Journal of Alzheimer’s Disease 22 (2010) 581–591 581 DOI 10.3233/JAD-2010-091549 IOS Press Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease Stefan F¨ orster a,* , Andreas Vaitl a , Stefan J. Teipel b,c , Igor Yakushev d , Mona Mustafa a , Christian la Foug` ere a , Axel Rominger a , Paul Cumming a , Peter Bartenstein a , Harald Hampel b,e , Thomas Hummel f , Katharina Buerger b,g , Walter Hundt h and Silke Steinbach f ,i a Department of Nuclear Medicine, Ludwig-Maximilian University, Munich, Germany b Dementia Research Section and Memory Clinic, Alzheimer Memorial Center and Geriatric Psychiatry Branch, Department of Psychiatry Ludwig-Maximilian University, Munich, Germany c Department of Psychiatry, University Rostock, Rostock, Germany d Department of Psychiatry, University Mainz, Germany e Department of Psychiatry, University Frankfurt, Germany f Smell & Taste Clinic, Department of Otorhinolaryngology, Technical University, Dresden, Germany g Institute for Stroke and Dementia Research, Klinikum Großhadern, Ludwig-Maximilian University, Munich, Germany h Department of Radiology, Philipps-University, Marburg, Germany i Department of Otorhinolaryngology, Philipps-University, Marburg, Germany Handling Associate Editor: Valeria Drago Accepted 6 July 2010 Abstract. We used [ 18 F]fluorodeoxyglucose (FDG) PET analysis to determine performance in different olfactory domains of patients with early AD compared to cognitively healthy subjects, and to map the functional metabolic representation of olfactory impairment in the patient sample. A cohort of patients with early AD (n = 24), consisting of 6 subjects with incipient AD and 18 subjects with mild AD, and a control group of 28 age-matched non-demented individuals were assembled. Patients and controls were tested for olfactory performance using the “Sniffin’ Sticks” test battery [odor identification (ID), discrimination (DIS) and threshold (THR)], while patients additionally underwent resting state FDG-PET. Voxel-wise PET results in the patients were correlated with olfaction scores using the general linear model in SPM5. Patients with early AD showed significantly reduced function in all three olfactory subdomains compared to controls. After controlling for effects due to patients’ age, gender, cognitive status, and treating scores in the two other olfactory subdomains as nuisance variables, ID scores correlated with normalized FDG uptake in clusters with peaks in the right superior parietal lobule, fusiform gyrus, inferior frontal gyrus, and precuneus, while DIS scores correlated with a single cluster in the left postcentral cortex, and THR scores correlated with clusters in the right thalamus and cerebellum. The subtests employed in the “Sniffin’ Sticks” test battery are complementary indicators of different aspects of olfactory dysfunction in early AD, and support the theory of a parallel organized olfactory system, revealed by FDG-PET correlation analysis. Keywords: Alzheimer’s disease, FDG PET, mild cognitive impairment, olfactory system, smell test * Correspondence to: Stefan F¨ orster, MD, Klinik und Poliklinik f¨ ur Nuklearmedizin, TU Munich, Ismaninger Str. 22, 81675 Munich, Germany. Tel.: +49 89 4140 2965; Fax: +49 89 4140 4950; E-mail: [email protected]. INTRODUCTION Decreases in olfactory function have been well docu- mented in patients with various neurodegenerative dis- orders, including Parkinson’s disease [1–3], mild cog- nitive impairment (MCI) [4–6] (a prodromal stage of ISSN 1387-2877/10/$27.50 2010 – IOS Press and the authors. All rights reserved

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Alzheimer’s Disease 22 (2010) 581–591 581DOI 10.3233/JAD-2010-091549IOS Press
Functional Representation of OlfactoryImpairment in Early Alzheimer’s Disease
Stefan Forstera,∗, Andreas Vaitla, Stefan J. Teipelb,c, Igor Yakushevd, Mona Mustafaa,Christian la Fougerea, Axel Romingera, Paul Cumminga, Peter Bartensteina, Harald Hampelb,e,Thomas Hummelf , Katharina Buergerb,g, Walter Hundth and Silke Steinbachf,iaDepartment of Nuclear Medicine, Ludwig-Maximilian University, Munich, GermanybDementia Research Section and Memory Clinic, Alzheimer Memorial Center and Geriatric Psychiatry Branch,Department of Psychiatry Ludwig-Maximilian University, Munich, GermanycDepartment of Psychiatry, University Rostock, Rostock, GermanydDepartment of Psychiatry, University Mainz, GermanyeDepartment of Psychiatry, University Frankfurt, GermanyfSmell & Taste Clinic, Department of Otorhinolaryngology, Technical University, Dresden, GermanygInstitute for Stroke and Dementia Research, Klinikum Großhadern, Ludwig-Maximilian University, Munich,GermanyhDepartment of Radiology, Philipps-University, Marburg, GermanyiDepartment of Otorhinolaryngology, Philipps-University, Marburg, Germany
Handling Associate Editor: Valeria Drago
Accepted 6 July 2010
Abstract. We used [18F]fluorodeoxyglucose (FDG) PET analysis to determine performance in different olfactory domains ofpatients with early AD compared to cognitively healthy subjects, and to map the functional metabolic representation ofolfactoryimpairment in the patient sample. A cohort of patients with early AD (n = 24), consisting of 6 subjects with incipient ADand 18 subjects with mild AD, and a control group of 28 age-matched non-demented individuals were assembled. Patients andcontrols were tested for olfactory performance using the “Sniffin’ Sticks” test battery [odor identification (ID), discrimination(DIS) and threshold (THR)], while patients additionally underwent resting state FDG-PET. Voxel-wise PET results in the patientswere correlated with olfaction scores using the general linear model in SPM5. Patients with early AD showed significantlyreduced function in all three olfactory subdomains compared to controls. After controlling for effects due to patients’ age,gender, cognitive status, and treating scores in the two other olfactory subdomains as nuisance variables, ID scores correlatedwith normalized FDG uptake in clusters with peaks in the right superior parietal lobule, fusiform gyrus, inferior frontal gyrus, andprecuneus, while DIS scores correlated with a single cluster in the left postcentral cortex, and THR scores correlated with clustersin the right thalamus and cerebellum. The subtests employedin the “Sniffin’ Sticks” test battery are complementary indicators ofdifferent aspects of olfactory dysfunction in early AD, andsupport the theory of a parallel organized olfactory system, revealedby FDG-PET correlation analysis.
Keywords: Alzheimer’s disease, FDG PET, mild cognitive impairment, olfactory system, smell test
∗Correspondence to: Stefan Forster, MD, Klinik und Poliklinikfur Nuklearmedizin, TU Munich, Ismaninger Str. 22, 81675 Munich,Germany. Tel.: +49 89 4140 2965; Fax: +49 89 4140 4950; E-mail:[email protected].
INTRODUCTION
Decreases in olfactory function have been well docu-mented in patients with various neurodegenerative dis-orders, including Parkinson’s disease [1–3], mild cog-nitive impairment (MCI) [4–6] (a prodromal stage of
ISSN 1387-2877/10/$27.50 2010 – IOS Press and the authors. All rights reserved

582 S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease
Alzheimer’s disease (AD), and in patients with clin-ically manifest AD [7,8]. The olfactory deficits oc-cur early in the course of AD and increase with dis-ease severity [5,7,9]. A recent meta-analysis of reportson olfactory functioning in AD patients showed severedeficits in different olfactory domains, including odoridentification, odor recognition, and discrimination. Ofthese three domains, odor threshold detection, whilestill impaired, was relatively better preserved [7]. Es-pecially in early stages of AD, poor performance inthe domains of odor identification and recognition weremost prominent [8,10]. Indeed, these findings led to thesuggestion that olfactory tasks with memory demandscould detect changes in AD earlier than olfactory tasksinvolving simply threshold detection [11,12]. Further-more, MCI patients with particularly poor odor identi-fication, who were unaware of their deficit, proved to bethe most likely to develop AD [4]. Recently, Devanandand colleagues showed that impairment of odor identi-fication at baseline, in conjunction with neuropsycho-logical deficits and MR-volumetric changes, togetherpredicted with high accuracy the conversion from MCIto manifest AD [6]. These consistent findings of anearly impairment of olfaction in AD seem consistentwith the early pathological changes in brain areas thatare strongly involved with processing of olfactory in-formation, as well as memory consolidation [13].
The cerebral processing of olfactory stimuli haswidely been studied using neurophysiological and neu-roanatomical methods. Odor-evoked responses are firstevoked in sensory neurons at the nasal mucosa, whichproject to mitral cells of the olfactory bulb, which inturn give rise to projections to the ipsilateral prima-ry olfactory areas, consisting of the anterior olfacto-ry nucleus, the piriform cortex, the nucleus corticalisof the amygdala, and the entorhinal cortex. Higher-order projections arising from each of these primaryolfactory brain structures converge on the orbital pre-frontal cortex, agranular insular cortex, other amyg-dala subnuclei, thalamus, hypothalamus, basal gangliaand hippocampus (for review, see [14]). This func-tional anatomic network was first deduced by classicalneuroanatomy, and has recently been investigated bynew imaging techniques. In particular, the pattern andsequence of brain activation evoked by odorants hasbeen studied with activation positron emission tomog-raphy (PET) and functional magnetic resonance imag-ing (fMRI), which have together provided new insightsin the topographic organization of olfactory processingin living human brain. In healthy subjects, exposure toseveral different odorants has consistently evoked acti-
vation of the right orbitofrontal cortex, amygdala, pir-iform cortex, insular cortex, anterior cingulate cortex,and also cerebellum [15,16].
Despite the well-known olfactory deficits of AD,few studies have so far investigated the relationshipbetween olfactory performance and brain metabolismin AD. One early PET study employed an activationparadigm, in which the utilization of the glucose ana-logue [18F]fluorodeoxyglucose (FDG) during perfor-mance of an olfactory memory task was impaired in theanterior portion of the middle temporal cortex of a smallAD group when compared to elderly controls [17]. Ina number of resting state studies, FDG PET has beenused to investigate neuronal networks subserving hu-man cognitive function. Thus, correlations betweenregional FDG uptake and overall memory performancein AD patients have been reported [18–20]. In this con-text, AD serves as a natural lesion model in which thespread of AD pathology manifests in impaired brainenergy metabolism, and consequently in impairmentof those cognitive functions subserved by the affectedregions. In particular, FDG-PET has revealed a char-acteristic pattern of hypometabolism relative to thatseen in healthy controls, which encompasses the bilat-eral parietotemporal association cortices and posteriorcingulate cortices of patients with prodromal and ear-ly stage AD [21,22], and also involves the prefrontalcortical areas in more advanced disease stages [23,24].
However, the relationship between olfactory deficitsin patients with early AD and resting state FDGmetabolism has yet to be investigated. We predictedthat (relative to the respective cognitive demand of thetest) olfactory performance in early AD patients shouldbe linked to impairment in a functional network sub-serving differing- order olfactory function. Therefore,we first defined performance in different olfactory do-mains, revealed by the “Sniffin’ Sticks” smell test bat-tery, in a well characterized sample of patients with ear-ly AD, in comparison to an age-matchedcontrol subjectsample. We then obtained resting state FDG recordingsin the patients, and performed voxelwise correlationwith individual scores in the olfactory tasks.
MATERIALS AND METHODS
Study subjects and study protocol
In a prospective design, we obtained resting FDGPET scans in 59 patients with suspected aMCI andAD. All patients had been referred from the Alzheimer

S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease 583
Memorial Center of the Department of Psychiatry, Lud-wig Maximilian University, of Munich from December2007 to April 2008. Diagnosis of aMCI was made ac-cording to Petersen’s criteria [25], whereas diagnosisof AD was based on NINCDS-ADRDA criteria [26].According to recent guidelines on AD [27] we appliedan AD-typical finding on FDG-PET as supportive di-agnostic marker. In the absence of a histopatholog-ical confirmation of AD, a “positive” PET scan wasshown to increase the probability of AD pathologyto 84% [28]. By this criterion, 24 right-handed pa-tients, 6 aMCI (MMSE= 26.2 ± 1.9) and 18 mildAD (MMSE = 21.8± 3.0), were finally included inthe present study. The AD-typical pattern was charac-terized by the presence of significant hypometabolism(> 5 SD from controls) in the posterior cingulate cor-tex, and not necessarily additional hypometabolism inparieto-temporal-, and/or prefrontal cortex, as assignedautomatically using the 3D-SSP single subject com-parison relative to age-matched non-demented controlgroups (Cortex ID, GE Healthcare) [29]. In the routineclinical follow-up until June 2009, all six patients ini-tially presenting with aMCI had converted to manifestprobable AD, according to NINCDS-ADRDA criteria.Therefore, they are referred to as subjects with incipi-ent AD hereafter in the paper, while the whole patientcohort (n = 24) is referred to as “early AD”. Overallexclusion criteria included any relevant co-morbidities,such as head trauma, stroke, acute rhinosinusitis, his-tory of nasal polyps or endonasal surgery, any neo-plasia, asthma, hyper- or hypoactivity of the thyroidgland, diabetes mellitus, liver or renal problems, neu-rological disorders, and present alcohol or drug abuse.In all patients, routine laboratory testing, consisting ofhaematologyand biochemistryscreening, thyroid func-tion tests, serum vitamin B12 and folate assays, wasperformed in order to exclude other causes of impairedcognitive function.
All patients underwent structural MRI of the brainto exclude the presence of focal cerebral atrophy andto exclude significant white matter hyperintensities, ac-cording to the Schelten scale [30]. MRI, apolipoproteinE ε4 genotyping, and cognitive testing with the Mini-Mental State Examination (MMSE) were all performedduring a two to three day period as part of the diagnosticwork-up at the Alzheimer Memorial Centre. A controlgroup consisting of 28 elderly non-demented subjectswas recruited by advertisement, with exclusion of de-mentia on the basis of MMSE score> 28. Control sub-jects were available for olfactory testing, MMSE andquestionnaires. Demographic variables such as age,
Table 1Demographic characteristics of control subjects and earlyADpatients
Control subjects Patients
N 28 24Mean age(years) 68.2± 3.9 71.4± 7.9Women(%) 50 50MMSE 29.0± 1.0 22.9± 3.3ApoEε4 status
03–03 (n) NA 503–04 (n) NA 1204–04 (n) NA 7
Antidepressant intake(n) 0 0Smoker(n) 0 0
NA = not available.
gender, MMSE score, intake of antidepressants, andsmoking habits of all subjects are described in Table 1.
The study protocol was approved by the local clin-ical institutional review board and complied with thedeclaration of Helsinki. Written and informed consentwas obtained from all subjects.
Olfactory testing
Olfactory function was measured in the morning be-fore breakfast for all subjects, which was on the day ofthe FDG PET examination for patients. The adminis-trator of the olfactory test advised the subjects to fillout a questionnaire for subjective assessment of theirown olfactory function, using an analogue scale from 0to 100. In order to evaluate different dimensions of ol-factory function, we administered the “Sniffin’ Sticks”test battery (Burghart Medizintechnik GmbH, Wedel,Germany), which is recommended by the “WorkingGroup Olfaction and Gustation” of the German Soci-ety for Otorhinolaryngology, Head and Neck Surgery.The test was introduced more than 10 years ago [31,32] and is very well validated [33] for measuring odoridentification (ID), odor discrimination (DIS), and odorthreshold (THR). In this test, odorants are presentedvia felt-tip pens, which are uncapped and placed ap-proximately two centimeters in front of the subject’snostrils for 3 s. We administered the test birhinally in awell-ventilated room to minimize interference with thetest odors. For ID, 16 odorants in suprathreshold in-tensity were presented, in a multiple forced-choice for-mat with four descriptions (4-alternative forced choice;written and verbal). For DIS, subjects were blindfold-ed, and 16 odor-triplets were presented with an intervalof 30 s between each triplet. Each triplet consisted oftwo identical and one different odorants, all present-ed at suprathreshold intensity. Subjects were blind-folded and asked to identify the non-matching odor in

584 S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease
the three-alternative forced choice, without needing torecognize or name the odors. For THR, sixteen seri-al dilutions of a single odorant were prepared in 4%n-butanol. Triplets consisting of two vehicle and oneodorant pen were presented in randomized order, in anascending sequence of the 16 odorant concentrations.After twice correctly recognizing the pen containingthe odor in a presented triplet, the pen triplets were pre-sented in descending order of concentration until thesubject could no longer identify the pen containing theodorant, where upon the sequence or presentation wasagain reversed. The THR was calculated as the meandilution coinciding with the last four of seven orderreversals. The ID and DIS score range is 0–16, andthe THR score range is 1–16. The sum of the individ-ual ID, DIS, and THR scores represents total olfactorytest performance (TDI; range: 1–48). Subtests werealways applied in the same sequence (first THR, thenDIS and finally ID) and administration of tests requiredone hour for the patients and approximately 30 min forthe control subjects.
FDG PET
All patients had fasted for at least 6 h prior to FDGPET. Recordings were made using a Philips AllegroPET scanner with a 128× 128 pixel matrix (pixel size2 mm), an axial field of view of 180 mm and a fullwidth at half maximum (FWHM) resolution of 5.5 mm.Approximately15 min after FDG administration (mean200 MBq, i.v.) while sitting in a dimly-lit room withminimal background noise, patients were asked to re-cline on the bed of the tomograph. Each patient’s headwas positioned within the aperture of the tomograph,and comfortably immobilized using a foam cushion.First, a brief attenuation scan was obtained with a ro-tating 137Cs point source. Then, a dynamic emissionrecording consisting of five six-minute frames was ob-tained in the interval 30 to 60 min following the FDGinjection. After visual inspection of the sinograms toexclude frames with unacceptable head motion, frameswere summed into a single frame and images were re-constructed iteratively using a three dimensional row-action maximum likelihood algorithm (3D-RAMLA).
Statistical analysisSPM5 routines (Wellcome Department of Cognitive
Neurology, London, UK) implemented in MATLAB(version 7.1) were used to perform basic image process-ing and voxel-based statistical analysis of the summedPET images, which were spatially normalized usingdefault transformation parameters to the SPM standard
PET template in the MNI space. Normalized imageswere represented on a 79× 95× 69 matrix with 2×2× 2 mm voxel size, and smoothed using an isotropicGaussian kernel (12 mm FWHM), which accommo-dates inter-individual anatomical variability, and thusimproves the sensitivity of the statistical analysis [34].FDG uptake scaling was performed applying the refer-ence cluster approach [35], which is described in detailelsewhere [36]. In our hands, this data-driven normal-ization algorithm is appropriate for the statistical analy-sis of FDG PET in patients with mild to moderate stagesof AD and Parkinson’s disease [35,37–39]. Within theentire patient group, normalized FDG uptake in eachvoxel was regressed separately for each olfactory testperformance scores as covariates of interest. In all ourstatistical models age, gender, and MMSE score wereadded as covariates of no interest, given that age andgender are known to affect odor perception [40], andthat cognition-related effects on FDG uptake are notthe present matter of interest. To increase specificityof the cognitive-metabolic relationships, we performedadditional partial correlation analyses, in which scoreson each subtest were correlated to FDG uptake, whilescores on the other two subtests were treated as nui-sance variables (in addition to age, gender, and MMSEscore). T-statistic maps were calculated for positivecorrelations, i.e., in the neurobiologically-expected di-rection, where impaired performance should predictdecreased FDG uptake. Due to the exploratory na-ture of the whole-brain analyses and after inclusion offive nuisance variables, we chose for FDG PET studiescommonly used uncorrected probability thresholds ofp < 0.005 [41,42] and a threshold for minimum spa-tial extent of 20 contiguous voxels. The coordinatesof the highest T-statistic peaks were automatically as-signed by the SPM5 software to the coordinate systemof the MNI space, and then converted to Talairach andTournoux coordinates for identification of the Brod-mann areas and anatomic designations using the Ta-lairach Daemon [43]. The output from the TalairachDaemon was visually checked with reference to theTalairach and Tournoux Atlas.
All clinical data analyses were performed with theSPSS software, version 13.0 (SPSS, Chicago, IL,USA). Unless stated otherwise unpaired t-tests wereused and p values6 0.05 were considered significant.
RESULTS
Subjective olfactory function
The subjective self-assessment of olfactory function(where 100 is perfect) tended to be lower in the pa-

S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease 585
Table 2Control subjects’ and early AD patients’ olfactory performance
Control subjects Patients P value
Olfactory function(mean)ID 13.07± 1.9 7.54± 3.9 < 0.001DIS 12.07± 2.4 8.70± 2.5 < 0.001THR 6.41± 2.1 4.33± 2.6 0.005TDI 31.55± 5.2 20.62± 7.6 < 0.001
tient subgroup with higher TDI performance (57± 23)than in the subgroup with lower performance (71±21; p = 0.13). The mean self-assessment score wasnon-significantly higher in patients with incipient AD(68 ± 17) than in the mild AD patients (65± 24),and significantly lower in both patient groups than inthe control group (85± 22; p < 0.01). None of thesubjects complained of phantosmia.
Olfactory testing
Scores of ID, DIS, and TDI revealed by the “Sniffin’Sticks” test battery were significantly lower in patientsin comparison with control subjects (see Table 2). Ofthe patients, those with mild AD showed a tendency forlower olfactory test scores than did those with incipientAD.
Correlation of subjective olfactory function andolfactory test performance
In patients but not in control subjects there was a neg-ative correlation between the subjective assessment ofolfactory function and the objective scores of the threesubtests. However, only THR performance showed asignificant negative correlation with subjective ratingof olfactory function in the patient group (Spearman’srho two-tailed:p = 0.038,r = −0.426).
Instead, in control subjects there were positive corre-lations between the subjective assessment of olfactoryfunction and the objective scores of ID, THR, and TDI(Spearman’s rho two-tailed:p = 0.0010;r = 0.724 forID; p = 0.0227,r = 0.548 for THR;p = 0.0075,r =
0.623 for TDI).
Correlation of FDG uptake and single olfactory testperformances(ID, DIS, THR) in patients with earlyAD
Of the three Sniffin’ sticks subtests, ID showed morewidespread correlations with normalized FDG uptakethan did DIS and THR.
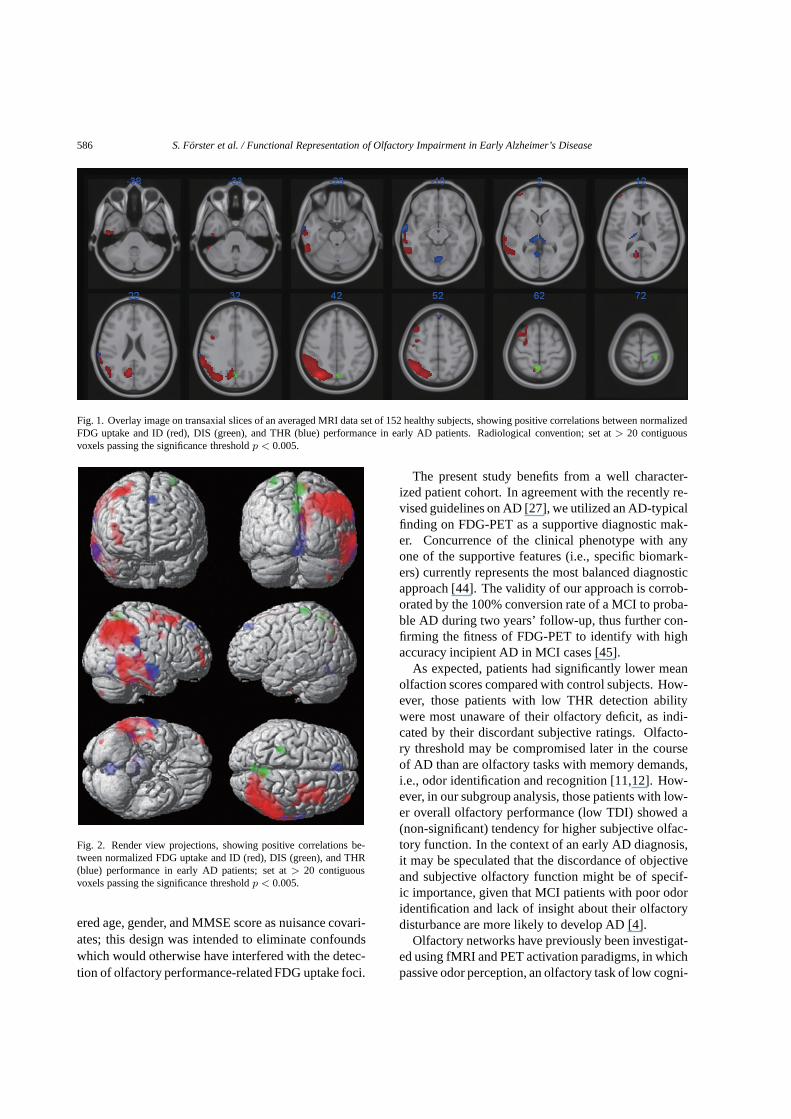
More specifically, regression of ID performance andnormalized FDG uptake showed clusters of major peakcorrelation in the right superior parietal lobule, rightfusiform gyrus, right middle frontal gyrus, right inferi-or frontal gyrus, right precuneus and right cerebellum.Minor peak correlations were found in the right infe-rior parietal lobule, adjacent supramarginal gyrus andprecuneus, as well as in the right inferior- and middletemporal gyrus (Figs 1 and 2: red color). Controllingfor DIS and THR in the additional partial correlationanalysis did not substantially change the pattern of thecorrelation. Clusters that survived such a correction aremarked with an asterisk in Table 3.
DIS performance correlated with normalized FDGuptake in three single clusters located in the rightprecuneus, left postcentral gyrus, and left precuneus(Figs 1 and 2: green color). When controlling forID and THR, one cluster in the left postcentral gyrussurvived.
THR performance showed major peak correlationswith normalized FDG uptake in the right middle tem-poral gyrus, right thalamus, right cerebellum (culmenand anterior lobe), right inferior parietal lobule, and leftsuperior frontal gyrus. Minor peak correlations werefound in the medial dorsal nucleus of the right thala-mus and in the left thalamus (Figs 1 and 2: blue col-or). After controlling for ID and DIS in the additionalpartial correlation analysis the clusters in the thalamus(including all subpeaks) and cerebellum survived.
A summary of detailed anatomical designations(AAL terminology) including Brodman areas and Ta-lairach coordinates is provided in Table 3.
DISCUSSION
In the first part of this study we compared perfor-mance in tests of olfactory function between patientswith early AD and an age-matched sample of controlsubjects. We then conducted in the patients a voxel-wise regression between olfactory test scores and brainFDG uptake. Unlike the approach in previous FDGstudies of cognition in AD patients [18–20], we consid-
586 S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease
Fig. 1. Overlay image on transaxial slices of an averaged MRIdata set of 152 healthy subjects, showing positive correlations between normalizedFDG uptake and ID (red), DIS (green), and THR (blue) performance in early AD patients. Radiological convention; set at> 20 contiguousvoxels passing the significance thresholdp < 0.005.
Fig. 2. Render view projections, showing positive correlations be-tween normalized FDG uptake and ID (red), DIS (green), and THR(blue) performance in early AD patients; set at> 20 contiguousvoxels passing the significance thresholdp < 0.005.
ered age, gender, and MMSE score as nuisance covari-ates; this design was intended to eliminate confoundswhich would otherwise have interfered with the detec-tion of olfactory performance-related FDG uptake foci.
The present study benefits from a well character-ized patient cohort. In agreement with the recently re-vised guidelines on AD [27], we utilized an AD-typicalfinding on FDG-PET as a supportive diagnostic mak-er. Concurrence of the clinical phenotype with anyone of the supportive features (i.e., specific biomark-ers) currently represents the most balanced diagnosticapproach [44]. The validity of our approach is corrob-orated by the 100% conversion rate of a MCI to proba-ble AD during two years’ follow-up, thus further con-firming the fitness of FDG-PET to identify with highaccuracy incipient AD in MCI cases [45].
As expected, patients had significantly lower meanolfaction scores compared with control subjects. How-ever, those patients with low THR detection abilitywere most unaware of their olfactory deficit, as indi-cated by their discordant subjective ratings. Olfacto-ry threshold may be compromised later in the courseof AD than are olfactory tasks with memory demands,i.e., odor identification and recognition [11,12]. How-ever, in our subgroup analysis, those patients with low-er overall olfactory performance (low TDI) showed a(non-significant) tendency for higher subjective olfac-tory function. In the context of an early AD diagnosis,it may be speculated that the discordance of objectiveand subjective olfactory function might be of specif-ic importance, given that MCI patients with poor odoridentification and lack of insight about their olfactorydisturbance are more likely to develop AD [4].
Olfactory networks have previously been investigat-ed using fMRI and PET activation paradigms, in whichpassive odor perception, an olfactory task of low cogni-

S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease 587
Table 3Correlations between ID / DIS / THR- performance and FDG uptake in early AD patients
Talairach and TournouxOlfactory Location BA x y z Peak Clustersubtests z-value extension
ID
R, Superior Parietal Lobule∗ 7 34 −72 42 4.52 4856R, Inferior Parietal Lobule 40 44 −56 50 3.87R, Supramarginal Gyrus∗ 40 66 -46 32 3.49R, Precuneus∗ 31 8 −66 24 3.86R, Fusiform Gyrus∗ 20 60 −38 −30 3.50 2078R, Inferior Temporal Gyrus∗ 20 52 −20 −38 3.36R, Middle Temporal Gyrus 37 60 −50 −10 3.14R, Middle Frontal Gyrus 6 38 18 60 3.29 809R, Inferior Frontal Gyrus∗ 9 46 2 34 3.04 60R, Precuneus∗ 7 8 −60 64 2.89 50R, Cerebellum, Culmen 10 −36 −6 2.69 72
DIS R, Precuneus 7 6 −58 60 3.59 259L, Postcentral Gyrus∗ 2 −28 −34 70 3.19 110L, Precuneus 7 −2 −72 36 3.00 158
THR R, Middle Temporal Gyrus 21 66 −8 −12 3.88 349R, Thalamus∗ 27 6 −30 2 3.72 538R, Thalamus, Med. Dorsal Ncl.* 10 −26 8 3.67L, Thalamus∗ −6 −34 0 3.24R, Cerebellum, Culmen∗ 4 −62 −6 3.61 614R, Inferior Parietal Lobule 40 68 −30 26 3.09 100L, Superior Frontal Gyrus 8 −4 42 48 3.06 108R, Cerebellum, Anterior Lobe 46 −36 −30 2.74 31
Cluster extension represents the number of contiguous voxels surpassing the threshold ofp < 0.005uncorrected controlling for age, gender and MMSE. Bold markings delineate a cluster and the peak z-valuewithin the cluster. Subsequent non-bold markings identifyfurther peaks within the same cluster. Asterisks“*” indicate surviving clusters/peaks after controlling for age, gender, MMSE and the respective two otherodor subtests. Associated anatomic structures are indicated, along with designations of Brodman area(BA); R: right hemisphere; L: left hemisphere.
tive complexity, evoked either symmetrical or predomi-nantly right-hemispheric activations in the orbitofrontalcortex, amygdala, piriform cortex, insular cortex, an-terior cingulate cortex, and cerebellum of healthy sub-jects [15,16]. These empirical findings suggest a cen-tral role for the non-dominant hemisphere in olfactoryprocessing, although others have noted an associationbetween left hemispheric traumatic injury and anos-mia [46]. The authors of one PET activation studyinvestigated the pattern of cerebral activation with ol-factory tasks of increasing cognitive complexity [16],and concluded that the olfactory system is organized ina parallel and hierarchical manner. Although not di-rectly comparable, due to methodological differencesand present investigation of AD patients, we likewiselink olfactory processing of different orders with a par-allel organized functional network. Considering ADas a natural perturbation of this network, we find thatthe separate components of olfactory performance, i.e.,odor identification, discrimination, and threshold de-tection, are mediated by different networks, which areonly partially overlapping. These networks includebrain regions known to be involved in somatosenso-
ry processing (post-central gyrus), olfactory sensoryprocessing (prefrontal-, inferior-/orbitofrontal cortex,thalamus (medial dorsal nucleus) and cerebellum, andalso brain regions plausibly engaged in episodic odorrecognition memory (precuneus, inferior temporal- andfusiform gyrus). Of course, the three measured olfac-tory characteristics are closely interdependent. For in-stance, tests of odor identification require odorant de-tection as well as discrimination. Accordingly, and asnoted above, there is a certain degree of overlap be-tween the correlation patterns. The issue of specificitywas addressed in additional analyses, in which eachsingle odor test was considered as a covariate of in-terest, while the two other tests were treated as nui-sance variables. Despite this rather conservative ap-proach, a number of clusters remained significant, thussupporting the robustness of our results, and corticalsegregation of aspects of olfactory function.
Arguably, the ID task reflects a higher cognitive do-main in olfactory processing, requiring an integrationof verbal or visual skills with olfactory skills. This hasrecently been shown by Hedner and colleagues, whodemonstrated that variation in odor discrimination was

588 S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease
best explained by cognitive variables followed by odoridentification, whereas odor thresholds were least de-pendent on the investigated cognitive functions [47].Therefore, our findings of an association between IDand FDG uptake in the right prefrontal and orbito-frontal cortex may reflect the contribution of executivefunction and odor working memory, as the identifica-tion task requires storage and comparison of odors,bothof which are needed to make a correct identification ofan odorant. Likewise the association between ID andFDG uptake in superior and inferior parietal corticalareas may reflect higher-order processing and integra-tion of the olfactory ID task with other modalities, es-pecially within tertiary areas of the parietal lobe. Ourfinding of a strong involvement of the precuneus (forID and DIS, but not THR) in early AD patients agreesanatomically with a PET activation study by Savic andcolleagues, investigating memory for recognition of fa-miliar odors in healthy subjects [16]. They found pre-cuneal and cerebellar activations, and in a more recentstudy they also found activation of the parahippocampalgyrus and parietal cortex, including the precuneus [48].
In contrast to odor identification, the odor thresholddetection task requires only the ability to detect thepresence of an odor and is least dependent on high-er cognitive functions [47]. Thus, the association be-tween THR and FDG uptake, especially in subcorticalstructures (thalamus and cerebellum), may reflect theinvolvement of phylogenetically ancient brain regionsin “central olfactory processing”. In concordance withour findings in AD patients, Kronenbuerger and col-leagues recently found that deep brain stimulation ofthe cerebellothalamic pathway impaired odor thresholdand, to a lesser extent, odor discrimination in patientssuffering from tremor disorders [49]. Olfactory infor-mation processing occurs via direct projections fromthe primary processing areas (piriform cortex) to neo-cortical structures (orbitofrontal cortex),as well as indi-rectly via the medial dorsal thalamic nucleus (MDTN;for review see [50]), perhaps revealed by the highlysignificant correlation between THR and FDG uptakein right MDTN of our AD patients.
Odor discrimination, a task of intermediate com-plexity, requires detection and comparison of differentodors, which entails short-term retention in modalityspecific memory. In this regard, the anatomical over-lap with ID (i.e., the clusters in the precuneus) mightreveal the substrate of short-term memory processing.While entailing some short-term memory, the DIS task,in contrast to ID task, requires no verbal or cross-modalintegration. However, the only task-specific surviving
cluster for DIS was located in the left postcentral gyrus,which subserves somatosensory processing, and hasnot previously been linked to complex discriminationtasks in humans.
Poor performance in odor identification and recog-nition is most prominent in early AD [8,10], leadingto the suggestion that performance of olfactory taskswith memory demands should be more impaired thanthreshold detection [11,12]. These observations linkthe neuropathology of early AD with specifically cog-nitive aspects of olfactory processing [13]. Likewise,of the three Sniffin’ sticks subtests, ID showed the mostwidespread clusters, a potentially relevant finding fordiagnostic workup in early AD patients. Although re-stricted to the right hemisphere, the ID-related patternoverlaps extensively with the pathology in postmortemstudies of AD [24,51,52], as well as with the AD-specific pattern of hypometabolism in previous FDG-PET studies [35,53].
Given that the earliest neurodegenerative changesof AD occur in the medial temporal lobes, in prox-imity to the primary olfactory cortex, we expected awidespread correlation network extending into the me-dial temporal cortex. However, clusters were seen onlyin the inferior/lateral temporal cortex. Despite the mainneurodegenerative burden of the medial temporal loberegions, some mismatch is noted in FDG-PET [54],which may be due to effects of partial volume in smallstructures [55]. Alternately, the present paucity of clus-ters in medial temporal structures may be due to flooreffects, given that a potentially strong functional im-pairment of the medial temporal lobe in our early ADpatients would reduce metabolic variation in that re-gion.
However, according to the disconnection theory, oc-currence of hypometabolism in association corticesmay represent disruption of functional input from distalregions (i.e., medial temporal lobe), being most severe-ly affected by AD pathology. The medial temporal lobeand the inferior parietal lobe are believed to retain con-siderable plasticity throughout healthy aging, in con-sideration of the complexity of the memory consoli-dation task. The particular requirement for plasticityin these regions may be a predisposing factor for ADpathology [56]. Insofar as olfactory memory entailsa distributed representation resembling that of gener-al memory in neocortical association cortex [57], ol-factory learning might be inextricably associated withvulnerability of medial temporal and inferior parietalstructures to early AD changes. Thus, early impairmentof olfactory processing is consistent with the hypoth-

S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease 589
esis of particular plasticity conferring vulnerability toAD pathology [58].
Although focusing on neurobiological issues, ourstudy might have clinical applications. Specifically,impaired performance on specific odor tests, togetherwith the AD-typical FDG pattern, may be helpful foridentification of incipient AD in subjects with MCI. Fordifferential diagnosis of AD, further studies are neces-sary to examine the accuracy of olfactory tests alone,or in combination with FDG-PET. Recently smell iden-tification function was found useful as a clinical mea-sure to assess treatment response with donepezil inAD [59]. However, the potential of olfactory testingfor screening of early AD might be compromised bythe occurrence of impaired olfactory performance inother non-AD neurodegenerativediseases [2,3], as wellas healthy aging, such that tests of verbal and spatiallearning probably remain standard in clinical practice.
LIMITATIONS
Because control subjects were not imaged with FDGPET, the present findings in AD patients are not readi-ly generalized to metabolic-functional relationships innormal subjects. Given that our control group was cog-nitively intact and had entirely normal olfactory testscores, we suppose that their cerebral FDG uptake waslikewise normal, and of relatively restricted range, inwhich event a correlation analysis might not have re-vealed significant clusters: there would have to be iden-tified specific factors accounting for systematic vari-ation in olfactory performance and brain metabolism.The present study assumes a lesion-based conceptualmodel of AD, such that covariance between progressivecognitive dysfunction and metabolic decline drives theassociation between olfactory performance and specif-ic cortical networks. Therefore, our approach need notnecessarily encompass the entire neuronal network in-volved in olfactory performance, but rather may iden-tify the brain regions in which dysfunction is mostcritically relevant to the specific cognitive changes inAD. As such, our approach may be more comparableto neuropsychological lesion studies than to functionalactivation studies in healthy subjects. As the olfactorysubtests utilized have different reliabilities, we cannotexclude that lower reliability in one subtest had pre-cluded identification of some correlations. However,as each subtest assesses partially distinct traits and hasdifferent complexity, it is hardly possible that all havethe same reliability. Although all subtests possess good
inter-rater reliability [60], there are a number of othermethodological factors (e.g., order and frequency ofodor presentation, pleasantness of odors, uni-/birhinalpresentation of odors) which might have confoundedthe relationships between “trait” measures and regionalFDG uptake. In our study olfactory testing was per-formed birhinally.
CONCLUSIONS
We combined resting state FDG-PET with olfactorytests of odor identification, discrimination and thresh-old detection to study the functional metabolic rep-resentation of impaired olfactory function in patientswith early AD. Notwithstanding some overlap due tothe interdependence of the three olfactory subdomains,the clusters in the right parietal association cortices,right precuneus, right inferior temporal cortex and rightorbitofrontal cortex emerged as a cortical network forodor identification. For the subtest of intermediatedifficulty (odor discrimination), metabolism in the leftsensorimotor cortex was most predictive of good taskperformance, whereas the cognitively less demand-ing odor threshold detection task was associated withmetabolism in subcortical structures, i.e. thalamus andcerebellum. Performance in the subtests of the “Snif-fin’ Sticks” test battery proved to be associated withmetabolic activity in distinct domains with a parallel-organized network of olfactory pathways, in a mannerconsistent with the cognitive complexity of the subtests.
ACKNOWLEDGMENTS
A substantial part of this work originated from thedoctoral thesis of Andreas Vaitl.
Authors’ disclosures available online (http://www.j-alz.com/disclosures/view.php?id=529).
REFERENCES
[1] Ward CD, Hess WA, Calne DB (1983) Olfactory impairmentin Parkinson’s disease.Neurology33, 943-946.
[2] Chaudhuri KR, Healy DG, Schapira AH (2006) Non-motorsymptoms of Parkinson’s disease: diagnosis and management.Lancet Neurol5, 235-245.
[3] Doty RL, Riklan M, Deems DA, Reynolds C, Stellar S (1989)The olfactory and cognitive deficits of Parkinson’s disease:evidence for independence.Ann Neurol25, 166-171.

590 S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease
[4] Devanand DP, Michaels-Marston KS, Liu X, Pelton GH, Padil-la M, Marder K, Bell K, Stern Y, Mayeux R (2000) Olfac-tory deficits in patients with mild cognitive impairment pre-dict Alzheimer’s disease at follow-up.Am J Psychiatry157,1399-1405.
[5] Djordjevic J, Jones-Gotman M, De Sousa K, Chertkow H(2008) Olfaction in patients with mild cognitive impairmentand Alzheimer’s disease.Neurobiol Aging29, 693-706.
[6] Devanand DP, Liu X, Tabert MH, Pradhaban G, Cuasay K,Bell K, de Leon MJ, Doty RL, Stern Y, Pelton GH (2008) Com-bining early markers strongly predicts conversion from mildcognitive impairment to Alzheimer’s disease.Biol Psychiatry64, 871-879.
[7] Mesholam RI, Moberg PJ, Mahr RN, Doty RL (1998) Olfac-tion in neurodegenerative disease: a meta-analysis of olfacto-ry functioning in Alzheimer’s and Parkinson’s diseases.ArchNeurol55, 84-90.
[8] Warner MD, Peabody CA, Flattery JJ, Tinklenberg JR (1986)Olfactory deficits and Alzheimer’s disease.Biol Psychiatry21, 116-118.
[9] Doty RL, Reyes PF, Gregor T (1987) Presence of both odoridentification and detection deficits in Alzheimer’s disease.Brain Res Bull18, 597-600.
[10] Kesslak JP, Cotman CW, Chui HC, Van den Noort S, Fang H,Pfeffer R, Lynch G (1988) Olfactory tests as possible probesfor detecting and monitoring Alzheimer’s disease.NeurobiolAging9, 399-403.
[11] Murphy C (1999) Loss of olfactory function in dementingdisease.Physiol Behav66, 177-182.
[12] Serby M, Larson P, Kalkstein D (1991) The nature and courseof olfactory deficits in Alzheimer’s disease.Am J Psychiatry148, 357-360.
[13] Braak H, Braak E (1997) Diagnostic criteria for neuropatho-logic assessment of Alzheimer’s disease.Neurobiol Aging18,S85-S88.
[14] Gottfried JA (2006) Smell: central nervous processing. AdvOtorhinolaryngol63, 44-69.
[15] Zatorre RJ, Jones-Gotman M, Evans AC, Meyer E (1992)Functional localization and lateralization of human olfactorycortex.Nature360, 339-340.
[16] Savic I, Gulyas B, Larsson M, Roland P (2000) Olfactoryfunctions are mediated by parallel and hierarchical processing.Neuron26, 735-745.
[17] Buchsbaum MS, Kesslak JP, Lynch G, Chui H, Wu J, SicotteN, Hazlett E, Teng E, Cotman CW (1991) Temporal and hip-pocampal metabolic rate during an olfactory memory task as-sessed by positron emission tomography in patients with de-mentia of the Alzheimer type and controls. Preliminary stud-ies.Arch Gen Psychiatry48, 840-847.
[18] Teipel SJ, Willoch F, Ishii K, Burger K, Drzezga A, EngelR, Bartenstein P, Moller HJ, Schwaiger M, Hampel H (2006)Resting state glucose utilization and the CERAD cognitivebattery in patients with Alzheimer’s disease.Neurobiol Aging27, 681-690.
[19] Desgranges B, Baron JC, de la Sayette V, Petit-Taboue MC,Benali K, Landeau B, Lechevalier B, Eustache F (1998)The neural substrates of memory systems impairment inAlzheimer’s disease. A PET study of resting brain glucoseutilization. Brain 121(Pt 4), 611-631.
[20] Desgranges B, Baron JC, Lalevee C, Giffard B, Viader F, de LaSayette V, Eustache F (2002) The neural substrates of episodicmemory impairment in Alzheimer’s disease as revealed byFDG-PET: relationship to degree of deterioration.Brain 125,1116-1124.
[21] Silverman DH, Small GW, Chang CY, Lu CS, Kung De AburtoMA, Chen W, Czernin J, Rapoport SI, Pietrini P, AlexanderGE, Schapiro MB, Jagust WJ, Hoffman JM, Welsh-BohmerKA, Alavi A, Clark CM, Salmon E, de Leon MJ, MielkeR, Cummings JL, Kowell AP, Gambhir SS, Hoh CK, PhelpsME (2001) Positron emission tomography in evaluation ofdementia: Regional brain metabolism and long-term outcome.Jama286, 2120-2127.
[22] Chetelat G, Desgranges B, de la Sayette V, Viader F, BerkoukK, Landeau B, Lalevee C, Le Doze F, Dupuy B, HannequinD, Baron JC, Eustache F (2003) Dissociating atrophy andhypometabolism impact on episodic memory in mild cognitiveimpairment.Brain 126, 1955-1967.
[23] Herholz K (2003) PET studies in dementia.Ann Nucl Med17,79-89.
[24] Friedland RP, Brun A, Budinger TF (1985) Pathological andpositron emission tomographic correlations in Alzheimer’sdisease.Lancet1, 228.
[25] Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC, RabinsPV, Ritchie K, Rossor M, Thal L, Winblad B (2001) Currentconcepts in mild cognitive impairment.Arch Neurol58, 1985-1992.
[26] McKhann G, Drachman D, Folstein M, Katzman R, Price D,Stadlan EM (1984) Clinical diagnosis of Alzheimer’s disease:report of the NINCDS-ADRDA Work Group under the aus-pices of Department of Health and Human Services Task Forceon Alzheimer’s Disease.Neurology34, 939-944.
[27] Dubois B, Feldman HH, Jacova C, Dekosky ST, Barberger-Gateau P, Cummings J, Delacourte A, Galasko D, Gauthier S,Jicha G, Meguro K, O’Brien J, Pasquier F, Robert P, Rossor M,Salloway S, Stern Y, Visser PJ, Scheltens P (2007) Researchcriteria for the diagnosis of Alzheimer’s disease: revising theNINCDS-ADRDA criteria.Lancet Neurol6, 734-746.
[28] Jagust W, Reed B, Mungas D, Ellis W, Decarli C (2007) Whatdoes fluorodeoxyglucose PET imaging add to a clinical diag-nosis of dementia?Neurology69, 871-877.
[29] Minoshima S, Frey KA, Koeppe RA, Foster NL, Kuhl DE(1995) A diagnostic approach in Alzheimer’s disease usingthree-dimensional stereotactic surface projections of fluorine-18-FDG PET.J Nucl Med36, 1238-1248.
[30] Scheltens P, Barkhof F, Leys D, Pruvo JP, Nauta JJ, Verm-ersch P, Steinling M, Valk J (1993) A semiquantative ratingscale for the assessment of signal hyperintensities on magneticresonance imaging.J Neurol Sci114, 7-12.
[31] Kobal G, Hummel T, Sekinger B, Barz S, Roscher S, Wolf S(1996) “Sniffin’ sticks”: screening of olfactory performance.Rhinology34, 222-226.
[32] Hummel T, Sekinger B, Wolf SR, Pauli E, Kobal G (1997)“Sniffin’ sticks”: olfactory performance assessed by the com-bined testing of odor identification, odor discrimination andolfactory threshold.Chem Senses22, 39-52.
[33] Hummel T, Kobal G, Gudziol H, Mackay-Sim A (2007) Nor-mative data for the “Sniffin’ Sticks” including tests of odoridentification, odor discrimination, and olfactory thresholds:an upgrade based on a group of more than 3,000 subjects.EurArch Otorhinolaryngol264, 237-243.
[34] Friston KJ, Frith CD, Liddle PF, Frackowiak RS (1991) Com-paring functional (PET) images: the assessment of significantchange.J Cereb Blood Flow Metab11, 690-699.
[35] Forster S, Teipel S, Zach C, Rominger A, Cumming P, FougereCL, Yakushev I, Haslbeck M, Hampel H, Bartenstein P, BurgerK (2010) FDG-PET mapping the brain substrates of visuo-constructive processing in Alzheimer s disease.J PsychiatrRes44, 462-469.

S. Forster et al. / Functional Representation of Olfactory Impairment in Early Alzheimer’s Disease 591
[36] Yakushev I, Hammers A, Fellgiebel A, Schmidtmann I,Scheurich A, Buchholz HG, Peters J, Bartenstein P, Lieb K,Schreckenberger M (2009) SPM-based count normalizationprovides excellent discrimination of mild Alzheimer’s diseaseand amnestic mild cognitive impairment from healthy aging.Neuroimage44, 43-50.
[37] Borghammer P, Jonsdottir KY, Cumming P, Ostergaard K,Vang K, Ashkanian M, Vafaee M, Iversen P, Gjedde A (2008)Normalization in PET group comparison studies – the impor-tance of a valid reference region.Neuroimage40, 529-540.
[38] Borghammer P, Cumming P, Aanerud J, Forster S, GjeddeA (2009) Subcortical elevation of metabolism in Parkinson’sdisease – A critical reappraisal in the context of global meannormalization.Neuroimage47, 1514-1521.
[39] Borghammer P, Cumming P, Aanerud J, Gjedde A (2009) Arte-factual subcortical hyperperfusion in PET studies normalizedto global mean: lessons from Parkinson’s disease.Neuroimage45, 249-257.
[40] Fusari A, Ballesteros S (2008) Identification of odors of edibleand nonedible stimuli as affected by age and gender.BehavRes Methods40, 752-759.
[41] Edison P, Archer HA, Hinz R, Hammers A, Pavese N, TaiYF, Hotton G, Cutler D, Fox N, Kennedy A, Rossor M,Brooks DJ (2007) Amyloid, hypometabolism, and cognitionin Alzheimer disease: an [11C]PIB and [18F]FDG PET study.Neurology68, 501-508.
[42] Alexander GE, Chen K, Pietrini P, Rapoport SI, Reiman EM(2002) Longitudinal PET evaluation of cerebral metabolic de-cline in dementia: a potential outcome measure in Alzheimer’sdisease treatment studies.Am J Psychiatry159, 738-745.
[43] Lancaster JL, Woldorff MG, Parsons LM, Liotti M, Freitas CS,Rainey L, Kochunov PV, Nickerson D, Mikiten SA, Fox PT(2000) Automated Talairach atlas labels for functional brainmapping.Hum Brain Mapp10, 120-131.
[44] Dubois B, Picard G, Sarazin M (2009) Early detection ofAlzheimer’s disease: new diagnostic criteria.Dialogues ClinNeurosci11, 135-139.
[45] Yuan Y, Gu ZX, Wei WS (2009) Fluorodeoxyglucose-positron-emission tomography, single-photon emission to-mography, and structural MR imaging for prediction of rapidconversion to Alzheimer disease in patients with mild cogni-tive impairment: a meta-analysis.AJNR Am J Neuroradiol30,404-410.
[46] Atighechi S, Salari H, Baradarantar MH, Jafari R, KarimiG, Mirjali M (2009) A comparative study of brain perfusionsingle-photon emission computed tomography and magneticresonance imaging in patients with post-traumatic anosmia.Am J Rhinol Allergy23, 409-412.
[47] Hedner M, Larsson M, Arnold N, Zucco GM, Hummel TCognitive factors in odor detection, odor discrimination,andodor identification tasks.J Clin Exp Neuropsychol, 1-6.
[48] Savic I, Berglund H (2004) Passive perception of odors andsemantic circuits.Hum Brain Mapp21, 271-278.
[49] Kronenbuerger M, Zobel S, Ilgner J, Finkelmeyer A, Reinach-er P, Coenen VA, Wilms H, Kloss M, Kiening K, Daniels C,Falk D, Schulz JB, Deuschl G, Hummel T Effects of deep brainstimulation of the cerebellothalamic pathways on the senseofsmell.Exp Neurol222, 144-152.
[50] Tham WW, Stevenson RJ, Miller LA (2009) The functionalrole of the medio dorsal thalamic nucleus in olfaction.BrainRes Rev62, 109-126.
[51] Braak H, Braak E (1991) Neuropathological stageing ofAlzheimer-related changes.Acta Neuropathol82, 239-259.
[52] Geddes JW, Tekirian TL, Soultanian NS, Ashford JW, DavisDG, Markesbery WR (1997) Comparison of neuropathologiccriteria for the diagnosis of Alzheimer’s disease.NeurobiolAging18, S99-105.
[53] Kumar A, Schapiro MB, Grady C, Haxby JV, Wagner E, Saler-no JA, Friedland RP, Rapoport SI (1991) High-resolution PETstudies in Alzheimer’s disease.Neuropsychopharmacology4,35-46.
[54] Mosconi L (2005) Brain glucose metabolism in the early andspecific diagnosis of Alzheimer’s disease. FDG-PET studiesin MCI and AD.Eur J Nucl Med Mol Imaging32, 486-510.
[55] Mosconi L, Tsui WH, De Santi S, Li J, Rusinek H, ConvitA, Li Y, Boppana M, de Leon MJ (2005) Reduced hippocam-pal metabolism in MCI and AD: automated FDG-PET imageanalysis.Neurology64, 1860-1867.
[56] Ashford JW, Shan M, Butler S, Rajasekar A, Schmitt FA(1995) Temporal quantification of Alzheimer’s disease sever-ity: ’time index’ model.Dementia6, 269-280.
[57] Ashford JW, Shih WJ, Coupal J, Shetty R, Schneider A, CoolC, Aleem A, Kiefer VH, Mendiondo MS, Schmitt FA (2000)Single SPECT measures of cerebral cortical perfusion reflecttime-index estimation of dementia severity in Alzheimer’sdis-ease.J Nucl Med41, 57-64.
[58] Ashford JW, Jarvik L (1985) Alzheimer’s disease: does neuronplasticity predispose to axonal neurofibrillary degeneration?N Engl J Med313, 388-389.
[59] Velayudhan L, Lovestone S (2009) Smell identification test asa treatment response marker in patients with Alzheimer diseasereceiving donepezil.J Clin Psychopharmacol29, 387-390.
[60] Haehner A, Mayer AM, Landis BN, Pournaras I, Lill K, Gudzi-ol V, Hummel T (2009) High test-retest reliability of the ex-tended version of the “Sniffin’ Sticks” test.Chem Senses34,705-711.
Related Documents











