1527 ISSN 1757-6180 Bioanalysis (2009) 1(9), 1527–1535 10.4155/BIO.09.112 © 2009 Future Science Ltd ReseaRch aRticle Interest in hepatocyte transplantation has been growing continuously in recent years and this treatment might represent an alternative clini- cal approach for patients with acute liver fail- ure and liver-based metabolic disorders, such as ornithine transcarbamylase deficiency (OTC) [1] . OTC is the most common urea cycle defect observed in humans and it can be a life-threat- ening X-linked inborn error of metabolism. It results in impaired urea formation and the ele- vation of endogenous ammonia, in severe cases to fatal levels. The indication and timing for liver transplantation in such metabolic disorders depends on the underlying cause. Some meta- bolic disorders cause progressive liver injury, eventually leading to cirrhosis [2] . In severe metabolic cases, it has been recommended that auxiliary partial orthotopic liver transplantation (APOLT) be made as early as possible to avoid liver failure [3,4] . Even in less-severe cases, when treated with nitrogen scavengers, impairment of the urea cycle leads to reduced bioavailability of de novo ornithine and arginine. Isolated dietary interventions are generally ineffective and so the use of liver cell infusions to replenish the deficient liver enzymes has been proposed [5–7] . For both cell and liver transplantation, there is a critical need to monitor and evaluate graft function and the biochemical effect of therapy. NMR-based metabonomic techniques can help to follow therapeutic response, since the use of 1 H NMR spectroscopy as a method for determin- ing profiles of endogenous metabolites present in biofluids such as urine, blood plasma and, more recently, intact tissues is well established [8–11] . As such, the technique has been widely employed in the characterization of the metabolic conse- quences of disease or toxic insult [12–15] and to several inborn errors of metabolism [16,17] . When combined with advanced methods of data pro- cessing and chemometrics, it has proved to be a useful method for disease diagnosis and biomarker identification [18] . This case study describes the use of 1 H NMR spectroscopy-based metabonomics to assess the metabolic consequences of the first com- bined treatment by hepatocyte infusion and APOLT performed on an infant with severe OTC deficiency. Materials & methods Patient An 18-year-old full-term primigravida, asymp- tomatic and heterozygous for OTC deficiency, was referred to the Pediatric Liver Centre. There was a significant history of OTC deficiency in her family. Her brother and niece had died within the first week of life of hyperammone- mic encephalopathy and severe cerebral edema. She was pregnant with a male fetus and the mutation IVS7 + 3A>G had been identified in a fetal blood sample, confirming the diagnosis of OTC deficiency. The infant was delivered at term in good condition (Apgar scores of 9 at 1 min and 10 at 5 min) with a birth weight of 3.85 kg. The initial blood ammonia level was First example of hepatocyte transplantation to alleviate ornithine transcarbamylase deficiency, monitored by NMR-based metabonomics We demonstrate the effective use of NMR spectroscopic profiles of urine and plasma from the first successful use of hepatocyte transplantation as a bridge to auxiliary partial orthotopic liver transplantation in a child antenatally diagnosed with severe ornithine transcarbamylase deficiency. In this single-patient study, NMR profiles indicated that the disrupted urea cycle could be normalized by hepatocyte cell infusion and this was confirmed using orthogonal partial least-squares- based chemometrics. However, despite dietary manipulations and adminstration of ammonia scavengers, the desired reduction in plasma ammonia was not consistently achieved between sessions of hepatocyte transplantation due to episodes of sepsis. A subsequent liver transplant corrected the metabolic abnormalities. The use of metabolic profiling has been shown to be a promising method for evaluating the efficacy of cell infusions and has demonstrated the capability for the early detection of response to therapy in real time, an approach that may be of use in wider clinical settings. Cristina Legido-Quigley 1,4† , Olivier Cloarec 1 , David A Parker 1 , Gerard M Murphy 1 , Elaine Holmes 1 , John C Lindon 1 , Jeremy K Nicholson 1 , Ragai R Mitry 2 , Hector Vilca-Melendez 2 , Mohamed Rela 2 , Anil Dhawan 3 & Nigel Heaton 2† † Authors for correspondence 1 Department of Biomolecular Medicine, Faculty of Medicine, Sir Alexander Fleming Building, Imperial College, London, UK E-mail: cristina.legido_quigley@ kcl.ac.uk 2 Liver Transplant Surgical Service, Institute of Liver Studies, King’s College Hospital, Denmark Hill, London, UK E-mail: [email protected] 3 Paediatric Liver Centre, King’s College Hospital, Denmark Hill, London, UK 4 Pharmaceutical Science Division, King’s College London, UK For reprint orders, please contact [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1527ISSN 1757-6180Bioanalysis (2009) 1(9), 1527–1535 10.4155/BIO.09.112 © 2009 Future Science Ltd
ReseaRch aRticle
Interest in hepatocyte transplantation has been growing continuously in recent years and this treatment might represent an alternative clini-cal approach for patients with acute liver fail-ure and liver-based metabolic disorders, such as ornithine transcarbamylase deficiency (OTC) [1]. OTC is the most common urea cycle defect observed in humans and it can be a life-threat-ening X-linked inborn error of metabolism. It results in impaired urea formation and the ele-vation of endogenous ammonia, in severe cases to fatal levels. The indication and timing for liver transplantation in such metabolic disorders depends on the underlying cause. Some meta-bolic disorders cause progressive liver injury, eventually leading to cirrhosis [2]. In severe metabolic cases, it has been recommended that auxiliary partial orthotopic liver transplantation (APOLT) be made as early as possible to avoid liver failure [3,4]. Even in less-severe cases, when treated with nitrogen scavengers, impairment of the urea cycle leads to reduced bioavailability of de novo ornithine and arginine. Isolated dietary interventions are generally ineffective and so the use of liver cell infusions to replenish the deficient liver enzymes has been proposed [5–7].
For both cell and liver transplantation, there is a critical need to monitor and evaluate graft function and the biochemical effect of therapy. NMR-based metabonomic techniques can help to follow therapeutic response, since the use of 1H NMR spectroscopy as a method for determin-ing profiles of endogenous metabolites present in
biofluids such as urine, blood plasma and, more recently, intact tissues is well established [8–11]. As such, the technique has been widely employed in the characterization of the metabolic conse-quences of disease or toxic insult [12–15] and to several inborn errors of metabolism [16,17]. When combined with advanced methods of data pro-cessing and chemometrics, it has proved to be a useful method for disease diagnosis and biomarker identification [18].
This case study describes the use of 1H NMR spectroscopy-based metabonomics to assess the metabolic consequences of the first com-bined treatment by hepatocyte infusion and APOLT performed on an infant with severe OTC deficiency.
Materials & methods�� Patient
An 18-year-old full-term primigravida, asymp-tomatic and heterozygous for OTC deficiency, was referred to the Pediatric Liver Centre. There was a significant history of OTC deficiency in her family. Her brother and niece had died within the first week of life of hyperammone-mic encephalopathy and severe cerebral edema. She was pregnant with a male fetus and the mutation IVS7 + 3A>G had been identified in a fetal blood sample, confirming the diagnosis of OTC deficiency. The infant was delivered at term in good condition (Apgar scores of 9 at 1 min and 10 at 5 min) with a birth weight of 3.85 kg. The initial blood ammonia level was
First example of hepatocyte transplantation to alleviate ornithine transcarbamylase deficiency, monitored by NMR-based metabonomics
We demonstrate the effective use of NMR spectroscopic profiles of urine and plasma from the first successful use of hepatocyte transplantation as a bridge to auxiliary partial orthotopic liver transplantation in a child antenatally diagnosed with severe ornithine transcarbamylase deficiency. In this single-patient study, NMR profiles indicated that the disrupted urea cycle could be normalized by hepatocyte cell infusion and this was confirmed using orthogonal partial least-squares-based chemometrics. However, despite dietary manipulations and adminstration of ammonia scavengers, the desired reduction in plasma ammonia was not consistently achieved between sessions of hepatocyte transplantation due to episodes of sepsis. A subsequent liver transplant corrected the metabolic abnormalities. The use of metabolic profiling has been shown to be a promising method for evaluating the efficacy of cell infusions and has demonstrated the capability for the early detection of response to therapy in real time, an approach that may be of use in wider clinical settings.
Cristina Legido-Quigley1,4†, Olivier Cloarec1, David A Parker1, Gerard M Murphy1, Elaine Holmes1, John C Lindon1, Jeremy K Nicholson1, Ragai R Mitry2, Hector Vilca-Melendez2, Mohamed Rela2, Anil Dhawan3 & Nigel Heaton2† †Authors for correspondence1Department of Biomolecular Medicine, Faculty of Medicine, Sir Alexander Fleming Building, Imperial College, London, UKE-mail: [email protected] Transplant Surgical Service, Institute of Liver Studies, King’s College Hospital, Denmark Hill, London, UK E-mail: [email protected] 3Paediatric Liver Centre, King’s College Hospital, Denmark Hill, London, UK 4Pharmaceutical Science Division, King’s College London, UK
For reprint orders, please contact [email protected]

ReseaRch aRticle | Legido-Quigley, Cloarec, Parker et al.
Bioanalysis (2009) 1(9)1528 future science group
76 µmol/l. Shortly after birth, an umbilical venous catheter and a peripheral venous can-nula were inserted. He was commenced on intravenous dextrose, sodium phenylbutyrate (250 mg/kg/day), sodium benzoate (250 mg/kg/day), arginine (100 mg/kg/day) supplementation and maintained on a restricted protein intake (0.75 g/kg/day) [3].
�� Infusion of hepatocytes Hepatocyte transplantation was performed in the pediatric intensive care unit, under continu-ous cardiovascular and transcutaneous oxygen saturation monitoring. Sedation of the patient was not required during the cell infusions. The infusion of hepatocytes was redirected into the portal vein under angiographic guidance. The infant received a total of 1.74 × 109 hepatocytes (1.57 × 109 viable cells), estimated to be equiva-lent to approximately 5% of his liver mass. Cell viability was assessed by the trypan blue exclusion test (median 93%; range 85–95%) before each infusion. Seven cell infusions were performed within the first month of life into the portal vein. One further infusion was performed 5 months later via percutaneous transhepatic puncture of the portal vein. Isolated hepatocytes were resuspended in transplant medium containing heparin (1 IU/ml) and human serum albumin (4% final concentration) at a concentration of approximately 10 × 106 cells/ml [3].
�� Collection & preparation of samples for 1H NMR spectroscopy Plasma samples were collected on 14 days over the 350-day treatment period: days 0, 2, 3, 4, 5, 6, 7, 10, 28, 35, 59, 98, 105 (before transplanta-tion) and 350 (after transplantation). On each of the study days 2–5, urine samples were collected at noon from urinary bags, which had accumu-lated sample over the previous night. Plasma sam-ples (150 µl) were placed in 5-mm NMR tubes together with 350 µl of aqueous 0.9% NaCl (20% D
2O). Urine samples for NMR spectroscopy were
made up from 400 µl of urine and 200 µl of buf-µl of urine and 200 µl of buf- of urine and 200 µl of buf-µl of buf- of buf-fer solution (0.2 M Na
2HPO
4/0.2 M NaH
2PO
4,
pH 7.4) mixed in a microcontainer and the result-ing solution left to stand for 10 min. The buffered urine samples were then centrifuged at 13,000 rpm for 10 min to remove any precipitates, and aliquots of the resulting supernatant (500 µl) were placed in 5-mm NMR tubes, to which 50 µl of a solution of sodium 3-trimethylsilyl-(2,2,3,3–2H
4)-1-propionate in D
2O was added (to a final
concentration of 1 mM).
�� NMR spectroscopic analysis of plasma & urine samplesThe samples were analyzed at 298 K by 1H NMR spectroscopy at 600.29 MHz using a Bruker Avance 600 spectrometer (Bruker Biospin Ltd, Coventry, UK). Standard 1D, Carr–Purcell–Meiboom–Gill (CPMG) spin-echo, J-resolved (JRES) and 1H-1H total correlation pulse sequences were used with presaturation of the water signal [9]. D
2O provided a deuterium lock
signal for the NMR spectrometer and the TSP served as a chemical-shift reference (d 0.0) in urine. Chemical shifts in the plasma NMR spec- Chemical shifts in the plasma NMR spec-Chemical shifts in the plasma NMR spec-tra were referenced to the doublet signal at d 1.33 from the methyl group of lactate.
1D 1H NMR spectra of urine were measured using a standard pulse sequence with solvent presaturation suppression (relaxation decay [RD]-90°-t
1-90°-mixing time [t
m]-90°-acquire
free-induction delay [FID], t1 = 3 µs, tm =
100 ms) [9]. A total of 128 FIDs were collected into 32 k data points using a spectral width of 12019 Hz, an acquisition time of 1.36 s and a relaxation delay of 2 s. An irradiation was applied to the water resonance frequency during the RD and the t
m. The FIDs were multiplied
by an exponential weighting function corre-sponding to a line broadening of 0.3 Hz prior to Fourier transformation (FT). Additionally, for plasma samples, CPMG spin-echo spectra were acquired (with presaturation water suppres-sion) with 128 scans after 16 dummy scans into 64 k data points with a total spin–spin relaxation delay (2nt) of 120 ms and a total pulse recycle delay of 6.25 s. The FIDs were multiplied by an exponential function, corresponding to a 0.3 Hz line broadening prior to FT.
To aid spectral assignment, 2D JRES spectra were recorded on all samples and 1H-1H total correlation spectra were recorded for selected samples. JRES spectra with water presaturation were measured by acquiring 8 k data points with 64 transients for each of 64 increments, using spectral widths of 6000 Hz in the F2 dimension and 60 Hz in the F1 (J-coupling) dimension. Prior to FT, the FIDs were weighted in both dimensions by a sine-bell function (SSB = 0) and zero-filled in the F1 dimension to 256 data points. The spectra were tilted by 45° to provide orthogonality of the chemical shift and coupling constant axes, and subsequently symmetrized about the F1 axis. 1H-1H TOCSY spectra were acquired for selected samples using 128 scans into 4 k data points per increment for 256 increments, with F1 and F2 spectral widths of
ORnithine tRanscaRbamylase deficiency
Condition that kills one in two newborns affected with this deficiency in the first month of life
metabOnOmics
Quantitative measurement of the dynamic multiparametric metabolic response of living systems to pathophysiological stimuli or genetic modification
hepatOcyte tRansplantatiOn
Proposed for two types of situations: as gene therapy for a variety of inherited disorders expressed in the liver and as a treatment for liver failure due to any cause. We should continue to explore its use as a treatment for a number of genetic and nongenetic diseases

First hepatocyte transplant to alleviate ornithine transcarbamylase deficiency | ReseaRch aRticle
www.future-science.com 1529future science group
10,000 Hz. The relaxation delay between suc-cessive pulse cycles was 2 s and the mixing time of the MLEV spin-lock was 80 ms. The FIDs were multiplied by a shifted sine-bell2 function in both dimensions prior to FT.
1H NMR spectra of plasma and urine were manually phased and baseline corrected using XWINNMR 3.5 (Bruker Analytik, Rheinstetten, Germany). The spectra over the range of d 0.2–10.0 were imported into Matlab (Version 7, The Mathworks Inc., Natwick, MA, USA), using 42,000 data points. The data points corresponding to the water resonance (d 4.65–5.03) were removed. Normalization to the total sum of spectral integrals was carried out prior to pattern-recognition analyses.
�� Pattern recognition: modeling & interpretationThe multivariate pattern-recognition techniques used are based on the orthogonal partial least-squares–discriminant analysis (O-PLS–DA)approach with unit variance scaling [19,20]. O-PLS is a method for relating two data matri-ces, X (NMR data) and Y (clinical class variables as defined by acceptable [<50 µM] and unac-ceptable [>50 µM] plasma ammonia levels), by a linear multivariate model. O-PLS–DA explains the maximum separation between defined class samples Y using the data X, by decomposing the covariance matrix (YTX) into several PLS components. The O-PLS algorithm is derived from the PLS-regression method. In the O-PLS algorithm, the variation in X is decomposed into three parts, namely the variation in X that is related to Y, any systematic variation in X and any residual variation [19–21]. This leads to a model with a minimal number of predictive components defined by the number of degrees of freedom. O-PLS modeling was performed on the NMR data using the response informa-tion (clinical data) to derive predictive loadings, which are presented using a back-scaling model and have a similar shape to NMR spectra [22]. Within loadings plots, the degree of covariance and the correlation coefficient for each NMR variable or loading is defined by magnitude and the combination of direction and the color scale, respectively. The strength of the discrimination between treatment stages is assessed by the pre-dictability power of the model through the R2 and Q2 parameters [21,22], which have a maxi-mum value of 1. R2 is the fraction of the sum of squares explained by the model, while Q2 is the cross-validated value of R2.
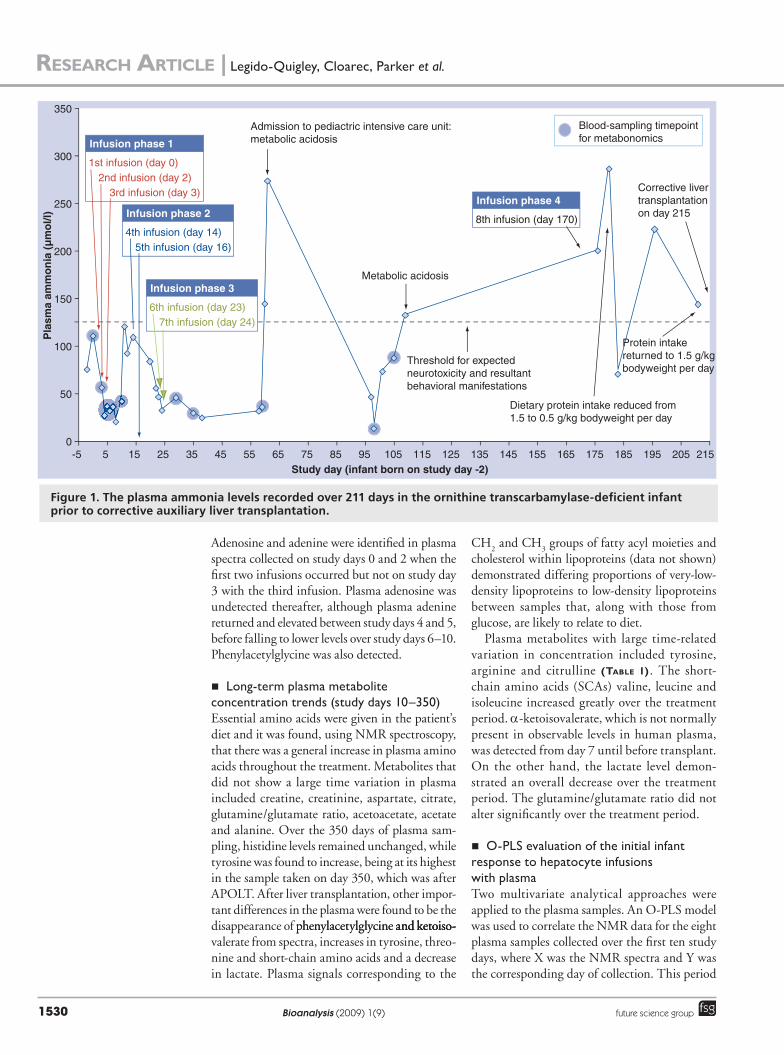
ResultsThe clinical procedure was regarded as suc-cessful by the medical team [3]. In patients with disturbances of the urea cycle, ammonia plasma levels lower than 50 µmol/l are desirable, with behavioral manifestations of neurotoxicity expected above 125 µmol/l. Following infusions, plasma ammonia levels were noted to initially fall (figuRe 1). The first-phase infusions reduced plasma ammonia to below 50 µmol/l for 8 days before an elevation, while the second-phase infu-infu-sions reduced and maintained plasma ammonia at 56 µmol/l. The third-phase infusions reduced plasma ammonia to below 50 µmol/l for 36 days. Periods of poor control of ammonia levels were observed during lapses of sepsis.
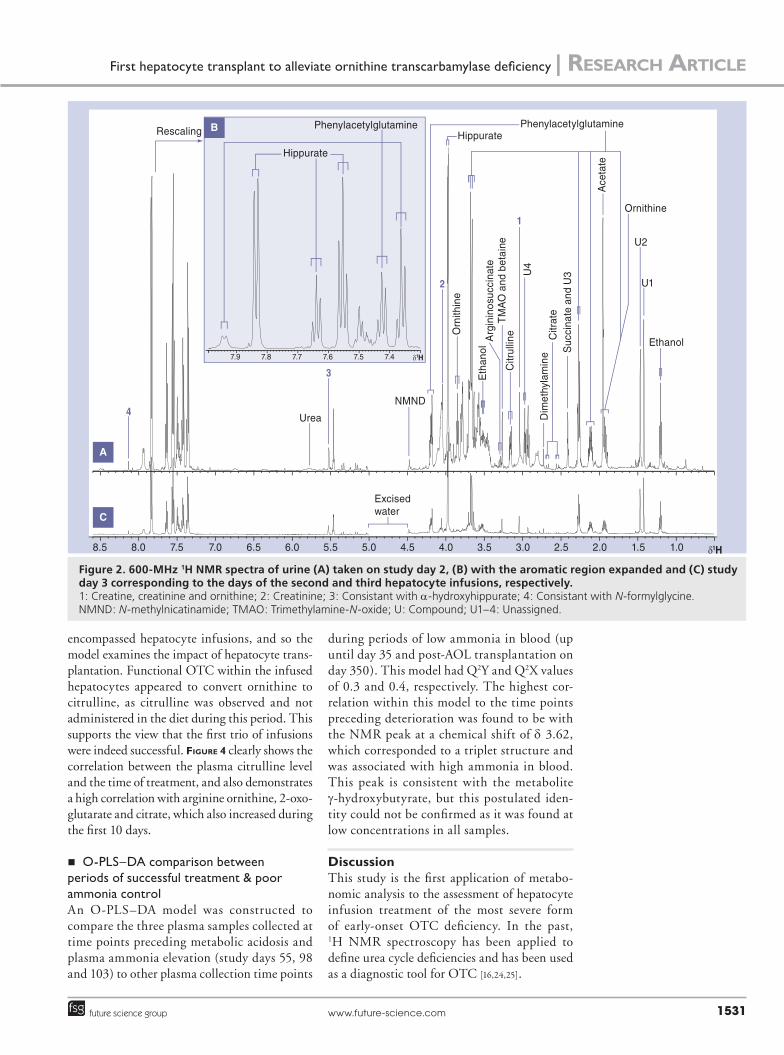
�� Short-term urinary metabolite concentration trends (study days 2–5)The metabolic response to the first phase of hepa-tocyte infusions (occurring on study days 0, 2 and 3) could be monitored through the varying metabolite profiles defined in the NMR spectra. Typical urine 1H NMR spectra are illustrated for study days 2 and 3 in figuRe 2. Increased urinary excretion of glucose, citrulline, arginosuccinate, succinate and acetate were observed after the first infusion phase. After the first urine sample, the urine NMR spectra remained constant for the 4 days subsequently sampled in terms of peak intensities for many endogenous metabolites. Citrulline was not administered during this time-span and so its initial presence suggests biochemical activity of functional OTC within infused hepatocytes. As urinary concentrating ability in humans is believed to be lowest at birth [23], the creatinine concentration of all the urine samples was determined and it was found that creatinine concentration was slightly lower in the first sample, hence the high concentration of the peaks seen in the first sample was not due to dehy-dration of the patient. From birth to day 5, oral benzoate and phenylbutyrate dosages remained constant. Hippurate was readily detected in all urine samples, a product in part from benzoate. Phenylacetylglutamine was also identified in the urine and was likely to derive, at least in part, from the sodium phenylbutyrate therapy.
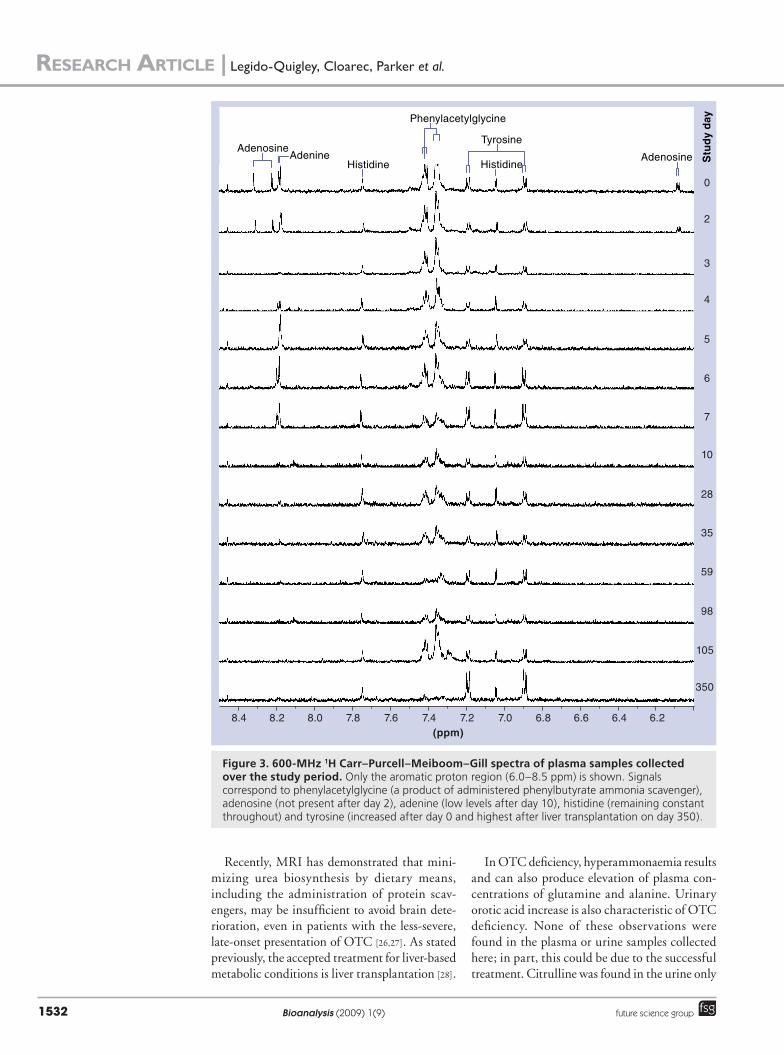
�� Short-term plasma metabolite concentration trends (study days 0–10)Partial 1H NMR spectra (6.5–8.5 ppm) for all collected plasma samples are shown in figuRe 3. Plasma spectra collected until study day 7 demon-strated consistent levels of tyrosine and histidine.
Infusion phase 1
1st infusion (day 0)
3rd infusion (day 3)2nd infusion (day 2)
Infusion phase 2
4th infusion (day 14)5th infusion (day 16)
Infusion phase 3
6th infusion (day 23)
Infusion phase 4
8th infusion (day 170)
7th infusion (day 24)
Admission to pediactric intensive care unit:metabolic acidosis
Metabolic acidosis
Threshold for expectedneurotoxicity and resultantbehavioral manifestations
Dietary protein intake reduced from 1.5 to 0.5 g/kg bodyweight per day
Protein intake returned to 1.5 g/kg bodyweight per day
Corrective livertransplantationon day 215
Blood-sampling timepointfor metabonomics
0
50
100
150
200
250
300
350
Pla
sma
amm
on
ia (
µm
ol/l
)
Study day (infant born on study day -2)-5 5 15 25 35 45 55 65 75 85 95 105 115 125 135 145 155 165 175 185 195 205 215
ReseaRch aRticle | Legido-Quigley, Cloarec, Parker et al.
Bioanalysis (2009) 1(9)1530 future science group
Adenosine and adenine were identified in plasma spectra collected on study days 0 and 2 when the first two infusions occurred but not on study day 3 with the third infusion. Plasma adenosine was undetected thereafter, although plasma adenine returned and elevated between study days 4 and 5, before falling to lower levels over study days 6–10. Phenylacetylglycine was also detected.
�� Long-term plasma metabolite concentration trends (study days 10–350)Essential amino acids were given in the patient’s diet and it was found, using NMR spectroscopy, that there was a general increase in plasma amino acids throughout the treatment. Metabolites that did not show a large time variation in plasma included creatine, creatinine, aspartate, citrate, glutamine/glutamate ratio, acetoacetate, acetate and alanine. Over the 350 days of plasma sam-pling, histidine levels remained unchanged, while tyrosine was found to increase, being at its highest in the sample taken on day 350, which was after APOLT. After liver transplantation, other impor-tant differences in the plasma were found to be the disappearance of phenylacetylglycine and ketoiso-phenylacetylglycine and ketoiso- and ketoiso-valerate from spectra, increases in tyrosine, threo-nine and short-chain amino acids and a decrease in lactate. Plasma signals corresponding to the
CH2 and CH
3 groups of fatty acyl moieties and
cholesterol within lipoproteins (data not shown) demonstrated differing proportions of very-low-density lipoproteins to low-density lipoproteins between samples that, along with those from glucose, are likely to relate to diet.
Plasma metabolites with large time-related variation in concentration included tyrosine, arginine and citrulline (table 1). The short-chain amino acids (SCAs) valine, leucine and isoleucine increased greatly over the treatment period. a-ketoisovalerate, which is not normally present in observable levels in human plasma, was detected from day 7 until before transplant. On the other hand, the lactate level demon-strated an overall decrease over the treatment period. The glutamine/glutamate ratio did not alter significantly over the treatment period.
�� O-PLS evaluation of the initial infant response to hepatocyte infusions with plasmaTwo multivariate analytical approaches were applied to the plasma samples. An O-PLS model was used to correlate the NMR data for the eight plasma samples collected over the first ten study days, where X was the NMR spectra and Y was the corresponding day of collection. This period
Figure 1. The plasma ammonia levels recorded over 211 days in the ornithine transcarbamylase-deficient infant prior to corrective auxiliary liver transplantation.
Citr
ate
Phenylacetylglutamine
δ1H
δ1H
Urea
Excisedwater
TM
AO
and
bet
aine
Citr
ullin
e
Suc
cina
te a
nd U
3
Rescaling
Ethanol
Ace
tate
PhenylacetylglutamineHippurate
2
Orn
ithin
e
Hippurate
3
NMND
Arg
inin
osuc
cina
te
Dim
ethy
lam
ine7.9 7.8 7.7 7.6 7.5 7.4
1
U4
U1
U2
Ornithine
4
Eth
anol
B
A
C
8.5 8.0 7.5 7.0 6.5 6.0 5.5 5.0 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0
First hepatocyte transplant to alleviate ornithine transcarbamylase deficiency | ReseaRch aRticle
www.future-science.com 1531future science group
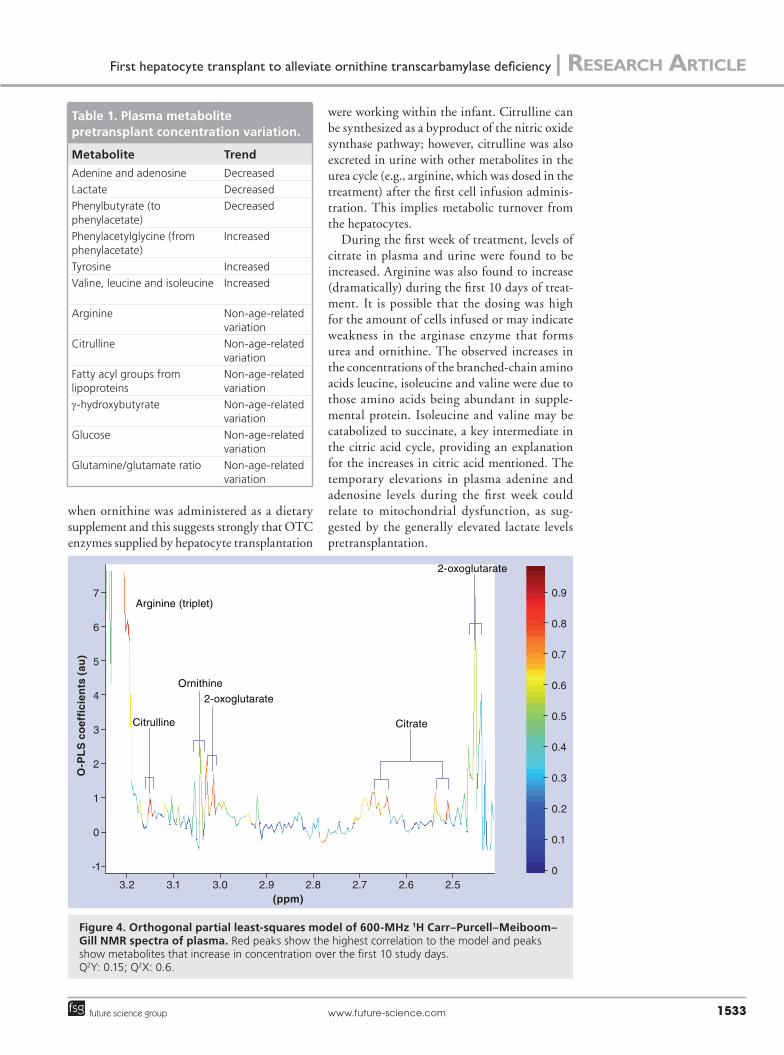
encompassed hepatocyte infusions, and so the model examines the impact of hepatocyte trans-plantation. Functional OTC within the infused hepatocytes appeared to convert ornithine to citrulline, as citrulline was observed and not administered in the diet during this period. This supports the view that the first trio of infusions were indeed successful. figuRe 4 clearly shows the correlation between the plasma citrulline level and the time of treatment, and also demonstrates a high correlation with arginine ornithine, 2-oxo-glutarate and citrate, which also increased during the first 10 days.
�� O-PLS–DA comparison between periods of successful treatment & poor ammonia controlAn O-PLS–DA model was constructed to compare the three plasma samples collected at time points preceding metabolic acidosis and plasma ammonia elevation (study days 55, 98 and 103) to other plasma collection time points
during periods of low ammonia in blood (up until day 35 and post-AOL transplantation on day 350). This model had Q2Y and Q2X values of 0.3 and 0.4, respectively. The highest cor-relation within this model to the time points preceding deterioration was found to be with the NMR peak at a chemical shift of d 3.62, which corresponded to a triplet structure and was associated with high ammonia in blood. This peak is consistent with the metabolite g-hydroxybutyrate, but this postulated iden-tity could not be confirmed as it was found at low concentrations in all samples.
DiscussionThis study is the first application of metabo-nomic ana lysis to the assessment of hepatocyte infusion treatment of the most severe form of early-onset OTC deficiency. In the past, 1H NMR spectroscopy has been applied to define urea cycle deficiencies and has been used as a diagnostic tool for OTC [16,24,25].
Figure 2. 600-MHz 1H NMR spectra of urine (A) taken on study day 2, (B) with the aromatic region expanded and (C) study day 3 corresponding to the days of the second and third hepatocyte infusions, respectively.1: Creatine, creatinine and ornithine; 2: Creatinine; 3: Consistant with a-hydroxyhippurate; 4: Consistant with N-formylglycine.NMND: N-methylnicatinamide; TMAO: Trimethylamine-N-oxide; U: Compound; U1–4: Unassigned.
Phenylacetylglycine
Tyrosine
Histidine Histidine
AdenosineAdenosineAdenine S
tud
y d
ay
0
2
3
4
5
6
7
10
28
35
59
98
105
350
8.4 8.2 8.0 7.8 7.6 7.4 7.2 7.0 6.8 6.6 6.4 6.2(ppm)
ReseaRch aRticle | Legido-Quigley, Cloarec, Parker et al.
Bioanalysis (2009) 1(9)1532 future science group
Recently, MRI has demonstrated that mini-mizing urea biosynthesis by dietary means, including the administration of protein scav-engers, may be insufficient to avoid brain dete-rioration, even in patients with the less-severe, late-onset presentation of OTC [26,27]. As stated previously, the accepted treatment for liver-based metabolic conditions is liver transplantation [28].
In OTC deficiency, hyperammonaemia results and can also produce elevation of plasma con-centrations of glutamine and alanine. Urinary orotic acid increase is also characteristic of OTC deficiency. None of these observations were found in the plasma or urine samples collected here; in part, this could be due to the successful treatment. Citrulline was found in the urine only
Figure 3. 600-MHz 1H Carr–Purcell–Meiboom–Gill spectra of plasma samples collected over the study period. Only the aromatic proton region (6.0–8.5 ppm) is shown. Signals correspond to phenylacetylglycine (a product of administered phenylbutyrate ammonia scavenger), adenosine (not present after day 2), adenine (low levels after day 10), histidine (remaining constant throughout) and tyrosine (increased after day 0 and highest after liver transplantation on day 350).
3.2 3.1 3.0 2.9 2.8 2.7 2.6 2.5(ppm)
O-P
LS
co
effi
cien
ts (
au)
7
6
-1 0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0
1
2
3
4
5
Arginine (triplet)
Citrulline
Ornithine
Citrate
2-oxoglutarate
2-oxoglutarate
First hepatocyte transplant to alleviate ornithine transcarbamylase deficiency | ReseaRch aRticle
www.future-science.com 1533future science group
Figure 4. Orthogonal partial least-squares model of 600-MHz 1H Carr–Purcell–Meiboom–Gill NMR spectra of plasma. Red peaks show the highest correlation to the model and peaks show metabolites that increase in concentration over the first 10 study days. Q2Y: 0.15; Q2X: 0.6.
when ornithine was administered as a dietary supplement and this suggests strongly that OTC enzymes supplied by hepatocyte transplantation
were working within the infant. Citrulline can be synthesized as a byproduct of the nitric oxide synthase pathway; however, citrulline was also excreted in urine with other metabolites in the urea cycle (e.g., arginine, which was dosed in the treatment) after the first cell infusion adminis-tration. This implies metabolic turnover from the hepatocytes.
During the first week of treatment, levels of citrate in plasma and urine were found to be increased. Arginine was also found to increase (dramatically) during the first 10 days of treat-ment. It is possible that the dosing was high for the amount of cells infused or may indicate weakness in the arginase enzyme that forms urea and ornithine. The observed increases in the concentrations of the branched-chain amino acids leucine, isoleucine and valine were due to those amino acids being abundant in supple-mental protein. Isoleucine and valine may be catabolized to succinate, a key intermediate in the citric acid cycle, providing an explanation for the increases in citric acid mentioned. The temporary elevations in plasma adenine and adenosine levels during the first week could relate to mitochondrial dysfunction, as sug-gested by the generally elevated lactate levels pretransplantation.
Table 1. Plasma metabolite pretransplant concentration variation.
Metabolite Trend
Adenine and adenosine Decreased
Lactate Decreased
Phenylbutyrate (to phenylacetate)
Decreased
Phenylacetylglycine (from phenylacetate)
Increased
Tyrosine Increased
Valine, leucine and isoleucine Increased
Arginine Non-age-related variation
Citrulline Non-age-related variation
Fatty acyl groups from lipoproteins
Non-age-related variation
g-hydroxybutyrate Non-age-related variation
Glucose Non-age-related variation
Glutamine/glutamate ratio Non-age-related variation

ReseaRch aRticle | Legido-Quigley, Cloarec, Parker et al.
Bioanalysis (2009) 1(9)1534 future science group
At 3 years of age, this child was healthy and neurologically well developed and was maintained on a normal diet. A comparison was therefore made between pre-APOLT and the correspond-ing post-transplant values. In the post-transplant plasma samples, the phenylacetylglycine was no longer present since the ammonia scavengers were not administered. The reason why the conjugated glycine metabolite was found in plasma in the pretransplant samples while the conjugated glu-tamine metabolite was excreted in urine is unclear. This could be related to the relative hydrophilic partition coefficient of these two metabolites in plasma. Another interesting observation is that the latter has two nitrogen atoms; in urine this would be a mechanism of nitrogen excretion running at the same magnitude as the urea cycle [29].
Using metabonomics, it has been possible to establish that a defective urea cycle can be corrected by hepatocyte transplantation, albeit temporarily, as shown by increases in urinary citrulline. We have shown that, by employing a nontargeted NMR approach, we were able to detect some expected results, in particular the increase of phenyl butyrate and benzoate metabo-lites in urine, such as phenylacetylglutamine and hippurate, respectively, urea cycle intermediaries and citrate in urine and in plasma and dietary amino acids. Some unexpected results, such as the detection of adenine and adenosine in plasma ornithine excreted in urine and ketoisovalerate in plasma, higher glycine conjugation in plasma and higher glutamine conjugation in urine, were also detected and will be evaluated in further studies.
Future perspectiveMetabonomic evaluation of hepatocyte therapy provided evidence that transplanted hepatocytes can function in a child with severe liver-based metabolic disease. Here, the metabolic profiling approach could be adopted for multiparametric monitoring of biochemical effects of cell trans-plantation and could potentially be implemented in real time in a clinical setting.
Ethical conduct of research The authors state that they have obtained appropriate insti tutional review board approval or have followed the princi ples outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addi-tion, for investi gations involving human subjects, informed consent has been obtained f rom the participants involved.
AcknowledgementsThe authors wish to thank the Roche Organ Transplant Research Foundation for its continuous support (CLQ and DAP) and the organ donors who helped this infant.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert t estimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
�� This case study describes the use of 1H NMR spectroscopy-based metabonomics to assess the metabolic consequences of the first combined treatment by hepatocyte infusion and auxiliary partial orthotopic liver transplantation performed on an infant with severe ornithine transcarbamylase deficiency.
�� While citrulline was not administered during the first cell transplant, initial presence in urine suggests biochemical activity of functional ornithine transcarbamylase within infused hepatocytes.
�� An NMR orthongonal partial least-squares model from the plasma samples collected over the first 10 study days shows an increase in citrulline and other urea cycle metabolites.
�� Plasma metabolites with large time-related variation in concentration included tyrosine, arginine, citrulline, valine, leucine and isoleucine ketoisovalerate. The glutamine/glutamate ratio did not alter significantly over the treatment period. Due to sepsis and dietary manipulations, assessing long-term effects of cell transplantation was not possible.
�� Using NMR-based metabonomics, it has been possible to establish that a defective urea cycle can be corrected by hepatocyte transplantation, albeit temporarily, as shown by increases in citrulline.
Bibliography1 Puppi J, Dhawan A. Human hepatocyte
transplantation overview. Methods Mol. Biol. 481, 1–16 (2009).
2 Sze YK, Dhawan A, Taylor RM et al. Pediatric liver transplantation for metabolic liver disease: experience at King’s College Hospital. Transplantation 87(1), 87–93 (2009).
3 Puppi J, Tan N, Mitry RR et al. Hepatocyte transplantation followed by auxiliary liver transplantation – a novel treatment for ornithine transcarbamylase deficiency. Am. J. Transplant 8(2), 452–457 (2008).
First hepatocyte transplant to alleviate ornithine transcarbamylase deficiency | ReseaRch aRticle
www.future-science.com 1535future science group
4 Ensenauer R, Tuchman M, El-Youssef M et al. Management and outcome-onset ornithine transcarbamylase deficiency following liver transplantation at 60 days of life. Mol. Genet. Metabol. 84, 363–366 (2005).
5 Horslen SP, McCowan TC, Goertzen TC et al. Isolated hepatocyte transplantation in an infant with a severe urea cycle disorder. Pediatrics 111(6), 1262–1267 (2003).
6 Strom SC, Fisher MA, Thompson MT et al. Hepatocyte transplantation as a bridge to orthotopic liver transplantation in terminal liver failure. Transplant. Proc. 63, 559–569 (1997).
7 Fox IJ. Treatment of the Crigler-Najjar syndrome type I with hepatocyte transplantation. N. Engl. J. Med. 338(20), 1422 (1998).
8 Nicholson JK, Wilson ID. High resolution proton magnetic resonance spectroscopy of biological fluids. Prog. Nucl. Magn. Reson. Spectrosc. 21(4–5), 449–501 (1989).
9 Nicholson JK, Spraul M, Farrant RD et al. 750 MHz 1H and 1H-13C NMR spectroscopy of human blood plasma. Anal. Chem. 67(5), 793–811 (1995).
10 Waters NJ, Garrod S, Farrant RD et al. High-resolution magic angle spinning 1H NMR spectroscopy of intact liver and kidney: optimization of sample preparation procedures and biochemical stability of tissue during spectral acquisition. Anal. Biochem. 282(1), 16 (2000).
11 Griffin JL, Williams HJ, Sang E et al. The initial pathogenesis of cadmium-induced renal toxicity. FEBS Lett. 478(1), 147 (2000).
12 Nicholson JK, Connelly J, Lindon JC et al. Metabonomics: a platform for studying drug toxicity and gene function. Nat. Rev. Drug Discov. 1, 153–161 (2002).
13 Robertson DG, Reily MD, Sigler RE et al. Metabonomics: evaluation of nuclear magnetic resonance (NMR) and pattern recognition technology for rapid in vivo screening of liver and kidney toxicants. Toxicol. Sci. 57(2), 326–337 (2000).
14 Griffin JL, Williams HJ, Sang E et al. Metabolic profiling of genetic disorders: a multi-tissue 1H nuclear magnetic resonance spectroscopic and pattern recognition study into dystrophic tissue. Anal. Biochem. 293(1), 16 (2001).
15 Nicholson JK, Lindon JC, Holmes E. ‘Metabonomics’: understanding the metabolic responses of living systems to pathophysiological stimuli via multivariate statistical analysis of biological NMR spectroscopic data. Xenobiotica 29(11), 1181 (1999).
16 Engelke UFH, Oostendorp M, Webers RA et al. Handbook of 1H-NMR Spectroscopy in Inborn Errors of Metabolism (2002).
17 Oostendorp M, Engelke UFH, Willemsen MA et al. Diagnosing inborn errors of lipid metabolism with proton nuclear magnetic resonance spectroscopy. Clin. Chem. 52(7), 1395–1405 (2006).
18 Nicholson JK, Wilson ID. Opinion: understanding ‘global’ systems biology: metabonomics and the continuum of metabolism. Nat. Rev. Drug Discov. 2(8), 668–676 (2003).
19 Trygg J. O2-PLS for qualitative and quantitative analysis in multivariate calibration. J. Chemometr. 16(6), 283–293. (2002).
20 Trygg J, Wold S. Orthogonal projections to latent structures (O-PLS). J. Chemometr. 16, 119–128 (2002).
21 Trygg J, Wold S. O2-PLS, a two-block (XY) latent variable regression (LVR) method with
an integral OSC filter. J. Chemometr. 17(1), 53–64 (2003).
22 Cloarec O, Dumas ME, Trygg J et al. Evaluation of the orthogonal projection on latent structure model limitations caused by chemical shift variability and improved visualization of biomarker changes in 1H NMR spectroscopic metabonomic studies. Anal. Chem. 77(2), 517–526 (2005).
23 Green AMI, Morgan I. Neonatology and Clinical Biochemistry. ACB Venture Publications (1993).
24 Burns SP, Wolff DA, Leonard JV et al. Investigation of urea enzyme disorders by 1H-NMR spectroscopy. Clin. Chim. Acta 209, 47–60 (1992).
25 Choi C-G, Yoo HW. Localized proton MR spectroscopy in infants with urea cycle defect. AJNR Am. J. Neuroradiol. 22(5), 834–837 (2001).
26 Kawagishi N, Satoh K, Enomoto Y et al. Improved quality of life and unchanged magnetic resonance brain imaging after living donor liver transplantation for late-onset ornithine transcarbamylase deficiency: report of a case. Surgery Today 35(12), 1087–1091 (2005).
27 Takanashi J-I, Barkovich AJ, Cheng SF et al. Brain MR imaging in neonatal hyperammonemic encephalopathy resulting from proximal urea cycle disorders. AJNR Am. J. Neuroradiol. 24(6), 1184–1187 (2003).
28 Dhawan A, Mitry RR, Hughes RD et al. Hepatocyte transplantation for inherited factor VII deficiency. Transplant. Proc. 78(12), 1812–1814 (2004).
29 Piscitelli S, Thibault A, Figg W et al. Disposition of phenylbutyrate and its metabolites, phenylacetate and phenylacetylglutamine. J. Clin. Pharmacol. 35(4), 368–373 (1995).
Related Documents




![t e c h n ol gy Journal of Biotechnology & Biomaterials · argF proB kgd) for L-ornithine production, which could produce 4.62 g/L of L-ornithine [13]. The level of L-ornithine production](https://static.cupdf.com/doc/110x72/5e22e2c1220ab9163b5a39e7/t-e-c-h-n-ol-gy-journal-of-biotechnology-biomaterials-argf-prob-kgd-for-l-ornithine.jpg)






