Fitness for Transplant Recipients How Important Is it? Patricia Painter, Ph.D. FACSM Associate Research Faculty Department of Physical Therapy University of Utah

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Fitness for Transplant RecipientsHow Important Is it?
Patricia Painter, Ph.D. FACSMAssociate Research Faculty
Department of Physical TherapyUniversity of Utah
REVISED and Updated : Physical Activity Guidelines Advisory Committee Report, 2008
Reduces the risk of dying prematurely
The Benefits of Regular Physical Activity
Surgeon General’s Report on Physical Activity and Health
Reduces the risk of dying from heart disease
Reduces the risk of developing diabetes
Reduces the risk of developing high blood pressure
Helps reduce blood pressure in people who already have high blood pressure
Reduces feelings of depression and anxiety Helps control body weight
Helps build and maintain healthy bones, muscles and joints
Helps older adults become stronger and better able to move about without falling
Regular physical activity can help people with chronic, disabling conditions:
improve their stamina and muscle strength
The Benefits of Regular Physical Activity
Surgeon General’s Report on Physical Activity and Health
improve psychological well-being and quality of life by increasing the ability to perform activities of daily life
So, why would transplant recipients be any different than the general population?
Exercise in Organ Transplantation
OR perhaps physical activity is MORE important for tx recipients because of: The deconditioning experienced prior to transplant High prevalence of CV risk factors Tendency for excessive weight gain Need for complete rehabilitation
FACT:
Exercise capacity as measured by peak oxygen uptake (VO2peak) is low in ESRD patients treated with hemodialysis. Over 45 studies that document low levels of
exercise capacity and/or physical functioning
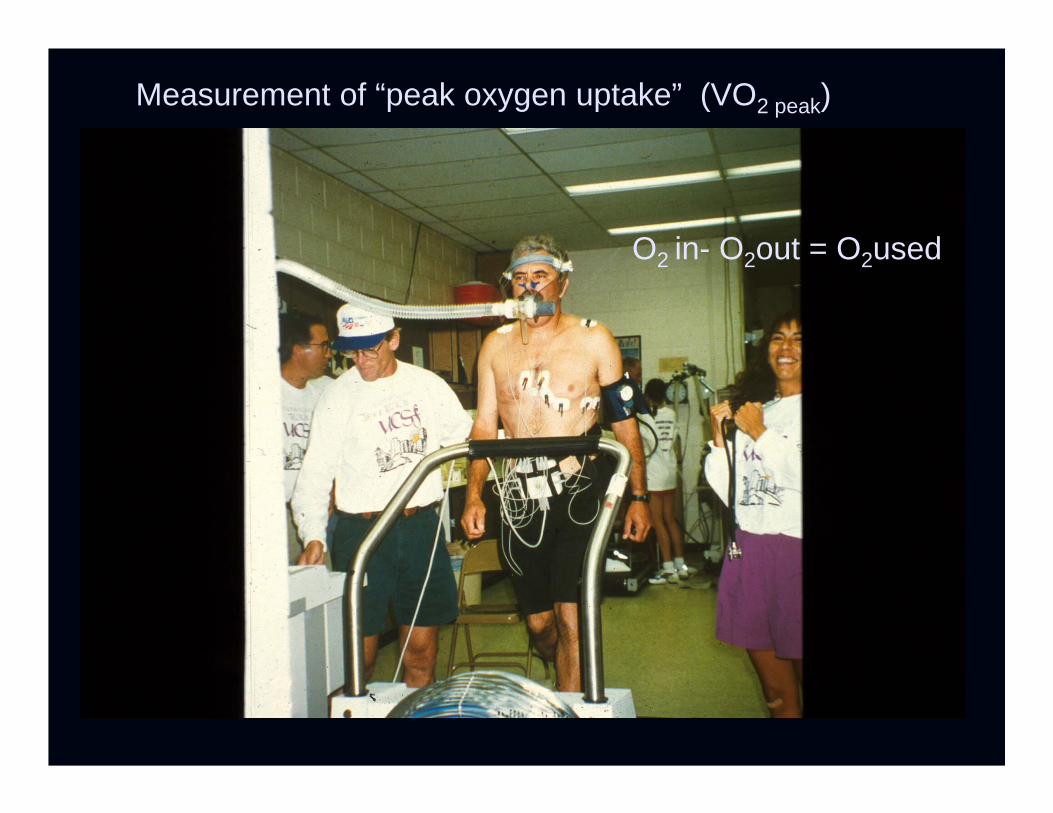
Measurement of “peak oxygen uptake” (VO2 peak)
O2 in- O2out = O2used

Untrained
sedentary normal males
sedentary normal females
50
40
30
20
10
0
max
imal
oxy
gen
upta
ke (m
l/kg/
min
)
20 30 40 50 60 70
age
Oxygen Uptake in Adult Hemodialysis Patients *
(*Average VO2peak in 14 studies - pre EPO )
FACT:
Exercise capacity as measured by peak oxygen uptake (VO2peak) increases soon after successful kidney transplant (~28% within 8 weeks post surgery, with no exercise training)
Painter, et al AJKD 10: 452-456, 1987

50
40
30
20
10
0max
imal
oxy
gen
upta
ke (m
l/kg/
min
)
20 30 40 50 60 70
age
sedentary normal males
sedentary normal females
Before TransplantAfter Transplant
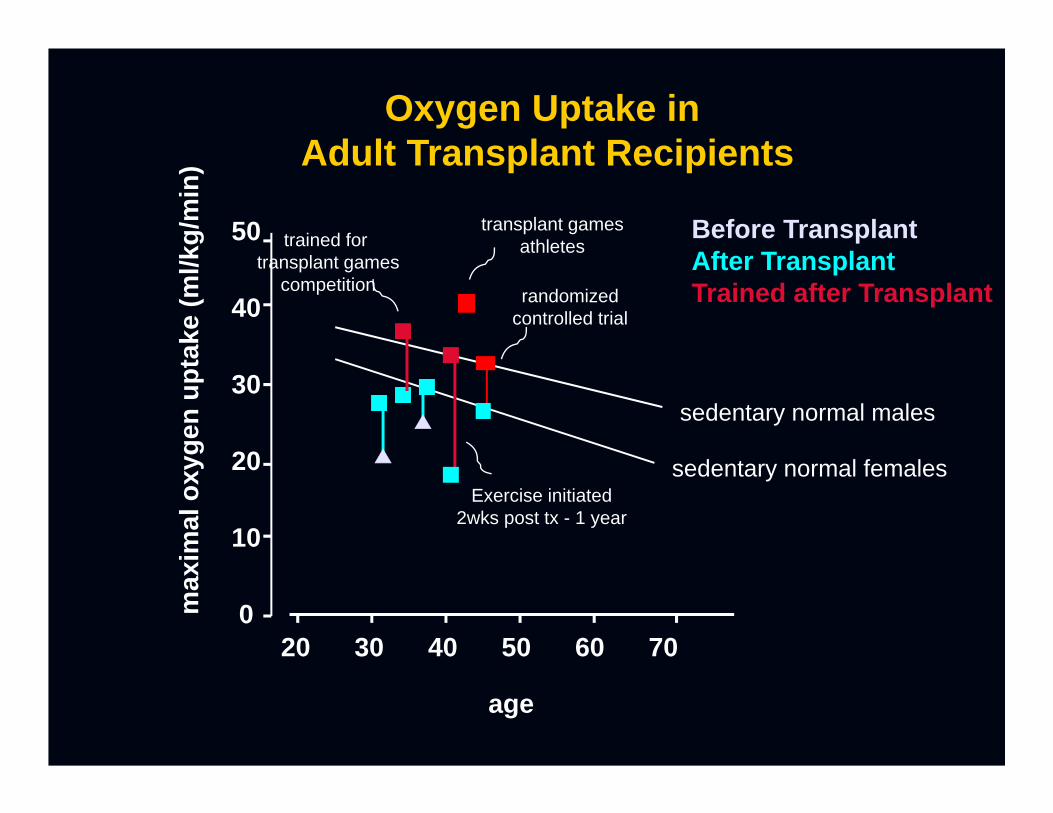
Oxygen Uptake in Adult Transplant Recipients
8 weeks12 weeks
FACT:
Exercise capacity as measured by peak oxygen uptake (VO2peak) increases with exercise training in kidney transplant recipients.
Kempeneers, et al 1990, Miller, et al 1987van De Hamm, 2006
50
40
30
20
10
0max
imal
oxy
gen
upta
ke (m
l/kg/
min
)
20 30 40 50 60 70
age
sedentary normal males
sedentary normal females
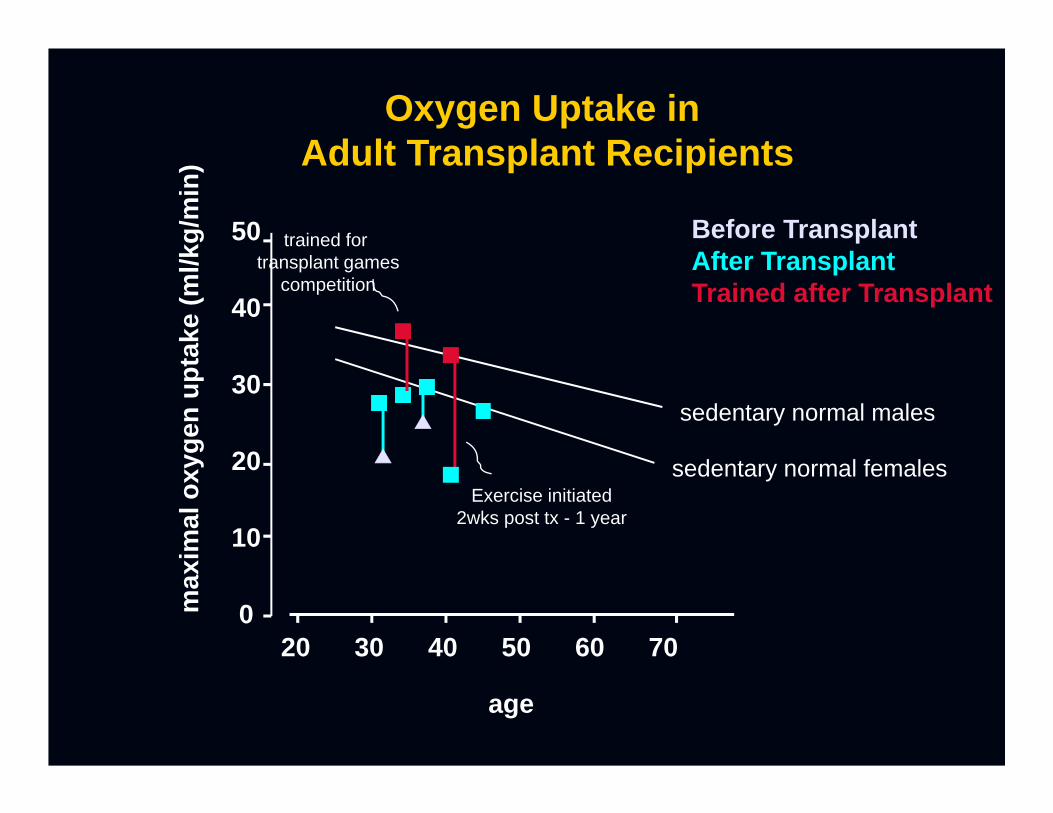
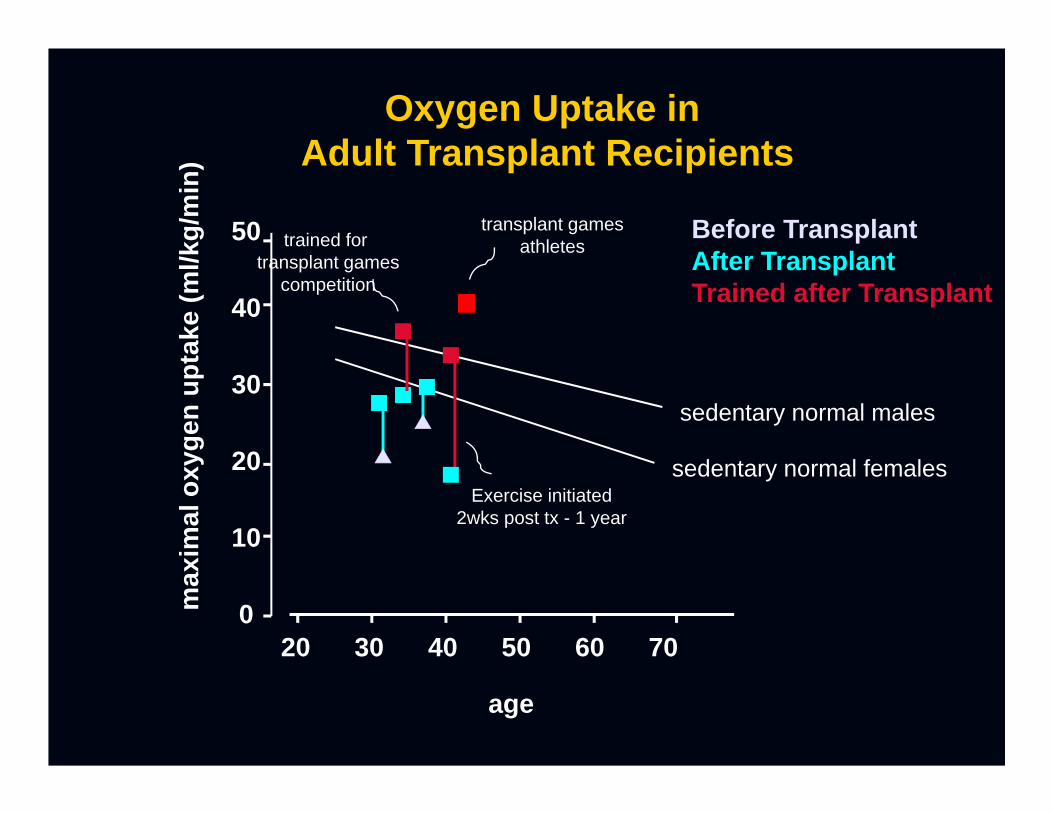
Before TransplantAfter TransplantTrained after Transplant
Oxygen Uptake in Adult Transplant Recipients
trained for transplant games
competition
Exercise initiated2wks post tx - 1 year
Health-Related Fitness and Quality of Life in Organ Transplant Recipients: Exercise testing of
Participants at the 1998 U.S. Transplant Games
P. PainterM. Luetkemeier
GE MooreS DibbleG Green
J MyllL Carlson
Transplantation 64: 1795-1800, 1997
DemographicsTransplant Games Testing
N= 128 (selected on order of receipt of registration: 412 registered)Kidney (n=76)Liver (n=16)Heart (n=19)Lung (n=6)P/K (n=7)Bone Marrow (n=4)
Ave age: 45.9±11.2 Time post tx: 8.1 ± 10.5 Highest level of education: 15.5 ± 2.3 Active 76.6%
“Active” Criteria
3 x per week or more of ‘aerobic’ activity >20 minutes per session intensity described as “somewhat hard” or greater

Testing Maximal Treadmill testing with VO2 measurements Isokinetic Muscle testing Underwater weighing (% fat, lean mass, fat mass) SF-36 Questionnaire
Transplant Rehab Intervention Project

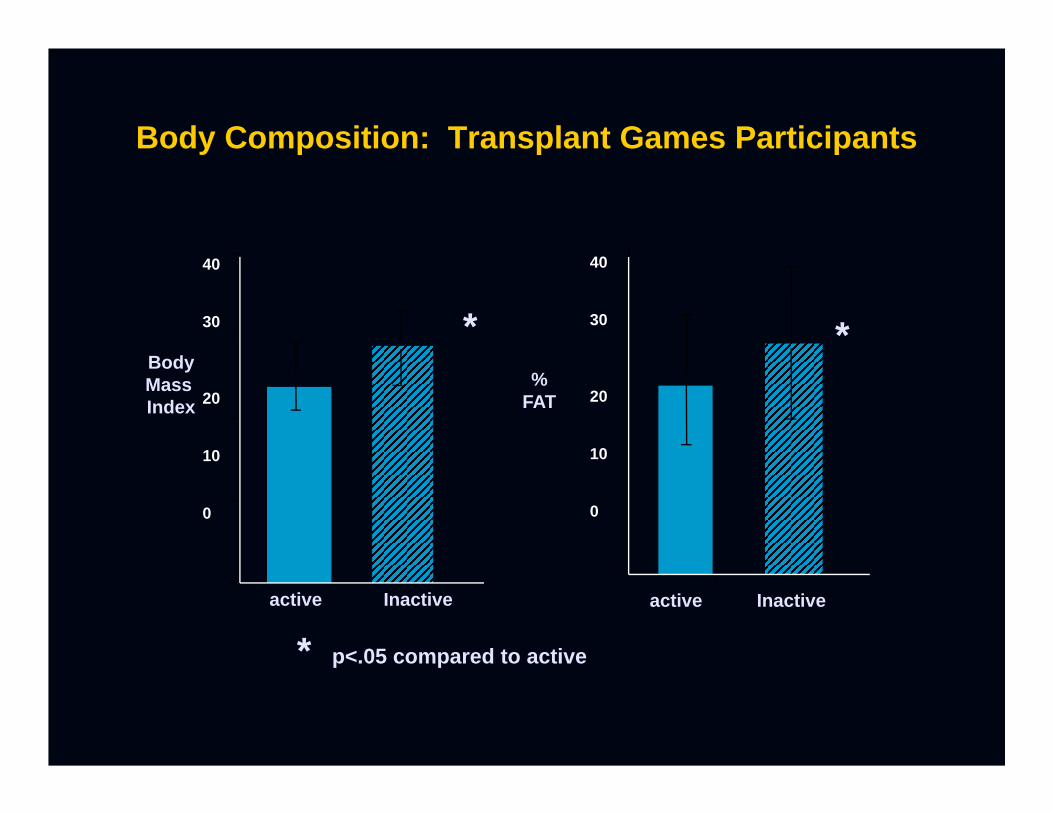
Body Composition: Transplant Games Participants
* p<.05 compared to active
BodyMass Index
40
30
20
10
0
*
active Inactive
40
30
20
10
0
%FAT
*
active Inactive

0
50
100
150
hemodialysis TxG
active
inactive
*##
* p<.01 compared to inactivep<.01 compared to HD
Perc
ent o
f Age
Pre
dict
ed V
O2
Differences in Exercise Capacity between
Active and Inactive RTX Recipients
0
20
40
60
80
100
120
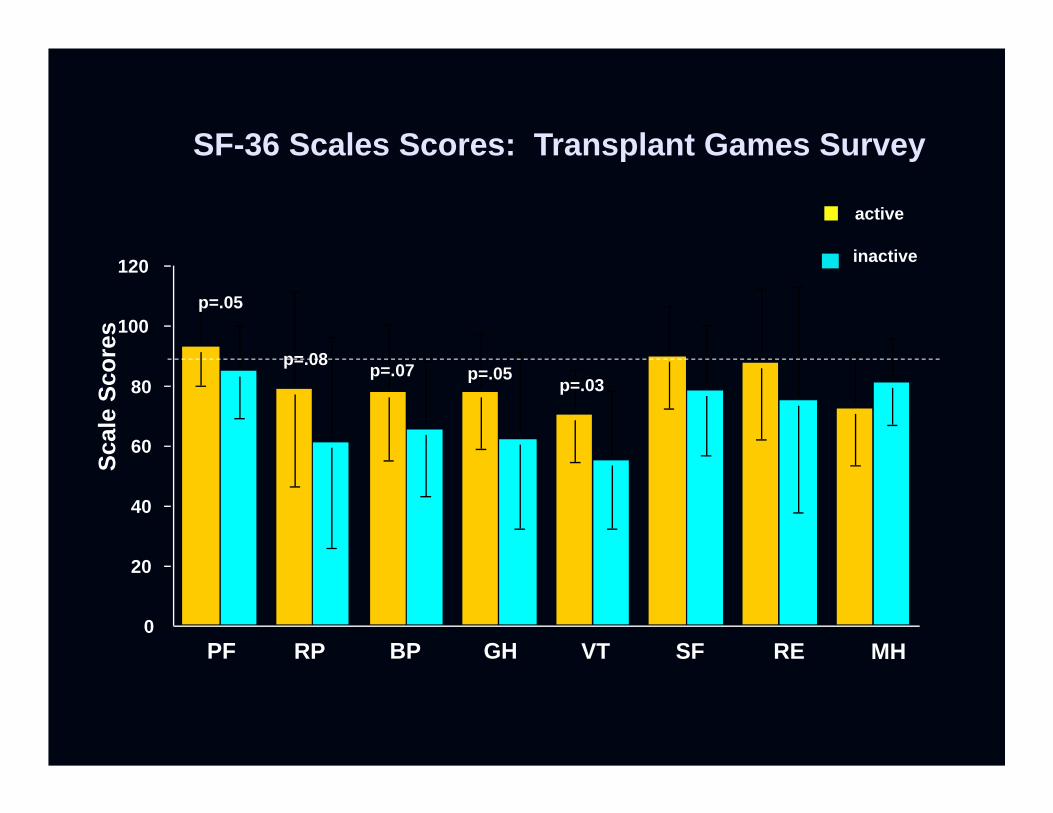
PF RP BP GH VT SF RE MH
p=.05
p=.08p=.05p=.07
p=.03
SF-36 Scales Scores: Transplant Games SurveySc
ale
Scor
es
active
inactive
50
40
30
20
10
0max
imal
oxy
gen
upta
ke (m
l/kg/
min
)
20 30 40 50 60 70
age
sedentary normal males
sedentary normal females
Before TransplantAfter TransplantTrained after Transplant
Oxygen Uptake in Adult Transplant Recipients
transplant gamesathletestrained for
transplant gamescompetition
Exercise initiated2wks post tx - 1 year
A Randomized Trial of Exercise Training following Renal Transplantation
Patricia Lynn Painter Lisa HectorKaren Ray
Liliana Lynes Suzanne Dibble Steven M. Paul
Stephen L. Tomlanovich Nancy L. Ascher
Painter, et al: Transplantation 74:42-48, 2002Transplant Rehab Intervention Project
NIH/NINR: RO1 NR02880
to determine the effects of exercise training over the first year post kidney transplant on
health-related fitness (cardiorespiratory fitness, muscle strength, body composition
and health-related quality of life).
Transplant Rehab Intervention Project
Purpose:
Study Design
Baseline testing (2 mo post tx) (n=177)
exercise* usual care
6 month retest
12 month retest (n=95)
randomize
Transplant Rehab Intervention Project
Testing Maximal Treadmill testing with VO2 measurements Isokinetic Muscle testing Dexa (% fat, lean mass, fat mass) SF-36 Questionnaire
Intervention Independent Home Exercise
cardiovascular 3x or more/week 30 min or more/session
Transplant Rehab Intervention Project
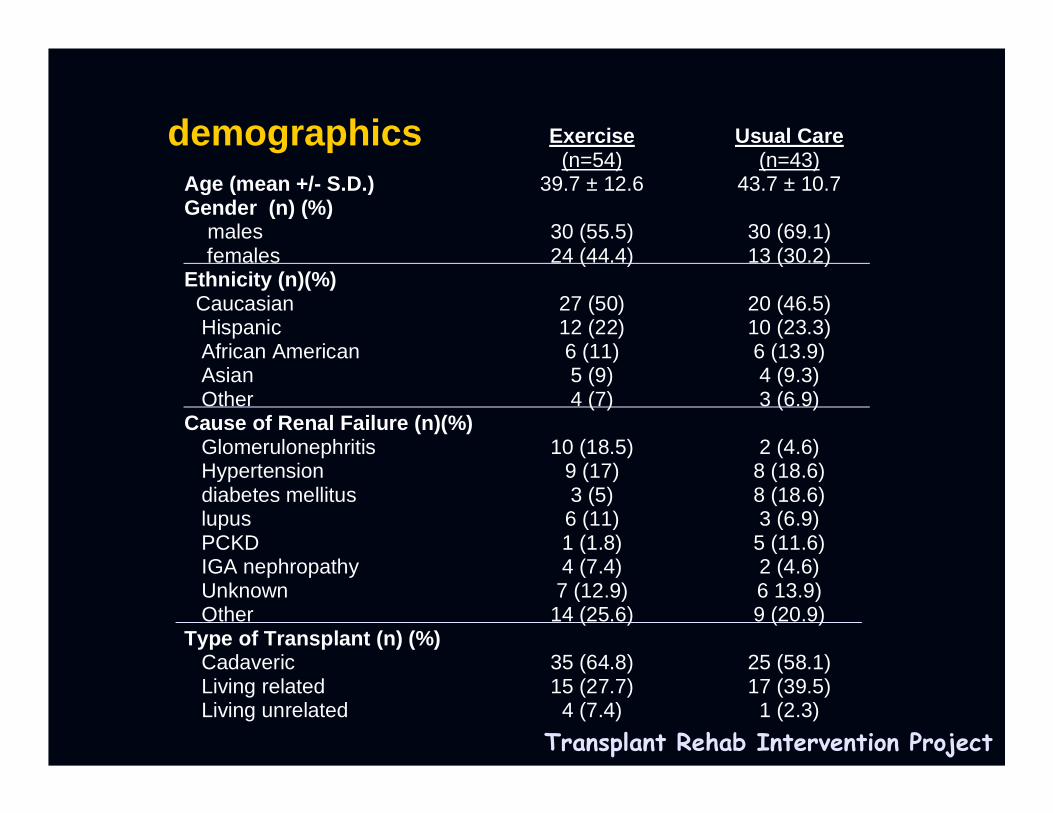
Exercise(n=54)
Usual Care(n=43)
Age (mean +/- S.D.) 39.7 ± 12.6 43.7 ± 10.7Gender (n) (%) males females
30 (55.5)24 (44.4)
30 (69.1)13 (30.2)
Ethnicity (n)(%) Caucasian Hispanic African American Asian Other
27 (50)12 (22)6 (11)5 (9)4 (7)
20 (46.5)10 (23.3)6 (13.9)4 (9.3)3 (6.9)
Cause of Renal Failure (n)(%) Glomerulonephritis Hypertension diabetes mellitus lupus PCKD IGA nephropathy Unknown Other
10 (18.5)9 (17)3 (5)6 (11)1 (1.8)4 (7.4)7 (12.9)
14 (25.6)
2 (4.6)8 (18.6)8 (18.6)3 (6.9)
5 (11.6)2 (4.6)6 13.9)9 (20.9)
Type of Transplant (n) (%) Cadaveric Living related Living unrelated
35 (64.8)15 (27.7)
4 (7.4)
25 (58.1)17 (39.5)
1 (2.3)
demographics
Transplant Rehab Intervention Project
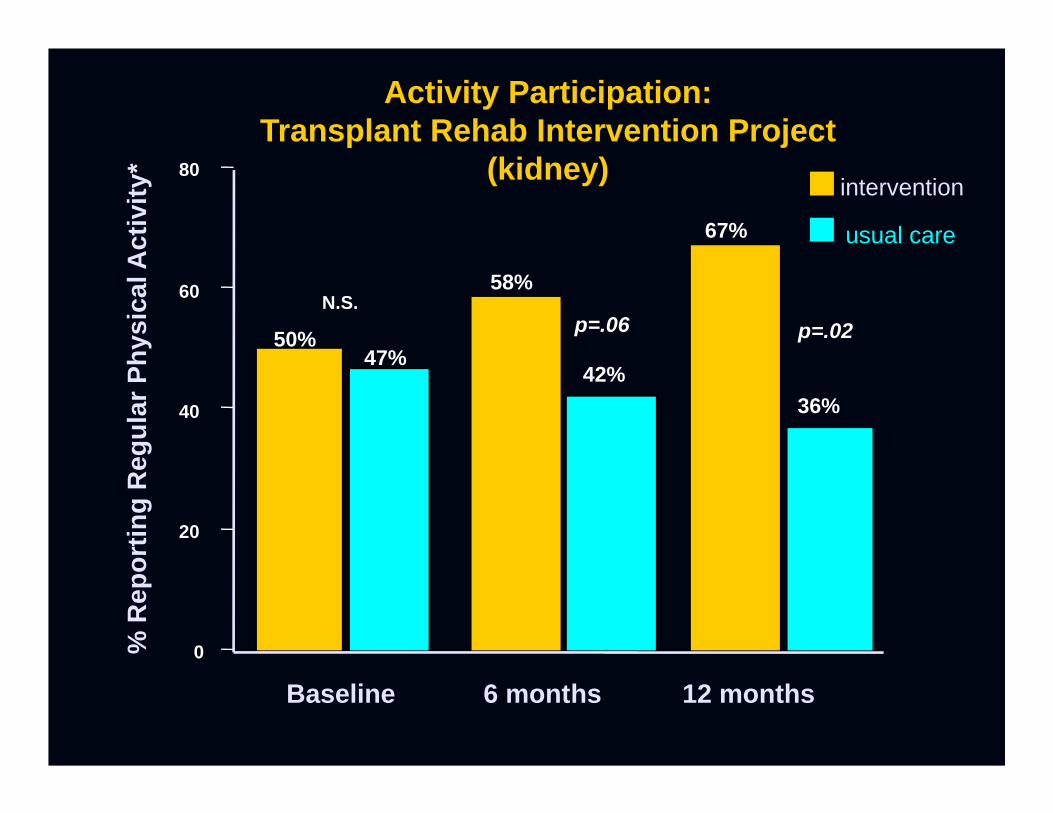
0
20
40
60
80
Baseline 6 months 12 months
50%47%
58%
67%
42%36%
% R
epor
ting
Reg
ular
Phy
sica
l Act
ivity
*
N.S.p=.06 p=.02
intervention
usual care
Activity Participation:Transplant Rehab Intervention Project
(kidney)
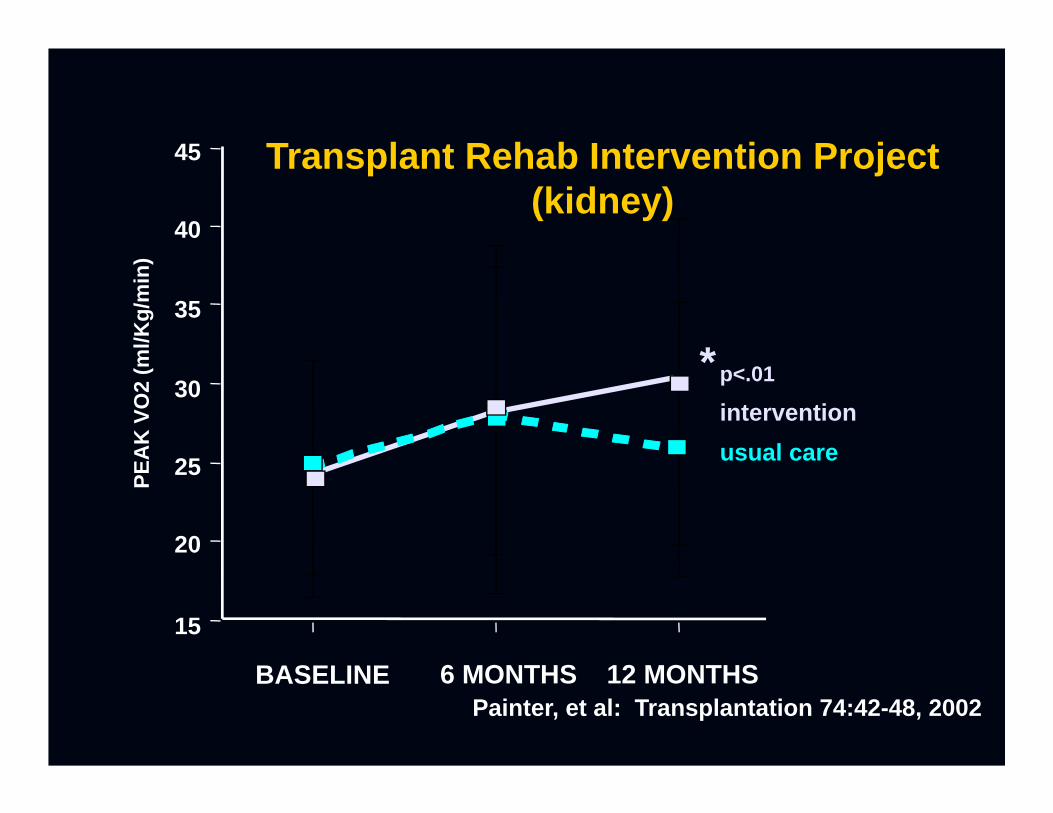
BASELINE 6 MONTHS 12 MONTHS
15
20
25
30
35
40
45PE
AK
VO
2 (m
l/Kg/
min
)
*
Transplant Rehab Intervention Project(kidney)
interventionusual care
p<.01
Painter, et al: Transplantation 74:42-48, 2002
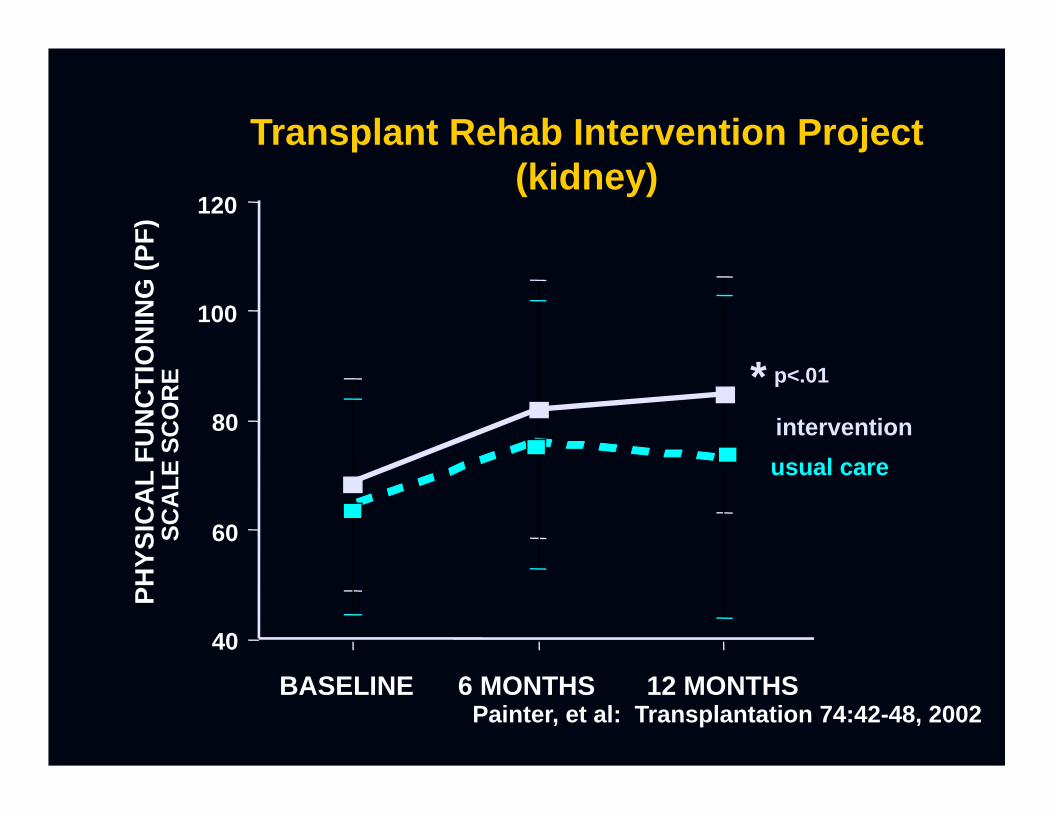
40
60
80
100
120
BASELINE 6 MONTHS 12 MONTHS
PHYS
ICA
L FU
NC
TIO
NIN
G (P
F)SC
ALE
SC
OR
E *interventionusual care
p<.01
Transplant Rehab Intervention Project(kidney)
Painter, et al: Transplantation 74:42-48, 2002
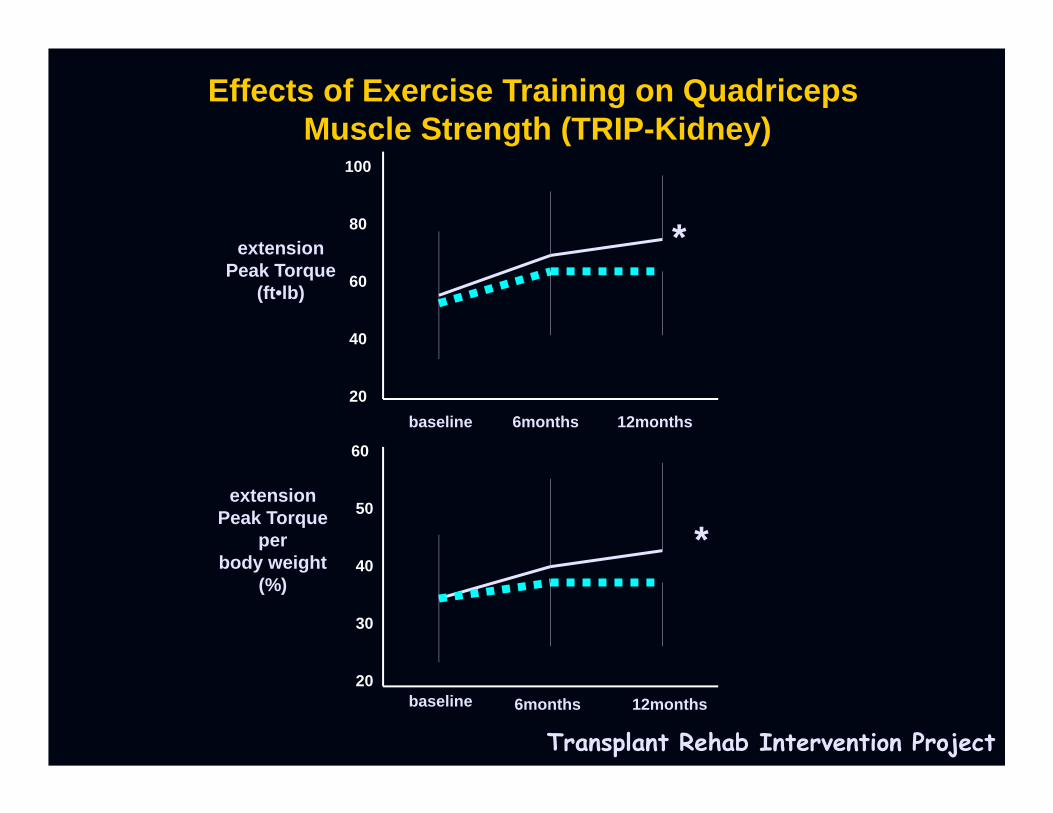
100
80
60
40
20
60
50
40
30
20
extensionPeak Torque
(ft•lb)
extensionPeak Torque
perbody weight
(%)
baseline
baseline
6months
6months
12months
12months
*
*
Transplant Rehab Intervention Project
Effects of Exercise Training on Quadriceps Muscle Strength (TRIP-Kidney)
50
40
30
20
10
0max
imal
oxy
gen
upta
ke (m
l/kg/
min
)
20 30 40 50 60 70
age
sedentary normal males
sedentary normal females
Before TransplantAfter TransplantTrained after Transplant
Oxygen Uptake in Adult Transplant Recipients
transplant gamesathletes
randomizedcontrolled trial
trained for transplant games
competition
Exercise initiated2wks post tx - 1 year
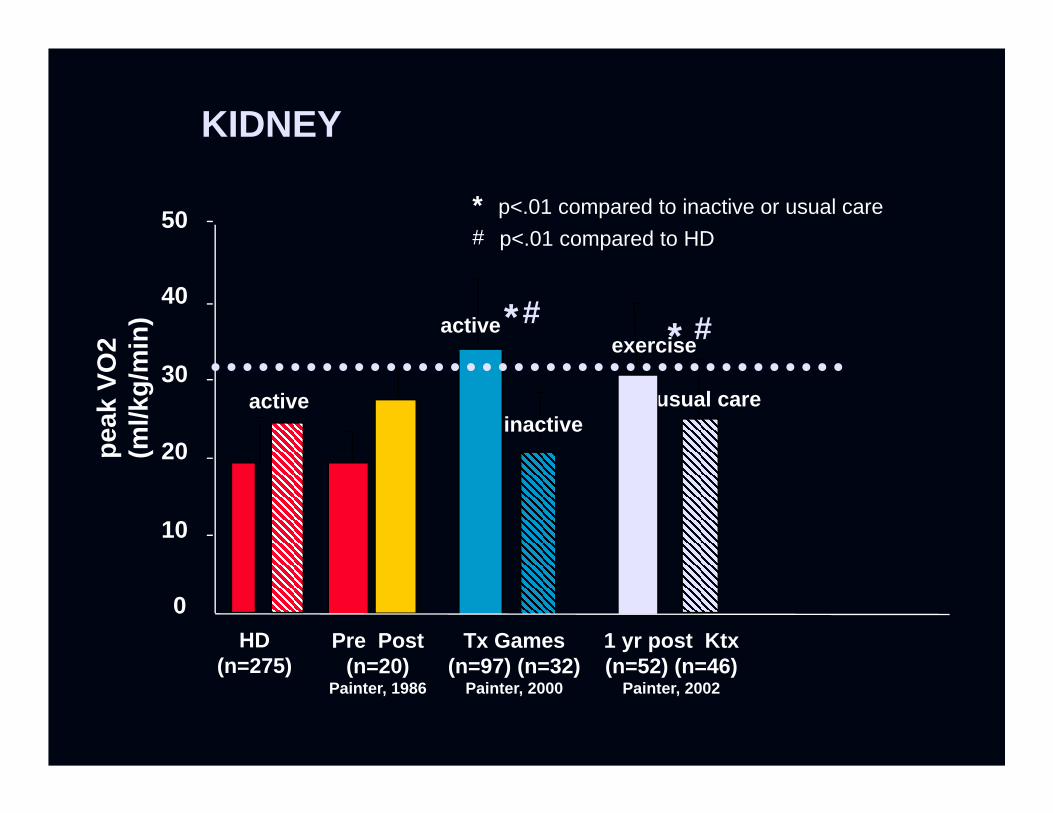
usual care
exercise
1 yr post Ktx(n=52) (n=46)
Painter, 2002
* #
HD(n=275)
Pre Post(n=20)
Painter, 1986
KIDNEY
inactive
active
Tx Games(n=97) (n=32)
Painter, 2000
*#
* p<.01 compared to inactive or usual care# p<.01 compared to HD
0
10
20
30
40
50
peak
VO
2(m
l/kg/
min
)
active
A Randomized Trial of Exercise Training following Liver
Transplantation
Patricia Lynn Painter Joanne B. Krasnoff
Andrea VintroMarylin DoddSteven Paul
Nancy Ascher
Krasnoff Transplantation 2006Transplant Rehab Intervention ProjectNIH-NINR R01 NR04120
to determine the effects of an intervention of diet and exercise training over the first year
post liver transplant on health-related fitness (cardiorespiratory fitness, muscle strength, body composition and health-related quality
of life).
Transplant Rehab Intervention Project
Purpose:
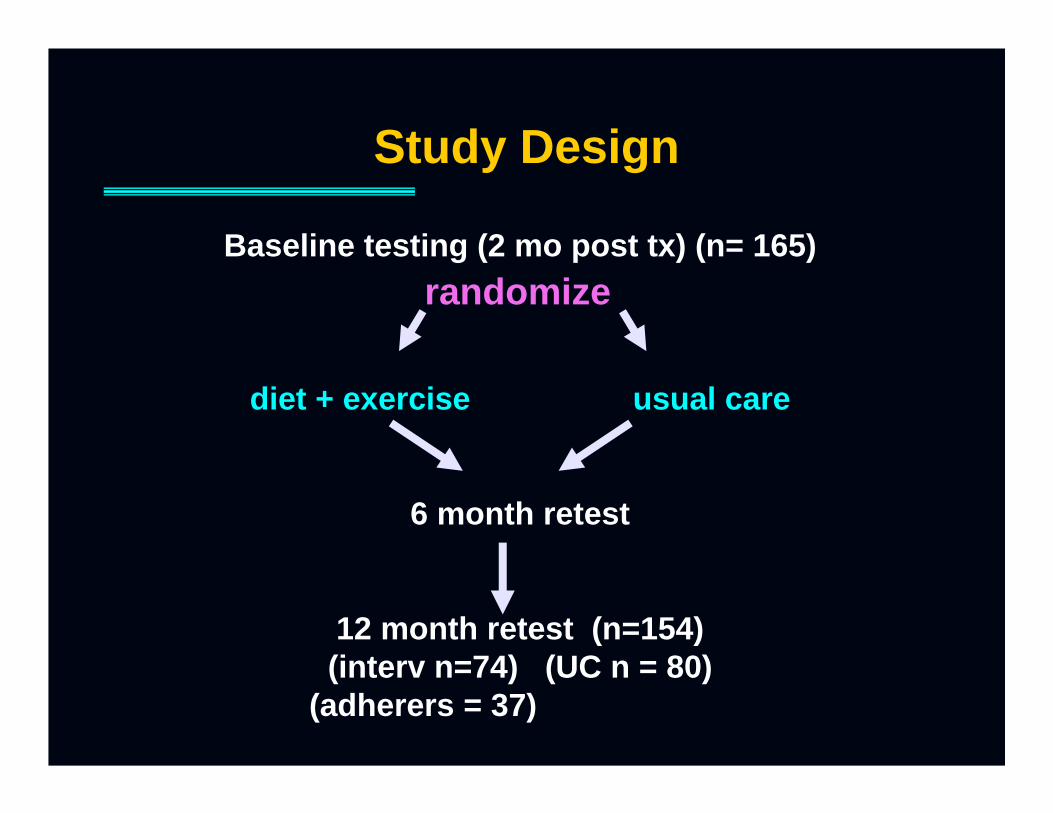
Study Design
Baseline testing (2 mo post tx) (n= 165)
diet + exercise usual care
6 month retest
12 month retest (n=154)(interv n=74) (UC n = 80)
(adherers = 37)
randomize
Testing Maximal Treadmill testing with VO2 measurements Isokinetic Muscle testing Dexa (% fat, lean mass, fat mass) SF-36 Questionnaire Food Frequency Questionnaire
Intervention Independent Home Exercise
cardiovascular 3x or more/week 30 min or more/session
AHA Step I-II diet Transplant Rehab Intervention Project
Bimonthly Phone Follow-up:
Exercise physiologistReg Dietitian
• Adherers: those who followed the exercise prescription for frequency, intensity and duration > 50%of the time. • Non adherers: those who participated in exercise at the prescribed frequency, intensity and duration <50% of the time.
Transplant Rehab Intervention Project(liver)
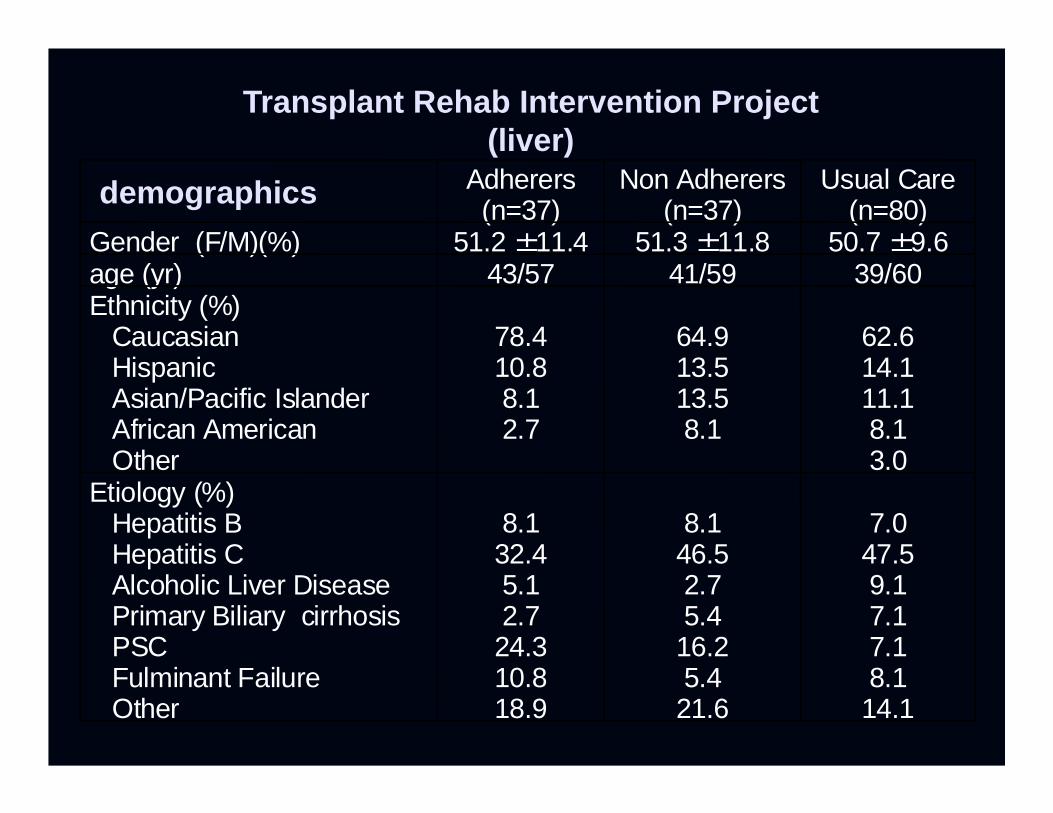
Adherers(n=37)
Non Adherers(n=37)
Usual Care(n=80)
Gender (F/M)(%) 51.2 ±11.4 51.3 ±11.8 50.7 ±9.6age (yr) 43/57 41/59 39/60Ethnicity (%)
CaucasianHispanicAsian/Pacific IslanderAfrican AmericanOther
78.410.88.12.7
64.913.513.58.1
62.614.111.18.13.0
Etiology (%)Hepatitis BHepatitis CAlcoholic Liver DiseasePrimary Biliary cirrhosisPSCFulminant FailureOther
8.132.45.12.7
24.310.818.9
8.146.52.75.4
16.25.4
21.6
7.047.59.17.17.18.1
14.1
Transplant Rehab Intervention Project(liver)
demographics

10
15
20
25
30
35
usual care
nonadherers
adherers
baseline 6 month 12 month
*p<.002
Transplant Rehab Intervention Project(liver)
Recommendations for Physical Activity for Treating Medical Conditions
Regular Exercise is Recommended in National Guidelines for the following conditions: Hypertension (JNC VII)
JAMA 289:2560-2572,2003 Hyperlipidemia (NCEP III)
JAMA 285:2486-2497, 2001 Cardiovascular Disease (NIH consensus Conference,
1993) American Diabetes Association
Ruderman N, Devlin JT, Schneider SH, Krisra A, (Ed) Handbook of Exercise in Diabetes. Alexandria, VA, American Diabetes Association, 2002
KDOQI (Kidney Disease outcomes Quality Initiative)Cardiovascular Disease Practice Guidelines
GUIDELINE 14.2:All dialysis patients should be counseled and regularly encouraged by nephrology and dialysis staff to increase their level of physical activity
Need Similar Practice Guideline for Post Transplant Care
Reasons for Recommending and Encouraging Physical Activity following Transplant
Present for transplant with low levels of functioning
Present for transplant physically inactive High prevalence of cardiovascular risk factors that
may be modified by physical activity May attenuate weight gain Will OPTIMIZE functioning
Will positively impact QOL
? Improve transplant outcomes?
Reasons for Recommending and Encouraging Physical Activity following Transplant
(and for having a trained exercise physiologist as part of the care team)
They are afraid to exert themselves
They don’t know what to do for exercise They are weak, low functioning - need appropriate
prescription for type, progression of exercise They need regular encouragement
Will be a part of an overall positive lifestyle expectation following transplant
Will provide an added level of medical surveillance
No information or encouragement is given for exercise...
MESSAGES: How they are interpreted byPatients and/or Families
No information or encouragement is given for exercise.
Exercise must not be important for people on dialysis or after transplant …..they didn’t say anything
hmmm ….????
“TAKE IT EASY”
Maybe I shouldn’t do anything…I need to takeit easy!!!
“DON’T OVERDO IT”
Wow, maybe I shouldn’tbe doing anything, sinceI might overdo it…???*
*Patients may not know what Their limits are, so they may feelThat anything may be ‘overdoing it”
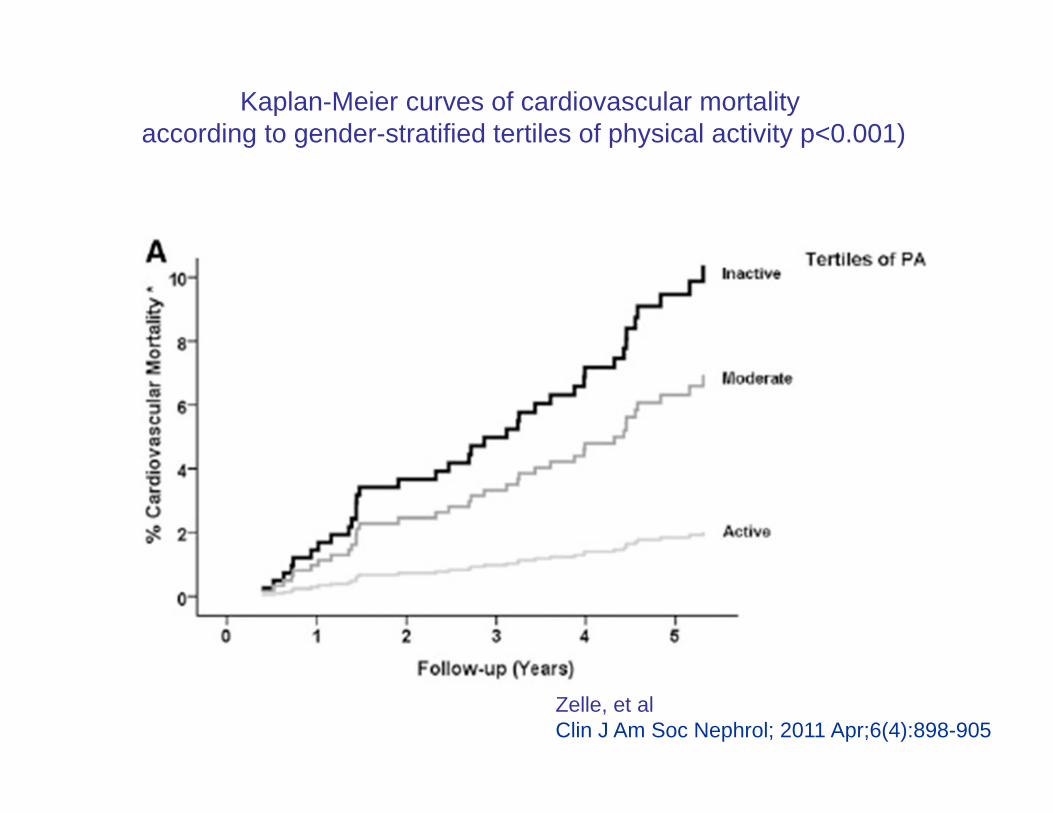
Kaplan-Meier curves of cardiovascular mortality
according to gender-stratified tertiles of physical activity p<0.001)
Zelle, et al Clin J Am Soc Nephrol; 2011 Apr;6(4):898-905
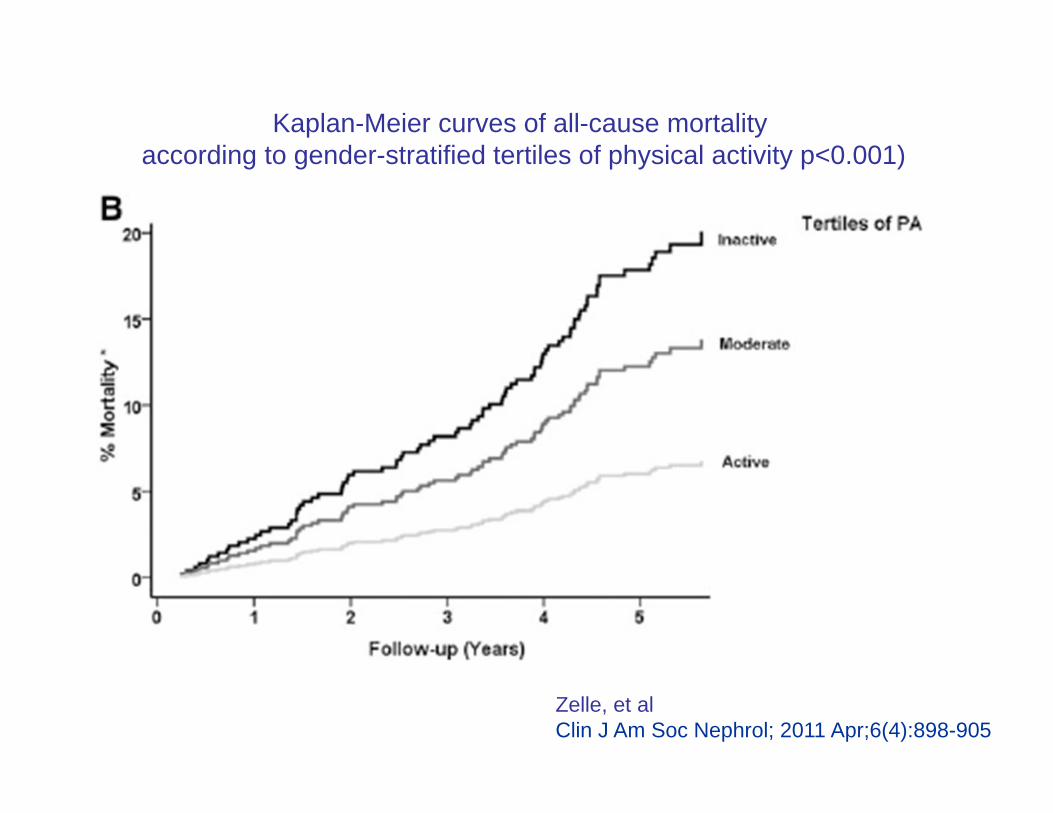
Kaplan-Meier curves of all-cause mortality according to gender-stratified tertiles of physical activity p<0.001)
Zelle, et al Clin J Am Soc Nephrol; 2011 Apr;6(4):898-905
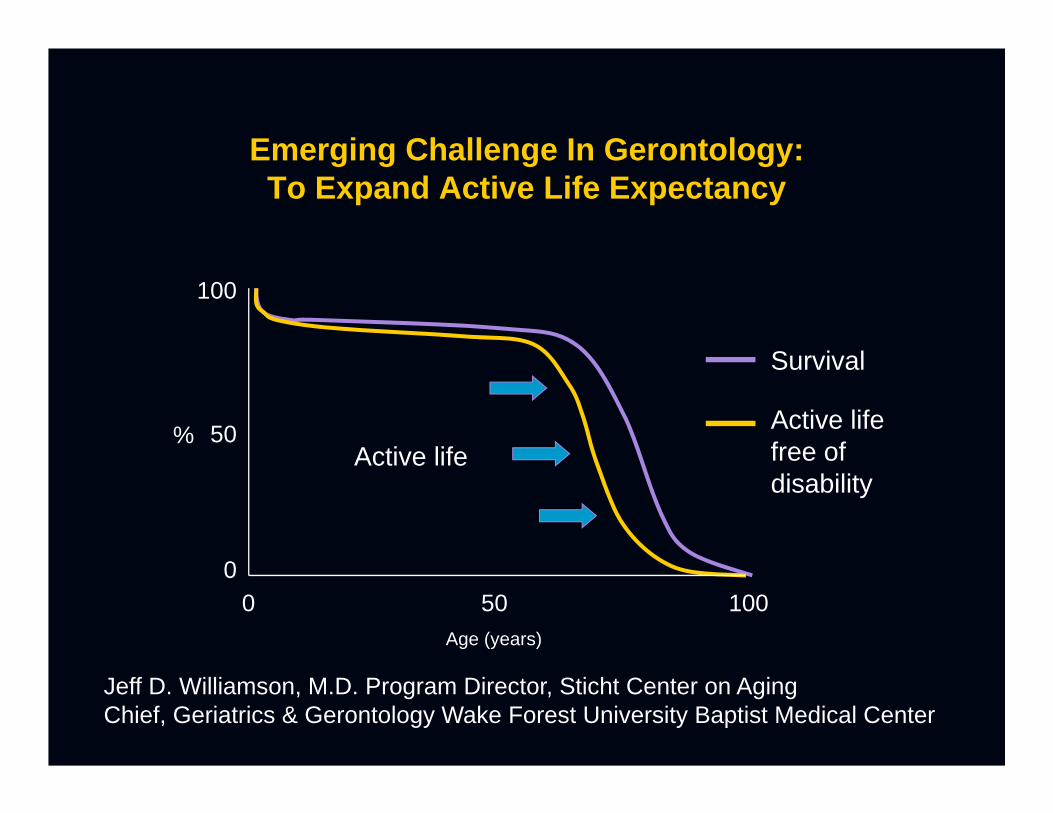
Emerging Challenge In Gerontology: To Expand Active Life Expectancy
0 10050Age (years)
0
100
50%Active life
Survival
Active life free of disability
Jeff D. Williamson, M.D. Program Director, Sticht Center on AgingChief, Geriatrics & Gerontology Wake Forest University Baptist Medical Center
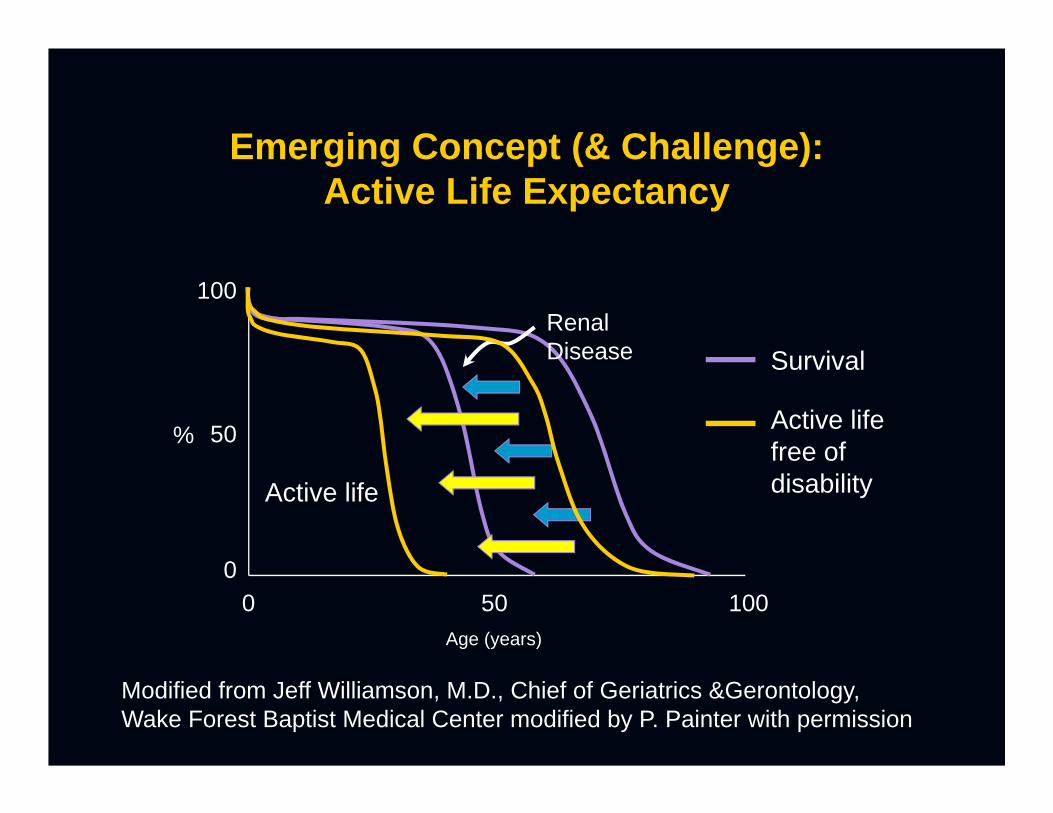
Emerging Concept (& Challenge): Active Life Expectancy
0 10050Age (years)
0
100
50%
Active life
Survival
Active life free of disability
Renal Disease
Modified from Jeff Williamson, M.D., Chief of Geriatrics &Gerontology,Wake Forest Baptist Medical Center modified by P. Painter with permission
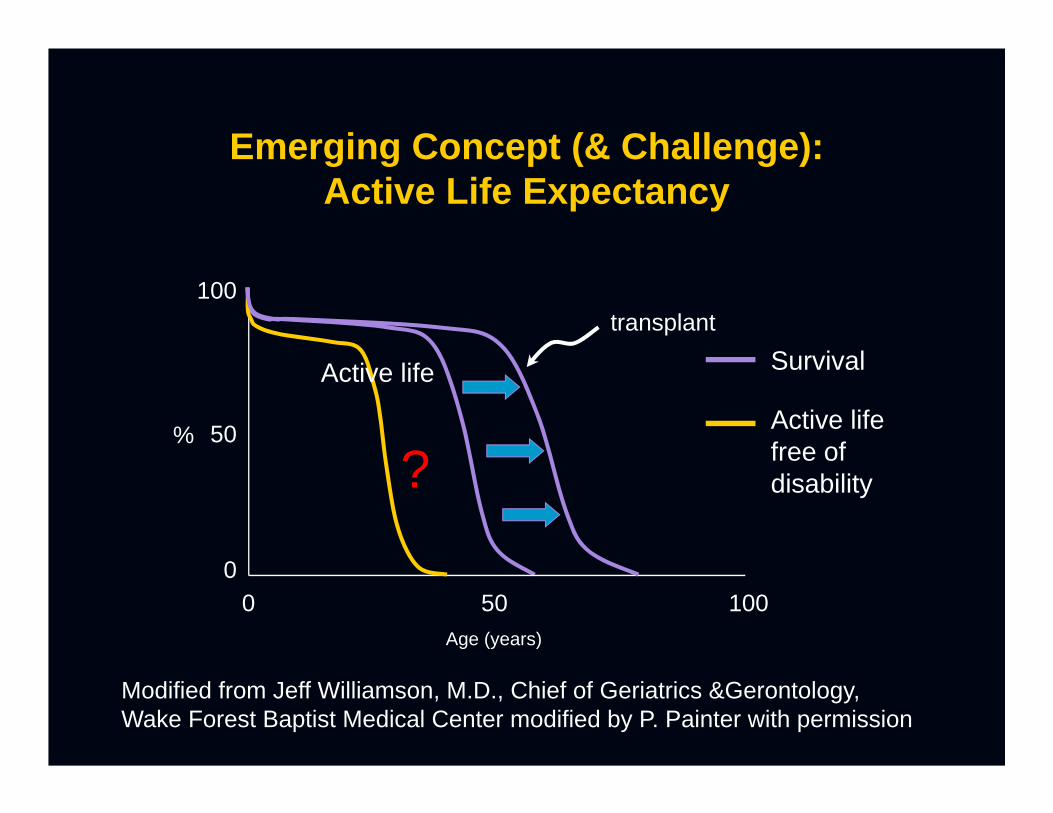
Emerging Concept (& Challenge): Active Life Expectancy
0 10050Age (years)
0
100
50%
Survival
Active life free of disability
transplant
Active life
?
Modified from Jeff Williamson, M.D., Chief of Geriatrics &Gerontology,Wake Forest Baptist Medical Center modified by P. Painter with permission
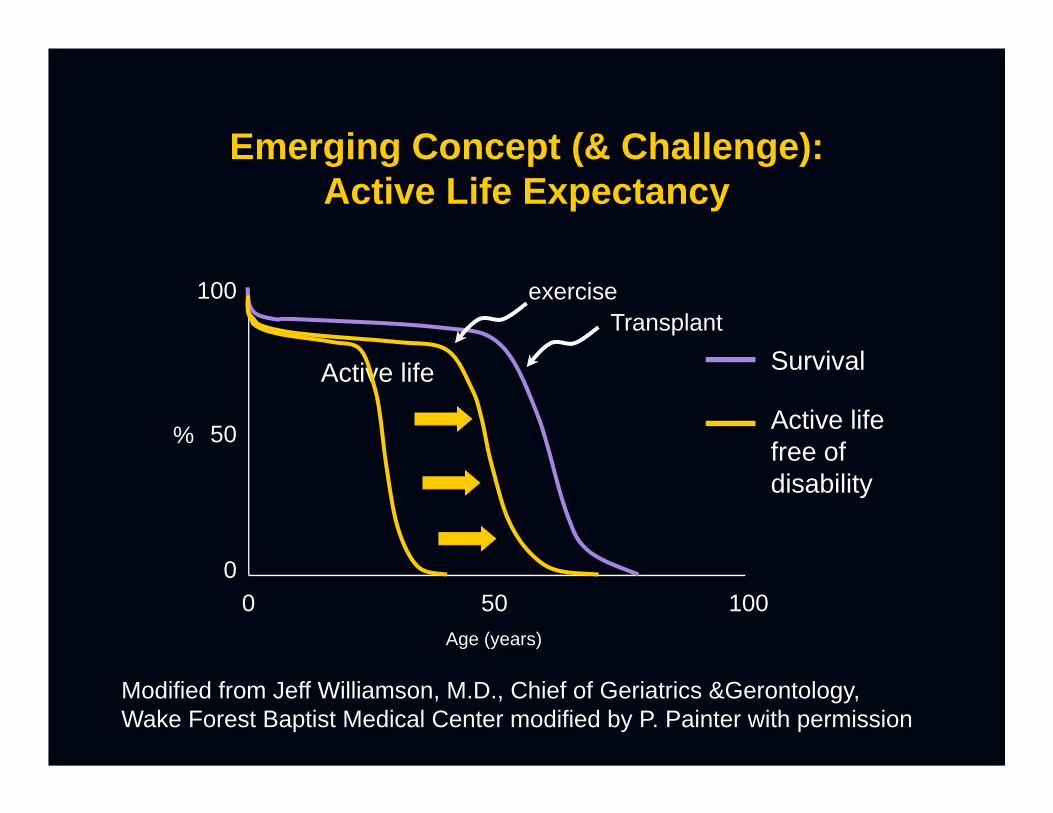
Emerging Concept (& Challenge): Active Life Expectancy
0 10050Age (years)
0
100
50%
Active life Survival
Active life free of disability
Transplant
Modified from Jeff Williamson, M.D., Chief of Geriatrics &Gerontology,Wake Forest Baptist Medical Center modified by P. Painter with permission
exercise


Thanks for your attention....
Let’s get them MOVING!
Related Documents











