
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

# 2008 University of South Africa
All rights reserved
Printed and published by theUniversity of South AfricaMuckleneuk, Pretoria
LCR403T/1/2009±2010
98331205
3B2
CONTENTS
Study units Page
PREFACE v
1. INTRODUCTION 1
2. BASIC ANATOMY AND PHYSIOLOGY 20
3. POST-MORTEM CHANGES 53
4. IDENTIFICATION 77
5. GENERAL TRAUMATOLOGY 94
6. COMPLICATIONS OF TRAUMA 106
7. HEAD INJURIES 116
8. ASPHYXIA 139
9. FIREARM INJURIES 160
10. THERMAL, ELECTRICAL, ATMOSPHERIC PRESSURE
AND RADIATION ASSOCIATED DEATHS 175
11. TOXICOLOGY AND ALCOHOL 185
12. PREGNANCY-ASSOCIATED DEATHS 216
13. PAEDIATRIC FORENSIC PATHOLOGY 221
14. SEXUAL OFFENCES 234
COLOUR SUPPLEMENT 241
BIBLIOGRAPHY 286
iii
LCR403T/1/2009±2010
iv

PREFACE
We welcome you to the course Forensic Medicine. We are sure that you will
find the course interesting, informative and of practical use.
Format of the study guide
This course consists of a number of chapters or study units. Each study unit
deals with a particular aspect of forensic medicine. It is important to note that
certain parts of some study units contain material which was inserted for
general background reading and need not be studied for examination
purposes. We shall draw your attention specifically to these parts.
Format of a study unit
Each study unit is presented as follows:
. a table of contents of the material discussed
. a list of desired outcomes you should bear in mind when studying the
study unit
. an exposition of the topic covered in the study unit
. activities
. feedback
Each activity may be regarded as an assignment relating to a particular study
unit. We suggest that you write down your answer to a specific activity. The
feedback will enable you to assess the correctness of your answer.
v
LCR403T/1

STUDY UNIT 1Introduction
Contents
1.1 The practice of forensic medicine
1.2 Cause of death
1.2.1 Natural or non-natural (unnatural) death
1.2.2 Non-natural (unnatural death)
1.3 The primary cause of death
1.3.1 Definition
1.3.2 Homicide, suicide, accident
1.3.3 Formulation of the cause of death
1.4 The inquest
1.4.1 How does the inquest court come to know of an alleged non-
natural death?
1.4.2 How does the medical practitioner become involved in the
medical investigation of death?
1.4.3 The post-mortem examination
1.4.4 Subsequent proceedings and findings
1.4.5 How do the findings affect the medical practitioner?
1.4.6 General reasons for censure of the medical practitioner at an
inquest
1.5 Violence and causes of death in South Africa
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. discuss the role of forensic medicine in medical science as well as in
the legal profession
. discuss the difference between natural and unnatural deaths
. discuss the classification of the different causes of unnatural deaths,
giving examples
. discuss the concept of the primary cause of death
. discuss the principles relating to inquests
1.1 The practice of forensic medicine
The practice of forensic medicine (medicina forensis) is largely focused on
the clinical aspects and pathology of medicine as they relate to the needs of
the courts of law [forensic (adjective) = of courts of law].
1
The terms ``forensic medicine'' and ``medical jurisprudence'' are often used
synonymously, but in fact differ in meaning. ``Medical jurisprudence'' is
sometimes used in a wide sense as also inclusive of medical law, in other
words the law pertaining to the practice of medicine, while ``forensic
medicine'' refers to the ``medical'' needs of the courts.
Clinical forensic medicine embraces the medical condition of the living
``victim'' and/or ``assailant'' arising out of assault and alcohol and drug usage,
as well as topics such as age determination, identity, abortion, sexual offences
and iatrogenic conditions (``iatrogenic'' means ``resulting from the activity of
doctors'').
Forensic pathology, on the other hand, involves largely the post-mortem
medical investigation of deaths which appear to be the result of causes other
than natural causes. It also involves pathology laboratory procedures and
investigations needed to support both clinical forensic medicine and the post-
mortem investigation. This includes, for example, microscopic examination
of tissue, microbiological and biochemical tests and blood and tissue
grouping.
Further support to both the clinical and pathology investigations is offered by
the analytical toxicologist who undertakes tests for the determination of
foreign chemical substances in body tissues and fluids. Not infrequently the
medico-legal investigation becomes a multi-disciplinary team-effort on the
part of a number of different categories of scientists, which may include the
forensic psychiatrist, odontologist, biologist, ballistic and other forensic
scientists of many different callings.
[The following need not be studied for examination purposes.]
In his inaugural lecture delivered at the University of South Africa in 1976 the
late Professor HA Shapiro addressed himself to the practice and scope of
forensic medicine. A slightly abridged version of his address follows:
The scope
Forensic medicine includes every aspect of medical practice which can assist the
courts in resolving an issue. There is a considerable civil sphere, arising largely
from non-fatal traffic accidents, in which any medical practitioner may become
involved as an expert at any time, in his capacity as a physician, a neurosurgeon,
a neurologist, a psychiatrist, an orthopaedic surgeon, and so on.
Here I include those medical examinations of persons alleged to be under the
influence of alcohol or other drugs; of assailants and victims in cases of
assault, including rape, etc. This kind of medico-legal examination is an
ordinary general clinical examination which all medical practitioners are
trained to do. In examining a person alleged to be under the influence of
alcohol or drugs, the emphasis would be on the reason for a transitory
disturbance of the nervous system. No special merit resides in the
examination or the opinion merely because it has been made by a district
surgeon.1 In this, as in all cases, it is the reasons for coming to a conclusion
Study unit 1
ÐÐÐÐÐÐÐÐÐÐÐ1 Note that the system of district surgeons was abolished in the early 2000s. District surgeons used to be
responsible for the majority of medico-legal post-mortem examinations.
2
that will, in due course, be scrutinised and tested in cross-examination in
court. Whether the expert is a district surgeon or a specialist, nothing can
avail him in these circumstances except his clinical competence, derived from
his general medical training and experience.
The practice
But there remains a field requiring knowledge which is not ordinarily within
the province of medical practitioners unless they have been exposed to a
special kind of training and experience. This is the area we can conveniently
describe as falling within Forensic Pathology. It is easier to describe than to
define Forensic Pathology, which is concerned largely with deaths not due to
natural causes. It includes a study of the fatal effects of poisons, under the title
of Toxicology.
There is sometimes a tendency to argue that an external examination of the
body reveals such severe injuries as to make a post-mortem examination
unnecessary. This attitude embraces the fallacy of accepting the obvious. The
need to do a careful post-mortem examination, despite what common sense
may dictate to the contrary, is well demonstrated in the case of Rex v Blom.
This case, as you all know, stresses the 2 cardinal rules of logic which cannot
be ignored when reasoning by inference:
1. The inference sought to be drawn must be consistent with all the proved
facts. If it is not, the inference cannot be drawn.
2. The proved facts should be such that they exclude every reasonable
inference from them save the one sought to be drawn. If they do not
exclude other reasonable inferences, then there must be a doubt whether
the inference sought to be drawn is correct (1939 AD 188, at 202±203).
In this case the body of the deceased had been mutilated by a train which had
passed over it. The post-mortem examination yielded evidence which was
consistent with the view that the deceased was dead before her body was
placed on the railway line and that she had been killed by an administration of
chloroform. This case strikingly demonstrates the importance of a careful
post-mortem examination on all occasions.
The forensic pathologist is, however, also confronted, to a considerable
extent, with deaths due to natural causes, but occurring in such circumstances
that the usual death certificate cannot be issued by a registered medical
practitioner.
In actual practice, therefore, an inquiry into the cause of death requires, to
begin with, an adequate knowledge of the abnormal signs encountered in
deaths due to natural causes. At the time of the post-mortem examination an
investigator cannot, in many cases, be sure in which category the death will fall.
The limitations on the inferences which can reasonably be drawn from
isolated, naked-eye post-mortem findings must be appreciated very clearly.
Nowhere are these limitations reflected better than, for example, in deaths
where an anaesthetic has been administered: in cases of fatal poisoning, where
it is the negative findings which should raise suspicion: in many cases of head
injury and in many deaths due to natural causes. The problem arises regularly
Introduction
3

where death is attributed to arteriosclerotic heart disease on the basis of the
solitary post-mortem findings. The deceased, after all, had been walking
around, harbouring his disease, until just before he died.
There need and should be no hesitation about declining to state the cause of
death on the post-mortem findings alone, when the autopsy observations
clearly do not permit the pathologist to do so. He may only be in a position to
give the answer when the results of other investigations are made available to
him, eg a clinical history of the case, the results of a toxicological or other
laboratory analysis, etc. The pathologist then acts as a consultant and
expresses an opinion on all the facts when these are put to him at the proper
time and in the proper place, eg in an inquest court or during a trial. The post-
mortem examination is really just a special investigation and is only one of the
items in the total collection of evidence which must be evaluated in coming to
a conclusion. It is important not to confuse the role of the consultant with
that of the observer carrying out the autopsy. Two separate operations are
involved in coming to a diagnosis.
The forensic pathologist cannot, however, express such a view without
relying on a general knowledge of medicine, which must be applied to the
circumstances of a particular case. This contribution is best made by those
who are, to begin with, well trained in all branches of medical knowledge.
This emphasises the need to ensure that he is, in the first place, a competent
medical practitioner. Any defects in his medical knowledge must inevitably be
reflected in the inadequacy of his opinion as a medico-legal expert.
There seems to be a view, which is fairly widely held in some quarters, that
the performance of a post-mortem examination necessarily provides the
answer to the cause of death. In fact, this is so only in a relatively small
percentage of cases in which the lesion observed is incompatible with life.
There is no reason for a medico-legal pathologist to feel obliged to pretend to
omniscience or papal infallibility. It may well be a matter of regret that post-
mortem findings are not always capable of providing those precise answers
which legal questions so often demand. But this is not the fault of the medical
witness, who must consequently guard with great care against pretending to a
knowledge which, in the nature of things, he cannot have. Should he make
such claims, he would merely demonstate that he stands alone in the
possession of unique talents which his colleagues in the rest of the scientific
world lack.
There is no duty upon him to become a kind of sniffing medical bloodhound
who naõÈvely considers it a compliment to be described as wearing the mantle
of a Spilsbury; nor can we allow Forensic Pathology to descend to the level at
which the pathologist may have to be equated in status with the ancient
Roman augur who, with prophetic insight, offers his soothsayers's opinion
after inspecting the entrails of a corpse. It is a matter of some concern that
many a forensic opinion in medico-legal pathology has virtually not advanced
beyond the stage of such ancient Roman quackery.
The unavoidable shortcomings in medical knowledge emphasise the
importance of instructing legal practitioners in the principles which should
guide us all in evaluating the observations made by practitioners and the
legitimate inferences they seek to draw from them.
Study unit 1
4
Ex Africa semper aliquid novi
Now it so happens that in South Africa all medico-legal post-mortem
examinations are carried out exclusively by employees of the State. They are
the only medical practitioners who are exposed to this kind of medico-legal
experience. It is therefore gratifying to know that from their ranks have come
research workers whose contributions have profoundly influenced the
teaching and practice of Forensic Medicine all over the world.
Perhaps the single, most fundamental and revolutionary contribution burst
upon the scene when, on 9 September 1944, Professor I Gordon published a
paper entitled A Classification of Deaths of Medico-Legal Importance, in the
British Medical Journal. Professor Gordon used to be a senior academic in this
field and his paper (written with Einsteinian conciseness and brevity) was
merely the forerunner of a series of observations which had 3 main
consequences. His work produced a startling impact on the practice of our
discipline; it rescued Forensic Pathology from the Cinderella role which had
overtaken it; and it ushered in a scientific era in the history of Forensic
Pathology. South African medico-legal research thus came to influence
forensic teaching and practice far and wide.
Alexander Pope has reminded us that the proper study of mankind is man. As
I will demonstrate, the proper studies which come from South Africa
contributed to a scientific evaluation of many problems that face us daily. The
research work was marked by its utilitarian character. This is not to say that
we are unsympathetic to fundamental inquiries which have no immediate
practical application Ð what we may call futilitarian research. Indeed, some
of my best friends in research are futilitarians! But the nature of the problems
which confronted us impressed on us the immediacy and the urgency of the
need to examine these practical issues. The liberty, if not the lives, of accused
persons were at stake because so-called expert opinions were being offered
which were without any scientific foundation and which reflected the
ignorance, the obstinacy, the bias and prejudice of those who are not
handicapped by a knowledge of the subject.
As you can well appreciate, a very considerable part of our practice is
concerned with violent deaths, eg deaths due to suffocation, throttling,
strangling, hanging, drowning, etc. These are the so-called asphyxias, where
death is due to a mechanical obstruction of the airway. Those who taught us
and wrote the textbooks on which we depended, led us to believe that it was
possible, on the basis of the post-mortem findings alone, both to recognise
that death was due to asphyxia and to determine its particular type. These
assertions are still made in some quarters and they comprise possibly the
biggest myth that has ever pervaded thinking, teaching and practice in this
field.
Professor Gordon pointed out the fallacies in these claims and the wholly
unwarranted inferences which were being drawn from observations made on
the dead. There was a failure to distinguish between clinical evidence derived
from the living and the totally different order of things seen in the dead. In
brief, he showed that asphyxia was not an entity which could be recognised
from the post-mortem findings alone and, with the perspicacity of a
Introduction
5
Mendeleeff, he constructed what was virtually a periodic table for the
classification of these deaths. On the basis of Gordon's observations, it
become possible to pigeon-hole the various kinds of asphyxial death in
categories which are acceptable scientifically and permit us to predict fairly
confidently the abnormal signs which we can expect to find and which will
give us an indication of how the chain of events leading to a fatal outcome
was initiated.
Although Gordon's classification requires us to abandon the use of the
scientifically inadequate term asphyxia (it means ``without a pulse'') and to
substitute for it the more appropriate term anoxia (which means ``without
oxygen''), this change in nomenclature has not yet been adopted universally,
even though it is today used very widely (if in some cases still apologetically)
in modern forensic writings. Our new generations of lawyers are becoming
familiar with the acceptable scientific nomenclature, so it will not be long
before the obsolete terminology is abandoned.
In the diagnosis of the so-called asphyxial deaths, our teachers set much store
by the presence of small haemorrhages, pin-point to pin-head in size, on the
surface of the lungs, the heart, and so on. These small haemorrhages are
called petechiae (from the Latin for freckles). They have been likened to flea-
bites. Indeed, their profusion in certain diseases of the kidney has led to the
rather apt description of the flea-bitten kidney.
Notwithstanding the presence of petechiae in various disease processes
unconnected with asphyxia, these small haemorrhages came to be regarded as
diagnostic of mechanical obstruction to the airway. They acquired this
asphyxial attribute largely as the result of the claims of the 19th Century
physician, Tardieu. Despite some contemporary criticisms of Tardieu's
assertions, the Tardieu spots (as they come to be known) were invested with
a significance exclusively indicative of asphyxia. They became the hall-mark
of the diagnosis.
Reliance on the Tardieu spots as evidence of asphyxia (indeed, of throttling)
reached its misguided culmination in the case of Rex v Carr, first heard in the
Port Elizabeth Circuit Local Division on 29 November 1948. In this case the
Appellate Court set aside a conviction for murder and a sentence of death,
after it had taken the unusual step of hearing new evidence. There were, of
course, other issues besides the petechiae, but they were relied on by the chief
witness for the Crown to support (on the evidence available) a wholly
insupportable diagnosis of death due to throttling.
The Carr case stimulated Professor Gordon to initiate a most intense and
fruitful programme of research in the field of forensic pathology. Careful
studies on the petechiae revealed that they can occur spontaneously in the
dead body and can even be produced as artefacts after death on the very
surfaces of the organs where their presence has been regarded as indicating
asphyxia.
It has, for example, long been observed that healthy infants have
unexpectedly been found dead in bed or in their cots. In such cases we
were taught that they had died from suffocation whether by smothering in the
6
Study unit 1
bedclothes or overlaying by parents. One of the signs relied on for calling
them asphyxial deaths was the presence of Tardieu spots of petechiae on the
surfaces of the lungs and the heart.
In the early 1960s it was realised that these deaths could not be explained in
this way and the entity of unexpected death in infancy (or UDI, as I may call
it) was recognised. We do not yet know why these apparently well infants die
unexpectedly and suddenly, but the petechiae which are observed in these
cases are no longer misinterpreted as evidence of mechanical obstruction to
the airway. This is the direct result of Gordon's recognition of their non-
specific character.
``... one thing is certain; they [the petechiae] cannot be accepted as indicating
an `asphyxial' termination if by the use of the term `asphyxia' we infer
mechanical obstruction to the entry of air into the alveoli. This was an
erroneous view held by our forebears, and it has persisted longer than most
other medico-legal myths. But it has now been discarded.''
The final touches to the work of Gordon in this area come with the
demonstration that bruises in the tissues of the neck can be produced during
the course of a post-mortem dissection and that it is not possible to
distinguish, even microscopically, between such bruises and bruises inflicted
recently before death. It is hardly necessary to point out that these
observations have a profound significance for the post-mortem diagnosis of
cases of throttling and other forms of violent death; nor is it surprising that
they led to a modification of the technique of dissecting the neck structures
that has been adopted widely.
It is fair to say today that the fundamental research work contributed by
Professor Gordon and other South Africans has been adopted (if at times
rather reluctantly, but adopted nevertheless), fairly generally in authoritative
textbooks of international repute.
Thus the truth of the old tag of Pliny the Elder prevails: Ex Africa semper
aliquid novi.
A few words in conclusion
It is clear from what I have said that, once they entered the medico-legal
theatre, South Africans did some major plastic and reconstructive surgery on
the face of Forensic Pathology. This has forced medico-legal pathologists all
over the world to take another, more informed look at the subject. They have
not always shown alacrity in trying to overcome their resistance to the
unsettling observations which our researches have forced them to adopt in
place of outworn shibboleths. How could such things come out of the jungles
of Africa? They did not apparently appreciate that a sophisticated medicine
flourished in the best tradition of Western civilisation at the extremity of this
vast continent.
This is why we have repeatedly, but politely, had to say to them, as Bernardo
said to Horatio before Hamlet's approach:
7
Introduction
``Sit down a while
And let us once again assail your ears,
That are so fortified against our story.''
Hamlet, Act I, Scene I.
If we approach our forensic problems in a scientific spirit, we will be able to
say, with all the humility of the Soothsayer in Anthony and Cleopatra:
``In nature's infinite book of secrecy
A little I can read.''
Act I, Scene II
Modest as this accomplishment may be, it is the only way in which we can
advance the practice of our discipline so that we can play our proper part in
the administration of justice.
Let us remind ourselves of what Sir Thomas Browne (1605±1682) said some
300 years ago in his treatise on Vulgar Errors:
``But the mortallest enemy unto knowledge, and that which hath done
the greatest execution upon truth, hath been a peremptory adhesion
unto authority; and more expecially, the establishing of our belief upon
the dictates of antiquity ... . Now hereby methinks we manifestly delude
ourselves, and widely walk out of the track of truth.''
Sir Thomas Browne, Pseudodoxia Epidemica; Enquiries into very many
commonly received Tenents and commonly presumed Truths (1646).
[Study from here for examination purposes.]
1.2 Cause of death
As the cause of death poses such a serious problem in the medico-legal
investigation, it is necessary to focus one's attention (through the eyes of the
forensic pathologist) on so-called ``natural'' and ``non-natural or unnatural''
deaths, particularly with regard not only to identifying them as such but also
to the formulation of the cause of death.
The importance of accurately identifying the cause of death is not only
relevant to criminal matters, but may also be of considerable importance for
the family of the deceased. In a specific case, the deceased's family was issued
with a death certificate in which it was stated that ``death was solely and
exclusively due to natural causes'', to wit tetanus. The deceased had taken out
substantial insurance against accidental death. It was the insurers who, when
presented with a copy of this certificate, identified the fact that tetanus had
been the direct consequence of an injury sustained by the deceased some six
weeks earlier. By the time tetanus had developed the initial injury had already
healed. (Tetanus has a variable incubation period which may vary in length
from days to a few months.)
The inquest often constitutes an essential element of the medico-legal
8
Study unit 1

investigation, and by the very nature of the provisions of the Inquests Act 58
of 1959, forms an effective audit of medical practice, especially where
medical treatment, or lack of it is identified in the course of the inquiry.
1.2.1 Natural or non-natural (unnatural) death2
The medical practitioner who completes a death certificate must decide
whether the death was solely and exclusively due to natural causes or whether
it should be reported to the magistrate.
The decision may be difficult because not all cases which appear to be the
result of natural causes are in fact natural deaths; similarly, a death which
initially appears to be the result of non-natural causes may eventually turn out
to have been caused by natural disease.
TABLE 1.1
Conditions which may be due to either natural or non-natural causes
Condition Causes
Natural Non-natural
Meningitis
Subarachnoid
haemorrhage
Intracerebral
haemorrhage
General infection
Berry aneurysm
Hypertension
Atherosclerosis
Head injury
Head injury
Head injury
Where the cause of death is obvious there is no problem in designating it
``non-natural'' or ``natural'', for example deaths following stab wounds,
multiple injuries sustained during an accident, and exposure to fire or deaths
due to myocardial infarction (necrosis of the heart muscle). Problems may
arise, however, if a diagnosis has to be made based on symptoms suggesting
gastro-enteritis, as they can also be caused by a poison. It is incorrect to record
the complication, terminal event or underlying condition as the primary cause
of death. Stating, for example, that the cause of death of a patient with a head
injury was bronchopneumonia (the terminal complication), implies that this
was a natural death.
The medical practitioner who is required to make a decision about what
constitutes a non-natural or natural death receives little guidance from
legislation in this respect. His dilemma can be illustrated by the death of a
newborn infant following meconium aspiration due to foetal distress. This
may be a natural complication. On the other hand, it may be the result of an
omission on the part of a midwife or medical practitioner. In the former case
there is no question of negligence, whereas in the latter there is.
Pneumoconiosis (a chronic condition resulting from dust inhalation) and
certain lung tumours are caused by the inhalation of foreign material; yet death
as a result of these conditions is traditionally considered to be natural but
compensatable. Death due to acute or chronic arsenic poisoning and death due
9
Introduction
ÐÐÐÐÐÐÐÐÐÐÐ2 TG SchwaÈr (1986). An adapted version is published here by kind courtesy of the author.
to acute alcohol intoxication are unnatural, whereas the chronic ingestion of
alcohol which eventually causes death as a result of liver failure is considered
natural! The general attitude of the legislature is that the medical practitioner is
required to exercise his professional discretion and, for purposes of completing
the death certificate, must decide on grounds of available information or
circumstances whether death is due to natural or unnatural causes.
1.2.2 Non-natural (unnatural) death
Unnatural death can be classified as follows:
1.2.2.1 Death due to violence to the body
1. physical (stab wounds, gunshot wounds), microbiological (biological
warfare) and chemical (poisoning)
2. trauma due to nature related events, including dog bites, lightning, snake
bites and anaphylaxis after a bee sting
3. conditions like tetanus and gas gangrene as complications of trauma
1.2.2.2 Death classified as unnatural by section 56 of the Health Professions Act
Any death whilst under the influence of a general or local anaesthetic agent,
or where the administration of such a drug played a role in the death of an
individual, is not regarded as natural.
1.2.2.3 Death due to an omission or commission
Meconium is the faecal content that a foetus sometimes passes in utero if it
experiences stress, especially a lack of oxygen (intra-uterine foetal distress).
The primary aim of the management of the birth process is to prevent intra-
uterine oxygen deficiency or hypoxia. If hypoxia does occur, it is expected
that the medical practitioner or midwife will either perform (or refer the
patient for) a Caesarian section to prevent hypoxic injury to the foetus. If the
labour process is already well advanced, all attempts must be made to hasten
the delivery of the baby. In addition, immediately after the delivery of the
head, the airways of the baby must be cleaned by suction to prevent any
aspiration of meconium-stained amniotic fluid. If aspiration does occur,
respiratory distress, lung infection and death will often occur. If a baby
aspirates meconium, and subsequently dies due to lung complications, the
circumstances of birth must be assessed. If a baby dies due to meconium
aspiration and this is a result of poor management of the mother in the
maternity ward, it must be regarded as a non-natural death. However, it may
be regarded as a natural death if the delivery occurred in the absence of
proper medical care, for instance in a remote village.
1.2.2.4 Sudden and unexpected death
Sudden and unexpected death occurs in two situations, namely so-called
sudden infant death syndrome or cot death, or where a young person
suddenly and unexpectedly dies, for instance while exercising:
1. In the case of cot death no obvious cause of death can be found. It is not
possible to exclude unnatural causes like trauma or poisoning, before a post-
10
Study unit 1
mortem examination has been performed and excluded any possible
unnatural causes. After exclusion of an unnatural cause with a post-mortem
examination, the death will then be classified and regarded as natural.
2. The same applies where a young athlete suddenly and unexpectedly dies
due to a previous undiagnosed heart condition. It is also important to
remember that the findings at the post-mortem examination are not only
of help in formulating the cause of death, but also benefit the family if a
possible hereditary and treatable condition is diagnosed. The other
siblings can then receive precautionary treatment.
Unnatural deaths are dealt with in terms of the Inquests Act 58 of 1959. This
Act determines action to be taken after someone has died due to non-natural
causes. We shall now discuss unnatural deaths and give some examples.
By and large unnatural deaths are deaths which follow injury. Death may
follow only weeks or months after the injury as a result of complications (eg
a patient with a spinal cord injury may survive for months). The length of
time between the original injury and death in no way influences the
decision.
Death due to infection following an injury caused by an animal with rabies,
for example, or an injury resulting in tetanus (including tetanus neonatorum),
cannot be regarded as natural. Similar considerations apply to snake and
spider bites, bee and scorpion stings. In contrast, fatal malaria infection
transmitted by a mosquito bite is usually considered a natural cause of death.
Yet if death is the consequence of an infected blood transfusion, it is
considered non-natural.
A further category of non-natural deaths is that of deaths caused by the effect
of physical agents or of chemical or biological substances. Physical agents
include lightning, electricity (causing electrocution), fire, steam, hot fluid
(causing burns), suffocation (causing obstruction of the respiratory passages),
natural heat or cold (causing hyperthermia or hypothermia), and submersion
in water or other fluids (causing drowning). Chemical substances may be
administered accidentally or deliberately (for therapeutic reasons or in cases
of suicide or murder). Biological substances that may play a role include sera
and micro-organisms, which may cause food poisoning.
In the course of medical practice acts or omissions may also cause death, for
example omitting to test sensitivity where indicated, or omitting to perform a
routine examination or prescribe routine treatment.
The fact that the medical practitioner cannot make a definite or satisfactory
diagnosis when her patient dies is no reason to label the case an unnatural
death. She may so decide if she is convinced that the death was not solely and
exclusively due to natural causes, that is, she must have a reasonable doubt
that the death was not due to natural causes and if so requested, must be
prepared to substantiate her decision.
Sudden unexpected death poses an additional problem. It may be due to
either natural or unnatural causes, and in the absence of any background
information or personal knowledge of the deceased (as in cot deaths) the
medical practitioner will be unable to certify that to the best of her knowledge
and belief the death was due solely and exclusively to natural causes.
11
Introduction
1.3 The primary cause of death
1.3.1 Definition
The primary medical cause of death is defined as the disease or injury that
began the sequence of events and that led directly to death.
The following are often confused with the primary cause of death and are
mistakenly indicated as such: mechanism of death, occurrence, place or
environment where the death occurred, contributory cause, precipitating
cause, underlying cause, predisposing cause and terminal cause.
1.3.1.1 The place, environment, circumstances or scene of death
Merely supplying these particulars does not provide the necessary informa-
tion about the primary medical cause of death. It is not incorrect to include
this information, but if the practitioner himself has not seen the place, this
must be indicated by the addition of the words ``as ascertained'' or ``as I am
informed'', otherwise it is hearsay evidence. The practitioner also has to be
consistent: if in some cases he indicates that someone died in a car accident,
he must also indicate a fall from stairs in a house or hospital, or an injury in a
garden elsewhere.
1.3.1.2 Mechanisms of death
Mechanisms causing death are those physiological mechanisms or changes
that ultimately cause death, such as a disturbance in the acid-base balance of
the body or neurogenic stimulation of the heart. These or other loose terms
such as ``cardiac arrest'' or ``respiratory arrest'' are not primary medical
causes of death. It is therefore inadvisable to use them as such because they do
not provide the necessary information about the cause which initiated the
mechanism.
1.3.1.3 Contributory conditions or causes
A contributory condition or cause does not in itself cause death, but rather
contributes to an earlier demise. A person may, for example, suffer from a
natural condition such as coronary atherosclerosis which on its own (but not
necessarily at any specific moment) may cause death. The same applies to
other diseases such as diabetes, where an infection following on an injury will
spread far quicker than it would in the case of a healthy person. In the above-
mentioned cases atherosclerosis and diabetes are the contributory causes.
1.3.1.4 Predisposing conditions or causes
Predisposing or underlying conditions or causes can trigger a certain
occurrence. They are very similar to contributory conditions or causes and
often cannot be separated from them. Examples are the imbibing of alcohol
or epileptic seizures which may lead to an accident where injuries are
sustained by the subject himself.
12
Study unit 1

1.3.1.5 Precipitating conditions or causes
Precipitating conditions or causes are responsible for the immediate
development of a particular illness or occurrence. They are closely related
to contributory or predisposing conditions. Excitement may precipitate a
cerebral haemorrhage or a myocardial ischaemia, the primary causes of which
are cerebral or coronary atherosclerosis respectively.
Please note that contributory, predisposing and precipitating conditions/
causes are closely related and often interchangeable.
1.3.1.6 Terminal cause of death
The terminal cause of death is usually the complication that eventually sets in.
A person with a head injury (the primary medical cause) often develops
bronchopneumonia (terminal cause).
1.3.1.7 Sole cause of death
The sole cause of death is the cause where no contributory or other factors
have played a role. In a case where a person has suffered a single injury such
as a stab wound in the aorta, that is the primary cause of death.
1.3.2 Homicide, suicide, accident
Having established the primary medical cause of death, the doctor must
decide, to the best of her knowledge and conviction, whether the death is
solely the result of natural causes.
1.3.3 Formulation of the cause of death
When the cause of death has been formulated, it must always be borne in
mind that the diagnosis is based solely on personal observation. Where death
from natural causes is concerned, the patient's history and the results of all
special investigations should be taken into consideration in order to establish
the cause of death. This is not permissible in a medico-legal case because
information from other sources could be considered as hearsay. Such
information could however be used as a clue, so that special attention can
be paid to specific aspects which may be important and which otherwise may
possibly have been overlooked in a routine examination.
If a diagnosis cannot be made in a medico-legal case on the grounds of the
findings of the investigation alone, this fact must be recorded on the relevant
form, for example ``cause of death could not be determined by the post
mortem'', or ``death could not be determined by the post-mortem
examination alone''.
Only if the cause of the injury has been indisputably determined may the
aetiological factors in the cause of death be mentioned. A bullet wound in the
head can only be diagnosed if the bullet fragments are found in the head, or
other findings make the diagnosis obvious. Furthermore, it is wrong to record
``penetrating knife-wound'' as the cause, because similar wounds can also be
inflicted by other instruments such as daggers, razor blades, swords, bayonets
or even long pieces of glass. The use of the term ``stab wound'' is preferable.
If further information is provided by the submission of a full investigation dossier
13
Introduction
of a case, together with all the statements to the doctor in the form of affidavits,
or the furnishing of background information to the court, the doctor will be able
to determine the primary medical cause of death by way of inferences based on
her general medical and medico-legal knowledge and background.
In medico-legal cases where death resulted from an acute neurogenic cardiac
arrest due to parasympathetic stimulation; an anoxia or other mechanism in
cases of strangulation, suffocation and choking; drowning; where the dying
person was under the influence of drugs; or in cases of poisoning, the primary
medical cause of death is determined by the court after an evaluation of the
following evidence:
1.3.3.1 The evidence of the doctor who carried out the post-mortem examination
This evidence relates to the following:
1. the findings which indicate a specific occurrence
2. the exclusion of any other possible cause of death
1.3.3.2 The evidence of personnel from a specific laboratory
This evidence relates to the special investigation carried out, such as the
following:
1. the result of an investigation of blood from the right and left ventricles in
a case of suspected drowning
2. the result of a histological investigation to confirm or exclude
macroscopic changes
3. the result of a toxicological investigation of organs and body fluids in the
case of a suspected poisoning
1.3.3.3 The doctor's opinion
If the doctor feels competent to give his opinion on the result of a laboratory
investigation and to testify to it, he may do so.
1.3.3.4 The evidence of others (``testimony'')
The evidence of others must be presented by the prosecutor, especially with
regard to the following:
1. the state of health of the deceased and indications whether a death was
expected or not
2. the course of events that led to the death
1.4 The inquest3
The Inquests Act provides, inter alia, for ``holding of inquests in cases of
deaths or alleged deaths apparently occurring from other than natural causes,
and for matters incidental thereto ...''
1.4.1 How does the inquest court come to know of an alleged non-natural death?
Where a medical practitioner is unable to certify that the death of his patient
(or other person) was solely and exclusively due to natural causes, he is
14
ÐÐÐÐÐÐÐÐÐÐÐ3This section is based on Smith (1986) and Strauss (1991:424).
Study unit 1
required to inform a policeman accordingly. In such cases the doctor does not
issue a death certificate. The police will inform a magistrate accordingly, who
will request the police to investigate the matter. The police will then report to
the public prosecutor.
The Act reads:
Any person [this includes the doctor or nurse] who has reason to believe
that ... a person has died ... due to other than natural causes shall report
accordingly to a policeman, unless he has reason to believe that a report
has or will be made by any other person.
Any policeman who has reason to believe that any person had died ...
from other than a natural cause shall investigate the circumstances of the
death or alleged death.
1.4.2 How does the medical practitioner become involved in the medical investigation ofdeath?
The magistrate to whom the death is reported must, if he deems it expedient
in the interests of justice, cause it to be examined by a medical practitioner (eg
a forensic pathologist) ``who may, if he deems it necessary for the purpose of
ascertaining with greater certainty the cause of death make or cause to be
made an examination of any internal organ, or any part or any contents of the
body, or any other substance or thing''. For the purpose of this examination
``any part or internal organ or contents of a body may be removed'' and
``removed to any place''.
If the pathologist or any medical practitioner has been involved in the treatment
of the deceased before death, it is the policy of the Department of Health that
he should advise the magistrate accordingly so that he can seek the assistance of
another pathologist or medical practitioner in order to conduct the post-
mortem examination. In practice he will generally consult with the forensic
consultant, in other words the chief pathologist for the region.
1.4.3 The post-mortem examination
The extent and nature of the post-mortem examination is not prescribed by
statute, but the medical practitioner undertaking this task would be well
advised to follow with discretion the procedure as laid out in the report form
provided for this purpose.
1.4.3.1 Who may be present at the post-mortem examination?
A police officer or another medical practitioner nominated by any person,
who satisfies the magistrate that he has a ``substantial and peculiar interest in
the issue of the examination may be present at the post-mortem examination,
as well as any other person permitted by the magistrate or the medical
practitioner conducting the post-mortem examination''. The attendance of
students is included in the latter provision. The doctor performing the
autopsy should welcome the presence of a colleague, who may be appointed
by the relatives to represent their interests, as he should have nothing to hide,
and a second opinion is generally helpful (Strauss 1991:424).
15
Introduction
1.4.3.2 Report of the examination
The findings at an autopsy, which are recorded as the autopsy is done, are
generally later transcribed on the prescribed form, with (it is hoped)
meticulous attention to relevant factual detail and accuracy; these findings
represent the personal factual observations of the medical practitioner
performing the examination (Nel 1986:5).
1.4.4 Subsequent proceedings and findings
The report is submitted to the investigating police officer in the form of an
affidavit. Together with the other relevant documents it is submitted to the
public prosecutor, who may call for additional information. If criminal
proceedings are not instituted, the prosecutor will submit the documents and
other information to the magistrate.
In terms of the Inquests Act the judicial officer shall record a finding on the
following:
1. the identity of the deceased
2. the date or likely date of death
3. the cause or likely cause of death
4. whether the death was brought about by any act or omission involving or
amounting prima facie to an offence on the part of any person
If the judicial officer is unable to record any such finding she shall record that
fact. It should be appreciated that the evidence which justifies a finding of a
likely cause of death may not stand the test of a criminal trial or a civil action.
Both competent medical acts and omissions may result in a death (eg death
during a heart transplant operation or following failure to institute specific
treatment in a case of cerebral haemorrhage), but such an act or omission
need not constitute an offence in the sense of criminal negligence.
If the body has been destroyed (eg by cremation) or if no body can be recovered
(eg in a sea disaster) and if the evidence proves beyond reasonable doubt that the
person has died, the judicial officer shall accordingly record a finding of death
and then proceed to make a finding as in the case of all inquests.
At the termination of the inquest the judicial officer is required to submit the
record to the Director of Public Prosecution in the following circumstances:
1. if she cannot make a finding
2. if she makes a finding that death was brought about by an act or omission
involving or amounting to an offence
3. if the Director of Public Prosecutions has requested that this be done
The Director of Public Prosecutions has the powers to re-open an inquest or
to permit exhumation of a body for further investigation.
16
Study unit 1
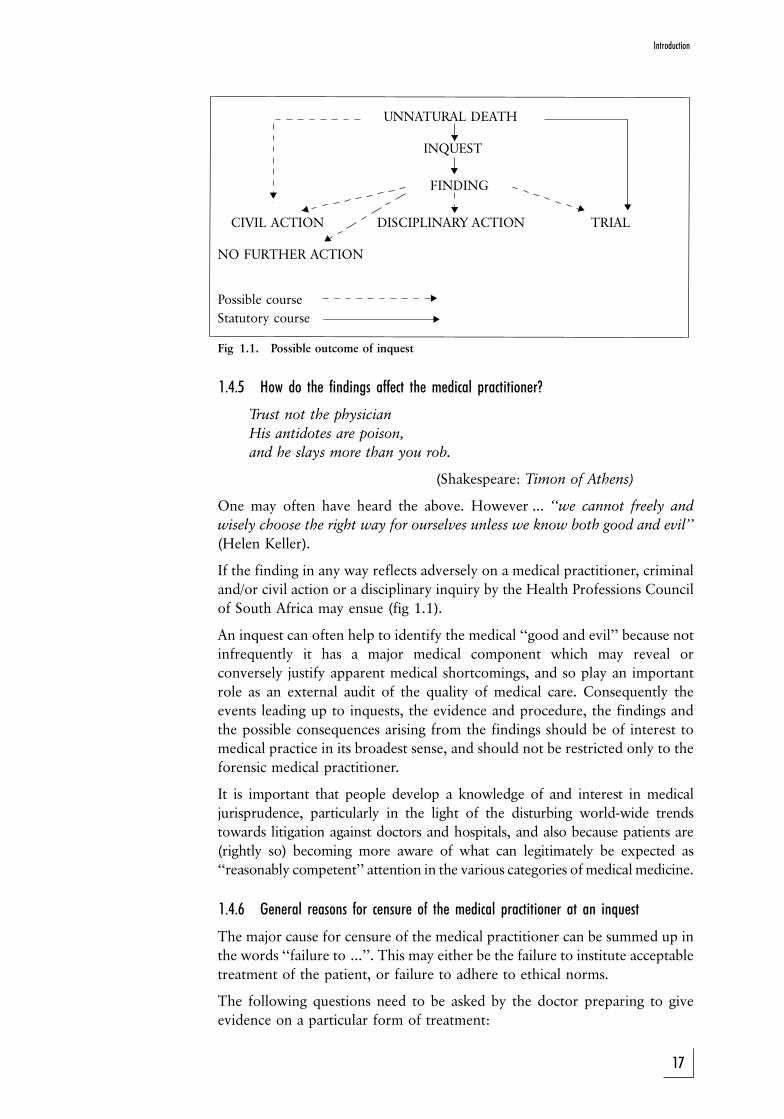
Fig 1.1. Possible outcome of inquest
1.4.5 How do the findings affect the medical practitioner?
Trust not the physician
His antidotes are poison,
and he slays more than you rob.
(Shakespeare: Timon of Athens)
One may often have heard the above. However ... ``we cannot freely and
wisely choose the right way for ourselves unless we know both good and evil''
(Helen Keller).
If the finding in any way reflects adversely on a medical practitioner, criminal
and/or civil action or a disciplinary inquiry by the Health Professions Council
of South Africa may ensue (fig 1.1).
An inquest can often help to identify the medical ``good and evil'' because not
infrequently it has a major medical component which may reveal or
conversely justify apparent medical shortcomings, and so play an important
role as an external audit of the quality of medical care. Consequently the
events leading up to inquests, the evidence and procedure, the findings and
the possible consequences arising from the findings should be of interest to
medical practice in its broadest sense, and should not be restricted only to the
forensic medical practitioner.
It is important that people develop a knowledge of and interest in medical
jurisprudence, particularly in the light of the disturbing world-wide trends
towards litigation against doctors and hospitals, and also because patients are
(rightly so) becoming more aware of what can legitimately be expected as
``reasonably competent'' attention in the various categories of medical medicine.
1.4.6 General reasons for censure of the medical practitioner at an inquest
The major cause for censure of the medical practitioner can be summed up in
the words ``failure to ...''. This may either be the failure to institute acceptable
treatment of the patient, or failure to adhere to ethical norms.
The following questions need to be asked by the doctor preparing to give
evidence on a particular form of treatment:
17
Introduction
!
!
! !!
!
!
!!
!
UNNATURAL DEATH
INQUEST
FINDING
CIVIL ACTION DISCIPLINARY ACTION TRIAL
NO FURTHER ACTION
Possible course
Statutory course

1. Was the drug or procedure the correct choice, and was I competent to
administer it?
2. Was there a clear indication for its use?
3. Was I aware of dangers involved and contra-indications?
4. Did I attempt to anticipate by generally acceptable methods the possibility
that the patient might exhibit any idiosyncrasy to such use?
5. Was I in a position to skilfully apply the necessary counteractants?
6. Was I in a position to skilfully manage any complications due to
intervention?
1.5 Violence and causes of death in South Africa
The incidence of violent deaths in South Africa is alarmingly high. No fewer
than 38,77% of all cases of unnatural death in 2005 were due to violence/
homicide, and almost the same percentage (38,78%) due to accidents of
which the majority was due to road accidents. Almost 10% of unnatural
deaths were due to suicide. These figures are according to the publication, A
profile of fatal injuries in South Africa, the Seventh Annual Report of the
National Injury Mortality Surveillance System in 2005. If you would like
more information on this subject, visit the website at:
http://www.sahealthinfo.org/violence/national2005.pdf
ACTIVITIES
1. Classify unnatural deaths.
2. Why is the sudden and unexpected death of a person always treated as an
unnatural death? Can these deaths also include natural causes?
3. A person under the influence of alcohol is involved in a motor vehicle
accident and sustains multiple injuries. During his stay in the intensive
care unit, ventilation is necessary due to his injuries. He develops a lung
infection (pneumonia) and dies due to lung (respiratory) failure. What is
the primary cause of death? What will you regard as the terminal cause of
death? And the mechanisms of death? Are there any predisposing causes?
4. In those cases where there are minimal or no signs of trauma to the body
of the deceased, such as drowning, certain evidence may be of value to
determine the cause of death. Discuss this statement.
5. Which findings must be made by the judicial officer during an inquest?
FEEDBACK
1. Unnatural deaths can be classified as follows:
(a) deaths as the result of violence to the body
(b) deaths governed by section 56 of the Health Professions Act, the
so-called ``anaesthetic deaths''
(c) deaths due to an omission or commission by someone else
(d) sudden and unexpected deaths.
2. When a person dies suddenly and unexpectedly, it is not obvious
18
Study unit 1
initially whether this death is the result of natural or unnatural
causes. It is important that any unnatural causes should be excluded
before the death is treated as a natural death. For this reason, it is
routine practice to treat these deaths as unnatural deaths, and to
perform a post-mortem examination. If the cause of death is
diagnosed at post-mortem, and if there are no obvious signs of
violence to the body visible during the post mortem, these deaths
can then be further dealt with as natural. This is done for both
babies (sudden infant death syndrome (SIDS or cot death) as well as
in younger persons (younger than 50±60 years) who suddenly and
unexpectedly die without a pre-existing medical history of
significance.
3. The primary cause of death is multiple injuries. The terminal cause
of death is pneumonia or lung infection and the mechanism of death
is respiratory or lung failure. Alcohol can be regarded as a
predisposing cause.
4. Circumstantial evidence is often of value in determining the cause of
death in this type of situation.
5. The follow findings must be recorded:
(a) the identity of the deceased
(b) the date or likely date of death
(c) the cause or likely cause of death
(d) whether the death is brought about by an act or omission prima
facie involving or amounting to an offence on the part of any
person
19
Introduction
STUDY UNIT 2Basic anatomy and physiology
[This chapter need not be studied for examination purposes. It is intended to
give lay persons a basic understanding of anatomy and physiology. It is
reproduced here in a somewhat adapted form by kind courtesy of the SA Red
Cross Society. Read it carefully. It will assist you in gaining a better
understanding of the study units that follow.]
Contents
2.1 General structure and working of the body
2.2 The skeleton
2.2.1 The central axial skeleton
2.2.2 The bones of the upper limb
2.2.3 The bones of the lower limb
2.2.4 The joints
2.2.5 The skeleton: medico-legal applications
2.3 The muscles
2.4 The nervous system
2.4.1 The brain
2.4.2 The spinal cord
2.4.3 The nerves
2.4.4 The autonomous or sympathetic system and parasympathetic
nerve system
2.5 Contents of the cavities of the chest and abdomen
2.5.1 The chest cavity or thorax
2.5.2 The abdominal cavity or belly
2.6 The skin
2.7 The working of the body
2.7.1 The digestion stage
2.7.2 Use of foods and oxygen in the body
2.7.3 Excretion of waste matter
2.8 Circulation of the blood
2.8.1 Introduction
2.8.2 The blood vessels
2.8.3 The heart
2.8.4 The portal circulation
2.8.5 Valves of the heart
2.8.6 The pulse
2.8.7 Bleeding from arteries and veins
20

2.9 Respiration
2.9.1 The respiratory organs
2.9.2 Respiration movements
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should
. have a basic knowledge of the anatomy of the body
. have a basic knowledge of the physiology of the body
2.1 General structure and working of the body
The body is composed of the bones, which together form the skeleton, and
the soft parts, namely the skin, fat, muscles, blood vessels, et cetera, which
cover and surround the bones. The internal organs of the body are also soft
parts. The body is subdivided into the head and neck, the trunk, the two
upper limbs, and the two lower limbs. It is usual to include with the bones of
the upper limb also the shoulder blade and the collar bone, which attach the
arm to the trunk, and with the bones of the lower limb the hip bone by which
each thigh is attached to the trunk. The vertical middle line of the body is an
imaginary line which, with the body in the erect position and the palms of the
hands facing forwards, runs from the middle of the crown of the head to
between the feet.
2.2 The skeleton (fig 2.1)
The skeleton forms the framework around which the body is built up and
which gives the body its general shape. The bones of the skeleton give the
muscles a place to attach to, and muscle contraction makes movement
possible.
A muscle starts out from one bone and is inserted into another bone across a
joint. When the muscle shortens or contracts, the joint is moved, permitting
movement or locomotion. Bones such as the skull, the spinal column, the ribs
and the hip bones protect some very important internal organs.
The main purpose of the limbs is to provide a system of levers to make body
movement possible. The limb bones are typically long bones with strong
shafts and large round ends.
On the other hand, bones whose main purpose is to protect important
internal organs are usually flat bones, for example the bones of the skull, the
ribs, the breastbone and the hip bones. Where a part of the skeleton is
designed for compactness, with limited movement, as at the wrist or the back
part of the foot, or in the backbone, the bones are typically short bones, and
are frequently very irregular in shape.
21
Basic anatomy and physiology
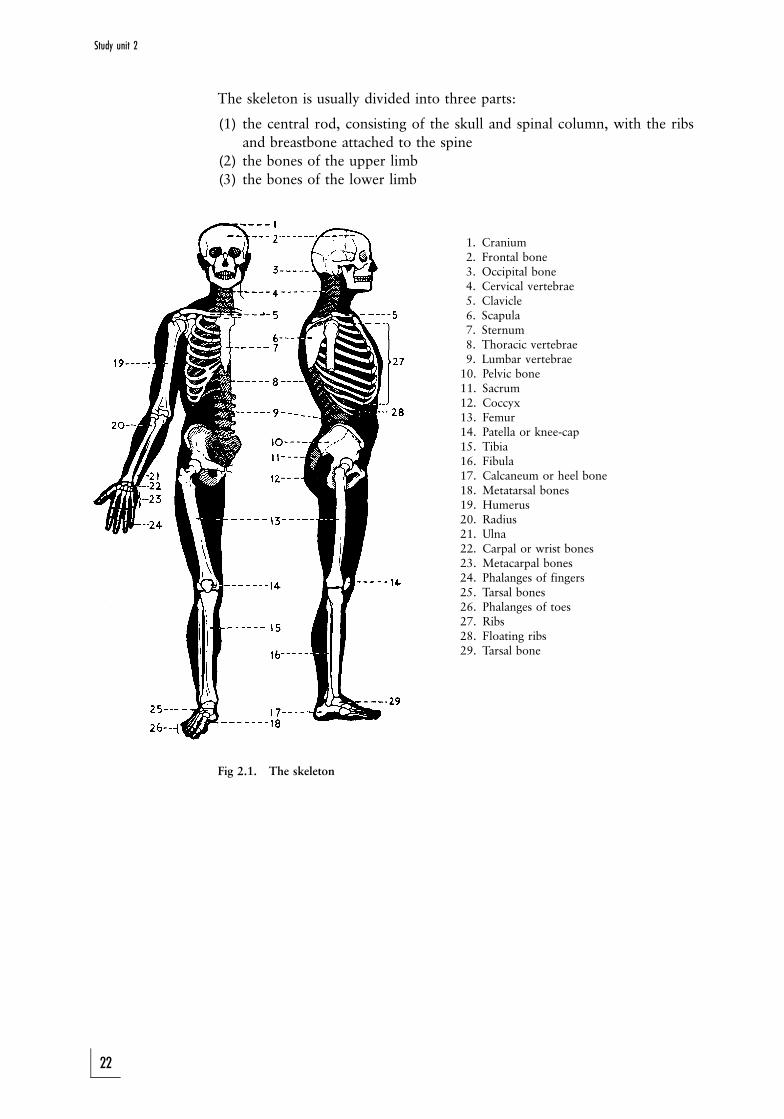
The skeleton is usually divided into three parts:
(1) the central rod, consisting of the skull and spinal column, with the ribs
and breastbone attached to the spine
(2) the bones of the upper limb
(3) the bones of the lower limb
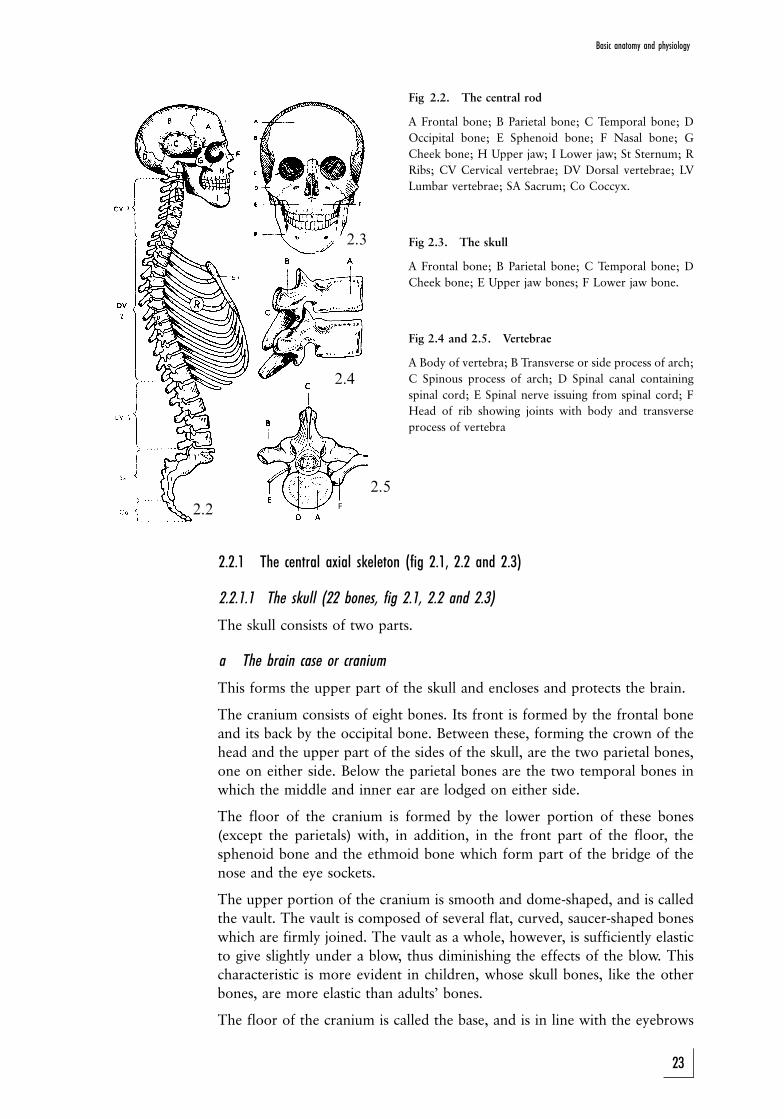
1. Cranium2. Frontal bone3. Occipital bone4. Cervical vertebrae5. Clavicle6. Scapula7. Sternum8. Thoracic vertebrae9. Lumbar vertebrae
10. Pelvic bone11. Sacrum12. Coccyx13. Femur14. Patella or knee-cap15. Tibia16. Fibula17. Calcaneum or heel bone18. Metatarsal bones19. Humerus20. Radius21. Ulna22. Carpal or wrist bones23. Metacarpal bones24. Phalanges of fingers25. Tarsal bones26. Phalanges of toes27. Ribs28. Floating ribs29. Tarsal bone
Fig 2.1. The skeleton
22
Study unit 2
2.3
2.4
2.5
2.2 F
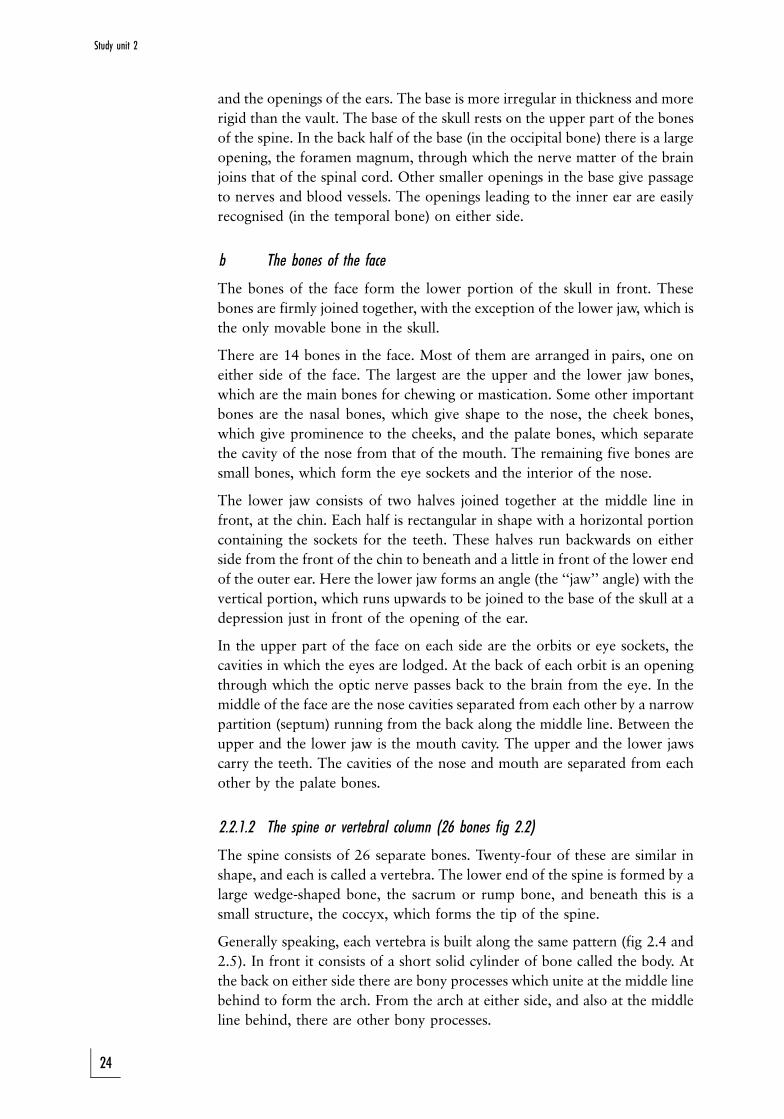
Fig 2.2. The central rod
A Frontal bone; B Parietal bone; C Temporal bone; D
Occipital bone; E Sphenoid bone; F Nasal bone; G
Cheek bone; H Upper jaw; I Lower jaw; St Sternum; R
Ribs; CV Cervical vertebrae; DV Dorsal vertebrae; LV
Lumbar vertebrae; SA Sacrum; Co Coccyx.
Fig 2.3. The skull
A Frontal bone; B Parietal bone; C Temporal bone; D
Cheek bone; E Upper jaw bones; F Lower jaw bone.
Fig 2.4 and 2.5. Vertebrae
A Body of vertebra; B Transverse or side process of arch;
C Spinous process of arch; D Spinal canal containing
spinal cord; E Spinal nerve issuing from spinal cord; F
Head of rib showing joints with body and transverse
process of vertebra
2.2.1 The central axial skeleton (fig 2.1, 2.2 and 2.3)
2.2.1.1 The skull (22 bones, fig 2.1, 2.2 and 2.3)
The skull consists of two parts.
a The brain case or cranium
This forms the upper part of the skull and encloses and protects the brain.
The cranium consists of eight bones. Its front is formed by the frontal bone
and its back by the occipital bone. Between these, forming the crown of the
head and the upper part of the sides of the skull, are the two parietal bones,
one on either side. Below the parietal bones are the two temporal bones in
which the middle and inner ear are lodged on either side.
The floor of the cranium is formed by the lower portion of these bones
(except the parietals) with, in addition, in the front part of the floor, the
sphenoid bone and the ethmoid bone which form part of the bridge of the
nose and the eye sockets.
The upper portion of the cranium is smooth and dome-shaped, and is called
the vault. The vault is composed of several flat, curved, saucer-shaped bones
which are firmly joined. The vault as a whole, however, is sufficiently elastic
to give slightly under a blow, thus diminishing the effects of the blow. This
characteristic is more evident in children, whose skull bones, like the other
bones, are more elastic than adults' bones.
The floor of the cranium is called the base, and is in line with the eyebrows
23
Basic anatomy and physiology
and the openings of the ears. The base is more irregular in thickness and more
rigid than the vault. The base of the skull rests on the upper part of the bones
of the spine. In the back half of the base (in the occipital bone) there is a large
opening, the foramen magnum, through which the nerve matter of the brain
joins that of the spinal cord. Other smaller openings in the base give passage
to nerves and blood vessels. The openings leading to the inner ear are easily
recognised (in the temporal bone) on either side.
b The bones of the face
The bones of the face form the lower portion of the skull in front. These
bones are firmly joined together, with the exception of the lower jaw, which is
the only movable bone in the skull.
There are 14 bones in the face. Most of them are arranged in pairs, one on
either side of the face. The largest are the upper and the lower jaw bones,
which are the main bones for chewing or mastication. Some other important
bones are the nasal bones, which give shape to the nose, the cheek bones,
which give prominence to the cheeks, and the palate bones, which separate
the cavity of the nose from that of the mouth. The remaining five bones are
small bones, which form the eye sockets and the interior of the nose.
The lower jaw consists of two halves joined together at the middle line in
front, at the chin. Each half is rectangular in shape with a horizontal portion
containing the sockets for the teeth. These halves run backwards on either
side from the front of the chin to beneath and a little in front of the lower end
of the outer ear. Here the lower jaw forms an angle (the ``jaw'' angle) with the
vertical portion, which runs upwards to be joined to the base of the skull at a
depression just in front of the opening of the ear.
In the upper part of the face on each side are the orbits or eye sockets, the
cavities in which the eyes are lodged. At the back of each orbit is an opening
through which the optic nerve passes back to the brain from the eye. In the
middle of the face are the nose cavities separated from each other by a narrow
partition (septum) running from the back along the middle line. Between the
upper and the lower jaw is the mouth cavity. The upper and the lower jaws
carry the teeth. The cavities of the nose and mouth are separated from each
other by the palate bones.
2.2.1.2 The spine or vertebral column (26 bones fig 2.2)
The spine consists of 26 separate bones. Twenty-four of these are similar in
shape, and each is called a vertebra. The lower end of the spine is formed by a
large wedge-shaped bone, the sacrum or rump bone, and beneath this is a
small structure, the coccyx, which forms the tip of the spine.
Generally speaking, each vertebra is built along the same pattern (fig 2.4 and
2.5). In front it consists of a short solid cylinder of bone called the body. At
the back on either side there are bony processes which unite at the middle line
behind to form the arch. From the arch at either side, and also at the middle
line behind, there are other bony processes.
24
Study unit 2

The process at the back of the arch is called the spinous process of the
vertebra; the processes on either side of the arch are called the transverse
processes.
The vertebrae are arranged one above the other in a column. In front the
bodies form a column of short solid cylinders which carry the weight of the
trunk and head, and are seen to increase in size and strength from the neck
downwards. Behind, the arches form a column or series of rings which
enclose a canal (the spinal canal) and in which lies the spinal cord (fig 2.5).
Between each pair of vertebrae is an opening on either side through which a
spinal nerve issues from the spinal cord. Throughout the whole length of the
spine the vertebrae are bound together by strong fibrous bands or ligaments,
but between the body of each vertebra and that of the vertebra above and
below it, is a pad or disc of cartilage or gristle (fig 2.4). These discs are elastic.
They allow slight movement between the bodies and act as buffers against
jolts caused by blows on the head or falls where the person lands on the lower
end of the spine or on the feet.
Although the amount of movement possible between any one pair of
vertebrae is small, the sum of these movements in the spine as a whole allows
bending forwards or backwards or to either side, and also to a lesser extent a
twisting of the spine.
There are seven vertebrae in the neck (cervical vertebrae). The 12 vertebrae in
the upper part of the trunk (dorsal vertebrae) give attachment to the ribs. In
the loin area there are five (lumbar vertebrae). The spine is curved slightly
forward in the neck, backward in the dorsal regions, and forward again in the
region of the loins (fig 2.2).
The sacrum or rump bone consists of five vertebrae, fused together, and much
altered in shape, to form one wedge-shaped bone. It fits between the hip
bones behind, transmitting the weight of the body to them, and so to the
lower limbs. The coccyx is a small bone attached to the lower end of the
sacrum, and forms the tip of the spine.
2.2.1.3 The ribs (12 pairs) and the breastbone (figs 2.1 and 2.2)
The ribs are flat curved bones, 12 on each side. They are numbered from top
to bottom. The ribs are joined at the back to the bodies and side transverse
processes of the dorsal vertebrae (fig 2.5), and arch forward, enclosing the
cavity of the chest. The upper seven are joined by means of small joints to the
breastbone, but between each rib and the breastbone is a short plate of elastic
cartilage or gristle, an arrangement which makes elastic chest movement
possible when breathing. The next three ribs are joined by similar plates of
cartilage to the cartilage of the seventh rib. The lowest two ribs are shorter
and have no attachment in front. They are therefore called floating ribs.
The breastbone (sternum) is a flat, dagger-shaped bone lying on the middle
line in front. It is joined by small joints to the two collar bones above, and at
either side to the ribs in the way already described.
The spine at the back, the ribs at the sides, and the breastbone in front
together form the bony portion of the chest (or thorax) and protect the
organs within.
25
Basic anatomy and physiology
2.2.2 The bones of the upper limb
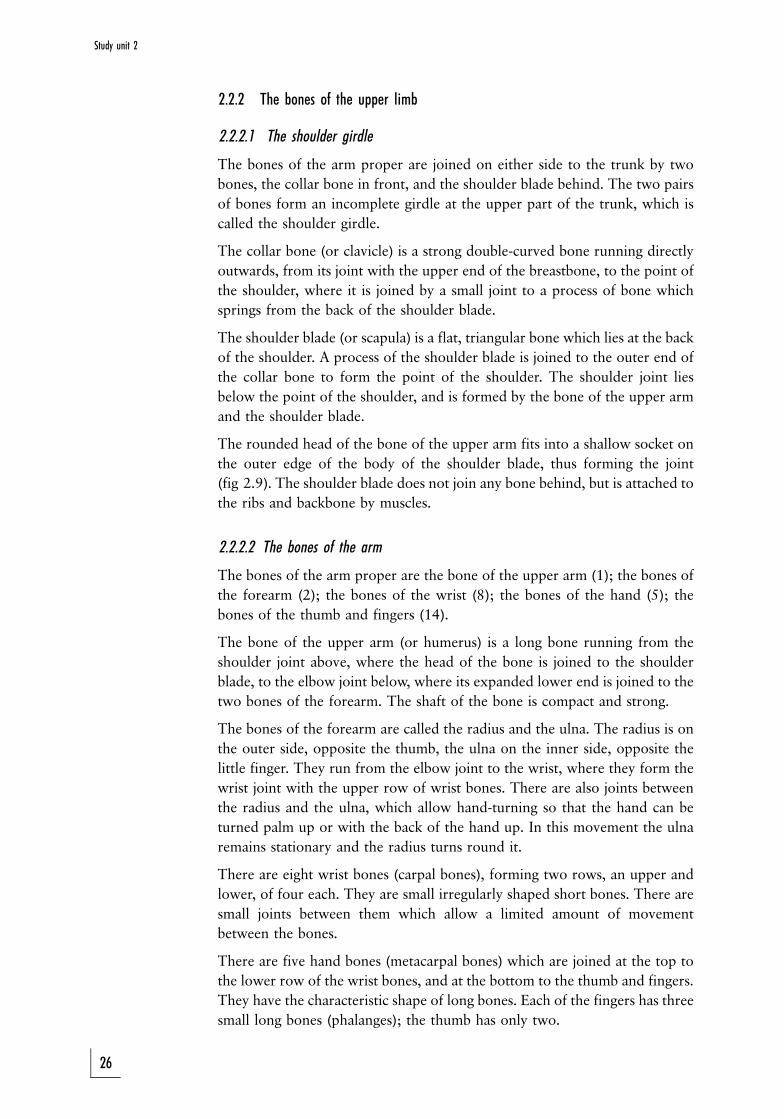
2.2.2.1 The shoulder girdle
The bones of the arm proper are joined on either side to the trunk by two
bones, the collar bone in front, and the shoulder blade behind. The two pairs
of bones form an incomplete girdle at the upper part of the trunk, which is
called the shoulder girdle.
The collar bone (or clavicle) is a strong double-curved bone running directly
outwards, from its joint with the upper end of the breastbone, to the point of
the shoulder, where it is joined by a small joint to a process of bone which
springs from the back of the shoulder blade.
The shoulder blade (or scapula) is a flat, triangular bone which lies at the back
of the shoulder. A process of the shoulder blade is joined to the outer end of
the collar bone to form the point of the shoulder. The shoulder joint lies
below the point of the shoulder, and is formed by the bone of the upper arm
and the shoulder blade.
The rounded head of the bone of the upper arm fits into a shallow socket on
the outer edge of the body of the shoulder blade, thus forming the joint
(fig 2.9). The shoulder blade does not join any bone behind, but is attached to
the ribs and backbone by muscles.
2.2.2.2 The bones of the arm
The bones of the arm proper are the bone of the upper arm (1); the bones of
the forearm (2); the bones of the wrist (8); the bones of the hand (5); the
bones of the thumb and fingers (14).
The bone of the upper arm (or humerus) is a long bone running from the
shoulder joint above, where the head of the bone is joined to the shoulder
blade, to the elbow joint below, where its expanded lower end is joined to the
two bones of the forearm. The shaft of the bone is compact and strong.
The bones of the forearm are called the radius and the ulna. The radius is on
the outer side, opposite the thumb, the ulna on the inner side, opposite the
little finger. They run from the elbow joint to the wrist, where they form the
wrist joint with the upper row of wrist bones. There are also joints between
the radius and the ulna, which allow hand-turning so that the hand can be
turned palm up or with the back of the hand up. In this movement the ulna
remains stationary and the radius turns round it.
There are eight wrist bones (carpal bones), forming two rows, an upper and
lower, of four each. They are small irregularly shaped short bones. There are
small joints between them which allow a limited amount of movement
between the bones.
There are five hand bones (metacarpal bones) which are joined at the top to
the lower row of the wrist bones, and at the bottom to the thumb and fingers.
They have the characteristic shape of long bones. Each of the fingers has three
small long bones (phalanges); the thumb has only two.
26
Study unit 2
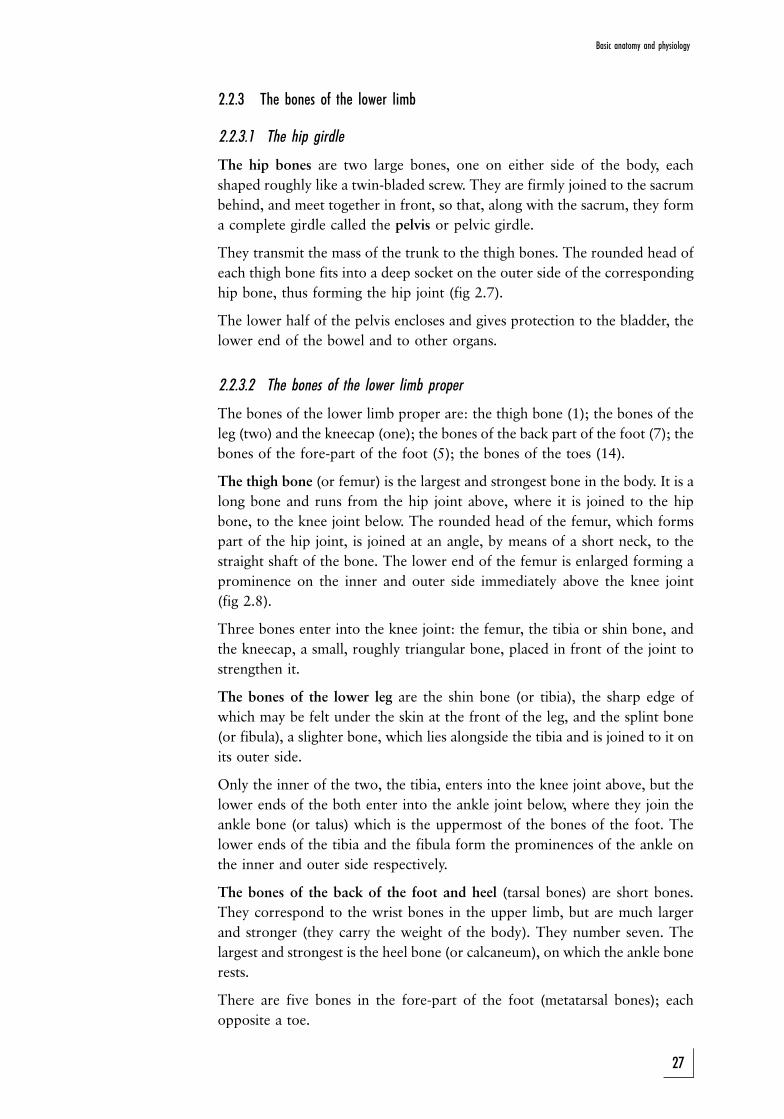
2.2.3 The bones of the lower limb
2.2.3.1 The hip girdle
The hip bones are two large bones, one on either side of the body, each
shaped roughly like a twin-bladed screw. They are firmly joined to the sacrum
behind, and meet together in front, so that, along with the sacrum, they form
a complete girdle called the pelvis or pelvic girdle.
They transmit the mass of the trunk to the thigh bones. The rounded head of
each thigh bone fits into a deep socket on the outer side of the corresponding
hip bone, thus forming the hip joint (fig 2.7).
The lower half of the pelvis encloses and gives protection to the bladder, the
lower end of the bowel and to other organs.
2.2.3.2 The bones of the lower limb proper
The bones of the lower limb proper are: the thigh bone (1); the bones of the
leg (two) and the kneecap (one); the bones of the back part of the foot (7); the
bones of the fore-part of the foot (5); the bones of the toes (14).
The thigh bone (or femur) is the largest and strongest bone in the body. It is a
long bone and runs from the hip joint above, where it is joined to the hip
bone, to the knee joint below. The rounded head of the femur, which forms
part of the hip joint, is joined at an angle, by means of a short neck, to the
straight shaft of the bone. The lower end of the femur is enlarged forming a
prominence on the inner and outer side immediately above the knee joint
(fig 2.8).
Three bones enter into the knee joint: the femur, the tibia or shin bone, and
the kneecap, a small, roughly triangular bone, placed in front of the joint to
strengthen it.
The bones of the lower leg are the shin bone (or tibia), the sharp edge of
which may be felt under the skin at the front of the leg, and the splint bone
(or fibula), a slighter bone, which lies alongside the tibia and is joined to it on
its outer side.
Only the inner of the two, the tibia, enters into the knee joint above, but the
lower ends of the both enter into the ankle joint below, where they join the
ankle bone (or talus) which is the uppermost of the bones of the foot. The
lower ends of the tibia and the fibula form the prominences of the ankle on
the inner and outer side respectively.
The bones of the back of the foot and heel (tarsal bones) are short bones.
They correspond to the wrist bones in the upper limb, but are much larger
and stronger (they carry the weight of the body). They number seven. The
largest and strongest is the heel bone (or calcaneum), on which the ankle bone
rests.
There are five bones in the fore-part of the foot (metatarsal bones); each
opposite a toe.
27
Basic anatomy and physiology
The bones of the back and the front of the foot together form a double arch at
the instep, an arrangement which gives a certain spring to the walk and
reduces the effects of jars in jumping or running.
The bones of the toes (phalanges) are arranged like those of the fingers Ð
two for the big toe, and three for the others. All the living bones, especially
the long bones, have great power of repair. Consequently, when a bone has
been broken, it is capable of becoming firmly joined together again by the
formation of new bone between and around the broken ends. This process of
bone union of a broken bone takes many days, and in the case of larger bones
often a good many weeks to complete. During the first part of that time the
broken bones must be kept totally immobile.
2.2.4 The joints
2.2.4.1 Varieties of joints
A joint is a structure which unites two or more bones, and commonly allows
movement between them. The joints are divided into three main groups in
accordance with their degree of movement.
(1) joints so firmly joined together that no movement can occur between
them, for example the bones of the cranium
(2) joints that allow a limited amount of movement, for example joints
between the vertebrae, between the bones at the back of the foot, or the
two joints between the skull (occipital bone) and the first vertebra of the
neck where the nodding movements of the head take place
(3) joints that move freely, such as the joints between the long bones of the
limbs. There are two main types:
(a) the hinge joint where there is backwards and forwards movement on
one level only, as in an ordinary hinge. The elbow (fig 2.9), the joints
of the fingers and toes and, broadly speaking, the knee (fig 2.6) and
the ankle are of this type.
(b) the ball and socket joint, or universal joint, which allows free
movement in all directions. Two joints, the hip (fig 2.7) and the
shoulder (fig 2.9) are of this type. The socket of the shoulder joint is
shallow and for this reason accidental dislocation or displacement of
the bone of the upper arm at this joint is not uncommon.
Although these are the more important types, there are also other types of
joints. The wrist joint is an example. It has a shallow oval socket or cup (the
lower end of the radius and ulna) and a shallow and oval head (the upper row
of wrist bones). The range of movement is not as free as that at the shoulder
or hip, but much freer than the movement in a simple hinge joint. The
movement of turning the head from side to side is performed at a ring and
pivot joint between the first and second vertebrae of the neck, the pivot being
formed by an upright peg of bone attached to the upper surface of the body of
the second vertebra, the first vertebra forming an incomplete ring round the
front and sides of the peg. The ring is completed behind by a fibrous ligament.
28
Study unit 2
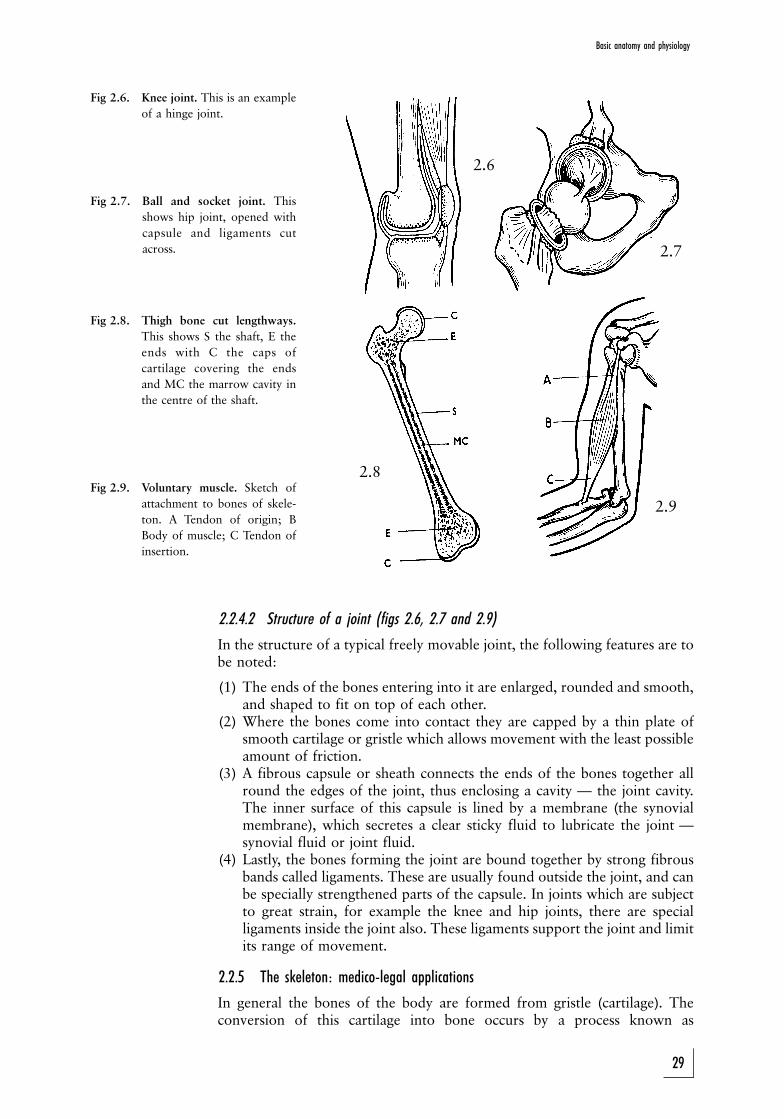
2.6
2.9
2.8
2.7
Fig 2.6. Knee joint. This is an example
of a hinge joint.
Fig 2.7. Ball and socket joint. This
shows hip joint, opened with
capsule and ligaments cut
across.
Fig 2.8. Thigh bone cut lengthways.
This shows S the shaft, E the
ends with C the caps of
cartilage covering the ends
and MC the marrow cavity in
the centre of the shaft.
Fig 2.9. Voluntary muscle. Sketch of
attachment to bones of skele-
ton. A Tendon of origin; B
Body of muscle; C Tendon of
insertion.
2.2.4.2 Structure of a joint (figs 2.6, 2.7 and 2.9)
In the structure of a typical freely movable joint, the following features are tobe noted:
(1) The ends of the bones entering into it are enlarged, rounded and smooth,and shaped to fit on top of each other.
(2) Where the bones come into contact they are capped by a thin plate ofsmooth cartilage or gristle which allows movement with the least possibleamount of friction.
(3) A fibrous capsule or sheath connects the ends of the bones together allround the edges of the joint, thus enclosing a cavity Ð the joint cavity.The inner surface of this capsule is lined by a membrane (the synovialmembrane), which secretes a clear sticky fluid to lubricate the joint Ðsynovial fluid or joint fluid.
(4) Lastly, the bones forming the joint are bound together by strong fibrousbands called ligaments. These are usually found outside the joint, and canbe specially strengthened parts of the capsule. In joints which are subjectto great strain, for example the knee and hip joints, there are specialligaments inside the joint also. These ligaments support the joint and limitits range of movement.
2.2.5 The skeleton: medico-legal applications
In general the bones of the body are formed from gristle (cartilage). Theconversion of this cartilage into bone occurs by a process known as
29
Basic anatomy and physiology
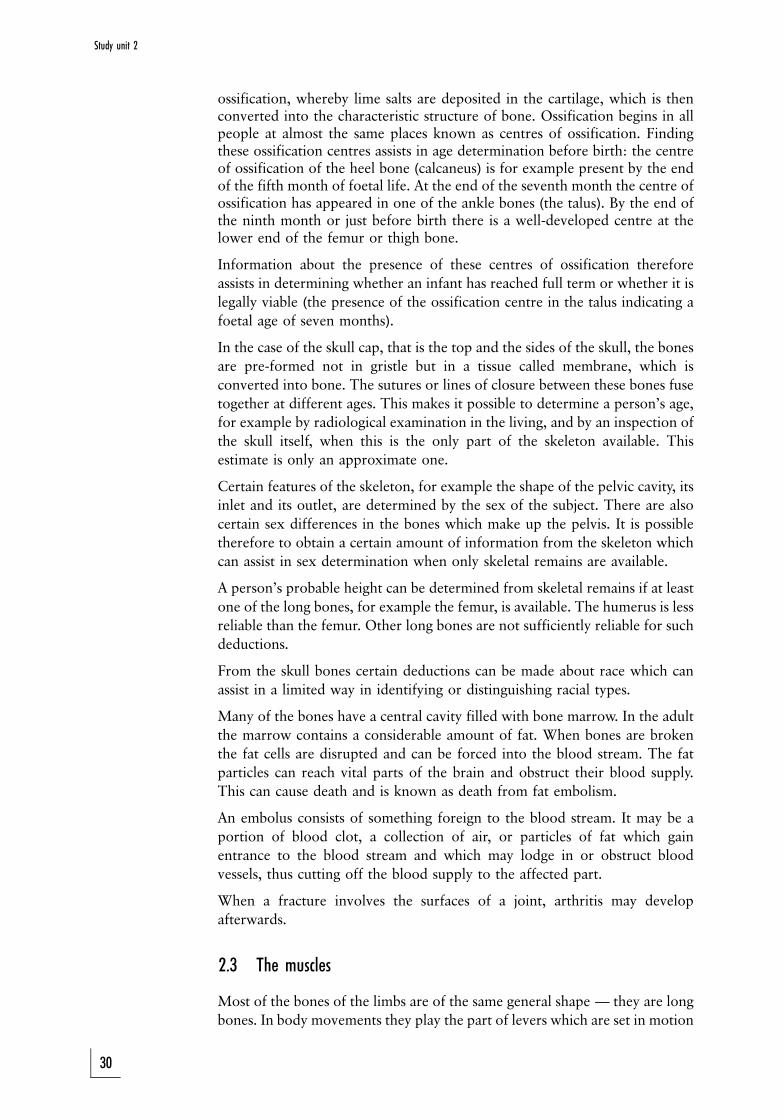
ossification, whereby lime salts are deposited in the cartilage, which is thenconverted into the characteristic structure of bone. Ossification begins in allpeople at almost the same places known as centres of ossification. Findingthese ossification centres assists in age determination before birth: the centreof ossification of the heel bone (calcaneus) is for example present by the endof the fifth month of foetal life. At the end of the seventh month the centre ofossification has appeared in one of the ankle bones (the talus). By the end ofthe ninth month or just before birth there is a well-developed centre at thelower end of the femur or thigh bone.
Information about the presence of these centres of ossification therefore
assists in determining whether an infant has reached full term or whether it is
legally viable (the presence of the ossification centre in the talus indicating a
foetal age of seven months).
In the case of the skull cap, that is the top and the sides of the skull, the bones
are pre-formed not in gristle but in a tissue called membrane, which is
converted into bone. The sutures or lines of closure between these bones fuse
together at different ages. This makes it possible to determine a person's age,
for example by radiological examination in the living, and by an inspection of
the skull itself, when this is the only part of the skeleton available. This
estimate is only an approximate one.
Certain features of the skeleton, for example the shape of the pelvic cavity, its
inlet and its outlet, are determined by the sex of the subject. There are also
certain sex differences in the bones which make up the pelvis. It is possible
therefore to obtain a certain amount of information from the skeleton which
can assist in sex determination when only skeletal remains are available.
A person's probable height can be determined from skeletal remains if at least
one of the long bones, for example the femur, is available. The humerus is less
reliable than the femur. Other long bones are not sufficiently reliable for such
deductions.
From the skull bones certain deductions can be made about race which can
assist in a limited way in identifying or distinguishing racial types.
Many of the bones have a central cavity filled with bone marrow. In the adult
the marrow contains a considerable amount of fat. When bones are broken
the fat cells are disrupted and can be forced into the blood stream. The fat
particles can reach vital parts of the brain and obstruct their blood supply.
This can cause death and is known as death from fat embolism.
An embolus consists of something foreign to the blood stream. It may be a
portion of blood clot, a collection of air, or particles of fat which gain
entrance to the blood stream and which may lodge in or obstruct blood
vessels, thus cutting off the blood supply to the affected part.
When a fracture involves the surfaces of a joint, arthritis may develop
afterwards.
2.3 The muscles
Most of the bones of the limbs are of the same general shape Ð they are long
bones. In body movements they play the part of levers which are set in motion
30
Study unit 2
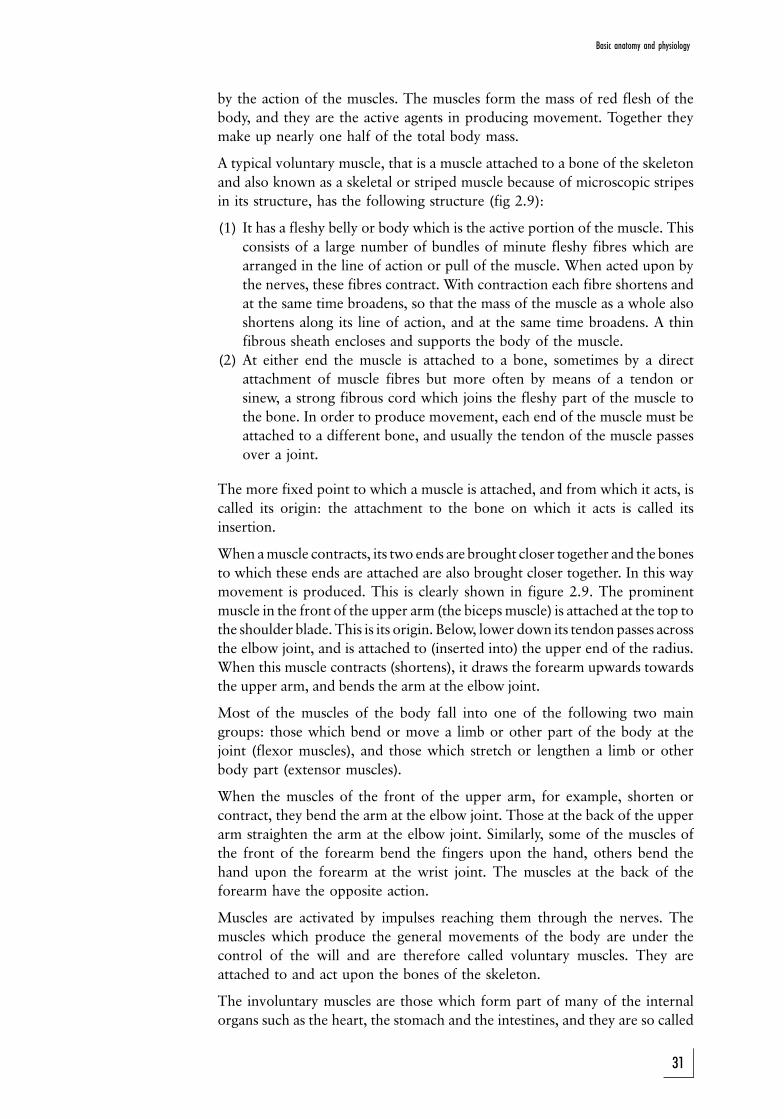
by the action of the muscles. The muscles form the mass of red flesh of the
body, and they are the active agents in producing movement. Together they
make up nearly one half of the total body mass.
A typical voluntary muscle, that is a muscle attached to a bone of the skeleton
and also known as a skeletal or striped muscle because of microscopic stripes
in its structure, has the following structure (fig 2.9):
(1) It has a fleshy belly or body which is the active portion of the muscle. This
consists of a large number of bundles of minute fleshy fibres which are
arranged in the line of action or pull of the muscle. When acted upon by
the nerves, these fibres contract. With contraction each fibre shortens and
at the same time broadens, so that the mass of the muscle as a whole also
shortens along its line of action, and at the same time broadens. A thin
fibrous sheath encloses and supports the body of the muscle.
(2) At either end the muscle is attached to a bone, sometimes by a direct
attachment of muscle fibres but more often by means of a tendon or
sinew, a strong fibrous cord which joins the fleshy part of the muscle to
the bone. In order to produce movement, each end of the muscle must be
attached to a different bone, and usually the tendon of the muscle passes
over a joint.
The more fixed point to which a muscle is attached, and from which it acts, is
called its origin: the attachment to the bone on which it acts is called its
insertion.
When a muscle contracts, its two ends are brought closer together and the bones
to which these ends are attached are also brought closer together. In this way
movement is produced. This is clearly shown in figure 2.9. The prominent
muscle in the front of the upper arm (the biceps muscle) is attached at the top to
the shoulder blade. This is its origin. Below, lower down its tendon passes across
the elbow joint, and is attached to (inserted into) the upper end of the radius.
When this muscle contracts (shortens), it draws the forearm upwards towards
the upper arm, and bends the arm at the elbow joint.
Most of the muscles of the body fall into one of the following two main
groups: those which bend or move a limb or other part of the body at the
joint (flexor muscles), and those which stretch or lengthen a limb or other
body part (extensor muscles).
When the muscles of the front of the upper arm, for example, shorten or
contract, they bend the arm at the elbow joint. Those at the back of the upper
arm straighten the arm at the elbow joint. Similarly, some of the muscles of
the front of the forearm bend the fingers upon the hand, others bend the
hand upon the forearm at the wrist joint. The muscles at the back of the
forearm have the opposite action.
Muscles are activated by impulses reaching them through the nerves. The
muscles which produce the general movements of the body are under the
control of the will and are therefore called voluntary muscles. They are
attached to and act upon the bones of the skeleton.
The involuntary muscles are those which form part of many of the internal
organs such as the heart, the stomach and the intestines, and they are so called
31
Basic anatomy and physiology
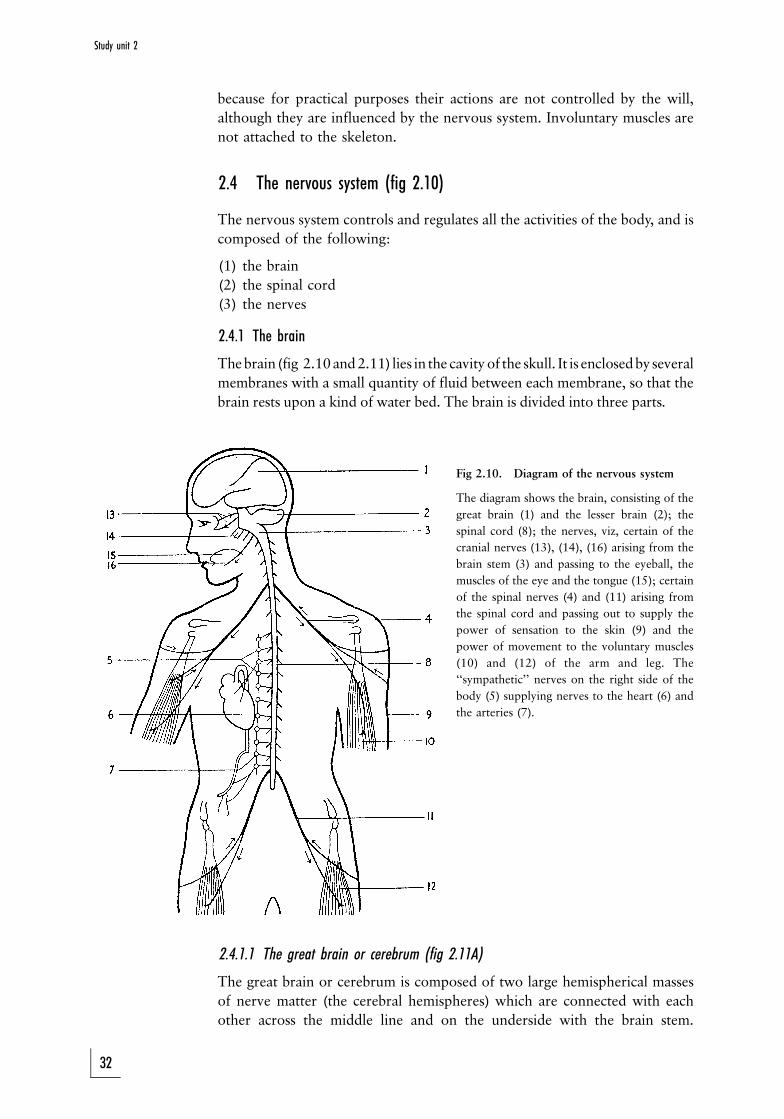
because for practical purposes their actions are not controlled by the will,
although they are influenced by the nervous system. Involuntary muscles are
not attached to the skeleton.
2.4 The nervous system (fig 2.10)
The nervous system controls and regulates all the activities of the body, and is
composed of the following:
(1) the brain
(2) the spinal cord
(3) the nerves
2.4.1 The brain
The brain (fig 2.10 and 2.11) lies in the cavity of the skull. It is enclosed by several
membranes with a small quantity of fluid between each membrane, so that the
brain rests upon a kind of water bed. The brain is divided into three parts.
Fig 2.10. Diagram of the nervous system
The diagram shows the brain, consisting of the
great brain (1) and the lesser brain (2); the
spinal cord (8); the nerves, viz, certain of the
cranial nerves (13), (14), (16) arising from the
brain stem (3) and passing to the eyeball, the
muscles of the eye and the tongue (15); certain
of the spinal nerves (4) and (11) arising from
the spinal cord and passing out to supply the
power of sensation to the skin (9) and the
power of movement to the voluntary muscles
(10) and (12) of the arm and leg. The
``sympathetic'' nerves on the right side of the
body (5) supplying nerves to the heart (6) and
the arteries (7).
2.4.1.1 The great brain or cerebrum (fig 2.11A)
The great brain or cerebrum is composed of two large hemispherical masses
of nerve matter (the cerebral hemispheres) which are connected with each
other across the middle line and on the underside with the brain stem.
32
Study unit 2
Together these two hemispheres fill the greatest part of the skull cavity. They
are the seat of our conscious life, and of thought and feeling. All voluntary
impulses that activate the voluntary muscles issue from them, and all impulses
that convey sensation and so give us knowledge of our surroundings go back
to them. Serious disruption of the working of the great brain results in
unconsciousness.
2.4.1.2 The lesser brain or cerebellum (fig 2.11C)
The lesser brain or cerebellum lies in the lower part of the back of the skull. It
is attached in front to the brain stem.
The lesser brain is involved in the (usually unconscious) maintenance of the
balance of the body when normal body movements are executed, for example
standing, running, walking, jumping, et cetera.
2.4.1.3 The brain stem (fig 2.11B)
The brain stem forms the stalk of the brain, lies within the skull and is
connected at the top to the cerebrum or great brain, at the back to the
cerebellum or lesser brain, and on the underside it runs continuous with the
spinal cord through the opening in the base of the skull as previously
described.
The nerve centres responsible for the involuntary regulation of breathing,
heart-beat and circulation, lie in the brain stem, which serves also to conduct
impulses to and from the great brain, the lesser brain and the spinal cord. An
intact brain stem is necessary for consciousness.
2.4.2 The spinal cord (fig 2.11(2))
The spinal cord is a long, rounded cord of nerve matter which begins at the
opening in the base of the skull, where it is continuous with the brain stem,
and runs down through a canal which is enclosed by the arches of the
vertebrae, to end at the level of the upper part of the loins. Its main function is
to conduct impulses to the muscles downwards from the brain via nerves (of
which it is made up), and also to conduct upwards impulses coming from the
skin and other parts of the body via the nerves, thus conveying sensations to
the various parts of the brain.
The spinal cord is no thicker than a finger, and the paths for the impulses to
and from both sides of the body are all contained within it, so that an injury to
the cord need not be extensive in order to damage or destroy these paths.
Consequently, tearing or compression of the spinal cord, which is liable to be
caused by a fracture of the vertebrae, is followed by more or less complete
loss of power of movement (or paralysis) and of feeling on both sides of the
body below the seat of injury.
2.4.3 The nerves
Between each pair of vertebrae a pair of nerves (fig 2.5E; fig 2.10) issues
33
Basic anatomy and physiology
from the spinal cord, one on either side. Thirty-one pairs of spinal nerves
arise in this way from the spinal cord. They are strong white cords of nerve
matter.
The nerves divide and subdivide. Some go to a skin area to which they supply
power of sensation, others to a certain group of muscles to which they supply
power of movement. The spinal nerves supply impulses in this way to the
whole of the trunk and limbs, the neck and the back of the scalp.
The organs of the special senses, the eyes (sight), the ears, (hearing), the nose
(smell), the tongue (taste), and also the skin and the muscles of the face are in
a similar way supplied by 12 pairs of cranial nerves (fig 2.10) which issue
from the brain stem and pass outward through openings in the base of the
skull.
Injury to a nerve (such as tearing or cutting) is followed by loss of power of
movement or paralysis of the particular muscles, and loss of feeling in the
particular area of skin supplied by that nerve.
The following points must be noted:
(1) The nerve matter of the great brain controls all voluntary movement and
sensation.
(2) All impulses conveying sensation from the skin or from the organs of
special sense pass by way of the nerves to the spinal cord, or brain stem,
respectively, and thence to the great brain.
(3) All impulses which produce voluntary movement of the muscles arise in
the great brain and pass through the brain stem and spinal cord and
thence by way of nerves to the muscles.
(4) The paths conducting these impulses from skin to brain and from brain to
muscle, cross over the middle line on their way through the brain stem, so
that the muscles of the left side of the body are set in action by impulses
from the right side of the brain, and vice versa. In the same way, sensation
arising in the left side of the body is received in the right half of the brain,
and vice versa. That is why an injury to one half of the brain may be
accompanied by paralysis or loss of muscle power on the opposite side of
the body.
2.4.4 The autonomous or sympathetic system and parasympathetic nerve system(fig 2.10(5))
The internal organs of the body (heart, lungs, liver, stomach, bowel, etc) are
also supplied by nerves which issue along with certain of the cranial nerves
and with most of the spinal nerves from the brain stem or the spinal cord
respectively. These nerves, however, function virtually independently of the
control of the will. We cannot control the movements of our internal organs
by simply willing them to do something, and regulation of the circulation of
the blood, of digestion and other processes, goes on whether we are asleep or
awake, independently of the will, and controlled by the action of these special
nerves. It is by means of these nerves also that emotional impulses, arising in
the brain or spinal cord, affect the action of the heart, blood vessels and other
internal organs.
Most of these nerves issue from the spinal cord, and, on leaving it, are
34
Study unit 2
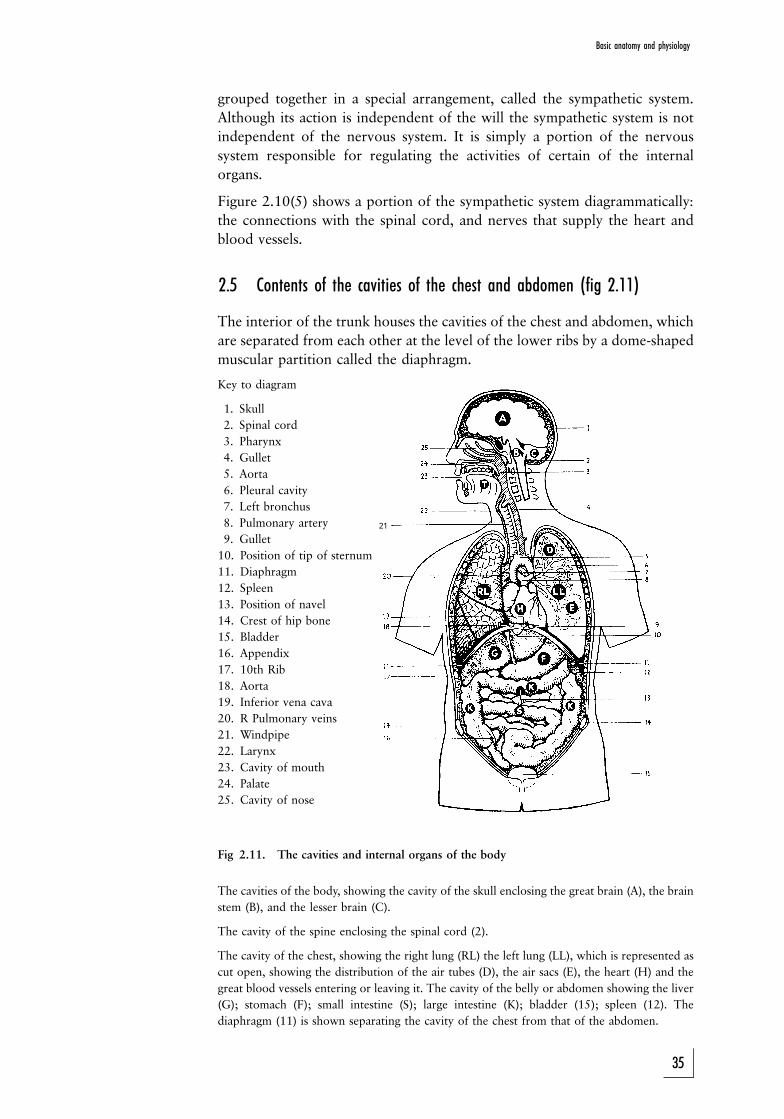
21
grouped together in a special arrangement, called the sympathetic system.
Although its action is independent of the will the sympathetic system is not
independent of the nervous system. It is simply a portion of the nervous
system responsible for regulating the activities of certain of the internal
organs.
Figure 2.10(5) shows a portion of the sympathetic system diagrammatically:
the connections with the spinal cord, and nerves that supply the heart and
blood vessels.
2.5 Contents of the cavities of the chest and abdomen (fig 2.11)
The interior of the trunk houses the cavities of the chest and abdomen, which
are separated from each other at the level of the lower ribs by a dome-shaped
muscular partition called the diaphragm.
Key to diagram
1. Skull
2. Spinal cord
3. Pharynx
4. Gullet
5. Aorta
6. Pleural cavity
7. Left bronchus
8. Pulmonary artery
9. Gullet
10. Position of tip of sternum
11. Diaphragm
12. Spleen
13. Position of navel
14. Crest of hip bone
15. Bladder
16. Appendix
17. 10th Rib
18. Aorta
19. Inferior vena cava
20. R Pulmonary veins
21. Windpipe
22. Larynx
23. Cavity of mouth
24. Palate
25. Cavity of nose
Fig 2.11. The cavities and internal organs of the body
The cavities of the body, showing the cavity of the skull enclosing the great brain (A), the brain
stem (B), and the lesser brain (C).
The cavity of the spine enclosing the spinal cord (2).
The cavity of the chest, showing the right lung (RL) the left lung (LL), which is represented as
cut open, showing the distribution of the air tubes (D), the air sacs (E), the heart (H) and the
great blood vessels entering or leaving it. The cavity of the belly or abdomen showing the liver
(G); stomach (F); small intestine (S); large intestine (K); bladder (15); spleen (12). The
diaphragm (11) is shown separating the cavity of the chest from that of the abdomen.
35
Basic anatomy and physiology
2.5.1 The chest cavity or thorax
The chest cavity is enclosed and protected by the doral ventebrae at the back
and the ribs and breastbone at the sides and in front.
It contains the following organs, most of which are involved in the circulation
of the blood or breathing:
1. On either side are the right and left lungs, which together fill the greater
part of the chest cavity.
2. The windpipe or trachea lies along the vertical middle of the neck and
divides into two smaller tubes, the right and left bronchus, each of which
enters the corresponding lung.
3. The central portion of the chest is occupied by the heart and the great
blood vessels which issue from it or enter it, namely the aorta and
pulmonary artery, and the corresponding great veins.
4. Behind the heart the gullet runs down from the neck where is lies behind
the windpipe, to the diaphragm through which it passes to enter the
stomach.
2.5.2 The abdominal cavity or belly
The abdominal cavity contains a large number of important organs most of
which are involved in the digestion of food. It is protected at the back by the
backbone, above by the lower ribs, and at its lowest portion by the pelvic
bones. This portion lies wholly within the pelvis and is called the pelvic cavity.
1. The stomach lies in the upper part of the abdomen immediately below the
diaphragm, and mainly to the left side of the middle line. It is continuous
with the gullet at the top and with the small intestine at its lower part.
2. The coils of the small intestine form a tube some six metres long, and
occupy the central portion of the abdomen.
3. In the right lower corner of the abdomen the small intestine joins the large
intestine, which passes up the right side of the abdomen, then across it just
below the stomach, and finally down the left side, and through the cavity of
the pelvis to end at the anus. The large intestine is about 1,5 m long.
A small worm-like blind tube about 10 cm long called the appendix is
affixed to the large intestine close to the point where the small intestine
enters it.
The mouth, throat, gullet, stomach, small intestine and large intestine
together form a continous tube, the digestive canal, through which the
food passes in digestion (fig 2.11, 2.12). Connected with the digestive
canal in the abdomen are two organs, the liver and the pancreas.
4. The liver occupies the right upper part of the abdomen, immediately
below the diaphragm, and extends across the middle line to the left. It lies
almost wholly under the lower ribs. This large organ produces the bile
which, after being stored in the gall bladder (a small sac at the lower end
of the liver) enters the small intestine not far from where the intestine
begins by a duct or tube (fig 2.12).
5. The pancreas lies in the angle between the stomach and the small
intestine. It produces an important digestive juice, and the duct which
conveys this juice to the small intestine enters the bowel at the same point
as the duct which carries the bile from the liver (fig 2.12).
6. To the left of the stomach, in the upper part of abdomen, covered by the
36
Study unit 2
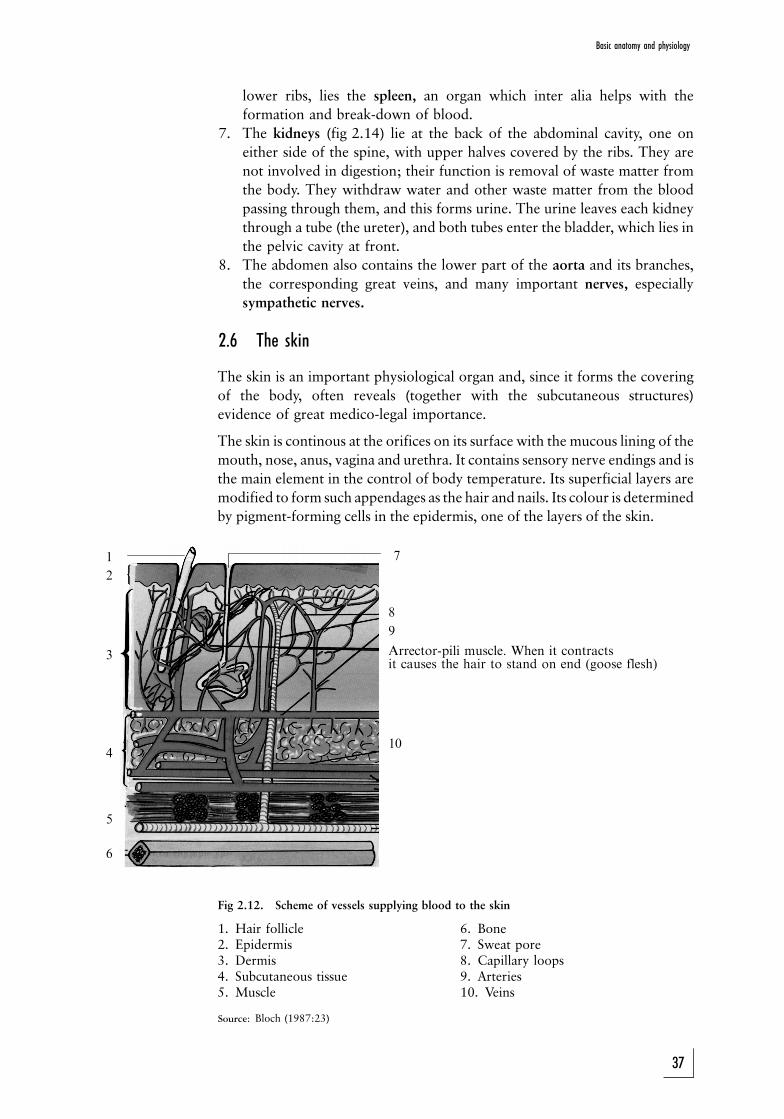
lower ribs, lies the spleen, an organ which inter alia helps with the
formation and break-down of blood.
7. The kidneys (fig 2.14) lie at the back of the abdominal cavity, one on
either side of the spine, with upper halves covered by the ribs. They are
not involved in digestion; their function is removal of waste matter from
the body. They withdraw water and other waste matter from the blood
passing through them, and this forms urine. The urine leaves each kidney
through a tube (the ureter), and both tubes enter the bladder, which lies in
the pelvic cavity at front.
8. The abdomen also contains the lower part of the aorta and its branches,
the corresponding great veins, and many important nerves, especially
sympathetic nerves.
2.6 The skin
The skin is an important physiological organ and, since it forms the covering
of the body, often reveals (together with the subcutaneous structures)
evidence of great medico-legal importance.
The skin is continous at the orifices on its surface with the mucous lining of the
mouth, nose, anus, vagina and urethra. It contains sensory nerve endings and is
the main element in the control of body temperature. Its superficial layers are
modified to form such appendages as the hair and nails. Its colour is determined
by pigment-forming cells in the epidermis, one of the layers of the skin.
Fig 2.12. Scheme of vessels supplying blood to the skin
1. Hair follicle 6. Bone2. Epidermis 7. Sweat pore3. Dermis 8. Capillary loops4. Subcutaneous tissue 9. Arteries5. Muscle 10. Veins
Source: Bloch (1987:23)
37
Basic anatomy and physiology
1
2
3
4
5
6
8
9
Arrector-pili muscle. When it contractsit causes the hair to stand on end (goose flesh)
10
7
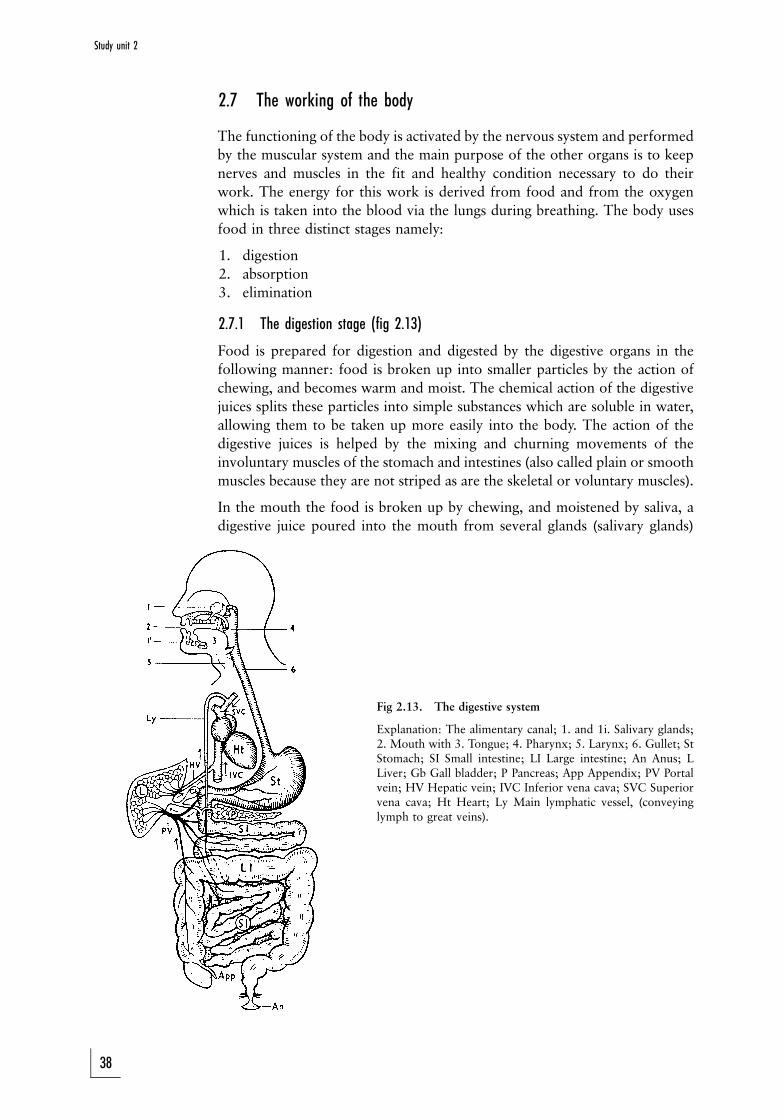
2.7 The working of the body
The functioning of the body is activated by the nervous system and performed
by the muscular system and the main purpose of the other organs is to keep
nerves and muscles in the fit and healthy condition necessary to do their
work. The energy for this work is derived from food and from the oxygen
which is taken into the blood via the lungs during breathing. The body uses
food in three distinct stages namely:
1. digestion
2. absorption
3. elimination
2.7.1 The digestion stage (fig 2.13)
Food is prepared for digestion and digested by the digestive organs in the
following manner: food is broken up into smaller particles by the action of
chewing, and becomes warm and moist. The chemical action of the digestive
juices splits these particles into simple substances which are soluble in water,
allowing them to be taken up more easily into the body. The action of the
digestive juices is helped by the mixing and churning movements of the
involuntary muscles of the stomach and intestines (also called plain or smooth
muscles because they are not striped as are the skeletal or voluntary muscles).
In the mouth the food is broken up by chewing, and moistened by saliva, a
digestive juice poured into the mouth from several glands (salivary glands)
Fig 2.13. The digestive system
Explanation: The alimentary canal; 1. and 1i. Salivary glands;2. Mouth with 3. Tongue; 4. Pharynx; 5. Larynx; 6. Gullet; StStomach; SI Small intestine; LI Large intestine; An Anus; LLiver; Gb Gall bladder; P Pancreas; App Appendix; PV Portalvein; HV Hepatic vein; IVC Inferior vena cava; SVC Superiorvena cava; Ht Heart; Ly Main lymphatic vessel, (conveyinglymph to great veins).
38
Study unit 2
situated near it. The act of swallowing passes the moistened food down the
gullet into the stomach. The stomach acts as a reservoir in which the food is
retained until it is thoroughly warmed and reduced to a fluid condition. The
walls of the stomach pour out a second juice (gastric juice) which also acts
upon the food. Upon leaving the stomach the partially digested food enters
the small intestine in a liquid state, and is there acted upon by the digestive
juice of the pancreas (pancreatic juice). The bile also acts to some extent upon
the food. At the same time the walls of the intestine also secrete a digestive
juice (the intestinal juice). The small intestine is the main area in which
digestion takes place.
Thus, in its passage through the digestive canal, food is continuously
undergoing change. Finally, after passing through the large intestine, the
undigested and unabsorbed remainder of the food is expelled from the body.
The passing of the food through the digestive canal takes about 24 hours.
A normal diet contains, in proportions suited to the needs of the body, the
following three main classes of nutrients:
1. Nitrogenous nutrients found mainly in animal foods (meat, fish, etc), and
which also form the main part of these foods. Several vegetable foods,
however, also contain a considerable amount of nitrogenous nutrients.
2. Starches and sugars, found mainly in vegetables, bread, potatoes, sugar,
fruits, etc. Meats contain virtually no starch or sugar.
3. Fats, found for example in butter, oil, meat, fat and cream.
While all these nutrients serve as sources of energy, it is chiefly starches,
sugars and fats which supply energy. In a normal diet starches, sugars and fats
amount to more than three-quarters of the total food intake. The main use of
nitrogenous nutrients is to repair the break-down in the living structures of
the body.
In addition to these nutrients a normal diet contains mineral salts and
vitamins. These are necessary to the body, but they are not sources of energy,
and the same is true of the water which we drink.
Digestive juices act upon the nutrients in different ways. Saliva only acts upon
starches in the food, and gastric juice mainly upon the nitrogenous nutrients.
Gastric juice is the only acid digestive juice, and for this reason it has an
important action in checking the development of any infective germs which
may have been swallowed.
Partially digested foodstuffs are acted upon in the small intestine by
pancreatic juice, bile, and intestinal juice. All these are alkaline juices, and
together they aid digestion, but the strongest is pancreatic juice. By the joint
action of these juices the digestion of all three classes of nutrients is continued
and completed in the small intestine where they are reduced to the simple
forms in which they can be absorbed into the body.
In the lower part of the small intestine and in the large intestine a certain
amount of putrefactive change also takes place. This is due not to the
digestive juices, but to the action of germs or bacteria.
39
Basic anatomy and physiology
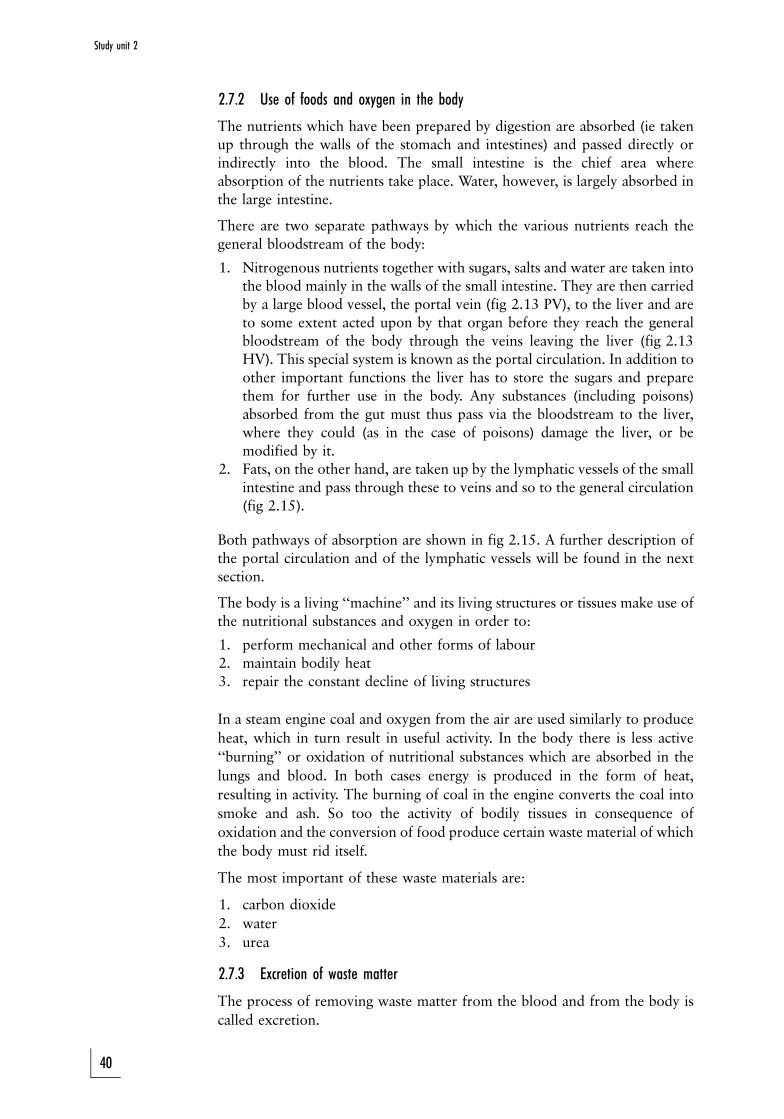
2.7.2 Use of foods and oxygen in the body
The nutrients which have been prepared by digestion are absorbed (ie takenup through the walls of the stomach and intestines) and passed directly orindirectly into the blood. The small intestine is the chief area whereabsorption of the nutrients take place. Water, however, is largely absorbed inthe large intestine.
There are two separate pathways by which the various nutrients reach thegeneral bloodstream of the body:
1. Nitrogenous nutrients together with sugars, salts and water are taken intothe blood mainly in the walls of the small intestine. They are then carriedby a large blood vessel, the portal vein (fig 2.13 PV), to the liver and areto some extent acted upon by that organ before they reach the generalbloodstream of the body through the veins leaving the liver (fig 2.13HV). This special system is known as the portal circulation. In addition toother important functions the liver has to store the sugars and preparethem for further use in the body. Any substances (including poisons)absorbed from the gut must thus pass via the bloodstream to the liver,where they could (as in the case of poisons) damage the liver, or bemodified by it.
2. Fats, on the other hand, are taken up by the lymphatic vessels of the smallintestine and pass through these to veins and so to the general circulation(fig 2.15).
Both pathways of absorption are shown in fig 2.15. A further description ofthe portal circulation and of the lymphatic vessels will be found in the nextsection.
The body is a living ``machine'' and its living structures or tissues make use ofthe nutritional substances and oxygen in order to:
1. perform mechanical and other forms of labour2. maintain bodily heat3. repair the constant decline of living structures
In a steam engine coal and oxygen from the air are used similarly to produce
heat, which in turn result in useful activity. In the body there is less active
``burning'' or oxidation of nutritional substances which are absorbed in the
lungs and blood. In both cases energy is produced in the form of heat,
resulting in activity. The burning of coal in the engine converts the coal into
smoke and ash. So too the activity of bodily tissues in consequence of
oxidation and the conversion of food produce certain waste material of which
the body must rid itself.
The most important of these waste materials are:
1. carbon dioxide
2. water
3. urea
2.7.3 Excretion of waste matter
The process of removing waste matter from the blood and from the body is
called excretion.
40
Study unit 2
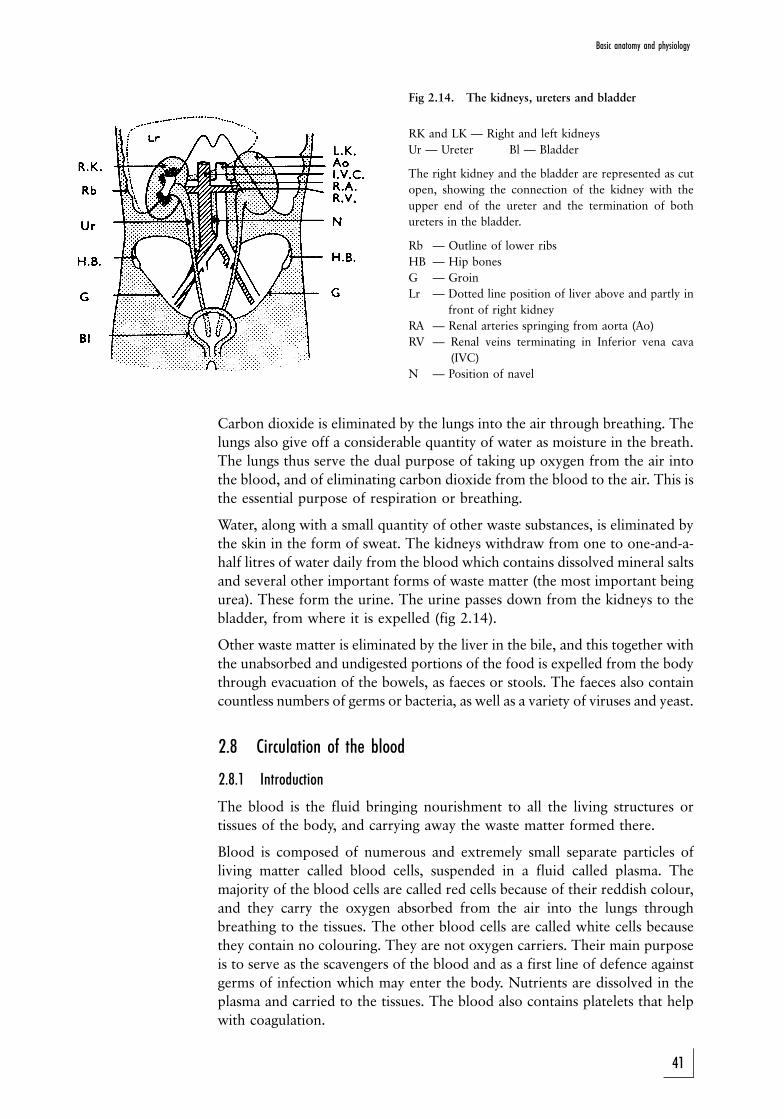
Fig 2.14. The kidneys, ureters and bladder
RK and LK Ð Right and left kidneys
Ur Ð Ureter Bl Ð Bladder
The right kidney and the bladder are represented as cut
open, showing the connection of the kidney with the
upper end of the ureter and the termination of both
ureters in the bladder.
Rb Ð Outline of lower ribs
HB Ð Hip bones
G Ð Groin
Lr Ð Dotted line position of liver above and partly in
front of right kidney
RA Ð Renal arteries springing from aorta (Ao)
RV Ð Renal veins terminating in Inferior vena cava
(IVC)
N Ð Position of navel
Carbon dioxide is eliminated by the lungs into the air through breathing. The
lungs also give off a considerable quantity of water as moisture in the breath.
The lungs thus serve the dual purpose of taking up oxygen from the air into
the blood, and of eliminating carbon dioxide from the blood to the air. This is
the essential purpose of respiration or breathing.
Water, along with a small quantity of other waste substances, is eliminated by
the skin in the form of sweat. The kidneys withdraw from one to one-and-a-
half litres of water daily from the blood which contains dissolved mineral salts
and several other important forms of waste matter (the most important being
urea). These form the urine. The urine passes down from the kidneys to the
bladder, from where it is expelled (fig 2.14).
Other waste matter is eliminated by the liver in the bile, and this together with
the unabsorbed and undigested portions of the food is expelled from the body
through evacuation of the bowels, as faeces or stools. The faeces also contain
countless numbers of germs or bacteria, as well as a variety of viruses and yeast.
2.8 Circulation of the blood
2.8.1 Introduction
The blood is the fluid bringing nourishment to all the living structures or
tissues of the body, and carrying away the waste matter formed there.
Blood is composed of numerous and extremely small separate particles of
living matter called blood cells, suspended in a fluid called plasma. The
majority of the blood cells are called red cells because of their reddish colour,
and they carry the oxygen absorbed from the air into the lungs through
breathing to the tissues. The other blood cells are called white cells because
they contain no colouring. They are not oxygen carriers. Their main purpose
is to serve as the scavengers of the blood and as a first line of defence against
germs of infection which may enter the body. Nutrients are dissolved in the
plasma and carried to the tissues. The blood also contains platelets that help
with coagulation.
41
Basic anatomy and physiology
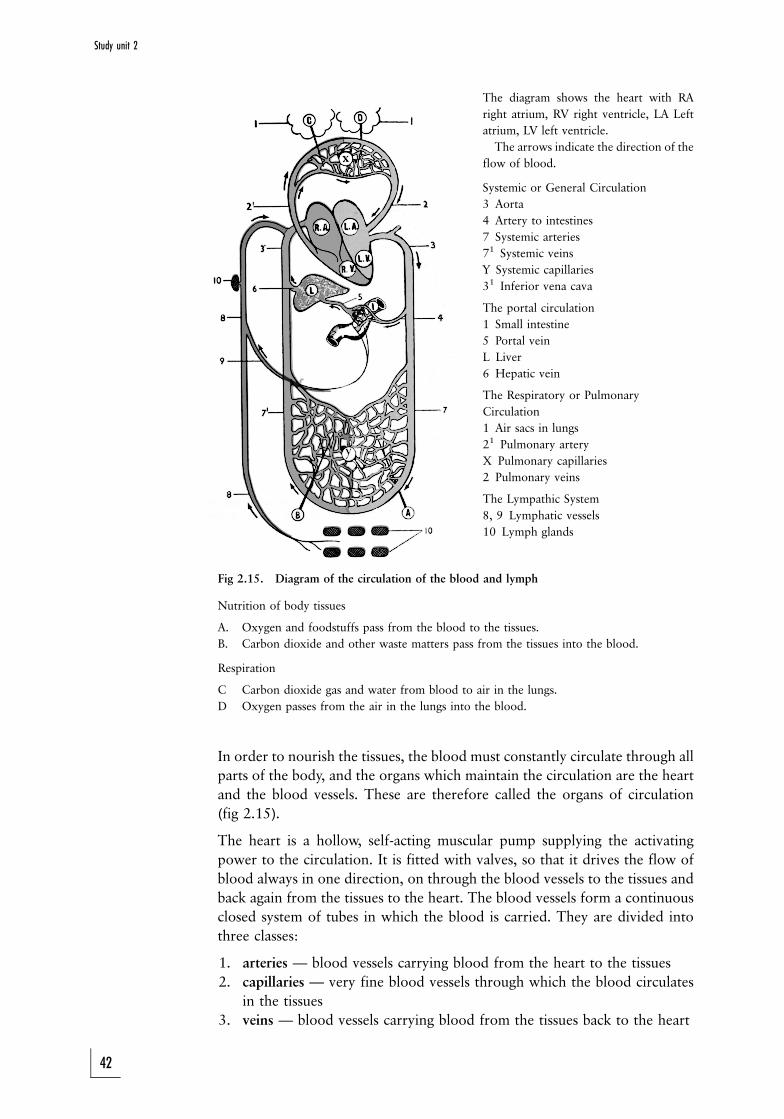
The diagram shows the heart with RA
right atrium, RV right ventricle, LA Left
atrium, LV left ventricle.
The arrows indicate the direction of the
flow of blood.
Systemic or General Circulation
3 Aorta
4 Artery to intestines
7 Systemic arteries
71 Systemic veins
Y Systemic capillaries
31 Inferior vena cava
The portal circulation
1 Small intestine
5 Portal vein
L Liver
6 Hepatic vein
The Respiratory or Pulmonary
Circulation
1 Air sacs in lungs
21 Pulmonary artery
X Pulmonary capillaries
2 Pulmonary veins
The Lympathic System
8, 9 Lymphatic vessels
10 Lymph glands
Fig 2.15. Diagram of the circulation of the blood and lymph
Nutrition of body tissues
A. Oxygen and foodstuffs pass from the blood to the tissues.
B. Carbon dioxide and other waste matters pass from the tissues into the blood.
Respiration
C Carbon dioxide gas and water from blood to air in the lungs.
D Oxygen passes from the air in the lungs into the blood.
In order to nourish the tissues, the blood must constantly circulate through all
parts of the body, and the organs which maintain the circulation are the heart
and the blood vessels. These are therefore called the organs of circulation
(fig 2.15).
The heart is a hollow, self-acting muscular pump supplying the activating
power to the circulation. It is fitted with valves, so that it drives the flow of
blood always in one direction, on through the blood vessels to the tissues and
back again from the tissues to the heart. The blood vessels form a continuous
closed system of tubes in which the blood is carried. They are divided into
three classes:
1. arteries Ð blood vessels carrying blood from the heart to the tissues
2. capillaries Ð very fine blood vessels through which the blood circulates
in the tissues
3. veins Ð blood vessels carrying blood from the tissues back to the heart
42
Study unit 2
2.8.2 The blood vessels
2.8.2.1 The arteries (fig 2.15, 2.16)
Blood going to all parts of the body from the heart leaves the left side of the
heart through one large vessel, the aorta. The aorta forms an arch above the
heart, and from this arch large branches are given off on either side, supplying
blood to the head and neck (right and left carotid arteries) and to the upper
limbs (right and left subclavian arteries). The aorta then runs downwards
behind the heart alongside the spine, passes through the diaphragm and enters
the abdomen, giving off branches on the way, mainly to the internal organs of
the abdomen, and to the muscles and skin of the trunk.
Just below the level of the navel the aorta divides into two large branches
(iliac arteries), one on either side, each of which goes on ultimately to supply
blood to the corresponding lower limb as the right or left femoral artery.
Each of these larger arteries gives off smaller branches, and these again
smaller and smaller branches, until finally in the tissues themselves the
smallest arteries break up into a network of very fine and short tubes which
are called the capillaries and which are so small that they can only be seen
through a microscope (fig 2.17).
Figure 2.16. The systemic and pulmonary circulations
Blue = Venous blood Red = Arterial bloodA. Heart D. LungsB. Main artery E. MuscleC. Main veins F. Stomach
2.8.2.2 Capillaries (fig 2,15, 2.17)
It is when blood is passing through the capillaries that the essential work of
the blood, namely the nourishment of the tissues is done. The walls of the
capillaries are extremely thin and a certain amount of the fluid portion of the
blood, containing the nutrients, passes through the thin walls of these very
fine tubes and so reaches the tissues. Oxygen also passes from the blood
through the walls of the capillaries in a similar way. In this way the tissues are
kept supplied both with food and oxygen. Conversely, much of the waste
matter formed by the activity of the tissues, such as carbon-dioxide gas, passes
from the tissues through the walls of the capillaries into the bloodstream and
is thus carried away.
43
Basic anatomy and physiology
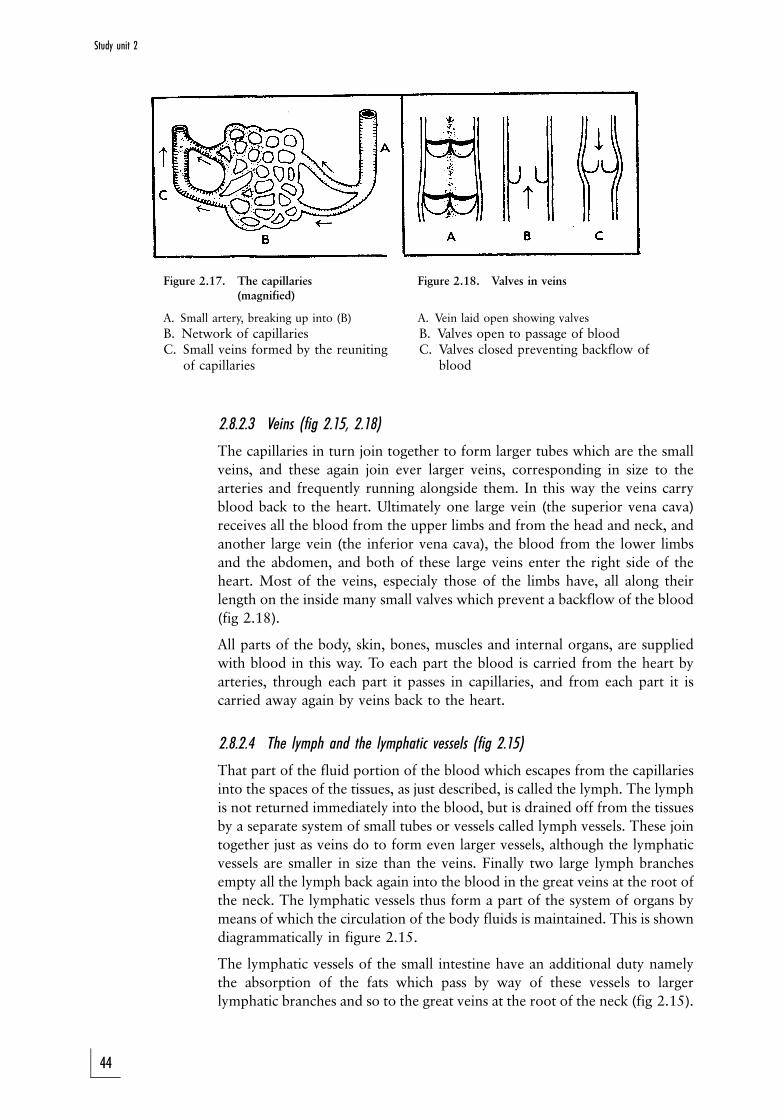
Figure 2.17. The capillaries Figure 2.18. Valves in veins(magnified)
A. Small artery, breaking up into (B) A. Vein laid open showing valves
B. Network of capillaries B. Valves open to passage of bloodC. Small veins formed by the reuniting C. Valves closed preventing backflow of
of capillaries blood
2.8.2.3 Veins (fig 2.15, 2.18)
The capillaries in turn join together to form larger tubes which are the small
veins, and these again join ever larger veins, corresponding in size to the
arteries and frequently running alongside them. In this way the veins carry
blood back to the heart. Ultimately one large vein (the superior vena cava)
receives all the blood from the upper limbs and from the head and neck, and
another large vein (the inferior vena cava), the blood from the lower limbs
and the abdomen, and both of these large veins enter the right side of the
heart. Most of the veins, especialy those of the limbs have, all along their
length on the inside many small valves which prevent a backflow of the blood
(fig 2.18).
All parts of the body, skin, bones, muscles and internal organs, are supplied
with blood in this way. To each part the blood is carried from the heart by
arteries, through each part it passes in capillaries, and from each part it is
carried away again by veins back to the heart.
2.8.2.4 The lymph and the lymphatic vessels (fig 2.15)
That part of the fluid portion of the blood which escapes from the capillaries
into the spaces of the tissues, as just described, is called the lymph. The lymph
is not returned immediately into the blood, but is drained off from the tissues
by a separate system of small tubes or vessels called lymph vessels. These join
together just as veins do to form even larger vessels, although the lymphatic
vessels are smaller in size than the veins. Finally two large lymph branches
empty all the lymph back again into the blood in the great veins at the root of
the neck. The lymphatic vessels thus form a part of the system of organs by
means of which the circulation of the body fluids is maintained. This is shown
diagrammatically in figure 2.15.
The lymphatic vessels of the small intestine have an additional duty namely
the absorption of the fats which pass by way of these vessels to larger
lymphatic branches and so to the great veins at the root of the neck (fig 2.15).
44
Study unit 2
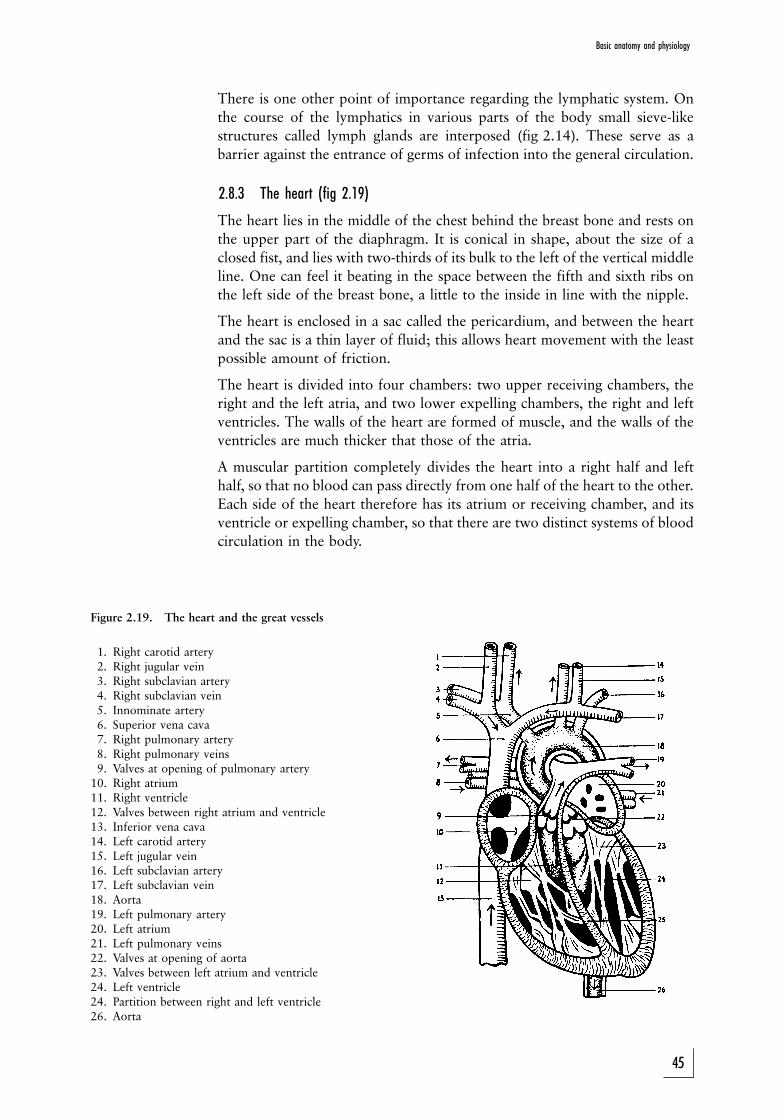
There is one other point of importance regarding the lymphatic system. On
the course of the lymphatics in various parts of the body small sieve-like
structures called lymph glands are interposed (fig 2.14). These serve as a
barrier against the entrance of germs of infection into the general circulation.
2.8.3 The heart (fig 2.19)
The heart lies in the middle of the chest behind the breast bone and rests on
the upper part of the diaphragm. It is conical in shape, about the size of a
closed fist, and lies with two-thirds of its bulk to the left of the vertical middle
line. One can feel it beating in the space between the fifth and sixth ribs on
the left side of the breast bone, a little to the inside in line with the nipple.
The heart is enclosed in a sac called the pericardium, and between the heart
and the sac is a thin layer of fluid; this allows heart movement with the least
possible amount of friction.
The heart is divided into four chambers: two upper receiving chambers, the
right and the left atria, and two lower expelling chambers, the right and left
ventricles. The walls of the heart are formed of muscle, and the walls of the
ventricles are much thicker that those of the atria.
A muscular partition completely divides the heart into a right half and left
half, so that no blood can pass directly from one half of the heart to the other.
Each side of the heart therefore has its atrium or receiving chamber, and its
ventricle or expelling chamber, so that there are two distinct systems of blood
circulation in the body.
Figure 2.19. The heart and the great vessels
1. Right carotid artery2. Right jugular vein3. Right subclavian artery4. Right subclavian vein5. Innominate artery6. Superior vena cava7. Right pulmonary artery8. Right pulmonary veins9. Valves at opening of pulmonary artery
10. Right atrium11. Right ventricle12. Valves between right atrium and ventricle13. Inferior vena cava14. Left carotid artery15. Left jugular vein16. Left subclavian artery17. Left subclavian vein18. Aorta19. Left pulmonary artery20. Left atrium21. Left pulmonary veins22. Valves at opening of aorta23. Valves between left atrium and ventricle24. Left ventricle24. Partition between right and left ventricle26. Aorta
45
Basic anatomy and physiology
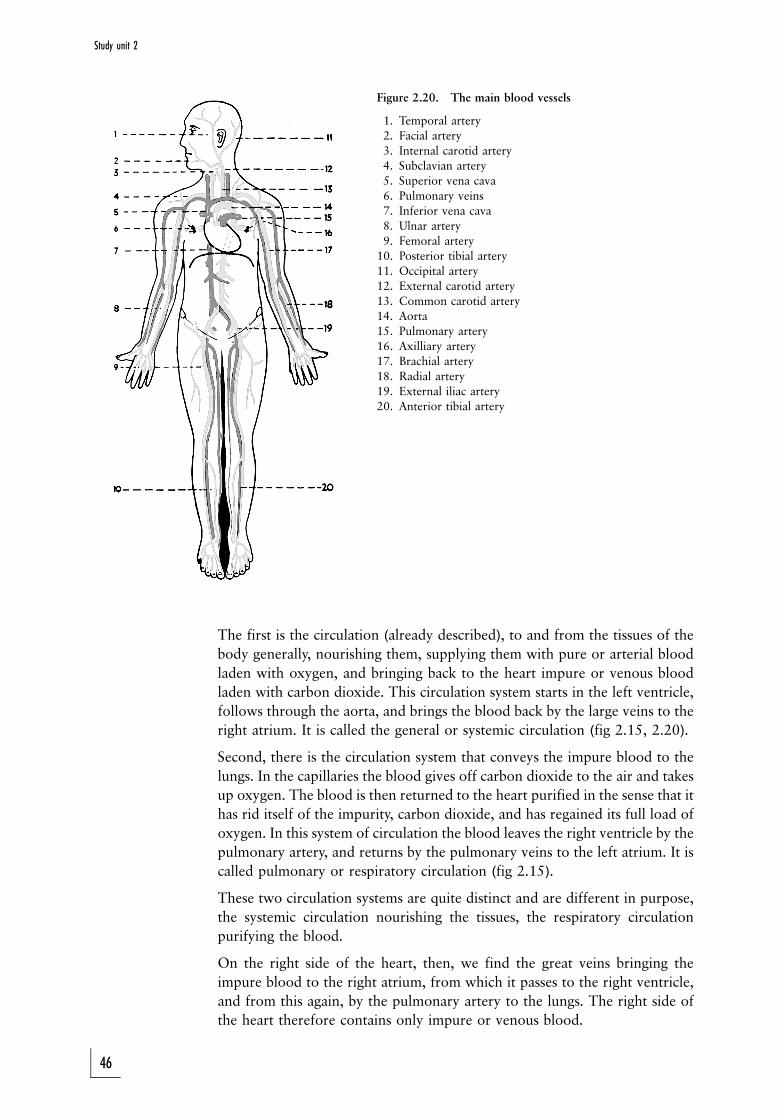
Figure 2.20. The main blood vessels
1. Temporal artery
2. Facial artery
3. Internal carotid artery
4. Subclavian artery
5. Superior vena cava
6. Pulmonary veins
7. Inferior vena cava
8. Ulnar artery
9. Femoral artery
10. Posterior tibial artery
11. Occipital artery
12. External carotid artery
13. Common carotid artery
14. Aorta
15. Pulmonary artery
16. Axilliary artery
17. Brachial artery
18. Radial artery
19. External iliac artery
20. Anterior tibial artery
The first is the circulation (already described), to and from the tissues of the
body generally, nourishing them, supplying them with pure or arterial blood
laden with oxygen, and bringing back to the heart impure or venous blood
laden with carbon dioxide. This circulation system starts in the left ventricle,
follows through the aorta, and brings the blood back by the large veins to the
right atrium. It is called the general or systemic circulation (fig 2.15, 2.20).
Second, there is the circulation system that conveys the impure blood to the
lungs. In the capillaries the blood gives off carbon dioxide to the air and takes
up oxygen. The blood is then returned to the heart purified in the sense that it
has rid itself of the impurity, carbon dioxide, and has regained its full load of
oxygen. In this system of circulation the blood leaves the right ventricle by the
pulmonary artery, and returns by the pulmonary veins to the left atrium. It is
called pulmonary or respiratory circulation (fig 2.15).
These two circulation systems are quite distinct and are different in purpose,
the systemic circulation nourishing the tissues, the respiratory circulation
purifying the blood.
On the right side of the heart, then, we find the great veins bringing the
impure blood to the right atrium, from which it passes to the right ventricle,
and from this again, by the pulmonary artery to the lungs. The right side of
the heart therefore contains only impure or venous blood.
46
Study unit 2

On the left side of the heart we find the pulmonary veins bringing pure or
arterial blood from the lungs to the left atrium and from there to the left
ventricle, from which it passes to the arteries of the body generally. The left
side of the heart therefore contains only pure or arterial blood.
If we follow the course of a drop of blood in the right atrium it must pass to
the right ventricle and through the pulmonary circulation to the left atrium,
then to the left ventricle and through some part of the systemic circulation,
before it can come back to the right atrium again.
In summary, all the blood from the lungs passes to the left atrium and all the
blood from the rest of the body passes to the right atrium.
2.8.4 The portal circulation (fig 2.15)
There is one portion of the systemic circulation which differs in an important
respect from the general circulation pattern, namely bloodflow in the veins
from the stomach and intestines.
The blood to the stomach and intestines is supplied by arteries derived from
the aorta. The arteries break up in the ordinary way into capillaries in the
walls of these organs and the capillaries reunite again into veins. Ultimately all
the veins coming from the stomach and intestines unite to form a single large
vein called the portal vein (fig 2.15).
So far this is in accordance with the general circulation pattern. But the portal
vein is peculiar in that instead of joining the inferior vena cava as might be
expected, it enters the liver, where it branches off just as an artery does, into
smaller branches and these again branch off into a second set of capillaries in
which the blood circulates through the liver. Only after the blood has passed
through the liver these capillaries reunite into several large veins (hepatic
veins, fig 2.15(6)) which enter the inferior vena cava. This special
arrangement is named the portal circulation. Its object is to enable nutrients
(excluding fats) absorbed from the stomach and intestines to pass through the
liver and be processed there, before they enter the general circulation.
2.8.5 Valves of the heart (fig 2.19)
To control the bloodflow and keep it constantly moving in one direction, the
heart contains valves. Each half of the heart has two sets of valves:
1. One set lies between the atrium and the ventricle, preventing the blood
from being forced back into the atrium when the ventricle contracts, thus
forcing the blood to enter the aorta or the pulmonary artery respectively.
2. The second set lies at the openings of the aorta and the pulmonary artery,
preventing the blood from passing back into the ventricles when the
ventricles relax.
When the heart beats both atria contract sumultaneously and fill the
ventricles. Immediately afterwards the ventricles contract simultaneously,
forcing the blood into the pulmonary artery and the aorta. Then the ventricles
relax and immediately the valves at the openings of these vessels close, so that
the blood is kept inside. It is the contraction of the ventricles which is felt as
the heartbeat.
47
Basic anatomy and physiology

2.8.6 The pulse
At each heartbeat a quantity of blood is shot into the aorta from the left
ventricle. The pressure in the aorta is therefore raised, its elastic walls are
distended, and the shock is transmitted along the aorta and its main branches
and so to the smaller arteries as a wave of increased pressure.
This wave of increased pressure travelling along the arteries is called the
pulse. It can be felt by the finger in any artery which is accessible, rising and
falling at regular intervals. It is usual to feel the pulse with two fingers lightly
placed over the radial artery just above the wrist and near the outer border of
the forearm.
By feeling the pulse we learn the rate, the force, and the regularity of the
heart's action. A rapid pulse means a rapidly beating heart; a weak pulse
indicates a weak heart; a strong slow pulse indicates a forcible slow
contraction of the heart. The pulse beats in adults from 60 to 80 times a
minute; it is faster in children.
Each beat of the ventricle ejects about 60 m: of blood into the circulation. At
an average heart rate of 72 beats per minute, this equals 4 320 m: or 4,320 :of blood per minute or nearly 260 : per hour, 6 240 : (almost 1 400 gallons)
every 24 hours. This illustrates dramatically the work done by the heart.
The pulse is only felt in the arteries. It does not pass through the capillaries
because the pulse wave is blocked by the resistance of the walls of a vast
network of very fine tubes which form the capillaries. This resistance is
sufficient to keep the blood in the arteries always under a certain amount of
pressure.
2.8.7 Bleeding from arteries and veins
In the arteries the blood is under comparatively high pressure, and if an artery
is cut or torn, the blood spurts out in a stream which comes in jets, each jet
corresponding to a pulse wave. Because of this high pressure bleeding from an
artery is more copious, and therefore more dangerous than bleeding from a
vein, and it is more difficult to stem such bleeding. The amount of blood lost
depends of course on the size of the artery damaged; a man can bleed to death
in a short time from a wound to one of the main arteries.
In the capillaries the blood is under steady and much lower pressure.
Consequently it flows through the tissues in a steady stream. Bleeding from
the capillaries is of no great consequence. Blood usually oozes slowly from the
skin after an abrasion, and can easily be stemmed by pressure.
In the veins the pressure is even lower; in fact, it can even be negative in the
large veins of the neck, owing to the suction caused by the act of breathing.
Therefore there is the danger of air being sucked into the veins during the act
of breathing when someone has a neck wound. When a vein is damaged the
blood flows out in a steady stream without jetting, and under comparatively
low pressure. Unless the vein is a large one, venous bleeding is readily
stemmed by pressure applied to the wound. However, a great deal of blood
can be quickly lost from a wound in a large vein.
48
Study unit 2
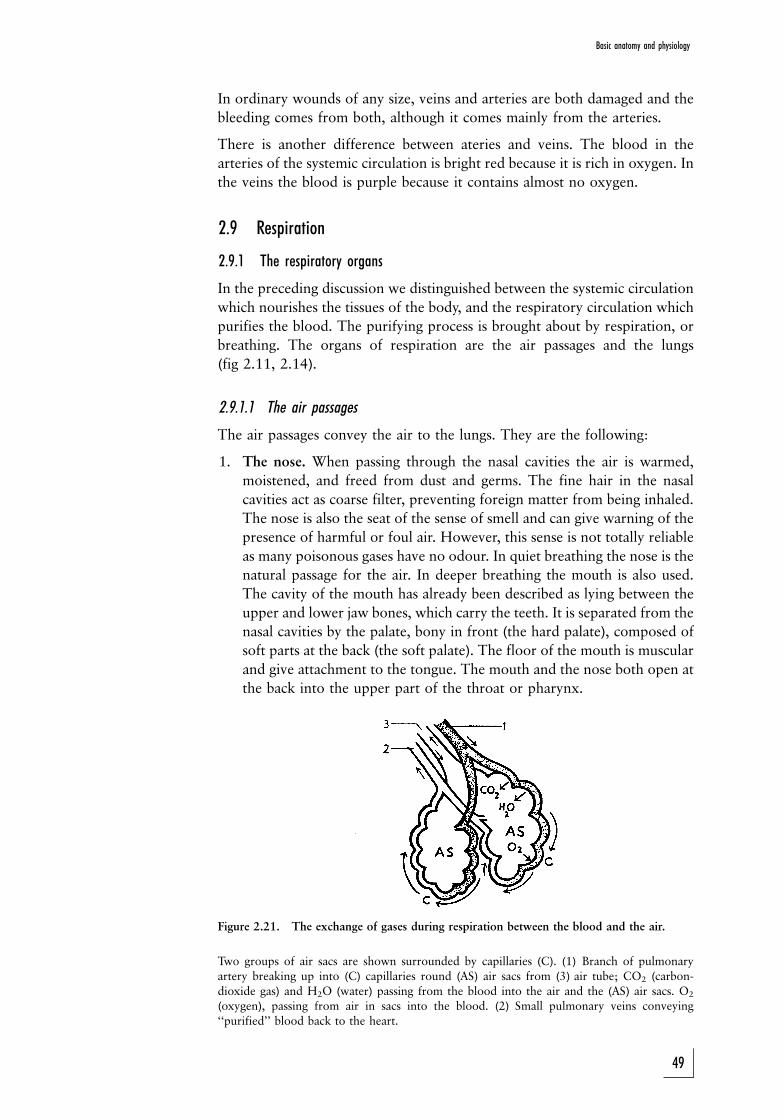
In ordinary wounds of any size, veins and arteries are both damaged and the
bleeding comes from both, although it comes mainly from the arteries.
There is another difference between ateries and veins. The blood in the
arteries of the systemic circulation is bright red because it is rich in oxygen. In
the veins the blood is purple because it contains almost no oxygen.
2.9 Respiration
2.9.1 The respiratory organs
In the preceding discussion we distinguished between the systemic circulation
which nourishes the tissues of the body, and the respiratory circulation which
purifies the blood. The purifying process is brought about by respiration, or
breathing. The organs of respiration are the air passages and the lungs
(fig 2.11, 2.14).
2.9.1.1 The air passages
The air passages convey the air to the lungs. They are the following:
1. The nose. When passing through the nasal cavities the air is warmed,
moistened, and freed from dust and germs. The fine hair in the nasal
cavities act as coarse filter, preventing foreign matter from being inhaled.
The nose is also the seat of the sense of smell and can give warning of the
presence of harmful or foul air. However, this sense is not totally reliable
as many poisonous gases have no odour. In quiet breathing the nose is the
natural passage for the air. In deeper breathing the mouth is also used.
The cavity of the mouth has already been described as lying between the
upper and lower jaw bones, which carry the teeth. It is separated from the
nasal cavities by the palate, bony in front (the hard palate), composed of
soft parts at the back (the soft palate). The floor of the mouth is muscular
and give attachment to the tongue. The mouth and the nose both open at
the back into the upper part of the throat or pharynx.
Figure 2.21. The exchange of gases during respiration between the blood and the air.
Two groups of air sacs are shown surrounded by capillaries (C). (1) Branch of pulmonaryartery breaking up into (C) capillaries round (AS) air sacs from (3) air tube; CO2 (carbon-dioxide gas) and H2O (water) passing from the blood into the air and the (AS) air sacs. O2
(oxygen), passing from air in sacs into the blood. (2) Small pulmonary veins conveying``purified'' blood back to the heart.
49
Basic anatomy and physiology
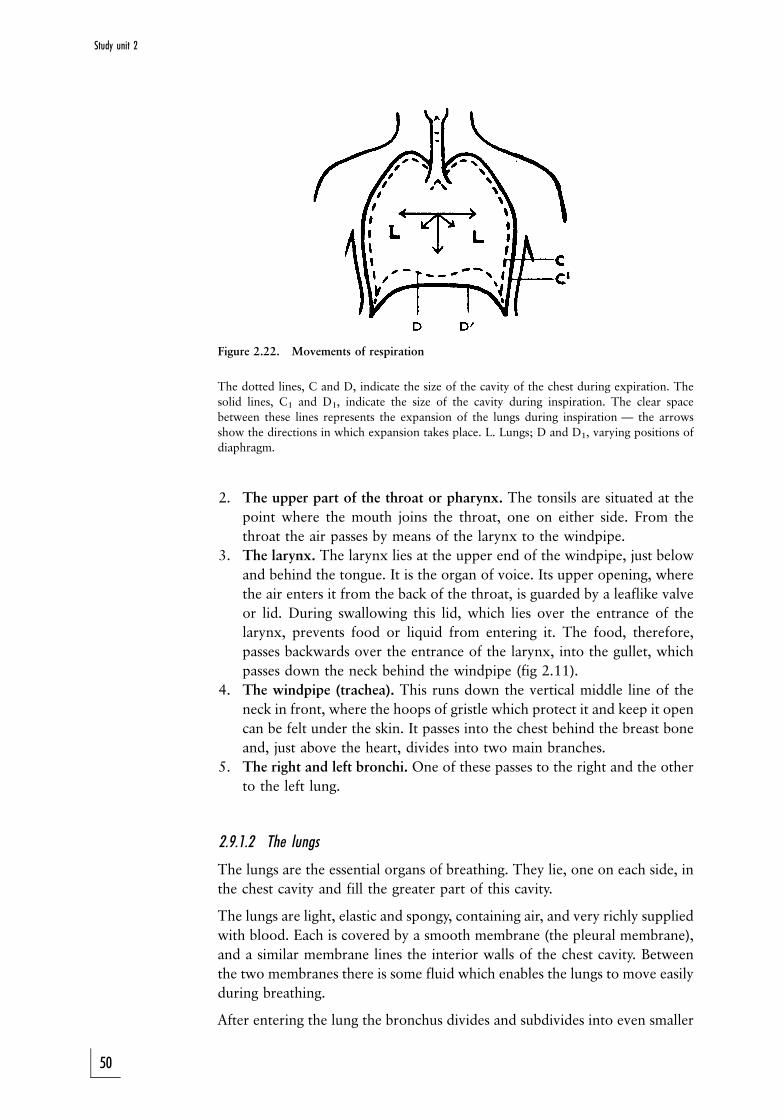
Figure 2.22. Movements of respiration
The dotted lines, C and D, indicate the size of the cavity of the chest during expiration. The
solid lines, C1 and D1, indicate the size of the cavity during inspiration. The clear space
between these lines represents the expansion of the lungs during inspiration Ð the arrows
show the directions in which expansion takes place. L. Lungs; D and D1, varying positions of
diaphragm.
2. The upper part of the throat or pharynx. The tonsils are situated at the
point where the mouth joins the throat, one on either side. From the
throat the air passes by means of the larynx to the windpipe.
3. The larynx. The larynx lies at the upper end of the windpipe, just below
and behind the tongue. It is the organ of voice. Its upper opening, where
the air enters it from the back of the throat, is guarded by a leaflike valve
or lid. During swallowing this lid, which lies over the entrance of the
larynx, prevents food or liquid from entering it. The food, therefore,
passes backwards over the entrance of the larynx, into the gullet, which
passes down the neck behind the windpipe (fig 2.11).
4. The windpipe (trachea). This runs down the vertical middle line of the
neck in front, where the hoops of gristle which protect it and keep it open
can be felt under the skin. It passes into the chest behind the breast bone
and, just above the heart, divides into two main branches.
5. The right and left bronchi. One of these passes to the right and the other
to the left lung.
2.9.1.2 The lungs
The lungs are the essential organs of breathing. They lie, one on each side, in
the chest cavity and fill the greater part of this cavity.
The lungs are light, elastic and spongy, containing air, and very richly supplied
with blood. Each is covered by a smooth membrane (the pleural membrane),
and a similar membrane lines the interior walls of the chest cavity. Between
the two membranes there is some fluid which enables the lungs to move easily
during breathing.
After entering the lung the bronchus divides and subdivides into even smaller
50
Study unit 2

branches or air tubes. The very finest of these tubes end by opening into a tiny
space surrounded by a cluster of air sacs that open into the space into which
the air is led in this way (fig 2.21).
Surrounding each air sac is a close network of blood capillaries with blood
coming from the heart through the pulmonary artery. The air sacs have very
thin walls, and as the blood flows round them, oxygen from the air in the air
sacs passes through their walls, and is taken into the blood in the capillaries.
At the same time carbon dioxide and water pass out of the blood in the
capillaries. In this way, the blood brought to the lungs by the pulmonary
ateries loses carbon dioxide and water, and takes up oxygen. It thus becomes
purified and is then returned to the heart by the pulmonary veins.
The air in the air sacs at the same gives off oxygen and takes up carbon
dioxide and water, thus becoming impure. When we breathe out, we expel a
certain amount of this impure air; when we breathe in, we draw in pure air to
take its place.
Anything that blocks or stops this exchange of gases between the blood and
the air in the lungs immediately endangers life, and soon causes death if it is
not removed.
2.9.2 Respiration movements
Breathing involves two movements, namely inspiration or breathing air in,
and expiration or breathing air out (fig 2.22).
Inspiration happens in two ways: by the action of muscles which act upon the
ribs, thereby raising the walls of the chest so that its capacity is increased both
from front to back and from side to side, and by the action of the diaphragm,
the dome-shaped muscle which separates the chest from the abdomen. The
diaphragm contracts during inspiration, and in doing so descends and flattens.
Thus the capacity of the chest is also increased from above downwards. The
lungs follow the movement of the walls of the chest and diaphragm, and
expand, and thus air is drawn into them. At the same time the capillaries of
the lungs are dilated, so that during inspiration more blood passes through the
lungs.
In ordinary quiet breathing, expiration is only a slight muscular act. When the
effort of inspiration ceases, the walls of the chest fall back again, the
diaphragm relaxes and rises, the elastic lungs contract, and air is thus driven
out of the chest. During exertion, when we exhale as much air as possible,
additional muscular effort is required, as is the case with inhalation under
such circumstances.
ACTIVITIES
This chapter is not for examination purposes, but you should study the blood
circulation in detail, and be able to differentiate between veins and arteries.
51
Basic anatomy and physiology
FEEDBACK
The importance of having a good and practical working knowledge of
the blood circulation, and specifically to be able to differentiate between
the arterial and venous systems, cannot be emphasised enough, as it
plays a central role in most of the study unit in this study guide.
52
STUDY UNIT 3Post-mortem changes
[Study from here for examination purposes]
Contents
3.1 Introduction
3.2 Early post-mortem changes
3.2.1 Post-mortem cooling (algor mortis)
3.2.2 Post-mortem muscle changes
3.2.3 Hypostasis (livores mortis)
3.3 Late post-mortem changes
3.3.1 Decomposition
3.3.2 Mummification
3.3.3 Maceration
3.3.4 Adipocere (wax) formation
3.3.5 Skeletisation
3.4 Relevant topics
3.4.1 Determination of the post-mortem interval
3.4.2 Entomology
3.4.3 Stomach contents
3.4.4 Decomposition/putrefaction in a submerged body
3.4.5 Post mortem: observation and interpretation of artefacts
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. discuss the concept of somatic and cellular death
. discuss the concept of brain death
. discuss the different changes which may occur post mortem
. discuss the different post-mortem artefacts which may occur, and
the different conditions they could resemble
3.1 Introduction
The process of death is a period during which the physiological and metabolic
functions of the body are permanently lost. These changes are due to the fact
that the human body and the tissues which constitute it, are dependent on
aerobic respiration and therefore oxygen. When oxygen does not reach the
body on cellular level any longer, the cells and therefore the tissues and
53
Basic anatomy and physiology
Fig 3.1. Ancient Aztec religion: A human sacrifice to the Sun God. The live sacrificial victim
is spread-eagled by four priests, while a fifth tears out his beating heart as an offering to the
god. In this way the god is propitiated with the best nutriment of the most precious of all
offerings.
Source: Vaillant JC 1972 Aztecs of Mexico New York: Pelican. Printed with acknowledgement to the
author.
organs, stop functioning. A single ``moment of death'' cannot always be
determined, unless regard is had to an event such as was described in respect
of the Aztecs of Mexico in ancient times (see fig 3.1).
Not all tissues or organs cease to function instantly at the moment of death;
muscles, for instance, can still contract for some time after death when
electrically or chemically stimulated (fig 3.2A and B, fig 3.3A and B).
Thus there is a difference between somatic death and cellular death. The
development of cellular death is determined, inter alia, by the dependence of
the type of tissue, and specifically the cell-type, on oxygen, and its capacity to
function at low or nonexistent levels of oxygen (hypoxia and anoxia).
Since organ transplants became general medical practice, it has become
imperative to formulate criteria for determining the diagnosis of brain death.
54
Study unit 3
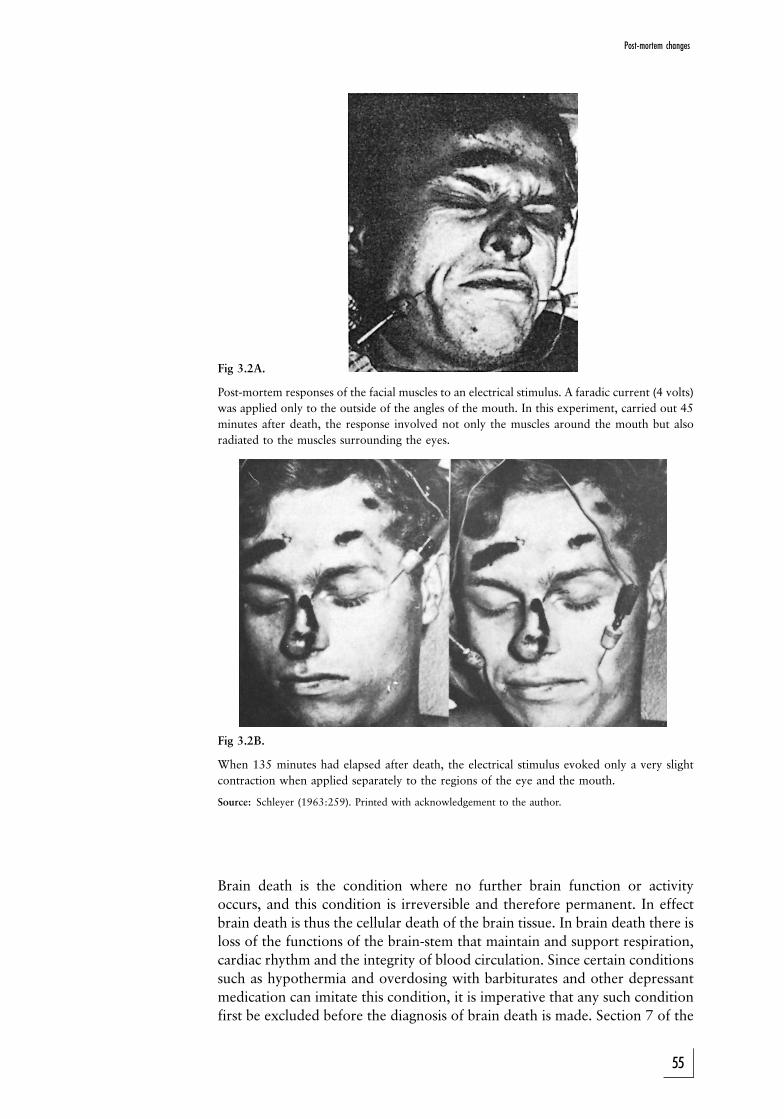
Fig 3.2A.
Post-mortem responses of the facial muscles to an electrical stimulus. A faradic current (4 volts)
was applied only to the outside of the angles of the mouth. In this experiment, carried out 45
minutes after death, the response involved not only the muscles around the mouth but also
radiated to the muscles surrounding the eyes.
Fig 3.2B.
When 135 minutes had elapsed after death, the electrical stimulus evoked only a very slight
contraction when applied separately to the regions of the eye and the mouth.
Source: Schleyer (1963:259). Printed with acknowledgement to the author.
Brain death is the condition where no further brain function or activity
occurs, and this condition is irreversible and therefore permanent. In effect
brain death is thus the cellular death of the brain tissue. In brain death there is
loss of the functions of the brain-stem that maintain and support respiration,
cardiac rhythm and the integrity of blood circulation. Since certain conditions
such as hypothermia and overdosing with barbiturates and other depressant
medication can imitate this condition, it is imperative that any such condition
first be excluded before the diagnosis of brain death is made. Section 7 of the
55
Post-mortem changes
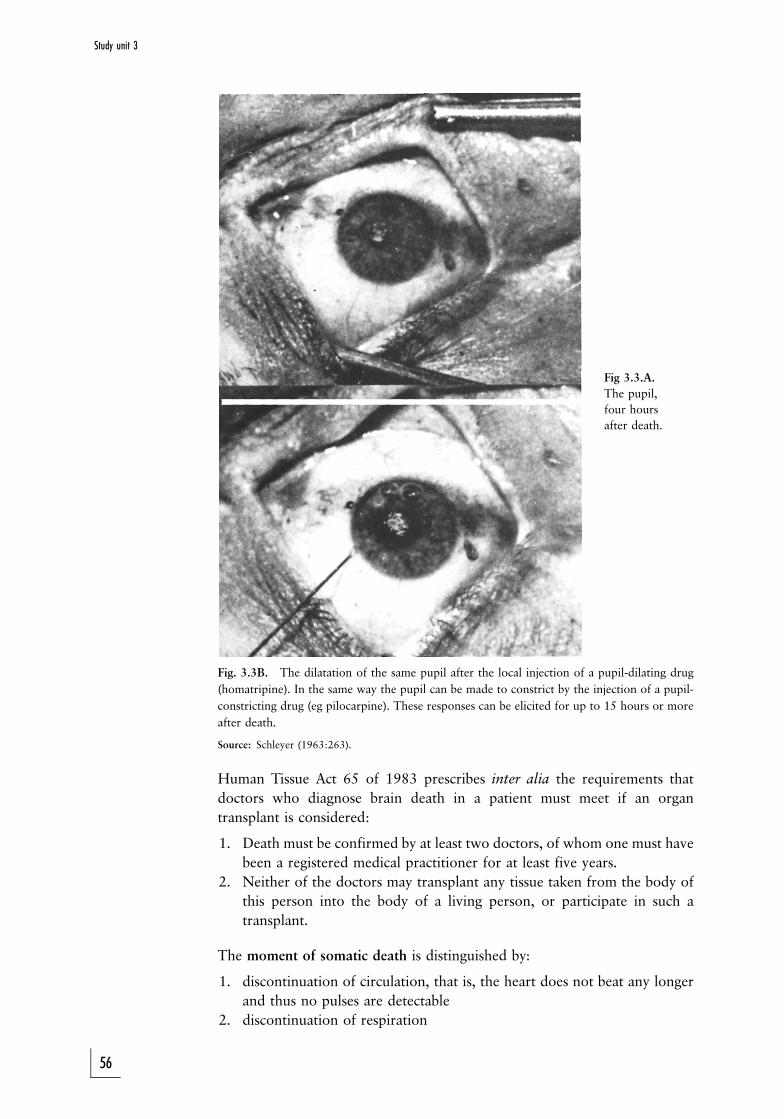
Fig 3.3.A.
The pupil,
four hours
after death.
Fig. 3.3B. The dilatation of the same pupil after the local injection of a pupil-dilating drug
(homatripine). In the same way the pupil can be made to constrict by the injection of a pupil-
constricting drug (eg pilocarpine). These responses can be elicited for up to 15 hours or more
after death.
Source: Schleyer (1963:263).
Human Tissue Act 65 of 1983 prescribes inter alia the requirements that
doctors who diagnose brain death in a patient must meet if an organ
transplant is considered:
1. Death must be confirmed by at least two doctors, of whom one must have
been a registered medical practitioner for at least five years.
2. Neither of the doctors may transplant any tissue taken from the body of
this person into the body of a living person, or participate in such a
transplant.
The moment of somatic death is distinguished by:
1. discontinuation of circulation, that is, the heart does not beat any longer
and thus no pulses are detectable
2. discontinuation of respiration
56
Study unit 3
3. loss of all reflexes
4. body relaxation due to loss of muscular tone (primary muscle flaccidity)
5. changes in the eyes: initially there is congestion of blood in the veins in
the back of the eyeball (fundal veins) and later changes occur because of
drying out of the cornea and conjunctiva
Please note that in the case of an organ donation, the deceased must be
certified as being brain dead. However, to preserve organs like the heart or
kidneys until such time they can be harvested, blood circulation and
respiration are artificially maintained, including by the administation of
drugs to stimulate heart function and prevent cellular death. The moment
these supportive measures are discontinued, the signs and features of somatic
death will present.
The post-mortem changes can be divided according to the changes taking
place in the first few hours or days, and those taking place at a later stage:
Changes taking place early after death are:
1. cooling of the body, so-called algor mortis
2. post-mortem muscle changes, namely stiffening or so-called rigor mortis,
followed by secondary muscle flaccidity
3. post-mortem colour changes, also known as hypostatic changes, lividity
or livores mortis
Changes taking place later are:
1. decomposition, including autolysis and putrefaction
2. mummification
3. adipocere-formation
4. maceration
5. skeletalisation
3.2 Early post-mortem changes
3.2.1 Post-mortem cooling (algor mortis)
Energy, therefore heat, is produced in the body by metabolic processes. The
temperature control mechanism in the brain is responsible for maintaining
normal oral temperature at between 36 and 37,28 C, regardless of fluctuation
in the outside temperature. Rectal temperature is about 0,3 to 0,48 C higher.
Heat is spread through the whole body by the circulation and is then lost
during different processes:
1. radiation or emission
2. conduction from the body to other substances or materials in contact with
it Ð this is not important in the living person, but becomes important
post mortem (eg heat transmitted and lost when a body is lying on a cold
cement floor)
3. convection or the process by which the air in immediate contact with a
warmer body is heated and expands in volume, becomes lighter (less
dense), rises and is replaced by colder and denser air
4. evaporation, mostly by perspiration
57
Post-mortem changes
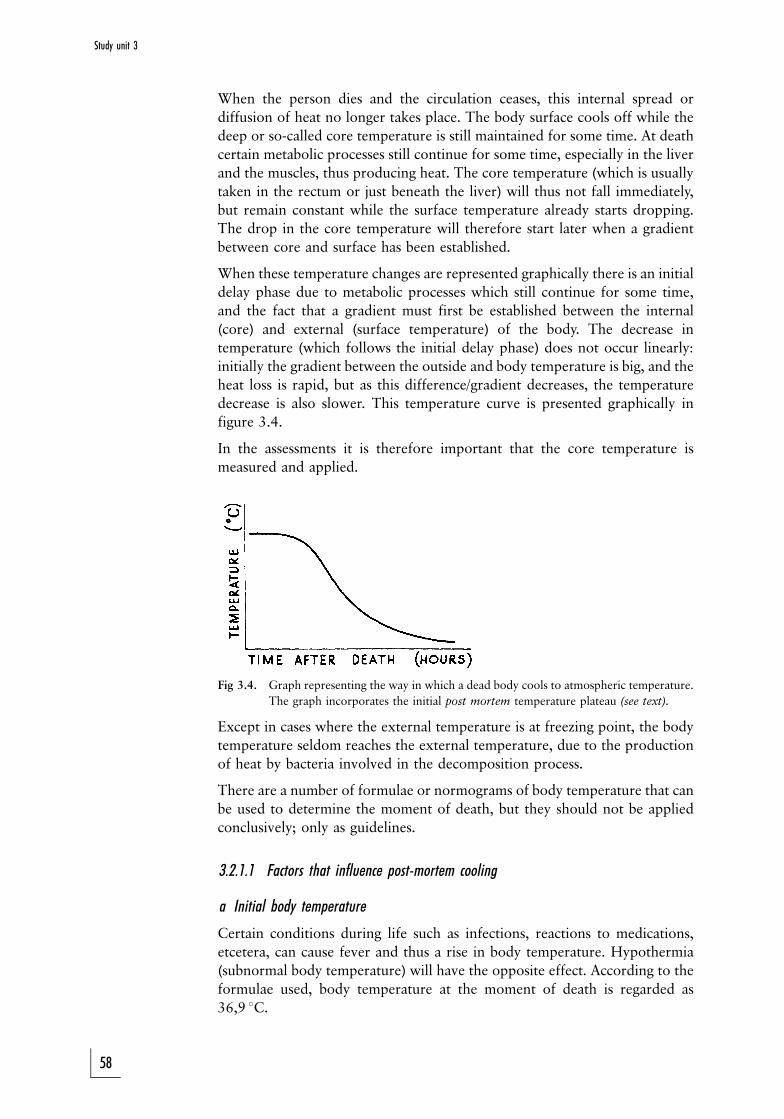
When the person dies and the circulation ceases, this internal spread or
diffusion of heat no longer takes place. The body surface cools off while the
deep or so-called core temperature is still maintained for some time. At death
certain metabolic processes still continue for some time, especially in the liver
and the muscles, thus producing heat. The core temperature (which is usually
taken in the rectum or just beneath the liver) will thus not fall immediately,
but remain constant while the surface temperature already starts dropping.
The drop in the core temperature will therefore start later when a gradient
between core and surface has been established.
When these temperature changes are represented graphically there is an initial
delay phase due to metabolic processes which still continue for some time,
and the fact that a gradient must first be established between the internal
(core) and external (surface temperature) of the body. The decrease in
temperature (which follows the initial delay phase) does not occur linearly:
initially the gradient between the outside and body temperature is big, and the
heat loss is rapid, but as this difference/gradient decreases, the temperature
decrease is also slower. This temperature curve is presented graphically in
figure 3.4.
In the assessments it is therefore important that the core temperature is
measured and applied.
Fig 3.4. Graph representing the way in which a dead body cools to atmospheric temperature.
The graph incorporates the initial post mortem temperature plateau (see text).
Except in cases where the external temperature is at freezing point, the body
temperature seldom reaches the external temperature, due to the production
of heat by bacteria involved in the decomposition process.
There are a number of formulae or normograms of body temperature that can
be used to determine the moment of death, but they should not be applied
conclusively; only as guidelines.
3.2.1.1 Factors that influence post-mortem cooling
a Initial body temperature
Certain conditions during life such as infections, reactions to medications,
etcetera, can cause fever and thus a rise in body temperature. Hypothermia
(subnormal body temperature) will have the opposite effect. According to the
formulae used, body temperature at the moment of death is regarded as
36,9 8C.
58
Study unit 3
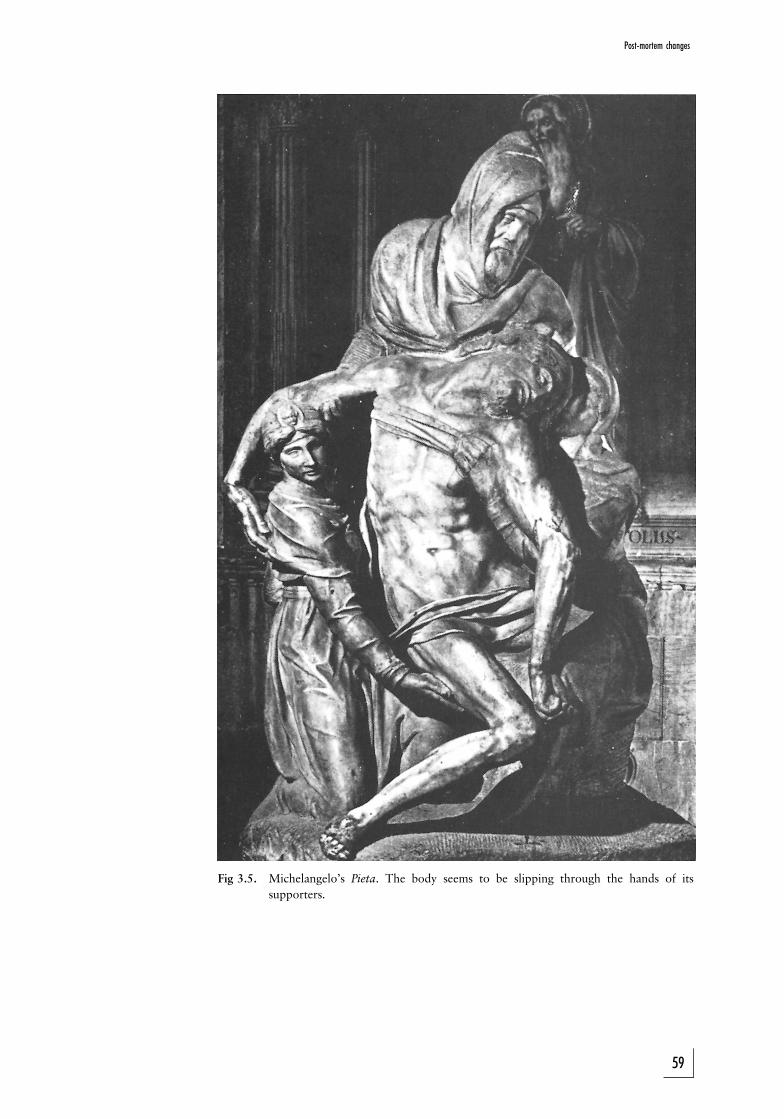
Fig 3.5. Michelangelo's Pieta. The body seems to be slipping through the hands of its
supporters.
59
Post-mortem changes
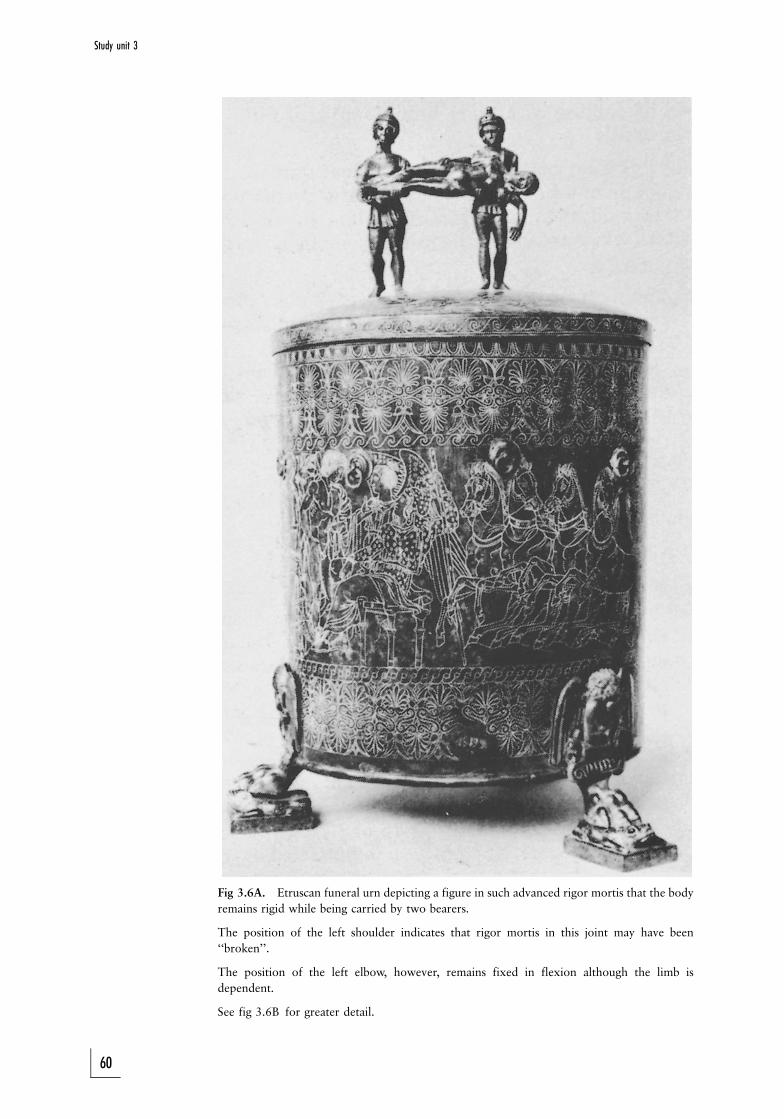
Fig 3.6A. Etruscan funeral urn depicting a figure in such advanced rigor mortis that the body
remains rigid while being carried by two bearers.
The position of the left shoulder indicates that rigor mortis in this joint may have been
``broken''.
The position of the left elbow, however, remains fixed in flexion although the limb is
dependent.
See fig 3.6B for greater detail.
60
Study unit 3
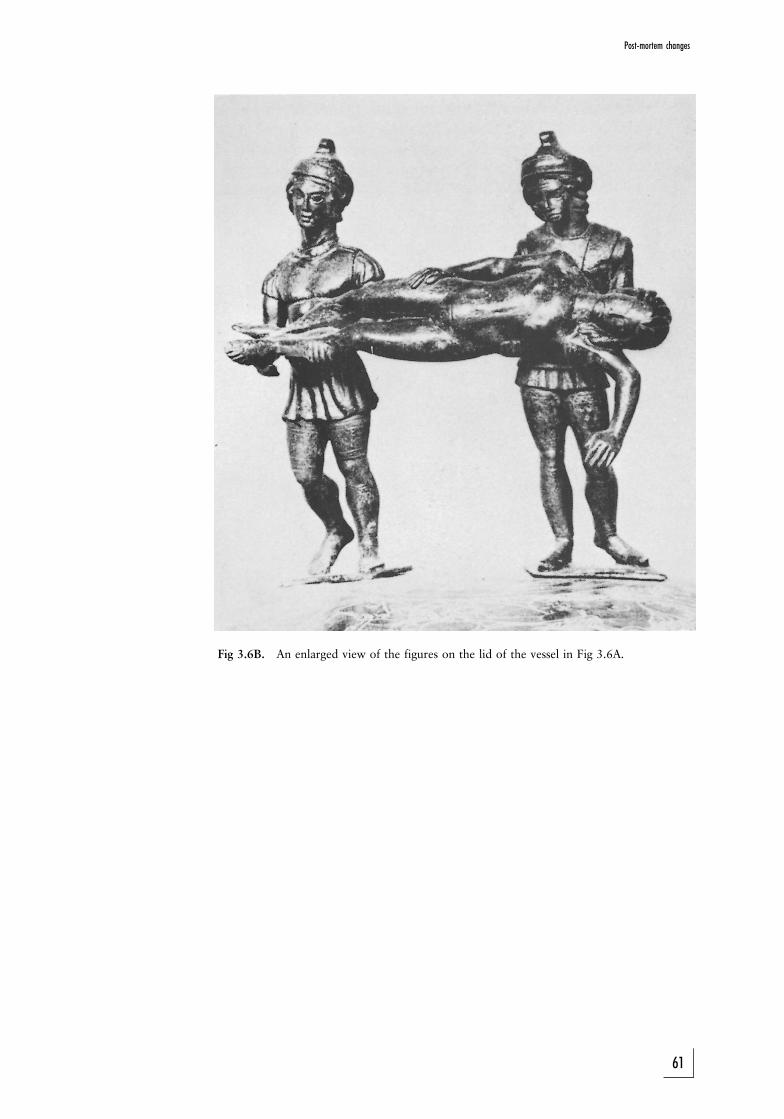
Fig 3.6B. An enlarged view of the figures on the lid of the vessel in Fig 3.6A.
61
Post-mortem changes
b External temperature
The external temperature determines the gradient and therefore the rate of
cooling. If the external temperature is higher than 37 8C, obviously no
cooling will take place.
c Physical characteristics
Fat provides good insulation against heat loss. An obese person therefore loses
heat more slowly than a lean person. Babies also have a large body surface
relative to their weight, and cool off more rapidly. Especially the surface of a
baby's head is disproportionately large compared to the rest of the body.
Oedema and dehydration also have an effect; heat loss is more rapid in a
dehydrated person.
d Body posture
Any position which minimises the area of the body surface exposed to air or a
cold surface will slow down the cooling process. A body curled up in the
foetal position will therefore cool off more slowly than a stretched-out body,
all the other factors being the same.
e Air movement and humidity
Air in motion can precipitate cooling, as it accelerates convection and
conduction. This is also called the wind factor. Humid air promotes heat loss.
f Clothing and other coverings
Clothes slow down heat loss by conduction and convection. Wet clothes
speed up heat loss.
g Medium in which body lies
A body lying in water loses body heat more rapidly than one outside due to
greater heat loss as a result of increased convection and conduction in water
as opposed to air. The type of water (fresh water or sea water) plays no role;
only the temperature of the water. Sewage water may have a higher
temperature due to heat produced by micro-organisms (see also section on
decomposition).
3.2.2 Post-mortem muscle changes
The muscles of the body go through three phases after death.
1. Primary muscle flaccidity occurs immediately at death, as a result of loss
of muscle tone. The body becomes limp. An exception, the so-called
cataleptic stiffness (rigor) is discussed elsewhere.
2. Rigor mortis or post-mortem stiffness then follows (fig 36A and B as well
as photo 1).
3. Secondary muscle flaccidity commences at the onset of the putrefaction
process when the muscles start to relax finally and permanently.
62
Study unit 3
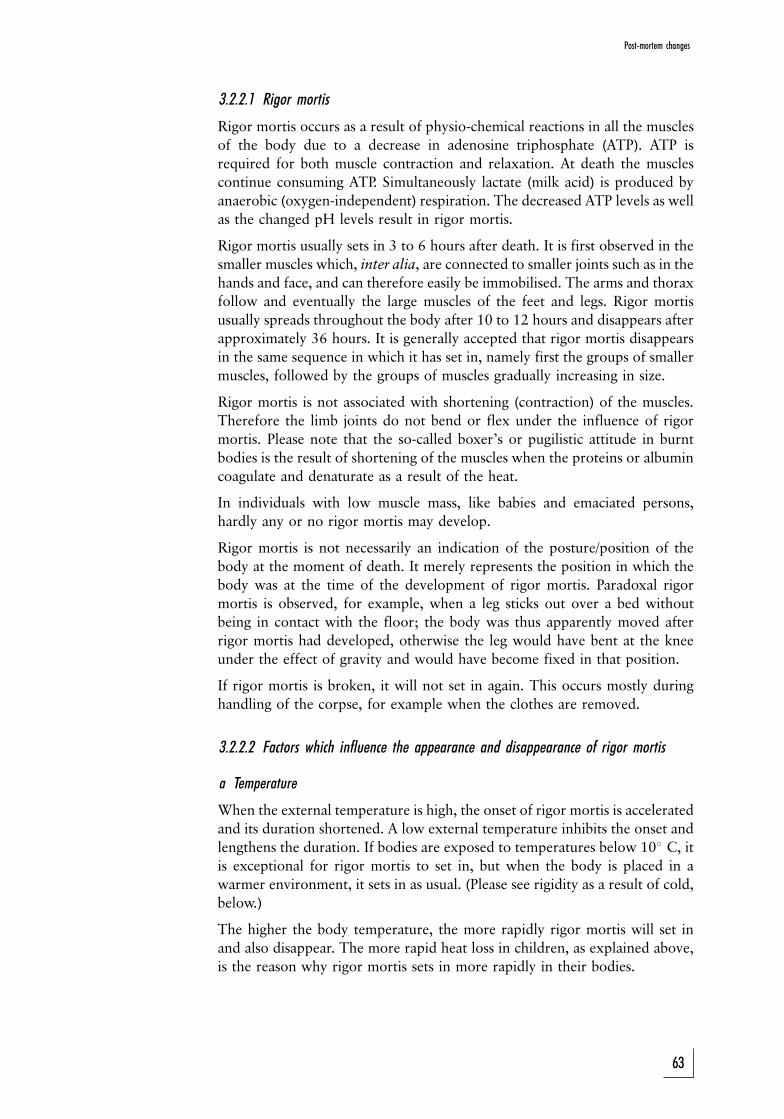
3.2.2.1 Rigor mortis
Rigor mortis occurs as a result of physio-chemical reactions in all the muscles
of the body due to a decrease in adenosine triphosphate (ATP). ATP is
required for both muscle contraction and relaxation. At death the muscles
continue consuming ATP. Simultaneously lactate (milk acid) is produced by
anaerobic (oxygen-independent) respiration. The decreased ATP levels as well
as the changed pH levels result in rigor mortis.
Rigor mortis usually sets in 3 to 6 hours after death. It is first observed in the
smaller muscles which, inter alia, are connected to smaller joints such as in the
hands and face, and can therefore easily be immobilised. The arms and thorax
follow and eventually the large muscles of the feet and legs. Rigor mortis
usually spreads throughout the body after 10 to 12 hours and disappears after
approximately 36 hours. It is generally accepted that rigor mortis disappears
in the same sequence in which it has set in, namely first the groups of smaller
muscles, followed by the groups of muscles gradually increasing in size.
Rigor mortis is not associated with shortening (contraction) of the muscles.
Therefore the limb joints do not bend or flex under the influence of rigor
mortis. Please note that the so-called boxer's or pugilistic attitude in burnt
bodies is the result of shortening of the muscles when the proteins or albumin
coagulate and denaturate as a result of the heat.
In individuals with low muscle mass, like babies and emaciated persons,
hardly any or no rigor mortis may develop.
Rigor mortis is not necessarily an indication of the posture/position of the
body at the moment of death. It merely represents the position in which the
body was at the time of the development of rigor mortis. Paradoxal rigor
mortis is observed, for example, when a leg sticks out over a bed without
being in contact with the floor; the body was thus apparently moved after
rigor mortis had developed, otherwise the leg would have bent at the knee
under the effect of gravity and would have become fixed in that position.
If rigor mortis is broken, it will not set in again. This occurs mostly during
handling of the corpse, for example when the clothes are removed.
3.2.2.2 Factors which influence the appearance and disappearance of rigor mortis
a Temperature
When the external temperature is high, the onset of rigor mortis is accelerated
and its duration shortened. A low external temperature inhibits the onset and
lengthens the duration. If bodies are exposed to temperatures below 108 C, it
is exceptional for rigor mortis to set in, but when the body is placed in a
warmer environment, it sets in as usual. (Please see rigidity as a result of cold,
below.)
The higher the body temperature, the more rapidly rigor mortis will set in
and also disappear. The more rapid heat loss in children, as explained above,
is the reason why rigor mortis sets in more rapidly in their bodies.
63
Post-mortem changes
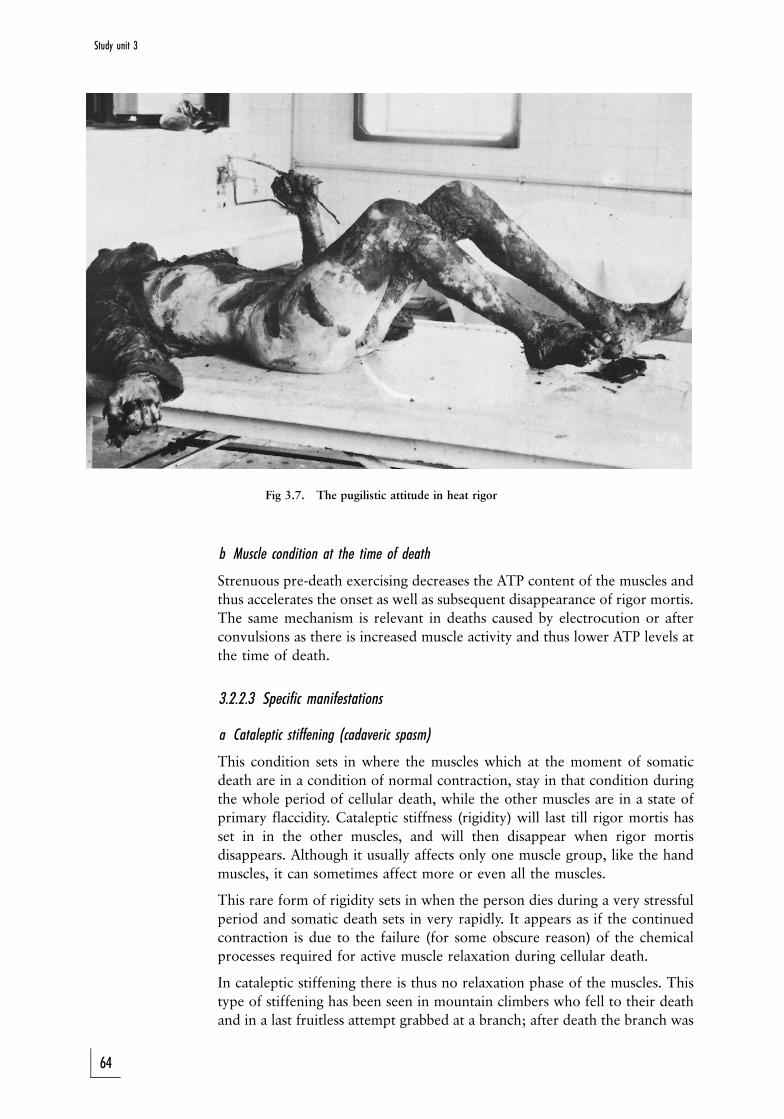
Fig 3.7. The pugilistic attitude in heat rigor
b Muscle condition at the time of death
Strenuous pre-death exercising decreases the ATP content of the muscles and
thus accelerates the onset as well as subsequent disappearance of rigor mortis.
The same mechanism is relevant in deaths caused by electrocution or after
convulsions as there is increased muscle activity and thus lower ATP levels at
the time of death.
3.2.2.3 Specific manifestations
a Cataleptic stiffening (cadaveric spasm)
This condition sets in where the muscles which at the moment of somatic
death are in a condition of normal contraction, stay in that condition during
the whole period of cellular death, while the other muscles are in a state of
primary flaccidity. Cataleptic stiffness (rigidity) will last till rigor mortis has
set in in the other muscles, and will then disappear when rigor mortis
disappears. Although it usually affects only one muscle group, like the hand
muscles, it can sometimes affect more or even all the muscles.
This rare form of rigidity sets in when the person dies during a very stressful
period and somatic death sets in very rapidly. It appears as if the continued
contraction is due to the failure (for some obscure reason) of the chemical
processes required for active muscle relaxation during cellular death.
In cataleptic stiffening there is thus no relaxation phase of the muscles. This
type of stiffening has been seen in mountain climbers who fell to their death
and in a last fruitless attempt grabbed at a branch; after death the branch was
64
Study unit 3

firmly grasped in the hand. The same applies to a small percentage of suicide
cases, where the firearm was grasped in the hand. More extreme cases of
cataleptic rigor have been noted in soldiers dying during a military charge.
Cataleptic spasm can be imitated after death if an object is placed in the hand
in such a way that the onset of rigor mortis will clench it in a grip: The
difference is that in cataleptic spasm only the hand that grips the object has
stiffened; the other muscles are limp.
b Rigidity due to heat
When a body is exposed to heat, the proteins denaturate and coagulate (break
up and solidify) in the muscles, and the muscles shorten. As the flexor muscles
are bigger and stronger than the extensor (stretch) muscles, they dominate the
smaller muscles, and the body takes on the typical posture of a boxer (fig 3.7).
The shortening can be such that the muscles tear, also causing laceration
wounds of the overlying skin and soft tissue.
Rigor mortis does not develop in muscles that stiffened due to heat, but the
latter can set in after rigor mortis.
Heat stiffening and the concomitant body posture is therefore a post-mortem
phenomenon, and not an indication of the body posture or position of the
limbs at the time of death.
c Rigidity due to cold
Cold rigidity sets in when the body is exposed to temperatures under 3,5o C.Babies and young children have a thick subcutaneous layer of fat, and thisrigidity is then often prominent because the fat ``stiffens'' and makes the bodyless flexible. This is also true of fat people where cold rigidity is moreprominent than in slim persons. When the body later heats up, true rigormortis can set in, although the ice crystals often damage the muscle cells andmay prevent rigor mortis.
3.2.3 Hypostasis (livores mortis)
There are several synonyms for this condition, namely lividity, death spotsand post-mortem discoloration. About one hour after death the blood in mostbodies becomes permanently fluid because of the release of fibrinolysin fromthe endothelial lining of the blood vessels. The blood cells gravitate to thedependent or lowest parts of the body (fig 3.8A and B). This gravity-dependent movement of blood discolours the skin as well as internal organsto a reddish-blue colour. In a body in the hanging position the hypostasis willtherefore appear in the hands/forearms and feet/lower legs.
The fluid component of blood (plasma) also gravitates to a lesser extent andcauses oedema and later even skin blistering. Sometimes the capillary veinscan also rupture, and then petechial haemorrhages set in, which can convergeand even form blood blisters. The colour of the complexion determines howreadily hypostasis will be visible on the skin.
In a person who was exsanguinated (``bled out'') before death, this conditionis often less obvious because of the fact that very little blood remained in thecirculation.
65
Post-mortem changes
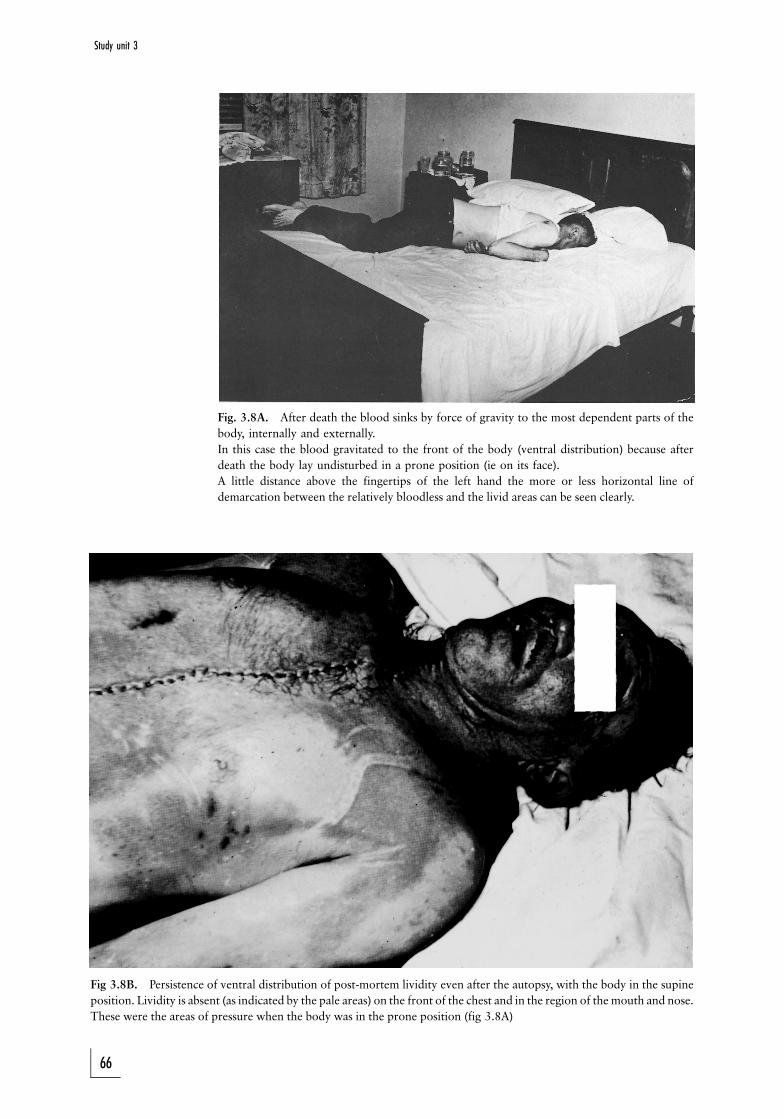
Fig. 3.8A. After death the blood sinks by force of gravity to the most dependent parts of the
body, internally and externally.
In this case the blood gravitated to the front of the body (ventral distribution) because after
death the body lay undisturbed in a prone position (ie on its face).
A little distance above the fingertips of the left hand the more or less horizontal line of
demarcation between the relatively bloodless and the livid areas can be seen clearly.
Fig 3.8B. Persistence of ventral distribution of post-mortem lividity even after the autopsy, with the body in the supine
position. Lividity is absent (as indicated by the pale areas) on the front of the chest and in the region of the mouth and nose.
These were the areas of pressure when the body was in the prone position (fig 3.8A)
66
Study unit 3
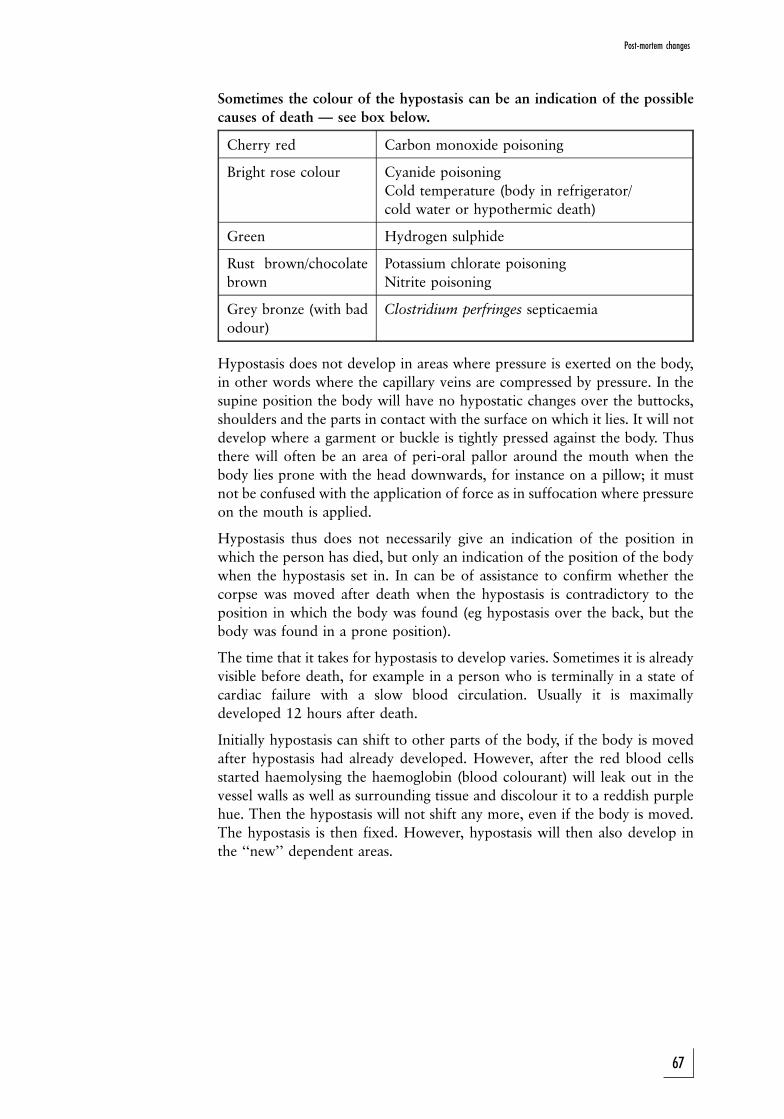
Sometimes the colour of the hypostasis can be an indication of the possible
causes of death Ð see box below.
Cherry red Carbon monoxide poisoning
Bright rose colour Cyanide poisoning
Cold temperature (body in refrigerator/
cold water or hypothermic death)
Green Hydrogen sulphide
Rust brown/chocolate
brown
Potassium chlorate poisoning
Nitrite poisoning
Grey bronze (with bad
odour)
Clostridium perfringes septicaemia
Hypostasis does not develop in areas where pressure is exerted on the body,
in other words where the capillary veins are compressed by pressure. In the
supine position the body will have no hypostatic changes over the buttocks,
shoulders and the parts in contact with the surface on which it lies. It will not
develop where a garment or buckle is tightly pressed against the body. Thus
there will often be an area of peri-oral pallor around the mouth when the
body lies prone with the head downwards, for instance on a pillow; it must
not be confused with the application of force as in suffocation where pressure
on the mouth is applied.
Hypostasis thus does not necessarily give an indication of the position in
which the person has died, but only an indication of the position of the body
when the hypostasis set in. In can be of assistance to confirm whether the
corpse was moved after death when the hypostasis is contradictory to the
position in which the body was found (eg hypostasis over the back, but the
body was found in a prone position).
The time that it takes for hypostasis to develop varies. Sometimes it is already
visible before death, for example in a person who is terminally in a state of
cardiac failure with a slow blood circulation. Usually it is maximally
developed 12 hours after death.
Initially hypostasis can shift to other parts of the body, if the body is moved
after hypostasis had already developed. However, after the red blood cells
started haemolysing the haemoglobin (blood colourant) will leak out in the
vessel walls as well as surrounding tissue and discolour it to a reddish purple
hue. Then the hypostasis will not shift any more, even if the body is moved.
The hypostasis is then fixed. However, hypostasis will then also develop in
the ``new'' dependent areas.
67
Post-mortem changes

Fig 3.9. The distribution of the post-mortem lividity is in keeping with the position in which the body was found.
The livid areas can be seen because the pigmented skin, as a result of post-mortem changes, easily peeled off (so-called
slip-skin), to expose the underlying blood vessels. These are visible as areas of reddish discoloration, because blood has
gravitated into the dependent parts.
3.2.3.1 Conditions that have to be distinguished from hypostasis
a Bruises
The location and shape of a discoloration can distinguish it from hypostasis,
but the indisputable evidence is only to be found when the skin is incised. In
the case of a bruise the blood is extravasated (ie discharged from a vessel) or
diffused into the tissue; in the case of hypostasis it is still limited to the vessels.
Microscopy can be of further assistance if the naked eye cannot detect the
difference.
b Inflammatory changes
Inflammation causes increased blood circulation in the affected tissue and it
can, for example, imitate hypostasis in a lung, where there was in fact
pneumonia, or in the heart, where there was in fact a myocardial infarction.
Microscopy is again necessary to find the final answer.
68
Study unit 3
3.3 Late post-mortem changes
3.3.1 Decomposition
Decomposition is a process originating as result of the breakdown of the body
by enzymes. These enzymes can be from the body itself (the process is then
called autolysis) or from other organisms, (heterolysis). Generally the process
is known as putrefaction.
Although both these processes set in immediately at death, the condition is
only visible at a later stage. The environmental temperature plays an
important role: in a refrigerator the process will be suppressed, while in a
warm environment it will be accelerated. There is therefore a considerable
amount of variation.
Autolysis is especially visible in the pancreas (racemose gland) where the
enzymes leak out of the cells after death and digest the surrounding tissue.
The spleen is often autolytic in cases of sepsis (autolysis means the
spontaneous disintegration of tissues of an organ see Ð above).
The bacteria which play the most important part in putrefaction originate
from the alimentary canal. They include oxygen-dependent (aerobic) and
non-oxygen-dependent (anaerobic) organisms. The latter group is mostly
responsible for the production of gas and the offensive odour of a
decomposing body. In persons who die due to septicaemia there already is
an abundance of organisms in the body at the time of death, which naturally
will accelerate the whole decomposition process.
During putrefaction the whole body discolours to greenish-black, becomes
bloated due to gas production, and the skin strips (slips) off (fig 3.9). The
blood vessels of the skin often show up prominently due to the broken-down
blood (haemolysis) which reacts with the hydrogen sulphide produced by
bacteria. This gives the effect of marbling. The process of liquefaction of the
soft tissue is often promoted by the activity of maggots.
3.3.2 Mummification
Mummification occurs in dry climates, where the body literally dries out like
biltong. This happens in hot as well as cold, dry climates, for example the
Namib desert and also on Mount Everest. It can also occur in cases where the
body is lying in an environment with a high acid content. In the case of the
Tollund man, who was found in the swamps of Jutland, which have a high
acid content, the features were exceptionally well preserved.
In the case of the bodies of newborn babies who are concealed shortly after
birth in a cardboard box, drying out also occurs. This is because newborns are
microbiologically sterile (they have not yet been colonised by micro-
organisms) and putrefaction is very slow.
3.3.3 Maceration
Maceration refers to autolysis (spontaneous disintegration) in a foetus which
dies while inside the mother (intra-uterine death). As the contents of the
uterus is sterile, there is no putrefaction. In maceration the skin softens and
69
Post-mortem changes

large fluid-containing blisters appear, and the skin then strips away. At thesame time the internal organs soften and the bones gradually loosen from thecartilage and tendon attachments.
3.3.4 Adipocere (wax) formation
In this condition water binds with the body fat and forms a wax-like substancewith a rancid odour. Bacterial enzymes contribute to the process. It is alsoknown as saponification or transformation of body fat into soap.
Wax formation usually develops over a period of weeks to months and itsuppresses further decomposition of the body. Should the process manifest inthe face, it can preserve the features to an extent. It can also preserve woundsand other signs of trauma.
3.3.5 Skeletisation
After all soft tissue has been destroyed, whether on account of decompositionor, amongst others, maggot and rodent activity, only the skeleton remains.Cartilage and ligaments can survive for some time. Exposure of the bones tothe elements eventually causes bleaching. Finally only porous brittle bone thatfragments into minute pieces during handling remains.
The skeleton can be useful for a considerable time for identification of thedeceased and determining how long the person has been dead.
3.4 Relevant topics3.4.1 Determination of the post-mortem interval
When a person is found dead, it is sometimes important to determine the time
of death as accurately as possible. Immediately or soon after death it is often
easy, but after putrefaction has set in, it becomes more difficult. This is
because so many factors come into play, such as temperature, movement of
air, clothes, bacterial activity in the body, and the person's physique.
The following table is a simple set of general rules to apply when examining a
corpse in the first few hours after death.
53 h Body warm and flaccid (primary muscle flaccid-
ity)
3±8 h Body warm and stiff (rigor mortis has set in)
8±36 h Body cold and stiff
436 h Body cold and soft (flaccid) (secondary muscle
flaccidity has set in)
3.4.2 Entomology
Insects, such as blue-bottles and flies, frequently attack the body. Various phasesof their life cycles are found on the body, for example eggs, maggots and adult(fully developed) insects (photo 3). Different insects are found in differentgeographic areas. The type of insect and the stage in the life cycle (eggs, maggots,etc) found on a body can assist the forensic entomologist to determine the time a
70
Study unit 3
body has been in an area. Bodies of persons who have died of organophosphateor other pesticide poisoning are often ``resistant'' to insect activity, as the insectsdie when they are exposed to the tissue or body fluids.
3.4.3 Stomach contents
The condition of the stomach contents does not give any indication as to thepost-mortem interval, because the digestive processes largely come to an endafter death.
The stomach contents can reveal the following information at the post-mortem examination:
1. what the person ate before death2. approximately how long he lived after eating.
Stomach contents digestion and emptying can, however, vary considerablyand can be unpredictable. Especially in comatose persons food can still berecognisable after two days.
Acids and other chemicals taken orally (eg in suicide cases) will continue tohave an effect; the changes observed at the post-mortem examination willtherefore be more advanced than they were at the time of death.
Gastromalacia is a post-mortem change where the stomach wall is destroyedby the process of autolysis (bearing in mind that the stomach contents ismainly acidic) and the stomach contents then leak into the abdominal cavity.This must be distinguished from ante-mortem pathological processes such as aruptured stomach ulcer or the effect of caustic substances taken by mouth.
3.4.4 Decomposition/putrefaction in a submerged body
A body decomposes more slowly in a liquid medium than in the air. Initiallywhen a body is submerged in a liquid medium, it often floats in a proneposition (face downwards), and putrefaction then first appears in the face and
frontal aspect of the neck. This can complicate identification. As gas
formation proceeds, the body rises to the surface.
The rate of putrefaction in a submerged body is determined by:
1. The temperature of the medium: Putrefaction occurs more rapidly in a
warm than in a cold medium.
2. The nature of the medium: Putrefaction occurs more rapidly in sewage
water than in fresh water as sewage water usually is warmer due to the
microbiological activity and therefore heat production. Putrefaction also
occurs more rapidly in fresh water than in seawater.
3. Movement of the liquid: Putrefaction usually occurs more rapidly in
stagnant water.
71
Post-mortem changes
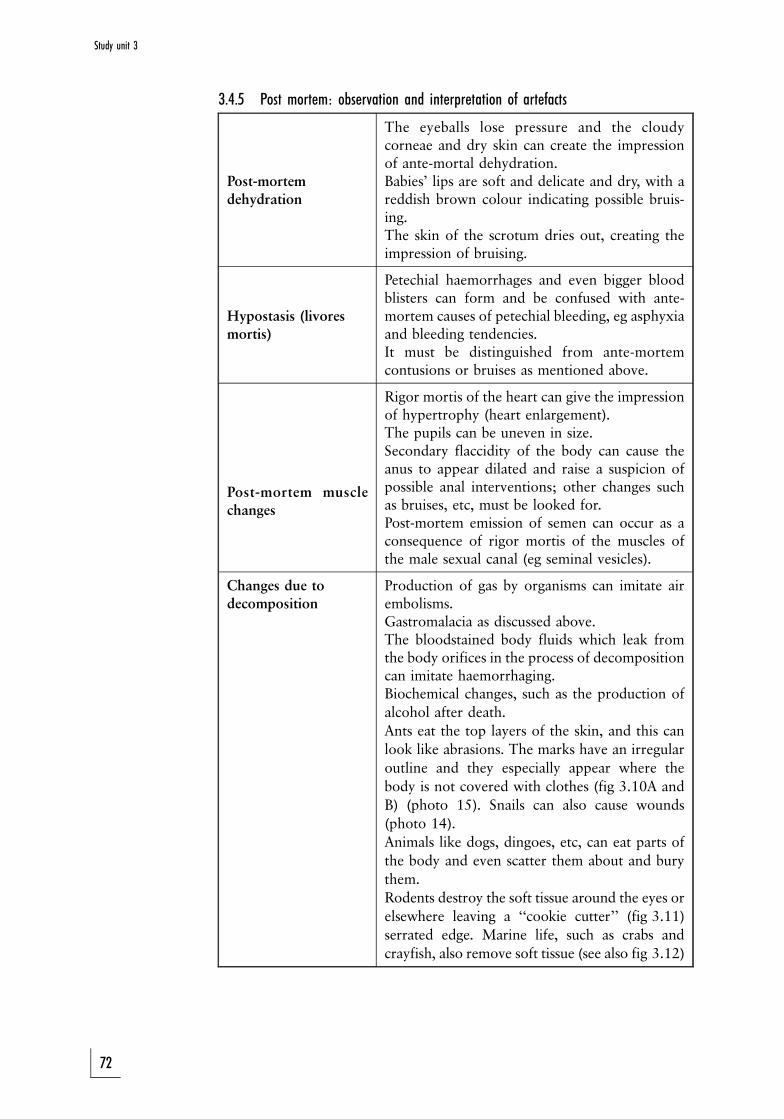
3.4.5 Post mortem: observation and interpretation of artefacts
Post-mortemdehydration
The eyeballs lose pressure and the cloudycorneae and dry skin can create the impressionof ante-mortal dehydration.Babies' lips are soft and delicate and dry, with areddish brown colour indicating possible bruis-ing.The skin of the scrotum dries out, creating theimpression of bruising.
Hypostasis (livoresmortis)
Petechial haemorrhages and even bigger bloodblisters can form and be confused with ante-mortem causes of petechial bleeding, eg asphyxiaand bleeding tendencies.It must be distinguished from ante-mortemcontusions or bruises as mentioned above.
Post-mortem musclechanges
Rigor mortis of the heart can give the impressionof hypertrophy (heart enlargement).The pupils can be uneven in size.Secondary flaccidity of the body can cause theanus to appear dilated and raise a suspicion ofpossible anal interventions; other changes suchas bruises, etc, must be looked for.Post-mortem emission of semen can occur as aconsequence of rigor mortis of the muscles ofthe male sexual canal (eg seminal vesicles).
Changes due todecomposition
Production of gas by organisms can imitate airembolisms.Gastromalacia as discussed above.The bloodstained body fluids which leak fromthe body orifices in the process of decompositioncan imitate haemorrhaging.Biochemical changes, such as the production of
alcohol after death.
Ants eat the top layers of the skin, and this can
look like abrasions. The marks have an irregular
outline and they especially appear where the
body is not covered with clothes (fig 3.10A and
B) (photo 15). Snails can also cause wounds
(photo 14).
Animals like dogs, dingoes, etc, can eat parts of
the body and even scatter them about and bury
them.
Rodents destroy the soft tissue around the eyes or
elsewhere leaving a ``cookie cutter'' (fig 3.11)
serrated edge. Marine life, such as crabs and
crayfish, also remove soft tissue (see also fig 3.12)
72
Study unit 3
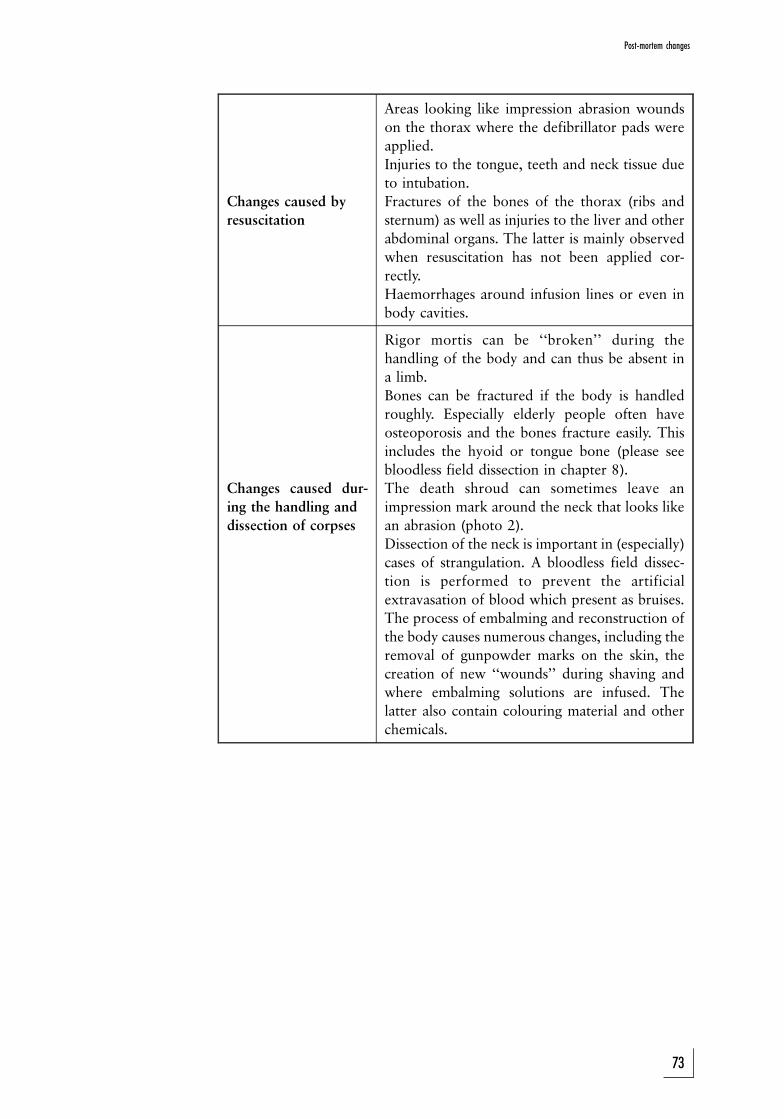
Changes caused by
resuscitation
Areas looking like impression abrasion wounds
on the thorax where the defibrillator pads were
applied.
Injuries to the tongue, teeth and neck tissue due
to intubation.
Fractures of the bones of the thorax (ribs and
sternum) as well as injuries to the liver and other
abdominal organs. The latter is mainly observed
when resuscitation has not been applied cor-
rectly.
Haemorrhages around infusion lines or even in
body cavities.
Changes caused dur-
ing the handling and
dissection of corpses
Rigor mortis can be ``broken'' during the
handling of the body and can thus be absent in
a limb.
Bones can be fractured if the body is handled
roughly. Especially elderly people often have
osteoporosis and the bones fracture easily. This
includes the hyoid or tongue bone (please see
bloodless field dissection in chapter 8).
The death shroud can sometimes leave an
impression mark around the neck that looks like
an abrasion (photo 2).
Dissection of the neck is important in (especially)
cases of strangulation. A bloodless field dissec-
tion is performed to prevent the artificial
extravasation of blood which present as bruises.
The process of embalming and reconstruction of
the body causes numerous changes, including the
removal of gunpowder marks on the skin, the
creation of new ``wounds'' during shaving and
where embalming solutions are infused. The
latter also contain colouring material and other
chemicals.
73
Post-mortem changes
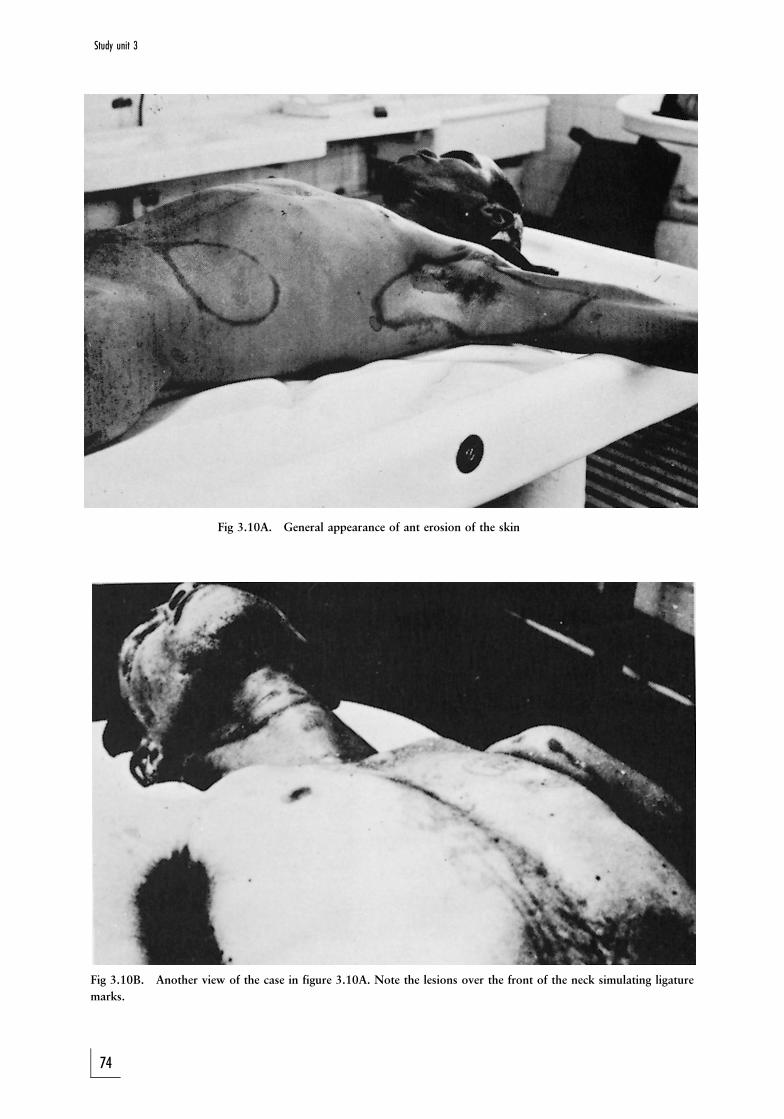
Fig 3.10A. General appearance of ant erosion of the skin
Fig 3.10B. Another view of the case in figure 3.10A. Note the lesions over the front of the neck simulating ligature
marks.
74
Study unit 3

Fig 3.11. Post-mortem rat-bite of the hand
ACTIVITIES
1. The body of a murdered person is found in the open veld. It is still warm
on contact, but rigor mortis has already developed. How long do you
estimate the post-mortem interval to be? What factors may affect the rate
of cooling of the body?
2. The body of a person who allegedly drowned is retrieved from water. A
branch of a tree is tightly gripped in the hand. How will you interpret
this?
3. A female dies a day after having been severely assaulted by her spouse.
During the post-mortem examination blue or reddish blue marks are
present over the back. The pathologist is convinced that this is only due to
hypostasis. How should this case be managed?
75
Post-mortem changes
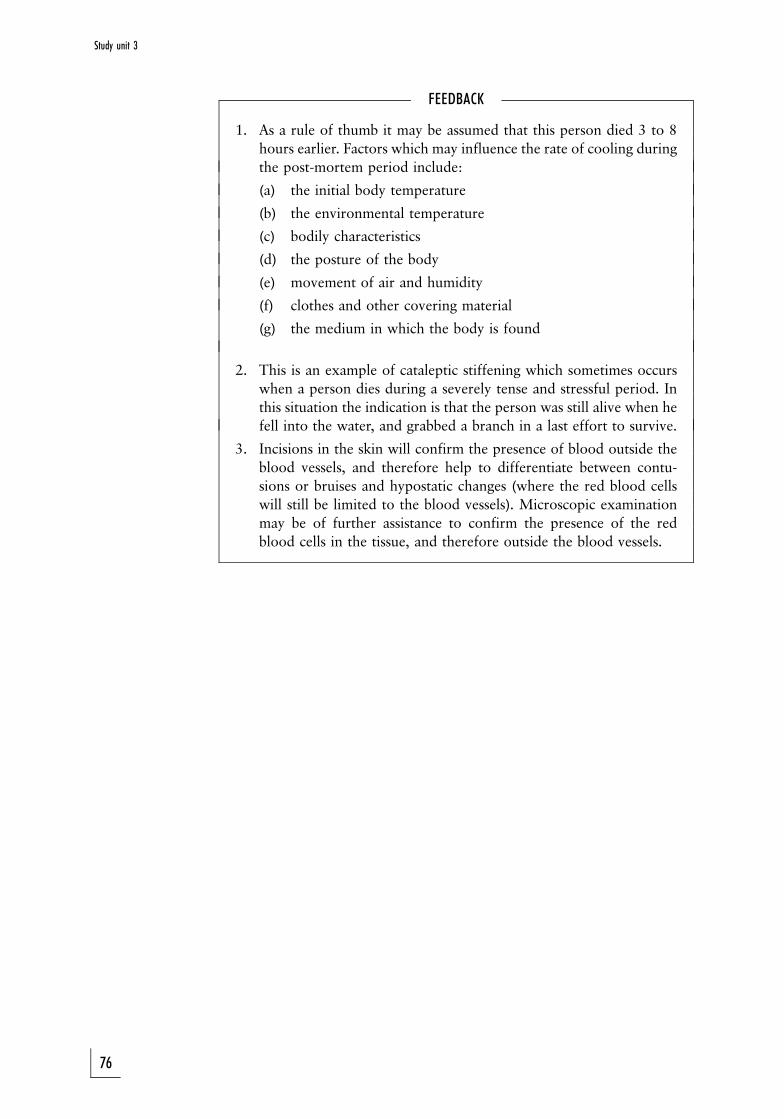
FEEDBACK
1. As a rule of thumb it may be assumed that this person died 3 to 8
hours earlier. Factors which may influence the rate of cooling during
the post-mortem period include:
(a) the initial body temperature
(b) the environmental temperature
(c) bodily characteristics
(d) the posture of the body
(e) movement of air and humidity
(f) clothes and other covering material
(g) the medium in which the body is found
2. This is an example of cataleptic stiffening which sometimes occurs
when a person dies during a severely tense and stressful period. In
this situation the indication is that the person was still alive when he
fell into the water, and grabbed a branch in a last effort to survive.
3. Incisions in the skin will confirm the presence of blood outside the
blood vessels, and therefore help to differentiate between contu-
sions or bruises and hypostatic changes (where the red blood cells
will still be limited to the blood vessels). Microscopic examination
may be of further assistance to confirm the presence of the red
blood cells in the tissue, and therefore outside the blood vessels.
76
Study unit 3
STUDY UNIT 4Identification
Contents
4.1 Introduction
4.1.1 Mass disasters
4.1.2 Skeletal remains
4.2 Age determination
4.2.1 Age determination before birth
4.2.2 Age determination during infancy, childhood and adolescence
4.3 Determination of sex
4.4 Determining height
4.5 Determining ethnic type (race)
4.6 Personal identity
4.7 Molecular biology
4.8 Case study
4.8.1 Comparison of skulls and photographs
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. discuss the circumstances where identification of the deceased may
be more difficult than usual
. discuss the basic principles regarding identification
. discuss the management of the identification of mass disaster victims
. discuss the most important aspects in the identification of the
skeleton
4.1 Introduction
If a person (dead or alive) cannot be identified correctly, it can have far-
reaching implications, and this is not true only for the legal process. Family
members have the need to dispose of the remains of their loved ones in a
suitable fashion and the insurance industry also needs unequivocal proof of
the deceased's identity before a claim can be settled.
Identification is usually not a major issue in most deaths, although it may be
traumatic for the next of kin to see the mutilated body of a loved one. It has
for example happened that under such emotional circumstances people have
been identified incorrectly.
77
Identification can be difficult in certain situations:
1. Where bodies are mutilated, especially where the head and limbs are
absent
2. Where bodies are decomposed.
3. If bodies are burnt and charred.
4. If there is only a skeleton, or parts thereof, left (photo 4).
5. In the case of mass disasters where mutilation and charring of bodies are
common, such as on 11 September 2001 in New York, and in aircraft and
mining accidents.
The identification of a living person is also important. A young individual, age
unknown, may be prosecuted for a crime in which the exact age of the
assailant may be an issue of importance, especially when it comes to an
appropriate sentence. It is sometimes also necessary to link the genetic
contents of a specimen, for example semen, with a specific individual.
Identification of the alleged father in cases of a paternity dispute is a common
occurrence.
Identification, both in the living and a dead person, is done according to one
or both of the following two basic principles:
1. Identification through reconstruction and classification. This involves
determining age, sex, race, height, et cetera. On the grounds of this
information one can place the individual in a group of individuals.
2. Identification through comparative studies. Certain features unique to an
individual can be compared with data available about that individual or
possible individuals. Fingerprints, photographs, scars, operation scars and
prostheses, or the absence of viscera (eg the uterus) can be of value. The
impression of a bite mark on the skin can be compared with the teeth of
an alleged assailant. In charred bodies the teeth are usually preserved, and
can be used in the identification of the deceased.
The use of molecular biology, specifically DNA analysis, offers unequivocal
proof in the identification of a specific individual. At present this technique is
extensively used in paternity testing, and has replaced blood group analysis.
Fingerprints (also palmprints) are still an important means to identify an
individual, but for this method comparative prints are needed.
We shall now discuss two situations where identification is often problematic
and difficult, and then we discuss general principles regarding age, race and
sex in skeletal and nonskeletal remains when it comes to identification.
4.1.1 Mass disasters
In a mass disaster the following issues are at stake:
1. the number of individuals involved
2. the identity of each individual based on
(a) age, sex and race
(b) personal identifying marks, such as scars, jewelry, tattoo's, finger-
prints
(c) forensic odontology or dentistry
(d) molecular biology (DNA)
78
Study unit 4
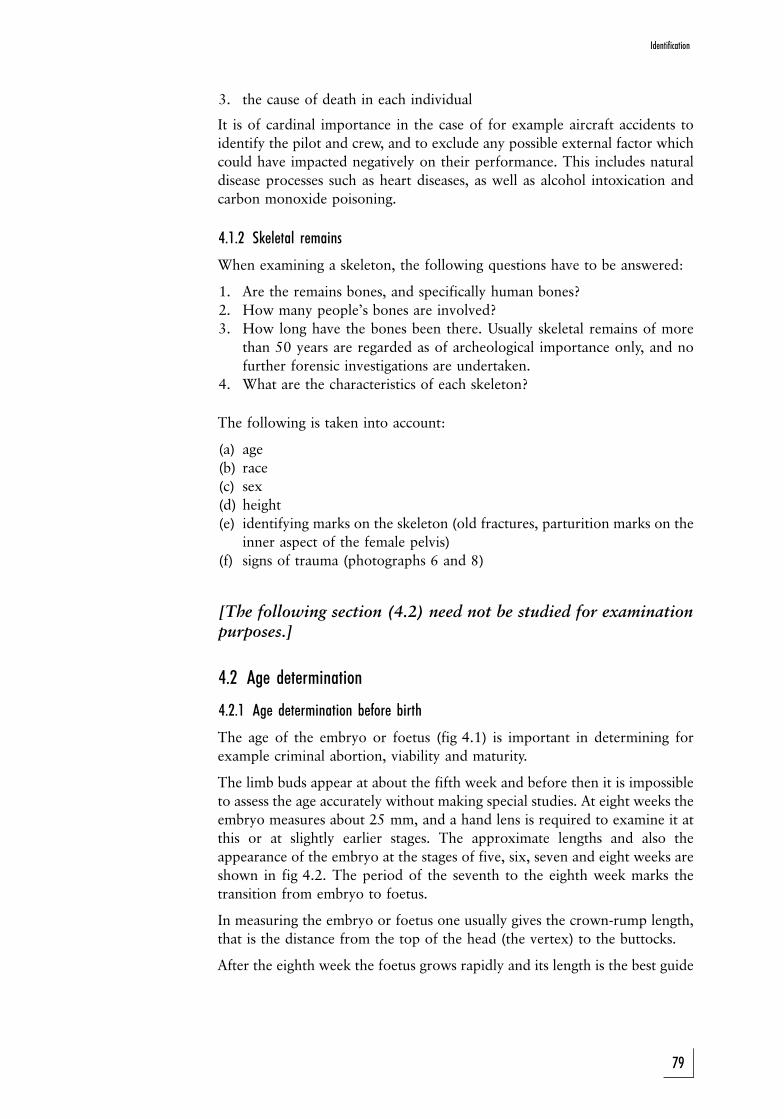
3. the cause of death in each individual
It is of cardinal importance in the case of for example aircraft accidents to
identify the pilot and crew, and to exclude any possible external factor which
could have impacted negatively on their performance. This includes natural
disease processes such as heart diseases, as well as alcohol intoxication and
carbon monoxide poisoning.
4.1.2 Skeletal remains
When examining a skeleton, the following questions have to be answered:
1. Are the remains bones, and specifically human bones?
2. How many people's bones are involved?
3. How long have the bones been there. Usually skeletal remains of more
than 50 years are regarded as of archeological importance only, and no
further forensic investigations are undertaken.
4. What are the characteristics of each skeleton?
The following is taken into account:
(a) age
(b) race
(c) sex
(d) height
(e) identifying marks on the skeleton (old fractures, parturition marks on the
inner aspect of the female pelvis)
(f) signs of trauma (photographs 6 and 8)
[The following section (4.2) need not be studied for examinationpurposes.]
4.2 Age determination
4.2.1 Age determination before birth
The age of the embryo or foetus (fig 4.1) is important in determining for
example criminal abortion, viability and maturity.
The limb buds appear at about the fifth week and before then it is impossible
to assess the age accurately without making special studies. At eight weeks the
embryo measures about 25 mm, and a hand lens is required to examine it at
this or at slightly earlier stages. The approximate lengths and also the
appearance of the embryo at the stages of five, six, seven and eight weeks are
shown in fig 4.2. The period of the seventh to the eighth week marks the
transition from embryo to foetus.
In measuring the embryo or foetus one usually gives the crown-rump length,
that is the distance from the top of the head (the vertex) to the buttocks.
After the eighth week the foetus grows rapidly and its length is the best guide
79
Identification
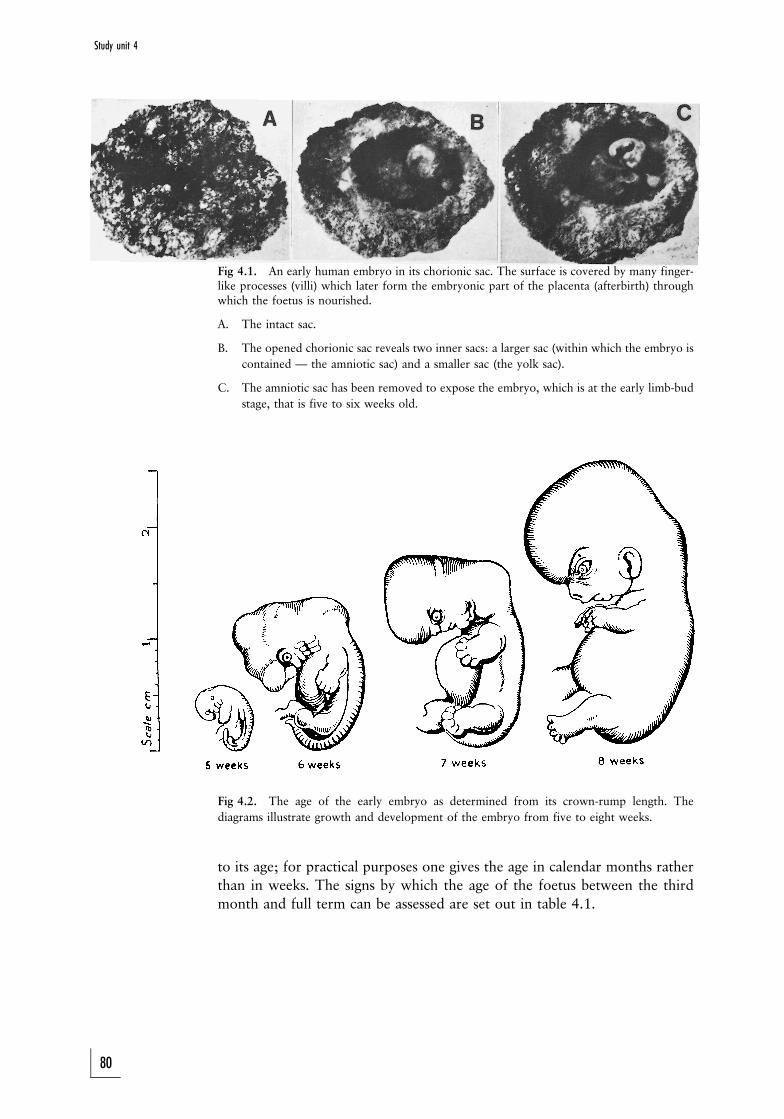
Fig 4.1. An early human embryo in its chorionic sac. The surface is covered by many finger-like processes (villi) which later form the embryonic part of the placenta (afterbirth) throughwhich the foetus is nourished.
A. The intact sac.
B. The opened chorionic sac reveals two inner sacs: a larger sac (within which the embryo is
contained Ð the amniotic sac) and a smaller sac (the yolk sac).
C. The amniotic sac has been removed to expose the embryo, which is at the early limb-bud
stage, that is five to six weeks old.
Fig 4.2. The age of the early embryo as determined from its crown-rump length. The
diagrams illustrate growth and development of the embryo from five to eight weeks.
to its age; for practical purposes one gives the age in calendar months rather
than in weeks. The signs by which the age of the foetus between the third
month and full term can be assessed are set out in table 4.1.
80
Study unit 4
TABLE 4.1
The main points by which to judge the age of the foetus between the third month of intra-uterine life and the time of birth
(Note: It is not required to memorise this table for examination purposes!)
Age of foetus in ca-lendar months
Crown rump lengthor sitting height
Other important signs
End of third month About 7 cm Ð
End of fourth month About 13 cm Ð
End of fifth month About 18 cm External genitalia suffi-ciently developed to en-a b l e t h e s e x t o b erecognised. Primary centreof ossification of calca-neum (heel bone) has ap-peared.
End of sixth month About 22 cm
End of seventh About 26 cm Primary centre of ossifica-tion of talus (ankle bone)has appeared. Foetus leg-ally viable.
End of eighth month About 30 cm
End of ninth monthor just before birth
About 34 cm The testes have descended.The centre of ossificationin the lower epiphysis (thesecondary bone-formingcentre separated from themain part of the bone bycartilage) of the femur hasappeared. The centre ofossification in the cuboid(a foot bone on the outsideof the foot), and some-times one in the upperepiphysis of the tibia (shinbone) has appeared.
The primary centres of ossification in the long bones, scapulae (shoulder
blades), hip bones, bodies of the vertebrae and in the skull bones begin to
appear about the eighth week. However, up to the end of the third month the
foetus is too small for this to be of great importance. By the sixteenth week,
that is during the fourth month, parts of the foetal skeleton can be shown on a
good X-ray of the mother's abdomen. From that time onwards the vertebral
column of the foetus becomes well defined, the approximate sitting height
can be determined from the X-ray, and the age judged by reference to table
4.1. If the remains of a pregnant uterus are removed from the pelvis, parts of
the foetal skeleton can be shown by X-ray somewhat earlier than the sixteenth
week.
81
Identification
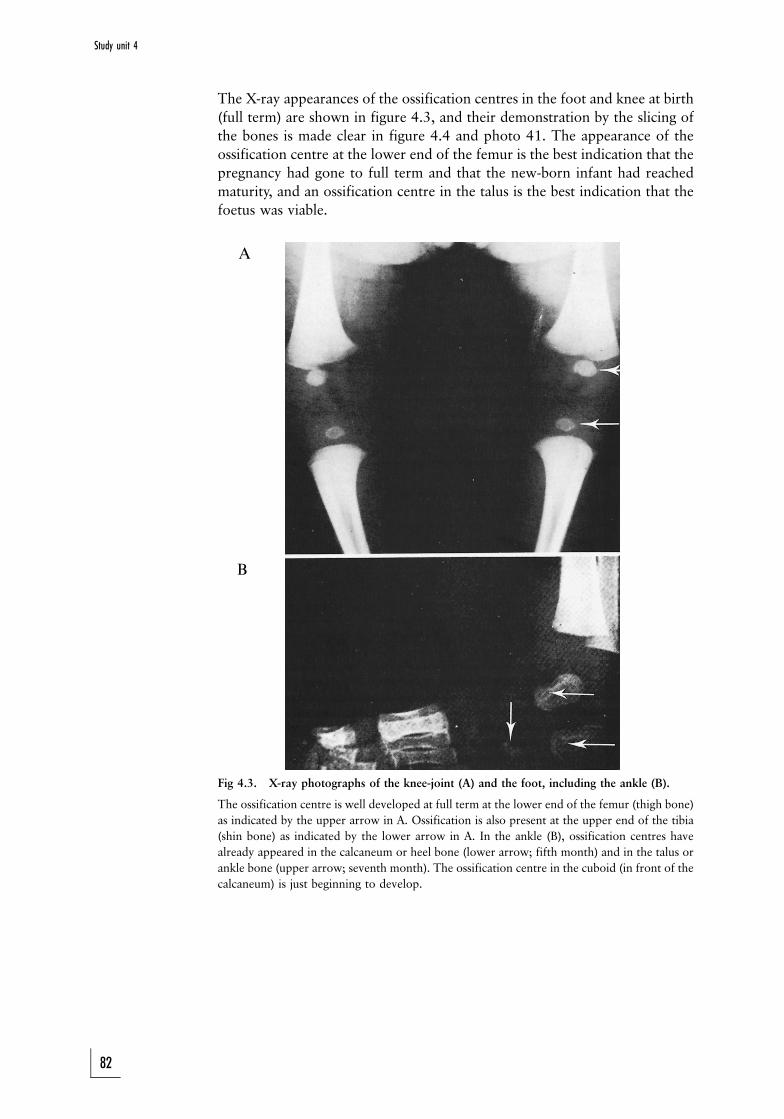
A
B
The X-ray appearances of the ossification centres in the foot and knee at birth
(full term) are shown in figure 4.3, and their demonstration by the slicing of
the bones is made clear in figure 4.4 and photo 41. The appearance of the
ossification centre at the lower end of the femur is the best indication that the
pregnancy had gone to full term and that the new-born infant had reached
maturity, and an ossification centre in the talus is the best indication that the
foetus was viable.
Fig 4.3. X-ray photographs of the knee-joint (A) and the foot, including the ankle (B).
The ossification centre is well developed at full term at the lower end of the femur (thigh bone)
as indicated by the upper arrow in A. Ossification is also present at the upper end of the tibia
(shin bone) as indicated by the lower arrow in A. In the ankle (B), ossification centres have
already appeared in the calcaneum or heel bone (lower arrow; fifth month) and in the talus or
ankle bone (upper arrow; seventh month). The ossification centre in the cuboid (in front of the
calcaneum) is just beginning to develop.
82
Study unit 4
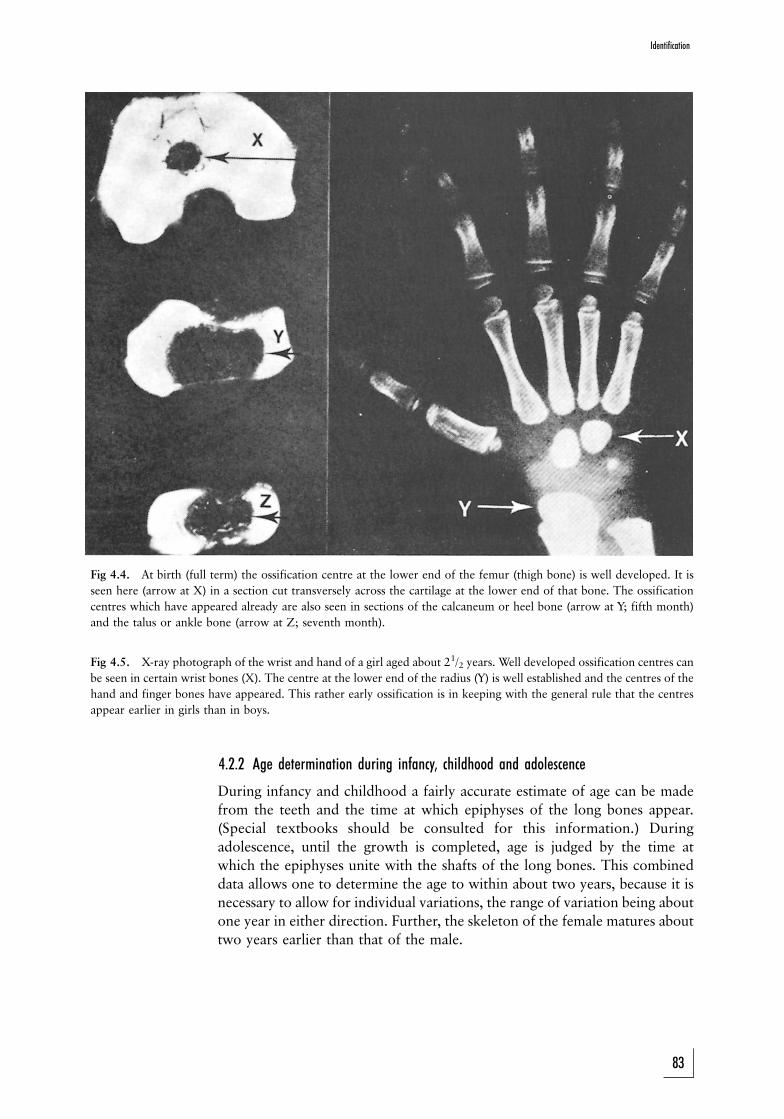
Fig 4.4. At birth (full term) the ossification centre at the lower end of the femur (thigh bone) is well developed. It is
seen here (arrow at X) in a section cut transversely across the cartilage at the lower end of that bone. The ossification
centres which have appeared already are also seen in sections of the calcaneum or heel bone (arrow at Y; fifth month)
and the talus or ankle bone (arrow at Z; seventh month).
Fig 4.5. X-ray photograph of the wrist and hand of a girl aged about 21/2 years. Well developed ossification centres can
be seen in certain wrist bones (X). The centre at the lower end of the radius (Y) is well established and the centres of the
hand and finger bones have appeared. This rather early ossification is in keeping with the general rule that the centres
appear earlier in girls than in boys.
4.2.2 Age determination during infancy, childhood and adolescence
During infancy and childhood a fairly accurate estimate of age can be made
from the teeth and the time at which epiphyses of the long bones appear.
(Special textbooks should be consulted for this information.) During
adolescence, until the growth is completed, age is judged by the time at
which the epiphyses unite with the shafts of the long bones. This combined
data allows one to determine the age to within about two years, because it is
necessary to allow for individual variations, the range of variation being about
one year in either direction. Further, the skeleton of the female matures about
two years earlier than that of the male.
83
Identification
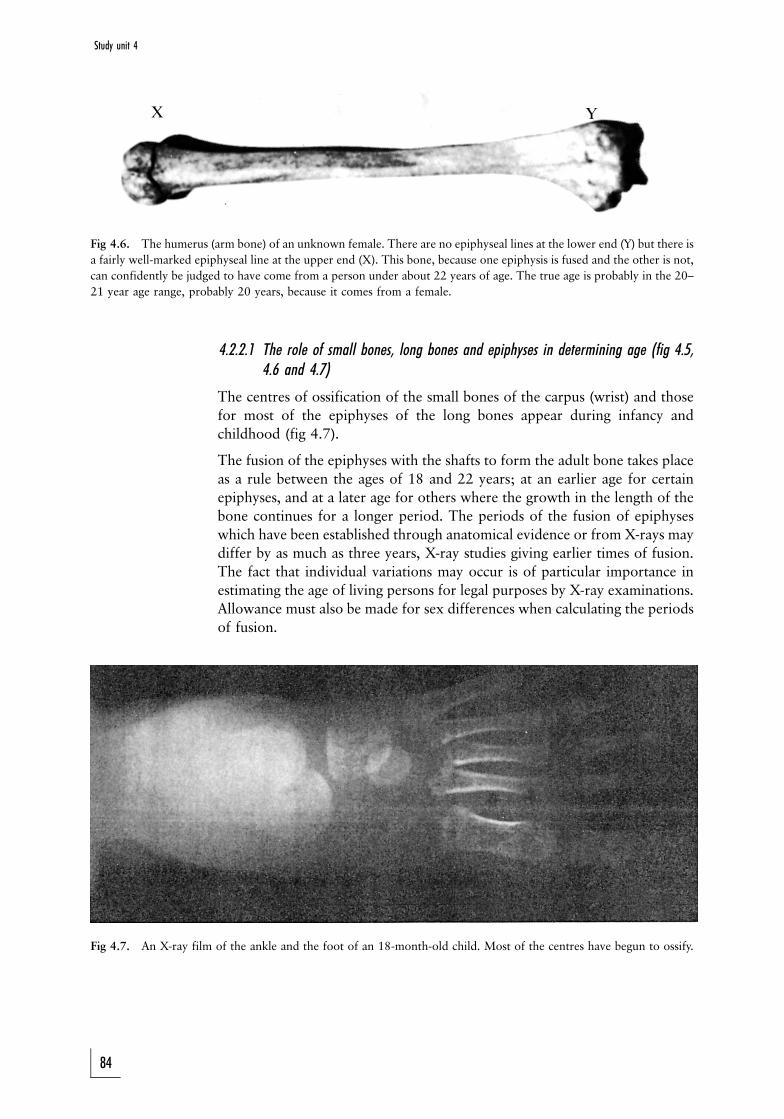
X Y
Fig 4.6. The humerus (arm bone) of an unknown female. There are no epiphyseal lines at the lower end (Y) but there is
a fairly well-marked epiphyseal line at the upper end (X). This bone, because one epiphysis is fused and the other is not,
can confidently be judged to have come from a person under about 22 years of age. The true age is probably in the 20±
21 year age range, probably 20 years, because it comes from a female.
4.2.2.1 The role of small bones, long bones and epiphyses in determining age (fig 4.5,4.6 and 4.7)
The centres of ossification of the small bones of the carpus (wrist) and those
for most of the epiphyses of the long bones appear during infancy and
childhood (fig 4.7).
The fusion of the epiphyses with the shafts to form the adult bone takes place
as a rule between the ages of 18 and 22 years; at an earlier age for certain
epiphyses, and at a later age for others where the growth in the length of the
bone continues for a longer period. The periods of the fusion of epiphyses
which have been established through anatomical evidence or from X-rays may
differ by as much as three years, X-ray studies giving earlier times of fusion.
The fact that individual variations may occur is of particular importance in
estimating the age of living persons for legal purposes by X-ray examinations.
Allowance must also be made for sex differences when calculating the periods
of fusion.
Fig 4.7. An X-ray film of the ankle and the foot of an 18-month-old child. Most of the centres have begun to ossify.
84
Study unit 4
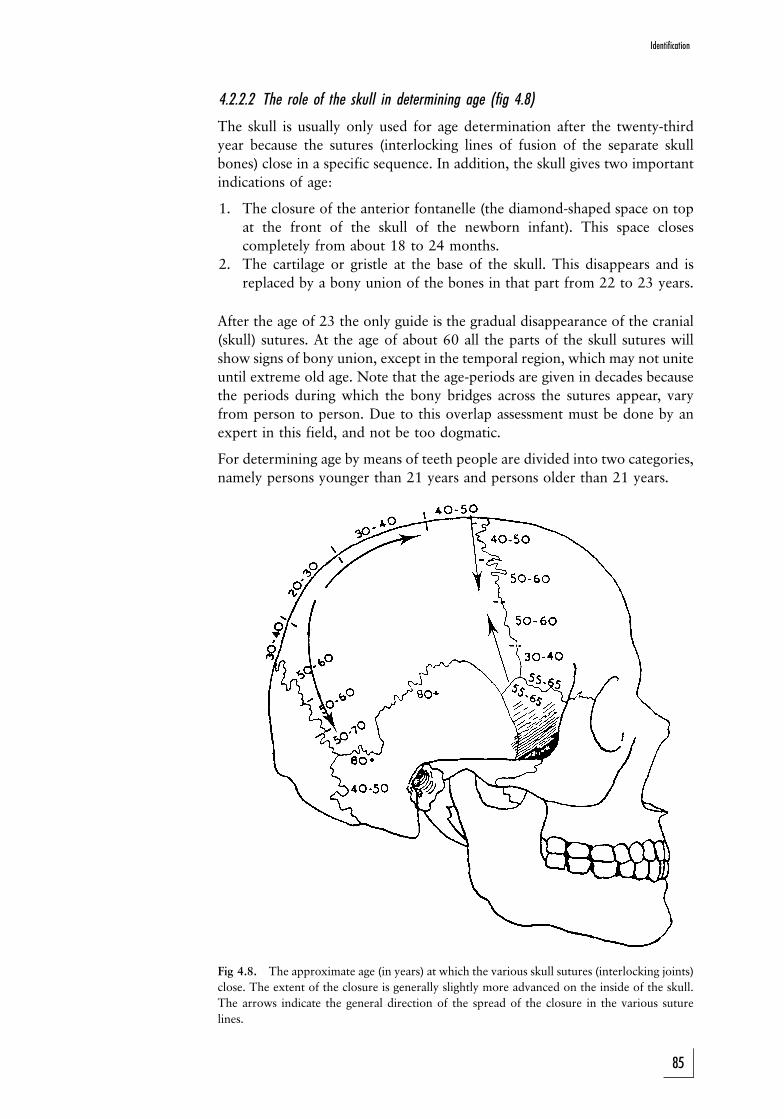
4.2.2.2 The role of the skull in determining age (fig 4.8)
The skull is usually only used for age determination after the twenty-third
year because the sutures (interlocking lines of fusion of the separate skull
bones) close in a specific sequence. In addition, the skull gives two important
indications of age:
1. The closure of the anterior fontanelle (the diamond-shaped space on top
at the front of the skull of the newborn infant). This space closes
completely from about 18 to 24 months.
2. The cartilage or gristle at the base of the skull. This disappears and is
replaced by a bony union of the bones in that part from 22 to 23 years.
After the age of 23 the only guide is the gradual disappearance of the cranial
(skull) sutures. At the age of about 60 all the parts of the skull sutures will
show signs of bony union, except in the temporal region, which may not unite
until extreme old age. Note that the age-periods are given in decades because
the periods during which the bony bridges across the sutures appear, vary
from person to person. Due to this overlap assessment must be done by an
expert in this field, and not be too dogmatic.
For determining age by means of teeth people are divided into two categories,
namely persons younger than 21 years and persons older than 21 years.
Fig 4.8. The approximate age (in years) at which the various skull sutures (interlocking joints)
close. The extent of the closure is generally slightly more advanced on the inside of the skull.
The arrows indicate the general direction of the spread of the closure in the various suture
lines.
85
Identification

To determine the age of someone younger than 21 years, two elements of
tooth development are used, namely calcification and formation, and
eruption. Although determining the stage of eruption is a popular method
of calculating age, it is not always accurate since there are meaningful
differences in the eruption times of teeth. The eruption time can be
influenced by, for example, genetic and environmental factors, socio-
economic status, hormonal imbalance and chronic diseases. Stages of tooth
eruption can be used as a general guideline, but must always be confirmed by
the developmental stage of the teeth. The development of the teeth is
generally reflected in their state of calcification and this can be observed in
roentgenological photos (X-rays). Published charts giving the stages of tooth
development assist in determining age precisely. The stage of development of
the first permanent molar, for example, is a good indication of age up to
about nine years. Between the ages of 14 and 20 years it is difficult to be
accurate and therefore the development stages of the second and third molars
are also taken into account. According to a study by Nortje in which the ages
of patients were compared with the radiographic appearances of the
developmental stage of the root of the third mandibular molar, the age of
an unknown person of between 15 and 21 years can be determined to within
an accuracy of 2 to 4 years.
It is even possible to determine the age of a foetus by studying the
development stage of the milk teeth roentgenologically and histologically. By
seven months the dentine of the top front milk teeth, for example, is 3 mm
thick. At birth there is a short period when the hard tissue of the teeth is
formed, and this is shown in the dentine and enamel as a clear neonatal line.
The quantity of dentine formed before birth thus gives an indication of the
age, since 4 micrometer dentine is formed daily until the tooth is fully
formed. The easiest method is, however, to take good roentgen photos of the
root areas of teeth and to use these to investigate the age.
When teeth formation has ended (by 21 years) a series of additional changes
in the teeth is used in the calculation of age. Some of these changes are the
wearing-away of the masticatory areas of the crowns, pulling away of the
gums, deposits of secondary dentine in the pulp, deposits of cement at the
point of the root, resorption at the point of the root, and an increase in the
translucency of the root as a result of intensified calcification in the dentine of
the root (fig 4.15). These changes are measured according to a detailed chart
and points are allocated. The total is then an indication of the person's age.
This technique has the advantage that age can be determined even when all
the bony sutures have closed and no other method remains than an
examination of the teeth.
4.3 Determination of sex
If soft parts are recognisable there is, as a rule, little difficulty in determining
sex. When only skeletal remains are available, however, sex determination is
difficult, unless the pelvis as a whole, or a hip bone or the sacrum is present.
Although the long bones and the skull show sexual differences, these are not
always sufficiently pronounced to enable the observer to say with certainty
86
Study unit 4
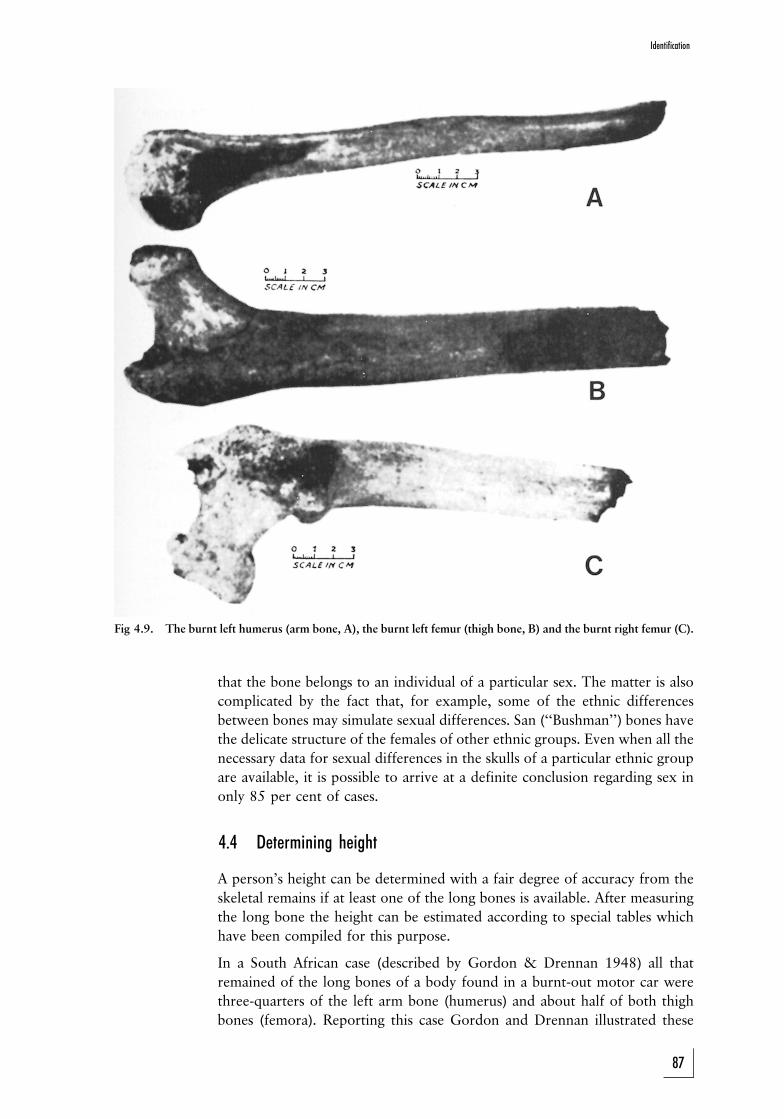
Fig 4.9. The burnt left humerus (arm bone, A), the burnt left femur (thigh bone, B) and the burnt right femur (C).
that the bone belongs to an individual of a particular sex. The matter is also
complicated by the fact that, for example, some of the ethnic differences
between bones may simulate sexual differences. San (``Bushman'') bones have
the delicate structure of the females of other ethnic groups. Even when all the
necessary data for sexual differences in the skulls of a particular ethnic group
are available, it is possible to arrive at a definite conclusion regarding sex in
only 85 per cent of cases.
4.4 Determining height
A person's height can be determined with a fair degree of accuracy from the
skeletal remains if at least one of the long bones is available. After measuring
the long bone the height can be estimated according to special tables which
have been compiled for this purpose.
In a South African case (described by Gordon & Drennan 1948) all that
remained of the long bones of a body found in a burnt-out motor car were
three-quarters of the left arm bone (humerus) and about half of both thigh
bones (femora). Reporting this case Gordon and Drennan illustrated these
87
Identification
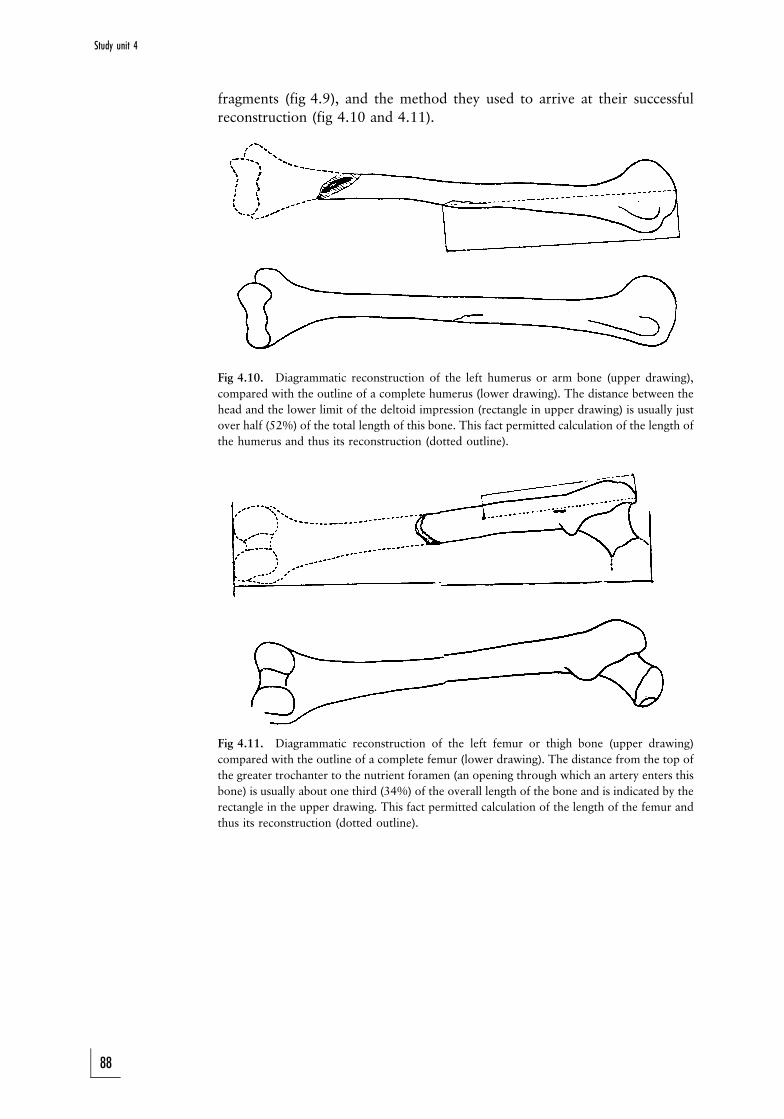
fragments (fig 4.9), and the method they used to arrive at their successful
reconstruction (fig 4.10 and 4.11).
Fig 4.10. Diagrammatic reconstruction of the left humerus or arm bone (upper drawing),
compared with the outline of a complete humerus (lower drawing). The distance between the
head and the lower limit of the deltoid impression (rectangle in upper drawing) is usually just
over half (52%) of the total length of this bone. This fact permitted calculation of the length of
the humerus and thus its reconstruction (dotted outline).
Fig 4.11. Diagrammatic reconstruction of the left femur or thigh bone (upper drawing)
compared with the outline of a complete femur (lower drawing). The distance from the top of
the greater trochanter to the nutrient foramen (an opening through which an artery enters this
bone) is usually about one third (34%) of the overall length of the bone and is indicated by the
rectangle in the upper drawing. This fact permitted calculation of the length of the femur and
thus its reconstruction (dotted outline).
88
Study unit 4
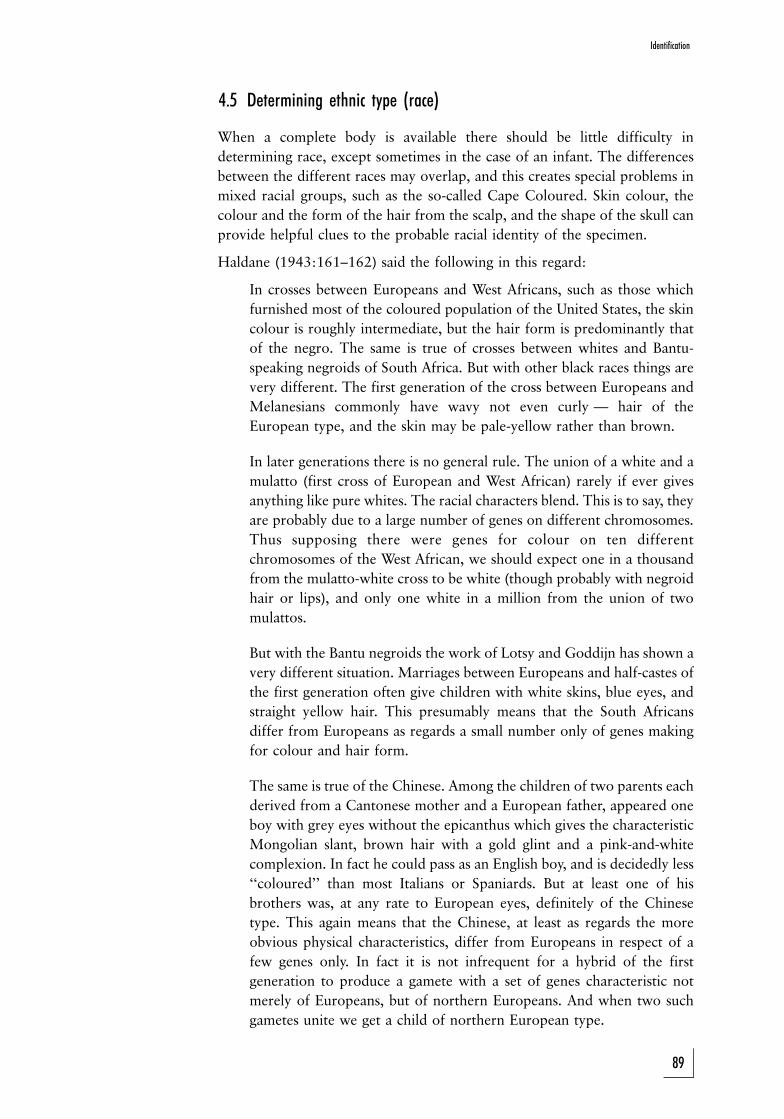
4.5 Determining ethnic type (race)
When a complete body is available there should be little difficulty in
determining race, except sometimes in the case of an infant. The differences
between the different races may overlap, and this creates special problems in
mixed racial groups, such as the so-called Cape Coloured. Skin colour, the
colour and the form of the hair from the scalp, and the shape of the skull can
provide helpful clues to the probable racial identity of the specimen.
Haldane (1943:161±162) said the following in this regard:
In crosses between Europeans and West Africans, such as those which
furnished most of the coloured population of the United States, the skin
colour is roughly intermediate, but the hair form is predominantly that
of the negro. The same is true of crosses between whites and Bantu-
speaking negroids of South Africa. But with other black races things are
very different. The first generation of the cross between Europeans and
Melanesians commonly have wavy not even curly Ð hair of the
European type, and the skin may be pale-yellow rather than brown.
In later generations there is no general rule. The union of a white and a
mulatto (first cross of European and West African) rarely if ever gives
anything like pure whites. The racial characters blend. This is to say, they
are probably due to a large number of genes on different chromosomes.
Thus supposing there were genes for colour on ten different
chromosomes of the West African, we should expect one in a thousand
from the mulatto-white cross to be white (though probably with negroid
hair or lips), and only one white in a million from the union of two
mulattos.
But with the Bantu negroids the work of Lotsy and Goddijn has shown a
very different situation. Marriages between Europeans and half-castes of
the first generation often give children with white skins, blue eyes, and
straight yellow hair. This presumably means that the South Africans
differ from Europeans as regards a small number only of genes making
for colour and hair form.
The same is true of the Chinese. Among the children of two parents each
derived from a Cantonese mother and a European father, appeared one
boy with grey eyes without the epicanthus which gives the characteristic
Mongolian slant, brown hair with a gold glint and a pink-and-white
complexion. In fact he could pass as an English boy, and is decidedly less
``coloured'' than most Italians or Spaniards. But at least one of his
brothers was, at any rate to European eyes, definitely of the Chinese
type. This again means that the Chinese, at least as regards the more
obvious physical characteristics, differ from Europeans in respect of a
few genes only. In fact it is not infrequent for a hybrid of the first
generation to produce a gamete with a set of genes characteristic not
merely of Europeans, but of northern Europeans. And when two such
gametes unite we get a child of northern European type.
89
Identification

4.6 Personal identity
The South African Police Service retains a record of all individuals who have
been found guilty of an offence. These records include fingerprints as well as
data about height and body mass, and information on build (physique), facial
characteristics, hair, teeth, disabilities, scars, tattoos (photo 7), et cetera.
Photographs are filed separately.
The importance of teeth in the estimation of age has been mentioned (fig
4.15). Comparative studies of the teeth of charred bodies and the dental
records of possible victims are of tremendous value.
Congenital abnormalities and birth defects can provide additional evidence.
Tattoos are often of value, even after other markings have been destroyed by
decomposition. Tattoos often show up better after the epidermis is lost
through the ``slip skin'' phenomenom.
Certain markings can be an indication of a person's occupation, such as
carbon scars on coal miners' skins.
4.7 Molecular biology
Every individual has a unique genetic profile and composition as result of the
combination of his or her inherited genetic profiles. As DNA analysis is so
conclusive, blood grouping and tissue typing are seldom used today.
Molecular biology can assist the forensic pathologist in a number of ways:
1. comparing biological material like semen or blood with an alleged
suspect's genetic material: this is of major importance in cases of sexual
assault
2. comparing an unknown individual's genetic profile with the profiles of
possible family members, for example parents or siblings
3. comparing the genetic profile of an infant with an alleged parent (usually
a father in a paternity dispute)
4.8 Case studies
In a South African case (discussed by Gordon and Drennan 1948), the only
remnants of the long bones found in a burnt-out vehicle were three quarters
of the left humerus and approximately half of each femur. Figure 4.9 shows
the remains, and figures 4.10 and 4.11 show the successful reconstruction.
4.8.1 Comparison of skulls and photographs
This procedure was first used in a criminal case by Glaister and Brash (1937)
in the case of R v Ruxton. In this case the dismembered remains of two
women were found in a ravine 160 km from the home of Dr Ruxton. Various
facts gave rise to the suspicion that the remains, which had been mutilated
beyond recognition, were those of Mrs Ruxton, the accused's wife, and of the
nursemaid, Mary Rogerson. Evidence of height and of age, as well as
fingerprints and the size of the feet, tended to confirm the suspicion. In
addition, photographs of the two skulls, of a size corresponding to their
90
Study unit 4

actual dimensions, were taken and compared with enlarged photographs of
the two missing women. The natural size of the faces on the photographs was
determined as accurately as possible so that the enlargements should be life-
size. When the orientation of the skulls had been adjusted, the outline of each
skull was shown to conform accurately to the features of the photographs of
one, but not of the other missing woman.
In the Dobkin case (Simpson 1969) a similar procedure was followed, with the
difference that no standard for the measurement of Mrs Dobkin's face in the
photograph was available. In this case photographs of skull and face were
superimposed by adjusting the magnification until the distances between the
pupils corresponded. Again, outline of skull and features corresponded closely.
In the case already described by Gordon and Drennan, this method was used
to show that outline drawings of the charred remainder of the skull which was
found in the burnt-out car, fitted reasonably well into life-size drawings of the
head of a Mr Wolkersdorfer, who owned the car and had disappeared since
the night of the burning.
In this case the only photographs of Wolkersdorfer that were available were
the three snapshots shown in the figures. The police were able to obtain the
tie which was worn by Wolkersdorfer, and its square pattern was used as a
scale to make a life-size drawing of this view of his head. In order to obtain
life-size drawings of his head the size of his left ear, determined by the tie scale
(fig 4.12 and 4.12A), was used.
In all three superimpositions there was quite good anatomical correspon-
dence, which supported other skeletal evidence regarding race, age and height
in suggesting that the remains could have been Wolkersdorfer's. The skull
fragment was sufficiently large to show that the individual's head had been
decidedly brachycephalic, that is very short and wide. The small circles in
figure 4.13A represent leadshot pellets placed at the entrance to each ear
opening of the skull. The width between the pellets was considerable in this
skull, and it was thought significant that this measurement fitted the
dimensions of Wolkersdorfer's head.
Fig 4.12. A snapshot of the deceased (oblique view) taken in Durban in 1946.
Fig 4.12A. Diagrammatic reconstruction of the skull and its superimposition on a drawing of
the head made from the appropriate photograph in fig 4.12.
91
Identification
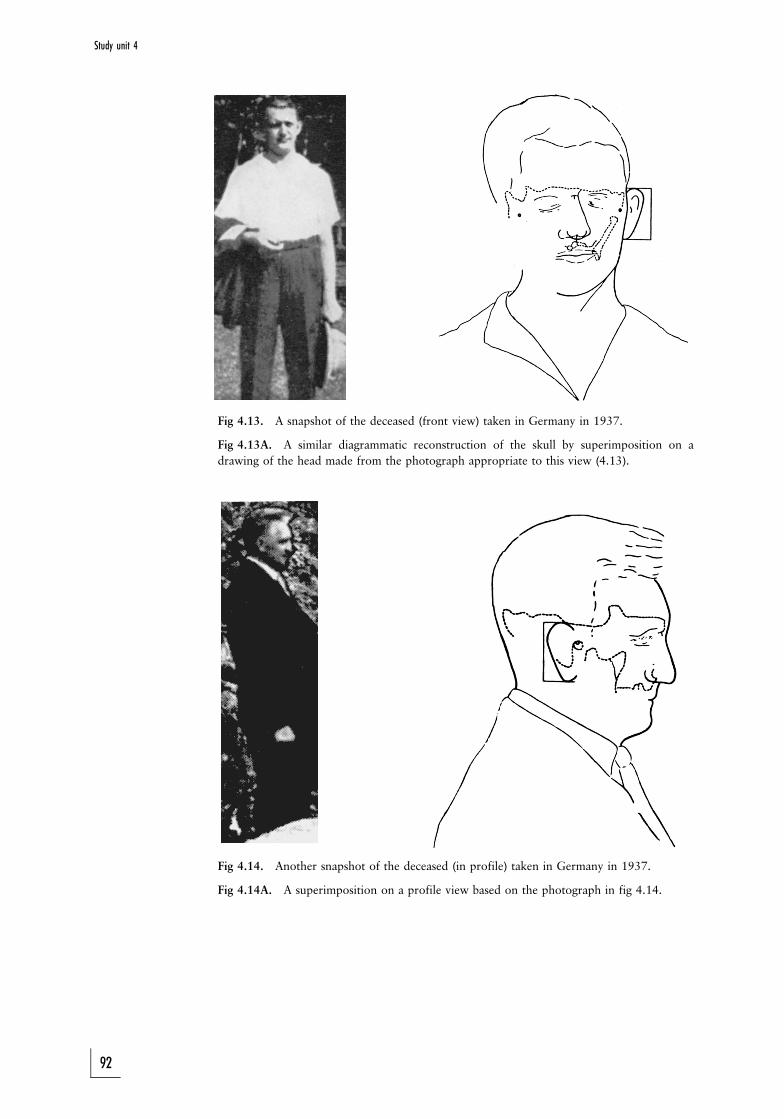
Fig 4.13. A snapshot of the deceased (front view) taken in Germany in 1937.
Fig 4.13A. A similar diagrammatic reconstruction of the skull by superimposition on a
drawing of the head made from the photograph appropriate to this view (4.13).
Fig 4.14. Another snapshot of the deceased (in profile) taken in Germany in 1937.
Fig 4.14A. A superimposition on a profile view based on the photograph in fig 4.14.
92
Study unit 4
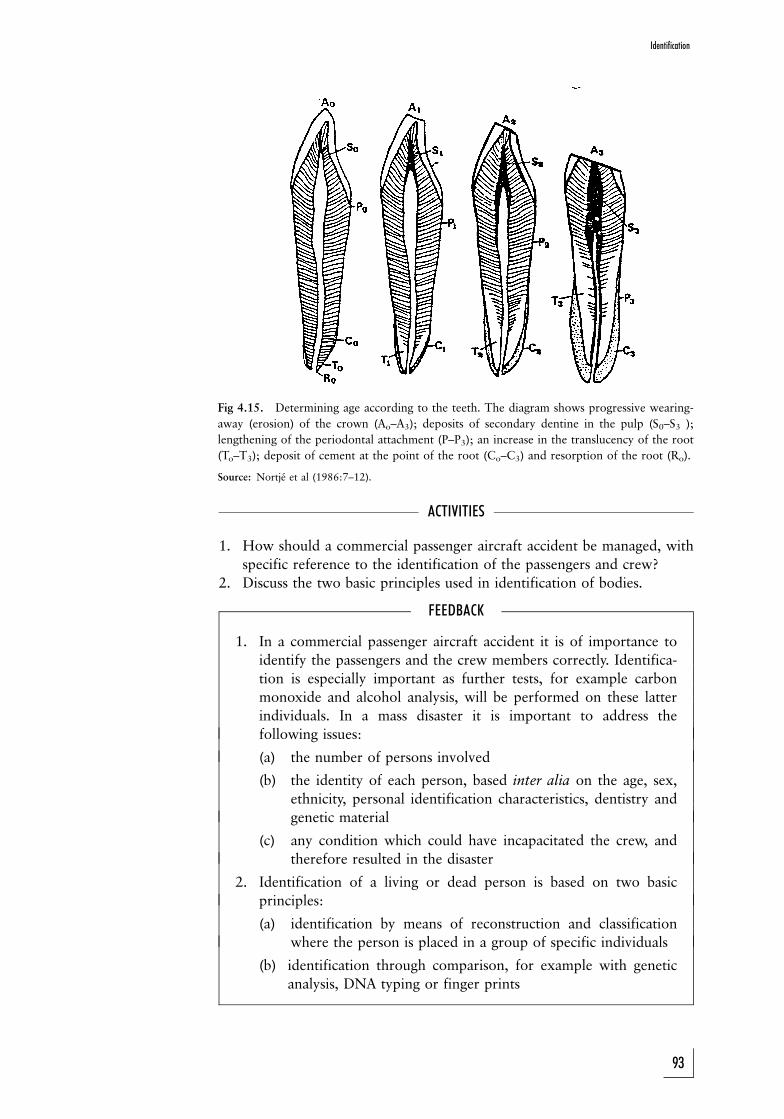
Fig 4.15. Determining age according to the teeth. The diagram shows progressive wearing-
away (erosion) of the crown (Ao±A3); deposits of secondary dentine in the pulp (S0±S3 );
lengthening of the periodontal attachment (P±P3); an increase in the translucency of the root
(To±T3); deposit of cement at the point of the root (Co±C3) and resorption of the root (Ro).
Source: Nortje et al (1986:7±12).
ACTIVITIES
1. How should a commercial passenger aircraft accident be managed, with
specific reference to the identification of the passengers and crew?
2. Discuss the two basic principles used in identification of bodies.
FEEDBACK
1. In a commercial passenger aircraft accident it is of importance to
identify the passengers and the crew members correctly. Identifica-
tion is especially important as further tests, for example carbon
monoxide and alcohol analysis, will be performed on these latter
individuals. In a mass disaster it is important to address the
following issues:
(a) the number of persons involved
(b) the identity of each person, based inter alia on the age, sex,
ethnicity, personal identification characteristics, dentistry and
genetic material
(c) any condition which could have incapacitated the crew, and
therefore resulted in the disaster
2. Identification of a living or dead person is based on two basic
principles:
(a) identification by means of reconstruction and classification
where the person is placed in a group of specific individuals
(b) identification through comparison, for example with genetic
analysis, DNA typing or finger prints
93
Identification

STUDY UNIT 5General traumatology
Contents
5.1 Definition of trauma
5.2 Types of trauma
5.3 Mechanical trauma
5.3.1 The effective wounding or injury force
5.3.2 Appearance of a wound
5.4 Classification of mechanical trauma
5.4.1 Blunt trauma
5.4.2 Sharp injuries
5.5 Description of wounds
5.6 Dating of wounds
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. discuss the different types of trauma which may involve a human
body
. identify different factors which may influence the appearance of a
wound
. discuss the different types of injuries due to blunt and sharp forces.
A basic knowledge of the general concepts regarding trauma to the skin is
important, as the latter is seen widely in forensic practice. Abrasions, for
instance, are not only seen in strangulated victims, but also in rape cases and
even in cases of child abuse. In this chapter trauma in general and the relevant
principles of importance in the examination of skin wounds are discussed.
5.1 Definition of trauma
Trauma can be defined as a wound or injury to the body as result of violence
or force applied to the body. This disrupts or destroys the integrity of the
body as a whole, or of an organ system or body part.
5.2 Types of trauma
We are all subject to different types of wounds or injuries in daily life. Some of
these wounds are the result of physical violence or physical factors.
Mechanical violence or trauma occurs during a fall, or when we are hit by
94

something; this can be a blunt or sharp object. Other wounds due to physical
trauma occur when heat or even cold affects the body, such as burn wounds
or thermal trauma. Electricity also causes wounds. Wounds due to radiation
were especially seen after the nuclear explosions in Japan during WWII.
Barotrauma occurs when the body is exposed to very high or low pressures,
especially if it is associated with sudden changes in atmospheric pressure.
Many chemical substances act as irritants to the body. Corrosive substances
like acids and alkalis often cause injuries to the mouth and oesophagus.
Poisoning can also be regarded as a form of chemical trauma to the body.
Trauma or violence can therefore be classified as follows:
PHYSICAL TRAUMA CHEMICAL TRAUMA
. Mechanical trauma: . Acid or alkaliBlunt forceSharp force
. Thermal factors: . PoisoningHeatCold
. Electrical trauma
. Barotrauma
. Radiation-associated trauma
. Ultrasound
Some of these wounds are discussed elsewhere in this study guide. The
primary aim of this study unit is to discuss wounds involving the skin and
underlying tissue which occur as a result of a mechanical force or violence
acting on the body.
5.3 Mechanical trauma
When the body is exposed to mechanical violence, certain factors will
determine the extent of the injury or trauma: This is also called the effective
wounding or injury force.
5.3.1 The effective wounding or injury force
The effective wounding force, that is the effective amount of force resulting
in a wound, and which will determine its extent and appearance, depends on
the following factors:
1. The amount of energy transferred to the tissue. Mechanical violence to
the body is the result of the relative movement of the body in relation to
another object, for example a knife or the road surface. It therefore
represents the kinetic energy of the object, which is represented by the
formula Ek = �mv2, available for acting on the body.
2. The duration of the application of the force. Cricket players know too well
that it is much more comfortable and less painful to catch a cricket ball
while the hand is moving in the same direction as the ball. As the ball is
stopped over a longer distance as well as time interval, the loss of energy by
the ball occurs more gradually. As the energy transfer from ball to hand thus
takes longer, energy and therefore the effective force that can cause trauma,
is all the time kept low and thus trauma is prevented. Scientifically speaking
energy loss per time unit is lower than it would have been if the ball stops
95
General traumatology

immediately, for example as in hitting a wall. The amount of force needed
to cause trauma (or pain) is thus never reached.
3. The surface of application of the force. When the body is hit by a flat
piece of wood (plank) or other material, energy loss occurs over a larger
surface area compared with the force exerted on the tip of a knife or on
its cutting edge. The amount of energy per surface area unit is therefore
much higher in the case of a knife tip compared with the larger flat
surface of a plank.
4. The behaviour of an object when it hits the body. If the object
disintegrates at the moment of impact, energy is lost, and less energy is
then available to cause injury.
5. The biomechanical features of the tissue. Certain tissue types, for example
the skin, can stretch before it is injured. Other types such as bone and
organs like the liver, do not have the same degree of elasticity. Fatty tissue
also bruises easily. The degree of resistance to injury by the skin varies. The
skin over the abdomen can undergo significant distortion before it tears;
the scalp is more easily torn because it is trapped between the object of
force and the underlying skull. Abnormal conditions can also influence the
effect of violence. If a person bleeds easily it will increase blood loss and
therefore the extent of contusions (bruises). Other diseases affecting
organs, for instance enlarged spleens in malaria cases also exacerbate
trauma.
6. Protective material. A helmet and thick leather clothes as well as thick
hair covering the scalp will diminish trauma.
5.3.2 Appearance of a wound
The appearance of a wound is determined of a number of factors:
1. The effective wounding or injury force, as described above.
2. The age of a wound. Certain changes occur after time Ð contusions
undergo a spectrum of colour changes, from purple to yellow-brown. The
edges of wounds are often swollen in the initial stage.
3. Therapeutic interventions. Suture material and other interventions
change the appearance of the wound. In some cases the wound can even
be excised, for instance where a plastic surgeon changes the appearance of
a wound to achieve a better cosmetic effect.
4. Complications. Certain wounds, for example wounds due to animal bites,
often become inflamed. The inflammation process can change the
appearance of a small wound dramatically.
5.4 Classification of mechanical trauma
Mechanical trauma or violence can be applied over a large surface area (blunt
trauma or violence), or it can be applied over a smaller area as seen with sharp
violence or trauma. These two main groups will be discussed in detail. Please
study photos 9, 10, 11, 12, 13, 16, 17, 18 for the different types of trauma.
5.4.1 Blunt trauma
Blunt trauma comprises a spectrum of wounds, such as contusions (bruises),
abrasions and laceration wounds resulting from blunt forces. This is also the
96
Study unit 5
sequence in which these wounds appear as the violence increases, in other
words the first wound is a contusion, when the small blood vessels in the soft
tissue in the subcutaneous region tear. With more violence the epidermis of
the skin will be lost, either partially or completely, and an abrasion will
appear. With even more violence the epidermis and the underlying
subcutaneous tissue will tear, resulting in a laceration.
5.4.1.1 Contusions (bruises)
Contusions or bruises are the result of damage to small blood vessels in the
subcutaneous tissue, which then rupture, with subsequent extravasation of
red blood cells (red blood cells leaking out of the blood vessels into the
surrounding soft tissue). Very small pin-point contusions are also known as
petechiae. Larger contusions are also called ecchymosis. A haematoma is an
even larger contusion where the blood collects in a cavity formed in the
damaged tissue.
The extent of a contusion is influenced by a number of factors:
1. The anatomical structure of the tissue. If the skin is well supported by the
underlying tissue, only a limited space exists in which the red blood cells
can accumulate outside the blood vessels (extravasation). This is the
reason why the palms of the hands as well as the sole of the feet are often
the preferred sites to which violence is applied during torturing, as it will
be less obvious. Contusions appear more readily in fatty tissue; this is one
of the reasons why females are more easily bruised than males.
2. The age of the individual. Elderly people and babies are more prone to
bruising as the smaller blood vessels are very fragile in older individuals,
while babies have a high percentage fatty tissue, which offer little support
for the smaller blood vessels.
3. Other medical conditions and drugs. Certain medicines that dilute the
blood cause people to bleed more readily and this increases the extent of
the contusions. This is often seen in individuals on anti-coagulation
therapy such as Warfarin. Malnutrition (eg scurvy due to vitamin C
deficiency) is also a predisposing factor as the bloodvessels are more
fragile.
4. Skin colour. Contusions are less readily visible in a person with a dark
complexion.
5. Age of the contusions. Contusions develop over a period of time. At first
the area may be quite small, but after some hours or days it becomes
bigger. It is therefore important in cases of alleged assault (eg sexual
offences) to re-examine the living victim a day or two after the assault, as
some of the contusions may than be more readily visible.
Contusions undergo a spectrum of colour changes over time as a result of
break-down of the blood. In older people contusions take longer to disappear.
Several factors influence the tempo of disappearance and colour changes in
contusions, and it is therefore important not to be too dogmatic when the age
of a contusion is determined. However, in general it can be assumed that a
contusion with no colour changes is less than two days old, except in the
elderly. It is also of importance to determine whether all contusions are more
or less of the same age.
97
General traumatology

During an autopsy post-mortem colour changes (hypostasis) must not be
confused with a contusion. An incision of the skin to determine whether the
blood is limited to the blood vessels (hypostasis) or whether it is present in
the surrounding tissue (contusion) will give verification.
It is important to know that contusions do not develop post mortem as an
active blood circulation is necessary for contusions to develop. Although red-
blood cells can leak out of the blood vessels during the post-mortem period,
this is limited and forms part of the process of hypostasis or livores mortis.
The following are characteristic contusions which can be of assistance in a
post-mortem examination:
1. Impression contusion. The shape of the object which caused the
contusion, for instance the buckle of a belt or motor vehicle tyre, can
be discerned.
2. Tramline contusions (fig 5.2) Typically caused by a cane. During contact
of a cane with the body, the skin and tissue in the central aspect are
compressed, while some degree of stretching occurs at the border region.
In this latter area the blood vessels can tear resulting in two parallel red
lines with a white area in between.
3. Abrasion due to fingers and finger tips. These contusions are seen on the
limbs of an abused child, the thighs of a rape victim or the neck of a
strangulation victim.
4. Contusions caused by teeth. The pattern left by the teeth can assist in
identifying an alleged assailant.
5. Contusions due to resuscitation. Substantial force is exerted during
cardiac massage, and this can result in contusions of the breast bone
(sternum) and even fractures of the bone.
5.4.1.2 Abrasions
Abrasions occur due to partial or complete loss of the epidermis after
violence. If the full thickness of the epidermis is lost, the small blood vessels
in the underlying tissue are exposed, and the wound will bleed. It is often
possible to determine the direction of force, as the small heaped-up skin
fragments will be present in the direction in which the force was applied.
The following types of abrasions occur:
1. Brush abrasions or grazes. These wounds occur due to a force applied
horizontally to the surface of the skin, for instance when the body moves
over a relatively rough surface such as grass or a tarred road. A so-called
grassburn is an example of this type of wound.
2. Impression abrasions. These wounds are similar in origin to impression
contusions, but the amount of force is greater and the force is exerted
vertical to the skin. The abrasion resulting from a safety belt or steering
wheel is an example of this type of wound.
3. Scratch wounds. Scratches are the result of a force applied linearly to the
skin, for instance when a fingernail moves over the skin surface. The skin
fragments will accumulate in the direction of the force. This type of
wound is often seen in assaults. In cases of strangulation with the hands,
scratch wounds in the neck may be caused by the assailant as well as the
victim. It is therefore important to collect any material below the finger
Study unit 5
98
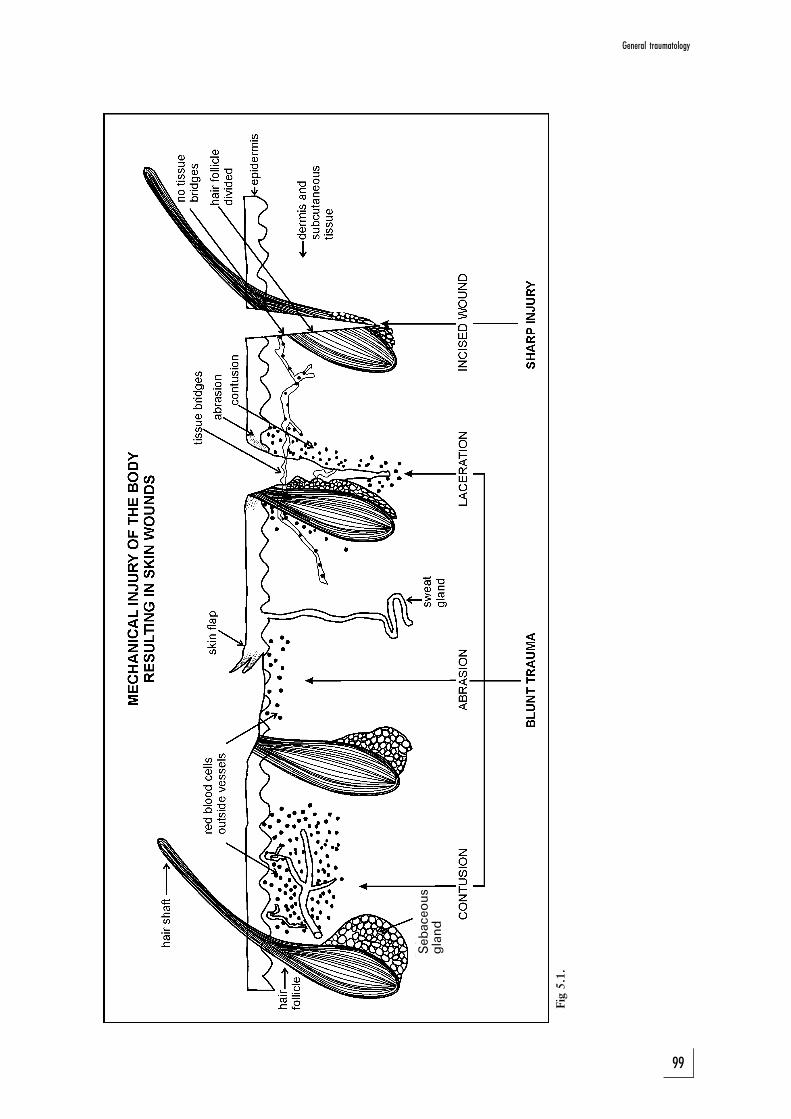
Sebaceous
gland
Fig
5.1
.
General traumatology
99

nails of the victim as well as the alleged assailant for forensic analysis, as it
may be of assistance in the identification process.
4. Localised friction abrasions. This type of wound is the result of force
applied linearly to the skin over a localised area. The energy loss per
surface area unit is therefore very high. An example is the wound on the
skin of the neck of a hanging victim after removal of the rope. It is also
seen in injuries made by a whip (sjambok).
Ante-mortem abrasions are usually covered by a scab. Abrasions arising in the
perimortem period often look like parchment, that is dry and leathery.
Abrasions can also appear in the post-mortem period, but then they are
yellow and transparent with no sign of a tissue response (eg no signs of
haemorrhage). Bite marks made by ants can also look like small abrasions.
5.4.1.3 Lacerated wounds
Lacerated wounds occur when the amount of force is such that the integrity
of the tissue is disrupted and the skin breaks. As the lacerated wound
develops at the site where the force is at the maximum, it is surrounded by an
area where the force was less, which then results in an abrasion. This abrasion
is then further surrounded by an area where there was even less energy per
unit area, resulting in a contusion or bruise. Therefore a lacerated wound is
always surrounded by the whole spectrum of injuries made by a blunt force
(ie abrasions and contusions).
A lacerated wound has a typical appearance, and differs from an incised
wound in the following ways:
LACERATED WOUNDS INCISED WOUNDS
. Wound edges irregular and ragged . Sharply outlined smooth edges
. Wound margin shows surrounding . No other injuries of woundabrasion and contusion, with loss margins, or hair lossof hair around wound
. Tissue bridges with blood vessels . All structures in the wound lineand nerve fibres present in wound transected
. Sometimes foreign material in . No foreign material in woundwound
The following typical lacerated wounds occur:
1. Split wounds. This type of wound occurs when the skin is trapped
between two hard objects. It often involves the scalp, when the skin is
Study unit 5
100
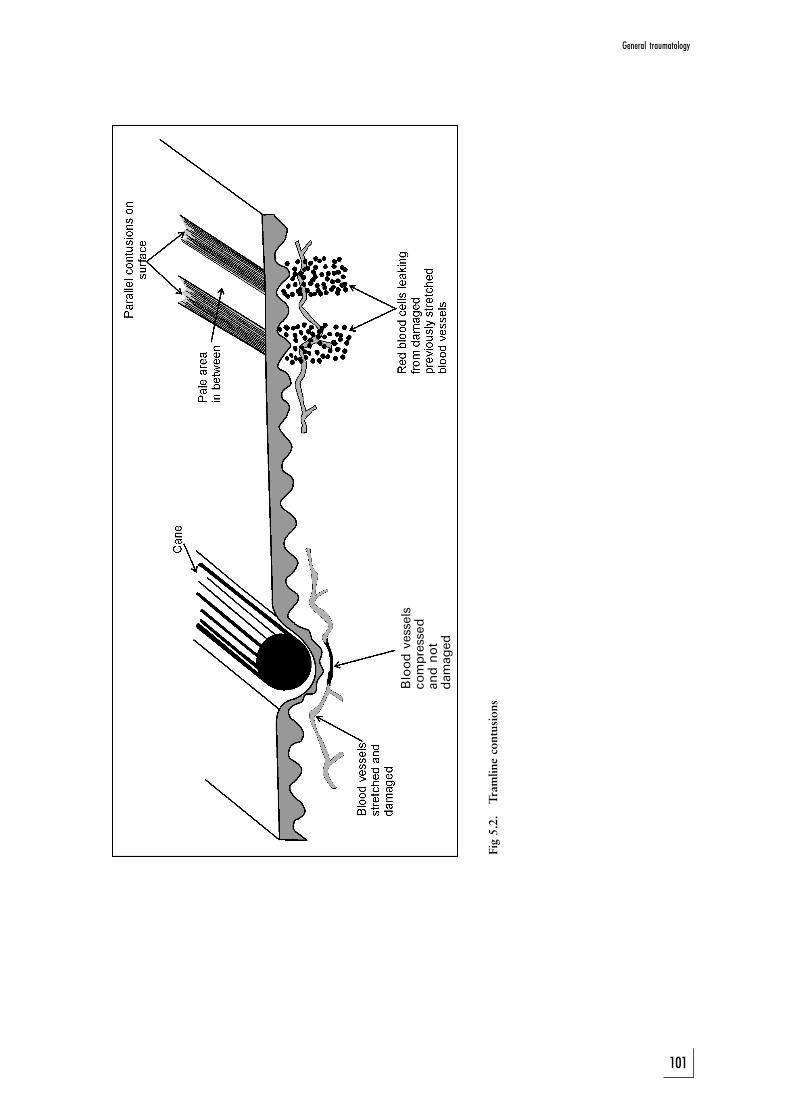
Bloodvessels
compressed
andnot
damaged
Fig
5.2
.T
ram
lin
eco
ntu
sio
ns
General traumatology
101
split between a hard object and the underlying skull. In these cases the
surrounding abrasion and contusion are often minimal. Sometimes loss
of hair can be seen surrounding the wound, due to the abrasion.
2. Hook lacerations. In this case a sharp object tears the skin and underlying
tissue from the body, leaving a linear appearance or angled flap. Animal
bite wounds belong to this category.
3. Subcutaneous tissue lacerations and degloving injuries. These wounds
occur when the different skin layers move against each other in such a
way that the tissue layers are torn apart. This is also known as
decollement injuries. The term ``degloving'' refers to the case where the
skin and soft tissue are literally pulled from the body like a glove.
4. Blunt penetration wounds. This group of wounds comprises a lacerated
wound on the surface, with a wound tract extending into the underlying
tissue. They are caused inter alia by garden forks, bicycle spokes and
screw drivers.
5.4.2 Sharp injuries
Sharp injuries occur when the force is concentrated on a very small surface
area, for instance the edge or tip of a knife. The tissue, and any other
structures in the skin, for instance a hair follicle, is transected. If the
underlying bone is involved there will be marks on the surface of the bone.
This is often seen with panga injuries to the head.
There are two types of sharp injuries, namely incised wounds and stab
wounds.
5.4.2.1 Incised wounds
These wounds are not as deep as they are long, and there is no wound track.
The location can give an indication of the circumstances in which they
occurred. For instance, tentative wounds over the front of the arms and wrist
are often seen in suicide cases. Wounds over the back of the forearms often
occur when the victim tries to protect him/herself (defence wounds).
5.4.2.2 Stab wounds or penetrating incised wounds
These wounds are not as long as they are deep, and there is a wound tract.
A stab wound has certain features: the skin wound looks like an incised
wound, and depending on the type of blade, both corners of the wound can
be sharp, or the one can be blunt and the other sharp. Sometimes the wound
seems to be branching out Ð this happens when the position of the blade is
changed while the knife is still in the body. If the whole blade penetrated the
body, an abrasion and contusion may be present on the skin where the hilt of
the knife hit the body.
The length of the wound tract is not necessarily an indication of the length of
the blade. Soft tissue (like the abdomen) can be compressed, and a relatively
short weapon may injure deep-lying organs. At post mortem, injuries could
be seen in an organ further away from the overlying skin surface than the
length of the blade.
It is important to describe the direction of the wound tract, and therefore the
Study unit 5
102
direction of the stab wound. It is also important to indicate whether any
important structures, such as arteries, are involved in the wound tract. The
tip of the weapon is sometimes found deep in the wound.
5.5 Description of wounds
It is important to describe wounds in detail. If possible, photos of wounds
should be included, but then a colour chart should also be added so that
colour changes can be judged objectively; sketches are also important.
The following must be indicated:
1. The number of wounds.
2. The time when the wound was inflicted. Except if the contrary is
indicated, it is usually assumed that the wounds occurred ante mortem.
However, if it is possible that a wound may have occurred in the post-
mortem period, it must be mentioned. This type of situation often occurs
with drowning victims, where injuries due to propellers of boats as well
as rocks may develop in the post-mortem period.
3. The precise location of every wound, measured from fixed reference
points (eg from the middle of the body in the horizontal level and specific
vertical points Ð like the height above the heel, level of the nipples, level
of the eyes, etc). It is also important to remember that the wounds are
described with the body in the anatomical position, that is in an upright
position with the palms of the hands facing forward. The wound tract of
a stab wound therefore does not necessarily represent the position of the
body at the time of the stabbing. (The same principle applies when the
body is hit by a bullet.)
4. The shape of every wound. For instance, is the abrasion an oval shape
with accumulation of skin on the one side? Are both corners of the stab
wound sharp (pointed), as those made by a knife with a double-edged
blade?
5. The size of the wound. Abrasions and contusions have two dimensions.
Lacerated wounds and incised wounds have only one dimension, namely
length, even if the wound is gaping. Stab wounds also have a depth
measurement.
6. Any additional wounds, for instance abrasions or contusions surrounding
a laceration wound.
7. The estimated age of the wound. It is important to decide whether the
wound is still fresh or whether it shows signs of healing.
8. Any signs of complications, for instance inflammation or abscess
formation.
9. Any signs of medical treatment, for example sutures
In the case of a stab wound, the direction of the wound tract, the depth as
well as any important structures involved, must be mentioned. Any other
additional factors of importance, including the impression sometimes seen in
contusions and abrasions, or the presence of foreign material in the wound,
must be mentioned. It is important to examine the entire body, also concealed
areas. Some pathologists will even indicate on the sketch with a tick mark
that they have examined the part in question and found no wounds.
General traumatology
103

The distribution of wounds can be of assistance to reconstruct the scenario.
Contusions and abrasions over the posterior aspects of the forearms are often
seen when the victim tries to protect his head by folding the arms over the
head (self-defence wounds). Sometimes incised wounds of the hands can be
seen if the victim tried to grab the knife from the assailant. Tentative wounds
in cases of suicide have already been mentioned.
5.6 Dating of wounds
Certain tests can be done to date wounds. However, wounds change over
time and there can therefore be a significant overlap, so that dating may not
be absolutely conclusive. Wound changes are due to the tissues' response in
trying to heal the wound.
The following is of importance in dating of wounds:
1. Macroscopic appearance, in other words colour changes, swelling, et
cetera, as seen with the naked eye.
2. Microscopic appearance, in other words cellular changes in the form of
inflammatory cells and connective tissue elements, visible under a
microscope.
3. Biochemical analysis, for example to detect enzyme changes. This is a
highly specialised field and it is seldom used?
ACTIVITIES
1. A person presents with a linear wound to his head. He alleges that he was
hit with a panga, although there is also evidence that he was only hit on
the head with a hard piece of wood (plank). How will you differentiate
between these two wounds?
2. You are involved in a trial where the victim was an elderly female who
was murdered. The post-mortem report states that numerous bruises/
contusions were present over the chest, and there were also fractures of
the ribs and sternum. These fractures were surrounded by fresh
haemorrhages. The defence alleges that these injuries were caused by
attempts at resuscitation by the assailant, and not by the assault itself.
How can the pathologist refute this allegation?
3. You are involved in a trial where the victim had allegedly died of a stab-
wound. What are the most important features regarding this wound
which you would look for in the post-mortem report.
FEEDBACK
1. A blow with a hard object over the head tends to cause skin
splitting. This occurs because the skin is caught between the hard
object on the one side and the skull bone on the other. Although not
necessarily prominent, detailed examination will still show the
features of a lacerated wound, that is a thin margin of abrasion and
contusion surrounding the wound, and tissue bridges in the wound.
With the abrasion there could also be loss of hair surrounding the
wound.
2. When injuries occur while a person is still alive, an effective blood
Study unit 5
104

circulation is still present. In other words, blood will leak from the
damaged vessels as well as from the fractures due to haemorrhaging
into the soft tissue. If resuscitation is unsuccessful, blood circulation
will not be reinstated, and therefore minimal leakage of blood from
the damaged vessels or fractures will occur. For this reason post-
mortem fractures are without surrounding haemorrhage.
If resuscitation was indeed successful, the wounds will have the
appearance of contusions and fractures as usually seen in the living
person. In this specific case, the resuscitation was unsuccessful, and
the contusions or fracture-associated haemorrhages are therefore
not expected. This statement is therefore most probably incorrect
or false.
3. The description of wounds consists of a number of important
aspects including the number of wounds, the appearance, et cetera.
This is discussed in section 5.5 of this study unit.
General traumatology
105
STUDY UNIT 6Complications of trauma
Contents
6.1 Shock
6.1.1 Definition
6.1.2 Classification of shock
6.1.3 Clinical presentation
6.1.4 The effect of shock on organ systems
6.2 Embolism
6.2.1 Definition
6.2.2 Thrombo-embolism
6.2.3 Air (gas) embolism
6.2.4 Fat embolism
6.2.5 Diverse conditions
6.3 Pneumothorax
6.3.1 Definition
6.3.2 Causes
6.3.3 Origin of pneumothorax
6.3.4 How to diagnose a pneumothorax
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. understand that shock often is the final mechanism causing the death
of a severely ill or injured person
. discuss the different types of embolism and the circumstances in
which they occur
. understand that pneumothorax is a common complication in the
trauma unit
The initial injury is often not severe enough to cause death, but complications
may follow which then become the terminal cause of death.
There can be many complications. Some are unique to a specific body part or
organ (eg pneumothorax in thoracic or chest injuries and herniations of brain
tissue after brain injuries), while others are more general. The two most
important general complications are shock and infection (sepsis, septicaemia,
endotoxaemia, septic shock).
This study unit will deal with the latter two general complications, as well as
some of the system-associated complications.
106
6.1 Shock
6.1.1 Definition
Shock is a condition where the circulatory system is not able to perfuse the
vital organs adequately, due to a discrepancy between the circulating blood
volume and the volume of the vascular bed.
6.1.2 Classification of shock
Shock can be caused by failure of different mechanisms.
(1) Cardiogenic shock. When the heart cannot contract effectively, forward
propulsion of blood in the circulation decreases, and organs such as the
brain and lungs do not receive any blood, and therefore oxygen and other
nutrients. This causes stagnation hypoxia. A massive myocardial infarct or
heart attack is the most common cause of cardiogenic shock. Insufficient
or decreased cardiac function further negatively affects the heart muscle,
as perfusion of the heart muscle itself also decreases, and the heart cannot
contract adequately.
(2) Hypovolemic shock. Severe blood loss or loss of other body fluids, either
externally (dehydration) or internally (for instance in the abdominal
cavity in cases of peritonitis or inflammation of the abdominal cavity), can
decrease the circulating blood volume. Trauma with blood loss, for
instance due to multiple injuries sustained in a motor-vehicle accident, or
due to stab wounds, is a common cause of hypovolemic shock. This
results in anaemic hypoxia of the tissue.
(3) Neurogenic shock. Loss of the normal tone of blood vessels can result in
dilatation of the vascular bed, which then increases dramatically in
volume. The circulating blood volume is not sufficient to fill the dilated
vascular bed. This type of shock is seen in spinal cord injuries, and
sometimes during anaesthetic procedures.
(4) Septic shock. Micro-organisms, especially bacteria, can produce sub-
stances which cause shock through certain mechanisms. The substances
are usually part of the structure of the micro-organism, and are then
called endotoxins. If the micro-organism produces and releases the
substance into the blood, they are called exotoxins. They affect different
mechanisms, for example blood-clotting mechanisms, resulting in DIC
(diffuse intravascular coagulopathy).
(5) Anaphylactic shock. Individuals who are highly allergic to substances like
penicillin or bee venom, will also experience a dramatic dilatation of the
vascular bed. The blood volume is not sufficient to fill this dilated
vascular bed. There is often additional loss of fluid due to increased
permeability of vessels.
Shock is therefore the result of an imbalance between the circulating blood
volume and the vascular bed which has to be perfused.
6.1.3 Clinical presentation
A person in shock is characteristically cold and sweaty, with a grey colour, low
Complications of trauma
107

blood pressure and weak pulse. The pulse rate is rapid, but as shock
progresses and becomes irreversible, the pulse rate will gradually drop. Shock
is initially reversible if managed optimally and timeously.
6.1.4 The effect of shock on organ systems
Shock affects many organs, but the degree of damage to vital organs will
determine whether or not the person in shock will survive. The normal
response of the body is to redistribute blood from the less important organ
systems, such as the skin and abdominal organs, to the more important vital
organs such as the brain and heart.
6.1.4.1 Brain
Some of the brain cells in specific regions of the brain (eg the neurons in the
hippocampus) are more susceptible to a lack of oxygen (hypoxia) than
elsewhere in the brain. In addition the watershed regions are also more
susceptible to hypoxia due to decreased blood flow, and are therefore often
involved in cases of severe hypotension (low blood pressure). The watershed
areas are present at the boundaries between the distribution areas of two
major cerebral arteries.
Because it is essential to fulfil the oxygen needs of the brain, blood flow to the
brain will be maintained almost until death occurs, unfortunately with the
sacrifice of other organ systems, for instance the lungs, kidneys and gastro-
intestinal system.
6.1.4.2 Lungs
Lung changes are also known as diffuse alveolar damage (DAD), shock lung
or adult respiratory distress syndrome (ARDS). Due to the changes oxygen
cannot be sufficiently absorbed by the small blood vessels surrounding the
lung sacs (alveolar capillaries). These patients often have to be ventilated, and
are susceptible to lung infections.
6.1.4.3 Kidneys
Decreased blood flow to the kidneys causes cell death in the small tubuli in
the kidneys. This is also known as acute tubular necrosis (ATN), and it causes
renal failure.
There are other causes of acute tubular necrosis which are not necessarily
associated with shock in the initial stages, such as poisons or the products
released by damaged red blood cells and muscle cells (haemoglobin and
myoglobin). The latter condition is often seen during marathons, and is the
combined effect of dehydration and damage to red blood cells and muscle
elements in the athletes' feet. ATN also commonly occurs after assault causing
multiple blunt injuries. These victims often have severe bruises or contusions,
causing two problems: blood loss into the soft tissue, with subsequent
hypovolemia, and at the same time destruction of the red blood cells trapped
in the tissue. Two or more days after the assault the victim presents in a
shocked state, with no urinary output, and dies.
Study unit 6
108
6.1.4.4 Gastro-intestinal system
Stomach ulcers can cause severe bleeding, which can be prevented by
administering antacids to the person in shock.
There can be necrosis of the intestinal mucosa, and sometimes even of the
entire bowel wall due to rechannelling of blood away from the gastro-
intestinal system towards the vital organs.
6.1.4.5 Liver
In a patient in shock the liver presents with a patchy red pattern against a
whitish background. The patchy pattern is caused by congestion of the
central blood vessels due to poor drainage against the background of early
fatty changes due to decreased oxygen supply. In some of the textbooks this
appearance is described as a nutmeg pattern.
6.1.4.6 Heart
There can be haemorrhages beneath the endocardium (the innermost
membrane covering the heart surface), especially in the left ventricle. These
sub-endocardial haemorrhages are also described in arsenic poisoning and
head injuries (see photo 49).
6.1.4.7 Adrenals
The adrenals can show haemorrhages and fat depletion. The latter is the
result of the release of the fat-containing stress hormones (adrenalin and
cortisone).
6.2 Embolism
6.2.1 Definition
An embolus is a foreign substance which forms in, or enters the blood
circulation: It can be a thrombo-embolus or blood clot, air or gas, fat,
amniotic fluid or even a bullet.
6.2.2 Thrombo-embolism
Blood clots or thrombi often develop in the veins of the lower legs of
individuals who are immobile, for example when sitting in one position for a
long time (as in the so-called economy-class syndrome as described in air
passengers). It can also develop in bedridden persons after an operation or
due to illness. Some people may also have a genetic predisposition for
developing blood clots.
If this blood clot (thrombus) detaches from the blood vessel wall, it can travel
in the venous system to the lungs, where a lung embolism can develop. This
presents with symptoms such as shortness of breath and coughing up of
blood. If the blood clot is large it can cause death.
Certain measures can prevent the formation of thrombi and consequently
Complications of trauma
109

embolism, inter alia moving the legs and contracting and relaxing leg muscles,
elevating the foot of the bed, and allowing patients to become mobile as soon
as possible.
6.2.3 Air (gas) embolism
6.2.3.1 Definition
Air embolism is the presence of air in the blood circulation.
6.2.3.2 Classification
Air embolisms can form in the arterial and/or venous systems, and therefore in
either the systemic blood vessels (eg the blood vessels of the brain) or the
pulmonary (lung) vessels. The terminology of veins and arteries is often
confusing, and you are referred to the basic anatomy as described in study unit 2.
The following general principles apply: a vein always carries blood towards
the heart, while an artery carries blood away from the heart. Arteries usually
contain oxygen-rich blood, and veins oxygen-poor blood. The two major
blood vessels of the lungs can cause confusion. The pulmonary artery
distributes oxygen-poor blood from the heart to the lungs; it is an artery as it
carries the blood away from the heart. The pulmonary vein brings the
oxygen-rich blood from the lungs to the heart.
6.2.3.3 How an air embolism originates
If an air bubble enters the circulation, it forms an air lock as the air is
compressed and therefore prevents forward movement of blood. The amount
of air necessary to create such an airlock depends on the diameter of the
blood vessel. An arterial vessel, for instance the carotid and coronary arteries,
can be blocked by as little as one millilitre air. Venous emboli are usually
larger, and approximately one hundred millilitre (100 ml) air is needed to
obstruct pulmonary outflow from the right ventricle.
The pathological features seen in cases of arterial air embolism are similar to
those seen in ischaemic damage, including infarctions in the brain and heart.
If the patient dies instantly, no changes, except for the presence of air in
vessels, will be noted.
Certain factors will determine whether air will enter a blood vessel after
damage to the vessel. With a venous air embolism the negative pressure in the
venous system during inspiration is the major factor. This is often seen in
cases where the defect in the blood vessel is at a higher level than the heart,
for instance in cases where a person remains standing after being stabbed in
the jugular vein. The size of the defect and the distance to the heart is also
important. Some veins also dilate due to the action of the adjacent muscles
during inspiration, for instance the subclavian vein.
A number of small emboli formed over time is not necessarily fatal. Air can
also enter the blood circulation but only spread to other organs after some
time (delayed air embolism).
Study unit 6
110
6.2.3.4 Causesa Venous air embolism (the most common type)
(1) Penetration of the jugular vein in the neck (eg due to a stab wound) and
especially when the person remains in the upright position. The air will
go via this vein to the superior vena cava and ultimately to the right side
of the heart.
(2) Criminal abortions. In some cases air may enter the uterus inadvertently,
especially if a syringe is used during the procedure. The placenta will
detach from the uterine wall. The air will enter the venous system
through the numerous blood vessels in the placental bed, and will then
spread via the pelvic veins to the inferior vena cava and eventually to the
right side of the heart.
(3) Neurosurgical procedures, especially with surgery in the occipital region
and the patient in the upright position.
(4) Iatrogenic or doctor-associated causes, for example intravenous lines.
This includes defective dialysis equipment.
b Arterial air embolism
(1) Barotrauma, where pressure changes or pressure waves may rupture or
lacerate the lungs allowing air to move from the alveolar spaces into the
lung blood vessels. Mostly seen in two situations:
. explosions, especially in confined spaces
. diving accidents, where a diver surfaces without exhaling while
surfacing.
The basic principle is that the volume of any gas, including air, is
inversely proportionate to the pressure. A given volume of air will
therefore occupy a small volume under water compared with at the
surface, due to the higher pressure under water. If the diver does not
gradually exhale while surfacing, the air in the lung will expand and
the lung will rupture.
(2) Stab wounds in the lung, where the lung tissue is damaged and the blood
vessels come into contact with air.
(3) Stab wounds in the neck, with damage to the carotid arteries. Air, and
sometimes even fat, may be sucked into the vessel through the so-called
Venturi-effect.
(4) Open heart surgery.
(5) Paradoxical air embolism. This is found in two situations, namely in
newborn babies and in adults. In the unborn baby (foetus) there is a
connection between the right and left heart chambers, the foramen ovale.
It is not necessary for blood to flow through the lungs, because the baby is
still intra-uterine and does not use its lungs.
In a newborn this opening is still open, and the circulation is also not yet
optimal. A small volume of air entering the venous circulation can go
through the foramen ovale to the left side of the heart, and from there
into the arterial circulation. This may obstruct blood flow to the heart and
the brain.
In approximately 20% of adults this potential right-to-left connection
may continue to exist. However, this opening will usually be occluded by
Complications of trauma
111
a membrane, as long as the pressure in the left heart chambers is higher
than in the right heart chambers.
If the pressure in the right heart chambers rises higher than that in the left
chambers, which happens when the patient exhales against a closed nose
and mouth (the Valsalva manoeuvre), this potential connection may open
due to the change in the pressure gradient, and blood (and air) may leak
from right to left. An air embolus can then move from the venous system
to the arterial circulation, with obstruction of the blood supply of the
brain and heart.
In other heart defects where there are openings in the septum, air emboli
can also occur.
6.2.3.5 How to diagnose an air embolism
In certain circumstances the possibility of an air embolism must be considered
before the post mortem is performed, for example when there is a stab wound
in the neck, or a young female dies suddenly and unexpectedly (criminal
abortion). In these cases it is advisable to take X-rays so that air in the heart
and blood vessels could be detected.
Often air is found in the tissues surrounding the defect, and this can result in a
crackling sound with palpation, so-called crepitus. The tissue can also appear
swollen, known as surgical emphysema.
If a young female in her fertile years dies suddenly and unexpectedly, it is
important to examine the uterus in situ, that is before it is removed. Any signs
of recent pregnancy must be noted, and the inferior vena cava must be
examined for air bubbles.
The next step is to open the pericardial sac and to examine the coronary
arteries for an air embolism. The pericardial sac is then filled with water and
the right heart chambers and thereafter the left heart chambers opened under
water with a knife or scissors. If there is an air embolism, air will bubble out of
the heart.
The cerebral arteries must also be inspected for air bubbles. It is important to
remember that air can be sucked into the cerebral veins during the removal of
the skull, and that this does then not indicate an air embolism, but is due to
human intervention. If decomposition has set in, air may either dissolve and
disappear if there indeed was an air embolism, or decomposition gases can be
produced, presenting as an air embolism. The gases then have to be analysed
in order to determine what they are.
6.2.4 Fat embolism
6.2.4.1 Definition
Fat embolism occurs when fat cells, and sometimes even bone-marrow tissue,
enter the circulation.
6.2.4.2 Causes
Certain conditions cause fat cells to enter the venous circulation and they can
then become trapped in the capillary vessels of the lung. This not only causes
Study unit 6
112
mechanical obstruction to the blood flow, but also activates the blood clotting
system. The fat cells then enter the arterial circulation, and eventually the
brain, after the vascular beds of the lungs had been saturated with fat.
Some of the causal conditions are:
(1) fractures of the shaft of long bones, for instance the femur
(2) soft tissue injuries
(3) burn wounds
6.2.4.3 Clinical presentation
Almost 90% of patients with severe skeletal injuries develop fat emboli, but
only 1% will present clinically. The clinical presentation is called the fat
embolism syndrome. It usually presents 24 to 72 hours after injury, and it is
fatal in 10% of cases. It has the following clinical features:
(1) lung insufficiency: the patient feels short of breath
(2) neurological symptoms: the patient is irritated, restless and suffers from
delirium
(3) anaemia
(4) decreased platelets (thrombocytopenia): the patient shows petechial
haemorrhages
6.2.4.4 Confirmation of fat embolism
Microscopic examination of the lung and brain tissue in the deceased can
indicate the presence of fat in the tissue. In a living person fat drops can be
detected in the sputum.
6.2.5 Diverse conditions
Two conditions which are not caused by complications due to injuries but
from part of the embolism spectrum, need to be mentioned. They are caisson
disease or decompression sickness and an amniotic fluid embolism.
(1) Caisson disease or decompression sickness is the condition which is
sometimes confused with air or gas embolism. It is seen in divers, when
the nitrogen and other gases in the blood come out of solution and form
minute air bubbles when decompression is too rapid. This is the cause of
the so-called bends.
(2) Amniotic fluid embolism is a dangerous, but fortunately rare, complica-
tion of pregnancy and labour. When the amniotic fluid enters the
maternal circulation (via a mechanism similar to that of air embolism), the
amniotic fluid does not only cause mechanical obstruction to the blood
flow in the lungs, but it also contains certain substances which can interact
with the blood clotting mechanism. It can also suppress cardiac function.
6.3 Pneumothorax
6.3.1 Definition
Pneumothorax is the condition where air is present in the thoracic cavity.
Complications of trauma
113
6.3.2 Causes
(1) Stab wounds and other penetrating wounds of the thorax. The negative
pressure in the thorax cavity will suck the air into the cavity.
(2) Barotrauma. If a diver surfaces without exhaling, the air in the lungs will
expand due to the lower pressure on the surface. This expansion can
rupture the lung and air will enter the thoracic cavity. This can also cause
an air embolism. Explosions causing shock waves can also result in
rupture of the lungs.
(3) Medical conditions. Lung pathology such as emphysema can cause
pneumothorax. Sometimes young people develop this condition sponta-
neously.
6.3.3 Origin of pneumothorax
The lungs need a negative intra-thoracic pressure for expansion. When a
pneumothorax originates, this negative pressure is lost, and the lung collapses.
In some conditions air may also enter the thoracic cavity, but be unable to
leave it again, usually because of a one-way valve-like action of the tissue. This
results in a life-threatening complication, the tension pneumothorax. The
increased positive pressure in the thoracic cavity causes decreased blood flow
to the heart, and the patient goes into shock and may die.
6.3.4 How to diagnose pneumothorax
In a living individual an X-ray of the chest will show the collapsed lung as well
as air in the thoracic cavity. In the deceased person the thoracic cavity must be
opened under water. This can easily be done by folding back the skin and
muscle on the sides of the thorax so that a small reservoir is formed, which is
then filled with water. An opening is made below the water level into the
thoracic cavity. If there is a pneumothorax, air bubbles will escape into the
water.
ACTIVITIES
1. During a fight one person stabs the other in the neck. While they are still
standing upright and arguing, the stabbed individual collapses and dies
almost immediately. How should the pathologist approach this death?
2. A scuba diver surfaces, coughs blood and dies. What condition will the
pathologist have to consider? What other complications may also be
caused by this mechanism?
FEEDBACK
1. This scenario is typical of an air embolism. During a fight a stab
wound or incised wound is often inflicted to the neck, which opens
(injures) the jugular vein(s), and sometimes also the carotid arteries.
While the patient is in the upright position, the wound is higher
Study unit 6
114

than the heart, and air is sucked into the vessel, especially during
inspiration.
In this type of death the presence or absence of air embolism must
be established. Although the majority of these deaths are caused by
venous air embolism, opening of the carotid arteries may also cause
arterial air embolism to the brain.
2. This scenario is that of pulmonary barotrauma with rupture of lung
tissue. This develops when a scuba diver surfaces after having
inhaled additional air while under water. If this extra volume of air
is not exhaled while he surfaces, the volume of air will increase at
the lower pressure, and rupture and damage the lung tissue. The
blood vessels rupture, and air enters the vessels causing arterial air
embolism. It develops because the air enters the pulmonary or lung
vein and is then distributed to the left side of the heart and
ultimately to the vital organs such as the brain and heart. Other
complications are pneumothorax and surgical emphysema as well as
unique complications such as ``the bends''.
Explosions in enclosed spaces may also result in pulmonary
barotrauma.
115
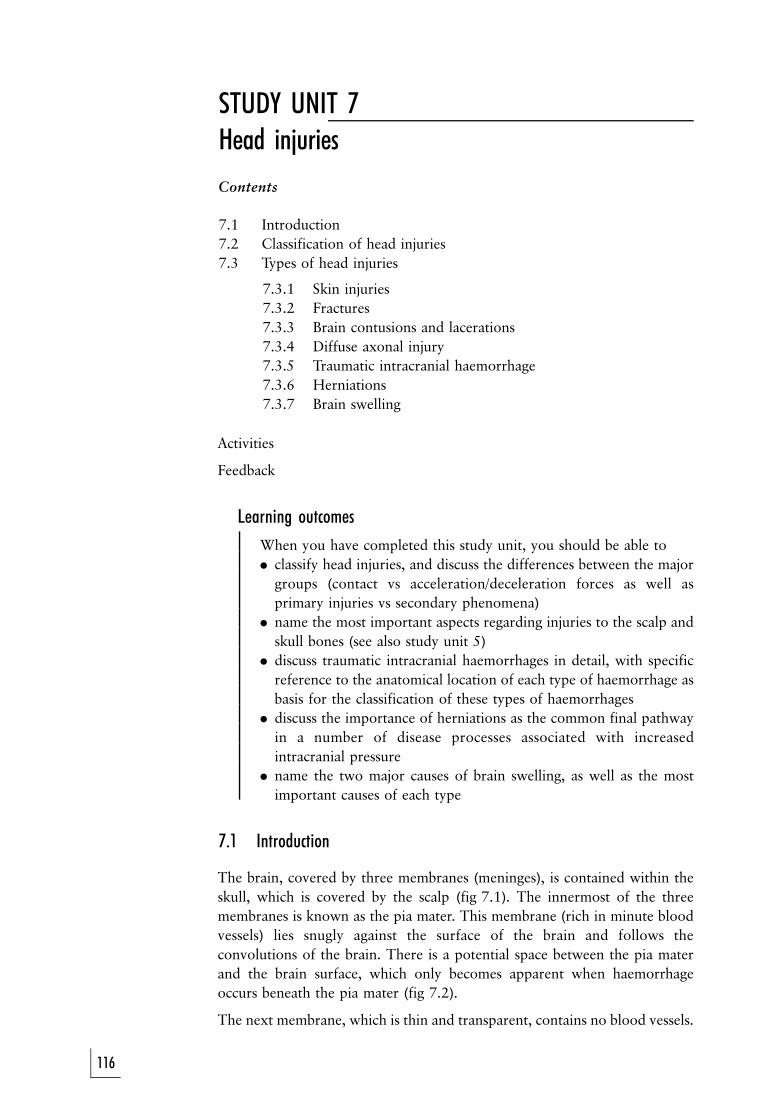
STUDY UNIT 7Head injuries
Contents
7.1 Introduction
7.2 Classification of head injuries
7.3 Types of head injuries
7.3.1 Skin injuries
7.3.2 Fractures
7.3.3 Brain contusions and lacerations
7.3.4 Diffuse axonal injury
7.3.5 Traumatic intracranial haemorrhage
7.3.6 Herniations
7.3.7 Brain swelling
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. classify head injuries, and discuss the differences between the major
groups (contact vs acceleration/deceleration forces as well as
primary injuries vs secondary phenomena)
. name the most important aspects regarding injuries to the scalp and
skull bones (see also study unit 5)
. discuss traumatic intracranial haemorrhages in detail, with specific
reference to the anatomical location of each type of haemorrhage as
basis for the classification of these types of haemorrhages
. discuss the importance of herniations as the common final pathway
in a number of disease processes associated with increased
intracranial pressure
. name the two major causes of brain swelling, as well as the most
important causes of each type
7.1 Introduction
The brain, covered by three membranes (meninges), is contained within the
skull, which is covered by the scalp (fig 7.1). The innermost of the three
membranes is known as the pia mater. This membrane (rich in minute blood
vessels) lies snugly against the surface of the brain and follows the
convolutions of the brain. There is a potential space between the pia mater
and the brain surface, which only becomes apparent when haemorrhage
occurs beneath the pia mater (fig 7.2).
The next membrane, which is thin and transparent, contains no blood vessels.
116
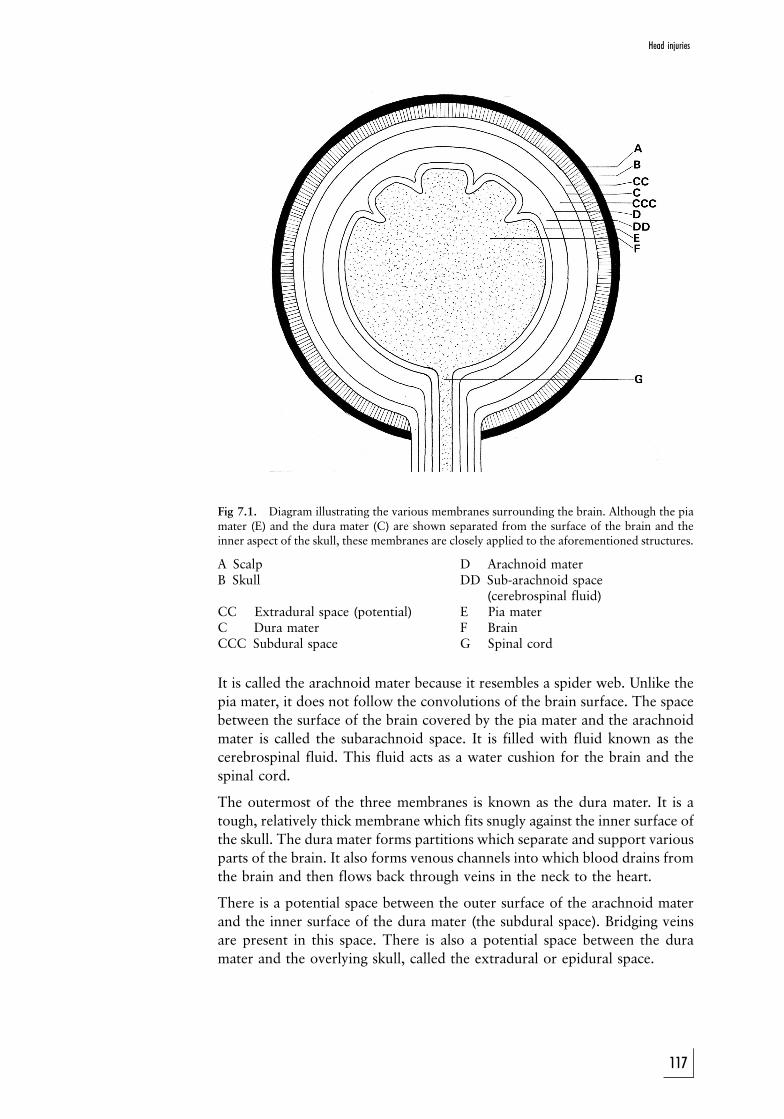
Fig 7.1. Diagram illustrating the various membranes surrounding the brain. Although the piamater (E) and the dura mater (C) are shown separated from the surface of the brain and theinner aspect of the skull, these membranes are closely applied to the aforementioned structures.
A Scalp D Arachnoid materB Skull DD Sub-arachnoid space
(cerebrospinal fluid)CC Extradural space (potential) E Pia materC Dura mater F BrainCCC Subdural space G Spinal cord
It is called the arachnoid mater because it resembles a spider web. Unlike the
pia mater, it does not follow the convolutions of the brain surface. The space
between the surface of the brain covered by the pia mater and the arachnoid
mater is called the subarachnoid space. It is filled with fluid known as the
cerebrospinal fluid. This fluid acts as a water cushion for the brain and the
spinal cord.
The outermost of the three membranes is known as the dura mater. It is a
tough, relatively thick membrane which fits snugly against the inner surface of
the skull. The dura mater forms partitions which separate and support various
parts of the brain. It also forms venous channels into which blood drains from
the brain and then flows back through veins in the neck to the heart.
There is a potential space between the outer surface of the arachnoid mater
and the inner surface of the dura mater (the subdural space). Bridging veins
are present in this space. There is also a potential space between the dura
mater and the overlying skull, called the extradural or epidural space.
Head injuries
117
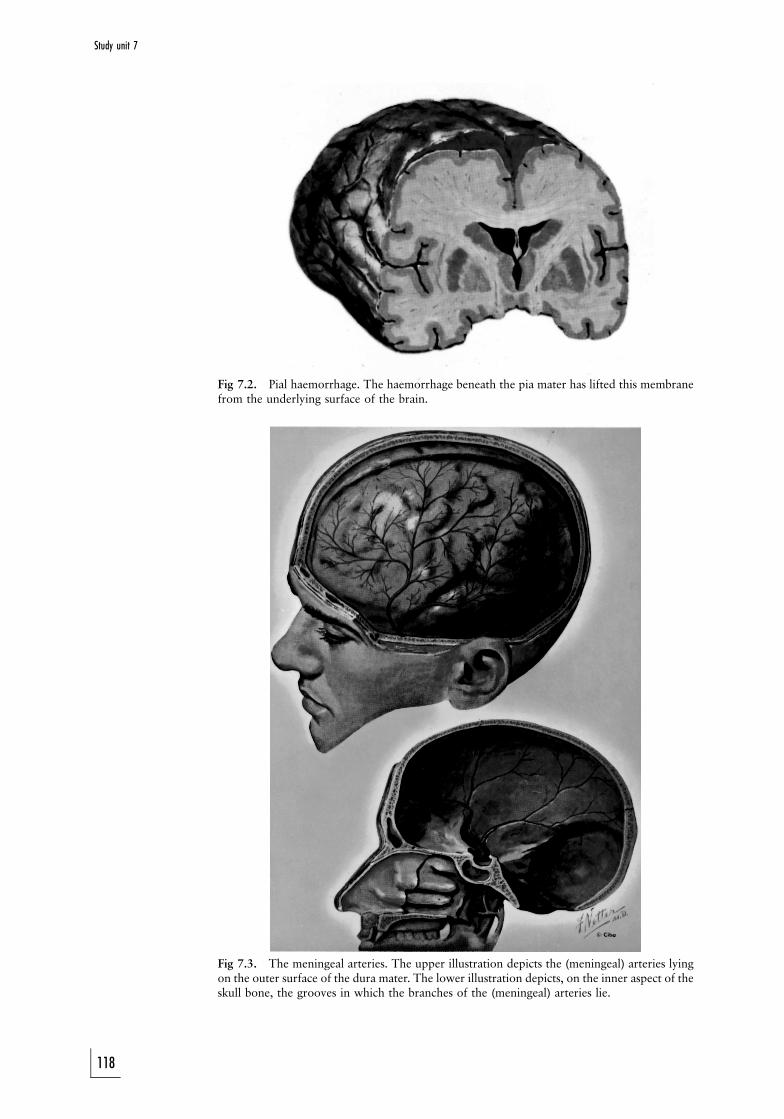
Fig 7.2. Pial haemorrhage. The haemorrhage beneath the pia mater has lifted this membranefrom the underlying surface of the brain.
Fig 7.3. The meningeal arteries. The upper illustration depicts the (meningeal) arteries lyingon the outer surface of the dura mater. The lower illustration depicts, on the inner aspect of theskull bone, the grooves in which the branches of the (meningeal) arteries lie.
Study unit 7
118
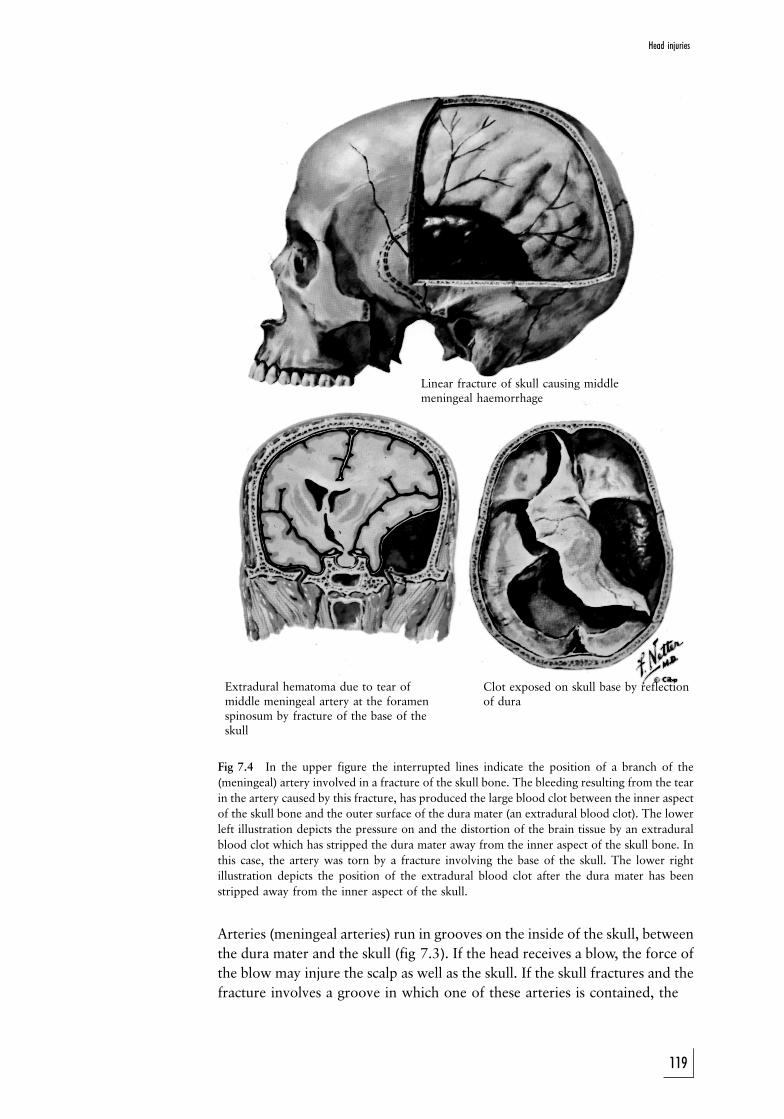
Linear fracture of skull causing middlemeningeal haemorrhage
Extradural hematoma due to tear ofmiddle meningeal artery at the foramenspinosum by fracture of the base of theskull
Clot exposed on skull base by reflectionof dura
Fig 7.4 In the upper figure the interrupted lines indicate the position of a branch of the
(meningeal) artery involved in a fracture of the skull bone. The bleeding resulting from the tear
in the artery caused by this fracture, has produced the large blood clot between the inner aspect
of the skull bone and the outer surface of the dura mater (an extradural blood clot). The lower
left illustration depicts the pressure on and the distortion of the brain tissue by an extradural
blood clot which has stripped the dura mater away from the inner aspect of the skull bone. In
this case, the artery was torn by a fracture involving the base of the skull. The lower right
illustration depicts the position of the extradural blood clot after the dura mater has been
stripped away from the inner aspect of the skull.
Arteries (meningeal arteries) run in grooves on the inside of the skull, between
the dura mater and the skull (fig 7.3). If the head receives a blow, the force of
the blow may injure the scalp as well as the skull. If the skull fractures and the
fracture involves a groove in which one of these arteries is contained, the
119
Head injuries
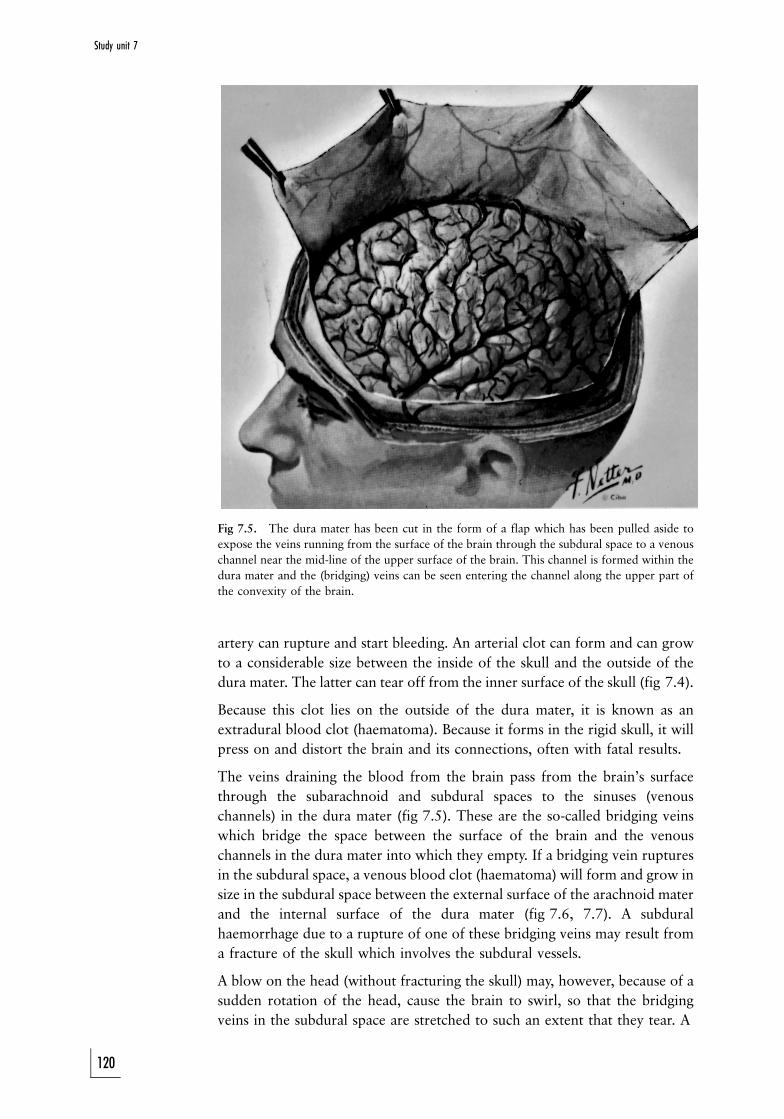
Fig 7.5. The dura mater has been cut in the form of a flap which has been pulled aside to
expose the veins running from the surface of the brain through the subdural space to a venous
channel near the mid-line of the upper surface of the brain. This channel is formed within the
dura mater and the (bridging) veins can be seen entering the channel along the upper part of
the convexity of the brain.
artery can rupture and start bleeding. An arterial clot can form and can grow
to a considerable size between the inside of the skull and the outside of the
dura mater. The latter can tear off from the inner surface of the skull (fig 7.4).
Because this clot lies on the outside of the dura mater, it is known as an
extradural blood clot (haematoma). Because it forms in the rigid skull, it will
press on and distort the brain and its connections, often with fatal results.
The veins draining the blood from the brain pass from the brain's surface
through the subarachnoid and subdural spaces to the sinuses (venous
channels) in the dura mater (fig 7.5). These are the so-called bridging veins
which bridge the space between the surface of the brain and the venous
channels in the dura mater into which they empty. If a bridging vein ruptures
in the subdural space, a venous blood clot (haematoma) will form and grow in
size in the subdural space between the external surface of the arachnoid mater
and the internal surface of the dura mater (fig 7.6, 7.7). A subdural
haemorrhage due to a rupture of one of these bridging veins may result from
a fracture of the skull which involves the subdural vessels.
A blow on the head (without fracturing the skull) may, however, because of a
sudden rotation of the head, cause the brain to swirl, so that the bridging
veins in the subdural space are stretched to such an extent that they tear. A
120
Study unit 7
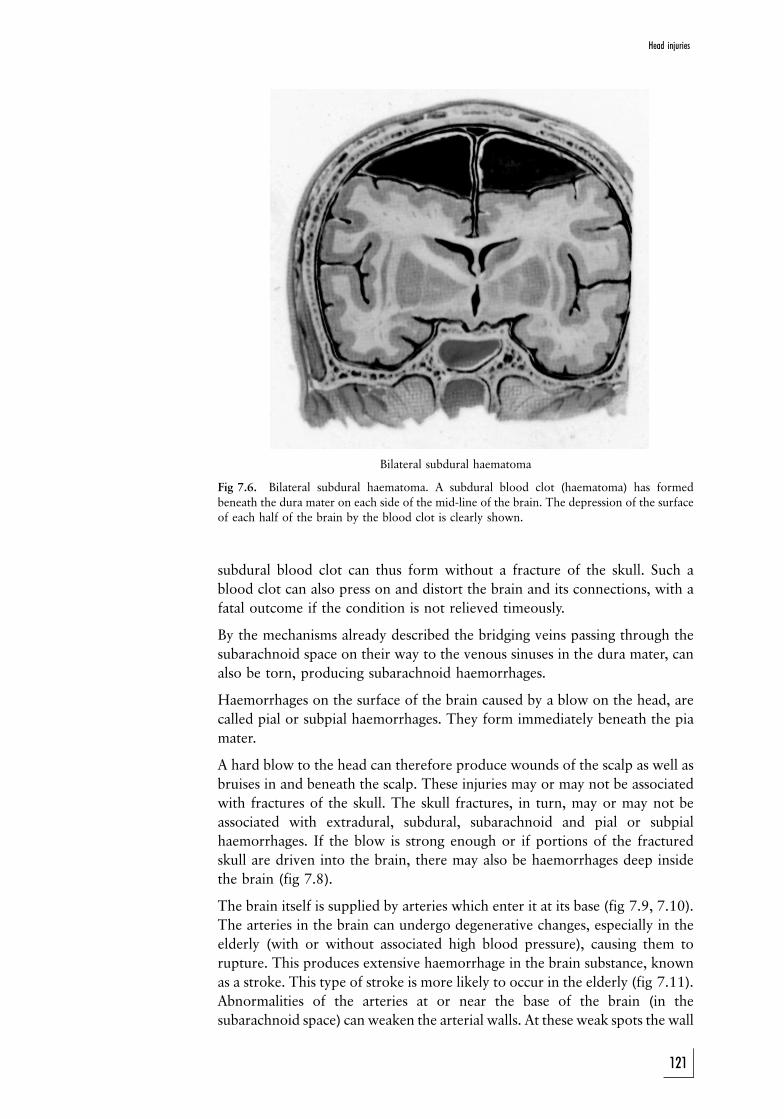
Bilateral subdural haematoma
Fig 7.6. Bilateral subdural haematoma. A subdural blood clot (haematoma) has formed
beneath the dura mater on each side of the mid-line of the brain. The depression of the surface
of each half of the brain by the blood clot is clearly shown.
subdural blood clot can thus form without a fracture of the skull. Such a
blood clot can also press on and distort the brain and its connections, with a
fatal outcome if the condition is not relieved timeously.
By the mechanisms already described the bridging veins passing through the
subarachnoid space on their way to the venous sinuses in the dura mater, can
also be torn, producing subarachnoid haemorrhages.
Haemorrhages on the surface of the brain caused by a blow on the head, are
called pial or subpial haemorrhages. They form immediately beneath the pia
mater.
A hard blow to the head can therefore produce wounds of the scalp as well as
bruises in and beneath the scalp. These injuries may or may not be associated
with fractures of the skull. The skull fractures, in turn, may or may not be
associated with extradural, subdural, subarachnoid and pial or subpial
haemorrhages. If the blow is strong enough or if portions of the fractured
skull are driven into the brain, there may also be haemorrhages deep inside
the brain (fig 7.8).
The brain itself is supplied by arteries which enter it at its base (fig 7.9, 7.10).
The arteries in the brain can undergo degenerative changes, especially in the
elderly (with or without associated high blood pressure), causing them to
rupture. This produces extensive haemorrhage in the brain substance, known
as a stroke. This type of stroke is more likely to occur in the elderly (fig 7.11).
Abnormalities of the arteries at or near the base of the brain (in the
subarachnoid space) can weaken the arterial walls. At these weak spots the wall
121
Head injuries
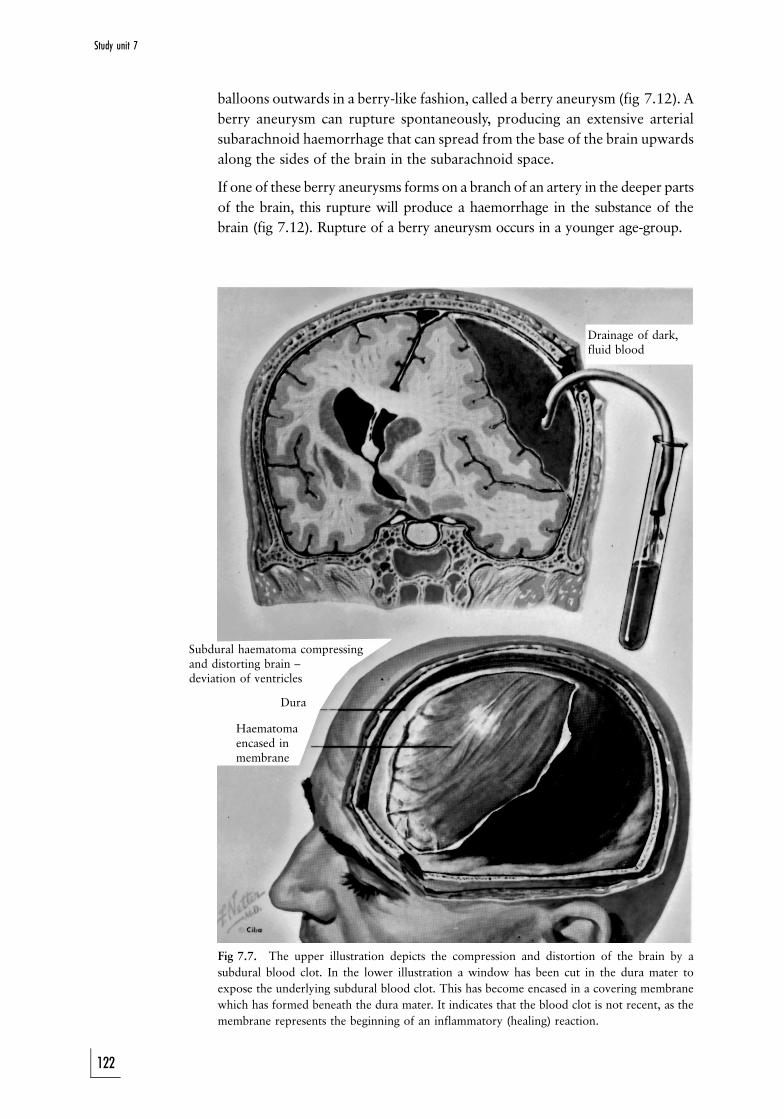
Drainage of dark,fluid blood
Subdural haematoma compressingand distorting brain ±deviation of ventricles
Dura
Haematomaencased inmembrane
balloons outwards in a berry-like fashion, called a berry aneurysm (fig 7.12). A
berry aneurysm can rupture spontaneously, producing an extensive arterial
subarachnoid haemorrhage that can spread from the base of the brain upwards
along the sides of the brain in the subarachnoid space.
If one of these berry aneurysms forms on a branch of an artery in the deeper parts
of the brain, this rupture will produce a haemorrhage in the substance of the
brain (fig 7.12). Rupture of a berry aneurysm occurs in a younger age-group.
Fig 7.7. The upper illustration depicts the compression and distortion of the brain by a
subdural blood clot. In the lower illustration a window has been cut in the dura mater to
expose the underlying subdural blood clot. This has become encased in a covering membrane
which has formed beneath the dura mater. It indicates that the blood clot is not recent, as the
membrane represents the beginning of an inflammatory (healing) reaction.
122
Study unit 7
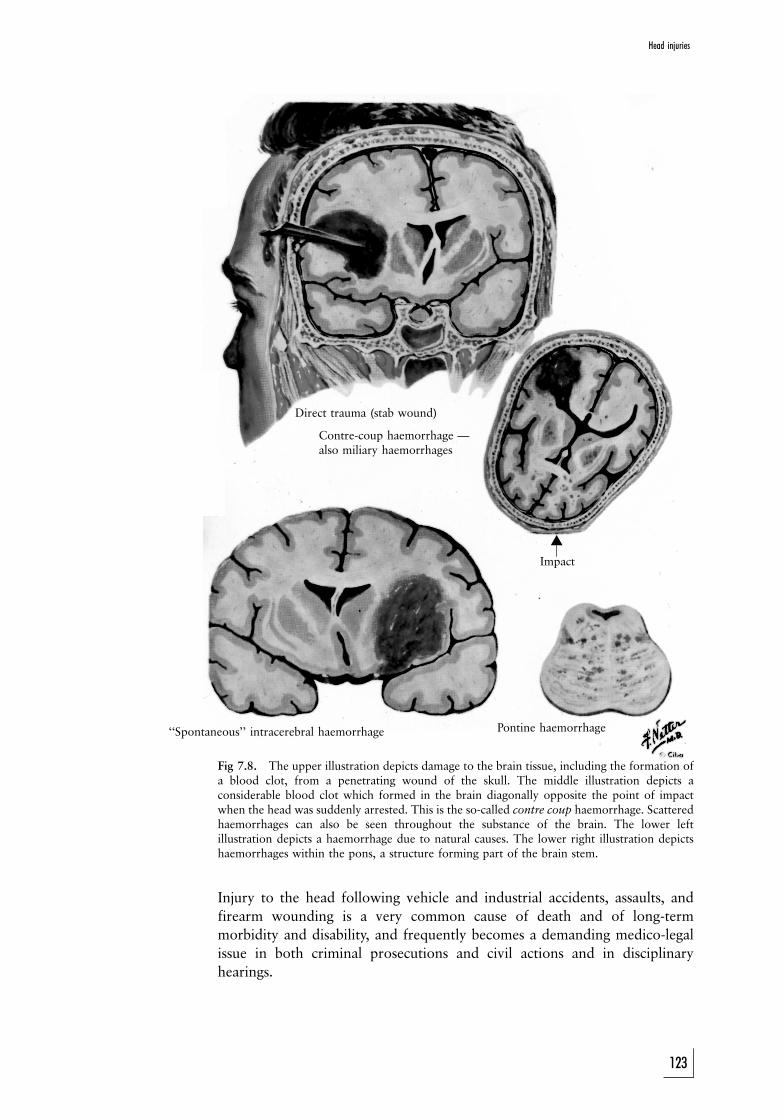
Direct trauma (stab wound)
Contre-coup haemorrhage Ðalso miliary haemorrhages
Impact
``Spontaneous'' intracerebral haemorrhage Pontine haemorrhage
!
Fig 7.8. The upper illustration depicts damage to the brain tissue, including the formation ofa blood clot, from a penetrating wound of the skull. The middle illustration depicts aconsiderable blood clot which formed in the brain diagonally opposite the point of impactwhen the head was suddenly arrested. This is the so-called contre coup haemorrhage. Scatteredhaemorrhages can also be seen throughout the substance of the brain. The lower leftillustration depicts a haemorrhage due to natural causes. The lower right illustration depictshaemorrhages within the pons, a structure forming part of the brain stem.
Injury to the head following vehicle and industrial accidents, assaults, and
firearm wounding is a very common cause of death and of long-term
morbidity and disability, and frequently becomes a demanding medico-legal
issue in both criminal prosecutions and civil actions and in disciplinary
hearings.
123
Head injuries
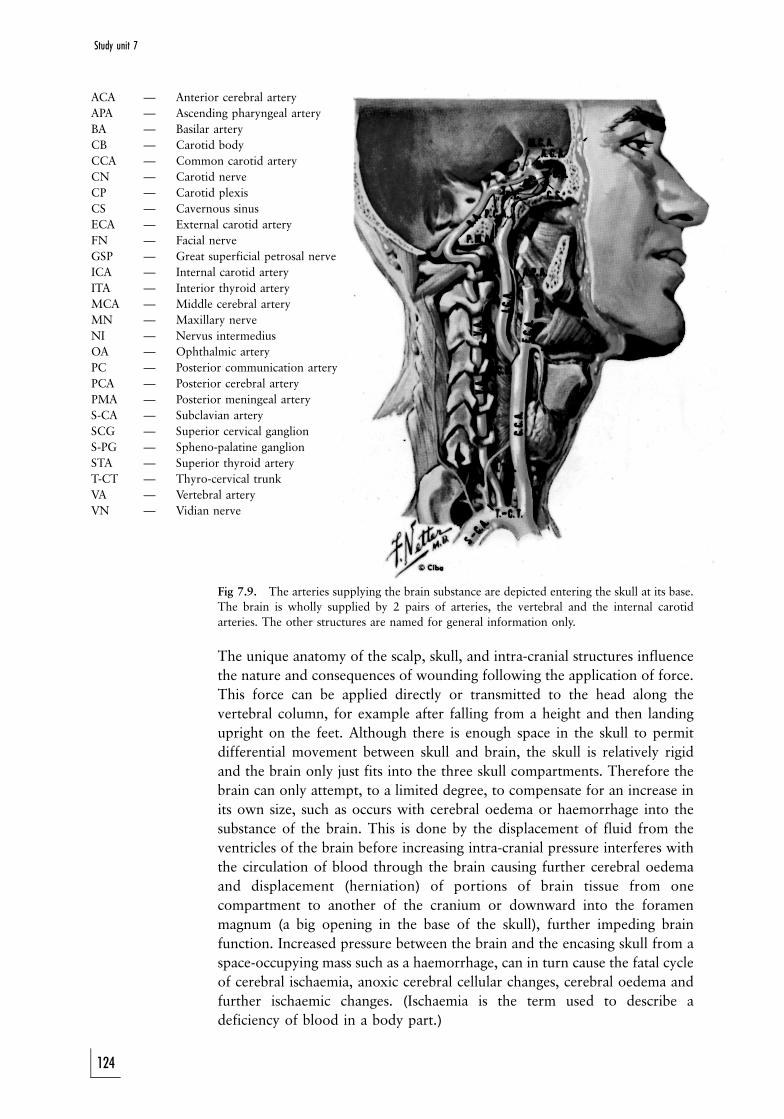
ACA Ð Anterior cerebral artery
APA Ð Ascending pharyngeal artery
BA Ð Basilar artery
CB Ð Carotid body
CCA Ð Common carotid artery
CN Ð Carotid nerve
CP Ð Carotid plexis
CS Ð Cavernous sinus
ECA Ð External carotid artery
FN Ð Facial nerve
GSP Ð Great superficial petrosal nerve
ICA Ð Internal carotid artery
ITA Ð Interior thyroid artery
MCA Ð Middle cerebral artery
MN Ð Maxillary nerve
NI Ð Nervus intermedius
OA Ð Ophthalmic artery
PC Ð Posterior communication artery
PCA Ð Posterior cerebral artery
PMA Ð Posterior meningeal artery
S-CA Ð Subclavian artery
SCG Ð Superior cervical ganglion
S-PG Ð Spheno-palatine ganglion
STA Ð Superior thyroid artery
T-CT Ð Thyro-cervical trunk
VA Ð Vertebral artery
VN Ð Vidian nerve
Fig 7.9. The arteries supplying the brain substance are depicted entering the skull at its base.
The brain is wholly supplied by 2 pairs of arteries, the vertebral and the internal carotid
arteries. The other structures are named for general information only.
The unique anatomy of the scalp, skull, and intra-cranial structures influence
the nature and consequences of wounding following the application of force.
This force can be applied directly or transmitted to the head along the
vertebral column, for example after falling from a height and then landing
upright on the feet. Although there is enough space in the skull to permit
differential movement between skull and brain, the skull is relatively rigid
and the brain only just fits into the three skull compartments. Therefore the
brain can only attempt, to a limited degree, to compensate for an increase in
its own size, such as occurs with cerebral oedema or haemorrhage into the
substance of the brain. This is done by the displacement of fluid from the
ventricles of the brain before increasing intra-cranial pressure interferes with
the circulation of blood through the brain causing further cerebral oedema
and displacement (herniation) of portions of brain tissue from one
compartment to another of the cranium or downward into the foramen
magnum (a big opening in the base of the skull), further impeding brain
function. Increased pressure between the brain and the encasing skull from a
space-occupying mass such as a haemorrhage, can in turn cause the fatal cycle
of cerebral ischaemia, anoxic cerebral cellular changes, cerebral oedema and
further ischaemic changes. (Ischaemia is the term used to describe a
deficiency of blood in a body part.)
124
Study unit 7
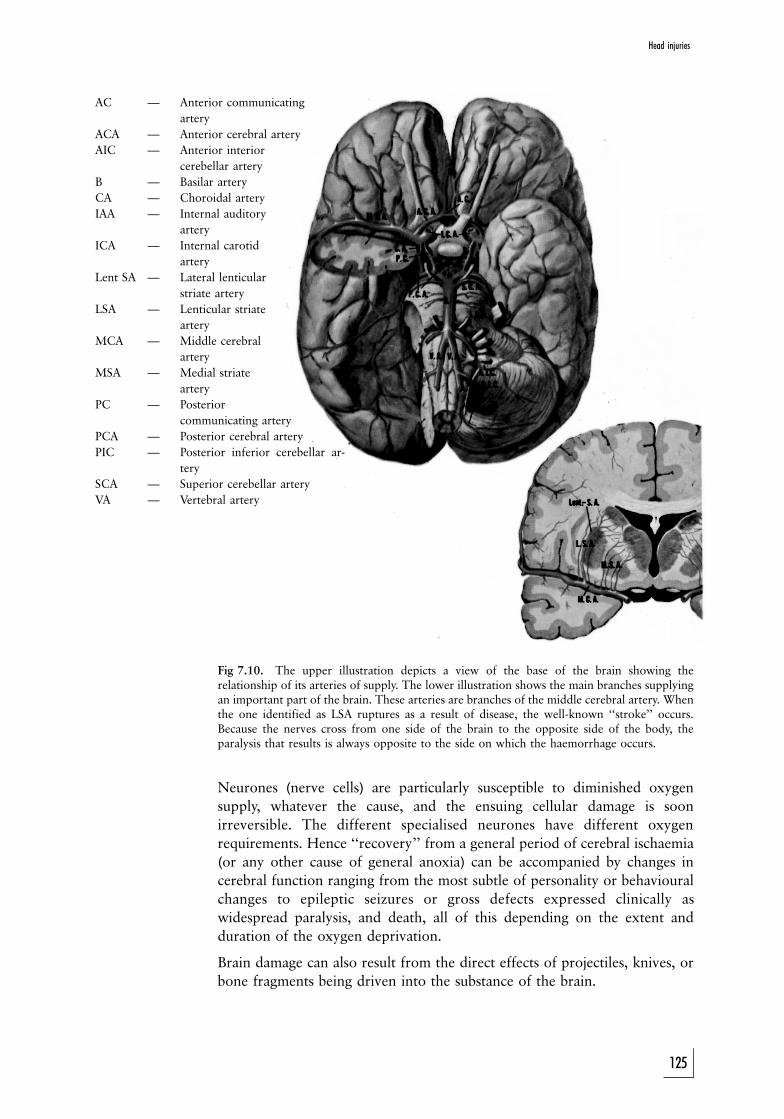
AC Ð Anterior communicating
artery
ACA Ð Anterior cerebral artery
AIC Ð Anterior interior
cerebellar artery
B Ð Basilar artery
CA Ð Choroidal artery
IAA Ð Internal auditory
artery
ICA Ð Internal carotid
artery
Lent SA Ð Lateral lenticular
striate artery
LSA Ð Lenticular striate
artery
MCA Ð Middle cerebral
artery
MSA Ð Medial striate
artery
PC Ð Posterior
communicating artery
PCA Ð Posterior cerebral artery
PIC Ð Posterior inferior cerebellar ar-
tery
SCA Ð Superior cerebellar artery
VA Ð Vertebral artery
Fig 7.10. The upper illustration depicts a view of the base of the brain showing therelationship of its arteries of supply. The lower illustration shows the main branches supplyingan important part of the brain. These arteries are branches of the middle cerebral artery. Whenthe one identified as LSA ruptures as a result of disease, the well-known ``stroke'' occurs.Because the nerves cross from one side of the brain to the opposite side of the body, theparalysis that results is always opposite to the side on which the haemorrhage occurs.
Neurones (nerve cells) are particularly susceptible to diminished oxygen
supply, whatever the cause, and the ensuing cellular damage is soon
irreversible. The different specialised neurones have different oxygen
requirements. Hence ``recovery'' from a general period of cerebral ischaemia
(or any other cause of general anoxia) can be accompanied by changes in
cerebral function ranging from the most subtle of personality or behavioural
changes to epileptic seizures or gross defects expressed clinically as
widespread paralysis, and death, all of this depending on the extent and
duration of the oxygen deprivation.
Brain damage can also result from the direct effects of projectiles, knives, or
bone fragments being driven into the substance of the brain.
125
Head injuries
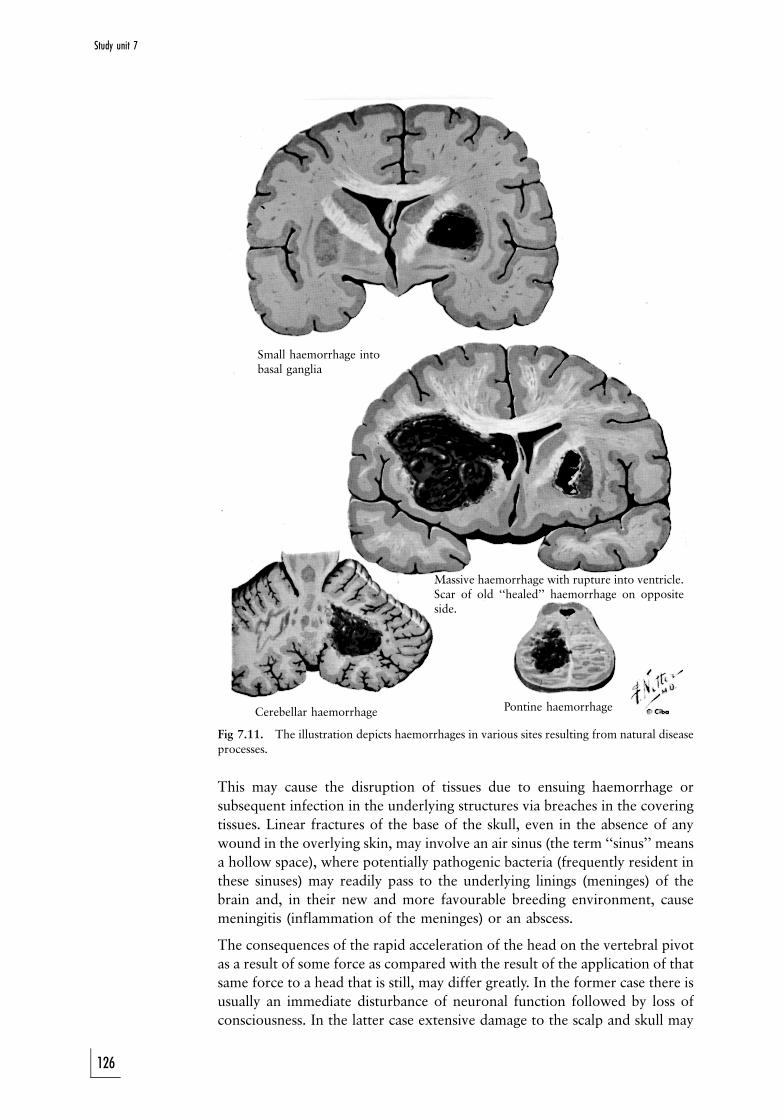
Small haemorrhage intobasal ganglia
Massive haemorrhage with rupture into ventricle.Scar of old ``healed'' haemorrhage on oppositeside.
Cerebellar haemorrhage Pontine haemorrhage
Fig 7.11. The illustration depicts haemorrhages in various sites resulting from natural diseaseprocesses.
This may cause the disruption of tissues due to ensuing haemorrhage or
subsequent infection in the underlying structures via breaches in the covering
tissues. Linear fractures of the base of the skull, even in the absence of any
wound in the overlying skin, may involve an air sinus (the term ``sinus'' means
a hollow space), where potentially pathogenic bacteria (frequently resident in
these sinuses) may readily pass to the underlying linings (meninges) of the
brain and, in their new and more favourable breeding environment, cause
meningitis (inflammation of the meninges) or an abscess.
The consequences of the rapid acceleration of the head on the vertebral pivot
as a result of some force as compared with the result of the application of that
same force to a head that is still, may differ greatly. In the former case there is
usually an immediate disturbance of neuronal function followed by loss of
consciousness. In the latter case extensive damage to the scalp and skull may
126
Study unit 7

Aneurysm ruptured intracerebrally
Aneurysm of anterior cerebral artery
Fig 7.12. The illustration on the right depicts the balloon-like swelling (aneurysm) which hasformed on one of the arteries at the base of the brain. The illustration on the left depicts theblood clot and destruction of the brain tissue resulting from the rupture of such an (berry)aneurysm.
Acknowledgements
Source: Figures 7.2±7.12 reproduced by courtesy of the Ciba collection of medical illustrations, vol 1,
Nervous systems. (Frank Netter 1972).
not be accompanied by immediate loss of consciousness and the patient may
be able to recall events up to the time of injury and relate them before lapsing
into unconsciousness as a result of the delayed effects of the injury.
The function of nerve cells is affected not only by trauma and its
consequences but also equally dramatically and often similarly by a variety
of therapeutic drugs, the abuse of drugs, natural disease processes such as
diabetes, and primary and secondary spreading of cancerous tumours of the
brain. Many of these conditions can be caused by a fall, a motor-vehicle
accident, or assault, and can add to the diagnostic problem, namely to
determine what caused the specific clinical picture.
The effects of alcoholic intoxication can closely resemble a post-concussional
state, and that the two cannot be easily differentiated, has been a bitter lesson
taught by experience; the answer is to keep the patient under observation.
This is particularly problematic when a person was involved in an accident
and apprehended for driving under the influence of alcohol. Many people
have died because a treatable head injury was confused with intoxication. It
happened that a driver once, after having been carefully medically examined
for ``driving under the influence'', was subsequently taken into custody. One
hour later the driver was seen to be ``sleeping'' deeply by someone who had
returned to the cells on an unrelated matter. An examination revealed blood-
127
Head injuries

stained fluid issuing from his ear Ð a sign of a possible fracture of the base of
the skull. The person was immediately transferred to a neurosurgical ward
and an emergency operation to evacuate an acute extradural haemorrhage
was successful. The blood-alcohol concentration was also far in excess of the
statutory level. This was thus a case where the suspect appeared to be ``under
the influence'' when he was apprehended, but had previously sustained
intracranial bleeding, which only presented later.
Certain prescription medications to inhibit blood clotting, chronic alcohol-
ism, and cerebral atrophy, can considerably increase the effect of even a trivial
force to the head and thus the risk of brain injury. The fact that even in the
most serious brain injuries there might be no outwardly visible evidence of
violence, compounds the problems of the medical practitioner. Furthermore,
clinical manifestation of brain damage may only appear many hours after the
injury was sustained; this is often the case with a subdural haemorrhage. Or
such a haemorrhage may follow a lucid interval subsequent to a period of
unconsciousness due to concussion; during the period of lucidity the victim
appears to have recovered from the effects of the injury.
It is these very real problems, especially in a busy hospital trauma unit, which
raise the question whether all head-injury patients (except those with very
minor head injuries) should not undergo X-rays of the skull, or other more
sophisticated investigations. No wonder, then, that Bernard Knight (1996)
one of the best-known medico-legal authors, a barrister-at-law and consultant
pathologist, is of the opinion that head injuries ``constitute one of the most
difficult problems in the realms of accident medicine both from the technical
and medico-legal points of view. Many actions for negligence have arisen
from failure to view head injuries with sufficient concern. The doctor's
procedure when dealing with a head injury must be coloured by his regard
not only for his patients' welfare but also for possible medico-legal
complications at a later date. Even if he considered that the clinical state
does not warrant further investigation, it is most unwise to proceed other
than with the greatest caution.''
In hospital practice, one of the most important facts to be determined is
whether the patient was unconscious for any period of time, however short. If
it is likely that this was the case, it would be most unwise to discharge the
patient. Wherever possible, the patient should be admitted for at least 24
hours so that the onset of symptoms and signs of a latent condition such as a
sub- or extradural haemorrhage can be observed. These conditions are usually
readily remediable if the diagnosis is made timeously. It is customary to issue a
``head-injury warning card'' to a patient's relative or friend to inform the
person of what action to take should the patient's condition deteriorate after
discharge. It would serve little purpose to issue such a card to the patient
himself, who may not be in a position to respond to such a warning, should
the need arise. It must also be remembered that an X-ray of the head will only
indicate fractures. Brain injury may be present even though there is no
fracture. Special investigations, such as a CT-scan, will be required to
diagnose this. However, it is not always practical to perform this.
128
Study unit 7
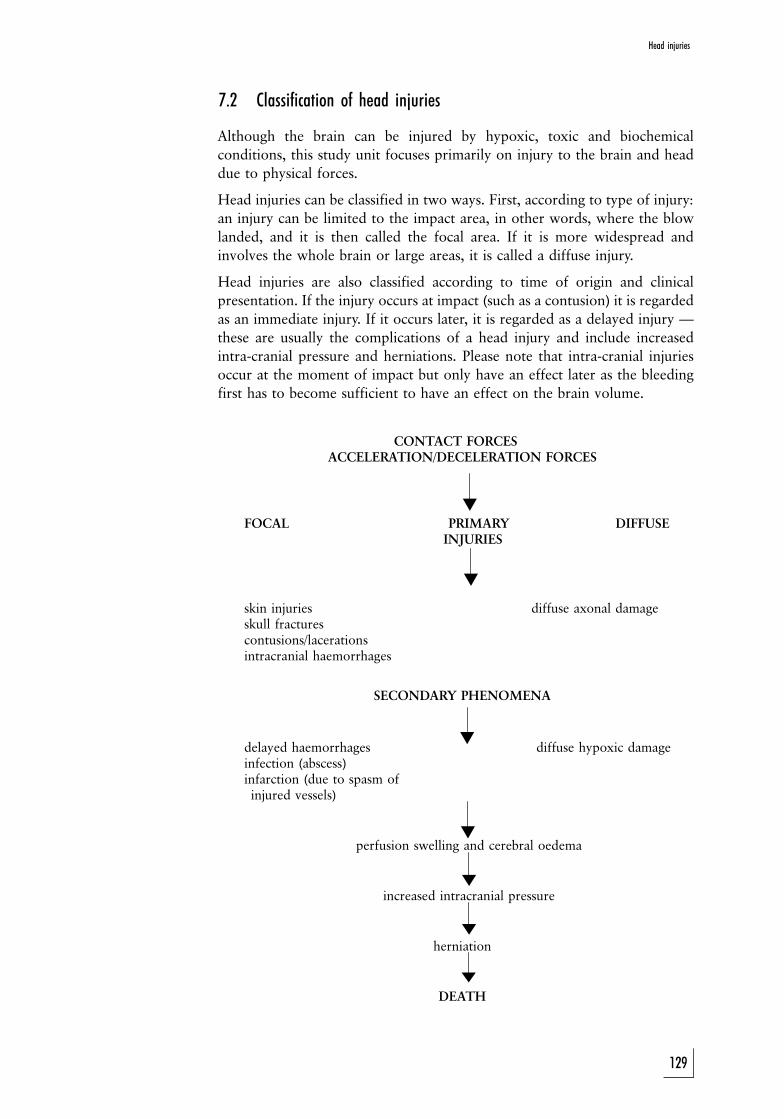
!
!
!
!
!
!
!
7.2 Classification of head injuries
Although the brain can be injured by hypoxic, toxic and biochemical
conditions, this study unit focuses primarily on injury to the brain and head
due to physical forces.
Head injuries can be classified in two ways. First, according to type of injury:
an injury can be limited to the impact area, in other words, where the blow
landed, and it is then called the focal area. If it is more widespread and
involves the whole brain or large areas, it is called a diffuse injury.
Head injuries are also classified according to time of origin and clinical
presentation. If the injury occurs at impact (such as a contusion) it is regarded
as an immediate injury. If it occurs later, it is regarded as a delayed injury Ð
these are usually the complications of a head injury and include increased
intra-cranial pressure and herniations. Please note that intra-cranial injuries
occur at the moment of impact but only have an effect later as the bleeding
first has to become sufficient to have an effect on the brain volume.
CONTACT FORCESACCELERATION/DECELERATION FORCES
FOCAL PRIMARY DIFFUSEINJURIES
skin injuries diffuse axonal damageskull fracturescontusions/lacerationsintracranial haemorrhages
SECONDARY PHENOMENA
delayed haemorrhages diffuse hypoxic damageinfection (abscess)infarction (due to spasm ofinjured vessels)
perfusion swelling and cerebral oedema
increased intracranial pressure
herniation
DEATH
129
Head injuries
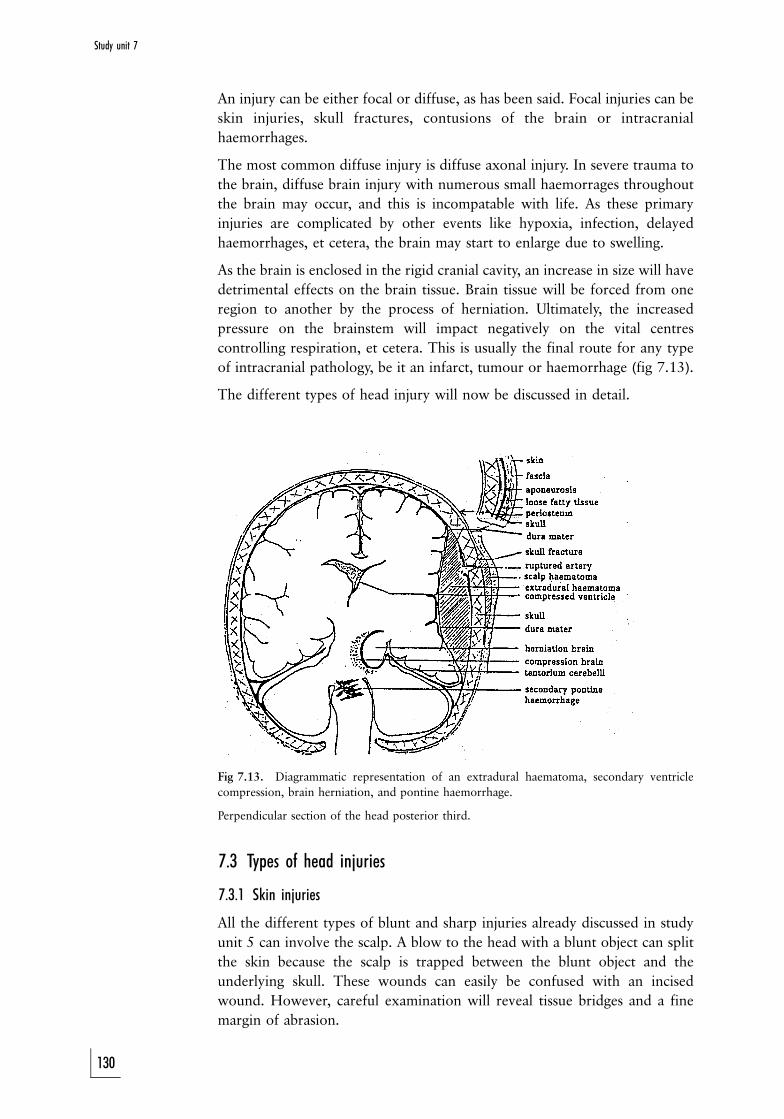
An injury can be either focal or diffuse, as has been said. Focal injuries can be
skin injuries, skull fractures, contusions of the brain or intracranial
haemorrhages.
The most common diffuse injury is diffuse axonal injury. In severe trauma to
the brain, diffuse brain injury with numerous small haemorrages throughout
the brain may occur, and this is incompatable with life. As these primary
injuries are complicated by other events like hypoxia, infection, delayed
haemorrhages, et cetera, the brain may start to enlarge due to swelling.
As the brain is enclosed in the rigid cranial cavity, an increase in size will have
detrimental effects on the brain tissue. Brain tissue will be forced from one
region to another by the process of herniation. Ultimately, the increased
pressure on the brainstem will impact negatively on the vital centres
controlling respiration, et cetera. This is usually the final route for any type
of intracranial pathology, be it an infarct, tumour or haemorrhage (fig 7.13).
The different types of head injury will now be discussed in detail.
Fig 7.13. Diagrammatic representation of an extradural haematoma, secondary ventricle
compression, brain herniation, and pontine haemorrhage.
Perpendicular section of the head posterior third.
7.3 Types of head injuries
7.3.1 Skin injuries
All the different types of blunt and sharp injuries already discussed in study
unit 5 can involve the scalp. A blow to the head with a blunt object can split
the skin because the scalp is trapped between the blunt object and the
underlying skull. These wounds can easily be confused with an incised
wound. However, careful examination will reveal tissue bridges and a fine
margin of abrasion.
130
Study unit 7
The appearance of entrance gunshot wounds is discussed elsewhere.
If someone wears a protective cap or even just has a thick head of hair, the
skin, but not necessarily the underlying brain, may be protected against injury.
Absence of skin injuries or fractures does therefore not exclude brain injury.
7.3.2 Fractures
Skull fractures can be classified as follows:
1. Simple fractures: the overlying scalp is intact
2. Open or compound fractures: the fracture and underlying tissue
communicate through a skin defect with the external environment.
These fractures can easily become infected.
3. Comminuted fracture: the bone is broken into many separate pieces.
Skull fractures have certain unique features:
1. Linear fractures are usually not associated with movement of the adjacent
bone plates.
2 Depressed fractures differ from the above. They are often more localised,
and result from impact against a smaller object. Knobkieries often cause a
depressed fracture.
3. Contre-coup fractures are found diagonally opposite the point of impact.
If someone falls on the back of his head, fractures may occur on the
frontal aspect of the skull, especially of the thin and delicate bone
overlying the orbital cavities (orbital plates).
4. A ring fracture is present around the hole at the base of the skull (the
foramen magnum). These fractures occur when someone lands forcefully
on his feet and the weight of the head propels the skull downward on the
spine.
5. Hinge fractures are severe and may display extensive fractures involving
the base of the skull. After removal of the cranial vault, the anterior and
posterior aspects of the skull base can be moved relative to one another.
It must be remembered that the skull of an infant toddler may deform
substantially without fracturing. Brain injuries could therefore occur without
any fractures. However, the sutures between the bony plates may be damaged
(diastasis).
7.3.3 Brain contusions and lacerations
Wherever the brain is brought forcefully into contact with the overlying bone
or even the free edges of the dural folds (eg the inferior aspect of the falx
cerebri, the dural fold dividing the brain in two halves), the tissue can become
contused. If the force is sufficient, the brain surface may even tear (lacerate).
As these lacerations are always surrounded by contusions, we often refer to
them as contusions/lacerations.
As can be expected, these injuries will be located at the points of contact with
the overlying bone. Contusions are therefore seen at the crest of the
convolutions (gyri), and not in the depth of the grooves (sulci). Those parts of
the brain in contact with rough and uneven bony elements are particularly
131
Head injuries
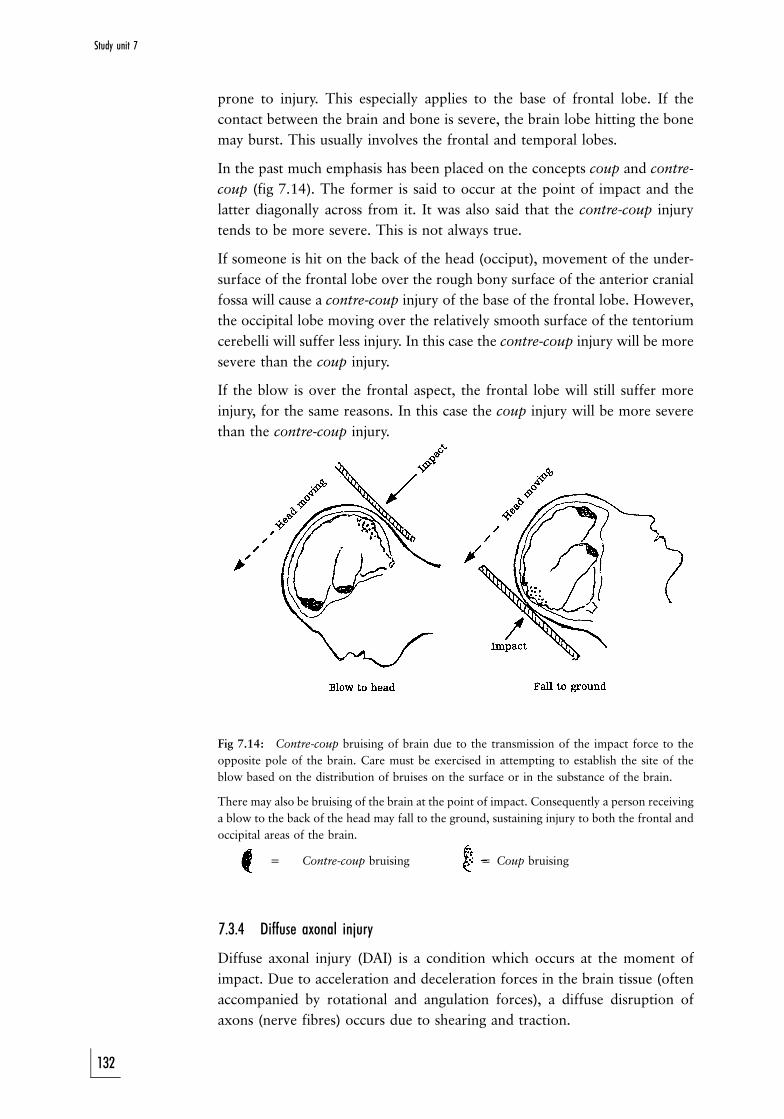
prone to injury. This especially applies to the base of frontal lobe. If the
contact between the brain and bone is severe, the brain lobe hitting the bone
may burst. This usually involves the frontal and temporal lobes.
In the past much emphasis has been placed on the concepts coup and contre-
coup (fig 7.14). The former is said to occur at the point of impact and the
latter diagonally across from it. It was also said that the contre-coup injury
tends to be more severe. This is not always true.
If someone is hit on the back of the head (occiput), movement of the under-
surface of the frontal lobe over the rough bony surface of the anterior cranial
fossa will cause a contre-coup injury of the base of the frontal lobe. However,
the occipital lobe moving over the relatively smooth surface of the tentorium
cerebelli will suffer less injury. In this case the contre-coup injury will be more
severe than the coup injury.
If the blow is over the frontal aspect, the frontal lobe will still suffer more
injury, for the same reasons. In this case the coup injury will be more severe
than the contre-coup injury.
Fig 7.14: Contre-coup bruising of brain due to the transmission of the impact force to the
opposite pole of the brain. Care must be exercised in attempting to establish the site of the
blow based on the distribution of bruises on the surface or in the substance of the brain.
There may also be bruising of the brain at the point of impact. Consequently a person receiving
a blow to the back of the head may fall to the ground, sustaining injury to both the frontal and
occipital areas of the brain.
= Contre-coup bruising = Coup bruising
7.3.4 Diffuse axonal injury
Diffuse axonal injury (DAI) is a condition which occurs at the moment of
impact. Due to acceleration and deceleration forces in the brain tissue (often
accompanied by rotational and angulation forces), a diffuse disruption of
axons (nerve fibres) occurs due to shearing and traction.
132
Study unit 7
7.3.4.1 Clinical presentation
DAI presents immediately at the moment of impact. Clinically it can present
with a spectrum of different grades, varying from mild, which presents
clinically as concussion, to severe. In the latter case the patient is immediately
unconscious with no lucid interval. In these cases the coma usually lasts more
than 6 hours.
7.3.4.2 Pathological changes
Macroscopically (with the naked eye) or with certain radiological procedures
(a CT scan or magnetic resonance (MR)) petechial haemorrhages are present
in the corpus callosum (the fibres joining the two halves of the brain) and in
the dorso-lateral aspects of the pons (a part of the brain stem). A tear of the
septum pellucidum and fornixes may also be present. This results in
haemorrhage in the two lateral ventricals of the brain (intraventricular
haemorrhage). The petechial haemorrhages are the result of rupture of the
small blood vessels running alongside the axons (nerve fibres) in the brain. As
these vessels are also damaged by the shearing forces experienced during DAI,
it is an indirect indicator of axonal injury, as the latter is not visible with the
naked eye. In the corpus callosum and dorso-lateral aspects of the pons, the
nerve fibres are more susceptible to damage as they are longer and are
therefore more prone to damage by shearing forces.
Microscopically a diffuse disruption of the axons can be seen. Depending on
the survival period certain changes will be evident, of which the first sign will
be retraction balls due to axonal swelling. Damage to axons (and neurons, ie
brain cells) is irreversible, and with time these damaged neurons disappear.
7.3.4.3 Associations
The method of injury (whether the brain decelerates or accelerates inside the
cranial cavity) can cause certain associations with other, but separate, brain
injuries. Gliding contusions occur almost in the midline of the brain
(parasagittal region) where the surface of the brain is fixed by means of the
arachnoid villi to the overlying dura mater. When movement of the brain
occurs relative to these points of fixation, small haemorrhages occur at the
interface between the white and grey matter as the latter is fixed by means of
the arachnoid villi, and cannot move with the white matter.
There are sometimes also haematomas (localised haemorrhages) in die deep
intra-cerebral matter, in the region of the basal ganglia. They are also known
as intermediary coup lesions.
It is important to note that DAI has no or minimal association with other
injuries which are normally the result of more localised impact, such as
fractures of the skull, contusions or lacerations of the brain matter, and
intracranial haemorrhages (other than those mentioned above). In addition
DAI is seldom associated with an increase in the intracranial pressure.
To summarise: DAI is a common injury due to acceleration and deceleration
of the brain, often concomitant with rotational and angulation forces. If
133
Head injuries
severe enough, it can cause a vegetative state, where a patient is unconscious,
but able to maintain his or her own vital functions (respiration and
cardiovascular status).
7.3.5 Traumatic intracranial haemorrhage
7.3.5.1 General
. This is often the result of non-missile injury, such as a blow to the head.
. These haemorrhages are the most common cause of deterioration in a
patient after a lucid (``awake'') period.
. More than 35 ml is a sufficient volume to act as a space-occupying lesion.
. These haemorrhages are often associated with fracture(s).
. There is often more than one type of haemorrhage.
. Although of primary origin, it often presents as a complication, in other
words as a secondary phenomenon.
7.3.5.2 Classification
. extradural haemorrhage
. subdural haemorrhage
. subarachnoidal haemorrhage
. intracerebral haemorrhage
. intraventricular haemorrhage
This classification is limited to traumatic haemorrhages, and does not include
spontaneous causes of haemorrhages, such as hypertensive haemorrhages or
haemorrhages due to rupture of a berry aneurysm (defect in the blood-vessel
wall).
a Extra(epi)dural haemorrhage (fig 7.3 and fig 7.4)
Extradural haemorrhages are also known as epidural haemorrhages. These
haemorrhages occur between the dura and the overlying skull. The dura is a
relatively thick membrane which lines the inner surface of the skull. A number
of arteries are present in the dura. They are often partially embedded in the
overlying skull bone. One of these arteries is the middle meningeal artery
which runs on the side of the head in the temporo-parietal region. This artery
can be damaged with subsequent haemorhage if a fracture occurs in that
region. Smaller fracture-associated extradural haemorrhages may also occur
elsewhere.
b Subdural haemorrhage (fig 7.5, fig 7.6 and fig 7.7)
A number of small veins run between the surface of the brain (arachnoid
mater or leptomeninges) and the dura. With sudden acceleration or
deceleration these small veins may rupture, with subsequent haemorrhage.
A relatively small brain compared with the cranial cavity will predispose to
such movement, and therefore injury with subsequent haermorrhage. This
condition is therefore often found in alcoholics with brain atrophy. In
addition, babies have relatively small brains compared with the cranial cavity.
134
Study unit 7
The muscles of a baby's neck are also not well developed, and if you shake a
baby, as is often seen in cases of child abuse, excessive movement of the brain
can occur in the cranial cavity, with subsequent damage to these vessels.
Subdural haemorrhages can also occur in cases of burst lobe, where severe
trauma to part of the brain will cause haemorrhage in the brain tissue (in a
brain lobe), as well as outside (in the subdural space). This usually
communicates via contusion/laceration. Subdural haemorrhage typically
present after a period of time, as they are venous in origin and therefore
take time to develop (longer compared with an extradural haemorrhage).
These patients are often called ``walk-talk-and-die'' patients, as the patient
will present to the trauma unit with a history of even relatively trivial trauma,
and after examination the doctor will send the patient home. The next day or
thereafter the patient presents in a comatose state and dies.
Subdural haemorrhages can be divided into acute, subacute and chronic
haemorrhages. An acute haemorrhage will consist of clotted blood, while a
chronic haemorrhage will consist of liquid blood. In addition there will often
be signs of membrane formation encapsulating these haemorrhages. Subdural
haemorrhages, like any other space-occupying lesion, will cause herniation of
brain tissue if of sufficient volume.
c Subarachnoidal haemorrhage
These haemorrhages occur below the leptomeninges (arachnoid mater) in the
subarachnoidal space, are quite common in head injuries, and can be diffuse
or focal. Subarachnoidal haemorrhages are also seen when there is rupture of
a berry aneurysm. Berry aneurysms occur because of weakening of the
vasculature of the brain. At these points the wall of the blood vessel forms
small balloons (aneurysms) which can rupture, with subsequent often fatal
haemorrhage. It is important to remember that this is not a trauma-related
haemorrhage.
d Intracerebral haemorrhage
Intracerebral haemorrhages may either be present in a lobe of the brain (lobar
haematoma), or in the basal ganglia region, as seen in cases of diffuse axonal
injury.
e Intraventricular haemorrhage
Intraventricular haemorrhages occur in the lateral ventricles of the brain.
They are often the result of rupture of the septum pellucidum or fornix.
These haemorrhages therefore occur in cases of diffuse axonal injury.
7.3.6 Herniations
The volume of the cranial cavity is fixed. The intracranial contents consist of
70% brain tissue, 15% blood and 15% cerebrospinal fluid. If there is an
increase in the volume occupied by the brain or blood, the cerebrospinal fluid
135
Head injuries
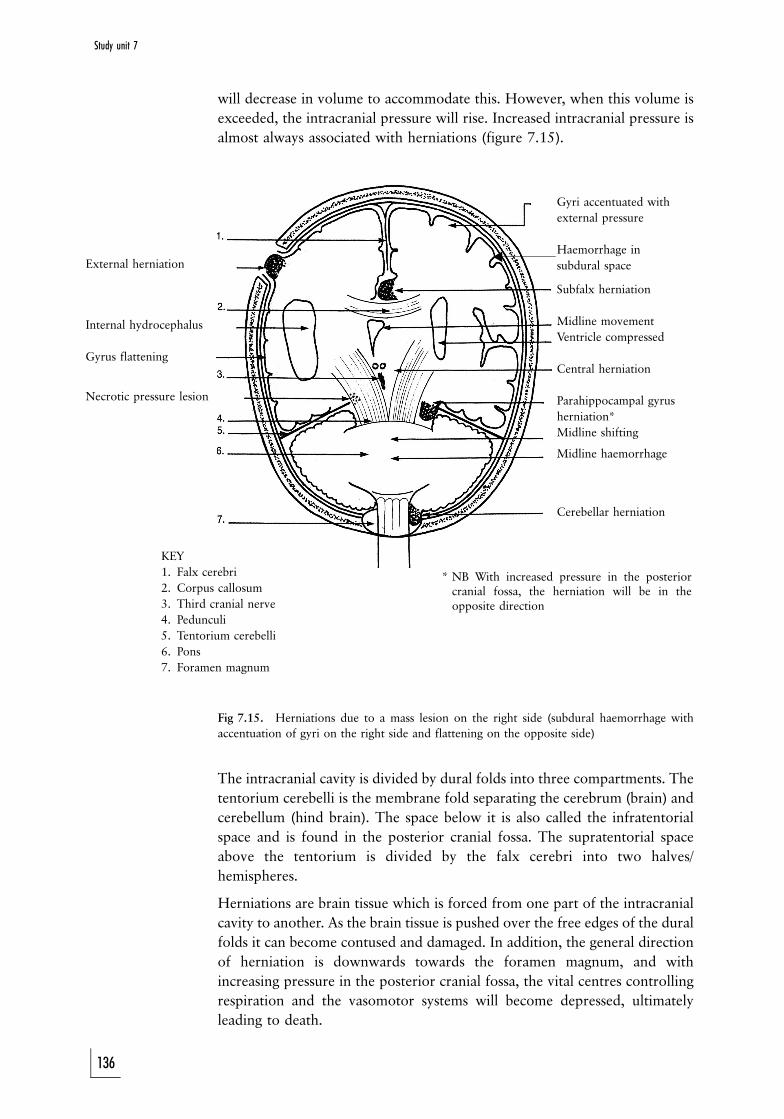
External herniation
Internal hydrocephalus
Gyrus flattening
Necrotic pressure lesion
Gyri accentuated with
external pressure
Haemorrhage in
subdural space
Subfalx herniation
Midline movement
Ventricle compressed
Central herniation
Parahippocampal gyrus
herniation*
Midline shifting
Midline haemorrhage
Cerebellar herniation
KEY
1. Falx cerebri
2. Corpus callosum
3. Third cranial nerve
4. Pedunculi
5. Tentorium cerebelli
6. Pons
7. Foramen magnum
* NB With increased pressure in the posteriorcranial fossa, the herniation will be in theopposite direction
!
will decrease in volume to accommodate this. However, when this volume is
exceeded, the intracranial pressure will rise. Increased intracranial pressure is
almost always associated with herniations (figure 7.15).
Fig 7.15. Herniations due to a mass lesion on the right side (subdural haemorrhage with
accentuation of gyri on the right side and flattening on the opposite side)
The intracranial cavity is divided by dural folds into three compartments. The
tentorium cerebelli is the membrane fold separating the cerebrum (brain) and
cerebellum (hind brain). The space below it is also called the infratentorial
space and is found in the posterior cranial fossa. The supratentorial space
above the tentorium is divided by the falx cerebri into two halves/
hemispheres.
Herniations are brain tissue which is forced from one part of the intracranial
cavity to another. As the brain tissue is pushed over the free edges of the dural
folds it can become contused and damaged. In addition, the general direction
of herniation is downwards towards the foramen magnum, and with
increasing pressure in the posterior cranial fossa, the vital centres controlling
respiration and the vasomotor systems will become depressed, ultimately
leading to death.
136
Study unit 7
The following herniations may occur see (fig 7.15). As herniation is a dynamic
process, more than one is often present, as it creates a domino effect.
1. Subfalx herniation. The medial aspect of the one cerebral hemisphere is
forced below (sub) the falx cerebri (falx) to the opposite side. As this is
located above the corpus callosum it is also called a supra-callosal
herniation. (The falx cerebri is the fold between the cerebral hemispheres.
Herniation means the abnormal protrusion of a body structure through a
defect in a membrane, muscle or bone.)
2. Central herniation. The central aspect of the brain is forced downwards
onto the brain stem. This may cause secondary haemorrhages in the brain
stem, with damage to the vital centres, and death.
3. Parahippocampal gyrus herniation. The medial aspect of the temporal
lobe (the parahippocampal gyrus) is forced over the free edge of the
opening in the tentorium cerebelli (incisura) into the posterior cranial
fossa. Traction and compression may cause damage to nerves and blood
vessels Ð the latter with infarction of brain tissue.
4. Tonsillar herniation. This is also known as coning. The cerebellum
(cerebellar tonsils) is forced downwards through the foramen magnum.
As this is a risk in cases of raised intracranial pressure, it is contra-
indicated to perform a lumbar puncture in patients expected to suffer
from raised intracranial pressure, as it lowers the pressure in the spinal
colum.
All these are internal herniations. External herniations occur when brain
tissue herniate through a defect in the skull. It appears as a mushroom of brain
tissue protruding from the head.
7.3.7 Brain swelling
Brain swelling is an increase in the size of the brain or parts thereof. It can be
due to an increase in the blood volume, ie perfusion swelling; the blood (and
therefore fluid) is still intravascular (in the vessels). This condition occurs in
two situations: in young children after brain trauma, and in the brain on the
same side as a subdural haemorrhage. It is the result of collapse of the system
which controls blood-flow in the brain.
If the fluid accumulates outside the vessels (extravascular) it is also called
cerebral oedema. There are different types of oedema.
Tumors and brain abscesses are often surrounded by new, immature blood
vessels. The walls leak, and fluid accumulates in the surrounding tissue. This
surrounding rim of oedema is called vasogenic oedema, and increases the size
of the tumor or abscess significantly.
The other important type of cerebral oedema is cytotoxic oedema. This is
caused by damage to cells, which then swell due to loss of the normal energy-
dependant fluid control of the cells. It is often seen in an infarction, where
loss of oxygen supply causes the energy-dependant processes to stop. Sodium
will then accumulate in the cell, it will attract water due to the osmotic
pressure, with concomitant swelling.
As a matter of interest it must be noted that both types of oedema are often
137
Head injuries
seen in an infarction. The central aspect shows cytotoxic oedema, and the
more peripheral aspect, where the blood vessel walls have been damaged by
the hypoxia, exhibits vasogenic oedema.
There are also other types of oedema, for example in cases of hypertension
(hydrostatic oedema) or due to rehydration after a period of diabetic coma or
hypertonic dehydration (osmotic oedema). These, however, fall beyond the
scope of this study guide.
ACTIVITIES
1. A 60 year old alcoholic falls and hits his head while under the influence of
alcohol. He is admitted to the local casualty department. Discuss possible
head injuries which may be caused by such a fall, as well as the problems
which may confront the doctor in diagnosing this condition.
2. A patient with a skull fracture over the temporal bone is initially
apparently normal, but over a period of 12 hours becomes gradually
more confused and drowsy. He dies before treatment can be adminis-
tered. Discuss the probable cause of death.
FEEDBACK
1. The possible head injuries which may occur in this case include
wounds to the scalp as well as fractures of the skull.
There is often a higher incidence of subdural haemorrhages in
alcoholics. These types of haemorrhages tend to occur often in
alcoholics, inter alia due to the presence of brain atrophy which may
occur and which may result in increased mobility of the brain in the
skull. This results in rupture of the bridging veins. The doctor is
often confronted in this situation with the fact that the patient is
under the influence of alcohol and it is therefore difficult to
differentiate findings due to alcohol intoxication from those due to
a head injury. Because subdural haemorrhages tend to take a while
before they present, it is advisible to admit these patients for
observation. Otherwise the individual can be discharged, but only if
he is in the care of a responsible person. This person must be
informed of any warning signs which may indicate increased
intracranial pressure due to the development of a subdural
haemorrhage.
2. (a) This most probably indicates an extradural haemorrhage. It is a
result of rupture of the middle meningeal artery which lies on
the inside of the temporal bone.
(b) The intracranial haemorrhage results in increased intracranial
pressure, which in time may be complicated by herniations.
138
Study unit 7
STUDY UNIT 8Asphyxia
Contents
8.1 Anoxia/hypoxia
8.1.1 Anoxic anoxia/hypoxia
8.1.2 Anaemic anoxia/hypoxia
8.1.3 Stagnation anoxia/hypoxia
8.1.4 Cytotoxic anoxia/hypoxia
8.2 Classification of asphyxic deaths
8.3 ``Classical'' signs of asphyxia
8.3.1 Petechial haemorrhages
8.3.2 Congestion and oedema
8.3.3 Cyanosis
8.3.4 Congestion and dilatation of the right heart chambers and
increased fluidity of blood
8.4 Causes of asphyxic deaths
8.4.1 Suffocation
8.4.2 Smothering
8.4.3 Choking
8.4.4 Restriction of respiratory movements
8.4.5 Deaths due to pressure on the neck
8.4.6 Hanging
8.4.7 Auto-erotic deaths
8.4.8 Drowning
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. understand the causes of anoxia/hypoxia
. critically assess the so-called classical signs of asphyxia
. discuss death due to suffocation, smothering, aspiration as well as
restriction of respiratory movement
. discuss the group of deaths due to violence or pressure applied to
the neck
. discuss possible causes (including drowning) of death in bodies
retrieved from water
Asphyxia is a misnomer. It actually refers to asphyxia neonatorum, a
condition which describes the absence of a pulse in a baby. Nevertheless, the
139
term asphyxia is generally used to describe the group of deaths due to a lack
of oxygen. It includes drowning, and some authors also regard carbon-
monoxide poisoning as a cause of asphyxia.
The primary physiological abnormality is a total or partial lack of oxygen.
Another important manisfestation is neurogenic cardiac arrest. The other
causes of death will be discussed in more detail below.
8.1 Anoxia/hypoxia
The availbility of oxygen plays a vital and central role in this group of
conditions. Anoxia refers to a total lack of oxygen, while hypoxia refers to a
partial lack or deficit. The causes of anoxia and hypoxia (please note not
necessarily asphyxia) can be classified as follows:
8.1.1 Anoxic anoxia/hypoxia
In this group the oxygen tension in the inhaled air is too low to oxygenate the
red blood cells sufficiently. This may be the result of low barometric pressure,
as found at high altitude. It may also be the result of lung pathology, where
the gas exchange capacity of the lungs is decreased, as seen in emphysema.
(Emphysema is a swelling due to presence of air, applied especially to a
morbid condition of the lungs.)
8.1.2 Anaemic anoxia/hypoxia
In this condition the oxygen-carrying capacity of the blood is decreased. This
may be the result of a low haemoglobin (the molecule which binds the oxygen
in the blood) level, also known as anaemia. Blood loss leads to acute anaemia.
In some cases the haemoglobin content may be normal but the molecules
cannot bind with oxygen, as another substance, such as carbon monoxide, has
already bonded with the haemoglobin molecule (carbon-monoxide poison-
ing).
8.1.3 Stagnation anoxia/hypoxia
This condition arises when the circulation cannot circulate the blood
sufficiently. The most common cause is heart failure, where the heart is not
contracting adequately. This may be the result of a myocardial infarct (the
heart muscle degenerates because of, for example, a blood clot in a coronary
artery which stops the flow of blood), high blood pressure or other cardiac
disease.
8.1.4 Cytotoxic anoxia/hypoxia
In this condition the oxygen delivery to the tissues is adequate, but the tissues
and the cells cannot use the oxygen. This may be due to a blockage of the
enzyme systems in the cell, so that oxygen cannot be used for cell metabolism.
Examples include cyanide poisoning. Carbon-monoxide poisoning causes
anaemic anoxic/hypoxia, as well as an element of cytotoxic hypoxia due to the
inhibition of the enzyme systems in the cells.
140
Study unit 8
8.2 Classification of asphyxic deaths
The following is a classification of the causes of asphyxic deaths. The fact that
this type of death occurs in so many situations indicates the importance of
asphyxia as cause of death.
1. Suffocation
decreased atmospheric oxygen tension (pressure)
Ð low barometric pressure
Ð displacement by inert gasses (nitrogen [N2]; carbon dioxide [CO2])
2. Smothering
obstruction of the external airways
3. Choking
obstruction of the internal airways
4. Impairment or respiratory movements (mechanical asphyxia)
5. Pressure on neck
(a) Throttling
pressure exerted by hands on the neck
(b) Strangulation
pressure exerted by a ligature on the neck (without the weight of the
body having an effect)
6. Hanging
pressure exerted by a ligature on the neck due to the effect of the body
weight
7. Auto-erotic deaths
8. Drowning
(a) Immersion without aspiration
(b) Drowning with aspiration
8.3 ``Classical'' signs of asphyxia
These signs are non-specific and are not only often absent in typical hypoxic
deaths, but may also sometimes be present in non-hypoxic deaths. The matter
is complicated further by the fact that some asphyxic deaths may occur
without hypoxia, for instance neurogenic cardiac arrest. Bernard Knight, a
well-known forensic pathologist, believes that the non-specific nature of these
signs are so obvious, that it forms part of forensic mythology. However, as it is
sometimes dogmatically advocated by some authors, it is discussed in this
study guide to give some perspective on this matter.
8.3.1 Petechial haemorrhages
Petechial, punctate or pinpoint haemorrhages originate from small venules
which are less than 2 mm in diameter. It may occur on the skin, eyes (sclera
and conjunctiva), as well as the thoracic organs and the membranes covering
the body cavities (pleura and pericardium). The petechial haemorrhages of
the pleural surface was first described by Tardieu, and are also noted in cases
of sudden infant death syndrome (SIDS or cot death). There is often also
141
Asphyxia
some degree of swelling of the tissue. Possible causes include increased venous
pressure, decreased intrapleural pressure and/or hypoxic damage to the walls
of the blood vessels. The pressure in the thoracic cavity is usually negative,
and this assists in keeping the lung in an inflated position. With airway
obstruction the individual will struggle to inhale air. The muscles of
respiration will contract more powerfully, and the negative pressure in the
thoracic cavity will increase even further. The blood will be ``sucked'' from
the small blood vessels in the pleural tissue. Petechial haemorrhages can also
occur in the post-mortem period, as discussed in the study unit on post-
mortem hypostasis (study unit 3).
8.3.2 Congestion and oedema
When there is obstruction of venous blood flow, blood will accumulate above
the level of obstruction. In the beginning there is congestion of blood in the
vessels, but later fluid from the vessels leak into the surrounding tissue,
causing swelling. In the lungs this oedema will produce a foamy fluid, as air
and fluid will be mixed during breathing. This is often pronounced in cases of
drowning.
8.3.3 Cyanosis
Cyanosis is a colour change which occurs when the haemoglobin concentra-
tion, saturated with oxygen, drops below 85%. The skin, lips and other
mucosal surfaces assume a blue hue or appearance. Post-mortem cyanosis is
controversial, because death is generally associated with lack of circulation,
and therefore insufficient oxygenation of the haemoglobin. The degree of
cyanosis is therefore not an indication of the type of death.
8.3.4 Congestion and dilatation of the right heart chambers and increased fluidity ofblood
This alleged characteristic of asphyxic death is often discussed in Asiatic
literature. It is however a non-specific phenomenon.
To summarise: There is no single sign which is indicative of asphyxic death.
The diagnosis therefore depends on circumstantial evidence, as well as other
external changes, such as scratch marks on the neck or fractures of the hyoid
bone.
8.4 Causes of asphyxic death
8.4.1 Suffocation
Suffocation is the result of a decreased oxygen tension in the inhaled air due
to lower atmospheric oxygen tension, or PAO2, or lower partial oxygen
pressure. An example of low atmospheric pressure is the sudden decompres-
sion of an aircraft cabin at high altitude, with a drop in the barometric
pressure in the cabin. The oxygen can also be consumed or displaced by other
inert gases such as carbon dioxide or nitrogen. This is seen when oxygen is
consumed by a fire, or in an enclosed space such as a fridge. An interesting
example which often occurs in the agricultural regions of our country, is when
142
Study unit 8

people die in wine tanks or silos. During the process of fermentation in these
tanks or silos, oxygen is consumed and carbon dioxide produced. This
process is similar to the fermentation process responsible for the production
of ginger beer or wine, or when yeast causes bread to rise. Carbon dioxide is a
heavy gas and it will accumulate at the bottom of the tank or silo. If the
person enters this space, the oxygen-poor/carbon-dioxide-rich air will
overwhelm him, and death will follow. A similar situation occurs in ships'
hulls. Rust is the product of iron oxidation. When steel rusts, (which is
common in ships) oxygen is consumed and replaced by inert gases. More
examples of an oxygen-poor atmosphere are wells in lime soil (lime contains
carbon dioxide, a heavy gas which will accumulate in the deeper parts of a
well), and defective scuba-diving gear.
Although hypoxia plays the most important role in these deaths, inert gases
like nitrogen and carbon dioxide may also caused death due to neurogenic
cardiac arrest. This condition will be discussed below.
On post-mortem examination there are seldom signs of asphyxia. Where the
death is due to a fire, signs of carbon monoxide poisoning may also be
present. Note that a fire does not only consume oxygen, but also produces
carbon dioxide and carbon monoxide, depending on the availability of
oxygen. Other poisonous products such as sulphur-containing substances are
also produced, depending on the type of material. These substances are toxic
and inter alia damage the airways.
8.4.2 Smothering
This is the result of occlusion of the external airways, namely the mouth and
nose. Examples include occlusion with a hand, impermeable material (a
plastic bag) or even solid material (sand and grain). The individual can also lay
face down on an impermeable surface, for instance when an intoxicated
person is lying face down on a wet cushion covered by vomit. Note that cot
death or SIDS is not caused by smothering.
Smothering can occur due to an accident, suicide or murder.
``Gagging'' refers to a situation where a piece of cloth is used to forcibly close
the mouth. It is often associated with the introduction of a piece (ball or plug)
of material into the mouth of the victim. This is common when intruders
overpower a person and gag him in an effort to silence him. The mandible is
often displaced backwards and fixed in that position so that the victim cannot
swallow. The saliva will with time cause the material over the mouth and nose
that was initially permeable, to become impermeable. At the same time
ineffective swallowing movements may cause the material in the mouth to
move backwards towards the throat. Ultimately the victim suffocates, and the
initial crime of theft and assault becomes an (unforeseen) case of culpable
homicide or murder.
The post-mortem examination often shows no signs of trauma or asphyxia.
Local trauma or injuries to the lips, nose and mucosa of the mouth may
sometimes be visible, especially when the airways were forcibly occluded. It is
important to remember that babies and some old people have no teeth, and
will therefore not necessarily have any mouth lesions. It is also important to
143
Asphyxia

remember that the inner aspects of the mouth must always be examined, as
the delicate membrane connecting the lips with the gingiva on the midline, is
often injured, even if the individual has no teeth. It is also important not to
confuse hypostasis and peri-oral pallor in cases where the body is lying in the
prone position.
` Asphyxic'' signs include petechiae of the face and conjunctiva, especially if
there was a struggle.
8.4.3 Choking
Choking is the result of occlusion of the internal airways, occurring at any
level from the pharynx (throat) to the bifurcation of the trachea (windpipe).
This obstruction may be caused by foreign bodies like teeth, food (eg beans),
or even marbles. There are also medical conditions which can cause severe
swelling of the epiglottis (valve-like structure over the larynx) with
subsequent obstruction of the airway, such as anaphylaxis (severe allergic
reaction) or certain bacterial infections (haemophilus influenzae). An example
from daily life is when someone drinks a cool drink from a can with a bee
trapped inside. When the person swallows the bee, and is stung in the throat,
the soft tissues of the throat can swell dramatically, causing narrowing and
obstruction of the airways. Fortunately this type of swelling responds rapidly
to the correct treatment.
The most important post-mortem findings is the presence of a foreign body in
the airway, or swelling of the mucosa and soft tissue. In cases of suspected
choking, it is important that the airways be incised with a knife, and not cut
open with scissors, as the foreign body will then be displaced, being pushed
downwards by the tip of the scissors. Signs of asphyxia are often absent.
When interpreting the presence of gastric contents in the airways during a
post-mortem examination, the following aspects need to be considered.
Gastric or stomach matter often gets into the airways due to regurgitation or
passive backflow from the stomach into the oesophagus and from there into
the airways. This occurs especially during handling of the body. It must not be
confused with aspiration of stomach contents. Aspiration of stomach contents
can only be diagnosed post mortem, if:
. it is present in the smaller airways (bronchial structures), as it can only
reach these structures if actively inhaled
. there is microscopic evidence of an inflammatory process in the lung tissue
due to the presence of foreign material
. it was witnessed by someone else
The only exception to this rule is when an individual with a high blood-
alcohol level has stomach contents in the airways at the post mortem.
Intoxicated individuals not only are more at risk to vomit, but are also more
at risk to aspirate due to their depressed protective upper-airway reflexes.
In the 1950s a condition known as bolus death (``cafe coronary syndrome'')
was described where someone died suddenly and unexpectedly while eating
(photos 53 and 54). Initially it was believed that he had a heart attack
(therefore the reference to coronary), but in reality the cause was neurogenic
144
Study unit 8

heart arrest. This condition occurs when a large piece of food stimulates the
back of the throat during swallowing. It then triggers vaso-vagal inhibition of
the heart.
8.4.4 Restriction of respiratory movements
This is also known as traumatic or positional asphyxia, although it is actually a
misnomer as no signs of trauma have to be present. Mechanical asphyxia is a
more appropriate term.
In this condition movement of the chest is restricted. This may occur when
the chest, and usually also the abdomen, is compressed. Movement of the
chest and diaphragm muscles is therefore prevented or restricted, and
inspiration cannot occur. This may occur when the chest is compressed by soil
or other material/objects, including a vehicle. In recent years disasters
occurred at a number of sporting and other events (eg at Ellis Park,
Johannesburg) when a panicking or excited crowd pushed forward and
individuals were trapped against gates or other obstructions during the
stampede. A comparable situation is where an intoxicated person loses
consciousness while in a position where the head is lower than the rest of the
body, and the intestines press downwards on the diaphragm, restricting its
movement. Cases were also reported where an intruder climbs over a high
fence, and then falls in such a way that his feet are caught in the security
spikes on top of the fence. In this upside-down position, the downward
pressure of his intestines on the diaphragm limits inhalation. Inhalation
against this gravity-effect on the diaphragm is tiring, and the individual
eventually develops ``asphyxia'' and dies.
Crucifixion is another example where someone dies due to restriction of
respiratory movement. During crucifixion in the upright position, the chest is
fixed in a state of inspiration. The individual therefore struggles to exhale. If
the individual is crucified upside down, the intestines press on the diaphragm
and the thoracic organs, and the individual cannot inhale without effort.
In this group of asphyxic deaths post-mortem signs, and especially the so-
called signs of ``asphyxia'' are well developed, with petechial haemorrhages,
congestion and swelling present above the level where the pressure was
applied. Bleeding from the mouth and ears may also be present, as well as
congestion of the lungs. The skin may show wounds due to the pressure of
the object on the body.
8.4.5 Deaths due to pressure on the neck
This group of deaths includes strangulation with the hands or throttling,
strangulation with a ligature, and hanging.
8.4.5.1 Causes of death
Death is caused by one or more of the following.
1. Airway obstruction. Direct pressure on the larynx and trachea (throat
and windpipe) or upward displacement of the larynx (throat) against the
pharynx can obstruct the airways. This results in hypoxic-anoxic anoxia.
145
Asphyxia
In a similar manner the base of the tongue may be displayed backwards
against the throat.
2. Compression of the veins in the neck. Compression of the internal and
external jugular veins (the veins at the side of the neck) prevents blood
flow from the head to the heart. This is especially serious if the carotid
arteries are still open, as blood flow into the head region is still possible,
but the blood cannot flow out of that region. This leads to stagnation of
inter alia blood flow to and from the brain.
3. Compression of the carotid arteries. This is less common than
compression of the veins, as more pressure is required. This results in
stagnation hypoxia. Compression of the vertebral arteries (the blood
vessels running through the vertebral column to the brain) is rare, as they
are protected by bone. With bilateral compression of the carotid arteries
loss of consciousness occurs almost immediately, as the vertebral arteries
are not able to supply sufficient blood to the brain to preserve
consciousness. In elderly individuals pressure on the carotid arteries
may damage the blood vessel walls and atheroma plaques may be
dislodged, which can then cause a stroke.
4. Neurogenic stimulation. This is a very important cause of death. At the
bifurcation of the carotid arteries in the neck, baro- or pressure receptors
are located in a slight dilation in the blood vessel, the carotid sinus.
Usually these receptors play a role in controlling blood pressure. If the
latter rises, the receptors are stimulated due to the higher pressure in the
blood vessels, and via a reflex arc the heartspeed is then suppressed or
inhibited. As the vagus nerve forms part of this reflex arc, this reflex is
also known as the vaso-vagal response. Mechanical stimulation of these
receptors by pressure triggers a parasympathetic response. The heart rate
drops (bradycardia), the person could faint, and if severe enough, reflex
cardiac arrest may occur. Alcohol, hypoxia, drugs such as cocaine, as well
as anxiety and fear can sensitise these receptors and cause an exaggerated
response.
Neurogenic cardiac arrest is more common in throttling and hanging than
in strangulation. The receptors are partially covered by the neck muscles.
During throttling the fingers dig below the muscles and can stimulate the
receptors directly. With hanging the knot in the cord often lies directly
over the receptors. With strangulation with a ligature, the ligature is
usually lower down over the neck, away from the receptors. Blows to the
neck can also stimulate the receptors directly or indirectly (like in martial
arts). In cases of bolus death, branches of the same nerves supplying these
receptors, are stimulated in the back of the throat, and this causes a
similar effect. In some individuals the receptors may be very sensitive, and
even stimulation by the collar of a shirt can cause the individual to faint.
5. Combination of the above mechanisms: Throttling is a dynamic process.
During the struggle the grip on the neck is continuously changed. More
than one of the above causes can therefore be involved. It is also
important to remember that hypoxia due to compression of the airways
will stimulate the carotid receptors, and therefore increase the risk of
neurogenic cardiac arrest.
146
Study unit 8

8.4.5.2 Throttling (strangulation with the hands)
Throttling is relatively common, especially in domestic murders, sex-associatedmurders and child murders. In order to overpower and throttle a person, theperpetrator has to have a physical advantage. Females therefore seldom throttlevictims (apart from children) and even men don't often succumb to throttling.As has been said throttling is a dynamic process with the hands changing the gripcontinously. Any of the above causes of death may therefore occur.
The post-mortem signs are local skin wounds, caused by the fingers of theassailant as well as those of the victim. The contusions and abrasions vary insize, and are usually round or oval in shape. They tend to be present mostlyon one side of the neck. The distribution (one mark on the one side and fourmarks on the opposite side) could indicate whether the assailant was left- orright-handed.
Abrasions may be caused by the fingers and nails of the assailant as well asthose of the victim. Many are caused by the victim himself, in an effort tobreak the grip of the assailant. It is therefore important always to examine thenails of the victim, and to collect any material under the nails. This materialcan be genetically analysed for comparison with the genetic profile of thealleged assailant.
Damage to the deep-lying structures, for instance haemorrhage into the softtissue and muscles of the neck, damage of the vascular structures as well asfractures of the bone and cartilage of the neck may also occur (fig 8.1).Haemorrhage into the thyroid gland may also occur.
Fig 8.1. Professor JJF Taljaard's case (Department of Forensic Medicine, University of the Witwatersrand,Johannesburg). A case of assault including throttling. There were hardly any injuries on the skin of the neck, butdissection revealed deep bruising in the soft parts, consistent with throttling. (Reproduced by permission ofProfessor Taljaard.)
147
Asphyxia
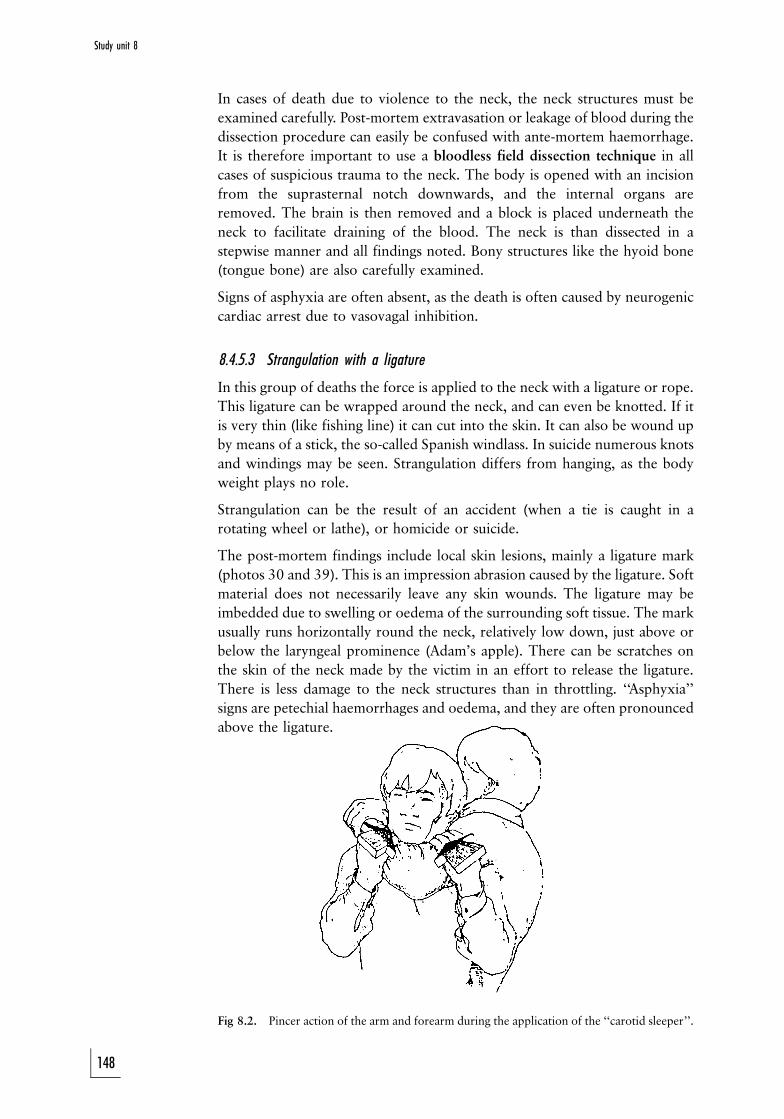
In cases of death due to violence to the neck, the neck structures must be
examined carefully. Post-mortem extravasation or leakage of blood during the
dissection procedure can easily be confused with ante-mortem haemorrhage.
It is therefore important to use a bloodless field dissection technique in all
cases of suspicious trauma to the neck. The body is opened with an incision
from the suprasternal notch downwards, and the internal organs are
removed. The brain is then removed and a block is placed underneath the
neck to facilitate draining of the blood. The neck is than dissected in a
stepwise manner and all findings noted. Bony structures like the hyoid bone
(tongue bone) are also carefully examined.
Signs of asphyxia are often absent, as the death is often caused by neurogenic
cardiac arrest due to vasovagal inhibition.
8.4.5.3 Strangulation with a ligature
In this group of deaths the force is applied to the neck with a ligature or rope.
This ligature can be wrapped around the neck, and can even be knotted. If it
is very thin (like fishing line) it can cut into the skin. It can also be wound up
by means of a stick, the so-called Spanish windlass. In suicide numerous knots
and windings may be seen. Strangulation differs from hanging, as the body
weight plays no role.
Strangulation can be the result of an accident (when a tie is caught in a
rotating wheel or lathe), or homicide or suicide.
The post-mortem findings include local skin lesions, mainly a ligature mark
(photos 30 and 39). This is an impression abrasion caused by the ligature. Soft
material does not necessarily leave any skin wounds. The ligature may be
imbedded due to swelling or oedema of the surrounding soft tissue. The mark
usually runs horizontally round the neck, relatively low down, just above or
below the laryngeal prominence (Adam's apple). There can be scratches on
the skin of the neck made by the victim in an effort to release the ligature.
There is less damage to the neck structures than in throttling. ` Asphyxia''
signs are petechial haemorrhages and oedema, and they are often pronounced
above the ligature.
Fig 8.2. Pincer action of the arm and forearm during the application of the ``carotid sleeper''.
148
Study unit 8
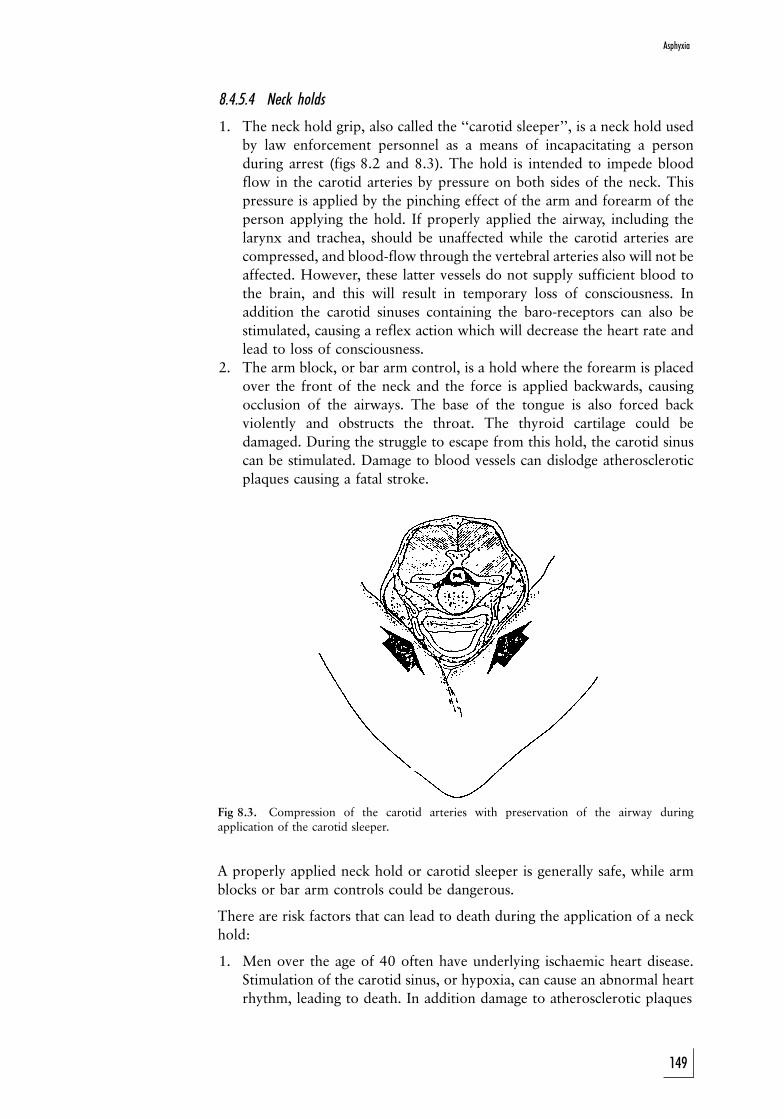
8.4.5.4 Neck holds
1. The neck hold grip, also called the ``carotid sleeper'', is a neck hold used
by law enforcement personnel as a means of incapacitating a person
during arrest (figs 8.2 and 8.3). The hold is intended to impede blood
flow in the carotid arteries by pressure on both sides of the neck. This
pressure is applied by the pinching effect of the arm and forearm of the
person applying the hold. If properly applied the airway, including the
larynx and trachea, should be unaffected while the carotid arteries are
compressed, and blood-flow through the vertebral arteries also will not be
affected. However, these latter vessels do not supply sufficient blood to
the brain, and this will result in temporary loss of consciousness. In
addition the carotid sinuses containing the baro-receptors can also be
stimulated, causing a reflex action which will decrease the heart rate and
lead to loss of consciousness.
2. The arm block, or bar arm control, is a hold where the forearm is placed
over the front of the neck and the force is applied backwards, causing
occlusion of the airways. The base of the tongue is also forced back
violently and obstructs the throat. The thyroid cartilage could be
damaged. During the struggle to escape from this hold, the carotid sinus
can be stimulated. Damage to blood vessels can dislodge atherosclerotic
plaques causing a fatal stroke.
Fig 8.3. Compression of the carotid arteries with preservation of the airway duringapplication of the carotid sleeper.
A properly applied neck hold or carotid sleeper is generally safe, while arm
blocks or bar arm controls could be dangerous.
There are risk factors that can lead to death during the application of a neck
hold:
1. Men over the age of 40 often have underlying ischaemic heart disease.
Stimulation of the carotid sinus, or hypoxia, can cause an abnormal heart
rhythm, leading to death. In addition damage to atherosclerotic plaques
149
Asphyxia
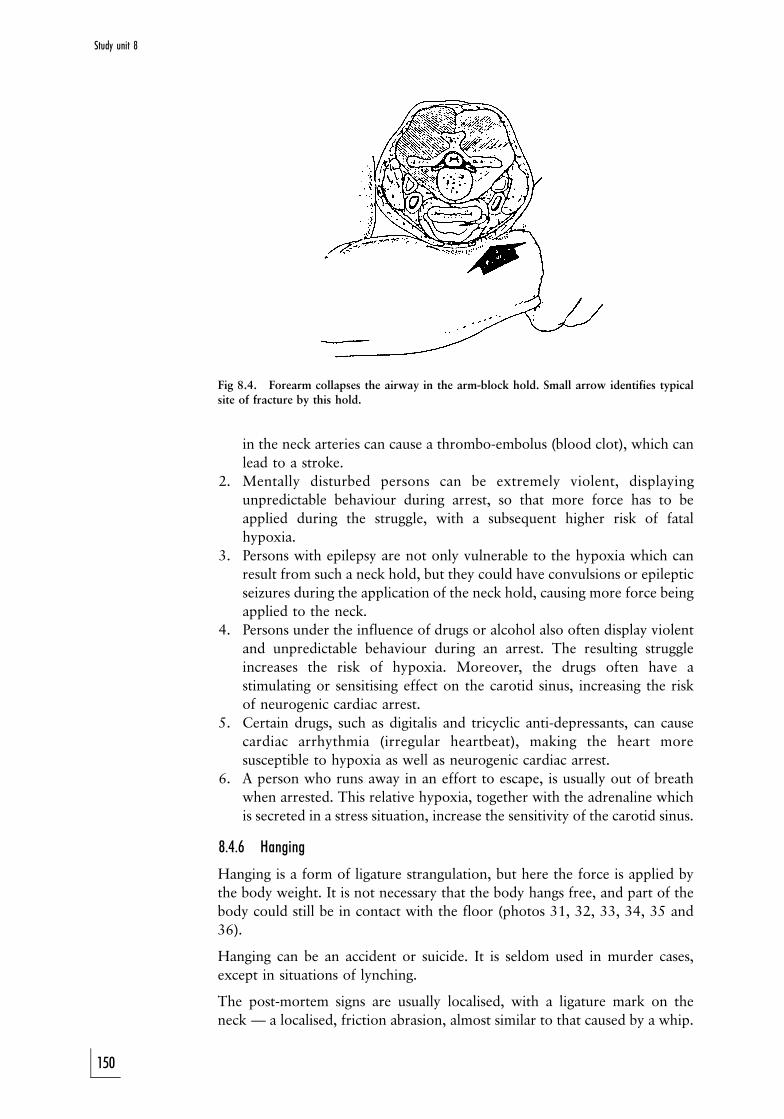
Fig 8.4. Forearm collapses the airway in the arm-block hold. Small arrow identifies typicalsite of fracture by this hold.
in the neck arteries can cause a thrombo-embolus (blood clot), which can
lead to a stroke.
2. Mentally disturbed persons can be extremely violent, displaying
unpredictable behaviour during arrest, so that more force has to be
applied during the struggle, with a subsequent higher risk of fatal
hypoxia.
3. Persons with epilepsy are not only vulnerable to the hypoxia which can
result from such a neck hold, but they could have convulsions or epileptic
seizures during the application of the neck hold, causing more force being
applied to the neck.
4. Persons under the influence of drugs or alcohol also often display violent
and unpredictable behaviour during an arrest. The resulting struggle
increases the risk of hypoxia. Moreover, the drugs often have a
stimulating or sensitising effect on the carotid sinus, increasing the risk
of neurogenic cardiac arrest.
5. Certain drugs, such as digitalis and tricyclic anti-depressants, can cause
cardiac arrhythmia (irregular heartbeat), making the heart more
susceptible to hypoxia as well as neurogenic cardiac arrest.
6. A person who runs away in an effort to escape, is usually out of breath
when arrested. This relative hypoxia, together with the adrenaline which
is secreted in a stress situation, increase the sensitivity of the carotid sinus.
8.4.6 Hanging
Hanging is a form of ligature strangulation, but here the force is applied by
the body weight. It is not necessary that the body hangs free, and part of the
body could still be in contact with the floor (photos 31, 32, 33, 34, 35 and
36).
Hanging can be an accident or suicide. It is seldom used in murder cases,
except in situations of lynching.
The post-mortem signs are usually localised, with a ligature mark on the
neck Ð a localised, friction abrasion, almost similar to that caused by a whip.
150
Study unit 8
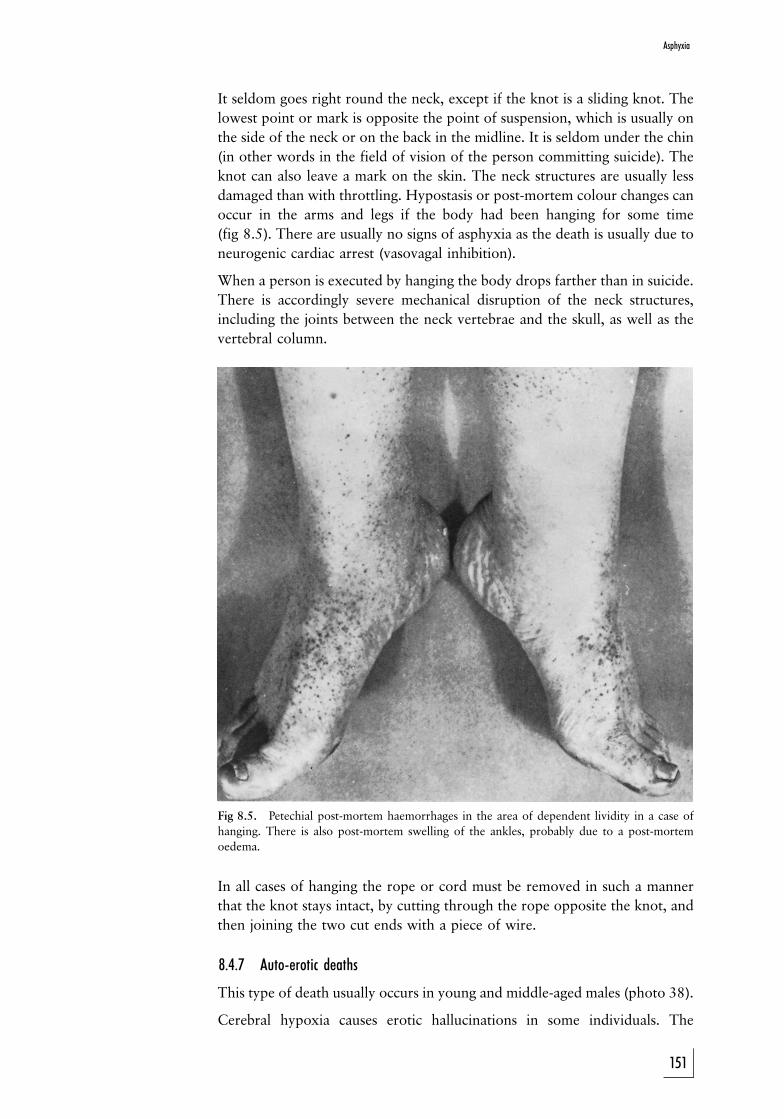
It seldom goes right round the neck, except if the knot is a sliding knot. The
lowest point or mark is opposite the point of suspension, which is usually on
the side of the neck or on the back in the midline. It is seldom under the chin
(in other words in the field of vision of the person committing suicide). The
knot can also leave a mark on the skin. The neck structures are usually less
damaged than with throttling. Hypostasis or post-mortem colour changes can
occur in the arms and legs if the body had been hanging for some time
(fig 8.5). There are usually no signs of asphyxia as the death is usually due to
neurogenic cardiac arrest (vasovagal inhibition).
When a person is executed by hanging the body drops farther than in suicide.
There is accordingly severe mechanical disruption of the neck structures,
including the joints between the neck vertebrae and the skull, as well as the
vertebral column.
Fig 8.5. Petechial post-mortem haemorrhages in the area of dependent lividity in a case of
hanging. There is also post-mortem swelling of the ankles, probably due to a post-mortem
oedema.
In all cases of hanging the rope or cord must be removed in such a manner
that the knot stays intact, by cutting through the rope opposite the knot, and
then joining the two cut ends with a piece of wire.
8.4.7 Auto-erotic deaths
This type of death usually occurs in young and middle-aged males (photo 38).
Cerebral hypoxia causes erotic hallucinations in some individuals. The
151
Asphyxia
hypoxia is usually induced by pressure to the neck, although a mask over the
face, occluding the mouth and nose, may also be used. There is usually a
ligature around the neck, placed in such a way that it will loosen, as the
person becomes unconscious. Unfortunately things may not always go
according to plan: the ligature may not loosen when the person loses
consciousness, causing eventual death.
It is important to inspect the scene of death for other sexual practices such as
bondage, transvestism and fetishism. Erotic literature is often found beside
the body. As these deaths are unplanned and unforeseen, suicide letters are
not found.
Remember that the emission of semen is a common post-mortem
phenomenon due to rigor mortis of the muscles surrounding the sexual
organs, and therefore not necessarily an indication of ante-mortal sexual
activity.
8.4.8 Drowning
If a body is retrieved from water (submersed bodies) the death could be due to:
(1) natural causes (eg myocardial infarct) before falling into the water; in
other words the person suffered a heart attack, died and then fell into the
water
(2) natural causes (eg heart attack) while in the water
(3) unnatural causes (eg gunshot wound) before falling into the water
(4) unnatural causes (eg multiple injuries after being hit by a boat or bitten by
a shark) while in the water
(5) the effects of submersion other than drowning
(6) drowning
The situations sketched in (1) to (4) are also known as pseudo-drowning. The
person may have died of natural or unnatural causes while outside the water,
and then fallen into the water, or these causes may occur in the water. The
most common natural cause is a myocardial infarct or heart attack. Certain
natural conditions, such as epilepsy can predispose a person to drowning. It is
often difficult to distinguish between ante- and post-mortem wounds, as the
blood is washed from the body and the wounds appear clean.
8.4.8.1 Signs of submersion
(1) Maceration of the skin. This condition develops rapidly in warm water,
but may take hours to develop in cold water. This skin is pale and
wrinkled, the so-called ``washer-woman's skin'', similar to what it looks
like after lying in the bath for a long period. Maceration appears first in
areas with a thick keratin layer, such as the fingertips, palms and toes
(photo 5). After days in warm water and weeks in cold water the sogged
keratin layers become detached, but they can still be used to identify the
deceased (eg finger prints), as the small skin grooves are preserved.
(2) Cutis anserina. This condition is non-specific. The skin looks like goose
flesh, as the small muscles of the hair follicles contract making the hairs
stand up. This can also be observed in other types of death.
152
Study unit 8
(3) Distribution of post-mortem hypostasis. In still water a body will float on
its abdomen with the limbs facing downwards. The post-mortem colour
changes or lividity will be present over the legs, arms and the ventral
(anterior) aspect of the abdomen. With much water movement the body is
constantly rolled around, causing more widespread and uniform
distribution. The hypostasis is often a pink colour.
(4) Foreign material in airways and upper gastro-intestinal system. Sand,
mud, crustaceans and plants are often present in the airways and
oesophagus, especially if the body was rolled around vigorously or the
water was very deep.
(5) Partial breaking of rigor mortis. Rigor mortis can be broken by the wave
movement. However, this will only be partial, as only certain muscle
groups will be involved.
8.4.8.2 Determination of the period of submersion
Water temperature is the most important factor determining the appearance
of the body. Water pollution per se plays a minor role, although the
temperature of sewage water could rise due to bacterial activity.
The following can be used as guideline to the duration of submersion:
5 12 hours wrinkling of fingers
12 hours ± 3 days increased wrinkling of hands, feet
4±10 days early decomposition (low-lying parts)
2±4 weeks severe decomposition; loss of epidermis (skin)
1±2 months loss of skin, muscles, liquefaction
The two groups of death where the death is a direct result of the submersion,
with or without aspiration of water or other liquid medium, will now be
discussed.
8.4.8.3 Drowning without the aspiration of fluid into the lungs
Some deaths occur without aspiration of water. Possible causes are:
(1) Acute neurogenic cardiac arrest. Sometimes a person dies instantly when
hitting the water, probably from acute neurogenic cardiac arrest. A
possible cause may be the sudden stimulation of the skin or the back of
the throat by cold water. Alcohol can predispose a person to this
condition because it dilates the blood vessels of the skin.
This condition, also known as hydrocussion, is often witnessed in
harbours when intoxicated sailors fall into the sea, and die instantly, even
before the bodies can be taken out of the water.
(2) Hypothermia. The effect of cold water and subsequent hypothermia is
discussed in study unit 10.
(3) Laryngospasm. We have already said that irritation due to the inhaled
water will cause a spasm of the vocal cords (laryngospasm). This will then
prevent airflow, as well as further aspiration of water, into the lungs. It is
not clear whether laryngospasm alone can cause death. Usually it will
153
Asphyxia
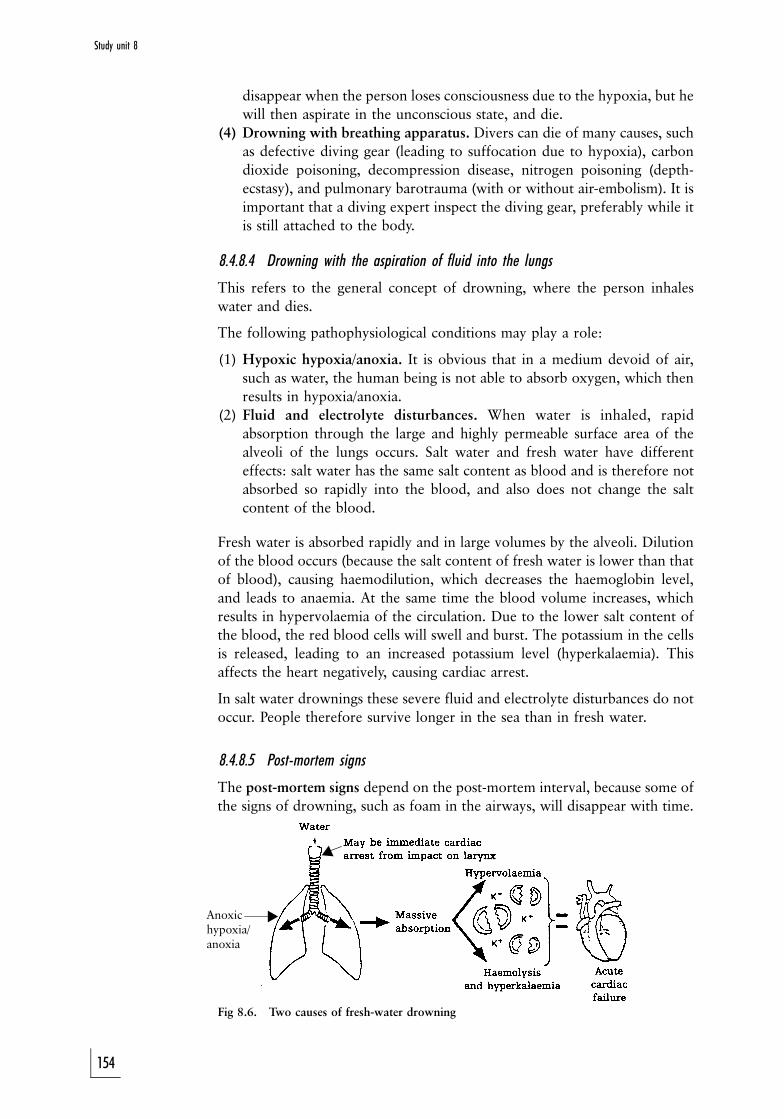
Anoxichypoxia/anoxia
!
!
disappear when the person loses consciousness due to the hypoxia, but he
will then aspirate in the unconscious state, and die.
(4) Drowning with breathing apparatus. Divers can die of many causes, such
as defective diving gear (leading to suffocation due to hypoxia), carbon
dioxide poisoning, decompression disease, nitrogen poisoning (depth-
ecstasy), and pulmonary barotrauma (with or without air-embolism). It is
important that a diving expert inspect the diving gear, preferably while it
is still attached to the body.
8.4.8.4 Drowning with the aspiration of fluid into the lungs
This refers to the general concept of drowning, where the person inhales
water and dies.
The following pathophysiological conditions may play a role:
(1) Hypoxic hypoxia/anoxia. It is obvious that in a medium devoid of air,
such as water, the human being is not able to absorb oxygen, which then
results in hypoxia/anoxia.
(2) Fluid and electrolyte disturbances. When water is inhaled, rapid
absorption through the large and highly permeable surface area of the
alveoli of the lungs occurs. Salt water and fresh water have different
effects: salt water has the same salt content as blood and is therefore not
absorbed so rapidly into the blood, and also does not change the salt
content of the blood.
Fresh water is absorbed rapidly and in large volumes by the alveoli. Dilution
of the blood occurs (because the salt content of fresh water is lower than that
of blood), causing haemodilution, which decreases the haemoglobin level,
and leads to anaemia. At the same time the blood volume increases, which
results in hypervolaemia of the circulation. Due to the lower salt content of
the blood, the red blood cells will swell and burst. The potassium in the cells
is released, leading to an increased potassium level (hyperkalaemia). This
affects the heart negatively, causing cardiac arrest.
In salt water drownings these severe fluid and electrolyte disturbances do not
occur. People therefore survive longer in the sea than in fresh water.
8.4.8.5 Post-mortem signs
The post-mortem signs depend on the post-mortem interval, because some of
the signs of drowning, such as foam in the airways, will disappear with time.
Fig 8.6. Two causes of fresh-water drowning
154
Study unit 8
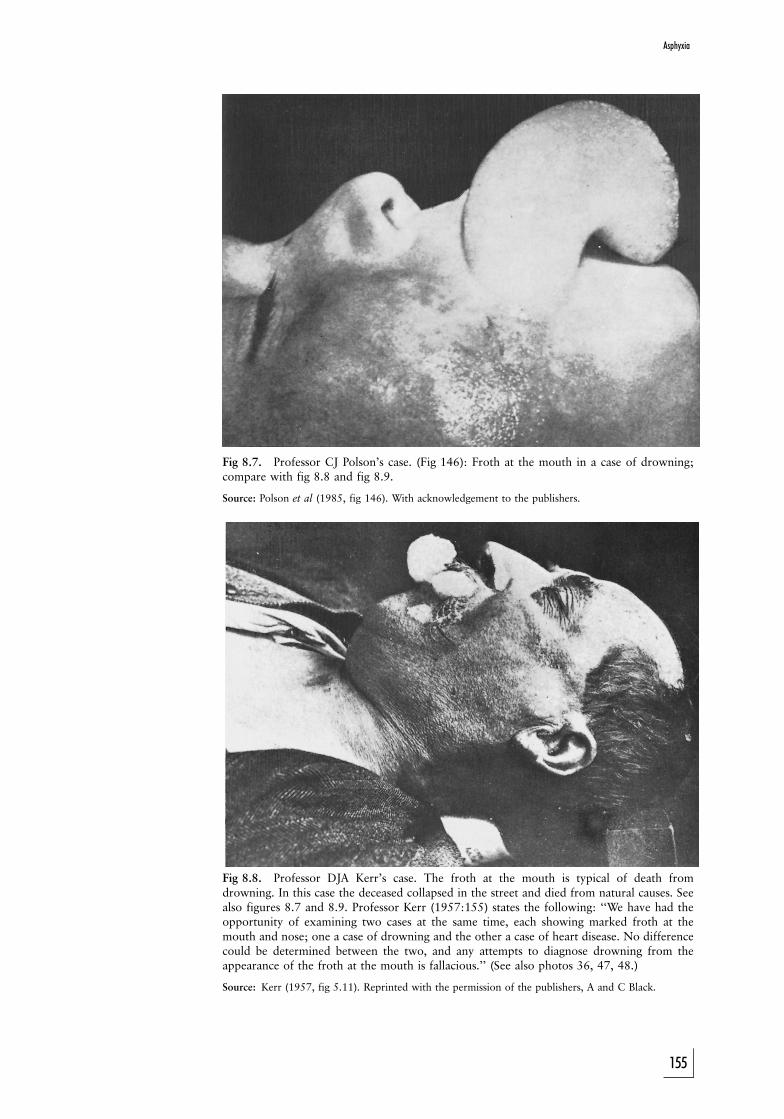
Fig 8.7. Professor CJ Polson's case. (Fig 146): Froth at the mouth in a case of drowning;compare with fig 8.8 and fig 8.9.
Source: Polson et al (1985, fig 146). With acknowledgement to the publishers.
Fig 8.8. Professor DJA Kerr's case. The froth at the mouth is typical of death fromdrowning. In this case the deceased collapsed in the street and died from natural causes. Seealso figures 8.7 and 8.9. Professor Kerr (1957:155) states the following: ``We have had theopportunity of examining two cases at the same time, each showing marked froth at themouth and nose; one a case of drowning and the other a case of heart disease. No differencecould be determined between the two, and any attempts to diagnose drowning from theappearance of the froth at the mouth is fallacious.'' (See also photos 36, 47, 48.)
Source: Kerr (1957, fig 5.11). Reprinted with the permission of the publishers, A and C Black.
155
Asphyxia
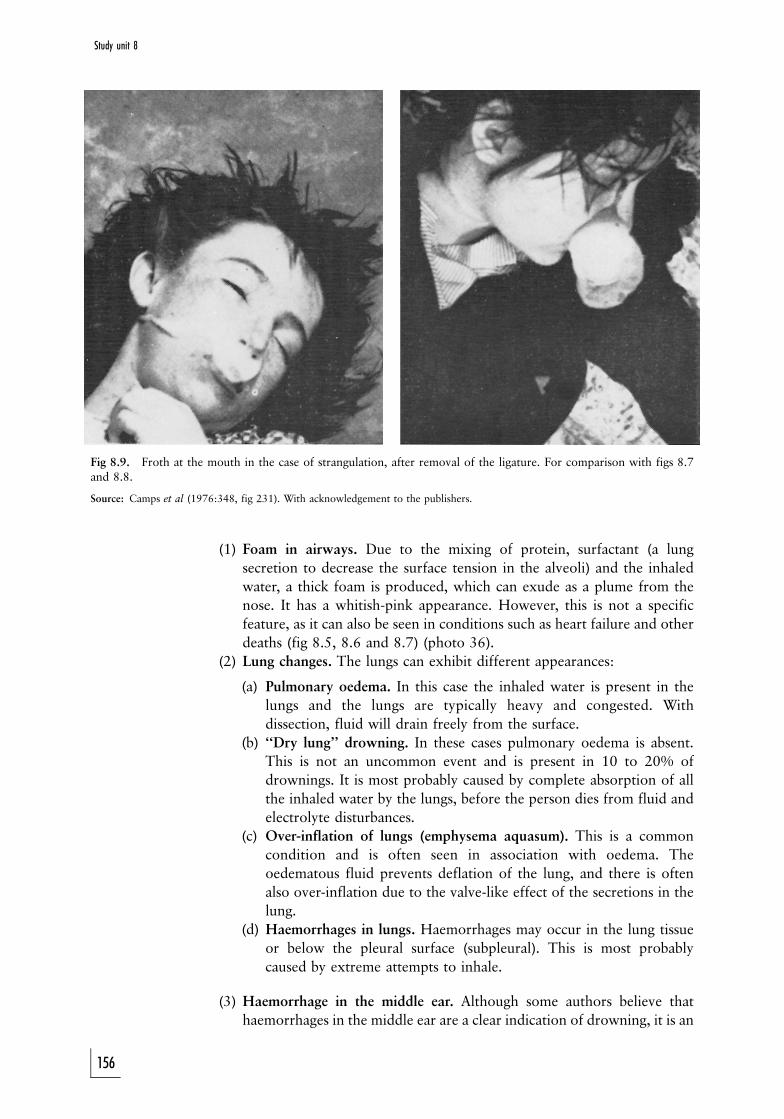
Fig 8.9. Froth at the mouth in the case of strangulation, after removal of the ligature. For comparison with figs 8.7and 8.8.
Source: Camps et al (1976:348, fig 231). With acknowledgement to the publishers.
(1) Foam in airways. Due to the mixing of protein, surfactant (a lung
secretion to decrease the surface tension in the alveoli) and the inhaled
water, a thick foam is produced, which can exude as a plume from the
nose. It has a whitish-pink appearance. However, this is not a specific
feature, as it can also be seen in conditions such as heart failure and other
deaths (fig 8.5, 8.6 and 8.7) (photo 36).
(2) Lung changes. The lungs can exhibit different appearances:
(a) Pulmonary oedema. In this case the inhaled water is present in the
lungs and the lungs are typically heavy and congested. With
dissection, fluid will drain freely from the surface.
(b) ``Dry lung'' drowning. In these cases pulmonary oedema is absent.
This is not an uncommon event and is present in 10 to 20% of
drownings. It is most probably caused by complete absorption of all
the inhaled water by the lungs, before the person dies from fluid and
electrolyte disturbances.
(c) Over-inflation of lungs (emphysema aquasum). This is a common
condition and is often seen in association with oedema. The
oedematous fluid prevents deflation of the lung, and there is often
also over-inflation due to the valve-like effect of the secretions in the
lung.
(d) Haemorrhages in lungs. Haemorrhages may occur in the lung tissue
or below the pleural surface (subpleural). This is most probably
caused by extreme attempts to inhale.
(3) Haemorrhage in the middle ear. Although some authors believe that
haemorrhages in the middle ear are a clear indication of drowning, it is an
156
Study unit 8
unreliable sign. It is most probably the result of pressure of the water on
the middle ear.
(4) Stomach content. The presence of water in the stomach is unreliable as a
sign of drowning; pressure of the water on the submersed body is
sufficient to force water into the stomach.
(5) Cataleptic stiffening or cadaver spasm. This phenomenon was discussed
in depth in study unit 3. It is an indication that the person was alive when
falling into the water.
(6) Post-mortem trauma. Propellers of boats and ships, as well as shells and
rocks can cause injury to the submerged body. It is often difficult to
differentiate between ante- and post-mortem trauma.
8.4.8.6 Tests
Special tests may be performed in cases of drowning.
(1) Test to determine biochemical changes.
Biochemical changes occur when water is inhaled. The chloride
concentration of the blood from the left and right ventricles is compared.
In a case of drowning in fresh water, the haemodilution effect will lower
the chloride concentration as the blood circulates through the lungs (ie
the level of chloride in the left ventricle will be lower than that in the right
ventricle). In the case of drowning in seawater, the opposite will occur.
However, in practice this does not always happen and the test should
therefore be interpreted with caution.
(2) Test to find diatoms in lung tissue (photo 37).
Diatoms are microscopically small silica-like organisms which occur freely
in nature. It is believed that isolation of a specific type of diatom in the
lung tissue, blood and bone-marrow of a deceased person confirms that
the person drowned in a specific body of water. However, diatoms are
freely found in a number of substances (including toothpaste), and
because of this, as well as the fact that isolating them from tissue is so
timeconsuming, this test has become obsolete.
It is important to remember that a finding of drowning is often made on
circumstantial evidence obtained during the inquest.
It is also important to remember that an individual could be rescued and
revived, only to die at a later stage due to lung complications (especially the
inhalation of water) or brain damage. This is called secondary or near-
drowning. Cases have been described where children had been submerged in
ice-cold water for some time, but after resuscitation and warming up,
survived with no or little brain damage. This is due to the protective effect of
hypothermia on the brain, as it decreases the oxygen requirements of the
brain.
ACTIVITIES
1. During a court case the one party alleges that the dark blue discoloration
of the hands and feet of the deceased's body (cyanosis) is a definite sign
that the person was throttled. How would you deal with this statement?
157
Asphyxia
2. During cleaning of a wine tank, one of the workers dies while climbing
into the tank. What is the probable cause of death?
3. A person is throttled with the hands during an assault. What could be the
causes of death?
4. The body of a young man is found in weird circumstances. There is a rope
with a sliding knot around his neck. The body is naked and pornographic
material is present on the scene. With what phenomenon are we faced
here?
5. Which risk factors may increase the risk of death during the application of
a neck grip?
6. A person may die during immersion with or without aspiration of water.
What are the causes of death in these two groups of death?
FEEDBACK
1. Post-mortem cyanosis is controversial, as all deaths are associated
with failure of the circulation with lack of oxygen delivery by the
haemoglobin to the peripheral tissues and cells. Therefore almost all
deaths present with blue discoloration or cyanosis. Exceptions
include bodies that have been refrigerated, cases of drowning and
also certain poisonings. In this case, the fact that cyanosis is present,
is no indication of the type or mode of death.
2. This is an example of suffocation due to fermentation in the wine
tank, which causes oxygen to decrease and carbon-dioxide to be
produced.
3. During the application of pressure to the neck, death may be caused
by the following:
(a) airway obstruction
(b) occlusion of the neck veins
(c) occlusion of the carotid arteries
(d) neurogenic stimulation
(e) a combination of the above
Especially in throttling, which is a dynamic process, the hands tend
to change their grip continuously, and therefore any one or a
combination of the above could play a role.
4. This is an example of an auto-erotic death.
5. The risk of neck grips is increased by the following factors:
(a) ischaemic heart disease
(b) psychiatric illness, epilepsy, drugs, alcohol and certain medica-
tion
(c) physical exercise preceding the application of pressure Ð this
increases the sensitivity of the carotid sinus due to adrenalin
sensitisation of the sinus
6. When there is aspiration of water, death is usually caused by
hypoxia or fluid electrolyte disturbances. The latter will be more
prominent in cases of drowning in fresh water than in salt water or
158
Study unit 8
seawater. Where death occurs without aspiration, possible causes
include neurogenic heart arrest, hypothermia or a defective
aspiration apparatus (scuba diving) or a diving accident. The latter
includes carbon-dioxide poisoning, decompression disease (``the
bends'') and barotrauma.
159
Asphyxia

STUDY UNIT 9Firearm injuries
Contents
9.1 Introduction
9.2 Pathophysiology of gunshot wounds and wound ballistics
9.3 Examination of the body
9.4 Cutaneous (skin) entrance wounds caused by rifled firearms
9.4.1 Introduction
9.4.2 Concealed and unusual entrance wounds
9.4.3 Classification of cutaneous gunshot entrance wounds
9.5 Cutaneous gunshot exit wounds caused by rifled firearms
9.5.1 Introduction
9.5.2 Case study
9.6 Gunshot wounds caused by smooth-bore firearms (shotguns)
9.7 Injury by rubber and plastic bullets
9.8 Industrial nailguns
9.9 Blank-cartridge injuries
9.10 Accident, suicide or homicide
9.10.1 Accidental shootings
9.10.2 Suicide wounds
9.10.3 Homicide gunshot wounds
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should
. have a basic knowledge of ballistics, including knowledge of the
changes occurring in the firearm itself, as well as the products of
combustion
. be able to classify firearms based on the characteristics of the barrel,
the way the firearm is handled (hand vs shoulder) as well as the type
of projectile fired
. be able to correlate the products emerging from the muzzle with the
features on the skin surrounding the firearm entrance wound
. be able to discuss the basic principles of wound ballistics
. be able to discuss in detail the entrance wounds caused by each of
the different types of firearms (rifled arms, smooth-bore firearms
(shotguns), pistols, etc)
. discuss firearm exit wounds
160

9.1 Introduction
Although firearms also include arms that can fire plastic and rubber bullets, as
well as industrial nailguns, it is especially pistols, revolvers and rifles which
are important. This group of firearms is divided into handarms and
shoulderarms, and also according to whether the barrel is rifled or not.
Rifled firearms have spiral grooves on the inner surface of the barrel which
gives the spinning movement to the projectile as it travels down the barrel.
This rotational movement or spin stabilises the projectile in flight. Handarms,
for example revolvers and pistols, as well as shoulderarms such as hunting
rifles, and automatic and semi-automatic machine guns, all have these
grooves. Smooth-bore firearms (eg shotguns) do not have grooves.
When the percussion pin activated by the trigger strikes the percussion cap,
the spark generated ignites the propellant powder in the bullet casing. This
powder has chemical and physical characteristics peculiar to the type of
ammunition. The gases which develop during the explosion have a potential
volume many times greater than that of the powder, generally in excess of
500 times under atmospheric pressure. It is this gas pressure which drives the
projectile along the barrel. While passing along the barrel the projectile is
soiled by oil and gas in the barrel. When it leaves the muzzle there is also a
flash and a gas emission, which includes carbon monoxide, as well as hot and
partially unignited powder particles, all of which impart to the recipient
surface characteristics which assist in determining the firing range for that
particular weapon and its ammunition.
Although the medical practitioner is not a ballistics expert the observations
made in the case of firearm injuries can be of considerable assistance in
establishing the range as well as the direction of fire, the type and calibre of
weapon and the nature of the wound, for example whether it points at
suicide, homicide or an accident. Then, and equally relevant, there is the
establishment of (in the case of fatal injury) the manner of death as well as the
period of survival and the extent of immobilisation of the victim and
restriction of volitional acts on account of the injury.
In order to measure up to the expectations of the court in this regard, close
attention must be paid to the size and shape of the entrance and exit
wound(s). Careful inspection of the skin around the entrance wound, noting
the presence, size and shape of any abrasion collar, smoke blackening,
tattooing and singeing of hair, is an essential element of the medical
investigation. Evidence should also be sought of any vital reaction, such as
erythema (a reddening of the skin) in the vicinity of hot-powder tattooing and
carboxyhaemoglobin in surrounding tissues (carbon monoxide is one of the
gases emitted by the explosion in the chamber of the firearm).
An X-ray examination of the body (both at the clinical examination and the
autopsy) can be of considerable assistance in retrieving projectiles for ballistic
examination, particularly in the case of multiple entrance wounds.
In siting both entrance and exit wounds it is helpful if measurements are
expressed as the perpendicular height above the base of the heel line.
Entrance and exit wounds must preferably be indicated on a diagram. This
can assist (when evidence is given) to relate the findings to circumstantial
161
Firearm injuries
evidence. It must be remembered that the direction of the wound track, with
the body in the anatomical position during the post-mortem examination, is
not necessarily representative of the position of the body when it was hit by
the projectile. For instance, if the individual was slightly bent over while
running away, and then hit by a projectile fired at a horizontal level, the
entrance wound in the back may be lower than the exit wound at the front if
the body is in the anatomical position.
Caution should be exercised when expressing an opinion on the pre-impact
direction of the projectile flight path based solely on the wound in the tissues
after impact, as there can be considerable deflection, not only through the
bony structures, but also through the soft tissues.
During clinical examination and autopsy other evidence should be sought,
such as powder marks on the hands of the victim and assailant and other
evidence of a struggle by either party. Clothing can absorb much of the
explosion residue and modify the shape of the entrance wound. Therefore it
should always form an integral part of the examination. Serious omissions in
the accumulation of medical evidence may result where no attempt is made to
anticipate the needs and priorities of the subsequent inquiry. This is what
happened initially at the autopsy of President Kennedy after his assassination.
(See Where Death Delights by Milton Helpern.)
Multiple firearm wounds do not necessarily rule out suicide. In one case the
deceased had three separate revolver wounds in the chest and all three bullets
had penetrated the ventricles of the heart. A suicide note was found, the
revolver was shown ballistically to have fired the shots, and swabs taken from
the deceased's right hand contained the specific powder residue.
The percussion effect set up in the tissue by shock waves during the
projectile's flight is well exemplified in the following case. A fugitive who was
running away from the scene of a burglary, was fired on at a range of about 40
metres while his trunk was flexed forward in a position customarily adopted
by escapees to reduce the target site. Despite being hit by a shot, he continued
to run for another 100 metres, before collapsing. He died half an hour later.
At the autopsy an entrance wound was indentified above the left iliac crest, on
the lateral side of the body. The bullet had tracked upward in the
subcutaneous tissues to enter the chest cavity between the eighth and ninth
ribs, and had then passed across the dome of the diaphragm, below the
parietal pleura, along the outer aspect of the pericardial sac to come to rest in
the apex of the left lung.
Neither the abdominal cavity nor the pericardial sac had been penetrated by
the projectile, yet the former contained 100 ml of free blood and the
pericardial sac 350 ml of blood, resulting from a 2 cm percussion rupture of
the liver, and 3 cm rupture of the left ventricle of the heart (see photo 52).
162
Study unit 9

Oil/Soot Gas SmokeHeat Gun powder
Fig 9.1.
A number of products are released when a shot is fired and leaves the muzzle of the firearm.The bullet or projectile is also coated with any oil or soot which may be present in the barrel.
Each of these products will travel for a certain distance from the muzzle. Burnt, unburnt andpartially burnt powder particles travel the furthest.
Wounds A to C are so-called intermediate wounds
Wound D is a distant wound, ie usually more than 75 cm from the muzzle
It is important to note that the appearance will differ with different firearms. Therefore eachcase must be compared with the relevant firearm by means of ballistic tests. If the shot is firedthrough clothes, some of the features will be visible on the clothing.
9.2 Pathophysiology of gunshot wounds and wound ballistics
Injuries caused by missiles entering live tissue are directly related to the
amount of kinetic energy transferred from the missile to the target tissue. This
energy is expressed by the equation Ek = � mv2, where the exponential
factor of velocity represents the greatest contribution to energy transferred.
The mass is also of importance. Therefore, the damage caused by a bullet is
determined not only by the velocity, but also by tissue resistance (the greatest
amount of energy is transferred at the point where tissue resistance is
maximal), the yaw (angle of the bullet in relation to its trajectory path), the
bullet's tumble effect after it hits the target tissue, the bullet weight, and the
extent of bullet fragmentation.
In shotgun injuries, especially those inflicted at close range, the total mass of
the individual projectiles is a very important factor in the kinetic energy
equation. At close range the pellets act as a solitary missile because of tight
clustering, and their total weight is much greater than that of individual rifle
or handgun bullets. Furthermore, the ballistically poor design of multiple
small, round balls does not favour maintenance of high kinetic energy at
considerable distances from the muzzle, nor does it permit great tissue
penetration. However, at close ranges (ie up to about 3 m in the case of
163
Firearm injuries
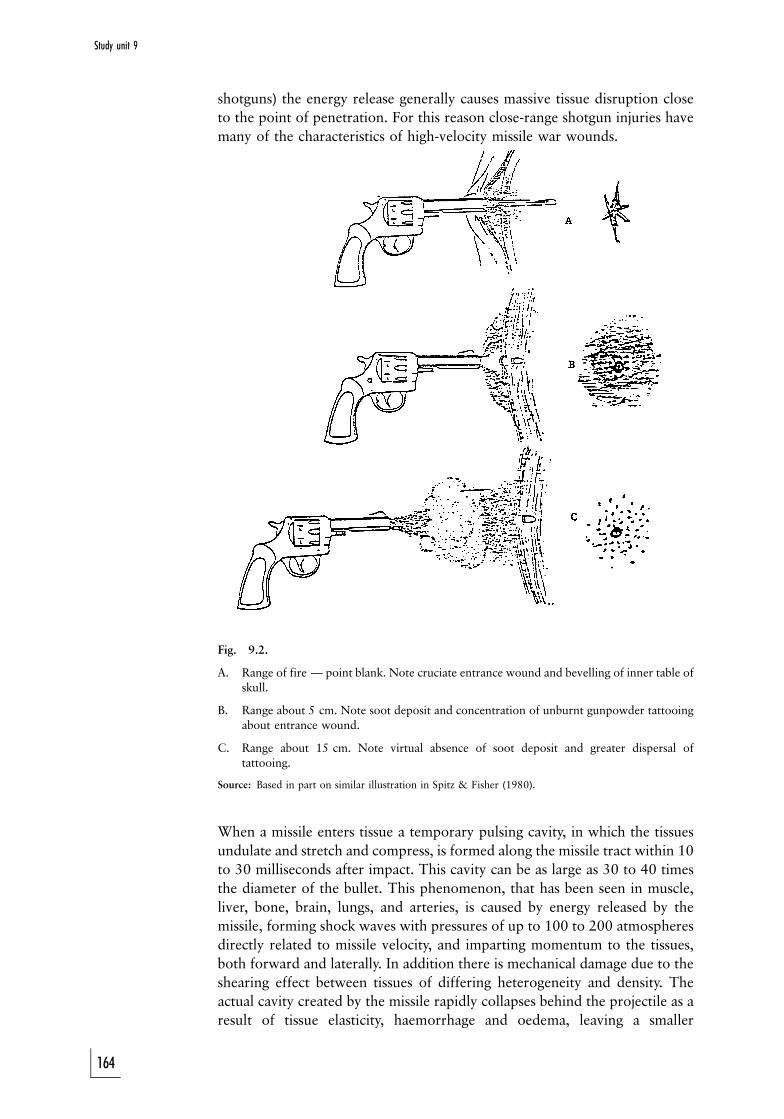
shotguns) the energy release generally causes massive tissue disruption close
to the point of penetration. For this reason close-range shotgun injuries have
many of the characteristics of high-velocity missile war wounds.
Fig. 9.2.
A. Range of fire Ð point blank. Note cruciate entrance wound and bevelling of inner table ofskull.
B. Range about 5 cm. Note soot deposit and concentration of unburnt gunpowder tattooingabout entrance wound.
C. Range about 15 cm. Note virtual absence of soot deposit and greater dispersal oftattooing.
Source: Based in part on similar illustration in Spitz & Fisher (1980).
When a missile enters tissue a temporary pulsing cavity, in which the tissues
undulate and stretch and compress, is formed along the missile tract within 10
to 30 milliseconds after impact. This cavity can be as large as 30 to 40 times
the diameter of the bullet. This phenomenon, that has been seen in muscle,
liver, bone, brain, lungs, and arteries, is caused by energy released by the
missile, forming shock waves with pressures of up to 100 to 200 atmospheres
directly related to missile velocity, and imparting momentum to the tissues,
both forward and laterally. In addition there is mechanical damage due to the
shearing effect between tissues of differing heterogeneity and density. The
actual cavity created by the missile rapidly collapses behind the projectile as a
result of tissue elasticity, haemorrhage and oedema, leaving a smaller
164
Study unit 9

permanent pathway usually marked by tissue loss, haemorrhage, bullet
fragments or sometimes bone fragments which can be seen during
radiological examination shortly after injury. Bullet fragmentation is a major
cause of tissue disruption and there is a close connection between large exit
wounds and bullet fragmentation.
The critical velocity at which bone is fractured is approximately 66 m/s.
Kinetic energy imparted to the tissue causes bone to fracture. Although some
bone fragments may be contained within the surrounding framework of the
periosteum (bone membrane), muscle and connective tissue, others may have
sufficient energy to act as secondary missiles, creating further destruction and
multiple exit-wounds. The medical examiner may thus be faced with a
discrepancy between the number of entrance and exit wounds.
In low-velocity gunshot wounds, defined as those inflicted by missiles
travelling at a velocity of less than 360 m/s (ie most handguns), the energy
transferred to the tissues is considerably less than that of high-velocity
missiles, resulting in less tissue destruction. As an interesting rider: the Soviet
AK-47 assault rifle, despite the high velocity (900 m/s at the muzzle) and
marked tendency of its bullet to yaw after penetration, causes relatively non-
dramatic wounds in the more elastic soft tissues (muscle, bowel wall, lung)
because of its nonfragmenting behaviour, but multiple fractures and massive
disruption in inelastic tissues such as bone and liver.
9.3 Examination of the body
The only fully reliable method of gaining definitive evidence on gunshot
fatalities is a complete autopsy. This entails correct description and accurate
localisation of all external wounds, exploration of the bullet track,
documentation of all injuries and recovery of bullets still in the body. In
addition to the anatomical examination a study of the victim's clothing,
photographs of entrance and exit wounds, and radiological screening to
detect missiles or bullet fragments which remain unaccounted for must be
done.
9.4 Cutaneous (skin) entrance wounds caused by rifled firearms
9.4.1 Introduction
Entrance wounds are usually round or ovoid (oval) with an abrasion ring
where the bullet abraded the skin during entrance. This abrasion ring is
caused by the force exerted by the projectile at entry, when the outermost
layers of the epidermis are stripped away. It is not caused by the rotational
movement of the projectile, as it is sometimes described in the literature, but
by the tangential force exerted on the skin. Similar abrasions are sometimes
seen surrounding the exit wound when the skin is pressed against a hard
object, for instance a belt buckle. After the bullet perforated the skin the
elasticity of the cutaneous tissue restores the skin's previous elasticity and the
skin defect contracts.
When bullets strike skin at a 908 angle (ie perpendicular to the skin surface)
they produce round entrance wounds with a more or less symmetrical collar
165
Firearm injuries

or abrasion ring. Oval or elliptical entrance wounds with asymmetrical
abrasion rings occur when bullets strike the skin at acute angles. The wider
area of abrasion is then located on the side of the entrance wound closest to
the gun.
Entrance wound shape (ie round, oval, star-shaped or cross-shaped) and size
must be described precisely. Cutaneous injury and its associated features, such
as soiling and rim abrasion ring, should be accurately measured and the
dimensions recorded. A circular wound requires only the diameter measure-
ment, whereas an elliptical wound is measured across its widest and narrowest
diameters and variations in width of the marginal abrasion are recorded.
Peripheral fouling or stippling due to unburnt powder residues should be
specifically noted.
9.4.2 Concealed and unusual entrance wounds
Entrance wounds occasionally occur in unusual sites or are not easily seen. If
the body is covered in blood, clots may obscure the injury. Similarly, scalp and
pubic wounds are not easily seen, and in these cases shaving the hair before
autopsy will reveal the injury. The possibility of wounds in concealed or
unusual sites should always be borne in mind. Such sites comprise the external
auditory meatus (opening), nostrils, umbilicus (navel), axillae (armpits),
perineum (pelvic floor), vagina and rectum. Oral wounds are sometimes
difficult to see as a bullet may have entered the open mouth, and after rigor
mortis set in the mouth could not be opened.
Injuries which do not look like gunshot wounds can be difficult to interpret.
This occurs for example when the missile passes through glass or if the bullet
strikes the body after it has ricocheted. If the bullet then glances off the body
without penetrating, only an abrasion or laceration may be produced.
A round penetrating defect similar to a bullet entrance wound can also be
produced by an instrument such as a screwdriver, but in this case no missile
will be found at the end of the track. Similar wounds can be produced if the
victim was beaten with a nail-studded plank.
9.4.3 Classification of cutaneous gunshot entrance wounds
The definitive factor determining the appearance of a cutaneous entrance
wound is the muzzle-to-skin distance, which accounts for the simple
classification of entrance wounds as ``contact'', ``intermediate'' and ``distant''.
However, estimates of the firing range cannot be made with accuracy unless
the exact type of firearm is known, and even then only by ballistic experts,
preferably after test shots were fired at varying distances under controlled
conditions.
166
Study unit 9

INTERMEDIATE ENTRANCE WOUND WITH FIREARM
PERPENDICULAR TO SKIN
Tattooing due to burnt, unburnt and partiallyburnt gun powder particles
Smoke (soot) deposits
Singeing of hair due to heat
Abrasion ring surrounds central entrance de-fect. The abrasion ring is the result of trauma tothe skin due to radial forces which act on theskin as it is pierced by the projectile/bulletSometimes oil, etc is also seen on the inneraspect
Central defect. This can have a smallerdiameter than the bullet, due to stretching ofthe skin
Fig 9.3. The appearance of an intermediate cutaneous entrance wound with the barrel 90degrees (perpendicular) to the skin. As the unburnt and partially burnt powder particles travelthe furthest, their distribution on the skin is therefore the widest.
9.4.3.1 Contact wounds
The margins of the skin perforation are charred by the flame coming from the
muzzle, and the abraded border is usually soiled with powder residue which
can also be clearly visible in the subcutaneous and deeper tissues. The
surrounding abrasion ring is of uniform width, and around this there can be
an additional abrasion ring from the gun barrel and gun sight. These muzzle
imprints result from expansion of the subcutaneous tissue when gas is blown
into the tissue, elevating the skin surface and pressing it tightly against the
muzzle. The subcutaneous tissues in and immediately adjacent to the bullet
track may have a cherry red colour due to localised carboxyhaemoglobin
formation from carbon monoxide in the muzzle gases. If the muzzle is at an
angle with the skin, the distribution is more elliptical.
Contact-range entrance wounds in the scalp look slightly different because
stellate (star-shaped) lacerations radiate from the central defect (fig 9.4). This
is due to expansion of the explosion gases between scalp and skull and within
the cranial cavity. Explosion skull fractures may result, producing bone
fragments which can act as secondary missiles.
9.4.3.2 Intermediate or medium distance entrance wounds
Entrance gunshot wounds are classified as intermediary when muzzle-to-
target distances are such that the target surface is still within range of the
muzzle blast although target and muzzle are not in contact. Maximum
muzzle-to-target distances at which flame and muzzle blast create dermal
damage and soiling vary according to the type of gun and ammunition.
Handguns and ammunition encountered in civilian homicides do not
ordinarily deposit powder on the target at ranges greater than 50 to 75 cm.
Close-range entrance wounds in unclothed areas may be surrounded by a
167
Firearm injuries
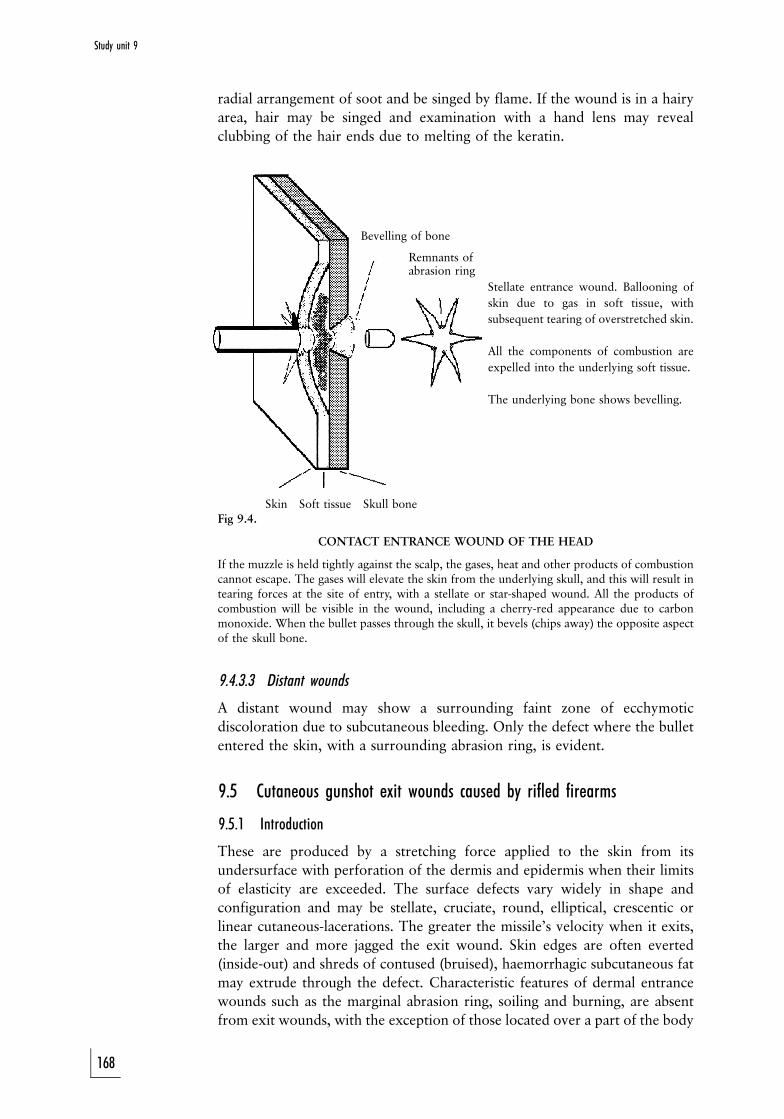
radial arrangement of soot and be singed by flame. If the wound is in a hairy
area, hair may be singed and examination with a hand lens may reveal
clubbing of the hair ends due to melting of the keratin.
Bevelling of bone
Remnants ofabrasion ring
Stellate entrance wound. Ballooning of
skin due to gas in soft tissue, with
subsequent tearing of overstretched skin.
All the components of combustion are
expelled into the underlying soft tissue.
The underlying bone shows bevelling.
Skin Soft tissue Skull boneFig 9.4.
CONTACT ENTRANCE WOUND OF THE HEAD
If the muzzle is held tightly against the scalp, the gases, heat and other products of combustioncannot escape. The gases will elevate the skin from the underlying skull, and this will result intearing forces at the site of entry, with a stellate or star-shaped wound. All the products ofcombustion will be visible in the wound, including a cherry-red appearance due to carbonmonoxide. When the bullet passes through the skull, it bevels (chips away) the opposite aspectof the skull bone.
9.4.3.3 Distant wounds
A distant wound may show a surrounding faint zone of ecchymotic
discoloration due to subcutaneous bleeding. Only the defect where the bullet
entered the skin, with a surrounding abrasion ring, is evident.
9.5 Cutaneous gunshot exit wounds caused by rifled firearms
9.5.1 Introduction
These are produced by a stretching force applied to the skin from its
undersurface with perforation of the dermis and epidermis when their limits
of elasticity are exceeded. The surface defects vary widely in shape and
configuration and may be stellate, cruciate, round, elliptical, crescentic or
linear cutaneous-lacerations. The greater the missile's velocity when it exits,
the larger and more jagged the exit wound. Skin edges are often everted
(inside-out) and shreds of contused (bruised), haemorrhagic subcutaneous fat
may extrude through the defect. Characteristic features of dermal entrance
wounds such as the marginal abrasion ring, soiling and burning, are absent
from exit wounds, with the exception of those located over a part of the body
168
Study unit 9
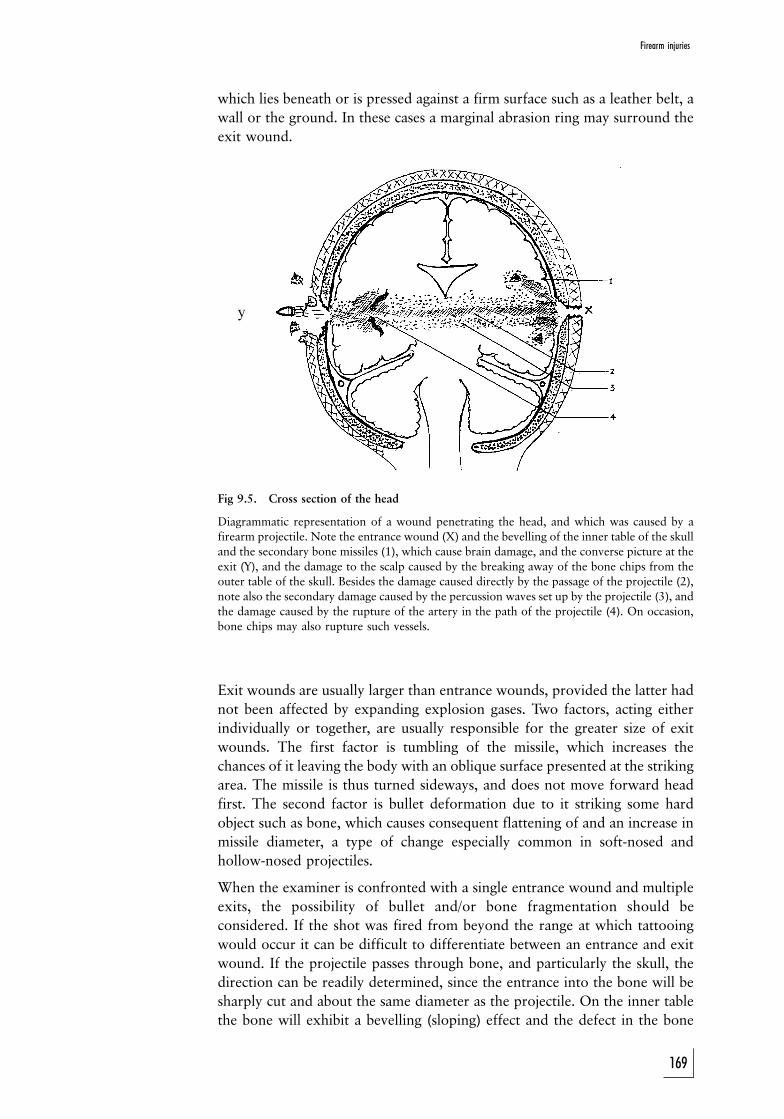
y
which lies beneath or is pressed against a firm surface such as a leather belt, a
wall or the ground. In these cases a marginal abrasion ring may surround the
exit wound.
Fig 9.5. Cross section of the head
Diagrammatic representation of a wound penetrating the head, and which was caused by afirearm projectile. Note the entrance wound (X) and the bevelling of the inner table of the skulland the secondary bone missiles (1), which cause brain damage, and the converse picture at the
exit (Y), and the damage to the scalp caused by the breaking away of the bone chips from theouter table of the skull. Besides the damage caused directly by the passage of the projectile (2),note also the secondary damage caused by the percussion waves set up by the projectile (3), and
the damage caused by the rupture of the artery in the path of the projectile (4). On occasion,bone chips may also rupture such vessels.
Exit wounds are usually larger than entrance wounds, provided the latter had
not been affected by expanding explosion gases. Two factors, acting either
individually or together, are usually responsible for the greater size of exit
wounds. The first factor is tumbling of the missile, which increases the
chances of it leaving the body with an oblique surface presented at the striking
area. The missile is thus turned sideways, and does not move forward head
first. The second factor is bullet deformation due to it striking some hard
object such as bone, which causes consequent flattening of and an increase in
missile diameter, a type of change especially common in soft-nosed and
hollow-nosed projectiles.
When the examiner is confronted with a single entrance wound and multiple
exits, the possibility of bullet and/or bone fragmentation should be
considered. If the shot was fired from beyond the range at which tattooing
would occur it can be difficult to differentiate between an entrance and exit
wound. If the projectile passes through bone, and particularly the skull, the
direction can be readily determined, since the entrance into the bone will be
sharply cut and about the same diameter as the projectile. On the inner table
the bone will exhibit a bevelling (sloping) effect and the defect in the bone
169
Firearm injuries

will be generally larger than that at the entrance. The bone breaking away
from the inner table will produce secondary missiles which may cause more
extensive tissue damage than the missile itself. As the projectile leaves the skull
the converse will apply, that is the wound on the outer table will be bevelled.
9.5.2 Case study
A patient was found to have a .22 bullet lodged in the occipital portion of his
skull immediately below the entrance wound in the scalp. He died later that
night. At post-mortem examination it was found that a small chip of bone
from the inner table of the skull had pierced the dural venous sinus, which
had given rise to a large subdural haemorrhage which, in turn had caused the
victim's demise. The small bone fragment was missed upon initial
examination of the X-ray plate.
9.6 Gunshot wounds caused by smooth-bore firearms (shotguns)
These wounds merit a separate discussion because shotguns and their
ammunition differ so markedly from rifled weapons and their ammunition.
As mentioned above, range, gauge (barrel diameter), degree of ``choke'' and
size and number of pellets in the shell play a role in determining the
characteristics of shotgun injuries. The explosive effect and the burns created
by the muzzle flame can cause additional damage to the damage created by
the shot if gun and victim are sufficiently close. Additional trauma may result
from the wadding striking the victim, a feature not seen in other types of
firearm injuries.
Contact and close-range cutaneous shotgun entrance wounds are round or
elliptical, depending on the angle between muzzle and skin. Smoke and
powder residue with scorching, surround the entrance wound, and marginal
abrasion similar to a single-bullet entrance is present. Occasionally, stellate
lacerations due to the muzzle blast are seen as gases expand beneath the skin
and lacerate the wound edges as they exit through the original entrance.
Contact shotgun wounds of the head commonly cause extreme mutilation.
With close-range shots of up to 120 to 150 mm the shotgun charge enters the
body as a single conglomerate mass producing a round defect somewhat
larger in diameter than the bore of the barrel. Wound margins in such cases
show abrasion as well as scalloped defects. The linear abrasions occasionally
seen in the immediate vicinity of these wounds are due to the impact of
clothing against the stretched skin during penetration of the shot.
Beyond this range, as muzzle-to-target distance increases, the major central
defect becomes progressively smaller and individual pellet wounds become
more numerous as the pellets begin to fan out. However, the minimal distance
at which this occurs varies considerably, ranging from 90 to 120 mm with
sawn-off shotguns, 180 mm with cylinder-bore guns and up to 540 mm with
full-choke guns. Wadding and plastic casing usually enter the wound when
muzzle-to-victim distance is less than 150 to 180 mm.
As a rough estimate it is usually accepted that for every meter the pellets will
170
Study unit 9
disperse 2,5 to 3,0 cm. If the diameter of the wound (the maximum distance
between the most remote pellet wounds on the skin) is therefore 30 cm, the
firing distance was approximately 10 meters.
9.7 Injury by rubber and plastic bullets
A rubber bullet or, more accurately a rubber baton round is a slightly fexible,
hard rubber missile introduced as a riot-control weapon in Northern Ireland
in 1970. It evolved from the wooden baton round used by security forces
during the Hong Kong riots of the 1950s and 1960s, and in turn gave rise to
the plastic baton round which was introduced in Northern Ireland in 1976.
The rubber baton round has a tapered blunt tip, weighs 135 to 140 g and is
15 cm long and 3,5 cm in diameter. It slides into a metal cartridge case which
has a powder propellant charge of 55 grains at its base and is fired from a riot
gun, the Webley-Schermully gun, at a muzzle velocity of about 73 m/s.
However, because its discharge from the barrel is inefficient, the muzzle
velocity varies considerably and the poor aerodynamic characteristics of the
missile render it unstable in flight, so that it soon tumbles. The disadvantage
of the missile is its inaccuracy, and it has been replaced in Northern Ireland by
a shorter plastic bullet (about 10 cm long and 3,7 cm in diameter). This
missile is blunt-ended and sealed into a canister with a charge of 45 grains in
the base. It is more accurate in flight than the rubber bullet and has a longer
range, so that it is regarded as a superior riot-control weapon. (It is not
expected of students to know these statistical details for examination
purposes.)
The severity of the injury produced by these missiles depends on the part of
the body struck. Cranial impact is the most serious and can result in fractures
of the skull and facial bones as well as injuries to the eyes. Of the 90 cases
reported by Millar et al, 35 involved the face and skull, while 24 patients
sustained injuries to the eye and adnexa (adjacent parts). Blindness or severe
loss of vision occurred in 14 of these cases. Further reports have confirmed
orbital and eye injuries due to plastic bullets. Furthermore, in a study which
compared the injuries caused by plastic bullets with those caused by rubber
bullets, it was found that while plastic bullets struck the head and chest less
often than rubber bullets, resulting in fewer facial fractures, the craniocerebral
injuries produced appeared to be more severe.
9.8 Industrial nail guns
These are firearm-like tools used in construction work for firing metal studs
into steel, wood or concrete. An interchangeable breech makes different
calibres possible, usually ranging from 0,22 to 0,38 and with marked
powers of penetration. The 0,22 charge, for example, can reach a velocity
of 150 to 180 m/s. The velocity of the stud, its size and shape, and its
tendency to tumble and ricochet all produce severe tissue disruption,
resulting in atypical and larger wounds than those normally produced by
ordinary bullets.
171
Firearm injuries

9.9 Blank cartridge injuries
A blank cartridge consists of primer, gunpowder or smokeless powder and
wadding but no bullet. Its function is to produce a loud noise like that of an
actual gunshot. Clinically and experimentally two types of injury are
produced. The first occurs where gunpowder is present in the cartridge and
consists of a penetration wound with the wadding and powder granules acting
as missiles. The second type of injury is a blast injury produced by expanding
combustion gases. This is seen when smokeless blank cartridges, which are
more combustible and have greater wounding power than ordinary
gunpowder, are used. Severe soft tissue and visceral injuries result. Although
shots fired from a distance with blank cartridges are harmless, skin contact
shots from 0,38 and 0,45 calibre blanks can produce severe and even fatal
wounds.
9.10 Accident, suicide or homicide?
The medical examiner is often called upon to assist the court in determining
whether the manner of death in a particular gunshot fatality was accidental,
suicidal or homicidal. While a number of helpful features pointing to a
specific manner of death may be present, few areas in forensic medicine
provide as much opportunity for misinterpretation as gunshot wounds. There
are nevertheless a number of well-recognised patterns that can be of help in
determining the manner of death.
9.10.1 Accidental shootings
These usually result from careless handling of firearms, and children, hunters
and inebriated persons are the most common victims. The wound sites and
firing ranges vary a great deal, depending on the circumstances of death, and
are therefore of paramount importance in determining whether the shooting
incident was truly accidental.
9.10.2 Suicide wounds
Suicide wounds, on the other hand, are usually contact or close-range wounds
and are found in classic locations, most often the temple area (right temple in
right-handed persons and left temple in left-handed persons), anterior left
chest, roof of mouth and center of forehead. Occasionally the epigastric
(upper middle region of the stomach) and submental (below the chin) areas
are chosen. Suicide gunshot wounds of the limbs are extremely rare but may
occur, and multiple suicide gunshot-wounds, although uncommon, may be
encountered, including wounds to the head.
The number of entry wounds in the body is not an important factor when
distinguishing between suicide and homicide, especially when the gun is in the
automatic firing mode. Because the safety-catch is usually set on a selected
mode, its position is significant in any firearm investigation. In a reported case
a person who committed suicide fired eight bullets with one pull of the
trigger. Perhaps he did not intend to fire that number of bullets, but
spasmodic movements, which usually accompany such a violent death, might
172
Study unit 9
have caused continuous depression of the trigger until the victim's muscle
tone was lost completely. (If this is true, a case of suicide with as many as 24
entry wounds should be possible, since the maximum capacity of a magazine
is usually 24 bullets.) In fact, the number of entry wounds is more likely to be
dictated by chance than by any other force. Even when the safety-catch is set
on the self-loading, single-shot mode, the number of shots alone, without
taking other factors or features into account, is not pathognominic (indicative
of the exact cause) because multiple suicide injuries still occur, however rarely.
An additional feature indicative of suicide rather than homicide is that the
clothing surrounding the wound may have been drawn back and neatly
arranged prior to infliction of the wound in order to avoid its being soiled by
blood. Finally, a suicide note may be found at the scene.
9.10.3 Homicide gunshot wounds
Homicide gunshot wounds are found on any part of the body and are mostly
inflicted from a distance beyond arm's reach (intermediate or distant).
Contact and close-range wounds are also found in homicide cases. These
wounds, if found in the classic suicide sites, may be very difficult to interpret.
Wounds found on the face, back or any inaccessible part of the body should
be presumed to be homicide wounds, until accidental infliction is definitely
ruled out.
Activities
1. Correlate the products produced during the firing of a cartridge with
their possible effect and appearance on the skin of the victim.
2. The examination of a firearm entrance wound shows an oval-shaped
central defect surrounded by an irregular abrasion ring, which is wider on
the right-hand aspect of the wound. There are no signs of soot deposits or
singeing/burning of the skin, but tattooing is present. This is also
irregularly distributed, with a more concentrated distribution over the
right-hand aspect compared with the left side. What conclusions can be
drawn from this?
3. Discuss the unique appearance of a contact firearm entrance wound to
the head.
4. Examination of the victim of a shotgun shooting accident shows a central
defect with a crenated margin surrounded by smaller individual entrance
wounds. The distance between the peripheral wounds is 30 cm. From
how far do you think the firearm was fired?
Feedback
1. The products expelled from the muzzle, and the corresponding
features on the skin or target, are illustrated in figure 9.1.
2. The two findings relate to direction and distance. The direction is
from right to left, and the distance is approximately an arm's length
(50±75 cm). However, in all cases experimental shots must be fired
with the same firearm and the same type of ammunition, as the
173
Firearm injuries

abovementioned method to determine the distance gives only a
rough estimate based on the absence of smoke and heat-related
changes, and the presence of tattooing on the skin.
3. The typical presence of a contact gunshot entrance wound to the
head is the result of the muzzle being closely and tightly applied to
the skin, while the underlying subcutaneous tissue is supported by
the skull. When the firearm is fired, the gas cannot escape. The skin
balloons and lacerates around the entrance wound, this is a typical
stellate wound. This is further illustrated in figure 9.4.
4. Pellets disperse approximately 3 cm for every 1 meter. In this case
the distance is therefore roughly 30/3 = 10 m. Again experimental
shots are essential, as the barrels and muzzles of shotguns often vary,
and distribution of the pellets may therefore vary accordingly.
174
Study unit 9
STUDY UNIT 10
Thermal, electrical, atmospheric pressure andradiation associated deaths
Contents
10.1 Deaths caused by abnormal temperatures
10.1.1 Hypothermia
10.1.2 Hyperthermia
10.1.3 Thermal wounds (burns)
10.2 Deaths caused by electricity
10.2.1 The features of electrical current
10.2.2 The features of the body
10.2.3 Causes of death
10.3 Death due to radiation
10.4 Disease due to atmospheric pressure
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. discuss deaths due abnormal temperatures
. discuss death caused by electricity with reference to the following:
(a) factors that can influence the effect of the electrical current on
the body
(b) causes of death
(c) skin wounds caused by domestic electrical currents
(d) the presentation of a victim of lightning
. discuss death caused by pressure changes
Although the injuries caused by stab wounds and motor vehicle accidents are
also strictly speaking due to physical violence, this study unit will deal
primarily with other physical forces, for instance heat, electricity, atmospheric
pressure and radiation. (You are reminded that study unit 5 deals with injuries
in general, as well as blunt and sharp violence. Burns may also be caused by
strong acids or alkali's, called chemical burns.)
175
10.1 Deaths caused by abnormal temperatures
These injuries may be due to exposure to cold (hypothermia), high
environmental temperatures (hyperthermia) or hot objects coming into
contact with the body (burns). All these deaths are unnatural.
10.1.1 Hypothermia
Hypothermia or low body temperature is defined as a condition where the
central or core body temperature is 35 8C or lower. Hypothermia is a
common complication where individuals are exposed to low environmental
temperatures. This often occurs amongst mountaineers and other adventurers
exposed to the environment. Although the environmental temperature as
such plays an important role, it is also important to remember that movement
of air (wind) lowers the temperature even further (wind factor).
Exposure to cold water, for instance after shipwrecks, increases the risk of
hypothermia. Should an intoxicated person fall into cold water, hypothermia
will be worse, as alcohol causes vasodilatation, which increases heat loss (see
study unit 11).
The elderly and the young are at greatest risk to develop hypothermia in the
domestic situation.
Within certain temperature ranges, hypothermia has a protective effect on
certain vital organs, like the brain, as it decreases the energy needs (including
oxygen) of the organs. This is one of the reasons why the body temperature is
usually lowered during open-heart surgery to protect the brain. Cooling
down and rewarming of the body in these circumstances are of course strictly
controlled to prevent complications.
Local changes due to hypothermia include frostbite, which can lead to loss of
fingers, toes or even parts of the face.
The post-mortem findings are often nonspecific. Typically the hypostasis has a
pink to rose-pink discoloration. It tends to be present over the extensor
surfaces and large joints. Pulmonary oedema, acute gastric erosions and acute
pancreatitis as well as perivascular haemorrhages and small micro-infarcts
(small foci of necrosis) may also be present.
Hypothermia can cause confusion and irrational behaviour; sufferers can
even take off their clothes due to a false perception that it is hot. This then
creates the impression that the person was assaulted or even raped. These
people often hide away from sight, the so-called ``hide-and-die'' syndrome.
10.1.2 Hyperthermia
Hyperthermia is a condition which occurs when the internal body
temperature rises above 40,5 8C, and is usually seen in the following two
situations:
1. Exposure to high environmental temperatures. In mines the temperature
and humidity are often very high. Physical activity in these circumstances
may cause hyperthermia in individuals who have not acclimatised
beforehand. It can be aggravated by drugs, that cause constriction of
176
Study unit 10
the blood vessels in the skin, for instance drugs that decrease mucus
secretion during a common cold (eg ephedrine). The capacity for giving
off heat is lost and the patient can become ``overheated''.
The post-mortem findings are often nonspecific, with signs of heart
failure (ie pulmonary oedema), internal haemorrhages due to clotting
abnormalities, and renal failure.
2. Malignant hyperthermia. This condition occurs in individuals who are
genetically susceptible to certain anaesthetic agents, especially if
halothane is used in conjunction with a muscle relaxant (succinylcholine).
Professor Harrison of the University of Cape Town developed an
antidote, Dantrolene, years ago. This resulted in a significant drop in the
mortality rate. In addition to the high body temperature the patient
develops an increased potassium level and other metabolic abnormalities.
Microscopic examination of the muscles shows myopathy (muscle
abnormality) with a moth-eaten appearance and with the nuclei located
centrally in the cells.
10.1.3 Thermal wounds (burns)
Strictly speaking frostbite is also a form of thermal injury, but it was discussed
under hypothermic injuries. This discussion will therefore focus on the
injuries resulting from the application of local heat to the body.
Burns are a common problem in South Africa because the majority of the
population use open fires for the preparation of food and heating. As was said
in the study unit on carbon monoxide poisoning, these open fires in enclosed
spaces are a major cause of death due to the production of carbon monoxide.
Deaths due to thermal injuries can be instantaneous or almost immediate if
severe, or can occur later due to complications, for instance infection. The
inhalation of smoke and toxic substances found in smoke can also cause death
from damage to the airways (heat inhalation syndrome). This may even occur
without any external thermal injuries to the body.
Old people and children are especially susceptible to thermal injuries. In
elderly people the skin is less sensitive, and they do not realise in time that
they are in contact with a hot object. For example hotwater bottles often
cause burns. Children sometimes pull containers with boiling water over
themselves, as they are inquisitive and cannot see what is happening on the
stove.
Deaths due to burns may thus be an accident, a homicide or a suicide.
A post-mortem examination of a severely charred body is often difficult as it
might be almost impossible to identify the person.
An important factor to be determined is whether the person was alive at the
time the fire started, or whether he or she was already dead at that time
(sometimes fires are started to conceal a murder).
These aspects will be discussed later.
10.1.3.1 Classification of thermal wounds
Burn wounds are classified according to depth:
177
Thermal, electrical, atmospheric pressure and radiation associated deaths
First degree Ð only the epidermis is involved
Ð often painful
Ð sunburn a possible cause
Ð heal without scar tissue formation
Second degree Ð the epidermis and part of the dermis are involved
Ð sometimes blisters may be present on the skin
Ð painful
Ð heal without scar tissue formation, except when
complicated by infection
Third degree Ð the epidermis and the full thickness of the dermis are
involved
Ð usually painless due to the destruction of the nerve-end
fibres in the skin
Ð heal with scar tissue formation
Some authors describe fourth-degree burns as charring of part of the body.
Skin burns may further be graded according to the percentage of skin surface
involved. In certain areas, for instance the face and perineum (genital region)
there is a high risk of complications.
10.1.3.2 The complications of burns
1. Local complications. The most important is sepsis due to infection of the
open wounds containing dead (necrotic) tissue. Over the flexor aspects of
joints, for instance the elbow and knee, fibrosis forms scars, which can
cause loss of movement. This is also known as a contracture.
2. Systemic complications. This is usually the result of fluid and electrolyte
loss through the raw and injured surface of the skin. In addition lung
complications can occur due to inhalation of hot air. Pulmonary thrombo-
emboli due to immobilisation of the patient, and stasis, may also occur.
The post-mortem findings will depend on the degree of charring. In cases
where charring did not occur, open, raw areas are seen. The pathologist must
give an estimate of the percentage of the body surface damaged by the burns.
In third-degree burns physicians often make incisions in the skin to release the
tension of the contracted skin on the underlying soft tissue (escharotomies).
This must not be confused with incised wounds.
With inhalation injuries the airways will show signs of damage, and the lungs
will be congested in the initial stages. Signs of diffuse alveolar damage or
shock lung will be found at a later stage.
In cases of charring the body will be in the so-called pugilistic or boxer stance
(see study unit 3) due to shortening of the muscles as the proteins break down
and coagulate as result of the heat. The flexor muscles have a larger mass and
are therefore stronger than the extensor muscles. The flexor muscles will
therefore dominate if all the muscles are shortened. The elbows and knees
will bend and the body will assume the stance of a boxer.
178
Study unit 10
The skull bone can fracture and a bloody fluid can ``cook up'' from the bone
into the extradural space. This is known as extradural burn haematoma. It
must not be confused with injuries of the skull and extradural haemorrhage
due to trauma in the ante-mortem period. The skin and soft tissue can also
tear, due to shortening of muscles (heat tears). This is not an indication of
ante-mortem injuries.
If a body is totally charred, X-rays for identification purposes as well as to
locate possible projectiles and other injuries are mandatory. Examination of
the teeth is also indicated for identification purposes. In aircraft accidents
charring is a common problem and correct identification often depends on
dental records (forensic odontology).
The following signs could indicate whether the person was alive when the fire
started:
1. the carbon monoxide in the body (by determining the carboxyhaemoglo-
bin level [COHB]): a level of more than 5% in a nonsmoker and more
than 10% in a smoker indicates that the person was alive when the fire
started
2. ash and soot in the airways, stomach and oesophagus
3. fat emboli in the pulmonary vessels (only indicated by some authors)
Boiling water and other hot liquids often cause scald wounds in children.
These wounds are characterised by the fact that the intensity of the scalding
decreases as the fluid runs over the body and cools. The presence of clothes
may also influence the extent and distribution of scald wounds caused by
boiling water.
10.2 Deaths caused by electricity
Domestic and to a lesser extent the industrial use of electricity cause a number
of deaths annually. Most of these deaths are the result of accidents, although
suicide by electrocution is also seen.
The effect of the exposure of the body to an electrical current will be
influenced by a number of factors:
10.2.1 The features of electrical current
1. The type of current (alternating current [AC] versus direct current [DC]).
The human body is four to six times more susceptible to an alternating
current than to a direct current. It is especially low frequencies between
39 to 150 cycles per second (39±150 Hertz) which are dangerous. The
higher the frequency, the less dangerous the current. It is important to
remember that household electricity is usually 50 to 60 Hertz!
2. The strength of the current, measured in ampere. The higher the current,
the more dangerous. A current of 1 mA (milli-amperes) will only result in
a sensation of shock, while a current of 15,0 mA will result in contraction
of the muscles and the person will not be able to release the wire. As a
matter of interest, the same principle underlying the so-called pugilistic or
boxer posture in charred bodies plays a role in this situation: all the
179
Thermal, electrical, atmospheric pressure and radiation associated deaths
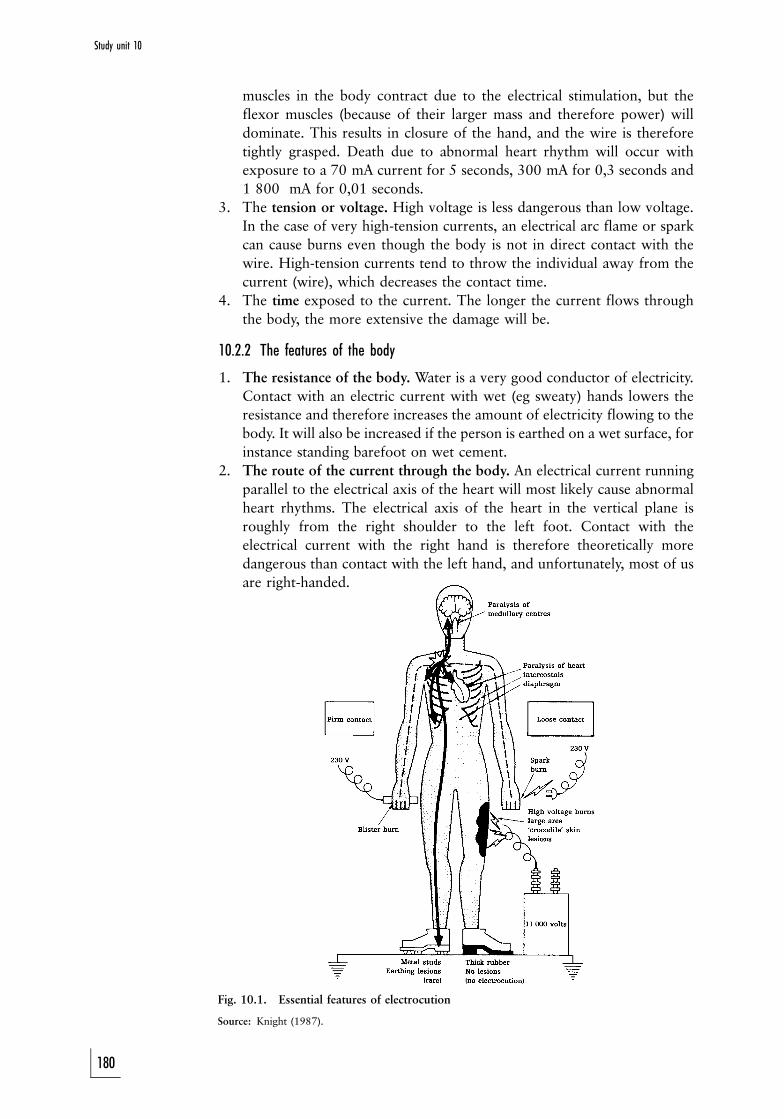
muscles in the body contract due to the electrical stimulation, but the
flexor muscles (because of their larger mass and therefore power) will
dominate. This results in closure of the hand, and the wire is therefore
tightly grasped. Death due to abnormal heart rhythm will occur with
exposure to a 70 mA current for 5 seconds, 300 mA for 0,3 seconds and
1 800 mA for 0,01 seconds.
3. The tension or voltage. High voltage is less dangerous than low voltage.
In the case of very high-tension currents, an electrical arc flame or spark
can cause burns even though the body is not in direct contact with the
wire. High-tension currents tend to throw the individual away from the
current (wire), which decreases the contact time.
4. The time exposed to the current. The longer the current flows through
the body, the more extensive the damage will be.
10.2.2 The features of the body
1. The resistance of the body. Water is a very good conductor of electricity.
Contact with an electric current with wet (eg sweaty) hands lowers the
resistance and therefore increases the amount of electricity flowing to the
body. It will also be increased if the person is earthed on a wet surface, for
instance standing barefoot on wet cement.
2. The route of the current through the body. An electrical current running
parallel to the electrical axis of the heart will most likely cause abnormal
heart rhythms. The electrical axis of the heart in the vertical plane is
roughly from the right shoulder to the left foot. Contact with the
electrical current with the right hand is therefore theoretically more
dangerous than contact with the left hand, and unfortunately, most of us
are right-handed.
Fig. 10.1. Essential features of electrocution
Source: Knight (1987).
180
Study unit 10
3. Underlying pathology. People with heart diseases are more vulnerable to
the effect of an electrical current than others. Ironically, electrical energy
is used in controlled conditions to treat abnormal heart rhythms.
10.2.3 Causes of death
Causes of death may either result in instantaneous death or death at a later
stage due to complications. It is therefore possible that the person may survive
initially and walk some distance after having been exposed to an electrical
current, but then collapses and dies due to an abnormal heart rhythm.
1. Abnormal heart rhythm (arrhythmia), especially ventricular fibrillation.
In this condition the heart contracts in an unco-ordinated manner, with
no forward propulsion of blood. It therefore results in cardiac arrest.
2. Respiratory failure due to contraction of the thoracic muscles (muscles of
the chest) and diaphragm. This is due to stimulation of the muscle by the
electric current causing spasm, so that the person cannot inhale of exhale.
3. Paralysis of the brain stem and the vital centres. These vital centres
control respiration as well as the cardiovascular system. The brain stem is
especially vulnerable if the current flows through these centres, in other
words when the person's head comes into contact with the current or it is
in the way of the current as it passes through the body.
Other injuries include burns with high-tension electricity currents, with the
presence of arc burns, and head injuries, which may occur when the person is
thrown from a ladder after receiving an electrical shock.
The post-mortem signs (excluding the burns and other injuries which we
already discussed) due to electrical current may be minimal and can easily be
overlooked, especially if they are in obscure places. In cases where the
resistance of the skin is very low, for instance due to being wet, the contact
wound may even be absent. The entrance or contact wound is usually found
on the hands, and the exit wounds on the soles of the feet.
The skin wounds are caused by heat production. The epidermis resists the
flow of the electrical current. The remainder of the body tissue consists of
water and electrolytes (salts), which are an ideal conduction medium. Due to
resistance to the flow of the electrical current, the skin is heated, and this heat
production creates a characteristic wound. The epidermis becomes white and
sometimes surrounds a vesicle containing fluid caused by production of steam
under the skin as it is heated by the current flowing through the tissue with a
high resistance (compare this with the principle applying to a kettle).
Histologically the cells of the basal layer of the epidermis are distorted. This
appearance is also known as Joule's wounds. When the contact is less firm,
small sparks may jump over the gap. This results in a spark lesion consisting of
a hard, brown nodule on the skin.
With special examination techniques the deposit of metal particles (metalisa-
tion) may be seen at the entrance wound.
Some authors have also noted that in an individual previously exposed to
electrical current, and who has survived, calcifications may develop in the
underlying tissue. This may be of importance in cases of alleged torture with
electricity.
181
Thermal, electrical, atmospheric pressure and radiation associated deaths
In the case of lightning a powerful electrical current acts over a very short
period of time.
The post-mortem signs in a lightning victim may include the following:
1. A fernlike or arborescent distribution of red or erythematous marks on
the body surface. Lightning usually occurs when the atmosphere is humid
or during rain storms. The wet body is drenched in water, which
accumulates in the body folds. It is along these ``paths'' of least resistance
that the electrical current will spread over the skin surface, with only
slight burning of the skin. This presents as arborising red lines.
2. More extreme burns and singed hair.
3. The shoes and clothes may be ripped from the body. This can raise
suspicion that the vicim was raped.
4. Rupture of the tympanum of the ear (ear drum) and injuries to the brain.
As a matter of interest, any metal objects on the body, for instance the buckle
of a belt or coins, can become magnetised and act like a magnet.
10.3 Death due to radiation
Depending on the amount as well as the period of exposure, radiation can
cause instantaneous death or delayed death. Tissues that divide rapidly are
most vulnerable because their DNA is more sensitive. This explains the
sensitivity of tissues such as bone marrow and the epithelial cells of the gastro-
intestinal system, that divide rapidly.
If the radiation dosage is low, or if the person survives the initial phase of
radiation disease, damage to the genetic content of the cells could later cause
tumours or leukaemia. This can take as long as 10 years or more. In a similar
manner damage to the reproductive organs and especially the embrionic cells
could cause genetic abnormalities in babies. The descendants of the survivors
of the atomic bomb explosions in Japan are living proof of the devastating
effect of radiation. In controlled situations radiation is an integral part of the
treatment of malignant tumours (radiotherapy).
10.4 Diseases due to atmospheric pressure
Although lengthy exposure to low atmospheric pressure (ie at high altitudes
in the Andes mountains) can cause cardio-respiratory pathological abnor-
malities and premature death, it is sudden changes in pressure that are more
dangerous and can lead to unnatural death. This is also called barotrauma.
When the atmospheric pressure drops, the volume of a given amount of air
increases. If a diver inhales any air while under water, be it ever so little, and
he does not exhale it again before he reaches the surface, the air will expand
in the lungs resulting in rupture of the lungs, especially the smaller air sacs or
alveoli. This can cause an air or gas embolism owing to barotrauma.
Exposure of the body to shock waves during an explosion may result in
similar types of trauma.
182
Study unit 10
ACTIVITIES
1. Discuss hypothermia and hyperthermia due to exposure to abnormally
low and high environmental temperatures.
2. Discuss the post-mortem findings in a burn victim, including problems
which may arise during identification. Discuss how you will determine
whether the victim was alive when the fire started.
3. Discuss factors which may have an effect when an individual is
accidentally exposed to a domestic electrical current.
4. A scuba diver surfaces. He coughs blood and dies instantly. What is the
most probable cause?
FEEDBACK
1. Hypothermia or low body temperature is defined as a condition
where the central or core temperature is 35 8C or less. It occurs
among mountaineers and other adventurers, as well as drowning
victims. Hyperthermia occurs when the internal body temperature is
higher than 40,5 8C. It occurs in two situations: exposure to high
environmental temperatures and malignant hyperthermia.
2. Identification may be difficult in charred bodies, and DNA analysis
as well as dental records and identification by comparison may be of
value. During the post-mortem examination, not only the degree of
the burn wounds, but also the percentage of body surface involved,
must be noted.
The following factors can play a role in establishing whether the
person was alive when the fire occurred:
(a) the carbon monoxide level in the body (by determining the
carboxyhaemoglobin level (COHb) Ð a level of more than 5%
in a nonsmoker and more than 10% in a smoker indicates that
the person was alive when the fire started
(b) soot and ash in the airways, stomach and oesophagus
(c) some authors also mention the presence of fat embolism in the
pulmonary vessels
3. The following factors may play a role (please see the text for more
details):
(a) the characteristics of the electric current
(i) the type of current (alternating current vs direct current)
(ii) the strength of the current (ampere)
(iii) the tension of the current (voltage)
(iv) the period of exposure to the current
(b) the characteristics of the body
(i) the resistance of the body
(ii) the route of the current through the body
183
Thermal, electrical, atmospheric pressure and radiation associated deaths

(iii) underlying pathological conditions, like heart disease with
rhythm disturbances or abnormalities
4. The appearance is that of pulmonary barotraumas with rupture
of the lung tissue. This is discussed in study unit 6.
184
Study unit 10
STUDY UNIT 11Toxicology and alcohol
Contents
11.1 Introduction
11.2 Toxicology in general
11.2.1 Classification
11.2.2 Factors affecting toxicity
11.2.3 The difference between a therapeutic and lethal dosage
11.2.4 Poisoning
11.2.5 Post-mortem examination
11.3 Carbon monoxide poisoning
11.3.1 Sources of carbon monoxide
11.3.2 Pathophysiology and pharmacology
11.3.3 Method of exposure
11.3.4 Clinical presentation
11.3.5 Toxicological analysis
11.3.6 Post-mortem signs
11.3.7 Case study
11.4 Alcohol
11.4.1 Production of alcohol
11.4.2 Pharmacodynamics of alcohol
11.4.3 Alcohol-level analysis
11.4.4 Calculations
11.4.5 Pharmacological effect
11.4.6 The role of alcohol in unnatural deaths
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. discuss the general principles of toxicology
. discuss carbon-monoxide poisoning in detail
. discuss all aspects of acute alcohol toxication in detail
11.1 Introduction
Pharmacology is the study of the use of drugs to improve the functioning of
the body of a living being. Toxicology is the study of the chemical and
physical characteristics of toxic substances (drugs and poisons) and the
185

physiological effects on the human body. This also includes the analytical
methods to determine the level of the substance in the body, as well as the
treatment of poisoning or overdosing.
Put simply, pharmacology refers to those cases where a drug is beneficial for
an individual, and may even cure the individual. However, if a drug is
consumed in too high a dosage, it has toxic effects, and that is toxicology. This
can be an over-simplification, but even Paracelsus (1493±1541) remarked:
` All drugs are poisons; there is not one which is not a poison. The right dose
differentiates a poison from a remedy''.
Toxicology and poisoning have formed part of human life since the beginning
of time. Diseases which are today treatable with medication with relatively
few if any side effects, were until not so long ago treated with drugs or
substances which few, if any, modern men will dare to ingest. The treatment
of syphilis, for instance, was with arsenic salts. Mercury was used for other
ailments.
The following inscription was found on a tomb in the Cross Kirk cemetery in
Eshaness, Shetland:
Donald Robertson
Born 11th January, 1785, Died 4th June, 1848,
aged 63 years.
He was a peaceable quiet man and to all
appearances a sincere Christian. His death was
very much regretted, which was caused by the
stupidity of Laurence Tulloch in Clothester,
who sold him nitre instead of Epsom salts,
by which he was killed in the space of 3 hours
after taking a dose of it.
If Donald Robertson did take the customary teaspoonful of what he thought
to be Epsom salts, he probably ingested about 5 g or more of nitre (saltpetre).
Severe abdominal pain, vomiting and diarrhoea probably commenced shortly
thereafter, leading to a state of shock, and death. Post-mortem lividity was
probably of a chocolate-brown colour due to the formation of methaemo-
globin. Saltpetre was and still is in use as a meat preservative and colourant,
and in small doses may give rise to reactions of hypersensitivity. One wonders
what the court would have awarded as damages in those times.
Prescribing drugs is not without risk, even in modern times. The doctor's
illegible handwriting, an incorrect unit, for instance gram instead of milligram
or an incorrect dose interval are but a few examples that can lead to
misinterpretation. In addition the pharmacist and the patient can also play a
role. The elderly are especially at risk when it comes to taking medicines.
Often their memories are not good any longer, and they forget whether they
already took their daily medication or not. Diabetics sometimes have bad
eyesight and cannot see exactly how much insulin they are administering to
themselves.
In this study unit a few general principles of pharmacology and toxicology
will be discussed, and two important substances (carbon monoxide and
alcohol) will be discussed in more detail.
186
Study unit 11

11.2 Toxicology in general
11.2.1 Classification
Toxicological substances (including medicines) can be classified according to
the following:
. chemical characteristics, for example organic, inorganic
. mode of action, for example corrosive, irritant
. target organ, for example lungs, heart
. intended use, for example solvent, insecticide
. field of use, for example agricultural, industrial
. origin, for example plant, bacterial, fungal
11.2.2 Factors affecting toxicity
A poison is a substance which, when absorbed by a living organism, results in
harm or death. There are many thousands of substances occurring naturally
or in synthesised form that exhibits this property. Medicines or even
beverages, if used in excess or inappropriately, can result in poisoning.
Furthermore, two innocuous substances could, after administration, combine
and so have a harmful synergistic effect.
Poisoning can be acute, subacute or chronic and its intensity as well as its signs
and symptoms can vary from person to person, appearing dramatically and
suddenly or as vague discomfort over a long time. It may also vary in the same
individual at different times.
The intensity and nature of the reaction to a poison often becomes an
important issue in court. The many variables which need to be considered
when attempting to solve this problem are best expressed as a functional
equation:
IR = DrA
SPrE
Where: IR = Intensity of reaction
D = Dose
rA = Absorption rate
rE = Elimination rate
S = Specific properties of subject
P = Physico-chemical nature of the poison
Intensity of the reaction ranges from the most insignificant to death.
Dose is the amount administered and the frequency of administration.
Rate of absorption will be influenced by the route of administration, that is
whether by mouth, intravenously, per vagina, per rectum, or by inunction
(rubbing in) or inhalation.
Rate of elimination may be accelerated by vomiting, diarrhoea or accelerated
metabolic pathways such as in people addicted to the particular substance or
habitually exposed to it in the workplace. Both absorption and elimination
may be delayed by a variety of medicines in use at the relevant time. The
converse is equally true.
187
Toxicology and alcohol
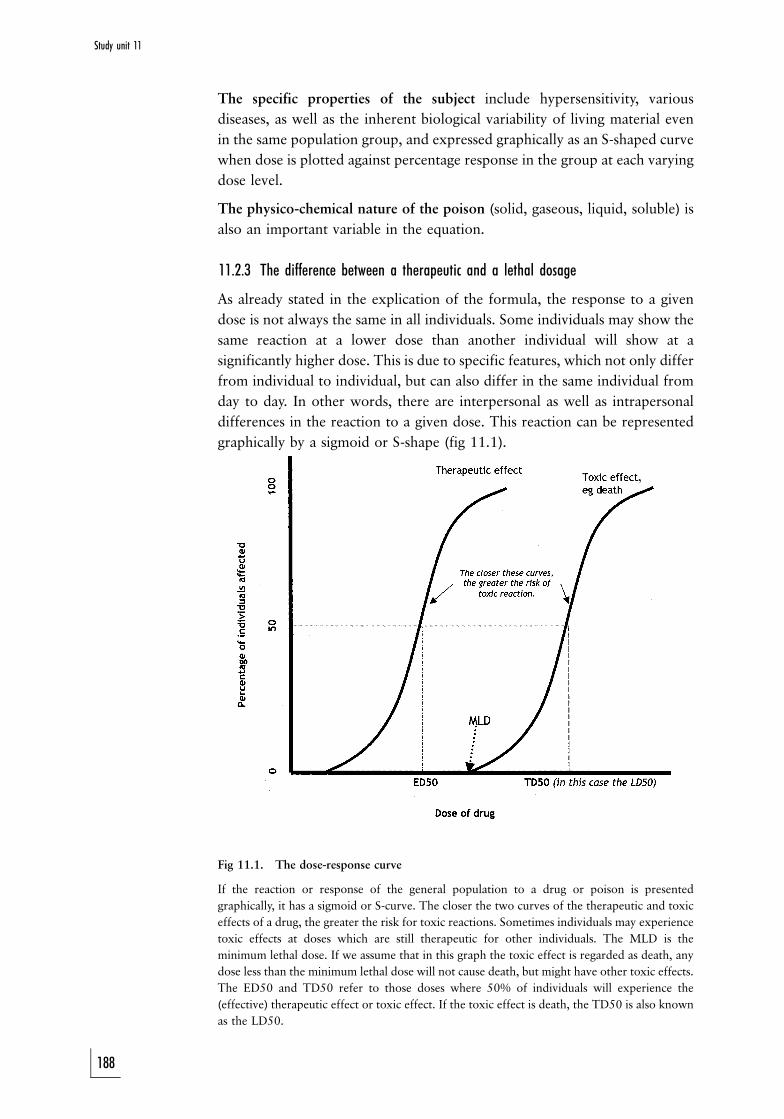
,
The specific properties of the subject include hypersensitivity, various
diseases, as well as the inherent biological variability of living material even
in the same population group, and expressed graphically as an S-shaped curve
when dose is plotted against percentage response in the group at each varying
dose level.
The physico-chemical nature of the poison (solid, gaseous, liquid, soluble) is
also an important variable in the equation.
11.2.3 The difference between a therapeutic and a lethal dosage
As already stated in the explication of the formula, the response to a given
dose is not always the same in all individuals. Some individuals may show the
same reaction at a lower dose than another individual will show at a
significantly higher dose. This is due to specific features, which not only differ
from individual to individual, but can also differ in the same individual from
day to day. In other words, there are interpersonal as well as intrapersonal
differences in the reaction to a given dose. This reaction can be represented
graphically by a sigmoid or S-shape (fig 11.1).
Fig 11.1. The dose-response curve
If the reaction or response of the general population to a drug or poison is presented
graphically, it has a sigmoid or S-curve. The closer the two curves of the therapeutic and toxic
effects of a drug, the greater the risk for toxic reactions. Sometimes individuals may experience
toxic effects at doses which are still therapeutic for other individuals. The MLD is the
minimum lethal dose. If we assume that in this graph the toxic effect is regarded as death, any
dose less than the minimum lethal dose will not cause death, but might have other toxic effects.
The ED50 and TD50 refer to those doses where 50% of individuals will experience the
(effective) therapeutic effect or toxic effect. If the toxic effect is death, the TD50 is also known
as the LD50.
188
Study unit 11

The therapeutic dose where 50% of individuals will experience the
therapeutic effect is also known as the ED50 (``effective dose''). The dose
where 50% of indiduals will die, is called LD50 (``lethal dose''). If a specific
toxic effect other than death is used, it is called TD50 (``toxic dose''). The
closer these doses are to one another, the higher the risk for toxic reactions.
The concept of the minimum lethal dose or MLD has been debated at length.
It is obvious from the sigmoid curve that we could say that the drug could not
have caused the individual's death if the level is lower than the MLD. The
contrary, however, is not possible; if an individual's blood level is somewhere
along this curve, it is not possible to state whether the individual indeed died
due to the effect of the drugs or substance. The higher the level of the
substance, the greater the chances that it could have played a role.
11.2.4 Poisoning
11.2.4.1 How is poisoning proved?
Poisoning can be proved from the symptoms and signs displayed by the victim
during his lifetime, together with a chemical analysis to test for the presence
of a particular poison or its metabolites in the vomit, bodily excretions, and
blood, or by determining specific target-organ changes. At a post-mortem
examination internal organs and tissues can be removed from the body for
chemical analysis.
If the poison is taken by mouth, it must (after absorption from the gut) pass to
the liver. The liver can destroy the poison or modify it, or the poison can
damage the liver. This can lead to symptoms and signs indicating liver
disorder, but often there is no clinical evidence to indicate whether the
damage is due to disease or poisoning. There could for example, be jaundice
(a yellow colouring of the skin, internal organs and tissues) because the ability
of the liver to handle the bile pigments could be sufficiently disrupted to push
the bile back into the blood. This is one of the ways in which jaundice can
originate regardless whether by disease or by a poison. One can now
understand why the liver is often one of the organs sent for chemical analysis
in a case of suspected poisoning.
After passing through the liver the poison reaches the heart and then goes to
the brain and all the other organs and tissues of the body. It is eventually
eliminated in the sweat, urine and the faeces. This is why the kidneys (which
produce the urine) are also often sent for analysis in the case of a deceased, or
the urine in the case of a living person.
The stomach and its contents can also be removed at a post-mortem
examination for analysis or, in the living patient, vomit can be examined.
Inspection of stomach contents can reveal recognisable items, for example
portions of the swallowed capsules which contained medicines, fragments of
the coloured wing cases of the beetles responsible for cantharadin (Spanish
fly) poisoning, et cetera. Some poisons have a greater affinity for certain
tissues. For example, arsenic is deposited in the hair and the nails, and hair
and nail clippings thus could provide evidence not only of this form of
poisoning, but also of the approximate period of time during which the
189
Toxicology and alcohol
arsenic was ingested, because the tempo at which hair and nails grow is
known. So, if these specimens are analysed in sections along the length of the
hair (or nails), the likely time of ingestion of the poison can be determined.
In 1955 a lock of Napoleon's hair was shown to contain arsenic. It was hinted
that this might purposely have been administered by his captors during the
latter part of his life on St Helena. He experienced health problems after the
Russian debacle, and evidence suggests that since arsenic was commonly
prescribed as a tonic at the time, this probably was the source of the arsenic.
If heavy metal poisons are found in tissues they should be evaluated carefully,
and the possibility that they may represent environmental contamination
before and after death must be carefully considered. In certain parts of South
Africa the soil is heavily contaminated by arsenic, and the presence of arsenic
in the hair or nails of exhumed bodies may mean no more than post-mortem
contamination of these tissues.
Post-mortem examinations seldom reveal any characteristic signs which can
be attributed to a particular poison. One of the few notable exceptions is the
bright, cherry-red colour of the blood in carbon-monoxide poisoning, due to
the formation of a special blood pigment called carboxyhaemoglobin
(COHb). Another example is the staining and destruction of the skin around
the lips and of the lining of the mouth, the gullet and the stomach, produced
by corrosive acids or caustic alkalis.
It is sometimes claimed that acute arsenic poisoning produces characteristic
haemorrhages beneath the inner lining of the left ventricle of the heart.
However, this is also seen in cases of death due to other causes. Therefore,
although such haemorrhages are not peculiar to arsenic poisoning only, they
may well arouse the suspicion of arsenic poisoning (in the absence of any other
satisfactory explanation for its appearance in the heart Ð see photo 49).
Lead and mercury poisoning can cause a dark blue-black line along the gum-
tooth margin, and in organophosphate poisoning the lungs may appear
markedly oedematous and frothy fluid may exude from the mouth and
nostrils (photo 47). Potassium dichromate can stain the tissues an orange
colour. It has also been observed that flies which feed from the body of a
person who died from insecticide poisoning also die. If there is a smell of
bitter almonds when the skull is opened, one should suspect cyanide
poisoning. Microscopic examination of the tissues could also indicate
poisoning. Certain changes in liver cells could indicate paracetamol
poisoning, and in kidney cells, glycol poisoning.
Remnants of capsule coverings, insects, and leaves in the stomach contents
could suggest the analytical procedure to be followed during toxicological
examination.
In general the post-mortem examination provides little evidence to indicate a
particular form of poisoning. The various organs and systems affected by a
poison however do display specific signs and symptoms. Whatever the poison
affecting the intestinal tract, the clinical features are usually nausea, retching,
vomiting, diarrhoea, constipation and cramp (colic). In the same way, the
effects of any poison acting on the respiratory system are manifested in
190
Study unit 11
interference with the breathing, for example the victim has difficulty in
breathing in or breathing out; he breathes rapidly or slowly; the breathing is
deep or shallow; there may be a cough, et cetera.
Arsenic acts on almost every system of the body. Hence, in chronic arsenic
poisoning, where arsenic has been ingested over a period of many weeks or
months, the victim may show evidence of vomiting and diarrhoea, thickening
of the skin, especially of the palms and the soles, uniform or spotty
pigmentation of the skin, rashes of one kind or another, inflammation of
nerves in different parts of the body, producing, for example, hoarseness of
the voice or weakness of the limbs, sometimes amounting to paralysis.
Arsenic poisoning has so many different faces that it can be mistaken for
many diseases. It could simulate laryngitis, scarlet fever (because of the type of
rash it produces), alcoholic neuritis, and attacks of diarrhoea and vomiting,
which could be (and often have been) mistaken for bacterial food poisoning.
The pigmentation of the skin could resemble certain natural diseases
associated with weakness of the limbs, vomiting, et cetera.
The problem is, therefore, to decide whether the different clinical signs as a
group could have been caused by a natural disease or by a poison. Otherwise
one has to decide how much each contributes to the total picture. The post-
mortem examination thus becomes important in excluding certain diseases,
and the chemical analysis can provide confirmation of the nature and amount
of the poison, which will indicate what condition the victim suffered from
and what caused his death.
It is often the virtually negative findings at a post-mortem examination which
arouse suspicion about poison as a possible explanation of the cause of death.
A negative post-mortem finding thus becomes a very important factor in the
investigation of a case of suspected poisoning.
The clinical history, the post-mortem findings and the results of any special
investigations (such as the chemical analysis for the presence of a poison) must
all be evaluated in order to arrive at a conclusion. The answer is not to be
found in one isolated part of the inquiry, but in a combination of all the steps
involved in making a medical diagnosis.
Since the final cause of death in a case of poisoning is often a condition such
as pneumonia, liver failure or kidney disease, it is understandable why, even
despite an autopsy, the true cause of death could easily be missed if
circumstantial evidence does not suggest a non-natural death. The value
placed on toxicological analysis adds to the problems relating to diagnosis.
The fact that a poisonous substance is found in the tissue does not necessarily
indicate that this was the cause of death. Such a finding could indicate that the
deceased was exposed to that poison, either in the environment or in his
workplace. Conversely, the opposite finding does not mean that poison was
not the cause of death, since death could be caused by some extremely
poisonous substances in such minute quantities as to defy routine chemical
analytical detection. In experimental animals the botulism toxin (a bacterial
toxin) can cause death in doses as small as 0,0001 mg/kg of body mass. Some
poisons are broken down so rapidly in the body that the metabolites cannot
be identified; others are present in the tissues as normal elements and only
relatively small additional quantities may cause death, particularly if given
191
Toxicology and alcohol
intravenously. Potassium chloride used as a resuscitative drug to replenish
tissue potassium after certain forms of cardiac collapse could have disastrous
consequences if administered incorrectly. Yet, on analysis the blood potassium
levels may have returned to normal at the time of death a little while later.
Various remedies are used by herbalists and medicine men for a variety of
ailments. The pharmacologically active substances in these preparations are
not always chemically identifiable.
Certain preparations are made from the wing cases of the Cantharides beetle
(Spanish fly), and concoctions are also made from the bulb of the candelabra
flower (Buphane disticha). The use of Cantharides as an abortifacient and an
aphrodisiac has led to fatal poisoning, as have concoctions made from the
bulb of Buphane disticha, given to adults for a variety of complications.
Understandably a death suspected to have been the result of poisoning may
only be brought to the notice of the appropriate authorities a considerable
time later. This could necessitate an exhumation, in which case special
precautions (in addition to the standard precautions) have to be taken when
sampling for poisons. While care must be taken to avoid contamination of
samples by extraneous chemical substances, steps must also be taken to
identify possible contamination after burial by sampling the soil above and
below the body, as well as the shrouds and the coffin.
11.2.4.2 Case studies
1. During a six-week period in 1969 seven young children died. Their illness
was heralded by fever, vomiting and diarrhoea, followed by severe liver
and kidney failure. Despite intensive medical supportive therapy, death
ensued within four days of admission to hospital. Initially the illness was
thought to be a ``natural disease'', probably viral in origin. An autopsy
(not medico-legal) was undertaken to confirm the clinical diagnosis.
However, the findings of a microscopic examination of tissues sampled at
the autopsy were suggestive of diethylene glycol poisoning. Epidemio-
logical studies revealed a single common factor in all the cases, namely a
proprietary brand of paediatric sedative mixture with a pharmaceutical
formulation which included propylene glycol as a solvent for the active
ingredients. An analysis of this medicine taken from the homes of the
victims established that these medicines did not contain propylene glycol,
but diethylene glycol Ð a related highly toxic anti-freeze agent used in
engine-cooling systems. The source of the diethylene glycol was a drum
(incorrectly) labelled propylene glycol, which contained diethylene
glycol. This had been supplied to the manufacturing pharmaceutical
company by the importers as propylene glycol.
2. In contrast with (1) above the death of a young male in 1977 following on
vomiting, delirium, jaundice, kidney failure and widespread tissue
haemorrhages was initially considered to have probably been the result
of poisoning. A medico-legal autopsy was therefore performed by
Professor N Scheepers. Microscopic examination of the tissues sampled
at the autopsy suggested that the condition was probably viral in origin.
Further virological studies subsequently confirmed this diagnosis; it was a
case of haemorrhagic fever caused by the Marburg virus. This was the
192
Study unit 11
first case reported in South Africa, and the second series of cases in the
world.
3. A party of forty-five adult males was given an ointment containing
mercury, then commonly known as ``blue-butter'' and formerly used for
treating pubic lice infestation. The week's supply of ointment was
(contrary to instructions) enthusiastically rubbed into the pubic area that
same evening by forty of the ``patients'', who all became acutely ill within
12 hours with signs of mercury poisoning, including nausea, burning
sensation in the chest, salivation, followed by a loosening of teeth in the
jaw, and kidney disturbances. Mercury was isolated in their urine samples.
All of them later developed the typical blue-line-on-the gum margins.
Specific antidote treatment was instituted, and after a ``stormy passage''
all the patients recovered. A variety of toxic substances (and medica-
ments) can be readily absorbed through the skin; amongst these are
mercury and various nitrites, such as TNT. Five patients who were not
poisoned had either not used the ointment, or had used it according to
instructions.
4. A middle-aged company director was admitted to hospital, acutely
shocked and with severe abdominal pain and vomiting. A year earlier he
had been treated for a peptic ulcer. An emergency operation was
considered necessary for a suspected perforation of the ulcer. The patient
died while still under general anaesthetic and before the abdomen could
be opened. In terms of the provisions of the Health Professions Act
relating to death while under, or in consequence of a general or local
anaesthetic, a medico-legal autopsy was performed. At the autopsy the
stomach lining had a velvety appearance, and a large subendocardial
haemorrhage was observed in the left ventricle of the heart. No other
significant signs which could account for death were found. The sub-
endocardial bleeding necessitated chemical analysis of the organs. Large
quantities of arsenic were discovered, enough to cause acute poisoning.
The source of the poison was never found, but in the light of
circumstantial evidence, suicide was suspected.
5. An asthmatic patient also suffering from high blood pressure was issued
with a prescription for an anti-hypertensive medicine, containing an
adrenalin-blocking agent, in small therapeutic quantities. Within minutes
of taking the first dose the patient suffered an acute attack of asthma
which did not respond to the adrenalin-like anti-asthmatic medicine she
had been accustomed to use, since the former blocked the cellular
receptor sites for the latter. The patient died in status asthmaticus despite
having been rushed to hospital, and despite the expeditious application of
resuscitative measures.
6. The deceased, a political defector form Eastern Europe, felt something
sting him on the back of his thigh whilst waiting for a bus in London. On
reaching home his suspicion that a wasp had stung him was ``confirmed''
by the discovery of a small puncture wound in the centre of a large
inflamed area of his thigh. He mentioned that he had noticed a man with
a furled umbrella hurrying away from the scene shortly after he had been
stung. At the subsequent autopsy a few days later a very small object
which resembled a ball-bearing through which a minute hole had been
bored was found in the depths of the affected tissues. It was later
193
Toxicology and alcohol
established that another defector in Paris had had a similar experience but
had not succumbed despite a stormy passage in hospital. He was traced,
his leg X-rayed and a similar object was revealed to be embedded in the
leg. This was removed, and both objects were identified as being of the
same composition and dimensions, and peculiar to an alloy used in the
country from which the two victims hailed. Subsequently it was
established that the hole in the object contained ricin in a concentrated
form. The substance had been the subject of research by a scientist in the
aforementioned country. Available evidence suggested that the furled
umbrella was a cover for an airgun-type weapon. The volume of ricin in
the hole constituted a possible lethal dose.
11.2.5 Post-mortem examination
In addition to the above signs of poisoning, it is also important to submit the
relevant specimens for toxicological analysis during the post mortem. Blood,
kidneys and urine, the liver and the stomach and stomach contents will be
routinely analysed. In some cases eye fluid or vitreous humour (for alcohol)
and other organs such as the brain, will also be analysed. Hair and nails will
also be examined especially in heavy metal poisoning.
11.3 Carbon-monoxide poisoning
Carbon monoxide (CO) is formed during the incomplete oxidation or
combustion of carbon-containing material (ie organic material). During
combustion of carbon-containing material in the presence of sufficient
oxygen (O2), each carbon atom will bind with two oxygen atoms to form
carbon dioxide (CO2). If sufficient oxygen atoms are not available, every
carbon atom will only bind with one oxygen atom. Carbon monoxide (CO)
instead of carbon dioxide (CO2) will be produced.
11.3.1 Sources of carbon monoxide
Carbon monoxide is produced wherever incomplete oxidation of carbon
occurs during combustion.
1. Household or domestic. Open fires in rooms or other shelters with an
insufficient oxygen supply, such as warm-water gas cylinders or fires in
enclosed spaces.
2. Transport. Transport vehicles produce CO. Petrol engines produce more
carbon monoxide than diesel engines. CO production is also increased if
the engine is not correctly tuned. It is alleged that a 1600cc engine in a
closed garage will produce deadly levels within 5 minutes.
3. Industrial. In certain types of industry, such as smelting-works.
4. General. Incomplete fermentation can also produce CO. Firing a firearm
at close range causes carbon monoxide emission, which can discolour the
underlying tissue.
11.3.2 Pharmacology
Carbon monoxide is a colourless, odourless and tasteless non-irritating gas. It
is slightly lighter then air. The gas is absorbed via the lungs and has the
following effects:
194
Study unit 11
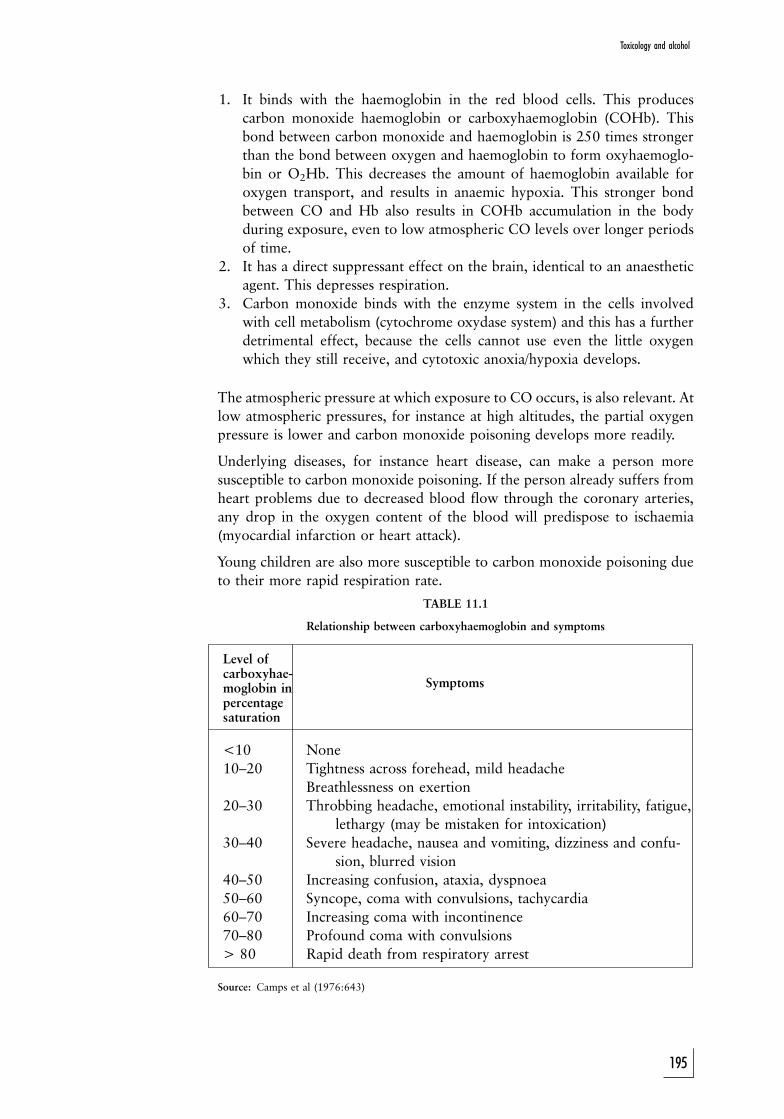
1. It binds with the haemoglobin in the red blood cells. This produces
carbon monoxide haemoglobin or carboxyhaemoglobin (COHb). This
bond between carbon monoxide and haemoglobin is 250 times stronger
than the bond between oxygen and haemoglobin to form oxyhaemoglo-
bin or O2Hb. This decreases the amount of haemoglobin available for
oxygen transport, and results in anaemic hypoxia. This stronger bond
between CO and Hb also results in COHb accumulation in the body
during exposure, even to low atmospheric CO levels over longer periods
of time.
2. It has a direct suppressant effect on the brain, identical to an anaesthetic
agent. This depresses respiration.
3. Carbon monoxide binds with the enzyme system in the cells involved
with cell metabolism (cytochrome oxydase system) and this has a further
detrimental effect, because the cells cannot use even the little oxygen
which they still receive, and cytotoxic anoxia/hypoxia develops.
The atmospheric pressure at which exposure to CO occurs, is also relevant. At
low atmospheric pressures, for instance at high altitudes, the partial oxygen
pressure is lower and carbon monoxide poisoning develops more readily.
Underlying diseases, for instance heart disease, can make a person more
susceptible to carbon monoxide poisoning. If the person already suffers from
heart problems due to decreased blood flow through the coronary arteries,
any drop in the oxygen content of the blood will predispose to ischaemia
(myocardial infarction or heart attack).
Young children are also more susceptible to carbon monoxide poisoning due
to their more rapid respiration rate.
TABLE 11.1
Relationship between carboxyhaemoglobin and symptoms
Level of
Symptomscarboxyhae-moglobin inpercentagesaturation
<10 None
10±20 Tightness across forehead, mild headache
Breathlessness on exertion
20±30 Throbbing headache, emotional instability, irritability, fatigue,
lethargy (may be mistaken for intoxication)
30±40 Severe headache, nausea and vomiting, dizziness and confu-
sion, blurred vision
40±50 Increasing confusion, ataxia, dyspnoea
50±60 Syncope, coma with convulsions, tachycardia
60±70 Increasing coma with incontinence
70±80 Profound coma with convulsions
> 80 Rapid death from respiratory arrest
Source: Camps et al (1976:643)
195
Toxicology and alcohol
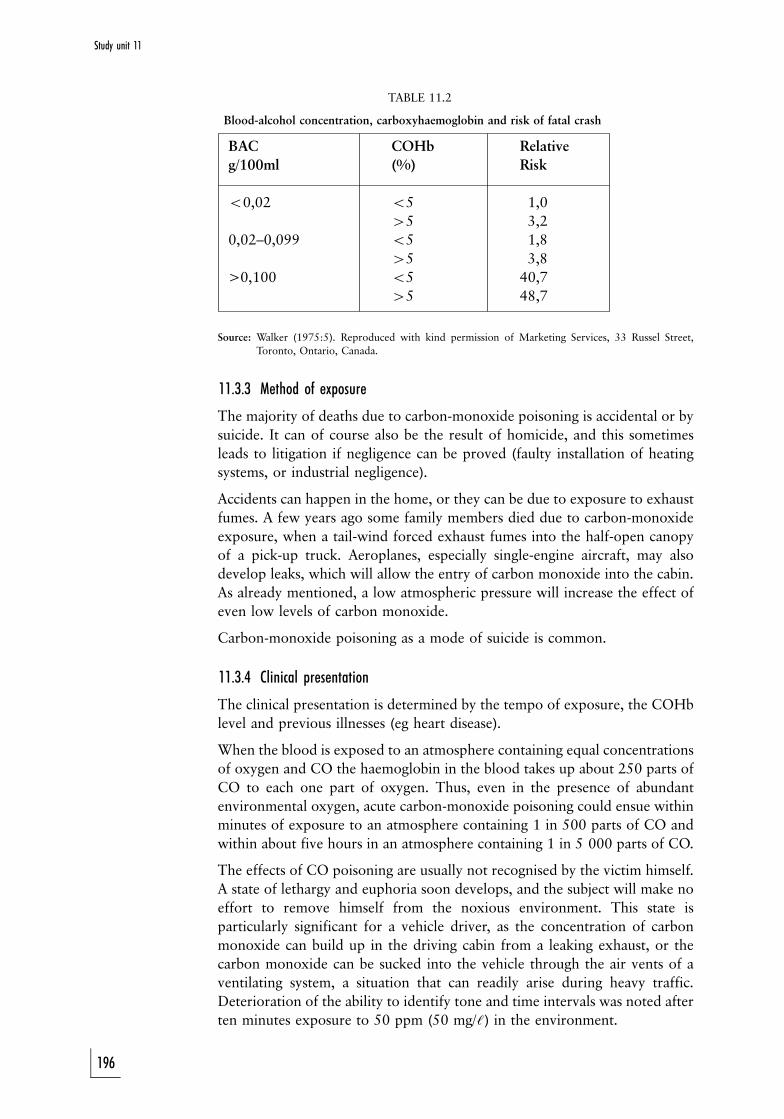
TABLE 11.2
Blood-alcohol concentration, carboxyhaemoglobin and risk of fatal crash
BAC COHb Relative
g/100ml (%) Risk
50,02 55 1,0
45 3,2
0,02±0,099 55 1,8
45 3,8
>0,100 55 40,7
45 48,7
Source: Walker (1975:5). Reproduced with kind permission of Marketing Services, 33 Russel Street,
Toronto, Ontario, Canada.
11.3.3 Method of exposure
The majority of deaths due to carbon-monoxide poisoning is accidental or by
suicide. It can of course also be the result of homicide, and this sometimes
leads to litigation if negligence can be proved (faulty installation of heating
systems, or industrial negligence).
Accidents can happen in the home, or they can be due to exposure to exhaust
fumes. A few years ago some family members died due to carbon-monoxide
exposure, when a tail-wind forced exhaust fumes into the half-open canopy
of a pick-up truck. Aeroplanes, especially single-engine aircraft, may also
develop leaks, which will allow the entry of carbon monoxide into the cabin.
As already mentioned, a low atmospheric pressure will increase the effect of
even low levels of carbon monoxide.
Carbon-monoxide poisoning as a mode of suicide is common.
11.3.4 Clinical presentation
The clinical presentation is determined by the tempo of exposure, the COHb
level and previous illnesses (eg heart disease).
When the blood is exposed to an atmosphere containing equal concentrations
of oxygen and CO the haemoglobin in the blood takes up about 250 parts of
CO to each one part of oxygen. Thus, even in the presence of abundant
environmental oxygen, acute carbon-monoxide poisoning could ensue within
minutes of exposure to an atmosphere containing 1 in 500 parts of CO and
within about five hours in an atmosphere containing 1 in 5 000 parts of CO.
The effects of CO poisoning are usually not recognised by the victim himself.
A state of lethargy and euphoria soon develops, and the subject will make no
effort to remove himself from the noxious environment. This state is
particularly significant for a vehicle driver, as the concentration of carbon
monoxide can build up in the driving cabin from a leaking exhaust, or the
carbon monoxide can be sucked into the vehicle through the air vents of a
ventilating system, a situation that can readily arise during heavy traffic.
Deterioration of the ability to identify tone and time intervals was noted after
ten minutes exposure to 50 ppm (50 mg/:) in the environment.
196
Study unit 11

At levels of 10% to 20% blood saturation, mild headache, breathlessness and
confusion can occur (table 11.1). At levels of 20% and more, emotional
instability, irritability, fatigue and marked lethargy, and at 30% severe
headache, nausea, vomiting, dizziness, confusion, blurred vision, ataxia,
tachycardia, nystagmus, Rombergism and a flushed face could be experienced
and this can mistakenly be attributed to alcohol intoxication. On recovery
from the poisoning there can be complete amnesia about the events at the
time of the incident. (Ataxia is unco-ordinated muscle movement. Tachycardia
is an excessively rapid heart-beat. Nystagmus is an involuntary rapid
movement of the eyeball. Rombergism is the tendency to sway when closing
the eyes while standing still with the feet close together.)
The rate of the build-up of carboxyhaemoglobin levels will affect the gravity
of the symptoms. The more rapid the saturation, the more intense the
symptoms will be at a given level. If other gases are also involved, the
haemoglobin levels could be far lower than anticipated from the clinical signs,
and if there is severe anaemia, cardiovascular disorders and alcohol
involvement, the effects may be more marked than the case of a healthy
person. Even at very low levels of carboxyhaemoglobin (3%) people with
coronary artery disease reveal electrocardiographic changes, and anginal pain
can arise sooner with mild exercise.
If there is alcohol involvement the risk increases. Some motor accidents are
due to the combined action of alcohol and CO on the driver (the source of the
latter being faulty exhausts) (table 11.2).
11.3.5 Toxicological analysis
To make a finding of carbon monoxide poisoning there must be evidence of
an abnormally high carboxyhaemoglobin or COHb level. Any blood sample
(arterial or venous) can be used, even a bloody fluid, as the percentage of
haemoglobin bound to the carbon monoxide (COHb) has to be determined.
A COHb of more than 5% in nonsmokers and more than 10% in smokers is
significant. As decomposition may affect COHb levels, the specimen must be
preserved with sodium fluoride and potassium oxalate. This is the same
preservative used for alcohol analysis, and the sodium fluoride is an enzyme
inhibitor which suppresses the production of carbon monoxide after the
collection of the specimen. As mentioned, other diseases, for instance pre-
existing anaemia or heart disease, as well as alcohol, have a negative effect.
11.3.6 Post-mortem signs
The body has a characteristic cherry-red appearance due to (even only
through one oxygen atom) the oxygenised state of the haemoglobin. The
muscles are also cherry-red as the process also involves the myoglobin in the
muscles. In individuals surviving for a period of time, damage to the brain and
heart will be evident.
11.3.7 Case study
A man and his wife made a suicide pact. They drove to the appointed place
and connected the exhaust of the car to a hosepipe so that the fumes could
flow into the car. Prior to leaving for the scene the husband had consumed
197
Toxicology and alcohol

half a bottle of brandy Ð this was approximately two hours before the
estimated time of his death. The following day the husband's body was found
slumped in the front passenger seat of the car. The driver's door was wide
open. The evening of the following day the wife phoned the police from a
hotel some 30 km from the suicide scene. On the same day their dog was
found wandering aimlessly about in the bush, and obviously blind (probably
the consequence of carbon-monoxide poisoning). The wife made a statement
to the effect that she and her husband had got into the car, he in the driver's
seat and she in the passenger seat. Their dog was asleep on the back seat.
Shortly after starting the car her husband asked her to move into the driver's
seat as he felt too drowsy to keep his foot on the accelerator pedal. This she
did. She had no further recollection of events up to the time she remembered
entering the hotel from where she had phoned the police.
A post-mortem examination of the husband's body revealed that his blood
contained 75% carboxyhaemoglobin. His blood-alcohol concentration was
0,25g%. The alcohol probably caused the initial drowsiness and made him
more susceptible to the effects of the carbon monoxide. The wife, in a state of
confusion, probably managed to open the door on her side and fell out of the
car, and at that time the dog must have escaped.
Note: Temporary confusion and amnesia are frequently encountered in
persons recovering from carbon-monoxide poisoning.
11.4 Alcohol
The term alcohol actually refers to a group of chemicals which all contain a
hydroxyl group. Depending on the number of carbon atoms it includes
methanol, ethanol, propanolol, et cetera. However, in general the term
alcohol refers to ethanol.
Ethanol (C2H5OH) is a colourless, odourless and volatile substance without
any taste. It is completely water soluble and burns easily. Ethanol itself does
not have a specific odour. The ``smell'' of alcohol is not due to the ethanol,
but rather to the additives which give each drink its characteristic taste and
odour. Ethanol is the most potent psycho-active anaesthetic drug that is
legally available without prescription. It is often abused, resulting in acute
intoxication or chronic alcoholism. In this study unit we discuss mainly acute
intoxication, although chronic alcoholism with its adverse effects on health
and society is equally important.
11.4.1 Production of alcohol
Alcohol is produced after fermentation of sugar (in grape, malt, etc) by yeasts.
This process will carry on spontaneously until the alcohol concentration is
15%. At this point the alcohol will inhibit the yeast and no further
fermentation will take place. The substances produced by this process are
inter alia natural wine, beer and cider.
Distillation is a process whereby the alcohol level can be increased to absolute
198
Study unit 11
or 95 to 100% alcohol. This process produces distilled beverages such as
brandy, whisky, et cetera. Fortified drinks are produced by fortifying natural
wine with distilled spirits (eg sherry and port).
The alcohol concentration of natural wine is therefore less than 15%, distilled
spirits more than 40 to 42% and fortified beverages in the mid 20%. This is
the reason why an opened bottle of distilled or fortified drink will retain its
taste, as the alcohol at that percentage inhibits the growth of all yeasts,
including those producing vinegar. The same does not apply to an opened
bottle of white or red wine, as the alcohol is easily transformed into vinegar.
11.4.2 Pharmacodynamics of alcohol
Pharmacodynamics is the study of the action of drugs on living organisms.
Although alcohol may be theoretically introduced into the body via the
rectum, intravenously or even by inhalation, the most common, and for all
practical purposes the only, route is by ingestion.
11.4.2.1 Absorption of alcohol by the body
a Ingestion of alcohol
Alcohol is usually taken by mouth in one or other form and is absorbed into
the body directly and unchanged by the process of diffusion. Alcohol, unlike
other substances like sugars, is not chemically modified in any way before it is
absorbed. The process of diffusion occurs through the mucous membranes (ie
the membranes coating the inner surface of the stomach, intestines, etc) into
the large network of capillary blood vessels in the alimentary canal.
The absorption of alcohol in the mouth and oesophagus is minimal and for
practical purposes nil, because the alcohol passes rapidly through these
structures. Absorption proceeds immediately in the stomach and small
intestine. Approximately 20% of alcohol which is ingested is absorbed in the
stomach, and the rest (80%) in the small intestine. Depending on the volume
of alcohol ingested, a small quantity may reach the colon and be absorbed
there. If alcohol is administered into the colon by means of an enema, the
absorption there is also rapid and complete.
i Anatomical and physical factors of importance
Alcohol absorbed by the stomach and small intestine is first absorbed into the
blood and then distributed to all the organs. The following anatomical and
physical factors determine not only the rate of absorption, but also the site of
maximum absorption:
. Surface of the mucous membrane
Due to its length the small intestine has a far greater surface area of
mucous membrane than the stomach. Thus alcohol is absorbed much
faster from the small intestine than from the stomach. If the mucous
membrane is covered by mucus or food this will delay the absorption
because the area of contact between the alcohol and the mucous
membrane is less.
199
Toxicology and alcohol
. Absorption capacity of the mucous membrane
The mucous membrane of the small intestine has a better supply of
blood vessels than that of the stomach, and therefore absorption in the
small intestine is greater than in the stomach. Any condition which
increases the blood supply in the mucous membrane will increase
absorption, for example congestion and/or gastritis or dilatation of the
capillaries by warm or hot liquids. The rate of absorption (diffusion)
of alcohol depends on the concentration gradient between the alcohol
in the stomach and the intestine, and the alcohol in the blood of the
capillaries in the stomach and intestinal wall. The smaller the gradient,
the slower the rate of absorption (Fick's law).
ii Factors influencing the rate of alcohol absorption
Using the above information as background it is possible to classify the
relevant factors. We discuss them in some detail.
1. The peristaltic movement of the alimentary canal and the functional
status of the stomach's pyloric sphincter. The forward propulsion of
food is due to rhythmic contractions called peristaltic movements or
peristalsis. A muscle forming a valve, the pyloric sphincter, is present
at the stomach outlet. It is this valve which controls the flow of food
out of the stomach and into the small intestine. Any condition which
stimulates contraction of this valve will therefore slow down the rate
of forward movement of food (and alcohol).
The greater the gastric motility and the more relaxed the pyloric
sphincter, the more rapid the absorption of alcohol because the gastric
contents (mixed with alcohol) pass more rapidly into the duodenum
(the first part of the small intestine). Gastric motility is decreased by
certain medicines, by very high alcohol concentrations (paralysis of
the smooth muscle of the gastric wall) and in cases of nausea and
shock. Gastric motility is increased by the intake of large volumes of
food and/or liquids. The rate at which the stomach is emptied is
increased by conditions of inflammation such as peptic ulcers, as these
cause gastric irritation.
Irritating substances in the stomach cause the pyloric sphincter to
contract and there is then a delay in the emptying of the stomach.
Psychological factors such as anxiety may influence the function of
the pyloric sphincter, but it is not possible to predict whether more or
less alcohol will then be absorbed because this differs from person to
person.
Surgical procedures of the stomach and the small intestine (eg
gastrectomy) will cause more rapid absorption of alcohol as the gastric
contents will pass more rapidly into the small intestine.
Thus, if the gastric contents are slowly released into the small
intestine, absorption will be slower and over a longer period.
Therefore the blood-alcohol level will not rise so high because the
body will have more time to eliminate the alcohol already absorbed,
in other words, it will be more able to cope with the absorbed alcohol.
200
Study unit 11

2. The nature, composition, amount and strength of the beverage
ingested. Optimal absorption of alcohol occurs when the beverage has
an alcohol concentration of between 10% and 20%. The higher the
concentration, the slower the absorption, because of the possible
secretion of excessive mucus, spasm of the pyloric sphincter and/or
suppression of gastric motility. Large volumes of beverage make
contact with the mucous membranes over a larger area and also
increase the gastric motility so that alcohol passes more rapidly into
the small intestine. Absorption of the alcohol in beer is delayed
because of the presence of carbohydrates in the beer. The alcohol in
beverages that contain gas or to which diluents containing gas (carbon
dioxide, bicarbonate) have been added, is absorbed faster. This is due
to the distension of the stomach with gas, and therefore increasing the
surface contact area due to flattening of the normal stomach folds,
almost similar to an inflated balloon.
Warm beverages are absorbed faster than cold ones and hence also the
alcohol in the beverage. This is due to an increase in the blood flow to
the intestines.
To summarise: the most ``potent'' drink (if someone is crazy enough
to drink it) will be a warm bottle of champagne (warm Ð absorbed
faster than cold; bottle Ð large volume; champagne Ð contains gas
and has an alcohol concentration between 10% and 20%)!
3. The contents of the alimentary canal. The absorption of alcohol from
the stomach and small intestine is influenced by the nature and
amount of their contents. Food ``dilutes'' alcohol and prevents
contact between the alcohol and the mucous membrane. This is
especially true of fatty foods and/or food with a high protein and/or
carbohydrate (sugar) content. Certain foods, especially fats, delay the
emptying of the stomach so that the food-alcohol mixture takes
longer to reach the small intestine with its large absorptive surface. It
therefore makes good sense not to drink on an empty stomach.
4. Medicines and other chemical substances. As mentioned above,
various substances influence gastric and intestinal peristalsis and the
activity of the pyloric sphincter, thus influencing the speed of
absorption. This is a specialised field, and often used in courts as a line
of defence; for this course it is sufficient to be aware of the possible
role pharmaceutical substances may play.
b Absorption through the airways and lungs
Although absorption through the airways and lungs can be rapid, it is highly
unlikely that significant blood concentrations will be reached, as the alcohol
irritates the airways. The maximum blood concentration reached through
inhalation is 0,02g%. People do not die of alcohol intoxication when they
enter a wine tank, but they die of anoxia (absence of oxygen) or the
accumulation of carbon dioxide (CO2).
201
Toxicology and alcohol
c Absorption through the skin
Alcohol is not absorbed through an intact skin.
d Intravenous and subcutaneous administration
This route is theoretically possible.
There is common misconception that the clinical effect of alcohol
intoxication is determined by the rate of absorption of alcohol. This is
wrong; a specific alcohol level will correspond with a specific clinical effect,
regardless of how rapidly that level was reached.
11.4.2.2 Distribution
After absorption from the gastro-intestinal system, alcohol is distributed
through the body via the blood circulation. Certain factors will affect the
distribution:
a Cardiac output
Any increase in cardiac output, such as caused by exercise or excitement, will
increase distribution.
b Water in tissues
Alcohol is water soluble. The water in an organ or tissue will therefore
determine the amount of alcohol which can dissolve in that specific tissue. In
tissues with a high water content more alcohol can dissolve. Males have
(supposedly) a higher muscle mass than females; the latter have a higher fat
content. Therefore males can redistribute more alcohol out of their blood
into their extra-vascular areas (muscles). That is why, all other factors being
equal, a male will have a lower blood-alcohol level than an identical female
counterpart after absorption of the same amount of alcohol. This factor is
also called the distribution factor or ``r'' factor in the Widmark formula (0,7
for males and 0,6 for females).
c General
Alcohol does not accumulate in any organ or tissue. If the blood-alcohol level
drops below the alcohol level in the tissues (brain or muscles), alcohol will
diffuse from the tissues (higher concentration) to the blood (lower
concentration). This enables the body to eventually get rid of all the absorbed
alcohol.
11.4.2.3 Metabolism and secretion of alcohol
About 85% to 90% of alcohol is metabolised by the liver. The enzyme,
alcoholdehydrogenase (ADH), plays a major role in this process. The
metabolites produced by this process include acetaldehyde, one of the causes
of a hangover. The rest is secreted unchanged via the lungs, kidneys and
perspiration. Alcohol is eliminated at a constant rate. The rate of elimination
is between 0,01 and 0,02g% per hour. Usually the average (0,015g% per
hour) is used, and this is called the B60 value.
202
Study unit 11
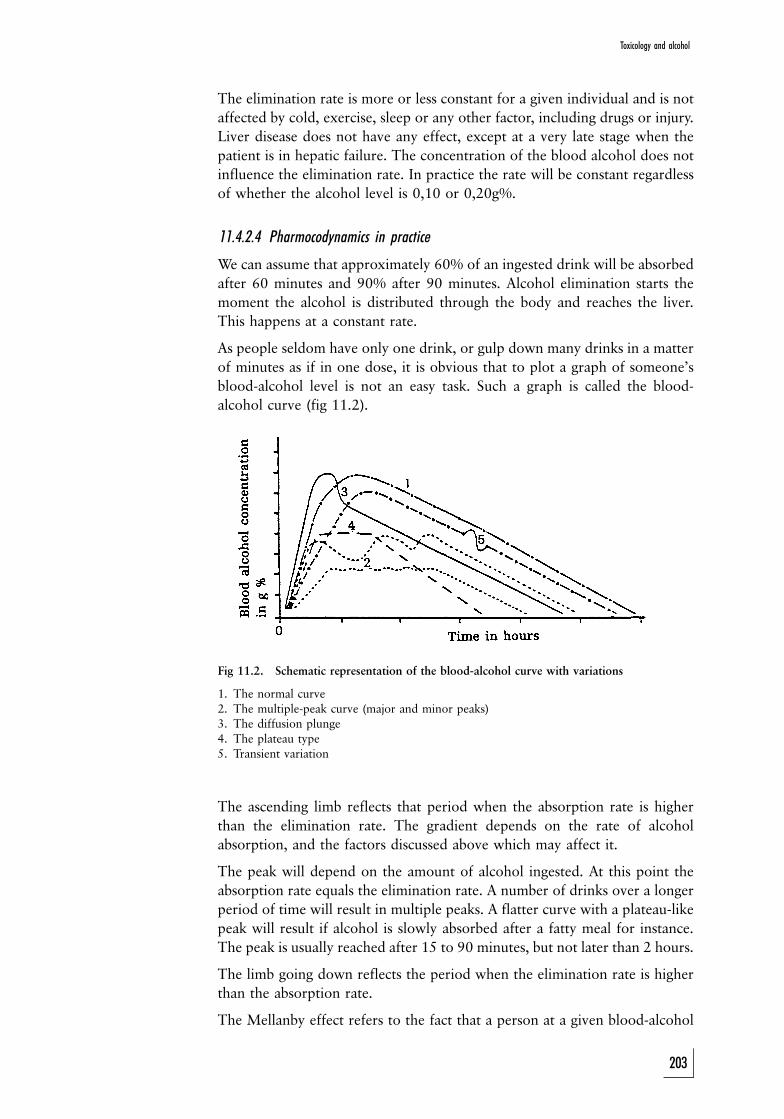
The elimination rate is more or less constant for a given individual and is not
affected by cold, exercise, sleep or any other factor, including drugs or injury.
Liver disease does not have any effect, except at a very late stage when the
patient is in hepatic failure. The concentration of the blood alcohol does not
influence the elimination rate. In practice the rate will be constant regardless
of whether the alcohol level is 0,10 or 0,20g%.
11.4.2.4 Pharmocodynamics in practice
We can assume that approximately 60% of an ingested drink will be absorbed
after 60 minutes and 90% after 90 minutes. Alcohol elimination starts the
moment the alcohol is distributed through the body and reaches the liver.
This happens at a constant rate.
As people seldom have only one drink, or gulp down many drinks in a matter
of minutes as if in one dose, it is obvious that to plot a graph of someone's
blood-alcohol level is not an easy task. Such a graph is called the blood-
alcohol curve (fig 11.2).
Fig 11.2. Schematic representation of the blood-alcohol curve with variations
1. The normal curve
2. The multiple-peak curve (major and minor peaks)3. The diffusion plunge
4. The plateau type
5. Transient variation
The ascending limb reflects that period when the absorption rate is higher
than the elimination rate. The gradient depends on the rate of alcohol
absorption, and the factors discussed above which may affect it.
The peak will depend on the amount of alcohol ingested. At this point the
absorption rate equals the elimination rate. A number of drinks over a longer
period of time will result in multiple peaks. A flatter curve with a plateau-like
peak will result if alcohol is slowly absorbed after a fatty meal for instance.
The peak is usually reached after 15 to 90 minutes, but not later than 2 hours.
The limb going down reflects the period when the elimination rate is higher
than the absorption rate.
The Mellanby effect refers to the fact that a person at a given blood-alcohol
203
Toxicology and alcohol

level will present a different clinical picture, depending on whether he/she is
on the rising or declining limb of the curve. The degree of intoxication will be
more pronounced on the rising than the declining limb because the brain will
adapt to alcohol after a while due to the development of acute alcohol
tolerance.
11.4.3 Alcohol-level analysis
11.4.3.1 Living person
The blood-alcohol level is usually determined in the living by means of a
venous blood sample collected from the cubital fossa (anterior aspect of the
elbow). However, any blood specimen can be used. It is important to prevent
contamination with alcohol-containing solutions, especially when the skin is
cleaned.
The specimen must be collected in a special test tube containing sodium
fluoride (NaF) and potassium oxalate. The former is an enzyme inhibitor that
inhibits the production and transformation of alcohol in the specimen. It is
also used for post-mortem specimens and for the analysis of carbon monoxide
(carboxyhaemoglobin).
Breath-alcohol analysis is at present widely used by law-enforcement agencies.
It is based on the principle that a certain amount of alcohol will be eliminated
via the lungs. Although technical factors (eg condensation in the mouthpiece,
the effect of temperature, etc) often had an effect on the functioning of the
older measuring instruments, modern equipment is more sensitive and
accurate. This method is often used as a screening procedure at roadblocks,
and the level of alcohol intoxication is then confirmed with a blood analysis.
11.4.3.2 The dead body
Alcohol levels are routinely measured in all individuals older than 16 years
who die unnaturally. A blood or vitreous humour (eye fluid) specimen is
tested. It is important to collect the specimen as far away as possible from the
stomach and liver. Post-mortem diffusion of ingested alcohol from the
stomach into adjacent tissues can lead to a false measurement. Therefore
specimens from the heart are not acceptable. The same applies to the liver,
where post-mortem fermentation of sugars by micro-organisms can produce
alcohol. The specimen is therefore collected from the femoral vein in the
groin, as the inferior vena cava has valves which will prevent backward
diffusion to the abdominal region.
Most forensic laboratories use vitreous humour. This fluid has certain
advantages. The eye is protected quite well by bony structures. Even in severe
mutilation eye fluid will still be available. Then the eyes are also
microbiologically quite sterile. Post-mortem alcohol production is therefore
less common. Lastly eye fluid is in a way chemically isolated from the body
and not so susceptible to biochemical changes with death.
Urine-alcohol levels only confirm alcohol ingestion. Urine-alcohol concentra-
tion is influenced by the volume of urine, and is therefore not a reliable
indication of the amount of alcohol ingested.
204
Study unit 11

If the specimen is analysed by a gas chromotograph other alcohols will also be
indicated on the graph. If an alcohol such as butanol is produced during
decomposition it will thus be indicated. The absence of other alcohol peaks
therefore further confirms the accuracy of the blood-alcohol level, as it
indicates that there was no post-mortem or post-collection production of
alcohol.
11.4.4 Calculations
11.4.4.1 The amount of alcohol in a drink
As a rule of thumb we can assume that a glass of wine, a beer and a tot of
spirits each contains roughly the same amount of alcohol, namely 10 grams.
However, it is often necessary to be more precise about the exact amount of
alcohol in a drink. If the strength of a beverage expressed as v/v% is known,
the amount of alcohol in gram can be calculated. As an example a 100 ml
glass containing white wine with an alcohol content of 12% will be used for
the following measurements: 100 ml wine will therefore contain 12 ml
alcohol. The specific gravity of alcohol is 0,79, in other words 1 ml alcohol
weighs 0,79 g. Therefore the alcohol content of 100 ml wine will be
12 6 0,79 = 9,48 g.
11.4.4.2 The Widmark formula
The Widmark formula is used to calculate the amount of alcohol in grams
ingested by an individual to produce a specific blood-alcohol concentration at
a given time. It is important to realise that it does not reflect any alcohol
already absorbed and eliminated, nor any alcohol ingested but not absorbed.
A = p 6 c 6 r 6 10
A: The amount of alcohol in gram in the body at a given time to cause
the blood alcohol concentration
P: the mass of the person in kg
C: the blood alcohol concentration in g% or g/dl
R: the Widmark or distribution factor
As mentioned above, alcohol is water-soluble. The higher the water
content of a tissue or body, the more alcohol can be dissolved in the
tissues, and the lower the blood-alcohol level will be. As males generally
have more muscle tissue than females, the same quantity of alcohol
ingested by a male and female of the same mass (all other factors being
equal) will result in a lower level in the male than in the female. This ``r''
or distribution factor is 0,6 for females and 0,7 for males.
10: The reason why this formula must be multiplied by 10 is its German
origin. In Germany an alcohol-level is expressed in promille, that is g/l. In
order to express the g% or g/dl value as used in South Africa, we multiply
by 10.
205
Toxicology and alcohol

Take the example of a man weighing 70 kg and a blood-alcohol level of
0,08g%. Based on the Widmark formula this level represents the following
amount of alcohol ingested:
A = p 6 c 6 r 6 10
= 70 6 0,08 6 0,7 6 10
= 39,20 g
This represents roughly 4 drinks
11.4.4.3 Reverse calculations
When using this formula it is important to remember that it also represents
alcohol already absorbed by the body. As we can safely assume that all alcohol
will be absorbed after 2 hours, this formula can only be applied if no alcohol
was ingested in the 2-hour period before specimen collection. If alcohol was
taken in during this period, the amount and its impact on the blood-alcohol
level must be taken into account.
This formula is based on the principle that alcohol elimination occurs at a
constant level of between 0,01 and 0,02g% per hour. This value is also called
the B60 value, and we generally use an average value of 0,015g%/h.
Let us take as example someone arrested at 22:00 with a blood-alcohol level
of 0,10g% at the time of the arrest. The incident occurred at 19:00, 3 hours
previously. If we use the formula:
Ci = Ca + (B60 6 t)
Ci: concentration at time of incident
Ca: concentration at time of arrest
t: hours between these events
m60: 0,015g%/h
We find that:
Ci = Ca + (B60 6 t)
= 0,10 g% + (0,015 g%/h 6 3h)
= 0,10 g% + 0,045 g%
= 0,145 g%
As said before, we can use this formula only if no more alcohol was consumed
during the period between the incident and the time of specimen collection,
except if we take that alcohol into account.
11.4.5 Pharmacological effect
11.4.5.1 General
The effect that alcohol has on the psyche, both pleasant and unpleasant, is
well-known. What is less well-known is that alcohol, in different quantities
206
Study unit 11

for different people, is a toxic drug. Alcohol has both an acute and chronic
effect on various organs of the body, including the brain, heart, lungs, liver,
the gastro-intestinal, genito-urinary and endocrine systems.
a Nervous system
The damage that alcohol causes to the central and peripheral nervous systems
is of particular importance when it comes to the driving of vehicles, as the
following quote (Shaw: 1978) makes clear:
The exact mode of action of alcohol on the central nervous system is
unclear and its study complex. The effects of acute administration of
alcohol are often quite at variance with the effects of chronic
administration and the effects caused by a steady blood-alcohol level
are often very different from the effects caused by a changing blood-
alcohol level. The rate of change may itself be an important factor.
Individual variation on whatever basis it may rest is also important.
Not only do we find that effects in the naõÈve subject are very different
from effects in the alcohol sophisticate, but it is well known that all
alcoholics do not suffer all the complications of alcoholism and indeed
some suffer none.
It appears that alcohol modifies the quality of nerve-impulse transmission by
stimulating the naturally occurring nerve-transmission inhibitor, GABA,
(gamma-amino-butyric acid) in the grey matter of the brain. Drugs like
Valium and barbiturates mimic this effect. Similarly, cross-tolerance between
these drugs and alcohol, when one of them is used over a long period, is
frequently observed. Furthermore, different types of nerve cells display
different degrees of sensitivity to the effects of alcohol and these drugs.
The fact that we have stressed the complexity of the effects of alcohol on the
body should make it clear that many factors, as yet poorly understood, could
influence the response elicited by alcohol, and that extreme caution should be
exercised before expressing any final opinion on individual behaviour and
responses of the users of alcohol. In the early stages of intoxication it is the
loss of the inhibitory effect exercised by the higher centres over the lower
centres which accounts for the characteristic behavioural changes such as the
feeling of euphoria and the excessive self-confidence which is out of all
proportion to reality (Shaw: 1978).
It produces loss of emotional restraint and diminishes the inhibitions
which civilisation imposes on human conduct. Because in a social
environment many people become more active, both in speech and
manner, it is widely (but incorrectly) regarded as a stimulant.
The effect of alcohol on the nervous system is, however, essentially
depression of function, the extent of which depends on the amount of
alcohol working in on the brain cells, and the susceptibility of these cells (or
groups of cells) to alcohol. The cortical brain cells (responsible for the higher
functions) generally display the effect of alcohol far sooner than those of the
lower centres in the basal ganglia and the midbrain. As blood-alcohol and thus
brain-alcohol levels rise, more functions of the nervous system are impaired,
until co-ordination is drastically disturbed and unconsciousness ensues. Death
207
Toxicology and alcohol

could follow due to depression of the respiratory and later the circulatory
control centres. It is said that alcohol is in fact the most powerful depressant
of the central nervous system that is freely available without a doctor's
prescription.
Furthermore, it seems as if alcohol prolongs recovery time of the retinal response,
and this is probably due to a direct effect on the nerve cells of the retina.
In broad terms it can be said that the effect of alcohol on the highly developed
frontal cortical regions of the brain (responsible, inter alia, for conscious
thought) can be seen with blood-alcohol levels as low as 0,01%. This is
manifested through altered judgment, talkativeness and lack of attention
(Shaw: 1978).
Early behavioural effects are much modified by personality factors in theuser and by the environmental situation in which drink is taken. In livelycompany, disinhibition is the rule. The drinker becomes less self-conscious, more talkative and less discreet. Judgment and restraintrapidly go and there is loss of emotional control, giving rise to thehumorous observation that the super-ego is readily soluble in alcohol. Asthe blood level rises, thinking becomes slowed and superficial andlearning and retention become faulty. Less attention is paid to stimuli sothat internal stimuli such as hunger and pain are ignored, sometimes withdire consequences. It becomes more difficult to attend and respond toexternal stimuli. Events at the periphery are ignored and only theimmediate situation is given attention. This impaired psychological stateis usually accompanied by feelings of increased confidence and skill.
b Muscular system
The detrimental effect on muscle activity is due to poor control by the central
nervous system (and the decrease in impulse conduction and transmission)
over the use and co-ordination of muscle potential, rather than to any direct
impact on muscle strength itself.
11.4.5.2 Factors affecting pharmacological effect
The pharmacological effect of alcohol can be modified by a number of
congenital and acquired factors, which could partly account for the different
reactions of individuals to alcohol. One of these is the elimination rate.
Certain organic, functional and degenerative diseases could render the brain
cells or parts of the brain more susceptible to the intoxicating effect of
alcohol. Severe liver disease, such as alcoholic cirrhosis, can have a significant
effect on the distribution and elimination of drugs, including alcohol, and this
makes it difficult to predict how such a person will respond to alcohol or
drugs in any dosage.
11.4.5.3 Degrees of intoxication: clinical features
(See also Kemp 1986:29±31.)
The clinical features of alcoholic intoxication are mainly caused by its effect
on the intellect, voluntary movement, speech content, sensation, reflexes,
cardio-vascular and gastrointestinal function.
208
Study unit 11
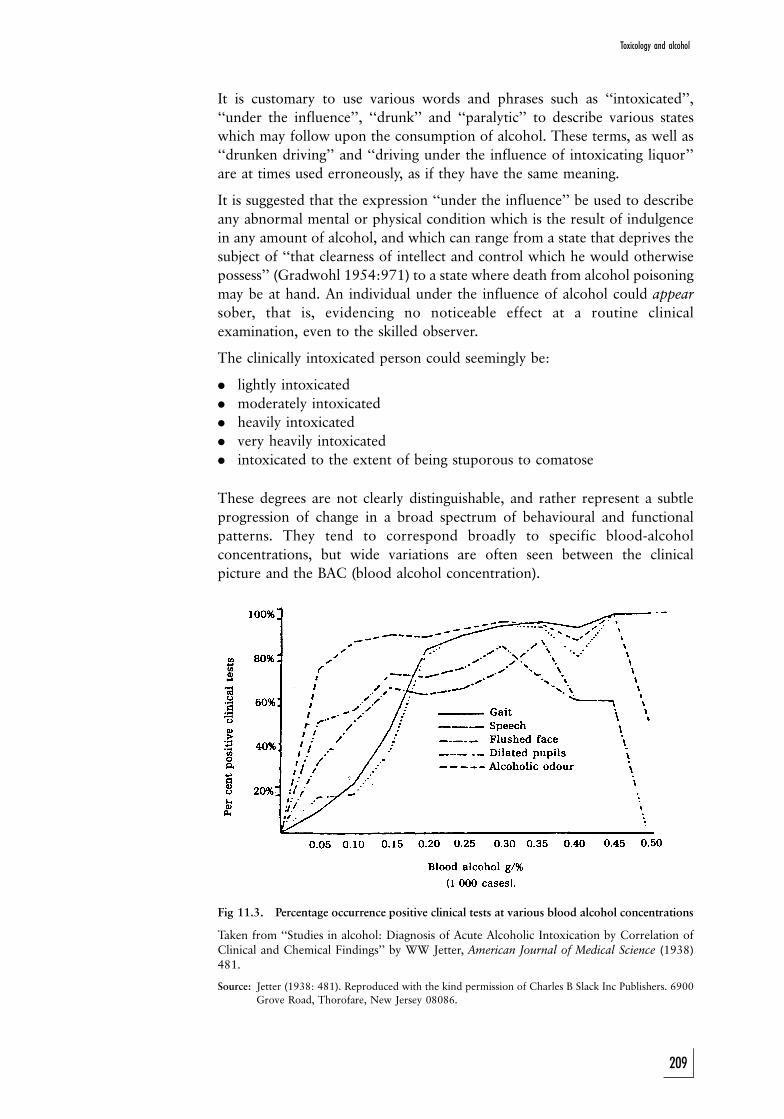
It is customary to use various words and phrases such as ``intoxicated'',
``under the influence'', ``drunk'' and ``paralytic'' to describe various states
which may follow upon the consumption of alcohol. These terms, as well as
``drunken driving'' and ``driving under the influence of intoxicating liquor''
are at times used erroneously, as if they have the same meaning.
It is suggested that the expression ``under the influence'' be used to describe
any abnormal mental or physical condition which is the result of indulgence
in any amount of alcohol, and which can range from a state that deprives the
subject of ``that clearness of intellect and control which he would otherwise
possess'' (Gradwohl 1954:971) to a state where death from alcohol poisoning
may be at hand. An individual under the influence of alcohol could appear
sober, that is, evidencing no noticeable effect at a routine clinical
examination, even to the skilled observer.
The clinically intoxicated person could seemingly be:
. lightly intoxicated
. moderately intoxicated
. heavily intoxicated
. very heavily intoxicated
. intoxicated to the extent of being stuporous to comatose
These degrees are not clearly distinguishable, and rather represent a subtle
progression of change in a broad spectrum of behavioural and functional
patterns. They tend to correspond broadly to specific blood-alcohol
concentrations, but wide variations are often seen between the clinical
picture and the BAC (blood alcohol concentration).
Fig 11.3. Percentage occurrence positive clinical tests at various blood alcohol concentrations
Taken from ``Studies in alcohol: Diagnosis of Acute Alcoholic Intoxication by Correlation ofClinical and Chemical Findings'' by WW Jetter, American Journal of Medical Science (1938)481.
Source: Jetter (1938: 481). Reproduced with the kind permission of Charles B Slack Inc Publishers. 6900
Grove Road, Thorofare, New Jersey 08086.
209
Toxicology and alcohol
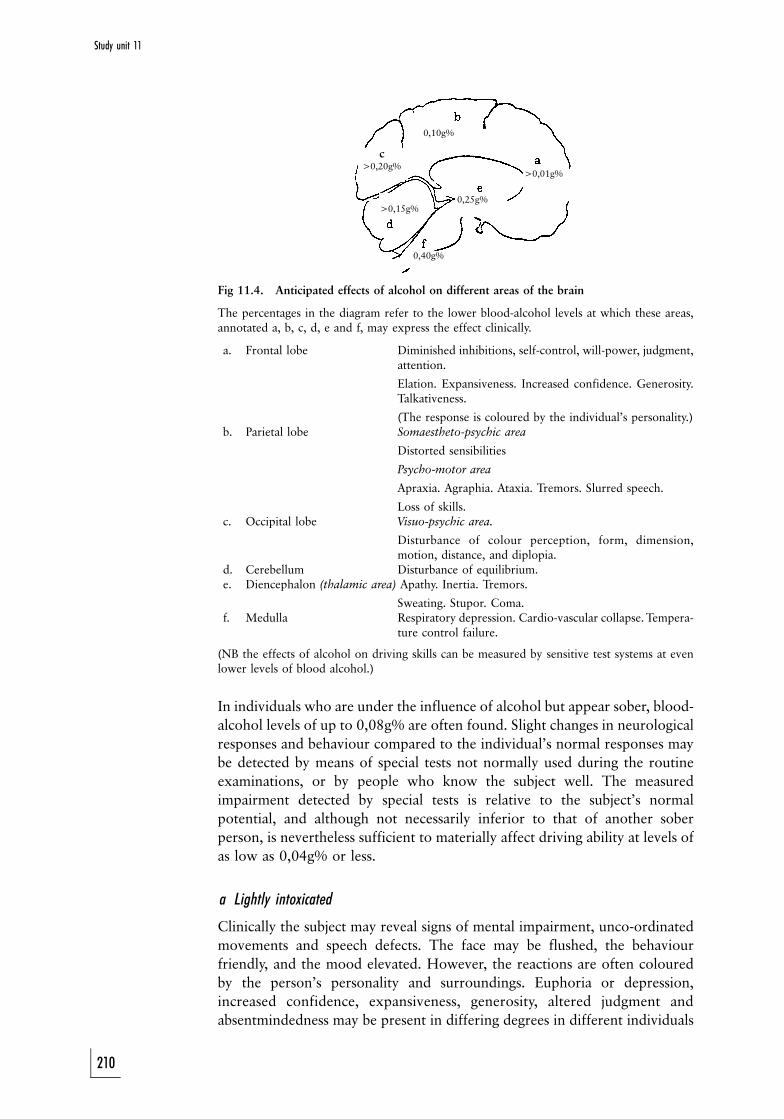
0,10g%
>0,01g%
0,40g%
>0,15g%
c>0,20g%
0,25g%
Fig 11.4. Anticipated effects of alcohol on different areas of the brain
The percentages in the diagram refer to the lower blood-alcohol levels at which these areas,annotated a, b, c, d, e and f, may express the effect clinically.
a. Frontal lobe Diminished inhibitions, self-control, will-power, judgment,attention.
Elation. Expansiveness. Increased confidence. Generosity.Talkativeness.
(The response is coloured by the individual's personality.)b. Parietal lobe Somaestheto-psychic area
Distorted sensibilities
Psycho-motor area
Apraxia. Agraphia. Ataxia. Tremors. Slurred speech.
Loss of skills.c. Occipital lobe Visuo-psychic area.
Disturbance of colour perception, form, dimension,motion, distance, and diplopia.
d. Cerebellum Disturbance of equilibrium.e. Diencephalon (thalamic area) Apathy. Inertia. Tremors.
Sweating. Stupor. Coma.f. Medulla Respiratory depression. Cardio-vascular collapse. Tempera-
ture control failure.
(NB the effects of alcohol on driving skills can be measured by sensitive test systems at evenlower levels of blood alcohol.)
In individuals who are under the influence of alcohol but appear sober, blood-
alcohol levels of up to 0,08g% are often found. Slight changes in neurological
responses and behaviour compared to the individual's normal responses may
be detected by means of special tests not normally used during the routine
examinations, or by people who know the subject well. The measured
impairment detected by special tests is relative to the subject's normal
potential, and although not necessarily inferior to that of another sober
person, is nevertheless sufficient to materially affect driving ability at levels of
as low as 0,04g% or less.
a Lightly intoxicated
Clinically the subject may reveal signs of mental impairment, unco-ordinated
movements and speech defects. The face may be flushed, the behaviour
friendly, and the mood elevated. However, the reactions are often coloured
by the person's personality and surroundings. Euphoria or depression,
increased confidence, expansiveness, generosity, altered judgment and
absentmindedness may be present in differing degrees in different individuals
210
Study unit 11

and in the same individual at different times at a given blood-alcohol level.
Clinical examinations generally reveal no other signs of impairment. Blood-
alcohol levels could reach 0,15g%. Subjectively the first noticeable changes
may be difficulty in visual accommodation and hearing, especially when these
functions are also impaired by disease or the ageing process. The first
movements to become visibly impaired are those requiring the greatest skill.
b Moderately intoxicated
Clinical examination generally reveals evidence of faculty impairment. The
mood becomes less self-critical, and behavioural changes, less tempered by
reason, tend to be accentuated and often accompanied by impulsive acts. The
person is more reckless but sometimes also more cautious. Unsteadiness when
standing, turning and walking may be present in varying degrees. Nystagmus
(an involuntary rapid movement of the eyeball) is usually present. The face is
often flushed and the eyes bloodshot. Blood-alcohol levels could reach
0,25g%, but generally range between 0,10 and 0,20g%.
c Heavily intoxicated
It is easy to detect functional impairment with this degree of intoxication.
Many aspects of behaviour are generally beyond self-control and self-
evaluation. The mind is dull and impairment of most faculties is obvious. The
faculties controlling the close co-ordination needed for walking and other
voluntary motor actions are markedly impaired. Staggering, slurred and thick
speech, the quality of which is shallow, confused and illogical, is present.
Movements are clumsy. Distance and position are misjudged. The subject may
attempt to conceal this impairment by performing tasks more slowly. Pain and
other sensations are dulled. Reflexes as tested clinically are depressed and
reaction time prolonged. The pupils become dilated and react sluggishly to
light. Co-ordination of eye movement is impaired. Balance is impaired. Heart
rate can increase. If nausea or vomiting is present, the subject could be pale.
Although intoxication is obvious to the observer, the cause may (as in all
degrees of intoxication) be difficult to determine. Blood-alcohol levels of up
to 0,30g% and very occasionally even higher are found.
d Very heavily intoxicated
There are confusion and disorientation with regard to both time and place,
apathy, drowsiness and marked disruption of both motor and functional co-
ordination. Confusion, disorientation and supressed sensibility, particularly
when accompanied by nausea and vomiting, could mask or resemble
underlying organic pathology. Blood-alcohol levels even in excess of 0,35g%
are found.
e Stuporous to comatose
It can be very difficult to determine the cause of the stupor or coma.
Unconsciousness, slow respiration, weak cardiac action and dilated pupils
with marked depression of all reflex reactions may be caused by many
different intoxicants and a great variety of diseases. Blood-alcohol levels of up
to 0,45g% and on rare occasions even higher may be found.
211
Toxicology and alcohol
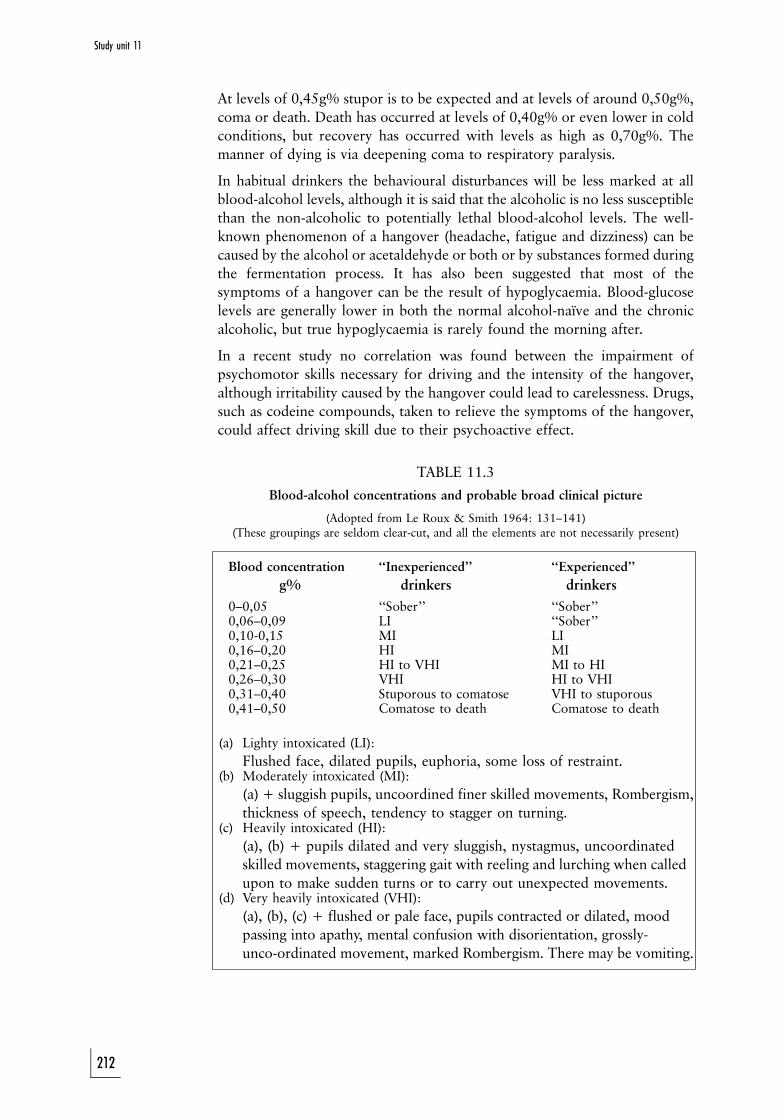
At levels of 0,45g% stupor is to be expected and at levels of around 0,50g%,
coma or death. Death has occurred at levels of 0,40g% or even lower in cold
conditions, but recovery has occurred with levels as high as 0,70g%. The
manner of dying is via deepening coma to respiratory paralysis.
In habitual drinkers the behavioural disturbances will be less marked at all
blood-alcohol levels, although it is said that the alcoholic is no less susceptible
than the non-alcoholic to potentially lethal blood-alcohol levels. The well-
known phenomenon of a hangover (headache, fatigue and dizziness) can be
caused by the alcohol or acetaldehyde or both or by substances formed during
the fermentation process. It has also been suggested that most of the
symptoms of a hangover can be the result of hypoglycaemia. Blood-glucose
levels are generally lower in both the normal alcohol-naõÈve and the chronic
alcoholic, but true hypoglycaemia is rarely found the morning after.
In a recent study no correlation was found between the impairment of
psychomotor skills necessary for driving and the intensity of the hangover,
although irritability caused by the hangover could lead to carelessness. Drugs,
such as codeine compounds, taken to relieve the symptoms of the hangover,
could affect driving skill due to their psychoactive effect.
TABLE 11.3
Blood-alcohol concentrations and probable broad clinical picture
(Adopted from Le Roux & Smith 1964: 131±141)(These groupings are seldom clear-cut, and all the elements are not necessarily present)
Blood concentration ``Inexperienced'' ``Experienced''
g% drinkers drinkers
0±0,05 ``Sober'' ``Sober''0,06±0,09 LI ``Sober''0,10-0,15 MI LI0,16±0,20 HI MI0,21±0,25 HI to VHI MI to HI0,26±0,30 VHI HI to VHI0,31±0,40 Stuporous to comatose VHI to stuporous0,41±0,50 Comatose to death Comatose to death
(a) Lighty intoxicated (LI):
Flushed face, dilated pupils, euphoria, some loss of restraint.(b) Moderately intoxicated (MI):
(a) + sluggish pupils, uncoordined finer skilled movements, Rombergism,
thickness of speech, tendency to stagger on turning.(c) Heavily intoxicated (HI):
(a), (b) + pupils dilated and very sluggish, nystagmus, uncoordinated
skilled movements, staggering gait with reeling and lurching when called
upon to make sudden turns or to carry out unexpected movements.(d) Very heavily intoxicated (VHI):
(a), (b), (c) + flushed or pale face, pupils contracted or dilated, mood
passing into apathy, mental confusion with disorientation, grossly-
unco-ordinated movement, marked Rombergism. There may be vomiting.
212
Study unit 11

11.4.6 The role of alcohol in unnatural deaths
According to the Fourth Annual Report of the National Injury Mortality
Surveillance System 2002, the blood-alcohol concentration was determined in
11 927 of the 32 227 cases. The average blood-alcohol concentration was
0,18 + 0,1 g/100 ml (g%).
Analysis of the different deaths in this report emphasises the important role of
alcohol in unnatural deaths. In 52,6% of the cases of manslaughter and
murder a positive blood-alcohol concentration with an average level of
0,17 g% was observed. In 52,3% of all transport-associated deaths a positive
level was found, with an average blood level of 0,19 g%. In 55,3% of all
drivers a positive blood-alcohol concentration with an average of 0,17 g%
was found. Approximately 60% of all pedestrians had a positive blood-
alcohol concentration with an average of 0,22 g%.
11.4.6.1 Alcohol and violent death
In line with the findings of Le Roux and Smith, it has now become almost
routine for blood to be drawn from the bodies of all persons over the age of
16 years who survived for less than 24 hours after a fatal injury.
During 1980 the blood of 1 617 bodies was sampled. Of these 1 510 had
died a non-natural death, and blood-alcohol tests in respect of 61% were
positive. An analysis of these deaths revealed that 41 persons had been driving
at the time of the accident which had caused their deaths, and that they had
died within one hour of the accident. Blood tests on 82% of them were
positive, and 70% had been driving with a blood-alcohol concentration
(BAC) in excess of 0,08%. Twenty-six per cent had probably been driving
with a BAC which had rendered them 25 times more likely to cause an
accident than when sober. Three of the 41 who had taken no alcohol were
involved in accidents in which the other driver had a BAC in excess of 0,15%.
Alcohol tests in respect of more than half the passenger fatalities and 62% of
pedestrian deaths were positive. In most cases levels were in excess of 0,20%.
About 73% of the 424 persons stabbed to death and about 63% of the 180
kicked or beaten to death had high blood-alcohol levels at the time of death.
In the case of the 61 drownings, 36 asphyxiations, and 128 firearm fatalities
62%, 50%, and 38% respectively were positive when tested for alcohol. The
findings for the other unnatural deaths were not significantly different.
Follow-up findings for the subsequent five years presented an essentially
similar picture.
11.4.6.2 Alcohol in drowning
a Possible factors leading to drowning
While the role of alcohol in the morbidity and mortality associated with
motor-vehicle and other accidents is virtually exclusively due to its effects on
the central nervous system, additional harmful physiological results could
213
Toxicology and alcohol
ensue in water. The effects of alcohol on the central nervous system must
certainly be accepted as one of the ways in which alcohol plays a role in
drowning.
There can be little doubt that when a person under the influence of alcohol
disregards pleas not to enter rough seas, alcohol not only influences his
decision to take such action but also reduces his awareness of the care
required to prevent an accident, and, finally, his capacity to save himself once
he is in difficulty.
Although the effects of alcohol on the central nervous system have been
documented very thoroughly, there is much less clarity regarding the effects
of alcohol on the cardiovascular system and temperature-regulating mechan-
isms of an immersed human body. Intoxicating doses produce a rise in pulse
rate, a fall in blood pressure, and cutaneous vasodilation with loss of body
heat and a fall in body temperature. The skin temperature rises and the
individual temporarily feels comfortably warm, even in cold surroundings.
The increase in skin temperature leads to an increase of the gradient between
the skin and the environmental temperature, thus causing hypothermia to
develop.
The thermal conductivity of water is about 1 000 times greater than that of
air at comparable temperatures. Alcohol ingestion and cold water immersion
should therefore produce an even more significant fall in body temperature.
There is little doubt that swimming hastens a fall in body temperature, so that
hypothermia develops more readily, and this in turn significantly hampers
swimming.
Exercise taken in the cold by normally healthy volunteers after the
consumption of only 25g alcohol showed a fall in the mean blood-glucose
concentration to 1,77 mmol/l. This was not observed when the same amount
of exercise was done without alcohol consumption. Therefore, any person
exercising strenuously in water while under the influence of alcohol could
develop hypoglycaemia that can lead to paralysis.
Alcohol therefore not only has an impact on the central nervous system but
probably also on the cardiovascular system and on glucose metabolism. All of
these facts must, we believe, be regarded as significant (either individually or
together) in a case of drowning.
ACTIVITIES
1. Which factors will influence the intensity of a reaction which a person
may experience after exposure to a specific drug or substance?
2. Discuss the effects of carbon monoxide on the physiological functions of
the human body.
3. Discuss the factors which may influence the absorption of alcohol from
the gastro-intestinal tract.
4. The legally acceptable blood-alcohol level is 0,05 g%. Does any risk of
danger and even death exist at a blood-alcohol concentration lower than
this legal limit?
5. An 80 kg female is arrested for alleged driving under the influence of
alcohol. Her blood-alcohol concentration is 0,14 g%. She alleges that she
214
Study unit 11
consumed three glasses of white wine, the last one two hours before
arrest. How will you confirm or refute her statement regarding alcohol
consumption?
6. How will the alcohol level of a deceased driver in a fatal motor accident
be determined?
FEEDBACK
1. These factors are best represented by a functional formula:
IR = D rA SPrE
Please see the text for a discussion of this formula, which may be
used for any drug or poison, including alcohol.
2. Carbon monoxide has the following effects:
(a) It binds with haemoglobin in the red blood cells. Subsequently
there is a decrease in the available haemoglobin for oxygen
transport, and anaemic hypoxia occurs.
(b) It has a direct depressing effect on the brain, similar to
anaesthetic drugs. It therefore causes depression of respiration.
(c) Carbon monoxide also combines with the enzyme systems in the
cells involved with cell metabolism (the cytochrome-oxydase
system). This results in cytotoxic anoxia/hypoxia.
3. Numerous factors influence alcohol absorption. See section
11.4.2.1.
4. Even at alcohol levels as low as 0,05 g%, depression of certain brain
functions that control the personality and inhibitions occurs. A false
feeling of self-confidence may increase the risk getting involved in a
fight that can be fatal. Interestingly, some studies show that there is a
decline in the risk for motor-vehicle accidents at levels less than
0,05 g%. This is most probably because these individuals will drive
more carefully and with more concentration, because they may be
afraid that their abilities are already affected by the alcohol.
5. The Widmark formula can be used to calculate the minimum
amount of alcohol, which in this specific case will result in an
alcohol level of 0,14 g%. As two hours had already passed, it can be
accepted that all the ingested alcohol had been absorbed.
A = p 6 c 6 r 6 10
A = 80 kg 6 0,14 g% 6 0,6 6 10
A = 67,2 g
She therefore consumed at least 7 units of alcohol. Although this
formula is a rough indication, it is obvious that her defence cannot
be upheld.
6. Eye fluid or venous blood may be used. The latter must be obtained
as far as possible from the heart, preferably from the thigh or
femoral vein. Cardiac blood is not acceptable. It must be preserved
in sodium fluoride to eliminate any changes due to decomposition
and therefore alcohol production or metabolism.
215
Toxicology and alcohol

STUDY UNIT 12Pregnancy-associated deaths
Contents
12.1 Causes of maternal death
12.1.1 Abortion
12.1.2 Lung embolism
12.1.3 Amniotic fluid embolism
12.1.4 Injuries and infection
12.1.5 Pre-eclampsia and eclampsia
12.1.6 Abnormalities of the placenta
12.1.7 Ectopic pregnancy
12.1.8 Pre-existing diseases
Activities
Feedback
LEARNING OUTCOMES
When you have completed this study unit, you should
. understand the basic classification of abortions (spontaneous vs
induced)
. be able to discuss the most important complications of induced
abortion
. be able to discuss other causes of maternal death during pregnancy
Please also see study unit 6.
The maternal and perinatal mortality rate is proof of the level of development of
a country, and it also reflects the availability and efficiency of the medical
services of such a country. Maternal mortality is the death of a mother during the
pregnancy, the labour process or the puerperium (ie within 42 days after giving
birth). The interval of 42 days is used, as it takes approximately 6 weeks for the
body of a post-pregnancy female to return to the non-pregnant condition.
12.1 Causes of maternal death
12.1.1 Abortion
Abortion is the expulsion of the product of conception, and specifically the
foetus, from the uterus. According to the Births and Deaths Registration Act
51 of 1992 a foetus of less than 6 months, in other words 26 weeks, is not
considered to be viable. Any foetus expelled before a gestational period of 26
weeks is thus by definition an abortion. It is, however, important to realise
that with the help of modern medical technology such a foetus (or rather
216
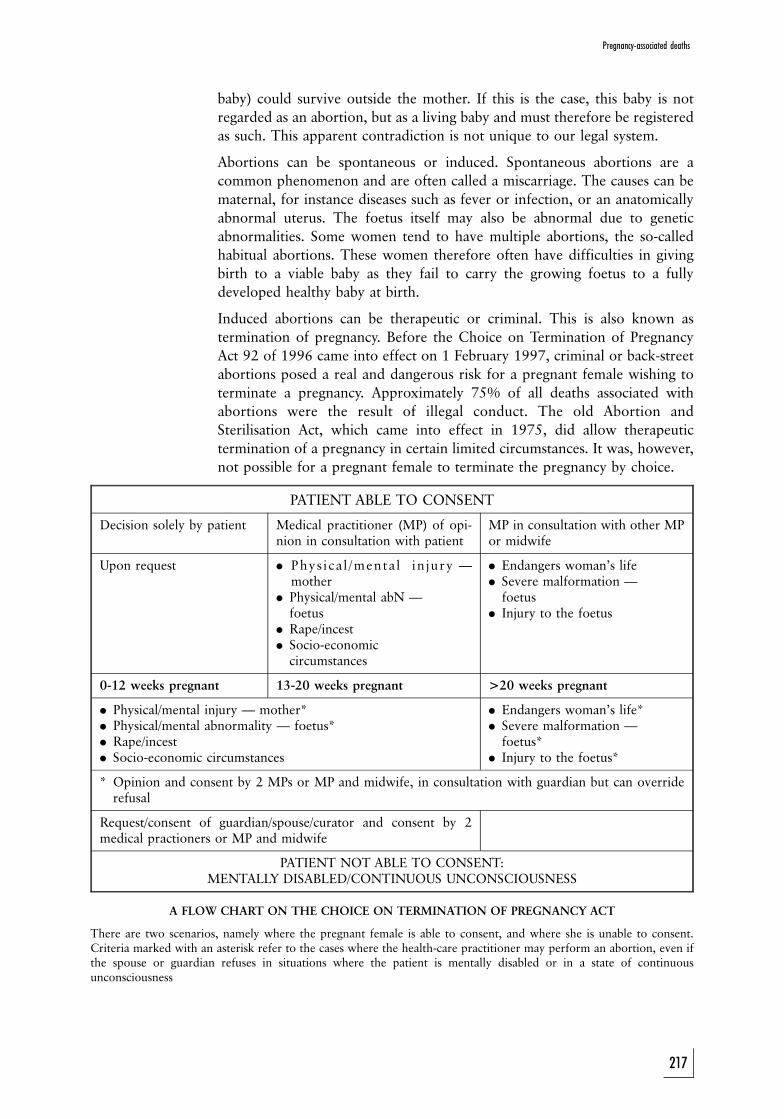
baby) could survive outside the mother. If this is the case, this baby is not
regarded as an abortion, but as a living baby and must therefore be registered
as such. This apparent contradiction is not unique to our legal system.
Abortions can be spontaneous or induced. Spontaneous abortions are a
common phenomenon and are often called a miscarriage. The causes can be
maternal, for instance diseases such as fever or infection, or an anatomically
abnormal uterus. The foetus itself may also be abnormal due to genetic
abnormalities. Some women tend to have multiple abortions, the so-called
habitual abortions. These women therefore often have difficulties in giving
birth to a viable baby as they fail to carry the growing foetus to a fully
developed healthy baby at birth.
Induced abortions can be therapeutic or criminal. This is also known as
termination of pregnancy. Before the Choice on Termination of Pregnancy
Act 92 of 1996 came into effect on 1 February 1997, criminal or back-street
abortions posed a real and dangerous risk for a pregnant female wishing to
terminate a pregnancy. Approximately 75% of all deaths associated with
abortions were the result of illegal conduct. The old Abortion and
Sterilisation Act, which came into effect in 1975, did allow therapeutic
termination of a pregnancy in certain limited circumstances. It was, however,
not possible for a pregnant female to terminate the pregnancy by choice.
PATIENT ABLE TO CONSENT
Decision solely by patient Medical practitioner (MP) of opi-nion in consultation with patient
MP in consultation with other MPor midwife
Upon request . Phys i ca l /menta l in jury Ðmother
. Physical/mental abN Ðfoetus
. Rape/incest
. Socio-economiccircumstances
. Endangers woman's life
. Severe malformation Ðfoetus
. Injury to the foetus
0-12 weeks pregnant 13-20 weeks pregnant >20 weeks pregnant
. Physical/mental injury Ð mother*
. Physical/mental abnormality Ð foetus*
. Rape/incest
. Socio-economic circumstances
. Endangers woman's life*
. Severe malformation Ðfoetus*
. Injury to the foetus*
* Opinion and consent by 2 MPs or MP and midwife, in consultation with guardian but can overriderefusal
Request/consent of guardian/spouse/curator and consent by 2medical practioners or MP and midwife
PATIENT NOT ABLE TO CONSENT:MENTALLY DISABLED/CONTINUOUS UNCONSCIOUSNESS
A FLOW CHART ON THE CHOICE ON TERMINATION OF PREGNANCY ACT
There are two scenarios, namely where the pregnant female is able to consent, and where she is unable to consent.Criteria marked with an asterisk refer to the cases where the health-care practitioner may perform an abortion, even ifthe spouse or guardian refuses in situations where the patient is mentally disabled or in a state of continuousunconsciousness
217
Pregnancy-associated deaths
A therapeutic abortion is associated with relatively low risk for the mother.
The sooner it is performed, the lower the risk. Criminal abortions, however,
have a very high risk, and numerous cases of death of the mother used to
occur. This was also one of the main reasons why the statutory grounds were
broadened and the procedure simplified.
The most important complications of a criminal abortion are:
1. local inflammation and infection, sometimes complicated by septic shock
2. haemorrhage, followed by hypovolaemic shock
3. neurogenic (nerve) shock, inter alia due to dilatation of the cervix
4. venous air embolism (see study unit 6)
5. the toxic effect of the solutions used to induce the abortion, for instance
soapy solutions
6. amniotic fluid embolism (see study unit 6)
Although the incidence of death due to criminal abortions has decreased since
1997, criminal abortions are still a real problem. Any female of child-bearing
age who dies suddenly and unexpectedly, must be regarded as pregnant, and
therefore a possible victim of a failed abortion attempt, until proven
otherwise.
12.1.2 Lung embolism
Lung or pulmonary embolism because of a blood clot (embolus) is a risk
during pregnancy and in the puerperium (the period following termination of
pregnancy). Risk factors include operative intervention, for example
caesarean section, or other trauma during delivery, high maternal age, obesity
and any other reason causing the mother to be immobilised for a period of
time.
12.1.3 Amniotic fluid embolism
Amniotic fluid embolism also occurs in full-term patients. It often occurs in
older females who have precipitous labour (ie where birth is given rapidly).
This condition is discussed in study unit 6.
12.1.4 Injuries and infection
After delivery blood loss due to injuries to the genital tract may also result in
the demise of the patient if not aggressively managed. Infection is also a risk
and puerperal sepsis could develop. As indicated above, criminal abortions are
often complicated by infection or sepsis.
12.1.5 Pre-eclampsia and eclampsia
Pregnant women can also die due to conditions unique to pregnancy. With
pre-eclampsia there is high blood pressure (hypertension), oedema and
protein in the urine. If the patient develops convulsions or epileptic fits, it is
known as eclampsia. These patients also have a risk of intracranial
haemorrhages (bleeding inside the skull).
218
Study unit 12
12.1.6 Abnormalities of the placenta
Two conditions which may threaten the life of the mother and the foetus are
associated with the placenta.
Late in pregnancy the placenta can become detached from the uterine wall.
Blood-clot abnormalities can develop, and death could follow. If the baby is
not delivered immediately, both the mother and baby could die. This
condition is known as abruptio placentae. In placenta praevia the placenta is
in a low-lying position. With the onset of labour the cervix or the neck of the
uterus dilates. The placenta can then become detached from the uterine wall,
causing possible death of the mother and foetus.
12.1.7 Ectopic pregnancy
Ectopic pregnancy is a condition where the foetus does not develop in the
uterine cavity, but on the outside, often in one of the Fallopian tubes. When
this thin-walled tube ruptures, it could cause haemorrhage into the abdominal
cavity, which could be fatal.
12.1.8 Pre-existing diseases
Pregnancy affects the female body in a number of ways. It inter alia affects the
haemodynamics (circulation and heart). This hyperdynamic circulation
induced by the pregnancy in a female with pre-existing heart diseases (eg
valvular abnormalities) may cause complications and even death.
ACTIVITIES
1. A young female undergoes a criminal abortion and dies during the
procedure. Discuss the possible causes of her death. Discuss also how a
post-mortem examination may be of assistance in determining the cause
of death.
2. A pregnant female in her last trimester of pregnancy dies suddenly and
unexpectedly. Which possibilities must be considered?
FEEDBACK
1. When a woman dies due to a criminal abortion it must be
remembered that certain causes will result in instant death, that is
during the procedure. Other causes will only present at a later stage.
These latter causes include conditions such as local inflammation or
infection, as well as the toxic effects of the drugs used to induce the
abortion.
Conditions where the death occurs during the procedure includes
haemorrhage due to hypovolemic shock, neurogenic shock due to
dilatation of the cervix, venous air embolism as well as amniotic
fluid embolism.
One of the primary aims of the post-mortem examination is to
exclude the above conditions. X-rays of the abdomen and chest may
be of assistance to establish the presence of air in the vascular
219
Pregnancy-associated deaths

system. The post mortem must also be performed in such a way that
air embolism can be excluded. This technique is discussed in more
detail in study unit 6.
A detailed examination of the genital system is necessary to identify
any damage to large blood vessels causing a fatal haemorrhage.
Amniotic fluid embolism can be excluded by histological assessment
of lung tissue. Amniotic fluid elements may be detected in the
maternal vessels.
Neurogenic shock can only be determined after exclusion of other
causes of sudden collapse and death.
2. Causes of death in a pregnant female during the last trimester of
pregnancy include conditions such as pre-eclampsia and eclampsia,
abnormalities of the placenta (abruptio placentae and placenta
praevia Ð see text for discussion of these conditions-), pulmonary
or lung embolism and any other pre-existing disease, for instance
heart disease, which are complicated by the pregnancy. Amniotic
fluid embolism, injuries and infections usually follow as a
complication of pregnancy or in the post-partum period. An
undiagnosed ectopic pregnancy seldom occurs in a third trimester
pregnancy, but may cause sudden death in the first trimester.
220
Study unit 12
STUDY UNIT 13Paediatric forensic pathology
Contents
13.1 Introduction
13.2 Infanticide and concealment of birth
13.2.1 Definitions and statutory provisions
13.2.2 Medico-legal problems
13.2.3 Case study
13.3 The battered-baby syndrome (Caffey's syndrome or non-accidental
injury syndrome)
13.3.1 Description
13.3.2 Injuries
13.3.3 Obligation to report: medical practitioners and other profes-
sionals
13.4 Sudden infant death syndrome (SIDS or cot-death)
13.4.1 Incidence
13.4.2 Predisposing factors
13.4.3 Appearance
Activities
Feedback
Learning outcomes
When you have completed this study unit, you should be able to
. name the different stages in the development of a baby and child and
the most important causes of death at each of these stages
. discuss the medico-legal problems regarding the alleged conceal-
ment of death
. discuss the non-accidental injury syndrome
. discuss unexpected deaths in babies, including cot deaths
13.1 Introduction
Many medico-legal problems arise when children die from what appears to be
unnatural causes. In the foetal period, mutations and developmental defects
arising from viral infections, drug abuse, medication and anoxic states in the
mother, as well as failed attempts to induce abortion, may become the subject
of litigation involving the medical practitioner, the pharmaceutical industry
and diagnostic laboratory personnel. During the neonatal period problems
221
can relate to stillbirth, viability, birth injuries, ``infanticide'', concealment of
birth and abandonment, as well as establishment of paternity in cases of
suspected nursery identification errors.
Infancy, representing life between 28 days and one year Ð an arbitarily
decided time interval Ð is a period where sudden, unexpected infant death
assumes disturbing proportions. From one to three years the toddler is at a
stage where accidental poisoning by medicines, household poisons and plant
toxins, drowning in a swimming-pool, falls, aspiration of foreign bodies,
motor-vehicle accidents and child abuse occur.
As the child passes into the pre-school age (four to five years) and school age
(five to ten years) and starts moving about relatively unprotected in the new
environment, transport accidents, drowning, burns and firearm injuries take
on greater significance.
During pre-adolescence (ten to twelve years) and adolescence (twelve to
eighteen years) accidents become even more significant, as do sport injuries,
alcohol and drug abuse, suicides and (as adulthood approaches) aberrations in
sexual behaviour.
13.2 Infanticide and concealment of birth
During the neonatal period most medico-legal problems relate to infanticide,
concealment of birth, and identity.
13.2.1 Definitions and statutory provisions
The medico-legal investigation of suspected infanticide and concealment of
birth will inter alia be influenced by the provisions of the Births and Deaths
Registration Act 51 of 1992, the Criminal Procedure Act 51 of 1977, and the
General Law Amendment Act 46 of 1935.
13.2.1.1 Definitions (s 1 of Act 51 of 1992)
``Birth'' in relation to a child means the birth of a child born alive.
``Still-born'', in relation to a child, means that it has had at least 26 weeks of
intra-uterine existence but showed no sign of life after complete birth, and
``stillbirth'' in relation to a child, has a corresponding meaning.
13.2.1.2 Other statutory provisions
` At criminal proceedings at which an accused is charged with the killing of a
newly-born child, such child shall be deemed to have been born alive if the
child is proved to have breathed, whether or not the child had an independent
circulation'' (s 239(1) of Act 51 of 1977).
` At criminal proceedings at which an accused is charged with the concealment
of the birth of a child, it shall not be necessary to prove whether the child died
before or at or after birth'' (s 239(2) of Act 51 of 1977).
` Any person who disposes of the body of any child with intent to conceal the
fact of its birth, shall be guilty of an offence'' (s 113(1) of Act 46 of 1935).
222
Study unit 13

13.2.2 Medico-legal problems
In cases of alleged infanticide or concealment of birth, it is necessary to
establish the following:
1. whether the infant was viable (ie its uterine age)
2. whether it had lived (ie whether it had breathed)
3. if it had lived, for how long
4. what the cause of death was
5. how long it had been dead when found
6. whether it could be identified as belonging to a particular mother (ie by
virtue of identity and evidence in the mother of a recent birth, compatible
with the age of the infant)
7. if stillborn, why it had not lived (ie cause of death)
Whereas the mass and length of the newborn infant can be used only for an
approximation of the uterine age, the presence and size of the centres in the
lower end of the femur and in the calcaneum (heel bone) and talus (ankle
bone) are a reliable measure of the uterine age from the fifth to the ninth
month (see photographs 41 and 44).
To establish whether the child breathed or not (besides general appearance,
photographs 46), the hydrostatic test is applied to the lungs. This involves
testing whether the lungs or portions of them float when immersed in water.
The inference here is that air breathed after birth is responsible for this
flotation.
This is a valid conclusion only if it can be established that putrefaction gases
did not cause flotation. By applying pressure to the portions of lung that float
the putrefaction gases are readily displaced, in contrast to air trapped in the
minute alveolae (lung pockets). This method of establishing whether the child
breathed is not reliable in the case of advanced putrefaction. Where the
newborn's lungs expanded fully, the appearance of the lungs as they fill the
chest cavity or confirmation from the microscopic picture is sufficient
evidence to justify the finding of a live birth. During the first few hours of life
the changes which are observable at the place of attachment of the umbilical
cord to the child's belly may assist in determining inter alia the duration of
life. The presence of breast secretions in the stomach are also indicative of live
birth. The presence of air in the middle ears confirms that the baby swallowed
and therefore was alive Ð air can only reach the middle ear cavity by entering
the cavity via the Eustachian tubes during the process of active swallowing.
See photograph 46 for the appearance of the lungs of a newborn.
13.2.3 Case study
The body of a newborn infant wrapped in newspaper (date of issue
decipherable) was found two days after the newspaper date.
At the post-mortem examination the body was free of vernix caseosa (the fatty
substance covering the foetal skin), 44 cm in length and 3 kg in mass. The
umbilical cord had been cleanly cut and tied, but revealed no observable
changes. Ossification centres were present in the calcaneum, talus and lower
end of the femur. The stomach was empty, and the lungs filled the pleural
223
Paediatric forensic pathology

cavity. The lungs floated in water before and after the pressure test. The
bronchial tree contained an abundance of markedly frothy fluid with a
fragrant odour. A sample of this fluid was taken for chemical analysis, and a
sample of infant blood for grouping.
The suspect mother was apprehended a week later, and on clinical
examination showed evidence of having recently given birth. In her room
at the address where she was employed as a domestic help a packet of
detergent powder was found, which chemically matched the fluid sample
taken at the post-mortem examination. Later the mother confessed that the
infant had cried after birth, that she had tied and cut the umbilical cord, and
that then, a little later, she had tried to bath the baby, which was fouled with
meconium, in a small bath of water to which she had added some of the
detergent powder. The baby had slipped from her hands into the bath and,
despite being promptly removed, had shortly thereafter ``choked'' and died.
Overcome by fear, she had attempted to dispose of the body.
13.3 The battered-baby syndrome (Caffey's syndrome or non-accidentalinjury syndrome)
13.3.1 Description
Violence against infants and children is as old as recorded history. Infanticide
was an accepted practice for dealing with unwanted children in prehistoric
and ancient cultures in the face of scarce resources. Darwin actually said that
one could correlate the beginning of human civilisation with infanticide.
``Our early semi-human progenitors would not have practised infanticide ... .
For the instincts of the lower animals are never so perverted as to lead them
regularly to destroy their own offspring''.
We now know that the first medical article on child abuse was written in Paris
in 1860 by Ambroise Tardieu, a professor of legal medicine. He reported on
autopsies of 32 children who had died violently, mainly at the hands of their
parents. Tardieu's article described the same medical lesions (multiple injuries
and traumatic lesions of skin, bone, and brain) and the same demographic and
social factors (the perpetrators were generally the parents who had
contradictory explanations for the injuries) as Kempe et al described more
than a hundred years later.
In 1946 the father of paediatric radiology, John Caffey, described six cases of
multiple fractures in the long bones of infants who had chronic subdural
haematomas Ð classic signs of physical abuse. At one time he stated that a
clotting defect as yet unrecognised was responsible for this phenomenon.
Caffey noted that there was no X-ray evidence of any underlying pathological
bone condition in these children, that subdural haematomas were best
explained by trauma, and that the bone lesions were traumatic in nature,
adding: ``[T]he injuries which caused the fractures in the long bones of these
patients were either not observed or were denied when observed. The motive
for denial has not been established.'' Dr Caffey believed that these children
were victims of inflicted injury but was concerned about legal repercussions.
In 1956 Caffey further made a statement which was in line with our thinking
224
Study unit 13
about child abuse in a speech before the congress of the British Institute of
Radiology by urging early diagnosis to save abused children from further
injury: ``The correct early diagnosis of injury may be the only means by which
the abused youngsters can be removed from their traumatic environment and
their wrongdoers punished.''
Dr Kempe wrote as follows:
``My involvement in child abuse was at first far from humane; it was,
candidly, intellectual, at least in part. Day after day, while making rounds
at the University of Colorado Medical School, I was shown children
with diagnoses by residents and by consultants and attending physicians
which simply were examples of either ignorance or denial. I thought
very much the latter. I was shown children who had thrived for seven
months and then developed `spontaneous subdural haematoma' ...
`multiple bruises of unknown aetiology' in whom all tests were normal,
who had no bleeding disorders and who did not bruise in the ward even
when they fell; `osteogenesis imperfecta tarda' ... in kids who had
normal bones by X-ray, except that they showed on whole-body X-ray
many healing fractures which could be dated; `impetigo' in kids with
skin lesions which were clearly cigarette burns; `accidental burns of
buttocks' in symmetrical form which could only occur from dunking a
child who had soiled into a bucket of hot water to punish soiling. In
these cases and many others, we did often learn from one or both
parents, in time and with patient and kindly approaches, that these were
all inflicted accidents or injury.''
Thanks to Drs Kempe and Caffey, the public as well as the medical profession
became aware that child abuse is a common problem and can occur in families
of any socio-economic status. Health professionals are generally cognisant of
the forms abuse takes, the causative factors, and the potentially lethal nature
of this ``disease'' of parenting.
We now understand that physical abuse requires four basic factors:
1. There is a parent with the potential for abuse. Such parents were usually
not parented well themselves, often were themselves victims of abuse, are
isolated, do not trust others, and have unrealistic expectations of
children.
2. There is a child who usually exhibits ``some behaviour ... which the
parent, correctly or incorrectly, justifiably or unjustifiably, perceives as
aversive and as requiring some intervention to change''.
3. There is a stressful situation or incident that serves as a trigger.
4. The family lives in a culture in which corporal punishment is sanctioned
or encouraged.
In one sense all parents have the potential to abuse, but most of us keep our
murderous inclinations in check because we have impulse control, inner
resources, and support systems.
The so-called ``battered baby'' or Caffey syndrome is associated with young
children who cannot give verbal evidence of the events.
The story of each case is so similar as to be almost a carbon copy of the other.
225
Paediatric forensic pathology
A child is taken to the doctor or hospital, and found to be injured or dead. In
the event of death, there may be a subdural haematoma with or without a
fracture of the skull, or there may be a fracture of a long bone or of the ribs,
and often multiple bruises on the trunk and head. A common explanation is
that the child sustained the injuries as a result of some accident, such as falling
from a table, or that ``it bruises easily''. What is usually significant is the
length of time which elapsed between the ``accident'' and the seeking of
medical assistance. This is often a clue to the situation, because the behaviour
of a normal parent is to seek help at once in case of any serious injury. In
many of the ``battered-baby'' cases some hours may have elapsed, possibly
spent in ``hoping for the best'' or thinking up an excuse.
The injuries usually follow a pattern: one or more localised bruises on the
head, quite inconsistent with a simple fall, apart from their severity; bruises
on the chest and face and sometimes on the trunk and limbs, consistent with
grip marks. If the doctor is alert he will arrange for a full X-ray examination
of the child. This may show other injuries such as fractured ribs or long bones,
or epiphyseal separations of different ages, of which some have closed again.
Further questioning will usually reveal that medical assistance was sought on
previous occasions quite commonly at some other hospital. Inevitably the
parents deny that they hit the child, although they may admit to one slap.
Often only one of the parents was present when the incident occurred. One
or both parents are usually of low intelligence, and the child is most
commonly the first or, if not, the youngest. If not illegitimate, the child will
usually be found to be not really ``wanted'' because the pregnancy was
accidental, the child interfered with freedom of movement or earning
capacity, or there are already too many children in the family. The child often
appears well cared for; the acts of violence are intermittent. The violence
could be the result of sudden loss of temper due to provocation by the crying
or disobedience when the parent was tired or worried.
In 1967 Simpson (Currie 1970: 635) defined the battered-child syndrome
according to six characteristics:
1. Infants, usually of two to three years of age, are subjected to
2. persistent or repeated violence at the hands of
3. either or both parents or guardians who
4. either fail to report Ð or delay reporting Ð the injuries they are aware
of, and who
5. affect ignorance or lie; offering a simple explanation for the injuries, and
who are usually
6. inadequate, subnormal or simple, but seldom under medical care.
We have to distinguish between the battered child and the neglected child, the
exploited child, the deprived child and the murdered child, although there is a
considerable overlap.
Out of a total of 208 battered children reported, 83% were three-year-olds or
younger and 36% were younger than six months. This is because children
older than 3 years can run away or tell others what happened to them.
226
Study unit 13

13.3.2 Injuries
13.3.2.1 Head injuries
When an infant falls from a table, hospital trolley, or bed (even onto a hard
floor) he is unlikely to sustain a fracture of the skull, and is almost certainly
assured of escaping major intracranial injury. Falls from greater heights
(between 1 and 2 meters), for example from a standing adult's shoulder, may
result in a single linear parietal hairline fracture of the skull. Serious
intracranial injury is extremely unlikely.
The force used in physical abuse, for example when swinging a child's head
against a wall, is so much greater that the pattern of injury is different.
Fractures are more likely to be extensive, multiple, depressed, involving
several individual skull bones. The occipital bone and base of the skull, which
are hardly ever fractured in simple falls, are common sites of injury. Children
who were shaken but who did not suffer blunt trauma to the head will have
no fracture but may share a similar pattern of intracranial injury to that
associated with acceleration/deceleration forces. The neck muscles of small
children are inadequately developed to support the relative heavy head when
they are shaken. There is often an associated brain injury in a child with a
head injury caused by physical abuse. Unexplained neurological deficit,
seizures, apnoeic attacks (inability to breathe), hydrocephalus and raised
intracranial pressure may be manifestions of child abuse.
a Subdural haematoma
Subdural haematoma in an infant that cannot be explained satisfactorily,
strongly suggests physical abuse, such as violent shaking. A simple fall is not
sufficient to explain such an injury. There is often no accompanying fracture,
and the haematoma arises from disrupted bridging veins spanning the surface of
the brain to the dura. The presentation may be immediate or delayed, with fits,
poor feeding, lethargy, drowsiness, or rapidly developing unconsciousness.
b Cerebral contusion, haemorrhage, and oedema
(Hobbs 1985:1169-1170)
Cerebral contusion, haemorrhage, and oedema are responsible for most of
the deaths and long-term illnesses resulting from physical abuse. Neurological
deficit after widespread neuronal damage from repeated shaking, parallels the
punch-drunk syndrome of professional boxers. Intraventricular haemorrhage
can present as late secondary hydrocephalus (an accumulation of fluid in the
skull). Focal or generalised convulsions may be a further sign of cerebral
injury.
c Retinal haemorrhages
Like subdural haematoma, the presence of retinal haemorrhage without
adequate explanation should create a strong suspicion of physical abuse.
However, this is not the case in the newborn. A short-term rise in intracranial
pressure Ð for example, after shaking Ð is responsible for the increased
pressure in the central retinal vein, causing retinal haemorrhages.
227
Paediatric forensic pathology
13.2.2.2 Bone fractures
These fractures are often of different ages and involve the ribs and long
bones.
13.3.2.3 Skin wounds
Most of the injuries will be caused by the hands of the adult, and contusions
due to the child having been slapped or marks due to grasping may be
present. The latter typically has a round or oval-shaped appearance and
appear on the upper arms and torso. Injuries caused by burning cigarettes may
also be present.
13.3.3 Obligation to report: medical practitioners and other professionals(Child Care Act 74 of 1983, s 42)
Every dentist, medical practitioner, nurse or social worker who examines or
deals with any child in circumstances giving rise to the suspicion that that
child has been ill-treated, or suffers from any injury, single or multiple, the
cause of which probably might have been deliberate, or suffers from a
nutritional deficiency disease, shall immediately notify the Director-General
of Health or any officer designated by him for the purposes of this section of
those circumstances.
On receipt of a notification in terms of subsection (1) the Director-General or
the said officer may issue a warrant in the prescribed form and manner for the
removal of the child concerned to a place of safety or a hospital.
The Director-General or the said officer shall thereupon arrange that the
child and his parents receive such treatment as the Director-General or the
said officer may determine.
This section shall not exclude any other action against or treatment of the
parent and his child in terms of this Act.
Any dentist, medical practitioner or nurse who contravenes any provision of
this section shall be guilty of an offence.
No legal proceedings shall lie against any dentist, medical practitioner, nurse
or social worker in respect of any notification given in good faith in
accordance with this section.
13.4 Sudden infant death syndrome (SIDS or Cot death)
This condition is defined as the sudden and unexpected death of a baby,
usually between 1 month and 1 year of age, who was clinically healthy before
the death or may have suffered from a mild or trivial disease or ailment, like
fever or upper respiratory tract infection. A complete post-mortem
examination, including histology and other relevant laboratory examinations,
fails to identify an obvious cause of death.
Because the death is unexpected and without obvious cause, it must be dealt
with according to the Inquests Act 58 of 1959. It is only after a post-mortem
examination has been performed, and other causes, like violence, have been
228
Study unit 13
excluded, that the death can be regarded as natural. After other obvious
morphological and even biochemical and microbiological causes of death
have been excluded, the death can be attributed to this syndrome (sudden
infant death syndrome or SIDS). This will therefore exclude conditions like
pneumonia or congenital heart abnormalities.
13.4.1 Incidence
It is the most common cause of death in developed countries in babies 28 days
to 1 year old. It involves approximately 2,3 babies per 1 000 live births in the
USA. In the United Kingdom the incidence is 3 per 1 000 live births.
13.4.2 Predisposing factors
1. Age. It occurs between the ages of 1 month and 2 years, with most deaths
between 2 months and 7 months. There is a peak at 3 months. True SIDS
does not occur in the neonatal period and is rare before the age of 1
month. There are exceptions, namely premature and low birth-weight
babies.
2. Sex. Females babies are more prone, with a ratio of 1,3:1.
3. Twins. Twins are twice as prone due to the higher incidence of
prematurity and low birth weight.
4. Seasonal distribution. Most cot deaths occur in the colder and wetter
months. Although attempts have been made to correlate the incidence of
SIDS with temperature changes and respiratory infection, the results are
contradictory. However, it has been proven that respiratory infections are
indeed a precipitating factor for SIDS.
5. Social status. There is a higher incidence in the lower socio-economic
group.
6. Other factors. Maternal factors:
Ð smoking and drug abuse
Ð anaemia
Ð urinary tract infections/venereal disease during pregnancy
Ð multiple pregnancies (twins)
Ð previous complications of pregnancy (prematurity, still-born babies
and miscarriage)
Ð a young mother, especially younger than 20 years
Ð poor antenatal clinic attendance
Ð limited education (no secondary school education
Ð short intervals between pregnancies (less than 6 months)
Ð sub-optimal weight increase during pregnancy
Child-related factors:
Ð prematurity
Ð low birth weight
Ð poor general condition at birth
Ð female babies (see above)
Ð twins (see above)
Ð lengthy stay in hospital
Ð poor postnatal clinic attendance
229
Paediatric forensic pathology
Ð poor weight increase
Ð babies who are not breastfed
13.4.3 Appearance
13.4.3.1 History and background
Most babies are healthy or may suffer from a mild upper respiratory tract
infection or gastro-intestinal condition. They are usually laid down in the cot
in an apparently healthy condition, just to be found dead the next morning.
The deaths may sometimes also occur after the morning feed.
13.4.3.2 Scene of death
In most cases the scene of death is not investigated, as the parents will rush
the child to the hospital for resuscitation. If the body of the baby is examined
in the cot, there are usually no external signs of any significance. There may
be a pink foam exuding from the nose and mouth, and the face and
fingernails may be blue or cyanotic while the face may also be pale. Petechial
or punctate (spotty) haemorrhages are usually not visible in the eyes or face.
It has been alleged that there is a higher incidence of SIDS in babies lying in
the prone (on their stomach) position. If the baby was indeed lying in the
prone position, the area of pallor surrounding the mouth and nose must not
be misinterpreted as the result of smothering. This is due to the normal
distribution of hypostasis, with a pale area surrounding the mouth due to
pressure of the face on the underlying pillow. The dried out and delicate lips
of the baby can also look like an abrasion. This is a normal post-mortem
finding.
13.4.3.3 Post-mortem examination
The post-mortem signs are non-specific, but some are relatively common.
1. Intra-thoracic petechial haemorrhages (punctate haemorrhages in the
chest cavity) are present in 50% of cases on the lung surface (pleura), the
external aspect of the heart (epicardium) and also on the thymus (a gland
in the upper chest cavity).
2. Respiratory infection as indicated by inflammation of the mucosal
surfaces of the trachea and larynx is present in 50% of cases.
3. The lungs show pulmonary congestion and oedema. The surface of the
lungs shows dark and light coloured areas consistent with patchy collapse
of the lung tissue. There can also be an increased number of inflammatory
cells, especially surrounding the airways.
4. Enlargement of lymphoid structures like the thymus and lymph nodes
may be present. Histological examination, however, shows only non-
specific signs of stimulation.
13.4.3.4 Theories
More than 2 000 articles have been published regarding possible causes of
sudden infant death syndrome. The following is a list of the most common
theories which have been postulated:
230
Study unit 13
1. Hyperthermia/hypothermia or temperature abnormalities. This theory is
based on the fact that SIDS occurs more frequently during winter
months because the risk of hypothermia due to the lower environmental
temperature, as well as the risk of hyperthermia is higher. The latter is
due to the fact that the child is often covered with too many blankets.
Hyperthermia will be further aggravated if the child has low-grade
infection associated with fever.
2. Poisoning Ð carbon monoxide/carbon dioxide (CO/CO2). This theory,
which is at present widely accepted, is based on the fact that babies lying
on their stomachs (prone) have a higher risk. The baby exhales carbon
dioxide, which is heavier than air, and this accumulates around its head
in the cot. Carbon dioxide is an anaesthetic agent and can cause apnoea
(inability to breathe).
3. Death due to ``overlying'' is no longer an accepted cause of SIDS. The
baby who died in the Bible story, where Solomon had to decide over the
plight of the surviving living baby, was most probably a victim of SIDS.
4. Allergies, for instance for cow's milk and also dust mites.
5. Infections Ð low-grade and otherwise slight infections of especially the
airways.
6. Metabolic disturbances such as metabolic enzyme defects, hypoglycae-
mia (low blood-glucose level) and hypothyroidism (inactive thyroid).
7. Vitamins and electrolyte deficiency, such as vitamin C, D and E,
thiamine, magnesium and calcium deficiencies.
8. Conduction system remodelling defects of the heart. The heart
undergoes a process of remodelling. During the intra-uterine period
the right ventricle is the most important heart chamber responsible for
the forward propulsion of blood. However, after birth the left ventricle
becomes more important, and the right ventricle only has to pump the
blood through a relatively low pressure system in the lungs. Due to this
the walls of the right ventricle will become thinner. This ``absorption'' of
heart muscle is associated with changes in the anatomy of the
conduction system, which increase the irritability of the heart system
and the risk of arrhythmia (irregular heart rate) and even death.
9. Abnormalities of the brain, including a narrow foramen magnum (the
opening at the base of the skull) causing pressure on the brain stem.
10. Obstruction of the upper airways, especially during sleep.
11. Immune deficiencies which lower the resistance of the baby.
During the period 1970 to 1980 the hypothesis was developed that all babies
experience normal episodes of apnoea during sleep. This re-establishing of
breathing after a period of apnoea is also known as auto-resuscitation. Some
babies have a poor respiratory drive (the mechanism allowing you to breathe
automatically), which may increase these episodes of apnoea. It has been
alleged that progressive hypoxia and the inability to respond timeously and
sufficiently to hypercapnia (increased carbon-dioxide levels in the blood) and
hypoxia cause death. Carbon dioxide is the normal stimulus or drive for
respiration. The sleeping baby will go into a downward spiral of hypoxia Ð
apnoea Ð which will ultimately result in bradycardia and cardiac arrest.
There are, however, also contradictions in this theory, as with each of the
other theories mentioned above.
231
Paediatric forensic pathology
At present it is accepted that SIDS has many causes and that it is only the final
situation leading to death in a child compromised by a number of factors
which all have to come together in a baby to result in death. These factors are:
1. sleep (it depresses the brain stem, which inter alia controls respiration)
2. viral infections (especially of the respiratory tract): viraemia causes
decreased oxygenation and narrowing of the airways due to swelling of
the mucosa as well as mucus secretion
3. other factors such as prematurity and low birth weight
4. lying in the prone position: these babies are more vulnerable to the
accumulation of carbon dioxide surrounding the head; carbon dioxide is
a heavy gas and will accumulate in the space surrounding the face; carbon
dioxide has an anaesthetic effect and depresses the respiration even more.
It has been proven that non-specific community health-care improvements (ie
ante- and postnatal clinics) lead to a decrease in the incidence of SIDS. It has
been also been proven that informing mothers about the position in which
babies should sleep (on the face or side) helped in lowering the incidence.
How can you prevent SIDS in your own family? One solution is to use a sleep
apnoea monitor or alarm, which is placed under the mattress in the cot. The
moment that the baby stops breathing, an alarm is triggered, and both baby
and mother are awakened. These monitors may be rented from most
pharmacies.
The main reason for performing a post-mortem examination in a case of SIDS
is to exclude murder and child abuse. Thereafter any morphological,
biochemical and microbiological cause of death has to be excluded. If a
significant abnormality cannot be demonstrated with a complete post mortem,
the death is attributed to SIDS. It is therefore a diagnosis made by exclusion.
ACTIVITIES
1. Which questions must be answered in cases where a newborn baby is
found dead and it is obvious that the birth was concealed?
2. A boy, three years of age, presents in the trauma unit with a fracture of the
skull and vague history of a fall off a chair.
a. Which condition must be considered by the medical practitioner?
b. Which other injuries must be excluded?
c. What is the medical practitioner's legal obligation?
3. A baby of four months of age dies unexpectedly in the cot. How should
such death be managed?
4. In cases of cot death the cause of death is obvious. Discuss this statement.
Feedback
1. In a case of alleged concealment of birth it is necessary to determine
the following:
. whether the child would have survived (ie the gestation period)
. whether the child indeed lived (ie established its own respiration)
. if the child did live, for how long
232
Study unit 13

. what the cause of death is
. how long the child had been dead when it was found
. whether it can be established whether the child belongs to a
specific mother (ie on the basis of identity and the fact that the
mother shows signs of a recent pregnancy which correlate with
the age of the child)
. if the child was stillborn, why it did not survive
2. This case raises suspicion about non-accidental injury syndrome or
child abuse. Other injuries include multiple bone fractures, often of
different ages, contusions and other skin wounds, retinal haemor-
rhages as well as intracranial haemorrhages, especially subdural
haemorrhages. The medical practitioner must report this case in
terms of the Child Care Act. Failure to do so constitutes an offence.
3. This case of unexpected death in a 4-month-old baby is highly
suggestive of the sudden infant death syndrome (SIDS) or cot death.
As there is no pre-existing history which may assist in defining a
possible cause of death, it must be initially managed as an unnatural
death. The sudden unexpected death in a baby may be the result of
other natural diseases, such as a lung infection, abnormalities of the
heart, meningitis, et cetera. SIDS can only be diagnosed after
violence and any other natural disease processes had been excluded.
During the (complete) post-mortem examination, which includes
histological or microscopical examination of vital organs, as well as
microbiology and other tests, the absence of any morphological
abnormalities will support this diagnosis.
4. The unique characteristic of cot death is the fact that there is no
obvious physiological or anatomical cause of death. Although there
are certain theories about the possible cause of death, no single
abnormality has been identified as a possible cause of this condition.
Cot death is the result of the exposure of an already compromised
young baby to a number of different stress situations, which may
lead to death. Apnea (ie cessation of respiration) plays a central role.
Research has also shown that when a normal person ceases to
inhale/exhale for whatever reason, an auto-resuscitative mechanism
will stimulate respiration. This is the reason why a person cannot
voluntarily commit suicide by just holding his/her breath. In time the
auto-resuscitative mechanism will re-establish respiration, if not
severely depressed by drugs or alcohol. This defence mechanism is
not yet effectively developed in babies. If their respiration stops due
to some or other stress factor, this mechanism does not optimally
operate to end the period of apnea, and the baby accordingly dies.
233
Paediatric forensic pathology
STUDY UNIT 14Sexual offences
Contents
14.1 Rape
14.1.1 Introduction14.1.2 Medical examination
14.2 Sexually transmitted diseases14.3 Interpretation of clinical findings
14.3.1 Extragenital injuries14.3.2 Genital injuries14.3.3 Laboratory test results14.3.4 General considerations
14.4 Sodomy (buggery; anal intercourse)
Activities
Feedback
Learning outcomesWhen you have completed this study unit, you should be able to
. discuss the impact of sexual offences and rape on the South Africancommunity
. interpret the clinical findings in rape victims
Sexual offences include rape and a variety of so-called ‘‘unnatural offences’’such as sodomy, incest, bestiality and masochism. Of these rape is the mostfrequently reported, and the medico-legal investigation of the victims andassailants forms one of the most frequent and important tasks of the districtsurgeon. The use of drugs to induce amnesia and also to suppress the level ofconsciousness, has become more popular during the last few years,particularly with so-called ‘‘date rape’’.
14.1 Rape
14.1.1 Introduction
According to statistics supplied by the South African Police Service thenumber of rapes increased with 20,6% between 1994 and 2002 (see the webpage of the South African Police Service www.saps.gov.za). NICRO alsomaintains that only one out of every 20 cases of rape or attempted rape isreported. If this is indeed true, the implications are shocking.
234
Number of rapes according to SAPS 1 052 107
Alleged number based on 1:20 ratio of reporting 1 042 140
Number of rapes per day 1 022 855
Number of rapes per hour 1 01 0119
Number of rapes per minute 1 01 01 1,98
If it is correct that only one out of every 20 rapes or attempted rapes isreported, one person is raped every 30,3 seconds somewhere in South Africa!Even with the official number of 52 107 cases per year, it reflects an incidenceof one rape every 10 minutes!
It is also of great concern that a large number of rape victims are children.This is often due to a misconception in the community that intercourse with avirgin will cure HIV/AIDS.
A survey of 163 alleged rape victims in the Cape Town region a number ofyears ago revealed that 46% of rape victims were younger than 20 years(5,6% younger than 10 years), 46% between the ages of 20 and 40, and theremainder older than 40 years.
No observable injuries were recorded in 33% of cases; tenderness andabrasions of the genitals in 37%; genital tears in 25%, and severe genitallacerations with or without extragenital traumatic lesions in 5%. Seventy-three per cent of the victims were allegedly assaulted by a single assailant.
14.1.2 Medical examinationThe medical examination should commence as soon as the complainant (or arepresentative) has given consent. The examination must be thorough, takingparticular note of even the most trivial of injuries, as well as the mental stateof the victim. The appropriate specimens (eg vaginal smears, blood, pubichair) must be routinely taken. It is often only much later, and usually at thetrial, that the relevance of a particular observation or laboratory resultrelating to the victim or assailant is revealed. It is important to bear in mindthat bruising may only appear some hours after the assault.
It is equally important to examine the alleged assailant thoroughly, both withregard to his physical and his mental state.
The examining doctor will not be in a position to say whether thecomplainant was raped from the medical findings alone. Although the verynature of the investigation demands a sympathetic approach, his or herfunction is to report objectively on the observations and to prepare him/herself adequately to interpret these during evidence, avoiding at all stagesand at all costs prejudgment of the case.
Note that section 335B of the Criminal Procedure Act 51 of 1977 containsspecial provisions enabling a magistrate or, in cases of extreme urgency, even apoliceman, to consent to medical examination of a minor who was probably avictim of a sexual offence. This may occur where, for example, a parentcannot be traced within a reasonable time, or unreasonably refuses to consent,or is himself or herself the suspected offender, or is deceased.
Sexual offences
235
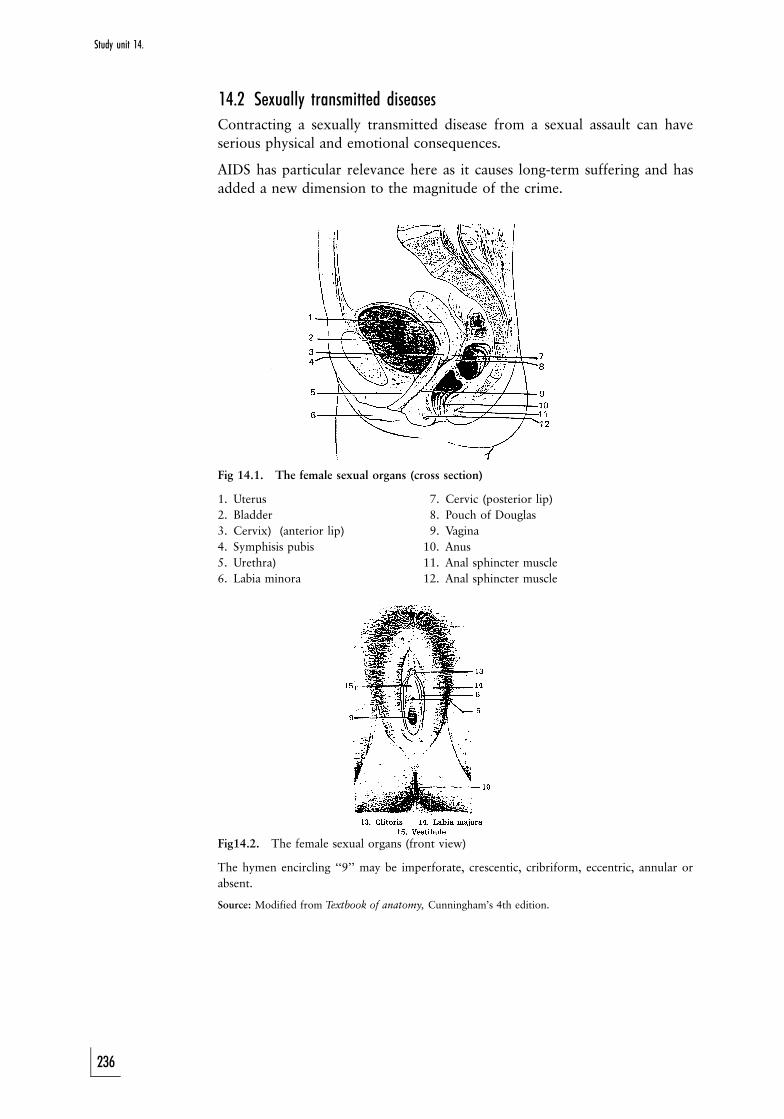
14.2 Sexually transmitted diseasesContracting a sexually transmitted disease from a sexual assault can haveserious physical and emotional consequences.
AIDS has particular relevance here as it causes long-term suffering and hasadded a new dimension to the magnitude of the crime.
Fig 14.1. The female sexual organs (cross section)
1. Uterus 17. Cervic (posterior lip)2. Bladder 18. Pouch of Douglas3. Cervix) (anterior lip) 19. Vagina4. Symphisis pubis 10. Anus5. Urethra) 11. Anal sphincter muscle6. Labia minora 12. Anal sphincter muscle
Fig14.2. The female sexual organs (front view)
The hymen encircling ‘‘9’’ may be imperforate, crescentic, cribriform, eccentric, annular orabsent.
Source: Modified from Textbook of anatomy, Cunningham’s 4th edition.
Study unit 14.
236

14.3 Interpretation of clinical findings
14.3.1 Extragenital injuriesThe absence of signs of injury on the complainant’s person should not beconstrued as consent to sexual relations. She may have been overcome by fear,submitted under threat of harm to her children or partner, or had beenheavily intoxicated. In gang rapes, where the victim is overcome by a numberof assailants, or if attacked from the back by a single person, it may be verydifficult to offer any resistance. Furthermore the victim may be examinedshortly after the event, in which case bruising, which may only appear manyhours later, is not evident. It is therefore sometimes indicated that the personmust be re-examined 24 hours later. Conversely, although the presence ofinjuries suggests that force was used to overcome resistance — and the moreexensive they are the more likely this is to be the case — it should be borne inmind that the injuries may be unrelated to the rape as such, the allegation ofrape being part of a trumped-up charge. The occasional bruise, nail scratch orbite mark is not infrequently inflicted during over-zealous intercourse withconsent. This includes a so called love-bite.
It is also important to examine the finger nails for any foreign material.
14.3.2 Genital injuries (fig 14.1 and 14.2)In the case of a marked disproportion in size between the assailant and thevictim (eg when a child was assaulted) the injuries to the genital organs may beextensive and extend into the abdominal cavity and rectum. If the victim hadborne children, no injuries may be detected in or about the vagina, despite thefact that force was used to penetrate the vagina. The presence of an intacthymen, depending on the type of hymen, is not necessarily an indication ofvirginity. Neither is it an indication that rape has not taken place. Onoccasion, rape is associated with other aberrant sexually perverse acts such assodomy, fellatio lingua (oral stimulation of the sexual organ) and genitalmutilation.
14.3.3 Laboratory test resultsThe results concerning injuries related to sexual assault should be evaluatedjust as critically as test results from any other type of injury. What the analystconveys to the reader should be what is read into the report, purely andsimply, namely that from the specimen a certain result was elicited. Inevaluating this finding relative to the subject under review the reader mustdetermine whether the following was carried out:
. The specimen submitted for analysis was drawn properly.
. It was adequately preserved in transit.
. It was suitably identified.
. It was not contaminated before or after collection.
. It was representative of the subject matter under consideration.
In addition, the method of testing should be known to the reader, and itsaccuracy, specificity and the ability to reproduce it, understood.
Molecular biology and the use of DNA analysis has made it much easier to
Sexual offences
237
identify an assailant. In the case of DNA typing the result can prove beyondany doubt that a single hair, drop of blood, sperm, minute fragment of tissue,et cetera, is derived from a particular person. This specificity, which makes itpossible to determine a person’s identity almost 100% accurately, is due to theuniqueness of each individual’s nucleic acid (DNA) structure of the cell, andhence the many different permutations of each of these characteristics in anyone individual.
14.3.4 General considerationsEjaculation may have occurred in the anus or on the perineal surface. Whereno ejaculation has occurred, despite penetration, there may be a considerableamount of secreted penile (urethral) mucous which the woman may mistakefor ejaculate. Intense emotion or depressants such as alcohol or drugs mayinhibit ejaculation.
The presence of smegma (secretion) below a free pepuce (foreskin) suggeststhat the male has not had intercourse for some days.
During sexual intercourse, where there is marked disproportion in the sexualorgans, the male may rupture the frenular artery, which passes below the headof the penis, and it may bleed profusely. In intercourse with consent this maybe a source of considerable embarrassment to both parties, and a revelation toa third party.
In studying the topic of rape it is important to bear in mind that mere contact,for example when the penis is placed on the vulva, constitutes penetration.Penetration, therefore, does not necessarily involve penetration of the hymen.
There are a number of different anatomical variations to the shape of the‘‘virginal’’ hymen, ranging from an imperforate to no more than a thin rim oftissue encircling the entrance to the vagina. The following examples shouldelucidate this point:
1. Strips of hymenal tissue may still be present in women who gave birthvaginally.
2. The hymen of the non-virginal non-parous (ie not giving birth) woman,depending on the type of hymen, generally reveals an old rupture at themid-posterior position.
3. A ruptured hymen may be the result of masturbation, and the hymen maybleed profusely.
4. Non-virginal women may have intact hymens, particularly of the annulartype. Cases have been reported of prostitutes where this type of hymenrevealed no evidence of having ever ruptured.
Spermatozoa may be found in the vagina for as long as five to ten days afterbeing introduced there. Although motile spermatozoa can retain their motilityfor as long as five to ten days after being introduced into the vagina, thisperiod is reduced to no more than an hour or two in the majority of cases.
The absence of spermatozoa in the vagina does not mean that there was noejaculation into the vagina. This absence may be the result of azoospermia(absence of sperm) in the ejaculate, or the use of a condom.
Study unit 14.
238

14.4 Sodomy (buggery; anal intercourse)
Sodomy may be a passing phase of homosexual behaviour during puberty.However, an estimated 5% of males remain exclusively homosexual, ofwhom one-third are said to be capable of heterosexuality, but often at theprice of instability in the heterosexual relationships. Situational homosexualbehaviour is common in prisons and often leads to crimes of violence arisingfrom jealousy. Homosexual behaviour is often associated with extremes ofpromiscuity. It has been found that 28% of homosexual males had more than1 000 partners (Berkow 1992).
It is not surprising, therefore, that homosexuals are at serious risk ofcontracting a variety of sexually transmissible conditions, ranging fromamoebic dysentery infections of the genital tract to AIDS. The prevalance ofdepression, paranoid states and suicide seems higher among homosexualsthan among those conducting ‘‘normal’’ lives. As a group, homosexuals areunderstandably vulnerable to blackmail, especially when in high office. Thusin a medico-legal investigation of what may appear to be a motiveless suicideor homicide, the possibility of homosexual associations should not beoverlooked. Taylor, quoted by Glaister in Medical Jurisprudence andToxicology found that of 96 prisoners in prison because of homosexualoffences (in England), 39 were charged with indecent assault on boys, 24 withimportuning, 17 with gross indecency, and 16 with the crime of sodomy. Inthe case of 5% of the 96 prisoners the offences involved boys. Taylorclassified the cases into four groups:
1. the pseudo-homosexual group, where homosexual acts were substitutedfor the preferred heterosexual act
2. the bisexual group, where there were strong bisexual tendencies3. prostitutes among pseudo-homosexuals for purposes of gain4. the true homosexual group, which included only thirteen of the 96. Five
were always passive, two always active, three both active and passive.Fellatio was admitted by four of this group of thirteen (Rentoul & Smith1973: 452).
In keeping with Taylor’s findings, an American investigation also found thatonly about 5% of group 4 had effeminate appearances.
As with cases of rape, the victim and the alleged assailant must be examinedthoroughly and attention must be directed especially at detecting anal tears,which may be extensive in the inexperienced partner. In the case of markeddisproportion (also with rape) the frenular artery of the active member maytear, and haemorrhaging may be surprisingly severe. Specimens for thedetection of seminal fluid and blood should be taken.
ACTIVITIES
1. Discuss the injuries which may be present in cases of rape.2. The absence of spermatozoa in the female genital tract or vagina excludes
rape. Discuss this statement.
Sexual offences
239
FEEDBACK
1. Injuries in cases of alleged rape may be of a general or genital nature.The general injuries may be any type of skin injury as describedelsewhere in this guide. Genital injuries may be minimal orextensive. They may even be absent. It is also important toremember that injuries may sometimes be caused by overenthusias-tic intercourse.
It is important to remember that injuries are not always visibleinitially, and if absent at the initial examination, the patient must bere-examined 24 hours later, as some contusions may only appear ata later stage.
2. This statement is incorrect. Ejaculation can occur outside the vagina,in a condom, or the ejaculate can be azoospermic (withoutspermatozoa), for instance after a vasectomy.
Study unit 14.
240
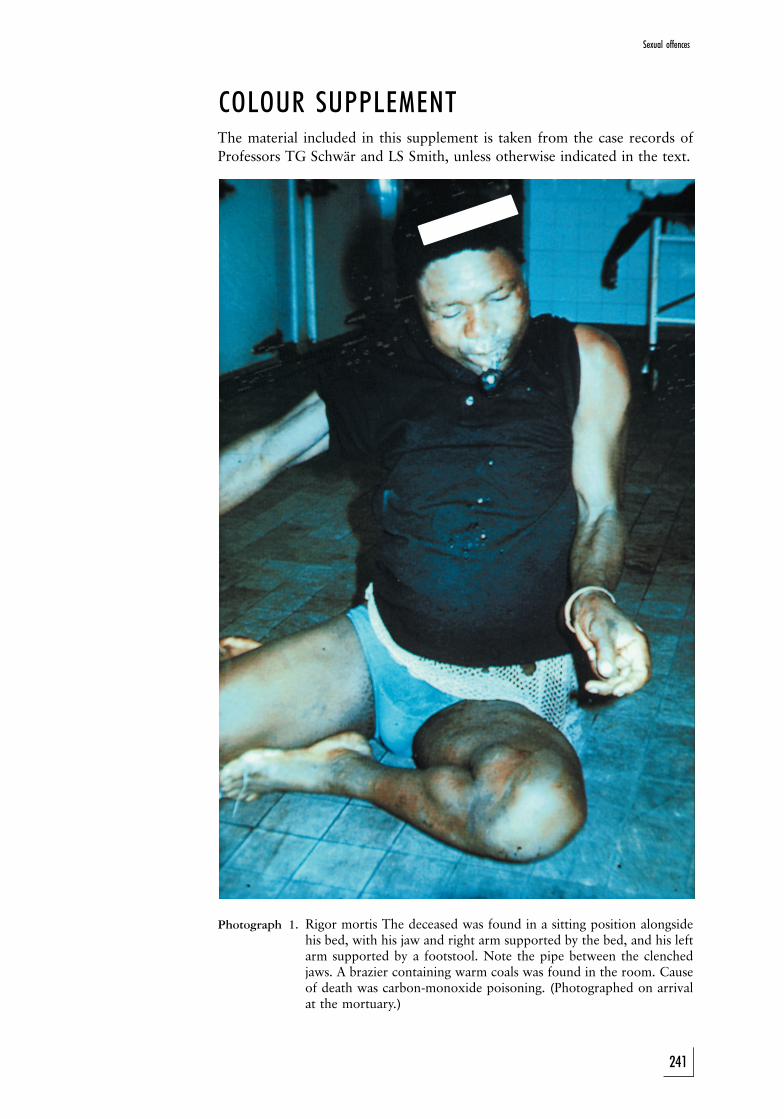
COLOUR SUPPLEMENTThe material included in this supplement is taken from the case records ofProfessors TG Schwar and LS Smith, unless otherwise indicated in the text.
Photograph 1. Rigor mortis The deceased was found in a sitting position alongsidehis bed, with his jaw and right arm supported by the bed, and his leftarm supported by a footstool. Note the pipe between the clenchedjaws. A brazier containing warm coals was found in the room. Causeof death was carbon-monoxide poisoning. (Photographed on arrivalat the mortuary.)
Sexual offences
241
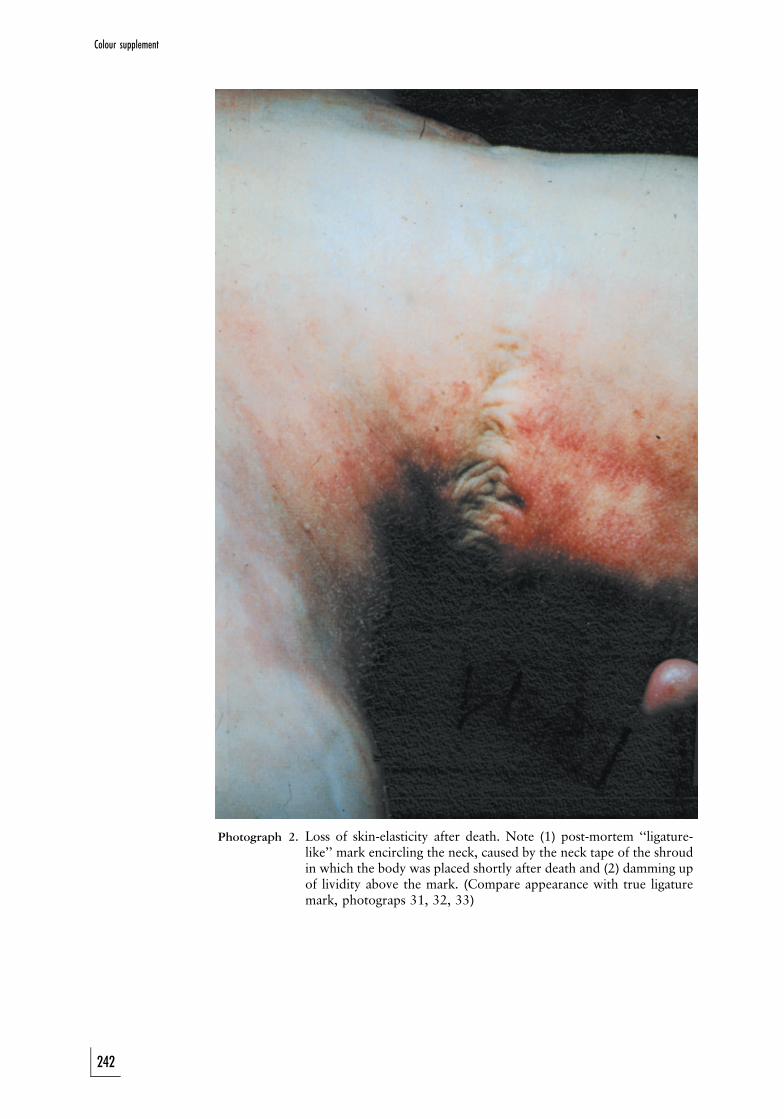
Photograph 2. Loss of skin-elasticity after death. Note (1) post-mortem ‘‘ligature-like’’ mark encircling the neck, caused by the neck tape of the shroudin which the body was placed shortly after death and (2) damming upof lividity above the mark. (Compare appearance with true ligaturemark, photograps 31, 32, 33)
Colour supplement
242
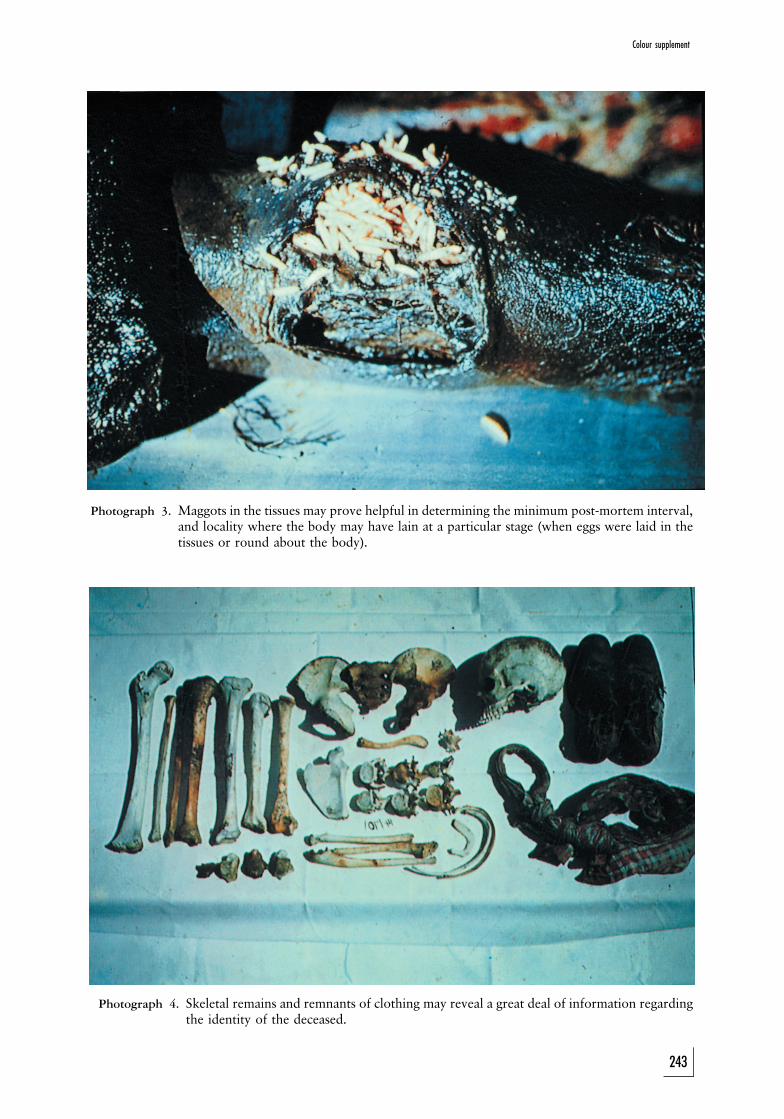
Photograph 3. Maggots in the tissues may prove helpful in determining the minimum post-mortem interval,and locality where the body may have lain at a particular stage (when eggs were laid in thetissues or round about the body).
Photograph 4. Skeletal remains and remnants of clothing may reveal a great deal of information regardingthe identity of the deceased.
Colour supplement
243
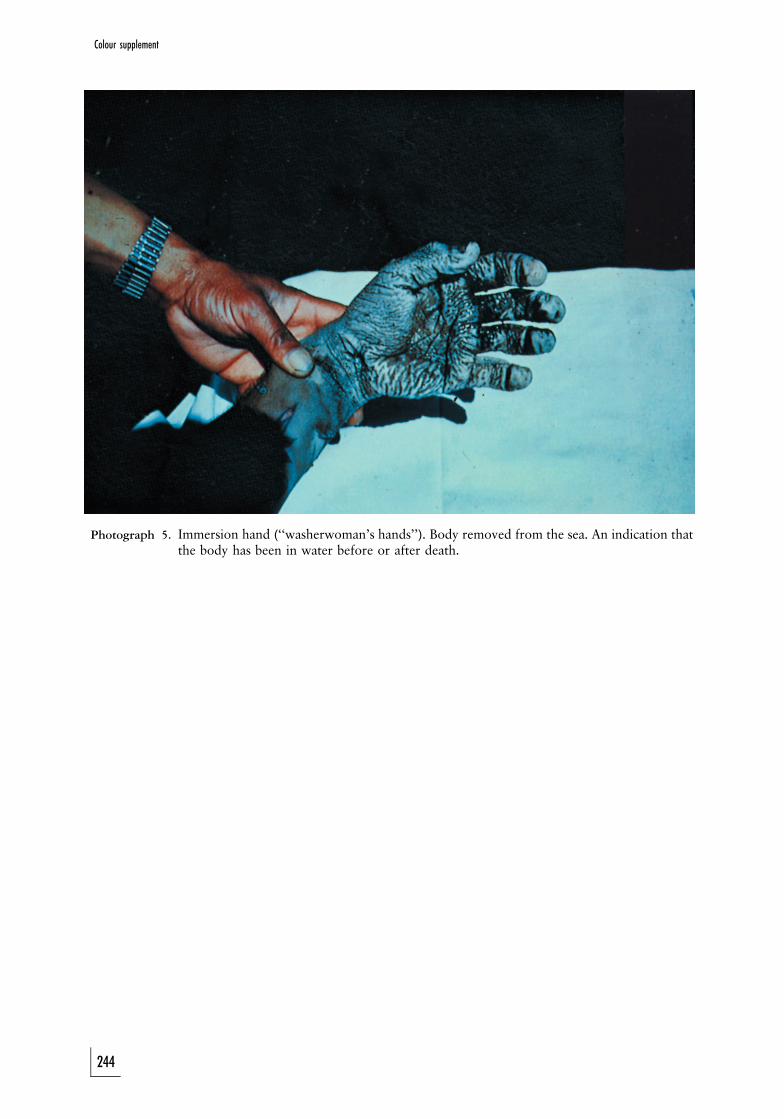
Photograph 5. Immersion hand (‘‘washerwoman’s hands’’). Body removed from the sea. An indication thatthe body has been in water before or after death.
Colour supplement
244
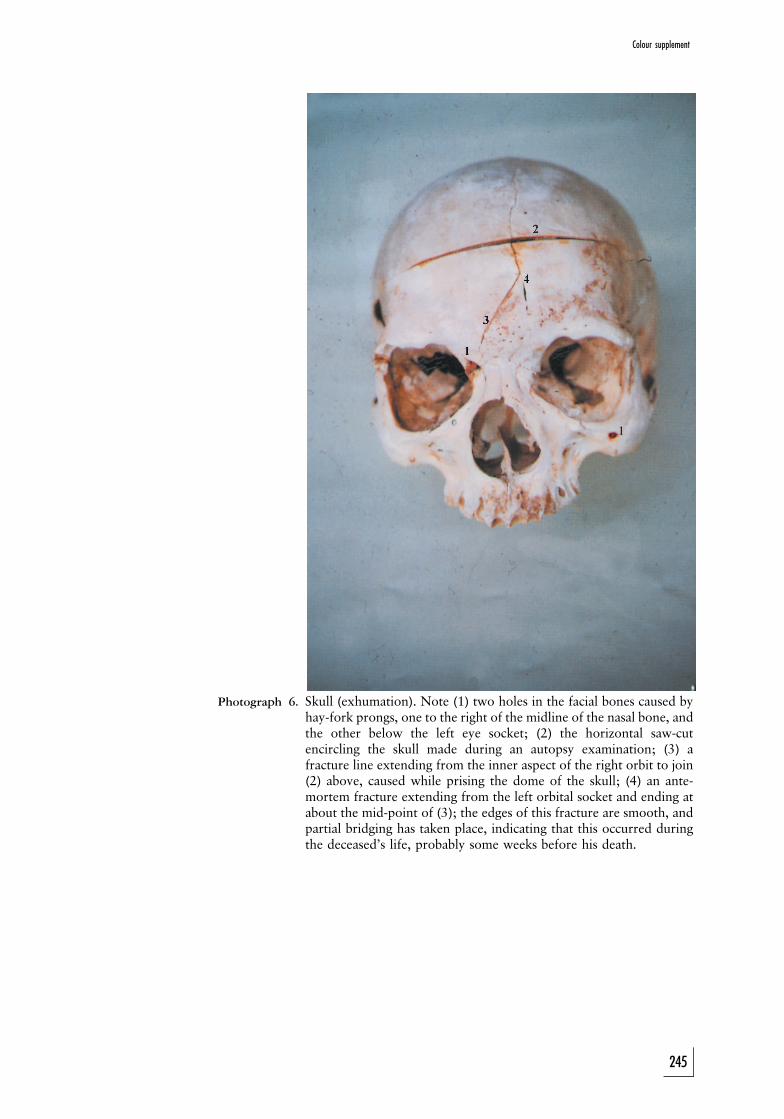
1
Photograph 6. Skull (exhumation). Note (1) two holes in the facial bones caused byhay-fork prongs, one to the right of the midline of the nasal bone, andthe other below the left eye socket; (2) the horizontal saw-cutencircling the skull made during an autopsy examination; (3) afracture line extending from the inner aspect of the right orbit to join(2) above, caused while prising the dome of the skull; (4) an ante-mortem fracture extending from the left orbital socket and ending atabout the mid-point of (3); the edges of this fracture are smooth, andpartial bridging has taken place, indicating that this occurred duringthe deceased’s life, probably some weeks before his death.
Colour supplement
245
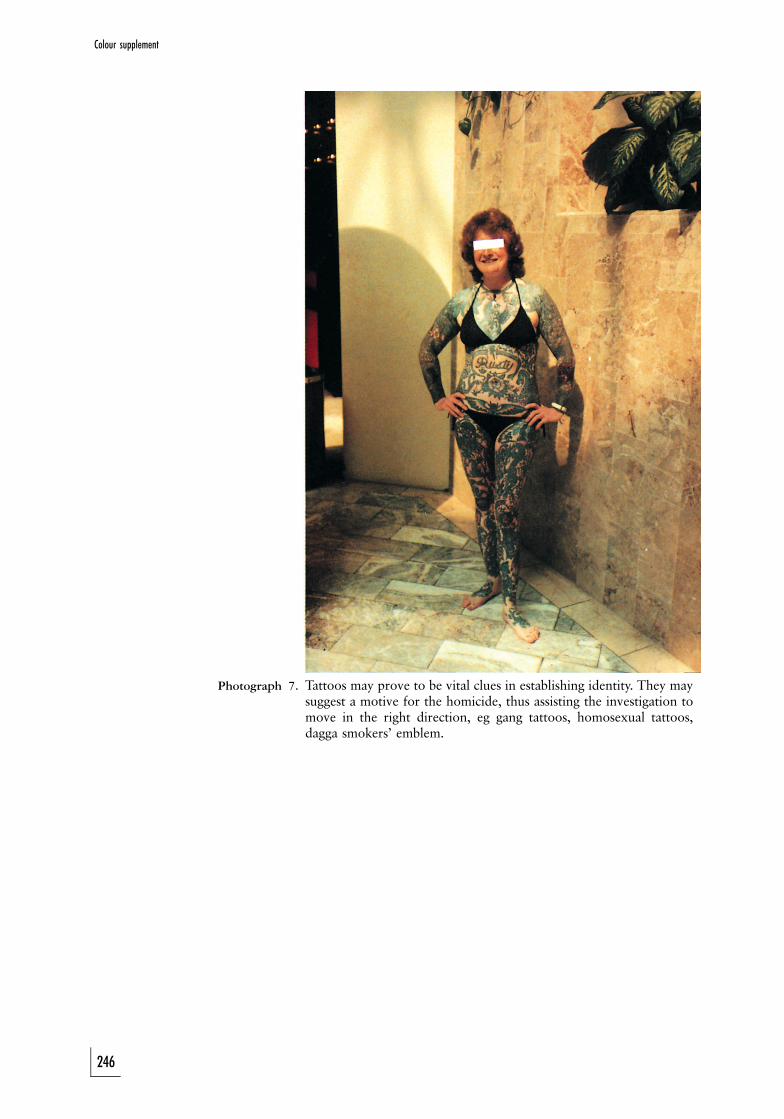
Photograph 7. Tattoos may prove to be vital clues in establishing identity. They maysuggest a motive for the homicide, thus assisting the investigation tomove in the right direction, eg gang tattoos, homosexual tattoos,dagga smokers’ emblem.
Colour supplement
246
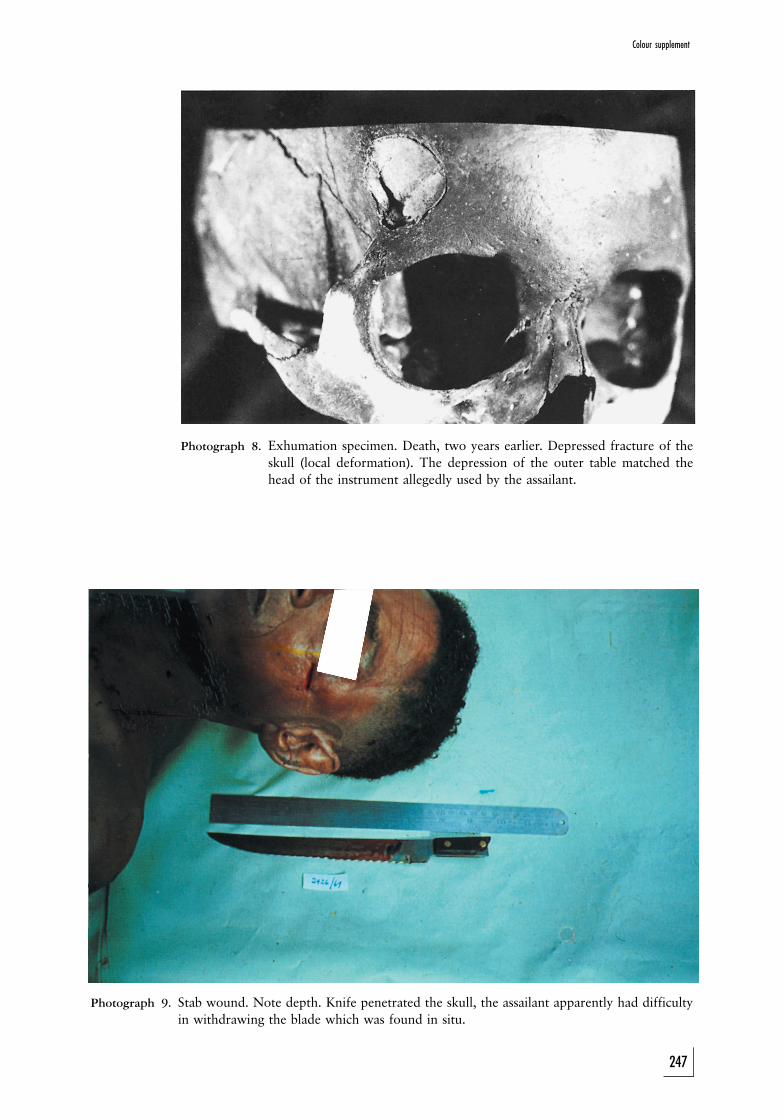
Photograph 8. Exhumation specimen. Death, two years earlier. Depressed fracture of theskull (local deformation). The depression of the outer table matched thehead of the instrument allegedly used by the assailant.
Photograph 9. Stab wound. Note depth. Knife penetrated the skull, the assailant apparently had difficultyin withdrawing the blade which was found in situ.
Colour supplement
247
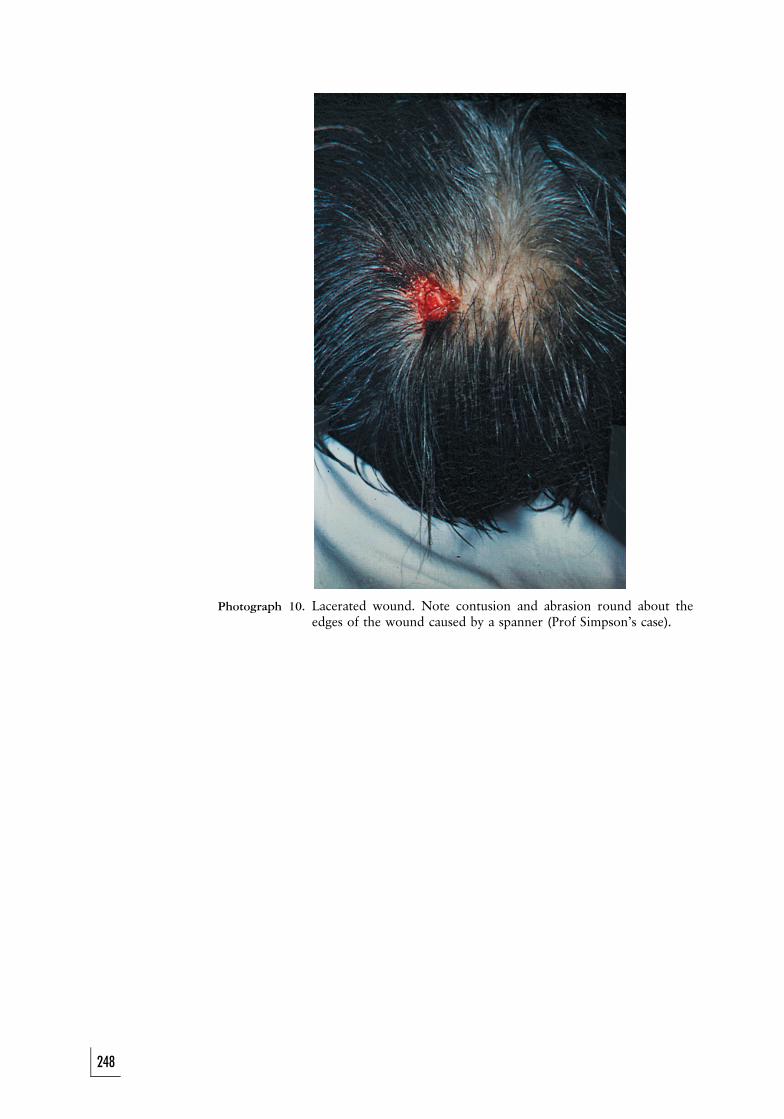
Photograph 10. Lacerated wound. Note contusion and abrasion round about theedges of the wound caused by a spanner (Prof Simpson’s case).
248
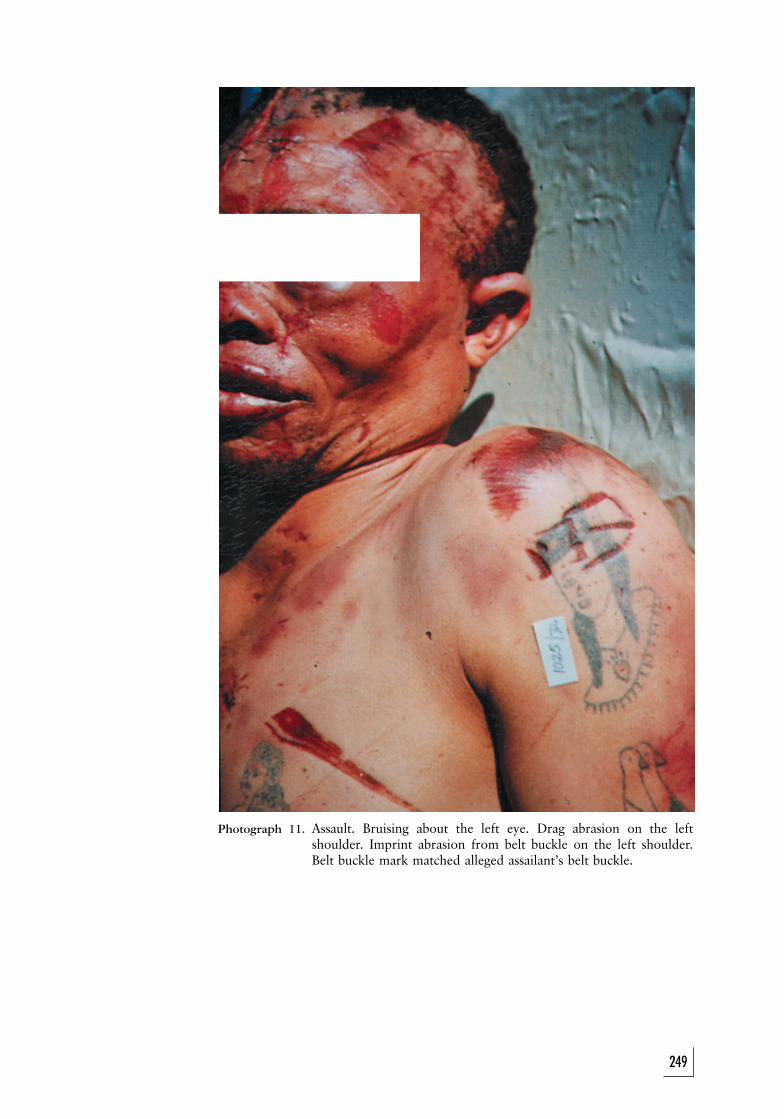
Photograph 11. Assault. Bruising about the left eye. Drag abrasion on the leftshoulder. Imprint abrasion from belt buckle on the left shoulder.Belt buckle mark matched alleged assailant’s belt buckle.
249
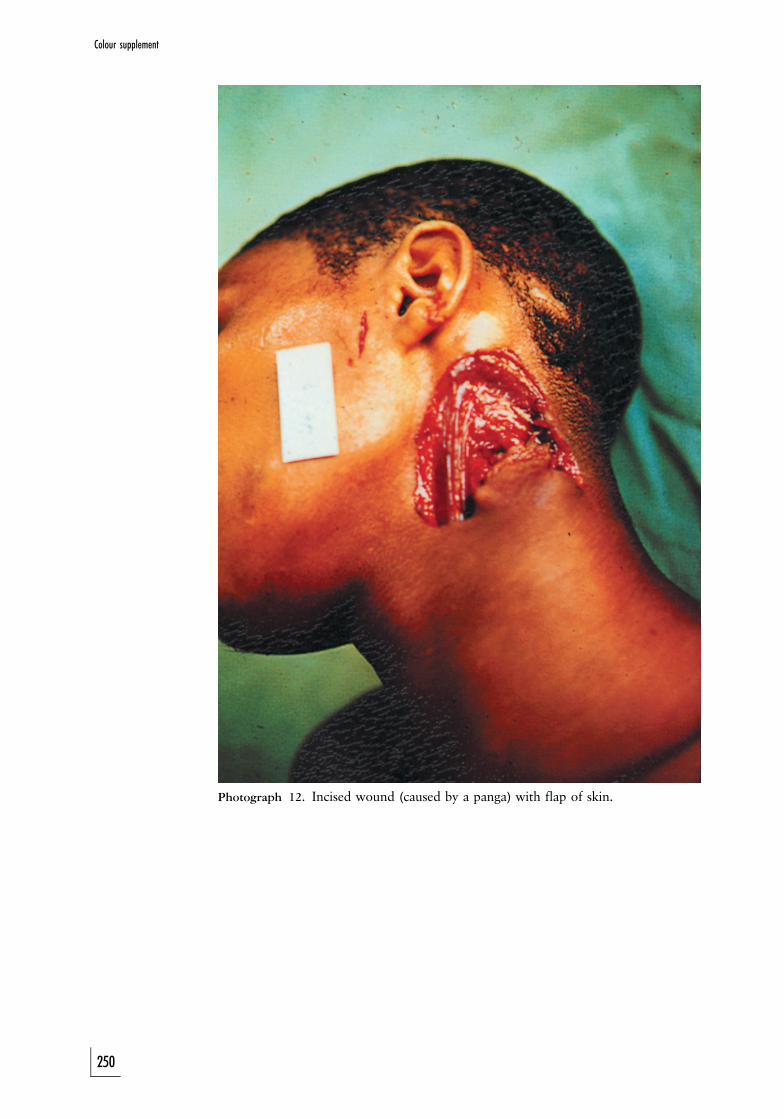
Photograph 12. Incised wound (caused by a panga) with flap of skin.
250
Colour supplement
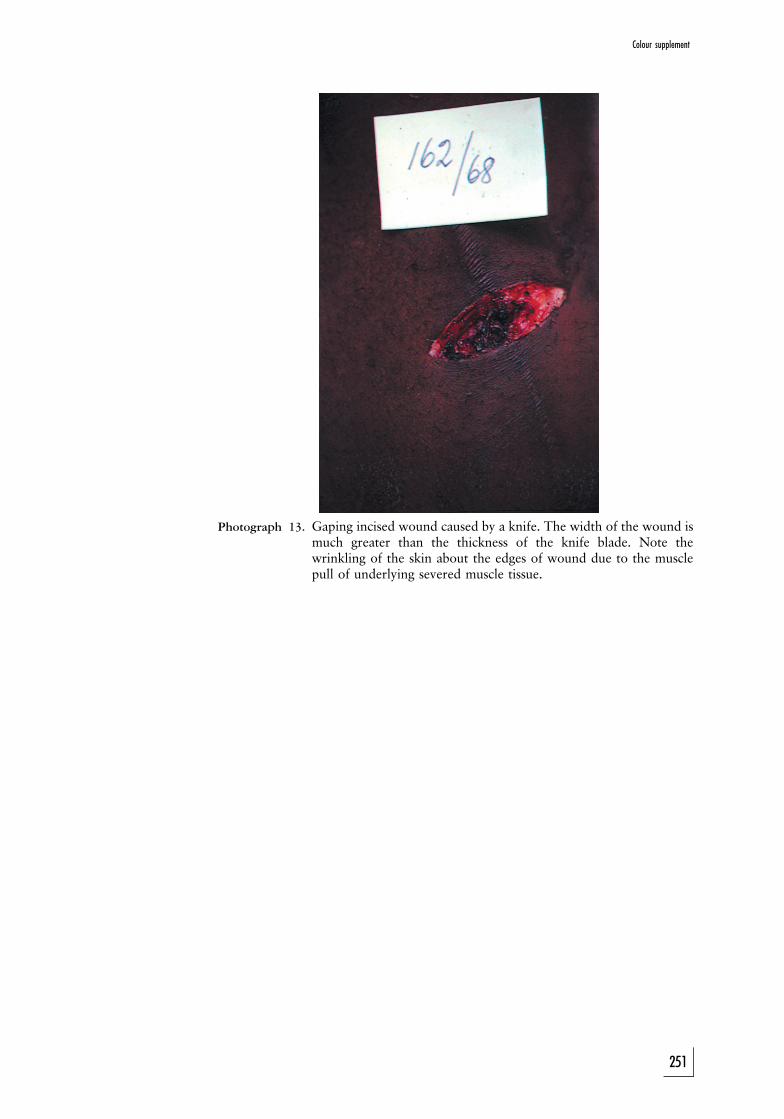
Photograph 13. Gaping incised wound caused by a knife. The width of the wound ismuch greater than the thickness of the knife blade. Note thewrinkling of the skin about the edges of wound due to the musclepull of underlying severed muscle tissue.
251
Colour supplement
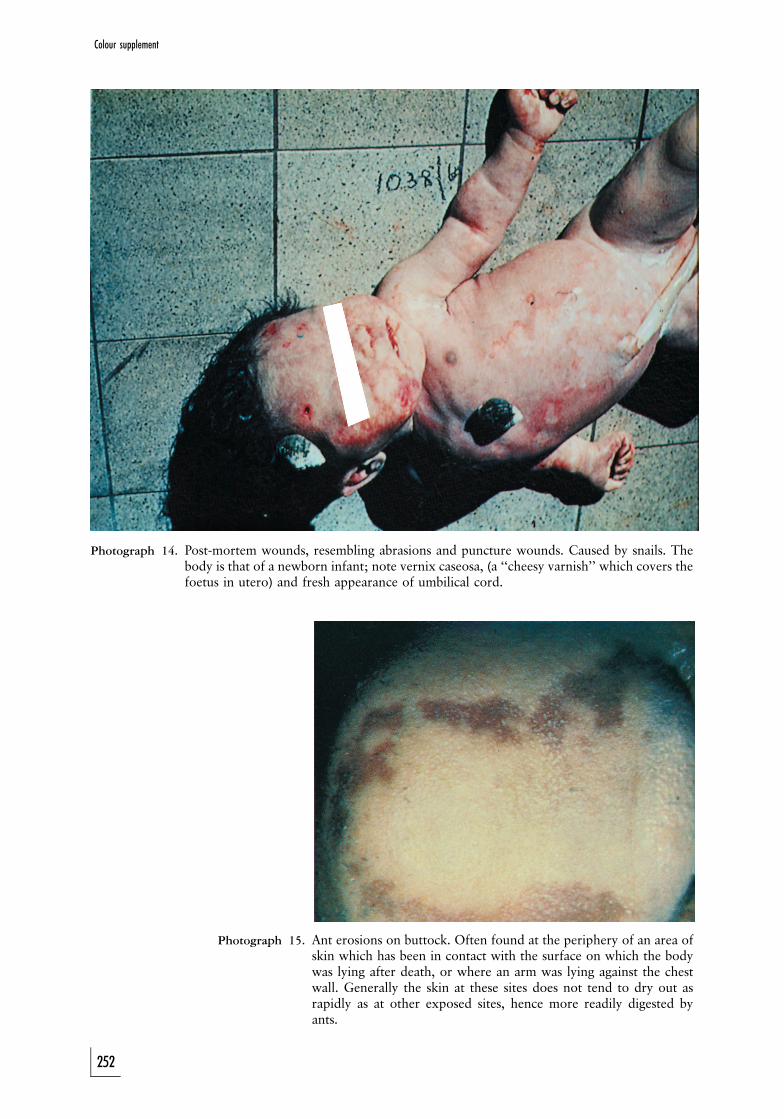
Photograph 14. Post-mortem wounds, resembling abrasions and puncture wounds. Caused by snails. Thebody is that of a newborn infant; note vernix caseosa, (a ‘‘cheesy varnish’’ which covers thefoetus in utero) and fresh appearance of umbilical cord.
Photograph 15. Ant erosions on buttock. Often found at the periphery of an area ofskin which has been in contact with the surface on which the bodywas lying after death, or where an arm was lying against the chestwall. Generally the skin at these sites does not tend to dry out asrapidly as at other exposed sites, hence more readily digested byants.
252
Colour supplement
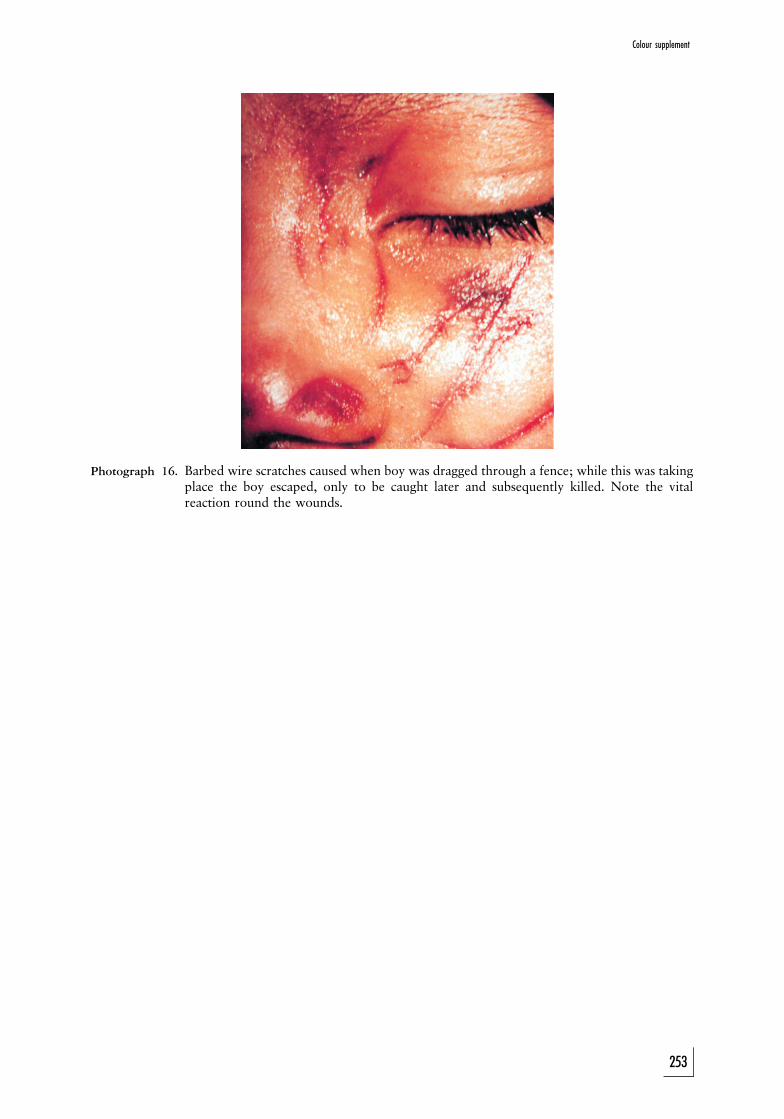
Photograph 16. Barbed wire scratches caused when boy was dragged through a fence; while this was takingplace the boy escaped, only to be caught later and subsequently killed. Note the vitalreaction round the wounds.
253
Colour supplement
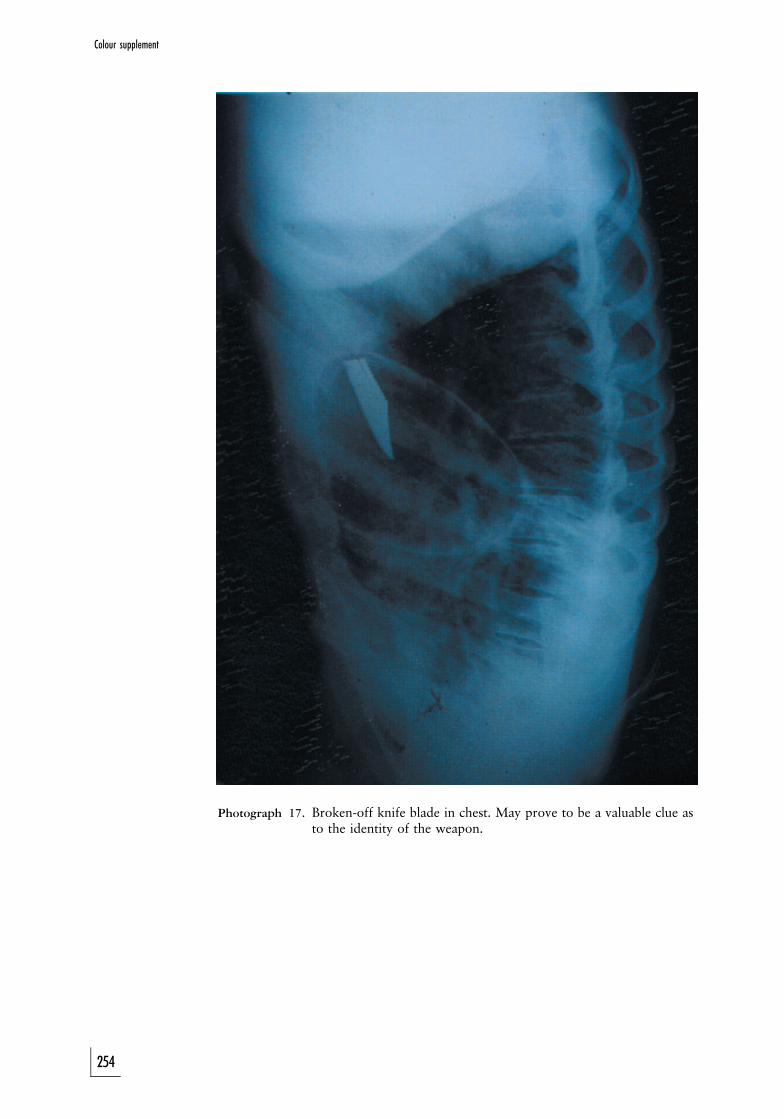
Photograph 17. Broken-off knife blade in chest. May prove to be a valuable clue asto the identity of the weapon.
254
Colour supplement
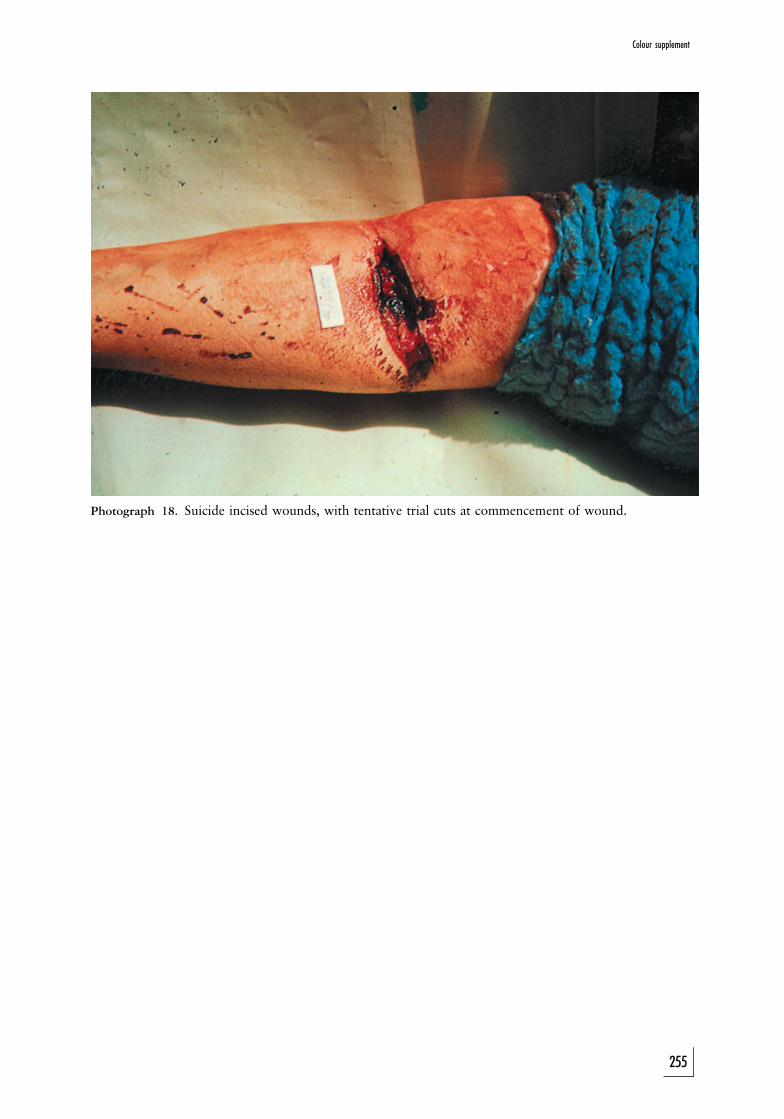
Photograph 18. Suicide incised wounds, with tentative trial cuts at commencement of wound.
255
Colour supplement
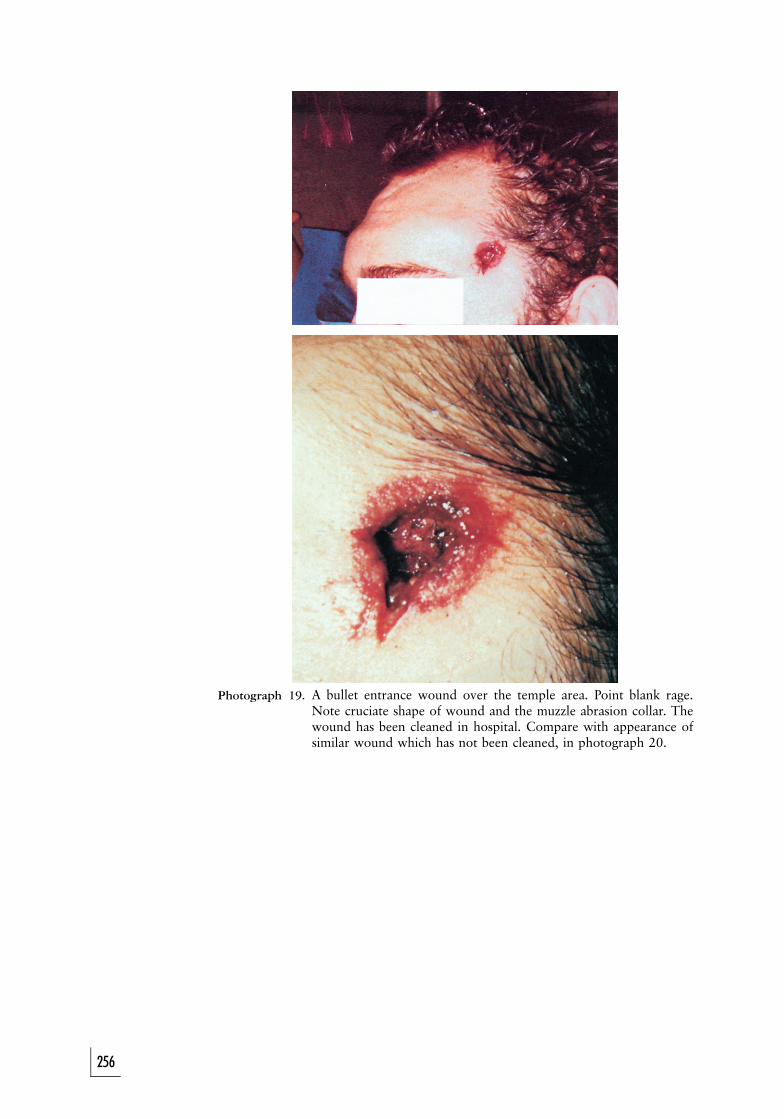
Photograph 19. A bullet entrance wound over the temple area. Point blank rage.Note cruciate shape of wound and the muzzle abrasion collar. Thewound has been cleaned in hospital. Compare with appearance ofsimilar wound which has not been cleaned, in photograph 20.
256
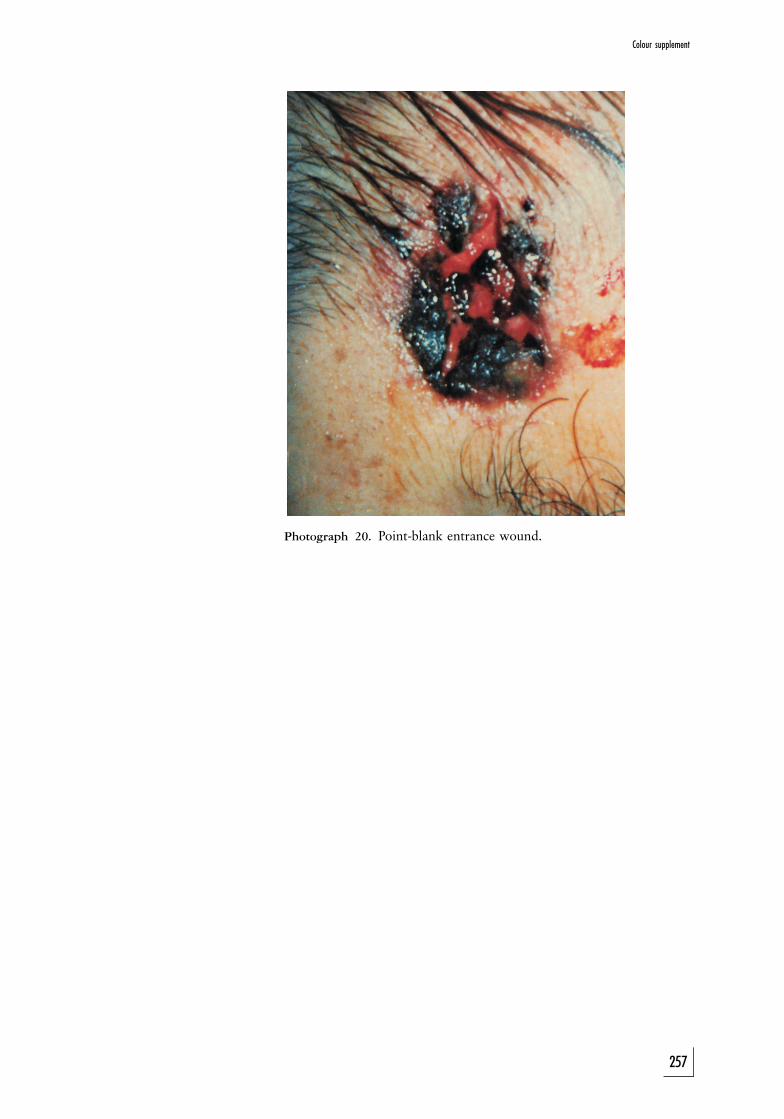
Photograph 20. Point-blank entrance wound.
257
Colour supplement
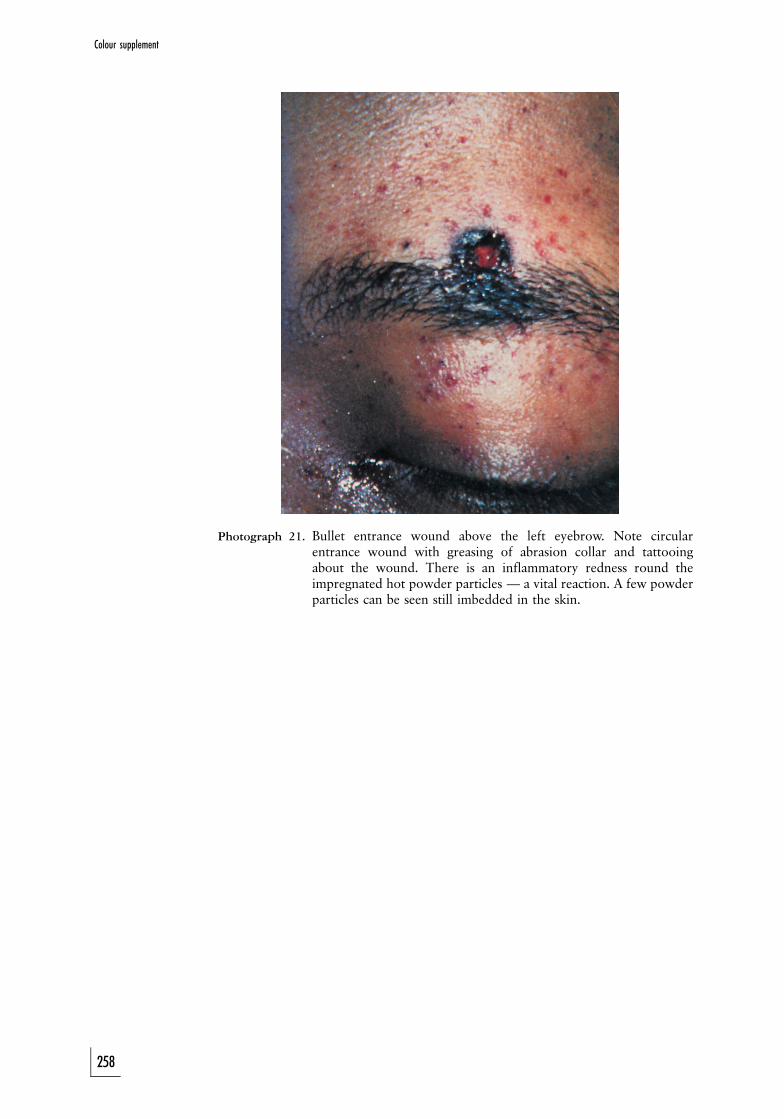
Photograph 21. Bullet entrance wound above the left eyebrow. Note circularentrance wound with greasing of abrasion collar and tattooingabout the wound. There is an inflammatory redness round theimpregnated hot powder particles — a vital reaction. A few powderparticles can be seen still imbedded in the skin.
258
Colour supplement
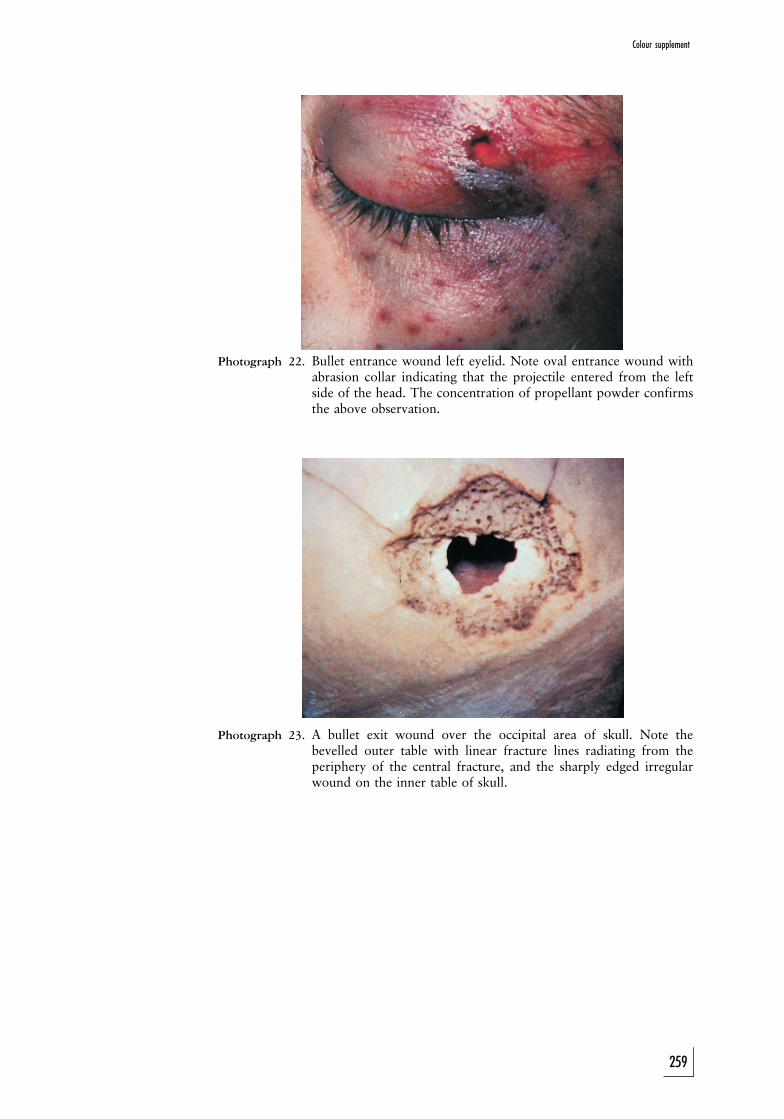
Photograph 22. Bullet entrance wound left eyelid. Note oval entrance wound withabrasion collar indicating that the projectile entered from the leftside of the head. The concentration of propellant powder confirmsthe above observation.
Photograph 23. A bullet exit wound over the occipital area of skull. Note thebevelled outer table with linear fracture lines radiating from theperiphery of the central fracture, and the sharply edged irregularwound on the inner table of skull.
259
Colour supplement
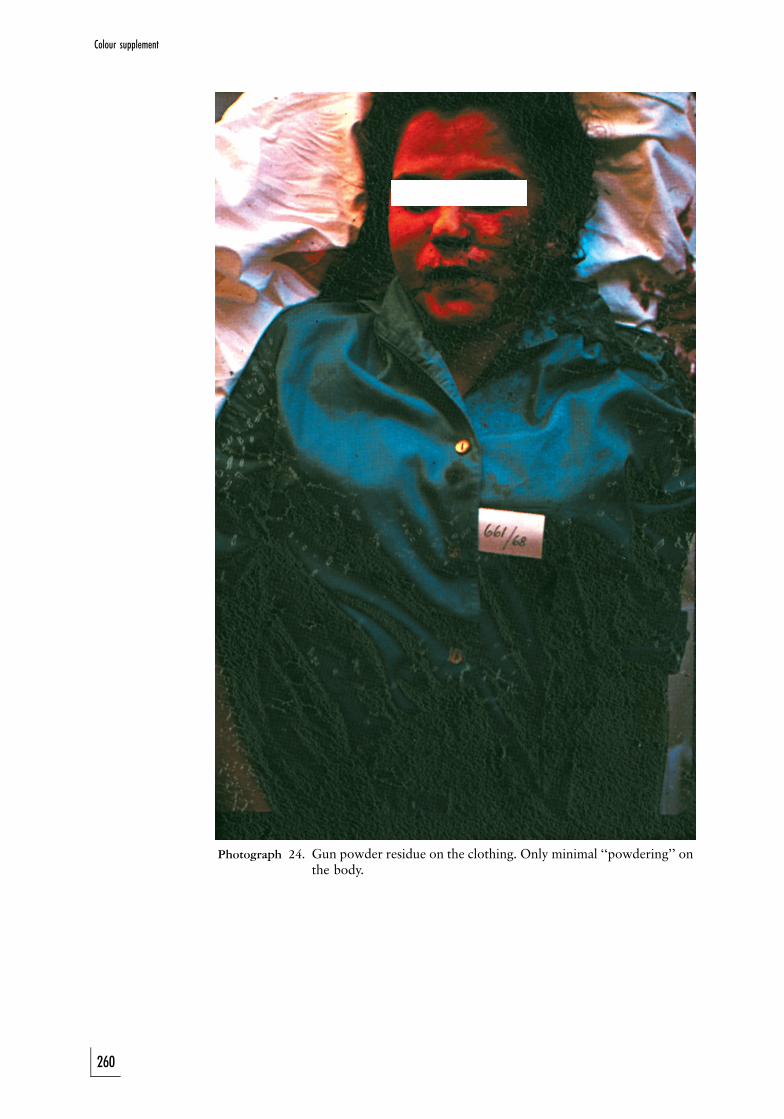
Photograph 24. Gun powder residue on the clothing. Only minimal ‘‘powdering’’ onthe body.
260
Colour supplement
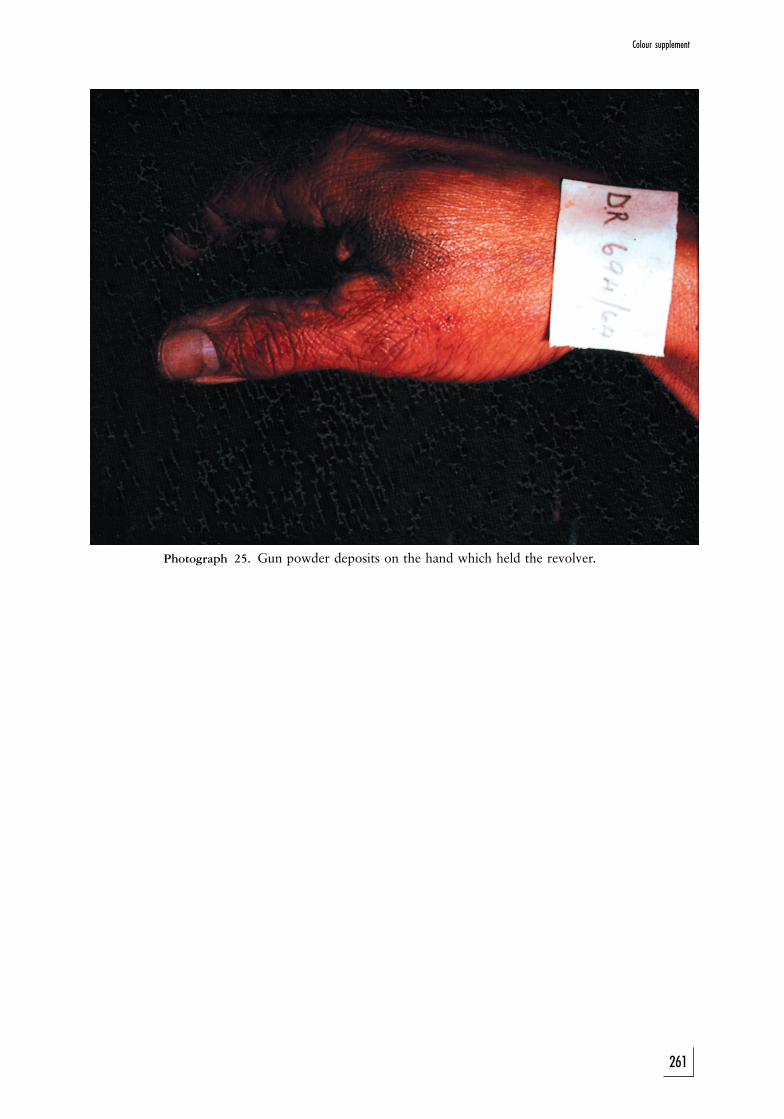
Photograph 25. Gun powder deposits on the hand which held the revolver.
261
Colour supplement
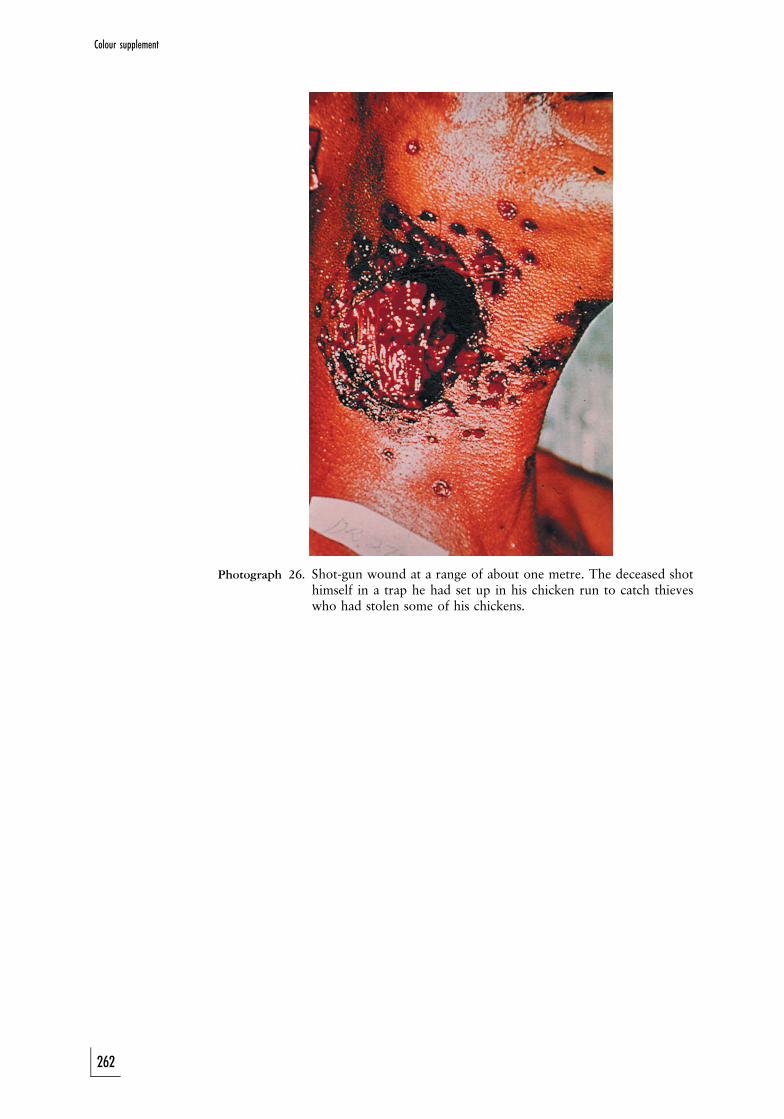
Photograph 26. Shot-gun wound at a range of about one metre. The deceased shothimself in a trap he had set up in his chicken run to catch thieveswho had stolen some of his chickens.
262
Colour supplement
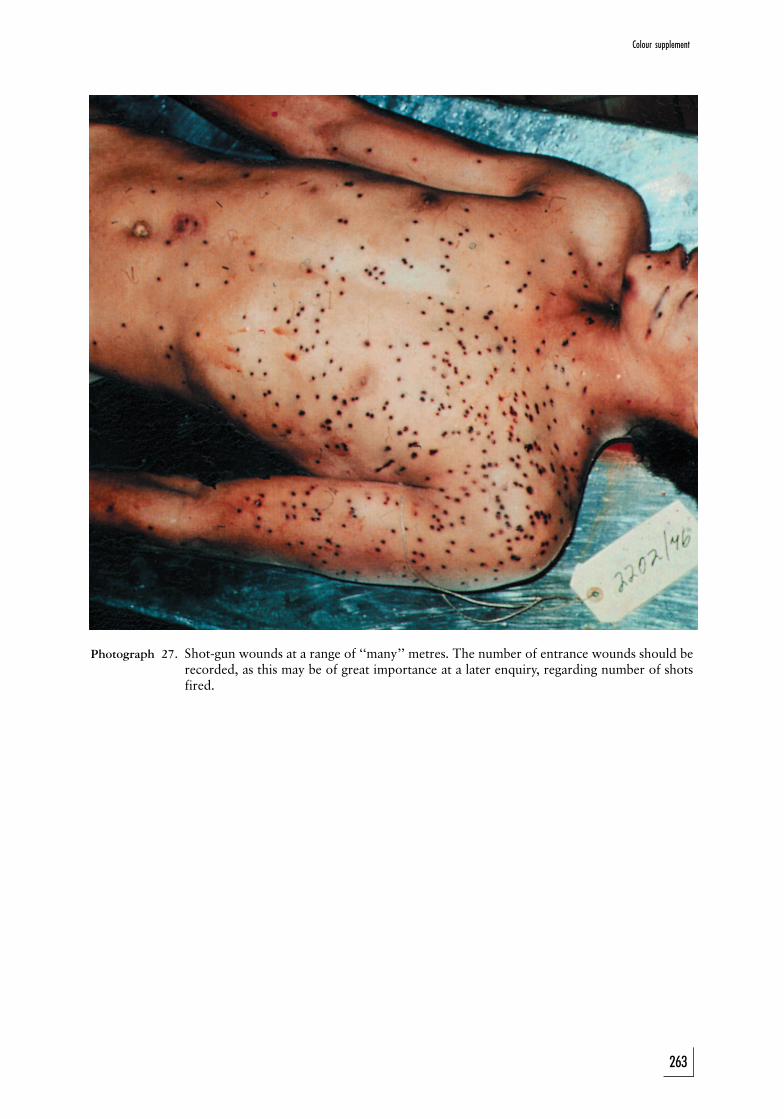
Photograph 27. Shot-gun wounds at a range of ‘‘many’’ metres. The number of entrance wounds should berecorded, as this may be of great importance at a later enquiry, regarding number of shotsfired.
263
Colour supplement
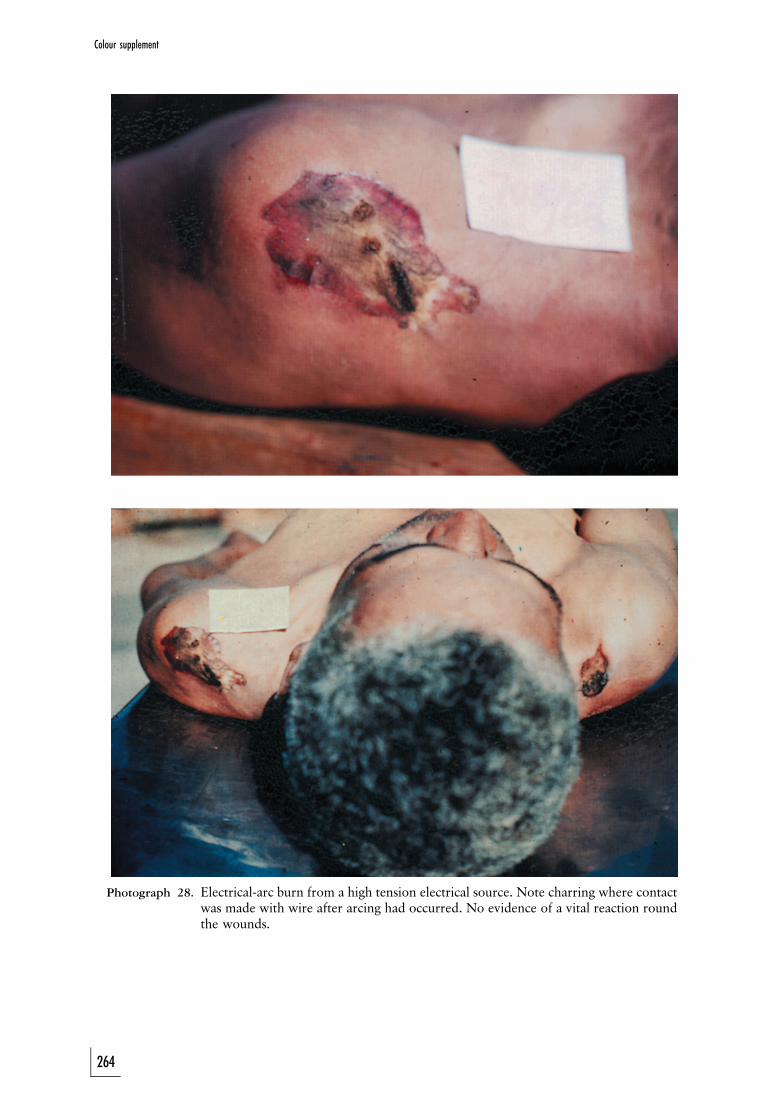
Photograph 28. Electrical-arc burn from a high tension electrical source. Note charring where contactwas made with wire after arcing had occurred. No evidence of a vital reaction roundthe wounds.
264
Colour supplement
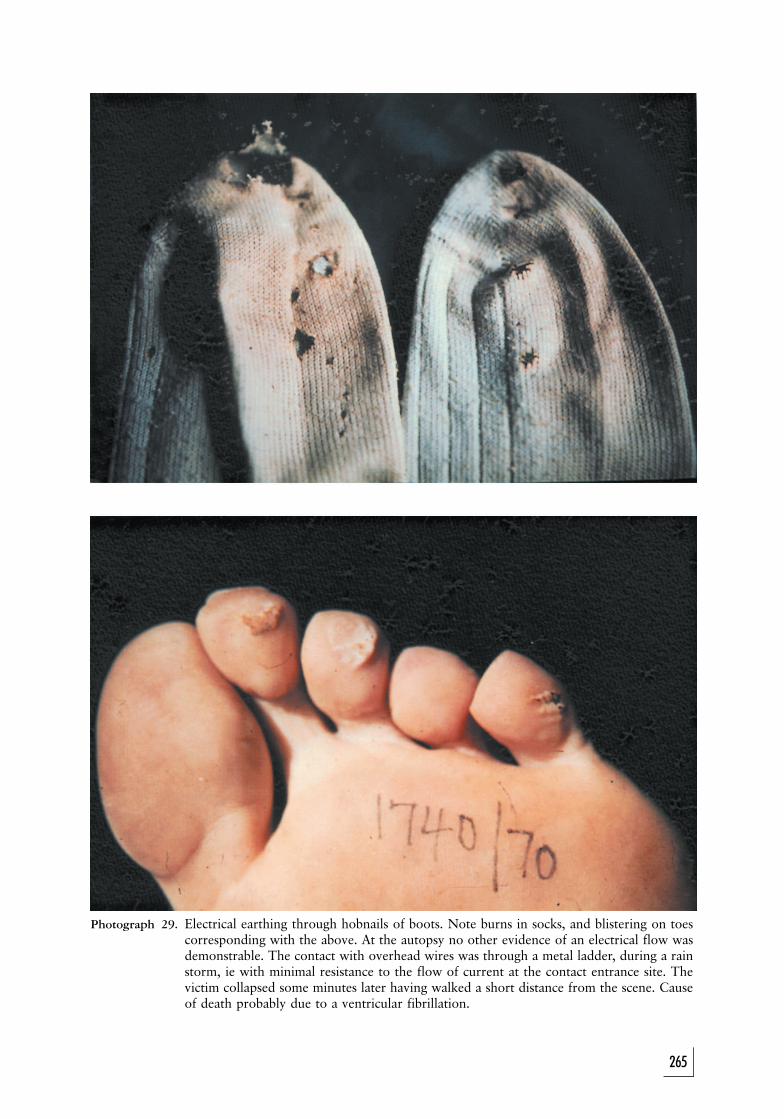
Photograph 29. Electrical earthing through hobnails of boots. Note burns in socks, and blistering on toescorresponding with the above. At the autopsy no other evidence of an electrical flow wasdemonstrable. The contact with overhead wires was through a metal ladder, during a rainstorm, ie with minimal resistance to the flow of current at the contact entrance site. Thevictim collapsed some minutes later having walked a short distance from the scene. Causeof death probably due to a ventricular fibrillation.
265
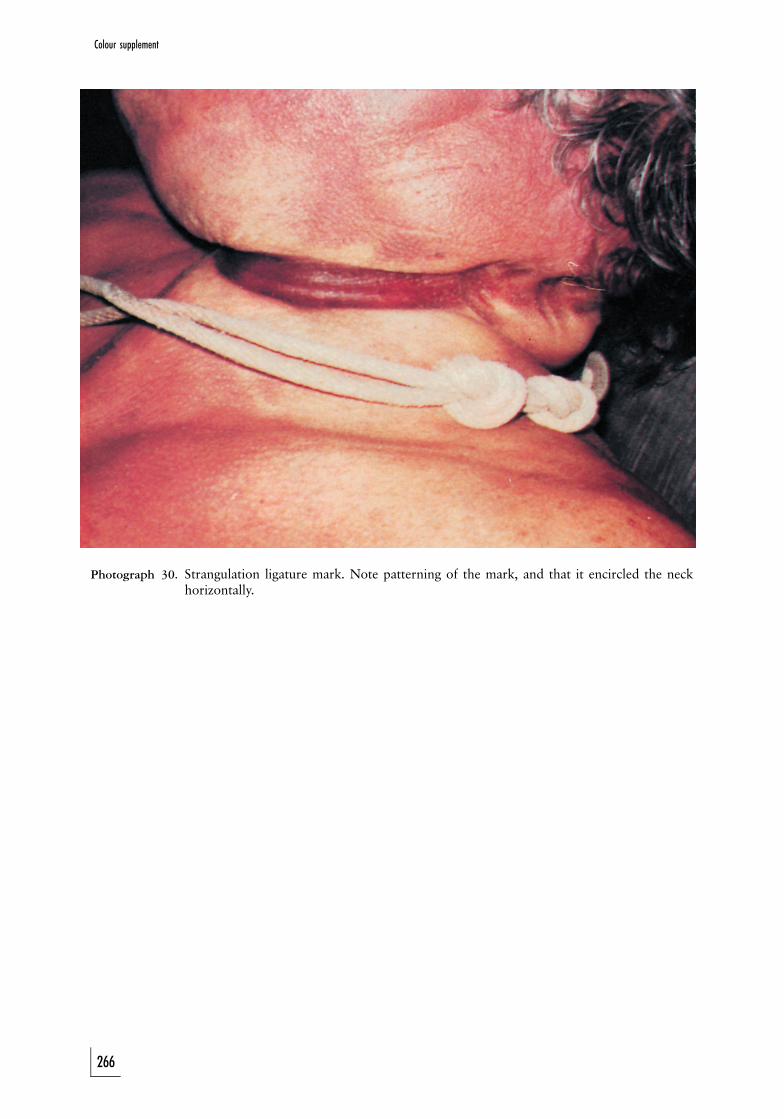
Photograph 30. Strangulation ligature mark. Note patterning of the mark, and that it encircled the neckhorizontally.
266
Colour supplement
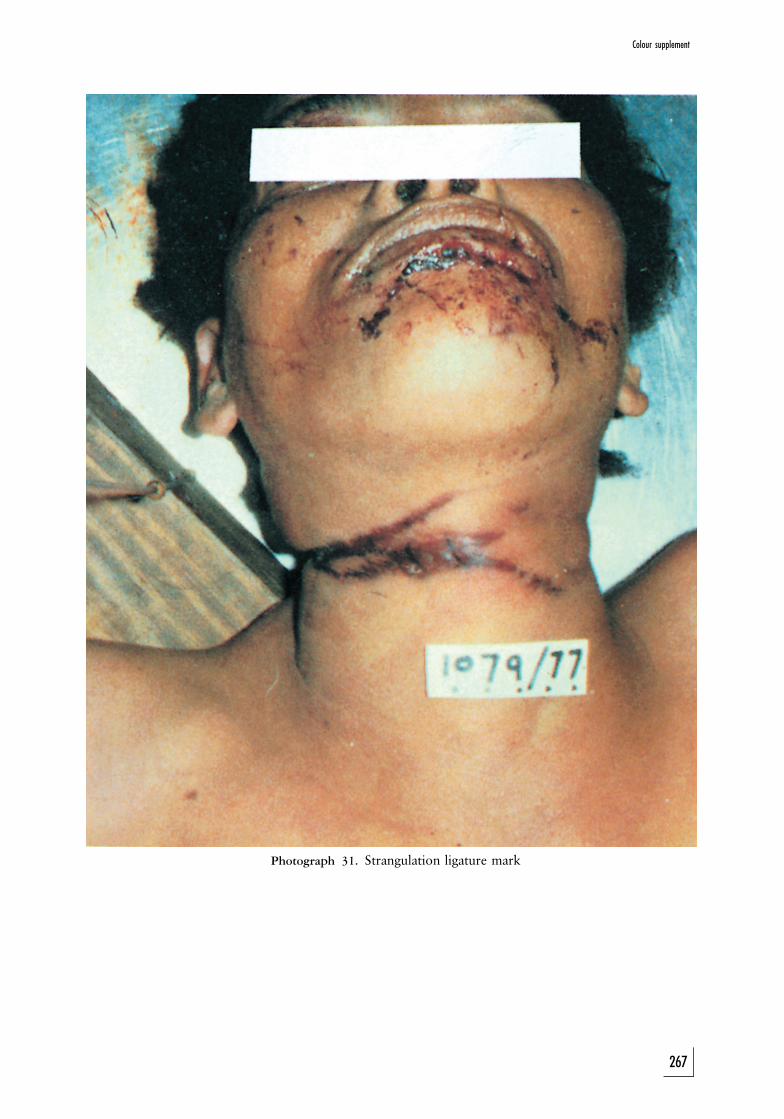
Photograph 31. Strangulation ligature mark
267
Colour supplement
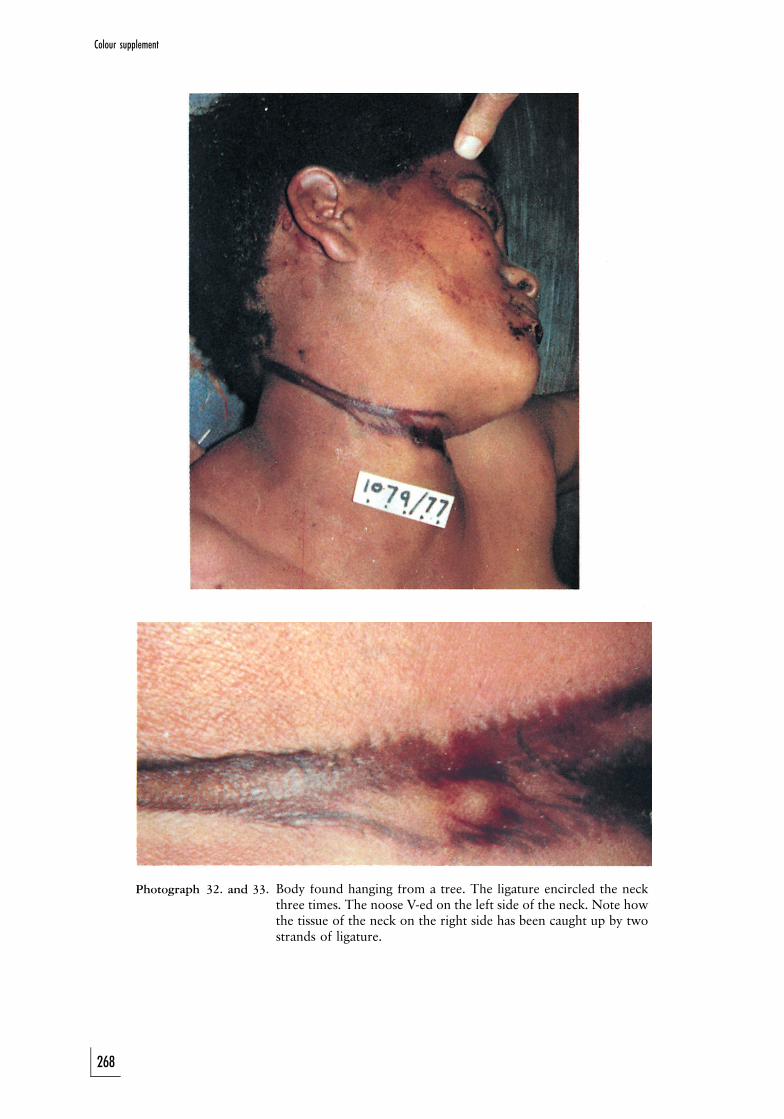
Photograph 32. and 33. Body found hanging from a tree. The ligature encircled the neckthree times. The noose V-ed on the left side of the neck. Note howthe tissue of the neck on the right side has been caught up by twostrands of ligature.
268
Colour supplement
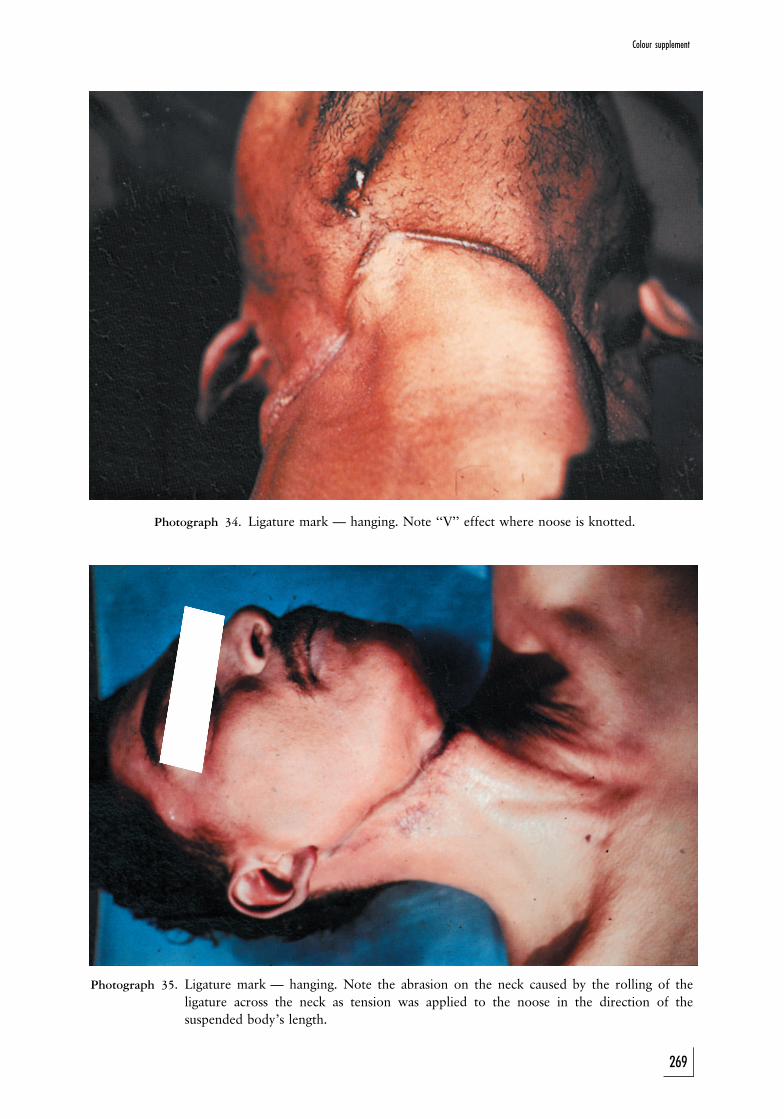
Photograph 34. Ligature mark — hanging. Note ‘‘V’’ effect where noose is knotted.
Photograph 35. Ligature mark — hanging. Note the abrasion on the neck caused by the rolling of theligature across the neck as tension was applied to the noose in the direction of thesuspended body’s length.
269
Colour supplement
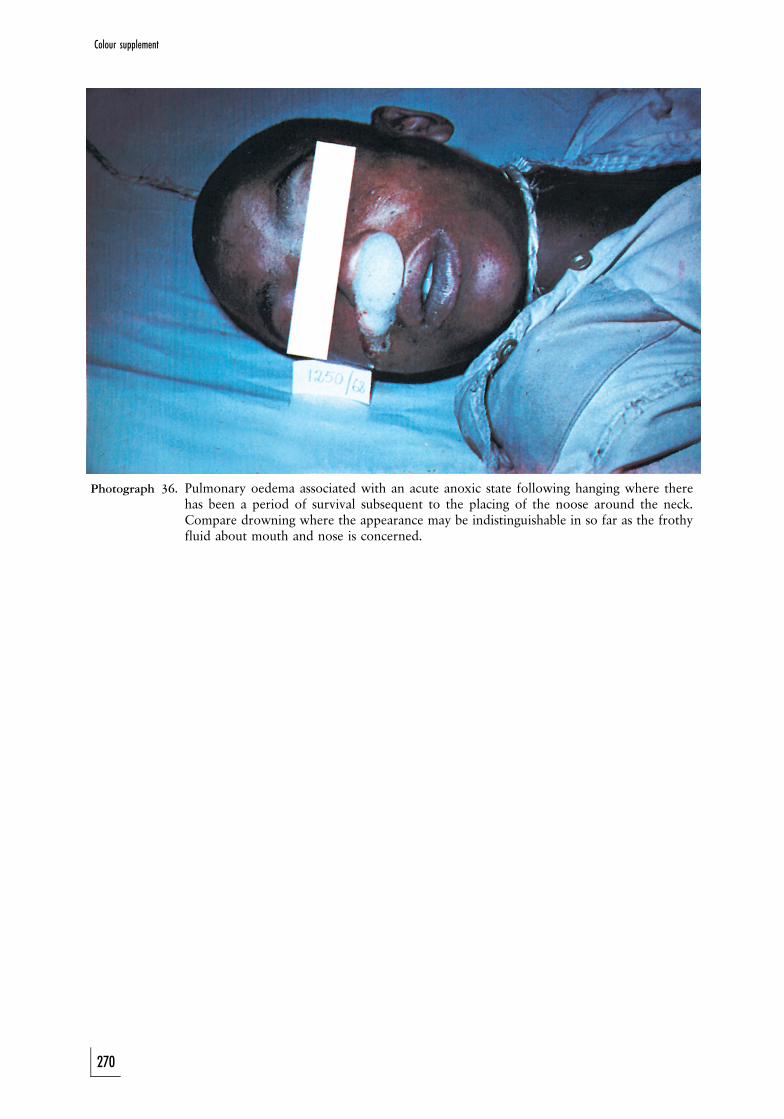
Photograph 36. Pulmonary oedema associated with an acute anoxic state following hanging where therehas been a period of survival subsequent to the placing of the noose around the neck.Compare drowning where the appearance may be indistinguishable in so far as the frothyfluid about mouth and nose is concerned.
270
Colour supplement

Photograph 37. Diatoms in the bone marrow of a case of drowning match thediatoms of the water in which the drowning occurred. Deceased wasa strong swimmer. Blood alcohol concentration — 0,30 g%. (Thepresence of diatoms is, of course, established microscopically. Thephotograph represents a huge enlargement.)
271
Colour supplement
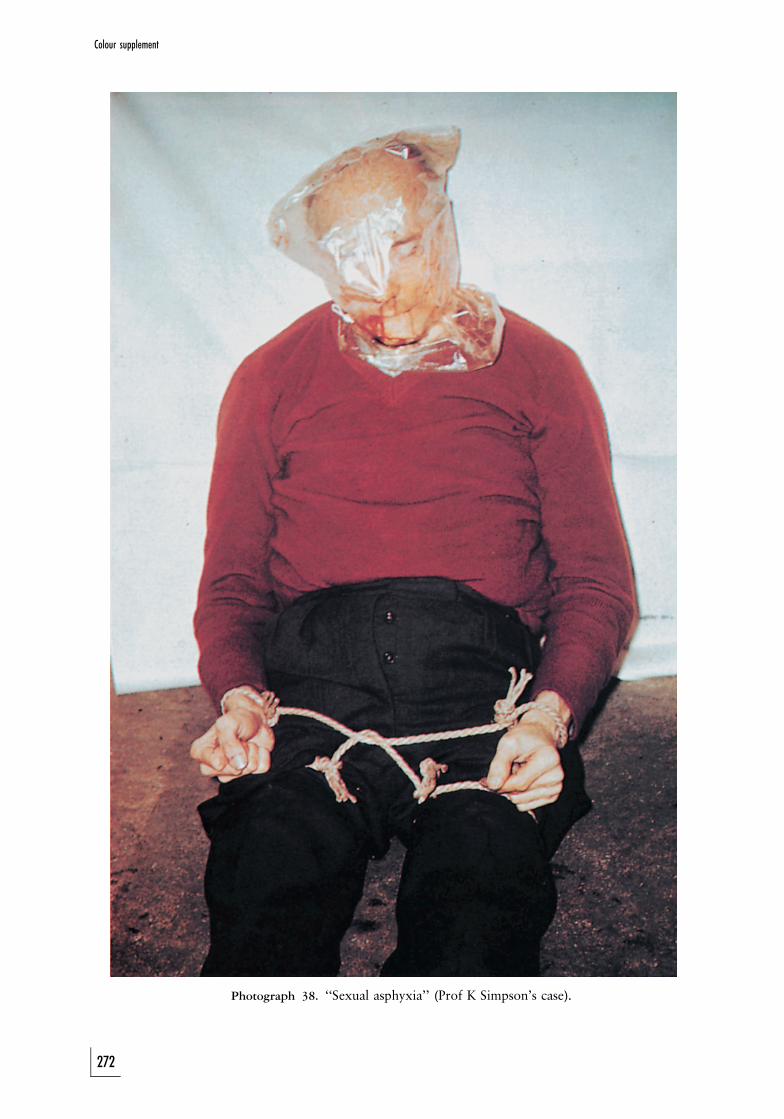
Photograph 38. ‘‘Sexual asphyxia’’ (Prof K Simpson’s case).
272
Colour supplement

Photograph 39. A ligature strangulation mark caused a week prior to death from inhalationpneumonia, which followed on inhalation of vomitus after the ‘‘strangulation’’
273
Colour supplement
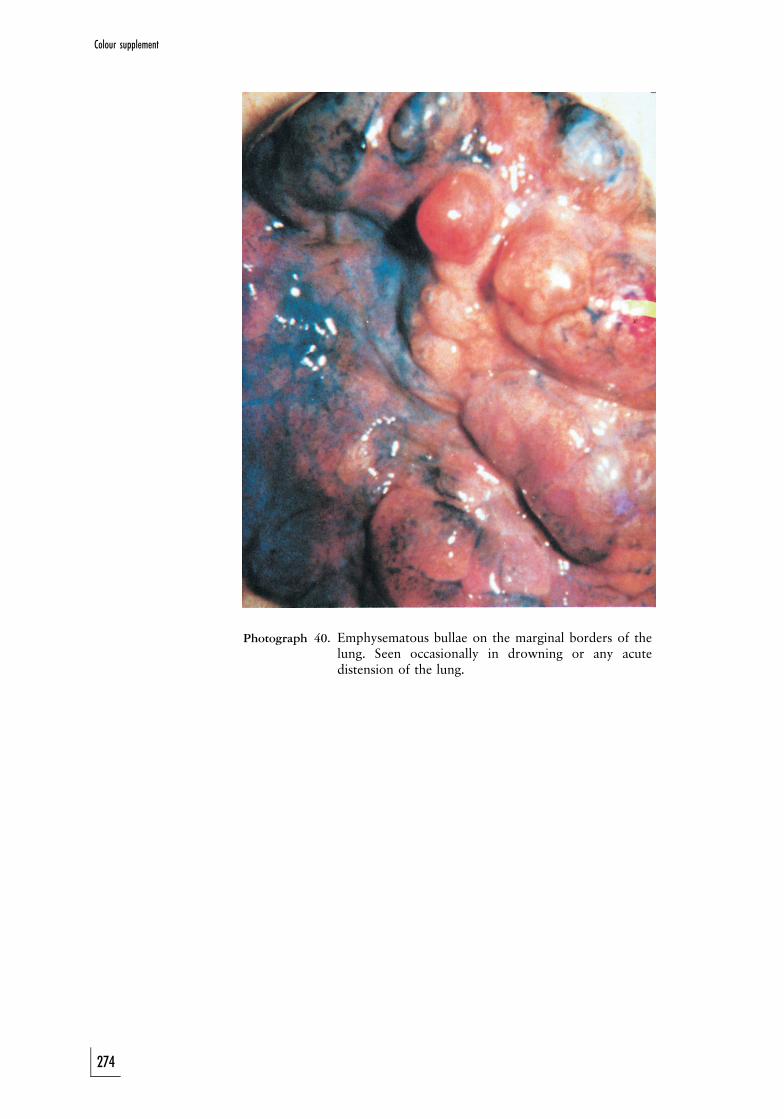
Photograph 40. Emphysematous bullae on the marginal borders of thelung. Seen occasionally in drowning or any acutedistension of the lung.
274
Colour supplement
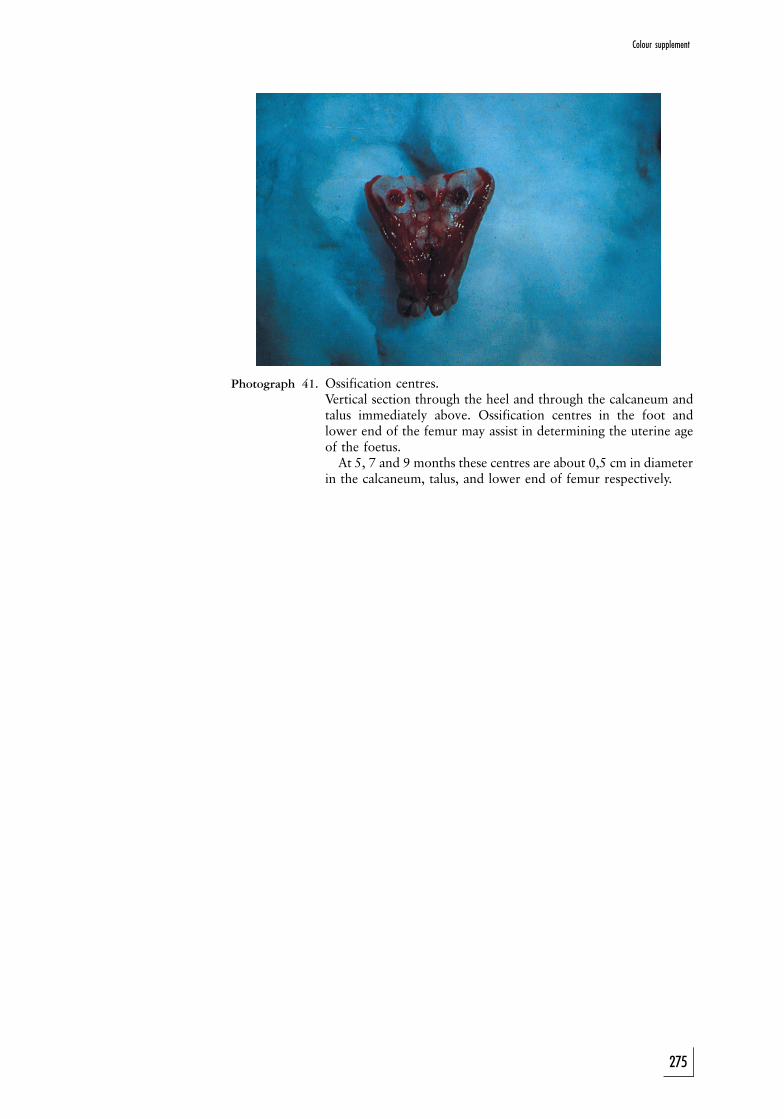
Photograph 41. Ossification centres.Vertical section through the heel and through the calcaneum andtalus immediately above. Ossification centres in the foot andlower end of the femur may assist in determining the uterine ageof the foetus.At 5, 7 and 9 months these centres are about 0,5 cm in diameter
in the calcaneum, talus, and lower end of femur respectively.
275
Colour supplement
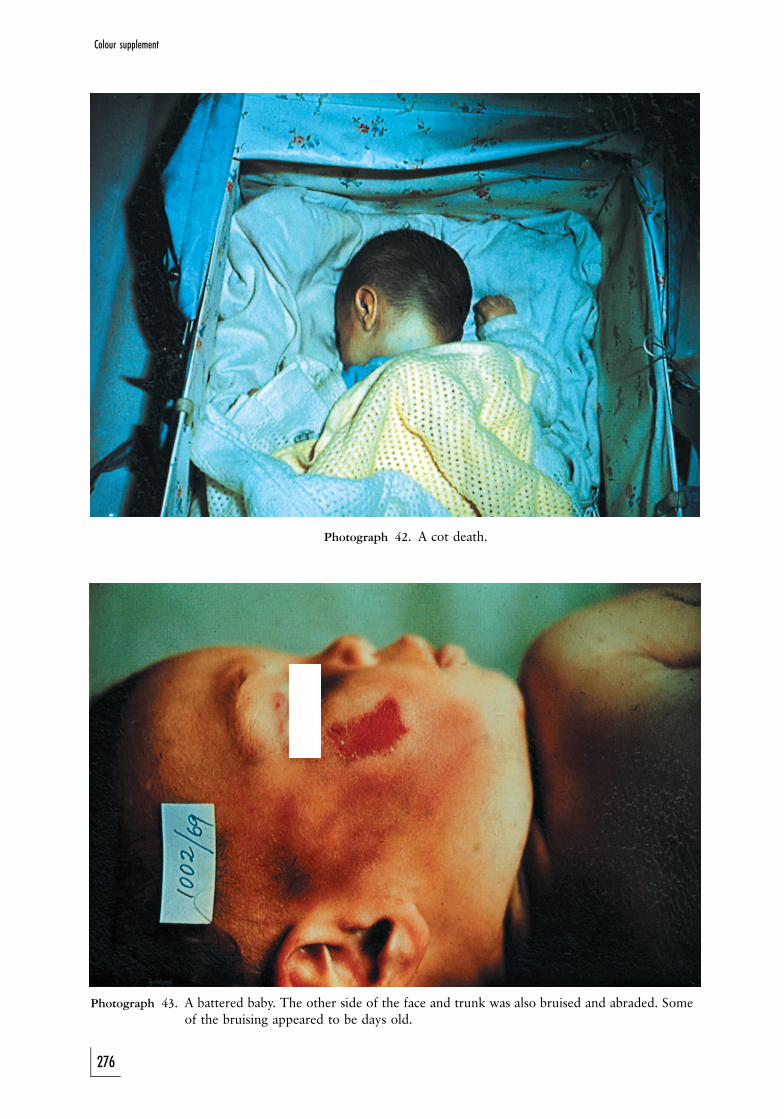
Photograph 42. A cot death.
Photograph 43. A battered baby. The other side of the face and trunk was also bruised and abraded. Someof the bruising appeared to be days old.
Colour supplement
276
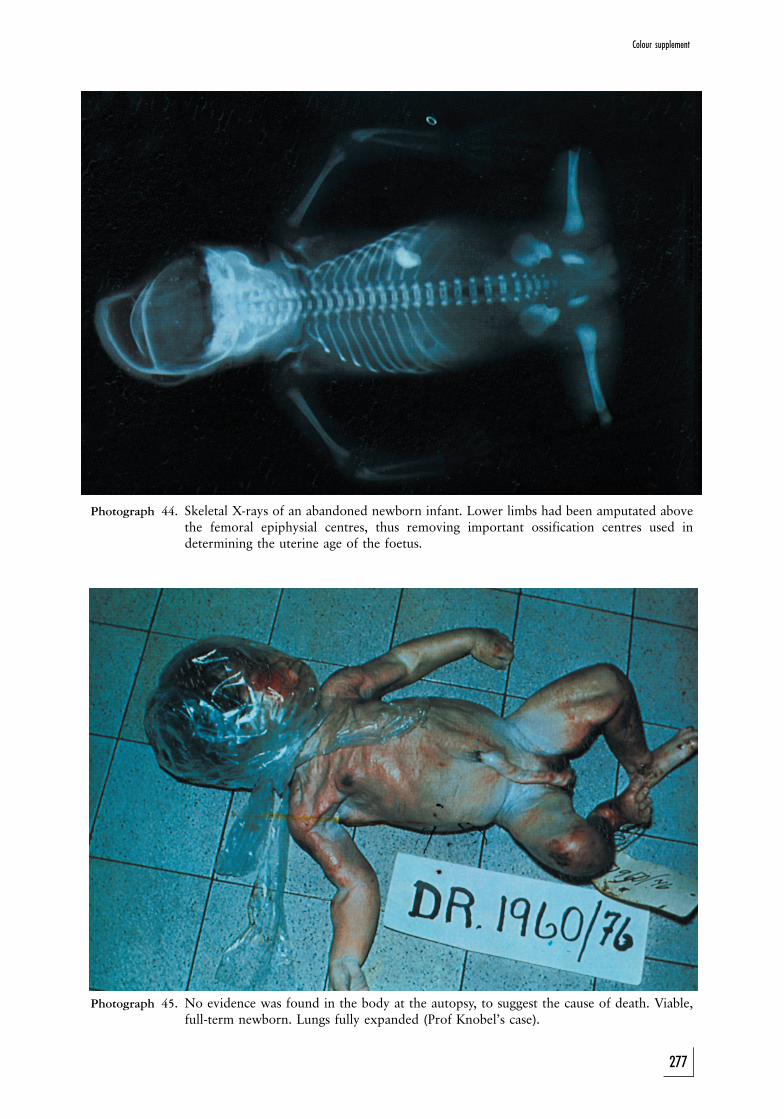
Photograph 44. Skeletal X-rays of an abandoned newborn infant. Lower limbs had been amputated abovethe femoral epiphysial centres, thus removing important ossification centres used indetermining the uterine age of the foetus.
Photograph 45. No evidence was found in the body at the autopsy, to suggest the cause of death. Viable,full-term newborn. Lungs fully expanded (Prof Knobel’s case).
Colour supplement
277
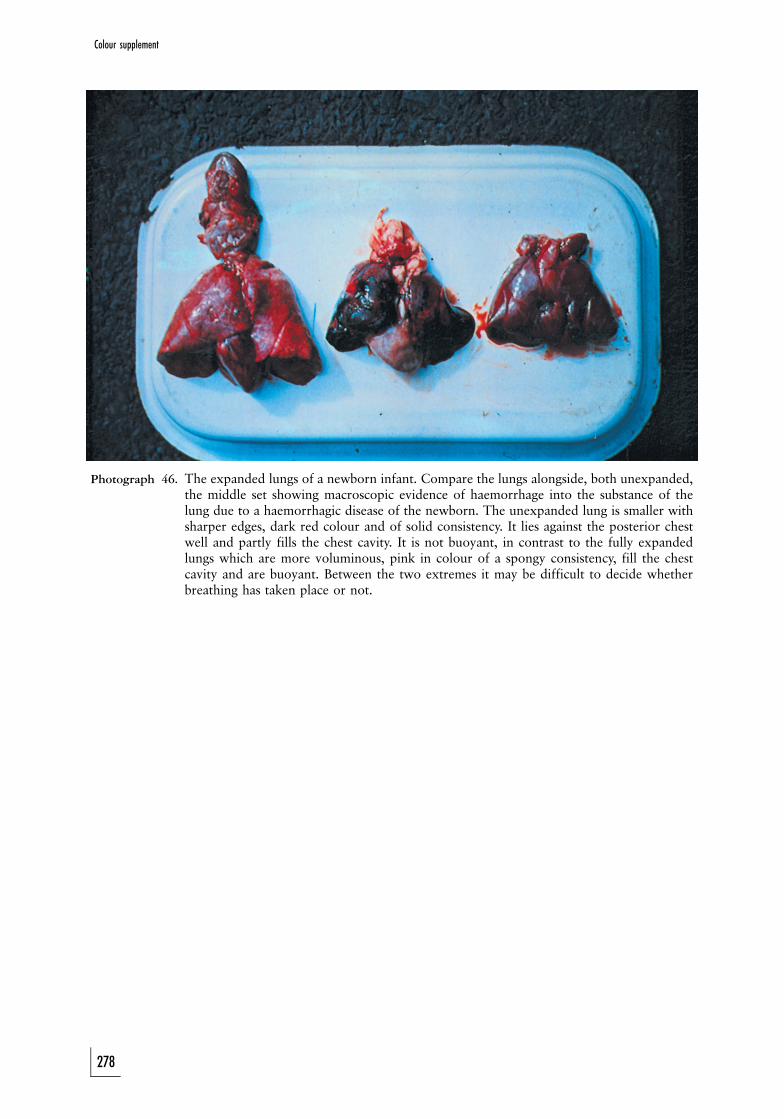
Photograph 46. The expanded lungs of a newborn infant. Compare the lungs alongside, both unexpanded,the middle set showing macroscopic evidence of haemorrhage into the substance of thelung due to a haemorrhagic disease of the newborn. The unexpanded lung is smaller withsharper edges, dark red colour and of solid consistency. It lies against the posterior chestwell and partly fills the chest cavity. It is not buoyant, in contrast to the fully expandedlungs which are more voluminous, pink in colour of a spongy consistency, fill the chestcavity and are buoyant. Between the two extremes it may be difficult to decide whetherbreathing has taken place or not.
Colour supplement
278

Photograph 47. Acute pulmonary oedema in a case of parathion poisoning.
Colour supplement
279

Photograph 48. Acute pulmonary oedema in drowning — a mixture of oedema and drowning fluid.
Colour supplement
280
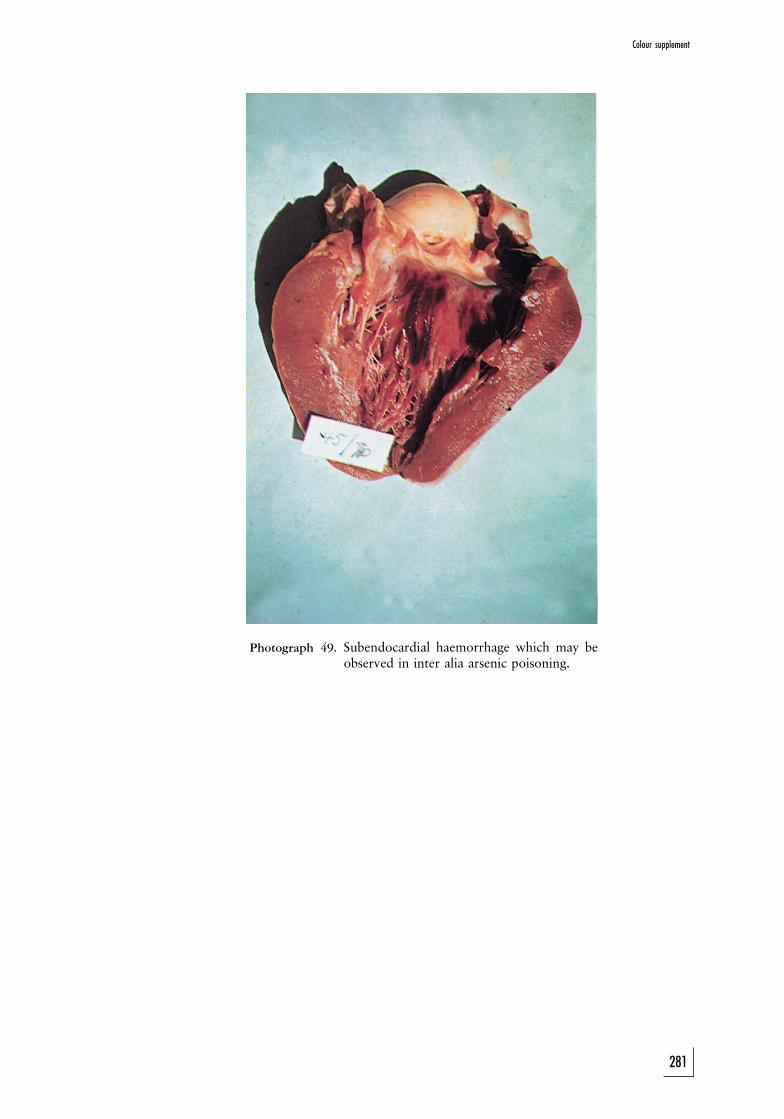
Photograph 49. Subendocardial haemorrhage which may beobserved in inter alia arsenic poisoning.
Colour supplement
281
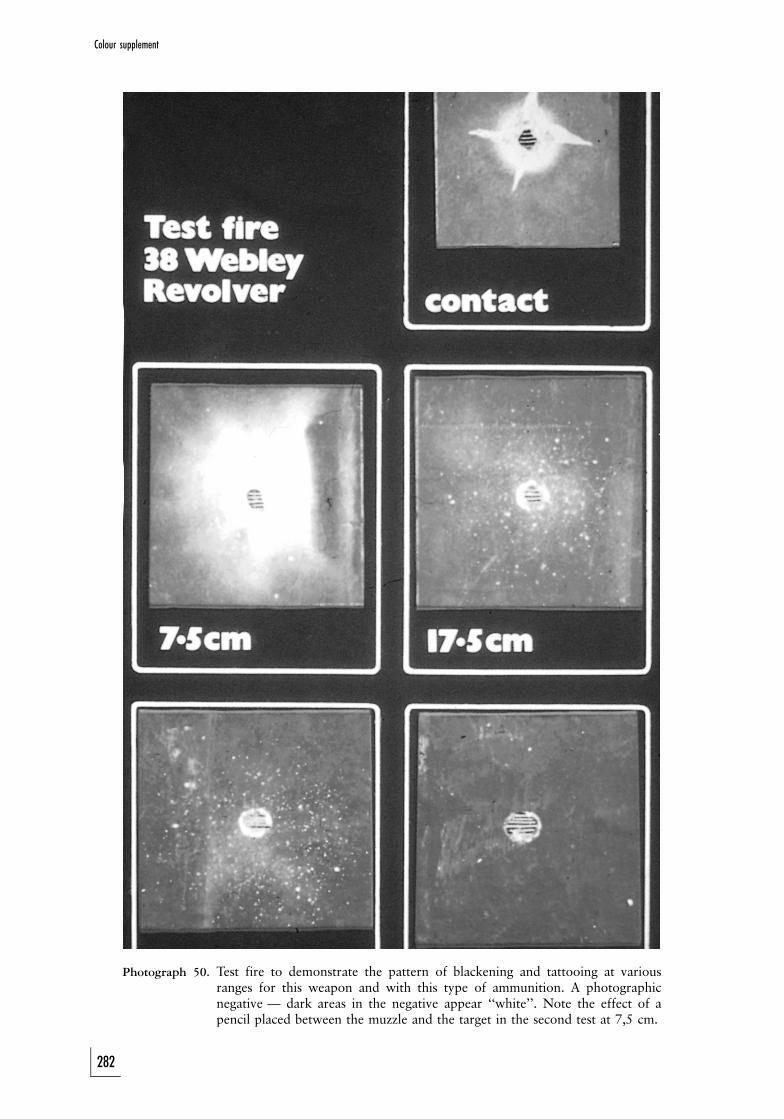
Photograph 50. Test fire to demonstrate the pattern of blackening and tattooing at variousranges for this weapon and with this type of ammunition. A photographicnegative — dark areas in the negative appear ‘‘white’’. Note the effect of apencil placed between the muzzle and the target in the second test at 7,5 cm.
Colour supplement
282
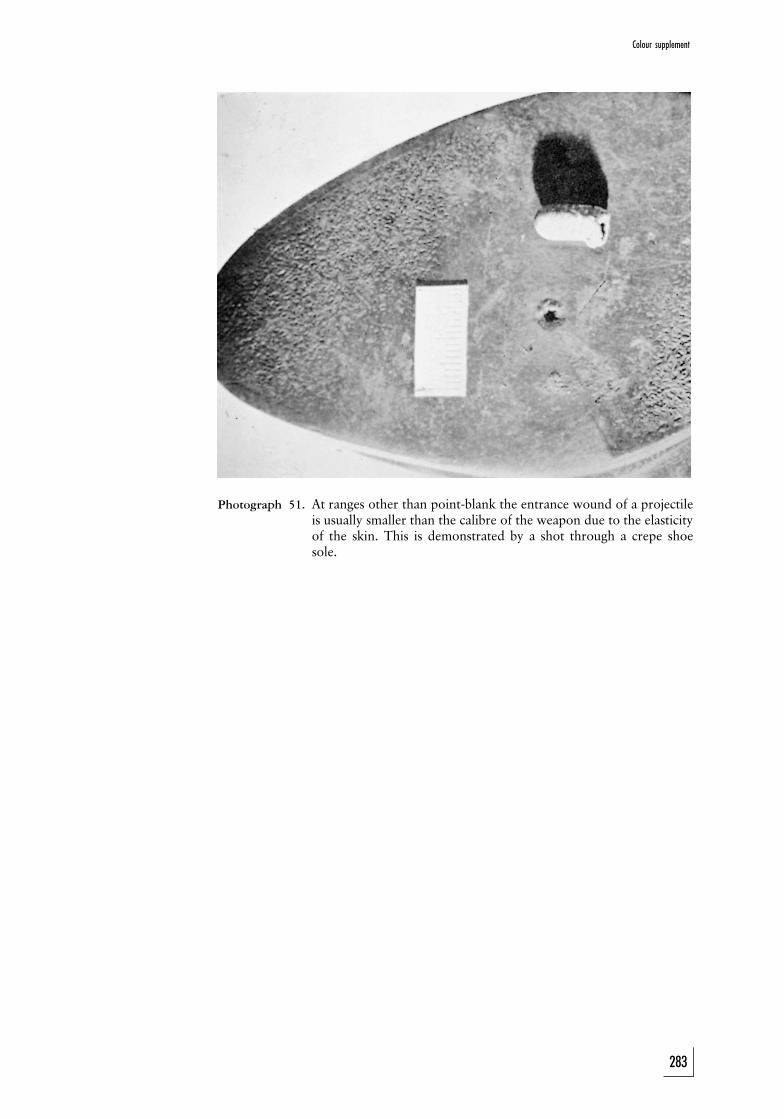
Photograph 51. At ranges other than point-blank the entrance wound of a projectileis usually smaller than the calibre of the weapon due to the elasticityof the skin. This is demonstrated by a shot through a crepe shoesole.
Colour supplement
283
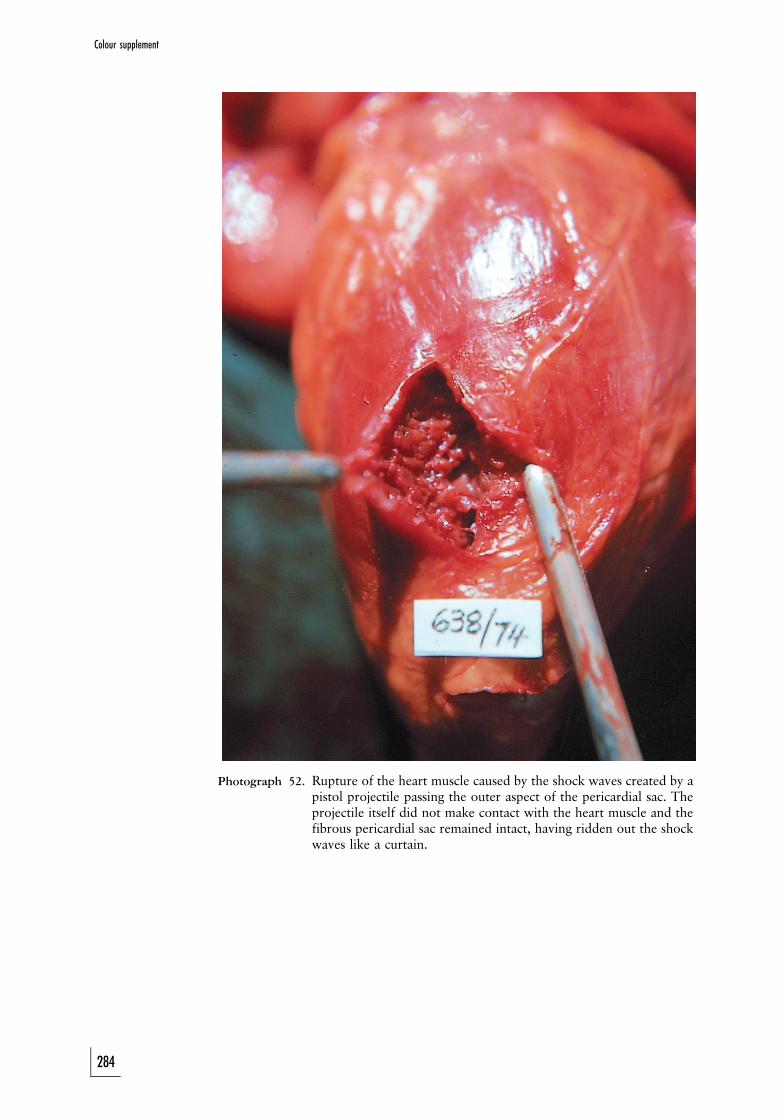
Photograph 52. Rupture of the heart muscle caused by the shock waves created by apistol projectile passing the outer aspect of the pericardial sac. Theprojectile itself did not make contact with the heart muscle and thefibrous pericardial sac remained intact, having ridden out the shockwaves like a curtain.
284
Colour supplement
Photograph 53. Cafe Death? Death in this case probably due to obstruction of the airway by abolus of steak. In the case of a neurogenic cardiac arrest it would be unlikely thatthe victim would appear cyanosed. The appropriate sudden compression of thelower chest often forces the obstruction out of the respiratory tract; the placing ofan oxygen mask over the nose and mouth serves no purpose, and iscontraindicated before the obstruction is removed. (With thanks to the Journalof the American Medical Association.)
Photograph 54. Cafe Death. Note the piece of steak which impacted in the pharynx.
285
Colour supplementColour supplement
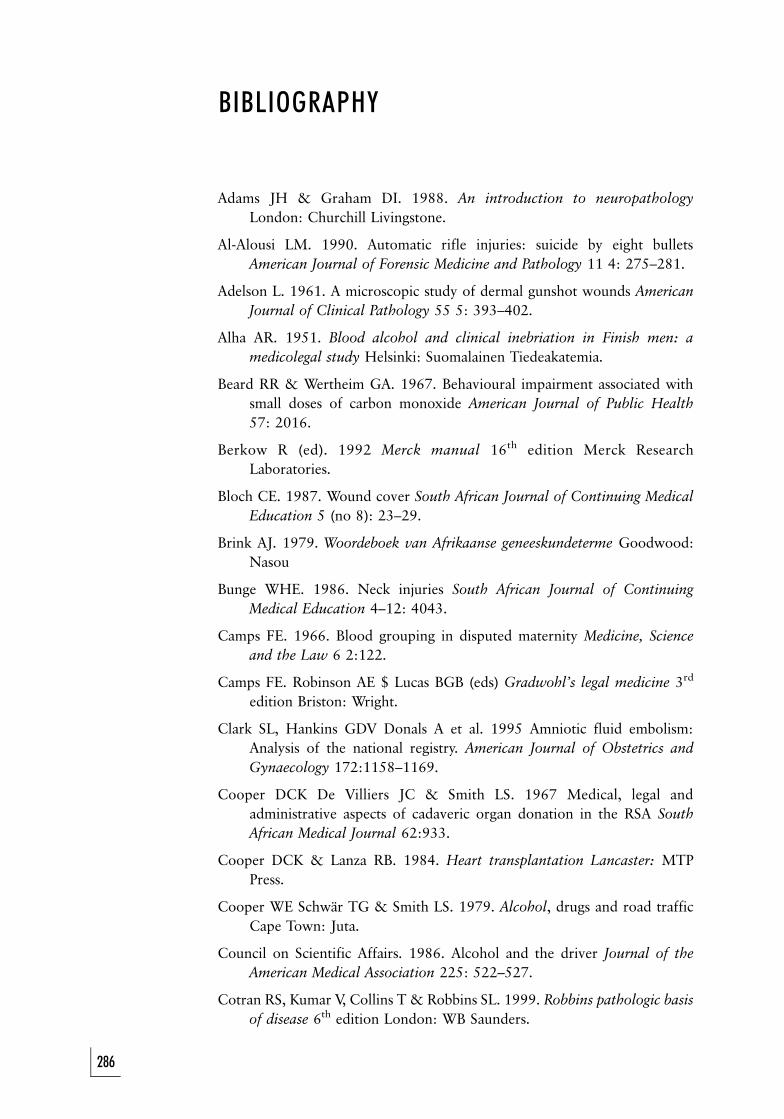
BIBLIOGRAPHY
Adams JH & Graham DI. 1988. An introduction to neuropathologyLondon: Churchill Livingstone.
Al-Alousi LM. 1990. Automatic rifle injuries: suicide by eight bulletsAmerican Journal of Forensic Medicine and Pathology 11 4: 275–281.
Adelson L. 1961. A microscopic study of dermal gunshot wounds AmericanJournal of Clinical Pathology 55 5: 393–402.
Alha AR. 1951. Blood alcohol and clinical inebriation in Finish men: amedicolegal study Helsinki: Suomalainen Tiedeakatemia.
Beard RR & Wertheim GA. 1967. Behavioural impairment associated withsmall doses of carbon monoxide American Journal of Public Health57: 2016.
Berkow R (ed). 1992 Merck manual 16th edition Merck ResearchLaboratories.
Bloch CE. 1987. Wound cover South African Journal of Continuing MedicalEducation 5 (no 8): 23–29.
Brink AJ. 1979. Woordeboek van Afrikaanse geneeskundeterme Goodwood:Nasou
Bunge WHE. 1986. Neck injuries South African Journal of ContinuingMedical Education 4–12: 4043.
Camps FE. 1966. Blood grouping in disputed maternity Medicine, Scienceand the Law 6 2:122.
Camps FE. Robinson AE $ Lucas BGB (eds) Gradwohl’s legal medicine 3rd
edition Briston: Wright.
Clark SL, Hankins GDV Donals A et al. 1995 Amniotic fluid embolism:Analysis of the national registry. American Journal of Obstetrics andGynaecology 172:1158–1169.
Cooper DCK De Villiers JC & Smith LS. 1967 Medical, legal andadministrative aspects of cadaveric organ donation in the RSA SouthAfrican Medical Journal 62:933.
Cooper DCK & Lanza RB. 1984. Heart transplantation Lancaster: MTPPress.
Cooper WE Schwar TG & Smith LS. 1979. Alcohol, drugs and road trafficCape Town: Juta.
Council on Scientific Affairs. 1986. Alcohol and the driver Journal of theAmerican Medical Association 225: 522–527.
Cotran RS, Kumar V, Collins T & Robbins SL. 1999. Robbins pathologic basisof disease 6th edition London: WB Saunders.
286
Currie JRB. 1970. Psychiatric assessment of the battered child syndromeSouth African Medical Journal 44: 635.
Curry AS 1972. Advances in forensic and clinical toxicology Cleveland: CRCPress.
Dada MA & McQuoid-Mason DJ. 2001. Introduction to medico-legalpractice Durban: Butterworths.
Dada MA Loftus IAJ & Rutherfoord GS Shotgun bullet embolism to the brainThe American Journal of Forensic Medicine and Pathology 14 1: 58–60.
Dada MA & Loftus IAJ. 1992. Stab wounds of the head: an autopsy study,presented at the 30th Annual Congress of the Federation of SouthAfrican Societies of Pathology in Cape Town, July 1990.
Davis S & Smith LS. 1982. Alcohol and drowning in Cape Town SouthAfrican Medical Journal 62: 931–933.
Davis S & Smith LS. 1985. The epidemiology of drowning in Cape Town.19801983. South African Medical Journal 68: 739–742.
Director-General, National Health and Population Development. 1990.Epidemiological comments 17 2.
Editor. 1990. Medical news and perspectives Journal of the American MedicalAssociation 263 21.
Evans TJ & Krausz T 1994. Pathogenesis and pathology of shock RecentAdvances in Histopathology 16 London: Churchill Livingstone 21–47.
Fackler ML. 1988. Wound ballistics Journal of the American MedicalAssociation 259 18: 2730–2736.
Gallagher PJ. 1994. The investigation of cardiac death Recent Advances inHistopathology 16 London: Churchill Livingstone 123–146.
Glaister J & Brash JC. 1937. Medico-legal aspects of the Ruxton case 48Edinburgh E & S Livingstone.
Gonzales T Vance M Helpern M & Umberger CJ 1954. Legal medicine,pathology and toxicology 2nd edition East Norwalk: Appleton-Century-Crofts.
Gordon J and Drennan MR. 1948. Medico-legal aspects of the Wolkersdorfercase S Afr Med J 22, 543–549.
Gordon I Shapiro HA & Berson SD. 1988. Forensic medicine: a guide toprinciples 3rd edition New York: Churchill Livingstone.
Haldane JBS. 1943. Heredity and politics London: Allen & Unwin.
Heins M. 1984. The battered child revisited Journal of the American MedicalAssociation 251 24: 32–95.
Hewlett RH. 1986. The forensic neurological examination South AfricanJournal of Continuing Medical Education 4 12:33–39.
287
BIBLIOGRAPHY
Hill IR. 1986. Toxicological findings in fatal aircraft accidents in the UnitedKingdom American Journal of Forensic Medicine and Pathology7 4: 322–326.
Hobbs CJ. 1985. ABC of head injuries British Medical Journal 292: 1169–1170.
Jetter WW. 1938. Studies in alcohol: diagnosis of acute alcoholic intoxicationby correlation of clinical and chemical findings American Journal ofMedical Science 196: 481.
Judex. 1949. Rex v Carr: medico-legal aspects of the trial and the appealSouth African Medical Journal 7: 647–651.
Kemp VD. 1986. Some random thoughts on the examination of ‘‘drunkendrivers’’ South African Journal of Continuing Medical Education: 29–31.
Kerr DJA. 1957. Forensic medicine 6th edition London: A and C Black.
Knight B. 1996. Forensic pathology 2nd edition London: Edward Arnold.
Knight B. 1987. Legal aspects of medical practice 4th edition London:Churchill Livingstone.
Loftus IAJ & Dada MA. 1992. A retrospective analysis of alcohol in medico-legal post-mortems over a period of five years The American Journal ofForensic Medicine and Pathology. 13 3: 248–252.
Loftus IAJ Nel JP & Rossouw DJ. The spectrum of pulmonary pathology infatal poisoning presented at the 2nd Medico-Legal Symposium, Durban,May 1993.
Loubser JD. 1986. Ophang as ’n oorsaak van dood — die post mortemdiagnose South African Journal of Continuing Medical Education4 12: 45–48.
Mason JK. 1983. Forensic medicine for lawyers 2nd edition London:Butterworths.
Medical defence Union Annual Report 1987: 16.
Merz B. 1988. DNA fingerprints come to court Journal of the AmericanMedical Association 259 15: 2193–2194.
Moar JJ. 1986. Forensic pathology of missile wounding South African JournalContinuing Medical Education 4 11: 44–48.
Nel JP. 1986. Sudden death South African Journal of Continuing MedicalEducation 4 11: 56.
Nortje CJ, Thomas CJ, Van Wyk CW & Philips VM. 1986. Forensieseodontologie: ’n bruikbare aspek van geregtelike geneeskunde SouthAfrican Journal of Continuing Medical Education 4 12: 712.
Olivier JA. 1986. Die farmakologiese uitwerking van etielalkohol op diemenslike liggaam South African Journal of continuing Medical education4 12: 23–28.
288
BIBLIOGRAPHY
Palmon SC, Moore LE, Lundberg J & Toung T. 1997. Venous air embolism:A review J Clinical Anesthesia 9:251–257.
Polson CJ, Gee DJ & Knight B 1985. The essentials of forensic medicine 4th
edition Oxford: Pergamon.
Raekallio J. 1980. Estimation of time in forensic biology and pathologyAmerical Journal of Forensic Medicine and Pathology 1 3: 213–218.
Reay DT & Eisele JW. 1982. Death from law enforcement neck holdsAmerican Journal of Forensic Medicine and Pathology 3 3: 252–258.
Rentoul E & Smith H. 1973. Glaister’s Medical jurisprudence and toxicologyEdinburgh: Churchill Livingstone.
Rhodes WF, Gordon I & Turner R. 1945. Medical jurisprudence 2nd editionEdinburgh: Postgraduate Press.
Schleyer F. 1963. Determination of the time of death in the early post-mortem interval, in Methods of forensic science vol 2 edited by FLindquist London: Interscience.
Schwar TG. 1986. Natural and non-natural death South African Journal ofContinuing Medical Education 4 11: 13–17.
Schwar TG, Loubser JD & Olivier JA. 1984. Die ABC van geregtelikegeneeskunde Kaapstad: HAUM.
Simpson K. 1969. Forensic medicine 6 ed, 34–38.
Sinclair-Smith CC & Kibel MA. 1986. Sudden infant death South AfricanJournal of Continuing Medical Education 4 12: 13–17.
Smith LS. 1981. Alcohol and violent death. Paper read at the conference‘‘Alcohol in perspective’’, held by the Department of Health in Pretoria.
Smith LS. 1986. The inquest as it relates to medical practice South AfricanJournal of Continuing Medical Education 4 11: 7–12.
Smith S. 1948. Taylor’s principles and practice of medical jurisprudence 10th
edition London: Churchill.
Snyman HW. 1981. Geneeskundewoordeboek 3de uitgawe Durban: Butter-worths.
Spitz WU & Fisher RS. 1980. Medico-legal investigation of death 2nd editionSpringfield: Thomas.
Strauss SA. 1991. Doctor, patient and the law 3rd edition Pretoria: Van Schaik.
Strauss SA. 1987. Regsgeneeskundige vrae en antwoorde SA Praktykbestuur/SA Practice Management 18 4: 13.
Tedeschi CG, Eckert W & Tedeschi L. 1977. Forensic medicine: a study intrauma and environmental hazards vol 13 Philadelphia: Saunders.
Toner PG & Crane J. 1994. Pathology of death in pregnancy Recent Advancesin Histopathology 16 London: Churchill Livingstone 189–211.
289
BIBLIOGRAPHY

Van Ieperen L. 1986. Kantaantekeninge by lugembolisme South AfricanJournal of Continuing Medical Education 4 11: 49–52.
Walker JA. 1975. Epidemiological issues about alcohol, other drugs andhighway safety, in Alcohol, drugs and road safety Toronto: ARF Books.
www.sahealthinfo.org/violence/national2005.pdf
www.saps.gov.za
www.sun.ac.za/anatpath/neuro_path/path/nphmpg2.html
BIBLIOGRAPHY
290

NOTES
291
NOTES
292

NOTES
293

NOTES
294

NOTES
295
Related Documents











