Formal and Informal Volunteer Activity and Spousal Caregiving Among Older Adults Namkee G. Choi University of Texas at Austin Jeffrey A. Burr Jan E. Mutchler Francis G. Caro University of Massachusetts, Boston On the basis of data from the 1998 and 2000 waves of the Health and Retirement Study, this study tested two alternative hypotheses, role overload and role exten- sion, about the relationship between volunteering and spousal caregiving among older married persons. Spousal caregiving was not significantly associated with the likelihood of formal or informal volunteering for men; however, female caregivers were found to be less likely than noncaregivers to have engaged in formal or informal volunteering to a certain extent, thus lending partial support to the role overload hypothesis. Functional health status and other human and cultural capital resources were significant predictors of both formal and infor- mal volunteering for both men and women. Future studies need to examine in more depth the effect of spousal caregiving on volunteering, taking caregiving burden and stress into consideration, to more fully understand these two types of productive activity in later life. Keywords: spousal caregiving; volunteer activity; informal helping; role theory A ccording to data collected through a supplement to the September 2005 Current Population Survey, 30.2% of persons aged between 55 and 64 years and 24.8% of those aged 65 years and older volunteered in a variety of Research on Aging Volume 29 Number 2 March 2007 99-124 © 2007 Sage Publications 10.1177/0164027506296759 http://roa.sagepub.com hosted at http://online.sagepub.com 99 Authors’ Note: We acknowledge the research support of the National Institute on Aging (R03 AG 18910). Correspondence concerning this article should be addressed to Namkee G. Choi, University of Texas at Austin, School of Social Work, 1 University Station, Mail Code D3500, Austin, TX 78712-0358; e-mail: [email protected]. at University of Texas Libraries on June 26, 2015 roa.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Formal and Informal Volunteer Activity and Spousal Caregiving Among Older AdultsNamkee G. ChoiUniversity of Texas at AustinJeffrey A. BurrJan E. MutchlerFrancis G. CaroUniversity of Massachusetts, Boston
On the basis of data from the 1998 and 2000 waves of the Health and RetirementStudy, this study tested two alternative hypotheses, role overload and role exten-sion, about the relationship between volunteering and spousal caregiving amongolder married persons. Spousal caregiving was not significantly associated withthe likelihood of formal or informal volunteering for men; however, femalecaregivers were found to be less likely than noncaregivers to have engaged informal or informal volunteering to a certain extent, thus lending partial supportto the role overload hypothesis. Functional health status and other human andcultural capital resources were significant predictors of both formal and infor-mal volunteering for both men and women. Future studies need to examine inmore depth the effect of spousal caregiving on volunteering, taking caregivingburden and stress into consideration, to more fully understand these two typesof productive activity in later life.
Keywords: spousal caregiving; volunteer activity; informal helping; roletheory
According to data collected through a supplement to the September 2005Current Population Survey, 30.2% of persons aged between 55 and 64
years and 24.8% of those aged 65 years and older volunteered in a variety of
Research on AgingVolume 29 Number 2March 2007 99-124
© 2007 Sage Publications10.1177/0164027506296759
http://roa.sagepub.comhosted at
http://online.sagepub.com
99
Authors’ Note: We acknowledge the research support of the National Institute on Aging (R03AG 18910). Correspondence concerning this article should be addressed to Namkee G. Choi,University of Texas at Austin, School of Social Work, 1 University Station, Mail Code D3500,Austin, TX 78712-0358; e-mail: [email protected].
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
100 Research on Aging
formal settings, such as hospitals, religious organizations, schools, seniorcenters, Meals on Wheels programs, and other educational and human serviceorganizations (U.S. Department of Labor, Bureau of Labor Statistics 2005).Many such organizations and groups have come to depend on older volun-teers as essential resources for carrying out their programs and deliveringservices (Caro and Bass 1997; Freedman 1999). Older adults also provideinformal assistance, such as babysitting and caregiving, to neighbors, friends,and relatives outside the household.
In addition to the significant societal economic benefits that they provide,older volunteers help themselves by volunteering (Johnson and Schaner 2005;Piliavin and Charng 1990). Studies have found that volunteering in later lifehas positive physical and functional health outcomes and offers a protectiveeffect against mortality (Lum and Lightfoot 2005; Musick, Herzog, and House1999; Oman, Thoreson, and McMahon 1999). Volunteering also contributes toenhanced self-esteem, sense of personal control, psychological well-being,and life satisfaction (Harlow and Cantor 1996; Herzog et al. 1998; Krause,Herzog, and Baker 1992; Thoits and Hewitt 2001; Van Willigen 2000; Wheeler,Gorey, and Greenblatt 1998).
With an increasing number of well-educated, healthy older adults in thiscountry, tapping the vast reservoir of their human capital resources is indeedan important issue, especially given the many beneficial effects of volunteeractivity for the helper and the helped as well as the community as a whole.Interest in older adults’ volunteering behavior led researchers to examinetheir reasons for and correlates of volunteering. Volunteer work has oftenbeen seen as “one of the few viable alternatives to complete social disen-gagement in lieu of major role losses in later life such as widowhood andretirement” (Krause et al. 1992:P300). Researchers have also often found thatemployed adults engage in volunteering as an extension of paid work, or “thelong arm of the job” (Wilson and Musick 1997b). Volunteering has thus beenfrequently examined in the context of role substitution or role extension.
To our knowledge, however, the relationship between formal and infor-mal volunteering and spousal caregiving, a role that many older adults carryout, has rarely been examined. The purpose of this study was to examine thequestion of whether spousal caregiving conditions the likelihood of volun-teering among older adults. Spousal caregiving is a unique form of produc-tive activity in part because it often requires a significant commitment ofindividuals’ time and effort on a daily basis, and unlike formal and informalvolunteering, caregiving occurs largely out of public view, within the carerecipient’s home. Empirical results from the sparse research literature thathas examined the relationship between caregiving and formal volunteering
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
as well as the relationship between caregiving and informal helping areequivocal. On one hand, one might expect spousal caregiving to suppress care-givers’ capacity to volunteer for organizations and extend help to otherpeople. On the other hand, spousal caregivers may be more likely to engagein informal and formal helping activities as an extension of their daily care-giving routines, because this activity brings them into increased contact withboth informal social networks and formal service networks.
Volunteering and Spousal Caregiving:An Application of Role Theory
The role extension hypothesis is one perspective that may be applied tohelp understand the relationship between formal and informal volunteeringand spousal caregiving. Spousal caregivers may be more likely to volunteerand do so at significant levels because their caregiver role brings them intocontact with people and organizations that provide more opportunities for vol-unteering. Although spouses tend to be the primary caregivers in coupledyads, studies also show that a large proportion of spousal caregivers havesecondary or tertiary helpers—adult children, other relatives, friends, andneighbors—who provide financial, instrumental, and/or emotional assistance(Burton et al. 1995; Mui, Choi, and Monk 1998). Thus, spousal caregivers arelikely to have bigger informal social networks and more opportunities toexchange favors and engage in reciprocal informal helping relationships thanthose who are not caregivers. Because caregivers are also likely to be linkedto formal support systems (e.g., hospitals, clinics, and home- and community-based service agencies), they may also be more likely than their peers who arenot caregivers to be exposed to opportunities to volunteer in formal settings.Farkas and Himes (1997) found that among middle-aged (mean age = 43years) women, caregiving was associated with significantly higher levels ofparticipation in social activities and visiting with friends. The authors alsofound that caregiving did not reduce the frequency of participation in formalvoluntary activities, both service and hobby- or garden-type clubs, for bothmiddle-aged and older female caregivers.
Caregivers may also be more likely to engage in volunteer activities becausethe latter offer time away from caregiving routines and the associated sense ofburden or stress, guilt, anxiety, and/or loneliness. Studies show that caregiversengaged in volunteer activities out of self-protective motivations and as partof their efforts to maintain or improve their own physical and emotional health(Bowen, Andersen, and Urban 2000; Morrow-Howell and Mui 1989; Okun,
Choi et al. / Volunteer Activity and Caregiving 101
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from

Barr, and Herzog 1998). A study of older caregivers providing care directly orarranging for care to be provided to friends or relatives found that those whoworked and/or volunteered reported better self-rated health, although being acaregiver while assuming another role was not significantly associated withthe level of functional impairment and depressive symptoms (Rozario,Morrow-Howell, and Hinterlong 2004). Adelman (1994a, 1994b) also foundthat multiple roles—employee, spouse, parent, volunteer, homemaker, grand-parent, caregiver, and student—were significantly associated with better phys-ical and emotional health for both genders and for both African Americansand Whites. This research suggests that caregivers may seek other activitiesoutside the home, such as helping others, to relieve some of the psychologi-cal burden that accompanies some forms of caregiving.
In contrast to the role extension hypothesis, the role overload hypothesis isanother perspective that may be applied to help understand the relationshipbetween volunteering and spousal caregiving. Although not without positiveaffective outcomes for some spousal caregivers, caring for a disabled spouseis, on balance, a stressful experience that often requires the commitment of alarge amount of time and effort and takes both a physical and an emotionaltoll. Spouses are the predominant sources of primary caregiving, and on aver-age, they spend more time on caregiving than do adult children, who providemost secondary assistance, and other relatives, who are more likely to assumea secondary caregiving role (Enright 1991; Kennedy, Walls, and Owens-Nicholson 1999). Study findings based on longitudinal surveys (the CaregiverHealth Effects Study) of a large population-based sample of adults aged 65years and older showed that spousal caregivers who provided assistance withany impairments to activities of daily living (ADLs) or instrumental ADLs(IADLs), especially those who were heavy caregivers, compared with non-caregiving spouses, showed more symptoms of depression and anxiety andpoorer self-reported health and health behaviors (Beach et al. 2000; Burton et al. 2003). A study based on the same data also showed that spousal care-givers, especially those reporting strain, were more likely to have lower edu-cation, lower incomes, and more functional impairments (Schulz et al. 1997).Other studies based on community samples have also shown that spousalcaregivers reported declines in preventive health and self-care activities,increases in at-risk health behaviors, and increased levels of loneliness anddepression with increasing caregiving burden (e.g., Beeson 2003; Connell1994; Strawbridge et al. 1997; see also Pinquart and Sorensen’s [2003] meta-analysis of caregiver burden and depressive symptoms).
Compared with people who freely engage in and freely disengage from lessobligatory forms of caregiving for friends, neighbors, and relatives outside the
102 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
household, most spousal caregivers do not feel that they have a choice to dis-engage from their caregiving responsibilities, for reasons of both affection andobligation. Previous studies have shown that adult children, especially thosewho provided nonresidential caregiving, and more distant relatives and nonkinassociates, who had lower levels of normative obligation, experienced lowercaregiving burden and more beneficial effects on well-being and developmentfrom caregiving than spousal caregivers did (Chumbler et al. 2003; Marks,Lambert, and Choi 2002; Raschick and Ingersoll-Dayton 2004).
Because of the time commitment required for caregiving, along with thephysical and mental health strain emanating from the caregiver role, somespousal caregivers may not be able to engage in volunteer activities, or theymay reduce commitments they already have. Especially when spousal care-givers also have to juggle other family- and work-related roles, they couldexperience role demand overload (time constraints) and role conflict (psy-chological tension and strain or disturbances) (see Goode 1960; Mui andMorrow-Howell 1993; Sieber 1974). In such circumstances, caregivers maychoose to avoid volunteer commitments or to withdraw from or reduce thevolunteer activities they already have in place to abate the competing roledemands associated with volunteering and caregiving. Although they didnot evaluate caregiving effects on nonpaid work, such as volunteering,Pavalko and Artis (1997) did find that caregiving women often found it nec-essary to reduce their work hours to meet caregiving demands. It is worthnoting that volunteering, unlike paid work, tends to be a discretionary activ-ity, which can be more easily avoided or reduced than can paid work.
Other Correlates of Volunteering
An increasing amount of research on volunteering frames analyses of thisbehavior around a “forms of capital” perspective (Wilson 2000). That is,researchers have found that indicators of cultural, human, and social capitalare related to levels and intensity of volunteering. Studies have demonstratedthat older volunteers tend to offer their services in an effort to increase theirfeelings of usefulness and productivity and that they are likely to be moremotivated than their younger counterparts by service or community obliga-tions as well as social values and beliefs, which may be referred to as culturalcapital (Chappell and Prince 1997; Okun et al. 1998; Omoto, Snyder, andMartino 2000; Wilson and Musick 1997b). This sense of moral obligation tohelp worthy organizations or other individuals may originate from a person’saltruistic disposition, prosocial personality orientation, early life experiencesof helping others, and/or religious faith (Hodgkinson and Weitzman 1994;
Choi et al. / Volunteer Activity and Caregiving 103
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from

Penner and Finkelstein 1998; Wilson 2000; Wilson and Janoski 1995; Wilsonand Musick 1997b).
In addition, studies have found that individuals’ human capital resourcesare associated with their likelihood of volunteering, especially in formalorganizational settings. Health status (including the presence of fewer func-tional impairments), higher levels of education and higher status occupa-tions, and higher socioeconomic status, in general, were found to have increaseda person’s likelihood of volunteering, because these assets equip people withthe resources and skills needed for certain types of volunteer work and openup more opportunities for them to volunteer (Fischer, Mueller, and Cooper1991; Gallagher 1994; Independent Sector 1990; Van Willigen 2000; Wilson2000; Wilson and Musick 1997a, 1997b).
Unlike the case of formal volunteering, some studies have found health,education, and other human capital resources to be insignificant or onlymarginally significant predictors of the informal volunteering that benefitsfriends, neighbors, and relatives outside the home (see Chambré 1993;Wilson and Musick 1997b). Informal helping of kith and kin is likely to bea function of social capital—the size of one’s social network and the degreeof social integration—and may be driven by affection and/or obligationtoward them (Wilson 2000). Insofar as these same individuals may haveprovided assistance in the past, obligation to reciprocate or exchange favorsis likely to play a substantial role in informal helping behavior (Amato1990; Wilson and Musick 1997b). People are aware that giving help to oth-ers increases the probability that their own needs will be met in the future(see Krause et al. 1992). The expectation of future return of favors may bea stronger motive for older adults with declining health than for younger,healthier ones. Although it was not the central objective of this study to testthe forms-of-capital perspective as it relates to volunteering, we controlledfor these characteristics in our multivariate analyses.
Study Hypotheses
Two alternative role hypotheses about the relationship between volun-teering and spousal caregiving were posited. On one hand, the literaturesuggests that it is possible that volunteering, in both of the forms identifiedherein, is an addendum to or extension of the caregiving role, and it may bethat caregivers choose to stay involved in roles other than caregiving forseveral reasons, including the protection of their psychological well-being.Thus, in the role extension hypothesis, spousal caregivers were assumed tobe more likely to volunteer than people who were not spousal caregivers.
104 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
On the other hand, given the possibility of role overload and the resultingconflict between roles among the activities associated with volunteeringand caregiving, a second hypothesis was that spousal caregivers would beless likely to volunteer than people who were not spousal caregivers. Ofcourse, a third possibility was that after other covariates known to influenceformal and informal helping behaviors were controlled for, there would beno statistical association between spousal caregiving and volunteering.
Methods
Data Source and Sample
The data for this study came from the 1998 and 2000 interview waves ofthe Health and Retirement Study (HRS), a nationally representative panelsurvey of noninstitutionalized older adults (and their spouses, in the case ofmarried respondents) that began in 1992. The biennial surveys collect detailedinformation on respondents’ demographic, housing, household and family,economic, and health status characteristics, among others. Detailed expla-nations of the data system, including its sampling methods, weights, andlist of variables, can be found in the machine-readable codebooks and man-uals produced by the Institute for Social Research (2001) at the Universityof Michigan.
Although the original HRS sample was chosen from among personsbetween 51 and 61 years of age in 1992, those belonging to different agecohorts have been added to the sample in later interview waves. The samplefor this study included married persons only who were aged 55 years andolder in 1998 and were interviewed in both 1998 and 2000 (n = 10,120). Ofthese, 321 persons whose racial or ethnic identifications were not AfricanAmerican, Hispanic, or non-Hispanic White were excluded (n = 9,799). Thesample was further reduced to 9,719 persons when those with missing dataon formal and informal volunteering hours were excluded. After we excludedthose who were proxy interviewed (mostly because of cognitive impair-ments), the final study sample consisted of 8,663 individuals, with 51.7%men and 48.3% women and 5.7% African Americans, 5.2% Hispanics, and89.1% non-Hispanic Whites. In terms of age distribution, 43.5% were aged55 to 64 years, 36.4% were aged 65 to 74 years, 17.7% were aged 75 to 84years, and 2.4% were aged 85 years and older. Because of missing data onsome predictor variables, the sample size for multivariate analyses was some-what smaller than 8,663.
Choi et al. / Volunteer Activity and Caregiving 105
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
Although the HRS did not ask respondents a direct question about whetherthey were spousal caregivers, all sample members with any ADL or IADLimpairments were asked who their primary and secondary helpers were. If arespondent said that his or her spouse was the primary or secondary caregiver,then for this study, we identified the husband or wife of the respondent as aspousal caregiver; otherwise, respondents were not considered to be spousalcaregivers. In the study sample, 9.4% of the respondents (8.5% of men and10.4% of women) were identified as spousal caregivers. Among the spousalcaregivers, 3.4% provided help to their spouses for both ADL and IADLimpairments, 2.2% provided help for ADL impairments only, and 4.1% pro-vided help for IADL impairments only. Preliminary analyses indicated nostatistically significant gender differences with respect to the kind of help thespousal caregivers provided. Further analysis also showed that 49.8% ofthose identified as spousal caregivers at the time of the 2000 interview wave(hereafter referred to as time 2) had also been spousal caregivers at the timeof the 1998 interview wave (hereafter referred to as time 1), while 50.2% hadbecome spousal caregivers since the time 1 interview. All the spousal care-givers at time 2 were married to the same spouses as at time 1. Unfortunately,the data on spousal caregiving did not include the number of hours of care-giving, and thus the extent and intensity of caregiving could not be factoredin. For this study, we assumed that assisting one’s spouse with his or her ADLand/or IADL impairments indicated daily involvement in caregiving.
Variables
The dependent variable was the amount of time (number of hours) commit-ted to formal and informal volunteer work during the 12 months preceding the2000 interview (time 2). At time 2, respondents were asked whether they hadspent “any time in the past 12 months doing volunteer work for religious, edu-cational, health-related, or other charitable organizations” and how many hoursthey had spent doing “volunteer work for such organizations.” In terms of infor-mal volunteering, respondents were asked about the hours they had spent in thepreceding 12 months “helping friends, neighbors, or relatives who did not livewith you and did not pay you for the help.” Because almost one fourth of thosewho had done volunteer work could not provide a specific number of hours,they were also asked whether the number of hours had been less than or morethan 100 or whether the number of hours had been less than or more than 200.Thus, the extent of volunteer activity in both formal and informal sectors ismeasured as (1) no volunteer work (the reference category), (2) 1 to 200 hoursannually, or (3) 201 or more hours annually. Two hundred hours of annual vol-unteer work translates to an average of nearly 4 hours per week.
106 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
The central independent variable was the target person’s status as a spousalcaregiver (1 = yes, 0 = no) at the time of the time 2 interview. For both spousalcaregivers and noncaregivers, the other variables in our models included con-trols for demographic characteristics as well as indicators of cultural capital,human capital, and social capital. Demographic characteristics included age infour categories (85 years and older, 75 to 84 years, 65 to 74 years, and 55 to64 years [the reference category]), race or ethnicity (African American,Hispanic, and non-Hispanic White [the reference category]), and nativity (notnative born or native born [the reference category]). The nativity variable wasincluded because an earlier study found that being foreign born was negativelyassociated with volunteering (Independent Sector 1990). For the cultural cap-ital resource variable, the perceived importance of religion (very important,somewhat important, and not too important [the reference category]) wasincluded. The HRS does not contain any information about respondents’ per-sonalities or altruistic disposition characteristics.
Human capital resource variables included the number of years of com-pleted education, family’s total income at the time of the 2000 interview (in$5,000 increments), the number of medical conditions ever diagnosed by adoctor by the time 2 interview (ranging from zero to seven conditions: highblood pressure or hypertension, diabetes, cancer, lung disease, heart disease,stroke, and arthritis), and the number of combined ADL and IADL impair-ments (ranging from 0 to 12 impairments) at time 2. The level of depressivesymptoms was measured by the 8-item Center for Epidemiologic StudiesDepression Scale (CES-D). Depressed people may want to engage in volun-teering activities for “protective” reasons, as discussed earlier, but they mayalso want to withdraw from such activities because of the nature of theirdepressed mood. Work status (working for pay at the time of the time 2 inter-view or not working for pay [the reference category]) may be considered aform of both human and social capital in the sense that working people arelikely to have accumulated skills needed for some types of volunteer posi-tions, and they are more likely to be exposed to volunteering opportunitiesthrough their employment. The number of living children (or the combinednumber of resident and nonresident children), a form of social capital, wasalso included in the regression model.
Analytic Strategy
Although we did not have a specific hypothesis regarding gender differ-ences for the association between spousal caregiving and volunteering, wenevertheless structured our analyses by gender group; regression models wereestimated for men and women separately. We took this approach because the
Choi et al. / Volunteer Activity and Caregiving 107
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
literature indicates that there are considerable gender differences in perceivedcaregiver stress and burdens (Atienza et al. 2001; Miller and Cafasso 1992;Yee and Schulz 2000).
Because our dependent variable had more than two categories, a multino-mial logistic regression technique was required. (Although the categories werealso rank ordered, tests of the proportionality of odds assumption did not war-rant the use of ordinal logistic regression.) This technique generated log-likelihood coefficients showing the relationship between a given independentvariable and the dependent variable, the categories of hours of volunteering.The model allowed us to estimate whether persons engaged in spousal care-giving were more likely than nonspousal caregivers to volunteer. This was ananalysis of the level of volunteering at a specific point in time, with lagged andcontemporaneous independent variables. We report two types of model fit sta-tistics: the –2 log-likelihood χ2 statistics for model fit and an estimate ofexplained variance for logistic regression models called pseudo-R2. Pseudo-R2,though reported to give readers another estimate of the goodness of fit of themodels, should be interpreted with caution, because it represents only roughestimates of the explained variances. Analyses were based on data weighted toaccount for the design characteristics of the HRS.
Given that spousal caregivers were significantly older than noncare-givers (refer to Table 1), we also examined the effect of interaction termsbetween caregiving status and age group on both formal and informal vol-unteering hours. None of the interaction terms was statistically significant,and thus we report only the results of our main-effects models. Given thestrong association between time 1 and time 2 volunteering hours, especiallyin the case of formal volunteering (refer to the “Results” section), we alsoexamined the question of whether the effects of the independent and con-trol variables were more likely to be statistically significant in the cross-sectional models because the very strong and overwhelming effect of thetime 1 level of volunteering had been removed. By including the time 1indicator of the dependent variable in the regression models, we were esti-mating residualized change models in which the coefficients represent thelog likelihood of a change in the level of volunteering between time 1 andtime 2, given a unit increase in a given explanatory variable (see Wilmothand Chen 2003 for a similar approach). The results of these change models,however, showed that most significant key predictors of the level of time 2volunteering in the cross-sectional model continued to be significant.Because of space constraints, we report the results of the change modelsonly briefly in the “Results” section (results of the change models are avail-able on request).
108 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
Choi et al. / Volunteer Activity and Caregiving 109
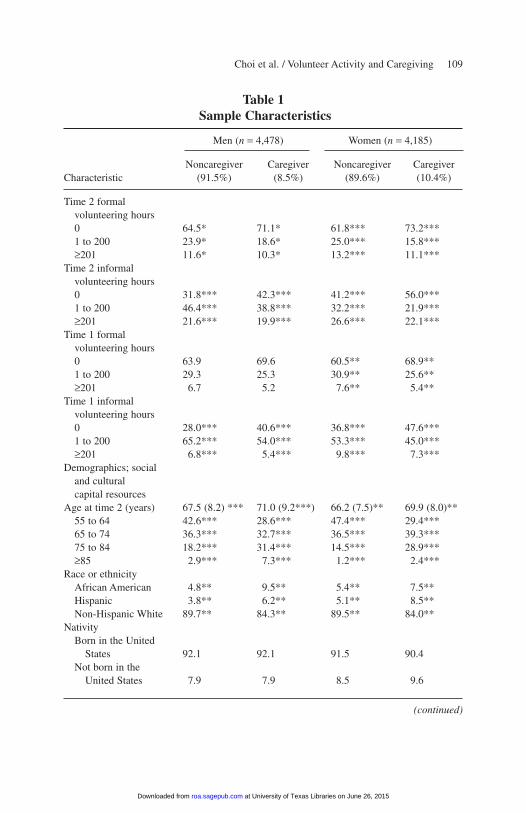
Table 1Sample Characteristics
Men (n = 4,478) Women (n = 4,185)
Noncaregiver Caregiver Noncaregiver Caregiver Characteristic (91.5%) (8.5%) (89.6%) (10.4%)
Time 2 formal volunteering hours0 64.5* 71.1* 61.8*** 73.2***1 to 200 23.9* 18.6* 25.0*** 15.8***≥201 11.6* 10.3* 13.2*** 11.1***
Time 2 informal volunteering hours0 31.8*** 42.3*** 41.2*** 56.0***1 to 200 46.4*** 38.8*** 32.2*** 21.9***≥201 21.6*** 19.9*** 26.6*** 22.1***
Time 1 formal volunteering hours0 63.9 69.6 60.5** 68.9**1 to 200 29.3 25.3 30.9** 25.6**≥201 6.7 5.2 7.6** 5.4**
Time 1 informal volunteering hours0 28.0*** 40.6*** 36.8*** 47.6***1 to 200 65.2*** 54.0*** 53.3*** 45.0***≥201 6.8*** 5.4*** 9.8*** 7.3***
Demographics; social and cultural capital resources
Age at time 2 (years) 67.5 (8.2) *** 71.0 (9.2***) 66.2 (7.5)** 69.9 (8.0)**55 to 64 42.6*** 28.6*** 47.4*** 29.4***65 to 74 36.3*** 32.7*** 36.5*** 39.3***75 to 84 18.2*** 31.4*** 14.5*** 28.9***≥85 2.9*** 7.3*** 1.2*** 2.4***
Race or ethnicityAfrican American 4.8** 9.5** 5.4** 7.5**Hispanic 3.8** 6.2** 5.1** 8.5**Non-Hispanic White 89.7** 84.3** 89.5** 84.0**
NativityBorn in the United
States 92.1 92.1 91.5 90.4Not born in the
United States 7.9 7.9 8.5 9.6
(continued)
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
Finally, we performed multinomial logistic regression analysis to examinethe predictors of the level of formal and informal volunteering within the care-giver group. This was an attempt to find out if there was any subgroup of care-givers who were more likely to volunteer than the other caregivers. Becausethe results were similar to those of the models that included both caregiversand noncaregivers, however, we briefly report them in the “Results” sectionwithout presenting the specifics in tables.
110 Research on Aging
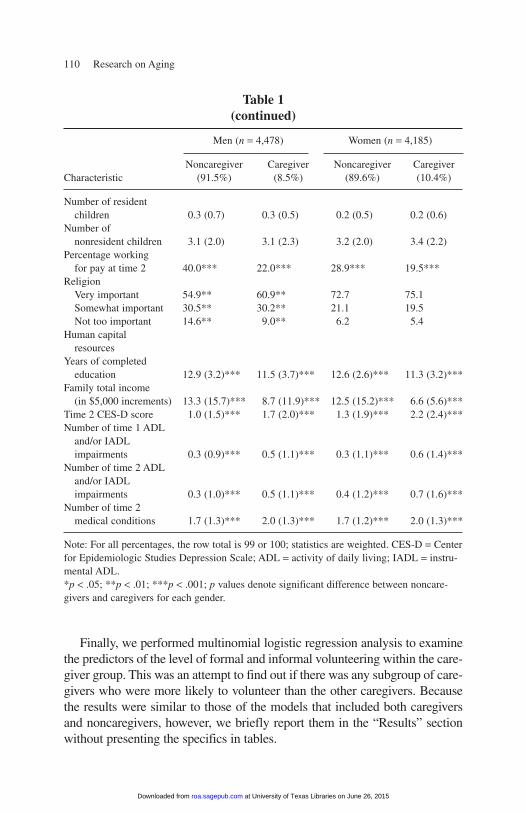
Table 1(continued)
Men (n = 4,478) Women (n = 4,185)
Noncaregiver Caregiver Noncaregiver Caregiver Characteristic (91.5%) (8.5%) (89.6%) (10.4%)
Number of resident children 0.3 (0.7) 0.3 (0.5) 0.2 (0.5) 0.2 (0.6)
Number of nonresident children 3.1 (2.0) 3.1 (2.3) 3.2 (2.0) 3.4 (2.2)
Percentage working for pay at time 2 40.0*** 22.0*** 28.9*** 19.5***
ReligionVery important 54.9** 60.9** 72.7 75.1Somewhat important 30.5** 30.2** 21.1 19.5Not too important 14.6** 9.0** 6.2 5.4
Human capital resources
Years of completed education 12.9 (3.2)*** 11.5 (3.7)*** 12.6 (2.6)*** 11.3 (3.2)***
Family total income (in $5,000 increments) 13.3 (15.7)*** 8.7 (11.9)*** 12.5 (15.2)*** 6.6 (5.6)***
Time 2 CES-D score 1.0 (1.5)*** 1.7 (2.0)*** 1.3 (1.9)*** 2.2 (2.4)***Number of time 1 ADL
and/or IADL impairments 0.3 (0.9)*** 0.5 (1.1)*** 0.3 (1.1)*** 0.6 (1.4)***
Number of time 2 ADL and/or IADL impairments 0.3 (1.0)*** 0.5 (1.1)*** 0.4 (1.2)*** 0.7 (1.6)***
Number of time 2 medical conditions 1.7 (1.3)*** 2.0 (1.3)*** 1.7 (1.2)*** 2.0 (1.3)***
Note: For all percentages, the row total is 99 or 100; statistics are weighted. CES-D = Centerfor Epidemiologic Studies Depression Scale; ADL = activity of daily living; IADL = instru-mental ADL.*p < .05; **p < .01; ***p < .001; p values denote significant difference between noncare-givers and caregivers for each gender.
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
Results
Bivariate Results
As shown in Table 1, 8.5% of men and 10.4% of women were identifiedas spousal caregivers. Of male noncaregivers, 23.9% and 11.6% reported thatthey had done 1 to 200 hours and 201 or more hours, respectively, of formalvolunteering during the 12-month period, while the corresponding percent-ages for male caregivers were 18.6% and 10.3%. Of female noncaregivers,25.0% and 13.2% reported that they had done 1 to 200 hours and 201 or morehours, respectively, of formal volunteering, while the corresponding percent-ages for female caregivers were 15.8% and 11.1%. For both caregivers andnoncaregivers, the proportion of those who had done informal volunteeringwas higher than that of those who had done formal volunteering. Again, a sta-tistically significant smaller proportion of caregivers than noncaregivers ofboth genders reported that they had done informal volunteering. Whetherthese statistical differences would remain after controlling for other covariatesis examined later in this article, in the discussion of our multivariate models.It is nonetheless noteworthy that more than 25% of caregivers (among bothmen and women) had provided some volunteer hours to formal organizationsin the year before the interview and that almost 60% of male spousal care-givers and 44% of female spousal caregivers provided informal help to per-sons in their social networks in the same time period.
Demographic data showed that caregivers were significantly older thannoncaregivers. Higher proportions of caregivers than of noncaregivers wereAfrican Americans and Hispanics. With respect to nativity, there was nosignificant difference between caregivers and noncaregivers for both gen-ders. Among men, a higher proportion of caregivers than noncaregiversreported that religion was very important to them, whereas no significantdifference in the perceived importance of religion was found among femalecaregivers. Caregivers and noncaregivers did not differ with respect to thenumbers of resident and nonresident children. A significantly lower pro-portion of caregivers than noncaregivers of both genders was working, andthe caregivers had significantly less education and lower family incomesthan noncaregivers. Consistent with earlier research, caregivers also hadsignificantly higher CES-D scores and significantly more physical andfunctional health problems than noncaregivers.
Further analysis showed that time 1 and time 2 formal volunteering hourswere significantly correlated among both caregivers and noncaregivers(Kendall’s τ-b = 0.585, p = .029 and .596, p = .009, respectively) and that time1 and time 2 informal volunteering hours were also significantly correlated
Choi et al. / Volunteer Activity and Caregiving 111
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
(Kendall’s τ-b = 0.324, p = .031 and .298, p = .010, respectively.) Furtheranalysis also showed that time 2 formal and informal volunteering hours werealso significantly correlated with each other (Kendall’s τ-b: 0.314, p = .030among caregivers and Kendall’s τ-b = 0.172, p = .010 among noncaregivers),suggesting the possibility that formal and informal volunteering may be mutu-ally reinforcing. These results show both that formal and informal volunteer-ing behaviors were stable over time and that informal volunteers were alsomore likely than those who did not report informal volunteering hours to vol-unteer for formal organizations. Thus, the finding suggests that time 1 volun-teering hours were likely to be a strong predictor of time 2 volunteering hoursin analyses of multivariate models.
Multivariate Results
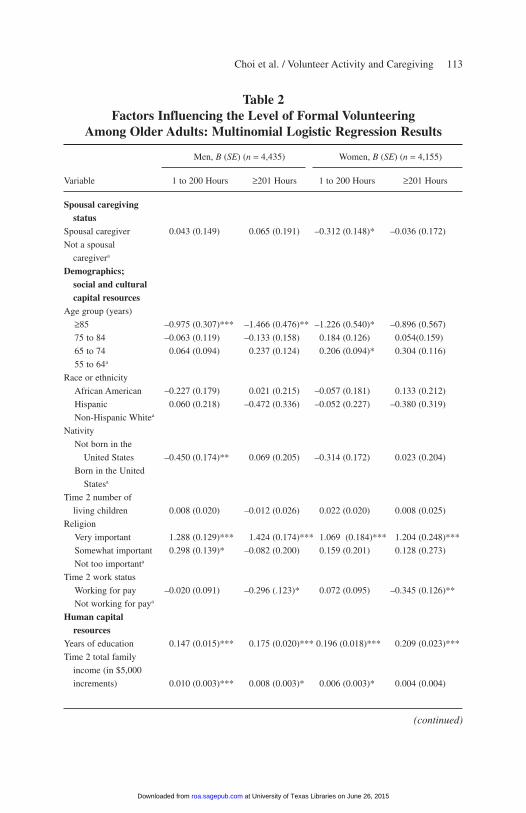
Tables 2 and 3 report the results of our cross-sectional analysis of formalvolunteering and informal volunteering, respectively, for men and womenseparately. As shown in Table 2, caregiving status was not significantly asso-ciated with the number of men’s formal volunteering hours, whereas it wassignificantly associated with women’s likelihood of volunteering 1 to 200hours annually but not with their likelihood of volunteering 201 or morehours annually, as opposed to not volunteering. Thus, the statistically sig-nificant differences between caregivers and noncaregivers in terms of vol-unteering for formal organizations found in the simple bivariate analyseswere eliminated among men after we controlled for their demographic char-acteristics and their human, cultural, and social capital. Neither the roleextension nor the role overload hypothesis was supported for men. On theother hand, limited support for the role overload hypothesis was offered inthe case of female caregivers, although the findings showed that no differ-ence was found between female caregivers and female noncaregivers at ahigher level of volunteering (201 or more hours annually).
Significant predictors of men’s formally volunteering 1 to 200 hours annu-ally, as opposed to not volunteering at all, were age, nativity, the perceivedimportance of religion, the number of years of education, the level of familyincome, CES-D scores, and the numbers of ADL and/or IADL impairmentsand diagnosed medical conditions. Compared with those who were aged 55to 64 years, those who were aged 85 years and older were less likely to havevolunteered. Foreign birth, higher CES-D scores, and greater numbers ofADL and/or IADL impairments and medical conditions were also negativelyassociated with the likelihood of a man’s having volunteered. On the other
112 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
Choi et al. / Volunteer Activity and Caregiving 113
Table 2Factors Influencing the Level of Formal Volunteering
Among Older Adults: Multinomial Logistic Regression Results
Men, B (SE) (n = 4,435) Women, B (SE) (n = 4,155)
Variable 1 to 200 Hours ≥201 Hours 1 to 200 Hours ≥201 Hours
Spousal caregiving status
Spousal caregiver 0.043 (0.149) 0.065 (0.191) –0.312 (0.148)* –0.036 (0.172)
Not a spousal
caregivera
Demographics; social and culturalcapital resources
Age group (years)
≥85 –0.975 (0.307)*** –1.466 (0.476)** –1.226 (0.540)* –0.896 (0.567)
75 to 84 –0.063 (0.119) –0.133 (0.158) 0.184 (0.126) 0.054(0.159)
65 to 74 0.064 (0.094) 0.237 (0.124) 0.206 (0.094)* 0.304 (0.116)
55 to 64a
Race or ethnicity
African American –0.227 (0.179) 0.021 (0.215) –0.057 (0.181) 0.133 (0.212)
Hispanic 0.060 (0.218) –0.472 (0.336) –0.052 (0.227) –0.380 (0.319)
Non-Hispanic Whitea
Nativity
Not born in the
United States –0.450 (0.174)** 0.069 (0.205) –0.314 (0.172) 0.023 (0.204)
Born in the United
Statesa
Time 2 number of
living children 0.008 (0.020) –0.012 (0.026) 0.022 (0.020) 0.008 (0.025)
Religion
Very important 1.288 (0.129)*** 1.424 (0.174)*** 1.069 (0.184)*** 1.204 (0.248)***
Somewhat important 0.298 (0.139)* –0.082 (0.200) 0.159 (0.201) 0.128 (0.273)
Not too importanta
Time 2 work status
Working for pay –0.020 (0.091) –0.296 (.123)* 0.072 (0.095) –0.345 (0.126)**
Not working for paya
Human capital resources
Years of education 0.147 (0.015)*** 0.175 (0.020)*** 0.196 (0.018)*** 0.209 (0.023)***
Time 2 total family
income (in $5,000
increments) 0.010 (0.003)*** 0.008 (0.003)* 0.006 (0.003)* 0.004 (0.004)
(continued)
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
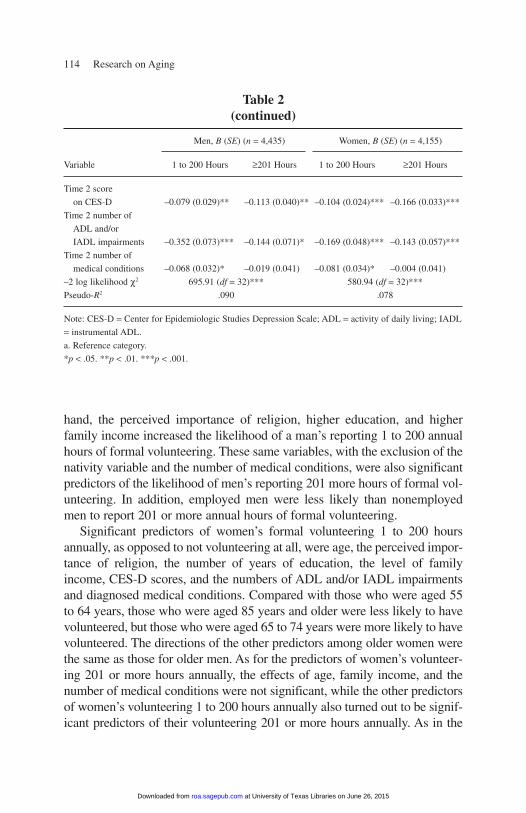
hand, the perceived importance of religion, higher education, and higher family income increased the likelihood of a man’s reporting 1 to 200 annualhours of formal volunteering. These same variables, with the exclusion of thenativity variable and the number of medical conditions, were also significantpredictors of the likelihood of men’s reporting 201 more hours of formal vol-unteering. In addition, employed men were less likely than nonemployedmen to report 201 or more annual hours of formal volunteering.
Significant predictors of women’s formal volunteering 1 to 200 hoursannually, as opposed to not volunteering at all, were age, the perceived impor-tance of religion, the number of years of education, the level of familyincome, CES-D scores, and the numbers of ADL and/or IADL impairmentsand diagnosed medical conditions. Compared with those who were aged 55to 64 years, those who were aged 85 years and older were less likely to havevolunteered, but those who were aged 65 to 74 years were more likely to havevolunteered. The directions of the other predictors among older women werethe same as those for older men. As for the predictors of women’s volunteer-ing 201 or more hours annually, the effects of age, family income, and thenumber of medical conditions were not significant, while the other predictorsof women’s volunteering 1 to 200 hours annually also turned out to be signif-icant predictors of their volunteering 201 or more hours annually. As in the
114 Research on Aging
Table 2(continued)
Men, B (SE) (n = 4,435) Women, B (SE) (n = 4,155)
Variable 1 to 200 Hours ≥201 Hours 1 to 200 Hours ≥201 Hours
Time 2 score
on CES-D –0.079 (0.029)** –0.113 (0.040)** –0.104 (0.024)*** –0.166 (0.033)***
Time 2 number of
ADL and/or
IADL impairments –0.352 (0.073)*** –0.144 (0.071)* –0.169 (0.048)*** –0.143 (0.057)***
Time 2 number of
medical conditions –0.068 (0.032)* –0.019 (0.041) –0.081 (0.034)* –0.004 (0.041)
–2 log likelihood χ2 695.91 (df = 32)*** 580.94 (df = 32)***
Pseudo-R2 .090 .078
Note: CES-D = Center for Epidemiologic Studies Depression Scale; ADL = activity of daily living; IADL
= instrumental ADL.
a. Reference category.
*p < .05. **p < .01. ***p < .001.
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
case of men, women who were working were also less likely to report 201 ormore annual hours of volunteering.
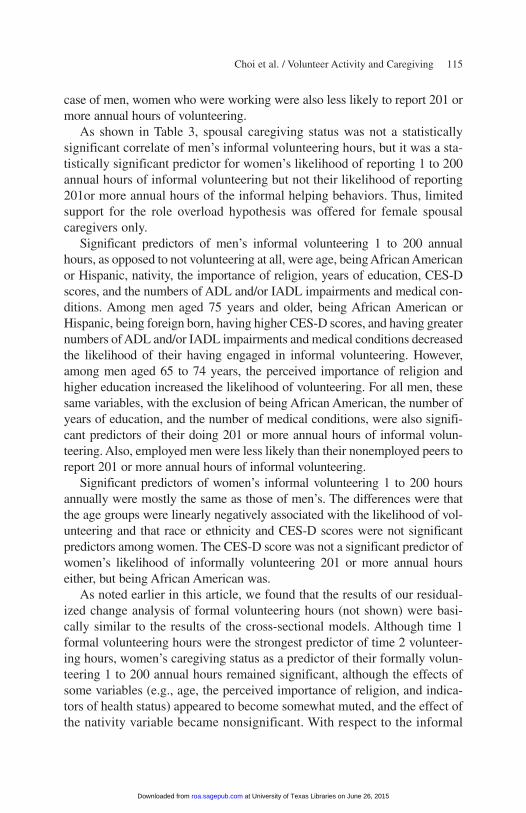
As shown in Table 3, spousal caregiving status was not a statisticallysignificant correlate of men’s informal volunteering hours, but it was a sta-tistically significant predictor for women’s likelihood of reporting 1 to 200annual hours of informal volunteering but not their likelihood of reporting201or more annual hours of the informal helping behaviors. Thus, limitedsupport for the role overload hypothesis was offered for female spousalcaregivers only.
Significant predictors of men’s informal volunteering 1 to 200 annualhours, as opposed to not volunteering at all, were age, being African Americanor Hispanic, nativity, the importance of religion, years of education, CES-Dscores, and the numbers of ADL and/or IADL impairments and medical con-ditions. Among men aged 75 years and older, being African American orHispanic, being foreign born, having higher CES-D scores, and having greaternumbers of ADL and/or IADL impairments and medical conditions decreasedthe likelihood of their having engaged in informal volunteering. However,among men aged 65 to 74 years, the perceived importance of religion andhigher education increased the likelihood of volunteering. For all men, thesesame variables, with the exclusion of being African American, the number ofyears of education, and the number of medical conditions, were also signifi-cant predictors of their doing 201 or more annual hours of informal volun-teering. Also, employed men were less likely than their nonemployed peers toreport 201 or more annual hours of informal volunteering.
Significant predictors of women’s informal volunteering 1 to 200 hoursannually were mostly the same as those of men’s. The differences were thatthe age groups were linearly negatively associated with the likelihood of vol-unteering and that race or ethnicity and CES-D scores were not significantpredictors among women. The CES-D score was not a significant predictor ofwomen’s likelihood of informally volunteering 201 or more annual hourseither, but being African American was.
As noted earlier in this article, we found that the results of our residual-ized change analysis of formal volunteering hours (not shown) were basi-cally similar to the results of the cross-sectional models. Although time 1formal volunteering hours were the strongest predictor of time 2 volunteer-ing hours, women’s caregiving status as a predictor of their formally volun-teering 1 to 200 annual hours remained significant, although the effects ofsome variables (e.g., age, the perceived importance of religion, and indica-tors of health status) appeared to become somewhat muted, and the effect ofthe nativity variable became nonsignificant. With respect to the informal
Choi et al. / Volunteer Activity and Caregiving 115
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
116 Research on Aging
Table 3Factors Influencing the Level of Informal Volunteering Among
Older Adults: Multinomial Logistic Regression Results
Men, B (SE) (n = 4,435) Women, B (SE) (n = 4,155)
Variable 1 to 200 Hours ≥201 Hours 11 to 200 Hours ≥201 Hours
Spousal caregiving status
Spousal caregiver –0.023 (0.118) –0.122 (0.158) –0.307 (0.136)* –0.211 (0.134)
Not a spousal
caregivera
Demographics; socialand cultural capitalresources
Age group (years)
≥85 –2.205 (0.246)*** –1.864 (0.284)*** –1.298 (0.437)** –0.922 (0.375)*
75 to 84 –1.183 (0.112)*** –1.290 (0.135)*** –0.798 (0.125)*** –0.835 (0.129)***
65 to 74 0.441 (0.094)*** 0.523 (0.110)*** –0.246 (0.091)** –0.145 (0.094)
55 to 64a
Race or ethnicity
African American –0.431 (0.163)** –0.311 (0.184) –0.214 (0.170) –0.539 (0.188)**
Hispanic –0.711 (0.190)*** –0.776 (0.231)*** –0.176 (0.207) –0.192 (0.203)
Non-Hispanic Whitea
Nativity
Not born in the
United States –0.346 (0.145)* –0.430 (0.180)* –0.401 (0.158)* –0.093 (0.152)
Born in the
United Statesa
Time 2 number of
living children 0.023 (0.018) –0.012 (0.026) –0.004 (0.019) –0.035 (0.020)
Religion
Very important 0.601 (0.109)*** 0.680 (0.134)*** 0.609 (0.164)*** 0.599 (0.173)***
Somewhat important 0.371 0.355 (0.143)* 0.188 (0.177) 0.265 (0.186)
Not too importanta
Time 2 work status
Working for pay –0.170 (0.091) –0.346 (0.108)** 0.033 (0.094) –0.055 (0.100)
Not working for paya
Human capital resources
Years of education 0.073 (0.013)*** 0.016 (0.021) 0.143 (0.017)*** 0.108 (0.017)***
(continued)
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
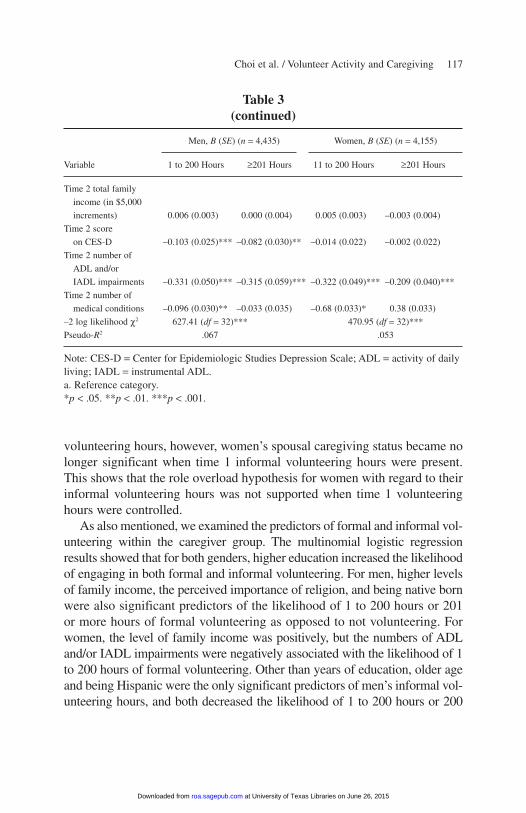
volunteering hours, however, women’s spousal caregiving status became nolonger significant when time 1 informal volunteering hours were present.This shows that the role overload hypothesis for women with regard to theirinformal volunteering hours was not supported when time 1 volunteeringhours were controlled.
As also mentioned, we examined the predictors of formal and informal vol-unteering within the caregiver group. The multinomial logistic regressionresults showed that for both genders, higher education increased the likelihoodof engaging in both formal and informal volunteering. For men, higher levelsof family income, the perceived importance of religion, and being native bornwere also significant predictors of the likelihood of 1 to 200 hours or 201or more hours of formal volunteering as opposed to not volunteering. Forwomen, the level of family income was positively, but the numbers of ADLand/or IADL impairments were negatively associated with the likelihood of 1to 200 hours of formal volunteering. Other than years of education, older ageand being Hispanic were the only significant predictors of men’s informal vol-unteering hours, and both decreased the likelihood of 1 to 200 hours or 200
Choi et al. / Volunteer Activity and Caregiving 117
Table 3(continued)
Men, B (SE) (n = 4,435) Women, B (SE) (n = 4,155)
Variable 1 to 200 Hours ≥201 Hours 11 to 200 Hours ≥201 Hours
Time 2 total family
income (in $5,000
increments) 0.006 (0.003) 0.000 (0.004) 0.005 (0.003) –0.003 (0.004)
Time 2 score
on CES-D –0.103 (0.025)*** –0.082 (0.030)** –0.014 (0.022) –0.002 (0.022)
Time 2 number of
ADL and/or
IADL impairments –0.331 (0.050)*** –0.315 (0.059)*** –0.322 (0.049)*** –0.209 (0.040)***
Time 2 number of
medical conditions –0.096 (0.030)** –0.033 (0.035) –0.68 (0.033)* 0.38 (0.033)
–2 log likelihood χ2 627.41 (df = 32)*** 470.95 (df = 32)***
Pseudo-R2 .067 .053
Note: CES-D = Center for Epidemiologic Studies Depression Scale; ADL = activity of dailyliving; IADL = instrumental ADL.a. Reference category.*p < .05. **p < .01. ***p < .001.
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from

and more hours of informal volunteering. For women, higher family income,the perceived importance of religion, and more children increased their likeli-hood of informally volunteering 1 to 200 hours, but the numbers of ADLand/or IADL impairments were negatively associated with such likelihood.Older age (75 years and older) also decreased women’s likelihood of 201 ormore hours of informal volunteering.
Discussion
Descriptive data from the HRS show that a significant proportion ofspousal caregivers, despite their commitments to spouses with ADL and IADLlimitations, engaged in volunteering for formal organizations and/or informalvolunteering, providing help to persons in their social networks. The propor-tions of caregiver volunteers were significantly lower than the proportions ofnoncaregiver volunteers among both genders. However, it is worth noting thatthe differences in formal and informal volunteering hours by caregiving statusamong men generally disappeared when we controlled for other personal char-acteristics and that neither the role extension nor the role overload hypothesisis supported with respect to the relationship between spousal caregiving andformal volunteering. For women, when their other characteristics were con-trolled for, there appears to be limited support for the role overload hypothe-sis, because the caregivers were found to be less likely than the noncaregiversto have reported volunteering 1 to 200 annual hours. It may be that wives whoare caregivers to their husbands may have less time and energy to volunteer forformal organizations. Because no gender difference was found in the types offunctional limitations for which care was provided, we are not sure of the rea-sons for the gender difference in the association between spousal caregivingand formal volunteering. When data become available, further research willneed to be done to determine whether the gender difference may be attribut-able to gender differences in the length of caregiving duration and intensity ofcaregiving burden or stress.
The findings of multivariate analysis also show that whether a woman wasa spousal caregiver or not was not associated with her likelihood of havingreported 201 or more annual hours of formal volunteering. Among those whoprovided many hours of formal volunteering, their caregiving status was nota deterrent to volunteering. Because 201 or more annual hours of volunteer-ing equals nearly 4 hours per week, it is a significant commitment of personaltime and effort. The fact that spousal caregiving duties apparently did not stopthese seriously committed volunteers from continuing their volunteering
118 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
shows that private caregiving behaviors and public formal volunteeringbehaviors are linked. A previous study, in fact, showed that those who pro-vided a greater number of hours of informal care were also likely to providea greater number of formal volunteering hours (Burr et al. 2005).
No association was found between men’s spousal caregiving status andtheir informal volunteering hours. On the other hand, spousal caregiving wasagain significantly negatively associated with women’s likelihood of havingengaged in 1 to 200 annual hours of informal volunteering, but it was not sig-nificantly associated with their likelihood of having done 201 or more annualhours of volunteering. Thus, there appears to be conditional support for the roleoverload hypothesis among women with respect to their informal volunteeringhours. As discussed, however, when previous informal volunteering hourswere also controlled for, the relationship between women’s spousal caregivingstatus and their informal volunteering hours was no longer significant.
In sum, the findings show in part that older persons, even those withspousal caregiving responsibilities, are capable of taking on multiple produc-tive activities. It appears that spousal caregiving for most caregivers is neithera deterrent to nor a conduit for formal or informal volunteering, whereas age,years of education, the importance of religion, and health status (and previousvolunteering history) are significant correlates of formal and informal volun-teering hours. Although spousal caregiving is an obligation requiring, moreoften than not, an intensive commitment of time and energy, it is an event andsituation that also needs to be understood in the broad context of each indi-vidual’s previous life course. Those who had previously volunteered are likelyto continue their volunteering behaviors, even with the added burden ofspousal caregiving, because they may have larger networks providing supportfor volunteering and opportunities to continue volunteering. Volunteers mayalso be persons who have the continuing desire and motivation to help othersbecause of their religious beliefs, as shown in the significance of perceivedimportance of religion as a predictor for volunteering hours, altruistic dispo-sition, or early socialization to volunteering.
As previous studies have shown, volunteering in late life may also needto be understood in the context of older adults’ human capital resources. Theconsistent significance of years of education as a predictor of both formaland informal volunteering among caregivers of both genders underscores theimportant role the level of education plays in volunteering. In addition to thesignificance of the number of years of education as determinants of volunteer-ing, the significant effect of health conditions on the likelihood of volunteeringin late life cannot be emphasized too much. With the onset and deterioration ofdisability with the progression of aging, older adults are less likely to be able
Choi et al. / Volunteer Activity and Caregiving 119
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
to engage in volunteer activities, both formal and informal. This study alsoshows that engagement in paid work is a deterrent to providing a large numberof hours of formal volunteering (201 or more annual hours) for both men andwomen. Time constraints (role overload) may be a reason. It is also a deterrentto men’s engaging in a large number of informal helping activities but not adeterrent to women’s informal volunteering. Unlike men, women may engage,by choice or because of a sense of obligation, in private helping activitiesdespite time constraints.
We also found that men with higher CES-D scores (or depressive symp-toms) were less likely to have done formal or informal volunteering. Womenwith higher CES-D scores were also less likely to have done formal volun-teering, but the relationship between women’s CES-D scores and informalvolunteering hours was not significant, suggesting that women, unlike men,may engage in private helping activities regardless of their own emotionalhealth status, because they may perceive these helping behaviors as anexpected duty. The significant relationship between CES-D scores and for-mal volunteering hours among both genders may indicate that those withpoor emotional health, like those with functional impairments, are less likelyto volunteer. Because this was a cross-sectional study, however, we were notable to examine the extent to which the relationship was a result of the pos-itive health effect of volunteering.
More studies on the relationship between volunteering and spousal care-giving are needed. To more effectively test the theories and hypotheses dis-cussed in this study, future studies need to examine the extent of thechanges in volunteer activities as a result of spousal caregiving. Futureresearch also needs to factor into the model the level of caregiving burdenor stress.
As shown in previous studies, volunteering offers older adults outletsand opportunities to continue to be active and strengthen existing socialbonds as well as assume new roles and meet new people. Because most vol-unteer work involves collective action, done with and for other people, vol-unteering can help strengthen or expand one’s informal and formal supportnetworks. Volunteering also helps older adults maintain or improve physi-cal and emotional well-being. Unlike volunteer activities, which tend toproduce positive physical and mental health effects, however, spousal care-giving, especially when done over a long period, tends to negatively affecta caregiver’s physical and mental health. Finding ways for caregivers tobalance the caregiving role with volunteer work may help them cope betterwith the physical and emotional toll exacted by caregiving.
120 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from

References
Adelman, Pamela K. 1994a. “Multiple Roles and Physical Health Among Older Adults.”Research on Aging 16:142-66.
Adelman, Pamela K. 1994b. “Multiple Roles and Psychological Well-Being in a NationalSample of Older Adults.” Journal of Gerontology: Social Sciences 49:S277-85.
Amato, Paul. 1990. “Personality and Social Network Involvement as Predictors of HelpingBehavior in Everyday Life.” Social Psychology Quarterly 53:31-43.
Atienza, Audie A., Patrick C. Henderson, Sara Wilcox, and Abby C. King. 2001. “GenderDifferences in Cardiovascular Response to Dementia Caregiving.” The Gerontologist 41:490-98.
Beach, Scott R., Richard Schulz, Jennifer Yee, and Sharon Jackson. 2000. “Negative andPositive Health Effects of Caring for a Disabled Spouse: Longitudinal Findings From theCaregiver Health Effects Study.” Psychology and Aging 15:259-71.
Beeson, Rose A. 2003. “Loneliness and Depression in Spousal Caregivers of Those WithAlzheimer’s Disease Versus Non-Caregiving Spouses.” Archives of Psychiatric Nursing17:135-43.
Bowen, Deborah J., M. Robyn Andersen, and Nicole Urban. 2000. “Volunteerism in aCommunity-Based Sample of Women Aged 50 to 80 Years.” Journal of Applied SocialPsychology 30:1829-42.
Burr, Jeffrey A., Namkee G. Choi, Jan E. Mutchler, and Francis G. Caro. 2005. “Caregiving andVolunteering: Are Private and Public Helping Behaviors Linked?” Journal of Gerontology60B:S247-56.
Burton, Lynda, Judith Kasper, Andrew Shore, Kathleen Cagney, Thomas Laveist, C. Cubbin,and P. German. 1995. “The Structure of Informal Care: Are There Differences by Race?”The Gerontologist 35:744-52.
Burton, Lynda, Bozena Zdaniuk, Richard Schulz, Sharon Jackson, and Calvin Hirsch. 2003.“Transitions in Spousal Caregiving.” The Gerontologist 43:230-41.
Caro, Francis G. and Scott A. Bass. 1997. “Receptivity to Volunteering in the ImmediatePostretirement Period.” Journal of Applied Gerontology 16:427-41.
Chambré, Susan M. 1993. “Volunteerism by Elders: Past Trends and Future Prospects.” TheGerontologist 33:221-28.
Chappell, Neena L. and Michael J. Prince. 1997. “Reasons Why Canadian Seniors Volunteer.”Canadian Journal of Aging 16:336-53.
Chumbler, Neale R., James W. Grimm, Marisue Cody, and Cornelia Beck. 2003. “Gender,Kinship and Caregiver Burden: The Case of Community-Dwelling Memory ImpairedSeniors.” International Journal of Geriatric Psychiatry 18:722-32.
Connell, Cathleen M. 1994. “Impact of Spouse Caregiving on Health Behaviors and Physicaland Mental Health Status.” American Journal of Alzheimer’s Care and Related Disordersand Research 9:26-36.
Enright, Robert B. 1991. “Time Spent Caregiving and Help Received by Spouses and AdultChildren of Brain-Impaired Adults.” The Gerontologist 31:375-83.
Farkas, Janice I. and Christine L. Himes. 1997. “The Influence of Caregiving and Employmenton the Voluntary Activities of Midlife and Older Women.” Journal of Gerontology 52B:S180-89.
Fischer, Lucy Rose, Daniel P. Mueller, and Philip W. Cooper. 1991. “Older Volunteers:A Discussion of the Minnesota Senior Study.” The Gerontologist 31:183-94.
Choi et al. / Volunteer Activity and Caregiving 121
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from

Freedman, Marc. 1999. Prime Time: How Baby Boomers Will Revolutionize Retirement andTransform America. New York: Public Affairs.
Gallagher, Sally K. 1994. “Doing Their Share: Comparing Patterns of Help Given by Olderand Younger Adults.” Journal of Marriage and the Family 56:567-78.
Goode, William J. 1960. “A Theory of Role Strain.” American Sociological Review 2:483-96.
Harlow, Robert E. and Nancy Cantor. 1996. “Still Participating After All These Years: A Studyof Life Task Participation in Later Life.” Journal of Personality and Social Psychology71:1235-49.
Herzog, A. Regula, Melissa M. Franks, Hazel R. Markus, and Diane Holmberg. 1998.“Activities and Well-Being in Older Age: Effects of Self-Concept and EducationalAttainment.” Psychology and Aging 13:179-85.
Hodgkinson, Virginia Ann and Murray S. Weitzman. 1994. Giving and Volunteering in theUnited States. Washington, DC: Independent Sector.
Independent Sector. 1990. Giving and Volunteering in the United States. Washington, DC:Independent Sector.
Institute for Social Research. 2001. “Health and Retirement Study 1998. Final Core DataRelease, Version 1: Data Description and Usage.” Ann Arbor: University of Michigan.
Johnson, Richard W. and Simone G. Schaner. 2005. “Value of Unpaid Activities by OlderAmericans Tops $160 billion per Year.” Washington, DC: Urban Institute Retirement Project.Available at http://www.urban.org
Kennedy, Jae, Craig Walls, and Dawn Owens-Nicholson. 1999. “National Profile of Primaryand Secondary Household Caregivers: Estimates From the 1992 and 1993 Surveys onIncome and Program Participation.” Home Health Care Services Quarterly 17:39-58.
Krause, Neal, A. Regula Herzog, and Elizabeth Baker. 1992. “Providing Support to Others andWell-Being in Later Life.” Journal of Gerontology 47:P300-11.
Lum, Terry Y. and Elizabeth Lightfoot. 2005. “The Effects of Volunteering on the Physical andMental Health of Older People.” Research on Aging 27:31-55.
Marks, Nadine F., James D. Lambert, and Heejeong Choi. 2002. “Transitions to Caregiving,Gender, and Psychological Well-Being: A Prospective U.S. Study.” Journal of Marriageand the Family 64:657-67.
Miller, Baila and Lynda Cafasso. 1992. “Gender Differences in Caregiving: Fact or Artifact?”The Gerontologist 32:498-507.
Morrow-Howell, Nancy and Ada C. Mui. 1989. “Elderly Volunteers: Reasons for Initiatingand Terminating Service.” Journal of Gerontological Social Work 13:21-34.
Mui, Ada C., Namkee G. Choi, and Abraham Monk. 1998. Long-Term Care and Ethnicity.Westport, CT: Auburn House.
Mui, Ada C. and Nancy Morrow-Howell. 1993. “Sources of Emotional Strain Among theOldest Caregivers: Differential Experiences of Siblings and Spouses.” Research on Aging15:50-69.
Musick, Marc A., A. Regula Herzog, and James S. House. 1999. “Volunteering and MortalityAmong Older Adults: Findings From a National Sample.” Journal of Gerontology54B:S173-80.
Okun, Morris A., Alicia Barr, and A. Regula Herzog. 1998. “Motivation to Volunteer by OlderAdults: A Test of Competing Measurement Models.” Psychology and Aging 13:608-21.
Oman, Doug, Carl A. Thoresen, and Kay McMahon. 1999. “Volunteerism and MortalityAmong the Community-Dwelling Elderly.” Journal of Health Psychology 4:301-16.
122 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
Omoto, Allen M., Mark Snyder, and Steven C. Martino. 2000. “Volunteerism and the Life Course:Investigating Age-Related Agendas for Action.” Basic and Applied Social Psychology 22:181-97.
Pavalko, Eliza K. and Julie E. Artis. 1997. “Women’s Caregiving and Paid Work: CasualRelationships in Late Midlife.” Journal of Gerontology 52B:S170-79.
Penner, Louis A. and Marcia A. Finkelstein. 1998. “Dispositional and Structural Determinantsof Volunteerism.” Journal of Personality and Social Psychology 74:525-37.
Piliavin, Jane Allyn and Hong-Wen Charng. 1990. “Altruism: A Review of Recent Theory andResearch.” Annual Review of Sociology 16:27-65.
Pinquart, Martin and Silvia Sorensen. 2003. “Associations of Stressors and Uplifts of CaregivingWith Caregiver Burden and Depressive Mood: A Meta-Analysis.” Journal of Gerontology:Psychological Sciences 58B:P112-28.
Raschick, Michael and Berit Ingersoll-Dayton. 2004. “Costs and Rewards of CaregivingAmong Aging Spouses and Adult Children.” Family Relations 53:317-25.
Rozario, Philip A., Nancy Morrow-Howell, and James E. Hinterlong. 2004. “Role Enhancementor Role Strain: Assessing the Impact of Multiple Productive Roles on Older Caregiver Well-Being.” Research on Aging 26:413-28.
Schulz, Richard, Jason Newsom, Maurice Mittelmark, Lynda Burton, Calvin Hirsch, andSharon Jackson. 1997. “Health Effect of Caregiving: The Caregiver Health Effects Study:An Ancillary Study of the Cardiovascular Health Study.” Annals of Behavioral Medicine19:110-16.
Sieber, Sam D. 1974. “Toward a Theory of Role Accumulation.” American SociologicalReview 39:567-78.
Strawbridge, William J., Margaret I. Wallhagen, Sarah J. Shema, and George A. Kaplan. 1997.“New Burdens or More of the Same? Comparing Grandparent, Spouse, and Adult-ChildCaregivers.” The Gerontologist 37:505-10.
Thoits, Peggy A. and Lyndi N. Hewitt. 2001. “Volunteer Work and Well-Being.” Journal ofHealth and Social Behavior 42:115-31.
U.S. Department of Labor, Bureau of Labor Statistics. 2005. “Volunteering in the UnitedStates, 2005.” Retrieved December 28, 2005, from http://www.bls.gov.news.releaase/volun.nr0.htm
Van Willigen, Marieke. 2000. “Differential Benefits of Volunteering Across the Life Course.”Journal of Gerontology 55B:S308-18.
Wheeler, Judith A., Kevin M. Gorey, and Bernard Greenblatt. 1998. “The Beneficial Effectsof Volunteering for Older Volunteers and the People They Serve: A Meta-Analysis.”International Journal of Aging and Human Development 47:69-79.
Wilmoth, Janet M. and Pei-Chun Chen. 2003. “Immigrant Status, Living Arrangements, andDepressive Symptoms Among Middle-Aged and Older Adults.” Journal of Gerontology58B:S297-313.
Wilson, John. 2000. “Volunteering.” Annual Review of Sociology 26:215-40.Wilson, John and Thomas Janoski. 1995. “The Contribution of Religion to Volunteer Work.”
Sociology of Religion 56:137-52.Wilson, John and Marc Musick. 1997a. “Who Cares: Toward an Integrated Theory of
Volunteer Work.” American Sociological Review 62:694-713.Wilson, John and Marc A. Musick. 1997b. “Work and Volunteering: The Long Arm of the
Job.” Social Forces 76:251-72.Yee, Jennifer L. and Richard Schulz. 2000. “Gender Differences in Psychiatric Morbidity
Among Family Caregivers: A Review and Analysis.” The Gerontologist 40:147-64.
Choi et al. / Volunteer Activity and Caregiving 123
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from

Namkee G. Choi is a professor of social work at the University of Texas at Austin. Her cur-rent research interests include mental health needs among low-income older adults and geri-atric mental health service utilization. She has recently published in the Journal of Health andAging, Aging & Mental Health, and Research on Aging.
Jeffrey A. Burr is a professor of gerontology and chair of the Department of Gerontology at theUniversity of Massachusetts, Boston. His current research interests include productive activity inlater life, living arrangements and household composition of older immigrants, and late-life laborforce participation. Some of his recent research appears in the Journal of Gerontology: SocialSciences, Demography, Population Research and Policy Review, Generations, and Journal ofAging and Social Policy.
Jan E. Mutchler is a professor of gerontology and associate director for social and demographicresearch at the Gerontology Institute, University of Massachusetts, Boston. Her current researchfocuses on grandparent caregiving in diverse populations and intergenerational living arrange-ments among immigrant populations. Her research is supported by grants from the NationalInstitute on Aging and the National Institute of Child Health and Human Development.
Francis G. Caro is a professor of gerontology and fellow in the Gerontology Institute at theUniversity of Massachusetts, Boston. He is a sociologist by training and has held a variety ofacademic and research positions. His research interests include productive aging, residentialadjustments among elders, and community-based long-term care.
124 Research on Aging
at University of Texas Libraries on June 26, 2015roa.sagepub.comDownloaded from
Related Documents











