Frequencies of different nuclear morphological features in prostate adenocarcinoma Farhat Rashid, MBBS ⁎ , Anwar Ul Haque, DABP Department of Histopathology, Pakistan Institute of Medical Sciences, Islamabad, Pakistan Received 26 May 2011; accepted 1 June 2011 Abstract Diagnosis of prostate adenocarcinoma is primarily based on morphological analysis. Nucleomegaly, prominent nucleoli, and hyperchromasia constitute current nuclear diagnostic parameters but are seen in benign conditions, vary with Gleason grade, and pose diagnostic challenge in well-differentiated tumors with accompanying inflammation or equivocal architectural features. In such cases, other pleomorphic nuclear features such as variation in size and shape, irregular contours, nuclear membrane infoldings, and nonuniform chromatin, which are not incorporated in formal evaluation, may prove helpful. Our aim was to study different nuclear morphological features of prostate adenocarcinoma (including currently practiced ones) and highlight their variation with Gleason grades. We examined 84 cases of prostate adenocarcinoma using oil immersion microscopy where necessary. Commonest Gleason pattern observed was grade 4a accounting for 42.8% of cases. Nuclear enlargement (moderate to marked in 93.8%), nucleolar enlargement (62.1%), and nonuniform chromatin distribution (100%) could serve as useful diagnostic features but did not vary with tumor differentiation. Pleomorphism (moderate in 58.6%), nuclear overlapping (62.8%), nuclear membrane infoldings (66.2%), and irregular contours (frequent in 94.5%) were significant diagnostic features that increased in frequency and extent with increasing grade and could be used to differentiate low-grade from high-grade tumors. Worsening of nuclear morphology with advancing tumor grades indicated that nuclear anaplasia accompanies poor architectural differentiation. Coexistence of pale and dark nuclei signified variable chromatin density of no diagnostic significance. © 2011 Elsevier Inc. All rights reserved. Keywords: Prostate adenocarcinoma; Nuclear morphology; Gleason grades 1. Introduction Prostate carcinoma is the second most common malignant tumor and sixth leading cause of cancer-related deaths in males, accounting for 903 500 new cases and 258 400 deaths in 2008 [1]. Despite recent advances in molecular genetics, light microscopic evaluation of archi- tectural and cytologic features on needle biopsy remains the gold standard for diagnosis of prostate adenocarcinoma [2-5]. However, approximately 18% to 28% [6-9] of clinically significant cancers are missed on primary biopsy, and to overcome this problem, efforts have always been made to study ongoing morphological changes and devise ancillary techniques that could help in early detection of prostate carcinoma, differentiate it from benign mimics, and predict its biologic behavior. Nuclei have been center of research for decades. Nuclear atypia of malignancy is morphological expression of ongoing genetic and epigenetic changes in carcinogenesis [10-13]. Most of the published textbooks and journal articles describe nuclear atypia of prostate adenocarcinoma in terms of prominent nucleoli, nucleomegaly, and hyperchromasia [2-5,8]. Although regarded as significant diagnostic features [2-5,8], these are nonspecific and often seen in many benign conditions such as atrophy, basal cell hyperplasia, and in reactive atypia caused by acute or chronic prostatitis, infarction, and irradiation [8,9,14]. In addition, appearance of nucleoli, nuclear size, and chromasia are often influenced Available online at www.sciencedirect.com Annals of Diagnostic Pathology 15 (2011) 414 – 421 ⁎ Corresponding author. Tel.: +92 512 202 090. E-mail address: [email protected] (F. Rashid). 1092-9134/$ – see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.anndiagpath.2011.06.002

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Available online at www.sciencedirect.com
Annals of Diagnostic Pathology 15 (2011) 414–421
Frequencies of different nuclear morphological features inprostate adenocarcinoma
Farhat Rashid, MBBS⁎, Anwar Ul Haque, DABPDepartment of Histopathology, Pakistan Institute of Medical Sciences, Islamabad, Pakistan
Received 26 May 2011; accepted 1 June 2011
Abstract Diagnosis of prostate adenocarcinoma is primarily based on morphological analysis. Nucleomegaly,
⁎ Corresponding aE-mail address: fr
1092-9134/$ – see frodoi:10.1016/j.anndiag
prominent nucleoli, and hyperchromasia constitute current nuclear diagnostic parameters but are seenin benign conditions, vary with Gleason grade, and pose diagnostic challenge in well-differentiatedtumors with accompanying inflammation or equivocal architectural features. In such cases, otherpleomorphic nuclear features such as variation in size and shape, irregular contours, nuclear membraneinfoldings, and nonuniform chromatin, which are not incorporated in formal evaluation, may provehelpful. Our aim was to study different nuclear morphological features of prostate adenocarcinoma(including currently practiced ones) and highlight their variation with Gleason grades. We examined84 cases of prostate adenocarcinoma using oil immersion microscopy where necessary. CommonestGleason pattern observed was grade 4a accounting for 42.8% of cases. Nuclear enlargement (moderateto marked in 93.8%), nucleolar enlargement (62.1%), and nonuniform chromatin distribution (100%)could serve as useful diagnostic features but did not vary with tumor differentiation. Pleomorphism(moderate in 58.6%), nuclear overlapping (62.8%), nuclear membrane infoldings (66.2%), andirregular contours (frequent in 94.5%) were significant diagnostic features that increased in frequencyand extent with increasing grade and could be used to differentiate low-grade from high-grade tumors.Worsening of nuclear morphology with advancing tumor grades indicated that nuclear anaplasiaaccompanies poor architectural differentiation. Coexistence of pale and dark nuclei signified variablechromatin density of no diagnostic significance.
© 2011 Elsevier Inc. All rights reserved.Keywords: Prostate adenocarcinoma; Nuclear morphology; Gleason grades
1. Introduction
Prostate carcinoma is the second most commonmalignant tumor and sixth leading cause of cancer-relateddeaths in males, accounting for 903 500 new cases and258 400 deaths in 2008 [1]. Despite recent advances inmolecular genetics, light microscopic evaluation of archi-tectural and cytologic features on needle biopsy remains thegold standard for diagnosis of prostate adenocarcinoma[2-5]. However, approximately 18% to 28% [6-9] ofclinically significant cancers are missed on primary biopsy,and to overcome this problem, efforts have always been
uthor. Tel.: +92 512 202 [email protected] (F. Rashid).
nt matter © 2011 Elsevier Inc. All rights reserved.path.2011.06.002
made to study ongoing morphological changes and deviseancillary techniques that could help in early detection ofprostate carcinoma, differentiate it from benign mimics, andpredict its biologic behavior.
Nuclei have been center of research for decades. Nuclearatypia of malignancy is morphological expression ofongoing genetic and epigenetic changes in carcinogenesis[10-13]. Most of the published textbooks and journal articlesdescribe nuclear atypia of prostate adenocarcinoma in termsof prominent nucleoli, nucleomegaly, and hyperchromasia[2-5,8]. Although regarded as significant diagnostic features[2-5,8], these are nonspecific and often seen in many benignconditions such as atrophy, basal cell hyperplasia, and inreactive atypia caused by acute or chronic prostatitis,infarction, and irradiation [8,9,14]. In addition, appearanceof nucleoli, nuclear size, and chromasia are often influenced

415F. Rashid, A. Ul Haque / Annals of Diagnostic Pathology 15 (2011) 414–421
by differences in fixation, processing, section thickness, andstaining [3,4,8,15]. Diagnosing carcinoma alone on thesefeatures is an extremely difficult task especially whenarchitectural features are equivocal or difficult to assessbecause of scanty tissue in small biopsy specimens. In suchcases, analysis of additional features such as variation innuclear size and shape, irregular nuclear contours withindentations, undulations and folds of nuclear membrane,nonuniform chromatin texture, as well as changes in size,shape, and number of nucleoli, which are of great value indiagnostic evaluation of other tumors [16-20], are likely tohelp. Because prostate carcinoma shows variable degrees ofdifferentiation, another concern is variation of nuclearmorphology in different tumor grades. Many researchershave studied changes in nuclear size, shape, contours,chromatin, nuclear cytoplasmic ratio, and nucleoli and foundsignificant changes in different Gleason grades, but most ofthem used morphometry, [21-30], which is difficult to use inroutine practice because of complexity of image analysis.Some articles address morphological changes but consideronly few characteristics such as variation in nuclear size,shape, chromatin distribution, and nucleoli [9,31,32].
Our aim was to determine frequencies of different nuclearmorphological features in prostate adenocarcinoma andhighlight their variation with different Gleason grades.This knowledge will be extremely useful in the evaluationof low-grade tumors, tumors with equivocal architecturalfeatures, presence of confounding factors such as inflamma-tory atypia, and in very small biopsies and cytologypreparations devoid of sufficient architectural details.
2. Material and methods
This study was done at the Department of Histopathology,Pakistan Institute of Medical Sciences, after approval byregional research and training monitoring cell. FromSeptember 2010 to February 2011, 84 cases of prostateadenocarcinomawere selected by nonprobability consecutivesampling. These included 9 needle biopsies, 64 transurethralresections, and 11 prostatectomy specimens. Patients receiv-ing radiotherapy, hormones, or chemotherapy were excludedfrom the study to avoid confusion with radiation and drug-induced atypia. Each case was subcategorized into primary,secondary, and tertiary Gleason grades (where applicable).To reduce statistical errors, each tumor with similar primaryand secondary grades was analyzed as single case. Hema-toxylin and eosin–stained sections with a thickness of 3 to5 μm were first examined at low (×100) and high (×400)powers and then at oil immersion microscopy (×1000).Analysis of nuclear enlargement, pleomorphism (variation innuclear size and shape), nuclear overlapping, prominentnucleoli, chromatin appearance, chromatin distributionpattern, nuclear membrane infoldings and thickening, andnuclear contours was done in comparison with benign glandsin the specimens to reduce variability caused by differences in
fixation, section thickness, and staining. Nucleomegaly andpleomorphism were subcategorized as mild, moderate, ormarked; nuclear overlapping and membrane infoldings asabsent, focal, or frequent; nuclear contours as uniform ornonuniform; and chromatin appearance as (1) light or pale(hypochromatic and vesicular), (2) dark (dense hyperchro-matic and coarse chromatin), or (3) a combination of these.Nucleoli were designated as “prominent nucleoli” when seeneasily on low power and as “visible nucleoli” when seen onhigh power. Statistical analysis was done using SPSSpackage program (version 17; SPSS Inc, Chicago, IL, USA).
3. Results
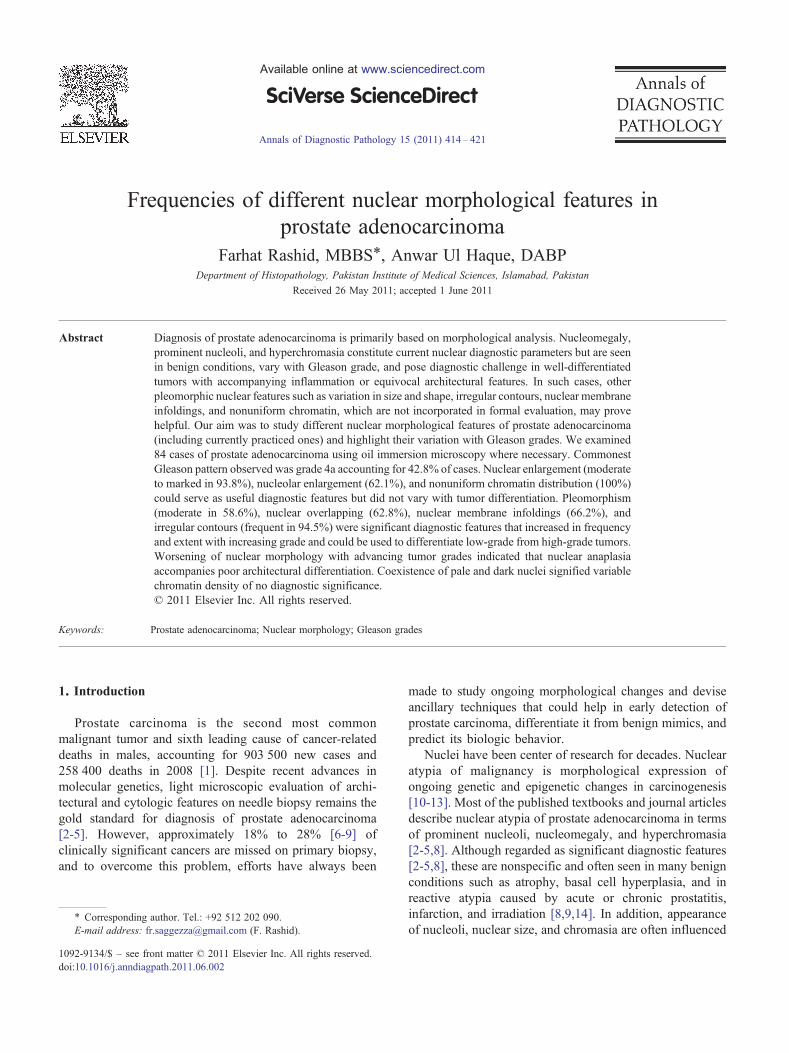
Mean age was 71.1 ± 10.6 years with an age range of 51to 101 years. Commonest Gleason pattern observed wasgrade 4a accounting for 42.8% of cases. Nucleomegaly,pleomorphism, nonuniform chromatin distribution, andirregular nuclear contours were constant features in allcases, but their degree varied with Gleason grades. Normalprostate acinar cell nuclei were small, roughly equal to, orslightly larger than a small lymphocyte nucleus or a maturered blood cell. Nuclei were round or slightly angulated withregular contours, uniform dark chromatin, and occasionallyobserved tiny nucleoli. In prostate carcinoma, nuclei were 2or more times enlarged. Largest nuclei seen were evengreater than nuclei of vascular smooth muscle cells (Fig. 1).Nuclear enlargement and pleomorphism of mild to moderatedegree were seen in grade 1 and 2 tumors and of mild tomarked degree with bizarre nuclei in grade 3 to 5 tumors. Anexception was grade 4b tumors that showed hyperchromaticmildly enlarged nuclei with minimal pleomorphism butirregular borders (Figs. 2 and 3). Tumors of all gradesshowed irregularly distributed chromatin with alternatingareas of clearing, dense condensation with prominentchromocenters and vacuoles or bubbles. Contours wereirregular with bumps and indentations. However, this featurewas more pronounced in nuclei depicting hyperchromasia orcoarse chromatin. Nuclear overlapping was observed in 91(62.8%) cases, most of which belonged to grade 3 to 5category. Nuclear membranes were irregularly thickenedshowing infoldings in 96 (66.2%) cases (Fig. 4). Both low-and high-grade tumors showed prominent nucleoli, which inmany cases were multiple, eosinophilic, and often margin-ated (Fig. 5). Of the cases, 67.6% showed a combination of 2types of nuclei (Fig. 6); one type, “light or pale nuclei,” hadmarkedly enlarged round to ovoid nuclei showing minimalpleomorphism, vesicular irregularly distributed chromatin,large prominent and often multiple eosinophilic nucleoli,irregularly thickened nuclear membrane, irregular contours,and nuclear overlapping. Because of vesicular chromatin,these nuclei appeared pale with prominent eosinophilicnucleoli and fulfilled the commonly designated termprostate carcinoma looks back at you. These were observedin both low- and high-grade tumors. The other type of nuclei
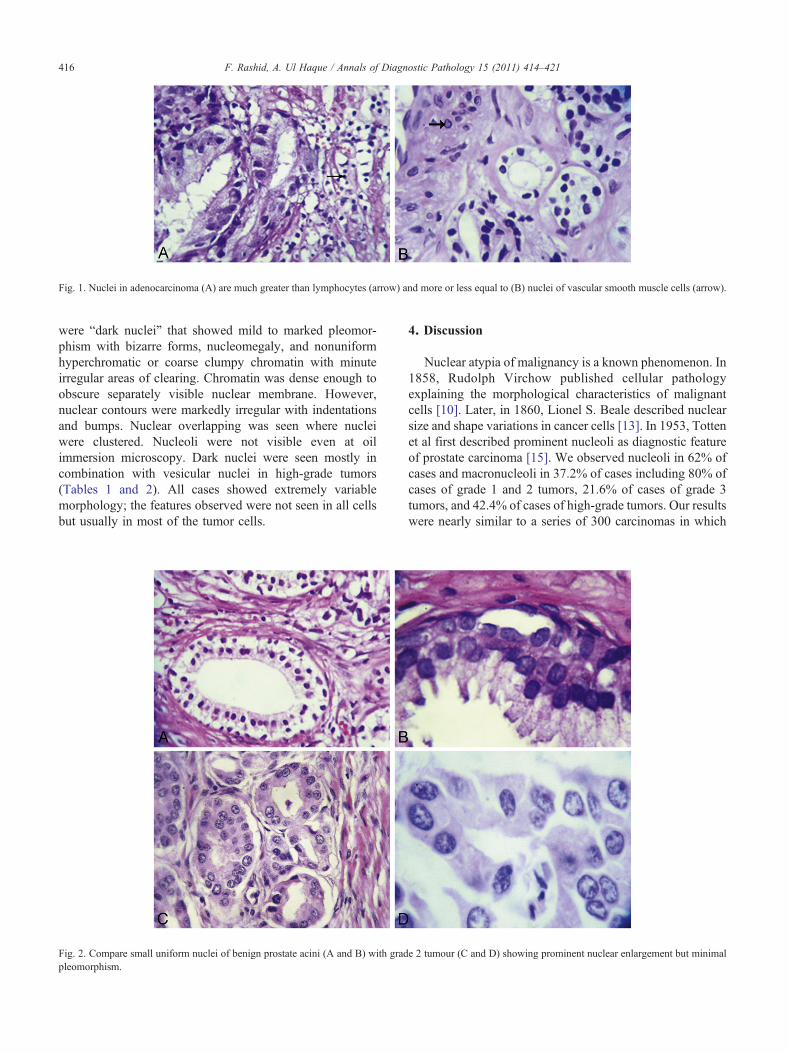
Fig. 1. Nuclei in adenocarcinoma (A) are much greater than lymphocytes (arrow) and more or less equal to (B) nuclei of vascular smooth muscle cells (arrow).
416 F. Rashid, A. Ul Haque / Annals of Diagnostic Pathology 15 (2011) 414–421
were “dark nuclei” that showed mild to marked pleomor-phism with bizarre forms, nucleomegaly, and nonuniformhyperchromatic or coarse clumpy chromatin with minuteirregular areas of clearing. Chromatin was dense enough toobscure separately visible nuclear membrane. However,nuclear contours were markedly irregular with indentationsand bumps. Nuclear overlapping was seen where nucleiwere clustered. Nucleoli were not visible even at oilimmersion microscopy. Dark nuclei were seen mostly incombination with vesicular nuclei in high-grade tumors(Tables 1 and 2). All cases showed extremely variablemorphology; the features observed were not seen in all cellsbut usually in most of the tumor cells.
Fig. 2. Compare small uniform nuclei of benign prostate acini (A and B) with gradpleomorphism.
4. Discussion
Nuclear atypia of malignancy is a known phenomenon. In1858, Rudolph Virchow published cellular pathologyexplaining the morphological characteristics of malignantcells [10]. Later, in 1860, Lionel S. Beale described nuclearsize and shape variations in cancer cells [13]. In 1953, Tottenet al first described prominent nucleoli as diagnostic featureof prostate carcinoma [15]. We observed nucleoli in 62% ofcases and macronucleoli in 37.2% of cases including 80% ofcases of grade 1 and 2 tumors, 21.6% of cases of grade 3tumors, and 42.4% of cases of high-grade tumors. Our resultswere nearly similar to a series of 300 carcinomas in which
e 2 tumour (C and D) showing prominent nuclear enlargement but minimal
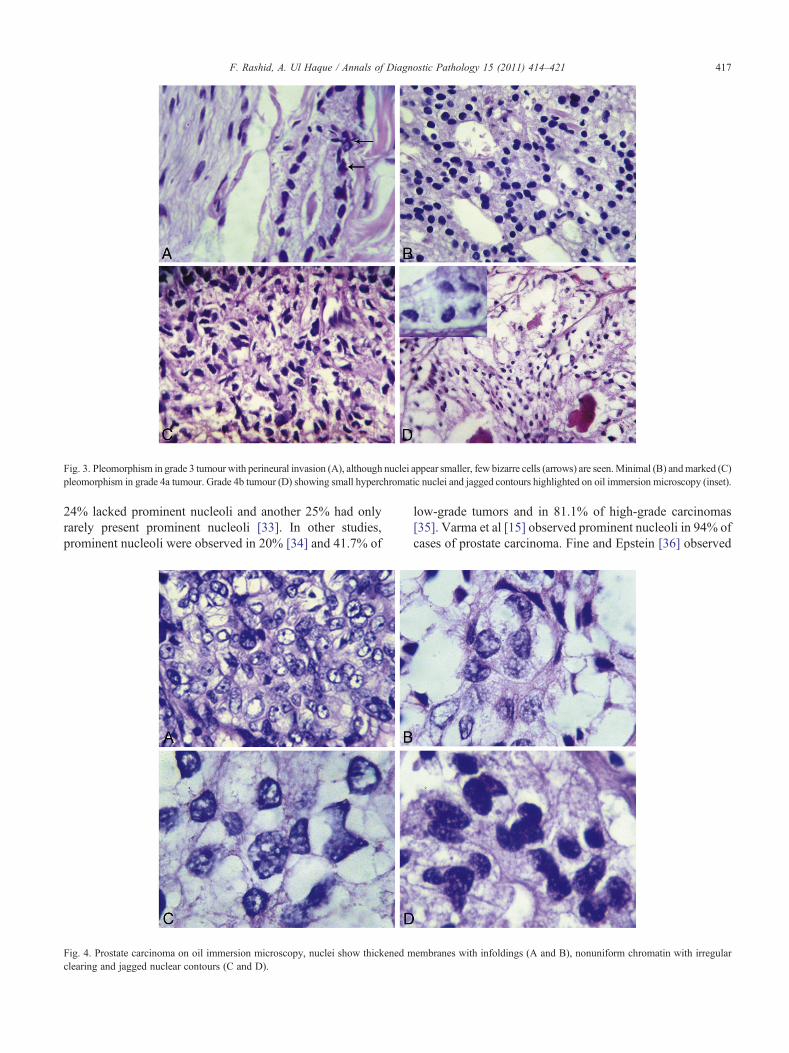
Fig. 3. Pleomorphism in grade 3 tumour with perineural invasion (A), although nuclei appear smaller, few bizarre cells (arrows) are seen.Minimal (B) andmarked (C)pleomorphism in grade 4a tumour. Grade 4b tumour (D) showing small hyperchromatic nuclei and jagged contours highlighted on oil immersion microscopy (inset).
417F. Rashid, A. Ul Haque / Annals of Diagnostic Pathology 15 (2011) 414–421
24% lacked prominent nucleoli and another 25% had onlyrarely present prominent nucleoli [33]. In other studies,prominent nucleoli were observed in 20% [34] and 41.7% of
Fig. 4. Prostate carcinoma on oil immersion microscopy, nuclei show thickened mclearing and jagged nuclear contours (C and D).
low-grade tumors and in 81.1% of high-grade carcinomas[35]. Varma et al [15] observed prominent nucleoli in 94% ofcases of prostate carcinoma. Fine and Epstein [36] observed
embranes with infoldings (A and B), nonuniform chromatin with irregular
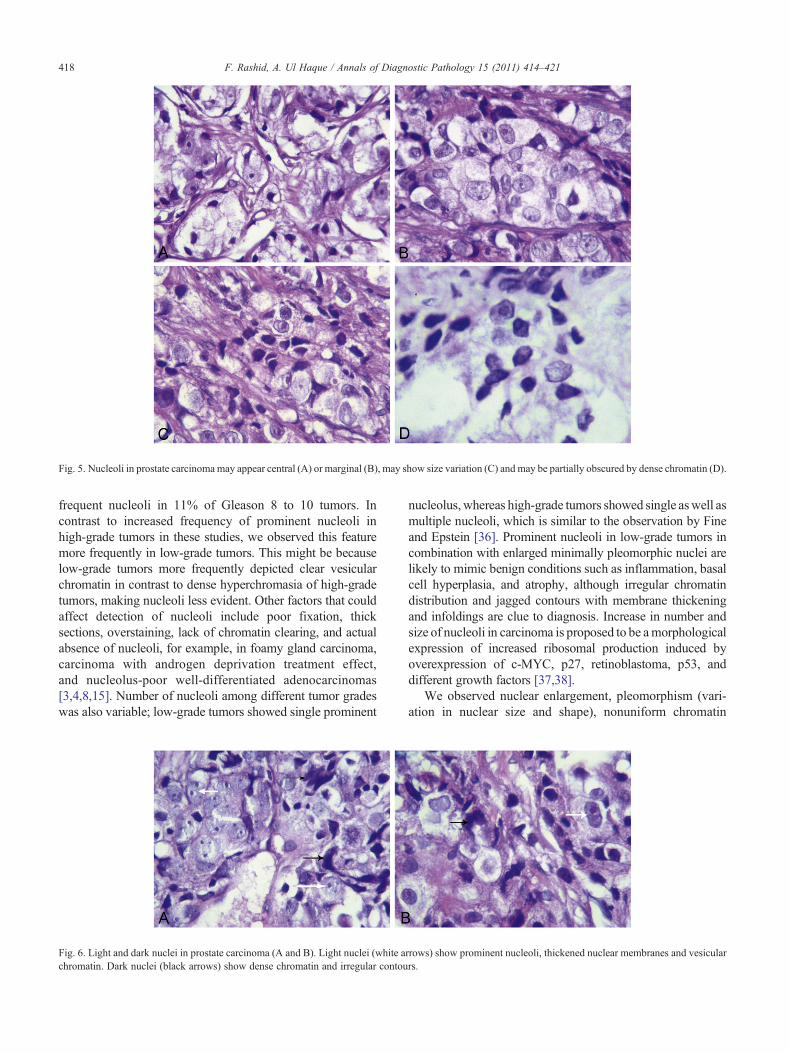
Fig. 5. Nucleoli in prostate carcinomamay appear central (A) or marginal (B), may show size variation (C) and may be partially obscured by dense chromatin (D).
418 F. Rashid, A. Ul Haque / Annals of Diagnostic Pathology 15 (2011) 414–421
frequent nucleoli in 11% of Gleason 8 to 10 tumors. Incontrast to increased frequency of prominent nucleoli inhigh-grade tumors in these studies, we observed this featuremore frequently in low-grade tumors. This might be becauselow-grade tumors more frequently depicted clear vesicularchromatin in contrast to dense hyperchromasia of high-gradetumors, making nucleoli less evident. Other factors that couldaffect detection of nucleoli include poor fixation, thicksections, overstaining, lack of chromatin clearing, and actualabsence of nucleoli, for example, in foamy gland carcinoma,carcinoma with androgen deprivation treatment effect,and nucleolus-poor well-differentiated adenocarcinomas[3,4,8,15]. Number of nucleoli among different tumor gradeswas also variable; low-grade tumors showed single prominent
Fig. 6. Light and dark nuclei in prostate carcinoma (A and B). Light nuclei (white achromatin. Dark nuclei (black arrows) show dense chromatin and irregular contou
nucleolus,whereas high-grade tumors showed single aswell asmultiple nucleoli, which is similar to the observation by Fineand Epstein [36]. Prominent nucleoli in low-grade tumors incombination with enlarged minimally pleomorphic nuclei arelikely to mimic benign conditions such as inflammation, basalcell hyperplasia, and atrophy, although irregular chromatindistribution and jagged contours with membrane thickeningand infoldings are clue to diagnosis. Increase in number andsize of nucleoli in carcinoma is proposed to be amorphologicalexpression of increased ribosomal production induced byoverexpression of c-MYC, p27, retinoblastoma, p53, anddifferent growth factors [37,38].
We observed nuclear enlargement, pleomorphism (vari-ation in nuclear size and shape), nonuniform chromatin
rrows) show prominent nucleoli, thickened nuclear membranes and vesicularrs.
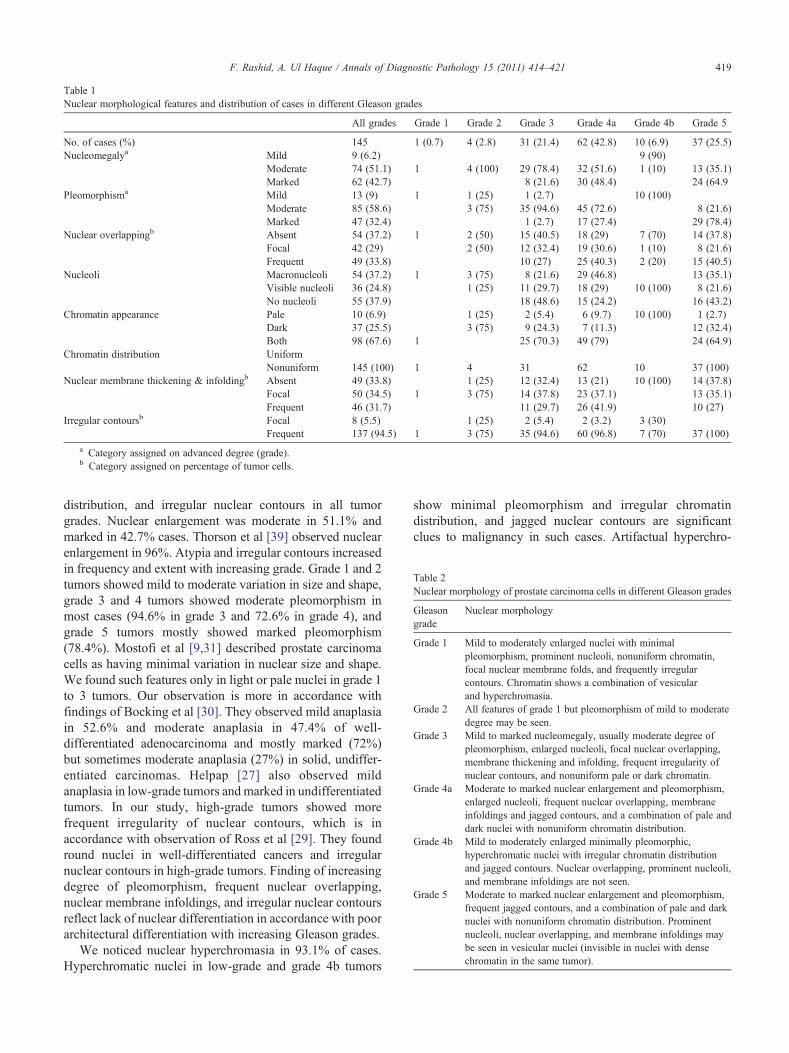
Table 1Nuclear morphological features and distribution of cases in different Gleason grades
All grades Grade 1 Grade 2 Grade 3 Grade 4a Grade 4b Grade 5
No. of cases (%) 145 1 (0.7) 4 (2.8) 31 (21.4) 62 (42.8) 10 (6.9) 37 (25.5)Nucleomegalya Mild 9 (6.2) 9 (90)
Moderate 74 (51.1) 1 4 (100) 29 (78.4) 32 (51.6) 1 (10) 13 (35.1)Marked 62 (42.7) 8 (21.6) 30 (48.4) 24 (64.9
Pleomorphisma Mild 13 (9) 1 1 (25) 1 (2.7) 10 (100)Moderate 85 (58.6) 3 (75) 35 (94.6) 45 (72.6) 8 (21.6)Marked 47 (32.4) 1 (2.7) 17 (27.4) 29 (78.4)
Nuclear overlappingb Absent 54 (37.2) 1 2 (50) 15 (40.5) 18 (29) 7 (70) 14 (37.8)Focal 42 (29) 2 (50) 12 (32.4) 19 (30.6) 1 (10) 8 (21.6)Frequent 49 (33.8) 10 (27) 25 (40.3) 2 (20) 15 (40.5)
Nucleoli Macronucleoli 54 (37.2) 1 3 (75) 8 (21.6) 29 (46.8) 13 (35.1)Visible nucleoli 36 (24.8) 1 (25) 11 (29.7) 18 (29) 10 (100) 8 (21.6)No nucleoli 55 (37.9) 18 (48.6) 15 (24.2) 16 (43.2)
Chromatin appearance Pale 10 (6.9) 1 (25) 2 (5.4) 6 (9.7) 10 (100) 1 (2.7)Dark 37 (25.5) 3 (75) 9 (24.3) 7 (11.3) 12 (32.4)Both 98 (67.6) 1 25 (70.3) 49 (79) 24 (64.9)
Chromatin distribution UniformNonuniform 145 (100) 1 4 31 62 10 37 (100)
Nuclear membrane thickening & infoldingb Absent 49 (33.8) 1 (25) 12 (32.4) 13 (21) 10 (100) 14 (37.8)Focal 50 (34.5) 1 3 (75) 14 (37.8) 23 (37.1) 13 (35.1)Frequent 46 (31.7) 11 (29.7) 26 (41.9) 10 (27)
Irregular contoursb Focal 8 (5.5) 1 (25) 2 (5.4) 2 (3.2) 3 (30)Frequent 137 (94.5) 1 3 (75) 35 (94.6) 60 (96.8) 7 (70) 37 (100)
a Category assigned on advanced degree (grade).b Category assigned on percentage of tumor cells.
able 2uclear morphology of prostate carcinoma cells in different Gleason grades
leasonrade
Nuclear morphology
rade 1 Mild to moderately enlarged nuclei with minimalpleomorphism, prominent nucleoli, nonuniform chromatin,focal nuclear membrane folds, and frequently irregularcontours. Chromatin shows a combination of vesicularand hyperchromasia.
rade 2 All features of grade 1 but pleomorphism of mild to moderatedegree may be seen.
rade 3 Mild to marked nucleomegaly, usually moderate degree ofpleomorphism, enlarged nucleoli, focal nuclear overlapping,membrane thickening and infolding, frequent irregularity ofnuclear contours, and nonuniform pale or dark chromatin.
rade 4a Moderate to marked nuclear enlargement and pleomorphism,enlarged nucleoli, frequent nuclear overlapping, membraneinfoldings and jagged contours, and a combination of pale anddark nuclei with nonuniform chromatin distribution.
rade 4b Mild to moderately enlarged minimally pleomorphic,hyperchromatic nuclei with irregular chromatin distributionand jagged contours. Nuclear overlapping, prominent nucleoli,and membrane infoldings are not seen.
rade 5 Moderate to marked nuclear enlargement and pleomorphism,frequent jagged contours, and a combination of pale and darknuclei with nonuniform chromatin distribution. Prominentnucleoli, nuclear overlapping, and membrane infoldings maybe seen in vesicular nuclei (invisible in nuclei with densechromatin in the same tumor).
419F. Rashid, A. Ul Haque / Annals of Diagnostic Pathology 15 (2011) 414–421
distribution, and irregular nuclear contours in all tumorgrades. Nuclear enlargement was moderate in 51.1% andmarked in 42.7% cases. Thorson et al [39] observed nuclearenlargement in 96%. Atypia and irregular contours increasedin frequency and extent with increasing grade. Grade 1 and 2tumors showed mild to moderate variation in size and shape,grade 3 and 4 tumors showed moderate pleomorphism inmost cases (94.6% in grade 3 and 72.6% in grade 4), andgrade 5 tumors mostly showed marked pleomorphism(78.4%). Mostofi et al [9,31] described prostate carcinomacells as having minimal variation in nuclear size and shape.We found such features only in light or pale nuclei in grade 1to 3 tumors. Our observation is more in accordance withfindings of Bocking et al [30]. They observed mild anaplasiain 52.6% and moderate anaplasia in 47.4% of well-differentiated adenocarcinoma and mostly marked (72%)but sometimes moderate anaplasia (27%) in solid, undiffer-entiated carcinomas. Helpap [27] also observed mildanaplasia in low-grade tumors andmarked in undifferentiatedtumors. In our study, high-grade tumors showed morefrequent irregularity of nuclear contours, which is inaccordance with observation of Ross et al [29]. They foundround nuclei in well-differentiated cancers and irregularnuclear contours in high-grade tumors. Finding of increasingdegree of pleomorphism, frequent nuclear overlapping,nuclear membrane infoldings, and irregular nuclear contoursreflect lack of nuclear differentiation in accordance with poorarchitectural differentiation with increasing Gleason grades.
We noticed nuclear hyperchromasia in 93.1% of cases.Hyperchromatic nuclei in low-grade and grade 4b tumors
show minimal pleomorphism and irregular chromatindistribution, and jagged nuclear contours are significantclues to malignancy in such cases. Artifactual hyperchro-
TN
Gg
G
G
G
G
G
G

420 F. Rashid, A. Ul Haque / Annals of Diagnostic Pathology 15 (2011) 414–421
matism could be caused by compression, cauterization, oroverstaining, but in such cases, nuclei appear crushed andcytoplasm is fragmented.
Nuclear membranes showed irregular thickenings andinfoldings in 66.2% cases in both low- and high-gradetumors where chromatin appeared vesicular or hypochro-matic and became inconspicuous focally in nuclei withchromatin condensation in the same tumor. Irregularmembrane thickening occurs because of peripheral conden-sation of chromatin in a haphazard manner. Infoldings andirregularity of nuclear envelop may develop dynamicallyduring interphase after oncogene expression in clonalevolution of prostate cancer and reflect cytoskeletal forcesexerted on the nuclear envelop (NE) during active celllocomotion. Furthermore, it could promote chromosomalinstability and impact replication competence, transcriptionalprogramming, and nuclear pore function [38].
5. Conclusions
Pleomorphism, nonuniform chromatin distribution, andirregular nuclear contours could serve as useful diagnosticfeatures in the evaluation of prostate adenocarcinoma inaddition to currently recommended prominent nucleoli,nucleomegaly, and hyperchromasia. Nuclear overlappingand nuclear membrane irregularities could also be helpful.Coexistence of pale vesicular/smudgy and dark hyperchro-matic nuclei signifies variable chromatin appearance of nodiagnostic significance.
Nuclear enlargement, prominent nucleoli, and nonuni-form chromatin distribution are important diagnostic featuresbut do not vary with Gleason grades, whereas pleomor-phism, nuclear overlapping, nuclear membrane infoldings,and irregular contours increased in frequency and extent withincreasing tumor grades. Moderate to marked variation innuclear size and shape with frequent overlapping, membraneinfoldings, and irregular contours signify high-grade tumorsin contrast to mild to moderate variation in nuclear size andshape with focal nuclear overlapping, membrane infoldings,and irregular contours in low-grade tumors.
Acknowledgment
Our sincere gratitude to Dr. Noor Khan Lakhnana for hiskind support in data collection.
References
[1] Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA CancerJ Clin 2011;61:69-90.
[2] Humphrey PA. Diagnosis of adenocarcinoma in prostate needle biopsytissue. J Clin Pathol 2007;60:35-42.
[3] Thorson P, Humphrey PA. Minimal adenocarcinoma in prostate needlebiopsy tissue. Am J Clin Pathol 2000;114:896-909.
[4] Epstein JI. Diagnosis and reporting of limited adenocarcinoma of theprostate on needle biopsy. Mod Pathol 2004;17:307-15.
[5] Humphrey PA. Prostate Pathology. Chicago, IL; ASCP Press; 2003.[6] Yuasa T, Tsuchiya N, Kumazawa T, et al. Characterization of prostate
cancer detected at repeat biopsy. BMC Urol 2008;8:14.[7] Bak JB, Landas SK, Haas GP. Characterization of prostate cancer
missed by sextant biopsy. Clin Prostate Cancer 2003;2:115-8.[8] Bostwick DG. Evaluating prostate needle biopsy: therapeutic and
prognostic importance. CA Cancer J Clin 1997;47:297-319.[9] Mostofi FK, Davis CJ, Sesterhenn IA. Pathology of carcinoma of the
prostate. Cancer 1992;70:235-53.[10] Berman JJ. Neoplasms: principles of development and diversity. USA:
Jones and Bartlett; 2009.[11] HuismanA,PloegerLS,DullensHFJ, et al. Racial differences in 3-Dnuclear
chromatin patterns of prostate cancer. Open Prost Cancer J 2009;2:32-7.[12] Bignold LP. Pathogenetic mechanisms of nuclear pleomorphism of
tumour cells based on the mutator phenotype theory of carcinogenesis.Histol Histopathol 2003;18:657-64.
[13] Zink D, Fischer AH, Nickerson JA. Nuclear structure in cancer cells.Nat Rev Cancer 2004;4:677-87.
[14] Srigley JR. Benign mimickers of prostatic adenocarcinoma. ModPathol 2004;17:328-48.
[15] Varma M, Lee MW, Tamboli P, et al. Morphologic criteria for thediagnosis of prostatic adenocarcinoma in needle biopsy specimens. Astudy of 250 consecutive cases in a routine surgical pathology practice.Arch Pathol Lab Med 2002;126:554-61.
[16] Bussolati G. Proper detection of the nuclear shape: ways andsignificance. Rom J Morphol Embryol 2008;49:435-9.
[17] Nickerson JA. Nuclear dreams: the malignant alteration of nucleararchitecture. J Cell Biochem 1998;70:172 (abstr).
[18] Ferris DG, Cox JT, O'Connor DM, et al. Modern colposcopy: textbookand atlas. 2nd ed. USA: Kendall Hunt Publishing Company; 2004.
[19] Rashid F, Haque AU. Nuclear morphological and morphometricfeatures of reactive versus neoplastic gastric mucosa. IJP 2009;7:66-72.
[20] Baloch ZW, LiVolsi VA. Etiology and significance of the opticallyclear nucleus. Endocr Pathol 2002;13:289 (abstr).
[21] Diamond DA, Berry SJ, Jewett HJ, et al. A new method to assessmetastatic potential of human prostate cancer: relative nuclearroundness. J Urol 1982;128:729-34.
[22] Kim D, Charlton JD, Coggins JM, et al. Semiautomated nuclear shapeanalysis of prostatic carcinoma and benign prostatic hyperplasia. AnalQuant Cytol Histol 1994;16:400 (abstr).
[23] Van der Poel HG, Oosterhof GO, Schaafsma HE, et al. Intratumoralnuclear morphologic heterogeneity in prostate cancer. Urology 1997;49:652 (abstr).
[24] Bartels PH, Montironi R, Hamilton PW, et al. Nuclear chromatintexture in prostatic lesions. I. PIN and adenocarcinoma. Anal QuantCytol Histol 1998;20:389-96.
[25] Christen R, Xiao J, Minimo C, et al. Chromatin texture features inhematoxylin and eosin–stained prostate tissue. Anal Quant CytolHistol 1993;15:383 (abstr).
[26] Van Brussel JP, Mickisch GH. Prognostic factors in prostate and testiscancer. BJU Int 1999;83:910-6.
[27] Helpap B. Cell kinetic and cytological grading of prostatic carcinoma.Virchows Arch A Pathol Anat Histol 1981;393:205 (abstr).
[28] Christens-Barry WA, Partin AW. Quantitative grading of tissue andnuclei in prostate cancer for prognosis prediction. Johns Hopkins APLTech Dig 1997;18:226-33.
[29] Ross JS, Jennings TA, Nazeer T, et al. Prognostic factors in prostatecancer. Am J Clin Pathol 2003;120(Suppl):S85-100.
[30] Böcking A, Kiehn J, Heinzel-Wach M. Combined histologic gradingof prostatic carcinoma. Cancer 1982;50:288-94.
[31] Mostofi FK, Sesterhenn IA, Davis Jr CJ. A pathologist's view ofprostatic carcinoma. Cancer 1993;71(3 Suppl):906-32.
[32] Murphy GP, Whitmore Jr WF. A report of the workshops on the currentstatus of the histologic grading of prostate cancer. Cancer 1979;44:1490-4.
[33] Epstein JI, Walsh PC, Carmichael M, et al. Pathological and clinicalfindings to predict tumor extent of non-palpable (stage T1c) prostatecancer. JAMA 1994;271:368-74.

421F. Rashid, A. Ul Haque / Annals of Diagnostic Pathology 15 (2011) 414–421
[34] Kramer CE, Epstein JI. Nucleoli in low-grade prostate adenocarcinomaand adenosis. Hum Pathol 1993;24:618 (abstr).
[35] Helpap B, Riede C. Nucleolar and AgNOR-analysis of prostaticintraepithelial neoplasia (PIN), atypical adenomatous hyperplasia(AAH) and prostatic carcinoma. Pathol Res Pract 1995;191:381(abstr).
[36] Fine SW, Epstein JI. Minute foci of Gleason score 8-10 on prostaticneedle biopsy: a morphologic analysis. Am J Surg Pathol 2005;29:962-8.
[37] Koh CM, Gurel B, Sutcliffe S, et al. Alterations in nucleolar structureand gene expression programs in prostatic neoplasia are driven by themyc oncogene. Am J Pathol 2011;178:1824 (abstr).
[38] Fischer AH, Bardarov Jr S, Jiang Z. Molecular aspects of diagnosticnucleolar and nuclear envelope changes in prostate cancer. J CellBiochem 2004;91:170 (abstr).
[39] Thorson P, Vollmer RT, Arcangeli C, et al. Minimal carcinoma inprostate needle biopsy specimens: diagnostic features and radicalprostatectomy follow-up. Mod Pathol 1998;11:543-51.
Related Documents











