GABA(A) alpha-1 subunit mediated desynchronization of elevated low frequency oscillations alleviates specific dysfunction in stroke – A case report Stephen D. Hall a, * , Naoki Yamawaki a , Alison E. Fisher b , Ralf P. Clauss c , Gavin L. Woodhall a , Ian M. Stanford a a School of Life and Health Sciences, Aston University, Aston Triangle, Birmingham, UK b Department of Experimental Psychology, University of Bristol, Bristol, UK c Nuclear Medicine Department, Royal Surrey County Hospital, Guildford, Surrey, UK article info Article history: Accepted 25 November 2009 Available online 25 January 2010 Keywords: Magnetoencephalography (MEG) GABA Theta Beta Stroke Pathological oscillations abstract Objective: The paradoxical effects of the hypnotic imidazopyridine zolpidem, widely reported in persis- tent vegetative state, have been replicated recently in brain-injured and cognitively impaired patients. However, the neuronal mechanisms underlying these benefits are yet to be demonstrated. We imple- mented contemporary neuroimaging methods to investigate sensorimotor and cognitive improvements, observed in stroke patient JP following zolpidem administration. Methods: We used Magnetic-Resonance-Imaging (MRI) and Magnetic-Resonance-Spectroscopy (MRS) to anatomically and chemically characterize stroke damage. Single-photon-emission-computed-tomogra- phy (SPECT) and magnetoencephalography (MEG) were used to identify changes in cerebrovascular per- fusion and neuronal network activity in response to sub-sedative doses of zolpidem, zopiclone and placebo. Cognitive improvements were measured using the WAIS-III and auditory-verbal tasks. Results: MRI and MRS revealed a lesion with complete loss of neuronal viability in the left temporal–pari- etal region; whilst SPECT indicated improved perfusion in the affected hemisphere following zolpidem. MEG demonstrated high-amplitude theta (4–10 Hz) and beta (15–30 Hz) oscillations within the peri- infarct region, which reduced in power coincident with zolpidem uptake and improvements in cognitive and motor function. Conclusions: In JP, functional deficits and pathological oscillations appear coincidentally reduced follow- ing administration of low-dose zolpidem. Significance: GABA(A) alpha-1 sensitive desynchronisation of pathological oscillations may represent a biomarker and potential therapeutic target in brain injury. Ó 2009 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. 1. Introduction The family of ‘z drugs’ which includes zolpidem, zopiclone and zaleplon are non-benzodiazepine sedative/hypnotic agents usually prescribed (10–30 mg) for insomnia (Dooley and Plosker, 2000; Holm and Goa, 2000), taking advantage of their fast absorption, short half-life and resultant limited duration of action. However, over recent years there have been an increasing number of reports that have highlighted the paradoxical ability of sub-sedative doses (2–5 mg) of zolpidem to improve cognitive and motor ability for patients not only in persistent vegetative state (Clauss and Nel, 2006), but also in brain injury (Cohen et al., 2004; Shames and Ring, 2008), idiopathic Parkinson’s disease (Daniele et al., 1997), drug-induced Parkinsonism (Farver and Khan, 2001), and dementia (Jarry et al., 2002). Previous single-photon-emission-computed-tomography (SPECT) studies have suggested that there is reduced regional blood perfusion in the affected brain area, with respect to the con- tralateral hemisphere, suggestive of diminished neuronal activity. Following administration of low-dose zolpidem, SPECT studies in a brain injured patient showed increased perfusion, implying recovery of cortical activity (Cohen et al., 2004). Here we report results from patient JP, who suffered a major ischemic stroke 6 years ago, causing left hemispheric damage to temporo-parietal regions of the brain. Whilst JP, as an ischemic stroke patient, is not an unusual case, the inhomogeneity of brain injury and consequently neurological deficits in this patient group pose particular difficulties in comparative analyses. JP is, how- ever, a representative example of a brain injury patient whose 1388-2457/$36.00 Ó 2009 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.clinph.2009.11.084 * Corresponding author. Address: Translational Neuroscience, School of Life and Health Sciences, Aston University, Birmingham B4 7ET, UK. Tel.: +44 (0) 121 204 4105; fax: +44 (0) 121 204 4090. E-mail address: [email protected] (S.D. Hall). Clinical Neurophysiology 121 (2010) 549–555 Contents lists available at ScienceDirect Clinical Neurophysiology journal homepage: www.elsevier.com/locate/clinph

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical Neurophysiology 121 (2010) 549–555
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
GABA(A) alpha-1 subunit mediated desynchronization of elevated lowfrequency oscillations alleviates specific dysfunction in stroke – A case report
Stephen D. Hall a,*, Naoki Yamawaki a, Alison E. Fisher b, Ralf P. Clauss c, Gavin L. Woodhall a,Ian M. Stanford a
a School of Life and Health Sciences, Aston University, Aston Triangle, Birmingham, UKb Department of Experimental Psychology, University of Bristol, Bristol, UKc Nuclear Medicine Department, Royal Surrey County Hospital, Guildford, Surrey, UK
a r t i c l e i n f o a b s t r a c t
Article history:Accepted 25 November 2009Available online 25 January 2010
Keywords:Magnetoencephalography (MEG)GABAThetaBetaStrokePathological oscillations
1388-2457/$36.00 � 2009 International Federation odoi:10.1016/j.clinph.2009.11.084
* Corresponding author. Address: Translational NeuHealth Sciences, Aston University, Birmingham B4 7E4105; fax: +44 (0) 121 204 4090.
E-mail address: [email protected] (S.D. Hall).
Objective: The paradoxical effects of the hypnotic imidazopyridine zolpidem, widely reported in persis-tent vegetative state, have been replicated recently in brain-injured and cognitively impaired patients.However, the neuronal mechanisms underlying these benefits are yet to be demonstrated. We imple-mented contemporary neuroimaging methods to investigate sensorimotor and cognitive improvements,observed in stroke patient JP following zolpidem administration.Methods: We used Magnetic-Resonance-Imaging (MRI) and Magnetic-Resonance-Spectroscopy (MRS) toanatomically and chemically characterize stroke damage. Single-photon-emission-computed-tomogra-phy (SPECT) and magnetoencephalography (MEG) were used to identify changes in cerebrovascular per-fusion and neuronal network activity in response to sub-sedative doses of zolpidem, zopiclone andplacebo. Cognitive improvements were measured using the WAIS-III and auditory-verbal tasks.Results: MRI and MRS revealed a lesion with complete loss of neuronal viability in the left temporal–pari-etal region; whilst SPECT indicated improved perfusion in the affected hemisphere following zolpidem.MEG demonstrated high-amplitude theta (4–10 Hz) and beta (15–30 Hz) oscillations within the peri-infarct region, which reduced in power coincident with zolpidem uptake and improvements in cognitiveand motor function.Conclusions: In JP, functional deficits and pathological oscillations appear coincidentally reduced follow-ing administration of low-dose zolpidem.Significance: GABA(A) alpha-1 sensitive desynchronisation of pathological oscillations may represent abiomarker and potential therapeutic target in brain injury.� 2009 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved.
1. Introduction
The family of ‘z drugs’ which includes zolpidem, zopiclone andzaleplon are non-benzodiazepine sedative/hypnotic agents usuallyprescribed (10–30 mg) for insomnia (Dooley and Plosker, 2000;Holm and Goa, 2000), taking advantage of their fast absorption,short half-life and resultant limited duration of action. However,over recent years there have been an increasing number of reportsthat have highlighted the paradoxical ability of sub-sedative doses(2–5 mg) of zolpidem to improve cognitive and motor ability forpatients not only in persistent vegetative state (Clauss and Nel,2006), but also in brain injury (Cohen et al., 2004; Shames and
f Clinical Neurophysiology. Publish
roscience, School of Life andT, UK. Tel.: +44 (0) 121 204
Ring, 2008), idiopathic Parkinson’s disease (Daniele et al., 1997),drug-induced Parkinsonism (Farver and Khan, 2001), and dementia(Jarry et al., 2002).
Previous single-photon-emission-computed-tomography(SPECT) studies have suggested that there is reduced regionalblood perfusion in the affected brain area, with respect to the con-tralateral hemisphere, suggestive of diminished neuronal activity.Following administration of low-dose zolpidem, SPECT studies ina brain injured patient showed increased perfusion, implyingrecovery of cortical activity (Cohen et al., 2004).
Here we report results from patient JP, who suffered a majorischemic stroke 6 years ago, causing left hemispheric damage totemporo-parietal regions of the brain. Whilst JP, as an ischemicstroke patient, is not an unusual case, the inhomogeneity of braininjury and consequently neurological deficits in this patient grouppose particular difficulties in comparative analyses. JP is, how-ever, a representative example of a brain injury patient whose
ed by Elsevier Ireland Ltd. All rights reserved.

550 S.D. Hall et al. / Clinical Neurophysiology 121 (2010) 549–555
neurological deficits are markedly improved by the administrationof low-dose zolpidem, therefore we investigated the changes in JPsneuronal network function using pharmaco-magnetoencephalog-raphy (Hall et al., 2009); consequently providing the first applica-tion of this method to the investigation of neurological disorder. JPpresented with fluent conversational speech but had difficultiescomprehending specific words (a specific auditory–verbal deficit)with word finding difficulties and semantic paraphasias. Unilateralsomatosensory diminution and abnormal gait were also observed.JP evinced marked cognitive and motor improvement in responseto zolpidem (5 mg), as reported by patient and consultant, suchthat a single daily dose provided symptomatic relief beginning atapproximately 40 min and lasting for up to 8 h, consistent withprevious reports (Cohen et al., 2004; Clauss and Nel, 2006). In addi-tion to symptomatic relief, previous psychometric assessment of JPsuggested improvements in IQ as a consequence of zolpidemadministration, although the specific nature of this ameliorationwas not identified. Similarly, initial SPECT imaging suggested re-duced cerebrovascular perfusion in posterior left temporal lobe,which was improved following zolpidem administration. These ini-tial observations formed the starting-point for the studies on JP de-scribed below, the ultimate purpose of which was to determine thechanges in brain activity underlying JP’s neurological deficits and,more importantly, to measure how neuronal network activitywas modulated by zolpidem in relation to recovery of sensorimo-tor and cognitive function. In order to investigate the specificityof zolpidem-mediated improvements, we used a double-blinded,repeated measures study including zolpidem, zopiclone and pla-cebo. Whilst zolpidem and zopiclone are both sedative hypnoticsthat act, primarily, by modulating activity at the GABAA receptor,zolpidem differs in its selectivity for the alpha-1 subunit, whereaszopiclone acts indiscriminately at alpha 1, 2, 3 and 5 receptors; acharacteristic which may be of particular Importance at low doses.
2. Methods
2.1. Patient
JP, a 60 year old right handed male with chronic stage strokesymptoms, presented with cognitive deficits, characterized by dif-ficulties comprehending specific words (a specific auditory–verbaldeficit) with word finding difficulties and semantic paraphasias. Inaddition, JP evinced specific sensorimotor deficits, specifically, uni-lateral somatosensory diminution leading to abnormal motor gaitand difficulties in modulating grip strength. These deficits showedmarked improvements, as reported qualitatively by the patient andconsultant, following a single daily dose (5 mg) of zolpidem, re-ported (JP) to occur approximately 45 min post administration.
2.2. Psychometric investigation
Cognitive improvements were examined extensively using a re-peated WAIS-III test, performed firstly when JP had taken his zolpi-dem medication; followed 6 months later when JP was offzolpidem. Test–retest gains in performance across WAIS-III Indexand IQ scores due to practice effects are well documented (Bassoet al., 2002), therefore the order of administration was chosen tounderestimate rather than overestimate gains due to zolpidem;specifically, changes during retest include any improvementsattributable to learning. Additionally, measures of covert letter flu-ency and category naming used in the MEG study were examinedoff-line before and during the period of zolpidem administration.The covert letter fluency task requires the participant to think of(during MEG) and verbalize (off-line) as many words beginningwith a specific letter within 30 s post letter presentation. Similarly,
the category naming task requires the participant to think of (dur-ing MEG) and verbalize (off-line) as many things within a specificcategory (e.g. furniture) as possible within 30 s of the category pre-sentation. It is important to note that due to the complex nature ofthe somatosensory-motor impairment, quantitative assessmentswere not obtained; rather, the improvements noted are qualitativeand observational reports by the patient and consultant.
2.3. Neuroimaging
2.3.1. Single photon emission computed tomography (SPECT)Previous 99mTc-hexamethylpropylene amine oxime (HMPAO)
SPECT imaging (see Clauss and Nel (2004) for details) of JP identi-fied reduced cerebrovascular perfusion in the region of the poster-ior left temporal lobe, with respect to normalized control data,which was observed to improve following 5 mg zolpidem adminis-tration (Supplementary Fig. S1).
2.3.2. Magnetic-Resonance-Imaging (MRI)In order to obtain a structural image of JP’s brain, to identify the
extent of any lesion and specific neuronal damage, we employed avariety of MRI approaches. A 3-Tesla MRI scanner (Siemens Trio:Erlangen, Germany) was used to acquire a detailed T1 weightedimage for subsequent neuroimaging reconstruction and co-regis-tration (Supplementary Fig. S2) and a series of T2 weighted gener-alized auto-calibrating partially parallel acquisition (GRAPPA)sequences were used to provide detailed information regardingthe grey and white matter structural integrity of the lesioned area.
2.3.3. Proton Magnetic Resonance Spectroscopy (1H MRS)1H MRS was used to obtain chemical information reflecting
structural integrity of the central lesion, lesion periphery and con-tralateral control region. These loci were selected based uponobservations of rCBF change in SPECT and lesion boundary identi-fied from anatomical MRI images. In summary, this method gener-ates a spectrum that reflects the presence or absence of typicalmetabolic substrates, which form markers of viable brain tissue.These substrates, including N-acetyl-aspartate (NAA), creatine(Cr), choline (Ch) and myo-inositol (mI) are reflected in stable ra-tios in healthy brain tissue. A variation in this ratio or the presenceof other abnormal metabolites, such as a lactate (Lac) peak, is areflection of altered neuronal tissue viability or altered metabo-lism, indicative of pathological conditions; these data were pro-cessed using LCModel software (http://www.s-provencher.com).
2.3.4. Magnetoencephalography (MEG)The study consisted of a double blind MEG study of three differ-
ent drug states, carried out over 3 days. On the morning of each dayour patient (JP), was instructed to consume breakfast, without caf-feine, 2 h prior to commencement of the study. At the same timeon each day (10.30am) JP was comfortably situated in a 275 chan-nel MEG system (CTF Systems, Canada) in a supine position whilsta continuous data acquisition was made for a period of 60 min at asampling rate of 600 Hz. At the beginning of this period JP wasadministered either zolpidem (5 mg), zopiclone (3.5 mg) or pla-cebo. Head position with respect to the sensors was determinedcontinuously with the use of three localization electrodes and athree-dimensional digitization of the patient’s scalp. This affordedthe ability to control for head movement and co-register the mea-sured MEG signal with the patient’s anatomical MRI (Adjamianet al., 2004).
During each session the 60 min acquisition was divided into sixidentical 10 min sessions. During these 10 min sessions JP was re-quired to perform five 30 s tasks: eye closure, isometric contractionof the left then right hands, covert letter fluency and category nam-ing tasks. These tasks were spread throughout the 10 min period,
S.D. Hall et al. / Clinical Neurophysiology 121 (2010) 549–555 551
therefore being interleaved by 7 min 30 s of passive period. Thisserved the purpose of spatially localizing right and left motor cor-tex (Taniguchi et al., 2000) and regions involved in letter fluency(Singh et al., 2002) and category naming paradigms and maintain-ing attention across the 60 min acquisition period.
2.4. Analysis
Data analyses were performed using the Synthetic ApertureMagnetometry (SAM) method (Vrba and Robinson, 2001; Hille-brand et al., 2005) to identify the spatial distribution of oscillatorypower changes in the theta (4–10 Hz), alpha (7–14 Hz), beta (15–30 Hz) and gamma (30–80 Hz) frequency bands between two timeperiods. Localization of task related change was determined bycomparing pre-task ‘passive’ and during task ‘active’ periods. Local-ization of drug action was performed by comparing the first 7 min30 s (considered to be ‘drug inactive’) with each of the subsequentfive periods (considered to be ‘drug active’). At the regions of inter-est (ROI) identified from the SAM analysis we placed virtual elec-trodes (Hall et al., 2005), which were band-pass filtered to thefrequency band of interest, which enabled us to reconstruct theoscillatory power change over the entire period of drug uptake.Data obtained from comparative locations in the intact contralat-eral hemisphere were used a controls. Further comparative analy-sis of synchronous change was performed at ROI showing changein response to zolpidem. Specifically, the mean oscillatory powerin bands of interest was calculated for each 10 min period follow-ing administration of zolpidem, zopliclone or placebo at an identi-cal cortical location. Further statistical analyses were performed toverify the differences observed between the zolpidem, zopicloneand placebo data. Mann–Whitney z-statistics were computed bothbetween and within drug conditions in frequency bands of interestto determine the statistical significance of observed changes. Fur-thermore, correlation coefficients were computed between fre-quency bands throughout the duration of the recordings todetermine interactions between frequencies.
3. Results
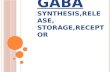
Psychometric evaluation of JP used the WAIS-III to evaluatedrug-enhanced cognitive performance, firstly with zolpidem andthen 6 months later without zolpidem. JP achieved highest scoreson the Perceptual Organization Index, with scores falling in thetop 12–18% of his age group. In the absence of zolpidem results re-vealed deterioration in performance across all Index and IQ scores
Fig. 1. Psychometric analyses. WAIS-III assessment results: (A) carried out with zolpidepercentiles. Results of covert letter fluency (blue) and category naming (red) tasks. (B) Otime 0 and tasks performed at 10 min intervals over a period of 80 min.
with the exception of the Working Memory Index, which remainedwithin the bottom 1% of the population across both test occasions.The greatest change was evident in the Verbal Comprehension In-dex and JP’s standardized score dropped by 27 percentile points,moving from the ‘average’ to the ‘low average’ range (Fig. 1A);these observations were consistent with clinical presentation.Additionally, off-line measures of covert letter fluency and cate-gory naming demonstrated improvements in language perfor-mance after the 40 min interval after zolpidem administration.These improvements were particularly pronounced in the categorynaming task, whereas covert letter fluency demonstrated onlyslight improvement over the pre-drug period (Fig. 1B).
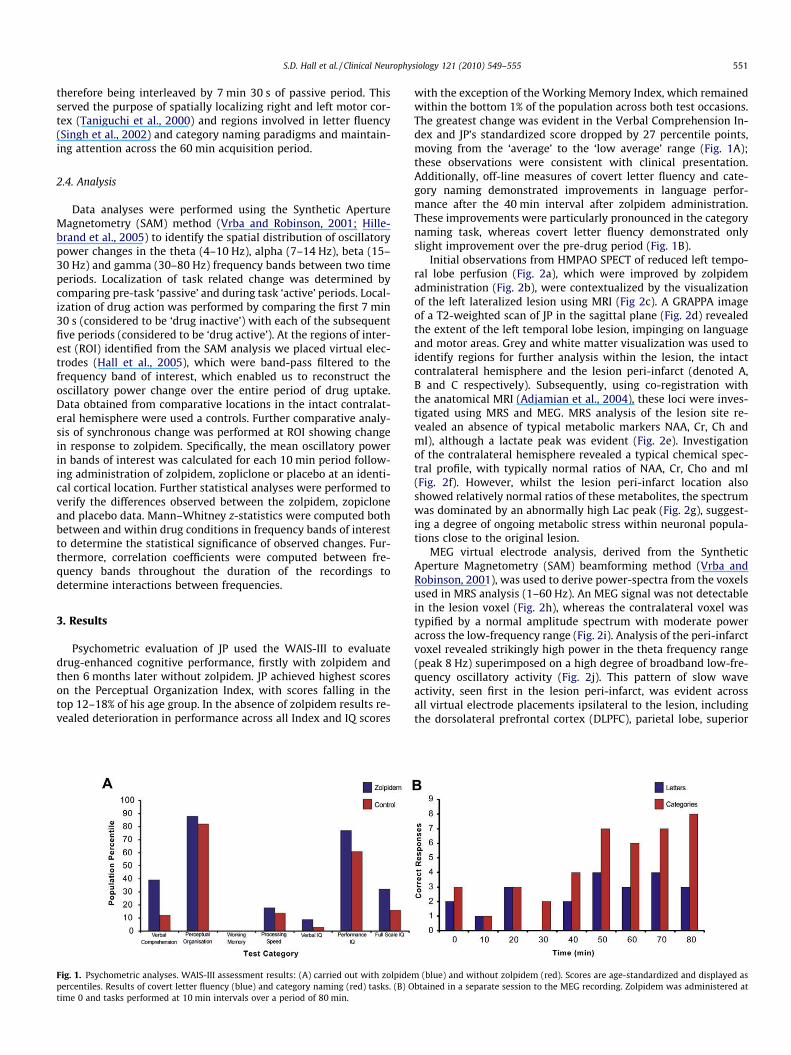
Initial observations from HMPAO SPECT of reduced left tempo-ral lobe perfusion (Fig. 2a), which were improved by zolpidemadministration (Fig. 2b), were contextualized by the visualizationof the left lateralized lesion using MRI (Fig 2c). A GRAPPA imageof a T2-weighted scan of JP in the sagittal plane (Fig. 2d) revealedthe extent of the left temporal lobe lesion, impinging on languageand motor areas. Grey and white matter visualization was used toidentify regions for further analysis within the lesion, the intactcontralateral hemisphere and the lesion peri-infarct (denoted A,B and C respectively). Subsequently, using co-registration withthe anatomical MRI (Adjamian et al., 2004), these loci were inves-tigated using MRS and MEG. MRS analysis of the lesion site re-vealed an absence of typical metabolic markers NAA, Cr, Ch andmI), although a lactate peak was evident (Fig. 2e). Investigationof the contralateral hemisphere revealed a typical chemical spec-tral profile, with typically normal ratios of NAA, Cr, Cho and mI(Fig. 2f). However, whilst the lesion peri-infarct location alsoshowed relatively normal ratios of these metabolites, the spectrumwas dominated by an abnormally high Lac peak (Fig. 2g), suggest-ing a degree of ongoing metabolic stress within neuronal popula-tions close to the original lesion.
MEG virtual electrode analysis, derived from the SyntheticAperture Magnetometry (SAM) beamforming method (Vrba andRobinson, 2001), was used to derive power-spectra from the voxelsused in MRS analysis (1–60 Hz). An MEG signal was not detectablein the lesion voxel (Fig. 2h), whereas the contralateral voxel wastypified by a normal amplitude spectrum with moderate poweracross the low-frequency range (Fig. 2i). Analysis of the peri-infarctvoxel revealed strikingly high power in the theta frequency range(peak 8 Hz) superimposed on a high degree of broadband low-fre-quency oscillatory activity (Fig. 2j). This pattern of slow waveactivity, seen first in the lesion peri-infarct, was evident acrossall virtual electrode placements ipsilateral to the lesion, includingthe dorsolateral prefrontal cortex (DLPFC), parietal lobe, superior
m (blue) and without zolpidem (red). Scores are age-standardized and displayed asbtained in a separate session to the MEG recording. Zolpidem was administered at
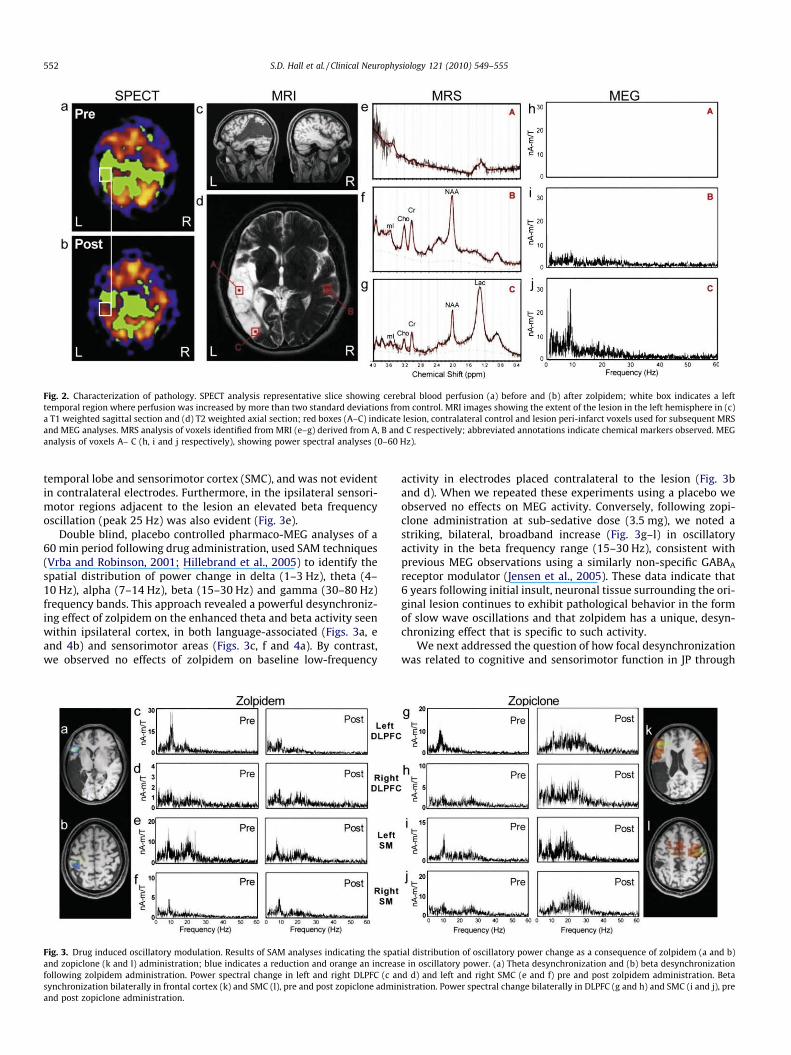
Fig. 2. Characterization of pathology. SPECT analysis representative slice showing cerebral blood perfusion (a) before and (b) after zolpidem; white box indicates a lefttemporal region where perfusion was increased by more than two standard deviations from control. MRI images showing the extent of the lesion in the left hemisphere in (c)a T1 weighted sagittal section and (d) T2 weighted axial section; red boxes (A–C) indicate lesion, contralateral control and lesion peri-infarct voxels used for subsequent MRSand MEG analyses. MRS analysis of voxels identified from MRI (e–g) derived from A, B and C respectively; abbreviated annotations indicate chemical markers observed. MEGanalysis of voxels A– C (h, i and j respectively), showing power spectral analyses (0–60 Hz).
552 S.D. Hall et al. / Clinical Neurophysiology 121 (2010) 549–555
temporal lobe and sensorimotor cortex (SMC), and was not evidentin contralateral electrodes. Furthermore, in the ipsilateral sensori-motor regions adjacent to the lesion an elevated beta frequencyoscillation (peak 25 Hz) was also evident (Fig. 3e).
Double blind, placebo controlled pharmaco-MEG analyses of a60 min period following drug administration, used SAM techniques(Vrba and Robinson, 2001; Hillebrand et al., 2005) to identify thespatial distribution of power change in delta (1–3 Hz), theta (4–10 Hz), alpha (7–14 Hz), beta (15–30 Hz) and gamma (30–80 Hz)frequency bands. This approach revealed a powerful desynchroniz-ing effect of zolpidem on the enhanced theta and beta activity seenwithin ipsilateral cortex, in both language-associated (Figs. 3a, eand 4b) and sensorimotor areas (Figs. 3c, f and 4a). By contrast,we observed no effects of zolpidem on baseline low-frequency
Fig. 3. Drug induced oscillatory modulation. Results of SAM analyses indicating the spatand zopiclone (k and l) administration; blue indicates a reduction and orange an increasfollowing zolpidem administration. Power spectral change in left and right DLPFC (c ansynchronization bilaterally in frontal cortex (k) and SMC (l), pre and post zopiclone adminand post zopiclone administration.
activity in electrodes placed contralateral to the lesion (Fig. 3band d). When we repeated these experiments using a placebo weobserved no effects on MEG activity. Conversely, following zopi-clone administration at sub-sedative dose (3.5 mg), we noted astriking, bilateral, broadband increase (Fig. 3g–l) in oscillatoryactivity in the beta frequency range (15–30 Hz), consistent withprevious MEG observations using a similarly non-specific GABAA
receptor modulator (Jensen et al., 2005). These data indicate that6 years following initial insult, neuronal tissue surrounding the ori-ginal lesion continues to exhibit pathological behavior in the formof slow wave oscillations and that zolpidem has a unique, desyn-chronizing effect that is specific to such activity.
We next addressed the question of how focal desynchronizationwas related to cognitive and sensorimotor function in JP through
ial distribution of oscillatory power change as a consequence of zolpidem (a and b)e in oscillatory power. (a) Theta desynchronization and (b) beta desynchronizationd d) and left and right SMC (e and f) pre and post zolpidem administration. Betaistration. Power spectral change bilaterally in DLPFC (g and h) and SMC (i and j), pre
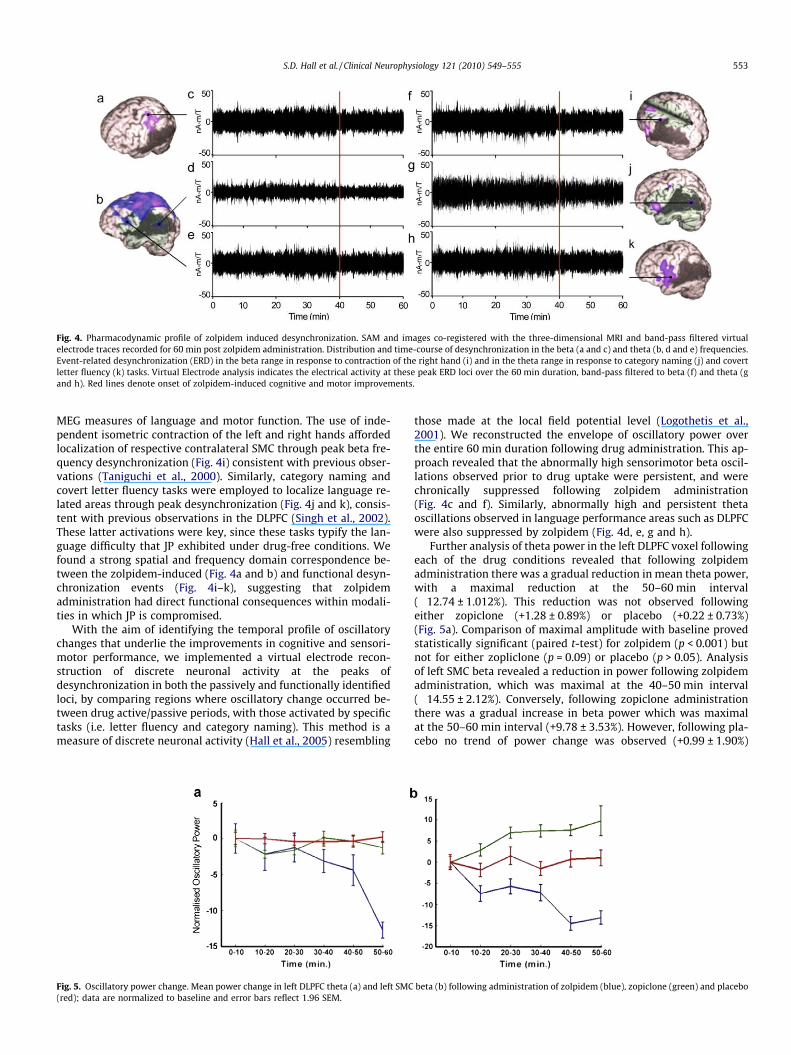
Fig. 4. Pharmacodynamic profile of zolpidem induced desynchronization. SAM and images co-registered with the three-dimensional MRI and band-pass filtered virtualelectrode traces recorded for 60 min post zolpidem administration. Distribution and time-course of desynchronization in the beta (a and c) and theta (b, d and e) frequencies.Event-related desynchronization (ERD) in the beta range in response to contraction of the right hand (i) and in the theta range in response to category naming (j) and covertletter fluency (k) tasks. Virtual Electrode analysis indicates the electrical activity at these peak ERD loci over the 60 min duration, band-pass filtered to beta (f) and theta (gand h). Red lines denote onset of zolpidem-induced cognitive and motor improvements.
S.D. Hall et al. / Clinical Neurophysiology 121 (2010) 549–555 553
MEG measures of language and motor function. The use of inde-pendent isometric contraction of the left and right hands affordedlocalization of respective contralateral SMC through peak beta fre-quency desynchronization (Fig. 4i) consistent with previous obser-vations (Taniguchi et al., 2000). Similarly, category naming andcovert letter fluency tasks were employed to localize language re-lated areas through peak desynchronization (Fig. 4j and k), consis-tent with previous observations in the DLPFC (Singh et al., 2002).These latter activations were key, since these tasks typify the lan-guage difficulty that JP exhibited under drug-free conditions. Wefound a strong spatial and frequency domain correspondence be-tween the zolpidem-induced (Fig. 4a and b) and functional desyn-chronization events (Fig. 4i–k), suggesting that zolpidemadministration had direct functional consequences within modali-ties in which JP is compromised.
With the aim of identifying the temporal profile of oscillatorychanges that underlie the improvements in cognitive and sensori-motor performance, we implemented a virtual electrode recon-struction of discrete neuronal activity at the peaks ofdesynchronization in both the passively and functionally identifiedloci, by comparing regions where oscillatory change occurred be-tween drug active/passive periods, with those activated by specifictasks (i.e. letter fluency and category naming). This method is ameasure of discrete neuronal activity (Hall et al., 2005) resembling
Fig. 5. Oscillatory power change. Mean power change in left DLPFC theta (a) and left SMC(red); data are normalized to baseline and error bars reflect 1.96 SEM.
those made at the local field potential level (Logothetis et al.,2001). We reconstructed the envelope of oscillatory power overthe entire 60 min duration following drug administration. This ap-proach revealed that the abnormally high sensorimotor beta oscil-lations observed prior to drug uptake were persistent, and werechronically suppressed following zolpidem administration(Fig. 4c and f). Similarly, abnormally high and persistent thetaoscillations observed in language performance areas such as DLPFCwere also suppressed by zolpidem (Fig. 4d, e, g and h).
Further analysis of theta power in the left DLPFC voxel followingeach of the drug conditions revealed that following zolpidemadministration there was a gradual reduction in mean theta power,with a maximal reduction at the 50–60 min interval(�12.74 ± 1.012%). This reduction was not observed followingeither zopiclone (+1.28 ± 0.89%) or placebo (+0.22 ± 0.73%)(Fig. 5a). Comparison of maximal amplitude with baseline provedstatistically significant (paired t-test) for zolpidem (p < 0.001) butnot for either zopliclone (p = 0.09) or placebo (p > 0.05). Analysisof left SMC beta revealed a reduction in power following zolpidemadministration, which was maximal at the 40–50 min interval(�14.55 ± 2.12%). Conversely, following zopiclone administrationthere was a gradual increase in beta power which was maximalat the 50–60 min interval (+9.78 ± 3.53%). However, following pla-cebo no trend of power change was observed (+0.99 ± 1.90%)
beta (b) following administration of zolpidem (blue), zopiclone (green) and placebo
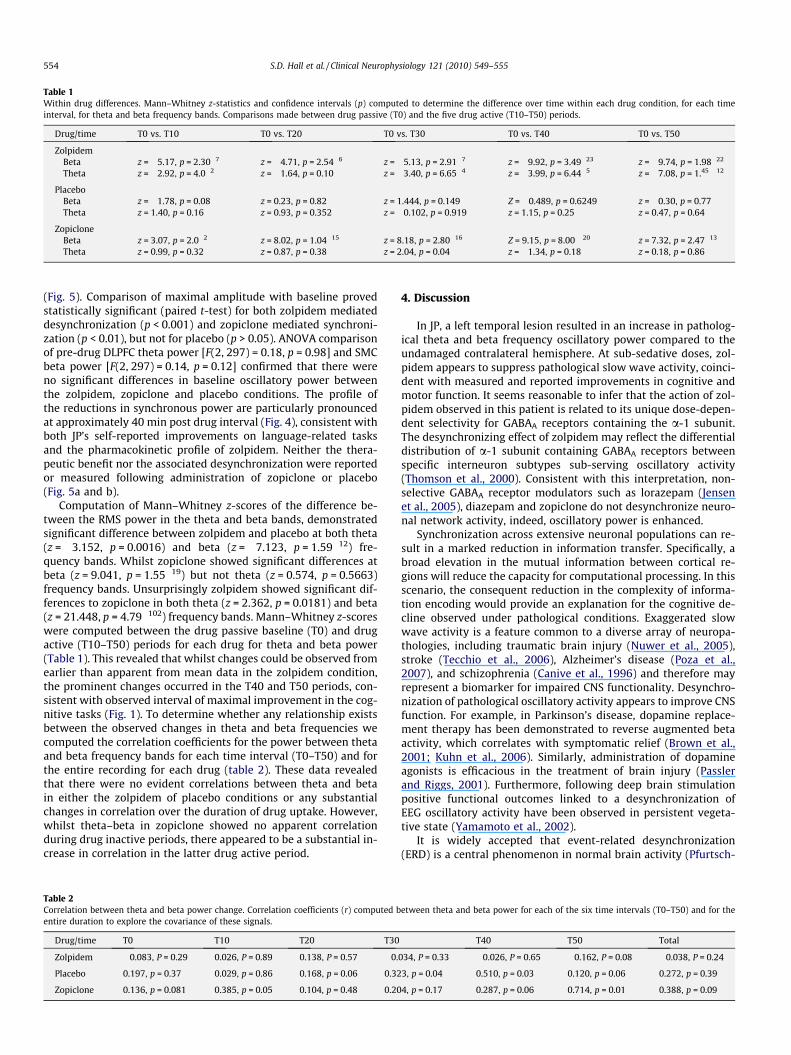
Table 1Within drug differences. Mann–Whitney z-statistics and confidence intervals (p) computed to determine the difference over time within each drug condition, for each timeinterval, for theta and beta frequency bands. Comparisons made between drug passive (T0) and the five drug active (T10–T50) periods.
Drug/time T0 vs. T10 T0 vs. T20 T0 vs. T30 T0 vs. T40 T0 vs. T50
ZolpidemBeta z = �5.17, p = 2.30�7 z = �4.71, p = 2.54�6 z = �5.13, p = 2.91�7 z = �9.92, p = 3.49�23 z = �9.74, p = 1.98�22
Theta z = �2.92, p = 4.0�2 z = �1.64, p = 0.10 z = �3.40, p = 6.65�4 z = �3.99, p = 6.44�5 z = �7.08, p = 1.45 �12
PlaceboBeta z = �1.78, p = 0.08 z = 0.23, p = 0.82 z = 1.444, p = 0.149 Z = �0.489, p = 0.6249 z = �0.30, p = 0.77Theta z = 1.40, p = 0.16 z = 0.93, p = 0.352 z = �0.102, p = 0.919 z = 1.15, p = 0.25 z = 0.47, p = 0.64
ZopicloneBeta z = 3.07, p = 2.0�2 z = 8.02, p = 1.04�15 z = 8.18, p = 2.80�16 Z = 9.15, p = 8.00 �20 z = 7.32, p = 2.47�13
Theta z = 0.99, p = 0.32 z = 0.87, p = 0.38 z = 2.04, p = 0.04 z = �1.34, p = 0.18 z = 0.18, p = 0.86
554 S.D. Hall et al. / Clinical Neurophysiology 121 (2010) 549–555
(Fig. 5). Comparison of maximal amplitude with baseline provedstatistically significant (paired t-test) for both zolpidem mediateddesynchronization (p < 0.001) and zopiclone mediated synchroni-zation (p < 0.01), but not for placebo (p > 0.05). ANOVA comparisonof pre-drug DLPFC theta power [F(2, 297) = 0.18, p = 0.98] and SMCbeta power [F(2, 297) = 0.14, p = 0.12] confirmed that there wereno significant differences in baseline oscillatory power betweenthe zolpidem, zopiclone and placebo conditions. The profile ofthe reductions in synchronous power are particularly pronouncedat approximately 40 min post drug interval (Fig. 4), consistent withboth JP’s self-reported improvements on language-related tasksand the pharmacokinetic profile of zolpidem. Neither the thera-peutic benefit nor the associated desynchronization were reportedor measured following administration of zopiclone or placebo(Fig. 5a and b).
Computation of Mann–Whitney z-scores of the difference be-tween the RMS power in the theta and beta bands, demonstratedsignificant difference between zolpidem and placebo at both theta(z = �3.152, p = 0.0016) and beta (z = �7.123, p = 1.59�12) fre-quency bands. Whilst zopiclone showed significant differences atbeta (z = 9.041, p = 1.55�19) but not theta (z = 0.574, p = 0.5663)frequency bands. Unsurprisingly zolpidem showed significant dif-ferences to zopiclone in both theta (z = 2.362, p = 0.0181) and beta(z = 21.448, p = 4.79�102) frequency bands. Mann–Whitney z-scoreswere computed between the drug passive baseline (T0) and drugactive (T10–T50) periods for each drug for theta and beta power(Table 1). This revealed that whilst changes could be observed fromearlier than apparent from mean data in the zolpidem condition,the prominent changes occurred in the T40 and T50 periods, con-sistent with observed interval of maximal improvement in the cog-nitive tasks (Fig. 1). To determine whether any relationship existsbetween the observed changes in theta and beta frequencies wecomputed the correlation coefficients for the power between thetaand beta frequency bands for each time interval (T0–T50) and forthe entire recording for each drug (table 2). These data revealedthat there were no evident correlations between theta and betain either the zolpidem of placebo conditions or any substantialchanges in correlation over the duration of drug uptake. However,whilst theta–beta in zopiclone showed no apparent correlationduring drug inactive periods, there appeared to be a substantial in-crease in correlation in the latter drug active period.
Table 2Correlation between theta and beta power change. Correlation coefficients (r) computed bentire duration to explore the covariance of these signals.
Drug/time T0 T10 T20 T30
Zolpidem �0.083, P = 0.29 0.026, P = 0.89 0.138, P = 0.57 �0.
Placebo 0.197, p = 0.37 0.029, p = 0.86 0.168, p = 0.06 0.32
Zopiclone 0.136, p = 0.081 0.385, p = 0.05 0.104, p = 0.48 0.20
4. Discussion
In JP, a left temporal lesion resulted in an increase in patholog-ical theta and beta frequency oscillatory power compared to theundamaged contralateral hemisphere. At sub-sedative doses, zol-pidem appears to suppress pathological slow wave activity, coinci-dent with measured and reported improvements in cognitive andmotor function. It seems reasonable to infer that the action of zol-pidem observed in this patient is related to its unique dose-depen-dent selectivity for GABAA receptors containing the a-1 subunit.The desynchronizing effect of zolpidem may reflect the differentialdistribution of a-1 subunit containing GABAA receptors betweenspecific interneuron subtypes sub-serving oscillatory activity(Thomson et al., 2000). Consistent with this interpretation, non-selective GABAA receptor modulators such as lorazepam (Jensenet al., 2005), diazepam and zopiclone do not desynchronize neuro-nal network activity, indeed, oscillatory power is enhanced.
Synchronization across extensive neuronal populations can re-sult in a marked reduction in information transfer. Specifically, abroad elevation in the mutual information between cortical re-gions will reduce the capacity for computational processing. In thisscenario, the consequent reduction in the complexity of informa-tion encoding would provide an explanation for the cognitive de-cline observed under pathological conditions. Exaggerated slowwave activity is a feature common to a diverse array of neuropa-thologies, including traumatic brain injury (Nuwer et al., 2005),stroke (Tecchio et al., 2006), Alzheimer’s disease (Poza et al.,2007), and schizophrenia (Canive et al., 1996) and therefore mayrepresent a biomarker for impaired CNS functionality. Desynchro-nization of pathological oscillatory activity appears to improve CNSfunction. For example, in Parkinson’s disease, dopamine replace-ment therapy has been demonstrated to reverse augmented betaactivity, which correlates with symptomatic relief (Brown et al.,2001; Kuhn et al., 2006). Similarly, administration of dopamineagonists is efficacious in the treatment of brain injury (Passlerand Riggs, 2001). Furthermore, following deep brain stimulationpositive functional outcomes linked to a desynchronization ofEEG oscillatory activity have been observed in persistent vegeta-tive state (Yamamoto et al., 2002).
It is widely accepted that event-related desynchronization(ERD) is a central phenomenon in normal brain activity (Pfurtsch-
etween theta and beta power for each of the six time intervals (T0–T50) and for the
T40 T50 Total
034, P = 0.33 �0.026, P = 0.65 �0.162, P = 0.08 �0.038, P = 0.24
3, p = 0.04 0.510, p = 0.03 0.120, p = 0.06 0.272, p = 0.39
4, p = 0.17 0.287, p = 0.06 0.714, p = 0.01 0.388, p = 0.09

S.D. Hall et al. / Clinical Neurophysiology 121 (2010) 549–555 555
eller, 2001) and ERD has been established as a feature of sensori-motor (Taniguchi et al., 2000) and cognitive processing (Singhet al., 2002). In JP, the high power and persistent nature of patho-logical oscillations appears to represent an obstacle to adequateERD; inability to desynchronize may represent a barrier to effectivecomputation in neuronal networks. Here we show that drug in-duced suppression of this functional barrier affords a return of cog-nitive performance, typically associated with ERD. An alternativeexplanation is that the observed reduction in synchronous poweris an epiphenomenon of increased neural activation, similar to thatobserved in ERD. However, this argument only emphasizes theinterpretation that normalization of the MEG signal permits regu-lar processing; albeit by a different mechanism. We would suggestthat pharmaco-MEG represents a powerful method for the identi-fication and development of future therapeutic interventions.
A potential limitation of the current study lies in the difficultiesassociated with generalizing from data obtained from brain inju-ries such as stroke. Specifically, the exact nature of the structural,functional and, almost certainly, chemical profile of each patientmay differ; leaving broad uncertainties. Therefore, it is not possibleto infer a specific mechanism of functional pathology or mode oftreatment from any single patient. Similarly, the exact modus offunctional abnormality, related to brain injury, will vary betweenindividuals; the measurement of which can be particularly prob-lematic. This is emphasized here in the observation that whilstboth category naming and covert letter fluency are both symptomsof JP that show improvement following zolpidem, cover letter flu-ency shows particular improvement following zolpidem adminis-tration (Fig. 1). Here our measurements are contingent upon thestability of WAIS-III test over time and anecdotal patient reportsof sensorimotor improvement. Similarly, measures of cognitiveimprovement are somewhat coarse and have limited repeatabilitydue to practice effects. Furthermore, whilst it is desirable that anystudy of neurological disorders be based around the observationsof a cohort of comparable cases, the individual differences in ische-mic stroke gives rise to an inhomogeneous group. However, wehave focused on an individual, representative of brain injury caseswhere zolpidem-mediated improvements are observed. Therefore,what we offer here is a potential electrophysiological basis for theobserved functional abnormalities in an individual, which formsthe basis for composing hypotheses for pertinent neurologicalquestions.
In conclusion, given the involvement of pathological slow waveoscillatory activity in a wide range of neurological disorders, andthe desynchronizing properties of zolpidem as measured usingpharmaco-MEG, it seems reasonable to suggest that the role of cor-tical GABA in pathological oscillations is one that requires furtherexploration.
Acknowledgements
This work was supported by Regen Therapeutics Plc. and anRCUK Fellowship (SDH). MEG work was supported by The Well-come Trust and The Dr. Hadwen Trust and the MRI work was sup-ported by The Lord Dowding Fund. We thank Dr. Peter Magill, forhelpful comments on the manuscript.
Appendix A. Supplementary material
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.clinph.2009.11.084.
References
Adjamian P, Barnes GR, Hillebrand A, Holliday IE, Singh KD, Furlong PL, et al. Co-registration of magnetoencephalography with magnetic resonance imagingusing bite-bar-based fiducials and surface-matching. Clin Neurophysiol2004;115:691–8.
Basso MR, Carona FD, Lowery N, Axelrod BN. Practice effects on the WAIS-III across3- and 6-month intervals. Clin Neuropsychol 2002;16:57–63.
Brown P, Oliviero A, Mazzone P, Insola A, Tonali P, Di L V. Dopamine dependency ofoscillations between subthalamic nucleus and pallidum in Parkinson’s disease. JNeurosci 2001;21:1033–8.
Canive JM, Lewine JD, Edgar JC, Davis JT, Torres F, Roberts B, et al.Magnetoencephalographic assessment of spontaneous brain activity inschizophrenia. Psychopharmacol Bull 1996;32:741–50.
Clauss R, Nel W. Drug induced arousal from the permanent vegetative state.NeuroRehabilitation 2006;21:23–8.
Clauss RP, Nel WH. Effect of zolpidem on brain injury and diaschisis as detected by99mTc HMPAO brain SPECT in humans. Arzneimittelforschung 2004;54:641–6.
Cohen L, Chaaban B, Habert MO. Transient improvement of aphasia with zolpidem.N Engl J Med 2004;350:949–50.
Daniele A, Albanese A, Gainotti G, Gregori B, Bartolomeo P. Zolpidem in Parkinson’sdisease. Lancet 1997;349:1222–3.
Dooley M, Plosker GL. Zaleplon: a review of its use in the treatment of insomnia.Drugs 2000;60:413–45.
Farver DK, Khan MH. Zolpidem for antipsychotic-induced parkinsonism. AnnPharmacother 2001;35:435–7.
Hall SD, Barnes GR, Furlong PL, Seri S, Hillebrand A. Neuronal networkpharmacodynamics of GABAergic modulation in the human cortexdetermined using pharmaco-magnetoencephalography. Hum Brain Mapp, inpress. Available online: 23 November 2009. doi:10.1002/hbm.20889.
Hall SD, Holliday IE, Hillebrand A, Singh KD, Furlong PL, Hadjipapas A, et al. Themissing link: analogous human and primate cortical gamma oscillations.Neuroimage 2005;26:13–7.
Hillebrand A, Singh KD, Holliday IE, Furlong PL, Barnes GR. A new approach toneuroimaging with magnetoencephalography. Hum Brain Mapp2005;25:199–211.
Holm KJ, Goa KL. Zolpidem: an update of its pharmacology, therapeutic efficacy andtolerability in the treatment of insomnia. Drugs 2000;59:865–89.
Jarry C, Fontenas JP, Jonville-Bera AP, utret-Leca E. Beneficial effect of zolpidem fordementia. Ann Pharmacother 2002;36:1808.
Jensen O, Goel P, Kopell N, Pohja M, Hari R, Ermentrout B. On the humansensorimotor-cortex beta rhythm: sources and modeling. Neuroimage2005;26:347–55.
Kuhn AA, Kupsch A, Schneider GH, Brown P. Reduction in subthalamic 8–35 Hzoscillatory activity correlates with clinical improvement in Parkinson’s disease.Eur J Neurosci 2006;23:1956–60.
Logothetis NK, Pauls J, Augath M, Trinath T, Oeltermann A. Neurophysiologicalinvestigation of the basis of the fMRI signal. Nature 2001;412:150–7.
Nuwer MR, Hovda DA, Schrader LM, Vespa PM. Routine and quantitative EEG inmild traumatic brain injury. Clin Neurophysiol 2005;116:2001–25.
Passler MA, Riggs RV. Positive outcomes in traumatic brain injury-vegetative state:patients treated with bromocriptine. Arch Phys Med Rehab 2001;82:311–5.
Pfurtscheller G. Functional brain imaging based on ERD/ERS. Vision Res2001;41:1257–60.
Poza J, Hornero R, Abasolo D, Fernandez A, Escudero J. Analysis of spontaneous MEGactivity in patients with Alzheimer’s disease using spectral entropies. In: ConfProc IEEE Eng Med Biol Soc 2007; 2007. p. 6180–3.
Shames JL, Ring H. Transient reversal of anoxic brain injury-related minimallyconscious state after zolpidem administration: a case report. Arch Phys MedRehab 2008;89:386–8.
Singh KD, Barnes GR, Hillebrand A, Forde EM, Williams AL. Task-related changes incortical synchronization are spatially coincident with the hemodynamicresponse. Neuroimage 2002;16:103–14.
Taniguchi M, Kato A, Fujita N, Hirata M, Tanaka H, Kihara T, et al. Movement-relateddesynchronization of the cerebral cortex studied with spatially filteredmagnetoencephalography. Neuroimage 2000;12:298–306.
Tecchio F, Zappasodi F, Pasqualetti P, Tombini M, Caulo M, Ercolani M, et al. Long-term effects of stroke on neuronal rest activity in rolandic cortical areas. JNeurosci Res 2006;83:1077–87.
Thomson AM, Bannister AP, Hughes DI, Pawelzik H. Differential sensitivity toZolpidem of IPSPs activated by morphologically identified CA1 interneurons inslices of rat hippocampus. Eur J Neurosci 2000;12:425–36.
Vrba J, Robinson SE. Signal processing in magnetoencephalography. Methods2001;25:249–71.
Yamamoto T, Katayama Y, Oshima H, Fukaya C, Kawamata T, Tsubokawa T. Deepbrain stimulation therapy for a persistent vegetative state. Acta Neurochir Suppl2002;79:79–82.
Related Documents