Author's personal copy Focused ultrasound and interleukin-4 receptor-targeted liposomal doxorubicin for enhanced targeted drug delivery and antitumor effect in glioblastoma multiforme Feng-Yi Yang a, ⁎, Tai-Tong Wong b, ⁎⁎, Ming-Che Teng a , Ren-Shyan Liu a, c, d , Maggie Lu e , Hsiang-Fa Liang e , Ming-Cheng Wei e a Department of Biomedical Imaging and Radiological Sciences, National Yang-Ming University, Taipei, Taiwan b Department of Neurosurgery, Neurological Institute, Taipei Veterans General Hospital, Taipei, Taiwan c Department of Nuclear Medicine, National PET/Cyclotron Center, Taipei Veterans General Hospital, Taipei, Taiwan d Molecular and Genetic Imaging Core, National Yang-Ming University Medical School, Taipei, Taiwan e Drug Delivery Lab, Biomedical Technology and Device Research Laboratories, Industrial Technology Research Institute, HsinChu, Taiwan abstract article info Article history: Received 14 September 2011 Accepted 26 February 2012 Available online 3 March 2012 Keywords: Focused ultrasound AP-1 Targeted drug delivery Blood–brain barrier Brain tumor The clinical application of chemotherapy to brain tumors has been severely limited because the blood–brain barrier (BBB) often prevents therapeutic levels from being achieved. Here we show that pulsed HIFU and human atherosclerotic plaque-specific peptide-1 (AP-1)-conjugated liposomes containing doxorubicin (AP- 1 Lipo-Dox) act synergistically in an experimental brain tumor model. We developed an intracranial brain- tumor model in NOD-scid mice using human brain glioblastoma multiforme (GBM) 8401 cells. Pulsed HIFU was used to transcranially disrupt the BBB in these mouse brains by delivering ultrasound waves in the pres- ence of microbubbles. Prior to each sonication, AP-1 Lipo-Dox or unconjugated Lipo-Dox was administered intravenously, and the concentration in the brains was quantified by fluorometer. Compared to control ani- mals treated with injections of AP-1 Lipo-Dox or unconjugated Lipo-Dox, animals receiving the drug followed by pulsed HIFU exhibited enhanced accumulation of the drug in tumor cells. Drug injection with sonication increased the tumor-to-normal brain doxorubicin ratio of the target tumors by about twofold compared with the control tumors. Moreover, the tumor-to-normal brain ratio was highest after the injection of AP-1 Lipo-Dox with sonication. Combining sonication with AP-1 Lipo-Dox also significantly inhibited tumor growth compared with chemotherapy alone. There was a modest but significant increase in the median sur- vival time in mice treated with AP-1 Lipo-Dox followed by pulsed HIFU, compared to those treated with AP-1 Lipo-Dox without sonication. The use of AP-1-conjugated liposomes carrying cytotoxic agents followed by pulsed HIFU represents a feasible approach for enhanced targeted drug delivery in brain tumor therapies. Crown Copyright © 2012 Published by Elsevier B.V. All rights reserved. 1. Introduction The concentration of chemotherapeutics required to achieve clin- ically effective cytotoxicity in tumors is limited by the associated tis- sue toxicity and by physiologic barriers that prevent the delivery of drug to the tumor [1]. Liposome-based drug-delivery systems have been designed to elevate tumor drug levels while limiting systemic drug exposure [2]. It is thought that targeted delivery of liposomes encapsulating cytotoxic drugs should increase the accumulation and retention of drugs at the tumor site. The employment of liposomal chemistry, such as liposomes conjugated to antibodies or targeting li- gands, can optimize and enhance the local delivery and better drug cell internalization compared with the free drug [3,4]. Glioblastoma multiforme (GBM) is an aggressive, high-grade brain tumor in humans, and patients have a poor prognosis even after che- motherapy and radiation therapy. Surgical resection is difficult due to the diffuse nature of the glioma. Current chemotherapies are either ineffective in treating the glioma completely or display a series of toxic side effects to normal tissues, limiting potentially effective treat- ments. New therapeutic strategies are therefore vital to improving the life expectancy of these patients. Previous work has shown that human brain tumor cell lines express high levels of plasma mem- brane interleukin-4 receptors (IL-4R) [5]. Furthermore, human brain tumors in situ overexpress IL-4R compared with normal brain tissues [6]. IL-4R-targeted cytotoxin has been shown to mediate a remark- able antitumor effect in immunodeficient xenograft models of human GBM tumors [7]. These observations show that selective Journal of Controlled Release 160 (2012) 652–658 ⁎ Correspondence to: F.Y. Yang, Department of Biomedical Imaging and Radiological Sciences, School of Biomedical Science and Engineering, National Yang-Ming University, Taipei, Taiwan, No. 155, Sec. 2, Li-Nong St., Taipei 11221, Taiwan. Tel.: +886 2 2826 7281; fax: +886 2 2820 1095. ⁎⁎ Correspondence to: T.T. Wong, Division of Pediatric Neurosurgery, Neurological In- stitute, Veterans General Hospital Taipei, Taiwan, No. 210, Sec. 2, Shih-Pai Road, Taipei 11217, Taiwan. Tel.: +886 2 28712121; fax: +886 2 28757587. E-mail addresses: [email protected] (F.-Y. Yang), [email protected] (T.-T. Wong). 0168-3659/$ – see front matter. Crown Copyright © 2012 Published by Elsevier B.V. All rights reserved. doi:10.1016/j.jconrel.2012.02.023 Contents lists available at SciVerse ScienceDirect Journal of Controlled Release journal homepage: www.elsevier.com/locate/jconrel NANOMEDICINE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Author's personal copy
Focused ultrasound and interleukin-4 receptor-targeted liposomal doxorubicin forenhanced targeted drug delivery and antitumor effect in glioblastoma multiforme
Feng-Yi Yang a,⁎, Tai-Tong Wong b,⁎⁎, Ming-Che Teng a, Ren-Shyan Liu a,c,d, Maggie Lu e,Hsiang-Fa Liang e, Ming-Cheng Wei e
a Department of Biomedical Imaging and Radiological Sciences, National Yang-Ming University, Taipei, Taiwanb Department of Neurosurgery, Neurological Institute, Taipei Veterans General Hospital, Taipei, Taiwanc Department of Nuclear Medicine, National PET/Cyclotron Center, Taipei Veterans General Hospital, Taipei, Taiwand Molecular and Genetic Imaging Core, National Yang-Ming University Medical School, Taipei, Taiwane Drug Delivery Lab, Biomedical Technology and Device Research Laboratories, Industrial Technology Research Institute, HsinChu, Taiwan
a b s t r a c ta r t i c l e i n f o
Article history:Received 14 September 2011Accepted 26 February 2012Available online 3 March 2012
Keywords:Focused ultrasoundAP-1Targeted drug deliveryBlood–brain barrierBrain tumor
The clinical application of chemotherapy to brain tumors has been severely limited because the blood–brainbarrier (BBB) often prevents therapeutic levels from being achieved. Here we show that pulsed HIFU andhuman atherosclerotic plaque-specific peptide-1 (AP-1)-conjugated liposomes containing doxorubicin (AP-1 Lipo-Dox) act synergistically in an experimental brain tumor model. We developed an intracranial brain-tumor model in NOD-scid mice using human brain glioblastoma multiforme (GBM) 8401 cells. Pulsed HIFUwas used to transcranially disrupt the BBB in these mouse brains by delivering ultrasound waves in the pres-ence of microbubbles. Prior to each sonication, AP-1 Lipo-Dox or unconjugated Lipo-Dox was administeredintravenously, and the concentration in the brains was quantified by fluorometer. Compared to control ani-mals treated with injections of AP-1 Lipo-Dox or unconjugated Lipo-Dox, animals receiving the drug followedby pulsed HIFU exhibited enhanced accumulation of the drug in tumor cells. Drug injection with sonicationincreased the tumor-to-normal brain doxorubicin ratio of the target tumors by about twofold comparedwith the control tumors. Moreover, the tumor-to-normal brain ratio was highest after the injection of AP-1Lipo-Dox with sonication. Combining sonication with AP-1 Lipo-Dox also significantly inhibited tumorgrowth compared with chemotherapy alone. There was a modest but significant increase in the median sur-vival time in mice treated with AP-1 Lipo-Dox followed by pulsed HIFU, compared to those treated with AP-1Lipo-Dox without sonication. The use of AP-1-conjugated liposomes carrying cytotoxic agents followed bypulsed HIFU represents a feasible approach for enhanced targeted drug delivery in brain tumor therapies.
Crown Copyright © 2012 Published by Elsevier B.V. All rights reserved.
1. Introduction
The concentration of chemotherapeutics required to achieve clin-ically effective cytotoxicity in tumors is limited by the associated tis-sue toxicity and by physiologic barriers that prevent the delivery ofdrug to the tumor [1]. Liposome-based drug-delivery systems havebeen designed to elevate tumor drug levels while limiting systemicdrug exposure [2]. It is thought that targeted delivery of liposomesencapsulating cytotoxic drugs should increase the accumulation and
retention of drugs at the tumor site. The employment of liposomalchemistry, such as liposomes conjugated to antibodies or targeting li-gands, can optimize and enhance the local delivery and better drugcell internalization compared with the free drug [3,4].
Glioblastomamultiforme (GBM) is an aggressive, high-grade braintumor in humans, and patients have a poor prognosis even after che-motherapy and radiation therapy. Surgical resection is difficult due tothe diffuse nature of the glioma. Current chemotherapies are eitherineffective in treating the glioma completely or display a series oftoxic side effects to normal tissues, limiting potentially effective treat-ments. New therapeutic strategies are therefore vital to improvingthe life expectancy of these patients. Previous work has shown thathuman brain tumor cell lines express high levels of plasma mem-brane interleukin-4 receptors (IL-4R) [5]. Furthermore, human braintumors in situ overexpress IL-4R compared with normal brain tissues[6]. IL-4R-targeted cytotoxin has been shown to mediate a remark-able antitumor effect in immunodeficient xenograft models ofhuman GBM tumors [7]. These observations show that selective
Journal of Controlled Release 160 (2012) 652–658
⁎ Correspondence to: F.Y. Yang, Department of Biomedical Imaging and RadiologicalSciences, School of Biomedical Science and Engineering, National Yang-Ming University,Taipei, Taiwan, No. 155, Sec. 2, Li-Nong St., Taipei 11221, Taiwan. Tel.: +886 2 28267281; fax: +886 2 2820 1095.⁎⁎ Correspondence to: T.T. Wong, Division of Pediatric Neurosurgery, Neurological In-
stitute, Veterans General Hospital Taipei, Taiwan, No. 210, Sec. 2, Shih-Pai Road, Taipei11217, Taiwan. Tel.: +886 2 28712121; fax: +886 2 28757587.
E-mail addresses: [email protected] (F.-Y. Yang), [email protected](T.-T. Wong).
0168-3659/$ – see front matter. Crown Copyright © 2012 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.jconrel.2012.02.023
Contents lists available at SciVerse ScienceDirect
Journal of Controlled Release
j ourna l homepage: www.e lsev ie r .com/ locate / jconre l
NANOMEDICIN
E

Author's personal copy
drug delivery may be achievable by binding chemotherapeutic agentsto IL-4R. It is noteworthy that IL-4R is also up-regulated in some dis-eases, such as ovarian cancer and lung cancer, and has already beenused as a target for tumor treatment [8,9].
Our previous study demonstrated that the concentration of Evansblue dye (EB) in tumors and the tumor-to-normal brain ratio of EB inthe brain are increased after blood–brain barrier (BBB) disruption(BBB-D) induced by pulsed high-intensity focused ultrasound (pulsedHIFU) with an ultrasound contrast agent (UCA) [10]. This disruptionto the BBB is transient and reversible and does not damage neurons[11–14]. Pulsed HIFU provides a more attractive approach for increas-ing local concentrations of therapeutic agents in the brain for thetreatment of GBM than do other methods involving modifiedchemicals. It has been shown that the use of focused ultrasoundachieves noninvasive targeted delivery of liposomal doxorubicin(Lipo-Dox) in the normal brain [15]. Another strategy is to usereceptor-targeted Lipo-Dox to improve the therapeutic efficacy, asdemonstrated in an intracranial brain tumor model [16,17].
A novel peptide we designed as a ligand from atheroscleroticplaque-specific peptide-1 (AP-1) was selected from phage display li-braries that can locate atherosclerotic plaque tissue and bind to the IL-4 receptor, since it has the same binding motif to the IL-4 protein [18].AP-1-labeled nanoparticles were used for the targeted drug deliveryto tumor [19,20]. In the present study, pulsed HIFU exposures werecombinedwith AP-1-conjugated liposomes to enhance the targeted de-livery of doxorubicin (Dox) into tumors (Fig. 1), and the results werecompared with that of the cytotoxic agent alone. The experimentswere carried out in vivo to evaluate the local drug accumulation andtherapeutic efficacy in a human brain tumor model. This technologycombines pulsed HIFU and targeted nanoparticles as a synergistic deliv-ery system for treating central nervous system diseases.
2. Materials and methods
2.1. Intracranial glioma xenograft model
All procedures were performed according to the guidelines of andwere approved by the Animal Care and Use Committee of the NationalYang-Ming University. Male 6- to 8-week-old NOD-scid mice wereanesthetized via an intraperitoneal administration of pentobarbital ata dose of 40 mg/kg body weight. Their heads were shaved above thenape of the neck, scrubbed with Betadine/alcohol, and immobilized ina Cunningham Mouse/Neonatal Rat Adaptor stereotactic apparatus(Stoelting, Wood Dale, IL, USA). A 5-mm skin incision was made alongthe sagittal suture and a burr hole drilled into the skull. Then, 2×105
human brainmalignant glioma cells (GBM8401) in 2 μl of culturemedi-um were injected stereotactically into a single location in each lefthemisphere (0.14 mm anterior and 2.0 mm lateral to the bregma) ofeach mouse at a depth of 3.5 mm from the brain surface. The burr
holes in the skull were then sealed with bone wax and the woundwas flushed with iodinated alcohol. Biophotonic imaging was used todetermine that a tumor was established.
2.2. Preparation of Lipo-Dox and AP-1-labeled Lipo-Dox
Lipo-Dox was prepared using a solvent injection method plusremote loading procedures. Briefly, hydrogenated soybean L-α-phosphatidylcholine (95.8 mg, Avanti Polar Lipids), cholesterol(31.9 mg, Sigma-Aldrich), and 1,2-distearoyl-sn-glycero-3-phos-phoethanolamine-N-[methoxy(polyethylene glycol)-2000] (DSPE-PEG2000, 31.9 mg, Avanti Polar Lipids) were dissolved and well mixedin 1 ml of absolute ethanol at 60 °C. The lipid and ethanol mixture wasthen injected into a 9-ml solution of 250 mM ammonium sulfate andstirred for 1 h at 60 °C. The mixture was then extruded five timesthrough polycarbonate membranes (Isopore Membrane Filter,Millipore) with pore sizes of 0.4, 0.2, 0.1, and 0.05 μm, consecutively,at 60 °C with high-pressure extrusion equipment (Lipex Biomem-branes) to produce small liposomes. The liposome suspension wasthen dialyzed five times against large amounts of 10% sucrose contain-ing 5 mMNaCl to remove the unentrapped ammonium sulfate and eth-anol. After dialysis, the liposome suspensionwas placed in a 50-ml glassbottle in a 60 °C water bath and mixed with Dox, to a final Dox concen-tration of 2 mg/ml in 10% sucrose solution. The bottle was intermittent-ly shaken in a 60 °C water bath for 1 h and then immediately cooleddown to 4 °C, culminating in the production of Lipo-Dox.
Due to the presence of a thiol group on each cystine of theAP-1 peptide (CRKRLDRNC), it is possible to couple AP-1 to lipo-somes via the thiol-maleimide reaction. Briefly, AP-1 peptide wasconjugated to 1,2-distearoyl-sn-glycero-3-phosphoethanolamine-N-[maleimide(polyethylene glycol)-2000] (DSPE-PEG2000-MAL, AvantiPolar Lipids) by adding AP-1 to the DSPE-PEG2000-MAL micelle solu-tion at a 2:1 molar ratio while mixing at 4 °C overnight. The free thiolgroups were measured with 5,5′-dithiobis-(2-nitrobenzoic acid)(Ellman's reagent, Sigma-Aldrich) at 420 nm to confirm that most ofthe AP-1 was conjugated with DSPE-PEG2000-MAL after the reaction.AP-1-conjugated DSPE-PEG2000 was transferred into the preformedLipo-Dox at a 1.5% molar ratio of total lipid components and incubat-ed at 60 °C for 1 h to obtain AP-1-labeled Lipo-Dox (AP-1 Lipo-Dox;Fig. 2).
The resulting unconjugated Lipo-Dox and AP-1 Lipo-Dox werefound to have particle diameters of 100–120 nm, as measured by adynamic light-scattering apparatus (Coulter N4 plus, Beckman), aswell as a surface zeta potential of between −20 and −30 mV, asmeasured by electrophoretic light scattering (ZetaPlus, Brookhaven).
2.3. Pulsed HIFU and the treatment protocol
Pulsed HIFU exposures were generated by a 1.0-MHz, single-element focused transducer (A392S, Panametrics, Waltham, MA,USA) with a diameter of 38 mm and a radius of curvature of63.5 mm. The focal zone of the therapeutic transducer was in theshape of an elongated ellipsoid, with a radial diameter (−6 dB) of3 mm and an axial length (−6 dB) of 26 mm. The ultrasound-driving system and equipment setup were the same as used in ourprevious study [21]. UCA (SonoVue, Bracco International, Amsterdam,The Netherlands) was injected into the tail vein of the mice about 10 sbefore each sonication. This agent contains phospholipid-coatedmicrobubbles at a concentration of 1–5×108 bubbles/ml, with thebubbles having a mean diameter of 2.5 μm. The sonication was pre-cisely targeted using a stereotaxic apparatus that utilized the bregmaof the skull as an anatomical landmark. The ultrasound beam was de-livered to one location in the left brain hemisphere, centered on thetumor injection site. The following sonication parameters wereused: an acoustic power of 2.86 W (corresponding to a peak negative
Fig. 1. Schematic depiction of the synergistic treatment strategy. (A) Tumor treatedwith liposomal doxorubicin (Lipo-Dox); Lipo-Dox diffusion was easier than in tumorstreated with free doxorubicin (Dox). (B) Lipo-Dox actively targeted the chemothera-peutics to the tumor via conjugation with human atherosclerotic plaque-specificpeptide-1 (AP-1). (C) Combining targeted Lipo-Dox (AP-1 Lipo-Dox) with pulsed high-intensity focused ultrasound (pulsed HIFU) in the presence of microbubbles significantlyincreases the amount of chemotherapeutics that reaches the tumor site. EC= endothelialcell, P = pericyte, BL = basal lamina, N = neuron, AE = astrocyte endfoot.
653F.-Y. Yang et al. / Journal of Controlled Release 160 (2012) 652–658
NANOMEDICIN
E

Author's personal copy
pressure of 0.7 MPa) with an injection of 300 μl/kg UCA, a pulse rep-etition frequency of 1 Hz, and a duty cycle of 5%.
A group of control mice was injected with GBM8401 glioma cells,but received no treatment. Five and 9 days after tumor cell implanta-tion, the other glioma-bearing mice received one of the following: (1)pulsed-HIFU exposure, (2) AP-1 Lipo-Dox, or (3) AP-1 Lipo-Dox fol-lowed by pulsed HIFU. The concentration of liposomes administeredto the mice via tail-vein injection corresponded to 5 mg/kg.
2.4. Quantitative analysis of Dox
An overdose of pentobarbital was used to put animals into a state ofdeep anesthesia. The brain was perfused by transcardiac methods withnormal saline 3.5 h after the Dox administration in order to flush unab-sorbed Dox from the cerebral vessels. The site of tumor tissue was har-vested along with its contralateral counterpart as a control. Dox wasextracted from the tumor and control tissues by homogenization andrefrigeration for 24 h in 20 volumes of acidified ethanol at 4 °C. Tissueswere centrifuged at 16,000×g for 25 min at 4 °C and the supernatantwas stored at −20 °C until being used in a fluorometric assay [22].The concentration of Dox present was measured using a spectropho-tometer (PowerWave 340, BioTek, USA; excitation at 480 nmand emis-sions measured at 590 nm), with the value determined by taking theaverage of at least three fluorometric readings. The Dox present in thetissue samples was quantified using a linear regression standard curvederived from seven different concentrations of Dox; the amount ofDox was quantified as the absorbance per gram of tissue.
2.5. Biophotonic tumor imaging
Tumor size was quantified by analyzing biophotonic imagesobtained from 5 to 16 days after tumor implantation. The GBM8401cell lines were transformed with the luciferase gene, and each mousewas injected with 4.29 mg of freshly prepared luciferin substrate sus-pended in phosphate-buffered saline (PBS). After anesthetic inductionwith isoflurane (1.5 l/min oxygen in 4% isoflurane), mice were imagedusing the Xenogen IVIS imaging system (Xenogen, Palo Alto, CA, USA)10 min after the intraperitoneal injection of luciferin, with a 1-min ac-quisition time in small-bin mode. Luciferase activity was viewed andquantified using Living Image Software from Xenogen within a region
of interest that encompassed the head of the mouse after administra-tion of luciferin substrate to the anesthetized mouse.
2.6. Magnetic resonance imaging
Magnetic resonance imaging (MRI) was performed using a 3-TMRI system (TRIO 3-T MRI, Siemens MAGNETOM, Germany) after fo-cused ultrasound sonication. The mice were anesthetized with iso-flurane mixed with oxygen during the imaging procedure. A loopcoil (Loop Flex Coil, approximately 4 cm in diameter) was used forRF reception. Tumor progression was monitored by means ofT2-weighted images obtained from 4 to 16 days after tumor implan-tation. The parameters for T2-weighted imaging were as follows:repetition time/echo time=3500/75 ms, matrix=125×256, field ofview=25×43 mm, and section thickness=1.0 mm. The imagingplane was located across the center of the tumor injection site.
2.7. Brain immunofluorescence
Mice were deeply anesthetized with pentobarbital and perfusedtranscardially with a solution of 0.9% saline followed by 4% paraformal-dehyde in PBS. Brains were dissected out and postfixed in 4% parafor-maldehyde for 24 h at 4 °C. They were then incubated in a 30%sucrose solution overnight at 4 °C. Coronal sections were serially cutat 30 μm using a freezing microtome. Serial sections were collected inPBS containing 0.05% sodium azide, and then stored at 4 °C. Immuno-histochemistry was performed on floating sections. Briefly, sectionswere first incubated in a blocking solution for 1 h and then transferredto the rabbit antiluciferase primary antibody (1:100; Santa Cruz Bio-technology), where they remained for 18 h at 4 °C. After washing, thesections were incubated with secondary DyLight488 fluorescently la-beled goat-antirabbit antibody (1:1000; Rockland Immunochemicals)for 2 h at room temperature. After secondary antibody staining, the sec-tions were counterstained with 4′-6-diamidino-2-phenylindole,mounted on glass slides using FluoreGuard mounting medium (ScyTekLaboratories), and then stored in the dark and cold until imaged. Six toeight coronal sections of each animal were analyzed using an OlympusFV1000 confocal microscope with a UPLSAPO ×20 air, ×40 air, or ×60oil lens, and FV10-ASW1.7 software (Olympus, Shinjuku-Ku, Tokyo,Japan). A vertical scanwas performed to determine the plane of greatestintensity of the fluorescent signal within the specimen; a single hori-zontal scan was subsequently performed at that plane [23]. For quanti-fication of Dox or luciferase immunoreactivity in each brain tumorregion, the images were analyzed offline using MetaMorph image-analysis software (Molecular Devices).
2.8. Statistical analysis
The statistical analysis of differences between treatment condi-tions was performed using an unpaired Student's t-test. TheKaplan–Meier method was used to plot an animal survival curve. Sig-nificance was assessed by using the Log-Rank test. The four treatmentgroups (i.e., control, pulsed-HIFU exposure alone, AP-1 Lipo-Doxalone, and AP-1 Lipo-Dox followed by pulsed HIFU) were comparedwith respect to mean survival time, percentage increase in mean sur-vival time, and maximal survival time. The level of statistical signifi-cance was set at P≤0.05.
3. Results
3.1. Accumulation of Dox in brains and tumors
Spectrophotometry was used to measure the average tumor Doxconcentration (in micrograms per gram of tissue) for three micefrom each group. Dox was extracted from the tumor and contralateralcontrol regions of the harvested brains treated with unconjugated
Fig. 2. Schematic diagram of the liposome and AP-1-conjugated liposome. Liposomeswere prepared containing maleimide-functionaled polyethylene glycol chains. Themaleimide was used to attach the AP-1 peptide through the thiol group on a cystine.Therapeutic liposomes were loaded with Dox. DSPE-PEG2000 = 1,2-distearoyl-sn-glycero-3-phosphoethanolamine-N-[methoxy(polyethylene glycol)-2000], MAL =maleimide.
654 F.-Y. Yang et al. / Journal of Controlled Release 160 (2012) 652–658
NANOMEDICIN
E
Author's personal copy
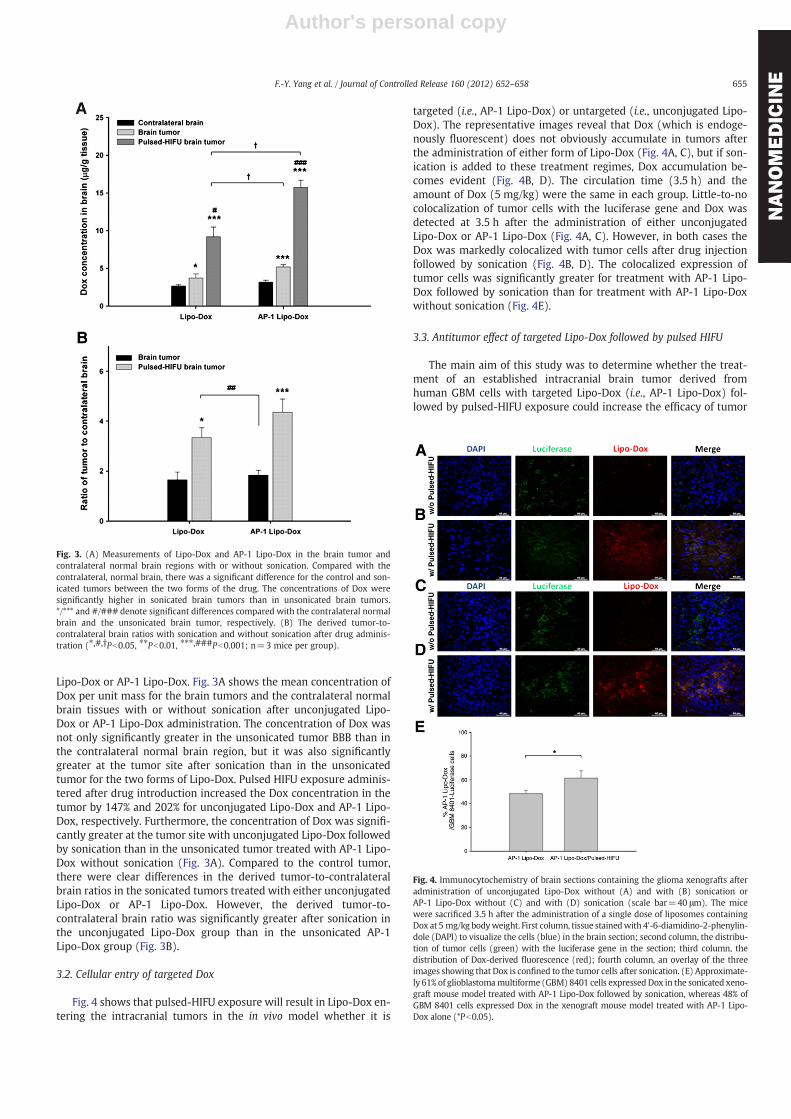
Lipo-Dox or AP-1 Lipo-Dox. Fig. 3A shows the mean concentration ofDox per unit mass for the brain tumors and the contralateral normalbrain tissues with or without sonication after unconjugated Lipo-Dox or AP-1 Lipo-Dox administration. The concentration of Dox wasnot only significantly greater in the unsonicated tumor BBB than inthe contralateral normal brain region, but it was also significantlygreater at the tumor site after sonication than in the unsonicatedtumor for the two forms of Lipo-Dox. Pulsed HIFU exposure adminis-tered after drug introduction increased the Dox concentration in thetumor by 147% and 202% for unconjugated Lipo-Dox and AP-1 Lipo-Dox, respectively. Furthermore, the concentration of Dox was signifi-cantly greater at the tumor site with unconjugated Lipo-Dox followedby sonication than in the unsonicated tumor treated with AP-1 Lipo-Dox without sonication (Fig. 3A). Compared to the control tumor,there were clear differences in the derived tumor-to-contralateralbrain ratios in the sonicated tumors treated with either unconjugatedLipo-Dox or AP-1 Lipo-Dox. However, the derived tumor-to-contralateral brain ratio was significantly greater after sonication inthe unconjugated Lipo-Dox group than in the unsonicated AP-1Lipo-Dox group (Fig. 3B).
3.2. Cellular entry of targeted Dox
Fig. 4 shows that pulsed-HIFU exposure will result in Lipo-Dox en-tering the intracranial tumors in the in vivo model whether it is
targeted (i.e., AP-1 Lipo-Dox) or untargeted (i.e., unconjugated Lipo-Dox). The representative images reveal that Dox (which is endoge-nously fluorescent) does not obviously accumulate in tumors afterthe administration of either form of Lipo-Dox (Fig. 4A, C), but if son-ication is added to these treatment regimes, Dox accumulation be-comes evident (Fig. 4B, D). The circulation time (3.5 h) and theamount of Dox (5 mg/kg) were the same in each group. Little-to-nocolocalization of tumor cells with the luciferase gene and Dox wasdetected at 3.5 h after the administration of either unconjugatedLipo-Dox or AP-1 Lipo-Dox (Fig. 4A, C). However, in both cases theDox was markedly colocalized with tumor cells after drug injectionfollowed by sonication (Fig. 4B, D). The colocalized expression oftumor cells was significantly greater for treatment with AP-1 Lipo-Dox followed by sonication than for treatment with AP-1 Lipo-Doxwithout sonication (Fig. 4E).
3.3. Antitumor effect of targeted Lipo-Dox followed by pulsed HIFU
The main aim of this study was to determine whether the treat-ment of an established intracranial brain tumor derived fromhuman GBM cells with targeted Lipo-Dox (i.e., AP-1 Lipo-Dox) fol-lowed by pulsed-HIFU exposure could increase the efficacy of tumor
Fig. 4. Immunocytochemistry of brain sections containing the glioma xenografts afteradministration of unconjugated Lipo-Dox without (A) and with (B) sonication orAP-1 Lipo-Dox without (C) and with (D) sonication (scale bar=40 μm). The micewere sacrificed 3.5 h after the administration of a single dose of liposomes containingDox at 5 mg/kg bodyweight. First column, tissue stainedwith 4'-6-diamidino-2-phenylin-dole (DAPI) to visualize the cells (blue) in the brain section; second column, the distribu-tion of tumor cells (green) with the luciferase gene in the section; third column, thedistribution of Dox-derived fluorescence (red); fourth column, an overlay of the threeimages showing that Dox is confined to the tumor cells after sonication. (E) Approximate-ly 61% of glioblastomamultiforme (GBM) 8401 cells expressed Dox in the sonicated xeno-graft mouse model treated with AP-1 Lipo-Dox followed by sonication, whereas 48% ofGBM 8401 cells expressed Dox in the xenograft mouse model treated with AP-1 Lipo-Dox alone (*Pb0.05).
Fig. 3. (A) Measurements of Lipo-Dox and AP-1 Lipo-Dox in the brain tumor andcontralateral normal brain regions with or without sonication. Compared with thecontralateral, normal brain, there was a significant difference for the control and son-icated tumors between the two forms of the drug. The concentrations of Dox weresignificantly higher in sonicated brain tumors than in unsonicated brain tumors.*/*** and #/### denote significant differences compared with the contralateral normalbrain and the unsonicated brain tumor, respectively. (B) The derived tumor-to-contralateral brain ratios with sonication and without sonication after drug adminis-tration (⁎,#,†Pb0.05, ⁎⁎Pb0.01, ⁎⁎⁎,###Pb0.001; n=3 mice per group).
655F.-Y. Yang et al. / Journal of Controlled Release 160 (2012) 652–658
NANOMEDICIN
E
Author's personal copy
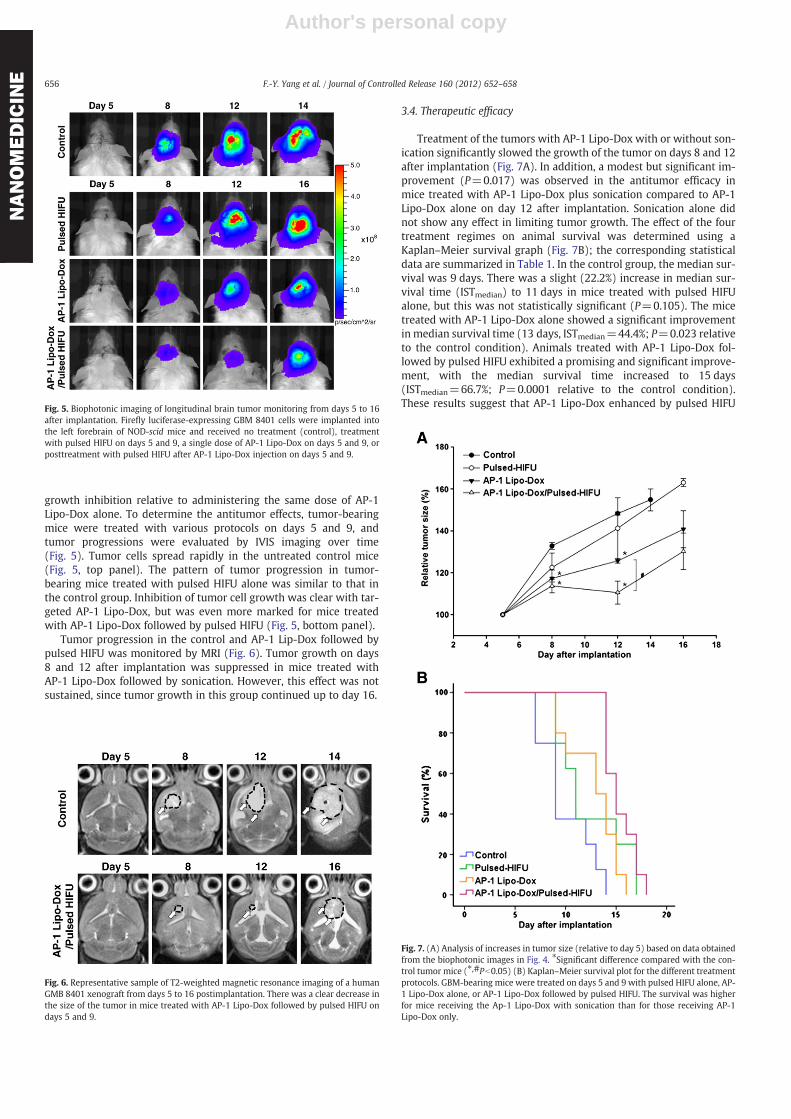
growth inhibition relative to administering the same dose of AP-1Lipo-Dox alone. To determine the antitumor effects, tumor-bearingmice were treated with various protocols on days 5 and 9, andtumor progressions were evaluated by IVIS imaging over time(Fig. 5). Tumor cells spread rapidly in the untreated control mice(Fig. 5, top panel). The pattern of tumor progression in tumor-bearing mice treated with pulsed HIFU alone was similar to that inthe control group. Inhibition of tumor cell growth was clear with tar-geted AP-1 Lipo-Dox, but was even more marked for mice treatedwith AP-1 Lipo-Dox followed by pulsed HIFU (Fig. 5, bottom panel).
Tumor progression in the control and AP-1 Lip-Dox followed bypulsed HIFU was monitored by MRI (Fig. 6). Tumor growth on days8 and 12 after implantation was suppressed in mice treated withAP-1 Lipo-Dox followed by sonication. However, this effect was notsustained, since tumor growth in this group continued up to day 16.
3.4. Therapeutic efficacy
Treatment of the tumors with AP-1 Lipo-Dox with or without son-ication significantly slowed the growth of the tumor on days 8 and 12after implantation (Fig. 7A). In addition, a modest but significant im-provement (P=0.017) was observed in the antitumor efficacy inmice treated with AP-1 Lipo-Dox plus sonication compared to AP-1Lipo-Dox alone on day 12 after implantation. Sonication alone didnot show any effect in limiting tumor growth. The effect of the fourtreatment regimes on animal survival was determined using aKaplan–Meier survival graph (Fig. 7B); the corresponding statisticaldata are summarized in Table 1. In the control group, the median sur-vival was 9 days. There was a slight (22.2%) increase in median sur-vival time (ISTmedian) to 11 days in mice treated with pulsed HIFUalone, but this was not statistically significant (P=0.105). The micetreated with AP-1 Lipo-Dox alone showed a significant improvementin median survival time (13 days, ISTmedian=44.4%; P=0.023 relativeto the control condition). Animals treated with AP-1 Lipo-Dox fol-lowed by pulsed HIFU exhibited a promising and significant improve-ment, with the median survival time increased to 15 days(ISTmedian=66.7%; P=0.0001 relative to the control condition).These results suggest that AP-1 Lipo-Dox enhanced by pulsed HIFUFig. 5. Biophotonic imaging of longitudinal brain tumor monitoring from days 5 to 16
after implantation. Firefly luciferase-expressing GBM 8401 cells were implanted intothe left forebrain of NOD-scid mice and received no treatment (control), treatmentwith pulsed HIFU on days 5 and 9, a single dose of AP-1 Lipo-Dox on days 5 and 9, orposttreatment with pulsed HIFU after AP-1 Lipo-Dox injection on days 5 and 9.
Fig. 6. Representative sample of T2-weighted magnetic resonance imaging of a humanGMB 8401 xenograft from days 5 to 16 postimplantation. There was a clear decrease inthe size of the tumor in mice treated with AP-1 Lipo-Dox followed by pulsed HIFU ondays 5 and 9.
Fig. 7. (A) Analysis of increases in tumor size (relative to day 5) based on data obtainedfrom the biophotonic images in Fig. 4. ⁎Significant difference compared with the con-trol tumor mice (⁎,#Pb0.05) (B) Kaplan–Meier survival plot for the different treatmentprotocols. GBM-bearing mice were treated on days 5 and 9 with pulsed HIFU alone, AP-1 Lipo-Dox alone, or AP-1 Lipo-Dox followed by pulsed HIFU. The survival was higherfor mice receiving the Ap-1 Lipo-Dox with sonication than for those receiving AP-1Lipo-Dox only.
656 F.-Y. Yang et al. / Journal of Controlled Release 160 (2012) 652–658
NANOMEDICIN
E

Author's personal copy
at the tumor site is more effective at inhibiting tumor growth and im-proving animal survival than either treatment regimen alone.
4. Discussion
Previous studies have shown that poor penetration and limited dis-tribution of Dox in solid tumors are themain causes of its inadequacy asa chemotherapeutic agent [24,25]. Long-circulating nanoparticles havebeen approved to deliver anticancer drugs into brain tumors via thepassive enhancement of permeability and the retention effect [26].The active targeting of the receptors that are overexpressed on braintumor cells is a novel approach for brain tumor therapy [16,17]. It hasbeen demonstrated that ultrasound sonication could facilitate the deliv-ery of various types of agents to solid tumors [27]. Moreover, this en-hancement could improve the therapeutic efficacy of Lipo-Dox in abreast cancer tumormodel [28]. The purpose of this studywas to deter-mine whether exposure to pulsed HIFU could enhance the delivery oftargeted Lipo-Dox to the tumor tissue and improve the antitumor effectin an intracranial human brain tumor model. In the present study, wedesigned active targeting nanoparticles by conjugating AP-1 to the sur-face of liposomes to provide a potential antitumor treatment for braintumors (Fig. 2). Our strategy was to use a ligand-conjugated liposomaldrug in conjunction with pulsed HIFU to deliver a concentrated highdose of a chemotherapeutic agent into brain tumors by using only theusual systemic dosage (Fig. 3A).
Pulsed HIFU not only significantly enhanced the concentration ofDox in the tumor, but also significantly elevated the tumor-to-normalbrain ratio at the sonicated tumor site (Fig. 3). By combining biology-directed and physically-assistedmethods, it is hoped that this synergis-tic technology can safely deliver high-dose chemotherapy specifically toa brain tumor without causing extra toxicity to the normal brain tissueor systemic side effects.
The possible mechanisms underlying the enhancing effect of pulsedHIFU on brain tumor chemotherapy are threefold. Firstly, cavitation ac-tivities can disrupt the BBB and acoustic waves can actually aid the pen-etration of drugs through the tumor tissue. Secondly, this technologyalso reduces interstitialfluid pressure in tissues,which in turn enhancesdiffusion through the interstitium [29]. Finally, ultrasound can increasethe porosity of the cell membrane [30] and enhance the delivery ofdrugs into the cells through these openings. Although the real mecha-nisms remain to be established, it is believed that the oscillatingbehavior of themicrobubbles causes rupture of the cell membrane, cre-ating hydrophilic pores that allow the transmembrane flux of fluid andmacromolecules [31], thus enhancing the cellular uptake of therapeu-tics. If the BBB is intact, only the endothelial cells may have increase po-rosity and this effect doesn't directly relate to tumor cells. While theultrasound pressure is so high that cavitation occurs, cells beyond thislayer may become more porous but the dominant mechanism is lessthan the cavitation itself. The colocalized enhancements of tumor drugconcentration and tumor-to-normal brain ratio noted in the presentstudy (Fig. 4E) are consistent with the idea that poration of the cellmembrane occurs. Amodest but significant difference in the colocalizedexpression of tumor cells in Fig.4E may be the possible reason that theamount of Doxwasmore than twice as high with sonication but no sig-nificant effects on the growth rate were found.
Furthermore, there were no significant differences in tumor Doxconcentration and tumor-to-contralateral brain ratio in the tumorstreated with AP-1 Lipo-Dox alone compared to the mice treated withunconjugated Lipo-Dox alone (Fig. 3). This could have been due to thecirculation time of this study, 3.5 h, being insufficient for the drugs toreach the maximum concentration in the tumor. However, the tumorDox concentration and tumor-to-contralateral brain ratio was signifi-cantly elevated in tumors treated with the two drugs followed by soni-cation at the same time point. The effect of pulsed HIFU on drug uptakeobserved herein is consistent with the findings of a previous report thatsonication could shorten peak tumor uptake time and increase peaktumor uptake values compared with those of unsonicated tumors [29].
One limitation of this study was that the use of a single-elementtransducer made it difficult to achieve identical pressure profiles in tu-mors of various sizes and shapes. Because the BBB-D is dependent onthe acoustic pressure, the variability in pressure probably contributedto the observed intragroup heterogeneity in drug delivery and tumorresponse. Therefore, pulsed HIFU also increased the accumulation ofDox in the surrounding tissues, but the net increase wasmarginal com-pared with the increase in tumor accumulation of the chemotherapeu-tic agent [10,29]. In the clinical setting, a phased-array transducer couldbe used to provide more localized sonication [32–34]. In addition,human tumors are much larger than mouse tumors, so these devicesmay be capable of directing pressure to more specific and focused re-gions of human tumors.
The findings of this study demonstrate that ligand-conjugated lipo-somal technology assisted by pulsed HIFU is able to concentrate high-dose chemotherapeutic drugs into brain tumors and improve their anti-tumor effects. The integration of targeted nano-anticancer drugs andpulsed-HIFU technology may open a window for achieving enhancedlocal drug delivery and treatment efficacy with minimal side effects inthe chemotherapy of high-grade gliomas and other brain diseases.
Acknowledgments
This studywas supported by grants from the National Science Coun-cil of Taiwan (no. NSC 100-2321-B-010-010 and NSC 99-2321-B-010-017), Cheng Hsin General Hospital Foundation (no. 100F117CY25),Veterans General Hospitals University System of Taiwan Joint ResearchProgram (#VGHUST100-G1-3-3 and V100E6-007), Yen Tjing LingMedical Foundation (grant CI-100-17), Department of Health of Taiwan(DOH101-TD-PB-111-TM012 and DOH101-TD-C-111-007).
References
[1] J.D. Floyd, D.T. Nguyen, R.L. Lobins, Q. Bashir, D.C. Doll, M.C. Perry, Cardiotoxicityof cancer therapy, J. Clin. Oncol. 23 (30) (2005) 7685–7696.
[2] T.M. Allen, P.R. Cullis, Drug delivery systems: entering the mainstream, Science303 (5665) (2004) 1818–1822.
[3] T.M. Allen, Liposomes. Opportunities in drug delivery, Drugs 54 (Suppl. 4) (1997)8–14.
[4] C.R. Dass, T.L. Walker, M.A. Burton, E.E. Decruz, Enhanced anticancer therapy me-diated by specialized liposomes, J. Pharm. Pharmacol. 49 (10) (1997) 972–975.
[5] R.K. Puri, P. Leland, R.J. Kreitman, I. Pastan, Human neurological cancer cells ex-press interleukin-4 (IL-4) receptors which are targets for the toxic effects ofIL4-Pseudomonas exotoxin chimeric protein, Int. J. Cancer 58 (4) (1994)574–581.
Table 1Efficacy of treatment protocols on brain tumor in mice.
Treatment group Median survival (d) ISTmedian (%) Mean survival (d)† Maximal survival (d) P value
Control (n=6) 9 … 10±0.9 14 …
Pulsed HIFU (n=6) 11 22.2 12.4±1.2 17 0.105AP-1 Lipo-Dox (n=10) 13 44.4 12.8±0.8 16 0.023AP-1 Lipo-Dox/pulsed HIFU (n=10) 15 66.7 15.4±0.5 18 0.0001‡
Note. Increases in ISTmedian and P value are relative to the control group.† Data are the mean±standard deviation.‡ P value is 0.017 between the AP-1 Lipo-Dox and the AP-1 Lipo-Dox/pulsed HIFU group.
657F.-Y. Yang et al. / Journal of Controlled Release 160 (2012) 652–658
NANOMEDICIN
E

Author's personal copy
[6] B.H. Joshi, P. Leland, A. Asher, R.A. Prayson, F. Varricchio, R.K. Puri, In situ expres-sion of interleukin-4 (IL-4) receptors in human brain tumors and cytotoxicity of arecombinant IL-4 cytotoxin in primary glioblastoma cell cultures, Cancer Res. 61(22) (2001) 8058–8061.
[7] S.R. Husain, N. Behari, R.J. Kreitman, I. Pastan, R.K. Puri, Complete regression ofestablished human glioblastoma tumor xenograft by interleukin-4 toxin therapy,Cancer Res. 58 (16) (1998) 3649–3653.
[8] M. Kioi, S. Takahashi, M. Kawakami, K. Kawakami, R.J. Kreitman, R.K. Puri, Expres-sion and targeting of interleukin-4 receptor for primary and advanced ovariancancer therapy, Cancer Res. 65 (18) (2005) 8388–8396.
[9] L. Garland, B. Gitlitz, S. Ebbinghaus, H. Pan, H. de Haan, R.K. Puri, D. VonHoff, R. Figlin, Phase I trial of intravenous IL-4 pseudomonas exotoxin pro-tein (NBI-3001) in patients with advanced solid tumors that express the IL-4 receptor, J. Immunother. 28 (4) (2005) 376–381.
[10] F.Y. Yang, H.E.Wang,G.L. Lin,M.C. Teng, H.H. Lin, T.T.Wong, R.S. Liu,Micro-SPECT/CT-based pharmacokinetic analysis of 99mTc-diethylenetriaminepentaacetic acid in ratswith blood–brain barrier disruption induced by focused ultrasound, J. Nucl. Med. 52(3) (2011) 478–484.
[11] F.Y. Yang, Y.S. Lin, K.H. Kang, T.K. Chao, Reversible blood–brain barrier dis-ruption by repeated transcranial focused ultrasound allows enhanced ex-travasation, J. Control. Release 150 (1) (2011) 111–116.
[12] K. Hynynen, N. McDannold, N. Vykhodtseva, F.A. Jolesz, Noninvasive MR imaging-guided focal opening of the blood–brain barrier in rabbits, Radiology 220 (3)(2001) 640–646.
[13] F.Y. Yang, S.C. Horng, Y.S. Lin, Y.H. Kao, Association between contrast-enhancedMR images and blood–brain barrier disruption following transcranial focused ul-trasound, J. Magn. Reson. Imaging 32 (3) (2010) 593–599.
[14] F.Y. Yang, S.H. Liu, F.M. Ho, C.H. Chang, Effect of ultrasound contrast agentdose on the duration of focused-ultrasound-induced blood–brain barrier dis-ruption, J. Acoust. Soc. Am. 126 (6) (2009) 3344–3349.
[15] L.H. Treat, N. McDannold, N. Vykhodtseva, Y. Zhang, K. Tam, K. Hynynen, Targeteddelivery of doxorubicin to the rat brain at therapeutic levels using MRI-guided fo-cused ultrasound, Int. J. Cancer 121 (4) (2007) 901–907.
[16] A.B. Madhankumar, B. Slagle-Webb, X. Wang, Q.X. Yang, D.A. Antonetti, P.A.Miller, J.M. Sheehan, J.R. Connor, Efficacy of interleukin-13 receptor-targeted lipo-somal doxorubicin in the intracranial brain tumor model, Mol. Cancer Ther. 8 (3)(2009) 648–654.
[17] A.B. Madhankumar, B. Slagle-Webb, A. Mintz, J.M. Sheehan, J.R. Connor, Interleu-kin-13 receptor-targeted nanovesicles are a potential therapy for glioblastomamultiforme, Mol. Cancer Ther. 5 (12) (2006) 3162–3169.
[18] H.Y. Hong, H.Y. Lee, W. Kwak, J. Yoo, M.H. Na, I.S. So, T.H. Kwon, H.S. Park,S. Huh, G.T. Oh, I.C. Kwon, I.S. Kim, B.H. Lee, Phage display selection of pep-tides that home to atherosclerotic plaques: IL-4 receptor as a candidate tar-get in atherosclerosis, J. Cell. Mol. Med. 12 (5B) (2008) 2003–2014.
[19] X.L. Wu, J.H. Kim, H. Koo, S.M. Bae, H. Shin, M.S. Kim, B.H. Lee, R.W. Park, I.S. Kim,K. Choi, I.C. Kwon, K. Kim, D.S. Lee, Tumor-targeting peptide conjugated pH-responsive micelles as a potential drug carrier for cancer therapy, Bioconjug.Chem. 21 (2) (2010) 208–213.
[20] J.H. Kim, S.M. Bae, M.H. Na, H. Shin, Y.J. Yang, K.H. Min, K.Y. Choi, K. Kim, R.W.Park, I.C. Kwon, B.H. Lee, A.S. Hoffman, I.S. Kim, Facilitated intracellular deliveryof peptide-guided nanoparticles in tumor tissues, J. Control. Release (2011).
[21] F.Y. Yang, G.L. Lin, S.C. Horng, T.K. Chang, S.Y. Wu, T.T. Wong, H.E. Wang, Pulsedhigh-intensity focused ultrasound enhances the relative permeability of theblood-tumor barrier in a glioma-bearing rat model, IEEE Trans. Ultrason. Ferroe-lectr. Freq. Control 58 (5) (2011) 964–970.
[22] N.R. Bachur, A.L. Moore, J.G. Bernstein, A. Liu, Tissue distribution and dispositionof daunomycin (NCS-82151) in mice: fluorometric and isotopic methods, CancerChemother. Rep. 54 (2) (1970) 89–94.
[23] A.O. Muda, S. Feriozzi, S. Rahimi, E. Ancarani, T. Faraggiana, Spatial arrangementof subepithelial deposits in lupus and nonlupus membranous nephropathy, Am.J. Kidney Dis. 34 (1) (1999) 85–91.
[24] A.J. Primeau, A. Rendon, D. Hedley, L. Lilge, I.F. Tannock, The distribution of theanticancer drug doxorubicin in relation to blood vessels in solid tumors, Clin.Cancer Res. 11 (24 Pt 1) (2005) 8782–8788.
[25] J. Lankelma, H. Dekker, F.R. Luque, S. Luykx, K. Hoekman, P. van der Valk, P.J. vanDiest, H.M. Pinedo, Doxorubicin gradients in human breast cancer, Clin. CancerRes. 5 (7) (1999) 1703–1707.
[26] U.S. Sharma, A. Sharma, R.I. Chau, R.M. Straubinger, Liposome-mediated therapyof intracranial brain tumors in a rat model, Pharm. Res. 14 (8) (1997) 992–998.
[27] Y. Manome, M. Nakamura, T. Ohno, H. Furuhata, Ultrasound facilitates transduc-tion of naked plasmid DNA into colon carcinoma cells in vitro and in vivo, Hum.Gene Ther. 11 (11) (2000) 1521–1528.
[28] V. Frenkel, A. Etherington, M. Greene, J. Quijano, J. Xie, F. Hunter, S. Dromi, K.C. Li,Delivery of liposomal doxorubicin (Doxil) in a breast cancer tumor model: inves-tigation of potential enhancement by pulsed-high intensity focused ultrasoundexposure, Acad. Radiol. 13 (4) (2006) 469–479.
[29] A. Khaibullina, B.S. Jang, H. Sun, N. Le, S. Yu, V. Frenkel, J.A. Carrasquillo, I. Pastan,K.C. Li, C.H. Paik, Pulsed high-intensity focused ultrasound enhances uptake ofradiolabeled monoclonal antibody to human epidermoid tumor in nude mice,J. Nucl. Med. 49 (2) (2008) 295–302.
[30] K. Tachibana, T. Uchida, K. Ogawa, N. Yamashita, K. Tamura, Induction of cell-membrane porosity by ultrasound, Lancet 353 (9162) (1999) 1409.
[31] A. van Wamel, K. Kooiman, M. Harteveld, M. Emmer, F.J. ten Cate, M. Versluis, N.de Jong, Vibrating microbubbles poking individual cells: drug transfer into cellsvia sonoporation, J. Control. Release 112 (2) (2006) 149–155.
[32] G.T. Clement, P.J. White, R.L. King, N. McDannold, K. Hynynen, A magnetic reso-nance imaging-compatible, large-scale array for trans-skull ultrasound surgeryand therapy, J. Ultrasound Med. 24 (8) (2005) 1117–1125.
[33] M. Pernot, J.F. Aubry, M. Tanter, J.L. Thomas, M. Fink, High power transcranialbeam steering for ultrasonic brain therapy, Phys. Med. Biol. 48 (16) (2003)2577–2589.
[34] K. Hynynen, F.A. Jolesz, Demonstration of potential noninvasive ultrasound braintherapy through an intact skull, Ultrasound Med. Biol. 24 (2) (1998) 275–283.
658 F.-Y. Yang et al. / Journal of Controlled Release 160 (2012) 652–658
NANOMEDICIN
E
Related Documents











