LEFT VENTRICULAR DYSSYNCHRONY Functional Mitral Regurgitation at Rest Determines the Acute Hemodynamic Response to Cardiac Resynchronization Therapy During Exercise: An Acute Exercise Echocardiographic Study Sylvestre Mare ´chaux, MD, Claire Pinc ¸on, PhD, Benjamin Gal, MD, Claude Kouakam, MD, Christelle Marquie ´, MD, Dominique Lacroix, MD, PhD, Pascal de Groote, MD, PhD, Fre ´de ´ric Mouquet, MD, PhD, Thierry Le Tourneau, MD, PhD, Ste ´phane Dennetie `re, MD, Yves Guyomar, MD, Alain Cohen Solal, MD, PhD, Damien Logeart, MD, PhD, Philippe Asseman, MD, Thierry H. Le Jemtel, MD, and Pierre Vladimir Ennezat, MD, PhD, Lille, Roubaix, and Paris, France; New Orleans, Louisiana Background: Cardiac resynchronization therapy (CRT) acutely enhances forward stroke volume (FSV) during exercise by reducing the severity of functional mitral regurgitation (MR) in patients with systolic chronic heart failure. Whether CRT increases FSV in patients without functional MR at rest is unknown. Accordingly, the aim of the study was to compare the effect of CRT on exercise-induced increase in FSV in patients with chronic heart failure with or without functional MR at rest. Methods and Results: Forty-one patients with systolic chronic heart failure who had recently undergone CRT performed 2 exercise stress echocardiography tests, the first with CRT On and the second with CRT Off. Twenty-six patients had more than trivial MR (effective regurgitant orifice [ERO] < 10 mm 2 in 16 patients, < 20 mm 2 in 8 patients, and $ 20 mm 2 in 2 patients), and 15 patients had no MR at rest. Mean exercise-in- duced change (D) in mitral ERO was reduced by CRT (8 6 7 mm 2 vs 1 6 4 mm 2 , P < .00001). In patients with functional MR at rest, D FSV during dynamic exercise was greater with CRT On than CRT Off (4 6 8 vs À2 6 7 mL, P = .0002), whereas CRT did not significantly affect D FSV in patients without MR at rest (9 6 9 mL vs 9 6 9 mL, P = .93). Similarly, D cardiac output was greater with CRT On than CRT Off (1.6 6 1.2 L/min vs 1.1 6 1.2 L/min, P = .002) in patients with functional MR at rest, whereas D cardiac output was similar with CRT On and CRT Off in patients without MR at rest (1.9 6 1.4 L/min vs 2.0 6 1.2 L/min, P = .59). Severity of functional MR decreased or failed to increase, whereas cardiac output improved during exercise in 9 of 26 patients (34%) with CRT On and in only 2 of 26 patients (8%) with CRT Off (P = .039). Conclusion: Functional MR at rest may be an important determinant of the acute hemodynamic response to CRT during exercise. (J Am Soc Echocardiogr 2009;22:464-471.) Keywords: Exercise echocardiography, Functional mitral regurgitation, Cardiac resynchronization therapy Functional mitral regurgitation (MR) is common in symptomatic patients with chronic heart failure (CHF) and predicts a poor out- come. 1-3 Functional MR results from an imbalance between decreased mitral closing forces and increased tethering forces. 4,5 During exercise, worsening of functional MR tends to decrease for- ward stroke volume (FSV) in patients with CHF. 6 Conversely, cardiac resynchronization therapy (CRT) acutely increases FSV during exer- cise by reducing the severity of functional MR. 7-9 Whether CRT similarly increases, FSV during exercise in patients without resting functional MR is unclear. Accordingly, the present study was undertaken to compare the ef- fects of CRTon exercise-induced changes in FSV in patients with CHF with or without functional MR at rest. The hypothesis behind the pres- ent study was that patients with CHF with or without functional MR at rest may derive contrasting acute hemodynamic benefits from CRT. MATERIALS AND METHODS Study Population Ambulatory stable patients with CHF caused by left ventricular (LV) systolic dysfunction (ejection fraction < 35%) who had undergone CRT no more than 3 weeks ago were eligible for the study. Patients with recent myocardial infarction (< 3 months), acute coronary From the Centre Hospitalier Re ´ gional et Universitaire de Lille, Departments of Ultrasound and Physiology (S.M., T.L.T.) and Cardiology (B.G., C.K., C.M., D.L., P.de G., F.M., T.L.T., P.A., P.V.E.), Lille, France; EA 2693, Universite ´ de Lille 2, Faculte ´ de Me ´decine, Lille, France (S.M., F.M., T.L.T., P.A., P.V.E.); Department of Biostatistics, Faculte ´ de Pharmacie, Universite ´ de Lille 2, Lille, France (CP); Centre Hospitalier de Roubaix (S.D.); Centre Hospitalier Saint Philibert, Faculte ´ Libre de Me ´decine de Lille (Y.G.); Ho ˆ pital Lariboisie `re, Assistance Publique-Ho ˆ pitaux de Paris, Paris, France (A.C.S., D.L.); and Division of Cardiology, Tulane University School of Medicine, New Orleans, Louisiana (T.H.LJ). Reprint requests: Pierre Vladimir Ennezat, MD, PhD, Intensive Care Unit, Cardiol- ogy Hospital, Bd Pr J Leclercq, 59037 Lille Cedex. (E-mail: [email protected]). 0894-7317/$36.00 Copyright 2009 by the American Society of Echocardiography. doi:10.1016/j.echo.2009.02.002 464

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

LEFT VENTRICULAR DYSSYNCHRONY
Functional Mitral Regurgitation at Rest Determines theAcute Hemodynamic Response to Cardiac
Resynchronization Therapy During Exercise: An AcuteExercise Echocardiographic Study
Sylvestre Marechaux, MD, Claire Pincon, PhD, Benjamin Gal, MD, Claude Kouakam, MD,Christelle Marquie, MD, Dominique Lacroix, MD, PhD, Pascal de Groote, MD, PhD, Frederic Mouquet, MD,PhD, Thierry Le Tourneau, MD, PhD, Stephane Dennetiere, MD, Yves Guyomar, MD, Alain Cohen Solal, MD,
PhD, Damien Logeart, MD, PhD, Philippe Asseman, MD, Thierry H. Le Jemtel, MD,and Pierre Vladimir Ennezat, MD, PhD, Lille, Roubaix, and Paris, France; New Orleans, Louisiana
Background: Cardiac resynchronization therapy (CRT) acutely enhances forward stroke volume (FSV) duringexercise by reducing the severity of functional mitral regurgitation (MR) in patients with systolic chronic heartfailure. Whether CRT increases FSV in patients without functional MR at rest is unknown. Accordingly, the aimof the study was to compare the effect of CRT on exercise-induced increase in FSV in patients with chronicheart failure with or without functional MR at rest.
Methods and Results: Forty-one patients with systolic chronic heart failure who had recently undergone CRTperformed 2 exercise stress echocardiography tests, the first with CRT On and the second with CRT Off.Twenty-six patients had more than trivial MR (effective regurgitant orifice [ERO] < 10 mm2 in 16 patients,< 20 mm2 in 8 patients, and $ 20 mm2 in 2 patients), and 15 patients had no MR at rest. Mean exercise-in-duced change (D) in mitral ERO was reduced by CRT (8 6 7 mm2 vs 1 6 4 mm2, P < .00001). In patientswith functional MR at rest, D FSV during dynamic exercise was greater with CRT On than CRT Off (4 6 8 vs�2 6 7 mL, P = .0002), whereas CRT did not significantly affect D FSV in patients without MR at rest (9 6
9 mL vs 9 6 9 mL, P = .93). Similarly, D cardiac output was greater with CRT On than CRT Off (1.6 6 1.2L/min vs 1.1 6 1.2 L/min, P = .002) in patients with functional MR at rest, whereas D cardiac output was similarwith CRT On and CRT Off in patients without MR at rest (1.9 6 1.4 L/min vs 2.0 6 1.2 L/min, P = .59). Severity offunctional MR decreased or failed to increase, whereas cardiac output improved during exercise in 9 of26 patients (34%) with CRT On and in only 2 of 26 patients (8%) with CRT Off (P = .039).
Conclusion: Functional MR at rest may be an important determinant of the acute hemodynamic response toCRT during exercise. (J Am Soc Echocardiogr 2009;22:464-471.)
Keywords: Exercise echocardiography, Functional mitral regurgitation, Cardiac resynchronization therapy
Functional mitral regurgitation (MR) is common in symptomaticpatients with chronic heart failure (CHF) and predicts a poor out-come.1-3 Functional MR results from an imbalance betweendecreased mitral closing forces and increased tethering forces.4,5
From the Centre Hospitalier Regional et Universitaire de Lille, Departments of
Ultrasound and Physiology (S.M., T.L.T.) and Cardiology (B.G., C.K., C.M., D.L.,
P.de G., F.M., T.L.T., P.A., P.V.E.), Lille, France; EA 2693, Universite de Lille 2,
Faculte de Medecine, Lille, France (S.M., F.M., T.L.T., P.A., P.V.E.); Department of
Biostatistics, Faculte de Pharmacie, Universite de Lille 2, Lille, France (CP); Centre
Hospitalier de Roubaix (S.D.); Centre Hospitalier Saint Philibert, Faculte Libre de
Medecine de Lille (Y.G.); Hopital Lariboisiere, Assistance Publique-Hopitaux de
Paris, Paris, France (A.C.S., D.L.); and Division of Cardiology, Tulane University
School of Medicine, New Orleans, Louisiana (T.H.LJ).
Reprint requests: Pierre Vladimir Ennezat, MD, PhD, Intensive Care Unit, Cardiol-
ogy Hospital, Bd Pr J Leclercq, 59037 Lille Cedex. (E-mail: [email protected]).
0894-7317/$36.00
Copyright 2009 by the American Society of Echocardiography.
doi:10.1016/j.echo.2009.02.002
464
During exercise, worsening of functional MR tends to decrease for-ward stroke volume (FSV) in patients with CHF.6 Conversely, cardiacresynchronization therapy (CRT) acutely increases FSV during exer-cise by reducing the severity of functional MR.7-9 Whether CRTsimilarly increases, FSV during exercise in patients without restingfunctional MR is unclear.
Accordingly, the present study was undertaken to compare the ef-fects of CRTon exercise-induced changes in FSV in patients with CHFwith or without functional MR at rest. The hypothesis behind the pres-ent study was that patients with CHF with or without functional MR atrest may derive contrasting acute hemodynamic benefits from CRT.
MATERIALS AND METHODS
Study Population
Ambulatory stable patients with CHF caused by left ventricular (LV)systolic dysfunction (ejection fraction < 35%) who had undergoneCRT no more than 3 weeks ago were eligible for the study. Patientswith recent myocardial infarction (< 3 months), acute coronary

syndrome according to European Society of Cardiology/AmericanHeart Association criteria,10 or coronary revascularization within thepast 3 months were ineligible for the study. Patients with primarymitral or aortic valvular disease were also ineligible for the study.The initial study population included 70 patients with ischemic andnonischemic cardiomyopathy. The ischemic cause of LV systolic dys-function was documented by the presence of a lesion > 50% in atleast 1 coronary artery. All patients were in sinus rhythm witha wide QRS (>120 ms) related to left bundle branch block (meanQRS duration 168 ms) before CRTand received a Guidant Corp (In-dianapolis, IN) or Medtronic (Minneapolis, MN) device. The LV leadwas advanced in an epicardial vein via the coronary sinus in all pa-tients. The preferred position was a lateral or posterolateral vein. Byusing pulsed Doppler mitral inflow, the atrioventricular delay (1256 26 ms) was selected to allow for adequate E and A-wave separationand termination of the Awave before mitral valve closure. Six patientswere excluded after implantation for lead dislodgement (n = 3) anddiaphragmatic stimulation (n = 3). In addition, 23 patients were ex-cluded for the following: poor acoustic window (n = 4), sinus or atrio-ventricular blocks (n = 6), atrial fibrillation (n = 6), presence of lateralwall scar on cardiac imaging (n = 4), or orthopedic limitation to exer-cise (n = 3). The study was approved by the Lille University MedicalCenter institution review board. All patients signed an informedconsent.
Exercise Echocardiography
Symptom-limited (fatigue, dyspnea, or both) exercise was performedon a semi-recumbent and tilting bicycle ergometer starting at a 25watts (W) workload and with 20 W increments every 3 minutes.Blood pressure was measured every 2 minutes. A 12-lead electrocar-diogram was continuously monitored. Patients received their routinemedications (including beta-adrenergic blockade) the morning of thestudy. Echocardiographic measurements were performed at baselineand at the end of the exercise with the following stepwise sequence:LVoutflow tract and velocity time integral), continuous-wave Dopplerrecording of tricuspid regurgitation, proximal isovelocity surface arearecording and continuous-wave Doppler recording of MR, and LVapical 4- and 2-chamber views. All patients performed 2 maximalsymptoms limited exercise tests. Patients exercised first with CRTOn. CRT was discontinued (CRT Off), and patients performed a sec-ond exercise at least 6 hours later.
Echocardiographic Analysis
Continuous 2-dimensional and Doppler echocardiography monitor-ing was performed with a scanner (SONOS 5500, Philips, Andover,MA) equipped with a 2- to 4-MHz transducer. All echocardiographicmeasurements were performed off-line by 2 experienced echocardi-ographers (BG and PVE). At least 3 cardiac cycles were used for eachmeasurement, and the average value was taken. LV volumes and ejec-tion fraction were calculated using the Simpson biplane method. Rest-ing LV diastolic function was assessed by peak velocities of the E wave(early diastole), A wave (late diastole), deceleration time of the Ewave, and E/A ratio. Aortic ejection delay was defined as the delaybetween the onset of the QRS and the onset of the systolic aorticflow. Pulmonary ejection delay was defined as the delay betweenthe onset of the QRS and the onset of the systolic pulmonary flowthat was recorded from the parasternal view. Interventricular dyssyn-chrony was evaluated as the difference between aortic and pulmo-nary ejection delays using standard pulsed-Doppler. Resting intra-LVdyssynchrony was assessed by pulsed-tissue Doppler imaging.11,12
Journal of the American Society of EchocardiographyVolume 22 Number 5
The septal, lateral, inferior, and anterior walls were analyzed fromthe apical 4- and 2-chamber views. Gains and filters were optimizedto eliminate background noise. Sample volume was placed in themiddle of the basal segment of each wall. The tissue Doppler imagingsignals were recorded at a sweep speed of 100 mm/s. Delays weremeasured between the onset of the QRS and the onset of the Swave. Intraventricular mechanical delays were calculated from thedifference between the earliest and the most delayed sites. Cardiacoutput was calculated as the product of the FSV (velocity time integral� (D2/ � p D being the diameter of the LV outflow tract) and heartrate. The trans-tricuspid pressure gradient was estimated from themaximal tricuspid regurgitation velocity using the modified Bernoulliequation (DP = 4 Vmax2, DP being the difference of pressure be-tween the right ventricle and the right atrium and Vmax being themaximal velocity of the regurgitant jet) in the absence of pulmonicstenosis.13 Mitral regurgitant flow volume (RV) and orifice area(ERO) at rest and exercise were measured by the proximal flow con-vergence technique.14 Depth, size, and sector settings were optimizedfor optimal color Doppler resolution. The Doppler color flow zerobaseline was shifted downward to obtain satisfactory hemisphericproximal isovelocity surface area. The proximal flow convergencewas imaged and expanded in the apical 4-chamber view. The aliasingvelocity (Vr) was carefully adjusted (20-40 cm/s) and left unchangedduring exercise. The midsystole radius of proximal flow convergenceregion (r) was measured from the point of aliasing to the leaflet tips.MR maximum regurgitant velocity and the regurgitant time-velocityintegral were obtained from continuous-wave Doppler echocardiog-raphy. The regurgitant flow was measured as 2 � p � r2 � Vr. Thefollowing parameters were calculated: ERO = regurgitant flow/max-imal regurgitant velocity, and RV = ERO � regurgitant time-velocityintegral. LV +dP/dt was defined as the slope trace between 1 and3 m/s on the MR continuous-wave Doppler jet recorded at a sweepspeed of 100 mm/s.15 The reproducibility in the measurement ofERO at rest and peak exercise, as assessed by the mean difference6 standard deviation among 10 studies (average of 3 cardiac cycles)on 2 occasions within a 24-hour period by the same investigator, was0.6 6 1.4 mm2 and 0.9 6 1.2 mm2, and intraobserver regression co-efficients were 0.95 and 0.97, respectively. Ten subjects were used forreliability analysis between 2 observers (average of 3 cardiac cycles).The mean difference 6 standard deviation for ERO at rest and peakexercise was 0.8 61.3 mm2 and 1.1 62 mm2, respectively, and inter-observer regression coefficients were 0.96 and 0.95, respectively.
Table 1 Demographic and clinical characteristics of studypopulation (n = 41)
Age (y) 65 6 10Male (%) 76
Diabetes mellitus (%) 17
Body mass index (kg/m2) 26 6 4
History of smoking (%) 58Systemic hypertension (%) 49
Hypercholesterolemia (%) 48
Ischemic (%) 37
ACE inhibitors/angiotensin II receptor antagonists (%) 100Beta-blockade (%) 88
Diuretics (%) 78
Spironolactone (%) 49Antiplatelet therapy (%) 37
Implantable cardiac defibrillator (%) 61
ACE, Angiotensin-converting enzyme.
Marechaux et al 465

Table 2A Acute hemodynamic and echocardiographic effects of cardiac resynchronization therapy at rest in patients with orwithout functional mitral regurgitation at rest
MR (n = 26) No MR (n = 15)
CRT Off CRT On Change CRT Off CRT On Change
Heart rate (bpm) 68 6 13 67 6 12 �1 6 1 73 6 16 72 6 15 �1 6 2
Systolic blood pressure (mm Hg) 111 6 15 115 6 15 4 6 2 120 6 23 127 6 21 7 6 3b
LV ejection fraction (%) 23 6 8 23 6 8 1 6 1 27 6 12 28 6 12 �1 6 1
LV end-diastolic volume (mL) 234 6 73 237 6 81 3 6 4 190 6 81 197 6 79 7 6 5E/A ratio 1.7 6 1.3 1.9 6 1.8 0.1 6 0.2 1.3 6 1.1 1.1 6 0.7 �0.1 6 0.1
Maximal velocity of the E wave (cm/s) 74 6 27 67 6 21 �7 6 3 65 6 19 61 6 20 �2 6 5
E-wave deceleration time (ms) 160 6 59 161 6 74 3 6 13 241 6 124a 220 6 79a �16 6 24
Left atrial area (cm2) 30 6 9 29 6 7 �1 6 1 26 6 8 25 6 8 �1 6 2FSV (mL) 44 6 12 42 6 10 �2 6 2 45 6 17 45 6 15 �1 6 2
Cardiac output (L/min) 3.0 6 1.0 2.8 6 0.8 �0.2 6 0.1 3.2 6 1.1 3.1 6 0.9 �0.1 6 0.2
Transtricuspid pressure gradient (mm Hg) 29 6 9 28 6 9 �1 6 1 22 6 8 25 6 8 2 6 1
Interventricular dyssynchrony (ms) 52 6 38 21 6 16 �32 6 7b 55 6 36 28 6 22 �27 6 9b
Intra-LV dyssynchrony (ms) 96 6 64 41 6 40 �55 6 14b 93 6 74 24 6 54 �70 6 19b
CRT, Cardiac resynchronization therapy; LV, left ventricular; MR, mitral regurgitation; FSV, forward stroke volume.
Values of hemodynamic and echocardiographic parameters are expressed as mean 6 standard deviation. Two-way ANOVA for repeated measureswas used for statistical comparisons. Values of changes are expressed as differences of least squares means 6 standard error. ANOVA showed no
significant interaction between those with or without functional MR at rest and CRT On or Off.aP # .05 for MR effect for all subjects.bP # .05 for CRT effect for all subjects.
466 Marechaux et al Journal of the American Society of EchocardiographyMay 2009
Statistical Analysis
Characteristics are presented as mean and standard error for continu-ous variables and as percentages for categoric variables. Effects of CRTand presence of MR were tested with a 2-way analysis of variance(ANOVA), with the presence of MR as the between-subject variableand CRT as the within-subject variable. To take into account the re-peated nature of the experiment (with or without CRT), the datawere analyzed with the MIXED procedure of the SAS system (SASv8, SAS Institute Inc, Cary, NC) with a repeated statement. The firststep was to select the within-subject covariance, based on likelihoodratio tests.16 Then, tests of the fixed effects were performed. Whena significant interaction between CRT On or Off and presence or nopresence of MR was found, the difference between means with orwithout CRT was tested to be equal to zero for each level of MR.Values of changes are subsequently expressed as differences of leastsquares means 6 standard error.
In the subsample of patients with MR, comparisons of means withor without CRTwere performed with paired Student t tests wheneverthe distribution of the data was found to be normal by a Shapiro-Wilktest. Otherwise, a Wilcoxon signed-rank test for paired data was used.
Effects of CRT and severity of MR at rest on LV FSV and cardiacoutput at rest and during exercise were tested with a repeated-mea-sures 2-way ANOVA as described above, severity of MR being de-fined using the median value of mitral ERO when the device is off.
The relationship between exercise-induced changes (D) in mitralERO and D cardiac output or D LV FSV was investigated again usingthe MIXED procedure with a repeated statement, nesting D cardiacoutput or D FSV with CRT. A separate regression line within eachlevel of CRT was obtained, modelizing D FSV or D cardiac outputas a function of D mitral ERO. For each level of CRT, the slope wastested to be equal to zero.
Last, we computed the proportions of patients for whom D mitralERO was lower than or equal to zero while D FSVor D cardiac outputwere greater than zero with CRT On and with CRT Off. To comparethese correlated proportions, we used the McNemar’s exact test(based on the cumulative binomial distribution), because the number
of discordant pairs was less than 20. Two-sided P values less than .05were deemed to be statistically significant.
RESULTS
The final study population consisted of 31 men and 10 women, withan average age of 65 610 years. The clinical characteristics and med-ical regimen of the study population are summarized in Table 1. Allpatients were receiving angiotensin-converting enzyme inhibitorsand beta-blockers except for 5 patients who could not toleratebeta-adrenergic blockade. LV systolic dysfunction was caused by cor-onary artery disease in 15 patients (37%).
Resting Parameters
Twenty-six patients had more than trivial MR at rest (ERO < 10 mm2
in 16 patients, < 20 mm2 in 8 patients, and $ 20 mm2 in the remain-ing 2 patients). The 2-way ANOVA showed that there was no
Table 2B Acute effects of cardiac resynchronization therapyon mitral regurgitation parameters at rest in patients withfunctional mitral regurgitation at rest
MR (n = 26)
CRT Off CRT On Change
Mitral ERO (mm2) 9 6 7 8 6 7 �2 6 4a
Mitral RV (mL) 15 6 11 12 6 10 �3 6 6a
LV + dP/dT (mm Hg/s) 435 6 173 578 6 139 143 6 129a
CRT, Cardiac resynchronization therapy; ERO effective regurgitant ori-
fice area; RV, regurgitant volume; LV, left ventricular; MR, mitralregurgitation.
Values and their changes are expressed as mean 6 standard deviation.
Paired t tests or Wilcoxon tests were used for statistical comparisons.aP # .05 for CRT effect.

Figure 1 Quantification of functional MR at rest and during exercise with CRT On and Off. In this patient, mitral ERO was mildly re-duced by CRT at rest and significantly reduced at peak exercise. CRT was associated with a clear increase in the LV + dP/dt andmitral regurgitant maximal jet velocity at peak exercise.
Table 3A Acute hemodynamic and echocardiographic effects of cardiac resynchronization therapy during exercise in patients withor without functional mitral regurgitation at rest
MR (n = 26) No MR (n = 15)
CRT Off CRT On Change CRT Off CRT On Change
Workload (W) 53 6 21 55 6 21 2 6 2 54 6 17 53 6 18 �1 6 2D Heart rate (bpm) 29 6 14 28 6 14 �2 6 2 27 6 16 25 6 16 �2 6 2
D Systolic blood pressure (mm Hg) 11 6 17 15 6 18 �4 6 4 17 6 17 7 6 18 �10 6 5
D LV ejection fraction (%) 1 6 8 3 6 6 2 6 2 1 6 6 1 6 9 0 6 2D LV end diastolic volume (mL) �6 6 20 �11 6 21 �5 6 5 3 6 19 �4 6 28 �7 6 6
D Forward stroke volume (mL) �2 6 7 4 6 8 7 6 2a 9 6 9 9 6 9 0 6 2
D Cardiac output (L/min) 1.1 6 1.1 1.6 6 1.2 0.5 6 0.2a 2.0 6 1.2 1.9 6 1.4 �0.1 6 0.2
D Trans-tricuspid pressure gradient (mm Hg) 21 6 16 16 6 13 �5 6 4 22 6 15 20 6 10 �1 6 5
CRT, Cardiac resynchronization therapy; MR, mitral regurgitation; LV, left ventricular.
Values of exercise-induced changes (D) are expressed as mean 6 standard deviation. Two-way ANOVA for repeated measures was used for statistical
comparisons. Values of changes are expressed as differences of least squares means 6 standard error.aP # .05 for mean changes in CRT On or Off for patients with MR.
Journal of the American Society of EchocardiographyVolume 22 Number 5
Marechaux et al 467
interaction between those with or without functional MR at rest andCRT On or Off for all resting parameters. No effect of the presence offunctional MR was found for all resting parameters but E-wave decel-eration time (Table 2A). Consequently, resting parameters were com-pared between CRT On and Off, except for E-wave deceleration timethat was compared in patients with or without MR (Table 2A). As ex-pected, CRT significantly reduced interventricular and intra-LV dys-synchrony in the whole population (54 6 38 ms vs 24 6 19 msand 95 6 70 ms vs 32 6 44 ms, respectively, both P < .001). Inter-ventricular and intra-LV dyssynchrony were also reduced by CRT inpatients with or without MR (Table 2A). Systolic blood pressurewas increased by CRT independently from the presence of MR(116 6 18 mm Hg vs 121 6 18 mm Hg, P = .005), whereas heartrate was unchanged. Similarly, LV ejection fraction, LV end-diastolicand end-systolic volumes, FSV, cardiac output, left atrial area, E/A ra-tio, E-wave velocity, and the trans-tricuspid pressure gradient werenot altered by CRT or the presence of functional MR (Table 2A).
The E-wave deceleration time was lower in patients with MR thanin patients without MR but was not altered by CRT (160 6 66 msvs 229 6 101 ms, P = .0078).
In the 26 patients with functional MR at rest, mitral ERO and RVwere both reduced at rest by CRT (9 6 7 mm2 vs 8 6 7 mm2, and 156 11 mL vs 12 610 mL, P = .05 and P = .015, respectively; Table 2B).CRT significantly increased LV + dP/dt in patients with MR (435 6
173 mm Hg/s vs 578 6 139 mm Hg/s, P < .00001; Figure 1 andTable 2B).
Exercise Parameters
No significant interaction was found in those with or without func-tional MR at rest and CRT On or Off for all exercise parameters ex-cept for D FSV and D cardiac output. Workloads achieved weresimilar during exercise performed with or without CRTand in patientswith or without functional MR (Table 3A). During dynamic exercise,
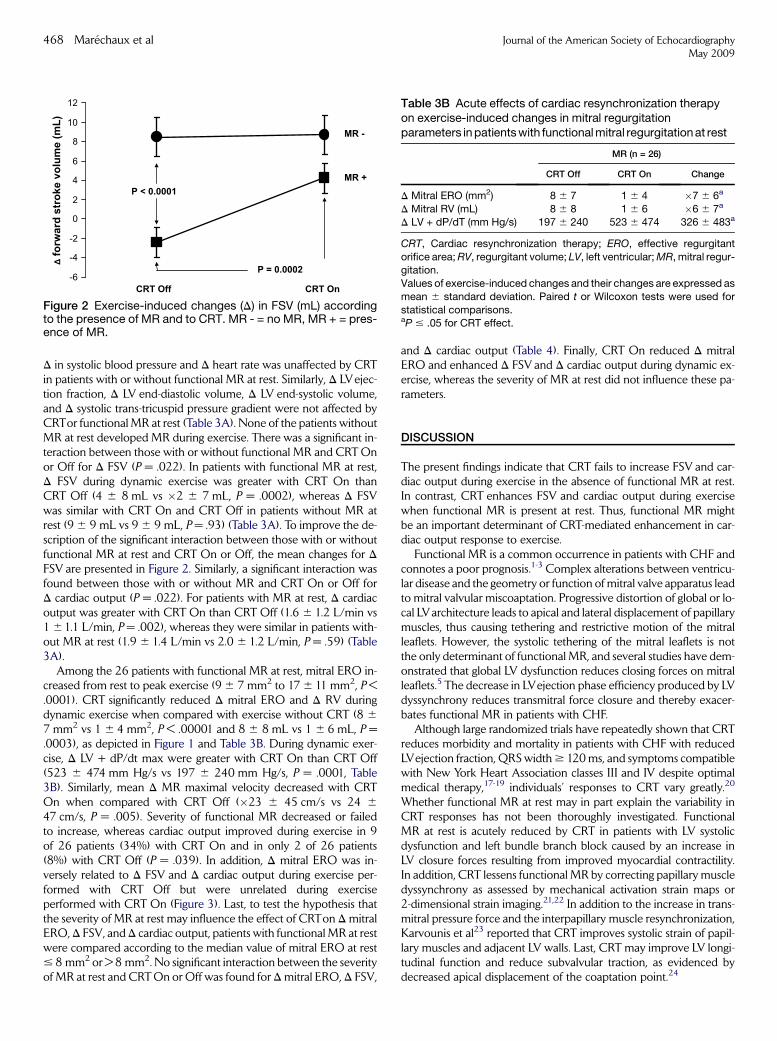
D in systolic blood pressure and D heart rate was unaffected by CRTin patients with or without functional MR at rest. Similarly, D LVejec-tion fraction, D LV end-diastolic volume, D LV end-systolic volume,and D systolic trans-tricuspid pressure gradient were not affected byCRTor functional MR at rest (Table 3A). None of the patients withoutMR at rest developed MR during exercise. There was a significant in-teraction between those with or without functional MR and CRT Onor Off for D FSV (P = .022). In patients with functional MR at rest,D FSV during dynamic exercise was greater with CRT On thanCRT Off (4 6 8 mL vs �2 6 7 mL, P = .0002), whereas D FSVwas similar with CRT On and CRT Off in patients without MR atrest (9 6 9 mL vs 9 6 9 mL, P = .93) (Table 3A). To improve the de-scription of the significant interaction between those with or withoutfunctional MR at rest and CRT On or Off, the mean changes for DFSV are presented in Figure 2. Similarly, a significant interaction wasfound between those with or without MR and CRT On or Off forD cardiac output (P = .022). For patients with MR at rest, D cardiacoutput was greater with CRT On than CRT Off (1.6 6 1.2 L/min vs1 61.1 L/min, P = .002), whereas they were similar in patients with-out MR at rest (1.9 6 1.4 L/min vs 2.0 6 1.2 L/min, P = .59) (Table3A).
Among the 26 patients with functional MR at rest, mitral ERO in-creased from rest to peak exercise (9 6 7 mm2 to 17 6 11 mm2, P <.0001). CRT significantly reduced D mitral ERO and D RV duringdynamic exercise when compared with exercise without CRT (8 6
7 mm2 vs 1 6 4 mm2, P < .00001 and 8 6 8 mL vs 1 6 6 mL, P =.0003), as depicted in Figure 1 and Table 3B. During dynamic exer-cise, D LV + dP/dt max were greater with CRT On than CRT Off(523 6 474 mm Hg/s vs 197 6 240 mm Hg/s, P = .0001, Table3B). Similarly, mean D MR maximal velocity decreased with CRTOn when compared with CRT Off (�23 6 45 cm/s vs 24 6
47 cm/s, P = .005). Severity of functional MR decreased or failedto increase, whereas cardiac output improved during exercise in 9of 26 patients (34%) with CRT On and in only 2 of 26 patients(8%) with CRT Off (P = .039). In addition, D mitral ERO was in-versely related to D FSV and D cardiac output during exercise per-formed with CRT Off but were unrelated during exerciseperformed with CRT On (Figure 3). Last, to test the hypothesis thatthe severity of MR at rest may influence the effect of CRTon D mitralERO, D FSV, and D cardiac output, patients with functional MR at restwere compared according to the median value of mitral ERO at rest# 8 mm2 or > 8 mm2. No significant interaction between the severityof MR at rest and CRT On or Off was found for D mitral ERO, D FSV,
-6
-4
-2
0
2
4
6
8
10
12
fo
rw
ard
stro
ke vo
lu
me (m
L)
CRT Off CRT On
MR +
MR -
P < 0.0001
P = 0.0002
Figure 2 Exercise-induced changes (D) in FSV (mL) accordingto the presence of MR and to CRT. MR - = no MR, MR + = pres-ence of MR.
468 Marechaux et al
and D cardiac output (Table 4). Finally, CRT On reduced D mitralERO and enhanced D FSV and D cardiac output during dynamic ex-ercise, whereas the severity of MR at rest did not influence these pa-rameters.
DISCUSSION
The present findings indicate that CRT fails to increase FSV and car-diac output during exercise in the absence of functional MR at rest.In contrast, CRT enhances FSV and cardiac output during exercisewhen functional MR is present at rest. Thus, functional MR mightbe an important determinant of CRT-mediated enhancement in car-diac output response to exercise.
Functional MR is a common occurrence in patients with CHF andconnotes a poor prognosis.1-3 Complex alterations between ventricu-lar disease and the geometry or function of mitral valve apparatus leadto mitral valvular miscoaptation. Progressive distortion of global or lo-cal LVarchitecture leads to apical and lateral displacement of papillarymuscles, thus causing tethering and restrictive motion of the mitralleaflets. However, the systolic tethering of the mitral leaflets is notthe only determinant of functional MR, and several studies have dem-onstrated that global LV dysfunction reduces closing forces on mitralleaflets.5 The decrease in LVejection phase efficiency produced by LVdyssynchrony reduces transmitral force closure and thereby exacer-bates functional MR in patients with CHF.
Although large randomized trials have repeatedly shown that CRTreduces morbidity and mortality in patients with CHF with reducedLVejection fraction, QRS width $ 120 ms, and symptoms compatiblewith New York Heart Association classes III and IV despite optimalmedical therapy,17-19 individuals’ responses to CRT vary greatly.20
Whether functional MR at rest may in part explain the variability inCRT responses has not been thoroughly investigated. FunctionalMR at rest is acutely reduced by CRT in patients with LV systolicdysfunction and left bundle branch block caused by an increase inLV closure forces resulting from improved myocardial contractility.In addition, CRT lessens functional MR by correcting papillary muscledyssynchrony as assessed by mechanical activation strain maps or2-dimensional strain imaging.21,22 In addition to the increase in trans-mitral pressure force and the interpapillary muscle resynchronization,Karvounis et al23 reported that CRT improves systolic strain of papil-lary muscles and adjacent LV walls. Last, CRT may improve LV longi-tudinal function and reduce subvalvular traction, as evidenced bydecreased apical displacement of the coaptation point.24
Table 3B Acute effects of cardiac resynchronization therapyon exercise-induced changes in mitral regurgitationparameters in patients with functional mitral regurgitation at rest
MR (n = 26)
CRT Off CRT On Change
D Mitral ERO (mm2) 8 6 7 1 6 4 �7 6 6a
D Mitral RV (mL) 8 6 8 1 6 6 �6 6 7a
D LV + dP/dT (mm Hg/s) 197 6 240 523 6 474 326 6 483a
CRT, Cardiac resynchronization therapy; ERO, effective regurgitant
orifice area; RV, regurgitant volume; LV, left ventricular; MR, mitral regur-gitation.
Values of exercise-induced changes and their changes are expressed as
mean 6 standard deviation. Paired t or Wilcoxon tests were used for
statistical comparisons.aP # .05 for CRT effect.
Journal of the American Society of EchocardiographyMay 2009

Table 4 Acute effects of cardiac resynchronization therapy during exercise on exercise-induced changes in forward stroke volumeand cardiac output according to the severity of functional mitral regurgitation at rest
Mitral ERO # 8 mm2 (n = 13) Mitral ERO > 8 mm2 (n = 13)
CRT Off CRT On Change CRT Off CRT On Change
D Mitral ERO (mm2) 8 6 6 3 6 3 �5 6 2a 8 6 8 0 6 5 �8 6 2a
D FSV (mL) 0 6 7 3 6 8 4 6 3a �5 6 7 5 6 8 9 6 3a
D Cardiac output (L/min) 1.5 6 1.1 1.8 6 1.5 0.2 6 0.2a 0.7 6 0.8 1.4 6 0.6 0.7 6 0.2a
CRT, Cardiac resynchronization therapy; ERO, effective regurgitant orifice area; RV, regurgitant volume; LV, left ventricular; MR, mitral regurgitation;FSV, forward stroke volume.
Values of parameters at rest and exercise-induced changes (D) are expressed as mean 6 standard deviation. Two-way ANOVA for repeated measures
was used for statistical comparisons. Values of changes are expressed as differences of least squares means 6 standard error. ANOVA showed no
significant interaction between mitral ERO > or # 8 mm2 at rest and CRT On or Off.aP # .05 for CRT effect for all patients.
Figure 3 Relationships between exercise-induced changes (D) in mitral ERO and D FSV according to CRT.
Journal of the American Society of EchocardiographyVolume 22 Number 5
Marechaux et al 469
Functional MR is a highly dynamic condition. Exercise variably af-fects functional MR, and the severity of functional MR at rest doesnot predict MR response to exercise.12 Exercise-induced MR resultsin a decrease in FSV and thereby exercise capacity in patients withLV systolic dysfunction.6 Resting and dynamic LV dyssynchrony (asassessed by tissue Doppler imaging) strongly predict worsening offunctional MR during exercise,12,25 in addition to inducible myocar-dial ischemia26 or local LV remodelling resulting in increased dy-namic leaflet tethering.27 By enhancing LV +dP/dt 2-fold, CRTincreases mitral force closures that offset the detrimental effects ofexercise on functional MR.7 In our patients with MR at rest, atten-uation of exercise-induced MR improved exercise FSV and exercisecardiac output, whereas CRT did not affect the FSV and cardiac out-put responses to exercise in patients without MR at rest. The presentdata support the findings of Lancellotti et al8 and Bordachar et al,9
who reported that CRT decreases functional MR at rest and duringdynamic exercise early after initiation of CRT. In contrast, Madaricet al28 reported that 3 months were required for CRT to counteractthe negative effect of dynamic exercise on functional MR. The rea-sons for this temporal disparity are not readily apparent. WhetherCRT-mediated attenuation of MR at rest and transient exercise-in-duced MR has any clinical correlate during long-term CRT remainsto be studied. Of note, Kang and coworkers29 found that the extent
of intraventricular dyssynchrony measured at peak exercise in pa-tients with nonischemic cardiomyopathy correlates with dynamic in-crease in mitral ERO and independently predicts unfavorable LVremodeling at follow-up with medical treatment. Therefore, one ex-pects that CRT-mediated attenuation in dyssynchrony and MR bothat rest and during exercise would often result in reverse remodeling,especially in patients with CHF with large QRS and functional MRat rest, as suggested by Gorcsan et al30 in the recent American So-ciety of Echocardiography expert consensus on echocardiographyfor CRT.
Acute CRT did not affect systolic pulmonary artery pressure at restor during dynamic exercise in our patients. The lack of acute effect ofCRTon pulmonary artery pressure was somewhat expected becausemultiple factors in addition to myocardial asynchronism affect theseverity of pulmonary hypertension in CHF.31,32
STUDY LIMITATIONS
Although the 2 symptom-limited maximal exercise tests were sepa-rated by a minimum of 6 hours, residual fatigue may have affectedthe second exercise. Acute CRT increased cardiac output during dy-namic exercise in patients with functional MR at rest. However, they

470 Marechaux et al Journal of the American Society of EchocardiographyMay 2009
were unable to achieve a greater workload than without CRT. Suchdissociation between fixed functional capacity and acute improve-ment in LV systolic performance has been reported in patients withCHF.33 Acute interventions do not immediately reverse the alter-ations in skeletal muscle metabolism, mass, and vasculature that pri-marily limit peak functional capacity in ambulatory patients withsevere CHF.34 One cannot evaluate CRT in a double-blind fashionby echocardiography. Last, our findings in a small patient populationneed to confirm by larger and longer term studies.
CONCLUSIONS
In the absence of functional MR at rest, CRT does not acutely increaseforward cardiac output during exercise. When functional MR is pres-ent at rest, CRT acutely increases FSV during exercise by lesseningfunctional MR. The contrasting acute hemodynamic effects of CRTduring exercise in patients with or without resting functional MRsuggest that functional MR is an important determinant of the acutehemodynamic response to CRT during exercise.
REFERENCES
1. Robbins JD, Maniar PB, Cotts W, Parker MA, Bonow RO, Gheorghiade M.Prevalence and severity of mitral regurgitation in chronic systolic heart fail-ure. Am J Cardiol 2003;91:360-2.
2. Grigioni F, Enriquez-Sarano M, Zehr KJ, Bailey KR, Tajik AJ. Ischemic mi-tral regurgitation: long-term outcome and prognostic implications withquantitative Doppler assessment. Circulation 2001;103:1759-64.
3. Ennezat PV, Marechaux S, Huerre C, Deklunder G, Asseman P, Jude B,et al. Exercise does not enhance the prognostic value of Doppler echocar-diography in patients with left ventricular systolic dysfunction and func-tional mitral regurgitation at rest. Am Heart J 2008;155:752-7.
4. Ennezat PV, Marechaux S, Asseman P, Lejemtel TH, Van Belle E,Bauters C, et al. Functional mitral regurgitation and chronic heart failure.Minerva Cardioangiol 2006;54:725-33.
5. He S, Fontaine AA, Schwammenthal E, Yoganathan AP, Levine RA. Inte-grated mechanism for functional mitral regurgitation: leaflet restrictionversus coapting force: in vitro studies. Circulation 1997;96:1826-34.
6. Lapu-Bula R, Robert A, Van Craeynest D, D’Hondt AM, Gerber BL,Pasquet A, et al. Contribution of exercise-induced mitral regurgitation toexercise stroke volume and exercise capacity in patients with left ventric-ular systolic dysfunction. Circulation 2002;106:1342-8.
7. Ennezat PV, Gal B, Kouakam C, Marquie C, LeTourneau T, Klug D, et al.Cardiac resynchronisation therapy reduces functional mitral regurgitationduring dynamic exercise in patients with chronic heart failure: an acuteechocardiographic study. Heart 2006;92:1091-5.
8. Lancellotti P, Melon P, Sakalihasan N, Waleffe A, Dubois C, Bertholet M,et al. Effect of cardiac resynchronization therapy on functional mitral re-gurgitation in heart failure. Am J Cardiol 2004;94:1462-5.
9. Bordachar P, Lafitte S, Reuter S, Serri K, Garrigue S, Laborderie J, et al.Echocardiographic assessment during exercise of heart failure patientswith cardiac resynchronization therapy. Am J Cardiol 2006;97:1622-5.
10. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction rede-fined—a consensus document of The Joint European Society of Cardiol-ogy/American College of Cardiology Committee for the redefinition ofmyocardial infarction. J Am Coll Cardiol 2000;36:959-69.
11. Bader H, Garrigue S, Lafitte S, Reuter S, Jais P, Haissaguerre M, et al. Intra-left ventricular electromechanical asynchrony. A new independent predic-tor of severe cardiac events in heart failure patients. J Am Coll Cardiol2004;43:248-56.
12. Ennezat PV, Marechaux S, Le Tourneau T, Lamblin N, Bauters C, VanBelle E, et al. Myocardial asynchronism is a determinant of changes in func-
tional mitral regurgitation severity during dynamic exercise in patients withchronic heart failure due to severe left ventricular systolic dysfunction. EurHeart J 2006;27:679-83.
13. Sorrell VL, Reeves WC. Noninvasive right and left heart catheterization:taking the echo lab beyond an image-only laboratory. Echocardiography2001;18:31-41.
14. Lebrun F, Lancellotti P, Pierard LA. Quantitation of functional mitralregurgitation during bicycle exercise in patients with heart failure. J AmColl Cardiol 2001;38:1685-92.
15. Bargiggia GS, Bertucci C, Recusani F, Raisaro A, de Servi S, Valdes-Cruz LM, et al. A new method for estimating left ventricular dP/dt by con-tinuous wave Doppler-echocardiography. Validation studies at cardiaccatheterization. Circulation 1989;80:1287-92.
16. Schwarz G. Estimating the dimension of a model. Ann Stat 1978;6:461-4.17. Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, et al.
Cardiac resynchronization in chronic heart failure. N Engl J Med 2002;346:1845-53.
18. Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, et al.Cardiac-resynchronization therapy with or without an implantable defi-brillator in advanced chronic heart failure. N Engl J Med 2004;350:2140-50.
19. Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D,Kappenberger L, et al. The effect of cardiac resynchronization on morbid-ity and mortality in heart failure. N Engl J Med 2005;352:1539-49.
20. Saxon LA, Boehmer JP, Hummel J, Kacet S, De Marco T, Naccarelli G,et al. Biventricular pacing in patients with congestive heart failure: two pro-spective randomized trials. The VIGOR CHF and VENTAK CHF Investi-gators. Am J Cardiol 1999;83(5B): 120D-3.
21. Kanzaki H, Bazaz R, Schwartzman D, Dohi K, Sade LE, Gorcsan J 3rd. Amechanism for immediate reduction in mitral regurgitation after cardiacresynchronization therapy: insights from mechanical activation strain map-ping. J Am Coll Cardiol 2004;44:1619-25.
22. Ypenburg C, Lancellotti P, Tops LF, Bleeker GB, Holman ER, Pierard LA,et al. Acute effects of initiation and withdrawal of cardiac resynchroniza-tion therapy on papillary muscle dyssynchrony and mitral regurgitation.J Am Coll Cardiol 2007;50:2071-7.
23. Karvounis HI, Dalamaga EG, Papadopoulos CE, Karamitsos TD,Vassilikos V, Paraskevaidis S, et al. Improved papillary muscle functionattenuates functional mitral regurgitation in patients with dilated cardio-myopathy after cardiac resynchronization therapy. J Am Soc Echocardiogr2006;19:1150-7.
24. Vinereanu D, Turner MS, Bleasdale RA, Mumford CE, Cinteza M,Frenneaux MP, et al. Mechanisms of reduction of mitral regurgitationby cardiac resynchronization therapy. J Am Soc Echocardiogr 2007;20:54-62.
25. Lafitte S, Bordachar P, Lafitte M, Garrigue S, Reuter S, Reant P, et al.Dynamic ventricular dyssynchrony: an exercise-echocardiography study.J Am Coll Cardiol 2006;47:2253-9.
26. Marechaux S, Ennezat PV. Myocardial ischemia might be an importantdeterminant of exercise-induced changes in mitral regurgitation in pa-tients with left ventricular systolic dysfunction. Am Heart J 2008;156:e29-30.
27. Lancellotti P, Lebrun F, Pierard LA. Determinants of exercise-inducedchanges in mitral regurgitation in patients with coronary artery diseaseand left ventricular dysfunction. J Am Coll Cardiol 2003;42:1921-8.
28. Madaric J, Vanderheyden M, Van Laethem C, Verhamme K, Feys A,Goethals M, et al. Early and late effects of cardiac resynchronization ther-apy on exercise-induced mitral regurgitation: relationship with left ventric-ular dyssynchrony, remodelling and cardiopulmonary performance. EurHeart J 2007;28:2134-41.
29. Kang S-J, Lim H-S, Choi B-J, Choi S-Y, Yoon M-H, Hwang G-S, et al. Theimpact of exercise-induced changes in intraventricular dyssynchrony onfunctional improvement in patients with nonischemic cardiomyopathy.J Am Soc Echocardiogr 2008;21:948-53.
30. Gorcsan J, Abraham T, Agler DA, Bax J, Derumeaux G, Grimm RA, et al.Echocardiography for cardiac resynchronization therapy: recommendationsfor performance and reporting. J Am Soc Echocardiogr 2008;21:191-213.

31. Marechaux S, Pincon C, Le Tourneau T, de Groote P, Huerre C,Asseman P, et al. Cardiac correlates of exercise induced pulmonary hyper-tension in patients with chronic heart failure due to left ventricular systolicdysfunction. Echocardiography 2008;25:386-93.
32. Tumminello G, Lancellotti P, Lempereur M, D’Orio V, Pierard LA. Deter-minants of pulmonary artery hypertension at rest and during exercise inpatients with heart failure. Eur Heart J 2007;28:569-74.
Journal of the American Society of EchocardiographyVolume 22 Number 5
33. Maskin CS, Forman R, Sonnenblick EH, Frishman WH, LeJemtel TH. Fail-ure of dobutamine to increase exercise capacity despite hemodynamic im-provement in severe chronic heart failure. Am J Cardiol 1983;51:177-82.
34. Jondeau G, Katz SD, Zohman L, Goldberger M, McCarthy M, Bourdarias JP,et al. Active skeletal muscle mass and cardiopulmonary reserve. Failure to at-tain peak aerobic capacity during maximal bicycle exercise in patients withsevere congestive heart failure. Circulation 1992;86:1351-6.
Marechaux et al 471
Related Documents











