COLLEGE OF CHIROPRACTORS OF ONTARIO PUBLIC INFORMATION PACKAGE FOR COUNCIL MEETING FRIDAY, JUNE 23, 2017 – 8:30 A.M.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

COLLEGE OF CHIROPRACTORS OF ONTARIO
PUBLIC INFORMATION PACKAGE FOR COUNCIL MEETING
FRIDAY, JUNE 23, 2017 – 8:30 A.M.
RHPA
Duties and Obiects of Colleges
Dufy of Collegez.l It is the duty of the College to work in consultation with the Minister to ensure, as a
matter of public urterest, that the people of Ontario have access to adequate numbers of
qualified, iLitl"¿ and competent regulated health professionals' 2008' c' l8' s- l'
Objects of College3. ( I ) The College has the following objects'
l. To regulate the practice of the profession and to govern the members in accordance
with the healttr profession Act, this Code and the Regulated Health Professions
Act, I991 and the regulations and by-,laws'
2. To.develop, establish and maintain standards of qualification lor persons to be issued
certificates o f registration.
3. To develop, establish and maintain programs and standards of practice to assure the
qualify of the practice of the profession'
4. 'I-o develop, establish and maintain standards of knowledge and skill and programs to
promoteãntinuing evaluation, competence and improvement among the members'
4.1 To develop, in collaboration and consultation with other Colleges, standards of
knowledgå, skill and judgment relating to the performance olcontrolled acts
"o-,ooriumong healih professions to enhance interprolessional collaboration, while
respecting the rinique character of individual health professions and their members'
5. To develop, establish and maintain standards of professional ethics for the members'
6- To develop, establish and rnaintain programs to assist individuals to exercise their
rights under this Code and the Regulated Heatth Professions Act, ] 991 '
T.Toadminister the health profession Act, this code and the Regulated Health
professions Act, lggl as it relates to the profession and to perform the other duties
and exercise the other po\Ãiers that are imposed or conlened on the College'
g- To promote and enhance relations befween the College and its members, other
health profession colleges, key stakeholders, and the pubtic.
9. To promote inter-professional collaboration with other health profession colleges'
10. To develop, establish, and maintain standards and programs to promote the ability
of members to respond to changes in practice environments, advances in
technolory and other emerging issues-
I l. Any other objects retating to human health care that the Council considers
desirable. t9é1, c. 18, SJrte¿. 2, s.3 (l); 2007, c- 10, Sched' M, s' l8; 2009, c'26'
s. 2a (l l)-
Dufy(2) In carrying out its objects, the College has a duty to serye and protect the public
interest. I991, c. 18, Sched. 2, s- 3 (2)'
.1
Version date: December 7, 2015
COLLEGE OF CHIROPRACTORS OF ONTARIO MISSION AND STRATEGIC OBJECTIVES
MISSION The College of Chiropractors of Ontario is the self-governing body of the chiropractic profession committed to improving the health and well-being of Ontarians by informing the public and assuring them of competent and ethical chiropractic care.
The College examines, registers and regulates the chiropractic profession and partners with other health professions, their licensing bodies, organizations and government.
Developed at the strategic planning session in September 2004 Approved by Council on February 8, 2005
STRATEGIC OBJECTIVES
1. Improve communication of the role, mandate and mechanism of CCO to key
internal and external stakeholders. 2. Strive for unity in the public interest, while respecting the diversity within the
profession. 3. Optimize chiropractic services in the public interest. 4. Continue to regulate in a fiscally responsible manner: Statutory mandate met
and priorities set and appropriately resourced (human and financial).
Developed at the strategic planning session: October 2010 Confirmed at the strategic planning sessions: September 2012, 2013, 2014, 2015
CCO Cooe or, CoruDUcT FOR CURRCruT ANDFoRnneR EI.eCreD AND PUELIC MCMSCNS OF
GouncrL AND Not¡-CouNcrL Conn¡vurree MemBERS
Executive CommitteeApproved by Council: September 28,2012Amended: February 23,2016, April 19,2016, September 15, 2016
Current and former elected and public members of Council and non-Council committeemembers must, at all times, maintain high standards of integrity, honesty and loyaltywhen discharging their College duties. They must act in the best interest of the College.They shall:
1. be familiar and comply with the provisions of the Regulated Health ProfessionsAct, l99l (RHPA), its regulations and the Health Professions Procedural Code,the Chiropractìc Act I 991 , its regulations, and the by-laws and policies of theCollege;
2. diligently take part in committee work and actively serve on committees as
elected and appointed by the Council;
3. regularly attend meetings on time and participate constructively in discussions;
4. offer opinions and express views on matters before the College, Council andcommittee, when appropriate;
5. participate in all deliberations and communications in a respectful, courteous andprofessional manner, recognizing the diverse background, skills and experience ofmembers on Council and committees;
6. uphold the decisions made by Council and committees, regardless of the level ofprior individual disagreement;
7. place the interests of the College, Council and committee above self-interests;
8. avoid and, where that is not possible, declare any appeatance of or actual conflictsof interestsl;
refrain fiom including or referencing Council or committee positions held at theCollege in any personal or business promotional materials, advertisements andbusiness cards;2
I There is a general assumption of real or perceived conflict unless confirmation of no conflict by theExecutive Committee and/or Council, which will be addressed promptly.2 This section does not preclude the use ofprofessional biographies for professional involvement.
9
CCO Code of Conduct
10. preserve conf,rdentiality of all information before Council or committee unlessdisclosure has been authorized by Council or otherwise exempted under s. 36(i)of the RHPA;
1 l. refrain from communicating to members, including other Council or committeemembers, on statutory committees regarding registration, complaints, reports,investigations, disciplinary or fitness to practise proceedings which could beperceived as an attempt to influence a statutory committee or a breach ofconhdentiality, unless he or she is a member of the panel or, where there is nopanel, of the statutory committee dealing with the matter;
12. refrain from communicating to members and stakeholder3 on behalf of CCOincluding on social medìa, unless authorized by Councila;
13. respect the boundaries of staff whose role is not to report to or work for individualCouncil or committee members; and
14. be respectful of others and not engage in behaviour that might reasonably beperceived as verbal, physical or sexual abuse or harassment.
Potential Breaches of the Code of Gonduct
15. An elected or appointed member of Council or non-Council committee memberwho becomes aware of any potential breach of this code of conduct shouldimmediately advise the President and Registrar, or if the potential breach involvesthe President, advise the Vice President and Registrar; and
16. Potential breaches will be addressed f,rrst through informal discussion with theCouncil member(s) or non-Council committee member(s), and subsequently bywritten communication expressing concerns and potential consequences.
I, , Council member or non-Council committee member of theCollege of Chiropractors of Ontario underlake to comply with the CCO Code of Conductfor Current and Former Elected and Public Members of Council and Non-CouncilCommittee Members, both during and following my term on CCO Council or acommittee
Signature Witness
Date
3 Stakeholders include professional associations, societies, and other organizations related to the regulation,education and practice of chiropractic.a This does not preclude Council members from communicating about CCO, provided they are notcommunicating on behalf of CCO.
2
1
2
Rules of Order of the Council of theGollege of Chiropractors of Ontario
Approved by Gouncil: September 20, 2014
ln this Schedule, "member" means a council member
Each agenda topic will be introduced briefly by the person or committeerepresentative raising it. Members may ask questions of clarification, then theperson introducing the matter shall make a motion and another member mustsecond the motion before it can be debated.
When any member wishes to speak, he or she shall so indicate by raising his orher hand and shall address the chair and confine himself or herself to the matterunder discussion.
Staff persons and consultants with expertise in a matter may be permitted by thechair to answer specific questions about the matter.
5
6
Observers at a council meeting are not allowed to speak to a matter that is underdebate.
A member may not speak again on the debate of a matter until every councilmember who wishes to speak to it has been given an opportunity to do so. Theonly exception is that the person introducing the matter or a staff person mayanswer questions about the matter. Members will not speak to a matter morethan twice without the permission of the chair.
A member may not speak longer than five minutes upon any motion except withthe permission of Council.
When a motion is under debate, no other motion can be made except to amendit, to postpone it, to put the motion to a vote, to adjourn the debate of the councilmeeting or to refer the motion to a committee.
A motion to amend the motion then under debate shall be disposed of first. Onlyone motion to amend the motion under debate can be made at a time.
3
4
7
B
I
10 When a motion is on the floor, a member shall make every effort to be presentand to remain in the room.
When it appears to the chair that the debate in a matter has concluded, whenCouncil has passed a motion to vote on the motion or when the time allocated tothe debate of the matter has concluded, the chair shall put the motion to a voteand no further debate is permitted.
11
Rules of Order of CouncilApproved by Council: September 20, 2014
12
13
14
15
16
17
18
19
2
A member is not entitled to vote upon any motion in which he or she has aconflict of interest, and the vote of any member so interested will be disallowed.
Any motion decided by the Council shall not be re-introduced during the samesession except by a two-thirds vote of the Council then present.
Whenever the chair is of the opinion that a motion offered to the Council iscontrary to these rules or the by-laws, he or she shall rule the motion out of orderand give his or her reasons for doing so.
The chair shall preserve order, etiquette and decorum, and shall decidequestions of order, which include addressing any distractions that interfere withthe business of the meeting, subject to an appeal to the Council without debate.
The above rules may be relaxed by the chair if it appears that greater informalityis beneficial in the particular circumstances unless the Council requires strictadherence.
Members are not permitted to discuss a matter with observers while it is beingdebated.
Members are to be respectful, courteous and professional while others arespeaking.
ln all cases not provided for in these rules or by other rules of Council, thecurrent edition of Robert's Rules of Order shall be followed so far as they may beapplicable.
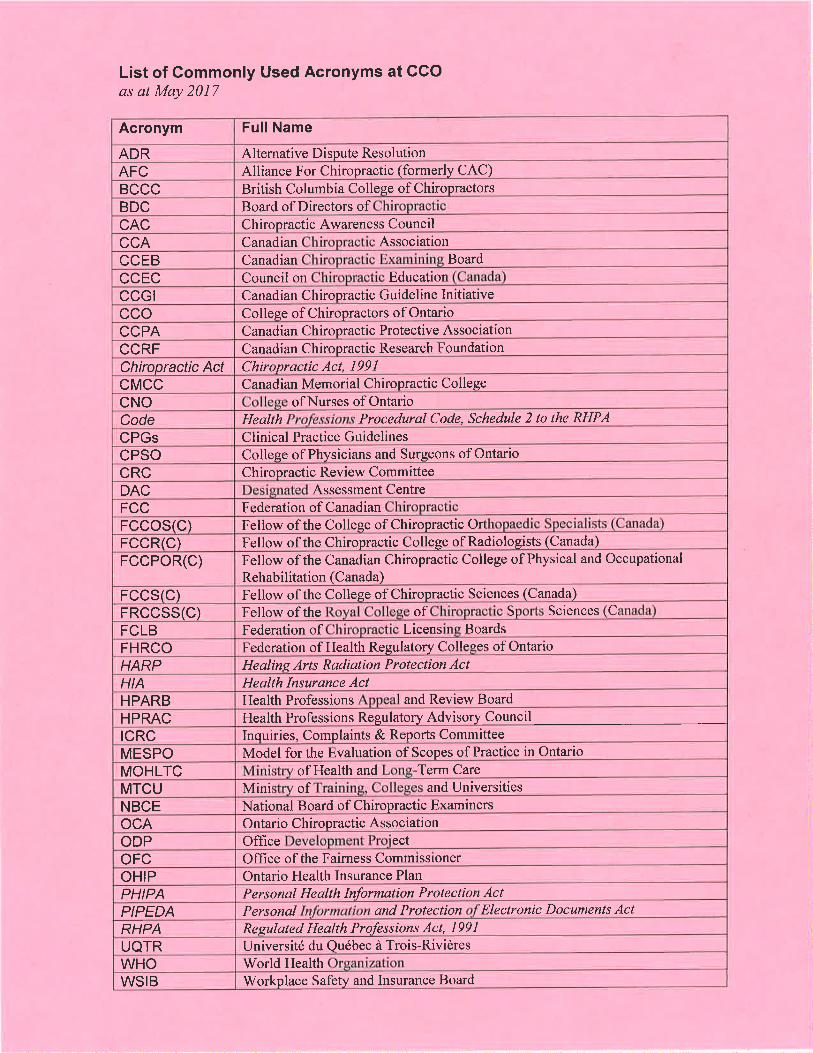
List of Commonly Used Acronyms at CCOas at May 2017
Acronym Full Name
ADR Alternative Dispute ResolutionAFC Alliance For Chiropractic (formerly cAC)BCCC British Columbia College of ChiropractorsBDC Board of Directors ofcAc Chiropractic Awareness Council
CCA Canadian Association
CCEB Canadian Board
CCEC Council on Education
cccr Canadian Chiropractic Guideline Initiativecco College of Chiropractors of OntarioCCPA Canadian Chiropractic Protective Association
CCRF Canadian Chiropractic Research Foundation
Chiropractic Act Chiropractic Act, I99lcMcc Canadian Memorial Chiropractic College
cNo of Nurses of OntarioCode Health Procedurql Code, Schedule 2 to the RHPA
CPGs Clinical Practice GuidelinesCPSO College of Physicians and Surgeons of Ontario
cRc Chiropractic Review CommitteeDAC Assessment Centre
FCC Federation of Canadian
FCCOS(C) Fellow of the College of Chiropractic Orthopaedic Speqralists (CanadÐ
FCCR(C) Fellow of the Chiropractic College of Radiologists (Canada)
FCCPOR(C) Fellow of the Canadian Chiropractic College of Physical and Occupational
Rehabilitation (Canada)
FCCS(C) Fellow of the College of Chiropractic Sciences (Canada)
FRCCSS(C) Fellow of the of S Sciences C
FCLB Federation of Licens Boards
FHRCO Federation of Health Regulatory Co llaccc of Ontario
HARP Healins Arts Radiation Protection ActHIA Health Insurance ActHPARB Health Professions and Review Board
HPRAC Health Professions Regulatory Advisory Council
tcRc Inquiries, Complaints & Reports Committee
MESPO Model for the Evaluation of Scopes of Practice in Ontario
MOHLTC of Health and Term Care
MTCU Mini of and Universities
NBCE National Board of Chiropractic Examiners
ocA Ontario Chiropractic AssociationODP Office ect
OFC Office of the Fairness CommissionerOHIP Ontario Health Insurance Plan
PHIPA Personal Health Information Protection ActPIPEDA Personal and Protection Electronic Documents ActRHPA Regulated Health Professions Act, l99IUQTR Université du Québec à Trois-RivièresWHO World HealthWSIB and Insurance BoardWorkplace Safety
ITEM 1.1SubmittedJune 12,2017
Gollege of Chiropractors of OntarioDiscipline Committee Report to GouncilFriday, June 23,2017
ICore Members: Ms Judith McCutcheon, Chair
Dr. Reginald GatesDr. David StarmerDr. Pat TavaresDr. Daniela Arciero, non-Council memberDr. Angela Barrow, non-Council memberDr. Liz Gabison, non-Council memberDr. Colin Goudreau, non-Council memberDr. Roberta Koch, non-Council memberDr. Matt Tribe, non-Council member
Staff Support: Ms Jo-Ann'Willson, Registrar and General Counsel
Since the last council meeting there have been no committee meetings or hearings.
The panel's decisions and reasons for the following hearing was released to the parties:. Dr. LizaBgbogah (heard - April 19,2017)
There have been a number of prehearings scheduled which will proceed to hearingsshortly. A hearing for the Dr. Ellis matter is scheduled for August 1,2017 . The panel willbe composed of Ms McCutcheon as chair, Drs. Gabison, Koch, Starmer and Mr. DougCressman. A hearing for the Dr. Sangster matter is scheduled for December 4--7,2017(inclusive). The panel will be composed of Ms McCutcheon as chair, Drs. Arciero,Barrow, Starmer and Mr. Doug Cressman.
The Federation of Health Regulatory Colleges of Ontario (FHRCO) held a
Discipline Orientation Basic on May 18,2017. The following persons attended:Dr. Matt Tribe, Mr. Craig Malcolm and Mrs. Kelly Malcolm (CCO Investigators).According to our bylaws, every member of Council is a member of the DisciplineCommittee and as such may be called upon to serve on an upcoming panel. Therefore, forany Council members who have not yet attended this basic training, there will be anothersession in the fall. Members should also be aware that the advanced course will also be
offered in the fall.
The work of the Discipline Committee is vital to protecting the public interest and Iwould like to thank the members of the Discipline Committee for their time andDedication: Dr. Daniela Arciero, Dr. Angela Barrow, Mr. Doug Cressman, Dr.LizGabison, Dr. Colin Goudreau, Dr. Roberta Koch, Dr. David Starmer, Dr. Pat Tavares andDr. Matt Tribe. In addition, I would also like to extend my thanks to all members ofcouncil who are willing to serve on panels.
Respectfully submitted,
Ms Judith McCutcheonChair, Discipline Committee
PANEL:
BETWEEN
COLLEGE OF CHI ROPRACTORSOF ONTARIO
-and-
Dr. Liza EgbogahRegistration #5414
|TEM 1.1.1
DISCIPLINE COMMITTEEOF THE COLLEGE OF CHIROPRACTORS OF
Ms. Judith McCutcheon, ChairDr. Angela BarrowMr. Douglas CressmanDr. Elisheva GabisonDr. Reginald Gates
Public MemberProfessional MemberPublic MemberProfessional MemberProfessional Member
10
)))))))))
Mr. Chris Paliare andMs. Karen Jones for theCollege of Chiropractors of Ontario
Ms. Valerie Wise and Ms. EstherNwator
))
Heard: April 19,2017
Also present at the hearing were
Mr. Paul Le Vay - lndependent Legal Counselto the PanelMs. Jo-Ann Willson - Registrar and General Counsel CCOMr. Robert Donnelly - Court Reporter
DECISION AND REASONS
Introduction
This was a hearing before a panelof the Disciplíne Committee (the "Panel") of the College
of Chiropractors of Ontario (the "College"). The College has a mandate to regulate the
practice of the chiropractic profession and to govern its members and, in so doing, serve
and protect the public interest.1 of19
RSÇEIVEDJtf{ 0û 10t7
;êbÏr.EGÈCIütçmsffãreffi
11
As outlined below, the hearing began with the presentation by the parties of an AgreedStatement of Fact ("ASF") upon which we were asked to make findings of professional
misconduct. We did so for the reasons set out below.
The Panel then heard a joint submission on penalty from the parties. For the reasonsset out below, we accepted the joint submission and made the order as to penalty setout in these reasons.
The Alleqations
The allegations against Dr. Liz Egbogah, (the "Member"), were set out in the two Noticesof Hearing.
Notice of Hearinq #1
Notice of Hearing #1 was dated June 2,2016 and was entered into evidence as Exhibit
The allegations in respect of the Member's conduct set out therein were as follows
1
1. You have committed 9n ac-t of professional misconduct as provided bysubsection 51(1)(c) of the Health Professionals Procedural Code of thechiropractic Act,1gg1, s.o. 1gg1, c. 21, asamended, and paragraph 1 (2) otontario Regulation a52/gg, in that during the period 2011 6 2016, youcontravened a standard of practice of the profession or failed to mãinta¡n thestandard of practice expected of members of the profession with respect to yourassessment, treatment, documentation and/or billing of professional servicesand products for patients of the [crinic] known as "H.L." and/or 'F.F.'
2. You have committed gn act of professional misconduct as provided bysubsection 51(1)(c) of the Health Professionals Procedural Code of thechiropractic Act,1gg1, s.o. 1gg1, c. 21, as amended, and paragraph I (14) ofO_ntario Regulation 852/93, in that during the period 2011 to 201É, you proúiOeO adiagnostic or therapeutic service that wãs not necessary with respect to patientsof the [clinic] known as "H.L." and/or 'F.F.'
2of19
123. You have committed an act of professional misconduct as provided by
subsection 51(1)(c) of the Health Professionals Procedural Code of theChiropractic Act, 1 991 , S.O. 1991 , c. 21 , as amended, and paragraph I (19) ofOntario Regulation 852/93, in that during the period 2011 to 2015, you failed tokeep records as required by the regulations regarding patients of the [clinic]known as "H.L." and/or uF.F."
4. You have committed an act of professional misconduct as provided bysubsection 51(1Xc) of the Health Professionals Procedural Code of theChiropractic Act, 1991 , S.O. 1991 , c. 21, as amended, and paragraph 1(20) ofOntario Regulation 852/93, in that during the period 2011 to 2015, you falsified arecord or records relating to your practice regarding the assessment, treatment,and/or billing for professional services for patients of the [clinic] known as "H.L."and/or uF.F."
5. You have committed an act of professional misconduct as provided bysubsection 51(1)(c) of the Health Professionals Procedural Code of theChíropractic Act, 1991 , S.O. 1991 , c. 21, as amended, and paragraph 1 (22) oÍOntarío Regulation 852/93, in that during the period 2011 to 2015, you signed orissued, in your professional capacity, a document or documents that you knewcontained false or misleading statements regarding the assessment, treatment,and/or billing for professional services for patients of the [clinic] known as "H.L."and/or "F.F."
6. You have committed an act of professional misconduct as provided bysubsection 51(1)(c) of the Health Professionals Procedural Code of theChiropractic Act,1991, S.O. 1991, c. 21, as amended, and paragraph 1(23) ofOntario Regulation 852/93, in that during the period 2011 lo 2015, you submittedan account or charge for services that you knew was false or misleadingregarding patients of the [clinic] known as "H.L." and/or *F.F."
7. You have committed an act of professional misconduct as provided bysubsection 51(1Xc) of the Health Professionals Procedural Code of theChiropracticAct,l99l, S.O. 1991, c.21,as amended, and paragraph 1(33) ofOntarío Regulation 852/93, in that during the period 2011 to 2015, you engagedin conduct or performed an act, that, having regard to all the circumstances,would reasonably be regarded by members as disgraceful, dishonourable orunprofessional with respect to your assessment, treatment, documentationand/or billing regarding patients of the [clinic] known as "H.L." and/or 'F.F.'
3 of19
Notice of Hearins #2 13
Notice of Hearing #2 was dated October 28, 2016 and was entered into evidence as
Exhibit 2.
The allegations in respect of the Member's conduct set out therein were as follows
1. You have committed an act of professional misconduct as provided bysubsec-tion 51(1)(c) of the Health Professionals Procedural Code of the Chiiopractic Act,1991, S.O. 1991, c. 21, as amended, and paragraph 1(2) of Ontario Regutation 852/g3,in that during the period 2013 to 2014, you contravened a standard of practice of theprofession or failed to maintain the standard of practice expected of members of theprofession with respect to your billing for professional services for a patient of the [clinic]known as "Patient X."
2. You have committed an act of professional misconduct as provided by9ylseclio_n 51(1)(c) of the Health Professionals Procedural Code of the Chiiopractic Act,1991, s.o. 1991 , c.21, as amended, and paragraph 1(20) of ontario Regutaiion852/93, in that during the period 2013 to 2014, you falsified a record or records relatingto your practice regarding the'billing for professional services for a patient of the [clinicjknown as "Patient X."
3. You have committed an act of professional misconduct as provided bysubseclion 51(1)(c) of the Health Professionals Procedural Code of the Chiropractic Act,1991, s.o. 1991 , c. 21, as amended, and paragraph 1(22) of ontario Regutaiion852/93, in that during the period 2019 to 2014, you signed or issued, in yourprofessional capacity, a document or documents that you knew contained false ormisleading statements regarding the billing for professíonal services for a patient of the[clinic] known as "Patient X."
4. You have committed an act of professional misconduct as provided by9ylgecJign 51(1)(c) of the Health Professionals Procedural Code of the Chiropractic Act,1991, s.o. 1991, c. 21, as amended, and paragraph 1(23) of ontario Regutaiion852/93, in that during the period 2013 to 2014, you submitted an accounior charge forservices that you knew was false or misleading regarding a patient of the [clinic] Ènownas "Patient X."
5. You have committed an act of professional misconduct as provided by9ylseclio_n 51(1)(c) of the Health Professionals Procedural Code of the Chiiopractíc Act,1991, s.o. 1991, c. 21, as amended, and paragraph 1(33) of ontario Regutation
4of19
14852/93, in that during the period 2013 to 2014, you engaged in conduct or performed anact, that, having regard to allthe circumstances, would reasonably be regarded bymembers as disgraceful, dishonourable or unprofessional with respect to your billingregarding a patient of the [clinic] known as "Patient X."
Member's Plea
As set out below and qualified in the Agreed Statement of Fact, the Member admitted the
following allegations:
1. Notice of Hearing #1:Allegations 1,3,4,5,6 and 7 (disgraceful, dishonourable
and unprofessional re patient H.L. and dishonourable and unprofessional re patient
F.F.)
2. Notice of Hearing #2: Allegations 1 and 5 (dishonourable and unprofessional only)
The other allegations were withdrawn by the College.
The Panel was satisfíed that the Member's admissions were voluntary, informed and
unequivocal.
Aqreed Statement of Facts
The following agreed facts were presented to the Panel and entered as Exhibit 3
Backqround
1. Dr. Liza Egbogah ("Member") became a member of the College of Chiropractors
of Ontario ("CCO') on September 4,2007.
2. During the relevant time, she practiced chiropractic at the [clinic] in Toronto
("Clinic").
3. Prior to October 2014, the Member owned and operated the Clinic. She sold the
Clinic on October 1,2014 and continued to work at the Clinic as a chiropractor until
November 28,2014
5of19
4 The Member has no previous discipline history at the CCO. 15
Re: H.L.
5. on December 6, 2011, the Member saw a patient known as "H.L." who wascomplaining of low back pain and arch pain. H.L. had a prescription for 1 pair of custom
orthotics. At the time, H.L.'s insurance covered orthopedic shoes and orthotics up to amaximum of $500.00. The Member conducted a gait analysis. The Member ordered
orthopedic shoes for her patients at the Cliníc from either The Orthotic Group ("TOG',) orWalking on a Cloud. ln H.L.'s case, the Member ordered a pair of orthotics and a pair ofboots for H.L. on December 6, 2011fromTOG. The Member billed the insurer $150.00for the December 6,2011 assessment, $500.00 for orthotics and $g0.00 for asubsequent assessment on December 21, 2011, when she documented the patientpicked up the orthotics and orthotic boots. The insurer paid the Member $657.00.
6. on November 6, 2012, the Member submitted a claim for $g0.00 to the insurerfor a chiropractic assessment for November 6,2T12for H.L.. On November g, 2012,the Member submitted claims to the insurer for two chiropractic visits ($80.00 and
$70.00) and a pair of custom orthotics ($50O.OO) for H.L. On Janua ry 25,2013, theMember submitted claims totalling $150.00 to the insurer for two chiropractic treatmentsfor H.L. that took place on the same day. The ínsurer paid the Member $7TT.OO. Thereare no patient records for the November 6,2012 assessment. There are no recordsindicating the Member ever ordered orthotics for H.L. There are no records indicatingthe patient received chiropractic treatment on any of the 2012 or 2013 dates. There is arecord that the Member ordered a pair of off the shelf boots in March 2O1g for H.L.
7. On December 24,2013, the Member submitted a claim to the insurer for achiropractic assessment and treatment ($150.00), orthotics ($S00.00) and orthopedicshoes ($500.00) for H.L. The Member provided the insurer with the same Gait Analysis
6of19
16for H.L. that she submitted in 2011 (with the original date whited out with what appears
to be liquid paper, and a new date written over the whitened-out portion), and a receipt
that is the same as the 2012 receipt (with the original date whited out and a new date
written over the whitened-out area). There is no documentation in the patient record
regarding the assessment or treatment and there are no records indicating orthotics or
orthopedic shoes were ever ordered. The insurer paid the Member $494.50.
8. On October 8,2014, the Member submitted hruo claims to the insurer regarding
H.L.: a $250.00 claim for a chiropractic assessment and treatment, and a $500.00 claim
for orthotics. The insurer paid $449.50 directly to the Member. There is no evidence
the Member ordered any orthotics for H.L. The Member provided the insurer wíth the
same Gait Analysis she submitted in 2011 (with the date whited out and a new date
written over the white out area and handwritten notes), and a receipt that is the same as
the receipt submitted in 2012 (with the date whited out and a new date written over the
whitened-out area). She also submitted an authorization from H.L. directing the insurer
to pay the Member directly. The authorization is the same authorization signed by H.L.
in 2013, with the date whited out and a new date written over the whitened-out aÍea.
The Expenses Statement, which is signed by H.L., is the same Expenses Statement
submitted to the insurer in 2013, with certain information and the date whitened out and
a new date written in.
Re: F.F.
9. The Member saw patient F.F. in 2012 for plantar fasciitis. She ordered
orthopedic shoes for him at that time.
10. The Member documented assessing F.F. on July 9, 2014. She made a claim to
the insurer for $100.00 for the assessment and was paid $100.00 directly by the insurer
On July 11, 2014, the Member submitted a claim to F.F.'s insurer for $500.00 for
7 of19
11
17orthotics and $600.00 for orthopedic shoes. The insurer denied both claims. On
September 18,2014, the insurer paid the Member $500.00 for the orthotics.
12. The Member documented seeing F.F. on October 7 , 2014, noting he was "sore
after last treatment but after that better". The Member billed the insurer for two separate
appointments on October 7,2014, one for assessment and one for treatment, each
costing $250.00. The insurer paid the Member $500.00 directly on October 7,2014.
13. On October 24,2014, the Member ordered two pair of non-custom shoes and
one pair of orthotics from TOG for F.F, which she documented he picked up on October
28,2014.
Admrcsíons
14. The Member admits, based on the facts set out above, that she committed acts
of professional misconduct as set out in the Notice of Hearing dated June 2,2016("NOH"), in that:
Re: Allegation #1 in the NOH:
a. during the period 2012 - 2014, she contravened a standard of practice of
the profession or failed to maintain the standard of practice expected of
members of the profession with respect to her assessment, treatment,
documentation and billing of professional services and products for a
patient of the [cliníc] known as "H.L."; and
b. in 2014, she contravened a standard of practice of the profession or failed
to maintain the standard of practice expected of members of the
profession with respect to documentation and billing of professional
services and products for a patient of the [clinic] known as "F.F."
Re: Allegation #3 in the NOH:
8of19
18a. during the period 2012 to 2014, she failed to keep records as requíred by
the regulations regarding a patient of the [clinic] known as "H.L."; and
b. in2014, she failed to keep records as required by the regulations regardíng
a patient of the [clinic] known as "F.F."
Re: Allegation #4 in the NOH:
o during the period 2012 - 2014, she falsified a record or records relating to her
practice regarding the assessment, treatment, and billing for professional
services for a patient of the [clinic] known as "H.L."
Re: Allegation #5 in the NOH:
. during the period 2012 - 2014, she signed or issued, in her professional
capacity, a document or documents that she knew contained false or
misleading statements regarding the assessment, treatment, and billing for
professional services for a patient of the [clinic] known as "H.L."
Re: Allegation #6 in the NOH:
o during the period 2012 - 2014, she submitted an account or charge for
services that she knew was false or misleading regarding a patient of the
[clinic] known as "H.L."
Re: Allegation #7
a. during the period 2012 -2014, she engaged in conduct or performed an act, that,
having regard to all the circumstances, would reasonably be regarded by
members as disgraceful, dishonourable and unprofessional with respect to her
assessment, treatment, documentation and billing regarding a patient of the
[clinic] known as "H.L."; and
9ofl9
19b. in 2014, she engaged in conduct or performed an act, that, having regard to all
the circumstances, would reasonably be regarded by members as dishonourable
and unprofessional with respect to her documentation and billing regarding a
patient of the [clinic] known as "F.F."
Notice of Hearinq #2 dated October 28, 2016
Background
15. on August 12, 2013, a patíent known as "patient X." started receiving
physiotherapy at the Clinic from a registered physical therapist (.RPT"). Patient X. had
been in a motor vehicle accident and injured her back and neck. She also had
massage therapy treatments from the Clinic's registered massage therapist. Patient X.
was not treated by the Member, who owned and operated the clinic.
16. Patient X. paid for her treatments personally, and was reimbursed for her
treatment from the Clinic by her private insurer. On occasion, the Clinic billed the
private insurer directly and was paid directly by the private insurer. Patient X. had
unlimited physical therapy and massage therapy benefits through her private insurer
17. ln November 2013, the RPT from the Clinic moved to another clinic. Patient X.
had her file transferred to the new clinic so she could continue receiving treatment from
the RPT. Patient X's account at the Clinic was fully paid before her file transferred tothe new clinic.
18. Patient X. continued to receive physiotherapy treatments from the RPT at the
new clinic, and continued to have her treatments paid for by her private insurer until
November 2014, when she divorced her husband and her extended private health
coverage ended. Thereafter, she relied on her auto insurance to pay for her
treatments.
10 of 19
2019. When Patient X. starting to rely on her auto insurance, she discovered that on
Arpril22,2014, the Member had, without her knowledge or consent, submitted an
invoice to her auto insurer and been directly paid $490.00 by the auto insurer for
treatment she had received at the Clinic.
20. The Member never met or treated Patient X. However, as the owner of the
Clinic, the Member admits she was responsible for submitting insurance claim forms
and for the billing at the Clinic.
The MIG
21. ln 2013, minor physical injuries resulting from a motor vehicle accident were
treated by insurers and health practitioners in accordance with the Minor lnjury
Guideline ("MlG') that was released by the Financial Services Commission of Ontario
(.FSCO"). The MIG provided a FSCO-approved process for the treatment of
uncomplicated musculoskeletal injuries. The purpose of the MIG was to help expedite
treatment by providing a pre-approved process, and as a result avoid delays due to
lengthy insurer approval requirements.
22. The first document provided to an insurer in such a situation by a health
practitioner was an OCF-23 (Treatment Confirmation Form) which was completed by a
claimant and their health practitioner. The OCF-23 was provided to the claimant's
insurer. An ínsurer would respond to the OCF-23, and inform the health practitioner
whether the claimant was covered by an insurance policy and whether the injuries
described fell within the MlG. The treatment permitted by an OCF-23 occurred over 12
weeks, which was divided into 3 blocks, each of a duration of 4 weeks
23. The insurer would pay for treatment under the MIG as follows:
o Fee for initial examination/consultation: $215. Fee for block one: $775
11 of19
. Fee for block two: 9500o Fee for block three: $225 21
24. When the treatment under the OCF-23 was completed, the health
practitioner would send the insurer an ocF-21 (standard lnvoice).
25- Section 47 (2) of the SABS provides that an auto insurer was not obliged to pay
for the portion of an expense allowable under the MIG if payment was reasonably
available under other insurance or health care coverage ("extended health care
benefits" or "EHCBs"). All EHCBs are deducted from amounts othen¡rise payable by
the auto insurer.
Patient X.'s Treatment and Billing at the Ctinic
26. Patient X. had an initial visit at the Clinic on August 12. She paid for that visitand three subsequent treatments on August 14, 16 and 19,2013 for a total of $960.00.When Patient X. started going to the CIinic, she was charged the Clinic's regular rate foran assessment and treatment. However, after her third treatment, when the Clinic
realized she had been injured as the result of an motor vehicle accident, the Clinic
increased the cost per treatment to the fee allowed by FSCO, and applied thatincreased amount retroactively.
27. On August 16,2013, the Clinic sent a Treatment Confirmation Form (OCF-23) toPatient X.'s auto insurer. That OCF-23 was not signed by Patient X., although her
signature was required on the document. The auto insurer approved the OCF-23 on
August 20,2013 and confirmed the maximum that would be paid pursuant to the MIG
was $2,200.00.
28. The Clinic sent extended health care claims to Patient X.'s private insurer on
August 21, August 23, August 30, September 4, September 6 and Septembe r g,2013,
each for $100.00.
12 of 19
2229. On September 23,2013, the Clinic issued a Statement of Accounts showing that
between the first visit on August 12,2013 and the treatment on September 11,2013,
Patient X. had incurred $1215.00 in fees, and had paid $360.00. This period coincides
with the assessment and Block 1 of the MlG.
30. On September 24,2013, the Clinic sent an explanation of benefits to the auto
insurer which indicated claims had been paid by the private insurer for $500.00 for
Patient X.'s treatments on August 21,23,30, and September 6 and 9,2013.
31. On September 24,2013, the Clinic also sent an Auto Insurance Standard lnvoice
("OCF-21") to the auto insurer. The OCF-21 indicated that the initial visit had been on
August 12,2013 and that Patient X. had received 10 physical rehabilitation treatments
between August 14,2013 and September 11,2013 for a total under the MIG of
$990.00. The OCF-21 indicated that another insurer had paid $500.00 and it requested
the auto insurer pay the difference, $490.00. The OCF-21 did not indicate that $360.00
had also been paid by Patient X., who was then reimbursed by the private insurer.
32. The auto insurer did pay the Clinic $490.00 by cheque, but later cancelled the
cheque because Patient X. advised her auto insurer that her private insurer was paying
for her treatment.
33. Patient X. paid the Clinic an additional $2,920.00 for treatment between
September 23 and November 28,2013. When Patient X. attended the Clinic for the last
time on November 8,2013, her account was paid in full, and the Clinic had received
$3,780.90 for her treatment.
34. The maximum that the Clinic could bill pursuant to the MIG was $2,200.00.
Therefore, as of November 8,2013, the Clinic had been paid more than the maximum it
was entitled to under the MIG and it had no claim against the auto insurer for Patient
X.'s treatment.
13 of 19
2335. However, even though Patient X.'s account had been fully paid, the Clinicresubmitted the OCF-21for $490.00 (dated September 24,2013) to the auto insurer on
December 9,2013, December 19, 2019, January 1s,2014, and April 22,2014.
36. On April 25,2014, the auto insurer paid the Clinic $490.00 by cheque. The Clinic
kept the payment, even though Patient X's. available money for treatment under theMIG has been depleted by $490.00 because of the payment.
37 ' Had she testified, the Member would have said that she does not know why theSeptember 24,2013 OCF-21was resubmitted by the Clinic or why the $4g0 cheque
was accepted on April 25, 2014, but she accepts responsibility for the mistakes as theowner of the Clinic at the time.
Admrcsíons
38. The Member admits, based on the facts set out above, that she committed actsof professional misconduct as set out in the Notice of Hearing dated October 2g,2016('NOH #2"), in that:
Re: Allegation #1 in NOH #2:
o during the period 2013 - 2014, she contravened a standard of practice of theprofession or failed to maintain the standard of practice expected of members ofthe profession with respect to her billing for professional services for a patient ofthe [clínic] known as "Patient X."
Re: Allegation #5 in NOH#2
during the period 2013 -2014, she engaged in conduct or performed an act,
that, having regard to allthe circumstances, would reasonabty be regarded by
a
14 of 19
24members as dishonourable and unprofessional with respect to her billing
regarding a patient of the [clinic] known as Patient X.
Acknowledqement
39. Dr. Egbogah acknowledges that she obtained independent legal advice from
her counsel, Valerie Wise, prior to entering into this Agreed Statement of Facts. She is
entering into this Agreed Statement of Facts freely and voluntarily.
Decision on Professional Misconduct
The Panel accepted the facts as set out in the Agreed Statement of Facts (Exhibit 3)
The Panel considered the Agreed Statement of Facts and the Member's admissions of
professional misconduct, found that the Member engaged in the forms of professional
misconduct described in Allegations 1, 3, 4, 5, 6 and 7 contained in the Notice of
Hearing dated June 2,2016 (Exhibit 1) and in Allegations 1 and 5 contained in the
Notice of Hearing dated October 28,2016 (Exhibit 2).
ln reaching its decision, the Panel relied exclusively on the evidence presented at the
hearing as contained in the Agreed Statement of Facts.
Penaltv
The penalty portion of the hearing then proceeded. The Panel received a joint submission
on penalty and entered it as Exhibit 4.
Joint Submíssion on Penaltv
Further to the pre-hearing conference of February 23,2017, held before Dr. Drew Potter
and in view of the Agreed Statement of Facts and of the Undertaking signed by Dr.
Egbogah which is attached to this Resolution Agreement as Exhib¡t uA', the College of
Chiropractors of Ontario ('CCO") and Dr. Liza Egbogah ("Member") jointly submit that
15 of 19
the panel of the Discipline Committee ("Panel") make an Order:25
1. Requiring Dr. Egbogah to appear before the Panel to be reprimanded.
2. Ordering the Registrar and General Counsel ("Registrar") to suspend Dr
Egbogah's Certificate of Registration ("Certificate") for a period of 9 months.
3. Ordering the Registrar to impose the following terms, conditions and limitations
on Dr. Egbogah's Certificate:
1. By November 19,2017, the Member must have:
(i) signed an undertaking to the Registrar confirming that
she has reviewed and will undertake to comply with al! CCO
regulations, standards, policies and guidelines, including but
not limited to CCO Standard 5-002: Record Keeping, CCO
Standard S-012: Orthotics, CCO Guideline G-008: Business
Practices and the business practices portion of the
Misconduct Regulation;
(ii) successfully completed an educational program
conducted by an expert chiropractor approved of in advance
by the Registrar regarding the standard of practice expected
of members of the profession with respect to billing
practices, record keeping and orthotics.
2. the Member's practice shall be monitored by the cco by means ofinspection(s) by a representative or representatives of the CCO a maximum offour times during the twenty-four (24) months following the lifting of the
súspension. The Member shall cooperate with the CCO during the inspections
and, further, shall pay to the CCO in respect of the cost of monitoring, the
16 of 19
26amount of $600.00 per inspection, such amount to be paid within thirty (30)
days of the completion of each of the inspections;
3. the Member must be peer assessed at her own expense within
six months after she returns to practice after the lifting of the
suspension.
4. Ordering the Registrar to suspend two months of the suspension if the Member
successfully completes the Conditions set out in paragraph 3a. above, by November 19,
2017.
5. Requiring the Member to pay a portion of CCO's investigative and legal costs in
the amount of $15,000.00 by December 31 ,2017, with post-dated cheques for the costs
to be provided to the Registrar at the hearing.
6. Requiring that the results of the proceeding be recorded in the register and
published in the Annual Report or other CCO publications at the discretion of the CCO.
The Member agrees that she obtained legal advice from her lawyer, Valerie Wise, prior
to entering into this Resolution Agreement. She is signing this Joint Submission on
Penalty freely and voluntarily.
Penaltv Decision and Reasons
The Panel carefully weighed the principles of general and specific deterrence,
rehabilitation, and protection of the public in accepting the Joint Submission on Penalty
Dr. Egbogah admitted to the acts of misconduct which obviated the need for a
contested hearing and therefore saved the College both time and money. By
acknowledging her conduct had fallen short of that expected by the public and the
17 of19
27profession, she accepted responsibility for her actions. Dr. Egbogah has no prior
disciplinary history with the college since her registration in 2007.
The serious nature of the penalty imposed demonstrates the consequences of this
behaviour to this Member and to members of the profession generally and therefore
satisfies the principles of specific and general deterrence. Falsifying records to deceive
a third-party payor is an egregíous violation of the relationship between a chiropractor
and an insurance company and will not be tolerated by the public and profession. The
terms of the penalty send a clear message to other chiropractors that failure to bíll forprofessional services and products in a proper manner or to maintain accurate records
in accordance with required standards is unacceptable.
Dr. Egbogah is required to complete several rehabilitative activities designed to
remediate her education in billing, recordkeeping, business practices and orthotícs. Thís
wíll help to ensure good practices by her in the future, to the benefit of the public. She
must complete an extensive review of the Standards of Practice with respect to billíng
practices, recordkeeping, and orthotics and she is atso required to meet with an expert
chiropractor, approved by the Regístrar, to complete successfully an educational
program. Dr. Egbogah attended CCO's Record Keeping Workshop and successfullypassed the Legislative and Ethics examination in october 2016.
Protectíon of the public is the paramount concern of the College and the Joint
Submission on Penalty provides a requirement for supervision of Dr. Egbogah's
practice. Once she returns to practice, she will be peer assessed within six months. In
addition, she will be required to have her practice monitored, at her expense, by a
representative or representatives of the College, a maximum of four times during the 24
months following the lifting of the suspension. The ability to monitor her practice, to
require peer and practice assessment, and to complete additional education in businesspractices will provide ongoíng protection of the public.
18 of 19
28The Panel found that the Joint Submission on Penalty to be within the range of
appropriate penalties given the nature of the admitted conduct. As well, the Panel is
hesítant to interfere in a penalty that has been negotiated between experienced counsel
representing the College and the Member and thus, by its nature, balances the interests
of the public and fairness to the Member. For the reasons outlined above, the Panel
accepts the Joint Submission on Penalty (Exhibit 4) signed by the parties and has made
the order requested.
REPRIMAN D ADMINISTERED
The Member expressly undertook not to appeal or seek judicial review if the Panel
accepted the Joint Submission. Consequently, at the conclusion of the hearing, the Panel
administered the oral reprimand required by its penalty order.
l, Judith McGutcheon, sign this decision and reasons for the decísion as Chair of this
Discipline Panel and on behalf of the members of the Discipline Panel as listed below:
{TTA-fú*o+*Judith McCutcheon, Chair June 1,2017
Panel Members:
Ms. Judith McCutcheonDr. Angela BarrowMr. Douglas CressmanDr. Elisheva GabisonDr. Reginald Gates
19 of 19
.¡üdl'ñt!rt!¡,tftñûç¡ñe,.|TEM 1.1.2 29
CONDUCTING ADISCIPTINE HEARING
0Rpsff,Federation of Health Regulatory
Colleges of OntarioThursday, fVlay tr"8, 2CI17
LIMITED SEATINGWEBCASTING AVAILABLE
Osgoode ProfessionaIDeveloprnent Centre
1 Dundas St W 26th FloorToronto ON MsG 1-23
Faculty:Brian Gover/Luisa Ritacca
Stockwoods LLP &Richard Steinecke
Steinecke Maciura LeBlanc
Discipline Orientation Committee¡ Tina Langlois, College
of Medical RadiationTechnologists of Ontario(Chair)
r Anita Ashton, College ofPhysiotherapists of Ontario
r Genevieve Plummer,Ontario College ofPharmacists
. Ravi Prathivathi, College ofNurses of Ontario
o lris Samson, College ofAudiologists and Speech-Language Pathologists ofOntario
''t:, :'' ;l:rt -, :.:!.;1itr,:r:i : l, :ì'. '1. ': . :. L
ltrr'-dtl
8:30 a.m. - 9:0CI a.m.Registration andLIGHT CONTINENTAL BREAKFAST
9:CIO a.rn. - 9:3t a.nr.lntroduction and Legal FrameworkTopics include: applicablelegislation, jurisd iction, the publicinterest, confi dentia lity, disclosu re,
allegations, penalties and costs
9:30 a.m. - Lü:00 a.rn.Video of a Discipline Hearing
10:00 ã.m. - 10:30 a.m.Principles of Administrative LawTopics include: nature of a hearing,natu ra I justice, transpa rency, burdenof proof and accountability
3"0:30 a.rn. * 10:45 a.rn" BREAK
L0:45 a.m. - l-1:00 a.m.Fitness to Practice (FTP)
Topics include: how the FTP processdiffers from discipline, definition ofinca pacity
LL:00 a.rn, -- L1:30 a.m.Pre-Hearing ProceduresRole play will focus on the Pre-Hearing Conference and the goalof narrowing the issues, coming toan agreed statement of fact, anddeveloping joint submissions onpenalty
11:30 a.m. - L2:1"5 p.m.Roles of Various Participants in theHearing ProcessDiscussion will focus on the rolesof panel members, prosecutionand defence counsel, independentlegal counsel, intervenors, media,experts, witnesses, court reporters,and staff
12:15 p.m" - 1:00 p.m. LUNCH(provided)
1":00 p.m" - 2:30 p"rn.The Discipline HearingThrough role play, attendeeswill experience an abbreviatedcontested hearing
2:30 p.rn. - 2:45 p.rn. BREAK
2:45 p.nr. - 3;00 p.m"The Discipline Hearing (continued)
3:00 p.m. - 4:00 p.m.Responsibilities of Panel MembersDiscussion will focus on panelmember conduct prior to, during,and after the hearing by usingreal case examples of situationswhere panel member conduct is
q uestioned
4:OCI p.nr. * 4:1"5 p.m.
Concluding Remarks and Evaluation
All registrations will be confirmed via fax or email within five (5) business days
of receipt of the form. lf you do not receive a confirmation, please contact theFederation office by phone (416-493-4076),fax (1--866-814-6456), or
e ma i I ( i nfo@ regu lated h ea lth p rofession s. o n. ca )
See Registration Fcrrn for rates and payment inforr*-ration'
Program ObjectivesThis program is designed toprovide professional regulatorswith a comprehensiveorientation to the disciplineprocess. At the conclusion ofthesess¡on, participants will have anunderstanding of:r Relevant principles of
administrative law. Roles of various participants
in the hearings process. Activities that occur prior to
a hearing. Procedures associated with
the hearings process. Responsibilities of panel
rnembers
ñ-lG oRFSo
Federation of Health RegulatoryColleges of Ontario
BAS|C SESSIONThursday, May 18,2017
30
Osgoode Professional Development Centre, 1 Dundas St W 26th Floor; Toronto ON MsG 123
Contact information: (for name badge) ODr. OMr. OMs. OMrs. OOther {Please specify-)Registrant's Name:
Organization:Street Address:
City: Province:Fax #:
Postal Code
Phone #:Registrant's Email :
Name of person completing form (if different from Registrant):Email/Phone # of person completing formSend registration information to:
Registrant lnformation :
Dieta ry restrictions (e.g., allergies):
ORegistrant OPerson completing form OBoth
Have you attended a Federation Discipline Hearing Program previously? OYes ONoHave you participated in one or more discipline hearings? OYes (1) OYes (between 2-5) OYes (6 or more) ONoAre you willing to participate in a scripted role play? OYes ONo
WEBCAST OPTION AVAILABI-E FOR BASIC SESSION: O attending in person O attending by webcast
*Member rates apply to all Council, Committee Members, and Staff of Federation Members
Submit completed forms to the Federation Office via:
email: , orFax: 1-866-814-6456, orMail: Federation of Health Regulatory Colleges of Ontario
Suite 301- 396 Osborne St, PO Box244Beaverton ON LOK 140
Make cheques payable to:Federation of Health Regulatory Colleges of Ontario
Payment Method:OCheque OVISA OMasterCard OAMEX
r lf by credit cardCard #: Exp: _
i Cardholder's Name:Signature:(lf completíng form electronically, cardholders not able toinclude e-Signature will be contacted far verification)
Policies: Concellotíons received in writing not less thqn ten (10) busíness days príor to the event will receive a full refund.
Cqncellotíons receíved less than ten (ß) business doys wílt not be refunded, but substitutions ore permitted, Registration in the
FHRCO Disciptine Orientotion Program is restricted to indivíduals who serve on or support a discipline committee ot o regulatorycollege and employees of reloted agencies ot the inv¡tatíon of a FHRCO member or odmínistration.
Confrrmotion: Al! registratíons will be confirmed via fax or email wíthín five (5) busíness doys of receipt of the form. lf you do nat
receive a confírmatíon, please contact the Federatíon offíce by phone (416-493-4076), fqx (1-866-874-6456)' or emoil
( i nÍo @ re g u I ated hea Ith profess i ons.o n. co )
Conducting a Þiscipline HearingResistra otl Forlrr
RATE SCHEDUTE fINCtUDES HST) Earlv Bird {to Mav 1) Resular (After Mav 1) Total
Federation Member* $s3 1.10 $ssz.oo
Non-Member $saz.oo S7oo.6o
Rates remain the same for both live session and webcast 0
Click here to submit by email(Please ensure you are sending from a secure system if you
øre including credit card informøtion.)HST #871-392825
ITEM 1.2Submitted, June 12, 2017
Gollege of Chiropractors of OntarioFitness to Practise Committee Report to GouncilThursday, June 23,2017
31
Members: Dr. Kristina Peterson, ChairMs Georgia AllanDr. Peter Amlinger
Staff Support: Jo-Ann Willson, Registrar ønd General CounselJoel Friedman, Director, Policy & Research
Committee Mandate
a To hear and determine allegations of mental or physical incapacity referred to thecommittee by the Inquiries, Complaints and Reports Committee.
To review applications for reinstatement following an incapacity finding.
The Committee held a brief teleconference meeting June 9,2017 to ensure we wereadequately prepared for this coming year.
No referrals \ryere received. If the Committee receives a referral, there will be furthertraining before the hearing.
I would like to thank the Fitness to Practise Committee members for their time; MsGeorgia Allan, Dr. Peter Amlinger and our staff support Ms. Jo-Ann Willson.
Respectfully submitted,
Dr. Kristina Peterson, ChairFitness to Practise Committee
a
ITEM 1 .3 Submítted to CCo on June 7, 2017
College of Ghiropractors of Ontariolnquiries, Complaints and Reports Committee Report to GouncilFriday, June 23,2017
32
Members: Ms Patrice Burke, Chair, Public MemberDr. Brian Schut, Council MemberDr. Gauri Shankar, Council MemberDr. Steve Gillis, non-Council MemberMr. Wendy Lawrence, Alternate Public Member
Staff Support: Ms Christine McKeown,Investigations, Compløints & Reports OfrìcerMs Tina Perryman, Manager, Inquiries, Complaints & Reports
Since the last Council meeting, the Inquiries, Complaints and Reports Committee (ICRC)met on two occasions, and reviewed 15 complaints and five reports. ICRC made decisions onsix complaints and one report. One section 75(a) investigators were approved by the ICRCand two section 75(c) investigators were requosted by the ICRC. Currently, the ICRC has sixongoing 75(a) Registrars investigations and 15 ongoing 75(c) investigations which wereappointment requests from the ICRC.
Thank you to members of the committee, Drs. Schut, Shankar and Gillis and special thankyou to the staff, Ms Tina Perryman and Ms Christine McKeown for their support and
expertise.
Respectfully submitted,
Ms Patrice Burke, Chair, Public MemberInquires, Complaints & Reports Committee
ITEM 1.4 Submittedto CCo onJune 12,2017
Gollege of Chiropractors of OntarioRegistration Committee Report to GouncilFriday, June 23,2017
33
Members:
Staff Support:
Dr. Pat Tavares, ChairMr. Shakil AkhterDr. Reginald GatesMr. Doug Cressman, Alternate
Mr. Joel Friedman, Director, Policy and ResearchMs Madeline Cheng, Registration CoordinatorMs Jo-Ann Willson, Registrar and General CounselMs Andrea Szametz, Recording Secretary
lntroduction
The committee has met once by teleconference since the first council meeting of thisyear. During that meeting members reviewed the application of two chiropractors whowished to be registered in Ontario. One in particular requested to be exempt from part Aboard exams, but the committee was in agreement that if accommodation could beprovided to the applicant by the examining body, that he could rewrite his part A boardexam again shortly as nearly one year has passed since his last exam.
Various documents pertaining to the committee were reviewed, and we will have our firstin-person meeting in July. For consideration atthat meeting will be various itemsincluding a review of the legislation & ethics examination and its format, reviewingregistration renewal and application forms for corporations, assessing the impact of theTechnology Upgrade Project on registration and noting the similarities and differences inregistration processes across Canada.
Current Member Status
Chart 1: Membership Statistics as at June912017
Status TotalActive 4378Active w/ Terms 0
Active-Non Resident 29
Inactive - Resident 157
Inactive - Non Resident 65
Retired r28All categories 4757
Registration Committee Report to Counci l: June 23,2017
Chart 2: Change in Registration statistics for Aprit ll,20l7- June 9,2017 34
Chart 3: Colleges of Graduation for New Registrants
CMCC 5
NYCC 1
Palmer (Florida) 1
UQTR I
I would like to thank the members of the registration committee and the support staff fortheir time and commitment: Dr. Reginald Gates, Mr. Shakil Akhter, Mr. Dõug Cressman,Mr. Joel Friedman, Ms Madeline Cheng, Ms Andrea Szametzand Ms Jo-AnnV/illson.
Respectfully submitted,
Dr. Pat Tavares,Chair, Registration Committee
2
Description TotalNew 8Female 2Male 6
rrEM 1.4.1Rose Bustria
From:Sent:To:Subject:Attachments:
Jo-Ann WillsonTuesday, May 09, 2017 12:47 PMRose BustriaFW: CCO FinalAssessment ReportCCO Report - final.docx; Action Plan lnstructions and template.docx
35
Registration and Council
Jo.Ann Wlllson, B.Sc., M.S.W., LL.B.Registrar & General Counsel
Collêge of Chiropractors of Ontarlo130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 exl 1 1 1
Fax: (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may contain confìdential ¡nformation and is ¡ntended only for the person(s) named above. Any olherdistribution, copying or disclosure is strictly prohibited. lf you have received this e-mail in error, please notify me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: Mendel, James (MCl) [mailto:[email protected]]Sent: Tuesday, May 09,2077 L2:44PMTo: Jo-Ann Willson <[email protected]>; Joel Friedman <[email protected]>
Cc: Jafri, N uzhat ( MCI) <Nuzhat.Jafri@onta rio.ca>
Subject: CCO Final Assessment Report
Dear Jo-Ann and Joel,,
Thank you for meeting with the OFC to discuss the assessment findings, recommendations and next
steps. Please find attached the final assessment report.
The OFC will post the assessment report, with any commendable practices or recommendations, on ourwebsite.
Because you have no more than 10 recommendations you have the option to submit a formal actionplan to the OFC or update the OFC on progress in meeting recommendations during semi-annual
meetings.o lf you choose to submit an action plan please use the attached action plan template which
includes instructions for completing them. Your Action Plan should be submitted to the OFC
within 60 days.¡ lf you choose semi-annual meetings, the first meeting will be scheduled no later than 4 months
from now, and subsequent meetings willtake place every 6 months until all recommendationsare implemented.
lf you have any questions, please do not hesitate to contact me
1
Regards,

James MendelPolicy and Program AdviserOffice of the Fairness Commissioner416-272-566rwww.fa irnesscom missio ner.ca
The information transmitted in this èmail is intended only forthe person to whom it is addressed and may containconfidential material. Any review, dissemination, or other useof this information by persons other than the lntendedreajpient is prohlbited, lf you received this message in error,please contact the sender and permanently delete it,including any attachments, without making a copy. Thanky0u.
36
2
Rose Bustria
From:Sent:To:Subject:Attachments:
Jo-Ann WillsonTuesday, May 02, 2017 10:35 AMRose BustriaFW: CCO / OFC Assessment MeetingCCO Assessment Meeting Agenda 020117.doc
37
Registration and Council.
Jo-Ann Willson, B.Sc., M.S.W., LL.B.Registrar & General Counsel
College of Chiropractors of Ontarlo130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. I 1 1
Fax: (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNI NG;This e-mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any otherdistributlon, copying or disclosure is strictly prohibited, lf you have rece¡ved this e-mail in enor, please notify me ¡mmediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: Mendel, James (MCl) [mailto:[email protected]]Sent: Tuesday, May 02,2OL7 9:48 AMTo: Joel Friedman <[email protected]>
Cc: Jafri, Nuzhat (MCl) <[email protected]>; Jo-Ann Willson <[email protected]>
Subject: CCO /OFC Assessment Meeting
Hi Joel,
Please find attached an agenda for our meeting this Thursday
ThanksJames
James MendelPolicy and Program AdviserOffice of the Fairness Commissioner4t6-212-566Lwww.fairnesscom missioner.ca
The ¡nformation transmitted in this email is intended only forthe person to whom it is addressed and may containconfidential material, Any review, dissemination, or other useof this information by persons other than the intendedrecipient is prohibited. lf you received this message in error,please contact the sender and permanently delete ¡t,
including any attachments, without making a copy. Thankyou.
1
Office of thc Bureau ducommissaire à
&i:,?,Í::, l'é quitéo
38
2016 - 2017 Assessment MeetingAgenda
Regulatory Body: Gollege of Ghiropractors of Ontario
Date: May 4th 20172pm -4 pm595 Bay St. - Suite 1201
Attendees:Joel Friedman - Director, Policy and Research, CCOMadeline Cheng - Registration Coordinator, CCONuzhat Jafri - Executive Director, OFCJames Mendel, - Policy and Program Advisor, OFC
Agenda Items
1. lntroduction2. Assessment Report3. FRP Report (data trends and changes)4. Regulation/by-law/policy changes5. Projects or activities undenruay6. Next Steps
Rose Bustria
From:Sent:To:Subject:Attachments:
Jo-Ann WillsonThursday, April20, 2017 5:21 PMRose BustriaFW: OFC Draft Assessment of CCO Registration Practices - Cycle 3CCO Report - draft#3 - CCO commentsApril2l2ll7.docx
39
Registration and Council.
Jo-Ann P. Willson, B.Sc., M.S.W., LL.B.
Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected] Site: www.cco.on.ca
CONFIDENTALITY WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copies includingany attachments without reading it or making a copy. Thank you.
From: Joel FriedmanSent: Thursday, April 20, 20t7 4:28 PM
To: [email protected]; [email protected]: Jo-Ann WillsonSubject: RE: OFC Draft Assessment of CCO Registration Practices - Cycle 3
Good Afternoon,
I am attaching an updated report with some comments from CCO following the recommendations
Regards,
Joel D. Friedman, BSc, LL.BDirector, Policy and ResearchGollege of Chiropractors of Ontario130 Bloor Street West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 104Toll Free: 1 -877 -577 -477 2Fax: (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any otherdistribution, copying or d¡sclosure is strictly prohibited. lf you have rece¡ved this e-mail in enor, please notify me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
1
From: Mendel, James (MCl) [mailto:[email protected]]Sent: Tuesday, April 04,2Ot7 L2:38 PMTo: Jo-Ann Willson <[email protected]>Cc: Joel Friedman <[email protected]>; Jafri, Nuzhat (MCl) <[email protected]>Subject: OFC Draft Assessment of CCO Registration Pract¡ces - Cycle 3
Dear Jo-Ann,
Please find attached the OFC's draft assessment report for the College of Chiropractors of Ontario.
The draft assessment report has been developed using the Resistration Practices Assessment Guide: ForResulated Professions and Health Regulatorv Colleges, and the material provided by the College in theself-assessment report.
The purpose of this stage of the assessment process is to allow regulators the opportunity to providetheir comments to the OFC about the content of the draft report. These comments may includeclarification, additional evidence and/or further information that may inform the content of the report.
Within the draft report, the OFC has identified text boxes in which regulators are to provide theircomments. These textboxes appear in the draft report under each practice for the specific duty sectionsof the report and under each principle for the general duty. You are encouraged to submit additionalcomments or evidence as attachments to the report at this time. Any comments you provide will beremoved in the finalized version of the assessment report.
Please provide comments by April 20th. lf you have any questions in the meantime, please do nothesitate to contact me.
Regards,
James
James MendelPolicy and Program AdviserOffice of the Fairness Commissioner4L6-2L2-566Lwww.fa irnesscom m issioner.ca
The information transmitted in this email is intended only forthe person to whom it is addressed and may containconf¡dential material. Any review, dissemination, or other useof this information by persons other than the intendedrecipient is prohib¡ted. lf you received this message in error,please contact the sender and permanently delete it,including any attachments, without mak¡ng a copy. Thankyou.
40
2
41
1
Office of the Bureau ducommissaire àfnirness l'équitécommlsstoner
REG ISTRATION PRACTICES ASSESSM E
College of Chiroproctors ol Ontorio
2OL6-20L7 Assessment Cycle
Off¡ce of the Fairness Commissioner595 Bay Street, Suite 1201
Toronto ON M7A2B4Canada
416 325-9380 or 1 877
Thethe Fa¡r
agency of the Ontario government, established under
lsoryTrades Act, 2006. lts mandate is to ensure that certa¡n
that are transparent, objective, impartial and fair
/////,,,1,
7Last
regulated
Fairness
latedhave
Office of the Fairness Commissioner
42
2
Contents
Focus of this Assessment and Report ..........,... ...........4
Assessment Summary ....,,,..,....... ...................,,...............5
Specific duties assessed,...,..,.....
General Duty....
Assessment Method............. ...........,..,,.,..,......5
Commendable Practices.,..,.......
General Duty:
Recommendations ................,.........
Assessment History,.,..,.................,.
1. Specific Duty * lnformation
2, Specific
3. Specific
4.
.................5
........,.......,5
...............6
6
7
,..8
...8
...8
6.
7.
Qualifications ...,.,....
10
8. Specific Records ......L4
General Duty,.,,,.... L4
Transparency 1"4
Assessment Methods,..,..,.... .....,.,..,20
Specif¡c Duties.. ............,..............20
Office of the Fairness Commissioner
Duty -
43
3
20Sources
AVAITABITITY OF REPORT
This report is provided by the OFC to the regulatory body assessed. The OFC will, upon request, release the report
to other part¡es. The OFC will also post the report on its website. ln the
the OFC encourages regulatory bodies to provide the report to its staff,
interested part¡es.
transpa rency and accountab¡lity,
the public, and other
Office of the Fairness Commissioner
44
4
IntroductionAssessment is one ofthe Fairness Commissioner's mandated roles under the FairAccess to ReÂulated Professionsand Compulsorv Trades Act, 2006 (FARPACTAI and the Resulated Health Professions Act, 1991 (RHPA) -collectively known as fair access legislat¡on.
Assessment CycleOne of the primary ways the OFC holds regulators accountable for continuous improvement is through theassessment of registration practices using a three -vear assessment cvcle.
Assessment cycles alternate between full assessments and targeted assessments:
Full assessmênts address all specific and general duties.described in the fa¡r-access legislation.
Targeted assessments focus on the areas where the OFC made recommendations in the previous fullassessment.
Focus of this Assessment and ReportThe 2016-2017 assessment is a full assessment.
The OFC'S detailed report captures the results of the full asséssment, However, practices related to provision ofinformation are excluded for regulators who have previously completed an assessment. For those regulators, thesepractices have been removed from the transparency section of the report. Th¡s includes: all practices fromlnformation for Applican8, practice 3 from lnternal Review and Appe.als, pract¡ce 1 from lnformat¡on on AppealRights, practice 1 from Documentation of Qual¡ficat¡ons, practlce 1 from Assessment of eualifications, practice 2
from Access to Records; and practices 4-11 from TÍansparency ofthe Registrat¡on Practices Assessment Guide.
The assessment summary pioyides ihe following kéy information from the detailed report:
duties that were assessed
an overview of assessment outcomes for specific duty practices
an overview of comments related to the general duty
commendable practices
recommendations
a
a
Office of the Fairness Commissioner
45
5
AssessmentSummary
Specifìc Duties
Specifìc duties assessedThe regulator has been assessed in all of the areas below. Recommendations are made for partially
demonstrated and non-demonstrated areas. These appear later ¡n this report.
Comments
The regulatory body has demonstrated all ofthe practices in the uty areas:
. lnternal Reviews and Appeals
. Assessment of Qualificationso Training. Access to Records
General Duty
Assessment MethodThe regulator selected
b. OFC practice based
Principles
Comments
The OFC found
measures to ensure
The
ngm assessment general duty:
(fol the practices in the Assessment Gu¡de)
the duty principles: transparency, objectivity,
assessment, the College of Chiropractors of Ontario (CCO) has taken
objective, impartial and fair registration processes.
Commendable PracticesA commendoble pract¡ce is a program, activity or strategy that goes beyond the minimum standards set
by the OFC assessment guides, considering the regulatory body's resources and profession-specif¡c
context. Commendable practices may or may not have potent¡al for transferability to another
regulatory body,
The regulatory body is demonstrating commendable practices in the follow¡ng areas:
Off¡ce of the Fairness Commissioner
46
6
General Duty:
Objectivity
1. The College has developed an internal Registration Comm¡ttee (Committee) flowchart to rev¡ewvarious scenarios that apply to applicants to ensure that similar applications are decided in aconsistent manner. (T13)
2. CCO's recogn¡tion of international accred¡ting bodies around the world allows applicants toreceive their educat¡on ¡n many chiropractic educational institutions around the world and meet
the requirements for registrat¡on with CCO; (O1)
Fairness
1. Some individuals that failed the legislation and ethics exam have been given an opportunity torewrite the examination earl¡er rather than wa¡t¡ng for the next scheduled exam¡nation s¡tting,ifthey had already passed the Canadian Chiropractic Examining Board (CCEB) examinations.
Recommendations
Transparency
1. Review the College's communication practices, including consideration of the College,s
statements and policies regarding applicants and individuals with disabilities.
2. Update the webs¡te to include improvements to how registrat¡on lnformation is commun¡cated.
3. Translate all standards of pract¡ce, policies and guidelines (including those relating toregistrationlinto French, ensuring published information is available ¡n both official languages.
4. Review Committee terms of reference to ensure that specif¡c Committeepract¡ces and timelines for reviewing applications for reg¡strat¡on are specified; (T3)
5. Undertake the following related to communicating with applicants: (T12)
a. review Committee terms of reference to ensure that communicat¡onpractices are referenced;
b. review Comm¡ttee letters of commun¡cat¡on to applicants;
c. enhance electronic commun¡cation systems to allow for online payments and membership
renewals.
Office of the Fairness Commissioner
47
7
6. Translate the Committee's decision-making flowchart into a policy that is ava¡lable to the public
and applicants. (T13)
Obiectivity
1. Consider evidence from other health regulatory colleges in developing Committee policies, such
as requiring applicants to submit a police reference check in the initial application. (O1)
lmpart¡al¡ty
1. Promote a decis¡on-making env¡ronment that is free of nd
a) develop a pol¡cy to reiterate the College's commitment being discrimination and
bias;
b) review Comm¡ttee terms of reference
discrimination and bias in dec¡sion
Fairness
1. Review and update terms ensure requirements are
reviewed for relevance at ntervals, (F2)
2. lnclude more of origin in College's annual report.
3. Review timelines for reg¡stration decisions in CCO
policy, (F8)
other colleges in an effort to make sure CCO is
(Fe)
it includes to be free of
¡n the registration process, sim¡lar to the policy statements
Policy P-045 - Leg¡slat¡on and Ethics Exam
Assessment Historyln the previous assessment, the OFC identified 17 recommendations for the regulator
They have all been implemented,
5
that
Office of the Fairness Commissioner
48
8
Deailed Reportl
Specific Duty
1, Specific Duty - Information for ApplicantsExempt as Previously Assessed
2. Specifìc Duty - Timely Decisions, Responses and Reasons,RHPA, Schedule 2, s.2O (Il*Only applies to regulotory bodies governed by FARPACTA
1. lfa regulator rejects an application, ¡t g¡ves wr¡tten.reaions to the appllcant. [Falrness,Transparencyl
2. The regulator makes registratlon dec¡sions, and gives úrltten decisions and reasons to applicants,w¡thout undue.delay*. [Fairness]
AssessmentOutcome
Not Appli¿able
3. The regulator responds to.applicants'lnquiries or requests w¡thout undue delay*. [Fairness]
AssessmentOutcome
Not Applicable
4' The regulator provides internal reviews of decisions, or appeals from decisions, w¡thout unduedelay*. IFairness]
Assessmentoutcome
Not Applicable
1 Please note: Suggestions for continuous improvement appear only in the detailed report. Suggestionsfor improvement are not intended to be recommendations for action to demonstrate a practice, but aremade solely to provide suggestions for areas that a regulatory body may consider improving in the future.
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed dur¡ng the f¡nalizotion oÍ the report)
Office of the Fairness Commiss¡oner
49
5. The regulator makes declslons about lnternal revlews and appeals, and glves wr¡tten declslons
and reasons to applicants, wlthout undue delay*. IFairness]
AssessmentOutcome
Not Applicable
3. Specific Duty - Intemal Review or AppealRHPA, Schedule 2, s, 15, s. 17, s. L9, s,22.3
'Only opplles to regulatory bodles governed by FARPACTA
1. The regulator provldes appllcants wlth an lnternal ol ordecislons. IFalrness]
2. The regulator rules anyone who acted as a decision-
maker in athât same
ln an lnternal revlew or appeal ofIlm
3. The regulator provldes lnformatlon on ¡ts webslte that lnforms appllcants about opportun¡tles foran lnternal review or appeal. [Transparency]Exempt as Previously Assessed
4. The regulator provldes lnformatlon on lts webslte about any l¡mlts or condltlons on an lnternal
revlew or appeal*, [fransparency]Exempt as Previously Assessed
Assessmentoutcome
Demonstrated ;i./1/
to removedRegulatorComments
AssessmentOutcome
RegulatorComments
(Fuutt; dur¡ng the f¡nallzot¡on the report)be
Office of the Fairness Commissioner
50
10
2. The regulator communicates the[Transparencyl
4. Specific Duty - Information on Appeal RightsExempt as Prev¡ously Assessed
5. Specific Duty - Documentation of QualificationsExempt as Previously Assessed
6. Speciñc Duty - Assessment of QualificationsRH PA, Schedule 2, s. 22.4(21*Only appl¡es to regulotory bodles thot develop ond odm¡n¡ster the¡r
1. On its webs¡te, the regulator lnforms appllcants the process, for theassessment of qualifications. [Transparency]Exempt as Previously Assessed
to eech ln writ¡ng.
3. The crlterla, pollcles and procedures.
4. The regulator shows that its tests and exams measure what they lntend to measure, [Objectivltyl
AssessmentOutcome
RegulatorComments
(Row to be of the
AssessmentOutcome
VéÐÅ.
'v4
(RowRegulatorComments
removed durlng the Ílnollzot¡on of the
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed durtng the Í¡nal¡zot¡on of the report)
Office of the Fairness Commissioner
51
11
5. The regulator states its assessment crlter¡a in ways that enable assessors to lnterpret them
consistently. f Objectivityl
6. The regulator ensures that the lnformatlon about ls used to develop orupdate assessment cr¡teria ls kept current and accurate.
7. The regulator links lts for entry to theprofesslon or trade.
consistently apply quallflcations assessment cr¡terla, policies
9. The regulator uses only quallfied assessors to conduct the assessmenB. lobiectlvltyl
AssessmentOutcomê
Demonstrated
Theand
8.
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed during the Íinolizot¡on of the report)
Demonstrated.../)
øø,AssessmentOutcome
oÍ the report)RegulatorComments
remweaffiai(Row to be
AssessmentOutcome
RegulatorComments 'E
oÍ the report)
to all
'l;H,"".AssessmentOutcome
RegulatorComments
¡Rõ61õ be removed during the finattzot¡on ol the report)
office of the Fairness Commissioner

52
T2
RegulatorComments
(Row to be removed during the Jinolizot¡on of the report)
10. The regulator monitors the consistency and accuracy of decisions, and takes corrective act¡ons asnecessary, to safeguard the objectivity of ¡ts assessment decisions. lObjectivity]
11. The regulator prohibits discrimination and informs assessors about the need to avoid. bias in theassessment. Ilmpartiality]
12. The regulator ¡mplements procedures to óafeguard the impartiality of its assessment methods andprocedures. Ilmpartial¡ty]
AssessmentOutcome
RegulatorComments
(Row to be removed during the linolizotion of the report)
13. The regulator gives applicants an opportun¡ty to appeal the results of a quallflcations assessmentorto have the results reviewed. [Fairness]
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed during the finol¡zotion of the report)
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed dur¡ng the finølízotion of the report)
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed dur¡ng the Í¡nal¡zot¡on of the report)
Office of the Fa¡rness Commissioner
53
13
14. The regulator assesses qualifications, communicates results to appl¡cants, and provides wr¡ttenreasons for unsuccessful applicants, w¡thout undue delay. IFairness]
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed during the finolizot¡on of the report)
t 5, Regulators that rely on th¡rd-pafi assessments establish polícies and procedures to hold third-party assessors accountable for ensuring that assessments are transparent, objectlve, impartialand falr. [Transparency, Objectivity, lmpart¡ality, Fairness]
7. Specific Duty - TrainingRHPA, Schedule 2, s.22.4(31
t . The regulator prov¡des tra¡níng for staff and volunteers who assess qualifications or make
registration, internal review or appeal decisions. [Objectivity, lmpart¡al¡ty, Fairness]
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed dur¡ng the finolizot¡on of the report)
2. The regulator addresses topics of objectivity and impartiality in the training ¡t provides toassessors and decision-makerc. [Objectivity, lmpartiality]
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed during the finolizot¡on of the report)
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed during the f¡nolizot¡on of the report)
Office of the Fa¡rness Commissioner
54
L4
3' The regulator identifies when new and incumbent staff and volunteers require training andprovides the training accordingly. [Objectiv¡ty, lmpartial¡ty, Fairness]
B. Specific Duty - Access to RecordsRHPA, Schedule 2, s. 16
1. The regulator provides each applicant with access to hls or her application records.
2. lf there is a fee for making records available, the regulatory body gives applicants an estimate ofthis fee. [Transparencyl
Exempt as previously assessed
3. lf there ls a fee for making records avâilable, the regulator reviews the fee to ensure that ¡t doesnot exceed the amount of reasonable cost recovery. IFairness]
General DutyRHPA, Schedule 2, S.22.2
Transparencyo Maintaining opennesso Providing access to, mon¡toring, and updating reg¡stration information
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed dur¡ng the Í¡nol¡zotion of the rcport)
AssessmentOutcome
Demonstrated
RegulatorComments
(Row to be removed during the finolizot¡on of the report)
AssessmentOutcome
Not Applicable
RegulatorComments
(Row to be removed during the Jinolizotion of the report)
Office of the Fairness Commissioner
55
15
o Communicating clearly w¡th appl¡cants about their status
AssessmentOutcome S¡nce the previous assessment, the College has increased transparency of registrat¡on processes,
through development of policy statements and registration mater¡als. The College has commiüedto further transparency in¡tiatives in the coming months.
Openness
The College continues to ma¡ntain a high degree of transparency with regard to College
processes, through publicat¡on of Council meetings and advertising stakeholder
consu ltations.
Access
lnformat¡on about the reg¡strat¡on process is clearly provided on the College's website,
and has been enhanced through the previous assessment cycle w¡th the posting of lettertemplates from the Registration Committee to applicants.
Clørity
The College has committed to review¡ng tools and methods of commun¡cat¡on w¡th
appl¡cants, and upgrading the information and technology infrastructure that supports
interaction with appl¡cants.
Recommendat¡ons L. Review the College's communication practices, including consideration of theCollege's statements and policies regarding applicants and individuals withdisabilities.
2. Update the webs¡te to include improvements to how registrat¡on information is
communicated.
3. Translate all standards of practice, policies and guidelines (including those relating toregistration) into French, ensuring published information is available in both officiallanguages.
4. Review Committee terms of reference to ensure that spec¡fic Comm¡tteepractices and timelines for reviewing applications for registration are specified; (T3)
5. Undertake the following related to communicat¡ng with applicants: (T12)
a. review Committee terms of reference to ensure that commun¡cationpractices are referenced;
b. review Committee letters of communicat¡on to appl¡cants;
c. enhance electronic commun¡cation systems to allow for online payments and
membership renewals.
Office of the Fa¡rness Commissioner

56
t6
Obiectivity. Des¡gn¡ng criter¡a and procedures that are reliable and valido Monitor¡ng and following up threats to validity and reliability
6. Translate the Comm¡ttee's decision-making flowchart into a policy that isavailable to the publ¡c and applicants. (T13)
RegulatorComments
CCO hos tronsloted oll reaulotions, stondords of proct¡ce, Ðolic¡es ond ou¡del¡nes ond w¡ll bepost¡nq ¡n on the webs¡te followino the next Execut¡ve Comm¡ttee meetino in Mov. CCO w¡llundettoke to complete the other recommendot¡ons followina the str¡k¡no of the new comm¡tteeson Aprìl 27, 2077. CCO ¡s currentlv work¡na on uporodino its dotobose to ollow for more onlinecommunicot¡on with apolicants ond members ond foresees thot this will be reodv to lounch ¡n thefoll of 2017.
Assessmentoutcome The College's practices were assessed aga¡nst the OFC's standards of object¡vity in 2OI2,
and were found to meet the standards. As a result, these practices were not assessed inthe second cycle in 2014.
The College uses a variety of methods to achieve objectivity in its assessment processes.These methods support a conslstent approach to assessments, by promot¡ng a sharedunderstanding of policies, procedures and methodologies. This is evident from policydocuments, examples of tools for decision-makers, and ¡nformation posted on theCollege's website.
Reliability
The College's Registrat¡on Committee relies on an internal flowchart that describesvarious applicant scenarios, providing decision-makers with supporting evidence as theyreview cases, and promoting consistency and reliability in the decision-making process.
Validiü
The Registration Committee revlews the legislation and ethics exam to ensure thequestions are fair and that the information is readily available in the Chirocare binder andinformationpostedonthewebs¡te. Thisreviewensuresthattheexamismeasuringknowledge of policies, concepts and competencies contained in the College's resourcematerials.
CommendablePract¡ces
1. The College has developed an internal Registration Committee (Committee)flowchart to review various scenarios that apply to applicants to ensure that similarapplications are decided in a consistent manner. (T13)
Office of the Fa¡rness Commissioner
57
T7
2. CCO's recognition of international accrediting bodies around the world allows
applicants to receive their education in many chiropract¡c educational inst¡tutionsaround the world and meet the requirements for registrat¡on with CCO; (O1)
Recommendations 1. Cons¡der evidence from other health regulatory colleges in developing Committeepolicies, such as requiring appllcants to submit a police reference check in the initialapplication. (O1)
RegulatorComments
Formatted I Superscript
Council meet¡no,
Impartialityo ldentifying bias, monitoring, and taking correct¡ve actiono lmplementingstrategies
AssessmentOutcome The College has processes to identify bias and deploys strategies to mitigate the impact
of potential bias.
ldent¡Í¡cotion of B¡as
The College provides training materials that identifo and define bias in various forms,including conflict of ¡nterest and discr¡m¡nat¡on.
Stroteg¡es
The College has demonstrated commitment to impartial decision making, by providing
annual training that addresses the potent¡al for bias and discr¡minat¡on in decision
making.. The training is delivered by legal counsel and covers a variety of scenarios thatcommittee members and staff may confront, including conflict of interest, and human
rights obligations.
Recommendat¡ons 1. Promote a decision-making env¡ronment that is free of bias and discr¡mination:
a) develop a pol¡cy to reiterate the College's commitment to being free ofd¡scrim¡nat¡on and bias;
b) review Committee terms of reference to ensure ¡t includes CCO'S commitment tobe free of discriminat¡on and bias in decision making.
Office of the Fa¡rness Commissioner
58
18
RegulatorComments
CCO will look ot develooino such o oolicv, similor in nøture to the policv that is opplicobte tomembers (Guidel¡ne G-07il.
Fairnesso Ensuring substantive fairnesso Ensuring procedural fairnesso Ensuring relational fairness
AssessmentOutcome
The College shows evidence of fairness ¡n ¡ts registratión practices, drawn from policies,annual reports, and FRP reports, and in commitments made under the self-assessment.
Substantive fairnessThe registration requirements were developed in 1991 and amended in 2011 inconsultation with members, stakehôlders, government, professional assoc¡at¡ons,malpractice protect¡on assoc¡at¡ons, and other jurisd¡ctions.
The Registrat¡on Regulation allows Council to consider and approve acceptablealternatives for the educational. and examination requirements.
Procedural fairnessTheCollegeendeavourstoprovideflexibilityinregistrationprocesses. Someindividualsthat failed the leg¡slation. and ethics exam have been given an opportunlty to rewritethe examination at an earlier time rather than wait for the next scheduled examinationsitting, ifthey had already passed the CCEB examinations.
Relationaf Falrnessln its policy on the lêgislative and ethics exam, the College describes how applicants mayrequest accommodation when writing the exam, to accommodate a disability. TheCollege has committed to writing a stand-alone policy on the accommodationprocess.
CommendablePfact¡ces
1. Some individuals that failed the legislation and eth¡cs exam have been given anopportun¡ty to rewrite the examination earlier rather than wait for the nextscheduled exam¡nation sitting, ifthey had already passed the Canadian ChiropracticExamining Board (CCEB) exam¡nat¡ons.
Recommendations Substantive Fairness
1. Review and update Registration Committee terms of reference to ensure reg¡strationrequ¡rements are reviewed for relevance and necess¡ty at regular intervals. (F2)
Office of the Fa¡rness Comm¡ssioner
59
19
Procedural Fairness
2. lnclude more data on members and applicants country of origin in College's annual
report.
3. Review Committee terms of reference to speciry the timelines for registrationdecisions in CCO policy. (F8)
4, Meet with individuals ¡n similar positions at other colleges in an effort to make sure
CCO is capturing the best practices of similar regulators. (F9)
statements that currently resi{g within Pollcy///2
process, similar to the policyand Eth¡cs Exam,
Relational Fairness
5, Develop a policy on accommodation i
Ident¡fv best practlces, //¿
RegulatorComments
Office of the Fairness Commissioner
60
20
Background
Assessment MethodsAssessments are based on the Res¡strat¡on Practices Assessment Guide: For Resulated Professions and HealthResulatorv Colleses. The guide presents registration practices relating to the spec¡fic duties and general duty in theRHPA.
A regulatory body's practices can be measured against the RHPA's specific duties in a straightforward way.However, the general duty is broad, and the principles it mentions (transparency, objectivity, ¡mpartiality andfairness) are not defined ¡n the legislation.
As a result, the spec¡f¡c-duty and general-duty obligations are assessed differently (see the Stroteav for Cont¡nuouslmÛrove me nt of Reaistrot¡on Prad¡ced.
Specific DutiesThe OFC can clearly determine whether a regulatory body demonstrates the specific-duty practices in theassessment guide. Therefore, for each specific-duty pract¡ce, the OFC provides one of the following assessmentoutcomes:
Demonstrated - all required elements of the practice are present or addressed
Partially Demonstrated - some but not all requlred elements are present or addressed
Not Demonstrated - none of the required elements are present or addressed
Not Applicable - this practice does not apply to the lo cronym of regulotory body)'s registration practices
General DutyBecause there are many ways that a regulatory body can demonstrate that ¡ts practices, overall, are meeting theprinciples of the general dúty, the OFC makes assessm ent commenß for the general duty, rather tha n identifyingassessment outcomes. For the same reason, assessment comments are made by principle, rather than by practice.
For informat¡on about the OFC's interpretat¡ons of the general-duty principles and the practices that the OFC usesas a guideline for assessment, See the OFCls website..
Commendable Practices and RecommendationsWhere applicable, the OFC ident¡fies commendable practices or recommendations for improvement related to thespecific duties and general duty.
SourcesAssessment outcomes, comments, and commendable practices and recommendations âre based on informationprovided by the regulatory body. The OFC relies on the accuracy of this information to produce the assessmentreport. The OFC comp¡les registrat¡on information from sources such as the following:
Fair Registration Practices Reports, aud¡ts, Entry-to-Practice Rev¡ew Reports, annual meetings
the regulatory body's:
. website
a
a
a
a
a
Office of the Fairness Commissioner
61
2T
. polic¡es, procedures, guidelines and related documentation templates for communication w¡th
applicants
. regulations and bylaws
o internal au'diting and report¡ng mechanisms
. third-party agreements and related monitor¡ng or reporting documentation
o qualifications assessments and related documentation
targeted questions/requests for evidence that the regulatory body demonstrates a practice or principle
For more information about the assessment cycle, assessment process, and legislative obligations, see the Sl/ateov
fol Contlnuous lmprovement of Reoistrot¡on Prdctlces.
Office of the Fairness Commissioner
RÐCEIJUN 0 e u0l7
VED
or
Office of the
&:(ni.::,Bureau ducommissaire à
l'éqaité
62CI
595 Bay Street, Suite 1201, Toronto ON M7A 2B4p t ;, t i r,' 416.725.938o li r.t 416.326.6o8t
595, rue Ba¡ Bureau 1201, Toronto ON M7A 284t,: l,; ¡¡ ! t, ¡ ¡',' 416 425.938o r ! I t: i a p í r u i 4t6 ¿26.6o8r
|TEM 1.4.2 [email protected] www'fairnesscommissioner.ca
I|lday 29,2017
Ms. Jo-Ann WillsonRegistrar and General CounselCollege of Chiropractors of OntarioSuite 902130 Bloor St WestToronto ON M5S 1N5
Dear Ms. Willson,
As you may know, I was appointed the Fairness Commissioner of Ontario in April of this
year. I am honoured to assume this important role in Ontario.
The team and I are committed to ensuring that we continue to provide impartial expertise
and advicc in a way that makes a meaningful sontribution to your regulatory body.
In this capacity,I will continue to advance Ontario's commitment to fair access
legislation and work with your organizationto ensure that licensing is transparent,
objective, impartial and fair.
As you recall, the Office of the Faimess Commissioner was established a decade ago to
help ensure fair access to regulated professions and compulsory trades for everyone who
is qualified, including those trained or educated outside of Canada.
One of my fîrst priorities as Commissioner will be outreach, as I look forward to working
together.
Sincerely,
A. JamesonFairness Commissioner
cc: Nuzhat Jafri, Executive Director, Office of the Fairness Commissioner
Þontrr¡o
No.
Co¡-lece oF CHrRopRAcroRS oF ONTAR¡o
Gouncil Meeting
Friday, June 23,2017 (8:30 a.m. - 4:30 p.m.l1 2
AGENDA (Public) 3
ActionRequired
Action By PriorityLevel a
SEcTtoNsOF THË
CooEFoRIN.CAMERA
SEsstoNs rFDIRECTEO AY
CouNcrL
Page ITEM
9
10
29
31
Cn¡l- To ORDER
Appoint P arliamentqrian
Opportunity to Declare any real orperceived conflicts of interest with respect
to any agenda item
1. ConsentAgenda
1.1 Discipline Committee Report1.1.1 CCO v. Dr. Liza Egbogah
Decision (received June8,2017)
1,1.2 FHRCO Conducting a
Discipline HearingProgram(Basic - May 18, 2016)
1.2 Fitness to Practise CommitteeReport
1.3 Inquiries, Complaints andReports Committee Report(rcRC)
1.4 Registration Committee Report
Council
Approve Council
Shankar Híeh
Shankar/ Híeh
33
1 Subject to Council's direction.2 Ms Wendy Lawrence has sent regrets. Mr. Shakil Akhter must leave by noon.3 lf you would like the complete background documentation relating to any item on the agenda, please speak to
Ms Willson.4 Sub.¡ect to Council's direction. Consider addressing all agreed upon high priority items first whether they are old
or new business items.
Council nda - June 23,2017 (Public) 2
SÊcÍoN8OF THECoDEFoRIN.CAMERA
SEsstoNs rF
OIRECTED BY
CouNcrL
Page ITEM
62
ActionRequired
VerbalReport/Approverecommendations/Ratifydecisionsmade in-camera
Considernext phase
of by-lawamendments
Action By
Shankar/Council
PriorityLevel 4
No.
94 4.1 Executive Committee RePort
Ss. 7(2)(bXc)(dXe)
Bylaws 6 Council Medium
s Only members present at the meeting should approve the minutes.6 Additional matters to be considered to enhance transparency and accountability: conflict of interest provisions
for other organizations, possibility of a ""cooling off" period if candidate has served in leadership position on
another organization wiih respeci to which theie ¡s a real or perceived conflict of interest, whether cco should be
able to invest in instruments others than banker's acceptance certificates, process re: appointment of noncouncil
committee members and what other information needs to go on the public register.
aflous
t.4.2
re: Ontario Faimess
Commissioner ReportCorrespondence dated May29,2017 from GrantJameson, Fairness
Commissioner
2. Adoption of Agenda
3. Adoption of Minutes 5
4. Committee Reports
Move In Camera/lVlove out of Cameraand ratify decisions
Adopt Committee Hieh

Council Agenda - June 23, 2017 (Pu blic) 3
SEcÏoNgOF IHECoDEFoRlN-CAMERA
SEsstoNs rF
DIRÉCTED BY
CouNcrL
No.Page ITEM
470 4.t.26
Amendments to By-law 17:
Public Register
Summary of PublicRegister Requirements
Current CCO By-lawsExtract from RHPA repowers of ExecutiveCommitteeExtract of Bill 87 re:
increasing information onthe public register
ActionRequired
pprovedistributionandfeedbackReviewConsidernext phase
of by-lawreview/Recommend-ations toCouncilFYIFYI
FYI
V/elcomeback!
FYI
FYI
Action By PriorityLevel 4
Council Medium
474523
4.1.274.r.28
524 4.1.29
529
531
s26
Minßtry of Heølth and Long-TermCare4.1.30 Reappointment of Mr.
Shakil Akhter dated MaY19,2017
4.1.31 Correspondence dated MaY19,2017 to Registrars fromDenise Cole re:
appointment of Deanna
Williams4.1.32 Other communication from
MOHLTC re: APPliedBehavioural AnalYsts, and
new policy advisor
CouncilAgenda -June 23,2017 (Public) 4
SEcïoNsOF THE
CoDEFoRlN-CAMÊRA
SEssroNs rF
DIRECTED BYCouNctL
PageNo.
535
571
574
576
ITEM ActionRequired
maFYI subiecttoquestionsand verbalreports
Action By PriorityLevel a
573
Related Stakeholders
Ontario ChiropracticAssociation(OCA)4.1.33 Miscellaneous
Bulletins/Communications(including survey)
4.1.34 Correspondence dated MaY8,2017 to Dr. Shankarfrom Dr. Azad
F e der at i on of C anadi an Chir opr act ic(FCC)4.1.35 Correspondencedated
ApriI25,2017 to MsDantas from Dr. Jean-
Francois Henry4.1.36 Communication dated MaY
5,2017 re: FCCSuccession Planning 7
Federation of ChiroPracticLicensing Boards (FCLB)
4.1.37 Communicationdated May 16, 20t7 re:affirmation from FCLB
C anadian Chir opr act ic As s o c i ation4.1.38 MediaAnnouncement
dated }l{ay 9,2017:Chiropractors included innew 2017 CanadianGuideline for OPioidTherapy and Chronic Non-Cancer Pain
C anadian Memorial Chir oPr acticCollege (CMCC)
579
7 Mr. Jim Duncan will be retiring before the Fall 2017 meetings'
Council a - June 23,2017 (Public) 5
SEcnoNsOF THE
CoDEFoRIN.CAMERA
SEssroNs rF
DIRECTED BY
CouNctL
PageNo.
607
614
631
634
636
650671
ActionRequired
Action By PriorityLevel a
ITEM
605
youBrian Gleberzon dated
};4lay 8,20174.1.40 Invitationto CMCC
graduation to Present Dr.Beasley award
4.L41 Article in PrimarY ContactChiropractic in 2017 andBeyond and feedback dated
June 13,2017 from Dr.Mike Staffen (CCO Peerassessor)
Federation of Health RegulatorYColleges of Ontario4.1.42 Legislative UPdates from
Richard Steinecke (March,April2017)
4.1.43 Communicationexchangebetween FHRCO and
Jacques Gallant, TorontoStar dated };/:aY 10,2017re: Bill 87
4.1.44 Information dated MaY 18,
2017) re:FHRCOcommunications Plan and
new public Portal
Review of Policies, Standards ofPractice, Guidelines etc.
4.1.45 ExecutiveCommitteepolicies, standards ofpractice, guidelines
4.1.46 InternalPolicies4.1.47 Code of Conduct/Rules of
Order4.1.48 Privacy Code (and
supporting documents)4.1.49 Table of Contents (French
Translation)
Reaffirm Council Medium
67s
739
Council a - June 23,2017 (Public) 6
SËcÏoNsOF lHECoDEFoRIN-CAMERA
SEssroNs rFDIRECTED BY
CouNctL
No.Page ITEM
Declaration for PubhcMembers
755 4.2 Advertising Committee RePort
ActionRequired
VerbalReport/Clarification
VerbalReporlApproveRecommend-ations
VerbalReport/ApproveRecommend-ationsFYI
Action By PriorityLevel a
Amlinger Medium
Gates Híeh
um
7s7762
773
4.2.r4,2.24.2.4
778
4.3.1
4.3.2
4.3.3
801 4.4.2
4.4.3
820 4.4.4
4.3 Patient Relations CommitteeReport
S-016: AdvertisingG-016: AdvertisingCommunication from OCAre: CCO Advertisingprovisions
Draft Amendments toPatient RelationsCommittee Terms ofReferencePatient RelationsCommittee Terms ofReference (current)Draft Communique re: Bill87
S-003: ProfessionalPortfolio (cunent)Information re: College ofVeterinarians Consultation5-009: Chiropractic Care
of AnimalsCCO survey of animalchiropractors
780
782
784
786 Anderson-Peacock
Híeh4.4 Quality Assurance CommitteeReport
808
830 4.4.6
Council a - June 23,2017 (Public) 7
SEcnoNsOF THE
CooEFoRIN.CAMERA
SEsstoNs rF
DIRECTED BY
CouNctL
Page ITEM
848
881
929
939
942
976
979
ActionRequired
Report/ReviewMaterial
FYI (subjecttoquestions)
Action By
Council
PriorityLevel 4
No.
933
us ness
5,1 Bill87, Protecting Patients Act,2017 I
5.2 News Release dated l|i{.aY 30,2017Ontario Strengthens Laws toPrevent Sexual Abuse of Patients
6. For Your lnformation
6.1 New York Times (MaY 1,2017):For Bad Baclcs, It MaY be Time to
Rethink Biases aboutChiropractors
Other RegulatorsCollege of Dental Technologists ofOntario6.2 Conespondence dated };4.aY 24,
2017, Circulation of ProPosed
Changes for 2017 -2018 Fees
College of Naturopaths of Ontario6.3 lNformeD Newsletter Spring 2017
College of Nurses of Ontario6.4 Announcement dated APril 19,
2017 NPs can now Prescribecontrolled substances
6.5 Various Media RePorts re: CNO
College of Physicians andSurgeons of Ontario
6.6 News Release dated lune 13,20t7"CPSO defends Patients'rights to
access health services"College of Physiotherapists of Ontario
6.7 May 2017 Issue of PersPectives
967
8 Richard Steinecke is scheduled to attend at 9:30 a.m. to provide an overview of Bill 87 and the implications for
cco.
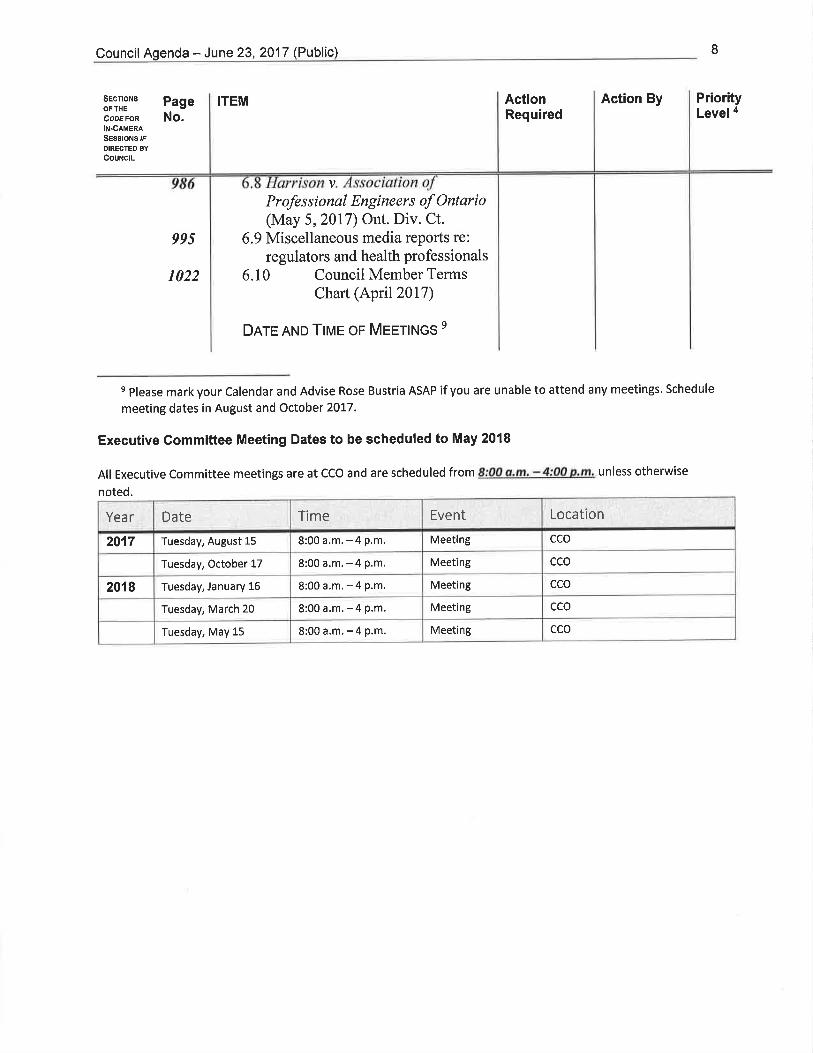
Council Agenda - June 23, 2017 (Public) 8
SEcfloNsOF THE
CoDE FoRlN-CaMERA
SEssroNs rFDIRECTEO BY
CouNctL
PageNo.
ITEM ActionRequired
Action By PriorityLevel a
v
995
1022
Professional Engineers of Ontario(May 5,2017) Ont. Div. Ct.
6.9 Miscellaneous media reports re:
regulators and health professionals
6.10 Council Member TermsChart (April 2017)
Dnre AND TIME oF MEETtNcs e
s please mark your Calendar and Advise Rose Bustria ASAP if you are unable to attend any meetings. Schedule
meeting dates in August and October 2017.
Executive Committee Meeting Dates to be scheduled to May 2018
All Executive Committee meetings are at CCO and are scheduled from 8:00 a.m, - 4:00 p,m, unless otherwise
noted.
Year Date Time Event Location
2017 Tuesday, August 15 8:00a.m.-4p.m. Meeting cco
Tuesday, October 17 8:00a.m.-4p.m. Meeting cco
2018 Tuesday, January 16 8:00 a.m, -4 p.m. Meeting cco
Tuesday, March 20 8:00a,m.-4p.m. Meeting cco
Tuesday, May 15 8:00a.m.-4p.m, Meeting cco
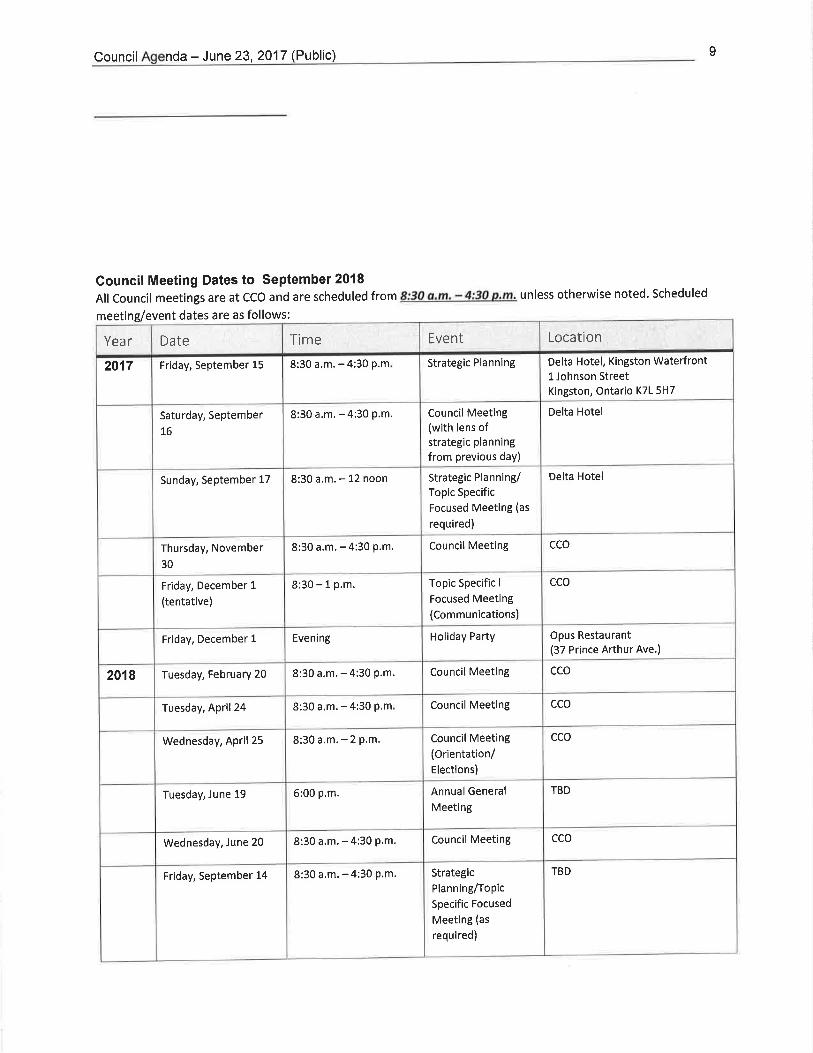
Council nda - June 23,2017 (Public)
Council Meeting Dates to September2018All Council meetings are at CCO and are scheduled from 8:30 a,m. - 4:30 p.m, unless otherwise noted. Scheduled
meeting/event dates are as follows:
I
Year Date Time Event Location
2017 Friday, September 15 8:30 a.m. - 4:30 p.m Strategic Planning Delta Hotel, Kingston WaterfrontI Johnson StreetKingston, Ontario K7L 5H7
Saturday, September
L6
8:30 a,m, -4:30 p.m. Council Meeting(with lens ofstrategic planning
from previous day)
Delta Hotel
Sunday, September 17 8:30 a.m. - 12 noon Strategic Planning/Topic Specific
Focused Meeting (as
required)
Delta Hotel
Thursday, November
30
8:30 a.m. - 4:30 p.m, Council Meeting cco
Friday, December 1
(tentative)
8:30 - 1 p.m. Topic Specific I
Focused Meeting(Communications)
cco
Friday, December 1 Evening Holiday Party Opus Restaurant(37 Prince Arthur Ave.)
2018 Tuesday, February 20 8:30 a.m. - 4:30 p.m. Council Meeting cco
Tuesday, April 24 8:30 a.m. - 4:30 P.m Council Meeting cco
Wednesday, April 25 8:30a.m,-2p,m. Council Meeting(Orientation/Elections)
cco
Tuesday, June 19 6:00 p.m. Annual General
Meet¡ng
TBD
Wednesday, June 20 8:30 a.m. - 4:30 P.m. Council Meeting cco
Friday, September 14 8:30 a.m, - 4:30 p.m. Strategic
Planning/Topic
Specific Focused
Meeting (as
required)
TBD
Council - June 23,2017 (Public) 10
SEcnoNgOF THE
CODEFOR
IN-CAMERA
SEsstoNg rF
DIRECTED BY
CouNctL
Page ITEM ActionRequired
Action By PriorityLevel a
No.
Ao¡oun¡¡nnett
Saturday, September
15
8:30 a.m. - 4:30 P.m. Council Meeting TBD
Sunday, September 16 Strategic
PlannlngÆopic
Specific Focused
Meeting (as
required)
TBD

ITEM 4.1 94Generated Internally
College of Chiropractors of OntarioExecutive Committee Report to CouncilJune23,2017
Members:
Staff Support:
Dr. Gauri Shankar, PrestdentDr. Cliff Hardick, Vice-PresidentMr. Shakil Akhter, TreasurerDr. Liz Anderson-PeacockMs Wendy LawrenceMs Judith McCutcheonDr. David Starmer
Mr. Joel Friedman, Director, Polícy and ResearchMs Jo-Ann V/illson, Registrar and General Counsel
I lntroduct¡on
a Thank you to all council members for your support as I present my firstreport to Council as President. Since the Council meetings on April 26 and27,2017, there was a meeting of the new Executive Committee("Committee") on l;4:ay 16,2017. The draft, confidential minutes for theMay 16, 2017 meeting are included in the council information package.
Executíve Comm¡ttee Report to Council-June 23,2017 5
98Other Communications
As part of CCO's commitment to more electronic communication, the
Executive is recommenciing a new process reiating speciÍicaiiy to
communication about amendments to CCO by-laws, standards, policies and
guidelines. Included in the council information package is the proposed
communication with respect to the amendments approved by Council on April27,2017 (reflected in the minutes to be approved on June 23, 2017:.
o
a
a
That Councíl approve the proposed e-maíl blast of amendments to the Policíes and
Guideltnes approved by Counctl on April 26, 2017 and that a símilar procedure be
adoptedfor the communí.cation offuture amendments to CCO documents.
Dr. Walton and Ms Willson have continued CCO's outreach with the
roadshows, and feedback generally is positive. I will ask any Council members
who have attended the recent events to provide any feedback (time permifiing).More roadshows are scheduled for the fall and at the conclusion of the year, the
Committee will review the project and consider what recommendations should
be made for 2018 and following. The consideration of this initiative will also
be informed by the facilitated communication discussion on December 1,2017.
For the first time on June 13,2077, CCO facilitated attendance at its record
keeping workshop remotely for an applicantwho is deaf. CCO has an obligation
to provide reasonable accommodation to individuals with disabilities. The
feedback from the applicant was very positive (included in the informationpackage).
Executíve Committee Report to Council - June 23,2017 6
a
99By-laws
CCO has been in the process of reviewing its various by-iaws, anci has
completed phase 1 of this-process which now-necessitates a consideration ofother items which were previously defened. Bill 87 includes a number ofamendments aimed to enhance transparency and accountability to the public,and fortunately, many of the recommended changes have already been
implemented. The Committee continues to review the by-laws for otherchanges that .will increase public accountability. At this time, there is a
recornmendation relating to increasing information on the public register whichwill be consistent with 8il1 87 and the by-laws of other health regulators.
Thtlt Council approve for dístríbution and feedback amendments to the publicregìster relating to offences and bail conditÌons known to CCO as outlined in the
draft proposed amendments to By-lmu 17: Publíc Regìster.
Vl Ministry of Health and Long-Term Gare (MOHLTC)
I am pleased to report that Mr. Shakil Akhter has been reappointed to CCO Counciluntil May 6,2078. Welcome back Shakil!
a
a Ms Deanna Williams, who presented to CCO Council in April2016, has been
appointed by MOHLTC to undertake work relating to the recommendations of the
Sexual Abuse Task Force. Deanna will be communicating with all colleges over the
next several months to seek opinions and perspectives as regulators on the various
recommendations from the task force.
Executíve Committee Report to Council -June 23,2OI7 7
vil
a
Chiropractic Organizations/Health Relatedcr¿- t-^ t- - l J ^ --arLilÁet tL,luer Ð
lncluded in the Council information package is a variety of informationrelating to various chiropractic orgartizations and other health regulatoryorganizations. Council members will note the following:
The CCO and OCA Presidents, Vice-Presidents and CEO's have adinner meeting on Tuesday, June 27,2017.Included on the agenda isan update on the OCA's new strategic plan and possible futuremeetings;
100
The FCC is in the process of recruiting for a new CEO in light of theretirement of Jim Duncan efîective suÍtmer 2017. Meetings are
scheduled for the fall,20t7 and Ms Willson and I will be attending onbehalf of CCO;
The CCA has announced that chiropractors are included inthe2017Canadian Guideline for Opioid Therapy and Chronic Non-CancerPain;
Ms Willson will be attending the June 16,2017 CMCC graduation topresent the Dr. Beasley Award;
CCO was copied on feedback relating to a¡r article in CMCC'spublication Chiropractic in20l7 and beyond;
FHRCO has distributed various legislative updates from RichardSteinecke; in addition, FRHCO has embarked on a comprehensivecommunication plan and strategy including a new public portal; CCOcan capitalize onthe efforts being made by FHRCO when updating itsown coÍrmunication strategies.
a
a
o
a
a
a
Executive Committee Report to Council - June 23,2OI7 8
101Vll¡ lnternal Policies
ml '-¿. - -----t- '--^-J --^--:^--- J^^--*^-+^ ^+ +L^ I\Á^.' 1 â, a^1 '7 Áâ^+i^ft. lne u0nullrtLgg Icvlcwçct v4rruuS LruuulllsuLù aL Lllç rvrc¿J rwr z¡vl ruvvruró,
and has thc follor,ving recommendation:
That Council reffirm the Executive Commíttee's standards, policíes, guidelines,
code of conduct, rules of order and prívacy code (as included ín the council
information package).
o The Committee is considering various strategies to address real or perceived
conflicts of interest before and during council and committee meetings to both
raise awareness of the importance of matters of real or perceived conflict and
to ensure there are specific action steps in place. There may be firtherrefinement of recommendations relating to conflict of interest, but at this time,
the Committee recommends that sta¡rdard agendas include wording with the
adoption of the agenda and before approval of the previous meeting minutes
to permit council members to declare real or perceived conflicts with respect
to any agenda item.
Executive Committee Report to Council - June 23,2At7 I
102lX Concf usion
In addition to the matters noted above, the Committee is dealing with avariety of other issues reflected in the draft minutes. Please note theExecutive and Council meeting dates included in the agenda for the June23, 2017 Council information package.
I appreciate the efforts of all council members and staff as we head intothe next term. I encourage anyone to contact me with any questions orconcerns. I look forward to working with all of you over the months tocome. Thank you.
a
Respectfully submitted by,
Dr. Gauri Shankar,President
6n/2017 RecentAmendments to Policies and Guidelines
College of Chiropractors of OntarioL'Ordre des Chiropratic¡ens dÊ I'Ontario 452
ITEM 4.1.23
Update to Policies and Guidelines
Please see the links below to access the updated documents, whichare also posted on the "What's New" section at www.cco.on.ca.
Approved on April 2q 2074 Came into Effect June 23' 2077
Minor Amendmenfs to GuÍdeline G'OO8: Business Practices
Council approved minor amendments to Guideline G-008: BusinessPractices, These amendments are intended to ensure members properlycommunicate information relating to a plan of care as it relates to feesand billings, including:
. the nature of care;
. who will be delivering the care;
. if any care is to be assigned or delegated to another individual; ando policies and procedures related to billing third-pafty payors
The purpose of these amendments is to ensure that patients are informedon the policies and procedures on fees for care, so that patients canmake an informed decision and are not taken by surprise by any fees orpractices related to billing third-pafty payors.
As well, the amendments include a more detailed example of how anunused portion of a block fee/payment plan is to be refunded. Theexample illustrates that if a patient opts out of the block fee/paymentplan, a member may not charge a patient any additional fees for anytreatments or services that Were discounted or complimentary as paft ofthe block fee/payment plan. A refund must always reference the unit costper service, which may be complimentary or discounted, of the blockfee/payment plan agreement. The example includes a scenario in whichmultiple services are included in the block fee.
New Policy P-O56: Requirement to Disclose Police Record Checks
Council approved a policy requiring new applicants for registration tosubmit a Canadian Police Information Centre Vulnerable Sector check orequivalent from the applicant's current jurisdiction in Canada, as well asany past jurisdictions in which the applicant has practised chiropractic.This requirement, which is applied by several other Ontario healthregulatory colleges will help to ensure that only competent, safe andethical applicants are registered with CCO.
This policy will only apply to new applicants for registration orapplicants who were previously suspended or revoked from a
https://ui.constantcontact.com/visualeditor/visual_editorjreviewjsp?agent.uid= 1128129988598&format=html&print=true 112
6n2U7 RecentAmendments to Policies and Guidelines
discipline hearing, and not to members renewing annually.
New Guideline G-O72: Use of Social Media 453Council approved a guideline on the use of social media, which clarifiesthe expectations regarding members' use of social media, including:
' exercising caution to maintain the privacy and confidentiality of thepatient;
' refraining from providing clinical advice or communicating adiagnosis;
' ensuring health related links are used with appropriate permissionand are within the chiropractic scope of practice;
' adhering to the advertising standard of practice and guideline whensocial media is used for advertising purposes;
. maintaining appropriate boundaries and avoiding posts that may beperceived as disgraceful, dishonourable or unprofessional; and
' using good judgement and caution before posting to social media,as information that is posted online cannot be removed easily.
College of Chiropractors of Ontario, 130 Bloor Street, Suite 902, Toronto, Ontario M551N5 Canada
SafeUnsubscribe" {recipient's email}Update Profile I About our service orovider
Sent by [email protected] in collaboration with
MantM',irt1Try it free today
https://ui.constantcontact.com/visualeditor/visual_editorjreview.jsp?agent.uid= 11281299885g8&formaFhtml&print=true z2

GuroeurueG-008
Quality Assurance CommitteeApproved by Councii: November 29, 2007
Amended: F'ebruary 26, 2013, April 26, 2017
Business Practices
454
a
a
a
Note to readers: In the suent of any inconsistency betzoeen this document and tlrc legislation that
affects chiropractic practice, the legislation 4laerns.
lrurerur
To advise members of acceptable business practices in a clinical practice, includingbut not limited to: the disclosure of fees to the patient for the delivery of care and
services, unit billing, block fees and/or payment plans as they relate to care or aplan of care delivered to the patient; and the billing of third-party payors.
Oe¡eclves
To clarify for members the sections of the Professional Misconduct Regulation852193 concerning Business Practices.
To ensure members provide accurate, complete information to patientsregarding fees, unit billing, block fees and/or payment plans, as they relate tothe delivery of care.
To ensure members clearly communicate to patients their right to choose and/orrefuse block fees and/or payment plans and their right to opt out of such plans
at any time during care.
To ensure members understand, comply with and communicate with patients
about the policies and procedures for billing third-party Payors'
DescnrploN oF GUtDELINE
Fees
When creating and implementing fees for service in clinical practice, members mustadhere to the following conditions:
. fees must be for care that is diagnostically or therapeutically necessary;
. fees must be fair and reasonable;
. billing practices, as they relate to patient care, must be disclosed to patients inadvance of any care. This includes, but is not limited to:
o the nature of the care or plan of care to be provided,o who is delivering the care,
o if any care is to be delegated,o the use of any adjunctive therapies and/or services,
1
College of Ch¡ropractors of Ontario
GuroeurueG-008
Business Practices
o the sale of any products, and/oro practices relating to billing third-party payors (see section on "Billing Third
Party Payors");an account for professional services must be itemized, if:o requested to do so by the patient or a person or agency who is to pay, in
whole or in part, for the services, oro if the account includes a fee for a product or device or a service other than
care;a re-assessment, as set out in Standard of Practice 5-002: Record Keeping, must:o be conducted when clinically necessary and, in any event, no later than
each 24th visit; ando be sufficiently comprehensive for the member to:
- evaluate the patient's current condition;- assess the effectiveness of the member's chiropractic care;- discuss with the patienÇ the patient's goals and expectations for
hislher ongoing care; and- affirm or revise the member's plan of management for the patient.
455
a
a
2
Fees for Service as Provided
A member charging and collecting a fee for the service as provided must complywith the conditions as set out above.
Unit Billing
Unit billing refers to charging and invoicing a patient for each component of theservice performed at a single visit, as opposed to charging and invoicing the patientfor the whole visit. A member engaging in unit billing shall:
o comply with CCO regulations, standards of practice, policìes and guidelinesrelating to business and billing practices; and
' ensure that the unit billing is fair and reasonable and be aware that charginga fee excessive to the service performed may constitute professionalmisconduct.
Block Fees and/or Payment Plans
A block fee and/or payment plan is any fee where the patient is charged formultiple services and/or treatments at any time other than when the services and/ortreatments are provided.
College of Chiropractors of Ontario
GuroeurueG-008
Business Practices
456
A member charging a block fee and/or payment plan must ensure that there is a
signed, written agreement between the member and the patient, which includes the
following provisions in which the member has:
r given the patient the option to pay for each service on a "pay per visit" basis;
. disclosed to the patient the regular unit cost per service and the unit cost per
service established by the block fee and/or payment plan if the fees differ; and
. fully inform the patient of his/her right to opt out of a block fee and/orpayment plan at any time during care, and the patient's right to a refund of any
unspent portion of the block fee and/or payment plan, calculated by reference to
the number of services provided multiplied by the block fee/payment plan unitcost per service.
A member shall not subject the patient to any undue pressure and/or duress when
offering a block fee and/or payment plan.
Repayment of Unused Block Fee and/or Payment Plan
. A patient may choose to opt out of a block fee and/or payment plan at any time
during care, even if an agreement has been previously signed.
. A member shall not subject the patient to any undue pressure and/or duress
when the patient chooses to opt out of a block fee and/or payment plan.
. A member must fully refund to the patient any unused portion of the block fee
and/or payment plan calculated by multiplying the number of services
provided by the established unit cost per service of the block fee/payment plan
agreement.
. If a patient opts out of the block fee/payment plary a member may not charge a
patient any additional fees for any treatments or services that were discountedõr complimentary as part of the block fee/payment plan. A refund must refer-
ence the unit cost per setvice, which may be complimentary or discounted, ofthe block fee/payment plan agreement.
3
College of Chiropractors of Ontario
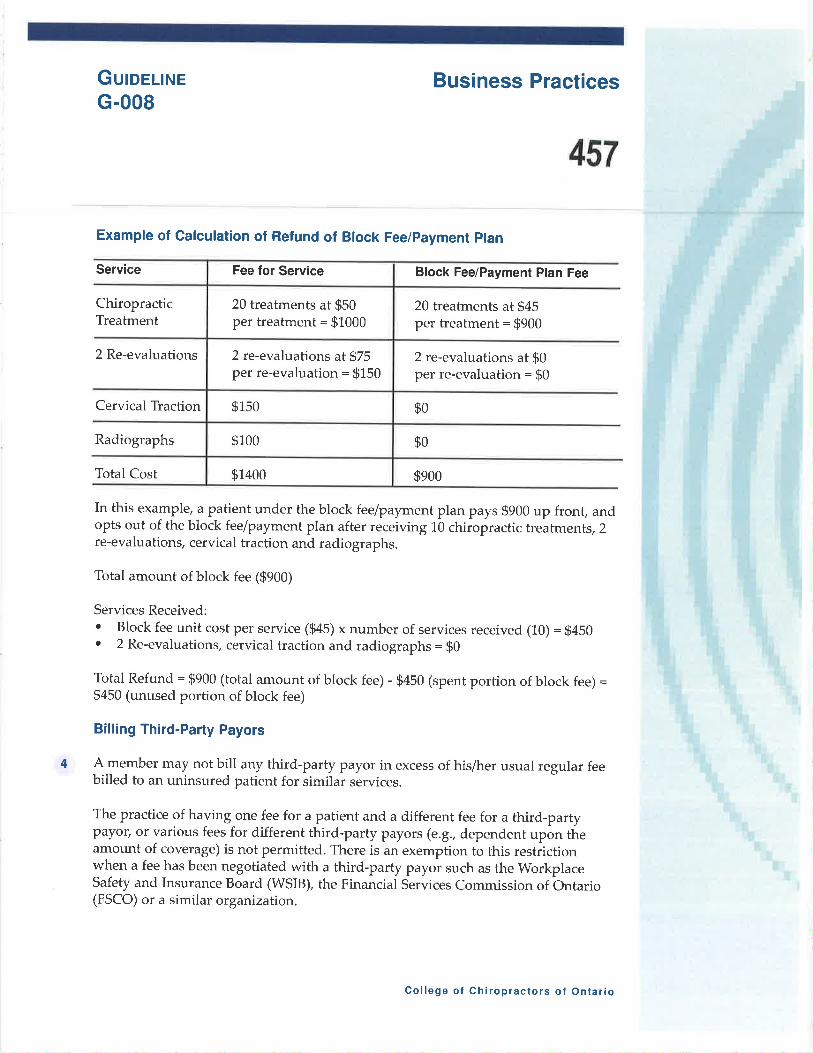
GuroeuneG-008
Business Practices
457
Example of Calculation of Refund of Block Fee/payment plan
Service Block Fee/Payment Plan Fee
ChiropracticTreatment
20 treatments at $45per treatment = $900
4
2 Re-evaluations 2 re-evaluations at $0per re-evaluation = $0
Cervical Traction $0
Radiographs $o
Total Cost $900
In this example, a patient under the block fee/payment plan pays $900 up front, andopts out of the block fee/payment plan after receiving 10 chiropractic treatments, 2re-evaluations, cervical traction and radiographs.
Total amount of block fee (9900)
Services Received:
' Block fee unit cost per service ($4S¡ x number of services received (10) = $450. 2 Re-evaluations, cervical traction and radiographs = $0
Total Refund : $900 (total amount of block fee) - $450 (spent portion of block fee) =$450 (unused portion of block fee)
Billing Third-Party Payors
A member may not bill any third-party payor in excess of his/her usual regular feebilled to an uninsured patient for similar services.
The practice of having one fee for a patient and a different fee for a third-partypayor/ or various fees for different third-party payors (e.g., dependent upon theamount of coverage) is not permitted. There is an exemption to this restrictionwhen a fee has been negotiated with a third-party payor such as the workplaceSafety and Insurance Board (WSIB), the Financial Services Commission of Ontario(FSCO) or a similar organization.
Fee for Service
20 treatments at $50per treatment: $1000
2 re-evaluations at $75per re-evaluu¡is¡ = $150
$150
$100
$1400
College of Chiropractors of Ontario
GuroeururG-008
Business Practices
458
A member should have a discussion with a patient of the member's involvementwith billing third-party payors to ensure the patient is fully aware of their ownresponsibilities regarding reimbursement from any third-party Payor.
LecrslnnvE CoNTExr
Regulation R-008: Professional Misconduct
1. The following are acts of professional misconduct for the purPoses of clause
51(1)(c) of the Health Professions Procedural Code:
The Practice of the Profession and the Care of and Relationship with Patients
1,. Contravening a standard of practice of the profession or failing to maintain the
standard of practice expected of members of the profession.
11. Breaching an agreement with a patient relating to professional services for the
patient or fees for such services14. Providing a diagnostic or therapeutic service that is not necessary.
Business Practices
23. Submitting an account or charge for services the member knows is false ormisleading.
24. Failing to disclose to a patient the fee for a service before the service is
provided, including a fee not payable by the patient.25. Charging a block fee unless,
i. the patient is given the option of paying for each service as it isprovided,
ii a unit cost per service is specified,iii. the member agrees to refund to the patient the unspent portion of the block
fee, calculated by reference to the number of services provided multipliedby the unit cost per service.
26. Failing to itemize an account for professional services,
i. if requested to do so by the patient or person or agency who is to pay, inwhole or in part, for the setvices, or
ii. if the account includes a fee for a product or device or a service other than a
treatment.27. Selling any debt owed to the member for professional services. This does not
include the use of credit cards to pay for professional services.
5
College of Chiropractors of Ontario
Guroel¡rueG-008
Business Practices
459
6
Miscellaneous Matters
28. contravening the Act, th.e Regulated Health professions Act, Lgg1or theregulations under either of those Acts.
29. Contravening a federal, provincial or territorial law, a municipal by-law or a by-law or rule of a hospital within the meaning of the Public HoÀpitais Ac! if thecontravention is relevant to the member's suitability to practise.
33. Engaging in conduct or performing an act that, having regard to all thecircumstances, would reasonably be regarded by members as disgraceful,dishonourable, or unprofessional.
A block fee and/or payment plan is any fee where the patient is charged formultiple services and/or treatments at any time other than when the servicesand/or treatments are provided.
College of Chiropractors of Ontar¡o
PoucvP-054
Approved by Council: April 26,2017
Requirement to DisclosePolice Griminal Record
Ghecks
460
Note to reøders: In tlrc eaent of any inconsistency between this document ønd the legisløtion thøt
affects chiropractic practice, the legislatíon 4laerns.
lrur¡rur
To clarify the College of Chiropractors of Ontario's (CCO) responsibility to protect
the public interest by ensuring that only competen! safe and ethical applicants are
registered.
To ensure that applicants for registration to CCO provide a police criminal record
check for the purposes of demonstrating good character and disclosing findings ofguilt in relation to an offence.
Oe¡eclves
As part of its mandate to regulate the chiropractic profession in the public interest,
CCO requires applicants for registration to demonstrate good character inaccordance with section 3(4) and disclose findings of guilt in relation to an offence
in accordance with section a(3) of Regulation 13711,1, under the Chiroprøctic Act,
L991, as follows:
Section 3(4): The applicant's past and present conduct must afford reasonable
grounds for belief that the applicant,i. is mentally and physically competent to practise chiropractic,ii. will practise chiropractic with decency, integrity, honesty and
in accordance with the lawiii. has sufficient knowledge, skill and judgment to engage in
chiropractic, andiv. will display professional behaviour.
Section 4(3): Every applicant is required to provide the College with details of the
following with respect to the applicant that occur or arise after the
applicant has submitted his or her application, and if the applicantbecomes a member, it is a condition of the member's certificate ofregistration that he or she provide such details:A finding of guilt in relation to any offence.
As part of its due diligence and efforts to promote openness and accountability,
CCO requires applicants for registration to provide a Canadian Police InformationCentre (CPIC) Vulnerable Sector (VS) check from the applicant's current jurisdiction
in Canada as well as any past jurisdiction(s) in which the applicant has practised.
1
College of Chiropractors of Ontario
PoucyP-054
Requirement to DisclosePolice Criminal Record
Checks
461
1,
The CPIC vs check verifies whether an applicant has a criminal record or anyrecord suspensions for sexual offences, and searches local police records forinformation relevant to the CPIC VS check.
Applicants who are applying from an international jurisdiction shall provide adocumentation from their jurisdiction that is substantially equivalent to the CPICVS.
DescnlploN oF Poltcy
Procedures
The following applicants and members shall submit a CpIC vs check withtheir application for registration:. all applicants for initial registration with CCO, including those
moving from another canadian jurisdiction under the Agreement onInternal Trade,
' individuals suspended from the findings of a discipline hearingseeking reinstatement with CCO, and
o Individuals with a revoked license seeking reinstatement with cco.The CPIC vs check can be obtained from a local police department or theRoyal Canadian Mounted Police (RCMP).
The cPIC vs check must show that the search of the CpIC database wasconducted no more than six months before the date of application forregistration.
The CPIC VS check must include the following information:' Records of discharge which have not been removed from the CpIC
system in accordance with the Criminal Records Ac! 1985, andrecords of outstanding criminal charges of which the police areaware;
. The name on the report must match the name that appears on theapplicant's registration application;
' The report must indicate that the search was completed on all namesthe applicant is currently using or has used;
' The date of birth that appears on the report must match that on theapplication;
The results of the CPIC vs check must be submitted to cCo directly fromthe police or RMCP or in a sealed envelope provided to the applicant by thepolice or RCMP.
2.
J
2
4.
College of Chiropractors of Ontario
Por-rcvP-054
Requirement to DisclosePolice Griminal Record
Ghecks
462
6.
5. If the report indicates a criminal record, applicants are required to submitsufficient documentation regarding the criminal charge to facilitate an
assessment of the report by the Registration Committee.
All reports indicating a criminal record will be referred to the RegistrationCommittee for review. The Registration Committee will review the reportand application, consistent with Policy P-054: Determination of Good
Character of an Applicant or Member http://cco.on.ca/site-documents/P-054.pdf.
For more resources and instructions on how to obtain a CPIC V$ please consult the
following websites:
. Canadian Police Information Centre www.cpic-cpic.ca
. Ontario Provincial Police: www.opp.ca
. RoyalCanadianMounted Police: http://www.rcmP-grc.gc.ca
LecrslRnvE CoNTEXT
Regulation l37l1L under th.e Chiroprøctic Act,1991
Section 3(4): The applicant's past and present conduct must affordreasonable grounds for belief that the applicant,i. is mentally and physically competent to practise
chiropractic,ii. will practise chiropractic with decency, integrity, honesty
and in accordance with the law,iii. has sufficient knowledge, skill and judgment to engage
in chiropractic, andiv. will display professional behaviour.
Section 4(3): Every applicant is required to provide the College with details
of the following with respect to the applicant that occur or arise after the
applicant has submitted his or her applicatiory and if the applicant becomes
a member, it is a condition of the member's certificate of registration that he
or she provide such details:A finding of guilt in relation to any offence.
3
College of Chiropractors of Ontario
Gu¡oeurueG-012Approved by Council: April 26,2017
Use of Social Media
463
a
Note to readers: In tlrc eoent of any inconsistency betzueen this document and the legisløtion that
fficts chiropractic practice, the legislntion Soaerns.
lrurerur AND OBJEcIvES
To fulfill the objective under the Regulated Heølth Professions Act, L99L (RHPA) to
develop, establistu and maintain standards and programs to promote the abilityof members to respond to changes in practice environments, advances intechnology and other emerging issues.
To outline the uses of social media in a professional context;
To provide guidelines to members on how to engage in social media while
continuing to meet legal, regulatory and professional obligations.
DescRrpnoN oF GUIDELINE
lntroduction
The term social media refers to all web and mobile technologies and practices thatare used to share conten! opinions, experiences and perspectives online. Social
media has become widely used by people as a means of communication and inmany instances, has become the preferred method of communication. Examples ofsocial media platforms include, but are not limited to: Webpages, Facebook, Twitter,Youtube, Linkedlru and blogging sites.
Social media may present opportunities to enhance patient care, education about
chiropractic, intra and inter-professional communication and collaboratiorç and
opportunities for continuing education and professional develoPment.
A member is expected to comply with all existing legal, regulatory and professional
obligations when engaging in the use of social media, including all relevantlegislatiory regulation, standards of practice, policies and guidelines. The followinoguidelines identify some of those obligations as they relate to the use of social
media.
1
College of Chiropractors of Ontario
GuroeurueG-012
Use of Social Media
464
a
Guidelines
A member must
comply with all legal and professional obligations to maintain privacy andconfidentiality in accordance with the Personal Health Information Protection Act,2004 (PHIPA) and cco standards of practice. A member may not divulgeinformation through social media that identifies a patient by name or through acombination of other identifying information.
a Any communication between a member and patient, such as providinginformation or scheduling an appointmen! must be done through secureprivate messaging only. A member must have a clear understanding of theprivacy settings available in any use of social media, and apply their useaccordingly. while patients or members of the public may make themselvespublically known through posting, a member must not breach the privacy orconfidentiality of a patient in any context. A member must also exercise cautionwhen blogging so as not to identify a patient.
not provide any clinical advice, communicate a diagnosis and/or guaranteeresults to a patient or any member of the public through social media. However,a member may provide general health information related to the chiropracticscope of practice for educational or informational purposes. All health relatedinformation and links posted must be related to the chiropractic scope of prac-tice.
The chiropractic scope of practice is defined in the chiropractic Act, 1gg1 andfurther explained in Standard of Practice 5-001: Chiropractic Scope of Practice.This includes adjunctive diagnostic and therapeutic procedures that are in thepublic domain, such as nutritional counselling, prescribing orthotics, givingadvice on lifestyle and exercise, providing therapeutic modalities.
A member must be cognizant of the risks of using social media for professionalreasons, such as a member of the public incorrectly applying information foundonline to their personal health situation. Whenever a member uses his/herprofessional designation or provides health related informatiory that member isviewed as acting in a professional capacity. A member must exercise cautionwhen posting health related information, so that it be clearly used for educationor informational purposes, and must not be used as clinical advice.
exercise caution when posting health related information and links to journalarticles or academic information to ensure he/she is not infringing on anycopyrighted material.
a
2
College of Chiropractors of Ontario
a
GuroeurueG-012
Use of Social Media
465
maintain appropriate professional boundaries, and avoid posting informatiorycomments or images that may be perceived as disgraceful, dishonourable orunprofessional. A member is further encouraged to have separate personal and
professional social media pages;
not post any information to social media that may be perceived as harassment,
bullying, or inflammatory comments. A member is expected to comply withGuideline G-009: Code of Ethics in use of social media;
comply with relevant advertising provisions in Standard of Practice 5-016:
Advertising when using social media for advertising purposes';
understand that information that is posted online cannot be removed easily. Amember must consider his/her legal, professional and regulatory obligationsand exercise good judgment and caution before posting material to social
media.
LecrslarvE CoNTEXT
Ontario Regulation 852193 under the Chiroprnctic Act,199L
The following are acts of professional misconduct for the Purposes of clause 51 (1)
(c) of the Health Professions Procedural Code:
10. Giving information about a patient to a person other than the patient, his orher authorized representative, or the member's legal counsel or insurer,
except with the consent of the patient or his or her authorized representative
or as required or allowed by law.1,6. Using a term, title or designation in respect of a member's practice contrary
to the policies of the College.17. Using a term, title or designation indicating a specialization in the
profession contrary to the policies of the College.28. Contravening the Act, the Regulated Health Professions Act, L991' or the
regulations under either of those Acts.29. Contravening a federal, provincial or territorial law, a municipal by-law or a
by-law or rule of a hospital within the meaning of the Public Hospitals Act,if the contravention is relevant to the member's suitability to practise.
33. Engaging in conduct or performing an act that, having regard to all the
circumstances, would reasonably be regarded by members as disgraceful,
dishonourable or unprofessional.
3
College of Chiropractors of Ontar¡o
Guroel¡rueG-012
Use of Social Media
466
This guideline should be read in conjunction with:¡ Standard of Practice 5-00L: Chiropractic Scope of practiceo Standard of Practice 5-0L6: Advertisingo Guideline G-001.: Communication with Patients. G-009: Code of Ethics
lAdvertising is defined in Standard of Practice 5-016: Advertising as "any messagecommunicated outside a member's office through a public medium that can be seenor heard by the public at large with the intent of influencing a person's choice ofservice or service provider."
#"ì!.1'

ø6/13/2917 08:23PM s6'¡9204921
Rating $cale DescriPtlon
H W4 Good
3 $atisfactory
¿ Fair
1 Unsatisfactory
ITEM 4-1'24
College of Chlroprac{ors of OntarioRecord KeePing WorkshoP
June 13, 2O17 "TorontoEvaluation Form
Yourfeedbøck í,s very iînporlant!
LCP Health PAGE Ø8/ø8
468
L Overall rating - On a scale of I to 5, I found the recorcl keeping workshop to be (cii'cle the
appropr{ate nruuber):
0hJectlvea
. Show the importance of high quality tecolds'
. Improve ur derstanding of stanclzuds ofproctice related to recorcl keeping.
. *Recgrd KeEing Made Easy''.,,. whatwotks and what doeorr't work.
. Have some fun!
2. Wliat did you {irnl most usefirl about the record keeping wot'kshop?
This was the first tirne I attencled a workshop without f.rllirrg asleep and irnpatientþ waiting
to end!
I must aclmit thnt I er¡ioYed readitrg the closed captionlng alongside wit'h llte vidso on the
satne screen. The we,Í9 IN their
Note to CCO book is the
3. What, if nny(hing, clo you think could be improved, in tlie record keepíng workshop?
Si¡ce the via LIVE IR tsroadcast ¡ft
be helpful to know what uÞt slide the speaker wåg ou at siven time druins thc worksho¡r
'Ihe clicl shift his to the üower point slidçs everv $o often which was
the uarne of the there is
ohange over. Or, the speaker can Eay their name bsforc speak for an hour o¡ so.
4. General Commçnts (tse back if necessaty)
I was for the entire and lear:red sot:te iusieht hr regarcls to the
importanco pf record , Even thoush the uumle CCO biuder is our Þractice bible.I
pratefi;l tbr havíne the onnorhrnilvto leanr more fi'om the speâkers. As aatn
result,Ihaveacle arer idea as to what is exPccted of nre going forwatd.
professionally, attendirg this workshop by means of IJVE IR Bloadcast & Vidco was
breath ficsh air!
(þThank yon.for yow ParlicîPation,
Name (optional)
rrtdÊtb,
/Ê)\-t
474|TEM 4.1.27
By-LAw 1: Den¡¡rnoNs AND lrurenpnETATroNApproved by Council: February 24, 2001Amended: September 24,2009, September 17,2015, February 23,2016, February 28,201 7
1.1 In these by-laws, unless the context otherwise dictates,
"Administrator" in the context of a chiropractic educational institution means one
who occupies an executive, management and/or policy'making position;
'.AFC" means the Alliance for Chiropractic
"Appointed Member" means a member of the Council appointed by theLieutenant Governor in Council;
o'By-laws'n means by-laws made by the Council;
"CCA" means the Canadian Chiropractic Association;
"CCEB" means the Canadian Chiropractic Examining Board;
"CCEC" means the Council on Chiropractic Education (Canada)
"CCPA" means the Canadian Chiropractic Protective Association;
"Chiropractíc Act" means the Chiropractic Act, 1991;
"CMCC" means the Canadian Memorial Chiropractic College;
"Code" means the Health Professions Procedural Code, Schedule 2 to theRegulated Health Professíons Act, 1991;
'oCouncil Member" means a member of the Council of CCO
"CSCE" means the Canadian Society of Chiropractic Evaluators;
"CCO" means the College of Chiropractors of Ontario;
"Council" means the Council of the CCO;
"Elected Member" means a member of the Council elected by the members of theCCO;
@ College of Chiropractors of Ontario

By-law 1: Definitions and lnterpretation
475"FCC" mean the Federation of Canadian Chiropractic;
"Member" means a member of the CCO;
"OCA" means the Ontario Chiropractic Association;
"Non-council Member" means a committee member who is not a member ofCouncil;
"Prescribed" means prescribed in the regulations or by-laws;
"Primary practice" is the member's practice address as identified in cco'sregister;
"Primary residence" is the member's residential address as identified in CCO'sregister;
"RHPA" means the Regulated Health Professions Act, I99I;
"UQTR" means Université du Quebéc à Trois-Rivières.
r.2 The definitions contained in the RHPA and Chiropractic Act are incorporated andadopted in the by-laws unless the context otherwise dictates.
1.3 Any act referred to by name shall mean that act in force at the relevant time asamended.
2
1.4
1.5
The by-laws shall be governed and construed in accordance with the laws ofOntario.
In the event of an inconsistency between the byJaws and the HHPA, ChiropracticAct, or the regulations under those acts, the KHPA, the Chiropractic Act and theregulations under those acts shall govern.
476Bv-lew 2: SenlApproved by Council: February 24, 2001
Amended: September 24, 2009, September 17, 201 5
2.2
2.I The seal shown on this page is the seal of CCO.
The registrar, president, vice-president and treasurer and such other person orpersons as may be authorized by Council shall each have authority to affix the
seal of CCO to any document.
@ College of Chiropractors of Ontario
477BY.LAW 3: EXTCUTION Or DOCUMENTSApproved by Council: February 24, 2001Amended: September 24, 2009, Septernber I 7, 20 I 5
3.1
3.2
Unless otherwise provided by law or the by-laws, a document of CCO shall be
signed by: the registrar or the deputy registrar and one of the president, vice-president or treasurer if the document has financial implications for CCO; and the
registrar or the deputy registrar, or someone authorized by him/her, if the
document does not have financial implications for CCO.
Minutes of Council meetings shall be signed by any two of the president, vice-president, treasurer or registrar.
Proposed regulations shall be signed by the registrar and one of the president,
vice-president or treasurer.
Decisions made by the panel of the Discipline Committee andlor the Fitness to
Practise Committee of CCO shall be signed by all members participating inthe decision.
Documents of a committee, such as a notice of a summons, shall be signed by arepresentative of the committee.
J.J
3.4
3.5
@ College of Chíropractors of Ontario
478BY.LAw 4: BaTXING AND FIruEruCEApproved by Councíl: February 24, 200 IAmended: September 24, 2009, September 17, 2015
4.1
4.2
4.3
4.4
4.6
4.7
4.5
The Executive Committee shall appoint a chartered bank where deposits are
insured by the Canadian Deposit Insurance Corporation for the use of CCO.
All money belonging to CCO shall be deposited in the name of CCO with thebank without deduction for any purpose whatsoever.
The registrar or deputy registrar may endorse any negotiable instrument forcollection on account of CCO through the bank for deposit to the credit of CCOwith the bank.
The registrar or deputy registrar and one of the president, vice-president ortreasurer may invest or reinvest funds of CCO, not immediately required, in:
(a) bonds, debentures, or other evidences ofindebtedness oforguaranteed by the Government of Canada or the Government ofOntario; or
(b) deposit receipts, deposit notes, certificates of deposit, and othersimilar instruments issued or endorsed by a chartered bank.
The Executive Committee may by resolution decide to invest or reinvest funds ofCCO, not immediately required, in securities outlined in ByJaw 4.4 above.
The registrar or deputy registrar and one ofthe president, vice-president ortreasurer shall sign documents to implement a decision made by the ExecutiveCommittee pursuant to By-law 4.5 above.
The Council may from time to time by resolution:
(a) borrow money on the credit of CCO;
(b) limit or increase the amount or amounts to be borrowed; and
(c) secure any present or future borrowing, or any debt, obligation, orliability of the College, by charging, mortgaging, hypothecating orpledging all or any of the real or personal property of CCO,whether present or future.
@ College of Chiropractors of Ontario
By-law 4: Banking and Finance
479
4.9
The Executive Committee shall not exercise the powers or duties of the Councilunder By-law 4.7 above or take any similar action.
The registrar or deputy regisfar and one ofthe president, vice-president ortreasurer shall sign documents to implement a decision made by the Councilpursuant to ByJaw 4.7 above.
2
4.8
4.10 Goods or services may be purchased or leased for the benefit of CCO if thepurchase or lease is approved by:
(a) the registrar or the deputy registrar, if the resulting obligationdoes not exceed $10,000;
(b) the registrar or the deputy registrar and one of the president, vice-president, or treasurer if the resulting obligation does not exceed $25,000;and
(c) the Executive Committee or the Council if the resultingobligation exceeds $25,000.
v rvullttgtt Ul ilr uPr 4urvt ù ut \,,l ttat tu
480BY.LAW 5: F¡ruEruCIRL YEIN AND AUO¡TIUCApproved by Council: February 24, 200 1
Amended: September 24, 2009, Septernber 17, 2015
5.1
5.2
5.3
5.4
5.5
The financi al year of CCO shall be from the I't of January of one year to the 3 l'tof December of the same year.
The Council shall at each annual meeting appoint one or more auditors who are
duly licensed (or hold a certiftcate of authorization under the Public Accounting
Act,2004) to hold office until the next annual meeting and, if an appointment is
not made, the auditor in office shall continue until a successor is appointed.
The Council shall fill any temporary vacancy in the office of auditorbut, whilesuch vacancy continues, the surviving or continuing auditor, if any, shall continue
as auditor.
The registrar shall give notice of every appointment and reappointment of an
auditor to the auditor in writing promptly after the appointment or reappointment
is made, together with a copy of this byJaw and any other relevant byJaws.
The auditor shall make such examination as will enable himlher to report to the
Council as required by law and under this byJaw.
The accounts and financial transactions of CCO shall be subject to annual audit
by the auditor(s) appointed or re-appointed annually by Council.
The auditor has a right of access at all reasonable times to all records, documents,
books, accounts and vouchers of CCO and is entitled to require from the council
members, officers and employees of CCO such information as in his/her opinion
is necessary to enable himlher to report as required by law or under this by-law.
The auditor is entitled to attend any meetings of the Council and to be heard at
any such meeting that he/she attends on any part of the business of the meeting
that concerns the financial affairs of CCO.
The auditor shall report to the Executive Committee upon reasonable request by
the Executive Committee and in any event at the last meeting of the Executive
Committee before the annual meeting of Council.
5.6
5.7
5.8
5.9
@ College of Chiropractors of Ontario
By-law 5: Financial Year and Auditing
481
5.1 I
The auditor shall report in writing to the Council at the annual meeting of Councilon the financial statement which shall be submiued to each annual meeting andshall state in the report whether, in his/her opinion, the fìnancial statemenipresents fairly the financial position of CCO and the results or its operations forthe period under review in accordance with generally accepted accóuntingprinciples applied on a basis consistent with that of the preceding period.
The Executive Committee shall not exercise the powers or duties of the Councilunder this by-law.
2
5.10
482By-LAw 6: EuecnoN or Gouucu MeUBERSApproved by Council: February 24, 2001Amended: February 12, 2002, September 24, 2009, September 17, 2015,February 23, 2016, February 28, 2017
6,1
6.2
Electoral District 1: Northern comprised of the districts of Kenora, Rainy River,Thunder Bay, Algoma, Cochrane, Manitoulin, Parry Sound, Nipissing,Timiskaming; the district municipality of Muskoka; and the city of GreaterSudbury.
Electoral District 2: Eastern comprised of the counties of Frontenac, Hastings,Lanark, Prince Edward, Renfrew, Lennox and Addington; the united counties ofLeeds and Grenville, Prescott and Russell, Stormont, Dundas and Glengarry; andthe city of Ottawa.
Electoral District 3: Central East comprised of the counties of Haliburton,Northumberland, Peterborough, and Simcoe, the city of Kawartha Lakes, theregional municipality of Durham and the township of Scugog.
Electoral District 4: Central bomprised of the city of Toronto and the regionalmunicipality of York.
Electoral District 5: Central West comprised of the counties of Brant, Dufferin,V/ellington, Haldimand and Norfolk, the regional municipalities of Halton,Niagara, Peel and Waterloo, and the city of Hamilton.
Electoral District 6: Western comprised of the counties of Essex, Bruce, Grey,Lambton, Elgin, Middlesex, Huron, Perth and Oxford, and the municipality ofChatham-Kent.
A member is eligible to vote in the electoral district in which the member, as ofJanuary ltt of the election year, has his/her primary practice, or if the member is
not engaged in the practice of chiropractic, in which the member has his/trerprimary residence.
@ College of Chiropractors of Ontario
By-law 6: Election of Council Members
For each electoral district referred to in column 1 of the following table, thereshall be elected to Council the number of members set out opposite in column 2.
Column 1 Column 2Electoral District Number of Members
1 1
2 1
3 1
4 35 26 1
The term of office of a member elected to Council is approximately three years,commencing with the first regular meeting of Council immediately following theelection. The member shall continue to serye in office until his/he. s.rc".ssoitakes office in accordance with this by-law.
6.5 A member who has served on Council for nine consecutive years is ineligible forelection to Council until a full three year term has passed since that memLer lastserved on Council.
6.6 An election of members to Council shall be held:
(a) in March, 1995, and in every third year after that for members fromelectoral districts 2 and 3 and for one member from electoral district 4;
(b) in March, 1996, and in every third year after that for members fromelectoral district 6 and for one member from electoral district 4 and,one member from electoral district 5; and
(c) in March, 1997, and in every third year after that for members fromelectoral district 1 and for one member from electoral district 4 andone member from electoral district 5.
The registrar, as directed by Council, shall set the date for the each election ofmembers to Council.
6.8 A member is ineligible to vote in a council election if he/she is in default ofpayment of any fees prescribed by by-law or any fine or order for costs to CCoimposed by a CCO committee or court of law or is in default in completing andretuming any form required by CCO.
483 2
6.3
6.4
6.7
By-law 6: Election of Council Members 3
4846.9 A member is eligible for election to Council in an electoral district, if on the
closing date of nominations and anytime up to and including the date of the
election:
(a) the member has hislher primary practice of chiropractic located in the
electoral district in which he/she is nominated or, if the member is notengaged in the practice of chiropractic, has his/her primary residence
located in the electoral district in which he/she is nominated;
(b) the member is not in default of payments of any fees prescribed by byJawor any fine or order for costs to CCO imposed by a CCOcommittee or court of law;
(c) the member is not in default in completing and returning any formrequired by CCO;
(d) the member is not the subject of any disciplinary or incapacity proceeding
(e) a finding of professional misconduct, incompetence or incapacity has notbeen made against the member in the preceding three years;
(Ð the member is not an employee, officer or director of any professionalchiropractic association such that a real or apparent conflict of interest
may arise, including but not limited to being an employee, officer ordirector of the OCA, CCA, CCPA, AFC, CCEB, CSCE or the CCEC ofthe FCC;
(g) the member is not an officer, director, or administrator of any chiropracticeducational institution, including but not limited to, CMCC and UQTR,such that a real or apparent conflict of interest may arise;
(h) the member has not been disqualified from the Council or a committee ofthe Council in the previous three years;
(Ð the member is not a member of the Council or of a committee of the
College of any other health profession; and
the member has not been a member of the staff of CCO at any time withinthe preceding three years.
6.10 The registrar shall supervise the nomination of candidates.
0)
@ College of Chiropractors of Ontario
By-law 6: Election of Council Members 4
4856.1 I No later than 60 days before the date of an election, the registrar shall noti$r every
member eligible to vote of the date, time and place of the election and of thenomination procedure.
6.12 The nomination of a candidate for election as a member of council, andundertaking to the CCO Registrar shall be in writing and shall be given to theregistrar at least 45 days before the date of the election (i.e., the nomination date).
6.13 The nomination shall be signed by the candidate and by at least l0 members whosupport the nomination and who are eligible to vote in the electoral district inwhich the election is to be held,
6.14 The candidate shall provide to the registrar by the nomination date or such laterdate as the registrar permits, biographical information in a manner acceptable tothe registrar for the pulpose of distribution to eligible members in accordancewith the by-laws.
6.15 The candidate may withdraw his or her nomination for election to Council nolater than 30 days before the date of the election.
6,16 If the number of candidates nominated for an electoral district is less than or equalto the number of members to be elected, the registrar shall declare the candidatisto be elected by acclamation.
6.17 The regishar shall supervise and administer the election of candidates and, for thepurpose of carrying out that duty, the registrar may, subject to the by-laws,
(a) appoint returning officers and scrutineers;
(b) establish a deadline for the receiving of electronic ballots;
(c) provide for the notification of all candidates and members of the results ofthe election;
(d) if there has been a non-compliance with a nomination or electionrequirement, determine whether the non-compliance should be waived incircumstances where the fairness of the election will not be affected; and
(e) provide for the destruction of electronic ballots following an election.
6.18 No later than 2l days before the date of an election, the registrar shall sendelectronically, or any other medium as determined by Council, to every membereligible to vote in an electoral district in which an election is to take place, a list ofthe candidates, the candidates' biographical information if provided, an
(Ò Colleoc of Chirnnranlnrc nf nô
By-law 6: Election of Council Members 5
486,explanation of the voting procedure, and electronic access to a ballot for voting.
6.19 Voting for elections of member to Council shall be by electronic method or any
other medium as determined by Council.
6.20 The instruction for voting shall contain the following:
a) a member may cast as many votes on a ballot in an election of members to
the Council as there are members to be elected to Council from the
electoral district in which the member is eligible to vote.;
b) a member shall not cast more than one vote for any one candidate;
c) a member shall clearly indicate the voter's choice in one of the appropriate
places on the electronic ballot to indicate the voter's choice;
the electronic vote shall be received by 4 pm on the date indicated in the
notice of election and voting guide; and
e) the electronic vote will not be counted in the election unless it has been
received in accordance with the instructions for voting.
6.21 On the date of the election, the registrar or his/her agent shall count the votes foreach candidate in each electoral district with a contested election.
6.22 The counting of the electronic votes shall be conducted so that no person knows
for whom any member voted.
6.23 Candidates or their representatives may be present when the electronic votes are
counted.
6.24 If there is a tie in an election of members to the Council, the registrar shall break
the tie by lot.
6.25 A candidate may require a recount by giving a written request and deposition the
sum or $150 with the registrar no more than 15 days after the date of an election.
6.26 The registrar shall hold the recount no more than 10 days after receiving the
request.
6.27 If the recount changes the election result, the full amount of the deposit shall be
refunded to the candidate, If the recount does not change the election result, CCO
will keep the deposit to partially ofßet recount costs, including staff time.
d)
@ College of Chiropractors of Ontario
By-law 6: Election of Council Members
487When there is an intemrption of mail service during a nomination or election, theregistrar shall extend the holding of nominations and election for such minimumperiod of time as the registrar considers necessary to compensate for theintemrption.
6.29 The Council shall disqualify an elected member from sitting on Council if theelected member:
(a) is subject of any disciplinary or incapacity proceeding;
(b) is found to have committed an actof professional misconduct or is foundto be incompetent by a panel of the Discipline Committee;
(c) is found to be an incapacitated member by a panel of the Fitness toPractice Committee;
(d) fails to attend two consecutive meetings of the Council or of a committeeor of a subcommittee in which helshe is a member, without reasonablecause in the opinion of Council;
(e) fails to attend a hearing or review of a panel for which he/she has beenselected, without reasonable cause in the opinion of council;
(Ð ceases to either have a primary practice of chiropractic or primaryresidence in the electoral district in which the member was electãd;
(g) becomes an employee, officer or director of any professional chiropracticassociation such that a real or apparent conflict of interest rnuy uiir.,including but not limited to being an employee, officer or director of theocA, ccA, ccPA, AFC, ccEB, cscE or the Accreditation standardsand Policies Committee or the CCEC of The FCC;
(h) becomes an ofÍicer, director or administrator of any chiropracticeducational institution, including but not rimited to cMCò and ueTR;
(Ð becomes a member of the council or a committee of the college of anyother health profession;
breaches the conflict of interest provision(s) for members of council andcommittees, in the opinion of the council after giving notice to themember of the concern and giving the member an opportunity to respondto the concern;
b
6.28
û)
By-law 6: Election of Council Members 7
488(k) fails to discharge properly or honestly any office to which he/she has been
elected or appointed, in the opinion of the Council, after being givennotice of the concern and an opportunity to respond;
becomes in default of payment of any fees prescribed by by-law or anyfine or order for costs imposed by a CCO committee or court of law; or
(m) becomes in default of completing and retuming any form required byCCO;
6.30 A council member shall resign from Council prior to applying for any CCO staffposition.
6.31 The seat of an elected Council member shall be deemed to be vacant upon thedeath, resignation or disqualification of the Council member.
632 If the seat of an elected council member becomes vacant in an electoral district nomore than 12 months before the expiry of the member's term of office, theCouncil may,
(a) leave a seat vacant;
O) appoint as an elected member the candidate, if any, who had the mostvotes of all the unsuccessful candidates in the last election of councilmembers for that electoral district; or
(c) direct the registrar to hold an election in accordance with this by-lawfor that electoral district.
6.33 If the seat of an elected council member becomes vacant in an electoral districtmore than 12 months before the expiry of the member's term of office, theregistrar shall hold an election in accordance with this by-law for that electoraldistrict.
6.34 The term of a member appointed under By-law 6.31(b) or elected in an electionunder By-law 6.31(c) shall continue until the time the former council member'sterm would have expired.
6.35 If, within 90 days from the date of the election, the Council is of the opinion thatthere is a reasonable ground for doubt or dispute as to the validity of the electionof any member of Council, the Council shall hold an inquiry and decide whetherthe election of the member is valid and, if an election is found to be invalid, the
Council shall direct another election to be held.
(l)
@ College of Chiropractors of Ontario
489BY-LAw 7: EucnoNs (wrnlru Couttcu)Approved by Council: February 24, 200 lAmended: September 24, 2009, September 17, 201 5
7.1 An elected member of the Council is eligible:
(a)
(b)
(c)
to vote for elections within Council;
for election to the position of president, vice-president or treasurer; and
for election to the position of chair or member of a statutory or non-statutory committee;
if the member is eligible for election to Council as of that date.
7.2 An appointed member of the Council is eligible:
(a) to vote for elections within Council;
O) for election to the position of president, vice-þresident or treasurer; and
(c) for election to the position of chair or member of a statutory or non-
statutory committee.
7.3 The Council shall at the first meeting of Council following the general election, oras soon thereafter as practicable, elect a president, vice-president and treasurer to
hold office until the first meeting of Council following the general election in the
subsequent yeag and if an election is not so held, the president, vice-president and
treasurer for the preceding year shall continue in office until their successors are
elected.
The election ofthe president, vice-president and treasurer shall be by secret ballotusing generally accepted democratic procedures, and where more than twocouncil members are nominated, the nominee who receives the lowest number ofvotes on each ballot shall be deleted from the nomination unless one nominee
receives a majority of the votes cast on the ballot, and this procedure shall be
followed until one nominee receives a majority of the votes cast'
7.4
7.5 Each member of Council has one vote with respect to each of the offtces ofpresident, vice-president and treasurer.
@ College of Chiropractors of Ontario
7.6
7.7
7.8
By-law 7: Elections (within Council) 2
490The president is the chief officer of CCO and the vice-president shall assist thepresident in the discharge of his/her duties.
The president, vice-president or treasurer, may be removed from office by a two-thirds vote of the Council at a special meeting called for that putpose, and theCouncil may elect a new president, vice-president or treasurer from its membersto hold office for the remainder of the year.
The office of president, vice-president or treasurer becomes vacantif the holder ofthe office dies, resigns or stops being a council member.
7.9 If the office of the president becomes vacant, the vice-president shall become thepresident for the unexpired term of the office and the office of vice-presidentthereby becomes vacant.
7 .I0 The Council shall fill any vacancy in the office of vice-president or treasurerusing the procedures in By-law 7.4 at a special meeting which the president shallcall for that purpose as soon as practicable after the vacancy occurs.
7.11 The president of the Council shall be the chair of the Executive Committee.
7.r2 The Council shall at the first meeting of Council following the general election, oras soon thereafter as is practicable, elect the chairs and members of all statutoryand non-statutory committees of CCO. If such elections are not so held, the chàirsand members of the committees for the preceding year shall continue until theirsuccessors are elected.
7.13 The election of chairs and members of statutory and non-statutory committeesshall be by secret ballot using generally accepted democratic procedures, andwhere more council members are nominated than available positions, the nomineewho receives the lowest number of votes on each ballot shall be deleted fromnomination and this procedures shall be repeated until each nominee receives amajority of the votes cast.
7.r4 Following the election of a particular committee, a member of that committeeshall be elected as chair. Each member of Council has one vote with respect to theposition of chairs of all statutory and non-statutory committees.
The chair of any statutory or non-statutory committee may be filled by an electedor appointed member of council but not by a non-council member ofcco.
A chair of a statutory or non-statutory committee may be removed from office bya two-thirds vote of the Council at a special meeting called for that purpose, and
7.r5
7,16
By-law 7: Elections (within Council)
491the Council may elect a new chair to hold the position for the remainder of theyeaf.
7.t7 The position of chair of a statutory or non-statutory committee becomes vacant ifthe holder of the position dies, resigns or stops being a Council member.
7.18 If the position of chair of a statutory or non-statutory committee becomes vacant,the Executive Committee shall appoint a chair for the unexpired term of theposition.
7.19 The duties and powers of the Council include:
(a) administering the RHPA, Chíropractic Act and the regulations and by-lawsunder those acts;
(b) reviewing the activities of statutory and non-statutory committees of theCouncil and requiring committees to provide reports and information tothe Council;
(c) requiring statutory and non-statutory committees of the Council to do
anything that, in the opinion of the Council, is necessary or advisable tocarry out the intent of the KHPA, Chiropractic Act, and the regulationsunder those acts;
(d) finalizing and proposing amendments to regulations and by-laws under theRHPA or the Chiropractíc Act.
7.20 The duties and powers of the president of the Council include:
(a) directing the activities of CCO;
(b) chairing meetings of Council;
(c) chairing meetings of the Executive Committee;
(d) approving agendas of the meetings of Council and meetings of the
Executive Committee;
(e) supervising the arrangements for the annual meeting;
(Ð taking all reasonable steps to ensure that orders and resolutions of the
Council and the Executive Committee are implemented;
(g) ensuring CCO is represented at all relevant meetings;
3
@ College of Chiropractors of Ontario
By-law 7: Elections (within Council)
492(h) presenting an Executive report at each Council meeting;
(i) acting as a liaison between cco and other professional organizations asappropriate; and
û) performing all acts and deeds pertaining to his/her office and such otheracts and deeds as may be decided by Council.
7.21 The president, while chairing a Council meeting or Executive Committeemeeting, votes only to break a tie.
1,22 The president of Council shall be eligible for election to a maximum of twoconsecutive one-year terms in the presidency.
7.23 The duties and powers of the vice-president include:
(a) assuming the role of president in the absence of the president or whenappointed to do so by the president; and
(b) performing all acts and deeds pertaining to his/her office and such otheracts and deeds as may be decided by Council.
7.24 The vice-president shall be eligible for election to a maximum of two consecutiveone-year terms in the vice-presidency.
7 ,25 The duties and powers of the treasurer of the council include:
(a) supervising all matters relating to the financial affairs of CCO; and
(b) performing all acts and deeds pertaining to his/her office and such otheracts and deeds as may be decided by Council.
7.26 The treasurer shall be eligible for election to a maximum of two consecutive one-year terms in the offrce.
7.27 The duties and powers of the secretary of the council include:
(a) preparing agendas for the meetings of council and meetings of theExecutive Committee and submitting such agendas to the president forapproval;
(b) keeping a record of matters that the council has referred to thecommittees;
4
@ Colleqe of Chirooractors of Ontario
By-law 7: Elections (within Council)
493
(c) having custody and care of the records and documents of the Council;
(d) giving or causing to be given notice of all council meetings and statutoryand non-statutory committees; and
(e) performing all acts and deeds pertaining to his/her office and such otheracts and deeds as may be decided by Council.
7.28 In preparing agendas for the meetings of Council, the secretary shall include aperiod during which council members may raise for discussion topics relevant tothe affairs of CCO.
7.29 The registrar shall be the secretary of the Council.
7.30 The duties and powers of the chairs of each committee shall include:
(a)
o)
(c)
(d)
directing the activities of the committee and reporting to Council;
chairing meetings of the committee;
preparing and approving agendas of the meetings of the committee;
taking all reasonable steps to ensure that orders and resolutions of thecommittee are implemented;
(e) acting as a liaison between the Council or Executive Committee and thecommittee;
(Ð reporting to the Executive Committee upon reasonable request by theExecutive;
(g) reporting in writing to the Council at the annual meeting of Council on theactivities of the committee for the preceding year;
(h) preparing a work plan for the subsequent year, which includes allbudgetary requirements for the committee, by November 1 of each and
every year, or by such other time as directed by Council;
ensuring the activities of the committee are conducted in a fiscallyresponsible manner within approved budgetary restraints; and
performing all acts and deeds pertaining to his/her office and such otheracts and deeds as may be decided by Council.
5
(ù
(')
@ College of Chiropractors of Ontario
By-law 7: Elections (within Council)
The chair of every statutory and non-statutory committee shall be eligible forelection to a maximum of two consecutive one-year terms.
6
4;947.3r
v vvlqve vt vr¡ilvPtar-[(',tù ut tql
495BY-LAW 8: CounCI¡. MeeTINGSApproved by Council: February 24, 2001Amended: September 24, 2009, September 17, 2015
8.1 The Council shall hold,
(a) an annual meeting which shall be called by the president between April 1
and June 30 ofeach year;
(b) regular meetings which shall be called by the president from time totime; and
(c) any special meetings which may be called the by the president, or amajority of council members, who deposit with the registrar a writtenrequest for the meeting containing specifìcs of the matter or matters fordecision at the meeting.
The registrar shall cause each council member to be notified in writing of theplace, date and time of a council meeting by sending such notification by ordinaryprepaid'mail, facsimile, e-mail or similarly effective method at least,
8.2
8.3
8.4
(a) 30 days before an annual meeting;
(b) 14 days before a regular meeting; and
(c) five days before a special meeting.
The registrar shall cause to be included in or with the notifïcation of all meetingsto council members, the agenda for the meeting.
The registrar shall cause to be included in or with the notification of a special
meeting to council members sufficient information about the matter or matters fordecision contained in the requisition of the meeting deposited with him/her topermit the member to form a reasonable judgment.
The registrar shall cause the public to be notified of council meetings inaccordance with any regulations under the RHPA and, if there are not applicable
regulations or not otherwise specified, in a generally accepted manner.
No annual, regular or special meeting shall be made void because of an
inadvertent or accidental error or omission in giving notice. In addition, any
council member may waive the notice requirements and ratify, approve and
8.5
8.6
@ College of Chiropractors of Ontario

By-law 8: Council Meetings 2
confirm any proceedings taken at the meeting. 496
8.7 Meeting of the Council shall take place in Ontario at aplace, date and timedesignated by the president or the majority of council members calling themeeting but, if a place, date or time is not designated or is incompatible with thebyJaws, the registrar shall select aplace, date and time compatible with the by-laws which is as close as he/she can reasonably select to the place, date and timedesignated by the person or people calling the meeting.
8.8 Unless otherwise required by law or by-law, every question which properly comesbefore the Council may be decided by a simple majority of the votes cast at themeeting by council members, and, if there is an equal number of votes on aquestion, the chair may cast a deciding vote.
8.9 voting at a council meeting shall be by a show of hands, or if appropriate, bysecret ballot.
8.10 Voting by proxy at council meetings shall not be permitted in any circumstances.
8.1 I The Council shall consider or transact at the annual meeting:
(a) the annual report for the preceding year;
(b) the reports of the committees established under the RHpA;
(c) the financial statement of CCO;
(d) the report of the auditor; and
(e) the appointment of the auditors for the ensuing year.
8.12 The Council may consider or transact at arcgtlar meeting:
(a) matters brought by the Executive Committee;
(b) interim reports by committees which have received prior review by theExecutive Committee; and
(a) any other business.
8.13 The Council may only consider or transact at aspecial meeting, the matter ormatters for decision at the meeting contained in the requisition deposited with theregistrar.
By-law 8: Council Meetings
8.19
3
497
8.14 The Council may consider or transact at any meeting, matters included in theagendaprepared by the secretary and approved by the president, androutine and procedural matters in accordance with the rules of the order.
8.15 The president shall cause the proceedings of the council meeting including allmotions and recommendations to be recorded, and the written record of theCouncil meeting, when signed by any two of the president, vice-president,treasurer or registrar, is prima facie proof of the accuracy of the contents of everysuch record.
8.16 The written record of the proceedings of a council meeting when accepted at asubsequent council meeting, subject to any corrections made at such subsequentmeeting, is conclusive proof of the accuracy of the contents of every such record.
8.17 'Whether or not a quorum is present, the president may adjoum any councilmeeting and reconvene it at any time and from time to time and, if a quorum ispresent at any reconvened meeting, any matter may be considered and transactedwhich could have been transacted at the original meeting which was adjourned.
8.18 Robert's Rules of Order are the rules of order for council meetings and form partof the by-laws. Where there is an inconsistency between Robert's Rules of Orderand CCO by-laws, CCO by-laws take precedence.
Any meeting of the Council or of a committee or of a panel that is held for anypurpose other than for the conducting of a hearing, except as permitted under theStatutory Powers Procedure Act,may be held in any manner that allows allpersons participating to communicate with each other simultaneously andinstantaneously.
8.20 Persons participating in the meeting, as outlined in By-law 8.19, are deemed to bepresent at the meeting.
8.2I A vote called at a meeting under By-law 8.19 shall be taken in such a manner as
determined by the chair unless a member of the council, committee or panel of thecommittee which is meeting, requests a roll call vote, in which case, a roll callvote shall be taken.
8.22 Notice of a meeting held under ByJaw 8.19 shall not specify a place for themeeting but rather the means by which the meeting will be conducted.
@ College of Chiropractors of Ontario
l1
By-law 8: Council Meetings 4
4988.23 The chair of any committee conducting meetings by conference call shall:
(a) noti$ CCO office of the meeting and the agenda for the meeting;
(b) ensure minutes are kept; and
(c) record the time spent on the meetings.
t6) Onllana nf Êhiranraatara af
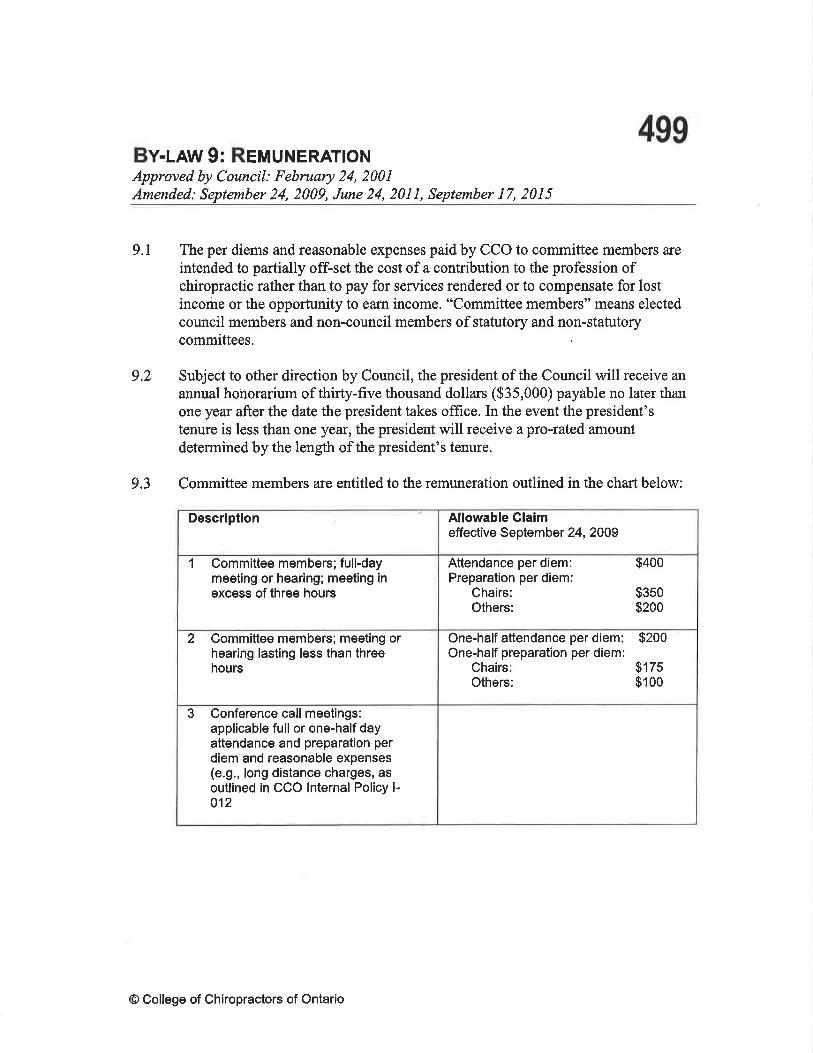
499Bv-uw 9: Ren¡uNERATToNApproved by Council: February 24, 2001Amended: September 24, 2009, June 24, 2011, September 17, 2015
9.1 The per diems and reasonable expenses paid by CCO to committee members are
intended to partially ofÊset the cost of a contribution to the profession ofchiropractic rather than to pay for services rendered or to compensate for lostincome or the opportunity to earn income. "Committee members" means electedcouncil members and non-council members of statutory and non-statutorycommittees
9.2 Subject to other direction by Council, the president of the Council will receive an
annual honorarium of thirty-five thousand dollars ($35,000) payable no later thanone year after the date the president takes office. In the event the president'stenure is less than one year, the president will receive a pro-rated amountdetermined by the length of the president's tenure.
9.3 Committee members are entitled to the remuneration outlined in the chart below:
Descriptlon Allowable Claimeffective September 24, 2009
I Committeemembers;full-daymeeting or hearing; meeting inexcess of three hours
Attendance per diem:Preparation per diem:
Chairs:Others:
$400
$350$200
2 Committee members; meeting orhearing lasting less than threehours
One-half attendance per diem:One-half preparation per diem:
Chairs:Others:
$2oo
$175$100
3 Conference call meetings:applicable full or one-half dayattendance and preparation perdiem and reasonable expenses(e.9., long distance charges, asoutlined in CCO lnternal Policy l-012
@ College of Chiropractors of Ontario
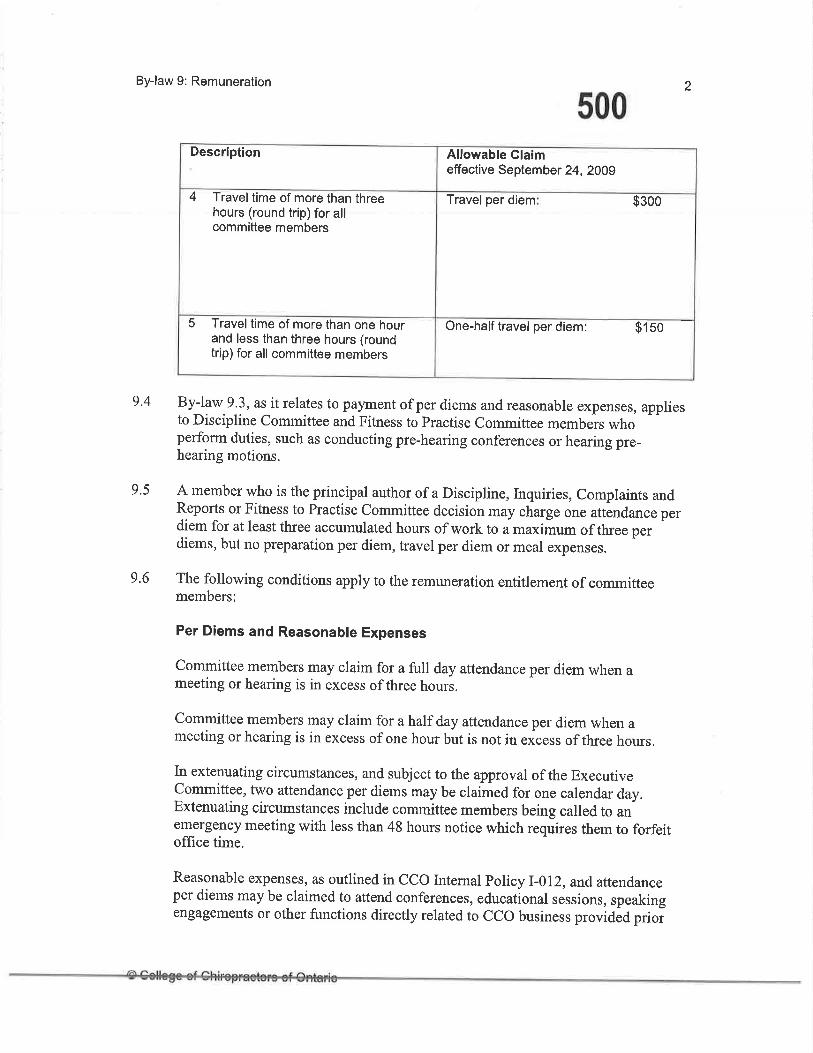
By-law 9: Remuneration
500
9.5
By-law 9.3, as it relates to pa¡rment of per diems and reasonable expenses, appliesto Discipline committee and Fitness to practise committee members whoperform duties, such as conducting pre-hearing conferences or hearing pre-hearing motions.
A member who is the principal author of a Discipline, Inquiries, complaints andReports or Fitness to Practise Committee decision may charge one attãndance perdiem for at least three accumulated hours of work to a maximum of three perdiems, but no preparation per diem, travel per diem or mear expenses.
2
9.4
9.6 The following conditions apply to the remuneration entitlement of committeemembers:
Per Diems and Reasonable Expenses
committee members may claim for a full day attendance per diem when ameeting or hearing is in excess of three hours.
committee members may claim for a half day attendance per diem when ameeting or hearing is in excess of one hour but is not in eir"ss of three hours.
In extenuating circumstances, and subject to the approval of the Executivecommittee, two attendance per diems may be claimed for one calendar day.Extenuating circumstances include committee members being called to anemergency meeting with less than 48 hours notice which requires them to forfeitoffice time.
Reasonable expenses, as outlined in CCo Internal policy l-012, and attendanceper diems may be claimed to attend conferences, educational sessions, speakingengagements or other functions directly related to CCO business provided prioi
Description Allowable Glaimeffective September 24, 2009
4 Travel time of more than threehours (round trip) for allcommittee members
Travel per diem $3oo
5 Travel time of more than one hour-and less than three hours (roundtrip)for all committee members
One-half travel per diem: 9150
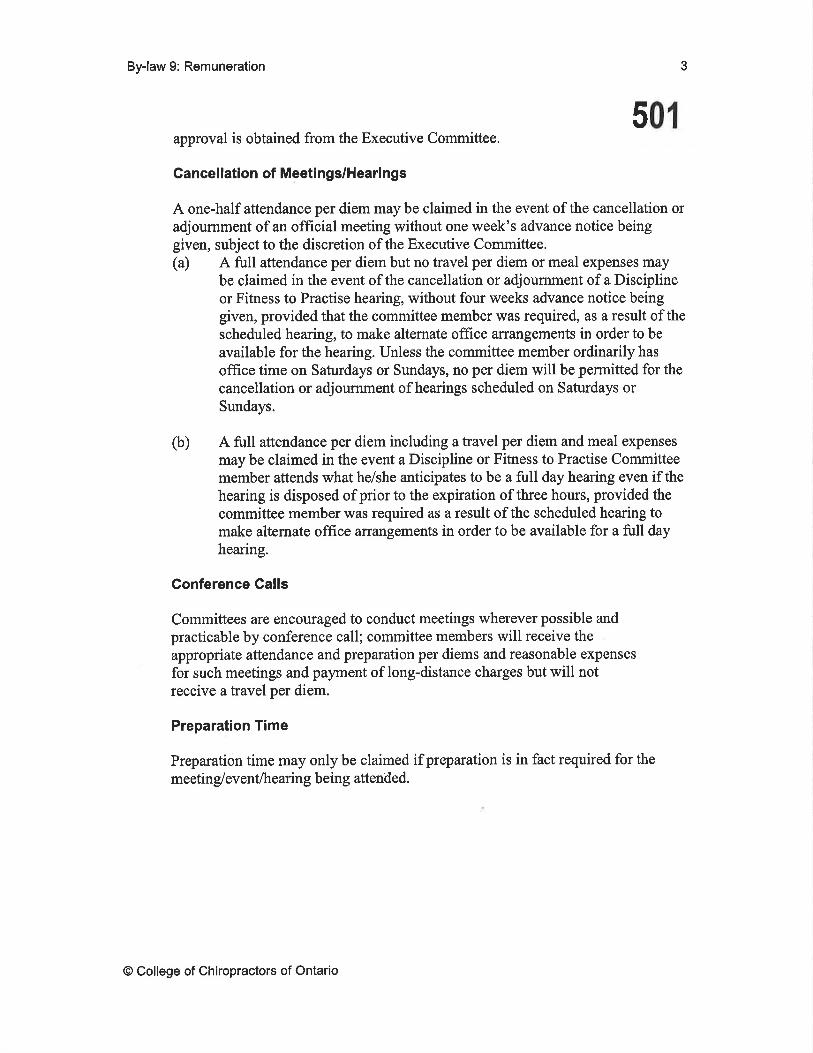
By-law 9: Remuneration 3
501approval is obtained from the Executive Committee.
Gancellation of Meetings/Heari ngs
A one-half attendance per diem may be claimed in the event of the cancellation oradjournment of an official meeting without one week's advance notice beinggiven, subject to the discretion of the Executive Committee.(a) A full attendance per diem but no travel per diem or meal expenses may
be claimed in the event of the cancellation or adjournment of a Disciplineor Fitness to Practise hearing, without four weeks advance notice beinggiven, provided that the committee member was required, as a result of thescheduled hearing, to make altemate office arrangements in order to be
available for the hearing. Unless the committee member ordinarily has
office time on Saturdays or Sundays, no per diem will be permitted for thecancellation or adjournment of hearings scheduled on Saturdays orSundays.
(b) A full attendance per diem including a travel per diem and meal expenses
may be claimed in the event a Discipline or Fitness to Practise Committeemember attends what he/she anticipates to be a full day hearing even if thehearing is disposed of prior to the expiration of three hours, provided thecommittee member was required as a result of the scheduled hearing tomake alternate office arrangements in order to be available for a full dayhearing.
Gonference Calls
Committees are encouraged to conduct meetings wherever possible andpracticable by conference call; committee members will receive theappropriate attendance and preparation per diems and reasonable expenses
for such meetings and payment of long-distance charges but will notreceive a travel per diem.
Preparation Time
Preparation time may only be claimed if preparation is in fact required for the
meeting/event/hearing being attended.
@ College of Chiropractors of Ontario
502BY-LAW I 0 : l¡¡oeMNtFtcATtoNApproved by Council: February 24, 2001Amended: September 24, 2009, September 17, 201 5
10.1 Every member of the Council and staff and their heirs, executors and
administrators, and estate and effects, shall from time to time and at all times be
indemnified and saved harmless out of the funds of CCO from and against:
(a) all costs, charges and expenses whatsoever that he/she sustains or incurs inor about any action, suit or proceeding that is brought, commenced orprosecuted against him/her, for or in respect of any act, deed, omission,
matter or thing whatsoever, made, done or permitted by him/trer, in orabout the execution of the duties of his/her office; and
(b) all other costs, charges and expenses that he/she sustains or incurs in orabout or in relation to the affairs thereof, except such costs, charges orexpenses as are occasioned by his/her own willful neglect or default.
@ College of Chiropractors of Ontario

Bv+Rw ll: GomMFTEE ComposrnoNApproved by Council: February 24, 2001Amended: September 24,2009, November 30,2012, September 17,2015
503
11.1 The Executive Committee, inclusive of the president, vice-president and treasurer,
shall be composed of the following:
(a) Four members of Council who are members of CCO;
(b) Three members of Council who are appointed by the Lieutenant Govemorin Council;
I1 z The president of the Council shall be the chair of the Executive Committee.
11.3 The Registration Committee shall be composed of:
(a) two members of Council who are members of CCO; and
(b) two members of Councils appointed to the Council by the LieutenantGovernor in Council.
ll.4 The Inquiries, Complaints and Reports Committee shall be composed of:
(a) two members of Council who are members of CCO;
(b) one member of Council appointed to Council by the Lieutenant Govemorin Council; and
(c) one member of CCO who is not a member of Council.
11.5 The Discipline Committee shall be composed of:
(a) every member of Council; and
(b) two or more members of CCO who are not members of Council.
11.6 The Fitness to Practise Committee shall be composed of every member ofCouncil.
Il.7 The Quality Assurance Committee shall be composed of:
(a) two members of Council who are member of CCO;
@ College of Chiropractors of Ontario
By-law 11: Committee Composition
504
I 1.8
(b) two members of Council appointed to Council by the Lieutenant Governorin Council; and
(c) one member of CCO who is not a member of Council.
The Patient Relations Committee shall be composed of:
(a) one member of Council who is a members of CCO;
(b) two members of Council appointed to Council by the Lieutenant Governorin Council; and
(c) two members of CCO who are not members of Council.
I 1.9 Council may, by resolution, establish non-statutory committees. For each non-statutory committee, Council shall specify in the resolution the duties andresponsibilities of the committee, its composition and its termination date orevent.
I 1. l0 A committee is still properly constituted if it has vacancies so long as a quorum
2
remalns
11.11 By-laws 8.19 to 8.22 (electronic meetings) applies to committee meetings
@ College of Chiropractors of Ontario
505By-LAW 12= AppotNTMENT oF No¡¡-CouNclL MennaeRsApproved by Council: Februøry 24, 2001Amended: September 24,2009, September 17,2015, February 23,2016, February 28,
2017
l2.l This byJaw applies with respect to the appointment of members who are notmembers of the Council to a committee of CCO.
1,2.2 The Council shall appoint members to committees in the numbers prescribed byByJaw 11.
I2.3 The Council shall make the appointments at the fìrst regular council meeting after
each regular council election or as soon thereafter as is practicable.
12.4 The Council may make appointments from time to time to fill any vacancy
created by the disqualification, death or resignation of a member appointed under
this byJaw.
L2.5 In making the appointments, the Council shall take into account location and type
ofpractice, experience, professional qualifications and skills, and otherqualifications and characteristics of members to complement the attributes ofmembers of the committees who are members of Council.
12.6 The term of office of a committee member who is not a member of the Council is
approximately one year starting on the date the appointment is made, except
where an appointment is made to fill a vacancy in which the person appointed
shall complete the term of the previous appointee.
I2.7 A non-council member may only serve on CCO committees for nine consecutive
years, whether the time is served as a council member or as a non council
member.
I2.8 A non-council member who has served on CCO committee (s) for nine
consecutive years is not eligible to be re-appointed to any CCO committee until at
least three years have passed since the member last served on a CCO Committee.
I2.9 A member is eligible for appointment to a committee if, on the date of the
appointment:
(a) The member has his/her primary practice of chiropractic located inOntario, or if the member is not engaged in the practice of chiropractic,has his/her primary residence located in Ontario;
@ College of Chiropractors of Ontario
By-law 12: Appointment of Non-Council Members
506
(b) the member is not in default of payment of any fees prescribed by byJawor any fine or order for costs to CCO imposed by a CCO committee orcourt of law;
(c) the member is not in default in completing and returning any formrequired by CCO;
(d) the member is not subject of any disciplinary or incapacity proceeding;
(e) a finding of professional misconduct, incompetence or incapacity has notbeen made against the member in the preceding three years;
(Ð the member is not an employee, offîcer or director of any professionalchiropractic association such that a real or apparent conflict ofinterestmay arise, including but not limited to being an employee, officer ordirector of the OCA, CCA, CCPA, AFC, CCEB, CSCE or theAccreditation Standards and Policies Committee or the CCEC of the FCC.
(g) the member is not an officer, director or administrator of any chiropracticeducational institution, including but not limited to CMCC òr uerR;
(h) the member has not been disqualified from the Council or a committee ofthe Council in the previous three years;
(Ð the member is not a member of Council or of a committee of the Collegeof any other health profession; and
6) the member has not been a member of CCO's staff at any time within thepreceding three years.
l2'I0 The Council shall disqualify a member appointed to a committee from sitting onthe committee if the member:
(a) is the subject of any disciplinary or incapacity proceeding;
(b) is found to have committed an actof professional misconduct or is foundto be incompetent by a panel of the Discipline Committee;
(c) is found to be an incapacitated member by a panel of the Fitness toPractice Committee;
2
By-law 12:Appointment of Non-Council Members 3
507(d) fails to attend two consecutive meetings of the committee or of a
subcommittee in which he/she is a member, without reasonable cause inthe opinion of Council;
(e) fails to attend a hearing or review of a panel for which he/she has been
selected; without reasonable cause in the opinion of the Council;
(Ð ceases to either have a primary practice of chiropractic or primaryresidence in the province of Ontario;
(g) becomes an employee, officer or director of any professional chiropracticassociation such that a real or apparent conflict of interest may arise,
including but not limited to being an employee, officer or director of the
OCA, CCA, CCPA, AFC, CCEB, CSCE or the Accreditation Standards
and Policies Committee or the CCEC of the FCC;
(h) becomes an offïcer, director or administrator of any chiropracticeducational institution, including but not limited to CMCC or UQTR;
becomes a member of the Council of CCO or a committee of any otherhealth profession;
û) breaches the conflict of interest provision(s) for members of Council and
committees, in the opinion of the Council after giving notice to the
member of the concern and giving the member an opportunity to respond
to the concem;
(k) fails to discharge properly or honestly any office to which he/she has been
appointed, in the opinion of the Council after giving notice to the member
of the concem and giving the member an opportunity to respond to the
concemr;
(1) becomes in default of payment of any fees prescribed by by-law or any
fine or order for costs imposed by the Discipline Committee;
(m) becomes in default of completing and returning any form required byCCO; or
Iz.lt A non-council committee member shall resign from a committee prior to applying
for any CCO staff position.
12.12 A member who is disqualified under this by-law from sitting on a committee
ceases to be a member of the committee'
(Ð
@ College of Chiropractors of Ontario
508BY-LAW 13: FresApproved by Council: November 28, 2003
Amended: September 24, 2009, September 17, 2015
13.1 The fee for applying for each class of certificate of registration is as follows:
(a) General certificate: $50
(b) Temporary certificate: $50
(c) Retired certificate: NIL
(d) Inactive certificate: $50, unless the applicant already has a general
certificate, in which case the application is NIL
The application fee is non-refundable.
t3.2 In addition to the application fee and the annual fee, an applicant for registration
must pay the following initial certificate fee.
(a) For a general certificate of registration: $325
(b) For a temporary certifi cate to actively practise chiropractic in Ontario ofregistration: $150
(c) For a temporary certificate of registration to participate in a specific event
in Ontario:NIL
(d) For an inactive certificate of registration: $325
(e) For a retired certifïcate of registration: NIL
13.3 An applicant for a general certificate of registration who has completed the
requirements for graduation from a chiropractic education program that is
accredited or the subject of reciprocal recognition by the CCEC within the six
months prior to his/her application is exempted from paying the prescribed annual
fee for the year in which the certificate is issued.
t3.4 A member who holds a general certificate of registration is exempted from paying
the prescribed certificate and annual fees for an inactive certificate of regishation
for the year in which the inactive certificate is issued.
@ College of Ghiropractors of Ontario
By-law 13: Fees
509i 3.s Every member except a member who holds a temporary certificate shall pay an
annual fee.
13.6 The annual fee is $1050 for a member who holds a general certificate ofregistration, $525 for a member who holds a general certificate of registrationwho is renewing his/her license for the first time, $475 for a membeiwho holdsan inactive certificate of registration and $100 for a member who holds a retiredcertifi cate of registration,
13,7 Council may, without, amending these by-laws, adjust the amount of any fees orpenalties in ByJaw 13 to reflect annual changes to the Cost of Living Adjustment(Ontario).
13.8 The annual fee for a member who holds a general certificate of registration maybe paid in two instalments on January I't and June l't of each y.ur1n amounts tobe set by the registrar.
13.9 No later than 60 days before the annual fee or the first instalment of the annual feeis due, the registrar shall notify the member of,
(a) the amount of the annual fee or, if the member is paying by instalment, theamounts of the first and second instalments;
(b) the date on which the annual fee or each of the instalments is due; and
(c) the penalty for late payment.
I 3. 1 0 If a member fails to pay the annual fee or an instalment on or before the day onwhich it is due, the member shall pay a penalty in addition to the annual feå.
I 3. 1 I The penalty is $ I 00 for a member who holds a general certificate of registration,$20 for a member who holds an inactive certificate of registration, andi2O for amember who holds a retired certificate of registration.
13.L2 Where a person requests the registrar to do anything the registrar is required orauthorized to do by statute or by regulation, the perion shaÍ pay the piescribedfee or the fee set by the regishar for doing so.
13.13 If the registrar suspends a member's certificate of registration for failure to pay aprescribed fee, the registrar may lift the suspension on payment of:
(a) the fee the member failed to pay;
2
@ Col lege of Chiropractors of Ontario
By-law 13: Fees 3
510(b) the annual fee for the year in which the suspension is to be lifted if it is
not the same fee as clause (a); and
(c) any applicable penalty.
13.14 A member whose certificate of registration was revoked for failure to pay a feeand who applies to be reinstated is required to pay:
(a) anapplication fee of $50;
(b) the annual fees and any applicable penalties the member failed to pay upto the date of revocation; and
(c) the annual fee for the year in which the member wishes to be reinstated.
But the member shall not be entitled to reinstate a general certificate ofregistration unless the member successful completes a refresher courseapproved by the Registration Committee or otherwise satisfies the RegistrationCommittee that he or she is currently competent to practice.
13.15 The Registration Committee may grant apartial exemption from the fees payable
by a member pursuant to this by-law if the committee is satisfied thatextraordinary circumstances exist which justit/ the exemption.
13.16 The amount payable by a member who applies for reinstatement of a retiredcertificate of registration is $50.
I3.I7 The fee for follow-up letters to a member who has not complied with a requestfrom CCO, such as a request:
(a) to make available the members'professional portfolio to the QualityAssurance Committee,
(b) to participate in the peer and practice assessment component of the
Quality Assurance Program,
(c) to explain an advertisement that does not appear to complywith CCOregulations or guidelines despite previous advice or caution to themember,
is $50 per letter.
13.18 Where CCO presents a continuing education or professional developmentprogram or course, CCO shall determine whether any fee shall be charged for that
@ College of Chiropractors of Ontario

By-law 13: Fees
course and if so, what the fee shall be.
4
511
@ College of Chiropractors of Ontario
512By-LAw 1 4: PnoFESstoNnl ConpoRATtoNSApproved by Council: February 24, 200 1
Amended: September 24, 2009, September 1 7, 201 5
l4.I The fee for the application for a certificate of authorization, including on anyreinstatement of a certificate of authorization, for a professional corporation is
$50.
I4.2 The fee for the issuance of a certifïcate of authorization is $600.
14.3 The fee for the annual renewal of a certificate of authonzation is $200.
I4.4 A professional corporation or a member listed in CCO's records as a shareholderof a professional corporation shall pay an administrative fee of $50 for each
notice sent by the registrar to the corporation or member for failure of thecorporation to renew its certificate of authorization on time. The fee is due within30 days of the notice being sent.
t4.5 The fee for the issuing of a document or certificate respecting a professionalcorporation, other than the first certificate of authorization or one annual renewal
of a certificate of authorization, is $50.
14.6 Every member of CCO shall, for every professional corporation of which the
member is a shareholder, provide in writing the following information on the
application and annual renewal forms for a certificate of authorization, upon the
written request of the registrar within 30 days and upon any change in the
information within 30 days of the change:
(a) the name of the professional corporation as registered with the Ministry ofGovemment Services;
(b) any business names used by the professional corporation;
(c) the name, as set out in the register, and registration number of each
shareholder of the professional corporation;
(d) the name, as set out in the register, of each officer and director of the
professional corporation, and the title or office held by each officer and
director;
(e) the principal practice address, telephone number, facsimile number and e-
mail address of the professional corporation;
@ College of Chiropractors of Ontario
By-law 1 4: Professional Corporations
513
(Ð the address and telephone number of all other locations, other thanresidences of clients, at which the professional services offered by theprofessional corporation are provided; and
(g) a brief description of the professional activities carried out by theprofes sional corporation.
The information specified in By-law 15.6 is designated as public for the purposesofparagraph 4 ofsubsection 23(3) ofthe Code.
14.7
@ College of Chiropractors of Ontario
514BY-LAW 15: TNERAPYAND COUruSELINGApproved by Council: November 30, 2002
Amended: September 24, 2009, September 17, 2015
15.1 CCO shall require a therapist or counselor who is providing therapy or counseling
that is funded through the program required under By-law 85.7 of the Code toprovide a written statement signed by him/trer containing details of his/hertraining and experience and confïrming that the therapy or counseling is beingprovided and that the funds received are being devoted only to that purpose.
15.2 CCO shall require a person who is receiving therapy or counseling that is funded
through the program required under ByJaw 85.7 of the Code to provide a writtenstatement signed by him/her acknowledging that he/she is aware of the details ofthe training and experience of the therapist or counselor and confirming that the
therapy or counseling is being provided and that the funds received are being
devoted only to that purpose.
@ College of Chiropractors of Ontario
Bv-¡-nw I 6: PnoFEsstoNnu LlRelLlrY ltrlsunRruceApproved by Council: September 24, 2009
515
Amended: September 17, 2015
16.I Each member holding a general or temporary certificate of registration mustprovide evidence satisfactory to the registrar of carrying professional liabilityinsurance in the applicable minimum amount per occurence and minimumaggregate amount per year, including coverage for claims after the member ceases
to hold a certificate relating to occurrences while holding a certificate, ormembership in a protective association that provides equivalent protection. Amember who is or will be when registered, an employee of a member, a health
facility or other body that has equivalent professional liability insurance coverage
or membership in a protective association that provides equivalent protection is
deemed to comply with this section.
16.2 The professional liability insurance referred to in By-law 16.1 must have:
(a) a minimum amount of $1,000,000 per occurrence, and
(b) a minimum aggregate amount of $3,000,000 per year.
16.3 When applying for a general or temporary certificate of registration or a renewal
of a general or temporary certificate of registration, an applicant must sign a
declaration that he/she complies with By-laws 16.1 and 16.2.
16.4 A member holding a general or temporary certificate of registration must have
available in his/her office, in written or electronic form, evidence that he/she
complies with ByJaws 1 6. I and 16.2, or may have the provider of the protection
under By-law 16.1 provide regular updates to CCO confïrming compliance withByJaws 16.l and 16.2.
@ College of Chiropractors of Ontario
51 6BY.LAW 17: PUgUC RECISTERApproved by Council: September 24, 2009Amended: September 17, 2015, April 19, 2016
17.l Subject to ByJaw 17.2, amember's name in the register shall be the fullnameindicated on the document used to support the member's initial registration withthe College
17.2 TheRegistrarmay enteranameotherthanthenamereferredtoinBy-law 17.1 inthe register if the Registrar:
(a) has received a written request from the member;
(b) is satisfied that the member has legally changed his or her name; and
(c) is satisfied that the name change is not for any improper purpose.
17.3 Subject to By-law 17.6(q)(i), a member's business address in the register shall be
the address of the location in Ontario where the member is employed or self-employed as a chiropractor. In the event that the member is employed or self-employed as a chiropractor in more than one location in Ontario, the member's
business address shall be then member's primary practice. ln the event that
the member is not employed or self-employed in Ontario as a chiropractor, the
registrar shall enter as the member's business address the location designated
by the member.
17.4 A member's business telephone number shall be the telephone number of the
location in Ontario where the member is employed or self-employed as a
chiropractor. In the event that the member is employed or self-employed as a
chiropractor in more than one location in Ontario, the member's business
telephone number shall be the telephone number of the member's primarypractice. ln the event that the member is not employed or self-employed inOntario as a chiropractor, the register shall not contain a business telephone
number for the member.
17.5 The Registrar shall maintain a register in accordance with section 23 of the Code.
@ College of Chiropractors of Ontario
By-law 17: Public Register
51717.6 In addition to the information set out in subsection23(2) of the Code, the register
shall contain the following publically available information with respect to eachmember:
(a) For every matter that has been referred by the Inquiries, complaints andReports Committee to the Discipline Committee under section 26 of theCode, or where the Registrar has referred an application for reinstatementto the Discipline Committee under section 73 of the Code, and the matterhas not been finally resolved, until the matter has been resolved,
(i) a notation of that fact, including the date of the referral;
(ii) a summary of each specified allegation; and
(iii) any hearing dates, including dates for the continuation of thehearing;
(iv) the notice of hearing ; and
(v) the status of the hearing.
(b) 'where the results of a disciplinary proceeding are contained in the
register, the date on which the panel of the Discipline Committee made thefinding of professional misconduct or incompetence and the date on whichthe panel made the order;
(c) After July 1,2016, a summary of any reprimand given publicly to aMember as part of a panel of the Discipline Committee, unless the resultsof the proceeding before the Discipline committee are not otherwiseavailable to the public under the Code.
(d) 'where a decision of a panel of the Discipline committee has been
published by the college with the member's or former member's nameincluded,
(Ð a notation ofthat fact; and
(ii) identification of, a link to, or a copy of the specifìc publicationcontaining that decision.
(e) where the member's certificate of registration is subject to an interimorder, a notation of that fact, the nature of the order and the date that theorder took effect;
2
By-law l7: Public Register
518(Ð Where the member's certifïcate of registration is subject to a suspension
for failure to pay a fee, the reason for the suspension and the date of the
suspension in addition to the fact of that suspension;
(g) Where, during or as a result of a proceeding under section 25 of the Code
a member has resigned, a notation of that fact.
(h) Where, on or after July l, 2016 , for a complaint or for a matter in whichan investigator is appointed under section 75(1Xa) or 75(1)(b) of the Code,
a panel of the Inquiries, Complaints and Reports Committee requires a
member to appear before a panel of the Committee to be cautioned,
(Ð a notation of that fact;
(ii) a summary of the caution;
(iii) the date of the panel's decision; and
(iv) if applicable, a notation that the panel's decision is subject toreview and is not yet final, which notation shall be removed once
the review and any reconsideration by the Committee is finallydisposed of.
(Ð The information required under ByJaw 17.6(h) shall be removed from the
register 12 months after the Registrar is satisfied that the member has
appeared before a panel of the lnquiries, Complaints and Reports
Committee and received the caution.
'Where, on or after July 1, 2016 , for a complaint or for a matter in whichan investigator is appointed under 75(1Xa) or 75(1)(b) of the Code, a
panel of the Inquiries, Complaints and Reports Committee takes other
action requiring a member to complete a specified continuing education orremediation program,
(i) a notation of that fact,
(iÐ a summary of the specified continuing education or remediationprogram,
(iiÐ
(iv)
the date of the panel's decision,
the date the specified continuing education or remediation program
is successfi.rlly completed, and
3
(')
By-law 17: Public Register
519(v) if applicable, a notation that the panel's decision is subject to
review and therefore is not yet final, which notation shall beremoved once the review and any reconsideration by theCommittee is finally disposed of.
(k) The information required under ByJaw 17.6(ù shall be removed from theregister 12 months after the Registrar is satisfied that the Member hassuccessfully completed the specified continuing education or remediationprogram.
(l) Where, on or after July 1, 2016, for a complaint or for amattq in whichan investigator is appointed under 75(1Xa) or 75(l)(b) of the Code, apanel of the Inquiries, complaints and Reports committee obtains anundertaking from the Member,
4
(Ð
(iÐ
(iii)
(iv)
a notation of that fact,
a summary of the terms of the undertaking,
the date of the panel's decision, and
if applicable, a notation that the panel's decision is subject toreview and therefore is not yet final, which notation shall beremoved once the review and any reconsideration by theCommittee is finally disposed of.
(m) The information required under ByJaw 17.6(l) shall be removed from theregister 12 months after the Registrar is satisfied that the Member hassuccessfully completed the all of the terms of the undertaking.
(n) Notwithstanding By-laws 17.6(h), O and (l), where, after areview, theInquiries, Complaints and Reports Committee has been required to removeor vary the appearance for a caution, specified continuing education orremediation program or undertaking, the notation may be removed oncethe Committee makes its new decision. Where the original requirement toappear for a caution or to complete a specified continuing education orremediation program has been varied, the Registrar may enter a summaryof the process leading up to and the results of the variation.
(o) A decision of any findings of guilt, of which the college is aware, madeby a court after July 1,2016, against a Member in respect of a criminaloffence.
By-law 17: Public Register 5
520(p) 'Where
the College is aware that amember is currently registered orlicensed to practise a profession inside of Ontario, a notation of that fact.
(Ð the following practice information related to a member:
(Ð The business address, business telephone number and businessemail of up to three practice locations;
(iÐ The member's gender;
(iÐ the name of the chiropractic education program graduated by themember and year of graduation from that program;
(iii) the year of initial registration with CCO; and
(iv) up to three languages in which the member offers professionalservices, as identified by the member.
17.7 If requested, the member shall immediately provide the College with thefollowing information, in the form requested by the College:
(a) information required to be maintained in the register in accordance withsubsection 23(2) oîthe Code andBy-law 17.6;
(b) the address and telephone number of the member's primary residence inOntario and, if the member does not reside in Ontario, the address and
telephone number of the member's primary residence;
(c) The member's email addresses;
(d) Proof of professional liability insurance;
(e) The member's areas of practice and categories of clients seen;
(Ð Information regarding the member's emplo¡rment including:
(Ð the member's title and position,
(ii) a description of the member's role, duties, and responsibilities, and
(iiÐ the member's employment category and status.
(g) any nicknames or abbreviations that the member uses in any place of
By-law 17: Public Register
521practice;
(h) information about the member's registration with any other body thatgoverns a profession, whether inside or outside of Ontario, including thename of the governing body, the member's registration or license numberand the date the member first became registered;
(i) information about any finding of professional misconduct or incompetenceor similar finding that has been made against he member by a body thatgoverns a profession, inside or outside of ontario, where the fînding hasnot been reversed on appeal, including;
(i) the finding,
(ii) the name of the governing body that made the finding,
(iiÐ a brief summary of the facts on which the finding was based,
(iv) the penalty and any other orders made relative to the finding,
(v) the date the finding was made, and
(vi) information regarding any appeals of the finding.
0) information about any finding of incapacity or similar finding that hasbeen made against the memberby abody that governs a profession, insideor outside of ontario, where that finding has not been reversed on appeal,including:
(Ð the finding
(ii) the name of the governing body that made the finding,
(iiÐ the date the finding was made,
(iv) a summary of any order made, and
(v) information regarding any appeals of the finding.
(k) information about the member's participation in the euality AssuranceProgram,
0) information for the purpose of compiling statistical data,
6
By-law 17: Public Register 7
52217.8 The member shall notify the College, in, writing, of any changes to the following
information within 30 days of the effective date of the change:
(a) the member's name,
(b) the address and telephone number of the member's primary residence inOntario and, if the member does not reside in Ontario, the address and
telephone number of the member's primary residence,
(c) the member's business address or business telephone number.
17.9 All of the information in the register is designated, under subsection 23(6) of the
Code, as information that may be withheld from the public if the Registrar has
reasonable grounds to believe that disclosure may jeopardize the safety of an
individual.
5111t2017 Regulated Health Professions Act, 1991, S.O. 1991, c. 18
Executive Committee's exercise of Council's powers
12 (1) Between the meetings of the Council, the Executive Committee has all the
powers of the Council with respect to any matter that, in the Committee's opinion,
requires immediate attention, other than the power to make, amend or revoke a
regulat¡on or by-law.
523|TEM 4.1.28Report to Council
(2)lf the Executive Committee exercises a power of the Council under subsection (1),
it shall report on its actions to the Council at the Council's next meeting. 1991, c. 18,
Sched. 2, s. 12.
https:/ /vww.ontario.callaws/statute/91 r 18 1t1
5t11t2017 Bill 97, Protect¡ng Patients Act, 2017 | Legislat¡ve Assemþly 01 Ontano I Hllls & LawmaKlng I Uurrem h'arllament
12. (11 Subsection 23 (21of Schedule 2 to the Act is repealed and the following substituted:
Contents of register
(2) The register shall contain the following' ITEM 4'1 '29 5241. Each member's name, business address and business telephone number, and, if applicable, the name of
every health profession corporation of which the member is a shareholder.
2. The name of each former member of the College, and where a former member is deceased, the date upon
which the former member died, if known to the Registrar.
3. The name, business address and business telephone number of every health profession corporation.
4. The names of the shareholders of each health profession corporation who are members of the College.
5. Each member's class of registration and specialist status.
6. The terms, conditions and limitations that are in effect on each certificate of registration.
7. A notation of every caution that a member has received from a panel of the lnquiries, Complaints and Reports
Committee under paragraph 3 of subsection 26 (1), and any specified continuing education or remedial progE¡ms
required by a panel of the lnquiries, Complaints and Reports Committee using its powers under paragraph 4 of
subsection 26 (1).
g. A notation of every matter that has been refened by the lnquiries, Complaints and Reports Committee to the
Disciptine Committee under section 26 and that has not been finally resolved, including the date of the refenal and
the status of the hearing before a panel of the Discipline Committee, until the matter has been resolved.
g. A copy of the notice of specified allegations against a member for every matter that has been refened by the
lnquiries, Complaints and Reports Committee to the Discipline Committee and has not been finally resolved'
i0. The result, including a synopsis of the decision, of every disciplinary and incapacity proceeding'
11. A notation and synopsis of any acknowledgements or undertakings in relation to professional misconduct and
incompetence that a member has entered into with the College.
12. A notation of every finding of professional negligence or malpractice, which may or may not relate to the
member's suitability to practise, made against the membeç unless the finding is reversed on appeal.
13. A notation of every revocation or suspension of a certificate of registration.
14. A notation of every revocation or suspension of a certificate of authorization.
1b. lnformation that a panel of the Registration Committee, Discipline Committee or Fitness to Practise
Committee specifies shall be included'
16. Where findings of the Discipline Committee are appealed, a notation that they are under appeal, until the
appeal is finally disPosed of.
17. Where, during or as a result of a proceeding under section 25, a member has resigned and agreed never to
practise again in ontario, a notation of the resignation and agreement.
1g. Where the College has an inspection program established under clause 95 (1) (h) or (h.1), the outcomes of
inspections conducted by the college.
19. lnformation that is required to be kept in the register in accordance with regulations made pursuant to clause
43 (1) (t) of the Regulated Health Professions Act, 1991'
20. lnformation that is required to be kept in the register in accordance with the by-laws.
(Zl Subsection 23 (41of Schedule 2to the Act is amended by striking out "paragraph 11" and substituting
"paragraph 15".
(3) Subsection 23 (5) of Schedule 2 to the Act is repealed and the following substituted:
Access to infomation by the Public
(S) All of the information required by paragraphs 1 to 19 of subsection (2) and all information designated as public in the
by-laws shall, subject to subsections (6), (7), (8), (9) and (11), be made available to an individual during normal business
hþ:/lwww.ontla.on.calweb/bills/bills_detail.do?locale=en&BilllD=4477&delailPage=bills-detail the-bill 1t2

-';;;, and sha,, * *;;:;ä:*;';ffi; ffi;;;,;:;" ff ;;ä*ï.i:î";äî;;ä, received the
information and in a manner that is accessible to the public or in any other manner and form specified by the Minister.(4) Subsection 23 (11) of Schedule 2 to the Act is amended by striking out "paragraph 7" in the portion before
clause (a) and substituting ',paragraph 10,'.
(5) Clause 23 (111(d) of Schedule 2 to the Act is amended by striking out "clause (a) or (b)" and substituting"clause (a), (b) or (c)."
(6) Section 23 of Schedule 2 to the Act is amended by adding the following subsection:Correction of informatíon
(13.1) The Registrar shall conect any information contained in the register where a member demonstrates, to thesatisfaction of the Registraç that the information contained in the register is incomplete or inaccurate and where the memberprovides the Registrar with the information that is necessary to enable the Registrar to conect the incomplete or inaccurateinformation.
(7) Subsection 23 (la) of Schedule 2 to the Act is repealed and the following substituted:Meaning of results of proceeding
(14) For the purpose of this section and section 56,
"result", when used in reference to a disciplinary or incapacity proceeding, means the panel's finding, particulars of thegrounds for the finding, and the order made, including any reprimand, and where the panel has made no finding, includes thefailure to make a finding.
13. Subsections 25 (2) and (3) of Schedule 2 to the Act are repealed and the following substituted:
525
http://www.ontla.on.ca/web/bills/bills detail.do?locale=en&BilllD=44V&dF'failPage=bills_detail the_bill 2t2
|TEM 4.1.30tllnlstry of llealthand Long-Term Cam
Office of the Mlnister
10h Floor, Hepbum Block80 Grosvenor StreetToronto ON M7A 2C4Tel. 418 3274300Fax 4't6 32S.1571un¡w. ontarlo. celhealth
Mlnl¡tå¡s de la Santéet des Solns de longue durðe
Bureau du ministe
Êdlfrce Hepbum, 10' étage80, rue GmsvenorToronto ON M7A 2C4Tér. 416 327-4300Téléô. 416 3211571un¡u¡¡.ontario.calsanle
!D 526
l,lAV r I 2017
Mr. ShakilAkhter20 GlenheatherTenaceScarborough ON M1B sHg
Dear Mr. Akhter:
Congratulations on your r€appointment to the Council of the College of Chiropractors ofOntario. I am looking forward to your continued serv¡ce beginning May 7,2017 untilMay 6, 2018.
I am very pleased that you have again taken on this important respons¡bility to serve thepeople of Ontario. We expect that you will continue to be committed to the principles
and values of public service and that you w¡ll perform your duty with integrity.
I have enclosed a copy of the Order in Council which was approved on May 1 0,2A17.
Again, please accept my congr:¡tulations
Yours sincerely,
Dr. Eric HoskinsMinister
Enclosure
c: RegistrarRaymond Sung Joon Cho, MPP
527Ontarlo
Executive Council of OntarioOrder in Council
On the recommendation of the undersigned, theLieutenant Governor of Ontario, by and with theadvice and concurrence of the Executive Councilof Ontario, orders that:
Conseil exécutif de I'OntarioDécret
Sur la recommandation de la personnesoussignée, la lieutenante-gouverneure deI'Ontario, sur I'avis et avec le consentement duConseil exécutif de I'Ontario, décrète ce quisuit :
PURSUANT TO clause 6(1Xb) of the Chiropractic Act' 1991,
Shakil Akhter of Scarborough
be reappointed as a part-time member of the Councll of the College of Chiropractors of Ontario for a
period of one year, effective May 7, 2017 to and including May 6, 2018.
EN VERTU DE I'alinéa 6 (1) b) de la Loide 1991 sur les chiropratícíens,
Shakil Akhter de Scarborough
1,003120 17I'
1O.C./Décret:
est reconduit au poste de membre à temps partiel du Conseil de l'Ordre des chiropraticiens de
I'Ontario pour une durée fixe d'un an à compter du 7 mai z}l7jusqu'au 6 maí 2O1g inclusivement.
528
Recommended: Minister of Health and Long-Term CareRecommandé par: le ministre de la santé et des soins de longue durée
Concurred: Chair of CabinetAppuyé par : le président/la présidente du conseildes ministres
Approved and Ordered:Approuvé et décrété le :
l,lAY 1 0 2017
Lieutenant GovernorLa lieutenante.gouverneure
2O.C./Décret:
Ministry of Healthand Long-Term Gare
Health Workforce Planning andRegulatory Affalrs Divlsion
|TEM 4.1.31Ministère de la Santéet des Soins de longue durée
Division de la planification et de la réglementationrelatives aux ressources humalnes dans ledomalne de la santé
529
Ontario12'h Floor56 Wellesley Street WestToronto ON MsS 2S3
Tel.: 416 212-6115Fax 416 327-0167
12u élage56, rue Wellesley OuestToronto ON M5S 2S3
Té1.: 416 212-6115Téléc.: 416 327-A167
HLTC2968lT-2017-110l.lAY 1 g ?017
Dear Regístrars:
As you are aware, the ministry has engaged Deanna Williams to undertake workrelating to the recommendations of the Sexual Abuse Task Force. I am writing to let you
know that Ms. Williams has officially begun her work with the ministry and may be
reaching out to you in the coming weeks and months to seek your opinions andperspectives as regulators.
Ms. Williams will be providing advice and expertise to the ministry on four key areas:
1. Best practices in Ontario and other jurisdictions in the intake of complaints,investigation and discipline of misconduct matters, including sexual abuse.
2. Best practices in Ontario and other jurisdictions with regards to patient supportsand patient relations provided at the college level.
3. Best practices in Ontario and other jurisdictions in college governance andcollege committee membershiP.
4. Review and analysis of the Task Force recommendations to establishindependent bodies responsible for the investigation and adjudication of sexualabuse matters.
While thematically similar to the proposed amendments to the Regulated HealthProfessions Act, l99l (RHPA) included in Bill 87, the Protecting Patients Aú, 2A16,1
want to stress that Ms. Williams'work is entirely independent from that Bill. The ministryanticipates that most of the advice resulting from her work would be implemented viapolicy and programmatic changes as well as through regulation-making authoritíes. Theministry is not contemplating, at this time, further amendments to the RHPA beyond theprovisions currently being debated as part of the legislative process around Bill 87.
...2
-2-530
I trust that you will provide Ms. Williams with the same supporl you have demonstratedto the ministry to date. I look forward to continued partnership and collaboration as wemove fonruard.
Sincerely,
ise ColeAssistant Deputy MinisterHealth Workforce Planning and Regulatory Affairs Division
Enclosure
c: Presidents, Health Regulatory CollegesDr. Robert Bell, Deputy Minister, Ministry of Health and Long-Term careDerrick Araneda, chief of staff, office of the Hon. Dr. Eric HoskinsAllison Henry, Director, Health System Labour Relations and Regulatory PolicyBranch
|TEM 4.1.32Rose Bustria
531From:Sent:To:Subject:
Jo-Ann WillsonFriday, June 09, 2017 2:49 PMRose BustriaFW: Clarification - Applied BehaviouralAnalysts (ABA)
lmportance High
Council
Jo.Ann Willson, B.Sc., M.S.W., LL.BReg¡strar & General Counsel
College of Chlropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext.111Fax: (416) 925-9610E-mail: ipwillson(ôcco.on.caWeb Site: www.cco.on.ca
CONFIDENTIALITY WARNIThis e-mail including any attachments may contain conf¡dential information and is intended only for the person(s) named above. Any otherdistribution, copying or disclosure is strictly prohibited. lf you have received this e-mail ¡n error, please notify me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: Cole, Denise (MOH LTC) [mailto:[email protected]]Sent: Friday, June 09, 2Ot7 2:36 PM
To: Allan Mak ([email protected]) <[email protected]>; Andrew Parr<[email protected]>; Anne Coghlan <[email protected]>; Basil Ziv
<[email protected]>; Brenda Kritzer <[email protected]>; Brian O'Riordan<[email protected]>; Corinne Flitton <[email protected]>; Dr. Rick Morris([email protected]) <rmorr¡[email protected]>; Elinor Larney <[email protected]>; Fazal Khan
<[email protected]>; Felecia Smith <[email protected]>; Glenn Pettifer (gpettifer@denturists-
cdo.com)<[email protected]>; lrwin Fefergrad <[email protected]>; Jo-Ann Willson<[email protected]>; Judy Rigby <[email protected]>; Kathy Wilkie ([email protected])
<[email protected]>; Kelly Dobbin <[email protected]>; Kevin Taylor <[email protected]>; Linda
Gough ([email protected]) <[email protected]>; Lisa Taylor <[email protected]>; Mark Pioro
([email protected]) <[email protected]>; Melisse Willems <[email protected]>;
Nancy Lum-Wilson ([email protected])<[email protected]>; Paula Garshowitz<[email protected]>; Rocco Gerace <[email protected]>; Shenda Tanchak
<[email protected]>; Andrew Lewarne <[email protected]>; Andrew Padmos
<[email protected]>; OHA, lnfo (MCl) <[email protected]>; Beth Witney <[email protected]>;
Blanca McArthur <[email protected]>; Bob Bond <[email protected]>; Carol Ford
<[email protected]>; Cedric K.T. Cheung <[email protected]>; Christie Brenchley
<[email protected]>; Dennis Darby <[email protected]>; Dianne Martin<[email protected]>; Dorianne Sauve <[email protected]>; Doris Grinspun <[email protected]>; Dr.
Bob Haig <[email protected]>; Dr. Francine Lemire <[email protected]>; Dr. James Hill
<[email protected]>; Frank Bevilacqua <[email protected]>; Franklin Parada <[email protected]>; Greg
Toffner <[email protected]>; OASW, JMD (MCl)<[email protected]>; John Kallitsis
<[email protected]>; John Wellner <[email protected]>; Kelly Stadelbauer<[email protected]>; Kim Stilwell<[email protected]>; Linda Haslam-Stroud
<[email protected]>; Lorne Kashin <[email protected]>; M. Janet Kasperski
<[email protected]>; Margaret Carter <[email protected]>; Marsha Sharp
1
<[email protected]>; Mary Cook <[email protected]>; Michael Decaire <[email protected]>;Stephen Laramee <[email protected]>; Stuart Moulton <[email protected]>; Sushila Lalsingh<info@ nupath.org>; Theresa Agnew <[email protected]>; Tom Magayrody <[email protected]>cc: Henry, Allison (MoHLTc) <[email protected]>; cheng, stephen (MoHLTc)
532<[email protected]>; Holm, Bruna E. (MOHtTC)<[email protected]>; Nolasque, Letitia(MOHLTC) <[email protected]>; Santolin, Anna (MOHLTC) <[email protected]>; deBraga nca, Lo rra ine ( MO H LTC) < Lorra ine.de Braga nca @onta rio.ca>Subject: Clarification - Applied Behavioural Analysts (ABA)lmportance: High
Dear Registrars, Executive Directors and Presidents,
A short note to prov¡de clarification on the recent media report that applied behaviouralanalysts (ABA) will be regulated health professionals in Ontario. The ministry is workingwith our colleagues in the Ministry of Children and Youth Services to ensure thatOntarians receive safe, quality ABA services and that individuals providing thoseservices do so within an appropriate accountability framework. Please notê that nodecisions have been made about what that framework will be and we recognize that anyscheme should be proportionate to the level of risk of harm to the public.
To assist with future decisíon-making, the ministry is working on a referral to HpRAC forthe Minister's consideration. The referral is under development and, as usual, allcolleges and associations will receive a copy of the referral after it is sent to HpRAC.
Should you have any questions, let me or Allison Henry know.
Regards,
Daa¿¿¿
Denise ColeAssrsfanf Deputy Minister, Health Workforce Ptanning & Regulatory Affairs DivisionMinistry of Health and Long-Term Care56 Wellesley Sfreef West, 12th FloorToronto ON M5S 2S3T: 416-212-7688f c; 647-282-86241F: 416-327-1B7BIE: [email protected] Support Coordinator: Lorraine de Braganca ¿I O-ZI i-PLEASE NOTE: The information contained ìn this e-mait message and any attachments is prìviteged and confidential, andis ¡ntended only for the use of the recipìent(s) named above. tf you have-receîved this e-mait in ãrror, ptease notify meimmediately and delete this e-mail and any attachments withou{copying, distrìbuting or aìsclosÍig theír comments.
2
Rose Bustria
From:Sent:To:Subject:
Jo-Ann WillsonTuesday, May 30, 2017 10:33 AMRose Bustria
533FW: New Policy Contact Person at the Health System Labour Relations andRegulatory Policy Branch, Health Workforce Planning and Regulatory AffairsDivision, Ministry of Health and Long-Term Care
Council.
Jo-Ann P. Wíllson, B.Sc., M.S.W., LL.B.
Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING :
This e-mail íncluding any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notiff me immediately by reply e-mail and delete all copies including
any attachments without reading it or making a copy. Thank you.
From: Jo-Ann WillsonSent: Tuesday, May 30, 20L7 10:32 AM
To: Chance, Melissa (MOHLTC)
Cc: Joel FriedmanSubject: RE: New Policy Contact Person at the Health System Labour Relations and Regulatory Policy
Branch, Health Workforce Planning and Regulatory Affairs Division, Ministry of Health and Long-Term
Care
Thank you very much. I'm away at the moment but we look forward to chatting wíth you
Jo-Ann P. Willson, B.Sc., M.S.W., LL.B
Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected] Site: www.cco.on.ca
CONFIDENTALITY WARNING :
This e-mail including any attachments may contain confidential ínformation and ís intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copies including
any attachments without reading it or making a copy. Thank you.
1
5:ä'r'J::å:i i,:'f:iji."#'L%ffie$ssa'cnance@ontario'car 534To: Jo-Ann WillsonSubject: New Policy Contact Person at the Health System Labour Relations and Regulatory policyBranch, Health Workforce Planning and Regulatory Affairs Division, Ministry of Health and iong-TermCare
Good morning Ms. Wilson,
I am the new policy analyst (acting) contact person for the College of Chiropractors of Ontario. I
will be with the Regulatory Policy Unit until November 30,z}tl.
Please feelfree to contact me for assistance. I look forward to working with you and your team!
Thank you.
Melissa
Melissa ChanceA/Policy AnalystHealth System Labour Relations and Regulatory policy BranchHealth Workforce Planning and Regulatory Affairs Division12th Flr. 56 Wellesley Street WestToronto ON M5S 2S3
Tel.: (416) 327-2s60Fax: (416) 327-0t67PlgnSe NOTE: The information contained in this e-ma¡l message and any attachments ¡s pr¡vileged and conf¡dential, and isintended only for the use of the recipient(s) named above. lf you have recéived th¡s e-mail ¡n erroi please notify me immediatelyand delete this e'mail and any attachments without copying, distributing or disclosing their contenis.
2
Rose Bustria ITEM 4.1.33 535From:Sent:lo:Subject
Jo-Ann WillsonMonday, April 17, 2017 7:27 PMRose BustriaFW: Member Survey Results
Exec and Council.
Jo-Ann P. Willson, B,Sc., M.S.W., LL.B.Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected] Site: wr /w.cco.on.ca
CONFIDENTALITY WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you havereceived this e-mail in error, please notify me ímmediately by reply e-mail and delete all copies includingany attachments without reading it or making a copy. Thank you.
Begin forwarded message:
From: Ontario Chiropractic Association <[email protected]>Date: April l7 ,2017 at 4:01:02 PM EDTTo: <[email protected]>
Subject: Member Survey ResultsReply-To: Ontario Chiropractic Association <[email protected]
We're Here For You.
View this email in your browser
OntarioChiropracticAssociation
1
--tbbb-O
536,
We would like to thank the hundreds of members that took the time to fill out our member
survey earlier this year. lt was a vital input to our upcoming strategic plan that will
determine our priorities and efforts for the next few years.
Tomorrow, we begin a series of regional member consultations that will take us to
Burlinqton, Toronto, sarnia, North Bay and ottawa. we hope to see many of you there!
Here are some survey highlights:
Trust and Satisfaction
The survey showed that over 600/o of survey respondents are satisfied with the OCA.
Over 70Vo trust the association and70% would recommend the OCA to other
chiropractors. We are grateful that so many of you see the value in our efforts to serve
you and we are focusing on increasing these numbers for our next survey!
Vision & Mission
360% û70% a70%
YhfrlrHÍI
The current Vision, "to be recognized as spinal
health care experts in the health care system",
resonated with over 75% of respondents. The
2
Member Survey Results
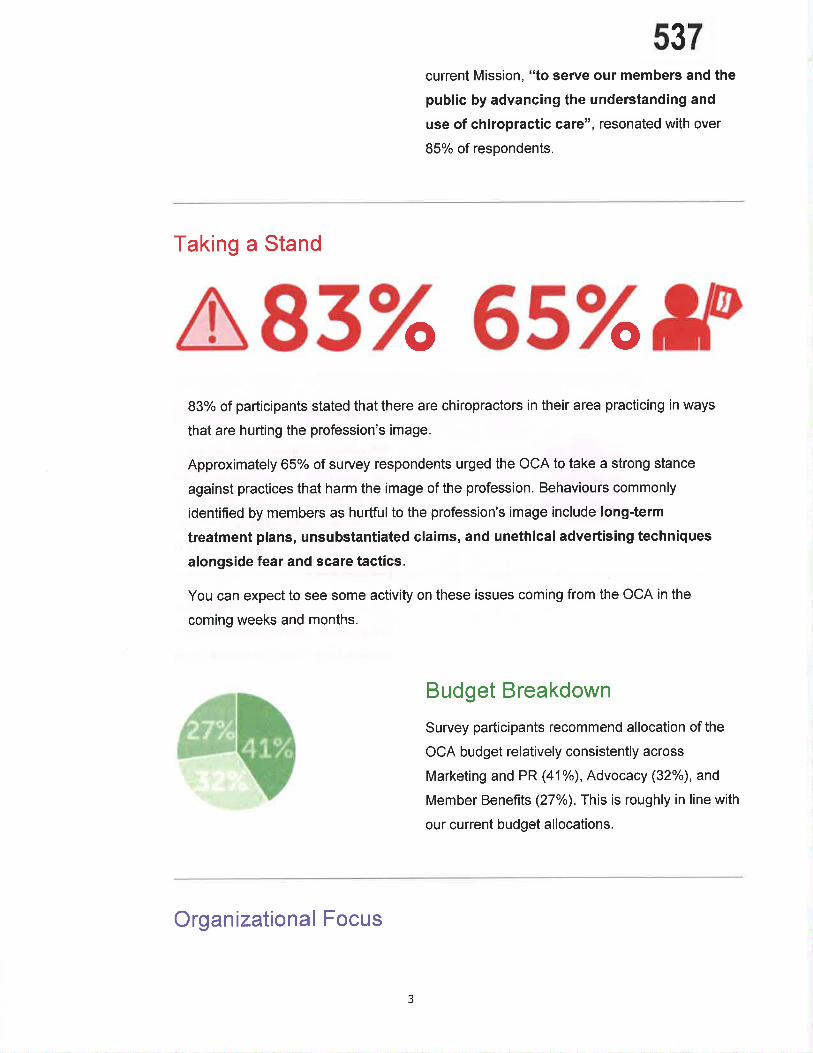
537current Mission, "to serve our members and the
public by advancing the understanding and
use of chiropractic care", resonated with over
85% of respondents.
Taking a Stand
a83 6s IPo o83% of participants stated that there are chiropractors in their area practicing in ways
that are hurting the profession's image.
Approximately 65% of survey respondents urged the OCA to take a strong stance
against practices that harm the image of the profession. Behaviours commonly
identified by members as hurtfulto the profession's image include long-term
treatment plans, unsubstantiated claims, and unethical advertising techniques
alongside fear and scare tactics.
You can expect to see some activity on these issues coming from the OCA in the
coming weeks and months.
Budget Breakdown
Survey participants recommend allocation of the
OCA budget relatively consistently across
Marketing and PR (41%), Advocacy (32%o), and
Member Benefits (27%). This is roughly in line with
our current budget allocations.
Organizational Focus
3
538
Members rated advocacy to ensure coverage within beneflts programs as most
important for the OCA to pursue. We will outline a dedicated strategy to address this
complex issue in the coming months.
The most important member programs and services to members were our webinars
and webinars on demand, foll'owed by business support resources and ourweekly informational updates.
Challenges to the Profession
Attracting patients emerged as a major theme for
our respondents, followed by challenges marketing
and advertising the services you provide, access to
insurance and benefits, and finally being
acknowledged and referred to by medical
professionals.
We are currently finalizing our strategic plan and
the priorities that we will focus on as an
organization. You can expect to see a focus on
addressing harmful business practices, a strategy
to engage with EHC providers and continued
efforts to enhance our webinar offerings alongside
tangible resources to help you in your practice.
We're here for you. Call us:
Local : 41 6-860-0070 | Toll-free: 1 -877 -327 -2273
Update your OCA membership preferences or unsubscribe from this list
Our mailing address is:
Ontario Chiropractic Association
4
Rose Bustria 539From:Sent:To:Subject:
Jo-Ann WillsonTuesday, April25, 2017 5:17 PMRose BustriaFW: Weekly News: Falls Prevention Tools, NationalVolunteer Week,Webinars
Exec and Council.
Jo-Ann P. Willson, B.Sc., M.S.W., LL.B,
Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : jpwillson@cco,on.caWeb Site: www.cco,on.ca
CONFIDENTALITY WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you havereceived this e-mail in error, please notify me immediately by reply e-mail and delete all copies includingany attachments without reading it or making a copy. Thank you.
From: Ontario Chiropractic Association [[email protected],net] on behalf ofOntario Ch i ropractic Association [OCA@ch iropractic.on.ca]Sent: Tuesday, April 25, 20L7 4:0I PM
To: Jo-Ann WillsonSubject: Weekly News: Falls Prevention Tools, NationalVolunteer Week, Webinars
We're Here For You.
View this email in your browser
OntarioChiropract¡cAssociation
-Otr-bb-
-
1
540DON'T LET A
FALL GETYoUDOWN.
A senior who's suffered an injury from a fall knows the dramatic impact it can have-notjust physically, but psychologically. Falls can swiftly sweep away the independence and
confidence that allow a senior to fully enjoy their life.
Unfortunately 1 in every 3 Canadians over the age of 65 will experience a fall, with hip,
wrist and pelvic fractures being the most common injuries. To help your patients reduce
their risk of fall-related injuries, we've collected and packaged some simple tips and
techniques for you to share.
Our Falls Prevention Presentation Toolkit, found exclusively in our Marketinq & Outreach
Library online, includes:
Falls Prevention Presentation (PowerPoint)
Patients Handouts:
o Don't Let a Fall Get You Down (Brochure)
o Seated Stretches for Older Adults (One Pager)
o lmprove Your Strength and Balance (Double-Sided)
o Prevent Falls in the Home (Double-Sided)
o Reduce Your Health Risks (Double-Sided)
o Watch Your Step (Double-Sided)
As an OCA member, you can download and print all of these materials for free or orderprofessionally printed copies delivered straight to your clinic.
2
Presentation & Patient Tools: Falls Prevention
Explore our Falls Prevention Presentation Toolkit
Celebrating National
Volunteer Week
pJf I
f!. -rr',1
\
541We are celebrating National Volunteer Week!
We'd like to thank all of our Communitv Enqaoement & Leadership Program Volunteers
who have engaged with the public, health care providers and community partners to help
increase the understanding and use of chiropractic care. Your contribution has influenced
interprofessional collaboration and chiropractic involvement in falls prevention programs,
ergonomics in the workplace, pain management strategies and more.
OCA volunteers have also engaged with government officials to advocate for provincial
support of chiropractic driven initiatives and programs such as inclusion of chiropractors in
provincially funded health care programs like the Primary Care Low Back Pain pilot. Our
volunteers connected with MPPs at Advocacy Day at Queen's Park last fall, and hosted
several clinic visits where MPPs were able to see chiropractic in action.
lf you've done community outreach with the OCA or another group this year, share your
pictures and tell us about your volunteer experiences on social media using the hashtag
#ChirosCare by Friday to be entered into a draw to win a $100 VISA gift card!
OCA members can save 30% on single-game tickets by using our discount code for this
week's Toronto Marlies Playoff Games on:
. Wednesday, April26
. Friday, April 28
3
Learn More About Volunteering With Us
Member Discount
30% Off Marlies
Playoffs Tickets
a Saturday, April 29 (if necessary)
542Get the Discount Code Now
UPCOM¡NGWEBINARS
Money Talk for NewGhiropractors(Rebroadcast)
Wed. Apr. 26,12-1PM
Saeed Ally (The Heritage Group,
Manulife Securities)
Welcome to life as a
chiropractor! ln your first five
years in practice, you may be
paying off school debt, looking
for employment, deciding where
to live, or thinking about starting
a family. This webinar will help
you navigate early career
decisions that can strengthen
your financial future.
Clinic GhangeManagement
Wed. May 3,12-1 PM
Lynsey Turchet (MD+A Health
Solutions)
Whether it's implementing new
products, expanding your clinic
team or introducing new
services, strategic
implementation of change is
important to maintaining a
successful practice. This
webinar will introduce some of
the main concepts of change
management and how you can
apply them to your clinic.
Upcominq CE & Events lWebinars On Demand
Brought to you by our CE Sponsor: S |NNæARE
4
Register Now Register Now

We're here for you. Call us:
Local: 41 6-860-0070 | Toll-free: I -877 -327 -227 3
Update your OCA membership preferences or unsubscribe from this list
Our mailing address is:
Ontario Chiropractic Association
200-20 Victoria St
Toronto, ON MsC 2N8
Canada
Add us to vour address book
I Twitter
in Linkedln
543
5
Rose Bustria544
From:Sent:To:Cc:Subject:
Jo-Ann WillsonWednesday,May 24,2017 2:15 AMRose BustriaBruce Walton; Joel FriedmanFW: Weekly News: Animal Chiropractors, Pregnancy Tools for Patients,Advocacy, Webinars
QA and Council.
Jo-Ann P. Willson, B.Sc., M.S.W., LL,B.
Registrar and General Counsel
College of Chiropractors of Ontarío130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected],caWeb Site: www.cco.on,ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copíes including
any attachments without reading it or making a copy' Thank you.
From: Ontario Chiropractic Association [[email protected],net] on behalf ofOntario Ch iropractic Association [OCA@ch iropractic.on.ca]Sent: Tuesday, May 23, 20L7 4z02PMTo: Jo-Ann WillsonSubject: Weekly News: Animal Chiropractors, Pregnancy Tools for Patients, Advocacy, Webinars
We're Here For You.
View this email in vour browser
OntarioChiropract¡cAssociation
-It¡bb-
-
1
The College of Veterinarians of Ontario (CVO) is undergoing an extensive legislative review
and consultation process to modernize the Veterinarians Acf including the development of a
scope of practice model. Some of our members were concerned that these legislative
changes would limit the scope of practice of animal chiropractors, and we have developed
a response to the CVO's consultation which outlines these concerns and how the CVO
could address them.
Along with close to 20 animal chiropractors, we have consulted with the CVO and the
College of Chiropractors of Ontario (CCO). A small working group of animal chiropractors
and representatives from the Veterinary Chiropractic Learning Centre assisted in drafting
the OCA response.
On May 12,we submitted an extensive response. Although the CVO draft scope of practice
model included an exemption to allow chiropractors to perform manipulation and use the
title'doctor'when treating animals, we recommended explicitly authorizing chiropractors toperform additional authorized acts in accordance with cco standards:
1. Communicating a diagnosis
2. Performing procedures on tissue on or below the dermis
3. Putting a finger beyond the anal verge for the purpose of manipulating the tailbone
4. Using forms of energy
We also requested clarification of the wording of the authorized act on 'assessment' to
allow chiropractors to perform an assessment for chiropractic treatment.
2
lf you have any questions about this submission or if you hear of any issues where you
would like support in advocating for the profession, please contact us.
546Read the OCA Submission to CVO
Patient Tools.
Preg nancy Stretches
& Exercises
)
Studies show that up to 90% of pregnant women will experience low back and/or pelvic
pain related to their pregnancy. Our own experience shows us that mommy bloggers are
one of the most active and passionate communities to engage with online. That is why we
created this patient toolkit, found exclusively in our Marketinq & Outreach Library online, to
help expectant mothers perform simple core strengthening exercises that can help reduce
stress on their back.
. Presentation: Pregnancy & Core Strength
. Handout: 9 Pregnancy Stretches for the Whole Body - illustrated stretches
. One Pager: Minimize Pregnancy-Related Back Pain - tips
. One Pager: Avoid New Mom Backache - tips and exercises
. Blog Post: Your Whole Wo¡ld is on Your Shoulders - technique for lifting children
Explore our Pregnancy Toolkit
3

Your membership with us strengthens our collective voice and enables us to advocate on
your behalf to the government. Today we'd like to update you on some of our current
advocacy work.
547Primary Care Low Back Pain Pilot
On April 25, we sent a letter to the Honorable Dr. Eric Hoskins, Minister of Health and
Long-Term Care, with an update on an evaluation of the impact of the PCLBP pilot which
was recently performed by the Centre for Effective Practice.
Getting Ready for An Election
The next Ontario election will be held on or before June 7, 2018. The pre-election season is
an active time in government, as they prepare to make a case for re-election. We are taking
every opportunity during this time to advocate for chiropractors regarding the expansion of
the lnter-professional Spine Education and Assessment Clinics (ISAEC), possible
integration of ISAEC with the PCLBP pilot, and the possibility of gaining access to X-ray
and lab services.
May 11-13. Pri-Med Conference
We hosted a tradeshow booth at the Pri-Med Conference which was attended by over
3,000 family physicians, nurse practitioners, pharmacists and students. Thank you to our
tradeshow volunteers!
Conference delegates were very interested in our public education resources, particularly
those on pain relief options for MSK issues, and we gave away 500 Easv Stretches for the
Whole Body toolkits. We surveyed 63 people who came by our booth and found that:
The most difficult complaints to manage effectively were back pain, motor vehicle
accidents including whiplash, neck pain and headaches.
Family physicians and nurse practitioners said they refer to chiropractors most
frequently for back pain, sports injuries and headaches.
While this is a small snapshot, it is helpful to keep these needs in mind and refer to our
Collaboration & Referral Resource Kit when building referral relationships.
Members are always welcome to volunteer at our tradeshow booths and contact us for an
update on advocacy issues.
a
a
4
UPCOMINGWEBINARS
Breaking the lce:Techniques forlnstantly Making a
Gonnection(Rebroadcast)
Wed. May 24,12-1 PM
lvan Wanis Ruiz, Dale Carnegie
Training
ln this webinar you will learn
tried and true techniques to
connect instantly and sincerely
with potential patients and
colleagues. Dale Carnegie
principles will be applied to
enhance the way you
communicate with new people
and build mutually beneficial
relationships.
Online Advertising forNew PatientAcquisition
Wed. May 31, 12-1 Pl\A
TechWyze
Just like TV, newspapers or
outdoor banners, online
advertising can bring you new
patients. U nlike traditional
advertising, online advertising
allows you to only pay when
someone clicks on your ad and
to collect all the data you could
ever need to see what return
you get for your investment. ln
this webinar we show you how
to use online advertising to grow
your patient caseload.
548
Uppominq CE & Events I Webinars On Demand
Brought to you by our CE Sponsor: # INNæARE
We're here for you. Call us:
Local : 4 1 6-860-0070 | Tol l-free : 1 -87 7 -327 -227 3
Update your OCA membership preferences or unsubscribe from this list
5
Register Now Register Now

Our mailing address is:
Ontario Chiropractic Association
200-20 Victoria St
Toronto, ON MsC 2N8
Canada
Add us to vour address book
f Facebook
V Twitter
in Linkedln
549
6

5t26t2017 Regulation & Government Relations - OCA
Q cHrRoonacronLocrron 550IÇ[gçp6p5tp¡fgrglÂV{ìrw.cnInopRAcrrc,oN.cA/MEMBERS/)>ADVERrrsrNG&ADVocAcy
(HTTPS://WWW,CHIROPRACTIC.ON.CA/MEMBERS/ADVERTISING-ADVOCACY4 > ADVOCACY
(HTTPS://WWW.CHIROPRACTIC.ON,CA/MEMBERS/ADVERTISING-ADVOCACY/ADVOCACYD > REGULATION
& GOVERNMENT RELATIONS
Select from l\4enu
REGULATION & GOVERNMENT RELATIONS
As the assoc¡ation mandated to promote and support the chiropractic profession, the OCA advocates to the Sovernment, legislature and regulatory colleges on issues
¡mp¿cting the profess¡on.
College of Chiropractors of Ontario. January21,2O16-OCAFeedbackonCCOBy-Laws6(ElectlonofCouncll Members)and17(Publ¡cRegister)(http://M.ch¡ropractlc.on.calwp-content/uPloads/CCO.
By-Laws-OCA-Submission-01 21 1 6.pd0
. March26,2015-OCAFeedbackonarangeofproposedamendmentsincludlng;(http://M.chlropractlc.on.calwp-content/uploads/201s-ocA.response-CCO-
consultation.pd0
o spousal Exemption toSexualAbuse Prov¡sions
o Advertis¡ng
o ProfessionalPortfolios
o Ass¡stive Dev¡ces
. April 25, 2014 - OCA Feedback on proposed amendment to Ståndard of Practlce S-016 Advertlsint (http://w.chlropractic.on.calwp-content/uploads/OCA-
Submission-Re-Proposed-Amendments-to-S-01 6.pdf)
College of Veterinarians of OntarioThe College of Veter¡narians of Ontario's extensive legislative rev¡ew and consultation process will modern¡ze the Veterinarians Actindud¡ng the development of a scope ofpractice model. Our response to the CVO'S consultat¡on outlined concerns relatìng to the ch¡ropract¡c scope of practice ¿nd the ability of chiropractors to treãt ¿n¡mãls in
Ontario.
. May12,2017-OCAResponsetoCollegeofVeter¡nar¡ansofOntarioConsultat¡on(http://w.chiropractlc.on.calwp-content/uploads/CVO-Let-Changes-OCA-
Response-Mây"'l 2-'l 7-FlNAL.pdf)
FSCO Service Provider LicensingThe OCA has continu¿lly advocated that wh¡le fraud reduction ¡s a worthy goal, it should not come at the expense of health c¿re providers. The OCA advocated that, as
members of a regulated health profession, chiropractors should be exempt from th¡s licensing process.
.lnlMay20l4,seruiceProviderLicensingbecameakeypriorityintheOCA'Sadvocarywithcandidatesforthe20l4OntarioElection.
. tn Apr¡l 20'14. the OCA partnered with the Ontario PhysiotherapyAssociat¡on (OPA) to make presentatlons on Bill 17'l to the Standlng Commlttee on General
Government. (http://w.chiropractic.on.calwp.content/uploads/2014.04.30-Presentation-on-Auto-lnsurance.pdf)
Ontario Ministry of Health & Long-Term CarePatients First Act. November 23, 2016 - OCA Presentation to the Standing Committee on the Legislative Assembly on Ontario's Pat¡ents F¡rst Act (http://M.ch¡ropractic.on.calwp.
content/uploads/B¡ll-41-Presentat¡on-Standlng-Ctte-Leglslative"Assembly-Nov.23.2016-FlNAL5.pd0: The OCA recommends two amendments to Bill 41 to remove
barr¡ers and enable patient-focused integrated care for low back pa¡n and other musculoskeletal conditions. The amendments would enable LHINs and other agencies to
ut¡l¡ze chiropractors.
. February 26, 2016 - OCA Feedback on Ontario's Pâtients F¡rst proposal (http;//M.chiropractic.on.calwp-content/uploads/Pät¡ents-First-Discussion-Paper-Response-
OCA-Response-1.pd0
Ontario's Opioid Strategyln a feedbäck process on the Ministry of Health and Long-Term Care's Op¡o¡d Strategy, the OCA supported a comprehensive approach to pa¡n manågement that will improve
health outgìes and decrease the reliance on opio¡ds. We advocated that, as MSK experts, chiropractors h¿ve a role in reducing and preventing reliance on opioj¡f¡p manage
r'ri<0"',Q (http://www.addthis.com/bookmark.php?v=300&pubid=ra-52c6c81212a89780) Ç)ff"ïl'H":ffî:î:ïî:î';ifJiil:i?ïJ,llî'tfihï'å'É'"üäÁi&Ëi:#ffiùtrÕNåHi¡'ìådiiËgtr¡iïls"o*o""dprogramswhchsupportpeoprewth. Decembers,2016-ocrStrtpr:rJl,rmmrunfat$o{fu4ufi{Íü"{t?dgchiropraethrüsgeÉffii$N}@(
tiËiliiü';ütr:TiÅiËåii s,"m/çoqrqa¡y/o¡tario-chiropractic-association I @ ft"l'rr 6-860-0070) OClihic Regulation Working Gróup r/Search)
F$gÊ€lPtilbLqt,3þtÑmtmggtiçgtUWngssion Resulatory colleses' includins the cco E@
512612017 Regulation & Government Relations - OCA. January 19,2016 - Feedbackon Proposed Cllntc Regulation Model (http://M.chlropractic.on.calwp-contenVuploads/Cllnlc.Regulation.OCA.Response-January-1 g-
2016-FlNAL.pdf)
551/Ch i ropractorLocator/)
Tweets
Prepar¡ng for #camoins (https://tw¡tter.com/search?o=campingì is just as ¡mportant as enjoying it. Here are 7 bãck-saving camping tips to follow!https://t.colwfmnRbThN O lhttps://t.colwf mnRbThNOthtto://www.tw¡tter.com/ON Chiropractíc (http://M.twitter.com/ON Chiropracticl22 hours aEo lhttp://twitter.com/ON Chíropract¡c/ståtuses/8677574704873676801
OCA membersl Get 209{ off @lnnoCareltd lhttÞ://twitter.com/lnnocareltdl's Connect call answering to extend your hours without added staffng cost.httþs://t.co/9pas8lklP6 (https://t.co/gpasBlklP6)httþ://www.twltter.com/ON Ch¡roÞractic lhttþ://www.twitter.com/ON ChiroÞracticlvesterdavlhttp://twitter.com/ON ChlroÞractlc/statuses/867440i5553i07i488ì
Ontario Chiropract¡c Association20 Victorið St., Su¡te 200Toronto, ON M5C 2N8Canada Tel: 41 6-860-0070 f tel:41 6-860-00701
1 ollÍ | eei 1 -877 -327 -2273 ltel:1 -877 -327 -221 3\Fax:41 6-860-0857oca@chirooract¡c,on,ca lma¡lto:oca@chirooract¡c.on.ca)
Regular Business HoursOCA: 9:00 to 5:00 EST - Monday to Fr¡dayPlvlP support: 7:30 to 5:00 EDf - Monday to Fridãy
@201 7 Ontar¡o Chiropractic Assoc¡ationPr¡vacv Poliw l/orivacv-oolicvlCustomer 5eru¡ce Standard Pol¡cv l/customer.service-standard-oolicv)
Q crrnornerron rocr:ion
@ {httR:Zwww.addthis.com/bookmark.php?v=300&pubid=ra- 52c6c81212a897lrir Ql(https;//twitter. com/ON-Ch i ropra ctic) O
(https://www.facebook.com/ontariochiropracticassociation) @ (
https://www.linkedin.com/company/ontario-chiropractic-association ) @ {tet:+f 6-860-0070) ø(/Search)
puBltc(/puBuc) | vevsensrrN4err4seRst [@https://trvww.chiropractic.on.calmembers/advertisingradvocacy/advocacy/regulation-government-relationsi?utm source=1+-+Members&utm campaign=dd505. 2t3
-¡a-bb-
OntarioChiropracticAssociation 552
lNlay 12,2017Ms. Jan RobinsonRegistrar & Chief Executive OfficerCollege of Veterinarians of Ontario2106 Gordon StreetGuelph, Ontario NIL 1G6
Dear Ms. Robinson
The Ontario Chiropractic Association (OCA) commends the College of Veterinarians of Ontario
(CVO) and the Ontario Association of Veterinary Technicians (OAVT) for undertaking an
extensive legislative review and consultation process to modernize the legislation governing the
care of animals in Ontario. We support the proposed scope of practice model that articulates how
a system of providers, including chiropractors, can deliver animal care in the province. Thisreflects both the current landscape of animal care and the public's expectation to access
chiropractic care directly for their animals.
Animal chiropractors report strong and positive relationships with veterinarians. By practising in
a shared care model, there is recognition of the unique scopes of practice of the two professions,
and the benefits of working collaboratively together for animals and their owners.
BACKGROUNDAs primary care practitioners regulated under the Regulated
Health Professions Act, 199j,(RHPA), chiropractors provide care
to patients with a variety of health concerns related to the spine
and joints and the effect on the nervous system, such as lumbar
spine, shoulder and knee pain, injuries, and overall wellness care.
Chiropractors focus on patient-centred care, using manual
therapies, and often work in collaboration with other regulated
health providers.
Depending on a patient's particular needs, treatment may combine
a range of options, including patient education, recommendations
for lifestyle modifications, the prescription of therapeutic exercise,
and other evidence based interventions such as manual therapy and
modalities to speed healing.
The goal of all treatment plans is to improve patient outcomes and
promote the patient's return to regular activity and work as quickly
Ch i ropractic P atient Care
1) Assessment
. Palient history
. Examirration. Observation. Range of nrotion testing. Neurologìcal testing. Odhopaed¡c testing. Palpation
2) Diagnosis
3) Treatment and Management
. Patient education
. Therapeutic exercise
. Lifestyle modificationso Manual therapy
Paflenls reqttiring care outside of the
chiropractic scope of practice are referredback to their primary care provider as
appropriate.
2OO - 2A Victoria St.
Toronto ONM5C 2NB
Tet 416-860-0070Tolt -f ree L- 877 - 327 - 227 3
Fax 416-860-0857
www. ch iropractic.on. ca
HOntarioChiropracticAssociation
Page 2
553and painlessly as possible.
The scope of practice of chiropractic as defined by the Regulated Heatth Professions Act, t 991 isthe assessment of conditions related to the spine, nervous system and joints and the diagnosis,prevention and treatment, primarily by adjustment of:
o dysfunctions or disorders arising from the structures of functions of the spine and theeffect of those dysfunctions or disorders on the nervous system; and
. dysfunctions or disorders arising from the structures or functions of the joints.
Under the RHPA, chiropractors have the authority to perform the following authorized acts:
1. Communicating a diagnosis identiÛiing, as the cause of a person's symptoms,i. A disorder arising from the structures or functions of the spine and their effects on
the nervous system, orii. A disorder arising from the structures or functions of the joints of the extremities.
2. Moving the joints of the spine beyond a person's usual physiological range of motionusing a fast, low amplitude thrust.
3. Putting a ftnger beyond the anal verge for the purpose of manipulating the tailbone
ANIMAL CHIROPRACTIC CAREChiropractors who treat animals have completed additional training beyond the four year postgraduate program that qualifies them to be chiropractors. The Veterinary Chiropractic LearningCentre (https://verterinarychiropractic.ca) is the Ontario program that educates both chiropractorsand veterinarians in animal chiropractic. It consists of a minimum of 220 hours of supervisedclassroom and hands-on instruction. The VCLC program is approved for certification by theCollege of Animal Chiropractors and the American Veterinary Chiropractic Association.Separate training in animal acupuncture will be described below.
In delivering care to animals, chiropractors must practice within the chiropractic scope ofpractice and adhere to all standards of practice of the profession. The College of Chiropractors ofOntario (CCO) has a standard of practice specifically related to the care of animals (Standard ofPractice 5-009 Chiropractic Care of Animals). One of the objectives of this standard is to ensureappropriate coordination and consultation between chiropractors and veterinarians in thechiropractic care of animals. The Standard of Practice 5-009 Chiropractic Care of Animals(201 5) clearly states that "primary responsibility for the health care of animals is with registrantsof the College of Veterinarians of Ontario."
Chiropractors must always practice based on their qualifications, skills, knowledge and level ofcompetence. There are safeguards in place to ensure that chiropractors providing animal care donot practice beyond their scope including professional misconduct regulations (described below)
E554Ontario
ChiropracticAssociation
Page 3
and standards of practice. Chiropractors recognize their role in animal care is focused on
musculoskeletal (MSK) conditions. It is through this lens that we are responding to the proposed
scope of practice model. Patient scenarios (in italics) are included to illustrate the nature of care
provided and to support the request for additional authorized acts.
PROPOSED SCOPE OF PRACTICE MODEL
Title protectionThe OCA supports the draft wording of the title protection clause which would enable
chiropractors to continue to use the title 'doctor' when treating animals. This is consistent withthe RHPA, which authorizes chiropractors to use the title 'Doctor' (Dr.).
Authorized ActsThe OCA supports the adoption of a regulatory model similar to the RHPA that recognizes there
are some specific activities that pose a significant risk to patients and, therefore, need to be
restricted. The OCA supports the exemption which would allow for chiropractors to performmanipulation (Authorized Act #1 1).
We are requesting additional (full or part of the) authorized acts of communicating a diagnosis,performing procedures on tissue on or below the dermis; putting a finger beyond the anus, and
using forms of energy. We are also recommending clarification and revision of wording of the
authorized act regarding assessment, or alternatively, an exemption to allow chiropractors toperform assessments for the purposes of chiropractic treatment.
RECOMMENDATIONS
Authorized Act #1: Communicating a DiagnosisChiropractors have the authority under the RHPA to communicate a diagnosis. The conditionsmay include, but are not limited to, such MSK conditions as a vertebral joint dysfunction, atemporomandibular (TMJ) joint disorder or a lumbo-sacral sprain. Animal chiropractors have the
expert knowledge, skill and judgement to determine if chiropractic care is indicated/contraindicated in animals and to communicate their MSK dysfunction related diagnosis to the
animals' owner(s), and when care is not indicated, to refer to their veterinarian.
There are safeguards in place to ensure that appropriate referrals to veterinarians are made. Theprofessional misconduct regulation (Ontario Regulation 852193) identifies that it is professional
misconduct to fail to advise a patient to consult with another health professional when the
member knows or ought to know that:o the patient's condition is beyond the scope of practice and competences for the members;o the patient requires the care ofanother health professional; oro the patient would be appropriately treated by another health professional.
H555Ontario
ChiropracticAssociation
Page 4
In seeking chiropractic care, animal owners are expecting chiropractors to communicate thenature of the MSK condition affecting their animal. Furthermore, the communication of adiagnosis is important to obtaining informed consent to treat. Animal owners must be aware oftheir animal's condition and circumstances to provide informed consent. In addition, the CCOstandard of practice (5-002 Record Keeping) requires that patient records include the chiropracticdiagnosis or clinical impression. Consequently, we request that an exemption be made to allowchiropractors treating animals to communicate a diagnosis that falls with the chiropractic scopeof practice. This would limit the diagnosis to MSK related conditions (spine, nervous system,and joints), thereby protecting the patients.
Scenario: A competitive hunter/jumper horse presents with an inability to "drivefrom behind"(ess power in hind end) and swaps leads when asked to transition between various gaits. Theowner reports no lmown trauma. The owner notices the horse is "cranþt" when she grooms himover the back and pelvis and drops away from pressure in the lumbosacral and sacropelvícregion. Gait analysis (at a walk, trot and canter) revealed the horse to be short striding on thehind leg and when cantering ro the right, would change leads and limit stance time on the righthind. Gross movements otherwise appeared bilaterally symmetrical and no head bob wasobserved. No heat or swelling was apparent in distal extremities. Static and motion palpationanalysis revealed q mild unlevelling of the pelvis with the right side being higher and restrictedin its movement to D-V challenge. Muscle hypertonicity was noted in the gluteal and erectorspinae muscles to the transition area of the spine on the right side, which was also restricted inits movement on palpation.
Chiropractic Diagnosis: right Sacroiliac Dysfunction/initation with secondary muscle pain &hypertonicity.
Recommendation: trial of manipulation (VSMT) +/- auxiliary chiropractic therapies (soft tissue,equitape, laser or acupuncture prn) to address associated soft issue pain and dysfunctionassociated with chiropractic Jindings.
POM: approx 3 visits then reøssess, if no signs of improvement, reassess determine if chiro careis still índicated and/or concurrent vet care is wananted
Notes: discuss findings with client, permission to contact vet if needed, and informed consent tocare.
Recommendation - Authorized Act # 1: Communicating a Diagnosis
An exemption be included to authorize chiropractors to communicate a diagnosis within thechiropractic scope of practice, in accordance with standards set by the College of Chiropractorsof Ontario.
H556Ontario
ChiropracticAssociation
Page 5
Authorized A,ct#22 Performing an Assessment to Determine the Fitness or Soundness of an
Animal, or Group of AnimalsThe CVO provideã clarification during the May 2nd webinar that this authorized act relates
specifically and exclusively to assessment for the purposes of fitness for slaughter and soundness
for sale. The term "fitness and soundness" may have particular meaning and be well known
within the veterinary medicine world; however, we believe the current wording of the proposed
authorized act may be unclear to the public.
We suggest it is critical to distinguish between assessment for fitness for slaughter and soundness
for sale, and a health assessment for the purposes of a differential diagnosis or treatment (which
chiropractors do). Providing additional specificity regarding the intent of the authorized act willhelp promote transparency for the public regarding the activities that pose a significant risk, and
therefore, need to be restricted.
Alternatively, if assessment is being defined more broadly and may include assessment for the
purpose of providing health treatment, then chiropractors would need to have access to this
authorized act. A comprehensive assessment is required to develop a differential diagnosis and
the appropriate treatment plan.
Animal chiropractors need to perform an assessment to determine soundness so they can decide
if chiropractic care is indicated. This is central to what chiropractors do. To clarify, this is notdiagnosing a'otrue lameness", but rather watching, for example, a horse move; assessing
biomechanics; and ruling out red flags to treatment.
Assessing gait and range of motion, along with neurological exams assist in doing this.
Soundness and fitness issues can be due to musculoskeletal issues, therefore a chiropractorworking on animals should be able to perform these assessments. Animal chiropractors observe
for improper movement patterns to assess and guide treatment on animals. It is imperative that
the animal chiropractor be able to assess the movement and function of an animal in order to
determine if there are any contraindications to treatment, such as signs of fracture or neurologicaldeficit. Cranial nerve exams, proprioceptive test and peripheral reflexes provide valuable
information regarding the integrity of the animal as well as pre and post treatment changes.
Screening for muscle asymmetry and faulty gaitlmovement pattems are covered in detail in the
training of animal chiropractors (see Attachment 1: VCLC Program Curriculum). Animal
chiropractors are trained to refer to a veterinarian for lameness workups when indicated by their
assessment. This assists in determining whether an animal is sound as well as to know when it is
a musculoskeletal diagnosis versus needing referral to a veterinarian. Allowing chiropractors to
assess an animal's fitness would be an adjunct to their clinical picture, and would never deter
from propet veterinarian referral and communication.
H557Ontario
ChiropracticAssociation
Page 6
Scenario: An owner of a competition agility dog presents indicating that the dog's jumpingmechanics have changed, causing it to knock down jump bars. The owner communicates herobservations. She sees that the dog is unable tofully extend its rightfront leg during the jumpingprocess. The chiropractor observes the gait to see if there is any noticeable short striding withthat right front limb. The chiropractor then takes that information to a hands-on assessment/palpation of this dog and determines the treatment from there. The chiropractor then asks theowner to walk the dog againfor a post treatment reassessmenl.
Authorized Act #5: Performing a procedure on tissue on or below the dermisAnimals can experience muscular and connective tissue tension, trigger points and weakness.Depending on an animal's condition(s), chiropractors perform muscle and soft tissue techniquesalone or in combination with spinal manipulation. Administering techniques to facilitate amuscular change can also help support the adjustment/manipulation. Some examples includemyofascial release, Logan basic technique and stretches. These are part of the curriculum at theVeterinary Chiropractic Learning Centre's program (which builds on the foundation acquiredthrough the four year chiropractic program) and provides the opportunity to learn thesetechniques specifically on animals.
Acupuncture is another treatment that can be an adjunct to spinal manipulation. V/hile theInternational Veterinary Acupuncture Society (IVAS) provides training in acupuncture toveterinarians, there are an international animal acupuncture courses that are accredited by theIVAS or IVAS affiliated organizations in which chiropractors can enroll. One example is the
Recommendation - Authorized Act #2: Performing an Assessment to Determine the Fitnessor Soundness of an Animal, or Group of Animals:
The wording of the authorized act related to assessment be revised as:
Performing an assessment to determine the fitness for slaughter or soundness for sale of ananimal, or group of animals, on which it is reasonably foreseeable that a person will rely on theassessment.
ALTERNATTVELY:
An exemption be included to authorize chiropractors to perform an assessment for the purposesof treatment within the chiropractic scope of practice, in accordance with standards set by theCollege of Chiropractors of Ontario.
H558Ontario
ChiropracticAssociation
Page 7
"Applied Animal Acupuncture for Animal Chiropractors" (Accreditation # CPD 1637) certified
by the Collectief Praktiserende Dierenartsen in Amsterdam.
Adjunctive therapies like massage, exercise prescription, acupuncture, ultrasound, laser,
vibration, et al. can be necessary, in addition to manipulation. Animal chiropractors who perform
acupuncture are accountable to the CCO and must practice according to two standards ofpractice: Care of Animals (5-009) and Acupuncture (S-017), and within the chiropractic scope ofpractice. The Acupuncfure standard notes that "CCO adopts the WHO Guidelines that a
combined (clinical and academic) minimum of 200 hours offormal training is required for a
member who intends to use acupuncture as an adjunctive procedure in his/her practice" (CCO
Standard of Practice S-017, 2016). The CCO has stipulated that specific clinical competency for
acupuncture on animals be obtained prior to use. That is, the CCO requires that animal
chiropractors first must qualiff to do acupuncture on humans (by meeting the requirements set
out in the Standard S-017) before being trained to perform it on animals. Demonstration of this
competency could be through examination, certification or proof of training. We believe this
requirement would provide the necessary safeguards for chiropractors to perform acupuncture on
animals.
Clarification is needed regarding the draft wording of the authorized act "performing a procedure
on tissue on or below the dermis, specifically whether it includes the use of "Equitape" (which is
applied to the epidermis). This is used in support of the care provided by animal chiropractors.
We understand from the webinar that, given the wording of this proposed authorized act,
chiropractors would continue to be able to perform procedures on the epidermis that would affect
tissue below the dermis.
Scenario 1: Dog with a chronically weak hind end, stifflower backwhile walking, slow
ipsilateral paw rightíng, absent skinflinch below L2 unilateral to the weakness, mild quadriceps
atrophy, poor thoracolumbar alignment. Veterinarian x-rays were unremarkable.
Treatment included spinal adjustment/manipulation to the thoracolumbar vertebraefor
alignment and the lumbør vertebrae to improve motion and take stress off the proximal segments
will remove the interference. Acupuncture would be appropriate to stimulate healing and
neuroplastic adaptation in the affected nerves and to reduce the hypertonicity of the lumbar
muscles. Pulsed microcurcent or transcutaneous electrical nerve stimulation €ENS) can help
with the quadriceps atrophy. Therapeutic ultrasound to provide specific deep and gentle heating
to help loosen the tight lumbar muscles would also be helpful'
Scenario 2: Dog presents in significant pain and discomfort and owner notices he "yelps" or
"screams" when trying to turn his head to the right. The pain is further aggravated by cervical
extension. The owner reports a previous episode last year after playing tug with a neighbour's
H559Ontario
ChiropracticAssociation Page I
dog. The dog had been seen by the veterinarian who prescribed an NSAID. X-rays were nottaken due to financial reasons.
Palpation revealed mechanical joint restriction/facet irritation at C3 and C4. Primarychiropractic therapy: Only a C4 body right adjustment/manipulation ancl mobilization whileacute. Auxiliary therapies: application of acupuncture to the dorsal left side of the neck,stímulating the needles with a high-frequency, low intensity TENS current. This stimulates thesegmental dorsal primary rami of the spinal nerves. This technique is highly ffictive atinhibiting pain because it stimulates the large nerve fibres which directly inhibit the c-type painnervefibres. Cervical icing was also done to calm inflammation and clecrease pain.
Authorized Act # 12: Putting an instrument, arm, hand or finger vi) beyond the anusIt may be necessary for a chiropractor to put his/her fìnger beyond the anal verge for thepurposes of manipulating the tailbone. This is an authorized act granted to chiropractors underthe fuHPA. As with humans, the only indication for putting afrnger beyond the anal verge wouldbe for a coccygeal adjustment/manipulation. This would be a last case scenario if extemaladjustment/manipulation procedures were unsuccessful, resulting in the persistence of a deviatedsacral apex and/or sacrotuberous ligament tautness. With trauma, fracture must first be ruled outby the veterinarian. Once this has been done, chiropractors can apply their expertise. Thesacrotuberous ligament and its treatment in both horses and dogs are discussed at length in theVCLC program.
Scenario: Sport dog comes in 2 weel<s after he has flipped over a piece of agility equipment (thetire) landing on his hind end and injured the sacrococcygeal area (tailbone). Vet examinationwas performed and diagnosed with "soft tissue injury"; X-rays were unremarkableforfractureor pathologlt; metacam was givenfor pain. Chiropractic exam revealed sacro pelvic jointrestrictions, muscle splintíng and the apex of the sacrum was deviated to the left (tail hung tol"ft...o new thingfor this dog) and associated soft tissue hypertonicity. Sacrotuberous ligament
Recommendationsdermis:An exemption be included to authorize chiropractors to perform a procedure on tissue on orbelow the dermis within the chiropractic scope of practice, in accordance with standards set bythe College of Chiropractors of Ontario.
An exemption be included to authorize chiropractors who have completed an accreditedacupunctwe course such as the Intemational Veterinary Acupuncture Society or equivalent inaccordance with standards set by the College of Chiropractors of ontario.
- Authorized Act #5: Performing a procedure on tissue on or below the
H560Ontario
ChiropracticAssociation
Page 9
was very tight and tender to touch on the right. Regular course of treatment was initiated using
VSMT to the sacro pelvis and myofascial release to the associated soft tissues and external
sacrotuberous ligament release is attempted; however, the sacrotuberous ligament remained
tight and apex deviated. A gentle, ínternal sacrococcygeal manipulation would be appropriate to
further release the sacrotuberous ligament internally and allow the sacrum to return to its
normal function/position and relieve pain.
Recommendation - Authorized Act #12 Putting an instrument' arm' hand or finger vi)beyond the anus.
An exemption be included to authorize chiropractors to put a fingerbeyond the anal verge for the
purpose of manipulating the tailbone, in accordance with standards set by the College ofChiropractors of Ontario.
Authorized Act #13: Forms of EnergYBased on the discussion at the May 2 webinar, we understand that additional work will be
undertaken to examine and identify the specific forms of energy that CVO and OAVT considers
may pose a risk of harm to animals. During this process, it would be possible to identify the
forms of energy that chiropractors should be authorized to use as part of chiropractic treatment.
As background, chiropractors have extensive training and skill in auxiliary chiropractic therapies
such as phototherapy (laser), mechanotherapy, and various electrotherapies (i.e. all those that do
not require sedation). The foundational knowledge is acquired in chiropractic college where
students are required to successfully complete a minimum of 96 modality treatments prior to
graduation. These therapies are further reviewed in the animal chiropractic training at VCLC
(indications, contraindications such as known or suspected cancer, theory) and in continuing
education courses offered to animal chiropractors. The emphasis for animal chiropractors would
be identifying red flags/contraindications and working with the veterinarian to rule out cancer),
and also if there is no improvement (as per standards of practice) to send back to the veterinarian
for further testing.
The theoretical component, including what occuts in the tissues at different wavelengths, and
commonly used classes of lasers, is taught at the VCLC as well as common indications/
contraindications to its use. The practical aspect is currently taught by the manufacturer of the
equipment since factors/settings vary with the type of laser used. 'We
have been informed by the
VCLC that auxiliary chiropractic therapies using forms of energy are aî area that can be further
developed and offered at the VCLC either into the basic animal program or via a separate
continuing education course. Work is underway by the VCLC regarding enhancing training in
these areas.
H561Ontario
ChiropracticAssociation Page 10
Performing X-rays on animals by animal chiropractors would not be appropriate and fall out ofscope because many animals require sedation for this procedure.
Scenario I: A dog presents with a hamstring strainfrom participating in dog sports. Theassociated vertebral ioint restrictions in the sacropelvis are addressed, but it is felt that properbiomechanics will be restored faster if the hamstring issue is addressed simultaneously. Usinglaser would facilitate this process and bring the dog back to futt function more quickly,minímizing the risk of aggravation of to the injury site.
Scenario 2: A horse is tense and reactive to attempts to adjust it. A massager (Thumper type ofmodality) is used which dampens the muscular tension, allowingfor more relaxed behaviour,more comfort and a more complete response from the treatment.
We look forward to participating in future consultations related to the proposed forms of energyauthorized act. Until such time, we recommend an exemption for chiropractors be included in therevised Act, and the details about which specif,rc forms of energy chiropractors would beauthorized to use could be stipulated in regulation.
Recommendation:
An exemption be included to authorize chiropractors to use fonns of energy within thechiropractic scope of practice, in accordance with standards set by the CoGge of Chiropractorsof Ontario.
CONCLUSIONThank you for the opportunity to provide input into the modernizationof the Veterinarians Actand the development of the scope of practice model. We believe the review has the opportunityto improve patient safety in the care of animals. Please do not hesitate to contact us if you haveany questions regarding our submission.
Sincerely,
Prç,Ç /c
Dr. Bob Haig, D.C.
Chief Operating OfficerOntario Chiropractic Association
Attachment: Appendix 1: Veterinary Chiropractic Learning Centre Program Curriculum
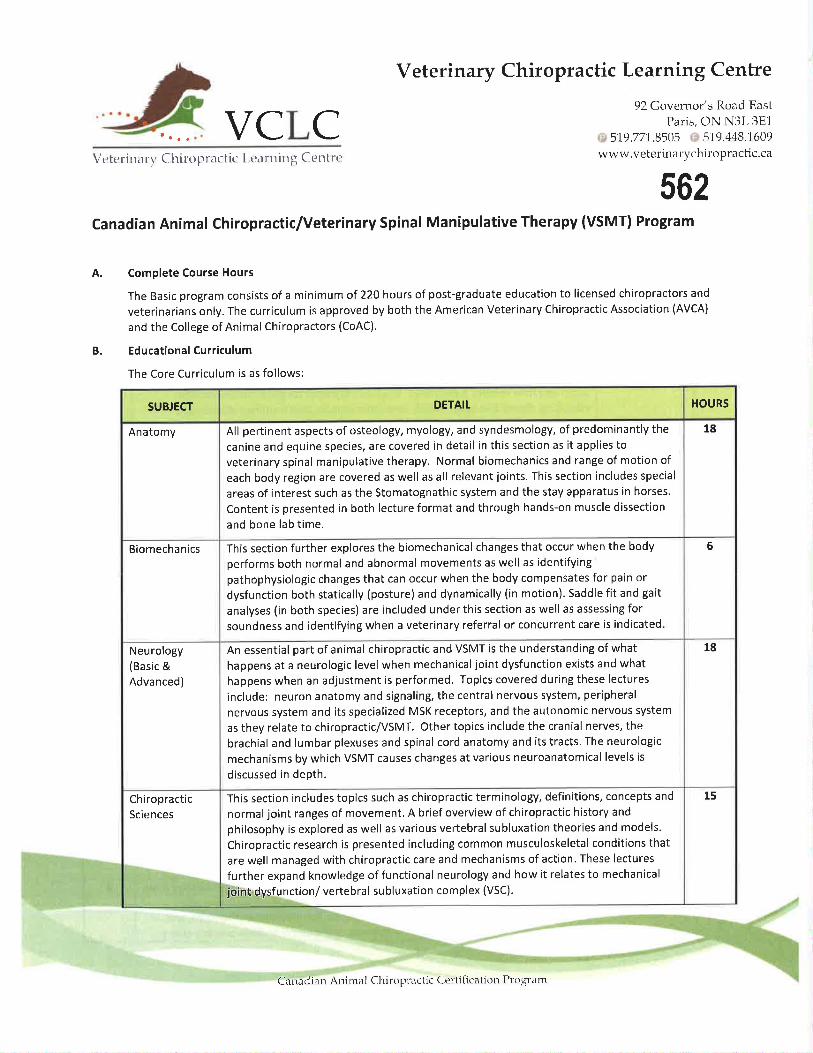
VCLC
Veterinary Chiropractic Learning Centre
92 Governor's Ro¿rd East
Paris, ON N3L 3E1
519.77'1.8505 519.448.1609wwr,v.veterinarychiropractic.caVe teri rr.r rt' C hirol-r r.rc tic [-eit rtriu g Ct'tr t rt'
B.
562Canadian Animal Chiropractic/Veterinary Sp¡nal Manipulative Therapy (VSMTI Program
A. Complete Course Hours
The Basic program consists of a minimum of 220 hours of post-graduate education to licensed chiropractors and
veterinarians only. The curriculum is approved by both the American Veterinary Chiropractic Association (AVCA)
and the College of Animal Chiropractors (CoAC).
Educational Curriculum
The Core Curriculum is as follows:
SUBJECT DETAIT HOURS
Anatomy All pertinent aspects of osteology, myology, and syndesmology, of predominantly the
canine and equine species, are covered in detail in this section as it applies to
veterinary spinal manipulative therapy. Normal biomechanics and range of motion of
each body region are covered as well as all relevant joints. This section includes special
areas of interest such as the Stomatognathic system and the stay apparatus in horses.
Content is presented in both lecture format and through hands-on muscle dissection
and bone lab time.
18
Biomechanics This section further explores the biomechanical changes that occur when the body
performs both normal and abnormal movements as well as identifyingpathophysiologic changes that can occur when the body compensates for pain or
dysfunction both statically (posture) and dynamically (in motion). Saddle fit and gait
analyses (in both species) are included under this section as well as assessing forsoundness and identifying when a veterinary referral or concurrent care is indicated
6
Neurology(Basic &Advanced)
An essential part of animal chiropractic and VSMT is the understanding of what
happens at a neurologic level when mechanical joint dysfunction exists and what
happens when an adjustment is performed. Topics covered during these lectures
include: neuron anatomy and signaling, the central nervous system, peripheral
nervous system and its specialized MSK receptors, and the autonomic nervous system
as they relate to chiropractic/VSMT. Other topics include the cranial nerves, the
brachial and lumbar plexuses and spinal cord anatomy and its tracts. The neurologic
mechanisms by which VSMT causes changes at var¡ous neuroanatomical levels is
discussed in depth.
18
ChiropracticSciences
This section includes topics such as chiropractic terminology, definitions, concepts and
normal joint ranges of movement. A brief overview of chiropractic history and
philosophy is explored as well as various vertebral subluxation theories and models.
Chiropractic research is presented including common musculoskeletal conditions that
are well managed with chiropractic care and mechanisms of action. These lectures
further expand knowledge of functional neurology and how it relates to mechanical
joint dysfunction/ vertebral subluxation complex (VSC).
15
Crrnarlian Ani tn¿rl Chiropractic Cer:tiiication Pt'o gram
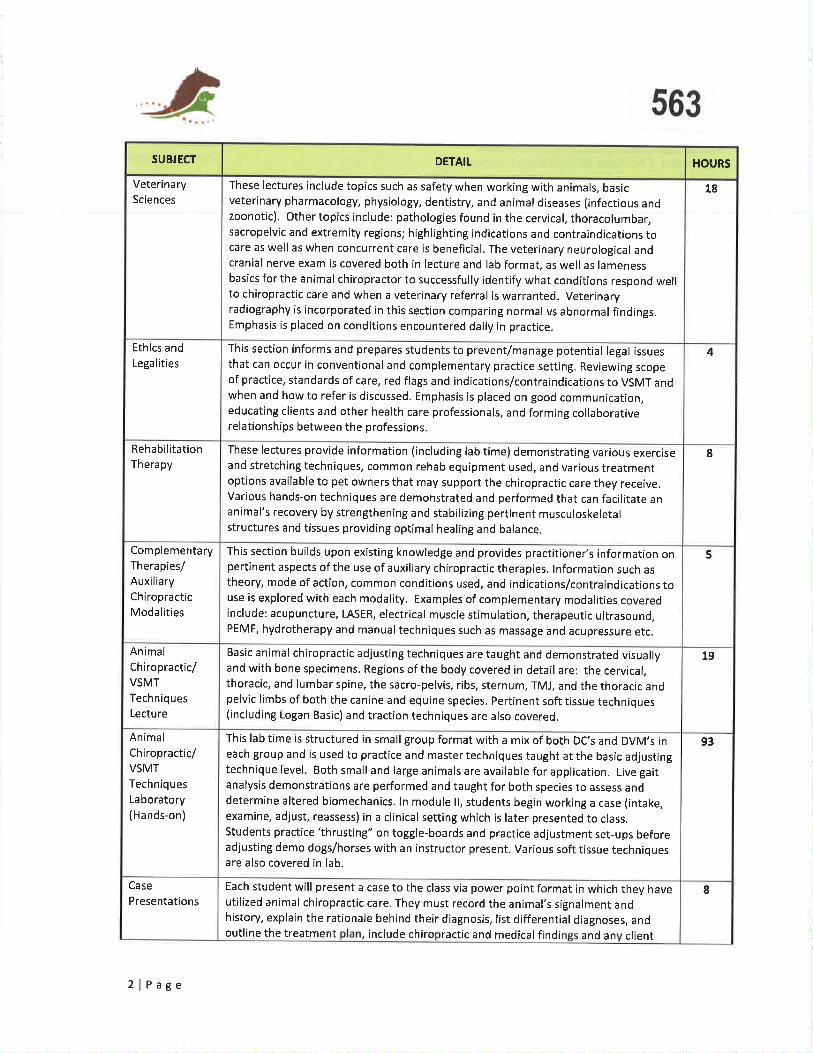
563
SUBJECT DETAIT HOURS
VeterinarySciences
These I ectures include topics such as safety when working with animals, basicveter¡nary pharmacology, physiology, dentistry, and animal diseases (infectious andzoonotic). other topics include: pathologies found in the cervical, thoracolumbar,sacropelvic and extremity regions; highlighting indications and contraindications tocare as well as when concurrent care is beneficial. The veterinary neurological andcranial nerve exam is covered both in lecture and lab format, as well as lamenessbasics for the animal chiropractor to successfully identify what conditions respond wellto chiropractic care and when a veterinary referral is warranted. Veterinaryradiography is incorporated in this sect¡on comparing normal vs abnormal findings.Emphasis is placed on conditions encountered daily in practice.
18
Ethics andLega lities
This section inform s and prepares students to prevent/manage potential legal issuesthat can occur in conventional and complementary practice settlng. Reviewing scopeof practice, standards of care, red flags and indications/contraindications to VSMT andwhen and how to refer is discussed. Emphasis is placed on good communication,educating clients and other health care professionals, and forming collaborativerelationships between the professions.
4
RehabilitationTherapy
These Iectures provide information (including lab time) demonstrating various exerciseand stretching techniques, common rehab equipment used, and various treatmentoptions available to pet owners that may support the chiropract¡c care they receive.Various hands-on techniques are demonstrated and performed that can facilitate ananimal's recovery by strengthening and stabilizing pertinent musculoskeletalstructures and tissues providing optimal healing and balance.
8
ComplementaryTherapies/AuxiliaryChiropracticModalities
This section builds upon existing knowledge and provides practitioner's information onpert¡nent aspects of the use of auxiliary chiropractic therapies. lnformation such astheory, mode of action, common conditions used, and indications/contraindications touse is explored with each modality. Examples of complementary modalities coveredinclude: acupuncture, LASER, electrical muscle stimulation, therapeutic ultrasound,PEMF, hydrotherapy and manual techniques such as massage and acupressure etc.
5
Animal
Chiropractic/VSMT
TechniquesLecture
Basic animal ch iropractic adjusting techniques are taught and demonstrated visuallyand with bone specimens. Regions of the body covered in detail are: the cervical,thoracic, and lumbar spine, the sacro-pelvis, ribs, sternum, TMJ, and the thoracic andpelvic limbs of both the canine and equine species. pertinent soft tissue techniques(including Logan Basic) and traction techniques are also covered.
19
AnimalCh iropractic/VSMTTechniques
La boratory(Hands-on)
This lab time is structured in small group format with a mix of both DC,s and DVM,s ineach group and is used to practice and mastertechniquestaught atthe basic adjustingtechnique level. Both small and large animals are available for application. Live gaitanalysis demonstrations are performed and taught for both species to assess anddetermine altered biomechanics. ln module ll, students begin working a case (intake,examine, adjust, reassess) in a clinical setting which is later presented to class.students practice'thrusting" on toggle-boards and practice adjustment set-ups beforeadjusting demo dogs/horses with an instructor present. Various soft tissue techniquesare also covered in lab.
93
Case
PresentationsEach student will present a case to the class via power point format in which they haveutilized animal chiropractic care. They must record the animal's signalment andhistory, explain the ratlonale behind their diagnosis, list differential diagnoses, andoutline the treatment include chiro ractic and medical findi and an client
8
2lPage
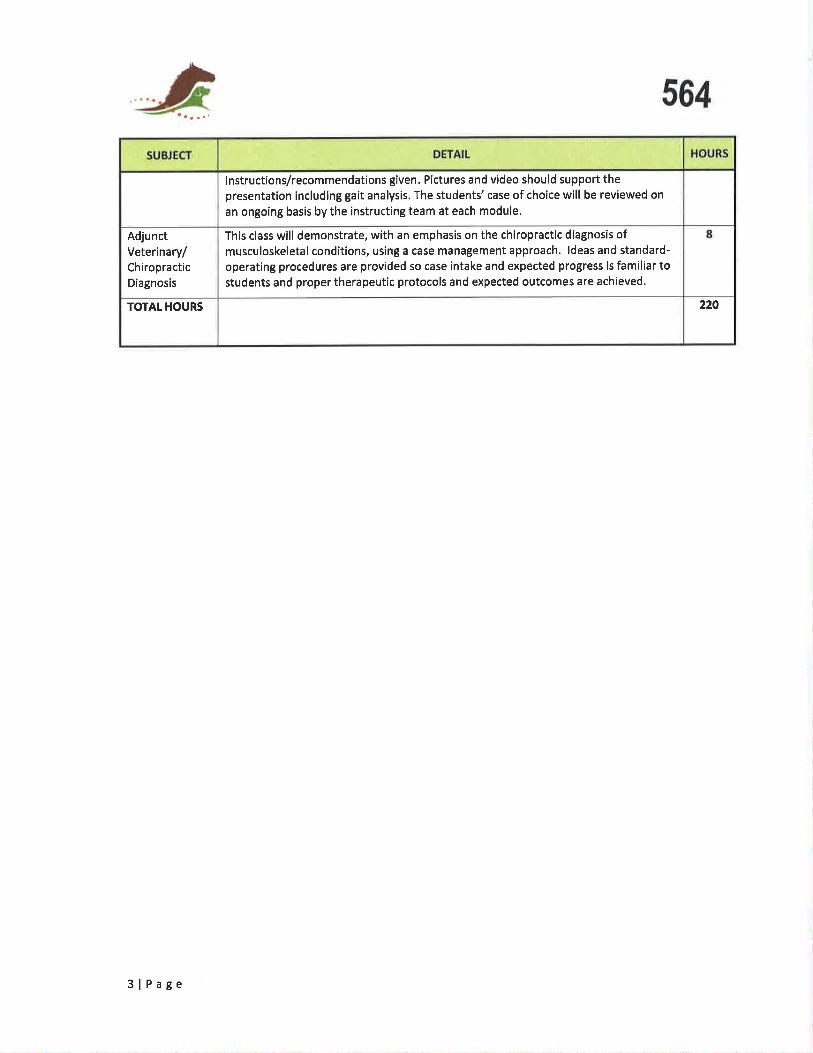
564
instructions/recommendations given. Pictures and video should support thepresentation including gait analysis. The students' case of choice will be reviewed on
an ongoing basis by the instructing team at each module.
AdjunctVeterinary/ChiropracticDiagnosis
This class will demonstrate, with an emphasis on the chiropractic diagnosis ofmusculoskeletal cond¡tions, using a case management approach. ldeas and standard-
operating procedures are provided so case intake and expected progress is familiar tostudents and proper therapeutic protocols and expected outcomes are achieved'
220TOTAT HOURS
3lPage
O¡a-bb--
OntarioChiropracticAssociation
April25,2Ot7
Hon. Dr. Eric Hoskins
Minister of Health and Long-Term Care
10th Floor, Hepburn Block
80 Grosvenor StreetToronto, Ontario M7 A 2C4
Dear Minister
Thank you for recognizing the significant value the Primary Care Low Back Pain (PCLBP) pilot brings to patients,
practitioners and the system by extending the program and funding for another year. We are very appreciative of
your ongoing support.
As you noted in our meeting in July 20t6, a ministry funded pilot must be supported by a relevant and robust
evaluation in order for the ministry to assess the impact on patient care, and the applicability of the program more
broadly. To that end, The Centre for Effective Practice (CEP) undertook an evaluation to examine the impact of the
PCLBP pilot. A summary of some of their key findings is attached. The findings demonstrate that the PCLBP pilot is
delivering not only on the Ministry's Low Back Pain Strategy, but also in the areas of health equity, opioid
mitigation strategíes, coordinated inter-professional care pathways, and patient education and empowerment.
The evaluation started late due to a lag in funding, captured only a portion of the fiscal year, and was comparing
seven different delivery models. Having an evaluation for the full fiscal 2Ot7 /2Ot8 extension that standardizes
some of the approaches to care will allow for a more comprehensive, quantifiable evaluation. Additionally, it will
enable a more detailed analysis of how the PCLBP impacts patient, provider and system oL.ltcomes, as well as its
alignment with the ministry's longer-term vision for low back pain and other related primary care priorities. This
can include quantifying the impact the PCLBP pilot has on reducing opioid use among patients, reducing
unnecessary diagnostic imaging and specialist referrals, improving patients' function and pain, improving patients'
ability to self-manage their conditions, and providing a more defined articulation of the ROl.
The PCLBP pilots provide an upstream approach to addressing low back pain, which fits very well with the more
downstream approaches of ISAEC, and the hip and knee surgical centralized assessment centres. Together, these
components can serve as the foundation for the development of a comprehensive approach to MSK conditions.
Thank you for your continued support and commitment to both the PCLBP pilot and the delivery of care models
that enhance health and wellbeing of Ontarians. We look forward to working with your team to ensure the
extended funding of these pilots provides the Ministry with the necessary data to inform how best to align the
PCLBP with the Ministry's MSK strategy and its broader primary care priorities.
Sincerely,
565
Prt(& flc
Dr. Bob Haig, D.C.
Ch ief Executive Officer
cc. Dr. Bob Bell, Deputy MinisterJust¡ne Walker, Senior Policy Advisor, Deputy Minister's Office
Alyson Rowe, Director of Policy, Minister's Office
lan Chesney, Policy Advisor, Minister's Office
2OO - 20 Victoria St.
Toronto ONMsC 2NB
Tet 416-860-0070Tolt -f ree L- 877 - 327 - 227 3
Fax 416-860-0857
www.chiropractrc.on.ca
H566Ontario
ChiropracticAssociation Page 2
Attachment
Summary of The Centre for Effective Practice,s phase 2 Report for 2Ot:6l2OL7
While the PCLBP pilot is part of the overall Provincial Low Back Pain Strategy, its approach alsocomprehensively supports the Patients First legislation, the Ministry's chronic pain and opioid mitigationstrategies, and the focus on health equity and vulnerable populations. The pilot is demonstrating positiveimpact on pat¡ents, providers and the health care system.
Patients ProfileThe pilot sites are serving some of Ontario's most vulnerable patients who would not otherwise haveaccess to care for low back pain due to financial barriers. The "typical" pcLBp patient:
. suffers from co-morbidities and yellow flags¡ has chronic pain and lack of overall wellness¡ often has mental health and addictions issues (specifically opioid and pain medication
dependencies). possesses the characteristics typical of high users ofthe health care system
Patient Experience and Outcomes:Preliminary patient experience and outcomes include:
¡ improved function and decreased pain;. less reliance on pain medication;¡ increased access to LBP programs that patients otherwise would not have received;. better ability to understand and self-manage their LBp; and. high level of satisfact¡on with assessment and treatment received.
Provider: lntegration & Clinical CareThe low rules nature of the pilot has allowed teams to hire and integrate MSK providers based oncommunitv needs and provider competencv.
r providers have been able to comprehensively address a patient's condition rather than relying onsymptom management, and address other co-morbid conditions, such as opioid dependency anddia betes
. there has been increased trust, communication, and relationship building among care providersthat has led to more coordinated care for patients, not only for their LBP, but also for otherunidentified/unmet needs (e.g. mental health concerns)
o all sites have leveraged services or formed linkages with community resources to enhance thevalue of the program for patients enrolled into the pilot. This integration across communityresources and services has been an important achievement of the pilot program from a healthcare delivery and policy perspective.
System: lmpacts & OutcomesBased on the anecdotal evidence and available narrat¡ves, the PCLBP pilot sites have(to varying degrees), had a positive impact on a range of system and patient outcomes, including:
¡ reducing unnecessary diagnostic imaging;¡ reducing specialist referrals; and. improving medication management by reducing opioids and NSAIDs.
While there is positive preliminary data, because this was a short-term, low rules pilot and there werelimitations related to the ability to access relevant ICES data, both a restructuring of the site models andfurther quantitative data will be important to allow for a more conclusive outcome assessment,
HOntarioChiropracticAssociation Page 3
567Going ForwardThese findings demonstrate the pilot is delivering not only on the Ministry's Low Back Pain Strategy, but
the focus on health equity, opioid mitigation strategies, coordinated inter-professional care pathways and
patient education and empowerment. lt will therefore be important to better understand:
¡ the impact of a more standardized primary care based program of care on patients, providers
and the system with a more defined articulation of ROI
o how best evidence conservative care for MSK conditions can lessen the use of and dependency
on opioids and other medications, including manual therapy as recommended in the recent
National Pain Centre Best Practice Draft Guidelinel. how best evidence conservative care for MSK condit¡ons, such as spinal manipulative therapy can
improve function and pain, as recommended in the recent American College of Physicians2
GUtOeltne
¡ how best to mitigate downstream speciality care referrals into ISAECs as they roll out across the
LHlNs.
t htto://nationalpaincentre.mcmaster.caiquidelines.html
- 2017 Draft Recommendations for Use of Opioids in Chronic Non-Cancer Pain
2 http://www.aafp.orslnews/health-of-the-public/2O17O214acp-backpain.html Ihe American College of Physicians issued a clinicalpiãctice guideline recommending physicians treat patients' nonradicular acute or subacute low back pain with nondrug
therapies,
Rose Bustria568
From:Sent:To:Subject:
Jo-Ann WillsonFriday, May 19, 2017 10:15 AMRose BustriaFW: CCO Advertising SoP Now Applies to Websites & Social Media
Advertising and Council.
Jo-Ann Willson, B.Sc., M.S.W., LL.B.Registrar & General Counsel
College of Ghiropractors of Ontario130 Bloor St. West, Su¡te 902Toronto, ON M5S lN5Tel: (416) 9226355 ext. 1 l1Fax (416) 925-9610E-ma¡l: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any otherdistribution, copying or disclosure ¡s strictly prohibited. lf you have received this e-mail in enor, please notify me immediately by reply e-mail
and delele all copies including any attachments w¡thout read¡ng it or making a copy. Thank you.
From: Ontario Chiropractic Association Imailto:[email protected]] On
Behalf Of Ontario Chiropractic Association
Sent: Friday, May L9, 2017 9:03 AMTo: Jo-Ann Willson <jpwillson @cco.on.ca>Subiect: CCO Advertising SoP Now Applies to Websites & Social Media
We're Here For You. View this email in vour browser
OntarioChiropracticAssociation
--trrb¡-
-
1
569
þ
Our websites and social media feeds can have a major impact on our collective ability to
protect the profession's reputation, as recent neoative media coverage of chiropractic
websites in Manitoba has demonstrated.
ln a very positive move, the CCO has amended its definition of Advertising in its Sfandard
of Practice S-016: Advertisina to include websites and social media (emphasis added):
"Advertising is any message communicated outside a member's
office through a public medium, including electronic mediasuch as websites and social media, that can be seen or heard
by the public at large with the intent of influencing a person's
choice of service or service provider. This standard applies equally
to members acting individually, as a group, or as a professional
health corporation."
With this amendment, websites and social media are now subject to the criteria of the
Standard. As such, they must be accurate, factual and contain information that is verifiable,
and must not contain:
. anything false or misleading;
. a guaranteed success of care;
. arìV comparison to another member's or other health care provider's practice,
qual ifications or expertise;
2
CCO Standard of Practice S-016: AdvertisingNow Applies to Websites & Social Media
569
Our websites and social media feeds can have a major impact on our collective ability to
protect the profession's reputation, as recent neqative media coveraoe of chiropractic
websites in Manitoba has demonstrated.
ln a very positive move, the CCO has amended its definition of Advertising in its Sfandard
of Prcctiæ *016: Adveñisinq to include websites and social media (emphasis added):
"Advertising is any message communicated outside a member's
office through a public medium, including electronic media
such as websites and social med.ia, that can be seen or heard
by the public at large with the intent of influencing a person's
choice of service or service provider. This standard applies equally
to members acting individually, as a group, or as a professional
health corporation."
With this amendment, websites and social media are now subject to the criteria of the
Standard. As such, they must be accurate, factual and contain information that is verifiable,
and must not contain:
. anything false or misleading;
. a guaranteed success of care;
. any comparison to another member's or other health care provider's practice,
qualifications or expertise;
2
CCO Standard of Practice S-016: Advertising
Now Applies to Websites & Social Media

Rose Bustria
568From:Sent:To:Subject:
Jo-Ann WillsonFriday, May 19, 2017 10:15 AMRose BustriaFW: CCO Advertising SoP Now Applies to Websites & Social Media
Advertising and Council.
Jo-Ann Uvllbon, B.Sc., M.S.W., LL.B.Registrar & General Counsel
College of Chiropr.ctor3 of Onterio130 Bloor Sl. West, Suib 902Toronto, ON MSS 1NsTel: (,{16) 922631tS ext. 1 I 1
Fax (,116) 92$9610E+nail: iowillsontÞcco.on.caWeb Site: www.cco.m.ca
CONFIDENTIALITY WARNI I{G:This e-mail induding eny ilaclùner{s may conta¡n coûfident¡al ¡nbmat¡on and b inter¡ded only br ttre person(s) narn€d abore. Any dnrdistih¡tion, cop$nS or cÌsdæue is st'tcily prolt¡bibd- lf you haræ reoeiìred thb email in enor, please rü'fy me inÍred¡aHy by repþ e{ailand delete all cop¡es ¡ndudng eny attaclments without reading it or making a copy. Thart you.
From: Ontario Chiropractic Association Ima ilto:OCA=chiropractic.on.ca @mail108.wdc01.mcdlv.net] OnBehalf Of Ontario Chiropractic AssociationSent: Friday, May 19, 2017 9:03 AMTo: Jo-Ann Willson <[email protected]>Subject: CCO Advertising SoP Now Applies to Websites & Social Media
We're Here For You View this email in vour browser
OntarioChiropracticAssociation
1
-Otrfb--f
any expressed or implied endorsement or recommendation for the exclusive use of
a product or brand of equipment used to provide services; and
materialthat, having regard to allthe circumstances, would reasonably be
regarded as disgraceful, dishonourable or unprofessional.
The OGA applauds the CCO for this significant and important update to S-016. We
encourage all members to review their websites and social media feeds today to ensure
compliance with Standard of Practice S-016: Adveñisinq.
a
a
570
We're here for you. Call us:
Local: 41 6-860-0070 | Toll-free: 1 -877 -327 -2273
Update your OCA membershio preferences or
unsubscribe from this list
Our mailing address is:
Ontario Chiropractic Association
200-20 Victoria St
Toronto, ON MsC 2N8
Canada
Add us to vour address book
+ Facebook I Twitter in Linkedln
CCO Standard of Practice S-016: Advertising
3
ITEM 4-1 -35
573THE FEDETIATIONFEDERAT¡ON OF C/TNADIÂN cHIRO PRACTIC
LA FEDERATIONFÈDÈRATIOñ1 CHIROPRATIQU T' C.ANADIENN E
April25,2OI7
Ms. Alison DantasChief Executive OfficerCanadian Chiropractic AssociationADa ntas @ ch iropractic.ca
Dear Ms. Dantas,
Your letter of March 22,2OI7 was discussed by the Federation's Regulatory Council members at theirApril 8, 2017 meeting in Toronto. The Council wishes to underline the following points with theCanadian Chiropractic Association's (CCA) ad ministrators.
The Federation of Canadian Chiropractic is a federation which brings together independent bodies, each
with its own enabling legislation and requirements under regulation, These bodies, which include
individual provincial/territorial regulators, are responsible to their own governments and to the public
within their areas of jurisdiction.
Matters related to chiropractic come forward in the media from time to time. FCC Regulatory Council
members are prepared to address such matters within the context of the appropriate jurisdictional and
regulatory environments and provide information to the media regarding the jurisdiction's mandate and
responsibilities under law. There are numerous examples of this. CCA's assistance in referring such
matters to the appropriate regulatory body would be appreciated.
To conclude, if you wish to find out more about the individual provincial and territorial regulators'
disciplinary actions, including those pertaining to false advertising/claims by their members, we would
kindly refer you to the regulators' respective annual reports, all of which contain information of thatnature.
Yours very truly,
Jean-François Henry
Co-Chair, Regulatory Council
c: FCC Executive, Regulatory Council, Registrars BC, AB, NL
30 Gloucester St., Suite 2301, Toronto, ON, Canada, M4Y 116 P 4t6-697-7458 W chirofed.ca
61z2017 2017 Resolutions
Home
::-:T-
lf Home Resolutions 2017 Resolutions liejll.'il. .. .Å,Visron Statement: The FCLB rs the premrer rnternatronal resource for rnformatron and consdìdated servrces for ensurrng
the safe, ethrcal practrce of chrropractic.
Mrssron Statement:
i quicr l-inrs
Resolutions Home
201ó Resotutions
2009 Resolutions
2008 Resolutions
200ó Resolutions
2m4 Resolutions
2001 Resotutions
1999 Resolutions'1998 Resolutions
1997 Resolutions
199ó Resolutions
ic by promotrng excellence rn chrropactrc regulatron through servrce to our member boar&.Orlando, Florida
MaV 6t 2OL7
Submitted for Consideration by FCLB Board of Directors
Ich¡ropractic Licensing Boards'Affirmat¡on on Ch¡ropract¡c Ped¡atr¡c Practice
Whereas, the Federation of Chiropractic Licensing Board (FCLB) is comprised of memberchiropractic licensing boards throughout the United States and across the globe; and
Whereas, the primary responsibility of a chiropractic licensing board is to protect thehealth, safety and welfare of the consumers of chiropractic services; and
Whereas doctors of chiropractic are taught and trained to evaluate and examine patients ofall ages for the purpose of determining the presence or absence of physical or physiologicillnesses, injuries, conditions or disorders of the body, including chiropractic subluxationsand somat¡c dysfunctions; and
Whereas, doctors of chiropractic are taught and trained to care for patients of all ages withillnesses, injuries, conditions or disorders, including chiropract¡c subluxations and somaticdysfunctions, through the administration of a chiropractic adjustment to the body for thepurpose of maintaining, restoring or ¡mprov¡ng biomechanical and/or physiological function;and
Whereas, a chiropract¡c adjustment often involves the application of manual andmechanical procedures, including when applicable, high-velocity, low-amplitudeadjustments; and
Whereas, doctors of chiropractic are taught and trained to tailor the application of a high-velocity, low-amplitude adjustment to the patient's condition or circumstance, includingthe maturity, size and structural integrity of the patient; and
Whereas, doctors of chiropractic routinely care for infants and children across the globe;and
Whereas, no FCLB member jurisdiction prohibits the practice of chiropractic on persons of a
certain age, including infants and children; now therefore be it
Resolved, that the Federation of Chiropractlc Licensing Boards (FCLB) supports the safeand effective care of patients of all ages, including infants and children, by doctors ofchiropractic.
Adopted by the delegate body without d¡ssent97st Annual CongressMay 6, 2017 . Orlando, Florida
RESOLUTION #1-17
http:/Âwww.fcl b.org/H om e/Resol uti ons/201 TResol utions.aspx 1t2
6122017 2017 Reso[¡tions
Contact Us
Privacy Statement Terms Of Use
CIN-BAD Login . IMPAK Login . For Our Members5401 W. 10th Street, Suite 101 . Greetey, CO 80ó34 . 970.356.3500
For Our BoardFAX: 970,356.3599
Site Map F
CopyrÌglrt 2017 by FCLB
578
http://www.fcl b.org/H om e/Resol uti ons/201 TResol ú¡ons.aspx a2
Rose Bustria579|TEM 4.1.38
Jo-Ann WillsonWednesday, May 10, 2017 7:12 AMRose BustriaFW: MEDIA ANNOUNCEMENT: Chiropractors included in new 2017Canadian Guideline for Opioid Therapy and Chronic Non-Cancer Pain
From:Sent:To:Subject:
Exec and Council
Jo-Ann P. Willson, B.Sc., M.S.W., LL.B.Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected] Site: www.cco.on.c¿t
CONFIDENTALIW WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other dístribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copies including
any attachments without reading it or making a copy. Thank you.
Begin forwarded message:
From: Canadian Chiropractic Association <[email protected]: MEDIA ANNOUNCEMENT: Chiropractors included in new 2017
Canadian Guideline for Opioid Therapy and Chronic Non-Cancer PainDate: May 9,2017 at 5:15:58 PM GMT-4To: [email protected]
Ghiropractors included in new 2017 Canadian Guideline for OpioidTherapy and Chron¡c Non-Cancer Pa¡n
HAssociation
chiropratiquecanadienne
CanadianChiropracticAssociation
Having tror-rble viewing this email? !.ìircl' lr'.rri:
I
580The Canadian Chiropractic Association (CCA) has released the following press release insupport of the new Canadian prescribing guidelines issued by The Michael G. DeGrooteNational Pain Centre at McMaster University on behalf of Health Canada yesterday. As part ofthe Joint Statement of Action to Address the Opioid Crisis, the CCA was invited to providefeedback on The 2017 Draft Recommendations for Use of Opioids in Chronic Non-CancerPain. We are pleased to announce that the new guidelines are in line with our feedback andwith the CCA's White Paper responding to Canada's opioid crisis, A Better Approach to PainManaqement.
Chiropractors were not included in the original draft guidelines. The CCA made a compellingcase for the professions' inclusion in the new guidelines and we were successful, highlightingthat Canada's chiropractors have an important role to play for patients with chronic non-cancerpain including those who are using opioids and are experiencing serious challenges intapering. We focused our feedback on the synergy between the need for a better approach topain management, and chiropractors' care approach which aims to relieve pain and improvefunction using non-invasive and non-pharmacologicaltechniques. We also stressed that spinalmanipulative therapy is recommended as a first-line intervention in numerous clinical practiceguidelines.
Dr. Jason Busse, DC, PhD was the lead author of lhe2017 Canadian Guideline for OpioidTherapy and Chronic Non-Cancer Pain. He is a graduate of Canadian Memorial ChiropracticCollege and is an Associate Professor in the Department of Anesthesia at McMasterUniversity. Ten recommendations for healthcare providers were published yesterday as part ofthe new guideline in the Canadian Medical Association Journal. We would like to highlight thefollowing two recommendations:
Recommendation l: When considering therapy for patients with chronic non-cancerpain, we recommend optimization of non-opioid pharmacotherapy and non-pharmacologictherapy, rather than a trial of opioids.
Recommendation 10: For patients with chronic non-cancer pain who are using opioidsand experiencing serious challenges in tapering, we recommend a formal multidisciplinaryprogram.
Recognizing the cost of formal multidisciplinary opioid reduction programs and theircurrent limited availability/capacity, an alternative is a coordinated multidisciplinarycollaboration that includes several health professionals whom physicians can accessaccording to their availability (possibilities include, but are not limited to, a primary carephysician,anurse,apharmacist,aphysicaltherapist,achiropractor,akinesiologist,an occupationaltherapist, an addiction specialist, a psychiatrist, and a psychologist).
a
This is a very important and necessary step foruvard for the profession and for the health ofmillions of Canadians living with chronic non-cancer pain.
Should you receive a call from a media outlet please contact Ronda Parkes for assistance atrparkes@ch i ropractic. ca or by phone al 647 -gT 1 -221 2.
Associationchiropratique
canadienne HCanadianChiropracticAssociation
416-585 7902 | 1377 222-9303 | [email protected]¡gpractic ca
2
186 Spaclina AvenLre, St¡ite 6 Toronto, Ontario I\45T 382 Carrada
If you no longer wish to receive ottr emails, click the link below
_LJ1 r s r r b :-, r;.r. i l-ic,
581
3
St1Ot2O17 The Canadian Chiropractic A.ssociation commends the newly released recommendations for opioid therapy and chronic non-cancer pain - Canadian Chir
doctors of chiropract¡c. Approximately 4.5 million Canadians usethe services of a chiropractor each year. The CCA advocates onbehalf of members and their patients to advance the quality andaccess¡bility of chiropractic care in Canada and to improve theeffectiveness and efficiency of the healthcare system. For moreinformation on the CCA or for a referral to a doctor of chiropractic,please visit www.chiropractic.ca
igzSOURCE Canadian Chiropract¡c Association
I
For further information: Vanessa Bennett, Senior Manager ofMarketing & Communications, [email protected] /41 6-585 -7902, ext. 235
RELATED LINKShttps : //www. ch i rop racti c. cal
https://www.chiropractic.calmedia-centrdthe-canadian-chiropractic-association-com mends-the-newly-releaseúrecom m endations-for-opioidtherapy-and-chro. 3/3
5t1Ot2O17 The Canadian Chiropractic Association commends the newly released recommendations for opioid therapy and chronic non-cancer pain - Canadian Chir
Home > Media Centre > News Releases > The CanadianChiropractic Association commends the newly releasedrecommendations for opioid therapy and chronic non-cancer pa¡n
The Ganadian Chiropractic Association commends the newly releasedrecommendations for opioid therapy and chronic non-cancer pain
TORONTO, May g,2017 /CNW/ - Canada's new opioid 583prescr¡bing guideline that was released yesterday is an importantstep fonruard in address¡ng Canada's opioid crisis. The opioid crisisis not only a challenge of Canadians struggling with addiction, it isalso a pa¡n management crisis.
Opioids rapidly emerged as a first-line treatment for non-cancerpa¡n. However, it is now clear the risks and harms of opioidsusually far outweigh the benefits, including dependency andaddiction. lt is also troubling that many illicit opioid users were firstintroduced through prescription opioids.
"Low back pa¡n and other musculoskeletal conditions are currentlykey drivers of non-cancer op¡oid prescribing," says Alison Dantas,CEO of the Canadian Chiropractic Association, "That is whyCanada's chiropractors are already playing a leading role inresponding to this crisis and are committed to being part of thesolution."
Chiropractors are one of five health professions that aresignatories of Health Canada's Joint Statement of Action and areworking to develop solutions to improve the integration and accessto non-pharmacological interprofessional pain management forCanadians.
In a press release from McMaster University, Dr. Jason Busse,principal investigator for developing the new guideline, associateprofessor at McMaster University, and a chiropractor, explains that"opioids are not first-line therapy for chronic non-cancer pain.There are important risks associated with opioids, such asunintentional overdose, and these risks increase with higherdoses."
The new guideline strongly recommends optimizing non-pharmacological therapy for patients with non-cancer pain such aslow back pain.
511012017 The Canadian Chiropractic Association commends the newly released recommendations for opioid therapy and chronic non-cancer pain - Canadian Chir
"The key to reducing the number of new opioid users is to ensureaccess to evidence-based, non-opioid alternatives," says Dr.Busse. Among the recommended non-pharmacological therapiesfor pain management is spinal manipulation, which is advised forthe treatment of neck pa¡n,1 headaches,l and chronic backpain.2'3
584"By working together to provide prompt access to clinicalalternatives like chiropractic care, ev¡dence suggests we canreduce reliance on opioids and achieve better outcomes forpatients," says Dantas.
The new and supporting guidelines are in line with the CanadianChiropractic Association's White Paper responding to Canada'sopioid crisis, A Better Approach to Pain Management.
The new recommendations on the use of opioids were publishedyesterday in the Canadian MedicalAssociation Journal, officiallytitled rhe 2017 canadian Guideline for opioid rherapv andChronic Non-Cancer Pain. These recommendations were issuedby The Michael G. DeGroote National Pain centre at McMasterUniversity and developed on behalf of Health Canada.
References
1. Nahin RL, Boineau R, Khalsa PS, Stussman BJ, Weben UrJl.Evidence-based evaluatÍon of complementary health approachesfon pain management in the united states. Mayo cLiníc proc.2Øt6; 91(9) : 1292-3Ø6. doi : Lø .tøL6/ j . mayocp .2ø16.ø6 .øø7 .
2. Chou R, Deyo R, Fniedly J, et aI. Systemic phanmacologicthenapies fon low back pain: a systematic neview fon anAmenican College of Physicians Clinical Practice Guideline. AnnIntern Med. 2ØL7; 166(7): 48Ø-92. doi: LØ.7326/t4L6-2458.3. chou R, Deyo R, Friedry J, et al. Noninvasive Tneatments fonLow Back Pain. AHRQ comparative Effectiveness Reviews. 2øL6.Rockville (MD): Agency fon Healthcane Research and Quality(US); 2øt6 Feb. Repont No.: L6-EHCøø4-EF.
About the Ganadian Chiropractic Association
The canadian chiropractic Association (ccA) is a national,voluntary association representing canada's 8,500 licensed

2017 Canadian Guideline for Opioids for Chronic Non-cancer Pain
Values & Preferences Statement585
On the basis of our review of the relevant published literature, our own focus group interviews with ourpatient panel, and the clinical experience of our expert consultants, we have concluded that for patients
living with chronic non-cancer pain receiving opioid therapy, achieving pain relief is the most important
consideration. We believe these results (and the subsequent importance ratings we present here) are
likely to generalize to patients considering opioid therapy, and we therefore use these values in
questions directed at this population.
When patients experience severe nausea, vomiting, or constipation as a result of opioid use, these
adverse effects are almost as important as pain relief, and thus may be more important than small
degrees of pain relief. Other opioid-related adverse events, such as sleep disturbance, personality
changes, dizziness, and mental fog are less important to patients with chronic non-cancer pain but are
not irrelevant and thus deserve consideration in making our recommendations.
When considering less common but more severe adverse events (addiction), and particularly rare but
very serious adverse events (unintentional overdose requiring hospitalization, fatal unintentional
overdose) we viewed societal values and preferences as very important. On the basis of decisions made
regarding other drugs with severe rare side effects, and on public and policy reactions to diversion,
addiction and death related to widespread opioid use by patients with chronic non-cancer pain, we have
concluded that society places a high value on minimizing these adverse events. As a result, we too place
a high value on avoiding these adverse events, even if less frequent or rare. We consider that their
avoidance may be more important than achieving modest pain reduction, particularly if that pain
reduction is associated with the adverse effects noted previously.
Superficial consideration of our interviews with members of the patient advisory panel would suggest
that these índividuals place little importance on avoiding addiction or the small likelihood of accidental
overdose or death. Our analysis, however, suggests that this may be a result of an attitude of "it won'thappen to me". That conclusion is based in part on the observation that the lived experience appears tohave an important framing effect on patient's values and preferences regarding use of opioids, thatserves to aligns patients' and societies' values over the long-term. Out of desperation for any relief from
chronic pain, patients with chronic non-cancer pain are often willing to trade rare but serious harms forsmall but important pain relief, and this may leave some patients vulnerable to short-term decisions
that are inconsistent with societal values. The patients on our advisory panel who had actually suffered
serious adverse events placed a much highervalue on their avoidance, consistentwith societal attitudes
toward such events.
Finally, our focus group interviews revealed that some patients usíng long term opioid therapy forchronic non-cancer pain were concerned about adverse consequences of opioid withdrawal that may
result from efforts to wean or discontinue their opioid use. For those using high doses of opioids in
whom weaning is undertaken, we continue to place a high value on societal considerations ofminimizing the risk of rare serious adverse events, but we also place a high value on avoiding severe
suffering, increased pain, and functional limitation that may accompany opioid reduction. We also place
a high value on patient autonomy under these circumstances.

---55O
O
A Better Approach to
Pain Management
Associationchiropratique
canadienne
CanadianChiropracticAssociation
Respond¡ng to
Canada's Opio¡d Cri ssa
I
Novem be r 201 6
Associationchiropratique
canadienne
CanadianChiropracticAssociationH
587
A BETTER APPROACH TO PAIN MANAGEMENT IN CANADA
EXECUTIVE SUMMARY
opioids have quickly emerged as one of the primary means for managing acute and chronic non-cancerpain in primary care settings. Available evidence points to back pain and other musculoskeletalconditions as a leading reason for opioid prescribing. As leading experts in the care of musculoskeletalconditions, Canada's chiropractors and the Canadian Chiropractic Association (CCA) are prepared to be apartner in the action plan to reduce the use of opioids.
The Canadian Minister of Health's National Opioids Conference is an important opportunity for thegovernment, healthcare providers, and others to address a long-overlooked and often-silent healthepidemic: chronic non-cancer pain. The challenge is to increase awareness and accessibility toalternatives to opioids for Canadians in pain. Evidence-informed guidance for prescribing professions onthese key alternatives, including chiropractic, is an important first step in a comprehensiveinterprofessional pain management strategy for Canada. Together, we can support and facilitateprogressive and innovative practices that will not only improve health outcomes but also decrease over-reliance on opioids as a first-line intervention.
/ssues.'
Pain is real, complex, and can be difficult to manage. Chronic pain can adversely affect an individual'sability to carry out daily activities, work productively, and maintain family commitments. ln the 1990s,opioids quickly emerged as one of the main ínterventions used to manage chronic non-cancer pain, withback pain being one of the leading reasons. This reliance on opioids occurred despite limited evidencesupporting their use or efficacy in treating acute and chronic musculoskeletal pain. The unforeseenconsequences of opioids are increasingly evident and constitute a major health concern. Evidence showsthat the risks from the first time that opioids are prescribed for back pain can be profound and includeaddiction, morbidity, and even death. As a result, effective solutions must include reducing the pressureto prescribe by prioritizing alternative approaches to pain management. Every year in Canada, over2,000 Canadians die from the overuse of opioids, which accounts for 50% of all annual drug-relateddeaths. The impact on vulnerable and marginalized populations is even graver, given the higherprevalence of both low back pain and incidence of opioíd use within this group.
Evidence shows that alternative approaches to managing back pain such as spinal manipulationprovided by chiropractors are effective. Yet, referrals to community-based providers are not commonlychosen as the first option for musculoskeletal conditions. Conservative care options, like manualtherapies for back pain and other musculoskeletal conditions, generally fall outside the publicly-fundedsystem, making access challenging for many people-particularly in vulnerable and marginalizedpopulations. Healthcare practitioners such as physicians may feel they have limited choices available tothem-without coverage or direct access, they may be less likely to refer patients for conservative care.
2
f (416) s85.7902 Í 1é71t222.930f r (416) 585-2970186 Spddind Avenue Suite 6, Toronto, ON ¡,45T:82
Associationchiropratique
canadienne
CanadianChiropracticAssociationH
588
Solutions:
To truly manage musculoskeletal conditions, all stakeholders need to better understand the burden ofpain related to musculoskeletal conditions. We need a comprehensive interprofessional pain
management strategy that relies less on opioids and reduces the pressures on healthcare practitioners
to prescribe. Evidence-based alternative approaches should be considered first. This is particularly
important as practice guidelines change over time and new evidence ís emerging that is moving away
from opioids, especíally for the treatment of chronic conditions. lncreasing access and referrals to
community-based providers like chiropractors and integrating them within the interprofessional
healthcare team is a posítive alternative.
lnterprofessional teams with a full range of assessment and treatment skills in pain management
approaches are quickly becoming widely accepted as being effective alternatives. There are a number ofinterprofessional and innovative models being piloted (e.g., Ontario's low back pain pilot programs) and
fully implemented (e.g., St. Michael's Hospital Family Health Team in Toronto, Ontario and Mount
Carmel Clinic in Winnipeg, Manitoba), which have shown great promise in effectively managing acute
and chronic musculoskeletal pain and reducing the pressure to prescribe opioids. This has been
accomplished by integrating community-based providers with chiropractors who are playing a central
role in providing conservative care. Currently, over 4.5 million Canadians annually choose to visit a
chiropractorto help prevent and treat musculoskeletal conditions. However, many others are either
unaware of this option or do not have access to it. As a further benefit, effective back pain triage and
access to appropriate care have been shown to reduce wait times and costs associated with unnecessary
services such as diagnostic imaging and specialist visits'
Recommendations:
The CCA strongly believes that to actually change the current course and to reduce reliance on opioids
we must take a broader approach to comprehensively manage pain. We assert that a better approach
must take into account best practices and innovations, including greater access to conservative care
options. We also assert that the evidence is clear that manual therapies, including chiropractic, should
be first-line options for the management of musculoskeletal conditions within the interprofessional
healthcare team. Such management offers a safe, effective, non-invasive, coordinated, and cost-
effective alternative to opioids. Further, we recommend:
1,, Collaborate with governments and other stakeholders to support and facilitate innovativepractices to improve the delivery of alternatives in primary care.
2. Expand access to alternat¡ve approaches to opioids such as conservative care modalities forall, but in particular for vulnerable populations. These approaches must be readily available
through interprofessional care teams for those suffering from musculoskeletal conditions.
3. Develop a better understanding, in partnership with third-party payers, on how to best
maximize health outcomes using currently available funding.3
f {4r6) 585.7902 t 1ß771222-9303 F (416) s85-2970! 86 Spadin¿ Avenue - Sùite 6, foronto, ON M5T 382
Associationchiropratique
canadienne
CanadianChiropracticAssociationH 589
4. lnvest in research to fully understand the breadth of the opioids cr¡s¡s and burden ofmusculoskeletal conditions. Furthermore, ¡nvest in health services research that would allowfor the creation of comprehensive approaches to managing chronic non-cancer pain.
A BETTER APPROACH TO PAIN MANAGEMENT IN CANADA
INTRODUCTION
Opioíds have quickly emerged as one of the primary means for managing chronic non-cancer pain inprimary care settings. There is now a growing awareness of the associated risks and widespreadrecognition that opioids are being prescribed far too often. Better approaches are needed to managechronic pain in Canada and reduce reliance on opioids as a first-line intervention.
Available evidence points to back pain and other musculoskeletal conditions as a leading reason foropioid prescribing; a recent British Medical Journalstudy found that 50% of those prescribed opioids inthe United States reported back pain.1
The canadian chiropractic Association (ccA)'? believes that to address theproblem of opioid abuse we must better understand the underlying Canadian chÍropractorscauses of overuse. Our approach must look at alternatives to manage the are musculoskeletøl pøîncauses of pain and how these alternatives can be better integrated into erqerts and provide careprimary care settings to help Canadians suffering, partícularly for those in to over 4.5 mÍllionchronic pain. As musculoskeletal experts, Canada's 8,500 chiropractors Canadiøns eøch yearcan play a greater role in the assessment and management ofmusculoskeletal-related pain and dysfunction by providing safe and effective care.
The CCA believes that one important solution is to develop a comprehensive pain management strategy,starting with innovative approaches to interprofessional care within primary care settings. This can beaccomplished in part by enhancing access to appropriate care alternatives such as chiropractic,physiotherapy, and psychology among others. Considering the tremendous burden that both opioidoveruse and musculoskeletal conditions have on society, and particularly on vulnerable andmarginalized populations, this strategy should also specifically address the needs of those that are atgreater risk.
This document is intended to support the development of a better approach to pain management inCanada. lt highlights:
The prevalence of musculoskeletal conditions as a leading cause of non-cancer pain.The current over-reliance on opioids to manage chronic non-cancer pain and the particularimpact on vulnerable populations,
a
a
4
r (,116)585 Ìtti.)2 It1(a/ll)tÌ rtìLlt | (41¡j)r85 2iìl0l3L 5f-,¡dr¡lr
^rrr.u. Sur(¡r ¡r, Irronto,(J¡ì l.irì jLl¿
Associationchiropratique
canad¡enne
CanadianChiropracticAssociationH 590
How better integration of evidenced-based alternative care options, such as chiropractic
services within interprofessional care teams, can help reduce the reliance on
pharmacotherapies while improving overall health outcomes.
The four key recommendations for the Opioid Action Plan that the CCA believes could help
governments achieve a more comprehensive approach to non-cancer pain management, but
particularly for Canada's most vulnerable populations.
MUSCULOSKELETAL CONDITIONS ARE A LEADING CAUSE OF CHRONIC PAIN
a
a
One in five Canadians suffers from chronic non-cancer pain3'a with back pain as the
leading condition. ln reality, the burden of chronic back pain is a silent epidemic in
Canada, Too often, people suffer in silence with little recourse. Every year, over
11 million Canadians suffer from back pain and other musculoskeletal conditions, such
as arthritis,s which rival cardiovascular disease as an overall health burden in terms ofdirect and indirect costs.6 Musculoskeletal conditions also significantly impact Canada's
productivity and disproportionally affect workforce participation among lower income
Canadians doing more physically demanding labour. Among the general population, up
to 85% of workers will suffer from back pain at least once in their lifetime. Often, thatback pain will reoccur or become chronic.T ln Canada, the disability costs related tomusculoskeletal conditions are the most significant of any chronic disease at S15
billion.s Over half of workdays lost due to injury are for musculoskeletal conditions.e
Today, onein fiveCanadionssuffer lromchronÍc non-cancer pøÍnwith backpøin øs theIeading type
Today, Canada is in the midst of a pain management crisis. This crisis has had a significant impact on
patients and society at large with consíderable implications for the healthcare system, including for
healthcare providers, administrators, and insurers. The CCA believes that non-cancer pain-musculoskeletal-related pain, in particular-is currently poorly managed in Canada due in part to limited
access to alternative care options.
OVERREL¡ANCE ON OPIOIDS TO MANAGE CHRONIC PAIN
The increasing use of opioids as a first-line treatment for chronic paín, and specifícally for mechanical
back pain, is a key contributorto the increasing use of opioids in Canada.10 Since 1999, prescription
opioid sales have increased fourfold.ll lt is reported that half of legitimate prescriptions of opioids are
prescribed to help manage back pain and other musculoskeletal conditions.l2 ln the United States,
opioids are reported as the leading cause of unintended death by overdose, also outnumbering those
attributable to cocaine and heroin combined (see Figures 1 and 2 below)'
5
r (4la)585 /932 rllt l/)222 1J0l I (41ô)t8519/018i' 5p¡drild
^!larue 5uitc ¿ Ioronto,0f! f/r5l -ltll
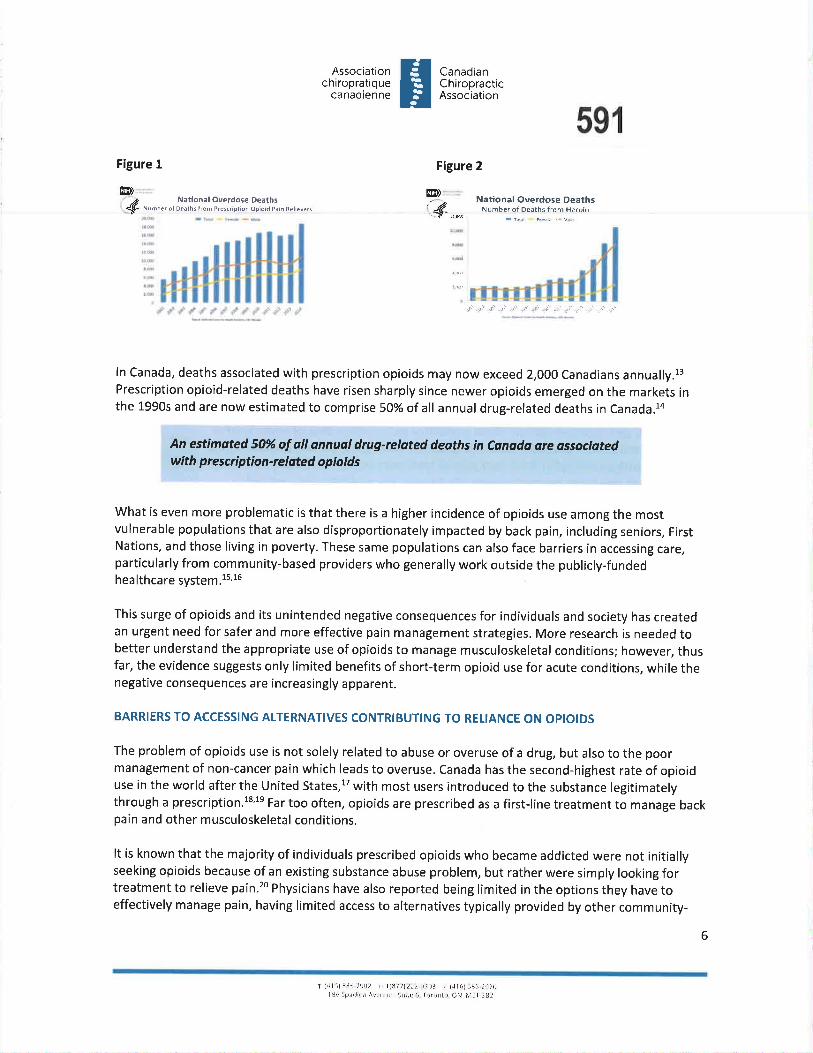
Associationchiropratique
canadienne
CanadianChiropracticAssociation
Figure 2
H591
Figure 1
4@) @)
National Overdos€ DeethsNuñber of Deàths fronì Prerc¡ipnon ôpþid P¿¡n Reli€ve11
rrll
,4"*. Nationel Overdose DeathsNumber of Deaths from H€roin
r. i ..¡ j ,. ¡J j. .,' ..: .,ìr :i -ìr ì) .rr .¡'.ç' d.¡ ,.r l+ j .r+ +¡ .J ,s i J ^¡'
ln Canada, deaths associated with prescription opioids may now exceed 2,000 Canadians annually.13Prescription opioid-related deaths have risen sharply since newer opioids emerged on the markets inthe 1990s and are now estimated to comprise 50% of all annual drug-related deaths in Canada.la
An estîmøted 50% of all annuøl drug-related deaths in canøda are øssociøtedwíth p re scríptî on-re I ated o p¡o ids
What is even more problematic is that there is a higher incidence of opioids use among the mostvulnerable populations that are also disproportionately impacted by back pain, including seniors, FirstNations, and those living in poverty. These same populations can also face barriers in accessing care,particularly from community-based providers who generally work outside the publicly-fundedhea lthcare system.1s,16
This surge of opioids and its unintended negative consequences for individuals and society has createdan urgent need for safer and more effective pain management strategies. More research is needed tobetter understand the appropriate use of opioids to manage musculoskeletal conditions; however, thusfar, the evidence suggests only limited benefits of short-term opioid use for acute conditions, while thenegative consequences are increasingly apparent.
BARRIERS TO ACCESSING ALTERNATIVES CONTRIBUTING TO RELIANCE ON OPIOIDS
The problem of opioids use is not solely related to abuse or overuse of a drug, but also to the poormanagement of non-cancer pain which leads to overuse. Canada has the second-highest rate of opioiduse in the world after the United States,17 with most users introduced to the substance legitimatelythrough a prescription.ls'1s Far too often, opioids are prescribed as a first-line treatment to manage backpain and other musculoskeletal conditions.
It is known that the majority of individuals prescribed opioids who became addicted were not initiallyseeking opioids because of an existing substance abuse problem, but rather were simply looking fortreatment to relieve pain.20 Physicians have also reported being limited in the options they have toeffectively manage pain, having limited access to alternatives typically provided by other community-
6
Ì (.i1,))!C5 t<i)/ 1ttl8l/)Ì2¿ 1l0l I (41.ì)rE!2!r70lgi5ptrrJlr¡^/crìùr 5r¡,tc I ì¡-,r,)¡ìto ON ¡,¡!l rlJ2
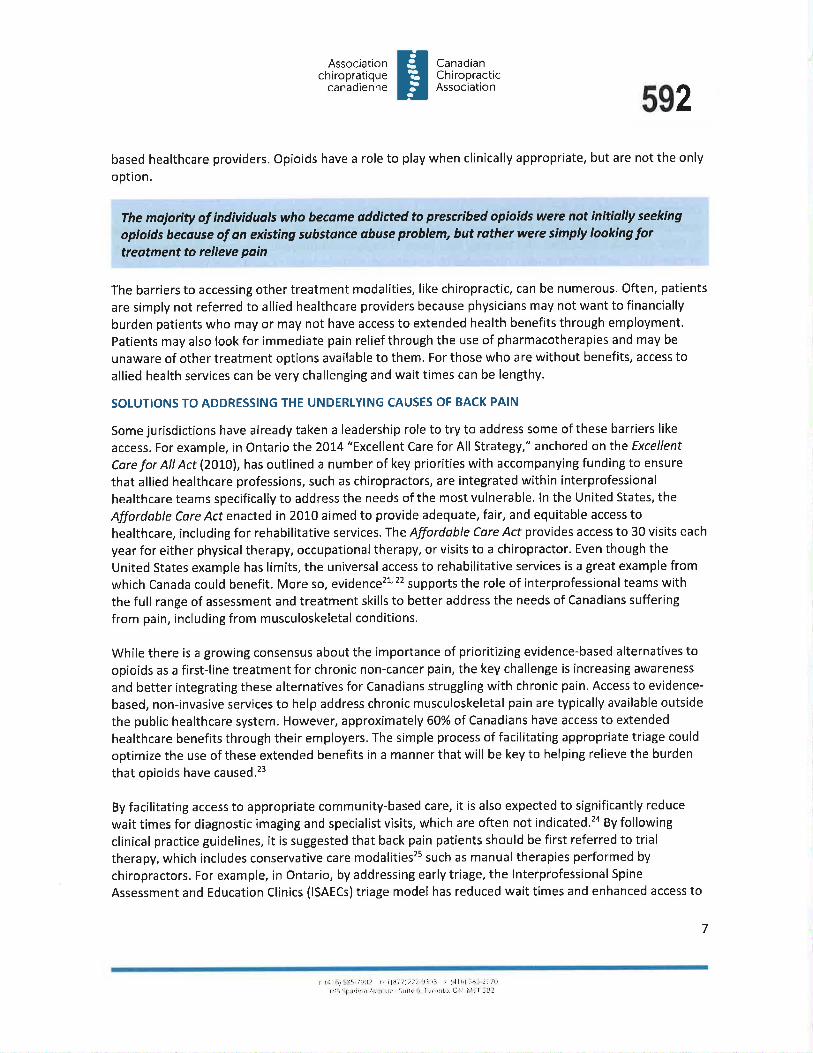
Associationchiropratique
canadienne
CanadianChiropracticAssociationH 592
based healthcare providers. Opioids have a role to play when clinically appropriate, but are not the only
option.
The majority of índÍviduals who becøme addìcted to prescribed opioids were not initíally seeking
opÍoÍds because of an existing suhstance obuse problem, but rather were simply lookÎng fortreøtment to relíeve paîn
The barriers to accessing other treatment modalities, like chiropractic, can be numerous. Often, patients
are simply not referred to allied healthcare providers because physicians may not want to financially
burden patients who may or may not have access to extended health benefits through employment.
Patients may also look for immediate pain relief through the use of pharmacotherapies and may be
unaware of other treatment options available to them. For those who are without benefits, access to
allied health services can be very challenging and wait times can be lengthy.
SOLUTIONS TO ADDRESSING THE UNDERLYING CAUSES OF BACK PAIN
Some jurisdictions have already taken a leadership role to try to address some of these barriers like
access. For example, in Ontario the 2014 "Excellent Care for All Strategy," anchored on the Excellent
Care for All Act (2OLO\, has outlined a number of key priorities with accompanying funding to ensure
that allied healthcare professions, such as chiropractors, are integrated within interprofessional
healthcare teams specifically to address the needs of the most vulnerable. ln the United States, the
Affordable Core Act enacted in 20L0 aímed to provide adequate, fair, and equitable access tohealthcare, including for rehabilitative services.lhe Affordoble Care Acf provides access to 30 visits each
year for either physical therapy, occupational therapy, orvisits to a chiropractor. Even though theUnited States example has limits, the universal access to rehabilitative services is a great example from
which Canada could benefit. More so, evidence2l'22 supports the role of interprofessional teams with
the full range of assessment and treatment skills to better address the needs of Canadians suffering
from pain, including from musculoskeletal conditions.
While there is a growing consensus about the importance of prioritizing evidence-based alternatives to
opioids as a first-line treatment for chronic non-cancer pain, the key challenge is increasing awareness
and better integrating these alternatives for Canadians struggling with chronic pain. Access to evidence-
based, non-invasive services to help address chronic musculoskeletal pain are typically available outside
the public healthcare system. However, approximatelV 60% of Canadians have access to extended
healthcare benefits through their employers. The simple process of facilitating appropriate triage could
optimíze the use of these extended benefits in a manner that will be key to helping relieve the burden
that opioids have caused.23
By facilitating access to appropriate community-based care, it is also expected to significantly reduce
wait times for diagnostic imaging and specialist visits, which are often not indicated.24 By followingclinical practice guidelines, it is suggested that back pain patients should be first referred to trialtherapy, which includes conservative care modalities2s such as manual therapies performed by
chiropractors. For example, in Ontario, by addressing early triage, the lnterprofessional Spine
Assessment and Education Clinics (lSAECs) triage model has reduced wait times and enhanced access to
7
r (.it;l'i'l Ì<)t\.1 1i ilAi i)/)Ì ¡)ril , 1.1ì6) rE' lll1rllS' !Jr,rd l¡ Á,,..r'u¡ !!rtL ., l,'rr)rìt,J, O:l I',ì :U.¿
Associationchiropratique
canadienne
CanadianChiropracticAssociationH 593
education for acute and chronic low back pain patients. The result was accomplished by employingchiropractors and advanced practice physiotherapists to assess patients early.
Chiropractors in the ISAECs and similar models are already adding their expertise to an increasingnumber of leading-edge pain management programs. Chiropractors are ideally suited to fill this role dueto their extensive education and training: four years of study in chiropractic and over a thousand hoursof theoretical and clinical studies, preceded by a minimum of three years of post-secondary education.Chiropractors have the knowledge, skills, and competencies to assess and diagnose the underlyingcauses of musculoskeletal pain. They also have the ability to develop an evidence-informed treatmentplan to improve pain and function and make referrals to other professionals as needed.
CASE TOR CONSERVATIVE26 CARE - ROLE OF THE CHIROPRACTOR
"...when considering effectiveness and cost together, chiropractic care for low back ond neck pain ishighly cost-effective ond represents good vø\ue..." 27
There is a growing consensus and supporting evidence that there are better approaches than opioids toaddress chronic musculoskeletal pain, including conservative care approaches provided by chiropractorsand by other healthcare professionals. The challenge is to make conservative care more accessible toCanadians in pain by facilitating appropriate referrals between primary care settings and community-based providers.
As discussed, chiropractors are trained to assess and manage a wide array of musculoskeletalconditions. Commonly, they use hands-on manual therapies, such as spinal manipulation, to help relievepain and improve function. Spinal manipulation has been shown to be effectíve in the management ofacute, subacute, and chronic low back pâín.28,29 Specifically, the literature supports that spinalmanipulation for chronic low back pain is statistically effective in terms of pain relief and improvementin function.30 Evidence suggests that prescribing opioids may actually delay return-to-work of injuredworkers and provides little to no benefit in terms of function.3l Spinal manipulation is alsorecommended as a first-line intervention for back pain in numerous clinical practice guidelines, includingthose by the U.S. Department of Veterans Affairs, the Bone and Joint Decade Task Force, the AmericanCollege of Physicians, the American Pain Society, and Britain's National lnstítute of Health and CareExcellence. The journal Sprne reported that evidence-based treatments such as spinal manipulation foracute mechanical low back pain were associated with "significantly greater improvement" in condition-specific functioning.32
Manipulation is often complemented by other manual therapies and modalities, as well as rehabilitationand exercise therapy. ln fact, spinal manipulation in addition to strengthening exercises have acomparable effect to the prescription of nonsteroidal antl-inflammatory drugs and exercise both forshort- and long-term pain relief.33 A study reported that exercise in conjunction with manipulation mightaccelerate the recovery and improve outcomes while decreasing the reoccurrence of injury.3a
Addíng manual therapy like spinal manipulation to standard medical care has been clinically shown to bea viable, non-invasive, and evidence-based approach to managing musculoskeletal-related pain anddysfunction.3s For example, the publicly-funded Mount Carmel Clinic in Winnipeg, Manitoba
8
r {4l6) 58s 7902 1ç lß77t222.9303 r {416) 585-2970186 Sp¿dind Avenue Suite 6, loronto. ON Msl 382

Associationchiropratique
canadienne
CanadianChiropracticAssociationH
594
demonstrated in a preliminary study that the primary source of referrals for chiropractic treatment was
from the clinic's physicians. As well, referrals were made for a variety of musculoskeletal conditions with
back pain as the leading cause. Among those patients treated by the clinic chiropractor, there was a
clinically significant reduction in musculoskeletal-related pain.36
CHIROPRACTORS STRENGTHEN INTERPROFESSIONAL PAIN MANAGEMENT TEAMS
"We need a culturoltronsformation thot places the patient ot the centre of o personalized, toilored,
integrated, multidisciplinary model of self-core and directed care drawing upon oll available evidence-
based modalities to relieve pain and improve function." 37
Pain is very complex and can be tremendously difficult to manage. Yet, for those in pain, the experience
is real and can have a devastating effect on their lives. One approach may not work for all patients.
Empowering patients to manage their care with the healthcare team of their choosing is an importantcomponent of recovery. To do so, providers must be encouraged to work collaboratively to ensure
prompt access to the right care at the right time.
Addressing the opioid crisis will require a broader understanding of the underlying issues and
reconsideration of the role(s) that all healthcare providers can play in appropriately managing patients'
needs. Better integration of allied healthcare providers, including chiropractors, is one solution toenhancing patient-centred care. As the health needs of the population evolve, so should healthcare
delivery. Within integrated healthcare teams, providers who are able to practice to the maximum of
their scope and abilities are better able to meet the health needs of Canadians. For musculoskeletal
conditions, the key is to prioritize non-invasive, conservative alternatives before prescribing opioids orother drugs for chronic pain. Accordingly, the U.S. Centers for Disease Control and Prevention
recommends access to alternative approaches38 that can be facilitated by interprofessional
collaboration. An early Ontario project has shown that integrating chiropractors into interprofessional
care teams reduced the use of pharmacotherapies and improved overall health outcomes. The 2010
study for the Ontario Ministry of Health found that including chíropractic in a team-based care pilot
reduced the use of narcotics by 57%.3e
Every year, millions of Canadians visit a chiropractor to help treat or prevent musculoskeletal conditions
The chiropractic profession also benefits from being governed by provincially-legislated regulatory and
licensing bodies ín all provinces. Each provincial regulatory body is responsible for granting a license topractice chiropractic in their jurisdiction, establishing standards of practice, and ensuring the protection
of the public. Chiropractors typically follow a methodological process to manage patients referred to as
The Roadmap to Care. The Roadmap to Care is currently taught as a best practice to reflect the flow ofinitial, subsequent, or re-evaluation visits. See Appendix 1 for additional information.
Commonly, chiropractors play the role of a primary care provider who assesses, diagnoses, and
conservatively manages musculoskeletal conditions using non-invasive, non-pharmacological manual
therapies (e.g., joint manipulation and mobilization, soft tissue therapy, and other modalities
complemented by exercise recommendations and rehabilitation). While some other healthcareprofessions have received training in performing spinal manipulation, it is an area of clinical strength forchiropractors, whose education focuses on hands-on learning with a particular interest in the spine.
9
f (4r 6) 585.7902 lF 1 ß77t222 9303 f (416) s85'2970186 Spadrnd Avenue -suite 6, loronto, ON M5T 382
Associationchiropratique
canadienne
CanadianChiropracticAssociationH
595
Canada's current reluctance to more fully coordinate between the public sector and community-basedservices is a critical limitation to ensuring fair and equitable access for all in need, especially vulnerablepopulations. Fortunately, Canada currently has a number of unique collaborative projects underwaywith organizational structures designed to best support collaborative care. Below are three examples ofsuccessful models of care where chiropractors were introduced and integrated into theinterprofessional healthcare team to help manage musculoskeletal-related pain:
Example 7: Føcilitating Triage
ln two Ontario low back pain pilot programs funded by the Government of Ontario, chiropractors andadvanced practice physiotherapists were employed to help triage and manage acute and chronic lowback pain patients. First, as mentioned previously, the lnter-professional Spine Assessment andEducation Clinics (ISAECs)40 have demonstrated that engaging chiropractors in the assessment and co-management role of low back pain decreases the need for unnecessary diagnostic ímaging and specialistvisits and their associated costs.al A second example is an ongoing project in the assessment stage calledthe Primary Care Low Back Pain Pilot program. This program aims to demonstrate the benefits of aninterprofessional approach to musculoskeletal management that includes chiropractors andphysiotherapists as part of the team. Anecdotal results show a reduced use of imaging, specialistreferrals, and use of opioids, while positively impacting patient function and mobility.
Example 2: lntegration into a Fdmìly Health Team
The Toronto-based St. Michael's Hospital Family Health Team integrative healthcare model wasrecognized as one of four centres of excellencea2 by the Council of the Federation in 2OI2.The team-based model includes nine provider groups, which include medical doctors, nurse practitioners, nurses,and chiropractors. Since the inception of the program, waiting lists for musculoskeletal assessmentshave grown exponentially because of the program's sLlccess in addressing chronic pain. Musculoskeletalconditions are now part of the primary care intake process and patients are readily referred tochiropractic interns, who are under the supervision of clinícians, early in the process. The programcontinues to operate successfully to meet the needs of patients and the community at large.
FøcilitøtÍng tr¡dge and the integration ol chìropractors ond other communíty-based providers íntoprimary healthcare teoms improves timely access, reduces relionce on opíoîds, ond improves overollhealth outcomes
Example 3: Meeting the Needs of Vulnerable Populations
ln 20L1, Manitoba initiated a pilot program providing public access to chiropractic care at the MountCarmel Clinic serving an inner-city community in Winnipeg. The services are now fully integrated andfunded by the province of Manitoba. Preliminary results demonstrated a significant reduction inmusculoskeletal pain and improvements in function for those patients referred for chiropracticservices.a3 Similar results have been demonstrated with chiropractic integration into hospital settingsaa
r (41ô) !85 /t1i) ú l\8/ /)2L!.fl Dl r (¿rrì) _iEtj 29/013r' 5lrrd rr ¡!tfuii 5uitc !, ¡,r',rrìtD, Ol'.1 l,1il jiJ2
10

Associationchiropratique
canadienne
CanadianChiropracticAssociationH 596
and healthcare teams serving military and veterans.4s Effective triage away from expensive and
unnecessary services has been reported to be cost-effective and sustainable,
These are the only three examples of the roles that chiropractors play in interprofessional
musculoskeletal care models and programming across Canada.
STRATEGIC PARTNERSHIP WITH THIRD-PARTY PAYERS AND THE PRIVATE SECTOR
Though a large number of medical services are publicly funded, roughly 3O% of healthcare services are
privately funded through private insurance or out-of-pocket payment.46 lt is estimated that 60% of
Canadians have access to extended health benefits through their employment and many rely on these
to accessvision, dental, pharmaceuticals, and paramedicals.ot By providing accessto health benefitsto
millions of Canadians, the insurance industry and third-party payers play a key role in health-related
policy matters. As a result, governments, policyholders, and Canadian consumers are increasingly
looking to the insurance industry to also take part in the development of solutions to help enhance
access to care and ensure productivity and economic prosperity. Unfortunately, the impact of chronic
disease continues to threaten the sustainability of both the public and private sectors, partly due to
rising costs of prescription drugs, lt is evident that a shared public-private responsibility is needed for
sustainable, long-term access to appropriate health services in Canada.
Third-party payers have the opportunity to be key players in ThÍrd-party payers have the
facilitating and supporting innovative practices that would enhance opportunity to he key pløyers ìn
access to community-based services. Accordingly, the Advisory Panel lacilÍtating and supporting
on Healthcare lnnovationas recommends breaking down silos Ínnovative practicesthatwouldbetween publicly- and privately-funded sectors to promote and enhance access to communÍty-
facilitate better integration of community-based providers. This bosed servíces
evolution should move away from supply-focused to need-focused
care which would improve outcomes and save costs. Currently, Canadians covered by extended health
benefits often have better, prompter access to the right care by the right provider. lndustry partners and
strategic partnerships are part of the solution to bridging the gap between primary care settings and
community-based services. Such a strategic partnership could improve the outcomes, efficiency, and
cost-effectíveness of the system. Canadians, governments, and industry partners would all benefit in
partnering to develop effective multidisciplinary approaches to managing conditions such as chronic
back pain which, in addition to being a primary reason for opioid use, is also a leading cause of disability
worldwide.as Enhancing access and referrals to appropriate conservative care could help in reducing the
reliance on opioids and decrease the ever-increasing cost pressure of pharmacotherapies on employers
and the system alike.
TOWARDS A BETTER APPROACH TO PAIN MANAGEMENT- OUR RECOMMENDATIONS
More can be done to approach pain management, starting by shifting away from opioids and highly
addictive pharmacotherapies as first-line options and increasing access to appropriate alternatives tohelp manage pain. The appropriate management of pain must become a focus, The 2016 CDC Guideline
for Prescribing Opioids for Chronic Pain clearly emphasizes the use of nonpharmacological therapies for
1t
r (4rit585./9O2 n 1ß/t)2229a\t r (416)385.2!70186 5p¿dilì¡ A?.arue Suilcrj, iororìto, ON ¡l5I:U2
Associationchiropratique
canadienne
CanadianChiropracticAssociationH 597
treating chronic pain. Similarly, the U.S. National Pain Strategy specifically recognizes the value ofchiropractic care for pain management.so
The aim is to look at developing a better approach that is based on a full understanding of why opioidsare being prescribed for non-cancer pain, accounts for best practices, and allows for greater access toconservatíve care options, including those traditionally outside the public healthcare system. Theevidence is clear that manual therapies, including chiropractic, should be first-line options for themanagement of musculoskeletal conditions like acute and chroníc back pain. For Canadians, chiropracticcare delivered as part of their interprofessional healthcare team offers a safe, effective, non-invasive,coordinated, and cost-effective alternative to opioids.
The CCA has four key recommendations emerging from this submission that we believe couldsignificantly reduce reliance on opioids and lead to major improvements in managing themusculoskeletal pain of Canadians. The recommendations are also intended to help improve overallhealth outcomes for those who are most vulnerable and for the general population.
1. Collaborate with governments and other stakeholders to support and facilitate innovativepractices to improve the delivery of alternatives in primary care.
The CCA has already begun to partner with other stakeholder groups to build a morecomprehensive approach to the management of musculoskeletal health conditions, initially bypromoting evidence-informed guidance for prescribing professions on appropriate referraltochiropractic care. Chiropractic care is an important alternative to opioids for back pain and manyother musculoskeletal conditions. The CCA believes that a broader approach is also needed andrecommends that in order to truly support and facilitate innovative practices furthercollaboration and partnerships are needed, including with governments, policy makers, insurers,primary care teams, regulators, professional associations, patients, and other interested parties.This is important to build a better understanding of the role that community-based províderssuch as chiropractors have in patient-centred care and in comprehensive pain management.
2. Ensure and expand access to alternative approaches to opioids such as conseruative caremodalities for all, but in particular for vulnerable populations. These approaches must bereadily available through interprofessional care teams for those suffering frommusculoskeletal conditions.
The evidence clearly shows the significant positive impact that effective integration ofalternative approaches have on reducing the burden of chronic musculoskeletal pain and thereliance on opioids. The CCA recommends that current models be expanded and new modelsexplored, particularly for the most vulnerable populations. These models must includeconservative care options provided by community-based providers such as chiropractors to helpensure that patients are served by the right care, at the right time, by the right provider.Further, ongoing study and evaluation of current and new models is important to promote bestpractices, share learnings, and provide opportunities to scale those models that prove effective.
72
I (416) 585.7902 v 1 ó771222.9303 F (416) 585.2970186 Sp¿dina Avenue .suite 6, Toronto, ON Msf 382
Associationchiropratique
canadienne
CanadianChiropracticAssociationH
59S
3. Develop a better understanding, in partnership with third-partv pavers. on how to best
maximize health outcomes using currently available funding.
Given the impact and burden of chronic disease on the sustainability of both the public and
private sectors, it is critical for all stakeholders to work together, including insurers, healthcareprofessionals, associations, governments, and other policy makers, to seek out solutions to help
enhance access to care within currently available funding.
4. lnvest in research to fully understand the breadth of the opioids crisis and burden ofmusculoskeletal conditions and allow for the øeation of comprehensive approaches tomanaging chronic non-cancer pa¡n.
To truly understand the impact of the opioids crisis, an investment in research is needed by
governments, private payers, and others. Research is needed to build on current evidence and
knowledge in order to gain a more in-depth understanding of the tremendous burden thatmusculoskeletal conditions have broadly (individuals and at the system level), including on
vulnerable populations. Further, there is a need for research that builds and supports thecreation of comprehensive approaches to managing non-cancer pain, Results should be shared
broadly, including to the public.
ln partnership with other stakeholder groups, the CCA is working to build a more comprehensive
approach to the management of musculoskeletal conditions, starting with working with otherhealthcare professionals to promote appropriate referrals. Building a better understanding of the role ofcommunity-based providers in patient-centred care is an important step leading to better health system
performance. However, for this work to be meaningful, we must first recognize the tremendous burden
of musculoskeletal conditions as a key driver in current over-reliance of opioids. Canada would benefit
from a better approach to the management of chronic non-cancer pain which would include theintegration of alternative care options, like chiropractic treatment, as a first-line treatment for those in
need.
L3
r {4l6)5E5'7902 v 1@771222-9303 r {416) 585-2970t 86 Spad¡ña Avenue . Suite 6, loronto, ON M5T 382
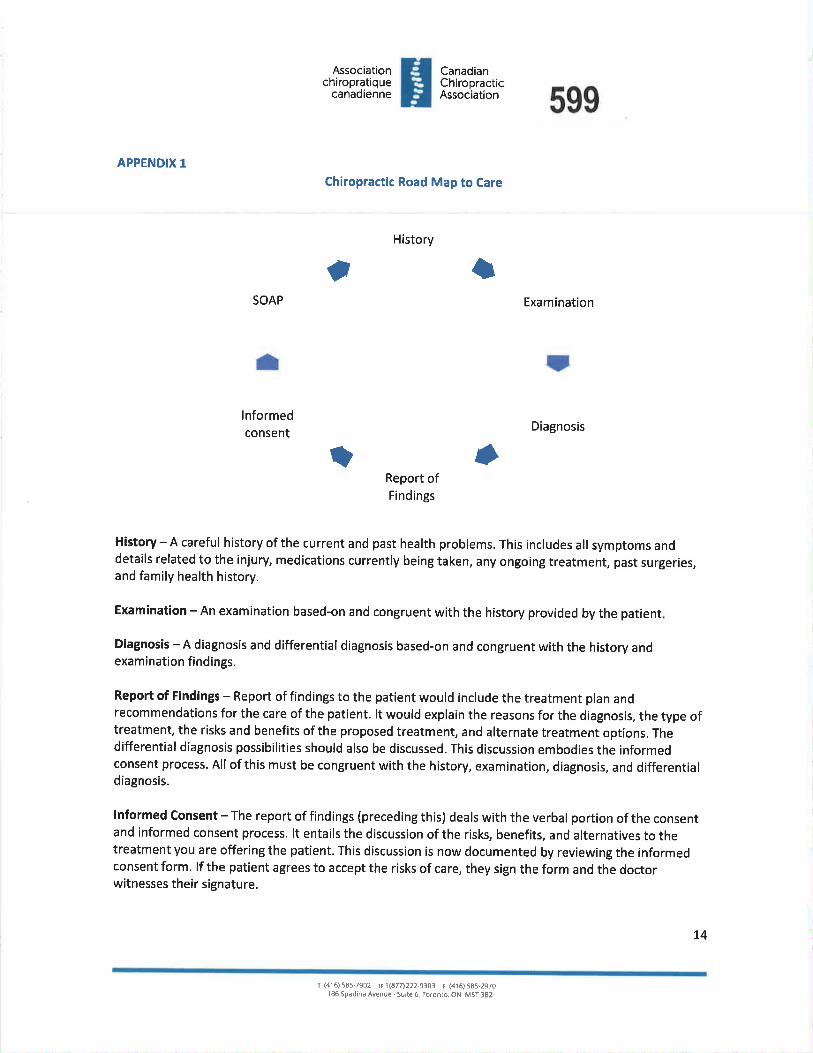
Associationchiropratique
canâdienne
CanadianChiropracticAssociationH 599
APPENDIX 1
Chiropractic Road Map to Care
History
SOAP Examination
lnformedconsent Diagnosis
rlReport ofFíndings
History - A careful history of the current and past health problems. This includes all symptoms anddetails related to the injur¡ medications currently being taken, any ongoing treatment, past surgeries,and family health history.
Examination - An examination based-on and congruent with the history provided by the patient
Diagnosis - A diagnosis and differential diagnosis based-on and congruent with the history andexamination findings.
Report of Findings - Report of fíndings to the patient would ínclude the treatment plan andrecommendations for the care of the patient. lt would explain the reasons for the diagnosis, the type oftreatment, the risks and benefits of the proposed treatment, and alternate treatment options. Thedifferential diagnosis possibílities should also be discussed. This discussion embodies the informedconsent process. All of thís must be congruent with the history, examination, diagnosis, and differentialdiagnosis.
lnformed Consent - The report of findings (preceding this) deals with the verbal portion of the consentand informed consent process. lt entails the discussion of the risks, benefits, and alternatives to thetreatment you are offering the patient. This discussion is now documented by reviewing the informedconsent form. lf the patient agrees to accept the risks of care, they sign the form and the doctorwitnesses their signature.
IÇ
rta
)
14
I (416)5E5.7902 t 1lé77)222.9303 f (416,5E5-2970186 Spdd¡na Avenue -Suite 6, loronto, ON M5f 382

Associationchiropratique
canadienne
CanadianChiropracticAssociationH 600
SOAP - This is the documentation of your treatment of the patient and their response to care:
S (subjective symptoms on the date of the treatment), O (your objective findings on the date of care),
A (the action you take on the date of care, treatment, and advice provided), and P (the plan for the care
going forward). The SOAP notes must justify that the care you are providing is accomplishing what you
set out in the treatment plan. lf the patient is not improving it is a signal that you must go back to basics
and review the original history, examination, and diagnosis. lt may mean that the treatment you are
providing needs to be modified, more testing might be required, or the díagnosis and treatment plan
need to be revisited. lf any new treatment options are being considered the process of informed
consent needs to be revisited with the patient.
15
r (416) 5E5.7902 tr 1 1a77t222-9303 r (416) 585-29701 86 Spadinð Avenue Suite 6, foronto, ON M5f 3B2
Associationchiropratique
canadienne
CanadianChiropracticAssociation 601H
Endnotes:
1 Deyo R, Von Korff M, Duhrkoop D. Opioids for low back pain. BMJ.2015; 350: 96380.2 The Canadian Chiropractic Association is a national, voluntary assoc¡ation representing Canada's 8,500 licensed/registereddoctors of chiropractic. The CCA advocates on behalf of members and their patients to advance the quality and accessibility ofchiropractic care in Canada and to improve the effectiveness and efficiency ofthe healthcare system.3 Schopflocher D, Taenzer P, Jovey R. The prevalence of chronic pain in Canada. Poin Res Monog. 2}lt; 76:445-50.a Moulin D, Clark AJ, Speechly M, Morley-Forster P. Chronic pain in Canada, prevalence, treatment, impact and the role ofopioid analgesia. Pain Res Manage,2O02;7: L79-84.s Building a Collective Policy Agenda for Musculoskeletal Health and Mobility; Canadian Orthopaedic Care Strategy Groupbackgrounder report. 2010.6 Desjardins, D. Le fardeau de la maladie lié aux troubles musculosquelett¡ques au Canada. Prévention l'incapacité au travail : unsymposium pour favoriser l'action concertée. lournées onnuelles de la santé publique,2006.7 Andersson G. The epidemiology of spinal disorders. ln: Frymoyer JW, ed. The adult spine: principles and practice, 2nd ed.P h i I a d e I ph i a : Li pp i n cott- Rave n; 1997 : 93 -t4L.8 Mirolla M. The Cost of Chronic Disease in Canada. 2004. Accessed November tS,2Ot6.http://www.eoiatlantic.orelpdf/health/chronicca nada. pdf .
e Occupational Health and Safety Council of Ontario. MSD Prevention Guidelines for ontario. Musculoskeletal Disorders. 2007.10 Hudson Tl, Edlund MJ, Steffick DE, Tripathi SP, Sullivan MD. Epidemiology of regular prescribed opioid use: results from anational, population-based survey. J Pain Symptom Manage.2OOS; 36(3): 280-288.11 Rudd RA, Aleshire N, zibbell JE, Gladden RM. lncreases in Drug and Opioid overdose Deaths-United States, 20oo-20i.4.MMWR Morb Mortol Wkly Rep.2016; 64(50-51): 1378-82.12 Hudson TJ, Edlund Mi, Steffick DE, Tripathi SP, Sullivan MD. Epidemiology of regular prescribed opioid use: results from anational, population-based survey. J Pøin Symptom Manage.2008; 36(3): 280-8.13 Picard, A. Opioid overuse is creating "lost generation," expert says. I/re Gtobe and Mait Accessed November 15,20L6.http://www.theslobeandmail.com/news/national/opioid-overuse-is-creatins-lost-generation-expert-savs/article31547148/1a Fischer, B. and Keates, A. Opioid drought', Canadian style? Potential implications of the'natural experiment'of delistingOxycontin in Canada. lnternat¡onol Journal of Drug Policy.2OL2; 23161: 495-497 .
1s Glazier R, Bradley EM, Gilbert JE, Rothman L. The nature of increased hospital use in poor neighbourhoods: findings from aCanad ian I n ner City. Ca n J P u blic H e d lth. 2OOO; 9Ll4l: 268-7 3.16 Kopansky-Giles D, Vernon H, Boon H, Steiman l, Kelly M, Kachan N. lnclusion of a CAM therapy (chiropractic care) for themanagement of musculoskeletal pain in an ¡ntegrative, inner city, hospital-based primary care setting../o urnol of AlternativeM ed ici n e Rese a rch. 2Ot0; 2lI): 6I-7 4.17 Fischer B, Argento E. Prescription opioid related misuse, harms, diversion and interventions in Canada: a review. PoinPhysiciøn. 2072; I5(3 Suppl): ES191-203.18 Fischer B, Jones W, Urbanoski K et al. Correlations between prescription opioid analgesic dispensing levels and relatedmortality and morbidity in Ontario, Canada, 2005-2011. Drug Alcohol Rev.20I;33(1): 19-26.ls Webber V. Opioid Use in Canada: Prevent¡ng Overdose with Education Programs & Naloxone Distribution. Montréal, Québec:National Collaborating Centre for Healthy Public Policy. 2016. Accessed November IS,2OL6.http://www.ncchpp.caldocs/2016 OBNL NGO OverviewOpioides En.pdf20 Martin L, Laderman M. A System Approach ls the Only Way To Address The Opioid Crisis. Heotth Affairs Blog.20t6. AccessedNovember t5,2016. htto://healthaffairs.orelbloe/2016/06/13/a-svstems-approach-is-the-onlv-wav-to-address-the-op¡oid-crisis/.21 Mior S, Gamble B, Barnsley J, Côté P, Côté E. Changes in primary care physician's management of low back pain in a model ofinterprofessional collaborative care: an uncontrolled before-after study. CtuTo Man Ther.2OI3;2!:6.22 Canadian MedicalAssociation, Achieving patient-centred collaborative care.2008. Accessed November 15,2016. https://www.cma.calAssets/assets-libra rvldocu ment/en/p D0B-02-e.pdf.23 Fraser Group. Canadians'Access to Prescription Medicines, Volume 2: The Un-lnsured and Under-lnsured. 2000. Access fromhttp://www.frasersroup.com/downloads/volume 2.pdf24 ISAEC. 2012. Accessed November 15, 2016. www.isaec.ors.2s Wong JJ, Cote P, Sutton DA, Yu H, et al. Clinical practice guidelines for the noninvasive management of low back pain: Asystematic review by the Ontario Protocol for Traffic lnjury Management (OTlMa) Collaboration. Eur J Pain.2016. doi:10.1002/ej p.931.
76
f (4¡6)58s.7902 tF 1ß77t222.9303 r (416) 5a5-2970186SpadínôAvenue suite6, loronlo,ON MsT3B2
602
26 Conservative management is an approach to treating back pain, neck pain and related spinal conditions utilizing non-surgical .
and non-pharmacological treatment options,zz Choudhry N, Milstein A. Do Chiropractic Physician Services for Treatment of Low-Back and Neck Pain lmprove the Value of
Health Benefit Plans? An Evidence-Based Assessment of lncremental lmpact on Population Health and Total Health Care
Spending. Harvard Medical School, Boston, Mercer Health and Benefits .2009. Accessed November t5,2OL6.
http://www.f4cp.com/files/white-papers/do-chiro-services-improve-va lue-of-health-benefit-plans. pdf.
28 Bronfort G, Haas M, Evans R et al. Effectiveness of manual therapies: the UK evidence report. BMC Chiro & Osteo.2010; 18: 3.
2e Dagenais S, Gay RE, Tricco AC et al. NASS Contemporary Concepts in Spine Care: Spinal manipulation therapy for acute low
back pain. Spine J.2010; 10: 918-40.30 van Tulder, M., Koes, B. & Malmivaara, A. Outcome of non-invasive treatment modalities on back pain: An evidence-based
review. European Spine Journol. 2006: 15(1).31 Deyo R, Von Korff M, Duhrkoop D. opioids for low back pain.ÙMJ.2015; 350(ian05 10): 96380.32 Bishop PB, Fisher CG, Dvorak MF, Quon JA, The Chiropractic Hospital-based lnterventions Research Outcomes (CHIRO) Study.
Spine.2OI0;1o(I2],.33 Bronfort G, Haas M, Evans R, Kawchuk G, Dagenais S. Evidence-informed management of chronic low back pain with spinal
manipulation and mobilization. Spine Journal. 2008; 8(1): 213-25.34 Lawrence RC, Felson DT, Helmick CG, Arnold LM, et al. Estimates of the prevalence of arthritis and other rheumatic conditions
in the United States. Artårifis Rheum.2008; 58(1): 26-35.3s Goertz CM, Long CR, Hondras MA, et al. Adding chiropractic manipulative therapy to standard medical care for pat¡ents with
acute low back pain: results of a pragmatic randomized comparative effectiveness study. Sp,ne. 2013; 38(8): 627-34.36 Passmore SR, Toth A, Kanovsky J, Olin G. lnitial integration of chiropractic services into a provincially funded inner city
community health centre: a program description. JCCA. 2015; 59(4): 363-72.37 Gordon S, Sakallaris B. Chronic Pain Breakthrough Collaborative Webinar. Collaboratives of the Samueli lnstitute. Accessed
November 15, 2016.http://www.samueliinstitute.ore/File%20Librarv/For%20Health%2OCare%20and%20Hospitals/Sl ChronicPainWebinar.pdf '38 CDC. CDC Guideline for Prescribing Opioids for Chronic Pain. 2016. Accessed November I9t 2016.
www.cdc.gov/drugoverdose/prescribing/ guideline.3e Mior S, Gamble B, Barnsley J, côté P, Côté E. Changes in primary care physician's management of low back pain in a model of
interprofessional collaborative care: an uncontrolled before-after study. Chiropr Man Ther.2OL3;2L:6.40 ISAEC. 2012. Accessed November 15, 2016. www.isaec.ors.41 lSAEc. 2012. Accessed November 15, 2016. www.isaec.ors.a2 Le Conseil De La Fédération. De l'innovation à l'action : premier rapport du Groupe de travail sur l'innovation en maitière de
santé. Accessed November 15,2076.http://www.pmprovincesterritoires.calphocadownload/publications/health innovation report fr'pdf'a3 Passmore SR, Toth A, Kanovsky J, Olin G. lnitial integration of chiropractic services into a provincially funded inner city
community health centre: a program descr:iption. JCCA. 2015; 59(4): 363-72'4 paskowski l, Schneider M, Stevans J, Ventura JM, Justice BD. A hospital-based standardized spine care pathway: report of a
multidisciplinary, evidence-based process. J Manipulotive Physiol Ther.2011 Feb;34(2):98-106.as Goertz CM, Long CR, Hondras MA, et al. Adding chiropract¡c manipulative therapy to standard medical care for patients with
acute low back pain: results of a pragmatic randomized comparative effectiveness study. Sprne. 2013; 38(8): 627-34.a6 ClHl. National Health Expenditures: Where does Canada's health care money come from? 2015. Accessed November 15,
2016. https://www.cihi.calen/spending-and-health-workforce/spendins/national-health-expenditure-trends/nhex2015-topic5'a7 Fraser Group. Canadians'Access to Prescript¡on Medicines, Volume 2: The Un-lnsured and Under-lnsured.2000' Access from
http:/lwww.frasergroup.com/downloads/volume 2.pdf 'a8 Naylor D, Girard F, Jack Mintz J, Fraser N, Jenkins T, Power C. Unleashing lnnovation: Excellent Healthcare for Canada. 2015.
Accessed November 15,2016. http://healthvcanadians.ec.calpublícations/health-svstem-svsteme-sante/report-healthcare-innovation-rapport-soins/index-eng.php.asVos T, Flaxman AD, Naghavi M et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-
2010:asystematicanalysisfortheGlobalBurdenofDiseaseStudy2010. Lancet.2OL2;380:2163-96.so CMA. Harms Associated with Opioids and the Other Psychoactive Prescription Drugs. CMA Policy.2016. Accessed November
t5, 2016. http://pol icvbase.cma.cald btw-wpd/Pol icvpdf/P015-06.pdf .
Associationchiropratique
canadienne
CanadianChiropracticAssociationH
77
T {4l6) 585'7902 1.11877)2229303 r (416) 585'2970I 86 Spddinð Avenue - Suite 6, loronto, ON M5l 382
Rose Bustria ITEM 4.1.39603From:
Sent:To:SubJect:
Jo-Ann WillsonMonday, May 08, 2017 3:24 PMRose BustriaFW: Thank you!
Exec and Council
Jo.Ann Wlllson, B.Sc., M.S.W., LL.B.Registrar & General Counsel
College of Chlropractors of Ontarlo130 Bloor St. West, Suite 902Toronto, ON M5S 'lN5Tel: (416) 922-6355 ext. I 1 1
Fax: (416) 925-9610E-ma¡l: [email protected],caWeb Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any otherdistribution, copying or d¡sclosure is str¡ctly prohibited. lf you have received this e-mail in error, please notify me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: Bria n Gleberzon [mailto: BG [email protected]]Sent: Monday, May 08,20L7 3:01 PM
To: lo-Ann Willson <[email protected]>; [email protected]: Thank you!
Good afternoon Jo-Ann and Chris:
I hope this email finds you both doing well.
I wanted to thank you both for being as grac¡ous as you are to the Year III students when they attend aDiscipline Hearing. To a person, the students tell me how insightful your comments are to them after theHearing is over.
In years past, since I was on Council, I could thank you each in person but since I'm seldom (if ever) atCCO head quarters now I thought it best to send a quick email.
Thank you again,Brian
Dr. Brian J. Gleberzon BA, MHSc, DC
ProfessorChair, Department of Chiropractic TherapeuticsCanadian Memorial Chiropractic College& Private Practitioner
"Democracy is Proximate Solutions to Insoluble Problems"
Reínhold Niebur
1
This communication together with any attachments is for the exclusive and confidential use ofthe addressee(s). Any other distribution, use or reproduction without the sender's prior consent isunauthorized and strictly prohibited. If you have received this message in error, please notify thesender immediately and delete or shred the message without making any copies.
604
2
McutccCanadian Memoriat Chiropractic Cottege
605
|TEM 4.1.40
May B, 2017
Ms. Jo-Ann WillsonRegistrar and General CounselCollege of Chiropractors of Ontario130 Bloor Street WestSuite 902Toronto, ON MsS 1N5
Dear Ms. Willson
The President and the Board of Governors of the Canadian Memorial ChiropracticCollege request the honour of your presence at the at the seventy-second Convocationon Friday, June 16,2017 at 11:00 am at Roy Thomson Hall with a reception tofollow. Please arrive no later than 10:30 am.
The Awards Committee would be pleased if you would agree to present the HaroldBeasley Award for Excellenae in Jurisprudence at the ceremony.
Please RSVP your attendance no later than May 26,2017 to Lynne Hodgson,Fundraising Development Specialist , at 416-482-2340 extension 270 or by email [email protected].
We look fon¡uard to seeing you there!
Regards,
Peter S.Y. Kim, BSc, DC, FCCS(C)Director, Development and Clinic Advancement
RECHIVBI)MAY I 5 2017
COí,T,EËE OF CHM,OPR.ACTISS
OFONTAruO
Canadian Memorial Chiropractic Collegeó100 Lestie Streei, Toronto, 0ntario M2H 3J1
f 416 482 2340 www.cmcc.ca
Canadian Memoriat Chiropractic Cottege
Seventy-secon d Co nvocatio nRoy Ihomson Haü.
ó0 Símcoe Street,Toronto, 0N MsJ 2HsFriday, June ló, 201T al lf :00 a.m.
606ïhe President and the Board of Governors of the
Canadian Memoriat Chiropractic Coll"ege
request the honour of your presence at the
Seventy-second Convocation
on Friday, June 1ó, 2017 al ll:00 a.m.
Roy Thomson Hat[
Admission to the Hal.l. from 10:30 a.m
Reception fottowing the ceremony in the foyer of
Roy Thomson Hatt
RSVP to Barbara a1416 4822340x290o r Þ-¡gu/þjggt ng@cmec.ç.A
#i*ۊ#*00.82
fil2H 3J1 2017 .05.13
Ms. Jo-Ann WillsonRegistrarCollege of Chiropractors of Ontario902-130 Bloor St WToronto ON M5S 1Ns
cYort-o)âNlfro-o>,v(oc.¡riÕ|f)coÈo(f, fr.- c\.tOC.le(ÐÕl.(.)o-oo
I1
I
ParkingUnderground & surface Lots avaitabte
Public TransitSt. Andrew station on yonge-University-spadina
Subway
For more information on parking, trans¡t, and other detail.s,ptease visit www.cmcc.ca/convocation
rFoyThornsor¡Hall
o
NECBTVEDHAY l7 ,;Wl
oo[¡DcEOrffinffßrct(m
PR Yi-$' ir .'.; ".:.:! r :! !1. ITEM 4.1 .41
607
ChÍropractic in 2017 and beyond
Exptoring prescription rightsand solutions to the opioidcrisis
lmproving Canada's responseto disabiLity
,fr. . *.*+.ts.à,.,ffiffi
6081O PRIMARYCONTACT
The role of chiropractic in 2017 -consideri ng prescri ption rights andsolutions to the opioid crisis
Chiropractic is guided by diversephitosophies and models of care.As we enter 2017, the profession isconsidering its identity as one thatcoutd heLp bring a sotution to theopioid crisis and as one which coutdreduce health care costs throughthe rights to prescribe anatgesics.
What are the implications ofmedication prescription rights forchiropractors and the profession'spotential rote in reducing Canada's
!.ött
struggle with opioid addiction?
Should chiropractors prescribe?Drs. Mark Erwin ICtass of '84] andSiephen Burnie f Ctass of '05) haveco-authored a journaI articte withDr. Peter Emary, et a[., examiningthe implications of a potentiaIchange of scope within chiropracticto inctude Limited medicationprescription right, presentlyincorporated into chiropractic scopeof practlce in some jurisdictions
wortdwide, such as USA, Denmarkand Austratia.
ln Burnie's words, "This artic[espeaks to an issue that is somewhatcontroversiaI in our profession butvery topicat, and an area wherescope of practice changes may becoming. We feel it is imperative tostart discussing the impticationsof prescribing rights so that ourprofession can work through theinherent issues it may come with."
PRIMARYCONTACT 11 -I
609"Limited prescription rights woutd be of great convenience to a patient who
woutd benefit from added relief between treatments or supplementary pain
retief, particutarly in the acute phase."
The paper, entitted 'A commentaryon the imptications of medicationprescription rights for thechiropractic profession," waspubl.ished in the Chiropractic andManuaI Therapies journaI andcan be found ontine on its site atwww.ch iromt. bio medcentra [. com/a rtictes/1 0.1 186 I s12998-01 6-01 1 4-y.
"Limited prescription rightswoutd be of great convenience toa patient who woutd benefit f rornadded retief between treatmentsor supplementary pain retief,particu[arty in the acute phase,"continues Dr. Burnie. "The practicewoutd potentialty save the patienttime and reduce costs to the medicaIsystem by ensuring they don'thave to see a general practitionerfor the same condition they arebeing treated for with chiropractic.Chiropractors are atso in an ideatposition to know when not toprescribe and to understand whenmanuaI treatment, exercise andother interventions woutd be morebeneficiaI and less harmfut. AsMSK speciatists, no one is betterpositioned to weigh the pros andcons of prescription for MSK issues."
Prescription rights and chiropracticin the 21st centuryEartier in his career, CMCCPresident Dr. David Wickes hetdpositions at NationaI Universityof Heatth Sciences in Lombard,ItLinois and University of WesternStates in Porttand, Oregon, wherechiropractic scope of practiceinctuded the abitity to order tests
such as EKGs and advancedimaging, and where studenteducation inctuded a foundationin non-pharmaceuticaI naturalmedicine. AdditionaLLy, throughhis administrative career, he hasstudied a variety of modets of careand studied the effects of differingscopes of practice. Drawing on thishistory, he weighs in on the presentquestion of chiropractic scope ofpractice in Canada, and considersthe question of prescription rights:
The debateAt one sìde of the debate isthe growing interest by manychiropractors in having access toat Least a limited prescriptton drugarmamentarium as part of themanage ment of m uscu Loske leta Idisorders. Perhaps even a furtheroutlier would be the push by someUS-based DCs to have access tomany prescription drugs used totreat those non-MSK disorderstraditionaLLy managed by medicaLprimary care physicia ns.
At the other end of the debatespectrum is the time-honouredp h i loso p h ica L sta n ce thatchiropractic was founded as adrugless professíon and mustremain so. However, it's farmore compLicated that just theseo pposi n g views. Co m petiti o namongst various health careproviders whose scopes ofpractice seem to be growing whilstch i ro p ractic's rema i ns u n cha n g edin many jurisdictions has led toeconomic concerns.
Patíent need and practitionerphilosophyThe positioning of chiropractic asa valuable component of a nationaLstrategy to address the opioidaddiction crisis is a balancing actbetween the argument that being adrugless practitioner reduces theIikelihood that a patient will becomehooked on anaLgesics, and therealization that some patients withacute and chronic pain syndromescannot be adequately managed bytrad itiona I ch iro p ra ctic methodsalone.
I spent decades in the US observingthe debates and heated argumentsabout prescription drug rights forDCs and know that there are fewissues more capabLe of enraging thetraditìonal, vitalistic segment of ourprofession. 0ur profession strugg leswith its identity, leading to confusionof the general public as well aslegisLators and policy makers.
An inconsistent approachEven in those parts of the worLd inwhich DCs have some prescriptiondrug privileges, there is noconsistent approach. ln New Mexico,the permitted formulary includesa d m i n istratio n of bioide ntica L
hormones and injections ofhomeopathic agents, whereasin Switzerland the formulary ismuch more consistent with a MSK-focused practíce. ln 0klahoma andldaho, DCs can administer vitamins,m i nera Is o r n utritiona I su p p Leme ntsvia injection, including intravenousinf usion.
SPRING 2017
I 12 PRIMARYCONTACT
Finding our footingl've been asked what CMCC woutddo if, for example, ALberta enactedLegisLation to permit Iimitedprescription drug use by DCs in thatprovince. My response is that CMCC
strives to prepare its graduatesfor successful practice Ìn alL of theprovinces, so our curricuLum wouldevolve to include the necessarytraining in science-based practicesalLowed by the various provinces andthe necessary elements to ensurepatient safety.
I encourage the thoughtful,deliberate debate of the prescriptiondrug issue and of the expansionof access to advanced imagingp roced u res a n d La bo ra to ry d ia g n ostictests. A profession that refuses toconsider change and that fails toa c k n owLed g e a dva n ce m e nts m a d e
in the scientific understandingof the body is likeLy to becomemarginaLized.
Conservative care options insteadof opioidsWhil.e chiropractors and chiropracticeducators consider the impticationsof prescription rights, the CanadianChiropractic Association [CCA] hasrecentty signed a joint statementof action with the federaI andprovinciaI governments to addressthe opioìd crisis Iin Canadai becauseof the recognition of back painas a key driver for current opioidprescri bi ng.
Dr. Brian Budgett, Director of CMCC
Life Sciences Labs agrees that "white
many patients turn to ana[gesicsas a f irst approach to pain, opioiduse is [ikety to be a laie response tosevere recurrent or chronic spinaIpain. Hence, treatment options [ikechiropractic, which prevent chronicityor mitigate pain and disabitity, maywe[[ reduce the number of patientswho turn to opioids."
Currentty, Canada is the secondhighest consumer of prescription
opioids in the world and ctearlyrecognizes the probtem. The jointstatement referred to above, wassigned by the federaI government,seven provincial. heatth ministries,four other heal.th professionaIassociations (medicine, nursing,pharmacy, and dentistry) and 30
other pariner organizations thathave a rote in reducing the impact ofopioids.
How chiropractic can hetpThe CCA has been advocating on
behatf of Canadian chiropractorsand their patients for greaieraccess to conservative care optionsas first-tine treatment of MSKconditions. "By providing promptaccess to clinicaI alternatives, [ikechiropractic care, evidence suggeststhat we can reduce retiance on
opioids to treat acute and chronicMSK-retated pain," says CCA ChairDr. David Peeace.
Ilndeed, according to Budgett, a
number of wet[-designed studieshave shown that spinal. manipulatíonis a competitive treatment option forchronic necktll and back painl2l, andcan atso be cost effectivel3l.l
CCA Chief Executive Officer AtisonDantas adds that the organization is"tooking to buil.d an understandingof how to better íntegrate carethat is atready avaitabte incommunities across Canada," andthat "integrating chi ropractors intointerprofessionaI care teams hasbeen shown to reduce the use ofpharmacotherapies and improveoveratl heatth outcomes. This effortis even more important now becausethe new draft Canadian prescribingguidetines strongty discourage firstuse of opioids."
For more information on thejoint statement of action, ptease
visit:www.ca nada.calen/heatth-ca nada/se rvices/su bsta nce-a buse/o p i o id -co nf e re n ce/j o i nt-state m e nt-action-add ress-o pio id -crisis. htm I
610Footnotes:tltsaayman, Hays and AbrahamseJ Manipulative PhysioL Ther. 2011
M a r-Ap r ;34(3J : 1 53 - 1 ó3)
t2tEnix et al. op Integr Health Care.2015; ó(1J:jnline access only 17 p;
Giles and Muller. J ManipulativePhysiol Ther. 2005 J an ;28( 1 J :3- 1 1 J
t3tVavrek, Sharma and Hass. JM a ni p u Lative Physi ol Th e r. 20 1 4
Jun;37[5J:300-31 1]
ln the joint statement,OCA commits to:
Devetoping ev¡dence basedprofess¡onat practicerecommendations and
guidetines to facititatethe appropriate triageand referrat of Canadians
suffering from chronic and
acute muscutosketetaIcond¡t¡ons and reduceretiance on opioids. The
recommendations wilt aim to:
better understand theburden of pa¡n retatedto muscutosketetatconditions;
a
develop keyrecommendations forthe appropriate roteof chiropractic care Íinanticipation of simitarefforts for other key
atternatives to opioidsl;and
facititate dissemination ofkey recommendations.
a
www.cmcc.ca
Rose Bustria trEM 4.1.44
-
From:Sent:To:Subject:
Attachments:
634Jo-Ann WillsonThursday, May 18, 2017 12:15 PMRose BustriaFW: FHRGO News: Help Spread the News about the New Ontario HealthRegulators WebsiteOHR Content for FHRCO Communicators- Final (002).docx
Anyreply
Council and Communications.
Jo-Ann Wlllson, B.Sc., M.S.W., LL.B.Registrar & General Counsel
College of Chhopractors of Ontario130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext. 1 1 1
Fax: (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may conta¡n confident¡al information and is intended only for the person(s) named above,distribution, copying or d¡sclosure is strictly prohibited. lf you have received this e-mail in error, please notify me immediately by
and delete all cop¡es including any attachments without reading it or making a copy. Thank you.
othere-mail
From: FHRCO - Beth Ann Kenny Imailto:[email protected]]Sent: Thursday, May L8,20L7 L2:11 PM
To: [email protected]: 'commcommr <[email protected]>; 'Monique Poirier'<monique.poirier@collegeofdietitia ns.org>Subject: FW: FHRCO News: Help Spread the News about the New Ontario Health Regulators Website
The following is being forwarded to you on behalf of FHRCO Communicotions Committee Chair MoniquePoirier.
Hí there,
We're looking for your help to spread the word about the new Ontario Health Regulators websitel This
is a unique resource designed for the public that we hope will become a one-stop gateway for anyone
trying to find information about their healthcare professional.
The purpose of the website is to
1.. Educate the public about the role of regulatory colleges, the value of regulation, and theimportance of a self-regulated system.
2. Help drive traffic and engagement to the college websites, where individuals can get moredetailed information about a regulated health professional.
3. Educate Ontarians about their rights as healthcare consumers.
4. Help people find a regulated health professional.
1
Here's how you can help: 635Distribute our attached background piece on this project to your members and stakeholders. ltintroduces the website and its purpose. Feel free to include it in an e-blast or print publication,or however else you communicate your college's updates.
lf your college is on social media, consider using one of our sample posts to promote the site toyour followers.
Review the information you provide on your website for members of the public. Perhapsconsider adding a section for the public if you do not have one.
Tell your family and friends about the site and ask them for their feedback. Ask them to visitwww.onta riohea lthregulators.ca
The success of this campaign rests on the shoulders of all colleges working together to get the news outto their members and stakeholders. Remember to ask them to spread the news.
lf you have suggestions to improve the message, let me know
Regards,
Monique Poirier, MA
Communications Manager
4l 6-598-1725 I 800-668-4990, ext.222
Video: How the College of Dietitians of Ontario protecls the public
I 8l 0, 5775 Yonge Street, Box 30Toronto, ON M2M 4Jl
a
a
a
,ø,Colhge c¿
lhilf¡n¡d ûrlrrlà
www.col I eoeofd ietitians. org
The College of Dietitians of Ontario is dedicated to public protection. We regulate and support Registered Dietitians for theenhancement of safe, ethical and competent nutr¡tion services in diverse practice environments.
L'Ordre des diététistes de I'Ontario se consacre à la protection du public.Nous réglementons et aidons les diététistes afin d'améliorer la sécurité, l'éthique et la compétence dans les servicesnutritionnels offerts dans divers milieux d'exercice.
2

PoucY ITEM 4.1.45P-009Executive Comrnittee ancl RegistrationCornmitteeApproved by Council; Septernber
-1.7, 1"994
Amended: November 30, 2002,Septernber 20,2073Re-affirmed: June 18, 2074
Dr. Harold BeasleyMemorial Award
636
Note to renders: In the eaent of any inconsistency betu¡een this document and the legislcrtion tlntfficts chiroprøctic practice, the legislatiot't gooerns.
lrurerur
To encourage chiropractic students at the Canadian Memorial Chiropractic College(CMCC) to develop a greater understanding of Ontario jurisprudence relating tochiropractic practice.
DescnrpnoN oF PoLtcY
CCO will present an annual award to a graduating student of CMCC, who intendsto practise in Ontario, for demonstrating excellence in Ontario jurisprudence. Theaward is named the Dr. Harold Beasley Memorial Award. The award will begranted to the graduating student who receives the top grade in CMCC'sjurisprudence course, who is registered for CCO's Legislation and Ethicsexamination, and demonstrating intent to practise in Ontario.
CCO will present the award arurually at the CMCC graduation. The winner shallhave his/her fees for application and registration in Ontario waived for the first yearof his/her registration with CCO.
1
College of Chiropractors of Ontario
PoucvP-010Executive CommitteeApproved by Council: January 20, 1995Re-afiirmed: June 18, 2014
Professional MisconductRelating to Orthopract¡c
637
f*r:'-n
Note to Readers: In the eaent of any inconsistency between this document and the legislation thal
fficts chiropractic pructice, the legisløtion governs.
lNrenr
To delineate the terms, titles or designations relating to orthopractic, the use ofwhich is prohibited by CCO.
Descn¡pr¡oN oF PoLtcY
Use of the following terms, titles or designations by members are contrary to thepolicies of CCO for the purposes of subsections L6 and 17 of. the ProfessionalMisconduct Regulation under tli.e Chiropractic Act, L991:
. orthopractice;¡ orthopractic;. orthopractor;o Orthopractic Manipulation Society International (OMSI); and. any similar term, title or designation.
tB
t,l t I
îEtå,
College of Chiropractors of Ontario
PoucvP-011Executive CommitteeApproved by Council: February 18, 1995Amended: November 15, 1996, November 26,2004,September 11,2007, June 16,2016
Conflict of lnterest forCouncil and Committee
Members
638
Note to renders: In the eaent of øny inconsistency between this document and the legislation thnt
fficts chiropractic practice, the legislation goaerns.
lrurer,¡r
To determine and define circumstances in which a potential and/or appearance ofconflict of interest or appearance of bias ("conflict of interest") may exist or arise fora CCO Council or a CCO non-council committee member so the council ornon-council committee member may declare the conflict and Council or a CCOcommittee can take appropriate action.
DescnrpnoN oF PoLtcY
A conflict of interest arises when a relationship or activity is reasonably seen as
influencing a council or non-council committee member's ability to make a decisionsolely in the public interest and/or consistent with the objectives of CCO.
Reporting and Responding to a Potential Conflict of lnterest
Where a Council member or non-council committee member has a potential conflictof interest in a matter coming before Council or a committee, the member shalldeclare the conflict prior to the matter being considered by Council or the commit-tee. Council or the committee will analyse the potential conflict of interest, withoutthat member present.
If Council or a committee determines that the member has a conflict of interest orappearance of conflict of interest on the matter, the member shall not participate inactivify, the discussion of the matter, nor vote on the matter, and if the particularmeeting is not open to the public, the member with the conflict shall leave the roomboth during the discussion and vote on the matter.
A member of the Inquiries, Complaints and Reports, Registration, Discipline and/orFitness to Practise Committees who finds himself/herself faced with a conflict ofinterest shall disclose the situation to the committee for decision and, in the case ofthe Discipline Committee, the disclosure will also be made to both counsel. Thedecision as to whether the member is in a conflict situation will be determined bythe committee as a whole.
1
College of Chiropractors of Ontario
PoucyP-011
Conflict of lnterest forGouncil and Committee
Members
2
639
An elected or appointed member of Council or non-Council committee memberwho becomes aware of any unreported potential conflict of interest shall immedi-ately advise the President and Registrar, or if the potential breach involves thePresident, advise the Vice President and Registrar
Reporting of Conflict in Minutes
The minutes of every meeting or hearing where a conflict of interest or a potentialconflict of interest has been disclosed shall record the information.
Conflicts of Interest Arising from Position on Council or Committee(s)
It is considered a conflict of interest for a Council member or non-CouncilCommittee member to use his/her position on Council or a committee to:
. further or promote any activity, service or product in which the member ofcouncil or a committee (or any member of hislher immediate family, employeror affiliated organizatron) has a financial interest;
o obtairL by virtue of his/her position on Council or a committee, any benefit,privilege, money, appointment, employment or any other personal gain;
' be employed (either full-time or part-time) by any chiropractic association/socie-ty, other health profession council or association, or other organization that maybe in conflict with the mandate of CCO (this excludes a teaching position at anychiropractic educational institution or the facilitation/presentation of a seminarconference or workshop for which a per diem and/or expenses will be paid);
' campaign publicly for or on behalf of any person, other than himself/herself:
o in any election to CCO Council; or
o in any other political election in Ontario.
(e.g., it would be inappropriate for a candidate to use election material whichincludes comments such as "endorsed by Dr. X, CCO Committee Chair," etc.);
receive information as a Council member or non-corlncil committee memberwhich is, in turry used for a personal benefiÇ
evaluate or take part in an evaluation of staff members when the Councilmember or non-council committee member has a personal or professionalrelationship with the staff member outside the office; or
a
a
College of Chiropractors of Ontario
PoucvP-011
Gonflict of lnterest forCouncil and Committee
Members
a
a
a
a
640
. makes threats or promises or agreements related to his/her position on Council.
Conflicts of lnterest Arising from Affiliations with other Organizations
A conflict of interest may arise where a council or non-colrncil committee member,
a close relative or friend or another close entity has a role or interest in an
organization that may be in conflict with CCO's mandate, such as a chiropracticorganization, society or specialty group, another health profession council orassociation, or government ("affiliated organization")'
It is considered a potential conflict of interest for a council member or non-councilcommittee member to:
be an employee, officer or director of any affiliated organizatiory as identified inBy-law 6.9;
have an interest in a specific issue before CCO that is related to an affiliatedorganization;
receive or use confidential information relevant to CCO from his/her role at an
affiliated organization; or
receive or use confidential information relevant to an affiliated organizationfrom his/her role at CCO;
Conflicts of lnterest Arising from Other Activities
A conflict of interest may arise where a council member or non-council committeemember engages in an activity or is approached by an affiliated organization to
engage in an activity that may be in conflict with CCO's mandate'
It is considered a potential conflict of interest for a council member or non-councilcommittee member to:
give a presentation or participate in a working grouP or task force for an
affiliated organization;
communicate with an affiliated organization on matters related to CCO,without the authorization of CCO;
communicate to the public, including on social media
3
a
a
College of Chiropractors of Ontario
Por-rcyP-011
Conflict of lnterest forGouncil and Committee
Members
641
on matters or opinions related to CCO without theauthorization of CCO, ormessages inconsistent with CCO's mandate; or
. engage in legal proceedings against CCO.
Conflicts of lnterest lnvolving Inquiries, Complaints and Reports
Where a Council member or non-council committee member or anyoneassociated in an official capacity with CCO:
has an official complaint registered against him/her,
that complaint has been validated by the Inquiries, Complaints and ReportsCommittee as being wiihin the jurisdiction of CCO, and
the complaint has been referred by the Inquiries, Complaints and Reportscommittee to either the Discipline or Fitness to Practise Committees,
that Council member or non-colrncil committee member shall be considered to be ina conflict of interest and shall not be active on Council or anycommittee until such time as the complaint has been disposed of. Should this occur,the Council member or non-council committee member has the right to an expedi-tious process.
conflicts of lnterest lnvolving lnvestigations, Assessments or Hearings ofRelated Members
A Council member or non-council committee member shall not participate in theinvestigation, assessment or hearing of a member to whom the member is relatedby blood, marriage, adoptiory or who is a partner or associate of the member beinginvestigated, or who is engaged in a relationship or strong friendship with themember being investigated, which might reasonably impair the member's objectivi-ty.
Conclusion
The reputation and high standards of the Council must be protected. Therefore,members of Council will avoid and/or report to Council any situation that couldlead to a real or apparent conflict of interest which exists or may arise.
o
o
a
4
College of Chiropractors of Ontario
Po¡-rcvP-0'17
Executive CommittêeApproved by Gouncil: June 2, 1995Re-affirmed: June 18, 2014
Concurrent Treatment:Physiotherapy
642
L,F.;
Note to readers: In the eoent of any incansistency betuseen this document and the legislation that
fficts chiropractic practice, the legislation governs.
l¡rre¡¡r
To encourage dialogue befween chiropractors and physiotherapists treating a
p atient simultaneously.
Descn¡pr¡oN oF PoLtcY
CCO will advise all members who complain about cooperation byphysiotherapists in the issue of concutrent care that they should dialogue withthese physiotherapists to determine if there is contraindication to concurrent careThis is in keeping with a letter from the College of Physiotherapists of Ontario,dated May 1.2,1995, which states:
The advice we give to callers is that client care should be coordinated and thismust be done by each provider, communicating with others involved in theclient's (patient's) care.
{H
t I I I
m *;,b
College of Chiropractors of Ontario

PoucvP-029Executive CommitteeApproved by Council: September 7, 1 996Amended: November 1, 1997, April20,2002June 22,2012Re-affirmed: June 18. 2014Amended: April 22,2015
Ghiropractic Specialties
643
Note to resders: In the eaent of øny inconsistency betuteen this docutnent ønd tlrc legísløtion tlmt
fficts chiroprøctic prøctice, the legislntion governs.
l¡¡re¡¡r
To delineate which specialty designations are recognizedby CCO for the purpose ofthe professional misconduct regulation and the advertising regulation.
DescnrpnoN oF PoLtcY
CCO recognizes the following as approved specialties:
FCCS(C) - Fellow of the College of Chiropractic Sciences (Canada)
FCCR(C) - Fellow of the Chiropractic College of Radiologists (Canada)
FRCCSS(C) - Fellow of the Royal College of Chiropractic Sports Sciences (Canada)
FCCOS(C) - Fellow of the College of Chiropractic Orthopaedic Specialists (Canada)
FCCPOR(C) - Fellow of the Canadian Chiropractic Specialty College of Physicaland Occupational Rehabilitation (Canada)
Procedure for Review
This policy will be reviewed annually by CCO's Executive Committee taking intoaccount the recommendations of the Canadian Federation of ChiropracticRegulatory and Educational Accrediting Boards.
1
College ot Chiropractors ot Ontario
ITEM 6.2
SrnruoRnD oF Pnacnce Cooperation and5-020 Communication with CCO
Executive CommitteeApproved by Council: December 1, 2011
Amended: February 11, 2014 644
Note to readers: In the eaent of any inconsistency betuteen this document and the legísløtion tkat
fficts chiroprøctic practice, the legislatioll Sonerns'
l¡¡rrrur
To communicate the importance of members' cooperation and timelycommunication with CCO.
Descn¡ploN oF STANDARD
CCO's ability to fulfil its mandate is depencient upon the cooperation and timelycommunication with all members
Members are required under tlne Regulated Health Professiorts Act, L99L (RHPA),
regulations made under the Chiroprøctic Act, L991and CCO by-laws to cooperate
with CCO and its statutory committees. It is tl-re professional responsibility of amember to cooperate in a timely marìner when CCO makes reasonable requests forinformatiorç when CCO requires a specific action from a member or CCO requests
attendance at a meeting or hearing to address an area of concern.
Such requests for information, cooperation and/or attendance from CCO include,but are not limited to, the following:
. a request for written submissions in response to an inquiry, complaint orreport to the Inquiries, Complaints and Reports Committee;
a request to appear before a panel of the Inquiries, Complaints and Reports
Committee for an oral caution or other disposition;
a request for disclosure regarding participation in initiatives of the QualityAssurance Committee, such as participation in peer and practice assessment,
attendance at a record keeping workshop, and participation in continuingeducation, professional development and self assessmenü
timely communication and cooperation with peer assessors;
complying with a signed undertaking or other agreement with CCO;
responding to allegations regarding improper advertising; and
requests for information on registration and renewal forms'
a
a
1
a
a
a
a
College of Chiropractors of Ontario
2
SraruonRD oF Pnnclces-020
Cooperation andCommunication with CCO
645
It may be considered an act of professional misconduct for a member to refuse toreasonably cooperate with CCO and could lead to a referral to the DisciplineCommittee.
LecrslalvE CoNTEXT
Health Professions Procedural code, schedule 2 to the Regutated HealthProfessions Act, 1991
section 25.2(1): A member who is the subject of a complaint or report may makewritten submissions to the Inquiries, Complaints and Reports Committee within 30days of receiving notice under subsection 25(6).
Section 81: The Quality Assurance Committee may appoint assessors for the pur-poses of a quality assurance program.
section 82(1): Every member shall co-operate with the euality AssuranceCommittee and with any assessor it appoints and in particular every member shall,
(a) permit the assessor to enter and inspect the premises where themember practises;
(b) permit the assessor to inspect the member's records of the care of patients;(c) give the Committee or the assessor the information in respect of the care of
patients or in respect of the member's records of the care of padents thecommittee or assessor requests in the form the committee or assessorspecifies;
(d) confer with the Committee or the assessor if requested to do so by either ofthem; and
(e) participate in a program designed to evaluate the knowledge, skill andjudgment of the member, if requested to do so by the Committee.
Section B2(2): Every person who controls premises where a member practises, otherthan a private dwelling, shall allow an assessor to enter and inspect the premises.
Section B2(3): Every person who controls records relating to a member's care ofpatients shall allow an assessor to inspect the records.
Section B2(4): Subsection (3) does not require a patient or his or her representativeto allow an assessor to inspect records relating to the patient's care.
Section B2(5): This section applies despite any provision in any Act relating to theconfidenfiality of health records.
College of Chiropraclors of Ontario
SrnruoRRD oF PnRclces-020
Cooperation andCommunication with CCO
646
Ontario Regulation 204194 made under lhe Chiropractíc Act, 1991
Section 13(1): Each year, the College shall select at random the names of membersreqtrired to undergo a peer assessment.
Section 13(2): A member shall undergo a peer assessment if selected at randomunder subsection (1).
Ontario Regulation 852193 made under lhe Chiropractic Act, 1991
The following are acts of professional misconduct for the purposes of clause 51(1)(c)
of the Health Professions Procedural Code:
28. Contravening the Act, the Regulated Healtlt Professions Act, L991, or theregulations under either of those Acts.
31. Failing to comply with an order ol or breaching an undertaking given to,
the Complaints, Discipline or Fitness to Practise Cornmittees or to theRegistrar of the College.
32. Failing to carry out an agreement entered into with the College.
33. Engaging in conduct or performing an act that, having regard to all thecircumstances, would reasonably be regarded by members as disgraceful,dishonourable or unprofessional.
By-law 13: Fees
By-law 13.16:
A member who has not complied with a request from the College shall pay a fee,
set by the Registrar, for any follow-up letters from the College. Such requestsinclude, but are not limited to, requests:
(a) to make available the members' professional portfolio to the Quality AssuranceCommittee,
(b) to participate in the peer assessment cotnponent of the Quality AssuranceProgram, and
(c) to explain an advertisement that does not appear to comply with the Collegeregulations or guidelines, despite previous advice or caution to the member.
3
College of Chiropractors of Ontario
Sm¡roanD oF Pnncnces-020
Cooperation andCommunication with CCO
647
4
(d) to respond to a letter from the College about a complain! report or otherinquiry.
ùÊ
:Jf
College of Chiropractors of Ontario
648
GuroelrNEs FoR OesenvERs nr CouNctL Mernrucs
GCO lnternal Policy l-016Executive GommitteeApproved by Council: September 15, 2016Amended: 2017
lxrenr
To provide guidelines for observers and guests at CCO Council meetings
Por-rcv
l. Meetings of the Council of the College of Chiropractors of Ontario are open to thepublic for purposes of to ensure transparency and openness regarding the decision-making process regarding the governance of the profession of chiropractic in theinterests of the public. This is subject to the capacity limits of the meeting space.
Members and the public may observe all proceedings except those noted under theRegulated Health Professions Act, 1991 (RHPA) as being more suitably held in-camera (members of the public and often staff are excluded). Observers are notpermitted to participate in meeting procedures or to lobby Council members or staffduring breaks.
2. Any member of the public wishing to attend a Council meeting may do so providedhis/her attendance is in accord with the following. Public observers are expected to:r Sit or stand in an area designated by the Council for public observers;r Not take part in any issue under debate by the Council;o Not speak to any member of Council while an issue is being debated or is slated
to be debated;o Exit the council meeting during arty in-camera sessions; ando Maintain dignity and decorum during the Council meeting; any disruptions caused
by a public observer can result in removal.
3. Public observers are requested to ensure they arrive on time for the commencement ofthe Council meeting and any other recommencements thereafter. If the meeting is atcapacity, the individual will be denied entry or re-entry into the meeting.
4. To guarantee admittance, an individual can email the College and reserve a spot up toone week prior to the commencement of the meeting. If your reservation is unable tobe secured because capacity has been filled, you will be notified by the College. Ifyou are unable to attend a meeting, we ask that you notifu our office to cancel yourreservation.
Internal Policy: I-016Guideline for Observers at Council Meetings 6495. If you are not able to secure a reservation, you are welcome to come to the meeting
location in the event that there are last minute cancellations. However, we cannotguarantee that seating will be available.
6. Individuals attending as observers are requested to:o Turn off any electronic device ringers;o Refrain from recording proceedings by any means, including taking of
photographs, video recordings, voice recordings or any other means;r Be quiet during the meeting and not engage in conversation, discussion or any
disruptive behavior;o Refrain from addressing Council, speaking to, or giving or passing notes,
documents or information to Council members while the meeting is in process;o Refrain from lobbying Council members during the meeting and/or during breaks;o Understand and respect that observers aÍe not allowed to participate in debate of
any matter before the Council;o Respect the authority of the presiding offrcer; ando Take their seats in the area designated to observers.
2
|TEM 4.1 .46650
MErr¡Ho Gu¡neuues
Executive CornmitteeApproved by Council: May 24, 1996Revísion Dates: November 15, 1ggô and August 16, 1gg7
CCO INTERNAL PoLIcY
| -'00f
lNteHr
Por-rcy
PRoceounesDefinition of'a
'Meeting"
Meetíngs with Staff
Duration ofMeetings
\
To clariff claiming of per-diems and expenses and to ênsure that allclaims areconsidered/reviewed fairly and equally.
ly'úhenever possible, the followíng procedures are to be followed regarding'ccorneetings.
A meeting of a statutory or non-statutory committee of the whole to concluÒt theaffairs of the cco held at the cco (or in some rare instances, at anotherlocation). The meeting rnust have an Agenda and-Mînutes_ (fìted with theRegistrar).
A meeting of two or more members of a committee to complete a task orprepâre a report etc., will also be c'oltsidered for remuneration, howeve¡ themeeting must have an fuend.agnd Minutes. (fited with the Registrar).and bedirectly related to a task or dirdction given in the Minutes of a meeting of theConlmittee of the whole.
conferencg-ø¡lls..shall also meet tl¡e above criteria to be considered forremuneration.
wfien a comrnittee chaír needs to meet with a member or members of the staffat the cco office, the following conditions shall apply (both for the purpose ofremuneration and for scheduling of time etc_):
. the meeting shall be arranged in advance with the Registrar, who will.approve the time.s.potand advise the staff person(s);
. the meeting must be directly related to the affairs of the co.ilege and/or atask direction given in the Minutes of the Committee of the whole; anä
. tlre meeting must have an Agenda and Mínutes (filed with the Registrar).
. Any -other
meeting with staff (cornmittee member) shall be arranged throughthe eommittee.thaír-and-follow.the above,gúidelines.
whenever possible, all business of the college wilf be conducted duríng regularbusiness hours, Monday through Friday, B a.m. to 5 p.m.
There should be reasonableness in claiming half per{iems for meetings of lessthan three hours duration.
Time spent may be prorated on an hourly basís up to the three hour period forhalf claims etc. For example, a one and a half hour meeting should be held andadded to another short duration meeting (i.e. another one hour meeting) beforethe half per'diem claim is submitted,
CCO POLICY I - 001 Meeting Guidelines 651Page 2
Preparation Time
Staff Support forCommítteeWork
(Agenda's, Reports,Minutes. Research,
lnfôrmation etc.)
Similarly, all conference calls and other brief "payable periods' should beaccumulated until a reasonable per{ieim claim iS sUbmitted.
ls intended to be claimed for time spent in preparation for meetings (reviewingall dooumsnts for the meeting, proparing position papers, reports, agendarsetc.).
Wren a Committee requires staff support:ò the rcquest shall be made by the Ccjmmitteê Chair, through the Registraf;. the reguest must be presented well in advance, ¡n a legible format and. information on what is required and accompanying documents or outl¡nes
should also be submitted to assist the ôtaff in öomplêting the work required.
I 1CHI ROCARU'OLICIES\INTÊRNAL\IOO 1 MTGI.DOC
This docurnênt has been provide{ for your assistance. lf you have further questÍons. please contact the côllege af.
(416) e22-635s. €ô
652PnoceouREs FoR Arrenor¡¡o Everurs/Fu rucroNs
GCO lnternal Policy: l-009Executive CommitteeApproved by Council: February 19, 2008
@Ð
lrurerur
To provide clarification to council members and staff on approved practices for attendingevents and functions as representatives of CCO:
Poucv
Council members and staff of CCO are often invited as representatives of CCO topolitical fundraisers, charitable functions and other events. Selection of representativesshall be made in the following manner:
Pnoceounes
Selecti n g GCO Representatives
The president and registrar have the discretion to approve how many and which councilmembers and staff will attend a specific evenVfunction.
Whenever possible:
a 'Where CCO is invited to attend an event or function, there shall be an equalrepresentation among elected council members, public council members and staffThe number of representatives will be based on the presence required at theevent/function.CCO representatives shall be invited to attend a specific event/function based ontheir knowledge base and special expertise as it relates to the event/function.where an evenVfunction is relevant to a specific CCO committee and/or workinggroup, representatives shall be invited to attend based on their participation as
chair and/or member of that committee andlor working group.
CCO representatives shall be invited to attend an evenlfunction based on theirgeographical proximity to the event/function.
Expenses
Once approved, CCO shall reimburse the member for reasonable expenses in attendingthe event consistent with CCO's budget.
a
o
@ College of Chiropractors of Ontario
653
PnoceouREs FoR Arreruol¡¡eE ouceroNAL S essto¡ls/PnoFEssl oNALDeveloPM ENT P noc Rervls
CCO lnternal Policy: l-010Executive Gommittee' Approved by Council: February 19, 2008
@Ð
lnrerur
To provide clarification to council members on approved practices for attending
educational sessions/professional development programs related to their duties and
responsibilities as council members of CCO:
Pou¡cres
Council members often attend edueational sessions/professional development programs
related to their duties and responsibilities as council members of CCO.
Where a council member wishes to attend such a program, the following procedures shall
be followed:
PnoceouRes
Written Request
The council member shall make a written request to the registrar describing the programhe/she wishes to attend and why this program is directly related to his/her duties and
responsibilities as a council member of CCO.
The president and registrar have the discretion to determine whether an educationalsession/professional development program is directly related to the council member'sduties and responsibilities as a council member of CCO.
Report to Counci l/Comm ittees
Following attendance at an educational session/professional development program, the
council member shall report to Council and/or any relevant committee(s), written ororally as appropriate, what was taught at the program.
@ College of Chiropractors of Ontario
Procedures for Attend ing Educational Sessions/Profess ional Development Programs 2
Expenses 654Once apþroved, CCO shall reimburse the member for reasonable expenses in attendingthe educational session/professional development program consistent with CCO,s budget.
@ College of Chiropractors of Ontario
655
PnoCeOURES FOR THE PrEN AND PNRCI¡CrAssessMENT or GoruMrrreE Merrreens
CCO lnternal Policy: l-011Executive GommitteeApproved by Council: December 11, 2008
lntent
To ensure that all CCO committee members have been peer and practice assessed. Forthe purpose of this policy,'ocommittee members" means elected council members andnon-council members of statutory and non-statutory committees.
Policy
The Quality Assurance (QA) Committee of CCO developed the Peer and PracticeAssessment Program to enhance members' learning opportunities and ensure theircompliance with CCO's regulations, standards of practice, policies and guidelines.
Committee members are expected to have thorough knowledge of CCO's regulations,standards of practice, policies and guidelines, as they are involved in the development ofpolicy, review of complaints and adjudication of discipline hearings. For this reason, it isin the public interest that all committee members be peer and practice assessed in atimely manner.
Procedures
Committee members, who have not previously been peer and practice assessed, shall be
assessed during the next cycle of peer and practice assessments following their election toCouncil or a committee.
Committee members who have not previously been peer and practice assessed shall signan undertaking at the first council meeting following election to Council or a committee,or as soon thereafter as practicable, that they will volunteer to be assessed during the nextcycle of peer and practice assessments.
@ College of Chiropractors of Ontario

656
REIMBURSËMENT oF REASONABLE EXPENSES AND
Pen Dreus
GCO lnternal Policy l-012Executive CommitteeApproved by Gouncil: December 11,2008Amended: September 24,2009, September 21,2010, September 22,2011,February 14,2012, February 28,2017
KÐ
Irurerr
To outline for CCO committee members CCO policies and procedures-for thereimbursement of reasonable expenses directly relating to CCO business.
To clarify CCO's policies and procedures for submitting per diem and expense claims forcommittee members.
For the purpose of this policy, "committee members" means elected council memberso
non-council members of statutory and non-statutory committees, and peer assessors.
PoucY
Committee members are entitled to per diems and expenses in accordance with CCO By-law 9 and this policy. CCO expense reimbursement policies are consistent with currentacceptable standards and will be reviewed and revised periodically.
CCO committee members may claim for reimbursement for reasonable expenses relatingdirectly to CCO business. All claims for reimbursement for expenses shall be supportedby receipts. Credit card vouchers will not be accepted as receipts for expenses without thebackup description of items purchased.
Committee members are encouraged to seek documented approval from the Registrar oran Executive Officer, if they have any questions or concerns regarding reimbursement forreasonable expenses.
For the purpose of this policy, "public members" means CCO council members who are
appointed by the Lieutenant Governor in Council. Public Members may be reimbursedfor reasonable expenses directly related to CCO business only if these expenses are notreimbursed by the Ministry of Health and Long-Term Care. Public members will be
reimbursed for these reasonable expenses consistent with the policies and procedures ofthe Ministry of Health and Long-Term Care.
657Public members shall seek documented approval with rationale from the Registrar or anExecutive Officer for any reasonable expenses directly related to CCO business that arenot reimbursed by the Ministry of Health and Long-Term Care..
General and M¡scellaneous Expenses
Committee member shall be reimbursed for miscellaneous reasonable expenses relatingto CCO business (e.g., eomrrrunication, accommodation, travel and meal'expenses), asdirected by Council and as supported by receipts.
Committee members shall not be reimbursed for the cost of entertainment (e.g. videos orpay movies), personal services (e.g., dry cleaning, personal grooming) or othér expensesunrelated to CCO business.
Receipts shall be attached to the expense claim form.
Communicat¡on Expenses
Committee members shall be reimbursed for reasonable communication expenses, asdirected by Council (e.g. long-distance charges, email and internet use during travel forCCO business) directly related to CCO business, as supported by receipts and otherdocumentation.
Committee members shall, whenever possible, use their CCO issued calling cards forlong-distance charges involving CCO business.
Accommodation Expenses
committee members who travel a distance of more than 40 kilometres to ameeting/event/hearing directly related to CCO business shall be reimbursed forreasonable hotel accommodations.
committee members who travel a distance of less than 40 kilometres to ameeting/eventlhearing directly related to CCO business may be reimbursed forreasonable hotel accommodation(s) on a specific occasiono only in the case ofextenuating circumstances, or only following documented approval with rationale.
All committee members are strongly encouraged to choose accommodation for whichfavourable rates may be obtained.
Travel Expenses
Committee members shall be reimbursed for reasonable expenses for transportation toand from meetings/events/trearings relating to CCO business.
2@ College of Chiropractors of Ontario
658When travelling in hisÆrer own vehicle, committee members shall be reimbursed formileage at a rate of $0.50 per kilometre
All committee members are strongly encouraged to book travel arrangements as far rnadvance as possible to obtain the most economical fares.
Meal Expenses
Reasonable meal expenses:
o shall be supported by receipts;
o shall not include reimbursement for alcoholic beverages;
shall only be claimed if the attendance of the member was required at a
meeting/event/hearing at which meals were not provided;
The maximum amount that may be expensed for each meal is as follows:
a
Breakfast:Lunch:Dinner:
$2s$3s$s0
A maximum of three meals may be claimed in one calendar day
Committee members may only claim for reasonable meal expenses when travelling toand from a meeting/event/hearing directly related to CCO business when a committeemember is required to travel from a location which is outside the boundary of the
municipality or metropolitan area in which the meeting/eventlhearing is convened. In theevent of a meeting/event/hearing at the CCO office, the municipality or metropolitan area
is the Greater Toronto Area.
PnoceounEs
Committee members shall comply with the following procedures when making claims forper diems and expenses.
Committee Members shall submit per diem and expenses claim statements using the formapproved by CCO entitled "Meeting Per Diem and Expenses Claim Statement".
Committee Members shall submit to CCO a completed Meeting Per Diem and Expenses
Claim Statement no later than the earlier of 90 days after the meeting/event/hearing towhich the claim is related, or 30 days following the year end of any given year. Thisincludes claims for per diems associated with conference calls lasting less than one hourthat are to be accumulated as outlined in By-law 9.
3@ College of Chiropractors of Ontario
659If a per diem and expenses claim statement is not received by CCO as described above,the committee member shall not be permitted to submit a claim and shall not receive aper diem and,/or expenses for this particular meeting/event/hearing.
If there are extenuating circumstances related to a claim for reasonable expenses,committee members shall identi$z and provide an explanation for these extenuatingcircumstances on the "Meeting Per Diem and Expenses claim statement,,.
If a claim for per diem or expenses is denied, a committee member may make writtensubmissions to the registrar, within 30 days of the denial of the claim, outlining thereasons why he/she is entitled to the claim for per diem or reasonable expenses. Allwritten appeals for per diem or expense claim received by the registrar shall be referredto the Executive Committee for review and decision.
4@ College of Chiropractors of Ontario
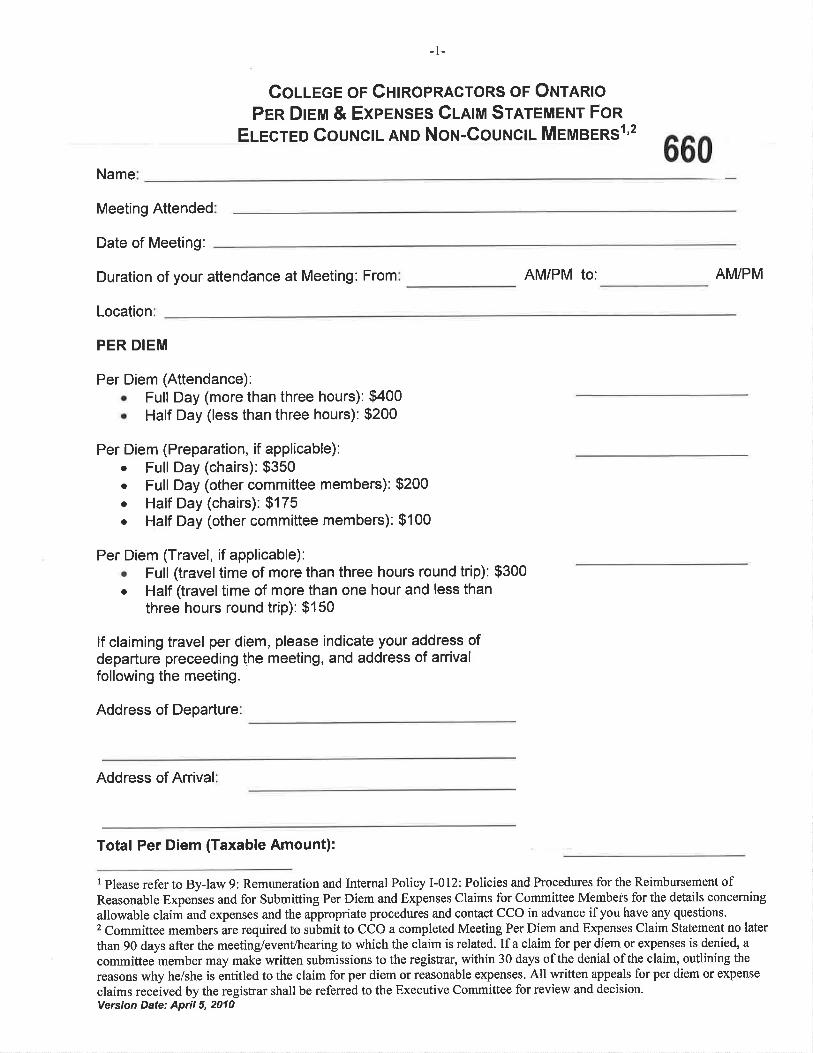
-1-
Couece or GntnoPRAcroRs oF Ouran¡oPEn Drem & Experuses Cnlm Srnreue¡¡r Fon
Euecreo CouNctL AND Not¡-Gou¡¡c¡¡- MeusERSr'2
Name660
Meeting Attended
Date of Meeting:
Duration of your attendance at Meeting: From AM/PM to: AM/PM
Location
PER DIEM
Per Diem (Attendance):o Full Day (more than three hours): $400o Half Day (less than three hours): $200
Per Diem (Preparation, if applicable):. Full Day (chairs): $350¡ Full Day (other committee members): $200o Half Day (chairs): $175o Half Day (other committee members): $100
Fer Diem (Travel, if applicable):. Full (traveltime of more than three hours round trip): $300. Half (travel time of more than one hour and less than
three hours round trip): $150
lf claiming travel per diem, please indicate your address ofdeparture preceeding the meeting, and address of arrivalfollowing the meeting.
Address of Departure
Address of Arrival
Total Per Diem (Taxable Amount):
I Please refer to By-law 9: Remuneration and Internal Policy I-012: Policies and Procedures for the Reimbursement ofReasonable Expenses and for Submitting Per Diem and Expenses Claims for Committee Members for the details concerning
allowable claim and expenses and the appropriate procedures and contact CCO in advance ifyou have any questions.2 Committee members are required to submit to CCO a completed Meeting Per Diem and Expenses Claim Statement no later
than 90 days after the meeting/event/hearing to which the claim is related. If a claim for per diem or expenses is denied, a
committee member may make written submissions to the registrar, within 30 days of the denial of the claim, outlining the
reasons why he/she is entitled to the claim for per diem or reasonable expenses. All written appeals for per diem or expense
claims received by the registrar shall be referred to the Executive Committee for review and decision.Version Date: April 5,2010
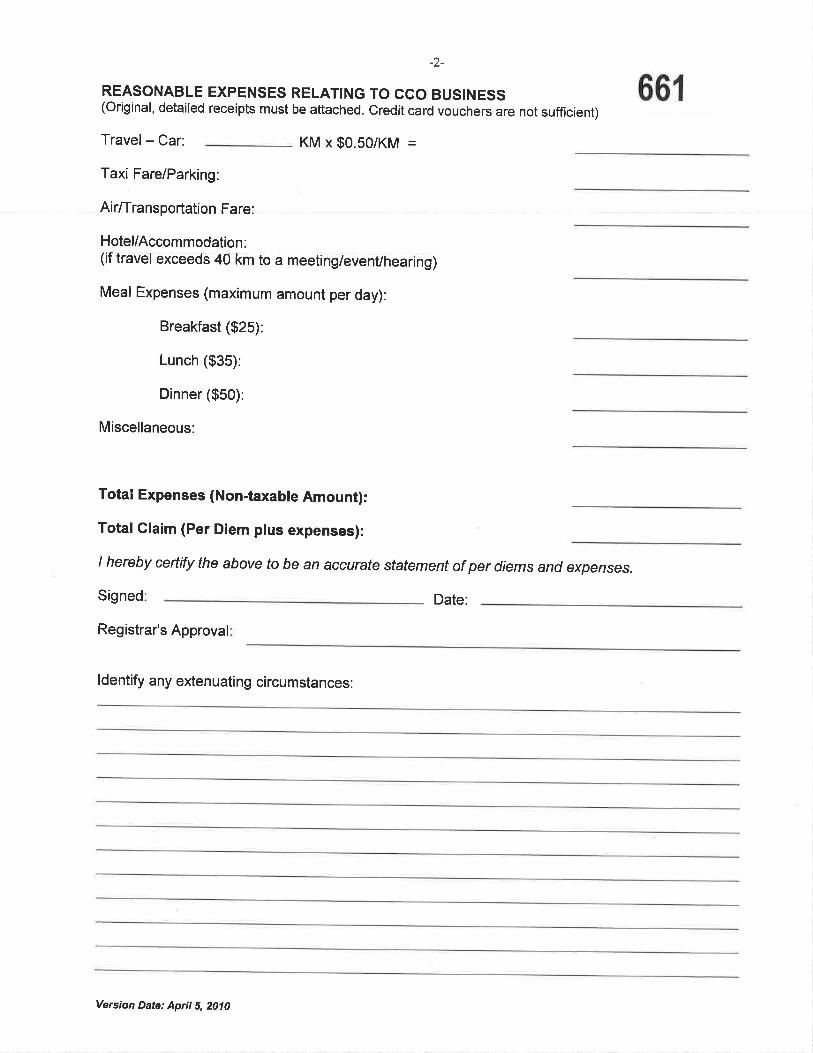
-2-
REASONABLE EXPENSES RELATING TO CCO BUSINESS(Original, detailed receipts must be attached. Credit card vouchers are not sufficient)
Travel - Car: KM x $0.50/KM =
Taxi Fare/Parking:
Air/Transportation Fare:
Hotel/Accommodation:(if travël èlcéedS 40 km to a meeting/evenVhearing)
Meal Expenses (maximum amount per day):
Breakfast ($2S¡:
Lunch ($3S¡:
Dinner ($S0):
Miscellaneous:
Total Expenses (Non-taxable Amount):
Total Glaim (Per Diem plus expenses):
I hereby certify the above to be an accurate statement of per diems and expenses.
Signed Date:
Registrar's Approval
66r
ldentify any extenuating circumstances:
Version Date: April 5,2010
662
PROCEOURES FOR SPCRrcNO EruEEGEMENTS FOR .Zã\Gour.¡crL MeMsERs
WÐCCO lnternal Policy: l-013Executive CommitteeApproved by Council: February 19, 2009
l¡¡rerur
To provide clarification to members of Council on approved practices concerning public
speaking engagements as representatives of CCO:
Polrcv
Members of Council may be invited or may choose to speak at various conferences and
events. Attendance at these events will be in one of two capacities, as representatives ofCCO or in some other capacity, including as private members of the chiropractioprofession.
Where a member of Council participates in a speaking engagement as a representative ofCCO, the following procedures shall be followed:
PnocEouRes
Written Request
All requests for representatives speaking on behalf of CCO must be made in writing tothe registrar. If a member of Council receives a personal invitation or chooses to speak as
a representative of CCO at an event, firnction or conference, he/she shall make a writtenrequest to the registrar.
The request shall include details of the speaking engagement, including, but not limitedto, the date, time, place, topic and anticipated length of presentation.
The president and registrar have the discretion to decide whether a speaking engagement
falls within the scope of CCO.
If it is determined thataspeaking engagement falls within the scope of CCO, the
member's speaking engagement will be as a representative of CCO.
@ College of Chiropractors of Ontario
lnternal Policy - Procedures for Speaki ng Engagements for Council Members
663If it is determined that a speaking engagement falls outside the scope of CCO, themember's speaking engagement will be in some other capacity, in;luditrg u. á privatemember of the chiropractic profession, and not as a representãtive of cCo. '
Attendance at Speaking Engagement
V/hen speaking as a representative of CCO, council members are expected to advocateexisting CCO policies and standards and refrain from offering p.rro^nul opinions.
If a member of Council speaks in Ontario as a private member of the chiropracticprofession and/or not as a representative of CCO on a subject related to chiropractic,regulation, or any other topic that may be reasonably assotiated with CCo, hå/she shall:
take reasonable steps to clearly communicate to hislher audience that he/she is notrepresenting CCO and that the information, opinions and views communicated inthe speaking engagement to do not necessarily represent those of CCO and do notconstitute legal advice; and
2
a
o take reasonable steps to refrain from representing himself/herself as a CCOcouncil member in any written communication piece relating to the speakingengagement, except as part of his/trer curriculum vitae
Per Dierns and Expenses
Where a member of Council speaks as a representative of CCO, the member may make aclalm for appropriate per diem and expenses, consistent with CCO's budget. V/henmaking a claim for appropriate per diem and expenses, council members must disclose tothe registrar any honorarium, per diem or expense payment received as part of thespeaking engagement.
@ College of Chiropractors of Ontario
664
PnoceoURES FOR STruXIN¡G AND
D¡ssor-vr Nc Su a-GomulrrEEs
GGO lnternal Policy: l-014Executive GommitteeApproved by Gouncil: April 16, 2009
lrure¡,¡r
To outline CCO's policies and procedures in striking and dissolving sub-committees,
sub-groups, workgroups, projects or alike (oosub-committee"). Sub-committees may be
formed to take on specific tasks andlor perform duties on behalf of CCO as directed byCouncil and/or a statutory committee.
Poucv
When CCO Council andlor a statutory committee require a sub-committee to assist in aspecific project requested by Council atdlor one of its statutory committees, the sub-
committee shall require the following approval:
If a sub-committee requires its own budget separate and apart from an existingstatutory committee, the striking of the sub-committee shall require the approval
of Council
If a sub-committee's budget falls within the allocated budget of a statutory
committee, the striking of the sub-committee shall require approval from thatstatutory committee
All sub-committees
shall report directly to a statutory committee and to Council as may be
required;
shall require terms of references outlining the purpose, goals, composition,reporting requirements, anticipated budget and authority of the sub-
committee;
shall typically be comprised of 3-5 members. Any additional member(s)
appointed to a sub-committee must be approved by Council;
a
o
o
@ College of Chiropractors of Ontario
lnternal Policy - Procedures for Striking and Dissolving Sub-Committees 2
665may include one or more non-council member;
shall include one ore more public members of Council in the same proportionas that of Council, within reason;
shall perform specific duties as directed by the statutory committee to which itreports and/or as directed by Council;
shall schedule meetings through CCO;
shall include an agendaandminutes with every meeting;
may hold meetings via teleconference or in person;
shall allocate per diems and reasonable expenses to the statutory committee towhich it reports, unless otherwise directed by council. All expenses mustremain in the allotted budget of the statutory committee unless Councilapproves extra expenditures for that specific committee or sub-committee.
Pnoceounes
Appointments
Vy'henever possible, appointments and re-appointments to sub-commiuees shall be madefollowing elections to Council and prior to the first committee meeting of the statutorycommittee to which the sub-committee reports. However, a newly required sub-committee may be struck and appointments may be made to this sub-committee at anytime during the year based on need, following the approval of Council and/or thestatutory committee to which the sub-committee will report.
Appointments and re-appointments to a sub-committee shall be made þ through thecollaboration of the president, registrar and the committee chair of the statutorycommittee to which the sub-committee reports. In cases where a sub-committee reportsdirectly to the Executive Committee, appointments shall be made þ through thecollaboration of the president, registrar and vice-president.
In making appointments to a sub-committee, the following criteria shall be taken intoaccount:
a council member's interest in the specific task of the sub-committee,
a council member's general knowledge relating to the specific task of the sub-committee,
o
a
a
a
a
a
a
a
@ College of Chiropractors of Ontario
lnternal Policy - Procedures for Striking and Dissolvíng Sub-Committees 3
666a council member's experience with similar tasks,
the balancing of different perspectives on the sub-committee,
the availability and time commitment of a council member to devote to thesub-committee, and
other relevant qualifications and characteristics to complement the othermembers' attributes on the sub-committee.
The chair of a sub-committee shall be selected through the collaboration of the president,
registrar and the committee chair of the statutory committee to which the sub-committeereports. In cases where the sub-committee reports directly to the Executive Committee,the chair shall be selected by the president, registrar and vice-president.
Dissolution of a sub-committee and/or discharge of a sub-comm¡tteemember
A sub-committee shall be dissolved if:
the sub-committee has completed its task, as determined by Council and/or thestatutory committee to which the sub-committee reports, or
the statutory committee to which the sub-committee reports and/or Councildetermines that the subcommittee is no longer necessary and/or has nothingfurther to add to the specific task/objective.
A member shall be discharged from a sub-committee if:
o the sub-committee has completed its specified task,
o the sub-committee is dissolved for any reason, or
o the member meets any of the conditions enumerated inBy-law 6.29.
Sub-committees are to be struck for specific objectives/tasks and to assist CCO incarrying out its statutory mandate to regulate the chiropractic profession in the publicinterest. A sub-committee's existence is time-limited and the time frame is to be decidedby Council and/or a statutory committee. V/hen a time-frame is not placed on a sub-
committee by Council, the sub-committee will dissolve automatically in five years fromthe date of its shiking unless an extension is approved by Council.
a
a
a
a
@ College of Chiropractors of Ontario
Record Retention and Destruction Policy(Approved by Council: September t5,2}t6l 667
Description of Policy
Objectives
¡ To ensure CCO's records are managed in an effective and efficient mannero To provide guidelines for the management, retention, maintenance and destruction of CCO records
This policy applies to all departments, committees and offices of.CCO, to all records of CCO and to all CCO staff, council and committeemembers, contractors and agents who create, receive or maintain reco¡:ds as part of their work on behalf of CCO.
While the records schedule prescribes the minimum period that CCO records shall be retained, CCO can keep records for a longer period of timeif it is deemed legally, contractually, regulatory or administratively necessary.
Records shall be retained in their original format, whether paper or electronic. CCO will not generally retain paper copies of electronicallygenerated records.
The following record retention schedule will apply to CCO records:
Retain onsite for 7 years after memberbecomes resigned, revoked or deceasedRetain permanently offsite and/or digitally
Retain 7 years from the date of receipt ofrenewal formRetain a record of renewal and paymentonline permanently
lncludes members' application, QA,complaints, discipline, communicationmaterials, and any other relevant documentsrelating to individual members.Members' annual renewal forms
Registration
Member Files
RenewalForms
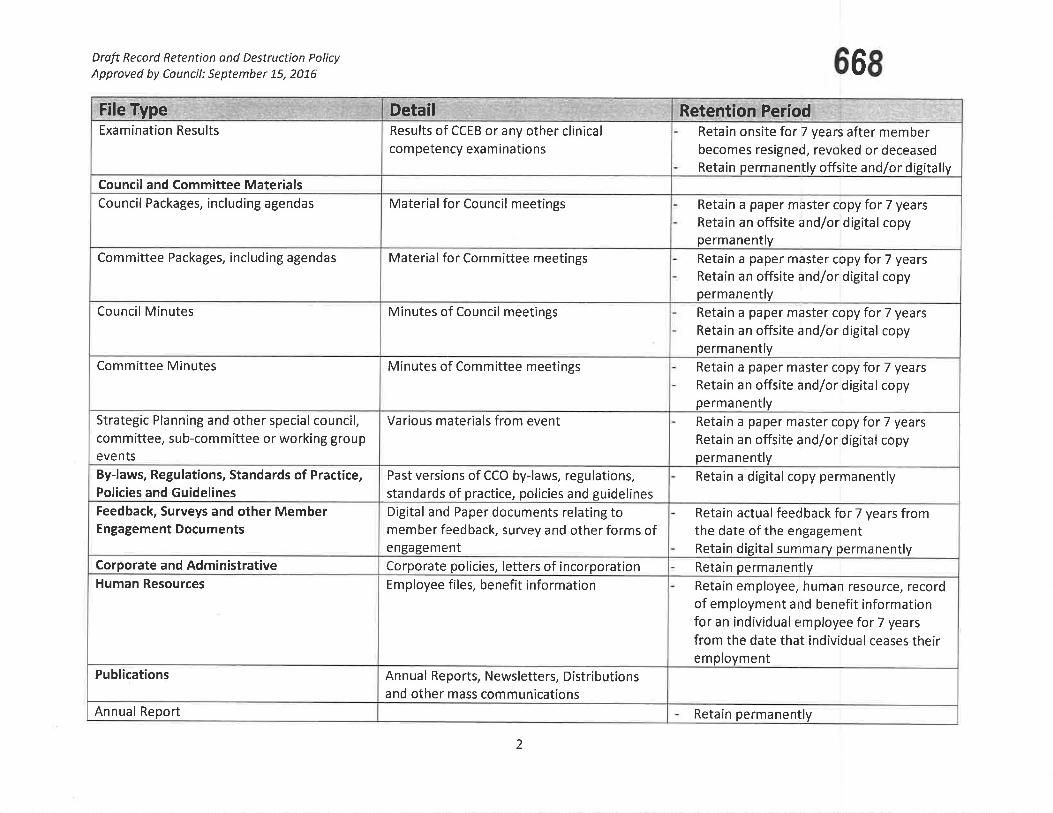
Draft Record Retention ond Destruction PolicyApproved by Council: September 75,2016 66S
Retention PeriodRetain onsite for 7 years after memberbecomes resigned, revoked or deceasedRetain permanently offsite and/or digitally
Retain a paper master copy for 7 yearsRetain an offsite and/or digital copypermanently
Retain a paper master copy for 7 yearsRetain an offsite and/or digital copypermanently
Retain a paper master copy for 7 yearsRetain an offsite and/or digital copypermanently
Retain a paper master copy for 7 years
Retain an offsite and/or digital copypermanently
Retain a paper master copy for 7 years
Retain an offsite and/or digital copypermanently
Retain a digital copy permanently
Retain actual feedback for 7 years fromthe date of the engagementRetain digital surnmary permanentlyRetain permanently
Retain employee, human resource, recordof employment and benefit informationfor an individual employee for 7 yearsfrom the date that individual ceases theiremployment
Retain permanenllly
DetailResults of CCEB or any other clinicalcom petency exam inations
Material for Council meetings
Material for Committee meetings
Minutes of Council meetings
Minutes of Committee meetings
Various materials from event
Past versions of CCO by-laws, regulations,standards of practice, policies and guidelinesDigital and Paper documents relating tomember feedback, survey and other forms ofengagementCorporate policies, letters of incorporationEm ployee files, benefit information
Annual Reports, Newsletters, Distributionsand other mass communications
File TypeExamination Results
Council and Committee Mater¡alsCouncil Packages, including agendas
Committee Packages, including agendas
Council Minutes
Committee Minutes
Strategic Planning and other special council,committee, sub-committee or working groupeventsBy-laws, Regulations, Standards of Practice,Policies and GuidelinesFeedback, Surveys and other MemberEngagement Documents
Corporate and AdministrativeHuman Resources
Publications
Annual Report
2
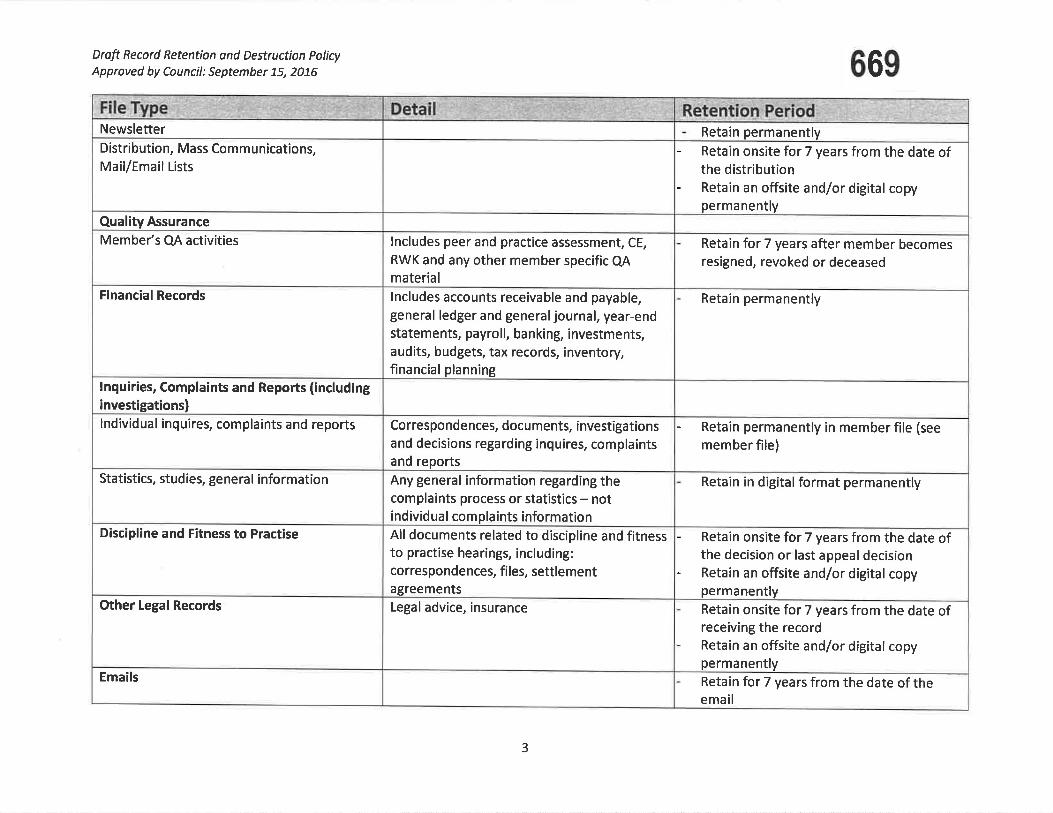
Droft Record Retention ond Destruction PolicyApproved by Council: September 75,2076 669
Retain permanentlyRetain ons¡te for 7 years from the date ofthe distributionRetain an offsite and/or digitalcopypermanently
Retain for 7 years after member becomesresigned, revoked or deceased
Retain permanently
Retain permanently in member file (see
member file)
Reta¡n in digital format permanently
Retain onsite for 7 years from the date ofthe decision or last appeal decisionRetain an offsite and/or digitalcopypermanentlyRetain onsite for 7 years from the date ofreceiving the recordReta¡n an offsite and/or digitalcopypermanently
Retain for 7 years from the date of theemail
lncludes peer and practice assessment, CE,
RWK and any other member specific QAmateriallncludes accounts receivable and payable,general ledger and generaljournal, year-endstatements, payroll, banking, investments,audits, budgets, tax records, inventory,financial planning
Correspondences, documents, investigationsand decisions regarding inquires, complaints
reportsand
Any general information regarding thecomplaints process or statistics - not
ividual complaints informationind
All documents related to discipline and fitnessto practise hearings, including:correspondences, files, settlementagreementsLegal advice, insurance
NewsletterDistribution, Mass Communications,Mail/Email Lists
Quality Assurance
Member's QA activities
Financial Records
lnquiries, Complaints and Reports (includinginvestigations)lndividual inquires, complaints and reports
Statistics, studies, general information
Discipline and Fitness to Practise
Other Legal Records
Emails
3
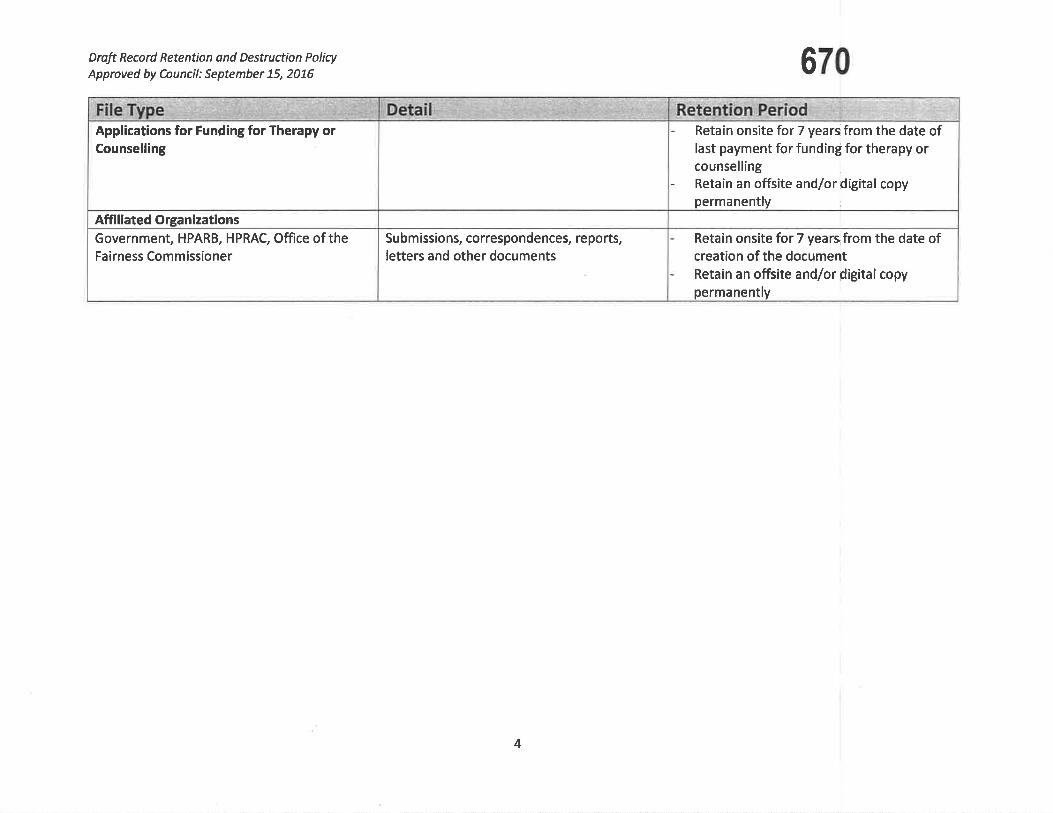
Draft Record Retention and Destruction Policy
Approved by Council: September 75, 2076 670
Retain onsite for 7 yearsifrom the date oflast payment for funding for therapy orcounsellingRetain an offsite and/or digital copypermanently
Reta¡n onsite for 7 years from the date ofcreation of the documentRetain an offsite and/or pigital copypermanently
Subm issions, correspondencet reports,letters and other documents
Applications for Funding for Therapy orCounselling
Affiliated OrganizationsGovernment, HPARB, HPRAC, Office of theFairness Commissioner
4
|TEM 4.1.47 671CCO Gooe Or GOruDUCT FOR CURRENT AND
FoRnaen EucreD AND PueL¡c MertneeRs oFCout¡crL AND Not¡-GouNctL Gortnn¡¡rree MeMBERs @ÐExecutive CommitteeApproved by Council: September 28,2012Amended: February 23,2016, April 19, 2016, Septembet 15,2O16
Current and former elected and public members of Council and non-Council committeemembers must, at all times, maintain high standards of integrity, honesty and loyaltywhen discharging their College duties. They must act in the best interest of the College.They shall:
l. be familiar and comply with the provisions of the Regulated Health Professíons
Act, 1991 (HHPA), its regulations and the Health Professions Procedural Code,the Chiropractic Act 1991, its regulations, and the byJaws and policies of the
College;
2. diligently take part in committee work and actively serve on committees as
elected and appointed by the Council;
3. regularly attend meetings on time and participate constructively in discussions;
4. offer opinions and express views on matters before the College, Council and
committee, when appropriate;
5. participate in all deliberations and communications in a respectful, courteous and
professional manner, recognizing the diverse background, skills and experience ofmembers on Council and committees;
6. uphold the decisions made by Council and committees, regardless of the level ofprior individual disagreement;
7. place the interests of the College, Council and committee above self-interests;
8. avoid and, where that is not possible, declare any appearance of or actual conflictsof interestsl;
9. refrain from including or referencing Council or committee positions held at theCollege in any personal or business promotional materials, advertisements and
business cards;2
t There is a general assumption of real or perceived conflict unless confirmation of no conflict by theExecutive Committee and/or Council, which will be addressed promptly.2 This section does not preclude the use ofprofessional biographies for professional involvement.
672CCO Code of Conduct
10. preserve confidentiality of all information before Council or committee unlessdisclosure has been authorized by Council or otherwise exempted under s. 36(1)ofthe RHPA;
11. refrain from communicating to members, including other Council or committeemembers, on statutory committees regarding registration, complaints, reports,investigations, disciplinary or fitness to practise proceedings which could beperceived as an attempt to influence a statutory committee or a breach ofconfidentiality, unless he or she is a member of the panel or, where there is nopanel, of the statutory committee dealing with the matter;
12. refrain from communicating to members and stakeholdef on behalf of CCO,including on social media, unless authorized by Councila;
13. respect the boundaries of staff whose role is not to report to or work for individualCouncil or committee members; and
14. be respectful of others and not engage in behaviour that might reasonably beperceived as verbal, physical or sexual abuse or harassment.
Potential Breaches of the Code of Gonduct
15. An elected or appointed member of Council or non-Council committee memberwho becomes aware of any potential breach of this code of conduct shouldimmediately advise the President and Registrar, or if the potential breach involvesthe President, advise the Vice President and Registrar; and
16. Potential breaches will be addressed first through informal discussion with theCouncil member(s) or non-Council committee member(s), and subsequently bywritten communication expressing concems and potential consequences.
I, , Council member or non-Council committee member of theCollege of Chiropractors of Ontario undertake to comply with the CCO Code of Conductfor Current and Former Elected and Public Members of Council and Non-CouncilCommittee Members, both during and following my term on CCo Council or acommittee
Signature: S/itness
Date:
3 Stakeholders include professional associations, societies, and other organizations related to the regulation,education and practice of chiropractic.a This does not preclude Council members from communicating about CCO, provided they are notcomniunicating on behalf of CCO.
2
Rules of Order of the Gouncil of theCollege of Chiropractors of Ontario
Approved by Gouncil: September 20, 2014
673
1
2
ln this Schedule, "member" means a council member
Each agenda topic will be introduced briefly by the person or committeerepresentative raising it. Members may ask questions of clarification, then theperson introducing the matter shall make a motion and another member mustsecond the motion before it can be debated.
When any member wishes to speak, he or she shall so indicate by raising his orher hand and shall address the chair and confine himself or herself to the matterunder discussion.
Staff persons and consultants with expertise in a matter may be permitted by thechair to answer specific questions about the matter.
4
5
6.
Observers at a council meeting are not allowed to speak to a matter that is underdebate.
A member may not speak again on the debate of a matter until every councilmember who wishes to speak to it has been given an opportunity to do so. Theonly exception is that the person introducing the matter or a staff person mayanswer questions about the matter. Members will not speak to a matter morethan twice without the permission of the chair.
A member may not speak longer than five minutes upon any motion except withthe permission of Council.
When a motion is under debate, no other motion can be made except to amendit, to postpone it, to put the motion to a vote, to adjourn the debate of the councilmeeting or to refer the motion to a committee.
A motion to amend the motion then under debate shall be disposed of first. Onlyone motion to amend the motion under debate can be made at a time.
10 When a motion is on the floor, a member shall make every effort to be presentand to remain in the room.
When it appears to the chair that the debate in a matter has concluded, whenCouncil has passed a motion to vote on the motion or when the time allocated tothe debate of the matter has concluded, the chair shall put the motion to a voteand no further debate is permitted.
3.
7
8
I
11.
Rules of Order of CouncilApproved by Council: September 20, 2014
12
13
14.
15
16
6742
)
A member is not entitled to vote upon any mot¡on in which he or she has aconflict of interest, and the vote of any member so interested will be disallowed.
Any motion decided by the Council shall not be re-introduced during the samesession except by a two-thirds vote of the council then present.
Whenever the chair is of the opinion that a motion offered to the Council iscontrary to these rules or the by-laws, he or she shall rule the motion out of orderand give his or her reasons for doing so.
The chair shall preserve order, etiquette and decorum, and shall decidequestions of order, which include addressing any distractions that interfere withthe business of the meeting, subject to an appeal to the Council without debate.
The above rules may be relaxed by the chair if it appears that greater informalityis beneficial in the particular circumstances unless the Council requires striitadherence.
17. Members are not permitted to discuss a matter with observers while it is beingdebated.
18. Members are to be respectful, courteous and professional while others arespeaking.
19 In all cases not provided for in these rules or by other rules of Council, thecurrent edition of Robert's Rules of Order shall be followed so far as they may beapplicable.
Approved by Council:June 18,2014
|TEM 4.1.48
PRIVACY CODE
Drafting Assumptions
675
This draft Privacy Code has been created based on the following assumptions:
a
The term "College" has the same meaning as it does in the RegulatedHealth Professions Act, 1991 (RHPA).
With respect to its regulatory activities, the College is not engaged in a'commercial activity' as set out in the Personal lnformation Protection andElectroníc Documenfs Acf (PIPEDA) and as such the College's collection,use and disclosure of personal information is not covered by PIPEDA.'Commercial activity' is defined in PIPEDA as "any particular transaction,act or conduct or any regular course of conduct that ís of a commercialnature, including the selling, bartering or leasing of donor, membership orother fund raising lists."
The Privacy Code endeavours to adapt the Canadian StandardsAssociation (CSA) principles included in Schedule 1 to PIPEDA in amanner that is appropriate for a regulatory body.
The Privacy Code is voluntary
The principles set out in the Privacy Code are not equivalent to the CSAPrinciples included in Schedule 1 to PIPEDA.
The principles set out in the Privacy Code do not comply with therequirements of PIPEDA.
The College is applying for designation as an 'investigative body' underPIPEDA in order to permit organizations that are (or will be) governed byPIPEDA to be able to provide personal information about members to theCollege on a voluntary basis.
The Privacy Code has been prepared in order to assist the process of theCollege being designated as an 'investigative body' under PIPEDA and,once customized and adopted by individual Colleges, is to be provided tolndustry Canada.
The Privacy Code does not deal with the personal information ofemployees of the College.
The Privacy Code is not intended for use by members of the College inconnection with their own obligations under PIPEDA or the PersonalHealth lnformation Protection Act, 2004 (PHIPA)
o
a
a
a
a
a
a
a
676REVISED PRIVACY CODE
COLLEGE OF CHIROPRACTORS OF ONTARIO(approved by Council: June 18,2014)
Preamble
Chiropractic is a self-governing health profession in Ontario under the Regu/a ted HeatthProfessions Acf, 1gg1 (RHPA). Under the RHpA, it is the duty of the MinJster of Healthand Long-Term Care to ensure that health professions are regulated and co-ordinatedin the public interest.
The College of Chiropractors of Ontario was established by the Chiropractic Act, 1gg1and has the following objects as set out in the Health Professions Procedural Code(being Schedule 2 to the RHPA) (RH?A procedural Code):
"1. To regulate the practice of the profession and to govern the members inaccordance with the health profession Act, this Code and the RegutatedHealth Professions Acú, 1991 and the regulations and by-laws.
2 To develop, establish and maintain standards of qualification for personsto be issued certificates of registration.
3. To develop, establish and maintain programs and standards of practice toassure the quality of the practice of the professíon.
4. To develop, establish and maintain standards of knowtedge and skill andprograms to promote continuing evaluation, competence, andimprovement among the members.
4.1 To develop, in collaboration and consultation with other coileges,standards of knowledge, skill and judgment relating to the performance ofcontrolled acts common among health professions to enhanceinterprofessional collaboration, while respecting the unique character ofindividual health professions and their members.
To develop, establish and maintain standards of professional ethics for themembers.
To develop, establish and maintain programs to assist individuals toexercise their rights under this Code and the Regulated HeatthProfessions Acf, 1991.
To administer the health profession Act, this Code and the RegutatedHealth Professions Acf, 1991 as it relates to the profession and to ferform
5
6
7
2
Approved by Councíl:June 18,2014
677the other duties and exercise the other powers that are imposed orconferred on the College.
8. To promote and enhance relations between the College and its members,other health profession colleges, key stakeholders, and the public.
9. To promote inter-professional collaboration with other health professioncolleges.
10. To develop, establísh, and maintain standards and programs to promotethe ability of members to respond to changes in practice environments,advances in technology and other emerging issues.
11 Any other objects relating to human health care that the Council considersdesirable.
ln carrying out its objects, the College has a duty to serve and protect the publicinterest.
The legal powers and duties of the College are set out in the RHPA, the RHPAProcedural Code and the Chiropractic Act, 1991. The activities of the College aresubject to a number of oversight mechanisms including both general and specificoversight by the Ontario Minister of Health and Long-Term Care and specific oversightby the Health Professions Appeal and Review Board, the Health Professions RegulatoryAdvisory Council and the .
In the course of fulfilling its mandate, the College may collect, use and disclose personalinformation regarding applicants for membership, members, members' patients andpersons employed, retained, elected or appointed for the purpose of the administrationof the Legislation. The personal information being collected is critical to the College'sability to effectively regulate the profession in the public interest.
lndividuals who are employed, retained or appointed by the College as well as everymember of College Council or a College committee are required by section 36 of theRHPA to maintain confidentiality with respect to all information that comes to theirknowledge. lndividuals who breach this provision face fines of up to $25,000.00 for afirst time offence and up to $50,000 for a second or subsequent offence. (Section 36 ofthe RHPA is attached as Schedule 1 to this Privacy Code.) ln addítion, personalinformation handled by the College is subject to the provisions of this Privacy Code.
The College's collection, use and disclosure of personal information in the course ofcarrying out its regulatory activities is done for the purpose of regulating the professionin the public interest. These regulatory activities are not of a commercial character.Accordingly, the performance of the College of its statutory duties is not covered byPIPEDA. The College has adopted this Privacy Code voluntarily to provide a voluntarymechanism through which the College can provide appropriate privacy rights toindividuals involved in the College's activities while still enabling the College to meet itsstatutory mandate under the RHPA, the RHPA Procedural Code and the ChiropractícAct, 1991.
Approved by Council:June 18, 2014
Definition of Terms 678The following terms used in this Privacy Code have the meanings set out below:
"Board" means the Health Professions Appear and Review Board.
"By'laws" ryeans the by-laws of the College passed under the authority ofsection g4 of the RHPA procedural Code.
"College" means College of Chiropractors of Ontario.
"Discipline Gommittee" means the Discipline Committee of the College asrequired by the RHPA Procedural Code.
"lnquiries, Complaints, and Reports Gommittee" (ICRC) means the lnquiries,Complaints and Reports Committee of the College as required by the RH7AProcedural Code.
"Legislation" means the RHPA, RHPA Procedural Code, Chiropractic Act, 1gg1,Regulations and By-laws.
J
"member" means a member of the College.
"organization" includes an individual, a corporation,partnership, and a trade union.
"patient" is deemed to include an individual to whom an applícant or member ofthe College has purported to provide professional services.
"personal information" means information about an identifiable individual butdoes not include the name, title, or business address or telephone number of anindividual.
"Privacy Committee" means the Executive Committee.
"Registration Committee" means the Registration Committee of the College asrequired bythe RHPA Procedural Code.
"Regulations" means the regulations made under the RHPA and/or regulationsmade under the Profession Specific Act.
"RHPA means the Regulated Health Professions Acf, 1gg1 as amended fromtime to time.
"RHPA Procedural Code" means the Health Professions Procedural Code(being Schedule 2 to the RHPA).
an assocíation, a

Approved by Councíl:June 18,2014
Principtel-Accountabitity 679
The Regrstrar and General Counsel is accountable for compliance with these policiesand procedures. Complaints or questions regarding the manner in which personalinformation is being handled by the College should be directed to the Registrar andGeneral Counselwho can be reached at 130 Bloor Street, W, Suite 902, Toronto, ON,M5S 1N5,416-922-6355.
The College will provide orientation and training to all new employees and appointeesas well as all members of Council, committees or working groups regarding theirobligations pursuant to section 36 of the RHPA and this Privacy Code.
The College's policies regarding privacy and information management are available onthe College's website at www.cco.on.ca and on request by phone at 416-922-6355 orby mail at 130 Bloor Street, Suite 902, Toronto, ON, MsS 1N5.
Principle 2 - ldentifyi ng Purposes
The purpose for which the College collects, uses and discloses personal informatíon is
to administer and enforce the Legislation.
lnformation About Members
The College collects and uses personal information regarding its members for thefollowing purposes:
o to assess whether a member continues to meet the standards of qualification fora certificate of registration;
to investigate complaints regarding the conduct or actions of a member of theCollege;
to investigate whether a member has committed an act of professionalmisconduct or is incompetent and to resolve such matters including through theimposition of a specified continuing education and remediation program andthrough undertakings;
to inquire whether a member is incapacitated;
to negotiate and implement informal resolutions, including acknowledgementsand undertakings that provide for reviewing samples of patient records;
to hold a hearing of allegations of a member's professional misconduct orincompetence or of allegations that a member is incapacitated;
to carry out the quality assurance program of the College, including anassessment of the records and practice of its members;
4
o
a
a
a

680Approved by Council:June 18, 2014
' to administer the program established by the College to provide funding fortherapy and counselling for persons who, while patients, were sexually abusedby members of the College;
o to investigate reports filed about members of the College under the RHpAProcedural Code;
' to assess whether a former member's certificate of registration should bereinstateci;
o to provide statistical information for human resource planning and demographicand research studies for regulatory purposes including providing that infoimationto the Ministry of Health and Long Term Care and other appropriate agencies;
o to provide information about members to the public for regulatory purposes onthe public register which is located on the college's website;
o to fulfill its duties under sectíon 3 of the Health Professions procedural Code,Schedule 2 of the RHPA;
. to administer or enforce the Legislation.
The.College may collect personal information regarding a member from the member,employers and colleagues of the member, patients of the member and other p"rson",for the purposes set out above. Personal information regarding members is collectedby the College from time to time and at regular intervals.
The College discloses personal information regarding its members only as permitted bysection 36 of the RHPA or as required by law. For example, the Cóttegé is requiredunder the RHPA Procedural Code to maintain a register containing informãtion about itsmembers. Such information includes, but is not restricted to: mèmbers' qualificationsand practice information; court findings of professional negligence or malpractice madeagainst the member unless the finding is reversed on appeál; referrals to the College'sDiscipline Committee until the matter has been finally resolved; and the result and asynopsis of the decision for every finding made against a member as a result of adisciplinary or incapacity proceeding. The RHPA Procedural Code and the By-lawsrequire the college to post the register on the college's website.
lnformation About Employers, Cotteagues and patients
The College collects and uses personal information regarding the employers,colleagues and patients of members of the College for the following purposes:
5
o to investigate complaints regarding the conduct or actions of a member of theCollege;
Approved by Council:June 18, 2014
to investigate whether a member has committed an act of professionalmisconduct or is incompetent;
to inquire whether a member is incapacitated; 681
6
a
a
a
a
a
o
a
o
a
to hold a hearing of allegations of a member's professional misconduct orincompetence or of allegations that a member is incapacitated;
to negotiate and implement informal resolutions, including acknowledgementsand undertakings or specified continuing education and remediation programs
that provide for reviewing samples of patient records;
to carry out the quality assurance program of the College, including an
assessment of the records and practice of its members;
to administer the program established by the College to provide funding fortherapy and counselling for persons who, while patients, were sexually abusedby members of the College;
to investigate reports filed about members of the College under the RHPAProcedural Code;
to assess whether a member continues to meet the standards of qualification fora certificate of registration;
to assess whether a former member's certificate of registration should bereinstated;
o to provide information about members to the public for regulatory purposes such
as public register information and information about discipline hearings;
o to administer or enforce the Legislation.
The College may collect personal information regarding an employer, colleague andpatient of a member of the College from the employer, the colleague, the patient, themember and other persons, for the purposes set out above.
The College discloses personal information regarding the employers, colleagues,patients of members of the College only as permitted by section 36 of the RHPA or as
required by law. For example, hearings of the Discipline Committee are required,
subject to certain exceptions, to be open to the public. Evidence at a hearing of theDiscipline Committee may include personal information regarding the member of theCollege who is the subject of the allegation of professional misconduct orincompetence, as well as personal information regarding the member's patients related
to the allegations of professional misconduct or incompetence. Another example ofdisclosure of personal information abqut patients of members of the College relates tocomplaints regarding the conduct or actions of members of the College. Where a
7
Approved by Council:June 18,2014682
complainant, who is frequently a patient of a member, or a member does not agree witha decision of the ICRC, subject to certain exceptions, either person can request areview by the Board. The RHPA Procedural Code requires that ihe College disilose tothe Board a record 9f t[e investigation and the documents and things up=on which thedecision was based. This disclosure of personal information abõut a patient of amember to the Board is required under the RHpA procedural code.
Information About Applicants For Registration and Potentiat Members
The College collects and uses personal information regarding applicants and potentialmembers and the patients of applicants and potential membérs't'o assess whether anapplicant or potential member meets, and continues to meet, the standards ofqualification to be issued a certificate of registration and to administer or enforce theLegislation. The College discloses personal information regarding applicants andpotential members, references about them and their patientJ only as' permitted bySection 36 of lhe RHPA or as required by law. For example, the R HpA proceduralCode provides a procedure for an applicant who does not agree with a decision of theRegistration Committee to request a review or a hearing Ùy the Board. The RH1AProcedural Code requires that the College disclose to the áoaø a copy of the order andreasons of the Registration Committee and the documents and thinþi upon which thedecision was based. This disclosure of personal information to thiBoard is requiredunder the RHPA Procedural Code.
lnformation Related to lJnauthorized practice and Holding outThe College collects and uses personal information regarding individuats who may bepractising the profession of chiropractic, using protected titles ór holding themselveé outas practicing the profession and their patientê to investigate whether tñe individual hascontravened or is contravening the Legislation and 1o admínister or enforce theLegislation. The College discloses personal information regarding such individuals onlyas permítted by section 36 of the RHpA or as required by law.
Information Related to Administering the Legislation
The College collects and uses personal information regarding individuals who areretained, elected or appointed for the purpose of the admlnistration of the ChiropracticAct, 1991 including the following:
o to review prospective candidates and retain or appoint persons for the purpose ofthe administration of the Act;
' to maintain records to ensure accurate remuneration and payment of expenses,and all documentation required by law and by the various levels of government inaccordance with sound accounting practices;
. to communicate with the person (e.g., home contact information);
683Approved by Council:June 18, 2014
o to maintain accurate and fair accounts of any disputes, possible conflicts ofinterest or misconduct involving a person retained or appointed for the purpose ofthe administration of the Act or a member of the Council or committee of theCollege;
. for purpose of making payments and providing benefits.
The College discloses personal information regarding the individuals referred to aboveonly as permitted by section 36 of the RHPA or as requíred by law.
Specifying the ldentified Purpose
Where practicable, the College will make a reasonable effort to specify the identifiedpurposes to the individual from whom the personal information is collected, either at thetime of collection or after collection but before use, except where to do so would defeatthe purpose of the Legislation or be inconsistent with the Legislation.
The College will state the identified purposes in such a manner that an individual can
reasonably understand how the information will be used or disclosed.
Where personal information is collected for one purpose, the College has the right touse and disclose the information for another regulatory purpose where it is in the public
interest to do so. For example, the ICRC will receive all information, documents and
reports concerning a member, no matter what the originating source. Further, the ICRC
is mandated to review and consider the prior history (i.e. previous complaints orreports), including prior decisions dismissing a complaint or concern. ln certainsituations, the complainant may also obtain access to the member's prior history.
Principle 3 - Consent
The College collects personal information for purposes related to its objects (see
Preamble for the College's objects) including for the purpose of the proper
administration and enforcement of the Legislation and for other related regulatorypurposes. ln carryíng out its objects, the College has a duty to serve and protect thepublic interest.
Where practicable, the College will make a reasonable effort to specify the identifiedpurposes to the individual from whom the personal information is collected as describedin Principle 2. However, obtaining consent of the individuals would, in many cases,
defeat the purposes of the College's collecting, using and disclosing the personalinformation. Personal information will only be collected, used and disclosed without theknowledge and consent of the individual for the purpose of the administration orenforcement of the Legislation and in accordance with any applicable provisions of theLegislation. For example, personal information about a patient may be collected and
used without the patient's consent for the purpose of the College's quality assuranceprogram regarding the assessment of a member's practice in accordance with theRHPA Procedural Code and the Regulations. Another example is that personal
8
684Approved by Council:June 18,2014
information about a patient may be collected and used without the patient's consent forthe purpose of an investigation of a member in accordance with tie RHpA proceduralCode and the Regulations.
Principle 4- Limiting Gollection
The College collects only the personal information that is required for the purposesidentified in Principle 2 of this Privacy Code. The College collects personal iniormationusing procedures that are fair and lawful
Personal informatiol regarding patients must be collected as pârt of the College'sregulatory function. This information is typically obtained by the bollege as part oi aninvestigation or quality assurance program. The focus of thése inquirieõ is the conduct,competence or capacity of the member and the protection of the public. The Collegeonly collects personal information regarding patients to satisfy thís regulatory purpose.
Principle 5 - Limiting lJse, Disclosure or Retention
The College uses personal information only for the purposes ídentified in Principle 2 andin accordance with the provisions of the Legislation. Personal information is onlydisclosed in accordance with the provisions of séction 36 of the RHPA or as required bylaw.
Ïhe RHPA Procedural Code and By-laws clearly designate the information regardingmembers that is publicly available and the By-laws can be accessed from the Collegãwebsite at www.cço.on..ca or by contacting the College at 416-922_6355. ln additio-n,under the RHPA Procedural Code, the College is requìred to publish certain informationregarding diseipline hearings conducted by the Discipline committee.
Under the RHPA Procedural Code, discipline hearings conducted by the DisciptineCommittee are open to the public. Evidence at a discipline heariñg may includepersonal information regarding the member and the member's patients, émptóyers andcolfeagues related to allegations of professional misconduct oi incompetence. Underthe RHPA Procedural Code, the panel of the Discipline Committee has the discretion toclose a hearing under certain prescribed circumstances and/or restrict the publication ofpersonal information where appropriate. Under the RHPA Procedural Code, reviews ofdecisions of the ICRC and Registration Committee by the Board are open to the public.Similarly, the Board has the discretion to restrict the disclosure of perional informationin its review process. The objectíve of these regulatory processes is always theprotection of the public.
The College has a record retention policy in place and conducts regular audits to ensurethat personal information that is no longer.required to be kept is ãestroyed, erased ormade anonymous. Specific information regarding the record retention polícy can beobtained by contacting the Registrar and General Counsel at the College.
9
10
Approved by Council:June 18, 2014
Principte 6- Accuracy 685It is in the best interest of the public that the College collect, use and disclose onlyaccurate personal information in regulating the profession. The College therefore uses
its best efforts to ensure that the information it collects, uses and discloses is accurate.However, in order to be accountable for its collection, use and dísclosure of information,the College makes corrections to information without obliterating the original entry.
Members are required to provide thê College with current name, contact and
employment information and to advise the College of changes within thirty (30) days ofany change. This information is updated annually when members renew theirregistration with the College.
Principle 7 - Safeguards
The College ensures that personal information it holds is secure
The College ensures that personal information is stored in electronic and physical filesthat are secure. Security measures are in place to safeguard this information whichinclude restricting access to personal information to authorized personnel, ensuring thatphysical files are under lock and key and ensuring that electronic files are passwordprotected. The College reviews its security measures periodically to ensure that allpersonal information is secure.
Employees of the College receive an orientation and ongoing training regarding theinformation safeguards required for personal information and their importance.
The College ensures that personal information that is no longer required to be retained
is disposed of in a confidential and secure fashion (i.e. shredding).
Principle 8 - Openness
The College's personal information management policies and procedures are availableto the public and its members via the College's website at www.cco.on.ca or can be
requested by phone at 416-922-6355 or by mail at 130 Bloor Street W., Suite 902.lnquiries concerning the College's policies and practices for collecting, using anddisclosing personal information may be directed to the Registrar and General Counselat 416-922-6355 or ccco. [email protected].
Principle I - lndividualAccess
Access
Where the College holds personal information about an individual, upon written request,
the College shall allow access to the information to that individual, unless providingaccess could reasonably be expected to interfere with the administration or enforcement
11 686Approved by Councìl:June 18,2014
of the Legislation or ¡t ¡s impracticable or impossible for the College to retrieve theinformation.
Examples of situations where access may be denied include:
' lnformation contains references to another individual(s) that cannot be severed;
' Disclosure may result in significant risk of harm to the requestor or a third party;
' lnformation was collected or created in the course of an inspection, investigation,inquiry, assessment or similar procedure;
o Disclosure may defeat the purposes for which the information was collected;
' lnformation cannot be disclosed for legal, security or commercial proprietaryreasons;
o lnformation is subject to solicitor-patient or other privilege;
' lnformation was generated in the course of a dispute or resolution process;
' The request is frivolous, vexatious, made in bad faith or otherwise an abuse ofprocess.
ln cases where the personal information forms part of a record created by anotherorganization, the College may refer the individual to the organization that created therecord (unless it is inappropriate to do so) so that the individual may obtain access tothe personal information from the organization rather than the college.
Whife the College's response will typícally be provided at no cost or minimal cost to theindividual, depending on the nature of the request and the amount of informationinvolved, the College reserves the right to impose a cost recovery fee. ln thesecircumstances, the College will inform the indívidual of the approximate cost to providethe response and proceed upon payment by the individual of ihe cost.
The College will make every effort to respond to the request within thirty days and toassist the individual in understanding the information.
lndividuals should send their written request for access, with contact information andsufficient information about themselves to identify them, to the Registrar and GeneralCounsel.
ln the event the College refuses to provide access to all of the personal information itholds, then the College will provide reasons for denying
"cc"ss. The índividual may
then choose to file a complaint with the Registrar and ôeñeral counsel.
challenqinq accuracy and completeness of personal information
687Approved by Council:June 18,2014
An individual has the right to request a correction of what in his or her view, is
erroneous information. Where the information forms part of a record created by anotherorganization, then the College may refer the individual to the organization that createdthe record (unless it is inappropriate to do so) so that the individual may challenge theaccuracy or completeness of the information.
Where an individual is able to successfully demonstrate that the personal information ofa factual nature (not, for example, the expression of an opiníon) is inaccurate orincomplete, the College will amend the information (i.e., correct, or add informatioit). lnaddition, where appropriate, the College will notify any third parties to whom the Collegehas disclosed the erroneous information. ln some cases, a correction may beinappropríate (e.g., where the fact that a person made or recorded such a statement isthe primary focus of the record rather than whether the statement is, in fact, accurate).
Where there is a dispute between the índividual and the College as to the accuracy orcompleteness of the information, then the College will document the details of thedisagreement, and, where appropriate, will advise any third party who received thecontested information from the College, of the unresolved disagreement.
Principle 10 - Challenging compliance
Complaints or questions regarding the College's compliance with this Privacy Codeshould be directed to the Registrar and General Counsel who can be reached at 416-922-6355.
, lf the Registrar and General Counsel cannot satisfactorily resolve a complaint, theCollege has a formal privacy complaints procedure which includes:
acknowledg ing the complaint;
review of the complaint by the College's Executive Committee;
providing a written decision and reasons to the complainant; and
. taking appropriate measures where the complaint is found to be justified.
Please note that there is a different process for handling complaints about the conductor actions of a member of the College. Please contact the Registrar and GeneralCounsel if you wish to file a complaint about the conduct or actions of a member of theCollege.
12
o
a
IApproved by Coancíl:June 18,2014
SCHEDULE 1
sEcTtoN 36 0F
THE REGULATED HEALTH PRoFEssto^rs Acr, r991, as amended(as of March 20101
39 (tl Every person employed, retained or appointed for the purposes of theadministration of this Act, a health profession Act or the Drug
'and pharmaciesRegulation Acf and every member of a Council or committee of a-College shall keepconfidential all information that comes to his or her knowledge in the course of his or herduties and shall not communicate any information to any other person except,
(a) to the extent that the information is available to the public under this Act, ahealth profession Act or the Drug and pharmacres Regutatíon Act;
(b) in connection with the administration of this Act, a health profession Act or theDrug and Pharmacies Regulation Acf, including, wíthout limiting the generality ofthis, in connection with anything relating to the registration oi membãrs,complaints about members, allegations of members' incaþacity, incompetence oracts of professional misconduct or the governing of the profeséion;
(c) to a body that governs a profession inside or outside of Ontario;
(d) as may be required for the administration of the Drug lnterchangeabitity andDispensing Fee Acf, the Healing Arts Radiation Prolection Act, tn" Heatthlnsurance 4"t, the lndependent Heatth Facitities Act, the Laboratory andSpecimen Collection Centre Licensing Acf, the Ontario Drug Benefit Aóf, theNarcotic control Acf (canada) and the Food and DrugsAcf (cãnada);
(e) to a police officer to aid an investigation undertaken with a view to a tawenforcement proceeding or from which a taw enforcement proceeding is likely toresult;
(0 to the counsel of the person who is required to keep the informationconfidential under this section (g) to confirm whether the College is investigatinga member, if there is a compelling public interest in the disclosure of tfialinformation
(h) where disclosure of the information is required by an Act of theLegislature or an Act of Parliament;
(i) if there are reasonable grounds to believe that the disclosure isnecessary for the purpose of eliminating or reducing a significant riskof serious bodily harm to a person or group of persons; or
688
689Approved by Council:June 18,2014
0) with the written consent of the person to whom the information relates.
2007, c. 10, Sched. M, s. 7 (1).
Reports required under Code
(1.1) Clauses (1) (c) and (d) do not apply with respect to reports required under section85.1 or 85.2 of the Code. 1993, c. 37, s. 1.
Definition
(1.2) ln clause (1) (e),
"law enforcement proceeding" means a proceeding in a court or tribunal that could
result in a penalty or sanction being imposed.
Limitation
(1.3) No person or member described in subsection (1) shall disclose, under clause (1)
(e), any information with respect to a person other than a member'
No requirement
(1.4) Nothing in clause (1) (e) shall require a person described in subsection (1) todisclose information to a police officer unless the information is required to be produced
under a warrant. 1998, c. 18, Sched. G, s. 7 (2).
Confirmation of investiqation
(1.5) lnformation disclosed under clause (l) (g) shall be limited to the fact that an
investigation is or is not underway and shall not include any other information.2007, c. 10, Sched. M, s. 7 (5).
Not compellable
(2) No person or member described in subsection (1) shall be compelled to give
testimony in a civil proceeding with regard to matters that come to his or her knowledgein the course of his or her duties. 1991, c. 18, s. 36 (2).
Evidence in civil proceedings
(3) No record of a proceeding under this Act, a health profession Act or the Drug andPharmacies Regulation Act, no report, document or thing prepared for or statementgiven at such a proceeding and no order or decision made in such a proceeding is
admissible in a civil proceeding other than a proceeding under this Act, a healthprofession Act or the Drug and Pharmacies Regulation Act or a proceeding relating to
2
, 690an order under section 11.1 or 11.2 of the ontario Drug Benefit Act.(3); 1996, c. 1, Sched. G, s. 2T (2).
Approved by Council:June 18,2014
1991, c. 18, s.36
Rose Bustria |TEM 4.1.50From:Sent:To:Subject:Attachments:
Jo-Ann WillsonWednesday, May 10, 2017 2:38PMRose BustriaFW: Conflict of lnterest DeclarationCOI_ENG.pdf
742
Exec
Jo-Ann Willson, B.Sc., M.S.W., LL.B.Registrar & General Counsel
College of Ch¡ropractor€ of Ontar¡o130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 1't1Fax (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any otherdistribution, copying or disclosure is strictly prohibited. lf you have received this e-mail in enor, please notiry me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: Joel FriedmanSent: Wednesday, May 10, 2Ot7 2:O6PMTo: Jo-Ann Willson <[email protected]>Subject: RE: Conflict of lnterest Declaration
Attached is the conflict of interest declaratíon form for public members and a link to variousinformation: https://www.pas.gov.on.calscripts/en/senerallnfo.asp?#5.
Thanks,
Joel D. Friedman, BSc, LL.BDirector, Policy and ResearchCollege of Chiropractors of Ontario130 Bloor Street West, Suite 902Toronto, ON MsS'lN5Tel: (416) 922-6355 e)d. 104Toll Free: 1 -877 -577 -477 2Fax (416) 925-9610E-mail: [email protected]¡.cgWeb Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any aftachments may contain confidential information and is intended only for the person(s) named âbove. Any otherdistribut¡on, copying or disclosure is strictly prohibited. lf you have received th¡s e-ma¡l in enor, please notifo me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: Jo-Ann WillsonSent: Wednesday, May 10, 2OL7 1:76 PM
To: Joel Friedman <[email protected]>
Subject: Conflict of lnterest Declaration
1
Hi Joel- apparently public members have to sign a conflict of interest declaration as part of theirapplication process (through the Health Board Secretariat). Can you try to track down any informationabout this including the form? Thanks
743Jo.Ann Willson, B.Sc., M.S.W., LL.BRegistrar & General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Su¡te 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This.e'mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any otherdistr¡bution, copying or disclosure is strictly prohib¡ted. lf you have received th¡s e-mail in eror, please notity mè Ímmediately by rep"ly e-mailand delete all copies including any attachments without read¡ng ¡t or making a copy. Thank you.
2
744PERSONAL AND CONFLICT OF INTEREST DISCLOSURE STATEMENT
//\ISTRUCT/OA/S FOR COMPLETING THE PERSONAL AND CONFLICT OF /NIEREST D/SC¿OSURE STATEMENT
PART 1
GoMPLEte, stGN AND DATE PART Iyou MUST srcN AND oere (Nor wee) rru rne SIcNATURE BLocK pRovrDED.
PART2
NOTE: lF YOU PROVIDE YOUR OWN CRIMINAL RECORDS CHECK THROUGH YOUR LOCAL POLICESERVICE YOU ARE NOT REQUIRED TO COMPLETE PART 2.
Houe loonessrs
You ¡vrusr pRovrDE THE ADDRESSES wHERE you HAVE RESTDED FoR THE FULL pAsr nve (5) yEARs TNGLUDTNG @g!!AND YEAR.
Teuepnone
You n¡usr tNcLUDE youR cURRENT RES|DENTIAL TELEpHoNE NUMBER.
VenrRcalon oF pERSoNAL tNFoRMATtoN
a YOU MUST SHOW TWO (2) PIECES OF ACCEPTABLE ID TO THE AUTHORIZED OFFICIAL (SEE PAGE 8).
a THE AUTHORIZED OFFICIAL CONFIRMS THAT THE PHOTO ON THE ID IS YOUR ¡MAGE, AND VERIFIES YOUR NAME, DATEOF BIRTH AND ADDRESS INFORMATION WTH THE ID PRESENTED.
YOU SIGN AND DATE THE CONSENT AND RELEASE PORTION PART 2 SECTION B ON THE PERSONAL AND CONFLICT OFINTEREST DISCLOSURE STATEMENT IN THE PRESENCE OF THE AUTHORIZED OFFICIAL.
THE AUTHORIZED OFFICIAL COII'IPLETES, SIGNS AND DATES SECTION C OF THE FORM.
THE AUTHORIZED OFFICIAL PHOTOCOPIES THE 2 PIECES OF ID AND CERTIFIES THE ID BY SIGNING AND DATING THEPHOTOCOPY.
a THE AUTHORIZED OFFICIAL RETURNS BOTH THE ORIGINAL ID AND CERTIFIED PHOTOCOPY TO YOU.
a YOU COMPLETE SECTION D OF THE PERSONAL AND CONFLICT OF INTEREST DISCLOSURE STATEMENT IN PRIVATEAND PLACE THE COMPLETED PART 2 IN A SEALED ENVELOPE MARKED'PAS"
a PART 1 AND PART 2 OF THE PERSONAL AND CONFLICT OF INTEREST DISCLOSURE STATEMENT ARE THEN SUBMITTEDTO YOUR MINISTRY/AGENCY CONTACT OR THE PUBLIC APPOINTMENTS SECRETARIAT.
Page 1 of 11
PERSONAL AND CONFLICT OF INTERESTDISCLOSURE STATEMENT
745
The Personal and Conflict of lnterest Disclosure Statement consists of two parts. The personalinformation requested on this form is being collected and used by the Public AppointmentsSecretariat (PAS) and the ministry that has jurisdiction for the agency for which you are beingconsidered in order to evaluate the suitability of your potential candidacy for apfointment to ãnontario agency, board, or commission. This information will not be disclosed éicept as requiredfor the above-noted purpose. Questions about the collection, use, or disclosure of
'personai
information requested on this form should be directed to the Senior Program Consultant, publicAppointments Secretariat at:
Room 2440, Whitney Block99 Wellesley St West
Toronto ON M7A 1W4Tel: 416-327-2640
lmportant: Do not alter this form. Do not fax your compteted form. An original formonly will be accepte!, You may submit your completed form to your miniãtry/agencycontact or to the Public Appointments secretariat at the above áddress.
Page2 ol 11
NAME OF APPLICANT:(last name, first name)
AGENCY, BOARD, COMMISSION(agency to which you are applying)
PART I
Conflict of lnterest
A conflict of interest arises where you have a personal interest that conflicts, might conflict, or may beperceived to conflict with the interests of the agency, board, or commission, including a conflict with yourduties as an appointee to the agency, board, or commission. A conflict of interest could arise in relation topersonal matters including:
. directorships or other employment;. interests in business enterprises or professional practices;
. share ownership;. beneficial interests in trusts;. existing professional or personal associations with the agency, board, or commission;. professional associations or relationships with other organizations; and. personal associations with other groups or organÞations, or family relationships.
Every potential appointee must disclose any obligation, commitment, relationship or interest that couldconflict or may be perceived to conflict with his or her duties to or interests of the agency, board orcommission to which the applicant is seeking appointment.
1. A direct or indirect conflict with my duty as an appointee to the agency may arise because,
a) I hold the following offíce(s) (appointed or elected):
b) l, or any trustee or any nominee on my behalf, own or possess, directly or indirectly, the followinginterest(s):
746
2. The nature and extent of the conflicting office, duty or interest is:
Page3ofl1
7473. A real or perceived conflict of interest with my duty as an appointee to the agency could arise because
I receive financial remuneration (either for services performed by me as an owner or part owner,trustee, or employee or othen¡vise) from the following source(s):
4. Other than disclosed above, do you have any relationships or interests that could compromise, or beperceived to compromise, your ability to exercise judgment or decision-making independen¡y andobjectively with a view to the best interests of the agency?
Yes El No tr
lf yes, describe:
You may also be bound by the Public Service of Ontario Act, 2006 and other statutes, regulations, rules,or directives that cunently exist or may be established which are applicable to agencies, úoards, orcommissions.
Page4of11
748lntegrity and Public Accountability
Note: An affirmative answer to any of the following questions does not disqualiff a potential applicant from being appointed. Eachcandidate's background will be considered in relation to the specific requirements of the appointment.
1. ln connection with your employment or business affairs, have you, or any company in which you havea direct or indirect controlling interest, in Ontario or elsewhere:
a) been charged with (where charges are still outstanding and unresolved) or convicted of an offenceunder the Criminal Code (Canada) in respect of which a pardon has not been granted or issued underlhe CriminalRecords Act (Canada)?
Yestr Notr
b) been charged with (where charges are still outstanding and unresolved) or convicted of an offenceunder any other Federal statute, including but not limited to the lncome Tax Act, in respect of which apardon has not been granted or issued under the CriminalRecords Act (Canada)?
Yestr Notr
2. Have you been charged with (where charges are still outstanding and unresolved) or been disciplinedby any professional association or body?
Yes tl No tr
3. Have you been involved in any issue or controversy in the past, or that may be subject to public reviewin the future, in which the government may have an interest?
Yes El No tr
lf yes to any of the above, please provide details below (attach additíonal page if required):
Page5of11
749Biography
lf you are appointed to the agency, the Public Appointments Secretariat may publish a biography thatstates the area of the Province in which you reside and contains general information (e.g., a summary ofemployment history and community involvement) provided on your application for appointment. You mayalso choose to attach separately or write below a short (i.e., 100 words) biography for publicationpurposes.
Do you agree to publication of your biography? Yes tr No tr
I have read the above information and understand the request for disclosure. The details are accurate to the best of my knowledge,lf at any time following the signing of this Personal and Conflict of lnterest Disclosure Statement there occurs any matérial changã tothe information given herein re-9qrging conflict of interest, either by way of addition or deletion, I shall forthwith fiÉ a supplementãrydisclosure statement w¡th the Public Appointments Secretariat deðcribing such change. I understand that if I am appointed to apublic body prescribed under the Public Service of Ontario Act, 2006lhave an obligátion to notify my ethics execuiive of intereststhat could raise an issue under the conflict of interest rules.
PART I
llirri i )
Page6ofl1

PART 2 - Personnel Screening Gheck 750Applicants must receive a personnel screening clearance before they may be offered a public appointment. As such,a personnel screening check is conducted upon your written consent, A personnel screening check involvesverification of personal information, a Declaration in respect of previous convictions for federal offences, and a policerecords check.
The Security Services and Contingency Planning Branch (SSCPB) of the Ministry of Government Services isresponsible for administering the personnel screening check process. The information you provide on the Declarationand the information that is obtained by the Ontario Provincial Police (OPP) as part of the police records check will becollected by the SSCPB and the Deputy Chief of Staff of the PAS for the purpose of conducting a personnelscreening clearance evaluation. All personal information collected by the SSCPB will be securely maintained withinthe branch in confidence; access to information will be restricted to only those employees in the SSCPB who requirethe information to conduct a clearance evaluation and government auditors. The SSCPB and the Deputy Chief ofStaff of the PAS will use your personal information only to evaluate your suitability for the appointment to which youhave applied in regard to the requirements of the position, and will not disclose any information obtained as part of apolice records check to any other person.
Verifìcation of personal information
An authorized official will verify your identity against the personal information you have provided. ln addition, ministrystaff may verify the accuracy of information you have provided in support of your application by contacting yourprevious employers, educational institutions, references, and other contacts as necessary. Only your personalinformation that is relevant to the individual or organization contacted will be disclosed. Additional information aboutyou may be collected from the individuals contacted where such collection is necessary to verifo the information youhave supplied.
Declaration
A Declaration (Section D) is required from you disclosing any unresolved charges and/or previous convictions foroffences under federal statutes (Federal Offences) for which a pardon has not been granted or issued under theCriminal Records Act (Canada). The information you supply in the Declaration will be used to compare against theresults of a police records check. lf a discrepancy is identified between your Declaration and the results of the policerecords check, you may be contacted and given an opportunity to explain this information before a clearance decisionis made.
Police records check
A police records check involves a search by the OPP of records maintained by the RCMP in the Canadian Policelnformation Centre (CPIC), and records maintained by provincial and municipal police forces, for information aboutyou relating to: Convictions under the offence provisions of federal statutes (Federal Offences) including, but notlimited to, the Criminal Code (Canada) and the Controlled Drugs and Substances Act (Canada); where a court hasmade a finding of guilt in respect of a Federal Offence, but has granted you a discharge; charges that have been laidunder the offence provisions of federal statutes but remain unresolved; records of judicial orders in effect made inrelation to Federal Offences.
Convictions for which a pardon has been issued or granted to you under the Criminal Records Act (Canada) will notbe collected. Records of discharges that have been removed from the CPIC system in accordance with the CriminalRecords Act (Canada) will not be collected. Charges that have been withdrawn by the Crown, or stayed or dismissedby a Court will not be collected.
The information collected in a police records check will be used only to assess your suitability for a publicappointment in relation to the requirements of the position. ln the event that adverse information is identified, you maybe contacted to discuss the results of the police records check before a clearance decision is made. The policerecords check will be conducted by the OPP using the personal information you have supplied on this form.lnformation you provide about your date and place of birth, gender, and legal status in Canada will be used only toverify your identity as part of the police records check, and will not be used for any other purpose. You will berequired to provide your fingerprints if a search of the CPIC database reveals that there may be a charge orconviction associated with you in order for the record to be released to the SSCPB. lf you provide paper basedfingerprints, a reduced copy will be returned to you and the original destroyed after 30 days; digital fingerprints arenot retained.
Certain public appointments may require additional personnel screening checks. Applicants to these positions will benotified by the Deputy Chief of Staff of the PAS of any further screening checks required.
Page7 of 11
751
I nstructions for Completin Part 2 ease read careful before completing this part)
You are required to provide all your applicable names and to complete all other parts of Section A.Remember to provide all addresses where you have resided within the last five (5) vears, starting withyour current address, and to provide your current residential telephone number.
2 You are required to sign Section B after an authorized official has verified your personal information.An authorized official may be a senior Ontario Public Service official, the chair of the agency, a notarypublic, a commissioner of oaths, a barrister and solicitor, or a doctor.
You are required to present two (2) pieces of identification, one of which must be government-issuedand include your name, date of birth, signature, and photo. The authorized official will return youridentification to you with a certified photocopy, which is to be included when you submit yourcompleted form.
3. The authorized official will complete Section C after veriñ7ing your personal information.
4. lt is important to note that Section D is confidential to you. Do not comptete this section in thepresence of the authorized official nor present lt to the authorized official.
5. The following procedure is required when submitting your completed Personal and Conflict of lnterestDisclosure Statement:
. Place Part2 in an envelope, including the certified photocopy of youridentification.
¡ Write "PAS' on the envelope and seal it.o Attach the envelope to Part 1.¡ Submit entire form (Parts 1 and 2 together).
Acceptable photo lD Acceptable non-photo lD. Driver's Licence - front and back.Passport' BYID (formerly Age of Majority card)' Canadian Citizenship Card. Permanent Residency Card. Certificate of lndian Status' Possession and Acquisition Licence (FirearmsAct) or PAL Card' Canadian National lnstitute of the Btind (CNIB)ldentification Card' Canadian Military EmploymenVCanadian MilitaryFamily ldentification Card
.Birth Certificate
. Baptismal Certificate
.Hunting Licence'Outdoors Card. Canadian Blood Donor Card'lmmigration Papers
A recent utility bill, property tax statement, or federal income tax statement can be used to verify addressif neither lD shows an addressNote: Health Cards cannot be accepted for purposes under the Personallnformation Protection Act, 2004. Social lnsurance Cards are not to be photocopied and, therefore, willalso not be accepted
Page8of11
752A. Applicant lnformation (to be completed by applicant)
mm ddMale tr Female tr
Couc Province/state
From mm/yy To mm/yyStreet address City, province/state, country, postal/zipcode
Present
Page9of11
753B. Consent and Release (to be co leted b icant)a
I have read and understand the requirements listed on this form for a personnel screening check.
' I consent to the verification of the personal information I have provided in support of this application.
' I consent to the collection and use of the personal information I have supplied in the Declaration by theSecurity Services and Contingency Planning Branch and the Deputy Chief of Staff of the publicAppointments Secretariat for the purpose of evaluating my application for the public appointment towhich I have applied.
' I consent to and authorize the Ontario Provincial Police to conduct a police records check, asdescribed on this form, and to provide the information collected to the Security Services andContingency Planning Branch and the Depug Chief of Staff of the Public Appointments Secretariat forthe purpose of evaluating my application for the public appointment to which I have applied.
' I hereby authorize and consent to the release of the records and information held by the RCMp, theOntario Provincial Police, and provincial and municipal police forces, that are required by the OntarioProvincial Police to conduct a police records check, and the Security Services and ContíngencyPlanning Branch and the Deputy Chief of Staff of the Public Appointments Secretariat to cônduct apersonnel screening check.
I further declare that all the answers provided in this application, as well as all the information contained inthe documents and materials submitted with it, are true and complete.
I hereby release and discharge forever Her Majesty the Queen in Right of Ontario and any or all herrespective directors, employees, servants, and agents, including their successors and asõigns, from anyand all actions, claims and demands for damages, loss or injury howsoever arising, exceptãs a result ofnegligence or wilful misconduct, which may hereafter be sustained by myself as a result of the collection,use and disclosure of information about me by the Ontario ProvinciaL Poiice, in the course of conductingpersonnel screening checks.
I confirm that the applicant's personal information including name, date of birth, and address has beenverified.
C. Verification of Personal lnformation (to be com leted authorized official)
Page 10 of 11
754licantato be com leted confidentiallD. Declaration
Please identify in the space provided below whether or not you have unresolved charges and/orconvictions received in relation to the offence provisions of federal statutes including, but not limited to,the Criminal Code (Canada) andthe Controlled Drugs and Substances Act (Canada), subiect to thefollowino exceptions:
lf you have received a pardon for a previous conviction in accordance with the Criminal Records Act(Canada), please do not disclose the conviction nor the fact that you have received a pardon for theconviction,lf you have been charged with or convicted of an offence under a provincial statute (ProvincialOffences), please do not disclose the charge or conviction.lf as a young person you were subject to charges that were dealt with under the Youth CriminalJustice Act or its predecessors the Young Offenders Acf or the Juvenile Delinquents,Acf, please donot disclose that information.
Please prov¡de below details of all unresolved outstanding charges and/or conv¡ctionsOR write "not applicable".
Page11of11
755ITEM 4.2
Submitted on June I 2, 20I7
Gollege of Ghiropractors of OntarioAdvertising Committee Report to GouncilFriday, June 23,2017
Members: Dr. Peter Amlinger, ChairMr. Douglas CressmanDr. Colin Goudreau, non-Council memberDr. Kristina Peterson
Staff Support: Mr. Joel Friedman, Director, Policy & Research
The Advertising Committee met once via teleconference on May 18, 2017 since the lastCouncil meeting.
The Committee reviewed the terms of reference, protocols, standard of practice, guidelineand policy for the Advertising Committee and discussed the procedure for reviewing andproviding feedback for proposed advertisements.
The Committee continues to review proposed advertisements submitted by members forreview, which now include websites and electronic media.
The Committee is interested in getting direction from Council concerning an amendmentthat was approved to Guideline G-016 at the February 28,2017 Council meeting, namely:
"All advertisements must be presented in a professional manner, maintain professionalintegrity, and serve the public's best interest. Although discountedfees may be ffired,online coupons, contests and giveawqys are inappropriate."
There have been inquiries to CCO on how this section is to be applied, whether it ismeant as a prohibition against online coupons, contests and giveaways or meant as adviceagainst using them. An extract from the minutes from the February 28,2017 Councilmeeting is included in the package.
At its next in-person meeting the Committee will review the feedback from the upcomingcirculation of Draft Policy P-016: Public Outreach.
I would like to thank Mr. Joel Friedman for the institutional knowledge and efficiency he
brings to the committee.
I would also like to thank my fellow committee members Mr. Doug Cressman and DrsGoudreau and Peterson. Their commitment to the work of this committee and toregulating the profession in the public interest is most appreciated.
2Advertisino Comm ittee Report to Council: June 23.2017
756Respectfully submitted,
Dr. Peter Amlinger,Chair, Advertising Committee
SrRruonRD oF PRRclces-016 |TEM 4.2.1Advertising CommitteeApproved by Council: September 7, 1996Amended: September 21,2002, June 22,2007, November 29,2007,September 24, 2009, February 28, 2017
Advertising
757
a
Note to renders: In the eaent of ttny inconsistency betuteen this document attd tlte legislntion tlntøffe c t s chir opr a c t i c p r a c t i c e, th e I e gisl at io n gott er n s.
lrurEt¡r
To provide members with advertising guidelines to ensure all advertisements
serve the public interest.
To educate the public on what is available for their chiropractic care.
To ensure advertisements are accurate, factual and contain information that isverifiable.
To ensure, as much as possible, that the public has the information to makerational choices for their care.
To assist the public in obtaining the services of members of their choice
To maintain a professional image.
Advertising Definition for the Purpose of Standard of Practice S-016Advertising
Advertising is any message communicated outside a member's office through a
public meclium, including electronic media such as websites and social media, thatcan be seen or heard by the public at large with the intent of influencing a person's
choice of service or service provider. This standard applies equally to members act-
ing individually, as a grovpt or as a professional health corporation.
DescnrpnoN oF STANDARD
1. An advertisement must be:
(a) accurate, factual and contain information that is verifiable; and
(b) readily comprehensible by the persons to whom it is directed.
a
a
a
I
College of Chiropractors of Onlario
2
Srn¡¡onnD oF PRRclces-016
Advertising
758
2. An advertisement may:
(a) name a specific diagnostic or therapeutic procedure or modality but cannotclaim superiorify or endorse the exclusive use of such procedures, services,techniques, modalities or products. References to specific diagnostic or ther-apeutic procedures must comply with Standard of Practice 5-001:Chiropractic Scope of Practice;
(b) make reference to the member being a specialist, providecl the member isrecognized pursuant to CCO's policy as a specialist, and the specialty isdisclosed. Refer to Policy P-029: Chiropractic Specialties, for the list ofspecialties currently recognized by CCO;
(c) make reference to the member being affiliated with any professionalassociation, society or body, other than CCO, only on a curriculum vitae,bnsiness stationery and recognized public displays;
(d) allow an individual or organization to endorse a member provided:
(i) the individual or organization proposing the endorsement has sufficientexpertise, according to CCO, relevant to the subject matter beingendorsed; and
(ii) the member has been appropriately assessed as providing the subjectmatter being endorsed; and
(e) offer an initial complimentary consultation'
(f) include testimonials that refer only to the benefits of chiropractic andnot to a particular member or office, with the exception of a member'swebsite which may include testimonials that refer to a particular member oroffice, provided the testimonials are:
(i) accurate, verifiable, and recorded in the patient health record;
(ii) used only in accordance with the written consent of the patient;
(iii) not obtained using any unclue pressure, duress, coercion or incentives;and
(iv) otherwise compliant and consistent with Standard of Practice 5-016:Advertising, the chiropractic scope of practice, other CCO standards ofpractice, policies and guidelines, and privacy legislation.
College of Chiropractors of Ontario
SraruoRRD oF PRnclces-016
Advertising
759
3. Any advertisement with respect to a member's practice must not contain:
(a) anything false or misleading;
(b) a guaranteed success of care;
(c) any comparison to another membet's or other health care provider'spractice, qualifications or expertise;
(d) any expressed or implied endorsement or recommendation for the exclusiveuse of a product or brand of equipment used to provicle services; and
(e) material that, having regard to all the circumstances, would reasonably be
regarded as disgraceful, dishonourable or unprofessional.
4. A member may advertise his/her fee for chiropractic services provided
(a) the advertisement contains accurate, complete and clear disclosure of whatis and what is not included in the fee;
(b) there are no hidden fees/costs;
(c) the member does not bill a thircl-party payor for the complimentary portionof the diagnostic or treatment service;
(d) the advertisement expressly states the timeframe to be honoured for anycomplimentary or discounted diagnostic or treatment service;
(e) the advertisement does not limit the offer to a certain number ofparticipants;
(f) no obligation is placed on the patient for follow-up appointments as a resultof the complimentary or discounted diagnostic or treatment service; and
(g) the advertisement is presented in a professional manner that maintains thedignity of the profession.
5. A member advertising the exchange of products/services for proceeds/d.onations to a charity may do so as follows:
(a) the proceeds/donations are being collectecl for a registered charity, school orother organization that, in the opinion of the Advertising Committee/ serves
the public's interest ("chaúly');
3
College of Chiropractors of Onlario
4
Srn¡¡onnD oF Pnncnces-016
Advertising
760
(b) the charity is disclosed in the advertisement;
(c) the member discloses the part of the proceeds/donations to be given to thedesignated charity ¿ind if he/she is taking any proceeds/donations to coverhis/her expenses;
(d) the member may not bill any third-party payor for the diagnostic or treat-ment services provided in exchange for the charitable proceeds/donation;and
(e) the member providing diagnostic or treatment services in exchange for thecharitable proceeds/donation must comply with all cCo standards ofpractice.
6. Public presentations or displays'are permissible provided
(a) a member adheres to CCO's regulations and standards of practice (e.g.,consent, record keeping);
(b) professional conduct is maintained at all times;
(c) material distributed complies with the advertising standarda;
(d) assessment(s) performed comply with CCo's Public Display protocol (policyP-016) and are for educational purposes;
(e) no controlled acts of diagnosis and/or acljustments are performed; and
(f) no coercion or pressure tactics are usecl..
7. A communication by a member to a patient or prospective patient for thepurPoses of soliciting business shall be appropriate to the standards of theprofession and shall be respectful of patient choice, and not involve unduepressure and not promote unnecessary products or services. A member mustnot contact or communicate with or allow any person to contact orcommunicate with potential patients via telemarketing or electronic methods.
I' A member must not advertise or permit advertising with respect to his/herpractice in contravention of the regulations or standards of practice.
College of Chiropraclors of Onlario
SrnruoanD oF PnaclcEs-016
Advertising
761
Lecrslnnve GoruTExr
It is an act of professional misconduct to contravene or fail to maintain a standardof practice.
For additional information regarding billing procedures, please refer to RegulationR-008: Professional Misconduct (Business Practices section) and Guideline G-008:
Business Practices.
'A consultation is a meeting to discuss how chiropractic may benefit the patient. Aconsultation does not include examination procedures, diagnostic tests(e.g., radiographs) or treatment services.
3 "Displays" include presentations or other visual material to members of thepublic, in a place normally frequented by the public, by a person or persons whoare physically present when such material is disturbed or presented.
a It is strongly recommended that material to be distributed be pre-approved by theAdvertising Committee.
5 Voluntary appointments are permitted - i.e., if potential patients ask for themember's business card or request an appointment.
5
College of Chiropractors of Ontario
GuroeurueG-016 ITEM 4.2.2
Advertising CommitteeApproved by Council: January L3, 1'996
Arnendcd and Approved by Council: September 21-, 2002, lttne 22, 20O7,
November 29,2007, September 24,2009, February 28,2017
Advertising
762
Note to readers: In tlrc eaent of øny inconsistency betuteen this document snd the legislntion tlnt
fficts chiropractic prøctice, the legislntiott goperns.
lrurerur
The advertising guideline is designed to detail Standard of Practice S-016:
Advertising, and to give members guidance when educating members of thepublic. Advertisements should help the public make informed choices regardingtheir health care. To assist members of the public in making knowledgeablechoices, advertisements must be informative and maintain a professional image.
DescnrproN oF GUIDEL¡NE
1. An aclvertisement must be:
(a) accurate, factual and contain information that is verifiable;
Proaidtttg the public zuith accurste, factual, objectiae and aerifiable informntiott to
rnnke nn inþrtned choice in henlth care is in the public's best interest, Subjectiue
opinions mny cûuse confusion and lack of trust.
(b) readily comprehensible by the persons to whom it is directed.
Adztertisements should be rendily understandnble so tlrc general public is not
confused by the message,
2. An aclvertisement may
(a) name a specific diagnostic or therapeutic procedure or modality but cannotclaim superiority or endorse the exclusive use of such procedures, services,
techniques, modalities or products. References to specific diagnostic or ther-apeutic procedures must comply with the Standard of Practice 5-001:
Chiropractic Scope of Practice;
Such references assist the publíc in fínding a particr.tlnr type of chiropractic care and
allow an informed clrcice.
Members nny adaertise seraices (e.g., autpu.ncture, ultrøsottnd, radiography),
adjustiue techniqtrcs, øttd other procedures zttithin tlrc public domøtn (e.g. ortlntics,nutritional products). Members should tntderstand exhaustiae lists of eaerythittg
possible may confuse the publíc nnd are not adztised.
1
College of Chiropractors of Ontario
Gu¡oeu¡leG-016
Advertising
2
763
(b) make reference to the member being a specialist, provided the member isrecognized pursuant to cCo's policy as a specialist, and the specialty isdisclosed. Refer to Policy P-029: Chiropractic specialties, for the list ofspecialties currently recognized by CCO;
Members may only use terms such as "specinlist" nnd "specializing itr" in referenceto the specialties recognized by cco. A tnentber cnnnot sdaertise ø specíalty inarea(s) not recognizedby cCo. Amentber may express nn "interest itr" or "focuson" an øreø ofpractice,
(c) make reference to the member being affiliated with any professionalassociatiory society or body, other than CCO, only on curriculum vitae,business stationery and recognized public displays;
Adaertising n mentber's ffiliatiorts in any other mediutn tnãy confuse the publicand nmy csuse contparisons to otlrcr mentbers, zuhich is not permitted. In electronicmedin, ø member may include professional nssociøtions other thøn CCO, only in thecurrinLlum uitaelbiograplty section of n zoebsíte or socittl media home page.
(d) allow an individual or organization to endorse a member, provided:
An utqualified endorsement from n solffce with little or no expertise is not in thepr.tblic's best interest and undermines tlrc public's trust.
(i) the individual or organization proposing the endorsement has sufficientexpertise, according to CCO, relevant to the subject matter beingendorsed;
(ii) the member has been appropriately assessed as providing the subjectmatter being endorsed;
(e) offer an initial complimentary consultation.l
Members may ndaertise complinrcntørylcourtesy initiøl consultations. Membersmay not bill any third'pnrty payors for contplimentørylcourtesy constiltations.
(f) include testimonials that refer only to the benefits of chiropractic andnot to a particular member or office, with the exception of a member'swebsite which may include testimonials that refer to a particular member oroffice, provided the testimonials are:
College of Chiropraclors of Onlario
GuroeurueG-016
Advertising
764
(i) accurate, verifiable, and recorded in the patient health record;
(ii) used only in accordance with the written consent of the patient, which maybe withdrawn at any time;
(iii) not obtainecl using any undue pressure, duress, coercion or incentives; and
(iv) otherwise compliant and consistent with Standard of Practice 5-016:
Advertising, the chiropractic scope of practice, other CCO standards ofpractice, policies and guidelines and privacy legislation.
Testintoninls that refer to the benefits of chiropractic øttd not to n particulnr mentber
or ffice ar"e pernissible; hozueaer, nrcmbers rnay contintrc to use specific testímoniøls
on their zoebsites.
Testímoninls must be truthful and aerífinble, nnd eaidenced in the patient health
record.
There must be documented pntient consent relnted to n pnrtiuúnr testimoninl,
documented in t!rc patient health record.
Patíents may only ffir a testimotùnl under tlrcir own free will and not dtte to øny
coercion or contpensat iott.
As zuitlt nll ndaertising, use of testimoninls must be consistent with the chiroprnctic
scope of prnctice, ns defined in the Chiropractic Act, 199L, and releaant legislntittn,
standnrds of practice, policies ønd guidelines.
3. Any advertisement with respect to a member's practice must not contain:
(a) anything false or misleading;
Fnlse or misleading statements undermine public trust in tlrc professíon and may
result in a complaint to CCO by ø collengue or n ntember of the ¡sublic'
(b) a guaranteecl sllccess of care;
Claims nnd gunrantees of success are often not aerifiable and møy appeßr
unprofessiorml. Members slntild not use expressiorts such as "utill help" and "does
relieue" which imply n gunrøntee. Mentbers may use expressions such as "may be
able to help" or "lns been slnntt to relieae."
3
Coflege of Chiropractors of Ontario
GuroeurueG-016
Advertising
765
4
(c) any comparison to another member's or other health care provider'spractice, qualifications or expertise;
Compnríson to any fncet of ønother member's practice is unprofessional. The publicnnd the professiott are better seraed by positiae and generic chiroprnctic føcts.
Members should not use adjectiaes zuith contparatiztes (e.g., "more" or "better") intheir adaertising because tlrcy imply a comparison, Members mßy use utords such ss"søfe" and "effectizte" to desuibe the chiropractic profession in general.
(d) any expressed or implied endorsement or recommendation for the exclusiveuse of a product or brand of equipment used to provide services;
Exclusiue endorsements of products suggest stryeriority nnd imply a cornparison,which is not permitted,
(e) material that, having regard to all the circumstances, would reasonably beregarded as disgraceful, dishonourable or unprofessional.
All adaertisenrcnts must maintøin professional integrity nnd sense the public's bestinterest.
It is an act of professionøl misconùrct to engage in conduct or perþrm an act that,hnaing regard to all the cirunnstances, zoottld reøsonably be regarded by nrcmbers nsdis gr acef ul, dishonour nble or unprofessional.
4. A member may advertise his/her fee for chiropractic services provided:
(a) the advertisement contains accurate, complete and clear disclosure of whatis and what is not included in the fee;
The public is entitled to full disclosure of whnt is nnd whnt is not included in theaduertised fee.
(b) there are no hidden fees/costs;
The puhlic is entitled to full disclosure of zohat is nnd what is not included in tlrcadaertised fee.
(c) the member does not bill a third-party payor for the complimentary portionof the diagnostic or treatment service;
A member is not pernúttecl to bill any third-party ¡tnyor for complimentarydiagnostic or treatment serztices as this prnctice is wtethical and møy be professional
College of Chiropractors of Ontario
GuroeurueG-016
Advertising
766
núsconduct
(d) the advertisement expressly states the timeframe to be honoured for anycomplimentary or discounted diagnostic or treatment service;
To ensure there is no confitsiott or núsunderstanding, the adrtertisement must
indicøte the exøct tirnefrnme in which the complimentary or discowtted diøgnostic
or treatment seruices apply.
(e) the advertisement does not limit the offer to a certain number ofparticipants;
Mentbers of the public mt¡st øll be giz,en øn equal opportwüty to obtain the
ødaertised complimentary or discounted diagnostic or trenfunent seraices. Anødaertísement that limits an offer to a certain nutnber of participønts møy be
núsleøding.
(f) no obligation is placed on the patient for follow-up appointments as a resultof the complimentary or discounted diagnostic or treatment service;
A member may not use an sdaertisement for cotn¡slitnentnry or discottnted
diøgnostic or trentnrcnt seruices to presxtre or clerce ø member of tlrc public toreturn for folloro -up nppointments.
(g) the advertisement is presented in a professional manner that maintains the
dignity of the profession.
All ødaertisements must be presented in n professional mmtner, maintninproþssionnl integrity, and s'erue the public's best interest.@tthottgtt discounted fees'miy
be offered, lntine coupot'ts, contests ancl giaeøztrøys nre inapproVriatel
5. A member aclvertising the exchange of products/services for proceeds/donations to a charity may do so as follows:
An ntiuertisement that encourages philnnthropy, if done professionølly ønd ethicølly,
seraes the pultlic's interest.
(a) the proceeds/donations are being collectecl for a registered charity, school orother organization that, in the opinion of the Advertising Committee/ serves
the public's interest ("chaúty");
The charity or organizntion must serrte tlrc public ínterest.
5
College of Chiropractors of Ontario
GuroeurueG-016
Advertising
6
767
(b) the charity is disclosed in the advertisement;
The public is entitled to fuII disclosure regarding the chnrity or orgmùzntion forwhich proceeds are being collected.
(c) the member discloses the part of the proceeds/donations to be given to thedesignated charity and if he/she is taking any proceeds/donations to coverhis/her expenses;
The publíc is entitled to full discloutre regørding horo the proceeds zuill be diaided.
(d) the member may not bill any third-party payor for the diagnostic or treat-ment services provided in exchange for the charitable proceeds/donation;
A member is not permitted to bill øny third-¡tarty pnyor for complimentarydingnostic or treatment seraices øs this practice is unethicnl and may constitute ntact of fratLd.
(e) the member providing diagnostic or treatment services in exchange for thecharitable proceeds/donation must comply with all CCo standards ofpractice.
Members must comply with all CCO stnndctrds of prøctice. If the member isuncertøin if tlrc proposed ndaertisement is nppropriate, helshe is encournged tosubmit it to the Adaertising Committee for reaiezp prior to publication. Turnaraundtime for a response is approximately 10 busíness døys.
6. Public presentations or displays'are permissible provided:
The ndoertising stnndnrd permits pttblic presentatiorts for educøtional or inþrmntionalpltl?oses. Being intrusiz¡e to the public within ø public place, hnrassing the public orusing pressure tnctics are unprofessional nnd undermines tlrc public's trust.
(a) member(s) adhere(s) to CCo's regulations and standarcls of practice (e.g.,consent, record keeping);
(b) professional conduct is maintained at all times;
(c) material distributed complies with the advertising standard;a
(d) assessment(s) performed comply with cco's public Display protocol (poticyP-016) and are for educational purposes;
College of Chiropractors of Ontario
GuloeurueG-016
Advertising
768
Assessment procedures, ns listed in CCO's Public Displny Protocol (Policy P-016),
øre pennitted, proaitled tlæ protocol is followed and consetú is obtained.
(e) no controlled acts of diagnosis and/or adjustments are performed;
Since a conryIete history nnd exnrninntion are innppropriate at a public display,
making a dingnosis or performing an adjustrnent is not pernütted. Adjustrnents st a
pubtic displny mny alnrm the public when obseraing a,n adjustment procedure
uitltout ø proper explanntion.
(f) no coercion or pressure tactics are used.n
7, A communication by a member to a patient or prospective patient for the
purposes of soliciting business shall be appropriate to the standards of the
profession and shall be respectful of patient choice, and not involve unduepressure and not promote unnecessary products or services. A member mustnot contact or communicate with or allow any Person to contact orcommunicate with potential patients via telemarketing or electronic methods.
Arty comnrunication to patients or prospectiue patients must be consistent with the
ødaertising standard of prnctice, within the cltiropractic scope of practíce, professional
øncl respectfut of the pttblic interest, nnd contplinnt zuith Cnnndinn anti-spøtn legislø-
tion, no matter zohøt the medium.
8. A member must advertise or permit advertising with respect to his/her practice
onnly in compliance with the regulations or standards of practice; and
A member is responsible for nll ødaertising that is directly or indirectly controlled by
that mentber.
LecrsllrvE CoNTEXT
For additional information regarding billing procedures, please refer to RegulationR-008: Professional Misconduct (Business Practices section) and Guideline G-008:
Business Practices.
' A consultation is a meeting to discuss how chiropractic may benefit the patient' Aconsultation does not include examination procedures, diagnostic tests (e.g., x-rays)
or treatment services.
7
College of Chiropractors of Ontario
Guroeu¡leG-016
Advertising
769
I
2 "Displays" include presentations or other visual material to members of thepublic, in a place normally frequented by the public, by a person or persons whoare physically present when such material is distributed or presenteã.
3It is strongly recommended that material to be distributed be pre-approved by theAdvertising Committee.
a voluntary appointments are permitted - i.e., potential patients ask for themember's business card or reguest an appointment.
fl I
College of Chiropractors of Ontar¡o
Rose Bustria trEM 4.2.4Jo'Ann WillsonMonday, May 08, 2017 9:37 AMRose BustriaFW:AttachedShankar LTR - Advertising SOP - May 2017.pdf
773From:Sent:To:Subject:Attachments:
Advertising and Executive.
Jo.Ann Wlllson, B.Sc., M.S.W., LL.BRegistrar & General Counsel
Gollege of Chlropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext. 'l 1 1
Fax (416) 925-9610E-mail: jujllsoû@cco. o!.caWeb Site: www.cco.on.ca
CONFIDENTIALITY WARNI NG:This e-mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any otherdistribution, copying or disclosure is strictly prohibited. lf you have received this e-mail in enor, please notify me immediately by reply e-mail
and delête all copies including any attachments without reading it or making a copy. Thank you.
From: Bob Haig Imailto:[email protected]]Sent: Monday, May 08,2017 9:35 AMTo: Jo-Ann Willson <[email protected]>Cc: Ayla Azad ([email protected]) <[email protected]>; Deborah Proudfoot<d pro udfoot @ch i ro p ra ctic.o n.ca >
Subject: Attached
Jo-Ann:
Attached please find a letter from Dr. Azad to Dr. Shankar
Dr. Bob HaigChief Executive OfficerOntario Chi ropractic AssociationTel: (41 6) 860-41 55 or 1 (877) 327 -2273 exl. 7204rdhaiq@chi ropractic.on.cawww. ch i rop ra cti c. o n. ca
Note: This email message is ¡ntended only for the named recipieni(s) above andmay conta¡n informat¡on that is privileged, confidential and/or exempt fromdisclosure under âpplicable larv. lf you have received this message in efror. or arenot the named rec¡pient(s). please ¡tnmediately notify the sender and delete thisellìa¡l message.
Bob
1
--¡aabbO-
-5atbbO-
OntarioChiropracticAssociation 774
May 8,2017
Gauri Shankar, DC
PresidentCollege of Chiropractors of Ontario130 Bloor Street West, Suite 902Toronto, ON M5S 1N5
Dear Dr. Shankar,
On behalf of the Ontario Chiropractic Association, I would like to acknowledge the dedicated
work of the CCO Advertising Committee and Council in revising the Advertising Standard of
Practice.
Websites and social media are a complex and ever evolving landscape and your actions will
undoubtedly help in the protection of the public.
Sincerely,
Ayla Azad, DC
President
+b("$>
200 - 20 Victoria St.
Toronto ONM5C 2N8
Tet 416-860-0070Toll -f ree 7- 877 -327 - 227 3
Fax 416-860-0857
www.ch iropractic.on.ca
Joel Friedman
From:Sent:To:Cc:Subject:
Heather Ann Kaldeway <[email protected]>Monday, May 08, 2017 1:14 PMJoelFriedmanMiguelPachecofoireview FW: [Test] CCO Advertising SoP Now Applies to Websites & Social Media
OntarioChiropracticAssociation
775
Joel,
We will be sharing the good news about the expansion of 5-016 with our members later this week (excellent work, by
the way!) and we were hoping you could review the email draft below to ensure that it is accurate'
We're aiming to send this out on Thursday this week, so feedback any time between now and Wednesday would be
lovely.
Many thanks, hope you are well,
Heather Ann
Heather Ann KaldewayCommunication Specialist, OCATel: (4'16) 860-7196 orI (877)327-2273 [email protected]
From: Ontario Chiropractic Association [mailto:[email protected]'mcdlv.net] On Behalf OfOntario Chiropractic AssocíationSent: May-08-17 12:42 PM
To: Heather Ann KaldewaySubject: fTest] CCO Advertising SoP Now Applies to Websites & Social Media
We're Here For You View this email in your browser
--¡rfbba
O
1
776
Our websites and social media feeds can have a major impact on our collective ability toprotect the profession's reputation, as recent neoative media coveraqe of chiropractic
websites in Manitoba has demonstrated.
ln a very positive move, the CCO has amended its definition of Advertising in its Sfandardof Practice S-016: Advertisinq to include websites and social media (emphasis added):
"Advertising is any message communicated outside a member's
office through a public medium, including electronie mediasuch as websites and social media, that can be seen or heard
bythe public at large with the intent of influencing a person's
choice of service or service provider. This standard applies equally
to members acting individually, as a group, or as a professional
health corporation."
With this amendment, websites and social media are now subject to the criteria of the
Standard. As such, they must be accurate, factual and contain information that is verifiable,
and must not contain:
. anything false or misleading;
o a guaranteed success of care;
. arìV comparison to another member's or other health care provider's practice,
qualifications or expertise;
2
CCO Standard of Practice S-016: AdvertisingNow Applies to Websites & Social Media
any expressed or implied endorsement or recommendation for the exclusive use of
a product or brand of equipment used to provide services; and
materialthat, having regard to allthe circumstances, would reasonably be
regarded as disgraceful, dishonourable or unprofessional. 777
The OCA applauds the CGO for this significant and important update to S-016. We
encourage all members to review their websites and social media feeds today to ensure
compliance wilh Standard of Practice S-016: Advertisino.
a
a
We're here for you. Call us:
Local: 41 6-860-0070 | Toll-free: 1 -877 -327 -227 3
Update your OCA membership preferences or
unsubscribe from this list
Our mailing address is:
Ontario Chiropractic Association
200-20 Victoria St
Toronto, ON MsC 2N8
Canada
Add us to your address book
f Facebook t Twitter in Linkedln
CCO Standard of Practice S-016: Advertising
3
ITEM 4.3 Submitted June 12, 2017
College of Chiropractors of OntarioPatient Relations Committee Report to GouncilFriday, June 23,2017
778
Members: Dr. Reginald Gates, ChairMs Georgia AllanMs Patrice BurkeDr. Janit Porter, non-Council memberDr. Matt Tribe, non-Council member
Staff Support Mr. Joel Friedman, Director, Policy and ResearchMs Jo-Ann Willson, Registrar and General Counsel
l. Introductionand Recommendations
The Patient Relations Committee has met once on June 8,2017 since the last meeting ofCouncil.
Recommendotìon 1
That Council approve amendments to the Patient Relations Committee Terms of Reference.
The Patient Relations Committee continued the work of the previous committee byreviewing its Terms of Reference. The Committee has included several bullets from theduties and objects of colleges from the Regulated Health Professions Act, l99I (RHPA) andCCO's strategic objectives.
The Committee is also recommending that CCO committees develop a consistent templatefor their terms of reference that reference the duties and objects of the colleges and CCO'sstrategic objectives.
ll. Report on Bill 87
Bill 87 Protecting Patients Act, 2006 received royal assent on May 30,2017. Most of theamendments come into effect upon the bill receiving royal assent, while some amendments,
such as the definition of a patient, will come into effect upon proclamation, the date ofwhich is unknown. The Patient Relations Committee continued the work of the previouscommittee in analysing relevant standards of practice, policies and guidelines foramendment to ensure consistency with the amendments to the RHPA. The Committee has
identified the following documents that will require amendments:o Standard of Practice S-014: Prohibition of a Sexual Relationship with a Patient
(incorporation of mandatory one year waiting period and inclusion of additional acts
of sexual abuse that will result in the revocation of a license)o P-018: Funding for Therapy and Counselling for Patients Sexually Abused by
Members (review of policy to ensure it is consistent with legislative amendmentsthat make funding for therapy available upon the filing of a complaint or report)
. Guideline G-001: Communication with Patients (inclusion of additional acts ofsexual abuse that will result in the revocation of a license)
Patient Relations Committee Report to Council: June 23,2017
The Committee foresees that it will have recommendations for the September Councilmeeting.
2
779Recommendatíon 2
That Council approve a communique to be distributed by email blast to CC} membersinforming them of the passing of Bill 87.
lll. Ongoing Funding for Therapy and Counselling
The Committee continues to monitor payments made for therapy and counselling. Thecommittee noted that one ongoing funding has reached its five year limit.
lV. Other Ongoing Business
CCO continues to be involved with the Federation of Health Regulatory Colleges ofOntario's (FHRCO) group on "Training for the Prevention of Sexual Abuse of Patients".The FHRCO group is preparing resources for the education health professionals in theprevention of sexual abuse of patients, and will be meeting next on June 29, 2017 .
The Committee also continues to review resources and information relating tocommunication with the public, including scripts for videos, radio ads and other e-Leamingopportunities. The Committee hopes that this will be part of Council's discussion aboutcommunication at a future strategic planning and/or focused Council meeting.
V. Acknowledgements
I wish to thank Ms. Georgia Allan, Ms. Patrice Burke, Dr. Janit Porter, Dr. Matt Tribe, fortheir continued commitment and insight. I wish to also thank Mr. Joel Friedman, Ms. Jo-Ann V/illson and Ms. Andrea Szametz for their excellent work in support of this committee.
Sincerely,Dr. Reginald GatesChair, Patient Relations
Approved by Council: April 14, 2010
ITEM 4.3.2 rP^rerur RelRnoNS coMMrrrEE 782
Vrsrot¡ Srereuerur
The Patient Relations Committee seeks to implement a proactive patient relationsprogram and promote confidence in the chiropractic profession by making the programvisible to the public, to chiropractors, to other health care professionals, and to thegovernment.
In particular, the Committee aims to ensure that members are fully informed regardingthe nature of professional relationships, that policy making and complaints processes ofthe College of Chiropractors of Ontario (CCO) are open and accessible to the public, and
that members of the public are fully informed regarding their rights to safe, effective, and
ethical chiropractic care.
Tennns oF REFERENcE
l. The Patient Relations Committee is a statutory committee of CCO
2. The Commiuee is composed of one elected member of Council, two public(appointed) members of Council, and two non-Council members of CCO. TheCommunications Officer is the staff resource person to the Committee.
3. Areas of Responsibility:
a. Develop and implement a program to enhance relations between the patient andthe member.
b. Develop and implement measures for preventing and dealing with sexual abuse ofpatients.
c. Report to HPRAC on the program and on any significant changes of the program
d. Develop and deliver educational requirements for the members and training forCCO staff.
e. Develop guidelines for the conduct of members with their patients.
f. Provide information to the public about their rights, for example, the Partnershipof Care (Patient's Charter of Rights and Responsibilities).
g. Administer the Funding Program.
@ College of Chiropractors of Ontario
Patient Relations Committee: Vision Statement and Terms of Reference 2
783h. Develop guidelines for CCO members to assist them in dealing with all aspects of
member-patient relationships.
i. Make recommendations to Council regarding new regulations, standards ofpractice, policies, or guidelines related to the Patient Relations mandate.
@ College of Chiropractors of Ontario
6t122017 Ontario Strengthens Laws to Prevent Sexual Abuse of Patients
ITEM 4.3.3
College of Chiropractor$ of OntarioL'Ordre des Chiropraticiens de I'Ontario
pRÃFnøÉÐ784
Ontario Stengthens Laws to Prevent Sexual Abuseof Patients
On May 30,2017, the Ontario government passed Bill 87: TheProtecting Patients Act, 2017, which amends several pieces oflegislation including the Regulated Health Professions Act, 1991.Please see the following link for the Ontario Government's newsrelease on the passage of the Pratecting Patients Act, 2077.
The amendments reinforce Ontario's zero tolerance policy on thesexual abuse of patients by any regulated health professional, andimplement new programs and policies to keep people healthy.
The Profecting Patients Act, 2A17 includes legislative amendmentsto:
. Expand the list of acts of sexual abuse that will result in themandatory revocation of a regulated health professional's certificateof registration
. Remove the ability of a health regulatory college to imposerestrictions that would allow a regulated health professional tocontinue practising on patients of a specific gender
. Ensure more timely access to therapy and counselling for patientswho make a complaint of sexual abuse by a regulated healthprofessional to a health regulatory college
. Define a patient to include a former patient to remain a "patient" forthe purposes of the sexual misconduct provisions for a period of oneyear from when the person would otherwise cease to be a patient(comes into force upon proclamation)
. Require that more information regarding the current and pastconduct of regulated health professionals is available to the public in
an easy-to-access and transparent way. Incorporate feedback from stakeholders, including establishing a
higher threshold for when third-party records may be ordered to beproduced in discipline hearings involving sexual abuse.
Please look out for future CCO communiques, circulations and newslettersfor more information on the impact of the passing of the ProtectingPatients Act, 2017.
College of Chiropractors of Ontario, 130 Bloor Street, Suite 902, Toronto, Ontario M551N5 Canada
https://ui.constantcontact.com/visualeditor/visual_editorjreview.jsp?agent.uid= 1128168001157&format=html&print=true 1t2
6t1212017 Ontario Strengtlrens Laws to Prevent Sexual Abuse of patients
SafeUnsubscribe'M { recioíent's email}Uodate Profile I About our service orovider
Sent by [email protected] in collaboration with
785
C-orcffittCottWt'VFTry it free today
https://ui.constantcontact.comfuisualeditor/visual-editor_¡reviorvjsp?agent.uid=1128168001157&format=html&print=tue 2t2
Submitted on June 9, 2017
ITEM 4.4
College of Chiropractors of OntarioQuality Assurance Committee Report to CouncilFriday, June 23,2017
786
Members:Dr. Elizabeth Anderson-Peacock, ChairDr. Kristina PetersonMs Patrice BurkeMr. Douglas CressmanDr. Joel V/eisberg, non-council member
Staff:Mr. Joel Friedman, Director, Policy & ResearchDr. Bruce Walton, Director of Professional PracticeMs. Jo-Ann'Willson, Registrar and General CouncilMs. Andre a Szametz, Recording Secretary
Chair's Report
l. lntroduction and Recommendations
Since the last meeting of Council, the Quality Assurance (QA) Committee has met once onMonday llv4.ay 29,2017.
Dr. Kristina Peterson and Mr. Doug Cressman were welcomed as new members to the QualityAssurance (QA) committee. Ms. Patrice Burke and Dr. Joel V/eisberg were welcomed back toserve another term with the committee.
Meetings have been scheduled for the 2017-2018 year along with a work plan.
Recommendøtion I
Standard of Practice 5-003: Professional Portfolio
Discussion on the document and it was agreed that the expectation in a new CE cycle is that amember complete their "Part 2: Self Assessment" within 90 days since it is that self assessment
which will dictate the education they pursue over the course of the cycle.
The wording be added to the Standard of Practice 5003: Professional Portfolio.
A member is required to complete CCO's self assessment process every two yeørs as set out by
CCO. It ìs highly recommended thìs be done within 90 days of a new cycle.
787Quality Assurance Committee Report to Council: June 2J,2O1Z
ll. QA lnitiatives
A. Review of Regulations, Standards of Practice, Policies and Guidelines
The QA committee reviewed all relevant regulations, standards of practice, policies andguidelines and identified the following documents for the upcoming year:
Review of regulation233105 to ensure the QA Committee is fulfilling its mandate under theregulation.
Standard of Practice 5001: Chiropractic Scope of Practice.
The committee discussed the possibly of incorporating elements of Guideline G-004 into the S-001 standard of practice as there were redundancies that could fit into this standard.The committee is working further on this and will report to council.
Stemming from this discussion was looking at replacing in QA documents "his/her" with genderneutral language. The committee felt it worthy of council discussion on whether this should bereflected in all documents. Instead of his/her, consider the patient. As a working example, suchas in a "consultation related to hisÆer the patientos presenting condition and or goals.'; Thecommittee felt council discussion was warranted to reflect the current sensitivity around genderidentification.
Discussion also arose around what a member of the public should expect when going to achiropractor, in light of the scope of practice. The committee felt if a chiropractor chose not toassess in the usual range scope, then the 'why" they did not should be reflected in the patient'spersonal health record. The committee recognizedthatwhile chiropractors have the right toperform controlled acts, they could choose not to. The committee felt the salient point was thediscussion the chiropractor has with the patient.
It was suggested that the Patient Relations Committee could consider a new distribution of thePartnership of Care document, perhaps againin tent folder or other format.
It was suggested that this warrants a broader discussion to develop ideas about how CCO cancommunicate what the public should expect when they visit a chiropractor.
The committee was of the view that an "upfront" placement of the Partnership of Care would behelpful to the public on the new website.
2
7883
Quality Assurance Committee Report to Council: June 23,2017
Standard of Practice 5-002: Record Keeping.
The committee is working on draft amendments to 5-002 based on the possible revocation of G-004. We are looking at minor wording changes in 5-002 and incorporating elements of G-004into this standard. The committee reviewed wording changes and additions to 5-002 including"location of service" and oowho" provided the service to be identified in the financial record.
Records Retention and Destruction: To increase clarity the committee suggested the addition ofooin its entirety" as there is some confusion that some members interpret this as only the last 7years of the record need to be retained rather than the whole record being maintained in itsentirety for 7 years subsequent to the last patient visit.
The prior QA committee began to look at whether there was a need to update the language toreflect when and the type or timing of re-evaluations. This committee reviewed the work that had
been developed by staff as a potential basis for developing a re-evaluation guideline. A summaryhas been developed by Dr. Walton as a basis to identify what forms of evaluations occur. 'We
wish to develop this further as we see the advantage of making the distinctions relevant topractice and patient care. Examples to which we considering are initial assessment/ examination,comparative assessment/examination, new complaint assessment/evaluation,assessment/examination after a stoppage of care and restart and, assessment/examination atdischarge when available.
The committee looked at Guidelines G-004 the documentation of a chiropractic visit as being apotential basis for the re-evaluation guideline.
The QA committee will develop further and report back to council.
Standard of Practice 5-004: Reporting of Diseases
Standard of Practice 5-005: Chiropractic Adjustment or ManipulationStandard of Practice 5-006: Ordering, Taking and Interpreting RadiographsStandard of Practice 5-007: Putting a Finger beyond the Anal Verge for the Purpose ofManipulating the TailboneStandard of Practice 5-008: Communicating a DiagnosisStandard of Practice 5-009: Chiropractic Care of Animals
Quality Assurance Committee Report to Council: June 23,2017789
Vy'e are continuing to monitor and respond to the proposed legislative model of the College ofVeterinarians of Ontario. Similar to the RHPA, the scope of practice and controlled acts will berestricted to veterinarians unless there is an exception carved into the legislation. Discussionsupported the general model proposed and we are monitoring the sense that chiropractors wouldlikely be exempted to perform the controlled acts under the RHPA they currently have onanimals. The chiropractors who perform animal chiropractic have provided feedback to theCVO. The CCO was requested to respond to the CVO which was reviewed by the committee.
The committee wonders if the Registration committee would consider a line added to theregistration form to identify chiropractors currently practicing animal chiropractic. We do nothave a list of who and how many chiropractors perform this. Something hkè'oDo you seeanimals?" would be helpful.
CCO corresponded with the CVO on June 14, 2017.
The committee will continue to receive, monitor and respond to incoming information and hasadded it to our work plan.
Standard of Practice 5-011: Members of More than One Health professionstandard of Practice s-012: standard of Practice s0r2: orthoticsStandard of Practice 5-013: ConsentStandard of Practice 5-017: AcupunctureStandard of Practice 5-018: Third Party Independent Chiropractic EvaluationsStandard of Practice 5-019: Conflict of Interest in Commercial Ventures
Standard of Practice S-021: Assistive DevicesFollowing a discussion on assisted devises it was noted that this needed to be added to the peerand Practice Assessment checklist as it was curïently missing.
Standard of Practice 5-022: Ownership, Storageo Security, and Destruction of Records ofPersonal Health Information
The committee discussed situations where a non-chiropractic staff personal is leaving and theyhave a requirement to follow their regulatory body's requirements with respect to paiient healihrecords. After discussion on situations where a change occurs in the primary care provider, it wasnoted that one person is required to be identified in the office/clinic to be the privácy officer andcustodian of all health information. The patient needs to be informed where their records can beassessed should any change arise such as the office closing, moving, or a new individual takeover their care.
4
790 5
Quality Assurance Committee Report to Council: June 23,2017
Draft Standards - Ordering Advanced Diagnostic Images/Laboratory Tests
Policies
Policy P-023: Participation in X-ray Peer Review Program
The committee received a verbal report and agreed to add it to our worþlan. This has beenfunneled into the PPA 2.0 stream which may make this policy redundant. 'We
have added this toour worþlan for further discussion and are not prepared to make any recommendations at thistime.
Policy P-051 Peer Assessors
The committee discussed mandating peer assessors to attend a current Record KeepingV/orkshop (RKW) within one year of their appointment. The Committee is looking at waivingthe cost for the workshop and reasonable expenses to be reimbursed but no per diem. We are notready to provide a recommendation to council at this time as discussion has been added to ourwork plan.
A greater discussion arose on whether members in general should have to attend another RKWover the span of their career, of if this should possibly be limited to council and committeemembers only.
'We are considering providing peer assessors an abbreviated RKV/ when they receive theirtraining on how to complete forms. However, additional expenses may be incurred with thisadditional training. Alternate forms of disseminating the modified RKV/ were also brieflydiscussed. The committee is looking at the best way to approach a shortened RKW.
Policy P-055: Non-compliance with Continuing Education Requirements
Guídelines
Guideline G-004: Documentation of A Chiropractic Visit The guidelines was noted and deferredto the next meeting.
G-008: Business Practices
There was a brief discussion about reflecting in the guideline that a member should refer to thecustomary office fee should there be refusal of a WSIB claim and the patient should be chargedfor the number of visits x that office fee. We felt the current wording was appropriate.
791Quality Assurance Committee Report to Council: June 23,2017
G-009: Code of Ethics
We are adding this into our work plan after a brief discussion of adding bullying.
G-012: Social Media
Core Competencies for CCO Members
The committee received introductory comments from Dr. Bruce Vy'alton, noting that it is a goodtool and members are regularly reminded about it.
Assignment of Care
The committee received a memorandum regarding the Assignment of Care of patients. Thecommittee reviewed materials from other regulatory colleges and discussed the definition of"assignment" of care, to non-regulated individuals vs the 'delegation" of care that is used in theRHPA to delegate a controlled act.The committee is of the opinion that clarity is in the public interest to ensure that assignment ofcare to an individual who has the skills, knowledge and training to deliver what they ãre asked todo. The committee agreed the patient health record of personal information should reflect "who,,deliveredoowhat" care. The committee will work further to develop a document and where it maybest be placed and report back to council.
B. Record Keeping Workshop (RKW)
The Committee continues to offer the RKW at least three times per year or on an "as requested"basis. The RKW material continues to be updated with CCO standards of Practice. The mostrecent RKV/ was held at xxx immediately following that Legislation and Ethic Examination.There were approximately xx in attendance. In addition, the director of Professional Practice, Dr.Bruce Walton and Mr. Joel Friedman are able to offer to groups a modified 3 hour RKV/ as partof the CCO's outreach.
C. Peer and Practice Assessment
o Staff continue to handle the internal processing of all Peer and Practice Assessment (PpA1.0) and (PPA 2.0) materials which includes:
¡ updating and streamlining the paperwork associated with ppA 1.0 and 2.0.o Selecting members to be assessed. Sending out selection materialso Processing incoming submissions for the members who are to be assessed.
6
792 7
Quality Assurance Committee Report to Council: June 23,2017
o Providing the assessors with their assignments and materials needed to conduct theassigned assessments.
o Processing all parts of the completed assessments.. Providing the final disposition of the member.
The committee was provided with an overview of the documentation received from peerassessors along with the final disposition of the member. The information received is betweenthe date of the previous meeting and this meeting for the QA committee to have eyes on thedocumentation and be afforded the opportunity to comment if necessary.
The committee also reviewed the feedback by both assessors on the AIT as well as the feedbackby the AIT themselves.
The previous QA committee anticipated appointment of the Assessors-in-Training (AIT) at thismeeting, The committee decided to hold on this as not all AIT have been fully trained. The delayhas been logistical with synching the schedules of three colleagues (the member being assessed,
the AIT plus the experienced assessor) to complete the assessments. They are in process. Manyreports have been returned and many are now scheduled. The director of Professional Practice,felt the committee would have more information to appoint by the next meeting, so this wasdeferred.
The minutes from the prior QA committee of March2,2017 reflected a motion by the QAcommittee to approve up to a maximum of 250 members to undergo PPA 2.0 in the upcomingschedule of peer assessments. This is in process. PPA 1.0 will continue to be used for memberswho are required to be assessed for the purposes of discipline, new registrants from otherjurisdictions and new graduates.
The committee received the materials for PPA 1.0 and PPA 2.0.
D. Other QA lnitiatives
Portfolio and Handbook
The committee received an overview of the Professional Portfolio Handbook and theProfessional Portfolio. Both documents have been added to the Committee's workplan for a fullreview.
Record Keeping Workshops
Record Keeping Workshops (RKW) continue to be delivered three times per year. Since theFebruary council meeting one, the RKV/ was delivered on June 13, 2017.
793Quality Assurance Committee Report to Council: June 23,2017
A verbal report was received in the RKW examination and the value of the in-person attendance.The Director of Professional Practice offered that an appreciated RKV/ can be available togroups. The committee supports this as it would be another opportunity to connect but differentfrom the roadshow. It would be a non-mandated 3 hour program.
Opportunity to Connect Roadshow
An opportunity to Connect Roadshow slideshow was included for review. Slides are updated toreflect the most current standards, policies, guidelines, current events and fine tuning of tneroadshow. Since the last council meeting, xxx roadshows have occurred.They continue to receive positive feedback from members in attendance.
E. Gommunication with Members and Stakeholders
The committee continues to respond to inquiries from members and other stakeholders.These inquiries include matters related to scope of practice for those chiropractors practicinganimal chiropractic with the veterinary scope review, and questions regarding assignment oicare.
lll. Acknowledgements
Our committee is off to a great start and is building on the work accomplished under theleadership of Dr. Bryan V/olfe. Many thanks to our public members, Ms. Patrice Burke and Mr.Doug Cressman and professional members Drs. Kristina Peterson and Joel Weisberg for yourpreparation and energy applied to the work of QA. As always our sincere thanks to the taient ofstaff Ms Andrea Szametz, Mr. Joel Friedman, Dr. Bruce V/alton and Ms. Jo-Ann Willson.
Respectfully submitted,
Dr. Elizabe th (Liz) Anderson-PeacockQuality Assurance Committee
SrnruoanD oF Pnacrlces-003
trEM 4.4.2Quality Assurance CommitteeApproved by Council: May 24, 1996Amended: February 28, 1998, November 30,2002, December 2'2009,September 17,2015
Professional Portfol io
801
Note to readers: ln tlrc eaent of nny inconsistency betueen this document and the legislation thnt
affe c t s chiropr nc t ic ¡t r ø c t i c e, th e Ie gis I n t io n 8071 er n s.
Note: For the ptrrposes of this standard of practice, "member" refers to a CCO
member registered in the "General" class of registration.
lrurrrur
To advise members of their government-legislatecl obligation to qualityimprovement by participation in peer and practice assessment, self-assessment and
seú-directecl, lifelong learning, through continuing education (CE) and professional
development.
To advise members that their professional portfolio is the file where they mustrecord and store information about their participation in quality asstlrance
initiatives.
Os¡ecrves
To fulfill the requirements of the Quality Assurance Committee as set out insection 80.1 of the Health Professions Procedural Code (the Code), Schedule 2 of
ttie Reguløted Health Professiorrs Act, 1'991- (RHP,A).
To facilitate continuous quality improvement through the concepts of peer and
practice assessmen! self assessment, self assessment action plans, and lifelonglearning.
To emphasize that each member is responsible for his/her own continuingcompetency and professional growth.
To enable the Quality Assurance Committee to assist a member with specific
remediation if it is requested or deemed necessary.
. To ensure the ongoing development of CCO's quality assurance Program.
DescnlploN oF STANDARD
Type of Portfolio to be Maintained
A member is required to maintain a professional portfolio, which will be made
College ol Chiropractors of Ontario
a
a
Ia
2
Sran¡oRnD oF Pnnclces-003
Professional Portfol io
802
available to the Quality Assurance Committee or a peer assessor upon request. Thecontents of the professional portfolio remain confidential within ttre çualityAssurance committee and will not be shared with any other committee.
A member is required to complete the four parts of the professional portfolio. Amember must maintain his/her professional portfolio, including CE materialsgatherecl in the current CE cycle and the immediate past complete CE cycle.Additional cycles may be discarded. However, cCO encoutag"s err"ry member toretain relevant materials for future use and reference.
Part 1: Professional Profile / Curriculum Vitae
. personal data: name, address, registration number¡ education: post-secondary/academic degrees/certificates; specialties/ fellowships
(if applicable). professional history: practice history and description' professional membership and service: names of professional organizations in
which the member holds current membership, and the services and activitiesprovided to professional organizations (including positions held)¡ volunteer work: service to profession; service to community
o awards /recognition' other professional activities: professional presentations; professional
publications. references (optional): a separate sheet may be attached.
Part 2: Self Assessment
The self-assessment process consists of two parts: the self-assessmentquestionnaire with a""ompur,ying handbooË and the plan of action summaÍy sheet.
A member is required to complete CCO's self-assessment process every two yearsas set out by CCO. The self-assessment questionnaire is completely confideniial andwill not be viewed by any committee.
once a member has completed the self-assessment questionnaire and hasidentifiecl areas that need improvement, the member should transfer theinformation to the self-assessment plan of action summary sheet. using thissummary sheet, a member shall develop a learning plan to help guide his/her CEand professional development.
The plan of action summary sheet is a component of the member's professionalportfolio and will be reviewed by a peer assessor during the peer and practiceassessment to monitor compliance with the self-assessment process. A member may
College of Chiropractors of Ontario
a
SrnruonnD oF PRacrlces-003
Professional Portfol io
803
identify areas from the self-assessment questionnaire which he/she desires to
strengthen and may incorporate these items into his/her CE activities.
Part 3: Gontinuing Education and Professional Development
CE activities should reflect the results of a member's self-assessment, and peer and
practice assessment, in adclition to any CE activities related to professional interests,
adding to a member's strength or changing a member's practice.
A member is required to participate in 40 hours of CE over a two-year period, as
determined by CCO. In accumulating the 40 hours, CCO requires members to:
participate in a minimum of 20 hours in structured CE activities (a1140 hoursmay be accumulated in structured activities);
record up to a maximum of 20 hours towards unstructured CE activities;
record participation in CE activities in his/her professional portfolio; and
maintain in his/her professional portfolio materials gathered while fulfilling CE
requirements (e.g., course outlines, brochures from conventions/conferences,certificates, letters of reference, receipts, etc.).
To monitor compliance with the quality assurance initiatives, a member who isregistered in the General class of registration for that entire cycle shall
complete and submit a one-page summary sheet of their CE activities (entitledContinuing Education and Professional Development Log) for that entire cycle. This
log will accompany CCO's registration renewal every two years,
CE activities must relate to a member's clinical practice and/or professionalactivitiesr, with the goal of enhancing a member's professional knowledge ancl skill.
A member is not permitted to bank hours over the two-year period (i.e., transfer
hours from one cycle to the next). The required 40 hours of CE is considered the
minimum standard for the two-year cycle. CCO encotlrages all members to
regularly participate in additional CE.
Structured Actiaities (20 hours minimum)
Structured activities are active/interactive learning programs. These activitiesgenerally have structured agenclas, specified learning objectives and interactionwith other members of the profession or other professions. Structured activitiesinclude:
a
a
a
3
College of Chiropractors ot Ontario
4
SrnruoRnD oF PRRclcEs-003
Professional Portfol io
804
o attending courses/ seminars, workshops, presentations, conferenceso participating in interactive internet courses, seminars, workshops, conferences,webinars
e participating in correspondence courseso participating in clinical rounds. participatingincomputer-assisted learning
Møncl.øtory Components of Struchred CE
As defined in the RHPA, the practice of chiropractic is the assessment of conditionsrelated to the spine, nervous system and joints, and the diagnosis, prevention andtreatment, primarily by adjustment, of: dysfunctions or disorders arising from thestrucfires or functions of the spine ancl the effects of those dysfunctions ordisorders on the nervous system; and dysfunctions or disorders arising from thestructures or ftrnctions of the joints.
In accorclance with section 4 of the Chiroprøctic Act,1991, a member is authorized toperform the following controlled acts:
L. Communicating a diagnosis identifying, as the cause of a persorl'ssymptorns,i. a disorder arising from the structures or functions of the spine ancl
their effects on the nervolrs system, orii. a disorder arising from the structures or functions of the joints of the
extremities.2. Moving the joints of the spine beyond a person's usual physiological range
of motion using a fast, low amplitude thrust.3. Putting a finger beyond the anal verge for the purpose of manipulating the
tailbone.
CCO requires that every mernber participate in a minimum of five hours of CE inevery CE cycle, that consists of structured activity on diagnostic or therapeuticprocedures related to any of the controlled acts within the chiropractic sôope ofpractice'?. These mandatory five hours should be relevant to the member's òlinicalpractice, but may not include adjunctive therapies, such as acupuncture, exercise ornutritional counseling.
CCO requires that every member successfully completes and remains current withemergency first aid/CPR certification.3
Unstructured Actiuities (20 hours møximum)
Unstructured activities are self-clirected, inclependent learning activities.Unstructured activities include:
College of Chiropractors of Ontario
Srn¡¡onnD oF Pnnclces-003
Professional Portfol io
805
. reading professional books, journals, articles, research paPers
. viewing/reading/listening to professional audio/video/ internet material
. reviewing CCO regulations, standards of practice, policies, guidelines, otherCCO material
. preparing/presenting professional presentations
. researching/writing/ecliting professional publications
. other (specify)
CCO requires that a member participate in CE activities that relate directly tohis/her clinical practice and/or professional activities. These activities may include,
bgt are not limited to, subjects such as communication, assessment, cliagnosis,
clinical impression, diagnostic imaging, patient care, and specialty training.
CCO will continue to review the CE Process and make appropriate changes as
necessary, which may include the introduction of mandatory elements to the
program and/or approval/disapproval of specific programs.
Doatmentøtion of CE Actiaities
Personal Data: Name, Registration Number
Every member is required to record his,4rer CE activities in the Continr"ring
Education & Professional Development section of the professional portfolio. Each
activity must include the following information:. date on which the member participated in the activity (month and year). activity code. learning objectives code. title and brief description of the activity. provider/sotrrce¡ total number of hourso outcome code
Part 4= Accompanying Folder
A member is required to maintain the following in his/her professional portfolio:
o materials gathered while ftrlfilling his/her CE requirements (e.g., course
outlines, brochures from conventions/conferences, certificates, letters ofreference, receipts, etc.);
. samples of his/her recent advertising (e.g., Yellozt, Pages advertisements,newspaper advertisements or other similar types of advertising); and
o the disposition reports following the member's peer and practice assessmeut.
5
College of Chiropractors of Ontario

6
Srnr,¡onnD oF PRncnces-003
Professional Portfol io
806
Lecrsulve CoTTEXT
Heafth Professions Procedural Code, Schedule 2 of the Regutated HealthProfessions Act, 19gl
The Quality Assurance program is defined in section 1 (1) of the code as ,,a
program to assure the quality of the practice of the profession and to promotecontinuing competency evaluatiory competence and improvement amongmembers."
Objects and Duties of GCO: Section 3 of the Code
Section 3(1): The College has the following obiects:
3. To develop, establish and maintain standards of practice to assure the quality ofthe practice of the profession.
4. To develop, establish and maintain standards of knowledge, skill and programsto promote continuing competence among the members.
section 80.1 of the code defines the minimum requirements for a quatityassurance program as follows:
(a) A qualify assurance program prescribed under section g0 shall include,continuing education or professional development designed to,
(i) promote continuing competence and continuing quality improvementamong the members,
(ii) address changes in practice environments, and
(iii)incorporate standards of practice, advances in technology, changes made toentry to practice competencies and other relevant issues in the discretion ofthe Council;
(b) self, peer and practice assessments; and
(c) a mechanism for the college to monitor members'participation irç andcompliance witþ the quatity assurance program.
{.!
i{ìti
College of Chiropractors of Ontario
SrauolnD oF Pnaclces-003
Professional Portfol io
807
Section 80.2 of the Code outlines the powers of the Quality Assurance Committeeas follows:
The Qualify Assurance Committee may do only one or more of the following:
1. Require individual members whose knowledge, skill and judgment have been
assessecl under section 82 ancl found to be unsatisfactory to participate in speci-
fied continuing education or remediation programs.
2. Direct the Registrar to impose terms, conditions or limitations for a specifiedperiod to be determinect by the Committee on the certificate of registration of amember,
l. whose knowledge, skill and judgment have been assessed or reassessed
under section 82 and have been found to be unsatisfactory, or
ii. who has been directecl to participate in specified continuing education orremediation pïograms as required by the Committee under paragraph 1 andhas not completed those programs successfully.
3. Direct the Registrar to remove terms, conditions or limitations before the end ofthe specified period, if the Committee is satisfied that the member's knowledge,skill and judgment are now satisfactory.
4. Disclose the name of the member and allegations against the member to theInquiries, Complaints and Reports Committee if the Quality AssuranceCommittee is of the opinion that the member may have committed an act ofprofessional misconduct, or may be incompetent or incapacitated.
I N.B. - a member's CE activities are separate and apart from daily professionalactivities. For example, if the member is an educator, the preparation andpresentation of classroom material would not be considerecl an acceptable CE
credit.
'?See Standard of Practice 5-001: Chiropractic Scope of Practice for an explanation of"diagnostic or therapeutic procedures". Controlled acts may include the authorizedactivities listed in section 4 of the Chiropractic Act, 199L or the authorization to oper-ate an X-ray machine or prescribe the operation of an X-ray machine undersections 5-6 of the Henling Arts Rndiation Protection Act, L990.
3The minimum requirement is emergency first aid: CPR Level C + CPR + AED. Thiscan be achieved through providers such as Red Cross and St John Ambulance as a
6.5 hour classroom instruction program.
7
College of Chiropractors ot Ontario
eYo ASSOCTATTONOFVETERNARYTECHNICIANS
THE COLLEGÊ OF
VETERINARIANS 808OF ONTAP'^
|TEM 4.4.3
An Open Consultationon the Evolving Scope of Practiceof Veterinary Medicine in Ontario
Veterinary medicine in Canada has historically been a profession with an exclusive scope of practice - meaning no one other than a veterinarian could
perform health care activities on animals unless under the delegation and supervision of a veterinarian. While this model made good sense 20 years ago
(and before), the public's expectations have changed.
The general discussion on what a profession should or should not protect within ¡ts scope of practice is increasingly focused on risk and harm - in
this case risk and harm to animals and to public health. ln the broader social context, the public realizes that high risk services (e.g. diagnosing illness,
prescribing medications, surgery) should only be performed by licensed veterinarians. On the other hand, the public expects to have direct access to low
risk services (e.g. massage therapy) without requiring a referral from a veterinarian. This, of course, is what individuals see and do in human medicine.
These shifts in practice, based on the public demand, require careful consideration of real, and not perceived, risk and/or potential harm.
While Ontario is, and has been, regulating under the premise of exclusive scope of practice for veterinarians, the reality is that there is no definitive
definition of the practice of veterinary medicine in the Veterinarians Act, merely a list of a few activities. Over the years, challenges to the current model
have come from other professions and trades - chiropractic, homeopathy, ultra-sonographers, trainers, breeders, etc. This confusion about what is and
is not the exclusive scope of practice of veterinarians is problematic for the public and the profession. Furthet the current model has at times proved
difficult to defend with respect to actual unauthorized and risky practice by lay persons.
ln recent years, the profession has also observed the strengthening of qualifications for veterinary technicians, and in particular the recognition of theRegistered Veterinary Technícian (RVT) as having credentials that represent quality and safety in veterinary practice. The growth in numbers of RVT's1 in
the province is a testament to their established place as a qualified team member within the system of veterinary medicine in Ontario.
The aim of this scope of practice review and proposal is to acknowledge that the world is not the same as when the Veterinarians Act was introduced in
1989. A model focused on the system of veterinary medicine and on protecting activities that pose the greatest risk of harm to animals is being proposed
The aim is to acknowledge changing public expectation and to balance this with the need for the protection of animals. Strengthening compliance
with the scope of practice of veterinary medicine by being clearer about where harm lies, and that both veterinarians and veterinary technicians are
accountable in that delivery is imperative for the future.
1 There are currently 3200 RVT's ¡n Ontario, an increase from 1200 in 2007
CollegeofVeterinariansofOntario. ontarioAssociationofVeterinaryTechnicians Page 1
eYo ONTARIOASSOCIATON OFVFTERINARYTECHNICIANS 809THE COLLEGE OF
VETERINARIANS
OF ONTARIO
So, whøt is proposed ond what wìll be dilferent ín a new piece of legislotion?
Key Features
o Both veterínarians and veterinary technicians are covered under the new definition of veterinary medicine
r Titles will be protected for both veterinarians and veterinary technicians. Anyone using these titles in French or English or a derivative mustbe licensed by the College
' The title 'doctor (Dr.)' will be protected for veterinarians, with conditions for its use by chiropractors treating animals
' The title 'Registered Veterinary Technician'wíll also be protected for licensed veterinary technicians
' The list of authorized activities applies to both veterinarians and veterinary technicians
' Unless identified in the list of exemptions, no one otherthan a veterinarian can perform the authorized activity independently
' Veterinarians will continue to be able to delegate authorized activities where appropriate and with an appropriate level of supervision
' Veterinary technicians will now be able to initiate certain specific subsets of authorized activities (see Appendix A)
' Veterinary technicians are also identified as the most appropriate individual to perform certain activities under an order from a veterinarianWhile this does not preclude delegation to an assistant, it does identify areas of competence of a veterinary technician on which aveterinarian can depend. (see Appendix A)
collegeofVeterinariansofontario. ontar¡oAssociationofveterinaryTechnicians Page 2
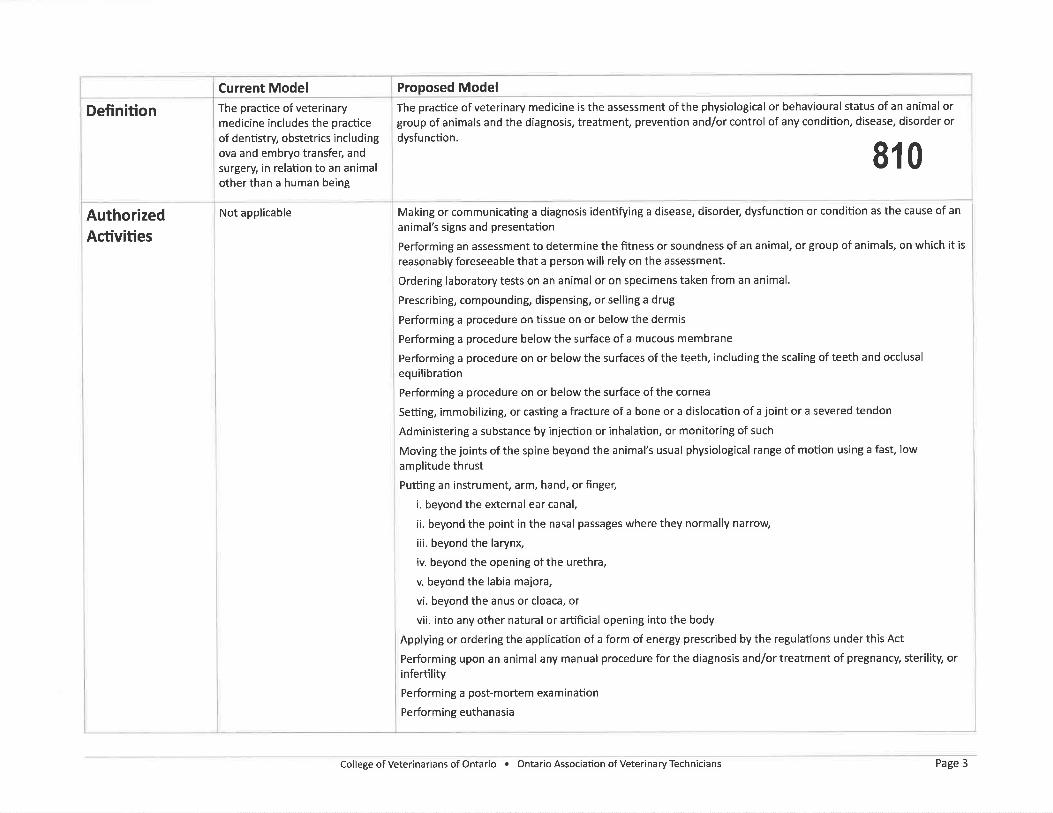
Proposed ModelThe practice of veterinary medicine is the assessment of the physiological or behavioural status of an animal orgroup of animals and the diagnosis, treatment, prevention and/or control of any condition, disease, disorder or
dysfunction.
810
Making or communicating a diagnosis identifying a disease, disorder, dysfunction or condition as the cause of an
animal's signs and presentation
Performing an assessment to determ¡ne the fitness or soundness of an animal, or group of animals, on which it is
reasonably foreseeable that a person will rely on the assessment.
Ordering laboratory tests on an animal or on specimens taken from an animal.
Prescribing, compounding, dispensing, or selling a drug
Performing a procedure on tissue on or below the dermis
Performing a procedure below the surface of a mucous membrane
Performing a procedure on or below the surfaces of the teeth, including the scaling of teeth and occlusal
equilibration
Performing a procedure on or below the surface of the cornea
Setting, immobilizing, or casting a fracture of a bone or a dislocation of a joint or a severed tendon
Administering a substance by injection or inhalation, or monitoring of such
Moving the joints of the spine beyond the animal's usual physiological range of motion using a fast, low
amplitude thrust
Putting an instrument, arm, hand, or finger,
i. beyond the external ear canal,
ii. beyond the point in the nasal passages where they normally narrow
iii. beyond the larynx,
iv. beyond the opening ofthe urethra,
v. beyond the labia majora,
vi. beyond the anus or cloaca, or
vii. into any other natural or artificial opening into the body
Applying or ordering the application of a form of energy prescribed by the regulations under this Act
Performing upon an animal any manual procedure for the diagnosis and/or treatment of pregnancy, sterility, orinfertility
Performing a post-mortem examination
Performing euthanasia
Current ModelThe practice of veterinarymedicine includes the practice
of dentistry, obstetrics includingova and embryo transfer, and
surgery, in relation to an animalother than a human being
Not appl¡cable
Definition
AuthorizedActivities
CollegeofVeterinariansofOntario. OntarioAssociationofVeterinaryTechnìcians Page 3
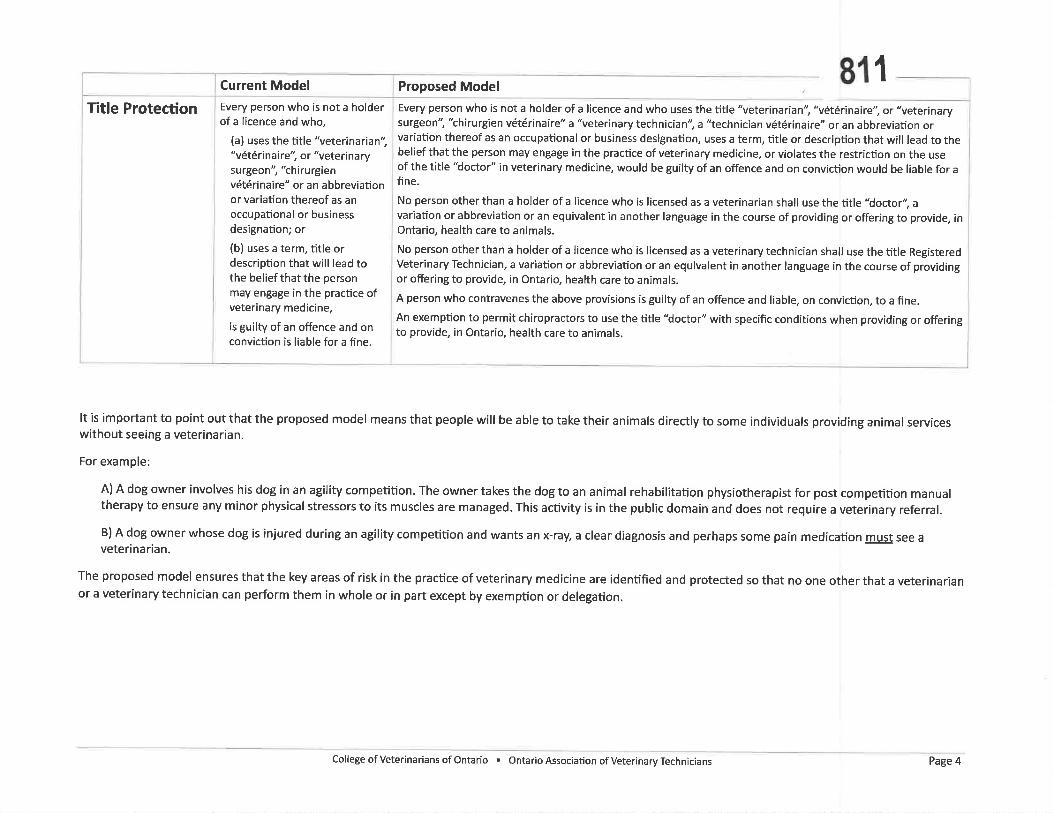
Current Model
Every person who is not a holderof a licence and who,
(a) uses the títle "veterinarian","vétérinaire", or "veterinarysurgeon", 'thirurgienvétérinaire" or an abbreviationor variation thereof as anoccupational or businessdesignation; or
(b) uses a term, title ordescription that will lead tothe belief that the personmay engâge in the practice ofveterinary medicine,
is guilty of an offence and onconviction is liable for a fine.
Title ProtectionProposed Model 81 1Every person who is not a holder of a licence and who uses the title "veterinarian", "vétérinairei or "veterinarysurgeon", 'thirurgien vétérinaire" a 'leterinary technician", a "technician vétérinaire" or an abbreviation orvariation thereof as an occupational or business designation, uses a term, title or description that will lead to thebelief that the person may engage in the practice of veterinary medicine, or violates the restr¡ction on the useof the title "doctor" in veterinary medicine, would be guilty of an offence and on conviction would be liable for afine.
No person other than a holder of a licence who is licensed as a veterinarian shall use the title 'loctori avariation or abbreviation or an equivalent in another language in the course of providing or offering to provide, inOntario, health care to animals.
No person other than a holder of a licence who is licensed as a veterinary technician shall use the title RegisteredVeterinary Technician, a variation or abbreviation or an equivalent in another language in the course of providingor offering to provide, in Ontario, health care to animals.
A person who contravenes the above provisions is guilty of an offence and liable, on conviction, to a fine.
An exemption to permit chiropractors to use the title "doctor" with specific conditions when providing or offeringto provide, in Ontario, health care to animals.
It is important to point out that the proposed model means that people will be able to take the¡r animals directly to some individuals providing animal serviceswithout see¡ng a veterinarian.
For example:
A) A dog owner involves his dog in an agility competition. The owner takes the dog to an animal rehabilitation physiotherapist for post competition manualtherapy to ensure any minor physical stressors to its muscles are managed. This activ¡ty is in the public domain and does not require a veterinary referral.
B) A dog owner whose dog is injured during an agility competition and wants an x-ray, a clear diagnosis and perhaps some pain medication roSl! see aveterinarian.
The proposed model ensures that the key areas of risk in the practice of veterinary medicine are identified and protected so that no one other that a veterinarianor a veterinary technician can perform them in whole or in part except by exemptíon or delegation.
collegeofVeterinariansofontario. ontarioAssociationofveterinaryTechnicians Page 4
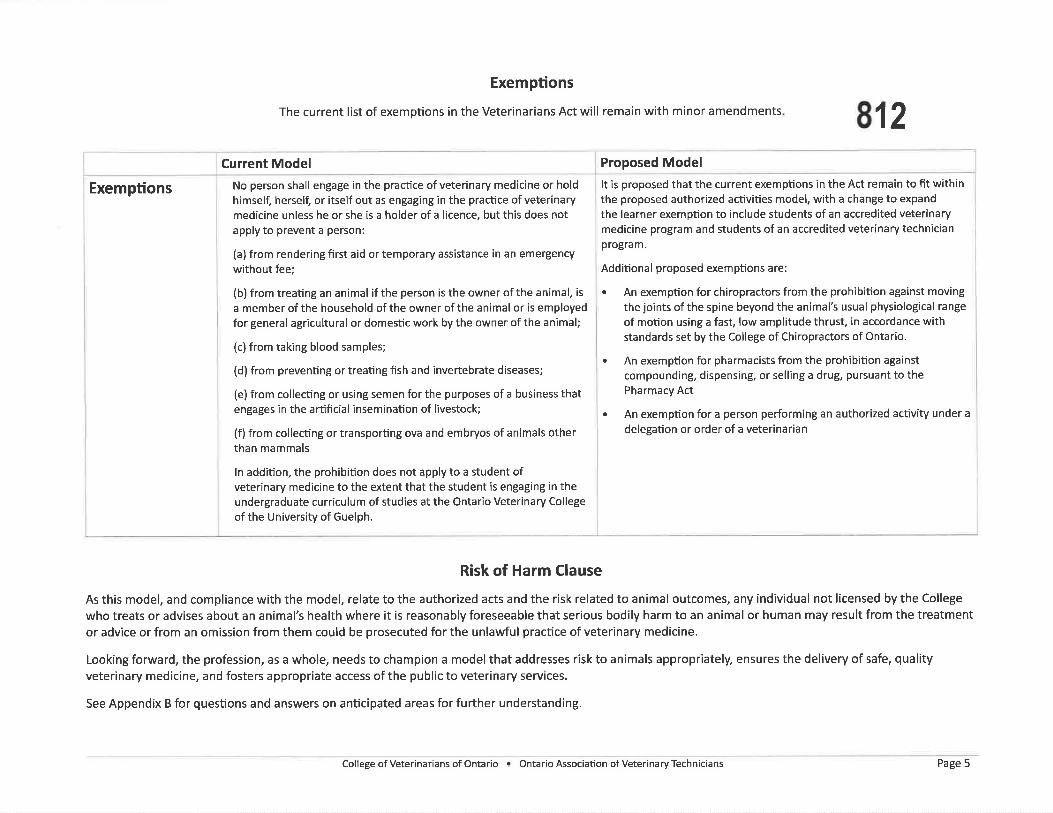
Exemptions
The current list of exemptions in the Veterinarians Act will remain with minor amendments 812Proposed Model
It is proposed that the current exemptions in the Act remain to fit withinthe proposed authorized activities model, with a change to expand
the learner exemption to include students of an accredited veterinarymedicine program and students of an accredited veterinary technicianprogram.
Additional proposed exemptions are:
. An exemption for chiropractors from the prohibition against moving
the joints of the spine beyond the animal's usual physiological range
of motion using a fast, low amplitude thrust, ¡n accordance withstandards set by the College of Chiropractors of Ontario.
. An exemption for pharmacists from the prohibition against
compounding, dispensing, or selling a drug, pursuant to thePharmacy Act
. An exemption for a person performing an authorized activity under a
delegation or order of a veterinarian
Current Model
No person shall engage in the practice of veterinary medicine or holdhimself, hersell or itself out as engaging in the practice of veterinarymedicine unless he or she is a holder of a licence, but this does notapply to prevent a person:
(a) from rendering first aid or temporary assistance in an emergency
without fee;
(b) from treating an animal if the person is the owner of the animal, isa member of the household of the owner of the animal or is employedfor general agricultural or domestic work by the owner of the animal;
(c) from taking blood samples;
(d) from preventing or treating fish and invertebrate diseases;
(e) from collecting or using semen for the purposes of a business thatengages in the artificial insemination of livestock;
(f) from collecting or transporting ova and embryos of animals otherthan mammals
ln addition, the prohibition does not apply to a student ofveterinary medicine to the extent that the student is engaging in theundergraduate curriculum of studies at the Ontario Veterinary College
of the University of Guelph.
Exemptions
Risk of Harm Clause
As this model, and compliance with the model, relate to the authorized acts and the risk related to animal outcomes, any individual not licensed by the College
who treats or advises about an animal's health where it is reasonably foreseeable that serious bodily harm to an animal or human may result from the treatmentor advice or from an om¡ssion from them could be prosecuted for the unlawful practice of veterinary medicine.
Looking forward, the profession, as a whole, needs to champion a model that addresses risk to animals appropriately, ensures the delivery of safe, qualityveterinary medicine, and fosters appropriate access of the public to veterinary services.
See Appendix B for questions and answers on anticipated areas for further understanding.
CollegeofVeterinariansofOntario r OntarioAssociationofVeterinaryTechnicians Page 5
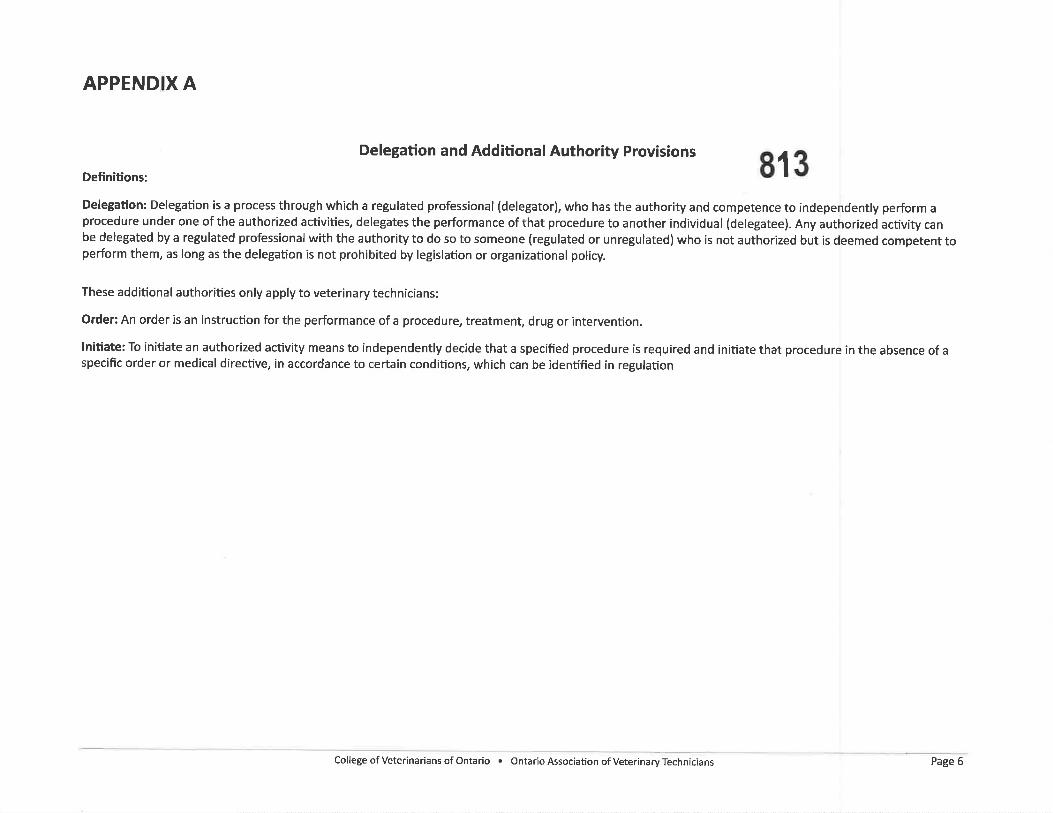
APPENDIX A
Delegation and Additional Authority Provisions
Definitions: r'ElEË'cL¡('l! cl¡lL¡ '.llu'LlLtrldl '.ulflctrlly rrgvlstons
813
Delegation: Delegation is a process through which a regulated professional (delegator), who has the authority and competence to independently perform aprocedure under one of the authorized activities, delegates the performance of that procedure to another individual (delegatee). Any authorized activity canbe delegated by a regulated professional with the authority to do so to someone (regulated or unregulated) who is not authorized but is deemed competent toperform them, as long as the delegation is not prohibited by legislation or organizational policy.
These additional authorities only apply to veterinary technicians:
Order: An order is an instruction for the performance of a procedure, treatment, drug or intervention.
lnitiate: To initiate an authorized activity means to independently decide that a specified procedure is required and initiate that procedure in the absence of aspecific order or medical directive, in accordance to certa¡n conditions, which can be identified ín regulation
college of Veterinarians of ontario . ontar¡o Associatíon of Veterinary Technicians Page 6
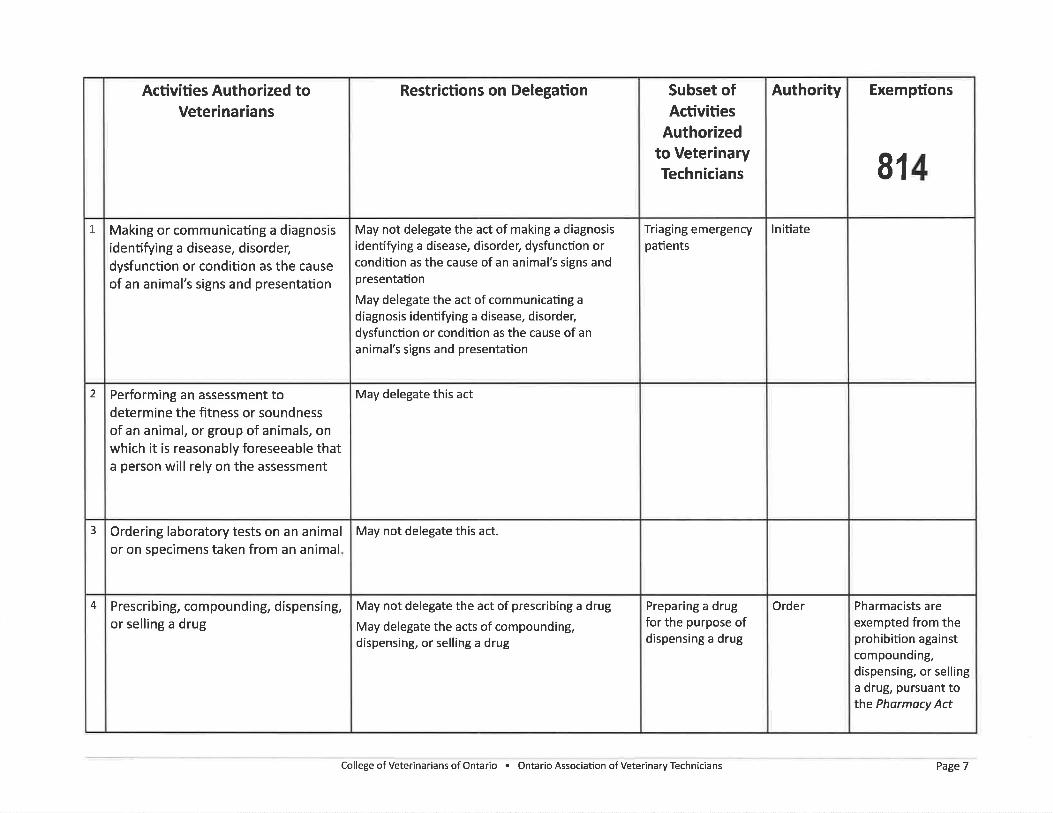
Exemptions
814
Pharmacists areexempted from theprohibition againstcompounding,dispensing, or sellinga drug, pursuant tothe Pharmacy Act
Authority
lnitiate
Order
Subset ofActivities
Authorizedto VeterinaryTechnicians
Triaging emergencypatients
Preparing a drugfor the purpose ofdispensing a drug
Restrictions on De¡egation
May not delegate the act of making a diagnosisidentifying a disease, disorder, dysfunction orcondition as the cause of an animal's signs andpresentation
May delegate the act of communicating a
diagnosis identifying a disease, disorder,dysfunction or condition as the cause of an
animal's signs and presentation
May delegate this act
May not delegate this act.
May not delegate the act of prescribing a drug
May delegate the acts of compounding,dispensing, or selling a drug
Activities Authorized toVeterinarians
Making or communicating a diagnosisidentifying a disease, disorder,dysfunction or condition as the causeof an animal's signs and presentation
Performing an assessment todetermine the fitness or soundnessof an animal, or group of animals, onwhich it ís reasonably foreseeable thata person will rely on the assessment
Ordering laboratory tests on an animalor on specimens taken from an animal,
Prescribing, compounding, dispensing,or selling a drug
1
2
3
4
College ofVeterinarians ofOntario . Ontario Assoc¡ation ofVeterinaryTechnicians Page 7
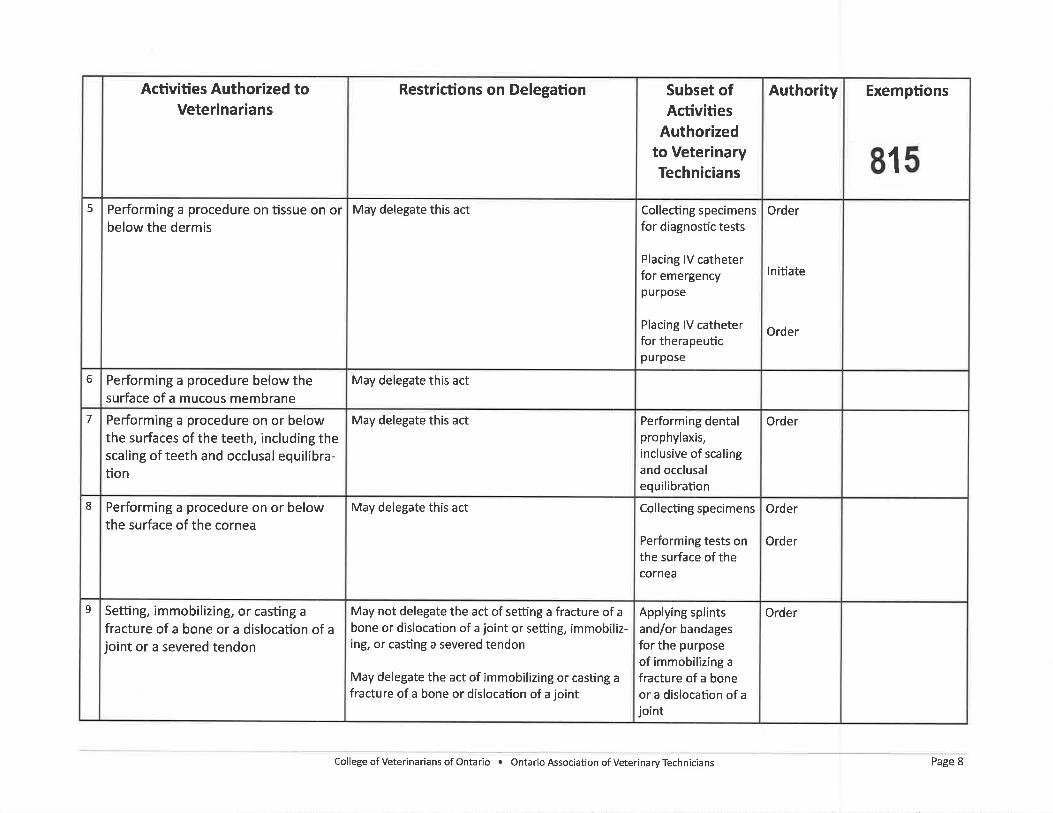
Exemptions
815
Authority
Order
lnitiate
Order
Order
Order
Order
Order
Subset ofActivities
Authorizedto VeterinaryTechnicians
Collecting specimensfor diagnostic tests
Placing lV catheterfor emergencypurpose
Placing lV catheterfor therapeuticpurpose
Performing dentalprophylaxis,inclusive of scalingand occlusalequilibration
Collecting specimens
Performing tests onthe surface of thecornea
Applying splintsand/or bandagesfor the purposeof immobilizing afracture of a boneor a dislocation of a
joint
Restrictions on De¡egation
May delegate this act
May delegate this act
May delegate this act
May delegate this act
May not delegate the act of setting a fracture of a
bone or dislocation of a joint or setting, immobiliz-ing, or casting a severed tendon
May delegate the act of immobilizing or casting a
fracture of a bone or dislocation of a joint
Activities Authorized toVeterinarians
Performing a procedure on tissue on orbelow the dermis
Performing a procedure below thesurface of a mucous membrane
Performing a procedure on or belowthe surfaces of the teeth, including thescaling of teeth and occlusal equilibra-tion
Performing a procedure on or belowthe surface of the cornea
Setting, immobilizing, or casting a
fracture of a bone or a dislocation of ajoint or a severed tendon
5
6
7
8
9
CollegeofVeterinariansofOntario. OntarioAssociationofVeterinaryTechnicians Page 8
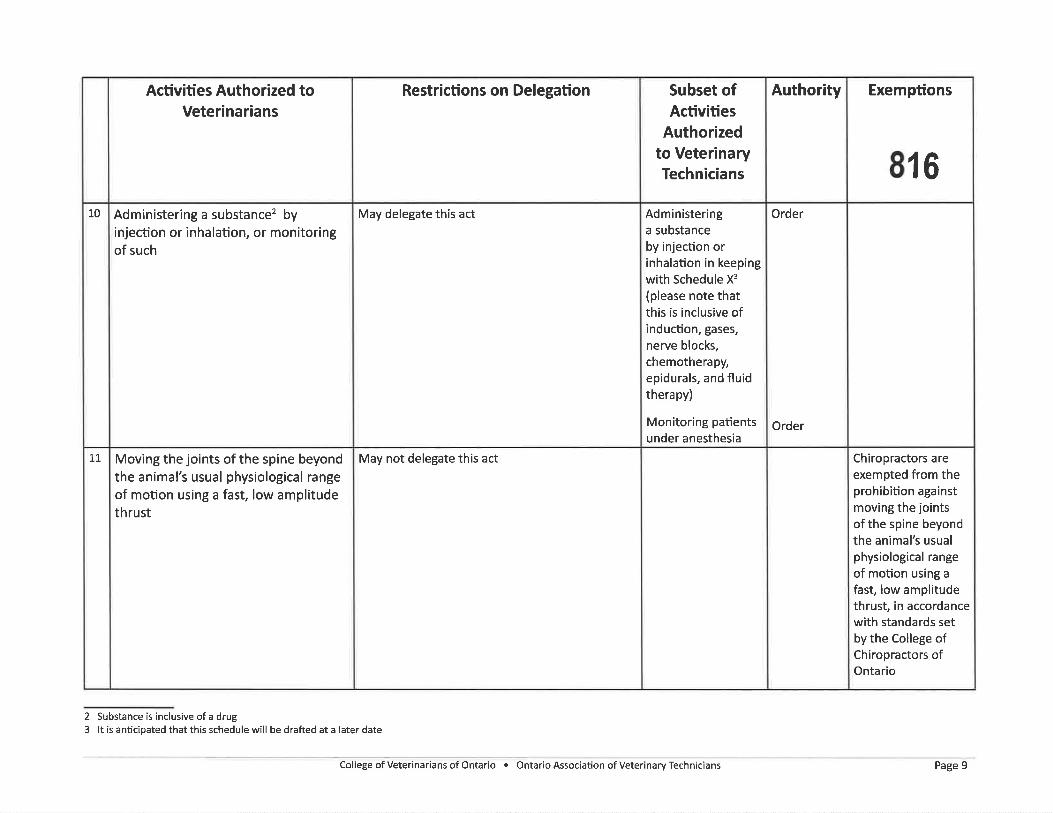
Exemptions
816
Chiropractors are
exempted from theprohibition againstmoving the jointsofthe spine beyondthe animal's usualphysiological range
of motion using a
fast, low amplitudethrust, in accordancewith standards setby the College ofChiropractors ofOntar¡o
Authority
Order
Order
Subset ofActivities
Authorizedto VeterinaryTechnicians
Administeringa substanceby injection orinhalation in keepingwith Schedule X3
(please note thatthis is inclusive ofinduction, gases,
nerve blocks,chemotherapy,epidurals, and fluidtherapy)
Monitoring patientsunder anesthesia
Restrictions on Delegation
May delegate th¡s act
May not delegate this act
Activities Authorized toVeterinarians
Administering a substance2 byinjection or inhalation, or monitoringof such
Moving the joints of the spine beyondthe animal's usual physiological rangeof motion using a fast, low amplitudethrust
10
tt
2 Substance is inclusive of a drug3 lt is anticipated that this schedule will be drafted at a later date
College of Veterinarians of Ontario . Ontario Association of Veterinary Technicians Page 9
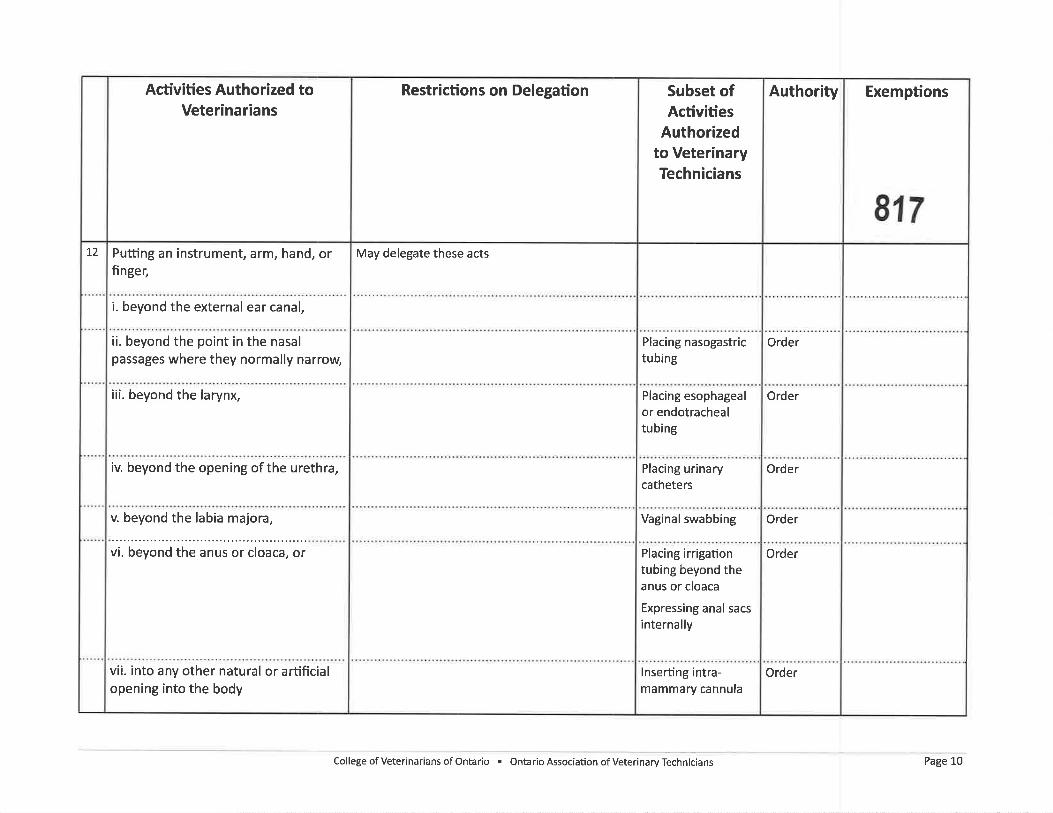
Exemptions
817
Authority
Order
Order
Order
Order
Order
Order
Subset ofActivities
Authorizedto VeterinaryTechnicians
Placing nasogastrictubing
Placing esophagealor endotrachealtubing
Placing urinarycatheters
Vaginal swabbing
Placing irrigationtubing beyond theanus or cloaca
Expressing anal sacs
internally
lnserting intra-mammary cannula
Restrictions on Delegation
May delegate these acts
Activities Authorized toVeterinarians
Putling an instrument, arm, hand, orfinger,
i. beyond the external ear canal,
ii. beyond the point in the nasalpassages where they normally narrow,
iii. beyond the larynx,
iv. beyond the opening of the urethra,
v. beyond the labia majora,
vi. beyond the anus or cloaca, or
vii. into any other natural or arfificialopening into the body
72
College of Veterinarians of Ontario . Ontario Association of Veterinary Technicians Page 10
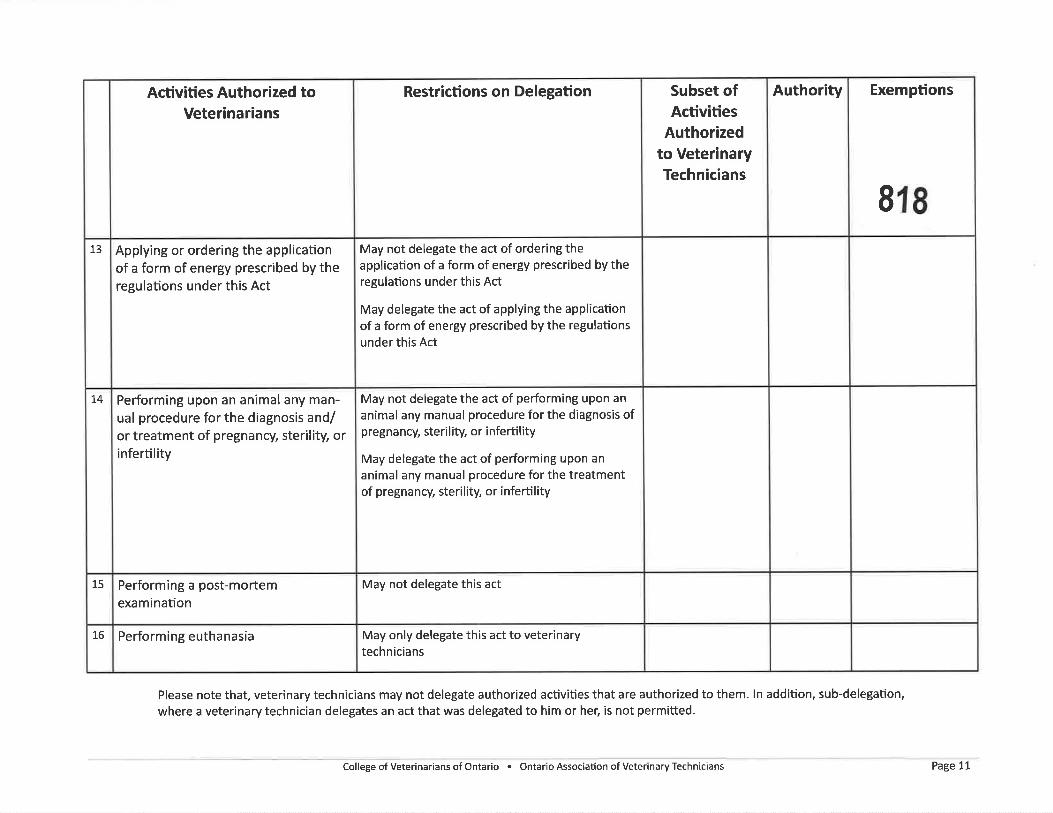
Exemptions
818
AuthoritySubset ofActivities
Authorizedto VeterinaryTechnicians
Restrictions on Delegation
May not delegate the act of ordering theapplication of a form of energy prescribed by theregulations under this Act
May delegate the act of applying the applicationof a form of energy prescribed by the regulationsunder this Act
May not delegate the act of performing upon an
animal any manual procedure for the diagnosis ofpregnancy, sterility, or infertility
May delegate the act of performing upon an
animal any manual procedure for the treatmentof pregnancy, steril¡ty, or infertility
May not delegate this act
May only delegate this act to veterinarytechnicians
Activities Authorized toVeterinarians
Applying or ordering the applicationof a form of energy prescribed by theregulations under this Act
Performing upon an animal any man-ual procedure for the diagnosis and/or treatment of pregnancy, ster¡lity, orinfertility
Performing a post-mortemexamination
Performing euthanasia
13
!4
15
16
Please note that, veterinary technicians may not delegate authorized activities that are authorized to them. ln addition, sub-delegation,
where a veterinary technician delegates an act that was delegated to him or her, is not permitted.
CollegeofVeterinariansofOntario. OntarioAssociatíonofVeterinaryTechnicians Page 11
ASSOCTATTONOFVFTERINARYTECHNICIANS
THE COLLEGE OFVETERINARIANS
OF ONTARIO
Questions and Answers
eYo APPENDIX B
819
Question: So how will this actually work, will veterinarians and veterinarytechnicians be legislated by one piece of legislation?
Answer: lf, after consultation, the model is finally approved by both theCollege and the OAVI) one piece of legislation will be proposed.
Question: lf it is one piece of legislation, how will this be administered?
Answer: While very early discussions have been hod between the Collegeand the OAVf,, there have been no proposals on how a new legislotivemodel might be administered. The focus currently is on the scope ofproctice model ond its appropriateness for the public, animals and thesafety of the proctice of veterinary medicine ¡n Ontdrio.
Question: The language in this model is not how I would talk in practice. Can'tmore commonly used medical terms be used?
Answer: lt is true thot not all of the lønguoge thot describes the authorizedactivities would be commanly used day to doy. The longuoge chosen isintentíonal, however, to provide a legal framework that is broad anddefensible. For exomple, the term surgery is not used, but all procedures ontissue that ore on or below the dermis would include surgery (authorizedøctivity #5)
Question: I am an RVT and I am confused when I read "veterinary technician"throughout this document. Why are both terms used?
Answer: This new model protects the term "veterinory technician" alongwith preserving use of the title 'RW". lt means thot they would becomeinterchangeoble. lt olso meons anyone using either term would have tohave met similor quolîfications.
Question: What about veterinary technicians that have graduated from anaccredited training program but have not chosen to join OAVT?
Answer: lt is acknowledged that this group of individuals exists in practice.It is unclear as to how many graduøte, non RW's there ore procticing inOntorio. The process for these individuals to be grandparented into o newpiece of legislation has not yet been determined. tt will be considered.
Question: What does an accredited program mean?
Answer: Accredited progroms refer to schools teaching either veterinarymedicine or veterinary technology. The accreditation process which isaccepted for either will be made at q loter date in policy. lt ¡s not a motterfor legislation.
Question: How is the feedback being tabulated?
Answer: The review of o professions scope of practice is on enormousundertaking ond hugely ímportont. As a result an independent consultanthos been hired to assist with the development of the feedback survey andthe onolysis of the responses. The final report will be shored with the twoorganizations for decision moking. The report will also be made public.
Question: So what happens after the consultation?
Answer: The consultatíon period ends May L2, 201_7. At that time both theCollege and the OAW will meet ond discuss the feedback received. Bothorgonizations will, however, hove independent discussíons on whether toproceed with the model as proposed.
college of veterinarians of ontario . ontario Association of Veterinary Technicians Page 12
SrnruoRRD oF Pnncr¡ces-009Quality Assurance CommitteeApproved by Council: April 25, 1998Amended: June 20, 2008, December 4,2015
Chiropract¡c Careof Animals
820
|TEM 4.4.4
a
a
a
a
Note to renders: ht tlrc eaent of any inconsistency betu,een this doøunent qnd tlrc legisløtion tlntafþct s chiropr øctic pr øc tice, the legisl atiotl 807,erns.
lrurerur
To advise members when and how they can conduct chiropractic care ofanimals, and to remind them that the primary responsibility for the health care ofanimals is with veterinarians.
Oe¡eclves
To promote professionalism, safety and effectiveness in the chiropractic care ofanimals.
To inform members of their obligations relating to the chiropractic care ofanimals.
To ensure appropriate coordination and consultation between members andveterinarians in the chiropractic care of animals.
To educate the public as to the appropriate nature of the chiropractic care ofanimals.
DrscnrproN oF STANDARÐ
A member is advised that:
The primary responsibility for the health care of animals is with registrants ofthe College of Veterinarians of Ontario (CVO), who are responsible forappropriate history taking, comprehensive examinatiorç including clinicalpathology, imaging, and the overall care/management of animals.
Consent to the chiropractic care of animals must be fully informed andvoluntarily given by the ownel of the animal, and registrants are required tocomply with all standards of practice and applicable legislation relating tochiropractic.
a
1
College of Chiropractors ot Onlario
SrnruoanD oF PRRclces-009
Chiropractic Careof Animals
821
In providing chiropractic care to an animal, a member shall:
demonstrate successful completion of a program in animal chiropractic of aminimum of 200 hours of formal training that includes, but is not limited to,studies in the following subject areas: anatomy, neurology, biomechanics,animal adjustment technique, diagnosis, pathology, chiropractic philosophy, andethics and legalities;
a
a
a
a
a
a
a
a
ensure the record of care includes the name of the treating registrant of CVoand the relevant portions of the veterinary record;
provide, upon request and only with the consent from the owner of the animalor otherwise in accordance with the Personal HeøIth Infonnation Protection Act,2004, a copy of relevant portions of the record to the treating registrant of CVOwithin a reasonable time of providing chiropractic care to an animal;
maintain separate appointment books, separate health and financial recordsand, where animals are provided with chiropractic care in the same office ashumans, maintain a separate portion of the office devoted to animalchiropractict; and
ensure that the owner of the animal(s) is fully informecl about the member'sinsurance coverage2.
Exemption
A member will be exempted from the first bulleted item above if he/she
is enrolled and participating in a program in animal chiropractic, leading to thesuccessful completion of a program in animal chiropractic of a minimum of 200hours of formal training that includes, but is not limited to, studies in thefollowing subject areas: anatomy, neurology, biomechanics, animal adjustmenttechnique, díagnosis, pathology, chiropractic philosophy, and ethics andlegalities;
completes the program in animal chiropractic within two years of his/herenrolment;
provides chiropractic care to animals within the parameters of hislher course ofstudy; and
informs the owner of the animal(s) that he/she has enrolled and is participatingin but has not yet graduated from a program in animal chiropractic.
a
2
College of Chiropractors of Ontario
SuruonnD oF PRncnces-009
Chiropractic Careof Animals
822
a
Lec¡slrlve ConrEXT
The governing legislation as it relates to human health care is lhe Regulated Heølth
Professions Act,199L, as amended (RHPA) and the Chiroprøctic Act,1"991.Thegoverning legislation as it relates to animal health care is the Veterinørians Act, 1990.
Specific relevant provisions are outlined below. The RHPÁ and the Chiroprnctic Actare administered by CCO and the Veterinarians Act is administered by CVO.
Sections of the RHPA
Objects and Duty of the CCO - Section 3 of the Health Professions ProceduralCode, Schedule 2lo RHPA=
(1) [CCO]has the following objects:
To develop, establish and maintain programs and standards of practice to
assure the quality of the practice of the profession.
¡ To develop, establish and rnaintain standards of knowledge, skill and programsto promote continuing comPetence among the members.
(2) In carrying out its objects, the [CCO] has a duty to serve and protect the publicinterest."
Sections of the Chiropractlc Act
Section 3: Chiropractic Scope of Practice
The practice of chiropractic is the assessment of conditions related to the spine,
nervous system and joints and the diagnosis, prevention and treatment primarilyby adjustment, of,
. dysfunctions or disorders arising from the structures or functions of the spine
and the effects of those dysfunctions or disorders on the nervous system; and
. dysfunctions or disorders arising from the structures or functions of the joints
Section 9: Restricted Titles for Chiropractic
(1) No person other than a member shall use the title "chiropractol", a variationor abbreviation or an equivalent in another language.
3
College of Chiropraclors of Ontario
Sra¡loano oF PnRcnces-009
Chiropractic Careof Animals
823
4
(2) No person other than a member shall hold himself or herself out as a personwho is qualified to practise in Ontario as a chiropractor or in a specialty ofchiropractic.
(3) In this section,'abbreviation' includes an abbreviation of a variation.
Sections of Regulation 852/93 under the Chiropractic Act
section 1 (2): Definition of Professional Misconduct for chiropractors(Standards of Practice)
The following are acts of professional misconduct for the purposes of clause 51 (1)(c) of tlre Health Proþssions Procedural Code: Contravening a standard of practice ofthe profession or failing to maintain the standard of practice expectecl ofmembers of the profession.
Sections of the Veterinarians Act
Subsection 1 (1): Definition of Veterinary Medicine
The'practice of veterinary medicine'includes the practice of dentistry, obstetrics(including ova and embryo transfer) and surgery in relation to an animal other thana human being.
Section 3: Objects of CVO
(1) The principal object of the [cvo] is to regulate the practice of veterinarymedicine and to govern its members in accordance with this Act, theregulations and the by-laws so as to serve and protect the public interest.
(2) For the purpose of carrying out its principal object, the [CVO] has thefollowing additional objects:
establisþ maintain and develop standards of knowledge and skill among itsmembers; and
a
a establisþ maintain ancl develop standarcls of qualification and standards ofpractice for the practice of veterinary medicine.
College of Chiropractors of Ontarío

Sr¡ruonRD oF Pnncr¡ces-009
Chiropractic Careof Animals
824
s&kftr'$
#tr
::
tri¡
.$ffi
itr
Subsection 11 (1): Licence Required to Practice Veterinary Medicine
No person shall engage in the practice of veterinary medicine or hold himself/herself out as engaging in the practice of veterinary medicine unless the person isthe holder of a license.
Sections of Regulation 1093 (General- Part ll Practice Standards) under theVeterinarians Act
Section 17: Definition of Professional Misconduct for Veterinarians (Standardsof Practice)
For the purposes of the AcÇ professional misconduct includes the following: Failingto maintain the standard of practice of the profession.
Maintenance of separate office space is a minimum requirement for health andsanitation reasons, particularly in light of the various communicablediseases common to humans and animals.
This requires the member to advise the owner of the animal if the member'spolicy of insurance or membership in a protective association does notprovide coverage for the chiropractic care of animals. The owner should be
informed about the member's insurance coverage as part of the generalrequirement that there be "informed" consent.
5
's-
College of Chiropractors of Ontar¡o
6t14t2017 CCO Survey on Chiropractic Care of Animals and CVO's Scope of Practice Consult¡ation
College of Chiropractor$ of OntarioL'Ordre dee Chiropraticiens de I'Ontario
|TEM 4.4.6
830
The College of Chiropractors of Ontario (CCO) is contacting you as amember of CCO who provides chiropractic care to animals in Ontario.
The College of Veterinarians of Ontario (CVO) has conducted aconsultation process on updating its scope of practice through proposedamendments to its legislation. Information about the process andconsultation can be found at the followlng link: htto://cvo.orglscope.
CVO is proposing adopting a regulatory model that includes authorizedacts with specific delegating authorities and exemptions. Please see theEvolving Scope of Practice of Veterinary Medicine in Ontario document formore information about this regulatory model.
CCO will be responding to the consultation from the perspective ofregulating chiropractors in Ontario in the public interest, and is interestedin collecting information and feedback from members who providechiropractic care to animals. Please complete the CCO survey on thechiropractic care of animals by June L3t 2017.
Thank you for your participation.
College of Chiropractors of Ontario, 130 Bloor Street,Suite 902, Toronto, Ontario M5S1N5 Canada
SafeU nsu bscribe" { recioient's email}
Update Profíle I About our service provider
Sent by [email protected] in collaboration with
CpnstarftCürtmtTry it free today
'r4lí
https://ui.constantcontact.comfuisualeditor/visual_editorSreviewjsp?agent.uid=1'1276%:692189&format=html&print=true 1t1
6t14t2017 Survey :Questions
CCO Consultation on Proposed CVO Scope of Practice Model
1. How long have you provided chiropractic care to animals in Ontario? 831O Under 5 years
Q 5-10years
Q 11-20years
O Over20 years
2. ls your practice exclusive to the care of animals (i.e. you do not provide chiropractic care to humans)?
C Only Animals
O Animals and Humans
3. lf you do provide chiropractic care to both humans and animals, roughly how many hours perweek is devoted toeach?
1000 characters left.
4. At which location do you provide chiropractic care to animals?g Chiropractic offce
Q Other (please specif, location, e.g. veterinary ofüce, barn, rehabilitation centre)
Comment:
(
,rll/,
http://survey.constantcont¡act.com lsurv ey I aO7 æ2Ofxgoj I gkc43l/ tm p/questions 1t4
6/14t2017 Survey :Questions
500 characters left.
8325. Where did you complete your training in order to comply with Standard of Practice 5-009: Chiropractic Care of
Animals?
1000 characters lefr.
6. lf you have not yet completed the training, where do you expect to complete it?
1000 characters left.
7. Which types of animals do you provide chiropractic care to? lf both, please list the percentage devoted to eachtYPe'
@ Small animals only
g Large animals only
http://survey.constantcontact.com/survey/aO7ee2Ofxgoj1gkc454/_tmp/questions z4

6114120't7 Survey : Questions
833
@ Both
Comment:
500 characters left.
8. Please listthe top 3 types of animals to which you provide chiropractic care.
1000 characters left.
9. Please describe your interactions with veterinarians in your practice:
g I work directly with a veterinarian
6 lwork independently but receive referrals from and provide referrals to veterinarians
@ | have no interaction with veterinarians
@ otter:
Comment:
(
500 characters left.
http://survey.constantcontact.com/survey/a07ee20fxgoj 1 gkc¿l9V tm p/quêst¡ons 3t4
611412017
1000 characters left.
Survey : Questions
10. My feedback to the CVO scope of oractice model would better protect the public interest and should beconsidered in any submission by CCO:
834
,11000 characters left.
11 . My feedback of the following amendments to St¡andard of Practice 3-009: Chirooractic would better protect thepublic interest:
Finish
http://survey.constantcontact.com/survey/aO7ee20fxgoj 1 gkc43l/ tm p/questions 414
6t14t2017 Survey :Questions
CCO Consultation on Proposed CVO Scope of Practice Model
1. How long have you provided chiropractic care to animals in Ontario? 835e underSyears
¡þ 5-10 years
g 11-20years
$ Over20years
2. ls your practice exclusive to the care of animals (i.e. you do not provide chiropractic care to humans)?
$ OnlyAnimals
e Animals and Humans
3. lf you do provide chiropractic care to both humans and animals, roughly how many hours perweek is devoted toeach?
1000 characters left.
4. Atwhich location do you provide chiropractic care to animals?g Chiropractic ofüce
Q Other (please speciff location, e.g. veterinary ofrce, barn, rehabilitation centre)
Comment:
http://survey. constantcontact. com/s urvey/aO7ee2Ofxgoj 1 gkc43V-tm p/questi ors 1t4
6t14t2017 Survey : Questions
500 characters left.
8365. Where did you complete your training in order to comply with Standard of Practice 5-009: Chiropractic Care of
Animals?
1000 characters left.
6. lf you have not yet completed the training, where do you expect to complete it?
41000 characters left.
7. Which types of animals do you provide chiropractic care to? lf both, please list the percentage devoted to eachtYPe'
@ Small animals only
@ Large animals only
http://survey. constantcontact. com /survey/a07ee20fxgoj 1 gkc4&t/_tm /questi ons 2!4
6t14t2017 Survey : Quest¡ons
@ Both
Comment:
)
I500 characters left.
837
500 characters left.
8. Please list the top 3 types of animals to which you provide chiropractic care.
1000 characters left.
9. Please describe your interactions with veterinarians in your practice
@ lwork directly with a veterinarian
@ lwork independently but receive referrals from and provide referrals to veterinarians
@ I have no interaction with veterinarians
€ oÛrer
Comment:
http://survey.constantcontact.com I surv ey I a07 æ20fxgoj 1 gkc43t/-tm p/questions
)v
3t4
6114t2017 Survey : Questions
10. My feedback to the CVO scooe of practice model would better protect the public interest and should beconsidered in any submission by CCO:
838
Ì¡t1000 characters left.
11. MyfeedbackofthefollowingamendmentstoStandardofPractice5-009:Chirooracticwouldbetterprotectthepublic interest:
1000 characters left.
:
,
http://s urvey.constantcontact com /s urvey/a07ee20fxgoj 1 gkc43l/_tm p/questi ons
m
4t4
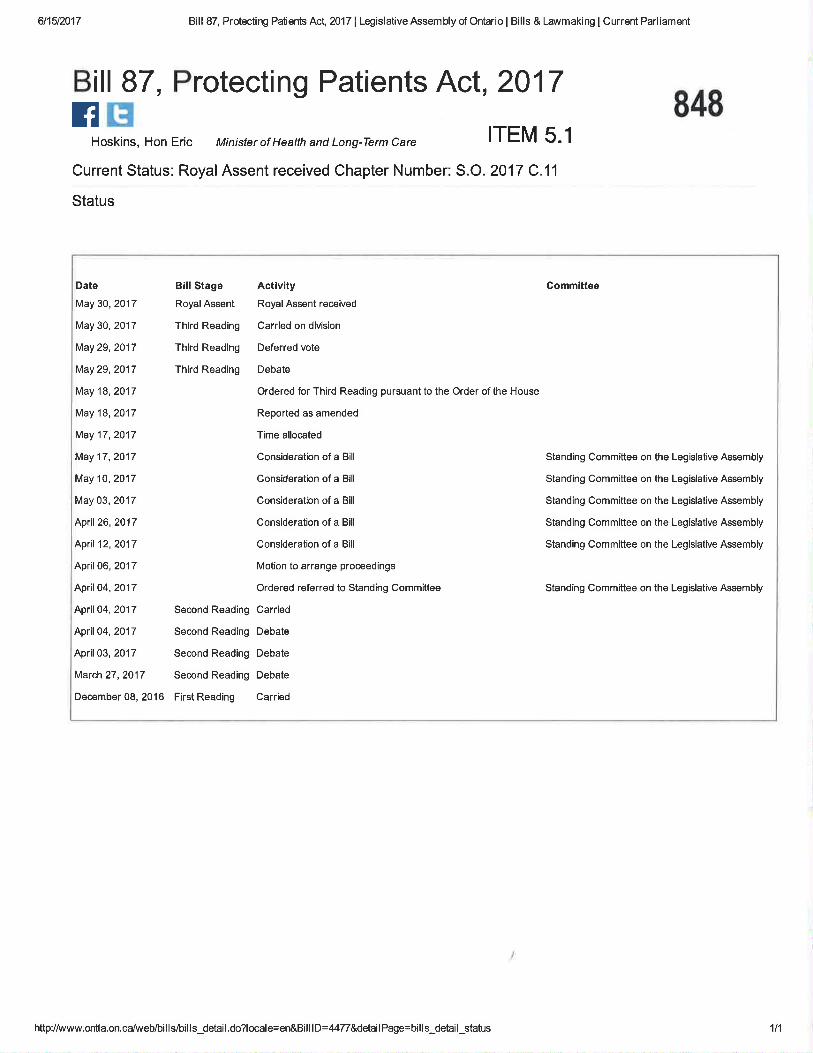
6t15t2017 Bill 87, Protecting Patients Act, 2017 | Legislative Assembly of Ontario I Bills & Lawmaking I Current Parliament
B¡ll 87, Protecting Patients Act, 2017fl Ët
Hoskins, Hon Eric Ministerof HeatthandLong-Termcare ITEM 5.1
Current Status: RoyalAssent received Chapter Number: S.O. 2017 C.11
Status
848
Date Bill Stage
May 30, 2017 Royal Assent
May 30,2017 Third Reading
May 29,2017 Third Reading
May29,2O'17 Third Reading
May 18,2017
May 18,2017
May 17,20'17
May 17,2017
May 10,2017
May 03, 201 7
April26,2O'17
April12,2017
April 06, 2017
April04,2017
April04,20'17 SecondReading
April04,2017 Second Reading
April 03, 2017 Second Reading
March 27,2017 Second Reading
December 08, 2016 First Reading
Actlvity
Royal Assent received
Carried on division
Deferred vote
Debate
Ordered for Third Reading pursuant to the Order of the House
Reported as amended
Time allocated
Consideration of a Bill
Consideration of a Bill
Consideration of a Bill
Consideration of a Bill
Consideration of a Bill
Motion to arrange proceedings
Ordered referred to Standing Committee
Carried
Debate
Debate
Debate
Carried
Committee
Standing Committee on the Legislative Assembly
Standing Committee on the Legislalive Assembly
Standing Committee on the Legislative Assembly
Standing Committee on the Legislative Assembly
Standing Committee on the Legislative Assembly
Standing Committee on the Legislative Assembly
http:/lwww.ontla.on.calweb/bills/bills_detail.do?locale=en&BilllD=4477&detailPage=bills_detail status 1t1
LegislativeAssemblyof Ontario
Assembléelégislativede I'Ontario
8492ND SESSION, 4l sr LEGISLATURE, ONTARIO
66 ELIZABETH II,2OI7
Bilt 87
(Chapter I I of the Statutes of Ontario, 2017)
An Act to implement health measures and measures relating to seniorsby enacting, amending or repealing various statutes
The Hon. E. HoskinsMinister of Health and Long-Term Care
lst Reading
2nd Reading
3rd Reading
Royal Assent
December 8,2016
April4,2017
NIay 30,2017
May 30,2017
@@
850EXPLANATORYNOTE
This Explanatory Note was written as a reader's aid to Bill 87 and does not form part of the law.Bill 87 has been enacted as Chapter 1l of the Stantes of Ontario, 2017.
SCHEDULE IDRUG AND PHARMACIES REGULATION ACT
Various amendments are made to the Drug and Pharmacies Regulation lct, including amendments to facilitateimplementation of interim orders regarding suspensions and the imposition of terms, conditions and limitations.
SCHEDULE 2
IMMUNIZATION OF SCHOOL PUPILS ACT
The Immunization of School Pupils Act is amended:
I . To require parents to complete an immunization education session before filing a statement of conscience or religiousbelief.
2. To expand the categories of persons who may provide statements regarding the administration of immunizing agents.
3. To require those who administer immunizing agents to provide information to the local medical officer of health.
SCHEDULE 3LABORATORY AND SPECIMEN COLLECTION CENTRE LICENSING ACT
A number of amendments are made to the Laboratory and Specímen Collection Centre Lícensing Act. Among them:
l. The two categories of "laboratory" and "specimen collection centre" are both provided for under the new term"laboratory facility", and the licensing provisions ofthe Act are amended accordingly.
2. Provision is made for the emergency suspension of licences.
3. The transfer oflicences is provided for.
4. The powers of inspectors under the Act are revised.
5. The collection, use and disclosure of personal information by the Ministry is provided for.
6. Revisions are made concerning the prosecution ofoffences under the Act.
The Animals for Research lcl is amended to correct a cross-reference.
The Health Insurance lct is amended to permit the Minister to enter into arrangements for the payment of remuneration tohealth facilities rendering insured services to insured persons on a basis other than fee for service, in addition to physiciansand practitioners.
The Public Hospitals Act is amended to permit the Minister to designate hospitals to provide community laboratory services.
SCHEDULE 4ONTARIO DRUG BENEFIT ACT
The Ontario Drug Benefit Act is amended to add new definitions for an "authorized prescriber" and a "registered nurse in the
extended class". Several amendments are made throughout the Act to accommodate prescriptions by authorized prescribers.A reference to a repealed Act is removed.
The Act is also amended to allow regulations to incorporate other documents by reference as they are amended from time totime after the regulation is made.
SCHEDULE 5REGULATED HEALTH PROFESSIONS ACT, 1991
The Regulated Health Professions Act, 1991 and its Health Professions Procedural Code are amended. Among the changes:
1. The purposes for which the Minister may require a College to collect information from members under section 36.1 ofthe Act are expanded to include health human resources research.
2. The Minister is given the power to make regulations respecting College committees and panels.
3. The matters that a College is required to note in its register are expanded.
4. For the purposes of the sexual abuse provisions of the Code, the definition of 'þatient", without restricting the ordinarymeaning of the term, is expanded to include an individual who was a member's patient within the last year or withinsuch longer period of time as may be prescribed from the date on which they ceased to be a patient, and an individualwho is determined to be a patient in accordance with the criteria set out in regulations.
ll
8515. The Inquiries, Complaints and Reports Committee and its panels may make an order for the interim suspension of a
member's certificate of registration at any time following the receipt of a complaint or after the appointment of aninvestigator, instead of only when a matter is referred for discipline or incapacityþroceedings,
6. The imposition of gender-based terms, conditions or limitations on a member's certificate of registration is prohibited.
7. The grounds for mandatory revocation of the certificate of registration of a msmber who has sexually abused a patientare expanded, and suspension is made mandatory in sexual abuse cases that do not involve conduct requiringmandatory revocation.
8. Members are required to report to the Registrar if they belong to professional bodies outside Ontario, and if there hasbeen a finding ofprofessional misconduct or incompetence against them by such a body.
9. Members are required to report to the Registrar if they are charged with an offence, and are required to provideinformation about bail conditions.
10. The mandatory program for Colleges to provide funding for therapy and counselling for patients who were sexuallyabused by members is expanded to apply to persons who are alleged to have been seiually abused while a patient, anãto provide funding for other purposes provided for in regulations.
I l. The penalties for failing to report sexual abuse ofpatients are increased.
sENroRS ""
truf ?ÏulTuåKrRE s Acr, 20 I 7
The Elderly Persons Centres Act is repealed and replaced with a new Act. Under the new Act, an operator that is not anindividual can obtain funding from the Minister Responsible for Seniors Affairs to establish, maintain oi operate a program ifa director appointed by the Minister approves both the operator and the program. The director approves a program oñ beingsatisfied that its ourpose is to promote active and healthy living, social engagement and leãrning for-persons who areprimarily seniors by providing them with activities and services.
If the operator operates the program in a municipality, any one municipality is required to make a contribution to theoperator. If the operator operates the program in a location that is not in a municipality, the regulations made under the Actcan prescribe what entities are required to make a contribution to the operator.
There is broad regulation-making power under the Act, including the power to make regulations governing contributions.
852Bil 87
l.2.3.Schedule ISchedule 2Schedule 3Schedule 4Schedule 5Schedule 6
2017
An Act to implement health measures and measures relating to seniorsby enacting, âmending or repealing various statutes
CONTENTS
Contents of this ActCommencementShort titleDrug and Pharmacies Regulation ActImmunization of School Pupils ActLaboratory and Specimen Collection Centre Licensing ActOntario Drug Benefit ActRegulated Health Professions Act, l99lSeniors Active Living Centres Act,2017
Her Majesty, by and with the advice and consent of the Legislative Assembly of the Province of Ontario, enacts as follows:
Contents of this Act
1 This Act consists of this section, sections 2 and 3 and the Schedules to this Act.
Commencement
2 (l) Subject to subsections (2) and (3), this Act comes into force on the day it receives Royal Assent.
(2) The Schedules to this Act come ¡nto force as provided in each Schedule.
(3) If a Schedule to this Act provides that any provisions are to come into force on a day to be named by proclamationof the Lieutenant Governor, a proclamation may apply to one or more of those provisions, and proclamations may beissued at different times with respect to any of those provisions.
Short title
3 The short title of this Act is the Protecting Patients Act' 2017.
2
853SCHEDULE 1DRUGAND PHARMACIES REGULATION ACT
1 The d_efinition of 6.registered pharmacy student" in subsection I (1) of the Drug ønd Phørmacies Regulation Acl isrepealed and the following substituted:
"intem technician" means a person registered as an intem technician under the Pharmacy Act, 1 99 1 ;
2 Subsections 139 (5) of the Act is amended by adding the following paragraph:
3. SubsectionslT (2) and(3).
3 (1) Subsection 140 (2) ofthe Act is amended by striking out rinterim orders where such allegations are referred tothe Committee".
(2) Section 140 of the Act is amended by adding the following subsections:
Interim order(2.0.1) The Accreditation Committee may at any time make an interim order directing the Registrar to suspend, or to imposeterms, conditions or limitations on, a certificate of accreditation, if it is of the opinion that the conducf or operation of apharmacy is likely to expose a patient, or a member of the public, to harm or injury.
Procedure
(2.0.2). The prwisions of the Health Professions Procedural Code dealing with interim suspension orders made by theInquiries, Complaints and Reports Committee or a panel of the Committee apply, with necessãry modifications, to inierimsuspension orders made by the Accreditation Committee under subsection (2.01).(3) Subsection f40 (2.1) of the Act is amended by striking out "section 37" and substituting "section 25.4".4 (1) Clause 149 (1) (c) of the Act is amended by striking out 'ra registered pharmacy student" at the beginning andsubstituting ú'a student who is in the course of fulfilling the educational requirements to become a member õf theCollege".
(2) Clause 149 (l) (d) of the Act is amended by adding "or an intern technician" after 6'a pharmacy technician',.(3) Subsection 149 (3) of the Act is repealed and the following substituted:
Remote dispensing locations
(3)_Despite clause (l) (d), a pharmacy technician may compound, dispense or sell a drug in a remote dispensing locationwithout a pharmacist being physically present to supervise, as long as a pharmacist is aõtively supervising the pharmacytechnician and,
(a) a certifrcate ofaccreditation has been issued permitting the operation ofthe remote dispensing location; and
(b) the remote dispensing location is operated in accordance with the regulations.
5 Subsection 15ó (2) of the Act is amended by striking out "two years'n at the end and substituting r'ten years".
6 This Schedule comes into force on a day to be named by proclamation of the Lieutenant Governor.
J
854SCHEDULE 2IMMUNIZATION OF SCHOOL PUPILS ACT
I (1) Section 1 of the Immunizutíon of School Pupils Actis amended by adding the following defÌnition:
"nurse" means a member of the College of Nurses of Ontario; ("infirmière ou infirmier")
(2) The definition of "physician" in section I of the Act is repealed and the following substituted:
'þhysician" means a member of the College of Physicians and Surgeons of Ontario; ("médecin")
2 Subsections 3 (3) and (4) ofthe Act are repealed and the following substituted:
Same, statement of conscience or religious belief
(3) Subsection (l) does not apply to a parent who has completed an immunization education session with a medical officerof health or with a medical officer of health's delegate that complies with the prescribed requirements, if any, and who has
fîled a statement of conscience or religious belief with the proper medical officer of health.
Transitional
(4) Subsection (l) does not apply to a parent who, before the coming into force ofsection 2 ofSchedule 2 to the ProtectingPatients Act, 20I 7, filed a statement of conscience or religious belief with the proper medical officer of health.
3 Clause 6 (2) (a) of the Act is repealed and the following substituted:
(a) that the medical officer ofhealth has not received,
(i) a statement from a physician, nurse or prescribed person showing that the pupil has completed the prescribedprogram of immunization in relation to the designated diseases,
(ii) an unexpired statement of medical exemption in respect of the pupil, or
(iii) a statement of conscience or religious belief in respect of the pupil and confirmation that the parent has
completed the education session described in subsection 3 (3); and
4 Section 10 of the Act is repealed and the following substituted:
Statements by providers of immunizing agents
10 (l) Every physician, nurse or prescribed person who administers an immunizing agent to a child in relation to a
designated disèase shall provide to a parent of the child a statement that shows that the immunizing agent has been
administered.
Information for M.O.H.
(2) Every physician, nurse or prescribed person who administers an immunizing agent to a child in relaÌion to a designated
disease sháll provide the prescribed information to the medical officer of health for the public health unit in which the
immunizing agent was administered.
5 Subclause 12 (2) (b) (i) of the Act is repealed and the following substituted:
(i) either a statement from a physician, nurse or prescribed person showing that the pupil has completed the' prescribed program of immunization in relation to the designated disease or other information satisffing the
medical officer of health that the pupil has completed the prescribed program, or
6 Subsection 17 (1) of the Act is amended by adding the following clause:
(f.l) respecting and goveming the information described in subsection l0 (2), including, without being limited to,speìifying one or more methods by which the information is to be provided, and requiring the information to beprovided by such a method;
Commencement
7 This Schedule comes into force on a day to be named by proclamation of the Lieutenant Governor.
4
855SCHEDULE 3LABORATORY AND SPECIMEN COLLECTION CENTRE LICENSING ÄCT
1 (1) Clause (a) of the definition of "laboratory" in section 5 of the Luborstory ønd Specímen Collection CentreLicensing Act is amended by striking out .'prophylaxistt and substituting .,preventiontr.
(2) Section 5 of the Act is amended by adding the following definition:
"laboratory facility" means a laboratory or a specimen collection centre; ("centre de laboratoire")
(3) The definition of "operator" in section 5 of the Act is repealed and the following substituted:
"operator" means a person having charge or control ofa laboratory facility; ("exploitant")
(4) Section 5 of the Act is amended by adding the following definition:'þersonal information" includes.personal information as defined inthe Freedom of Information and Protection of privacy Act
and personal health information as defined inthe Personal Health Information Protectíon Act, 2004; ('teiseignementspersonnels")
(5) The definition of "specÍmen collection centre" in section 5 of the Act is amended by striking out ..prophylaxis" inthe portion before clause (a) and substituting ..prevention,'.
(6) Clauses (a) to (d) of the definition of "specimen collection centre" in section 5 of the Act are repealed.
2 Section 9 of the Act is repealed and the following substituted:
Licence required
9 (l) No person shall establish, operate or maintain a laboratory facility except under the authority of a licence issued by theDirector under this Act.
Issuing licences
(2) The Director may issue a licence for a laboratory facilify to,
(a) perform one or more classes oftests specified in the licence;
(b) perform tests specified in the licence within one or more classes of tests;
(c) take or collect specimens or one or more classes of specimens specified in the licence; or(d) take or collect specimens specified in the licence within one or more classes of specimens.
Conditions
(3) A licence is subject to the conditions, ifany, specified by the Director in the licence.
Issuance of licence
(4) S_ubject to subsection (10), any person who applies in accordance with this Act and the regulations for a licence toestablish, operate or-maintain a laboratory facility and who meets the requirements of this Act and the regulations and whopays the prescribed fee is entitled to be issued the licence.
Where proposal not in public interest, issuance of licence
(5) -Despite subsection (4), tlre following applies where an application is made for a licence and the Minister states in writing
to the Director that it is not in the public interest to issue a licence to establish, operate or maintain the laboratory facility iìrthe area where the applicant proposes to establish, operate or maintain the laboratory facility:
l. Section 1l doesnotapply.
2. The Director shall not issue the licence to the applicant.
3. The Director shall give written notice to the applicant of the refi¡sal and of the Minister's statement.
\ühere proposal not in public interest, tests, specimens, etc.
(6) Despite subsection (4), where an application is made for a licencç and the Minister states in writing to the Director that itis not in the public interest to issue a licence, either,
(a) in the case of a laboratory, for any classes of tests or any of the tests within a class or classes of tests in respect ofwhich the application is made; or
(b) in^the.case of a specimen collection centre, to take or collect any specimens or class or classes of specimens in respectof which the application is made:
then,
5
(c) sections l0 and I I do not apply; 856
(d) where the Director issues a licence to the applicant upon the application, the Director shall give written notice to theapplicant of the Minister's statement; and
(e) the licence shall not be for the classes of tests or the tests within a class or classes of tests or for taking or collecting the
specimens or class or classes of specimens that are set out in the Minister's statement.
Matters to be considered by Minister(7) In making a decision as to what is in the public interest for the purposes of subsection (5) or (6), the Minister mayconsider any matter the Minister regards as relevant, including, without being limited to,
(a) the number and type of laboratory facilities that operate under the authority of licences issued under this Act,
(i) in the area, or
(ii) in the area and any other area;
(b) the tests and classes of tests performed or the specimens or class or classes of specimens taken or collected in thelaboratory facilities,
(i) in the area, or
(ii) in the area and any other area;
(c) the utilization ofexisting laboratory facilities and their capacity to handle increased volume;
(d) the availability offacilities for the transportation ofpersons and specimens to laboratory facilities,
(i) in the area, or
(ii) in the area and any other area; or
(e) the funds available to provide payment for laboratory tests that are insured services under the Health Insurance Act.
Blood collection facilities
(8) Despite subsection (4), where an application is made for a licence to establish, operate or maintain a laboratory facilitywhich will operate as a blood collection facility within the meaning of the Voluntary Blood Donations Act, 2014 and theMinister statés in writing to the Director that it is not in the public interest to issue such a licence, section 11 shall not applyand the Director shall not issue the licence to the applicant and shall give written notice to the applicant of the refusal and ofthe Minister's statement.
Same
(9) In making a decision in the public interest in subsection (8), the Minister may consider any matter the Minister regards as
relevant, including, without being limited to, the principles set out inthe Voluntary Blood Donations Act, 2014.
Grounds for refusal
(10) Subject to section I l, the Director may refuse to issue a licence where in the Director's opinion,
(a) the past conduct of the applicant or, where the applicant is a corporation, of its off,icers or directors affords reasonablegroùnds for belief that the laboratory facility will not be operated in accordance with the law and with honesty and
integrity;
(b) the proposed laboratory facility or its operation would contravene this Act or the regulations or any other Act orregulation or any municipal by-law respecting its establishment or location;
(c) the applicant is not competent to operate a laboratory facility in accordance with this Act and the regulations;
(d) the equipment and premises are not suitable for the performance of the tests or the taking or collecting of the
specimens for which the licence is sought; or
(e) any other ground for refusal that is prescribed in the regulations exists.
Provisional licence
(11) V/here the applicant for a licence does not meet all the requirements for issuance of the licence and requires time tomeet such requirements, the Director may issue a provisional licence for the laboratory facility.
Expiration and renewal of provisional licence
(12) A provisional licence expires on the date specified on the licence, which shall not be later than 12 months after the date
of its isiue, but the provisional licence may be renewed for one further period of no more than 12 months where, in theopinion of the Director, sufficient progress in complying with the requirements for issuance of a licence has been made.
6
Expiration and renewat of licence 857( I 3) A licence that is not a provisional licence expires on the date specified on the licence, which shall not be later than fiveyears from the date ofits issue or renewal. A renewal shall be issued where the applicant is not disqualified under subsection(20).
Transitional
(14) Despite subsections ( 12) and ( l3), a licence or provisional licence that is in existence immediately before section 2 ofSchedule 3 to the Protecting Patients Act, 2017 comes into force expires when it would have otherwise expired.
Stay of refusal to renew
(15) Where the Director refuses to renew a licence, the laboratory facility shall be deemed to continue to be licensed until anorder is made by the Review Board or until the time for requiring a heaiing by the Review Board expires, whichever occursfirst.
Operator to be named in licence
( l6) I.t is a condition of a licence that the operation of the laboratory facility be under the charge and control of the operatornamed in the licence as operator and that the ownership ofthe laboiatory fácility be only in thé person or persons narned inthe licence as owners.
Conditions re quality management
(17) It is a condition ofa licence for a laboratory facility that,
(a) the operation of the laboratory facility meet the requirements of a quality management program;
(b) the owner and the operator of the laboratory facility permit an agency designated in the regulations to carry out aquality management program; and
(c) the owner of the laboratory facility pay lhe fees for an assessment under a quality management program, if any, thatare prescribed by the regulations or established by an agency designated in thè regulations.
Failure to meet program requirements
(.18) Where an_agency designated in the regulations to carry out a quality management program reports to the Director thatthe operation of a laboratory facility does not meet the requirementsbf thè progrãm, the Director mäy impose any conditionsupon the laboratory facility's licence that the Director considers necessarybr ãdvisable in order thaithe health of the publicbe protected.
Notice of changes
(19). Where.the operator or the owner named in the licence is a corporation, the corporation shall notiff the Director inwriting within l5 days of any change in the officers or directors of the corporation.
Revocation, suspension, renewal refusal
(20) The Director may revoke, suspend or refuse to renew a licence where,
(a) any person has made a false statement in the application for the licence or its renewal or in any report, document orother information required to be furnished by this Act or the regulations or any other Act or regglatîon ihat applies tothe laboratory facility;
(b) any test authorized by the licence is incompetently performed;
(c) any specimen taking or collecting authorizcd by the licence is incompetently carried out;
(d) there is a breach of a condition ofthe licence;
(e) the owner or the operator does not comply with this Act or the regulations or any other Act or law relevant to theoperation or maintenance of a laboratory facility;
(Ð the services that can be provided by the laboratory facility are misrepresented;
(g) a change in the officers,or directors of any corporation which is an operator or owner of a laboratory facility named inthe licence would afford grounds for refusing to issue a licence undeiclause (10) (a); or
(h) any other ground for revoking, suspending or refusing renewal that is prescribed in the regulations exists.
Emergency suspension
9.1 (l) If the Director is of the opinion upon reasonable grounds that a laboratory facility is being operated or will beoperated in a.manner that poses an immçdiate th¡eat to the health or safefy of any person, the Director by a written order maysuspend the licence ofthe laboratory facility.
7
858Order effective immediately
(2) Anorderundersubsection(l)takeseffectimmediatelyuponnoticeoftheorderbeingservedonthelicensee.
Notice requirÍng hearing by Review Board
(3) The Director shall deliver with the order under subsection (1) notice that the licensee is entitled to a hearing by theReview Board if the licensee mails or delivers, within 15 days after the notice is served on the licensee, notice in writingrequiring a hearing to the Director and the Review Board, and the licensee may so require such a hearing.
Power of Review Board where hearing
(4) Section I I applies, with necessary modifications, to a suspension under subsection (l).
Service of notice
(5) The Director may serve notice ofan order under subsection (l) by sending the notice by any means that produces a paperrecord or by any other method ofdelivery that is prescribed in the regulations.
Deemed receipt
(6) If the Director serves notice in a manner described in subsection (5), the licensee shall be deemed to have received the
notice on the day it is sent.
No stay
(7) Despite section 25 of the Statutory Powers Procedure Act, arequest for a hearing by the Board made in accordance withsubsection (3) of this section or an appeal to Divisional Court of the Review Board's decision under section 13 does notoperate as a stay ofa suspension ofa licence ordered under subsection (l) ofthis section.
No interim order to stay
(8) Despite section 16.l of the Støtutory Powers Procedure Act,the Review Board shall not make an interim orderto staythe suspension ofa licence ordered under subsection (l) ofthis section.
Powers are additional
(9) For greater certainty, the powers ofthe Director under this section are in addition to, and not in place of, the powers ofthe Minister under the Health Facilities Special Orders Act.
Transfer of licence
9.2 (l) A licence issued under this Act is not transferrable without the consent of the Director.
How dealt with(2) In deciding whether to consent to the transfer ofa licence, the Director shall treat the proposed transferee ofthe licenceas if the proposed transferee were an applicant for a licence and, for the purpose, section 9 applies with necessarymodifications.
Limitations and conditions
(3) In consenting to the transfer of a licence, the Director may attach to the licence such conditions as the Director considersnecessary in the circumstances.
3 Subsection 11 (1) of the Act is repealed and the following substituted:
Proposal to refuse to issuen suspend, revoke or impose condition
(1) Where the Director proposes to suspend, revoke or to refuse to issue or renew a licence or to impose a condition on an
existing licence under this Act, the Director shall serve notice of the proposal, together with written reasons, on the applicantin the õase ofa proposal to refuse to issue or renew the licence and on the owner and operator in the case ofa proposal tosuspend, revoke or to impose a condition on the licence.
4 Section 15 ofthe Act is repealed.
5 Section ló of the Act is repealed and the following substituted:
Appointment of inspectors
16 (1) The Minister may appoint, in writing, one or more persons as inspectors for the purposes of this Act and theregulations.
Certilicate of appointment
(2) The Minister shall issue every inspector appointed under subsection (l) a certificate of appointment and every inspector,in the execution ofhis or her duties under this section and the regulations, shall produce the certificate ofappointment uponrequest.
8
859Director is an inspector
(3) The Director is an inspector by virtue ofoffice, and when acting as an inspector shall, on request, produce evidence ofbeing appointed as Director instead of the certificate of appointment required under subsection (2).
-
Inspections
(4) For the purpose of determining whether this Act and the regulations are being complied with, an inspector may, without awarrant? enter and inspect,
(a) a licensed laboratory facility;
(b) any business premises of a company that owns or operates one or more licensed laboratory facilities; and
(c) any place that the Director reasonably believes is being operated as a laboratory facility without a licence.
Time of entry(5) The power under this section to enter and inspect without a warrant may be exercised only during the regular businesshours of the laboratory facility, business premises orplace.
Dwellings
(6) The power to enter and inspect under this section shall not be exercised to enter and inspect a place or a part ofa placethat is used as a dwelling.
Use of force
(7) An inspector is not entitled to use force to enter and inspect a laboratory facility, business premises or place.
Powers of inspector
(8) An inspector conducting an inspection may,
(a) examine records or anything else that is relevant to the inspection;
(b) demand the production of a record or any other thing that is relevant to the inspection;
(c) remove a record or any other thing that is relevant to the inspection for review, examination or testing;
(d) remove a record or any other thing that is relevant to the inspection for copying;
(e) in order to produce a record in readable form, use data storage, information processing or retrieval devices or systemsthat are normally used in carrying on business in the place;
(f) take photographs or make any other kind ofrecording; and
(g) question a person on matters relevant to the inspection.
Written demand
(9) A demand under this section that a record or any other thing be produced must be in writing and must include a statementofthe nature ofthe record or thing required.
Obligation to produce and assist
(10) Ifan inspector demands that a record or any other thing be produced under this section, the person who has custody ofthe record or thing shall produce it and, in the case of a record, shall on request provide any assistance that is reasonáblynecessary to interpret the record or to produce it in a readable form.
Records and things removed from place
(l l) A record or other thing that has been removed for review, examination, testing or copying,
(a) shall be made available to the person from whom it was removed on request and at a time and place that areconvenient for the person and for the inspector; and
(b) shall be returned to the person wlthln a reasonable time, unless, in the case of a thing that has been subject to testing,the thing has been made unsuitable for return as a result of the testing.
Copy admissible in evidence
(1_2).4-c9nV of.a, record or other thing that purports to be certified by an inspector as being a true copy of the original isadmissible in evidence to the same extent as the original and has the same evideitiary value. -
Obstruction(13) No person shall hinder, obstruct or interfere with or attempt to hinder, obstruct or interfere with an inspector conductingan inspection, refuse to answer questions on matters relevant to the inspection or provide the inspector witlt false informadoàon matters relevant to the inspection.
9
860Personal information in records
( I 4) For greater certainty, a reference to a record in this section includes a record that contains personal information.
6 The Act is amended by adding the following section:
Personal information
17.1 (1) The Ministry may directly or indirectly collect personal information for purposes related to the administration orenforcement of this Act, subject to any requirements or conditions provided for in the regulations.
Use of personal information
(2) The Ministry may use personal information for purposes related to the administration or enforcement of this Act, subjectto any requirements or conditions provided for in the regulations.
Disclosure of personal information
(3) The Ministry may disclose personal information for purposes related to the administration or enforcement of this Act,subject to any requirements or conditions provided for in the regulations'
Personal health information not to be used for administration
(4) Despite the defrnition of 'þersonal information" in section 5, 'þersonal information" for purposes related to the
administration of this Act does not include personal health information as defined in the Personal Health InformationProtection Act, 2004.
7 Section 18 of the Act is repealed and the following substituted:
Regulations
1S (l) The Lieutenant Governor in Council may make regulations for carrying out the purposes and provisions of this Act.
Same
(2) Without restricting the generality of subsection (l), the Lieutenant Governor in Council may make regulations,
(a) providing for the issuance and renewal of licences and provisional licences and prescribing their terms and conditions;
(b) excluding institutions, buildings or places from the definitions of "laboratory" and "specimen collection centre" insection 5, and providing for additional institutions, buildings or places that are laboratories and specimen collectioncentres for the purposes ofthose definitions;
(c) prescribing examinations for the purpose of the definition of "laboratory" in section 5;
(d) prescribing grounds for the purposes of subsections 9 ( I 0) and 9 (20);
(e) prescribing classes oftests for the purposes ofthis Act and the regulations;
(f) respecting the officers and employees of laboratory facilities and prescribing their duties, responsibilities andqualifications;
(g) prescribing the classes ofpersons who may perform tests in a laboratory;
(h) prescribing the classes ofpersons who may take or collect specimens in a specimen collection centre;
(i) prescribing classes ofpersons who shall not be owners oflaboratory facilities or ofany interest in a laboratory facility;
O respecting the management and operation of laboratory facilities;
(k) requiring laboratory facilities to keep any records and make any reports that are prescribed;
(l) respecting and governing the promotion and advertising of laboratory facilities;
(m) prescribing fees for licences, provisional licences and renewals and for laboratory services performed by the Ministry;
(n) exempting laboratory facilities or any class oflaboratory facilities or any class ofpersons from the application ofanyprovision of this Act or the regulations;
(o) prescribing tests to which this Act does not apply;
þ) prescribing other duties and powers of the Director and the Review Board, including the approval of educationalqualifications of officers and employees of laboratory facilities ;
(q) instituting a system for the payment by the Province ofall or any part ofthe annual expenditures oflaboratories in lieuof amounts payable under the Health Insurance Act;
(r) prescribing fees for assessments under a quality management program;
10 961
(s) designating an_agency o^r agencies to carry out a quality management program, and permitting the agency or agenciesto establish and charge fees for assessments under the quality managementprogram;
(t) requiring an agency designated under clause (s) to submit reports to the Director, and goveming the contents of thosereports;
(u) prescribing, providing for and goveming any other matter that this Act refers to as being prescribed or provided for inthe regulations.
I Section 21 of the Act is repealed.
9 (1) Subsection22 (3) of the Act is repealed and the foltowing substituted:I)irectors, officers, etc.
(3) Whether or not a corporation has been convicted ofan offence under subsection (l), each director, officer, employee oragent of.the corporation who authorized, permitted, acquiesced in or participated in the commission of an offenõe úy thecorporation under subsection (l) or failed to take reasonable care to prevent the corporation from committing an offenceunder subsection (l) is a party to and guilty of the offence, and on conviction is liable to the punishment providãd for undersubsection (1).
(2) Section 22 of the Act is amended by addÍng the following subsections:
Provincial Judge required(5) The _Attomey General or an agent of the Attorney General may, by notice to the clerk of the Ontario Court of Justice,require that a provincial judge preside over a proceeding in respect of an offence under this Act.Publication re convictions
(6) -If a person is convicted of an offence under thisAct, the Minister may publish or otherwise make available to the general
public the name ofthe person, a description ofthe offence, the date ofthe-cõnviction and the person's sentence.
Restraining order not necessary
(7)-A person may be prosecuted under this section whether or not a restraining order has been previously made with respectto the subject matter ofthe prosecution.
Certificates
(8)_In any-prosecution or other proceeding under this Act, a certificate ofan analyst stating that the analyst has made ananalysis ofa sample and stating the result ofthat analysis is evidence ofthe facts alleged in the certiflrcate without proofofthe signature or the official character ofthe person appearing to have signed the certificãte.
Axrun,s FoR RESEÀRCH AcT1,0 _9ubsection 20 (13) ol the Anímals for Reseørch Act is amended by striking out "the Løhorøtory and SpechnenCollection Centre Licensíng Acf' andl substituting "the Health Protection ønd Promotion Acf,.
HnlI rn lxsunancnAcr11- Clause 2 (2) (a) of the Health Insurance lcf is amended by striking out 'sphysicians and practitioners" andsubstituting r6physicians, practitioners and health facilities".
PUBLIC HOSPITALS ACT
12 Section I of the Public Hospìtøls Act is amended by adding the following definition:
"co^mmunity laboratory services" means the services of a laboratory or specimen collection centre under the Laboratory øndSpecimen Collection Centre Licensing Act that are provided by a hospital designated under subsection 22 (l) of this Áct topersons who are neither in-patients nor out-patients; ("services de laboratoire cõmmunautaire")
13 The Act is amended by adding the following section:
Community laboratory services
22 (1) The Minister may designate one or more hospitals to provide community laboratory services.
Same
(2) A hospital that is designated under subsection (l) may provide community laboratory services, subject to any conditions,restrictions or requirements that may be prescribed in the regulations.
14 Subsection 32 (1) of the Act is amended by adding the following clauses:
(c. I ) prescribing conditions, restrictions and requirements for the purposes of subsection 22 (2);
l1
(c.2) providing for provisions of this Act or the regulations that do not apply with respect to community laboratory servicesprovided by a hospital designated under subsection 22 (1);
Commencement
15 (1) Subject to subsection (2), this Schedule comes into force on the day the Protectíng Pstíents Act,2017 receivesRoyal Assent.
(2) Sections 1 to 9 and 12 to 14 come into force on a day to be named by proclamation of the Lieutenant Governor.
862
12
863SCHEDULE 4
ONTARIO DRUG BENEFIT ACT
1 Subsection I (1) of the Ontørío Drug ßenefttlcf is amended by adding the following definitions:"authorized prescriber" means a physician, registered nurse in the extended class, a prescribed person or a member of a
prescribed class; þrescripteur autorisé)
"registered nurse in the extended class" means a registered nurse who holds an extended certihcate ofregistration under theNursing Act, I99I; ("infrmière autorisée ou infirmier autorisé de la catégorie supérieure")
2 Subsection 2 (2) of the Act is amended by striking out *the FamìIy Beneftts Act',.3 Subsections 9 (1) and (2) of the Act ¡re amended by striking out ooa physician'o wherever it appears and substitutingin each case ooan authorized prescriber".
4 subsections 16 (1), (3) and (4) ofthe Act are repealed and the foltowing substituted:
Unlisted drugs, special case
(l) If an authorized prescriber informs the executive officer that the proper treatment of a patient who is an eligible personrequires the administration of a drug for which there is not a listed drug product, the executive officer may mãke this Actapply in respect of the supplying of that drug as if it were a listed drug product by so notifying the prescriber.
Listed drugs, special case
(3) If an authorized prescriber informs the executive officer that the proper treatment of a patient who is an eligible personrequires the adminishation of a drug for which there are one or more listed drug products but for which the conditións forpayment under section 23 are not satisfied, the executive officer may make this Act apply in respect of the supplying of thoselisted drug products as if the conditions were satisfied.
Notice to operator
(4) An- operator of a pharmacy is not liable for contravening this Act or the regulations in respect of supplying a drugreferred to in subsection (1) or a listed drug product referred to in subsection (3) unless the operatoi has receivéd-notice fromthe authorized prescriber or from the executive officer that this Act applies to that supplying.
-
5 (1) Section l8 of the Act is amended by adding the following subsection:
Authorized prescribers
(1.1) The Minister may make regulations prescribing persons or classes of persons for the purpose of the definition of"authorized prescriber" in subsection I (1).
(2) Subsection 18 (8) of the Act is amended by adding "and the Minister shall not make any regulation undersubsection (L.l)" before ttunless" in the portion before clause (a).
(3) Subsection 18 (8) of the Act is amended by striking out '6and" after clause (c) and by repealing clause (d) andsubstituting the following:
(d) the Minister has considered whatever comments and submissions that members of the public have made on theproposed regulation in accordance with clause (9) (b) or (c); and
(e) in the case of regulations made by the Lieutenant Govemor in Council, the Minister has reported to the LieutenantGovernor in Council on what, if any, changes to the proposed regulation the Minister consideri appropriate.
(4) Section 18 of the Act is amended by adding the foltowing subsection:
Discretion to make regulations, Minister(ll.l) After considering the comments and submissions mentioned in clause (8) (d), the Minister, without further noticeunder subsection (8), may make the proposed regulation under subsection (1.1) with the changes that the Minister considersappropriate, whether or not those changes are mentioned in the comments and submissions.
(5) Subsection f8 (12) of the Act is amended by striking out 6rclause I (d)" and substituting "clause 8 (e)',.
(6) Section 18 of the Act is amended by adding the following subsection:
Rolling incorporation
( I 6) A regulation made under subsection ( 1 ) that incorporates another document by reference may provide that the referenceto the document includes amendments made to the document from time to time after the regulation ii made.
13
864Commencement
6 This Schedule comes into force on a day to be named by proclamation of the Lieutenant Governor
t4
865SCHEDULE 5
REGULATED HEALTII PROFESSIONS ACT, 1991
1 Subsection I (1) of the Regaløted Heøllh Professions Act, I99t is amended by adding the following definition:"personal health information" has the same meaning as in section 4 of the Personal Health Inþrmation Protection Act, 2004;
("renseignements personnels sur la santé")
2 (1) Clause 36 (1) (d) of the Act is repealed and the following substituted:
(d) 1s ryay be required for the administration of the Drug Interchangeability and Díspensing Fee Act, the Healing ArtsRadiation Protection Act, the Heahh Insurance Act, the Health Protection and Protnotion Act, the Independent lfeahhþ'acilitíes Act, lhe Laboratory and Specimen Collection Centre Licensing Act, the Long-Term Care Homes Act, 2007,the Retirement Homes Act, 2010, the Ontario Drug BeneJìt Act, the Coroners Alt, the Controlled Drugs andSubstances Act (Canada) andthe Food and Drugs Acl (Canada);
(2) Subsection 36 (1) of the Act is amended by striking out 610r" at the end of clause (i), by adding ..or,, ^tthe
end ofclause (i) and by adding the following clause:
(k) to the Minister in order to allow the Minister to determine,
(i) whether the College is fulhlling its duties and carrying out its objects under this Act, a health profession Act, theDrug and Pharmacies Regulation Act or the Drug Interchangeability and Dispensing Fee Act, or
(ii) whether the Minister should exercise any power of the Minister under this Act, or any Act mentioned insubclause (i).
(3) Section 36 of the Act is amended by adding the following subsection:
Restriction
(1.6) Information disclosed to the Minister under clause (l) (k) shall only be used or disclosed for the purpose for which itwas provided to the Minister or for a consistent purpose.
3 (1) Subsection 36.1 (1) of the Act is repealed and the following substituted:
Collection of personal information by College
(l) At the-request of the Minister, a College shall collect information directly from members of the College as is reasonablynecessary for the purpose ofhealth human resor¡rces planning or research.
(2) Subsections 36.1 (5) and (6) ofthe Act are repealed and the following substituted:
Use, collection, disclosure and publication
(5) The following applies to information collected under subsection (1):
1. The information may only be used for the purposes set out under subsection (l).2. The Minister shall not collect personal information if other information will serve the purposes set out under
subsection (1).
3. The Minister shall not collect more personal information than is necessary for the purposes set out under subsection(l).
4. The Minister may disclose the information only for the purposes set out in subsection (l).5. Reports and other documents using information collected under this section may be published for the purposes set out
under sutsection (1), and for those purposes only, but personal information about a member of a Collège shall not beincluded in those reports or documents.
(3) The definition of "informatÍonoo in subsection 36.1 (9) of the Act is repealed and the following substituted:
"information" includes personal information about members, but does not include personal health information.(,,renseignements,,) r -------^
(4) Subsection 3é.1 (9) of the Act is amended by adding the fotlowing defïnition:
"research" means the study ofdata and information in respect ofhealth human resources planning. ("recherche")
4 The delinition of "personal health information" in subsection 36.2 (6) of the Act is repealed.
5 (1) Subsection 43 (1) of the Act is amended by adding the following clause:
(o) establishilg criteria for the definition of"patient" in relation to professional misconduct involving the sexual abuse ofa patient forthe purposes ofsubsection I (3) ofthe Code.
l5
866(2) Subsection 43 (1) of the Act is amended by adding the following clauses:
(p) respecting the composition of committees that a College is required to have pursuant to subsection l0 (1) of the Codeand governing the relationship between such regulations and the by-laws of the College;
(q) respecting the qualification, selection, appointment and terms of office of members of committees that a College isreq-uired to have pursuant to subsection l0 (l) ofthe Code and governing the relationship between such regulationsand the by-laws of the College;
(r) prescribing conditions that disqualify committee members from sitting on committees that a College is required tohave pursuant to subsection l0 (l) of the Code and governing the removal of disqualified committee members andgoverning the relationship between such regulations and the by-laws of the College;
(s) speci$ing the composition of panels selected from amongst the members of the Registration Committee, Inquiries,Complaints and Reports Committee, Discipline Committee and Fitness to Practise Committee for the purposes ofsubsections 17 (2),25 (2),38 (2) and 64 (2) ofthe Code, and providing for quorum for such panels.
(3) Subsection a3 (1) of the Act is amended by adding the following clause:
(t) prescribing additional information to be contained in a College's register for the purposes of paragraph 19 of' iubsection 23 (2) of the Code and designating such information as information subject to subsection 23 (13.1) of the
Code.
(4) Subsection 43 (f) of the Act is amended by adding the following clauses:
(u) prescribing conduct for the purposes of subparagtaph 3 vii of subsection 5 I (5) of the Code;
(v) prescribing offences for the purposes of clause 5l (5.2) (a) of the Code.
(5) Subsection 43 (1) of the Act is amended by adding the following clause:
(w) clarifying how a College is required to perform its functions under sections 25 to 69 and 72 to 74 of the Code withrespect tõ matters involving allegations of a member's misconduct of a sexual nature, and providing for furtherfunctions and duties that are not inconsistent with those functions.
(6) Subsection 43 (1) of the Act is amended by adding the following clause:
(x) prescribing additional functions of the patient relations program for the purposes of subsection 84 (3. I ) of the Code.
(7) Subsection 43 (1) of the Act is amended by adding the following clause:
(y) prescribing additional purposes for which funding may be provided under the program which Colleges are required to- maintain under section 85.7 of the Code, and prescribing additional persons or classes of persons to whom fundingmay be paid for the purposes of subsection 85.7 (8) of the Code.
(8) Subsection 43 (1) of the Act is amended by adding the following clause:
(z) governing transitional matters arising from the enactment of Schedule 5 to the Protecting Patients Act, 2017.
6 Subsection 1 (6) of Schedule 2 to the Act is repealed and the following substituted:
Delinitions
(6) For the purposes of subsections (3) and (5),
"patient", without restricting the ordinary meaning of the term, includes,
(a) an individual who was a member's patient within one year or such longer period of time as may be prescribed from the
date on which the individual ceased to be the member's patient, and
(b) an individual who is determined to be a patient in accordance with the criteria in any regulations made under clause 43
(l) (o) ofthe Regulated Health Professions Act, 1991; ("patient")
"spouse", in relation to a member, means,
(a) a person who is the member's spouse as defined in section I of the Famíly Law Act, or
(b) a person who has lived with the member in a conjugal relationship outside of marriage continuously for a period of notless than three years. ("conjoint")
7 Section 1.1 of Schedule 2 to the Act is repealed and the following substituted:
Statement of purposeo sexual abuse provisions
1.1 The purpose of the provisions of this Code with respect to sexual abuse of patients by members is to encourage the
reporting ofsuch abuse, to provide firnding for therapy and counselling in connection with allegations of sexual abuse bymembers and, ultimately, to eradicate the sexual abuse of patients by members.
l6
8 Section 7 of Schedule 2 to the Act is amended by adding the following subsections:
Posting of meeting information(1.1) The College shall post on its website information regarding upcoming meetings of the Council, including the dates ofthose_ meetings, matters to be discussed at those meetings, and informatiõn and ãocumentation that will bã provided tomembers of the Council for the purpose of those meetings.
Items where public excluded
(1.2) If the Registrar anticipates that the Council will exclude the public from any meeting or part of a meeting undersubsection (2), th9 grgund.s for doing so shall be noted in the informatìon posted undèr subsection (i.t¡ and informat-ion anddocumentation related to that meeting or part of that meeting shall not be pòsted under subsection ( I . I ).-9 Subsection 10 (3) of Schedule 2 to the Act is repealed and the following substituted:
Composition
(3) The_composition of the committees shall be in accordance with the by-laws and with any regulations made pursuant toclauses 43 (1) (p) to (r) of the Regulated Health Professions Act, 1991.
10 Subsections 17 (2) and (3) ofSchedule 2 to the Act are repealed and the following substituted:Composition of panels
(Z) Ttt: panel selected by-the chair shall be composed in accordance with regulations made pursuant to clauses a3 (l) (p) to(s) of the Reguløted Health Professions Act, l99L
Quorum
Q) 9uorum for the,panel shall be in accordance with regulations made pursuant to clause 43 (l) G) of the Regulated HeahhProfessions Act, i,991.
1l (1) Subsection 23 (2) of Schedule 2 to the Act is repealed and the following substituted:Contents of register
(2) The register shall contain the following:
l. Each member's name, business address and business telephone number, and, if applicable, the name of every healthprofession corporation of which the member is a shareholder.
2. Vy'here a member is deceased, the name of the deceased member and the date upon which the member died, if knownto the Registrar.
3. The name, business address and business telephone number ofevery health profession corporation.
4. The names of the shareholders of each health profession corporation who are members of the College.
5. Each member's class of registration and specialist status.
6. The terms, conditions and limitations that are in effect on each certificate of registration.
7. A notation of every caution,that, a member has received from a panel of the Inquiries, Complaints and ReportsCommittee under paragraph 3 o{subsection 26 (l), and any speciñed continuing èducation of remedial programsrequired by a panel of the Inquiries, Complaints and Reports Committee using-its powers under paragrãptt-¿ ofsubsection 26 (1).
8. A notation of every matter that has been referred by the Inquiries, Complaints and Reports Committee to theDiscipline Committee under section 26 and that has not been flrnally resolved, including the dáte of the referral and thestatus of the hearing before a panel of the Discipline Committee, until the matter has beên resolved.
9. A copy.of the-specified allegations against a member for every matter that has been referred by the Inquiries,Complaints and Reports Committee to the Discipline Committee under section 26 and that has not been ïnallyresolved.
I 0. Every result of a disciplinary or incapacity proceeding.
I l. A notation and synopsis of any acknowledgements and undertakings in relation to matters involving allegations ofprofessional misconduct or incompetence before the Inquiries, Complaints and Reports Committee oi the ÚisciplineCommittee that a member has entered into with the College and that ale in effect.
12. A notation of every finding of professional negligence or malpractice, which may or may not relate to the member'ssuitability to practiie, madðagainst the membei u-nless the nnding is réversed on áppeal. "
I 3. A notation of every revocation or suspension of a certificate of registration.
I 4. A notation of every revocation or suspension of a certificate of authorization.
867
t7
15. Information that a panel of the Registration Committee, Discipline Committee or Fitness to Practise Committeespecifies shall be included.
16. Where findings of the Discipline Committee are appealed, a notation that they are under appeal, until the appeal isfinally disposed of.
17. Where, during or as a result of a proceeding under section 25, a member has resigned and agreed never to practiseagain in Ontario, a notation of the resignation and agreement.
18. Where the College has an inspection program established under clause 95 (l) (h) or (h.l), the outcomes of inspectionsconducted by the college.
19. Information that is required to be kept in the register in accordance with regulations made pursuant to clause 43 (l) (t)of the Regulated Health Professions Act, 1991.
20. Information that is required to be kept in the register in accordance with the byJaws.
(2) Subsection23 (4) of Schedute 2 to the Act is amended by striking out 6rparagraph 11" and substituting "paragraph1.5'.
(3) Subsection 23 (5) of Schedule 2 to the Act is repealed and the following substituted:
Access to information by the public
(5) All of the information required by paragraphs I to l9 of subsection (2) and all information designated as public in the by-laws shall, subject to subsectirons (6), (?), (8), (9) and (l l), be made available to an individual during normal business hours,
and shall be posted on the College's website within a reasonable amount of time of the Registrar having received the
information and in a manner that is accessible to the public or in any other manner and form specified by the Minister.
(4) Subsection 23 (11) ofSchedule 2 to the Act is amended by striking out "paragraphT" in the portion before clause(a) and substituting "paragraph 10".
(5) Clause 23 (11) (d) of Schedule 2 to the Act is amended by striking out 'oclause (a) or (b)" and substituting o'clause
(a), (b) or (c)."
(6) Section 23 of Schedule 2 to the Act is amended by adding the following subsection:
Other cases when information may be withheld
( I I . I ) The Registrar shall refuse to disclose to an individual or to post on the College's website information required byparagraph 10 ofsubsection (2) if,
(a) the result of a discipline proceeding was that no finding of professional misconduct or incompetence was made against
the member; and
(b) more than 90 days have passed since the information was prepared or last updated, unless before the expiry of the 90' days the member to whom the information relates specifically requests in writing that the Registrar continue tomaintain public access to the information.
(7) Section 23 of Schedule 2 to the Act is amended by adding the following subsection:
Correction of information
(13.1) The Registrar shall correct any information contained in the register that is required by paragraph l2 ofsubsection (2)
or thát is bothiequired by paragrapli 19 of subsection (2) and designated as subject to this subsection in a regulation.madeunder clause 43 (i ) (t) oi the nègalated Health Professions Act, I 99 I , where a member demonstrates, to the satisfaction ofthe Registrar, that the information contained in the register is incomplete or inaccurate and where. the member-provides the
Registrar with the information that is necessary to enable the Regishar to correct the incomplete or inaccurate information.
(8) Subsection23 (14) of Schedule 2 to the Act is repealed and the following substituted:
Meaning of results of proceeding
(14) For the purpose of this section and section 56,
"result",
(a) when used in reference to a disciplinary proceeding, means the panel's finding that the member committed an act ofprofessional misconduct or was incompetent, particulars of the grounds for the finding, a synopsis of the decision andihe order made, including any reprimand, and where the panel has made no such finding, includes a notation that no
such fînding was made and the reason why no such finding was made, and
(b) when used in reference to an incapacity proceeding, means the panel's finding that the member is incapacitated and the
order made by the panel.
12 Subsections25 (2) and (3) of Schedule 2tothe Act are repealed and the following substituted:
868
18
869Composition of panels
(z) Ttt: panel selecled by-the chair shall be composed in accordance with regulations made pursuant to clauses a3 (l) (p) to(s) of the Regulated Health Proþssions Act, 199i,.
Quorum
Q) 9uorum for the panel shall be in accordance with regulations made pursuant to clause 43 (l) (Ð of the Regulated HealthProfessions Act, 1991.
L3 Subsection 25.1 (4) of Schedule 2 to the Act is repealed and the fottowing substituted:Ratification of resolution
(4) If the complainant and the member reach a resolution of the complaint through alternative dispute resolution, they shalladvise the Registrar of the resolution, and the Registrar may,
(a) adopt the proposed resolution; or
(b) refer the decision of whether or not to adopt the proposed resolution to the panel.
Referral to panel
(5) where the Registrar makes a referral to the panel under clause (4) (b), the panel may,
(a) adopt the proposed resolution; or
(b) continue with its investigation of the complaint.
Time limit for ADR(6) If the complainant and the member do not reach a resolution of the complaint within 60 days of a referral to alternativedispute resolution under subsection (l), the Registrar or the panel shall not ádopt any resolution reached after that date andthe panel shall proceed with its investigation of the complaint.
Extension of time
(7) - Despite subsection (6), the Regìs-trar or the panel may, where the Registrar or the panel believes it is in the public interest
to do so, a.nd ¡i1th the agreement of the complainant and the membero adópt a resolutiôn reached within 120 days of a referralto alternative dispute resolution under subsection (l).14 Schedule 2 to the Act is amended by adding the following sections:
Withdrawal of complaint by Registrar25.3 (1) At any timeaction being taken bymayn at the request of
following the receipt of a complaint regarding the conduct or actions of a member and prior to anyI Panel ofthe Inquiries, Complaints and Reports Committee under subsection26 (l), tire Registrarthe complainant, withdraw the complaint if the Registrar believes that the withdrawal is in the þublic
interest.
Notice
(2) T,h9 Registrar shall give the complainant and the member, within 14 days of the Registrar having withdrawn thecomplaint, notice that the complaint has been withdrawn.
Interim suspension
25.4.(l) The Inquiries, Co^mplaints and Reports Commjttee may, subject to subsections (2) and (6), at any time following thereceipt.of a complaint or.following the appointment of an investigatór pursuant to subsêciion Zi (i¡ or (2¡, make an inñrimorder directing the Registrar to suspend, or to impose terms,-conditions or limitations on, à'-embér's certificate ofregishation if it is of the opinion that the conduct of the member exposes or is likely to expose the member's patients to harmor lnJury.
No gender-based terms, conditions, limitations
(2) Despite subsection (1), the Jnquiries, Complaints and Reports Committee shall not make an interim order directing theRegistrar to impose any gender-based terms, çonditions or limitations on a member's certificate of registrationProcedure following interim suspension
(3) If an order is made under subsection (l) by the Inquiries, Complaints and Reports Committee,
(a) the matter shall be investigated and prosecuted expeditiously; and
(b) the Inquiries, Complaints and Reports Committee, the Discipline Committee or the Fitness to Practise Committee, asthe case may be, shall give precedence to the matter.
t9
870Duration of order
(a) An order under subsection (l) continues in force until it is varied by the Inquiries, Complaints and Reports Committee oruntil the matter is withdrawn, resolved by way of an altemative dispute resolution process or otherwise finally disposed ofby a panel of the Inquiries, Complaints and Reports Committee, the Discipline Committee or the Fitness to PractiseCommittee.
Panelts order
(5) In a matter in which an order under subsection (l) was made, an order of a panel of the Discipline Committee or theFitness to Practise Committee directing the Registrar to revoke, suspend or impose conditions on a member's certificate takeseffect immediately despite any appeal.
Restrictions on orders
(6) No order shall be made under subsection (l) unless the member has been given,
(a) notice of the intention to make the order;
(b) at least 14 days to make written submissions to the Committee; and
(c) a copy ofthe provisions ofthis section.
Extraordinary action to protect public
(7) Despite subsection (6), an order may be made under subsection (l) without notice to the member, subject to the right ofthe member to make submissions while the suspension or the terms, conditions or limitations are in place, if the Committee isof the opinion, on reasonable and probable gtounds, that the conduct of the member exposes or is likely to expose themember's patients to harm or injury and urgent intervention is needed.
15 Subsection 2E (2) of Schedule 2 to the Act is repealed and the following substituted:
Impact of ADR on timelines
(2) Time spent by a complainant and member in an altemative dispute resolution process pursuant to a referral under section25.1 shall not be included in the calculation of time under this section.
16 Section 37 of Schedule 2 to the Act is repealed.
17 (1) Subsections 38 (2) and (3) ofSchedule 2 to the Act are repealed and the following substituted:
Composition
(2) The panel selected by the chair shall be composed in accordance with regulations made pursuant to clauses a3 (l) (p) to(s) of the Regulated Health Professions Act, i,991.
(2) Subsection 38 (5) of Schedule 2 to the Act is repealed and the following substituted:
Quorum(5) Quorum for the panel shall be in accordance with regulations made pursuant to clause 43 (1) G) of the Regulated HealthProfessions Act, 1991.
18 Schedule 2 to the Act is amended by adding the following section:
Production orders
42.2 (l) Where, in relation to a hearing involving allegations of a member's misconduct of a sexual nature, the memberseeks an order of the panel of the Discipline Committee for the production and disclosure of a record that containsinformation for which there is a reasonable expectation of privacy from a person who is not a party to the hearing, any one ormore of the following assertions made by the member are not sufficient on their own to establish that the record is likelyrelevant to an issue in the hearing or to the competence of a witness to testiff:
l. That therecord exists.
2. That the record relates to medical or psychiatric treatment, therapy or counselling that the complainant or a witness has
received or is receiving.
3. That the record relates to the incident that is the subject-matter ofthe proceedings.
4. That the record may disclose a prior inconsistent statement of the complainant or a witness.
5. That the record may relate to the credibility of the complainant or a witness.
6. That the record may relate to the reliability of the testimony of the complainant or a witness merely because thecomplainant or witness has received or is receiving psychiatric treatment, therapy or counselling.
7. That the record may reveal allegations of sexual abuse of the complainant or a witness by a person other than themember.

20 8718. That the record relates to the sexual activity of the complainant or a witness with any person, including the member.
9. That the record relates to the presence or absence of a recent complaint.
10. That the record relates to the sexual repuktion of the complainant or a witness.
I 1. That the record was made close in time to a complaint or report or to the activity that forms the subject-matter of theallegation against the member.
Same
(2) A panel of the Discipline_Committee may order the person who has possession or control of the record to produce therecord or Pfrt of the record if the panel is satisfied that the member has established that the record is likely reievant to anissrte in the hearing or to the competence ofa witness to testify in the hearing and the production ofthe recorá is necessary inthe interest ofjustice.
Factors to be considered
(3) In determining whether to grant an order for the production of records in accordance with this section, the panel shallconsider,
(a) the regulatory nature ofthe proceedings;
(b) the primary purpose ofthe proceedings, which is to protect the public and regulate the profession in the public interest;
(c) the privacy interest ofthe complajnant or a witness in the record sought; and
(d) the nature and purpose of tlte record sought in the motion.
Standing
(4) Despite subsection 4ljl (1)? the panel shall, upon the application ofany person who has a privacy interest in the recordsreferred to in subsection (l) of this section, grant the person standing on the member's motion fôr production of the records.Interpretation
(5) In subsection (l),"allegations,of a member's misconduct of a sexual nature" include, but are not limited to, allegations that the member
sexually abused a patient.
19 (1) Clause 51 (1) (b) of Schedule 2 to the Act is repealed and the fotlowing substituted:(b) the. governing body of another health profession in Ontario, or the governing body of a health profession in a
jurisdiction other than Ontario, has found that the member committed anlct of professiônal misconducì that would, inthe opinion ofthe panel, be an act ofprofessional misconduct under this section or an act ofprofessional misconductas defined in the regulations;
(2) Section 51 of Schedule 2 to the Act is amended by adding the following subsections:
No gender-based terms, conditions, limitations(4.1) In making an order under paragraph 3 of subsection (2), a panel shall not make any order directing the Registrar toimpose any gender-based terms, conditions or limitations on a member's certificate of regisiration.
Interim suspension of certificate(!.2) Th: panel shall immediately make an interim order suspending a member's certifrcate of registration until such time asthe panel makes an order under subsection (5) or (5.2) if the panel finds that the member has comrñitted an act of professionalmisconduct,
(a) 1r1rdgl clause (l) (a) and the offence is prescribed for the purposes of clause (5.2) (a) in a regulation made under clausea3 (l) (v) of the Regulated Health Professions Act, t99t;
(b) under clause (l) (b) and the misconduct includes or consists ofany ofthe conduct listed in paragraph 3 ofsubsection(5); or
(c) by sexually abusing a patient and the sexual abuse involves conduct listed under subparagraphs 3 i to vii ofsubsection(s).
Non-application to mandatory orders
(4.3) For greater certainty, subsection (4) does not apply to a mandatory order made under subsection (5) or a mandatoryorder made under subsection (5.2).
(3) Subsection 5l (5) of Schedule 2 to the Act is repealed and the following substituted:

2l
872Orders relating to sexual abuse
(5) If a panel finds a member has committed an act of professional misconduct by sexually abusing a patient, the panel shall
do the following in addition to anything else the panel may do under subsection (2):
L Reprimand the member.
2. Suspend the member's certificate of registration if the sexual abuse does not consist of or include conduct listed inparagraph 3 and the panel has not otherwise made an order revoking the member's certificate of registration under
subsection (2).
3. Revoke the member's certificate of registration if the sexual abuse consisted of, or included, any of the following:
i. Sexual intercourse.
ii. Genital to genital, genital to anal, oral to genital or oral to anal contact.
iii. Masturbation of the member by, or in the presence of, the patient.
iv. Masturbation of the patient by the member.
v. Encouraging the patient to masturbate in the presence of the member.
vi. Touching ofa sexual nature ofthe patient's genitals, anus, breasts orbuttocks.
vii. Other conduct of a sexual nature prescribed in regulations made pursuant to clause a3 ( I ) (u) of the RegulatedHealth Professions Act, l99l .
Interpretation
(5. I ) For greater certainty, for the purposes of subsection (5),
"sexual nature" does not include touching or conduct of a clinical nature appropriate to the service provided.
Mandatory revocation
(5.2) The panel shall, in addition to anything else the panel may do under subsection (2), reprimand the member and revoke
the member's certificate of registration if,
(a) the member has been found guilty of professional misconduct under clause (1) (a)and the offence is prescribed in aregulation made under clause 43 (l) (v) ofthe Regulated Health Professions Act, I99Ii or
(b) the member has been found guilty of professional misconduct under clause (1) (b) and the misconduct includes or
consists ofany ofthe conduct listed in paragraph 3 ofsubsection (5).
20 Section 62 of Schedule 2 to the Act is repealed and the following substituted:
Interim suspension
62 (l) The panel may, subject to section 63, make an interim order directing the Registrar to suspend or impose terms,
"o.tàiiionr oi limitatiois onâ member's certificate of registration if it is of the opinion that the physical or mental state of the
member exposes or is likely to expose his or her patients to harm or injury.
No gender-based terms
(2) Despite subsection (l), the panel shall not make an interim order directing the Registrar to impose any gender-based
terms, conditions or limitations on a member's certificate of registration.
Procedure following interim suspension
(3) If an order is made under subsection (l) in relation to a mattern
(a) the College shall inquire into and prosecute the matter expeditiously; and
(b) the Inquiries, Complaints and Reports Committee and the Fitness to Practise Committee shall give precedence to the
matter.
Duration of order
(4) An order under subsection (l) continues in force until it is varied by the panel of the.Inquiries, Complaints and Reports
Òómmittee or until the matter is hnally disposed of by a panel of the Inquiries, Complaints and Reports Committee or the
Fitness to Practise Committee.
2L subsection 63 (l) of Schedule 2 to the Act is repealed and the following substituted:
Restrictions on orders
(l) No order shall be made with respect to a member under subsection 59 (2) or subsection 62 (1) unless the member has
been given,
22
(a) noticeoftheintentionromaketheorder; 873(b) at least 14 days to make written submissions to the panel; and
(c) in the case of an order under subsection 62 (1), a copy of the provisions of section 62.
22 Subsections 64 (2) and (3) ofSchedule 2 to the Act are repealed and the following substituted:Composition of panels
(2) T!" panel selected by the chair shall be composed in accordance with regulations made pursuant to clauses a3 (l) (p) to(s) ofthe Regulated Health Professions Act, 1991.
Quorum(3) 9uorum for thepanel shall be in accordance with regulations made pursuant to clause 43 (l) G) of Ihe Regulated HealthProfessions Act, I99L
23 Section 71.1 of schedule 2 to the Act is repealed and the following substituted:No stay ofcertain orders pending appeal
71.1 Section 7l also applies to an order ma{9 by.a panel of the Discipline Committee because of a finding that a member hascommitted sexual abuse of the kind described in paragraph 3 of subsection 51 (5) or an act of profe"ssional mlsãn¿uctdescribed in subsection 51 (5.2).
24 Paragraph 3 of subsection 73 (3) of Schedule 2 to the Act is repealed.
25 Section 84 of Schedule 2 to the Act is amended by adding the following subsection:Other functions
(],t) rh9 patlent relations Plogram-shall perform any other functions that are prescribed in regulations made under clause 43(l) (x) of the Regulated Health Professions Act, .l99 j.26 Schedule 2 to the Act is amended by adding the following section:
Reporting by members re: other professional memberships and fìndings85.6.3 (l) A member shall advise -the Registrar in writing if the member is a member of another body that governs aprofession inside or outside of Ontario.
F'indings of misconduct or incompetence
(2) A member shall file a report in- writing with the Registrar if there has been a finding of professional misconduct orincompetence made against the member by inother body th-=at governs a profession inside or õuæide of Ontario.Timing of report(3) The report must be filed as soon as reasonably practicable after the member receives notice of the finding made againstthe member.
Contents of report(4) The report must contain,
(a) the name of the member filing the report;
(b) the nature of, and a description of; the finding;
(c) the date that the finding was made against the member;
(d) the name and location of the body that made the finding against the member; and
(e) the status of any appeal initiated respecting the finding made against the member.
Publication ban
(5) The report shall not contain any information that violates a publication ban.
Same
(6) No action shall be taken under this section which violates a publication ban and nothing in this section requires orauthorizes the violation ofa publication ban.
Additional reports
(7) A member who files a report under subsection (l) shall file an additional report if there is a change in status of thefinding made against the member as the result of an appeal.
27 Schedule 2 to the Act is amended by adding the following section:
23
874Reporting by members re: charges and bail conditions, etc.
85.6.4 (l) A member shall file a report in writing with the Registrar if the member has been charged with an offence, and the
report ihall include information abòut every bail condition or other restriction imposed on, or agreed to, by the member inconnection with the charge.
Timing of report(2) The report must be filed as soon as reasonably practicable after the member receives notice of the charge, bail condition
or restriction.\
Contents of report(3) The report must contain,
(a) the name of the member filing the report;
(b) the nature of, and a description of, the charge;
(c) the date the charge was laid against the member;
(d) the name and location of the court in which the charge was laid or in which the bail condition or restriction was
imposed on or agreed to by the member;
(e) every bail condition imposed on the member as a result of the charge;
(Ð any other restriction imposed on or agreed to by the member relating to the charge; and
(g) the status of any proceedings with respect to the charge.
Publication ban
(4) The report shall not contain any information that violates a publication ban'
Same
(5) No action shall be taken under this section which violates a publication ban and nothing in this section requires orauthorizes the violation of a publication ban.
Additional reports
(6) A member who files a report under subsection ( I ) shall flrle an additional report if there is a change in the status of the
charge or bail conditions.
28 (1) Subsection 85.7 (1) of Schedule 2 to the Act is repealed and the following substituted:
Funding provided by College
(l) There shall be a program, established by the College, to provide funding for the following pulposes in connection withallegations of sexual abuse by members:
L Therapy and counselling for persons alleging sexual abuse by a member.
2. Any other purposes prescribed in regulations made under clause 43 (l) (y) of the Regulated Health Professions Act,
1991.
(2) Subsections 85.7 (4) and (5) of Schedule 2 to the Act are repealed and the following substituted:
Eligibility(4) A person is eligible for fi.rnding if,
(a) it is alleged, in a complaint or report, that the person was sexually abused by a member while the person was a patient
of the member; or
(b) the alternative requirements prescribed in the regulations made by the Council are satisfied.
Timing(5) Where a request is made for funding pursuant to subsection (1), a determination of the person's eligibility for suchfirnding in accoidance with subsection (4¡ shall be made within a reasonable period of time of the request having been
received.
Not a finding
(5.1) The determination of a person's eligibility for funding in accordance with subsection (4) does not constitute a findingagainst the member and shall not be considered by any other committee of the College dealing with the member.
24
875Cessation of eligibility(5'2) Despite subsection (4), a person's eligibility to receive funding pursuant to subsection (1) ceases upon the occuffenceof any of the prescribed circumstances.
(3) Subsections 85.7 (8) to (12) of Schedule 2 to the Act are repealed and the following substituted:Payment
(8) Funding shall bc paid only to the therapist o-r counsellor chosen by the person or to other persons or classes ofpersonsprescribed in any regulation made under clause a3 (1) (y) of the Regulaied Hèalth Professions Act, 1991 .
10 p_ay f9r thJrapl or counselling and for any other puryoses prescribed in any regulationthe Regulated Health Professions Act, l99l and shall not be applied directly or iñdirectly for
Use of funding
(9) Funding shall be used onlymade under clause 43 (l) (y) ofany other pulpose.
Same
(10) Funding may be used to pay for therapy or counselling that was provided at any time after the alleged sexual abuse tookplace.
Other coverage
(!t)_ I!" funding that is provided to a person for therapy and counselling shall be reduced by the amount that the OntarioHealth Insurance Plan or a private insureris-required to pay for therapy ór counselling for the person during the period oftime during which funding may be provided for the person under the prõlram.
Right of recovery
(12) The College is entitled to recover from the member, in a proceeding brought in a court of competent jurisdiction, moneypaid in accordance with this section for an eligible person refeñed to in subsection (4).
29 Subsection 93 (2) of Schedule 2 to the Act is repealed and the following substituted:Same
(2) Every person.who contravenes subsection 35.l (l) or 85.4 (l) is guilty ofan offence and on conviction is liable to a fineof not more than $50,000.
Sexual abuse reporting by facilities(3) Despite subsection (l), every_person who contravenes subsection S5.2 (l) in respect of a matter concerning the sexualabuse ofa patient is guilty ofan offence and on conviction is liable,
(a) in the case of an individual to a fine of not more than $50,000; or
(b) in the case of a corporation to a fine of not more than $200,000.
30 (l) Clauses 94 (1) (h.1) to (h.4) of Schedule 2 to the Act are repealed and the following substituted:(h.1) subject to the regulations made under clauses 43 (l) (p) to (s) ofthe Regulated Health Professions Act, 1991,
(i) respecting the filling of vacancies on the Council or on committees,
(ii) providing for the composition of committees,
(iii) respecting the qualification, selection, ap-pointment and terms of office of members of committees required bysubsection 10 (l) who are not members of the Council,
(iv) prescribing conditions that disquali& committee members from sitting on committees required under subsectionl0 (l) and governing the removal of disqualified committee members;-
(2) Clause 94 (1) (1.2) of Schedule 2 to the Act is repealed and the following substituted:(1.2) Tecifying information as information to be kept in the register for the purposes of paragraph 20 of subse ction 23 (2),
designating information kept in the_.register as public for the purposès of subsectlion 23 (5), and designatìíginformation kept in the register
_as public for the purposes of subsection2: 1S¡ that may be withheld from ttre pu6lic foì
the purposes ofsubsection 23 (6);
3l Subsection 95 (1) of Schedule 2 to the Act is amended by adding the following clause:
(q.1) prescribing the circumstances in respect of which a person's eligibility for funding ceases for the purposes ofsubsection 85.7 (5.2);
25
876Commencement
32 (1) Subject to subsection (2), this Schedule comes into force on the day the Protectíng Patíents Act, 2017 receives
Royal Assent.
(2) The following provisions come into force on a day to be named by proclamation of the Lieutenant Governor:
1. Subsections 5 (1), (2) ¡nd (7).
2. Section 6.
3. Section 7.
4. Section 9.
5. Section 10.
6. Section 12.
7. Section 17.
8. Section 18.
9. Section 22.
10. Section 24.
11. Section 26.
12. Section 27.
13. Section 28.
14. Subsection 30 (1).
15. Section 31.
26
SCHEDULE 6sENroRS ACTTVE LTVING CENTRES ACT,2017
INTSRPRETeTIoN ¡¡Io AINTINISTRATION
Definitions
I In this Act,
"approval" means an approval ofan operator or a program issued under section 4; ("agrément")
"director" means the director appointed under section 2; (,.directeur,,)
"MinisteC' means the Minister Responsible for Seniors Affairs or any other member of the Executive Council to whom theresponsibility for the administration of this Act is assigned under the Executive Council Act;("ministre")
"operator" means a. corporation_ that establishes, -maintains or operates a program, where the corporation is a corporation
without share capital having objects ofa charitable nature,
(a) to which Part III of the Corporøtions Act applies, or
(b) that is incorporated under a general or special Act of the Parliament of Canada; ('þrestataire')
'þrogram" means a program whose purpose is described in subsection 4 (3); ('þrogramme'n)
"regulations" means the regulations made under this Act. ('.règlemenf')
Director
2 ( I ) The Minister shall appoint an individual, in writing, as the director for the purposes of this Act and the regulations fromamong the public_servants who are employed under Part III of the Pubtic Sert¡ice of Ontario Act, 2006 and wño work in theOntario Seniors' Secretariat.
Restrictions on appointment
(2) The Minister may specify, in the appointment, conditions or restrictions to which the appointment is subject.
Delegation of powers and duties
(3) The director may delegate his or her powers or duties under the appointment.
APPRoVALS
Approvals required for grants
3 No operator shall receive a payment under section 8 to establish, maintain or operate a program unless the director hasapproved both the operator and the program.
Issuance of approvals
¿ ( I ) Il order to obtain an aqProval of itself or an approval of a program, an operator shall apply to the director in accordancewith this Act and the regulations and .sh¿ll provide the directoi with the documents and'information specified in theregulations and the other documents and information that the director reasonably requires.
Approval ofoperator(2) The director shall approve an operator that applies for approval if the director is satisfied that the operatorn
(a) is financially capable of establishing, maintaining and operating a program;
(b) will carry on the program under competent management in good faith; and
(c) meets the other criteria, if any, that are prescribed by the regulations.
Approval ofprogram(3) The director shall approve a program ifthe operator ofthe program applies for the approval and ifthe director is satisfiedthat,
(a) the pulpos_e of the program is_ to promote active and healthy living, social engagement and learning for persons whoare primarily seniors by providing them with activities and sèrvicesl and
(b) the program meets the other criteria, if any, that are prescribed by the regulations.
Refusal to approve an operator(4) Sutject to section 5, the director shall refuse to approve an operator if, in the opinion ofthe director, the operator has notcomplied with subsection (l) or the criteria set out iniubsection (2) have not been met.
877
27
878Refusal to approve a program
(5) Subject to section 5, the director shall refuse to approve a program if, in the opinion ofthe director, the operator has not
complieã with subsection (l) or the criteria set out in subsection (3) have not been met.
No hearing required
5 (1) The director is not required to hold an oral hearing or to afford a person an opportunity for a hearing before doing
anything under section 4.
Non-application of Statutory Powers Procedure Act
(2) The Statutory Powers Procedure Act does not apply to anything done by the director under section 4.
Notice of intent to make decision
(3) The director shall not make a decision to refuse to issue an approval to an applicant unless, before doing so, the director,
(a) serves a notice of intent to make the decision on the applicant in accordance with subsection (4);
(b) gives the applicant an opportunity to make written submissions with respect to the proposed decision in accordance
with subsection (5); and
(c) reviews the written submissions, if any, made by the applicant in accordance with subsection (5).
Content of notice of intent
(4) A notice of intent shall,
(a) set out the proposed decision and the reasons for it; and
(b) state that the applicant may provide written submissions to the director in accordance with subsection (5).
Written submissions
(5) An applicant that is served with a notice of intent may provide written submissions to the director with respect_ to any
àátte. sei ärrt in the notice, within 15 days after the day the notice of intent was served on the applicant or within whatever
other period is specified in the notice.
Refusal of approval
6 If the director makes a decision to refuse to issue an approval to an applicant,
(a) the director shall serve the applicant with a notice of decision setting out the decision and the reasons for it; and
(b) the applicant may reapply to the director for approval ifthe applicant satisfies the director that new or other evidence is
available or that material circumstances have changed.
Director's decision final
7 (l) A decision made by the director under section 4 is frnal and not subject to appeal.
No judicial review
(2) Despite any other Act or law, no person may bring an application for judicial review of a decision made by the director
under section 4.
PAYMENT OF GRANTS
Maintenance and operating grants
8 (l) Subject to subsections (3) and (4), the Minister may direct that an amount be paid, out of the money appropriated forthàtþurpoie by the Legislature,'to an approved operator towards the cost of maintaining and operating an approved program.
Amount of payment
(2) The Minister has discretion to determine the amount of the payment.
Contribution if program in a municipality
(3) No payment shall be made to an approved operator with respect to an approved progfam that the operator will maintain
àíO opeiaie in a municipality unless oìè of the lollowing, as the Minister determines,. direct! ?aYment to the operator of a
sum équal to at least the arirount determined in accordãnce with subsection (5) or, if the Minister approves, contributespersonãl property or services that are equivalent in value to at least that amount:
l. The council of any one municipality.
2. The council of any one municipality, together with the councils of one or more contiguous municipalities.
3. The other entities, ifany, that are prescribed.
28
879Contribution if program not in a municipality(4)- No payment shall be made to an apprgv.ed gperator with respect to an approved program that the operator will maintainand operate in a location, other than a municipality, unless the eniities, ifany, ihat are preãcribed,
(a) direct payment to the operator of a sum equal to at least the amount determined in accordance with subsection (5); or(b) if the ìvfinister approves, contribute personal property or services that are equivalent in value to at least the amount
described in clause (a).
Amount of contribution(5) Subject to the regulations, the amount mentioned in subsection (3) or (4) is,
(a) the amount equal to.20 per cent of the net annual cost to the approved operator of maintaining and operating theapproved program, if the operator-was approved on or after Aprìl 1,200b under this Act or lne na"rty peísonsCentres Act, as it read at tåe time of the approval; or
(b) th: amount equal to 20 per.cent_ofthe net annual cost to-the approved operator in the operator's 2007-2008 fiscal yearof majntaining and operating the approved program, if the ãperator was approved bifore April l, 2008 under"theElderþ Persons Centres Acl, as it read at the aimé of the approvàI.
Special grants
9 (l) If the Minister directs that an amount be paid to an approved operator under subsection 8 (l) towards the cost ofmaintaining and operating an approved program, the Ministei-may, in àddition, direct that an amouát be paid, out of themolley appropriated for that purpose by the Legislature, on a one-time basis to the operator towards the cosi of maintainingand operating the program.
No contributions(2) For greater certainty, subsections 8 (3) and (4) do not apply to a payment made under subsection (l).Repayment of grants if approval ceases
10 If an approved operator ceases to meet the criteria for approval set out in subsection 4 (2) or if the program that theoperator,operates ceases to meet the criteria for approval set out in subsection 4 (3), the director may-detãrmine, on areasonable basis, what part of any payment that the operator has received under this Acì is to be repaid to the Crown.
GeNsnetRegulations
11 (l) The Lieutenant Governor in Council may make regulations,
(a) specifying anything that this Act describes as prescribed or specified in the regulations or done by or in accordancewith the regulations;
(b) goveming applications for approvals;
(c) setting a percentage for the purposes of subsection 8 (5) that differs from the one set out in that subsection;
(d) governing how the annual cost mentioned in subsection I (5) is to be determined;
(e) governing repayments described in section 10.
Scope
(2)^A regulation may be general or specific in its application to any person, place or thing or any class of them, may imposedifferent requirements, conditions or restrictions on or in respect ofäny class ãnd may ¡e limite¿äs to time and ptace'.
Classes
(3) A class described in a regulation may be described according to any characteristic or combination of characteristics andmay be described to include or exclude any specified member, whether ór not with the same characteristics.
AMENDMENT To THIs AcT12 Subsection I (5) of this Act is repealed and the following substituted:Amount of contribution(5) Subject to the regulations, the amount mentioned in subsection (3) or (a) is the amount equal to 20 per cent of the netannual cost to the approved operator ofmaintaining and operating the approved program.
CoxsnqunxrrAl AMENDMENTs
29
Not-for-Projit Corporatìons Act, 2 0 I 0
13 (1) Sectio n 222 oI the Not-for-Protìt Corporøtions Act, 2 0 I 0 is repealed.
(2) Subsection (1) applies only if section 222 ol the Not-for-Proftt Corporatíons Act, 2010 does not come into forcebefore subsection (1) comes into force.
Pay Equity Act
14 Clause I (p) under the heading o'Ministry of Community and Social Services" in the Appendix to the Schedule tothe Pøy Equìty lcl is repealed and the following substituted:
(p) operates a program that receives a payment under the Seniors Active Living Centres Act, 2017;
RDrEAL, Coun¡nxcrMENT AND Snonr TrrlnRepeal and revocation
15 (1) The Eldeþ Persons Cenlres Acf is repealed.
(2) Regulation 314 of the Revised Regulations of Ontario, 1990 (General) made under the Elderly Persons Centres Actis revoked.
Commencement
16 (1) Subject to subsection (2), the Act set out in this Schedule comes into force on a day to be named byproclamation of the Lieutenant Governor.
(2) Sections 13 and 14 and subsection 15 (2) come into force on the day subsection 15 (1) comes into force.
Short title
17 The short title of the Act set out in this Schedule is the Seníors Actíve Lìving Centres Act, 2017.
880
Rose Bustria ITEM 5.2Jo-Ann WillsonWednesday, May 31 ,2017 7:32 AMRose BustriaFW: Ontario Strengthens Laws to Prevent SexualAbuse of Patients
881From:Sent:To:Subject:
Patient Relations and Council.
Jo-Ann P. Willson, B.Sc., M.S.W., LL.B.
Registrar and General Counsel
College of Chíropractors of Ontario130 Bloor St, West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected] Site: www.cco.on,ca
CONFIDENTALITY WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copies including
any attachments without reading it or making a copy. Thank you.
From: FHRCO - Beth Ann Kenny [email protected]]Sent: Tuesday, May 30, 20L7 L:27 PM
To: [email protected]; legandpolí[email protected]:'Richard Steinecke'Subject: FW: Ontario Strengthens Laws to Prevent Sexual Abuse of Patients
FYI
Beth Ann Kenny, Executive CoordinatorFederation of Health Regulatory Colleges of Ontario (FHRCOI
301-396 Osborne St, PO Box244, Beaverton ON LOK 140
Email: [email protected]: www.regulatedhealthprofessions.on.caPhone: 4L6-493-4O7 6 / tax: 1-866-814-6456
Confidentiality notice: This emoil, including any attachments, is for the sole use of the intended recipient(s) ond moy conto¡n
pr¡vate,
confidential, and/or privileged informotion. Any unouthorized review, use, disclosure, or distribution is prohibited. lf you are not
the
1
intended recipient or th¡s information has been inappropriotely forworded to you, please contact the sender by reply emai! onddestroyoll copies of the original,
882From: Ontario News [mailto:[email protected]]Sent: May 30,20L7 t:22PMTo: bakenny@regulated healthprofessions.on.caSubject: Ontario Strengthens Laws to Prevent Sexual Abuse of patients
News Re/ease
ontario strenqthens Laws to Prevent sexual Abuse of patients
May 3Q,2017
Protecting Patients Act Ensures Health and Safety of Patients and Families
Ontario has reinforced its zero tolerance policy on the sexualabuse of patients by any regulated healthprofessional, and implemented new programs and policies to keep people healthy.
The province passed the Protecting Patients Act today, which includes legislative amendments to:
Expand the list of acts of sexual abuse that will result in the mandatory revocation of a
regulated health professional's certificate of registration
Remove the ability of a health regulatory college to impose restrictions that would allow a
regulated health professional to continue practisíng on patients of a specific gender
Ensure more timely access to therapy and counselling for patients who make a complaint ofsexualabuse by a regulated health professional to a health regulatory college
Require that more information regarding the current and past conduct of regulated healthprofessionals is available to the public in an easy-to-access and transparent way
lncorporate feedback from stakeholders, including establishing a higher threshold for when
third-party records may be ordered to be produced in discipline hearings involving sexual
abuse.
Additional amendments passed today to help people in Ontario stay healthy and safe include:
lmproving the way immunizations are reported, which will help prevent children from being
suspended from school for required school immunizations
Helping parents make informed decisions about immunizing their children if they are
considering a non-medical exemption
2
a
a
a
a
a
a
a
f*-ú¡--Ontario Newsroom
. lmproving and modernizing Elderly Persons Centres to help seniors stay healthy, active and
engaged
o Making it easier and more convenient for people to receive coverage under the Ontario Drug
Benefit (ODB) Program for prescriptions that are written by nurse practitioners, and in the
future, other authorized prescribers for products such as diabetes testing strips and nutritional
products
o Continuing to ensure that community laboratory services are safe and effective by updating
inspection provisions and streamlining licensing requirements. 883
Ontario is increasing access to care, reducing wait times and improving the patient experience tnrough
its Patients First Action Plan for Health Care and OHIP+: Children and Youth Pharmacare - protecting
health care today and into the future.
QUICK FAGTS
With the passage of the Protecting Patients Act, the government is able to make legislative
amendments to several statutes that will ensure that patients in Ontario are healthy and safe.
Ontario's health care budget will total $53.8 billion in 2017-18 - a 3.8 per cent increase from
the previous year.
As part of the 2017 Budget, Ontario is providing $8 million over the next three years to allow
for an additional 40 new Elderly Persons Centres by 2018-19, to meet the growing needs of
seniors and help support some of Ontario's most vulnerable populations.
BACKGROUND INFORMATION
The Protectinq Patients Act, 2017
a
a
a
a
a
a
ADDITIONAL RESOURCES
Patients First: Action Plan for Health Care
Patients First: Action Plan for Health Care Year Two Results
a
3
Elderlv Persons Centres
a
QUOTES
"Today marks an important milestone for our government. The passage of this legislation
reinforces our commitment to putting patients first and protecting Ontario's health care
system for generations to come. The Protecting Patients Act will help ensure that people inOntario remain healthy and safe."
- Dr. Eric Hoskins, Minister of Health and Long-Term Care
"We commend the government on the passage of the Protecting Patients Act. Thislegislation is an important step in protecting patients and supporting survivors of sexual
abuse. We look fonryard to working with the government to implement recommendations
from To Zero: lndependent Report of the Minister's Task Force on the Prevention of Sexual
Abuse of Patients and the Regulated Health professions Act.,'
- Farrah Khan and Sly Castaldi, co-chairs of Ontario's Roundtabte on Violence AgainstWomen, and Sheila Macdonald, member of Ontario's Task Foree on the Prevention ofSexual Abuse of Patients and the Regulated Heatth professions Act
Questions about your subscription? Contact us.
Edit your subscription preferences.
Unsubscribe from News on Demand.
I ,o,,o* Us on Twitter.
Visit the Newsroom.
Disponible en français.
@ Queen's Printer for Ontario, 2008 - 2017
99 Wellesley Street West 4th floor, Room 4620 Toronto ON M7A 1Al
To Zero: Independent Report of the Minister's Task Force on the Prevention of Sexual Abuse
of Patients and the Requlated Health Professions Act
884
4
5t31t2017 Newsroom : Ontario Strengthens La¡¡s to Prevent Sexual Abuse of Patients
News Release 885
Ontario Strengthens Laws to PreventSexua I Abuse of PatientsProtecting Patients Act Ensures Health and Safety ofPatients and Families
May 30, 2017 1:00 P.M. I Vlinistry of Health and Long-Term Care
Ontario has reinforced its zero tolerance policy on the sexual abuse of patients by
any regulated health professional, and implemented new programs and policies to
keep people healthy.
The province passed the Protecting Patients Act today, which includes legislative
amendments to:
. Expand the list of acts of sexual abuse that will result in the mandatoryrevocation of a regulated health professional's certificate of registration
. Remove the ability of a health regulatory college to impose restrictions
that would allow a regulated health professional to continue practising
on patients of a specific gender
. Ensure more timely access to therapy and counsellin gf or patients who
make a complaint of sexual abuse by a regulated health professionalto
a health regulatory college
. Require that more information regarding the current and past conduct
of regulated health professionals is available to the public in an easy-to-
access and transparent way
. lncorporate feedback from stakeholders, including establishing a higher
threshold for when third-party records may be ordered to be produced
in discipline hearings involving sexual abuse.
Additional amendments passed today to help people in Ontario stay healthy and
safe include:
https://news.ontario.calmohltc/enl21lTtOSlontario-strengthens-laws-toprevent-sexual-abuseof-patients.htnr l?utm-sourcæondemand&utm-medium=email&ut. 'U4
5131t20'17 Newsroom : Ontario Strengthens Laws to prevent Sexual Abuse of pat¡ents
' lmproving the way immunizations are reported, which will help preventchildren from being suspended from school for required schoolimmunizations 886
. Helping parents make informed decisions about immunizing theirchildren if they are considering a non-medical exemption
' lmproving and modernizing Elderly Persons Centres to help seniors stayhealthy, active and engaged
. Making it easier and more convenient for people to receive coverageunder the Ontario Drug Benefit (ODB) Program for prescriptions thatare written by nurse practitioners, and in the future, other authorizedprescribers for products such as diabetes testing strips and nutritionalproducts
' Continuing to ensure that community laboratory services are safe andeffective by updating inspection provisions and streamlining licensingrequirements.
Ontario is increasing access to care, reducing wait times and improving the patientexperiencethrough its Patients First Action Plan for Health Care and OHlp+:Children and Youth Pharmacare - protecting health care today and into thefuture.
Qu ick Facts
. With the passage of the Protecting Patients Act, the government is ableto make legislative amendments to several statutes that will ensure thatpatients in Ontario are healthy and safe.
. ontario's health care budget willtotal $53.8 billion in2017-19 - a 3.gper cent increase from the previous year.
' As part of the 2017 Budget, Ontario is providing $8 million overthe nextthree years to allow for an additional 40 new Elderly Persons Centres by2418-19, to meet the growing needs of seniors and help support someof Ontario's most vulnerable populations.
Background lnformation
. The Protecting Patients Act,2017https://news.ontario'ca/mohltc/enl2O17l05lonta¡io-stren$hens-laws-to-prevent-sexual-abus+of-patients.html?r¡tm source=ondemand&utm_medium=email&ut. 2t4
5t31120',17 Nerrusroorn : Ontario Strengthens Laws to Prevent Sexual Abuse of Patients
Additional Resources
. Patients First: Action Plan for Health Care 887
. Patients First: Action Plan for Health Care Year Two Results
. Elderly Persons Centres
. To Tero: lndependent Report of the Minister's Task Force on thePrevention of Sexual Abuse of Patients and the Regulated Health
Professions Act
Quotes
'Today marks an important milestone for our government. The
passage of this legislation reinforces our commitment to
putting patients first and protecting Ontario's health care
system for generations to come. The Protecting Patients Act will
help ensure that people in Ontario remain healthy and safe."
Dr. Eric HoskinsMínister of Health and Long-Term Care
"We commend the government on the passage of the Protecting Patients Act. This
legislation is an important step in protecting patients and supporting survivors of
sexual abuse. We look forward to working with the government to implement
recommendations from To Zero: lndependent Report of the Minister's Task Force on
the Prevention of SexualAbuse of Patients and the Regulated Health Professions
Act."
Farrah Khan and Sly Castaldi, co-chairs of Ontario's Roundtable on
Violence Against Women
and Sheila Macdonald, member of Ontario's Task Force on the
Prevention of Sexual Abuse of Patients and the Regulated Health
Professions Act
Members ofThunder Bay's Regionàl llealth s(ien(es (entre
Patient and tam¡ly Âdvisory (ouncil are sharing
their ¡rput and ideas to shape the (are ¿nd services
th¿t people receive.
Working with theeHe¿lth (entre ofEx(ellence, patients in
Wateloo can now usean online e+efenal systemto reduce
waittimes by connectinglhem Ìo spec¡àlists ¿nd other
health c¿re servìres in theìr commun¡ty.
ontaf ¡o.ca/pat¡entsf ¡fst
In the Mississauga ll¿lton LHIN, p¿lients ¿re receiving
¿dvift and services from a l0(¡l càre coofdinatol who ìs
helping them (onnect w¡th the c¿re they need. tor ex¿mple,
a pat¡ent le¿ving the hosplt¿l can be conne(ted wìth home
care services, including peßonal support, nußing ¿nd
rehabilit¿tion as àppropriate.
The m¡nislry h¿s comrnìtted t0 the rest0råtion ofthe ment¿l
health un¡tat Laker¡dge Heallh Ajax¿nd Pidering, whi(h
indudes ¿t le¿st20 new mental health inpatient beds.
V¡SION FOR THE FUTURE
"As we reflect on the acconplishments we
have ¿chieved in year two of oùr PûtientsFi,rsL: Action PIan ior Hea,l.th Cdre, ¿'nd
continue to improve the health care system,
we will ensure that patients and theirfamilies have a strong voice and role toplay in health care planning ând services."
-Dr. EricHoskins,
Minister of Health and Long-Term Care
PATIENTS FIRST IN ACT¡ON
As we transform Ontario's health care system, initiatives âre underway across the provincedemonstrating how we are putting patients flrst, such ¿s:
888PAIIEiITS FIRST:Afil0l{ PtAl{ FOR HEATTH CARE
Ye¿r{wo Resulte lApril 2017
MESSAGE FROM THE MINISTER
Our heatth care system belongs to everyone in Ontario. In February 201ã, we larmched ow Po'tiëntsFírst: Action Planfor Health, Care to transform our health care syst€m into one that puts patients
at the centre. lve are working with our partners in health care to make the system more aecessible,
equitable and integrated-
Du¡ing the last two years, we've made great strides to iûrprove the health care experience whiledelivering high quality care for patients, their families and caregivers.
For example:
. 94 per cent of people in Ontario now have a family doctor or other primary healthcare provide¡ and we are recruiting more health care professionals in high-needs andremote communities.
. According to a 2016 Frase¡ Institute report, Ontario h¡s the shorteet wait tines formedical procedures in the country with media¡ wait times more than four weeks lorn¡er
than the r¡ationâl average.
. We ¿re providing rnore hours of care ¿t home including 350,000 more hours of nursingcare, 1.3 million more hours ofpersonal support care, as well as 600,000 more hours of respitesewices for caregivers.
. We a¡e creating a provincial Patient and Farnily Advisory Council to ensure that thevoices ofpatients and caregivers are hea¡d in decisions about the health care system.
As we move forward, we remain committed to focusing on the needs of patients and improvingtheir health cåre experience by working with our health care partners across the system to ensure
that patients have access to the services they need, where and when they need them.
Sincerely,
6:/r.<Dr. Erie Hoskirs, Minister
Catalogue No 025682 |SBN 97&1-4606-9229-5 (PDF) April 2017@Queen3 PrÌnterforontario 2017Þ' ontar¡o
889
lnvest¡ng $12 billion over'10 years ¡n hosp¡tal ¡nfrastructure, with ¿bout 35 major hospit¿l
project5 underc0nstruct¡0n 0r being pl¿nned.
Proy¡ding ¿¡ additional $4E5 million in new fund¡ng h 2016/17t0 support new and redeveloped
hospitals enhance and m¿intain access t0 targeted priority iervi(es su(h ¿s organ ¿nd t¡ssue tr¿nsplants,
improve ð(cess ànd w¿¡t times for òdd¡tion¿l pro(edures such as (¿t¿r¿ct surger¡es, knee and hip
repl¿cements, aswdl ¿s to iupportsmall, nofthern and rural hospit¿ls, spec¡alty mental heàlth hospit¿ls
and t0 ensure the (ont¡nued provision ofservices p¿rticul¿rly in hoipitals experiencing h¡gh growth t0provide better patient¿rcess to high-quality health càre serv¡(es.
f4and¡nga(cesst0 quality(an(er(ðreservices forp¿t¡ents by investing¿n ¿dd¡tion¿l 5130million
overthe nextthreeyeaß;forexample, a new cancer(entre in Waterlo0 regìon, funding t0 rupport¿ new
PET-II sGnner in sudbury and new funding for stem cell research.
txpanding free dental care through Healthy 5m¡les ontar¡o; makìng it e¿sier for m0re thàn
323,000 eligible children and youth Írom low-inromÊ families l0 getfree dental care.
C0ntinuing to ¡mprove¿fford¿b¡lity ¿nd ¿ccess for ¿ssisted reprodudive serv¡(es - including fundingin vitro fertilization (lvt) - through the 0nt¿rio tertility Progr¿m, which has helped more than
6,500 pãt¡ents sin(ethe progr¿m's launch in De(ember 2015.
Passed the Pat¡ents F¡ßt Ad, 2016 th¿t wìll help p¿tients ¿nd theìr fàmil¡es obt¿in better
arcesslo a more lot¿l ¿nd integràled he¿hh care system, improvingthe p¿tientexper¡en(e ¿nd deliyering
higheÊqu¿lity càre.
Insuring lndigen0us people haveaccessto moreculturally approprialec¿re¿nd improved health outcomes
through 0ntafio'r Fkst l{ations Heahh Action Plan, which is support¡ng more d0ct0ß ¿nd other
health professionals ¡r northemfemote lndigenous (omnuo¡ties and ¡mpro'/ing ¿ccess to di¿betes and
h0me ¿nd (ommun¡ty (are iervi(es. lhrough th¡s plðn, 0ntar¡o is ¡0vef¡ng nearly 5222 mìllion in new
fuoding overthree yeaß. plus àn ¿dd¡tìo¡¿l S104.5 million ¿flnually 0fsüfained funding thereafter
Prov¡ding faster¡((ess to mentãl he.lth and addictions se¡vices by ¡nvesting in:
- 1,150 additional supportive hous¡ng un¡ts to reduce the risk of homelessness,
' Structured psy<hothelapy th¿t will help thousands of people learn stràtegiÊj to ¡mprove
theirmental heàlth ¿nd be more successful ¡n the¡rd¿ily lives.
' Up to nine youth servi(e hubs where y0ung people aged 12 t0 25 cn rece¡ve walk-in,
one-stop ac(ess to serv¡(es.
lmproving the quality of life for long-tem care home res¡dents by frengthening Ont¿rio's
quality¿nds¿fety inspect¡0n program by ¡mplementing enf0rcementtooh-indudìng Ínanriål pen¿lties
- to eniureall longlerm c¿re home operators address concerns promptly.
@
$75m
3,000
Moving fonrard with lmmun¡zat¡on 2020, Ont¿rio's five-ye¿rstràtegy to improve itr publi(ly funded
immunizàtion progr¿m, by offer¡ng:
' Theshingles vaccine free of chalgeto senloß between ó5 ¿nd 70.
' The Human Pal¡llomavir¡s (HPV) vaccine to boys as well as g¡rls in Gr¿de 7 to protect
more peoplefrom flPv-rel¿ted cancers and diseases.
(ontinuing to support children's health and well-being through the Healthy l(¡ds Community
thallengewìth programs in 45 commuRitiesth¿ten(ourage healthy e¡ting ¿nd physic¿j ¿(t¡vity.
Helping people qu¡lsmok¡ng through ¿ 55 mill¡on invefmentfrom t0bà((o t¿x revenues f0r:
' tree Niotine Replacement Therapy for patients being distharged from hospitah.
' 15 lndigenous (ommunities to develop new cess¿tion progr¿ms ¿nd enhance existing servies.
' Extra rupport ¡n (ommunit¡es uyith h¡ghersmoking rates ¿nd ¡n hospit¿ls that serve
pr¡ority popul¿tioûs.
opening the Pat¡€nt 0mbudsman office to help patients, former patients ¿nd câreg¡vers who
have an unresolved compl¿inlàb0ut thei0r their loved onel care¿t ð hospital, long-tefm care h0me or
[ommunity Care Ac(ess Centre.
lntrodu(ing leg¡sl¿t¡on th¿t v{ould strengthen measures to preventand respond to thesexualabuse ofpatients by any regulated he¿lth profess¡onal.
Passedthe HealthlnfoÌmation ProtectionA(tto help betterprotectthe personål health inform¿tion
0fp¿t¡ents¿ndensureth¿tont¿rlo m¿intains lts poslti0n ¿s¿ lÊ¿derin he¿lth ¡nform¿tion priv¿ry pr0teit¡on.
Passeda new QualityofCare lnformôtion ProtectionAdt0 help ensuretr¿05paren(y forpatients
and theirf¿milies during the ¡nvestig¿t¡on 0f(ritic¿l ¡n(idents.
lmplementing a comprehens¡ve opioid str¿tegyto prevent opio¡d addiction and overdose
inaluding the ¿ppo¡ntment 0f 0ntario'i i ßt-ever Prov¡ nci¿l Overdose (o-0 rdinato r a nd expanding atces
l0 nðloxone overdose medication free ofcharge for elig¡ble ont¿r¡ans.
o@
ln(feased bf eastfeed¡ng supports,indüding a 2417 breastfeeding
telephone servicq, and lo<al
programs for mothers.
Reducing the financial burdenon pat¡ents and th€irloved ones by
capping hospital pa*ing fees and
offering dis(ounted parking passes.
Pharmacists can now administervaccines for an additional
13preventable diseases - including
common travel va((inet - making iteasierand more convenient fol people
in 0ntario to ptotedthemselvesat home and abroad.
of tlnir lives by investing
Requir¡ng regulated food serv¡cepremises w¡th 20 or more locations inontar¡o to display calor¡es on menus
forstandard food items - helping(oîsumers make better-informed
choices when choosing whatto eat¿nd feed thekfam¡l¡es.
rú
È
$130
for up to 2m new hospice bed¡ in 54 more
commünities a('06s OnÞrio, while providing
continued funding for existing hospice beds.
Home and communig-based palliative
and end-of-life ca¡e for
lnvesting in
17chronic pain clinics ensuring
that pat¡ents re(eive t¡rnelyandappropr¡ate (aÌe.
Savings on prescription drugsfor approximately
30,ooomore sen¡orsannuallt through the0ntario Drug BenefitProgr¿m -
saving each ofthem approx¡mately
more pðt¡eîts afiojs 0ntario.
Redeveloping more than 3Q000 long-temorc beds in3(l0lonçtem (are homes by2025.
h
"*u"n$54mtop,ovidebehaviounl suppors for older adults livingwith dementia orognitive impairmenÈ.
peryeaf,
5t31t20',t7 Newsroom : Ontario to Provide Free Prescription Drugs for Children and Youth
News Release 890
O nta rio to P rovid e Free P rescriptio n D rugsfor Children and YouthProvince lntroduces a Balanced Budget for a Stronger,Healthier Ontario
April27,2017 4:0O P.M. I Ministry of Finance
Today, Finance Minister Charles Sousa released the 2017 Ontario Budget: A
Stronger, Heolthier Ontorio, which includes significant investments in health care
and education. Ontario's first balanced budget since the global recession -- thanks to
a strong economy and responsible fiscal management -- introduces free prescription
drug coverage for everyone aged 24 and under, makes important investments to
reduce wait times and improve access to care, helps students and makes life more
affordable for Ontario families.
As a leader in economic growth, the Province is set to balance the budget this year
and maintain a balanced budget for the next two years. A balanced budget means
more funding for the programs and services people rely on most.
Strengthening Ontario's Health Care
The balanced 2017 Budget launches OHIP+: Children and Youth Pharmacare, a new
drug benefit program that fully covers the cost of prescription medications for
everyone aged 24 and under, regardless of family income. This program -- the first of
its kind in Canada -- will ensure that young adults have access to universal drug
coverage and parents never have to choose between paying for their children's
prescription drugs and providing other essentials.
Ontario is increasing health care investments by $1 1.5 billion over the next three
years. The 2017 balanced Budget plan includes a new $7-billion booster shot to
health care, building on the commitment made in the 2016 Budget. This investment
will improve access to care, expand mental health and addiction services, and
enhance the experience and recovery of patients. lt includes $1.3 billion to further
reduce wait times.
https://news.ontario.calmoflenl2}lTl%lonlario-to-provid+fræprescription-drugs-for-children-and-youth.html 1t5
5131120'17 Newsroom : Ontario to Provide Free Prescription Drugs for Children and youth
With the balanced 2017 Budget, Ontario is committing to several new major hospitalprojects across the province, adding to the 34 underway.An additional $9-bíllíoncapital investment over 10 years will provide faster access to care and help to meetthe needs of the growing aging population. gg lThe Province is expanding home and community care programs, including homenursing, personal support and physiotherapy services, with an additional investmentof $250 million this year. Family and friends caring for loved ones will be bettersupported through access to respite care, education and traíning, and a new OntarioCaregiver Tax Credít.
Ontario's new Dementia Strategy will improve and better coordinate services forthose living with dementia and their caregivers by providing more than $100 míllionover three years.This will include funding to expand provincewide access tocommunity programs and other investments to enhance access to care, informationand support when a diagnosis is made.
lmproving Education
With an additional investment of $6.4 billion over three years, the balan ced 2017Budget reflects the government's commítment to help learners reach their fullpotential by supporting them from full-day kindergarten to postsecondary educationand beyond.
The Province continues to construct new schools and renew existing ones to createnurturing envíronments where children can learn and grow. The Province is
providing almost $16 billion over 10 years to help build and improve schools.
The government is rolling out the new Ontario Student Assistance Program, whichmeans free tuition for more than 2i 0,000 students in postsecondary educationstarting thís fall.
Creating Opportu n ities
Ontario's new Career Kick-Start Strategy will provide nearly $190 million over threeyears to create 40,000 new work-related opportunities for students and recentgraduates to give them the experience they need to help land a good job.
With the balanced 2017 Budget, Ontario is ensuring it remains at the forefront ofresearch and development in transformative technologies that will lead tomorrow'sgrowth. ln doing so, Ontario's new investments in artificial intelligence, fifth-
https://naivs.ontario.calmollenl2}lTl%lonlarielo-provide-fr+prescription-drugs-for-children-and-youth.html z5
St31t2O'17 Newsroom : Ontario to Provide Free Prescription Drugs for Children and Youth
generation wireless technology, advanced computing, autonomous vehicles and
quantum technologies will make the province's economy more innovative and create
more well-paying jobs.
Making Lire More Affordable 892
To make everyday life more affordable, the balanced 2017 Budget is strengthening
the public services that matter most to people while lowering costs.
The Province is helping 100,000 more children get affordable, quality licensed child
care. ln 201 7-18, Ontario will support child care for 24,AA0 more children up to four
years old through new fee subsidy spaces and support for new licensed child care
spaces in schools. The government will continue to work with schools and
municipalities to fund the expansion of school-, community- and home-based
licensed care that is convenient, flexible and in line with parents' needs.
The government is also taking action to make housing more affordable for
homebuyers and renters with Ontario's Fair Housing Plan. This plan introduces a
comprehensive package of measures to help more people find affordable homes, as
well as increase supply, protect buyers and renters, and bring stability to the real
estate market.
These proposed measures include a new non-resident speculation tax of 15 per cent
on the price of homes in the Greater Golden Horseshoe purchased by non-Canadian
citizens, non-permanent residents and non-Canadian corporatíons buying properties
that contain at least one and not more than six single-family residences.
The plan also proposes to expand rent control to all private rental units -- including
those built after 1991 -- and to empower Toronto and potentially other municipalities
to introduce a tax on vacant homes to encourage owners to sell or rent them.
The government is committed to lowering household electricity bills by 25 per cent,
on average, beginning this summer, and to holding rate increases over the next four
years to inflation. ln addition, the government is also proposing to lower energy
costs by expanding access to natural gas to communities that do not currently have
service, including rural, northern Ontario and First Nation communities.
The government is delivering on its commitment to balance the budget this year,
building on a successful track record of prudent fiscal management, which has made
Ontario an economic leader in Canada and the world.
https://news.ontario.catmoflent2}lT/04/ontariotoprovidefreeprescription-drugs-for-children-and-youth.htrnl 3/5
513112017 Newsroom : Ontario to Provide Free Prescription Drugs for Children and youth
Quick Facts893
' The Province's investment ¡n public infrastructure of more than $190billion over a 1 3-year period, which started in 2014-15, is the largestinfrastructure investment in the province's history. lt is supportingprojects such as building child care spaces, schools, hospitals, publictransit, highways and roads.
. over the last three years, ontario's real GDp growth has outpaced thatof all G7 countries. Exports and business investments are increasing,household incomes are rising and the unemployment rate continues todecline - and has been below the national average for 24 consecutivemonths.
. Employment in 2017 is forecast to increase by r.3 per cent, or 94,000net new jobs, following 1.1 per cent growth in 2016. These gains areexpected to continue at 1.1 per cent annually, on average, from 2o1g-20. This would result in 900,000 net new jobs created between 2010 and2020, the majority in industries that pay above-average wages, in theprivate sector and in full-time positions.
Additional Resources
. Read the full 2017 Ontario Budget
. Read the Budget Speech
. Read the 2017 Budget in Brief
. Path to a Balanced Budget
. Helping You and Your Family
. Strengthening Health Care
. lmproving Education
. Creating Opportunity and Security
. lnfrastructure and Housing
Quotes
https://news.ontario.ca/mof/en/2O17l04/ontariotoprovid+freeprescription-drugs-for-children-and-youth.html 4t5

5t3112017
Charles Sousa
Minister of Finance
Newsroom : Ontario to Provide Free Prescription Drugs for Children and Youth
"A balanced budget is more than just the bottom line number.
It's about finding new ways to help you and your family. lt's
about creating opportunities and providing the supports people
need to succeed. This balanced budget is dedicated toproviding young people with free prescription medications,
providing free tuition and helping businesses grow. We are
delivering on our commitment to ensure that everyone has
equal opportunities for success."
894
https://news.ontario.calmof/en/2O17l0¿Vontariotoprovide-fræprescription-drugs-for-children-and-youth.html 5/5
5t3112017 Neru¡sroom :The Protecting Patients Act, 2017
Backgrounder 895The Protecting Patients Act, 2017
May 30, 2017 1:00 P.M. Ministry of Health and Long-Term Care
The Pr.otecting Patients Act supports Ontario's Patients First: Action Plan for
Health Care and ensures that patients in Ontario remain healthy and safe.
Regulated Health Professions Act
Ontario has strengthened its zero tolerance policy on patient sexual abuse by any
regulated health professional.
Acts of professional misconduct involving the sexual abuse of a patient are always
unacceptable. The relationship between a patient and their regulated health
professional must be built upon a foundation of trust, confidence and safety.
The act strengthens the prevention of, and response to, incidents of patient sexual
abuse, increases supports for victims of sexual abuse by regulated health
professionals and improves regulatory oversight and accountability of health
regulatory colleges. Specifically, the act will:
. Expand the list of acts that would result in the mandatory revocation ofa regulated health professional's certificate of registration
. Remove the ability of a college to impose gender-based restrictíons on a
regulated health professional's certificate of registration
. lncrease fines for health professionals and organizations that fail to
report an allegation of patient sexual abuse to a college
. lncrease the required information that colleges must post on theirpublic registers
. Establish a minimum time period of one year after the end of a patient-
professional relationship during which activities of a sexual nature
between professionals and former patients are prohib¡ted
https://news.ontario.calmohltc/enl2017l}5lth*protecting.patients-act-2017.htm1 1t3
513112017 Ner¡¡sroom : The protecting patients lr}t,2}17
. Ensure more tímely access to funding for patient therapy andcounselling in relation to sexual abuse by a regulated healthprofessional.
896lmmunization of School pupils Amendment Act
There are some immunízations that chíldren are required to receive in order toattend school to protect themselves, as well as the other children at their school,against certain vaccine-preventable diseases. Ontario will support parents who areseeking to exempt their children from these immunizations to make informed andevidence-based decisions. The act will requíre parents to complete an educationsession before they submit a request to exempt their child from requiredimmunizations for non-medical reasons.
ln addition, ontario wíll also help parents by improving the way immunizations arereported. Currently, parents and guardians are responsible for reporting thevaccines that their child has received to their local public health unit. Thegovernment will now require doctors and other health care providers whoadminister vaccines that are needed to attend school in Ontarío to report vaccinesthat they administer to children and youth directly to their local public health unít.
Seniors Active Living Centres Act
Ontario is modernizing the Elderly Persons Centres network across the province, tohelp seniors stay healthy, active and engaged. These Centres support more than100,000 seniors per year with social and recreational activities ranging from fitnessand cooking classes, to Meals-on-Wheels, falls prevention classes and transportationservices.
Modernizing the legislation will give Centres more flexibility to be more responsive tocommuníty needs and to strengthen the services they offer. Modernized legislationwill also encourage them to act as community hubs that provide a central accesspoint for a range of health, social and cultural services.
Ontario Drug Benefit Act
Ontario wilf make it easier for people to receive coverage for certain prescriptionsthat are written by nurse practitioners, and in the future, other authorizedprescribers.
https://narvs.ontario.calmohltc/en/2O17lOsithe-protectingFpatients-act-2017.htm1213
5lg1t2117 Nervr¡sroom : The Protecting Patients Act, 2017
The province is amending the Ontario Drug Benefit Act to allow products such as
diabetes testing strips and nutritional products prescribed by nurse practitioners,
and in the future, other authorized prescribers, to be reimbursed under the Ontario
Drug Benefit (oDB) Program. 897The amendments will also enable nurse practitioners, and in the future, other
authorized prescribers, to submit a funding application to the Ministry of Health and
Long-Term Care for drug products for specific ODB recipients under the Exceptional
Access Program (EAP), which facilitates patient access to drugs not listed on the ODB
Formulary/Comparative Drug lndex, or where no listed alternative is available.
Laboratory and Specimen Collection Centre Licensing Act; Health lnsurance Act;
and Public Hospitals Act
To support modernization of the community laboratory sector, amendments to the
Laboratory and Specimen Collection Centre Licensing Act and the Health lnsurance
Act will give the ministry more flexibility in regulating and funding the community
laboratory sector.
Amendments to the Public Hospitals Act will allow for hospitals to be designated to
provide community laboratory services in addition to the laboratory services they
currently provide to admitted ín-patients and registered out-patients.
https://news.ontario.calmohltc/en/2017l05ith+protecting'patients-act-2017.hhm! 3l/3

St3l,t2}17 Minister's Task Force on the Prevention of Sexual Abuse of Patients and the Regulated Health Professions Act, 1991 - Public lnformation - MOHLTC
ÞO*rio . nrr"' tt***."rr,MrN'srRYoF HEALTH AND LONG-TERM CARE
<http : / /www. health.aov.on.ca / en/ >898
Minister's Task Force on the Prevention of SexualAbuse of Patients and the Regulated Health ProfessionsAct, 1991
Ontario is taking concrete act¡on to uphold and reinforce a zero tolerance policy on sexual abuse of patients by any
regulated heath professional.
As part of the Ontario overnment's commitment to Prevent and better respond to the sexual abuse of pat¡ents,
a report titled To Zero: IndependentPatients and the Reoulated Healthe government's actions are based on the
task force's recommendations from this report.
Resources
a To Zero: Independent Report of the Minister's Task Force on the Prevent¡on of Sexuâl Abuse of Patients and
the Regulated Health Professions Act. 1991ThttoJ/**i.h.atth.aov.olia/en/càmmoin/n'¡i¡'tistr:t/oub!¡cat¡ons/reoorts/sexual health/taskforce prevention of sexual abu:
[PDF Version | 8.44 Mb]
To Zero: Independent RepoÉ of the Min¡ster's Task Force on the Prevention of Sexual Abuse of Patients
and ahe Reoulated Health profess¡ons Act. 1991 - Append¡x B: Recommendations7äl1Twiw.heali:i,oov.on.ca/en/comnon/min¡strv/publications/reports/sexual health/default.aspx>
News Release - ontario Takino Action to Prevent sexual Abuse of Patients<htto: // news.onta rio.ca/m/4 J736>
For More Information
Call Serviceontãr¡o, INFOI¡ne at:1-866-532-3 16 1 (Toll-free)In Toronto, (416) 314-5518TTY 1-800-387-5559.In Toronto, ITY 416-327'42A2Hours of operation : Monday to Friday, 8:30am - 5:00pm
http://www.health. gov.on.calen/publ i c/program s/sexual healttt/ 1t2

511t2017 For Bad Backs, lt May Be Time to Rethink Biases Abotf Chiropractors - The Neur York Times
ITEM 6.1
Aaron E. Carroll
THE NEW HEALTH CARE MAY', zorT
About two of every three people wiìl probably experience significant low back pain at
some point. A physician like me might suggest any number of potential treatments
and therapies. But one I never considered was a referral for spinal manipulation.
It appears I may have been mistaken. For initial treatment of lower back pain, itmay be time for me (and other physicians) to rethink our biases.
Spinal manipulation - along with other less traditional therapies like heat,
meditation and acupuncture - seems to be as effective as many other more medical
therapies we prescribe, and as safe, if not safer.
Most back pain resolves over time, so interventions that focus on relief of
symptoms and allow the body to heal are ideal. Many of these can be
nonpharmacological in nature, Iike the work done by chiropractors or physical
therapists.
Physicians are traditionally wary of spinal manipulation (applying pressure on bones
and joints), in part because the practitioners are often not doctors and also because a
few chiropractors have claimed they can address conditions that have little to do
with the spine. Patients with back pain haven't seemed as skeptical. A large survey of
929
glte Nctu Snrk@imer https:i/nyti.ms/2pmtucx
The Upshot
For Bad Backs, It May Be Time to RethinkBiases About Chiropractors
hþs:i/www.nytimes.com/2017105/01/upshoVfor-badbacks-its-timetorethink-biases-about-chiropractors.html 114
5t'U2017 For Bad Backs, lt May Be Time to Rethink Biases Abor¡t Chiropractors - The Neriv York Times
them from 2oo2 through 2oo8 found that more than 3o percent sought chiropracticcare, significantly more than those who sought massage, acupuncture orhomeopathy. 930
Researchers have been looking at the evidence supporting spinal manipulationfor some time. Almost gS years ago, a systematic review evaluated the available
research, most of which was judged to be low in quality, and found that there mightbe some short-term benefits from the procedure. Two reviews from 2oo3 agreed forthe most patr, finding that spinal manipulation worked better than a "sham
procedure", or placebo, but no better or worse than other options.
Almost a decade later, a Cochrane review assessed the literature once more, andfound 12 new trials had been conducted. This review was more damning. It foundthat spinal manipulation was no better than sham interventions.
But since then, data have accumulated, as more higher-quality studies have
been performed. Recentþ, in The Journal of the American Medical Association,researchers looked for new studies since 2011, as well as those that had beenperformed before.
The evidence from r5 randomized controlled trials, which included more thant,7oo patients, showed that spinal manipulation caused an improvement in pain ofabout ro points on a loo-point scale. The evidence from tz randomized controlledtrials - which overlapped, but not completely with the other trials - of almost t,4oopatients showed that spinal manipulation also resulted in improvements in ftinction.
In February, in Annals of Internal Medicine, another systematic review ofnonpharmacologic therapies generally agreed with the other recent trials. Based
upon this review, and other evidence, the American College of Physicians released
new clinical practice guidelines for the noninvasive treatment of subacute back painThey recommended that patients should try heat, massage, acupuncture or spinalmanipulation as first-line therapies.
The only things that might detract from the use of spinal manipulation in thissituation would be its cost and potential harms.
htþs:/Á¡truw.nytimes.com/2017105/0'1/upshoVfor-baûbacks-its-tim+terethink-biases-about-chiropractors.html 214
5t',U2017 For Bad Backs, lt May Be Time to Rethink Biases About Chiropractors - The New York Times
931Because they fear those potential harms, some physicians are hesitant to rerer'
patients to chiropractors or physical therapists for care. But in all the studies
summarized above, there were really no serious adverse events reported. It's
possible to find anecdotes of harm to the spinal cord from improper manipulations,
but these are rare, and almost never involve the lower spine.
Some physicians are concerned about the cost of spinal manipulation, especially
since most insurance carriers don't cover it. Visiting a chiropractor costs more than
taking many non-narcotic pain medications. But more invasive interventions can
cost a lot of money. In addition, studies have shown that, in general, users of
complementary and alternative medicine spend less over all for back pain than users
of only traditional medicine.
Medication and surgery can also lead to harms. We shouldn't forget that
prescription pain medications, Iike opioids, can lead to huge costs, especially when
they're misused.
Some physicians are uncomfortable that we don't have a clear picture of how
spinal manipulation actually works to reduce pain. It's also possible that some
chiropractors do it "better" than others, and we can't tell. This concern should be
tempered by the fact that we don't have a great understanding of why many other
therapies work either. Some of the more traditional things we recommend don't
even work consistentþ.
Still, there is no merit to many other claims about spinal manipulation - that ithas been proved to work for things like infantile colic, painful periods, asthma,
gastrointestinal problems, and more. For most conditions, the therapy lacks a good
evidence base.
But given the natural course of back pain - that most of it goes away no matter
what you do - the ideal approach is to treat the symptoms and let the body heal.
Noninvasive therapies seem to do that well enough.
A¿rron E. Carroil is a prot'essor of pediatrics at Indiana UniversitySchool of Medicine u,Ìro blogs on health research ancl policy ¿rt The
htþs://www.nytimes.com/2017105/01/upshoVfor-ba*backs-its{im+torethink-biases-abouþchiropractors.html 3t4
51112017 For Bad Backs, lt May Be Time to Rethink Biases About Chiropractors - The Ner¡¡ York Times
Incidental Economist and makes videos at Healthcare Triage. Follolr'hinr on Tl\ritter at @aaronecarroll. W2The Upshot provides news, analysis and graphics about politics, policyand everyday life. Follow us on Facebook and Twitter. Sign up for ournewsletter.
@ 2017 The New York Tmes Company
https:/Árrtww.nytimes.com2017105/01/upshotlfor-baúbacks-its{imetorethink-biases-about-chiropractors.html 414
ITEM 6.2Rose Bustria
From:Sent:To:Subject:
Jo-Ann WillsonWednesday,May 24,2017 2:14 AMRose BustriaFW: Circulation of Proposed Changes for 2017-2018 Fees
933
Council.
Jo-Ann P. Willson, B.Sc., M,S.W., LL.B.Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected] Site: www.cco.on.ca
CONFIDENTALITY WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copies including
any attachments without reading it or making a copy. Thank you.
From: College of Dental Technologists of Ontario [[email protected]] on behalf ofCollege of Dental Technologists of Ontario [email protected]]Sent: Tuesday, May 23,2017 3:35 PM
To: Jo-Ann WillsonSubject: Circulation of Proposed Changes for 2017-2018 Fees
Proposed Changes for 2017-2018 Fees
View this email in vour browser
Col,lege of Dental Technologists of OntarioOrclre cies Tecl.nologues Dentaire:s cle ['Ontario
PROPOSED CHANGES FOR 2017-2018 FEES
1
The College is seel<ing feedback on a draft amendment to Schedule 5 to the
College By-Laws, Fees, that would see an average increase of 2.4% for all
applicable fees that a Member or person shall pay ro rhe College. This
increase would bring the fee that a dental technologist pays to renew their
General Certificate of Registration from $ I ,520 to g I ,556.
934
BACKGROUND
Annually the college reviews the currency, quality, and transparency of its
Programs and services in place for the Public, Members and Prospective Members
and recommends operational improvements to achieve Council approved strategic
priorities, Ministry of Health and Long-Term Care (MoHLTc) directives, and
service level enhancements. To the extent possible the funding for these
improvements comes from cost savings due to operational efficiencies, favourable
contract negotiations and reallocat¡on of approved existing budget dollars. Any
shortfall in funding to support day to day operations is recovered through
justifiable fee increases.
Each year each fee described in the By-Laws is increased by the percentage
increase in the Consumer Price lndex (CPl) for goods and services in Canada as
published by Statics Canada. Any fee increase above the CPI increase is circulated
to Members and Stakeholders for feedback.
2017 -2018 PROPOSED FEES :
The proposed fee increases have been reviewed by the Executive Committee and
are now being circulated to Members and Stakeholders for comment for a period
2
of sixty days. To comment on the proposed changes, please send an email to the
College at [email protected] on or before the deadline: Tuesday, July 18, 2017.
Schedule 5 to the By-laws can be accessed by clicking this LINK. 935
Judith (Judy) M. Rigby, CPA, CGA
Registrar and GEO
Phone:416438 5003
Copyright A 2U7 The College of Ðental Technologists of Ontario, AII rights reserved.
CDTO Stakeholder
Our mailing address is:The College of Dental Technologists of Ontario
2100 Ellesmere Road
Toronto, ON M1H 387Canada
Add us to your address book
unsubscribe from this list update subscription oreferences
3
512612017 The College of Dental Technologists of Ontario: Frequently Asked Questions
936FAQs CON'
OffDRE ÛES TECHNOLOGUES DENTAIRES DE L'ONTARIO
:: About the College
i¡ Regulations & Guide
!r StandardsofPractice
ir Publications
!¡ Registration
i: Complaints & Discipline
ir Qualitl Assur'ànce
i:' Patient Relations
,
1.
¡
CONSULTATION ON FEES FOR 2017.2018
What's New H
Council Meeting:January 14,2011
Les réunions au Conseil:Le 14 janvier 2011
"--
PROPOSED CHANGES FOR 20I7-20I8 FEES
READ N{ORE
The Colleee is seekins feedback on a draft amendment. to Schedule 5 to the College By-Laws, Fees, that would see anaverase inãrease of 2.'4% for all applicable fees that a Member or Þerson shall pay lo die Collese. This increase wouldbring"rhe fee rhar a denral techndlbgist pays to renew the¡r Genei-al Certificat'e óf Registration"from $1,520 to $1,556.
BACKGROUND
Annually the College reviews the currency, qualiry, and transparency of ics programs and servíces in place for che PublicMembers and Prospective Members and recommends operational improvements to achieve Council approved strategicÞriorities, Ministrybf Health and Lonq-Term Care (MOHLTC) direcdves, and service level enhancemencs. To the exterbossible the fundihg for these imÞrovéments comei from cost savings due to operational efficiencies, favourable concrachegoriacions and re"allocation of åppro¡ed existing budger dollars. A"ny shorcfalf in funding to supporc day to dayoperatrons rs recovered through lustrlrable lee rncreases.
Member Self-SerPublic Register
!4.T
com
iÕNS ACT 1991 to
ctísing inOntario.
The College is a regulatorydy establíshed under the
REGULATtD.ItALTH
COLLEGE OF DENTAL TECHNOLOGISTS OF ONTARIO
hþ://cdto. calfee_consul tati on.aspx 1t3
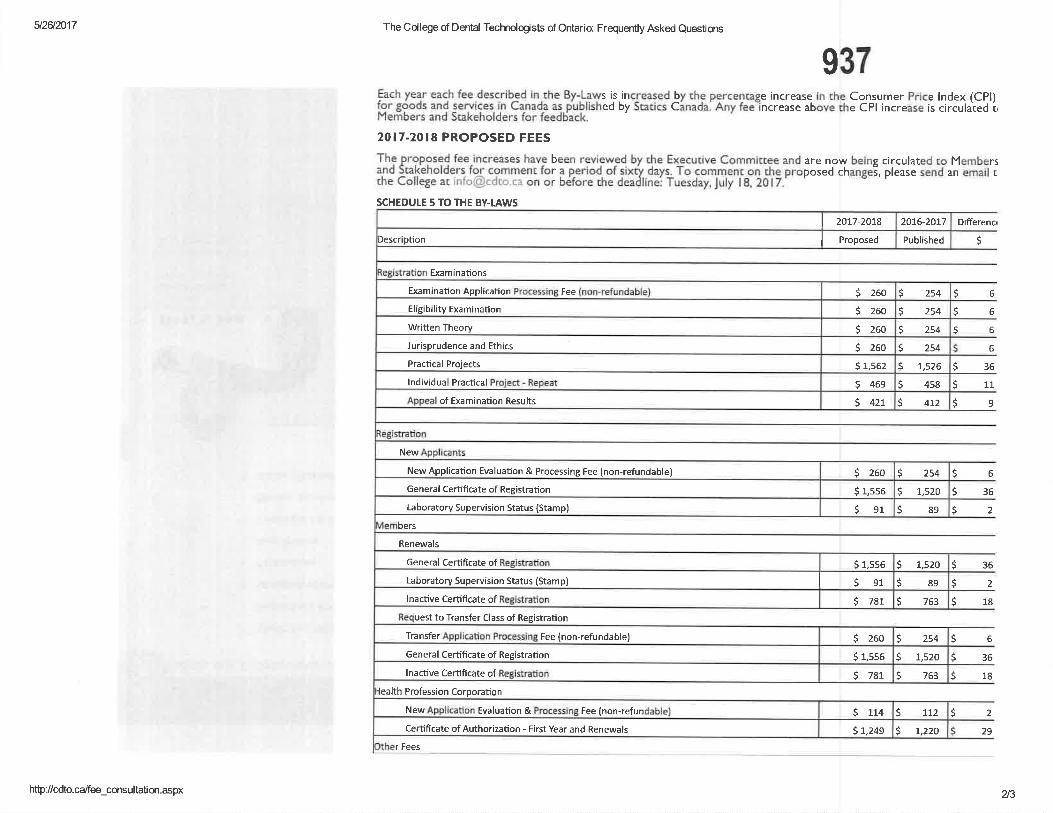
(Ðñ@
(omæ
oNN
(omN
æ
lUt
ø
@óN
roC
rl(o
@(o
(oro
d
øltl
coçN.EGxr
ooô
-È
2eô-=
r oE
Ug
+E
vir È
!x=
oq
+E
E
55'ü
9-P
si E
fi+
fr sË
qb giù
¡-c iô-
=.-ru
äåiU
o¡ -oã
Ëi
ð:-a.=(J
üq-.-o
L o:{ñ
(Ëô-
Ëo
roQ
)6 F
LLd
ãO-
EE
õcñ
sË
g:R(Ë
c, çô
-!
oJ =
-@L9
tsg-l,)-
:ceâ
,Yq->
ã¿
vE:t
Áì
q¡ çlc€
ÈÞ
àu^q
à'ri iP
g
is ïå!
g,ä àà*
C >
\ -.4
0J'--O
X
øE
îx X
t:>
-c .:!
eã.e
à.9 g,
"*I gffi
H(Ë
õ -o!L
ÈaO
1^
"'OO
-þ: u¡ ;:
-'=
FX
uJ !E
õ-oã.È
t! -o-
8ur n
úÊq g
;:ü ú. ph€ 3€s+
I Ë;ó å
-üÈÈ
ö si€ ï*Ë
i É riË
Þ
qr (!ã co
2YaJ
râ
k€r ã Ëþö -'
90(, N
iJã;
l
ËË
$ ì ËïE
t
l\aoct)
øø
oo4
coooqo.9ooÀ
qog'Eoo&,oG(JocßFoof,
Iooc@@¡
3oz
ØcôFEføRvØco)rl!.Þ(ItcobøU
'
BõoPEc)oo0)Ðo=oC
)ct-ct--
xcrØ(õio(t= o5orlp(goct!,oäc
t-oõt(oôt6
NoN(ooN
Eo.9!o
+nN\tnN
+nNsf6N
(oñulæn$
Nsf<
tN
oNrno00
ø
oNhoæ
ó6È<
t6N
ONhd4
(orN
Ø
oNN
o@No(oNØ
\oNø
o@NN@h
o@<f
Itr
N<f
ooN@hh
do(oúød
æoNÈÈON
t¡J
oooèço
goß.9oçaEou ooq
ço€çÈa4Ës.go
o5¡-coF=
.usUEñocot5d'-=
@Þ'
4oIßa
rFoÀGJp!s
!foú,goGçÈoqo
o= o@qocoo4üc.GooÀdçoFeõucoo.9oo3q)
=]
oFo,9b¡oÉ,ooortrEoU6oco('
aEo5oo.øCJ
looo¡oJ
oooE(J(J6otro(9
oo.Ëoc.9.9UoIooo¡oJ
dæÈo€No¡o!çfocooog
ooGçEoC)oGc
oqßl--
(on6çg'ú0e,ooGEoU6oço(J
coçocoouo¿oçoJ6uoaooEoUoFaç
3oz3!oo
æF.
ÉO
lstN!o= ocoú.!cño*iIço6Nooo6gEo(J
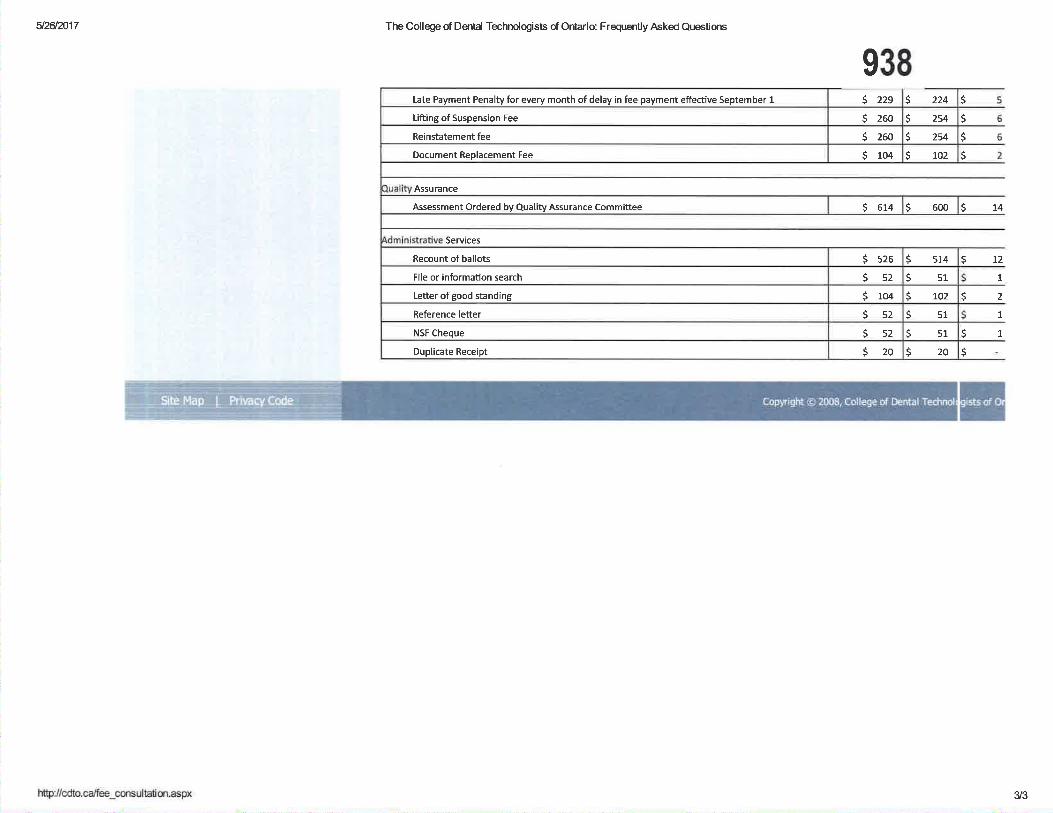
512612017 The College of Dental Technologists of Ontario: Frequently Asked Questions
Assurance
Services
938s
s
s
S14
s
t2s
1
2
IL
s
s
s
s 224
s 2s4
S zsq
S 102
S 600
S sr¿
SsrS 102
Ssrss1s20
Seu
S szs
5szS 104
$szss2520
s 229
s 260
5 zoo
S 104
Duplicate Rece¡pt
Late Payment Penalty for every month of delay in fee payment effective September 1
Lifting of Suspension Fee
Reinstatement fee
Document Replacement Fee
Assessment Ordered by Quality Assurance Committee
Recount of ballots
File or information search
Letter of good standinE
Reference letter
NSF Cheque
@
3/3
ITEM 6.3Rose Bustria
From:Sent:To:Subject:
Jo-Ann WillsonFriday, June 02, 2017 11:37 AMRose BustriaFW: iNformeD Newsletter Spring 2017
939
Council.Jo-Ann P, Willson, B.Sc., M,S.W., LL.B.Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : jpwillson@cco,on,caWeb Site: www,cco,on.ca
CONFIDENTALITY WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copies includingany attachments without readÍng it or making a copy. Thank you.
From: College of Naturopaths [email protected]]Sent: Friday, June 02, 2017 10:40 AM
To: Jo-Ann WillsonSubject: iNformeD Newsletter Spring 2017
Click here to view this online I Please add our email address to your contacts
lNformeD News¡etterSpri ng 2017
1
Read the latest issue here. 940
Feature articles include:
Council election resu/fs & Committee appointmenfs
September 30 CE reporting deadline
Delegations, referrals, consu ltations and assignments of care
New grads working for a College Member
Practising without reg istration
Discipline decision
Registration process overuiew
and more....
ls there something you'd like to see in a future issue of iNformeD?Please let us know.
Gollege of Naturopaths of OntarioT: 416-583-60f 0 | F: 416-583-6011 | info(ôcolleqeofnaturopaths.on.ca
150 John St., 1Oth Floor Toronto ON MSV 3E3
E DO NOT UNSUBSCRI BE IF YO U ARE A MEM BER oF TH E COLLEGE. tf members unsubscribe,wil be contacted by staff to re-subscribe as the Col lege pnmarily commun icates to members vta email
strive to keep communications relevant and to a m tn imum nformation regardi ng registration mattersual renewa dead ne, qual ity assurance requ irements etc. ), and important news and upd ates are
assumption rmun icated vi email The Co lege works on the that al members receive and revtew a il of ou
2
941The College of Naturopaths of Ontario
Appointment of Margot White
(Toronto, ON) - The College of Naturopaths of Ontario is pleased to announce the appointmentof Margot White as Director of Gommunications and Lead of Community Engagement.
Margot joins the College with over 20 years' experience in the private, public and non-profitsectors. She recently relocated to Toronto from Vancouver, where she led majorcommunications initiatives with Doctors of BC (BC MedicalAssoc.), the Canadian BarAssociation and other member service and regulatory organizations. Margot also spent sixyears with the College of Dental Surgeons of BC as Director of Communications and PolicyDevelopment and was part of the team that led their transition to regulation under the HealthProfessions Act.
"l am delighted to welcome Margot to our team. Her extensive experience and collaborativestyle represent important assets, particularly as we move forward with our communications,community engagement and educational initiatives to reinforce our role as a regulator working inthe public interest", said Andrew Parr, Registrar and CEO.
Margot will take a leadership role in moving fonrvard the College's communications orientedstrategic i nitiatives.
"l am excited about creating impactful communications strategies and programs that support alllevels of the organization, including a strong focus on community engagement and education,"said Margot.
She can be reached by email or by phone at 416-583-6012.
The College of Naturopaths of Ontario rs esfab/ished under provincial legislation and regulatesnaturopathic doctors in the public interest. To fulfill its mandate, the College establishes andmaintains standards of practice, ensures individuals wishing to enter into practice meet therequirements, operates a quality assurance program to ensure members maintain theircompetency and holds the profession accountable through the complaints and disciplineprocesses.
For more information, please contact:
Margot WhiteDirector of CommunicationsCollege of Naturopaths of OntarioPhone: 416.583.6012E-mail: [email protected]
May 1 5,2017
150 John St., 1O'h Floor, Toronto, ON MsV 383
T 416.583.6010 F 416.583.6011
Rose Bustria ITEM 6.4
Jo-Ann WillsonWednesday, April 19, 2017 5:00 PMRose BustriaFW: NPs can now prescribe controlled substances
From:Sent:To:Subject: 942
Exec and Council
Jo-Ann P. Willson, B.Sc., M.S.W., LL.B.
Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext. 111Fax: (416) 925-9610E-mail : [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited, If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copies including
any attachments without reading it or making a copy. Thank you'
From: The College of Nurses of Ontario [[email protected]]Sent: Wednesday, April 19, 20L7 4:22PMTo: Jo-Ann WíllsonSubject: NPs can now prescribe controlled substances
NPs can now prescribe controlled substances
CoLI.EGE OF NURSESor ONrlnrooRDRE ors rNHR¡¡tÈn¡sET INFIRMIERS DE gONTARIO
View Online
NPs can now prescr¡be controlledsubstances
On April 19,2017, the Ontario government approved changes toregulations under the Nursing Act, 1991. With this change, Ontario NPswho have successfully completed approved controlled substanceseducation can now prescribe controlled substances.
NPs who have not completed this education are not authorized toprescribe controlled substances. Their profile on Frnd a Nurse willstate: "Entitled to practise with restrictions. This member cannotprescribe controlled substances. They have not completed theeducation needed to do so."
ln additional to the education requirement and information posted onFind a Nurse, the College is implementing the following mechanismswith the public's interest in mind:
1

a 943A revised Nurse Pracflfioner practice standard that andincludes new content related to controlled substances andsets out expectations for NP practice in Ontario. For example,NPs are accountable for "informing clients of the unique risksassociated with medication misuse, addiction and diversion,and provide them with education and strategies for mitigatingrisk."Evidence-informed resources on the College's website tosupport clinical decision-making. This includes links tonational guidelines and documents developed by expertorganizations including Health Canada and other regulators.As part of the Quality Assurance program's continuingcompetence requirements Íor 2017, NPs are required toidentiff a learning goal and activities related to controlledsubstances, relevant to their role and setting.New national entry-to-practice competencies for NPs, whichintegrate content related to controlled substances, will takeeffect in January 2018. For example, one competency statesthat NPs must "apply strategies to reduce risk of harminvolving controlled substances, including medication misuse,addiction, and diversion." Entry{o-practice competencies areused to develop curriculum and exam content. Thev've beenreleased earlv to give stakeholders time to prefrre andintegrate them. ln the next couple of years, controlledsubstances content will be integrated into entry requirements.Once that happens, applicants will only be able to register withthe College as NPs when they have acquired competenciesrelated to controlled substances.
Privacv PolicyCollege Of Nurses Of Ontario | 101 Davenport Road I Toronto I ON I
MsR 3P1 | Canada
a
a
a
2
CANAD¡ANNURSESASSOCIATION
944-
Canadian Nurse Practitioner
Gore Gompetency
Framework
945
This document has been developed collaborarively by the canadian Nurses Association andrcpresentatives of the provincial/territorial regulatory organizations, with assist¿nce from
Canadat Testing Compan¡ Assessment Scrategies Inc.
All rights reservcd. No part of this document may be reproduced, srored in a retrieval system,or transcribed, in any form or by any means, electronic, mechanical, photocopying, recording,
or otherwise, without written permission of the publisher.
@ Cânadian Nurses Association
50 Driveway
Ottawa, ON K2P 182
Tel.: 613-237 -2133 or l -80O-361 -8404
Fax: 613-237-3520
cna-aiic.ca
May 2010
ISBN 978-r-55 I t9-329-8
946
TABTE OT GONTENTS
Preface
Acknowledgements .
Introduction
Purpose of the Framework .
ProÊle of the Nurse Practitioner
Overview of Comperencies .
Assumptions
Competer-rcies
l. Professional Role, Responsibiliry and Accountability .
2. Health Assessment and Diagnosis
3. Therapeutic Management
4. Health Promotion and Prevention of Illness and Injury
Glossary oITerms
Bibliography
Appendix A: Represenratives and Facilitators .
3
4
5
5
5
6
7
8
8
11
l2r3
L4
L9
2l
CANADIAN NURSES ASSOCIATION cna-ai¡c.cA
947
PREFACE
The respective execurive directors ofthe registered nursing regulatory bodies in Canada requested the
Canadian Nurses Association and Canadat Testing Compan¡ Assessment Strategies Inc., to facilitace
the update and revision of the core entry-level competencies for nurse practitioner practice in Canada.
Through a series of teleconferences, electronic communications, subgroup work and one face-to-face
meeting, rhe Canadian Nurse Practitioner Cow Competency Frameworþ (2010) was completed.
the Canadian Nurse Practitioner Core Competency Frømework (2010) was developed for use by
participating jurisdicrions. Each regulatory body may adopt this document or publish the entry-level
competencies approved in accordance with their context, policies and requirements. Anyone seeking
information about rhe nurse practitioner competencies that are in effect in a particular province or
territory is advised to contact the applicable regulatory body.
This framework defines rhe core competencies required for safe, competent and erhical nurse Practitioner
pracrice. The core competencies are transferable across diverse practice settings and client populations.
As a result, rhe framework is fundamental to all nr¡rse practitioner practice in Canada.
The firsr Canadian Nurse Practitioner Core Cotnpetency Frameworh, published in 2005, was developed in
collaboration with rhe Canadian jurisdictions through the support of the Canadian Nurse Practitioner
Initiative.r This document updates and replaces the 2005 publication.
The framework was revised using a consensus-building approach involving provincial/territorial nursing
regulators and expert nurse practitioners ¿cross Canada.2 The collaborative approach used to revise the
document promotes consistency of registration requirements across the country' facilitating compliance
with the Agreement on Internal Tiade.s
Nurse practitioner practice is clynamic, and the competencies will change over time in response to
population health needs, evolving practice and health-care environments. Hence, this document
will be reviewed at least once every five years to ensure that it keeps pace with chan¡Jes in nurse
practitioner practice.
llrc -{iiiL.ììln0iJ rteiJi,ii (,j-1 ttí ill:: '¡t;r:t' l! :i)ltl:t)lt')! rrìlj il (lirlri:ì(la
' il;:-:l;i :n tL¡,:l:::':.
3CANADIAN NURSES ASSOCIATION CNA-AiiC.CA
948ACKN OWLED G EM ENTS
Appreciation and thanks are extended to the regulatory aurhoriries, the Canadian Nurse Practitioner CoreCompetency Committee (see Appendix A), the Regisrered Nurses' Association of Ontario, and nursepractitioners across Canadawho participated in rhe development of this documenr. In particular, therevision of the framework was made possible by the collaborarive efforrs of the following organizations:
' Association of Registered Nurses of Newfoundland and Lalrraclor (ARNNL)
. Association of Regisrered Nurses of Prince Edward Island (ARNpEI)
. College of Registered Nurses of Nova Scotia (CRNNS)
' Nurses Association of New Brunswick / fusociation des infirmières et inÊrmiers du NouveauBrunswick (NANB)
. College of Nurses of Ontario (CNO)
. College of Registered Nurses of Manitoba (CRNM)
. Saskatchewan Registered Nurses' Associarion (SRNA)
. College and Association of Registered Nurses ofÁlberta (CARNA)
. College of Registered Nurses of British Columbia (CRNBC)
' Registerecl Nurses Association of the Northwest Terrirories and Nunavut (RNANT/NU)
. Yukon Registered Nurses Association (YRNA)
4 CANADIAN NURSE PRACTITIONER CORE COMPETENCY FFAMEWORK
949
INTRODUCTION
Purpose of the Framework
The Canadian Nurse Practitioner Core Competency Framework (2010) can be either adopted as is or
modified by regularory bodies to suit the particular context of each body. Nursing regulatory bodies
may use this document alone or in combination with additional provincial/territorial nurse practitioner
documents to support regulatory processes such as:
. reviewing and approving/recognizing nurse practitioner education Progralns;
. developing/approving regulatory examinations for nurse practitioner registration;
. assessing individual nurse practitioners for initial competence when applying for registration; and
. assessing continuing competence and providing for ongoing registration of nurse practitioners.
The competency sraremenrs describe the integrated knowledge, skills, judgment and attributes thac
guide nurse practirioner practice. Safe, competent, ethical nurse practitioner practice requires the
integration and performance of many competencies simultaneously. This document may be used by nurse
pracririoners ro srlpporr their self-reflection, selÊevaluation and continuing comPetence, as well as to
educate others about their role. Nurse practitioner educators may use it for curriculum development. And
it is a useful resource for helping others - including government agencies, employers, health providers and
the public - to understand what they can expect of nurse practitioners.
Profile of the Nurse Practitioner
Nurse practitioners, âs autonomous health professionals with advanced education, provide essential health
services grounded in professional, ethical and legal standards. Nurse practitioners integrate their in-depth
knowledge of advanced nursing practice and theor¡ health management, health promotion, disease/injury
prevenrion, and orher relevant biomedical and psychosocial cheories to provide comprehensive health
services. Nurse practirioners work in collaboration with their clients and other health-care providers in the
provision of high-quality pacient-centred care. They work with diverse client populations in a variety of
contexts and practice settings.
CANADIAN NUHSES ASSOCIATION cna.ai iC.CA
950Nurse practitioners have the competence to provide comprehensive health assessmenr, to diagnose health/illness condition's, ancl to treat and manage acute and chronic illness within a holistic model of care.
Nurse practitioners order and interpret screening and diagnostic tesrs, perform procedures and prescribemedications, while integrating the principles of resource allocation and cost-effecriveness, in accordancewith federal, provincial and territorial legislation and policy.
Nurse practitioners are accountable for their own practice and communicate wirh clients about heakhassessment Êndings and diagnoses, further required testìng and referral to orher health-care professionals;they are also responsible for client follow-up. Nurse practitioners counsel clients on symptommanagement, health maintenance, pharmacotherap¡ alternative therapies, rehabilitation strategies andother health programs.
Nurse practitioners have the knowledge to assess populacion health trends and parterns and to designservices that promote healthy living. They provide leadership in the developmenr, implementationand evaluation of strategies to promote health and prevenr illness and injur¡ and they work withinterprofessional teams, other health-care providers and secto¡s and community members. Nursepractitioners collaborate in che development of policy to influence healrh services and healthypublic policy.
0verview of Competenc¡es
Nurse practitioner competencies reflect advanced nursing practice by building and expandingupon rhe competencies required of a registered nurse. This document expands on the competenciesdefined in Aduønced Nursing Practice: A National Frameworþa as rhese comperencies apply ro nursepractitioners. The co¡e competencies in this framework are organized inro four categories:
. Professional Role, Responsibiliry and Accountability;
. Health Assessmenr and Diagnosis;
. Therapeuric Management; and
. Health Promotion and Prevention of Illness and Injury.
The competencies were developed according to certain assumptions and terms; thus, interpretarionof the competencies requires an understanding of the assumprions and the key terms found in theglossary of terms.
' Canacll:ì \lIlsíls A:rsoci.iltor,. 2009
o CANADIAN NURSE PRACTITIONER CORE COMPETENCY FRAMEWORK
951
ASSUMPTIONS
Familiariry with rhe âssumprions used to develop the core competencies is e.ssential to the understanding
of how these competencies may be applied to the nurse practitioner practice in all roles and settings, not
only those specific to a parricular clienr population or pracrice environment.
In developing rhe core competencies listed in this document, the following assumPtions were made:
1. The practice of nurse pracririoners is grounded in the values, knowledge and theories of
professional nursing practice.
Z. Nurse practitioner core competencies build and expand Lrpon the competencies required of a
registered nurse.
3. Nurse practitioner core competencies require additional nursing education, usually achieved at
the graduate level, with a substantial clinical component.
4, Nurse practitioner core competencies are the foundation for all areas of nurse Practitioner
pracrice, ancl are applicable across diverse practice settings and client populations.
S. Nurse praccitioner core competencies are an essential element of nurse Practitioner
competence assessment.
G. Nurse practitioner practice is grounded in the Êve SØorld Health Organization (\fHO)
principles of primary health care: accessibiliry public participation, health promotion,
appropriate technology and intersectoral collaboration.
7. Nurse pracririon€rs provide services relating to health promotion' illness and injury
prevenrion, rehabilitarive care, curâtive and supportive care, and palliative/end-oÊlife care.
L The identifìed core competencies incorporate the competencies identified for advanced nursing
pracrice and specifically address the activities that are includecl in the legislated scope of
pracrice of nurse prâcririoners (e.g., health assessment, diagnosis of acute and chronic illnesses
and their therapeutic management).
g. Nurse practitioners work in collaboration with other health-care providers to provide safe,
high-qualiry health-care services.
iO. Newly graduated nurse practitioners gain proÊciency in the breadth and depth of their Practice
over rime, with support from employers, mentors and health-care team members.
CANADIAN NURSES ASSOCIATION CNA-AiiC.CA
COMPETENGIES952
1. Professional Role, Responsibility and Accountability
This nurse practicioner competency category encompasses the core comperencies for the followingfour categories of advanced nursing practice: clinical praccice; collaboration, consultation andreferral; research; and leadership.t Nurse practitioner practice is characrerized by the simulraneousinteraction and blending of competencies at a level of complexity thar reflects the nursepracticionert highly developed critical rhinking skills, clinical nursing experience, and advancededucation that incorporares a subsrantial clinical component.
The competencies listed below are fundamental to advanced nursing pracrice and are integrated, intothe practice of nurse practitioners. Therefore, the competencies listed in rhis category also apply toeach of the three other competency categories in rhis framework: Health Assessmenr and. Diagnosis,Therapeutic Management, and Health Promotion and Prevention of Illness ancl Injury.
Glinical Practice
The nurse pracririoner:
1.1 Practises in accordance with federal and provincial/territorial legislation, professional andethical standards, and policy relevanr ro nurse practirioner practice.
1'2 Understands the changes in scope of practice from rhat of a regisrered nurse and the ways thatthese changes afFect responsibilities and accountabiliries when assuming rhe reservecl title andscope ofpractice ofa nurse practitioner.
1'3 Incorporates knowledge of diversit¡ cultural safety and determinants of health in theassessment, diagnosis and therapeutic management of clients and in the evaluationof outcomes.
1'4 Incorporates knowledge of developmental and life stages, pathophysiology, psychoparhology,epidemiology, enviroumental exposure, infectious diseases, behavioural sciences, demographicsand family processes when performing health assessmenrs, making diagnoses and providingoverall therapeutic managemenr.
:' Cirl¡\. -;iijv.;¡rcca r)t.tísrt(l at.:t,-i;:í:): /\ t.:în¡v! lra::tt)¡¡.t;,!, À,llnôij 2i'li)il
8 CANADIAN NURSE PRACTITIONËR CORE COMPETENCY FFAMEWORK
9531.5 Incorporates knowledge of the clinical manifestations of normal health events, âcute illness/
injuries, chronic diseases, comorbidities and emergency health needs, including the effects of' multiple etiologies in rhe assessment, diagnosis and therapeutic management of clients and in the
evaluation of outcomes.
1.G Integrates rhe principles of resource allocation and cost-effectiveness into clinical decision-making.
1.7 Provides client diagnostic information and education that are relevant, theory-based and evidence-
informed, using appropriate teaching/learning strategies.
i.g Promores safe clienr care by mitigating harm and addressing immediate risks for clients and others
affected by adverse events and near misses.
l.g Discloses the facts of adverse events to clients, and reports adverse events to appropriate
aurhoriries, in keeping with relevant legisladon and organizational policies.
l.l0 Documents clinical data, assessment Êndings, diagnoses, plans of care, therapeutic interventions,
client responses and clinical rationale in a timely and accurate manner.
l.1l Adheres to federal and provincial/territorial legislacion, policies and standards related to
privacy, documentarion and informarion management (this applies to verbal, written or
electronic records).
1.12 Engages in ongoing professional development and accepts personal responsibiliry for
maintaining nurse practitioner competence.
Collahoration, Gonsultation and ReÍerral
The nurse practitioner:
1.13 Consults with and/or refers clients to other health-care providers at any point in the care
continuum when the client's condition is not within the nurse practitioner scope of practice
or the individual nurse practitioner's competence.
1.14 Acts as a consultant to and/or refers and accepts referrals from health-care providers, communiry
agencies and allied non-health-care professionals.
f.1S Advocares for clients in relation to therapeutic intervention, health-care access' the health-care
system and policy decisions that affect health and qualiry oflife.
1.16 Collaborates with members of the health-care team to provide and promote interprofessional
client-centred care at the individual, organizational and systems levels.
1.17 Collaborates with members of the health-care team to promote and guide continuous qualiry
improvemenr initiarives at the individual, organizational and systems levels.
l.lB Applies advanced knowledge and skills in communication, negotiation, coalition building,
change managemenr and conflict-resolution, including the ability to analyze, manage and
negoriare conflict.
ICANADIAN NURSES ASSOCIATION CNA-AiiC.CA
Besearch
The nurse practitioncr: 9541.19 Engages in evidence-informed practice by critically appraising and applying relevant research,
best practice guidelines and theorywhen providing health-care services.
1.20 Develops, utilizes and evaluates processes within the practice setring to ensure rhat clientsreceive coordinated health services rhat idenri$r clienr outcomes and contribute to knowledgedevelopment.
1'21 Identifies and implements research-based innovarions for improving client care ar the individual,organizational and systems levels.
1'22 ldentifies, collects data on, and evaluates the ourcomes of, nurse practitioner pracrice for clientsand the healrh-care sysrem.
1.23 Collaborates with other members of the heahh-care ream or rhe communiry to identi$r research
opportuniries and to conduct and/or supporr research.
t.24 Acts as a change agent through knowledge translation and disseminarion of new knowledge thatmay include formal presentations, publication, informal discussions and rhe development of bestpracrice guidelines and policies.
Leadership
The nurse practitioner:
1.25 Provides leadership in the management of clinical care and is a resource person, educarorand role model.
1.26 Acts as a Preceptot mentor ¿nd coach to nursing colleagues, other members of the health-careteam and srudents.
1.21 Articulates and promotes the role of the nurse pracririoner to clients, other health-care providers,social and public service secrors, rhe public, legislators and policy-makers.
1'28 Provides leadership in the development and integration of rhe nurse practitioner role within thehealth-care system.
1'29 Advocates for and participates in creating an organizational envi¡onment that supporrs safe clientcare, collaborative practice and professional growth.
f .30 Guides, initiates and provides leadership in the development and implementation of standards,
practice guidelines, qualiry assurance, and education and research initiatives.
1.31 Guides, initiates and provides leadership in policy-related activiries to influence pracrice, heahhservices and public policy.
10 CANADIAN NURSE PRACTITIONÊR CORF COMPETENCY FRAMEWORK
2. Health Assessment and Diagnosis
The nurse practitioner integrates a broad knowledge base with cridcal appraisal to obtain the required
information for determining diagnoses and client needs. Throughout the process, the nurse practitioner
works collaboratively with clienrs co identify and mitigate health risks, promote understanding of
health issues and support healthy behaviours.
The nurse practitioner:
2,1 Performs a focused health assessment and/or an advanced comprehensive health assessment,
using and adapting assessment tools and techniques based on client needs and relevance to client
stage oflife.
2.2 Performs a complete or focused health history appropriate to the clientt situation, including
physical, psychosocial, emotional, ethnic, cultural and spiritual dimensions of health.
2.g Performs a complere or focused physical examination, and idendfies and interprets normal and
abnormal ñndings as appropriate to client presentation.
2.4 Synthesizes heakh assessment informacion using critical inquiry and clinical reasoning to
diagnose health risks and states ofhealth/illness.
2.5 Formulates differential diagnoses through the integration of client information and evidence-
informed practice.
2.6 Anticipates and diagnoses emergent, urgent and life-threatening situations.
2.7 Orders and/or performs screening and diagnostic investigations, interprets results using
evidence-informed clinical reasoning and critical inquiry, and assumes responsibility for
follow-up.
2.g Diagnoses diseases, disorders, injuries and conditions, and identiÊes health needs, while
considering the clientt response to the health/illness experience.
z.g Communicates with clients about health assessment findings and/or diagnosis, including
outcomes and prognosis.
955
CANADIAN NUBSES ASSOCIATION CNA-AiiC.CA 11
3. TherapeuticManagement 956Nurse practitioners collaborate with clients to set priorities for the provision and overall coordinationof care along the health/illness continuum. The nurse practitioner selects appropriare inrervenrionsfrom a range of non-pharmacological and pharmacological intervenrions to assist clienrs in restoringor maintaining functional, physiological and mental stabiliry ro achieve oprimal health.
The nurse practitioner:
3.1 Creates an environment in which effective communication of diagnostic and therapeuticintervention can take place.
3.2 Explores therapeutic options, considering implications for clients through the inregration ofclient informarion and evidence-informed practice.
3.3 Determines care options and initiates therapeutic inrerventions in collaboration with clienrs,while considering client perspecrives, feasibiliry and best ourcomes.
3.4 Initiates inte¡ventions for the purpose of stabilizing clients in emergenr, urgenr and life-threatening situarions.
3.5 Supports, educates, coaches and counsels clients regarding diagnoses, prognoses and self-management, including their personal responses to diseases, disorders, conditions, injuries,risk factors, lifesryle changes and therapeutic inrerventions.
3.6 Promotes client selÊefficacy in navigating rhe health-care sysrem and in identifying and
accessing the necessary resources.
3.7 Coordinates and facilitates client care with other health-care providers, agencies andcommunity resources.
3.8 Performs invasive/non-invasive procedures for the clinical managemenr and/o¡ prevention ofdisease, injuries, disorders or conditions.
3'9 Prescribes pharmacotherapy based on the clienr's healrh histor¡ disease, disorder, conditionand stage of life, and individual circumsrances.
3'10 Applies knowledge of pharmacotherapy and evidence-informed pracrice in prescribing,
monitoring and dispensing drugs.6
3.11 Counsels clients on medication therapy, benefirs, potendal side effecrs, interactions, importanceof compliance and recommended follow-up.
3'12 Demonstrates awareness oÇ and is mindful of, marketing strategies used to promote heakhproducts, medical devices, medications, alternarive therapies and healrh programs.
rn (lal::rl¡
12 CANADIAN NURSE PRACTITIONER CORE COMPETENCY FRAMEWORK
9573.13 Intervenes, as appropriate, when potential or actual problematic substance use and/or fitrsuo-
of drugs, including complementary and alternative therapies, is identified.
3.14 Prescribes and/or dispenses drugs in accordance with provincial, territorial and/or federal
standards and legisladve requirements.
3.15 Uses an evidence-informed approach in the selection or consideration of complementary and
alternative therapies, and considers the benefits and risks to clients' health and safety.
3.16 Collaborares with clients in monitoring their response to th€rapeutic interventions and in
adjusting interventions, as needed.
g,17 Monirors, evaluates and revises the plan of care and therapeutic intervencion based on current
evidence-informed practice and on client goals, preferences, health status and outcomes.
4. Health Promotion and Prevention of lllness and lniury
Nurse practirioners in all practice settings focus on improving and restoring health. The nurse
practitioner leads or collaborates with other health-care team members, other sectors and/or the
communiry in initiatives that promote health and reduce the risk of complications, illness and injury
for their individual clients, client groups and/or the population as a whole.
The nurse practitioner:
4.1 Assesses, identifies and critically analyzes information from a variety of sources to determine
clienr and/or population rrends and patterns that have health implications.
4.2 Initiates or participates in the development of strategies to address identiÊed client and/or
population health implications.
4.3 Initiaces or participares in the design of services/interventions for health promodon, health
prorecrion, and the prevention of injur¡ illness, disease and complications.
4.4 Initiares or parricipates in the development and implementation of evaluation Processes,
including identificadon of indicators for ongoing monitoring of stracegies, services and
interventions.
CANADIAN NURSES ASSOCIATION CN A-A iiC,CA 1â
958
GTOSSARY OF TERMS
Accountability
The obligation to answerforthe professional, ethical and legal responsibilities of one'sactivities and duties.
Advanced nursíng practíce
An umbrella term describing an advanced level of clinical nursing practice that maximizesthe use of graduate educational preparation; in-depth nursing knowledge; and expertise inmeet¡ng the health needs of individuals, families, groups, communities and populations. ltinvolves analyzing and synthesizing knowledge; understanding, interpreting and applyingnursing theory and research; and developing and advancing nursing knowledge and theprofession as a whole.
Adverse event
An event that results in unintended harm to the patient and is related to the care and/orservice provided to the patient rather than the patient's underlying condition.
Advocate
Actively supporting a right and good cause; supporting others in speaking for themselves;or speaking on behalf of those who cannot speak for themselves.
At.tributes
Characteristic qualities that include, but are not limited to, att¡tudes, values and beliefs.
Client
The beneficiary of care; may be an individual, family, group, population or entire community.
14 CANADIAN NURSE PRACTITIONER CORE COMPETËNCY FRAMEWORK
959Collaboratíon
Client care involving joint communication and decision-making processes among the client,
nurse practitioner and other members of a health-care team who work together to use their
individual and shared knowledge and skills to provide optimum client-centred care.The health-
care team works with clients toward the achievement of identified health outcomes, while
respecting the unique qualities and abilities of each member of the group or team.
Collaborate
Building consensus and working together on common goals, processes and outcomes
Competence
The integrated knowledge, skills, judgment and attributes required of a registered nurse to
practise safely and ethically in a designated role and setting.
Competencies
The specific knowledge, skills and personal attributes required for a nurse practitioner to
practise safely and ethically in a designated role and setting.
Complementary and alternative therapies
Those modalities or interventions that complemenl mainstream medicine, that are used to
address clients' health needs across the continuum of health care, and that are not met by
conventional approaches. Complementary therapies tend to be those that are used alongside
traditional health care, while alternative therapies tend to be those used in place of traditional
health care.
Consultation
Seeking the advice of others who have the required expertise
Critícal appra¡sal
The process of systematically examining research evidence to assess its validity, reliability,
results and relevance before using it to make an informed decision. lt is an essential part of
evidence-informed practice.
CANADIAN NURSES ASSOCIATION 15
cutturat sarety 960Addresses power relationships between the service provider and the people who use theservice. A manner that affirms, responds to and fosters the cultural expression of clients.This usually requires nurses to have undertaken a process of reflection on their own culturalidentity and to have learned to practise in a way that affirms the culture of clients and nursesUnsafe cultural practice is any action that demeans, diminishes or disempowers the culturalidentity and well-being of people.
Determinants of health
Definable entities that are associated with or induce health outcomes.These entities includehealth behaviours, lifestyles, coping abilities, biology, gender and genetics, income and socialstatus, culture, education, employment and working conditions, access to appropriate healthservices, and the physical environment.
Disease and injury prevention
Measures taken both to prevent the occurrence of disease and injury, such as risk-factorreduction, and to arrest the progress and reduce the consequences of disease or injuryonce established.
Diversity
The variation between people with respect to such factors as ethnicity, national origin, race,gender, ability, age, physical characteristics, religion, values, beliefs, sexual orientation, socio-economic class or life experiences.
Ev i d e n ce- i nfo rm ed p ra cti ce
An approach to decision-making in which the clinician conscientiously integrates criticallyappraised evidence, clinical practice experience, and knowledge of contextual factors in
consultation with the patient, in order to decide upon the option that best suits the patient'sneeds. Evidence may include, but is not limited to, published research, grey literatureresearch, clinical practice guidelines, consensus statements, clinical experts, qualityassurance and patient safety data.
Health
A state of complete physical, mental lspirituall and social well-being, and not merely theabsence of disease.T
'. Wor.l.i Health Organtzatton def inition oT health. Fror¡ the Prearrble t,) the Constjtut'on of the \,Vorl.l Health Orq¿nizalon as âdopted iry thelnlerrratronal Health ConTetence, frlev':York, June lg-22, 1946; siqnerJ on July 22. 1946. by the represenrarives of 6j ståtes {offici¿l recordsol the \Â/orl¿j Health OrEanization, no. 2, D. 100) and eniere.l ín¡o torce on April 7, 1948.
lb CANADIAN NURSE PRACÍITIONER CORE COMPETENCY FRAMEWORK
961Health promotion
The process of enabling people to increase control over and improve their health. lt embraces
actions directed not only at strengthening the skills and capabilities of individuals, but also at
changing social, environmental, political and economic conditions to alleviate their impact on
public and individual health.
Health protection
Activities in food hygiene, water purification, environmental sanitation, drug safety and other
areas that, as far as possible, eliminate the risk of adverse consequences to health that are
attributable to environmental hazards.
I nterp rofessi o n a I c a re
The provision of comprehensive health service to patients by multiple health caregivers who
work collaboratively to deliver quality care within and across settings.
Near miss
An event with the potential for harm that did not result in harm because it did not reach the
client due to timely intervention or good fortune (sometimes called a close call).
Pharmacotherapy
Treatment and prevention of diseases, disorders and/or symptoms by means of drug therapy.
This includes consideration of the characteristic interactions of a drug with the body in terms
of absorption, distribution, metabolism and excretion, and the interactions that may occur
between drugs.
Population health
Entails understanding the health of populations and the factors that influence health and
health risks.
Problematic substance use
The use of a substance that negatively affects a person's work or personal life (e.9., relationships,
financial situation, problems with the law). ln some individuals, it can develop into chemical
dependency and/or addiction.
Referral
The practice of requesting a consultation or service from another health-care provider on behalf
of a client.
17CANADIAN NURSES ASSOCIATION
Safe client care 962Reduction or mitigation of unsafe acts within the health-care system, as well as through theuse of best practices, shown to lead to optimal patient outcomes.
Scope of practice
The activities that nurses are educated and authorized to perform, as established throughlegislated definitions of nursing practice, complemented by standards, guidelines and policypositions issued by professional nursing bodies.
Standard
An authoritative statement that describes the required behaviour of every nurse and is usedto evaluate individual performance.
Th era peutic m a nagem ent
The pharmaceuticals, non-pharmaceuticals, therapies and interventions that nursepractitioners prescribe to provide health promotion and protection; disease prevention;and treatment of diseases, injuries, illnesses and conditions.
18 CANADIAN NURSE PRACTITIONER COFE COMPETENCY FRAMEWORK

963
BIBLIOGRAPHY
Baker, G. R., et al. (2007).Appendix B: Reuiew of prouincial, tenitorial øndfederal hgisktion and policy
related to the reporting and reuiew ofaduerse euents in heølthcare in Canada. Canadian Patient Safery
Insritute. Retrieved Apri|23,2009, from http://www.patientsaferyinstitute.calFrench/toolsresources/
ReportingAndlearning/CanadianAdverse EventsRepordngAndlearningSystem/Documents/CAERLSo/020
Consulration Vo20P apero/o20AppendixB.pdf
Bandolier. Glossary: Evidence-based medicine. Retrieved Aprl| 23,2009, from http://www.medicine.
ox. ac. uk/bandolieri booth/glossary/EBM.html
Canadian Nurses Associarion. (2005). Cønadian nurse practitioner cole competency fameworþ.
Ottawa: Author.
Canadian Nurse s Association. (2008). Aduanced nursing practice: A national frameworþ. Ottawa: Author
Canadian Nurses Associarion. (2008). Code of ethics for registered nurses. Ottawa: Author.
Canaclian Nurses Association and Canadian Association of Schools of Nursing. (2004). Ioint ?osition
statement: Promoting continuing competence for registered nurses. Ottawa: Authors.
Canadian Patient Safety Institute . (2008). The safety com?etencies ftulnteworþ: Bachgrounder. Retrieved
Apri| 22, 2009, from http://www.patientsafetyinstitute.calEnglish/education/safetyCompetencies/
Pages/Backgrounder. aspx
The Cochrane Collaborarion. (2010). Euidence-based heahhcare. Retrieved Aprll 23,2009, from
http : //www. cochrane. org/docs/ebm. htm
College of Registered Nurses of British Columbia. (December 200S). Complementary ønd alternatiue
health care [Practice srandard]. Retrieved April 23,2009, from: https:/iwww.crnbc.caldown\oadsl43T.pdf
College of Registered Nurses of Nova Scotia. (2008). Problematic substance use in the worhplace:
A rcsource guide þr registereà nurses. Halifax: Author.
Colle ge of Registered Nurses oF Nova Scotia. (2009) . Nurse practitioner comPeteltcies. Fl^alifax: Author.
Ellis, J. R., & Hartley, C.L. (2005). Managing and coordinating nursing care, 4th ed. Philadelphla
Lippincott Villiams E¿ Wilkins.
Guyatt, G., Rennie, D., Meade, M. O., E¿ Cook, D. (2003). Users'guides to the me¿lical literature:
Essentials of euidence-based clinical practice,2nd Edition. New York: McGraw-Hill.
CANADIAN NURSES ASSOCIATION CNA-AiiC.CA 19
964Health Canada. About primary heøhh care. Retrieved April 23,2009, from http:i/www.hc-sc.gclhcs-sss/prim/abour-apropos-eng.php
Hill, A. & Spittlehouse, C. (2009). \X/hat is critical appraisal? ln Euidence-basedrnedicine,2nd Edition. Oxford, U.K.: Hayward Medical Communications. Rerrieved April 22,2009, fromhttp://www.me dicine .ox.ac.uk/bandolier/painres/download/whatis/\7har-is-crirical_appraisal.pdf
Indigenous Physicians Association of Canada and Associarion of Faculties of Medicine of Canad.a.(2008). First Nations, Inuit, Métis health core competencies: A curricalumframeworhþr undergraduatemedical education. Retrieved April 23,2009, from htrp://www. afmc.calpdflCoreCompetenciesEng.pdf
Interprofessional Care Steering Committee. (JuIy 2007). Interprofessional care: A blueprintfor actionin Ontario. Toronto: Ministry of Health and Long-Term Care. Rerieved ApriI 23,2009, fromhttp://www.healthForceontario.calupload/en/whatishfo/ipc%20blueprint%20final.pdf
Muir Gra¡ J. A. (1997). Euidence-based ¡nedicine: Hout to mahe heølth policlt and management decisions.
London: Churchill Press.
National Framework for Nursing Standards lüØorking Group. (2003). Nationalframework for narsings tandard¡. [Unpublished report] . Toronro : Author.
Public Health Agency of Ontario. (August 2007). Glossary of terms releuant to the core cornpetencies forpubllc heabh. Retrieved April 22,2009, from http://www.phac-aspc.gc.calccph-cesp/glos-a-d-eng.php
Public Health Agency of Ontario. (200S). Core competencies for public health in Cønada. RetrievedApriI 23,2009, from http://www.phac-aspc.gc.calccph-cesp/pdfs/cc-manual-engO90407.pdf
Ramsden, I. (1990). Cultural safety. New Zeøland NurcingJournø|, 83, 18-19.
University ofVictoria. Cuhurøl safety: Module 1: Peoplei experiences of colonizatioz. Rerrieved April 22,2009, from hctp://web2.uvcs.uvic.calcourses/csafety/modl /index.htm
'sl'ilson, R. M., Harrison, B. T., Gibberd, R. \ø, & Hamilton J. D. (1999). An analysis of the causes
of adverse events from the Quality in Australia Health Care Study [Electronic version]. Medical Journalof Australia, I 70, 4tt-4t5.
20 CANADIAN NURSE PRACTITIONER CORE COMPÊTENCY FRAMEWORK

965APPENDIX A: REPRESENTATIVES AND FACILITAT0RS
The following individuals and groups committed their time and expertise to the development of the
Cønadian Nurse Practitioner Core Competency Fratneworþ.
Ganadian Nurse Practitioner Gore Gompetency Gommittee
Practice/Education Representatives Regulatory Representatives
Luisa Barton, NB Ontario
Margaret Dykeman, NB New Brunswick
Pamela Fald, NB Alberta
Cherie Gilbert, NB Nova Scotia
Lynn Guengrich, NB British Columbia
Lee Holliday, NB Yukon
Manuel James, NB Saskatchewan
Connie-Marie Lapadat, NB British Columbia
Janet Loo, NB Prince Edward Island
Patricia Nymark, NP, Northwest Territories
and Nunavut
Donnie Sampson, NB Newfoundland
Jennifer \Wellborn, NR Manitoba
Marsha'Wood, NB Nova Scoda
Joyce Black, RN, CRNBC
Paul Boudreau, RN, ARNPEI
Teri Crawford, RN, CRNNS
Donna Hogg, RN, CARNA
Rosanne Jabbour, RN, CNO
Steven, Leck, RN, RNANT/NU
Patrick Livingstone, RN, SRNA
Beverley Mclsaac, NB ARNNL
Susanne Priesc, RN, NANB
Ruth Rogers, RN, NANB
Jo \Øearing, RN, CRNBC
Suzanne tVowchuk, RN, CRNM
Co-chairs
Christine fueck Buckle¡ CNA
Barbara \Øaters, CARNA
Facilitators
Carole Dazé, ASI
Charles Mayenga, ASI
CANADIAN NURSES ASSOCIATION cna-aiic.ca 21
CANADIANNURSESASSOC¡ATTON
966v
cna-aiic.ca
star.com
This copy is for your personal non-commercial use only. To order presentation-ready copies of
Toronto Star content for distribution to colleagues, clients or customers, or inquire about
permissions/licensing, please go to: www.TorontoStarReprints.com
ITEM 6.5967
College of Nurses shouldn't letapr¡vacy trump safety: Editorial
Privacy for nurses cannot be allowed to trump the safety of patients
Premier Kathleen Wynne says she is open to calling an inquiry into the Elizabeth
Wettlaufer murders. The inqury should focus its sights on the College of Nurses
of Ontario. (CHR¡STOPHER KATSAROV I THE CANADIAN PRESS)
By STAR EDITORIAL BOARD
Tues., June t 3, 2c17
It has been more than three years since the College of Nurses of Ontario received a letter
from Woodstock's Caressant Care nursing home sayrng it had fired Elizabeth Wettlaufer
over a life-threatening "medication error."
But only now - after the former nurse pleaded guilty to killing eight patients with insulin
overdoses and assaulting or tryrng to murder six others - has the college "accelerated" an
investigation into her professional conduct.
Too Ìittle, too late comes to mind. Consider that after the college was notified of the life-threatening medication error, Wettlaufer admits she killed 75-year-old Arpa,il Horvath ata London nursing home, tried to kill a nursing home resid.ent in Paris, Ont., and. tried tokill again while providing in-home care.
968What the college was doing during all that time remains unknown. It won't say whatactions it took when it learned of Wettlaufer's firing, citing legislation it insists extendsconfidentialþ protection even to confessed serial killers.
If that is indeed the case, the legislation must be changed as soon as possible. privacy fornurses cannot be allowed to trump the safety of patients.
Nor is it clear why the college couldn't suspend Wettlaufer's licence, place her und.ersupervision or ban her from administering medication until the investigation wascompleted.
Instead, as the Star's Sandro Contenta reports, Wettlaufer's public record remainedunblemished, allowing her to continue to be employed and harm patients until sheresigned on her ovm and confessed her crimes.
How that could be allowed to happen is a question that may not be answered until anexpected public inquiry is underway. For nowthe college insists it "can't provide anyfurther information."
But, disturbingly, it wouldn't be the first time the college was slow to respond to seriouscomplaints.
Consider the drug-addicted nurse fired by Toronto's Sunnybrook Health Sciences Centrein February 2o1g for stealing medication and altering medical records over the course offive years. The college didn't place restrictions on her ability to practise until November2015, almost three years later, according to the lawyer who represented the hospital.
In fact, the college's website indicates disciplinary orders issued more than two yearsafter incidents of bad performance are commonplace. Indeed, the college informedCaressant to keep all documents relevant to Wettlaufer's firing for up to two years"pending investigation."
Really? The college is informed of a nurse administering a life-threatening medicationerror and it doesn't immediately ask for all documentation? If it had it would havelearned from Caressant's termination letter to Wettlaufer that the error that got her fired.was par[ of "a pattern of behaviours that are placing residents at risk."
While the college's actions will almost certainly come under the microscope at any publicinquiry into the Wettlaufer case, that does not mean it should wait to correct delays ininvestigations - not to mention a lack of transparency that is so bad one health careemployer referred to the college as a "black hole."
But there seems little chance of that. In the college's newly released annual report,
executive director Anne Coghlan actually stated that "safety is at the forefront of the
stand.ards we set and uphold."
Instead of patting itsetf on the back, the college should be alerting the public to steps it is
taking right now to protect patients from errant nurses. It should not wait to be forced.
Read more abouû Elizabeth Wettlaufer, Kathleen Wynne969
Copyright owned or licensed by Toronto Star Newspapers Limited. All rights reserved.
Republication or distribution of this content is expressly prohibited without the prior writtenconsent of Toronto Star Newspapers Limited and/or its licensors. To order copies of Toronto
Star articles, please go to : www.TorontoStarReprints.com
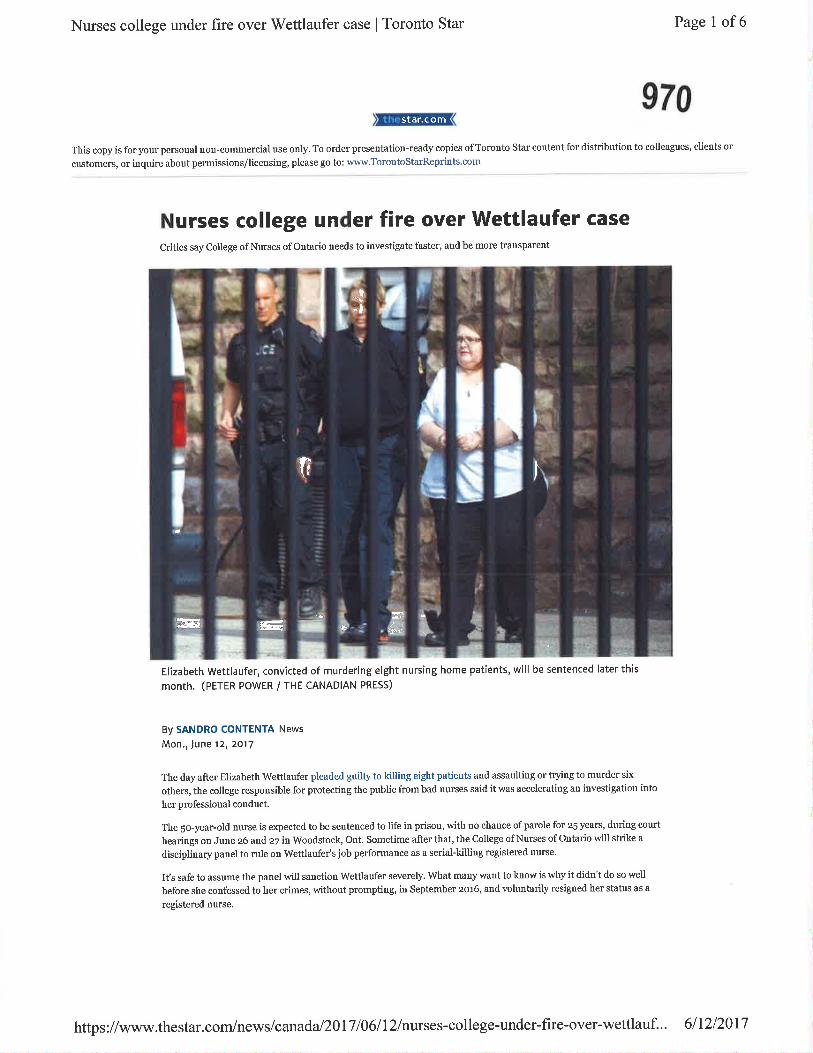
Nurses college under fire over V/ettlaufer case I Toronto Star Page 1 of6
970
This copy is for your personal non-commercial use only. To order preseutatiou-ready copies ofToronto Star content for distribution to colleagues, clients or
clßtomers, or inquire about permissions/licensing, please go to: www.TorontoStarReprints.com
Nurses college under fire over Wettlaufer caseCritics say Coltege of Nurses of Ontario needs to investigate faster, and be more transparent
Elizabeth Wettlaufer, convicted of murdering eight nursing home patients, will be sentenced later this
month. (PETER POWER / THE CANADIAN PRESS)
By SANDRO CONTENTA News
Mon., June 12t 2Q17
The day after Elizabeth Wettlaufer pleaded guilty to killing eight patients aùd assaulting or trying to mnrder six
others, the college respousible for protecting the public from bad nurses said it was accelerating an investigation into
her professioual conduct.
The 5o-year-old nurse is expected to be sentenced to life in prison, with no chance of parole for z5 years, during court
hearings on June z6 and z7 in Woodstock, Ont. Sometime after that, the College of Nurses of Ontario will strike a
discipliuary panel to mle on Wettlaufefs job performance as a serial-killing registered uurse.
It s safe to ass¡me the panel will sanction Wettlaufer severcly. Wrat many want to know is why it didn't do so well
before she confessed to her crimes, without prompting, in September zo16, an<l voluntarily resigned her status as a
registered nurse.
star.com
¡,.ì¡ rar ;*
h; i
¡
;{ id,
"¡ :'
ültfùt'll
¡
I.I
r ItF'--:rG
|\,,t$Tïr$
https://www.thestar.com/news/canada/20171061l2/nurses-college-under-fire-over-wettlauf... 6l12l2017
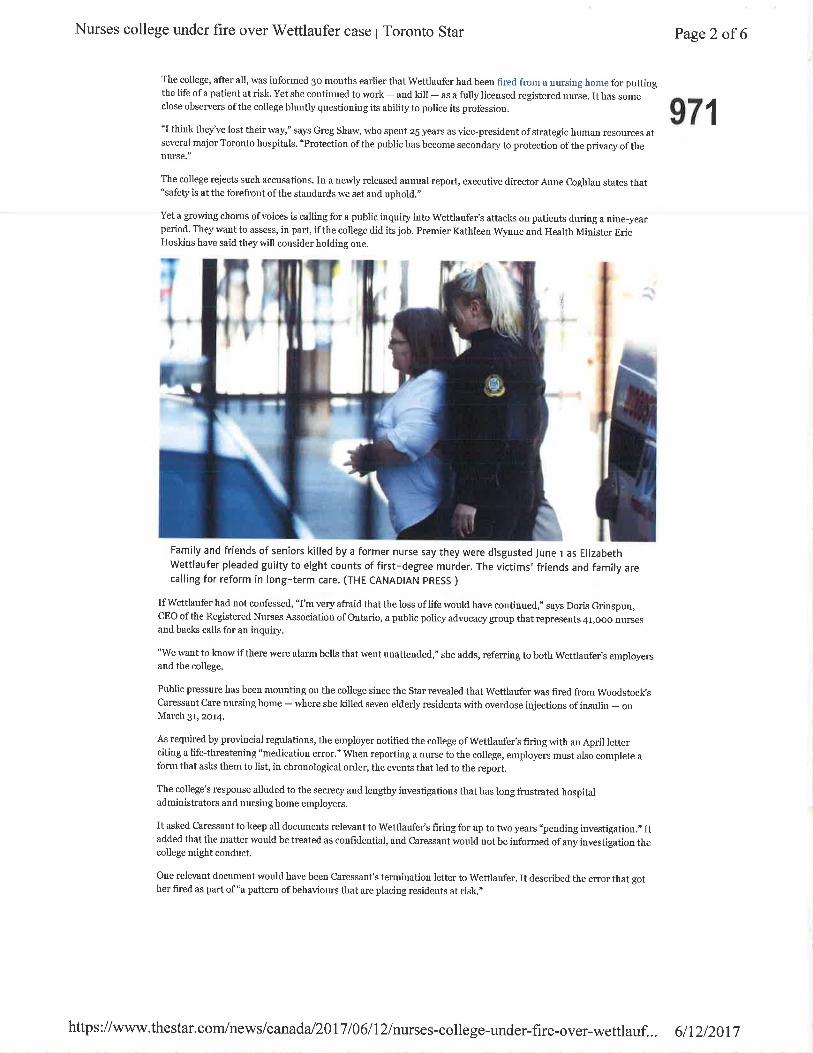
Nurses college under fire over V/ettlaufer case I Toronto Star
The college, after all, was informed 3o months earlier that wettlaufer had been fired from a nursing home for p¡ttingthe life of a patient at risk. Yet she continued to work - and kill - as a fully licensed registered nurse. It has someclose observers ofthe college bluntly questioning its ability to police its profession.
"I think they've lost their way," says Greg Shaw, who spent 2s years as vice-president ofstrategic human resources atseveral major Torouto hospitals. "Protection ofthe public has become secondary to protection ofthe privacy oftheuurse."
Page2 of 6
971
The college rejects such accusatious. In a newly released annual report, executive director ADne Coghla[ states that"safety is at the forefront of the standards we set and uphold."
Yet a growing chorus ofvoices is calling for a public iuquiry into Wettlaufer's attacks on patierts during a niue-yearperiod. They want to assess, in part, if the college did its job. Premier Kathleen Wynne ancl Health Minister EricHoskins have said they will consider holding one.
Family and friends of seniors killed by a former nurse say they were disgusted June r as ElizabethWettlaufer pleaded guilty to eight counts of first-degree murder. The victims'fríends and family arecalling for reform in long-term care. (THE CANADTAN PRESS )
IfWettlaufer hacl not confessed, "I'm very afraid that the loss oflife would have coutinued," says Doris Grinsp¡n,CEO ofthe Registered Nurses Association of Ontario, a public policy advocacy group that represents 41,ooo nr¡rsesand backs calls for an inquiry.
"We want to know ifthere were alarm bells that went unattended," she adds, referring to both Wettlaufer's ernployersaud the college.
Public pressure has been monuting ou the college siuce the Star revealed that Wettlaufer was {ired from Woodstock sCaressaut Ca¡e nursilg home - where she killed seven elderþ residents with overdose injections of insulin - onMarch 3r, zor4.
As required by provincial regulatious, the employer notified the college of Wettlauftr's firiug with an April letterciting a life-threatening "medication error." When reporting a nurse to the college, employers must also complete aform tlìat asks them to list, in chronological order, the events that led to the report.
The college's response alluded to the secrecy aud leugthy iuvestigations that has long frustrated hospitaladministrators and nursiug home employers.
It asked Caressant to keep all documents relevant to Wettlar.rfet's firing for up to two years "pending investigation.,, Itadded that the matter would be treated as confidential, and Caressant would not be informed of any investigation thecollege might conduct.
One relevant document would have been Caressant's termination letter to Wettlaufer. It described the error that gother fired as part of"a pattern ofbehaviours that are placiug residents at risk.,,
{
I
https://www.thestar.com/news/canada/2017106112/nurses-college-under-fire-over-wettlauf... 6lI2l20l7
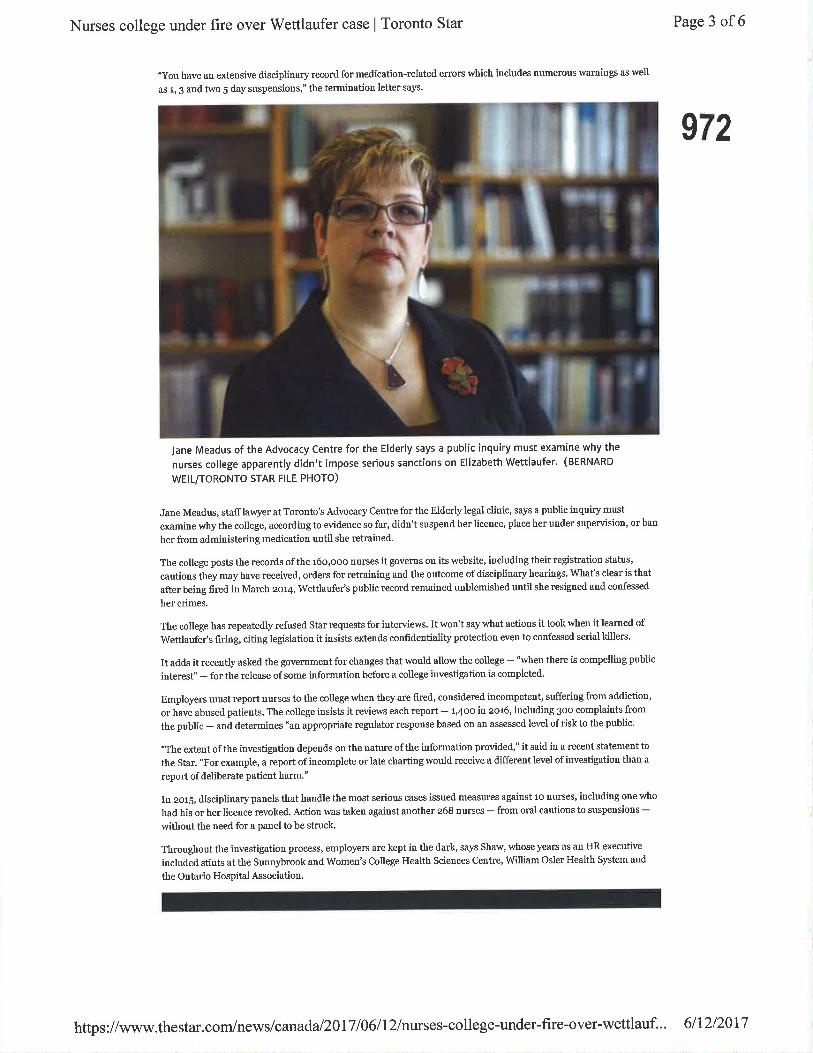
Nurses college under fire over Wettlaufer case I Toronto Star
"yo1 have an extensive discipliuary record for medication-relatetl erncrs which includes uumerous warniugs as well
as r, g and two 5 day suspensions," the termination letter says.
Page 3 of6
972
Jane Meadus of the Advocacy Centre for the Elderly says a public inquiry must examine why the
nurses college apparently didn't impose serious sanctions on Elizabeth Wettlaufer. (BERNARD
wEtL/TORONTO STAR FILE PHOTO)
Jane Meaclus, stafflawyer at Torouto's Advocacy Ceutre for the Elderly legal cliuic, says a public inquiry must
exami¡e why the college, according to evidence so far, didn't suspend her licence, place her under supervision, or ban
her fncm administering medication until she retrained'
The college posts the rrecords ofthe 16o,ooo nurses it governs on its website, including their registration stahls,
cautions they may have received, orders for retraining and the outcome ofdisciplinary hearings. What's clear is that
after being firecl in March 2o4, Wettlaufer's public record remained unblemished until she resigned aucl confessed
her crimes.
The college has repeatedly refused Star r€quests for iuterviews. It won't say what actions it took when it learned of
Wettlaufer's firing, citiug legislation it iusists extends confidentiality protection even to confessed serial killers.
It adds it recently asked the government for changes that would allow the college - "when there is compelling public
interest" - for the release ofsome information before a college investigation is completed.
Employers must report rurses to the college when they are fired, consiclered iucompeteut, suffering from addiction'
or have abused patients. The college insists it reviews each report - l,4oo in zo16, including 3oo complaints from
the p¡blic - anrl determines "an appropriate regulator response based on an assessed level of risk to the public.
"The exteut ofthe investigation depends on the nature ofthe information providecl," it said in a recent statement to
the Star. "For example, a report of incomplete or late charting would neceive a tlifferent level of iuvestigation than a
report of deliberate patient harm."
In zor5, discipliuary panels that hanclle the most serious cases issuecl measures against 10 nurses, incluiling one who
had his or her liceuce revoked. Action was taken agaiust another 268 nurses - from oral cautions to suspensions -without the need for a panel to be struck'
Throughout the investigation process, employers are kept in the dark, says Shaw, whose years as an HR executive
incl¡ded stints at the Sunnybrook ancl Women's College Health Scieuces Centre, William Osler Health System aud
the Outario Hospital Association.
https://www.thestar.com/news/canad a/2017 10611 2/nurses-college-under-fire-over-wettlauf.. . 6ll2l20l7

Nurses college under fire over Wettlaufer case I Toronto Star Page 4 of 6
I 973
three long-term care homes where she worked betweenraw video includes part of her confession. (ClTy NEWS)
zooT and zor4, and at a private house. This
"IMrett an employer files a cornplaint with the college, as they're obliged to clo, it goes into a black hole,,' adds Shaw,now a consttltant iu the sector. "You don't know if it's going to go to a disciplinary hearilg or whether they're dealingwith it. You have no idea what's going on.
"l'rn aware of a nuntber of circumstances where the college took more than two years for it to be dealt with, in whichtime the nnrse h¿ìs lìo notatiou on their liceuce, so they're free to seek alternative employnent ancl fi.ee to work in afull capacity."
Disciplilary orders issned rnore than two years after incitlents ofbad per{onnauce are easiìy found o¡ the college,swebsite.
"'l'he College has acknowledged that the timelines to adclress complailts antl reports is long, and i¡ some cases toolong," it said in a statetnelt to the Star on Thursday. "We cortinue to review our processes ard. add resorlrces toshorten the tinÌe to complete these cases. All rn¿ìtters that pose serious risk are triagecl and given priority."
Laboür lawyer Briau Smeenk has long called for the college to place interirn restrictions on nurses whe¡ an employerflags practices that clearþ put the public at risk.
He representecl Totouto's Sruurybrook Heerlth Sciences Centre when it fired a tlrug-acldictecl nnrse in F'ebruary zor3for stealing tnedication frotn the hospital, and altering rneclical records, over the course offive years. The collegedidn't place restrictions on her ability to practise until Novernber zo15, sr.neenk says.
"In the tneautine tlìe hospital hadu't heard a word from the college about the case," he says. "lt was a nystery to usItow the college came to a decisiou, becanse they never he¿rrd from (hospital) managernent abont what eictuirllyhappened."
'Ihe college says it "did rot have the legal right to restrict or suspencl a nurse without first completing aninvestigation" until the provincial Protecting Patients Act became law this rnonth. The college, which advocate¿ forthe change, says it can now impose interitn restrictions when it has "reasonable and probabìe grounds that a nurse,spractice poses a risk or is likely to pose a risk of hann or injury to a patient.,'
Less thau a mouth after losing her Caressant job in March 2o14, Wettlaufer lancled one at the Meadow park 1¡rsinghome ill Londoti, Ont. Il August, she killecl 75-year-old Arpacì Horvath with a¡ i¡s¡lin overdose.
She resignecl from Meadow Park iu October zor4 to be treated for abuse of alcohol and the clmgs she stole from therrrtrsiug hotne. Wherr she resnmed work with other ernployers, she tried to kill two more patieltts witlì irsulinoverdoses, one at a nrtrsing horne iu Paris, Ont., in Septernber zor5, and anotlÌer at a private resiclence in i¡gersolì inAugust 2o16.
https://www.thestar.com/news/canad a/2017106112/nurses-college-under-fire-over-wettlauf... 6112/2017
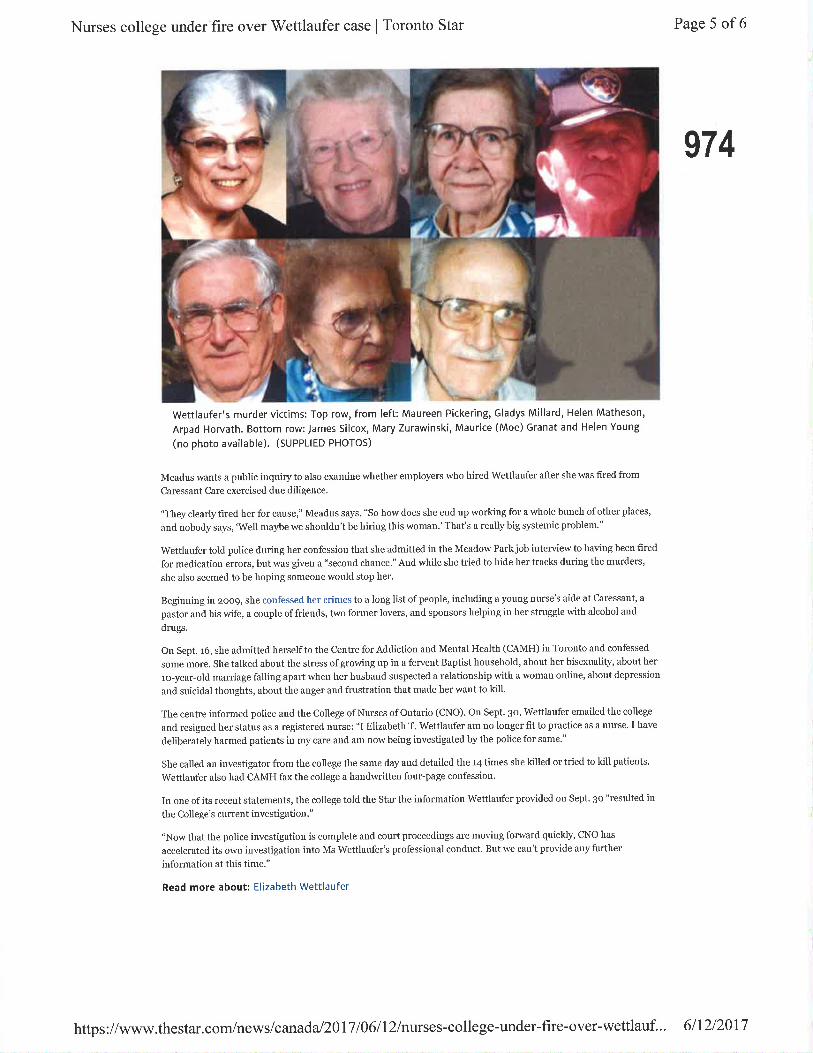
Nurses college under fire over Wettlaufer case I Toronto Star Page 5 of6
974
Wettlaufer's murder victims: Top row, from left: Maureen Pickering, Gladys Millard, Helen Matheson,
Arpad Horvath. Bottom row: James Silcox, Mary Zurawinski, Maurice (Moe) Granat and Helen Young
(no photo available). (suPPLlED PHoTos)
Meadus wa¡ts a public inquiry to also examine whether employers who hired Wettlaufer after she was fired from
Caressant Care exercised due diligence.
"They clearly fired her for cause," Meadus says. "So how does she end up working for a whole bunch of other places,
and nobody says, 'Well maybe we shouldn't be hiring this woman.' That's a really big systemic problem."
Wettla¡fer told police during her confession that she admitted in the Meadow Parkjob interview to having been fired
for medication errors, but was given a "second chance." And while she tried to hide her tracks dnring the murders,
she also seemed to be hoping someone would stop her.
Begiuning i¡ zoo9, she confessed her crimes to a long list of people, including a yonng nnrse's aide at Caressant, a
pastor and his wife, a couple of friends, two former lovers, and sponsors helping iu her stmggle with alcohol and
dmgs.
Ou Sept. 16, she admitted herselfto the Centre for Addiction and Mental Health (CAMH) in Toronto ald coufessed
some more. She talked about the stress of growing up in a fervent Baptist household, about her bisexuality, about her
ro-year-old maniage falling apart when her husband suspected a relationship with a woman online, about depression
and suicidal thoughts, about the anger and fntstration that made her want to kill'
The centre infonned police and the College ofNurses ofOntario (CNO). Ou Sept. 30, Wettlaufer emailed the college
and resignerl her status âs â registered nurse: "I Elizabeth T. Wettlaufer am no longer fit to practice as a nurse. I have
deliberately harmed patients in my care and am now bei[g investigated by the police for same."
She called an iuvestigator from the college the same day and detailed the 14 times she killed or tried to kill patients.
Wettlauftr also had CAMH fax the college a handwritten four-page confessiou.
Iu one of its receùt statements, the college told the Star the information Wettlaufer provided on Sept. 30 "resulted in
the College's current investigatioD."
"Now that the police investigation is complete and court proceediugs are moving folward qnickly, CNO has
accelerated its own investigation into Ms Wettlaufer's professional conduct. But we can't provide auy ftlrther
information at this time."
Read more about: Elizabeth Wettlaufer
https://www.thestar.com/news/canada/20I7106112/nurses-college-under-fire-over-wettlauf... 6ll2l20l7

Nurses college under fire over Wettlaufer case I Toronto Star Page 6 of6
975 KffiÈ,{dir+,i
Copyright owned or licensed by Tomnto star NeìÀ'spapers timitetl. AII rights reserved. Republicatiou or distributiôr of this content is expre¡sþ probibiteitwithout the prior written consent ofToronto Star Newspapers Limitecl and/or its licensors, To order copies ofToronto Star artictes, pleâsego iotwww.TorontostarReprints,com
https://www.thestar.com/newslcanada/2Al7l\6lDlnurses-college-under-fire-over-wettlauf... 6/12/2017
Rose Bustria ITEM 6.6
Jo-Ann WillsonTuesday, June 13, 2017 3:10 PMRose BustriaFW: CPSO defends patients' rights to access health services
From:Sent:To:Subject:
976
Council
Jo-Ann Willson, B.Sc., M.S.W., LL.B.Registrar & General Counsel
Collêgê of Ch¡ropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (41 6) 922-6355 ext. 1 1 1
Fax: (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any otherdistribut¡on, copying or disclosure is str¡ctly prohibited. lf you have received this e-mãil in error, please notify me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: FHRCO - Beth Ann Kenny Imailto:bakenny@regulatedhealthprofess¡ons.on.ca]Sent: Tuesday, June 13,20L7 3:08 PM
To: [email protected]; [email protected]:'Richard Steinecke'<[email protected]>;'Louise Verity'<[email protected]>Subject: FW: CPSO defends patients' rights to access health services
The following is being forworded to you on behalf of Louise Verity at CPSO.
As you may be aware, two applications are being heard in the Divisional Court this week
regard¡ng the CPSO's Human Rights and MedicalAssistance in Dying policies. The College is
vigorously defending patients' rights to access care. lnterveners in support of the College
position include the Attorney General of Ontario, Dying with Dignity Canada, the Canadian Civil
Liberties Association as well as a number of others.
Our news release can be accessed via the link below
http://www.cpso.on.ca/Whatsnew/Newç-Releases/2017lCPSO-defends-patients%E2%80%99-rights-to-a ccess-hea lth-se r
Louise
LOUISE VERITYASSOCTATE REGTSTRAR, DIRECTOR I POLICY AND COMMUNICATIONSCollege of Physicians and Surgeons of Ontario | 80 College Street I Toronto, Ontario I M5G 2E2r'. 41 6-967 -2600 l 1 -800-268-7096 ext. 466
1
977ill?ft*?kk.-+-- ORPSO
Beth Ann Kenny, Executive CoordinatorFederation of Health Regulatory Colleges of Ontario (FHRCO)301-396 Osborne St, PO Box244, Beaverton ON LOK 1AOEmail: [email protected]: www.requlated hea lth professions.on.caPhone: 4t6-493-4O7 6 / Fax: 1-866-814-6456
Confidentiølity notice: This emoil, includìng ony ottachments, is for the sole use of the intended recipient(s) ond møy contoinpr¡vote,
confidentiol, ond/or privileged informotion. Any unouthorized review, use, disc!osure, or distribution is prohibited, lf you ore nottheintended recipient or this informotion hos been inappropriotely forwarded to you, pleose contqct the sender by reply email ond
destroyoll copies of the original.
2
The College of Physicians and Surgeons of Ontario
News Release
Share 978a
a
a
a
a
CPSO defends patients' rights to access health services
Jun 13, 2017
Two applications are scheduled to be heard in the Divisional Court on June 13, 14 and 15 relating to theCollege of Physicians and Surgeons of Ontario's Human Rights and Medical Assistance in Dying(MAID) policies.
The College is vigorously defending patients' rights to access care. The College requires that physicrans
who do not want to provide a medical service for reasons of conscience or religion establish a
mechanism to connect their patients with an available, non-objecting healtþ'care provider with whom thepatient can explore all options ("effective referral")
This Challenge against the College's expectations of physicians has been initiated by the ChristianMedical and Dental Society of Canada, The Canadian Federation of Catholic Physicians' Societies,CanadianPhysicians for Life as well as five other individual physicians.
"rùy'e believe that our policies balance patients' rights to access all health services with any physician'sconscience or religious beliefs." said Dr. David Rouselle, College President. "Although an effectivereferral does not guarantee a patient will receive a treatment, it ensures access to care and demonstrates
respect for patient autonomy."
Interveners in support of the College position include the Attorney General of Ontario, Dying withDignity Canada,the Canadian Civil Liberties Association as well as a number of others.
The applications are being heard: June 13, 14 and 15,2017 at the Superior Court of Justice - DivisionalCourt, Osgoode Hall, 130 Queen Street West, Toronto in Courtroom 3. The start time is 10:00 a.m.
Media Inquiries:Jill [email protected]
Tracey [email protected]
416-967-2600 ext.611
Rose BustriaITEM 6.7 979 -
From:Sent:To:Subject:
Jo-Ann WillsonThursday, I'Aay 25,2017 10'.54 AMRose BustriaFW: Ultrasound Update, Patient Website, Case of the Month, and More
Exec and Council
Jo-Ann P. Willson, B.Sc,, M.S.W., LL.B.
Registrar and General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext. 111
Fax: (416) 925-9610E-mail : [email protected]
Web Site: www.cco.on.ca
CONFIDENTALITY WARNING :
This e-mail including any attachments may contain confidential information and is intended only for theperson(s) named above. Any other distribution, copying or disclosure is strictly prohibited. If you have
received this e-mail in error, please notify me immediately by reply e-mail and delete all copies including
any attachments without reading it or making a copy. Thank you.
From: The College of Physiotherapists of Ontario [[email protected]] on behalf of The College
of Physiotherapists of Ontario [[email protected]]Sent: Thursday, May 25,2017 10:33 AM
To: Jo-Ann WillsonSubject: Ultrasound Update, Patient Website, Case of the Month, and More...
View the web version of this Persoect¡ves Newsletter
www collegept.org
1
l,llay 2017 | info@colleqepû.oro õE¡egl
Welcome to the May lssue of perspectives! 980 æAs I mentioned ín last month's newsletter, the College has started reviewing pTweþsites to identify any departures from the Advertising standard. lf we seãsomething that doesn't quite fit, you can expect to receive an email suggesting sometweaks.
Ïo help you better understand if your website is compliant with the Standard or not,we've included a checklist below outlining what is okay to include on a websíte andwhat is not.
Next, head over to the Case of the Month and read all about a physiotherapist whobelieved that general exercise routines were an acceptable form óf "physiotherapy"treatment for 27 patients. Do you agree? what do you think the DisciplineCommittee did?
S€.;-LShenda
Ïhe use of ultrasound for diagnostic and biofeedback purposes is an issue that hasmade its way on to the College's radar.
We think it is important that you understand the legal aspects of how you are andare not permitted to use it.
Get the Details
Htppv PnvsroTH E RApy Morurn I
a
Ultrasound Update
New Patient Website - Protecting the public
2
There's a brand new website (https.//ontariohealthrequlators.ca)to help better equippatients with the information needed when making informed decisions surrounding n¿r ¡their health care and health care providers. Be sure to let your patients know. Võ'l
Have a Look
The College will be reviewing all physiotherapist websites to make sure they are
meeting the recently released Advertising Standard.
lf your site does not meet the Standard, you will receive an email from the College
flagging the issues and giving you time to make changes.
To help you out, we've created a resource, giving examples of what you can and
cannot do. Start by reading the Standard.
Advertisinq Answered
A PT student on a placement with me has been regularly having coffee with one of
the patients. What should I do?
Get The Answer
Over 80% of all health care workers surveyed revealed they experienced abusive
behaviour from a colleague. Click on the link below to learn more about the issue of
workplace abuse and how you can become a part of the solution.
Take a Sta nd
ln May's Case of the Month, we take a look at a PT who repeatedly seemed to
"confuse" general exercise with physiotherapy treatment for 27 of his patients.
Read the Storv
As a physiotherapist, you may be asked to provide medical information for a patient
who is undergoing a medical review for the Ontario Disability Support Program(oDSP).
3
Advertising Review
Practice Advice Question
Things Need to Change: Workplace Abuse
Gase of the Month
Changes to Medical Reviews for Ontario Disability SupportProgram
\.t¡Jùf \rflAtlq€ls
lllyth vs. Fact: Practice assessments are punitive and only look to find things wrongwith your practice.
Mvth vs. Fact? F ind Out
council meetings are open to the public and we'd love to see you there.
Join us on June 21-22,2017, to get a first hand look at how the rules and regulationsthat govern your profession are made.
About Council
982
The Electronic Health Library provides PTs with access to the most recent healthcare literature. Make use of the over 2,800 full text medicaljournals, 22 millioncitations for biomedical literature from MEDLINE, life science journals, and onlinebooks today!
EI ic Health ibrarv
Myth vs. Fact
Council: Join Us ln June
Free Access to Electron¡c Health Library
You
lnterviewing A Potential Employer?What Should PTs Know? Fees, Billing and Accounts
Read the Standard
I lrqÌ1ii:11¡.',i
Watch the eo
õE¡eBQuestions, comments or suggestions related to e-perspectives?
Get in touch at [email protected]'16-591 -3828 ext. 234 or 1-800-593-5gg5 extl3a
www.collegept.org
4
STANDARD
Þtzotzv't I uur ouy rs to protect me puÞilc. Here's no/v we oo ll. - FeoeraÛon of Flealm Keguatory uolleges ol untaflo
983
Our duty is to protect the public. Here's how we do it.There are more than 300,000 healthcare professionals in Ontario. They include doctors, dentists,nurses, kinesiologists, massage therapists, and many more. Ontario's health regulators are the26 health colleges that oversee them. We are not schools or professional associatíons.
This is how Ontario health regulators protect the public:
. We set the requirements for becoming a regulated health professional in
Ontario. Only qualified health professionals are registered to practise.
o We set and enforce practice standards so that you and your family can
receive safe, ethical, and competent healthcare from qualified healthprofessionals.
. We have quality assurance programs so that registered healthprofessionals keep their knowledge and skills up-to-date so they can
provide safe, ethical and competent healthcare throughout theír career.
. We provide public registers so that you can verify that your healthcareprofessional is qualified to practise.
. We are there to help should you have a concern and complaint aboutyour healthcare professíonal.
From this website you can access the following services from eachcollege:
> View online information about your healthcare professional(https://onta ri o h ea lth regu I ato rs.calfi nd-h ea lth-ca re-profession a l/)
> Find a regulated healthcare professional(https://o nta ri o h ea lth regu I ato rs. calfi nd-h ea lth-ca re-professio n a l/)
https ://ontariohealthregul ators.calwho-w+arel 1t3
512612017 Our duÇ is to protect the public. Here's how we do it. - Federation of Health Regulatory Colleges of Ontario
> Learn your rights as a health consumer(https://o nta rio hea lth regu lato rs.callea rnl) 984> Learn how to file a complaint about your healthcare professional(https://o nta rio h ea lth regu I ato rs. calget-he I p-us-co n ce rn s-co m p la i nts-ca rel)
Below is a list of websites for all 26 Ontario health regulators. There,you can get more detailed and reliable information about eachone. (Clicking on the links below will re-direct you to another website.)
> Acu pu n ctu rists (https://www.ctcm pa o.o n.ca)
> Au d iologists (http://www.caslpo.com)
> Ch i ropod ists (http://www.cocoo.on.ca)
> Ch i ropractors (http://www.cocoo.on.ca )
> Dental Hygienists (http://www.cdho.org)
> Dental Technologists (http://www.cdto.ca)
> Dentists (http://www.rcdso.org)
> De ntu rists (http ://www. d entu rists-cd o.com)
> D i etitia n s (http://www"co I I egeofd íetitia ns. o rg)
> H o m eo path s (http://www.co I I egeofh o m eopath s.o n.ca )
> Kin esíologists (http://www.coko.ca)
> Massage Therapists (http://www.cmto.com)
> M ed ica I La bo ratory Tech no logists (http://www.cm lto.com)
> Medical Radiation Technologists (http://www.cmrto.org)
> M idwives (http://www.cmo.on.ca)
> N atu ro paths (http ://www. co I I egeofnatu ro paths. on.ca)
> Nu rses (http://www.cno.org)
> Occupational Therapists (http://www.coto.org)
> O pticia ns (http://www.coptont.o rg)
> O ptom etrists (http ://www. co I I egeo pto m. o n.ca)
> Pharmacists (http://www.ocpinfo.com)
> Physicians and Surgeons (http://www.cpso.on.ca)
> P hys i oth e ra p ists ( http ://www. co I I ege pt. o rglH o m e)
> Psych ol ogica I Associates (http ://www.cpo. on. ca )
> Psychologists (http://www.cpo.on.ca)
> Psychotherapists (http://www.crpo.cal)https ://ontari ohealthregul ators.carlw ho-we-ard z3

vut uuly t5 tu pt utwt u tÞ puut¡!. n6 E 5 iluw wE uu ¡t. - rwEr duuil ur nËdlu l nclJuldtul y uurcgeù ul vntd ru
> Respi ratory Th e ra pists (http://www.crto.o n. ca)
> Speech-La ngu age Pathol ogists (http ://www.cas lpo.com)
> Trad itiona I Chinese Medicine Practitioners (https://www.ctcmpao.on.ca)
985H ow (https://o nta ri o h ea lth regu lators.calwh o-we-a rel)
Lea rn (https://onta riohealth regu lators.call ea rnl)
Find (https://ontariohealthregulators.calfind-health-care-professional/)
Get help (https://ontariohealthregulators.calget-help-us-concerns-complaints-care/)
English (https://onrariohealthregulators.calwho-we-are/) Françats (https://ontarjohealthregulators.calfrlwho-we-are/)
'F?fFi?Å,[[!'9,'#g#!3fl3!Êßf'gsÉil"E¿:,:t{-lT"'3,',in';1,f"-,'."n
P',iB#[,o[%[ìË8tiJ3[]f;S8!5ÊllfáÊ5lJ,*P{?StiRrr!:X?u8r1J-?2-,'..,r
r.-931fr?,Fçf¿fn5hdLe6rtLçeË1h.îAg{3,Sftfiff,-llËSå8r onRr¡Fbi (htps://onrar¡ohearthregurators calpa/who-we-are/)
Tamil (https://ontariohealthregulators.calta/who-we-are/) riJl (https://ontariohealthregulators.calurlwho-we-are/)
<AC ÞLupd-JA., (https://ontariohealthregulators.caloc/who-we-are/) Tagalog (https://ontarjohealthregulators.calt8/who-we-are/)
https ://ontari ohealthregul ators.calwho-w+arel 313
Rose Bustria ITEM 6.8Jo-Ann WillsonMonday, May 08, 2017 2:46 PMRose BustriaFW: New Divisional Court case on duty of complaints committee to givereasons when not referring to discipline
From:Sent:To:Subject:
986
Exec and Council.
Jo.Ann Willson, B.Sc., M,S.W., LL.B.Registrar & General Counsel
College of Chiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON M5S 1N5Tel: (416) 922-6355 ext.111Fax: (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-mail including any attachments may contain confidential information and is intended only for the person(s) named above. Any other
distr¡bution, copying or disclosure is strictly prohibited. lf you have received this e-mail in error, please notify me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: [email protected] Imailto:[email protected]]Sent: Monday, May 08,2OL7 2:45 PM
To: Jo-Ann Willson <[email protected]>; Tina Perryman <[email protected]>
Subject: New Divisional Court case on duty of complaints committee to give reasons when not referring
to discipline
You might find this Divisional Court case regarding a Complaints Committee decision of the Professional
Engineers of Ontario interesting:https://www.ca nlii.orelen/on/onscdc/doc/2017l2017onsc2569/2017onsc2569.html
The applicant, Jim Harrison, applied for judicial review of a decision of the Complaints Committee of the
respondent, the Association of Professional Engineers of Ontario. The Compla¡nts Committee refused to
refer the applicant's compla¡nt against the intervenors, David. W. Downey and David W. Downey
Engineering Ltd. to the Discipline Committee, finding that there was "no evidence of professional
misconduct of a significant nature on the part of Downey or David W Downey Engineering Ltd.".
The Divisional Court concluded that the complaints committee did not fail to give reasons and that the
decision was reasonable. The court noted:
tlgl lt becomes clear when looking at the material before the Complaints Committee that Downey
offered the Complaints Committee a response to every allegation advanced by the applicant. ln
addition, the evidence on this judicial review application establishes that both the applicant's and the
respondent Downey's versions of events were before the Committee. Therefore, it was open to the
Complaints Committee to accept Downey's explanation and decide that Downey's conduct did not merit
a referralto the Discipline Committee.
t29l The reasons of the Complaints Committee should have indicated that it accepted the
explanations provided to it by Downey. We are satisfied that the Complaints Committee must have done
so because Downey's explanations are a complete answer to the applicant's complaints and supported
the Complaints Committee's conclusion that "there was no evidence of professional misconduct of asignificant nature on the part of Downey"
987
[23] While we have decided to dismiss the application, we wish to make certain observations. TheComplaints Committee is expected to issue appropriate reasons. The applicable principles forappropriate reasons are set out in decisions of the Supreme Court of Canada. A helpful explanation ofthese principles can be found in the jurisprudence created after Dunsmuir. For example,in Jokutavicius ,..
l24l While the court can look to the material before the Complaints Committee to see if it explainstheir Reasons, the Complaints Committee should not assume that the material before it will alwayssatisfactorily explain its written reasons. For example, the Complaints Committee successfullymaintained before this Court that it was not required to produce a"record" because its refusalto referthe complaint to the Discipline Committee was not the exercise of the statutory power of decision. ThisCourt was able to conclude from the Decision and the material filed by the respondent and thelntervenors that Mr. Downey's response to the applicant's complaint was before the ComplaintsCommittee.
t25l Finally, while the court can consider the material before the Complaints committee to'see if itexplains the Committee's Reasons, the court cannot uphold a decision by writing reasons andsubstituting them for defective reasons.
Karen
2
988CITATION: Harrison v. Association ofProfessional Engineers of Ontario, 2017 ONSC2569
DIVISIONAL COtiRT FILE NO.: 14-1999DATE: 20170505
ONTARIO
ST]PERIOR COT]RT OF JUSTICE
DIVISIONAL COI]RT
MARROCCO A.C.J.S.C., ITEENEY R.S.J. & ELLTES J.
BETWEEN:
JIM HARzuSONJohn D. Dempster, for the Applicant
Applicant
-and-Leah Price and Nick Hambleton, for the
Respondent Association of ProfessionalEngineers
Respondent
-and-
DAVID W DOWNEY and DAVID 'W
DOWNEY ENGINEERING LTD.
Intervenors Scott Howardt,for the lntervenors
IIEARD at Ottawa: February 22, 23, 2017
MARROCCO A.C.J.S.C.
tll The applicant, Jim Harrisor¡ applies to judiciaþ review a decision of the Conplaints
Conrnittee of the respondent, the Association of Professional Engineers of Ontario. The
Conplaints Conrnittee refi¡sed to refer the applicant's complaint against the intervenors,
David. W. Downey and David W. Downey Engineering Ltd. to tfrc Discþline
Corrnittee, findlng tl:rrt there was 'ho evidence of professional misconduct of a
significant nature onthe part of Downey orDavid WDowney Engineering Ltd.".
l2l The applicant asks for an order
-=c(gOO)(olr)(\OU)zÞ.-
ON
ASSOCIATION OF PROFESSIONALENGINEERS OF ONTARIO
))))))))))))))))))))))
Page:2 989a setting aside the Decision and Reasons of the respondent's Conplaints Committee
dated Deceniber 19, 2013 conceming a conplaint of professional misconductagainst David w. Downey and David w. Downey Engineering Ltd.('Conplaint');
requiring the Conplaints Cornrnittee to refer his Conplaint to the respondent'sDiscþline Committee pursuant to s. 24Q)(a) of the Professional Enginèers Act,R.S.O. 1990,c. P.28 ('?EA'); or
Aftematively, refening his Conplaint back to the Conplaints Corrrnittee for re-determination.
-:lcõL)o)(Ou')c{OU)zot-ON
a
o
t3l The respondent resists the application maintaining tlre inpWned decision is reasonable.
l4l In February 2005, the Linrestone Dishict School Board retained David W. DowneyEngineering Ltd. to perform all engineering services and oversee all rnechanic al andelectrical fades hired to renovate Frontenac Secondary School in Kingsto4 Ontario.Allen Mechanical Inc. was awarded the heating ventilation and air-conditioning sub-confact. In November 2006, Allen Mechanical awarded Longhil Energy Products Ltd.(.'Longhilf) fte contract to sryply four heating ventilation and air-cõnditioning units,conditional upon receþt by Allen of Longþill's shop drawings approved by DavidDowney ('Downey'). In December 2006, Downey rejected l.ongtritts nitial shopdrawings because crucial information about the refrþerant systems was missing. In orabout May 2007, Downey rejected Longhill's resubmitted shop drawings. Laþa in May2007, Allen Mechanical Inc. cancelled the Longhil Purchase Ordei and issued ;Purchase Order to Engineered Air for the heating ventilation and air-conditioning units.
t5] The applicant is a professional engineer in Ontario. He was, at alI nntenal times, theowner, president and representative of lnngffi in ttre dealinp with Downey that led tohis corrplaint.
t6l In his conplaint, the applicant alleged that Downey sent Longhill's confidential shopdrawings for review and cornrnent to Engineered Air, one of Longhill's conpetitors whòhad also bid on the Project. Harrison alleged that Downey used Engineered Air'sconrnents to repeatedþ reject Longffi's heating ventilation and air-conditioning shopdrawings, resulting in Engineered Air eventuaþ replacing longhill as the supplieiof theunits. Harrison alleged Downey and Engineered Air mutually benefitted from inforrnaland inappropriate specification changes after ttre mechanical subconfractor issued itspurchase order to Engineered Air. Iastþ, the applicant conplained that Downey and hiswife, during the rnaterial time, went on vacation to Ireland with Darren Trenhokn ofEngineered Air and his wife.
l7l The applicant provided the respondent with evidence of his allegations, which includedaffdavits, expert reports and email exchanges. Innghi[ had used these materials topursue a civil claim against Downey. tnnghill settled that litþtion in Octob er 2011 and
Page: 3 990
then made the conplaint to the respondent with which we are concemed, in February20t2.
t8] Downey, wittr the assistance of coursel, responded to each allegation in the Conplaintapproximately one rnonth later, on March 30,2012.
tel On December 19, 2013, the Conplaints Corrrnittee found that "there was no evidence ofprofessional misconduct of a significant nafl¡re on the part of Downey..." and declined torefer the corrplaint to the Discþline Conn:nittee.
tl0] The applicant submits that the Conplaints Conmittee dismissed his conplaint withoutaddressing any of his allegations or providing any reasons as to why his allegations didnot constibte professional misconduct by Downey. Faih¡re to give reasons incircurnstances where they are required may constitute a breach of procedural åirness andan effor of law: Newfoundland and Labrador Nurses' Union v. Newfoundland andLabrador (Treasury Board), 201 1 SCC 62 at para. 22.
[11] When corsidering whether the procedure followed by the Conplaints Conrnittee was
åir, the Court nnrst keep in mind section 2a$) of the PEA, which provides tlrat the
Corrplaints Cormnittee '1s not required to hold a hearing or to afford any person anoppornniry for a hearing or an opporMity to make oral submissions before making a
decision or giving a direction".
U2l The Conplaints Corrrnittee is required by s. 2a() of the PEA to corsider and investþate
the applicant's corrplaint. It clearly did this, For exarrple, the applicant refened in his
complaint to the åct that Downey went to Ireland with Mr. Trenhohn of Engineered Air.The Corrplaints Cornrnittee in a December 19, 2013 document entitled 'Decisions and
Reasons of the Conplaints Committee of the Association of Professional Engineers ofOntario", comrnented on this trþ. Specificaþ, the Corplaints Committee indicated that
the timing and circumstances of Downey's vacation to heland could appear unusual and
that Downey should maintain ùn arm's lengh relationshþ with equþment suppliers
when working on public projects. In tlìis regard, it also sent Mr. Downey a Letter ofAdvice.
U3l The Corrplaints Cornrnittee is required by ss. 24(3) and 2a@) of the PEA to give itsdecision in writing to the Registrar and the Registrar must forward a copy of that decisionto the applicant. As indicated, the Conplaints Corrrnittee issued a document onDecember 19, 2013 which purported to be its reasons. The evidence disclosed that the
Regisnar forwarded a copy of this letter to the applicant.
[14] Accordingþ, I am satisfied that this is not a case in which there was a åihre to give
reasons and any challenge to the decision of the Conplaints Corr¡rnittee must be rnade
within the reasonableness anaþis: Newfoundland and Labrador NLtrses' Union at para,
22.
[15] Reasonableness is concerned rrnstþ with the existence of justificatior¡ hansparency and
inteligþility within the decision-making process. It is also concemed with whether the
âJ
oc)
La)C.l
(f)zot-ON
Page:4 991decision falls within a range of possible acceptable outcomes which are defensible on theåcts and the law: see Dunsmuir v, New Brunswick,2008 SCC 9 atpwa.47.
[16] The reasons of the Conplaints Conrnittee are defective because they state the centralconch.tsiorl nameþ that "there was no evidence of professional misconduct of asignificant naflire on the part of Downey..." without explaining why the ConplaintsConnnittee thougþt so. The Comrnittee's reasons lack tansparency: see Jakutavicius v.Canada (Attorney General) ,201 1 FC 3 1 1 at para. 3 1 .
ll7l However, the adequacy of teasons is not a stand-alone basis for quashing the decision.The approach to be taken by this court in considering the suffciency of the reasons givenby an administrative decision-maker was discussed n Dunsmuir, and more recentlyclarified n Newfoundland and Labrador Nurses' (Jnion. Abella J., speaking for the courtin tlre latter decisior¡ says this, at para. 12:
It is important to emphasize the Court's endorsement of Professor Dyzenhaus'sobservation that the notion of deference to administrative tribunal decision-makingrequires "a respectñf attention to the reasons offered or which could be offered insupport of a decision". In his cited article, Professor Dyzenhaus explains howreasonableness applies to reasons as follows:
"Reasonable" means here that the reasons do in fact or in princþle support theconclusion reached. That is, even if the reasons in fact given do not seem whollyadequate to support the decision, the court must first seek to supplement thembefore it seeks to subvert them. For if it is right that among the reasons fordeference are the appointment of the tribunal and not the court as the front lineadþdicator, the tribunals proximity to the dispute, its expertise, etc, then it is alsothe case that its decision should be presumed to be correct even if its reasons arein some respects defective. fEmphasis added.]
(David Dyzenhaus, 'The Politics of Deference: Judicial Review and Democracy",in Michael Taggart, ed, The Province of Administrative Law (1997),279, atp.304)
u8l
See also David Mullan, 'Dunsmuir v. New Brunswicþ Standard of Review andProceúnal Faimess for Public servants: Let's Try Again!" (2008), 21 c.J.A.L.p . rl7, atp, 136; David Phiþ Jones, Q.C., and Anne S. de Villars, e.C., princþles ofAdministrative Law (5th ed. 2004), at p, 380; andCarnda (Citizenshþ and Immigration)v. Khosa,2009 SCC 12,120091I S.C.R. 339,atpara.63,
In considering what reasons 'bould be offered" in srpport of the decision urder review,the law requires us to look at the record that was before the Conplaints Conrnittee to seeif its decision ålls within a range of possible acceptable outcomes which are defensibleon the facts and the law: see Newfoundlqnd ønd Løbrador Nurses' (Jnion at para.Il.
It beconres clear when looking at the rnaterial before the Conplaints Comrnittee thatDowney ofered the Conplaints Corrrnittee a response to every allegation advanced bythe applicant. In additior¡ the evidence on thls judicial review application esúablishes that
â=coOO)(oLa)(\Oc/)zoNc)N
[1e]
Page: 5
both the applicant's and the respondent Downey's versions of events were before t}rcConrnittee. Therefore, it was open to the Corrplaints Conrnittee to accept Downey'sexplanation and decide that Downey's conduct did not nrerit a referral to the DiscþlineCornrnittee.
Í201 The reasons of the Corplaints Conrnittee should have indicated that it accepted theexplanations provided to it by Downey. We are satisfied that the Conplaints Committeemust have done so because Downey's explanations are a conplete answer to the
applicant's conplaints and supported the Conplaints Connniuee's conch¡sion that 'there\Mas no evidence of professional misconduct of a significant natwe on the part ofDowney''.
[2lJ In additior¡ the essence of the applicant's allegation was that Mr. Downey's relatiorshþwrth Engnreered Air was comrpt. He suggests that none of the srrypliers could meet Mr.Downey's specifications "and so it was ineviøble that Engineered Air would receive thecontract at whatever price they wanted to charge". This allegation is not strpported by the
evidence. It is true that the project specifications at the time of tender were mostþ inconformance with those of Engineered Air. This is disclosed in Mr. Downey's email toMr. Trerihokn of Engineered Air dated November 7,2006. However, in a letter to AllenMechanical dated November 6, 2006, Iongþill's representative stated that after thereview of the drawings, specifications and sormd requirements for the project, he was
confident th;at Longhil would be able to meet the requirements indicated in the biddocwnents. The applicant was awarded the purchase order two days later. The applicantwas unable to meet those specifications and as a result was replaced on the project byEngineered Air
[22] Accordingþ, a review of the materials that were before the Corrplaints Conrnittee leads
to the conch¡sion tl:ø;t the Conplaint Comrnittee's Decision t}nt Downey actedappropriateþ even though the 'timing and circunutance of Downey's vacation withothers from the Project rnay be perceived as unusuaï' is within the range of possible
acceptable outcomes "defensible on the åcts and the law".
l23l 'While we have decided to dismiss the applicatior¡ we wish to make certain observations.
The Corrplaints Conrnittee is expected to issue appropriate reasons. The applicableprincþles for appropriate reasons are set out in decisions of the Suprenre Court ofCatnda. A heþfirl explanation of these princþles can be fornd in the jurisprudence
created after Dunsmuir. For exarple, n Jakutavicius l:[l4r. Justice Zin of the FederalCourt made the following observation atpara.3l:
The reasons provided for a decision rnay firlfll the requirements ofprocedural faimess in the sense that the reasons meet the goals of focusingthe decision maker on the relevant åctors and evidence, providing parties
with the assr¡rance tbat their representations have been considered,allowing parties to effectuate any right of appeal or judicial review they
might have and allowing reviewing bodies to determine whether the
decision maker erred, and providing guidance to others who are subject to
992
-=c(úOCt)(oLa)C\t
C)U)zol..r
c)N
Page: 6 993the decision maker's jurisdiction: VU Rail Canada v NationalTransportation Agency, 2000 CanLII 16275 (FCA), [2001] 2 F.C. 25(CA), at paras. l7-2I. Yet the same reasons which meet procedural musternriay render the decision unreasonable as a matter of substantive review. Itis in this context that one examines, based on the reasons provided, thejustificatior¡ transparency and intelligbilrty of the decision. Justificationrequires a decision nraker to focus on relevant åctors and evidence.Transparency requires a decision rnaker to clearþ state the basis for thedecision reached. Intelligibility requires a decision maker to reach a resultthat clearþ follows from the reasons provided.
l24l While the court can look to the material before the Conplaints Corrrnittee to see if itexplains their Reasons, the Conplaints Committee should not assume that the materialbefore it will always satisñctoriþ explain its written reasons. For exanple, theConplaints Conrnittee successflrlly maint¿ined before this Court that it was not requiredto produce a 'Îecord" because its refi;sal to refer the conplaint to the DiscþlineConn:nittee was not the exercise of the statutory power of decision. This Court was ableto conclude from the Decision and the material filed by the respondent and theIntervenors that Mr. Downey's response to the applicant's corrplaint was before theConplaints Connnittee.
125) Finally, while the court can consider the material before the Conplaints Conrnittee to seeif it explains the Cornrnittee's Reasons, the court cannot trphold a decision by writingreasons and substih¡ting ttrem for defective reasons.
126l The Conplaints Corn¡ittee was well represented in this matter by experienced counselwho could have, in a legally appropriate way, provided advice conceming the adequacyof the Reasons before they were released.
l27l This application is dismissed. Parties are not seeking costs and accordingþ there will beno order conceming costs.
MARROCCO A.C.J.S.C.
I agree:
HEENEY R.S. J
I agree:
ELLIES J.
-Jcñrìo)(orONOU)zof..-
ON
Released: 20170505
994
CITATION: Harrison v. Association ofProfessional Engineers of Ontario, 2017 ONSC 2569DMSIONAL COURT FILE NO.: 14-1999
DATE: 20170505
ONTARIO
SI]PERIOR COURT OF JUSTICE
DTVISIONAL COTIRT
MARROCCO A.C.J.S.C., ITEENEY R.S.J. &ELLIES J.
BETWEEN:
JIM HARRISON
Applicant
-and-ASSOCIATION OF PROFES SIONAL ENGINEERSOF ONTARIO
Respondent
-and-
DAVID W DOWNEY and DAMD W DOWNEYENGINEERING LTD.
Iftervenors
REASONS FOR JT]DGMENT
-=c(g(J
O)(oroc.,t
O(/)zoF.-
<>N
Released: 20170505
A6llORONto STAR FRIDA Y, MAY 19
Even th o u gh th "
p,ou i n." h a s i n t ro d rllc#lå il''#ilf:iil:t:iR Fr tE P'oro
Progressive Conservative MPP Laurie Scott sals it doesn't go far enough.
Critics push training forjudges on sexual assaultCurrent jurists 'need some
upgrading in their education'
NDP and Conservatives say.
KRISTIN RUSHOTYYQUEÊN's PARK SUREAU
Ontario needs to expand mandatorytraining on sexual-assault law to alljudges because it is the ci¡¡rent oneswho "apparently need some upgmd-ing in their educâtion' says NDPIæader Andrea Horu¡atì-'ï would hope that the government
and thè attorneygeneral make it re-ally, really clear that that needs to bea priority because there's no waythat a woman should have to go
througþ the insei'rsitivity or igno-rance, frankly, of ajustice when deal-inC with a sexual-assault situationthafs alieady dítrcutt and painfrn,"she said.Ontariot chief justice recently up-
dated the edircation plan for newjudges, compellingthem to take partin trai4ing that includes sexual-as-saultlaw.
The changes come amid wider con-cerns about how sexual-assault cases
are handled in courtrooms acrossthe country from the trial of formerCBC radio host Jian Ghomeshi to the"knees together"judge in Calgary -who has since resigned. Then, ajudge in Halifax found a taxi drivernot guilty, saying the severely intox-icated complainant could have con-sented.Progressive Conservative MPP
Lawie Scott, her parffs women's is-sues critig questioned whether the
training really is mandatory - butregardlesg sen-assault complairuntsdeservebetter.
She is one of two MPPs v*rohaveproposed private-membe¡'s bills,with hers oncompassing training onsex-assault laws, evidence, sexualconsent and skreot¡pes for all onthebend¡-The governmenfs stance "dearly
doesnt meet the e4pectations forsu¡vivors of se¡<ual assault, who wantto be sure that the court systemwilltreat thei¡ cases fairþ," she said at thelegislature.
'T'do know thdt (Attorney GeneralYasir Naqvi) cares aboutthis iszug somyquestionto þmis, wiil he finallyagree that mandated sexual-assar¡lttraining needs to be legislated, andwill he support rnybill?'
Naqvi said currentjudges have ac-cess to ongoing training and that ifsup to the court to decide what isprovided andwhat is mandatory.'Ifs a very integral part of our ho-
nour system to have judicial inde-pendencei Naqvi told reporters atQueen's Parlr."I had communicated with the
chief justice, letting her lanow of thedesire of the house that the trainingfor judges be mandatory - but thatdecision is up toher.
'tsut shehadinformed me, andl'mvery happy to note, that she hasworked with her education counseland updated the education plan, ex-pressly mandating trainíng for newjudges around social norms and so-cial contexts, including sexual as-saull'
ttt r tr 't&d tt¡
995
ITEM 6.9
Rose Bustria
From:Sent:To:Subject:
Jo-Ann WillsonMonday, May 15, 2017 9:51 AMRose BustriaFW: Doctor's pharma links raise fears of bias on opioid panel
996
Exec and Council
Jo-Ann Willson, B.Sc., M.S.W., LL.BRegistrar & General Counsel
College of Ghiropractors of Ontario130 Bloor St. West, Suite 902Toronto, ON MsS 1N5Tel: (41 6) 922-6355 ext. 1 1 IFax: (416) 925-9610E-mail: [email protected] Site: www.cco.on.ca
CONFIDENTIALITY WARNING:This e-ma¡l including any attachments may contain confidential information and is intended only for the person(s) named above. Any other
distribution, copying or disclosure is strictly prohib¡ted, lf you have received this e-mail in enor, please notify me immediately by reply e-mail
and delete all copies including any attachments without reading it or making a copy. Thank you.
From: Liz Anderson-Peacock Imailto:[email protected]]Sent: Monday, May L5,2Ot7 9:35 AMTo: Jo-An n Willson <jpwillson @cco.on.ca>Subject: Doctor's pharma links raise fears of bias on opioid panel
Jo-Ann,
Thought I'd pass along as this was an interesting art¡cle today in light of increasing scrutiny for
conflicts of interest.Liz
From the Globe and Mail:Doctor's pharma links raise fears of bias on op¡oid panel -
http://www.t slobeand mail.com/news/natio alldoctors-oharma-links-raise- rs-of-bias-on-
opioid-panel/a rticle3498478 U
Liz Anderson-Peacock. 705J94.L874 Sent from my mobile device
1

F$ii* N-s rultt 7 - T0R0ilïo
LAYNAFTAI
61212017 The Globe and Mail: Doctor's pharma links raise fears of bias on opioid panel
* 997
May 14,2017
Doctor's pharma links raise fears of bias on opioid panelBy KAREN HOWLETTGlobe and Mail Update
Decision to accept Ontario doctor as a panel member has shrouded the new prescribing
standards in controversy because of promise to ensure no one had any conflícts of interest
Officials overseeing new national standards for prescribing opioids did not honour a pledge to exclude medical
experts who receive income from drug companies from voting on the measures.
Sol Stern, a family doctor in Oakville, Ont., and one of 13 panel members who voted on the standards, has been a
paid speaker and advisory board member for drug companies, including the pharmaceutical giant whose pain pill
iriggeied Canada's deadly opioid epidemic, according to his declaration form posted online last week.
Jason Busse, an associate professor at McMaster University's department of anesthesia and co-lead of the group
that drafted the standards, said the group made an exception for Dr. Stern because his industry-sponsored talks
represented a "balanced approach" to opioids. Dr. Stern "reassured us he had no overt bias either strongly in
favour or strongly opposed to opioids for chronic pain," Dr. Busse said in an e-mail response to The Globe.
lnvestigation: How Canada got addicted to fentanyll
lnvestigation: How a littte-known patent sparked Ganada's opioid crisis2
Opinion: Why legalize pot, but shy away from addressing opioids?3
But the decision to accept Dr. Stern as a panel member has shrouded the new prescribing standards in
controversy because of promises made by the McMaster group to avoid a repeat of what happened in 2010, when
one-third oÎthe panel members working on an earlier version had ties to Big Pharma, and to ensure that no one
had any conflicts of interest this time around.
McMaster received $433,243 from Health Canada in 2O15 to revise prescribing guidelines that were out of date fora drug whose risks are substantial and benefits uncertain. The new standards unveiled last week by the school's
Micháel G. DeGroote National Pain Centre are aimed at reversing practices developed two decades ago, when
doctors began prescribing opioids to relieve moderate to severe pain as pharmaceutical companies promoted theirbenefits. Aioniinuing Globe investigation has traced the roots of Canada's opioid epidemic to the introduction ofthe prescription painkiller OxyContin in 1996.
Of the 49 members on the 2010 guideline panel, 17 received remuneration from OxyContin maker Purdue Pharma
and other drug companies. Purdue paid doctors, known as key opinion leaders, to help spread the word in the
medical community that OxyContin posed a lower threat of abuse and dependence to patients than otherpainkillers becausé of its slow-release formula. The drug was the top-selling long-acting opioid in Canada for more
than a decade.
Medical experts said anyone who gets paid to produce educational seminars about opioids by a company thatmakes the drugs has a conflict and should not be allowed to vote on guidelines that advise doctors on how toprescribe painkillers.
"We got into this problem because we listened to pharma-funded physicians," said Rupa Patel, a family doctor in
Kingðton who took over a practice with many patients on high doses of prescription opioids. "We're not going to be
http://license.icopyright.neUuser/viewFreeUse.act?fuid=MjU0NjQ3OTY%3D
.IT[Iì GIOßH Ä"]t{D IVIÂII,
1t2
612/2017 The Globe and Mail: Doctor's pharma links raise fears of bias on opioid panel
able to get out of this by listening to pharma-funded physicians.,, 998ln its application to Health Canada for funding, McMaster says "the key to developing conflict-freerecommendations" is to require all voting panel members to "have no iinancial or'intéllectual conflicts" and "refrainfrom particìpating in activities sponsored by the marketing departments of commercial entities." Dr. Busse echoedthat commitment in an interview with The Globe a year ago, saying that leaders had gone to great lengths toensure that no one who votes on the standards has conflicts of intérest. "We believe iery strongly thaiit is quitepossible for people making recommendations on guidelines to have strong conflicts of inierest i-nãt can very wellbias the recommendations that they make,,, he said.
Dr. Stern names four drug companies he has received remuneration from, including purdue. lnitially, those workingon the prescribing guidelines were to declare any conflicts dating back five years, aäcorOinj to the Health Canadaapplication. But the declaration forms ask individuals to discloselheir indusiry ties for only ä+ months. ln frinOsithì,the forms should have expanded the timeline to five years, Dr. Busse told The Globe. "Nót doing so was anoversight."
A spokeswoman at Health Canada said McMaster had a responsibility to craft prescribing standards ',according tothe highest ethicaland technicalstandards." Questions regarding contt¡ct issues relatingio any panelmemberðwould be best addressed by McMaster, the spokeswoman said. ór. Stern also referred-questions to McMaster.
Three doctors who worked on the standards, including one who was disqualified from voting because of her ownties to Big Pharma, Questioned the process for deciding who got to be a panel member, according to copies of e-mails obtained by The Globe.
Lydia Hatcher, chief of family medicine at St. Joseph's Healthcare in Hamilton, said in an interview it's "upsetting,,that her conflicts disqualified her while Dr. Stern, whom she described as a good friend, was allowed on ine pañet.
"lt doesn't make sense," she said. "Why can't I have a vote? l'm no different than Sol?"
Dr. Hatcher said she gives educational talks for a variety of pharmaceutical companies that produce everythingfrom opioids and medical marijuana to hypertension drúgs.
'Because she represänts so many companies, she-said,
she feels she is "not truly biased."
Dwight Moulin, a professor in the departments of clinical neurological sciences and oncology at the University ofWestern Ontario, says in an e-mail to Dr. Busse that he is "confuõed" about the process foiäeciding who haávoting. privileges. "My understanding was that individuals were relegated to the Ëxpert Committee if-they had anyassociation with Pharma," the e-mail says. Nav Persaud, a family dãctor at Toronto's St. Michae¡s Uosfitat anO ämember of the voting panel, also asks Dr. Busse in an e-mail whether the original plan had been to excludeanyone with a financial conflict from the voting panel.
pr..lusse acknowledged the decision to accept Dr. Stern as a panel member "may be controversial.,'But heinsisted in his e-mail responses to panel members and to The
'Globe that Dr. Stern's votes did not change any of
the recommendations on opioid prescribing. Dr. Persaud asks in his e-mail to Dr. Busse, "did you really-mean tostate that [Dr. stern's] 'participation did not change any of the recommendations?,,,
Meldon Kahan, medical director of the Substance Use Service at Women's College Hospital in Toronto and amember of the 2010 advisory panel, said whether Dr. Stern's participation influericed the results is impossible tosay. Regardless, he added, "lf you have rules on no conflicts of inteiest, he should not have been on the panel.,'
References
1 . www.theglobeandmail.com/news/investigations/a-killer-high-how-canada-got-addicted-tofenta n ylla rticle2g 57 0O2S
2. www.theglobeandmail.com/news/investigations/oxycontin/article3344g40g3. www.theglobeandmail.com/opinion/why-legalize-pot-but-shy-away-from-addressing-opioids/article34gg1926
The Globe and Mail, lnc.
dilJ,h" Globe and Mail lnc. All Rights Reserved.. Permission granted for up to 5 copies. Allrights reserved.s You may forward this article or get additional permissions by typingh-utp:/,/license.icopyright. ner-/3.8425'?ícx ict:3498478r intoãnyweb browser. The Globe and Mail, lncand The Globe and Mail logos are registered trademarks of The Globe and Mail, lnc. The iCopyright logo is aregistered trademark of iCopyright, lnc.
http://license.icopyright.neVuser/viewFreeUse.act?fuid=MjU0NjO3OTy%3D2t2
5t112017 Sarnia doctor still practising after court ruling he sexually assaulted colleague I Toronto Star
999This copy is for your personal non-commercial use only. To order presentation-ready
copies of Toronto Star content for distribution to colleagues, clients or customers, or
inquire about permissions/licensing, please go to: www.TorontoStarReprints.com
Sarn¡a doctor st¡ll pract¡sing aftercourt ruling he sexually assaultedcolleagueDr. Syed Nasir Ali was ordered last month by Superior Court Justice Johanne
Morissette to pay $zoo,ooo in damages to a colleague for the 1999 incident.
The College of Physicians and Surgeons of Ontario would not confirm or
deny if Dr. Syed Nasir Ali is being investigated. (DREAMSTIME / TORONTO
STAR ILLUSTRATION)
By JACQUES GALLANT Legal Affairs Reporter
Sun., April 30,2017
A Sarnia physician who was found by a civil court to have pinned down a fellow
doctor in her home and sexually assaulted her has continued to practise medicine
https://www.thestar.com/nevvs/gta/2017t%l3}lsarniædoctor-still-practising-after-court-ruling-he-raped-colleague.hlml
star.com
1t4
51112017 Sarnia doctor still practising after court ruling he sexually assaulted colleague I Toronto Star
"without consequence," a judge said.
Dr. Syed Nasir Ali was ordered in ApriÌ by superior Court Justice JohanrMorissette to pay Dr. B gzoo,ooo i' damages for thc 1999 incident.
re I 000
Ali was never criminally charged for the assault. (Dr. B did report the incident topolice). Ali's profile on the public register of the College of Physicians and Surgeonsof ontario shows no discipline history or restrictions on his licence.
"The fact is that Dr. Ali has not had to atone for his actions since Lggg;'Morissettewrote. "He has continued to practise medicine and live in Sarnia withoutconsequence for the sexual assault he committed on (Dr. B)."
A civil case requires a lower burden of proof than criminal cases, which is proofbeyond a reasonable doubt. In civil court, it must be proven that it was more likelythan not that the alleged incident occurred.
Ali's lawyer, Nina Perfetto, declined to comment to the Star as Ali intends to appealthe ruling.
The Star is not naming Dr. B as it does not identifii victims of sexual assault withouttheir consent.
"In reaction to the verdict, I felt an extreme sense of relief as I had suffered.humiliationfor t7 years," Dr. B told the Star in an emailed statement. "I believe thatDr. Ali's conduct should result in serious professional consequences. I hope that theCollege of Physicians and Surgeons deals with this situation appropriately."
The college has the power to discipline physicians for conduct that took place in theirprivate life, and Dr. B's case highlights the lack of information shared publicly by themedical regulator regarding its investigations.
A college spokesperson said she could not confïrm or deny that Ati is in fact beinginvestigated.
"Certainly I would expect in the face of a decision like this that the college wouldwant to launch their ovrn independent investigation," said medical malpracticelawyer Paul Harte, who was not involved in the case.
"In my view, the college should indicate whether they are in fact investigating thecivil findings. Such a statement would reassure the public and it would create little orno prejudice to the doctor (Ali) given the public finding of the civil court."
Ali and Dr. B first met in the early 199os when they were both married with youngchildren, court heard. Dr. B said they would speak regularly as they shared much incommon.
https://www.thestar.com/news/gta/2017l%l3Olsarni+doctor-still-practising-after-court-rulingrhe-raped-colleague.lrtml2t4
5/1t2017 Sarnia doctor still practising after court ruling he sexually assaulted colleague I Toronto Star
Ali testified that the two had had an extramarital affair that began around Lgg2,
which included sex in his car, in a park - "he remembered that the leaves werê
changing colour," Morissette wrote - and" at North York General Hospital. 1001Dr. B denied the affair and Ali's testimony on that point carried no weight in thejudge's findings. Morissette noted that an affair was never mentioned in any of AIi's
statements of defence.
"Dr. Ali's explanation for the change in evidence was that he was hopeful that the
matter would resolve itself without public disclosure and was concerned that he and
(Dr. B) could be victims of honour killings" by their families if the information came
out, Morissette wrote.
Ali and Dr. B presented two very different versions in court of the 1999 incident. The
judge ultimately sided with Dr. B.
She testifîed that Ali came over to her home under the pretense of an "urgent
matter," and then proceeded to remove his shoes and shirt at her door, telling her
"that he was hot." It turned out he wanted her to help complete a life insurance form
for the renewal of his office lease, court heard.
At one point, while Dr. B was bent down in her den plugging in the air conditioning,
Ali came into the doorway naked. He then tripped her and lowered her onto a rug.
While she pleaded for him to stop, he penetrated her and then ejaculated on the
carpet, Dr. B testified.
He then put his clothes back on and asked for a ride back to the hospital, to which
Dr. B agreed.
In Ali's version of events, he was the one who received the call from Dr. B to come to
her home so she could help him with the insurance form. He testifÏed that she was
examining his abdomen, as part of a physical examination for the form. He testified
Dr. B said to him "I want you now," but he got up and left the house.
(Dr. B denied performing an exam, saying she had no medical equipment at her
home.)
The rug would prove to be an important piece of evidence. Ali denied at trial that he
had any contact with it. But in 2oo1, Dr. B had the rug tested, which confirmed the
presence of semen. She then had a friend take a ceramic mug which Ali had been
using at a department meeting.
Court heard that the DNA on the rug was a match to the DNA on the mug. Alicontinued to deny ejaculating on the rug, but refused to provide a DNA sample.
The judge concluded that on a balance of probabilities, the sexual assault occurred.
She found Dr. B's evidence of the assault over the last 15 years to be consistent, and
https://www.thestiar.com/news/gat2}lTl%l30lsarnia-doctor-still-practising-after-court-rulingihe'raped-colleague.html 314
511t2017 Sarnia doctor still practising after court ruling he sexually assaulted colleague I Toronto Star
was corroborated by several friends and colleagues to whom she confided followingthe incident. 1002She also found that Ali's evidence was undermined by the failurc to chsclose analleged affair until the eve of the trial.
"(Dr. B) testified that she was in shock, horrified and humiliated by the assaultiveconduct of a person she considered to be a friend and work colleague," Morissettewrote.
"She testified that she felt violated. Her pride and dignity and sense of self-worthwere attacked. She felt like he treated her like a prostitute in her o\ m home."
Copy'right owned or licensed by Toronto Star Newspapers Limited. All rights reserved.Republication or distribution of this content is expressly prohibited without the priorwritten consent of Toronto Star Newspapers Lirnited and/or its licensors. To order copiesof Toronto star articles, please go to: www.TorontostarReprints.com
https://www.thestar.com/news/gital2017l%l30lsarnia-doctor-still-practising-afrer-court-rulinghe-raped-colleague.htm I 4t4
'sexually abusive' dentist was once voted best in Vaughan I Toronto Star Page I of2
I 003This copy is for your personal non-commercial use only. To order presentation-ready copies ofToronto Star content for distribution to colleagues, clients or
crstomers, or inquire about permissions/licensing, please go to: www.ToroutoStarReprints.com
tsexually abusivet dentist was once voted best inVaughanA Vaughan dentist has lost his licence to practise after admitting to having had sex with one patient, while acting in a
"predatory and sexuaìly abusive manner" toward another former patient.
Dr. Paul Sclodnick has had his dental licence revoked. He once served as president of the York Region
Dental Society and reportedly counted actress Neve Campbell among his pat¡ents. (BERNARD WEIL /TORONTO STAR) I ORDER THIS PHOTO
By IACQUES GALLANT Legal Affairs Reporter
Wed., April 26,2c17
Dr. Paul Sclodnick claims ou his website that it's the "positive atmosphere he creates with his cariug tnanner and
extensive dental experience" that has brought so many patieuts into his Maple clinic, inclndiug actress Neve
Campbell.
Ask some of Sclodnick's former patieuts and employees about atmosphere and you might get ar eutirely different
resporÌse.
Sclodnick, the principal dentist at Maple Dental Health, admitted this week to having had sex with one patient, while
acting in a "predatory and sexually abnsive mannef' toward auother former patient/employee'
The dentist, who was once voted "best in Vaughan" by readers of the Vaughan Citizen and is a past president of the
York Region Dental Society, is now finished.
The discipline panel of the Royal College of Dental Surgeons of Outario yanked his licence following a joint
snbmission from lawyers for the college and Scloduick.
https://www.thestar.com/news/gtal2017l04126lsexually-abusive-dentist-was-once-voted-be... 412612017

'Sexually abusive' dentist was once voted best in Vaughan I Toronto Star Page2 of2
Lawyer Matthew Wilton acknowledged that tlìere was no other penalty available for his client. Sex with a patient is acartlinal siu in the health professions and the law calls for the rnandatory revocation ofthe practitiouer's licence.
"Yonr professional misconduct is a matter ofprofound concern," the panel's chair, Dr. Richard Hunter, toldSclodnick in a public reprimand.
"It is completely nnacceptable to your fellow dentists and to the public. You have brought discredit to the entireprofessiou aud to yourself. Public confideuce in this profession has beeu put in jeopardy."
Sclodnick, who received his licencein rg7g, declined to address the panel.
One day while he was in the office with a now-fonner employee, whose identity is covered by a publication ban, hepulled back the woman's scrub pants and tlìen tugged at the waistband o{ her underwear, safng he wanted to seewhat colour they were, according to an agreed statement of{acts.
In another instance, he was alone with the woman in an elevator wheu he said "we have eight seconds alonetogether," and then kissed her without her consent.
And theu there was the time she gave him a drive home aud he "inappropriately put his haud on her leg," accordingto the statement offacts. When he got out ofthe car, he told her "he did not know how he would be able to workbecause he had a boner."
The woman recalled that Sclodnick tnade other sexually inappropriate comments and gestures in her presence atother times as well, according to the statement,
The panel noted that the woman was l'ulnerable after her husband died, leaving her the sole wage-eamer andcaregiver for her daughter.
"This episode had a negative impact on her life, and left her physically and emotionally drained and deeplytraumatized," said the college's lawyer, Christine Mainville, reading from a victim impact statemerìt.
The woman sought counselling as a result of Sclodnick's actions, she said.
Regarding the patient Sclodnick had sex with, the statement offacts said he was involved in a sexual relationship withher over a number ofyears.
In relation to a third complainant, also a former patient and ernployee, Slodnick admitted to toilching her hip whileshe was reaching for a binder, aud that this constituted professional misconduct.
"This is deeply concerning behaviour tlìat has spauned a number ofyears and targeted more thau one patient andemployee,' Mainville told the panel.
Scloduick was convicted in criminal court ofsimple assault on a former patient and given a conditioual discharge andrz mouths probation, accordiug to the Ministry of the Attomey General.
He had been required to practise il the preseuce ofa college-approved mouitor pending the outcome at the disciplinehearing.
Copyrigltt owned or liceDsed by Toronto Star Newspapers Limited. All rights reserved. Republication or distribution ofthis conteût is expressly prohibitedwithout the prior written cousent ofToronto Star Newspapers Limited and/or its licensors. To order copies ofToronto Star articles, please go to:www.TorontoStarRepriuts.com
1004
https://www.thestar.com/newslgtal2}lT l04126lsexually-abusive-dentist-was-once-voted-be.. . 412612017

rmmNmßñtr SATURDAY, APRIL 22,2017 SECTION GT ON ONO
dinic, Spear said, in the woman's pres-enct: "She is abeautiñ¡l woman and noJjust fromthe neckup. . . You shouldput a
ring on it before somebody snatches herup."And then came the statement about
beards.According to a recent discipline deci-
sion from tlre College of Optometrists,Spear then broached another topic withthe patient when she returned to the ex-amination rroom after having introducedher boyfriend to the optometrist
'The member also made aconunenttothe patient regarding an a¡tide that he
A SCI-FI LOVE STORYSure, the Gardiner is ugly. But it's useful, and as
Shawn Micallef says, maybe even beautiful, GT3
qì, ; \"i'i': li.i'{}ti.l '.\*"å'qi
Patient left doctor's omce in tearshad recently read about rnen's beards.The member told the patient that thearticle stated men's bcards are frrll of fe'ces," saidthe decision
"Tlre member eommented flrrther thatmen touclt their crotdr area and ttrentheir bea¡ds and then said that the pa-tient stror¡ld tlink about this when shethinks about her boyfriend, who the.membe¡had just met, (who) had abeardatthetime."Sþar, who opened the Toronto Eye
Clinic at Yonge SL and Eglinton Ave.about 3O years ago, admitted before adiscipline panel that his remarks about
I 005
the beard constituted professional mis-conducl He also admittedto makingthecornments about the patienfs looks,which the panel found to be sexual abuse.
He was handed afive-week suspension,ordered to take training on et}ics, andmade to pay $f6gOO for the patienfscounselling fees, should she require ilalong with a fr:rther $68,000 in costs tothecollege.
Toronto lawyer Bria¡r Greenspan, whorepresented Spear in the proceedings,objected to the term "sexual abuse.'
Toronto optometrist suspended formaking sexual remarks to woman
¡¡ceù¡s cAttAHTLEGAL AFFAIRS REPORTER
The patient went into the optometrisfs er<aminationroomwith conc€Íts aboutred eyes and a "circle" inher left eye. She left shaken and on the verge oftears.
"I'm not looki4g" Dr. Peter Spear told the 25-year-oldwoma¡l when he asked her to uncross her legs toconduct an examination "If only I was younger," hetold her at another poinl
To the patienfs boyfriend, who had a:rived at the
May 5-7,2017
60 Tal¡le Ganes .535 Slots
Port Perry, 0N::: grealblueherollcas¡no.conì
Ploy. SmoÉ Must be 19 or older
ptlt(Tr;ta I
BLUEGBÉAf
J noot
EYE EXAM continued on GT6

Doctor had'unblemished recordo II 006
awyer saysarp appropriately vieræd*¡s;-such*t"n
"o"tì¿eypd obiectivelv' "anù ts
-¡whoie, in all of the circurnrt4'P:'tritt" o*ut told SPear in a Public.ániu"a that his behaviour had
brãu$rt the profession of optometry
into disrepute.-fV" vi"',"tfris case involving sexual
abuse as serious- W-e are concerned
that, as a practitioner, you failed to
nrovide ari environment w-here your
pÀtie"t felt safe and comfortable'"
the panel saidItå¿i"rl malPractice lawYer Paul
Ha¡te, who \¡/as not involved in thiscase. said the college sent an impor-
iÃt'*".t"g" of zero tolerance, and
ouestioned whether the same com-
olaint about a physician would even
make it to "
ösciPline hearing'"I dobelieve that tlre use of the term
'sexual abuse' may have been unduly
strong for the facts ofthis case' This
does nottake awayfromthe inexcus-
able natr-rre of the conducl'' Harte
said-"The optometrist clearlywent over
urãUn" *¿ tnoot¿nothave engaged
in ttris trarassingbehaviour' He paid a
siørificant penalty reflecting the im-
oõrt"tt." of boundaries between
ireaìth workers and their patients'"
EYE EXAM from GTl
Greenspan also higtrlightêd Speat's
'f-Ut"*ittt"¿, 3O-plus-year record'
inhisfield.'TIe's higtrtY regarded' He is a very
rurã "*tãttiott"i.
H" has mentored
.ã""U"tt PeoPle, has mentored
countless women optometrists' Two
ái nis aos"st associates, within his
oractice, a-re women. He has gfeat'resnect and sensitivity toward wom-
en,'^' GreensPan told the Star'- rie said the term "sexual abuse" is a
"misnomet'' in this case, while ac-
Ltto*t"Agittg tttut provincial legisla-
ãã" *rÈ"t ãlea¡ that remarks alone
can constitute sexual abuse of a pa-
tient.*"üã *^ always honest and candid
about what had occun ed and he was
not as sensitive in terms of his lan-
guæ" *¿ his resPonsiveness to his
ñ*d""t as he ought to have been"'
GreensPansaid-,tf aüirg said that, the words'sexual
aUnsej it""se¿ outside the context of
the health professions ' ' ' t-hen one
would think he is a Predator' or
somebodY who took advantage ot
someone, or someone who PhYsical-
ly invaded somebody's sPaee'
F
Dr. Peter Spear was g¡ven a five-week suspension'.ordered to take ethics
iätr*i t.ã *v S1ã:0oo t"t *" ptiitnt's counielling fees' if she requires it'
"That's why the words 'sexual ofwhattookolace'"
abusd are such a misnomer ior the In an agreãd statement of facts'
typeofbehaviour*",t"t'ä"ãitä" spear suià'trt"t he did not intend for
'The conduct *"" u"toJåttfî *ã his comments or behaviour to be
admittedly insensitive, il;î th; sexual-innature' but admitted that'
sametime,thafsut"*tt"íä'iätpä"t øtrt trt" benefit of hindsight' "they
Advertising by some Manitoba chiropractorsundermines public health, exp ert says . , 10OTCBC News found many chiropractor websites containing ' - - - 'statements at odds with public health advice
CBC Investigates Posted: Mar 20' 2017 4:00 AM CT
Jacques Marcoux. Katie Pedersen' Katie Nicholson'CBC News
Several chiropractors in Manitoba disseminate inforn¡ation that is at odds with public
health advice. (Shutterstock)
345 shares
,l15 comments
Should chiropracfors åe weighing in on the vaccine debate? Who do you take
advice from? Te[us what vou thiltk in a video comment in ournew QggdTalk experinlgnt.
Statements circulated by dozens of Manitoba chiropractors are misleading and
potentially harmful, says a public health expert.
1 008"There is no evidence that chiropractic is effective in treating cancer and autism and anyof those things that they are apparently claiming that they can treat," said Dr. Atan KaÞ,director of the Manitoba Centre for Health policy.
A CBC News analysis of company websites and Facebook pages of every registeredchiropractor in Manitoba found several dozen examples of statements, claims andsocial media content at odds with many public heatth policies or medical research.
Examples include:
Offers of treatments for autism, Tourette's syndrome, Alzheimer's disease, colic,infections and cancer.
Anti-vaccination literature and recently published letters to the editor fromchiropractors that d iscourage vaccination.
An article claiming vaccines have caused a 200 to 600 per cent increase inautism rates.
A statement that claims the education and training of a chiropractor is "virtuallyidentical" to that of a medical doctor.
Discouraging people from getting díagnostic tests such as cr scans,colonoscopies and mammograms.
An informational video discouraging the use of sunscreen.
a
a
a
a
a
a
1009
Dr, {an Katz is the _direc_tor of the Manitoba Centrg for Heatth Policy. (CBC News )
Based on the Manitoba Chiropractors Association membership listing, there are
approximately 2TS licensed practitioners working out of 215 offices. CBC News found
questionable online content linked to more than 30 chiropractic offices.
Dr. Katz reviewed the examples gathered by the CBC l-Team and labelled most of them
"misinformation."
"tt misleads the public in two areas. Firstly, those who choose to go for chiropractic
care, particularly for things like infection and autísm and things that we know they're not
going to be beneficial for, it mísleads those individuals and gives them false hope for
treatment that will not be effective," he said.
"Putting these things up on their website also puts the doubt in the minds of others
about what we do know works, and as a result those people may not seek the right type
of care for conditions that could deteriorate if they don't seek that care'"
Vaccination and immunizations outside scope ofpract¡ce
1010The Manitoba Chiropractors Association declined an interview request but did say itwould review the content.
This irnage disparaEinE medicalclinic Facebook page.
tneatments and physicians appeared on a chiropractor's
"As the regulatory body that oversees the practice of chiropractic in Manitoba, we willreview the material you have shared with us in a thorough manner as provided for byour internal processes," said Ernie Miron, a chiropractic doctor and the associationregistrar.
ggilnlTilGlnIU$
hrnrcümcrhrffitËrürlrcdnænrlrnrhtrnütütüthfrJü
îrrlmnnlrhp;rrrfmmfDi¡r¡sr ¡s düct lrl hct ü tül lrn¡
h¡ntæ¡¡olhJllrtSonucnü¡ml mrtcln h ffirnlilrnr¡¡r¡rclmrl¡stlrtnflr¡
rawforbeau .comlol¡ftgl:
1011The Manitoba Chiropractors Association has previously addressed certain issues with
its membership through an internal communication.
"ln Manitoba, the administration of 'vaccination and immunization' currently falls outside
the scope of chiropractic practice," the communication said. lt also cautioned members
that:
. "Ch¡ropractors may be liable for opinions they provide to patients/public in
circumstances where it would be reasonably foreseeable that the individual
receiving the opinion would rely on it.
. "Providing professional opinions on the issue of vaccination and immunization
would likely be found by a court to be outside the scope of practice of a
chiropractor."
The association also said, "The degree to which a chiropractor can or cannot discuss
'vaccination and immunization'or other health-care procedures that are outside the
scope of practice with a patient is currently being reviewed by the board of directors."
'We encourage Manitobans to get vacc¡nated':prov¡nce
Manitoba is the only province in the country that universally covers a portion of
chiropractic treatments for all residents, to a limit of 12 visits per year.
ln 2016, the province paid out $11.9 million for a total of 984,432 claims from 166,897
unique patients.
1012
A local chiropractor shared this nnes sage on their company Facebook page. HealthCanada says fluoride concentration s in drinking water do not pose a risk to humanhealth and are endorsed by over 90 national and international professional healthorgan izations. (Facebook)
The fact that members of a regulated health profession are actively disseminatingquestionable medical information while benefiting from public funds ís cause forconcern, Katz said.
"Should we as a society be paying for the services of professionals, and I use that wordloosely, that are advocating care that is contrary to the official public policy?"
Manitoba's health minister didn't comment on the issue, but Manitoba Health provided astatement after it was given examples of the information.
"We offer a publicly funded vaccine program that follows national guidelines onimmunization and we encourage Manitobans to get vaccinated. But vaccination isalways a matter of informed consent between a practitíoner and a patient, based on an
- ' .r', i (.RI S'l L.,ee ¿rrle tlre f rrsl f t.(.r dr l.r¡tfrf;a:le+ i -,.)ttle CAl.-:i iS ll't e pirìea'ç a'.:-: clher.,,¿rse hnit.,,r., ¿..
¡C.'th,rd eye,tÞ ¡i' terally nas.CíiS A^Õ cones -sl (eì:t,. otlìfÌr r,lytst
+ : ..t .ì.
a, (ì ¡r, r,¡1 l'í)X,' l,'rìt ll t(, CO,ì..,.1 n.e._r:l il¿l/lJi,(:(.,(*cl\lr' fly llre i Í)A
a 't:T. i [ì flucrr;Cale3 ,lr.,e w,atr:r r, lf.e ccncr:ntrírl o.r ca^.ps:: Si ")ÂIt tl-,r- cr r:-ers
+ r.joiide rS 1þe sA-e ^qredleni useC " rat POlSC.r a^CF'o¿ac
¿cc,,';,' ,'l l,-' {)r fl; ,-'s''.,,'s()/;. ll,t,,t, ,, f f,¿' s.t.,.t,(.(Jii r.i r,..: r, .)/ll¡1¡;, ,1r' ,r' .lrt Íl ()t.tt:i'.r,Ç.115 ,tl l!¡¡1¡¡,¡t,¡t,'J i,tt.' ,r,.tl¿,, .tr f/.r..r, :t .n ,t
"p(a 5 ¿e,1 ,tflto¡Jtrl .ec¡rr!1t ,,() C¿¡l lhe P.¡ 5,_r¡r ¡-'çr¡1 f¡9l ( ?./):f.. J\/tìac,n! ":c,ndcx ¿o th6, l¡.:¡r c.1 ,)î ¡ t t,c. .l ,)l(d f¡)¡tf lr!,.lsie
L
Ditl t'ou knrlu'.)
rL0ffRlDr

1013informed evaluation of the benefits and risks. lf any practitioner provides advice that ts
contrary to our position, we do not agree with it."
,i'
lo ttre Amerlcon Journol d Ch¡ldhood Dl¡eo¡c¡ ondJoumol of the Amerlcon O¡leopolhic A¡¡oclollon
TRUfII R¡
,,. lI
l..d ,f'
A F¡ver IS rHE BODY'S PERTECT IESPONSE TO TIGHNNG INTECIION
2.S'. .,i-5 Sit<J!',' Tl'¡^'l i?Ll-^.j( ,1.(; [ [.','í.i' !', ]ltr . f 'lt-t ¡.{AV il"'i(,llLAStlrli :tVil¿ l,r & t,):lRAIrc)|.. (,)i Ti:i l,"tr'.i )s
3.l3 o¡rreRENI sTUDtEs sxow IHAT YouR cxllo's Rlsl orPERAAANENÍ DAMAGE TIOM A ÍEVET ARE NOT REDUCED ¡Y USING
ANT|-fEVIR DRUGS (N.V.OUlt, TYTENOI, ^^OtRlN,
l0U.?RQfllJ, EIC.)
f. t) ii-)iJ I,t.i(),'i !f iÁi ¡\ rIvl-? (- i:I Air.5 ¡\l¡ [ Ìi,' I'iì:,i'.'i'il ¡" ili' :;
i ,,rl)Y i¡',i 'iii: i..ii iìr\Cì[:] ¡r ,i:.1-) V,irl.',lS ( ¡\'.1,(.-\' 5.;'^'vitf ?
õ.To supponT n FrvrR: Gn YouR Spl¡¡e Ao¡usTED, DnlxxPtrrury oF WATER, Ear LlGHt, AND Gsr AoeouATE REsT
| ¡øa æ fr ,,*r I'ù.tr#r. J 'g'aY't
H t'|ñ ln¡r¡ ,trr¡$ d ù¡¡ñ¡+f O¡r¡¡r¡ lto h, f tl, , h't,r J ¡lü f årl t ¡Ð¡al ,, ¡traSr< rr¡rçJar trrr¡n¡¡ I rrrrlry mør¡bùlrt I ltt¡. . ¡ ¡t;1¡.4
t+¡lått fDt rúi.| I ia ¡¡r¡<¡ o¡te¡r$rc Aü,*rlDrl
Information on fevers posted online by a Manitoba chiropractor. The College of FamilyFhysicians of Canada says that if a infant has a temperature of 100.4"F (38"C) or htgherto call the doctor or immediately go to an emergency roorn. (Website)
Anti-vax letters to the editor prompted CBCinvestigationA letter by Winnipeg chiropractor Henri Marcoux was published last February in
Manitoba's francophone weekly newspaper La Liberté, in response to an article in which
a regional health authority expert was interviewed about influenza immunizations.
1014. Read translated version of the exchanse of letters in La Liberté
Marcoux wrote that he does not recommend flu vaccines, calling them "toxic." Hefurther stated that the flu virus actually "purifies our systems" and said that he believesflu vaccines are "driven by a vast operation orchestrated by pharmaceuticalcompanies."
People should instead focus on general wellness - which includes chiropractictreatment - to stave off the flu, he wrote.
Claims by a chiropractor that he orand Asperger's syndronne is not suthe Manitoba Centre for l-lealth Fol
she can treat disorders such as autism, Alzheimer'spported by evidence, says Dr. Alan Katz, director oficy.
Now-retired chiropractor and long-tíme anti-vaccination advocate Gérald Bohémierwrote a later letter in support of Marcoux that also appeared in La Liberte.
. chiropractic neck procedures cause strokes. sav suryivors
. Manitoba clinic avoidins opioidP in chronic pain malaqement
Letters then poured in from members of the community, including a resident and twophysicians who took exception to these statements.
Marcoux told the CBC's French service, Radio-Canada, that he does not believe hisviews are at odds with public health.
i'fa:l ix:tri. .ì:c --i .ì,!.ì.r i-:: :3aìe ;- :acr.ì:t:r.
íl:rt-.'I lre.ìt1 :¡e r:i 3r, -:: ::-:
r :.r .'i f;Ì aJ, !: .:.r_it..
'.,,t .l :fX':.ì ;f: P(1. a ,r
-
l¡r,J1:, t^o'3 ;.1¡,..;;lf J! ellÞ Ê._ t''f,". ::, :.e.:1 ^t,_.: CJ Pt-r¡ -,'

1015He stands by his letter, he said, adding if society as a whole took health and wellness
more seriously - rather than trying to treat symptoms - the need for vaccines would
dissipate or never would have existed in the first place.
Facts on chiropractic seruices
. Chiropractors in Manitoba are authorized by the Chiropractic Act to use the title
"doctor," but only if the individual displays or makes use of the word "chiropractic"
or "chiropractor" immediately before or after the name.
. ln 2016, Manitoba Public lnsurance spent $7.5 million on 176,820 chiropractic
treatments.
. ln 2016, the Worke/s Compensation Board spent $1.9 million on 48,226
chiropractic treatments.
. Chiropractic services have been covered by Manitoba Health since 1969.
. British Columbia, Alberta and Saskatchewan all offer some form of public
coverage, but only for limited groups, such as seniors and people on social
assistance.
. Ontario delisted chiropractic coverage in 2004 in a wave of health-care cuts.
Got a tip for the CBC l-Team? Email [email protected] or call the confidential tip line at204-788-3744.
Note to readers: 1016The letters below are in chronological order. They were written by:
o HenriMarcoux,chiropractoro Gérald Bohémier (retired chiropractor)o Dr. Denis Fortier, Southern Health Region
o Lucien Chaput, residento Dr. Philippe Erhard, family and sport medicine physician
o They were pubtished over the past four weeks in the French Manitoba newspaper La Liberté.
o The first tetter (by Henri Marcoux) was in response to an interview with Southem Health vice-president
of medical seruices Dr. Denis Fortier, tast January about the importance of flu immunizations.
o The letters below were translated from French to English.
Letter to the editor, La Liberté, February 1, 2017
Title: A denunciation of the the flu vaccine
To the editor,
Allow me to express a view on the flu vaccine that differs from those held by Dr. Denis Fortier,
published on the third page of the January 25 to 31 edition ot La Liberté.
f do not recommend vaccines because the immunization process is a naturalprocess of the
human body. The body uses all sorts of strategies to ¡mmunize itself against all possible harms
that coutd cause it to become sick. Vaccines can create a temporary immunization reaction,
however natural immunization creates antibodies that are permanent'
It is clear that there are benefits with certain vacc¡nes that have reduced the incidence of serious
diseases, such as malaria or tuberculosis. However, it's ridiculous to to think that we can
immunize the public against all the so-called "infectious" diseases. Especially when such a large
number of these illnesses are simply a manifestation of a life under stress, to poor nutrition, to
milk products, to a lack of exercise, among others.
This applies also to the flu, which I view as a cleansing of the body. Does it not generally arise
when we are exhausted, consume too much caffeine or alcohol, lack sleep, for example? Whether
young or very old, the flu is an inconvenience that requires more than a vaccine.
The vaccine against the flu does not help us develop a strong immune system that is strong when
it's the result of proper bodily functions. The absence of illness is a strength of well-being that
enables us to prevent illness.
a
1017Convinced of these beliefs, I believe that vaccines against the flu are driven by a vast operationorchestrated by pharmaceutical companies with the support of a majority of the medicalcommunity. But not all, because the medical community does not unanimously agree on the issueof the mass vaccinations of populations.
I understand those who are hesitant since the flu vaccine only provides protection against virusesfrom past seasons, not against the flu season underway. Why inject ourselves with a toxicsubstance that contaíns mercury or other poisons? lt's best to become aware of the fact thatviruses associated with the cold and flu are always present in our bodies. They operate in a waythat does not cause diseases. ln fact, they purify our systems as our bodies become too full oftoxins.
So what are we to do when we give ourselves a cold or the flu because of our lack of properwellness? You need to rest, consume liquids (pure water, tea), use heat to stimulate the immuneand circulatory systems (hot baths, sauna, massage, chiropractic treatment), have proper nutritionto create a bodily environment that can combat toxins, take vitamin C (2,000 to 5,000mg per day)and commit to a healthy life.
For those who want to know more, I recommend the documentary series called "VaccinesRevealed" ([email protected]) that scientifically exposes the absurdity of globalimmunization programs.
Henri Marcoux, chiropractorSaint-Boniface, ManitobaJanuary 27,2017
Letter to the editor, La Liberté, February B, 2017Title: Vaccines are not sacred injections
To the editor,
It is with consternation that I read in the January 25to January 31 edition of La Liberté the viewsexpressed by Dr. Denis Fortíer regarding the flu vaccine. Hence my response that opposes hispropaganda ín favour of this quasi religious rite that are flu vaccinations as well as these heavenlypraises in favour of vaccines in general.
Ïoday, one of the best scientific sources to take a step back from doctor Fortier's darling vaccinesís the report called "Cochrane Collaboration". These independent researchers do not share thesame views as the good doctor. Their conclusion assures us that science does not support theconclusion that vaccines is a valid tool to prevent seasonal flu, especially amongst the elderly.
1018Of concern, among others, is the presence of mercury in vaccines. Because of the neurotoxicity ofthe chemical compound in question (thiomersal or thimerosal), the vaccine is considered to be
one of the possible factors in autism rates among young children.
Let's dig a little deeper into the question of autism in children. The rate of autism was 3 per 10,000
in the 1950s to I in 68 today. M.l.T. professor Stéphanie Seneff estimates that if this trend
continues, in 2025 50 per cent of children could be affected and 80 per cent of boys. Horrible!
How can the human race hope to survive if we reach a point where half of our children are in
perpetual need special care? One does not have to be a mathematician to understand this
situation is unsustainable.
I would also note that the most recent generations of children are increasingly suffering from
allergies, asthma, learning difficulties, cancer, neurologicaldiseases, auto-immune problems,
gastrointestinal problems and much more. They are notably less healthy than their parents and
grandparents. Has the time not come to seriously question the role the ever increasing
vaccination rates of our population?
tn fact, the link between our children's health and vaccines seems to be increasingly more certain.
ln 2014, an experienced researcher with the U.S. Center for Disease Control, Dr. William
Thompson, blew the whistle on the situation. He presented thousands of pages of documents to
the U.S. Congress showing links dating back to 2004 between autism and the Measles, Mumps,
Rubella (MMR) VAccine. But this information was systematically suppressed.
Sadly, the CSC and U.S. Congress continue to sit on a pile of evidence proving this is a fraud.
Thankfully other independent researchers have received copies and have disseminated this
information (6). lt's really time to take a step back regarding the love affair certain people have for
vaccines that they consider to be sacred injections; and of course let's understand that they are
not.
Gérald Bohémier(retired doctor of chiropractic)Beauséjour, ManitobaJanuary 31,2017
Letter to the edítor, La Liberté, February 15, 2017
Title: Dr. Denis Fortier's recommendations regarding vaccines
To the editor,
How does one know if information contained in an article is credible or not? ln this era where
people in positions of authority speak of facts and alternative facts, how does a memþer of the
1019public searching for a clear and truthful answer avoid drowning in a sea of information found onthe Web? Regarding vaccínes in general or the flu vaccine in particular, the question to ask is:Where can we source information that is credible regarding the risks and benefits of vaccines?
ln the scientífic world, research results from individuals or teams must be presented to peers andmust pass an examination by these peers (other scientists with the necessary expertise in thefield in question) to ensure that the conclusions are considered credible. This review process is farmore rigorous than, for example, the opinion of an expert.
Once the work of a scientist has been validated by his or her peers, the research can then beaccepted for publication in a reputable scientific journal. After the publication, the study can becriticized and corrected down the road. The published study can also lead to other research thatcan either confirm or contradict the original conclusíons.
This then begs another question: who has the time, the education or the interest to spend hoursand hours reviewing scientific literature to confirm the validity of this research? Regardingresearch on vaccines, or flu vaccines and the associated risks and benefits, I recommend visitingnationally and internationally renowned websites that have taken the time to rigorously review thisscientific literature.
lf you are looking for more information, I recommend as a starting point Health Canada's websiteor the U.S. Center for Disease Control. Or at the international level, what the World HealthOrganization has to say about vaccines.
Dr. Denis FortierFebruary 11,2017
Lefter to the editor, La Liberté, February 15, 2017Title: ln response to Gérald Bohémier
To the editor,
Unbelievable!
A retired chiropractor turned comedian! How else to react to the fact that the wise anti-vaccinationdoctor champions information that has been long been circulating on Facebook that claims that S0per cent of children (and 80 percent of boys!) could be autistic by 202s.
Of course, don't take his word for it. lt's a professor from the prestigious MIT lnstitute that said it.He referenced it in a note at the end of his letter - it's all so very scientific. ln fact StephanieSeneff, an anti-vaccination and anti-GMO advocate, is a computer scientist with no background in
1020epidemiology. The chart that she produced to support her claims simply illustrates a correlation,
not causation. Using data for the same years, one could also produce an even stronger
correlation between autism and the increase in organic food sales. Better watch out for organic
products!
The reality is actually much simpler. Changes in the way autism is diagnosed explains the growth
in cases. Today we talk about autism spectrum disorder. Basically there are as many forms of
autism as there are autistic people.
Unfortunately it's not just Facebook that peddles this type of false information repurposed by
Gérald Bohémier in his letter to the editor. lt seems all of Hollywood is in on it. Even the president
of the United States Donald Trump buys into this hypothesis. "l've known cases," he said.
For these people, we can forgive their ígnorance. Like many have pointed out: they don't know
what they're doing. But when one signs off on a statement with "Doctor of chiropractic" to give an
air of authority, that person should know better. Retired or not, it dangerously borders on
professional misconduct.
Lucien ChaputBelair, ManitobaFebruary 8,2017
Letter to the editor, La Liberté, February 22, 2017
Title: A warning from Dr. Philippe Erhard
To the editor,
The letters from Mr. Gérald Bohémier and Mr. Henri Marcoux regarding vaccines warrant a
response.
The belief that vaccines cause autism is founded on a pseudo-study from 2003 that used a
sample of only 12 cases and has since been completely discredited. The author, Andrew
Wakefield, falsified the results and was condemned (four charges for dishonesty and 12 charges
involving the abuse of developmentally challenged children).
What's more, numerous scientific studies have been conducted across the globe. None could
ever demonstrate a link behueen autism and vaccines (or between mercury and autism).
There are severalerrors in Mr. Marcoux's letter. I won't list them all, but here are a few important
points:
1021M' Marcoux is confusing the common cold with influenza. He describes influenza as a simpleinconvenience. But it's an illness that, in the best of cases, is associated with an elevated fever,intense levels of fatigue and severe muscular pain. lt can also lead to myocarditis, encephalitisand can lead to death. Estimates show that 12,OOO Canadians are hospitalized each yearbecause of the flu and 3,500 people die from it. Pregnant women, children under five and theelderly are among the most vulnerable to complicatíons. But the flu can affect each and every oneof us. Living a perfectly healthy lifestyle is not enough to avoid the illness.
Also M. Marcoux adds that the virus is always present in our systems and serves to purify or tocleanse the body. Thís "idea" is not founded in any scientific study.
I'll note that chiropractic treatments do nothing to fight off the flu.
I ask readers to not make any important decisions on their health or the health of their childrenbased on personal opinions or on falsified pseudo-scientific studies. Serious diseases such asmeasles are reappearing due to a lack of vaccinations.
Dr. Philippe ErhardFebruary 13,2017
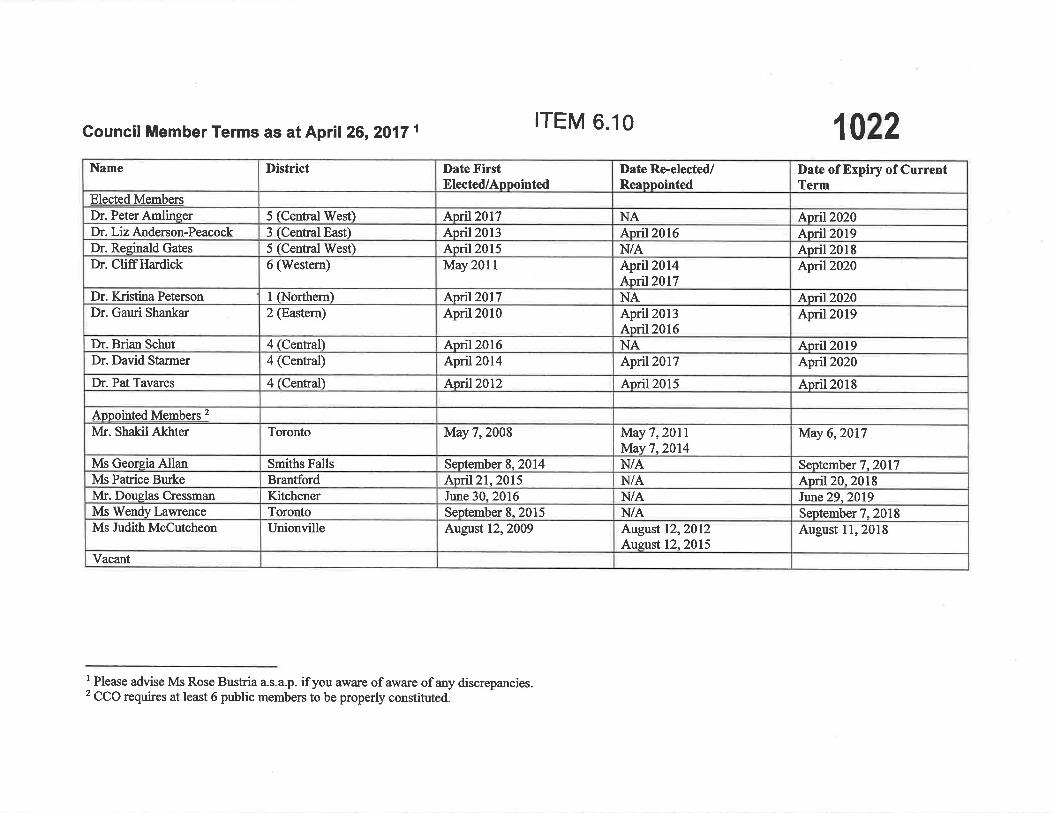
|TEM 6.10 1022Council Member Terms as at April 26,2017 1
I Please advise Ms Rose Bustria a.s.a.p. if you aware of aware of any discrepancies.2 CCO requires at least 6 public members to be properly constituted.
Date of Expiry of CurrentTerm
April2020April2019April2018Ãpnl2020
April2020April2019
April2019April2020
April2018
May 6,2017
September 7,2017April20.2018Jtur¿ie29,2019
September 7,2018August I l, 2018
Date Re-elected/Reappointed
NAApril2016N/AApril2014April2017NAApril2013April2016NAApril2017
April2015
ivlay7,20llM¡ay7,2O14N/AN/AN/AN/AAugust 12,2Ol2Auzust 12,2015
Date FirstElected/Appointed
April2017April2013April2015May201l
Apnl2017April2010
April2016April20l4
Apnl2012
May 7,2008
September 8.2014April2l, 2015June 30,2016September 8,2015August 12,2009
District
5 (Central West)3 (Central East)5 (Central West)6 (Westem)
I CNorthern)2 @astenr)
4 (Central)
4 (Central)
4 (Central)
Toronto
Smiths FallsBrantfordKitchenerTorontoUnionville
Name
Elected MembersDr. Peter AmlingerDr. Liz Anderson-PeacockDr. Reeinald GatesDr. CliffHardick
Dr. KristinaPetersonDr. Garni Shankar
Dr. Brian SchutDr. David Stanner
Dr. Pat Tavares
Apoointed Menbçrs 2
Ivk. Shakil Akhter
Ms Georeia AllanMs Patrice BurkeMr. Douglas CressmanMs Wendy LawrenceMs Judith McCutcheon
Vacant
Related Documents











