manner [26, p. 52 and Appendix A]. The GHQ is a screening instrument and is not diagnostic of mental illness. Subjects scoring over a certain level are regarded as possible ‘cases’ of non-psychotic psychiatric disorder. In our analysis we took a cut off point of 5 or more positive responses to the GHQ items to denote the presence of a minor affective disorder. Justification for using the GHQ as a measure of ‘present state’ in the way adopted here is discussed by Stanley and Gibson [30] and Goodchild and Duncan Jones [31].
The third dimension of health that required measurement was health status, which, to use Blaxter’s terminology again, refers to health over the longer term [28]. This was necessary in order to allow for the effects of underlying disease and of ‘health selection’, when examining any relationship between social position, affect state and physical morbidity. Using information available in HALS, subjects were defined as ‘healthy if they were not suffering from a limiting long-standing illness and the analysis was repeated for this group which excluded 12.6% of the sample. In some instances in this paper, only the results of the analysis for the healthy are shown.
Finally, consideration had to be given as to how best to measure different dimensions of social pos- ition. As already noted, the literature on sex differ- ences in the experience of ill-health contains much discussion of the influence of different social positions and/or roles, but it is not always clear precisely what is being measured. Variables such as marital status, parental status, household structure, employment status and occupational class have been used as measures of social position, social roles and social
conditions. Particular attention has focused on the inadequacies of existing occupationally based measures as proxies of the social class position of women [see for example 91. ‘Additionally, concepts such as power, control, self esteem, role demands, material resources, social integration and social support have all featured in the research.
Clearly, what is required is more sophisticated measurement of the risks to health associated with the material, social and psychological environments in which people live and we are presently engaged in research which we hope will contribute to this en- deavour [32-341. However, in common with other researchers we have limited this analysis to the fam- iliar, somewhat crude measures of individual social circumstances or social positions as we have termed them: marital status, occupational class, employment status and household income.
The income data in the HALS data set relate to a question on household income in which respondents were asked to choose from 11 income categories. We have collapsed these into 4 categories: low, lower middle, upper middle and high.
The distribution of women and men within these different social positions is shown in Table 1 for the two age groups considered in the paper: 18-39 and 4&59. A predictable concentration of younger women in the clerical class is apparent, albeit that this is perhaps somewhat less than might have been expected. Otherwise the distribution for women and men across the Registrar General’s classes is broadly similar. A higher proportion of the older groups are in Social Class I and a lower proportion, in particular amongst women, are in the clerical class.
Women are more likely than men to be in low income households regardless of age. In the other income groups there is some suggestion that women are more likely to be in the high income group when they are older whilst the opposite appears to be the
Table I. Distribution of women and men within each social position
Regisfrar General’s .social class
Age Women MelI
Professional/ Managerial
It-39 40-59 26 35 26 32
ClerGA
It-39 40-59 20 II 14 II
Skilled Semi-unskilled
I a-39 4&59 I t-39 40-59 32 34 21 20 38 37 22 20
Age Women MelI
Age Women MelI
Age Women
Household income High Upper middle Lower middle ~___~
I t-39 4&59 I t-39 40-59 It-39 4G-59 39 46 22 I7 I7 13 44 39 24 25 16 I8
Marital sfulus Married Single Previously married
It-39 4&59 It-39 4c-59 It-39 40-59 67 83 24 4 9 I3 59 86 36 7 5 7
Employment s,a,us Full-time Part-time
employment employment Unemployed
It-39 40-59 It-39 4&59 I u-39 4&59 40 32 21 32 4 2
Low
It-39 40-59 23 24 16 I8
Housewife
18-39 4&59 35 34
MelI 88 90 4 IO

Gender inequalities in health 25
case for men. In terms of marital status women are more likely than men to be previously married in both age groups but particularly so amongst the older group, whilst younger women are less likely than men to be single.
Comparisons across work status groups are of course problematic. One third of women are housewives and between a fifth and a third are part-time employed: categories which in this sample contain no men. Women are predictably much less likely to be in full-time employment than men. The proportion falls with age for women but raises mar- ginally for men. A similar proportion of younger women and men are unemployed but the proportion of older men in this group is much higher than the proportion of older women.
Analysis of the statistical significance of the influ- ence of different factors including social position and sex on the presence of minor physical illness and of affective disorder was carried out using logit models. These are a version of loglinear models [see e.g. 351. When one variable can be considered the ‘response’ (in this case the presence of minor physical illness or affective disorder) logit models are used to assess the effects of various factors by modelling the relative odds of the two possible outcomes on the response variable.
The analysis was carried out with the LOG- LINEAR procedure in SPSS. The response variable was fitted first. For each analysis the factors were then fitted one by one. The tables show the change in the likelihood ratio x2 and the change in its degrees of freedom for each main effect. For the interaction term in the table the change in likelihood ratio x2 for fitting the interaction after all main effects is given. This is often referred to as the analysis of deviance.
In the next section we present our findings. The section is divided into four parts. First, we demon- strate that the familiar female excess of both minor physical morbidity and affective disorders are appar- ent in the data set we were using. Second, we test the hypothesis that the female morbidity excess is caused by problems associated with menstruation and the menopause. Third, we consider the relationship be- tween minor physical morbidity, affective disorders and four dimensions of social position: occupational class, income, marital status and work status. Here
Table 2. Proportions of women and men reporting an affective disorder and minor physical morbidity
women: Younger
(18-39) Older
w-59) 4een : ounger (18-39) br !&59)
Affective disorder
% n
28.6 (440)
21.5 (304)
21.6 (245)
19.6 (167)
Physical morbidity
% n
25.3 (519)
31.1 (469)
14.5 (224)
15.4 (174)
we are concerned to describe the broad contours of these relationships, to consider whether they differ for women and men, and to explore the extent to which any variations that do exist might contribute to the overall female morbidity excess. We have controlled to some extent for the possibility that the patterns identified could be due to health related selection into particular social positions by looking separately at ‘healthy’ people-that is those not reporting the presence of a limiting long standing illness.
Finally, we consider the relationship between affec- tive disorders and minor physical morbidity. First we ask to what extent the experience of one might explain, at least in statistical terms, the experience of the other and second, if this relationship is different for women and men.
FINDINGS
(i) Gender inequalities in the health and lifestyles data set
The much reported female excess of both affective disorders and minor physical morbidity is clearly evident in the Health and Lifestyles survey data. As Table 2 shows, women reported both affective dis- orders (more than 5 GHQ items) and minor physical morbidity (3 or more physical symptoms) signifi- cantly more often than men. The female excess does not change significantly when younger (18-39) and older (4&59) women and men are considered separately. So how might this excess be explained?
(ii) Explanation 1: women’s problems
One explanation for this pattern is that the female excess of both affective disorders and minor physical morbidity is a measure of minor health problems associated with menstruation and the menopause- often termed ‘women’s problems’. In the HALS survey women were specifically asked whether they experienced any such problems, so we were able to look separately at these women compared with those reporting no problems.
The data in Table 3 show that rates of affective disorders and minor physical morbidity are consider- ably higher amongst women reporting menstrual or menopause problems. By removing these women some part of the female excess of both types of ill health therefore disappears. However, women who report no problems still show a significant excess on both measures compared to men.
Table 3. Proportion of women reporting an affective disorder or physical morbidity controlling for reports of problems with
With
menstruation or menopause and for age
Affective disorder Minor physical illness
18-39 &59 18-39 4ck-59 % % % %
37.8 35.1 38.1 41.9 problems
Without problems
26.2 25.8 22.4 28.7

26 JENNIE POPAY et al.
The theory behind this particular explanation is biochemical. It could therefore be argued that it cannot be adequately tested using women’s subjective perceptions. It is plausible that hormonal changes may be associated with minor illness, without women making this connection themselves. However, the much higher rates of minor physical illness and affective disorders reported by women experiencing problems associated with menstruation and meno- pause suggests that a sizable group of women do make this connection. On this basis it seems reason- able to argue that women’s perceptions are at least a partial test of this explanation and our analysis suggests that a female excess remains to be explained.
(iii) Explanation 2: social causation
What then of the relationship between various dimensions of social position and the experience of affective disorders and minor physical morbidity? Is this relationship different for women and men and to what extent could differences identified be expected to contribute to the overall female morbidity excess?
As already noted, the four social positions we considered were occupational social class, household income, marital status and work status. Our main findings are summarized in Tables 4 and 5.
In general affective disorders were more strongly related to these social position variables than minor physical illness, though in no case was the relation- ship as strong as has been demonstrated for mortality and social position by other researchers [36, 371. For both dimensions of ill health with which we were considered, there was a stronger relationship with household income than with occupational class. However, as is clear from Tables 4 and 5 the detailed patterning of both dimensions of ill-health across the four social position variables and within age, sex and health status groups is extremely complex. For example, whilst marital status was strongly associated with reports of affective disorders, there was no significant relationship with minor physical illness.
One of the most important aspects of the data in Tables 4 and 5, from the perspective of this paper is that in most cases the relationships that do exist do not differ significantly between the sexes. In general, both women and men in the most disadvantaged social positions report higher rates of both affective disorders and minor physical illnesses than women and men in more advantaged social positions.
That said, there do appear to be three instances where significant sex differences exist-all of them in relation to the reporting of affective disorders. How- ever, only two of these, the interaction between sex and occupational social class, and that between sex and work status, could be argued to contribute to the overall female excess of ill-health. As Fig. 1 illus- trates, amongst healthy older women, those in the skilled class reported the highest rates of affective disorders, a class which accounted for just over a third of all older women in this sample. Amongst

Gender inequalities in health 21
healthy older men, in contrast, the highest rates were reported in the clerical class, which accounted for only 11% of these men.
The significant interaction between sex and work status was also apparent only in the older age group. Additionally, it was obviously only possible to com- pare women and men who were unemployed or full-time employed, as we had no men in our sample who were housewives or part-time employed. As Fig. 2 illustrates, this sex difference appears to be due to the particularly high rates of affective disorders reported by older unemployed men compared to employed men. Older unemployed women reported only marginally more affective disorders than their full time employed contemporaries. The contribution this pattern might make to the overall female excess of affective disorders is somewhat less clear than it is in relation to the pattern associated with occu- pational class discussed above. Whilst 10% of older men in this sample were exposed to the very high risk of affective disorders evident amongst the unem- ployed some 32% of older women were exposed to the lower but still raised risk associated with full-time employment amongst older women.
In the sample as a whole, significant sex differences were also found in the relationship between affective disorders and income in both age groups. Figure 3 suggests that these can be accounted for by the particularly high rates reported by low income older men and high income younger men. Given that younger high income men account for 44% of all young men in the sample, this pattern would be expected to detract from an overall female excess of affective disorders. However, as can be seen in Table 4, the interactions between sex and income became insignificant when the analysis was repeated for the healthy, though the x2 are approaching significance.
Even when the relationship between social position and ill health is the same for women and men, their different distributions within the various social positions can be expected to contribute to women’s higher rates of both affective disorders and minor physical morbidity. For example, both women and men in low income households have a higher than expected rate of both types of ill health. However, as Table 1 shows a greater proportion of women (22%
healthy older women and men
L 01 5 I I I
Semi/ Skilled Clerical Prof unskilled
- Older women
- - - Older men
Registrar geneml’s social class
Fig. 1. Affective disorders by social class.

28 JENNIE POPAY et al.
Affective disorders by work status Affective disorders by work status healthy younger women and men healthy older women and men _
0 Younger women 0 Older women m Younger men m Older men
Physrcal symptoms by work status Physical symptoms by work status z
550
healthy younger women and men healthy older women and men
II?40
i - Full time Part time Unemployed Housewives Full time Part time Unemployed Houeewives e a
employed employed employed employed Work status
Fig. 2. Affective disorders and physical symptoms by work status.
of younger women and 24% of older) are exposed to these increased risks compared to men (16% for younger and 18% of older men). Similarly, amongst both women and men the previously married report the highest rates of affective disorders (see Fig. 4) but a greater proportion of women are previously mar- ried than men (9% of younger and 13% of older women compared to 5% of younger and 7% of older men).
Finally, some part of the higher rates of affective disorders and minor physical morbidity reported by women will undoubtedly be due to the fact that they occupy social positions which are not commonly occupied by men and which are associated with high rates of both kinds of ill health. This is particularly apparent in relation to housewives. As Fig. 2 illus- trates, in the healthy sample housewives report a higher rate of affective disorders than any other work status group except young unemployed women and
men and older unemployed men. These latter how- ever, account for only 4, 4 and 10% of the respective groups, compared to around a third of younger and older women in the housewife groups. A similar pattern is also apparent in relation to rates of physical morbidity reported by older women and men.
Our exploration of the social causation explanation for the female excess of ill-health therefore suggests that the excess cannot be fully explained by sex differences in the relationship between social position and either affective disorders or minor physical ill- ness. It would appear that some part of the excess is due to women’s concentration in social positions associated with particularly high rates of ill-health- social position which men rarely occupy. Addition- ally, however, it seems that within social positions occupied by both women and men, almost without exception, women report higher rates of both affective disorders and minor physical morbidity.
younger ages 18-39 (all) Older ages 40-59 (all)
~~~~ p+j
LOW Lower Upper High LOW Lower Upper High middle mrddle middle middle
- Younger women Income - Older women - - - Younger men - - - Older men
Fig. 3. Affective disorders by income.
Gender inequalities in health 29
Atfectlve disorders by marital status healthy younger women and men
Affective disorders by marital status healthy alder wamen and men
- Younger women --- Younger men
- Older wamen
--- Older men
g Physical symptoms by marital status Physical disorders by marital status
E healthy younger women and men healthy alder women and men
H ot I I
E Married Single Prev Married Single PmV married married
Marital status
Fig. 4. Affective disorders and physical symptoms by marital status.
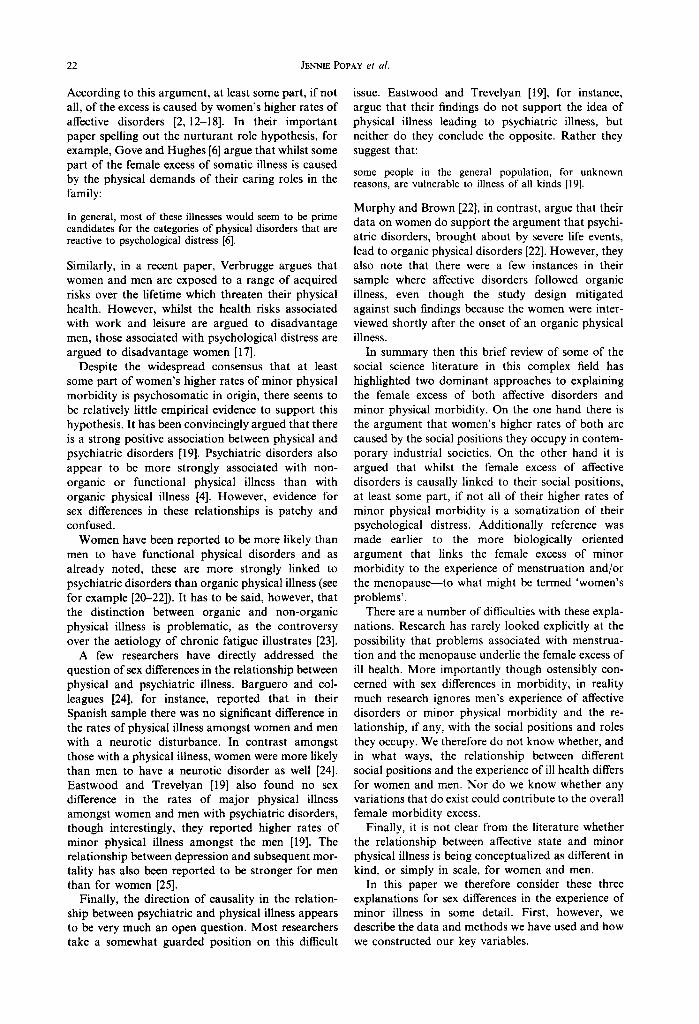
One of the most striking illustrations of this is the different rates of both affective disorders and minor physical illness amongst the previously married group shown in Fig. 4. Here over 44% of healthy young women reported an affective disorder and 21% a minor physical illness compared to 22 and 13% of young previously married men. Similarly, in the healthy sample around 27% of full-time employed women in both age groups reported an affective disorder compared to 19.6% of younger men and 16.9% of older men. This pattern is replicated for minor physical illness across income groups. In the healthy low income groups, for instance, as Fig. 5 illustrates, 25.3% of younger women and 33.7% of older women reported a minor illness compared to 14.6 and 19.6% amongst men. The equivalent figures for the high income groups were 22 and 23.5% for women compared to 12.2 and 9.9% for men. These findings suggest that the experience of a particular social position may be qualitatively different for
hoolthy younger women ond men
middle middle
women and men, an issue we return to in the discussion.
(iv) Explanation 3: somatising psychological distress
The third prominent explanation for a female excess of ill-health considered here can be termed the affect state hypothesis. According to this hypothesis, the minor physical illnesses that women experience are psychosomatic, originating in their experience of affective disorders which are in turn caused by the social positions they occupy. However, it is not clear from the existing literature whether the argument is that women are more likely than men to somatise their psychological distress or whether women and men are considered to be equally likely to do this, but that because women have higher rates of affective disorders they will inevitably have higher rates of minor physical illness. We have explored both of these possible explanations to some extent in the HALS data set.
healthy alder women and men
---:_-1
LOW Lower middle
Upper middle
High
- Youngor wamon Inccnne groups - Older women - - - Younger men - -- Older men
Fig. 5. Physical symptoms by income.
30 JENNIE PopAy et al
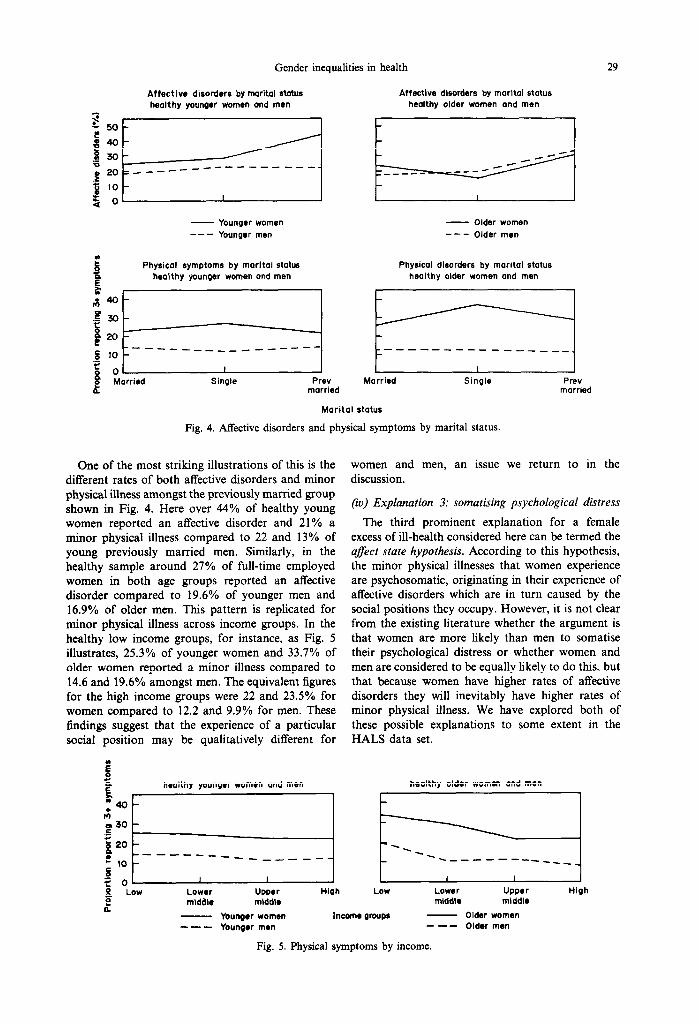
Table 6. Analysis of deviance tables resulting from loglinear analysis of physical symptoms as a function of affect
Attributable to P
Parameters All Healthy df All Healthy
I&79 FEU~-S old Physical symptoms 108.46 16.25 3 Main effects
Sex 44.09 40.04 I to.001 <O.OOl Affect 71.45 42.02 I <O.OOl <O.OOl
Interactions Sex x affect 0.38 0.21 I “S “S
4G 59 Jears okf Physical symptoms 152.36 10489 3 Main effects
Sex 64.32 52.12 2 <O.OOl 10.001 Afkct 98.82 58.45 2 < 0.00 I t0.ool
Interaction Sex x atfect 0.41 0.37 I ns IlS
The loglinear results shown in Table 6 indicate that reports of minor physical illness are significantly related to affective state, but that there is no inter- action with sex in either age group. This pattern remains unchanged amongst healthy women and men. Whatever the nature and direction of the re- lationship between affective disorders and minor physical illness, therefore, this suggests that it is the same for women and men. Is it then simply that the higher rates of affective disorder reported by women explain their higher rates of minor physical illness?
The data presented in Table 7 do not support this argument. As can be seen, in both age groups women are more likely to report a minor physical illness than men regardless of the presence or absence of an affective disorder. Interestingly these data provide some indication that the relationship between affec- tive disorders and minor physical illness may be stronger for men than for women. Within both age groups and both sexes the proportion reporting physical illness is significantly higher amongst those also reporting an affective disorder. However the difference in the rates is greater for men than for women. There is also some suggestion that in both age groups the ratio of women’s rates to men’s is smaller amongst those with an affective disorder.
There is therefore little support in these data for the argument that the excess of minor physical illness reported by women is causally linked to their experi- ence of affective disorders. It is of course just as plausible that women’s experience of minor physical morbidity causes them to suffer from affective dis- orders but this possibility has been given much less attention in the research literature. Interestingly, our
Tabk 7. Presence of minor physical morbidity (3+ symptoms) controlling for presence of a” affective disorder. Proportion reports
minor physical morbidity by age group
18-39 years 40-59 years
Affectwe WO”E” Me” WO”E” Me” disorder % n % n % n % n
No 21.0(231) 12.1 (108) 24.1 (193) 11.5(79) Yes 36.8 (162) 25.7 (63) 47.7 (145) 30.5 (51)
Loglinear results for interaction: sex by case x 2 = 0.38, df = I. P = “S.
Table 8. Sex differences in rate of affective disorders controlling for experience of minor physical morbidity and age. % reporting a”
affective disorder
No. of physical symptoms reported
18-39 40-59
Women Me” WO”E” Me” % n % n % n % n
0 14.7 (60) 15(61) 13.5 (34) 12.7 (40) 1 23.5 196) 18.8 (681 22.6 164) 18.2 (471 2 36.9 i12i) 27.5 <53j* 26.2 ;61 j 19.3 i29j 3+ 41.2 (162) 36.8 (63) 42.9 (145) 39.2 (51)
*Significance 0.05.
findings provide more support for this proposition, as the data in Table 8 illustrate. When the number of physical symptoms are held constant, the sex differ- ence in reports of affective disorders are dramatically reduced in both age groups-and with only one exception they become non-significant.
DISCUSSION
We have been concerned in this paper to consider three prominent explanations for the female excess of minor morbidity consistently reported in research: that it is due to problems associated with menstru- ation and the menopause; that it is ‘caused’ by the social positions women occupy in contemporary western society; that it is the result of a complex interaction between physical and psychological dis- tress such that women’s experience of depressive disorders (which result from their social position as mothers and wives in particular) lead them to report an excess of psychosomatic physical disorders.
Our analysis has been limited in a number of ways by the data we have used. As already noted, the health related measures were self reports. Though none of these were proxy answers by women for men, as has been the case with some previous research, this does mean that our results may reflect sex differences in willingness to report symptoms.
There is at present very little evidence that differen- tial symptom reporting by sex occurs on a scale sufficient to explain the considerable female excess of minor morbidity reported here and elsewhere. In a 1979 review of the literature, for example, Gove and Hughes [6] argued that there was an impressive array of evidence to suggest that women are no more willing to report symptoms than men and that the existing literature arguing the contrary:
is based on the beliefs of the authors who provide the appearance of empirical support for their assertions by a process of mutual citation [6, p. 1281.
Some 8 years later, Verbrugge and Wingard similarly concluded that evidence to support the argument that women have a different orientation towards illness than men was limited [16]. More recently still, Gijsbers van Wijk et al. [38] have again argued that:
differences in symptom sensitivity between men and women can probably be held responsible for part of the sex difference found in surveys.

Gender inequalities in health 31
Like other authors, these writers, do not provide any convincing new evidence for the existence of such differences. This therefore remains an important un- resolved issue for those concerned with the gendered patterning of health and illness. However, it is im- portant that social scientists do not allow this debate to become narrowly focused on methodological issues. As one of us has argued elsewhere:
Rather than engaging in a debate about the validity or otherwise of subjective accounts of ill-health and health, sociologists should be paying more attention to the tbeoreti- cal potential inherent in these accounts. . . which can enrich our understanding of the processes which may generate gendered differences in the experience of health and illness [34].
A second limitation of the data used in this paper is that it is cross-sectional. Though relationships may be identified between social positions and reported health state, or between different dimensions of ill health, the question of the direction of causality cannot be answered. By repeating our analysis ex- cluding women and men reporting a limiting long standing illness we have been able to explore the role of health related selection processes to some extent, albeit crudely, and our findings suggest that most of the relationships we have been concerned with are not significantly influenced by such processes. However, definitive answers to ‘causal’ questions must await analysis of longitudinal data. Finally we have had to rely on crude measures of the social positions people occupy.
There are however also advantages to the data set we have used. Perhaps the most important is its relatively large size and the availability of valid and reliable measures for three different dimensions of the experience of ill health-physical and psycho- logical or affective health state and long term health status. Previous research on sex differences in ill health has often ignored the issue of chronic illness and selection and the two dimensions of health state-the physical and the psychological are often confounded.
What then of our findings? Our analysis suggest that the female excess of minor ill health cannot be fully explained as the result of menopausal or menstruation problems. Similarly, though the ex- perience of both minor physical illness and affective disorders are associated with the four social positions considered here--albeit weakly-the relationships are broadly the same for women and men. We did identify some sex differences in these relation- ships which could be expected to contribute to the female excess of both affective disorders and physical morbidity. However, these would not be sufficient to explain it away. More importantly, the different distributions of women and men across the various social positions is such that a higher pro- portion of women than men are exposed to the relatively high risks associated with certain disadvan- taged positions, notably those related to low income
and being previously married. There are however instances where the reverse is the case. For example 36% of younger men are exposed to the relatively high risk of affective disorder attaching to single marital status.
By far the most important aspects of the analysis of the relationship between social position and health status is that almost without exception, within each category of social position occupied by women and men, women report higher rates of both affective disorders and minor physical morbidity. This cannot be explained in terms of the occupancy of a particular social position per se. At the very least then, it would appear that the experience of a particular social position must be different for women and men in ways which are not captured by the crude measures of class, household income, marital status and work status used here.
Finally, we found no evidence to support the argument that women’s reports of minor physical morbidity are the result of their experience of affec- tive disorders. Rather there is evidence that quite the opposite might be the case-our findings suggest that at least in statistical terms, women’s higher rates of minor physical morbidity explain their higher rates of affective disorders.
But we are still left with at least part of the original question-what causes women to report higher rates of minor physical morbidity? As we have already suggested the answer to this question depends partly on access to longitudinal data. Of equal if not greater importance, however, is the need for more sensitive measures of the nature of and interaction between the social positions that women and men occupy in modem societies.
We need to ask why the experience of living on a low income, for example, or of being previously married, or of being in full-time employment would have a different meaning for women than for men and in what ways these differences might explain the higher rates of morbidity that women report. Answers to these questions at a theoretical level will inform the development of more sensitive measures of social positions which can then be used in quantitat- ive research. We have suggested elsewhere that one place to start would be to move beyond the tra- ditional but artificial distinction between paid and unpaid work when considering the conditions of labour that may be relevant to our understanding of gendered patterns of ill-health [34]. What is needed is a reconceptualisation of labour conditions to take account of women’s unpaid work; of the possible interactions between formal and domestic labour in women’s lives; and of both the material and the psycho-social aspects of labour conditions. Such a reconceptualisation would also facilitate the develop- ment of an integrated theory of the relationship between social class and gender, which in turn is a pre-requisite if we are to fully understand gendered patterns of health and illness.

32 JENNIE POPAY et al.
Acknowledgements-This research was undertaken as part 23. Ridsdale L. Chronic fatigue in family practice. J. Fam. of an ESRC funded project at the Thomas Coram Research Pratt. 29, 5, 486-488 (1989). Unit, under grant number ROOO 23 1774. We are grateful to 24. Barquero J., Munoz P. and Madoz-Jaurequi V. The the ESRC Data Archive for the use of the Health and interaction between physical illness and neurotic mor- Lifestyles Survey. bidity in the community. Br. J. Psychiat. 139, 328-335
(1981).
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
REFERENCES
Studd J., Brincat M., Magos A. and Montgomery J. Women and mental illness. L&t. BMJ 292, 201 (1986). Gove W. Sex differences in mental illness amongst adult men and women: an evaluation of four questions raised regarding the evidence on the higher rates of women. Sot. Sci. Med. 12B, 187-198 (1978). Brown G. and Harris T. Social Origins of Depression: A Study of Psychiatric Disorder in Women. Tavistock, London (1978). Brown G. and Harris T. (Eds) Life Euenfs and Illness. Unwin Hyman, London (1989). Jenkins R. Sex differences in minor osvchiatric morbid- ity. Psychological Medical Monograph, Suppl. 7. CUP, Cambridge, (1985). Gove W. and Hughes W. Possible causes of the appar- ent sex differences in physical health: an empirical investigation. Am. Sot. Reo. 44, 126146 (1979). Graham H. Coping and how mothers are seen and not heard. In On the Position of Men (Edited by Friedmarsh S. and Sarah E.). Womens Press (1982). Graham H. Cat&g for the Family, Health Education Council, Research Report No. 1 (1986). Arber S., Gilbert G. N. and Dale A. Paid employment and women’s health: a benefit or a source of role strain? Social. Hlth Illness I. 3. 375400 (1985). Arber S. Gender and class inequalities in health: under- standing the differentials. In Health Inequalities in Euro- pean Countries (Edited bv Fox J.). Aldershot, Gower (1989). . . Popay J. and Jones G. Patterns of health and illness amongst lone parents. J. Sot. Policy 19, 4, 499-534 (1990). Hinkle L., Redmont R., Plummer N. and Wolff H. An examination of the relation between symptoms, disabil- ity and serious illness in two homogenous groups of men and women. Am. J. Public Hlth 50, 1327-1336 (1960). Nathanson C. Illness and the female role: a theoretical review. Sot. Sci. Med. 9, 57-62 (1975). Nathanson C. Social roles and health status amongst women: the significance of employment. Sot. Sci. Med. 14A, 463471 (1980). Marcus A. and Seeman T. Sex differences in health status: a re-examination of the nurturant role hypoth- esis. Am. Social. Rev. 46, 119-123 (1981). Verbrugge L. Multiple roles and physical health of women and men. J. Hllh Sot. Behav. 24. 16-30 (19831. Verbrugge L. The twain meet: empirical explanations of sex differences in health and mortality. J. Hlth Sot. Behav. 30, 282-304 (1989). Verbrugge L. and Wingard. Sex differentials in health and mortality. Women Hlth 12, 2, 103-143 (1987). Eastwood M. and Trevelyan M. Relationship between physical and psychiatric disorder. Psychol. Med. 2, 363-372 (1972). Creed F. Appendectomy. In op cit. (Edited by Brown G. and Harris T.), pp. 213-232 (1989). Craig T. Abdominal pain. In op cit. (Edited by Brown G. and Harris T.), pp. 233-260 (1989). Murphy E. and Brown G. Life events, psychiatric disturbance and physical illness. Br. J. Psychiat. 136, 326-338 (1980).
25. Murphy J., Manson R., Oliver D., Sobol A. and Leighton A. Affective disorders and mortality. Arch. gen. Psychiar. 44, 473480 (1987).
26. Cox B. D., Blaxter M., Buckle J., Fenner N., Golding J., Gore M., Huppert F., Nichson J., Roth, Sir M., Stark J., Wadsworth M. and Whichelow M. The Health and Lifestyles Survey: Preliminary Report. The Health Promotion Research Trust (1987).
27. Blaxter M. Health and Lifestyles,. Routledge, London (1990).
28. Blaxter M. Self definitions of health status and consult- ing rates in primary care. Quart. J. Sot. Afiirs 1, 131-171 (1985).
29. Goodberg D. The Detection of Psychiatric Illness by Quesrionnaire. Maudesley Monograph 2 1. OUP, London (1972).
30. Stanley B. and Gibson A. The prevalence of chronic psychiatric morbidity: A community sample. Br. J. Psychiat. 146, 372-376 (1985).
31. Goodchild M. E. and Duncan-Jones P. Chronicity and the General Health Questionnaire. Br. J. Psych. 146, 5561 (1985).
32. Popay .J. and Bartley M. Conditions of labour and women’s health. In Readings for a New Public Health (Edited by Martin C. and I&Queen D.), pp. 89-97. Edinburgh University Press, Edinburgh (1989).
33. Bartley M., Popay J. and Plewis I. Domestic work- load, paid employment and women’s experience of ill-health. In Sociology of Health and Illness. In press.
34. Popay J. and Bartley M. Conditions of formal and domestic labour. Paper presented to the BSA Annual Conference, Manchester (February 1990).
35. Fienberg S. E. The Analysis of Cross-Classified Categ- orical Data, 2nd edn. MIT Press, London (1980).
36. Wilkinson R. (Ed.) Class and Health: Research and Longitudinal Dais. Tavistock, London (1986).
37. Davev Smith G.. Bartlev M. and Blane D. The Black Report on socioeconomic inequalities in health: 10 years on. Br. Med. J. 301, 373 (1990).
38. Gijsbers van Wijk C. M., van Vliet K. P., Kolk A. M. and Everaerd W. T. Symptom sensitivity and sex differ- ences in physical morbidity: a review of health surveys in the United States and the Netherlands. Women HIrh 17, 1, 91-124 (1991).
39. Ponav J. Mv health’s alright I’m iust tired all the time: __ _ women’s accounts of health and illness. In Women’s Health Matfers (Edited by Roberts H.) Routledge Kegan Paul (1992).
40. Craig T. and Brown G. Goal frustration and life events in the aetiology of painful gastro-intestinal disorder. J. Psychosomat. Res. 28, 5, 411421 (1984).
41. Grant I., McDonald W., Patterson T. and.Trimble M. Multinle Sclerosis. In OD cit. (Edited bv Brown G. and Harris T.), pp. 295-312’ (1989). -
42. Jenkins R. and Clare A. Women and mental illness. Br. Med. J. 291, 6508, 1521-1522 (1985).
43. Kreitman N., Pearce K. and Ryle The relationship of psychiatric, psychosomatic and organic illness in a general practice. Br. J. Psychiat. 112, 569-579 (1966).
44. Mechanic D. Sex, illness behaviour and the use of health services. J. Human Stress 2, 29-40 (1976).
45. Rosenfeld S. The effects of womens employment: per- sonal control and sex differences in mental health. J. Hlth Sot. Behav. 30, 77-91 (1989).
Related Documents