FLUIDS AND ELECTROLYTES MALIK ALQUB MD. PhD.

FLUIDS AND ELECTROLYTES MALIK ALQUB MD. PhD.. The Cell Has a Limited Repetoire K+140 meq/L 280 milliosmoles/L H 2 0 moves passively Across cell membrane.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

FLUIDS ANDELECTROLYTES
MALIK ALQUB MD. PhD.

The Cell Has a Limited Repetoire
K+140 meq/L280 milliosmoles/L
H20 moves passivelyAcross cell membraneAccording to the osmotic gradient
Na+140 meq/L280 milliosmoles/L

High Osmolality Outside The Cell=Shrinkage
Na+150 meq/L300 milliosmoles/L
K+140 meq/L280 milliosmoles/L
H2O

Low Osmolality Outside The Cell=Swelling
K+140 meq/L280 milliosmoles/L
H20
Na+120 meq/L240 milliosmoles/L
RUPTURE

Body Fluid Compartments
2/3 (65%) of TBW is intracellular (ICF) 1/3 extracellular water
25 % interstitial fluid (ISF) 5- 8 % in plasma (IVF intravascular fluid) 1- 2 % in transcellular fluids – CSF,
intraocular fluids, serous membranes, and in GI, respiratory and urinary tracts;

Body Fluids
•Water is most abundant body compound“Average” body water volume in reference tables based on healthy, nonobese 70-kg male• Volume averages 42 L in a 70-kg male• Plasma (3.5 L)• Interstitial fluid (10.5 L)• Intracellular fluid (28 L)
•Water is about 80% of body weight in newborn; about 60% in adult males; and about 50% in adult females

7

Fluid compartments are separated by membranes that are freely permeable to water.
Movement of fluids due to: hydrostatic pressure osmotic pressure
Capillary filtration (hydrostatic) pressure Capillary colloid osmotic pressure Interstitial hydrostatic pressure Tissue colloid osmotic pressure
Movement of fluids

Osmotic Pressure When a solution containing non-penetrating solutes is
separated from pure water by a membrane, the pressure that must be applied to the solution to prevent the net flow of water into the solution (prevent osmosis) is termed the osmotic pressure of the solution.
The greater the osmolarity, the greater its osmotic pressure.
The lower the water concentration, the higher the osmotic pressure.
Osmotic pressure of a solution is directly proportional to the concentration of osmotically active particles in that solution

OSMOSIS
Movement of the solvent or water across a membrane
Involves solution or water Equalizes the concentration of ions
on each side of membrane Movement of solvent molecules
across a membrane to an area where there is a higher concentration of solute that cannot pass through the membrane


OSMOLALITY
Measure of solution’s ability to create osmotic pressure & thus affect movement of water
Number of osmotically active particles per kilogram of water
Plasma osmolality is 280-300* mOsm/ kg
ECF osmolality is determined by sodium MEASURE used in clinical practice to
evaluate serum & urine

Osmolality In Clinical Practice
Serum 280-300mOsm/kg; Urine 50-1400mOsm/kg
Serum osmolality can be estimated by doubling serum sodium More prescisely 2X Na + urea + glucose
Values are in mmol/L

Osmolarity Regulation
ICF Osm. = ECF Osm. Interstitial Osm = Serum Osm. Hypothalamus is the serum osmostat. It
stimulates thirst and ADH secretion. Primary Defense for Osmolarity =
Thirst Primary Defense for Osmolarity =
Renal excretion of water via ADH effect

Osmolarity Regulation
Maximum concentrating ability of kidney is approximately 800-1600mOsm/kg H20
Max. ADH effect decreases urine output to approximately 500 cc/day
No ADH release increases urine output to 15-20 Liters per day. Uosm = 40 – 80 mOsm/kg H20

Fluid Balance

Fluid Balance
Water circulates freely in ECF compartment
ECF and ICF are normally in osmotic equilibrium and no large-scale circulation occurs between compartments
If abnormal amounts of water move from plasma into interstitial fluid called?
Increases in plasma osmolality trigger thirst and release of antidiuretic hormone (ADH)

Primary Regulatory Hormones Affect fluid and electrolyte balance:
1. antidiuretic hormone (ADH)
2. aldosterone 3. natriuretic peptides

Antidiuretic Hormone (ADH)
Stimulates water conservation at kidneys: reducing urinary water loss concentrating urine
Stimulates thirst center: promoting fluid intake

ADH Production
Osmoreceptors in hypothalamus monitor osmotic concentration of ECF (plasma, CSF)
Change in osmotic concentration in plasma and CSF alters osmoreceptor activity
Osmoreceptor neurons secrete ADH in proportion to osmotic concentraiton via the posterior pituitary

Aldosterone
Is secreted by adrenal cortex in response to: rising K+ (sensed at the adrenal cortex) or falling
Na+ levels in blood activation of renin–angiotensin system (usually
due to changes in blood volume) Determines rate of Na+ absorption and K+
loss along DCT and collecting system “Water Follows Salt”
High plasma aldosterone concentration causes kidneys to conserve salt
Conservation of Na+ by aldosterone also stimulates water retention

Aldosterone
Figure 26.8

Natriuretic Peptides
ANP and BNP are released by cardiac muscle cells in response to abnormal stretching of heart walls due to elevated blood pressure or volume Reduce thirst Block release of ADH and aldosterone Cause diuresis Lower blood pressure and plasma volume

Fluid Shifts
Rapid water movements between ECF and ICF in response to an osmotic gradient
If ECF osmotic concentration increases: ECF becomes hypertonic to ICF water moves from inside cells to ECF
If ECF osmotic concentration decreases: ECF becomes hypotonic to ICF water moves from ECF into cells

Water Losses
Dehydration develops when water losses exceed water gains
If water is lost, but electrolytes retained: ECF osmotic concentration rises water moves from ICF to ECF in a fluid shift Both ECF and ICF will be slightly more
concentrated than before but they will be osmotically balanced
net change in ECF is small homeostatic responses will occur to replace
lost water

Water Losses
If water is lost, but electrolytes retained, ECF (and ICF) have higher concentrations, lower volumes
hypothalamus senses elevated ECF osmolarity this and releases ADH to restore fluid balance
New water in the ECF will shift into ICF and restore volumes and concentrations

Severe Water Loss
Causes: excessive perspiration inadequate water consumption repeated vomiting diarrhea

Water Gains If water is gained, but electrolytes are
not: ECF volume increases ECF becomes hypotonic to ICF fluid shifts from ECF to ICF Basically the opposite of water loss:
Reach osmotic balance but at lower concentrations, higher volumes
may result in overrhydration: distorts cells changes solute concentrations around enzymes disrupts normal cell functions

Water Gains
If water is gained, but electrolytes are not:
ECF is at lower concentration, higher volume
This triggers decrease in ADH release, fluid is lost and ICF will lose some water back to ECF, restoring both volume and concentration balance

Causes of Overhydration
Ingestion of large volume of fresh water Injection into bloodstream of hypotonic
solution Endocrine disorders like excessive ADH
production Inability to eliminate excess water in
urine: chronic renal failure heart failure cirrhosis

Disorders of Water Balance:
Figure 26.7a

Hypervolemia Hypovolemia
peripheral and presacral edema pulmonary edema jugular venous distension hypertension Decreased hematocrit decr. serum protein
poor skin turgor dry mucous membranes flat neck veins hypotension increased hematocrit Increased serum prot.
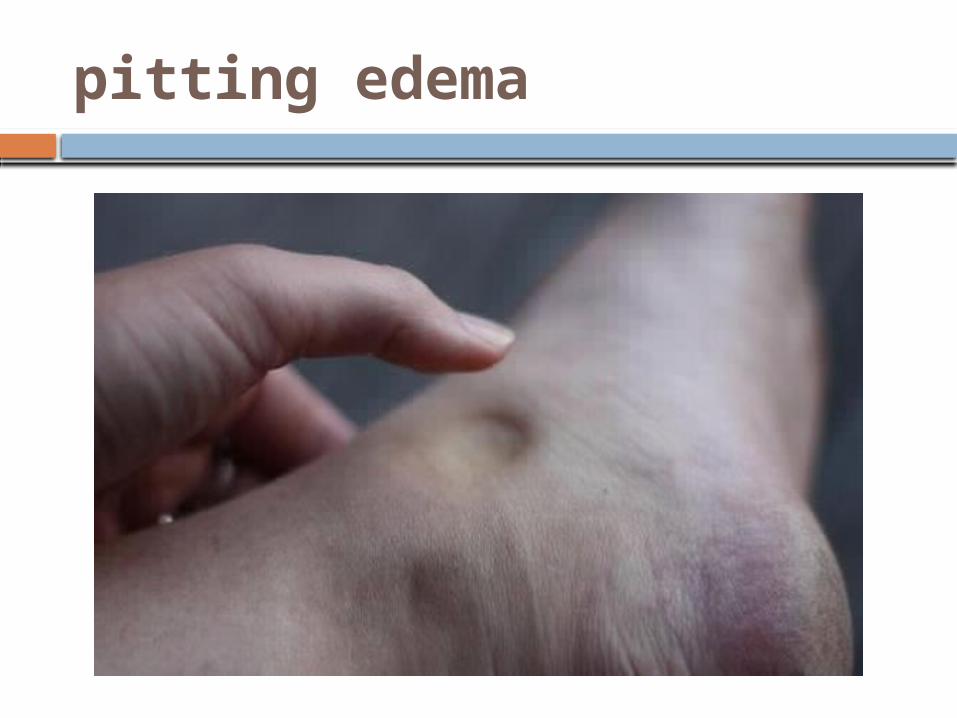
pitting edema

jugular venous distension

Electrolyte Balance

Electrolyte Balance
Requires equal rates of gain and loss for each electrolyte in the body
Electrolyte concentration directly affects water balance
Concentrations of individual electrolytes affect cell functions

37
Solutes – dissolved particles
Electrolytes – charged particles Cations – positively charged ions
Na+, K+ , Ca++, H+
Anions – negatively charged ionsCl-, HCO3
- , PO43-
Non-electrolytes .Proteins, urea, glucose, O2, CO2

Rules of Electrolyte Balance
• Most common problems with electrolyte balance are caused by imbalance between gains and losses of sodium ions
• Problems with potassium balance are less common, but more dangerous than sodium imbalance
• Changes in plasma sodium levels affect: Plasma volume, blood pressure ICF and interstitial fluid volumes

Na+, K+
Sodium holds a central position in fluid and electrolyte balance
Sodium is the dominant cation in ECF Sodium salts provide 90-95% of ECF
osmolarity (concentration): sodium chloride (NaCl) sodium bicarbonate
Sodium concentration in the ECF normally remains stable
Potassium Is the dominant cation in ICF

SODIUM (NA)
Main extracellular fluid (ECF) cation Helps govern normal ECF osmolality Helps maintain acid-base balance Activates nerve & muscle cells Influences water distribution (with
chloride)
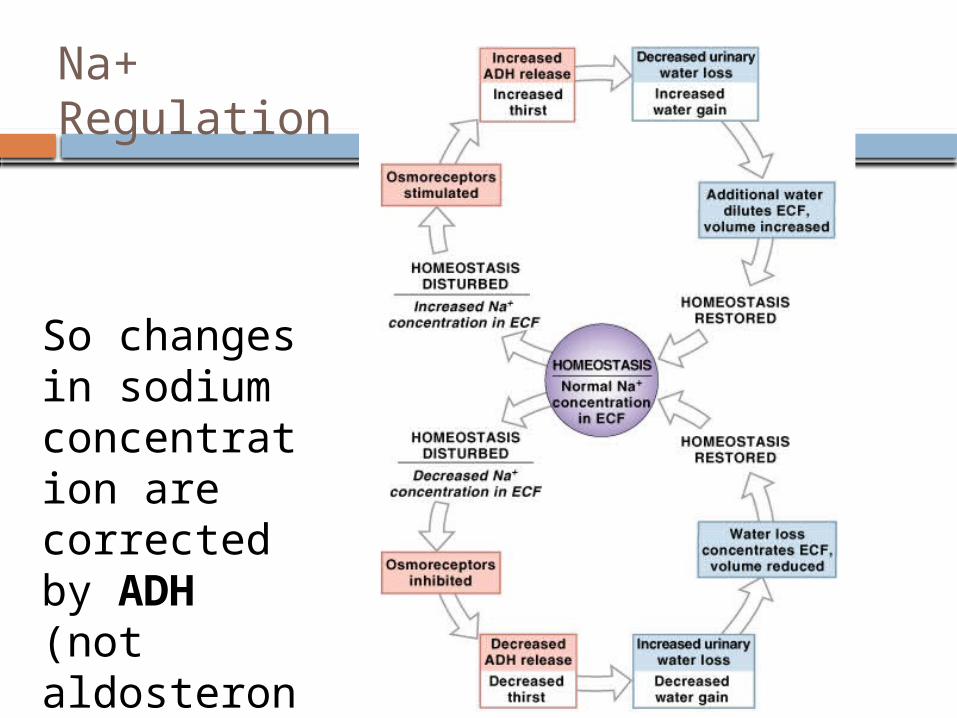
Figure 27–4
Na+ Regulation
So changes in sodium concentration are corrected by ADH (not aldosterone)

Abnormal Na+ Concentrations in ECF
Hyponatremia: usu. body water content rises (overhydration)
Hypernatremia: usu. body water content declines
(dehydration)
Severe problems with electrolyte concentrations almost always occur secondary to fluid balance problems

HYPERNATREMIA
Serum Na + level > 148 mEq/L serum osmolality > 295 mOsm/kg

Etiologies of Hypernatremia
Primary Sodium Excess
Excess Intake of Sodium
Decreased Urinary Excretion of SodiumHyperaldosteronism
Primary Water LossPoor Intake of Water
Impaired access to water (i.e. infants, elderly patients with dementia or whom are bedbound)
Impaired thirst sensation
Hypothalamic lesions
Increased Urinary Loss of Water
ADH deficiency (Central Diabetes Isipidus DI)
ADH resistance (Nephrogenic DI)
Increased GI Loss of Water
Increased Transcutaneous Loss of Water
Transmembrane Shift of Water (most often due to rapid production of intracellular lactate)

HYPONATREMIA
Serum Na+ < 135 mEq/L (patient may be asymptomatic until level drops below 125)

Etiologies of Hyponatremia
Poor Intake of Sodium
Increased Urinary Loss of Sodium
Diuretics
Proximal RTA
Aldosterone deficiency/resistance
Increased GI Loss of Sodium (Fluid loss must be followed by repletion with free water).
Vomitting
Diarrhea
Increased Transcutaneous Loss of Sodium (Fluid loss must be followed by repletion with free water).
Excessive Intake of Water (1° polydipsia)
Psychosis
Decreased Urinary Excretion of Water
Decreased GFR
Increased ADH
Heart failure
Cirrhosis
SIADH
Transmembrane Shift of Water
Hyperglycemia
Primary Sodium Loss Primary Water Excess

Potassium Balance
98% of potassium in the human body is in ICF
Cells expend energy to recover potassium ions diffused from cytoplasm into ECF
Factors Rate of gain across digestive epithelium Rate of loss into urine, regulated along
distal portions of nephron and collecting system as Na+ from tubular fluid is exchanged for K+ in peritubular fluid

Mechanisms of regulation
Renal regulation
Transcellular shift between the intracellular and extracellular compartments

Factors in Tubular Secretion of K+
1. Changes in concentration of ECF: higher ECF concentration increases rate of
secretion (just because there’s more of it)2. Aldosterone levels affect K+ loss in urine
ion pumps reabsorb Na+ from filtrate in exchange for K+ from peritubular fluid
High K+ plasma concentrations stimulate aldosterone release, lower K+ but Na+ stays
3. Changes in pH: low ECF pH lowers peritubular fluid pH H+ rather than K+ is exchanged for Na+
in tubular fluid so ECF K+ increases

Transcellular shifts
Sodium-potassium ATPase Both insulin and epinephrine increase the
activity of sodium-potassium pump. (An increase in potassium level stimulates
insulin release. --- a feedback mechanism)
Potassium-hydrogen exchange to maintain electrical neutrality In acidosis In alkalosis

POTASSIUM (K+)
DOMINANT INTRACELLULAR ELECTROLYTE
NL SERUM LEVEL 3.5-5.5 *mEq/L

POTASSIUM (K)
Dominant cation in intracellular fluid (ICF)
Regulates cell excitability Permeates cell membranes, thereby
affecting cell’s electrical status Helps control ICF osmolality & ICF
osmotic pressure

HYPERKALEMIA
K+ > 5.5 mEq/L Dangerous due to potential for fatal
dysrhythmias, cardiac arrest Major cause is renal disease Beware of pseudohyperkalemia due
to prolonged tourniquet, hemolysis of blood, sampling above KCl infusion
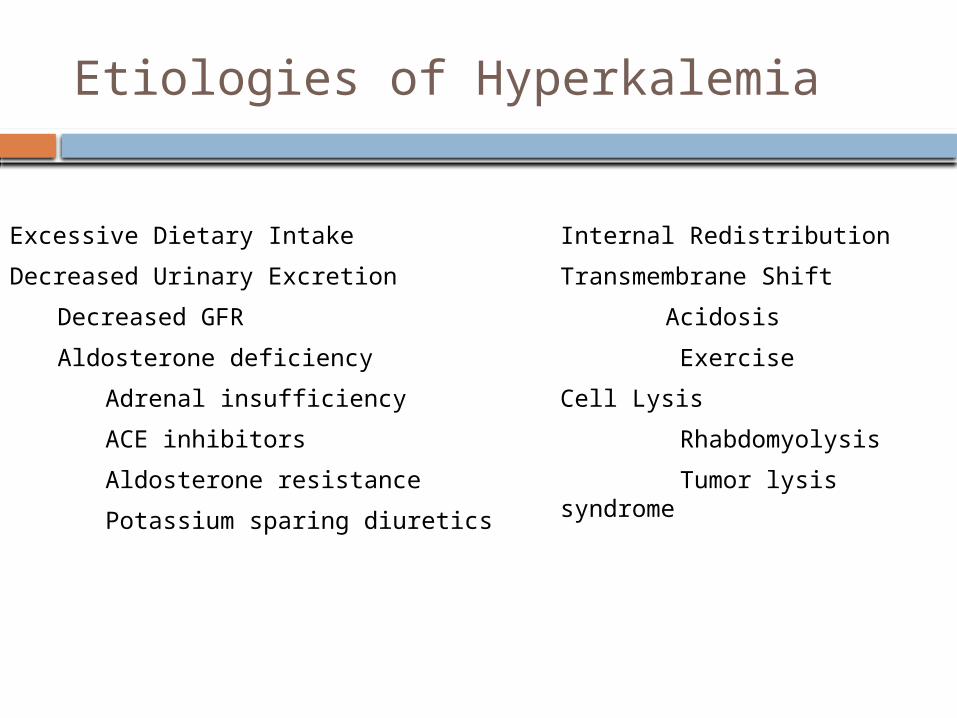
Etiologies of Hyperkalemia
Excessive Dietary Intake
Decreased Urinary Excretion
Decreased GFR
Aldosterone deficiency
Adrenal insufficiency
ACE inhibitors
Aldosterone resistance
Potassium sparing diuretics
Internal Redistribution
Transmembrane Shift
Acidosis
Exercise
Cell Lysis
Rhabdomyolysis
Tumor lysis syndrome

HYPOKALEMIA
K+ < 3.5mEq/L Most common type of electrolyte
imbalance Major cause is increase renal loss
most often associated with diuretics
Can increase the action of digitalis

Etiologies of Hypokalemia
Poor Intake
Increased Urinary Excretion
Decreased reabsorption in loop of Henle
Furosemide
Hyperaldosteronism
Primary hyperaldosteronism
Adrenal adenoma
Adrenal hyperplasia
Secondary hyperaldosteronism
Renovascular hypertension
Renin-secreting tumor
Increased GI Losses
Diarrhea
Laxative abuse
Vomiting / NG drainage
Increased Transcutaneous Losses
sweating
Transmembrane ShiftAlkalosis
Insulin treatment for DKA
High catecholamine states

FLIUD IMBALANCES
The five types of fluid imbalances that may occur are:
Extracellular fluid imbalances(ECFVD) Extracellular fluid volume excess(ECFVE) Extracellular fluid volume shift Intracellular fluid vloume excess(ICFVE) Intrcellular fluid volume deficit(ICFVD)
EXTRACELULLAR FLUID VOLUME DEFICIT
An ECFVD, commonly called as dehydration , is a decrease in intravascular and interstitial fluids
An ECFVD can result in cellular fluid loss if it is sudden or severe

ETIOLOGY AND RISK FACTORS Severe vomiting Diaphoresis Traumatic injuries Third space fluid shifts [percardial, pleural,
pertonial and joint cavities] Fever Gatrointestinal suction Burns
Hyperventilation Decresed ADH secretions Diabetes insipidus Diuretic phase of acute renal failure Use of diuretics

ELDERLY ARE HIGH RISK OF ECFVD DUE TO Decreased thirst response Decreased renal concentration of urine Altered ADH response Increased drug – drug interaction Multiple chronic diseases Decreased access to fluids due to financial
or transportation barriers Chemical or physical restraint Changes in mental status

CLINICAL MANIFESTATION
In Mild ECFVD, 1to 2 L of water or 2% of the body weight is lost
In Moderate ECFVD, 3 to 5L of water loss or 5%weight loss
IN Severe ECFVD , 5 to 10 L of water loss or 8% of weight loss

CLINICAL MANIFESTATION
Thirst Muscle weakness Dry mucus
membrane;dry cracked lips or furrowed tongue
Eyeballs soft and sunken (severe deficit)
Apprehension , restlessness, headache , confusion, coma in severe deficit
Elevated temperature Tachycardia, weak
thready pulse
Postural systolic BP falls >25mm Hg and diastolic fall > 20 mm Hg , with pulse increases > 30
Narrowed pulse pressure, decreased
Flattened neck veins in supine position
Weight loss Oliguria(< 30 mlper
hour) Decreased number and
moisture in stools

LABORATORY FINDINGS
Increased osmolality(> 295 mOsm/ kg) Increased or normal serum sodium level
(> 145mEq/ L ) Increase BUN (>25 mg / L ) Hyperglycemia ( >120 mg /dl ) Elevated hematocrit (> 55%)

MANAGEMENT
Mild fluid volume loss can be corrected with oral fluid replacement
-if client tolerates solid foods advice to take 1200 ml to 1500ml of oral fluids
-if client takes only fluids, increase the total intake to 2500 ml in 24 hours

EXTRACELLULAR FLUID VOLUME EXCESS
ECFVE is increased fluid retention in the intravasular and interstitial spaces

ETIOLOGY AND RISK FACTORS
Heart failure Renal disorders Cirrhosis of liver Increased ingestion of high sodium foods Excessive amount of IV fluids containing
sodium Electrolyte free IV fluids SIADH,Sepsis decreased colloid osmotic pressure lymphatic and venous obstruction

CLINICAL MANIFESTATION
Constant irritating cough Dyspnea & crackles in lungs Cyanosis, pleural fffusion Neck vein obstruction Bounding pulse &elevated BP Pitting & sacral edema Weight gain Change in level of consiousness

LAB INVESTIGATION
serum osmolality <275mOsm/ kg Low , normal or high sodium Decreased hematocrit [ < 45%] Specific gravity below 1.010 Decreased BUN [< 8mg/ dl]

MANAGEMENT
Diuretics [combination of potassium sparing and potassium depleting diuretics]
In people with CHF, ACE inhibitors and low dose of beta blockers are used
A low sodium diet
Related Documents











![Welcome [s3-eu-west-1.amazonaws.com] · We don’t know about you, but we’re pretty fed up with our own repetoire of dishes at home - we can’t wait to have our chefs’ cooking](https://static.cupdf.com/doc/110x72/5fb82b623593350b9b22bcdb/welcome-s3-eu-west-1-we-donat-know-about-you-but-weare-pretty-fed-up-with.jpg)