Fungal and Parasitic Infections Clinical and Neuroimaging Features Tomás Freddi, Laiz Laura de Godoy, Fabricio Guimaraes Goncalves, César Augusto Alves, and Prasad Hanagandi Contents Parasitic Infections ....................................................................... 2 Introduction ................................................................................ 2 Hydatid Disease (Echinococcosis) ......................................................... 3 Schistosomiasis ............................................................................ 6 Malaria ..................................................................................... 9 This publication is endorsed by: European Society of Neuroradiology (www.esnr.org). T. Freddi (*) Hcor - Hospital do Coração, São Paulo, Brazil e-mail: [email protected] L. L. de Godoy Neuroradiology Section, Hospital das Clínicas- HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, Brazil e-mail: [email protected] F. G. Goncalves Neuroradiology Department, Children’ s Hospital of Brasília, Brasília, DF, Brazil e-mail: [email protected] C. A. Alves Neuroradiology division, Children’ s Hospital of Philadelphia, Philadelphia, PA, USA e-mail: [email protected] P. Hanagandi Department of Diagnostic Imaging, Division of Pediatric Neuroradiology, Sidra Medical and Research Center, Doha, Qatar e-mail: [email protected] © Springer Nature Switzerland AG 2019 F. Barkhof et al. (eds.), Clinical Neuroradiology , https://doi.org/10.1007/978-3-319-61423-6_47-1 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Fungal and Parasitic Infections
Clinical and Neuroimaging Features
Tomás Freddi, Laiz Laura de Godoy,Fabricio Guimaraes Goncalves, César Augusto Alves, andPrasad Hanagandi
ContentsParasitic Infections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Hydatid Disease (Echinococcosis) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Schistosomiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Malaria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
This publication is endorsed by: European Society ofNeuroradiology (www.esnr.org).
T. Freddi (*)Hcor - Hospital do Coração, São Paulo, Brazile-mail: [email protected]
L. L. de GodoyNeuroradiology Section, Hospital das Clínicas-HCFMUSP, Faculdade de Medicina, Universidade de SaoPaulo, Sao Paulo, Brazile-mail: [email protected]
F. G. GoncalvesNeuroradiology Department, Children’s Hospital ofBrasília, Brasília, DF, Brazile-mail: [email protected]
C. A. AlvesNeuroradiology division, Children’s Hospital ofPhiladelphia, Philadelphia, PA, USAe-mail: [email protected]
P. HanagandiDepartment of Diagnostic Imaging, Division of PediatricNeuroradiology, Sidra Medical and Research Center,Doha, Qatare-mail: [email protected]
© Springer Nature Switzerland AG 2019F. Barkhof et al. (eds.), Clinical Neuroradiology,https://doi.org/10.1007/978-3-319-61423-6_47-1
1

Neurocysticercosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Amebiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Trypanosomiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Fungal Infections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Aspergillosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Mucormycosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26South American Blastomycosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Histoplasmosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Candidiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
AbstractParasitic and fungal infections of the centralnervous system (CNS) can cause significantmorbidity or mortality, and risk factors includeimmunodeficiency and living in endemicareas. Neuroimaging studies play a criticalrole in the diagnosis and clinical assessmentof these patients. This chapter discusses themost common patterns of magnetic resonanceimaging (MRI) found in parasitic and fungalinfections.
KeywordsParasitic · Fungal · Cysticercosis · Hydatic ·Magnetic Resonance Imaging (MRI)
List of Abbreviations3D-TOF
Three-dimensional time of flight
ADC Apparent diffusion coefficientAIDS Acquired immunodeficiency
syndromeASL Arterial spin labelCISS Constructive interference steady
stateCNS Central nervous systemCSF Cerebrospinal fluidCT Computed tomographyDCE Dynamic contrast enhancedDSC Dynamic susceptibility contrastDWI Diffusion-weighted imagingFIESTA Fast imaging employing steady-
state acquisitionFLAIR Fluid attenuation inversion recoveryHAT Human African trypanosomiasisHIV Human immunodeficiency virus
MRI Magnetic resonance imagingMRS Magnetic resonance imaging
spectroscopyNC NeurocysticercosisNECT Nifurtimox-eflornithine combina-
tion therapyPAM Primary amebic
meningoencephalitisPAM Primary amebic
meningoencephalitisSPECT Single photon emission computed
tomographySWI Susceptibility-weighted imagingWI Weighted images
Parasitic Infections
Introduction
Parasitic diseases affecting the central nervoussystem (CNS) cause significant morbidity andmortality worldwide. Cysticercosis is the mostcommon CNS parasitic infection (Carpio et al.2018). Other less frequent infections include toxo-plasmosis, echinococcosis, and schistosomiasis.Children and adults from developing countriesare the most affected subjects. Sporadic cases,however, may also occur in nonendemic areas asthe result of a boost in international travel andimmunosuppression caused by posttransplantationtherapy or by the human immunodeficiency virus(HIV) infection.
Parasites are a heterogeneous group of organ-isms that can be widely classified into single-celled organisms (i.e., protozoa) or multicellularhelminths (i.e., metazoa) (Carpio et al. 2016).
2 T. Freddi et al.

Many kinds of severe opportunistic infections inHIV patients are caused by protozoan parasites,due to its capability to multiply in theimmunosuppressed patient. Helminths have thepropensity to cause disease by physical disruptionof tissue as they migrate, provoking an intense,often eosinophilic, inflammatory response. Allparasites affecting humans might involve theCNS (Carpio et al. 2018). Parasitic infection ofthe CNS can produce a variety of symptoms andsigns, making the diagnostic challenging. Famil-iarity with the geographic origin of the patient,clinical features, serologic tests, and neuroimag-ing findings can increase the detection rate andappropriate treatment. Neuroimaging studiesplay a critical role in the diagnosis and manage-ment of these patients. MRI can accurately detectthe location and assess the extent of the parasitesand also characterize the lesion and define theamount of the surrounding parenchymal changes.CT scan, however, is better than MRI for thedetection of small calcifications (Kimura-Hayamaet al. 2010).
Hydatid Disease (Echinococcosis)
Definition of EntityThere are two major forms in human hosts:cystic echinococcosis, caused by Echinococcusgranulosus, and, less frequently, alveolar echino-coccosis, caused by Echinococcus multilocularis, amore severe and dangerous form of echinococcosis.The larval stage is the cause of hydatid disease inhumans.
Epidemiology/DemographicsCerebral hydatid disease is a rare parasitic infes-tation and accounts for 1–2% of all cystic echino-coccosis. It is a severe health problem indeveloping countries, endemic in the MiddleEast, South America, and Australia.
Pathology and PathogenesisHuman and sheep are intermediate hosts andacquire the parasite by ingesting eggs that areeliminated by the definitive hosts, especiallydogs. After being ingested, the eggs reach the
gastrointestinal tract, liberating embryos that typ-ically infest the liver and lungs, and rarely thebrain parenchyma (approximately 2–5% ofcases). Then the embryo evolves to a cystic larva(hydatid cyst).
Clinical FeaturesSymptoms of cerebral lesions result from cystenlargement when it compresses the brain tissueor intracerebral blood vessels (Walker and Zunt2005). The consequence is intracranial pressureincrease, and the patients present with headache,nausea, vomiting, and seizures. However, the cystcan cause more devastating symptoms if it rup-tures or becomes superinfected. Rarely, the lesionmay involve the dura, subarachnoid space, ven-tricular system, brainstem, and spinal canal. Sero-logical and imaging tests can suggest thediagnosis of echinococcosis.
Imaging Features
Cystic EchinococcosisNeuroimaging of hydatid disease is characterizedby well-defined oval mass in the brain tissue, oftenin the territory of the middle cerebral artery, due toits embolic nature. The cysts show attenuation andsignal intensity that resemble those of CSF and acharacteristic but not so common hypointense rimon T2WI, without contrast enhancement (Shih andKoeller 2015). The lesion is usually single andunilocular; however, the presence of multiplecysts may indicate the rupture of a preexistingsingle cyst. Sometimes, a discrete surroundinghalo of hyperintensity on T2WI can be observedand corresponds to the outermost layer of the cyst,composed of inflammatory cells and brous tissue.Eventually surrounding edema may also be pre-sent, and the absence of it may help in the differ-ential diagnosis with cerebral abscesses and alsoother infectious cysts, such as neurocysticercosis(Rocha et al. 2005).
MRI may show particulate materials within thecyst that represent daughter scolices and hydatidsand (aggregates of scolices). When the cystsrupture or infect, they change their signal patterns,with slightly decreased signal intensity at T2WIand increased signal intensity at T1WI, and there
Fungal and Parasitic Infections 3

may be discrete peripheral enhancement of thefibrous capsule. A single case report of a hydatidcyst in a human host demonstrated at MR spec-troscopy (MRS) elevated succinate, lactate, ala-nine, acetate, and pyruvate levels (Shih andKoeller 2015) (Fig. 1).
Alveolar EchinococcosisNeuroimaging findings of alveolar echinococco-sis are different from cystic echinococcosis andoften mimic brain tumor. The lesions appear likeheterogeneous solid or cystic masses with calcifi-cation at CT and corresponding T1- andT2-hypointensity. The mass is commonly associ-ated with prominent surrounding edema, and theenhancement is typically heterogeneous ring-like,nodular, and cauliflower-like. Perfusion MRimaging may demonstrate decreased relative cere-bral blood volume in the central portion of thelesion and higher relative cerebral blood volumein the periphery, a finding related to chronicinflammation. MRS of alveolar echinococcosisin an animal model presented a similar pattern
compared with cystic echinococcosis describedabove. Other investigators have demonstratednormal N-acetylaspartate-to-creatine and choline-to-creatine ratios, finding that can help distinguishthese lesions from neoplasms. Although the pres-ence of multicystic liver disease also contributesto the diagnosis (Rocha et al. 2005) (Fig. 2).
Interpretation Checklist• Hydatid disease of the CNS is rare and should be
suspected in patients with intraparenchymal cys-tic lesion with positive epidemiologicaldata.
• Cysts are usually isointense to CSF on MRI.• Presence of a hypointense rim on T2WI,
daughter cysts, and hydatid sand support thediagnosis.
• Alveolar echinococcosis is a more serious anddangerous form and lesions may have acauliflower-like appearance with typicalperipheral nodular enhancement associatedwith prominent surrounding edema.
Fig. 1 A 42-year-old male presented with headache.Leucocyte counts showed an increase of eosinophil.(a–d) Axial and coronal T2WI and FLAIR images showa single lesion in the left centrum semiovale with hyper-intense signal containing septation and mild mass effect.
(e) Axial T1WI shows the same lesion with a hypointensesignal similar to CSF. (f, g) Axial and sagittal postcontrastT1WI shows no enhancement. (h) DWI does not demon-strate restricted diffusion
4 T. Freddi et al.
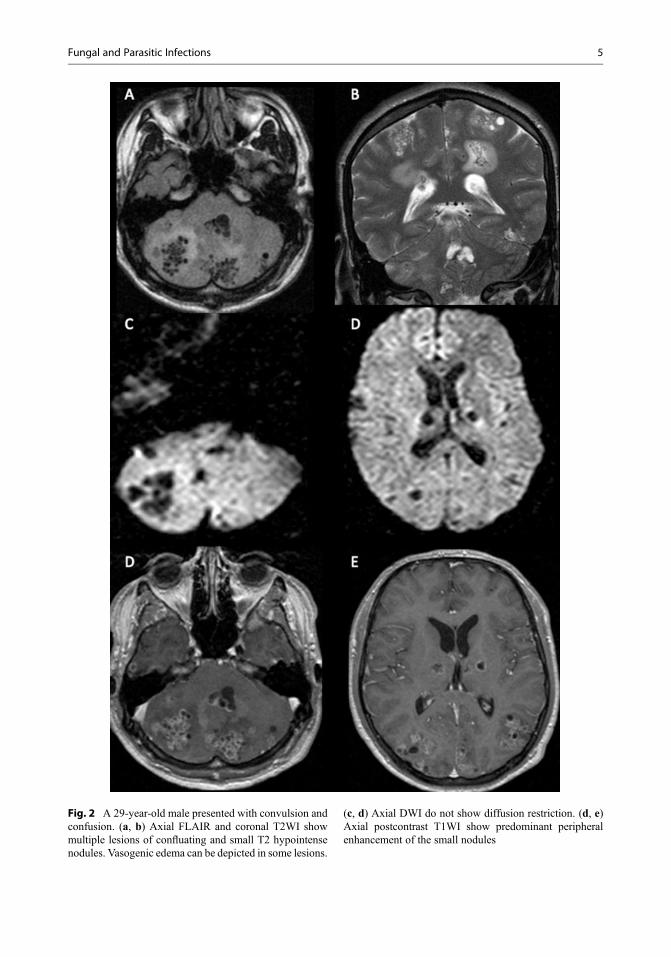
Fig. 2 A 29-year-old male presented with convulsion andconfusion. (a, b) Axial FLAIR and coronal T2WI showmultiple lesions of confluating and small T2 hypointensenodules. Vasogenic edema can be depicted in some lesions.
(c, d) Axial DWI do not show diffusion restriction. (d, e)Axial postcontrast T1WI show predominant peripheralenhancement of the small nodules
Fungal and Parasitic Infections 5
TreatmentSurgery is the most effective treatment forechinococcal infection, since preserving the integ-rity of their walls to prevent anaphylactic reactions.Clinical treatment with anthelmintic therapy hasbeen described to be effective, although experienceis limited, with some reports of exacerbation ofsymptoms related to intracranial hypertension dueto the local inflammatory reaction.
Clinical Case and Sample ReportPatient history: 42-year-old male patient pre-senting with headache. Immigrant from CentralAmerica.
Clinical diagnosis: Cerebral infection –Hyda-tid disease.
Purpose of MRI study: To scrutinize possibleinfection lesions in the CNS and rule outfocalbrainmass.
Imaging technique: Axial FLAIR, T1WI,T2WI, postcontrast T1WI, DWI, and SWI.
Full findings: A and B. Axial and coronalT2WI and C. Axial FLAIR show a single lesionin the right parietal lobe with signal intensity thatresembles those of CSF containing septation andmoderate mass effect. D, E, and F. Axial, sagittal,and coronal T1WI postcontrast show no enhance-ment. G. DWI does not demonstrate restricteddiffusion.
Interpretation: Intraparenchymal cysticlesion isointense to CSF without surroundingvasogenic edema or contrast enhancement, in apatient from a high risk zone raised the hypothesisof hydatic cyst (Fig. 3).
Schistosomiasis
Definition of EntityThe most remarkable species of Schistosomaresponsible for human disease are Schistosomamansoni and Schistosoma haematobium, almostalways associated with spinal infection, and
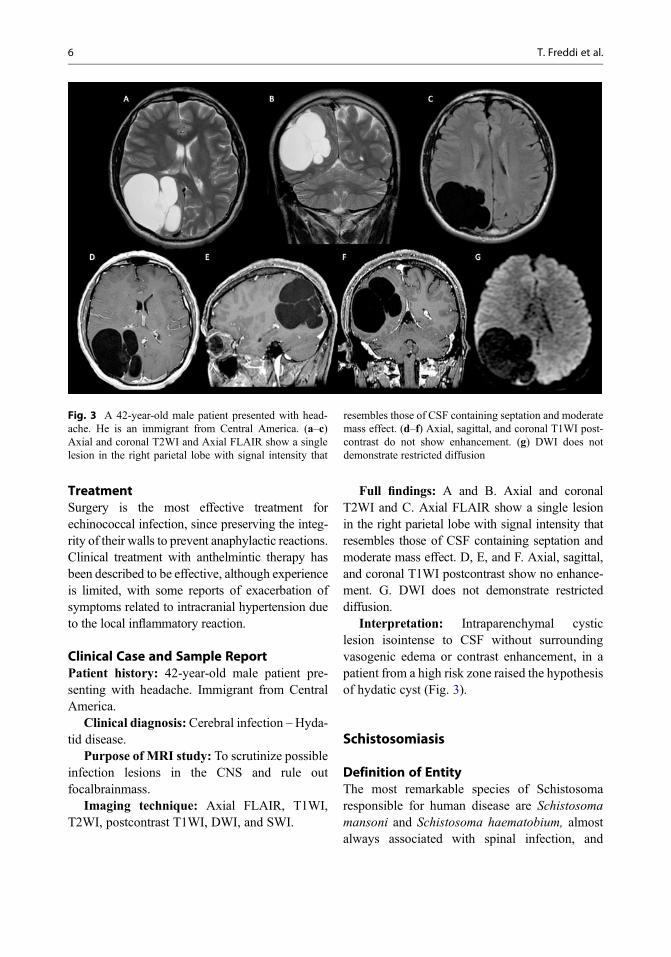
Fig. 3 A 42-year-old male patient presented with head-ache. He is an immigrant from Central America. (a–c)Axial and coronal T2WI and Axial FLAIR show a singlelesion in the right parietal lobe with signal intensity that
resembles those of CSF containing septation and moderatemass effect. (d–f) Axial, sagittal, and coronal T1WI post-contrast do not show enhancement. (g) DWI does notdemonstrate restricted diffusion
6 T. Freddi et al.

Schistosoma japonicum typically related to braininfection (Walker and Zunt 2005).
Epidemiology/DemographicsSchistosomiasis is a serious public health problemin developing countries, especially in tropical andsubtropical areas estimated to affect more than200 million persons in Africa, Asia, and theAmericas (Shih and Koeller 2015).
Pathology and PathogenesisSpecific snails carry the larvae (cercariae) in fresh-water and infect human penetrating the skin. Afterunfolding, the juvenile worms spread into thecirculatory system. It is believed that the eggsreach the CNS through the retrograde arterial orvenous blood flow or by anomalous migration ofadult worms, possibly through the vertebralvenous (Batson) plexus. The type of schistosomedetermines the final chronic organ-specific stageand is characterized by a granulomatous reactionand a host immune response (Walker and Zunt2005).
Clinical Features
Cerebral SchistosomiasisPatients with cerebral schistosomiasis are com-monly asymptomatic and may present with signssecondary to mass effect, such as headache, sei-zures, papilledema, and visual and oral distur-bances. The symptoms may vary from a fewweeks to over 1 year, depending on the locationand increased intracranial pressure. Cerebralinvolvement is caused by granuloma formationaround the eggs in the brain parenchyma andleptomeninges.
Spinal SchistosomiasisThe types of pathologic processes involved deter-mine the clinical findings: myelitic, granuloma-tous, radicular, and vascular. In practice, themajority of patients manifest with cord and radic-ular disease. Acute or subacute transverse myelitispresents with lumbalgia, muscular weakness, ves-ical dysfunction, and motor and sensory distur-bances. Focal granulomas determine symptomsrelated to spinal cord compression; symptoms of
vascular disease can be due to anterior spinalartery syndrome (a rare complication).
The clinical findings are not specific, but mustbe considered in patients with relevant epidemio-logical background. The remarkable clinical char-acteristic is the location in medullary cone orcauda equina related to granulomatous involve-ment; it can be explained by free anastomosisbetween the pelvic veins and vertebral venousplexus. It is characterized by rapid clinical pro-gression and overlap of medullary and radicularinvolvement.
Imaging Features
Cranial SchistosomiasisNeuroimaging findings are variable and non-specific. Brain CT often shows single or multiplehyperdense lesions surrounded by edema withvariable contrast enhancement that reflect a focalgranulomatous reaction in the cerebellum, cere-bral hemispheres, thalamus, or dura. MRI presentswith one or more foci of hypointense on T1 andhyperintense on T2WI. A linear enhancement,surrounded by multiple nodular tree-likepunctiform foci has been reported as “arborized”enhancement pattern (Rocha et al. 2005).Although this pattern is not always observed,when present in patients coming from endemicareas it justifies a proper treatment, even withouta biopsy.
Spinal SchistosomiasisSpinal cord involvement shows hyperintensity onT2WI with varying degrees of expansion of themedullary cone and irregular thickness of theroots. Enhancing pattern is characterized by het-erogeneous enhancement with a micronodularand multifocal converging aspect (Saleem et al.2005). CSF and blood analysis usually showeosinophilia and intrathecal specific antibodies.Identification of the Schistosoma is not commonand occurs in only about one-quarter of thepatients with myelopathy (Fig. 4).
Fungal and Parasitic Infections 7

Interpretation Checklist• Schistosomiasis is endemic in developing
countries, with the spinal form being morecommon.
• Diagnosis should always be suspected inpatients from endemic areas with long-standing cauda equina syndrome.
• Typical MRI findings are abnormal signalintensity with micronodular contrast enhance-ment of the medullary cone.
• Brain MRI may show a linear nodular tree-like“arborized” enhancement pattern.
TreatmentPraziquantel is used with good effectivenessagainst all Schistosoma spp. However, patientswho continue to shed eggs in feces should beretreated and if it is ineffective, oxamniquinemay be used. Steroids are recommended forpatients with edematous lesions or rapidly
progressive neurological deficits. Surgical proce-dure is the best choice when large granulomas arepresent.
Clinical Case and Sample ReportPatient history: A 15-year-old male patient withlow back pain and muscular weakness in the lowerlimbs for 7 months. History of swimming in freshwater contaminated with Schistosoma mansoni.CSF analysis demonstrated hypereosinophilia.
Clinical diagnosis: Spinal cord infection-Schistosomiasis.
Purpose of MRI study: Clarify neurologicmanifestations.
Imaging technique: MRI of lumbar spine,sagittal T1WI, T2WI, T2WI fat sat. Axial T2WI.Sagittal and axial postcontrast T1WI.
Full findings: A and B. Sagittal T2WI revealpatchy hyperintense lesions with mass effect in theconus medullaris of the spinal cord. C. Sagittal
Fig. 4 A 23-year-old female patient presented with head-ache and partial complex seizures, who has a history of arecent trip to South America. (a) Axial FLAIR showingsubcortical white matter edema in the right opercularregion. (b–d) Axial postcontrast T1WI demonstrates
multiple “punctate,” “spotty,” and “nodular” enhancinglesions. (e) DWI does not show restricted diffusion. (f, g)The patient was submitted to a biopsy that showed granu-loma with Schistosoma ova
8 T. Freddi et al.

T1WI postcontrast shows heterogeneous enhance-ment with a multinodular converging aspect (whitearrows). D. Axial T1WI postcontrast showsenhancement and thickening of the nerve roots.
Interpretation: Multinodular contrastenhancement of the caudal segment of the spinalcord is highly suggestive of spinal schistosomiasis(Fig. 5).
Malaria
Definition of EntityMalaria is considered a multisystem disease, withhepatic dysfunction, thrombocytopenia, andcoagulopathies. Four species of Plasmodiummay cause a systemic infection: P. Falciparum,P. vivax, P. malariae, and P. ovale and the first twoagents (P. Falciparum, P. vivax) are responsiblefor almost all cases.
Epidemiology/DemographicsMalaria is reported as the most important andcommon parasitic disease worldwide. It affectsprimarily sub-Saharan Africa children, where thedisease is endemic, and also Asian and SouthAmerican adults. The vast majority (>90%) ofcases occur in children younger than 5 years old.However, it was observed an increasing numberof cases in Europe and North America, particu-larly into the subgroup of travelers who visitedendemic tropical countries.
Pathology and PathogenesisThe infection is transmitted to the man through thebite of the infected female Anopheles mosquito.The incubation period ranges from 1 to 3 weeks;thus, some individuals will only develop the dis-ease when they reach their own countries. Cere-bral Malaria can be demonstrated through thesequestration of infected erythrocytes in themicrocirculation, particularly compromising
Fig. 5 A 15-year-old male patient presented with lowback pain and muscular weakness in the lower limbs for7 months. CSF analysis demonstrated hypereosinophilia.(a, b) Sagittal T2WI reveals patchy hyperintense lesionswith mass effect in the conus medullaris. (c) Sagittal T1WI
postcontrast shows heterogeneous enhancement with amultinodular converging aspect (white arrows). (d) AxialT1WI postcontrast shows enhancement and thickening ofthe nerve roots
Fungal and Parasitic Infections 9

cortical and perforating arterial branches, leadingto perivascular hemorrhage and white matternecrosis. Cerebral malaria is a lethal complicationexpressly caused by Plasmodium falciparum,occurring in 2% of infected patients.
Clinical FeaturesThe most common clinical features are epilepsyand encephalopathy evolving with coma. Themortality rate ranges among of 15%–25%.
Imaging FeaturesNeuroimaging is often not performed in thesecases because of the severity and rapid evolutionof these patients. Brain CT has low sensitivity andit is badly correlated to the degree of parasitemia.Increased brain volume and brain swelling inpatients with cerebral malaria have been describedand can be attributed to a growth in the volume ofintracerebral blood related to sequestration of par-asitized erythrocytes and compensatory vasodila-tion, rather than by edema (Rasalkar et al. 2011).
MRI can also show cortical infarcts or whitematter lesions, represented by hyperintense onT2WI that are usually multifocal. MRI can dem-onstrate the involvement of the thalamus andbasal ganglia as a consequence of encephalitis,disclosing typical features of hemorrhagic infarc-tions (Rasalkar et al. 2011). Besides, a classicalpattern of multifocal petechial hemorrhage at
subcortical and periventricular white matter canbe found at susceptibility sequences. Further-more, acute hemorrhagic infarctions are alsoencountered in the brainstem, cerebellum, andhippocampus (Fig. 6).
Bilateral thalamic hemorrhages are due to acritical reduction in cerebral perfusion pressure,hypoglycemia, and widespread blockage of smallvessels by the parasitized erythrocytes and anemia.
Interpretation Checklist• Cerebral malaria should be suspected in
patients with positive epidemiological historyand brain MRI demonstrating thalamicinvolvement or subcortical multifocal pete-chial hemorrhage.
TreatmentAntimalarial drugs are the only interventions thatcertainly reduce mortality in patients with malaria.The cinchoids (quinine and quinidine) andartemisinin compounds are most commonlyused, and artemisinins are becoming the drugs ofchoice, particularly for the treatment of severemalaria. A loading dose is recommended toenable parasiticidal levels to be achieved rapidly.Both the cinchoids and artemisinins are usuallycombined with other antimalarial drugs to shortenthe duration of therapy (in the case of quinine) andprevent resistance.
Fig. 6 A 25-year-old male patient presented with episodesof high-grade fever and abnormal behavior after visitingAmazon rainforest (Brazil). Peripheral blood smear shows
malarial parasites. (a–c) Bilateral thalamic hemorrhagesare noted on axial FLAIR, axial T1WI, and coronal gradi-ent echo WI images, respectively
10 T. Freddi et al.

Clinical Case and Sample ReportPatient history: 18-year-old male patient withepisodes of high-grade fever and epilepsy. Periph-eral blood smear shows malarial parasites. Patientfrom sub-Saharan Africa.
Clinical diagnosis: Cerebral infection –Malaria.
Purpose of MRI study: To scrutinize possibleinfection lesions in the CNS and rule out structurallesion that could be associated with epilepsy.
Imaging technique: Axial FLAIR, T1WI,T2WI, postcontrast T1WI, DWI, SWI, andgradient-echo WI.
Full findings: A and B. SWI-WI show diffuseand extensive linear and punctate foci of T2WI
shortening in the central deep white matter andsubcortical regions. C and D. The imaging find-ings are better seen on the SWI as compared togradient echo sequence. E. SPECT shows hypo-metabolism in both cerebral hemispheres.
Interpretation: Diffuse petechial hemorrhageoccurs when infected erythrocytes occlude cere-bral capillaries and small veins. Although themortality rate of cerebral malaria has been esti-mated between 20% and 50%, those patients whosurvive often have a full recovery with no long-term sequelae (Fig. 7).
Fig. 7 An 18-year-old male patient presented with epi-sodes of high-grade fever and epilepsy. Peripheral bloodsmear shows malarial parasites. (a, b) SWI-WI showsdiffuse and extensive linear and punctate foci of T2WI
shortening in the central deep white matter and subcorticalregions. (c, d) The imaging findings are better seen on theSWI as compared to gradient echo sequence. (e) SPECTshows hypometabolism in both cerebral hemispheres
Fungal and Parasitic Infections 11
Neurocysticercosis
Definition of EntityNeurocysticercosis (NC) is a parasitic infection ofthe central nervous system (CNS) caused by thelarval phase of tapeworm Taenia solium. It is themost common worldwide parasitic diseaseinvolving the CNS with substantial socioeco-nomic impact (Carpio et al. 2018).
Epidemiology/DemographicsNC affects both immunosuppressed and immuno-competent individuals and is endemic in LatinAmerican, African, and Asian countries. Withrecent trends in mass global migration, there isan increasing incidence in developed countries.Approximately more than 50% of infected peopleremain asymptomatic in underprivileged nations.Due to financial paucity to conduct elaborateresearch in underdeveloped countries, NC stillremains a neglected disease and its real prevalenceis hard to ascertain.
Pathology and PathogenesisHumans are the definitive host of Taenia solium.The adult worm (solitary) is located in the intes-tine and discharges the mature proglottidcontaining embryonated eggs (embryophytes)into the feces. The eggs are ingested by the inter-mediate host (pig). The embryos (oncospheres)penetrate the gastric mucosa and enter the blood-stream and migrate to distant tissues where theydevelop into cysticerci. Ingestion of undercookedcontaminated pork or water leads to the develop-ment of tapeworm in the human intestine, therebycompleting the cycle. Humans can be the interme-diate host when Taenia solium eggs are acciden-tally ingested and gain access to the systemiccirculation through gastric mucosa. The embryosare disseminated throughout the body tissues andevolve into the larval forms within organs thatprovide a favorable microenvironment especiallythe CNS being most common.
NC infection can be distinctly divided intoparenchymal, extraparenchymal, and mixedforms (Carpio et al. 2018). Parenchymal locationis defined as infection of the brain substance orcord and extraparenchymal location is an
infection of ventricular system or subarachnoidspaces. Although some authors believe that theparenchymal form is actually subarachnoid space,located in deep sulci or in perforating branches ofperivascular spaces (Kimura-Hayama et al. 2010).However, this type is still considered a separateand distinct form of neurocysticercosis, mainlybecause of the relatively easier treatment and bet-ter prognosis.
Clinical FeaturesParenchymal and extraparenchymal forms differin clinical presentation and imaging findings.Clinical manifestations of parenchymal NC areoften related to inflammation and include sei-zures, headache, motor deficits, and cognitiveimpairment. Seizures are the most common symp-toms and usually do not progress to epilepsy.Extraparenchymal NC symptoms are more fre-quently related to the mass effect due to parasiticobstruction of CSF drainage pathways and maypresent with intracranial hypertension, cranialnerve abnormalities, meningitis, and hydrocepha-lus (Carpio et al. 2018).
Imaging FeaturesThe pathophysiology of parenchymal form is betterunderstood, and the imaging findings reflectanatomical-pathological evolution and are broadlydivided into vesicular, colloidal, granular-nodularand calcified stages (Carpio et al. 2018).
Standard MRI protocol should include T2WIand FLAIR, gradient echo or susceptibilityweighted imaging, DWI, T1 postcontrastsequences and if available, heavily T2WI multi-planar sequences (i.e., FIESTA, CISS,BALANCE).
The vesicular stage is usually asymptomaticdue to minimal or no inflammatory reaction inthe parenchyma. Imaging demonstrates a cystwith an eccentric scolex and minimal or absentcontrast enhancement (Hanagandi et al. 2015;Venkat et al. 2016). Cysts are hypodense on com-puted tomography (CT) and usually isointense tocerebrospinal fluid (CSF) on magnetic resonance(MR) sequences; scolex may characteristicallyshow restricted diffusion on diffusion-weightedimages (DWI) or eventually show a blooming on
12 T. Freddi et al.

gradient echo or SWI sequences. Heavily T2WIthree-dimensional multiplanar sequences can bet-ter demonstrate the cyst morphology and the sco-lex (Del brutto et al. 2017) (Fig. 8).
In the colloidal stage, the scolex begins todegenerate with resultant thickening of the cystwall and thereby inciting significant inflammatoryreaction (Venkat et al. 2016). On imaging, the cysthas a distinct density or signal intensity to CSFwith a thin peripheral rim of enhancement associ-ated with perilesional vasogenic edema in thesurrounding parenchyma (Hanagandi et al. 2015)(Fig. 9).
The granular-nodular stage is characterizedby partial involution of inflammatory reactionwith a granulomatous nodule that usually hashypointense signal on T2WI and may show ringor solid enhancement with resolving perilesionalvasogenic edema (Venkat et al. 2016). In the last
stage, there is scarring and complete resolution ofedema with evolution into a calcified granuloma(Hanagandi et al. 2015) (Fig. 10).
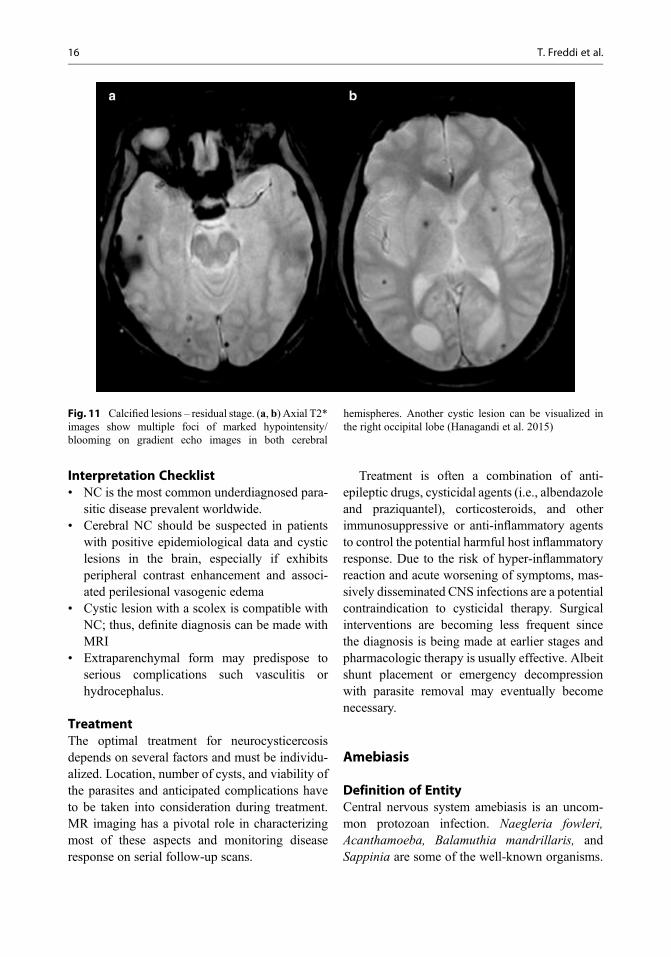
Calcified lesions are better detected by CT butcan be seen as hypointense foci on T2WI andespecially on gradient-echo- SWI sequences(Venkat et al. 2016). A thin rim of contrastenhancement may be evident but does not neces-sarily reflect active inflammation (Fig. 11).
Reactivation may be characterized when peri-lesional edema appears around a calcified lesionand can be associated with contrast enhancement.Several theories have been proposed, the mostwidely accepted being the calcified lesion stillcontains antigens that are somehow inaccessibleto the immune system and trigger a delayedinflammatory reaction (Fig. 12).
Atypical parenchymal presentations can beseen as pseudotumoral and miliary forms.
Fig. 8 Vesicular stage. (a–c) Axial T2WI and FLAIRimages show a single cystic lesion located in the leftopercular region, isointense to CS. (d) Axial DWI imageshows an eccentric scolex inside of the lesion with
restricted diffusion. (e) Axial T2* image demonstrateshypointense dot of the scolex. (f) Axial T1 postcontrastimage reveals mild peripheral enhancement
Fungal and Parasitic Infections 13
Pseudotumoral form presents as a single lesionwith multicystic appearance, variable contrastuptake, and perilesional edema, thereby mimick-ing brain tumors (Fig. 13).
Milliary form represents massive cysticercusinfestation of the CNS and is characterized bymultiple small cystic lesions disseminatedthroughout the brain parenchyma and at timescan be difficult to differentiate from metastaticlesions (Rocha et al. 2005).
MR Spectroscopy through the region of inter-est can demonstrate decreased N-acetylaspartateand creatine peaks and elevated choline peak. Inaddition, other notable peaks that can be appreci-ated are lactate, pyruvate, succinate, acetate, andamino acids like alanine and threonine. The pres-ence of succinate alone or increased levels of bothsuccinate and acetate indicates the probability ofdegenerating cysticerci. Perfusion techniquessuch as dynamic susceptibility-contrast (DSC),dynamic contrast-enhanced (DCE), and arterialspin label (ASL) usually demonstrate normal ordecreased values in and around NC and therebyhelp to differentiate them from tumoral patholo-gies. The extraparenchymal disease varies in itssymptoms and the prognosis depending on thelocation of parasites. It also considerably differs
from the parenchymal form by the absence ofestablished temporal degenerative changes. Theextraparenchymal form is characterized by cysticlesions with scolex or the racemose form and iswidely distributed in the subarachnoid spaceand/or the ventricular system.
Racemose NC appear as a cluster of cysts with-out scolex and usually located in suprasellar,sylvian, perimesencephalic, and other basal cis-terns. They resemble a bunch of grapes, with orwithout contrast uptake and can causeventriculitis and obstructive hydrocephalus(Hanagandi et al. 2015) (Fig. 14).
The fourth ventricle is the most common loca-tion for intraventricular cysticercosis and is pre-sumably due to gravity and CSF flow patterns.Although clinically silent this type can be poten-tially lethal due to higher risk of acute obstructivehydrocephalus, basal meningitis, and herniationsecondary to mass effect. Cysts and the scolexare better visualized on MR and may demonstrateenhancement. At times, the mobile intraventricu-lar cyst can cause intermittent or positional CSFobstruction leading to acute and transient increasein intracranial pressure with relapsing/remittingsymptoms. This phenomenon is called Bruns’
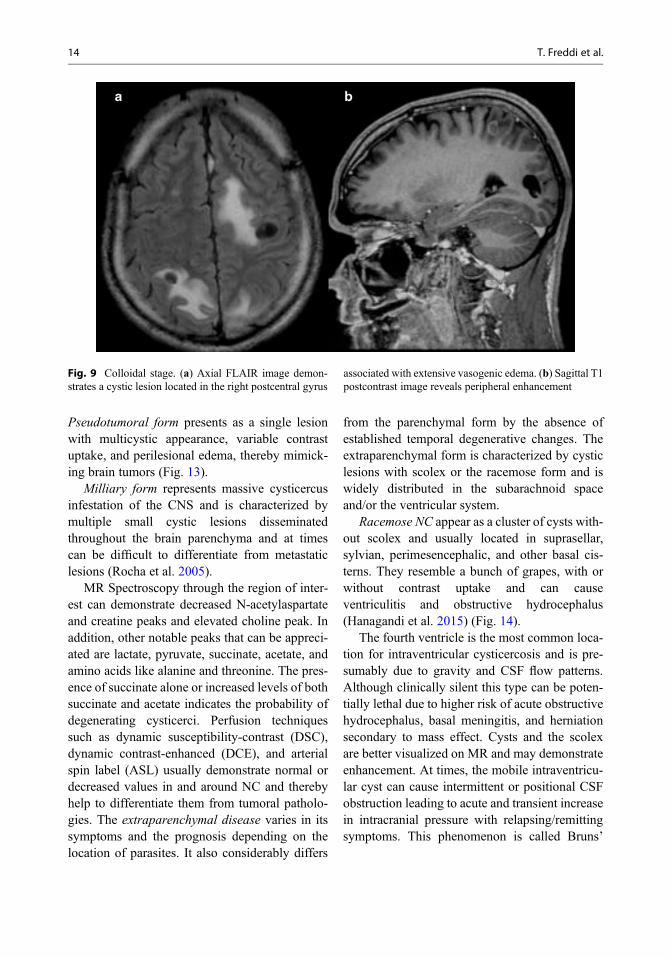
Fig. 9 Colloidal stage. (a) Axial FLAIR image demon-strates a cystic lesion located in the right postcentral gyrus
associated with extensive vasogenic edema. (b) Sagittal T1postcontrast image reveals peripheral enhancement
14 T. Freddi et al.

syndrome and is triggered by abrupt movement ofthe head.
Chronic meningitis and/or ventriculitis arelongstanding processes possibly due to leakageof cysticercus antigens into the CSF and mayresult in communicating hydrocephalus withenhancement of the basal cisterns and enlargedventricles (Fig. 15).
Vasculitis is a well-known complication of NCand must be suspected when segmentalnarrowing, beaded appearance, or abrupt vascularobstruction is depicted at three-dimensional time-
of-flight (3D-TOF) MR angiography. Vessel wallMR imaging usually demonstrates a concentricpattern of wall enhancement giving a “tramtrack” appearance. Arteritis can be seen in up to53% of patients with subarachnoid neurocysti-cercosis. It can also be observed in asymptomaticpatients and commonly involves posterior andmiddle cerebral arteries. Multivessel involvementaffects nearly 50% of cases and infarction associ-ated with arteritis is seen in about 10% (Fig. 16).
Fig. 10 Granular nodular stage. (a–c) Axial FLAIR,T2WI, and T2WI* images demonstrate a granulomatousnodule in the right precuneus, with hypointense signal on
all sequences. (d) Sagittal T1 postcontrast image revealsmild peripheral enhancement
Fungal and Parasitic Infections 15
Interpretation Checklist• NC is the most common underdiagnosed para-
sitic disease prevalent worldwide.• Cerebral NC should be suspected in patients
with positive epidemiological data and cysticlesions in the brain, especially if exhibitsperipheral contrast enhancement and associ-ated perilesional vasogenic edema
• Cystic lesion with a scolex is compatible withNC; thus, definite diagnosis can be made withMRI
• Extraparenchymal form may predispose toserious complications such vasculitis orhydrocephalus.
TreatmentThe optimal treatment for neurocysticercosisdepends on several factors and must be individu-alized. Location, number of cysts, and viability ofthe parasites and anticipated complications haveto be taken into consideration during treatment.MR imaging has a pivotal role in characterizingmost of these aspects and monitoring diseaseresponse on serial follow-up scans.
Treatment is often a combination of anti-epileptic drugs, cysticidal agents (i.e., albendazoleand praziquantel), corticosteroids, and otherimmunosuppressive or anti-inflammatory agentsto control the potential harmful host inflammatoryresponse. Due to the risk of hyper-inflammatoryreaction and acute worsening of symptoms, mas-sively disseminated CNS infections are a potentialcontraindication to cysticidal therapy. Surgicalinterventions are becoming less frequent sincethe diagnosis is being made at earlier stages andpharmacologic therapy is usually effective. Albeitshunt placement or emergency decompressionwith parasite removal may eventually becomenecessary.
Amebiasis
Definition of EntityCentral nervous system amebiasis is an uncom-mon protozoan infection. Naegleria fowleri,Acanthamoeba, Balamuthia mandrillaris, andSappinia are some of the well-known organisms.
Fig. 11 Calcified lesions – residual stage. (a, b) Axial T2*images show multiple foci of marked hypointensity/blooming on gradient echo images in both cerebral
hemispheres. Another cystic lesion can be visualized inthe right occipital lobe (Hanagandi et al. 2015)
16 T. Freddi et al.

On the contrary, Entamoeba histolytica rarely pre-sents with neurological complications.
Epidemiology/DemographicsIt has a reported incidence of 0.7–0.8% and isoften noted in patients during second to fourthdecade of life with male preponderance.
Pathology and PathogenesisCNS amebiasis manifests as granulomatousamebic encephalitis and primary amebicmeningoencephalitis.
Primary Amebic Meningoencephalitis (PAM)Primary amebic meningoencephalitis is an acuteonset (usually 48–72 h) and rapidly progressivefulminant infection caused by Naegleria fowleri. Itis common in nonimmunocompromised patientslike children and young adults. Naegleria fowleri
is a thermophilic organism and relatively ubiquitousand found in stagnant swimming pools, dust, or soilespecially during warm weather and CNS infectionoccurring through the olfactory epithelium (AbdelRasek et al. 2011). The brain pathologic changes aredue to sequelae of direct invasion of the paren-chyma, meninges, subarachnoid space, and bloodvessels. Histopathology demonstrates areas ofnecrosis and hemorrhage in the cerebral hemi-spheres, brainstem, cerebellum, and the spinal cordwith leptomeningeal exudates.
Granulomatous Amoebic Encephalitis (GAE)Unlike primary amebic meningoencephalitis GAEis a subacute onset and chronic progressive diseasecaused by Acanthamoeba, Balamuthia man-drillaris, and Leptomyxida species. This pattern ofdisease is frequent in debilitated patients receivingchemotherapeutic agents, steroid therapy, organ
Fig. 12 Reactivation. (a–d) Axial T2WI, axial and sagit-tal FLAIR, and axial T2WI* images demonstrate a hypo-intense nodule in the left superior frontal gyrus with slight
edema associated. (e) Axial T1 postcontrast image showsperipheral enhancement
Fungal and Parasitic Infections 17
transplantation, and immunocompromised individ-uals suffering from AIDS. Contrary to Naegleriafowleri, CNS infection is secondary to skin, lowerrespiratory, and genitourinary tract colonization(Abdel Rasek et al. 2011).
Clinical Features
Primary Amebic Meningoencephalitis (PAM)The clinical symptoms can be severe headache,fever, ataxia, vomiting, diplopia/photophobia, andneck stiffness eventually progressing to comawith high mortality.
Granulomatous Amoebic Encephalitis (GAE)The clinical scenario comprises of long durationfocal neurologic deficits mimicking an intracra-nial space-occupying lesion.
Imaging Features
Primary Amebic Meningoencephalitis (PAM)The CT and MR imaging features are usuallynonspecific and merely reflect the histopathologychanges. Imaging findings may be negative dur-ing the early phase and can demonstrate brainedema, hydrocephalus, and abnormal meningealenhancement on follow-up scan. Basal gangliainfarctions are well documented in the imagingliterature and attributable to obliteration of thelenticulostriate vessels in the basal cisterns(Akgoz et al. 2012).
Granulomatous Amoebic Encephalitis (GAE)CT and MR imaging can either demonstrate multi-focal or solitary pseudotumoral pattern. The formeris characterized by granulomatous inflammatory
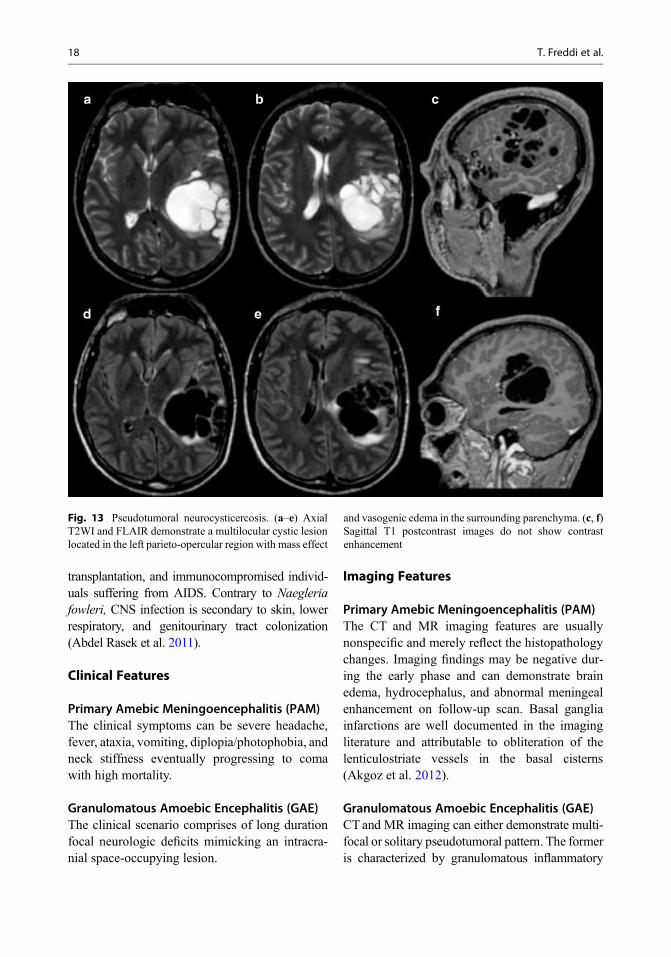
Fig. 13 Pseudotumoral neurocysticercosis. (a–e) AxialT2WI and FLAIR demonstrate a multilocular cystic lesionlocated in the left parieto-opercular region with mass effect
and vasogenic edema in the surrounding parenchyma. (c, f)Sagittal T1 postcontrast images do not show contrastenhancement
18 T. Freddi et al.

changes resulting in brain edema, necrosis withabscess formation. On MRI, heterogeneous T2WIhyperintense lesions with ring enhancing lesionsare preferentially seen involving the posteriorfossa, thalamus, and the brainstem. Hemorrhagedue to necrotizing angiitis can further complicatethe imaging features (Singh et al. 2006). Thepseudotumoral pattern demonstrates discretegyriform or linear nodular enhancement withinvolvement of the overlying meninges and under-lying corticomedullary junction and can serve as arelevant imaging clue to the diagnosis. A mixedpattern can be a dilemma and may resemble oppor-tunistic infections like toxoplasmosis, fungal gran-uloma, multiple septic emboli or can evenimpersonate neoplasms like low-grade glioma orlymphoma (Akgoz et al. 2012) (Fig. 17).
Interpretation Checklist• CNS amebiasis is rare with a few case reports
with imaging findings.
• On MRI can demonstrate multifocal nodularlesions with hemorrhage and variable contrastuptake.
TreatmentAlthough no consistently effective treatmentexists, the mainstay pharmacologic therapy isamphotericin B, rifampicin, and miconazole. Thecombined treatment with surgical removal ofgranulomatous mass lesions supports the bestchance of.
Clinical Case and Sample Report 2Patient history: 20-year-old male patient withacute onset of fever and confusion progressingto coma.
Clinical diagnosis: CNS infection.Purpose of MRI study: To evaluate structural
brain lesions that could justify the clinical picture.Imaging technique: Multiplanar FLAIR,
T1WI, T2WI, DWI, SWI, and postcontrast T1WI.
Fig. 14 Racemose form. (a–d) Sagittal T1 and axialT2WI and FLAIR images show multiple cysts withoutscolex located in suprasellar and parasellar cisterns and in
the left choroidal fissure with mass effect. (e, f) Sagittal T1postcontrast images do not show abnormal enhancement
Fungal and Parasitic Infections 19

Full findings: A and B. axial T1 and phaseimages demonstrate hemorrhagic peripherallesions in left frontal and right occipital lobes. C.Axial Flair image demonstrates signal hyper-intensity within the lesions and vasogenic edemaassociated. D and E. Axial ADC and DWI imagesreveal peripheral restricted diffusion. F. Axial T1postcontrast image shows gadoliniumenhancement.
Interpretation: Multiple hemorrhagic lesionswith peripheral restricted diffusion in associationwith encephalitis signs should raise the possibilityof amebiasis. Hemorrhagic lesions are due to nec-rotizing angiitis, a complication of the disease.Postmortem anatomopathological study con-firmed the diagnosis (Fig. 18).
Trypanosomiasis
Definition of EntityTrypanosomiasis is a parasitic infection catego-rized into two subtypes. The American trypano-somiasis commonly referred to as “Chagasdisease” and the African form also called as“sleeping sickness.”
Epidemiology/Demographics
Chagas DiseaseAmerican trypanosomiasis is a parasitic infectioncaused by Trypanosoma cruzi and is widely prev-alent in Latin American countries, especially inrural areas and in poor socio-economic statuspopulations. About 15–18 million people world-wide are affected with approximately 50,000deaths per year. The disease is transmitted by the
Fig. 15 Intraventricular neurocysticercosis. (a–c) SagittalT1, axial FLAIR, and T2WI images demonstrate a largecystic lesion with a scolex inside the IV ventricle. (d)
Coronal T2WI image depicts the marked enlargement ofIV ventricle. (e) Axial T1 postcontrast image do not showabnormal enhancement
20 T. Freddi et al.
bite of reduviid bug or by rubbing its feces onopen wounds.
Sleeping SicknessHuman African trypanosomiasis (HAT) is a flag-ellated protozoan infection caused by two differ-ent strains of Trypanosoma brucei transmitted bythe bite of tsetse fly (genus Glossina).Trypanosoma brucei gambiense is prevalent inWest Africa and the more virulent formTrypanosoma brucei rhodesiense in East Africa.The annual incidence averages 300,000 caseswith approximately 50 million population span-ning several countries being at risk across theAfrican continent. Cases detected in the westernworld are becoming common in travellers andmigrants. Recent case report regarding vertical
transmission has been documented in nonendemiccountries. Brain involvement is by haematogenousspread and dissemination across the CNS occurs byCSF seeding of choroid plexus and cerebral capil-laries (Lury and Castillo 2005).
Imaging Features
Chagas DiseaseMR imaging features typically manifest as menin-goencephalitis with focal or diffuse T1 hypo-intense, T2WI hyperintense lesions with nodularor ring pattern of enhancement. The corpuscallosum, periventricular, deep, and subcorticalwhite matter may be symmetrically involved.Likewise, intramedullary spinal cord lesions canexhibit focal or diffuse enhancing patterns.
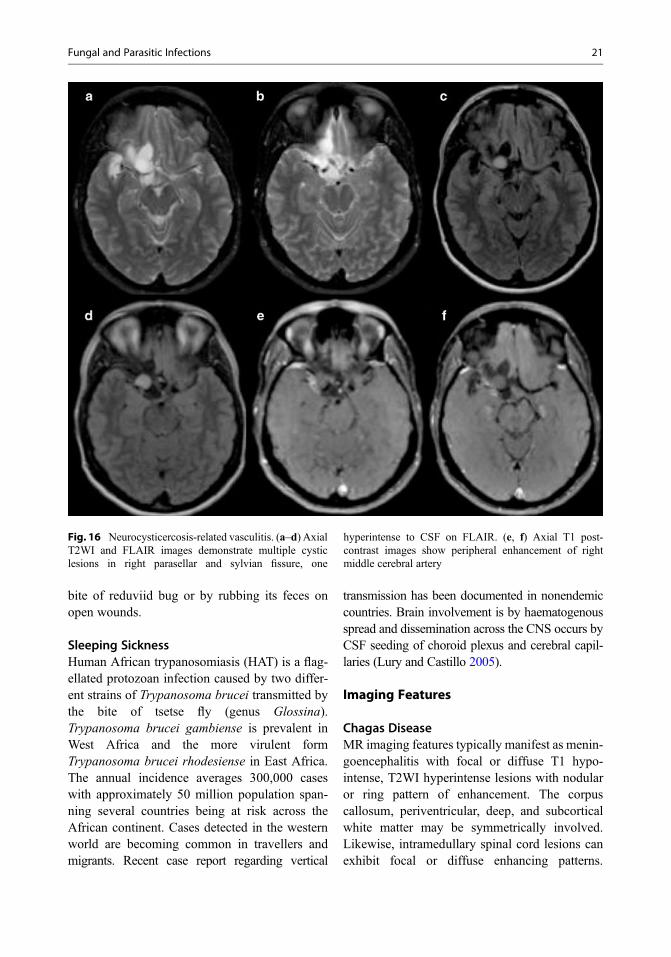
Fig. 16 Neurocysticercosis-related vasculitis. (a–d) AxialT2WI and FLAIR images demonstrate multiple cysticlesions in right parasellar and sylvian fissure, one
hyperintense to CSF on FLAIR. (e, f) Axial T1 post-contrast images show peripheral enhancement of rightmiddle cerebral artery
Fungal and Parasitic Infections 21

Necrotizing pseudotumoral or tumoral lesionscalled as “brain chagomas” can be difficult todifferentiate from toxoplasmosis or lymphoma(Razek et al. 2011). Definitive diagnosis isachieved by serology, CSF demonstration of theparasite or biopsy/autopsy.
Sleeping SicknessMRI demonstrates minimally enhancing andoften symmetrically confluent T2WI hyperintenselesions in the gray and white matter. Involvementof periventricular and subcortical white matter,corpus callosum, internal-external capsule, basalganglia, thalami, corticospinal tracts, and cerebel-lar peduncles has been elaborated in the imagingliterature. Other notable features include menin-geal thickening and enhancing perivascularspaces. The imaging findings can be misleadingas they overlap with post infectious demyelin-ation, gliomatosis, leukodystrophies, lymphoma,and tuberculosis. Residual T2WI signal
abnormalities with generalized brain atrophyensue on posttreatment follow-up (Lury andCastillo 2005).
Interpretation Checklist• CNS trypanosomiasis is rare with a few case
reports with imaging findings.• MRI findings are variable and can demonstrate
brain chagomas.
Treatment
Sleeping SicknessThe treatment of late-stage HAT is more compli-cated than is the case for an early-stage diseasebecause the drugs have a potential toxic effect forthe host. The only drug that is effective at presentfor treating late-stage T b rhodesiense is the triva-lent organic arsenical intravenously melarsoprol.An abridged 10-day course of intravenousmelarsoprol was successfully developed and thenadopted in 2005 for treatment of late-stage
Fig. 17 A 42-year-old male immunocompromised patientpresented with seizures and altered mental status, also withcutaneous erythematous nodules and ulcerations. (a, b)Axial FLAIR and T2WI show nonspecific white matterchanges. (c–g) Multiplanar T1 postcontrast images
demonstrate enhancing lesions in the left frontal corticaland subcortical areas and in the splenium of corpuscallosum (white arrows). (h) DWI does not show restricteddiffusion. Skin and brain biopsy were suggestive ofacanthameba with granulomatous meningitis
22 T. Freddi et al.

Tbgambiense and TbrhodesienseHAT. Melarsoprolis very toxic, producing a posttreatment reactiveencephalopathy in 10% of patients and half ofwhom die. A large trial showed that oral predniso-lone administration before treatment reduced bothmorbidity and death associated with melarsoprol-induced encephalopathy, but not the incidence ofother complications of melarsoprol treatment.
The standard first-line treatment for CNS-stageT b gambienseHAT is the nifurtimox–eflornithinecombination therapy (NECT), with intravenousmelarsoprol now being used as second-line treat-ment for this disease form. However, NECT isineffective against T b rhodesiense HAT.
Moreover, it can have many side-effects, such asbone marrow toxicity, alopecia, seizures, and gas-trointestinal symptoms.
Antiparasitic treatment is recommended forpatients in the acute phase. They are treated orallywith nifurtimox or with benznidazole; further-more, higher doses are recommended (up to25 mg/kg day) for patients with meningoenceph-alitis and/or myocarditis. In severe acute cases, ahigh mortality rate is reported, and combinedtherapy with corticosteroids and parasitologicaltreatment should be attempted. Side adverseeffects include gastrointestinal intolerance,
Fig. 18 A 20-year-old male patient presented with acuteonset of fever and confusion progressing to coma. (a, b)Axial T1 and phase images demonstrate hemorrhagicperipheral lesions in left frontal and right occipital lobes.(c) Axial FLAIR image demonstrates signal hyperintensity
within the lesions and vasogenic edema associated. (d, e)Axial ADC and DWI images reveal peripheral restricteddiffusion. (f) Axial T1 postcontrast image shows gadolin-ium enhancement. (Courtesy of Daniela Aguiar Dias-HCUF Ceará)
Fungal and Parasitic Infections 23
hypersensitivity, bone marrow depression, andperipheral polyneuropathy.
The parasites disappear from peripheral bloodafter the fifth day of treatment when is possible toan identified improvement of symptoms. Manage-ment with anticonvulsants, such as phenobarbital,and benzodiazepines, is indicated if seizures arepresent. Mannitol should be added when signs ofcritically elevated intracranial pressure are pre-sent. With appropriate therapy, the rate of cure inpatients with isolated central nervous systeminvolvement is nearly 50%.
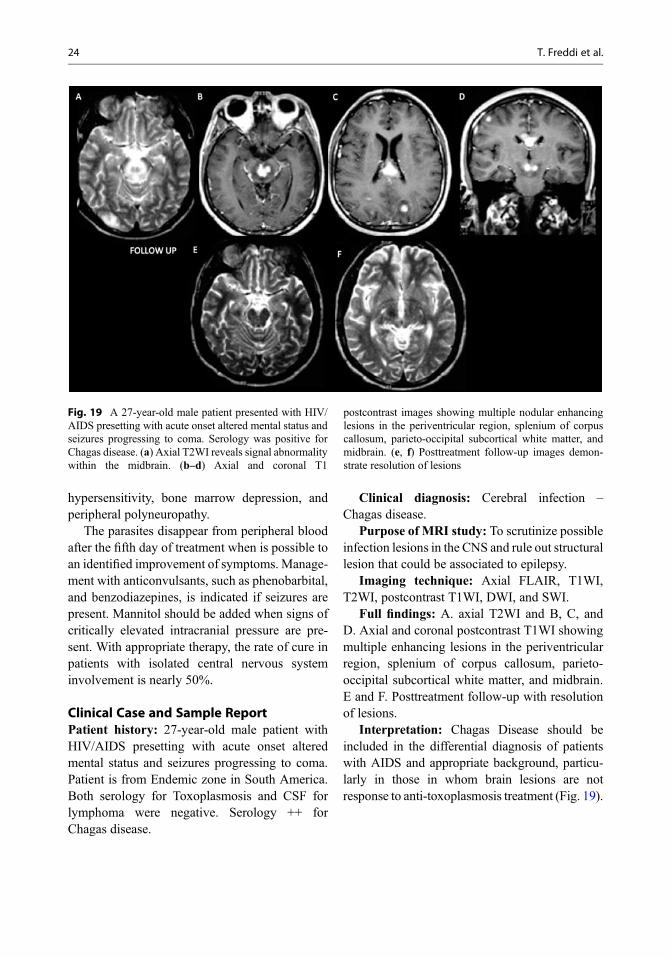
Clinical Case and Sample ReportPatient history: 27-year-old male patient withHIV/AIDS presetting with acute onset alteredmental status and seizures progressing to coma.Patient is from Endemic zone in South America.Both serology for Toxoplasmosis and CSF forlymphoma were negative. Serology ++ forChagas disease.
Clinical diagnosis: Cerebral infection –Chagas disease.
Purpose of MRI study: To scrutinize possibleinfection lesions in the CNS and rule out structurallesion that could be associated to epilepsy.
Imaging technique: Axial FLAIR, T1WI,T2WI, postcontrast T1WI, DWI, and SWI.
Full findings: A. axial T2WI and B, C, andD. Axial and coronal postcontrast T1WI showingmultiple enhancing lesions in the periventricularregion, splenium of corpus callosum, parieto-occipital subcortical white matter, and midbrain.E and F. Posttreatment follow-up with resolutionof lesions.
Interpretation: Chagas Disease should beincluded in the differential diagnosis of patientswith AIDS and appropriate background, particu-larly in those in whom brain lesions are notresponse to anti-toxoplasmosis treatment (Fig. 19).
Fig. 19 A 27-year-old male patient presented with HIV/AIDS presetting with acute onset altered mental status andseizures progressing to coma. Serology was positive forChagas disease. (a) Axial T2WI reveals signal abnormalitywithin the midbrain. (b–d) Axial and coronal T1
postcontrast images showing multiple nodular enhancinglesions in the periventricular region, splenium of corpuscallosum, parieto-occipital subcortical white matter, andmidbrain. (e, f) Posttreatment follow-up images demon-strate resolution of lesions
24 T. Freddi et al.

Fungal Infections
Abstract
Fungal infections affecting the CNS are relativelyrare and extremely threatening diseases. The twomain risk factors include any cause ofimmunocompromise and to inhabit in endemicareas. Healthy individuals can also be infected,however much less frequently.
Currently, it is possible to observe a relativelyhigh incidence of this disorder, which may beexplained by an increasing rate of mass migration,tourism, AIDS, and the use of chemotherapy andimmunosuppressive drugs. Aspergillosis, crypto-coccosis, mucormycosis, and candidiasis areamong the most common CNS fungal infections.
Morphologically, fungi are divided intohyphae or yeast types. Hyphae form multicellularcolonies of organisms that reproduce by formingspores or budding, whereas yeasts are colonies ofunicellular organisms. Furthermore, some fungimay be dimorphic, and hyphae and yeast maycoexist.
Hyphae proliferation tends to form colonies,and due to their relatively long size, they havelimited access to the microvascular system. Con-sequently, retrograde dissemination along thelarger vessels, mainly from the orbits and para-nasal sinuses, are the most common disseminationpathways. In the case of yeasts, their smaller sizein comparison with other fungi enables them topropagate with predominant involvement of themicrovasculature.
Intracranial fungal infections occur via ahaematogenous spread, CSF infection, or directextension from sinonasal disease, each route dis-closing some typical imaging features. Addition-ally, each organism has some distinctive imagingpatterns that can narrow the differential diagnosis.Parenchymal or meningeal involvement occursthrough dissemination by the walls of the vessels.Fungal infections represent a broad spectrum ofdiseases; however, some typical MRI featuresmay be observed, such as ring lesions patternwith various or reduced diffusion on DWI andsome subtle ring contrast enhancement.
Clinical signs and symptoms may be non-specific, and laboratory cultures are often nega-tive. The delayed diagnosis or inadequatetreatment of these diseases tends to evolve witha critical prognosis and commonly a fatal course.Regarding neuroimaging differential diagnosis,attention must be taken to some other diseasesthat may demonstrate some imaging similarities.Advanced MRI sequences may also corroboratethe hypothesis of fungal infection. Particularimportance must be awarded to MRS in the eval-uation of fungal abscess.
Potentially curative treatments for fungal infec-tion include administration of amphotericin B,voriconazole, or other newer agents at high enoughdoses to cross the blood-brain barrier. Eradication ofany underlying predisposing conditions and surgicaldebridement when possible and neuroimaging arealso essential to guide the efficacy of the treatmentand in the disease follow-up.
Aspergillosis
Definition of EntityAspergillus is a monomorphic abundant fungus innature, with several species found. These haveseptate branching hyphae that show dichotomousbranching, and irregular, nonparallel cell walls.The main opportunistic agents responsible foraspergillosis in humans are Aspergillus fumigatusand Aspergillus flavus.
Epidemiology/DemographicsAlthough Aspergillus infection is considered anopportunistic disease, it rarely affects the CNS ofindividuals with AIDS, due to the sparing of poly-morphonuclear cell function in these patients. Incontrast, aspergillosis is more common in condi-tions that course with neutropenia, chronic steroiduse, and in children with chronic granulomatousdisease.
Pathology and PathogenesisThe lungs and paranasal sinuses are the gatewayof these pathogens and the brain, a common sitefor hematogenous pathway dissemination. Asper-gillus species frequently strike vessels leading to
Fungal and Parasitic Infections 25

focal microhemorrhage as a consequence of ahigh-level production of elastase enzyme, whichdestroys of the internal elastic lamina of arteries(all arteries sizes are involved). Digested and con-sequently weakened walls may also facilitate theformation of a mycotic aneurysm and subarach-noid hemorrhage, which are characteristic fea-tures in aspergillosis and can be conspicuouslydemonstrated by angiography studies.
Clinical FeaturesClinical presentation is variable, which frequentlyincludes altered mental status, weakness, and sei-zures and may or not be associated to fever. Mor-tality can reach 100% if left untreated.
Imaging FeaturesAspergillus abscesses have a characteristicperipheral T2WI intermediate to low hypointensesignal and central hyperintensity, with a “target-like” appearance. Peripheral T2WI low signalprobably reflects an increased level of iron com-ponents related to fungal elements and hemor-rhage (Starkey et al. 2014). A basal ganglia,thalamus, and corpus callosum predispositioncan be noted.
DWI is a very useful tool in diagnosing fungalabscesses. Typically the center of these lesionsshow hypointense signal surrounded by a ring ofrestricted diffusion with a pattern of ring. Subtleor no enhancement of the peripheral part of thelesion “the ring” is the most common featurebeing an important diagnostic clue (Smith et al.2008). When a more evident ring enhancement ispresent, it is correlated with capsule formationfrom chronic inflammation and presence of gran-ulation tissue. Calcifications can also be presentand being better observed in susceptibilitysequences or by CT, and it is likely linked withhealing or healed granulomas, which are seenmore often in patients who survive after acuteinfection (Fig. 20).
Interpretation Checklist• Aspergillus CNS infection is commonly seen
in immunosuppressed patients.
• A brain mass with a “target-like” appearanceon T2WI and SWI with peripheral diffusionrestriction are suggestive findings.
TreatmentCNS aspergillosis is treated with intravenousvoriconazole, possibly in combination withcaspofungin or liposomal amphotericin B. Neuro-surgical procedures may also be sought in immu-nocompromised hosts, which encompasses nearlyall cases.
Clinical Case and Sample ReportPatient history: 40-year-old male patient pre-senting with a headache and hemoptysis. Historyof leukemia and neutropenia.
Clinical diagnosis: Cerebral infection –Angioinvasive aspergillosis.
Purpose of MRI study: To scrutinize possibleinfection lesions in the CNS and rule outfocalbrainmass.
Imaging technique: Axial FLAIR, T1WI,T2WI, postcontrast T1WI, DWI, and gradient-echo sequence.
Full findings: A and B. Axial CT scans shownodular hyperdense lesions in the subcorticalregions and the cerebellar hemispheres. C. AxialT2WI shows multiple hypointense lesions in thesubcortical regions with perilesional edema andmass effect. D. Gradient-echo sequence demon-strating components of hemorrhage in theselesions. E. Sagittal precontrast T1WI, and F andG. Axial postcontrast T1WI sequences showhyperintensities in the same lesionscorresponding to hemorrhage (meta-hemoglobin)without enhancement. Signs of leptomeningitiscan also be noted. H. Chest radiograph disclosingright upper lobe consolidation. I. Chest CTconfirming a right upper lobe cavitated mass(Fig. 21).
Mucormycosis
Definition of EntityMucormycosis is caused by molds from theMucor, Rhizopus, and Absidia genera. These ubiq-uitous pathogens subsist on decaying vegetation
26 T. Freddi et al.

and diverse organic material. In the proper setting,fungal spores can invade the nasal mucosa, whichare often not phagocytized due to an inadequateimmune response. Within tissue, they grow asnonseptate molds and have right-angle branchingand irregular, nonparallel cell walls. Like Asper-gillus, they are monomorphic.
Epidemiology/DemographicsMucormycosis also called as zygomycosis, ismainly associated with diabetes mellitus, intrave-nous drug abuse, and chronic alcoholism. Inimmunodeficiency, they multiply, and the sporesgerminate, forming hyphae, which become inva-sive and can disseminate. It is a deadly condition,with a mortality rate near from 100% (Palacios etal. 2014).
Pathology and PathogenesisInoculation occurs by inhalation when sporesreach the nasal cavity and/or nasopharynx. Thefungus spread primarily, by direct extension, tothe paranasal sinuses and subsequently to theorbit, through the nasolacrimal duct and medialorbital wall (Therekathu et al. 2018). They alsocan spread to the meninges, and brain, particularlyin the frontal lobes, via the orbital apex or thecribriform plate.
Mucormycosis may also disseminate through ahematogenous pathway, closely similar to that ofAspergillus. Once again, they invade the walls ofthe blood vessels resulting in vascular occlusion,thrombosis, and infarction. Spread to the brainmay occur via orbital vessels (Palacios et al.2014).
Fig. 20 A 60-year-old female patient presented withweakness in the upper and lower limbs for 2 months andfocal neurological signs for 3 weeks. The patient is immu-nocompromised due to prolonged high-dose corticosteroiduse and has a recent history of lung infection. (a, b) AxialT2WI shows multiple hypointense lesions in the
subcortical regions and the right basal ganglia (whitearrows) with perilesional edema. (c, d) Axial SWI demon-strating focal hemorrhage in these lesions. (e) Axial T1WIreveals T1-hyperintensity in the right basal gangliacorresponding to hemorrhage (meta-hemoglobin).(f) Axial postcontrast T1WI shows no enhancement
Fungal and Parasitic Infections 27

Clinical FeaturesWith CNS involvement mortality rates are greaterthan 70% and clinical manifestations includeheadache, sinusitis, fever, facial pain, numbness,unilateral periorbital cellulitis, and proptosis.When cranial neuropathy occurs, cavernoussinus thrombosis or invasion must be ruled outand, if let untreated can rapidly progress to comaor death. Laboratory studies are limited becauseMucor is rarely isolated from blood or CSF, andthere are no reliable serologic tests. Therefore,definitive diagnosis depends on tissue biopsy,but the association between orbital cellulitis andsinusitis in the context of immunosuppressionshould always raise the suspicion.
Imaging FeaturesMucormycosis neuroimaging findings have simi-lar pattern to that seen in aspergillosis. Comparedto aspergillosis, mucormycosis usually shows amore aggressive involvement of the cerebralparenchyma, characterized by areas of T2WIhyperintense signal that include vasogenic
edema and foci of annular enhancement, espe-cially in the basal ganglia and frontal lobes(Starkey et al. 2014).
Intracranial spread can be depicted on T1WIcontrast-enhanced images by meningeal thicken-ing or abnormal enhancement of skull base foram-ina and cavernous sinus (Therekathu et al. 2018).Parenchymal involvement may exhibit cerebritiswith low signal on ADC map. Nasal fossamucormycosis may characteristically showT2WI low signal of the mucosa without signifi-cant contrast enhancement, also known as theblack turbinate sign (Safder et al. 2010) (Fig. 22).
Interpretation Checklist• Mucormycosis is frequently associated to dia-
betes mellitus, intravenous drug abuse, andchronic alcoholism.
• The “black turbinate sign” is a characteristicfinding and intracranial spread should alwaysbe excluded.
Fig. 21 A 40-year-old male patient presented with aheadache and hemoptysis who has a history of leukemiaand neutropenia. (a, b) Axial CT scans show nodularhyperdense lesions in the subcortical regions and the cer-ebellar hemispheres. (c) Axial T2WI shows multiple hypo-intense lesions in the subcortical regions with perilesionaledema and mass effect. (d) Gradient-echo sequence
demonstrating components of hemorrhage in these lesions.(e–g) Sagittal precontrast T1WI and axial postcontrastT1WI images show hyperintensities in the same lesionscorresponding to hemorrhage (meta-hemoglobin) withoutenhancement. (h) Chest radiograph disclosing right upperlobe consolidation. (i) Chest CT confirming a right upperlobe cavitated mass
28 T. Freddi et al.

TreatmentManagement options include reversal of immuno-suppression, systemic amphotericin B, and surgi-cal debridement in selected cases.
South American Blastomycosis
Definition of EntitySouth American blastomycosis is a systemicmycotic infection caused by the dimorphic fungusParacoccidioides brasiliensis, which exists as amold in the environment and a yeast at bodytemperatures.
Epidemiology/DemographicsP. Brasiliensis is endemic in subtropical mountainforests, as well as, countries of Central and SouthAmerica, particularly in Brazil, Argentina,Colombia, and Venezuela. The infection is still arelevant health problem in Latin America.
Pathology and PathogenesisInfection is predominantly acquired via inhala-tion, making the lung the most common organaffected. The disease is usually chronic, oftenasymptomatic, which may mimic tuberculosis.Extrapulmonary dissemination most frequentlyinvolves the skin, bones, and the genitourinarysystem. CNS involvement is a deadly and uncom-mon complication.
Clinical FeaturesNeurological symptoms are nonspecific, withheadache being the most common presentation.Less frequently, the patients can present with focalneurological deficits, altered mental status, visionchanges, or seizures.
South American blastomycosis has beenreported as an AIDS-related opportunistic infec-tion, with lower incidence in comparison withother fungal diseases. AIDS patients tend to pre-sent the infection similarly to the subacute juve-nile form, with fast dissemination.
Fig. 22 A 38-year-old male patient presented with head-ache, chronic sinusitis, and right orbital cellulitis withproptosis with a history of type II diabetes mellitus. (a–c)Axial T2WI shows diffuse paranasal infection (maxillar,sphenoidal and ethmoidal sinusitis) extending to the orbits(red arrows), mainly on the right side. Note that the contentof bilateral sphenoid and ethmoid sinus presents with lowsignal intensity. (d) Sagittal T1WI confirms paranasal
infection (also frontal sinusitis) compromising also theright frontobasal region. (e) Axial T2WI shows signalhyperintensity within the right frontobasal region. (f, g)Axial postcontrast T1WI images show dural thickeningand no significant contrast enhancement in the rightfrontobasal region (white arrows). (h) DWI demonstratesrestricted diffusion, compatible with cerebritis
Fungal and Parasitic Infections 29
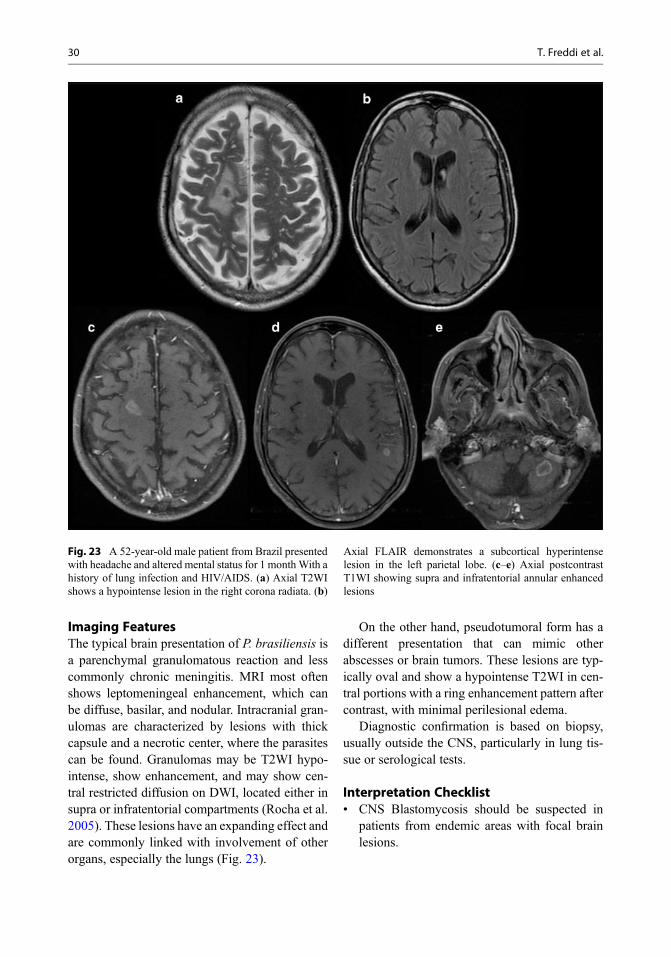
Imaging FeaturesThe typical brain presentation of P. brasiliensis isa parenchymal granulomatous reaction and lesscommonly chronic meningitis. MRI most oftenshows leptomeningeal enhancement, which canbe diffuse, basilar, and nodular. Intracranial gran-ulomas are characterized by lesions with thickcapsule and a necrotic center, where the parasitescan be found. Granulomas may be T2WI hypo-intense, show enhancement, and may show cen-tral restricted diffusion on DWI, located either insupra or infratentorial compartments (Rocha et al.2005). These lesions have an expanding effect andare commonly linked with involvement of otherorgans, especially the lungs (Fig. 23).
On the other hand, pseudotumoral form has adifferent presentation that can mimic otherabscesses or brain tumors. These lesions are typ-ically oval and show a hypointense T2WI in cen-tral portions with a ring enhancement pattern aftercontrast, with minimal perilesional edema.
Diagnostic confirmation is based on biopsy,usually outside the CNS, particularly in lung tis-sue or serological tests.
Interpretation Checklist• CNS Blastomycosis should be suspected in
patients from endemic areas with focal brainlesions.
Fig. 23 A 52-year-old male patient from Brazil presentedwith headache and altered mental status for 1 monthWith ahistory of lung infection and HIV/AIDS. (a) Axial T2WIshows a hypointense lesion in the right corona radiata. (b)
Axial FLAIR demonstrates a subcortical hyperintenselesion in the left parietal lobe. (c–e) Axial postcontrastT1WI showing supra and infratentorial annular enhancedlesions
30 T. Freddi et al.
• The granulomatous lesions usually show lowsignal on T2WI, contrast enhancement, andcentral diffusion restriction.
TreatmentThe recommended treatment for CNS blastomy-cosis is a lipid formulation of amphotericin B for4–6 weeks, followed by an oral azole, preferablyvoriconazole, for at least 1 year.
Clinical Case and Sample Report 1Patient history: 45-year-old male patient pre-senting with headache and vision changes. His-tory of lung infection and HIV/AIDS. Patientfrom South America.
Clinical diagnosis: Cerebral infection – SouthAmerican blastomycosis.
Purpose of MRI study: To rule out brainmass, in particular to exclude CNS infections.
Imaging technique: Axial FLAIR, T1WI,T2WI, postcontrast T1WI, DWI, and SWI.
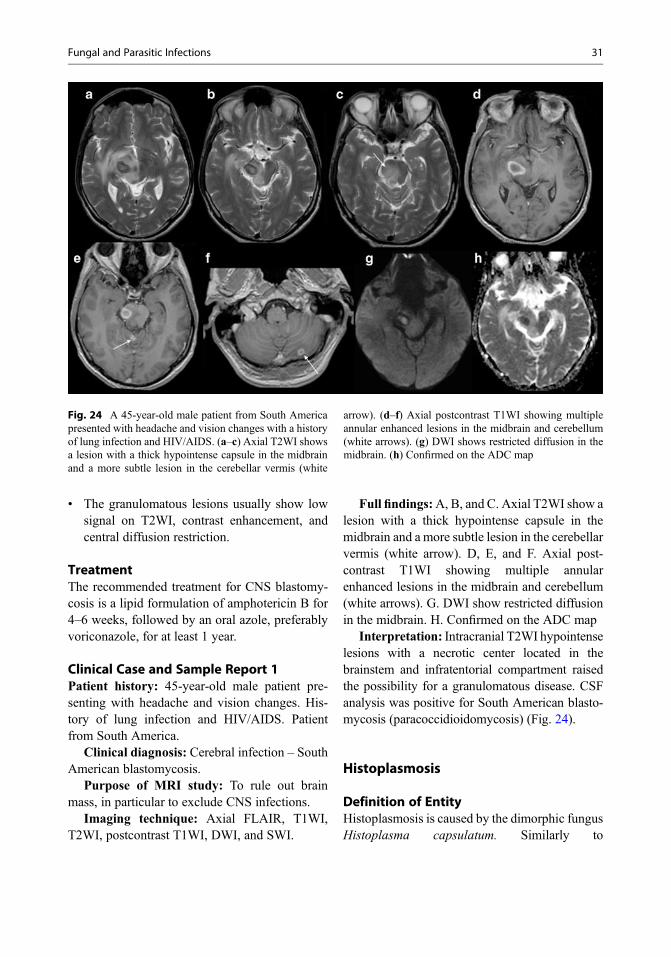
Full findings:A, B, and C. Axial T2WI show alesion with a thick hypointense capsule in themidbrain and a more subtle lesion in the cerebellarvermis (white arrow). D, E, and F. Axial post-contrast T1WI showing multiple annularenhanced lesions in the midbrain and cerebellum(white arrows). G. DWI show restricted diffusionin the midbrain. H. Confirmed on the ADC map
Interpretation: Intracranial T2WI hypointenselesions with a necrotic center located in thebrainstem and infratentorial compartment raisedthe possibility for a granulomatous disease. CSFanalysis was positive for South American blasto-mycosis (paracoccidioidomycosis) (Fig. 24).
Histoplasmosis
Definition of EntityHistoplasmosis is caused by the dimorphic fungusHistoplasma capsulatum. Similarly to
Fig. 24 A 45-year-old male patient from South Americapresented with headache and vision changes with a historyof lung infection and HIV/AIDS. (a–c) Axial T2WI showsa lesion with a thick hypointense capsule in the midbrainand a more subtle lesion in the cerebellar vermis (white
arrow). (d–f) Axial postcontrast T1WI showing multipleannular enhanced lesions in the midbrain and cerebellum(white arrows). (g) DWI shows restricted diffusion in themidbrain. (h) Confirmed on the ADC map
Fungal and Parasitic Infections 31
blastomycosis, histoplasma exists as a mold in theenvironment and yeast at body temperatures.
Epidemiology/DemographicsHistoplasma capsulatum is worldwide dissemi-nated, notably in the USA mid-western.Histoplasma infections are usually sporadic.Patients with AIDS are prone to developing dis-seminated histoplasmosis, with 5–10% of casesprogressing to CNS involvement.
Pathology and PathogenesisThe disease is commonly originated from theinhalation of bird or bat droppings, often foundin bat-inhabited caves, chicken coops, and soilsenriched with feces. If the patient is immunocom-petent, usually the disease is manifested as a mildrespiratory disease. On the other hand, immuno-compromised individuals are vulnerable for a dis-seminated form of disease, particularly those withAIDS and living in endemic areas.
Clinical FeaturesPatients generally present with confusion, leth-argy, weakness, and fever. Cerebral involvementis associated with hematogenous dissemination of
the disease and is especially characterized by cis-ternal meningitis and less frequently by parenchy-mal granulomas (histoplasmomas). Diffusemeningitis, abscess, and cerebritis may occuras well.
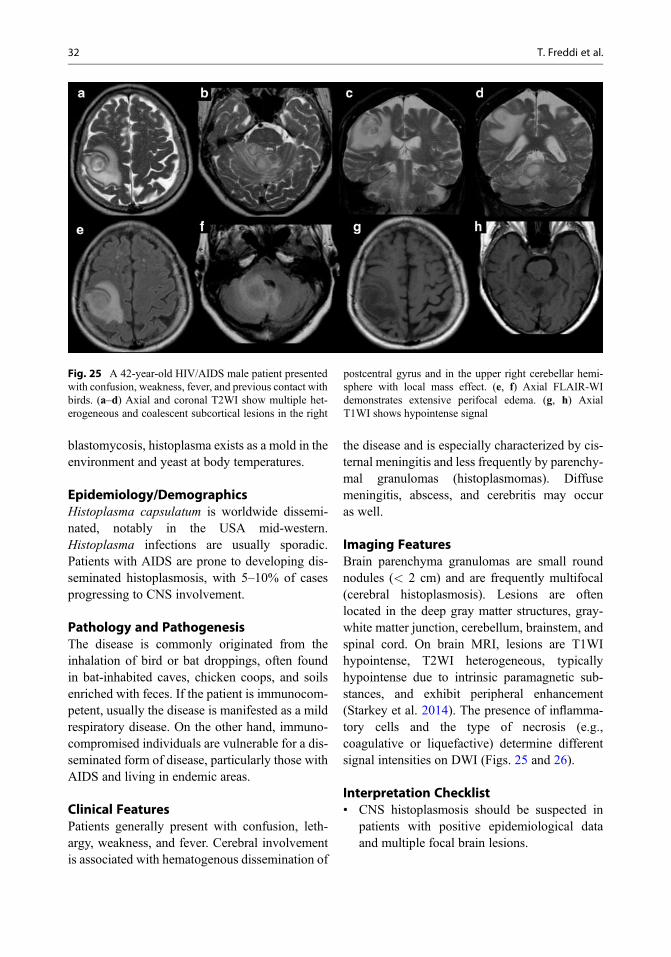
Imaging FeaturesBrain parenchyma granulomas are small roundnodules (< 2 cm) and are frequently multifocal(cerebral histoplasmosis). Lesions are oftenlocated in the deep gray matter structures, gray-white matter junction, cerebellum, brainstem, andspinal cord. On brain MRI, lesions are T1WIhypointense, T2WI heterogeneous, typicallyhypointense due to intrinsic paramagnetic sub-stances, and exhibit peripheral enhancement(Starkey et al. 2014). The presence of inflamma-tory cells and the type of necrosis (e.g.,coagulative or liquefactive) determine differentsignal intensities on DWI (Figs. 25 and 26).
Interpretation Checklist• CNS histoplasmosis should be suspected in
patients with positive epidemiological dataand multiple focal brain lesions.
Fig. 25 A 42-year-old HIV/AIDS male patient presentedwith confusion, weakness, fever, and previous contact withbirds. (a–d) Axial and coronal T2WI show multiple het-erogeneous and coalescent subcortical lesions in the right
postcentral gyrus and in the upper right cerebellar hemi-sphere with local mass effect. (e, f) Axial FLAIR-WIdemonstrates extensive perifocal edema. (g, h) AxialT1WI shows hypointense signal
32 T. Freddi et al.

• Imaging findings are nonspecific and multiplesmall granulomas with diffusion restrictionmay be seen, mimicking bacterialmicroabscesses.
TreatmentThe recommended treatment for CNS histoplas-mosis is amphotericin B for 4–6 weeks, followedby triazole (e.g., fluconazole, itraconazole, orvoriconazole) for at least 12 months, with variablesuccess. In immunosuppressed patients lifelongantifungal therapy may be needed to preventrelapse. Liposomal amphotericin B is preferredover standard amphotericin B formulation for itsgreater CNS penetration and lower toxicity.
Candidiasis
Definition of EntityCandida albicans is the mainly species responsi-ble for candidal infections. Nevertheless, approx-imately half of infections are caused by otherspecies including Candidaglabrata and Candidaparapsilosis. Candida species are small, round tooval, thin-walled, yeast-like fungi that lack a
sexual cycle, which reproduce by budding orfusion. Pseudohyphae predominate, but occasion-ally true hyphae are also seen.
Epidemiology/DemographicsCandida albicans is part of the normal flora of theskin, gastrointestinal tract, and other mucousmembranes. Cerebral infection is often causedby haematogenous spread with disseminated sys-temic infection in immunosuppressed patients.Risk factors include broad spectrum antibiotictreatment, diabetes, lymphoproliferative disease,intravenous drug abuse, parenteral hyperalimen-tation, AIDS, immunosuppression, hematologicmalignancy, and prematurity.
Pathology and PathogenesisThe gastrointestinal tract is the gateway for sys-temic infection in individuals with risk factorssuch as diabetes, lymphoproliferative disease,intravenous drug abuse, and broad-spectrum anti-biotics. Broad-spectrum antibiotic treatment maylead to microbial selection due to an imbalancebetween candida and other normal flora. The birthcanal is another potential route of infection. Dur-ing pregnancy vaginal flora overgrows which
Fig. 26 (a–d) Axial postcontrast T1WI shows multiple lesions with peripheral contrast enhancement. (e–h) DWI andADC show central restricted diffusion
Fungal and Parasitic Infections 33
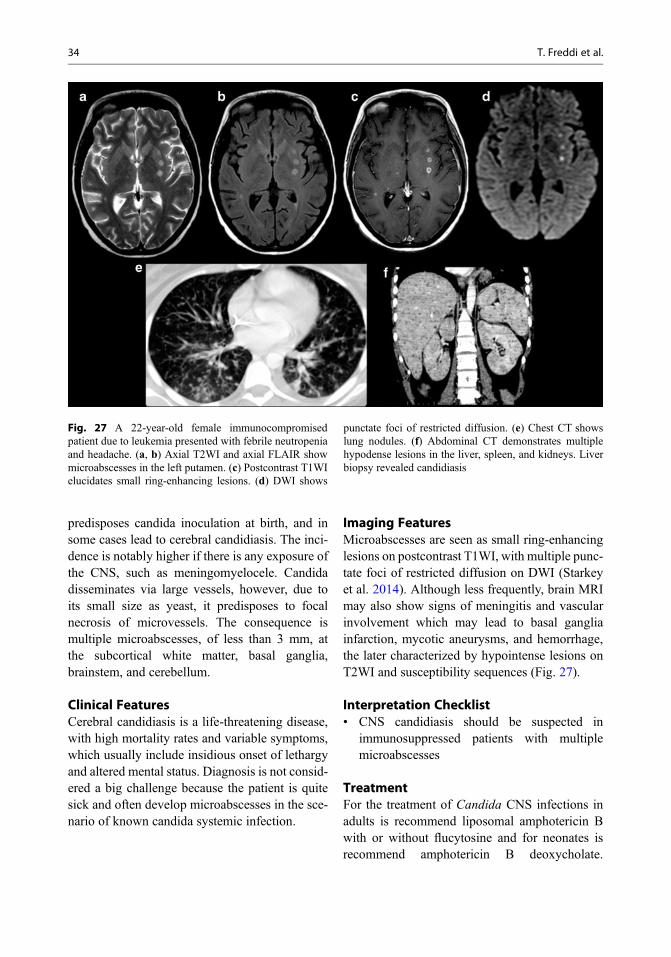
predisposes candida inoculation at birth, and insome cases lead to cerebral candidiasis. The inci-dence is notably higher if there is any exposure ofthe CNS, such as meningomyelocele. Candidadisseminates via large vessels, however, due toits small size as yeast, it predisposes to focalnecrosis of microvessels. The consequence ismultiple microabscesses, of less than 3 mm, atthe subcortical white matter, basal ganglia,brainstem, and cerebellum.
Clinical FeaturesCerebral candidiasis is a life-threatening disease,with high mortality rates and variable symptoms,which usually include insidious onset of lethargyand altered mental status. Diagnosis is not consid-ered a big challenge because the patient is quitesick and often develop microabscesses in the sce-nario of known candida systemic infection.
Imaging FeaturesMicroabscesses are seen as small ring-enhancinglesions on postcontrast T1WI, with multiple punc-tate foci of restricted diffusion on DWI (Starkeyet al. 2014). Although less frequently, brain MRImay also show signs of meningitis and vascularinvolvement which may lead to basal gangliainfarction, mycotic aneurysms, and hemorrhage,the later characterized by hypointense lesions onT2WI and susceptibility sequences (Fig. 27).
Interpretation Checklist• CNS candidiasis should be suspected in
immunosuppressed patients with multiplemicroabscesses
TreatmentFor the treatment of Candida CNS infections inadults is recommend liposomal amphotericin Bwith or without flucytosine and for neonates isrecommend amphotericin B deoxycholate.
Fig. 27 A 22-year-old female immunocompromisedpatient due to leukemia presented with febrile neutropeniaand headache. (a, b) Axial T2WI and axial FLAIR showmicroabscesses in the left putamen. (c) Postcontrast T1WIelucidates small ring-enhancing lesions. (d) DWI shows
punctate foci of restricted diffusion. (e) Chest CT showslung nodules. (f) Abdominal CT demonstrates multiplehypodense lesions in the liver, spleen, and kidneys. Liverbiopsy revealed candidiasis
34 T. Freddi et al.

Antifungal therapy should continue until allabscesses have resolved on MRI; the CSF glu-cose, pleocytosis, protein, and culture havereturned to normal, beyond the patient’s symp-toms and signs improvement.
References
Abdel Rasek AA, Watcharakorn A, Castillo M. Parasiticdiseases of the central nervous system. NeuroimagingClin N Am. 2011;21(4):815–41.
Akgoz A, Mukundan S, Lee TC. Imaging of rickettsial,spirochetal, and parasitic infections. NeuroimagingClin N Am. 2012:22(4):633–57
Carpio A, Romod ML, Parkhousef RME, Shortg B, DuagT. Parasitic diseases of the central nervous system:lessons for clinicians and policy makers. Expert RevNeurother. 2016;16(4):401–14.
Carpio A, Fleury A, Romo ML, Abraham R. Neurocysti-cercosis: the good, the bad, and the missing. Expert RevNeurother. 2018;18(4):289–301.
Del Brutto OH, et al. Revised diagnostic criteria forneurocysticercosis. J Neurol Sci. 2017;15(372):202–10.
Hanagandi, et al. Multidisciplinary approach to tropicaland subtropical infectious diseases: imaging with path-ologic correlation. Neurographics. 2015;5(21):258–78.
Kimura-Hayama, et al. Neurocysticercosis: radiologic-pathologic correlation. Radiographies. 2010; 30(6):1705–19.
Lury KM, Castillo M. Chagas’ disease involving the brainand spinal cord: MRI findings. AJR Am J Roentgenol.2005;185(2):550–2.
Palacios E, Rojas R, Rodulfa J, Gonzalez-ToledoE. Magnetic resonance imaging in fungal infections ofthe brain. Top Magn Reson Imaging. 2014;23(3):199–212.
Rasalkar DD, Paunipagar BK, Sanghvi D, Sonawane BD,Loniker P. Magnetic resonance imaging in cerebral
malaria: a report of four cases. Br J Radiol. 2011;84(1000):380–5.
Razek AAA, Watcharakorn A, Castillo M. Parasitic dis-eases of the central nervous system. Neuroimaging ClinN Am, 2011;21(4): 815–41, viii.
Rocha AJ, et al. Granulomatous diseases of the centralnervous system. Top Magn Reson Imaging. 2005;16(2):155–87.
Safder S, Carpenter JS, Roberts TD, Bailey N. The “BlackTurbinate” sign: an early MR imaging finding of nasalmucormycosis. AJNR Am J Neuroradiol.2010;31:771–4.
Saleem S, Belal AI, El-Ghandour NM. Spinal cord schis-tosomiasis: MR imaging appearance with surgical andpathologic correlation. AJNR Am J Neuroradiol.2005;26(7):1646–54.
Shih RY, Koeller KK. Bacterial, fungal, and parasitic infec-tions of the central nervous system: radiologic-pathologic correlation and historical. Perspectives.2015;35(4):1141–69.
Singh P, et al. Amebic meningoencephalitis: spectrum ofimaging findings. AJNR Am J Neuroradiol. 2006;27(6):1217–21.
Smith AB, Smirniotopoulos JG, Rushing EJ. From thearchives of the AFIP: central nervous system infectionsassociated with human immunodeficiency virus infec-tion: radiologic-pathologic correlation. Radiographics.2008;28(7):2033–58.
Starkey J, Moritani T, Kirby P. MRI of CNS fungal infec-tions: review of aspergillosis to histoplasmosis andeverything in between. Clin Neuroradiol. 2014;24(3):217–30.
Therekathu J, et al. Imaging features of rhinocerebralmucormycosis: a study of 43 patients. Egypt J RadiolNucl Med. 2018;49:447–52.
Venkat B, Aggarwal N, Makhaik S, Sood R. A compre-hensive review of imaging findings in human cysticer-cosis. Jpn J Radiol. 2016;34(4):241–57.
Walker MD, Zunt JR. Neuroparasitic infections: cestodes,trematodes, and protozoans. Semin Neurol. 2005;25(3):262–77.
Fungal and Parasitic Infections 35
Related Documents











