BioMed Central Page 1 of 19 (page number not for citation purposes) BMC Psychiatry Open Access Study protocol Folate Augmentation of Treatment – Evaluation for Depression (FolATED): protocol of a randomised controlled trial Seren Haf Roberts* 1 , Emma Bedson 1 , Dyfrig Hughes 2 , Keith Lloyd 3 , Stuart Moat 4 , Munir Pirmohamed 5 , Gary Slegg 1 , Richard Tranter 6 , Rhiannon Whitaker 7 , Clare Wilkinson 8 and Ian Russell 9 Address: 1 North Wales Section of Psychological Medicine, Institute of Medical and Social Care Research (IMSCaR), Bangor University, Academic Unit, Wrexham Technology Park, Wrexham, LL13 7YP, UK, 2 Centre for Economics and Policy in Health, IMSCaR, Bangor University, Dean Street, Bangor, Gwynedd, LL57 1UT, UK, 3 Psychological Medicine, Swansea University, Clinical School, Room 213, Grove Building, Swansea, SA2 8PP, UK, 4 Department of Medical Biochemistry and Immunology, University Hospital of Wales, Health Park, Cardiff, CF14 4XW, UK, 5 Department of Pharmacology and Therapeutics, University of Liverpool, Ashton Street, Liverpool, L69 3GE, UK, 6 North West Wales NHS Trust, Ysbyty Gwynedd, Bangor, Gwynedd, LL57 2PW, UK, 7 North Wales Organisation for Randomised Trials in Health (NWORTH), Institute of Medical and Social Care Research (IMSCaR), Bangor University, Ardudwy, Normal Site, Bangor, Gwynedd, LL57 2AS, UK, 8 Department of General Practice, Cardiff University, Gwenfro Building, Wrexham Technology Park, Wrexham, LL13 7YP, UK and 9 Institute of Medical and Social Care Research (IMSCaR), Bangor University, Brigantia Building, Bangor, Gwynedd, LL57 2AS, UK Email: Seren Haf Roberts* - [email protected]; Emma Bedson - [email protected]; Dyfrig Hughes - [email protected]; Keith Lloyd - [email protected]; Stuart Moat - [email protected]; Munir Pirmohamed - [email protected]; Gary Slegg - [email protected]; Richard Tranter - [email protected]; Rhiannon Whitaker - [email protected]; Clare Wilkinson - [email protected]; Ian Russell - [email protected] * Corresponding author Abstract Background: Clinical depression is common, debilitating and treatable; one in four people experience it during their lives. The majority of sufferers are treated in primary care and only half respond well to active treatment. Evidence suggests that folate may be a useful adjunct to antidepressant treatment: 1) patients with depression often have a functional folate deficiency; 2) the severity of such deficiency, indicated by elevated homocysteine, correlates with depression severity, 3) low folate is associated with poor antidepressant response, and 4) folate is required for the synthesis of neurotransmitters implicated in the pathogenesis and treatment of depression. Methods/Design: The primary objective of this trial is to estimate the effect of folate augmentation in new or continuing treatment of depressive disorder in primary and secondary care. Secondary objectives are to evaluate the cost-effectiveness of folate augmentation of antidepressant treatment, investigate how the response to antidepressant treatment depends on genetic polymorphisms relevant to folate metabolism and antidepressant response, and explore whether baseline folate status can predict response to antidepressant treatment. Seven hundred and thirty patients will be recruited from North East Wales, North West Wales and Swansea. Patients with moderate to severe depression will be referred to the trial by their GP or Psychiatrist. If patients consent they will be assessed for eligibility and baseline measures will be undertaken. Published: 15 November 2007 BMC Psychiatry 2007, 7:65 doi:10.1186/1471-244X-7-65 Received: 1 May 2007 Accepted: 15 November 2007 This article is available from: http://www.biomedcentral.com/1471-244X/7/65 © 2007 Roberts et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

BioMed CentralBMC Psychiatry
ss
Open AcceStudy protocolFolate Augmentation of Treatment – Evaluation for Depression (FolATED): protocol of a randomised controlled trialSeren Haf Roberts*1, Emma Bedson1, Dyfrig Hughes2, Keith Lloyd3, Stuart Moat4, Munir Pirmohamed5, Gary Slegg1, Richard Tranter6, Rhiannon Whitaker7, Clare Wilkinson8 and Ian Russell9Address: 1North Wales Section of Psychological Medicine, Institute of Medical and Social Care Research (IMSCaR), Bangor University, Academic Unit, Wrexham Technology Park, Wrexham, LL13 7YP, UK, 2Centre for Economics and Policy in Health, IMSCaR, Bangor University, Dean Street, Bangor, Gwynedd, LL57 1UT, UK, 3Psychological Medicine, Swansea University, Clinical School, Room 213, Grove Building, Swansea, SA2 8PP, UK, 4Department of Medical Biochemistry and Immunology, University Hospital of Wales, Health Park, Cardiff, CF14 4XW, UK, 5Department of Pharmacology and Therapeutics, University of Liverpool, Ashton Street, Liverpool, L69 3GE, UK, 6North West Wales NHS Trust, Ysbyty Gwynedd, Bangor, Gwynedd, LL57 2PW, UK, 7North Wales Organisation for Randomised Trials in Health (NWORTH), Institute of Medical and Social Care Research (IMSCaR), Bangor University, Ardudwy, Normal Site, Bangor, Gwynedd, LL57 2AS, UK, 8Department of General Practice, Cardiff University, Gwenfro Building, Wrexham Technology Park, Wrexham, LL13 7YP, UK and 9Institute of Medical and Social Care Research (IMSCaR), Bangor University, Brigantia Building, Bangor, Gwynedd, LL57 2AS, UK
Email: Seren Haf Roberts* - [email protected]; Emma Bedson - [email protected]; Dyfrig Hughes - [email protected]; Keith Lloyd - [email protected]; Stuart Moat - [email protected]; Munir Pirmohamed - [email protected]; Gary Slegg - [email protected]; Richard Tranter - [email protected]; Rhiannon Whitaker - [email protected]; Clare Wilkinson - [email protected]; Ian Russell - [email protected]
* Corresponding author
AbstractBackground: Clinical depression is common, debilitating and treatable; one in four peopleexperience it during their lives. The majority of sufferers are treated in primary care and only halfrespond well to active treatment. Evidence suggests that folate may be a useful adjunct toantidepressant treatment: 1) patients with depression often have a functional folate deficiency; 2)the severity of such deficiency, indicated by elevated homocysteine, correlates with depressionseverity, 3) low folate is associated with poor antidepressant response, and 4) folate is required forthe synthesis of neurotransmitters implicated in the pathogenesis and treatment of depression.
Methods/Design: The primary objective of this trial is to estimate the effect of folateaugmentation in new or continuing treatment of depressive disorder in primary and secondarycare. Secondary objectives are to evaluate the cost-effectiveness of folate augmentation ofantidepressant treatment, investigate how the response to antidepressant treatment depends ongenetic polymorphisms relevant to folate metabolism and antidepressant response, and explorewhether baseline folate status can predict response to antidepressant treatment.
Seven hundred and thirty patients will be recruited from North East Wales, North West Walesand Swansea. Patients with moderate to severe depression will be referred to the trial by their GPor Psychiatrist. If patients consent they will be assessed for eligibility and baseline measures will beundertaken.
Published: 15 November 2007
BMC Psychiatry 2007, 7:65 doi:10.1186/1471-244X-7-65
Received: 1 May 2007Accepted: 15 November 2007
This article is available from: http://www.biomedcentral.com/1471-244X/7/65
© 2007 Roberts et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Page 1 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
Blood samples will be taken to exclude patients with folate and B12 deficiency. Some of the bloodtaken will be used to measure homocysteine levels and for genetic analysis (with additionalconsent). Eligible participants will be randomised to receive 5 mg of folic acid or placebo. Patientswith B12 deficiency or folate deficiency will be given appropriate treatment and will be monitoredin the 'comprehensive cohort study'. Assessments will be at screening, randomisation and 3subsequent follow-ups.
Discussion: If folic acid is shown to improve the efficacy of antidepressants, then it will provide asafe, simple and cheap way of improving the treatment of depression in primary and secondarycare.
Trial registration: Current controlled trials ISRCTN37558856
BackgroundClinical depression is common, debilitating and treatable;one in four people experience it during their lives. By2020, unipolar major depression is predicted to be thesecond leading cause of disability worldwide [1].Impaired physical, social and occupational functioningare characteristic of depression, as is increased mortalityvia suicide, alcohol and drug misuse, and increased ratesof cardiovascular disease [2]. Depression thus burdensindividuals, families, the NHS, and the national economy[3]. Sub-optimal treatment of depressive disorders istherefore of great public health concern. Mental health is,like cardiovascular disease, the subject of a National Serv-ice Framework and thus reflects the priority given to therecognition and management of depression.
Despite a striking increase in the number of antidepres-sant options over the last 50 years their effectivenessremains largely unchanged. In line with National Instituteof Clinical Excellence (NICE) guidance [4] the greatmajority of recognised sufferers are treated in primarycare. However only half respond well to active treatment,while one-third respond to placebo [5]. According toNICE guidelines [4] selective serotonin reuptake inhibi-tors (SSRIs) are as effective in outpatient depression as tri-cyclic antidepressants (TCAs); since SSRIs generally havefewer side effects, they are recommended as first-line treat-ment in primary care.
The monoamine hypothesis of depression implicates afunctional deficiency of noradrenaline (NA) or serotonin(5-hydroxytryptamine, 5-HT) in neurotransmission; vir-tually all antidepressants are thought to act by prolongingthe activity of these neurotransmitters or by modulatingreceptor sensitivity [6]. Folate is an essential cofactor forthe biosynthesis of both 5-HT and NA. Thus folate defi-ciency leads to impaired 5-HT synthesis in the humanbrain [7]. Moreover, studies demonstrate that up to one-third of patients with depressive illness have decreasedplasma and red cell folate levels [8]. This may result frompoor nutrition or socio-economic disadvantage, both
common in chronic mental illness. Patients with lowfolate respond less well to antidepressant therapy [9].However, current clinical measures of folate status do notdetect patients who may have functional rather than abso-lute deficiency.
Homocysteine, a toxic amino-acid metabolite elevated infunctional folate deficiency, is a highly sensitive marker offolate status. A recent cohort study demonstrated thathyperhomocysteinaemia (plasma level >15 μmol/L), butnot total serum folate or vitamin B12, is significantlyrelated to depression severity (odds ratio = 1.90; 95% con-fidence interval = 1.11–3.25)[10]. Another study thatexamined 412 people aged between 60 and 64 yearsfound that low folate and high homocysteine, but not lowvitamin B12 levels, are correlated with depressive symp-toms [11]. Further evidence of a possible role of impairedfolate metabolism in depression is suggested by a findingthat patients homozygous for an abnormal variant of themethylenetetrahydrofolate reductase gene experiencemore severe depression (odds ratio = 1.69; 95% confi-dence interval = 1.09–2.62)[12]. This study has not beenreplicated, however, and was associated with a relativelymodest odds ratio, less than expected with homocysteine.The use of genotyping to predict the effectiveness of folatesupplementation of antidepressants thus needs furthercritical examination in appropriately powered studies thatalso take into account functional measures such as homo-cysteine level. Such a strategy should also acknowledgethat folate metabolism in the human body is extraordi-narily complex; 27 enzymes are involved, many of whichexhibit polymorphisms [13].
A variety of evidence thus suggests that folate may be auseful adjunct to antidepressant treatment: 1) patientswith depression often have a functional folate deficiency;2) the severity of such deficiency, indicated by elevatedhomocysteine, correlates with depression severity, 3) lowfolate is associated with poor antidepressant response,and 4) folate is required for the synthesis of neurotrans-mitters implicated in the pathogenesis and treatment of
Page 2 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
depression. Despite such suggestive evidence few attemptshave been made to determine the effect of folic acid sup-plementation on drug treatment of depression. ACochrane systematic review and meta-analysis identifiedonly two randomised controlled trials (combined n =151) examining the role of folate augmentation in depres-sion [14,15]. The trials differed substantially in recruit-ment criteria and provide little evidence for or against theroutine use of folic acid in antidepressant treatment. Inonly one of the studies was folate given in its dietary form,in this case combined with fluoxetine [16]. Folic acid atonly 0.5 mg per day was adequate to change serum homo-cysteine status, and to enhance antidepressant action, infemales but not males. Thus the differential effect in menand women may have been due to the low dose of folicacid used in the study. In addition, abnormal clinicalchemistry, (e.g. raised mean corpuscular volume as seenin folate deficiency) was used to exclude patients. Theother study utilised a higher dose of methylfolate (15 mg)and selected patients with low red cell folate (<200 μg/L)but was of low power, with only 24 patients [17]. Nostudy to date has used pharmacological doses of folic acid(i.e., 5 mg daily) to augment pragmatic antidepressanttherapy. Hence there is a clear need for a trial with suffi-cient power to examine the effect of folic acid supplemen-tation in the treatment of clinical depression. The effectsof folic acid supplementation may vary across differentclinical populations encountered in primary and second-ary care; in particular, the clinical and cost effectiveness offolate augmentation for new cases may differ from that ofcases with continuing but ineffective antidepressant pre-scription. In addition, the biological mechanism of folateaugmentation may differ across different antidepressanttreatments; accordingly, a comparison of SSRI versusother antidepressants is of interest.
The evidence, reviewed above, suggests that folic acid sup-plementation may augment antidepressant response. Thisis consistent with the finding that baseline levels of folatewithin the normal range predict antidepressant response[18]. In addition, there is evidence to suggest that folatedeficiency, (e.g., as may be produced by inflammatory dis-orders or anticonvulsant drug treatment [19]), may aggra-vate depression or impair response to treatment.
Since dose-response relationship for folic acid as anadjunct to antidepressant treatment is not known, it isnecessary to consider other evidence with regard to appro-priate dose choices for use with antidepressant. Based onknown pharmacology of folate, including its penetrationinto the central nervous system and effects on neurotrans-mitter metabolism, there is little chance that 5 mg wouldbe less effective than lower dose (e.g., 0.5 mg/day) folicacid, whereas it could well be more effective. This argu-ment is bolstered by findings [20,21] that 5 mg/day is
more effective than 0.4 mg/day with respect to both clini-cal and pre-clinical outcomes in the human cardiovascu-lar system. There is little available information regardingthe mechanism that may underlie a possible antidepres-sant-adjuvant effect, although suppression of homo-cysteine (Hcy) and clinical improvement were both morecommon in women than men treated with fluoxetinecombined with folic acid [16]. This result suggests thathigher doses of folic acid may be more effective, especiallyin men. Further evidence regarding potential mechanismsmay be inferred from cardiovascular data. In this systemthere is growing evidence that Hcy elevation is a marker offunctional folate deficiency, but suppression of Hcy byfolic acid does not correlate with the latter's beneficialeffects. For example, 0.4 mg/day folic acid is adequate tosuppress elevated Hcy, but not to restore disturbedendothelial function measured using the technique offlow mediated dilatation of human forearm artery [22].
Furthermore, despite high doses (5 mg) of folic acid beingsubstantially above the FDA's recommended daily dose(0.4 mg), there are few risks associated with such highdoses other than for those with B12 deficiency, epilepsy ormalignant disease. Even with lower doses of folic acid,consultant haematologists advise that vitamin B12 screen-ing, and exclusion of those found deficient, would berequired. With the exception of patients with malignantdisease and some patients with epilepsy, high dose folateis known to be safe in various clinical populations, includ-ing pregnant women and the elderly, provided B12 defi-ciency is screened and excluded [23]. Thus providingthose patients with contraindicated conditions or treat-ments are excluded there is no experimental or clinicaldisadvantage to using 5 mg/day folic acid dose.
Thus consideration of the appropriate folic acid dose fortrial participants with normal baseline serum folate is lim-ited by the lack of prior trials of folate augmentation ofantidepressant treatment with essentially no informationavailable on the nature of the dose-response relationshipapart from the observation that women appear to respondbetter than men to low dose (0.5 mg/day) folic acid aug-mentation of fluoxetine [16]. Accordingly, the decisionregarding folic acid dose depends on considerations ofsafety and possible effectiveness of various doses, rangingfrom 0.4 mg/day (as is used routinely pre-conception andin early pregnancy) to 5 mg/day (as is used routinely totreat folate deficiency). Of the two available tablet doses,we chose a pharmacological dose of 5 mg/day to improveour chances of detecting an effect of folate supplementa-tion in depression.
Methods/DesignThe primary objective of this trial is to estimate the effectof folate augmentation in new or continuing treatment of
Page 3 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
depressive disorder in primary and secondary care. Sec-ondary objectives are to evaluate the cost-effectiveness offolate augmentation of antidepressant treatment, investi-gate how the response to antidepressant treatmentdepends on genetic polymorphisms relevant to folatemetabolism and antidepressant response, and explorewhether baseline folate status can predict response to anti-depressant treatment.
This is a multi-centred double blind, placebo-controlled,randomised trial of folic acid augmentation of pragmaticantidepressant treatment of moderate-to-severe depres-sion. The trial investigates the effect of folic acid augmen-tation on new and continuing antidepressant treatmentover 3 months. Assessments will be at week -2 (baseline 1– antidepressant initiation if required), week -1 (tele-phone contact for tolerability of antidepressant), week 0(baseline 2 – randomisation to folate or placebo), andweeks 4, 12 and month 6 (outcome measures). Figure 1shows the flow diagram of the trial.
Outcome measuresTo estimate the effectiveness of folic acid in augmentingantidepressant treatment the trial will measure changes indepressive symptoms both from the participant's ownexperience and from the clinical perspective. The primaryoutcome measure is symptom severity as estimated by theself-rated Beck Depression Inventory (BDI). Clinician-rated Montgomery-Asberg Depression Rating Scale(MADRS) and the clinical global impression (CGI) ofchange will also measure symptom severity as secondarymeasures. Secondary outcome measures will include:health status (mental and physical aspects of quality oflife) through the SF-12; recording and appropriatelyreporting of adverse events (e.g. psychiatric inpatientadmission, attempted or completed suicide, and othermortality); and side effects as measured by the UKU sideeffects scale [24]. Cost-utility analysis will use the Euro-QoL (EQ-5D), a self complete resource use instrumentand relevant medication history from GPs.
Blood samples at baseline and each follow-up will meas-ure folate and B12 status. Homocysteine levels will bedetermined from blood samples taken at baseline, week12 and month 6. Pharmacogenetic analysis will be carriedout on blood samples obtained at baseline only.
Compliance will be measured using the following fourmethods:
(1) The number of tablets remaining at each follow upwill give a crude estimate of maximum compliance.
(2) Dispensing records for folic acid (or placebo) will bereviewed to measure persistence with therapy; and dates
on antidepressant medication containers to indicate delayin collecting repeat prescriptions.
(3) Patients will be asked to complete the Morisky ques-tionnaire [25], a validated tool for assessing compliancewith tricyclic antidepressants [26] at the 12-week visitonly.
(4) Red cell folate and homocysteine levels will be used asbiochemical measures of compliance.
Referral and recruitmentPatients will be recruited from primary and secondary carein three NHS Trusts areas – North East Wales, North WestWales and Swansea, covering a population of about800,000. A feasibility study in North West Wales estab-lished two ways of improving the recruitment of patientsfrom primary care into antidepressant trials: (a) research-ers visited general practices to register, consent, randomiseand follow-up patients; and (b) responsibility for pre-scribing shifted from general practitioners to trial psychi-
Flow diagram of trialFigure 1Flow diagram of trial.
Randomisation appointment
1. Treat as usual & count 2. Refer back to GP & count
No
Screening interview
Yes
GP appointment
No
No
Yes
Patients with depression who either need 1st prescription, change or optimisation of antidepressant treatment, or are not responding well to current antidepressant treatment
are identified as suitable for trial
Yes
No Does patient meet inclusion
criteria?
Exclude2
No Does the patient
consent? Exclude2
Blood & first baseline measures taken by researcher Randomisation appointment made within 2 weeks
Yes Does patient meet locally agreed B12
deficiency criterion?
B12 treatment and second baseline measures taken
Does patient meet locally agreed folate deficiency criterion?
Treat for folate deficiency and second baseline measures taken
RANDOMISATION stratified by centre, sex, new or continuing antidepressant,
antidepressant type and counselling Second baseline measures taken
Receive placebo Receive folate
Repeat outcome measures at follow-ups • 1 (4 weeks post randomisation appointment) • 2 (12 weeks post randomisation appointment) • 3 (6 months post randomisation appointment)
Exclude1
Yes
GP or psychiatrist refers patient to trial via fax /email and provides an information sheet
Psychiatrist and researcher clarifies trial process, answers questions, assesses eligibility and obtains consent
Is patient willing to be screened?
Trial phase
Trial psychiatrist screens for depression, confirms patient meets ICD-10 criteria for moderate to severe depression, & takes appropriate clinical action. If necessary an antidepressant will be prescribed, changed or optimised
Researcher telephones patient to arrange screening appointment
Trial referral process
Yes
Page 4 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
atrists. As a result the study recruited 155 patients in 18months at a single centre with fewer resources than pro-posed for FolATED. Where appropriate this study willadopt a similar model in order to reach our recruitmenttarget. In addition to minimising the barriers to recruit-ment we have developed two further strategies. First, GPswill be reimbursed for the administration costs for eachpatient recruited into the trial and second, patients willcomplete a depression rating scales (BDI, HADS orPHQ9) in accordance with GP preferences. These strate-gies will ensure the proposed sample size is achievable.
Research interested general practices will be identified ineach of the three Trust areas, from the All-Wales PrimaryCare Research Database managed by the North WalesDepartment of General Practice. Inviting general practiceswith a proven interest in research to refer patients to thestudy can be an effective way of enhancing recruitmentrates. The feasibility study in North West Wales demon-strated that research interested practices can recruit up to20 patients each over a 2-year recruitment period. Thus365 patients will be recruited from primary care.
The remaining 365 patients will be recruited from second-ary care. Although most cases of depression are managedin primary care across Wales, additional diagnostic andmanagement support is available in somewhat differentconfigurations in the three target regions. At North EastWales NHS Trust, patients with common mental healthproblems unable to be managed by the GP are referred tothe First Access Mental Health Service; by contrast onlypatients with severe and enduring mental illness arereferred to the Community Mental Health Teams(CMHTs). At North West Wales NHS Trust, patients withdepression requiring referral are directed either to thepractice counsellor, to research projects (e.g. the feasibilitystudy previously mentioned), or to the local CMHT. Sim-ilarly, at Swansea NHS Trust patients with depression notmanaged effectively in primary care are seen by liaisonpsychiatric nurses and may be referred to the Psychiatristwithin the local CMHT.
The Consultant Psychiatrists at each centre will ensurethat their respective teams recruit 122 patients over the18-month recruitment period, giving a total of 366patients recruited from secondary care. It is anticipatedthat patients recruited from secondary care will predomi-nantly be continuing cases that have already been initi-ated on antidepressant treatment. To maximiserecruitment the study will be adopted by the MentalHealth Research Network Cymru (MHRN-Cymru).
Participating GPs will identify patients with depressionand will give them a study booklet if they are interested inentering the trial. The study booklet will contain details of
the trial in the patient information leaflet and consentform. Patients willing to be screened will be referred to thetrial using a standardised referral form which will be faxedto the regional research team. In addition to the patients'demographic details, the form will also ask the GPs tonote their first and second choice antidepressant in eachinstance if they have not been prescribed an antidepres-sant. Patients not responding adequately to existing anti-depressant treatment will also be referred to the trial in asimilar manner. Patients with moderate or severe depres-sion routinely referred to secondary care will also berecruited into the trial using the same referral process. Thelocal research professional will contact referred patientswithin three days to discuss the study, answer any ques-tions and to arrange an appointment for a screening inter-view at the GP surgery or local research centre. Patientswho do not wish to be screened or are ineligible for otherreasons will be offered usual treatment by the GP. Toavoid withholding treatment an appointment will bemade within three working days for new patients whohave yet to be prescribed an antidepressant. For patientsalready prescribed an antidepressant an appointment willbe made as soon as possible.
ScreeningAt the screening interview the Psychiatrist explains whatwill happen and will ask the patient if they are happy tobe assessed. Patients will be assessed for depression by thepsychiatrist and asked to complete the BDI as part of thescreening process. (If the GP requests HADS or PHQ9patients will be asked to complete them in addition to theBDI.)
The Psychiatrist will take an appropriate clinical actionbased on the patients needs such as prescribing or opti-mising an antidepressant, or onward referral. If the patientmeets ICD-10 criteria for moderate to severe depressionthe Psychiatrist will ask the patient if they are willing to bescreened for eligibility. See planned inclusion and exclu-sion criteria.
Inclusion and exclusion criteriaInclusionOnly patients aged 18 or over with an ICD-10 diagnosis ofmoderate to severe depression [confirmed by the trial psy-chiatrists during the screening interview using BDI] willbe included. Only patients able to give informed consent(not delirious, actively psychotic or with severe communi-cation or learning disability) and able to complete theresearch assessments will be included.
ExclusionPatients will be excluded from the trial if they:
Page 5 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
(a) are folate deficient: they cannot be randomisedbecause they need to be treated with folic acid but can beincluded in the comprehensive cohort
(b) are B12 deficient: they cannot be randomised becausethey need to be treated with B12 injections but can beincluded in the comprehensive cohort
(c) have knowingly taken supplements containing folicacid within 2 months because this will mask any effects offolic acid given during the study
(d) suffer from psychosis because additional treatment forpsychosis may mask any benefit of folic acid with antide-pressants. Plus people suffering from psychosis are lessable to give informed consent and will require referralthrough to secondary services.
(e) are already participating in another research project
(f) are pregnant or planning to become pregnant as it isimportant for pregnant women to take folic acid so theycannot be randomised to placebo
(g) are taking anticonvulsants as in very rare circum-stances folic acid can react with certain anticonvulsants
(h) serious, advanced or terminal illness with a life expect-ancy of less than 1 year
(i) have recently started treatment for a medical conditionwhich has not yet been stabilised
(j) are taking lithium
(k) have had a diagnosis or treatment for any malignantdisease or any related condition such as intestinal polypo-sis
Informed consentOnce eligibility is determined the research professionaland psychiatrist will provide information about the trialand the patient will be given the opportunity to ask anyquestion regarding the trial. The patient is told that theycan withdraw from the study at any time without theirusual care being affected. The research team will checkthat the patient understands all aspects of the trial includ-ing the genetics part. The psychiatrist must be happy thatthe patient is willing to consent to the trial. Patients willthen be asked to give informed consent to participate inthe trial. If the patient agrees to enter the trial, the patientmust complete two copies of the consent form indicatingwhich parts of the study they are consenting to. Once thepatient has completed the consent form the Psychiatristmust sign and date it. One copy of the study booklet with
completed consent form will be given to the patient andone copy will be kept by the research team. Patients whodo not wish to enter the trial will be referred back to theirGPs.
Baseline measures and blood samplesFirst baseline measures will be undertaken during thisscreening appointment. For new cases of depression, theGPs can initiate according to their usual practice or theycan refer the patients to the study and the trial psychia-trists can initiate treatment. To be pragmatic, prescriptionswill take account of preferences expressed by GPs. Wherethe GP does not state a preference one of two availablegeneric SSRIs, namely citalopram or fluoxetine, will beprescribed. SSRIs will be prescribed according to NICE rec-ommendations. For depression not responding ade-quately to treatment, the trial psychiatrist will continuewith the current prescription where appropriate andadjust dosage in accordance with the current BritishNational Formulary [27]. If optimisation is required,patients will be given an optimal dose for 4 weeks beforerandomisation.
Note that two key exclusion criteria, namely B12 or folatedeficiency, will be determined via a blood test. For thisreason, blood samples will be taken at the screening inter-view to determine eligibility in the first instance.
Blood samples (40 ml in total) will be split into three, col-lected in EDTA tubes (plus a serum gel tube for haematol-ogy):
(1) Routine haematology. Full blood count, red cellfolate, serum folate and B12, to be analysed in local NHSlaboratories in Bangor, Wrexham and Swansea.
(2) Homocysteine. Samples will be centrifuged within 1hour and plasma taken off red cells. The resulting plasmawill be stored at -20°C and sent batch-wise to the Univer-sity Hospital of Wales, Cardiff.
(3) Genetic analysis (if consent is given). Samples will besent, as and when taken, to the University of Liverpool.
A further research appointment will be arranged betweenthe research professional and the patient within 14 days,in which time the folate and B12 results will be con-firmed. A copy of the results will be sent to the patient'sGP, again using a standardised form.
Patients who are ineligible or who do not consent to par-ticipate in the trial will be referred back to their GP forusual care. When needed an antidepressant will be pre-scribed to avoid further delays in treatment and any
Page 6 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
appropriate clinical action will be taken. A standardisedform will be used for referrals back to GPs.
Blood results and randomisationUpon receipt of the blood results, the research profession-als will liaise with the trial psychiatrist to determine B12and folate status based on locally determined values. Thepsychiatrist will then prescribe the appropriate action tobe taken at the second appointment between the researchprofessional and the participant. At this appointment theresearch professionals will inform the participant of theirblood test results and their eligibility to continue in thetrial. Patients whose blood results show B12 deficiencywill be referred back to their GP for immediate treatmentwith B12 injections. GPs will be informed of the defi-ciency with a copy of the blood results. Those patients willbe excluded from the principal trial but will continue inthe 'comprehensive cohort study' of recruited patients.Thus antidepressant response will be monitored at eachfollow-up.
Patients whose serum folate results suggest folate defi-ciency will have their red cell folate levels reviewed to con-firm the deficiency. If red cell folate is also below thenormal range for the local laboratory, then we shallexclude the participant from the trial, but include him orher in the 'comprehensive cohort study' for follow-up dur-ing (unblinded) folate supplementation. We shall theninform the GPs of the required treatment with copies ofthe blood results and continue to monitor treatmentresponses at each follow-up.
Randomisation, stratification and blindingFollowing baseline observations, patients with B12 andfolate levels within the normal range will be randomisedand allocated to folic acid or matching placebo. Partici-pants will thus receive either a folic acid or placeboadjunct to their antidepressant treatment. Randomisationto FoLATED will be achieved by telephone to the remoterandomisation centre at North Wales Organisation forRandomised Trials in Health (NWORTH) at Bangor Uni-versity. The randomisation will be performed by dynamicallocation to protect against subversion while ensuringthat each arm of the trial is balanced for the stratificationvariables. Participants will be stratified by (1) centre(Swansea/Wrexham/Bangor); (2) sex (male/female); (3)patient type [new/continuing (i.e. having taken the samedaily antidepressant for at least two months with a stabledose in the therapeutic range (BNF) for at least onemonth)] (4) the type of antidepressant prescribed (SSRI/other) and (5) whether or not they have ever receivedcounselling for depression.
For validation purposes, additional information is alsorequested including the participant's trial number, date of
birth, and the name of the person requesting the randomi-sation. The following questions will be asked during therandomisation process:
1. Has consent been given?
2. Does the patient meet ICD10 criteria?
3. Is the patient B12 deficient?
4. Is the patient folate deficient?
If a person requesting the randomisation responds 'Yes' tothe first two questions and then 'No' to the second twoquestions the participant can be randomised.
Identically packaged folic acid and placebo will be codedrandomly for each stratification group by NWORTH. Bothfolic acid and placebo tablets will appear identical. In thisway the patient, doctor, researchers and pharmacists willbe blind to the intervention. The research professionals ateach centre will hold the trial drugs and distribute as nec-essary. Each patient's prescription will indicate his or hertrial number and package serial number in addition to therandomisation code generated by NWORTH. This willdetermine the appropriate trial package to be dispensed.The allocated codes will be recorded in the research notesand the patient's clinical record. The key to the randomi-sation code will be held centrally by NWORTH and by thelocal pharmacies. A telephone number of the local phar-macy will also be available so that the code can be brokenin an emergency.
Follow-UpsThere are clinical and methodological reasons for follow-ing up after 4 weeks, 12 weeks and 6 months. Evidencesuggests that all antidepressants show a delayed and vari-able onset of clinical improvements in depression [28-30]. Although some antidepressants reportedly producesignificant improvements within the first week, this typi-cally continues over subsequent weeks; variability inresponse measures also affects the reported timing ofonset of response [28,29]. Available evidence indicatesthat around half of eventual responders (judged in week8) to fluoxetine treatment started to respond within twoweeks and that 75% started to respond within four weeks.A lack of response within four or six weeks was associatedwith 75% or 88% chance respectively of non-responsewithin eight weeks. However no predictors of responsetiming were found. Thus the onset of antidepressantresponse, if any, will most likely have occurred by week 6.We therefore propose to undertake the first outcomemeasures follow-up at week 4 (6 weeks after initiation ofantidepressant treatment, or optimisation for continuingpatients) to ensure sufficient time for likely treatment
Page 7 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
effects whilst retaining sensitivity to clinical change. Inaddition non-response at this point allows for possiblechanges to the antidepressant treatment in accordancewith the British National Formulary and NICE guidelinesas stipulated below. Given this early follow-up, we pro-pose to undertake later follow-up at 12 weeks to measurelate and continued responses to antidepressant treatment.It is important to monitor relapse rates during the main-tenance phase of treatment and to identify any effects offolate on late responders to antidepressants. Evidence sug-gests that SSRIs are associated with higher rates of relapse(tachyphylaxis) than other antidepressant classes includ-ing tricyclic antidepressants (TCAs) and selectivenoradrenaline reuptake inhibitors (SNRIs) [31]. Thus fol-low-up at 12 weeks monitors, not only the effects of folicacid on clinical outcomes, but also its effect on relapserates.
For new patients or continuing patients undertaking opti-misation, additional telephone follow-ups in week -1 willgauge tolerability of treatment and suicidality. Where nec-essary, changes to antidepressant type or dose will bemade. These changes will be the subject of regular sum-mary reports to the trial Data Monitoring and Ethics Com-mittee (DMEC).
There are two methodological reasons for follow-up after4 weeks, 12 weeks and 6 months. First, one of these is dur-ing treatment with folate, one and the end of treatmentand the final one after some time has lapsed post treat-ment. Second, the combination of short-, medium- andlong-term measures yields better estimates of the cost-effectiveness of treatment.
With consent, serum folate, homocysteine and B12 levelswill be assessed at week 12 and at the final follow-up. Asummary of the baseline and follow-up assessments canbe seen in Table 1.
WithdrawalA participant can withdraw or can be withdrawn from thetreatment. Participants who withdraw from the trial treat-ment will be asked to attend all the follow-up appoint-ments. Local research co-ordinators will notify the trial co-ordinator in writing about all trial participants who wishto withdraw from all future follow-ups.
Pharmacogenetics StudyThere is increasing realisation of the potential importanceof pharmacogenetics in maximising the benefits of medi-cines and to this end, most commercial trials and anincreasing number of non-commercial trials, now containa pharmacogenetic arm. For this reason, a major strand ofthis trial is to characterise the role of genetically deter-mined variation in folate metabolism in clinical outcome.
Prior to the completion of the human genome project, theconventional strategy utilised for pharmacogeneticsinvolved the analysis of single variants in single genes.This has been practiced since the 1960s and unfortunatelyhas not led to major breakthroughs. Indeed the literatureis littered with contradictory data on pharmacogenetics,which has made it impossible to translate any benefitsinto clinical practice. As stated earlier, folate metabolismis complex involving 27 different enzymes [13]. The com-plexity is exacerbated by the fact that folate requires activetransport into cells, and the facilitated transporters showgenetic polymorphisms [32]. To date, only the commonfunctional genetic polymorphism (C677T) in methylene-tetrahydrofolate reductase (MTHFR) gene has beenrelated to depression [12], although no study has yetrelated the occurrence of this polymorphism to the effec-tiveness of folate treatment. No other genes in the folatepathway have been investigated either in relation to theseverity of depression, response to antidepressant treat-ment, or to folate supplementation.
Concentrating on just one gene (for example MTHFR, themost widely studied gene in the folate pathway) would beunnecessarily restrictive and would ignore the variance inthe other pathways. On the other hand, in the timescaleavailable in this study, it would not be possible to under-take an analysis of all 27 genes involved in folate metabo-lism because (a) the genetic variability has not beenadequately characterised, (b) the functional effects of allgenetic polymorphisms has not been investigated, and (c)the study has not been powered to look at this number ofgenes with an insufficient sample size.
Furthermore, this would also be prohibitively expensive atthis stage. A practical strategy has been adopted, as fol-lows:
(a) analysis of the most important pathways based on pre-vious studies in other diseases areas, for example responseto methotrexate;
(b) we will adopt a genetic strategy that involves using tag-ging SNPs to determine the overall genetic diversity of thechosen genes. The tagging SNPs will be determined fromthe data that are publicly available via the HapMapproject;
(c) we will genotype patient samples for the common pol-ymorphisms (>10% population frequency) that haveeither a known functional effect or can be predicted tohave a functional effect and would therefore be in accord-ance with the sample size and hence power of the study;and
Page 8 of 19(page number not for citation purposes)

BM
C P
sych
iatry
200
7, 7
:65
http
://w
ww
.bio
med
cent
ral.c
om/1
471-
244X
/7/6
5
Page
9 o
f 19
(pag
e nu
mbe
r not
for c
itatio
n pu
rpos
es)
Table 1: FolATED Baseline and follow-up assessments
Assessment Outcome measure Respondent Trial entry – Baseline Follow-ups
Week -2 (baseline 1)
Week -1(Telephone contact)
Week 0 (baseline 2)
Week 4 Week 12 Month 6
Blood testing Routine haematology
FBC Clinician
Serum folate Clinician
Red Cell folate Clinician
B12 Clinician
Homocysteine Clinician
Genetics Clinician
(needs extra consent)
Depression status BDI Patient
MADRS Clinician/researcher
Health status and quality of life CGI Clinician/researcher
SF-12 Patient
EQ-5D Patient
Health economics Resource usage Patient
Compliance and side effects Morisky Questionnaire Patient
UKUside effects scale Clinician/researcher

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
(d) DNA will be stored for future analysis for other vari-ants in the same and other genes.
This strategy is currently being tested by Prof. Pirmo-hamed as part of 3 large projects funded through theDepartment of Health Pharmacogenetics Initiative. Thisstrategy will provide the highest chance of identifyinggenetic predictors of responsiveness to folate whilst simul-taneously provide us with a resource, as knowledge of thegenetics of these pathways increases, for future refinementand identification of other associations.
Thus, although this is a feasible strategy, it will neverthe-less be the most thorough investigation to date by allow-ing us to determine critically whether the interactionbetween any of the genetic polymorphisms in the folatepathway predicts the severity of depression, response toantidepressants per se, and the response to folate supple-mentation. Furthermore, this will allow us to determinewhether such a strategy has an impact on patient out-come, and therefore whether it is clinically and cost-effec-tive in a real-world setting. With this in mind, thefollowing 7 (out of the possible 27) genes in the folatepathway will be investigated in the first instance:
• methylenetetrahydrofolate reductase
• thymidylate synthase
• dihydrofolate reductase
• methionine synthase
• methionine synthase reductase
• gamma glutamyl hydrolase
• reduced folate carrier (SLC19A1).
The choice of genetic variant within each gene will bebased on (a) literature review of the functionally impor-tant common polymorphisms; (b) a search of the publiclyavailable databases including dbSNP http://www.ncbi.nlm.nih.gov/SNP/; and (c) a search of the Hap-Map database.
DNA will be extracted according to standard procedure.Genotyping for polymorphisms will be undertaken usinga medium throughput platform utilising TaqMan technol-ogy – available in the Department of Pharmacology, Uni-versity of Liverpool [33]. It is difficult to provide realisticpower calculations in advance since little is known aboutthe frequency of genetic variants in patients with depres-sion and the statistical methodology for the analysis ofgenetic association studies is still being developed. A key
variable in such studies is the frequency (among cases) ofthe SNP minor allele frequency. For rarer variants to beclinically important, their effect size (measured by theallelic odds ratio, OR) must be large. We therefore specifydistinct benchmarks for the power analyses: we seek tohave good power for (a) OR = 3 and a variant with a fre-quency of 10%; (b) OR = 2 for a common variant (>20%).Note that these effect sizes are for a single causal variant;we expect to realise much larger effect sizes via combina-tions of causal variants. The assumed type 1 error is 5%.Adjustment for multiple testing will be performed by per-mutation analysis [34]. As indicated above, multipleregression models will be used to evaluate the importanceof genetic factors in determining clinical outcomes inpatients.
InterventionGiven the increased efficacy of higher folic acid doses inother body systems and the very low risk of adverseeffects, we have opted for a pharmacological 5 mg/dayfolic acid dose or matching placebo to supplement antide-pressant treatment, the same dose as is routinely used totreat folate deficiency. This dose is the treatment of choicefor folate deficiency and well tolerated in various clinicalpopulations, including the elderly and pregnant women[35,36]. There is no evidence that pharmacological folatewill have a deleterious effect on either methylation statusor mood, nor that it will lead to sub-acute combineddegeneration of the spinal cord or other neurologicalcomplications, provided that B12 deficiency is excluded.Individuals identified with B12 or folate deficiency will beexcluded from the folate/placebo trial, but will be treatedappropriate and asked to continue to participate in the'comprehensive cohort study'. People who have beendiagnosed or treated for malignancy will not be able toreceive folic acid. Although there is evidence that highfolate intake lowers the risk of developing cancer if a per-son has already had a malignant disease there is some evi-dence that high folate intake may increase cancer growth.In summary,
• 5 mg/day folic acid is safe in working age adults and theelderly, provided B12 deficiency and diagnosed or treatedmalignancy is excluded.
• 5 mg/day folic acid is more likely than lower doses to beeffective as an antidepressant adjuvant, based on limitedtrial data and folate's known effects in other body systems.
Additional advantages include simplicity, low cost andready availability of the 5 mg preparation [27]. The folicacid dose-response relationship in clinical populations, inparticular those with depression, will need to be deter-mined in subsequent studies. Patients with folate defi-ciency continuing in the comprehensive cohort study will
Page 10 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
be treated with a 5 mg dose of folic acid. Patients with aB12 deficiency also continuing in the comprehensivecohort study, will be treated with B12 injections as neces-sary by the GP. Patients not wishing to continue will bereferred back to their GP for appropriate treatment usingthe designated form.
Risks and anticipated benefits for trial participants and society, including how the benefits justify the risksThere is suggestive evidence that folate may enhance theeffects of antidepressants for those suffering depression.Thus patients requiring antidepressant treatment maybenefit from supplementing their treatment with folicacid. The associated risks with folic acid supplementationare very low. Folic acid is normally well tolerated but occa-sionally nausea, allergic reactions, anorexia and abdomi-nal distension can occur. However, there is a potential riskfor patients with B12, folate deficiency or malignancy.Those patients with B12 deficiency must not receive folateand will be excluded from the trial. They will be asked tocontinue to participate as part of the 'comprehensivecohort study' and will be referred back to their GP forimmediate treatment with B12 injections. Similarly,patients with folate deficiency must be treated with folicacid and it would be unethical to randomise thesepatients to receive placebo. For this reason, they will alsobe invited to continue to participate as part of the compre-hensive cohort in an unblinded folate group and moni-tored as appropriate.
Patients with mental health problems might be viewed asa vulnerable population and therefore appropriate meas-ures will be taken to ensure that they fully understand thenature of the trial and the risks and benefits of the treat-ment. We recognise that people suffering from moderateto severe depression may have reduced capacity to assim-ilate information and we will thus ensure that all informa-tion is clear, user friendly, honest, and precise.Information will be given verbally in addition to writteninformation sheets and the research professionals will beavailable to answer any question. If folic acid augmenta-tion is shown to be beneficial, it would be a cheap, safeand simple method of improving treatment of a common,debilitating illness in primary care.
Informing potential trial participants of possible benefits and known risks of the intervention (or of no intervention or a placebo)Information sheets will be given to patients to keep whichwill explain in detail all the benefits and risk of participat-ing in the trial. Research professionals will be available toanswer any questions and respond to any difficulty expe-rienced during the trial. Patients will be given the oppor-tunity to nominate an advocate (e.g., family member) ifthey wish. Participants will be asked not to take folic acid
supplements (including multivitamin preparations con-taining folic acid) outside of the trial and any individualthat becomes pregnant during the trial will be asked toinform the appropriate research professional. Thesepatients will be followed-up as intention to treat. At eachappointment participants will also be asked if they are tak-ing any additional supplements.
Safety monitoring and reportingTo ensure that the safety of folic acid is properly moni-tored and reported this protocol stipulates the definitionsused to identify different types of adverse events (AE) andthe associated reporting requirements (adapted from theEU Directive [37]). All adverse events will be assessed forcausality, seriousness and expectedness. That is whetherthe AE is related to the drug; whether the AE is serious; andwhether the AE was unexpected. Table 2 shows how thesethree features apply to the main types of AEs.
CausalityCausality is the degree to which an untoward medicaloccurrence can be attributed to the trial drug and can beclassed as either unrelated, unlikely to be related, possiblyrelated, probably related or definitely related. Only unto-ward medical occurrences that are considered to be eitherpossibly, probably or definitely related to the trial drugwill be reported as having a causal relationship.
If the untoward medical occurrence is not considered tohave a causal relationship with the treatment at the timeof the event (i.e. it is not believed to be a consequence oftaking folic acid or placebo) this will be classified as anAdverse Event. However, if it is considered to have a causalrelationship with folic acid or placebo at the time of theevent it will be classified as an Adverse Reaction.
SeriousnessAny untoward medical occurrence will deemed serious ifit:
• results in death
• is life-threatening
• requires hospitalisation or prolongation of existing hos-pitalisation
• results in persistent or significant disability or incapacity
• results in a congenital anomaly or birth defect
Self harm or attempted suicide will also be consideredserious in this study.
Page 11 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
All serious events not considered to have a causal relation-ship with the treatment will be classified and reported asa Serious Adverse Event (SAE). All serious events that areconsidered to have a causal relationship with the treat-ment will be classified and reported as a Serious AdverseReaction (SAR).
ExpectednessAn untoward medical occurrence will be considered to be'unexpected' if its nature and severity are not consistentwith the information in the summary of product charac-teristics for that treatment. If an adverse event is consid-ered 1) to be related to the folic acid or placebo 2) isserious and 3) unexpected then is will be classed as a Sus-pected Unexpected Serious Adverse Reaction (SUSAR).
Known undesirable effects reported in the summary ofproduct characteristics include nausea, anorexia, abdomi-nal distension and allergic reaction.
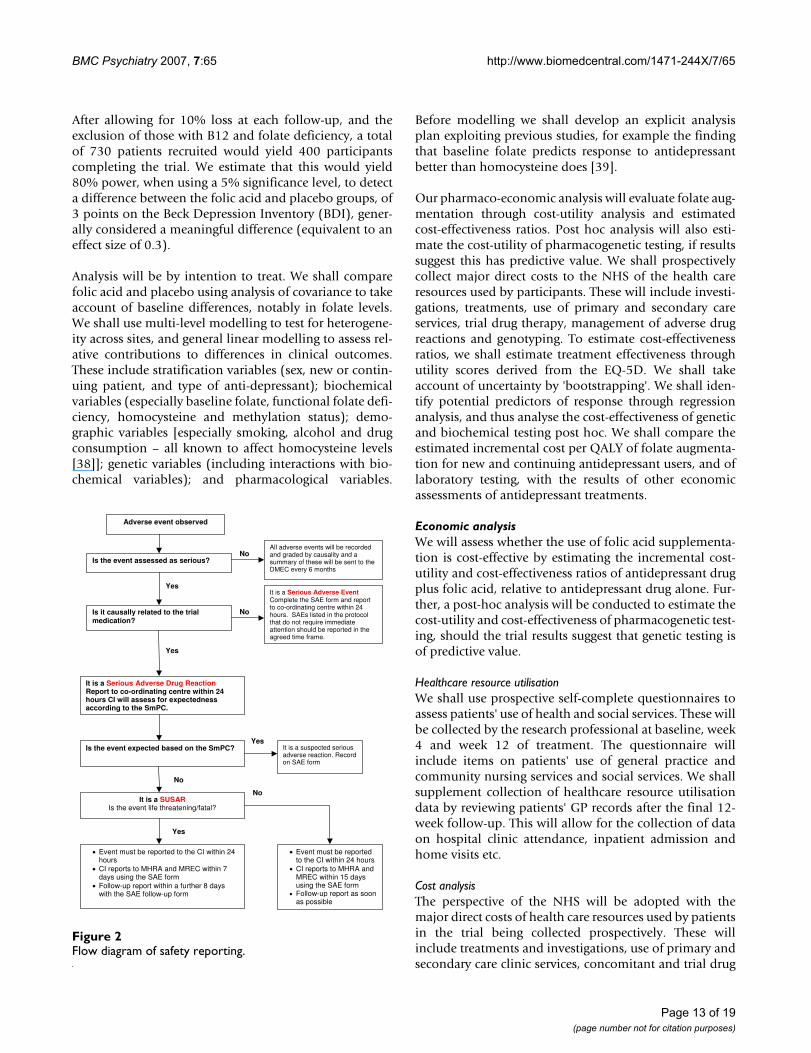
Responsibility for reportingThe reporting requirements differ depending on the cau-sality, seriousness and expectedness of the medical occur-rence as summarised in the flow diagram of safetyreporting (Figure 2).
All adverse events will be recorded on the trial database,evaluated by the principal investigator or other designatedperson responsible for the clinical aspect of the trial ineach centre and included in the annual safety report to theMREC and MHRA.
However, for all events considered serious additionalreporting is required. The trial co-ordinating centre mustbe informed within 24 hours of investigator's knowledgeof the event. A Serious Adverse Event Form must be com-pleted and sent to the trial co-ordinating centre as soon aspossible. The trial co-ordinator will immediately contactthe clinical and methodological chief investigators whohave been delegated the responsibility of reporting anyserious adverse events on behalf of the sponsor (BangorUniversity). A decision must then be made by the investi-gator with the clinical responsibility for aspects of thepatient's care which are relevant to the trial as to whetheran adverse event is related to folic acid or placebo. The
investigator should decide the degree to which the eventis caused by the trial drug. If a decision cannot be made,the investigator must contact the co-ordinating centre.Advice will be sought from the clinical chief investigatorand other clinicians may be asked if a decision cannot bereached.
If it is decided that the adverse event is a serious adversereaction then it must be determined whether the reactionis expected. If it is unexpected and thus considered aSUSAR then the SAE form will be completed and reportedto the MHRA and MREC.
For fatal or life-threatening SUSARs the MHRA and MRECwill be notified as soon as possible but no later than 7 cal-endar days after the sponsor has first knowledge of theevent. In each case relevant follow-up information will besought and a report completed as soon as possible. Thefollow-up information will be sent to the MHRA and theMREC within an additional eight calendar days.
Non-fatal and non life-threatening SUSARs will bereported to the MHRA and the MREC as soon as possiblebut no later than 15 calendar days after the sponsor hasfirst knowledge of the event. Further relevant follow-upinformation will be given as soon as possible.
Serious but expected reactions or non-serious adversereactions will be recorded in the database and reported inthe usual way.
StatisticsWith national collaboration and adoption of the projectby the Mental Health Research Network Cymru, it is esti-mated that 730 patients from 3 participating centres canbe randomised to folic acid 5 mg daily or placebo over 1to 2 years. We estimate that 5% will present with B12 defi-ciency and 10% with folate deficiency at baseline. Thesepatients will not enter the main trial but will be treatedappropriately and followed-up as part of the comprehen-sive cohort. Although up to 33% of patients with depres-sive illness have decreased plasma and red cell folatelevels [8], not all will be considered folate deficient.
Table 2: Types of adverse events
Adverse Events (AE)
Adverse Reactions (AR)
Serious Adverse Events (SAE)
Serious Adverse Reactions (SAR)
Suspected Unexpected Serious Adverse
Reactions (SUSAR)
Is the medical occurrence considered to be related to trial drug?
N Y N Y Y
Is the medical occurrence serious? N N Y Y YIs the medical occurrence unexpected? N N N N Y
Page 12 of 19(page number not for citation purposes)
BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
After allowing for 10% loss at each follow-up, and theexclusion of those with B12 and folate deficiency, a totalof 730 patients recruited would yield 400 participantscompleting the trial. We estimate that this would yield80% power, when using a 5% significance level, to detecta difference between the folic acid and placebo groups, of3 points on the Beck Depression Inventory (BDI), gener-ally considered a meaningful difference (equivalent to aneffect size of 0.3).
Analysis will be by intention to treat. We shall comparefolic acid and placebo using analysis of covariance to takeaccount of baseline differences, notably in folate levels.We shall use multi-level modelling to test for heterogene-ity across sites, and general linear modelling to assess rel-ative contributions to differences in clinical outcomes.These include stratification variables (sex, new or contin-uing patient, and type of anti-depressant); biochemicalvariables (especially baseline folate, functional folate defi-ciency, homocysteine and methylation status); demo-graphic variables [especially smoking, alcohol and drugconsumption – all known to affect homocysteine levels[38]]; genetic variables (including interactions with bio-chemical variables); and pharmacological variables.
Before modelling we shall develop an explicit analysisplan exploiting previous studies, for example the findingthat baseline folate predicts response to antidepressantbetter than homocysteine does [39].
Our pharmaco-economic analysis will evaluate folate aug-mentation through cost-utility analysis and estimatedcost-effectiveness ratios. Post hoc analysis will also esti-mate the cost-utility of pharmacogenetic testing, if resultssuggest this has predictive value. We shall prospectivelycollect major direct costs to the NHS of the health careresources used by participants. These will include investi-gations, treatments, use of primary and secondary careservices, trial drug therapy, management of adverse drugreactions and genotyping. To estimate cost-effectivenessratios, we shall estimate treatment effectiveness throughutility scores derived from the EQ-5D. We shall takeaccount of uncertainty by 'bootstrapping'. We shall iden-tify potential predictors of response through regressionanalysis, and thus analyse the cost-effectiveness of geneticand biochemical testing post hoc. We shall compare theestimated incremental cost per QALY of folate augmenta-tion for new and continuing antidepressant users, and oflaboratory testing, with the results of other economicassessments of antidepressant treatments.
Economic analysisWe will assess whether the use of folic acid supplementa-tion is cost-effective by estimating the incremental cost-utility and cost-effectiveness ratios of antidepressant drugplus folic acid, relative to antidepressant drug alone. Fur-ther, a post-hoc analysis will be conducted to estimate thecost-utility and cost-effectiveness of pharmacogenetic test-ing, should the trial results suggest that genetic testing isof predictive value.
Healthcare resource utilisationWe shall use prospective self-complete questionnaires toassess patients' use of health and social services. These willbe collected by the research professional at baseline, week4 and week 12 of treatment. The questionnaire willinclude items on patients' use of general practice andcommunity nursing services and social services. We shallsupplement collection of healthcare resource utilisationdata by reviewing patients' GP records after the final 12-week follow-up. This will allow for the collection of dataon hospital clinic attendance, inpatient admission andhome visits etc.
Cost analysisThe perspective of the NHS will be adopted with themajor direct costs of health care resources used by patientsin the trial being collected prospectively. These willinclude treatments and investigations, use of primary andsecondary care clinic services, concomitant and trial drug
Flow diagram of safety reportingFigure 2Flow diagram of safety reporting.
Is the event assessed as serious?
All adverse events will be recorded and graded by causality and a summary of these will be sent to the DMEC every 6 months
No
Yes
Is it causally related to the trial medication?
It is a Serious Adverse Event Complete the SAE form and report to co-ordinating centre within 24 hours. SAEs listed in the protocol that do not require immediate attention should be reported in the agreed time frame.
It is a Serious Adverse Drug Reaction Report to co-ordinating centre within 24 hours CI will assess for expectedness according to the SmPC.
Is the event expected based on the SmPC? It is a suspected serious adverse reaction. Record on SAE form
It is a SUSAR Is the event life threatening/fatal?
• Event must be reported to the CI within 24 hours
• CI reports to MHRA and MREC within 7 days using the SAE form
• Follow-up report within a further 8 days with the SAE follow-up form
• Event must be reported to the CI within 24 hours
• CI reports to MHRA and MREC within 15 days using the SAE form
• Follow-up report as soon as possible
No
Yes
Yes
Yes
No
No
Adverse event observed
Page 13 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
therapy, management of adverse drug reactions and geno-typing. Unit costs will be sought from appropriate sources[27,40,41].
Cost-utility analysisFor the purposes of estimating the cost-utility ratio, treat-ment effectiveness will be assessed by eliciting utilityscores from trial participants. Patients will be asked tocomplete the EQ-5D questionnaire and Visual AnalogueScale at the time points specified. We shall also conduct acost-effectiveness analysis by considering the incrementalcost per depression-free week. The number of weeks freefrom depression will be calculated from analysis of thedepression symptom rating scales, and by assuming linearinterpolation between time points.
Uncertainty analysisSensitivity analyses will be conducted to test the robust-ness of our findings. We shall use such analyses based onthe observed distributions of outcome and costs to testwhether, and to what extent, the incremental cost-utilityand cost-effectiveness ratios are sensitive to key assump-tions in the analysis. Uncertainty will also be addressed bymeans of probabilistic sensitivity analysis with results pre-sented as cost-effectiveness acceptability curves.
Subgroup analysisPutative predictors of response, adverse reactions andhigh cost episodes will be tested by means of generalisedlinear regression models. These will be used to inform thepost-hoc analysis of the cost-effectiveness of pharmacoge-netic testing.
Generalisability and policy implicationsThe findings of the economic evaluation will be comparedwith the results of other health economic assessments ofantidepressant drug treatments, including the AHEADtrial, a randomised control trial to compare the cost-effec-tiveness of tricyclic antidepressants, selective serotonin re-uptake inhibitors and lofepramine, funded by the HTAprogramme [42]. The estimated cost per QALY (and costper depression-free week) of folate supplementation, andof pharmocogenetic testing, will be compared with otherhealth care interventions to place into context the valuefor money they may offer.
Direct access to source data/documentsTrial related monitoring, audits, Research Ethics Commit-tee reviews and regulatory inspections will be permitted,allowing access to data and documents where required.
Quality control and quality assuranceThe conduct of this trial will follow the principles of goodclinical practice outlined by the ICH-GCP and will com-ply with the EU directive 2001/20/EC. The research is
underpinned by the MRC guidelines for clinical trials [43-46] and the Research Governance Frameworks for Eng-land and Wales [47,48].
A Trial Steering Committee (TSC) will be established tooversee the running of the trial, and will meet annually,with the first meeting being in Month 3. A Data Monitor-ing and Ethics sub-Committee (DMEC) will also be estab-lished. This committee will meet independently of theTSC but will be responsible for reporting to it.
Two other related work groups will be established to man-age the project, a Trial Management Group (TMG) and aResearch Team (RT). The lead applicant will chair theTMG which will meet every three months and consist ofco-applicants, collaborators, the trial co-ordinator andservice user and public involvement representatives. TheTMG will report to the TSC, and oversee the work of theRT. The RT, chaired by the trial co-ordinator and consist-ing of the three research professionals, will be responsiblefor the day-to-day research activities. The RT will meet andobtain input from particular members of the TMG whenrelevant. Members of the TMG will also have the opportu-nity to comment on draft questionnaires, draft papers andany other trial material. The existing close working rela-tionship between members of the proposed TMG willensure the aims and objectives of the project will be metwithin the time specified.
Full ethical approval has been sought from the Multi-cen-tre Research Ethics Committee (MREC) for Wales andfrom the Local Research Ethics Committees (LRECs) ateach centre. An Eudract Number (2006-004647-37) andclinical trial authorisation (CTA) have been received viathe Medicines and Healthcare products RegulatoryAuthority (MHRA). We have ensured that there is appro-priate insurance/indemnity to cover the liability of theinvestigators. In addition, we will ensure that we obtainwritten informed consent from all patients entering intothe trial and monitor, record and report any serious unex-pected adverse reactions to the TSC and DMEC, the spon-sor, the MHRA and ethics committees as appropriate. Anannual safety report will be provided.
Data Monitoring and Ethics Committee (DMEC)The role of the DMEC is to consider the need for interimanalyses of trial data, the implications of such analyses,and requests for release of interim data. It will report tothe TSC about these issues and after each meeting. As thisis a health technology assessment rather than a pharma-ceutical trial it is less likely that the DMEC will requireinterim analysis of trial data.
If two or more serious adverse events (SAEs) occur ineither of the folic acid and placebo groups, the research
Page 14 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
team will report this to the chair of the DMEC. The DMECwill examine the evidence, and if there is evidence ofimbalance in SAEs between the treatment groups thatrequires further action, report this to the TSC.
If new evidence becomes available during the course ofthe trial, for example suggesting that folic acid is substan-tially better or worse than no supplement, it is the respon-sibility of the DMEC to consider such issues and makerecommendations on the continuation of the trial to theTSC.
EthicsMREC for Wales and appropriate LREC approval havebeen sought. All trial documentation, including patientinformation leaflet and consent form, referral forms andtemplate GP letters have been submitted for approval. Toconform to the data protection and freedom of informa-tion acts, all data will be anonymised and stored securely.No published material will contain patient identifyinginformation.
Obtaining informed consent from participantsOnly patients 18 years of age or over and giving informedconsent will participate in the trial. Informed consent willbe obtained during the screening interview where both apsychiatrist and research professional will be present toensure that the patient fully understands the nature of thetrial and answer any questions. Patients will also beinformed that they can withdraw from the trial at anypoint and that doing so would not affect the care theyreceived. Patients will be given a copy of their consentform to keep.
Patients unable to give informed consent will be excludedfrom the trial.
Ethical issues of DNA testingAll genetic studies to be undertaken in the trial will besubject to approval by a research ethics committee accred-ited to deal with multi-domain studies. It is also impor-tant to note that the studies will be conducted under astrict ethical framework that adheres to guidelines devel-oped by Department of Health, MRC and the NuffieldCouncil on Bioethics. The studies will also be in accord-ance with the Human Tissue Act [49]. The following arethe key points of the study to be undertaken, as raised bythe reviewers:
• The DNA samples will be transported from the site ofpatient recruitment to Liverpool in a coded form wherethey will be extracted and stored. The laboratory will onlyknow the samples by code numbers, and will not be toldof clinical details including the study arm into which thepatient has been randomised, until after all the genotyp-
ing has been completed, and the results analysed. There-fore all genotyping will be blinded.
• The DNA will be stored in a coded form until the end ofthe study. When the DNA has been linked to the ano-nymised clinical details, the DNA sample will be irrevers-ibly anonymised and the original code destroyed.
• All patients will be asked to take part in the geneticstudy. In other genetic studies being undertaken in Liver-pool, no patient has yet refused on the basis of the factthat DNA was being collected. Furthermore the refusalrate in studies involving a single blood sample for DNAanalysis is <1%. However, as the trial progresses, we willcontinue to monitor the situation, and if there are prob-lems associated with recruitment which can be related tothe genetic testing, then steps will be undertaken to rectifythe situation after consultation with the ethics committee.
All patients will be asked to give informed consent for thegenetic study. Thus additional consent, separate from con-senting to the main study, will be required. Participantswill be asked to give specific consent to allow us to use theparticipant's DNA samples to investigate the specific genesmentioned in the protocol and broad consent to allow usto use their anonymised samples for further genetic test-ing. Anonymised DNA samples will be used in the futureto look at other genes relevant to responsiveness to folate,as and when these are identified. Participants who con-sent to the specific genetic testing will be invited to givebroad additional consent to anonymise their DNA sam-ples for analysis conducted once the FolATED trial is com-plete. Where no additional consent is given, the DNAsample will be destroyed at the end of the study. Thepatient information leaflet will state that these DNA sam-ples will be considered to be a gift and will be storedunder the custodianship of University of Liverpool. Noinformation on the genetic analysis will be passed ontothe patients individually or to their GPs.
Data handling and record keepingPatient information will only be accessible to the researchteam. All data will be link anonymised so that no patientidentifying information will be kept with raw data. Allfiles will be kept with the local research teams in a lockedand secure cabinet. It is our intention however, to attemptto make this trial as paperless as possible, thus most of thedata will be recorded electronically. Electronic data will bestored on a central computer at each centre. Field investi-gators will use laptops that will be cleared of data afterevery visit once uploaded to the central database. Thedatabase will be designed to ensure only valid data can beentered. Anonymised data will be collated by NWORTHcentrally from the three participating sites on a regularbasis for ongoing analysis and quality assurance monitor-
Page 15 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
ing. Since NWORTH will also be coordinating the ran-domisation procedures, the randomisation codes will bekept on a separate database by NWORTH.
With regard to blood samples, they will be split for differ-ent analyses depending on the consent given by the par-ticipant. The first sample will be sent to the localpathology laboratory for routine haematology analysis(FBC, red cell folate, serum folate and B12), the sampleswill then be destroyed. A second sample will be sent toCardiff for analysis of homocysteine levels, these sampleswill also be destroyed following analysis. A third sample,only taken with additional consent, will be used for DNAanalysis at the University of Liverpool and will be viewedas a gift to the University. The samples will be stored at theGenetic laboratory within the University with no identify-ing information for the duration of the study. Blood sam-ples used for genetic analyses and homocysteine will becoded so that no patient identifying information will beavailable with the sample. Blood samples used for routinehaematology will have patient details for clinical reasonsso that results can be forwarded to appropriate GPs and todetect folate deficiency during the course of the trial. Tosafeguard the research team's blindness to treatment, acollaborating GP will monitor blood results for changesin folate levels during the trial. We shall keep an extrasample of the plasma at each research site as a back up forhomocysteine analysis. This is to safeguard against loss ofsamples through unforeseen events like equipment fail-ure. We shall destroy these stored samples at the end ofthe study.
Anonymised electronic data will be stored by NWORTHfollowing the trial completion. This allows future access toraw data. Consent forms will be stored securely at localsites according to local research governance procedures.All blood samples retained for genetic analysis will bedestroyed after five years unless participants give broadconsent to allow anonymised samples to be kept indefi-nitely for future analysis. The database linking subjectidentity to anonymisation codes will be stored securely ateach local site for a period of five years following the com-pletion of the trial. This database will then be destroyed,ensuring trial data are permanently and irreversibly ano-nymised.
DiscussionFinanceThe FolATED trial is funded by a grant from the NHSHealth Technology Assessment Programme to BangorUniversity. No drug manufacturing company is sponsor-ing the trial. Folic acid manufactures have had no involve-ment with the design nor will they be involved with themanagement or reporting of the trial. DHP Ltd are manu-facturing the study drugs folic acid 5 mg and matching
placebo specifically for the study on a commercial basis.This ensures that adequate objectivity with regard to thestudy findings.
Cost implicationsFolATED has been designed to minimise costs for partici-pating hospitals, GPs and Community Mental HealthTeams (CMHTs). The drugs are supplied to patients free-of-charge. Folic acid is a simple out-patient treatment andthe follow-ups scheduled for the study are only margin-ally more than those that would be required with standardantidepressants treatment outside the trial. To reimbursethe administration costs for GPs to refer patients to thetrial a payment of £50 will be made to GPs for eachpatient recruited into the trial.
IndemnityNo special arrangements have been made for compensa-tion for non-negligent harm suffered by patients as aresult of participating in the study. Folic acid 5 mg islicensed for use as a treatment for folate deficiency. Alower dose, folic acid 400 mcg is available over-the-coun-ter as a vitamin supplement and often used by pregnantwomen. The NHS indemnity liability arrangements willapply for negligence on the part of any healthcare profes-sional involved in the study.
Publication policyA detailed publication strategy will be devised once thetrial has started. We are committed to publishing in aswide afield as possible in peer reviewed journals and toensuring that appropriate recognition is given to anyonewho has worked on trial. We are also committed to mak-ing research finding accessible for secondary analysis.
ConclusionIf folic acid is shown to improve the efficacy of antidepres-sants, then it will provide a safe, simple and cheap way ofimproving the treatment of depression in primary andsecondary care.
AbbreviationsAE: Adverse Event;
AR: Adverse Reactions;
BDI: Beck Depression Inventory;
BNF: British National Formulary;
BU: Bangor University;
CGI: Clinical Global Impression;
CMHTs: Community Mental Health Teams;
Page 16 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
CTA: Clinical Trial Authorisation;
DMEC: Data Monitoring and Ethic Committee;
EDTA: Ethylenediaminetetraacetic acid;
EQ-5D: EuroQol scale;
EU: European Union;
FBC: Full Blood Count;
FDA: Food and Drug Agency;
GP: General Practitioners;
HADS: Hospital Anxiety and Depression Scale;
Hcy: Homocysteine;
ICD-10: International Statistical Classification of Diseasesand Related Health Problems 10th RevisionICH-GCP –Good Clinical Practice;
LREC: Local Research Ethics Committee;
MADRS: Montomergy-Asberg Depression Rating Scale;
MHRA: Medicines and Healthcare product RegulatoryAgency;
MHRN-C: Mental Health Research Network Cymru;
MRC: Medical Research Council;
MREC: Mulitcentre Research Ethics Committee;
MTHFR: Methylenetetrahydrofolate reductase:
NA: Noradrenaline;
NEW: North East Wales;
NHS: National Health Service;
NICE: National Institute of Clinical Exellence;
NWORTH: North Wales Organisation for RandomisedTrials in Health;
NWW: North West Wales;
OR: Odds Ratio;
PHQ9: Patient Health Questionnaire 9;
QALY: Quality Adjusted Life Years;
RT: Research Team;
SAE: Serious Adverse Events;
SAR: Serious Adverse Reactions;
SNRI: Selective Noradrenaline Reuptake Inhibitor;
SNP: Single Nucleotide Polymorphisms;
SSRI: Selective Serotonin Reuptake Inhibitor;
SUSAR: Suspected Unexpected Serious Adverse Reaction;
TCA: Tricyclic Antidepressants;
TMG: Trial Management Group;
TSC: Trial Steering Committee;
UWB: University of Wales Bangor;
UKU: Udvalg for Kliniske Undersogelser (UKU side effectrating scale).
Competing interestsThe author(s) declare that they have no competing inter-ests.
Authors' contributionsITR contributed methodological and health servicesresearch expertise and was responsible for the first studyprotocol leading to funding. SHR was responsible for thesecond and subsequent versions of the protocol, as well ascoordinating and contributing to the development of thestudy design and protocol. All other named authors con-tributed to the study design and protocol in complemen-tary ways: KL and RT contributed clinical and healthservices research expertise; EB and GS contributed trialmanagement expertise; DH contributed the health eco-nomics component; MP contributed the genetics compo-nent; SM contributed expertise in the biochemistry offolate and homocysteine; RW contributed methodologi-cal and statistical expertise; and CW contributed primarycare research expertise. All authors have seen and agreedthis protocol manuscript.
AcknowledgementsThe development of this protocol has benefited from support from (1) the three participating NHS Trusts (North East Wales, North West Wales and Swansea), in particular the Research and Development Departments and collaborators at the haematology laboratories and pharmacies; (2) collabo-rating GPs; and (3) Dr Lindy Miller, Prof. David Menkes and Dr Johannes Thome.
Page 17 of 19(page number not for citation purposes)

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
This project is funded by the NHS R&D Programme Health Technology Assessment (HTA) Programme (project number 04/35/08). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Department of Health.
References1. Murray CJL, Lopez AD: Global mortality, disability and the con-
tribution of risk factors. Global Burden of Disease Study. Lan-cet 1997, 349:1436.
2. Musselman DL, Evans DL, Nemeroff CB: The Relationship ofDepression to Cardiovascular Disease: Epidemiology, Biol-ogy, and Treatment. Arch Gen Psychiatry 1998, 55:580-592.
3. Royal College of Psychiatrists Council: The psychological care ofmedical patients: A practical guide. In Report of a joint workingparty of the Royal College of Physicians and the Royal College of Psychia-trists London, Royal College of Physicians of London and Royal Col-lege of Psychiatrists; 2003.
4. National Institute for Clinical Excellence: Depression: Manage-ment of depression in primary and secondary care. London,National Institute for Clinical Excellence; 2004.
5. Agency for Health Care Policy and Research: Treatment forDepression - newer pharmocotherapies. Summary, Evi-dence Report. 1999.
6. Parker G, Mitchell P, Wilhelm K, Menkes DB, Snowdon J, SchweitzerI, Grounds D, Skerrit P, Roy K, Hadzi-Pavlovic D: Are the newerantidepressant drugs as effective as established physicaltreatments? Results from an Australasian clinical panelreview. Australian and New Zealand Journal of Psychiatry 1999,33:874-881.
7. Botez MI, Young SN, Bachevalier J, Gauthier S: Folate deficiencyand decreased brain 5-hydroxytryptamine synthesis in manand rat. Nature 1979, 278:182-183.
8. Carney MWP: Serum folate values in 423 psychiatric patients.British Medical Journal 1967:512.
9. Fava M, Borus JS, Alpert JE, Nierenberg AA, Rosenbaum JF, BottiglieriT: Folate, vitamin B12, and homocysteine in major depres-sive disorder. American Journal of Psychiatry 1997, 154:426-428.
10. Tiemeier H, van Tuijl HR, Hofman A, Meijer J, Kiliaan AJ, Breteler MM:Vitamin B12, folate, and homocysteine in depression: theRotterdam Study. American Journal of Psychiatry 2002,159:2099-2101.
11. Sachdev PS, Parslow RA, Lux O, Salonikas C, Wen W, Naidoo D,Christensen H, Jorm AF: Relationship of homocysteine, folicacid and vitamin B12 with depression in a middle-aged com-munity sample. Psychological Medicine 2005, 35:529-538.
12. Bjelland I, Tell GS, Vollset SE, Refsum H, Ueland PM: Folate, vitaminB12, homocysteine, and the MTHFR 677C->T polymor-phism in anxiety and depression: the Hordaland Homo-cysteine Study. Arch Gen Psychiatry 2003, 60:618-626.
13. Lucock M: Folic acid: nutritional biochemistry, molecular biol-ogy, and role in disease processes. Molecular Genetics & Metabo-lism 2000, 71:121-138.
14. Taylor MJ, Carney SM, Goodwin GM, Geddes JR: Folate for depres-sive disorders: systematic review and meta-analysis of rand-omized controlled trials. Journal of Psychopharmacology 2004,18:251-256.
15. Taylor MJ, Carney S, Geddes J, G. G: Folate for depressive disor-ders. The Cochrane Database of Systematic Reviews 2003.
16. Coppen A, Bailey J: Enhancement of the antidepressant actionof fluoxetine by folic acid: a randomised, placebo controlledtrial. Journal of Affective Disorders 2000, 60:121-130.
17. Godfrey PS, Toone BK, Carney MW, Flynn TG, Bottiglieri T, LaundyM, Chanarin I, Reynolds EH: Enhancement of recovery from psy-chiatric illness by methylfolate. Lancet 1990, 336:392-395.
18. Alpert M, Silva RR, Pouget ER: Prediction of treatment responsein geriatric depression from baseline folate level: interactionwith an SSRI or a tricyclic antidepressant. J Clin Psychopharma-col 2003, 23:309-313.
19. Harden CL, Goldstein MA: Mood disorders in patients with epi-lepsy: epidemiology and management. CNS Drugs 2002,16:291-302.
20. Moat SJ, Doshi SN, Lang D, McDowell IFW, Lewis MJ, Goodfellow J:Treatment of coronary heart disease with folic acid: Is therea future? American Journal of Physiology Heart & Circulatory Physiology2004, 287:H1-H7.
21. Moat SJ, McDowell IFW: Homocysteine and endothelial func-tion in human studies. Seminars in Vascular Medicine 2005,5:172-182.
22. Moat SJ, Madhavan A, Taylor SY, Payne N, Allen RH, Stabler SP,Goodfellow J, McDowell IFW, Lewis MJ, Lang D: High- but not low-dose folic acid improves endothelial function in coronaryartery disease. European Journal of Clinical Investigation 2006,36:850–859.
23. Campbell NR: How safe are folic acid supplements? Archives ofInternal Medicine 1996, 156:1638-1644.
24. Lingjaerde O, Ahlfors UG, Bech P, Dencker SJ, Elgen K: The UKUside effect rating scale. A new comprehensive rating scale forpsychotropic drugs and a cross-sectional study of side effectsin neuroleptic-treated patients. Acta Psychiatrica Scandinavica,Supplementum 1987, 334:1-100.
25. Morisky DE, Green LW, Levine DM: Concurrent and predictivevalidity of a self-reported measure of medication adherence.Medical Care 1986, 24:67-74.
26. George CF, Peveler RC, Heiliger S, Thompson C: Compliance withtricyclic antidepressants: the value of four different methodsof assessment. British Journal of Clinical Pharmacology 2000,50:166-171.
27. British Medical Association and Royal Pharmaceutical Society ofGreat Britain: British National Formulary Vol. Volume 50. Vol-ume September 2005. London, British Medical Association; 2007.
28. Parker G, Roy K, Menkes DB, Snowdon J, Boyce P, Grounds D, Hugh-son B, Stringer C: How long does is take antidepressant thera-pies to work? Australian and New Zealand Journal of Psychiatry 2000,34:65-70.
29. Nierenberg AA, Farabaugh AH, Alpert JE, Gordon J, Worthington JJ,Rosenbaum JF, Fava M: Timing of Onset of AntidepressantResponse with Fluoxetine Treatment. American Journal of Psychi-atry 2000, 157:1423-1428.
30. Gershon S: Antidepressants: can we determine how quicklythey work? Psychopharmacology Bulletin 1995, 31:21-22.
31. Posternak MA, Zimmerman M: Dual Reuptake Inhibitors IncurLower Rates of Tachyphylaxis Than Selective SeretoninReuptake Inhibitors: A retrospective Study. Journal of ClinicalPsychiatry 2005, 66:705-707.
32. Dervieux T, Kremer J, Lein DO, Capps R, Barham R, Meyer G, SmithK, Caldwell J, Furst DE: Contribution of common polymor-phism in reduced folate carrier and gamma-glutamylhydro-lase to methotrexate polyglutamate levels in patients withrheumatoid arthritis. Pharmacogenetics 2004, 14:733-739.
33. Owen A, Goldring C, Morgan P, Chadwick D, Park BK, PirmohamedM: Relationship between the C3435T and G2677T(A) poly-morphisms in the ABCB1 gene and P-glycoprotein expres-sion in human liver. British Journal of Clinical Pharmacology 2005,59:365-370.
34. Seaman SR, Muller-Myhsok B: Rapid simulation of P values forproduct methods and multiple-testing adjustments in associ-ation studies. American Journal of Human Genetics 2005, 76:399-408.
35. Moat SJ, Doshi SN, Lang D, McDowell IFW, Lewis MJ, J. G: Treat-ment of coronary heart disease with folic acid: is there afuture? Am J Physiol Heart Circ Physiol 2004, 287:H1-H7.
36. Office of Dietary Supplements: Dietary Supplement Fact Sheet:Folate. [http://www.ods.od.nih.gov/factsheet/folate.asp].
37. The European Parliament and the Council of the European Union:Directive 2001/20/EC of the European Parliament and of theCouncil of 4 April 2001. Official Journal of European Union 2001,Article 2:L121/36-L121/37.
38. Coppen A, Bolander-Gouaille C: Treatment of depression: timeto consider folic acid and vitamin B12. Journal of Psychopharma-cology 2005, 19:59-65.
39. Papakostas GI, Petersen T, Mischoulon D, et al: Serum folate, vita-min B12, and homocystine in major depressive disorder. JClin Psychiatry 2004, 65:1090-1098.
40. Department of Health: Reference Costs 2004 Collections: Cost-ing and Activities Guidance and Requirements. London,Department of Health,; 2005.
41. Curtis L, Netten A: Unit Costs of Health and Social Care 2004., Personal Social Services Research Unit, University of Kent; 2004.
42. Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, M M,Chatwin J, Goddard J, Thornett A, Smith H, Campbell M, ThompsonC: A randomised controlled trial to compare the cost-effec-tiveness of tricyclic antidepressants, selective serotonin
Page 18 of 19(page number not for citation purposes)
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=9164317
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=9164317
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=9672048
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=9672048
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=9672048
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=6065984
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=9054796
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=9054796
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=1974941
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=1974941
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=8694661
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=3945130

BMC Psychiatry 2007, 7:65 http://www.biomedcentral.com/1471-244X/7/65
Publish with BioMed Central and every scientist can read your work free of charge
"BioMed Central will be the most significant development for disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
reuptake inhibitors and lofepramine. Health Technology Assess-ment, 2005, 9:.
43. Majumdar SK, Shaw GK, Offerman EL, Thomson AD: Relationshipbetween depression and haematological status in chronicalcoholics. Neuropharmacology 1981, 20:1351-1352.
44. Medical Research Council: MRC Guidelines For Good ClinicalPractice In Clinical Trials. London, Medical Research Council;1998:1-49.
45. Medical Research Council: A framework for development andevaluation of RCTs for complex interventions to improvehealth. London, Medical Research Council; 2000:1-18.
46. Medical Research Council: Good Research Practice. London,Medical Research Council; 2000:1-18.
47. Department of Health: Research Governance Framework forHealth and Social Care. London, Department of Health;2001:1-50.
48. Wales Office for Research and Development in Health and SocialCare: Research Governance Framework for Health andSocial Care in Wales. Cardiff, Welsh Assembly Government;2001:1-43.
49. Great Britain: Human Tissue Act 2004 Elizabeth II. Chapter30,. London, The Stationery Office.; 2004.
Pre-publication historyThe pre-publication history for this paper can be accessedhere:
http://www.biomedcentral.com/1471-244X/7/65/prepub
Page 19 of 19(page number not for citation purposes)
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=7322307
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=7322307
Related Documents











