Supplementary materials Food Allergy and Anaphylaxis Guidelines European Academy of Allergy and Clinical Immunology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
European Academy of Allergy and Clinical Immunology
Supplementary materials
Food Allergy and Anaphylaxis Guidelines
European Academy of Allergy and Clinical Immunology
-
EAACI GUIDELINES Food Allergy and Anaphylaxis
Editors
Antonella Muraro
Graham Roberts
Editorial BoardIoana Agache
Carsten Bindslev-JensenAndy Clark
Anthony DuboisSusanne Halken
Karin Hoffmann-Sommergruber Aziz Sheikh
Thomas WerfelMargitta Worm
Supplementary materials
-
EAACI
Hagenholzsltrasse 111
3rd Floor
8050 Zurich
Switzerland
The European Academy of Allergy and Clinical Immunology, EAACI, is a non-profit organisation active in the field of allergic and immunologic diseases such as asthma, rhinitis, eczema, occupational allergy, food and drug allergy and anaphylaxis. EAACI was founded in 1956 in Florence and has become the largest medical association in Europe in the field of allergy and clinical immunology. It includes over 7800 members from 121 countries, as well as 47 National Allergy Societies.
- European Academy of Allergy and Clinical Immunology (EAACI) 2014
All rights reserved.
-
To all the members of EAACIand to our patients
-
Contents
Food allergy: diagnosis and managementE-3 The epidemiology of food allergy in Europe: systematic review and meta-analysisE-35 Prevalence of common food allergies in Europe: systematic review and meta-
analysisE-65 The diagnosis of food allergy: systematic review and meta-analysisE-75 Acute and long-term management of food allergy: systematic review
1
2 Primary prevention of food allergyE-109 Primary prevention of food allergy in children and adults: systematic review3 Quality of life in food allergy E-139 Disease-specific health-related quality of life instruments for IgE-mediated food allergy: systematic review4 Anaphylaxis E-151 The epidemiology of anaphylaxis in Europe: systematic reviewE-185 Management of anaphylaxis: systematic review
-
FOOD ALLERGY DIAGNOSIS
AND MANAGEMENT
1SECTION
Supplementary materials
-
BI Nwaru1, L Hickstein2, SS Panesar3, A Muraro4, T Werfel5, V Cardona6, AEJ Dubois7, S Halken8, K Hoffmann-Sommergruber9, LK Poulsen10, G Roberts11-13, R Van Ree14, BJ Vlieg-Boerstra15, A Sheikh3, 16 on
behalf of The EAACI Food Allergy & Anaphylaxis Guidelines Group
EAACI Food Allergy & Anaphylaxis Guidelines Group: CA Akdis, R Alvarez, K Beyer, C Bindslev-Jensen, V Cardona, P Demoly, A Dubois, P Eigenmann, M Fernandez Rivas, A Host, E Knol, G Lack, MJ Marchisotto, B
Niggeman, N Papadopolous, I Skypala, M Worm
1.1THE EPIDEMIOLOGY
OF FOOD ALLERGY IN EUROPE
SYSTEMATIC REVIEW AND META-ANALYSIS
Supplementary materials
-
AFFILIATIONS1 School of Health Sciences, University of Tampere, Finland
2 Institute for Medical Informatics, Biometry and Epidemiology, University of Munich, Germany3 Allergy & Respiratory Research Group, Center for Population Health Sciences, The University of Edinburgh, UK
4 Department of Pediatrics, Center for Food Allergy Diagnosis and Treatment, Veneto Region, University of Padua, Italy5 Hannover Medical School, Hanover, Germany
6 Hospital ValldHebron, Barcelona, Spain7 Department of Paediatrics, Division of Paediatric Pulmonology and Paediatric Allergy, University Medical Centre Groningen,
University of Groningen, Groningen, The Netherlands8 Odense University Hospital, Odense C, Denmark
9 Department of Pathophysciology and Allergy Research Medical University of Vienna, Vienna, Austria10 Laboratory of Medical Allergology, Allergy Clinic, Copenhagen University Hospital, Hellerup, Denmark
11 David Hide Asthma and Allergy Research Centre, St Marys Hospital, Newport, Isle of Wight, UK12 NIHR Southampton Respiratory Biomedical Research Unit, University of Southampton and University Hospital Southampton
NHS Foundation Trust, UK13 Human Development and Health and Clinical and Experimental Sciences Academic Units, Faculty of Medicine, University of
Southampton, UK14 Departments of Experimental Immunology and of Otorhinolaryngology, Academic Medical Center, University of Amsterdam,
The Netherlands15 Department of Pediatric Respiratory Medicine and Allergy, Emma Childrens Hospital, Academic Medical Center, University of
Amsterdam, The Netherlands16 Division of General Internal Medicine and Primary Care Brigham and Womens Hospital/Harvard Medical School, Boston, MA,
USA
-
E-5EAACI
Epidemiology of food allergy in Europe: a review
Supplementary materials
METHODSSearch strategyArticles were retrieved using a highly sensitive search strategy implemented in four electronic databases (OVID MEDLINE, OVID EMBASE, CINAHL, and ISI Web of Science). The search strategy was devised on OVID MEDLINE and then adapted for the other databases (see Box E1). Systematic reviews were retrieved by using the systematic review filter developed at McMaster University Health Information Research Unit (HIRU) (http://hiru.mcmaster.ca/hiru/HIRU_Hedges_MEDLINE_Strategies.aspx#Reviews). We also adapted the search filter from York University Centre for Reviews and Dissemination (http://www.york.ac.uk/inst/crd/intertasc/epidemiological_studies.html) to retrieve the characteristics describing the epidemiology of FA. The McMaster filter (http://hiru.mcmaster.ca/hiru/HIRU_Hedges_EMBASE_Strategies.aspx#Prognosis) was applied for retrieving studies on prognostic factors. Additional references were located byhand search. Unpublished work and research in progress were searched through discussion with experts in the field. There were no language restrictions, and where possible the literature in languages other than English was translated. The literature we were unable to translate is shown in the PRISMA flow diagram (Figure 1).
Inclusion and exclusion criteriaAs per the study design, we included systematic reviews and meta-analyses, cohort studies, case-control studies, cross-sectional studies, and routine healthcare studies. We excluded review and discussion papers, non-research letters and editorials, case studies and case series, animal studies, and all randomized controlled trials. Our initial inclusion criteria were broad by including studies published worldwide between January 1990 and September 2012. However, after assessing the large amount of articles, we made further restrictions to include studies published only in Europe (based on the United Nations definition (http://unstats.un.org/unsd/methods/m49/m49regin.htm#europe accessed on December 28, 2012) between January 1, 2000 and September 30, 2012, with the exception of Greenland and Turkey, which were included in the review because we believe they are culturally and politically more European than North American and Asia, respectively.
Term Definition
1 exp Food Hypersensitivity/
2 food allerg*.mp.
3 food hypersensitivity.mp.
4 food hypersensitivities.mp.
5 allergy, food.mp.
6 (rat or rats or cow or cows or chicken? or horse or horses or mice or mouse or bovine or animal$).ti.
7 exp animals/ not humans.sh.
8 6 or 7
9 *Incidence/
10 *Prevalence/
11 (incidence or prevalence or epidemiol$).ti.
12 epidemiologic methods/
13 *cohort studies/
14 controlled clinical trial.pt.
15 *case-control studies/
16 exp Food Hypersensitivity/ep [Epidemiology]
17 exp Hospitalization/
18 exp Hospitalization/sn, td [Statistics & Numerical Data, Trends]
19 exp Mortality/sn, td [Statistics & Numerical Data, Trends]
20 exp Epinephrine/ad, tu, th [Administration & Dosage, Therapeutic Use, Therapy]
21 exp "Cause of Death"/
22 ((adrenaline or epinephrine) adj3 (dispens$ or prescrib$)).tw.
23 or/9-22
24 or/1-5
25 23 and 24
26 25 not 8
27 limit 26 to yr="1990 - 2012"
Box E1 Ovid Medline search strategy
http://hiru.mcmaster.ca/hiru/HIRU_Hedges_MEDLINE_Strategies.aspx#Reviewshttp://hiru.mcmaster.ca/hiru/HIRU_Hedges_MEDLINE_Strategies.aspx#Reviewshttp://www.york.ac.uk/inst/crd/intertasc/epidemiological_studies.htmlhttp://www.york.ac.uk/inst/crd/intertasc/epidemiological_studies.htmlhttp://hiru.mcmaster.ca/hiru/HIRU_Hedges_EMBASE_Strategies.aspx#Prognosishttp://hiru.mcmaster.ca/hiru/HIRU_Hedges_EMBASE_Strategies.aspx#Prognosishttp://unstats.un.org/unsd/methods/m49/m49regin.htm#europehttp://unstats.un.org/unsd/methods/m49/m49regin.htm#europe
-
Epidemiology of food allergy in Europe: a review
E-6 EAACI Supplementary materials
Analysis, synthesis and reportingWe recalculated all the frequency estimates of FA occurrence if adequate data were provided by authors. If any discrepancies were observed between our recalculated estimates and those of the authors, we reported our recalculated estimates. Our recalculated estimates were based on the minimal measured events rather than extrapolated estimates. In studies where inadequate data were given to enable recalculation, we reported the estimates provided by the authors. Where needed and possible, we contacted authors of primary studies for clarifications. The 95% confidence intervals (95% CI) of our recalculations were computed by using the Wilson score method without continuity correction (15). Different reports from the same primary study were reported as one study. Although several specific food allergies were reported across the studies, the focus of the current report is to present the estimates for any FA. The other specific foods will be presented in a future report. In studies reporting estimates of sensitization to food allergy alongside cross-reactivity to pollen (wheat and grass), we always used the true estimates without pollen cross-reactivity, where possible.
We performed a random-effects meta-analysis for clinically and methodologically comparable studies to estimate the frequency of FA. The following outcomes were considered: 1. point and life-time prevalence of self-reported FA; 2. point prevalence of specific IgE positivity; 3. point prevalence of SPT positivity; 4. point prevalence of symptoms plus IgE positivity; 5. point prevalence of symptoms plus SPT positivity; 6. point prevalence of clinical history or OFC/DBPCFC-positivity; 7. point prevalence of positive response to food challenge (open food challenge [OFC] or DBPCFC). For outcomes 6 and 7 above, where a study reported estimates for both OFC and DBPCFC, the DBPCFC estimates were always used; otherwise OFC estimates were used if DBPCFC was not done in the study. We did not present pooled estimates for cumulative incidence of FA due to inconsistencies and very few data across studies.
We aimed to present stratified pooled estimates by different age groups (1 year and under, 2-5 years, 6-10 years, 11-17 years, 18-60 years, and older than 60 years). However, due to several overlapping ages of participants across the studies, the age-stratified pooled estimates were more feasibly computed for the age groups 0-17 years (children) and 18 years
and over (adults). A study with overlap between these two age groups was included in either age group if the age distribution was skewed to that age group. For studies that gave frequency estimates at different ages for the same individuals, we used the estimates for the highest age in computing the pooled estimates. We also present the pooled estimates stratified by geographical region in Europe (i.e., East, West, South, North, and Europe; the last group being for studies that included several European countries and gave overall estimate for all the countries and in which it was not possible to calculate the frequency for each country studied) using the classification by the UN (http://unstats.un.org/unsd/methods/m49/m49regin.htm#europe accessed December, 2012). Due to methodological differences across the studies investigating the risk and prognostic factors for FA (varied risk and prognostic factors studied, differences in study design, differences in statistical methods employed across studies, differences in factors considered for adjustment, and others), we did not perform meta-analysis for these studies.
RESULTS
Study characteristicsThe characteristics, main results, and the overall risk of bias grading of the studies included for review are shown in Table E1. Of the 56 studies reviewed, 31 were cross-sectional, 19 cohort, three were systematic reviews, and three case-control studies. Over 50% of the studies were conducted in northern European countries. A majority of the studies (n=37) were undertaken only in children. Ten studies assessed FA only by self-report, 10 only by specific-IgE or SPT positivity, while the remainder was a combination of self-report, specific-IgE or SPT sensitization, and food challenge. Twenty-six of the studies undertook food challenges for verifying FA, and 22 of these employed DBPCFC. A majority of the studies (n=49) reported point prevalence as the occurrence measure for estimating the frequency of FA. The majority of studies had a moderate risk of bias (Table E2).
Frequency of FASelf-reported FA: details of studiesEighteen of the 27 studies on self-reported FA included children (i.e., < 18 years). Two studies
http://unstats.un.org/unsd/methods/m49/m49regin.htm#europehttp://unstats.un.org/unsd/methods/m49/m49regin.htm#europe
-
E-7EAACI
Epidemiology of food allergy in Europe: a review
Supplementary materials
reported cumulative incidence in children: one study from Denmark reported the cumulative incidence of self-reported FA by the age of 6 years as 11.6% (27-29), whereas one study from the UK reported estimate of 25.8% by the age of 1 year and 28.1% by the age of 3 years (85-87). The lowest (1.6%) and highest (38.7%) point prevalence of FA were reported in Italy (20) and Norway (52), respectively (Figure E1). The lowest and highest life-time prevalence of FA was found in Turkey (5.7%) (59) and Poland (41.8%) (53), respectively (Table E3). The range of point prevalence of self-reported FAfor all age groups was 1.6% to 38.7% and the highest point prevalence was found in the age group 2-5 years (Table 1). The range of life-time prevalence of self-reported FA for all age groups was 5.7% to 41.8% and the highest life-time prevalence was found in the age group 6-10 years (Table E3).
FA by positive SPT or IgE to specific food allergens: details of studies
Of the 18 studies (17-19,27-29,35-42,47,50-52,61-64,67-70,76,77,81,82,85-88) that defined FA by means of specific sensitization (positive SPT or IgE) to food allergens, 12 were undertaken among children (Table E4). The frequency of FA as defined by positive specific-IgE was generally higher than corresponding positive SPT, and often the correlation between the two types of tests was low. The cumulative incidence of positive SPT or specific-IgE to at least one food by the age of 4 years was reported to be 5.5% in Finland (69). The cumulative incidence of positive specific-IgE by 6 years was 47.3% in Denmark (27-29), while that of positive SPT was 5.3% by the age of 3 years in the UK (Table E4) (85-87). The point prevalence of positive SPT to at least one food was lowest in France (1.8%) (67) and highest in the UK (7.7%) (88). In general, the point prevalence of SPT positivity was highest in Northern Europe than other regions (Figure E3), with only one study each being undertaken in Western and Southern Europe. No study was found from Eastern Europe on FA by SPT positivity to any specific food allergen. Studies on specific-IgE positivity to food allergens were from only Northern and Western Europe. The point prevalence of positive specific-IgE was lowest in Finland (2.0%) (41) and highest in Germany, Italy, Norway, and Denmark (each country having approximately 22%) (Table E4) (18). In general, the point prevalence was higher in Western than in Northern Europe (Figure E2), although only
one study was undertaken in Western Europe. The range of the prevalence of positive SPT positivity for all age groups was 1.8% to 6.1%, with the highest prevalence in the age group the 6-10 years; that of positive specific-IgE ranged from 2.0% to 52.0%, the age group 6-17 also having the highest prevalence (Table 1).
FA defined by symptoms plus allergic sensitization and by clinical history or food challenge
Nine studies (23,48,53,60,67,68,78-80,85-88) defined FA based on symptoms plus sensitization (SPT and IgE) to specific food allergens (n=5) or based on convincing clinical history or positivity to food challenge (OFC or DBPCFC) (n=4) (Table E5). All of these studies were among children and a majority from Northern Europe (n=6) (23,48,53,68,85-88). FA based on symptoms plus sensitization involved subjects who were symptomatic for FA (usually by self-report) and subsequently had positive results when they underwent SPT or IgE tests. On the other hand, FA based on clinical history or food challenge was defined as either having a convincing clinical history (without any food challenge) or being positive with food challenge.
The pooled point prevalence of symptoms plus positive IgE to at least one food was similar in Northern and Western Europe (Figure 3). The lowest (2.2%) and highest (4.6%) point prevalence of symptoms plus positive specific-IgE to at least one food were both found in Germany (78-80). The range of the point prevalence of symptoms plus positive specific-IgE by age group was 1.3% to 4.6%, those 1 year and less having the lowest frequency (Table 1).
The point prevalence of symptoms plus SPT positivity was just highest in Southern Europecompared toother regions (Figure 4). The lowest point prevalence was found in France (0.1%) (66) and the highest in Germany (13.1%) (77-79). The range of the point prevalence of symptoms plus positive SPT by age group was0.1% to 13.1%, the age groups 6-10 and 11-17 years having the lowest estimates.
The overall pooled point prevalence of clinical history or food challenge positivity was lowest in the UK (1.1%) (87) and highest in Norway (6.8%) (53) (Table E5). The range of the point prevalence of clinical history or food challenge by age group was 1.1% to 6.8%, the age group 2-5 years having the highest frequency (Table 1). Differences may be explained by the use of
-
Epidemiology of food allergy in Europe: a review
E-8 EAACI Supplementary materials
OFC versus DBPCFC.
There was significant heterogeneity between the studies (P < 0.05 for I2) despite stratification by age and region.
Challenge-verified FA: details of studies
Of the 12 primary studies (23,27-29,34,48,60,65,66,68-70,78-80,85-88) that assessed FA by performing food challenge (OFC or DBPCFC), eight only included children (23,27-29,48,60,68-70,85-88) and nine came from Northern Europe (23,27-29,48,65,66,68-70,85-88), two from Southern Europe (34,60), and one from Western Europe (78-80) (Table E6). Three of the studies reported cumulative incidence of challenge positive FA by 1 year (1.5% [95% CI 0.9-2.5]) (27-29), by 4 years (3.3% [95% CI 2.8-3.9]) (69,70), and by 6 years (3.6% [95% CI 2.3-5.4]) (85-87). The lowest point prevalence of challenge-verified FA was found in the UK (almost zero per cent) (85-87) while the highest was found in Germany (5.7%) (78-80) (Table E6). The range of the point prevalence of challenge-verified FA was from 0% to 5.7%, with the age group 11-17 having the highest frequency (Table 1). There was significant heterogeneity between the
studies (P < 0.05 for I2) even after stratification by age and region.
Cumulative incidence
Only one of the nine studies in these categories reported estimates for cumulative incidence (84-86), showing that the cumulative incidence of FA by the age of 3 years was 6.0% (95% CI 4.6-6.7) based on clinical history or OFC positivity and 5.0% (95% CI 3.8-6.5) based on clinical history or DBPCFC positivity.
Risk and prognostic factors for FAAlthough a number of the reviewed studies examined the risk and prognostic factors for self-reported FA and sensitization to specific food allergen, a priori, we were interested in studying the risk and prognostic factors for clinician-diagnosed or objectively-verified FA, which is expected to give stronger evidence for causality and would be more meaningful for clinical intervention. Thirteen studies (22,24-26,32,34,40,46,53,58,68-70,73,84-87) were found of which 11 were among children (Table 3). Due to several methodological differences between the studies, they were not combined in a meta-analysis.
-
E-9EAACI
Epidemiology of food allergy in Europe: a review
Supplementary materials
Tabl
e E1
The
mai
n fe
atur
es, m
ain
resu
lts o
f fre
quen
cy o
f FA
, and
ove
rall
risk
of b
ias
asse
ssm
ent o
f the
stu
dies
incl
uded
in th
e sy
stem
atic
revi
ew
on th
e ep
idem
iolo
gy o
f FA
in E
urop
e: s
tudi
es p
ublis
hed
1 J
anua
ry 2
00
0 -
30
Sep
tem
ber
20
12
Refe
renc
e,
coun
try
Stud
y de
sign
Stud
y po
pula
tion
N (c
hild
ren/
adul
ts; s
ourc
e of
st
udy
popu
latio
n)A
ge o
f su
bjec
tsO
utco
me
stud
ied
and
asse
ssm
ent m
etho
dO
ccur
renc
e m
easu
re(s
)
Mai
n re
sults
of t
he
freq
uenc
y of
FA
(FA
)Pe
rcen
tage
(95
% C
I)
Ove
rall
risk
of b
ias
asse
ssm
ent
Num
ber
appr
oach
edN
umbe
r pa
rtic
ipat
edO
utco
me(
s) s
tudi
edM
etho
d of
out
-co
me
asse
ssm
ent1
Ban
t et a
l. 2
00
8,
Pola
nd
Cros
s-se
ctio
nal
stud
y
Not
in
dica
ted
15
61
8-2
7
year
s ol
dA
ny fo
od a
llerg
enSP
T, s
IgE
Poin
t pr
eval
ence
Poin
t pre
vale
nce
of
sIgE
pos
itivi
ty to
ast
le
ast o
ne F
A: 1
1%
Mod
erat
e
Bur
ney
et a
l. 2
01
0; W
oods
et
al. 2
00
1, E
urop
e,
Uni
ted
Stat
es
of A
mer
ica,
A
ustr
alia
, New
Ze
alan
d
Cros
s-se
ctio
nal
stud
y
Not
in
dica
ted
17
28
02
0-4
4
yrs
old
Any
FA
, fish
, egg
, cow
s
milk
, mus
tard
, mel
on, p
op-
py s
eed,
soy
a, s
unflo
wer
, w
alnu
t, ba
nana
, pea
nut,
buck
whe
at, r
ice,
tom
ato,
co
rn, c
eler
y, k
iwifr
uit,
car-
rot,
sesa
me,
app
le, w
heat
, sh
rim
p, p
each
, haz
elnu
t
Self-
repo
rted
, sI
gE
Poin
t and
lif
e-tim
e pr
eval
ence
Poin
t pre
vale
nce
of
sIgE
pos
itivi
ty to
at
leas
t one
FA
for
all
coun
trie
s 1
2.3
%
Mod
erat
e
Caffa
relli
et a
l. 2
01
1, I
taly
Cros
s-se
ctio
nal
stud
y9
00
62
55
-14
ye
ars
old
Any
FA
, cow
s m
ilk,
egg,
tom
ato,
pea
nut,
whe
at, c
hoco
late
, kiw
i, st
raw
berr
y, m
elon
, or
ange
, haz
elnu
t, se
sam
e
Self-
repo
rted
Poin
t and
lif
e-tim
e pr
eval
ence
Poin
t pre
vale
nce
of
self-
repo
rted
FA
:1
.6%
(0.9
-2.9
)M
oder
ate
Chaf
en e
t al.
20
10
, Wor
ld-
wid
e
Syst
emat
ic
revi
ew
12
37
8
stud
ies
iden
tified
72
stu
dies
in
clud
edA
ll ag
e gr
oups
Cow
s m
ilk, e
gg, p
eanu
t, fis
h, s
hellfi
sh
Self-
repo
rted
, ph
ysic
ian-
diag
nosi
s, S
PT,
sIgE
, OFC
, D
BPC
FC
Poin
t, pe
riod
, lif
e-tim
e pr
eval
ence
; cu
mul
ativ
e in
cide
nce,
in
cide
nce
rate
The
sam
e fr
eque
ncy
estim
ates
as
give
n in
Ro
na e
t al.
20
07
Stro
ng
Colv
er e
t al.
20
05
, UK
and
Ir
elan
d
Cros
s-se
ctio
nal
stud
y 1
30
28
93
31
30
28
93
3Ch
ildre
n3
9
year
s ol
d
Any
FA
, fre
sh fr
uits
, m
eat,
fish,
egg
s, o
ctop
us
and
squi
d, c
hoco
late
, m
ilk, s
pice
s, le
gum
es
Self-
repo
rted
Poin
t pr
eval
ence
Poin
t pre
vale
nce
of
self-
repo
rted
FA
: 5
.2%
(3.7
-7.1
)M
oder
ate
Flok
stra
-de
Blo
k et
al.
20
11
, The
N
ethe
rland
s
Cros
s-se
ctio
nal
stud
y
No
info
rmat
ion
22
84
11
-20
ye
ars
old
Any
FA
Self-
repo
rted
Poin
t pr
eval
ence
Poin
t pre
vale
nce
of
self-
repo
rted
FA
: 2
.1%
(1.6
-2.8
)W
eak
Fox
et a
l. 2
00
9,
UK
Case
-co
ntro
l st
udy
13
3 c
ases
, 3
10
co
ntro
ls
13
3 c
ases
, 3
10
con
trol
s
10
0
year
s ol
d
Stra
wbe
rrie
s, b
anan
as, o
r-an
ges,
egg
s, p
eppe
r, ga
rlic,
ch
amom
ile, i
ce c
ream
Self-
repo
rted
Poin
t pr
eval
ence
Poin
t pre
vale
nce
of
FA: 3
.3%
(1.8
-6.0
)M
oder
ate
Tabl
e E1
(co
ntin
ued)
-
E-13EAACI
Epidemiology of food allergy in Europe: a review
Supplementary materials
Refe
renc
e,
coun
try
Stud
y de
sign
Stud
y po
pula
tion
N (c
hild
ren/
adul
ts; s
ourc
e of
st
udy
popu
latio
n)A
ge o
f su
bjec
tsO
utco
me
stud
ied
and
asse
ssm
ent m
etho
dO
ccur
renc
e m
easu
re(s
)
Mai
n re
sults
of t
he
freq
uenc
y of
FA
(FA
)Pe
rcen
tage
(95
% C
I)
Ove
rall
risk
of b
ias
asse
ssm
ent
Num
ber
appr
oach
edN
umbe
r pa
rtic
ipat
edO
utco
me(
s) s
tudi
edM
etho
d of
out
-co
me
asse
ssm
ent1
Nic
olao
u et
al.
20
10
, UK
Coho
rt
stud
y1
49
91
08
58
yea
rs
old
Pean
ut, m
ilk, e
gg, fi
sh,
tree
nut
Self-
repo
rted
, SP
T, s
IgE,
OFC
, D
BPC
FC
Poin
t and
lif
etim
e pr
eval
ence
Poin
t pre
vale
nce
of O
FC-c
onfir
med
pe
anut
alle
rgy:
0.7
%
(0.3
-1.4
)
Mod
erat
e
Nig
gem
ann
et a
l. 2
01
1, G
erm
any
Cros
s-se
ctio
nal
stud
y2
67
87
17
64
10
-17
ye
ars
old
Pean
ut a
llerg
ysI
gEPo
int
prev
alen
ce
Poin
t pre
vale
nce
of
sIgE
pos
itivi
ty to
pea
-nu
t alle
rgen
10
.9%
Mod
erat
e
Orh
an e
t al.
20
09
, Tur
key
Cros
s-se
ctio
nal
stud
y3
50
02
73
96
-9
year
s ol
d
Any
FA
, coc
oa, h
ens
egg
, be
ef, c
ows
milk
, fish
, to-
mat
o, h
azel
nut,
kiw
i, bl
ack
pepp
er, c
hick
pea,
pea
nut,
wal
nut,
corn
, ban
ana,
st
raw
berr
y, p
otat
o
Self-
repo
rted
, SP
T, O
FC,
DB
PCFC
Life
-tim
e an
d po
int
prev
alen
ce
Poin
t pre
vale
nce
of
DB
PCFC
-con
firm
ed
FA 0
.7%
(0.5
-1.1
)M
oder
ate
st
blom
et a
l. 2
00
8a,
20
08
b,
20
08
c an
d A
lmqv
ist e
t al.
20
05
, Sw
eden
Coho
rt
stud
y7
22
14
08
94
-8
year
s ol
d
Any
FA
, cow
s m
ilk, c
itrus
, pe
anut
, tre
e nu
ts/a
lmon
d,
hen
s eg
g, s
tone
frui
t, ch
oc-
olat
e, fi
sh, p
ea, s
oy b
ean,
w
heat
, ban
ana,
cod
fish
Self-
repo
rted
, sI
gE
Poin
t and
pe
riod
pr
eval
ence
Poin
t pre
vale
nce
of
sIgE
pos
itivi
ty to
at
leas
t one
FA
at 8
ye
ars:
13
.8%
(12
.5-
15
.4)
Mod
erat
e
Ost
erba
lle e
t al.
20
09
, Den
mar
k
Cros
s-se
ctio
nal
stud
y1
09
48
43
Mea
n ag
e 2
2
year
s
Any
FA
, ad
ditiv
es, c
odfis
h,
cow
s m
ilk, h
ens
egg
, oc
topu
s, p
eanu
t, sh
rim
p,
soy,
whe
at,
beer
, che
ese,
re
d w
ine
(oth
er s
econ
dary
fo
od a
llerg
ies
also
repo
rt-
ed in
the
pape
r
Self-
repo
rted
, SP
T, O
FC,
DB
PCFC
Poin
t pr
eval
ence
Poin
t pre
vale
nce
of O
FC/D
BPC
FC-
confi
rmed
FH
S: 1
.8%
(1
.1-2
.9)
Mod
erat
e
Ost
erba
lle e
t al.
20
05
, Den
mar
kCo
hort
st
udy
Not
in
dica
ted
18
34
Child
ren
and
adul
ts
Any
FA
, add
itive
s,
codfi
sh, c
ows
milk
, hen
s
egg,
pea
nut,
shri
mp,
soy
, w
heat
, fru
it/ve
geta
bles
Self-
repo
rted
, ph
ysic
ian
diag
nosi
s, S
PT,
sIgE
, OFC
, D
BPC
FC
Poin
t pr
eval
ence
Poin
t pre
vale
nce
of
OFC
/DB
PCFC
-con
-fir
med
FH
S: a
t 3 y
ears
2
.3%
(1.3
-4.0
); ad
ults
3
.2%
(2.3
-4.5
)
Mod
erat
e
Pena
rd-M
oran
d et
al.
20
05
, Fr
ance
Cros
s-se
ctio
nal
stud
y9
61
57
78
19
-11
ye
ars
old
Any
FA
, nut
s, fr
uits
or
vege
tabl
es, e
gg, m
ilk,
pean
ut, fi
sh, s
eafo
od
Self-
repo
rted
, SP
TPo
int
prev
alen
ce
Poin
t pre
vale
nce
of
sym
ptom
s pl
us S
PT
posi
tivity
to a
t lea
st o
ne
FA: 0
.1%
(0.1
-0.3
)
Mod
erat
e
Tabl
e E1
(co
ntin
ued)
-
Epidemiology of food allergy in Europe: a review
E-14 EAACI Supplementary materials
Refe
renc
e,
coun
try
Stud
y de
sign
Stud
y po
pula
tion
N (c
hild
ren/
adul
ts; s
ourc
e of
st
udy
popu
latio
n)A
ge o
f su
bjec
tsO
utco
me
stud
ied
and
asse
ssm
ent m
etho
dO
ccur
renc
e m
easu
re(s
)
Mai
n re
sults
of t
he
freq
uenc
y of
FA
(FA
)Pe
rcen
tage
(95
% C
I)
Ove
rall
risk
of b
ias
asse
ssm
ent
Num
ber
appr
oach
edN
umbe
r pa
rtic
ipat
edO
utco
me(
s) s
tudi
edM
etho
d of
out
-co
me
asse
ssm
ent1
Pere
ira e
t al.
20
05
, UK
Cros
s-se
ctio
nal
stud
y3
14
41
53
21
1 a
nd
15
yea
r ol
d
Any
FA
, milk
, egg
, whe
at,
fish,
pea
nut,
sesa
me,
tr
ee n
uts,
add
itive
s,
shel
lfish
Self-
repo
rted
, ph
ysic
ian
diag
nosi
s, S
PT,
OFC
, DB
PCFC
Poin
t pr
eval
ence
Poin
t pre
vale
nce
for
all c
hild
ren:
OFC
-con
-fir
med
FA
2.3
% (1
.6-
3.2
) DB
PCFC
-con
-fir
med
1.8
% (1
.2-2
.6
Mod
erat
e
Pyrh
nen
et a
l. 2
01
1 a
nd 2
00
9,
Finl
and
Coho
rt
stud
y 5
97
33
89
90
-4
year
s ol
d
Any
FA
, milk
, egg
, whe
at,
barle
y or
rye
, nu
t, fis
h,
citr
us fr
uit
Self-
repo
rted
, ph
ysic
ian-
diag
nosi
s, S
PT,
sIgE
, OFC
Life
-tim
e pr
eval
ence
, cu
mul
ativ
e in
cide
nce
Life
time
prev
alen
ce o
f se
lf-re
port
ed p
hysi
-ci
an-d
iagn
osed
FA
3
0.3
% (2
8.7
-31
.9)
Cum
ulat
ive
inci
denc
e of
O
FC-c
onfir
med
FA
by
4
year
s: 3
.3%
(2.8
-3.9
)
Mod
erat
e
Pyzi
ak a
nd
Kam
er 2
01
1,
Pola
nd
Cros
s-se
ctio
nal
stud
y1
15
83
6-1
7
year
s ol
d
Any
FA
, cow
s m
ilk, h
ens
eg
g, s
oy, p
ork,
bee
fSe
lf-re
port
ed,
sIgE
, SPT
, OFC
Poin
t pr
eval
ence
Freq
uenc
y es
timat
es
not g
iven
in th
e st
udy
Mod
erat
e
Ran
ce e
t al.
20
05
, Fra
nce
Cros
s-se
ctio
nal
stud
y3
50
02
71
6M
ean
age
8.9
ye
ars
Any
FA
, cow
s m
ilk, e
gg,
kiw
i, pe
anut
, fish
, tre
e nu
t, sh
rim
pSe
lf-re
port
edPo
int a
nd
life-
time
prev
alen
ce
Poin
t pre
vale
nce
of
self-
repo
rted
FA
: 4.7
(3
.9-5
.5)
Mod
erat
e
Robe
rts
et a
l. 2
00
5 a
nd L
ack
et a
l. 2
00
3, U
K
Coho
rt
stud
y1
39
71
12
09
0
0-7
ye
ars
Egg,
milk
, cod
fish
, soy
a,
sesa
me,
pea
nut,
tree
nut
, ca
shew
, alm
ond,
wal
nut,
haze
lnut
, bra
zil n
ut, p
ecan
nu
t
Self-
repo
rted
, SP
T, D
BPC
FCPo
int
Prev
alen
ce
Poin
t pre
vale
nce
of
DB
PCFC
-con
firm
ed
pean
ut a
llerg
y: 0
.2%
(0
.1-0
.3)
Mod
erat
e
Rona
et a
l. 2
00
7,
Wor
ld-w
ide
Syst
emat
ic
revi
ew9
34
stu
dies
id
entifi
ed
Num
ber
of s
tudi
es
incl
uded
in
revi
ew n
ot
indi
cate
d
All
age
grou
ps
Any
FA
, cow
s m
ilk,
hen
s eg
g, p
eanu
t, fis
h,
shel
lfish
Self-
repo
rted
, ph
ysic
ian-
diag
nosi
s, S
PT,
sIgE
, OFC
, D
BPC
FC
Poin
t, pe
riod
, lif
e-tim
e pr
eval
ence
, cu
mul
ativ
e in
cide
nce
and
inci
denc
e ra
te
Ran
ge o
f pre
vale
nce
of S
PT o
r sI
gE to
at
leas
t one
FA
: 2%
-5%
SPT
only
: 7%
-17
%
IgE
only
: 4%
-6%
Mod
erat
e
Ronc
hett
i et a
l. 2
00
8, I
taly
Cros
s-se
ctio
nal
stud
y
Not
in
dica
ted
38
0
9 a
nd
13
ye
ars
old
Any
FA
, cow
s m
ilk, h
ens
eg
g, to
mat
o, w
heat
flou
rSP
TPo
int
prev
alen
ce
Poin
t pre
vale
nce
of
SPT
posi
tivity
to a
t le
ast o
ne F
A fo
r all
chil-
dren
4.2
% (2
.6-6
.7)
Mod
erat
e
Tabl
e E1
(co
ntin
ued)
-
E-15EAACI
Epidemiology of food allergy in Europe: a review
Supplementary materials
Refe
renc
e,
coun
try
Stud
y de
sign
Stud
y po
pula
tion
N (c
hild
ren/
adul
ts; s
ourc
e of
st
udy
popu
latio
n)A
ge o
f su
bjec
tsO
utco
me
stud
ied
and
asse
ssm
ent m
etho
dO
ccur
renc
e m
easu
re(s
)
Mai
n re
sults
of t
he
freq
uenc
y of
FA
(FA
)Pe
rcen
tage
(95
% C
I)
Ove
rall
risk
of b
ias
asse
ssm
ent
Num
ber
appr
oach
edN
umbe
r pa
rtic
ipat
edO
utco
me(
s) s
tudi
edM
etho
d of
out
-co
me
asse
ssm
ent1
Sand
in e
t al.
20
05
, Sw
eden
an
d Es
toni
a
Case
-co
ntro
l st
udy
All
98
5Sw
eden
6
45
Esto
nia
34
0
All
77
0Sw
eden
48
3Es
toni
a 2
87
10
-11
ye
ars
old
Any
FA
; app
le, p
each
, ki
wi,
or c
arro
t; nu
t or
pea
nut;
oran
ge,
man
dari
n or
tom
ato;
m
ilk, e
gg, fi
sh o
r w
heat
Self-
repo
rt, s
IgE
Poin
t pr
eval
ence
Poin
t pre
vale
nce
of s
IgE
posi
tivity
to
at le
ast o
ne F
A fo
r Es
toni
a an
d Sw
eden
1
3.9
% (1
1.3
-16
.9)
Mod
erat
e
Sch
fer
et a
l. 2
00
1, G
erm
any
Nes
ted
case
-co
ntro
l st
udy
25
39
15
37
25
-74
Any
FA
Self-
repo
rted
, SP
T
Poin
t pr
eval
ence
, lif
etim
e pr
eval
ence
Poin
t pre
vale
nce
of S
PT
posi
tivity
to a
t lea
st o
ne
FA in
the
popu
latio
n of
the
alle
rgy
MO
NIC
A
stud
y: 1
6.8
%
Mod
erat
e
Schn
abel
et a
l. 2
01
0, G
erm
any
Coho
rt
stud
y3
09
71
08
26
yea
rs
old
Any
FA
Self-
repo
rted
, sI
gEPo
int
prev
alen
ce
Poin
t pre
vale
nce
of
sIgE
pos
itivi
ty to
at
leas
t one
FA
at 6
ye
ars:
11
.7%
(10
.0-
13
.8)
Mod
erat
e
Soos
t et a
l. 2
00
9
and
Zube
rbie
r et
al
. 20
04
, Roe
hr
et a
l. 2
00
4,
Ger
man
y
Cros
s-se
ctio
nal
stud
y1
33
00
All:
40
93
Age
0-1
7
year
s: 7
39
Age
18
-79
ye
ars:
32
27
0-7
9
year
s ol
d
Any
FA
, veg
etab
les,
leg-
umes
, soy
, spi
ces,
fish
, ce
real
s, m
eat a
nd fa
t, st
onef
ruit,
cho
cola
te/
swee
ts, c
ows
milk
, hen
s
egg,
pip
frui
t, nu
ts, v
eg-
etab
le o
il, c
arro
t, ce
lery
, se
sam
e, a
pple
, app
le,
haze
lnut
, pot
ato,
whe
at,
pean
ut, w
alnu
t, sh
rim
p
Self-
repo
rted
, ph
ysic
ian
diag
nosi
s, S
PT,
sIgE
, OFC
, SB
PCFC
, DB
PCFC
Poin
t and
lif
e-tim
e pr
eval
ence
Poin
t pre
vale
nce
of O
FC/D
BPC
FC-
confi
rmed
FA
:A
ll: 2
.8%
(2.4
-3.4
)Ch
ildre
n: 4
.2%
(3.0
-5
.9)
Adu
lts: 2
.9%
(2.3
-3
.5)
Mod
erat
e
Stei
nke
et a
l. 2
00
7, E
urop
e
Cros
s-se
ctio
nal
stud
y
Not
in
dica
ted
40
42
6
18
DB
PCFC
-con
firm
ed F
A/N
AFA
: 0.1
% (0
.1-0
.2)
DB
PCFC
-con
firm
ed F
A: 0
.1%
(0.1
-0.2
)D
BPC
FC-c
onfir
med
NA
FA: 0
.1%
(0.1
-0.2
)
Dat
a al
so re
port
ed f
or to
mat
o, e
gg, o
rang
e, e
ggpl
ant,
pean
ut, s
traw
berr
y, c
arro
t, ba
nana
, haz
elnu
t, pe
ar,
spin
ach,
red
chili
, bla
ck p
eppe
r, fo
od a
dditi
ves,
ch
ocol
ate,
wal
nut,
pota
to, fi
sh
Kri
stin
sdot
tir e
t al
. 20
11
, Ice
land
Child
ren
at 1
ye
arD
BPC
FC-c
onfir
med
FA
: 1.9
% (1
.3-2
.7)
Dat
a al
so re
port
ed f
or m
ilk, e
gg, fi
sh, w
heat
, pea
nut,
soya
Orh
an e
t al.
20
09
, Tur
key
Child
ren
6-9
yea
rsD
BPC
FC-c
onfir
med
FA
0.7
% (0
.5-1
.1)
Dat
a al
so re
port
ed fo
r eg
g, m
ilk, fi
sh, h
azel
nut,
pean
ut,
wal
nut,
beef
, coc
oa. A
utho
rs u
sed
num
ber
of p
ositi
ve
chal
leng
es (2
2) i
nste
ad o
f num
ber
of c
hild
ren
(20
) as
the
num
erat
or. O
ur e
stim
ates
are
bas
ed o
n nu
mbe
r of
po
sitiv
e ch
ildre
n.
Ost
erba
lle e
t al.
20
09
,D
enm
ark
Youn
g ad
ults
mea
n 2
2O
FC/D
BPC
FC-c
onfir
med
FH
S:
1.8
% (1
.1-2
.9)
Dat
a al
so re
port
ed f
or fi
sh, m
ilk, p
eanu
t, sh
rim
p, s
oy
Ost
erba
lle e
t al.
20
05
, Den
mar
kCh
ildre
n an
d ad
ults
OFC
/DB
PCFC
-con
firm
ed p
rim
ary
food
hy
pers
ensi
tivity
A
ll: 2
.4%
(1.8
-3.2
)Ch
ildre
n: 1
.6%
(0.9
-2.6
)
Age
3 y
ears
: 2.3
% (1
.3-4
.0)
A
ge
3 y
ears
: 1.0
% (0
.3-2
.9)
Adu
lts: 3
.2%
(2.3
-4.5
)
Child
ren
from
the
DA
RC
birt
h co
hort
and
thei
r si
blin
gs
(you
nger
and
old
er) a
nd a
dults
wer
e ex
amin
ed
-
Epidemiology of food allergy in Europe: a review
E-30 EAACI Supplementary materials
Refe
renc
e,
coun
try
Age
(s) o
f su
bjec
ts
Freq
uenc
y of
occ
urre
nce
of a
ny fo
od a
llerg
y (F
A)
Com
men
tCu
mul
ativ
e in
cide
nce
Perc
enta
ge (9
5%
CI)
Poin
t pre
vale
nce
Perc
enta
ge (9
5%
CI)
Pere
ira e
t al.
20
05
, UK
Child
ren
at 1
1
and
15
yea
rs
All:
OFC
-con
firm
ed F
A 1
.0%
(0.6
-1.7
)
DB
PCFC
-con
firm
ed 0
.3%
(0.1
-0.8
)A
t 11
yea
rs:
O
FC-c
onfir
med
FA
: 1.0
% (0
.5-2
.0)
D
BPC
FC-c
onfir
med
FA
: 0.1
% (0
-0.7
)A
t 15
yea
rs
O
FC-c
onfir
med
FA
: 1.1
% (0
.5-2
.1)
D
BPC
FC-c
onfir
med
FA
: 0.5
% (0
.2-1
.4)
Pyrh
onen
et a
l.
20
11
and
20
09
,Fi
nlan
d
Child
ren
by 4
yea
rs
OFC
-con
firm
ed a
ny
FA b
y 4
yea
rs: 3
.3%
(2
.8-3
.9)
Rona
et a
l. 2
00
7,
UK
All
ages
Ran
ge o
f pre
vale
nce
of a
llerg
y to
any
food
bas
ed
on fo
od c
halle
nge:
1%
-10
.8%
Resu
lts in
clud
e al
so n
on-E
urop
ean
stud
ies
Estim
ates
pre
sent
ed if
at l
east
4 s
tudi
es o
f the
food
ite
m w
ere
avai
labl
e Th
ere
was
sig
nific
ant h
eter
ogen
eity
am
ong
the
stud
ies.
Dat
a is
repo
rted
ava
ilabl
e fo
r m
ilk, e
gg, fi
sh, s
hellfi
sh
and
pean
ut
Soos
t et a
l. 2
00
9
and
Zube
rbie
r et
al.
20
04
an
d Ro
ehr
et a
l. 2
00
4, G
erm
any
Child
ren
and
adul
ts 0
-79
ye
ars
OFC
/DB
PCFC
-con
firm
ed F
A:
Tota
l pop
ulat
ion
(0-7
9 y
ears
):
2.8
% (2
.4-3
.4)
2
.6%
(2.1
-3.2
) (w
eigh
ted
for
Ger
man
y)A
dults
18
-79
yea
rs:
A
ll 2
.9 (2
.3-3
.5)
Ig
E m
edia
ted
1.9
% (1
.4-2
.4)
N
on Ig
E m
edia
ted
1.0
% (0
.7-1
.4)
Child
ren:
0-1
7 y
ears
: 4.2
% (3
.0-5
.9)
0
-14
yea
rs: 3
.8%
(2.6
-5.7
)
15
-17
yea
rs: 5
.7%
(2
.9-1
0.8
)
IgE-
med
iate
d (0
-17
yea
rs):
3.5
% (2
.4-5
.1)
N
on-I
gE-m
edia
ted
(0-1
7 y
ears
): 0
.7%
(0.3
-1
.6)
Food
alle
rgy
was
con
firm
ed b
y D
BPC
FC in
adu
lts a
nd
OFC
or
one
blin
ded
FC o
r D
BPC
FC in
chi
ldre
n.
Tabl
e E6
(co
ntin
ued)
-
E-31EAACI
Epidemiology of food allergy in Europe: a review
Supplementary materials
Refe
renc
e,
coun
try
Age
(s) o
f su
bjec
ts
Freq
uenc
y of
occ
urre
nce
of a
ny fo
od a
llerg
y (F
A)
Com
men
tCu
mul
ativ
e in
cide
nce
Perc
enta
ge (9
5%
CI)
Poin
t pre
vale
nce
Perc
enta
ge (9
5%
CI)
Vent
er e
t al.
20
08
and
20
06
, D
ean
et a
l. 2
00
7,
UK
Child
ren
1-6
yea
rs
OFC
-con
firm
ed a
ny
FA b
y 1
yea
r: 3
.6%
(2
.5-5
.0)
DB
PCFC
-con
firm
ed
any
FA b
y 1
yea
r:
1.5
% (0
.9-2
.5)
At a
ge 1
yea
r:
O
FC-c
onfir
med
FA
: 2.8
% (1
.9-4
.1)
D
BPC
FC-c
onfir
med
FA
: 1.3
% (0
.8-2
.3))
At a
ge 2
yea
rs:
O
FC-c
onfir
med
FA
: 1.0
% (0
.6-2
.0)
D
BPC
FC-c
onfir
med
FA
: 0
.1%
(0.0
-0.7
)A
t age
3 y
ears
:
OFC
-con
firm
ed F
A: 0
.8%
(0.4
-1.6
)
DB
PCFC
-con
firm
ed F
A: 0
.0%
Cum
ulat
ive
inci
denc
e al
so g
iven
for
age
1 a
nd 2
yea
rs
in th
e pa
per.
Vent
er e
t al.
20
06
, UK
Child
ren
at6
yea
rs
OFC
and
DB
PCFC
-con
firm
ed fo
od a
llerg
y O
FC-c
onfir
med
FA
: 1.3
% (0
.7-2
.3)
DB
PCFC
-con
firm
ed F
A :
0.4
% (0
.1-1
.1)
Tabl
e E6
(co
ntin
ued)
-
Epidemiology of food allergy in Europe: a review
E-32 EAACI Supplementary materials
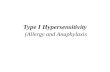
Figure E1 Pooled life-time prevalence of self-reported food allergy stratified by age (PANEL 1) and geograph-ical region (PANEL 2) in studies published in Europe between January 2000 and September 2012. Markers
represent percentages and 95%CI and boxes represent the study size
.
.
Overall (I-squared = 99.8%, p = 0.000)
Woods (2001)
Adults (>= 18 years)
Subtotal (I-squared = 99.8%, p = 0.000)
Frongia (2005)
Soost (2009)
Orhan (2009)
Roehr (2004)
Rance (2005)
Majkowska_Wojciechowska (2009)
Study
Caffarelli (2011)
Gelincik (2008)
Pyrhnen (2009)
Children (0-17 years)
Subtotal (I-squared = 99.9%, p = 0.000)
17.29 (16.96, 17.61)
19.20 (18.60, 19.80)
17.42 (16.88, 17.96)
7.80 (7.00, 8.60)
34.90 (33.60, 36.50)
5.70 (4.80, 6.60)
38.40 (35.00, 42.00)
6.70 (5.80, 7.70)
41.60 (39.50, 43.70)
10.60 (8.40, 13.20)
Percentage (95% CI)
9.50 (8.90, 10.00)
30.30 (28.70, 31.90)
17.22 (16.82, 17.63)
.
53.46
100.00
27.07
9.98
16.32
4.40
16.18
12.58
%
3.72
Weight
36.56
19.71
100.00
10 20 30 40 5000
.
.
.
.
.
Overall (I-squared = 99.8%, p = 0.000)
Eastern Europe
Subtotal (I-squared = 94.7%, p = 0.000)
Study
Caffarelli (2011)Sourthern Europe
Frongia (2005)
Woods (2001)Subtotal (I-squared = .%, p = .)
Gelincik (2008)
Pyrhnen (2009)Subtotal (I-squared = .%, p = .)
Soost (2009)Roehr (2004)Rance (2005)
Europe
Subtotal (I-squared = 99.9%, p = 0.000)
Subtotal (I-squared = .%, p = .)
Northern Europe
Western Europe
Majkowska_Wojciechowska (2009)
Orhan (2009)
17.29 (16.96, 17.61)
8.62 (8.21, 9.02)
10.60 (8.40, 13.20)
Percentage (95% CI)
7.80 (7.00, 8.60)
19.20 (18.60, 19.80)19.20 (18.60, 19.80)
9.50 (8.90, 10.00)
30.30 (28.70, 31.90)30.30 (28.70, 31.90)
34.90 (33.60, 36.50)38.40 (35.00, 42.00)6.70 (5.80, 7.70)
23.82 (22.94, 24.71)
41.60 (39.50, 43.70)41.60 (39.50, 43.70)
5.70 (4.80, 6.60)
.
100.00
%
3.17
Weight
23.03
100.00100.00
59.91
100.00100.00
48.2911.0640.65
100.00
100.00100.00
13.89
10 20 30 40 5000PANEL 2
PANEL 1
-
E-33EAACI
Epidemiology of food allergy in Europe: a review
Supplementary materials
Figure E2 Pooled point prevalence of specific immunoglobulin E (IgE) positivity to at least one food allergen stratified by age (PANEL 1) and geographical region (PANEL 2) in studies published in Europe between January
2000 and September 2012. Markers represent percentages and 95%CI and boxes represent the study size
.
.
Overall (I-squared = 97.7%, p = 0.000)
Subtotal (I-squared = 97.8%, p = 0.000)
Isolauri (2004)
Schnabel (2010)
Isolauri (2004)
Sandin (2005)
Isolauri (2004)
Krause (2002)
Ostblom (2008)
Subtotal (I-squared = 56.5%, p = 0.075)
Study
Adults (>= 18 years)
Johansson (2005)
Kjaer (2008)
Isolauri (2004)
Children (0-17 years)
10.07 (9.39, 10.76)
12.22 (11.35, 13.08)
9.00 (5.00, 18.00)
11.70 (10.00, 13.80)
2.00 (0.10, 7.00)
13.90 (11.30, 16.90)
9.00 (5.00, 18.00)
4.10 (3.00, 5.50)
13.80 (12.50, 15.40)
4.11 (3.15, 5.07)
3.60 (2.80, 4.70)
15.10 (11.70, 19.20)
52.00 (41.00, 62.00)
Percentage (95% CI)
.
100.00
5.55
21.58
5.55
11.81
5.55
20.57
37.04
100.00
%
83.35
7.00
1.99
Weight
10 20 30 40 50 600
.
.
Overall (I-squared = 97.7%, p = 0.000)
Ostblom (2008)
Isolauri (2004)
Sandin (2005)
Schnabel (2010)
Isolauri (2004)
Johansson (2005)
Subtotal (I-squared = 97.8%, p = 0.000)
Isolauri (2004)
Northern Europe
Western Europe
Kjaer (2008)
Krause (2002)
Isolauri (2004)
Subtotal (I-squared = .%, p = .)
Study
10.07 (9.39, 10.76)
13.80 (12.50, 15.40)
9.00 (5.00, 18.00)
13.90 (11.30, 16.90)
11.70 (10.00, 13.80)
9.00 (5.00, 18.00)
3.60 (2.80, 4.70)
9.77 (9.04, 10.50)
2.00 (0.10, 7.00)
Percentage (95% CI)
15.10 (11.70, 19.20)
4.10 (3.00, 5.50)
52.00 (41.00, 62.00)
11.70 (9.80, 13.60)
.
32.39
1.74
10.33
100.00
1.74
26.20
100.00
1.74
Weight
6.12
17.98
1.74
100.00
%
10 20 30 40 50 6000
PANEL 1
PANEL 2
-
Epidemiology of food allergy in Europe: a review
E-34 EAACI Supplementary materials
Figure E3 Pooled point prevalence of skin prick test (SPT) positivity to at least one food allergen stratified by age (only studies among children were available) (PANEL 1) and geographical region (PANEL 2) in studies
published in Europe between January 2000 and September 2012. Markers represent percentages and 95%CI and boxes represent the study size
.
Overall (I-squared = 91.5%, p = 0.000)
Venter (2006)
Venter (2008)
Penard_Morand (2005)
Pereira (2005)
Kjaer (2008)
Subtotal (I-squared = 91.5%, p = 0.000)
Ronchetti (2008)
Children (0-17 years)
Study
2.68 (2.38, 2.99)
3.60 (2.30, 5.20)
4.50 (3.20, 6.40)
1.80 (1.50, 2.10)
Percentage (95% CI)
5.00 (4.00, 6.30)
3.70 (2.20, 6.00)
2.68 (2.38, 2.99)
4.20 (2.60, 6.70)
.
6.91
6.34
65.89
Weight
13.31
3.79
100.00
3.75
%
2 4 6 8 1000
.
.
.
Overall (I-squared = 91.5%, p = 0.000)
Subtotal (I-squared = 0.0%, p = 0.430)
Sourthern Europe
Subtotal (I-squared = .%, p = .)
Venter (2008)
Subtotal (I-squared = .%, p = .)
Penard_Morand (2005)
Pereira (2005)
Ronchetti (2008)
Kjaer (2008)
Western Europe
Venter (2006)
Northern Europe
Study
2.68 (2.38, 2.99)
4.41 (3.69, 5.14)
1.80 (1.50, 2.10)
4.50 (3.20, 6.40)
4.20 (2.15, 6.25)
1.80 (1.50, 2.10)
5.00 (4.00, 6.30)
4.20 (2.60, 6.70)
3.70 (2.20, 6.00)
Percentage (95% CI)
3.60 (2.30, 5.20)
.
100.00
100.00
20.88
100.00
100.00
43.85
100.00
12.49
Weight
22.77
%
2 4 6 8 1000
PANEL 1
PANEL 2
-
BI Nwaru1, 2, L Hickstein3, SS Panesar2, G Roberts4-6, A Muraro7, A Sheikh2, 8, 9 on behalf of The EAACI Food Allergy & Anaphylaxis Guidelines Group
1.2PREVALENCE OF COMMON FOOD
ALLERGIES IN EUROPE
SYSTEMATIC REVIEW AND META-ANALYSIS
EAACI Food Allergy & Anaphylaxis Guidelines Group: S Halken, K Hoffmann-Sommergruber, T Werfel, C Bindslev-Jensen, M Worm, K Beyer, A Dubois, P Eigenmann, R van Ree, L Poulsen, V Cardona, I Agache,
N Papadopoulos, CA Akdis, G DuToit, M Fernandez Rivas, A Hst, E Knol, G Lack, MJ Marchisotto, B Niggemann, I Skypala, A Schoepfer, C Venter, B Vlieg-Boerstra, B Ballmer- Weber, C Nilsson
Supplementary materials
-
AFFILIATIONS1 School of Health Sciences, University of Tampere, Finland
2 Allergy & Respiratory Research Group, Center for Population Health Sciences, The University of Edinburgh, UK3 Institute for Medical Informatics, Biometry and Epidemiology, University of Munich, Germany
4 David Hide Asthma and Allergy Research Centre, St Marys Hospital, Newport, Isle of Wight, UK5 NIHR Southampton Respiratory Biomedical Research Unit, University Hospital Southampton NHS Foundation Trust, UK6 Human Development and Health and Clinical Experimental Sciences Academic Units, Faculty of Medicine, University of
Southampton, UK7 Department of Pediatrics, Center for Food Allergy Diagnosis and Treatment, Veneto Region, University of Padua, Italy
8 Division of General Internal Medicine and Primary Care, Brigham and Womens Hospital, Boston, MA, USA9 Department of Medicine, Harvard Medical School, Boston, MA, USA
-
E-37EAACI
Prevalence of common food allergies in Europe
Supplementary materials
Tabl
e E1
Sum
mar
y of
evi
denc
e on
the
freq
uenc
y of
alle
rgy
to c
ows
milk
, hen
s e
gg, w
heat
, and
soy
in E
urop
e: s
tudi
es p
ublis
hed
1 J
anua
ry
20
00
- 3
0 S
epte
mbe
r 2
01
2
Refe
renc
e,
coun
try
Estim
ates
of t
he fr
eque
ncy
of
cow
s m
ilk a
llerg
yPe
rcen
tage
(95
% C
I)
Estim
ates
of t
he fr
eque
ncy
of
hen
s eg
g al
lerg
yPe
rcen
tage
(95
% C
I)
Estim
ates
of t
he fr
eque
ncy
of w
heat
alle
rgy
Perc
enta
ge (9
5%
CI)
Estim
ates
of t
he
freq
uenc
y of
soy
alle
rgy
Perc
enta
ge (9
5%
CI)
Com
men
t
Bur
ney
et
al. 2
01
0;
Woo
ds e
t al.
20
01
, Eur
ope,
U
nite
d St
ates
of
Am
eric
a,
Aus
tral
ia, N
ew
Zeal
and
sIgE
poi
nt p
reva
lenc
e fo
r al
l co
untr
ies
0.7
%sI
gE p
oint
pre
vale
nce
for
all
coun
trie
s 0
.2%
sIgE
poi
nt p
reva
lenc
e fo
r al
l co
untr
ies
3.4
%sI
gE p
oint
pre
vale
nce
for
all c
ount
ries
1.4
%
Estim
ate
of s
ensi
tizat
ion
is a
wei
ghte
d av
erag
e ov
er a
ll co
untr
ies
in th
e st
udy
excl
udin
g bi
rth
posi
tivity
. No
wei
ghtin
g fa
ctor
or
base
line
data
giv
en, s
o w
e w
ere
unab
le to
reca
lcul
ate
the
estim
ate
Caffa
relli
et a
l. 2
01
1, I
taly
SR li
fetim
e pr
eval
ence
3.5
%
(2.3
-5.3
)SR
life
time
prev
alen
ce: 2
.4%
(1
.5-3
.9)
SR li
fetim
e pr
eval
ence
: 1.0
%
(0.4
-2.1
)
Chaf
en e
t al.
20
10
, Wor
ld-
wid
e
The
sam
e fr
eque
ncy
estim
ates
as
give
n in
Ro
na e
t al.
20
07
Du
Toit
et a
l. 2
00
8, U
K a
nd
Isra
el
SR p
oint
pre
vale
nce
2.2
%
(1.8
-2.7
) in
UK
SR p
oint
pre
vale
nce
1.5
%
(1.1
-1.9
) in
UK
Stud
y in
volv
ed U
K a
nd
Isra
el.
Dub
akie
ne
et a
l. 2
01
2,
Lith
uani
a
Poin
t pre
vale
nce
at 6
mo:
H
isto
ry +
sen
sitiz
atio
n 1
.0%
(0
.6-1
.6);
DB
PCFC
0.1
%
(0.0
-0.5
); Po
int p
reva
lenc
e at
12
mo:
His
tory
+
sens
itiza
tion
1.7
% (1
.1-2
.4)
Poin
t pre
vale
nce
at 6
mo:
H
isto
ry +
sen
sitiz
atio
n 0
.8%
(0.4
-1.3
); D
BPC
FC
0.1
% (0
.00
-0.0
4),
Poin
t pr
eval
ence
at 1
2 m
o: H
isto
ry
+ s
ensi
tizat
ion
1.7
% (1
.1-
2.5
)
Poin
t pre
vale
nce
at 6
mo:
H
isto
ry +
sen
sitiz
atio
n 0
.1%
(0.0
-0.5
); D
BPC
FC
0.1
% (0
.00
-0.0
4);
Poin
t pr
eval
ence
at 1
2 m
o:
His
tory
+ s
ensi
tizat
ion
0.5
% (0
.3-1
.0)
Egge
sb
et a
l. 2
00
3, 2
00
1a
and
20
01
b,
Nor
way
Po
int p
reva
lenc
e SR
3.6
%
(3.0
-4.4
);
By
hist
ory
and
sIgE
: 0.1
%
(0.0
-0.3
)
His
tory
or
OFC
/DB
PCFC
0
.5%
(0.3
-0.8
); H
isto
ry o
r D
BPC
FC 0
.4%
(0.2
-0.7
); O
FC/D
BPC
FC 0
.4%
(0.2
-0
.7);
DB
PCFC
0.3
% (0
.2-
0.6
)
Po
int p
reva
lenc
e
SR 2
.4%
(1.9
-3.0
);
By
hist
ory
and
sIgE
: 0.5
%
(0.3
-0.8
)
His
tory
or
OFC
/DB
PCFC
0
.8%
(0.5
-1.2
); H
isto
ry o
r D
BPC
FC 0
.7%
(0.4
-1.0
); O
FC/D
BPC
FC 0
.3%
(0.2
-0
.6);
DB
PCFC
0.2
% (0
.1-
0.4
)
-
Prevalence of common food allergies in Europe
E-38 EAACI Supplementary materials
Refe
renc
e,
coun
try
Estim
ates
of t
he fr
eque
ncy
of
cow
s m
ilk a
llerg
yPe
rcen
tage
(95
% C
I)
Estim
ates
of t
he fr
eque
ncy
of
hen
s eg
g al
lerg
yPe
rcen
tage
(95
% C
I)
Estim
ates
of t
he fr
eque
ncy
of w
heat
alle
rgy
Perc
enta
ge (9
5%
CI)
Estim
ates
of t
he
freq
uenc
y of
soy
alle
rgy
Perc
enta
ge (9
5%
CI)
Com
men
t
Elle
r et
al.
20
09
, Kja
er
et a
l. 2
00
8,
John
ke e
t al.
20
06
, Den
mar
k
Poin
t pre
vale
nce:
A
t 3 m
o: s
IgE
0.7
% (0
.2-
2.0
); SP
T 0
.4%
(0.1
-1.4
)
At 6
mo:
sIg
E 1
.6%
(0.7
-3
.4);
SPT
, 0.8
% (0
.3-2
.1)
A
t 12
mo:
sIg
E 1
.3%
(0.6
-3
.0);
SPT
1.3
% (0
.6-2
.8)
A
t 18
mo:
sIg
E , 0
.9%
(0.3
-2
.6);
SPT
0.7
% (0
.2-2
.0)
A
t 6 y
ears
by
OFC
/DB
PCFC
: 0
.0%
(0.0
-0.9
)
Cum
ulat
ive
inci
denc
e by
18
m
o: s
IgE
3.4
% (2
.1-5
.4);
SPT
2.0
% (1
.1-3
.5)
Poin
t pre
vale
nce:
A
t 3 m
o: s
IgE
1.1
% (0
.5-
2.6
); SP
T 0
.4%
(0.1
-1.4
)
At 6
mo:
sIg
E 3
.4%
(2.0
-5
.7);
SPT
, 1.9
% (1
.0-3
.5)
A
t 12
mo:
sIg
E 3
.6%
(2.2
-5
.9);
SPT
3.6
% (2
.3-5
.8)
A
t 18
mo:
sIg
E 6
.0%
(3.9
-9
.1);
SPT
2.6
% (1
.4-4
.5)
A
t 6 y
ears
by
OFC
/DB
PCFC
: 0
.7%
(0.3
-2.2
)
Cum
ulat
ive
inci
denc
e by
18
m
o: s
IgE
6.6
% (4
.7-9
.1);
SPT
4.5
% (3
.1-6
.6)
Falc
a e
t al.
20
04
,Po
rtug
al
SR p
oint
pre
vale
nce
0.3
%
(0.1
-1.1
)SR
poi
nt p
reva
lenc
e 0
.6%
(0
.2-1
.6)
Fron
gia
et a
l 2
00
5, I
taly
SR li
fetim
e pr
eval
ence
5.4
%
(4.8
-6.1
)Es
timat
es n
ot g
iven
in th
e pa
per
Gel
inci
k et
al.
20
08
, Tur
key
SR li
fetim
e pr
eval
ence
2.0
%
(1.8
-2.3
)Po
int p
reva
lenc
e:
His
tory
+ S
PT 0
.1%
(0.0
-0.1
)
His
tory
+ s
IgE
0.1
% (0
.0-0
.1)
D
BPC
FC 0
.1%
(0.0
-0.1
)
Estim
ates
for
SR li
fetim
e pr
eval
ence
for
othe
r fo
ods
give
n in
a fi
gure
in
the
pape
r.
Gru
ndy
et a
l. 2
00
2, U
KSP
T po
int p
reva
lenc
e 0
.7%
(0
.4-1
.4)
SPT
poin
t pre
vale
nce
1.4
%
(0.9
-2.2
)
Hs
t et a
l. 2
00
2, D
enm
ark
Clin
icia
n di
agno
sed
poin
t pr
eval
ence
2.2
% (1
.6-3
.0)
Tabl
e E1
(co
ntin
ued)
-
E-39EAACI
Prevalence of common food allergies in Europe
Supplementary materials
Refe
renc
e,
coun
try
Estim
ates
of t
he fr
eque
ncy
of
cow
s m
ilk a
llerg
yPe
rcen
tage
(95
% C
I)
Estim
ates
of t
he fr
eque
ncy
of
hen
s eg
g al
lerg
yPe
rcen
tage
(95
% C
I)
Estim
ates
of t
he fr
eque
ncy
of w
heat
alle
rgy
Perc
enta
ge (9
5%
CI)
Estim
ates
of t
he
freq
uenc
y of
soy
alle
rgy
Perc
enta
ge (9
5%
CI)
Com
men
t
Isol
auri
et a
l. 2
00
4, F
inla
nd
SR li
fetim
e pr
eval
ence
:
7-y
ear
olds
14
% (7
.9-2
2.4
)
27
-yea
r ol
ds 1
0%
(4.9
-17
.6)
4
7-y
ear
olds
14
% (8
.0-2
2.6
)
67
yea
r ol
ds 1
3%
(7.1
-21
.2)
sIgE
poi
nt p
reva
lenc
e
7-y
ear
olds
9%
(4.2
-16
.4)
2
7-y
ear
olds
4.4
% (1
.2-1
0.8
)
47
-yea
r ol
ds 1
.0%
(0.0
3-5
.5)
6
7-y
ear
olds
7.1
% (2
.9-1
4.0
)
No
abso
lute
dat
a w
here
pr
esen
ted
to re
calc
ulat
e th
e es
timat
es
Joha
nsso
n et
al.
20
05
, Sw
eden
and
N
orw
ay
sIgE
poi
nt p
reva
lenc
e:
Swed
en 0
.7%
(0.3
-1.4
)
Nor
way
0%
Sw
eden
+ N
orw
ay 0
.5%
(0
.2-1
.0)
sIgE
poi
nt p
reva
lenc
e:
Swed
en 0
.5%
(0.2
-1.2
)
Nor
way
0.6
% (0
.2-1
.8)
Sw
eden
+ N
orw
ay 0
.5%
(0
.3-1
.1)
sIgE
poi
nt p
reva
lenc
e:
Swed
en 2
.0%
(1.3
-3.1
)
Nor
way
0.4
% (0
.1-1
.5)
Sw
eden
+ N
orw
ay 1
.5%
(1
.0-2
.2)
sIgE
poi
nt p
reva
lenc
e:
Swed
en 2
.0%
(1.3
-3
.1)
N
orw
ay 0
%
Swed
en +
Nor
way
1
.3%
(0.9
-2.1
)
Julg
e et
al.
20
01
, Vas
ar
et a
l. 2
00
0,
Esto
nia
SPT
poin
t pre
vale
nce:
A
t 6 m
o 1
.7%
(0.6
-5.0
)
At 1
2 m
o 0
.9%
(0.2
-3.3
)
At 2
4 m
o 0
.0%
(0.0
-0,0
)
SPT
poin
t pre
vale
nce:
A
t 6 m
o 5
.2%
(2.8
-9.6
)
At 1
2 m
o 4
.1%
(2.2
-7.6
)
At 2
4 m
o 1
.8%
80
.7-4
.5)
sIgE
est
imat
es a
re a
vaila
-bl
e bu
t the
se a
re s
elec
tive
beca
use
they
incl
uded
onl
y ch
ildre
n w
ho to
ok p
art i
n al
l 3 s
tudy
ass
essm
ents
.
Kra
use
et
al. 2
00
2,
Gre
enla
nd
sIgE
poi
nt p
reva
lenc
e 0
.5%
(0
.2-1
.1)
sIgE
poi
nt p
reva
lenc
e 0
.4%
(0
.2-1
.0)
sIgE
poi
nt p
reva
lenc
e 0
.7%
(0
.3-1
.4)
sIgE
poi
nt p
reva
lenc
e 1
.2%
(0.7
-2.0
)
Kri
stin
sdot
tir
et a
l. 2
01
1,
Icel
and
Poin
t pre
vale
nce:
SR
4.2
% (3
.2-5
.4)
H
isto
ry +
SPT
0.7
% (0
.4-
1.4
)
His
tory
+ s
IgE
1.7
% (1
.2-
2.6
)
Poin
t pre
vale
nce:
SR
0.5
% (0
.3-1
.1)
H
isto
ry +
SPT
1.3
% (0
.8-2
.0)
H
isto
ry +
sIg
E 2
.2%
(1.5
-3.1
)
His
tory
+ S
PT o
r sI
gE 2
.4%
(1
.7-3
.3)
D
BPC
FC 1
.4%
(0.9
-2.2
)
Poin
t pre
vale
nce
SR
0.5
% (0
.3-1
.1)
H
isto
ry +
SPT
0%
H
isto
ry +
sIg
E 0
.6%
(0.3
-1
.2)
H
isto
ry +
SPT
or
sIgE
0.6
%
(0.3
-1.2
)
DB
PCFC
0.1
% (0
.0-0
.5)
Poin
t pre
vale
nce
SR
0.1
% (0
.0-0
.5)
H
isto
ry +
SPT
0%
H
isto
ry +
sIg
E 0
.3%
(0
.1-0
.8)
H
isto
ry +
SPT
or
sIgE
0
.3%
(0.1
-0.8
)
DB
PCFC
0.1
% (0
.0-0
.4)
Kuc
osm
anog
lu
et a
l. 2
00
8,
Turk
ey
SPT
poin
t pre
vale
nce
1.9
%
(1.2
-2.9
)
Tabl
e E1
(co
ntin
ued)
-
Prevalence of common food allergies in Europe
E-40 EAACI Supplementary materials
Refe
renc
e,
coun
try
Estim
ates
of t
he fr
eque
ncy
of
cow
s m
ilk a
llerg
yPe
rcen
tage
(95
% C
I)
Estim
ates
of t
he fr
eque
ncy
of
hen
s eg
g al
lerg
yPe
rcen
tage
(95
% C
I)
Estim
ates
of t
he fr
eque
ncy
of w
heat
alle
rgy
Perc
enta
ge (9
5%
CI)
Estim
ates
of t
he
freq
uenc
y of
soy
alle
rgy
Perc
enta
ge (9
5%
CI)
Com
men
t
Kur
ulaa
ratc
hy
et a
l. 2
00
5,
Ars
had
et a
l. 2
00
1, T
ariq
et
al. 2
00
0, U
K
SP
T po
int p
reva
lenc
e at
4 y
rs
0.8
% (0
.4-1
.6)
SP
T cu
mul
ativ
e in
cide
nce
by
2 y
rs 1
.9%
(1.3
-2.7
)
Estim
ates
for
othe
r fo
ods
give
n in
a fi
gure
in th
e pa
per.
Kven
shag
en
et a
l. 2
00
9,
Nor
way
Poin
t pre
vale
nce
by C
linic
ian
hist
ory
or O
FC 5
.5%
(3.8
-7.9
)
Clin
icia
n hi
stor
y or
OFC
:po
int p
reva
lenc
e 1
.0%
(0.4
-2
.3)
Estim
ates
not
giv
en in
the
pape
r.Es
timat
es n
ot g
iven
in
the
pape
r.
Maj
kow
ska-
Woj
ciec
how
ska
et a
l. 2
00
9,
Pola
nd
SR li
fetim
e pr
eval
ence
15
.0%
(13
.6-1
6.6
)SR
life
time
prev
alen
ce2
.9%
(2.3
-3.7
)
Aut
hors
rep
ort o
f res
ults
di
fficu
lt to
follo
w, h
ence
we
wer
e un
able
to re
calc
ulat
e th
e es
timat
es b
ased
on
num
bers
giv
en in
the
pape
r.
Mar
klun
d et
al.
20
04
, Sw
eden
SR p
oint
pre
vale
nce
1.3
% (0
.8-2
.0)
SR p
oint
pre
vale
nce
1.0
%
(0.6
-1.6
)SR
poi
nt p
reva
lenc
e 1
.3%
(0.8
-2.0
)
Thes
e ar
e in
dire
ct-
reca
lcul
ated
est
imat
es a
s th
e au
thor
s pr
ovid
ed o
nly
the
perc
enta
ge e
stim
ates
.
Mat
rica
rdi e
t al.
20
07
, Ger
man
ysI
gE p
oint
pre
vale
nce
at a
ge
10
1.0
% (0
.5-2
.3)
sIgE
poi
nt p
reva
lenc
e at
age
1
0: 0
.9%
(0.4
-2.0
)sI
gE p
oint
pre
vale
nce
8.8
%
(6.8
-11
.4)
sIgE
poi
nt p
reva
lenc
e 6
.1%
(4.4
-8.3
)
Mos
sako
wsk
a et
al.
20
08
, Po
land
SR p
oint
pre
vale
nce
0.3
%
(0.1
-1.9
)
Nic
olao
u et
al.
20
10
, UK
SR li
fetim
e pr
eval
ence
1.5
%
(0.9
-2.4
)SR
life
time
prev
alen
ce 2
.3%
(1
.6-3
.4)
Orh
an e
t al.
20
09
, Tur
key
SR li
fetim
e pr
eval
ence
0.9
%
(0.6
-1.4
)Po
int p
Related Documents