Frequency and Correlates of Gambling Problems in Depressed and Bipolar Outpatients Journal: The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie Manuscript ID: CJP-2009-163-OR.R1 Manuscript Type: Original Research Date Submitted by the Author: Complete List of Authors: Kennedy, Sidney; University Health Network, Psychiatry Key Words: gambling, bipolar disorder, major depressive disorder For Peer Review The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Frequency and Correlates of Gambling Problems in Depressed and Bipolar Outpatients
Journal: The Canadian Journal of Psychiatry/La Revue canadienne de
psychiatrie
Manuscript ID: CJP-2009-163-OR.R1
Manuscript Type: Original Research
Date Submitted by the Author:
Complete List of Authors: Kennedy, Sidney; University Health Network, Psychiatry
Key Words: gambling, bipolar disorder, major depressive disorder
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 1
Frequency and Correlates of Gambling Problems in Depressed and Bipolar Outpatients
Sidney H. Kennedy, MD, FRCPC 1*
Brenda R. Welsh, HBHSc 2
Kari Fulton, BA BScN RN2
Joanna K. Soczynska, HBSc.3
Roger S. McIntyre, MD, FRCPC 4
Claire O’Donovan, MD, FRCPC 5
Roumen Milev, MD, FRCPC 6
Jean-Michel le Melledo MD FRCPC 7
Jean-Claude Bisserbe MD FRCPC 8
Mark Zimmerman, MD 9
Neasa Martin BSc OT 10
1. Psychiatrist in Chief, University Health Network and Professor of Psychiatry, University
of Toronto, Toronto, ON, Canada
2. Research Coordinator, Mood Disorders Psychopharmacology Unit, University Health
Network, Toronto, ON, Canada
3. PhD Student, Institute of Medical Science, University of Toronto, Toronto, ON, Canada
4. Associate Professor of Psychiatry and Pharmacology, University of Toronto, Toronto,
ON, Canada
5. Associate Professor of Psychiatry, Dalhousie University, Halifax, NS, Canada
6. Head, Department of Psychiatry, Providence Care, Queen’s University, Kingston, ON,
Canada
7. Associate Professor of Psychiatry, University of Alberta, Edmonton, AB, Canada
Page 1 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 2
8. Clinical Director, Department of Psychiatry, Royal Ottawa Hospital, Professor of
Psychiatry, University of Ottawa, ON, Canada
9. Director of Outpatient Psychiatry, Rhode Island Hospital and Associate Professor,
Psychiatry & Human Behaviour, Brown University, RI, USA
10. Mental Health Consultant, Neasa Martin and Associates, Toronto, ON, Canada
Address for Correspondence: Sidney H. Kennedy, MD, FRCPC
EN8-222 - 200 Elizabeth Street
Toronto, Ontario M5G 2C4
Email: [email protected]
Page 2 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 3
ABSTRACT
OBJECTIVE: The primary objective of this study was to investigate the frequency of gambling
in individuals who have been diagnosed with major depressive disorder (MDD) or bipolar
disorder (BD). Secondary objectives were to examine: 1.) sex differences in the rates of
gambling behaviour, 2.) the temporal relationship between onset of mood disorders and problem
gambling, 3.) psychiatric comorbidities associated with problem gambling, and, 4.). the
influences of problem gambling on quality of life.
METHOD: Individuals (>18 years of age) who met criteria for lifetime DSM-IV-TR-defined
major depressive disorder (MDD) or bipolar I/II disorder (BD), confirmed by the Mini
International Neuropsychiatric Interview (M.I.N.I) were enrolled. Participants were recruited
from five sites in Canada and one in the United States. Prevalence of past-year problem
gambling was assessed with the Canadian Problem Gambling Index (CPGI). Associated
comorbidities with problem gambling are presented.
RESULTS: A total of 579 participants were enrolled (female: n = 379, male: n = 200).
Prevalence of problem gambling did not differ significantly between MDD (12.6%) and BD
(12.3%) group. There was a significant difference in the prevalence of problem gambling
between males (19.5%) and females (7.8%) in the BD group (χ2
=8.695, P = 0.003). Amongst
individuals meeting criteria for problem gambling, the mood disorder was the primary onset
condition in 71% of cases. Individuals with a mood disorder with comorbid current panic
disorder (OR = 1.96, 95% CI 1.02 to 3.75), obsessive-compulsive disorder (OR = 1.86, 95% CI
1.01 to 3.45), specific phobia (OR = 2.36, 95% CI 1.17 to 4.76), alcohol dependence (OR = 5.73,
95% CI 3.08 to 10.65) or lifetime substance dependence (OR = 2.05, 95% CI = 1.17 to 3.58), had
a significantly increased odds of problem gambling. Problem gambling across MDD and BD
Page 3 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 4
populations was also associated with lower quality of life ratings.
CONCLUSION: These results reaffirm a higher prevalence of gambling in both BD and MDD
populations compared to previously published community samples. The study also identifies risk
factors for gambling behaviours within these populations.
Key Words: gambling, bipolar disorder, major depressive disorder
Word count: ABSTRACT: 328
BODY TEXT: 3627
Page 4 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 5
Clinical implications
- Clinicians should assess gambling problems in patients who have a mood disorder and
include this in their comprehensive treatment programs.
- Problem gambling in individuals with a mood disorder contributes to diminished quality
of life and is a detractor from a full functional recovery.
- Routine screening for suicide risk is warranted as problem gamblers are more than twice
as likely to report suicidal ideation
Study Limitations
- The cross-sectional design cannot infer causality
- Not all psychiatric diagnoses were assessed
- The sample was predominantly Caucasian
- The temporal relationship scales have not been validated
Page 5 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 6
INTRODUCTION
Problem gambling involves a pattern of repeated gambling behaviour that disrupts the
individual’s life including, but not limited to, family life, occupational functioning, finances, and
personal well-being1. The prevalence of problem gambling in Canada is estimated at
approximately 2%2, while a further 3% of Canadians are at low risk for problem gambling3.
Studies have shown that problem gamblers frequently exhibit symptoms of mood disorders.
Despite the significant association between mood disorders and problem gambling, there have
been few explorations of the temporal relationship and comorbid risk factors of problem or
pathological gambling in psychiatric populations. Extant studies evaluating MDD and BD are
limited by the small sample size, failure to consider the temporal relationship between gambling
problems and mood disorders, or inconsistent findings on the comorbidities or determinants of
gambling behaviours4-6. There is little research that explores the risk of gambling in mood
disorder populations and the contribution of psychiatric comorbidity to treatment outcome or
quality of life.
Through a unique partnership involving the Mood Disorders Society of Canada, the
Canadian Network for Mood and Anxiety Treatments and Brown University, USA, the mutually-
defined primary objective of this study was to investigate the frequency of gambling problems in
individuals who have been diagnosed major depressive disorder (MDD) or bipolar disorder
(BD). The secondary objectives were to examine; (i) sex differences in the rates of gambling
behaviour; (ii) the temporal relationship between the onset of mood disorders and problem
gambling in the two groups; (iii) the influence of anxiety and substance use comorbidity on
gambling behaviours in both MDD and BD populations; (iv) the influence of gambling
behaviours on quality of life in MDD and BD populations.
Page 6 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 7
METHOD
Study Design
This was a single-visit, multi-site study involving five sites in Canada (University Health
Network in Toronto, Walter C. Mackenzie Health Sciences Centre in Edmonton, Queen
Elizabeth II Health Sciences Centre in Halifax, the Providence Continuing Care Centre in
Kingston, and the Royal Ottawa Hospital in Ottawa) and one site in the United States (Rhode
Island Hospital, Rhode Island). Over 60% of subjects were recruited from the three sites in
Ontario (see Table 1). Prior to initiation of any site, an inter-rater reliability session was held for
all study coordinators and standardised instructions for questionnaire administration were
provided for use at each centre.
Sample
Individuals (N = 606; > 18 years of age) meeting criteria for lifetime MDD or BDI/II
defined according to the Diagnostic and Statistical Manual of Mental Disorders, 4th
Edition
(DSM-IV-TR)7 were recruited from outpatient mood disorder and general psychiatric clinics and
advertisements posted in local hospitals. Posters invited participants who had a diagnosed mood
disorder to complete interviews and questionnaires on lifestyle and mood symptoms. Subjects
were excluded from the study if they met criteria for schizophrenia or other psychotic disorders.
The study was approved by local Research Ethics Boards at each of the recruiting sites. All
enrolled subjects provided written informed consent.
Primary Measures
Psychiatric diagnoses were confirmed using the short version of the Mini International
Neuropsychiatric Interview, version 5.0.0 M.I.N.I.PLUS8 for DSM-IV. The structured interview
was administered by a trained research coordinator, and included modules for mood and anxiety
Page 7 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 8
disorders, current suicide risk, alcohol and other substance dependence and abuse. The
researchers at the Rhode Island Hospital site applied the Structured Clinical Interview for DSM
diagnoses (SCID-P) in place of the M.I.N.I. The M.I.N.I. has been validated against the
Structured Clinical Interview for DSM diagnoses (SCID-P)8 as well as the Composite
International Diagnostic Interview for ICD-10 (CIDI)9. At the time of interview, depressive and
hypo/manic symptom severities were assessed respectively using the clinician-rated Hamilton
Depression Rating Scale 7-item (HAM-D-7)10 and the Young Mania Rating Scale (YMRS)11 .
The prevalence of problem gambling was assessed with a self-report questionnaire; The
Canadian Problem Gambling Index (CPGI)1. The CPGI is a 9-item self-report questionnaire
scored using a 4-point Likert scale that assesses problem gambling severity in the past year. The
CPGI divides scores into categories to indicate four severity levels of gambling (O = Non-
problem Gambler, 1-2 = Low risk gambler, 3-7 = Moderate risk gambler, 8 -27 = Problem
Gambler). This study classified individuals scoring >3 on the CPGI as problem gamblers. The
decision to collapse ‘moderate risk’ and ‘problem gambler’ categories was performed to increase
sample size as has been done previously10,12.
Sociodemographic data were collected and included age, sex, ethnicity, marital status,
education and income. Other measures included the Quality of Life Enjoyment and Satisfaction
Questionnaire (Q-LES-Q), a 16-item self-report questionnaire, was used to evaluate current
quality-of-life13; The NEO-FFI Personality Inventory14, a 60-item self report questionnaire, was
used to assess personality according to the Five Factor (Neuroticism, Conscientiousness,
Extraversion, Openness, Agreeableness) model; The Trimodal Anxiety Questionnaire (TAQ)15 is
a 36-item self-report questionnaire that was used to separately assess the cognitive, somatic, and
behavioural domains of anxiety; The Quick Inventory of Depressive Symptomatology (QIDS-
Page 8 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 9
SR16)16 is a 16-item self-report scale that was used to assess severity of depression, and has been
applied in many depression treatment trials: In order to capture the temporal relationship
between mood disorder and gambling, two scales were developed based on the DSM-IV-TR
criteria7 for MDD and Pathological Gambling Disorder; The Temporal Assessment of Mood
(TAM) and the Temporal Assessment of Gambling (TAG). These two scales provide a
chronological account of milestones for onset of mood disorder and onset of gambling problems.
Mean age scores were calculated for the TAM and the TAG and subsequently used in the
analysis of temporal relationship between mood and gambling pathology.
Statistical Analysis
The analysis herein focuses on past-year problem gambling, which is defined as moderate
risk or severe problem gambling (i.e., CPGI a score of >3). Analyses were first conducted for:
any mood disorder (including all subjects) and then separately for major depressive disorder
(MDD) and bipolar I/II disorder (BD) populations. The chi-square statistic was employed to
compare demographic characteristics, rates of problem gambling and psychiatric comorbidity.
Logistic regressions were performed to identify risk factors associated with problem gambling.
The independent t-test was implemented to compare mean scores between gamblers and non-
gamblers on continuous variables such as the HAM-D-7, YMRS, QIDS, TAQ, NEO-FFI.
Stepwise multiple logistic regressions were performed to identify a set of significant and unique
correlates of problem gambling behaviour. Variables included in the multiple logistic regressions
were first identified as significant individual covariates associated with problem gambling. Two
separate multiple logistic regressions were applied (i) MDD; and, (ii) BD. The variables included
in the MDD group included educational attainment, lifetime alcohol dependence, current
obsessive-compulsive disorder, risk for suicide in the past month, HAM-D-7 score, TAQ total
Page 9 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 10
score, Q-LES-Q, and the personality factors of neuroticism, openness, agreeableness, and
conscientiousness. The variables included in the BD group were sex, ethnicity, lifetime alcohol
dependence, lifetime substance dependence, current specific phobia, HAM-D-7, TAQ-somatic
subscale, Q-LES-Q, and the personality factors of agreeableness and conscientiousness. The
QIDS was excluded from the logistic regression because it was highly correlated with the HAM-
D-7. All tests were two-tailed with statistical significance set at alpha <0.05.
RESULTS
A total of 606 respondents were enrolled, of whom 27 withdrew consent, leaving a
sample of 579 (female: n = 379, male: n = 200) for analysis (mean age = 44.8, SD = 12.1). A
positive diagnosis for lifetime bipolar disorder (BD) was confirmed in 52.5% (BD-I = 227, BD-
II = 77) of the subjects; 5.3% (n = 16) of bipolar subjects met criteria for a current manic or
hypomanic episode at the time of interview, and 29.5% (n = 86) met criteria for a major
depressive episode. 47.5% (n = 275) of subjects met diagnostic criteria for major depressive
disorder (MDD) and 55.5% presented in a current major depressive episode at the time of
interview.
The prevalence of low risk problem gambling was 11.0% (n = 61), moderate risk 7.0% (n
= 39) and problem gambler 5.4% (n = 30). The prevalence of problem gambling as defined by
greater than 3 on the CPGI for the total mood disorder sample was 12.4% (n = 69). The
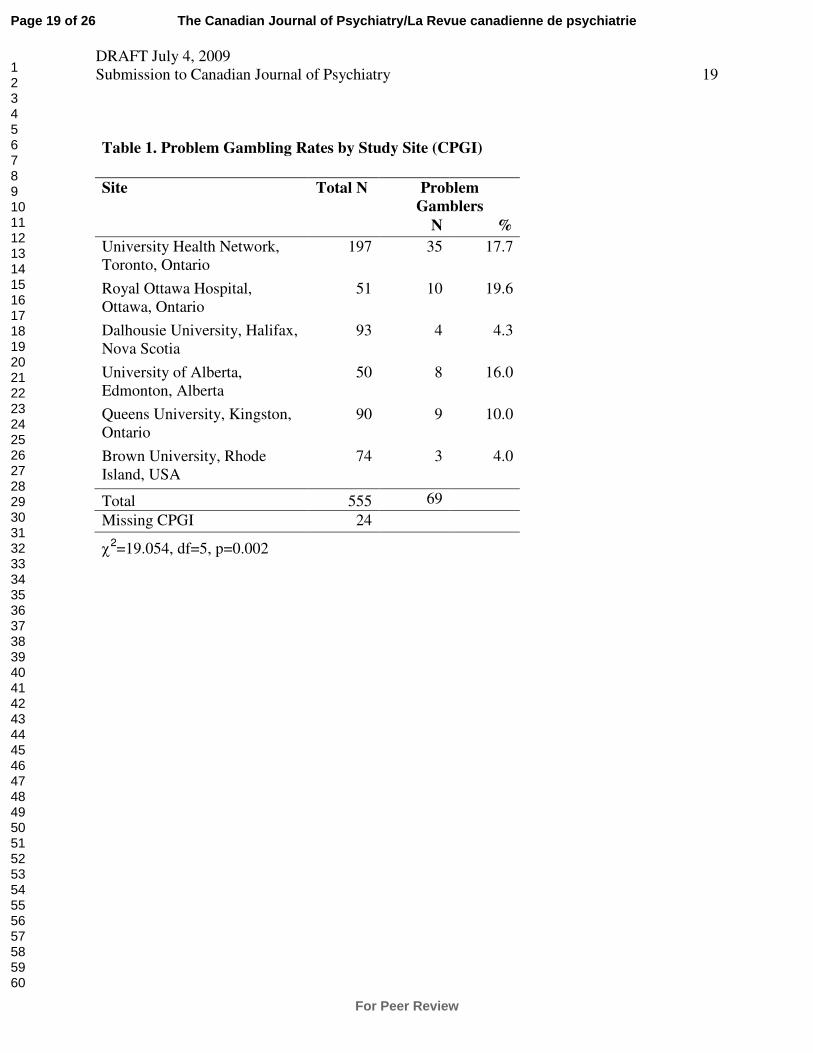
prevalence of problem gambling was significantly higher in three Canadian sites: Ottawa,
Toronto, and Edmonton (Ottawa = 19.6%, Toronto = 17.8%, Edmonton = 16.0%) compared to
the other three sites (Kingston = 10.0%, Halifax = 4.3%, Rhode Island = 4.1%) (χ2 =19.054, df =
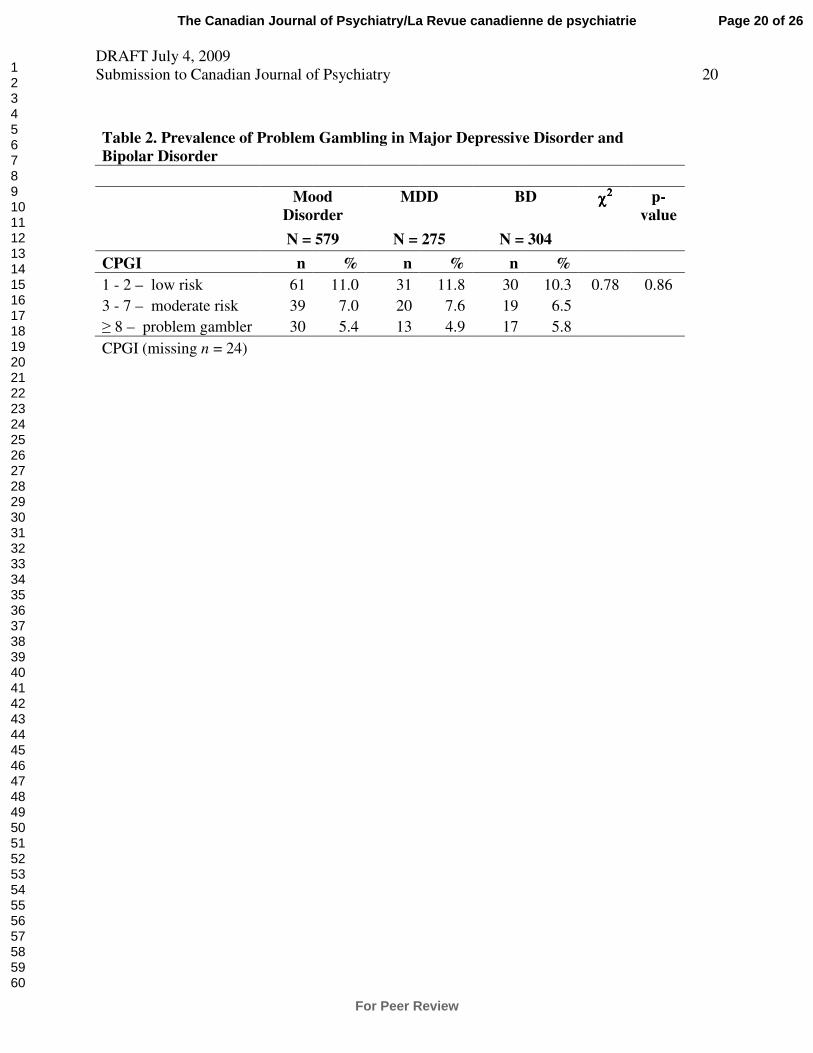
5, P = 0.002) (see Table 1). There were no significant differences in the prevalence rates of
problem gambling by the type of mood disorder diagnosis (see Table 2).
Page 10 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 11
Sex differences were identified in the BD group; a significantly higher prevalence of
problem gambling was identified in males (19.5%) versus females (7.8%) with BD (χ2 =8.695, P
= 0.003). No significant sex differences with respect to problem gambling were found in the
MDD group.
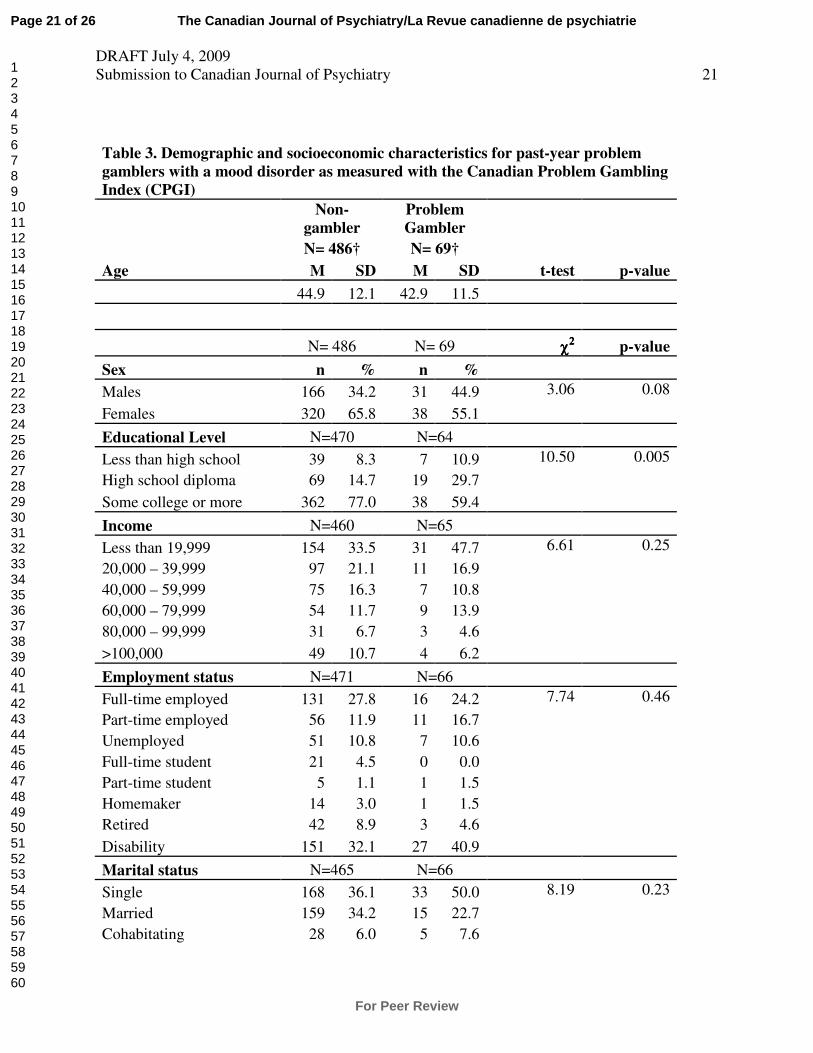
The prevalence of problem gambling was significantly associated with several
sociodemographic characteristics in individuals with a mood disorder (see Table 3). Individuals
with MDD and problem gambling were significantly more likely to lack any post-secondary
education compared to non-gamblers (37.5% vs. 15.4%; χ2 = 9.26, P = 0.01); this was not the
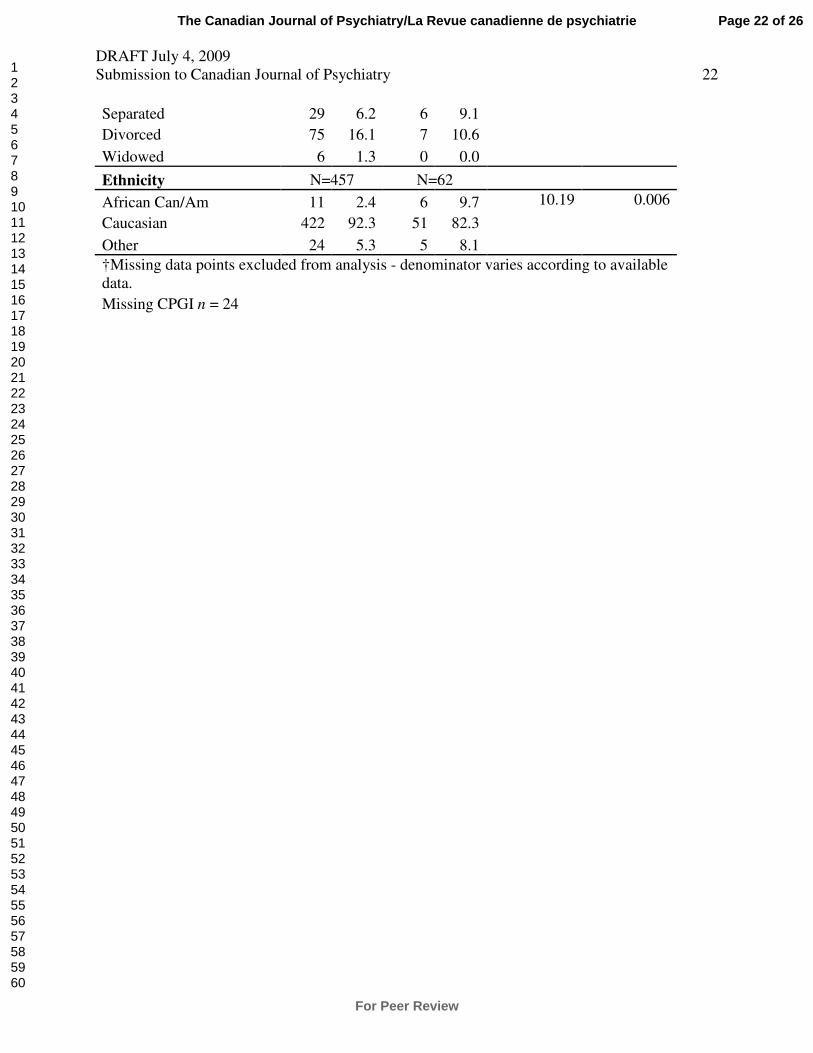
case for individuals with BD. Individuals with BD and problem gambling were significantly
more likely to be of non-Caucasian ethnicity compared to non-gamblers with BD (36.1% vs.
14.5%; χ2 = 10.43, P = 0.001). The presence of problem gambling was not significantly
associated with annual income, employment status, or marital status in the MDD or BD groups.
Temporal assessment of problem gambling
The temporal assessment of problem gambling questionnaire identified that the onset of
the mood disorder preceded the onset of gambling pathology in 80.6% of females, and 57.7% of
males (χ2 =3.83, P =0.05). In the MDD group, the onset of mood disorder preceded the onset of
gambling pathology in 77.3% of females, and 25.0% of males (χ2 = 6.903, P =0.009). In the BD
group, the onset of mood disorder preceded the onset of gambling pathology in 85.7% of females
and 72.2% of males, though the difference was not statistically significant.
Psychiatric comorbidities
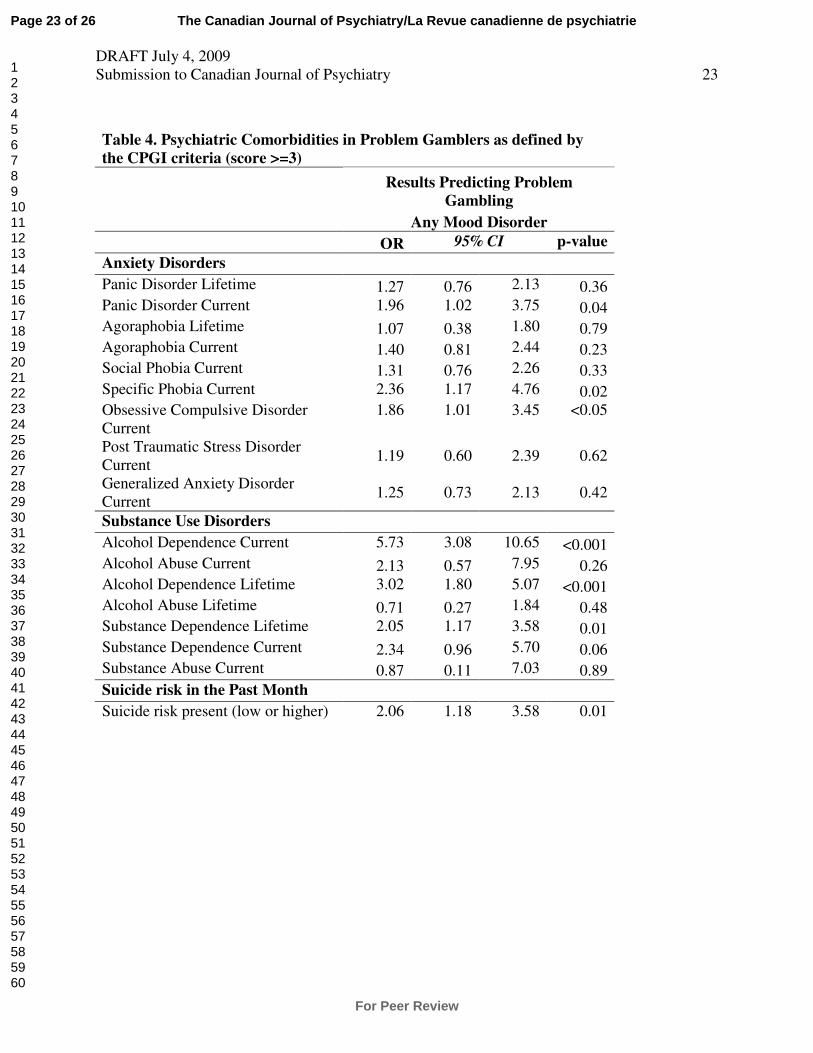
Individuals with a mood disorder who met CPGI criteria for problem gambling had
significantly increased odds of current panic disorder (OR = 1.96, 95% CI = 1.02-3.75), current
specific phobia (OR = 2.36, 95% CI 1.17 to 4.76), current obsessive-compulsive disorder (OCD)
Page 11 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 12
(OR = 1.86, 95% CI 1.01 to 3.65), current (OR = 5.73, 95% CI 3.08 to 10.65) as well as lifetime
(OR = 3.02, 95% CI 1.80 to 5.07) alcohol dependence, lifetime substance dependence (OR =
2.05, 95% CI 1.17 to 3.58), and risk for suicide in the past month (OR = 2.06, 95% CI 1.18 to
3.58). An increased odds of current OCD (OR = 2.67, 95% CI 1.13 to 6.31) as well as current
(OR = 2.92, 95% CI 1.05 to 8.09) and lifetime (OR = 2.12, 95% CI 0.99 to 4.51) alcohol
dependence, and risk for suicide (OR = 2.52, 95% CI 1.06 to 5.72) remained significant for
individuals with MDD. Individuals with BD had a significantly increased odds of current
specific phobia (OR = 2.96, 95% CI 1.08 to 8.15) as well as current (OR = 9.33, 95% CI 4.12 to
21.13) and lifetime (OR = 4.34, 95% CI 2.04 to 9.23) alcohol dependence and current (OR =
4.00, 95% CI 1.40 to 11.44) and lifetime (OR = 2.89, 95% CI 1.39 to 6.00) substance
dependence. Psychiatric comorbidities are shown in Table 4.
Quality of Life
Individuals meeting criteria for problem gambling reported lower quality of life on the Q-
LES-Q compared to non-problem gamblers both for the MDD (M = 22.94, SD = 8.85 vs. M =
31.47, SD = 11.65; t = 4.95, p < 0.001) and BD (M = 29.69, SD = 13.32 vs. M = 35.29, SD =
13.47; t = 2.334, P = 0.02) groups.
Anxiety Symptoms
Individuals with MDD who met criteria for problem gambling scored significantly higher
on self-reported anxiety as measured with the total TAQ score (M = 154.94, SD = 51.45 vs. M =
123.59, SD = 54.14; t = -3.127, P = 0.002) and all of its subscales: behavioural (M = 53.73, SD =
17.43 vs. M = 42.73, SD = 20.25; t = -2.964, P = 0.003), cognitive (M = 42.21, SD = 12.53 vs.
M = 32.30, SD = 14.59; t = -3.707, P < 0.001) and somatic (M = 59.00, SD = 29.00 vs. M =
48.56, SD = 26.63; t = -2.080, P = 0.04) as compared to non-problem gamblers. In the BD
Page 12 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 13
group, problem gamblers scored significantly higher on the somatic subscale only (M = 57.49,
SD = 26.80 vs. M = 46.43, SD = 30.26; t = -2.053, P = 0.04).
Personality
Individuals with MDD meeting criteria for problem gambling scored significantly higher
on the NEO-FII factor of neuroticism (M = 33.64, SD = 5.87 vs. M =29.82, SD = 8.36; t = -
2.532, P = 0.01), and lower on openness (M = 25.24, SD = 5.54 vs. M = 28.02, SD = 6.32; t =
2.394, P = 0.02), agreeableness (M = 27.85, SD = 6.57 vs. M = 31.71, SD = 5.87; t = 3.482, P =
0.001), and conscientiousness (M = 23.91, SD = 6.69 vs. M = 28.08, SD = 7.71; t = 2.951, P =
0.003) as compared to non-problem gamblers. Individuals with BD who met criteria for problem
gambling had significantly lower scores on the agreeableness (M = 26.31, SD = 6.66 vs. M =
31.65, SD = 6.59; t = 4.549, P < 0.001) and conscientiousness subscales (M = 25.17, SD = 7.44
vs. M = 28.61, SD = 7.85; t = 2.482, P = 0.01) as compared to non-problem gamblers. There
were no significant findings for the NEO-FFI factor of extraversion in either mood disorder
group.
Mood Symptom Severity
Individuals with MDD meeting criteria for problem gambling scored significantly higher
on depressive symptom severity as measured with the mean HAM-D-7 score as compared to
non-problem gamblers with MDD (M = 10.45, SD = 5.59 VS. M = 7.73, SD = 5.67, t = -2.585 P
= 0.010). This finding remained significant for individuals with BD (M = 7.67, SD = 5.29 vs. M
= 5.41, SD = 5.33; t = -2.386, P = 0.018). Within the BD group, there were no significant
difference between problem gamblers and non-gamblers in manic symptom severity as measured
with the mean YMRS score. Individuals with MDD meeting criteria for problem gambling had a
significantly higher mean score on the QIDS than those without problem gambling (M = 15.52,
Page 13 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 14
SD = 4.35 vs. M = 11.95, SD = 5.86; t = -4.198, P < 0.001). These results were not significant
for the BD group.
Predictors of problem gambling – results from a multiple logistic regression
Results from a multiple logistic regression indicate that for individuals with MDD, past-
year problem gambling was significantly predicted by having an educational attainment of high
school diploma or less (OR = 2.57, 95% CI 1.07 to 6.17), the personality factor of agreeableness
(OR = 0.92, 95% CI 0.86 to 0.90), and quality of life (OR = 0.94, 95% CI 0.90 to 0.98). For the
BD group, problem gambling was significantly predicted by being of non-Caucasian ethnicity
(OR = 2.82, 95% CI 1.21 to 6.57), lifetime alcohol dependence (OR = 4.20, 95% CI 1.85 to
9.50), and the personality factor of agreeableness (OR = 0.90, 95% CI 0.85 to 0.95).
DISCUSSION
This study confirmed a high prevalence of problem gambling in outpatients with a mood
disorder. The prevalence of past-year problem gambling was equally high in BD (12.3%) and
MDD (12.6%) populations. The rate of gambling was more than twice as high in men (19.5%)
compared to women (7.8%) with BD, although men and women did not differ significantly in
rates of gambling in the MDD population.
Problem gambling affects approximately 2% of individuals in the Canadian general
population2, which would suggest that individuals with a mood disorder are six more likely to
meet criteria for problem gambling.
Problem gamblers in this study were more likely to have had no post-secondary
education than were non-problem gamblers. This is consistent with a large epidemiological
survey in which problem gamblers had lower level of educational attainment and individuals
Page 14 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 15
with post-graduate degrees reported the lowest rates for gambling17.
There were also significant differences between gamblers and non-gamblers in several
areas of psychiatric comorbidity. Alcohol dependence conferred the highest risk for problem
gambling in individuals with BD and MDD. The problem gambling population was also more
than twice as likely to be at higher risk for suicide in the past month and have higher rates of
anxiety disorders such as OCD and specific phobias as compared to non-problem gamblers.
Using the Five-Factor Model of Personality, the study also showed a consistent profile of
high neuroticism, low openness, low agreeableness and low conscientiousness in the gambling
populations compared to non-gambling population, although the differences in neuroticism and
openness were largely accounted for by the MDD population. These findings have implications
for identifying individuals at high risk for gambling pathology, as well as generating hypotheses
regarding the etiology of gambling behaviour. For example, personality factors may mediate the
risk for substance dependence and gambling in patients with a mood disorder.
To our knowledge our study is the first to report on the temporal relationship between
onset of gambling behaviour and onset of mood disorders. Our investigation documents that
most (71%) individuals with a mood disorder experienced the problems with gambling following
the onset of mood disorder. The onset of problem gambling behaviour occurred earlier in men as
compared to women with MDD but not BD. These observations corroborate with a previous
report that documented an earlier age at onset of gambling problems in males18.
Individuals meeting criteria for problem gambling also had lower self-reported quality of
life, similar to Grant and Kim (2005)19, who reported that a diminished quality of life affects the
ability of individuals to interact socially, work effectively and manage their home life. The Banff
Consensus20, an expert panel invited by the Alberta Gambling Research Institute, concluded that
Page 15 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 16
quality of life is an important index of morbidity associated with gambling. This study confirms
that quality of life is indeed an important issue that needs to be addressed by clinicians for
individuals with problem gambling and mood disorders.
Individuals with MDD and problem gambling had higher self-reported anxiety
(behavioural, cognitive, and somatic) than non-problem gamblers, while individuals with BD and
problem gambling had higher anxiety as captured by the somatic subscale only. These results
substantiate the evidence from a previous report that anxiety is often a salient component of
problem and pathological gambling behaviour21.
Individuals meeting criteria for problem gambling also had higher levels of clinician-
rated depression, as quantified by the HAM-D-7 and self-reported levels of depression as
measured by the QIDS. This indicates the importance of exploring potential gambling behaviour
in individuals with depression and, in addition, to address the level of depression in individuals
with problem or pathological gambling.
There were a number of strengths to this study including the large sample size,
administration of ‘in-person’ interviews, the use of reliable and structured diagnostic instruments
and symptom scales. On the other hand, several methodological issues should be acknowledged.
First subjects were not randomly selected which limits generalizability of these findings to
indivividuals with a mood disorder in the general population. Second, the M.I.N.I.-PLUS was
shortened and did not include diagnoses for ADHD andpersonality disorders,andlifetime
incidence of anxiety disorders (with the exception of panic disorder and agoraphobia). Third,the
Temporal Assessment of Mood (TAM) and the Temporal Assessment of Gambling (TAG) scales
are not validated measures. The two scales include a series of subjective questions that mirrored
each other to ensure that a temporal onset could be extracted for comparisons. Fourth, causality
Page 16 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 17
of problem gambling cannot be inferred from the results of this study. Finally, the sample was
predominantly Caucasian, which limited exploration of increased gambling pathology in non-
Caucasian ethnic groups.
CONCLUSION
There is a higher prevalence of problem gamblers in both the BD and MDD populations
as compared to community populations in Canada. These results also identify that gambling in
mood disorder patients is highly comorbid with substance use and anxiety disorders, suggesting
that detection of one condition should trigger an assessment and relevant concomitant treatment
for all comorbid conditions. Problem gamblers suffer a diminished quality of life and this affects
their psychological, social, and occupational well being.
It is possible that individuals with depression engage in gambling in an attempt to
enhance their mood. Some individuals with problem gambling become depressed due to
decreased quality of life and financial ruin. Mood symptoms are certain to affect motivation to
gamble. The manic state involves pleasure-seeking and risk-taking with little regard for
consequences. Problem gambling can be viewed as sharing features with addictions and impulse-
control disorders, both of which affect individuals with depression and bipolar disorder more
frequently22,23.
The results of this study highlight the need for a greater focus on gambling problems in
the mood disorder population. It is recommended that clinicians initiate screening for problem
gambling in addition to substance disorders in their practice. These findings suggest that a
screening tool such as the CPGI can be used to help clinicians identify patients at higher risk for
problem gambling. Recommendations for future studies are to explore the temporal onset and
comorbities of problem gambling and mood disorders and also to differentiate between different
Page 17 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 18
gambling severities of risk.
FUNDING AND SUPPORT
This project was funded by the Ontario Problem Gambling Research Centre. The Mood
Disorders Society of Canada and the Canadian Network for Mood and Anxiety Treatments
provided administrative and financial project oversight.
ACKNOWLEDGMENTS
The authors recognize the contribution from the following research coordinators: Jessica
Ridgway, Julie Garnham, Janisse Khudabux-Der, Judy Joannette, and Mandi Peterson. Also, we
wish to acknowledge Dr. Gerald M. Devins and Dr. Anthony L. Vaccarino for their statistical
advice during this project.
Page 18 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 19
Table 1. Problem Gambling Rates by Study Site (CPGI)
Problem
Gamblers
Site Total N
N %
University Health Network,
Toronto, Ontario
197 35 17.7
Royal Ottawa Hospital,
Ottawa, Ontario
51 10 19.6
Dalhousie University, Halifax,
Nova Scotia
93 4 4.3
University of Alberta,
Edmonton, Alberta
50 8 16.0
Queens University, Kingston,
Ontario
90 9 10.0
Brown University, Rhode
Island, USA
74 3 4.0
Total 555 69
Missing CPGI 24
χ2=19.054, df=5, p=0.002
Page 19 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 20
Table 2. Prevalence of Problem Gambling in Major Depressive Disorder and
Bipolar Disorder
Mood
Disorder
MDD BD
N = 579 N = 275 N = 304
χχχχ2222 p-
value
CPGI n % n % n %
1 - 2 – low risk 61 11.0 31 11.8 30 10.3 0.78 0.86
3 - 7 – moderate risk 39 7.0 20 7.6 19 6.5
≥ 8 – problem gambler 30 5.4 13 4.9 17 5.8
CPGI (missing n = 24)
Page 20 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 21
Table 3. Demographic and socioeconomic characteristics for past-year problem
gamblers with a mood disorder as measured with the Canadian Problem Gambling
Index (CPGI)
Non-
gambler
Problem
Gambler
N= 486† N= 69†
Age M SD M SD t-test p-value
44.9 12.1 42.9 11.5
N= 486 N= 69 χχχχ2222 p-value
Sex n % n %
Males 166 34.2 31 44.9 3.06 0.08
Females 320 65.8 38 55.1
Educational Level N=470 N=64
Less than high school 39 8.3 7 10.9 10.50 0.005
High school diploma 69 14.7 19 29.7
Some college or more 362 77.0 38 59.4
Income N=460 N=65
Less than 19,999 154 33.5 31 47.7 6.61 0.25
20,000 – 39,999 97 21.1 11 16.9
40,000 – 59,999 75 16.3 7 10.8
60,000 – 79,999 54 11.7 9 13.9
80,000 – 99,999 31 6.7 3 4.6
>100,000 49 10.7 4 6.2
Employment status N=471 N=66
Full-time employed 131 27.8 16 24.2 7.74 0.46
Part-time employed 56 11.9 11 16.7
Unemployed 51 10.8 7 10.6
Full-time student 21 4.5 0 0.0
Part-time student 5 1.1 1 1.5
Homemaker 14 3.0 1 1.5
Retired 42 8.9 3 4.6
Disability 151 32.1 27 40.9
Marital status N=465 N=66
Single 168 36.1 33 50.0 8.19 0.23
Married 159 34.2 15 22.7
Cohabitating 28 6.0 5 7.6
Page 21 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 22
Separated 29 6.2 6 9.1
Divorced 75 16.1 7 10.6
Widowed 6 1.3 0 0.0
Ethnicity N=457 N=62
African Can/Am 11 2.4 6 9.7 10.19 0.006
Caucasian 422 92.3 51 82.3
Other 24 5.3 5 8.1
†Missing data points excluded from analysis - denominator varies according to available
data.
Missing CPGI n = 24
Page 22 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 23
Table 4. Psychiatric Comorbidities in Problem Gamblers as defined by
the CPGI criteria (score >=3)
Results Predicting Problem
Gambling
Any Mood Disorder
OR 95% CI p-value
Anxiety Disorders
Panic Disorder Lifetime 1.27 0.76 2.13 0.36
Panic Disorder Current 1.96 1.02 3.75 0.04
Agoraphobia Lifetime 1.07 0.38 1.80 0.79
Agoraphobia Current 1.40 0.81 2.44 0.23
Social Phobia Current 1.31 0.76 2.26 0.33
Specific Phobia Current 2.36 1.17 4.76 0.02
Obsessive Compulsive Disorder
Current
1.86 1.01 3.45 <0.05
Post Traumatic Stress Disorder
Current 1.19 0.60 2.39 0.62
Generalized Anxiety Disorder
Current 1.25 0.73 2.13 0.42
Substance Use Disorders
Alcohol Dependence Current 5.73 3.08 10.65 <0.001
Alcohol Abuse Current 2.13 0.57 7.95 0.26
Alcohol Dependence Lifetime 3.02 1.80 5.07 <0.001
Alcohol Abuse Lifetime 0.71 0.27 1.84 0.48
Substance Dependence Lifetime 2.05 1.17 3.58 0.01
Substance Dependence Current 2.34 0.96 5.70 0.06
Substance Abuse Current 0.87 0.11 7.03 0.89
Suicide risk in the Past Month
Suicide risk present (low or higher) 2.06 1.18 3.58 0.01
Page 23 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 24
Page 24 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 25
References
1. Ferris J, Wynne H. The Canadian Problem Gambling Index: Final report. Ottawa, ON:
Canadian Center on Substance Abuse; 2001.
2. Cox BJ, Yu N, Afifi TO, et al. A national survey of gambling problems in Canada. Can J
Psychiatry 2005 Mar;50(4):213-217.
3. Rush BR, Bassani DG, Urbanoski KA, et al. Influence of co-occurring mental and substance
use disorders on the prevalence of problem gambling in Canada. Addiction 2008
Nov;103(11):1847-1856.
4. Dannon PN, Lowengrub K, Sasson M, et al. Comorbid psychiatric diagnoses in kleptomania
and pathological gambling: a preliminary comparison study. Eur Psychiatry 2004
Aug;19(5):299-302.
5. el-Guebaly N, Patten SB, Currie S, et al. Epidemiological associations between gambling
behavior, substance use & mood and anxiety disorders. J Gambl Stud 2006 Fall;22(3):275-
287.
6. Petry NM, Stinson FS, Grant BF. Comorbidity of DSM-IV pathological gambling and other
psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and
Related Conditions. J Clin Psychiatry 2005 May;66(5):564-574.
7. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders,
Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.
8. Sheehan DV, Lecrubier Y, Harnett-Sheehan K, et al. Reliability and Validity of the MINI
International Neuropsychiatric Interview (M.I.N.I.): According to the SCID-P. European
Psychiatry 1997;12:232-241.
9. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric
Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric
interview for DSM-IV and ICD-10. J Clin Psychiatry 1998;59 Suppl 20:22-33;quiz 34-57.
10. McIntyre RS, Konarski JZ, Mancini DA, et al. Measuring the severity of depression and
remission in primary care: validation of the HAMD-7 scale. CMAJ 2005 Nov
22;173(11):1327-1334.
11. Young RC, Biggs JT, Ziegler VE, et al. A rating scale for mania: reliability, validity and
sensitivity. Br J Psychiatry 1978 Nov;133:429-435.
Page 25 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
DRAFT July 4, 2009
Submission to Canadian Journal of Psychiatry 26
12. Wiebe J, Single E, Falkowski-ham A. Measuring gambling and problem gambling in
Ontario. Ottawa, ON: Canadian Centre on Substance Abuse and Responsible Gambling
Council; 2001.
13. Endicott J, Nee J, Harrison W, et al. Quality of Life Enjoyment and Satisfaction
Questionnaire: a new measure. Psychopharmacol Bull 1993;29(2):321-326.
14. Costa P, McCrae RR. Revised NEO Personality Inventory (NEO-PI-R) and the Five Factor
Inventory (NEO-FFI) - Professional Manual. Odessa, FL: Psychological Assessment
Resources Inc.; 1992.
15. Lehrer PM, Woolfolk RL. Self-report assessment of anxiety: Somatic, cognitive, and
behavioural modalities. Behavioural Assessment 1982;4:167-177.
16. Rush AJ, Carmody T, Reimitz PE. The Inventory of Depressive Symptomatology (IDS):
Clinician (IDS-C) and Self-Report (IDS-SR) ratings of depressive symptoms. International
Journal of Methods Psychiatry Research 2000;9:45-49.
17. McIntyre RS, McElroy SL, Konarski JZ, et al. Problem gambling in bipolar disorder: results
from the Canadian Community Health Survey. J Affect Disord 2007 Sep;102(1-3):27-34.
18. Martins SS, Tavares H, da Silva Lobo DS, et al. Pathological gambling, gender, and risk-
taking behaviors. Addict Behav 2004 Aug;29(6):1231-1235.
19. Grant JE, Kim SW. Quality of life in kleptomania and pathological gambling. Compr
Psychiatry 2005 Jan-Feb;46(1):34-37.
20. Walker M, Toneatto T, Potenza MN, et al. A framework for reporting outcomes in problem
gambling treatment research: the Banff, Alberta Consensus. Addiction 2006
Apr;101(4):504-511.
21. Zimmerman M, Chelminski I, Young D. Prevalence and Diagnostic Correlates of DSM-IV
Pathological Gambling in Psychiatric Outpatients. J Gambl Stud 2006 Jul 1;22:255-262.
22. Krishnan KR. Psychiatric and medical comorbidities of bipolar disorder. Psychosom Med
2005 Jan-Feb;67(1):1-8.
23. Kessler RC, Chiu WT, Demler O, et al. Prevalence, severity, and comorbidity of 12-month
DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry
2005 Jun;62(6):617-627.
Page 26 of 26
For Peer Review
The Canadian Journal of Psychiatry/La Revue canadienne de psychiatrie
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Related Documents