LOGO Fluid, Electrolyte and Acid-base Disturbance Sirirat Reungjui, MD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

LOGO
Fluid, Electrolyte and
Acid-base Disturbance
Sirirat Reungjui, MD

Body Fluid
TBW
ECF
1/3
Extravascular
3/4
Intravascular
1/4
ICF
2/3
• Total body water
- Male (60%) > Female (50%)
- Higher in slim than fat
- Steadily decrease with age

Ionic composition
ICF
K,
PO4, Protein
ISF Plasma
Na, Cl,
HCO3
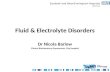
Input Output Ingested water: 1000 mL
Urine 1000 mL
Water in food: 800 mL
Skin 500 mL
Respiratory tract 400 mL
Water of oxidation: 300 mL
Stool 200 mL
Input - Output
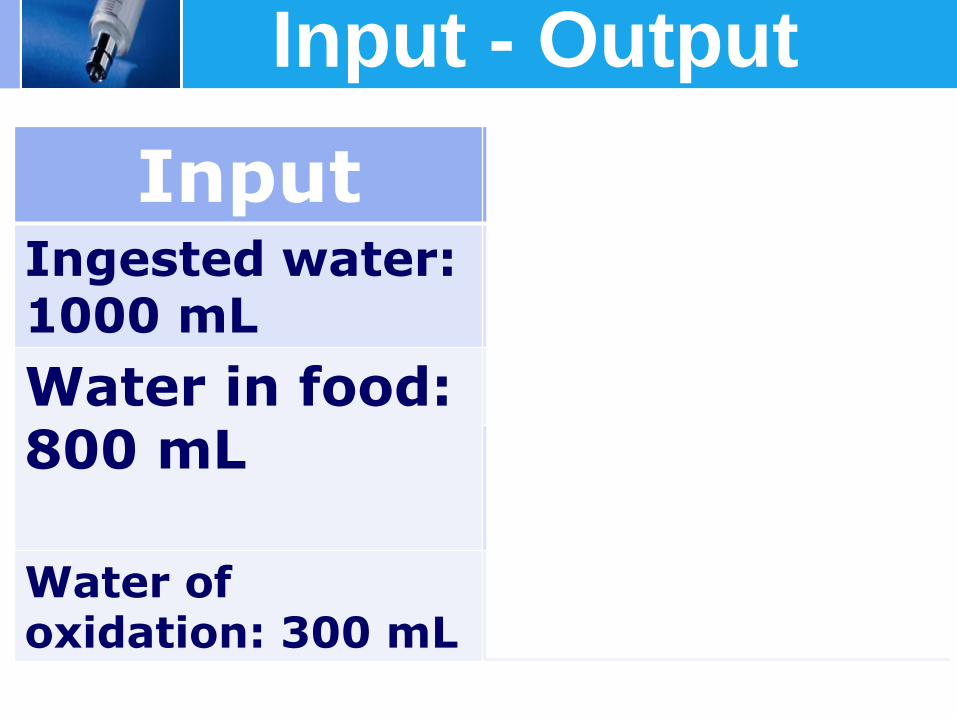
Water Turnover in the Bowel (ml/day)
Water from diet 2000-3000
Saliva 1000-2000
Gastric juice 1000-2000
Bile 500-1000
Pancreatic juice 1000-2000
Intestinal secretions 1000-2000

www.themegallery.com
Composition of GI secretion
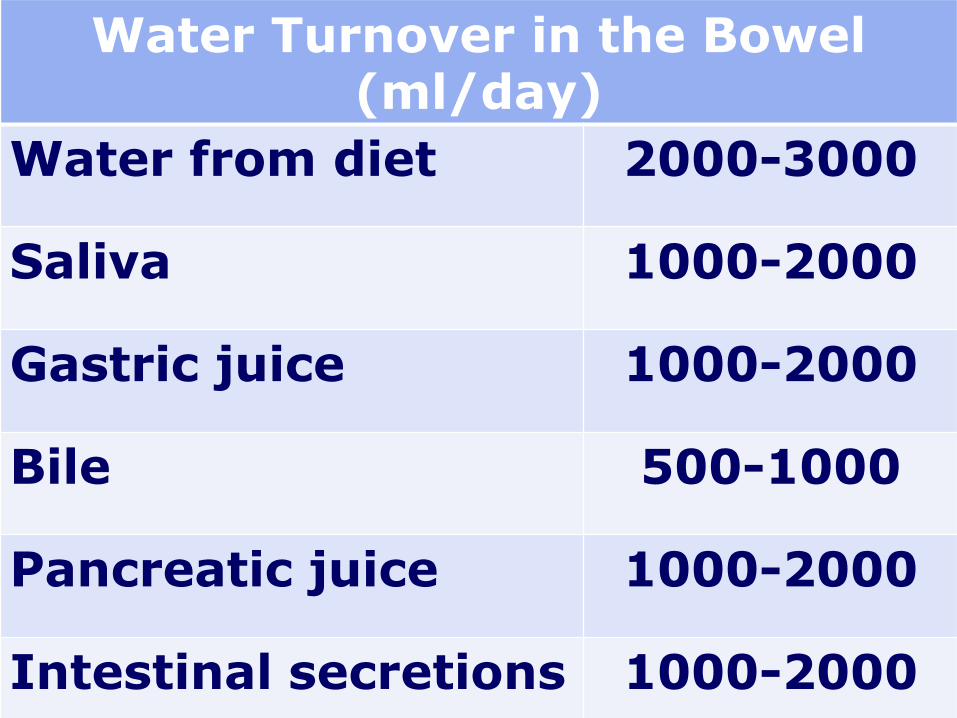
Fluid replacement
Fluid therapy = Maintenance + Fluid loss
Maintenance • Holiday & Segar’s Law 1st 10 kg = 100 cc/kg/day 2nd 10kg = 50 cc/kg/day > 20 kg = 20 cc/kg/day

www.themegallery.com
Dehydration
Mild dehydration (3–5%) - Thirsty
- Dry lip and tongue
Moderate dehydration (6–9 %) - tachycardia - orthostatic hypotension - decreased skin turgor - dry mucous membranes - irritability - delayed capillary refill (2 -3 s) - reduced urine output
Severe dehydration (≥10 %) - hypotension - capillary refill > 3 s - cool and mottled extremities - lethargy - deep respirations with rate
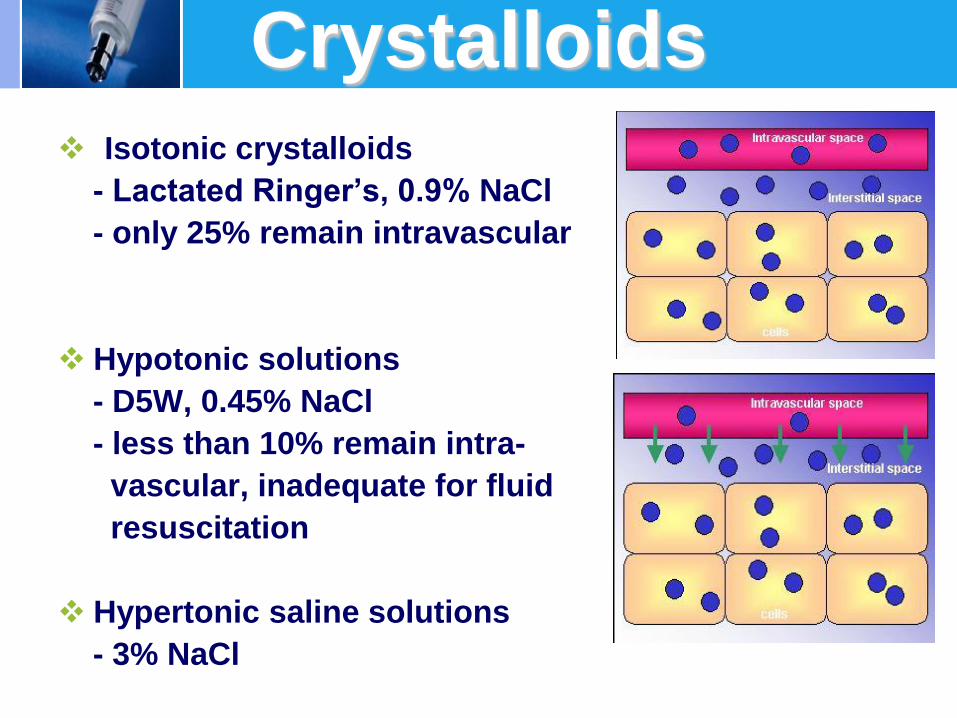
Crystalloids Isotonic crystalloids
- Lactated Ringer’s, 0.9% NaCl
- only 25% remain intravascular
Hypotonic solutions
- D5W, 0.45% NaCl
- less than 10% remain intra-
vascular, inadequate for fluid
resuscitation
Hypertonic saline solutions
- 3% NaCl
0500
100015002000250030003500400045005000
Infused
Volume
PV IFV ICV
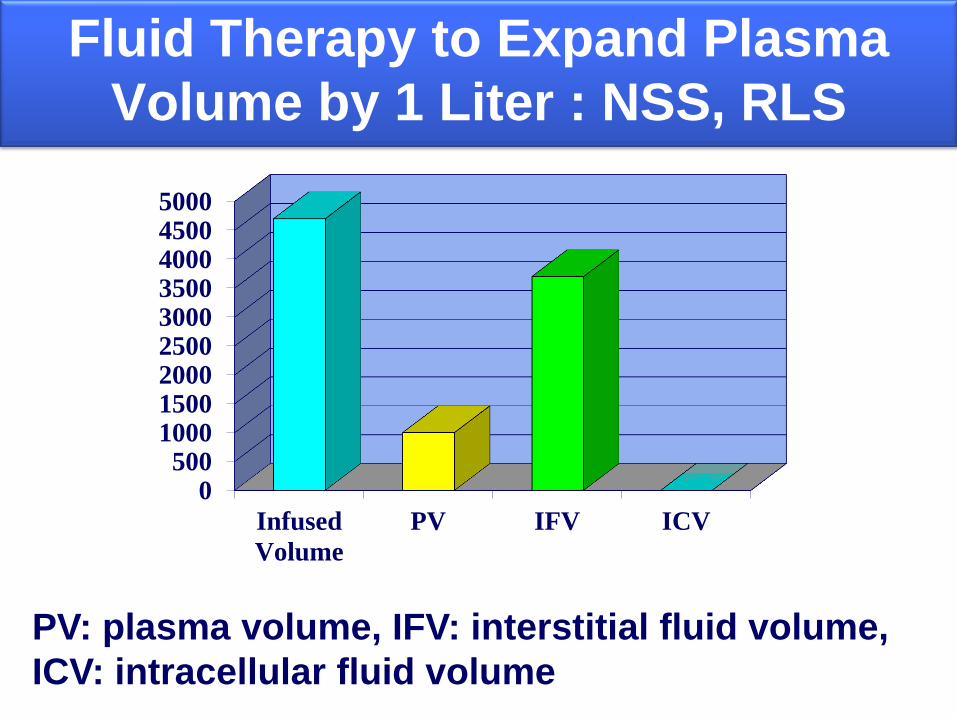
Fluid Therapy to Expand Plasma
Volume by 1 Liter : NSS, RLS
PV: plasma volume, IFV: interstitial fluid volume,
ICV: intracellular fluid volume
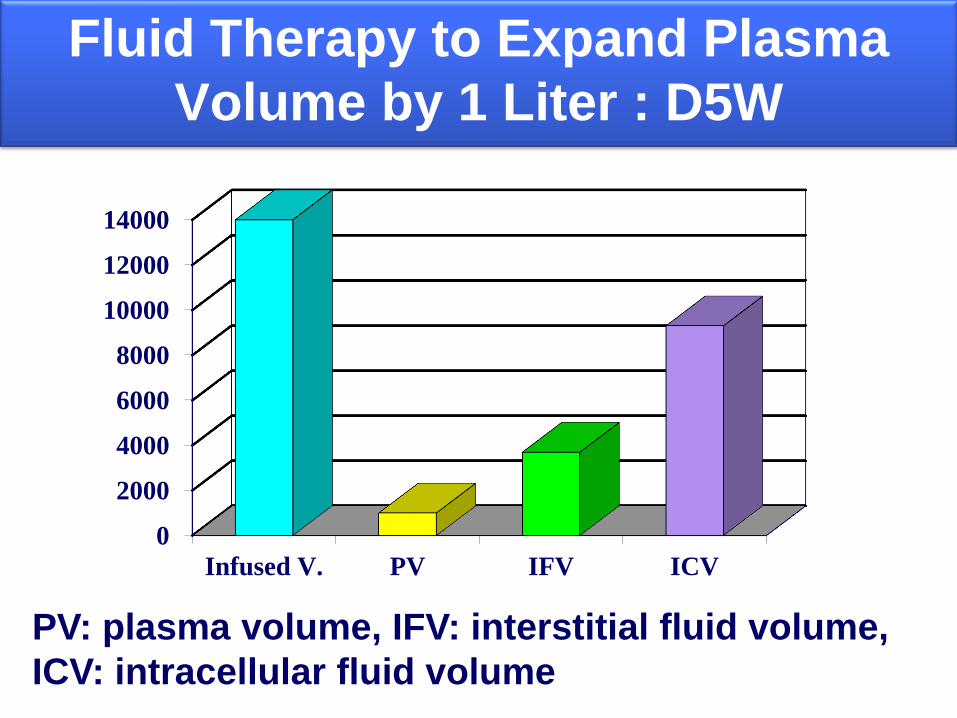
Fluid Therapy to Expand Plasma
Volume by 1 Liter : D5W
0
2000
4000
6000
8000
10000
12000
14000
Infused V. PV IFV ICV
PV: plasma volume, IFV: interstitial fluid volume,
ICV: intracellular fluid volume
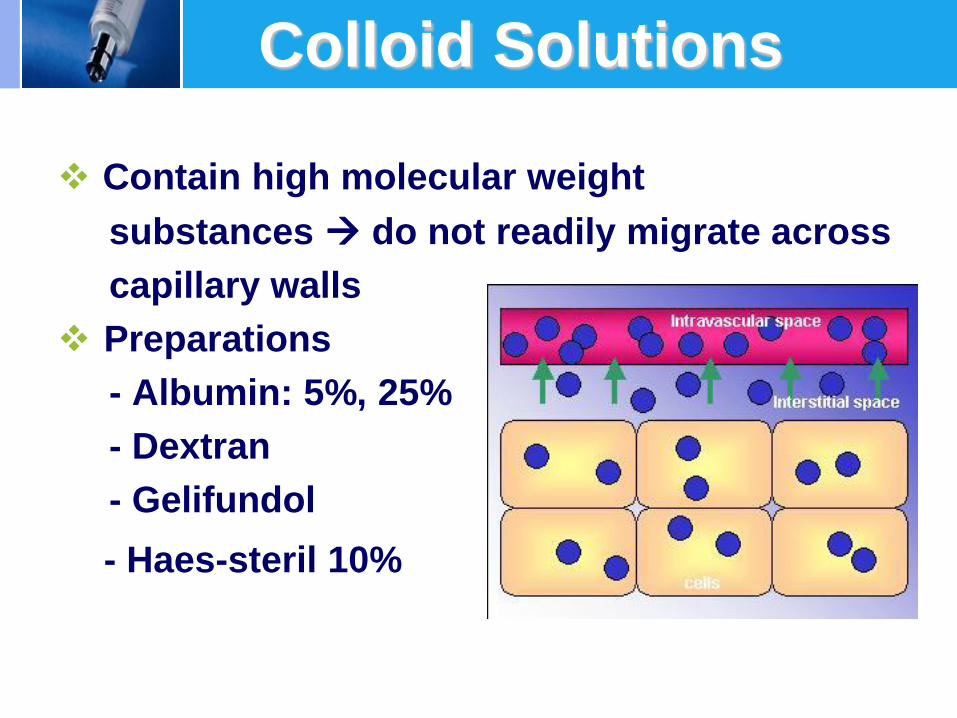
Colloid Solutions
Contain high molecular weight
substances do not readily migrate across
capillary walls
Preparations
- Albumin: 5%, 25%
- Dextran
- Gelifundol
- Haes-steril 10%

Fluid diffusion after intravascular infusion: to
achieve 1 liter of plasma volume expansion
Fluid Infused Volume(ml) PV IFV(ml) ICV(ml) D5W 14,000 1,000 3,700 9,300
NSS 4,000 1,000 3,000 0
RLS 4,700 1,000 3,700 0
3%NaCl 650 1,000 (-)120 (-)230
7.5%NaCl 140 1,000 (-)285 (-)575
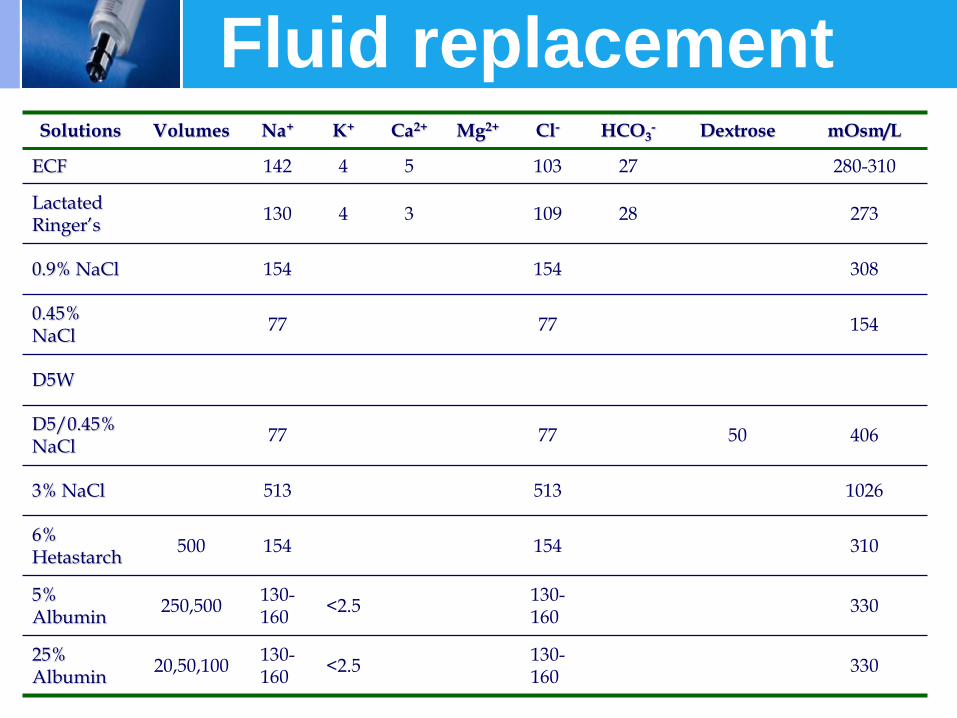
Fluid replacement Solutions Volumes Na+ K+ Ca2+ Mg2+ Cl- HCO3
- Dextrose mOsm/L
ECF 142 4 5 103 27 280-310
Lactated Ringer’s
130 4 3 109 28 273
0.9% NaCl 154 154 308
0.45% NaCl
77 77 154
D5W
D5/0.45% NaCl
77 77 50 406
3% NaCl 513 513 1026
6% Hetastarch
500 154 154 310
5% Albumin
250,500 130-160
<2.5 130-160
330
25% Albumin
20,50,100 130-160
<2.5 130-160
330
LOGO
Diuretics
www.themegallery.com

Metabolic Emergencies
Alteration of concious hyponatremia , hypernatremia
hypocalcemia , hypercalcemia hypomagnesemia , hypermagnesemia ,
metabolic alkalosis Convulsion hyponatremia , hypernatremia
hypomagnesemia , hypocalcemia metabolic alkalosis
Metabolic Emergencies
Muscle weakness
hypokalemia , hyperkalemia hypermagnesemia , hypomagnesemia hypercalcemia , metabolic alkalosis
Arrythmia or EKG changes
hypokalemia , hyperkalemia hypomagnesemia , hypermagnesemia, hypocalcemia , hypercalcemia
metabolic acidosis
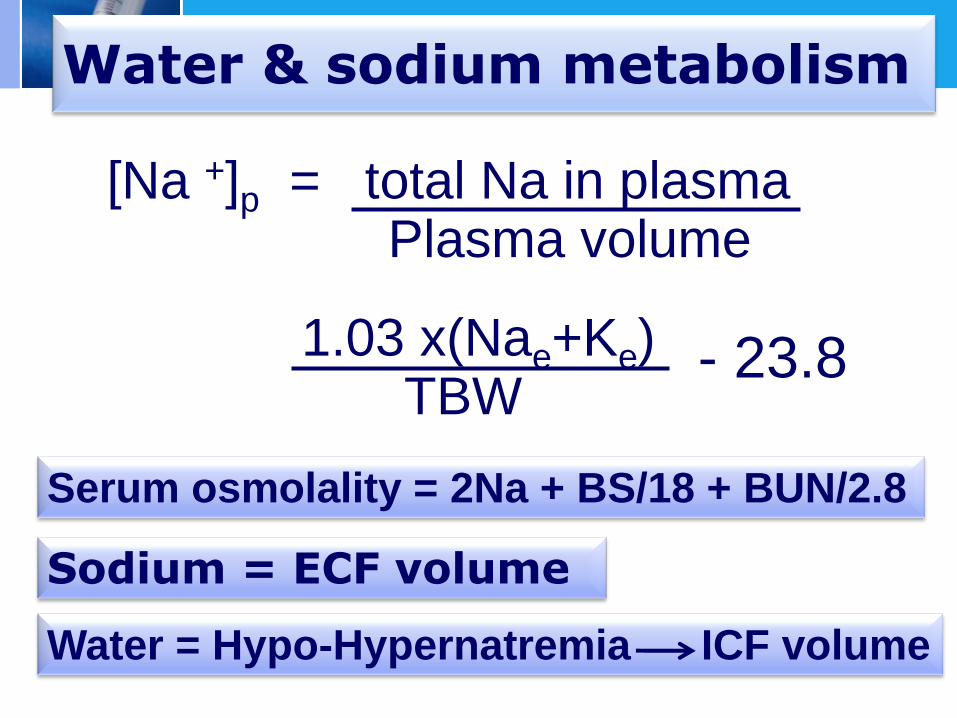
Water & sodium metabolism
1.03 x(Nae+Ke) TBW
[Na +]p = total Na in plasma Plasma volume
- 23.8
Serum osmolality = 2Na + BS/18 + BUN/2.8
Sodium = ECF volume
Water = Hypo-Hypernatremia ICF volume
www.themegallery.com
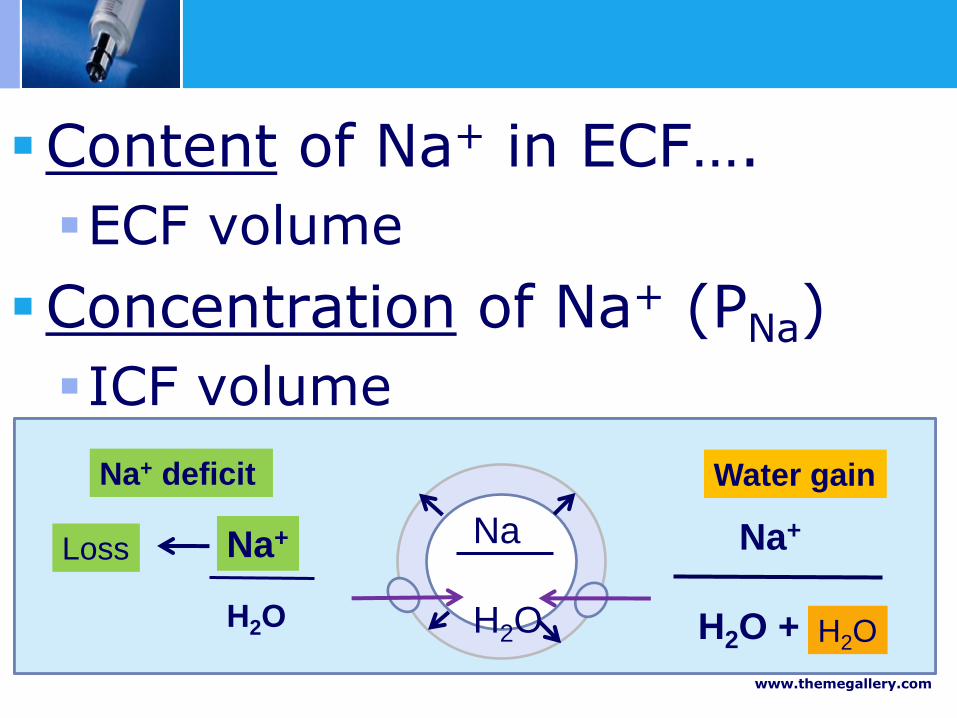
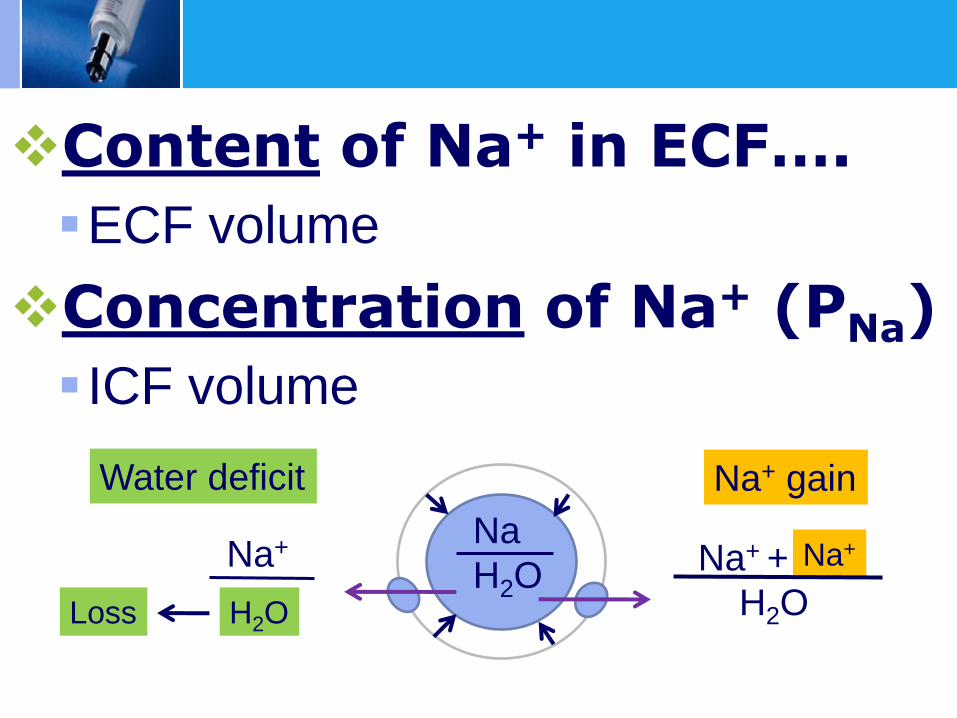
Content of Na+ in ECF….
ECF volume
Concentration of Na+ (PNa)
ICF volume
Na+ +
H2O
Na
H2O
Na+ gain
Na+
Na+
Loss
Water deficit
H2O
Na+
H2O +
Na
H2O
Water gain
Na+
Loss
Na+ deficit
H2O
Na+
H2O

www.themegallery.com

•Serum sodium < 135 mEq/l
•Severity…. rapidity and level
Acute vs Chronic hyponatremia
( 48 hr)
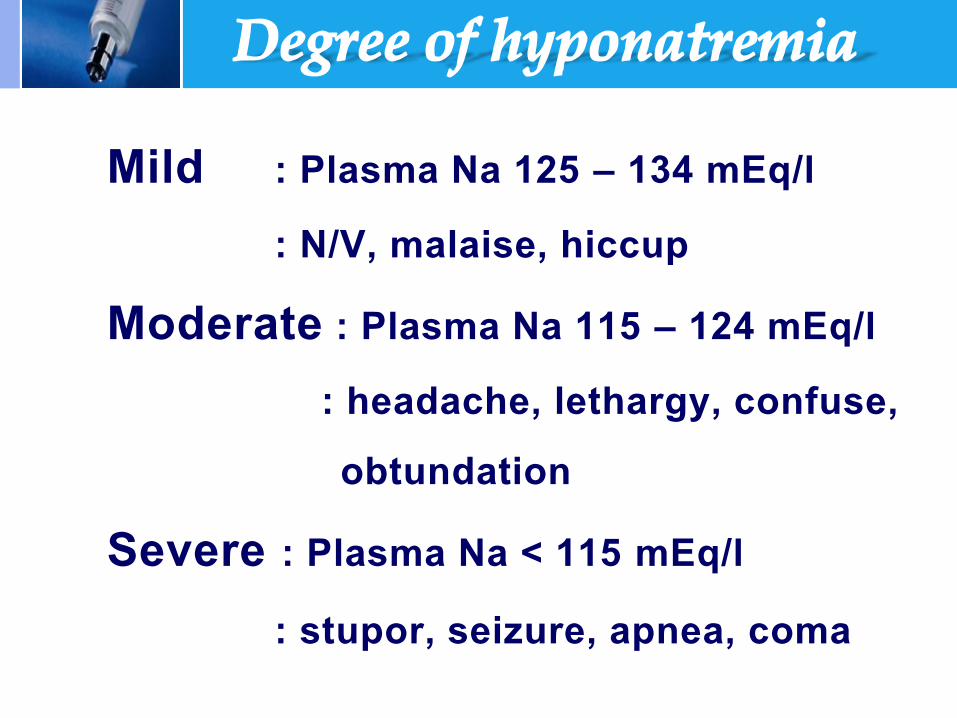
Mild : Plasma Na 125 – 134 mEq/l : N/V, malaise, hiccup Moderate : Plasma Na 115 – 124 mEq/l : headache, lethargy, confuse, obtundation Severe : Plasma Na < 115 mEq/l : stupor, seizure, apnea, coma

www.themegallery.com www.themegallery.com
Osmotic demyelination syndrome

serum
osmolarity
Normal
(280-295 mOsm)
Isotonic hyponatremia
Hyperlipidemia Hyperproteinemia
Low
(< 280 mOsm)
Uosm > 100
Uosm < 100
Psychogenic polydipsia
Elevate
(>295 mOsm)
Hypertonic hyponatremia
-hyperglycemia
-hypertonic infusion e.g.
glucose mannitol,ethanol

Uosm > 100
hypovolemia
UNa < 10
(extrarenal loss)
Vomiting
Diarrhea
Third space
loss
UNa > 20
Diuretics
Mineralocorticoid def.
Salt losing nephritis
Bicarbonaturia
Ketonuria
Osmotic diuresis
Euvolemia
UNa > 20
SIADH
Hypothyroidism
Glucocorticoid def.
Renal failure
Physical or emotional
stress
Post Op.
Hypervolemia
UNa < 10
Nephrotic syndrome
Cirrhosis
CHF
UNa >20
Acute or
chronic renal failure

Lab test
Blood sugar, serum osmole?
BUN/cr, uric acid
Causes of SIADH, TFT, Cortisol level
urine osmole less than 100 mosm/kg..shut down of ADH
more than 100 impaired free water excretion
(ADH still effect)
urine sodium
www.themegallery.com
Criteria for SIADH
Hypotonic hyponatremia
Urine osmolality >100 mOsm/kg
Urine Na > 40 mEq/L (usually)
Absence of ECV depletion
Normal thyroid and adrenal function
Normal cardiac, hepatic, renal function
www.themegallery.com
Causes of SIADH
www.themegallery.com
Drugs That Can Cause SIADH
Carbamazepine (Tegretol)
Chlorpropamide (Diabinese)
Clofibrate (Atromid-S)
Cyclophosphamide (Cytoxan)
Opiates
Oxytocin (Pitocin)
Phenothiazines
Tricyclic antidepressants
Vincristine
www.themegallery.com
1 Improve underlying condition
2 Increase PNa concentration - Acute vs chronic, symptom - Rate and type of fluid
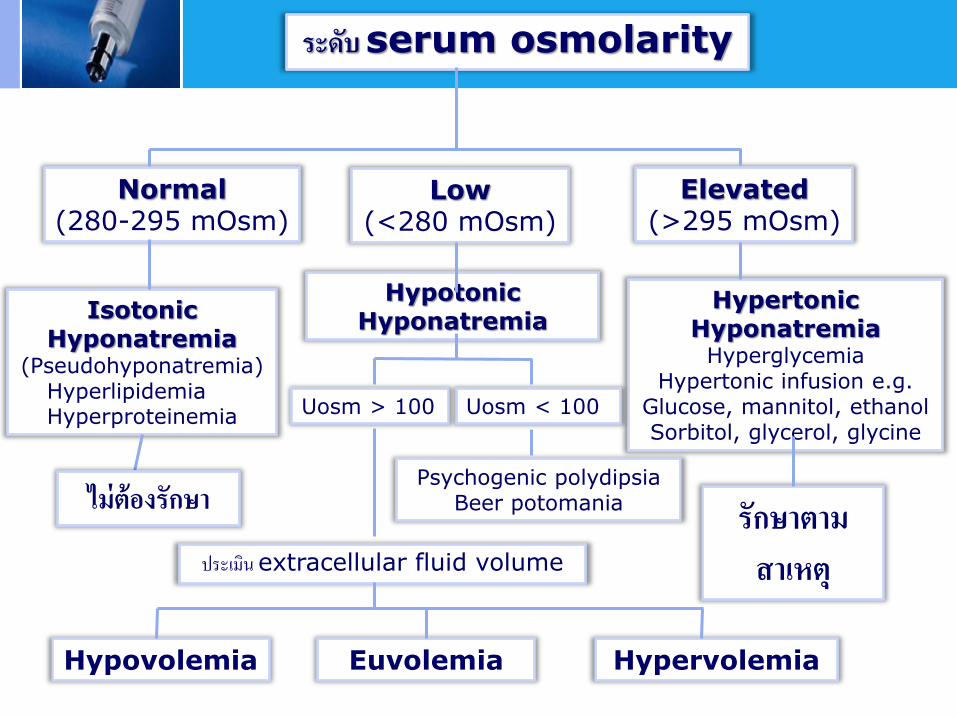
ระดบ serum osmolarity
Normal (280-295 mOsm)
Elevated (>295 mOsm)
Low (<280 mOsm)
Isotonic Hyponatremia
(Pseudohyponatremia) Hyperlipidemia Hyperproteinemia
Hypotonic Hyponatremia
Hypertonic Hyponatremia
Hyperglycemia Hypertonic infusion e.g.
Glucose, mannitol, ethanol Sorbitol, glycerol, glycine
Uosm > 100 Uosm < 100
Psychogenic polydipsia Beer potomania
ประเมน extracellular fluid volume
Hypovolemia Euvolemia Hypervolemia
ไมตองรกษา รกษาตาม สาเหต
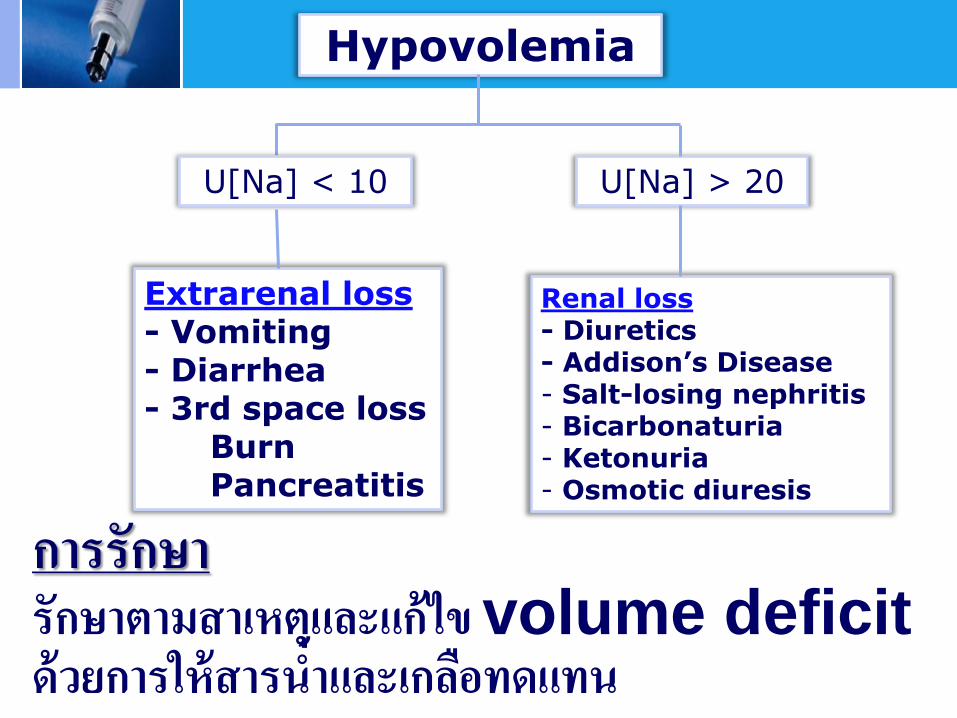
Hypovolemia
Extrarenal loss - Vomiting - Diarrhea - 3rd space loss Burn Pancreatitis
U[Na] > 20 U[Na] < 10
Renal loss - Diuretics - Addison’s Disease - Salt-losing nephritis - Bicarbonaturia - Ketonuria - Osmotic diuresis
การรกษา รกษาตามสาเหตและแกไข volume deficit ดวยการใหสารน าและเกลอทดแทน

Euvolemia
สงตรวจระดบ urine osmolality
< 100 mOsm/L > 100 mOsm/L
- Primary polydypsia - Water intoxication
Water loading test (ดมน า 15 cc/kg)
ขบน าออก > 80% ของน าทดมใน 4 ชม.
ขบน าออก < 80% ของน าทดมใน 4 ชม.
Reset osmostat
ตดตามอาการ ไมตองรกษา
SIADH มอาการ : ให 3%Nac ไมมอาการ : จ ากดน าดม 500-1000 ซซ/วน
ลดน ำดม รกษำทำงจตเวช

Treatment of chronic SIADHs
Restrict water intake (osmolol load/Uosm)
A high-sodium, high-protein diet
Loop diuretic
Urea
V2 receptor antagonists
Demeclocycline (rarely used)
Lithium is not used anymore
www.themegallery.com
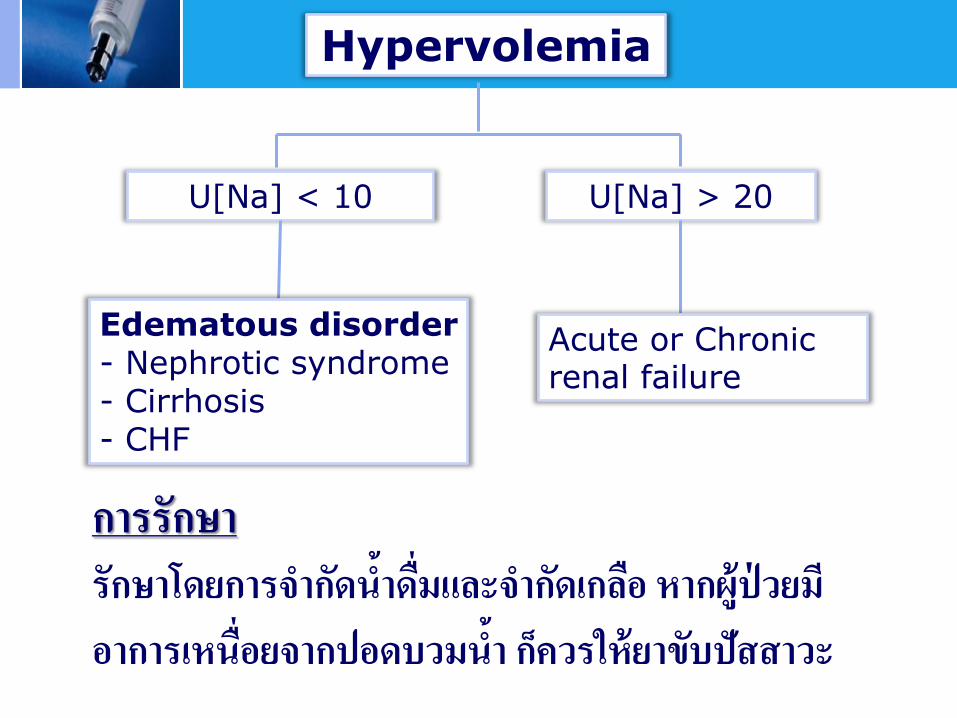
Hypervolemia
U[Na] > 20 U[Na] < 10
Edematous disorder - Nephrotic syndrome - Cirrhosis - CHF
Acute or Chronic renal failure
การรกษา รกษาโดยการจ ากดน าดมและจ ากดเกลอ หากผปวยมอาการเหนอยจากปอดบวมน า กควรใหยาขบปสสาวะ

www.themegallery.com
Rate and degree of correction

Na for 1 L of IVF = [(infusate Na + infusate K) – SNa]
TBW + 1
Na requirement (mEq) = (Desired Na - Serum Na)
x TBW
24 L
Water … L
Na + K ……….
Na + K
………
Water … L
Na
H20
+ …… mEq
……..
PNa 120 mEq/L
PNa 130 mEq/L
Tonicity balance
www.themegallery.com
Type of fluid replacement
• Hypovolemia : isotonic,0.9% saline • Euvolemia, Hypervolemia : hypertonic solution, 3% saline
- 2-6 days after Na treatment
- Dysarthria, dysphagia, paraparesis, quadriparesis, alteration of conscious, seizure, coma
• Risks..rapid correction (>20 mEq/first 24 hrs)
seizure, respiratory failure,
alcoholism, malnutrition,
chronic thiazide use, burn
Osmotic Demyelination Syndrome

LOGO
Hypernatremia Sirirat Reungjui, MD.
Content of Na+ in ECF….
ECF volume
Concentration of Na+ (PNa)
ICF volume
Na+ +
H2O
Na
H2O
Na+ gain
Na+
Na+
Loss
Water deficit
H2O
Plasma Na > 145 mEq/L Common in elderly, debilitated, esp. acute
(febrile) illness Risk factors Advanced age Mental or physical impairment Uncontrolled DM Underlying polyuria disorders Diuretic therapy Inadequate nursing care Hospitalization

www.themegallery.com
Characteristics of hypernatremia
Symptoms
Cognitive dysfunction ( neuronal cell shrinkage)
Lethargy, obtundation, confusion, abn. speech, irritability, myoclonic jerks, nystagmus, seizures
Dehydration (volume depletion)
Orthostatic BP changes, tachycardia, oliguria, dry oral mucosa, skin turgor
Other clinical findings Weight loss, generalized weakness

ADH
Osmostat
Thirst center
Uvol
Uosm
ADH
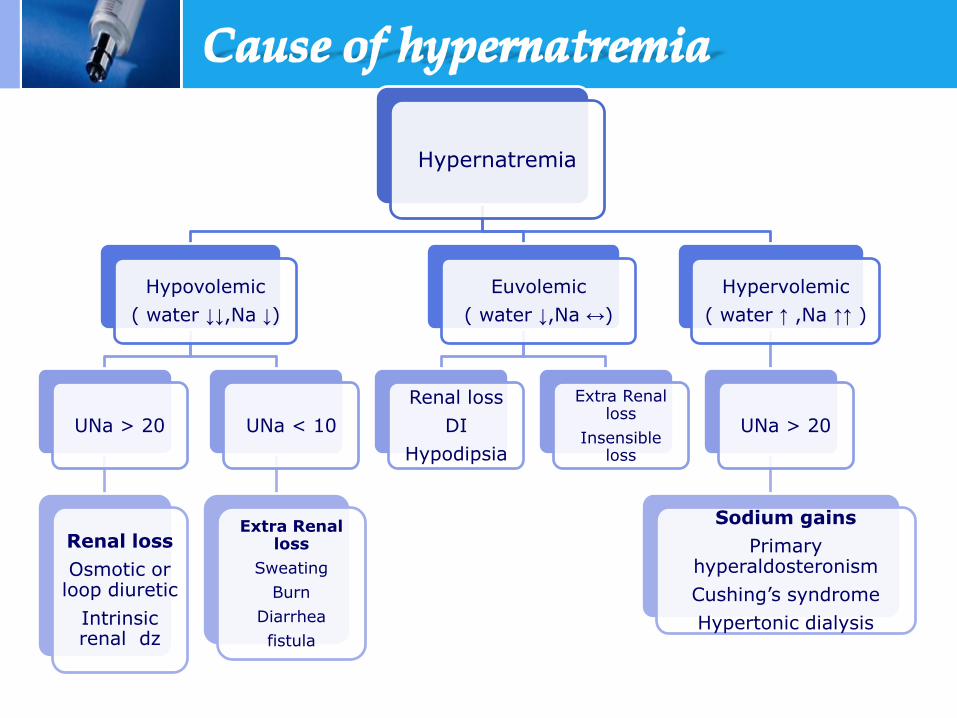
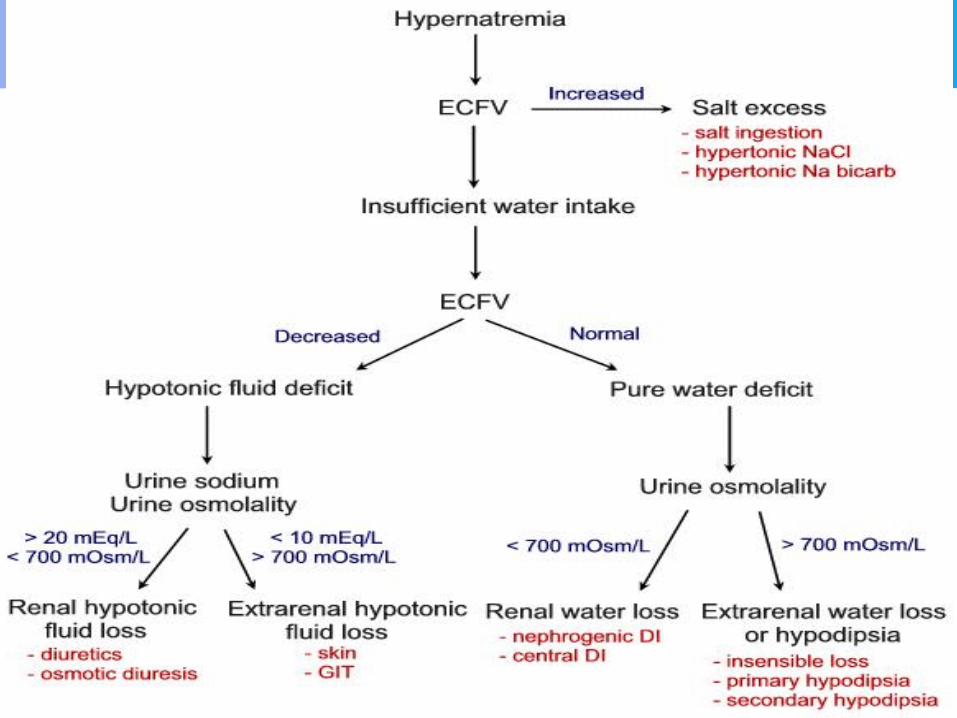
Hypernatremia
Hypovolemic
( water ↓↓,Na ↓)
UNa > 20
Renal loss
Osmotic or loop diuretic
Intrinsic renal dz
UNa < 10
Extra Renal loss
Sweating
Burn
Diarrhea
fistula
Euvolemic
( water ↓,Na ↔)
Renal loss
DI
Hypodipsia
Extra Renal loss
Insensible loss
Hypervolemic
( water ↑ ,Na ↑↑ )
UNa > 20
Sodium gains
Primary hyperaldosteronism
Cushing’s syndrome
Hypertonic dialysis

• Correct underlying diseases
• Correct water deficit =
TBW x ( PNa - 1 )
140
• 50 % in 12-24 hr and 50% later in 48-
72 hr ( < 0.5 mEq/L/hr )
www.themegallery.com
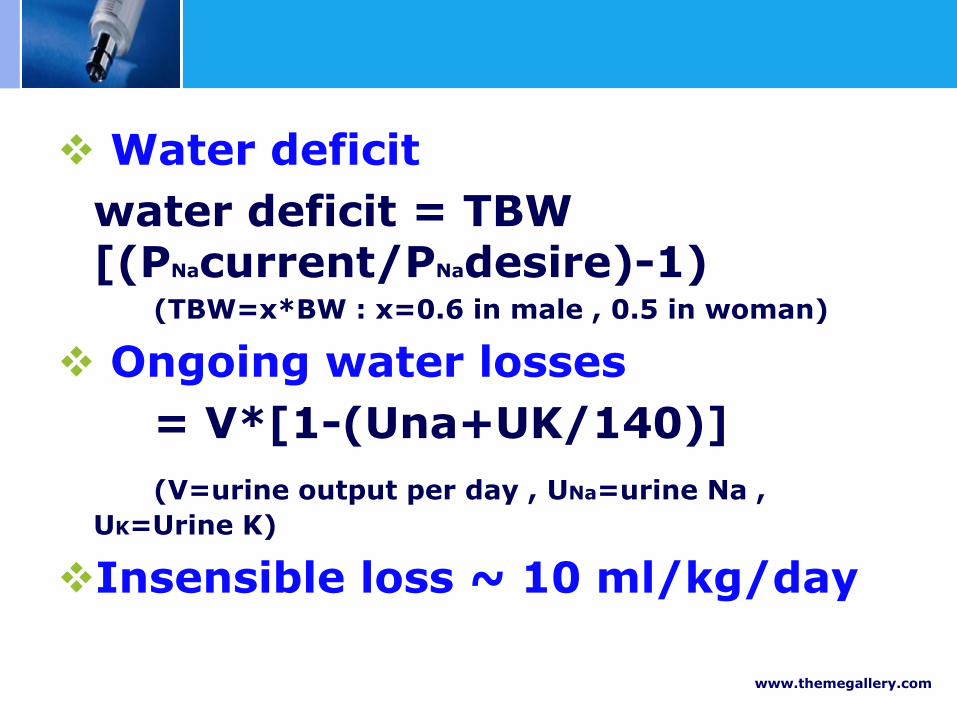
Water deficit
water deficit = TBW [(PNacurrent/PNadesire)-1)
(TBW=x*BW : x=0.6 in male , 0.5 in woman)
Ongoing water losses
= V*[1-(Una+UK/140)]
(V=urine output per day , UNa=urine Na ,
UK=Urine K)
Insensible loss ~ 10 ml/kg/day
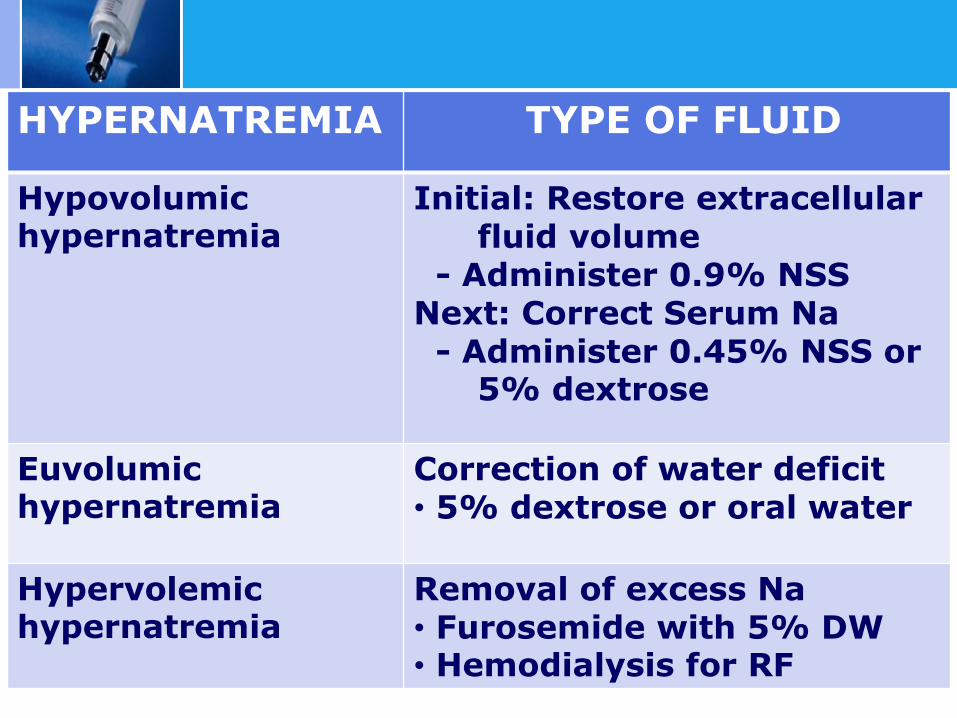
HYPERNATREMIA TYPE OF FLUID
Hypovolumic hypernatremia
Initial: Restore extracellular fluid volume
- Administer 0.9% NSS Next: Correct Serum Na - Administer 0.45% NSS or
5% dextrose
Euvolumic hypernatremia
Correction of water deficit • 5% dextrose or oral water
Hypervolemic hypernatremia
Removal of excess Na • Furosemide with 5% DW • Hemodialysis for RF
www.themegallery.com
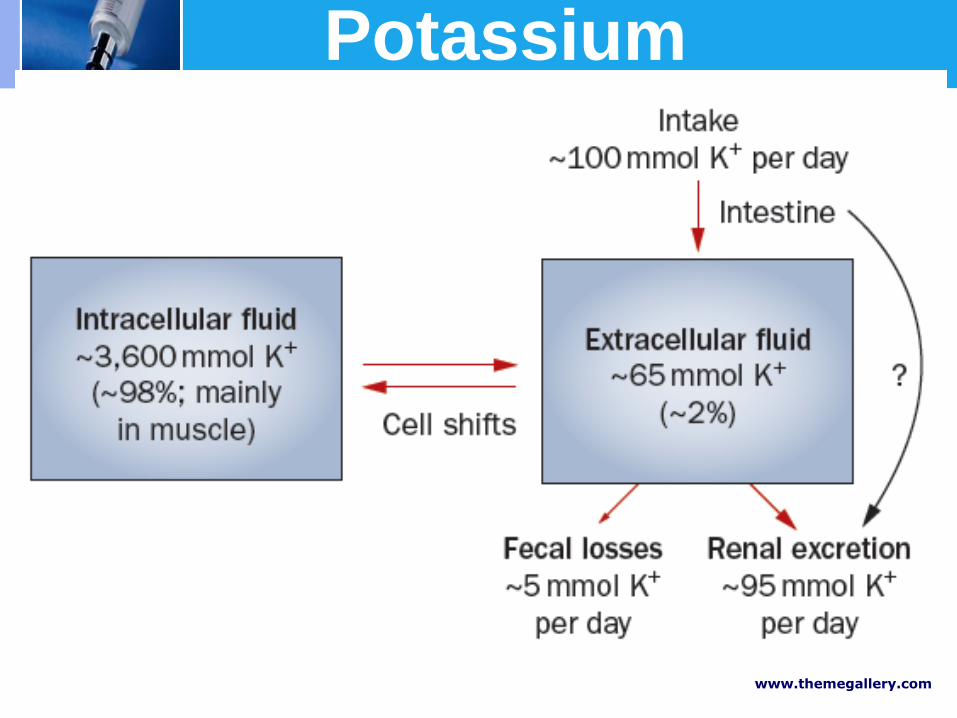
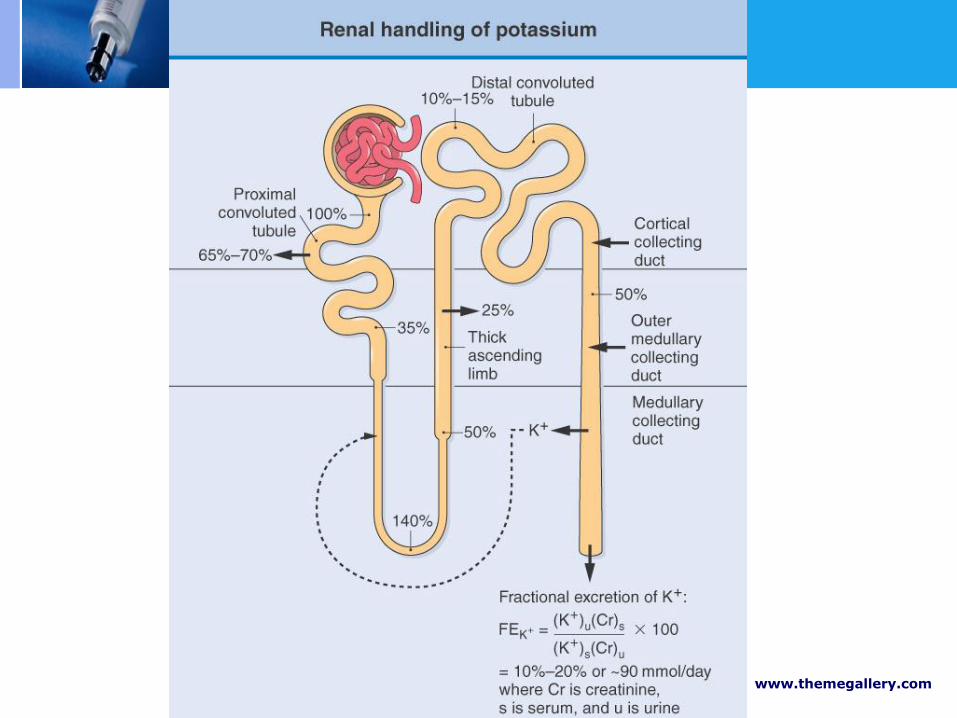
Potassium

www.themegallery.com
Transcellular shift Insulin, 2 agonist,
antagonist, alkalosis
Acidosis, hyperglycemia, 2 antagonist ,
agonist, exercise
www.themegallery.com
• plasma K< 3.5 mEq/l • Mild hypokalemia ………… 3-3.5 mEq/L Moderate hypokalemia ….. 2.5-3 mEq/L Severe hypokalemia ……… < 2.5 mEq/L.

www.themegallery.com
Moderate
Severe
Mild
Cardiac arrhythmia (digitalis)
•Atrial & Ventricular arrythmia •Flat T wave,PR prolong, U wave,PVC •constipation •Muscle weakness, Fatique,muscle cramp
•Flaccid paralysis •Hyporeflexia •Hypercapnia •Tetany •Rhabdomyolysis •Bowel ileus •Respiratory mucle weakness→arrest
< 3.5 2.5 - 3.5
< 2.5

www.themegallery.com
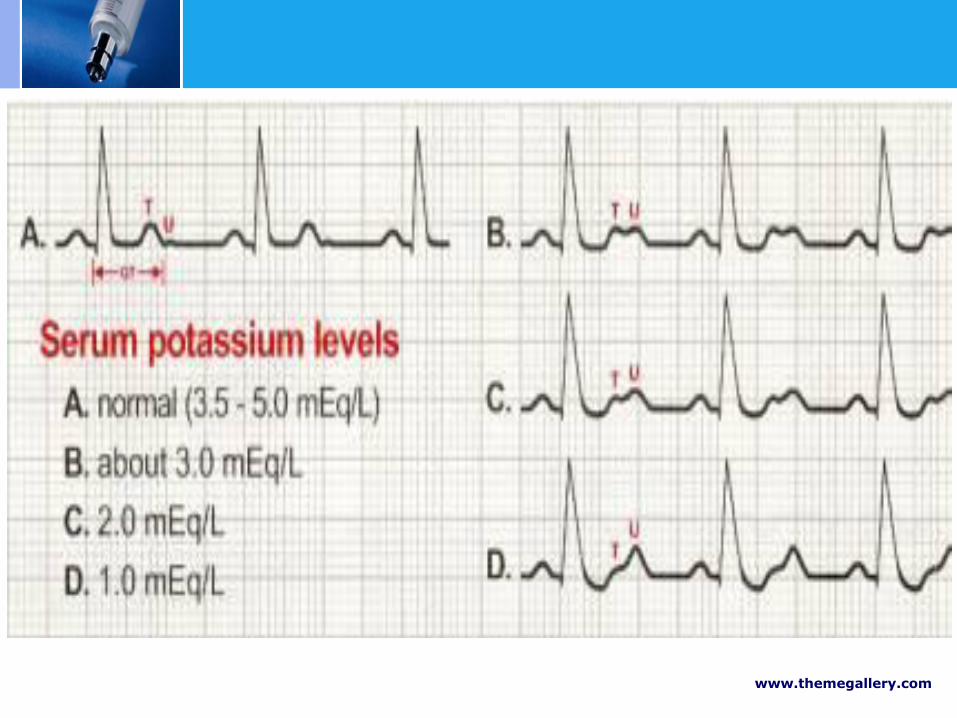
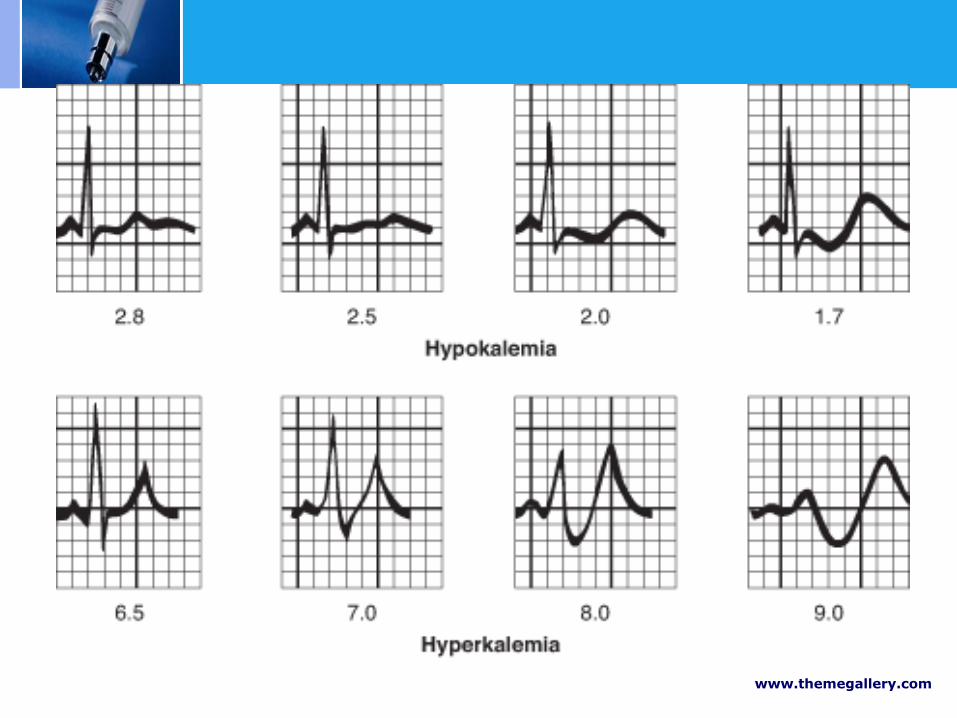
ECG OF HYPOKALEMIA
www.themegallery.com
Approach hypoK
Transcellular shift
Renal or extrarenal loss
..urine K (>20 mEq/day)
..TTKG
Acid-base..acidosis,alkalosis
Blood pressure

Hypokalemia
Extrarenal loss
TTKG < 3
Metabolic acidosis
Diarrhea
GI fistula
Laxative abuse
Normal acid-base
GI loss
Laxative abuse
Metabolic alkalosis
chloride losing diarrhea
Renal loss
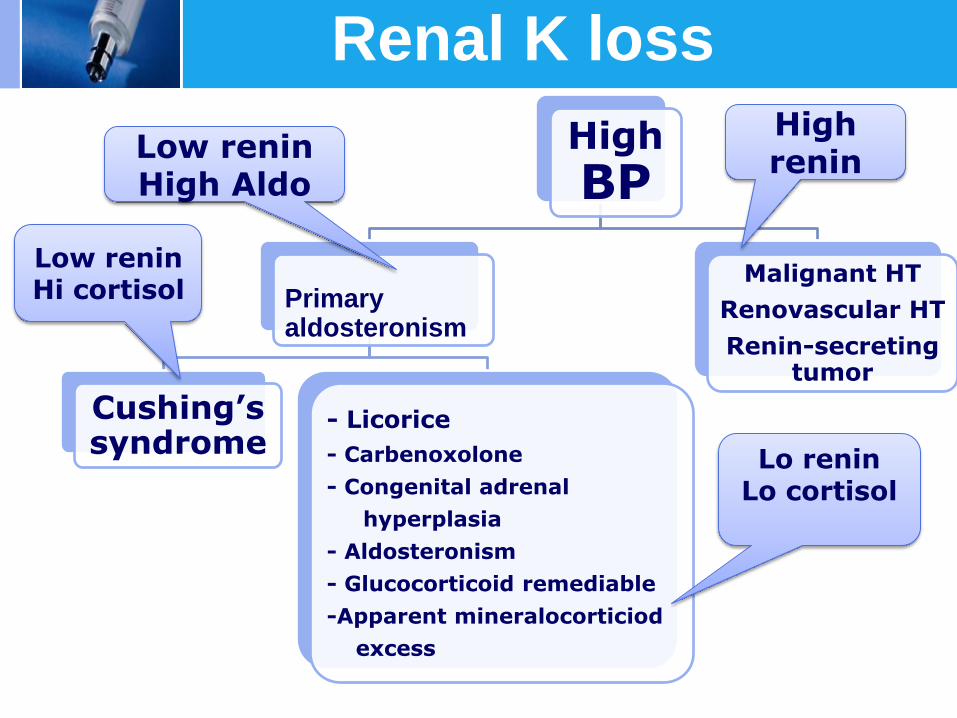
High
BP
Cushing’s syndrome
- Licorice
- Carbenoxolone
- Congenital adrenal
hyperplasia
- Aldosteronism
- Glucocorticoid remediable
-Apparent mineralocorticiod
excess
Malignant HT
Renovascular HT
Renin-secreting tumor
High renin
Low renin High Aldo
Primary aldosteronism
Low renin Hi cortisol
Lo renin Lo cortisol
Renal K loss
www.themegallery.com
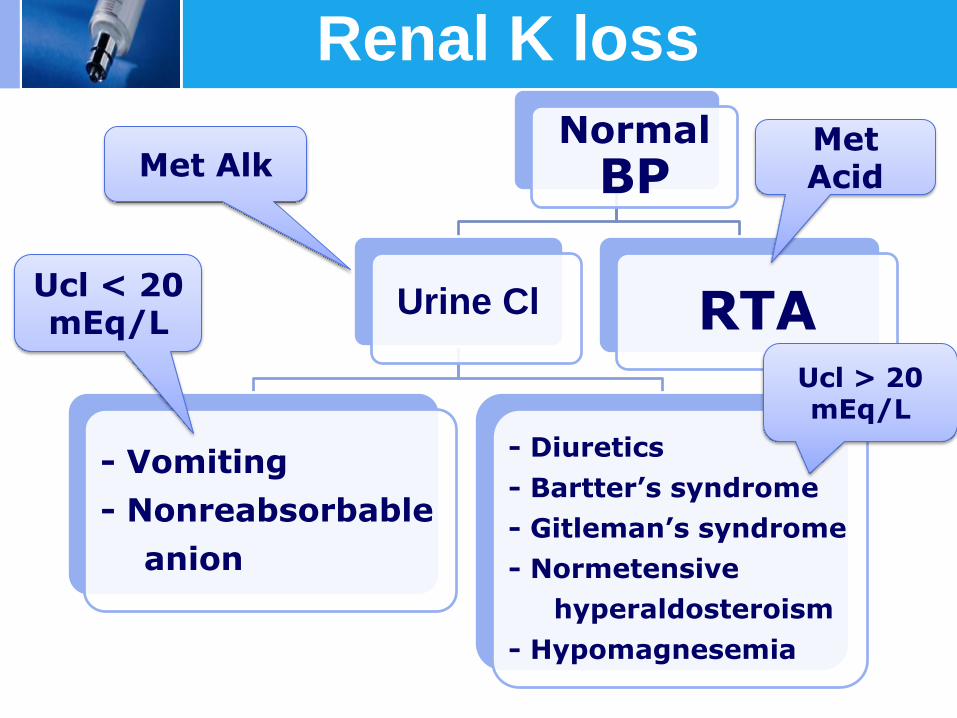
Normal
BP
- Vomiting
- Nonreabsorbable
anion
- Diuretics
- Bartter’s syndrome
- Gitleman’s syndrome
- Normetensive
hyperaldosteroism
- Hypomagnesemia
RTA
Met Acid Met Alk
Urine Cl Ucl < 20 mEq/L
Ucl > 20 mEq/L
Renal K loss
1. Treat cause 2. K supplement Mild to moderate hypokalemia ↓ K 1 mEq/L = K deficit 200-400 mEq/L Oral : elixir KCl (40-120 mEq/day) E.KCl 30 ml = K 20 mEq Follow K+ level Severe hypokalemia Intravenous : KCl in 0.9% NaCl (< 40-60 mEq/L) monitor EKG if replace > 10 mEq/hr

www.themegallery.com
100-400 (>200) mEq
> 500 mEq

• Plasma K > 5 mEq/l • Mild hyperkalemia….. 5 - 6 mEq/L
Moderate hyperkalemia …6 - 6.5 mEq/L Severe hyperkalemia …. > 6.5-7 mEq/L
1. Cardiovascular system ; arrhythmia, EKG change - Pk 5-6.5 mEq/l → tall peak T - Pk 6.5-8 mEq/l → P wave flattening, PR prolong, widening of QRS complex - Pk >8 mEq/l → biphasic sine wave, ventricular fibrillation, cardiac arrest
2. Numbness, muscle weakness, flaccid paralysis 3. Nausea, vomiting, abdominal pain, bowel ileus
www.themegallery.com

www.themegallery.com
Approach hyperK
Transcellular shift
Renal causes
..renal failure
..aldosterone deficiency
or resistance
..inhibit ENAC
..decrease distal flow
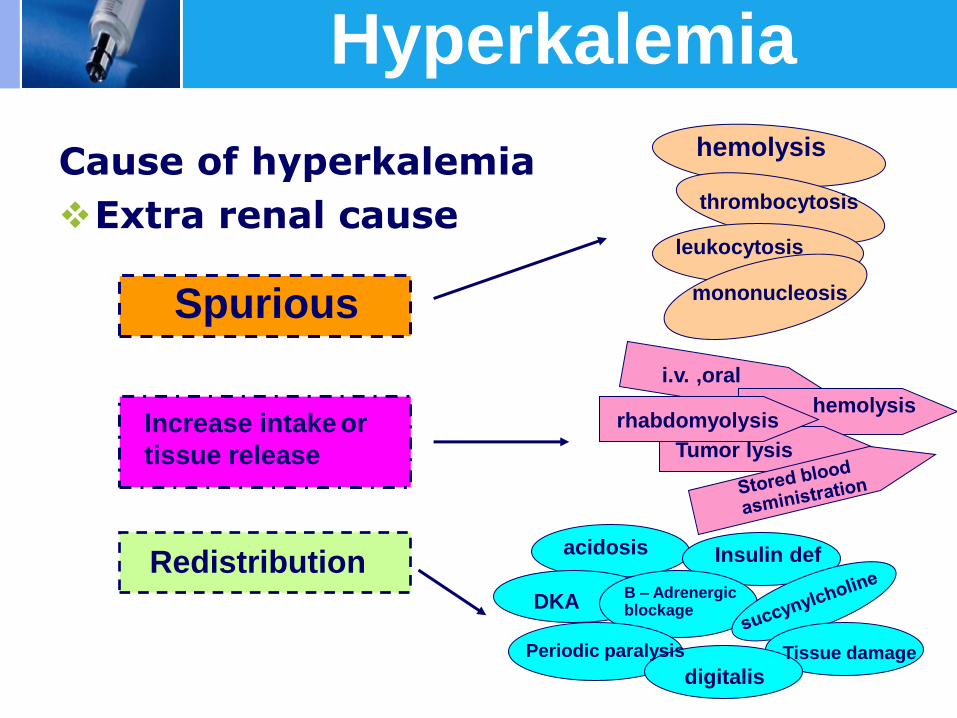
Hyperkalemia
Cause of hyperkalemia
Extra renal cause
Spurious
Increase intake or
tissue release
Redistribution
hemolysis
thrombocytosis
leukocytosis
mononucleosis
i.v. ,oral
hemolysis rhabdomyolysis
Tumor lysis
acidosis Insulin def
DKA B – Adrenergic blockage
Periodic paralysis
digitalis Tissue damage
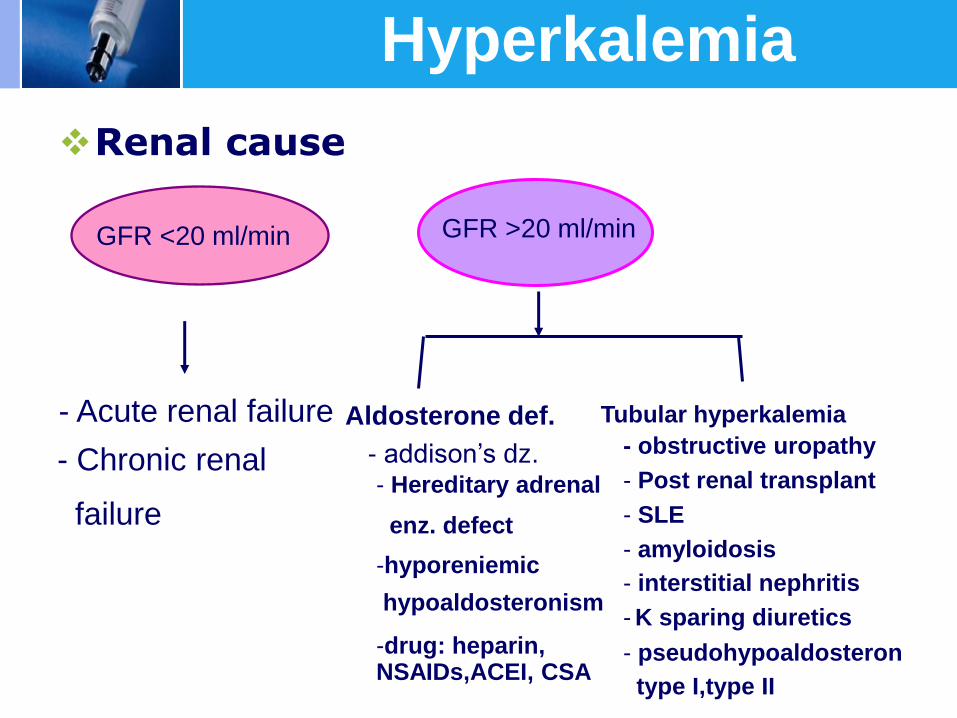
Hyperkalemia
Renal cause
GFR <20 ml/min GFR >20 ml/min
- Acute renal failure Aldosterone def. Tubular hyperkalemia
- addison’s dz. - Hereditary adrenal
enz. defect
-hyporeniemic
hypoaldosteronism
-drug: heparin, NSAIDs,ACEI, CSA
- obstructive uropathy
- Post renal transplant
- SLE
- amyloidosis
- interstitial nephritis
- K sparing diuretics
- pseudohypoaldosteron
type I,type II
- Chronic renal
failure
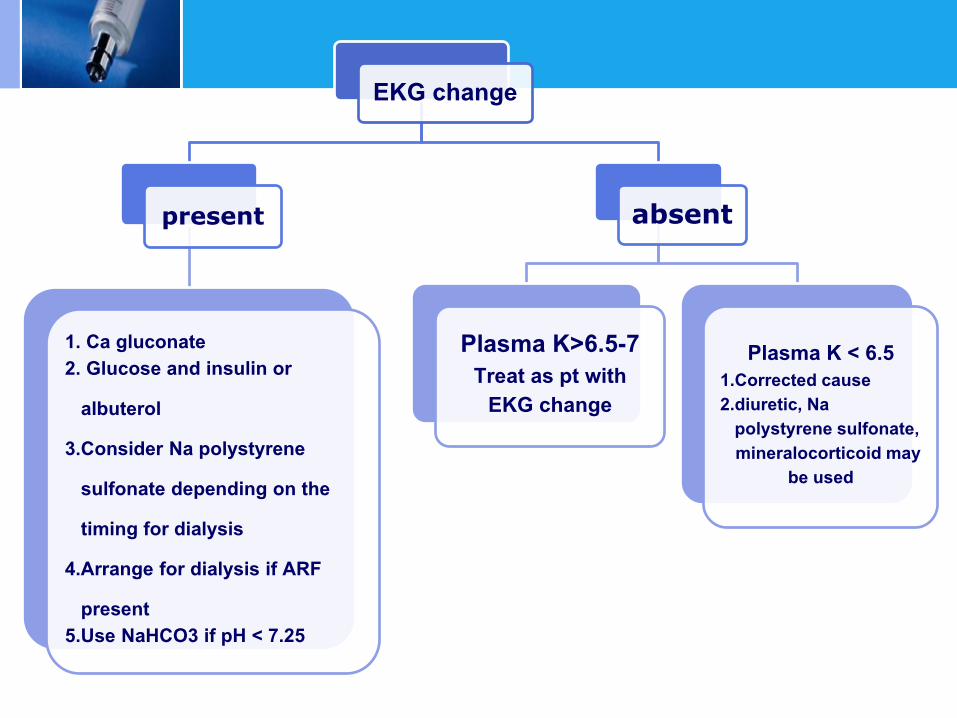
EKG change
present
1. Ca gluconate 2. Glucose and insulin or albuterol 3.Consider Na polystyrene sulfonate depending on the timing for dialysis 4.Arrange for dialysis if ARF present 5.Use NaHCO3 if pH < 7.25
absent
Plasma K>6.5-7 Treat as pt with
EKG change
Plasma K < 6.5 1.Corrected cause 2.diuretic, Na polystyrene sulfonate, mineralocorticoid may
be used
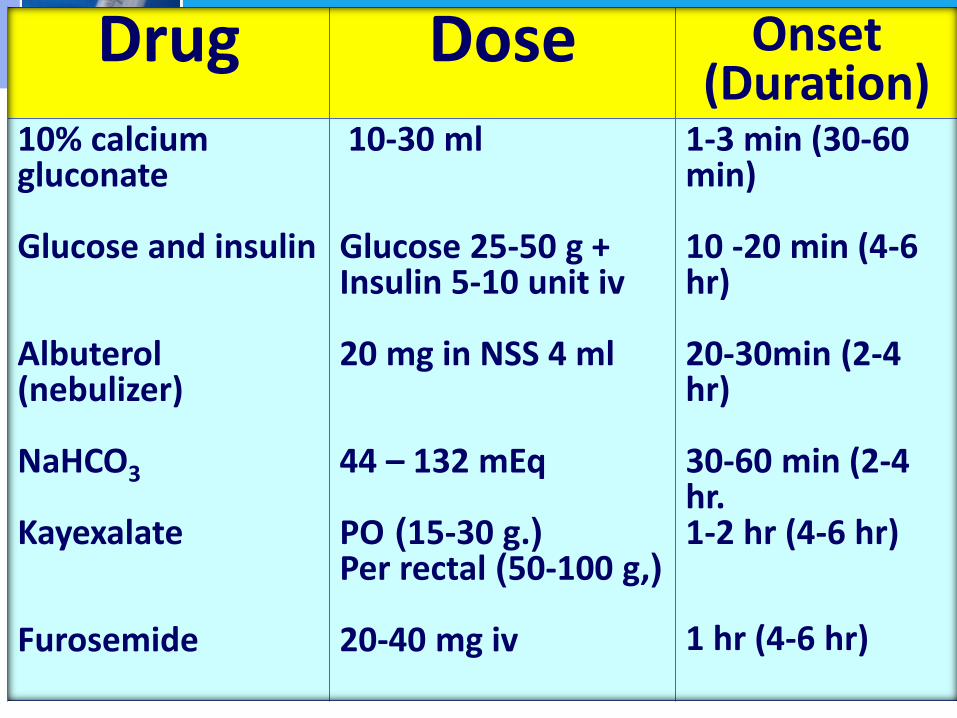
Drug Dose Onset (Duration)
10% calcium gluconate Glucose and insulin Albuterol (nebulizer) NaHCO3 Kayexalate Furosemide
10-30 ml Glucose 25-50 g + Insulin 5-10 unit iv 20 mg in NSS 4 ml 44 – 132 mEq PO (15-30 g.) Per rectal (50-100 g,) 20-40 mg iv
1-3 min (30-60 min) 10 -20 min (4-6 hr) 20-30min (2-4 hr) 30-60 min (2-4 hr. 1-2 hr (4-6 hr) 1 hr (4-6 hr)
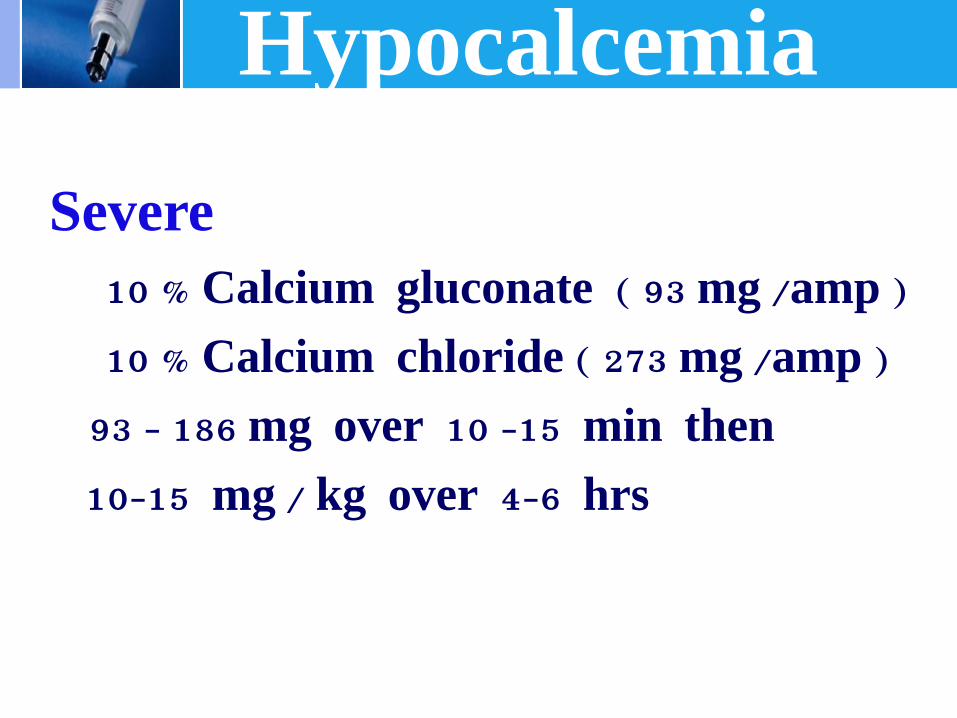
Hypocalcemia
Severe
10 % Calcium gluconate ( 93 mg /amp )
10 % Calcium chloride ( 273 mg /amp )
93 - 186 mg over 10 -15 min then
10-15 mg / kg over 4-6 hrs
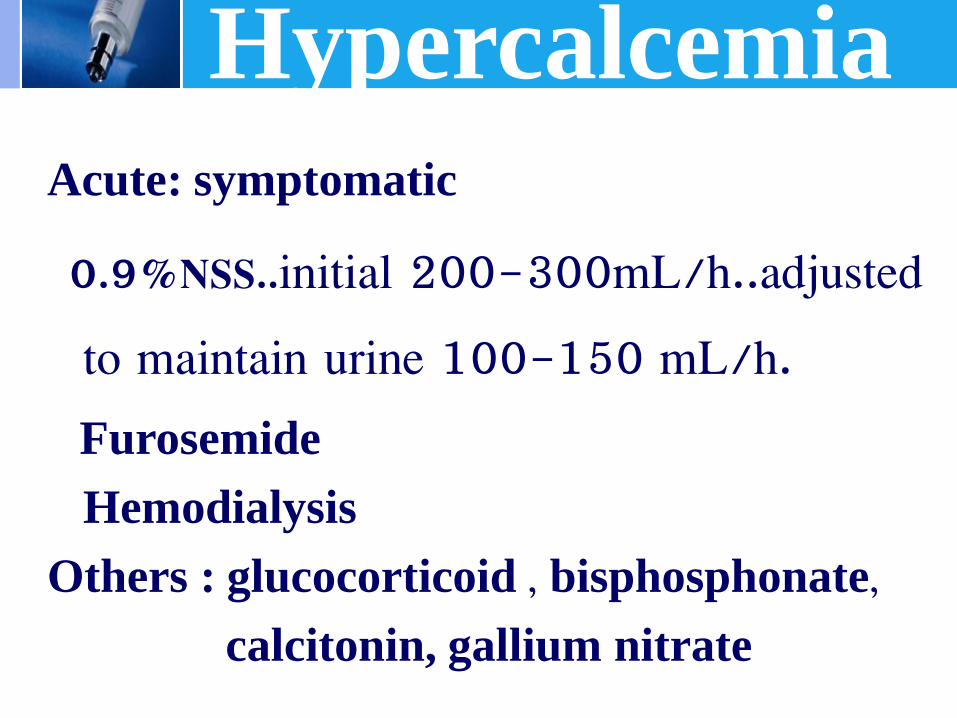
Hypercalcemia
Acute: symptomatic
0.9%NSS..initial 200-300mL/h..adjusted
to maintain urine 100-150 mL/h.
Furosemide
Hemodialysis
Others : glucocorticoid , bisphosphonate,
calcitonin, gallium nitrate
Hypomagnesemia
Mild - moderate deficiency (1.2 -1.7 mg/dL)…diet or oral Mg supplement
Symptomatic pts… 3 - 4 g (24 mEq to 32 mEq) of iv MgSO4 over 12-24 hrs
Repeated dose..maintain Smg > 1.2 mg/dL
Renal insufficiency.. reduce dose (25-50%)
Treatment of RTA
Underlying disease
Proximal RTA…alkali Rx, K replacement, thiazide, vit D , phosphate
Distal RTA…alkali Rx, K
Aldosterone deficiency.. mineralocorticoid
Calculated Bicarbonate Dose = 0.3 x Wt x BE BE = base excess Bicarbonate deficit = (0.5 x LBW) x (24 – HCO3) LBW = lean body weight
Alkali Treatment
Replace 50 % of the deficit over the first 24 hours
LOGO
Related Documents