Treatment of fistula in ano Abhilash

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Treatment of fistula in ano
Abhilash


Principles
• Control sepsis– EUA– Laying open abscesses and secondary tracts.– Adequate drainage- seton insertion.
• Define anatomy– Openings and tracts
• Internal and external• Single vs. multiple• Extensions / Horseshoe
– Relation to sphincter complex• High vs. low
• Exclude co-existent disease.

Complex fistulas.• Any fistula involving more than 30 percent of the external sphincter• Suprasphincteric fistulas• Extrasphincteric or high fistulas, proximal to the dentate or pectinate line• Women with anterior fistulas• Fistulas with multiple tracts• Recurrent fistulas• Fistulas related to inflammatory bowel disease• Fistulas related to infectious diseases including tuberculosis and human
immunodeficiency virus• Fistulas secondary to local radiation treatments• Patients with a history of anal incontinence• Rectovaginal fistulas

• Simple fistulas– Fibrin glue– Fistulotomy.
• Complex fistulas– Fistulotomy and seton.– LIFT– Advancement flaps.– Fistula plug.

Fistulotomy
• Fistula tract identified with probe
• E0xtent of external sphincter involvement assessed.
• laying open the fistula tract.
• Secondary tracts laid open• +/- marsupialization

• Success rates range from 79-100 percent in various studies.
• Recurrence rate in simple fistulas – 3- 7%• Incontinence varies from 0-18%.

• No difference in results between Fistulotomy and fistulectomy.
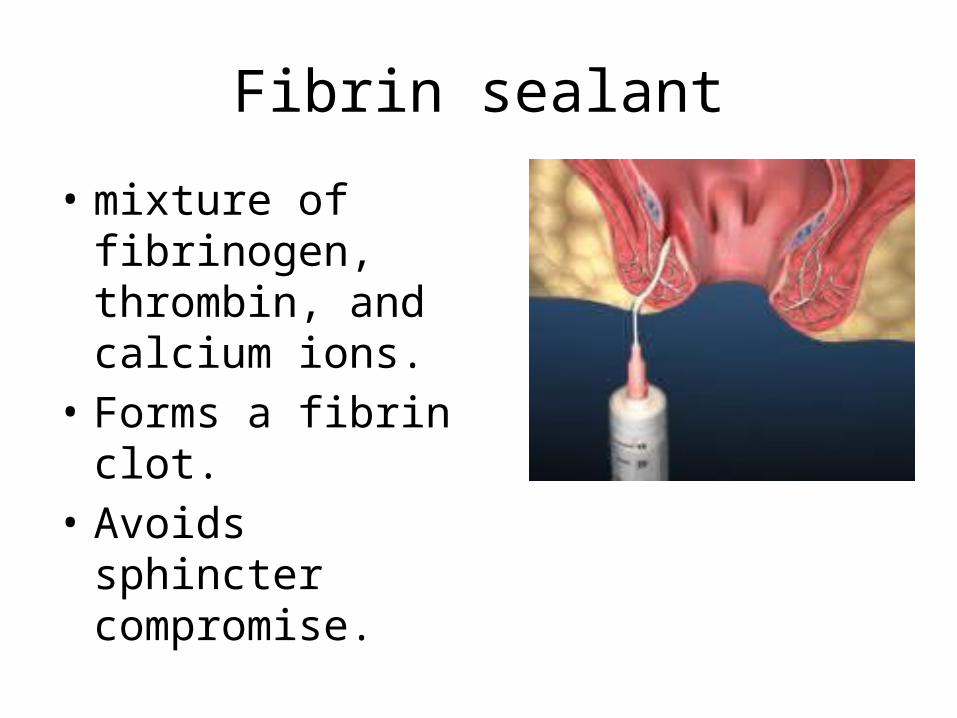
Fibrin sealant
• mixture of fibrinogen, thrombin, and calcium ions.
• Forms a fibrin clot.• Avoids sphincter
compromise.

• Recurrence rates of 14-69%.• Most recurrences are evident within 3
months.• Not recommended for complex fistulas.

Seton
• Any foreign material that encircles the sphincter complex.
• Silk, penrose drains, sialastic vessel tubes, nylon, polypropylene, braided steel wire., rubber band.
• Useful in complex fistulas, crowns, anterior fistulas and chronic diarrheal states.
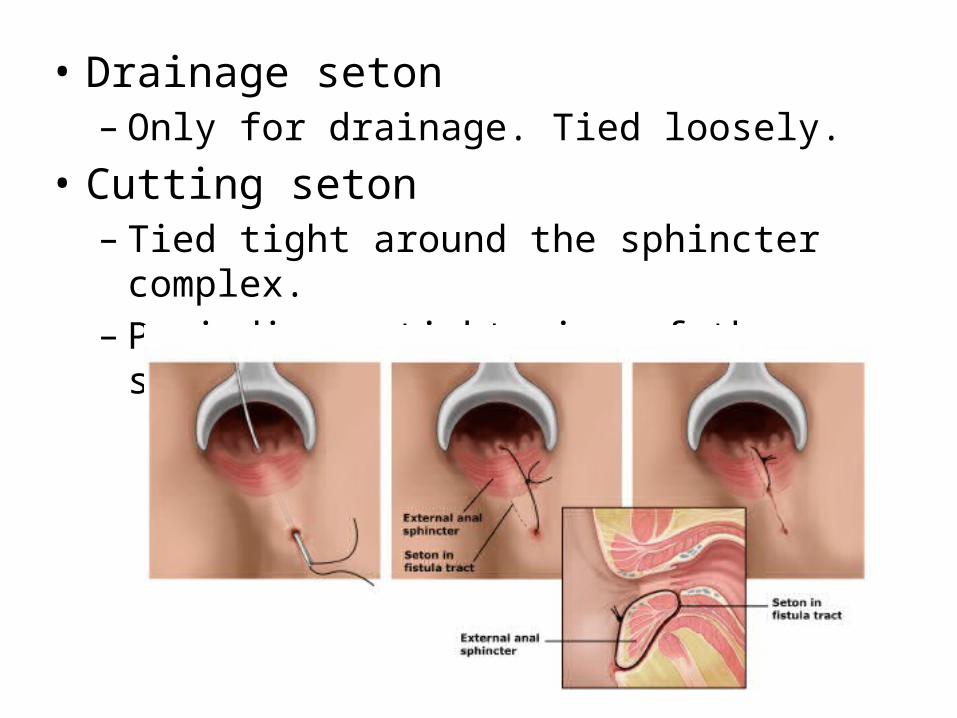
• Drainage seton– Only for drainage. Tied loosely.
• Cutting seton– Tied tight around the sphincter complex.– Periodic re-tightening of the seton.

• Success rates from 80-100 %.• Long term incontinence rate – 30%• Draining seton – poor quality of life and low
grade incontinence.

Fistula plug
• bio absorbable xenograft made of lyophilized porcine intestinal submucosa.
• Success rate of 35% to 87%.• Expensive
Advancement flap
• Consists of mucosa, submucosa and internal sphincter.
• Advantages.– One stage procedure.– Quicker healing– Minimal risk of anal canal deformity– Limited damage to sphincter.


• Success rate in literature 29-95%.• Cleveland clinic – 64% success rate.• Success rate drops with successive attempts.• Good functional results in most reports.

LIFT (Ligation of intersphincteric fistula tract)
• Sphincter sparing procedure.
• For complex transsphincteric fistulas
• Primary healing rate-62%
• No incontinence.


Other options
• Cutaneous flaps– V-Y flap– Island flap
• Chemical seton

References
• Shackelfords Surgery of the alimentary tract.• Jacob TJ, Perakath B, Keighley MR. Surgical
intervention for anorectal fistula. Cochrane Database of Systematic Reviews 2010, Issue 5.
• Dis Colon Rectum. 2013 Mar;56(3):343-7.• Dis Colon Rectum. 2008;51(10):1475.
Related Documents











