Eur Radiol (2005) 15: 468–484 DOI 10.1007/s00330-004-2555-2 NEURO G. Wilms Ph. Demaerel S. Sunaert Received: 7 July 2004 Revised: 11 October 2004 Accepted: 14 October 2004 Published online: 31 December 2004 # Springer-Verlag 2004 Intra-axial brain tumours Abstract The radiological diagnosis and differential diagnosis of intra- axial tumours no longer relies on CT scan and routine MR sequences alone. Standard multiplanar imaging has to be combined with fMRI to allow the exact anatomic location of the lesion and precise determination of the ex- tension of the tumour. Perfusion and diffusion MR is becoming more and more important in the differential diagnosis of cerebral mass lesions and in the grading and typing of gliomas. More sophisticated techniques such as diffusion tensor imaging and spec- troscopy will further enhance the value of the radiological studies. Keywords Brain neoplasms . Diagnosis . Computed tomography . Magnetic resonance imaging . Comparative studies Introduction Neuroradiology plays a key role in the diagnosis and pre- operative set-up of patients with brain tumours. State-of- the-art imaging requires a standardised imaging protocol, careful and systematic study of the images and finally an attempt at characterisation of the lesion. Imaging protocols for the study of (intra-axial) brain tumours In modern neuroradiology, magnetic resonance (MR) is the method of choice to study lesions of the brain. Since computed tomography (CT) is more widely available, it can be used as a first screening method if a patient is suspected of having an intracranial mass lesion. Routinely, precon- trast and postcontrast CT is performed. Nevertheless, if on plain CT a mass lesion is evident, one might consider not giving IV-contrast for economic and medical reasons and immediately going to MR [1, 2]. A routine MR examination of the brain starts with a long TR/long TE (T2-weighted) sequence, a short TR/short TE (T1-weighted) sequence and a fluid-attenuated (FLAIR) sequence. These images are mostly performed in the trans- verse direction, but for specific locations other incidences can be used. Gadolinium-enhanced series are routinely per- formed in the transverse, coronal and sagittal plane, com- pleted if necessary by more selective slices. We routinely include diffusion weighted imaging (DWI) in our imaging protocol for the study of intracranial mass lesions, since it can have important differential diagnostic implications [3, 4]. Perfusion CT or MR, although not routinely used in most centres, can offer valuable information on tumoral vascularity and grading and should be included in the imaging protocol [5–7]. If the tumour is situated in an eloquent area, functional MR (fMRI) will better locate the lesion and define its relations to the functional areas [8, 9]. In institutions where 3-T equipment is available, the use of diffusion tensor imaging for the study of white matter invasion of brain tumours is under investigation [10–12]. For the study of vessel displacement and to assess gross tumour vascularity, magnetic resonance angiography (MRA) G. Wilms (*) . P. Demaerel . S. Sunaert Department of Radiology, U.Z. Gasthuisberg, Herestraat 49, 3000 Leuven, Belgium e-mail: [email protected] Tel.: +32-1634-8781 Fax: +32-1634-8765

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Eur Radiol (2005) 15: 468–484DOI 10.1007/s00330-004-2555-2 NEURO
G. WilmsPh. DemaerelS. Sunaert
Received: 7 July 2004Revised: 11 October 2004Accepted: 14 October 2004Published online: 31 December 2004# Springer-Verlag 2004
Intra-axial brain tumours
Abstract The radiological diagnosisand differential diagnosis of intra-axial tumours no longer relies on CTscan and routine MR sequences alone.Standard multiplanar imaging has tobe combined with fMRI to allow theexact anatomic location of the lesionand precise determination of the ex-tension of the tumour. Perfusion anddiffusion MR is becoming more andmore important in the differentialdiagnosis of cerebral mass lesions andin the grading and typing of gliomas.More sophisticated techniques such as
diffusion tensor imaging and spec-troscopy will further enhance thevalue of the radiological studies.
Keywords Brain neoplasms .Diagnosis . Computed tomography .Magnetic resonance imaging .Comparative studies
Introduction
Neuroradiology plays a key role in the diagnosis and pre-operative set-up of patients with brain tumours. State-of-the-art imaging requires a standardised imaging protocol,careful and systematic study of the images and finally anattempt at characterisation of the lesion.
Imaging protocols for the study of (intra-axial) braintumours
In modern neuroradiology, magnetic resonance (MR) isthe method of choice to study lesions of the brain. Sincecomputed tomography (CT) is more widely available, it canbe used as a first screening method if a patient is suspectedof having an intracranial mass lesion. Routinely, precon-trast and postcontrast CT is performed. Nevertheless, if onplain CT a mass lesion is evident, one might consider notgiving IV-contrast for economic and medical reasons andimmediately going to MR [1, 2].
A routine MR examination of the brain starts with a longTR/long TE (T2-weighted) sequence, a short TR/short TE(T1-weighted) sequence and a fluid-attenuated (FLAIR)sequence. These images are mostly performed in the trans-verse direction, but for specific locations other incidencescan be used. Gadolinium-enhanced series are routinely per-formed in the transverse, coronal and sagittal plane, com-pleted if necessary by more selective slices. We routinelyinclude diffusion weighted imaging (DWI) in our imagingprotocol for the study of intracranial mass lesions, sinceit can have important differential diagnostic implications[3, 4]. Perfusion CT or MR, although not routinely usedin most centres, can offer valuable information on tumoralvascularity and grading and should be included in theimaging protocol [5–7]. If the tumour is situated in aneloquent area, functional MR (fMRI) will better locate thelesion and define its relations to the functional areas [8, 9].
In institutions where 3-T equipment is available, the useof diffusion tensor imaging for the study of white matterinvasion of brain tumours is under investigation [10–12].For the study of vessel displacement and to assess grosstumour vascularity, magnetic resonance angiography (MRA)
G. Wilms (*) . P. Demaerel .S. SunaertDepartment of Radiology, U.Z.Gasthuisberg,Herestraat 49,3000 Leuven, Belgiume-mail: [email protected].: +32-1634-8781Fax: +32-1634-8765
has replaced catheter angiography, which is only performed inextra-axial tumours [13, 14]. MR spectroscopy is only per-formed in selective cases, mainly for the differential diagnosisbetween tumours and non-tumoural mass lesions.
How to examine the images of a patient with a cerebral masslesion?
Today, with the availability of CTandMRI, the radiologicaldiagnosis of a brain tumour includes more than the simpleidentification of an intracranial mass. The diagnosis of abrain tumour includes multiple steps that have to be care-
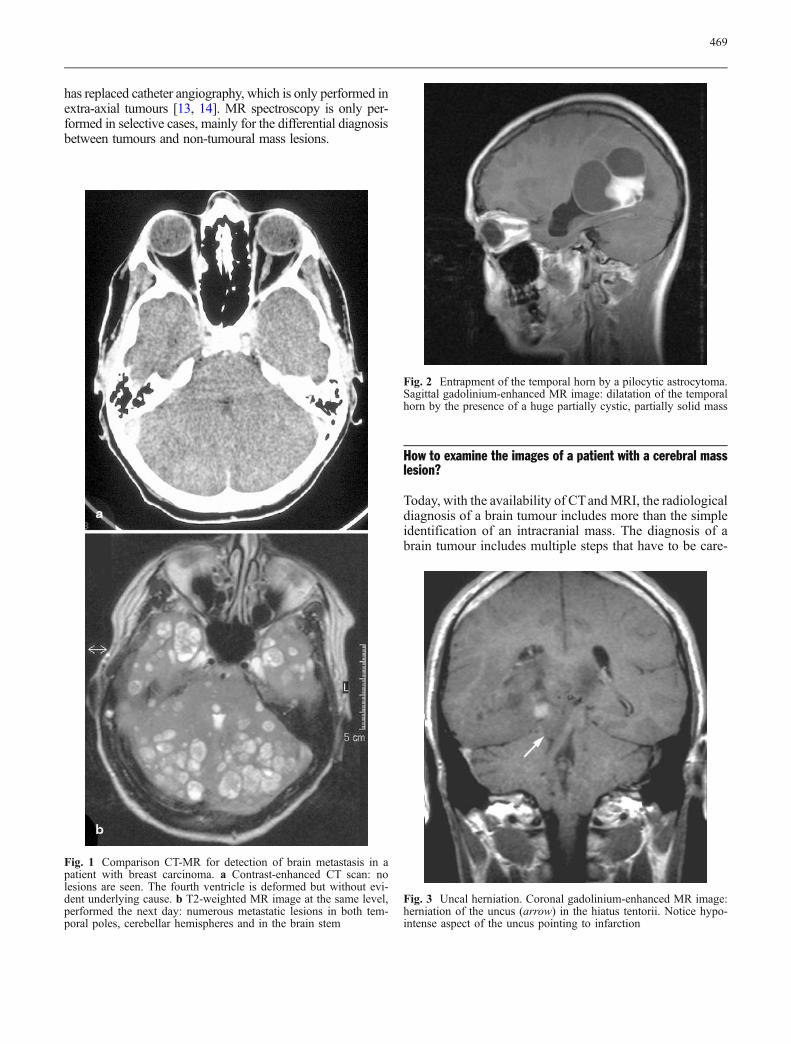
Fig. 1 Comparison CT-MR for detection of brain metastasis in apatient with breast carcinoma. a Contrast-enhanced CT scan: nolesions are seen. The fourth ventricle is deformed but without evi-dent underlying cause. b T2-weighted MR image at the same level,performed the next day: numerous metastatic lesions in both tem-poral poles, cerebellar hemispheres and in the brain stem
Fig. 2 Entrapment of the temporal horn by a pilocytic astrocytoma.Sagittal gadolinium-enhanced MR image: dilatation of the temporalhorn by the presence of a huge partially cystic, partially solid mass
Fig. 3 Uncal herniation. Coronal gadolinium-enhanced MR image:herniation of the uncus (arrow) in the hiatus tentorii. Notice hypo-intense aspect of the uncus pointing to infarction
469
fully examined. These steps are: detection, evaluation of itseffect on the brain and the ventricles, localisation especiallywith regard to eloquent areas and definition of the extentof the tumour. Finally the type and grade of the tumourhave to be described, together with its differential diagno-sis, especially with non-tumoural lesions.
The first and of course limiting step is the detection ofan intracerebral mass. This will first depend on the volumeof the lesion: smaller lesions will bemore easilymissed thanlarger ones. Nowadays with appropriate techniques andproper clinical suspicion, very small lesions such as tinymetastases or microadenomas of the hypophysis can bedetected with CT. Detection will depend on the difference inCT characteristics, meaning the atomic number or radio-density. Tumours such as low grade glioma, metastasis orlymphoma can be almost isodense with the surrounding
brain on CT (Fig. 1a). Artefacts in the posterior fossa or onthe highest slices can mask subtle lesions [15].
With MRI, detection will depend on the difference inMRI characteristics, such as T1, T2, proton density, flow,etc. It is known that the sensitivity for pathological con-ditions is higher with MR than with CT. Lesions producinglittle or no change in CT density tend to be more con-spicuous on MR (Fig. 1b) [15]. This is due to the highsensitivity of MR for changes in water content, almost in-variably present in or accompanying brain tumours, leadingto hyperintensity on T2-images and FLAIR images. Isoin-tensity of a lesion is extremely infrequent with higher fieldmagnets and, if seen, is rarely present on all sequences.Small metastasis, though, still can be missed if only ascreening transaxial T2-weighted sequence is performed.
If contrast medium is administered, detection will de-pend on the difference in vascularity and on the damage to
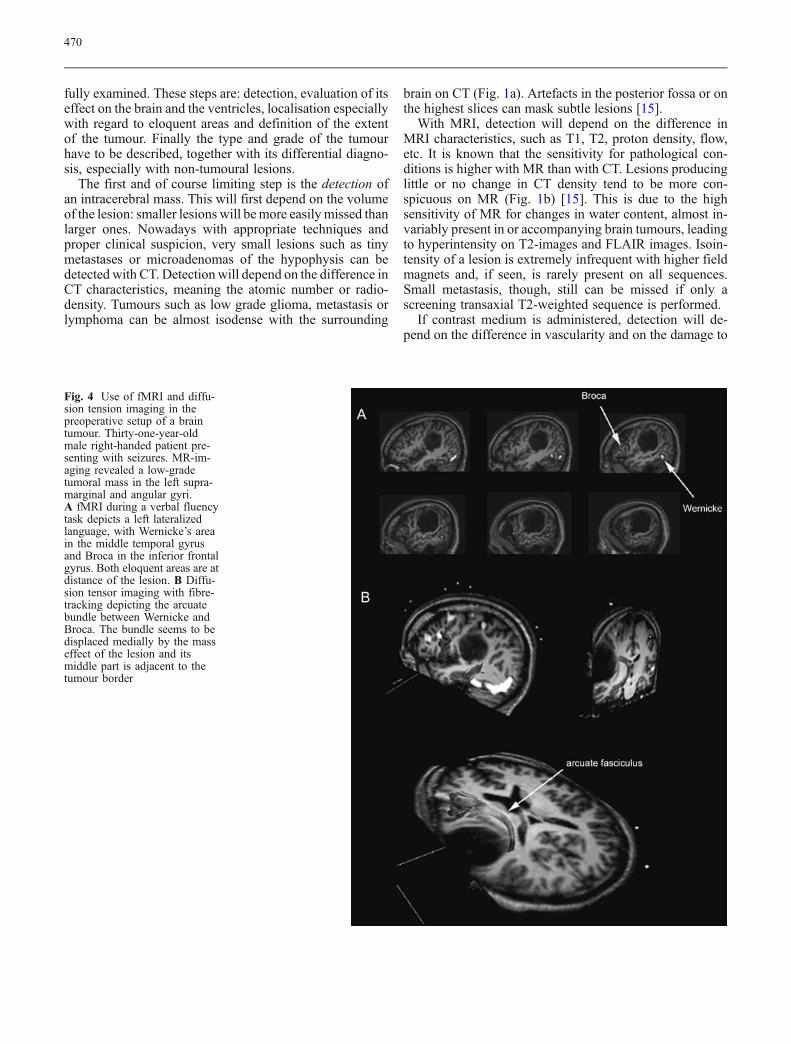
Fig. 4 Use of fMRI and diffu-sion tension imaging in thepreoperative setup of a braintumour. Thirty-one-year-oldmale right-handed patient pre-senting with seizures. MR-im-aging revealed a low-gradetumoral mass in the left supra-marginal and angular gyri.A fMRI during a verbal fluencytask depicts a left lateralizedlanguage, with Wernicke’s areain the middle temporal gyrusand Broca in the inferior frontalgyrus. Both eloquent areas are atdistance of the lesion. B Diffu-sion tensor imaging with fibre-tracking depicting the arcuatebundle between Wernicke andBroca. The bundle seems to bedisplaced medially by the masseffect of the lesion and itsmiddle part is adjacent to thetumour border
470
the blood-brain barrier. Since the mechanisms of enhance-ment are the same with CT and MRI, there will be a similarsensitivity for both techniques. Nevertheless, MRI will pickup smaller foci of contrast enhancement by its higher spa-tial resolution, or by the absence of artefacts or volume-
averaging from the overlying bone, especially if backgroundsuppression is enhanced by magnetic transfer prepulses[16, 17].
The second step is the evaluation of the effect of thetumour on the brain and the ventricles. This includesthe presence of hydrocephalus or of isolation of parts ofthe ventricular system, evaluation of midline shift, herni-ation of the cingulate gyrus under the falx, of the uncusthrough the incisura tentorii and of the cerebellar tonsilsthrough the foramen magnum, and the compression anddisplacement of functional brain tissue [18]. The evaluationof the impact of the tumour on brain and ventricles is im-portant for several reasons. First of all, in the acute setting,the presence of hydrocephalus, midline shift and herniationcan frequently better explain the actual clinical condition ofthe patient rather than the exact type or location of thetumour. Therefore, almost invariably it will be more im-portant to perform ventricular drainage or decompressionof an isolated “trapped” temporal horn (Fig. 2), rather thanactually to remove the tumour at a stage where little isknown about its histology. Associated brain herniation,especially of the uncus through the tentorial incisura, cancause secondary ischemic lesions and can largely deter-mine the final prognosis of the patient (Fig. 3).
The next step is the localization of the tumour. It has to bedetermined if the lesion is intra-axial or extra-axial, supra-or infratentorial and intraventricular or extraventricular.Also of concern is the localisation in specific brain struc-tures such as the hypophysis, the pineal gland or the brainstem, localisation with regard to functional brain regionsand localisationwith regard to vascular structures. To obtainthis information, multiplanar MR is without a doubt ofutmost importance.
Both for the understanding of the symptoms of the patientand for preoperative planning, it is tremendously important
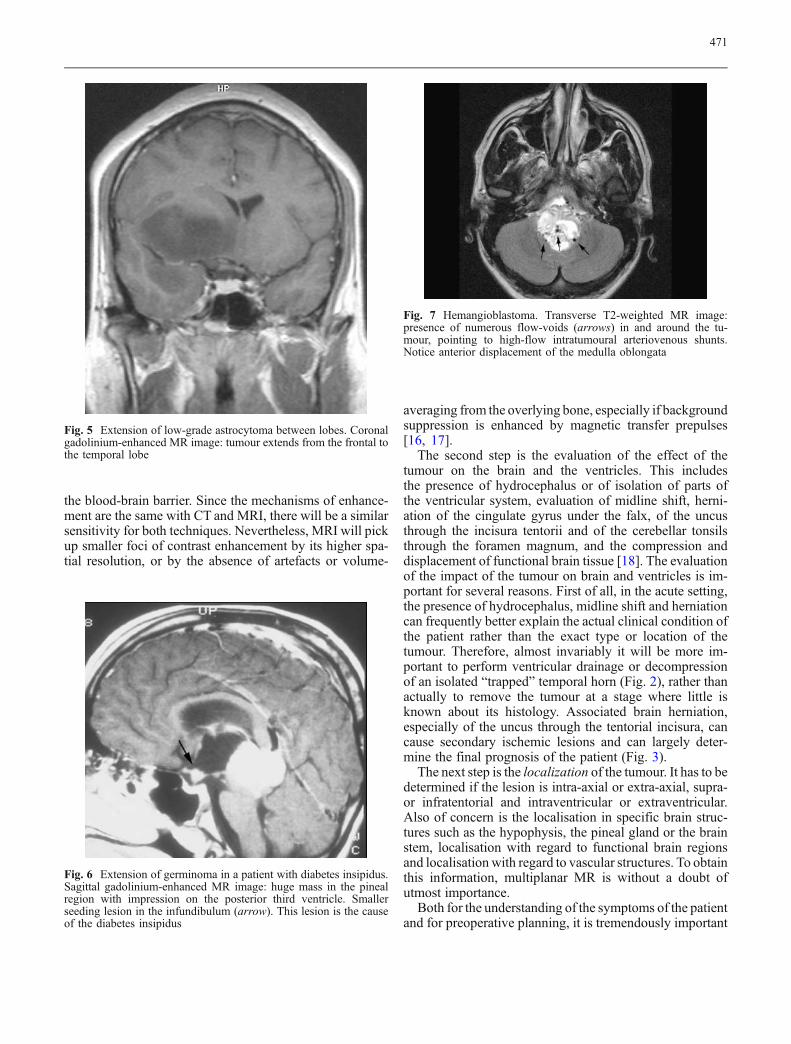
Fig. 5 Extension of low-grade astrocytoma between lobes. Coronalgadolinium-enhanced MR image: tumour extends from the frontal tothe temporal lobe
Fig. 6 Extension of germinoma in a patient with diabetes insipidus.Sagittal gadolinium-enhanced MR image: huge mass in the pinealregion with impression on the posterior third ventricle. Smallerseeding lesion in the infundibulum (arrow). This lesion is the causeof the diabetes insipidus
Fig. 7 Hemangioblastoma. Transverse T2-weighted MR image:presence of numerous flow-voids (arrows) in and around the tu-mour, pointing to high-flow intratumoural arteriovenous shunts.Notice anterior displacement of the medulla oblongata
471

to determine in which anatomic and functional region thetumour is situated. Morphologically, this is performed bythe study of the location of the tumour with regard to an-atomic fissures and sulci, such as the Sylvian (sensory andmotor speech), Rolandic (sensorimotor cortex) or calcarine(visual cortex) fissures.
Functional MR nowadays plays a major role in thelocalisation of a brain tumour or any other operative lesion,with regard to functional brain tissue, by the actual visual-isation of functional activity of motor function, speech orvisual activity (Fig. 4) [8, 9]. This activation can be present
Fig. 8 Cystic anaplastic astrocytoma grade 3. a Transverse T2-weighted MR image: the intensity of the cyst is higher than that ofthe cerebrospinal fluid in the ventricles and the subarachnoid spaces.b FLAIR-MR image: unlike the cerebrospinal fluid in the ventriclesand the subarachnoid spaces, the fluid in the cyst is not attenuateddue to its high protein content
Fig. 9 Ependymoma grade 2 of the fourth ventricle in a 2-year-oldchild. Coronal and sagittal gadolinium-enhanced MR images: inho-mogeneously enhancing tumour filling up the entire fourth ventricle.The tumour extends through the foramen of Magendie to the fora-men magnum (large white arrows) and through the foramina ofLuschka (black arrows) to the inferior cerebellar peduncle. There ismarked compression of the brainstem. In the most inferior aspect ofthe tumour the brainstem seems clearly invaded (arrowheads)
472
in the tumour itself, at its edges, or can be displaced by themass. The exact distance between the eloquent area and thetumour can be determinant in the assessment of the opera-bility of the tumour. Lack of cooperation by the patientbecause of tumour symptoms (paresis, aphasia, blindness)will of course interfere with this method.
Finally, the tumour has to be located with regard tovascular structures. Here, the display of the cortical venousanatomy will have important implications for the deter-mination of the surgical approach. While formerly this wasdone with angiography, the combination of surface imag-
ing and magnetic resonance angiography now offers therequired anatomical information to the surgeon. In the sameway, arterial encasement, invasion or occlusion of themajor vessels, such as, for example, the carotid artery andthe middle cerebral artery in cavernous sinus lesions, iseasily diagnosed by MRA [13].
The next step is the determination of the extent of thetumour. This answers the question whether or not the lesion
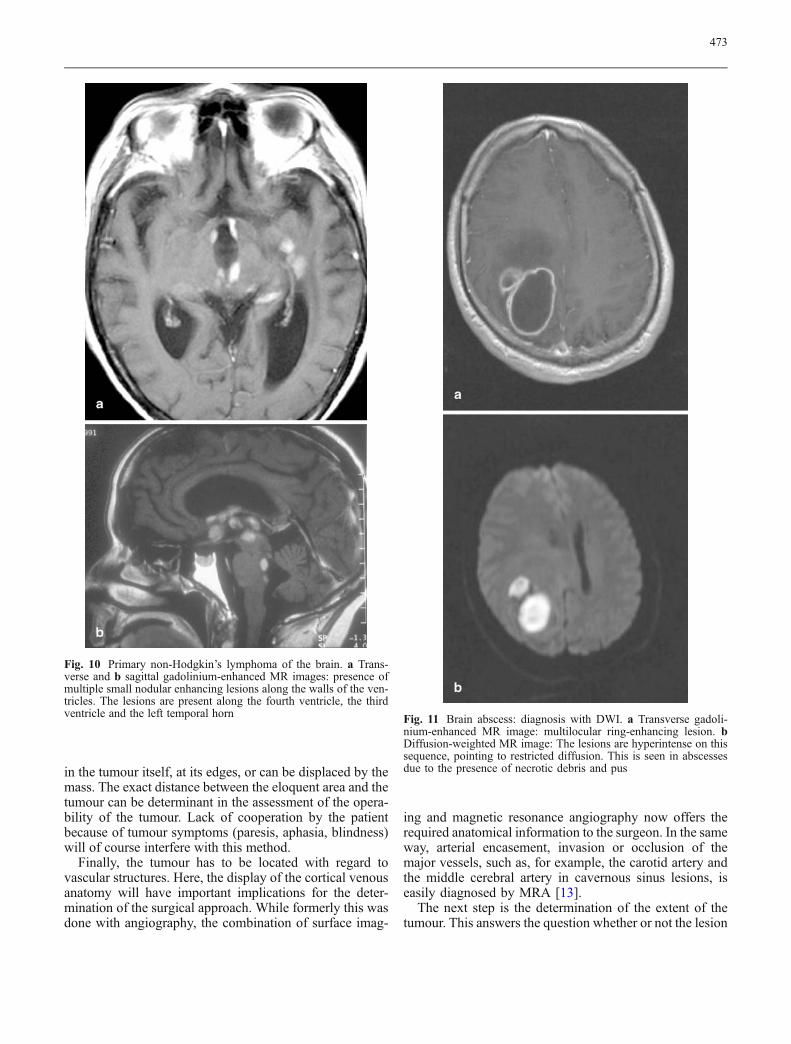
Fig. 10 Primary non-Hodgkin’s lymphoma of the brain. a Trans-verse and b sagittal gadolinium-enhanced MR images: presence ofmultiple small nodular enhancing lesions along the walls of the ven-tricles. The lesions are present along the fourth ventricle, the thirdventricle and the left temporal horn Fig. 11 Brain abscess: diagnosis with DWI. a Transverse gadoli-
nium-enhanced MR image: multilocular ring-enhancing lesion. bDiffusion-weighted MR image: The lesions are hyperintense on thissequence, pointing to restricted diffusion. This is seen in abscessesdue to the presence of necrotic debris and pus
473
is confined to one lobe or extends over a fissure to an-other lobe (for instance, a frontotemporal lesion) (Fig. 5),if the tumour involves the brain stem, basal ganglia, crossesthe midline, extends through the incisura tentorii, throughthe foramen magnum or seeds to specific anatomic areas. Inthis regard, the metastasis of pineoblastoma to the infun-dibulum of the hypophysis is a pathognomonic finding ina patient with diabetes insipidus (Fig. 6). Here too, mul-tiplanar imaging with MRI, with depiction of the ana-tomic relations in the axial, coronal and sagittal planes, ismandatory.
The final step in the examination of patients with acerebral mass lesion is the differential diagnosis or the
specification of the nature of the lesion. We have to dif-ferentiate between primary and metastatic lesions, menin-gioma and neurinoma, lymphoma and metastasis, benignand malignant character, glioma and other kinds of braintumours. This differential diagnosis is based on CT or MRcharacteristics (density-intensity), extension or localisation,contrast enhancement and classical signs [19, 20].
The first is the CT density of the lesion or the intensityon MR. The presence of calcification can point to oligo-dendroglioma or ependymoma. Flow voids because ofhypertrophic draining veins or hypervascularity can sug-gest hemangioblastoma (Fig. 7). The signal from cysticcomponents, such as hyperintense cholesterol-containing
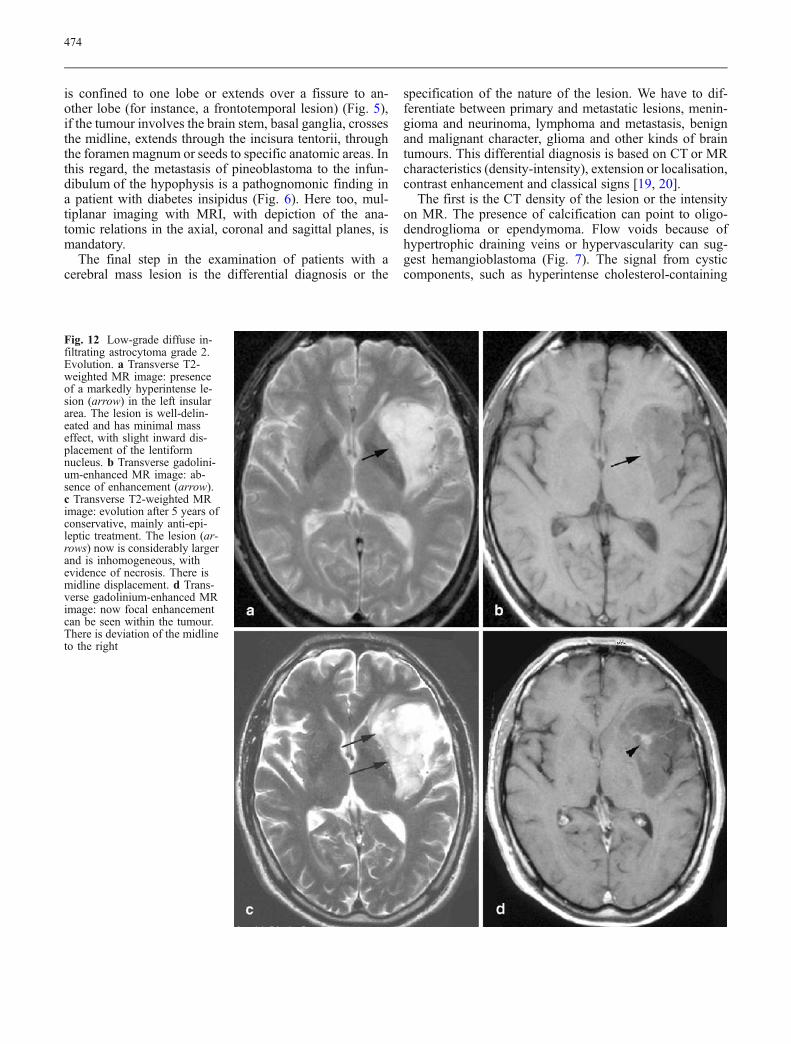
Fig. 12 Low-grade diffuse in-filtrating astrocytoma grade 2.Evolution. a Transverse T2-weighted MR image: presenceof a markedly hyperintense le-sion (arrow) in the left insulararea. The lesion is well-delin-eated and has minimal masseffect, with slight inward dis-placement of the lentiformnucleus. b Transverse gadolini-um-enhanced MR image: ab-sence of enhancement (arrow).c Transverse T2-weighted MRimage: evolution after 5 years ofconservative, mainly anti-epi-leptic treatment. The lesion (ar-rows) now is considerably largerand is inhomogeneous, withevidence of necrosis. There ismidline displacement. d Trans-verse gadolinium-enhanced MRimage: now focal enhancementcan be seen within the tumour.There is deviation of the midlineto the right
474
cysts in craniopharyngioma, can be diagnostic. MRI can bevery helpful in the specification of tumour necrosis and thedifferentiation between cystic versus non-cystic and hem-orrhagic versus non-hemorrhagic neoplasms. The identifi-cation of cystic areas on MRI also requires careful scrutinyof lesion intensity relative to CSF on all of the three rou-tinely obtained images: short TR/TE, long TR/short TE andlong TR/long TE. If a lesion is exactly isointense to CSF onall three of these sequences, then one can state very con-fidently that the lesion is cystic. Tumour cysts, however,can also be of slightly higher intensity than pure CSF dueto highly proteinaceous debris (Fig. 8). Finally, the recog-nition of fat in a tumour, by negative density on CT and theshort T1 and short T2 on MRI, is of utmost value in thediagnosis of lipoma, teratoma and dermoid cysts.
The second point to allow differential diagnosis is thelocation and the extension of the tumour. Some tumours,such as craniopharyngioma, show typical suprasellar loca-tion and extension. Midline masses in the posterior fossa inchildren are very hard to differentiate from one another. Incases of ependymoma, very frequently we will see that thetumour extends not only through the foramen of Magendieto the cisterna magna, but also through the lateral foraminaof Lushka to the cerebellopontine angle (Fig. 9) [21, 22]. Inastrocytoma, the most common glial neoplasm with calci-fication, it is not uncommon to identify cortical involve-ment by these tumours with thickening of the corticalmantle. This can mimic cortical infarction, but in astrocy-toma the lesion does not follow a vascular territory. Inpatients with temporal lobe epilepsy, diffusely hyperin-tense lesions in the uncus of the temporal lobe frequentlycorrespond to ganglioglioma. Multiple contrast-enhancingnodules over the hemispheres can correspond to multifocalglioblastoma, to metastasis or to lymphoma. If the lesionsare situated adjacent to the ventricles, lymphoma is highlyprobable (Fig. 10).
A third factor of interest is the degree of contrast en-hancement. Classically, it is said that with a higher degreeof malignancy, contrast enhancement will increase. Duringthe evolution of a lesion, we frequently will see not onlythat there is an increase in the oedema, but also in contrastenhancement. This can be a sign of anaplastic transforma-tion of the tumour. Nevertheless, striking changes in thecontrast enhancement of a lesion, without any change in thedegree of malignancy at biopsy, are seen in oligoden-drogliomas [23]. On the other hand, in some series, malig-nancy was found at biopsy in non-enhancing lesions in upto 40% of gliomas [20, 24, 25]. PerfusionMR in these casescan show tumour hypervascularity, reflecting the malignantnature of the lesion.
Finally, the differential diagnosis has to be made withnon-tumoral lesions, such as abscesses, multiple sclero-sis, radionecrosis, infarction, aneurysms, etc. Here, DWI,perfusionMR andMR-spectroscopy are important (Fig. 11)[3, 26, 27].
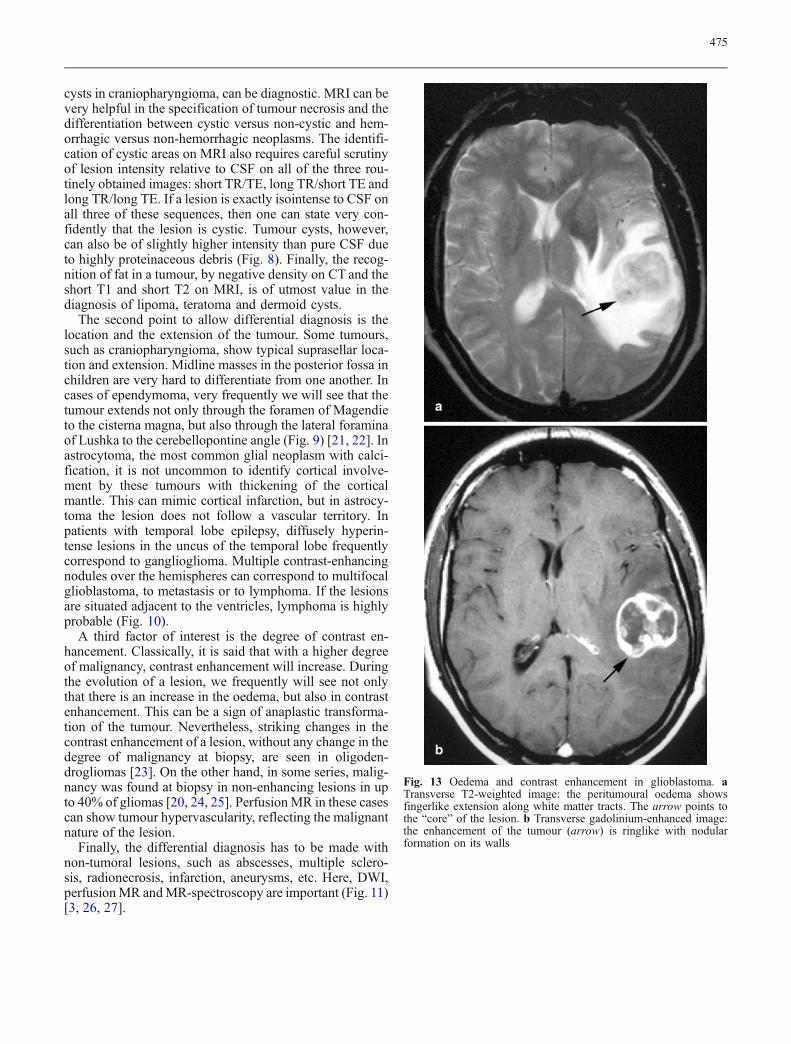
Fig. 13 Oedema and contrast enhancement in glioblastoma. aTransverse T2-weighted image: the peritumoural oedema showsfingerlike extension along white matter tracts. The arrow points tothe “core” of the lesion. b Transverse gadolinium-enhanced image:the enhancement of the tumour (arrow) is ringlike with nodularformation on its walls
475
The radiological diagnosis of intra-axial brain tumours
Here, we will discuss the imaging aspects of the most fre-quent intra-axial tumours: the neuro-epithelial tumours, theembryonal tumours and the metastases.
The World Health Organisation (WHO) Classificationof Brain Tumours was profoundly changed in 1993 andwas updated recently in 2000 [28, 29]. For the typing andgrading of brain tumours, no longer only standard patho-logical features are used, but besides information on immu-nohistochemistry and genetics, imaging findings are takeninto account.
The most important change concerned the large group ofthe astrocytic tumours, accounting for more than 60% ofprimary brain tumours. Here, a distinction is made betweendiffusely infiltrating and circumscribed astrocytomas, re-ferring to both gross pathological and imaging features.The diffusely infiltrating astrocytomas are at least grade 2and have an inherent tendency for anaplastic progression.Circumscribed astrocytomas are benign, and malignanttransformation is extremely rare.
Low grade astrocytomas are hypodense on CT and havelong T1 and T2 on MRI. Classically, there is no contrastenhancement. The diffusely infiltrating character is reflect-ed in a replacement rather than a displacement of brainstructures leading to a mass-effect that is less then expected
from the tumour volume and by crossing the borders of thecerebral lobes (Fig. 12a, b).
Progressive malignant transformation is characterised bya progressive increase in tumoral necrosis, intratumoralhaemorrhage and peritumoural oedema, with appearance ofcontrast enhancement. In this way the low-grade astrocyto-ma becomes anaplastic and finally displays the very “mul-tiform” aspect of glioblastoma multiforme (Fig. 12c, d)[20, 24]. It has to be stressed that in some gliomas anaplastictransformation is not translated into an increase of contrastenhancement [25].
The peritumoural vasogenic oedema is typically “finger-like”, dissecting white matter tracts (Fig. 14a). This oede-ma reflects the break-down of the blood-brain barrier, butis also related to angiogenesis, as proven by the presenceof vascular endothelial growth factors (VEGF). There-fore, oedema is more pronounced in malignant tumours[30, 31].
Tumoral contrast enhancement is mostly anarchic, areasof homogeneous enhancement alternating with ringlikebands of enhancement with nodular formations in the wall(Fig. 13b). It reflects both the blood-brain barrier break-down, but also is correlated with tumoral angiogenesis.This “malignant hypervascularity” has been known for along time from angiography, but is now easily demon-strated by perfusion CT or MRI [5–7] (Fig. 14a). Demon-
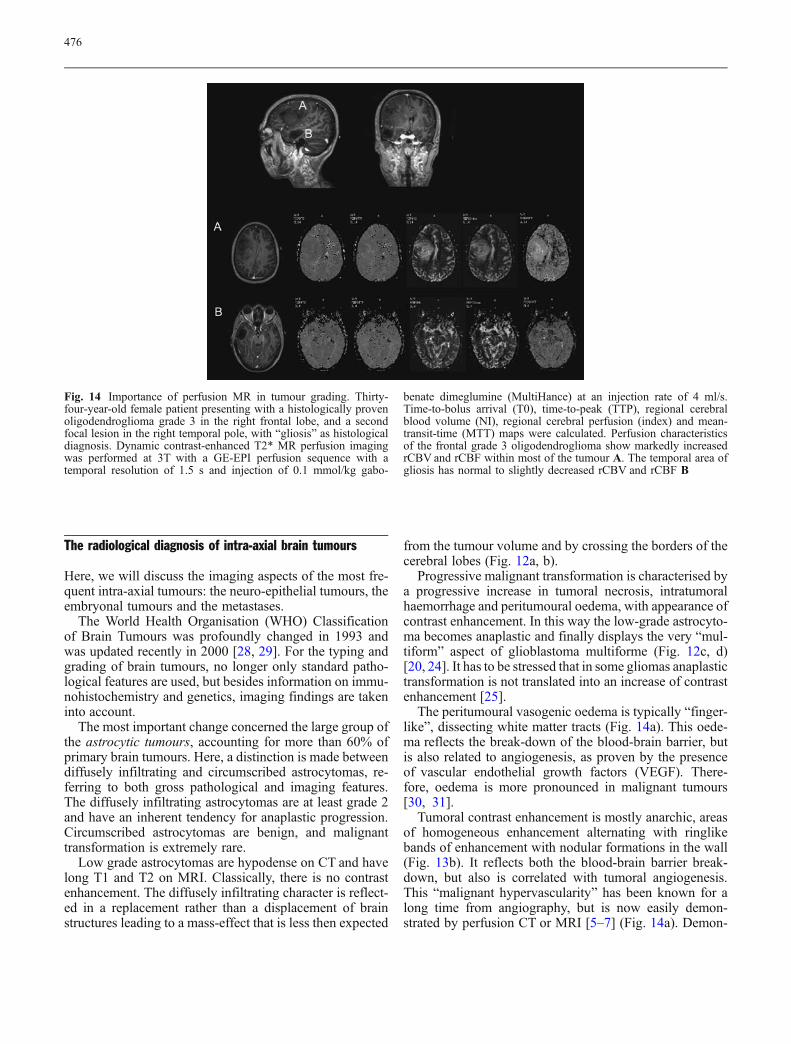
Fig. 14 Importance of perfusion MR in tumour grading. Thirty-four-year-old female patient presenting with a histologically provenoligodendroglioma grade 3 in the right frontal lobe, and a secondfocal lesion in the right temporal pole, with “gliosis” as histologicaldiagnosis. Dynamic contrast-enhanced T2* MR perfusion imagingwas performed at 3T with a GE-EPI perfusion sequence with atemporal resolution of 1.5 s and injection of 0.1 mmol/kg gabo-
benate dimeglumine (MultiHance) at an injection rate of 4 ml/s.Time-to-bolus arrival (T0), time-to-peak (TTP), regional cerebralblood volume (NI), regional cerebral perfusion (index) and mean-transit-time (MTT) maps were calculated. Perfusion characteristicsof the frontal grade 3 oligodendroglioma show markedly increasedrCBV and rCBF within most of the tumour A. The temporal area ofgliosis has normal to slightly decreased rCBV and rCBF B
476
stration of hypervascularity in non-enhancing lesions is asign of malignancy. It is noteworthy that the areas of maxi-mal perfusion do not necessarily correspond to the areas ofmaximal enhancement, which offers perspectives for guid-ed tumour biopsy. Finally, it has to be stressed that thetumour not only may extend beyond the margins of en-hancement, but even outside the T2-hyperintense area.Again, this is confirmed by perfusion CT or MRI. Resec-
tion of the enhancing area, therefore, is not sufficient toassure the cure of the patient. Diffusion-weighted imagingcan be of interest in diffusely infiltrating tumours by dem-onstrating displacement or invasion of white matter tracts(Fig. 14b).
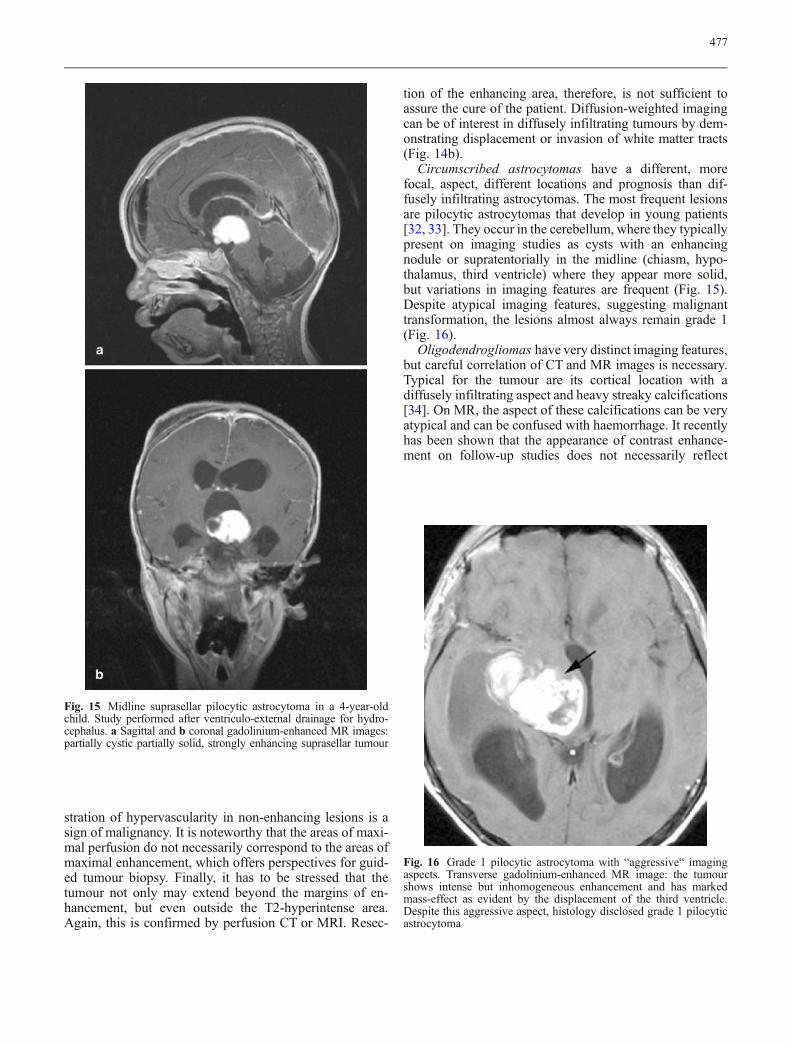
Circumscribed astrocytomas have a different, morefocal, aspect, different locations and prognosis than dif-fusely infiltrating astrocytomas. The most frequent lesionsare pilocytic astrocytomas that develop in young patients[32, 33]. They occur in the cerebellum, where they typicallypresent on imaging studies as cysts with an enhancingnodule or supratentorially in the midline (chiasm, hypo-thalamus, third ventricle) where they appear more solid,but variations in imaging features are frequent (Fig. 15).Despite atypical imaging features, suggesting malignanttransformation, the lesions almost always remain grade 1(Fig. 16).
Oligodendrogliomas have very distinct imaging features,but careful correlation of CT and MR images is necessary.Typical for the tumour are its cortical location with adiffusely infiltrating aspect and heavy streaky calcifications[34]. On MR, the aspect of these calcifications can be veryatypical and can be confused with haemorrhage. It recentlyhas been shown that the appearance of contrast enhance-ment on follow-up studies does not necessarily reflect
Fig. 15 Midline suprasellar pilocytic astrocytoma in a 4-year-oldchild. Study performed after ventriculo-external drainage for hydro-cephalus. a Sagittal and b coronal gadolinium-enhanced MR images:partially cystic partially solid, strongly enhancing suprasellar tumour
Fig. 16 Grade 1 pilocytic astrocytoma with “aggressive“ imagingaspects. Transverse gadolinium-enhanced MR image: the tumourshows intense but inhomogeneous enhancement and has markedmass-effect as evident by the displacement of the third ventricle.Despite this aggressive aspect, histology disclosed grade 1 pilocyticastrocytoma
477

malignant transformation, as in astrocytic tumours (Fig. 17)[23].
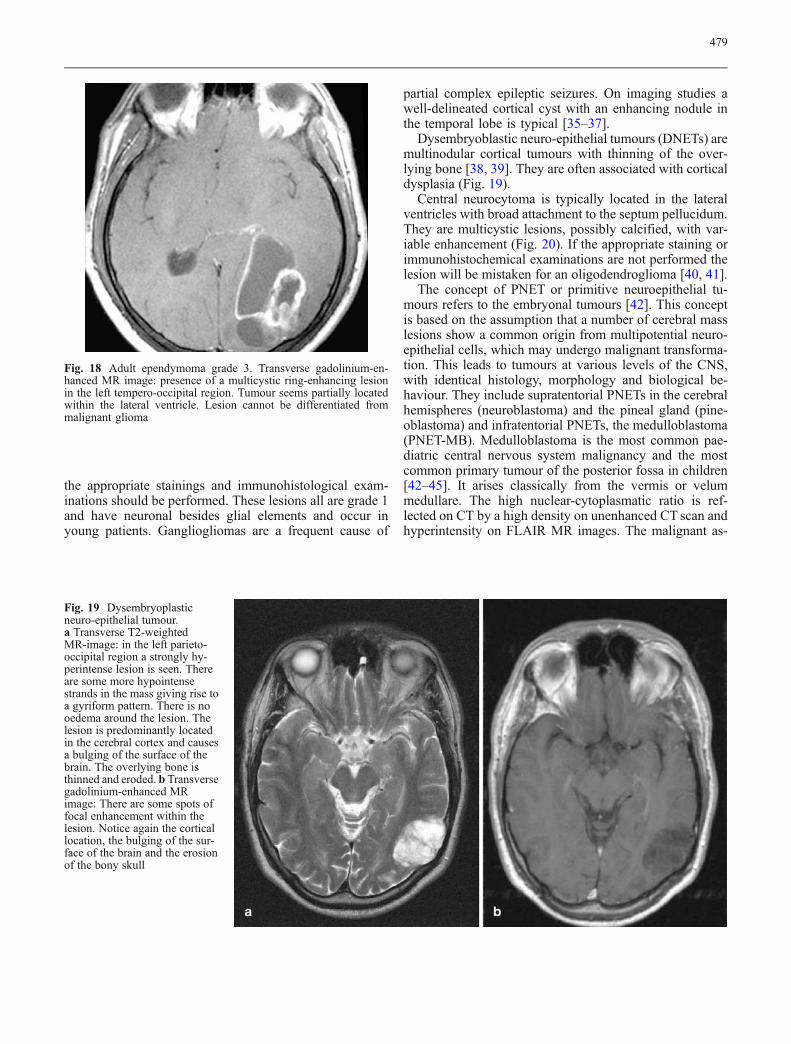
Ependymomas originate from the ependymal or sub-ependymal cells that line the ventricular walls and thecentral canal of the spinal cord. Ependymomas are mul-tilobulated, well-demarcated, frequently calcified massesthat are by definition intraventricular in location [22]. Mostcases occur in the fourth ventricle. They occur most fre-quently in children from 1 to 5 years of age. In adults theyoccur in the 3rd decade and are supratentorial. In thesupratentorial compartment, extraventricular locations arecommon (Fig. 18). On non-contrast CT ependymomas areisodense with calcification in 50%. Enhancement is mildto moderate. On MR ependymomas are hyperintense on
T2 WI and iso- to hypointense on T1 WI. Calcificationcan be less conspicuous than on CT, whereas cysts andsmall hemorrhagic foci are better demonstrated on MRI.Enhancement is moderate. Fourth ventricular ependymo-mas fill up the fourth ventricle and show lateral extensionto the cerebellopontine angle cisterns. This is consideredas a major differential diagnostic feature with medullo-blastoma.
Neuronal and mixed neuronal-glial tumours are a rela-tively new group of lesions, based on the detection by newimmunohistochemical techniques of neuronal elements insome primary brain tumours. Therefore, in our opinion, itis a specific responsibility for the (neuro-) radiologist tomention these tumours in the differential diagnosis, so that
Fig. 17 Oligodendrogliomagrade 2: CT and MR-aspect ofcalcifications. Enhancement ina low-grade lesion. a Contrast-enhanced CT scan: space-occupying lesion in the leftparieto-occipital area with ante-rior displacement of the calci-fied choroid plexus of the leftlateral ventricle. Presence ofdense streaky calcifications(arrow) in the lesion. Moderateenhancement of the dorsal as-pect of the lesion. b TransverseT2-weighted MR image: thelesion is inhomogeneously hy-perintense. The calcificationsare seen as hypointense streaks(arrows). c Transverse T1-weighted MR image: Thetumour now shows overall hy-pointense signal. Calcification(arrows) is seen as markedlyhyperintense foci. d Transversegadolinium-enhanced MRimage: the posterior part of thetumour is inhomogeneously en-hancing (arrow). In the anteriorpart some small foci of en-hancement are seen (arrow-heads)
478
the appropriate stainings and immunohistological exam-inations should be performed. These lesions all are grade 1and have neuronal besides glial elements and occur inyoung patients. Gangliogliomas are a frequent cause of
partial complex epileptic seizures. On imaging studies awell-delineated cortical cyst with an enhancing nodule inthe temporal lobe is typical [35–37].
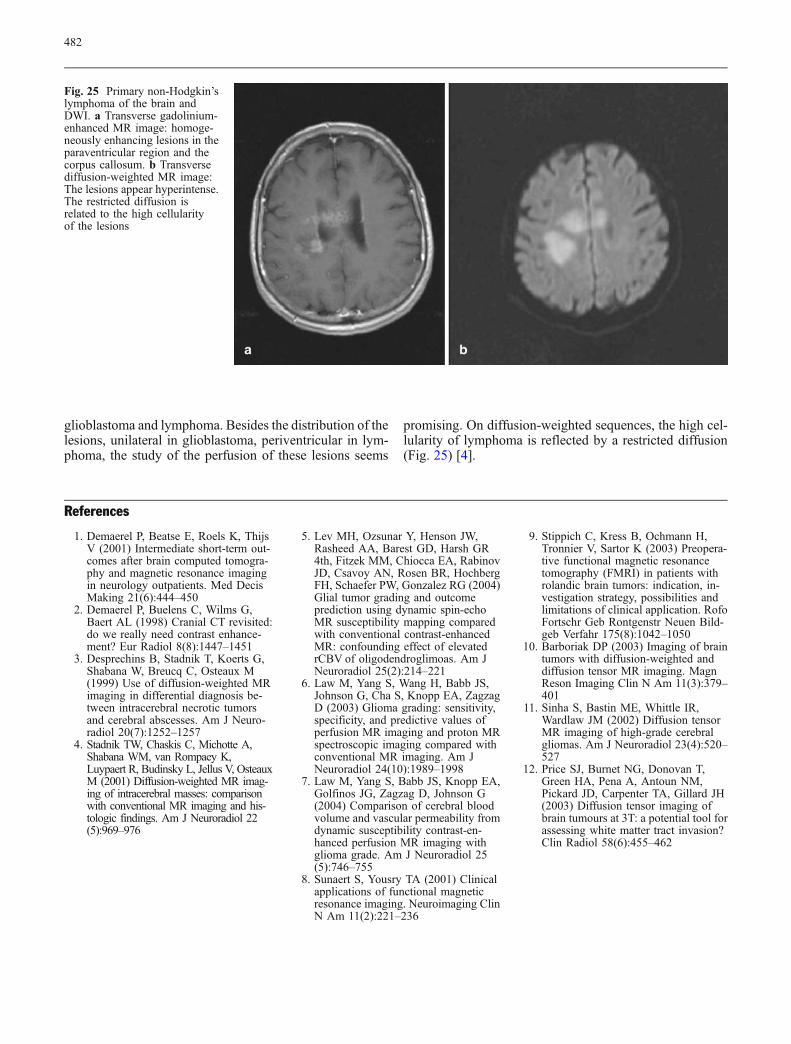
Dysembryoblastic neuro-epithelial tumours (DNETs) aremultinodular cortical tumours with thinning of the over-lying bone [38, 39]. They are often associated with corticaldysplasia (Fig. 19).
Central neurocytoma is typically located in the lateralventricles with broad attachment to the septum pellucidum.They are multicystic lesions, possibly calcified, with var-iable enhancement (Fig. 20). If the appropriate staining orimmunohistochemical examinations are not performed thelesion will be mistaken for an oligodendroglioma [40, 41].
The concept of PNET or primitive neuroepithelial tu-mours refers to the embryonal tumours [42]. This conceptis based on the assumption that a number of cerebral masslesions show a common origin from multipotential neuro-epithelial cells, which may undergo malignant transforma-tion. This leads to tumours at various levels of the CNS,with identical histology, morphology and biological be-haviour. They include supratentorial PNETs in the cerebralhemispheres (neuroblastoma) and the pineal gland (pine-oblastoma) and infratentorial PNETs, the medulloblastoma(PNET-MB). Medulloblastoma is the most common pae-diatric central nervous system malignancy and the mostcommon primary tumour of the posterior fossa in children[42–45]. It arises classically from the vermis or velummedullare. The high nuclear-cytoplasmatic ratio is ref-lected on CT by a high density on unenhanced CT scan andhyperintensity on FLAIR MR images. The malignant as-
Fig. 18 Adult ependymoma grade 3. Transverse gadolinium-en-hanced MR image: presence of a multicystic ring-enhancing lesionin the left tempero-occipital region. Tumour seems partially locatedwithin the lateral ventricle. Lesion cannot be differentiated frommalignant glioma
Fig. 19 Dysembryoplasticneuro-epithelial tumour.a Transverse T2-weightedMR-image: in the left parieto-occipital region a strongly hy-perintense lesion is seen. Thereare some more hypointensestrands in the mass giving rise toa gyriform pattern. There is nooedema around the lesion. Thelesion is predominantly locatedin the cerebral cortex and causesa bulging of the surface of thebrain. The overlying bone isthinned and eroded. b Transversegadolinium-enhanced MRimage: There are some spots offocal enhancement within thelesion. Notice again the corticallocation, the bulging of the sur-face of the brain and the erosionof the bony skull
479

pect of the tumour on gross pathology with cyst formation,haemorrhage and calcification is reflected by its heteroge-neous aspect on imaging studies (Fig. 21a, b). Invasionof the brain stem and extension through the foramen ofMagendie towards the cisterna magna and the spinal sub-
arachnoid space is well demonstrated by MRI. Evidence ofleptomeningeal spread is evident in one-third to one-halfof the patients (Fig. 21c) [46, 47]. Imaging of the spinalcanal therefore is part of the routine preoperative imagingprotocol of children with tumours of the posterior fossa.
Fig. 20 Central neurocytoma.a Transverse T2-weighted MRimage: lesion in the left lateralventricle broadly attached to theseptum pellucidum. Noticesmall intratumoural cysts.b Transverse gadolinium-enhanced MR image: moderateand homogeneous enhancement
Fig. 21 Medulloblastoma in a 5-year-old child. a Sagittal gadolin-ium-enhanced MR image: huge tumour, originating from the inferiorvermis with upward displacement of the fourth ventricle. Clearinvasion of the brain stem (arrows). Notice seeding to the spinalsubarachnoid space. b Transverse gadolinium-enhanced MR image:
The tumour extends to the inferior cerebellar peduncles, being mostpronounced on the right (arrow). c Sagittal gadolinium-enhancedMR image of the spinal canal: presence of a large seeding lesion onthe surface of the spinal cord
480

The desmoplastic variant of medulloblastoma would arisefrom the external granular layer. These tumours typicallyoccur in older patients and are often off-midline (Fig. 22)[48].
The relative incidence of intracerebral metastases is ra-pidly growing and now approaches nearly 50% of all brainneoplasms [49]. This is due to the growing effectivenessof therapies for malignant tumours and increasing de-tection with the new imaging modalities. Most frequentare metastases from lung cancer and breast cancer, frommalignant melanoma, from gastro-intestinal and genito-urinary primaries. They can be solitary or multiple. Onimaging studies enhancement can be solid or ring-like.Important peritumoural oedema is frequent. Brain metas-tases frequently present with short T2 [50]. This is seen inmetastases from mucoid neoplasms of the GI-tract (Fig. 23)and in hemorrhagic metastases from lung carcinoma orrenal carcinoma. Metastases from malignant melanomatypically present with short T1 and T2 due to the presenceof paramagnetic melanin (Fig. 24). Perfusion MR showspromising results in differentiating metastases from dif-ferent primaries from each other and in the differentiationbetween glioma and metastasis [51, 52]. In the presenceof multiple enhancing lesions in the brain, the differentialdiagnosis has to be made between metastases, multifocal
Fig. 23 Cerebellar metastasis from mucinous adenocarcinoma ofthe sigmoid colon. Transverse T2-weighted MR image: The lesionshows marked hypo-intensity pointing to T2-shortening
Fig. 24 Metastases from malignant melanoma. Transverse T1-weighted MR image: multiple spontaneously hyperintense noduliover both cerebral hemispheres. T1-shortening is due to the para-magnetic effect of melanin and/or the presence of blood-degradationproducts
Fig. 22 Desmoplastic medulloblastoma in a 34-year-old patient.Sagittal gadolinium-enhanced MR image: presence of a mass in thesuperior vermis. The tumour abuts the undersurface of the tentoriumand extends towards the hiatus tentorii (arrowheads). The aqueductand fourth ventricle (arrows) are anteriorly and inferiorly displaced.There is overall intense enhancement of the tumour, with evidenceof small cystic components. The lesion has a multilobulated aspect
481
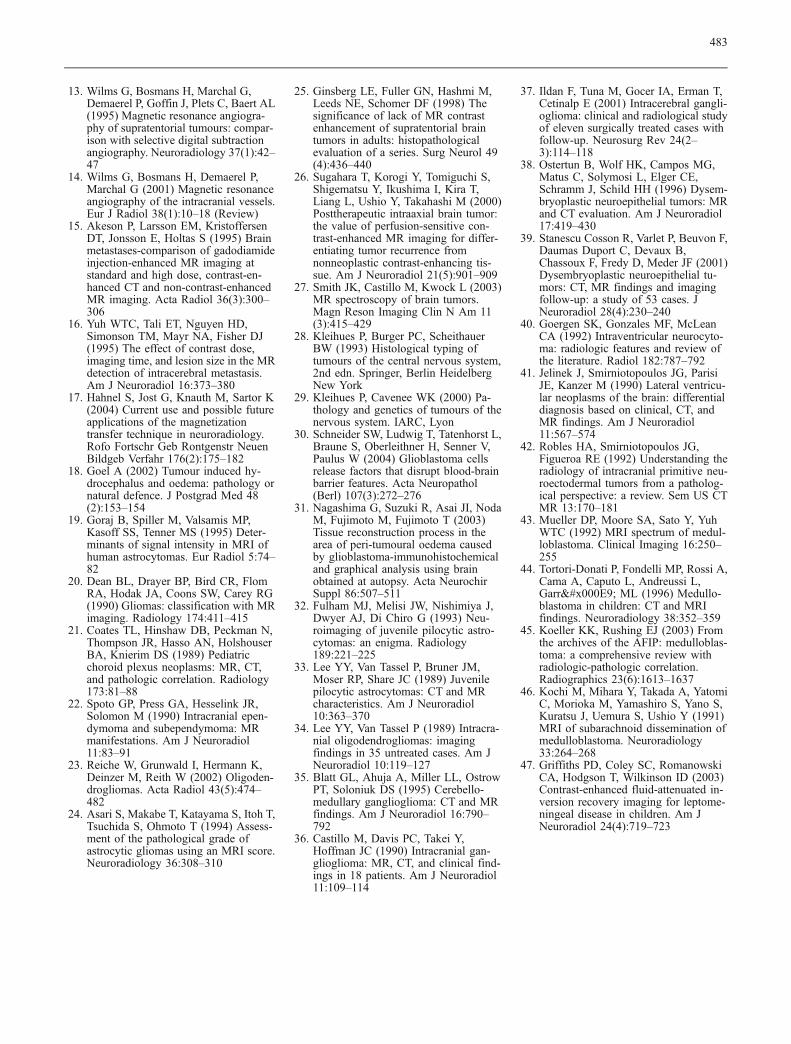
glioblastoma and lymphoma. Besides the distribution of thelesions, unilateral in glioblastoma, periventricular in lym-phoma, the study of the perfusion of these lesions seems
promising. On diffusion-weighted sequences, the high cel-lularity of lymphoma is reflected by a restricted diffusion(Fig. 25) [4].
Fig. 25 Primary non-Hodgkin’slymphoma of the brain andDWI. a Transverse gadolinium-enhanced MR image: homoge-neously enhancing lesions in theparaventricular region and thecorpus callosum. b Transversediffusion-weighted MR image:The lesions appear hyperintense.The restricted diffusion isrelated to the high cellularityof the lesions
References
1. Demaerel P, Beatse E, Roels K, ThijsV (2001) Intermediate short-term out-comes after brain computed tomogra-phy and magnetic resonance imagingin neurology outpatients. Med DecisMaking 21(6):444–450
2. Demaerel P, Buelens C, Wilms G,Baert AL (1998) Cranial CT revisited:do we really need contrast enhance-ment? Eur Radiol 8(8):1447–1451
3. Desprechins B, Stadnik T, Koerts G,Shabana W, Breucq C, Osteaux M(1999) Use of diffusion-weighted MRimaging in differential diagnosis be-tween intracerebral necrotic tumorsand cerebral abscesses. Am J Neuro-radiol 20(7):1252–1257
4. Stadnik TW, Chaskis C, Michotte A,Shabana WM, van Rompaey K,Luypaert R, Budinsky L, Jellus V, OsteauxM (2001) Diffusion-weighted MR imag-ing of intracerebral masses: comparisonwith conventional MR imaging and his-tologic findings. Am J Neuroradiol 22(5):969–976
5. Lev MH, Ozsunar Y, Henson JW,Rasheed AA, Barest GD, Harsh GR4th, Fitzek MM, Chiocca EA, RabinovJD, Csavoy AN, Rosen BR, HochbergFH, Schaefer PW, Gonzalez RG (2004)Glial tumor grading and outcomeprediction using dynamic spin-echoMR susceptibility mapping comparedwith conventional contrast-enhancedMR: confounding effect of elevatedrCBV of oligodendroglimoas. Am JNeuroradiol 25(2):214–221
6. Law M, Yang S, Wang H, Babb JS,Johnson G, Cha S, Knopp EA, ZagzagD (2003) Glioma grading: sensitivity,specificity, and predictive values ofperfusion MR imaging and proton MRspectroscopic imaging compared withconventional MR imaging. Am JNeuroradiol 24(10):1989–1998
7. Law M, Yang S, Babb JS, Knopp EA,Golfinos JG, Zagzag D, Johnson G(2004) Comparison of cerebral bloodvolume and vascular permeability fromdynamic susceptibility contrast-en-hanced perfusion MR imaging withglioma grade. Am J Neuroradiol 25(5):746–755
8. Sunaert S, Yousry TA (2001) Clinicalapplications of functional magneticresonance imaging. Neuroimaging ClinN Am 11(2):221–236
9. Stippich C, Kress B, Ochmann H,Tronnier V, Sartor K (2003) Preopera-tive functional magnetic resonancetomography (FMRI) in patients withrolandic brain tumors: indication, in-vestigation strategy, possibilities andlimitations of clinical application. RofoFortschr Geb Rontgenstr Neuen Bild-geb Verfahr 175(8):1042–1050
10. Barboriak DP (2003) Imaging of braintumors with diffusion-weighted anddiffusion tensor MR imaging. MagnReson Imaging Clin N Am 11(3):379–401
11. Sinha S, Bastin ME, Whittle IR,Wardlaw JM (2002) Diffusion tensorMR imaging of high-grade cerebralgliomas. Am J Neuroradiol 23(4):520–527
12. Price SJ, Burnet NG, Donovan T,Green HA, Pena A, Antoun NM,Pickard JD, Carpenter TA, Gillard JH(2003) Diffusion tensor imaging ofbrain tumours at 3T: a potential tool forassessing white matter tract invasion?Clin Radiol 58(6):455–462
482
13. Wilms G, Bosmans H, Marchal G,Demaerel P, Goffin J, Plets C, Baert AL(1995) Magnetic resonance angiogra-phy of supratentorial tumours: compar-ison with selective digital subtractionangiography. Neuroradiology 37(1):42–47
14. Wilms G, Bosmans H, Demaerel P,Marchal G (2001) Magnetic resonanceangiography of the intracranial vessels.Eur J Radiol 38(1):10–18 (Review)
15. Akeson P, Larsson EM, KristoffersenDT, Jonsson E, Holtas S (1995) Brainmetastases-comparison of gadodiamideinjection-enhanced MR imaging atstandard and high dose, contrast-en-hanced CT and non-contrast-enhancedMR imaging. Acta Radiol 36(3):300–306
16. Yuh WTC, Tali ET, Nguyen HD,Simonson TM, Mayr NA, Fisher DJ(1995) The effect of contrast dose,imaging time, and lesion size in the MRdetection of intracerebral metastasis.Am J Neuroradiol 16:373–380
17. Hahnel S, Jost G, Knauth M, Sartor K(2004) Current use and possible futureapplications of the magnetizationtransfer technique in neuroradiology.Rofo Fortschr Geb Rontgenstr NeuenBildgeb Verfahr 176(2):175–182
18. Goel A (2002) Tumour induced hy-drocephalus and oedema: pathology ornatural defence. J Postgrad Med 48(2):153–154
19. Goraj B, Spiller M, Valsamis MP,Kasoff SS, Tenner MS (1995) Deter-minants of signal intensity in MRI ofhuman astrocytomas. Eur Radiol 5:74–82
20. Dean BL, Drayer BP, Bird CR, FlomRA, Hodak JA, Coons SW, Carey RG(1990) Gliomas: classification with MRimaging. Radiology 174:411–415
21. Coates TL, Hinshaw DB, Peckman N,Thompson JR, Hasso AN, HolshouserBA, Knierim DS (1989) Pediatricchoroid plexus neoplasms: MR, CT,and pathologic correlation. Radiology173:81–88
22. Spoto GP, Press GA, Hesselink JR,Solomon M (1990) Intracranial epen-dymoma and subependymoma: MRmanifestations. Am J Neuroradiol11:83–91
23. Reiche W, Grunwald I, Hermann K,Deinzer M, Reith W (2002) Oligoden-drogliomas. Acta Radiol 43(5):474–482
24. Asari S, Makabe T, Katayama S, Itoh T,Tsuchida S, Ohmoto T (1994) Assess-ment of the pathological grade ofastrocytic gliomas using an MRI score.Neuroradiology 36:308–310
25. Ginsberg LE, Fuller GN, Hashmi M,Leeds NE, Schomer DF (1998) Thesignificance of lack of MR contrastenhancement of supratentorial braintumors in adults: histopathologicalevaluation of a series. Surg Neurol 49(4):436–440
26. Sugahara T, Korogi Y, Tomiguchi S,Shigematsu Y, Ikushima I, Kira T,Liang L, Ushio Y, Takahashi M (2000)Posttherapeutic intraaxial brain tumor:the value of perfusion-sensitive con-trast-enhanced MR imaging for differ-entiating tumor recurrence fromnonneoplastic contrast-enhancing tis-sue. Am J Neuroradiol 21(5):901–909
27. Smith JK, Castillo M, Kwock L (2003)MR spectroscopy of brain tumors.Magn Reson Imaging Clin N Am 11(3):415–429
28. Kleihues P, Burger PC, ScheithauerBW (1993) Histological typing oftumours of the central nervous system,2nd edn. Springer, Berlin HeidelbergNew York
29. Kleihues P, Cavenee WK (2000) Pa-thology and genetics of tumours of thenervous system. IARC, Lyon
30. Schneider SW, Ludwig T, Tatenhorst L,Braune S, Oberleithner H, Senner V,Paulus W (2004) Glioblastoma cellsrelease factors that disrupt blood-brainbarrier features. Acta Neuropathol(Berl) 107(3):272–276
31. Nagashima G, Suzuki R, Asai JI, NodaM, Fujimoto M, Fujimoto T (2003)Tissue reconstruction process in thearea of peri-tumoural oedema causedby glioblastoma-immunohistochemicaland graphical analysis using brainobtained at autopsy. Acta NeurochirSuppl 86:507–511
32. Fulham MJ, Melisi JW, Nishimiya J,Dwyer AJ, Di Chiro G (1993) Neu-roimaging of juvenile pilocytic astro-cytomas: an enigma. Radiology189:221–225
33. Lee YY, Van Tassel P, Bruner JM,Moser RP, Share JC (1989) Juvenilepilocytic astrocytomas: CT and MRcharacteristics. Am J Neuroradiol10:363–370
34. Lee YY, Van Tassel P (1989) Intracra-nial oligodendrogliomas: imagingfindings in 35 untreated cases. Am JNeuroradiol 10:119–127
35. Blatt GL, Ahuja A, Miller LL, OstrowPT, Soloniuk DS (1995) Cerebello-medullary ganglioglioma: CT and MRfindings. Am J Neuroradiol 16:790–792
36. Castillo M, Davis PC, Takei Y,Hoffman JC (1990) Intracranial gan-glioglioma: MR, CT, and clinical find-ings in 18 patients. Am J Neuroradiol11:109–114
37. Ildan F, Tuna M, Gocer IA, Erman T,Cetinalp E (2001) Intracerebral gangli-oglioma: clinical and radiological studyof eleven surgically treated cases withfollow-up. Neurosurg Rev 24(2–3):114–118
38. Ostertun B, Wolf HK, Campos MG,Matus C, Solymosi L, Elger CE,Schramm J, Schild HH (1996) Dysem-bryoplastic neuroepithelial tumors: MRand CT evaluation. Am J Neuroradiol17:419–430
39. Stanescu Cosson R, Varlet P, Beuvon F,Daumas Duport C, Devaux B,Chassoux F, Fredy D, Meder JF (2001)Dysembryoplastic neuroepithelial tu-mors: CT, MR findings and imagingfollow-up: a study of 53 cases. JNeuroradiol 28(4):230–240
40. Goergen SK, Gonzales MF, McLeanCA (1992) Intraventricular neurocyto-ma: radiologic features and review ofthe literature. Radiol 182:787–792
41. Jelinek J, Smirniotopoulos JG, ParisiJE, Kanzer M (1990) Lateral ventricu-lar neoplasms of the brain: differentialdiagnosis based on clinical, CT, andMR findings. Am J Neuroradiol11:567–574
42. Robles HA, Smirniotopoulos JG,Figueroa RE (1992) Understanding theradiology of intracranial primitive neu-roectodermal tumors from a patholog-ical perspective: a review. Sem US CTMR 13:170–181
43. Mueller DP, Moore SA, Sato Y, YuhWTC (1992) MRI spectrum of medul-loblastoma. Clinical Imaging 16:250–255
44. Tortori-Donati P, Fondelli MP, Rossi A,Cama A, Caputo L, Andreussi L,Garré ML (1996) Medullo-blastoma in children: CT and MRIfindings. Neuroradiology 38:352–359
45. Koeller KK, Rushing EJ (2003) Fromthe archives of the AFIP: medulloblas-toma: a comprehensive review withradiologic-pathologic correlation.Radiographics 23(6):1613–1637
46. Kochi M, Mihara Y, Takada A, YatomiC, Morioka M, Yamashiro S, Yano S,Kuratsu J, Uemura S, Ushio Y (1991)MRI of subarachnoid dissemination ofmedulloblastoma. Neuroradiology33:264–268
47. Griffiths PD, Coley SC, RomanowskiCA, Hodgson T, Wilkinson ID (2003)Contrast-enhanced fluid-attenuated in-version recovery imaging for leptome-ningeal disease in children. Am JNeuroradiol 24(4):719–723
483

48. Malheiros SM, Carrete H Jr, StavaleJN, Santos AJ, Borges LR, GuimaraesIF, Pelaez MP, Franco CM, Gabbai AA(2003) MRI of medulloblastoma inadults. Neuroradiology 45(7):463–467
49. Sawaya R (2001) Considerations in thediagnosis and management of brainmetastases. Oncology (Huntingt) 15(9):1144–1154 (See also pages 1157–1158 Discussion 1158, 1163–1165)
50. Carrier DA, Mawad ME, KirkpatrickJB, Schmid MF (1994) Metastatic ad-enocarcinoma to the brain: MR withpathologic correlation. Am J Neuro-radiol 15:155–159
51. Kremer S, Grand S, Berger F,Hoffmann D, Pasquier B, Remy C,Benabid AL, Bas JF (2003) Dynamiccontrast-enhanced MRI: differentiatingmelanoma and renal carcinoma metas-tases from high-grade astrocytomas andother metastases. Neuroradiology 45(1):44–49
52. Law M, Cha S, Knopp EA, Johnson G,Arnett J, Litt AW (2002) High-gradegliomas and solitary metastases: differ-entiation by using perfusion and protonspectroscopic MR imaging. Radiology222(3):715–721
484
Related Documents











