1992;52:3901-3907. Cancer Res Isabelle Marcillac, Frédéric Troalen, Jean-Michel Bidart, et al. Nongonadal Neoplasms Subunit in Gonadal and β Free Human Chorionic Gonadotropin Updated version http://cancerres.aacrjournals.org/content/52/14/3901 Access the most recent version of this article at: E-mail alerts related to this article or journal. Sign up to receive free email-alerts Subscriptions Reprints and . [email protected] Department at To order reprints of this article or to subscribe to the journal, contact the AACR Publications Permissions . [email protected] Department at To request permission to re-use all or part of this article, contact the AACR Publications Research. on October 26, 2014. © 1992 American Association for Cancer cancerres.aacrjournals.org Downloaded from Research. on October 26, 2014. © 1992 American Association for Cancer cancerres.aacrjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1992;52:3901-3907. Cancer Res Isabelle Marcillac, Frédéric Troalen, Jean-Michel Bidart, et al. Nongonadal Neoplasms
Subunit in Gonadal andβFree Human Chorionic Gonadotropin
Updated version
http://cancerres.aacrjournals.org/content/52/14/3901
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

[CANCER RESEARCH 52, 3901-3907, July 15, 1992]
Free Human Chorionic Gonadotropin ßSubunit in Gonadal and NongonadalNeoplasms1
Isabelle Mamilar, FrédéricTroalen, Jean-Michel Bidart, Pascale Giuliani, Vincent Ribrag, Bernard Escudier,Benoit Malassagne, Jean-Pierre Droz, Catherine I homme, Philippe Rougier, Pierre Duvillard, Michel Prade,Pierre-Marie Lugagne, FrançoisRichard, Thierry Poynard, Claude Bohuon, Jack Wands, and Dominique Bellet2
Departments of Molecular Immunology [I. M., F. T., J-M. B., P. G., B. M., C. B., D. B.J. Medicine ¡J-P.D., C. L., P. R.]. and Pathology B ¡P.D., M. P.], and theUnit of Intensive Care [f. R., B. E.], Institut G. Koussy, 38 Rue Camille Desmoulins, 94805 Villejuif, France; Hôpital de la Pitié,Boulevard de l'hôpital, 75013Paris, France /P-M. L., F. R.]; Hôpital Antoine Béclère,157 Rue de la Porte de Trivaux, 92140 Claman, France [T. P.J; Department of Immunology, CNRS, URA1484, Facultéde Pharmacie, 6 Avenue de l'Observatoire, 75006 Paris, France [J-M. B., T. P., D. B./; and the Molecular Hepatology Laboratory, MassachusettsCenerai Hospital Cancer Center, Charlestown, Massachusetts 02129 ¡J.H'.]
ABSTRACT
The diagnostic value of elevated human chorionic gonadotropi(hCG) and its free a (hCGa) and .; (hCG/3) subunit serum levels asspecific tumor markers for nongonadal malignancies is controversial. Inthe present report, different monoclonal based immunoradiometric assays specific for hCG and its free hCGa and hCGtf subunits have beenused to reevaluate the presence of these molecules in the serum ofpatients with a wide variety of tumors. Serum samples from patientswith newly diagnosed, persistent, or recurrent malignancies of eitherknown (n = 717) or unknown in = 32) primary site, healthy blooddonors (n = 309), and nonmalignant disease controls (n = 86) were
studied using four highly specific and sensitive monoclonal based immunoradiometric assays to hCG and its free subunits. Low level hCGelevations (< 11)0(1pg/ml) were found to be common in cancer patients,normal subjects, and disease controls. However, serum levels > 1(100pg/ml were highly diagnostic of gonadal tumors and specifically identified nonseminomatous testicular tumors. Significant serum elevationsof free hCGor subunit (as high as 3000 pg/ml) were found in approximately 96% of cancer patients, normal individuals, and disease controls.In contrast, free hCG/3 subunit levels ( •¿�100 pg/ml) were detected in 70
and 50% of patients with nonseminomatous and seminomatous testicular cancers, respectively, and in 47% of bladder, 32% of pancreatic, and30% of cervical carcinomas. All normal subjects and disease controlshad free hCG0 levels <100 pg/ml. Thus, the detection of the free hCG/8subunit in serum of nonpregnant subjects was highly diagnostic of malignancy in general and specifically defines a subgroup of aggressivenongonadal malignancies.
INTRODUCTION
Human chorionic gonadotropin is a glycoprotein hormonenormally secreted by the placenta and composed of two nonco-valently linked molecules, the a and the •¿�'>subunits. It is one
member of a family of glycoproteins including the three pituitary hormones, namely human luteinizing, human follicle-stimulating, and human thyroid-stimulating hormones. Theamino acid sequences of the a subunits of the hormones areidentical whereas the individual /3-subunit sequences diverge(1), and it is the ßsubunit which confers the biological andimmunological specificity to each hormone. These subunits areencoded by independent genes and consequently the freehCGa1 and hCG0, which are biologically inactive, are produced
Received 2/26/92; accepted 5/6/92.The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Supported in part by grants from Association pour la Recherche sur le Cancer.Villejuif, and CA-35711 and HD-20469 from the N1H.
2 To whom requests for reprints should be addressed.3 The abbreviations used are: hCG. human chorionic gonadotropin: hCG«,n
subunit of hCG; hCG/i, ßsubunit of hCG; m-IRMA, monoclonal immunoradiometric assay: hill, human luteinizing hormone; hill... .; subunit of hill
by trophoblastic cells in addition to the biologically active hCGduring normal pregnancy (2-4).
There is an extensive documentation of the presence of eitherhCG, hCG-like material, or free hCG subunits in the serum ofnormal adults as well as in patients with either trophoblastic ornontrophoblastic tumors (5-13). For example, several studieshave shown that such molecules may be localized to a variety ofnontrophoblastic tissues and further was extractable from virtually all normal and malignant human tissues (14-23). How
ever, most of these studies were based on the recognition ofhCG, hCG-like material, or free hCG subunits by either poly-
clonal or monoclonal antibodies that were not totally specificfor these glycoproteins (24, 25). Consequently, the productionof hCG-related molecules by nontrophoblastic cells remainedcontroversial and only indirect evidence has been provided thata hCG-like material was secreted by these cells. Recently, theutilization of monoclonal antibodies highly specific for hCGprovided direct evidence that this hormone was secreted by thenormal human pituitary and was present in the serum of normaladults (26-29). Moreover, monoclonal antibodies specific foreither the free hCGa or hCG/3 subunit have proved to be usefulin assessing the production of free subunits by normal andmalignant trophoblastic cells (4, 30). In the present investigation, different m-IRMAs specific for hCG, and its free hCGaand hCG/3 subunits, respectively, have been utilized to reevaluate the presence of these molecules in the serum of patientswith a wide variety of nontrophoblastic tumors. In the presentreport, we will present direct evidence demonstrating that thedetection of the free hCG/3 subunit in serum of nonpregnantsubjects is highly diagnostic of malignancy in general andspecifically defines a subgroup of aggressive nongonadalmalignancies.
MATERIALS AND METHODS
Subjects. Serum samples from 309 apparently healthy blood donorswere obtained through the blood transfusion services of Creteil, France.Healthy donors included men (rti= 147) and women (n = 162) with amedian age of 41 years. Among these women, 44 subjects were olderthan 45 years of age. From our serum banks at HôpitalAntoine Béclèreand at Institut Gustave Roussy, we selected a panel of 86 serum samplesfrom patients with nonmalignant diseases including gynecological(n = 19), pulmonary (n = 3), and gastrointestinal (n = 64) disorders.
Serum samples from patients with newly diagnosed, persistent, orrecurrent malignancies of either known (n = 717) or unknown (n = 32)primary site were retrospectively obtained from the serum banks of theInstitut Gustave Roussy and the Hôpital Antoine Béclèreas well asprospectively from patients treated at the Institut Gustave Roussy usingprotocols previously approved by the human studies committee. Thediagnoses were confirmed by review of operative notes and pathologyreports. Table 1A depicts the primary site of disease and the histology
3901
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
SERUM FREE hCGff MEASUREMENT AND CANCER
Table 1 Primary site and histology of (A) cancer patients included in this studyand (B) patients with detectable serum level (> 100 pg/ml) of free HCGfi subunit
as measured with the m-IRMA 11-9
PrimarysiteTestisOvaryBladderUterusCervixCorpusBreastLungHead
andneckProstateColorectalLiverPancreasStomachEsophagusUnknownHistologySeminomaNon-seminomaEmbryonal
carcinomaChoriocarcinomaTeratocarcinomaMixed
tumorGerm
cellDysgerminomaTeratocarcinomaMixed
tumorEpithelialTransitional
cellcarcinomaAdenocarcinomaEpidermoid
carcinomaAdenocarcinomaLeiomyosarcomaAdenocarcinomaNon-Hodgkin's
lymphomaAdenocarcinomaLarge-cell
carcinomaSmall-cellcarcinomaEpidermoidcarcinomaPoorly
differentiatedcarcinomaEpidermoid
carcinomaAdenocarcinomaPoorly
differentiatedcarcinomaAdenocarcinomaAdenocarcinomaHepatocellular
carcinomaHepatoblastomaAdenocarcinomaIslet
cellcarcinomaLeiomyosarcomaAdenocarcinomaNon-Hodgkin's
lymphomaRhabdomyosarcomaEpidermoid
carcinomaAdenocarcinomaAdenocarcinomaEpidermoid
carcinomaPoorlydifferentiated carcinomaA(total
no.)1219113726514338324207411202327284712326445743314311322129B(No.with
free hCG/3)6111299181742381511511324611
Total 749 139
of the tumor in the 749 patients. There were 380 females and 369 malesin this study. The primary tumor site was either the testis (n = 70), theovary (n = 156), the bladder (n = 38), the uterine cervix (n = 27), theuterine corpus (n = 27), the breast (n = 42), the lung (n = 102), the heador the neck (n = 10), the prostate (n = 32), the colon or the rectum(n = 64), the liver (n = 52), the pancreas (n = 47), the stomach (n = 45),the esophagus (n = 5), or unknown origin (n = 32). Serum samples werestored at -20'C before analysis.
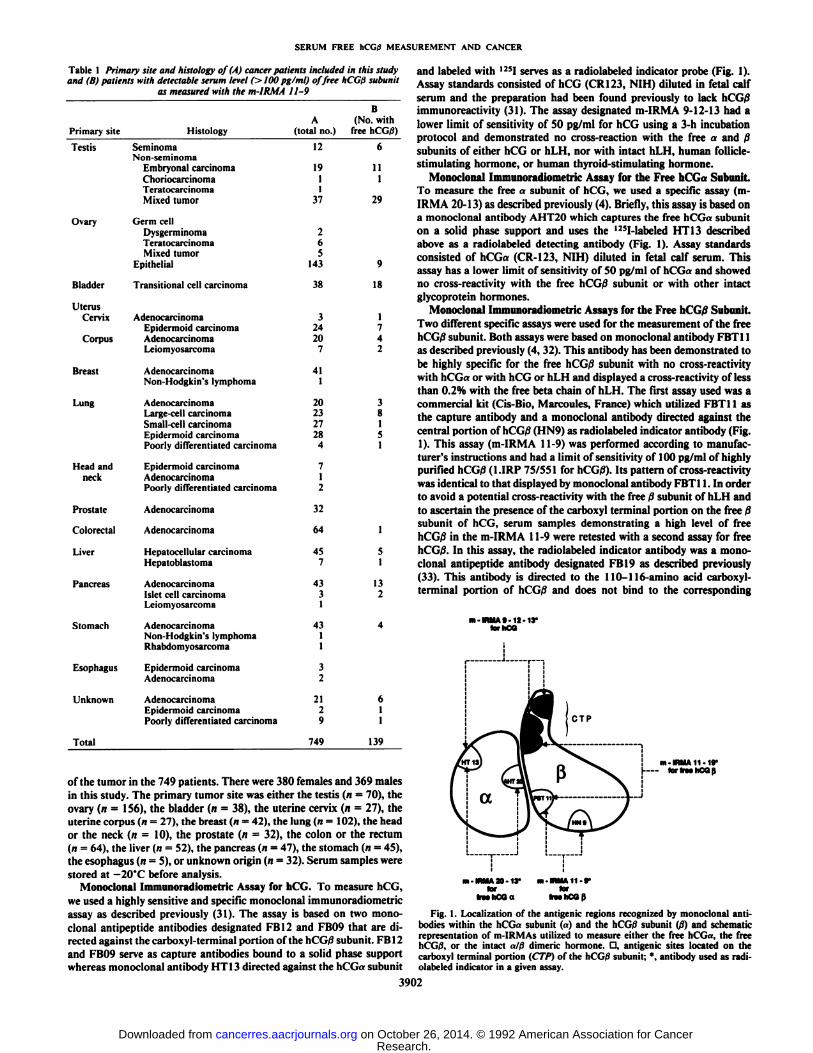
Monoclonal Immunoradiometric Assay for hCG. To measure hCG,we used a highly sensitive and specific monoclonal immunoradiometricassay as described previously (31). The assay is based on two monoclonal antipeptide antibodies designated FBI2 and FB09 that are directed against the carboxyl-terminal portion of the hCG/3 subunit. FBI 2and FB09 serve as capture antibodies bound to a solid phase supportwhereas monoclonal antibody HT 13 directed against the hCGa subunit
and labeled with 12SIserves as a radiolabeled indicator probe (Fig. 1).
Assay standards consisted of hCG (CR123, NIH) diluted in fetal calfserum and the preparation had been found previously to lack hCG/3imiminon-acti\ ily (31). The assay designated m-IRMA 9-12-13 had alower limit of sensitivity of 50 pg/ml for hCG using a 3-h incubationprotocol and demonstrated no cross-reaction with the free a and ßsubunits of either hCG or hLH, nor with intact hLH, human follicle-stimulating hormone, or human thyroid-stimulating hormone.
Monoclonal Immunoradiometric Assay for the Free hCGa Subunit.To measure the free a subunit of hCG, we used a specific assay (inIRMA 20-13) as described previously (4). Briefly, this assay is based ona monoclonal antibody AHT20 which captures the free hCGa subuniton a solid phase support and uses the 125I-Iabeled HT 13 described
above as a radiolabeled detecting antibody (Fig. 1). Assay standardsconsisted of hCGa (CR-123, NIH) diluted in fetal calf serum. Thisassay has a lower limit of sensitivity of 50 pg/ml of hCGa and showedno cross-reactivity with the free hCG/3 subunit or with other intactglycoprotein hormones.
Monoclonal Immunoradiometric Assays for the Free hCG0 Subunit.Two different specific assays were used for the measurement of the freeli( (..; subunit. Both assays were based on monoclonal antibody FBT11as described previously (4, 32). This antibody has been demonstrated tobe highly specific for the free hCG/3 subunit with no cross-reactivitywith hCGa or with hCG or hLH and displayed a cross-reactivity of lessthan 0.2% with the free beta chain of hLH. The first assay used was acommercial kit (Cis-Bio, Marcoules, France) which utilized FBT11 asthe capture antibody and a monoclonal antibody directed against thecentral portion of hCG/3 (HN9) as radiolabeled indicator antibody (Fig.1). This assay (m-IRMA 11-9) was performed according to manufacturer's instructions and had a limit of sensitivity of 100 pg/ml of highlypurified hCG|8 (l.IRP 75/551 for hCG/3). Its pattern of cross-reactivitywas identical to that displayed by monoclonal antibody FBT11. In orderto avoid a potential cross-reactivity with the free ßsubunit of hLH and
to ascertain the presence of the carboxyl terminal portion on the free 0subunit of hCG, serum samples demonstrating a high level of freehCG/3 in the m-IRMA 11-9 were retested with a second assay for freehCG/3. In this assay, the radiolabeled indicator antibody was a monoclonal antipeptide antibody designated FBI9 as described previously(33). This antibody is directed to the 110-116-amino acid carboxyl-terminal portion of hCG/3 and does not bind to the corresponding
m-IRMA 9-12-13-forhCQ
m -IRMA 11-WlorflMhCQß
m-IRMA 20-13*for
iTMhCOa
m-IRUAII-9-lar
frwhCOß
Fig. 1. Localization of the antigenic regions recognized by monoclonal antibodies within the hCG«subunit (a) and the li( <..; subunit (ß)and schematicrepresentation of m-IRMAs utilized to measure either the free hCGa, the freeh< <,,;. or the intact o/(j dimeric hormone. D, antigenic sites located on thecarboxyl terminal portion (CTP) of the hCGff subunit: *, antibody used as radiolabeled indicator in a given assay.
3902
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
SERUM FREE hCGtÃMEASUREMENT AND CANCER
region of hLHß(data not shown). Consequently, the m-IRMA 11-19based on FBT11 as capture antibody and FBI9 as tracer was entirelyspecific for hCGßwith no cross-reactivity with hLHfi. Moreover, thisassay will measure any free hCG/3 subunit containing the carboxyl-terminal portion of hCGi) (Fig. 1). The coefficient of variation withinthe assays (m-IRMA 11-19) averaged 8.4%; the coefficient of variationbetween assays averaged 6.4%. The sensitivity was 100 pg/ml of highlypurified hCGß(1.IRP 75/551 for hCG/3).
RESULTS
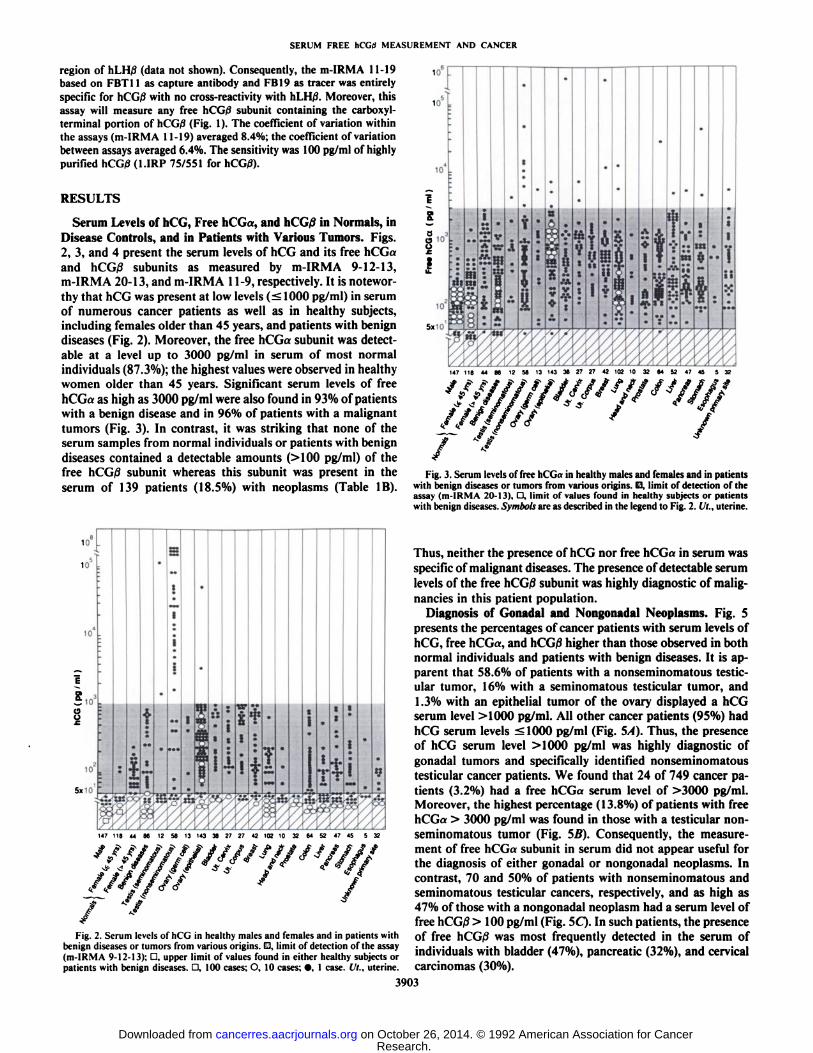
Serum Levels of hCG, Free hCGa, and hCG/8 in Normals, inDisease Controls, and in Patients with Various Tumors. Figs.2, 3, and 4 present the serum levels of hCG and its free hCGaand hCG/îsubunits as measured by m-IRMA 9-12-13,m-IRMA 20-13, and m-IRMA 11-9, respectively. It is noteworthy that hCG was present at low levels (< 1000 pg/ml) in serumof numerous cancer patients as well as in healthy subjects,including females older than 45 years, and patients with benigndiseases (Fig. 2). Moreover, the free hCGa subunit was detectable at a level up to 3000 pg/ml in serum of most normalindividuals (87.3%); the highest values were observed in healthywomen older than 45 years. Significant serum levels of freehCGa as high as 3000 pg/ml were also found in 93% of patientswith a benign disease and in 96% of patients with a malignanttumors (Fig. 3). In contrast, it was striking that none of theserum samples from normal individuals or patients with benigndiseases contained a detectable amounts (>100 pg/ml) of thefree hCG/3 subunit whereas this subunit was present in theserum of 139 patients (18.5%) with neoplasms (Table IB).
to
V
47 45 5 32
Fig. 3. Serum levels of free hCGa in healthy males and females and in patientswith benign diseases or tumors from various origins. D, limit of detection of theassay (m-IRMA 20-13). - limit of values found in healthy subjects or patientswith benign diseases. Symbols are as described in the legend to Fig. 2. It., uterine.
10
K
10
a
5x10
It
.
T
Fig. 2. Serum levels of hCG in healthy males and females and in patients withbenign diseases or tumors from various origins. G, limit of detection of the assay(m-IRMA 9-12-13); O, upper limit of values found in either healthy subjects orpatients with benign diseases. D, 100 cases; O, 10 cases; •¿�.1 case. Ut., uterine.
Thus, neither the presence of hCG nor free hCGa in serum wasspecific of malignant diseases. The presence of detectable serumlevels of the free hCG/3 subunit was highly diagnostic of malignancies in this patient population.
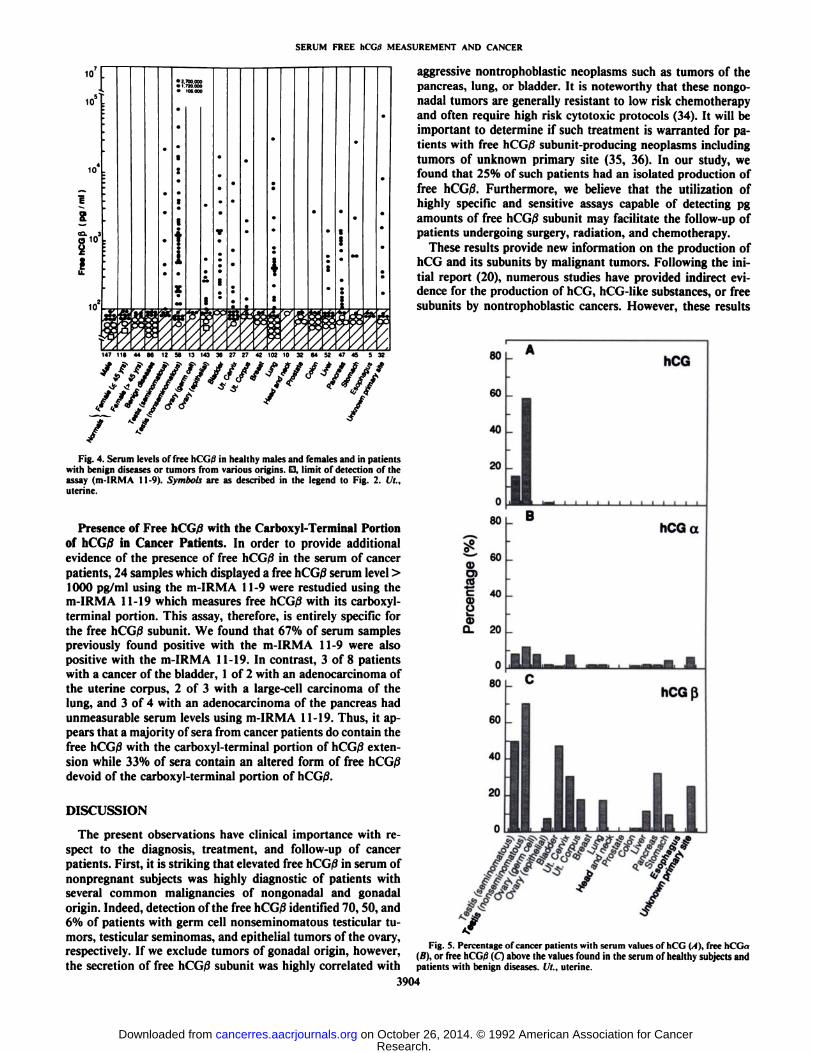
Diagnosis of Gonadal and Nongonadal Neoplasms. Fig. 5presents the percentages of cancer patients with serum levels ofhCG, free hCGa, and hCGßhigher than those observed in bothnormal individuals and patients with benign diseases. It is apparent that 58.6% of patients with a nonseminomatous testic-ular tumor, 16% with a seminomatous testicular tumor, and1.3% with an epithelial tumor of the ovary displayed a hCGserum level >1000 pg/ml. All other cancer patients (95%) hadhCG serum levels <1000 pg/ml (Fig. 5A). Thus, the presenceof hCG serum level >1000 pg/ml was highly diagnostic ofgonadal tumors and specifically identified nonseminomatoustesticular cancer patients. We found that 24 of 749 cancer patients (3.2%) had a free hCGa serum level of >3000 pg/ml.Moreover, the highest percentage (13.8%) of patients with freehCGa > 3000 pg/ml was found in those with a testicular nonseminomatous tumor (Fig. SB). Consequently, the measurement of free hCGa subunit in serum did not appear useful forthe diagnosis of either gonadal or nongonadal neoplasms. Incontrast, 70 and 50% of patients with nonseminomatous andseminomatous testicular cancers, respectively, and as high as47% of those with a nongonadal neoplasm had a serum level offree hCG/3 > 100 pg/ml (Fig. 5C). In such patients, the presenceof free hCG/3 was most frequently detected in the serum ofindividuals with bladder (47%), pancreatic (32%), and cervicalcarcinomas (30%).
3903
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
SERUM FREE hCGji MEASUREMENT AND CANCER
u? tie 44 ee 12 se 13 143 3e 2? 2? 42 10210 32 64 52 47 45 s 32
Fig. 4. Serum levels of free h<'<;., in healthy males and females and in patients
with benign diseases or tumors from various origins. D, limit of detection of theassay (m-IRMA 11-9). Symbols are as described in the legend to Fig. 2. Ut..uterine.
Presence of Free hCG/îwith the Carboxyl-Terminal Portionof hCG/8 in Cancer Patients. In order to provide additionalevidence of the presence of free hCG/3 in the serum of cancerpatients, 24 samples which displayed a free hCGßserum level >1000 pg/ml using the m-IRMA 11-9 were restudied using them-IRMA 11-19 which measures free hCG/S with its carboxyl-terminal portion. This assay, therefore, is entirely specific forthe free hCG/3 subunit. We found that 67% of serum samplespreviously found positive with the m-IRMA 11-9 were alsopositive with the m-IRMA 11-19. In contrast, 3 of 8 patientswith a cancer of the bladder, 1 of 2 with an adenocarcinoma ofthe uterine corpus, 2 of 3 with a large-cell carcinoma of thelung, and 3 of 4 with an adenocarcinoma of the pancreas hadunmeasurable serum levels using m-IRMA 11-19. Thus, it appears that a majority of sera from cancer patients do contain thefree hCG/3 with the carboxyl-terminal portion of hCG/3 extension while 33% of sera contain an altered form of free hCG£idevoid of the carboxyl-terminal portion of hCG/3.
DISCUSSION
The present observations have clinical importance with respect to the diagnosis, treatment, and follow-up of cancerpatients. First, it is striking that elevated free hCGßin serum ofnonpregnant subjects was highly diagnostic of patients withseveral common malignancies of nongonadal and gonadalorigin. Indeed, detection of the free hCG/3 identified 70, 50, and6% of patients with germ cell nonseminomatous testicular tumors, testicular seminomas, and epithelial tumors of the ovary,respectively. If we exclude tumors of gonadal origin, however,the secretion of free hCG/3 subunit was highly correlated with
aggressive nontrophoblastic neoplasms such as tumors of thepancreas, lung, or bladder. It is noteworthy that these nongonadal tumors are generally resistant to low risk chemotherapyand often require high risk cytotoxic protocols (34). It will beimportant to determine if such treatment is warranted for patients with free hCGßsubunit-producing neoplasms includingtumors of unknown primary site (35, 36). In our study, wefound that 25% of such patients had an isolated production offree hCG/8. Furthermore, we believe that the utilization ofhighly specific and sensitive assays capable of detecting pgamounts of free hCG/3 subunit may facilitate the follow-up ofpatients undergoing surgery, radiation, and chemotherapy.
These results provide new information on the production ofhCG and its subunits by malignant tumors. Following the initial report (20), numerous studies have provided indirect evidence for the production of hCG, hCG-like substances, or freesubunits by nontrophoblastic cancers. However, these results
a>O)
60
40
20
0
80
60
40
O)O- 20
O
80
60
40
20
O
hCG
lili
hCGa
hCGß
Fig. 5. Percentage of cancer patients with serum values of hCG (A), free hCGn(B), or free hCGtf (Q above the values found in the serum of healthy subjects andpatients with benign diseases. Ut., uterine.
3904
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
SERUM FREE hCG/i MEASUREMENT AND CANCER
were controversial since most investigations used polyclonaland monoclonal antibodies lacking the required specificity. Oneof the major problems was that most antibodies cross-reactedwith hLH. For example, antibody SB6 had a cross-reactivity of7 to 11% with hLH and therefore was not a highly specificreagent for hCG and hCG/3 (9, 24, 25). Recently developedassays based on monoclonal antibodies still displayed a low butsignificant cross-reactivity with hLH (37-39). More impor
tantly, most assays did not distinguish between the intact hCGmolecule and the free hCG/3 subunit (14, 37-41). Finally, thenomenclature for "hCG0" assays has been ambiguous since the
same designation has been given to at least two types of assayswith widely different specificities including those measuringonly the free hCGßsubunit and those measuring both intacthCG and the free hCG/3 subunit (34). Similarly, the nomenclature for "hCG" assays may be misinterpreted since these assays
may also measure the free hCG/3 subunit in addition to hCG(42).
Recently, mIRMAs entirely specific for intact hCG and thefree hCGa or hCG/3 subunit have enabled investigators to re-
evaluate the production of hCG and free subunits by normalindividuals, during pregnancy, and in patients with gestationaltrophoblastic diseases (4, 26, 29-31). The present study hastaken advantage of the specificity of such assays and assessedthe production of hCG and free subunits by gonadal as well asnongonadal and nontrophoblastic malignancies. In this context, we have used four different assays that are entirely specificfor the molecules of interest, namely hCG, free hCGa, andhCG/3 and the free hCG/3 with the CTP extension. The latterassay is the first described for free hCG/3 that displays no cross-reaction with the free hLH/3 subunit. The results from thisinvestigation demonstrate using these four highly specific mlR-MAs that neither the production of free hCGa nor low levelhCG was specific of malignant tumors. Indeed, the levels ofboth free hCGa and hCG were marginally raised in most patients with tumors but were within the range of values generallyfound in healthy individuals and those with benign diseases (29,30). In this regard, a common cause of marginally raised hCGalevels has been shown to be due to production of free a subunitsby the pituitary gland which will cross-react in the free hCGaassay (38). In addition, recent studies have provided direct evidence for production of the intact hCG molecule by the pituitary (27, 28, 43). It is highly likely that the low level hCG andthe free hCG« subunit found in the blood of patients withvarious tumors originates from the pituitary gland and not fromthe tumor (44-48). This observation may explain in part thefinding of elevated free hCG«and hCG levels in females olderthan 45 years with gynecological or breast cancers since serumlevels relating to a pituitary origin have been found to increasewith age (29, 30). Finally, in contrast to the insignificance of alow level hCG in patients with malignancy with respect to itsvalue to a specific tumor marker, we found that a serum level ofhCG >1 ng/ml was highly suggestive of a testicular tumor (seeFigs. 2 and 5A).
The finding of the free hCGßsubunit in patients with nongonadal and nontrophoblastic malignancies is at odds with previous results suggesting that the free hCG0 is rarely, if ever,produced by such tumors and that the free hCG/3 secretionoccurs only in association with the synthesis of high levels ofintact hCG (37, 49, 50). In the present investigation, 139 patients with various tumors had elevated free hCG0 levels.Among these patients, 92 had either an isolated secretion of
free hCG/3 or a predominant production of this free subunit inexcess of hCG. This pattern of secretion contrasts with thatobserved in pregnant women who display a predominant secretion of hCG in large excess of free hCG/3 (4). Since the initialcase report in 1973 (8), we have found only three other well-
documented published examples of either an isolated or predominant production of free hCG/ìin cancer patients (24, 50,51). In these four prior cases, such a production was associatedwith a pancreatic adenosquamous carcinoma (8), an adenocar-cinoma of the stomach (24), a carcinoma of the uterine cervix(50), and an epidermoid carcinoma of unknown primary site(51). Using the highly specific and sensitive mIRMAs, it appears that the presence of elevated serum levels free hCG/3 isnot rare and may be relatively common particularly in patientswith bladder tumors. This finding was not totally unexpectedsince the in vivo production of either hCG or free hCG/3 by suchneoplasms had been reported previously (52-56). Moreover, invitro studies performed on culture media derived from urothe-
lial cell lines strongly suggest that the material excreted by thesecells consisted principally of free hCG0 subunit or fragmentsthereof (57, 58).
There is accumulating evidence indicating that the isolatedproduction of free hCG/3 may be associated with aggressivenongonadal and nontrophoblastic malignancies. For example,we have found that the isolated production of free hCG/3 sub-
unit was associated with tumors of poor prognosis such ascancers of the lung, pancreas, and liver. This observation is inagreement with prior documented cases in which the presenceof free hCG/3 was associated with aggressive malignancies asmeasured by a duration of survival of 2 weeks to 3 months (8,51).
The histológica! origin of free hCG/3-producing cells in thesetumors (Table 1B) deserves comment. Several hypotheses havebeen proposed to explain the origin of hCG/3-producing cellsand include the following: (a) displaced totipotential or gonadalcells (extragonadal choriocarcinomas); (b) metastasis from anintrauterine or gonadal lesion; and (c) an evolution from asomatic cell that underwent a morphological and functionaltransformation (metaplasia) into a cell functionally similar tothe trophoblast. Since the pioneering work of Pick (59) in 1926,most authors favor the concept of a trophoblastic metaplasiawithin the carcinomatous tissues (54, 60-63). Indeed, the pathway of cytotrophoblast differentiation ensures that hCGamRNA accumulates before hCG/3 mRNA, resulting in increasing hCG production as hCG/3 synthesis is initiated (39). Ourresults are in agreement with this pathway; most gonadal andextragonadal choriocarcinomas as well as metastatic choriocarcinomas produce both hCG and the free hCG/3 subunit and thusdiffer from nongonadal cells producing predominantly the freehCG/3 subunit (34, 39, 40). In addition, it has been shown thatin the early stages of implantation as well as in trophoblasticdisease, the origin of free hCG/3 production may be due topoorly differentiated trophoblastic tissue (40, 64). These observations suggest that the origin of nongonadal malignant cellsinvolves a metaplasia of the carcinomatous tissues into a tissuesimilar to poorly differentiated trophoblasts. Finally, recognition of a secretion of free hCG/3 by nongonadal tumors such asbladder may become increasingly important inasmuch as thisfree subunit may represent a unique biological marker of malignancies that do not produce and secrete an identifiable tumorcell product.
3905
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
SERUM FREE hCGf) MEASUREMENT AND CANCER
ACKNOWLEDGMENTS
We are indebted to the National Pituitary Program of the NationalInstitute of Arthritis and Metabolic Diseases and the National Instituteof Child Health and Human Development for supplying hCG and itssubunits used in these studies and to Christine Bombled and Josyane LeCalvez for their excellent technical assistance.
REFERENCES
1. Pierce, J. G.. and Parsons. T. F. Glycoprotein hormones: structure andfunction. Annu. Rev. Biochem.. 50:465-495. 1981.
2. Fiddes. J. C.. and Goodman, H. M. The gene encoding the common a subunitof the four human glycoprotein hormones. J. Mol. Appi. Genet., /: 3-18,1981.
3. Boorstein, W. R., Vamvakopoulos. N. C., and Fiddes, J. C. Human chorionicgonadotropi •¿�-.nimmt is encoded by at least eight genes arranged in tandemand inverted pairs. Nature (Lond.). 300: 419-423, 1982.
4. Ozturk. M., Bellet. D., Manil, L., Hennen. G., Frydman, R., and Wands, J.R. Physiological studies of human chorionic gonadotropi (hCG), nhCG, andÕJhCGas measured by specific monoclonal immunoradiometric assays. Endocrinology. 120: 549-558. 1987.
5. Borkowski. A., and Muquardt. C. Human chorionic gonadotropi in theplasma of normal nonpregnant subjects. N. Engl. J. Med.. 301: 298-302.1979.
6. Kahn. C. R.. Rosen, S. W„Wcintraub. B. D.. Fajans. S. S., and Corden. P.Ectopie production of chorionic gonadotropin and its subunits by islet-celltumors. N. Engl. J. Med.. 297: 565-569, 1977.
7. Rosen. S. W., and Weintraub. B. D. Ectopie production of the isolated asubunit of the glycoprotein hormones. N. Engl. J. Med., 290: 1441-1447,1974.
8. Weintraub. B. D.. and Rosen. W. S. Ectopie production of the isolated lìsubunil of human chorionic gonadotropin. J. Clin. Invest.. 52: 3135-3142,1973.
9. Tormey, D. C, Waalkes. T. P., and Simon, R. M. Biological markers inbreast carcinoma. Cancer (Phila.), 39: 2391-2396, 1977.
10. Gailani. S., Chu, T. M., Nussbaum, A.. Ostrander. M., and Christoff. N.Human chorionic gonadotrophins (hCG) in nontrophoblastic neoplasms.Cancer (Phila.), 38: 1684-1686. 1976.
11. Blackman, M. R.. Weintraub. B. D., Rosen, S. W., and Kourides. I. A.,Steinwascher. K., and Gail, M. H. Human placenta! and pituitary glycoprotein hormones and their subunits as tumor markers: a quantitativeassessment. J. Nati. Cancer Inst.. 65: 81-93. 1980.
12. Hussa, R. O. Clinical applications of hCG tests: tumors. In: R. O. Hussa(ed.). The Clinical Marker hCG, pp. 119-136. New York: Praeger. 1987.
13. Hussa, R. O. Subunits of hCG. In: R. O. Hussa (ed.). The Clinical MarkerhCG, pp. 161-178. New York: Praeger, 1987.
14. Hussa. R. O. Tissue localization of hCG. In: R. O. Hussa (ed.). The ClinicalMarker hCG. pp. 151-160. New York: Praeger, 1987.
15. Burg-Kurland. C. L., Purnell. D. M., Combs, J. W.. Hillman, E. A., Harris.C. C., and Trump. B. F. Immunocytochemical evaluation of human esoph-ageal neoplasms and preneoplastic lesions for ^-chorionic gonadotropin. pla-cental lactogen. a-fetoprotein, carcinoembryonic antigen, and nonspecificcross-reacting antigen. Cancer Res., 46: 2936-2943, 1986.
16. Campo, E.. Palacin, A., Benasco. C., Quesada, E., and Cardesa, A. Humanchorionic gonadotropin in colorectal carcinoma. Cancer (Phila.). 59: 1611-1616. 1987.
17. Yakeishi. Y., Mori. M.. and Enjoji. M. Distribution of (¡-humanchorionicgonadotropin-positive cells in noncancerous gastric mucosa and in malignantgastric tumors. Cancer (Phila.). 66: 695-701. 1990.
18. Braunstein. G. D.. Rasor, J., and Wade, M. E. Presence in normal humantestes of a chorionic-gonadotropin-like substance distinct from human lutein-izing hormone. N. Engl. J. Med., 29.J: 1339-1343, 1975.
19. McGregor. W. G., Kühn.R. W.. and Jaffe, R. B. Biologically active chorionicgonadotropin: synthesis by the human fetus. Science (Washington DC), 220:306-308. 1983.
20. Reeves. R. L., Tesluk. H., and Harrison, C. E. Precocious puberty associatedwith hepatoma. J. Clin. Endocrinol. Metab., 19: 1651-1660, 1959.
21. Odell, W. D.. Wolfsen, A., Yoshimoto, Y.. Weitzman, R., Fisher. D., andHirose, F. Ectopie peptide synthesis: a universal concomitant of neoplasia.Tr. Assoc. Am. Physicians. 90: 204-227. 1977.
22. Yoshimoto. Y., Wolfsen, A. R.. and Odell. W. D. Human chorionic gona-dotropin-like substance in nonendocrine tissues of normal subjects. Science(Washington DC), 797: 575-577. 1977.
23. Braunstein, G. D., Kamdar, V.. and Rasor, J.. Swaminathan, N.. and Wade,M. E. W ¡despreaddistribution of a chorionic gonadotropin-like substance innormal human tissues. J. Clin. Endocrinol. Metab., 49: 917-925. 1979.
24. Papapetrou. P. D., Sakarelou. N. P., Braouzi. H., and Fessas, P. H. Ectopieproduction of human chorionic gonadotropin (hCG) by neoplasms: the valueof measurements of immunoreactive hCG in the urine as a screeningprocedure. Cancer (Phila.), 45: 2583-2592. 1980.
25. Monteiro, J. C. M. P.. Ferguson. K. M., McKinna, J. A., Greening, W. P.,and Neville. A. M. Ectopie production of human chorionic gonadotrophin-
26.
27.
28.
29.
30.
31.
32.
33.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
like material by breast cancer. Cancer (Phila.), 53: 957-962, 1984.Griffin, J., and Odell, W. D. Ultrasensitive immunoradiometric assay forchorionic gonadotropin which does not cross-react with luteinizing hormonenor free ßchain of hCG and which detects hCG in blood of non-pregnanthumans. J. Immunol. Methods. 103: 275-283. 1987.Odell. W. D.. Griffin, J.. Bashey, H. M., Snyder, P. J. Secretion of chorionicgonadotropin by cultured human pituitary cells. J. Clin. Endocrinol. Metab.,71: 1318-1321, 1990.Hammond. E.. Griffin, J.. and Odell, W. D. A chorionic gonadotropin-secreting human pituitary cell. J. Clin. Endocrinol. Metab.. 72: 747-754,1991.Odell. W. D., and Griffin. J. Pulsatile secretion of human chorionic gonadotropin in normal adults. N. Engl. J. Med.. 317: 1688-1691, 1987.Ozturk. M., Berkowitz, R., Goldstein. D., Bellet. D., and Wands, J. R.Differential production of human chorionic gonadotropin and free subunitsin gestational trophoblastic disease. Am. J. Obstet. Gynecol., 158: 193-198,1988.Bellet, D. H.. Ozturk, M.. Bidart, J. M., Bohuon. C. J., and Wands, J. R.Sensitive and specific assay for human chorionic gonadotropin (hCG) basedon ami-peptide and anti-hCG antibodies: construction and clinicalimplications. J. Clin. Endocrinol. Metab., 63: 1319-1327. 1986.Bidart. J. M.. Troalen. F., Salesse, R.. Bousfield. G. R., Bohuon, C, andBellet, D. Topographic antigenic determinants recognized by monoclonalantibodies on human choriogonadotropin (J-subunit. J. Biol. Chem., 262:8551-8556, 1987.Bidart. J. M.. Bellet. D. H.. Alberici, G. F.. Van Besien. F., and Bohuon. C.The immune response to a synthetic peptide analogous to the 109-145 (ihCGcarboxyl-terminus is directed against two major and two minor regions. Mol.Immunol.. 24: 339-345, 1987.Case records of the Massachusetts General Hospital (case 34-1983). N. Engl.J. Med.. 309: 477-487. 1983.Richardson. R. L., Schoumacher, R. A., and Fer, M. F. The unrecognizedextragonadal germ cell cancer syndrome. Ann. Intern. Med., 94: 181-186,1981.Greco, A., Vaughn, W. K., and Hainsworth. J. D. Advanced poorly differentiated carcinoma of unknown primary site: recognition of a treatablesyndrome. Ann. Intern. Med.. 104: 547-553. 1986.Sailer. B.. Clara. R.. Spottl, G., Siddle, K., and Mann. K. Testicular cancersecretes intact human choriogonadotropin (hCG) and its free ßsubunit: evidence that hCG (+hCG-rf) assays are the most reliable in diagnosis andfollow-up. Clin. Chem., 36: 234-239. 1990.Hay, D. L., and Murphy. J. R. Evaluating human choriogonadotropin heterogeneity in nongestational malignancy with monoclonal immunoassays.Oncology (Basel). 44: 174-179, 1987.Hay, D. L. Histological origins of discordant chorionic gonadotropin secretion in malignancy. J. Clin. Endocrinol. Metab.. 66: 557-564. 1988.Fan, C., Goto, S., Furuhashi, Y., and Tomoda. Y. Radioimmunoassay of theserum free /i-subunit of human chorionic gonadotropin in trophoblasticdisease. J. Clin. Endocrinol. Metab., 64: 313-318, 1987.Mann. K.. and Siddle. K. Evidence for free /J-subunit secretion in so-calledhuman chorionic gonadotropin-posilive seminoma. Cancer (Phila.), 62:2378-2382. 1988.Cole. L. A., and Kardana. A. Discordant results in human chorionic gonadotropin assays. Clin. Chem., 38: 263-270. 1992.Hoermann, R.. Spoettl. G., Moncayo. R., and Mann. K. Evidence for thepresence of human chorionic gonadotropin (hCG) and free iJ-subunit of hCGin the human pituitary. J. Clin. Endocrinol. Metab., 71: 179-186, 1990.Fusco. F. D., and Rosen. S. W. Gonadotropin-producing anaplastic large-cellcarcinomas of the lung. N. Engl. J. Med.. 275: 507-515, 1966.Broder. L. E., Weintraub, B. D., Rosen, S. W., Cohen, M. H., and Tejada. F.Placental proteins and their subunits as tumor markers in prostaticcarcinoma. Cancer (Phila.), 40: 211-216, 1977.Yamaguchi, A.. Ishida. T.. and Nishimura. G. Human chorionic gonadotropin in colorectal cancer and its relationship to prognosis. Br. J. Cancer, 60:382-384. 1989.Morinaga. S.. Yamaguchi. M.. Watanabe, I., Kasai, M., Ojima, M., andSasano, N. An immunohistochemica! study of hepatoblastoma producinghuman chorionic gonadotropin. Cancer (Phila.). 51: 1647-1652, 1983.Hattori. M., Yoshimoto, Y.. Matsukura, S.. and Fujita. T. Qualitative andquantitative analyses of human chorionic gonadotropin and its subunits produced by malignant tumors. Cancer (Phila.). 46: 355-361, 1980.Heitz. P. U., von Herbay, G., and Klöppel,G. The expression of subunits ofhuman chorionic gonadotropin (hCG) by nontrophoblastic, nonendocrine.and endocrine tumors. Am. J. Clin. Pathol.. 88: 467-472. 1987.Papapetrou, P. D., and Nicopoulou, S. Ch. The origin of a human chorionicgonadotropin tf-subunit-core fragment excreted in the urine of patients withcancer. Acta Endocrinol.. 112: 415-422. 1986.Nagelberg, S. B., Marmorstein, B., Khazaeli, M. B., and Rosen, S. W. Isolated ectopie production of the free beta subunit of chorionic gonadotropin byan epidermoid carcinoma of unknown primary site. Cancer (Phila.), 55:1924-1930, 1985.Dexeus. F.. Logothetis. C.. Hossan, E.. and Samuels, M. L. Carcinoembryonic antigen and .<huni.ui chorionic gonadotropin as serum markers foradvanced urothelial malignancies. J. Urol.. 136: 403-407, 1986.lies. R. K., Jenkins. B. J., Oliver. R. T. D.. Blandy, J. P., and Chard, T. ß
3906
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
SERUM FREE hCGfJ MEASUREMENT AND CANCER
human chorionic gonadotrophin in serum and urine. A marker for metastaticurothelial cancer. Br. J. Urol., 64: 241-244, 1989.
54. Vahlensieck. W., Riede. U., Wimmer, B., and Ihling. C. rf-Human chorionicgonadotropin-positive extragonadal germ cell neoplasia of the renal pelvis.Cancer (Phila.), 67: 3146-3149, 1991.
55. lies. R. K., and Chard. T. Human chorionic gonadotropin expression bybladder cancers: biology and clinical potential. J. Urol., 145:453-458, 1991.
56. Fetissof, F., Bellet, D.. Guilloteau, D„and Maillot, O. Hormone gonado-tropine chorionique et carcinome à cellules traditionnelles de la vessie. Ann.Pathol.. 8: 276-280, 1988.
57. Iles. R. K., Oliver. R. T. D.. Kitau, M., Walker. C., and Chard. T. In vitrosecretion of human chorionic gonadotropin by bladder tumour cells. Br. J.Cancer, 55: 623-626, 1987.
58. lies, R. K., and Chard, T. Immunochemical analysis of the human chorionicgonadotrophin-like material secreted by "normal" and neoplastic urothelialcells. J. Mol. Endocrino!., 2: 107-112, 1989.
59. Pick, L. Über die chorionepitheliomätnlich metastasierende Form des
Magencarcinoms. Klin. Wochenschr., 5: 1728-1729, 1926.60. Park, C. H., and Reid, J. D. Adenocarcinoma of the colon with choriocarci-
noma in its métastases.Cancer (Phila.), 46: 570-575, 1980.61. Obe, J. A., Rosen, N., and Koss, L. G. Primary choriocarcinoma of the
urinary bladder. Cancer (Phila.). 52: 1405-1409. 1983.62. Kubosawa, H.. Nagao, K., Kondo. Y., Ishigc, H., and Inaba, N. Coexistence
of adenocarcinoma and choriocarcinoma in the sigmoid colon. Cancer(Phila.). 54:866-868. 1984.
63. Campo, E., Algaba, F., Palacin, A., Germa, R., Sole-Balcells, F. J., andCardesa, A. Placental proteins in high-grade urothelial neoplasms. An im-munohistochemical study of human chorionic gonadotropin, human placen-tal lactogen, and pregnancy-specific /J-1-glycoprotein. Cancer (Phila.), 63:2497-2504. 1989.
64. Hay, D. L. Discordant and variable production of human chorionic gonadotropin and its free «-and /J-subunits in early pregnancy. J. Clin. Endocrinol.Metab., 61: 1195-1200, 1985.
3907
Research. on October 26, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
Related Documents







![HUMAN CHORIONIC GONADOTROPIN AND GONADOTROPIN … · B before a resynchronized fixed-timed AI (TAI)] on pregnancy rates in cows diagnosed not pregnant and pregnancy survival in cows](https://static.cupdf.com/doc/110x72/5eb7d9b299fd5235ef45b97b/human-chorionic-gonadotropin-and-gonadotropin-b-before-a-resynchronized-fixed-timed.jpg)



