BEHAVIOR THERAPY 32, 85--102, 2001 Further Tests of a Cognitive Model of Generalized Anxiety Disorder: Metacognitions and Worry in GAD, Panic Disorder, Social Phobia, Depression, and Nonpatients ADRIAN WELLS University of Manchester KARIN CARTER Salford NHS Trust Advances in treating generalized anxiety disorder (GAD) are likely to result from a better understanding of the dysfunctional cognitive mechanisms underlying persis- tent worrying. In a cognitive model of GAD, Wells (1995) proposed that pathologi- cal worry is maintained by maladaptive metacognitions (negative beliefs about worry concerning uncontrollability and danger, and negative appraisal of worrying [meta-worry]) and linked behaviors. Twenty-four patients with GAD were compared with sex-matched groups--social phobia, panic disorder, and nonpatients--on mea- sures of negative metacognitions and worry. It was hypothesized that patients with GAD would obtain higher negative metacognitive belief scores and higher meta- worry scores than the other groups; differences in negative metacognitions would be independent of the general frequency of worry. A group of individuals with major depression was also examined as a subsidiary exploration of relative metacognitive and worry characteristics of this disorder. All of the hypotheses were upheld in the univariate ANOVAs. There was a loss of one hypothesized significant difference be- tween the GAD and panic disorder groups in meta-worry when general worry fre- quency was controlled. However, the GAD group still had higher meta-worry scores than the panic group. This effect appears to be the result of patients with panic hav- ing intermediate meta-worry scores falling between the GAD and other groups. Dif- ferences between the GAD group and all other groups in negative metacognitive beliefs concerning uncontrollability and danger remained when general worry was controlled. The results add further support to the cognitive model, and treatment im- plications are briefly discussed. Generalized anxiety disorder (GAD) is a common and disabling condition. It is one of the most common anxiety disorders, accounting for 12% of pre- sentations at primary care clinics (DSM-IV; American Psychiatric Associa- Address correspondence to Adrian Wells, University of Manchester, Department of Clinical Psychology, Rawnsley Building, MRI, Manchester M13 9WL UK; e-mail: adrian.wells@ man.ac.uk. 85 005-7894/01/0085~) 10251.00/0 Copyright2001 by Association for Advancement of Behavior Therapy All rights for reproductionin any form reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

BEHAVIOR THERAPY 32, 85--102, 2001
Further Tests of a Cognitive Model of Generalized Anxiety Disorder: Metacognitions and Worry in GAD,
Panic Disorder, Social Phobia, Depression, and Nonpatients
ADRIAN WELLS
University of Manchester
KARIN CARTER
Salford NHS Trust
Advances in treating generalized anxiety disorder (GAD) are likely to result from a better understanding of the dysfunctional cognitive mechanisms underlying persis- tent worrying. In a cognitive model of GAD, Wells (1995) proposed that pathologi- cal worry is maintained by maladaptive metacognitions (negative beliefs about worry concerning uncontrollability and danger, and negative appraisal of worrying [meta-worry]) and linked behaviors. Twenty-four patients with GAD were compared with sex-matched groups--social phobia, panic disorder, and nonpatients--on mea- sures of negative metacognitions and worry. It was hypothesized that patients with GAD would obtain higher negative metacognitive belief scores and higher meta- worry scores than the other groups; differences in negative metacognitions would be independent of the general frequency of worry. A group of individuals with major depression was also examined as a subsidiary exploration of relative metacognitive and worry characteristics of this disorder. All of the hypotheses were upheld in the univariate ANOVAs. There was a loss of one hypothesized significant difference be- tween the GAD and panic disorder groups in meta-worry when general worry fre- quency was controlled. However, the GAD group still had higher meta-worry scores than the panic group. This effect appears to be the result of patients with panic hav- ing intermediate meta-worry scores falling between the GAD and other groups. Dif- ferences between the GAD group and all other groups in negative metacognitive beliefs concerning uncontrollability and danger remained when general worry was controlled. The results add further support to the cognitive model, and treatment im- plications are briefly discussed.
Generalized anxiety disorder (GAD) is a common and disabling condition. It is one of the most common anxiety disorders, accounting for 12% of pre- sentations at primary care clinics (DSM-IV; American Psychiatric Associa-
Address correspondence to Adrian Wells, University of Manchester, Department of Clinical Psychology, Rawnsley Building, MRI, Manchester M13 9WL UK; e-mail: adrian.wells@ man.ac.uk.
85 005-7894/01/0085~) 10251.00/0 Copyright 2001 by Association for Advancement of Behavior Therapy
All rights for reproduction in any form reserved.
86 W E L L S & CARTER
tion, 1994). The problem is often lifelong, and although cognitive-behavioral treatments are effective, only about 50% of patients improve (Fisher & Durham, 1999). Moreover, there is a high degree of variability in improve- ment across treatment studies (Borkovec & Costello, 1993; Butler, Fennell, Robson, & Gelder, 1991; Durham & Allan, 1993; Durham et al., 1994). Wells (1995) suggested that the treatment of GAD would be improved if treatment was based on a model of the development and maintenance of the problem.
Worry is a central feature of GAD, and it is experienced as excessive and uncontrollable. The uncontrollability dimension has been added with the advent of DSM-IV. A model of GAD should therefore explain the maladap- tive mechanisms that contribute to and maintain pathological worrying in this disorder. Worrying and other forms of negative perseverative thinking such as rumination have been conceptualized as part of a maladaptive cognitive- attentional syndrome associated with vulnerability to and the maintenance of psychological disorder (Wells & Matthews, 1994, 1996). Rather than viewing worry as merely a symptom of anxiety, Wells and Matthews (1994; Wells, 1994a) assert that individuals hold positive beliefs about worrying and some people use this as a strategy for contemplating threats and planning coping strategies. However, in pathological worry or ruminative states, individuals appear to hold conflicting negative metacognitive beliefs concerning the potential consequences of this type of thinking. Beliefs about thinking belong to a class of cognition labeled metacognitions. Metacognitions are the ele- ments of thinking that are involved in the appraisal and control of thinking itself (e.g., Flavell, 1979).
Building on a metacognitive framework, Wells (1994a, 1995) advanced a cognitive model of pathological worry and GAD. In this model, individuals with GAD use worrying as a means of coping with threat. This is stimulated by positive metacognitive beliefs about worrying. Positive beliefs about worry are normal and most individuals possess them to some degree. In GAD in particular, these beliefs are linked to the maintenance of worrying as a cop- ing strategy. However, it is the development of negative beliefs about worry, associated negative appraisal of worry (meta-worry), and linked responses that contribute centrally to distress and the development of pathological worry that is presented by GAD patients. Figure 1 represents the central fac- tors and processes that contribute to the development and maintenance of GAD in this model.
In this model, two types of worry are distinguished: Type 1 and Type 2. Type 1 worry concerns external events and noncognitive internal events (e.g., worrying about one's partner being involved in an accident; worrying about one's own competence at work; worrying about one's own physical health). Type 2 worry is concerned with thoughts themselves and centers on themes of uncontrollability of worry and its dangerous consequences for mental and physical well-being (e.g., appraising worry as uncontrollable; leading to mental breakdown; causing bodily damage). Type 2 worry is essentially worry about worry: a negative metacognitive appraisal closely linked to the

COGNITIVE MODEL OF GAD 87
Behaviour]
Trigger J . . . . .
(lbositive meta-beliefs activated': " ' - - . (Strategy selection) ...--"
Worry ~, ............. Type 1
,'.Negative meta-beliefsactivated . , . . . . . . . . . . . . . . . . . . . . .
Type 2 Worry (ieta-worry)
Thought Control
mo:on FIG. 1. A cognitive model of generalized anxiety disorder. From Cognitive Therapy of
Anxiety Disorders: A Practice Manual and Conceptual Guide (p. 204), by A. Wells, 1997, Chichester, UK: Wiley. Reprinted with permission.
individual's negative beliefs about worry. Elsewhere Type 2 worry has also been termed "meta-worry" (Wells, 1994b). The experience of Type 2 worry is tied to the activation of negative metacognitive beliefs, and can be viewed as the transient situational on-line output of their activation.
Type 1 worrying consists of catastrophizing sequences of thoughts in which the person with GAD contemplates a range of negative scenarios in a "what if" questioning style, and attempts to generate and/or plan coping options. This worrying continues until it is displaced by goals that compete for attention, or until the individual thinks that it is safe or appropriate to stop worrying. Internal cues, often in the form of a "felt sense" or knowing that most possibilities have been contemplated, signal that it is safe to terminate the worry process. However, when negative beliefs and Type 2 worry develop, anxiety symptoms are intensified so that it is difficult for the individ- ual to attain the internal state signaling that worry can cease. This contributes
88 WELLS & CARTER
to the prolongation and generalization of worrying, depicted by the bidirec- tional dotted line in Figure 1. Anxiety symptoms may be interpreted as a sign that catastrophe is imminent, for example, in the form of mental breakdown. Under such circumstances, anxiety increases rapidly and panic attacks can result.
The use of worrying as a strategy is problematic since it can lead to a potentially limitless range of negative scenarios, each of which can act as an internal trigger for continued worrying. Furthermore, it may disrupt more adaptive cognitive processes such as those involved in emotional processing, and thereby contribute to symptoms of failed emotional processing such as intrusive thoughts. Thus, worrying can create its own problems that contrib- ute to the need for further worrying in order to cope, and contribute to the strengthening of negative beliefs about thought processes. For instance, intru- sive thoughts resulting from worry may be interpreted as a sign of loss of mental control.
Negative beliefs about worry are not only strengthened by the appraisal of worry consequences, external factors such as the provision of information about the harmful consequences of stress can contribute to a negative reap- praisal of worrying. Once negative beliefs are established, individuals are prone to negatively appraise their Type 1 worrying, which contributes to anx- iety. Moreover, anxiety symptoms can be misinterpreted as a sign of danger associated with worrying, thereby maintaining Type 2 worry and contributing to further increases in anxiety as depicted by the feedback loop linking Type 2 worry to emotion in Figure 1.
Two further processes in the domains of behavioral and thought control re- sponses contribute to problem maintenance. Because the person with GAD has negative beliefs about worrying and also feels that it is necessary to worry in response to negative thought triggers, a self-regulatory conflict exists. This can be avoided by engaging in behaviors that are intended to avert the need to worry in the first place, and thereby avoid the dangers associated with worry- ing. These behaviors include avoidance of triggers for worry such as news items or situations, reassurance seeking, and checking. The range of behav- iors is idiosyncratic, but these responses can be problematic. First, some behaviors increase the range of worry triggers experienced. For instance, reassurance seeking can give rise to conflicting information, and reassuring information may not be delivered when required. Second, avoidance of situa- tions that trigger worrying, such as reading the newspaper, deprive the in- dividual of opportunities to discover that negative beliefs about the uncon- trollability of worry and its dangers are unrealistic. Moreover, it removes opportunities to practice nonworry response strategies that could strengthen alternatives to worry-based coping. In summary, some strategies increase worry triggers; the individual with GAD does not encounter evidence that can disconfirm negative beliefs and Type 2 worries; and avoidance of situa- tions that trigger the need to worry removes an opportunity to practice alter- native, non-worry-based coping routines.

COGNITIVE MODEL OF GAD 89
A further mechanism operates in the form of thought control. This is con- sidered separately from other forms of behavior since there are two aspects to this strategy that are relevant in formulating GAD mechanisms: (a) In many cases patients with GAD make few attempts to interrupt the Type 1 worry sequence once it is activated before reaching internal goals (this is because not worrying is similar to not attempting to cope); (b) a more common strat- egy occurs in the form of attempts to suppress or remove from consciousness thoughts that may trigger worrying. Unfortunately, suppression is rarely com- pletely effective, and its failure can reinforce negative beliefs such as those concerning lack of mental control. Furthermore, a lack of attempts to inter- rupt the iterative Type 1 worry process once it is initiated reduces opportuni- ties to discover that worrying is subject to voluntary control. In the model, an important distinction is made between trying to remove the content of Type 1 worry triggers from awareness (e.g., thoughts about accidents) and interrupt- ing the worry (catastrophizing) process. Patients with GAD tend to engage more in the former rather than the latter strategy when the latter strategy would provide evidence that worry is subject to control and therefore provide information that could challenge negative beliefs concerning the uncontrolla- bility of worry.
Research on nonpatient worriers and individuals meeting criteria for GAD has provided support for several key aspects of the model. It has been demon- strated that individuals meeting criteria for GAD report positive reasons for worrying (Borkovec & Roemer, 1995), and that proneness to pathological worry characteristic of GAD is associated with both positive and negative beliefs about worry (Cartwright-Hatton & Wells, 1997; Wells & Papageor- giou, 1998). Similarly, several authors have suggested that worriers treat worrying as a problem-solving task (Davey, 1994), and they hold beliefs about worrying as an activity that can avert catastrophes (Davey, Tallis, & Capuzzo, 1996).
In a test of one of the central predictions of the model, Wells and Carter (1999) showed that Type 2 worry was a stronger predictor of pathological worry than Type 1 worry when the interrelationships between these variables was controlled. Furthermore, even when the uncontrollability of worry and trait anxiety were used as simultaneous predictors, Type 2 worry emerged as a significant predictor of pathological worrying. In another test of the model, Nassif (1999) examined the causal role of negative metacognitions in patho- logical worry. In this study negative beliefs about the uncontrollability and dangers of worrying predicted the development of GAD 12 to 15 weeks later in nonpatients.
The model assumes that when worrying is used as a coping strategy it can have problematic consequences in some situations. Several studies that have examined the emotional and cognitive consequences of worrying are consis- tent with this hypothesis. Borkovec, Robinson, Pruzinsky, and DePree (1983) and York, Borkovec, Vasey, and Stern (1987) have demonstrated that brief periods of worry can increase the frequency of subsequent negative thought
90 WELLS & CARTER
intrusions. Butler, Wells, and Dewick (1995) investigated the effects of post- stress worry on intrusive images following exposure to a gruesome film. They showed that brief periods of worry were associated with an increased fre- quency of intrusive images about the film over a subsequent 3-day period. In a larger scale follow-up study, Wells and Papageorgiou (1995) found further support for an effect of post-event processing strategies on intrusions follow- ing a stressful film. Worrying for 4 minutes after exposure to the film was associated with an increase in intrusive images about the film over the next 3 days. These data were interpreted in terms of worrying blocking emotional processing and producing a "tagging" of film-related memories. In summary, the results of these studies are consistent with the hypothesis that worrying can have negative consequences and increase negative thoughts under some circumstances.
A study by Purdon (2000) examined the effects of in-vivo negative apprais- als of worry in nonpatients. Situational negative appraisals correlated posi- tively with trait measures of meta-worry and negative metacognitive beliefs. Greater in-situation negative appraisals of worry were associated with greater anxiety. Moreover, of particular relevance to the thought control aspects of the GAD model, whilst negative appraisals of worry were associated with greater thought control, positive beliefs about worry were concurrent predic- tors of reduced motivation to get rid of thoughts. These results provide sup- port for the anxiety-arousing effects of negative meta-appraisals and support the differential and potentially conflicting effects of metacognitions on use of thought control.
In the present study, we aimed to test further Wells's model of GAD by examining the metacognitions of GAD patients against patients with anxiety disorders in which intrusive thoughts or worries are not the central defining feature. The model predicts the following: GAD patients should report greater negative metacognitions concerning worry than patients with social phobia, panic disorder, or nonpatient controls. More specifically, since nega- tive beliefs concerning uncontrollability and the mental and physical health dangers of worry are hypothesized as central in the model, patients with GAD should report higher negative beliefs in this domain. However, individuals with GAD will continue to endorse positive beliefs about worry, and therefore we did not expect to find differences in positive beliefs. We extended the assess- ment of negative beliefs to explore potential differences in another negative belief domain--superstition, punishment, and responsibility--associated with thoughts. Although this domain is not implicated in the present model, such differences might provide a useful extension to exploring metacognitive belief domains in GAD. We also predicted that patients with GAD should endorse higher Type 2 worries (meta-worries) than patients with panic disor- der, social phobia, or nonpatient controls; however, there should be fewer dif- ferences across groups in Type 1 worry content. Higher levels of negative metacognitions (beliefs and Type 2 worry) in GAD are not merely a reflec- tion of a greater frequency of Type 1 worry. When Type 1 worry is controlled,

COGNITIVE M O D E L OF G A D 91
GAD patients should show greater negative metacognition scores than other anxious patients.
Maladaptive metacognitions also appear to relate to other disorders of intrusive thought (Emmelkamp & Aardema, 1999; Wells & Matthews, 1994; Wells & Papageorgiou, 1998). For instance, Rachman and Shafran (1999) have formulated Thought Action Fusion (TAF) in obsessional disorder as a belief that intrusive thoughts can directly influence external events, and Pur- don and Clark (1999) have explicitly considered the implications of a meta- cognitive approach to obsessional problems, emphasizing the importance of conceptualizing ego-dystonicity within a framework of this kind. In the present study, we had a subsidiary aim of exploring negative metacognitions in patients suffering from major depressive episode. Depression is associated with chains of intrusive negative thinking or rumination, which is similar to worry (Papageorgiou & Wells, 1999). Positive and negative beliefs about rumi- nation may be to depression what positive and negative beliefs about worry are to GAD. Metacognitions of this type have been demonstrated in depressed individuals (Papageorgiou & Wells, 2001; Papageorgiou & Wells, in press). However, at the time of conducting this study, no specific measure of beliefs about rumination existed. Therefore, we relied on a more general measure of beliefs about thoughts and worry. If metacognitions are involved in depres- sion, at the general level of metacognitive belief assessment available in this study, GAD and depression should be closer on negative metacognitions than GAD and the two other anxiety disorders tested: panic and social phobia.
Method Participants
Five groups of participants were recruited for this study: nonpatients with no history of psychological treatment, patients with primary GAD, social phobia, panic disorder, and major depression. All patients were screened from consecutive referrals for psychological treatment. All patients met crite- ria for their specified DSM-III-R disorder. Diagnosis was made following administration of the Structured Clinical Interview for DSM-III-R (SCID; Spitzer, Williams, Gibbon, & First, 1990). Interviews were conducted by qualified clinical psychologists who had been trained in using the SCID and were experienced with its usage. Patients were excluded if they had received previous treatment for the current presenting problem and if they also met criteria for any of the comparison disorders in this study (i.e., GAD patients could not also have panic disorder, social phobia, or major depression; patients with panic disorder could not have GAD, social phobia, or major depression; patients with social phobia could not have panic disorder, GAD, or major depression; patients with major depression could not have any of the comparison anxiety disorders).
In total, 24 individuals were recruited in each group with the proviso that groups were sex matched. Nonpatients were recruited by convenience sam-
92 WELLS & CARTER
pling from hospital and university employees. All of these individuals were asked if they had ever received treatment or counseling for a psychological problem, and only if they reported no history of treatment for psychologi- cal problems were they included in the study. Mean age for each group was as follows (range in parentheses): GAD = 37.90 (18 to 60); panic disorder = 38.00 (24 to 69); social phobia = 33.50 (16 to 58); nonpatients = 30.13 (19 to 61); depression = 34.63 (16 to 58). There were no significant differences in age between groups, F(4, 119) = 2.02, p -- ns. Each group was comprised of 10 men.
Procedure Following initial screening and interview, participants were asked to com-
plete a battery of questionnaires consisting of a number of self-report scales. The scales were as follows:
Anxious Thoughts Inventory (ANTI," Wells, 1994b). This instrument is a multidimensional trait measure of worry consisting of three empirically derived subscales that separately measure social worry, health worry, and meta (Type 2) worry. These subscales appear factorially reliable. The scale consists of 22 items measuring these domains. Test-retest over a 6-week period and alpha coefficients for each of the subscales are as follows (test- retest in parentheses): social worry alpha = 0.84 (0.76); health worry alpha = 0.81 (0.84); meta-worry alpha = 0.75 (0.77). The scales correlate meaningfully with a range of measures of emotional vulnerability.
Meta-Cognitions Questionnaire (MCQ; Cartwright-Hatton & Wells, 1997). The MCQ measures a range of beliefs about worry and intrusive thoughts and metacognitive processes. It consists of five factorially derived subscales that measure positive beliefs about worry (e.g., "Worrying helps me cope"); negative beliefs concerning themes of danger and uncontrollabil- ity (e.g., "Worrying is dangerous for me"); cognitive confidence (e.g., "I have a poor memory"); negative beliefs, including themes of weakness, supersti- tion, punishment, and responsibility (SPR; e.g., "Not being able to control my thoughts is a sign of weakness"); cognitive self-consciousness (e.g., "I pay close attention to the way my mind works"). Alpha coefficients and test- retest correlations (in parentheses) for a 5-week period are as follows: positive beliefs = 0.87 (0.85); uncontrollability and danger = 0.89 (0.89); cognitive confidence = 0.84 (0.84); SPR = 0.74 (0.76); cognitive self-consciousness = 0.72 (0.89). The subscales are meaningfully correlated with other measures. For purposes of testing the present hypotheses, only the positive belief and the two negative belief subscales were analyzed. The other MCQ dimensions are not implicated in the GAD model. While the model emphasizes the role of negative beliefs concerning uncontrollability of worry and its dangerous consequences for physical and mental health, the present analyses were extended to the more general negative belief subscale -- Superstition, Punish- ment, and Responsibility (SPR)--since this subscale captures additional neg- ative outcomes of worrying.

COGNITIVE MODEL OF GAD 93
Results Overview
To test our predictions concerning differences between patients with GAD, other anxiety patients, and nonpatient controls, one-way ANOVAs were run and followed by a-priori pairwise comparisons (Fisher's LSD). Following this analysis we tested for the hypothesized differences between groups in negative metacognitions while controlling for Type 1 worry using ANCO- VAs. Finally, our exploratory analyses comprising the depressed group con- sisted of a multigroup discriminant function analysis to examine which com- bination of metacognitive and worry factors were the best indicators of separation between the groups, and to enable a plot of the relative positions of the groups in discriminant space.
Tests of Hypothesized Group Effects One-way analyses of variance were computed to test for differences
between diagnostic groups (excluding the depressed group), followed by Fisher's LSD post hoc comparisons to locate pair-wise differences. Mean scores on the AnTI and MCQ and the results of pair-wise analyses are sum- marized in Table 1.
Significant differences between groups (GAD, panic, social phobia, nonpa- dents) emerged for MCQ negative beliefs concerning uncontrollability and danger, F(3, 95) = 16.20, p < 0.001. Fisher's LSD showed that, consistent with predictions, GAD patients reported higher negative beliefs in this domain than patients with panic disorder, social phobia, or nonpatients (ps < 0.001). The results for beliefs concerning superstition, punishment and responsibility followed the same pattern, F(3, 95) = 5.52, p < 0.003, with GAD patients scoring higher on this subscale than any of the other anxious groups or nonpatients (ps < 0.02). Significant overall differences were found
T A B L E 1 MEANS AND STANDARD DEVIATIONS (IN PARENTHESES) FOR
WORRY AND METACOGNITION VARIABLES
GAD Panic Social Control Depressed
AnTI Health worry 14.3 a (3.6) 15.5 a (5.6) 9.2 b (2.7) 10.0 b (3.3) 11.0 (4.4) Social worry 24.0 a (5.1) 18.0 b (3.8) 24.9a(5.7) 17.5b (4.6) 24.1 (6.5) Meta-worry 19.7 a (3.9) 15.7 b (4.6) 15.5 b (4.5) 12.8 ° (3.8) 18.0 (3.7)
MCQ Positive beliefs 33.1 (10.6) 32.3 (6.4) 29.7 (6.0) 32.3 (10.1) 33.0 (8.9) Negative danger 50.4 a (9.0) 40.2 b (10.9) 38.8 b (9.3) 31.4 c (8.6) 45.4 (9.3) Negative SPR 30.2 a (7.9) 24.6 b (5.8) 25.3 b (6.8) 22.7 b (6.1) 30.1 (7.8)
Note. Depressed group included here for reference only. Means with different superscripts differ significantly (ps ~< 0.03).
94 WELLS & CARTER
for meta-worry, F(3, 95) = 10.82, p < 0.001, in which patients with GAD obtained higher scores than the other anxious patients or nonpatients (ps < 0.002). Comparisons of Type 1 worry showed that significant differences emerged among the groups in social worry, F(3, 95) = 15.59,p < 0.001, and health worry, F(3, 95) = 14.83, p < 0.001. Patients with GAD obtained higher social worry scores than patients with panic or nonpatients (ps < 0.001), but they did not differ significantly from patients with social phobia. Patients with GAD also obtained higher scores for health worry compared with patients with social phobia or nonpatients (ps < 0.001). However, they did not differ significantly from patients with panic disorder on this worry dimension.
There were no significant group differences in the endorsement of positive beliefs about worry. As would be expected, patients with panic disorder endorsed higher health worries than patients with social phobia or nonpa- tients (ps < 0.001), patients with social phobia obtained higher social worry scores than patients with panic disorder or nonpatients (ps < 0.001). Patients with panic and those with social phobia did not differ in meta-worry, but both groups obtained higher scores than nonpatients in meta-worry (ps < 0.03).
In summary, the results of the univariate ANOVAs support the hypothe- sized differences between patients with GAD and the other groups with respect to negative metacognitive beliefs and meta-worry. Consistent with pre- dictions, GAD appears to be characterized more by elevated negative meta- cognitions than by the content of Type 1 worry. Patients with panic, while having lower meta-worry scores than patients with GAD, showed intermedi- ate levels of meta-worry, falling between GAD and the other groups.
It could be that patients with GAD merely worry more about social and physical health concerns (Type 1 worry) than other individuals, and this accounts for their elevated negative metacognitions, particularly those con- cerning uncontrollability. In order to test for the independence of differences in negative metacognitions from differences in Type 1 social and health worry, a series of ANCOVAs were run. Here, Type 1 worries (social and health) were entered as covariates in testing for group effects on negative metacognitions: negative beliefs (uncontrollability and danger), meta-worry, and SPR. For negative beliefs concerning uncontrollability and danger, group differences remained significant, F(3) = 8.40, p < 0.001. The adjusted group means showed that GAD patients retained the highest score on nega- tive beliefs concerning uncontrollability and danger (M = 48.29) compared to patients with panic (M = 41.08), social phobia (M = 37.45), or nonpa- tients (M = 33.97). Fisher's LSD tests showed that patients with GAD were significantly higher on this dimension than patients with panic (p < 0.02), social phobia (p < 0.001), and nonpadents (p < 0.001).
In the case of meta-worry, the overall group effect was significant, F(3) = 4.10, p < 0.01, and patients with GAD retained the highest scores. Pairwise comparisons showed that patients with GAD (M = 18.07) differed signifi- cantly from patients with social phobia (M = 14.42, p < 0.003) and nonpa-
COGNITIVE M O D E L OF G A D 95
tient controls (M = 14.68, p < 0.006). Differences between GAD patients (M = 18.07) and panic patients (M = 16.38) were not significant (p = 0.15). Finally, for SPR, the main group effect was not significant, F(3) = 1.83, p >0.1 .
Results of the ANCOVAs suggest that higher negative metacognitive beliefs (uncontrollability and danger) in GAD are not merely a function of the elevated Type 1 worries measured. Since the AnTI Type 1 worry sub- scales can be interpreted as a frequency measure, this result suggests that GAD patients differ from other anxious individuals assessed here in terms of particular negative metacognitions, and this is not solely a function of the fre- quency of Type 1 social and health worry. Differences were also sustained for Type 2 worry in all but the GAD versus panic comparison. However, patients with GAD still had higher meta-worry scores than the patients with panic (adjusted means = 18.07 and 16.38, respectively). The loss of significance in the panic comparison reflects the fact that patients with panic have elevated and intermediate levels of meta-worry. The absence of any differences in SPR in the ANCOVA suggests that group differences in these beliefs are depen- dent on the level of Type 1 worry.
Finally, a multigroup discriminant function analysis was performed to compare the characteristics of the groups on the basis of a combination of independent (Type 1 worry and metacognition) variables. Multigroup Dis- criminant Analysis (MDA) allows the identification of combinations of vari- ables that classify groups, and is appropriate for attempting to assess which factors are the best indicators of separation between the groups. The tech- nique can uncover the most powerful sets of contrasts between clusters of variables on a data-driven basis, and the results can be used to visually repre- sent the position of groups relative to each other in discriminant space. We included the patients with major depression in this analysis so that we could examine their relative position to the GAD and other groups with respect to the discriminant functions obtained.
First, potential discriminating variables were identified on the basis of the previous univariate F tests. The variables identified were social worry, health worry, meta-worry, negative beliefs, and SPR. Since there are five groups and five variables, the maximum number of discriminant functions that can be estimated is four. Only two discriminant functions (out of four) were signifi- cant: Function 1, X2(20) = 116.3,p < 0.0001, and Function 2, ×a(12) = 55.0, p < 0.0001, and were retained. These functions accounted for 96.1% of the variance between groups. Table 2 shows that social and health worry have the highest loadings on Function 1, while meta-worry and negative beliefs load most highly on Function 2. SPR loaded on Function 3, but as this Func- tion was nonsignificant it was not retained. The loadings show that Function 1 is a Type 1 worry content dimension that contrasts health worry with social worry (health worry loads negatively on this factor), while Function 2 is a negative metacognition dimension.
Since an aim of the discriminant analysis was to further examine differ-
96 WELLS & CARTER
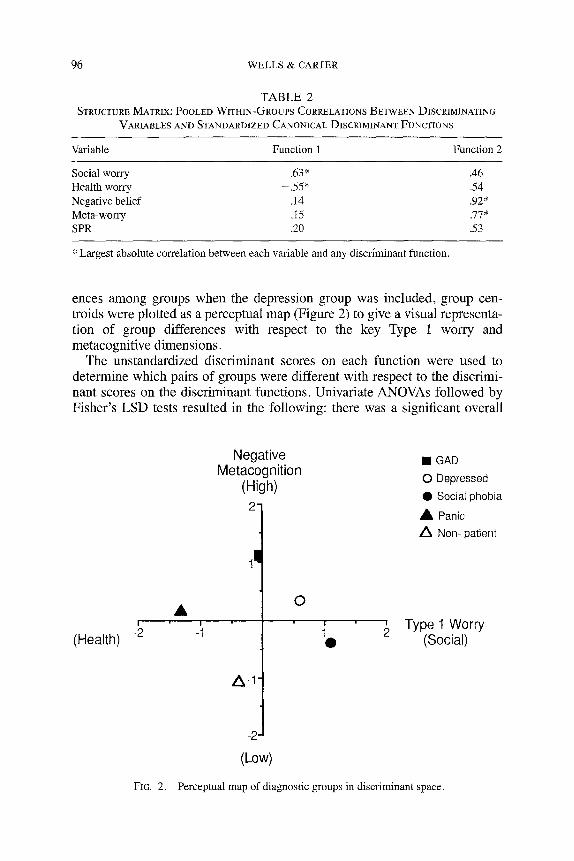
TABLE 2 STRUCTURE MATRLX: POOLED WITHIN-QROUPS CORRELATIONS BETWEEN DISCRIMINATING
VARIABLES AND STANDARDIZED CANONICAL DISCRIMINANT FUNCTIONS
Variable Function 1 Function 2
Social worry .63" .46 Health worry - 5 5 * .54 Negative belief .14 .92* Meta-worry .15 .77" SPR .20 .53
* Largest absolute correlation between each variable and any discriminant function.
ences among groups when the depression group was included, group cen- troids were plotted as a perceptual map (Figure 2) to give a visual representa- tion of group differences with respect to the key Type 1 worry and metacognitive dimensions.
The unstandardized discriminant scores on each function were used to determine which pairs of groups were different with respect to the discrimi- nant scores on the discriminant functions. Univariate ANOVAs followed by Fisher's LSD tests resulted in the following: there was a significant overall
(Health)
Negative • GAD Metacognition (High) o Depressed
• Social phobia
21 • Panic
/~ Non- patient
0 ~ Type 1 Worry
• (Social)
-2
(Low)
FIG. 2. Perceptual map of diagnostic groups in discriminant space.
COGNITIVE MODEL OF GAD 97
main effect for Function 1, F(4, 119) = 20.50, p < 0.0001, and Function 2, F(4, 119) = 15.55,p < 0.0001. Post hoc comparisons located the differences as follows: With respect to Function 1 (Type 1 worry) GAD patients differed from each of the other patient groups (ps < 0.03), but not from nonpatients. That is, the other anxious groups were characterized by greater levels of con- trasting health or social worry. As can be seen from Figure 2, GAD patients were not characterized specifically by health or social worry. Patients with depression differed from each of the other groups, apart from social phobia, in Function 1 (ps < 0.03).
With respect to Function 2, patients with GAD differed from all other groups (ps < 0.02). Depressed patients did not differ from patients with panic on this dimension, but they did differ from patients with social phobia and nonpatients (ps < .02). Summarizing these data with respect to patients with depression, it appears that these patients show elevated negative metacogni- tions concerning worry that are significantly lower than those of patients with GAD, similar in level to those of panic patients, but significantly higher than those of patients with social phobia or nonpatients. An incidental finding was that patients with depression showed elevated levels of social worry that sig- nificantly distinguished them from all other groups except for the social pho- bia group.
The following conclusions can be drawn from the univariate analysis of discriminant scores and from inspecting the perceptual map in Figure 2:
1. Patients with GAD report high negative metacognition scores, which sets them apart from the other anxious, depressed, and nonpatient groups. The depressed patients show a level of negative metacognitions that falls between the other anxious patients and patients with GAD. They do not differ significantly from patients with panic, but they do show higher scores than patients with social phobia or nonpatients.
2. Patients with panic or social phobia are different from patients with GAD in having a more specific health or social worry content rather than an elevated, nonspecific combination of both. Thus, the dimension that most clearly distinguishes GAD from these other anxiety disorders is specific negative metacognition.
3. Examination of Figure 2 shows that GAD can be characterized as a high negative metacognition problem, with nonspecific combinations of health and social worry. High health worry and intermediate levels of negative metacognitions characterize panic disorder, and high social worry and low negative metacognition as measured here characterize social pho- bia. Depressed patients appear to have moderate levels of negative metacognitions and high levels of social worry.
In summary, the results of the discriminant function analysis provide fur- ther support for the hypothesis that GAD is most specifically characterized by particular negative metacognitions, while panic and social phobia are dis- tinguished most by the content of Type 1 worry. Taken in combination with
98 WELLS & CARTER
the results of the ANCOVA in which Type 1 social and health worry was con- trolled, the results suggest that negative metacognitive beliefs concerning uncontrollability and danger in GAD are a characteristic feature distinct from at least two dimensions of Type 1 worry.
Conclusions The present study set out to test for differences in metacognitions as pre-
dicted by Wells's model of GAD. The first hypothesis, that patients with GAD should obtain higher scores on negative beliefs about uncontrollability and danger than the other anxious or nonpatient groups, was supported by the ANOVA and MDA computations. The subsidiary hypothesis, that there would be no group differences in the endorsement of positive metacognitive beliefs, was also supported. The second hypothesis, that patients with GAD should report higher Type 2 worries than patients with panic, social phobia, or nonpatients, was supported in the univariate analyses. Moreover, as pre- dicted, patients with GAD were discriminated more by negative metacogni- tions than by the content of specific Type 1 worry, as demonstrated in the univariate and discriminant analyses. The third hypothesis, that differences in negative metacognitions would be independent of Type 1 worry, was upheld for negative beliefs concerning uncontrollability and danger. Here patients with GAD remained higher on the negative belief dimension than all compar- ison groups. Differences between the GAD and other groups were predomi- nantly upheld in the case of meta-worry; however, the difference between the GAD and panic group was lost. One explanation for this loss of effect is that some negative appraisals in panic are synonymous with meta-worry. For instance, analyses of thought content in panic show that these patients misin- terpret mental symptoms as a sign of mental catastrophe (e.g., Ottaviani & Beck, 1987). Therefore, the difference in meta-worry between patients with GAD and some patients with panic is likely to be less pronounced.
The present study attempted to extend the analysis of domains of negative metacognitive beliefs that might be associated with GAD to beliefs about thoughts concerning superstition, punishment, and responsibility. While this domain is not an explicit feature of the GAD model, it is possible that a range of negative metacognitive beliefs could contribute to pathological worry. Patients with GAD obtained significantly higher SPR scores than the other anxious patients or nonpatients. However, when Type 1 worry was controlled, patients with GAD did not differ significantly from any of the comparison groups. This result suggests that differences in SPR may be a function of the occurrence of Type 1 worries. Further research is required to determine the relevance of this dimension to pathological worry.
In summary, the results are supportive of the predictions based on the GAD model. Only one result involving the GAD-panic comparison of meta-worry while controlling for Type 1 worry was discrepant from initial predictions. Nevertheless, patients with GAD still had higher meta-worry scores than
COGNITIVE MODEL OF GAD 99
patients with panic when Type 1 worry was controlled. The loss of signifi- cance can most probably be accounted for by overlaps between patients with GAD and patients with panic in the occurrence of meta-worry. Such overlap does not threaten the current model; indeed, the model assumes that patients with GAD will have panic attacks when their meta-worries represent inter- pretations of imminent catastrophe resulting from worry. Similar misinterpre- tations of mental events are found in cases of panic disorder (e.g., Ottaviani & Beck, 1987). Despite the finding that meta-worry no longer discriminated patients with GAD from those with panic when Type 1 worry was controlled, the results of another study support the independence of meta-worry from Type 1 worry in predicting pathological worry processes. In particular, Wells and Carter (1999) demonstrated that meta-worry remained a significant posi- tive predictor of pathological worry in nonpatients when its relationship with Type 1 worry, trait anxiety and the controllability of worry was controlled.
Our exploratory analysis of depressed patients supports the continued exploration of the role of metacognitive beliefs in depression. These patients were relatively close to patients with GAD in the negative metacognition domain. The results concerning metacognition derived from patients with major depression are particularly interesting for theory building. The phe- nomena of worry and metacognitions may offer a bridge in conceptualizing underlying cognitive dysfunction that unifies generalized anxiety and depres- sion. A clinical implication of this assertion is that it may be worth adapting metacognitive-focused therapy of GAD (Wells, 1997, 2000) to treat chronic rumination in depression. An incidental finding was that patients with depres- sion endorsed more social than health worries. This is a potentially interest- ing finding that could be worthy of future investigation. If depression is asso- ciated with elevated levels of social concern, it may be that depression may in part be a particular manifestation of worry about the self as a social object.
The present results show that GAD is characterized more by differences in certain meta-cognitions than by differences in social or health worry. The content specificity hypothesis in cognitive theory (Beck, Brown, Steer, Eidel- son, & Riskind, 1987) proposes that anxiety and depression can be distin- guished in terms of the content of thought. However, there appears to be little content specificity of negative thoughts in GAD at the Type 1 level, thus con- firming that worry in these patients is indeed generalized. The present model suggests that greater specificity can be found by examining metacognitions.
A number of limitations should be considered when interpreting the results of the present study. With the introduction of DSM-1V, a criterion of uncon- trollability of worry has been included as a diagnostic feature of GAD. Since the recruitment of individuals to the present study commenced before the advent of DSM-IV interview schedules, and DSM-III-R schedules were used, the participants with GAD were not asked about the uncontrollability of worry. Although this rules out circularity in the study (note also that the model was developed before the advent of DSM-IV), this may mean that the GAD sample tested here may differ from a sample diagnosed in accordance

100 WELLS & CARTER
with DSM-IV. Other changes in DSM-IV include the requirement of "exces- sive anxiety and worry" rather than "unrealistic or excessive anxiety and worry." In addition, DSM-III-R requires a minimum of 6 symptoms from a list of 18, while DSM-IV requires a minimum of 3 from a list of 6. It remains to be determined if these modifications lead to substantial differences in the characteristics of DSM-III-R- versus DSM-IV-diagnosed samples of patients with GAD. A further limitation of the present study is that reliability data on the diagnoses performed are not available. However, diagnoses were made by fully qualified and experienced clinical psychologists who had been trained in using the SCID.
The clinical implications of the cognitive model of GAD are that treatment should focus on eliciting and modifying negative metacognitive beliefs about worry rather than concentrating on challenging the content of Type 1 worries. This treatment, described in detail elsewhere (Wells, 1997, 1999), should also modify inflexible positive beliefs and examine alternative strategies for pro- cessing and coping with threat that do not rely on worry. Despite the fact that individuals with GAD do not differ from nonanxious individuals in endorsing positive beliefs about worry, the model proposes that in GAD the relationship between positive beliefs and worrying is usually different from that in nonanxious individuals. More specifically, as depicted in Figure 1, positive beliefs are linked to selection and maintenance of worrying as a coping strat- egy ("strategy selection"), while in nonpatients positive beliefs may not typi- cally lead to the active maintenance of worrying in order to "work through" problems. In treating GAD, it is helpful to challenge positive beliefs as a means of motivating patients to explore and develop alternative non-worry- based coping strategies. Moreover, residual positive beliefs are a marker for the potential continued use of worrying as a strategy, which itself can become problematic for self-regulation. Preliminary data on the outcome of such a metacognitive-focused cognitive therapy is in preparation, and it appears that the treatment is both efficient and effective. It is likely that treatment based on a specific model of the maintenance of pathological worry in GAD, like the model presented here, will improve treatment outcome.
References American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disor-
ders (3rd ed., rev.). Washington, DC: Author. American Psychiatric Association. (1994). Diagnostic and statistical manual of mental dis-
orders (4th ed.). Washington, DC: Author. Beck, A. T., Brown, G., Steer, R. A., Eidelson, J. I., & Riskind, J. H. (1987). Differentiating
anxiety and depression: A test of the cognitive content specificity hypothesis. Journal of Abnormal Psychology, 96, 179.
Borkovee, T. D., & Costello, E. (1993). Efficacy of applied relaxation and cognitive-behavioral therapy in the treatment of generalised anxiety disorder. Journal of Consulting and Clini- cal Psychology, 61, 611-619.

COGNITIVE MODEL OF GAD 101
Borkovec, T. D., Robinson, E., Pruzinsky, T., & DePree, J. A. (1983). Preliminary exploration of worry: Some characteristics and processes. Behaviour Research and Therapy, 21,9-16.
Borkovec, T. D., & Roemer, L. (1995). Perceived functions of worry among generalized anxiety disorder subjects: Distraction from more emotionally upsetting topics? Behavior Therapy and Experimental Psychiatry, 26, 25-30.
Butler, G., Fennell, M., Robson, R, & Gelder, M. (1991). Comparison of behavior therapy and cognitive behavior therapy in the treatment of generalized anxiety disorder. Journal of Consulting and Clinical Psychology, 59, 167-172.
Butler, G., Wells, A., & Dewick, H. (1995). Differential effects of worry and imagery after exposure to a stressful stimulus: A pilot study. Behavioural and Cognitive Psychotherapy, 23, 45-56.
Cartwright-Hatton, S., & Wells, A. (1997). Beliefs about worry and intrusions: The Metacogni- tions Questionnaire and its correlates. Journal of Anxiety Disorders, 11,279-296.
Davey, G. C. L. (1994). Pathological worry as exacerbated problem solving. In G. C. L. Davey & F. Tallis (Eds.), Worrying, perspectives on theory, assessment and treatment (pp. 35-59). Chichester, UK: Wiley.
Davey, G, C. L., Tallis, F., & Capuzzo, N. (1996). Beliefs about the consequences of worrying. Cognitive Therapy and Research, 20, 599-520.
Durham, R. C., & Allan, T. (1993). Psychological treatment of generalized anxiety disorder: A review of the clinical significance of results in outcome trials since 1980. British Journal of Psychiatry, 163, 19-26.
Durham, R. C., Murphy, T., Allan, T., Richard, K., Treliving, L. R., & Genton, G. (1994). Cog- nitive therapy, analytic psychotherapy and anxiety management training for generalized anxiety disorder. British Journal of Psychiatry, 165,315-323.
Emmelkamp, R M. G., & Aardema,A. (1999). Metacognition, specific obsessive-compulsive beliefs and obsessive-compulsive behaviour. Clinical Psychology and Psychotherapy, 6, 139-145.
Fisher, R L., & Durham, R. C. (1999). Recovery rates in generalized anxiety disorder following psychological therapy: An analysis of clinically significant change in STAI-T across out- come studies since 1990. Psychological Medicine, 29, 1425-1434.
Flavell, J. H. (1979). Metacognition and cognitive monitoring: A new area of cognitive-devel- opmental inquiry. American Psychologist, 34,906-911.
Nassif, Y. (1999). Predictors of pathological worry. Unpublished M.Phil thesis, University of Manchester, UK.
Ottaviani, R., & Beck, A. T. (1987). Cognitive aspects of panic disorders. Journal of Anxiety Disorders, 1, 15-28.
Papageorgiou, C., & Wells, A. (1999). Process and metacognitive dimensions of depressive and anxious thoughts and relationships with emotional intensity. Clinical Psychology and Psy- chotherapy, 6, 156-162.
Papageorgiou, C., & Wells, A. (2001). Positive beliefs about depressive rumination: Develop- ment and preliminary validation of a self-report scale. Behavior Therapy, 32, 13-26.
Papageorgiou, C., & Wells, A. (in press). Metacognitive beliefs about rumination in recurrent major depression. Cognitive and Behavioral Practice.
Purdon, C. (2000, July). Metacognition and the persistence of worry. Paper presented at the annual conference of the British Association of Behavioural and Cognitive Psychotherapy, Institute of Education, London, UK.
Purdon, C., & Clark, D. A. (1999). Metacognition and obsessions. Clinical Psychology and Psychotherapy, 6, 102-110.
Rachman, S., & Shafran, R. (1999). Cognitive distortions: Thought action fusion. Clinical Psy- chology and Psychotherapy, 6, 80-85.
Spitzer, R. L., Williams, J. B. W., Gibbon, M., & First, M. B. (1990). Structured Clinical Inter- view for DSM-III-R--Patient Edition (SCID-P, version 1.0). Washington, DC: American Psychiatric Press.

102 WELLS & CARTER
Wells, A. (1994a). Attention and the control of worry. In G. C. L. Davey & F. Tallis (Eds.), Wor- rying: Perspectives on theory, assessment, and treatment (pp. 91-114). Chichester, UK: Wiley.
Wells, A. (1994b). A multidimensional measure of worry: Development and preliminary valida- tion of the Anxious Thoughts Inventory. Anxiety, Stress and Coping, 6, 289-299.
Wells, A. (1995). Metacognition and worry: A cognitive model of generalized anxiety disorder. Behavioral and Cognitive Psychotherapy, 23,301-320.
Wells, A. (1997). Cognitive therapy of anxiety disorders: A practice manual and conceptual guide. Chichester, UK: Wiley.
Wells, A. (1999). A metacognitive model and therapy of generalized anxiety disorder. Clinical Psychology and Psychotherapy, 6, 86-95.
Wells, A. (2000). Emotional disorders and metacognition: Innovative cognitive therapy. Chich- ester, UK: Wiley.
Wells, A., & Carter, K. (1999). Preliminary tests of a cognitive model of generalized anxiety disorder. Behavior Research and Therapy, 37, 585-594.
Wells, A., & Matthews, G. (1994). Attention and emotion: A clinical perspective. Hove, UK: Lawrence Erlbaum.
Wells, A., & Matthews, G. (1996). Modelling cognition in emotional disorder: The S-REF model. Behaviour Research and Therapy, 34, 881-888.
Wells, A., & Papageorgiou, C. (1995). Worry and the incubation of intrusive images following stress. Behaviour Research and Therapy, 33,579-583.
Wells, A., & Papageorgiou, C. (1998). Relationships between worry, obsessive-compulsive symptoms, and recta-cognitive beliefs. Behaviour Research and Therapy, 36, 899-913.
York, D., Borkovec, T. D., Vasey, M., & Stem, R. (1987). Effects of worry and somatic anxiety induction on thoughts, emotion and physiological activity. Behaviour Research and Ther- apy, 25,523-526.
RECEIVED: April 11, 2000 ACCEPTED: September 25, 2000
Related Documents