Joumal of Advanced Nursing, 1996,23,430-440 From research to practice: one organizational model for promoting research-based practice Ahson Kitson RGN FRCN BSc{Hons) D Phil Professor and Director Laila Bana Ahmed BA(Hons) MA(Hons) MA Psychology Men Handicap PhD Senior Research Fellow Gillian Harvey RGN BNurs DN RHV PhD Senior Research and Development Officer Kate Seers RGN BSc{Hons) PhD Senior Research Fellow, National Institute for Nursing, Radchff'e Infirmary, Oxford and David R Thompson RGN RMN ONC FRGN BSc MA PhD Professor of Nursing Studies (formerly Reader in Cardiac Rehabilitation, National Institute for Nursing), Institute of Nursmg Studies, University of Hull, Hull, England KITSON A , AHMED L B , HARVEY G , SEERS K & THOMPSON D R (1996) Journal of Advanced Nursing 23, 430-440 From research to practice, one organizational model for promoting research- based practice This paper describes aframew^orkused by the National Institute for Nursing m Oxford to mtegrate research, development and practice With the increasing attention given to the topic of how research findings are implemented into clinical practice, it v^ras felt important to share the challenges that have arisen m attempting to combine traditional research activities wiih more practice-based development work The emerging conceptual framework, structures and functions are described, highlighting the variety of partnerships to be established in order to achieve the goal of integrating research into practice While the underpinning principles ofthe framework — generating knovirledge, implementing research into practice and evaluating the effectiveness of programmes — are not new, it is the way they have been combined v\rithin an organizational structure that could be helpful to others considering such a strategy Both the strengths and w^eaknesses ofthe framework are discussed, a number of conclusions drawn as to its robustness and consideration given to its replication rTTfiM Interest m the topic of getting research into practice seems INTRODUCTION ^^ j^^^^ reached a new pitch within the health service The NHS Research and Development programme has emharked Transforming research into practice is a demanding task requiring ^^ ^ ^^^^^^j ^^^^^^ ^^ ^^^^^^ designed to reduce the gap intellectual rigour and disciphne as well as creativity, clinical ^^^^^ ^^ generaUon of research and getting it into prac- judgement and skill, organisational savvy and endurance ^^^^ (Department of Health 1991) An increasing numher (Horsley et al 1983) ^^ aj^^les are heing published on the topic in both medical and nursing journals (Stocking 1992, Watt 1993, Closs & Correspondence Professor A Kitson, National Institute for Nursmg Cheater 1994, Dunning et al 1994, Haines & Jones 1994), Radchffe Infirmary, Woodstock Road Oxford OX2 6HE England and in spnng 1994 an maugural meeting was held at the 430 ® 1996 Blackwell Science Ltd

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Joumal of Advanced Nursing, 1996,23,430-440
From research to practice: one organizationalmodel for promoting research-based practice
Ahson Kitson RGN FRCN BSc{Hons) D PhilProfessor and Director
Laila Bana Ahmed BA(Hons) MA(Hons) MA Psychology MenHandicap PhDSenior Research Fellow
Gillian Harvey RGN BNurs DN RHV PhDSenior Research and Development Officer
Kate Seers RGN BSc{Hons) PhDSenior Research Fellow, National Institute for Nursing, Radchff'e Infirmary, Oxford
and David R Thompson RGN RMN ONC FRGN BSc MA PhDProfessor of Nursing Studies (formerly Reader in Cardiac Rehabilitation, NationalInstitute for Nursing), Institute of Nursmg Studies, University of Hull, Hull, England
KITSON A , AHMED L B , HARVEY G , SEERS K & THOMPSON D R (1996) Journal of
Advanced Nursing 23, 430-440From research to practice, one organizational model for promoting research-based practiceThis paper describes a framew^ork used by the National Institute for Nursing mOxford to mtegrate research, development and practice With the increasingattention given to the topic of how research findings are implemented intoclinical practice, it v̂ ras felt important to share the challenges that have arisen mattempting to combine traditional research activities wiih more practice-baseddevelopment work The emerging conceptual framework, structures andfunctions are described, highlighting the variety of partnerships to beestablished in order to achieve the goal of integrating research into practiceWhile the underpinning principles ofthe framework — generating knovirledge,implementing research into practice and evaluating the effectiveness ofprogrammes — are not new, it is the way they have been combined v\rithin anorganizational structure that could be helpful to others considering such astrategy Both the strengths and w^eaknesses ofthe framework are discussed, anumber of conclusions drawn as to its robustness and consideration given to itsreplication
rTTfiM Interest m the topic of getting research into practice seemsINTRODUCTION ^̂ j ^ ^ ^ ^ reached a new pitch within the health service The
NHS Research and Development programme has emharkedTransforming research into practice is a demanding task requiring ^^ ̂ ̂ ^^^^^j ^^^^^^ ^^ ̂ ^^^^^ designed to reduce the gapintellectual rigour and disciphne as well as creativity, clinical ^^^^^ ^^ generaUon of research and getting it into prac-judgement and skill, organisational savvy and endurance ^̂ ^̂ (Department of Health 1991) An increasing numher
(Horsley et al 1983) ^^ aj^^les are heing published on the topic in both medicaland nursing journals (Stocking 1992, Watt 1993, Closs &
Correspondence Professor A Kitson, National Institute for Nursmg Cheater 1994, Dunning et al 1994, Haines & Jones 1994),Radchffe Infirmary, Woodstock Road Oxford OX2 6HE England and in spnng 1994 an maugural meeting was held at the
430 ® 1996 Blackwell Science Ltd

Research-based practice
King's Fund Centre in London, which brought togetherpeople interested m assemhling systematic reviews onchanging the behaviour of health care professionals andthe puhhc (Wyatt & Oliver 1995)
There is growmg consensus regarding factors known toinhibit the uptake of research in practice These mcludethe cultural divide perceived to exist between researchers,practitioners and educators (Haines & Jones 1994), the per-sonal characteristics of the doctor and nurse (Hunt 1981,Eisenberg 1986), practitioners feeling that research is eso-teric and irrelevant to their everyday practice (Lomas &Haynes 1988, Luker & Kenrick 1992, Webh & MacKenzie1993), and practical difficulties in the application of validprocedures (Lomas & Haynes 1988), for example problemsof access to research literature, pressure of work, and per-ceived support from other colleagues and managers inembracing the new activity (Luker & Kenrick 1992,Bostrom et al 1989, Champion & Leach 1989)
MELking a judgement ahout the sort of research evidencethat ought to he implemented is not straightforward Ofparamount importance are the strength and generaliz-ahility of the evidence Ideally systematic reviews of allthe research evidence available should have been carriedout before implementation plans are dravm up (Haines &Jones 1994) The degree of risk to patients involved m thechange must be assessed with the potential benefits of newpractice outweighing the nsks The feasibility of theimplementation should also be assessed together withsome assessment of its cost-effectiveness (Horsley et al1983, Haines & Jones 1994)
Principles thought to be important in facilitating the useof research m practice include the acknowledgement thatresearch utilizaUon is an organizational issue rather thanan individual response alone (Brett 1987, Hunt 1987,Stocking 1992), and that modifying practice can involveeducational input, procedure and policy changes, theacquisition of resources, and the need for skills and knowl-edge concerning climcal practice, research, plannedchange, problem solving, organizational analysis, interper-sonal behaviour and decision making (Brett 1987) Morespecifically, Haines & Jones (1994) encourage the use ofevidence-based guidelines which are locally owned alongwith the influence of opinion leaders, computer-baseddecision support systems, clinical audit activity and moreinnovative forms of continuing (medical) education
There continues to be a paucity of well-designed studiestesting the effectiveness of different approaches toimplementing research findings This deficit has beenrecognized and a number of initiatives are underway toexpand the existmg knowledge (For example a NationalAdvisory Group on Research mto the Implementation ofProven Research Findings has been set up and the reviewgroup will also begm to produce systematic reviews ofcurrent reseeirch)
The research community is becommg more aware that
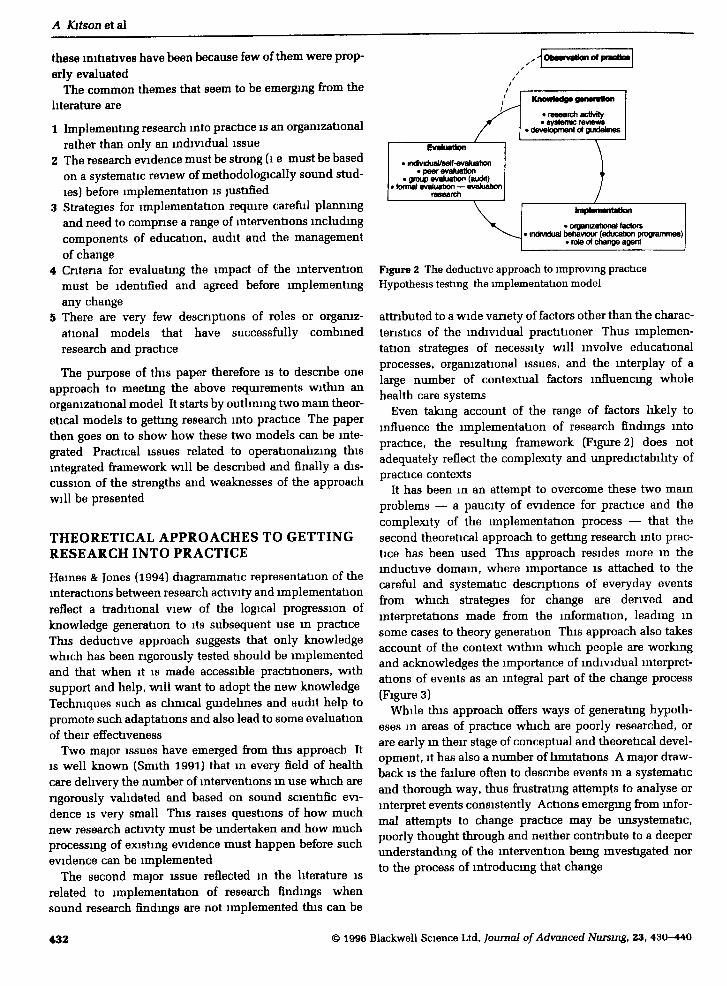
knowledge generation and dissemination are distinctactivities, good researchers are not necessarily good disse-minators or lmplementors and vice versa (Watt 1993) Thecomplex skills required for both jobs need to be clarifiedWatt (1993) recommends that research units should begiven resources and opportunities to develop expertise mdissemination He goes on to suggest that health authorit-ies should begin to identify local contacts for promotingdissemination activities which should themselves beevaluated withm the local audit process Hames & Jones(1994) illustrate how they perceive the interaction betweencontinuing education, audit and research findings(Figure 1) They see the professional associations playinga key role in promoting and developing evidence-basedguidelines and also ensuring that such knowledge feedsinto continuing education programmes
Within the nursing literature, a number of models havebeen documented as being used to bring researchers andresearch closer to the work setUng (CURN Project 1983,Funk et al 1989) Closs & Cheater (1994) identified themain initiatives as including the establishment of nursingdevelopment units, clmical nurse specialist roles, usingquality, audit and standard setting methodologies, settmgup secondments for clinicians and the testing out of com-bined roles such as researcher-change agent (Webb 1989,Titchen & Bmnie 1993a), researcher-teacher (Wilson-Bamett et al 1990) and researcher-clinician (Thompson &Cordle 1988, Tiemey & Taylor 1991) Closs & Cheater con-clude that It was difficult to judge how successful any of
Research activity
Systematic reviews of research findings
Development of evidence-based dimcal guidelines
Continuing medical education programmes
AdeMJtation of clinical guidelines and use aslocal standards for practice and audit
Understanding cntical appraisal techniques
Audit cyde
Figure 1 Interactions between continumg education, audit andresearch findmgs
© 1996 Blackwell Science Ltd, Joumal of Advanced Nursing, 23, 430-440 431
A Kitson ei si
these initiatives have been because few of them were prop-erly evaluated
The common themes that seem to be emerging from thehterature are
1 Implementing research into practice is an organizationalrather than only an individual issue
2 The research evidence must be strong (l e must be basedon a systematic review of methodologically sound stud-ies) before implementation is justified
3 Strategies for implementation require careful planningand need to comprise a range of mterventions lncludmgcomponents of education, audit and the managementof cheuige
4 Cntena for evaluating the impact of the mterventionmust be identified and agreed before implementingany change
5 There are very few descnptions of roles or organiz-ational models that have successfully combinedresearch and practice
The purpose of this paper therefore is to describe oneapproach to meeting the above requirements within anorganizational model It starts by outlining two mam theor-etical models to getting research mto practice The paperthen goes on to show how these two models can be inte-grated Practical issues related to operationalizmg thisintegrated framework will be described and finally a dis-cussion of the strengths euid weaknesses of the approachwill be presented
THEORETICAL APPROACHES TO GETTINGRESEARCH INTO PRACTICE
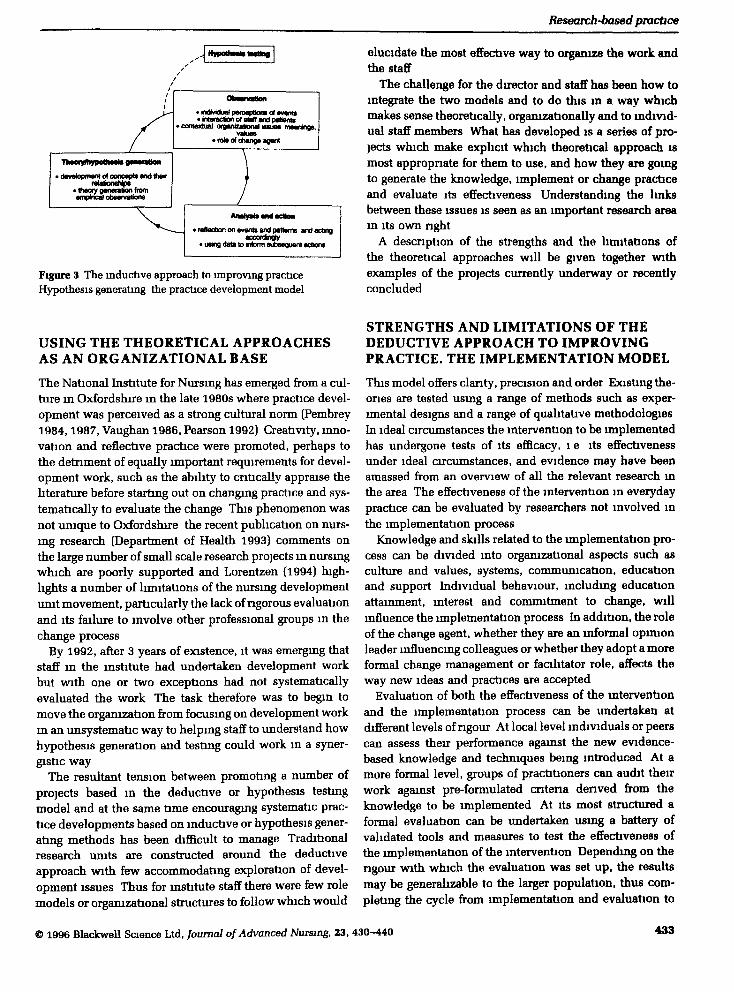
Haines & Jones (1994) diagrammatic representation oftheinteractions between research activity and implementationreflect a traditional view of the logical progression ofknowledge generation to its subsequent use m practiceThis deductive approach suggests that only knowledgewhich has been rigorously tested should be implementedand that when it is made accessible practitioners, withsupport and help, will want to adopt the new knowledgeTechniques such as clinical guidelines and audit help topromote such adaptations and also lead to some evaluationof their effectiveness
Two major issues have emerged from this approach ItIS well known (Smith 1991) that m every field of healthcare delivery the number of interventions m use which arerigorously validated and based on sound scientific evi-dence IS very small This raises questions of how muchnew research activity must be undertaken and how muchprocessing of existing evidence must happen before suchevidence can be implemented
The second major issue reflected in the literature isrelated to implementation of research findings whensound research findings are not implemented this can be
ObMfwHon of pracIlM
KnonHadg* g*raralian
• research acHvtty• systemic reviews
> develapinent of guidelines
• mdKndual/self-evaluation• peer evaluation
• group evaluation (audit)• forma) evaluation — evaluation
research
• organizational factors• individual twhavnur (education ptogiaimnes)
• role of change agent
Figure 2 The deductive approach to improving practiceHypothesis testing the implementation model
attributed to a wide variety of factors other than the charac-teristics of the individual practitioner Thus implemen-tation strategies of necessity will involve educationalprocesses, organizational issues, and the mterplay of alarge number of contextual factors infiuencing wholehealth care systems
Even taking account of the range of factors likely toinfiuence the implementation of research findings mtopractice, the resulting framework (Figure 2) does notadequately refiect the complexity and unpredictability ofpractice contexts
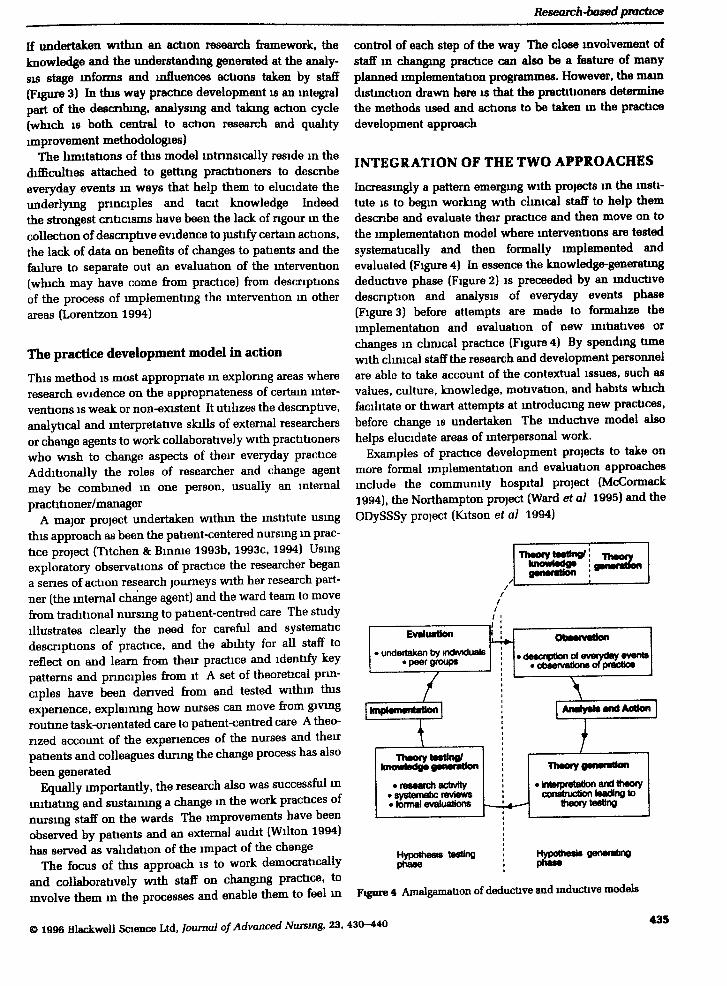
It has been in an attempt to overcome these two mamproblems — a paucity of evidence for practice and thecomplexity of the implementation process — that thesecond theoretical approach to getting research into prac-tice has been used This approach resides more m themductive domam, where importance is attached to thecareful and systematic descnptions of everyday eventsfrom which strategies for change are denved andinterpretations made from the information, leading msome cases to theory generation This approach also takesaccount of the context vnthm which people are workingand acknowledges the importance of individual interpret-ations of events as an integral part of the change process(Figure 3)
While this approach offers ways of generating hypoth-eses in areas of practice which are poorly researched, orare early m their stage of conceptual and theoretical devel-opment, it has also a number of limitations A major draw-back IS the fsulure often to describe events m a systematicand thorough way, thus frustrating attempts to analyse ormterpret events consistently Actions emerging from infor-mal attempts to change practice may be unsystematic,poorly thought through and neither contribute to a deeperunderstandmg of the intervention being mvestigated norto the process of introducing that change
432 © 1996 Blackwell Science Ltd, Joumal of Advanced Nursing, 23, 430-440
Research-based practice
^ J HypofliMlt iHttng j
p dsvvlopmai^ of oonoapts and thetrt H N
tfwoiy owincmctu o
• ndMdual paiGepUons ol rnwts. Maraclion of staR and pauentt
motlual oraamzMonal asuM iiiMn
.rate of change agent
. wflaclionon wenisandpadwnt andacbngaccofdinQly
. usmg dKa to nform subnquent actons
Figure 3 The mductive approach to improving practiceHypothesis generating the practice development model
elucidate the most effecbve way to organize the work andthe staff
The challenge for the director and staff has heen how tomtegrate the two models and to do this m a way whichmakes sense theoretically, organizationally and to mdivid-ual staff memhers What has develop)ed is a series of pro-jects which make explicit which theoretical approach ismost appropnate for them to use, and how they are goingto generate the knowledge, implement or change practiceand evaluate its effectiveness Understandmg the hnksbetween these issues is seen as an important research aream Its own nght
A description of the strengths and the limitations ofthe theoretical approaches will he given together withexamples of the projects currently underway or recentlyconcluded
USING THE THEORETICAL APPROACHESAS AN ORGANIZATIONAL BASE
The National Institute for Nursmg has emerged from a cul-ture in Oxfordshire in the late 1980s where practice devel-opment was perceived as a strong cultural norm (Pembrey1984,1987, Vaughan 1986, Pearson 1992) Creativity, inno-vation and reflective practice were promoted, perhaps tothe detriment of equally important requirements for devel-opment work, such as the ability to cntically appraise theliterature before startmg out on changmg practice and sys-tematically to evaluate the change This phenomenon wasnot unique to Oxfordshire the recent publication on nurs-ing research (Department of Health 1993) comments onthe large number of small scale research projects m nursmgwhich are poorly supported and Lorentzen (1994) high-lights a number of limitations of the nursing developmentunit movement, particularly the lack of rigorous evaluationand its failure to involve other professional groups in thechange process
By 1992, after 3 years of existence, it was emergmg thatstaff in the institute had undertaken development workbut with one or two exceptions had not systematicallyevaluated the work The task therefore was to begin tomove the oi^anization from focusmg on development workm an unsystematic way to helping staff to understand howhypothesis generation and testmg could work in a syner-gistic way
The resultant tension between promoting a number ofprojects based in the deductive or hypothesis testingmodel and at the same time encouragmg systematic prac-tice developments based on inductive or hjrpothesis gener-ating methods has been difficult to manage Traditionalresearch units are constructed around the deductiveapproach with few accommodating exploration of devel-opment issues Thus for mstitute staff there were few rolemodels or orgamzational structures to follow which would
STRENGTHS AND LIMITATIONS OF THEDEDUCTIVE APPROACH TO IMPROVINGPRACTICE. THE IMPLEMENTATION MODEL
This model offers clarity, precision and order Existing the-ories are tested using a range of methods such as exper-imental designs and a range of qualitative methodologiesIn ideal circumstances the intervention to be implementedhas undergone tests of its efficacy, l e its effectivenessunder ideal circumstances, and evidence may have beenamassed from an overview of all the relevant research mthe area The effectiveness of the intervention in everydaypractice can be evaluated by researchers not mvolved inthe implementation process
Knowledge and skills related to the implementation pro-cess can be divided into organizational aspects such asculture and values, systems, communication, educationand support Individual behaviour, including educationattainment, interest and commitment to change, willinfluence the implementation process In addition, the roleof the change agent, whether they are an informal opmionleader influencing colleagues or whether they adopt a moreformal change management or facilitator role, affects theway new ideas and practices are accepted
Evaluation of both the effectiveness of the mterventionand the implementation process can be undertaken atdifferent levels of rigour At local level individuals or peerscan assess their performance against the new evidence-based knowledge and techniques being introduced At amore formal level, groups of practitioners can audit theirwork against pre-formulated cntena denved from theknowledge to be implemented At its most stnictured aformal evaluation can be undertaken usmg a battery ofvahdated tools and measures to test the effectiveness ofthe implementation of the intervention Depending on thengour with which the evaluation was set up, the resultsmay be generalizable to the lai^er population, thus com-pletmg the cycle from implementation and evaluation to
© 1996 Blackwell Science Ltd, Joumal of Advanced Nursing, 23, 430-440 433

knowledge generation (Figure 2) If results are notgeneralizable at this point further detailed observation ofpractice is required
One weakness ofthe implementation phase has been thelack of careful observation as to how effective change canbe introduced Often it was assumed that when prac-titioners were presented with the facts they could applythem This we know not to be the case Also m its purestform this model can only be used to implement knowledgethat IS ngorously tested It is becommg increasingly clearthat the number of clmical interventions tested in a rigor-ous way IS small These factors would reinforce the needm this model for careful description ofthe implementationand evaluation stages
Practical considerations include the time and com-plexity of properly conducted implementations and evalu-ations, the problems with selecting methodologies whichare not too cumbersome and expensive and actually man-aging such projects
The implementabon model m action
The mam distinguishing characteristic of this approach isthe separation of the development of knowledge from theareas and subjects upon which it will subsequently beimplemented The national clmical guidelines initiativesillustrate this principle multidisciplmary groups cometogether to review the hterature and develop rigorous state-ments on the most effective practice for a certain conditionThe statements are checked for appropriateness, accept-ability, ngour and measurability and are available to clm-icians to use
Research has shown that such guidance is rarelyaccepted uncopditionally (Grol 1992, Grimshaw & Russell1993) and a senes of implementation strategies can be usedto encourage staff at local level to adopt the practice rec-ommended by such guidance Evaluation of such initia-tives can be undertaken usmg clmical audit or local peerreview approaches, or be part of a research programme
The stages va. the model are first to develop the guidance,second to decide upon the method(s) for aidmg the accept-ance and utilization of the guidance at local level andthirdly to evaluate its effect on patie(nt care and staffbehaviour
In the National Institute for Nursing a number of projectsare following this method national guidelines have beendeveloped for cardiac rehabilitation (Thompson 1994,Thompson et al 1996) emd the management of acute pain(NHS ME 1994), and the RCN DQI Programme has devel-oped guidance on nutntion m older hospitalized adults(Duff et al 1993) Each of these projects has undergone acareful process of devising the guidelines and undertakingthe implementation and evaluation stages
Another project located m this approach is the work onpatients' views of the service prior to hospitalization
(Ahmed & Stamszewdta 1994a, 1994b) and how themeasurement tool can be used as a method for evaluatingclients' views routinely as part of the audit cycleSimilarly, a project evaluating the impact of a continencetraimng programme on nurses' reported practice and sub-sequent care of patients with lncontmence (Williams et al1995) has utilized an mtervention to test changes m bothreported nursing and documented clmical practice
For mstitute staff undertaking such projects there mustbe a commitment to complete the cycle of generating theknowledge, implementing it and evaluatmg its effects onpatients and health care professionals This is a lengthyprocess if undertaken ngorously and it requires a wholerange of different skills and abihties Partnerships withclinical areas are also essential if careful documentationof the processes involved m implementation is to beachieved
STRENGTHS AND LIMITATIONS OF THEINDUCTIVE APPROACH TO IMPROVINGPRACTICE. THE PRACTICE DEVELOPMENTMODEL
The theoretical base for this model resides m the inductiveapproach to knowledge generation Through the carefuland painstsiking description of everyday practice connec-tions between events etre made Through analysis andinterpretation of such events theones can be constructedand thence tested This approach generates theory andhjrpotheses for subsequent testing
An addition to this traditional description of the induc-tive approach has been the acknowledgement that often atthe stage of systematically analysing events m practiceindividuals will adapt their behaviour according to theirunderstanding and interpretation of events Enhancedunderstandmg of the area being investigated mforms criti-cal debate amongst participants who move towards agreater understemdmg of the situation they are trying tochange and hence can change it If such processes remainimplicit then the mdividual practitioner cannot explainrationally or logically why they chose to behave in certainways By making such a process more explicit, individualscan be helped to formalize and systematize what they seearound them, how they analyse events and how they bothtake action to improve tbe situation and move on to makebroader interpretations regarding the underlying or tacitknowledge underpinning their practice
Attempts to encourage practitioners to describe every-day events m nursing have led to an expansion of infor-mation on the importance of concepts such as the nurse-patient relationship, the physical presence of the nursewith the patient, comfort, autonomy, digmty and canng(Lawler 1991) The ngour with which such observationshave been carried out and their subsequent analysis andinterpretation have led to new theones being developed
434 © 1996 Blackwell Science Ltd, Joumal of Advanced Nursing, 23, 430-440
Research-based practice
If undertaken withm an action research framework, theknowl^ge and the understanding generated at the analy-sis stage mfoims and influences actions taken hy staff(Figure 3) In this way practice development is an mtegralpart of the descnbing, analysing and takmg action cycle(which IS both central to action research and qualityimprovement methodologies)
The limitations of this model mtnnsically reside m thedifficulties attached to gettmg practitioners to descnbeeveryday events m ways that help them to elucidate theunderlying prmciples and tacit knowledge Indeedthe strongest cnticisms have been the lack of ngour m thecollection of descnptive evidence to justify certam actions,the lack of data on benefits of changes to patients and thefeilure to septarate out an evaluation of the mtervention(which may have come from practice) from descnptionsof the process of lmplementmg the intervention in otherareas (Lorentzon 1994)
The practice development model in action
This method is most appropnate m exploring areas whereresearch evidence on the appropnateness of certain inter-ventions IS weak or non-existent It utihzes the descnptive,analytical and interpretative skills of external researchersor change agents to work collaboratively with practitionerswho wish to change aspects of their everyday practiceAdditionally the roles of researcher and change agentmay be combmed m one person, usually an internalpractitioner/manager
A major project undertaken withm the institute usmgthis approach as been the patient-centered nursmg m prac-tice project (Titchen & Bmnie 1993b, 1993c, 1994) Usingexploratory observations of practice the researcher begana senes of action research journeys with her research part-ner (the internal change agent) and the ward team to movefrom traditional nursmg to patient-centred care The studyillustrates clearly the need for careful and systematicdescnpUons of practice, and the abihty for all staff toreflect on and learn from their practice and identify keypatterns and prmciples from it A set of theoretical prm-ciples have been denved from and tested withm thisexpenence, explainmg how nurses can move from givingroutme task-onentated care to patient-centred care A theo-rized account of the expenences of the nurses and theirpatients and colleagues during the change process has alsobeen generated
Equally importantly, the research also was successful inmitiatmg and sustaining a change m the work practices ofnursing staff on the wards The nnprovements have beenobserved by patients and an external audit (Wilton 1994)has served as validation of the impact of the change
The focus of this approach is to work democraticallyand coUaborabvely with staff on changmg practice, tomvolve them m the processes and enable them to feel m
control of each step of the way The close mvolvement ofstaff m changmg practice can also he a feature of manyplanned implementation pn^prammes. Howe\%3r, the maindistmction drawn here is that the practitioners determinethe methods used and actions to be taken m the practicedevelopment approach
INTEGRATION OF THE TWO APPROACHES
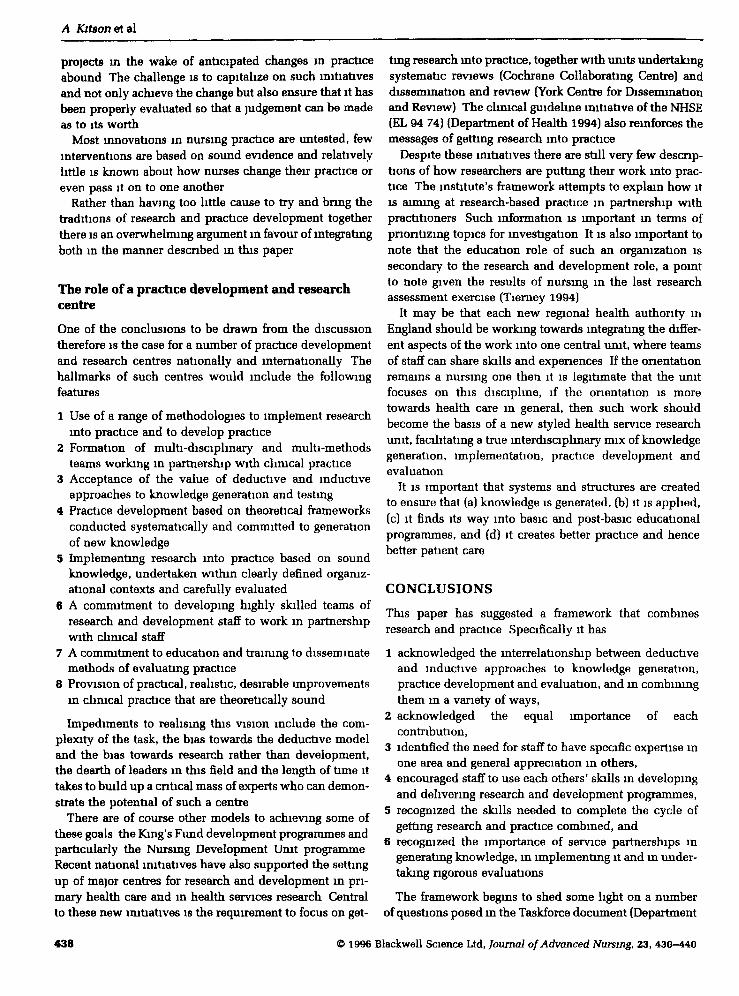
Increasingly a pattern emergmg with projects m the msti-tute IS to begin working with chmcal staff to help themdescnbe and evaluate their practice and then move on tothe implementation model where mterventions are testedsystematically and then formally implemented andevaluated (Figure 4) In essence the knowledge-generatingdeductive phase (Figure 2] is preceeded by an inductivedescnption and analysis of everyday events phase(Figure 3) before attempts are made to formalize theimplementation and evaluation of new initiatives orchanges in climcal practice (Figure 4) By spending tunewith climcal staff the research and development personnelare able to take accoimt of the contextual issues, such asvalues, culture, knowledge, motivation, and habits whichfacilitate or thwart attempts at mtroducing new practices,hefore change is undertaken The mductive model alsohelps elucidate areas of interpersonal work.
Examples of practice development projects to take onmore formal implementation and evaluation approachesinclude the community hospital project (McCormack1994), the Northampton project (Ward et al 1995) and theODySSSy project (Kitson et al 1994)
Evaluation
> undertaken by individuals• peer groups
I hnplaiiiaiitaUon I
•niaory i M gknoMrtadge ganarallon
• research actfvity• systematic reviews• formal evalutfions
ObMnwUon
• descnption of eMiyday events• observations of piactice
AnaiyaiaandAcllan
ITheory ganar
• brterpr^ation and theorycofwtruction leading to
ttiaorytesllrtg
Hypothesisphase
Hypothesis testingphase
Figure 4 AmalgamflUon of deducUve and inductive models
© 1996 BlackwBll Science Ltd, Joumal of Advanced Nursing, 23, 430-440435

A Kitson etei
The community hospital project
The commimity hospital project was set up as a practicedevelopment project ongmally m one of the eleven com-mimity hospitals in Oxfordshire The prmcipal researchand development fellow held a joint appointment betweenthe institute, the commumty unit and Oxford BrookesUmversity Dunng the first year he imdertook a carefuldescnption of practice, focusing on patient expenences,staff and the organization of care These data were analysedand presented to staff as a potential work plan for changeThis was followed by a prolonged penod of discussionand negotiation about pnonties and practices of cetre
Having changed the orgamzational structure and the pre-vaihng culture a senes of traimng programmes were under-taken and a community hospital wide audit was used toidentify current practice and set targets for improvementThis phase of work coincided with a decision to evaluatethe change process more formally by using a battery ofprocess and outcome measures The research and develop-ment fellow has moved m to the role of external evaluatoras he has trained other staff to operate as internal changeagents
The ongms of this project are clearly m the inductivepractice development model The role of the research anddevelopment fellow permitted a systematic analysis ofevents in order to inform subsequent actions A secondevaluation now seeks to test the on-gomg effect of thechange process by undertaking a formal before andafter test using process and outcome measiires based onresearch evidence
A similar pattern emerged witb the development workwithin the dermatology services The lead research anddevelopment fellow undertook an extensive penod oforganizational change, working with staff m clarifyingtheir roles and responsibilities, detailing patient and ser-vice needs tmd then beginning to test out differentapproaches to care delivery (Ersser 1992) Having estab-hshed tbe new role of a dermatology liaison nurse m thecommunity, the research team are settmg up a controlledtnal to test the effectiveness of this new interventionagainst traditional services (Ersser et al 1995)
Other examples of combining the models include theNorthampton project (Ward et al 1995) where staff mNorthamptonshire selected as key change agents have beensupervised by institute staff to introduce and evaluate tbeimplementation of one evidence-based clmical inter-vention While the local staff are being encouraged to useeither the implementation model or the practice develop-ment model, institute staff are using the practice develop-ment model to help them descnbe what is happening andto denve some general statements from it
The ODySSSy project (Kitson et al 1994) used an induc-tive approach to standard settmg and audit as the depen-dent vanable m a formal evaluation project ofthe effect of
local standard setting and audit on nursing actions andpatient outcomes In developmg objective measuresagamst which patient expenences could be evaluated, aset of national standards for post-operative pam manage-ment were constructed against which local standards werecompared The formal evaluation also took account of thelocal progress of each team m standard setting hy col-lecting data on group processes and nursmg staffs' viewsof the change process The results of the evaluation con-tnhuted to the knowledge around implementation of auditmethods and their impact on staff and patients
What has emerged from these expenences is thatpractice development should not be separated from syste-matic evaluations of those changes, nor should only oneapproach be advocated, more important is the clarity andngour with which the projects are set up
DISCUSSION
Staff in the mstitute have been workmg on ways of mte-gratmg research and practice since its inception m 1989This central goal is reflected m the institute's missionstatement which is to promote improvements in patientcare by critically evaluating the effectiveness of changesm care through the development of mtegrated theory,research and practice Important questions to he raisedinclude whether the models described have anythingadditional to offer m the debate on getting research intopractice, whether the organizational structure and staffarrangements promote opportunities for closer partner-ships between practice and research, whether the modelshave multi-professional application and are cost-effective,and finally whether there is a role for more practicedevelopment and research centres
Getting research into practice
The argument put forward in this paper is that there are anumber of conceptual models that can be used to tacklethe challenge of getting research into practice Thosemvolved in such activity should be aware of the strengthsand limitations of both the deductive and inductiveapproaches Important for both approaches is the way inwhich contextual issues are accommodated and how staffare mvolved m the process of change
Such contextual issues must be tackled before staff areable to respond to new knowledge and new ways ofworking The examples cited m the paper illustrate howmtensive penods of orgamzational development workneed to be undertaken before staff are ready to change theirpractice How these two requirements are managed, whofacilitates them and how they are evaluated will oftendetermine the success or otherwise of attempts to get newknowledge into practice Thus skills m methodologiesrelated to the deductive and the mductive traditions must
436 © 1996 Blackwell Science Ltd, Joumal of Advanced Nursing, 23, 430-440

Research-based {oactice
he available to practitioners who want or have to changepractice
The weakness of much of the strategic planmng withmthe research and development agenda at the moment isthat little attention is bemg paid to the importance of theinductive approach embodied m the practice developmentmodel and the mterpersonal and facihtative skills of theresearcher-change agent Possible reasons mclude scien-tific discourse is more familiar with the deductiveapproach, it has been successful m generating knowledge,and a wide repertoire of reliable and vahd tools has beendeveloped Conversely, the methods used m the mductivetradition are perceived as less ngorous, more suhjectiveand less likely to lead to generalization of findings Thisview has been perpetuated by development work that hasbeen undertaken unsystematically and opportunistically
The dearth of well trained research and developmentstaff, knowledgeable and confident m the use of a range ofmethodologies, also contnbutes to the tension Whilst itmay be unrealistic to expect individuals to master therange of appropnate methodologies to successfully inte-grate the two models, it may be more feasible to worktowards developing teams of research and developmentpersonnel with the range of expenence and skill neededto successfully mtroduce more clinically effectivepatient care
Partnerships hetween practice and research
The perceived gap between theory and practice andresearchers and climcal staff is often cited as a reason forresearch not being implemented By establishing closerlinks between knowledge generation and its implemen-tation, and between systematic descriptions of practiceand subsequent interpretation and theory generation, thegaps may begin to dimmish Practical problems, however,include the difficulty in ftmdmg and supporting such inte-grated posts at practice level Nursmg roles such as theclinical nurse specialist, chmcal practice developmentnurse, joint appointments and lecturer-practitioners haveall attempted to combine theory, research and practiceConsistent linutations have heen lack of preparation ofthepostholders m research methods and practice develop-ment techniques, lack of support and a paucity of aca-demic lmks with units or departments conversant with theorganizational and theoretical issues
Successful partnerships hetween academic units andservice areas relate to how well the research and develop-ment personnel meet the immediate needs of staff, howthey operate as facilitators of change without taking theownership and direction away from staff Providing mfor-mation on recent climcal care and equippmg staff withbasic evaluation and problem solvmg skills are alsopart of the relationship Equally important is the ngourwith which implementation strategies are planned and
executed, with acknowledgement of the importance ofcareful evaluation
Often the picture is very different, poorly trained andsupported staff are given practice development andresearch roles without appropnate supervision and guid-ance and with no strategic view of what problems to tacklefirst Such roles often are extinguished leaving clirucal staffmore cymcal of the value of research or researchers totheir practice
Partnerships between institute staff and local providerunits have developed in the last few years Research anddevelopment fellows work collaboratively with their ciim-cal tmit and on other related projects m the mstitute Clearprojects are negotiated with chmcal staff, incorporatingrealistic objectives and time-frames The progress of theproject IS shared with staff and managers and outcomesmust be tangible, realistic and relevant to everyday prac-tice One problem has been the desire of provider units toachieve improvements in practice in a relatively shortpenod of time, without regard for any remedial work need-ing to be done, team buildmg and careful assessment ofbaseline data before begmning the work There is a wide-spread view that development work does not require tobe undertaken ngorously or systematically and thusmanagers understandably are reluctant to mvest in morecostly development progreimmes that do follow ngorousmethodologies
Multi-disciplinary application and cost-effectiveness
The theoretical frameworks descnbed are relevant to allmembers of the health care team Traditionally, medicalresearch and development has favoured the deductiveapproach while nursing research and development has inrecent years tended to concentrate on the mductivedomain What is required is the transference of skills onboth sides with fully integrated teams working multi-professionally and with multi-methods
One potential drawback to such collaboration could bethe reluctance of policy makers to explore practice devel-opment approaches other than the straight deductiveapproach The reality, however, is that with relatively littleresearch-beised knowledge upon which to base practice itIS necessary to ensure that all other approaches to knowl-edge generation are utilized The case has already beenmade for systematic descnptions and evaluations of prac-tice, as has the argument for a more ngorous approach toclimcal audit (Russell & Wilson 1992)
The rapid changes in health care delivery, the trendtowards community care and greater emphasis on preven-tion will require careful evaluation Questions of appro-pnate care and who should be providmg it will alsocontinue to exercise not only pohcy makers but also theresearch community Opportunities to set up evaluation
© 1996 Blackwell Science Ltd, Joumal of Advanced Nursing, 23, 430-440 437
projects m the wake of anticipated changes m practiceabound The challenge is to capitalize on such mitiativesand not only achieve the change hut also ensure that it hasbeen properly evaluated so that a judgement can be madeas to Its worth
Most innovations m nursing practice are untested, fewinterventions are based on sound evidence and relativelylittle IS known about how nurses change their practice oreven pass it on to one another
Rather than having too little cause to try and bnng thetraditions of research and practice development togetherthere is an overwhelming argument m favour of lntegratmgboth in the manner descnbed in this paper
The role of a practice development and researchcentre
One of the conclusions to be drawn from the discussiontherefore is the case for a number of practice developmentand research centres nationally and mtemationally Thehallmeirks of such centres would include the followingfeatures
1 Use of a range of methodologies to implement researchinto practice and to develop practice
2 Formation of multi-disciplinary and multi-methodsteams working in partnership with clmical practice
3 Acceptance of the value of deductive and inductiveapproaches to knowledge generation and testing
4 Practice development based on theoretical frameworksconducted systematically and committed to generationof new knowledge
5 Implementing research into practice based on soundknowledge, undertaken within clearly defined organiz-ational contexts and carefully evaluated
6 A commitment to developmg highly skilled teams ofresearch and development staff to work m partnershipwith climcal staff
7 A commitment to education and traimng to disseminatemethods of evaluating practice
8 Provision of practical, realistic, desirable improvementsin clinical practice that Eire theoretically sound
Impediments to realismg this vision include the com-plexity of the task, the bias towards tbe deductive modeland the bias towards research rather than development,the dearth of leaders in this field and the length of time ittakes to build up a cntical mass of experts who can demon-strate the potential of such a centre
There are of course other models to achieving some ofthese goals the King's Fund development programmes andparticularly the Nursing Development Unit programmeRecent national lmtiatives have also supported the settingup of major centres for research and development in pn-mary health care and m health services research Centralto these new lmtiatives is the requirement to focus on get-
tmg research mto practice, together with units undertakmgsystematic reviews (Cochrane Collaboratmg Centre) anddissemination and review (York Centre for Dissemmationand Review) The clinical guideline initiative of the NHSE(EL 94 74) (Department of Health 1994) also reinforces themessages of getting research into practice
Despite these mitiatives there are still very few descnp-tions of how researchers are puttmg their work mto prac-tice The mstitute's framework attempts to explain how itIS aimmg at research-based practice m partnership withpractitioners Such information is important m terms ofpriontizmg topics for mvestigation It is also important tonote that the education role of such an organization issecondary to the research and development role, a pointto note given the results of nursing m the last researchassessment exercise (Tiemey 1994)
It may be that each new regional health authority mEngland should be working towards integrating the differ-ent aspects of the work into one central tmit, where teamsof staff can share skills and experiences If the onentationremains a nursing one then it is legitimate that the unitfocuses on this discipline, if the onentation is moretowards health care in general, then such work shouldbecome the basis of a new styled health service researchtmit, facilitating a true interdisciplinary mix of knowledgegeneration, implementation, practice development andevaluation
It IS important that systems and structures are createdto ensure that (a) knowledge is generated, (b) it is applied,(c) it finds its way mto basic and post-basic educationalprogrammes, and (d) it creates better practice and hencebetter patient care
CONCLUSIONS
This paper has suggested a framework that combinesresearch and practice Specifically it has
1 acknowledged the interrelationship between deductiveand inductive approaches to knowledge generation,practice development and evaluation, and m combiningthem m a variety of ways,
2 acknowledged the equal lmportemce of eachcontribution,
3 identified the need for staff to have specific expertise mone area and general appreciation m others,
4 encouraged staff to use each others' skills m developmgand dehvermg research and development programmes,
5 recogmzed the skills needed to complete the cycle ofgetting research and practice combmed, and
6 recognized the importance of service partnerships mgenerating knowledge, in implementing it and m under-taking ngorous evaluations
The framework begins to shed some light on a ntimberof questions posed in the Taskforce document (Department
438 © 1996 Blackwell Science Ltd, Joumal of Advanced Nursmg, 23, 430-440
Research-based practice
of Health 1993), particularly in developing a strategic planfor nursing research, career development m nursmg, link-ing research to clinical practice and integrating nursingresearch mto mainstream research and development workMost importantly the framework begins to elucidate thecomplexities of development work and skills needed foraction
Acknowledgements
We would wish to acknowledge the help of Angie Titchenin reviewing and making suggestions on tbe content ofthis paper
References
Ahmed L B & Staniszewska S (1994a) Patients expectations ofand satisfaction with health care a comparative study of whiteand ethnic minority populations Unpublished report, NationalInstitute for Nursing, Oxford
Ahmed LB & Staniszewska S (1994b) Development of measuresof Datient expectations and satisfaction a tool for consumeraudit Unpuhlished report, National Institute for NursmgOxford
Bostrom A C , Malmght M , McDougall J & Hargis D (1989) Staffnurses' attitudes towards nursing research a descriptive surveyJoumal of Advanced Nursmg 14 915-922
Brett J L L (1987) Use of nursmg practice research findingsNursmg Research 36, 344-349
Champion V L & Leach A (1989) Variables related to researchutilisation m nursing Joumal of Advanced Nursmg 14,704-710
Closs S J & Cheater F M (1994) Utihsation of nursmg researchculture, interest and support Joumal of Advanced Nursing19, 762-773
CURN (Conduct and Utilisation of Research in Nursing) Project(1983) Using Research to Improve Nursing Practice MichiganNurses Association, Grune and Stratton, Michigan
Department of Health (1991) Research for Health A Research andDevelopment Strategy for the NHS HMSO, London
Department of Health (1993) Report ofthe Taskforce on the Strat-egy for Research m Nursmg, Midwifery and Health VisitingDepartment of Health, London
Department of Health (1994) NHS Executive Improving theEffectiveness of the NHS Circular EL (94) 74 Department ofHealth, London
Duff L A , Kitson A L , Edgson R , Watson R & Bakewell J (1993)Nutritional Standards for the Older Adult in Continuing CareA Report of the Development and Initial Pilot-Testing of theStandards RCN Dynamic Quahty Improvement Programme,Oxford
Dunning M , McQuay H & Milne R (1994) Getting a grip HealthServices Joumal 104(5400), 24-26
Eisenberg J M (1986) Doctors' Decisions and the Cost of MedicalCare Health Admmistration Press, Ann Arbor, Michigan
Ersser S J (1992) An account of the work and role of a clinicallecturer based in the Department of Dermatology, Oxford
1990-1992 Unpublished report, NaUonal IntUtuta forNursing, Oxford
Ersser S J Venables J & Kaur V (1995) Report of the work of adermatology liaison nursmg service No 1 analytical descrip-Uon of role, its development and evaluation research strategyUnpublished report National Institute for Nursing/OxfordDepartment of Dermatology, Oxford
Funk S G , Tomquist E M & Champague M T (1989) A model forimproving the dissemination of research Western Joumal ofNursing Research 11, 361-367
Grimshaw J M & Russell IT (1993) Effect of clinical guidelineson medical practice a svstematic review of rigorous evalu-ations The Lancet 342, 1317-1322
Grol R (1992) Implementing guidelines m general practice careQualitv m Health Care Joumal 1, 184-191
Haines A & Jones R (1994) Implementing findings of researchBntish Medical Journal 308, 1488-1492
Horsley J A , Crane ) , Crabtree M K & Wood D J (1983) UsingResearch to Improve Nursing Practice A Guide Grune andStratton, New York
Hunt J (1981) Indicators for nursing practice the use of researchfindmgs Journal of Advanced Nursing 6, 189-194
Hunt M (1987) The process of translating research findings intonursing practice Joumal of Advanced Nursing 12 101-110
Kitson A L , Harvey G Hyndman S , Smdhu F & Yerrell P (1994)The Impact of a Nursing Quality Assurance Approach, theDynamic Standard Settmg System (DySSSy) on Nursing Prac-tice and Patient Outcomes The ODySSSy Pro/ect, Report No 4,Vols I, II &• III National Institute for Nursing, Oxford
Lawler J (1991) Behind the Screens Nursmg, Somology and theProblem of the Body Churchill Livingstone, London
Lomas J & Haynes R B (1988) A taxonomy and critical review oftested strategies for the application of clinical practice rec-ommendations from 'official' to 'individual' clmical policyAmerican Joumal of Preventative Medicine 4(suppl), 77-95
Lorentzon M (1994) Guest editorial Nursing development unitsprofessionalization strategy for nurses cheap service option orgenuine improvement in patient care' Joumal of AdvancedNursing 19, 835-836
Luker K A & Kennck M (1992) An exploratory study of thesources of influence on the clinical decisions of communitynurses Joumal of Advanced Nursing 17, 457-466
McCormack B (1994) A Report of the Work of the CommunityHospital Nursing Development Unit 1993/1994 Unpublishedreport, Oxfordshire Community NHS Trust, Oxford
NHS Management Executive Nursmg Directorate (1994) Strategyfor Mamly Nursmg-led Major Clmical Cuidehnes — ProjectUpdate Health Services Management Unit, Manchester
Pearson A (1992) Nursing af Burford A Story of Change ScutariPress, London
Pembrey S (1984) Nursing care professional progress Joumal ofAdvanced Nursmg 9, 539-547
Pembrey S (1987) District guidance on professional nursing prac-tice m Oxfordshire Unpublished paper, Oxfordshire HealthAuthonty, Oxford
Russell IT & Wilson BJ (1992) Audit the third clinical scienceQuahty m Health Care Journal 1(1), 51-55
Smith R (1991) Where is the wisdom' Editonal Bntish MedicalJoumal 303, 798-799
Stockmg B (1992) PromoUng change mto clinical care Qualitym Health Care Joumal 1, 56-60
© 1996 Blackwell Science Ltd, Joumal of Advanced Nursing, 23, 430-440 439

A Kitson et al
Thompson D R. & Cordle C J (1988) Supjx)rt of wives of myocar-dial infarction patients Joumal of Advanced Nursing 13,223-229
Thompson D R (1994) Cardiac rehabilitation services the needto develop guidelines Quahty in Health Care Joumal 3,169-172
Thompson D R , Bowman G S , Kitson A L , de Bono D P &Hopkins A (1996) Cardiac rehabilitation guidelines and auditstandards Submitted for publication
Tiemey A J & Taylor J (1991) Research in practice 'an experi-ment' in research-practitioner collaboration Joumal ofAdvanced Nursing 16, 506—570
Tiemey A J (1994) An analysis of nursing's pierformance in the1992 assessment of research in British Universities Joumal ofAdvanced Nursing 19, 593-602
Titchen A & Binnie A (1993a) Research partnerships collahor-ative action research m nursing Joumal of Advanced Nursing18, 858-865
Titchen A & Binnie A (1993b) What am I meant to be doing'Puttmg practice mto theory and back again Joumal ofAdvanced Nursing 18, 1054-1065
Titchen A & Binnie A (1993c) A 'double-act' co-actionresearcher roles in an acute hospital setting In ChangingNursing Practice through Action Research (Titchen A ed),Report No 6, National Institute for Nursmg, Oxford
Titchen A & Bmnie A (1994) Action research a strategy for
theory generation and testing Intemationaljoumal of NursingStudies 31(1), 1-12
Vaughan B (1986) Bndgii^ the gap, teaching roles in nursmgeducaUon Senior Nurse 6(5), 31
Ward M , Titchen A , Morrell C McCormack B & Kitson A (1995)The Northampton Practice Development Project NationalInstitute for Nursing, Oxford
Watt G C M (1993) Making research make a difference HealthBulletin 57, 187-195
Webh C (1989) Action research philosophy methods and personalexpenences Joumal of Advanced Nursing 14, 403—410
Webb C & MacKenzie J (1993) Where are we now' Researchmindedness m the 1990s Joumal of Clinical Nursing 2,129-133
Williams K , Roe B & Sindhu F (1995) The Continence CareProject An Evaluation of Nursing Developments m ContinenceCare Report No 10, National Institute for Nursmg, Oxford
Wilson-Bamett J , Comer J & De Carle B (1990) Integrating nurs-mg research and practice the role of the researcher as teacherJoumal of Advanced Nursing 15, 621-662
Wilton L (1994) The John Radchffe Hospital Audit of Accounts1992/3 A Review of the Management and Utilization of WardNursing Resources District Audit Service, Oxford
Wyatt J & Olivers (eds) (1995) Reviews of Behavioural Researchwithin the Cochrane Collahoration Newsletter 2, Jnly
440 © 1996 Blackwell Science Ltd, Joumal of Advanced Nursing, 23, 430-440

Related Documents











