Fluids in ICU JMO teaching 5th July 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Fluids in ICUJMO teaching 5th July 2016
Objectives• Physiology of fluid infusion
• History of fluid resuscitation
• Physiology of fluid resuscitation
• Types of resuscitation fluid
• The ideal resuscitation fluid
• Fluid overload and how to avoid it
Physiology of fluid infusion
• What are the effects of rapid infusion of a litre of 5% dextrose into a patient?
Physiology of fluid infusion
• What are the effects of rapid infusion of a litre of 0.9% saline (Normal saline) into a patient?

Physiology of fluid infusion
• What are the effects of rapid infusion of a litre of 5% normal serum albumin solution into a patient?

Physiology of fluid infusion
• Which of the 3 infusions would be excreted the quickest and why?

History of fluid resuscitation
• 1832 = Robert Lewis administered “Saline injections into the vines” vs cholera pandemic
“… the quantity necessary to be infected will probably be found to depend upon the quantity of serum lost; the object being to place the patient in nearly his ordinary state as to the quantity of blood circulating in the vessels”
History of fluid resuscitation
• Sidney Ringer (1834-1910) developed solution 1884
• Alexis Hartmann (1989-1964) modified solution by addition of lactate
• 1941 => blood fractionation => development of Albumin … used at Pearl Harbour same year
Physiology of fluid resuscitation
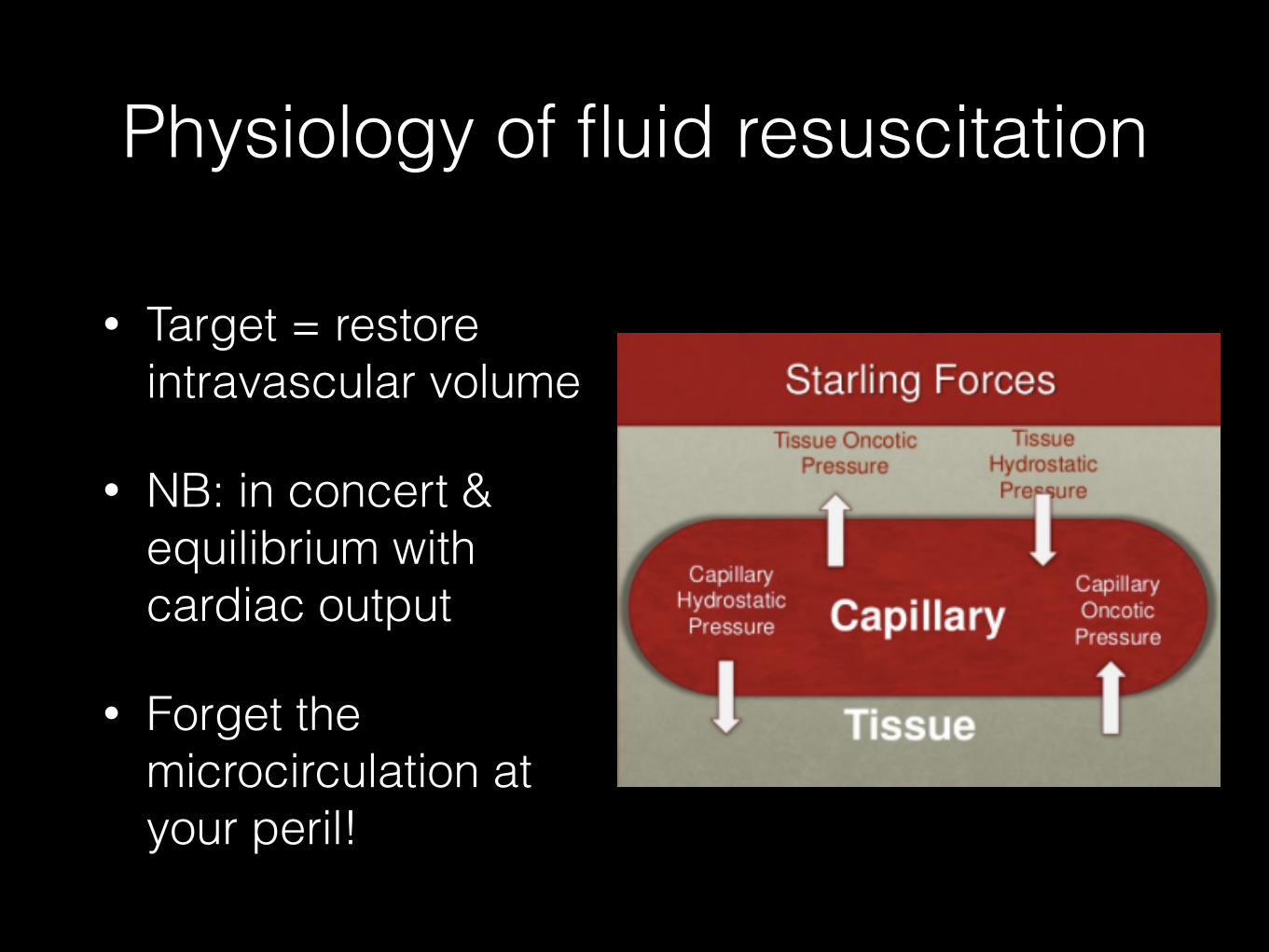
• Target = restore intravascular volume
• NB: in concert & equilibrium with cardiac output
• Forget the microcirculation at your peril!
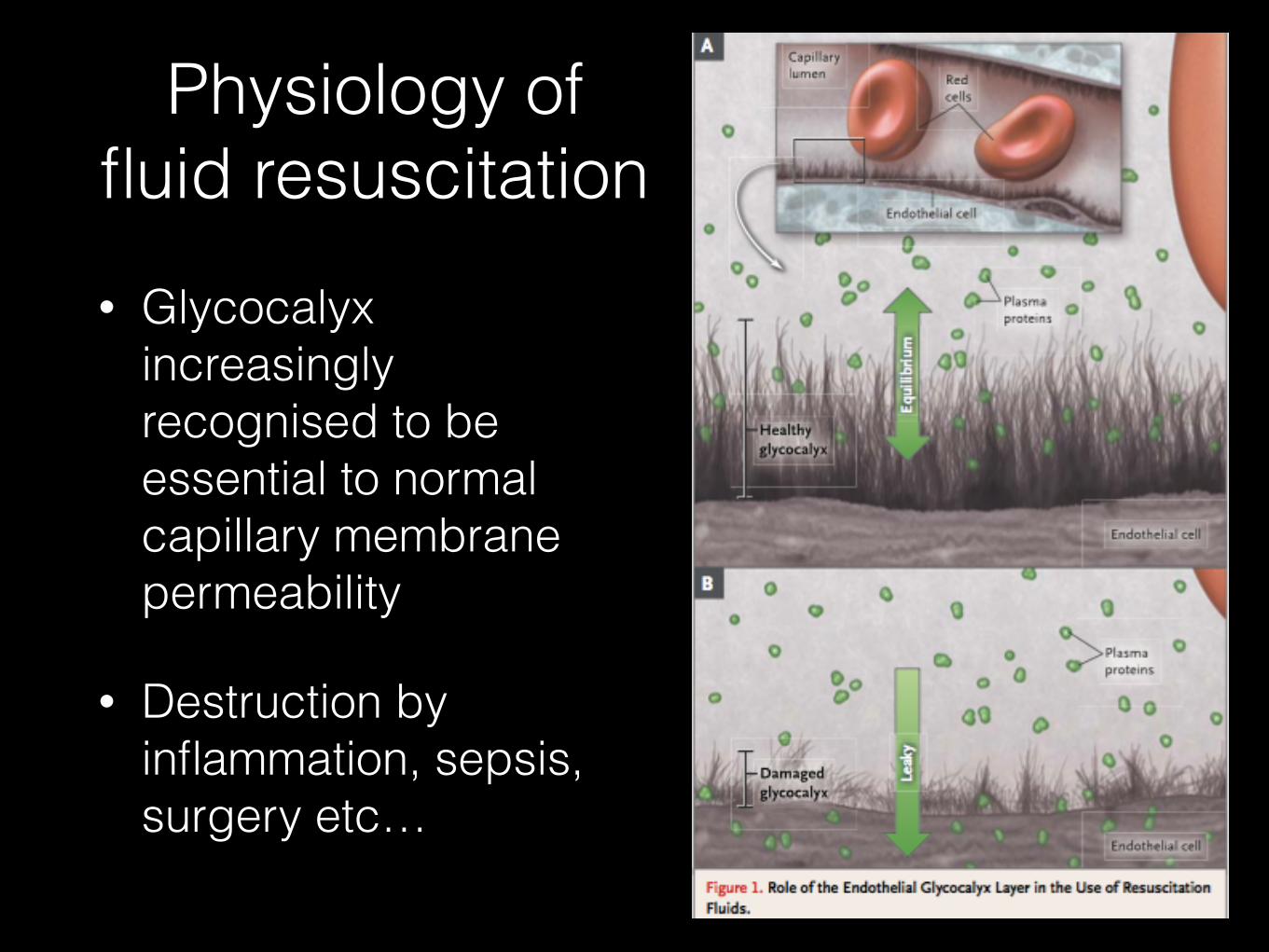
• Glycocalyx increasingly recognised to be essential to normal capillary membrane permeability
• Destruction by inflammation, sepsis, surgery etc…
Physiology of fluid resuscitation
Types of resuscitation fluid
Colloids
• Albumin
• HES (10%, 6%)
• Synthetic starch
Crystalloids
• 0.9% saline
• Hartman’s / CSL
• Plasmalyte
NB: huge variation in global use of these solutions

Ideal resuscitation fluid• Predictable response
• Sustained increase in intravascular volume
• Truely balanced vs ECF
• Metabolised and exerted without accumulation
• No adverse metabolic or systemic effects
• Cheap
• NB: this does not exists currently
Albumin• Reference colloid solution
• Fractionation blood => heat treated
Advantages:
• Safe
• Not as much coagulopathy / renal failure as other colloids
Disadvantages:
• Expensive (not so much in Australia)
• Limited availability in low/middle income countries
• Short shelf life (~1yr)

Albumin• 1998 Cochrane meta-analysis, 24 trials,1419 patients, albumin vs
N/S in hypovolaemia, burns and hypovolaemia => increased mortality (6% increase in absolute risk of death)
• SAFE trial (NEJM, 2004): MRCT, n = 6997, vs 28 day mortality, powered for 3% absolute reduction in mortality
• 4% albumin ‘safe’ compared to normal saline
• Post hoc analysis = TBI and major trauma had worse outcomes with albumin and patients with septic shock tended to better with albumin.
• Martin (CCM, 2005) = pts hypoproteinaemic with ARDS given albumin + frusemide vs frusemide alone => improved oxygenation & CVS stability
AlbuminAn approach …
• Use in
• Spontaneous bacterial peritonitis
• Early resuscitation of ICU patients esp sepsis (further studies pending)
• ARDS in patients with low albumin with frusemide
• NOT to be used in TBI
• ???
• To correct hypoalbuminaemia (<20)

0.9% NaCl• Isotonic
• Not that ‘normal’
• Adverse effects
• Hyperchloraemic metabolic acidosis (strong ion difference = 0)
• Immune and renal dysfunction
0.9% NaCl
• vs HES
• CHEST (NEJM 2012): MRCT, 7000 pts, no significant difference in mortality at 90 days
• HES => pruritus and 21% relative increase in RRT
Plasmalyte solution• Not truely ‘balanced’
• Recommended first line in surgery, DKA, burns, ? trauma
• Single centre trials indicate significant decrease in rate of major complications, infections, CRRT, transfusions
• Adverse effects
• Metabolic alkalosis
• Hyperlactaemia
• Hypotonic (low Na+)
• Micro thrombi (Ca2+ with citrate containing blood transfusions)
• Large RCT about to start …

Fluid administration
• How do you decide to administer a fluid bolus?
• What measures do you use to predict fluid responsiveness?



Fluid administration
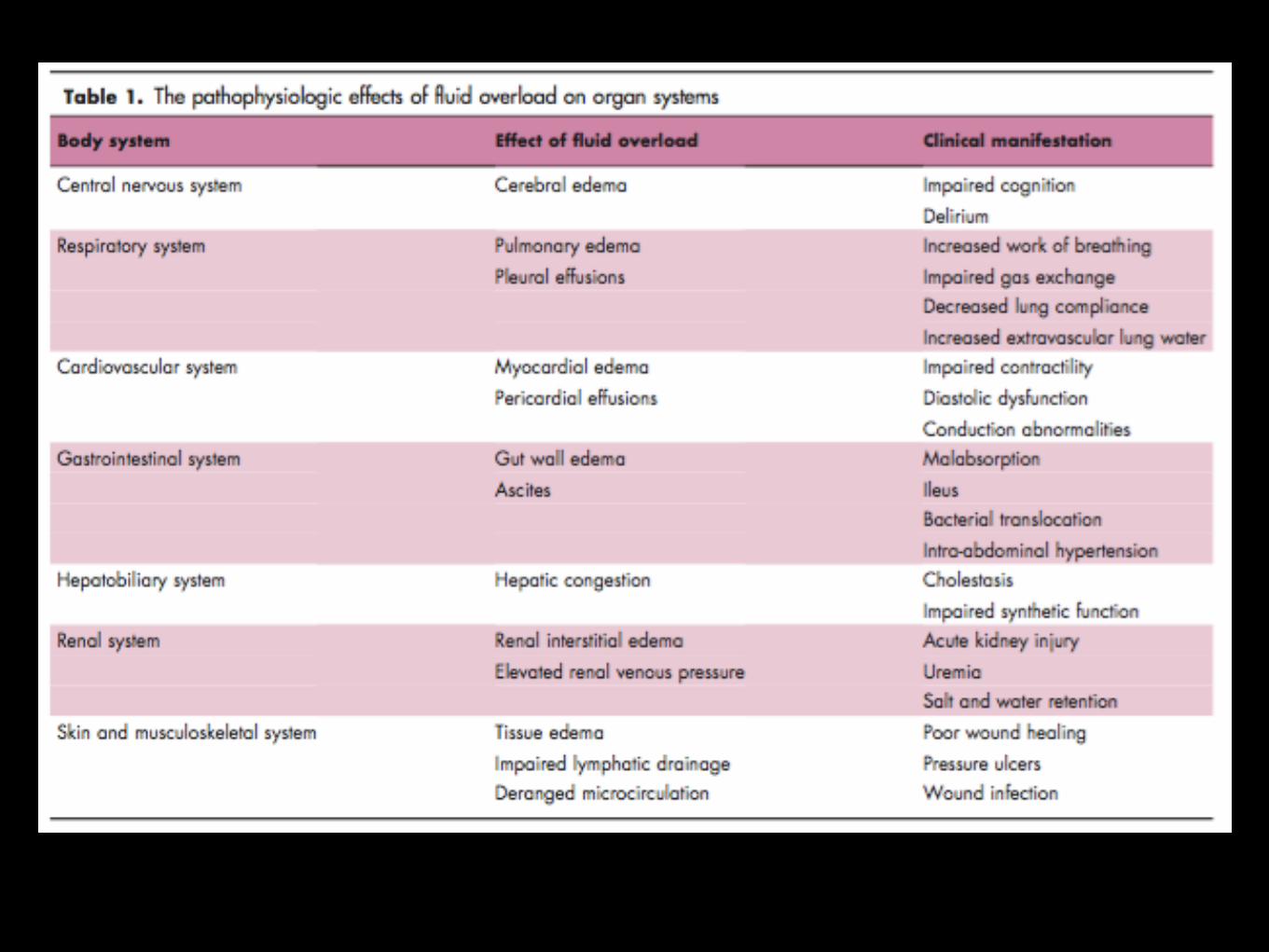
• What are the adverse effects of excessive fluid administration?

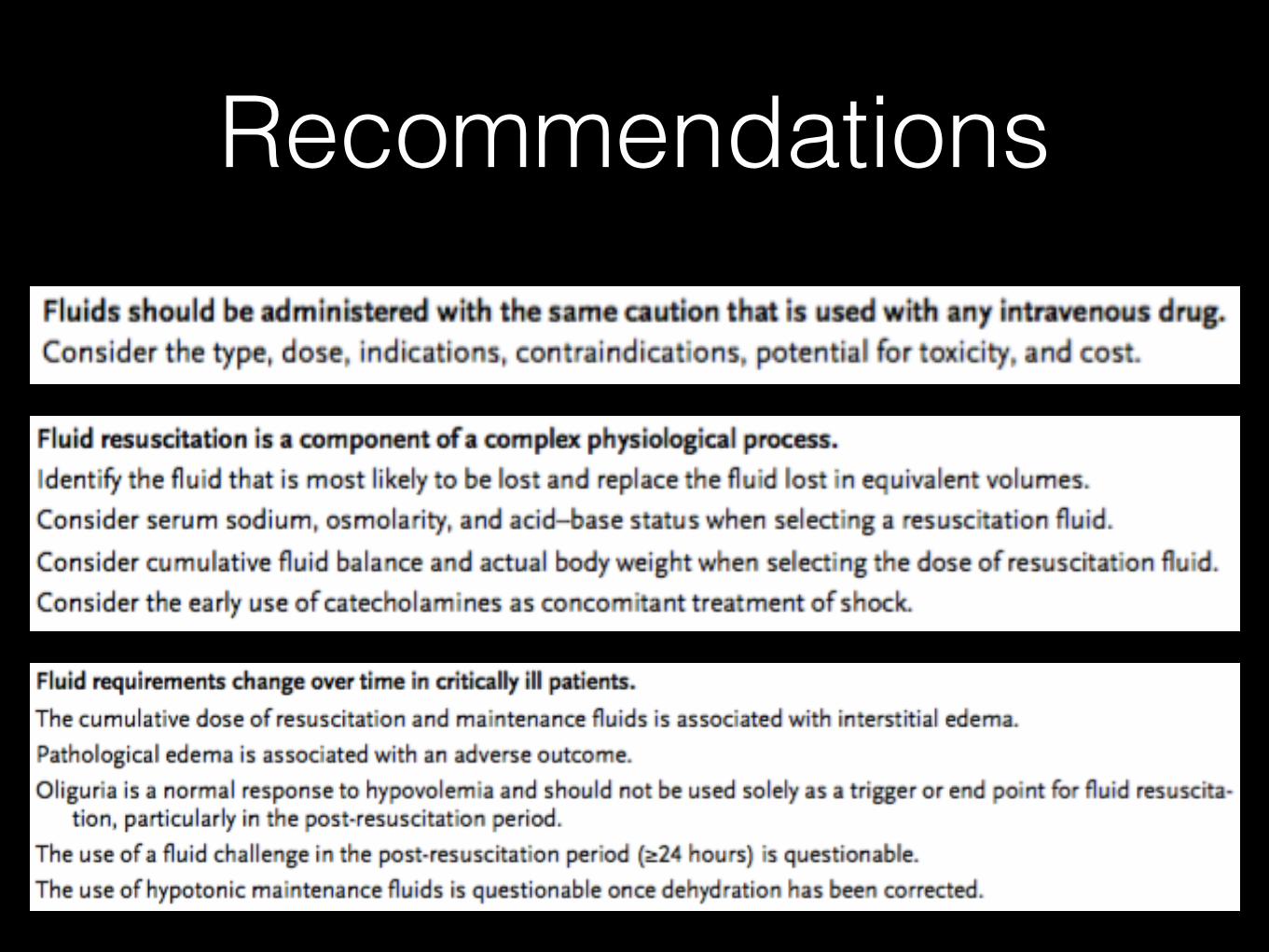
Recommendations

Recommendations

Thank you …• Myburgh JA, Mythen MG. Resuscitation Fluids.
N Engl J Med. 2013 Sep 26;369(13):1243–51.
• Ogbu OC, Murphy DJ, Martin GS. How to avoid fluid overload. Curr Opin Crit Care. 2015 Aug;21(4):315–21.
• CICM part II exams
• “The physiology viva” Kerry Brandis (2003)
Related Documents











