Future Directions in ALK Negative Anaplastic Large Cell Lymphoma
Jan 18, 2018
Future Directions in ALK Negative Anaplastic Large Cell
Lymphoma
Andrs Quesada Fellow, Hematopathology, MDACC Updates in
Hematopathology: 3rd Annual Meeting for Alumni and Friends of the
Department of Hematopathology Clinical History 33 year old
man
Right cervical and axillary lymphadenopathy Night sweats and fever
Duration: Several months PMH: Sleep apnea Family history: No
significant family history Right axillary lymph node excisional
biopsy 100x 100x 400x 400x 400x 1000x 1000x CD3 CD4 CD43 CD15 CD30
ALK1 Ki67 CD 43 20x CD43 Positive Negative CD15 (subset) CD1a ALK
CD30 (diffuse, strong) CD3 BCL2 CD43 CD4 BCL6 Ki67 (~90%) CD5 PAX5
CD7 Granzyme B CD10 EMA CD20 S100 CD45 CAM5.2 CD68 Final Diagnosis
Right axillary lymph node, excisional biopsy:
ALK NEGATIVE ANAPLASTIC LARGE CELL LYMPHOMA 1. Right axillary lymph
node (NAC , 8/25/2015): The cell block shows blood clot with
admixed lymphoid tissue. Within the lymphoid tissue are occasional
large atypical cells. Direct smears show lymphoid tissue with
scattered large highly atypical cells. On submitted
immunohistochemical stains, CD3 shows scattered predominantly
mature appearing T lymphocytes. Pancytokeratin and CAM 5.2 are
negative. 2. Right axillary lymph node and upper limb (SAC ,
9/25/2015): Per submitted surgical pathology report, sections of
the lymph node reportedly showed sheets of large neoplastic
lymphocytes with areas of geographic necrosis.Lymph node
architecture was not appreciated.The neoplastic lymphocytes
displayed large pleomorphic nuclei, finely dispersed chromatin,
prominent nucleoli and moderate amount of cytoplasm.Hallmark cells
were seen focally. Mitotic figures were conspicuous. We also
reviewed immunohistochemical stains performed elsewhere:
CD1a:Negative CD3:Negative in large cells CD4:Negative in large
cells CD5:Negative in large cells CD7:Negative in large cells
CD10:Negative in large cells CD15:Positive in subset of large cells
CD20:Negative in large cells CD30:Positive, diffuse, strong in most
cells in the infiltrate CD43:Positive in ~50% of large cells
CD45:Negative in large cells CD68:Negative in large cells
ALK:Negative in large cells BCL2:Negative in large cells
BCL6:Negative in large cells PAX5:Negative in large cells Ki67:~90%
of cells in the infiltrate are positive Granzyme B:Negative in
large cells; scattered small cells are positive EMA:Rare large
cells are faintly positive S100: Loose clusters of dendritic cells
are positive CAM5.2:Negative According to outside pathology report,
additional studies were performed at UCLAand reportedly showed the
lymphoma cells positive for CD2 (occasional low), and TIA-1
(occasional few); negative for CD8, TCR gamma/delta, TCR F1, TdT,
PD1, and EBER (extremely rare positive small cells). Polymerase
chain reaction (PCR) performed at Neogenomics showed the presence
of monoclonal T-cell receptor gene rearrangements. It was negative
for B-cell gene rearrangements. Per submitted pathology report,
flow cytometric analysis of the right axillary lymph node showed no
evidence of a lymphoproliferative disorder. The findings were
reported to be diagnostic of ALK negative anaplastic large cell
lymphoma. Please note that specimen SAC is not received for review.
3. Bone marrow, (FAC , 10/15/2015): A complete blood count and
peripheral blood smear shows white blood cell count 9.7, hemoglobin
10.7, and platelets The red blood cells are normocytic and
normochromic with slight polychromasia.The white blood cells are
adequate in number and morphology.There is no left-shift,
dysplasia, circulating blasts or lymphoma cells seen. The platelets
are normal in number with unremarkable morphology. The bone marrow
aspirate smear demonstrates trilineage hematopoiesis. There is a
sequential maturation in the erythroid and granulocytic lineages.
The erythrocytes show some dysplastic features including nuclear
budding and nuclear to cytoplasmic asynchrony. There is no increase
in blasts.No obvious lymphoma cells are seen.Megakaryocytes are
present and slightly increased in number.An iron stain shows
decreased iron storage.No ring sideroblasts are seen. The bone
marrow bone marrow and clot demonstrate 70% cellular
marrow.Trilineage hematopoiesis is evident.Megakaryocytes are
present and slightly increased in number (up to 9 per high-power
field).Occasional hypolobated forms are seen.No lymphoid aggregates
or sheets of lymphoid cells are seen. On submitted
immunohistochemical stains performed on the bone marrow biopsy, CD3
and CD20 highlight scattered small and mature appearing T and B
lymphocytes, respectively.The CD3-positive lymphocytes outnumber
the CD20-positive lymphocytes. CD30 fails to demonstrate the
presence of large cells. Per report, flow cytometric analysis of
the bone marrow showed no evidence of a monoclonal B-cell
population, but showed a mildly inverted CD4/CD8 ratio (0.8). Per
report, cytogenetics performed at Neogenomics, showed a normal male
karyotype (46,XY[20]). Per report, PCR performed on the bone marrow
was positive for a monoclonal T-cell receptor gene rearrangement.
In summary, we agree with the diagnosis of ALK negative anaplastic
large cell lymphoma rendered on the right axillary lymph node. The
bone marrow is not involved morphologically, but there is a T-cell
gene rearrangement reportedly present by PCR. Although this is may
be suggestive of involvement by ALCL, it is alone inconclusive to
render a diagnosis of bone marrow involvement especially in the
complete absence of CD30 positive large cells. RM:AQ/kma 12/3/2015
4:18 PM Comment UCLA additional studies: Polymerase chain reaction
(PCR)
Lymphoma cells positive for CD2 (occasional low), and TIA-1
(occasional few) Negative for CD8, TCR gamma/delta, TCR F1, TdT,
PD1, and EBER (extremely rare positive small cells). Polymerase
chain reaction (PCR) Monoclonal T-cell receptor gene
rearrangements. Negative for B-cell gene rearrangements. Per
submitted pathology report, flow cytometric analysis of the right
axillary lymph node showed no evidence of a lymphoproliferative
disorder. 1. Right axillary lymph node (NAC , 8/25/2015): The cell
block shows blood clot with admixed lymphoid tissue. Within the
lymphoid tissue are occasional large atypical cells. Direct smears
show lymphoid tissue with scattered large highly atypical cells. On
submitted immunohistochemical stains, CD3 shows scattered
predominantly mature appearing T lymphocytes. Pancytokeratin and
CAM 5.2 are negative. 2. Right axillary lymph node and upper limb
(SAC , 9/25/2015): Per submitted surgical pathology report,
sections of the lymph node reportedly showed sheets of large
neoplastic lymphocytes with areas of geographic necrosis.Lymph node
architecture was not appreciated.The neoplastic lymphocytes
displayed large pleomorphic nuclei, finely dispersed chromatin,
prominent nucleoli and moderate amount of cytoplasm.Hallmark cells
were seen focally. Mitotic figures were conspicuous. We also
reviewed immunohistochemical stains performed elsewhere:
CD1a:Negative CD3:Negative in large cells CD4:Negative in large
cells CD5:Negative in large cells CD7:Negative in large cells
CD10:Negative in large cells CD15:Positive in subset of large cells
CD20:Negative in large cells CD30:Positive, diffuse, strong in most
cells in the infiltrate CD43:Positive in ~50% of large cells
CD45:Negative in large cells CD68:Negative in large cells
ALK:Negative in large cells BCL2:Negative in large cells
BCL6:Negative in large cells PAX5:Negative in large cells Ki67:~90%
of cells in the infiltrate are positive Granzyme B:Negative in
large cells; scattered small cells are positive EMA:Rare large
cells are faintly positive S100: Loose clusters of dendritic cells
are positive CAM5.2:Negative According to outside pathology report,
additional studies were performed at UCLAand reportedly showed the
lymphoma cells positive for CD2 (occasional low), and TIA-1
(occasional few); negative for CD8, TCR gamma/delta, TCR F1, TdT,
PD1, and EBER (extremely rare positive small cells). Polymerase
chain reaction (PCR) performed at Neogenomics showed the presence
of monoclonal T-cell receptor gene rearrangements. It was negative
for B-cell gene rearrangements. Per submitted pathology report,
flow cytometric analysis of the right axillary lymph node showed no
evidence of a lymphoproliferative disorder. The findings were
reported to be diagnostic of ALK negative anaplastic large cell
lymphoma. Please note that specimen SAC is not received for review.
3. Bone marrow, (FAC , 10/15/2015): A complete blood count and
peripheral blood smear shows white blood cell count 9.7, hemoglobin
10.7, and platelets The red blood cells are normocytic and
normochromic with slight polychromasia.The white blood cells are
adequate in number and morphology.There is no left-shift,
dysplasia, circulating blasts or lymphoma cells seen. The platelets
are normal in number with unremarkable morphology. The bone marrow
aspirate smear demonstrates trilineage hematopoiesis. There is a
sequential maturation in the erythroid and granulocytic lineages.
The erythrocytes show some dysplastic features including nuclear
budding and nuclear to cytoplasmic asynchrony. There is no increase
in blasts.No obvious lymphoma cells are seen.Megakaryocytes are
present and slightly increased in number.An iron stain shows
decreased iron storage.No ring sideroblasts are seen. The bone
marrow bone marrow and clot demonstrate 70% cellular
marrow.Trilineage hematopoiesis is evident.Megakaryocytes are
present and slightly increased in number (up to 9 per high-power
field).Occasional hypolobated forms are seen.No lymphoid aggregates
or sheets of lymphoid cells are seen. On submitted
immunohistochemical stains performed on the bone marrow biopsy, CD3
and CD20 highlight scattered small and mature appearing T and B
lymphocytes, respectively.The CD3-positive lymphocytes outnumber
the CD20-positive lymphocytes. CD30 fails to demonstrate the
presence of large cells. Per report, flow cytometric analysis of
the bone marrow showed no evidence of a monoclonal B-cell
population, but showed a mildly inverted CD4/CD8 ratio (0.8). Per
report, cytogenetics performed at Neogenomics, showed a normal male
karyotype (46,XY[20]). Per report, PCR performed on the bone marrow
was positive for a monoclonal T-cell receptor gene rearrangement.
In summary, we agree with the diagnosis of ALK negative anaplastic
large cell lymphoma rendered on the right axillary lymph node. The
bone marrow is not involved morphologically, but there is a T-cell
gene rearrangement reportedly present by PCR. Although this is may
be suggestive of involvement by ALCL, it is alone inconclusive to
render a diagnosis of bone marrow involvement especially in the
complete absence of CD30 positive large cells. RM:AQ/kma 12/3/2015
4:18 PM Comment Sheets of large neoplastic lymphocytes with areas
of geographic necrosis. Lymph node architecture was not
appreciated. The neoplastic lymphocytes displayed large pleomorphic
nuclei, finely dispersed chromatin, prominent nucleoli and moderate
amount of cytoplasm. Hallmark cells were seen focally. Mitotic
figures were conspicuous. 1. Right axillary lymph node (NAC ,
8/25/2015): The cell block shows blood clot with admixed lymphoid
tissue. Within the lymphoid tissue are occasional large atypical
cells. Direct smears show lymphoid tissue with scattered large
highly atypical cells. On submitted immunohistochemical stains, CD3
shows scattered predominantly mature appearing T lymphocytes.
Pancytokeratin and CAM 5.2 are negative. 2. Right axillary lymph
node and upper limb (SAC , 9/25/2015): Per submitted surgical
pathology report, sections of the lymph node reportedly showed
sheets of large neoplastic lymphocytes with areas of geographic
necrosis.Lymph node architecture was not appreciated.The neoplastic
lymphocytes displayed large pleomorphic nuclei, finely dispersed
chromatin, prominent nucleoli and moderate amount of
cytoplasm.Hallmark cells were seen focally. Mitotic figures were
conspicuous. We also reviewed immunohistochemical stains performed
elsewhere: CD1a:Negative CD3:Negative in large cells CD4:Negative
in large cells CD5:Negative in large cells CD7:Negative in large
cells CD10:Negative in large cells CD15:Positive in subset of large
cells CD20:Negative in large cells CD30:Positive, diffuse, strong
in most cells in the infiltrate CD43:Positive in ~50% of large
cells CD45:Negative in large cells CD68:Negative in large cells
ALK:Negative in large cells BCL2:Negative in large cells
BCL6:Negative in large cells PAX5:Negative in large cells Ki67:~90%
of cells in the infiltrate are positive Granzyme B:Negative in
large cells; scattered small cells are positive EMA:Rare large
cells are faintly positive S100: Loose clusters of dendritic cells
are positive CAM5.2:Negative According to outside pathology report,
additional studies were performed at UCLAand reportedly showed the
lymphoma cells positive for CD2 (occasional low), and TIA-1
(occasional few); negative for CD8, TCR gamma/delta, TCR F1, TdT,
PD1, and EBER (extremely rare positive small cells). Polymerase
chain reaction (PCR) performed at Neogenomics showed the presence
of monoclonal T-cell receptor gene rearrangements. It was negative
for B-cell gene rearrangements. Per submitted pathology report,
flow cytometric analysis of the right axillary lymph node showed no
evidence of a lymphoproliferative disorder. The findings were
reported to be diagnostic of ALK negative anaplastic large cell
lymphoma. Please note that specimen SAC is not received for review.
3. Bone marrow, (FAC , 10/15/2015): A complete blood count and
peripheral blood smear shows white blood cell count 9.7, hemoglobin
10.7, and platelets The red blood cells are normocytic and
normochromic with slight polychromasia.The white blood cells are
adequate in number and morphology.There is no left-shift,
dysplasia, circulating blasts or lymphoma cells seen. The platelets
are normal in number with unremarkable morphology. The bone marrow
aspirate smear demonstrates trilineage hematopoiesis. There is a
sequential maturation in the erythroid and granulocytic lineages.
The erythrocytes show some dysplastic features including nuclear
budding and nuclear to cytoplasmic asynchrony. There is no increase
in blasts.No obvious lymphoma cells are seen.Megakaryocytes are
present and slightly increased in number.An iron stain shows
decreased iron storage.No ring sideroblasts are seen. The bone
marrow bone marrow and clot demonstrate 70% cellular
marrow.Trilineage hematopoiesis is evident.Megakaryocytes are
present and slightly increased in number (up to 9 per high-power
field).Occasional hypolobated forms are seen.No lymphoid aggregates
or sheets of lymphoid cells are seen. On submitted
immunohistochemical stains performed on the bone marrow biopsy, CD3
and CD20 highlight scattered small and mature appearing T and B
lymphocytes, respectively.The CD3-positive lymphocytes outnumber
the CD20-positive lymphocytes. CD30 fails to demonstrate the
presence of large cells. Per report, flow cytometric analysis of
the bone marrow showed no evidence of a monoclonal B-cell
population, but showed a mildly inverted CD4/CD8 ratio (0.8). Per
report, cytogenetics performed at Neogenomics, showed a normal male
karyotype (46,XY[20]). Per report, PCR performed on the bone marrow
was positive for a monoclonal T-cell receptor gene rearrangement.
In summary, we agree with the diagnosis of ALK negative anaplastic
large cell lymphoma rendered on the right axillary lymph node. The
bone marrow is not involved morphologically, but there is a T-cell
gene rearrangement reportedly present by PCR. Although this is may
be suggestive of involvement by ALCL, it is alone inconclusive to
render a diagnosis of bone marrow involvement especially in the
complete absence of CD30 positive large cells. RM:AQ/kma 12/3/2015
4:18 PM Comment 1. Right axillary lymph node (NAC15-7058,
8/25/2015):
The cell block shows blood clot with admixed lymphoid tissue.
Within the lymphoid tissue are occasional large atypical cells.
Direct smears show lymphoid tissue with scattered large highly
atypical cells. On submitted immunohistochemical stains, CD3 shows
scattered predominantly mature appearing T lymphocytes.
Pancytokeratin and CAM 5.2 are negative. 1. Right axillary lymph
node (NAC , 8/25/2015): The cell block shows blood clot with
admixed lymphoid tissue. Within the lymphoid tissue are occasional
large atypical cells. Direct smears show lymphoid tissue with
scattered large highly atypical cells. On submitted
immunohistochemical stains, CD3 shows scattered predominantly
mature appearing T lymphocytes. Pancytokeratin and CAM 5.2 are
negative. 2. Right axillary lymph node and upper limb (SAC ,
9/25/2015): Per submitted surgical pathology report, sections of
the lymph node reportedly showed sheets of large neoplastic
lymphocytes with areas of geographic necrosis.Lymph node
architecture was not appreciated.The neoplastic lymphocytes
displayed large pleomorphic nuclei, finely dispersed chromatin,
prominent nucleoli and moderate amount of cytoplasm.Hallmark cells
were seen focally. Mitotic figures were conspicuous. We also
reviewed immunohistochemical stains performed elsewhere:
CD1a:Negative CD3:Negative in large cells CD4:Negative in large
cells CD5:Negative in large cells CD7:Negative in large cells
CD10:Negative in large cells CD15:Positive in subset of large cells
CD20:Negative in large cells CD30:Positive, diffuse, strong in most
cells in the infiltrate CD43:Positive in ~50% of large cells
CD45:Negative in large cells CD68:Negative in large cells
ALK:Negative in large cells BCL2:Negative in large cells
BCL6:Negative in large cells PAX5:Negative in large cells Ki67:~90%
of cells in the infiltrate are positive Granzyme B:Negative in
large cells; scattered small cells are positive EMA:Rare large
cells are faintly positive S100: Loose clusters of dendritic cells
are positive CAM5.2:Negative According to outside pathology report,
additional studies were performed at UCLAand reportedly showed the
lymphoma cells positive for CD2 (occasional low), and TIA-1
(occasional few); negative for CD8, TCR gamma/delta, TCR F1, TdT,
PD1, and EBER (extremely rare positive small cells). Polymerase
chain reaction (PCR) performed at Neogenomics showed the presence
of monoclonal T-cell receptor gene rearrangements. It was negative
for B-cell gene rearrangements. Per submitted pathology report,
flow cytometric analysis of the right axillary lymph node showed no
evidence of a lymphoproliferative disorder. The findings were
reported to be diagnostic of ALK negative anaplastic large cell
lymphoma. Please note that specimen SAC is not received for review.
3. Bone marrow, (FAC , 10/15/2015): A complete blood count and
peripheral blood smear shows white blood cell count 9.7, hemoglobin
10.7, and platelets The red blood cells are normocytic and
normochromic with slight polychromasia.The white blood cells are
adequate in number and morphology.There is no left-shift,
dysplasia, circulating blasts or lymphoma cells seen. The platelets
are normal in number with unremarkable morphology. The bone marrow
aspirate smear demonstrates trilineage hematopoiesis. There is a
sequential maturation in the erythroid and granulocytic lineages.
The erythrocytes show some dysplastic features including nuclear
budding and nuclear to cytoplasmic asynchrony. There is no increase
in blasts.No obvious lymphoma cells are seen.Megakaryocytes are
present and slightly increased in number.An iron stain shows
decreased iron storage.No ring sideroblasts are seen. The bone
marrow bone marrow and clot demonstrate 70% cellular
marrow.Trilineage hematopoiesis is evident.Megakaryocytes are
present and slightly increased in number (up to 9 per high-power
field).Occasional hypolobated forms are seen.No lymphoid aggregates
or sheets of lymphoid cells are seen. On submitted
immunohistochemical stains performed on the bone marrow biopsy, CD3
and CD20 highlight scattered small and mature appearing T and B
lymphocytes, respectively.The CD3-positive lymphocytes outnumber
the CD20-positive lymphocytes. CD30 fails to demonstrate the
presence of large cells. Per report, flow cytometric analysis of
the bone marrow showed no evidence of a monoclonal B-cell
population, but showed a mildly inverted CD4/CD8 ratio (0.8). Per
report, cytogenetics performed at Neogenomics, showed a normal male
karyotype (46,XY[20]). Per report, PCR performed on the bone marrow
was positive for a monoclonal T-cell receptor gene rearrangement.
In summary, we agree with the diagnosis of ALK negative anaplastic
large cell lymphoma rendered on the right axillary lymph node. The
bone marrow is not involved morphologically, but there is a T-cell
gene rearrangement reportedly present by PCR. Although this is may
be suggestive of involvement by ALCL, it is alone inconclusive to
render a diagnosis of bone marrow involvement especially in the
complete absence of CD30 positive large cells. RM:AQ/kma 12/3/2015
4:18 PM Diagnosis Bone marrow, left iliac, biopsy, clot sections,
aspiration and peripheral blood: Normocellular bone marrow with
trilineage hematopoiesis and sequential maturation No morphologic
support for involvement by lymphoma 1. Right axillary lymph node
(NAC , 8/25/2015): The cell block shows blood clot with admixed
lymphoid tissue. Within the lymphoid tissue are occasional large
atypical cells. Direct smears show lymphoid tissue with scattered
large highly atypical cells. On submitted immunohistochemical
stains, CD3 shows scattered predominantly mature appearing T
lymphocytes. Pancytokeratin and CAM 5.2 are negative. 2. Right
axillary lymph node and upper limb (SAC , 9/25/2015): Per submitted
surgical pathology report, sections of the lymph node reportedly
showed sheets of large neoplastic lymphocytes with areas of
geographic necrosis.Lymph node architecture was not appreciated.The
neoplastic lymphocytes displayed large pleomorphic nuclei, finely
dispersed chromatin, prominent nucleoli and moderate amount of
cytoplasm.Hallmark cells were seen focally. Mitotic figures were
conspicuous. We also reviewed immunohistochemical stains performed
elsewhere: CD1a:Negative CD3:Negative in large cells CD4:Negative
in large cells CD5:Negative in large cells CD7:Negative in large
cells CD10:Negative in large cells CD15:Positive in subset of large
cells CD20:Negative in large cells CD30:Positive, diffuse, strong
in most cells in the infiltrate CD43:Positive in ~50% of large
cells CD45:Negative in large cells CD68:Negative in large cells
ALK:Negative in large cells BCL2:Negative in large cells
BCL6:Negative in large cells PAX5:Negative in large cells Ki67:~90%
of cells in the infiltrate are positive Granzyme B:Negative in
large cells; scattered small cells are positive EMA:Rare large
cells are faintly positive S100: Loose clusters of dendritic cells
are positive CAM5.2:Negative According to outside pathology report,
additional studies were performed at UCLAand reportedly showed the
lymphoma cells positive for CD2 (occasional low), and TIA-1
(occasional few); negative for CD8, TCR gamma/delta, TCR F1, TdT,
PD1, and EBER (extremely rare positive small cells). Polymerase
chain reaction (PCR) performed at Neogenomics showed the presence
of monoclonal T-cell receptor gene rearrangements. It was negative
for B-cell gene rearrangements. Per submitted pathology report,
flow cytometric analysis of the right axillary lymph node showed no
evidence of a lymphoproliferative disorder. The findings were
reported to be diagnostic of ALK negative anaplastic large cell
lymphoma. Please note that specimen SAC is not received for review.
3. Bone marrow, (FAC , 10/15/2015): A complete blood count and
peripheral blood smear shows white blood cell count 9.7, hemoglobin
10.7, and platelets The red blood cells are normocytic and
normochromic with slight polychromasia.The white blood cells are
adequate in number and morphology.There is no left-shift,
dysplasia, circulating blasts or lymphoma cells seen. The platelets
are normal in number with unremarkable morphology. The bone marrow
aspirate smear demonstrates trilineage hematopoiesis. There is a
sequential maturation in the erythroid and granulocytic lineages.
The erythrocytes show some dysplastic features including nuclear
budding and nuclear to cytoplasmic asynchrony. There is no increase
in blasts.No obvious lymphoma cells are seen.Megakaryocytes are
present and slightly increased in number.An iron stain shows
decreased iron storage.No ring sideroblasts are seen. The bone
marrow bone marrow and clot demonstrate 70% cellular
marrow.Trilineage hematopoiesis is evident.Megakaryocytes are
present and slightly increased in number (up to 9 per high-power
field).Occasional hypolobated forms are seen.No lymphoid aggregates
or sheets of lymphoid cells are seen. On submitted
immunohistochemical stains performed on the bone marrow biopsy, CD3
and CD20 highlight scattered small and mature appearing T and B
lymphocytes, respectively.The CD3-positive lymphocytes outnumber
the CD20-positive lymphocytes. CD30 fails to demonstrate the
presence of large cells. Per report, flow cytometric analysis of
the bone marrow showed no evidence of a monoclonal B-cell
population, but showed a mildly inverted CD4/CD8 ratio (0.8). Per
report, cytogenetics performed at Neogenomics, showed a normal male
karyotype (46,XY[20]). Per report, PCR performed on the bone marrow
was positive for a monoclonal T-cell receptor gene rearrangement.
In summary, we agree with the diagnosis of ALK negative anaplastic
large cell lymphoma rendered on the right axillary lymph node. The
bone marrow is not involved morphologically, but there is a T-cell
gene rearrangement reportedly present by PCR. Although this is may
be suggestive of involvement by ALCL, it is alone inconclusive to
render a diagnosis of bone marrow involvement especially in the
complete absence of CD30 positive large cells. RM:AQ/kma 12/3/2015
4:18 PM PET Imaging Multiple sites of disease above and below the
diaphragm
Diffuse hypermetabolic activity in the axial skeleton, pelvis and
humerus Treatment CHOP (Cyclophosphamide, Doxorubicin, Vincristine,
Prednisone) x 3 cycles with good response Plan: CHOP plus Etoposide
x 3 additional cycles followed by autologous stem cell transplant
WHO Definition 2008 WHO provisional entity CD30+ T-cell
neoplasm
Not reproducibly distinguishable on morphologic grounds from ALK+
ALCL Lacks ALK protein Blood 1999 Apr 15;93(8):
Immunohistochemistry and FISH
73 ALK- ALCL 32 ALK+ ALCL ALK- ALCL (n=73) 22 (30%) had DUSP22
rearrangements 6 (8%) had TP63 rearrangements Events were mutually
exclusive Not seen in any ALK+ ALCL 45 (62%) lacked both, termed
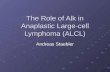
triple negative Survival Analysis by ALK Status
ALK+ ALCL N=29 5 yr OS: 85% ALK- ALCL N=67 5 yr OS: 52% Figure 1.
Outcomes in patients with ALCL based on genetic subtype. (A) OS
rates in patients with ALCL, stratified by ALK status only (ALK
positive, N = 29; ALK negative, N = 67). Survival Analysis ALK-
ALCL by Genetic Subtype
5 yr OS: 85% DUSP22 rearranged N=21 5 yr OS: 90% TP63 rearranged
N=6 5 yr OS: 17% Triple Negative ALCL N=40 5 yr OS: 42% Figure 1.
Outcomes in patients with ALCL based on genetic subtype (B) OS
rates in patients with ALCL, stratified by rearrangements of ALK (N
= 29), DUSP22 (N = 21), and TP63 (N = 6). -/-/-, triple-negative
cases lacking all 3 rearrangements (N = 40). Survival Analysis Only
non-transplanted cases DUSP22 rearranged
ALK+, N=21 DUSP22, N=15 TP63, N=5 -/-/-, N=34 DUSP22 rearranged 5
yr OS: 87% Figure 1. Outcomes in patients with ALCL based on
genetic subtype. (C) OS rates in patients with ALCL who did not
undergo transplantation, stratified by rearrangements of ALK (N =
21), DUSP22 (N = 15), and TP63 (N = 5). -/-/-, N = 34. Author
Recommendations
All ALK negative ALCL undergo FISH testing for rearrangements
involving DUSP22 and TP63 Include in the pathology report if
present Mention prognostic implication IHC for p63 and cytotoxic
markers are not specific and cant substitute for FISH
DUSP22rearrangements in pcALCL have an overall frequency of
approximately 30% Take Home Points ALK(-) ALCL
No longer a provisional entity More heterogeneous than once thought
Future risk stratification may include studies to determine DUSP22
and TP63 status Will ALK(-) ALCL be further sub-classified by
mutational status? Thank You! Thank You!