Final Report Implementation of Mental Health Promotion and Prevention Policies and Strategies in the EU member states and appplicant countries (EMIP) Volume I 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Final Report
Implementation of Mental Health Promotion and Prevention Policies and Strategies
in the EU member states and appplicant countries
(EMIP)
Volume I
1

IMPLEMENTATION OF MENTAL HEALTH PROMOTION AND PREVENTION POLICIES AND STRATEGIES
IN EU MEMBER STATES AND APPLICANT COUNTRIES
Grant Agreement Number - 2003301
Final Report
EuroHealthNet (Belgium), European Public Health Alliance (EPHA, Belgium)
Federal Institute for Occupational Safety and Health (FIOSH, Germany) IMHPA Network
(Network on Mental Health Promotion and Mental Disorder Prevention, Netherlands) Mental Health Europe (MHE, Belgium), STAKES (Finland)
WHO/Euro Network for Suicide Research and Prevention (Germany) WHO/Collaborating Centre for Health Promotion in Hospitals and Health Care
(Austria)

CONTENTS Volume I: 1. Introduction .......................................................................................... 5 1.1. Main objectives and results of the project ............................................ 6 1.2. Responsibilities ..................................................................................... 7 1.2.1. Consortium Partners .............................................................................. 7 1.2.2. National Partners ................................................................................... 8 2. Achievements ........................................................................................ 9 2.1. Calendar of Meetings ............................................................................ 9 2.2. Project Documents ................................................................................12 2.3. National reports .....................................................................................13 2.4. Dissemination of information on the project ........................................14 2.5. Translation of the WHO Declaration and Action Plan .........................17 3. EMIP: Achievements…………………................................................18 3.1. Introduction ..........................................................................................18 3.2. EMIP in the context of the WHO Mental Health Action Plan
and EC Green Paper ..............................................................................19 3.3. Common challenges ..............................................................................21 3.3.1. Competing priorities .............................................................................21 3.3.2. Predominant focus on prevention rather than promotion .....................21 3.3.3. Difficulty of engaging stakeholders beyond health ..............................22 3.3.4. Limited capacity and resources ............................................................22 3.3.5. Lack of public involvement in mental health promotion ......................22 3.3.6. Stigma/exclusion has greater focus than other elements of
mental health promotion .......................................................................22 3.3.7. Lack of evidence and evaluation .........................................................23 3.3.8. Public lack of awareness of mental health ..........................................23 3.3.9. Lack of focus on the wider determinants of mental health
and well-being ......................................................................................23 3.4. Key determinants of effective implementation .....................................24 3.4.1. Mental health promotion policy: national and regional ........................24 3.4.2. Cross sector ownership .........................................................................25 3.4.3. Marketing mental health and well-being ............................................26 3.4.4. Mental health promotion contributes to improved outcomes
for people with mental health problems ................................................27

3.4.5. Governance, performance management and accountability .................28 3.4.6. Clear definition of success and how it will be measured ......................28 3.4.7. Capacity building across all sectors ...................................................... 29 3.4.8. MHP intelligence/data, evidence base and evaluation ..........................29
4. Recommendations and conclusion ........................................................30
5. Financial Statements of Revenue and Expenditure ..............................33 Annexes I. Consortium Partners II. National Partners III. Project Experts IV. Dates of the National Workshops V. EMIP Implementation Road Map VI. EMIP Postcard VII. EMIP Response to EC Mental Health Green Paper VIII. EMIP Matrices EMIP Final Report Volume II: EMIP National Reports EMIP Final Report Volume III: Final Financial Report
1. INTRODUCTION The purpose of this final project report is to describe the development of the 30 months of the project running from 1 July 2004 – 31 December 2006. It includes:
• the objectives of the project and its main achievements during this period of time; • an overview of the project meetings and activities and their outcomes; • conclusions and recommendations for the future development of mental health
promotion in Europe; • a final financial report.
Due to the fact that the initial project application to the EC was submitted by Mental Health Europe and FIOSH took over the role of the Main Partner and became responsible for the overall project management, the actual start of the project had to be delayed for several months. This lead to the application for a six month no-cost prolongation that has been approved by the European Commission, so that the project now covers 30 months, instead of the originally planned 24, and will officially run until 31 December 2006.
5
1.1. Main objectives and results of the project The overall objective of this project is to build and support good practice in the development and effective implementation of mental health promotion and prevention, policy and strategy in the Member States of the European Union and in applicant countries.
Main Objectives
Expected Results
1. Develop a European strategy to initiate
and implement actions on mental health promotion and mental disorder prevention;
2. Support the creation of national networks
and assist National Partners in the organisation, implementation and evaluation of the national workshops.
3. Identify opportunities in the participating
countries (MS, NMS and CC) for promotion and prevention in key settings and target populations
4. Share with Member States and applicant countries information and expertise on effective practice developed from previous EC projects on Mental Health Promotion and Prevention of mental illness.
5. Develop and carry out an integrated
strategy for communication and dissemination of the aims, process and outcomes of the project, using all appropriate media most likely to: - raise awareness among relevant professionals, policy makers and the general public - encourage effective policy development and implementation within Member States and applicant countries.
1. European matrix on the determinants of
effective development and implementation of mental health promotion and prevention, based on the information acquired from the participating countries
2. Series of National Workshops for the
exchange of information and action planning at national, regional and local level in each participating country;
3. National reports summarising the results
of the National Workshops in order to contribute to a comparison of the MH situations in the participating countries;
4. Final report for mental health promotion
and prevention to put forward the national, regional and local implementation of consensus policy and action;
5. Range of communication products
including website, press releases, publications in peer, reviewed journals and publicity resources.
Table 1: Main objectives and expected results
6
1.2. Responsibilities Altogether 8 Consortium Partners and 12 National Partners are involved in the project. 1.2.1. Consortium Partners FIOSH created a Project Consortium with 7 partner networks:
• Mental Health Europe (MHE, Belgium) • STAKES (Finland) • WHO/Euro Network for Suicide Research and Prevention (Germany) • WHO/Collaborating Centre for Health Promotion in Hospitals and Health Care
(Austria) • EuroHealthNet (Belgium) • IMHPA Network (Network on Mental Health Promotion and Mental Disorder
Prevention, Netherlands) • European Public Health Alliance (EPHA, Belgium).
For a detailed list of the Consortium Partners, please see Annex I or http://www.emip.org/consortium_partners.html FIOSH undertook the management and co-ordination of the project, the financial management, the progress assessment and liaison with all participating partners. Among other tasks the Consortium Partners agreed to contribute to the project by • contacting national partners and assisting in the planning and the follow-up of national
workshops and supporting the involvement of key national stakeholders in order to develop a national network;
• using existing contacts and networks in order to disseminate the information about the project among relevant actors and stakeholders;
• providing a short report on their networks with a special focus on examples of best practice in the mental health promotion field;
• assisting in monitoring and evaluating the project; • providing input for the Final Report about the implementation of Mental Health
promotion and prevention policies and strategies as a final result of the project. STAKES and Mental Health Europe provided additional input by contributing to the development of the project documents (Guidelines, Manual, Action Plan, Interim Report, Final Report, etc.) in close co-operation with FIOSH.
7

1.2.2. National Partners National Partners from Austria, the Czech Republic, Estonia, Finland, Germany, Hungary, Ireland, the Netherlands, Poland, Portugal, Romania and Slovenia participated in the project. They agreed to undertake the following tasks: • organising a National Workshop and identifying relevant target groups (about 35
participants); • evaluating the National Workshop and preparing a national report based on the output of
the National Workshop; • participating in and contributing to a National Partners Meeting and a benchmarking
conference held at the end of the project cycle with the aim of analysing and presenting a framework for the more effective implementation of mental health promotion and prevention policies and strategies (which was developed as the EMIP Matrix and recommendations – see section 5).
For a detailed list of the National Partners1, please see Annex II or http://www.emip.org/national_partners.html
1 Due to internal reasons Slovakia withdrew from the project in autumn 2005
8

2. EMIP: Achievements “The influence of EMIP on the development of Estonian mental health policy and strategy in line with developments in WHO and EU has been remarkable.” (Estonia National Report) “Workshops following the EMIP model and utilising its experienced will be continued under the auspices of the WHO Collaborating Centre for Mental Health Promotion, Prevention and Policy (located in STAKES)”. (STAKES Report) “We conclude that the national workshop has contributed to bring prevention of depression to a higher level …… the participation in the two international conferences organised by EMIP were very useful as well. A lot could be learned from experiences in other countries and the international collaboration is still going on”. (The Netherlands National Report) “As a result of the EMIP project, the institutions, units and persons involved in mental health promotion/mental disorder prevention in Poland were identified”. (Poland National Report) “The EMIP Workshops strongly enhanced the necessary linking of various areas of the health service as well as among networks, self-help groups, policy actors and stakeholders”. (Germany National Report) 2.1. Calendar of Meetings a. Consortium Meeting, Brussels, 29/30 September 2004
At the first meeting of the project Consortium, a provisional list of National Partners was agreed upon and a rough outline for the structure of the National Workshops was established.
b. Consortium Meeting Vienna, 16/17 December 2004
All National Partners to participate in the project were established. Due to the fact that the MH situations in the partner countries seemed to show a very wide variety it was decided to change the original project timeline and at first arrange a National Partners Meeting with all the project partners to find a common way to conduct and structure the National Workshops that would be suitable for all countries.
c. Consortium and National Partners Meeting Brussels, 16/17 March 2005
Under the influence of the recent Ministerial Conference on MH “Facing the Challenges,
Building Solutions” held just two months before in Helsinki, the general atmosphere of the meeting was rather confident concerning future project activities within EMIP.
9

All partners agreed to tackle the following three main tasks in the National Workshops:
Conducting a mapping exercise: To outline the present situation of mental health with a special focus on promotion and prevention.
Defining: How do we create a critical mass?
Identifying push and pull factors i.e. the determinants of effective implementation of mental health promotion and prevention e.g. supporting policies, ownership by key stakeholders/sectors, networks or collaboration, national/regional initiatives, adequate data and resources
Streamlining the results:
Creating a national profile for the future development of mental health and mental health promotion and prevention i.e. specific challenges and opportunities facing each national partner
FIOSH also presented an “EMIP Implementation Road Map” summarising in a graphic layout an important part of the project strategy that aims at improving mechanisms for co-ordinating mental health promotion and prevention policies and programmes (see Annex V). A new time scale for the project was approved, indicating that all National Workshops should be held before the end of November 2005. The National Reports were to be presented and discussed with all participating partners in a final project conference (“baseline conference”) in March 2006. d. Consortium Meeting
Vienna, 9/10 December 2005 This Consortium meeting was the first opportunity to review the preliminary results of the EMIP National Workshops that had been conducted in the participating countries. The general impression of the workshop results was very positive. In some countries, for example Portugal and Estonia, added value was achieved because the EMIP workshop was supported by the Ministries of Health or Social Affairs.
It was agreed that a summary of the National Reports should be presented in the form of a
matrix at the EMIP “Baseline Conference” in Hungary in March 2006. The purpose of the Matrix was to strengthen collaboration and mutual support between partner countries and the exchange of information and best practices on addressing key challenges and taking advantage of specific opportunities.
In order to contribute to the EC Mental Health Green Paper consultation process, the
Consortium Partners agreed to formulate a joint EMIP commentary and submit it to the Commission in March 2006 in Budapest (please. see Annex VII for the complete text).2
2 A full list of contributions to the consultation on:
http://ec.europa.eu/health/ph_determinants/life_style/mental/green_paper/mentalgp_contributions_en.htm#3
10

In addition, the EMIP Matrix was presented by Lynne Friedli and Karl Kuhn at the third consultation meeting for the Green Paper: Research and Information in Mental Health in Luxembourg in May 2006 (http://www.ec.europa.eu/health/ph_determinants/life_style/mental/docs/ev_20060518_co08_en.pdf). In order to ensure that the EMIP website reflected the current development of the project and would provide a source of information and guidance for national partners and others, it was decided to re-edit the website content. Lynne Friedli, one of the project experts, agreed to manage this task. For the second period of the project she will take over the task of editing the website, in consultation with national partners and consortium members and prepare a new version to be presented at the next meeting in Budapest.
e. “Baseline Conference” and Consortium Meeting Budapest, 22-25 March 2006 The conference was attended by the Consortium Members and the National Partners from
the participating countries, as well as a number of invited experts. Considerable progress was made in identifying common determinants of effective implementation and sharing information on key challenges and barriers. Key issues included:
• the significant East-West differential in the standard of mental health services • a lack of sound epidemiological data on both mental illness and mental health • many countries do not have specific action plans or strategies for MH
promotion on the national level • shortages of funding and other resources • insufficient infrastructure, notably opportunities for collaboration and
networking • crucial role of international support and the EC in driving MH
promotion/prevention work forward, especially in the new Member States. John Henderson from the Consortium Partner Mental Health Europe summarised the learning from present EMIP developments in his presentation: “Mental Health Promotion and Prevention Implementation”. Copies of all the presentations from the Budapest conference “Creating a Momentum for Change” are available on http://www.emip.org/latest_news.html . f. Final Project Conference and Consortium Meeting Tallinn, 22/23 September 2006 The meeting of Consortium members and National Partners provided an opportunity for
sharing experiences about advocacy and policy development for mental health promotion at EU and national levels during the period of the project, and how the lessons learnt could be taken forward. Several suggestions were discussed on how the useful development of the website and its links could be sustained, together with ideas for advocacy and policy initiatives at EU levels.
11

Mental health was one feature of Health in All Policies (HiAP), the main health theme of the Finnish European Union Presidency3. Clive Needle from EuroHealthNet was a Rapporteur at the Health in all Policies event in Kuopio, Finland, and therefore led the discussion in Tallinn on key strategies for taking forward and making the best use of the outputs and conclusions of the EMIP project.
The key issue to arise from the final project conference and meeting was the added value
of the opportunities to exchange information, expertise and mutual support presented by EMIP and other EC projects. This is particularly the case in an emerging field such as mental health promotion, where ‘increased exchange and collaboration’, a key theme to emerge in the EC Green Paper consultation, is essential to moving forward.
2.2. Project Documents Two background documents were prepared: Project Guidelines - to be used internally by the project Consortium Members - including definitions of mental health, mental health promotion, implementation - providing a general guideline for the project alignment and quality assurance Project Manual (“EMIP Manual”) a more comprehensive background paper, especially to be used by the National Partners (http://www.emip.org/pdf/EMIP_Manual_050307.pdf) - providing extensive coverage of contemporary research in the field of MH promotion and
mental disorder prevention in Europe - meant to serve as a practical reference document summarising all the necessary
information the National Partners might need to conduct and evaluate their National Workshops
- providing a basic common structure for the National Reports
3 See Stahl T, Wismar M, Ollila E, Lahtinen E and Leppo K (2006) Health in all policies: prospects and potentials Helsinki: Ministry of Social Affairs and Health http://www.stm.fi/Resource.phx/eng/subjt/inter/eu2006/hiap/index.htx.i1153.pdf
12
2.3. National Reports After having held their National Workshops all EMIP country partners provided summary reports on the results achieved. Each of these National Reports includes the following issues: • mental health data • key stakeholders • strengths and weaknesses in mental health promotion and prevention • mental health policy environment • push and pull factors • most urgent needs/priorities • barriers to implementation • programme and list of participants The National Reports and their analyses are the core parts of EMIP (http://emip.org/national_reports.html)4. In order to summarise the results and assist in interpreting the similarities and differences between national partners, an individual matrix was developed for each participating country (see Annex VIII). An analysis of the findings, together with recommendations, is presented in section 3 of this report.
4 All the National Reports can also be found in Volume II of this report
13
2.4. Dissemination of information on the project With the help of the EMIP Consortium Partner EPHA, a structure and layout for a website presentation was developed in the first half of the project. It contained general information on the project, its co-operating partners, published documents and links to EC and other websites of relevance for MH issues. In the course of the project the EMIP Consortium Partners decided that more detailed information and background documents should be added to the website and that there should be a special focus on providing broader and more in-depth knowledge to its visitors. With the assistance and expertise from the EMIP project expert Dr. Lynne Friedli from London this goal could be accomplished in a very short period of time. In March 2006 the new content of the website was made available under the following address: http://www. emip.org EMIP has also been featured in several articles on the EPHA website and in the EPHA Newsletter, an important source of information for a wide number of health actors throughout the world. The website receives about 30 000 visits per month. Although initially EPHA committed to develop a system for internal and external communication for the project, later on, due to internal changes and restructuring of the organisation, EPHA limited its contribution to raising the profile of the project through its website and Newsletter and through participation and feed-back from various European mental health meetings. EMIP project-related website and Newsletter articles: - A general article about the EMIP project explaining the aims and objectives and its structure
(339 visits). http://www.epha.org/a/2217 - An article on EMIP Response to the Green Paper on Mental Health, which outlines that
actions to promote the mental health and well-being of the whole population, in schools, in the workplace, in the community, in the health care sector and among vulnerable groups in society are essential to achieving social cohesion and better social and economic welfare (256 visits).
http://www.epha.org/a/2282 - An article on the Mental Health baseline Conference, held in Budapest in March 2006,
which provided an opportunity for partners to meet and present their work at national seminars (792 visits).
http://www.epha.org/a/2170
14

- A press release at the “EMIP Baseline Conference” in Budapest calling for real commitment from EU Governments on mental health promotion – sent to about 100 journalists across Europe via EPHA php mailing system. This promoted the key EMIP message: “Positive mental health and well-being is essential to put Europe back on the path to long term prosperity”.
http://www.epha.org/a/2170 - Two articles on Tallinn partners meeting outlining the importance of involving NGOs in
action at every level and the need to create coalitions of interests for mental health promotion (and 174 visits).
http://www.epha.org/a/2390 http://www.epha.org/a/2370 EPHA also prepared a response to the European Commission Green Paper on Mental Health, which reinforces key aspects promoted by the EMIP Response to the Green Paper: addressing mental health and well-being requires a multi-faceted public policy approach. http://www.epha.org/a/1903 Wherever possible, EPHA has sought to provide added value to the EMIP project and raise its visibility to external audiences. The project has been presented as an example of a strong multi-disciplinary partnership (health professionals, academics, civil servants, and NGOs). EPHA promoted a holistic approach to mental health, particularly about increasing actions on mental health in the health policy (especially non-health policy) and underlining that promoting mental health is the responsibility of all sectors and will contribute to their benefit. EPHA also shared information and experiences about advocacy practices and best ways to raise political attention. All these different aspects were promoted not only in meetings with EU officials and other NGOs, but also in meetings with several foundations (Calouste Gulbekian Foundation and Medical Assistance International – in Lisbon, Egmond Fond and Health Insurance Fund in Copenhagen, Fondation de France). EuroHealthNet as one of the Consortium Partners established an EMIP sub-site under their own internet presentation: http://www.eurohealthnet.eu/content/blogcategory/11/26/ EuroHealthNet also disseminated information on the project progress and the important EMIP developments via its Health Action Memo. Mental Health Europe (MHE), yet another Consortium Partner, posted a presentation of EMIP on the MHE website (http://www.mhe-sme.org/en/projects_implementation.htm). MHE also included several articles informing on the project development in the MHE monthly Newsletters and presented the EMIP project at several occasions (internal and external meetings, seminars, etc.).
15

EMIP Leaflet With the help of MHE, EuroHealthNet and EPHA a project leaflet has been edited and designed. It addresses the general public and therefore tries to explain in a short and clear way what the EMIP project is about. In a certain way its headline alone already helps to summarise this: “Creating a momentum for change - bringing together individuals and organisations committed to implementing an integrated mental health strategy in selected European countries” Copies of the printed leaflet have been sent to all National Partners and the Consortium members for further distribution. EMIP Postcard A postcard format was developed and widely disseminated by all the EMIP Partners and affiliates in order to distribute and spread the information of EMIP and its aims more widely. By doing so the newly edited internet-site (www.emip.org) shall be promoted as well. The complete text and design can be found in Annex VI. Publications on EMIP in peer reviewed journals Two papers from EMIP national partners, describing EMIP findings in Slovenia and in the Czech Republic, were accepted for publication in the Journal of Public Mental Health. In a special issue on Europe (issue 5.1) EMIP was also featured in the editorial. • Tanja Kamin (2006) Mental health promotion: a perspective from Slovenia Journal of Public Mental Health 5.1: 24-28 • Ivan David,Vladimír Kebza, Ivo Paclt, Jirí Raboch, Jaroslav Volf (2006) Mental health in the Czech Republic Journal of Public Mental Health 5.2: 43-47 Also published was Karl Kuhn (2006) Mental Health promotion in the workplace: a European perspective Journal of Public Mental Health 5.1: 29-34 Journal of Public Mental Health http://www.pavpub.com/pavpub/journals/JPMH/index.asp Further papers produced as a result of the EMIP project could include further contributions from Slovenia, Estonia, Poland and Austria.
16
2.5. Translation of the WHO Declaration and the Action Plan At the Ministerial Conference in Helsinki in January 2005, 52 States endorsed the MH Declaration and Action Plan for Europe. Since these documents were regarded as very important for shaping the future development of MH activities in Europe it was decided to make them available to all the EMIP partners in their own language. After negotiating with the WHO about the copyright, FIOSH was then able to provide translated versions for all the National Partners. These were very well received and helped to address special issues in the National Workshops. Several National Partners reported a rise in demand for these translated copies and they have been widely distributed in the course of the project. The newly available languages of the documents now are: Czech, Dutch, Estonian, Finnish, Hungarian, Polish, Portuguese, Romanian, Slovenian and Slovakian.
17

3. EMIP: FINDINGS AND RECOMMENDATIONS 3.1. Introduction The analysis of the findings of EMIP is drawn from:
• outcomes of national workshops and networks developed at a national level
• EMIP conferences and consortium meetings held in Dortmund, Budapest, Vienna and Tallinn
• national reports submitted by partner countries
Analysis is based on the objectives and goals of the project as follows:
The overall objective of this project is to build and support good practice in the development and effective implementation of mental health promotion and prevention policy and strategy in the Member States of the European Union and in applicant countries.
The specific goals of the project are to:
• support the creation of national networks and assist National Partners in the organisation, implementation and evaluation of the national workshops; • identify opportunities in the participating countries for promotion and prevention in key settings and target populations; • share with Member States and applicant countries information and expertise on effective practice developed from previous EC projects on Mental Health Promotion and Prevention of mental illness; • develop a European framework on the determinants of effective development and implementation of mental health promotion and prevention, based on the information acquired from the participating countries; • produce a National Report for Mental Health Promotion and Prevention
• develop and carry out an integrated strategy for communication and dissemination of the aims, process and outcomes of the project, using all appropriate media most likely to: - raise awareness among relevant professionals, policy makers and the general public - encourage effective policy development and implementation within Member States and applicant countries.
For the purposes of the EMIP project, the scope of mental health promotion has been defined as follows:
• promote mental well-being • prevent mental health problems • improve quality of life for people with a mental illness diagnosis.
This broad field is commonly described as ‘public mental health’ to reflect its focus on improving the mental health of the whole population and an emphasis on understanding and addressing the wider determinants of mental health (Friedli 2004).
18

The scope of the project is therefore consistent with the population wide approach to mental health reflected in the WHO Mental Health Action Plan and the EC Green Paper Improving the Mental Health of the Population.5 In addition, the EMIP project provides further evidence, in the National Reports, of the central relevance of the mental health of the population to the EU’s strategic policy objectives.6 It also supports the growing commitment among EU member states to a greater focus on mental health promotion and prevention, a commitment very much reflected in the responses to the EC Green Paper. 7 3.2 EMIP in the context of the WHO Mental Health Action Plan and EC Green
Paper Ministers of health have endorsed the WHO Mental Health Action Plan for Europe and “support its implementation in accordance with each country’s needs and resources”. The priorities are:
• raise awareness of the importance of mental well-being • tackle stigma, discrimination and inequality, and empower and support people
with mental health problems and their families to be actively engaged in this process
• design and implement comprehensive, integrated and efficient mental health systems that cover promotion, prevention, treatment and rehabilitation, care and recovery
• address the need for a competent workforce, effective in all those areas; • recognise the experience and knowledge of service users and carers as an
important basis for planning and developing services. The twelve areas for action that should be reflected in countries’ own strategies and plans are:
1. Promote mental well-being for all 2. Demonstrate the centrality of mental health 3. Tackle stigma and discrimination 4. Promote activities sensitive to vulnerable life stages 5. Prevent mental health problems and suicides 6. Ensure access to good primary care for mental health problems 7. Offer effective care in community based services for people with severe mental
health problems 8. Establish partnerships across sectors 9. Create a sufficient and competent workforce 10. Establish good mental health information 11. Provide fair and adequate funding 12. Evaluate effectiveness and generate new evidence
5 Copies of the declaration and action plan can be found on: http://www.euro.who.int/document/mnh/edoc07.pdfhttp://www.euro.who.int/document/mnh/edoc06.pdf6 See EMIP’s response to the Green Paper consultation in Annex VII 7 http://ec.europa.eu/health/ph_determinants/life_style/mental/green_paper/mentalgp_report.pdf
19

The WHO Action Plan states: “the challenges over the next five to ten years are to develop, implement and evaluate policies and legislation that will deliver mental health activities capable of improving the well-being of the whole population, preventing mental health problems and enhancing the inclusion and functioning of people experiencing mental health problems”. In the Green Paper the Commission proposed that an EU-strategy should focus on the following:
promote mental health for all action to prevent mental ill health
improve quality of life of people with mental ill health or disability through social inclusion and the protection of their rights and dignity develop a mental health information, research and knowledge system for the EU 8
In response to the themes of the WHO Action Plan and the EC Green Paper, the key focus of EMIP has therefore been on delivery, i.e.:
• to identify, based on the experiences of 12 partner countries, what we have called the determinants of effective implementation.
In this respect, we should also note the response of the European Parliament as the EC will be obliged to take account of the Resolution in formulating the mental health strategy.9 While EMIP has identified a clear need for greater understanding of the determinants of mental health and for the development of the evidence base and evaluation of mental health promotion/prevention, there is still considerable work to be done in convincing stakeholders across all sectors of the importance and relevance of public mental health. Section 3.3 below outlines the common challenges identified by national partners in:
• making mental health and well-being a policy priority nationally and across key settings (mental health in policy)
• developing a whole population/population wide approach to promoting mental health and well-being (mental health for all)
8 COM (2005) 484 final of 14 October 2005, OJ (2006) C49/28 of 28 February 2006 http://europa.eu.int/eurlex/ lex/LexUriServ/LexUriServ.do?uri=CELEX:52005DC0484:EN:Not 9 European Parliament (2006) European Parliament resolution on improving the mental health of the population: Towards a strategy on mental health for the European Union (2006/2058(INI)) http://www.europarl.europa.eu/sides/getDoc.do?pubRef=-//EP//TEXT+TA+P6-TA-2006-0341+0+DOC+XML+V0//EN&language=EN
20
3.3. Common challenges Analysis of the National Project Reports suggests the following challenges or barriers in moving mental health promotion/prevention up the agenda and gaining the commitment and resources that make implementation possible. Tackling these barriers is crucial if mental health promotion is to make meaningful progress. For some of these challenges, action and support at an EU level, e.g. through the forthcoming Mental Health Strategy, would be of great value. For others, member states would like to consider the most effective strategies and actions for moving forward, taking account of the circumstances of individual countries in relation to mental health. The common challenges identified are as follows. These should be read in conjunction with section 3.4 on key determinants in order to provide a comprehensive overview of EMIP findings: 3.3.1. Competing priorities. For example, the need to reform mental illness services or legislation may take precedence over action on promotion/prevention. In some countries, physical health problems such as coronary heart disease, cancer and diabetes are seen as the most immediate health issues and the links between improved mental health and improved physical health outcomes have not been widely accepted. • Recommendation: Provide short, targeted briefings ‘making the case’ There is robust evidence that mental health promotion supports improved outcomes for people with long term mental health problems and aids recovery. There is also a growing body of evidence on the relationship between mental health and physical health. This evidence should be provided as part of a series of short briefings on the ‘case for mental health promotion’. 3.3.2. Predominant focus on prevention rather than promotion, which may limit action to targeted interventions with at risk and vulnerable groups, rather than a population wide strategy which includes action to promote mental health for all. While the benefits of physical health promotion are widely understood, there is much less awareness of the benefits of promoting mental health. • Recommendation: Raise awareness of benefits of promotion, as well as prevention There should be a greater focus on the benefits of promoting mental health and well-being10 for all (public mental health), linked to evidence of the relationship between improved mental well-being and wider outcomes, notably in: education, productivity, relationships, social cohesion, crime reduction, health behaviours and quality of life (see also section 3.4.8 below).
10 see for example World Health Organization, (2004). Promoting mental health: Concepts, emerging evidence, practice: summary report. A Report from the World Health Organization, Department of Mental Health and Substance Abuse in collaboration with the Victorian Health Promotion Foundation (VicHealth) and The University of Melbourne. Geneva, WHO
21

3.3.3. Difficulty of engaging stakeholders beyond health This involves demonstrating the contribution that mental health promotion can make to improving outcomes across a wide range of domains. Work is needed to forge partnerships with other sectors and to strengthen awareness of how mental health promotion is relevant to the achievement of wider goals e.g. in employment, criminal justice, environment, sustainable development, regeneration, social justice and the reduction of inequalities. Too often, mental health colleagues in promotion, prevention and treatment are simply ‘talking to each other’, rather than reaching out to other sectors. • Recommendation: cross sector events and briefings to address ‘why mental health
matters’ and the contribution mental health promotion can make to tackling some of the key challenges facing Europe
3.3.4. Limited capacity and resources, which includes knowledge, skills, motivation and training among professionals, lay workers and communities, notably in relation to promoting mental health and well-being. Germany stated that there is basically no specific training on preventing psychological illness. Germany also noted, for example, that the financial system may be a major barrier “most part of the money, if not everything, is foreseen for treating illnesses, and only a very limited amount for prevention”. • Recommendation: develop training, including train the trainers, with a focus on
promoting mental health and well-being and integrating ‘mental health impact’ within all practice e.g. in schools, hospitals, workplace, prisons, residential care, communities
3.3.5. Lack of public involvement in mental health promotion. Lack of political commitment/interest is often related to lack of understanding of the potential benefits of improving mental health, but also to the view that the general public are not interested in issues of mental health and well-being. • Recommendation: action to involve local communities and generate greater public and
media debate about mental health and well-being and how to promote it 3.3.6. Stigma/exclusion has greater focus than other elements of mental health promotion Tackling the stigma, exclusion and discrimination experienced by people with mental health problems is an important priority. However, in some countries it has proved difficult to achieve a focus on the wider elements of mental health promotion for example with parents and pre-school children, in schools, in the workplace, with older people, with black and minority ethnic groups, refugees and asylum seekers and those who have experienced violence and abuse. • Recommendation: build stronger partnerships with consumer and mental health service
user/survivor groups
22

3.3.7. Lack of evidence and evaluation remains a barrier, although evidence of the effectiveness of mental health promotion is growing (WHO 2004a; 2004b)11
Recommendation: continue to encourage collation and dissemination of data on evidence of effectiveness, as well as greater participation in debates about what constitutes evidence of effectiveness; strengthen investment in evaluation 3.3.8 Public lack of awareness of mental health: while in most countries there is a common awareness of key factors that influence physical health e.g. smoking, alcohol, exercise and diet, there is very limited awareness of ‘positive steps’ for mental health and well-being and very few examples of public education campaigns on what the public can do to promote their own mental health and well-being and that of others, including children. • Recommendation: include mental health in all public health campaigns; consider the
application of social marketing techniques to strengthen awareness of mental health (see 3.4.3 ‘marketing mental well-being’)
3.3.9 Lack of focus on the wider determinants of mental health and well-being: there is an apparent lack of balance between understanding and addressing individual level risk factors (and their biological mediators) and population level influences, including a life course (rather than life stage) analysis of mental health impact and influences. This theme is also reflected in responses to the EC Green Paper, where the need to put emphasis on tackling inequalities and reducing social exclusion as part of mental health promotion was noted. There is an important role for mental health promotion in generating greater debate about the relative contribution of individual (biological/genetic/psychological), material and cultural determinants of mental health outcomes and the impact of inequalities on mental health at both an individual and ecological level. • Recommendation: ensure that research addresses determinants of mental health
through the lifespan at an individual, community and structural/environmental level
11 See also IUHPE Special Issue http://www.imhpa.net/uploads/media/Special_Issue_IUHPE.pdf
23
3.4. Key determinants of effective implementation Many countries across the EU have policies, strategies and action plans that include a commitment to mental health promotion and prevention (see EMIP National Reports in Volume II of this report and also IMHPA Country Stories; http://www.imhpa.net).12
Unfortunately, this does not necessarily result in action. Developing a strategy and action plan may be only one element of what is needed to achieve effective implementation, just as ‘evidence of effectiveness’ is only one factor in influencing policy makers and practitioners. Indeed, there are examples of good practice in promotion and prevention in member states and applicant countries that do not yet have a national action plan. Although each country will have its own unique challenges and opportunities in moving from ‘policy’ to ‘delivery’, there are some common factors that support effective implementation. The following determinants of effective implementation have been drawn from analysis of the experiences of national partners in the EMIP project. The determinants of effective implementation are the factors or conditions that influence the scope, level and quality of mental health promotion and prevention activity in a given country. They include:
1. Mental health promotion policy: national and regional 2. Cross sector ownership of mental health promotion/prevention 3. Marketing mental health and well-being 4. Mental health promotion is seen to contribute to improved outcomes for people
with mental health problems 5. Governance, performance management and accountability 6. Clear definition of success and how it will be measured 7. Capacity building across all sectors 8. MHP intelligence/data, evidence base and evaluation
3.4.1. Mental health promotion policy: national and regional The need to increase the visibility and priority of mental health in policy is a recurring theme in EMIP National Reports and it was stressed that EC projects may assist centrally in achieving this. For example, EMIP goals were introduced twice to the Estonian Ministry of Social Affairs and were accepted and highly valued. Many member states consider the existence of a specific public mental health strategy and action plan to be essential. However, unless mental health is also mainstreamed and integrated across all relevant policy areas, consistent with the Health in all policies model, it is likely that mental health promotion will remain marginal. It is hoped that the EU level policies will provide leadership here by incorporating mental health across, for example, education, employment, nutrition, alcohol. A key consideration might be to address the issue: what would policy look like with a well-being focus?13
12 Some of the debates about the relative importance of national strategies/action plans are discussed in Kamin 2006 and issue 5.1 Journal of Public Mental Healthhttp://www.pavpub.com/pavpub/journals/JPMH/index.asp13 See, for example http://www.sustainable-development.gov.uk/publications/pdf/Wellbeing%20Project%202%20Final%20report.pdf
24

In some member states, ensuring that mental health is included within sub-national and regional policy is also an important determinant of effective implementation, notably in relation to the role of local or municipal government. The Netherlands, Estonia, Slovenia, Germany, Finland and Poland all specifically highlighted the importance of the municipalities. Many of the determinants of mental health fall within local government’s areas of responsibility. Equally, low levels of mental well-being have significant implications for the services and infrastructures provided by municipalities. Some local authorities/municipalities are already making a contribution to mental health and there is scope for strengthening local partnerships in this area. The fact that it has been agreed that mental health promotion will become one of the eight priority topics for further policy development work by EuroHealthNet and the IUHPE is also a positive outcome in terms of taking forward some of the learning from EMIP. 3.4.2. Cross sector ownership Improving the mental health of the population contributes to achieving a wide range of outcomes in addition to health outcomes, for both children and adults. Cross sector ownership involves building partnerships with non health sectors and demonstrating how mental health promotion can contribute to policy goals in other sectors, or vice versa i.e.
• policy goals that contribute to improving mental health and well-being (in areas like nutrition, physical activity, arts and creativity)
• policy goals that improving mental health will contribute to (e.g. education, employment, crime reduction, physical health and quality of life).
It involves embedding mental health promotion within existing structures for improving health and social outcomes, both at an EU level, and in ways that are appropriate within each individual member state. As recognised by a number of EMIP partners (e.g. Czech Republic), it also means acknowledging the contribution of NGO’s and planning future collaboration. The wide range of institutions who might be involved in mental health promotion is illustrated in the Estonia National Report which includes national, regional and local government departments, NGOs, including mental health organisations, Alcohol Free Estonia and the Estonian Council of Churches, professional organisations, community based organisations e.g. in schools, prisons, primary care, police and military, the media and research. Issues such as alcohol, violence, parenting, unemployment, work/life balance, community cohesion, sustainable development, and preparation for ageing are high on the policy agenda and so provide opportunities to strengthen awareness about what a greater focus on mental health promotion could contribute in these areas, as well as how specific issues impact on mental health. For example, Ireland, Poland, Slovenia and Austria all raise concerns about alcohol (see EMIP Matrices Annex VIII). Portugal is developing a specific programme on alcohol related problems. The Austrian Health Promotion Foundation´s 2007 activities will focus on the prevention of violence and addiction, as well as mental health promotion in kindergartens, schools and among the elderly. These issues also provide opportunities to build partnerships with non-health sectors.
25
Many existing programmes across all sectors are directly relevant to mental health and examples where mental health has been integrated into Healthy City Networks, Health Promoting Hospitals (for example, the WHO Collaborating Centre for Health Promotion in Hospitals and Health Care, in Austria, has specifically addressed the question: What can hospitals contribute to mental health promotion?) and Schools Networks and business networks (e.g. ENWHP14) are encouraging. Action on housing, noise, traffic congestion, fear of crime and cleaning and greening the environment all contribute to promoting mental health. Even small improvements in mental well-being will achieve significant cost benefits through improvements in physical health, productivity and quality of life. Strengthening cross sector ownership should build on the recommendations of Health in All Policies, with specific reference to mental health, and also identify mechanisms for engaging and establishing formal links with stakeholders across all sectors. Joint funding, where improving mental health can be demonstrated to be of value to a range of stakeholders, is a significant indicator of cross sector ownership. In Estonia for example, the Estonian Ministry of Social Affairs and the Estonian Board of Gambling Tax provided co-funding for the EMIP National Workshop. 3.4.3. Marketing mental health and well-being A recurring theme in the EMIP National Reports is the lack of public awareness in relation to mental health, which includes familiar concerns about stigma and lack of understanding about mental disorders, as well as very low levels of awareness of how to promote ‘positive mental health and well-being’. A precondition for improving the mental health of the population and in improving the quality of life of people with mental health problems is to increase the level of awareness of mental health and to establish it as a common interest and responsibility. As Estonia observed ‘people still equate mental health and psychiatry’. In the past decade, considerable progress has been made in raising awareness of mental health and a wide range of EC funded projects have contributed to this progress. At the same time, evidence from EMIP suggests that levels of mental health literacy i.e. levels of public knowledge on what harms and what protects mental well-being, remain low. Overall, the public is much better informed about physical health. At the same time, in many partner countries (for example Finland, Slovenia, and Ireland), there has been considerable media interest in ‘well-being’ generally, stimulated by debates about ‘happiness’ and quality of life15, as well as in the causes and consequences of anxiety and depression (http://www.eaad.net/).The proposed organization by the EC of a European Year of the Mind could make an extremely valuable contribution to moving these debates forward and placing mental health and well-being at the centre.
14 http://www.enwhp.org15 See for example the MTV youth happiness survey http://www.merinews.com/catFull.jsp?articleID=123782&category=Lifestyle&catID=7&rtFlg=rtFlg and the Happy Planet Index http://www.happyplanetindex.org/list.htm which addresses the relative success or failure of countries in supporting good life for their citizens, whilst respecting the environmental resource limits upon which our lives depend.
26

Marketing mental health and well-being involves strengthening people’s knowledge, skills and capacity to achieve positive mental health. In situations of sustained social, economic and psychological stress, most people experience symptoms of mental illness. What might be called the ‘five fruit and vegetables’ of mental health help to protect mental well-being for everyone, whether they have symptoms or not. They include:
• keeping physically active, • eating well • drinking in moderation • valuing yourself and others • talking about your feelings • keeping in touch with friends and loved ones • caring for others • getting involved and making a contribution • learning new skills • doing something creative • taking a break • asking for help
These ‘positive steps’ for mental health are familiar themes in a wide range of research on what people who experience mental health problems find helpful. They provide a foundation for everyone’s mental health and now need to be much more widely disseminated to the general public. Progress could be measured through data on mental health literacy i.e. levels of public knowledge on what harms and protects mental well-being, in addition to existing data on public attitudes to mental illness. Marketing mental well-being will only be effective if it is matched by greater opportunities for support, for families, in schools, in the workplace and in the community. The Netherlands, for example, in their work on the prevention of depression, have particularly highlighted the importance of using as much as possible, a community approach (Netherlands National Report). This will also involve working with primary care and the voluntary and community sector (VCS) to expand the range of therapeutic options for the promotion of mental health and the prevention of mental health problems and also addressing the wider determinants of mental health. In this way, marketing mental well-being can contribute to building community alliances and networks (similar to those developed to promote smoke free environments) with a commitment to working to counter global and local trends that are toxic to mental health and well-being. 3.4.4. Mental health promotion contributes to improved outcomes for people
with mental health problems As outlined in the responses to the EC Green Paper, in many member states, the reform of mental illness services and work to address the stigma, discrimination and denial of human rights and civil liberties experienced by people with mental health problems remain central and urgent priorities. It is important to demonstrate that the goals of mental health promotion are complementary, providing a framework for building hospitable communities where people with mental health problems can live, socialise, study, work, participate and enjoy the same opportunities and access to resources as everyone else.
27

Recovery agenda 3.4.5. Governance, performance management and accountability Governance, performance management and accountability refer to the need for a mechanism or framework for ensuring that action to improve mental health is not simply ‘optional’. Such a framework might include legislation, targets and clear lines of accountability for delivering mental health promotion, or the development of quality criteria, as suggested by the WHO-CC for Health Promotion in Hospitals and Health Care, arguing that the ‘Mental Health Promotiveness’ of a setting can be understood as a quality criterion. 3.4.6. Clear definition of success and how it will be measured
In order to assess progress in promoting mental well-being, there is a need to develop indicators that can be used to measure different dimensions of positive mental health, in addition to existing indicators of psychiatric morbidity, which are used to determine prevalence of mental illness (Stewart Brown, 2002). Currently, a personal and social well-being module is being developed for the third wave of the European Social Survey. This will include questions designed to capture personal and social well-being and adopts a definition of well-being which incorporates not only how people feel, i.e. hedonic aspects of well-being such as pleasure, enjoyment, satisfaction, but also how people function, i.e. eudaimonic aspects of well-being, such as competency, interest or engagement, meaning or purpose in life. It gives equal emphasis to personal well-being and to inter-personal or social well-being (Huppert et al, 2005). In some countries, there is an obligation to survey the health of the population, providing opportunities to include mental health. This is the case in the Netherlands, where the next round in 2007 will include questions on emotional problems, and in Portugal, where the 4th National Health Survey will strengthen both alcohol and mental health information. In Scotland, a wide ranging programme is addressing the development of national public mental health indicators and is currently assessing national and international datasets (www.wellscotland.info and http://www.healthscotland.com/understanding/population/mental-health-indicators.aspx). More broadly, European Commission funded programmes (European Commission & STAKES, 2004) concerned with establishing mental health indicators include:
• Establishment of a set of mental health indicators for the European Union (1999-2001)
which aimed to propose a set of feasible and reliable indicators for monitoring mental health that could be easily integrated into the European Community Health Indicators (ECHI) system (Korkeila, 2000; STAKES, 2001)
• Mental health information and determinants for the European level (MINDFUL) (2004-2006) established to tackle the shortage in available indicators (STAKES, 2005) http://www.stakes.fi/mentalhealth/mindful.html. This includes a partnership project concentrating on macro level structural positive mental health indicators led by the University of Deusto in Bilbao and currently piloting an extensive set of potential indicators
28

Mental Heath Impact Assessment provides a further framework for establishing a baseline and measuring success and a number of such projects are established or planned, for example a European Project co financed by the EC and the Portuguese National Health Plan.
3.4.7. Capacity building across all sectors As noted in section 3.3.4 Common Challenges, many member states have noted a shortage of mental health promotion skills across all sectors, including health and health promotion. Building public mental health capacity through training in different settings and sectors, including within the community, and at all levels, will be essential to achieve sustained improvements in effective delivery. As was noted during the informal consultation meeting on the Green Paper chaired by EuroHealthNet, even within health promotion, there is not necessarily expertise on mental health and on the extent to which areas like nutrition, physical activity and alcohol impact on mental health. Some countries do include promotion and prevention in the vocational training of health professionals – this is compulsory in Portugal, although still needs to be developed further. In a number of member states, it was noted that the EMIP project provided the first opportunity to bring colleagues together to address mental health promotion/prevention. The Czech Republic used the National Workshop to begin to build a National Coalition in Mental Health Promotion (NIPH). Austria stated that the workshop ‘provided the possibility to link experts working in different areas’. This kind of national collaboration, exchange of information and debate contributes centrally to building capacity. In Finland, for example, it has been agreed that workshops following the EMIP model will be continued under the auspices of the WHO Collaborating Centre for Mental Health Promotion, Prevention and Policy (located in STAKES), in partnership with the Finnish Public Health Institute and the Finnish Institute of Occupational Health. 3.4.8. MHP intelligence/data, evidence base and evaluation The need for significantly improved public mental health intelligence is widely recognised: in particular, further research is needed on:
• the determinants of mental health (see section 3.3.9.), • the relative contribution of different risk and protective factors to mental health
outcomes • mental health impact and mental health impact assessment • indicators (see section 3.4.6.) • effective interventions, notably in the area of non medical and non pharmacological
interventions, (sometimes called ‘community referrals or social prescribing) which has been under-researched relative to clinical interventions
Greater advantage should be taken of learning from those countries that have made considerable progress in these areas. The Netherlands, for example, has a tradition of large scale epidemiological studies and is leading the way in areas like e-prevention, epidemiological support and an integrated approach. There is also a need to strengthen awareness of and debate about a new range of research on what constitutes mental health - what Keyes has called the ‘symptoms and diagnostic criteria’ for mental health, as opposed to mental illness (Keyes 2002; 2005; 2006; Gilleard et al 2005).
29

Such research helps to demonstrate the case for a whole population approach to mental health and to provide a rationale for the focus on positive mental health and well-being. Keyes’ research confirms that individuals who fit the criteria for a DSM IV/ICD 10 mental disorder may have the presence of mental illness plus the absence of mental health, but equally may have moderate mental health or be flourishing. Keyes also argues, based on a longitudinal study of adolescents, that children without mental illness are not necessarily mentally healthy. Flourishing youth were found to be functioning better than moderately mentally healthy or languishing youth (Keyes 2006). Using measures of emotional well-being, psychological well-being and social well-being as three distinct but correlated factors, Keyes found that as mental health increased, prevalence of conduct problems decreased (arrests, truancy, alcohol, tobacco and marijuana use) and measures of psychosocial functioning (self determination, closeness to others and school integration) increased. The growing focus on positive mental health at an individual level is matched by research demonstrating the value of a model focusing on assets, as opposed to deficits.16 Research in the field of health assets has the potential to make a valuable contribution to enhancing understanding that mental health and well-being are precious assets, to be protected and promoted. 4. RECOMMENDATIONS AND CONCLUSIONS Recommendations for future mental health promotion activity fall into four categories:
• the future direction of mental health promotion policy • expanding the mental health promotion community of interest and building capacity
for mental health promotion • developing and supporting effective delivery of mental health promotion • mainstreaming mental health promotion
Mental health promotion moving up the agenda This is a time of significant policy developments in mental health promotion within the EC, WHO Europe and individual countries (WHO 2004a; WHO 2004b; Jane Llopis and Anderson 2006). Mental health promotion now has a much higher status on the policy agenda and it is clear from the EMIP project that colleagues in many countries are using European commitment to ‘mental health for all’ to develop or strengthen national policy and action to promote mental well-being. The focus on “mental health activities capable of improving the well-being of the whole population” marks an important shift towards including promotion, rather than an exclusive focus on prevention and treatment.
16 WHO defines a health asset as any factor (or resource) that enhances the ability of individuals, communities, populations etc to maintain health and well-being. Evidence shows that interventions to maximize and take advantage of health assets can counter negative social and economic determinants of health, especially among vulnerable groups. The result is improved health outcomes (http://www.euro.who.int/socialdeterminants/assets/20050623_1?language=French
30

EC Social Agenda and Green Paper It is important to demonstrate the contribution of mental health to the European Commission’s new Social Agenda, (part of the revamped Lisbon Strategy) with its focus on jobs and growth, with two key priorities: prosperity and solidarity. However, making the economic case in terms of the ‘burden of mental illness’ can suggest that prevention is the main goal and detract attention from the fact that promoting mental health is a worthwhile goal for Europe in its own right.17 A crucial step at an EU and national and/or regional level is to incorporate the promotion of mental health and well-being into general health and mental health policies. This can help ensure that strategies to reduce the consequences of depression and other mental disorders do not just focus on treating people who are already ill. Effective mental health policy requires a commitment to health improvement, prevention and indeed to wider goals and principles within society, such as social justice. Official support for these wider objectives can also help in developing programmes and strategies to improve coordination between agencies and also in raising the profile and priority of mental health promotion. We can see emerging in policy, practice and debate across the EU and within EU member states and applicant countries, some of the following key themes and areas of interest:
• positive well-being rather than illness; a focus on an assets, as opposed to a deficit, model
• research on the determinants of mental health, in addition to the determinants of mental illness
• the contribution mental health promotion makes to recovery and improved quality of life for people with mental health problems
• links between well-being and outcomes in health, education, crime, employment, quality of life, social cohesion and relationships
• relevance of well-being to non health sectors e.g. economic development, regeneration, sustainable development
Key themes across all policy areas that are relevant to the future direction of public mental health and where mental health promotion has a special contribution to make include:
• reducing inequalities • regenerating deprived communities • building the confidence that individuals and communities need, to be able to thrive
socially and economically • increasing participation among those most deprived and marginalised • reducing social exclusion • helping people to take more responsibility for actively managing their own health
17 While the Council of Europe’s European Convention on Human Rights (http://www.fco.gov.uk/Files/kfile/COE-EuropeanHumanRightsConvention.pdf) has been crucial in addressing abuses in mental health services, it is the EC’s economic growth agenda that is influencing new trends in mental health policy.
31

32
Table 2 Matrix for recommendations
National EU Level
Future directions
Population wide approach; Positive mental health and well-being
Determinants of mental health; mental health impact
Capacity building
Develop training and support infrastructures; Mechanisms for involving communities
Support opportunities for EU wide education, training, networking, exchange of information
Support for delivery
Adequate resources; strategy/action plans
EC Mental Health Strategy Trans-national research; EU-wide projects
Mainstreaming
Mental health in all policies; Cross sector partnerships
Mental health in all policies Mental health impact assessments
5. FINANCIAL STATEMENTS OF REVENUE AND EXPENDITURE (Please see following pages)

References David I, Kebza V, Paclt I , Raboch J, Volf J (2006) Mental health in the Czech Republic Journal of Public Mental Health 5.2: 43-47 European Commission (2005) Communication from the Commission on the Social Agenda http://europa.eu.int/comm/employment_social/social_policy_agenda/social_pol_ag_en.html European Commission (2005) Green Paper: Improving the mental health of the population. Towards a strategy on mental health for the EU Brussels: Health and Consumer Protection Directorate General http://europa.eu.int/comm/health/ph_determinants/life_style/mental/green_paper/mental_gp_en.pdf Friedli, L. (2004). Editorial. Journal of Mental Health Promotion, 3(1), 2-6. http://www.pavpub.com/pavpub/journals/JPMH/index.asp Gilleard C, Pond C, Scammell A, Lobo R, Simporis K and Rawaf S (2005) Well-being in Wandsworth: a public mental health audit Journal of Public Mental Health 4.2: 14-22 Jané-Llopis, E. & Anderson, P. (2005). Mental Health Promotion and Mental Disorder Prevention. A policy for Europe. Nijmegen: Radboud University Nijmegen. Journal of Public Mental Health http://www.pavpub.com/pavpub/journals/JPMH/index.asp Kamin T (2006) Mental health promotion: a perspective from Slovenia Journal of Public mental health 5.1: 24-28 Keyes, CLM. (2002) The mental health continuum: from languishing to flourishing in life. J Health Soc Res 43:207-22 Keyes CLM (2005) Mental illness and/or mental health? Investigating axioms of the complete state model of health Journal of Consulting and Clinical Psychology 73:539-548 Keyes CLM (2006) Mental health in youth: is America’s youth flourishing? American Journal of Orthopsychiatry (in press) Kuhn K (2006) Mental health promotion in the workplace: a European perspective Journal of Public mental Health 5.1:29-34 McAllister F (2005) Wellbeing Concepts and Challenges: Discussion paper Sustainable Development Research Network http://www.sd-research.org.uk/documents/SDRNwellbeingpaperfinal-20December2005_v3_000.pdf McMichael AJ (1999) Prisoners of the proximate: loosening the constraints on epidemiology in an age of change American Journal of Epidemiology 149:10 887-897 World Health Organization. (2004a). Prevention of mental disorders: Effective interventions and policy options, Summary Report. A report of the World Health

Organization, Department of Mental Health and Substance Abuse in collaboration with the Prevention Research Centre of the Universities of Nijmegen and Maastricht. Geneva: World health Organization http://www.who.int/mental_health/evidence/en/prevention_of_mental_disorders_sr.pdf World Health Organization, (2004b). Promoting mental health: Concepts, emerging evidence, practice :summary report. A Report from the World Health Organization, Department of Mental Health and Substance Abuse in collaboration with the Victorian Health Promotion Foundation (VicHealth) and The University of Melbourne. Geneva, WHO http://www.who.int/mental_health/evidence/en/promoting_mhh.pdf WHO European Declaration and Action Plan http://www.euro.who.int/document/mnh/edoc07.pdfhttp://www.euro.who.int/document/mnh/edoc06.pdf http://www.europa.eu.int/comm/health/ph_projects/2002/promotion/fp_promotion_2002_frep_16_en.pdf

Annexes: I. Consortium Partners II. National Partners III. Project Experts IV. Dates of the National Workshops V. EMIP Postcard VI. EMIP Response to EC Mental Health Green Paper VII. EMIP Matrices

Annex I: EMIP Consortium Partner addresses as at Dec. 06
Henderson, John Dr. Mental Health Europe Boulevard Clovis 7 1000 Bruxelles Belgium Tel.: +32-2-280 04 68 Fax: +32-2-280 16 04 mailto:[email protected]
Van Dievel, Mary Mental Health Europe Boulevard Clovis 7 1000 Bruxelles Belgium Tel.: +32-2-280 04 68 Fax: +32-2-280 16 04 mailto:[email protected] www.mhe-sme.org
Jané-Llopis, Eva PhD Van Alst, Sjoerd Prevention Research Centre, Academic Centre for Social Sciences and Department of Clinical Psychology Radboud University P.O. Box 9104 6500HE Nijmegen The Netherlands Tel: + 31 24 361 26 67 Fax: + 31 24 361 55 94 mailto:[email protected]:[email protected] www.preventioncentre.net
Pelikan, Juergen Prof. Dietscher, Christina Mag. WHO Collaborating Centre for Health Promotion in Hospitals and Health Care Ludwig Boltzmann Institut für Medizin- und Gesundheitssoziologie Rooseveltplatz 2/4 1090 Wien Austria Tel.: +43-1-4277- 48208 (-48203, -48230) Fax: +43-1-4277-48-290 mailto:[email protected]/mailto:[email protected]/ www.univie.ac.at
Lavikainen, Juha Dr. National Research and Development Centre for Welfare and Health (STAKES) P.O. Box 220 00531 Helsinki Finland Tel.:+358-9-3967 - 2184 Fax: +358-9-3967 – 2155 mailto:[email protected]
Katila-Nurkka, Ulla National Research and Development Centre for Welfare and Health (STAKES) P.O. Box 220 00531 Helsinki Finland Tel: +358-9-3967-2331 Fax: +358-9-3967-2155 mailto:[email protected]/mentalhealth
Kiikkala, Irma Dr. National Research and Development Centre for Welfare and Health (STAKES) P.O. Box 220 00531 Helsinki Finland Tel.:+358-9-3967 -2337 Fax: +358-9-3967 - 2155 mailto:[email protected]/mentalhealth
Needle, Clive EuroHealthNet Rue Philippe Le Bon 6 1000 Bruxelles Belgium Tel.:+32-2-235-03-20 Fax: +32-2-235-03-39 maito:[email protected]://www.eurohealthnet.eu
Schmidtke, Armin Prof. Dr. Sell, Roxane Psychologist WHO/Euro Network for Suicide Research and Prevention Department of Psychiatry and Clinical Psychology University of Wuerzburg Fuechsleinstr. 15 97080 Wuerzburg Germany Tel.: +49-931-201-76-670/680 Fax: +49-931-201-76-690 mailto:[email protected]

Radulescu, Roxana European Public Health Alliance (EPHA) 39-41 rue d´Arlon 1000 Bruxelles Belgium Tel.: +32-2-230-30-56 (-3873) Fax: +32-2-230-38-80 mailto:[email protected]
Kuhn, Karl Dr Kampstein, Claudia De León, Lucrecia Roos, Matthias Federal Institute for Occupational Safety and Health Friedrich-Henkel-Weg 1 – 25 44149 Dortmund Germany Tel.: +49 231 – 9071 – 2711/2303 Fax: +49 231 – 9071 – 2537 mailto:[email protected]:[email protected]:[email protected]:[email protected] www.baua.de
Annex II: EMIP National Partner addresses as at Dec. 06
Austria Rohrauer, Gerlinde Mag.a Fonds Gesundes Österreich Mariahilferstraße 176 1150 Wien Tel.: +43 (0)1-89-50-400-19 Fax: +43(0)1-8950400-20 mailto:[email protected] http://www.fgoe.org/
Czech Republic Janatova, Hana Dr. Kebza, Vladimir Dr. National Institute of PH Srobarova 48 100 42 Prague Tel.: +420-2670-829-69 Fax: +420-2670-829-69 mailto:[email protected]:[email protected]://www.szu.cz/
Estonia Värnik, Airi Dr., Head Prof. Sisask, Merike Estonian-Swedish Suicidology Institute Pärnu mnt. 104 Tallinn 11312 Tel.: +372-65-16-550 Fax: +372-62-155-80 mailto: [email protected]: [email protected]
Finland Irma Kiikkala National Research and Development Centre for Welfare and Health (STAKES) Mental Health P.O. Box 220 00531 Helsinki Tel.:+358-9-396 71 Fax: +358-9-761-307 mailto:[email protected]
Germany Beerman, Beate Dr. Federal Institute for Occupational Safety and Health Friedrich-Henkel-Weg 1 – 25 44149 Dortmund Tel.: +49 231 – 9071 – 2238 Fax: +49 231 – 9071 – 2537 mailto:[email protected]
Hungary Plette, Richard Dr. National Institute of Occupational Health Nagyvarad ter 2, P.O. Box 51 1450 Budapest Tel.:+(361)-476-1162 Fax: +(361)-216-9907 mailto:[email protected]
Ireland Wynne, Richard Dr. Work Research Centre 1 Greenlea Drive Dublin 6W Tel.: +353-1-49270-42 (office) Tel.: +353-87-9978-402 (mobile) Fax:+353-1-4927-046 mailto:[email protected] http://www.wrc-research.ie/
The Netherlands Bohlmeijer, Ernst Drs. Trimbos-Instituut Postbus 725 3500 AS Utrecht Tel.:0031-30-2971-100 Fax: 0031-30-2971-111 mailto:[email protected] http://www.trimbos.nl/
Poland Mroziak, Barbara PhD Okulicz-Kozaryn, Katarzyna Ph.D. Institute of Psychiatry and Neurology Sobieskiego 9 02-957 Warsaw Tel.: (48-28) 45-82-534 Fax: (48-28) 45-82-630 mailto:[email protected]:[email protected]://www.ipin.edu.pl/

Portugal Santos, Maria Joao Heitor dos Dr. Directorate General of Health Alameda D Alfonso Henriques 45 P-1049-005 Lisbon Tel.: +35- 121-843-0635 Fax.: +35-121-843-0655 mailto:[email protected]
Romania Haratau, Mihaela Dr. Haratau, Theodor Dr. Romtens Foundation Aleea Stanila Nr. 3 32707 Bucharest Tel.: + 4021 – 34 833 90 Fax::+ 4021 – 34 833 90 mailto:[email protected] mailto:[email protected] http://www.romtens.ro/
Slovenia Kamin, Tanja PhD Zorko, Maja Psychologist Institute of Public Health of the Republic of Slovenia Trubarjeva 2, PO box 260 1000 Ljubljana Tel.: 00386-1-4323-245 0038-612-441-402/404 Fax: 0038-612-441-447 mailto :[email protected]:[email protected]:[email protected]://www.sigov.si/ivz/
Annex III: Project experts Contact Data Dr. Lynne Friedli Mental health promotion specialist 22 Mayton Street UK-London N7 6QR Tel.: +44 (0)20 - 7700 - 5035 mobile: 07812- 52 83 07 mailto:[email protected] Dr. Gregor Henderson Director National Programme for Improving Mental Health and Well-Being - Scottish Executive 3EN St Andrew´s House Regent Road UK-Edinburgh EH1 3DG Scotland Tel.: ++ 0131 - 244 0109 mobile: 07973 - 53-88-37 Fax: ++ 0131 244 2846 mailto:[email protected] Czeslaw Czabala, Ph.D. Institute of Psychiatry and Neurology Sobieskiego 9 PL-02-957 Warsaw Tel.: (48-22) 45-82-621 (-800) mailto:[email protected] Prof. Dr. Hartmut Berger Task Force on Health Promoting Psychiatric Services Medical Director ZSP Philippshospital - Walter-Picard-Klinik Postfach 1362 DE - 64550 Riedstadt mailto:[email protected].: ++49 – (0)- 6158 - 183-201 Fax: ++49 – (0)- 6158 - 183-243 Prof. Dr. Ulrich Hegerl Klinik und Poliklinik für Psychiatrie Universitätsklinikum Leipzig Johannisallee 20 DE-04317 Leipzig Tel.: ++49 – (0)- 341 – 97-245-30 Fax: ++49 – (0)- 341 – 97-245-39 mailto:[email protected]
Prim. Univ. Doz. Dr. Christian Haring Psychiatric State Hospital of Tyrol Thurnfeldgasse 14 AT-6060 Hall Tel.: ++43 – (0) 5223 – 508-2030 mailto:[email protected] Jude Stansfield Care Services Improvement North West Development Centre Hyde Hospital, 2nd Floor Grange Road South UK- Hyde, Cheshire, SK14 5NY mailto:[email protected] Dr. Harry Vertio Cancer Society of Finland Liisankatu 21 B Universitätsklinikum Leipzig FI- 00170 Helsinki Tel.: ++358 9 135 331 Fax: ++358 9 135 1093 mailto:[email protected] More contact and background information can be found on the following websites: Members of the EC Working Party on MH http://europa.eu.int/comm/health/ph_information/implement/wp/mental/docs/ev_20050530_lp_en.pdf The National Programme for Improving Mental Health and Well-being in Scotland: http://www.wellontheweb.net Institute of Psychiatry and Neurology in Warsaw, Poland http://www.ipin.edu.pl Task Force on Health Promoting Psychiatric Services http://www.hpps.net/ European Alliance Against depression http://www.eaad.net/http://europa.eu.int/comm/health/ph_projects/2003/action3/action3_2003_14_en.htm
Annex IV: Dates of National Workshops EMIP National Workshops: 2005 September Netherlands October 4/5 Estonia October 14/15 Poland October 19 Slovenia October 31 Finland November 3/4 Portugal November 4 Hungary November 4 Germany November 7 Austria November 22 Czech Republic November 29 Ireland 2006 January 26 Romania (postponed from November 24/2005)
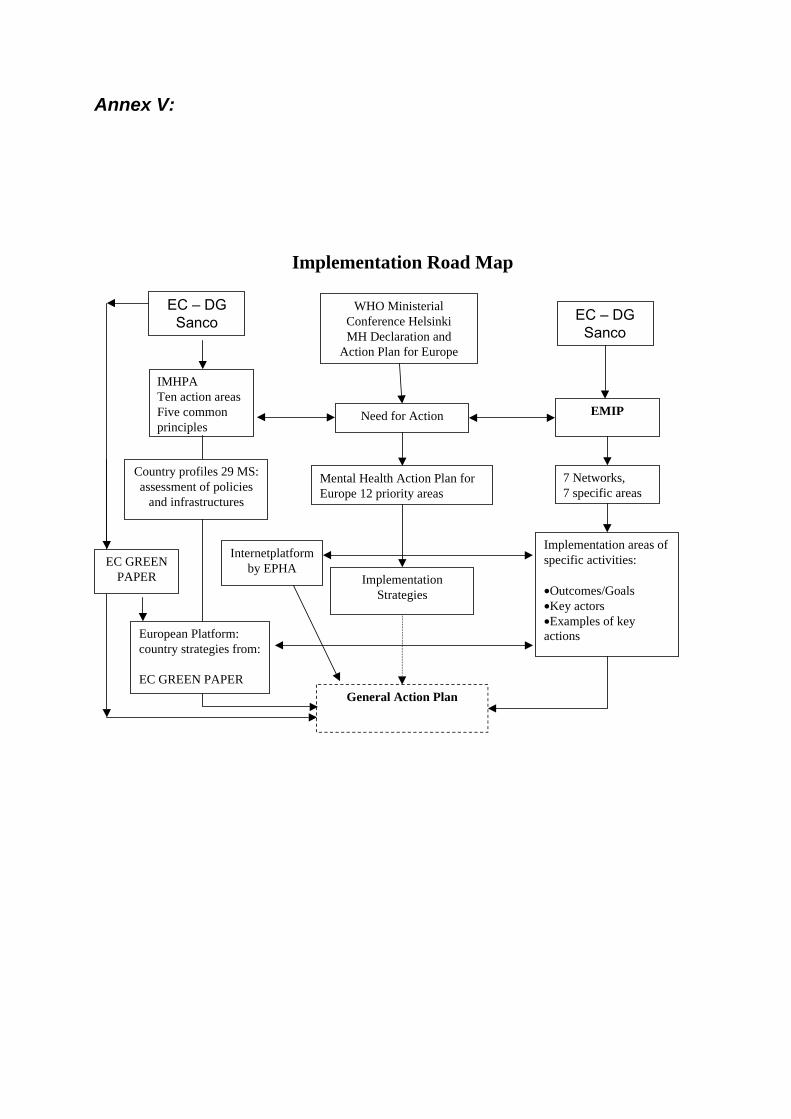
Annex V:
Implementation Road Map
EMIP
WHO MinisterialConference HelsinkiMH Declaration and
Action Plan for Europe
Need for Action
7 Networks,7 specific areas
Mental Health Action Plan forEurope 12 priority areas
Implementation areas ofspecific activities:
•Outcomes/Goals•Key actors•Examples of keyactions
General Action Plan
IMHPATen action areasFive commonprinciples
ImplementationStrategies
Internetplatformby EPHA
Country profiles 29 MS:assessment of policies
and infrastructures
EC – DGSanco
European Platform:country strategies from:
EC GREEN PAPER
EC – DGSanco
EC GREENPAPER
Annex VI: EMIP Postcard
Annex VII: EMIP Response to EC Mental Health Green Paper
“Implementation of Mental Health Promotion and Prevention Strategies in EU Member States and Applicant Countries” (EMIP) Response to EC Green Paper on Mental Health EMIP welcomes and supports the proposal for the development of an EU strategy for mental health. We are aware that progress in improving the mental health of the European population will depend not only on improving quality of life and protecting the rights and dignity of people with mental health problems, but also on action to promote mental health and prevent mental ill-health. The mental health of the European population is a resource to put Europe back on the path to long-term prosperity. Action to promote and protect mental well-being – of individuals, families, organisations and communities – will be crucial in achieving the European Commission’s New Social Agenda, with its focus on solidarity and prosperity. There is abundant robust evidence that the skills and attributes associated with positive mental health lead to improved physical health, better quality of life, reduced crime, higher educational attainment, economic well-being and personal dignity. Mental well-being also contributes fundamentally to the extent to which people feel able and motivated to exercise choice and control and to adopt healthy lifestyles. It is essential to enabling individuals, families and communities to realise their full potential and to make a positive contribution.18
18 World Health Organization (2004a) Prevention of mental disorders: Effective interventions and policy options Geneva: WHO http://www.who.int/mental_health/evidence/en/prevention_of_mental_disorders_sr.pdfhttp://www.who.int/mental_health/evidence/en/promoting_mhh.pdfWorld Health Organization (2004b) Promoting mental health: Concepts, emerging evidence, practice Geneva: WHO http://www.who.int/mental_health/evidence/en/promoting_mhh.pdf

We particularly welcome the support offered through the strategy to increase the coherence of actions in the health and particularly non-health policy sectors in member states and at the community level and the proposals for the development of information and knowledge on mental health. EMIP’s work with 12 EU partner countries has clearly demonstrated to us the need for a comprehensive, holistic approach that builds partnerships and demonstrates that promoting mental health is the responsibility of, and will benefit, all sectors.19
Specific responses to the consultation questions How relevant is the mental health of the population for EU’s strategic policy objectives?
EMIP supports the view taken in the 2005 WHO declaration on mental health which states that: “there is no health without mental health. Mental health is central to the human, social and economic capital of nations and should therefore be considered as an integral and essential part of other public policy areas such as human rights, social care, education and employment”. Mental health underpins the achievement of the EU’s strategic policy objectives. Without a mentally healthy society, we will not achieve prosperity, solidarity, social justice or quality of life for citizens. The case for tackling the factors that exclude people with mental health problems and for action to prevent mental health problems is significant. The social and economic costs of mental ill health are wide ranging: one in four Europeans experience a significant episode of mental illness during their lifetime and mental health problems account for approximately 20% of the total burden of ill-health in Europe.20 The loss to European GDP is 3-4% per annum and suicide has been identified as the third highest cause of death for young people. These are robust reasons to have an EU strategy. . However, a greater focus is needed on the development of a strategy to support the mental health and well-being of the whole community. Action to promote the mental health and well-being of the whole population, in schools, in the workplace, in the community, in the health care sector, and reaching out to at risk and vulnerable groups, will be essential to achieving social cohesion, better social and economic welfare and the transition of the EU into a knowledge society. This means involving those beyond traditional mental health services and integrating the priorities across generic strategies and programmes. It is important that mental health be integrated into EU strategic policy objectives and other EU strategies and programmes.
19 http://www.emip.org20 European Commission (2005) Green Paper: Improving the mental health of the population. Towards a strategy on mental health for the EU Brussels: Health and Consumer Protection Directorate General http://europa.eu.int/comm/health/ph_determinants/life_style/mental/green_paper/mental_gp_en.pdf

A comprehensive approach to mental health at every level is needed and an EU strategy will help to achieve this within member states. Key areas of importance include the following:
• Work and workplace: The need to support people with mental health problems to return to work and to create more mentally healthy workplaces. The need to provide more active, work oriented rehabilitation in order to boost social inclusion and return people to mental well-being. The need to recognise the contribution of those who contribute through unpaid work e.g. volunteering, caring and being active citizens, as well as supporting and creating opportunities for those who are unable to enter paid employment and to recognise the valuable contributions of all citizens.
• Health care sector: In terms of mental health, the health care sector is both a high-
risk workplace for staff, a stressful life event for patients and a key player in supporting promotion and prevention for the general population.
• Access to mainstream opportunities: Inclusion and recovery are particularly
significant to achieving the EU’s objectives of solidarity and social justice. It will be important to identify and address barriers to participation for people with mental health difficulties and to do so in the context of a recovery model.
• Quality of life is a significant health and mental health outcome. Consistent
monitoring of quality of life/mental health and well-being is therefore needed across Europe.
• Determinants of mental health and well-being: greater clarity on the wider
determinants of mental health and well-being is needed. Mental health problems are not a random misfortune: across the spectrum of disorders, poor mental health is associated with inequality, material deprivation, unemployment, low educational attainment, violence and abuse, neglect in childhood. “Inequality and exclusion are both a cause and consequence of mental health problems”.21
Would an EU strategy add value to existing and envisaged actions and are the proposed priorities adequate? The findings of the EMIP national workshops demonstrate that a framework which creates coherence of actions in different policy sectors across member states and provides a platform for involving stakeholders across all settings and sectors in building solutions around the four priorities would add value to and help to build on action being taken forward in member and applicant states.
21 Rogers A and Pilgrim D (2003) Mental Health and Inequality Basingstoke: Palgrave; Melzer D, Fryers T and Jenkins R (2004) Social inequalities and the distribution of common mental disorders Maudsley Monographs Hove: Psychology Press
It is already clear from responses to the Green Paper consultation that a comprehensive EU strategy would help to raise the profile of the importance of mental health within member states as well as within the EU and other European and international bodies. It would potentially lead to further actions and a consistent and evidence-based approach across member states. It is envisaged that, once developed, the strategy would need co-coordinated implementation and evaluation with the commitment of resources to do so and agreed timescales for action. EMIP fully supports the four priorities to:
(1) promote the mental health of all; (2) address mental ill health through preventive action; (3) improve the quality of life of people with mental ill health or disability through social inclusion and the protection of their rights and dignity; and (4) develop a MH information, research and knowledge system for the EU.
The balance of these four issues is most welcomed. Priorities that move us away from solely addressing population mental health through provision of health and social care services to ones that re-orient health services and address the determinants of mental health are long overdue. The feasibility of such approaches has been demonstrated by EU and WHO projects and networks such as the Implementing Mental Health Promotion Action project (IMHPA), the European Network .of Smoke-Free Hospitals or the WHO Network of Health Promoting Hospitals. The determinants of effective implementation, identified by the EMIP project, demonstrate that the following factors support the development and delivery of mental health promotion in member states:
Mental health promotion policy (national and local) Cross sector ownership Marketing mental well-being MHP contributes to service reform/improved outcomes for people with mental
health problems Governance/performance management/accountability Clear definition of success and how it will be measured Capacity building across all sectors Evidence base, evaluation and MHP intelligence/data
Are the proposed initiatives appropriate to support the co-ordination between member states? The initiatives proposed appear to be appropriate although more detail on this would be useful. The development of an action plan would be welcome. It would be beneficial for both the dialogue with member states and the EU platform to address all the priorities. Key issues of importance include the following: • Cost-benefit analysis of promotion and prevention would be welcome. • Greater opportunities for networking, sharing of information, partnership working.
Care should be taken that these opportunities are open, transparent and inclusive.

Conclusion In conclusion, EMIP welcomes and supports the proposals as set out in the Green Paper. The proposals in our view could be strengthened through a stronger emphasis within the proposed options for action on tackling the broader determinants of mental ill health, action to strengthen the determinants of effective implementation of mental health promotion and engaging the non-health policy sectors. This statement has been endorsed by all EMIP partners and experts22: Dr. Karl Kuhn EMIP Project Leader Federal Institute of Occupational Safety and Health (FIOSH) Friedrich-Henkel Weg 1- 25 D – 44139 Dortmund mailto:[email protected]
22 For contact details please see Annexes I, II, III.
Annex VIII: EMIP Matrices Guide to the EMIP Matrices 1.0 Introduction The EMIP Matrices are based on an analysis of the experiences of national partners identified during the EMIP project and described in the National Reports. The aims of the EMIP Matrices are to:
• identify common factors that support the development and effective implementation of mental health promotion and prevention
• provide a framework for identifying and mapping opportunities and challenges • provide a basis for partner countries to offer mutual support, exchange of information
and experience in moving mental health promotion forward The matrices should be read in conjunction with the National Reports (EMIP Final Report Volume 2), which provide more detail on the policy environment, strengths and weaknesses and examples of implementation. List of tables: Table 1 Matrix One: framework for recording challenges, opportunities, implementation
and legislation (Page 55) Table 2 Highlighted Issues by specific partner countries (Pages 56 – 58) Table 3 Determinants of effective implementation by partner country (Page 59, Romania, Poland, Slovenia, Hungary, Austria, Czech Republic) (Page 60, Germany. Estonia, Finland, Netherlands, Portugal, Ireland) Table 4 European Level Added Value (Page 61)
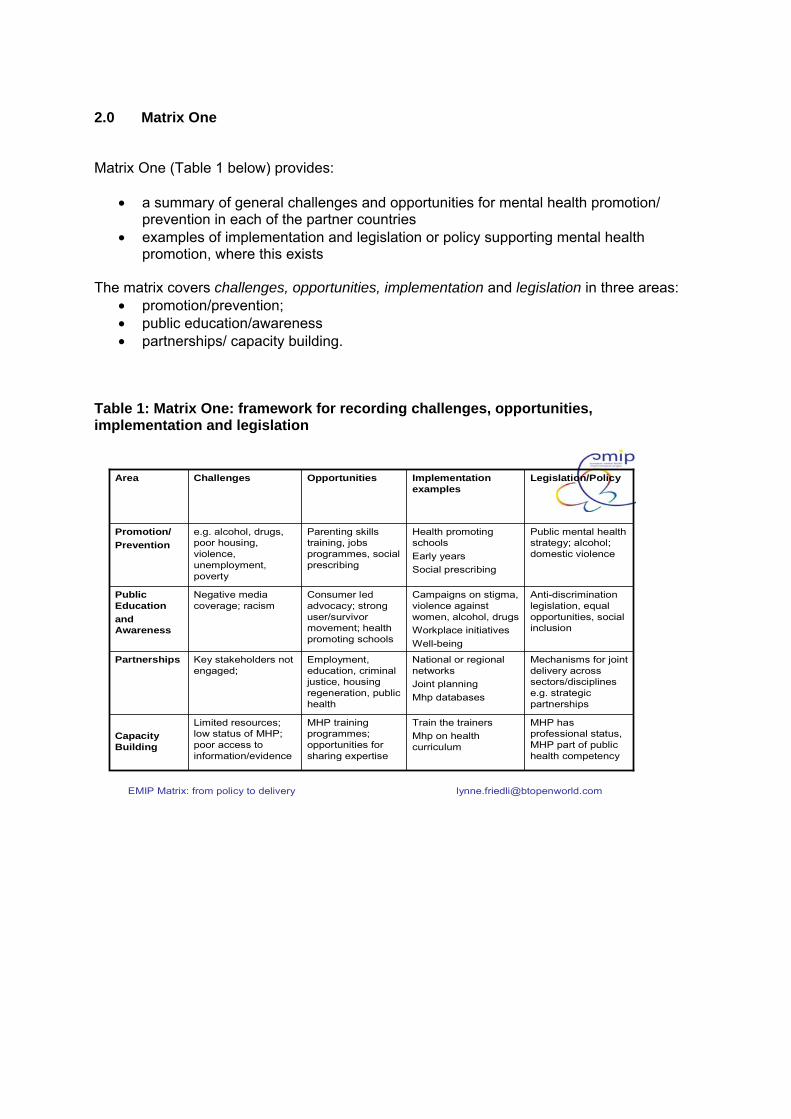
2.0 Matrix One Matrix One (Table 1 below) provides:
• a summary of general challenges and opportunities for mental health promotion/ prevention in each of the partner countries
• examples of implementation and legislation or policy supporting mental health promotion, where this exists
The matrix covers challenges, opportunities, implementation and legislation in three areas:
• promotion/prevention; • public education/awareness • partnerships/ capacity building.
Table 1: Matrix One: framework for recording challenges, opportunities, implementation and legislation
EMIP Matrix: from policy to delivery [email protected]
Mechanisms for joint delivery across sectors/disciplines e.g. strategic partnerships
National or regional networksJoint planning Mhp databases
Employment, education, criminal justice, housing regeneration, public health
Key stakeholders not engaged;
Partnerships
Train the trainersMhp on health curriculum
Campaigns on stigma, violence against women, alcohol, drugsWorkplace initiativesWell-being
Health promoting schoolsEarly yearsSocial prescribing
Implementation examples
MHP has professional status, MHP part of public health competency
MHP training programmes; opportunities for sharing expertise
Limited resources; low status of MHP; poor access to information/evidence
Capacity Building
Anti-discrimination legislation, equal opportunities, social inclusion
Consumer led advocacy; strong user/survivor movement; health promoting schools
Negative media coverage; racism
Public Educationand Awareness
Public mental health strategy; alcohol; domestic violence
Parenting skills training, jobs programmes, social prescribing
e.g. alcohol, drugs, poor housing, violence, unemployment, poverty
Promotion/Prevention
Legislation/PolicyOpportunitiesChallenges Area

2.1 Challenges: an overview - promotion/prevention The challenges identified by partner countries are divided into:
• key risk and protective factors that threaten or promote population mental well-being and vulnerable or neglected target groups
• issues that need to be addressed if mental health promotion/prevention is to be effectively implemented
Table 2 on the following pages below provides a summary of which issues were specifically highlighted by different partner countries. Table 2: Highlighted issues by specific partner countries Issue
Partner country
Sickness absence/stress Unemployment Labour protection Suicide Alcohol/Drugs Chronic physical illness Promoting Volunteering Promoting healthy lifestyles Social, environmental determinants Older people Early years/young people Carers
Finland, Germany, Portugal, Hungary Austria, Estonia Portugal Hungary, Austria Ireland, Germany, Hungary, Slovenia, Austria Ireland, Poland, Slovenia, Austria Poland Germany, Portugal, Austria Portugal Austria Ireland, Poland, Finland, Germany, Portugal, Hungary Portugal, Austria, Estonia, Poland Czech Republic

Table 2 ctd. : Highlighted issues by specific partner countries Barriers to implementation
Partner Country
Lack of national government engagement Local government not engaged Absence of national policy/strategy guidelines Legislation needed Co ordination/co operation lacking Mainstreaming MHP into health promotion and health care system Lack of knowledge/specialist resources/costs (e.g. of counselling) Mental health service reform needs
Ireland, Finland, Romania Netherlands Slovenia, Austria, Estonia, Czech Republic, Finland, Portugal Romania, Czech Republic Ireland, Slovenia, Czech Republic Ireland, Slovenia, Hungary, Austria Ireland, Estonia, Czech Republic Czech Republic, Romania
Public education/awareness – challenges and priorities
Partner country
General public/employees
Stigma
Family, parenting, early years
Schools Media
Migration issues
Integrate MH into public health campaigns e.g. on smoking
Ireland, Finland, Poland, Slovenia, Romania, Germany Germany, Portugal, Slovenia, Romania, Czech Republic Austria Germany, Portugal, Austria, Estonia Finland, Poland, Portugal, Hungary Germany Austria

Table 2 ctd.: Highlighted issues by specific partner countries Partnerships/capacity: key needs
Partner countries
Greater collaboration – regional/ national/international Coalitions with other sectors e.g. local government, community, disability rights, education Technical assistance/ programme development Evaluation information Research, education, training Community based mh services Partnership with Primary care
Ireland, Slovenia, Portugal, Romania, Netherlands, Estonia Poland, Romania, Germany, Portugal Romania Estonia, Poland Austria Romania Germany, Portugal, Austria
(For more details see Table 4)

Table 3: Determinants of effective implementation by partner country
EMIP Matrix: from policy to delivery [email protected]
New National Public Health prevention programme (forthcoming)
Ordinance of PM on Mental Health Promotion and Prevention 1996
National MH strategy (Phare)Anti drug strategy 2005-8
Location of mental health promotion policy (national/local)
Mental health and promotion research at University of Ljubljana
KidscreenStability Pact MH programmeEvidence base, evaluation and MHP intelligence/data
Mental health and promotion research at University of Ljubljana
National Programme on prevention of social maladjustment
Education for health programme in schools (ministries of health and education)
Capacity building across all sectors
MH law (in process)Action Plan on Social Inclusion (NGO)
Order no 10; framework agreement; MH centres; MH reform action plan
MHP contributes to service reform/improved outcomes for people with mh problems
Council for MHPMinistry of Health Governance/performance management/accountability
Mh monitoring; Social Diagnosis
Clear definition of success and how it will be measured
Regional anti stigma Depression campaign
Slovenia
Schools with class media campaign
Romanian League for Mental Health campaigns
Marketing mental well-being
Adaption of Strangers among us for preventing xenophobia
Cross sector ownership
PolandRomaniaKey Determinants of Effective Implementation
EMIP Matrix: from policy to delivery [email protected]
Public Health Law (not specific to mh or mhpromotion)
Austrian Health Promotion Act; Law on Social Insurance
Constitution; Labour Safety Act (but not specific to mental health promotion)
Location of mental health promotion policy (national/local)
Well-being research (Blatny et al 2005)
Implementation of evidence based programmes
Kopp study on role of family and workplace in mh of changing society
Evidence base, evaluation and MHP intelligence/data
Matra project ICT’s technologies: e-learning; potential mental health promotion alliance
6 universities train psychologists; activities of civil organisations increasing
Capacity building across all sectors
NGO advocacy, rehabilitation and education
MHP contributes to service reform/improved outcomes for people with mh problems
National Public Health Programme
Ministries for: Health and Women, Social Affairs, Education, Justice; Health Promotion Foundation
National Programme of Labour Safety; National Health Progarmme
Governance/performance management/accountability
Clear definition of success and how it will be measured
NGO campaigns
Czech Republic
Healthy Ageing; Toy-free nurseries; It’s up to you
Marketing mental well-being
Partnership: Ministries of Health & Education
Co operation with EU member states on EC funded programmes
Cross sector ownership
AustriaHungaryKey Determinants of Effective Implementation

EMIP Matrix: from policy to delivery [email protected]
Mental health policy (not mental health promotion); Public health law
Public Health Act; Occupational Health & Safety (some aspects of mh)
Social insurance law (SGB);Legislation protecting children and young people; prevention legislation in progress
Location of mental health promotion policy (national/local)
Estonian Swedish Mental Health & Suicidology Institute focal point for research
Network for mental health; prevention networks (DGPPN)
Evidence base, evaluation and MHP intelligence/data
Mental health first aid; NGO’s active in field of MH; WHO Safe Communities Network
Media training; Workplace network (ENWAP); Suicide prevention (Monsue)
Capacity building across all sectors
Psychiatric and psycho-social services for children and adolescents focus on promotion/prevention
Health care reform; anti stigma programmes; health promoting psychiatric services; psychiatry enquete; DGSP patient as partner
MHP contributes to service reform/improved outcomes for people with mh problems
Ministry of Social Affairs and Health
Ministry of Social AffairsCode of ethnics for Journalists
Federal German MinistryGovernance/performance management/accountability
Clear definition of success and how it will be measured
National programmes on suicide, depression, violence against women; school health surveys
EMIP workshops
Finland
EMIP; IMHPA, EEAD; regional and local initiatives
Suicide prevention (NaSPRO); MindMatters; alliances against depression; healthy ageing
Marketing mental well-being
EMIP workshops; Meaningful Life; Intersectoral MH partnership
Cross sector ownership
EstoniaGermanyKey Determinants of Effective Implementation
EMIP Matrix: from policy to delivery [email protected]
Vision for Change; MH Services Policy framework (forthcoming); Health Promotion Strategy; Suicide Action Plan
National Mental Health Plan (forthcoming)
Social Support Act (2006); general Special Illness Costs Act
Location of mental health promotion policy (national/local)
Psychological distress survey; drug & alcohol use surveys; public attitude survey
Programmes in pregnancy, early years, schools, workplace (forthcoming)3rd National Health Survey
Large scale scientific fund; National Prevention Support Centre; RadboudUniversity
Evidence base, evaluation and MHP intelligence/data
Training for health care professionals; e-learning
National Prevention Support Centre; Radboud University
Capacity building across all sectors
MH integrated into Acute Hospitals;
GGZ Nederland has made prevention a priority
MHP contributes to service reform/improved outcomes for people with mh problems
Department of Health; Ministry of health and 5 regional health authorities
Ministry of Public Health, Regional mental health care centres; municipal health services
Governance/performance management/accountability
Clear definition of success and how it will be measured
Primary Minds; Mind Matters; Move to Wellness; Positive ageing campaigns
Social Partnership Agreements (local)
Ireland
School curriculum; NGO activities with older people
Marketing mental well-being
Ministries of Health and Education
National prevention network to be created
Cross sector ownership
PortugalNetherlandsKey Determinants of Effective Implementation

Table 4: European Level Added Value
EMIP Matrix: from policy to delivery [email protected]
National researchSocial diagnosis/well-being e.g. Poland; ScotlandRisk/protective factor prevalence e.g. Netherlands
Trans-national research (via FP7)•Mh impact of environmental factors•Community interventions•Determinants of mental health
National ProjectsEU wide projectsGenerating co operation Visibility, moral supportUser friendly, web based dissemination
Building shared agendas: •drugs/alcohol (Poland)•Links with recovery/consumers (Czech)•Social inclusion (Ireland)•Workplace (Germany/Poland)
Data/knowledge needs •Indicators (positive mental health)•Evidence of effectiveness•Cost benefits of MHP
CollaborationNetworking Joint initiativesWider stakeholder/grass roots involvementInvolving public
Using existing structures for delivery:•Schools (Poland)•Psychological & educational centres (Czech Republic)•Regions (Celje, Slovenia; MH care centres, Netherlands)•Self-help (Hungary)
PolicyEC MH Green PaperLisbon Strategy: Social AgendaEU Disability Strategy
Co-production/ collaboration within and across countries
National Level(Examples of what supports implementation)
European Level Added Value

LIST OF ALL EMIP COUNTRY MATRICES
Country Matrices • Austria • Czech Republic • Estonia • Finland • Germany • Hungary • Ireland • Netherlands • Poland • Portugal • Romania • Slovenia
Austria

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Austria Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
Reduce psychological complaints.
Promotion of mental health in early childhood.
Reduce the suicide rate. Promote well-being at work
in order to reduce the sickness leave days
Fight against drugs. The substantial need for
research and training in Austria
The lack of specific national policies on MHP and MDP in Austria
Promote voluntary social activities.
Development of social and environmental conditions and settings which are supportive for mental health
The lack of cooperation between the “Labour Protection” and “Workplace Health Promotion”
The inclusion of MDP and Stigma in the agenda of the Ministry and the Austrian Health Promotion Foundation
Support by the social health insurance institutions.
Support by the federal-level associations in Austria.
In workplace settings, there are some local programs on stress management.
Increasing number of NGO´s activities aiming mental health
A Federal Drug Forum, which is responsible for putting in place interventions to prevent addiction and co-ordinate such activities.
A few MHP or MDP programmes relating to family, parenting and early childhood e.g.: • courses for parents,
financed by the Ministry for Social Affairs
• support and counselling for socially disadvantaged families provided by youth welfare institutions
• Implementation of evidence-based programmes during pregnancy and early childhood, in schools, in health care services, in the general public and at the workplace.
Since 1998 Austria has a law on promoting health (BGBI. No. 51/1998). The Austrian Health Promotion Act, is based on a comprehensive view of health and the principles contained in the Ottawa Charter of the WHO.
Health promotion and prevention are defined in the Allgemeines Sozialversicherungsgesetz (General law on social insurance)
A legal framework for health promotion (Art. 15a B-VG) (Federal Constitutional Law). This agreement between the federal government and the states, defined health promotion as a responsibility of the health care system of health system for the period 2005/2008. The preamble to the agreement mentions the importance of health promotion.

Austria Page 2 Public Education and awareness
Schools
1) Reduction of psychological and psychosomatic complaints among school-aged children 2) Reduction of tiredness and/or exhaustion (ca.45% of school children)
Increase MHP and MDP programs relating to family, parenting and early childhood
A lack of MHP activities in the Austrian research, education and training landscape
-Spielzeugfreier Kindergarten
(Pre-school without toys), a project in the area of addiction prevention
In the sector “healthy ageing” there are some projects running e.g.: Plan 60, Life-Worlds Worth Living for Older People, etc
In the sector “Addiction prevention” only the following projects have been implemented nation-wide: An internet event calendar, it’s up to you, a flyer for young people, becoming independent
Partnerships and capacity building
Training of primary health
professionals on mental health issues.
ICT’s technologies (namely
e- learning). New training models. Intersectorial Partnership –
Ministry of Health & Ministry of Education.
EMIP project.
Activities developed within
the EMIP project, namely the National Mental Health Workshop

Czech Republic

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Czech Republic Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
The lack of a specific policy on MHP
The low financing from health care budget on psychiatric care (3,9%) and also on health promotion programmes (0,2%)
The weak collaboration among community centres for MH and psychiatric care
The lack of resources (personal, financial) in Regional Public Health Institutes
The lack of collaboration and co-ordination among institution and agencies acting in MH
To increase the amount of projects aimed on family members and care givers of people with mental problems.
To gain the support of the EC in providing with a regulation committing the Czech government to take action and to co-ordinate implementation of MHP and with a specific funding program aimed on MHP
the international documents on MHP signed by government
the NGOs campaign to increase public awareness to mental health and decrease stigmatisation of people with mental health problems and diseases
the projects running in the EU and the support of the EC
The many NGOs which are involved in advocacy, promotion, prevention, rehabilitation and education
The National Public Health Promotion Programme
Healthy Ageing Projects and Projects for Disabled
There is no specific law on MH and no specific MHP policy. The legislative regulation in the field of MH is covered by the Law on Health Care. The Public Health Law was adopted in 2000 and it is a fundamental law for HP
The Base for HP Policy is the document Health 21, which objective is mental health improvement.
Policy in a social support field, disabled people are under social benefit from the government.
There are also MH Policies in the specific fields:
• Healthy School Network • Healthy Cities Network and
their Mh programmes • Healthy Company Network
and its specific activities • Substance abuse policy is a
part of a law amended in 1999
• National Therapeutic Drug Policy
• National Environment and Health Plan
• National Programme of Preparation for Ageing

Czech Republic Page 2 Public Education and awareness
decrease Stigmatisation
Partnerships and capacity building
EMIP Project and its workshop
Estonia
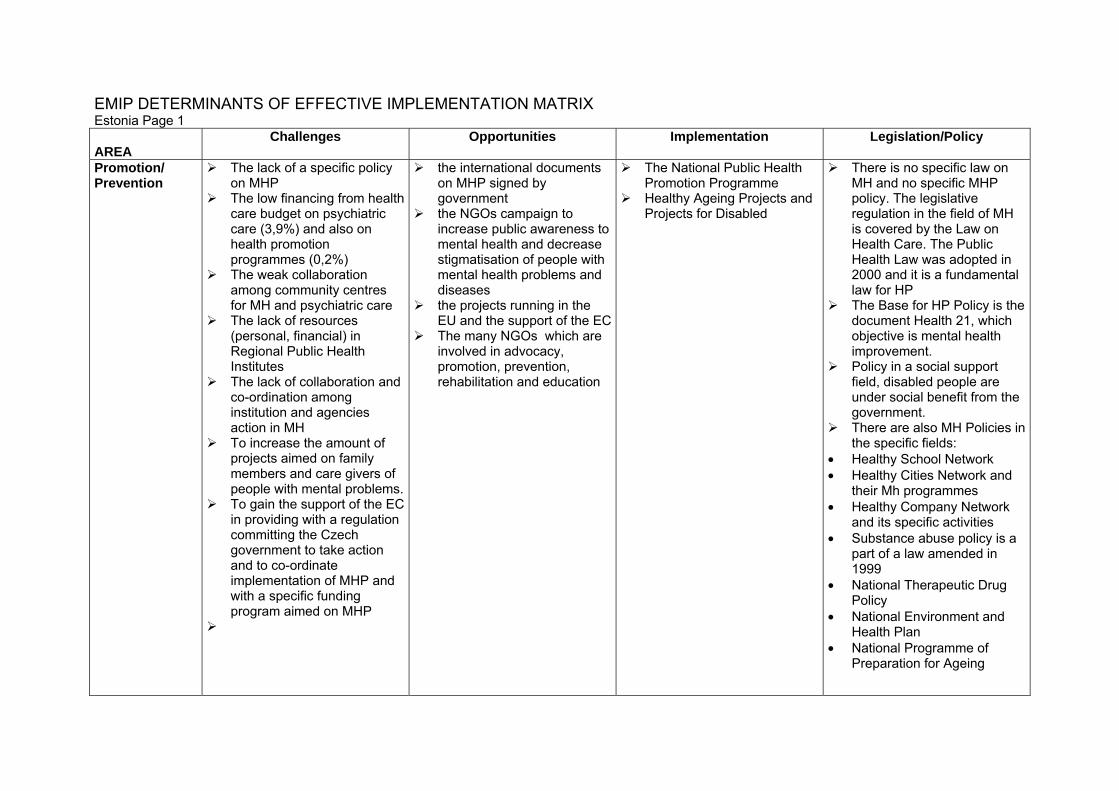
EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Estonia Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
The lack of a specific policy on MHP
The low financing from health care budget on psychiatric care (3,9%) and also on health promotion programmes (0,2%)
The weak collaboration among community centres for MH and psychiatric care
The lack of resources (personal, financial) in Regional Public Health Institutes
The lack of collaboration and co-ordination among institution and agencies action in MH
To increase the amount of projects aimed on family members and care givers of people with mental problems.
To gain the support of the EC in providing with a regulation committing the Czech government to take action and to co-ordinate implementation of MHP and with a specific funding program aimed on MHP
the international documents on MHP signed by government
the NGOs campaign to increase public awareness to mental health and decrease stigmatisation of people with mental health problems and diseases
the projects running in the EU and the support of the EC
The many NGOs which are involved in advocacy, promotion, prevention, rehabilitation and education
The National Public Health Promotion Programme
Healthy Ageing Projects and Projects for Disabled
There is no specific law on MH and no specific MHP policy. The legislative regulation in the field of MH is covered by the Law on Health Care. The Public Health Law was adopted in 2000 and it is a fundamental law for HP
The Base for HP Policy is the document Health 21, which objective is mental health improvement.
Policy in a social support field, disabled people are under social benefit from the government.
There are also MH Policies in the specific fields:
• Healthy School Network • Healthy Cities Network and
their Mh programmes • Healthy Company Network
and its specific activities • Substance abuse policy is a
part of a law amended in 1999
• National Therapeutic Drug Policy
• National Environment and Health Plan
• National Programme of Preparation for Ageing

Estonia Page 2 Public Education and awareness
decrease Stigmatisation
Partnerships and capacity building
EMIP Project and its
workshop

Finland

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Finland Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
The biggest challenge is the maintenance or preservation of the Finnish welfare society, although the basic infrastructure is firmly in place (eg. in day care and education)
The Finnish society will soon witness a reform in the structure of both the municipalities and health services, the purpose of which is to keep up adequate services as well as to coordinate and make the services more effective
To gain a stronger momentum for mental health on the national level.
While preparing for the forthcoming demographic changes, there is a need to prepare and implement specific programmes targeted at older people.
More sustainable funding should be ensured to promotion and prevention activities.
Structures and funding which exceed the normal project approach, need to be set up and adequately supported.
Specific funding from the Ministry of Social Affairs and Health can be applied for health promotion (incl. mental health)
Strong interest and influential work of the various NGOs active in the field plays an important role
The Finnish stakeholders have participated actively in EC-funded projects
The decreasing trend in the number of suicides (although the number is still quite high).
Corporate Social Responsibility seems to be moving forward in the country
By educating the teachers, principles and actions on promotion and prevention can be taken on board.
Starting in autumn 2006 every school is obliged to design and implement an "anti-bullying" programme
National programmes have been carried out on suicide ("Suicide can be prevented") in mid-1990s and on tackling depression ("Chin up!"). An example of a large multisectorial programme is the “Meaningful Life” programme (1999-2002). At the same time, a project on "Prevention of violence against women" was carried out.
A nation-wide project on Early Intervention (to support the interaction between parents and their infants) has been carried out.
Ear-marked funding into psychiatric and psychosocial services of children and adolescents, including a focus on promotion and prevention, has been provided from the State budget from the year 2000 onwards.
Regional projects (about 150) are underway through ear-marked funding by the Ministry or the Regional Offices.
The Quality
Although there exists a general mental health policy, an overall policy of mental health promotion is lacking and a policy of mental health promotion and prevention does not exist at national level. Mental health is not always taken into consideration in general health promotion policies. However, a national programme is being planned according to the experiences and results of large regional projects (due in 2008).
The Mental Health Act (1116/1990) outlines the contents of mental health work. The legislation list below is relevant with the provision of mental health services:
A new Public Health Law has been in place from the beginning of 2006. It deals with health promotion.
Primary Health Care Act, Act on Specialised Medical
Care, Act on the planning of the
State subsidies for social welfare and health care
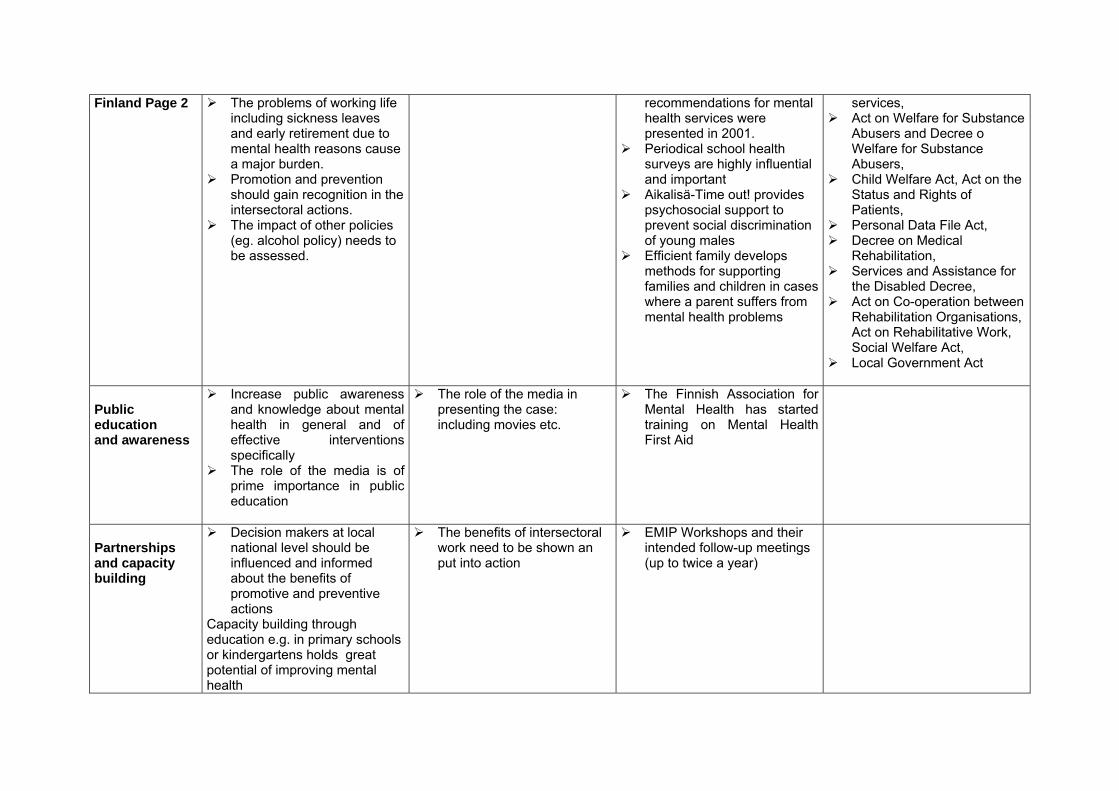
Finland Page 2 The problems of working life including sickness leaves and early retirement due to mental health reasons cause a major burden.
Promotion and prevention should gain recognition in the intersectoral actions.
The impact of other policies (eg. alcohol policy) needs to be assessed.
recommendations for mental health services were presented in 2001.
Periodical school health surveys are highly influential and important
Aikalisä-Time out! provides psychosocial support to prevent social discrimination of young males
Efficient family develops methods for supporting families and children in cases where a parent suffers from mental health problems
services, Act on Welfare for Substance
Abusers and Decree o Welfare for Substance Abusers,
Child Welfare Act, Act on the Status and Rights of Patients,
Personal Data File Act, Decree on Medical
Rehabilitation, Services and Assistance for
the Disabled Decree, Act on Co-operation between
Rehabilitation Organisations, Act on Rehabilitative Work, Social Welfare Act,
Local Government Act
Public education and awareness
Increase public awareness and knowledge about mental health in general and of effective interventions specifically
The role of the media is of prime importance in public education
The role of the media in presenting the case: including movies etc.
The Finnish Association for Mental Health has started training on Mental Health First Aid
Partnerships and capacity building
Decision makers at local national level should be influenced and informed about the benefits of promotive and preventive actions
Capacity building through education e.g. in primary schools or kindergartens holds great potential of improving mental health
The benefits of intersectoral work need to be shown an put into action
EMIP Workshops and their intended follow-up meetings (up to twice a year)
Germany

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Germany Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
Reduce psychological complaints
Promote well-being at work in order to reduce the sickness leave days
Suicide prevention The substantial need for
evaluation of prevention programmes
Reduce stigmatization of people with psychiatric disorders
Encourage liaisons between different initiatives
Promote voluntary social activities
Support by the social health insurance institutions
A special prevention legislation is currently in progress
Rising awareness for importance of prevention in Germany
Reform of health care is in progress
German network for mental health (register of already existing programmes sorted by themes) www.gnmh.de
Programme against stimatization (psychotic disorders)
Comprehensive networks for prevention of mental illness (DGPPN)
European and national alliances against depression (EAAD) www.eaad.net, special programmes for persons with migration background
National programme for suicide prevention in Germany (NaSPro) www.suizidpraevention-deutschland.de
The New Quality of Work Initiative www.inqa.de
Non-smoking campagne for teenagers www.rauchfrei.de
MindMatters- components of healthy schools (Bausteine einer psychisch gesunden Schule)
Initiative of the DGSP „Patient as a Partner“ www.patient-als-partner.de
Network of non-smoking hospitals www.rauchfreie-krankenhaueser.de
Network of hospitals with good treatment for migrants (Netzwerk migrantenfreundli-cher Krankenhäuser)
General law on social insurance (SGB) Book No. V): health promotion as obligation for the health insurance funds in Germany; to provide a basic definition of the appropriate provision of health care
General law on social insurance (SGB) Book No. IX: duty of cost providers in the field of rehabilitation is to avoid the occurrence of disability
For example: reintegration of employees after 6 weeks of illness (SGB Book No. IV, §84)
The legislation in the field of children and youth is established as prevention legislation
A special prevention legislation is currently in progress (second approach)

Germany Page 2
Network for health promotion in hospitals for children (Netzwerk zur Gesundheitsförderung in Kinderkrankenhäusern)
Task force on health promoting psychiatric services http://www.hpps.net/
Various programmes for the prevention of work related pain (for example OSI Mannheim)
Various regional initiatives
Public Education and awareness
A lack of MHP activities in the German research, education and training landscape
Create a specific education for the field of prevention
Increase MHP and MDP programs relating to working place
Increase MHP and MDP programs relating to migration background
Increase MHP and MDP programs relating to elderly
> Education of different multiplicators in the field of depression (alliances against depression in Germany)
European and national alliances against depression (EAAD) www.eaad.net
National programme for suicide prevention in Germany (NaSPro) www.suizidpraevention-deutschland.de
Various projects running (for example in the sector of healthy ageing: 55+)
Partnerships and capacity building
Training of primary health
professionals on mental health issues
Creating coalitions for raising of awareness for mental health problems at the work place
Training of the media
on reporting about suicide (NaSPro)
EMIP project German and
European network for workplace health promotion (ENWHP) www.enwhp.de
Activities developed within the EMIP
project, namely the National Mental Health Workshop
Activities developed within the MONSUE project (suicide prevention)

Hungary

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Hungary Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
Increase well-being at the
workplace Reduce workload Reduce stress at the
workplace Stick to the recommended 8
hours work per day. Reduce intimidation at the
workplace Reduce discrimination Create opportunities on
occupational health psychologist training
Reduce the suicide rate among young people
Increase attention to age-related special issues
Increase promotion of equal opportunity
Increase the role of the occupational health services
Support from the Government by:
-enforcing laws, -amending labour protection law, -integration of the health promotion into the health care system -reforming the health care system
The co-operation with EC countries on the implementation
The many programms running in the EC
The support of the EC
Health issues (also mental health) are included in the Labour Safety Act. However preservation of mental health and prevention is not specified.
National Programme of Labour Safety
National Health Programme
National Geriatric Council Laws and statutes to prevent mental disorders:
Constitution of the Republic of Hungary, 70/a.§.
Labour Code Law no. XI of 1991, on
handling and protection of health care and related personal data
Law XLII of 1999, on the protection of non-smokers
Law no. CXXV of 2003, on equal treatment and the promotion of equal opportunity
Law

Hungary Page 2 Public Education and awareness
The role of the media in the
promotion and influencing of mental health culture
Role of the media in demonstrating workplace intimidation, raising awareness in the society
improve work environments for women
in order to have success, health promotion campaigns on smoking and alcohol consumption, should target the psychological issues
Partnerships and capacity building
EMIP’s Workshop
Ireland
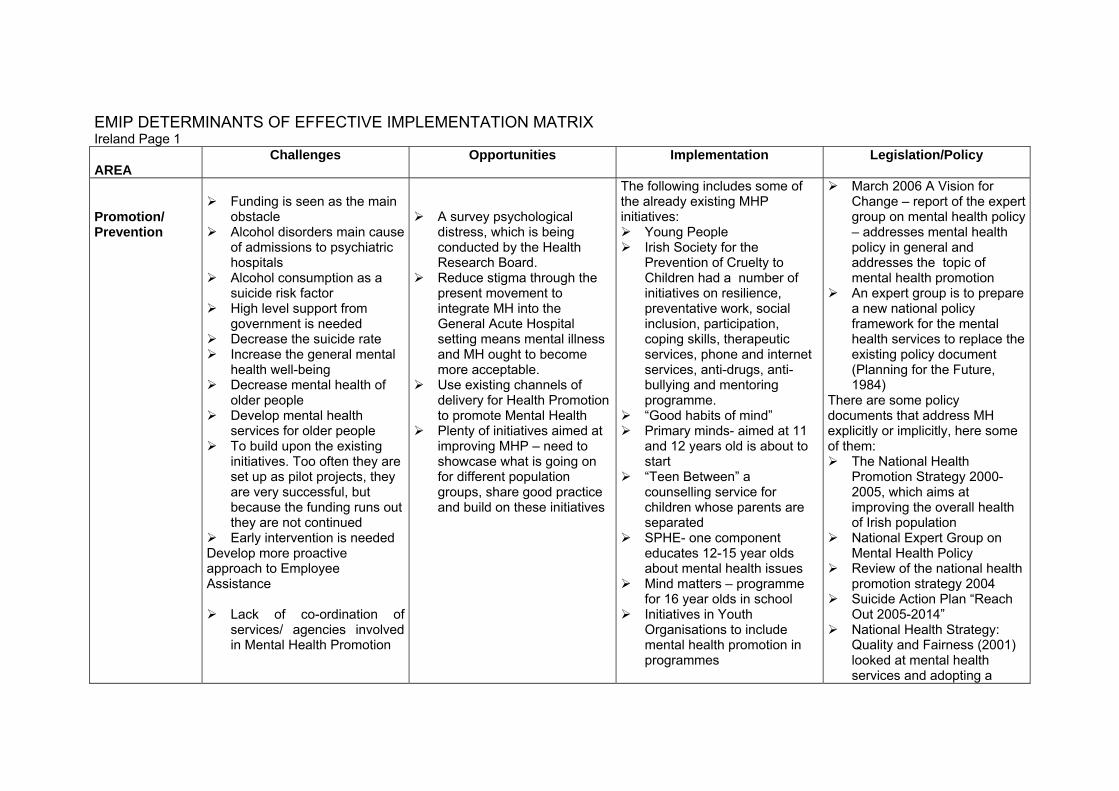
EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Ireland Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
Funding is seen as the main
obstacle Alcohol disorders main cause
of admissions to psychiatric hospitals
Alcohol consumption as a suicide risk factor
High level support from government is needed
Decrease the suicide rate Increase the general mental
health well-being Decrease mental health of
older people Develop mental health
services for older people To build upon the existing
initiatives. Too often they are set up as pilot projects, they are very successful, but because the funding runs out they are not continued
Early intervention is needed Develop more proactive approach to Employee Assistance
Lack of co-ordination of services/ agencies involved in Mental Health Promotion
A survey psychological distress, which is being conducted by the Health Research Board.
Reduce stigma through the present movement to integrate MH into the General Acute Hospital setting means mental illness and MH ought to become more acceptable.
Use existing channels of delivery for Health Promotion to promote Mental Health
Plenty of initiatives aimed at improving MHP – need to showcase what is going on for different population groups, share good practice and build on these initiatives
The following includes some of the already existing MHP initiatives:
Young People Irish Society for the
Prevention of Cruelty to Children had a number of initiatives on resilience, preventative work, social inclusion, participation, coping skills, therapeutic services, phone and internet services, anti-drugs, anti-bullying and mentoring programme.
“Good habits of mind” Primary minds- aimed at 11
and 12 years old is about to start
“Teen Between” a counselling service for children whose parents are separated
SPHE- one component educates 12-15 year olds about mental health issues
Mind matters – programme for 16 year olds in school
Initiatives in Youth Organisations to include mental health promotion in programmes
March 2006 A Vision for Change – report of the expert group on mental health policy – addresses mental health policy in general and addresses the topic of mental health promotion
An expert group is to prepare a new national policy framework for the mental health services to replace the existing policy document (Planning for the Future, 1984)
There are some policy documents that address MH explicitly or implicitly, here some of them:
The National Health Promotion Strategy 2000-2005, which aims at improving the overall health of Irish population
National Expert Group on Mental Health Policy
Review of the national health promotion strategy 2004
Suicide Action Plan “Reach Out 2005-2014”
National Health Strategy: Quality and Fairness (2001) looked at mental health services and adopting a
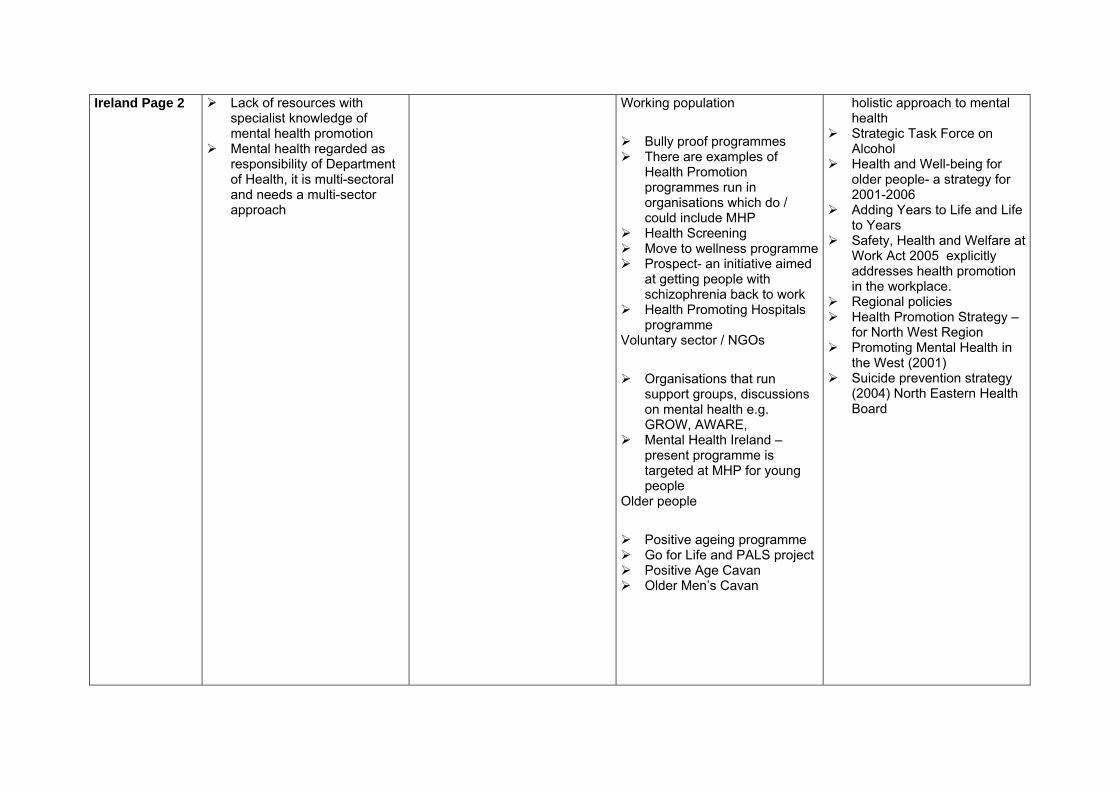
Ireland Page 2
Lack of resources with specialist knowledge of mental health promotion
Mental health regarded as responsibility of Department of Health, it is multi-sectoral and needs a multi-sector approach
Working population
Bully proof programmes There are examples of
Health Promotion programmes run in organisations which do / could include MHP
Health Screening Move to wellness programme Prospect- an initiative aimed
at getting people with schizophrenia back to work
Health Promoting Hospitals programme
Voluntary sector / NGOs
Organisations that run support groups, discussions on mental health e.g. GROW, AWARE,
Mental Health Ireland – present programme is targeted at MHP for young people
Older people
Positive ageing programme Go for Life and PALS project Positive Age Cavan Older Men’s Cavan
holistic approach to mental health
Strategic Task Force on Alcohol
Health and Well-being for older people- a strategy for 2001-2006
Adding Years to Life and Life to Years
Safety, Health and Welfare at Work Act 2005 explicitly addresses health promotion in the workplace.
Regional policies Health Promotion Strategy –
for North West Region Promoting Mental Health in
the West (2001) Suicide prevention strategy
(2004) North Eastern Health Board
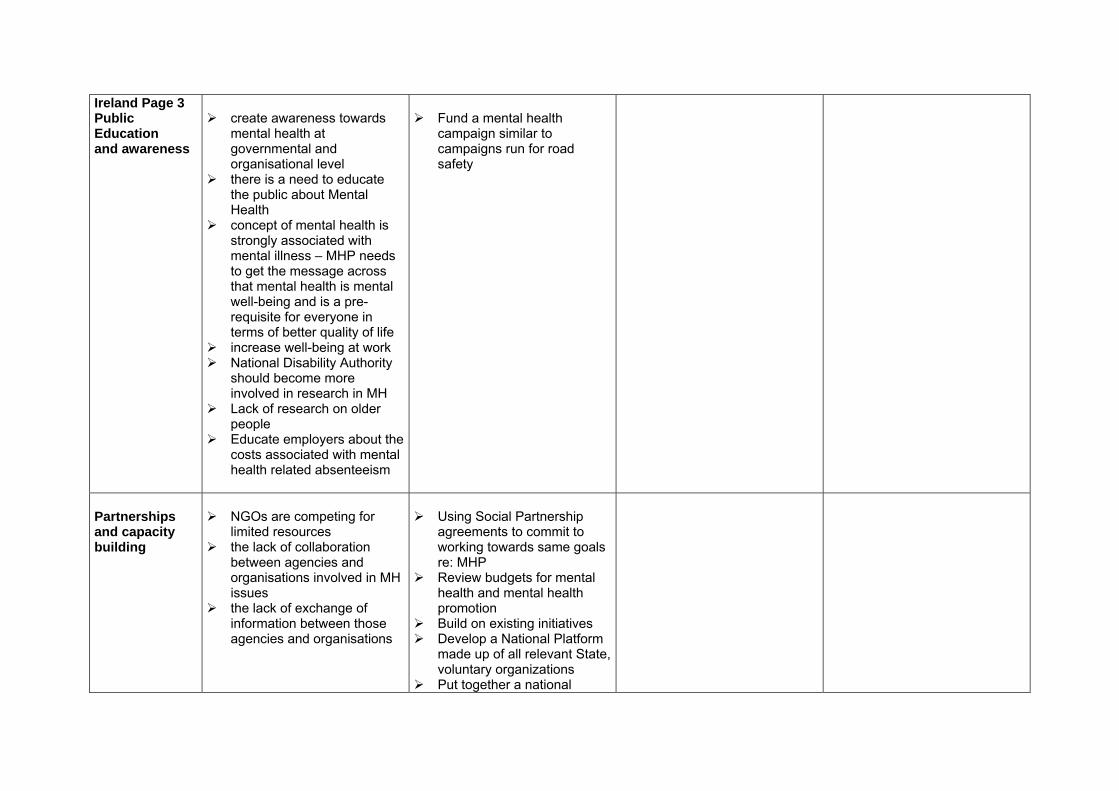
Ireland Page 3 Public Education and awareness
create awareness towards
mental health at governmental and organisational level
there is a need to educate the public about Mental Health
concept of mental health is strongly associated with mental illness – MHP needs to get the message across that mental health is mental well-being and is a pre-requisite for everyone in terms of better quality of life
increase well-being at work National Disability Authority
should become more involved in research in MH
Lack of research on older people
Educate employers about the costs associated with mental health related absenteeism
Fund a mental health
campaign similar to campaigns run for road safety
Partnerships and capacity building
NGOs are competing for
limited resources the lack of collaboration
between agencies and organisations involved in MH issues
the lack of exchange of information between those agencies and organisations
Using Social Partnership
agreements to commit to working towards same goals re: MHP
Review budgets for mental health and mental health promotion
Build on existing initiatives Develop a National Platform
made up of all relevant State, voluntary organizations
Put together a national

database of successful projects / initiatives

Netherlands

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Netherlands Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
The prevalence of
psychological disorders among the population needs to be more effectively made visible to the municipalities.
Knowledge on the part of the municipal administration on what mental health promotion and prevention entail needs to be enhanced.
for the first time in twenty years, GGZ Nederland, the umbrella organization for all the MH care facilities in the Netherlands, has made prevention the spearhead of its policy.
There is an ample opportunity for research. The state has launched a large scientific fund, which makes it possible to launch large-scale, scientifically founded innovation, research and implementation projects in the field of prevention and health promotion. Various universities and national knowledge institutes are extremely active in this field.
There is a high level of basic care (general practitioners, home care, infant health centres and so forth) in the Netherlands. This provides any number of opportunities to implement preventive and health- promoting interventions.
Prevention practice is reasonably extensive in the Netherlands, prevention is mainly implemented at regional mental health care centres. Most of them have separate prevention divisions. Each prevention division carries out a large number of projects. The main themes are:
Children of parents with psychiatric problems and/or addicted parents
Depression/ anxiety disorders
Work-related psychological problems
Social psychiatry, care provided by volunteers and psychology education
Other Projects carried out by
NGOs and Universities such as
IMHPA
Part of the prevention (individual secondary prevention) is to be regulated by the General Special Illness Costs Act. This form of prevention is to be diagnosis-related. Collective prevention is to be part of municipal policy and will be implemented in the framework of the Social Support Act, and covers the following aspects: -identifying and combating risk factors in the field of public mental health care -reaching and counseling vulnerable groups and high risk groups - serving as a spot where people can report crises or impending crises -providing psychosocial assistance after disasters -stimulating agreements between relevant organization about the implementation of public mental health care.
In the implementation of local health care the Social Support Act the municipalities play the role of director.
Since the 1st of January

Page 2 2006, a new Social Support Act is going into effect, which includes: - promoting social
cohesion and livability at the neighbourhood and district level
- supporting volunteer care and aid workers
- providing support in raising children
- providing facilities to people with chronic psychiatric problems
- providing ambulant addiction care
-
Public Education and awareness
Partnerships and capacity building
Imhpa Emip
Poland

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Poland Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
To decrease stress levels in young people
To reduce alcohol consumption rates, responsible for a high number of traffic accidents, suicides, and family violence cases.
To recognize young parents/ young families as one of the issues in mental health development
To develop mental health (MHP) promotion programmes for adults, especially for the elderly
To increase MHP efforts designed for and targeted to people with various health problems
To evaluate MHP programmes
Interest of the EC in MHP The variety of projects
running in the EU Numerous programmes and
projects running in Poland Mental health monitoring by
various institutions and agencies: Institute of Psychiatry and Neurology, National Institute of Hygiene, Central Statistical Office, Public Opinion Research Centre, Institute of Applied Social Sciences, University of Warsaw
Institutions and agencies dealing with mental health promotion/prevention: Departments of Health Psychology at all Polish Universities; Departments of Health Promotion at: the Institute of Cardiology, Institute of Occupational Medicine, the National Sick Fund, National Centre of Health System Management, and Municipal Councils of Warsaw and many other cities.
Department of Mental Health Promotion, at Institute of Psychiatry and Neurology
National Council for Mental Health Promotion, NCMHP,
The Network of 1200 Health-Promoting Schools all over Poland
The National Network of Health Promotion in the Workplace
Healthy Cities Network of Health
Promoting and Child-Friendly Hospitals
Implementation and evaluation of promotion and prevention programmes carried out in Polish schools
National anti-stigmatisation campaign “Schizophrenia- Open the Doors”
MH monitoring: global and thematic annual reports, yearbooks, specific projects- e.g. Social Diagnosis, survey repeated annually since 1991, or the European School Project on Alcohol and Drugs (ESPAD), international serial study
MHP programmes implemented at worksite, e.g. stress management for the police, debriefing for firemen as PTSD prevention.
Mass media & billboard
The Mental Health Act The Act on Upbringing in
Sobriety and Counteracting Alcoholism
The Act on Preventing Drug Dependence
The Ordinance of the Prime Minister on Mental Health Promotion and Mental Disorders Prevention
The National Program of Prevention and Resolving Alcohol-Related Problems
The National Program for Counteracting Drug Addiction (National Bureau for Drug Prevention)
National Action Plan on behalf of Children 2004 – 2012 (Ministry of Education)
National Programme on Prevention of Minors’ Maladjustment and Delinquency
National Health Programme 1996-2005 (Ministry of Health) – new version for the next 10 years is under the preparation
National Mental Health Programme (Institute of Psychiatry and Neurology)

Poland Page 2
appointed in 1997, an interdisciplinary advisory body to the Minister of Health
campaign against family violence
Crisis intervention and psychological support provision to disaster victims (e.g. of flood or a supermarket roof collapse)
Public Education and awareness
To promote the ideas of mental health promotion among politicians, mass-media workers, decision-makers, employers, health professionals
To popularise the already existing programs and possibilities
To heighten MHP awareness among the general public
Press conferences organised regularly e.g. on the World Mental Health Day Nationwide actions organised on the World Mental Health Day (reported in detail to MHE-SME)
Inclusion of MHP issues into training courses for various groups of professionals
Inclusion of MHP issues into school curricula
Mass media campaigns – e.g. in 2004-2005 how to recognise and manage SAD and depression
Attracting attention of mass media through the EMIP workshop
Participation of MHP experts in scientific conferences and/or training courses
Publication of articles in scientific journals and popular magazines/newspapers
Publication of books (e.g. Mental Health – Risks and Promotion, 2002
Publication and dissemination of: WHO guides on suicide prevention for various target groups, WHO posters and flyers “Do something good for your mental health”
Monitoring of TV violence and preparing a report for public TV authorities
The importance of public awareness and psychoeducation is acknowledged in the above-listed legislation/policies
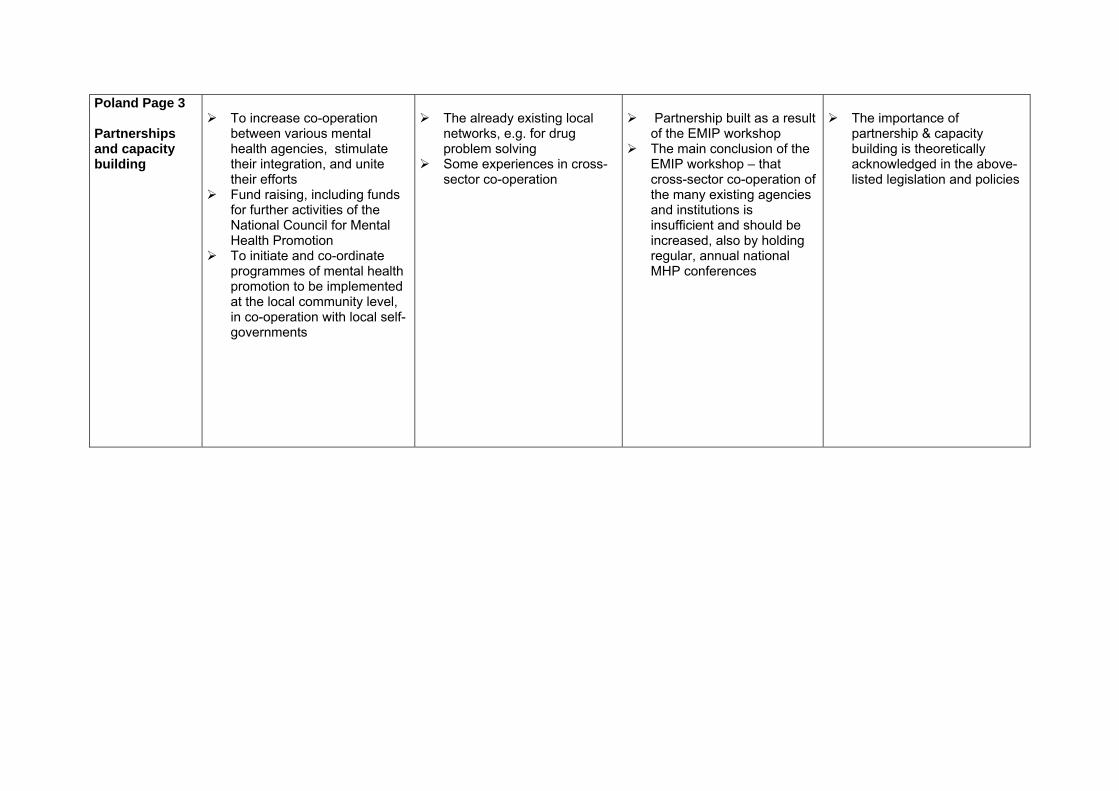
Poland Page 3 Partnerships and capacity building
To increase co-operation
between various mental health agencies, stimulate their integration, and unite their efforts
Fund raising, including funds for further activities of the National Council for Mental Health Promotion
To initiate and co-ordinate programmes of mental health promotion to be implemented at the local community level, in co-operation with local self-governments
The already existing local
networks, e.g. for drug problem solving
Some experiences in cross-sector co-operation
Partnership built as a result
of the EMIP workshop The main conclusion of the
EMIP workshop – that cross-sector co-operation of the many existing agencies and institutions is insufficient and should be increased, also by holding regular, annual national MHP conferences
The importance of
partnership & capacity building is theoretically acknowledged in the above-listed legislation and policies

Portugal

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Portugal Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
Promotion of healthy early childhood development.
Fight against Stigma. Promotion of healthy life
styles.
Reduce work stress.
Reduce unemployment stress.
Promote unemployed vocational training and new skills acquisition.
Promote elderly learning and sense of usefulness.
Promote voluntary social activities.
Development of policy and
practice guidelines on mental health promotion and mental disorder prevention.
School Curricula may contemplate subjects such as fight against stigma and healthy life styles.
In workplace settings, there are some local programmes on stress management.
Ministry of Social Solidarity
and Labour implements unemployed vocational training activities.
Increasing number of NGO´s activities aiming the elderly.
Implementation of evidence-based programmes during pregnancy and early childhood, in schools, in health care services, in the general public and at the workplace.
Training programmes for
health care professionals, which include promotion and prevention in mental health, started in 2005, funded through the National Health Plan.
An official governmental written policy for mental health promotion and mental disorder prevention is in preparation (National Mental Health Plan). This policy will include a national strategy on training, interventions by primary care professionals, school interventions integrated in the curriculum, interventions for groups at risk and interventions for the general public.
Several programmes, namely for the elderly, children and adolescents, depression, post-traumatic stress disorder (PTSD) and alcohol related problems are being prepared.
The country has specific programmes for disaster affected populations, elderly people and children.
The Institute for Employment and Vocational Training sponsors active employment.
Guidelines on mental health promotion and mental disorder prevention are under development.

Portugal Page 2 Public Education and awareness
Schools
1) Reduction of stigma associated with M.H. disorders. 2) Development of Programsof Personal Development Skills.
Media - promoting media awareness on M.H. subjects.
Portugal is a member of an
European Network of Health Promoting Schools. Mental Health is a priority subject.
Workgroup developing a
capacity building programme on interpersonal relation skills to be implemented in all public schools.
Seminars and workshops on
M.H. subjects.
This programme’s
attendance will be compulsory in all schools of the public sector.
Partnerships and capacity building
Training of primary health
professionals on mental health issues.
Training teachers and education personnel.
International partnerships
promoting the development of common promotion and prevention strategies and the creation of M.H. indicators.
ICT’s technologies (namely
e- learning). New training models.
Intersectorial Partnership – Ministry of Health & Ministry of Education.
EMIP project.
Since the 80’s – articulation
between Primary Care & M. Health Services, namely through training of primary health professionals on M.H. subjects.
Development of new models of training & development of new tools.
Activities developed within the EMIP project, namely the National Mental Health Conference.
Mental health promotion and
mental disorders prevention are integrated in the professional vocational training of general practitioners and family doctors, public health physicians and nurses or doctors’ assistants working in general practice, and it is compulsory, although not sufficiently developed.

Romania

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Romania Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
Increase the interest for MH
issues at the governmental level
The reduced budget for MH care and support
The development of MH services in the communities
The lack of legislative norms regarding MH promotion and prevention
Change the actual MH care model into one based on the multidisciplinary team and individual care plan
Setting up a network of MH community service
Gaining the interest and support of the Ministry of Health
Reduce stigma and discrimination
The long term monitoring by the EC, Amnesty International
The various projects in the EU
The Green Paper will be the starting point for the Romanian policy on prevention
The Twinning Light wit technical assistance from the Netherlander Government _(2005)
Mantra Project for the improvement of norms for hospitalisation in the psychiatric and hospitals and hospitals applying security measures
In Romania, mental Health was approached as a field exclusively related to the health sector for many years. The following is the existing legislation for MH promotion and prevention:
the National Strategy regarding MH and the Action Plan for the Implementation of the MH Policy of the Romanian Ministry of Health_ result of the PHARE Project Twining Light
Health Minister Order no. 661/2005
Law no. 522/204 Governmental Decision no.
73 of January 27, 2005 Action Plan of r implementing
the National Anti-drug Strategy 2005-2008
Ministry of Health Order no. 10/2005 regarding the implementation of national health programs and sub-programs funded for the state budget
The Order regarding the setting up and organising of the MH Centre which will be approved by the Ministry of Health in the next days
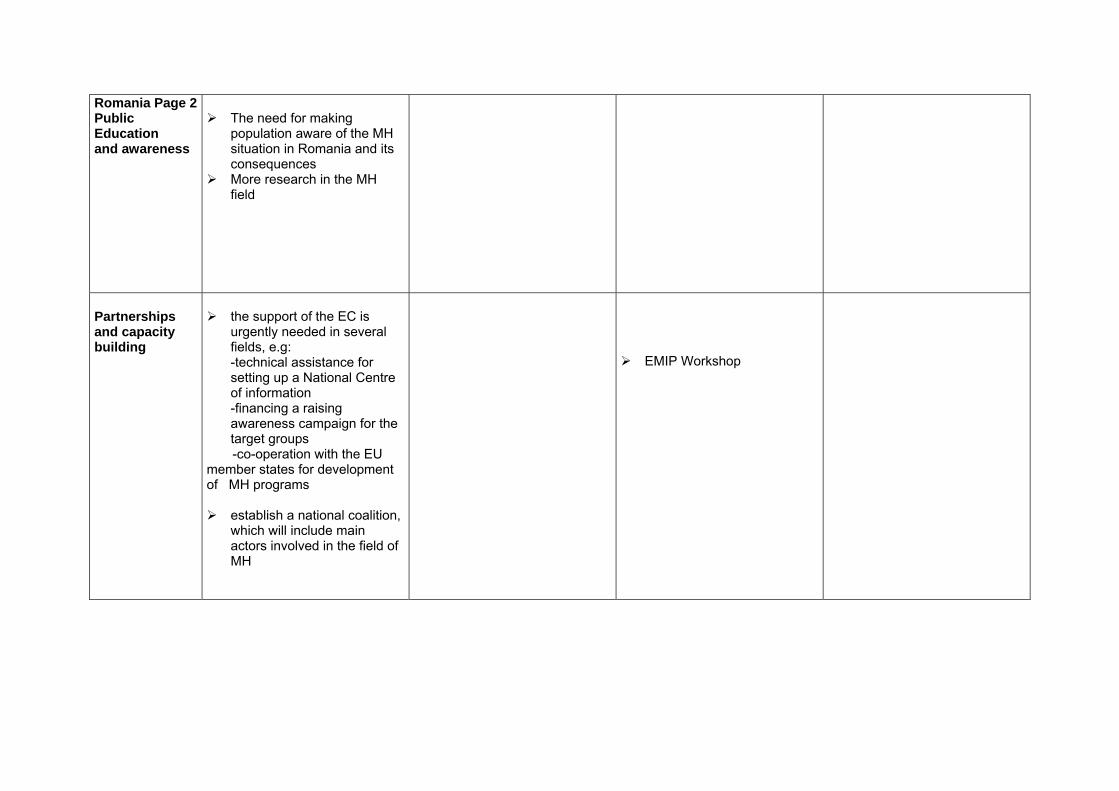
Romania Page 2Public Education and awareness
The need for making
population aware of the MH situation in Romania and its consequences
More research in the MH field
Partnerships and capacity building
the support of the EC is
urgently needed in several fields, e.g: -technical assistance for setting up a National Centre of information -financing a raising awareness campaign for the target groups
-co-operation with the EU member states for development of MH programs
establish a national coalition,
which will include main actors involved in the field of MH
EMIP Workshop
SLOVENIA
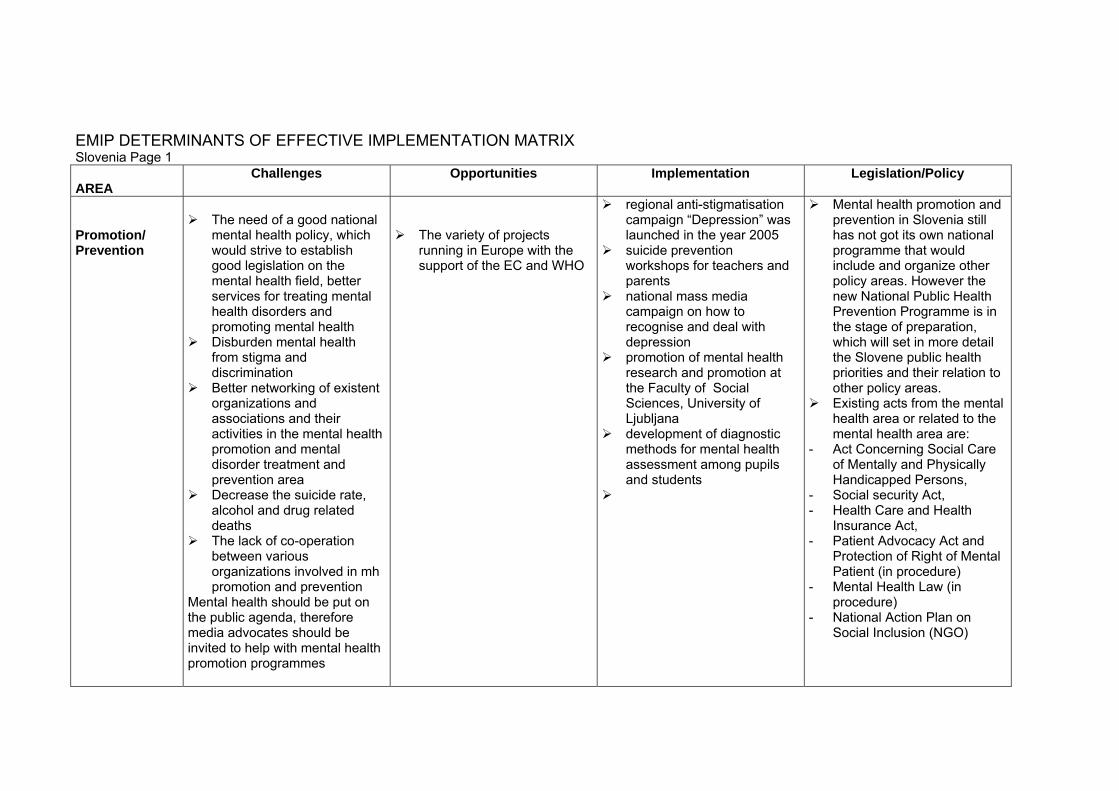
EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Slovenia Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
The need of a good national
mental health policy, which would strive to establish good legislation on the mental health field, better services for treating mental health disorders and promoting mental health
Disburden mental health from stigma and discrimination
Better networking of existent organizations and associations and their activities in the mental health promotion and mental disorder treatment and prevention area
Decrease the suicide rate, alcohol and drug related deaths
The lack of co-operation between various organizations involved in mh promotion and prevention
Mental health should be put on the public agenda, therefore media advocates should be invited to help with mental health promotion programmes
The variety of projects running in Europe with the support of the EC and WHO
regional anti-stigmatisation campaign “Depression” was launched in the year 2005
suicide prevention workshops for teachers and parents
national mass media campaign on how to recognise and deal with depression
promotion of mental health research and promotion at the Faculty of Social Sciences, University of Ljubljana
development of diagnostic methods for mental health assessment among pupils and students
Mental health promotion and prevention in Slovenia still has not got its own national programme that would include and organize other policy areas. However the new National Public Health Prevention Programme is in the stage of preparation, which will set in more detail the Slovene public health priorities and their relation to other policy areas.
Existing acts from the mental health area or related to the mental health area are:
- Act Concerning Social Care of Mentally and Physically Handicapped Persons,
- Social security Act, - Health Care and Health
Insurance Act, - Patient Advocacy Act and
Protection of Right of Mental Patient (in procedure)
- Mental Health Law (in procedure)
- National Action Plan on Social Inclusion (NGO)
Slovenia Page 2Public Education and awareness
Partnerships and capacity building
Emip’s workshop

Portugal Page 2 Public Education and awareness
Schools
1) Reduction of stigma associated with M.H. disorders. 2) Development of Programsof Personal Development Skills.
Media - promoting media awareness on M.H. subjects.
Portugal is a member of an
European Network of Health Promoting Schools. Mental Health is a priority subject.
Workgroup developing a
capacity building programme on interpersonal relation skills to be implemented in all public schools.
Seminars and workshops on
M.H. subjects.
This programme’s
attendance will be compulsory in all schools of the public sector.
Partnerships and capacity building
Training of primary health
professionals on mental health issues.
Training teachers and education personnel.
International partnerships
promoting the development of common promotion and prevention strategies and the creation of M.H. indicators.
ICT’s technologies (namely
e- learning). New training models.
Intersectorial Partnership – Ministry of Health & Ministry of Education.
EMIP project.
Since the 80’s – articulation
between Primary Care & M. Health Services, namely through training of primary health professionals on M.H. subjects.
Development of new models of training & development of new tools.
Activities developed within the EMIP project, namely the National Mental Health Conference.
Mental health promotion and
mental disorders prevention are integrated in the professional vocational training of general practitioners and family doctors, public health physicians and nurses or doctors’ assistants working in general practice, and it is compulsory, although not sufficiently developed.

Romania

EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Romania Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
Increase the interest for MH
issues at the governmental level
The reduced budget for MH care and support
The development of MH services in the communities
The lack of legislative norms regarding MH promotion and prevention
Change the actual MH care model into one based on the multidisciplinary team and individual care plan
Setting up a network of MH community service
Gaining the interest and support of the Ministry of Health
Reduce stigma and discrimination
The long term monitoring by the EC, Amnesty International
The various projects in the EU
The Green Paper will be the starting point for the Romanian policy on prevention
The Twinning Light wit technical assistance from the Netherlander Government _(2005)
Mantra Project for the improvement of norms for hospitalisation in the psychiatric and hospitals and hospitals applying security measures
In Romania, mental Health was approached as a field exclusively related to the health sector for many years. The following is the existing legislation for MH promotion and prevention:
the National Strategy regarding MH and the Action Plan for the Implementation of the MH Policy of the Romanian Ministry of Health_ result of the PHARE Project Twining Light
Health Minister Order no. 661/2005
Law no. 522/204 Governmental Decision no.
73 of January 27, 2005 Action Plan of r implementing
the National Anti-drug Strategy 2005-2008
Ministry of Health Order no. 10/2005 regarding the implementation of national health programs and sub-programs funded for the state budget
The Order regarding the setting up and organising of the MH Centre which will be approved by the Ministry of Health in the next days
Romania Page 2Public Education and awareness
The need for making
population aware of the MH situation in Romania and its consequences
More research in the MH field
Partnerships and capacity building
the support of the EC is
urgently needed in several fields, e.g: -technical assistance for setting up a National Centre of information -financing a raising awareness campaign for the target groups
-co-operation with the EU member states for development of MH programs
establish a national coalition,
which will include main actors involved in the field of MH
EMIP Workshop

SLOVENIA
EMIP DETERMINANTS OF EFFECTIVE IMPLEMENTATION MATRIX Slovenia Page 1 AREA
Challenges Opportunities Implementation Legislation/Policy
Promotion/ Prevention
The need of a good national
mental health policy, which would strive to establish good legislation on the mental health field, better services for treating mental health disorders and promoting mental health
Disburden mental health from stigma and discrimination
Better networking of existent organizations and associations and their activities in the mental health promotion and mental disorder treatment and prevention area
Decrease the suicide rate, alcohol and drug related deaths
The lack of co-operation between various organizations involved in mh promotion and prevention
Mental health should be put on the public agenda, therefore media advocates should be invited to help with mental health promotion programmes
The variety of projects running in Europe with the support of the EC and WHO
regional anti-stigmatisation campaign “Depression” was launched in the year 2005
suicide prevention workshops for teachers and parents
national mass media campaign on how to recognise and deal with depression
promotion of mental health research and promotion at the Faculty of Social Sciences, University of Ljubljana
development of diagnostic methods for mental health assessment among pupils and students
Mental health promotion and prevention in Slovenia still has not got its own national programme that would include and organize other policy areas. However the new National Public Health Prevention Programme is in the stage of preparation, which will set in more detail the Slovene public health priorities and their relation to other policy areas.
Existing acts from the mental health area or related to the mental health area are:
- Act Concerning Social Care of Mentally and Physically Handicapped Persons,
- Social security Act, - Health Care and Health
Insurance Act, - Patient Advocacy Act and
Protection of Right of Mental Patient (in procedure)
- Mental Health Law (in procedure)
- National Action Plan on Social Inclusion (NGO)

Slovenia Page 2Public Education and awareness
Partnerships and capacity building
Emip’s workshop

This report was produced by a contractor for Health & Consumer Protection Directorate General and represents the views of thecontractor or author. These views have not been adopted or in any way approved by the Commission and do not necessarilyrepresent the view of the Commission or the Directorate General for Health and Consumer Protection. The EuropeanCommission does not guarantee the accuracy of the data included in this study, nor does it accept responsibility for any use madethereof.
Related Documents