Filing at a Glance Company: BCBSVT Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing State: VermontGMCB TOI: ML02 Multi-Line - Other Sub-TOI: ML02.000 Multi-Line - Other Filing Type: GMCB Trend / Admin Charge Date Submitted: 02/23/2017 SERFF Tr Num: BCVT-130935599 SERFF Status: Assigned State Tr Num: State Status: Co Tr Num: Implementation Date Requested: On Approval Author(s): Pam Young, Jude Daye, Martine Brisson-Lemieux, Andrew Proulx Reviewer(s): Thomas Crompton (primary), David Dillon, Judith Henkin, Jacqueline Lee, Marisa Melamed, Noel Hudson Disposition Date: Disposition Status: Implementation Date: State Filing Description: SERFF Tracking #: BCVT-130935599 State Tracking #: Company Tracking #: State: VermontGMCB Filing Company: BCBSVT TOI/Sub-TOI: ML02 Multi-Line - Other/ML02.000 Multi-Line - Other Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing Project Name/Number: / PDF Pipeline for SERFF Tracking Number BCVT-130935599 Generated 02/27/2017 09:45 AM

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Filing at a Glance
Company: BCBSVT
Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing
State: VermontGMCB
TOI: ML02 Multi-Line - Other
Sub-TOI: ML02.000 Multi-Line - Other
Filing Type: GMCB Trend / Admin Charge
Date Submitted: 02/23/2017
SERFF Tr Num: BCVT-130935599
SERFF Status: Assigned
State Tr Num:
State Status:
Co Tr Num:
ImplementationDate Requested:
On Approval
Author(s): Pam Young, Jude Daye, Martine Brisson-Lemieux, Andrew Proulx
Reviewer(s): Thomas Crompton (primary), David Dillon, Judith Henkin, Jacqueline Lee, Marisa Melamed,Noel Hudson
Disposition Date:
Disposition Status:
Implementation Date:
State Filing Description:
SERFF Tracking #: BCVT-130935599 State Tracking #: Company Tracking #:
State: VermontGMCB Filing Company: BCBSVT
TOI/Sub-TOI: ML02 Multi-Line - Other/ML02.000 Multi-Line - Other
Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number BCVT-130935599 Generated 02/27/2017 09:45 AM

General Information
Project Name: Status of Filing in Domicile:
Project Number: Date Approved in Domicile:
Requested Filing Mode: Domicile Status Comments:
Explanation for Combination/Other: Market Type: Group
Submission Type: New Submission Group Market Size: Large
Group Market Type: Employer Overall Rate Impact:
Filing Status Changed: 02/24/2017
State Status Changed: Deemer Date:
Created By: Martine Brisson-Lemieux Submitted By: Martine Brisson-Lemieux
Corresponding Filing Tracking Number:
Filing Description:
February 23, 2017
Noel HudsonDirector of Health PolicyGreen Mountain Care Board89 Main Street, Third Floor, City CenterMontpelier, Vermont 05620
Subject:Blue Cross and Blue Shield of Vermont - NAIC # 53295Q3 2017 Large Group Rating Program Filing
Dear Mr. Hudson:
Attached for the Green Mountain Care Board’s review and approval is Blue Cross and Blue Shield of Vermont’s Q3 2017Large Group Rating Program Filing. As directed by the Board, this filing combines the various factor filings for large grouprating components (trend, large claims, benefit relativity, administrative fees and contribution to reserve, and the formula itself)into a single filing.
Please let me know if we can answer any questions or provide further information during your review.
Sincerely,
Ruth Greene
cc:Tom Crompton/GMCBPaul Schultz/BCBSVT Martine Lemieux/BCBSVT
SERFF Tracking #: BCVT-130935599 State Tracking #: Company Tracking #:
State: VermontGMCB Filing Company: BCBSVT
TOI/Sub-TOI: ML02 Multi-Line - Other/ML02.000 Multi-Line - Other
Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number BCVT-130935599 Generated 02/27/2017 09:45 AM

Company and Contact
Filing Fees
Filing Contact InformationJude Daye, Executive Assistant [email protected]
445 Industrial Lane
Montpelier, VT 05601
802-371-3244 [Phone]
Filing Company InformationBCBSVT
PO BOX 186
Montpelier, VT 05601
(802) 371-3450 ext. [Phone]
CoCode: 53295
Group Code:
Group Name:
FEIN Number: 03-0277307
State of Domicile: Vermont
Company Type: HospitalService Corp
State ID Number:
Fee Required? No
Retaliatory? No
Fee Explanation:
SERFF Tracking #: BCVT-130935599 State Tracking #: Company Tracking #:
State: VermontGMCB Filing Company: BCBSVT
TOI/Sub-TOI: ML02 Multi-Line - Other/ML02.000 Multi-Line - Other
Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number BCVT-130935599 Generated 02/27/2017 09:45 AM

Supporting Document Schedules Satisfied - Item: Actuarial MemorandumComments:Attachment(s): Q3 2017 BCBSVT Large Group Rating Program Filing - Actuarial Memorandum.pdfItem Status:Status Date:
Bypassed - Item: Civil Union Rating RequirementsBypass Reason: Not RequiredAttachment(s):Item Status:Status Date:
Satisfied - Item: Filing Compliance CertificationComments:Attachment(s): Q3 2017 BCBSVT Large Group Rating Program - Certification.pdfItem Status:Status Date:
Bypassed - Item: Third Party Filing AuthorizationBypass Reason: BCBSVT does not use a Third Party to submit filingsAttachment(s):Item Status:Status Date:
Satisfied - Item: Plain Language SummaryComments:Attachment(s): Q3 2017 BCBSVT Large Group Rating Program Filing - Plain Language Summary.pdfItem Status:Status Date:
Satisfied - Item: ExhibitsComments:
Attachment(s): Q3 2017 BCBSVT Large Group Rating Program Filing - Exhibits.pdfQ3 2017 BCBSVT Large Group Rating Program Filing - Exhibits.xlsx
Item Status:
SERFF Tracking #: BCVT-130935599 State Tracking #: Company Tracking #:
State: VermontGMCB Filing Company: BCBSVT
TOI/Sub-TOI: ML02 Multi-Line - Other/ML02.000 Multi-Line - Other
Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number BCVT-130935599 Generated 02/27/2017 09:45 AM

Status Date:
SERFF Tracking #: BCVT-130935599 State Tracking #: Company Tracking #:
State: VermontGMCB Filing Company: BCBSVT
TOI/Sub-TOI: ML02 Multi-Line - Other/ML02.000 Multi-Line - Other
Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number BCVT-130935599 Generated 02/27/2017 09:45 AM

Attachment Q3 2017 BCBSVT Large Group Rating Program Filing - Exhibits.xlsx is not a PDF documentand cannot be reproduced here.
SERFF Tracking #: BCVT-130935599 State Tracking #: Company Tracking #:
State: VermontGMCB Filing Company: BCBSVT
TOI/Sub-TOI: ML02 Multi-Line - Other/ML02.000 Multi-Line - Other
Product Name: BCBSVT Q3 2017 Large Group Rating Program Filing
Project Name/Number: /
PDF Pipeline for SERFF Tracking Number BCVT-130935599 Generated 02/27/2017 09:45 AM

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
1
Table of Contents
1. PURPOSE ........................................................................................................................................... 2
2. OVERVIEW AND RATE IMPACT ................................................................................................. 2
2.1. Overview ........................................................................................................................................ 2
2.2. Impact of Formula and Factor Changes .................................................................................. 2
3. FORMULA DESCRIPTION .............................................................................................................. 4
4. FACTORS APPLICABLE TO ALL LARGE GROUPS ................................................................. 7
4.1. Large Claims Factors ................................................................................................................... 7
4.2. Trend Factors ............................................................................................................................... 8
4.3. Benefit Relativity Factors ........................................................................................................ 16
4.4. Manual Rate ................................................................................................................................. 22
4.5. Administrative Charges ............................................................................................................ 23
4.6. Net Cost of Reinsurance ........................................................................................................... 25
4.7. Pharmacy Rebates ..................................................................................................................... 25
4.8. Contribution to Reserve ........................................................................................................... 25
4.9. State Mandates and Assessments ........................................................................................... 26
4.10. Federal Assessments ............................................................................................................. 27
5. FACTORS APPLICABLE ONLY TO SPECIFIC PRODUCTS................................................. 28
5.1. Stop Loss Coverage for Cost Plus products .......................................................................... 28
5.1.1. Individual Stop Loss ........................................................................................................... 28
5.1.2. Aggregate Stop Loss........................................................................................................... 28
5.2. Risk and Administrative Charges for Experience Refund Eligible products ................ 30
6. HISTORICAL FINANCIAL RESULTS ......................................................................................... 31
7. ACTUARIAL OPINION .................................................................................................................. 33

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
2
1. Purpose
Blue Cross and Blue Shield of Vermont (BCBSVT) performs large group rating on a case-by-case basis. Rating is accomplished through a formulaic approach that blends recent group experience with a manual rate according to a credibility formula. Formula results may be adjusted for underwriting judgment and/or management decisions. This filing establishes the formula, manual rate, and accompanying factors that will be used for renewals beginning upon approval of this filing, most notably January 2018 renewals. Once approved, this filing will be used for large group and grandfathered small group renewals (we will refer to them collectively as Large Groups for the remainder of the filing) prepared for business under the jurisdiction of the Green Mountain Care Board (GMCB) until superseded by a subsequent filing. This filing will apply beginning with rates communicated 10 business days after the date of its approval, and continuing until 10 business days after the date of approval of the next BCBSVT Large Group Rating Program Filing. The term “communicated,” for this purpose, means a written proposal delivered to a large group account.
2. Overview and Rate Impact 2.1. Overview This filing includes a description of the renewal formula and the development of each of the factors used in it. This formula is used for both Fully Insured and Cost Plus customers. BCBSVT projects that about 15,908 members (8,159 subscribers) in 67 groups will be impacted by this filing. These totals include members of both BCBSVT and The Vermont Health Plan (TVHP), and we will refer to the combined population as BCBSVT throughout this memorandum. We will describe in detail the formula used in the renewals. The formula has been modified from the currently approved version (BCVT-130453174). The changes, described in detail below, pertain to the credibility formula, calculation of ISL factors, and development of ASL and Refund-Eligible charges. We will then detail the factors applicable to all Large Groups (Fully Insured and Cost Plus). The factors included in the build-up of the projected claims cost include the Large Claims Factors, Trend Factors, Benefit Relativities, and the Manual Rate. In addition to the projected claims cost, we will explain the calculation of administrative charges, the net cost of reinsurance, contribution to reserve, and State and Federal Assessments, all of which are included in the rate development. Finally, we will discuss factors applicable only to specific products. Cost Plus customers purchase Individual and Aggregate Stop Loss from BCBSVT. We also offer an Experience Refund Eligible product for which risk charges and settlement administration changes apply. 2.2. Impact of Formula and Factor Changes To compute the impact of changes to the rating formula and the various factors in this filing on large group premium rates, we produce two renewals for each of the 59 large groups we expect to enroll in 2018 (excluding eight groups without a complete 12 months experience period with

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
3
two months of runout). The first renewal uses the approved factors currently in force (BCVT-130453174) with an effective date of January 1, 2017. The rates in these renewals are used as a baseline for the comparison with the rates produced by the new factors. The second renewal uses the same experience period as the first but has an effective date of January 1, 2018 and uses the factors and formulas detailed in this filing. The new trend factors are applied for 12 months to represent an additional year of trend with the new trend assumption. The result of comparing the renewals across all 59 large groups is an average 8.0 percent rate increase excluding the impact of the Federal Insurer Fee and 10.7 percent when including the impact of the fee. Reasons for the rate increase can be attributed to two main causes: changes in the rating formula and filed factors, and changes mandated due to the Affordable Care Act (ACA). The largest component of the increase due to changes in the filed factors is the additional year of trend applied to the experience and manual claims. The trend is responsible for a 6.8 percent increase in projected claims, which results in a 6.1 percent increase in premium. Administrative charges are increasing by 25.0 percent, which increases required premium by 1.5 percent. The average rate increase from all changes to the formula and factors is 8.0 percent. Changes in federal programs under the ACA work to increase the average rate increase by 2.7 percent. The federal insurer fee is assessed to insured groups and goes to pay for some provisions of the ACA. The Consolidated Appropriation Act of 2016 temporarily suspended this fee for 2017. We estimate the fee is 2.6 percent of premium in 2018 and 2.6 percent of premium in 2019. The overall 10.7 percent rate increase translates to a $50.74 PMPM increase. The PMPM increase can be broken down as follows:
Component 2017 PMPM
2018 PMPM
PMPM Change
Impact on Premium Increase
Projected Paid claims1 $415.34 $443.87 $28.52 6.0%
Administrative charges $28.98 $36.22 $7.24 1.5%
Contribution to Reserve $9.05 $10.05 $1.00 0.2%
Federal Programs $0.19 $13.08 $12.89 2.7%
Additional Items2 $18.66 $19.74 $1.08 0.2%
Total $472.22 $522.96 $50.74 10.7% (1) Projected paid claims include manual claims (5.9 percent increase), experience claims (7.4 percent increase), and projected rebates (5.6 percent increase). (2) Additional Items includes net cost of reinsurance, Cost Plus stop loss, broker commissions, State mandates and assessments, fees paid to outside vendors, and the Refund-Eligible margin & risk charge.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
4
3. Formula Description We are modifying our rating formula to rate Medicare Primary members separately from Active members. Previously, experience from both populations was combined in the rating formula. This resulted in the experience for active members being reflected in the premium for Medicare Primary members. We will use the same formula and factors for each population but the required premiums will be developed independently. Thus the Medicare Primary rates will be based on a blend of the group’s own Medicare Primary experience and the Medicare Primary experience of all BCBSVT Medicare Primary members as reflected in the manual claims. Benefit-Adjusted Projected Single Claims Rate A sample calculation of this quantity can be found as Exhibit 1A. Page 1 of the exhibit applies to active members and page 2 applies to Medicare Primary members. For each case, we start the rating with a twelve month experience period with two months of runout1. We determine a pooling point based on the size of the case at the end of the runout period and split the experience period claims (line A) into amounts above (line B) and below (referred to as Capped Claims, line C) the pooling point. We apply completion factors (line D) developed from the monthly financial reporting process to Capped Claims to produce Completed Capped Claims (line E). We multiply the completed capped claims by the pooling factor (line F, described in section 4.1) to calculate the expected claims above the pooling point (line G). The expected claims above the pooling limit are added to the Completed Capped Claims to produce large-claim-adjusted experience period claims. We do not expect Medicare Primary members to reach the group’s pooling point, so we do not remove actual claims above pooling or add in expected claims above pooling for Medicare Primary members. We then multiply the large-claim-adjusted experience claims by an adjustment factor (line H) to reflect structural changes in the benefit plan from the experience period to the rating period. This is to adjust for such things as mandated benefit changes, contractual provision changes, etc., that, in the judgment of the underwriter, are necessary to make the experience appropriate for the estimation of the expected claims in the rating period. We divide the result (line I) by the number of member months during the experience period (line J) to produce Adjusted Experience Period Claims per member per month (line K). The Adjusted Experience Period Claims per member per month (PMPM) is then divided by a seasonally-adjusted benefit relativity value to neutralize any effect of seasonality and benefits on the paid claims. To determine this factor, we first determine a benefit relativity factor for each benefit plan (using the factors described in section 4.3) and contract tier type (single, 2-person, family, etc.). Based on the seasonal patterns observed as part of the reserving process for each calendar month, we determine seasonal factors for CDHPs and for non-CDHPs and normalize them so that they total to 12. We combine these factors to calculate seasonal benefit relativity factors for each combination of benefit plan, contract tier type, and month. We apply these factors to the number of contracts for each benefit plan, contract tier type, and month in the experience period. We total the results and divide the resultant sum by the number of member months in the experience period. This produces the Average Experience Period Seasonal Adjusted Benefit Relativity Factor (line L).
1 For first year renewals, where twelve months of experience is not available, we generally use claims incurred in nine months with no runout.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
5
Dividing the Adjusted Experience Period Claims PMPM (line K) by the Average Experience Period Seasonal Adjusted Benefit Relativity Factor (line L) produces the Benefit-Adjusted Experience Period Single Claims Rate (line M), which is the expected cost for a single contract in the experience, neutral of benefit and seasonality. We then multiply this by a trend factor (line N, as calculated in section 4.2) to project the claims from the experience period to the rating period. We also multiply by a factor (line O) to account for differences in contracted pharmacy discounts between the experience period and the projection period. The resulting Projected Single Contract Rate (line P) is then blended (using the credibility formula described below) with the Adjusted Manual Rate (line Q, as described in section 4.4). The credibility factor (line R) is calculated as follows:
���������� = � ����� ���ℎ����������� The upper bound is determined based on pooling point as follows:
Pooling Point Member Months
$70,000 14,002
$90,000 16,127
$110,000 17,923
If member months are greater than the upper bound, the credibility factor will be 1. The credibility formula has been modified from the currently approved version. We periodically review the credibility formula to ensure that it is expected to produce reasonable results and that it is appropriate for its intended use and purpose2. The development of a credibility procedure has two parts: the determination of the threshold for full credibility and the selection and parametrization of a survival function to assign partial credibility. To determine the threshold for full credibility, we used classical (limited fluctuation) credibility theory. According to this theory, full credibility is achieved when, for selected values P and k, the probability that the sample mean differs from its expected value by less than a fraction k of the expected mean is equal to P. Formulaically, for a given distribution X, the number of observations of X required for full credibility is:
�� ∗ ���(�)( (�))! , where �� = "#$% &' and yp is the (()*)' percentile of the standard normal distribution.
Using the tables created from the combined BCBSVT projected claims file described in section 4.1, the mean and variance of claims by pooling point is calculated. This is then multiplied by ��, where P = 90% and k = 0.10. To assign partial credibility, the square root of member months divided by the upper bound is calculated. If a group’s pooling point is not in the table, identical
2 http://www.actuarialstandardsboard.org/wp-content/uploads/2014/02/asop025_174.pdf

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
6
data, assumptions and methodology as described above will be used to calculate the upper bound for the required pooling point. To blend the Projected Single Contract Rate with the Adjusted Manual Rate, we use the following equation: ����+��--�.�����/��.�0���1��2����3���43�� = /��.�0���1��2�������30�43�� ×(����������) + -�.����� 3��3�43�� × (1 − ����������) Required premium by Plan, Tier Type A sample calculation of premium can be found as Exhibit 1B. For each plan and contract tier type anticipated in the rating period, we calculate projected claims (line B1) as the product of the Benefit-Adjusted Projected Single Claims Rate (S) and the BRV for the plan and contract tier (line A). The members per contract tier during the last month of the runout period is the basis for the projected members per tier in the rating period. The underwriter will adjust this if, in their opinion, the result is not representative of the expected values in the rating period.3 The calculation for the total required premium by (plan, tier) is as follows:
{ Projected Claims by plan and tier (line B1) + Expected Net Cost of Reinsurance (line B2, as described in section 4.6) + Projected Pharmacy Rebates (line B3, as described in section 4.7) + Administrative Charges (line E, as described in section 4.5) + State Mandates (line C1 to C3, as described in section 4.9) + Federal Mandates } (line D, as described in section 4.10) / { 1 – Contribution to Reserve (line G, as described in section 4.8) – Broker Commissions (line F) - Federal Insurer Fee (line H, as described in section 4.10)}
=
Required premium by plan and tier (line I)
Underwriting Judgment Adjustments If, in the underwriter’s professional judgment, the specific properties of the case being rated are such that the standard formula would not produce appropriate rates for the rating period, the underwriter will make such modifications as needed to produce appropriate rates. The underwriter will document in the case file the reason(s) for the adjustment(s) and the method of determining the appropriate adjustment(s). Management Discretionary Adjustments For marketing or other reasons, management may decide to modify the rates on a specific case or block of cases. The underwriter will document in the case file the adjustment(s) made, along with a description of the nature of the adjustment(s). 3 E.g., the number of contracts in a particular tier may be small (or even 0). In such instances, the underwriter should use appropriate values based on total block of business or other appropriate source.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
7
4. Factors applicable to all Large Groups 4.1. Large Claims Factors
As described in section 3, experience claims above a certain pooling level are removed from the calculation and replaced by the expected claims above the pooling level. In order to develop the large claims factors used to calculate the expected claims above a pooling level, allowed charges and paid claims through September 30, 2016 were analyzed for the experience years ended December 31, 2013, December 31, 2014, and December 31, 2015. The data includes claims from BCBSVT Cost Plus groups, BCBSVT ASO Groups, BCBSVT Insured Large Groups, and TVHP Insured Large Groups. Combining these homogeneous populations creates greater consistency and credibility within the large claim factor development. Fee-for-Service equivalents were used for capitated services and claims incurred by Medicare Primary members were excluded. Any groups that do not include prescription drugs as a covered expense under their BCBSVT/TVHP benefit plan were also excluded. The source of the data is BCBSVT’s data warehouse, except where noted below. To ensure accuracy of claims information, the data used has been reconciled against internal reserving, enrollment, and other financial reports. For each experience year, allowed charges and paid claim amounts were totaled for each claimant. These were then sorted into categories by the amount of allowed charges. The categories used were:
- $0 up to $50 - $50 up to $100 - $100 up to $200…$1,900 up to $2,000 - $2,000 up to $2,500…$9,500 up to $10,000 - $10,000 up to $15,000…$995,000 up to $1,000,000 - Further categories in $5,000 increments as necessary for claims above $1,000,000
For each category, paid-to-allowed ratios were calculated. The ratios for each year were averaged for each category, while the resulting ratios at allowed amounts greater than $1,000 were smoothed. The high-to-low-to-high pattern of the ratios observed at allowed amounts less than $1,000 was maintained; presumably this pattern is due to the increased provision and use of preventive benefits covered at no charge. Different factors were created for use with Insured groups (based on data from BCBSVT and TVHP Insured Large Groups) and Self-Funded groups (based on data from Cost Plus and ASO groups). These factors were blended with factors generated by two other distributions of claims to generate the final factors used in the rating program. One set of factors was based on data from the 2014 Milliman Health Cost Guidelines and the other was based on the combined experience of BCBSVT and TVHP Insured Groups, Cost Plus groups, and ASO groups. We calculated the charge factors assuming experience periods begin on the first day of the quarter. To project the charges for future experience periods, the allowed amounts by claimant for 2013 and 2014 were trended by the observed trends to 2015, and then by 6.9 percent per annum (see section 4.2 for details). The allowed amounts for 2015 were also trended forward at 6.9 percent per annum. For each claimant record, a claim amount was calculated by applying the appropriate factor from the paid/allowed amount factor table. A projected claim file was built by combining the trended 2013 records with two copies of the trended 2014 records and three copies of the 2015 records (thus weighting the 2014 experience twice as heavily and the

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
8
2015 experience three times as heavily as the 2013 experience). For a set of limits (in increments of $5,000), the amounts in excess of the limit for each claim and the amounts under the limit for each claim were totaled and the ratio of these calculated. This produced a factor for each limit value expressing claims above the limit in terms of claims below the limit. A distribution of claims by amount was generated from the 2014 Milliman Health Cost Guidelines distribution of allowed charges (adjusted for Vermont) by trending the distribution to produce the same expected average annual allowed charge per member as the trended BCBSVT/TVHP distribution and then applying the paid-to-allowed factors calculated above. Factors for claims above the limit as a percentage of those below the limit were calculated from this distribution. As discussed in Section 3, we develop a credibility procedure using classical credibility. We let X be the paid claims per member-year in our blended experience and select P = 95% and k = 0.10. With these values, the standard for full credibility for the various experience groups is summarized below:
Groups in Base Data Member-Years for
Full Credibility Claims Threshold
for Full Credibility Insured 8,463 $20,000 Self-Funded 5,452 $50,000 Combined 6,392 $60,000
To determine partial credibility for limits above the threshold, we fit our distribution of claimants above that limit to a Pareto distribution. We selected the Pareto distribution due to
its decreasing, thick-tailed survival function, given by the formula 1(9) = ":;&< for x > θ, where
θ is the threshold for full credibility and q is a parameter estimated from the data. For each limit, two credibility factors were calculated to blend the three pooling factors. Credibility factor Z is the credibility given to the pooling factor for the appropriate category (Insured or Self-Funded) and Credibility Factor Y is the credibility of the remaining (1-Z) given to the combined BCBSVT experience. The blended pooling factor is calculated by the formula Z*(Category Factor) + (1-Z)*Y*(BCBSVT Combined Factor) + (1-Z)*(1-Y)*(Milliman Factor). This calculation is demonstrated in Exhibit 2A.
Exhibit 2B shows the factors that will be applied to the experience claims under the pooling limit to calculate the expected claims above the limit for Insured groups. These factors are calculated for each experience period starting quarter expected to be covered by this filing. Exhibit 2C shows the factors for Self-Funded groups.
4.2. Trend Factors Medical Trend Development The source of the data is BCBSVT’s data warehouse, except where noted below. To ensure accuracy of claims information, the data used has been reconciled against internal reserving, enrollment, and other financial reports. Claims incurred between November 1, 2012 and August

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
9
31, 2016, paid through October 31, 2016, were used in the analysis. Completion factors are applied to estimate the ultimate incurred claims for each period shown in the exhibits. The data includes claims from BCBSVT Cost Plus groups, BCBSVT ASO Groups, BCBSVT Insured Large Groups, and TVHP Insured Large Groups. CDHP and Non-CDHP claims are combined. The data from one large ASO group has been excluded from the medical analysis because they were not active for the entire experience period. Additionally, ASO groups with special pricing arrangements are excluded. Claims from Medicare Primary members are excluded. Medicare Primary trend is discussed in section 4.3. BCBSVT and TVHP cover substantially similar populations under similar benefit packages. Combining these homogeneous populations creates greater consistency and credibility within the trend factor development. Using the historical contracted reimbursement schedules, we calculated network factors that represent the different contracts and modify the claims to reflect a single contract. By making these adjustments we can observe the historical cost increases using all large group claims information. Medical trend is composed of three pieces: cost, utilization, and intensity. In our analysis, we combined utilization and intensity within the utilization metric and analyzed the unit cost separately. Historical experience was normalized for contract changes and then analyzed to derive a utilization trend in the absence of unit cost changes. Future unit cost trends were developed on a discrete basis using the most recent round of contract negotiations as a starting point. The overall trend is the product of these two components. Utilization Historical utilization trend patterns were examined by first normalizing claims for unit cost increases. Contract changes for the entirety of the experience period were measured explicitly for each facility within our service area as well as the three largest physician groups. Increases were measured for fee schedules and other Chargemasters by applying each schedule to a market basket of services. The market basket was defined by using Current Procedural Terminology (CPT) codes & CPT modifier combinations that were present in each of the effective periods the schedules covered. Using the same experience period data used throughout the trend analysis, total allowed costs for the selected CPT & CPT modifier combinations were compared under each schedule to estimate the percentage increase. For contracts under DRG arrangements, we compared the charge for the 1.000 DRG service for each period. Finally, for services under a discount of charge arrangement, we used the contracted chargemaster increase provided by our Provider Contracting department. This accounted for over 85 percent of allowed claims dollars during the experience period. Costs for other claims are primarily for out-of-area services. Contracting changes for these claims were derived from the Fall 2016 Blue Trend Survey, which is a proprietary and confidential dissemination of the BlueCross BlueShield Association. Claims were normalized to the October 2016 contract at each unique provider by applying a factor equal to the product of the impact of each contracting change from the experience month through October 2016. The derived trend for other claims was assumed to be continuous. Please see Exhibit 3A for an illustration of this approach.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
10
Exhibit 3B shows the resulting array of allowed PMPM claims costs, before and after normalization for contract changes. We performed a 24-month regression on monthly PMPM costs to match the length of the period used in the calculation of the cost trend (described below). We believe the resulting utilization trend of 1.5 percent to be overstated. The 24-month regression can be unduly influenced by the beginning and end months in the experience period. We observed utilization trends ranging from 0.3 percent to 1.7 percent by shifting the experience period used to calculate the regression. Alternatively, a regression on rolling PMPM costs can be too slow to capture shifts in utilization. We also calculated a year-over-year rolling PMPM utilization trend of 0.9 percent for the year ended August 2016. We have selected a utilization trend of 1.0 percent. This is lower than the trend calculated by our standard methodology, but balances the shifts noted in the monthly regressions and is consistent with the utilization trend of 1.0 percent in the most recently approved Large Group Rating Program filing.
We also investigated the impact of benefit changes throughout the experience period on utilization. Large groups have engaged in a benefit buy-down strategy over the last several years as a means of limiting rate increases. This manifests itself in a lower actuarial value over time and a dampening effect on trend due to decreases in induced utilization, as shown in the table below:
Year Ended Paid-to-Allowed
Ratio Induced
Utilization Percent Change
October 2013 86.5% 0.981
August 2014 84.7% 0.965 -1.6%
August 2015 83.6% 0.955 -1.0%
August 2016 84.1% 0.960 0.5% To account for the impact of the benefit buy-downs in the trend, we normalized claims to the mix of benefits present during the year ended August 2016. We did this by using a factor for each month equal to the ratio of the induced utilization for benefits present in the year ended August 2016 to the induced utilization for benefits present in the year ended that particular month. Exhibit 3C shows that the impact of induced utilization on the utilization trend is 0.3 percent. Applying this adjustment to our selected trend of 1.0 percent results in a final utilization trend of 1.3 percent when accounting for benefit changes. The concept of induced utilization is discussed further in section 4.3. Unit Cost Unit cost trends were largely derived from observations of recent contracting and provider budgetary changes. During the year ended July 2016, roughly 55 percent of total claims dollars were provided by Vermont facilities and providers impacted by the hospital budget review process of the Green Mountain Care Board (GMCB). We started with the assumption that the GMCB would approve hospital budgets for October 1, 2017 and October 1, 2018 that support identical commercial increases as that approved for October 1, 2016. While the GMCB, through increased oversight, has limited the overall increase of hospital budgets in recent years, the cost shift from Medicare and Medicaid has accelerated, driving commercial increases higher. We have little reason to believe that the cost shift will not continue at current levels. Based upon that

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
11
assumption, Provider Contracting and Actuarial worked together to assess the impact such an increase would have on contract negotiations for BCBSVT Managed Care, BCBSVT Non-Managed Care, and TVHP Managed Care contracts. Provider Contracting provided estimates for specific facilities in 2017 and 2018 that supplanted the assumptions noted above. Similarly, we assumed for other providers within the BCBSVT service area that overall 2017 and 2018 budget increases would be identical to those implemented during calendar 2016, except when Provider Contracting provided a specific estimate. Again, Provider Contracting and Actuarial worked together to assess the impact these increases would have on contracts for BCBSVT Managed Care, BCBSVT Non-Managed Care, and TVHP Managed Care contracts. Finally, unit cost increases for providers outside the BCBSVT service area were derived from the Fall 2016 Blue Trend Survey, which is a proprietary and confidential dissemination of the BlueCross BlueShield Association. For marketing reasons, Provider Contracting has been negotiating different unit cost increases for each of the three contracts. To reflect this, we calculated three different cost trends, one for each contract. Normalized claims were trended forward using expected increases. Unit cost trend is calculated by dividing claims year-ending December 2018 by claims year-ending June 2017 and converting to an annual factor.
The results of the analysis are summarized in the below chart: Annual Unit Cost Trend Assumption BCBSVT
Managed Care BCBSVT Non-Managed Care
TVHP Managed Care
Vermont facilities and providers impacted by GMCB’s Hospital Budget Review
4.4% 4.4% 4.4%
Other facilities and providers 4.9% 5.0% 5.0%
Total 4.6% 4.7% 4.7%
Total Medical Trend The total medical trend factors are the product of the utilization trend and the unit cost trend factors. BCBSVT
Managed Care BCBSVT Non-Managed Care
TVHP Managed Care
Cost Trend 4.6% 4.7% 4.7% Utilization Trend 1.3% 1.3% 1.3% Total Medical Trend 6.0% 6.0% 6.0%

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
12
To calculate the overall medical total trend to be applied in the renewal formula, we trended the manual rate (see section 4.4) experience medical claims based on the network to calendar year 2018. We then divided the projected claims cost by the experience claims cost to get the overall medical trend. BCBSVT
Managed Care
BCBSVT Non-Managed
Care
TVHP Managed
Care
Total
Experience Allowed Claims (Medical Only)
$7,288,679 $51,065,123 $15,209,332 $73,563,134
Trend Factors for 27 months 1.140276 1.140735 1.140735
Trended Claims $8,311,108 $58,251,774 $17,349,818 $83,912,701
Annual Trend 6.0% Pharmacy Trend Development The source of the data is BCBSVT’s data warehouse, except where noted below. To ensure accuracy of claims information, the data used has been reconciled against internal reserving, enrollment and other financial reports. The data includes claims from BCBSVT Cost Plus groups, BCBSVT ASO Groups, BCBSVT Insured Large Groups, and TVHP Insured Large Groups. Combining these homogeneous populations creates greater consistency and credibility within the trend factor development. CDHP and Non-CDHP claims are combined. Claims from Medicare Primary members are excluded. The data from ASO groups whose pharmacy benefits are not administered through the BCBSVT contract with ESI are excluded. We used claims incurred from October 1, 2014 to September 30, 2016, paid through October 31, 2016. Completion factors were applied to estimate the ultimate incurred claims for each period shown in the exhibits. ESI has been the pharmacy benefits manager for BCBSVT and TVHP since July 2009. The initial ESI contract was for a period of 3 years; new contracts became effective July 2012 and July 2015. Similar to the Q3 2016 Large Group Rating Program Filing, we base our cost trend calculation on Average Wholesale Price (AWP) and apply a factor to the rating formula to account for the contracting changes. With the emergence of new and expensive specialty drugs, as well as the ongoing shift to generics as more brand drugs come off patent, we analyzed the components of trend (cost and utilization) separately for brands, generics, and specialty drugs. We have projected the generic dispensing rate (GDR) based on the brand drugs that are scheduled to lose patent in the projection period. Specialty drugs are very high cost drugs with low utilization. Because of their relative infrequency, it is more appropriate to look at the overall PMPM trends for these drugs rather than separate cost and utilization components. The overall pharmacy trend is calculated by combining the separate projections. Non-Specialty Drugs Exhibit 3D provides the monthly and the 12-month rolling data, along with the corresponding year-over-year and exponential regression trends, for non-specialty drugs. These are shown separately for the generic cost, brand cost, and overall non-specialty utilization categories. The number of days supply, rather than the number of scripts, was used to normalize for changes in the days supply per script (e.g. increased use of 90-day fills). Because there are

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
13
several popular brand drugs that have become generic during the experience period, or will become generic during the projection period, we combined the data for generic and brand drugs for the purpose of analyzing utilization patterns (the separate GDR projection is applied to the total projected utilization to arrive at brand and generic components). The regressions use 24 data points on the monthly data, in order to best capture an adequate amount of the most recent history of drug costs. We selected annual trends of 5.1 percent for generic cost, 15.6 percent for brand cost, and 0.7 percent for total non-specialty utilization. Based on our current distribution of days supply and a list of brands expected to move to generic in the period during which these trend rates will be in effect, as provided by ESI, we estimate that GDR will reach 89.0 percent in the projected period. It is important to note that care must be taken in projecting the GDR to avoid the simplistic assumption that generic shift will continue at historical levels. Generic conversion is a very discrete function – while specific dates for generic launches may be impacted by ongoing litigation, the list of brand drugs losing their patent protection is well-recognized in the industry. Furthermore, generic substitution protocols have increased generic substitution rates to well over 99 percent where such switches are clinically viable. For the above reasons, it would be actuarially inappropriate to base a future GDR assumption on a linear projection of past increases, which is why we have chosen to take a far more detailed, and more discrete, approach. Exhibit 3E shows the calculation of the 89.0 percent GDR in the projection period. Utilization for brand drugs losing or expected to lose their patent protection from November 2014 through the projection period is summarized by month. Because Average Wholesale Price (AWP) and effective discounts do not change significantly for most new generic drugs until the six-month exclusivity period has closed (that is, when the generic becomes “multi-source”), monthly utilization for the year ended October 2016 is repeated through six months following each generic launch date (i.e. we assume the same days of supply in November 2016 as we had in November 2015, and so on). After that time, all utilization is expected to shift to generic. We assume drugs with no generic exclusivity period will switch to generic immediately after the patent expires. Exhibit 3F summarizes the trends for non-specialty drugs and calculates our total non-specialty allowed drug trend as 6.2 percent. Specialty Drugs The introduction of new specialty drugs for the treatment of hepatitis C in January 2014 required an adjustment to the trend calculation for specialty drugs. Other high-cost or high-utilization drugs have also entered the market recently, such as Orkambi, a treatment for cystic fibrosis with an annual cost of almost $250,000, and PCSK9 inhibitors like Repatha, used to treat high cholesterol in patients with the genetic disease familial hypercholesterolemia (FH) who have failed one statin and patients who have suffered a heart attack and failed two different statins. To accurately capture the effect of these new drugs on specialty trend, we removed their claims from the experience to calculate a trend rate to apply to these non-excluded claims. We trended those claims forward at the calculated rate for 27 months, then added back in our projections of claims for the new treatments (hepatitis C drugs, Orkambi, and PCSK9 inhibitors). We used the total restated projected claims to calculate a restated specialty trend. Exhibit 3G, Page 1 shows the calculation of specialty trend both for all specialty drugs and for specialty drugs excluding the new treatments described above. For our regressions, we chose 24 points of 12-month rolling data to capture the most recent history of drug costs. Rolling 12-

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
14
months regression is more appropriate for specialty drugs because of the low-frequency, high-cost nature of these drugs. The total specialty trend is 17.3 percent. Removing the large cost increases associated with the new treatments results in a 14.9 percent trend for the remaining specialty drugs. To project the cost of hepatitis C treatments in the rating period, we began by looking at actual hepatitis C claimants in 2015 and year-to-date 2016. We project 30 hepatitis C claimants in 2018 based on the ratio of claimants to members in 2015. There are several different drugs available for the treatment of hepatitis C (Sovaldi, Viekira Pak, Harvoni, Olysio, and Epclusa are in our experience). Hepatits C drugs are available in 3- and 6-month treatments. We project the distribution amongst the drugs in 2018 will be similar to our experience in 2015. In our experience, roughly 4/5s of claimants receive the 3-month treatment and 1/5 receive the 6-month treatment, so the average claimant receives 3.65 months of the drug. At an average monthly cost of $30,200, 30 claimants with an average treatment of 3.65 months have a projected 2018 cost of $3.30 million. PCSK9 inhibitors such as Repatha are used to treat high cholesterol. BCBSVT’s current policy is to approve PCSK9 inhibitors for the treatment of familial hypercholesterolemia (FH), a genetic disease characterized by very high levels of cholesterols in the blood, after failure of one high-does statin for 60 days. Current incidence studies suggest that 200 persons per 100,000 lives are diagnosed with FH. Another indication for these drugs is for patients who have had a heart attack and then failed two different high-dose statins for 60 days. Based on current membership, we project 16 members will use a PCSK9 inhibitor in 2018. With an annual cost of about $14,000, the projected total is $225,000. Orkambi is a drug used in the treatment of cystic fibrosis. In particular, it is used to treat a specific mutation of the disease that is found in roughly 50 percent of cystic fibrosis patients. Orkambi is prescribed to patients age 12 and older. We assumed that 50 percent of our members diagnosed with cystic fibrosis who are at least age 12 will take Orkambi. Orkambi has an annual cost of $247,000 and we project 8 members will use it. The projected cost for those members is $1.97 million. In our previous filing, we made an adjustment for the expected impact of biosimilars. We now do not expect biosimilars to have a cost impact until at least 2020, so the adjustment has been removed. To calculate the effective specialty trend, we started with the pharmacy claims from the year ended September 30, 2016 experience period and removed the claims for hepatitis C drugs, PCSK9 inhibitors, and Orkambi. We then trended the remaining claims at a 17.3 percent rate for 27 months and added the incremental cost of hepatitis C treatments, PCSK9 inhibitors, and Orkambi for a total restated projected claims. Using this method, the restated effective specialty drug trend is 19.3 percent. See Exhibit 3G, Page 2 for details. Total Pharmacy Trend Using the PMPM claims as weights between Non-Specialty and Specialty claims for the 12 months ended September 2016, we calculate the following:

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
15
Category PMPM Overall Trend
Generic $20.14 7.2%
Brand $41.25 5.7%
Specialty $32.34 19.3%
Total $93.73 11.0%
Contract Adjustment Factors Exhibit 3H contains the contract adjustment factors that will be applied to the drug claims in a group’s renewal. For drug claims in the year ended September 30, 2016, we took the AWP of the claims and applied the contracted discounts and dispensing fees for each potential renewal experience period and rating period to calculate adjusted allowed charges. The contract adjustment factor for each experience and rating period combination is the ratio of the adjusted allowed charges. These factors assume that both the experience period and rating period are 12 months. For cases where this is not true, we will calculate an appropriate factor using analogous methodology. Overall Total Trend Using the year ended September 2016 for the groups included in the manual rate (see section 4.4), the overall allowed trend is
Category Allowed PMPM Allowed Trend Medical $ 424.24 6.0%
Pharmacy $ 89.13 11.0% Total $ 513.37 6.9%
While we have included no implicit or explicit margin in our trend selections, we recognize that an environmental change may create a significant shift in either direction. As we have suggested in past years, we would submit an interim trend filing should information become available that meaningfully differs from the underpinnings of the trend analysis in this filing. Leveraged Trends The above trends are based on allowed charges and do not account for the leveraging effect of deductibles and copays. We utilized our Benefit Relativity models (see section 4.3 for a description of the methodology) to calculate the impact of leveraging on each benefit. To do so, we calculated the Paid PMPM with and without the trend (as described above). The ratio between the two paid PMPMs is the paid trend for that benefit, and the difference between the paid trend and the allowed trend is the leverage factor. See Exhibits 3I and 3J for example of leverage factors. Applying the leverage factors for benefits present in the year ended September 2016 for the groups included in the manual rate, we calculate the following paid trends:

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
16
Category Paid PMPM Paid Trend Medical $ 338.51 7.1% Pharmacy $ 76.36 12.2% Total $ 414.87 8.0%
Medicare Secondary Trends Medicare Secondary plans cover two categories of services: Medicare-covered services which are subject to member cost share (deductible/coinsurance) and services which are not covered by Medicare. Services subject to Medicare cost sharing were not adjusted for network, as the allowed charges are determined by Medicare, whereas the services not covered by Medicare were adjusted using the contract factors described above to bring all charges to a single network. For Medicare claims, cost trends were developed for the different types of service using trends from CMS4. Increases for 2018 were assumed to be the same as the 2017 increases. We assumed a 0.0 percent utilization trend for Medicare claims.
Category Allowed Trend Inpatient 1.4% Outpatient 1.6% Professional 0.5%
The trends used for services not covered by Medicare are the same as the trends developed for use with Active benefits. We use the same pharmacy trends for Medicare Secondary plans as we use for Active plans.
4.3. Benefit Relativity Factors
Overview To determine standardized premium rate relationships, also called relativities, BCBSVT has created models that simulate the impact of member benefits for all types of plans. The models determine the allowed charges for the completed 12 months of claims included in the study and “re-adjudicate” the claims, thereby simulating the impact of member cost sharing for a given benefit plan. Claims data is from BCBSVT’s data warehouse. To ensure accuracy, the claims data used has been reconciled against internal reserving, enrollment and other financial reports. The starting point of the analysis is allowed charges as determined by the BCBSVT claims adjudication system. The claims data includes benefit codes that enable us to identify the services and benefit structures (copays, deductibles, and coinsurance) for each claim. For each benefit plan of interest, the models produced the simulated PMPM values of the benefits. The PMPM for each plan was then divided by the manual rate, as calculated in section 4.4 but without adjustment for changes in the pharmacy contract, to produce its relativity.
4 https://www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/Downloads/FFS-Trends-2015-2017.pdf

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
17
Relativities are included for medical only plans, Rx only plans, and integrated CDHP plans. In addition, relativities have been produced for both Active Under 65 employees and Age 65+ Medicare Primary Employees. Incurred allowed charges from July 2015 to June 2016, paid through September 2016, were used in the models. The allowed charges were trended to July 1, 2018, which is the midpoint of the 12-month period that begins January 1, 2018. The majority of the business that will be renewed using these relativity factors has a January 1 renewal date; the rating formula adjusts the trend for non-January renewals (see section 4.4). The data includes claims from BCBSVT Cost Plus Groups, BCBSVT ASO Groups, BCBSVT Insured Large Groups, and TVHP Insured Large Groups. Combining these homogeneous populations creates greater consistency and credibility within the relativity factor development. CDHP and Non-CDHP claims are combined. We also excluded groups that have special benefits. This predominantly refers to groups that have specific reimbursement with particular providers outside of BCBSVT’s contracts and/or claims processing function. We created separate models for active members and Medicare Primary members. Models for Active Employees Benefit Relativity Model: Medical The trends used were the total medical trend, by type of service. Cost trends for each type of service were calculated by the discrete unit cost trend method above, while the same utilization trends were used for all types of service (see section 4.2). Using the contracted reimbursement schedules, we calculated network factors that represent the different network contracts. Using these factors, we can include all claims in each of the three networks by adjusting each claim to the basis of a single network. This enables us to combine all the experience for each plan design. The claims were categorized according to how benefits are paid, and one record was generated for each member, date of service, and type of service. Each record was then assigned a cost share (deductible/coinsurance, copay, covered in full) for each plan available. The plan designs modeled are:
• Vermont Freedom Plan (VFP) • Comprehensive (COMP) • J Plan (JPLAN) • Vermont Health Partnership (VHP) • Consumer Driven Health Plan (CDHP)
For all products, claims for preventive mandated benefits were assigned a “covered in full” cost share, independently of the product that is being modeled. The model tested one benefit design at a time. It determined the member portion of the allowed charges, and from this, a total simulated paid PMPM for each benefit design. The impact of copay, deductible, coinsurance, out-of-pocket maximum, and preventive mandated

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
18
benefits were all considered. If the average allowed cost of a category was less than the copay being examined, it was assumed that the member paid the full cost of the service. VFP and VHP plans have two levels of benefits, In-Network and Out-of-Network. For VFP plans, the In-Network benefit levels are applied to providers in the BlueCard© network and the Out-of-Network benefits are applied to non-participating providers. For VHP plans, the In-Network benefit levels are applied to providers in the BCBSVT Managed Care network and the Out-of-Network benefits are applied to both providers in the BlueCard© network and non-participating providers. In the administration of both VFP and VHP benefits, there is no overlap between the In-Network and Out-of-Network deductible and coinsurance. For COMP and JPLAN, the same overall benefits are applied to the BlueCard© and non-BlueCard©
networks. The underlying benefits in the experience have different splits between BlueCard©
and non-BlueCard© networks as part of the “freedom” of the benefit. The “freedom” represents the portion of providers in the service area that participate in the BlueCard© network. We use BRVs in two places in the rating formula described in section 3. The Average Experience Period Seasonal Adjusted Benefit Relativity Factor (line L in Exhibit 1A) is calculated using BRVs for the benefits in the experience period, while the Projected Claims for the rating period (line B1 in Exhibit 1B) uses BRVs for the benefits in the rating period. The relativities for active employees for the medical products currently in our book of business are displayed on Exhibits 4A and 4B. Benefit Induced Utilization: Medical An independent analysis was performed to measure the correlation between the benefit design and the overall health care spending. The correlation used the paid-to-allowed ratio as the independent variable and the total allowed charges (capped at $30,000 per member per year) as the dependent variable. A 2nd order polynomial was found to best fit the data. The polynomial was then normalized such that the average paid-to-allowed (PA) ratio underlying the base BRV experience returned a utilization adjustment of 1.00. In other words, if a simulated benefit has a paid-to-allowed ratio less than that of the average, then utilization will be reduced (i.e. factor < 1.00). If a simulated benefit has a paid-to-allowed ratio greater than the average, then the benefit will have induced utilization (i.e. factor > 1.00). The resulting formula is ���03������=3���� ∶ 0.5670 × (/-)' − 0.0652 × (PA) + 0.6133, with a minimum set at 0.74 and a maximum of 1.20. Benefit Relativity Model: Pharmacy The trends used were the total trend, by type of drug, as described above (section 4.2) for Brand, Generic, and Specialty drugs. Within the model, all pharmacy scripts, including specialty, are assigned to one of six categories: Retail Generic, Retail Preferred Brand, Retail non-Preferred Brand, Mail Generic, Mail Preferred Brand, and Mail non-Preferred Brand. We apply flags to identify several categories of drugs that are either required to be covered in full (ACA contraceptives and vaccines) or for which a group may purchase a rider to offer additional coverage (some fertility drugs) or exclusion (lifestyle drugs). We also flag drugs for which a group may offer special cost-sharing arrangements, such a diabetic medications and wellness drugs. We assign these flags by National Drug Codes as reported to us by ESI.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
19
The experience period data was adjusted to reflect the major brands that are expected to become generic during 2017 and 2018. The list was based on a report provided by ESI. For these brands, in the first 6 months (the exclusivity period), we reduced the Average Wholesale Price (AWP) by 10 percent and kept the brand discount. For the months after the exclusivity period, we reduced the AWP by 10 percent and changed the discount to the generic discount. The 10 percent reduction in AWP is based upon industry standard assumptions, supported by our own analysis of AWP changes for drugs that have moved from brand to generic over the past several years.
One record was created for each member and date of service combination. One record can have more than one script category. The model tested one benefit design at a time. It determined the member portion of the allowed charges and a total simulated paid PMPM for each benefit design. The impact of the deductible, coinsurance, copays and out-of-pocket maximum (OOPM) were considered. Following the ACA, contraceptives and vaccines were excluded from the cost sharing. If the average allowed cost of a category is less than the copay being examined, it is assumed that the member pays only the full cost of the script. With Vermont Act 171, all pharmacy benefits effective January 1, 2017 or later will have an OOPM of $1,300. It is possible that this limit will increase effective January 1, 2018, following the IRC rules for Health Savings Account and High Deductible Plans. The exhibits include the $1,300 OOPM benefit on pharmacy for benefits. The relativities for active employees for the pharmacy products currently in our book of business are displayed on Exhibit 4D. Benefit Induced Utilization: Pharmacy Independent analysis was performed to measure the correlation between the benefit design and the quantity of pharmacy prescriptions consumed. The pharmacy benefits are adjusted in two ways. First, the generic utilization varies with the benefit design. Claims and membership data from January 2012 through June 2016 were examined, and a table was created to adjust the base generic utilization up or down depending on the difference in the Generic and Brand copays of the member’s drug plan. Second, a separate analysis was done to adjust for the overall pharmacy benefit. A modeled paid-to-allowed (PA) ratio was assigned to every benefit in the experience period. The correlation used the paid-to-allowed ratio as the independent variable and total allowed charges as the dependent variable. A line was found to best fit the data. The line was then normalized such that the paid-to-allowed ratio underlying the base BRV benefit (manual rate) returned a utilization adjustment of 1.00. The resulting formula is /ℎ3��30�����=3���� ∶1.6201 × (PA) − 0.4589, with a minimum set at 0.65 and a maximum of 1.20. Although we use two steps to calculate the induced utilization, we are not adjusting the data twice. The adjustment for difference in Generic/Brand copays changes the mixture of scripts (i.e. generic dispensing rate) without adjusting the overall frequency of scripts. The richness or leanness of the plan, as measured by the paid to allowed ratio, drives an adjustment to the overall frequency of scripts without changing the mixture of scripts.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
20
Integrated Benefit Relativity Model (CDHP) The CDHP model combines both the medical and pharmacy models described above. One record was created for each member, date of service and type of service combination. A separate medical and pharmacy paid-to-allowed ratio was calculated, and the appropriate utilization adjustment was made. The relativities for active employees for the CDHP products currently in our book of business are displayed on Exhibit 4C. Tier Factors The BRV models calculate the average paid claims of a single member on a particular benefit design. BCBSVT sells products with rate tiers for multiple members. These rate tiers feature family deductibles and out-of-pocket maximums either in addition to or in place of the individual limits. We refer to products that have family limits in addition to individual limits as Stacked and to products with only family limits as Aggregate. For products renewing after January 1, 2016, members on Aggregate plans are subject to the federal maximum allowed individual out-of-pocket, even if the aggregate out-of-pocket maximum is higher. We refer to these plans as Hybrid. To price benefits for rate tiers with multiple members, we calculated tier factors to apply to the BRV for the benefit. We used the BRV models to calculate member paid amounts for each member in the model and used every combination of members to create “families” in the following categories:
• One Adult • Two Adults • One Adult and One Child, … , One Adult and Seven Children • Two Adults and One Child, … , Two Adults and Seven Children
For each category of family, we calculated the average plan paid amount subject to the family cost sharing. Then we combined the categories of families into rate tiers using the proportion of each category in the experience period membership as a weight. The ratio of plan paid amount for each rate tier to the single rate tier is the tier factor. For Aggregate and Hybrid factors, we grouped products together into three ranges of out-of-pocket maximums and calculated tier factors for each range. We calculated different factors for products with separate medical and drug benefits and for products with integrated benefits (CDHPs). The Hybrid factors are applicable to benefits with a $7,150 individual out-of-pocket maximum. The tier factors calculated for each range and type of benefit are shown in Exhibit 4H. These factors assume a family multiplier of two. If a group requests a benefit with a non-standard multiplier, out-of-pocket maximum, or individual out-of-pocket maximum (for a Hybrid plan) that is not in the exhibit, identical data, assumptions and methodology as described above will be used to calculate appropriate tier factors for the requested benefit.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
21
Models For Age 65+ Medicare Secondary Plans Benefit Relativity Model: Medical Benefit relative values are needed for Medicare Secondary plans. We use the same method to develop Medicare Secondary benefit relative values as we do for the active factors. For the claims base, we used allowed charges incurred between July 2015 and June 2016, paid through September 2016, for members whose primary insurance is Medicare. Medicare Secondary plans cover two categories of services: Medicare-covered services which are subject to member cost share (deductible/coinsurance) and services which are not covered by Medicare. Services subject to Medicare cost sharing were not adjusted for network, as the allowed charges are determined by Medicare, whereas the services not covered by Medicare were adjusted using the contract factors described above to bring all charges to a single network. The allowed charges were trended to July 1, 2018, which is the midpoint of the 12-month period that begins January 1, 2018. The trends used were the total medical trend, by type of service as described in section 4.2. As with the active benefits, the model simulates the effects of a benefit design on the trended allowed charges and calculates a simulated paid PMPM. This paid PMPM is divided by the manual rate (without the adjustment for changes to the pharmacy contract) to produce the benefit relative value. Unlike the active benefits, there is no adjustment for induced utilization due to the richness of the benefit. As Medicare is the primary insurance for these plans and Medicare-covered claims make up 97 percent of the trended allowed charges, we do not believe that the richness of the secondary insurance will have any influence on utilization. The relativities for the Medicare Secondary medical products currently in our book of business are displayed on Exhibit 4E. Benefit Relativity Model: Pharmacy To calculate relativities for pharmacy benefits for plans that are secondary to Medicare, we used allowed charges incurred between July 2015 and June 2016, paid through September 2016, for members whose primary insurance is Medicare. The allowed charges are trended to July 1, 2018 using the same trends as used for active members. Pharmacy scripts are assigned to the same categories as for the active members and allowed charges are adjusted for brands going generic between the experience period and the rating period. The benefit designs are modeled to produce a simulated paid PMPM, which is adjusted for mixture and frequency of scripts as described for the active relativities above. The adjusted paid PMPM is then divided by the manual rate (without the adjustment for changes to the pharmacy contract) to produce the relativity. The relativities for the Medicare Secondary pharmacy products currently in our book of business are displayed on Exhibit 4G. Integrated Benefit Relativity Model (CDHP) The Medicare Secondary CDHP model combines both the medical and pharmacy Medicare Secondary models described above. One record was created for each member, date of service and type of service combination. A separate medical and pharmacy paid-to-allowed ratio was calculated, and the appropriate utilization adjustment was made.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
22
The relativities for the Medicare Secondary CDHP products currently in our book of business are displayed on Exhibit 4F. 4.4. Manual Rate
The Manual Rate is the experience paid claims PMPM from the groups impacted by this filing, trended to calendar year 2018 using the trends and pharmacy contracts adjustments described in section 4.2.
Calculation of the Manual Rate
Experience Paid Claims, capped at $750,000 and completed A $ 72,137,723 Overall Paid Trend factor (8.0% for 27 months) B1 1.190
Pharmacy Contract Adjustment B2 0.995 Projected Total Paid Claims C = A x B1 x B2 $ 85,410,917 Total Member Months D 173,473 Manual Rate E = C / D $ 492.36
As noted in section 4.3 above, we use a version of the manual rate without the pharmacy contract adjustment as the denominator of the relativity calculation. Per the above calculation, this value is $494.76. We multiply the benefit relativity by the manual rate to calculate projected manual claims. If both the denominator of the relativity and the manual rate included the pharmacy contract adjustment, they would cancel in the multiplication and the projected claims would not reflect the discounts in the new pharmacy contract. The Manual Rate is adjusted to reflect a group’s particular characteristics, as demonstrated in Exhibit 5A. An adjustment is made for the average age/gender factor (line B) of the group. For active members, we used factors from the 2014 Milliman Health Cost Guidelines. For Medicare Primary members, we used factors from the SOA’s report Health Care Costs – From Birth to Death5. In each case, the factors were normalized such that the membership in the Manual Rate experience period has an age/gender factor of one. The case’s industry factor (line C) is developed based on the SIC and a standard table that has been updated based on BCBSVT experience data from October 2014 through September 2015 to reflect relationships between industries. See Exhibit 5B for the schedule of industry factors. These have also been normalized such that the Manual Rate has a factor of one. We do not apply an industry adjustment to the Manual Rate for Medicare Primary members. For groups with a projection period other than calendar year 2018, the manual rate will be adjusted for trend to reflect the group’s projection period (line D) and the additional impact of pharmacy contract changes (line E). Finally, a contract conversion factor (line F) is calculated based on member distribution and tier factors in order to convert from a PMPM to a single rate basis (necessary because the Adjusted Manual Rate is blended with the Projected Single Contract Rate, which is not on a PMPM basis).
5 https://www.soa.org/Research/Research-Projects/Health/research-health-care-birth-death.aspx The factors for the age curve are in Chart 21 of the databook linked on the page.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
23
4.5. Administrative Charges The sources of actual expense data in this filing are BCBSVT’s data warehouse and accounting records. The Experience Base period for this filing is November 2015 to October 2016. Actual BCBSVT administrative expenses for the Experience Base period are compiled on a GAAP reporting basis. During 2015, BCBSVT completed a comprehensive cost accounting study. The results were refreshed during 2016 to reflect known operational changes. Allocations to specific lines of business on a GAAP reporting basis were updated for the results of this study, beginning in December 2015. In order to normalize experience period data to the same allocation methodology, November 2015 expenses were reallocated according to the results of the cost accounting study. Exhibit 6A provides a reconciliation of the Experience Base period to restated GAAP financial report data. Experience Base of Actual Expenses Administrative expenses are allocated under BCBSVT’s cost accounting system to lines of business. Overhead expenses are allocated to lines of business on the basis of relative capital requirements, which were measured as each line’s relative impact on Risk-Based Capital (RBC). In past filings, we have combined BCBSVT Large Group Insured, BCBSVT Cost Plus and TVHP Large Group Insured actual administrative expenses to calculate the base administrative charges. A Cost Plus group with over 98 percent of the membership of that line of business is moving to an ASO arrangement as of January 1, 2018. We therefore only used Insured Group information for the base administrative charges. This is the main reason for the large increase in administrative charges. The remaining Cost Plus groups will continue to use the same administrative charge factors as the Insured groups. The cost accounting data by cost center is then allocated into Cost Categories for purposes of determining administrative charges for each specific BCBSVT group account, given that account’s characteristics.6 As noted above, BCBSVT updated the allocation methodology to reflect the results from the cost accounting study. With this filing, we are also updating the Group Cost Categories to align with the rules used in the cost allocation model. The Group Cost Categories include: Account − those expenses that are allocated to specific group accounts on a per group account basis. Member – those expenses that are allocated on a per member basis. Contract – those expenses that are allocated on a per contract (subscriber) basis. Medical Claims – those expenses that are allocated on a per medical claim basis. Total Projected Claims – those expenses that are allocated on a Capital Requirement basis. For each of the Group Cost Categories described above, the respective number of unit months during the Experience Base period is tabulated for the Insured Large Group (both BCBSVT and TVHP). These segments are combined in this filing for marketing considerations. The unit months include the number of account months, number of member months, number of contract months and number of medical claims by months. For the expenses allocated on a Capital Requirement basis, the experience administrative charges were divided by total paid claims to calculate a percent of claims factor.
6 PUPM costs for Cost Plus members having Medicare Supplement plans are set equal to the corresponding values for conventionally funded Medicare Supplement members. The resulting costs are removed from the Cost Plus cost accounting charges before dividing by the (non-Medicare Supplement) Cost Plus units.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
24
Fees paid to our vendor GHI for the electronic processing of Medicare Supplement claims are not being assigned correctly to all members whose claims go through the GHI system. These members are in the following product categories: Individual Medicare Supplement, Group Medicare Secondary, Cost Plus Medicare Supplement, Cost Plus Medicare Secondary, and TVHP Medigap Blue. They are currently only booked to Individual Medicare Supplement and TVHP Medigap Blue. The GHI fees are reallocated to the appropriate product categories using membership as a weight. This reclassification is reflected in Exhibit 6A. Other reclassifications reflected in the exhibit include the removal of federal fees (these are added to premium rates separately; see section 4.10) and fees paid to our vendor Health Equity for the administration of Health Savings Accounts and Health Reimbursement Accounts linked to our insurance products (participation in this service is optional and we assign these fees to groups who select the service). For this filing, we have also removed any expenses incurred due to one-time, non-recurring events, as these fees are not expected to continue to occur in the projection period. Using the adjusted Experience Base administrative expenses and unit months, per unit per month (PUPM) values are calculated. For the group segments included in this filing, there are four such PUPM values and one percent of claims value − one for each of the Cost Categories indicated above. The Experience Base administrative expenses PUPM are shown in Exhibit 6B, line C. Projection Factors Actual administrative costs PUPM from the Experience Base period are projected to each of the rating periods. Projection factors are based on a 2.4 percent annual trend. These projection factors are intended to make reasonable but modest provision for increases in overall operating costs PUPM. Note that there are no known extraordinary or mandate-related costs at this time which require separate provision for the rating periods involved in this filing. We are assuming that personnel costs (wages and benefits) will increase by 3 percent, the budgeted wage increase for 2017, over the projection period. Other operating costs are assumed to remain flat. Based on year-to-date October 2016 information, we have calculated that 81.4 percent of our administrative costs are for salaries and benefits. We are therefore increasing our projected administrative expenses by the weighted average of 2.4 percent per annum.
YTD Oct 2016 Percent of Total
Employee costs A 35,159,939 56.2%
Purchased service B 19,326,059 30.9%
Other operating costs C 8,046,148 12.9%
Subtotal administrative expenses D = A+B+C 62,532,147 100.0%
Total Personnel Cost E = A / (A + C) 81.4%
Trend for Personnel Cost F 3.0%
Total Trend G = {(1+F) x E + (1.00) x (1-E)} - 1 2.4%

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
25
An examination of historical administrative charges shows a decreasing trend in recent years, driven primarily by membership increases. For 2018, we project total BCBSVT membership will also increase. We calculated PMPM admin charges with experience period enrollment and projected 2018 enrollment and found they decreased by 0.7 percent with the projected increased 2018 enrollment. We assumed that variable costs represent half of the increase, and therefore applied a decrease of 0.4 percent to the base PUPM charges to account for the reduction in membership. Charges for Group Accounts The Administrative Charge PUPM figures shown in Exhibit 6B are the values to be applied on an account by account basis, along with each group account’s corresponding unit count, to produce account-specific administrative charges. These amounts will then be expressed as equivalent PMPM amounts for each group account. Amounts for special items or unique services not part of BCBSVT’s standard scope of administrative services (e.g., special booklets, certificates, or reports) are to be determined and applied separately on an account-specific basis. Commissions based on the commission scale applicable to the account are not reflected in the schedule of admin charges in Exhibit 6B; they are to be calculated and applied separately.
4.6. Net Cost of Reinsurance
BCBSVT has purchased reinsurance for claims in excess of $750,000 for 2017, and expects to purchase similar reinsurance in future years with limits approximately equal to the 2017 limit increased by trend. We estimate that the target loss ratio for the reinsurance is approximately 75 percent, which implies a cost of reinsurance of approximately 33 percent of claims above the reinsurance limit. For each pricing period starting quarter, we determined an annual cost of reinsurance for the trended reinsurance limit by multiplying the expected annual claims cost above the limit by 33 percent. Dividing this by 12 produces the PMPM cost of reinsurance. The table of these PMPM’s, based on pricing period starting quarter, is shown in the table below.
Pricing Period Starting Quarter
Q2 2017 Q3 2017 Q4 2017 Q1 2018 Q2 2018 Q3 2018
$1.55 $1.59 $1.61 $1.65 $1.67 $1.69 4.7. Pharmacy Rebates
Pharmacy rebates are calculated by taking the experience period rebates and trending them using the Brand Cost trend (from Exhibit 3D). Pharmacy rebates are paid with an average six-month delay from the time of the original claims. For months in the experience for which we do not have detailed rebate information, an estimated rebate amount is included in the calculation. 4.8. Contribution to Reserve The administrative charges developed are for administrative expenses only, and contain no provision for reserve contribution. Contribution to reserves (CTR) supports the overall financial

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
26
health of the company for the benefit of all members. CTR is required in order to maintain an adequate level of members’ surplus. Surplus is a critical consumer protection that allows members to receive needed care and providers to continue to receive payments in the event of unforeseen adverse events that may otherwise impact BCBSVT’s ability to pay claims. BCBSVT must remain financially strong in order to continue to provide Vermonters with outstanding member experiences, responsible cost management and access to high value care. BCBSVT also believes that CTR should be managed to an adequate long-term level, rather than fluctuating significantly from year to year. We believe that maintaining the currently approved CTR of two percent for Insured Groups and 0.5 percent for Cost Plus Groups represents an adequate long-term, yet not excessive, CTR. While this may fall above or below that required to maintain RBC in this or any given future year, consistently maintaining an adequate long-term assumption will allow us to avoid rate shocks in years of high growth in membership or high increases in health care cost trend. Using these long-term assumptions maintains consistency across product lines, which promotes fairness to ratepayers. 4.9. State Mandates and Assessments
Vermont Vaccine Purchasing Program Payments The Vermont Vaccine Purchasing Program7 offers health care providers state-supplied vaccines at no charge by collecting payments from Health plans, insurers, and other payers. The program’s assessment is a PMPM for each Vermont resident. The approved assessment for 2017 is $0.50 for Adults and $11.95 for Children. We will use these rates until new rates are approved. New Hampshire Purchasing Program Payments The New Hampshire Purchasing Program8 offers health care providers state-supplied vaccines at no charge by collecting payments from Health plans, insurers, and other payers. The assessment for 2017 is $10.30 for each child that is a New Hampshire resident. We will use this rate until a new rate is approved. New York Graduate Medical Education (GME) Program BCBSVT pays the New York GME Covered Lives Assessment9 for all members who are New York residents. The assessment varies based on the county of residence. We will use the approved 2017 rates until new rates are approved. Health Care Claims Tax The Health Care Claims Tax of 0.8 percent applies to all claims or capitations incurred by members with Vermont zip codes. We used the percentage of current members with Vermont
7 http://www.vtvaccine.org/ 8 http://www.nhvaccine.org/nhvaccine.nsf/pages/home.html 9 https://www.health.ny.gov/regulations/hcra/gme/2017_surcharges_and_assessments.htm
Line of Business Contribution to Reserve
BCBSVT Insured Groups 2% of premium
BCBSVT Cost Plus Groups 0.5% of equivalent premium

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
27
zip codes to estimate the percentage of rating period claims expected to be incurred by Vermont members.
Blueprint BCBSVT participates in the Vermont Blueprint for Health program. The current assessments for this program, applied to members who are attributed to a Blueprint provider as of the month the renewal is produced, are $2.77 PMPM for the Community Health Team and $3.00 PMPM for the Patient Centered Medical Homes (PCMH). PCMH are eligible for up to $0.50 for performance. We project that our total PMPM for PCMH will be $3.25. Any updates made to the Blueprint Manual10 will be incorporated in renewals. Other Assessments Other state mandates and assessments will be included in the calculation as applicable. 4.10. Federal Assessments Patient-Centered Outcomes Research Institute Fee: This fee is part of the Affordable Care Act and applies to all plan years ended after September 30, 2012. We estimate the fee to be $2.44 annually and therefore, we will include a $0.20 PMPM charge in the rate calculation. This estimate will be updated once additional information is received. Federal Insurer Fee The Federal Insurer Fee is intended to help pay for some provisions in the Affordable Care Act. This fee is only applicable to Fully Insured Groups. The Consolidated Appropriation Act of 2016 temporarily suspended this fee for 2017 only. For groups renewing in 2017, we will include the projected 2018 fee, currently estimated at 2.6 percent of premium, prorated for the months in 2018 that the policy will be effective. Please see below for the estimate of the 2018 and 2019 fee, which will be updated once additional information is received.
2018 2019
Projected Fully Insured Premium subject to the Federal Insurer Fee
a $593,391,000 $630,230,000
Total Industry Assessment for Federal Insurer Fee
b $14,300,000,000 $15,600,000,000
BCBSVT Portion of Total Assessment (based on 2016 information)
c 0.1% 0.1%
Projected BCBSVT Federal Insurer Fee, grossed up for Federal Income Tax (20%)
d = b x c / 0.8 $12,130,000 $13,230,000
Estimated Required Charge as a percent of Total Premium
e = d / a 2.6% 2.6%
10 http://blueprintforhealth.vermont.gov/implementation_materials

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
28
Other Assessments Other federal mandates and assessments will be included in the calculation as applicable. 5. Factors applicable only to specific Products
5.1. Stop Loss Coverage for Cost Plus products Cost Plus Groups are at risk for the claims incurred by their members. To protect themselves from high claims, they must purchase both Individual Stop Loss (ISL) and Aggregate Stop Loss (ASL) from BCBSVT11 .
5.1.1. Individual Stop Loss Stop Loss charge factors for a Cost Plus group are to be applied to the benefit-neutral claims for the group. Using the tables created from the combined BCBSVT projected claims file described in section 4.1 (including BCBSVT Cost Plus Groups, BCBSVT ASO Groups, BCBSVT Insured Groups, and TVHP Insured Groups) and the Milliman Guidelines, the ratio of expected claims above the limit divided by the total claims was calculated. Using the same credibility formula as described in section 4.1, the BCBSVT and Milliman factors were blended. These factors (see Exhibit 7A) also include a load for a 70 percent expected loss ratio (to include the cost of reinsurance). If a group requests an Individual Stop Loss limit that is not in Exhibit 7A, identical data, assumptions and methodology as described above will be used to calculate the appropriate Individual Stop Loss Rating Factor for the requested limit. 5.1.2. Aggregate Stop Loss Distribution of Individual Claims by Amount The distribution of individual claims by amount was stochastically modeled using the tables created from the combined BCBSVT projected claims file described in section 4.1 (including BCBSVT Cost Plus Groups, BCBSVT ASO Groups, BCBSVT Insured Groups, and TVHP Insured Groups). For each number of members (N) 25, 50, 100, 150, 200 to 1000 (at 100 increments), 1,500, 2,000 to 5,000 (by 1,000 increments) and 10,000 to 40,000 (by 10,000 increments), 5,000 simulations were run. For each specific stop loss level, the expected claims amount and standard deviation of the distribution of claims less than the specific stop loss level are calculated.
11 With the exception that with the approval of BCBSVT’s Executive staff, Cost Plus groups can shop their reinsurance in accordance with strict guidelines set forth by BCBSVT.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
29
Expected Claims Factors
For each number of members (N) noted above and for each ISL limit, a preliminary expected fraction of aggregate claims in excess of 110%, 115%, 120%, 125% and 130% of expected aggregate claims was calculated. These were then adjusted for uncertainty in the projection of expected claims as described in the table below:
Expected to projected expected
>107.5% 107.5%
- 102.5%
102.5% -
97.5%
97.5% -
92.5%
< 92.5%
Fraction of projections F1* F2* F3* F4* F5*
* Estimated for distribution
The factors developed above were then divided by 0.7 to produce an expected loss ratio (net of the provision for default) of 70 percent. To protect BCBSVT against potential default situations (i.e. to cover the risk of the group failing to fund claims), the proposed ASL rates include an additional fixed risk charge of 0.5 percent of expected claims under the ISL limit for groups with less than 20,000 members, and a reduced fixed risk charge of 0.4 percent of expected claims under the ISL limit for groups of 20,000 members or more. The resulting factors were then multiplied by ratios of claims under the limit to total claims at the various ISL limits. Thus the final factors are applicable to total expected claims. To assure that the factors on each line were strictly decreasing with increasing stop loss percentage, in cases where the ratio for a 130% stop loss percentage was less than 0.0001:
- the calculated value for 130% was increased by 0.00001 - the calculated value for 125% was increased by 0.00002 - the calculated value for 120% was increased by 0.00003 - the calculated value for 115% was increased by 0.00004 - the calculated value for 110% was increased by 0.00005.
The tables of factors are contained in Exhibit 8A. If the expected number of members (N) in the rating period is not one of the values in either table, the value is determined by interpolating linearly between the entries in the table for the numbers of members immediately below and above N. If a group requests an ISL limit or aggregate attachment point that is not in the exhibit or there are more than 40,000 members, identical data, assumptions and methodology as described above will be used to calculate the appropriate Aggregate Stop Loss Rating Factor for the required attachment point.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
30
5.2. Risk and Administrative Charges for Experience Refund Eligible products Risk Charges for Experience Refund Eligible Plans The BCBSVT Experience Refund Eligible products involve pricing margins of 10% or 5% (i.e. expected claims below the pooling limit will be increased by 10% or 5% in the determination of the premium). The risk charge factors are developed in the same way as the ASL factors described in the previous section, except that the loadings for the 70 percent expected loss ratio and for default (the charges of either 0.5 percent or 0.4 percent of expected claims) do not apply. These factors are applied to total expected claims (before adjustment for pricing margin) and the retention is increased by the risk charge (both in the prospective pricing and in the refund calculation). The tables of factors are contained in Exhibit 9A. If the expected number of members (N) in the rating period is not one of the values in either table, the value is determined by interpolating linearly between the entries in the table for the numbers of members immediately below and above N.
If a group requests a pooling limit that is not in the exhibit or there are more than 40,000 members, identical data, assumptions and methodology as described above will be used to calculate the appropriate risk charge for the required attachment point. Settlement Administration Charge An administration charge equal to a settlement administration charge, offset by an investment income credit, will be added to the group’s administrative charges (described in section 4.5).
1. Settlement Administration Charge: An additional administrative charge of $1,740 will be included to offset the costs of administering the retrospective arrangement. This amount is based on the 2017 settlement administration charge of $1,700 increased by 2.4 percent trend to reflect the assumed increase for the direct staff cost.
2. Investment Income Adjustment: A credit of 0.2 percent of the margin at 5% and 0.4
percent of the margin at 10% will be applied to the settlement administrative charge to reflect investment income earned on the margin.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
31
6. Historical Financial Results
Below is the combined medical and pharmacy experience for the prior five calendar years. This only includes BCBSVT Large Group (Insured and Self Funded) experience. The Self Funded experience includes our Cost Plus groups and one ASO group whose experience we are unable to separate. All other ASO groups are excluded.
Year Incurred Claims Earned Premium Loss Ratio
Number of Groups
Member Months
2012 $394,390,754 $425,696,914 92.6% 129 952,538
2013 $399,543,340 $428,024,970 93.3% 115 1,130,966
2014 $398,416,821 $428,215,842 93.0% 128 913,833
2015 $410,671,695 $438,023,593 93.8% 129 897,529
2016 $335,400,839 $356,244,218 94.1% 82 685,984
The incurred claims and earned premium are from BCBSVT’s GAAP financials. The claims include capitations, fee-for-services claims, certain assessments, and other claims expenses. The premium includes premium equivalent for Self Funded groups. Note that the 2016 financials have not been finalized at the time of this filing; the 2016 results above are preliminary.
The chart below shows the expected and actual contribution to reserves from the previous five years for Insured Large Groups. The expected contribution to reserves is based on our forecasting model, which incorporates final premiums including amendments ordered by regulators.
Year Expected Actual 2012 1.2% 0.0% 2013 -0.4% -1.0% 2014 -2.0% 1.6% 2015 -1.2% -2.5% 2016 -0.6% -3.4%
We used the factors and formula in this filing to project a Medical Loss Ratio (MLR) for 2018. Using the manual rate as a proxy for projected claims, we project a 2018 MLR of 90.7 percent. The BCBSVT credibility-adjusted MLR for Large Group was 93.2 percent in 2014 and 96.8 percent in 2015.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
32
(A) Manual Rate $490.37 Exhibit 5A
(B) Rebates $12.71 2015 MLR Filing, untrended
(C) Estimated HCQ $2.96 2015 MLR Filing, untrended
(D) State Mandates and Assessments
$8.64 Calculation as described on Exhibit 1B, using latest actual PMPM as needed
(E) MLR Numerator $489.27 = (A) – (B) + (C) + (D)
(F) Projected Claims $486.31 = (A) – (B) + (D)
(G) Net Cost of Reinsurance $1.65 Actuarial Memorandum, Section 4.6
(H) PCORI $0.20 Actuarial Memorandum, Section 4.10
(I) Administrative Charge $36.10 Calculation as of January 2018, from Exhibit 6B
(J) Subtotal $524.26 = (F) + (G) + (H) + (I)
(K) Total Premium $554.18 = (J) / (1-0.026-0.008-0.02)
(L) Federal Insurer Fee $14.41 = (K) x 2.6% (from Actuarial Memorandum, Section 4.10)
(M) Commissions $4.43 = (K) x 0.8% (from 2015 MLR filing)
(N) Contribution to Reserve $11.08 = (K) x 2.0% (from Actuarial Memorandum, Section 4.8)
(O) MLR Denominator $539.58 = (K) – (H) – (L)
(P) MLR 90.7% = (E) / (O)
The above calculation represents an estimate assuming that all pricing assumptions hold true, and assuming no change from 2015 values for various quantities (e.g. rebates, commissions).

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Actuarial Memorandum
33
7. Actuarial Opinion The purpose of this filing is to establish the formula, manual rate and accompanying factors that will be used for renewals of Blue Cross and Blue Shield of Vermont large group plans. This filing is not intended to be used for other purposes. The data used in this analysis has been reviewed for reasonableness and consistency; however, it has not been audited. It is my opinion that the rating formula and factors presented in this filing are reasonable, and have been prepared in accordance with applicable Actuarial Standards of Practice. The formula and factors will produce premium rates that are reasonable in relation to the benefits provided, and will not be excessive, deficient or unfairly discriminatory. I am a Fellow of the Society of Actuaries and a Member of the American Academy of Actuaries, and I meet the Academy’s Qualification Standards to render this opinion.
___________________________
Paul A Schultz, F.S.A., M.A.A.A.
February 23, 2017


Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Plain Language Summary
Blue Cross and Blue Shield of Vermont (BCBSVT) is committed to the health of Vermonters, outstanding member experiences and responsible cost management for all of the people whose lives we touch. By pooling the populations covered by our products, we protect individuals from the unaffordable and potentially ruinous costs associated with significant illnesses or injuries. Our products promote preventive care, health maintenance, and health improvement, and we have in place strong utilization management programs that support members who require medical care and assure that they have access to high value care while avoiding unnecessary costs. BCBSVT also works with providers to dampen cost increases through reimbursement strategies that include incentives to both provide and properly manage care. BCBSVT’s vision is a transformed health care system in which every Vermonter has health care coverage, and receives timely, effective, affordable care. None of this work is possible unless BCBSVT remains financially strong, and that requires that we be allowed to charge rates that cover the medical expenses of the populations it serves. BCBSVT performs large group premium rating on a case-by-case basis. Rating is accomplished through a formulaic approach that blends recent group claims experience with a manual rate according to a credibility formula. This filing establishes the rating formula, manual rate and accompanying factors that will be used for large group renewals beginning upon approval of this filing, most notably January 2018 renewals. The filing describes in detail the formula used in the renewals, along with each of the factors included in that formula. These include large claims pooling factors, medical and pharmacy trends, and benefit relativities, along with the development of the manual rate. In addition, the filing details the calculation of administrative charges, the net cost of reinsurance, contribution to reserve, and state and federal assessments, all of which are included in the rate development. Finally, the filing discusses certain factors applicable only to specific products. Key results include the following:
• BCBSVT is proposing paid trends of 7.1 percent for medical claims and 12.2 percent for pharmacy claims, for a total combined trend of 8.0 percent.
• Administrative charges have increased by 25.0 percent from the previous filing on a per member per month basis for the groups impacted by this filing.
• We are proposing a contribution to member reserves of 2 percent for insured groups. • Our proposed manual rate, the projected average calendar year 2018 paid claims per
member per month for groups impacted by this filing, is $492.36. • There are an estimated 6,700 contracts (13,200 members) currently enrolled in one of
50 BCBSVT large group plans that will be affected by this filing.
Our proposed medical trend is higher than what was approved in our most recent large group rating program filing, 6.7 percent. Cost trends have increased from the previous filing due to increases at hospitals not subject to the Green Mountain Care Board’s hospital budget review. The pharmacy trend is also higher than the 11.9 percent approved in the previous filing due to higher specialty drug trends.

Blue Cross and Blue Shield of Vermont Q3 2017 Large Group Rating Program Filing
Plain Language Summary
Administrative charges have increased by 25.0 percent from the previous filing, which increases premium by 1.5 percent. In the previous filing, we grouped together all Insured and Cost Plus administrative charges. We expect significant migration from Cost Plus arrangements to ASO before the effective date of this filing, therefore we used only Insured group data to develop the administrative charges. The exclusion of Cost Plus data removes a source of subsidization for the Insured groups. A contribution to reserves is required in order to maintain an adequate level of surplus. Surplus is a critical consumer protection that allows subscribers to receive needed care and providers to continue to receive payments in the event of unforeseen adverse events that may otherwise impact BCBSVT’s ability to pay claims. We believe that the levels established in this filing represent an adequate, yet not excessive, contribution to reserves. We have changed our large group rating formula from the time of previous filing by modifying our credibility formula, changing the way we apply Individual Stop Loss factors, and changing the development of Aggregate Stop Loss and Refund-Eligible Risk Factors. There were no other material changes. Other factors, including large claim pooling charges and benefit relativities, have been updated but by their nature have neither an inflationary nor deflationary impact on rates across our entire book of business.

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Exhibit 1A
Page 1
Example Calculation of Projected Single Claims Rate for Active Members
Benefit-Adjusted Projected Single Claims Rate:
Experience Period Paid Claims $987,000 A
Experience Period Claims Amount above $70,000 Pooling Limit $53,000 B
Capped Claims $934,000 C = A — B
Completion Factor 1.011 D
Completed Capped Claims $940,000 E = C x D
Pooling Charge Factor 0.206 F
Expected Claims above $70,000 Pooling Limit $190,000 G = E x F
Experience Adjustment Factor 1.000 H
Adjusted Experience Period Claims $1,130,000 I = (E + G) x H
Experience Period Member Months 3,270 J
Adjusted Experience Period Claims PMPM $345.57 K = I ÷ J
Average Experience Period Seasonal Adjusted Benefit Relativity Factor 0.761 L
Benefit-Adjusted Experience Period Single Claims Rate $453.88 M = K ÷ L
Trend 7.2% per annum for 18 months 1.110 N
Pharmacy Contract Adjustment 0.990 O
Projected Single Contract Rate $498.73 P = M x N x O
Adjusted Manual Rate $590.97 Q
Credibility factor 48% R
Benefit-Adjusted Projected Single Claims Rate $546.44 S = (P x R) + { Q x ( 1 — R)}
Credibility Calculation
Active Member Months 3,264 a
Member Months for Full Credibility at $70,000 Pooling Limit 14,002 b
Credibility 48% c = (a / b) ^ 0.5

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Exhibit 1A
Page 2
Example Calculation of Projected Single Claims Rate for Medicare Primary Members
Benefit-Adjusted Projected Single Claims Rate:
Experience Period Paid Claims $11,000 A
Experience Period Claims Amount above $70,000 Pooling Limit $0 B
Capped Claims $11,000 C = A — B
Completion Factor 1.011 D
Completed Capped Claims $11,100 E = C x D
Pooling Charge Factor - F
Expected Claims above $70,000 Pooling Limit $0 G = E x F
Experience Adjustment Factor 1.000 H
Adjusted Experience Period Claims $11,100 I = (E + G) x H
Experience Period Member Months 96 J
Adjusted Experience Period Claims PMPM $115.63 K = I ÷ J
Average Experience Period Seasonal Adjusted Benefit Relativity Factor 0.446 L
Benefit-Adjusted Experience Period Single Claims Rate $259.31 M = K ÷ L
Trend 7.2% per annum for 18 months 1.110 N
Pharmacy Contract Adjustment 0.990 O
Projected Single Contract Rate $284.93 P = M x N x O
Adjusted Manual Rate $523.39 Q
Credibility factor 8% R
Benefit-Adjusted Projected Single Claims Rate $503.64 S = (P x R) + { Q x ( 1 — R)}
Credibility Calculation
Medicare Primary Member Months 96 a
Member Months for Full Credibility at $70,000 Pooling Limit 14,002 b
Credibility 8% c = (a / b) ^ 0.5

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Example Calculation of Required Premium by Product and Tier
Illustrative Only
Exhibit 1B
From Exhibit 1A : Active Benefit-Adjusted Projected Single Claims Rate (S) $546.44
Medicare Primary Benefit-Adjusted Projected Single Claims Rate (S) $503.64
Plan A Single 2-Person Family
Medicare
Secondary
Members per contract 1.000 2.000 3.940 1.000
BRV: A 0.929 1.859 2.549 0.439
Projected Claims: B1 = A x S $507.80 $1,015.61 $1,392.91 $220.90
Net Cost of Reinsurance: B2 $1.50 $3.00 $5.91 $0.00
Projected Rx Rebate: B3 -$4.00 -$8.00 -$15.76 -$4.00
State Mandates and Assessments
Vaccines for Vemonters C1 $2.50 $5.00 $9.85 $2.50
Blue Print for Health C2 $2.50 $5.00 $9.85 $2.50
Health Care Claims Tax C3 = 0.8% * B1 $4.06 $8.12 $11.14 $1.77
Federal Mandates and Assements
PCORI D $0.20 $0.40 $0.79 $0.20
Administrative Charge E $25.00 $50.00 $98.50 $25.00
Commission (% premium) F 3.00%
Contribution to Reserve G 2.00%
Federal Insurer Fee H 2.60%
Required Premium: $583.95 $1,167.89 $1,637.65 $269.33
Plan B Single 2-Person Family
Medicare
Secondary
Members per contract 1.000 2.000 3.938 1.000
BRV: A 1.023 2.046 2.806 0.453
Projected Claims: B1 = A x S $559.01 $1,118.01 $1,533.35 $228.25
Net Cost of Reinsurance: B2 $1.50 $3.00 $5.91 $0.00
Projected Rx Rebate: B3 -$4.00 -$8.00 -$15.76 -$4.00
State Mandates and Assessments
Vaccines for Vemonters C1 $2.50 $5.00 $9.85 $2.50
Blue Print for Health C2 $2.50 $5.00 $9.85 $2.50
Health Care Claims Tax C3 = 0.8% * B1 $4.47 $8.94 $12.27 $1.83
Federal Mandates and Assements
PCORI D1 $0.20 $0.40 $0.79 $0.20
Administrative Charge E $25.00 $50.00 $98.50 $25.00
Commission (% premium) F 3.00%
Contribution to Reserve G 2.00%
Federal Insurer Fee H 2.60%
Required Premium: $639.80 $1,279.61 $1,790.86 $277.36
I = [ ∑(Bi) + ∑(Ci) + D + E ] / (1 -
F - G - H)
I = [ ∑(Bi) + ∑(Ci) + D + E ] / (1 -
F - G - H)

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Expected Large Claims Factor Development
Experience Period Starting Q4 2015
Exhibit 2A
a b c d Z Y
g = b*Z + c*(1-Z)*Y
+ d*(1-Z)*(1-Y)
Limits Insured Groups
BCBSVT
Combined Milliman
Credibility
(Insured)
Credibility (BCBSVT
Combined)
Insured net
claim factor
$30,000 48.5% 45.0% 43.0% 59.5% 100.0% 47.1%
$35,000 42.4% 39.3% 37.9% 48.8% 100.0% 40.8%
$40,000 37.7% 34.8% 33.9% 41.1% 100.0% 36.0%
$45,000 34.0% 31.1% 30.6% 35.4% 100.0% 32.1%
$50,000 30.8% 28.2% 27.9% 30.9% 100.0% 29.0%
$55,000 28.2% 25.7% 25.6% 27.3% 100.0% 26.4%
$60,000 26.0% 23.5% 23.6% 24.5% 100.0% 24.1%
$65,000 24.1% 21.7% 21.9% 22.1% 87.6% 22.2%
$70,000 22.4% 20.1% 20.4% 20.1% 77.4% 20.6%
$75,000 20.9% 18.7% 19.1% 18.4% 69.1% 19.2%
$80,000 19.6% 17.4% 17.9% 16.9% 62.1% 17.9%
$85,000 18.4% 16.3% 16.9% 15.6% 56.1% 16.8%
$90,000 17.3% 15.3% 16.0% 14.5% 51.0% 15.9%
$95,000 16.4% 14.4% 15.1% 13.6% 46.7% 15.0%
$100,000 15.5% 13.6% 14.4% 12.7% 42.9% 14.2%
$105,000 14.8% 12.8% 13.7% 11.9% 39.5% 13.5%
$110,000 14.0% 12.2% 13.0% 11.2% 36.6% 12.8%
$115,000 13.4% 11.5% 12.4% 10.6% 34.0% 12.3%
$120,000 12.8% 11.0% 11.9% 10.1% 31.7% 11.7%
$125,000 12.2% 10.5% 11.4% 9.5% 29.6% 11.2%
$130,000 11.7% 10.0% 10.9% 9.1% 27.7% 10.7%
$135,000 11.2% 9.5% 10.4% 8.6% 26.0% 10.3%
$140,000 10.8% 9.1% 10.0% 8.3% 24.5% 9.9%
$145,000 10.4% 8.7% 9.6% 7.9% 23.1% 9.5%
$150,000 10.0% 8.3% 9.3% 7.6% 21.9% 9.1%
$155,000 9.6% 8.0% 8.9% 7.2% 20.7% 8.8%
$160,000 9.2% 7.6% 8.6% 7.0% 19.7% 8.5%
$165,000 8.9% 7.3% 8.3% 6.7% 18.7% 8.2%
$170,000 8.6% 7.0% 8.0% 6.4% 17.8% 7.9%
$175,000 8.3% 6.7% 7.8% 6.2% 16.9% 7.6%
$180,000 8.0% 6.5% 7.5% 6.0% 16.2% 7.4%
$185,000 7.7% 6.2% 7.2% 5.8% 15.4% 7.1%
$190,000 7.4% 6.0% 7.0% 5.6% 14.8% 6.9%
$195,000 7.2% 5.8% 6.8% 5.4% 14.2% 6.7%
$200,000 7.0% 5.6% 6.6% 5.2% 13.6% 6.5%
$205,000 6.7% 5.4% 6.4% 5.1% 13.0% 6.3%
$210,000 6.5% 5.2% 6.2% 4.9% 12.5% 6.1%
$215,000 6.3% 5.0% 6.0% 4.8% 12.0% 5.9%
$220,000 6.1% 4.8% 5.8% 4.6% 11.6% 5.7%
$225,000 5.9% 4.6% 5.7% 4.5% 11.2% 5.6%
$230,000 5.8% 4.5% 5.5% 4.4% 10.8% 5.4%
$235,000 5.6% 4.3% 5.4% 4.2% 10.4% 5.3%
$240,000 5.4% 4.2% 5.2% 4.1% 10.0% 5.1%
$245,000 5.3% 4.1% 5.1% 4.0% 9.7% 5.0%
$250,000 5.1% 3.9% 4.9% 3.9% 9.4% 4.9%
$255,000 5.0% 3.8% 4.8% 3.8% 9.1% 4.7%
$260,000 4.9% 3.7% 4.7% 3.7% 8.8% 4.6%
1

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Expected Large Claims Factor Development
Experience Period Starting Q4 2015
Exhibit 2A
a b c d Z Y
g = b*Z + c*(1-Z)*Y
+ d*(1-Z)*(1-Y)
Limits Insured Groups
BCBSVT
Combined Milliman
Credibility
(Insured)
Credibility (BCBSVT
Combined)
Insured net
claim factor
$265,000 4.7% 3.6% 4.6% 3.6% 8.5% 4.5%
$270,000 4.6% 3.5% 4.5% 3.6% 8.2% 4.4%
$275,000 4.5% 3.4% 4.4% 3.5% 8.0% 4.3%
$280,000 4.4% 3.3% 4.2% 3.4% 7.8% 4.2%
$285,000 4.3% 3.2% 4.1% 3.3% 7.5% 4.1%
$290,000 4.2% 3.1% 4.0% 3.2% 7.3% 4.0%
$295,000 4.1% 3.0% 3.9% 3.2% 7.1% 3.9%
$300,000 3.9% 2.9% 3.9% 3.1% 6.9% 3.8%
$305,000 3.8% 2.8% 3.8% 3.0% 6.7% 3.7%
$310,000 3.7% 2.7% 3.7% 3.0% 6.6% 3.6%
$315,000 3.6% 2.7% 3.6% 2.9% 6.4% 3.5%
$320,000 3.5% 2.6% 3.5% 2.9% 6.2% 3.4%
$325,000 3.5% 2.5% 3.4% 2.8% 6.1% 3.4%
$330,000 3.4% 2.4% 3.4% 2.7% 5.9% 3.3%
$335,000 3.3% 2.4% 3.3% 2.7% 5.8% 3.2%
$340,000 3.2% 2.3% 3.2% 2.6% 5.6% 3.2%
$345,000 3.1% 2.2% 3.1% 2.6% 5.5% 3.1%
$350,000 3.0% 2.2% 3.1% 2.6% 5.4% 3.0%
$355,000 3.0% 2.1% 3.0% 2.5% 5.2% 2.9%
$360,000 2.9% 2.1% 2.9% 2.5% 5.1% 2.9%
$365,000 2.8% 2.0% 2.9% 2.4% 5.0% 2.8%
$370,000 2.8% 2.0% 2.8% 2.4% 4.9% 2.8%
$375,000 2.7% 1.9% 2.8% 2.3% 4.8% 2.7%
$380,000 2.6% 1.9% 2.7% 2.3% 4.7% 2.7%
$385,000 2.6% 1.8% 2.6% 2.3% 4.6% 2.6%
$390,000 2.5% 1.8% 2.6% 2.2% 4.5% 2.6%
$395,000 2.5% 1.7% 2.5% 2.2% 4.4% 2.5%
$400,000 2.4% 1.7% 2.5% 2.1% 4.3% 2.4%
$405,000 2.4% 1.6% 2.4% 2.1% 4.2% 2.4%
$410,000 2.3% 1.6% 2.4% 2.1% 4.1% 2.3%
$415,000 2.3% 1.5% 2.3% 2.0% 4.0% 2.3%
$420,000 2.3% 1.5% 2.3% 2.0% 4.0% 2.2%
$425,000 2.2% 1.5% 2.2% 2.0% 3.9% 2.2%
$430,000 2.2% 1.4% 2.2% 2.0% 3.8% 2.2%
$435,000 2.1% 1.4% 2.1% 1.9% 3.7% 2.1%
$440,000 2.1% 1.4% 2.1% 1.9% 3.7% 2.1%
$445,000 2.0% 1.3% 2.1% 1.9% 3.6% 2.0%
$450,000 2.0% 1.3% 2.0% 1.8% 3.5% 2.0%
$455,000 2.0% 1.3% 2.0% 1.8% 3.5% 2.0%
$460,000 1.9% 1.2% 2.0% 1.8% 3.4% 1.9%
$465,000 1.9% 1.2% 1.9% 1.8% 3.3% 1.9%
$470,000 1.8% 1.2% 1.9% 1.7% 3.3% 1.9%
$475,000 1.8% 1.2% 1.8% 1.7% 3.2% 1.8%
$480,000 1.8% 1.1% 1.8% 1.7% 3.2% 1.8%
$485,000 1.7% 1.1% 1.8% 1.7% 3.1% 1.7%
$490,000 1.7% 1.1% 1.7% 1.7% 3.1% 1.7%
$495,000 1.7% 1.1% 1.7% 1.6% 3.0% 1.7%
2

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Expected Large Claims Factor Development
Experience Period Starting Q4 2015
Exhibit 2A
a b c d Z Y
g = b*Z + c*(1-Z)*Y
+ d*(1-Z)*(1-Y)
Limits Insured Groups
BCBSVT
Combined Milliman
Credibility
(Insured)
Credibility (BCBSVT
Combined)
Insured net
claim factor
$500,000 1.6% 1.0% 1.7% 1.6% 3.0% 1.6%
$505,000 1.6% 1.0% 1.6% 1.6% 2.9% 1.6%
$510,000 1.6% 1.0% 1.6% 1.6% 2.9% 1.6%
$515,000 1.5% 1.0% 1.6% 1.6% 2.8% 1.6%
$520,000 1.5% 0.9% 1.6% 1.5% 2.8% 1.5%
$525,000 1.5% 0.9% 1.5% 1.5% 2.7% 1.5%
$530,000 1.5% 0.9% 1.5% 1.5% 2.7% 1.5%
$535,000 1.4% 0.9% 1.5% 1.5% 2.7% 1.5%
$540,000 1.4% 0.9% 1.4% 1.5% 2.6% 1.4%
$545,000 1.4% 0.8% 1.4% 1.4% 2.6% 1.4%
$550,000 1.4% 0.8% 1.4% 1.4% 2.5% 1.4%
$555,000 1.3% 0.8% 1.4% 1.4% 2.5% 1.3%
$560,000 1.3% 0.8% 1.3% 1.4% 2.5% 1.3%
$565,000 1.3% 0.8% 1.3% 1.4% 2.4% 1.3%
$570,000 1.3% 0.8% 1.3% 1.4% 2.4% 1.3%
$575,000 1.2% 0.7% 1.3% 1.3% 2.4% 1.3%
$580,000 1.2% 0.7% 1.2% 1.3% 2.3% 1.2%
$585,000 1.2% 0.7% 1.2% 1.3% 2.3% 1.2%
$590,000 1.2% 0.7% 1.2% 1.3% 2.3% 1.2%
$595,000 1.2% 0.7% 1.2% 1.3% 2.2% 1.2%
$600,000 1.1% 0.7% 1.2% 1.3% 2.2% 1.2%
$605,000 1.1% 0.7% 1.1% 1.3% 2.2% 1.1%
$610,000 1.1% 0.6% 1.1% 1.3% 2.1% 1.1%
$615,000 1.1% 0.6% 1.1% 1.2% 2.1% 1.1%
$620,000 1.1% 0.6% 1.1% 1.2% 2.1% 1.1%
$625,000 1.0% 0.6% 1.1% 1.2% 2.1% 1.1%
$630,000 1.0% 0.6% 1.0% 1.2% 2.0% 1.0%
$635,000 1.0% 0.6% 1.0% 1.2% 2.0% 1.0%
$640,000 1.0% 0.6% 1.0% 1.2% 2.0% 1.0%
$645,000 1.0% 0.6% 1.0% 1.2% 1.9% 1.0%
$650,000 1.0% 0.5% 1.0% 1.2% 1.9% 1.0%
$655,000 0.9% 0.5% 1.0% 1.1% 1.9% 1.0%
$660,000 0.9% 0.5% 0.9% 1.1% 1.9% 0.9%
$665,000 0.9% 0.5% 0.9% 1.1% 1.8% 0.9%
$670,000 0.9% 0.5% 0.9% 1.1% 1.8% 0.9%
$675,000 0.9% 0.5% 0.9% 1.1% 1.8% 0.9%
$680,000 0.9% 0.5% 0.9% 1.1% 1.8% 0.9%
$685,000 0.8% 0.5% 0.9% 1.1% 1.8% 0.9%
$690,000 0.8% 0.5% 0.9% 1.1% 1.7% 0.8%
$695,000 0.8% 0.5% 0.8% 1.1% 1.7% 0.8%
$700,000 0.8% 0.4% 0.8% 1.0% 1.7% 0.8%
$705,000 0.8% 0.4% 0.8% 1.0% 1.7% 0.8%
$710,000 0.8% 0.4% 0.8% 1.0% 1.7% 0.8%
$715,000 0.8% 0.4% 0.8% 1.0% 1.6% 0.8%
$720,000 0.7% 0.4% 0.8% 1.0% 1.6% 0.8%
$725,000 0.7% 0.4% 0.7% 1.0% 1.6% 0.7%
$730,000 0.7% 0.4% 0.7% 1.0% 1.6% 0.7%
3
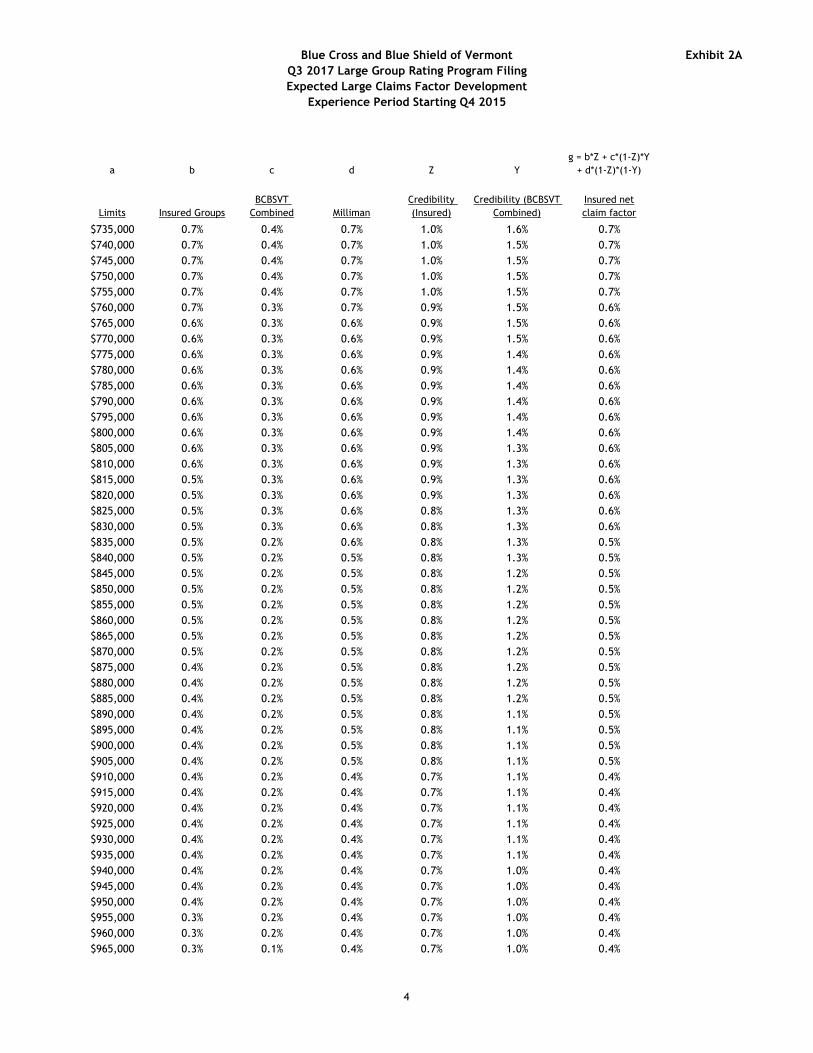
Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Expected Large Claims Factor Development
Experience Period Starting Q4 2015
Exhibit 2A
a b c d Z Y
g = b*Z + c*(1-Z)*Y
+ d*(1-Z)*(1-Y)
Limits Insured Groups
BCBSVT
Combined Milliman
Credibility
(Insured)
Credibility (BCBSVT
Combined)
Insured net
claim factor
$735,000 0.7% 0.4% 0.7% 1.0% 1.6% 0.7%
$740,000 0.7% 0.4% 0.7% 1.0% 1.5% 0.7%
$745,000 0.7% 0.4% 0.7% 1.0% 1.5% 0.7%
$750,000 0.7% 0.4% 0.7% 1.0% 1.5% 0.7%
$755,000 0.7% 0.4% 0.7% 1.0% 1.5% 0.7%
$760,000 0.7% 0.3% 0.7% 0.9% 1.5% 0.6%
$765,000 0.6% 0.3% 0.6% 0.9% 1.5% 0.6%
$770,000 0.6% 0.3% 0.6% 0.9% 1.5% 0.6%
$775,000 0.6% 0.3% 0.6% 0.9% 1.4% 0.6%
$780,000 0.6% 0.3% 0.6% 0.9% 1.4% 0.6%
$785,000 0.6% 0.3% 0.6% 0.9% 1.4% 0.6%
$790,000 0.6% 0.3% 0.6% 0.9% 1.4% 0.6%
$795,000 0.6% 0.3% 0.6% 0.9% 1.4% 0.6%
$800,000 0.6% 0.3% 0.6% 0.9% 1.4% 0.6%
$805,000 0.6% 0.3% 0.6% 0.9% 1.3% 0.6%
$810,000 0.6% 0.3% 0.6% 0.9% 1.3% 0.6%
$815,000 0.5% 0.3% 0.6% 0.9% 1.3% 0.6%
$820,000 0.5% 0.3% 0.6% 0.9% 1.3% 0.6%
$825,000 0.5% 0.3% 0.6% 0.8% 1.3% 0.6%
$830,000 0.5% 0.3% 0.6% 0.8% 1.3% 0.6%
$835,000 0.5% 0.2% 0.6% 0.8% 1.3% 0.5%
$840,000 0.5% 0.2% 0.5% 0.8% 1.3% 0.5%
$845,000 0.5% 0.2% 0.5% 0.8% 1.2% 0.5%
$850,000 0.5% 0.2% 0.5% 0.8% 1.2% 0.5%
$855,000 0.5% 0.2% 0.5% 0.8% 1.2% 0.5%
$860,000 0.5% 0.2% 0.5% 0.8% 1.2% 0.5%
$865,000 0.5% 0.2% 0.5% 0.8% 1.2% 0.5%
$870,000 0.5% 0.2% 0.5% 0.8% 1.2% 0.5%
$875,000 0.4% 0.2% 0.5% 0.8% 1.2% 0.5%
$880,000 0.4% 0.2% 0.5% 0.8% 1.2% 0.5%
$885,000 0.4% 0.2% 0.5% 0.8% 1.2% 0.5%
$890,000 0.4% 0.2% 0.5% 0.8% 1.1% 0.5%
$895,000 0.4% 0.2% 0.5% 0.8% 1.1% 0.5%
$900,000 0.4% 0.2% 0.5% 0.8% 1.1% 0.5%
$905,000 0.4% 0.2% 0.5% 0.8% 1.1% 0.5%
$910,000 0.4% 0.2% 0.4% 0.7% 1.1% 0.4%
$915,000 0.4% 0.2% 0.4% 0.7% 1.1% 0.4%
$920,000 0.4% 0.2% 0.4% 0.7% 1.1% 0.4%
$925,000 0.4% 0.2% 0.4% 0.7% 1.1% 0.4%
$930,000 0.4% 0.2% 0.4% 0.7% 1.1% 0.4%
$935,000 0.4% 0.2% 0.4% 0.7% 1.1% 0.4%
$940,000 0.4% 0.2% 0.4% 0.7% 1.0% 0.4%
$945,000 0.4% 0.2% 0.4% 0.7% 1.0% 0.4%
$950,000 0.4% 0.2% 0.4% 0.7% 1.0% 0.4%
$955,000 0.3% 0.2% 0.4% 0.7% 1.0% 0.4%
$960,000 0.3% 0.2% 0.4% 0.7% 1.0% 0.4%
$965,000 0.3% 0.1% 0.4% 0.7% 1.0% 0.4%
4

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Expected Large Claims Factor Development
Experience Period Starting Q4 2015
Exhibit 2A
a b c d Z Y
g = b*Z + c*(1-Z)*Y
+ d*(1-Z)*(1-Y)
Limits Insured Groups
BCBSVT
Combined Milliman
Credibility
(Insured)
Credibility (BCBSVT
Combined)
Insured net
claim factor
$970,000 0.3% 0.1% 0.4% 0.7% 1.0% 0.4%
$975,000 0.3% 0.1% 0.4% 0.7% 1.0% 0.4%
$980,000 0.3% 0.1% 0.4% 0.7% 1.0% 0.3%
$985,000 0.3% 0.1% 0.3% 0.7% 1.0% 0.3%
$990,000 0.3% 0.1% 0.3% 0.7% 1.0% 0.3%
$995,000 0.3% 0.1% 0.3% 0.7% 0.9% 0.3%
$1,000,000 0.3% 0.1% 0.3% 0.7% 0.9% 0.3%
5

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Insured Pooling Charge Factors
Exhibit 2B
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
$30,000 47.05% 47.71% 48.38% 49.06% 49.74% 50.43%
$35,000 40.81% 41.40% 42.00% 42.61% 43.22% 43.85%
$40,000 35.99% 36.53% 37.07% 37.62% 38.17% 38.73%
$45,000 32.14% 32.63% 33.13% 33.63% 34.14% 34.65%
$50,000 28.99% 29.44% 29.90% 30.36% 30.83% 31.30%
$55,000 26.37% 26.79% 27.21% 27.64% 28.07% 28.51%
$60,000 24.13% 24.52% 24.92% 25.32% 25.73% 26.14%
$65,000 22.24% 22.61% 22.97% 23.35% 23.73% 24.11%
$70,000 20.60% 20.95% 21.30% 21.66% 22.01% 22.37%
$75,000 19.19% 19.52% 19.84% 20.18% 20.51% 20.85%
$80,000 17.92% 18.23% 18.55% 18.88% 19.20% 19.53%
$85,000 16.85% 17.14% 17.42% 17.71% 18.00% 18.33%
$90,000 15.87% 16.15% 16.43% 16.71% 16.99% 17.28%
$95,000 14.98% 15.25% 15.52% 15.80% 16.07% 16.35%
$100,000 14.22% 14.47% 14.71% 14.96% 15.21% 15.49%
$105,000 13.50% 13.75% 13.99% 14.24% 14.48% 14.73%
$110,000 12.84% 13.07% 13.31% 13.56% 13.79% 14.05%
$115,000 12.27% 12.49% 12.70% 12.91% 13.14% 13.39%
$120,000 11.71% 11.93% 12.14% 12.36% 12.57% 12.79%
$125,000 11.20% 11.40% 11.61% 11.83% 12.04% 12.26%
$130,000 10.73% 10.93% 11.13% 11.32% 11.53% 11.75%
$135,000 10.28% 10.49% 10.68% 10.88% 11.07% 11.27%
$140,000 9.88% 10.06% 10.25% 10.45% 10.64% 10.84%
$145,000 9.50% 9.68% 9.86% 10.04% 10.22% 10.43%
$150,000 9.13% 9.31% 9.49% 9.67% 9.85% 10.03%
$155,000 8.80% 8.96% 9.13% 9.32% 9.49% 9.68%
$160,000 8.48% 8.65% 8.81% 8.97% 9.14% 9.34%
$165,000 8.17% 8.34% 8.50% 8.67% 8.83% 9.00%
$170,000 7.89% 8.05% 8.20% 8.37% 8.53% 8.71%
$175,000 7.62% 7.78% 7.93% 8.08% 8.24% 8.42%
$180,000 7.36% 7.52% 7.67% 7.82% 7.97% 8.14%
$185,000 7.11% 7.26% 7.41% 7.57% 7.72% 7.88%
$190,000 6.90% 7.03% 7.16% 7.32% 7.47% 7.64%
$195,000 6.69% 6.83% 6.96% 7.09% 7.22% 7.39%
$200,000 6.48% 6.62% 6.75% 6.89% 7.02% 7.16%
$205,000 6.28% 6.42% 6.55% 6.69% 6.82% 6.96%
Experience Period Starting Quarter
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
1

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Insured Pooling Charge Factors
Exhibit 2B
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$210,000 6.07% 6.22% 6.35% 6.49% 6.62% 6.77%
$215,000 5.89% 6.02% 6.15% 6.30% 6.43% 6.57%
$220,000 5.74% 5.85% 5.96% 6.10% 6.24% 6.38%
$225,000 5.58% 5.70% 5.81% 5.92% 6.05% 6.20%
$230,000 5.43% 5.55% 5.66% 5.78% 5.88% 6.01%
$235,000 5.28% 5.40% 5.51% 5.63% 5.74% 5.86%
$240,000 5.13% 5.25% 5.37% 5.48% 5.60% 5.72%
$245,000 4.98% 5.10% 5.22% 5.34% 5.45% 5.57%
$250,000 4.85% 4.96% 5.08% 5.20% 5.31% 5.43%
$255,000 4.74% 4.84% 4.93% 5.05% 5.17% 5.30%
$260,000 4.62% 4.72% 4.82% 4.92% 5.03% 5.16%
$265,000 4.51% 4.61% 4.71% 4.80% 4.90% 5.02%
$270,000 4.39% 4.50% 4.59% 4.69% 4.79% 4.89%
$275,000 4.28% 4.38% 4.48% 4.58% 4.68% 4.79%
$280,000 4.17% 4.27% 4.37% 4.47% 4.57% 4.68%
$285,000 4.07% 4.16% 4.26% 4.37% 4.47% 4.57%
$290,000 3.98% 4.06% 4.15% 4.26% 4.36% 4.47%
$295,000 3.88% 3.97% 4.06% 4.15% 4.25% 4.36%
$300,000 3.79% 3.88% 3.97% 4.06% 4.15% 4.26%
$305,000 3.70% 3.80% 3.88% 3.97% 4.06% 4.15%
$310,000 3.61% 3.71% 3.80% 3.89% 3.97% 4.06%
$315,000 3.52% 3.62% 3.71% 3.80% 3.89% 3.98%
$320,000 3.45% 3.53% 3.62% 3.71% 3.80% 3.90%
$325,000 3.38% 3.45% 3.54% 3.63% 3.72% 3.81%
$330,000 3.30% 3.38% 3.46% 3.54% 3.63% 3.73%
$335,000 3.23% 3.31% 3.39% 3.47% 3.55% 3.65%
$340,000 3.16% 3.24% 3.32% 3.40% 3.47% 3.56%
$345,000 3.08% 3.17% 3.25% 3.33% 3.40% 3.49%
$350,000 3.01% 3.10% 3.18% 3.26% 3.34% 3.42%
$355,000 2.94% 3.03% 3.11% 3.19% 3.27% 3.35%
$360,000 2.88% 2.96% 3.04% 3.12% 3.20% 3.29%
$365,000 2.82% 2.89% 2.97% 3.05% 3.13% 3.22%
$370,000 2.77% 2.84% 2.90% 2.98% 3.07% 3.15%
$375,000 2.71% 2.78% 2.85% 2.92% 3.00% 3.09%
$380,000 2.66% 2.73% 2.79% 2.86% 2.93% 3.02%
$385,000 2.61% 2.68% 2.74% 2.81% 2.87% 2.95%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
2

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Insured Pooling Charge Factors
Exhibit 2B
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$390,000 2.55% 2.62% 2.69% 2.76% 2.82% 2.89%
$395,000 2.50% 2.57% 2.64% 2.70% 2.77% 2.84%
$400,000 2.44% 2.52% 2.58% 2.65% 2.72% 2.79%
$405,000 2.39% 2.46% 2.53% 2.60% 2.67% 2.74%
$410,000 2.34% 2.41% 2.48% 2.55% 2.62% 2.69%
$415,000 2.28% 2.36% 2.43% 2.50% 2.57% 2.64%
$420,000 2.23% 2.30% 2.38% 2.45% 2.52% 2.59%
$425,000 2.19% 2.25% 2.32% 2.40% 2.47% 2.54%
$430,000 2.16% 2.21% 2.27% 2.35% 2.42% 2.49%
$435,000 2.12% 2.17% 2.23% 2.30% 2.37% 2.44%
$440,000 2.08% 2.14% 2.19% 2.24% 2.32% 2.39%
$445,000 2.04% 2.10% 2.15% 2.21% 2.27% 2.34%
$450,000 2.00% 2.06% 2.12% 2.17% 2.22% 2.29%
$455,000 1.96% 2.02% 2.08% 2.13% 2.19% 2.24%
$460,000 1.93% 1.99% 2.04% 2.10% 2.15% 2.21%
$465,000 1.89% 1.95% 2.00% 2.06% 2.12% 2.17%
$470,000 1.85% 1.91% 1.97% 2.02% 2.08% 2.13%
$475,000 1.81% 1.87% 1.93% 1.99% 2.04% 2.10%
$480,000 1.77% 1.83% 1.89% 1.95% 2.01% 2.06%
$485,000 1.74% 1.80% 1.86% 1.92% 1.97% 2.03%
$490,000 1.70% 1.76% 1.82% 1.88% 1.94% 1.99%
$495,000 1.67% 1.72% 1.78% 1.84% 1.90% 1.96%
$500,000 1.65% 1.69% 1.75% 1.81% 1.87% 1.92%
$505,000 1.62% 1.66% 1.71% 1.77% 1.83% 1.89%
$510,000 1.59% 1.64% 1.68% 1.73% 1.79% 1.85%
$515,000 1.56% 1.61% 1.66% 1.70% 1.76% 1.82%
$520,000 1.53% 1.58% 1.63% 1.67% 1.72% 1.78%
$525,000 1.51% 1.56% 1.60% 1.65% 1.69% 1.75%
$530,000 1.48% 1.53% 1.57% 1.62% 1.67% 1.71%
$535,000 1.45% 1.50% 1.55% 1.60% 1.64% 1.69%
$540,000 1.42% 1.47% 1.52% 1.57% 1.61% 1.66%
$545,000 1.40% 1.45% 1.49% 1.54% 1.59% 1.64%
$550,000 1.37% 1.42% 1.47% 1.52% 1.56% 1.61%
$555,000 1.34% 1.39% 1.44% 1.49% 1.54% 1.58%
$560,000 1.32% 1.36% 1.41% 1.46% 1.51% 1.56%
$565,000 1.30% 1.34% 1.39% 1.44% 1.48% 1.53%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
3

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Insured Pooling Charge Factors
Exhibit 2B
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$570,000 1.27% 1.31% 1.36% 1.41% 1.46% 1.51%
$575,000 1.25% 1.29% 1.33% 1.38% 1.43% 1.48%
$580,000 1.23% 1.27% 1.31% 1.36% 1.41% 1.46%
$585,000 1.21% 1.25% 1.29% 1.33% 1.38% 1.43%
$590,000 1.19% 1.23% 1.27% 1.31% 1.36% 1.41%
$595,000 1.17% 1.21% 1.25% 1.29% 1.33% 1.38%
$600,000 1.15% 1.19% 1.23% 1.27% 1.31% 1.35%
$605,000 1.13% 1.17% 1.21% 1.25% 1.29% 1.33%
$610,000 1.11% 1.15% 1.19% 1.23% 1.27% 1.31%
$615,000 1.09% 1.13% 1.17% 1.21% 1.25% 1.29%
$620,000 1.07% 1.11% 1.15% 1.19% 1.23% 1.27%
$625,000 1.05% 1.09% 1.13% 1.17% 1.21% 1.25%
$630,000 1.03% 1.07% 1.11% 1.16% 1.19% 1.23%
$635,000 1.02% 1.05% 1.10% 1.14% 1.18% 1.22%
$640,000 1.00% 1.04% 1.08% 1.12% 1.16% 1.20%
$645,000 0.99% 1.02% 1.06% 1.10% 1.14% 1.18%
$650,000 0.97% 1.01% 1.04% 1.08% 1.12% 1.16%
$655,000 0.96% 0.99% 1.02% 1.06% 1.10% 1.14%
$660,000 0.94% 0.98% 1.01% 1.04% 1.08% 1.12%
$665,000 0.93% 0.96% 0.99% 1.02% 1.06% 1.10%
$670,000 0.91% 0.94% 0.98% 1.01% 1.04% 1.08%
$675,000 0.90% 0.93% 0.96% 1.00% 1.03% 1.07%
$680,000 0.88% 0.91% 0.95% 0.98% 1.01% 1.05%
$685,000 0.86% 0.90% 0.93% 0.97% 1.00% 1.03%
$690,000 0.85% 0.88% 0.92% 0.95% 0.98% 1.02%
$695,000 0.83% 0.87% 0.90% 0.94% 0.97% 1.00%
$700,000 0.82% 0.85% 0.89% 0.92% 0.96% 0.99%
$705,000 0.80% 0.84% 0.87% 0.91% 0.94% 0.97%
$710,000 0.79% 0.82% 0.86% 0.89% 0.93% 0.96%
$715,000 0.77% 0.81% 0.84% 0.88% 0.91% 0.95%
$720,000 0.76% 0.79% 0.83% 0.86% 0.90% 0.93%
$725,000 0.74% 0.78% 0.81% 0.85% 0.88% 0.92%
$730,000 0.73% 0.76% 0.80% 0.83% 0.87% 0.90%
$735,000 0.71% 0.75% 0.78% 0.82% 0.86% 0.89%
$740,000 0.70% 0.73% 0.77% 0.81% 0.84% 0.88%
$745,000 0.68% 0.72% 0.76% 0.79% 0.83% 0.86%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
4

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Insured Pooling Charge Factors
Exhibit 2B
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$750,000 0.67% 0.70% 0.74% 0.78% 0.81% 0.85%
$755,000 0.66% 0.69% 0.73% 0.76% 0.80% 0.83%
$760,000 0.65% 0.67% 0.71% 0.75% 0.78% 0.82%
$765,000 0.64% 0.66% 0.70% 0.73% 0.77% 0.81%
$770,000 0.63% 0.65% 0.68% 0.72% 0.76% 0.79%
$775,000 0.63% 0.65% 0.67% 0.70% 0.74% 0.78%
$780,000 0.62% 0.64% 0.66% 0.69% 0.73% 0.76%
$785,000 0.61% 0.63% 0.65% 0.68% 0.71% 0.75%
$790,000 0.61% 0.63% 0.64% 0.66% 0.70% 0.74%
$795,000 0.60% 0.62% 0.64% 0.65% 0.68% 0.72%
$800,000 0.59% 0.61% 0.63% 0.65% 0.67% 0.71%
$805,000 0.59% 0.61% 0.62% 0.64% 0.66% 0.69%
$810,000 0.58% 0.60% 0.62% 0.63% 0.65% 0.68%
$815,000 0.57% 0.59% 0.61% 0.63% 0.64% 0.66%
$820,000 0.57% 0.59% 0.60% 0.62% 0.64% 0.65%
$825,000 0.56% 0.58% 0.60% 0.61% 0.63% 0.65%
$830,000 0.55% 0.57% 0.59% 0.61% 0.62% 0.64%
$835,000 0.55% 0.56% 0.58% 0.60% 0.62% 0.64%
$840,000 0.54% 0.56% 0.58% 0.59% 0.61% 0.63%
$845,000 0.53% 0.55% 0.57% 0.59% 0.61% 0.62%
$850,000 0.53% 0.54% 0.56% 0.58% 0.60% 0.62%
$855,000 0.52% 0.54% 0.56% 0.58% 0.59% 0.61%
$860,000 0.51% 0.53% 0.55% 0.57% 0.59% 0.60%
$865,000 0.51% 0.52% 0.54% 0.56% 0.58% 0.60%
$870,000 0.50% 0.52% 0.54% 0.56% 0.57% 0.59%
$875,000 0.49% 0.51% 0.53% 0.55% 0.57% 0.59%
$880,000 0.48% 0.50% 0.52% 0.54% 0.56% 0.58%
$885,000 0.48% 0.50% 0.52% 0.54% 0.55% 0.57%
$890,000 0.47% 0.49% 0.51% 0.53% 0.55% 0.57%
$895,000 0.46% 0.48% 0.50% 0.52% 0.54% 0.56%
$900,000 0.46% 0.48% 0.50% 0.52% 0.54% 0.55%
$905,000 0.45% 0.47% 0.49% 0.51% 0.53% 0.55%
$910,000 0.44% 0.46% 0.48% 0.50% 0.52% 0.54%
$915,000 0.44% 0.46% 0.48% 0.50% 0.52% 0.54%
$920,000 0.43% 0.45% 0.47% 0.49% 0.51% 0.53%
$925,000 0.42% 0.44% 0.46% 0.48% 0.50% 0.52%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
5

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Insured Pooling Charge Factors
Exhibit 2B
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$930,000 0.42% 0.44% 0.46% 0.48% 0.50% 0.52%
$935,000 0.41% 0.43% 0.45% 0.47% 0.49% 0.51%
$940,000 0.40% 0.42% 0.45% 0.47% 0.48% 0.50%
$945,000 0.40% 0.42% 0.44% 0.46% 0.48% 0.50%
$950,000 0.39% 0.41% 0.43% 0.45% 0.47% 0.49%
$955,000 0.38% 0.40% 0.43% 0.45% 0.47% 0.49%
$960,000 0.38% 0.40% 0.42% 0.44% 0.46% 0.48%
$965,000 0.37% 0.39% 0.41% 0.43% 0.45% 0.47%
$970,000 0.36% 0.38% 0.41% 0.43% 0.45% 0.47%
$975,000 0.36% 0.38% 0.40% 0.42% 0.44% 0.46%
$980,000 0.35% 0.37% 0.39% 0.41% 0.43% 0.45%
$985,000 0.34% 0.36% 0.39% 0.41% 0.43% 0.45%
$990,000 0.34% 0.36% 0.38% 0.40% 0.42% 0.44%
$995,000 0.33% 0.35% 0.37% 0.39% 0.42% 0.44%
$1,000,000 0.32% 0.35% 0.37% 0.39% 0.41% 0.43%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
6

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Self-Funded Pooling Charge Factors
Exhibit 2C
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
$30,000 43.31% 43.93% 44.56% 45.20% 45.85% 46.50%
$35,000 37.72% 38.29% 38.86% 39.44% 40.02% 40.61%
$40,000 33.32% 33.84% 34.36% 34.89% 35.42% 35.96%
$45,000 29.78% 30.25% 30.72% 31.21% 31.69% 32.19%
$50,000 26.86% 27.29% 27.73% 28.18% 28.63% 29.09%
$55,000 24.60% 25.00% 25.41% 25.83% 26.25% 26.67%
$60,000 22.64% 23.02% 23.40% 23.79% 24.19% 24.59%
$65,000 20.94% 21.30% 21.66% 22.03% 22.40% 22.77%
$70,000 19.46% 19.80% 20.14% 20.49% 20.84% 21.20%
$75,000 18.16% 18.48% 18.81% 19.14% 19.47% 19.80%
$80,000 17.00% 17.31% 17.62% 17.94% 18.25% 18.58%
$85,000 16.00% 16.29% 16.57% 16.86% 17.15% 17.47%
$90,000 15.10% 15.37% 15.65% 15.93% 16.20% 16.49%
$95,000 14.27% 14.53% 14.80% 15.08% 15.34% 15.63%
$100,000 13.56% 13.81% 14.05% 14.29% 14.54% 14.82%
$105,000 12.89% 13.14% 13.37% 13.62% 13.85% 14.10%
$110,000 12.28% 12.51% 12.74% 12.98% 13.22% 13.46%
$115,000 11.74% 11.96% 12.17% 12.39% 12.61% 12.86%
$120,000 11.22% 11.44% 11.65% 11.86% 12.07% 12.29%
$125,000 10.74% 10.94% 11.15% 11.37% 11.57% 11.79%
$130,000 10.30% 10.50% 10.69% 10.89% 11.09% 11.31%
$135,000 9.88% 10.08% 10.27% 10.47% 10.66% 10.86%
$140,000 9.50% 9.68% 9.87% 10.06% 10.25% 10.46%
$145,000 9.14% 9.32% 9.50% 9.68% 9.86% 10.06%
$150,000 8.79% 8.97% 9.15% 9.33% 9.50% 9.69%
$155,000 8.48% 8.64% 8.81% 8.99% 9.17% 9.36%
$160,000 8.18% 8.34% 8.50% 8.67% 8.84% 9.03%
$165,000 7.88% 8.05% 8.21% 8.38% 8.54% 8.71%
$170,000 7.62% 7.78% 7.93% 8.09% 8.25% 8.43%
$175,000 7.37% 7.52% 7.67% 7.82% 7.98% 8.15%
$180,000 7.12% 7.27% 7.43% 7.58% 7.73% 7.89%
$185,000 6.89% 7.03% 7.18% 7.34% 7.49% 7.65%
$190,000 6.68% 6.82% 6.95% 7.10% 7.25% 7.41%
$195,000 6.48% 6.62% 6.75% 6.88% 7.01% 7.18%
$200,000 6.29% 6.42% 6.55% 6.69% 6.82% 6.95%
$205,000 6.09% 6.23% 6.36% 6.50% 6.63% 6.77%
Experience Period Starting Quarter
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
1

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Self-Funded Pooling Charge Factors
Exhibit 2C
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$210,000 5.90% 6.04% 6.17% 6.31% 6.44% 6.58%
$215,000 5.72% 5.85% 5.98% 6.12% 6.26% 6.40%
$220,000 5.58% 5.69% 5.80% 5.94% 6.07% 6.21%
$225,000 5.43% 5.54% 5.65% 5.76% 5.89% 6.03%
$230,000 5.28% 5.40% 5.51% 5.62% 5.73% 5.86%
$235,000 5.14% 5.25% 5.37% 5.48% 5.59% 5.71%
$240,000 4.99% 5.11% 5.23% 5.34% 5.45% 5.57%
$245,000 4.85% 4.97% 5.09% 5.20% 5.32% 5.44%
$250,000 4.73% 4.83% 4.95% 5.07% 5.18% 5.30%
$255,000 4.62% 4.72% 4.81% 4.93% 5.05% 5.17%
$260,000 4.51% 4.61% 4.70% 4.80% 4.91% 5.04%
$265,000 4.40% 4.50% 4.59% 4.69% 4.78% 4.90%
$270,000 4.29% 4.39% 4.49% 4.58% 4.68% 4.78%
$275,000 4.18% 4.28% 4.38% 4.48% 4.57% 4.68%
$280,000 4.07% 4.17% 4.27% 4.37% 4.47% 4.57%
$285,000 3.97% 4.07% 4.17% 4.27% 4.37% 4.47%
$290,000 3.89% 3.97% 4.06% 4.16% 4.26% 4.37%
$295,000 3.80% 3.89% 3.97% 4.06% 4.16% 4.27%
$300,000 3.71% 3.80% 3.89% 3.97% 4.06% 4.17%
$305,000 3.62% 3.71% 3.80% 3.89% 3.97% 4.07%
$310,000 3.54% 3.63% 3.72% 3.81% 3.89% 3.98%
$315,000 3.45% 3.54% 3.63% 3.72% 3.81% 3.90%
$320,000 3.38% 3.46% 3.55% 3.64% 3.73% 3.82%
$325,000 3.31% 3.39% 3.47% 3.56% 3.65% 3.74%
$330,000 3.24% 3.32% 3.39% 3.47% 3.56% 3.66%
$335,000 3.17% 3.25% 3.32% 3.40% 3.48% 3.58%
$340,000 3.10% 3.18% 3.26% 3.33% 3.41% 3.50%
$345,000 3.03% 3.11% 3.19% 3.27% 3.34% 3.42%
$350,000 2.96% 3.04% 3.12% 3.20% 3.28% 3.36%
$355,000 2.89% 2.97% 3.05% 3.13% 3.21% 3.29%
$360,000 2.83% 2.90% 2.98% 3.07% 3.14% 3.23%
$365,000 2.77% 2.84% 2.92% 3.00% 3.08% 3.16%
$370,000 2.72% 2.79% 2.85% 2.93% 3.01% 3.10%
$375,000 2.67% 2.73% 2.80% 2.87% 2.95% 3.03%
$380,000 2.61% 2.68% 2.75% 2.81% 2.88% 2.97%
$385,000 2.56% 2.63% 2.70% 2.76% 2.83% 2.91%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
2

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Self-Funded Pooling Charge Factors
Exhibit 2C
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$390,000 2.51% 2.58% 2.64% 2.71% 2.78% 2.84%
$395,000 2.46% 2.53% 2.59% 2.66% 2.73% 2.79%
$400,000 2.40% 2.47% 2.54% 2.61% 2.68% 2.74%
$405,000 2.35% 2.42% 2.49% 2.56% 2.63% 2.69%
$410,000 2.30% 2.37% 2.44% 2.51% 2.58% 2.65%
$415,000 2.25% 2.32% 2.39% 2.46% 2.53% 2.60%
$420,000 2.20% 2.27% 2.34% 2.41% 2.48% 2.55%
$425,000 2.16% 2.22% 2.29% 2.36% 2.43% 2.50%
$430,000 2.12% 2.18% 2.24% 2.31% 2.38% 2.45%
$435,000 2.08% 2.14% 2.19% 2.26% 2.33% 2.40%
$440,000 2.05% 2.10% 2.16% 2.21% 2.28% 2.35%
$445,000 2.01% 2.07% 2.12% 2.17% 2.23% 2.31%
$450,000 1.97% 2.03% 2.08% 2.14% 2.19% 2.26%
$455,000 1.94% 1.99% 2.05% 2.10% 2.16% 2.21%
$460,000 1.90% 1.96% 2.01% 2.07% 2.12% 2.17%
$465,000 1.86% 1.92% 1.98% 2.03% 2.08% 2.14%
$470,000 1.82% 1.88% 1.94% 2.00% 2.05% 2.10%
$475,000 1.79% 1.85% 1.90% 1.96% 2.02% 2.07%
$480,000 1.75% 1.81% 1.87% 1.92% 1.98% 2.04%
$485,000 1.71% 1.77% 1.83% 1.89% 1.95% 2.00%
$490,000 1.68% 1.74% 1.79% 1.85% 1.91% 1.97%
$495,000 1.65% 1.70% 1.76% 1.82% 1.88% 1.93%
$500,000 1.62% 1.67% 1.72% 1.78% 1.84% 1.90%
$505,000 1.60% 1.64% 1.69% 1.75% 1.81% 1.86%
$510,000 1.57% 1.62% 1.66% 1.71% 1.77% 1.83%
$515,000 1.54% 1.59% 1.63% 1.68% 1.74% 1.80%
$520,000 1.51% 1.56% 1.61% 1.65% 1.70% 1.76%
$525,000 1.49% 1.54% 1.58% 1.63% 1.67% 1.73%
$530,000 1.46% 1.51% 1.56% 1.60% 1.65% 1.69%
$535,000 1.43% 1.48% 1.53% 1.58% 1.62% 1.67%
$540,000 1.41% 1.45% 1.50% 1.55% 1.60% 1.64%
$545,000 1.38% 1.43% 1.48% 1.52% 1.57% 1.62%
$550,000 1.35% 1.40% 1.45% 1.50% 1.54% 1.59%
$555,000 1.32% 1.37% 1.42% 1.47% 1.52% 1.57%
$560,000 1.30% 1.35% 1.40% 1.45% 1.49% 1.54%
$565,000 1.28% 1.32% 1.37% 1.42% 1.47% 1.52%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
3

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Self-Funded Pooling Charge Factors
Exhibit 2C
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$570,000 1.26% 1.30% 1.34% 1.39% 1.44% 1.49%
$575,000 1.24% 1.28% 1.32% 1.37% 1.42% 1.47%
$580,000 1.22% 1.26% 1.30% 1.34% 1.39% 1.44%
$585,000 1.20% 1.24% 1.28% 1.32% 1.37% 1.42%
$590,000 1.18% 1.22% 1.26% 1.29% 1.34% 1.39%
$595,000 1.16% 1.20% 1.24% 1.28% 1.31% 1.37%
$600,000 1.14% 1.18% 1.22% 1.26% 1.29% 1.34%
$605,000 1.12% 1.16% 1.20% 1.24% 1.28% 1.31%
$610,000 1.10% 1.14% 1.18% 1.22% 1.26% 1.29%
$615,000 1.08% 1.12% 1.16% 1.20% 1.24% 1.28%
$620,000 1.06% 1.10% 1.14% 1.18% 1.22% 1.26%
$625,000 1.04% 1.08% 1.12% 1.16% 1.20% 1.24%
$630,000 1.02% 1.06% 1.10% 1.14% 1.18% 1.22%
$635,000 1.01% 1.04% 1.08% 1.12% 1.16% 1.20%
$640,000 0.99% 1.02% 1.06% 1.11% 1.14% 1.18%
$645,000 0.98% 1.01% 1.05% 1.09% 1.13% 1.17%
$650,000 0.96% 0.99% 1.03% 1.07% 1.11% 1.15%
$655,000 0.95% 0.98% 1.01% 1.05% 1.09% 1.13%
$660,000 0.93% 0.97% 1.00% 1.03% 1.07% 1.11%
$665,000 0.92% 0.95% 0.98% 1.01% 1.05% 1.09%
$670,000 0.90% 0.94% 0.97% 1.00% 1.03% 1.07%
$675,000 0.89% 0.92% 0.95% 0.99% 1.02% 1.06%
$680,000 0.87% 0.91% 0.94% 0.97% 1.00% 1.04%
$685,000 0.86% 0.89% 0.92% 0.96% 0.99% 1.02%
$690,000 0.84% 0.88% 0.91% 0.94% 0.98% 1.01%
$695,000 0.83% 0.86% 0.89% 0.93% 0.96% 0.99%
$700,000 0.81% 0.85% 0.88% 0.91% 0.95% 0.98%
$705,000 0.80% 0.83% 0.87% 0.90% 0.93% 0.97%
$710,000 0.78% 0.82% 0.85% 0.89% 0.92% 0.95%
$715,000 0.77% 0.80% 0.84% 0.87% 0.90% 0.94%
$720,000 0.75% 0.79% 0.82% 0.86% 0.89% 0.92%
$725,000 0.73% 0.77% 0.81% 0.84% 0.88% 0.91%
$730,000 0.72% 0.76% 0.79% 0.83% 0.86% 0.90%
$735,000 0.70% 0.74% 0.78% 0.81% 0.85% 0.88%
$740,000 0.69% 0.73% 0.76% 0.80% 0.83% 0.87%
$745,000 0.67% 0.71% 0.75% 0.78% 0.82% 0.85%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
4

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Self-Funded Pooling Charge Factors
Exhibit 2C
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$750,000 0.66% 0.70% 0.73% 0.77% 0.81% 0.84%
$755,000 0.65% 0.68% 0.72% 0.76% 0.79% 0.83%
$760,000 0.64% 0.67% 0.70% 0.74% 0.78% 0.81%
$765,000 0.64% 0.65% 0.69% 0.73% 0.76% 0.80%
$770,000 0.63% 0.65% 0.68% 0.71% 0.75% 0.78%
$775,000 0.62% 0.64% 0.66% 0.70% 0.73% 0.77%
$780,000 0.62% 0.63% 0.65% 0.68% 0.72% 0.76%
$785,000 0.61% 0.63% 0.64% 0.67% 0.71% 0.74%
$790,000 0.60% 0.62% 0.64% 0.65% 0.69% 0.73%
$795,000 0.60% 0.61% 0.63% 0.65% 0.68% 0.72%
$800,000 0.59% 0.61% 0.62% 0.64% 0.66% 0.70%
$805,000 0.58% 0.60% 0.62% 0.63% 0.65% 0.69%
$810,000 0.58% 0.59% 0.61% 0.63% 0.65% 0.67%
$815,000 0.57% 0.59% 0.60% 0.62% 0.64% 0.66%
$820,000 0.56% 0.58% 0.60% 0.62% 0.63% 0.65%
$825,000 0.56% 0.57% 0.59% 0.61% 0.63% 0.64%
$830,000 0.55% 0.57% 0.58% 0.60% 0.62% 0.64%
$835,000 0.54% 0.56% 0.58% 0.60% 0.61% 0.63%
$840,000 0.53% 0.55% 0.57% 0.59% 0.61% 0.62%
$845,000 0.53% 0.55% 0.57% 0.58% 0.60% 0.62%
$850,000 0.52% 0.54% 0.56% 0.58% 0.59% 0.61%
$855,000 0.51% 0.53% 0.55% 0.57% 0.59% 0.61%
$860,000 0.51% 0.53% 0.55% 0.56% 0.58% 0.60%
$865,000 0.50% 0.52% 0.54% 0.56% 0.58% 0.59%
$870,000 0.49% 0.51% 0.53% 0.55% 0.57% 0.59%
$875,000 0.49% 0.51% 0.53% 0.55% 0.56% 0.58%
$880,000 0.48% 0.50% 0.52% 0.54% 0.56% 0.58%
$885,000 0.47% 0.49% 0.51% 0.53% 0.55% 0.57%
$890,000 0.47% 0.49% 0.51% 0.53% 0.54% 0.56%
$895,000 0.46% 0.48% 0.50% 0.52% 0.54% 0.56%
$900,000 0.45% 0.47% 0.49% 0.51% 0.53% 0.55%
$905,000 0.45% 0.47% 0.49% 0.51% 0.53% 0.54%
$910,000 0.44% 0.46% 0.48% 0.50% 0.52% 0.54%
$915,000 0.43% 0.45% 0.47% 0.49% 0.51% 0.53%
$920,000 0.43% 0.45% 0.47% 0.49% 0.51% 0.53%
$925,000 0.42% 0.44% 0.46% 0.48% 0.50% 0.52%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
5

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Self-Funded Pooling Charge Factors
Exhibit 2C
Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017
Limit
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
claim*
factor
Experience Period Starting Quarter
$930,000 0.41% 0.44% 0.45% 0.47% 0.49% 0.51%
$935,000 0.41% 0.43% 0.45% 0.47% 0.49% 0.51%
$940,000 0.40% 0.42% 0.44% 0.46% 0.48% 0.50%
$945,000 0.39% 0.42% 0.44% 0.46% 0.48% 0.49%
$950,000 0.39% 0.41% 0.43% 0.45% 0.47% 0.49%
$955,000 0.38% 0.40% 0.42% 0.44% 0.46% 0.48%
$960,000 0.37% 0.40% 0.42% 0.44% 0.46% 0.48%
$965,000 0.37% 0.39% 0.41% 0.43% 0.45% 0.47%
$970,000 0.36% 0.38% 0.40% 0.42% 0.44% 0.46%
$975,000 0.35% 0.38% 0.40% 0.42% 0.44% 0.46%
$980,000 0.35% 0.37% 0.39% 0.41% 0.43% 0.45%
$985,000 0.34% 0.36% 0.38% 0.40% 0.43% 0.45%
$990,000 0.33% 0.36% 0.38% 0.40% 0.42% 0.44%
$995,000 0.33% 0.35% 0.37% 0.39% 0.41% 0.43%
$1,000,000 0.32% 0.34% 0.36% 0.39% 0.41% 0.43%
*Percentages to be applied to experience claims below limit, to derive expected claims over limit.
6

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Medical Trend Development
Exhibit 3A
Month
Contract
Increase
Normalization
Factor
Experience
Claims
Normalized
Claims
Dec-12 1.1699 $1,000,000 $1,169,859
Jan-13 1.1699 $1,000,000 $1,169,859
Feb-13 1.1699 $1,000,000 $1,169,859
Mar-13 1.1699 $1,000,000 $1,169,859
Apr-13 1.1699 $1,000,000 $1,169,859
May-13 1.1699 $1,000,000 $1,169,859
Jun-13 1.1699 $1,000,000 $1,169,859
Jul-13 1.1699 $1,000,000 $1,169,859
Aug-13 1.1699 $1,000,000 $1,169,859
Sep-13 1.1699 $1,000,000 $1,169,859
Oct-13 1.0400 1.1249 $1,000,000 $1,124,864
Nov-13 1.1249 $1,000,000 $1,124,864
Dec-13 1.1249 $1,000,000 $1,124,864
Jan-14 1.1249 $1,000,000 $1,124,864
Feb-14 1.1249 $1,000,000 $1,124,864
Mar-14 1.1249 $1,000,000 $1,124,864
Apr-14 1.1249 $1,000,000 $1,124,864
May-14 1.1249 $1,000,000 $1,124,864
Jun-14 1.1249 $1,000,000 $1,124,864
Jul-14 1.1249 $1,000,000 $1,124,864
Aug-14 1.1249 $1,000,000 $1,124,864
Sep-14 1.1249 $1,000,000 $1,124,864
Oct-14 1.0400 1.0816 $1,000,000 $1,081,600
Nov-14 1.0816 $1,000,000 $1,081,600
Dec-14 1.0816 $1,000,000 $1,081,600
Jan-15 1.0816 $1,000,000 $1,081,600
Feb-15 1.0816 $1,000,000 $1,081,600
Mar-15 1.0816 $1,000,000 $1,081,600
Apr-15 1.0816 $1,000,000 $1,081,600
May-15 1.0816 $1,000,000 $1,081,600
Jun-15 1.0816 $1,000,000 $1,081,600
Jul-15 1.0816 $1,000,000 $1,081,600
Aug-15 1.0816 $1,000,000 $1,081,600
Sep-15 1.0816 $1,000,000 $1,081,600
Oct-15 1.0400 1.0400 $1,000,000 $1,040,000
Nov-15 1.0400 $1,000,000 $1,040,000
Dec-15 1.0400 $1,000,000 $1,040,000
Jan-16 1.0400 $1,000,000 $1,040,000
Feb-16 1.0400 $1,000,000 $1,040,000
Mar-16 1.0400 $1,000,000 $1,040,000
Apr-16 1.0400 $1,000,000 $1,040,000
May-16 1.0400 $1,000,000 $1,040,000
Jun-16 1.0400 $1,000,000 $1,040,000
Jul-16 1.0400 $1,000,000 $1,040,000
Aug-16 1.0400 $1,000,000 $1,040,000
Sep-16 1.0400 $1,000,000 $1,040,000
Oct-16 1.0400 1.0000 $1,000,000 $1,000,000
Nov-16 1.0000 $1,000,000 $1,000,000
Illustration of Contract Normalization

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Medical Trend Development
Exhibit 3B
Utilization Trend Calculation
Month Membership
Original Claims Original PMPM
Adjusted Claims -
Normalized for
Contract Changes
Adjusted
PMPM
Regression on Adjusted
PMPM - 24 Months
Rolling 12
PMPM
Nov-12 88,923 $33,095,262 $372.18 $38,965,529 $438.19 $414.25
Dec-12 88,775 $29,730,346 $334.90 $33,285,444 $374.94 $414.76
Jan-13 87,454 $34,727,441 $397.09 $39,000,528 $445.95 $415.29
Feb-13 87,369 $33,110,638 $378.97 $37,426,849 $428.38 $415.81
Mar-13 87,378 $34,592,332 $395.89 $38,778,941 $443.81 $416.29
Apr-13 87,188 $34,288,529 $393.27 $38,313,206 $439.43 $416.82
May-13 87,414 $34,874,532 $398.96 $39,353,818 $450.20 $417.33
Jun-13 87,331 $32,427,235 $371.31 $36,512,475 $418.09 $417.86
Jul-13 87,446 $33,666,958 $385.00 $37,416,998 $427.89 $418.37
Aug-13 87,399 $34,050,390 $389.60 $37,890,167 $433.53 $418.90
Sep-13 87,802 $30,058,347 $342.34 $33,491,069 $381.44 $419.43
Oct-13 87,792 $35,010,312 $398.79 $38,608,348 $439.77 $419.95 $426.74
Nov-13 87,664 $32,424,576 $369.87 $35,866,630 $409.14 $420.48 $424.30
Dec-13 87,613 $35,281,176 $402.69 $39,268,940 $448.21 $420.99 $430.47
Jan-14 86,608 $36,259,154 $418.66 $39,556,165 $456.73 $421.53 $431.35
Feb-14 86,619 $31,781,025 $366.91 $34,688,530 $400.47 $422.06 $429.04
Mar-14 86,439 $33,999,473 $393.33 $37,117,279 $429.40 $422.54 $427.84
Apr-14 86,104 $36,049,659 $418.68 $39,348,385 $456.99 $423.08 $429.27
May-14 86,606 $33,368,019 $385.29 $36,255,868 $418.63 $423.60 $426.64
Jun-14 86,367 $34,598,001 $400.59 $37,503,072 $434.23 $424.14 $427.98
Jul-14 85,471 $34,197,792 $400.11 $37,105,045 $434.12 $424.66 $428.50
Aug-14 85,426 $32,095,838 $375.72 $34,732,067 $406.57 $425.20 $426.27
Sep-14 86,092 $32,655,694 $379.31 $35,163,816 $408.44 $425.73 $428.58
Oct-14 86,136 $36,676,567 $425.80 $39,482,709 $458.38 $426.26 $430.11
Nov-14 86,037 $32,923,542 $382.67 $35,285,374 $410.12 $426.80 $430.23
Dec-14 86,185 $35,977,416 $417.44 $38,528,134 $447.04 $427.32 $430.10
Jan-15 84,280 $35,478,032 $420.95 $37,171,528 $441.05 $427.86 $428.76
Feb-15 84,304 $33,234,409 $394.22 $34,750,964 $412.21 $428.41 $429.79
Mar-15 84,197 $35,657,416 $423.50 $37,219,684 $442.05 $428.90 $430.83
Apr-15 83,735 $35,977,302 $429.66 $37,496,951 $447.80 $429.44 $430.02
May-15 83,665 $31,951,087 $381.89 $33,272,811 $397.69 $429.97 $428.33
Jun-15 83,926 $36,697,322 $437.26 $38,185,603 $454.99 $430.51 $430.03
Jul-15 83,032 $35,521,369 $427.80 $36,898,056 $444.38 $431.04 $430.86
Aug-15 82,740 $31,851,061 $384.95 $33,030,471 $399.21 $431.59 $430.32
Sep-15 82,840 $33,112,956 $399.72 $34,338,973 $414.52 $432.13 $430.89
Oct-15 82,757 $35,203,678 $425.39 $36,324,701 $438.93 $432.66 $429.20
Nov-15 82,866 $34,449,927 $415.73 $35,506,233 $428.48 $433.21 $430.77
Dec-15 82,966 $34,906,225 $420.73 $35,926,918 $433.03 $433.74 $429.56
Jan-16 71,911 $29,105,306 $404.74 $29,357,977 $408.25 $434.29 $427.03
Feb-16 71,491 $28,899,540 $404.24 $29,064,196 $406.54 $434.84 $426.81
Mar-16 71,433 $33,294,413 $466.09 $33,468,500 $468.53 $435.36 $428.57
Apr-16 71,293 $30,468,308 $427.37 $30,587,810 $429.04 $435.91 $426.92
May-16 70,642 $30,583,144 $432.93 $30,751,184 $435.31 $436.45 $430.15
Jun-16 70,409 $33,417,790 $474.62 $33,570,861 $476.80 $437.00 $431.45
Jul-16 69,594 $28,766,447 $413.35 $28,851,451 $414.57 $437.54 $428.98
Aug-16 69,465 $31,962,821 $460.13 $32,013,565 $460.86 $438.09 $434.19
Annual Increase 1.5% 0.9%

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Medical Trend Development
Exhibit 3C
Impact of Benefit Changes on Utilization
Month Membership
Adjusted Claims -
Normalized for
Contract Changes
Adjusted
PMPM
Regression on
Adjusted PMPM - 24
Months
Average
Induced
Utilization
Factor
Normalization
Factor for
Induced
Utilization
Adjusted Claims -
Normalized for
Contract Changes and
Induced Utilization
Factor
Adjusted
PMPM
Regression on
Adjusted PMPM - 24
Months
Sep-14 86,092 $35,163,816 $408.44 $425.73 0.9644 0.9952 $34,996,237 $406.50 $425.45
Oct-14 86,136 $39,482,709 $458.38 $426.26 0.9634 0.9963 $39,335,167 $456.66 $426.08
Nov-14 86,037 $35,285,374 $410.12 $426.80 0.9621 0.9977 $35,204,089 $409.17 $426.73
Dec-14 86,185 $38,528,134 $447.04 $427.32 0.9608 0.9990 $38,490,020 $446.60 $427.36
Jan-15 84,280 $37,171,528 $441.05 $427.86 0.9606 0.9992 $37,141,190 $440.69 $428.01
Feb-15 84,304 $34,750,964 $412.21 $428.41 0.9604 0.9994 $34,729,571 $411.96 $428.66
Mar-15 84,197 $37,219,684 $442.05 $428.90 0.9590 1.0009 $37,253,415 $442.46 $429.25
Apr-15 83,735 $37,496,951 $447.80 $429.44 0.9577 1.0022 $37,579,204 $448.79 $429.90
May-15 83,665 $33,272,811 $397.69 $429.97 0.9574 1.0026 $33,357,753 $398.71 $430.54
Jun-15 83,926 $38,185,603 $454.99 $430.51 0.9568 1.0031 $38,305,798 $456.42 $431.19
Jul-15 83,032 $36,898,056 $444.38 $431.04 0.9562 1.0038 $37,039,933 $446.09 $431.83
Aug-15 82,740 $33,030,471 $399.21 $431.59 0.9554 1.0047 $33,184,253 $401.07 $432.49
Sep-15 82,840 $34,338,973 $414.52 $432.13 0.9546 1.0055 $34,526,130 $416.78 $433.14
Oct-15 82,757 $36,324,701 $438.93 $432.66 0.9534 1.0068 $36,570,962 $441.91 $433.78
Nov-15 82,866 $35,506,233 $428.48 $433.21 0.9525 1.0077 $35,780,818 $431.79 $434.44
Dec-15 82,966 $35,926,918 $433.03 $433.74 0.9516 1.0086 $36,237,005 $436.77 $435.08
Jan-16 71,911 $29,357,977 $408.25 $434.29 0.9544 1.0057 $29,524,771 $410.57 $435.75
Feb-16 71,491 $29,064,196 $406.54 $434.84 0.9549 1.0051 $29,213,733 $408.64 $436.41
Mar-16 71,433 $33,468,500 $468.53 $435.36 0.9567 1.0033 $33,579,663 $470.09 $437.03
Apr-16 71,293 $30,587,810 $429.04 $435.91 0.9574 1.0026 $30,665,877 $430.14 $437.70
May-16 70,642 $30,751,184 $435.31 $436.45 0.9582 1.0017 $30,802,782 $436.04 $438.34
Jun-16 70,409 $33,570,861 $476.80 $437.00 0.9586 1.0013 $33,613,591 $477.40 $439.01
Jul-16 69,594 $28,851,451 $414.57 $437.54 0.9589 1.0010 $28,879,207 $414.97 $439.66
Aug-16 69,465 $32,013,565 $460.86 $438.09 0.9598 1.0000 $32,013,565 $460.86 $440.33
Annual Increase 1.5% 1.8%
Impact of Benefit Chages 0.3%
Selected Utilization Trend 1.0%
Final Utilization Trend 1.3%

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3D
Page 1
Generic Drugs - Cost Trend
Incurred
Date Supply
Average
Wholesale
Price AWP / Supply
Monthly
Cost Trend Supply
Average
Wholesale
Price AWP / Supply
Rolling 12
Cost Trend
Monthly
Data
Rolling 12
Data
Oct-13 2,265,302 $7,253,442 $3.20
Nov-13 2,121,453 $6,890,535 $3.25
Dec-13 2,330,331 $7,748,884 $3.33 $3.37 $3.22
Jan-14 2,208,744 $7,255,217 $3.28 $3.38 $3.24
Feb-14 1,981,483 $6,649,735 $3.36 $3.39 $3.26
Mar-14 2,169,186 $7,275,654 $3.35 $3.41 $3.27
Apr-14 2,142,425 $7,197,330 $3.36 $3.42 $3.29
May-14 2,201,938 $7,439,808 $3.38 $3.44 $3.30
Jun-14 2,177,681 $7,418,853 $3.41 $3.45 $3.32
Jul-14 2,183,364 $7,407,211 $3.39 $3.46 $3.34
Aug-14 2,125,774 $7,322,894 $3.44 $3.48 $3.35
Sep-14 2,143,936 $7,480,135 $3.49 26,051,616 $87,339,698 $3.35 $3.49 $3.37
Oct-14 2,269,593 $7,892,387 $3.48 8.6% 26,055,907 $87,978,642 $3.38 $3.51 $3.39
Nov-14 2,074,398 $7,272,032 $3.51 7.9% 26,008,853 $88,360,139 $3.40 $3.52 $3.40
Dec-14 2,366,560 $8,426,439 $3.56 7.1% 26,045,082 $89,037,694 $3.42 $3.54 $3.42
Jan-15 2,149,349 $7,563,049 $3.52 7.1% 25,985,687 $89,345,527 $3.44 $3.55 $3.44
Feb-15 2,007,242 $7,092,856 $3.53 5.3% 26,011,446 $89,788,648 $3.45 $3.57 $3.46
Mar-15 2,236,538 $8,036,412 $3.59 7.1% 26,078,798 $90,549,407 $3.47 $3.58 $3.47
Apr-15 2,162,941 $7,733,894 $3.58 6.4% 26,099,314 $91,085,971 $3.49 $3.59 $3.49
May-15 2,133,558 $7,647,472 $3.58 6.1% 26,030,934 $91,293,634 $3.51 $3.61 $3.51
Jun-15 2,228,960 $8,096,823 $3.63 6.6% 26,082,213 $91,971,604 $3.53 $3.62 $3.53
Jul-15 2,148,547 $7,834,374 $3.65 7.5% 26,047,396 $92,398,766 $3.55 $3.64 $3.54
Aug-15 2,117,362 $7,737,849 $3.65 6.1% 26,038,984 $92,813,721 $3.56 $3.65 $3.56
Sep-15 2,106,914 $7,743,606 $3.68 5.3% 26,001,963 $93,077,192 $3.58 6.8% $3.67 $3.58
Oct-15 2,181,592 $8,093,134 $3.71 6.7% 25,913,962 $93,277,940 $3.60 6.6% $3.68 $3.60
Nov-15 2,088,172 $7,838,378 $3.75 7.1% 25,927,736 $93,844,285 $3.62 6.5% $3.70 $3.61
Dec-15 2,337,915 $9,071,729 $3.88 9.0% 25,899,090 $94,489,575 $3.65 6.7% $3.71 $3.63
Jan-16 1,936,583 $7,198,354 $3.72 5.6% 25,686,324 $94,124,880 $3.66 6.6% $3.73 $3.65
Feb-16 1,887,392 $7,103,542 $3.76 6.5% 25,566,473 $94,135,566 $3.68 6.7% $3.75 $3.67
Mar-16 2,045,241 $7,687,932 $3.76 4.6% 25,375,176 $93,787,086 $3.70 6.4% $3.76 $3.69
Apr-16 1,939,781 $7,270,927 $3.75 4.8% 25,152,016 $93,324,119 $3.71 6.3% $3.78 $3.71
May-16 1,983,834 $7,505,022 $3.78 5.5% 25,002,292 $93,181,669 $3.73 6.3% $3.79 $3.72
Jun-16 2,004,386 $7,623,343 $3.80 4.7% 24,777,719 $92,708,189 $3.74 6.1% $3.81 $3.74
Jul-16 1,876,262 $7,103,515 $3.79 3.8% 24,505,434 $91,977,331 $3.75 5.8% $3.82 $3.76
Aug-16 2,001,917 $7,602,330 $3.80 3.9% 24,389,989 $91,841,812 $3.77 5.6% $3.84 $3.78
Sep-16 1,894,923 $7,231,781 $3.82 3.8% 24,177,997 $91,329,988 $3.78 5.5% $3.85 $3.80
Exponential Trend: 5.1% 6.2%
MONTHLY DATA ROLLING 12 EXPONENTIAL FIT
$0.00
$0.50
$1.00
$1.50
$2.00
$2.50
$3.00
$3.50
$4.00
$4.50
Oct-13 Jan-14 Apr-14 Jul-14 Oct-14 Jan-15 Apr-15 Jul-15 Oct-15 Jan-16 Apr-16 Jul-16
AWP per Day of Supply - Generic Drugs
Monthly Rolling 12 24 mths on Monthly (5.1%) 24 mths on rolling (6.2%)

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3D
Page 2
Brand Drugs - Cost Trend
Incurred
Date Supply
Average
Wholesale
Price AWP / Supply
Monthly
Cost Trend Supply
Average
Wholesale
Price AWP / Supply
Rolling 12
Cost Trend
Monthly
Data
Rolling 12
Data
Oct-13 449,136 $3,917,276 $8.72
Nov-13 419,342 $3,601,759 $8.59
Dec-13 449,080 $4,056,350 $9.03 $9.03 $8.76
Jan-14 389,997 $3,563,790 $9.14 $9.14 $8.85
Feb-14 358,317 $3,388,787 $9.46 $9.25 $8.94
Mar-14 382,954 $3,609,302 $9.42 $9.35 $9.03
Apr-14 380,892 $3,563,526 $9.36 $9.47 $9.12
May-14 376,034 $3,831,644 $10.19 $9.58 $9.22
Jun-14 379,367 $3,753,958 $9.90 $9.70 $9.31
Jul-14 372,535 $3,845,503 $10.32 $9.82 $9.41
Aug-14 364,386 $3,652,956 $10.02 $9.94 $9.51
Sep-14 377,225 $3,689,243 $9.78 4,699,265 $44,474,094 $9.46 $10.06 $9.61
Oct-14 402,087 $3,961,315 $9.85 13.0% 4,652,216 $44,518,133 $9.57 $10.18 $9.71
Nov-14 358,298 $4,046,277 $11.29 31.5% 4,591,172 $44,962,652 $9.79 $10.31 $9.81
Dec-14 433,833 $4,590,200 $10.58 17.1% 4,575,924 $45,496,502 $9.94 $10.43 $9.91
Jan-15 350,411 $3,765,256 $10.75 17.6% 4,536,339 $45,697,968 $10.07 $10.56 $10.02
Feb-15 333,424 $3,567,558 $10.70 13.1% 4,511,445 $45,876,739 $10.17 $10.69 $10.13
Mar-15 361,017 $3,903,314 $10.81 14.7% 4,489,508 $46,170,751 $10.28 $10.81 $10.22
Apr-15 352,702 $3,771,503 $10.69 14.3% 4,461,318 $46,378,728 $10.40 $10.94 $10.33
May-15 345,506 $3,873,970 $11.21 10.0% 4,430,790 $46,421,054 $10.48 $11.07 $10.44
Jun-15 355,405 $3,929,707 $11.06 11.7% 4,406,828 $46,596,803 $10.57 $11.21 $10.55
Jul-15 339,242 $3,831,948 $11.30 9.4% 4,373,535 $46,583,249 $10.65 $11.34 $10.66
Aug-15 345,400 $4,008,551 $11.61 15.8% 4,354,550 $46,938,844 $10.78 $11.48 $10.77
Sep-15 337,809 $3,888,175 $11.51 17.7% 4,315,133 $47,137,776 $10.92 15.4% $11.63 $10.88
Oct-15 362,989 $4,132,427 $11.38 15.6% 4,276,035 $47,308,888 $11.06 15.6% $11.76 $11.00
Nov-15 352,014 $4,045,734 $11.49 1.8% 4,269,751 $47,308,345 $11.08 13.1% $11.91 $11.11
Dec-15 398,340 $4,575,528 $11.49 8.6% 4,234,259 $47,293,673 $11.17 12.3% $12.05 $11.23
Jan-16 310,221 $3,722,816 $12.00 11.7% 4,194,068 $47,251,232 $11.27 11.8% $12.20 $11.35
Feb-16 295,201 $3,493,853 $11.84 10.6% 4,155,845 $47,177,527 $11.35 11.6% $12.35 $11.47
Mar-16 335,856 $4,159,306 $12.38 14.5% 4,130,684 $47,433,520 $11.48 11.7% $12.49 $11.58
Apr-16 310,301 $3,820,001 $12.31 15.1% 4,088,284 $47,482,018 $11.61 11.7% $12.65 $11.70
May-16 294,829 $3,754,412 $12.73 13.6% 4,037,607 $47,362,460 $11.73 12.0% $12.80 $11.82
Jun-16 303,728 $4,227,512 $13.92 25.9% 3,985,930 $47,660,265 $11.96 13.1% $12.96 $11.95
Jul-16 276,328 $3,773,739 $13.66 20.9% 3,923,016 $47,602,055 $12.13 13.9% $13.11 $12.07
Aug-16 291,426 $3,930,361 $13.49 16.2% 3,869,042 $47,523,864 $12.28 14.0% $13.27 $12.20
Sep-16 288,062 $3,971,983 $13.79 19.8% 3,819,295 $47,607,672 $12.47 14.1% $13.44 $12.33
Exponential Trend: 15.6% 13.3%
MONTHLY DATA ROLLING 12 EXPONENTIAL FIT
$0.00
$2.00
$4.00
$6.00
$8.00
$10.00
$12.00
$14.00
$16.00
Oct-13 Jan-14 Apr-14 Jul-14 Oct-14 Jan-15 Apr-15 Jul-15 Oct-15 Jan-16 Apr-16 Jul-16
AWP per Day of Supply - Brand Drugs
Monthly 12 mths Rolling 24 mths on Monthly (15.6%) 24 mths on rolling (13.3%)

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3D
Page 3
Non-Specialty Drugs - Utilization Trend
Incurred
Date Membership Supply
Supply per
Member
Monthly
Utilization
Trend Membership Supply
Supply per
Member
Rolling 12
Utilization
Trend Monthly Data
Rolling 12
Data
Oct-13 87,012 2,714,438 31.196
Nov-13 86,891 2,540,795 29.241
Dec-13 86,846 2,779,411 32.004 30.074 29.407
Jan-14 85,955 2,598,741 30.234 30.093 29.448
Feb-14 85,896 2,339,800 27.240 30.111 29.488
Mar-14 85,753 2,552,141 29.762 30.127 29.525
Apr-14 85,467 2,523,316 29.524 30.145 29.566
May-14 85,847 2,577,972 30.030 30.163 29.605
Jun-14 85,598 2,557,048 29.873 30.181 29.646
Jul-14 84,696 2,555,899 30.177 30.198 29.686
Aug-14 84,609 2,490,160 29.431 30.217 29.727
Sep-14 85,288 2,521,161 29.561 1,029,858 30,750,881 29.859 30.235 29.768
Oct-14 85,329 2,671,680 31.310 0.4% 1,028,175 30,708,123 29.867 30.252 29.808
Nov-14 85,265 2,432,696 28.531 -2.4% 1,026,549 30,600,024 29.809 30.270 29.849
Dec-14 85,377 2,800,393 32.800 2.5% 1,025,080 30,621,006 29.872 30.288 29.889
Jan-15 83,503 2,499,760 29.936 -1.0% 1,022,628 30,522,026 29.847 30.306 29.930
Feb-15 83,568 2,340,666 28.009 2.8% 1,020,300 30,522,892 29.916 30.325 29.971
Mar-15 83,423 2,597,555 31.137 4.6% 1,017,970 30,568,306 30.029 30.341 30.008
Apr-15 82,990 2,515,643 30.313 2.7% 1,015,493 30,560,632 30.094 30.359 30.050
May-15 82,836 2,479,064 29.927 -0.3% 1,012,482 30,461,724 30.086 30.377 30.090
Jun-15 83,112 2,584,365 31.095 4.1% 1,009,996 30,489,042 30.187 30.395 30.131
Jul-15 82,266 2,487,789 30.241 0.2% 1,007,566 30,420,932 30.192 30.413 30.172
Aug-15 81,946 2,462,762 30.053 2.1% 1,004,903 30,393,534 30.245 30.431 30.213
Sep-15 82,038 2,444,723 29.800 0.8% 1,001,653 30,317,096 30.267 1.4% 30.449 30.255
Oct-15 81,970 2,544,581 31.043 -0.9% 998,294 30,189,997 30.242 1.3% 30.467 30.295
Nov-15 82,047 2,440,186 29.741 4.2% 995,076 30,197,486 30.347 1.8% 30.485 30.337
Dec-15 82,123 2,736,255 33.319 1.6% 991,822 30,133,349 30.382 1.7% 30.503 30.378
Jan-16 75,134 2,246,804 29.904 -0.1% 983,453 29,880,392 30.383 1.8% 30.522 30.420
Feb-16 74,713 2,182,593 29.213 4.3% 974,598 29,722,319 30.497 1.9% 30.540 30.462
Mar-16 74,629 2,381,097 31.906 2.5% 965,804 29,505,860 30.551 1.7% 30.557 30.501
Apr-16 74,503 2,250,082 30.201 -0.4% 957,317 29,240,300 30.544 1.5% 30.575 30.543
May-16 73,846 2,278,664 30.857 3.1% 948,327 29,039,899 30.622 1.8% 30.593 30.584
Jun-16 73,597 2,308,114 31.362 0.9% 938,812 28,763,649 30.638 1.5% 30.612 30.626
Jul-16 72,790 2,152,590 29.573 -2.2% 929,336 28,428,450 30.590 1.3% 30.629 30.667
Aug-16 72,698 2,293,343 31.546 5.0% 920,088 28,259,030 30.713 1.5% 30.648 30.709
Sep-16 73,391 2,182,984 29.745 -0.2% 911,441 27,997,292 30.718 1.5% 30.666 30.751
Exponential Trend: 0.7% 1.6%
MONTHLY DATA ROLLING 12 EXPONENTIAL FIT
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
Oct-13 Jan-14 Apr-14 Jul-14 Oct-14 Jan-15 Apr-15 Jul-15 Oct-15 Jan-16 Apr-16 Jul-16
Days of Supply per Member per Month - Non-Specialty Utilization
Monthly 12 mths Rolling 24 mths on Monthly (0.7%) 24 mths on rolling (1.6%)

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3E
Month
Generic
Supply
Brand
Supply
Total Non-
Specialty
Supply Monthly Rolling 12
Nov-14 2,074,398 358,298 2,432,696 85.3%
Dec-14 2,366,560 433,833 2,800,393 84.5%
Jan-15 2,149,349 350,411 2,499,760 86.0%
Feb-15 2,007,242 333,424 2,340,666 85.8%
Mar-15 2,236,538 361,017 2,597,555 86.1%
Apr-15 2,162,941 352,702 2,515,643 86.0%
May-15 2,133,558 345,506 2,479,064 86.1%
Jun-15 2,228,960 355,405 2,584,365 86.2%
Jul-15 2,148,547 339,242 2,487,789 86.4%
Aug-15 2,117,362 345,400 2,462,762 86.0%
Sep-15 2,106,914 337,809 2,444,723 86.2%
Oct-15 2,181,592 362,989 2,544,581 85.7% 85.8%
Nov-15 2,088,172 352,014 2,440,186 85.6% 85.9%
Dec-15 2,337,915 398,340 2,736,255 85.4% 85.9%
Jan-16 1,936,583 310,221 2,246,804 86.2% 86.0%
Feb-16 1,887,392 295,201 2,182,593 86.5% 86.0%
Mar-16 2,045,241 335,856 2,381,097 85.9% 86.0%
Apr-16 1,939,781 310,301 2,250,082 86.2% 86.0%
May-16 1,983,834 294,829 2,278,664 87.1% 86.1%
Jun-16 2,004,386 303,728 2,308,114 86.8% 86.1%
Jul-16 1,876,262 276,328 2,152,590 87.2% 86.2%
Aug-16 2,001,917 291,426 2,293,343 87.3% 86.3%
Sep-16 1,894,923 288,062 2,182,984 86.8% 86.4%
Oct-16 2,252,562 342,844 2,595,406 86.8% 86.5%
Nov-16 2,133,542 320,081 2,453,624 87.0% 86.6%
Dec-16 2,390,866 362,116 2,752,982 86.8% 86.7%
Jan-17 1,978,372 280,393 2,258,765 87.6% 86.8%
Feb-17 1,928,317 266,759 2,195,076 87.8% 86.9%
Mar-17 2,089,105 306,814 2,395,919 87.2% 87.0%
Apr-17 1,985,263 277,972 2,263,235 87.7% 87.2%
May-17 2,018,120 274,535 2,292,655 88.0% 87.2%
Jun-17 2,040,174 283,117 2,323,290 87.8% 87.3%
Jul-17 1,911,491 254,896 2,166,387 88.2% 87.4%
Aug-17 2,037,234 271,679 2,308,913 88.2% 87.5%
Sep-17 1,928,497 268,544 2,197,041 87.8% 87.6%
Oct-17 2,287,862 319,680 2,607,542 87.7% 87.6%
Nov-17 2,153,119 300,505 2,453,624 87.8% 87.7%
Dec-17 2,433,105 319,877 2,752,982 88.4% 87.9%
Jan-18 2,009,333 249,432 2,258,765 89.0% 88.0%
Feb-18 1,958,308 236,767 2,195,076 89.2% 88.1%
Mar-18 2,123,874 272,044 2,395,919 88.6% 88.2%
Apr-18 2,009,634 253,601 2,263,235 88.8% 88.3%
May-18 2,041,750 250,904 2,292,655 89.1% 88.4%
Jun-18 2,067,128 256,162 2,323,290 89.0% 88.5%
Jul-18 1,935,135 231,252 2,166,387 89.3% 88.6%
Aug-18 2,065,835 243,078 2,308,913 89.5% 88.7%
Sep-18 1,954,591 242,450 2,197,041 89.0% 88.7%
Oct-18 2,321,031 286,511 2,607,542 89.0% 88.9%
Nov-18 2,182,474 271,150 2,453,624 88.9% 89.0%
Dec-18 2,446,790 306,192 2,752,982 88.9% 89.0%
Generic Dispensing Rate
Generic Dispensing Rate Development

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3F
For the 12 months ending September 2016: Generic Brand
Non-Specialty
Total
# Days Supply a 24,177,997 3,819,295 27,997,292
Allowed Charge per Supply b $0.76 $9.84
Total Allowed Charges c=a*b $18,353,253 $37,599,104 $55,952,357
Utilization Trends d 0.7%
Projected # Days Supply (12 months ending December 2018) e=a*(1+d)^(27/12) 28,447,952
Projected Rolling-12 dispensing rate (Generic and Brand split) f 89.0% 11.0%
Non-Specialty Projected # Days Supply: Generic and Brand g=e*f 25,322,865 3,125,088
Utilization Trends: Generic and Brand h=g/a-1 4.7% -18.2%
Cost Trends i 5.1% 15.6%
Projected Allowed Charge per Supply j=b*(1+i)^(27/12) $0.85 $13.64
Projected Total Allowed Charges k=g*j $21,475,915 $42,624,282 $64,100,198
Total Trends l=k/c-1 17.0% 13.4% 14.6%
Annual Trends 7.2% 5.7% 6.2%
PMPM Calculation
Member Months for the 12 months ending September 2016 m 911,441
PMPM by category n=c/m $20.14 $41.25 $61.39
Non-Specialty Drugs

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3G
Page 1
Specialty Drug Trend
Incurred
Date Members
New
Treatment1
Allowed
Charges
All Other
Specialty
Allowed
Charges
Total
Specialty Drug
Allowed
Charges
Total Specialty
PMPM
All Other
Specialty
PMPM Members
New
Treatment
Allowed
Charges
All Other
Specialty
Allowed
Charges
Total Specialty
Drug Allowed
Charges
Total
Specialty
PMPM
All Other
Specialty
PMPM
Total
Specialty
Specialty
Excluding
New
Treatments
10/1/2013 87,012 $ - $ 1,746,295 1,746,295$ $20.07 $20.07
11/1/2013 86,891 $ - $ 1,523,786 1,523,786$ $17.54 $17.54
12/1/2013 86,846 $ - $ 1,784,687 1,784,687$ $20.55 $20.55
1/1/2014 85,955 $ - $ 1,845,451 1,845,451$ $21.47 $21.47
2/1/2014 85,896 $ 58,804 $ 1,708,823 1,767,627$ $20.58 $19.89
3/1/2014 85,753 $ 309,530 $ 1,819,461 2,128,991$ $24.83 $21.22
4/1/2014 85,467 $ 473,065 $ 1,994,594 2,467,659$ $28.87 $23.34
5/1/2014 85,847 $ 508,910 $ 1,944,555 2,453,465$ $28.58 $22.65
6/1/2014 85,598 $ 175,741 $ 1,985,454 2,161,195$ $25.25 $23.20
7/1/2014 84,696 $ 235,897 $ 1,863,302 2,099,199$ $24.79 $22.00
8/1/2014 84,609 $ 202,631 $ 1,864,951 2,067,582$ $24.44 $22.04
9/1/2014 85,288 $ 148,700 $ 1,788,982 1,937,682$ $22.72 $20.98 1,029,858 $ 2,113,278 $ 21,870,342 23,983,620$ $23.29 $21.24 $24.03 $20.51
10/1/2014 85,329 $ 89,227 $ 1,870,387 1,959,614$ $22.97 $21.92 1,028,175 $ 2,202,505 $ 21,994,434 24,196,939$ $23.53 $21.39 $24.31 $20.78
11/1/2014 85,265 $ 158,347 $ 1,755,053 1,913,400$ $22.44 $20.58 1,026,549 $ 2,360,852 $ 22,225,700 24,586,553$ $23.95 $21.65 $24.60 $21.06
12/1/2014 85,377 $ 350,235 $ 2,024,003 2,374,238$ $27.81 $23.71 1,025,080 $ 2,711,087 $ 22,465,017 25,176,104$ $24.56 $21.92 $24.88 $21.34
1/1/2015 83,503 $ 347,594 $ 1,788,031 2,135,625$ $25.58 $21.41 1,022,628 $ 3,058,682 $ 22,407,596 25,466,278$ $24.90 $21.91 $25.18 $21.63
2/1/2015 83,568 $ 552,364 $ 1,724,714 2,277,078$ $27.25 $20.64 1,020,300 $ 3,552,242 $ 22,423,487 25,975,729$ $25.46 $21.98 $25.47 $21.92
3/1/2015 83,423 $ 665,468 $ 2,079,407 2,744,874$ $32.90 $24.93 1,017,970 $ 3,908,180 $ 22,683,432 26,591,612$ $26.12 $22.28 $25.75 $22.19
4/1/2015 82,990 $ 788,700 $ 1,907,186 2,695,886$ $32.48 $22.98 1,015,493 $ 4,223,815 $ 22,596,023 26,819,839$ $26.41 $22.25 $26.05 $22.49
5/1/2015 82,836 $ 476,284 $ 2,346,535 2,822,820$ $34.08 $28.33 1,012,482 $ 4,191,190 $ 22,998,004 27,189,194$ $26.85 $22.71 $26.35 $22.79
6/1/2015 83,112 $ 480,145 $ 2,018,695 2,498,839$ $30.07 $24.29 1,009,996 $ 4,495,593 $ 23,031,245 27,526,838$ $27.25 $22.80 $26.66 $23.10
7/1/2015 82,266 $ 344,839 $ 1,951,380 2,296,219$ $27.91 $23.72 1,007,566 $ 4,604,535 $ 23,119,323 27,723,858$ $27.52 $22.95 $26.97 $23.40
8/1/2015 81,946 $ 266,075 $ 1,909,255 2,175,330$ $26.55 $23.30 1,004,903 $ 4,667,979 $ 23,163,626 27,831,606$ $27.70 $23.05 $27.29 $23.72
9/1/2015 82,038 $ 86,564 $ 2,093,005 2,179,569$ $26.57 $25.51 1,001,653 $ 4,605,843 $ 23,467,649 28,073,492$ $28.03 $23.43 $27.61 $24.04
10/1/2015 81,970 $ 86,567 $ 2,115,863 2,202,430$ $26.87 $25.81 998,294 $ 4,603,183 $ 23,713,125 28,316,308$ $28.36 $23.75 $27.93 $24.36
11/1/2015 82,047 $ 53,096 $ 1,992,876 2,045,972$ $24.94 $24.29 995,076 $ 4,497,932 $ 23,950,949 28,448,881$ $28.59 $24.07 $28.26 $24.69
12/1/2015 82,123 $ 171,659 $ 2,471,061 2,642,720$ $32.18 $30.09 991,822 $ 4,319,356 $ 24,398,006 28,717,362$ $28.95 $24.60 $28.58 $25.01
1/1/2016 75,134 $ 21,720 $ 1,900,826 1,922,546$ $25.59 $25.30 983,453 $ 3,993,481 $ 24,510,802 28,504,283$ $28.98 $24.92 $28.92 $25.36
2/1/2016 74,713 $ 261,291 $ 1,982,160 2,243,450$ $30.03 $26.53 974,598 $ 3,702,407 $ 24,768,247 28,470,655$ $29.21 $25.41 $29.26 $25.70
3/1/2016 74,629 $ 264,538 $ 2,413,995 2,678,533$ $35.89 $32.35 965,804 $ 3,301,478 $ 25,102,836 28,404,314$ $29.41 $25.99 $29.59 $26.03
4/1/2016 74,503 $ 365,601 $ 2,080,534 2,446,134$ $32.83 $27.93 957,317 $ 2,878,378 $ 25,276,184 28,154,562$ $29.41 $26.40 $29.94 $26.38
5/1/2016 73,846 $ 241,535 $ 2,245,938 2,487,473$ $33.68 $30.41 948,327 $ 2,643,629 $ 25,175,587 27,819,216$ $29.34 $26.55 $30.28 $26.73
6/1/2016 73,597 $ 299,695 $ 2,451,161 2,750,856$ $37.38 $33.31 938,812 $ 2,463,179 $ 25,608,053 28,071,233$ $29.90 $27.28 $30.64 $27.09
7/1/2016 72,790 $ 207,874 $ 2,239,625 2,447,499$ $33.62 $30.77 929,336 $ 2,326,214 $ 25,896,299 28,222,513$ $30.37 $27.87 $30.99 $27.45
8/1/2016 72,698 $ 339,138 $ 2,608,184 2,947,322$ $40.54 $35.88 920,088 $ 2,399,277 $ 26,595,228 28,994,505$ $31.51 $28.91 $31.36 $27.82
9/1/2016 73,391 $ 399,975 $ 2,258,931 2,658,906$ $36.23 $30.78 911,441 $ 2,712,688 $ 26,761,154 29,473,842$ $32.34 $29.36 $31.73 $28.20
1. New treatments are hepatitis C drugs, PCSK9 inhibitors, and Orkambi Exponential Trend: 14.9% 17.3%
MONTHLY DATA PMPM ROLLING 12 PMPM EXPONENTIAL FIT
$0.00
$5.00
$10.00
$15.00
$20.00
$25.00
$30.00
$35.00
$40.00
$45.00
10/1/2013 1/1/2014 4/1/2014 7/1/2014 10/1/2014 1/1/2015 4/1/2015 7/1/2015 10/1/2015 1/1/2016 4/1/2016 7/1/2016
Allowed Cost per Member per Month - Specialty Drugs
Total Specialty PMPM All Other Specialty PMPM Total Specialty, 24 mths on Rolling 12 (14.9%) All Other Specialty, 24 mths on Rolling 12 (17.4%)

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3G
Page 2
Restated Specialty Drug Trend
Pharmacy Specialty Claims in the Experience A 29,473,842$
Claims Removed from the Experience
Hepatitis C B1 $2,393,099
PCSK9 Inhibitors1 B2 $51,939
Orkambi B3 $267,651
Total B = B1+B2+B3 $2,712,688
Pharmacy Specialty Claims without Excluded Drugs C = A - B 26,761,154$
Projected Specialty Claims using a 14.1% trend for 27 months D = C x (1.141)^(27/12) $38,313,061
Adding Incremental Cost of Excluded Treatments for the Projection Period
Hepatitis C E1 $3,297,770
PCSK9 Inhibitors E2 $225,344
Orkambi E3 $1,973,878
Total E = E1+E2+E3 $5,496,992
Restated Projected Specialty Claims F = D + E $43,810,053
Restated Specialty Trend G = (F/A)^(12/27) -1 19.3%
1. PCSK9 inhibitors in the formulary include Praluent, which was approved by the FDA on July 24, 2015, and Repatha,
which was approved by the FDA on August 27, 2015.

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3H
Contract Adjustment Factors
7/1/2017 8/1/2017 9/1/2017 10/1/2017 11/1/2017 12/1/2017 1/1/2018 2/1/2018 3/1/2018 4/1/2018 5/1/2018 6/1/2018 7/1/2018
10/1/2015 0.9782 0.9775 0.9767 0.9759 0.9752 0.9744 0.9736 0.9729 0.9721 0.9713 0.9706 0.9698 0.9690
11/1/2015 0.9796 0.9788 0.9781 0.9773 0.9765 0.9758 0.9750 0.9742 0.9735 0.9727 0.9719 0.9712 0.9704
12/1/2015 0.9810 0.9802 0.9794 0.9787 0.9779 0.9771 0.9764 0.9756 0.9748 0.9741 0.9733 0.9725 0.9718
1/1/2016 0.9823 0.9816 0.9808 0.9800 0.9793 0.9785 0.9777 0.9770 0.9762 0.9754 0.9747 0.9739 0.9731
2/1/2016 0.9837 0.9830 0.9822 0.9814 0.9807 0.9799 0.9791 0.9783 0.9776 0.9768 0.9760 0.9753 0.9745
3/1/2016 0.9851 0.9843 0.9836 0.9828 0.9820 0.9813 0.9805 0.9797 0.9790 0.9782 0.9774 0.9766 0.9759
4/1/2016 0.9865 0.9857 0.9850 0.9842 0.9834 0.9827 0.9819 0.9811 0.9803 0.9796 0.9788 0.9780 0.9773
5/1/2016 0.9879 0.9871 0.9864 0.9856 0.9848 0.9840 0.9833 0.9825 0.9817 0.9810 0.9802 0.9794 0.9786
6/1/2016 0.9893 0.9885 0.9878 0.9870 0.9862 0.9854 0.9847 0.9839 0.9831 0.9823 0.9816 0.9808 0.9800
7/1/2016 0.9899 0.9892 0.9884 0.9876 0.9868 0.9861 0.9853 0.9845 0.9837 0.9830 0.9822 0.9814
8/1/2016 0.9899 0.9891 0.9884 0.9876 0.9868 0.9860 0.9853 0.9845 0.9837 0.9829 0.9822
9/1/2016 0.9899 0.9891 0.9884 0.9876 0.9868 0.9860 0.9853 0.9845 0.9837 0.9829
10/1/2016 0.9899 0.9891 0.9884 0.9876 0.9868 0.9860 0.9852 0.9845 0.9837
11/1/2016 0.9899 0.9891 0.9883 0.9876 0.9868 0.9860 0.9852 0.9845
12/1/2016 0.9899 0.9891 0.9883 0.9876 0.9868 0.9860 0.9852
1/1/2017 0.9899 0.9891 0.9883 0.9875 0.9868 0.9860
2/1/2017 0.9899 0.9891 0.9883 0.9875 0.9868
3/1/2017 0.9899 0.9891 0.9883 0.9875
4/1/2017 0.9899 0.9891 0.9883
5/1/2017 0.9899 0.9891
6/1/2017 0.9898
Projection Beginning
E
x
p
e
r
i
e
n
c
e
B
e
g
i
n
n
i
n
g

Blue Cross and Blue Shield of VermontQ3 2017 Large Group Rating Program Filing
Medical Trend Development
Exhibit 3I
Benefit Leverage Factors
Vermont Freedom Plan (VFP), Comprehensive (COMP), and Indemnity J-Plan (JPLAN)
index Product Deductible Coinsurance Out-of-
Office
Copay
Specialist
CopayER1 Copay AMB
Copay
Deductible Coinsurance Out-of-
Leverage
Factor
1 VFP $200 20% $750 $15 $15 $400 30% $1,200 0.3%
2 VFP $400 20% $1,200 $10 $10 $800 30% $2,400 0.4%
3 VFP $500 20% $1,750 $20 $20 $1,000 30% $3,000 0.6%
4 VFP $1,000 20% $2,300 $20 $20 $100 $2,000 30% $4,600 0.8%
5 VFP $2,500 0% $2,500 $20 $30 $200 $5,000 30% $5,000 0.8%
6 VFP $3,000 0% $4,000 $30 $50 $150 $6,000 30% $8,000 1.1%
7 VFP $5,000 0% $5,000 $25 $25 $10,000 30% $10,000 1.3%
8 COMP $500 20% $1,500 0.5%
9 COMP $2,500 0% $2,500 1.1%
10 COMP $2,500 30% $5,000 1.3%
11 COMP $5,000 0% $5,000 1.5%
12 JPLAN2$100 20% $6,850 $10 $10 0.1%
13 JPLAN2$100 20% $6,850 $25 $35 0.2%
1. ER Copay: the displayed member copay goes toward the facility allowed charges. Associated physician and ancillary charges are the covered at 100%.
2. The J Plan deductible applies only to infusion therapy, DME and prosthetics ambulance.
Vermont Health Partnership (VHP) Medical Plans
VHP In-Network Benefits VHP Out-of-Network Benefits
index Product Inpatient
Care
Deductible2
Outpatient
Surgery
Copay
Office
Copay
Specialist
CopayER3 Copay AMB Copay Out-of-
Deductible Coinsurance Out-of-
Leverage
Factor
1 VHP1 $0 $0 $10 $20 $50 $50 $6,850 $500 30% $13,700 0.1%
2 VHP1 $250 $100 $10 $20 $50 $50 $6,850 $500 30% $13,700 0.1%
3 VHP1 $750 $750 $20 $30 $50 $50 $6,850 $500 30% $13,700 0.3%
4 VHP1 $1,000 $1,000 $20 $30 $50 $50 $6,850 $500 30% $13,700 0.3%
1. All VHP Plans have a DME rider benefit of: $100 deductible, 20% coinsurance, built into the relativity.
2. Maximum of 3/yr per family
3. ER Copay: the displayed member copay goes toward the facility allowed charges. Associated physician and ancillary charges are then covered at 100%.
Consumer Driven Health Plans (CDHP's)
index Product Deductible Coinsurance Out-of-
RX OOPM
Limit3
Wellness
Rx1
Drugs After
Deductible2
Diabetic
Supplies
Medical Rx
1 CDHP $1,500 0% $1,500 $1,300 0% N/A SAAO 0.8% 0.9%
2 CDHP $2,500 0% $2,500 $1,300 0% N/A SAAO 1.1% 1.1%
3 CDHP $3,000 0% $3,000 $1,300 0% N/A SAAO 1.2% 1.1%
4 CDHP $4,000 0% $4,000 $1,300 0% N/A SAAO 1.4% 1.2%
5 CDHP $5,000 0% $5,000 $1,300 0% N/A SAAO 1.5% 1.2%
6 CDHP $6,600 0% $6,600 $1,300 N/A N/A SAAO 1.7% 2.0%
1. Wellness Rx: if applicable, cost sharing rules apply before the deductible is satisfied.
The member’s cost share for Wellness Rx accumulates toward the Out-of-Pocket Maximum.
2. All other drugs are subject to deductible. Once the deductible is met, drugs are subject to the Drugs After Deductible
cost share until the Out-of-Pocket Maximum is met.
3. The Rx OOPM Limit is as described in Vermont Act 171.
In-Network Benefits Out-of-Network Benefits
Leverage FactorIn-Network

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Pharmacy Trend Development
Exhibit 3J
Benefit Leverage Factors
Index Type DeductibleRetail
Generic
Retail
Preferred
Brand
Retail Non-
Preferred
Brand
Mail Order
Generic
Mail Order
Preferred
Brand
Mail Order
Non-
Preferred
Brand
OOPMDiabetic
Supplies
Leveraging
Factor
1 CM1 $100 $5 40% 60% $10 40% 60% $1,300 SAAO 1.3%
2 COI $0 50% 50% 50% 50% 50% 50% $1,300 SAAO 1.2%
3 COP $0 $10 $20 $40 $20 $40 $80 $1,300 SAAO 0.8%
4 COP $0 $10 $25 $25 $20 $50 $50 $1,300 SAAO 0.8%
5 COP $0 $10 $25 $40 $20 $50 $80 $1,300 100% 0.8%
6 COP $0 $10 $25 $50 $20 $50 $100 $1,300 SAAO 0.9%
7 COP $0 $10 $25 $60 $20 $50 $120 $1,300 SAAO 0.9%
8 COP $0 $10 $30 $50 $20 $60 $100 $1,300 SAAO 0.9%
9 COP $0 $10 $35 $60 $20 $70 $120 $1,300 SAAO 1.0%
10 COP $0 $15 $25 $40 $30 $50 $80 $1,300 100% 0.8%
11 COP $0 $15 $25 $40 $30 $50 $80 $1,300 SAAO 0.9%
12 COP $0 $15 $30 $45 $30 $60 $90 $1,300 SAAO 1.0%
13 COP $0 $20 $40 $60 $40 $80 $120 $1,300 SAAO 1.2%
14 COP $0 $5 $20 $35 $10 $40 $70 $1,300 SAAO 0.7%
15 COP $0 $5 $20 $45 $10 $40 $90 $1,300 100% 0.6%
16 COP $0 $5 $30 $50 $10 $60 $100 $1,300 SAAO 0.8%
17 COP $0 $5 $45 $90 $10 $90 $180 $1,300 SAAO 1.0%
18 COP $100 $10 $15 $30 $20 $30 $60 $1,300 SAAO 1.0%
19 COP $100 $10 $25 $45 $20 $50 $90 $1,300 SAAO 1.1%
20 COP $100 $10 $30 $50 $20 $60 $100 $1,300 100% 1.0%
21 COP $100 $10 $30 $50 $20 $60 $100 $1,300 SAAO 1.2%
22 COP $100 $15 $30 $45 $30 $60 $90 $1,300 SAAO 1.2%
23 COP $100 $15 $40 $60 $30 $80 $120 $1,300 SAAO 1.4%
24 COP $100 $5 $20 $40 $10 $40 $80 $1,300 SAAO 1.0%
25 COP $100 $5 $25 $50 $10 $50 $100 $1,300 SAAO 1.0%
26 COP $50 $10 $20 $35 $20 $40 $70 $1,300 SAAO 0.9%
27 COP $50 $10 $25 $35 $20 $50 $70 $1,300 SAAO 1.0%
28 COP $50 $10 $25 $40 $20 $50 $80 $1,300 SAAO 1.0%
29 COP $50 $10 $30 $50 $20 $60 $100 $1,300 SAAO 1.0%
30 COP $50 $5 $10 $25 $10 $20 $50 $1,300 SAAO 0.7%
* Type: COI = coinsurance; COP = copay; CM1 = combined
* Diabetic: If "100%" then Diabetic medications and supplies are covered at 100% of allowed charges;
If "SAAO" then Diabetic medications and supplies are subject to cost sharing same as any other prescription drug.
Copay ($) / Coinsurance (%)

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Benefit Plan Relative Value Factors
Exhibit 4A
Vermont Freedom Plan (VFP), Comprehensive (COMP), and Indemnity J-Plan (JPLAN)
Relativity Factor
index Product Deductible Coinsurance Out-of-
Office
Copay
Specialist
CopayER1 Copay AMB
Copay
Deductible Coinsurance Out-of-
Active
1 VFP $200 20% $750 $15 $15 $400 30% $1,200 1.0145
2 VFP $200 20% $800 $20 $20 $400 30% $1,200 1.0061
3 VFP $200 20% $600 $30 $30 $150 $150 $400 50% $1,200 1.0222
4 VFP $400 20% $1,200 $10 $10 $800 30% $2,400 0.9653
5 VFP $500 20% $1,750 $10 $10 $1,000 30% $3,500 0.9272
6 VFP $500 20% $1,500 $20 $20 $1,000 30% $3,000 0.9284
7 VFP $500 20% $1,500 $20 $20 $250 $50 $1,000 30% $3,000 0.9347
8 VFP $500 20% $1,750 $20 $20 $1,000 30% $3,000 0.9159
9 VFP $500 20% $1,850 $20 $30 $100 $100 $1,000 30% $3,700 0.9202
10 VFP $1,000 20% $2,300 $20 $20 $100 $2,000 30% $4,600 0.8725
11 VFP $1,000 20% $3,500 $25 $25 $2,000 30% $7,000 0.8122
12 VFP $1,000 20% $3,500 $25 $45 $150 $150 $2,000 30% $7,000 0.8222
13 VFP $2,500 0% $2,500 $20 $30 $200 $5,000 30% $5,000 0.8251
14 VFP $2,500 20% $5,300 $20 $30 $5,000 30% $10,600 0.6999
15 VFP $3,000 0% $4,000 $30 $50 $150 $6,000 30% $8,000 0.7579
16 VFP $3,000 20% $6,000 $40 $40 $150 $6,000 30% $12,000 0.6861
17 VFP $5,000 0% $5,000 $25 $25 $10,000 30% $10,000 0.6595
18 VFP $5,000 0% $5,000 $25 $25 $10,000 30% $15,000 0.6592
19 VFP $5,000 0% $5,300 $25 $25 $10,000 30% $15,000 0.6515
20 VFP $5,000 0% $5,000 $30 $60 $10,000 0% $10,000 0.6464
21 COMP $500 20% $1,500 0.9108
22 COMP $2,500 0% $2,500 0.7485
23 COMP $2,500 30% $5,000 0.6407
24 COMP $5,000 0% $5,000 0.5970
25 JPLAN $100 20% $500 $10 $10 1.1232
26 JPLAN $100 20% $500 $25 $35 1.0867
1. ER Copay: the displayed member copay goes toward the facility allowed charges. Associated physician and ancillary charges are then covered at 100%.
2. The J Plan deductible applies only to infusion therapy, DME and prosthetics ambulance.
In-Network Benefits Out-of-Network Benefits

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Benefit Plan Relative Value Factors
Exhibit 4B
Vermont Health Partnership (VHP) Medical Plans
VHP In-Network Benefits VHP Out-of-Network Benefits Relativity Factor
index Product IP OP PCP SCP ER AMB OOPM Deductible Coinsurance Out-of-Pocket Active
1 VHP1 $0 $0 $0 $10 $50 $50 $6,850 $500 30% $13,700 1.0746
2 VHP1 $0 $0 $10 $20 $50 $50 $6,850 $500 30% $13,700 1.0536
3 VHP1 $250 $100 $10 $20 $50 $50 $6,850 $500 30% $13,700 1.0471
4 VHP1 $250 $100 $15 $25 $50 $50 $6,850 $500 30% $13,700 1.0368
5 VHP1 $750 $750 $20 $30 $50 $50 $6,850 $500 30% $13,700 1.0011
6 VHP1 $1,000 $1,000 $20 $30 $50 $50 $6,850 $500 30% $13,700 0.9918
7 VHP1 $1,500 $750 $20 $30 $50 $50 $6,850 $3,000 30% $13,700 0.9906
8 VHP1 $2,000 $1,000 $20 $30 $50 $50 $6,850 $500 30% $13,700 0.9815
PCP Primary Care Physician Copay
SCP Specialist Physician Copay
IP Inpatient Care Deductible (max of 3/yr per family)
OP Outpatient Surgery Copay
ER Emergency Room Copay
AMB Ambulance Copay
OOPM Per ACA, all copays accumulate toward the Out of Pocket Maximum
1. All VHP Plans have a DME rider benefit of: $100 deductible, 20% coinsurance, built into the relativity.

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Benefit Plan Relative Value Factors
Exhibit 4C
Consumer Driven Health Plans (CDHP's)
Relativity Factor
index Product Deductible Coinsurance Out-of-Pocket RX OOPM
Limit3Wellness Rx1 Drugs After
Deductible2
Diabetic
Supplies
Active
1 CDHP $1,500 0% $1,500 $1,300 0% N/A SAAO 1.0475
2 CDHP $1,500 0% $1,500 $1,300 N/A N/A SAAO 1.0362
3 CDHP $1,500 20% $2,500 $1,300 0% N/A SAAO 0.9669
4 CDHP $1,500 20% $2,500 $1,300 N/A N/A SAAO 0.9525
5 CDHP $2,000 0% $2,000 $1,300 0% N/A SAAO 0.9835
6 CDHP $2,000 0% $2,000 $1,300 N/A N/A SAAO 0.9696
7 CDHP $2,000 20% $3,000 $1,300 0% N/A SAAO 0.9150
8 CDHP $2,250 0% $2,250 $1,300 0% N/A SAAO 0.9562
9 CDHP $2,250 0% $2,250 $1,300 N/A N/A SAAO 0.9412
10 CDHP $2,500 0% $2,500 $1,300 0% N/A SAAO 0.9312
11 CDHP $2,500 0% $2,500 $1,300 N/A N/A SAAO 0.9154
12 CDHP $2,500 20% $5,000 $1,300 0% N/A SAAO 0.8308
13 CDHP $2,600 20% $5,000 $1,300 0% N/A SAAO 0.8256
14 CDHP $3,000 0% $3,000 $1,300 N/A $10/$35/$50 SAAO 0.8704
15 CDHP $3,000 0% $3,000 $1,300 0% N/A SAAO 0.8874
16 CDHP $3,000 0% $3,000 $1,300 $10/$30/$50 N/A SAAO 0.8808
17 CDHP $3,000 0% $3,000 $1,300 N/A N/A SAAO 0.8704
18 CDHP $3,000 20% $5,000 $1,300 0% N/A SAAO 0.8071
19 CDHP $3,000 20% $5,500 $1,300 0% 10%/25%/25% SAAO 0.7981
20 CDHP $4,000 0% $4,000 $1,300 0% N/A SAAO 0.8172
21 CDHP $4,000 20% $6,450 $1,300 0% N/A SAAO 0.7434
22 CDHP $5,000 0% $5,000 $1,300 0% N/A SAAO 0.7632
23 CDHP $5,000 0% $5,000 $1,300 N/A N/A SAAO 0.7432
24 CDHP $6,000 0% $6,000 $1,300 0% N/A SAAO 0.7195
25 CDHP $6,450 0% $6,450 $1,300 0% N/A SAAO 0.7023
26 CDHP $6,450 0% $6,450 $1,300 N/A N/A SAAO 0.6813
27 CDHP $6,550 0% $6,550 $1,300 0% N/A SAAO 0.6988
28 CDHP $6,550 0% $6,550 $1,300 N/A N/A SAAO 0.6776
29 CDHP $6,600 0% $6,600 $1,300 N/A N/A SAAO 0.6759
30 CDHP $6,850 0% $6,850 $1,300 0% N/A SAAO 0.6882
3. The Rx OOPM Limit is as described in Vermont Act 171.
1. Wellness Rx: if applicable, cost sharing rules apply before the deductible is satisfied.
The member’s cost share for Wellness Rx accumulates toward the Out-of-Pocket Maximum.
2. All other drugs are subject to deductible. Once the deductible is met, drugs are subject to the Drugs
After Deductible cost share until the Out-of-Pocket Maximum is met.
In-Network

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Benefit Plan Relative Value Factors
Exhibit 4D
Prescription Drug Cards
Relativity
Index Type DeductibleRetail
Generic
Retail
Preferred
Brand
Retail Non-
Preferred
Brand
Mail Order
Generic
Mail Order
Preferred
Brand
Mail Order
Non-
Preferred
Brand
OOPMDiabetic
SuppliesActive
1 CM1 $100 $5 40% 60% $10 40% 60% $1,300 SAAO 0.1566
2 COI $0 50% 50% 50% 50% 50% 50% $1,300 SAAO 0.1394
3 COP $0 $10 $20 $40 $20 $40 $80 $1,300 SAAO 0.2208
4 COP $0 $10 $25 $25 $20 $50 $50 $1,300 SAAO 0.2157
5 COP $0 $10 $25 $40 $20 $50 $80 $1,300 100% 0.2183
6 COP $0 $10 $25 $50 $20 $50 $100 $1,300 SAAO 0.2118
7 COP $0 $10 $25 $60 $20 $50 $120 $1,300 SAAO 0.2105
8 COP $0 $10 $30 $50 $20 $60 $100 $1,300 SAAO 0.2100
9 COP $0 $10 $35 $60 $20 $70 $120 $1,300 SAAO 0.1892
10 COP $0 $15 $25 $40 $30 $50 $80 $1,300 100% 0.2157
11 COP $0 $15 $25 $40 $30 $50 $80 $1,300 SAAO 0.2106
12 COP $0 $15 $30 $45 $30 $60 $90 $1,300 SAAO 0.2026
13 COP $0 $20 $40 $60 $40 $80 $120 $1,300 SAAO 0.1923
14 COP $0 $5 $20 $35 $10 $40 $70 $1,300 SAAO 0.2282
15 COP $0 $5 $20 $45 $10 $40 $90 $1,300 100% 0.2312
16 COP $0 $5 $30 $50 $10 $60 $100 $1,300 SAAO 0.2039
17 COP $0 $5 $45 $90 $10 $90 $180 $1,300 SAAO 0.1964
18 COP $100 $10 $15 $30 $20 $30 $60 $1,300 SAAO 0.2095
19 COP $100 $10 $25 $45 $20 $50 $90 $1,300 SAAO 0.1983
20 COP $100 $10 $30 $50 $20 $60 $100 $1,300 100% 0.2017
21 COP $100 $10 $30 $50 $20 $60 $100 $1,300 SAAO 0.1960
22 COP $100 $15 $30 $45 $30 $60 $90 $1,300 SAAO 0.1908
23 COP $100 $15 $40 $60 $30 $80 $120 $1,300 SAAO 0.1687
24 COP $100 $5 $20 $40 $10 $40 $80 $1,300 SAAO 0.2095
25 COP $100 $5 $25 $50 $10 $50 $100 $1,300 SAAO 0.2063
26 COP $50 $10 $20 $35 $20 $40 $70 $1,300 SAAO 0.2139
27 COP $50 $10 $25 $35 $20 $50 $70 $1,300 SAAO 0.2064
28 COP $50 $10 $25 $40 $20 $50 $80 $1,300 SAAO 0.2057
29 COP $50 $10 $30 $50 $20 $60 $100 $1,300 SAAO 0.2026
30 COP $50 $5 $10 $25 $10 $20 $50 $1,300 SAAO 0.2301
* Type: COI = coinsurance; COP = copay; CM1 = combined (COP/COP/COI)
* Diabetic: If "100%" then Diabetic medications and supplies are covered at 100% of allowed charges;
If "SAAO" then Diabetic medications and supplies are subject to cost sharing same as any other prescription drug.
Copay ($) / Coinsurance (%)

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Benefit Plan Relative Value Factors
Exhibit 4E
Medicare Secondary Vermont Freedom Plan (VFP), Comprehensive (COMP), and Indemnity J-Plan (JPLAN)
Relativity Factor
index Product Deductible Coinsurance Out-of-
Office
Copay
Specialist
CopayER1 Copay AMB
Copay
Deductible Coinsurance Out-of-
Medicare
Secondary
1 VFP $0 0% $6,850 $20 $20 $50 $250 20% $1,000 0.2363
2 VFP $100 20% $500 $10 $10 $200 30% $1,000 0.2174
3 VFP $200 20% $800 $20 $20 $400 30% $1,200 0.1963
4 VFP $400 20% $1,200 $10 $10 $800 30% $2,400 0.1817
5 VFP $500 20% $1,600 $10 $10 $1,000 30% $3,000 0.1719
6 VFP $500 20% $1,750 $10 $10 $1,000 30% $3,500 0.1708
7 VFP $500 20% $1,750 $20 $20 $1,000 30% $3,000 0.1644
8 VFP $500 20% $1,750 $20 $20 $1,000 30% $3,500 0.1643
9 VFP $500 20% $1,750 $20 $30 $100 $50 $1,000 30% $3,500 0.1635
10 VFP $1,000 0% $2,350 $25 $25 $50 $50 $2,000 30% $3,500 0.1573
11 VFP $1,000 20% $2,350 $25 $25 $50 $50 $2,000 30% $3,500 0.1405
12 VFP $1,000 20% $3,500 $25 $25 $2,000 30% $7,000 0.1328
13 VFP $5,000 0% $5,000 $25 $25 $10,000 30% $15,000 0.0710
14 COMP $300 20% $900 0.1909
15 COMP $5,000 0% $5,000 0.0617
16 JPLAN $100 20% $500 $10 $10 0.2464
17 JPLAN $100 20% $500 $20 $20 0.2391
1. ER Copay: the displayed member copay goes toward the facility allowed charges. Associated physician and ancillary charges are then covered at 100%.
2. The J Plan deductible applies only to infusion therapy, DME and prosthetics ambulance.
In-Network Benefits Out-of-Network Benefits

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Benefit Plan Relative Value Factors
Exhibit 4F
Medicare Secondary Consumer Driven Health Plans (CDHP's)
Relativity Factor
index Product Deductible Coinsurance Out-of-Pocket RX OOPM
Limit3Wellness Rx1 Drugs After
Deductible2
Diabetic
Supplies
Medicare
Secondary
1 CDHP $1,500 0% $1,500 $1,300 0% N/A SAAO 0.4785
2 CDHP $1,500 0% $1,500 $1,300 N/A N/A SAAO 0.4320
3 CDHP $2,500 0% $2,500 $1,300 0% N/A SAAO 0.4209
4 CDHP $3,000 0% $3,000 $1,300 $10/$30/$50 N/A SAAO 0.3763
5 CDHP $3,000 0% $3,000 $1,300 N/A N/A SAAO 0.3496
6 CDHP $4,000 0% $4,000 $1,300 0% N/A SAAO 0.3776
7 CDHP $5,000 0% $5,000 $1,300 0% N/A SAAO 0.3607
8 CDHP $5,000 0% $5,000 $1,300 N/A N/A SAAO 0.3050
9 CDHP $6,450 0% $6,450 $1,300 0% N/A SAAO 0.3449
10 CDHP $6,450 0% $6,450 $1,300 N/A N/A SAAO 0.2883
11 CDHP $6,550 0% $6,550 $1,300 N/A N/A SAAO 0.2875
In-Network
1. Wellness Rx: if applicable, cost sharing rules apply before the deductible is satisfied.
The member’s cost share for Wellness Rx accumulates toward the Out-of-Pocket Maximum.
2. All other drugs are subject to deductible. Once the deductible is met, drugs are subject to the Drugs
After Deductible cost share until the Out-of-Pocket Maximum is met.
3. The Rx OOPM Limit is as described in Vermont Act 171.

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Benefit Plan Relative Value Factors
Exhibit 4G
Medicare Secondary Prescription Drug Cards
Relativity
Index Type DeductibleRetail
Generic
Retail
Preferred
Brand
Retail Non-
Preferred
Brand
Mail Order
Generic
Mail Order
Preferred
Brand
Mail Order
Non-
Preferred
Brand
OOPMDiabetic
Supplies
Medicare
Secondary
1 COI $0 50% 50% 50% 50% 50% 50% $1,300 SAAO 0.2591
2 COP $0 $10 $20 $35 $20 $40 $70 $1,300 100% 0.4111
3 COP $0 $10 $20 $40 $20 $40 $80 $1,300 SAAO 0.3992
4 COP $0 $10 $25 $40 $20 $50 $80 $1,300 100% 0.3939
5 COP $0 $10 $30 $60 $20 $60 $120 $1,300 100% 0.3862
6 COP $0 $15 $30 $45 $30 $60 $90 $1,300 SAAO 0.3561
7 COP $0 $5 $25 $50 $10 $50 $100 $1,300 100% 0.4276
8 COP $0 $5 $30 $50 $10 $60 $100 $1,300 SAAO 0.3729
9 COP $100 $10 $30 $45 $20 $60 $90 $1,300 SAAO 0.3637
10 COP $100 $10 $30 $50 $20 $60 $100 $1,300 SAAO 0.3625
11 COP $100 $15 $30 $45 $30 $60 $90 $1,300 SAAO 0.3444
12 COP $100 $5 $25 $50 $10 $50 $100 $1,300 100% 0.4063
13 COP $100 $5 $25 $50 $10 $50 $100 $1,300 SAAO 0.3953
14 COP $50 $10 $25 $35 $20 $50 $70 $1,300 SAAO 0.3772
15 COP $50 $5 $10 $25 $10 $20 $50 $1,300 SAAO 0.4403
* Type: COI = coinsurance; COP = copay; CM1 = combined (COP/COP/COI)
* Diabetic: If "100%" then Diabetic medications and supplies are covered at 100% of allowed charges;
If "SAAO" then Diabetic medications and supplies are subject to cost sharing same as any other prescription drug.
Copay ($) / Coinsurance (%)

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Benefit Plan Relative Value Factors
Exhibit 4H
Tier Factors for Benefits with Separate Medical and Pharmacy Deductibles
Out-of-Pocket
Range Type Single Family Single 2-Person Family Single
Subscriber
& Spouse
Subscriber
& Children Family
NA/Stacked Stacked 1.000 2.379 1.000 2.000 2.743 1.000 2.000 1.653 2.810
$0 - $3,499 Aggregate 1.000 2.319 1.000 1.839 2.690 1.000 1.928 1.598 2.757
$3,500 - $4,999 Aggregate 1.000 2.249 1.000 1.791 2.605 1.000 1.877 1.552 2.669
$5,000 - $7,150 Aggregate 1.000 2.210 1.000 1.749 2.568 1.000 1.836 1.504 2.633
$0 - $3,499 Hybrid 1.000 2.322 1.000 1.840 2.696 1.000 1.928 1.603 2.762
$3,500 - $4,999 Hybrid 1.000 2.252 1.000 1.794 2.607 1.000 1.881 1.555 2.671
$5,000 - $7,150 Hybrid 1.000 2.260 1.000 1.812 2.608 1.000 1.902 1.547 2.674
Tier Factors for Benefits with Integrated Medical and Pharmacy Deductibles
Out-of-Pocket
Range Type Single Family Single 2-Person Family Single
Subscriber
& Spouse
Subscriber
& Children Family
NA/Stacked Stacked 1.000 2.379 1.000 2.000 2.743 1.000 2.000 1.653 2.810
$0 - $3,499 Aggregate 1.000 2.282 1.000 1.783 2.669 1.000 1.877 1.517 2.740
$3,500 - $4,999 Aggregate 1.000 2.195 1.000 1.718 2.565 1.000 1.811 1.442 2.636
$5,000 - $7,150 Aggregate 1.000 2.116 1.000 1.662 2.468 1.000 1.753 1.383 2.538
$0 - $3,499 Hybrid 1.000 2.282 1.000 1.783 2.669 1.000 1.877 1.517 2.740
$3,500 - $4,999 Hybrid 1.000 2.208 1.000 1.735 2.574 1.000 1.828 1.455 2.645
$5,000 - $7,150 Hybrid 1.000 2.235 1.000 1.799 2.572 1.000 1.895 1.493 2.642
2-Tier 3-Tier 4-Tier
2-Tier 3-Tier 4-Tier

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Example of Manual Rate Adjustment
Exhibit 5A
Manual Rate $490.37
Average Age/Gender Factor 1.000
Average Industry Factor 1.000
Projection Period 7/1/2018
Trend Factor 8.40%
Group Information Active Medicare Primary
Age/Gender Factor 0.940 1.030
Industry Factor 0.965 1.000
Projection Period 7/1/2018
Contract Conversion Contract Distribution Members Tier Factor "Contract Tiers"
Single 25 25 1 25
Two-Person 25 50 2 50
Family 50 197 2.743 137.15
100 272 212.2
Active Medicare Primary
Manual Rate A $490.37 $490.37
Adjustment for Age/Gender B = 0.94 / 1 0.9400 1.0300
Adjustment for Industry C = 0.965 / 1 0.9650 1.0000
Adjustment for Trend D = 8.4% for 2 months 1.0412 1.0412
Pharmacy Contract Adjustment E = 0.9953 0.9953
Contract Conversion Factor F = 212.15 / 272 1.2821 1.0000
Adjusted Manual Rate G = A x B x C x D x E x F $590.97 $523.39

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program FilingExhibit 5B
Industry Factors
2-Digit Normalized
SIC Code Industry Description Factor
01 Agricultural Production - Crops 0.972
02 Agricultural Production - Livestock And Animal Specialties 0.979
07 Agricultural Services 0.973
08 Forestry 0.978
09 Fishing, Hunting And Trapping 1.057
10 Metal Mining 1.113
12 Coal Mining 1.121
13 Oil And Gas Extraction 1.025
14 Mining And Quarrying Of Nonmetallic Minerals, Except Fuels 1.090
15 Building Cnstrctn - General Contractors & Operative Builders 0.992
16 Heavy Cnstrctn, Except Building Construction - Contractors 0.986
17 Construction - Special Trade Contractors 0.987
20 Food And Kindred Products 0.940
21 Tobacco Products 1.005
22 Textile Mill Products 0.957
23 Apparel, Finished Prdcts From Fabrics & Similar Materials 0.969
24 Lumber And Wood Products, Except Furniture 1.003
25 Furniture And Fixtures 0.957
26 Paper And Allied Products 0.967
27 Printing, Publishing And Allied Industries 0.947
28 Chemicals And Allied Products 0.996
29 Petroleum Refining And Related Industries 0.997
30 Rubber And Miscellaneous Plastic Products 0.953
31 Leather And Leather Products 0.983
32 Stone, Clay, Glass, And Concrete Products 0.990
33 Primary Metal Industries 0.975
34 Fabricated Metal Prdcts, Except Machinery & Transport Eqpmnt 0.956
35 Industrial And Commercial Machinery And Computer Equipment 0.953
36 Electronic, Elctrcl Eqpmnt & Cmpnts, Excpt Computer Eqpmnt 0.938
37 Transportation Equipment 0.985
38 Mesr/Anlyz/Cntrl Instrmnts; Photo/Med/Opt Gds; Watchs/Clocks 0.937
39 Miscellaneous Manufacturing Industries 0.951
40 Railroad Transportation 0.997
41 Local, Suburban Transit & Interurbn Hgwy Passenger Transport 1.039
42 Motor Freight Transportation 1.039
43 United States Postal Service 0.965
44 Water Transportation 1.017
45 Transportation By Air 0.963
46 Pipelines, Except Natural Gas 0.981
47 Transportation Services 0.945
48 Communications 0.920
49 Electric, Gas And Sanitary Services 0.989
50 Wholesale Trade - Durable Goods 0.967
51 Wholesale Trade - Nondurable Goods 0.957
52 Building Matrials, Hrdwr, Garden Supply & Mobile Home Dealrs 0.956
53 General Merchandise Stores 0.955
54 Food Stores 0.958
55 Automotive Dealers And Gasoline Service Stations 1.031
56 Apparel And Accessory Stores 0.957
57 Home Furniture, Furnishings And Equipment Stores 0.949
58 Eating And Drinking Places 1.083
59 Miscellaneous Retail 0.988
60 Depository Institutions 0.941
61 Nondepository Credit Institutions 0.910
62 Security & Commodity Brokers, Dealers, Exchanges & Services 0.941
63 Insurance Carriers 0.965
64 Insurance Agents, Brokers And Service 0.965
65 Real Estate 0.989
67 Holding And Other Investment Offices 0.941
70 Hotels, Rooming Houses, Camps, And Other Lodging Places 1.031

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program FilingExhibit 5B
Industry Factors
2-Digit Normalized
SIC Code Industry Description Factor
72 Personal Services 1.011
73 Business Services 0.954
75 Automotive Repair, Services And Parking 1.003
76 Miscellaneous Repair Services 0.967
78 Motion Pictures 0.980
79 Amusement And Recreation Services 1.053
80 Health Services 1.109
81 Legal Services 1.001
82 Educational Services 0.958
83 Social Services 1.109
84 Museums, Art Galleries And Botanical And Zoological Gardens 0.965
86 Membership Organizations 1.014
87 Engineering, Accounting, Research, Management & Related Svcs 0.916
88 Private Households 0.965
89 Services, Not Elsewhere Classified 0.969
91 Executive, Legislative & General Government, Except Finance 1.109
92 Justice, Public Order And Safety 1.109
93 Public Finance, Taxation And Monetary Policy 1.023
94 Administration Of Human Resource Programs 1.029
95 Administration Of Environmental Quality And Housing Programs 1.021
96 Administration Of Economic Programs 1.023
97 National Security And International Affairs 1.054
99 Nonclassifiable Establishments 0.965

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Administrative Charges Development
Exhibit 6A
11/15 - 10/16 Reconciliation to GAAP (1)
Experience Reclassification Reported
Business Segment Base Commissions Items(2)Expenses
Large Group
BCBSVT Insured $6,054 $1,347 ($2,165) $9,566
BCBSVT Cost Plus and ASO $23,401 $267 ($830) $24,497
TVHP Insured $2,512 $474 ($623) $3,609
Large Group Subtotal $31,967 $2,088 ($3,617) $37,672
Individual/Other
BCBSVT Small Group (QHP and Non-QHP) $15,151 $34 ($5,463) $20,647
BCBSVT Individual (QHP and Non-QHP) $13,188 $0 ($3,497) $16,685
TVHP Small Group $1 $0 $1 $0
Medicare Supplement $1,216 $0 ($106) $1,322
Cost Plus Medicare Supplement(3)$342 $0 $342
TVHP Medigap Blue $1,988 $0 ($125) $2,113
Other Member Categories
FEP $3,956 $0 ($1,735) $5,691
Blue MedicareRx $878 $0 ($83) $961
Other Categories
CBA $9,411 ($29) ($159) $9,541
Host $1,624 $0 ($222) $1,847
Total $79,722 $2,093 ($14,664) $96,478
Notes:
(3) Allocation of expenses for Cost Plus members with Med Supp coverage based on cost PMPM for insured Med Supp
members. In GAAP financials, expenses are included in Large Group Cost Plus.
Reconciliation of Experience Base Administrative Expense to Restated GAAP Expenses
(Dollars in 000's)
(1) Sources: Commissions and Reclassification Items are from Internal BCBSVT reports. Reported Expenses are from
Underwriting Results GAAP Basis, restated for the new allocation, for the Experience Base period.
(2) Reclassification Items include the allocation of GHI expenses across relevant member categories and the removal of
federal fees.

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Administrative Charges Development
Exhibit 6B
Unit Account Member Contract Medical Claim Projected Claims
Large Group
Subtotal CP Medsup
Administrative Expenses A $1,143,714 $3,667,679 $220,754 $665,378 $2,868,147 $8,565,672
Unit Months B 1,339 239,980 122,259 567,115 $96,639,491
Expense PUPM C = A / B $854.16 $15.28 $1.81 $1.17 3.0% $27.85
Increase for Membership D -0.4% -0.4% -0.4% -0.4% -0.4%
Updated Expense PUPM E = (1+D) x C $850.97 $15.23 $1.80 $1.17 $27.75
Annual Trend F 2.4% 2.4% 2.4% 2.4% 2.4%Monthly Trend Factor G = (1+F)^(1/12) 1.0020 1.0020 1.0020 1.0020 1.0020
Months of Trend to First Effective Period H 20 20 20 20 20
Projection PeriodsEffective Date Account Member Contract Medical Claim Projected Claims
Jul-17 I = E x G ^ (H/12) $853.82 $15.28 $1.81 $1.17 3.0% $27.84
Aug-17 J = I x G $855.54 $15.31 $1.81 $1.17 3.0% $27.90
Sep-17 K = J x G $857.26 $15.34 $1.81 $1.18 3.0% $27.95
Oct-17 $858.99 $15.37 $1.82 $1.18 3.0% $28.01
Nov-17 $860.72 $15.40 $1.82 $1.18 3.0% $28.06
Dec-17 $862.45 $15.43 $1.82 $1.18 3.0% $28.12
Jan-18 $864.18 $15.46 $1.83 $1.19 3.0% $28.18
Feb-18 $865.92 $15.49 $1.83 $1.19 3.0% $28.23
Mar-18 $867.66 $15.52 $1.83 $1.19 3.0% $28.29
Apr-18 $869.41 $15.56 $1.84 $1.19 3.0% $28.35
May-18 $871.16 $15.59 $1.84 $1.20 3.0% $28.40
Jun-18 $872.91 $15.62 $1.85 $1.20 3.0% $28.46
Jul-18 $874.67 $15.65 $1.85 $1.20 3.0% $28.52
Aug-18 $876.43 $15.68 $1.85 $1.20 3.0% $28.58
Sep-18 $878.19 $15.71 $1.86 $1.21 3.0% $28.63
Oct-18 $879.96 $15.74 $1.86 $1.21 3.0% $28.69
Administrative Charges PUPM

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Individual Stop Loss Charge Factors for Cost Plus
Exhibit 7A
Q2 2017 Q3 2017 Q4 2017 Q1 2018 Q2 2018 Q3 2018
Limit
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
$30,000 45.78% 46.22% 46.66% 47.11% 47.55% 48.00%
$35,000 41.69% 42.12% 42.55% 42.98% 43.42% 43.85%
$40,000 38.20% 38.62% 39.05% 39.47% 39.90% 40.32%
$45,000 35.20% 35.61% 36.02% 36.44% 36.85% 37.27%
$50,000 32.59% 32.99% 33.39% 33.79% 34.19% 34.60%
$55,000 30.46% 30.85% 31.23% 31.63% 32.02% 32.41%
$60,000 28.57% 28.94% 29.32% 29.69% 30.07% 30.45%
$65,000 26.85% 27.22% 27.58% 27.95% 28.32% 28.69%
$70,000 25.33% 25.68% 26.03% 26.38% 26.73% 27.10%
$75,000 23.95% 24.29% 24.63% 24.97% 25.31% 25.66%
$80,000 22.71% 23.04% 23.36% 23.69% 24.03% 24.37%
$85,000 21.56% 21.89% 22.21% 22.53% 22.85% 23.18%
$90,000 20.52% 20.82% 21.13% 21.46% 21.77% 22.10%
$95,000 19.60% 19.89% 20.18% 20.48% 20.76% 21.08%
$100,000 18.73% 19.03% 19.31% 19.60% 19.89% 20.19%
$105,000 17.92% 18.20% 18.49% 18.78% 19.07% 19.36%
$110,000 17.21% 17.48% 17.73% 18.00% 18.28% 18.58%
$115,000 16.53% 16.80% 17.06% 17.32% 17.58% 17.84%
$120,000 15.88% 16.15% 16.41% 16.67% 16.93% 17.19%
$125,000 15.31% 15.55% 15.78% 16.04% 16.30% 16.57%
$130,000 14.76% 15.01% 15.24% 15.48% 15.71% 15.96%
$135,000 14.22% 14.48% 14.71% 14.95% 15.18% 15.43%
$140,000 13.74% 13.97% 14.19% 14.44% 14.67% 14.92%
$145,000 13.28% 13.52% 13.73% 13.95% 14.17% 14.42%
$150,000 12.83% 13.07% 13.29% 13.51% 13.73% 13.96%
$155,000 12.43% 12.64% 12.85% 13.08% 13.30% 13.53%
$160,000 12.04% 12.25% 12.45% 12.66% 12.88% 13.11%
$165,000 11.65% 11.87% 12.07% 12.28% 12.48% 12.70%
$170,000 11.30% 11.50% 11.70% 11.92% 12.12% 12.33%
$175,000 10.96% 11.17% 11.35% 11.55% 11.76% 11.98%
$180,000 10.63% 10.84% 11.03% 11.22% 11.41% 11.62%
$185,000 10.33% 10.52% 10.71% 10.91% 11.10% 11.30%
$190,000 10.04% 10.23% 10.40% 10.59% 10.79% 10.99%
$195,000 9.76% 9.95% 10.12% 10.31% 10.48% 10.69%
$200,000 9.47% 9.67% 9.85% 10.03% 10.21% 10.40%
Pricing Period Starting Quarter
*Applied to Projected Benefit-Neutral Claims1

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Individual Stop Loss Charge Factors for Cost Plus
Exhibit 7A
Q2 2017 Q3 2017 Q4 2017 Q1 2018 Q2 2018 Q3 2018
Limit
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
Pricing Period Starting Quarter
$205,000 9.21% 9.39% 9.57% 9.76% 9.94% 10.13%
$210,000 8.98% 9.15% 9.30% 9.49% 9.68% 9.87%
$215,000 8.75% 8.92% 9.08% 9.24% 9.41% 9.60%
$220,000 8.53% 8.70% 8.86% 9.02% 9.18% 9.34%
$225,000 8.30% 8.47% 8.64% 8.80% 8.96% 9.13%
$230,000 8.08% 8.25% 8.42% 8.59% 8.75% 8.91%
$235,000 7.85% 8.03% 8.20% 8.37% 8.53% 8.70%
$240,000 7.68% 7.82% 7.98% 8.16% 8.32% 8.50%
$245,000 7.51% 7.65% 7.79% 7.94% 8.11% 8.29%
$250,000 7.34% 7.48% 7.62% 7.76% 7.90% 8.08%
$255,000 7.17% 7.32% 7.45% 7.59% 7.73% 7.87%
$260,000 7.00% 7.15% 7.29% 7.43% 7.57% 7.71%
$265,000 6.83% 6.98% 7.12% 7.27% 7.41% 7.55%
$270,000 6.66% 6.82% 6.96% 7.11% 7.25% 7.39%
$275,000 6.51% 6.65% 6.80% 6.95% 7.09% 7.24%
$280,000 6.37% 6.50% 6.63% 6.78% 6.93% 7.08%
$285,000 6.24% 6.37% 6.49% 6.62% 6.77% 6.92%
$290,000 6.11% 6.24% 6.36% 6.48% 6.61% 6.77%
$295,000 5.98% 6.11% 6.23% 6.36% 6.48% 6.61%
$300,000 5.85% 5.98% 6.10% 6.23% 6.35% 6.48%
$305,000 5.72% 5.85% 5.98% 6.11% 6.23% 6.36%
$310,000 5.59% 5.73% 5.85% 5.98% 6.11% 6.24%
$315,000 5.47% 5.60% 5.73% 5.86% 5.98% 6.12%
$320,000 5.37% 5.48% 5.60% 5.73% 5.86% 5.99%
$325,000 5.26% 5.38% 5.49% 5.61% 5.74% 5.87%
$330,000 5.16% 5.28% 5.38% 5.50% 5.62% 5.75%
$335,000 5.05% 5.17% 5.28% 5.40% 5.50% 5.63%
$340,000 4.95% 5.07% 5.18% 5.30% 5.41% 5.52%
$345,000 4.84% 4.97% 5.08% 5.20% 5.31% 5.42%
$350,000 4.74% 4.86% 4.98% 5.10% 5.21% 5.32%
$355,000 4.66% 4.76% 4.88% 5.00% 5.11% 5.23%
$360,000 4.57% 4.68% 4.78% 4.90% 5.01% 5.13%
$365,000 4.49% 4.59% 4.69% 4.80% 4.91% 5.03%
$370,000 4.40% 4.51% 4.61% 4.71% 4.82% 4.94%
$375,000 4.32% 4.42% 4.52% 4.63% 4.72% 4.84%
*Applied to Projected Benefit-Neutral Claims2

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Individual Stop Loss Charge Factors for Cost Plus
Exhibit 7A
Q2 2017 Q3 2017 Q4 2017 Q1 2018 Q2 2018 Q3 2018
Limit
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
Pricing Period Starting Quarter
$380,000 4.23% 4.34% 4.44% 4.54% 4.64% 4.74%
$385,000 4.14% 4.26% 4.36% 4.46% 4.56% 4.67%
$390,000 4.06% 4.17% 4.27% 4.38% 4.48% 4.59%
$395,000 3.97% 4.09% 4.19% 4.30% 4.40% 4.51%
$400,000 3.90% 4.00% 4.11% 4.22% 4.32% 4.43%
$405,000 3.84% 3.93% 4.03% 4.14% 4.24% 4.35%
$410,000 3.77% 3.86% 3.94% 4.06% 4.16% 4.27%
$415,000 3.71% 3.80% 3.88% 3.98% 4.08% 4.19%
$420,000 3.64% 3.73% 3.82% 3.91% 4.00% 4.12%
$425,000 3.58% 3.67% 3.76% 3.84% 3.93% 4.04%
$430,000 3.51% 3.61% 3.69% 3.78% 3.87% 3.96%
$435,000 3.45% 3.54% 3.63% 3.72% 3.81% 3.89%
$440,000 3.38% 3.48% 3.57% 3.66% 3.75% 3.83%
$445,000 3.32% 3.41% 3.50% 3.60% 3.68% 3.77%
$450,000 3.25% 3.35% 3.44% 3.53% 3.62% 3.71%
$455,000 3.19% 3.29% 3.38% 3.47% 3.56% 3.65%
$460,000 3.12% 3.22% 3.32% 3.41% 3.50% 3.59%
$465,000 3.06% 3.16% 3.25% 3.35% 3.44% 3.53%
$470,000 3.02% 3.09% 3.19% 3.29% 3.38% 3.48%
$475,000 2.97% 3.05% 3.13% 3.23% 3.32% 3.42%
$480,000 2.93% 3.00% 3.07% 3.16% 3.26% 3.36%
$485,000 2.88% 2.95% 3.02% 3.10% 3.20% 3.30%
$490,000 2.83% 2.91% 2.98% 3.05% 3.14% 3.24%
$495,000 2.79% 2.86% 2.93% 3.01% 3.08% 3.18%
$500,000 2.74% 2.82% 2.89% 2.96% 3.03% 3.12%
$505,000 2.69% 2.77% 2.84% 2.92% 2.99% 3.06%
$510,000 2.65% 2.73% 2.80% 2.88% 2.95% 3.02%
$515,000 2.60% 2.68% 2.75% 2.83% 2.90% 2.98%
$520,000 2.55% 2.63% 2.71% 2.79% 2.86% 2.93%
$525,000 2.51% 2.59% 2.66% 2.74% 2.82% 2.89%
$530,000 2.46% 2.54% 2.62% 2.70% 2.77% 2.85%
$535,000 2.41% 2.50% 2.57% 2.65% 2.73% 2.81%
$540,000 2.37% 2.45% 2.53% 2.61% 2.69% 2.76%
$545,000 2.33% 2.41% 2.49% 2.57% 2.64% 2.72%
$550,000 2.30% 2.36% 2.44% 2.52% 2.60% 2.68%
*Applied to Projected Benefit-Neutral Claims3

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Individual Stop Loss Charge Factors for Cost Plus
Exhibit 7A
Q2 2017 Q3 2017 Q4 2017 Q1 2018 Q2 2018 Q3 2018
Limit
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
Pricing Period Starting Quarter
$555,000 2.27% 2.33% 2.40% 2.48% 2.56% 2.64%
$560,000 2.23% 2.30% 2.35% 2.43% 2.51% 2.59%
$565,000 2.20% 2.26% 2.32% 2.39% 2.47% 2.55%
$570,000 2.16% 2.23% 2.29% 2.35% 2.43% 2.51%
$575,000 2.13% 2.19% 2.26% 2.32% 2.38% 2.47%
$580,000 2.09% 2.16% 2.22% 2.29% 2.35% 2.42%
$585,000 2.06% 2.13% 2.19% 2.25% 2.31% 2.38%
$590,000 2.03% 2.09% 2.16% 2.22% 2.28% 2.34%
$595,000 1.99% 2.06% 2.12% 2.19% 2.25% 2.31%
$600,000 1.96% 2.03% 2.09% 2.16% 2.22% 2.28%
$605,000 1.92% 1.99% 2.06% 2.12% 2.19% 2.25%
$610,000 1.89% 1.96% 2.02% 2.09% 2.15% 2.22%
$615,000 1.86% 1.93% 1.99% 2.06% 2.12% 2.19%
$620,000 1.83% 1.89% 1.96% 2.03% 2.09% 2.16%
$625,000 1.80% 1.86% 1.92% 1.99% 2.06% 2.12%
$630,000 1.78% 1.83% 1.89% 1.96% 2.03% 2.09%
$635,000 1.75% 1.80% 1.86% 1.93% 1.99% 2.06%
$640,000 1.73% 1.78% 1.83% 1.90% 1.96% 2.03%
$645,000 1.70% 1.75% 1.80% 1.86% 1.93% 2.00%
$650,000 1.68% 1.73% 1.78% 1.83% 1.90% 1.97%
$655,000 1.65% 1.71% 1.76% 1.81% 1.87% 1.94%
$660,000 1.63% 1.68% 1.73% 1.78% 1.83% 1.90%
$665,000 1.60% 1.66% 1.71% 1.76% 1.81% 1.87%
$670,000 1.57% 1.63% 1.68% 1.74% 1.79% 1.84%
$675,000 1.55% 1.61% 1.66% 1.71% 1.76% 1.82%
$680,000 1.52% 1.58% 1.63% 1.69% 1.74% 1.79%
$685,000 1.50% 1.56% 1.61% 1.67% 1.72% 1.77%
$690,000 1.47% 1.53% 1.59% 1.64% 1.69% 1.75%
$695,000 1.45% 1.51% 1.56% 1.62% 1.67% 1.72%
$700,000 1.43% 1.48% 1.54% 1.59% 1.65% 1.70%
$705,000 1.41% 1.46% 1.51% 1.57% 1.62% 1.68%
$710,000 1.39% 1.44% 1.49% 1.55% 1.60% 1.65%
$715,000 1.37% 1.42% 1.46% 1.52% 1.58% 1.63%
$720,000 1.35% 1.40% 1.44% 1.50% 1.55% 1.61%
$725,000 1.33% 1.38% 1.42% 1.47% 1.53% 1.59%
*Applied to Projected Benefit-Neutral Claims4

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Individual Stop Loss Charge Factors for Cost Plus
Exhibit 7A
Q2 2017 Q3 2017 Q4 2017 Q1 2018 Q2 2018 Q3 2018
Limit
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
Pricing Period Starting Quarter
$730,000 1.32% 1.36% 1.41% 1.45% 1.51% 1.56%
$735,000 1.30% 1.34% 1.39% 1.43% 1.48% 1.54%
$740,000 1.28% 1.32% 1.37% 1.41% 1.46% 1.52%
$745,000 1.26% 1.31% 1.35% 1.40% 1.44% 1.49%
$750,000 1.24% 1.29% 1.33% 1.38% 1.42% 1.47%
$755,000 1.22% 1.27% 1.31% 1.36% 1.40% 1.45%
$760,000 1.20% 1.25% 1.29% 1.34% 1.39% 1.43%
$765,000 1.18% 1.23% 1.28% 1.32% 1.37% 1.41%
$770,000 1.16% 1.21% 1.26% 1.30% 1.35% 1.39%
$775,000 1.14% 1.19% 1.24% 1.29% 1.33% 1.38%
$780,000 1.12% 1.17% 1.22% 1.27% 1.31% 1.36%
$785,000 1.10% 1.15% 1.20% 1.25% 1.30% 1.34%
$790,000 1.08% 1.14% 1.18% 1.23% 1.28% 1.32%
$795,000 1.07% 1.12% 1.16% 1.21% 1.26% 1.31%
$800,000 1.05% 1.10% 1.15% 1.19% 1.24% 1.29%
$805,000 1.03% 1.08% 1.13% 1.18% 1.22% 1.27%
$810,000 1.01% 1.06% 1.11% 1.16% 1.21% 1.25%
$815,000 0.99% 1.04% 1.09% 1.14% 1.19% 1.24%
$820,000 0.97% 1.02% 1.07% 1.12% 1.17% 1.22%
$825,000 0.95% 1.00% 1.05% 1.10% 1.15% 1.20%
$830,000 0.93% 0.98% 1.03% 1.09% 1.13% 1.18%
$835,000 0.92% 0.96% 1.02% 1.07% 1.12% 1.17%
$840,000 0.91% 0.95% 1.00% 1.05% 1.10% 1.15%
$845,000 0.90% 0.93% 0.98% 1.03% 1.08% 1.13%
$850,000 0.89% 0.92% 0.96% 1.01% 1.06% 1.11%
$855,000 0.89% 0.91% 0.94% 0.99% 1.04% 1.09%
$860,000 0.88% 0.90% 0.92% 0.98% 1.03% 1.08%
$865,000 0.87% 0.89% 0.92% 0.96% 1.01% 1.06%
$870,000 0.86% 0.88% 0.91% 0.94% 0.99% 1.04%
$875,000 0.85% 0.88% 0.90% 0.92% 0.97% 1.02%
$880,000 0.84% 0.87% 0.89% 0.91% 0.95% 1.01%
$885,000 0.83% 0.86% 0.88% 0.91% 0.94% 0.99%
$890,000 0.83% 0.85% 0.87% 0.90% 0.92% 0.97%
$895,000 0.82% 0.84% 0.87% 0.89% 0.91% 0.95%
$900,000 0.81% 0.83% 0.86% 0.88% 0.91% 0.94%
*Applied to Projected Benefit-Neutral Claims5

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Individual Stop Loss Charge Factors for Cost Plus
Exhibit 7A
Q2 2017 Q3 2017 Q4 2017 Q1 2018 Q2 2018 Q3 2018
Limit
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
charge
factor*
Pricing Period Starting Quarter
$905,000 0.80% 0.83% 0.85% 0.87% 0.90% 0.92%
$910,000 0.79% 0.82% 0.84% 0.87% 0.89% 0.91%
$915,000 0.78% 0.81% 0.83% 0.86% 0.88% 0.90%
$920,000 0.77% 0.80% 0.82% 0.85% 0.87% 0.90%
$925,000 0.76% 0.79% 0.82% 0.84% 0.87% 0.89%
$930,000 0.76% 0.78% 0.81% 0.83% 0.86% 0.88%
$935,000 0.75% 0.77% 0.80% 0.82% 0.85% 0.87%
$940,000 0.74% 0.77% 0.79% 0.82% 0.84% 0.87%
$945,000 0.73% 0.76% 0.78% 0.81% 0.83% 0.86%
$950,000 0.72% 0.75% 0.77% 0.80% 0.82% 0.85%
$955,000 0.71% 0.74% 0.77% 0.79% 0.82% 0.84%
$960,000 0.70% 0.73% 0.76% 0.78% 0.81% 0.83%
$965,000 0.70% 0.72% 0.75% 0.78% 0.80% 0.83%
$970,000 0.69% 0.72% 0.74% 0.77% 0.79% 0.82%
$975,000 0.68% 0.71% 0.73% 0.76% 0.78% 0.81%
$980,000 0.67% 0.70% 0.72% 0.75% 0.78% 0.80%
$985,000 0.66% 0.69% 0.72% 0.74% 0.77% 0.79%
$990,000 0.65% 0.68% 0.71% 0.74% 0.76% 0.79%
$995,000 0.64% 0.67% 0.70% 0.73% 0.75% 0.78%
$1,000,000 0.64% 0.66% 0.69% 0.72% 0.74% 0.77%
*Applied to Projected Benefit-Neutral Claims6

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$30,000 25 9.110% 7.561% 6.252% 5.143% 4.215%
$30,000 50 5.758% 4.424% 3.370% 2.553% 1.931%
$30,000 100 3.549% 2.436% 1.657% 1.137% 0.805%
$30,000 150 2.783% 1.824% 1.202% 0.812% 0.586%
$30,000 200 2.180% 1.351% 0.861% 0.589% 0.450%
$30,000 300 1.671% 0.962% 0.597% 0.432% 0.367%
$30,000 400 1.241% 0.694% 0.456% 0.369% 0.344%
$30,000 500 1.086% 0.597% 0.409% 0.352% 0.338%
$30,000 600 0.923% 0.517% 0.380% 0.344% 0.337%
$30,000 700 0.799% 0.463% 0.365% 0.342% 0.336%
$30,000 800 0.716% 0.428% 0.353% 0.339% 0.336%
$30,000 900 0.648% 0.404% 0.347% 0.338% 0.336%
$30,000 1,000 0.612% 0.392% 0.345% 0.338% 0.336%
$30,000 1,500 0.460% 0.353% 0.339% 0.337% 0.336%
$30,000 2,000 0.403% 0.343% 0.338% 0.337% 0.336%
$30,000 3,000 0.355% 0.339% 0.338% 0.337% 0.336%
$30,000 4,000 0.344% 0.339% 0.338% 0.337% 0.336%
$30,000 5,000 0.342% 0.339% 0.338% 0.337% 0.336%
$30,000 10,000 0.340% 0.339% 0.338% 0.337% 0.336%
$30,000 20,000 0.273% 0.272% 0.271% 0.270% 0.269%
$30,000 30,000 0.273% 0.272% 0.271% 0.270% 0.269%
$30,000 40,000 0.273% 0.272% 0.271% 0.270% 0.269%
$35,000 25 10.179% 8.539% 7.133% 5.939% 4.928%
$35,000 50 6.427% 5.002% 3.858% 2.959% 2.266%
$35,000 100 3.976% 2.776% 1.921% 1.338% 0.952%
$35,000 150 3.125% 2.084% 1.395% 0.952% 0.682%
$35,000 200 2.456% 1.547% 0.993% 0.674% 0.505%
$35,000 300 1.880% 1.098% 0.679% 0.481% 0.397%
$35,000 400 1.402% 0.790% 0.510% 0.401% 0.364%
$35,000 500 1.235% 0.679% 0.451% 0.375% 0.356%
$35,000 600 1.054% 0.586% 0.414% 0.365% 0.353%
$35,000 700 0.910% 0.518% 0.392% 0.360% 0.352%
$35,000 800 0.814% 0.474% 0.377% 0.356% 0.352%
$35,000 900 0.736% 0.444% 0.368% 0.354% 0.351%
$35,000 1,000 0.691% 0.427% 0.364% 0.353% 0.351%
$35,000 1,500 0.510% 0.376% 0.355% 0.352% 0.351%
$35,000 2,000 0.441% 0.361% 0.353% 0.352% 0.351%
$35,000 3,000 0.376% 0.355% 0.353% 0.352% 0.351%
* Applied to total projected claims1

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$35,000 4,000 0.362% 0.354% 0.353% 0.352% 0.351%
$35,000 5,000 0.359% 0.354% 0.353% 0.352% 0.351%
$35,000 10,000 0.355% 0.354% 0.353% 0.352% 0.351%
$35,000 20,000 0.285% 0.284% 0.283% 0.282% 0.281%
$35,000 30,000 0.285% 0.284% 0.283% 0.282% 0.281%
$35,000 40,000 0.285% 0.284% 0.283% 0.282% 0.281%
$40,000 25 11.102% 9.398% 7.925% 6.663% 5.585%
$40,000 50 7.011% 5.515% 4.301% 3.336% 2.582%
$40,000 100 4.351% 3.083% 2.165% 1.528% 1.094%
$40,000 150 3.425% 2.316% 1.571% 1.083% 0.775%
$40,000 200 2.693% 1.718% 1.109% 0.751% 0.555%
$40,000 300 2.063% 1.221% 0.755% 0.525% 0.423%
$40,000 400 1.546% 0.880% 0.563% 0.430% 0.382%
$40,000 500 1.367% 0.755% 0.490% 0.397% 0.369%
$40,000 600 1.168% 0.647% 0.445% 0.382% 0.365%
$40,000 700 1.010% 0.568% 0.416% 0.375% 0.364%
$40,000 800 0.904% 0.517% 0.397% 0.369% 0.363%
$40,000 900 0.817% 0.480% 0.386% 0.366% 0.363%
$40,000 1,000 0.763% 0.459% 0.380% 0.365% 0.363%
$40,000 1,500 0.555% 0.394% 0.367% 0.364% 0.362%
$40,000 2,000 0.475% 0.376% 0.365% 0.363% 0.362%
$40,000 3,000 0.395% 0.366% 0.364% 0.363% 0.362%
$40,000 4,000 0.376% 0.366% 0.364% 0.363% 0.362%
$40,000 5,000 0.371% 0.365% 0.364% 0.363% 0.362%
$40,000 10,000 0.367% 0.365% 0.364% 0.363% 0.362%
$40,000 20,000 0.294% 0.293% 0.292% 0.291% 0.290%
$40,000 30,000 0.294% 0.293% 0.292% 0.291% 0.290%
$40,000 40,000 0.294% 0.293% 0.292% 0.291% 0.290%
$45,000 25 11.953% 10.188% 8.659% 7.340% 6.203%
$45,000 50 7.554% 5.995% 4.721% 3.698% 2.887%
$45,000 100 4.704% 3.377% 2.403% 1.712% 1.234%
$45,000 150 3.703% 2.535% 1.741% 1.213% 0.868%
$45,000 200 2.920% 1.885% 1.225% 0.829% 0.606%
$45,000 300 2.234% 1.339% 0.830% 0.569% 0.448%
$45,000 400 1.684% 0.968% 0.615% 0.460% 0.400%
$45,000 500 1.493% 0.829% 0.530% 0.418% 0.382%
$45,000 600 1.273% 0.705% 0.475% 0.398% 0.377%
$45,000 700 1.104% 0.616% 0.441% 0.389% 0.375%
* Applied to total projected claims2

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$45,000 800 0.991% 0.560% 0.418% 0.381% 0.373%
$45,000 900 0.894% 0.516% 0.404% 0.377% 0.373%
$45,000 1,000 0.831% 0.489% 0.395% 0.376% 0.372%
$45,000 1,500 0.598% 0.412% 0.378% 0.373% 0.372%
$45,000 2,000 0.508% 0.390% 0.375% 0.373% 0.372%
$45,000 3,000 0.412% 0.377% 0.374% 0.373% 0.372%
$45,000 4,000 0.389% 0.375% 0.374% 0.373% 0.372%
$45,000 5,000 0.383% 0.375% 0.374% 0.373% 0.372%
$45,000 10,000 0.376% 0.375% 0.374% 0.373% 0.372%
$45,000 20,000 0.302% 0.301% 0.300% 0.299% 0.298%
$45,000 30,000 0.302% 0.301% 0.300% 0.299% 0.298%
$45,000 40,000 0.302% 0.301% 0.300% 0.299% 0.298%
$50,000 25 12.728% 10.921% 9.341% 7.973% 6.785%
$50,000 50 8.052% 6.441% 5.113% 4.043% 3.184%
$50,000 100 5.034% 3.655% 2.630% 1.892% 1.371%
$50,000 150 3.960% 2.741% 1.899% 1.334% 0.959%
$50,000 200 3.136% 2.047% 1.342% 0.908% 0.659%
$50,000 300 2.393% 1.450% 0.902% 0.612% 0.474%
$50,000 400 1.813% 1.052% 0.665% 0.489% 0.417%
$50,000 500 1.612% 0.902% 0.570% 0.439% 0.395%
$50,000 600 1.372% 0.761% 0.504% 0.414% 0.388%
$50,000 700 1.194% 0.664% 0.464% 0.403% 0.385%
$50,000 800 1.073% 0.602% 0.438% 0.393% 0.382%
$50,000 900 0.968% 0.551% 0.420% 0.388% 0.381%
$50,000 1,000 0.896% 0.519% 0.410% 0.385% 0.381%
$50,000 1,500 0.640% 0.429% 0.388% 0.382% 0.381%
$50,000 2,000 0.541% 0.403% 0.384% 0.382% 0.381%
$50,000 3,000 0.429% 0.386% 0.383% 0.382% 0.381%
$50,000 4,000 0.401% 0.384% 0.383% 0.382% 0.381%
$50,000 5,000 0.393% 0.384% 0.383% 0.382% 0.381%
$50,000 10,000 0.385% 0.384% 0.383% 0.382% 0.381%
$50,000 20,000 0.309% 0.308% 0.307% 0.306% 0.305%
$50,000 30,000 0.309% 0.308% 0.307% 0.306% 0.305%
$50,000 40,000 0.309% 0.308% 0.307% 0.306% 0.305%
$55,000 25 13.444% 11.602% 9.980% 8.563% 7.333%
$55,000 50 8.519% 6.863% 5.489% 4.373% 3.470%
$55,000 100 5.342% 3.917% 2.848% 2.067% 1.508%
$55,000 150 4.199% 2.934% 2.049% 1.450% 1.045%
* Applied to total projected claims3

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$55,000 200 3.339% 2.202% 1.455% 0.987% 0.711%
$55,000 300 2.542% 1.557% 0.973% 0.656% 0.500%
$55,000 400 1.934% 1.133% 0.715% 0.518% 0.434%
$55,000 500 1.725% 0.972% 0.610% 0.459% 0.407%
$55,000 600 1.466% 0.815% 0.532% 0.430% 0.398%
$55,000 700 1.278% 0.710% 0.487% 0.415% 0.394%
$55,000 800 1.151% 0.643% 0.458% 0.404% 0.390%
$55,000 900 1.039% 0.587% 0.437% 0.398% 0.389%
$55,000 1,000 0.958% 0.549% 0.424% 0.394% 0.389%
$55,000 1,500 0.682% 0.446% 0.397% 0.390% 0.388%
$55,000 2,000 0.573% 0.415% 0.392% 0.389% 0.388%
$55,000 3,000 0.445% 0.394% 0.390% 0.389% 0.388%
$55,000 4,000 0.413% 0.392% 0.390% 0.389% 0.388%
$55,000 5,000 0.403% 0.391% 0.390% 0.389% 0.388%
$55,000 10,000 0.392% 0.391% 0.390% 0.389% 0.388%
$55,000 20,000 0.315% 0.314% 0.313% 0.312% 0.311%
$55,000 30,000 0.315% 0.314% 0.313% 0.312% 0.311%
$55,000 40,000 0.315% 0.314% 0.313% 0.312% 0.311%
$60,000 25 14.100% 12.223% 10.567% 9.111% 7.839%
$60,000 50 8.952% 7.253% 5.841% 4.684% 3.740%
$60,000 100 5.624% 4.159% 3.050% 2.231% 1.638%
$60,000 150 4.424% 3.117% 2.192% 1.559% 1.128%
$60,000 200 3.530% 2.350% 1.565% 1.064% 0.763%
$60,000 300 2.675% 1.653% 1.038% 0.697% 0.525%
$60,000 400 2.044% 1.208% 0.762% 0.545% 0.451%
$60,000 500 1.828% 1.038% 0.647% 0.479% 0.418%
$60,000 600 1.554% 0.867% 0.560% 0.445% 0.407%
$60,000 700 1.358% 0.755% 0.509% 0.427% 0.402%
$60,000 800 1.225% 0.682% 0.477% 0.414% 0.398%
$60,000 900 1.107% 0.621% 0.454% 0.407% 0.396%
$60,000 1,000 1.017% 0.577% 0.437% 0.403% 0.396%
$60,000 1,500 0.722% 0.463% 0.406% 0.397% 0.395%
$60,000 2,000 0.604% 0.427% 0.399% 0.396% 0.395%
$60,000 3,000 0.461% 0.402% 0.397% 0.396% 0.395%
$60,000 4,000 0.424% 0.398% 0.397% 0.396% 0.395%
$60,000 5,000 0.412% 0.398% 0.397% 0.396% 0.395%
$60,000 10,000 0.399% 0.398% 0.397% 0.396% 0.395%
$60,000 20,000 0.320% 0.319% 0.318% 0.317% 0.316%
* Applied to total projected claims4

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$60,000 30,000 0.320% 0.319% 0.318% 0.317% 0.316%
$60,000 40,000 0.320% 0.319% 0.318% 0.317% 0.316%
$65,000 25 14.702% 12.794% 11.106% 9.616% 8.305%
$65,000 50 9.356% 7.621% 6.172% 4.979% 3.995%
$65,000 100 5.890% 4.389% 3.243% 2.388% 1.763%
$65,000 150 4.634% 3.289% 2.326% 1.663% 1.207%
$65,000 200 3.712% 2.493% 1.670% 1.139% 0.814%
$65,000 300 2.806% 1.748% 1.104% 0.738% 0.551%
$65,000 400 2.149% 1.282% 0.808% 0.573% 0.467%
$65,000 500 1.927% 1.102% 0.684% 0.500% 0.429%
$65,000 600 1.637% 0.917% 0.586% 0.459% 0.417%
$65,000 700 1.434% 0.798% 0.531% 0.438% 0.410%
$65,000 800 1.294% 0.720% 0.496% 0.424% 0.405%
$65,000 900 1.172% 0.655% 0.470% 0.416% 0.403%
$65,000 1,000 1.073% 0.604% 0.450% 0.410% 0.402%
$65,000 1,500 0.761% 0.479% 0.414% 0.403% 0.401%
$65,000 2,000 0.633% 0.439% 0.406% 0.402% 0.401%
$65,000 3,000 0.477% 0.409% 0.403% 0.402% 0.401%
$65,000 4,000 0.434% 0.405% 0.403% 0.402% 0.401%
$65,000 5,000 0.420% 0.404% 0.403% 0.402% 0.401%
$65,000 10,000 0.405% 0.404% 0.403% 0.402% 0.401%
$65,000 20,000 0.325% 0.324% 0.323% 0.322% 0.321%
$65,000 30,000 0.325% 0.324% 0.323% 0.322% 0.321%
$65,000 40,000 0.325% 0.324% 0.323% 0.322% 0.321%
$70,000 25 15.269% 13.334% 11.617% 10.094% 8.745%
$70,000 50 9.738% 7.968% 6.489% 5.262% 4.244%
$70,000 100 6.138% 4.605% 3.426% 2.540% 1.886%
$70,000 150 4.831% 3.454% 2.456% 1.763% 1.285%
$70,000 200 3.884% 2.628% 1.773% 1.213% 0.866%
$70,000 300 2.932% 1.841% 1.169% 0.780% 0.577%
$70,000 400 2.249% 1.352% 0.853% 0.600% 0.484%
$70,000 500 2.021% 1.163% 0.720% 0.520% 0.441%
$70,000 600 1.715% 0.964% 0.613% 0.474% 0.425%
$70,000 700 1.507% 0.840% 0.553% 0.449% 0.418%
$70,000 800 1.359% 0.756% 0.514% 0.433% 0.411%
$70,000 900 1.233% 0.686% 0.485% 0.425% 0.409%
$70,000 1,000 1.127% 0.631% 0.463% 0.418% 0.408%
$70,000 1,500 0.798% 0.495% 0.421% 0.409% 0.406%
* Applied to total projected claims5

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$70,000 2,000 0.662% 0.450% 0.412% 0.407% 0.406%
$70,000 3,000 0.492% 0.415% 0.408% 0.407% 0.406%
$70,000 4,000 0.445% 0.410% 0.408% 0.407% 0.406%
$70,000 5,000 0.428% 0.409% 0.408% 0.407% 0.406%
$70,000 10,000 0.411% 0.409% 0.408% 0.407% 0.406%
$70,000 20,000 0.329% 0.328% 0.327% 0.326% 0.325%
$70,000 30,000 0.329% 0.328% 0.327% 0.326% 0.325%
$70,000 40,000 0.329% 0.328% 0.327% 0.326% 0.325%
$75,000 25 15.801% 13.843% 12.098% 10.545% 9.165%
$75,000 50 10.105% 8.303% 6.796% 5.540% 4.495%
$75,000 100 6.379% 4.815% 3.605% 2.691% 2.009%
$75,000 150 5.021% 3.611% 2.583% 1.860% 1.358%
$75,000 200 4.043% 2.756% 1.872% 1.286% 0.917%
$75,000 300 3.054% 1.932% 1.233% 0.822% 0.604%
$75,000 400 2.343% 1.418% 0.895% 0.626% 0.500%
$75,000 500 2.109% 1.221% 0.756% 0.539% 0.451%
$75,000 600 1.789% 1.010% 0.639% 0.488% 0.434%
$75,000 700 1.577% 0.881% 0.575% 0.461% 0.425%
$75,000 800 1.421% 0.790% 0.531% 0.443% 0.417%
$75,000 900 1.290% 0.717% 0.500% 0.433% 0.414%
$75,000 1,000 1.179% 0.658% 0.475% 0.425% 0.413%
$75,000 1,500 0.834% 0.510% 0.429% 0.414% 0.411%
$75,000 2,000 0.689% 0.461% 0.418% 0.412% 0.411%
$75,000 3,000 0.507% 0.422% 0.413% 0.412% 0.411%
$75,000 4,000 0.455% 0.415% 0.413% 0.412% 0.411%
$75,000 5,000 0.436% 0.414% 0.413% 0.412% 0.411%
$75,000 10,000 0.416% 0.414% 0.413% 0.412% 0.411%
$75,000 20,000 0.333% 0.332% 0.331% 0.330% 0.329%
$75,000 30,000 0.333% 0.332% 0.331% 0.330% 0.329%
$75,000 40,000 0.333% 0.332% 0.331% 0.330% 0.329%
$80,000 25 16.309% 14.330% 12.557% 10.975% 9.567%
$80,000 50 10.454% 8.625% 7.092% 5.810% 4.738%
$80,000 100 6.609% 5.016% 3.778% 2.837% 2.130%
$80,000 150 5.201% 3.762% 2.704% 1.953% 1.429%
$80,000 200 4.196% 2.879% 1.967% 1.356% 0.966%
$80,000 300 3.170% 2.019% 1.293% 0.862% 0.629%
$80,000 400 2.427% 1.478% 0.934% 0.649% 0.515%
$80,000 500 2.195% 1.279% 0.791% 0.559% 0.462%
* Applied to total projected claims6

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$80,000 600 1.861% 1.055% 0.665% 0.502% 0.442%
$80,000 700 1.643% 0.921% 0.596% 0.472% 0.432%
$80,000 800 1.478% 0.823% 0.548% 0.452% 0.423%
$80,000 900 1.344% 0.746% 0.514% 0.441% 0.420%
$80,000 1,000 1.229% 0.684% 0.488% 0.431% 0.418%
$80,000 1,500 0.868% 0.525% 0.436% 0.419% 0.416%
$80,000 2,000 0.716% 0.472% 0.423% 0.417% 0.415%
$80,000 3,000 0.522% 0.428% 0.418% 0.416% 0.415%
$80,000 4,000 0.464% 0.420% 0.417% 0.416% 0.415%
$80,000 5,000 0.443% 0.419% 0.417% 0.416% 0.415%
$80,000 10,000 0.420% 0.418% 0.417% 0.416% 0.415%
$80,000 20,000 0.336% 0.335% 0.334% 0.333% 0.332%
$80,000 30,000 0.336% 0.335% 0.334% 0.333% 0.332%
$80,000 40,000 0.336% 0.335% 0.334% 0.333% 0.332%
$85,000 25 16.783% 14.785% 12.991% 11.381% 9.947%
$85,000 50 10.779% 8.928% 7.369% 6.064% 4.969%
$85,000 100 6.827% 5.210% 3.944% 2.977% 2.249%
$85,000 150 5.366% 3.901% 2.818% 2.042% 1.496%
$85,000 200 4.336% 2.992% 2.055% 1.423% 1.014%
$85,000 300 3.276% 2.099% 1.350% 0.901% 0.654%
$85,000 400 2.509% 1.537% 0.973% 0.674% 0.531%
$85,000 500 2.276% 1.334% 0.825% 0.579% 0.473%
$85,000 600 1.928% 1.098% 0.690% 0.515% 0.450%
$85,000 700 1.704% 0.958% 0.617% 0.483% 0.438%
$85,000 800 1.530% 0.853% 0.564% 0.460% 0.428%
$85,000 900 1.395% 0.774% 0.528% 0.448% 0.424%
$85,000 1,000 1.276% 0.708% 0.499% 0.437% 0.422%
$85,000 1,500 0.900% 0.540% 0.443% 0.423% 0.420%
$85,000 2,000 0.741% 0.482% 0.428% 0.421% 0.419%
$85,000 3,000 0.536% 0.433% 0.422% 0.420% 0.419%
$85,000 4,000 0.473% 0.425% 0.421% 0.420% 0.419%
$85,000 5,000 0.450% 0.423% 0.421% 0.420% 0.419%
$85,000 10,000 0.424% 0.422% 0.421% 0.420% 0.419%
$85,000 20,000 0.340% 0.339% 0.338% 0.337% 0.336%
$85,000 30,000 0.340% 0.339% 0.338% 0.337% 0.336%
$85,000 40,000 0.340% 0.339% 0.338% 0.337% 0.336%
$90,000 25 17.241% 15.226% 13.414% 11.777% 10.322%
$90,000 50 11.083% 9.213% 7.629% 6.301% 5.186%
* Applied to total projected claims7

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$90,000 100 7.040% 5.398% 4.106% 3.114% 2.366%
$90,000 150 5.527% 4.037% 2.929% 2.129% 1.563%
$90,000 200 4.471% 3.103% 2.141% 1.488% 1.061%
$90,000 300 3.379% 2.177% 1.405% 0.939% 0.679%
$90,000 400 2.589% 1.595% 1.012% 0.699% 0.547%
$90,000 500 2.354% 1.387% 0.859% 0.598% 0.483%
$90,000 600 1.993% 1.140% 0.714% 0.528% 0.457%
$90,000 700 1.763% 0.994% 0.637% 0.493% 0.444%
$90,000 800 1.579% 0.882% 0.580% 0.469% 0.434%
$90,000 900 1.444% 0.801% 0.542% 0.455% 0.429%
$90,000 1,000 1.321% 0.732% 0.510% 0.443% 0.427%
$90,000 1,500 0.932% 0.554% 0.449% 0.428% 0.424%
$90,000 2,000 0.765% 0.492% 0.433% 0.425% 0.423%
$90,000 3,000 0.549% 0.439% 0.426% 0.424% 0.423%
$90,000 4,000 0.482% 0.429% 0.425% 0.424% 0.423%
$90,000 5,000 0.457% 0.427% 0.425% 0.424% 0.423%
$90,000 10,000 0.428% 0.426% 0.425% 0.424% 0.423%
$90,000 20,000 0.343% 0.342% 0.341% 0.340% 0.339%
$90,000 30,000 0.343% 0.342% 0.341% 0.340% 0.339%
$90,000 40,000 0.343% 0.342% 0.341% 0.340% 0.339%
$95,000 25 17.675% 15.648% 13.819% 12.166% 10.689%
$95,000 50 11.369% 9.484% 7.879% 6.527% 5.394%
$95,000 100 7.238% 5.575% 4.260% 3.246% 2.477%
$95,000 150 5.680% 4.168% 3.036% 2.214% 1.628%
$95,000 200 4.599% 3.208% 2.223% 1.551% 1.108%
$95,000 300 3.476% 2.251% 1.459% 0.976% 0.703%
$95,000 400 2.664% 1.650% 1.050% 0.724% 0.563%
$95,000 500 2.428% 1.439% 0.891% 0.617% 0.494%
$95,000 600 2.055% 1.180% 0.738% 0.542% 0.465%
$95,000 700 1.820% 1.029% 0.656% 0.503% 0.450%
$95,000 800 1.627% 0.911% 0.595% 0.477% 0.439%
$95,000 900 1.491% 0.828% 0.555% 0.462% 0.434%
$95,000 1,000 1.364% 0.756% 0.522% 0.449% 0.431%
$95,000 1,500 0.962% 0.568% 0.455% 0.432% 0.427%
$95,000 2,000 0.788% 0.501% 0.438% 0.428% 0.427%
$95,000 3,000 0.562% 0.444% 0.429% 0.428% 0.427%
$95,000 4,000 0.491% 0.433% 0.429% 0.428% 0.427%
$95,000 5,000 0.463% 0.431% 0.429% 0.428% 0.427%
* Applied to total projected claims8

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$95,000 10,000 0.432% 0.430% 0.429% 0.428% 0.427%
$95,000 20,000 0.346% 0.345% 0.344% 0.343% 0.342%
$95,000 30,000 0.346% 0.345% 0.344% 0.343% 0.342%
$95,000 40,000 0.346% 0.345% 0.344% 0.343% 0.342%
$100,000 25 18.083% 16.043% 14.202% 12.537% 11.042%
$100,000 50 11.642% 9.742% 8.120% 6.747% 5.596%
$100,000 100 7.424% 5.743% 4.407% 3.372% 2.583%
$100,000 150 5.821% 4.288% 3.136% 2.293% 1.689%
$100,000 200 4.720% 3.307% 2.303% 1.611% 1.152%
$100,000 300 3.567% 2.321% 1.510% 1.011% 0.726%
$100,000 400 2.735% 1.702% 1.086% 0.748% 0.578%
$100,000 500 2.498% 1.488% 0.923% 0.636% 0.505%
$100,000 600 2.114% 1.219% 0.761% 0.555% 0.472%
$100,000 700 1.872% 1.062% 0.675% 0.513% 0.456%
$100,000 800 1.671% 0.938% 0.610% 0.485% 0.443%
$100,000 900 1.535% 0.853% 0.568% 0.469% 0.438%
$100,000 1,000 1.406% 0.779% 0.532% 0.454% 0.434%
$100,000 1,500 0.991% 0.581% 0.461% 0.435% 0.430%
$100,000 2,000 0.810% 0.510% 0.442% 0.431% 0.430%
$100,000 3,000 0.574% 0.448% 0.433% 0.431% 0.430%
$100,000 4,000 0.500% 0.436% 0.432% 0.431% 0.430%
$100,000 5,000 0.469% 0.434% 0.432% 0.431% 0.430%
$100,000 10,000 0.435% 0.433% 0.432% 0.431% 0.430%
$100,000 20,000 0.348% 0.347% 0.346% 0.345% 0.344%
$100,000 30,000 0.348% 0.347% 0.346% 0.345% 0.344%
$100,000 40,000 0.348% 0.347% 0.346% 0.345% 0.344%
$105,000 25 18.485% 16.435% 14.580% 12.903% 11.397%
$105,000 50 11.914% 10.001% 8.361% 6.968% 5.797%
$105,000 100 7.610% 5.910% 4.553% 3.498% 2.689%
$105,000 150 5.959% 4.405% 3.233% 2.371% 1.750%
$105,000 200 4.839% 3.406% 2.381% 1.672% 1.197%
$105,000 300 3.658% 2.391% 1.562% 1.047% 0.750%
$105,000 400 2.805% 1.754% 1.122% 0.772% 0.593%
$105,000 500 2.563% 1.532% 0.951% 0.653% 0.515%
$105,000 600 2.172% 1.258% 0.784% 0.568% 0.479%
$105,000 700 1.924% 1.096% 0.693% 0.523% 0.461%
$105,000 800 1.716% 0.965% 0.625% 0.493% 0.448%
$105,000 900 1.579% 0.879% 0.581% 0.476% 0.442%
* Applied to total projected claims9

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$105,000 1,000 1.447% 0.801% 0.543% 0.460% 0.438%
$105,000 1,500 1.020% 0.594% 0.467% 0.439% 0.433%
$105,000 2,000 0.832% 0.519% 0.446% 0.434% 0.433%
$105,000 3,000 0.586% 0.453% 0.436% 0.434% 0.433%
$105,000 4,000 0.508% 0.440% 0.435% 0.434% 0.433%
$105,000 5,000 0.475% 0.437% 0.435% 0.434% 0.433%
$105,000 10,000 0.438% 0.436% 0.435% 0.434% 0.433%
$105,000 20,000 0.350% 0.349% 0.348% 0.347% 0.346%
$105,000 30,000 0.350% 0.349% 0.348% 0.347% 0.346%
$105,000 40,000 0.350% 0.349% 0.348% 0.347% 0.346%
$110,000 25 18.873% 16.816% 14.948% 13.259% 11.741%
$110,000 50 12.173% 10.245% 8.591% 7.178% 5.988%
$110,000 100 7.788% 6.069% 4.692% 3.617% 2.791%
$110,000 150 6.094% 4.520% 3.329% 2.449% 1.811%
$110,000 200 4.956% 3.503% 2.459% 1.732% 1.242%
$110,000 300 3.748% 2.460% 1.613% 1.083% 0.775%
$110,000 400 2.872% 1.803% 1.157% 0.795% 0.608%
$110,000 500 2.628% 1.578% 0.982% 0.672% 0.526%
$110,000 600 2.227% 1.295% 0.807% 0.581% 0.487%
$110,000 700 1.974% 1.128% 0.712% 0.533% 0.467%
$110,000 800 1.759% 0.991% 0.640% 0.501% 0.453%
$110,000 900 1.622% 0.904% 0.594% 0.483% 0.446%
$110,000 1,000 1.487% 0.824% 0.554% 0.465% 0.441%
$110,000 1,500 1.048% 0.608% 0.473% 0.442% 0.436%
$110,000 2,000 0.853% 0.528% 0.451% 0.438% 0.435%
$110,000 3,000 0.598% 0.458% 0.439% 0.436% 0.435%
$110,000 4,000 0.516% 0.444% 0.438% 0.436% 0.435%
$110,000 5,000 0.482% 0.440% 0.437% 0.436% 0.435%
$110,000 10,000 0.442% 0.438% 0.437% 0.436% 0.435%
$110,000 20,000 0.353% 0.352% 0.351% 0.350% 0.349%
$110,000 30,000 0.353% 0.352% 0.351% 0.350% 0.349%
$110,000 40,000 0.353% 0.352% 0.351% 0.350% 0.349%
$115,000 25 19.232% 17.175% 15.298% 13.598% 12.070%
$115,000 50 12.417% 10.476% 8.809% 7.380% 6.172%
$115,000 100 7.951% 6.216% 4.823% 3.730% 2.888%
$115,000 150 6.218% 4.627% 3.419% 2.523% 1.868%
$115,000 200 5.066% 3.594% 2.533% 1.790% 1.286%
$115,000 300 3.831% 2.526% 1.662% 1.118% 0.799%
* Applied to total projected claims10

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$115,000 400 2.935% 1.849% 1.190% 0.818% 0.622%
$115,000 500 2.689% 1.622% 1.010% 0.690% 0.536%
$115,000 600 2.280% 1.331% 0.829% 0.594% 0.494%
$115,000 700 2.021% 1.158% 0.729% 0.542% 0.472%
$115,000 800 1.799% 1.016% 0.654% 0.509% 0.457%
$115,000 900 1.662% 0.928% 0.607% 0.489% 0.450%
$115,000 1,000 1.524% 0.845% 0.564% 0.470% 0.444%
$115,000 1,500 1.074% 0.620% 0.479% 0.445% 0.439%
$115,000 2,000 0.873% 0.536% 0.454% 0.440% 0.438%
$115,000 3,000 0.610% 0.462% 0.441% 0.439% 0.438%
$115,000 4,000 0.524% 0.447% 0.440% 0.439% 0.438%
$115,000 5,000 0.487% 0.443% 0.440% 0.439% 0.438%
$115,000 10,000 0.444% 0.441% 0.440% 0.439% 0.438%
$115,000 20,000 0.354% 0.353% 0.352% 0.351% 0.350%
$115,000 30,000 0.354% 0.353% 0.352% 0.351% 0.350%
$115,000 40,000 0.354% 0.353% 0.352% 0.351% 0.350%
$120,000 25 19.578% 17.521% 15.640% 13.930% 12.394%
$120,000 50 12.660% 10.707% 9.025% 7.582% 6.358%
$120,000 100 8.113% 6.362% 4.953% 3.844% 2.985%
$120,000 150 6.341% 4.733% 3.507% 2.596% 1.926%
$120,000 200 5.174% 3.685% 2.607% 1.848% 1.330%
$120,000 300 3.912% 2.590% 1.710% 1.152% 0.822%
$120,000 400 2.997% 1.896% 1.224% 0.841% 0.636%
$120,000 500 2.749% 1.664% 1.039% 0.708% 0.547%
$120,000 600 2.331% 1.366% 0.851% 0.606% 0.501%
$120,000 700 2.066% 1.188% 0.746% 0.551% 0.477%
$120,000 800 1.838% 1.041% 0.668% 0.516% 0.462%
$120,000 900 1.703% 0.952% 0.620% 0.496% 0.453%
$120,000 1,000 1.561% 0.866% 0.575% 0.475% 0.447%
$120,000 1,500 1.100% 0.633% 0.484% 0.448% 0.441%
$120,000 2,000 0.892% 0.544% 0.458% 0.443% 0.440%
$120,000 3,000 0.621% 0.466% 0.444% 0.441% 0.440%
$120,000 4,000 0.531% 0.450% 0.442% 0.441% 0.440%
$120,000 5,000 0.493% 0.445% 0.442% 0.441% 0.440%
$120,000 10,000 0.447% 0.443% 0.442% 0.441% 0.440%
$120,000 20,000 0.356% 0.355% 0.354% 0.353% 0.352%
$120,000 30,000 0.356% 0.355% 0.354% 0.353% 0.352%
$120,000 40,000 0.356% 0.355% 0.354% 0.353% 0.352%
* Applied to total projected claims11

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$125,000 25 19.916% 17.858% 15.974% 14.257% 12.714%
$125,000 50 12.899% 10.934% 9.237% 7.781% 6.541%
$125,000 100 8.271% 6.505% 5.081% 3.957% 3.080%
$125,000 150 6.461% 4.837% 3.594% 2.667% 1.983%
$125,000 200 5.282% 3.776% 2.681% 1.907% 1.375%
$125,000 300 3.993% 2.653% 1.758% 1.187% 0.846%
$125,000 400 3.059% 1.943% 1.257% 0.863% 0.651%
$125,000 500 2.807% 1.706% 1.068% 0.726% 0.558%
$125,000 600 2.381% 1.401% 0.873% 0.619% 0.508%
$125,000 700 2.110% 1.217% 0.763% 0.561% 0.482%
$125,000 800 1.877% 1.065% 0.682% 0.524% 0.466%
$125,000 900 1.742% 0.976% 0.633% 0.502% 0.457%
$125,000 1,000 1.597% 0.887% 0.585% 0.480% 0.450%
$125,000 1,500 1.125% 0.645% 0.490% 0.451% 0.444%
$125,000 2,000 0.912% 0.553% 0.462% 0.445% 0.443%
$125,000 3,000 0.632% 0.470% 0.446% 0.444% 0.442%
$125,000 4,000 0.539% 0.453% 0.445% 0.444% 0.442%
$125,000 5,000 0.498% 0.448% 0.445% 0.443% 0.442%
$125,000 10,000 0.449% 0.446% 0.444% 0.443% 0.442%
$125,000 20,000 0.358% 0.357% 0.356% 0.355% 0.354%
$125,000 30,000 0.358% 0.357% 0.356% 0.355% 0.354%
$125,000 40,000 0.358% 0.357% 0.356% 0.355% 0.354%
$130,000 25 20.232% 18.173% 16.289% 14.568% 13.018%
$130,000 50 13.126% 11.151% 9.440% 7.972% 6.718%
$130,000 100 8.418% 6.638% 5.201% 4.062% 3.171%
$130,000 150 6.574% 4.934% 3.676% 2.735% 2.038%
$130,000 200 5.387% 3.865% 2.753% 1.965% 1.419%
$130,000 300 4.069% 2.714% 1.804% 1.219% 0.868%
$130,000 400 3.118% 1.988% 1.290% 0.885% 0.665%
$130,000 500 2.864% 1.746% 1.095% 0.743% 0.568%
$130,000 600 2.424% 1.430% 0.891% 0.629% 0.514%
$130,000 700 2.151% 1.244% 0.779% 0.570% 0.487%
$130,000 800 1.913% 1.088% 0.695% 0.531% 0.471%
$130,000 900 1.779% 0.999% 0.645% 0.509% 0.461%
$130,000 1,000 1.632% 0.907% 0.595% 0.485% 0.453%
$130,000 1,500 1.149% 0.657% 0.495% 0.454% 0.446%
$130,000 2,000 0.931% 0.561% 0.465% 0.447% 0.445%
$130,000 3,000 0.643% 0.474% 0.449% 0.446% 0.445%
* Applied to total projected claims12

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$130,000 4,000 0.546% 0.455% 0.447% 0.446% 0.445%
$130,000 5,000 0.504% 0.450% 0.447% 0.446% 0.445%
$130,000 10,000 0.452% 0.448% 0.447% 0.446% 0.445%
$130,000 20,000 0.360% 0.359% 0.358% 0.357% 0.356%
$130,000 30,000 0.360% 0.359% 0.358% 0.357% 0.356%
$130,000 40,000 0.360% 0.359% 0.358% 0.357% 0.356%
$135,000 25 20.534% 18.475% 16.590% 14.869% 13.313%
$135,000 50 13.345% 11.359% 9.637% 8.159% 6.891%
$135,000 100 8.559% 6.767% 5.316% 4.163% 3.259%
$135,000 150 6.680% 5.026% 3.754% 2.798% 2.089%
$135,000 200 5.488% 3.951% 2.824% 2.022% 1.463%
$135,000 300 4.142% 2.773% 1.849% 1.252% 0.891%
$135,000 400 3.174% 2.031% 1.321% 0.907% 0.679%
$135,000 500 2.918% 1.786% 1.122% 0.760% 0.578%
$135,000 600 2.469% 1.462% 0.911% 0.640% 0.520%
$135,000 700 2.191% 1.271% 0.795% 0.578% 0.492%
$135,000 800 1.948% 1.111% 0.708% 0.539% 0.475%
$135,000 900 1.815% 1.021% 0.657% 0.515% 0.464%
$135,000 1,000 1.665% 0.926% 0.605% 0.490% 0.456%
$135,000 1,500 1.173% 0.669% 0.500% 0.457% 0.448%
$135,000 2,000 0.950% 0.569% 0.469% 0.450% 0.447%
$135,000 3,000 0.653% 0.478% 0.451% 0.448% 0.446%
$135,000 4,000 0.553% 0.458% 0.449% 0.447% 0.446%
$135,000 5,000 0.509% 0.452% 0.449% 0.447% 0.446%
$135,000 10,000 0.454% 0.449% 0.448% 0.447% 0.446%
$135,000 20,000 0.361% 0.360% 0.359% 0.358% 0.357%
$135,000 30,000 0.361% 0.360% 0.359% 0.358% 0.357%
$135,000 40,000 0.361% 0.360% 0.359% 0.358% 0.357%
$140,000 25 20.833% 18.776% 16.890% 15.168% 13.610%
$140,000 50 13.560% 11.565% 9.832% 8.343% 7.061%
$140,000 100 8.698% 6.894% 5.432% 4.264% 3.347%
$140,000 150 6.783% 5.116% 3.831% 2.861% 2.141%
$140,000 200 5.589% 4.036% 2.894% 2.077% 1.506%
$140,000 300 4.215% 2.831% 1.893% 1.284% 0.914%
$140,000 400 3.228% 2.074% 1.352% 0.928% 0.693%
$140,000 500 2.972% 1.825% 1.149% 0.777% 0.588%
$140,000 600 2.515% 1.493% 0.931% 0.652% 0.527%
$140,000 700 2.230% 1.297% 0.811% 0.587% 0.497%
* Applied to total projected claims13

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$140,000 800 1.984% 1.133% 0.722% 0.546% 0.479%
$140,000 900 1.851% 1.043% 0.670% 0.521% 0.468%
$140,000 1,000 1.697% 0.945% 0.615% 0.494% 0.458%
$140,000 1,500 1.196% 0.681% 0.506% 0.460% 0.450%
$140,000 2,000 0.968% 0.577% 0.472% 0.452% 0.448%
$140,000 3,000 0.664% 0.482% 0.453% 0.449% 0.448%
$140,000 4,000 0.560% 0.461% 0.451% 0.449% 0.448%
$140,000 5,000 0.514% 0.455% 0.450% 0.449% 0.448%
$140,000 10,000 0.456% 0.451% 0.450% 0.449% 0.448%
$140,000 20,000 0.363% 0.362% 0.361% 0.360% 0.359%
$140,000 30,000 0.363% 0.362% 0.361% 0.360% 0.359%
$140,000 40,000 0.363% 0.362% 0.361% 0.360% 0.359%
$145,000 25 21.116% 19.061% 17.176% 15.454% 13.894%
$145,000 50 13.767% 11.764% 10.022% 8.521% 7.228%
$145,000 100 8.834% 7.017% 5.545% 4.362% 3.432%
$145,000 150 6.883% 5.203% 3.906% 2.923% 2.192%
$145,000 200 5.685% 4.118% 2.963% 2.131% 1.548%
$145,000 300 4.285% 2.887% 1.937% 1.317% 0.936%
$145,000 400 3.281% 2.115% 1.382% 0.949% 0.707%
$145,000 500 3.023% 1.863% 1.175% 0.793% 0.598%
$145,000 600 2.558% 1.523% 0.950% 0.663% 0.533%
$145,000 700 2.267% 1.323% 0.826% 0.596% 0.501%
$145,000 800 2.018% 1.155% 0.735% 0.553% 0.484%
$145,000 900 1.886% 1.065% 0.682% 0.528% 0.471%
$145,000 1,000 1.729% 0.964% 0.625% 0.499% 0.461%
$145,000 1,500 1.218% 0.692% 0.511% 0.462% 0.452%
$145,000 2,000 0.986% 0.585% 0.476% 0.454% 0.450%
$145,000 3,000 0.674% 0.485% 0.455% 0.451% 0.450%
$145,000 4,000 0.567% 0.463% 0.453% 0.451% 0.450%
$145,000 5,000 0.519% 0.457% 0.452% 0.451% 0.450%
$145,000 10,000 0.458% 0.453% 0.452% 0.451% 0.450%
$145,000 20,000 0.364% 0.363% 0.362% 0.361% 0.360%
$145,000 30,000 0.364% 0.363% 0.362% 0.361% 0.360%
$145,000 40,000 0.364% 0.363% 0.362% 0.361% 0.360%
$150,000 25 21.375% 19.324% 17.441% 15.720% 14.160%
$150,000 50 13.965% 11.955% 10.203% 8.693% 7.390%
$150,000 100 8.961% 7.134% 5.651% 4.456% 3.514%
$150,000 150 6.978% 5.286% 3.978% 2.984% 2.242%
* Applied to total projected claims14

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$150,000 200 5.777% 4.197% 3.027% 2.182% 1.590%
$150,000 300 4.351% 2.940% 1.978% 1.347% 0.957%
$150,000 400 3.332% 2.154% 1.410% 0.969% 0.720%
$150,000 500 3.072% 1.900% 1.200% 0.808% 0.608%
$150,000 600 2.598% 1.552% 0.968% 0.674% 0.539%
$150,000 700 2.303% 1.347% 0.841% 0.604% 0.506%
$150,000 800 2.051% 1.177% 0.747% 0.560% 0.488%
$150,000 900 1.919% 1.086% 0.694% 0.534% 0.475%
$150,000 1,000 1.759% 0.983% 0.635% 0.504% 0.463%
$150,000 1,500 1.239% 0.703% 0.516% 0.465% 0.454%
$150,000 2,000 1.003% 0.593% 0.479% 0.456% 0.452%
$150,000 3,000 0.684% 0.489% 0.457% 0.453% 0.452%
$150,000 4,000 0.573% 0.466% 0.454% 0.453% 0.452%
$150,000 5,000 0.524% 0.459% 0.454% 0.453% 0.452%
$150,000 10,000 0.460% 0.455% 0.454% 0.453% 0.452%
$150,000 20,000 0.366% 0.365% 0.364% 0.363% 0.362%
$150,000 30,000 0.366% 0.365% 0.364% 0.363% 0.362%
$150,000 40,000 0.366% 0.365% 0.364% 0.363% 0.362%
$155,000 25 21.620% 19.573% 17.692% 15.973% 14.412%
$155,000 50 14.156% 12.139% 10.380% 8.860% 7.547%
$155,000 100 9.085% 7.248% 5.754% 4.547% 3.593%
$155,000 150 7.071% 5.368% 4.050% 3.045% 2.293%
$155,000 200 5.864% 4.272% 3.089% 2.232% 1.630%
$155,000 300 4.415% 2.992% 2.018% 1.377% 0.979%
$155,000 400 3.381% 2.192% 1.438% 0.988% 0.733%
$155,000 500 3.120% 1.936% 1.225% 0.824% 0.617%
$155,000 600 2.638% 1.580% 0.987% 0.685% 0.545%
$155,000 700 2.337% 1.370% 0.856% 0.612% 0.510%
$155,000 800 2.083% 1.197% 0.759% 0.567% 0.492%
$155,000 900 1.951% 1.106% 0.705% 0.540% 0.478%
$155,000 1,000 1.789% 1.001% 0.645% 0.509% 0.466%
$155,000 1,500 1.260% 0.714% 0.521% 0.467% 0.455%
$155,000 2,000 1.020% 0.601% 0.482% 0.458% 0.454%
$155,000 3,000 0.693% 0.492% 0.459% 0.454% 0.453%
$155,000 4,000 0.580% 0.468% 0.456% 0.454% 0.453%
$155,000 5,000 0.529% 0.461% 0.455% 0.454% 0.453%
$155,000 10,000 0.462% 0.456% 0.455% 0.454% 0.453%
$155,000 20,000 0.367% 0.366% 0.365% 0.364% 0.363%
* Applied to total projected claims15

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$155,000 30,000 0.367% 0.366% 0.365% 0.364% 0.363%
$155,000 40,000 0.367% 0.366% 0.365% 0.364% 0.363%
$160,000 25 21.856% 19.810% 17.932% 16.216% 14.655%
$160,000 50 14.343% 12.320% 10.553% 9.024% 7.702%
$160,000 100 9.204% 7.358% 5.853% 4.635% 3.669%
$160,000 150 7.163% 5.449% 4.120% 3.104% 2.341%
$160,000 200 5.948% 4.344% 3.150% 2.280% 1.668%
$160,000 300 4.478% 3.043% 2.058% 1.408% 1.000%
$160,000 400 3.429% 2.229% 1.466% 1.008% 0.746%
$160,000 500 3.168% 1.972% 1.250% 0.840% 0.627%
$160,000 600 2.676% 1.607% 1.005% 0.696% 0.551%
$160,000 700 2.365% 1.388% 0.866% 0.618% 0.514%
$160,000 800 2.115% 1.218% 0.772% 0.574% 0.496%
$160,000 900 1.983% 1.126% 0.717% 0.547% 0.482%
$160,000 1,000 1.817% 1.018% 0.654% 0.514% 0.468%
$160,000 1,500 1.281% 0.725% 0.527% 0.470% 0.457%
$160,000 2,000 1.036% 0.608% 0.486% 0.459% 0.455%
$160,000 3,000 0.702% 0.496% 0.460% 0.456% 0.455%
$160,000 4,000 0.586% 0.470% 0.458% 0.456% 0.455%
$160,000 5,000 0.534% 0.462% 0.457% 0.456% 0.455%
$160,000 10,000 0.464% 0.458% 0.457% 0.456% 0.455%
$160,000 20,000 0.368% 0.367% 0.366% 0.365% 0.364%
$160,000 30,000 0.368% 0.367% 0.366% 0.365% 0.364%
$160,000 40,000 0.368% 0.367% 0.366% 0.365% 0.364%
$165,000 25 22.074% 20.030% 18.156% 16.444% 14.884%
$165,000 50 14.520% 12.493% 10.719% 9.181% 7.850%
$165,000 100 9.319% 7.464% 5.948% 4.722% 3.744%
$165,000 150 7.251% 5.527% 4.189% 3.162% 2.390%
$165,000 200 6.027% 4.414% 3.207% 2.327% 1.706%
$165,000 300 4.537% 3.093% 2.098% 1.437% 1.021%
$165,000 400 3.475% 2.266% 1.492% 1.027% 0.758%
$165,000 500 3.214% 2.006% 1.275% 0.856% 0.636%
$165,000 600 2.713% 1.633% 1.022% 0.706% 0.557%
$165,000 700 2.396% 1.410% 0.880% 0.626% 0.518%
$165,000 800 2.145% 1.238% 0.784% 0.581% 0.499%
$165,000 900 2.013% 1.146% 0.728% 0.553% 0.485%
$165,000 1,000 1.843% 1.035% 0.663% 0.518% 0.471%
$165,000 1,500 1.301% 0.735% 0.531% 0.472% 0.459%
* Applied to total projected claims16

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$165,000 2,000 1.052% 0.615% 0.489% 0.461% 0.456%
$165,000 3,000 0.711% 0.499% 0.462% 0.457% 0.456%
$165,000 4,000 0.593% 0.473% 0.459% 0.457% 0.456%
$165,000 5,000 0.538% 0.464% 0.458% 0.457% 0.456%
$165,000 10,000 0.466% 0.459% 0.458% 0.457% 0.456%
$165,000 20,000 0.369% 0.368% 0.367% 0.366% 0.365%
$165,000 30,000 0.369% 0.368% 0.367% 0.366% 0.365%
$165,000 40,000 0.369% 0.368% 0.367% 0.366% 0.365%
$170,000 25 22.280% 20.239% 18.368% 16.660% 15.101%
$170,000 50 14.691% 12.662% 10.881% 9.335% 7.995%
$170,000 100 9.429% 7.566% 6.041% 4.806% 3.818%
$170,000 150 7.337% 5.604% 4.255% 3.219% 2.438%
$170,000 200 6.104% 4.480% 3.263% 2.371% 1.742%
$170,000 300 4.595% 3.141% 2.136% 1.467% 1.041%
$170,000 400 3.521% 2.301% 1.519% 1.046% 0.771%
$170,000 500 3.258% 2.040% 1.298% 0.872% 0.646%
$170,000 600 2.749% 1.659% 1.039% 0.717% 0.563%
$170,000 700 2.427% 1.431% 0.893% 0.634% 0.523%
$170,000 800 2.175% 1.257% 0.796% 0.588% 0.503%
$170,000 900 2.042% 1.164% 0.739% 0.559% 0.488%
$170,000 1,000 1.869% 1.051% 0.672% 0.522% 0.473%
$170,000 1,500 1.320% 0.746% 0.536% 0.475% 0.460%
$170,000 2,000 1.067% 0.623% 0.492% 0.463% 0.458%
$170,000 3,000 0.720% 0.502% 0.464% 0.459% 0.458%
$170,000 4,000 0.599% 0.475% 0.460% 0.459% 0.458%
$170,000 5,000 0.542% 0.466% 0.460% 0.459% 0.458%
$170,000 10,000 0.468% 0.461% 0.460% 0.459% 0.458%
$170,000 20,000 0.370% 0.369% 0.368% 0.367% 0.366%
$170,000 30,000 0.370% 0.369% 0.368% 0.367% 0.366%
$170,000 40,000 0.370% 0.369% 0.368% 0.367% 0.366%
$175,000 25 22.482% 20.443% 18.574% 16.869% 15.313%
$175,000 50 14.859% 12.828% 11.041% 9.487% 8.139%
$175,000 100 9.538% 7.668% 6.133% 4.889% 3.891%
$175,000 150 7.424% 5.681% 4.323% 3.277% 2.486%
$175,000 200 6.178% 4.545% 3.317% 2.415% 1.777%
$175,000 300 4.652% 3.189% 2.174% 1.496% 1.062%
$175,000 400 3.565% 2.336% 1.545% 1.065% 0.784%
$175,000 500 3.300% 2.072% 1.321% 0.887% 0.655%
* Applied to total projected claims17

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$175,000 600 2.785% 1.685% 1.056% 0.727% 0.569%
$175,000 700 2.458% 1.453% 0.907% 0.642% 0.527%
$175,000 800 2.205% 1.277% 0.807% 0.594% 0.507%
$175,000 900 2.071% 1.183% 0.750% 0.565% 0.492%
$175,000 1,000 1.894% 1.067% 0.680% 0.527% 0.475%
$175,000 1,500 1.340% 0.756% 0.541% 0.477% 0.462%
$175,000 2,000 1.082% 0.630% 0.495% 0.465% 0.459%
$175,000 3,000 0.729% 0.505% 0.465% 0.460% 0.459%
$175,000 4,000 0.605% 0.477% 0.462% 0.460% 0.459%
$175,000 5,000 0.547% 0.467% 0.461% 0.460% 0.459%
$175,000 10,000 0.469% 0.462% 0.461% 0.460% 0.459%
$175,000 20,000 0.371% 0.370% 0.369% 0.368% 0.367%
$175,000 30,000 0.371% 0.370% 0.369% 0.368% 0.367%
$175,000 40,000 0.371% 0.370% 0.369% 0.368% 0.367%
$180,000 25 22.670% 20.633% 18.767% 17.066% 15.513%
$180,000 50 15.019% 12.988% 11.196% 9.635% 8.280%
$180,000 100 9.638% 7.761% 6.219% 4.966% 3.960%
$180,000 150 7.508% 5.756% 4.389% 3.334% 2.534%
$180,000 200 6.248% 4.606% 3.369% 2.457% 1.810%
$180,000 300 4.707% 3.235% 2.211% 1.524% 1.082%
$180,000 400 3.608% 2.370% 1.570% 1.083% 0.796%
$180,000 500 3.342% 2.104% 1.344% 0.902% 0.664%
$180,000 600 2.819% 1.709% 1.072% 0.737% 0.575%
$180,000 700 2.488% 1.474% 0.920% 0.649% 0.531%
$180,000 800 2.233% 1.296% 0.819% 0.601% 0.510%
$180,000 900 2.098% 1.201% 0.760% 0.570% 0.495%
$180,000 1,000 1.918% 1.082% 0.688% 0.531% 0.477%
$180,000 1,500 1.359% 0.766% 0.546% 0.479% 0.463%
$180,000 2,000 1.096% 0.636% 0.498% 0.466% 0.460%
$180,000 3,000 0.737% 0.508% 0.467% 0.461% 0.460%
$180,000 4,000 0.611% 0.479% 0.463% 0.461% 0.460%
$180,000 5,000 0.551% 0.469% 0.462% 0.461% 0.460%
$180,000 10,000 0.471% 0.463% 0.462% 0.461% 0.460%
$180,000 20,000 0.372% 0.371% 0.370% 0.369% 0.368%
$180,000 30,000 0.372% 0.371% 0.370% 0.369% 0.368%
$180,000 40,000 0.372% 0.371% 0.370% 0.369% 0.368%
$185,000 25 22.856% 20.821% 18.957% 17.260% 15.710%
$185,000 50 15.178% 13.146% 11.350% 9.782% 8.420%
* Applied to total projected claims18

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$185,000 100 9.736% 7.853% 6.303% 5.042% 4.027%
$185,000 150 7.591% 5.830% 4.455% 3.390% 2.582%
$185,000 200 6.316% 4.666% 3.419% 2.498% 1.843%
$185,000 300 4.760% 3.281% 2.247% 1.552% 1.102%
$185,000 400 3.651% 2.404% 1.596% 1.101% 0.809%
$185,000 500 3.382% 2.135% 1.366% 0.917% 0.674%
$185,000 600 2.852% 1.733% 1.088% 0.747% 0.580%
$185,000 700 2.517% 1.494% 0.933% 0.657% 0.536%
$185,000 800 2.256% 1.311% 0.827% 0.605% 0.513%
$185,000 900 2.125% 1.219% 0.771% 0.576% 0.498%
$185,000 1,000 1.941% 1.096% 0.697% 0.535% 0.480%
$185,000 1,500 1.377% 0.776% 0.550% 0.481% 0.465%
$185,000 2,000 1.111% 0.643% 0.501% 0.468% 0.462%
$185,000 3,000 0.745% 0.511% 0.468% 0.463% 0.461%
$185,000 4,000 0.616% 0.481% 0.464% 0.462% 0.461%
$185,000 5,000 0.555% 0.471% 0.463% 0.462% 0.461%
$185,000 10,000 0.472% 0.464% 0.463% 0.462% 0.461%
$185,000 20,000 0.373% 0.372% 0.371% 0.370% 0.369%
$185,000 30,000 0.373% 0.372% 0.371% 0.370% 0.369%
$185,000 40,000 0.373% 0.372% 0.371% 0.370% 0.369%
$190,000 25 23.038% 21.005% 19.143% 17.449% 15.901%
$190,000 50 15.332% 13.298% 11.501% 9.926% 8.557%
$190,000 100 9.833% 7.943% 6.386% 5.117% 4.095%
$190,000 150 7.672% 5.902% 4.518% 3.445% 2.628%
$190,000 200 6.383% 4.725% 3.469% 2.539% 1.876%
$190,000 300 4.812% 3.325% 2.282% 1.579% 1.122%
$190,000 400 3.693% 2.437% 1.621% 1.119% 0.821%
$190,000 500 3.423% 2.166% 1.389% 0.932% 0.683%
$190,000 600 2.885% 1.756% 1.104% 0.756% 0.586%
$190,000 700 2.546% 1.515% 0.946% 0.665% 0.540%
$190,000 800 2.284% 1.329% 0.838% 0.611% 0.517%
$190,000 900 2.152% 1.237% 0.781% 0.582% 0.501%
$190,000 1,000 1.965% 1.111% 0.705% 0.540% 0.482%
$190,000 1,500 1.395% 0.786% 0.555% 0.484% 0.466%
$190,000 2,000 1.125% 0.650% 0.504% 0.469% 0.463%
$190,000 3,000 0.754% 0.514% 0.470% 0.464% 0.462%
$190,000 4,000 0.622% 0.483% 0.466% 0.464% 0.462%
$190,000 5,000 0.560% 0.472% 0.465% 0.463% 0.462%
* Applied to total projected claims19

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$190,000 10,000 0.474% 0.466% 0.464% 0.463% 0.462%
$190,000 20,000 0.374% 0.373% 0.372% 0.371% 0.370%
$190,000 30,000 0.374% 0.373% 0.372% 0.371% 0.370%
$190,000 40,000 0.374% 0.373% 0.372% 0.371% 0.370%
$195,000 25 23.210% 21.179% 19.320% 17.629% 16.083%
$195,000 50 15.477% 13.442% 11.644% 10.065% 8.688%
$195,000 100 9.927% 8.031% 6.467% 5.190% 4.160%
$195,000 150 7.750% 5.972% 4.580% 3.499% 2.673%
$195,000 200 6.447% 4.781% 3.517% 2.578% 1.908%
$195,000 300 4.862% 3.368% 2.317% 1.605% 1.142%
$195,000 400 3.734% 2.469% 1.646% 1.137% 0.834%
$195,000 500 3.463% 2.197% 1.411% 0.947% 0.693%
$195,000 600 2.917% 1.780% 1.120% 0.766% 0.592%
$195,000 700 2.574% 1.535% 0.959% 0.672% 0.544%
$195,000 800 2.311% 1.347% 0.849% 0.617% 0.521%
$195,000 900 2.178% 1.254% 0.791% 0.587% 0.504%
$195,000 1,000 1.987% 1.126% 0.713% 0.544% 0.484%
$195,000 1,500 1.413% 0.796% 0.560% 0.486% 0.467%
$195,000 2,000 1.139% 0.656% 0.506% 0.471% 0.464%
$195,000 3,000 0.762% 0.517% 0.471% 0.465% 0.464%
$195,000 4,000 0.627% 0.485% 0.467% 0.465% 0.464%
$195,000 5,000 0.564% 0.473% 0.466% 0.465% 0.464%
$195,000 10,000 0.475% 0.467% 0.466% 0.465% 0.464%
$195,000 20,000 0.375% 0.374% 0.373% 0.372% 0.371%
$195,000 30,000 0.375% 0.374% 0.373% 0.372% 0.371%
$195,000 40,000 0.375% 0.374% 0.373% 0.372% 0.371%
$200,000 25 23.372% 21.343% 19.486% 17.799% 16.255%
$200,000 50 15.619% 13.585% 11.785% 10.203% 8.820%
$200,000 100 10.019% 8.118% 6.547% 5.262% 4.225%
$200,000 150 7.826% 6.040% 4.641% 3.552% 2.718%
$200,000 200 6.510% 4.837% 3.564% 2.617% 1.940%
$200,000 300 4.911% 3.410% 2.351% 1.632% 1.161%
$200,000 400 3.774% 2.501% 1.671% 1.155% 0.846%
$200,000 500 3.501% 2.227% 1.433% 0.962% 0.702%
$200,000 600 2.949% 1.803% 1.136% 0.776% 0.597%
$200,000 700 2.602% 1.555% 0.973% 0.680% 0.548%
$200,000 800 2.337% 1.365% 0.860% 0.624% 0.524%
$200,000 900 2.203% 1.271% 0.801% 0.593% 0.507%
* Applied to total projected claims20

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$200,000 1,000 2.010% 1.140% 0.721% 0.548% 0.486%
$200,000 1,500 1.430% 0.805% 0.564% 0.488% 0.469%
$200,000 2,000 1.152% 0.663% 0.509% 0.472% 0.465%
$200,000 3,000 0.770% 0.520% 0.472% 0.466% 0.465%
$200,000 4,000 0.633% 0.487% 0.468% 0.466% 0.465%
$200,000 5,000 0.568% 0.475% 0.467% 0.466% 0.465%
$200,000 10,000 0.477% 0.468% 0.467% 0.466% 0.465%
$200,000 20,000 0.376% 0.375% 0.374% 0.373% 0.372%
$200,000 30,000 0.376% 0.375% 0.374% 0.373% 0.372%
$200,000 40,000 0.376% 0.375% 0.374% 0.373% 0.372%
$205,000 25 23.530% 21.504% 19.649% 17.964% 16.422%
$205,000 50 15.758% 13.724% 11.923% 10.339% 8.950%
$205,000 100 10.112% 8.205% 6.627% 5.334% 4.290%
$205,000 150 7.902% 6.108% 4.702% 3.604% 2.764%
$205,000 200 6.572% 4.892% 3.612% 2.656% 1.973%
$205,000 300 4.959% 3.451% 2.384% 1.658% 1.181%
$205,000 400 3.813% 2.532% 1.696% 1.172% 0.859%
$205,000 500 3.540% 2.258% 1.455% 0.977% 0.712%
$205,000 600 2.981% 1.826% 1.152% 0.786% 0.603%
$205,000 700 2.631% 1.575% 0.986% 0.688% 0.553%
$205,000 800 2.364% 1.383% 0.871% 0.630% 0.528%
$205,000 900 2.228% 1.287% 0.811% 0.598% 0.510%
$205,000 1,000 2.032% 1.154% 0.729% 0.552% 0.488%
$205,000 1,500 1.448% 0.814% 0.569% 0.490% 0.470%
$205,000 2,000 1.165% 0.669% 0.512% 0.474% 0.466%
$205,000 3,000 0.777% 0.523% 0.474% 0.467% 0.466%
$205,000 4,000 0.638% 0.488% 0.469% 0.467% 0.466%
$205,000 5,000 0.572% 0.476% 0.468% 0.467% 0.466%
$205,000 10,000 0.478% 0.469% 0.468% 0.467% 0.466%
$205,000 20,000 0.377% 0.376% 0.375% 0.374% 0.373%
$205,000 30,000 0.377% 0.376% 0.375% 0.374% 0.373%
$205,000 40,000 0.377% 0.376% 0.375% 0.374% 0.373%
$210,000 25 23.682% 21.657% 19.804% 18.122% 16.581%
$210,000 50 15.894% 13.860% 12.058% 10.472% 9.078%
$210,000 100 10.202% 8.291% 6.706% 5.405% 4.353%
$210,000 150 7.976% 6.176% 4.762% 3.656% 2.808%
$210,000 200 6.634% 4.946% 3.659% 2.694% 2.004%
$210,000 300 5.006% 3.491% 2.417% 1.683% 1.200%
* Applied to total projected claims21

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$210,000 400 3.853% 2.563% 1.720% 1.190% 0.871%
$210,000 500 3.578% 2.288% 1.477% 0.992% 0.722%
$210,000 600 3.012% 1.849% 1.168% 0.796% 0.609%
$210,000 700 2.659% 1.595% 0.999% 0.696% 0.557%
$210,000 800 2.390% 1.401% 0.882% 0.636% 0.532%
$210,000 900 2.247% 1.300% 0.818% 0.602% 0.512%
$210,000 1,000 2.054% 1.168% 0.737% 0.556% 0.490%
$210,000 1,500 1.465% 0.824% 0.573% 0.492% 0.471%
$210,000 2,000 1.179% 0.676% 0.515% 0.475% 0.467%
$210,000 3,000 0.785% 0.526% 0.475% 0.468% 0.467%
$210,000 4,000 0.644% 0.490% 0.470% 0.468% 0.467%
$210,000 5,000 0.577% 0.478% 0.469% 0.468% 0.467%
$210,000 10,000 0.479% 0.470% 0.469% 0.468% 0.467%
$210,000 20,000 0.378% 0.376% 0.375% 0.374% 0.373%
$210,000 30,000 0.377% 0.376% 0.375% 0.374% 0.373%
$210,000 40,000 0.377% 0.376% 0.375% 0.374% 0.373%
$215,000 25 23.829% 21.805% 19.953% 18.274% 16.735%
$215,000 50 16.024% 13.990% 12.187% 10.601% 9.204%
$215,000 100 10.287% 8.372% 6.780% 5.473% 4.414%
$215,000 150 8.048% 6.241% 4.820% 3.707% 2.852%
$215,000 200 6.692% 4.998% 3.703% 2.731% 2.034%
$215,000 300 5.051% 3.529% 2.449% 1.708% 1.219%
$215,000 400 3.890% 2.593% 1.743% 1.207% 0.883%
$215,000 500 3.615% 2.317% 1.498% 1.007% 0.732%
$215,000 600 3.042% 1.872% 1.183% 0.805% 0.615%
$215,000 700 2.686% 1.615% 1.012% 0.703% 0.562%
$215,000 800 2.415% 1.419% 0.892% 0.642% 0.536%
$215,000 900 2.271% 1.316% 0.828% 0.607% 0.515%
$215,000 1,000 2.075% 1.182% 0.745% 0.560% 0.492%
$215,000 1,500 1.481% 0.833% 0.578% 0.495% 0.472%
$215,000 2,000 1.191% 0.682% 0.518% 0.476% 0.468%
$215,000 3,000 0.793% 0.529% 0.476% 0.469% 0.467%
$215,000 4,000 0.649% 0.492% 0.471% 0.469% 0.467%
$215,000 5,000 0.581% 0.479% 0.470% 0.468% 0.467%
$215,000 10,000 0.481% 0.471% 0.469% 0.468% 0.467%
$215,000 20,000 0.378% 0.377% 0.376% 0.375% 0.374%
$215,000 30,000 0.378% 0.377% 0.376% 0.375% 0.374%
$215,000 40,000 0.378% 0.377% 0.376% 0.375% 0.374%
* Applied to total projected claims22

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$220,000 25 23.967% 21.945% 20.096% 18.419% 16.882%
$220,000 50 16.147% 14.113% 12.311% 10.723% 9.324%
$220,000 100 10.367% 8.449% 6.852% 5.538% 4.472%
$220,000 150 8.117% 6.303% 4.875% 3.755% 2.893%
$220,000 200 6.747% 5.048% 3.745% 2.766% 2.063%
$220,000 300 5.094% 3.567% 2.480% 1.732% 1.237%
$220,000 400 3.927% 2.622% 1.765% 1.223% 0.894%
$220,000 500 3.650% 2.344% 1.518% 1.021% 0.741%
$220,000 600 3.071% 1.893% 1.198% 0.815% 0.621%
$220,000 700 2.712% 1.634% 1.024% 0.711% 0.566%
$220,000 800 2.440% 1.436% 0.903% 0.648% 0.539%
$220,000 900 2.293% 1.331% 0.837% 0.612% 0.518%
$220,000 1,000 2.095% 1.195% 0.752% 0.564% 0.494%
$220,000 1,500 1.497% 0.842% 0.582% 0.497% 0.474%
$220,000 2,000 1.204% 0.688% 0.520% 0.478% 0.469%
$220,000 3,000 0.800% 0.531% 0.477% 0.470% 0.468%
$220,000 4,000 0.654% 0.494% 0.472% 0.469% 0.468%
$220,000 5,000 0.585% 0.480% 0.471% 0.469% 0.468%
$220,000 10,000 0.482% 0.471% 0.470% 0.469% 0.468%
$220,000 20,000 0.379% 0.378% 0.377% 0.376% 0.375%
$220,000 30,000 0.379% 0.378% 0.377% 0.376% 0.375%
$220,000 40,000 0.379% 0.378% 0.377% 0.376% 0.375%
$225,000 25 24.102% 22.083% 20.235% 18.561% 17.025%
$225,000 50 16.268% 14.235% 12.434% 10.846% 9.444%
$225,000 100 10.444% 8.523% 6.920% 5.601% 4.528%
$225,000 150 8.183% 6.363% 4.928% 3.803% 2.933%
$225,000 200 6.800% 5.095% 3.786% 2.800% 2.091%
$225,000 300 5.136% 3.603% 2.510% 1.756% 1.255%
$225,000 400 3.962% 2.650% 1.787% 1.239% 0.906%
$225,000 500 3.685% 2.371% 1.538% 1.035% 0.750%
$225,000 600 3.098% 1.913% 1.212% 0.823% 0.626%
$225,000 700 2.737% 1.652% 1.037% 0.719% 0.570%
$225,000 800 2.463% 1.452% 0.913% 0.654% 0.543%
$225,000 900 2.315% 1.346% 0.846% 0.617% 0.520%
$225,000 1,000 2.114% 1.207% 0.760% 0.568% 0.496%
$225,000 1,500 1.512% 0.850% 0.586% 0.499% 0.475%
$225,000 2,000 1.215% 0.694% 0.523% 0.479% 0.470%
$225,000 3,000 0.807% 0.534% 0.479% 0.471% 0.469%
* Applied to total projected claims23

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$225,000 4,000 0.659% 0.495% 0.473% 0.470% 0.469%
$225,000 5,000 0.589% 0.482% 0.471% 0.470% 0.469%
$225,000 10,000 0.483% 0.472% 0.471% 0.470% 0.469%
$225,000 20,000 0.380% 0.378% 0.377% 0.376% 0.375%
$225,000 30,000 0.379% 0.378% 0.377% 0.376% 0.375%
$225,000 40,000 0.379% 0.378% 0.377% 0.376% 0.375%
$230,000 25 24.233% 22.215% 20.369% 18.697% 17.163%
$230,000 50 16.384% 14.352% 12.551% 10.963% 9.560%
$230,000 100 10.521% 8.597% 6.989% 5.664% 4.584%
$230,000 150 8.247% 6.421% 4.980% 3.849% 2.972%
$230,000 200 6.852% 5.141% 3.824% 2.832% 2.118%
$230,000 300 5.177% 3.638% 2.539% 1.779% 1.273%
$230,000 400 3.995% 2.677% 1.808% 1.255% 0.917%
$230,000 500 3.718% 2.397% 1.556% 1.048% 0.759%
$230,000 600 3.125% 1.933% 1.225% 0.832% 0.631%
$230,000 700 2.762% 1.670% 1.049% 0.726% 0.574%
$230,000 800 2.486% 1.468% 0.924% 0.660% 0.546%
$230,000 900 2.336% 1.360% 0.855% 0.622% 0.523%
$230,000 1,000 2.133% 1.220% 0.767% 0.572% 0.498%
$230,000 1,500 1.527% 0.859% 0.590% 0.501% 0.476%
$230,000 2,000 1.226% 0.699% 0.525% 0.480% 0.471%
$230,000 3,000 0.814% 0.536% 0.480% 0.471% 0.470%
$230,000 4,000 0.664% 0.497% 0.474% 0.471% 0.470%
$230,000 5,000 0.592% 0.483% 0.472% 0.471% 0.470%
$230,000 10,000 0.484% 0.473% 0.472% 0.471% 0.470%
$230,000 20,000 0.380% 0.379% 0.378% 0.377% 0.376%
$230,000 30,000 0.380% 0.379% 0.378% 0.377% 0.376%
$230,000 40,000 0.380% 0.379% 0.378% 0.377% 0.376%
$235,000 25 24.359% 22.342% 20.498% 18.827% 17.294%
$235,000 50 16.496% 14.465% 12.665% 11.076% 9.672%
$235,000 100 10.597% 8.670% 7.057% 5.727% 4.640%
$235,000 150 8.310% 6.479% 5.031% 3.894% 3.011%
$235,000 200 6.903% 5.186% 3.863% 2.865% 2.144%
$235,000 300 5.218% 3.673% 2.567% 1.801% 1.290%
$235,000 400 4.027% 2.704% 1.829% 1.270% 0.928%
$235,000 500 3.750% 2.422% 1.575% 1.061% 0.767%
$235,000 600 3.151% 1.952% 1.239% 0.841% 0.637%
$235,000 700 2.786% 1.688% 1.061% 0.734% 0.578%
* Applied to total projected claims24

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$235,000 800 2.508% 1.484% 0.934% 0.666% 0.549%
$235,000 900 2.356% 1.374% 0.864% 0.627% 0.526%
$235,000 1,000 2.151% 1.232% 0.774% 0.576% 0.500%
$235,000 1,500 1.542% 0.867% 0.594% 0.503% 0.477%
$235,000 2,000 1.237% 0.705% 0.528% 0.481% 0.472%
$235,000 3,000 0.821% 0.539% 0.481% 0.472% 0.471%
$235,000 4,000 0.668% 0.499% 0.475% 0.472% 0.471%
$235,000 5,000 0.596% 0.484% 0.473% 0.472% 0.471%
$235,000 10,000 0.485% 0.474% 0.473% 0.472% 0.471%
$235,000 20,000 0.381% 0.380% 0.379% 0.378% 0.377%
$235,000 30,000 0.381% 0.380% 0.379% 0.378% 0.377%
$235,000 40,000 0.381% 0.380% 0.379% 0.378% 0.377%
$240,000 25 24.480% 22.464% 20.622% 18.952% 17.420%
$240,000 50 16.606% 14.576% 12.777% 11.188% 9.783%
$240,000 100 10.672% 8.742% 7.125% 5.789% 4.696%
$240,000 150 8.372% 6.537% 5.083% 3.939% 3.049%
$240,000 200 6.955% 5.232% 3.901% 2.898% 2.170%
$240,000 300 5.259% 3.708% 2.596% 1.824% 1.308%
$240,000 400 4.060% 2.730% 1.850% 1.285% 0.938%
$240,000 500 3.781% 2.447% 1.593% 1.074% 0.776%
$240,000 600 3.177% 1.971% 1.252% 0.850% 0.642%
$240,000 700 2.809% 1.705% 1.072% 0.741% 0.582%
$240,000 800 2.530% 1.500% 0.944% 0.672% 0.553%
$240,000 900 2.376% 1.388% 0.873% 0.632% 0.529%
$240,000 1,000 2.169% 1.244% 0.781% 0.580% 0.502%
$240,000 1,500 1.556% 0.875% 0.598% 0.505% 0.478%
$240,000 2,000 1.248% 0.710% 0.530% 0.482% 0.472%
$240,000 3,000 0.827% 0.541% 0.482% 0.473% 0.471%
$240,000 4,000 0.673% 0.500% 0.476% 0.473% 0.471%
$240,000 5,000 0.600% 0.486% 0.474% 0.472% 0.471%
$240,000 10,000 0.487% 0.475% 0.473% 0.472% 0.471%
$240,000 20,000 0.382% 0.380% 0.379% 0.378% 0.377%
$240,000 30,000 0.381% 0.380% 0.379% 0.378% 0.377%
$240,000 40,000 0.381% 0.380% 0.379% 0.378% 0.377%
$245,000 25 24.596% 22.581% 20.739% 19.070% 17.540%
$245,000 50 16.712% 14.683% 12.885% 11.295% 9.889%
$245,000 100 10.745% 8.813% 7.191% 5.850% 4.750%
$245,000 150 8.433% 6.594% 5.133% 3.984% 3.088%
* Applied to total projected claims25

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$245,000 200 7.005% 5.276% 3.939% 2.929% 2.196%
$245,000 300 5.299% 3.742% 2.624% 1.846% 1.325%
$245,000 400 4.091% 2.755% 1.870% 1.300% 0.949%
$245,000 500 3.812% 2.471% 1.611% 1.087% 0.785%
$245,000 600 3.203% 1.990% 1.265% 0.858% 0.647%
$245,000 700 2.832% 1.721% 1.083% 0.748% 0.586%
$245,000 800 2.551% 1.515% 0.953% 0.678% 0.556%
$245,000 900 2.396% 1.402% 0.881% 0.637% 0.532%
$245,000 1,000 2.187% 1.255% 0.788% 0.583% 0.504%
$245,000 1,500 1.570% 0.883% 0.602% 0.507% 0.479%
$245,000 2,000 1.259% 0.716% 0.533% 0.484% 0.473%
$245,000 3,000 0.833% 0.544% 0.483% 0.474% 0.472%
$245,000 4,000 0.678% 0.502% 0.476% 0.473% 0.472%
$245,000 5,000 0.604% 0.487% 0.475% 0.473% 0.472%
$245,000 10,000 0.488% 0.475% 0.474% 0.473% 0.472%
$245,000 20,000 0.382% 0.381% 0.380% 0.379% 0.378%
$245,000 30,000 0.382% 0.381% 0.380% 0.379% 0.378%
$245,000 40,000 0.382% 0.381% 0.380% 0.379% 0.378%
$250,000 25 24.702% 22.689% 20.849% 19.181% 17.652%
$250,000 50 16.807% 14.780% 12.983% 11.394% 9.988%
$250,000 100 10.815% 8.881% 7.254% 5.909% 4.803%
$250,000 150 8.491% 6.648% 5.181% 4.027% 3.125%
$250,000 200 7.052% 5.318% 3.976% 2.960% 2.221%
$250,000 300 5.337% 3.775% 2.651% 1.868% 1.342%
$250,000 400 4.121% 2.780% 1.889% 1.315% 0.959%
$250,000 500 3.841% 2.494% 1.628% 1.099% 0.793%
$250,000 600 3.226% 2.008% 1.277% 0.867% 0.652%
$250,000 700 2.853% 1.737% 1.094% 0.755% 0.590%
$250,000 800 2.571% 1.529% 0.963% 0.683% 0.559%
$250,000 900 2.415% 1.415% 0.890% 0.642% 0.534%
$250,000 1,000 2.204% 1.266% 0.795% 0.587% 0.506%
$250,000 1,500 1.584% 0.891% 0.606% 0.509% 0.480%
$250,000 2,000 1.269% 0.721% 0.535% 0.485% 0.474%
$250,000 3,000 0.839% 0.546% 0.484% 0.475% 0.473%
$250,000 4,000 0.682% 0.503% 0.477% 0.474% 0.473%
$250,000 5,000 0.608% 0.488% 0.475% 0.474% 0.473%
$250,000 10,000 0.489% 0.476% 0.475% 0.474% 0.473%
$250,000 20,000 0.383% 0.382% 0.381% 0.380% 0.379%
* Applied to total projected claims26

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$250,000 30,000 0.383% 0.382% 0.381% 0.380% 0.379%
$250,000 40,000 0.383% 0.382% 0.381% 0.380% 0.379%
$255,000 25 24.802% 22.790% 20.952% 19.285% 17.757%
$255,000 50 16.896% 14.872% 13.077% 11.488% 10.082%
$255,000 100 10.883% 8.946% 7.317% 5.966% 4.855%
$255,000 150 8.547% 6.700% 5.228% 4.069% 3.161%
$255,000 200 7.097% 5.360% 4.011% 2.990% 2.246%
$255,000 300 5.374% 3.807% 2.677% 1.889% 1.358%
$255,000 400 4.150% 2.804% 1.908% 1.329% 0.969%
$255,000 500 3.868% 2.516% 1.645% 1.111% 0.800%
$255,000 600 3.249% 2.025% 1.289% 0.874% 0.657%
$255,000 700 2.873% 1.752% 1.104% 0.761% 0.594%
$255,000 800 2.591% 1.543% 0.972% 0.688% 0.562%
$255,000 900 2.433% 1.427% 0.897% 0.646% 0.537%
$255,000 1,000 2.220% 1.277% 0.801% 0.590% 0.507%
$255,000 1,500 1.597% 0.899% 0.610% 0.511% 0.481%
$255,000 2,000 1.278% 0.726% 0.537% 0.486% 0.475%
$255,000 3,000 0.845% 0.548% 0.485% 0.475% 0.474%
$255,000 4,000 0.686% 0.505% 0.478% 0.475% 0.473%
$255,000 5,000 0.611% 0.489% 0.476% 0.474% 0.473%
$255,000 10,000 0.490% 0.477% 0.475% 0.474% 0.473%
$255,000 20,000 0.383% 0.382% 0.381% 0.380% 0.379%
$255,000 30,000 0.383% 0.382% 0.381% 0.380% 0.379%
$255,000 40,000 0.383% 0.382% 0.381% 0.380% 0.379%
$260,000 25 24.901% 22.891% 21.054% 19.388% 17.862%
$260,000 50 16.985% 14.962% 13.169% 11.581% 10.176%
$260,000 100 10.950% 9.012% 7.379% 6.024% 4.908%
$260,000 150 8.603% 6.753% 5.275% 4.111% 3.198%
$260,000 200 7.143% 5.401% 4.048% 3.021% 2.272%
$260,000 300 5.411% 3.839% 2.704% 1.910% 1.374%
$260,000 400 4.179% 2.828% 1.927% 1.343% 0.979%
$260,000 500 3.896% 2.538% 1.661% 1.122% 0.808%
$260,000 600 3.272% 2.042% 1.301% 0.882% 0.662%
$260,000 700 2.893% 1.766% 1.114% 0.767% 0.597%
$260,000 800 2.610% 1.557% 0.981% 0.694% 0.565%
$260,000 900 2.450% 1.440% 0.905% 0.651% 0.539%
$260,000 1,000 2.237% 1.288% 0.808% 0.594% 0.509%
$260,000 1,500 1.610% 0.906% 0.614% 0.512% 0.482%
* Applied to total projected claims27

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$260,000 2,000 1.287% 0.731% 0.539% 0.487% 0.475%
$260,000 3,000 0.850% 0.550% 0.486% 0.476% 0.474%
$260,000 4,000 0.691% 0.506% 0.479% 0.475% 0.474%
$260,000 5,000 0.614% 0.490% 0.477% 0.475% 0.474%
$260,000 10,000 0.491% 0.477% 0.476% 0.475% 0.474%
$260,000 20,000 0.384% 0.382% 0.381% 0.380% 0.379%
$260,000 30,000 0.383% 0.382% 0.381% 0.380% 0.379%
$260,000 40,000 0.383% 0.382% 0.381% 0.380% 0.379%
$265,000 25 24.999% 22.990% 21.155% 19.491% 17.965%
$265,000 50 17.072% 15.051% 13.261% 11.673% 10.268%
$265,000 100 11.016% 9.077% 7.441% 6.083% 4.961%
$265,000 150 8.657% 6.804% 5.321% 4.152% 3.234%
$265,000 200 7.189% 5.442% 4.084% 3.052% 2.297%
$265,000 300 5.448% 3.870% 2.730% 1.932% 1.391%
$265,000 400 4.208% 2.851% 1.946% 1.357% 0.989%
$265,000 500 3.923% 2.560% 1.678% 1.134% 0.816%
$265,000 600 3.294% 2.059% 1.313% 0.890% 0.666%
$265,000 700 2.913% 1.782% 1.125% 0.774% 0.601%
$265,000 800 2.630% 1.572% 0.990% 0.699% 0.568%
$265,000 900 2.468% 1.452% 0.913% 0.655% 0.542%
$265,000 1,000 2.253% 1.299% 0.815% 0.597% 0.511%
$265,000 1,500 1.623% 0.914% 0.618% 0.514% 0.483%
$265,000 2,000 1.297% 0.735% 0.541% 0.488% 0.476%
$265,000 3,000 0.856% 0.553% 0.487% 0.477% 0.475%
$265,000 4,000 0.695% 0.508% 0.479% 0.476% 0.475%
$265,000 5,000 0.618% 0.491% 0.477% 0.476% 0.475%
$265,000 10,000 0.492% 0.478% 0.477% 0.476% 0.475%
$265,000 20,000 0.384% 0.383% 0.382% 0.381% 0.380%
$265,000 30,000 0.384% 0.383% 0.382% 0.381% 0.380%
$265,000 40,000 0.384% 0.383% 0.382% 0.381% 0.380%
$270,000 25 25.098% 23.090% 21.256% 19.593% 18.069%
$270,000 50 17.158% 15.140% 13.351% 11.765% 10.360%
$270,000 100 11.084% 9.143% 7.504% 6.142% 5.015%
$270,000 150 8.713% 6.857% 5.369% 4.194% 3.271%
$270,000 200 7.236% 5.484% 4.122% 3.084% 2.324%
$270,000 300 5.485% 3.902% 2.757% 1.953% 1.408%
$270,000 400 4.237% 2.875% 1.965% 1.371% 0.999%
$270,000 500 3.951% 2.582% 1.695% 1.146% 0.824%
* Applied to total projected claims28

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$270,000 600 3.316% 2.076% 1.325% 0.898% 0.671%
$270,000 700 2.933% 1.797% 1.135% 0.780% 0.605%
$270,000 800 2.651% 1.586% 0.999% 0.705% 0.571%
$270,000 900 2.486% 1.465% 0.921% 0.660% 0.544%
$270,000 1,000 2.265% 1.306% 0.819% 0.599% 0.512%
$270,000 1,500 1.637% 0.922% 0.622% 0.516% 0.484%
$270,000 2,000 1.307% 0.740% 0.543% 0.489% 0.477%
$270,000 3,000 0.862% 0.555% 0.488% 0.477% 0.475%
$270,000 4,000 0.699% 0.509% 0.480% 0.476% 0.475%
$270,000 5,000 0.621% 0.492% 0.478% 0.476% 0.475%
$270,000 10,000 0.493% 0.478% 0.477% 0.476% 0.475%
$270,000 20,000 0.385% 0.383% 0.382% 0.381% 0.380%
$270,000 30,000 0.384% 0.383% 0.382% 0.381% 0.380%
$270,000 40,000 0.384% 0.383% 0.382% 0.381% 0.380%
$275,000 25 25.193% 23.186% 21.354% 19.692% 18.168%
$275,000 50 17.243% 15.227% 13.440% 11.856% 10.451%
$275,000 100 11.149% 9.206% 7.565% 6.199% 5.066%
$275,000 150 8.768% 6.909% 5.415% 4.236% 3.309%
$275,000 200 7.282% 5.526% 4.158% 3.115% 2.350%
$275,000 300 5.521% 3.934% 2.784% 1.975% 1.425%
$275,000 400 4.266% 2.899% 1.984% 1.386% 1.010%
$275,000 500 3.979% 2.604% 1.711% 1.158% 0.832%
$275,000 600 3.339% 2.093% 1.337% 0.906% 0.676%
$275,000 700 2.953% 1.811% 1.145% 0.787% 0.609%
$275,000 800 2.670% 1.601% 1.009% 0.710% 0.574%
$275,000 900 2.503% 1.477% 0.929% 0.664% 0.547%
$275,000 1,000 2.282% 1.317% 0.825% 0.602% 0.513%
$275,000 1,500 1.650% 0.930% 0.626% 0.518% 0.485%
$275,000 2,000 1.316% 0.745% 0.546% 0.490% 0.477%
$275,000 3,000 0.868% 0.557% 0.489% 0.478% 0.476%
$275,000 4,000 0.704% 0.511% 0.481% 0.477% 0.476%
$275,000 5,000 0.625% 0.493% 0.479% 0.477% 0.476%
$275,000 10,000 0.494% 0.479% 0.478% 0.477% 0.476%
$275,000 20,000 0.385% 0.384% 0.383% 0.382% 0.381%
$275,000 30,000 0.385% 0.384% 0.383% 0.382% 0.381%
$275,000 40,000 0.385% 0.384% 0.383% 0.382% 0.381%
$280,000 25 25.285% 23.279% 21.447% 19.787% 18.264%
$280,000 50 17.327% 15.313% 13.528% 11.946% 10.541%
* Applied to total projected claims29

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$280,000 100 11.212% 9.268% 7.624% 6.254% 5.117%
$280,000 150 8.822% 6.959% 5.461% 4.277% 3.345%
$280,000 200 7.327% 5.566% 4.195% 3.147% 2.376%
$280,000 300 5.556% 3.965% 2.810% 1.996% 1.441%
$280,000 400 4.294% 2.923% 2.002% 1.400% 1.020%
$280,000 500 4.006% 2.626% 1.727% 1.170% 0.840%
$280,000 600 3.361% 2.110% 1.349% 0.914% 0.681%
$280,000 700 2.972% 1.826% 1.155% 0.793% 0.612%
$280,000 800 2.690% 1.615% 1.018% 0.716% 0.577%
$280,000 900 2.520% 1.489% 0.937% 0.669% 0.549%
$280,000 1,000 2.299% 1.328% 0.832% 0.606% 0.515%
$280,000 1,500 1.663% 0.937% 0.630% 0.520% 0.486%
$280,000 2,000 1.325% 0.750% 0.548% 0.491% 0.478%
$280,000 3,000 0.874% 0.560% 0.490% 0.478% 0.477%
$280,000 4,000 0.708% 0.512% 0.481% 0.478% 0.476%
$280,000 5,000 0.628% 0.494% 0.479% 0.477% 0.476%
$280,000 10,000 0.495% 0.480% 0.478% 0.477% 0.476%
$280,000 20,000 0.386% 0.384% 0.383% 0.382% 0.381%
$280,000 30,000 0.385% 0.384% 0.383% 0.382% 0.381%
$280,000 40,000 0.385% 0.384% 0.383% 0.382% 0.381%
$285,000 25 25.375% 23.370% 21.540% 19.880% 18.358%
$285,000 50 17.410% 15.397% 13.615% 12.033% 10.629%
$285,000 100 11.275% 9.330% 7.683% 6.310% 5.168%
$285,000 150 8.875% 7.010% 5.507% 4.318% 3.382%
$285,000 200 7.372% 5.606% 4.230% 3.177% 2.402%
$285,000 300 5.591% 3.996% 2.835% 2.016% 1.457%
$285,000 400 4.323% 2.947% 2.021% 1.414% 1.030%
$285,000 500 4.033% 2.648% 1.744% 1.181% 0.848%
$285,000 600 3.383% 2.126% 1.360% 0.922% 0.686%
$285,000 700 2.991% 1.840% 1.165% 0.800% 0.616%
$285,000 800 2.709% 1.629% 1.027% 0.721% 0.581%
$285,000 900 2.537% 1.501% 0.945% 0.673% 0.552%
$285,000 1,000 2.315% 1.339% 0.839% 0.609% 0.517%
$285,000 1,500 1.676% 0.945% 0.634% 0.522% 0.487%
$285,000 2,000 1.335% 0.755% 0.550% 0.492% 0.479%
$285,000 3,000 0.879% 0.562% 0.491% 0.479% 0.477%
$285,000 4,000 0.712% 0.514% 0.482% 0.478% 0.477%
$285,000 5,000 0.631% 0.495% 0.480% 0.478% 0.477%
* Applied to total projected claims30

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$285,000 10,000 0.496% 0.480% 0.479% 0.478% 0.477%
$285,000 20,000 0.386% 0.385% 0.384% 0.383% 0.382%
$285,000 30,000 0.386% 0.385% 0.384% 0.383% 0.382%
$285,000 40,000 0.386% 0.385% 0.384% 0.383% 0.382%
$290,000 25 25.459% 23.455% 21.626% 19.967% 18.446%
$290,000 50 17.488% 15.477% 13.696% 12.117% 10.713%
$290,000 100 11.336% 9.389% 7.740% 6.365% 5.219%
$290,000 150 8.927% 7.059% 5.552% 4.358% 3.418%
$290,000 200 7.414% 5.645% 4.265% 3.207% 2.427%
$290,000 300 5.625% 4.025% 2.860% 2.037% 1.473%
$290,000 400 4.351% 2.970% 2.039% 1.428% 1.040%
$290,000 500 4.060% 2.669% 1.760% 1.193% 0.856%
$290,000 600 3.404% 2.142% 1.371% 0.929% 0.691%
$290,000 700 3.010% 1.854% 1.175% 0.806% 0.620%
$290,000 800 2.728% 1.642% 1.035% 0.726% 0.583%
$290,000 900 2.553% 1.513% 0.952% 0.678% 0.554%
$290,000 1,000 2.331% 1.350% 0.845% 0.613% 0.519%
$290,000 1,500 1.688% 0.952% 0.638% 0.524% 0.488%
$290,000 2,000 1.344% 0.760% 0.552% 0.493% 0.479%
$290,000 3,000 0.885% 0.564% 0.492% 0.480% 0.478%
$290,000 4,000 0.717% 0.515% 0.483% 0.479% 0.478%
$290,000 5,000 0.635% 0.496% 0.480% 0.479% 0.478%
$290,000 10,000 0.496% 0.481% 0.480% 0.479% 0.478%
$290,000 20,000 0.387% 0.385% 0.384% 0.383% 0.382%
$290,000 30,000 0.386% 0.385% 0.384% 0.383% 0.382%
$290,000 40,000 0.386% 0.385% 0.384% 0.383% 0.382%
$295,000 25 25.539% 23.536% 21.709% 20.051% 18.532%
$295,000 50 17.560% 15.551% 13.772% 12.195% 10.792%
$295,000 100 11.395% 9.446% 7.796% 6.418% 5.269%
$295,000 150 8.975% 7.105% 5.595% 4.396% 3.453%
$295,000 200 7.456% 5.682% 4.298% 3.236% 2.452%
$295,000 300 5.657% 4.053% 2.884% 2.056% 1.489%
$295,000 400 4.378% 2.993% 2.057% 1.442% 1.050%
$295,000 500 4.085% 2.690% 1.775% 1.204% 0.863%
$295,000 600 3.424% 2.158% 1.382% 0.937% 0.696%
$295,000 700 3.028% 1.867% 1.184% 0.812% 0.624%
$295,000 800 2.745% 1.655% 1.044% 0.731% 0.586%
$295,000 900 2.570% 1.525% 0.959% 0.682% 0.557%
* Applied to total projected claims31

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$295,000 1,000 2.346% 1.360% 0.851% 0.616% 0.521%
$295,000 1,500 1.700% 0.959% 0.642% 0.526% 0.489%
$295,000 2,000 1.352% 0.764% 0.555% 0.494% 0.480%
$295,000 3,000 0.890% 0.566% 0.493% 0.480% 0.478%
$295,000 4,000 0.721% 0.516% 0.483% 0.479% 0.478%
$295,000 5,000 0.638% 0.497% 0.481% 0.479% 0.478%
$295,000 10,000 0.497% 0.481% 0.480% 0.479% 0.478%
$295,000 20,000 0.387% 0.386% 0.385% 0.384% 0.383%
$295,000 30,000 0.387% 0.386% 0.385% 0.384% 0.383%
$295,000 40,000 0.387% 0.386% 0.385% 0.384% 0.383%
$300,000 25 25.615% 23.613% 21.787% 20.130% 18.612%
$300,000 50 17.631% 15.624% 13.847% 12.271% 10.870%
$300,000 100 11.454% 9.504% 7.852% 6.472% 5.319%
$300,000 150 9.023% 7.151% 5.637% 4.434% 3.486%
$300,000 200 7.497% 5.720% 4.331% 3.265% 2.476%
$300,000 300 5.688% 4.081% 2.907% 2.075% 1.504%
$300,000 400 4.405% 3.015% 2.075% 1.456% 1.060%
$300,000 500 4.110% 2.710% 1.790% 1.215% 0.871%
$300,000 600 3.444% 2.173% 1.393% 0.944% 0.700%
$300,000 700 3.045% 1.880% 1.193% 0.818% 0.627%
$300,000 800 2.763% 1.668% 1.052% 0.736% 0.589%
$300,000 900 2.586% 1.536% 0.967% 0.686% 0.559%
$300,000 1,000 2.361% 1.370% 0.857% 0.619% 0.522%
$300,000 1,500 1.711% 0.966% 0.645% 0.527% 0.489%
$300,000 2,000 1.361% 0.769% 0.557% 0.495% 0.480%
$300,000 3,000 0.896% 0.568% 0.493% 0.481% 0.479%
$300,000 4,000 0.725% 0.518% 0.484% 0.480% 0.478%
$300,000 5,000 0.641% 0.498% 0.481% 0.479% 0.478%
$300,000 10,000 0.498% 0.482% 0.480% 0.479% 0.478%
$300,000 20,000 0.387% 0.386% 0.385% 0.384% 0.383%
$300,000 30,000 0.387% 0.386% 0.385% 0.384% 0.383%
$300,000 40,000 0.387% 0.386% 0.385% 0.384% 0.383%
$305,000 25 25.687% 23.687% 21.862% 20.206% 18.688%
$305,000 50 17.700% 15.695% 13.920% 12.346% 10.946%
$305,000 100 11.511% 9.559% 7.907% 6.523% 5.367%
$305,000 150 9.071% 7.195% 5.678% 4.470% 3.519%
$305,000 200 7.538% 5.757% 4.364% 3.294% 2.501%
$305,000 300 5.719% 4.108% 2.930% 2.094% 1.519%
* Applied to total projected claims32
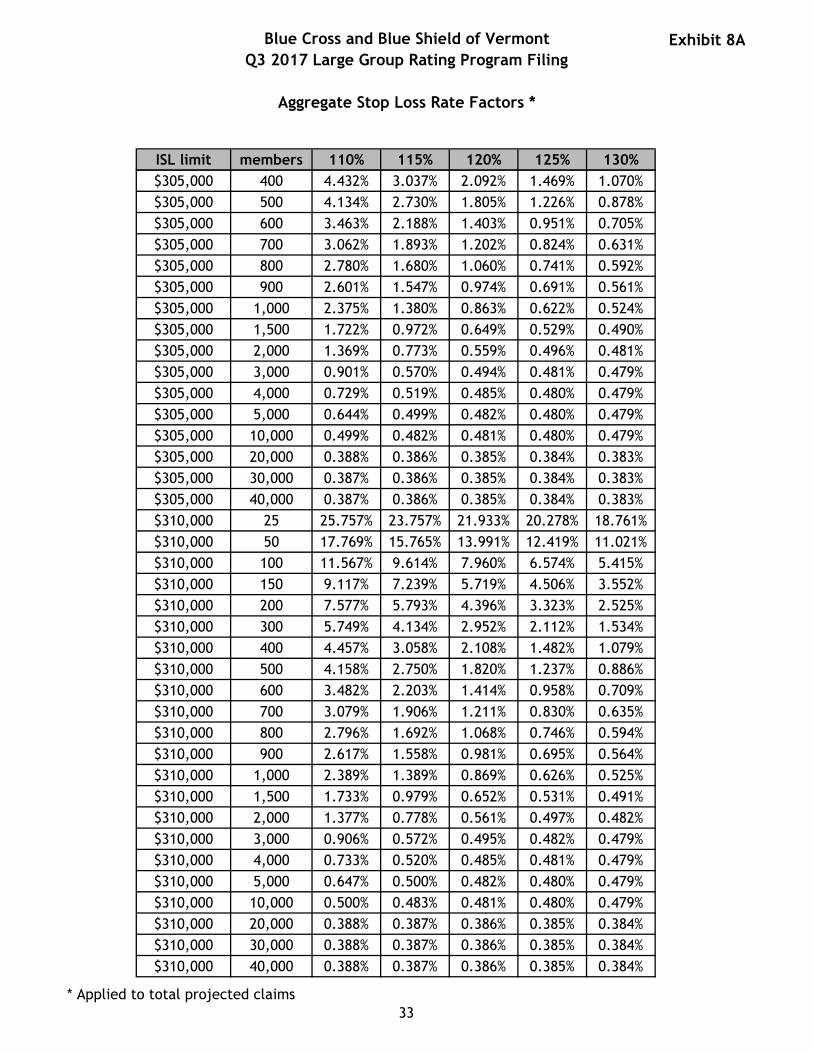
Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$305,000 400 4.432% 3.037% 2.092% 1.469% 1.070%
$305,000 500 4.134% 2.730% 1.805% 1.226% 0.878%
$305,000 600 3.463% 2.188% 1.403% 0.951% 0.705%
$305,000 700 3.062% 1.893% 1.202% 0.824% 0.631%
$305,000 800 2.780% 1.680% 1.060% 0.741% 0.592%
$305,000 900 2.601% 1.547% 0.974% 0.691% 0.561%
$305,000 1,000 2.375% 1.380% 0.863% 0.622% 0.524%
$305,000 1,500 1.722% 0.972% 0.649% 0.529% 0.490%
$305,000 2,000 1.369% 0.773% 0.559% 0.496% 0.481%
$305,000 3,000 0.901% 0.570% 0.494% 0.481% 0.479%
$305,000 4,000 0.729% 0.519% 0.485% 0.480% 0.479%
$305,000 5,000 0.644% 0.499% 0.482% 0.480% 0.479%
$305,000 10,000 0.499% 0.482% 0.481% 0.480% 0.479%
$305,000 20,000 0.388% 0.386% 0.385% 0.384% 0.383%
$305,000 30,000 0.387% 0.386% 0.385% 0.384% 0.383%
$305,000 40,000 0.387% 0.386% 0.385% 0.384% 0.383%
$310,000 25 25.757% 23.757% 21.933% 20.278% 18.761%
$310,000 50 17.769% 15.765% 13.991% 12.419% 11.021%
$310,000 100 11.567% 9.614% 7.960% 6.574% 5.415%
$310,000 150 9.117% 7.239% 5.719% 4.506% 3.552%
$310,000 200 7.577% 5.793% 4.396% 3.323% 2.525%
$310,000 300 5.749% 4.134% 2.952% 2.112% 1.534%
$310,000 400 4.457% 3.058% 2.108% 1.482% 1.079%
$310,000 500 4.158% 2.750% 1.820% 1.237% 0.886%
$310,000 600 3.482% 2.203% 1.414% 0.958% 0.709%
$310,000 700 3.079% 1.906% 1.211% 0.830% 0.635%
$310,000 800 2.796% 1.692% 1.068% 0.746% 0.594%
$310,000 900 2.617% 1.558% 0.981% 0.695% 0.564%
$310,000 1,000 2.389% 1.389% 0.869% 0.626% 0.525%
$310,000 1,500 1.733% 0.979% 0.652% 0.531% 0.491%
$310,000 2,000 1.377% 0.778% 0.561% 0.497% 0.482%
$310,000 3,000 0.906% 0.572% 0.495% 0.482% 0.479%
$310,000 4,000 0.733% 0.520% 0.485% 0.481% 0.479%
$310,000 5,000 0.647% 0.500% 0.482% 0.480% 0.479%
$310,000 10,000 0.500% 0.483% 0.481% 0.480% 0.479%
$310,000 20,000 0.388% 0.387% 0.386% 0.385% 0.384%
$310,000 30,000 0.388% 0.387% 0.386% 0.385% 0.384%
$310,000 40,000 0.388% 0.387% 0.386% 0.385% 0.384%
* Applied to total projected claims33

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$315,000 25 25.825% 23.826% 22.003% 20.348% 18.832%
$315,000 50 17.835% 15.834% 14.061% 12.490% 11.093%
$315,000 100 11.622% 9.667% 8.012% 6.624% 5.461%
$315,000 150 9.163% 7.281% 5.759% 4.541% 3.583%
$315,000 200 7.617% 5.829% 4.428% 3.351% 2.550%
$315,000 300 5.779% 4.160% 2.974% 2.130% 1.548%
$315,000 400 4.483% 3.079% 2.125% 1.495% 1.089%
$315,000 500 4.182% 2.770% 1.835% 1.247% 0.894%
$315,000 600 3.501% 2.217% 1.424% 0.965% 0.713%
$315,000 700 3.096% 1.919% 1.220% 0.836% 0.638%
$315,000 800 2.812% 1.704% 1.076% 0.751% 0.597%
$315,000 900 2.631% 1.569% 0.988% 0.699% 0.566%
$315,000 1,000 2.403% 1.398% 0.875% 0.629% 0.527%
$315,000 1,500 1.744% 0.986% 0.656% 0.532% 0.492%
$315,000 2,000 1.385% 0.782% 0.563% 0.498% 0.482%
$315,000 3,000 0.911% 0.574% 0.496% 0.482% 0.480%
$315,000 4,000 0.737% 0.521% 0.486% 0.481% 0.480%
$315,000 5,000 0.649% 0.501% 0.483% 0.481% 0.480%
$315,000 10,000 0.501% 0.483% 0.482% 0.481% 0.480%
$315,000 20,000 0.388% 0.387% 0.386% 0.385% 0.384%
$315,000 30,000 0.388% 0.387% 0.386% 0.385% 0.384%
$315,000 40,000 0.388% 0.387% 0.386% 0.385% 0.384%
$320,000 25 25.892% 23.893% 22.071% 20.417% 18.902%
$320,000 50 17.899% 15.898% 14.127% 12.558% 11.162%
$320,000 100 11.676% 9.720% 8.063% 6.673% 5.508%
$320,000 150 9.208% 7.324% 5.799% 4.578% 3.615%
$320,000 200 7.656% 5.866% 4.460% 3.379% 2.574%
$320,000 300 5.809% 4.186% 2.997% 2.148% 1.563%
$320,000 400 4.508% 3.101% 2.142% 1.508% 1.098%
$320,000 500 4.205% 2.789% 1.849% 1.258% 0.901%
$320,000 600 3.520% 2.232% 1.434% 0.972% 0.718%
$320,000 700 3.112% 1.931% 1.229% 0.841% 0.642%
$320,000 800 2.828% 1.715% 1.084% 0.755% 0.600%
$320,000 900 2.646% 1.580% 0.995% 0.703% 0.568%
$320,000 1,000 2.417% 1.408% 0.881% 0.632% 0.529%
$320,000 1,500 1.755% 0.992% 0.659% 0.534% 0.493%
$320,000 2,000 1.393% 0.786% 0.565% 0.499% 0.483%
$320,000 3,000 0.916% 0.577% 0.497% 0.483% 0.480%
* Applied to total projected claims34

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$320,000 4,000 0.740% 0.523% 0.486% 0.482% 0.480%
$320,000 5,000 0.652% 0.502% 0.483% 0.481% 0.480%
$320,000 10,000 0.501% 0.484% 0.482% 0.481% 0.480%
$320,000 20,000 0.389% 0.387% 0.386% 0.385% 0.384%
$320,000 30,000 0.388% 0.387% 0.386% 0.385% 0.384%
$320,000 40,000 0.388% 0.387% 0.386% 0.385% 0.384%
$325,000 25 25.957% 23.959% 22.138% 20.485% 18.970%
$325,000 50 17.960% 15.961% 14.191% 12.622% 11.228%
$325,000 100 11.729% 9.772% 8.113% 6.721% 5.553%
$325,000 150 9.254% 7.367% 5.839% 4.614% 3.648%
$325,000 200 7.695% 5.901% 4.492% 3.407% 2.598%
$325,000 300 5.838% 4.212% 3.019% 2.166% 1.577%
$325,000 400 4.533% 3.122% 2.158% 1.520% 1.108%
$325,000 500 4.228% 2.808% 1.863% 1.269% 0.909%
$325,000 600 3.538% 2.246% 1.444% 0.978% 0.722%
$325,000 700 3.128% 1.944% 1.238% 0.847% 0.646%
$325,000 800 2.844% 1.727% 1.091% 0.760% 0.603%
$325,000 900 2.660% 1.590% 1.002% 0.707% 0.570%
$325,000 1,000 2.430% 1.417% 0.887% 0.635% 0.530%
$325,000 1,500 1.765% 0.999% 0.663% 0.536% 0.494%
$325,000 2,000 1.401% 0.791% 0.567% 0.500% 0.483%
$325,000 3,000 0.921% 0.579% 0.497% 0.483% 0.481%
$325,000 4,000 0.744% 0.524% 0.487% 0.482% 0.481%
$325,000 5,000 0.655% 0.503% 0.484% 0.482% 0.481%
$325,000 10,000 0.502% 0.484% 0.483% 0.482% 0.481%
$325,000 20,000 0.389% 0.388% 0.387% 0.386% 0.385%
$325,000 30,000 0.389% 0.388% 0.387% 0.386% 0.385%
$325,000 40,000 0.389% 0.388% 0.387% 0.386% 0.385%
$330,000 25 26.015% 24.018% 22.197% 20.544% 19.030%
$330,000 50 18.015% 16.017% 14.248% 12.681% 11.287%
$330,000 100 11.780% 9.822% 8.161% 6.768% 5.598%
$330,000 150 9.296% 7.407% 5.876% 4.648% 3.678%
$330,000 200 7.731% 5.934% 4.521% 3.433% 2.620%
$330,000 300 5.865% 4.236% 3.039% 2.183% 1.590%
$330,000 400 4.556% 3.141% 2.174% 1.532% 1.117%
$330,000 500 4.249% 2.826% 1.876% 1.279% 0.916%
$330,000 600 3.554% 2.258% 1.453% 0.984% 0.726%
$330,000 700 3.143% 1.955% 1.246% 0.852% 0.649%
* Applied to total projected claims35

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$330,000 800 2.858% 1.738% 1.098% 0.764% 0.605%
$330,000 900 2.673% 1.599% 1.008% 0.711% 0.572%
$330,000 1,000 2.442% 1.425% 0.892% 0.638% 0.532%
$330,000 1,500 1.775% 1.005% 0.666% 0.538% 0.495%
$330,000 2,000 1.408% 0.794% 0.568% 0.501% 0.484%
$330,000 3,000 0.926% 0.580% 0.498% 0.484% 0.481%
$330,000 4,000 0.748% 0.525% 0.488% 0.482% 0.481%
$330,000 5,000 0.658% 0.504% 0.484% 0.482% 0.481%
$330,000 10,000 0.503% 0.485% 0.483% 0.482% 0.481%
$330,000 20,000 0.390% 0.388% 0.387% 0.386% 0.385%
$330,000 30,000 0.389% 0.388% 0.387% 0.386% 0.385%
$330,000 40,000 0.389% 0.388% 0.387% 0.386% 0.385%
$335,000 25 26.069% 24.072% 22.252% 20.600% 19.086%
$335,000 50 18.067% 16.070% 14.302% 12.736% 11.343%
$335,000 100 11.828% 9.870% 8.207% 6.813% 5.641%
$335,000 150 9.336% 7.445% 5.913% 4.680% 3.707%
$335,000 200 7.766% 5.967% 4.550% 3.459% 2.642%
$335,000 300 5.890% 4.258% 3.058% 2.198% 1.603%
$335,000 400 4.578% 3.159% 2.189% 1.544% 1.126%
$335,000 500 4.269% 2.843% 1.889% 1.288% 0.923%
$335,000 600 3.570% 2.271% 1.462% 0.990% 0.730%
$335,000 700 3.157% 1.966% 1.254% 0.858% 0.652%
$335,000 800 2.871% 1.748% 1.105% 0.769% 0.607%
$335,000 900 2.686% 1.608% 1.014% 0.714% 0.574%
$335,000 1,000 2.454% 1.433% 0.897% 0.641% 0.533%
$335,000 1,500 1.785% 1.011% 0.669% 0.539% 0.495%
$335,000 2,000 1.415% 0.798% 0.570% 0.502% 0.484%
$335,000 3,000 0.930% 0.582% 0.499% 0.484% 0.482%
$335,000 4,000 0.751% 0.527% 0.488% 0.483% 0.482%
$335,000 5,000 0.660% 0.505% 0.485% 0.483% 0.482%
$335,000 10,000 0.504% 0.485% 0.484% 0.483% 0.482%
$335,000 20,000 0.390% 0.388% 0.387% 0.386% 0.385%
$335,000 30,000 0.389% 0.388% 0.387% 0.386% 0.385%
$335,000 40,000 0.389% 0.388% 0.387% 0.386% 0.385%
$340,000 25 26.120% 24.124% 22.304% 20.653% 19.139%
$340,000 50 18.115% 16.119% 14.352% 12.787% 11.395%
$340,000 100 11.876% 9.917% 8.253% 6.858% 5.683%
$340,000 150 9.373% 7.481% 5.946% 4.711% 3.735%
* Applied to total projected claims36

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$340,000 200 7.799% 5.997% 4.578% 3.483% 2.664%
$340,000 300 5.914% 4.280% 3.076% 2.214% 1.615%
$340,000 400 4.600% 3.177% 2.203% 1.555% 1.135%
$340,000 500 4.289% 2.859% 1.902% 1.297% 0.930%
$340,000 600 3.585% 2.283% 1.471% 0.996% 0.733%
$340,000 700 3.171% 1.976% 1.261% 0.863% 0.655%
$340,000 800 2.884% 1.757% 1.112% 0.772% 0.610%
$340,000 900 2.698% 1.617% 1.020% 0.718% 0.576%
$340,000 1,000 2.466% 1.441% 0.902% 0.644% 0.535%
$340,000 1,500 1.794% 1.016% 0.672% 0.541% 0.496%
$340,000 2,000 1.421% 0.802% 0.572% 0.502% 0.485%
$340,000 3,000 0.935% 0.584% 0.499% 0.484% 0.482%
$340,000 4,000 0.755% 0.528% 0.489% 0.483% 0.482%
$340,000 5,000 0.663% 0.505% 0.485% 0.483% 0.482%
$340,000 10,000 0.504% 0.485% 0.484% 0.483% 0.482%
$340,000 20,000 0.390% 0.389% 0.388% 0.387% 0.386%
$340,000 30,000 0.390% 0.389% 0.388% 0.387% 0.386%
$340,000 40,000 0.390% 0.389% 0.388% 0.387% 0.386%
$345,000 25 26.168% 24.172% 22.353% 20.701% 19.189%
$345,000 50 18.161% 16.166% 14.400% 12.835% 11.444%
$345,000 100 11.922% 9.963% 8.298% 6.900% 5.724%
$345,000 150 9.410% 7.517% 5.979% 4.742% 3.762%
$345,000 200 7.832% 6.027% 4.604% 3.507% 2.685%
$345,000 300 5.938% 4.300% 3.094% 2.228% 1.627%
$345,000 400 4.620% 3.194% 2.217% 1.566% 1.143%
$345,000 500 4.308% 2.875% 1.914% 1.306% 0.936%
$345,000 600 3.599% 2.294% 1.479% 1.001% 0.737%
$345,000 700 3.184% 1.986% 1.269% 0.867% 0.658%
$345,000 800 2.897% 1.767% 1.118% 0.776% 0.612%
$345,000 900 2.709% 1.625% 1.025% 0.721% 0.578%
$345,000 1,000 2.477% 1.449% 0.907% 0.647% 0.536%
$345,000 1,500 1.802% 1.021% 0.675% 0.542% 0.497%
$345,000 2,000 1.427% 0.805% 0.574% 0.503% 0.485%
$345,000 3,000 0.939% 0.585% 0.500% 0.485% 0.482%
$345,000 4,000 0.758% 0.529% 0.489% 0.484% 0.482%
$345,000 5,000 0.665% 0.506% 0.486% 0.483% 0.482%
$345,000 10,000 0.505% 0.486% 0.484% 0.483% 0.482%
$345,000 20,000 0.390% 0.389% 0.388% 0.387% 0.386%
* Applied to total projected claims37

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$345,000 30,000 0.390% 0.389% 0.388% 0.387% 0.386%
$345,000 40,000 0.390% 0.389% 0.388% 0.387% 0.386%
$350,000 25 26.216% 24.220% 22.401% 20.750% 19.238%
$350,000 50 18.205% 16.211% 14.445% 12.881% 11.492%
$350,000 100 11.967% 10.008% 8.341% 6.942% 5.763%
$350,000 150 9.447% 7.552% 6.012% 4.772% 3.789%
$350,000 200 7.864% 6.057% 4.631% 3.530% 2.705%
$350,000 300 5.961% 4.321% 3.112% 2.243% 1.638%
$350,000 400 4.640% 3.211% 2.230% 1.577% 1.151%
$350,000 500 4.328% 2.891% 1.926% 1.316% 0.943%
$350,000 600 3.614% 2.306% 1.487% 1.007% 0.741%
$350,000 700 3.197% 1.996% 1.276% 0.872% 0.661%
$350,000 800 2.910% 1.776% 1.124% 0.780% 0.614%
$350,000 900 2.721% 1.634% 1.031% 0.724% 0.580%
$350,000 1,000 2.488% 1.456% 0.912% 0.649% 0.538%
$350,000 1,500 1.811% 1.026% 0.678% 0.544% 0.498%
$350,000 2,000 1.434% 0.809% 0.575% 0.504% 0.486%
$350,000 3,000 0.943% 0.587% 0.501% 0.485% 0.483%
$350,000 4,000 0.761% 0.530% 0.490% 0.484% 0.483%
$350,000 5,000 0.668% 0.507% 0.486% 0.484% 0.483%
$350,000 10,000 0.506% 0.486% 0.485% 0.484% 0.483%
$350,000 20,000 0.391% 0.389% 0.388% 0.387% 0.386%
$350,000 30,000 0.390% 0.389% 0.388% 0.387% 0.386%
$350,000 40,000 0.390% 0.389% 0.388% 0.387% 0.386%
$355,000 25 26.264% 24.268% 22.450% 20.799% 19.287%
$355,000 50 18.249% 16.255% 14.491% 12.928% 11.538%
$355,000 100 12.011% 10.052% 8.384% 6.984% 5.803%
$355,000 150 9.483% 7.588% 6.046% 4.803% 3.816%
$355,000 200 7.896% 6.086% 4.658% 3.554% 2.725%
$355,000 300 5.983% 4.341% 3.130% 2.257% 1.650%
$355,000 400 4.661% 3.229% 2.245% 1.588% 1.159%
$355,000 500 4.347% 2.907% 1.939% 1.325% 0.949%
$355,000 600 3.629% 2.317% 1.496% 1.013% 0.744%
$355,000 700 3.210% 2.006% 1.283% 0.877% 0.665%
$355,000 800 2.922% 1.785% 1.130% 0.784% 0.616%
$355,000 900 2.732% 1.642% 1.036% 0.728% 0.582%
$355,000 1,000 2.499% 1.464% 0.917% 0.652% 0.539%
$355,000 1,500 1.819% 1.032% 0.681% 0.545% 0.498%
* Applied to total projected claims38

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$355,000 2,000 1.440% 0.812% 0.577% 0.505% 0.486%
$355,000 3,000 0.947% 0.589% 0.501% 0.486% 0.483%
$355,000 4,000 0.765% 0.531% 0.490% 0.484% 0.483%
$355,000 5,000 0.670% 0.508% 0.486% 0.484% 0.483%
$355,000 10,000 0.507% 0.486% 0.485% 0.484% 0.483%
$355,000 20,000 0.391% 0.390% 0.389% 0.388% 0.387%
$355,000 30,000 0.391% 0.390% 0.389% 0.388% 0.387%
$355,000 40,000 0.391% 0.390% 0.389% 0.388% 0.387%
$360,000 25 26.312% 24.316% 22.498% 20.848% 19.336%
$360,000 50 18.293% 16.300% 14.536% 12.974% 11.585%
$360,000 100 12.056% 10.097% 8.428% 7.026% 5.844%
$360,000 150 9.521% 7.624% 6.080% 4.835% 3.844%
$360,000 200 7.928% 6.116% 4.685% 3.578% 2.746%
$360,000 300 6.007% 4.362% 3.148% 2.272% 1.662%
$360,000 400 4.682% 3.246% 2.259% 1.599% 1.168%
$360,000 500 4.366% 2.923% 1.951% 1.334% 0.956%
$360,000 600 3.643% 2.329% 1.504% 1.018% 0.748%
$360,000 700 3.223% 2.017% 1.291% 0.882% 0.668%
$360,000 800 2.935% 1.794% 1.136% 0.788% 0.618%
$360,000 900 2.744% 1.651% 1.042% 0.731% 0.584%
$360,000 1,000 2.510% 1.472% 0.922% 0.655% 0.541%
$360,000 1,500 1.827% 1.037% 0.684% 0.546% 0.499%
$360,000 2,000 1.446% 0.816% 0.579% 0.506% 0.486%
$360,000 3,000 0.951% 0.590% 0.502% 0.486% 0.484%
$360,000 4,000 0.768% 0.532% 0.491% 0.485% 0.483%
$360,000 5,000 0.673% 0.509% 0.487% 0.484% 0.483%
$360,000 10,000 0.507% 0.487% 0.485% 0.484% 0.483%
$360,000 20,000 0.391% 0.390% 0.389% 0.388% 0.387%
$360,000 30,000 0.391% 0.390% 0.389% 0.388% 0.387%
$360,000 40,000 0.391% 0.390% 0.389% 0.388% 0.387%
$365,000 25 26.360% 24.364% 22.547% 20.897% 19.386%
$365,000 50 18.336% 16.343% 14.580% 13.019% 11.631%
$365,000 100 12.100% 10.142% 8.472% 7.068% 5.884%
$365,000 150 9.558% 7.661% 6.114% 4.866% 3.872%
$365,000 200 7.960% 6.146% 4.712% 3.602% 2.767%
$365,000 300 6.030% 4.383% 3.166% 2.286% 1.674%
$365,000 400 4.703% 3.264% 2.273% 1.611% 1.176%
$365,000 500 4.385% 2.940% 1.964% 1.344% 0.963%
* Applied to total projected claims39

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$365,000 600 3.658% 2.341% 1.513% 1.024% 0.752%
$365,000 700 3.236% 2.027% 1.298% 0.887% 0.671%
$365,000 800 2.948% 1.804% 1.142% 0.792% 0.620%
$365,000 900 2.756% 1.659% 1.048% 0.735% 0.586%
$365,000 1,000 2.521% 1.480% 0.927% 0.658% 0.542%
$365,000 1,500 1.836% 1.042% 0.687% 0.548% 0.500%
$365,000 2,000 1.452% 0.819% 0.580% 0.506% 0.487%
$365,000 3,000 0.955% 0.592% 0.503% 0.487% 0.484%
$365,000 4,000 0.771% 0.533% 0.491% 0.485% 0.484%
$365,000 5,000 0.675% 0.509% 0.487% 0.485% 0.484%
$365,000 10,000 0.508% 0.487% 0.486% 0.485% 0.484%
$365,000 20,000 0.392% 0.390% 0.389% 0.388% 0.387%
$365,000 30,000 0.391% 0.390% 0.389% 0.388% 0.387%
$365,000 40,000 0.391% 0.390% 0.389% 0.388% 0.387%
$370,000 25 26.405% 24.410% 22.594% 20.944% 19.433%
$370,000 50 18.376% 16.385% 14.623% 13.062% 11.675%
$370,000 100 12.143% 10.185% 8.515% 7.109% 5.924%
$370,000 150 9.594% 7.696% 6.147% 4.897% 3.900%
$370,000 200 7.991% 6.175% 4.738% 3.625% 2.787%
$370,000 300 6.053% 4.404% 3.183% 2.301% 1.686%
$370,000 400 4.723% 3.282% 2.288% 1.622% 1.185%
$370,000 500 4.404% 2.956% 1.976% 1.353% 0.970%
$370,000 600 3.673% 2.353% 1.522% 1.030% 0.756%
$370,000 700 3.249% 2.037% 1.305% 0.892% 0.674%
$370,000 800 2.960% 1.813% 1.149% 0.796% 0.622%
$370,000 900 2.767% 1.667% 1.053% 0.738% 0.588%
$370,000 1,000 2.532% 1.487% 0.932% 0.661% 0.544%
$370,000 1,500 1.844% 1.047% 0.689% 0.549% 0.501%
$370,000 2,000 1.458% 0.822% 0.582% 0.507% 0.487%
$370,000 3,000 0.959% 0.594% 0.503% 0.487% 0.484%
$370,000 4,000 0.774% 0.535% 0.491% 0.485% 0.484%
$370,000 5,000 0.678% 0.510% 0.488% 0.485% 0.484%
$370,000 10,000 0.509% 0.488% 0.486% 0.485% 0.484%
$370,000 20,000 0.392% 0.390% 0.389% 0.388% 0.387%
$370,000 30,000 0.391% 0.390% 0.389% 0.388% 0.387%
$370,000 40,000 0.391% 0.390% 0.389% 0.388% 0.387%
$375,000 25 26.446% 24.451% 22.635% 20.986% 19.475%
$375,000 50 18.414% 16.423% 14.662% 13.102% 11.715%
* Applied to total projected claims40

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$375,000 100 12.182% 10.224% 8.554% 7.147% 5.960%
$375,000 150 9.627% 7.729% 6.178% 4.926% 3.926%
$375,000 200 8.020% 6.202% 4.762% 3.647% 2.806%
$375,000 300 6.075% 4.423% 3.200% 2.315% 1.698%
$375,000 400 4.742% 3.298% 2.301% 1.632% 1.193%
$375,000 500 4.422% 2.970% 1.988% 1.361% 0.976%
$375,000 600 3.687% 2.364% 1.530% 1.036% 0.760%
$375,000 700 3.260% 2.046% 1.312% 0.896% 0.677%
$375,000 800 2.971% 1.821% 1.154% 0.799% 0.624%
$375,000 900 2.778% 1.675% 1.058% 0.741% 0.590%
$375,000 1,000 2.542% 1.494% 0.937% 0.663% 0.545%
$375,000 1,500 1.852% 1.052% 0.692% 0.551% 0.501%
$375,000 2,000 1.464% 0.826% 0.583% 0.508% 0.488%
$375,000 3,000 0.963% 0.595% 0.504% 0.487% 0.485%
$375,000 4,000 0.778% 0.536% 0.492% 0.486% 0.484%
$375,000 5,000 0.680% 0.511% 0.488% 0.485% 0.484%
$375,000 10,000 0.509% 0.488% 0.486% 0.485% 0.484%
$375,000 20,000 0.392% 0.391% 0.390% 0.389% 0.388%
$375,000 30,000 0.392% 0.391% 0.390% 0.389% 0.388%
$375,000 40,000 0.392% 0.391% 0.390% 0.389% 0.388%
$380,000 25 26.485% 24.491% 22.675% 21.026% 19.516%
$380,000 50 18.451% 16.461% 14.701% 13.141% 11.755%
$380,000 100 12.221% 10.263% 8.593% 7.184% 5.996%
$380,000 150 9.661% 7.761% 6.209% 4.954% 3.951%
$380,000 200 8.048% 6.229% 4.786% 3.669% 2.825%
$380,000 300 6.097% 4.443% 3.217% 2.329% 1.709%
$380,000 400 4.761% 3.314% 2.315% 1.643% 1.202%
$380,000 500 4.439% 2.985% 1.999% 1.370% 0.982%
$380,000 600 3.701% 2.375% 1.538% 1.041% 0.764%
$380,000 700 3.272% 2.055% 1.318% 0.900% 0.680%
$380,000 800 2.983% 1.830% 1.160% 0.803% 0.627%
$380,000 900 2.788% 1.683% 1.063% 0.744% 0.592%
$380,000 1,000 2.552% 1.501% 0.941% 0.666% 0.546%
$380,000 1,500 1.859% 1.057% 0.695% 0.552% 0.502%
$380,000 2,000 1.470% 0.829% 0.585% 0.509% 0.488%
$380,000 3,000 0.967% 0.597% 0.505% 0.488% 0.485%
$380,000 4,000 0.781% 0.537% 0.492% 0.486% 0.485%
$380,000 5,000 0.682% 0.512% 0.488% 0.486% 0.485%
* Applied to total projected claims41

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$380,000 10,000 0.510% 0.488% 0.487% 0.486% 0.485%
$380,000 20,000 0.392% 0.391% 0.390% 0.389% 0.388%
$380,000 30,000 0.392% 0.391% 0.390% 0.389% 0.388%
$380,000 40,000 0.392% 0.391% 0.390% 0.389% 0.388%
$385,000 25 26.524% 24.530% 22.715% 21.066% 19.556%
$385,000 50 18.489% 16.500% 14.740% 13.181% 11.796%
$385,000 100 12.259% 10.302% 8.631% 7.221% 6.032%
$385,000 150 9.693% 7.793% 6.239% 4.982% 3.977%
$385,000 200 8.076% 6.255% 4.811% 3.691% 2.843%
$385,000 300 6.118% 4.462% 3.234% 2.343% 1.721%
$385,000 400 4.780% 3.331% 2.328% 1.654% 1.210%
$385,000 500 4.456% 3.000% 2.011% 1.378% 0.988%
$385,000 600 3.715% 2.386% 1.546% 1.047% 0.767%
$385,000 700 3.283% 2.064% 1.325% 0.905% 0.682%
$385,000 800 2.994% 1.838% 1.166% 0.807% 0.629%
$385,000 900 2.798% 1.690% 1.068% 0.747% 0.594%
$385,000 1,000 2.561% 1.508% 0.945% 0.668% 0.548%
$385,000 1,500 1.867% 1.061% 0.697% 0.553% 0.503%
$385,000 2,000 1.475% 0.832% 0.586% 0.509% 0.489%
$385,000 3,000 0.971% 0.598% 0.505% 0.488% 0.485%
$385,000 4,000 0.784% 0.538% 0.493% 0.486% 0.485%
$385,000 5,000 0.684% 0.512% 0.489% 0.486% 0.485%
$385,000 10,000 0.510% 0.488% 0.487% 0.486% 0.485%
$385,000 20,000 0.393% 0.391% 0.390% 0.389% 0.388%
$385,000 30,000 0.392% 0.391% 0.390% 0.389% 0.388%
$385,000 40,000 0.392% 0.391% 0.390% 0.389% 0.388%
$390,000 25 26.562% 24.568% 22.753% 21.105% 19.595%
$390,000 50 18.527% 16.538% 14.779% 13.221% 11.836%
$390,000 100 12.296% 10.339% 8.668% 7.257% 6.067%
$390,000 150 9.725% 7.824% 6.269% 5.010% 4.002%
$390,000 200 8.103% 6.281% 4.834% 3.712% 2.862%
$390,000 300 6.139% 4.481% 3.251% 2.357% 1.732%
$390,000 400 4.799% 3.346% 2.341% 1.664% 1.218%
$390,000 500 4.472% 3.013% 2.022% 1.386% 0.994%
$390,000 600 3.729% 2.397% 1.554% 1.052% 0.771%
$390,000 700 3.293% 2.072% 1.331% 0.909% 0.685%
$390,000 800 3.005% 1.847% 1.172% 0.810% 0.631%
$390,000 900 2.808% 1.698% 1.073% 0.750% 0.595%
* Applied to total projected claims42

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$390,000 1,000 2.571% 1.515% 0.950% 0.671% 0.549%
$390,000 1,500 1.874% 1.066% 0.700% 0.555% 0.503%
$390,000 2,000 1.480% 0.835% 0.588% 0.510% 0.489%
$390,000 3,000 0.974% 0.600% 0.506% 0.488% 0.485%
$390,000 4,000 0.787% 0.539% 0.493% 0.487% 0.485%
$390,000 5,000 0.687% 0.513% 0.489% 0.486% 0.485%
$390,000 10,000 0.511% 0.489% 0.487% 0.486% 0.485%
$390,000 20,000 0.393% 0.391% 0.390% 0.389% 0.388%
$390,000 30,000 0.392% 0.391% 0.390% 0.389% 0.388%
$390,000 40,000 0.392% 0.391% 0.390% 0.389% 0.388%
$395,000 25 26.598% 24.604% 22.789% 21.141% 19.631%
$395,000 50 18.565% 16.576% 14.817% 13.260% 11.876%
$395,000 100 12.330% 10.373% 8.703% 7.291% 6.099%
$395,000 150 9.756% 7.855% 6.298% 5.037% 4.026%
$395,000 200 8.129% 6.305% 4.856% 3.732% 2.879%
$395,000 300 6.159% 4.500% 3.267% 2.370% 1.743%
$395,000 400 4.816% 3.361% 2.354% 1.674% 1.225%
$395,000 500 4.488% 3.027% 2.032% 1.394% 0.999%
$395,000 600 3.741% 2.407% 1.562% 1.057% 0.774%
$395,000 700 3.304% 2.080% 1.337% 0.913% 0.688%
$395,000 800 3.015% 1.854% 1.177% 0.814% 0.633%
$395,000 900 2.818% 1.705% 1.078% 0.753% 0.597%
$395,000 1,000 2.580% 1.521% 0.954% 0.673% 0.550%
$395,000 1,500 1.881% 1.070% 0.702% 0.556% 0.504%
$395,000 2,000 1.486% 0.838% 0.589% 0.511% 0.489%
$395,000 3,000 0.978% 0.601% 0.506% 0.489% 0.486%
$395,000 4,000 0.789% 0.540% 0.494% 0.487% 0.486%
$395,000 5,000 0.689% 0.514% 0.489% 0.487% 0.486%
$395,000 10,000 0.512% 0.489% 0.488% 0.487% 0.486%
$395,000 20,000 0.393% 0.392% 0.391% 0.390% 0.389%
$395,000 30,000 0.393% 0.392% 0.391% 0.390% 0.389%
$395,000 40,000 0.393% 0.392% 0.391% 0.390% 0.389%
$400,000 25 26.633% 24.639% 22.824% 21.176% 19.666%
$400,000 50 18.600% 16.613% 14.854% 13.297% 11.913%
$400,000 100 12.363% 10.406% 8.736% 7.323% 6.130%
$400,000 150 9.786% 7.884% 6.326% 5.063% 4.050%
$400,000 200 8.154% 6.329% 4.878% 3.752% 2.896%
$400,000 300 6.179% 4.517% 3.282% 2.383% 1.753%
* Applied to total projected claims43

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$400,000 400 4.833% 3.376% 2.366% 1.683% 1.232%
$400,000 500 4.503% 3.040% 2.042% 1.401% 1.005%
$400,000 600 3.753% 2.417% 1.569% 1.062% 0.778%
$400,000 700 3.313% 2.088% 1.343% 0.917% 0.690%
$400,000 800 3.025% 1.862% 1.182% 0.817% 0.634%
$400,000 900 2.827% 1.712% 1.083% 0.756% 0.599%
$400,000 1,000 2.588% 1.527% 0.957% 0.675% 0.551%
$400,000 1,500 1.888% 1.074% 0.704% 0.557% 0.505%
$400,000 2,000 1.490% 0.840% 0.591% 0.511% 0.490%
$400,000 3,000 0.981% 0.603% 0.507% 0.489% 0.486%
$400,000 4,000 0.792% 0.541% 0.494% 0.487% 0.486%
$400,000 5,000 0.691% 0.514% 0.490% 0.487% 0.486%
$400,000 10,000 0.512% 0.489% 0.488% 0.487% 0.486%
$400,000 20,000 0.393% 0.392% 0.391% 0.390% 0.389%
$400,000 30,000 0.393% 0.392% 0.391% 0.390% 0.389%
$400,000 40,000 0.393% 0.392% 0.391% 0.390% 0.389%
$405,000 25 26.669% 24.674% 22.860% 21.212% 19.702%
$405,000 50 18.635% 16.647% 14.889% 13.332% 11.949%
$405,000 100 12.394% 10.438% 8.767% 7.354% 6.160%
$405,000 150 9.816% 7.913% 6.354% 5.089% 4.074%
$405,000 200 8.179% 6.353% 4.900% 3.771% 2.913%
$405,000 300 6.198% 4.535% 3.298% 2.396% 1.764%
$405,000 400 4.850% 3.390% 2.377% 1.693% 1.239%
$405,000 500 4.518% 3.052% 2.052% 1.409% 1.010%
$405,000 600 3.766% 2.427% 1.576% 1.067% 0.781%
$405,000 700 3.323% 2.096% 1.349% 0.921% 0.693%
$405,000 800 3.035% 1.869% 1.187% 0.820% 0.636%
$405,000 900 2.837% 1.719% 1.088% 0.759% 0.601%
$405,000 1,000 2.597% 1.533% 0.961% 0.677% 0.553%
$405,000 1,500 1.894% 1.079% 0.707% 0.558% 0.505%
$405,000 2,000 1.495% 0.843% 0.592% 0.512% 0.490%
$405,000 3,000 0.984% 0.604% 0.507% 0.489% 0.486%
$405,000 4,000 0.795% 0.541% 0.494% 0.488% 0.486%
$405,000 5,000 0.693% 0.515% 0.490% 0.487% 0.486%
$405,000 10,000 0.513% 0.490% 0.488% 0.487% 0.486%
$405,000 20,000 0.394% 0.392% 0.391% 0.390% 0.389%
$405,000 30,000 0.393% 0.392% 0.391% 0.390% 0.389%
$405,000 40,000 0.393% 0.392% 0.391% 0.390% 0.389%
* Applied to total projected claims44

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$410,000 25 26.704% 24.710% 22.896% 21.248% 19.738%
$410,000 50 18.669% 16.682% 14.924% 13.367% 11.984%
$410,000 100 12.424% 10.468% 8.798% 7.385% 6.189%
$410,000 150 9.846% 7.943% 6.382% 5.115% 4.098%
$410,000 200 8.204% 6.376% 4.921% 3.791% 2.930%
$410,000 300 6.218% 4.553% 3.313% 2.409% 1.774%
$410,000 400 4.867% 3.404% 2.389% 1.702% 1.246%
$410,000 500 4.534% 3.065% 2.062% 1.416% 1.016%
$410,000 600 3.778% 2.436% 1.583% 1.072% 0.784%
$410,000 700 3.333% 2.104% 1.355% 0.925% 0.695%
$410,000 800 3.045% 1.877% 1.192% 0.824% 0.638%
$410,000 900 2.846% 1.725% 1.092% 0.762% 0.602%
$410,000 1,000 2.605% 1.539% 0.965% 0.680% 0.554%
$410,000 1,500 1.901% 1.083% 0.709% 0.560% 0.506%
$410,000 2,000 1.500% 0.846% 0.593% 0.513% 0.490%
$410,000 3,000 0.987% 0.605% 0.508% 0.490% 0.487%
$410,000 4,000 0.797% 0.542% 0.495% 0.488% 0.486%
$410,000 5,000 0.695% 0.516% 0.490% 0.487% 0.486%
$410,000 10,000 0.513% 0.490% 0.488% 0.487% 0.486%
$410,000 20,000 0.394% 0.392% 0.391% 0.390% 0.389%
$410,000 30,000 0.393% 0.392% 0.391% 0.390% 0.389%
$410,000 40,000 0.393% 0.392% 0.391% 0.390% 0.389%
$415,000 25 26.741% 24.746% 22.933% 21.284% 19.775%
$415,000 50 18.702% 16.715% 14.957% 13.401% 12.019%
$415,000 100 12.454% 10.498% 8.828% 7.415% 6.218%
$415,000 150 9.875% 7.972% 6.410% 5.142% 4.122%
$415,000 200 8.228% 6.399% 4.942% 3.810% 2.947%
$415,000 300 6.237% 4.570% 3.328% 2.422% 1.785%
$415,000 400 4.883% 3.418% 2.401% 1.711% 1.253%
$415,000 500 4.548% 3.078% 2.072% 1.424% 1.021%
$415,000 600 3.789% 2.446% 1.590% 1.077% 0.787%
$415,000 700 3.343% 2.111% 1.360% 0.928% 0.698%
$415,000 800 3.055% 1.884% 1.197% 0.827% 0.640%
$415,000 900 2.855% 1.732% 1.097% 0.765% 0.604%
$415,000 1,000 2.613% 1.545% 0.969% 0.682% 0.555%
$415,000 1,500 1.908% 1.087% 0.712% 0.561% 0.507%
$415,000 2,000 1.505% 0.848% 0.595% 0.513% 0.491%
$415,000 3,000 0.991% 0.607% 0.509% 0.490% 0.487%
* Applied to total projected claims45

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$415,000 4,000 0.800% 0.543% 0.495% 0.488% 0.487%
$415,000 5,000 0.697% 0.516% 0.491% 0.488% 0.487%
$415,000 10,000 0.514% 0.490% 0.489% 0.488% 0.487%
$415,000 20,000 0.394% 0.393% 0.392% 0.391% 0.390%
$415,000 30,000 0.394% 0.393% 0.392% 0.391% 0.390%
$415,000 40,000 0.394% 0.393% 0.392% 0.391% 0.390%
$420,000 25 26.774% 24.779% 22.966% 21.318% 19.808%
$420,000 50 18.733% 16.746% 14.989% 13.433% 12.051%
$420,000 100 12.481% 10.526% 8.856% 7.443% 6.245%
$420,000 150 9.904% 8.000% 6.438% 5.168% 4.146%
$420,000 200 8.251% 6.421% 4.963% 3.828% 2.964%
$420,000 300 6.255% 4.587% 3.343% 2.434% 1.795%
$420,000 400 4.899% 3.432% 2.412% 1.720% 1.260%
$420,000 500 4.563% 3.090% 2.082% 1.431% 1.026%
$420,000 600 3.800% 2.455% 1.597% 1.081% 0.790%
$420,000 700 3.352% 2.119% 1.366% 0.932% 0.700%
$420,000 800 3.064% 1.891% 1.202% 0.830% 0.642%
$420,000 900 2.864% 1.739% 1.101% 0.768% 0.606%
$420,000 1,000 2.621% 1.550% 0.973% 0.684% 0.556%
$420,000 1,500 1.914% 1.091% 0.714% 0.562% 0.507%
$420,000 2,000 1.509% 0.851% 0.596% 0.514% 0.491%
$420,000 3,000 0.994% 0.608% 0.509% 0.490% 0.487%
$420,000 4,000 0.802% 0.544% 0.496% 0.488% 0.487%
$420,000 5,000 0.699% 0.517% 0.491% 0.488% 0.487%
$420,000 10,000 0.514% 0.491% 0.489% 0.488% 0.487%
$420,000 20,000 0.394% 0.393% 0.392% 0.391% 0.390%
$420,000 30,000 0.394% 0.393% 0.392% 0.391% 0.390%
$420,000 40,000 0.394% 0.393% 0.392% 0.391% 0.390%
$425,000 25 26.804% 24.810% 22.997% 21.349% 19.839%
$425,000 50 18.762% 16.776% 15.019% 13.464% 12.082%
$425,000 100 12.508% 10.553% 8.883% 7.470% 6.271%
$425,000 150 9.931% 8.028% 6.465% 5.193% 4.170%
$425,000 200 8.273% 6.443% 4.983% 3.847% 2.980%
$425,000 300 6.273% 4.604% 3.358% 2.447% 1.805%
$425,000 400 4.915% 3.445% 2.423% 1.729% 1.267%
$425,000 500 4.577% 3.102% 2.092% 1.438% 1.032%
$425,000 600 3.811% 2.463% 1.603% 1.086% 0.793%
$425,000 700 3.361% 2.126% 1.371% 0.936% 0.702%
* Applied to total projected claims46

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$425,000 800 3.073% 1.898% 1.207% 0.833% 0.644%
$425,000 900 2.872% 1.745% 1.106% 0.771% 0.607%
$425,000 1,000 2.629% 1.556% 0.976% 0.686% 0.557%
$425,000 1,500 1.920% 1.095% 0.716% 0.563% 0.508%
$425,000 2,000 1.513% 0.853% 0.597% 0.515% 0.492%
$425,000 3,000 0.997% 0.609% 0.510% 0.491% 0.487%
$425,000 4,000 0.805% 0.545% 0.496% 0.489% 0.487%
$425,000 5,000 0.701% 0.518% 0.491% 0.488% 0.487%
$425,000 10,000 0.515% 0.491% 0.489% 0.488% 0.487%
$425,000 20,000 0.395% 0.393% 0.392% 0.391% 0.390%
$425,000 30,000 0.394% 0.393% 0.392% 0.391% 0.390%
$425,000 40,000 0.394% 0.393% 0.392% 0.391% 0.390%
$430,000 25 26.834% 24.840% 23.027% 21.379% 19.869%
$430,000 50 18.790% 16.804% 15.048% 13.493% 12.111%
$430,000 100 12.533% 10.578% 8.908% 7.495% 6.296%
$430,000 150 9.958% 8.054% 6.491% 5.217% 4.192%
$430,000 200 8.295% 6.463% 5.002% 3.864% 2.996%
$430,000 300 6.291% 4.619% 3.372% 2.459% 1.815%
$430,000 400 4.930% 3.458% 2.434% 1.737% 1.273%
$430,000 500 4.591% 3.114% 2.101% 1.445% 1.037%
$430,000 600 3.822% 2.472% 1.609% 1.090% 0.796%
$430,000 700 3.369% 2.133% 1.376% 0.939% 0.705%
$430,000 800 3.081% 1.904% 1.211% 0.835% 0.645%
$430,000 900 2.881% 1.752% 1.110% 0.773% 0.609%
$430,000 1,000 2.636% 1.561% 0.979% 0.688% 0.558%
$430,000 1,500 1.926% 1.099% 0.718% 0.564% 0.508%
$430,000 2,000 1.518% 0.856% 0.598% 0.515% 0.492%
$430,000 3,000 1.000% 0.610% 0.510% 0.491% 0.488%
$430,000 4,000 0.807% 0.546% 0.496% 0.489% 0.487%
$430,000 5,000 0.702% 0.518% 0.491% 0.488% 0.487%
$430,000 10,000 0.515% 0.491% 0.489% 0.488% 0.487%
$430,000 20,000 0.395% 0.393% 0.392% 0.391% 0.390%
$430,000 30,000 0.394% 0.393% 0.392% 0.391% 0.390%
$430,000 40,000 0.394% 0.393% 0.392% 0.391% 0.390%
$435,000 25 26.862% 24.868% 23.055% 21.407% 19.898%
$435,000 50 18.816% 16.831% 15.075% 13.520% 12.139%
$435,000 100 12.556% 10.601% 8.931% 7.519% 6.319%
$435,000 150 9.983% 8.079% 6.515% 5.240% 4.213%
* Applied to total projected claims47

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$435,000 200 8.315% 6.482% 5.020% 3.880% 3.010%
$435,000 300 6.307% 4.634% 3.384% 2.469% 1.824%
$435,000 400 4.944% 3.470% 2.443% 1.745% 1.279%
$435,000 500 4.603% 3.124% 2.110% 1.452% 1.041%
$435,000 600 3.832% 2.480% 1.615% 1.094% 0.799%
$435,000 700 3.377% 2.139% 1.381% 0.943% 0.707%
$435,000 800 3.089% 1.910% 1.216% 0.838% 0.647%
$435,000 900 2.889% 1.757% 1.114% 0.776% 0.610%
$435,000 1,000 2.643% 1.566% 0.982% 0.690% 0.559%
$435,000 1,500 1.932% 1.102% 0.720% 0.565% 0.509%
$435,000 2,000 1.521% 0.858% 0.599% 0.516% 0.492%
$435,000 3,000 1.003% 0.612% 0.511% 0.491% 0.488%
$435,000 4,000 0.810% 0.547% 0.497% 0.489% 0.488%
$435,000 5,000 0.704% 0.519% 0.492% 0.489% 0.488%
$435,000 10,000 0.516% 0.491% 0.490% 0.489% 0.488%
$435,000 20,000 0.395% 0.393% 0.392% 0.391% 0.390%
$435,000 30,000 0.394% 0.393% 0.392% 0.391% 0.390%
$435,000 40,000 0.394% 0.393% 0.392% 0.391% 0.390%
$440,000 25 26.890% 24.896% 23.083% 21.435% 19.926%
$440,000 50 18.843% 16.858% 15.102% 13.548% 12.167%
$440,000 100 12.579% 10.625% 8.955% 7.542% 6.343%
$440,000 150 10.008% 8.104% 6.539% 5.262% 4.235%
$440,000 200 8.336% 6.502% 5.038% 3.897% 3.025%
$440,000 300 6.322% 4.648% 3.397% 2.480% 1.833%
$440,000 400 4.958% 3.482% 2.453% 1.753% 1.286%
$440,000 500 4.615% 3.135% 2.118% 1.458% 1.046%
$440,000 600 3.842% 2.488% 1.621% 1.098% 0.802%
$440,000 700 3.385% 2.145% 1.386% 0.946% 0.709%
$440,000 800 3.098% 1.917% 1.220% 0.841% 0.648%
$440,000 900 2.897% 1.764% 1.118% 0.778% 0.612%
$440,000 1,000 2.649% 1.570% 0.986% 0.692% 0.560%
$440,000 1,500 1.937% 1.106% 0.722% 0.567% 0.510%
$440,000 2,000 1.525% 0.860% 0.601% 0.516% 0.493%
$440,000 3,000 1.005% 0.613% 0.511% 0.491% 0.488%
$440,000 4,000 0.812% 0.548% 0.497% 0.489% 0.488%
$440,000 5,000 0.706% 0.519% 0.492% 0.489% 0.488%
$440,000 10,000 0.516% 0.492% 0.490% 0.489% 0.488%
$440,000 20,000 0.395% 0.393% 0.392% 0.391% 0.390%
* Applied to total projected claims48

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$440,000 30,000 0.394% 0.393% 0.392% 0.391% 0.390%
$440,000 40,000 0.394% 0.393% 0.392% 0.391% 0.390%
$445,000 25 26.918% 24.924% 23.111% 21.464% 19.954%
$445,000 50 18.870% 16.885% 15.130% 13.576% 12.195%
$445,000 100 12.602% 10.648% 8.979% 7.566% 6.367%
$445,000 150 10.033% 8.128% 6.563% 5.285% 4.256%
$445,000 200 8.357% 6.521% 5.056% 3.914% 3.040%
$445,000 300 6.338% 4.662% 3.410% 2.491% 1.842%
$445,000 400 4.972% 3.495% 2.463% 1.761% 1.292%
$445,000 500 4.628% 3.146% 2.127% 1.465% 1.051%
$445,000 600 3.852% 2.496% 1.627% 1.103% 0.805%
$445,000 700 3.393% 2.152% 1.391% 0.949% 0.711%
$445,000 800 3.106% 1.923% 1.224% 0.843% 0.650%
$445,000 900 2.905% 1.770% 1.123% 0.781% 0.614%
$445,000 1,000 2.656% 1.575% 0.989% 0.694% 0.561%
$445,000 1,500 1.943% 1.110% 0.724% 0.568% 0.510%
$445,000 2,000 1.529% 0.862% 0.602% 0.517% 0.493%
$445,000 3,000 1.008% 0.614% 0.512% 0.492% 0.488%
$445,000 4,000 0.814% 0.548% 0.497% 0.490% 0.488%
$445,000 5,000 0.707% 0.520% 0.492% 0.489% 0.488%
$445,000 10,000 0.517% 0.492% 0.490% 0.489% 0.488%
$445,000 20,000 0.395% 0.394% 0.393% 0.392% 0.391%
$445,000 30,000 0.395% 0.394% 0.393% 0.392% 0.391%
$445,000 40,000 0.395% 0.394% 0.393% 0.392% 0.391%
$450,000 25 26.945% 24.950% 23.138% 21.490% 19.981%
$450,000 50 18.897% 16.912% 15.157% 13.603% 12.223%
$450,000 100 12.625% 10.671% 9.002% 7.589% 6.390%
$450,000 150 10.057% 8.152% 6.586% 5.307% 4.277%
$450,000 200 8.377% 6.541% 5.074% 3.930% 3.055%
$450,000 300 6.354% 4.677% 3.422% 2.502% 1.851%
$450,000 400 4.986% 3.507% 2.473% 1.768% 1.298%
$450,000 500 4.640% 3.156% 2.135% 1.471% 1.056%
$450,000 600 3.863% 2.504% 1.633% 1.107% 0.808%
$450,000 700 3.400% 2.158% 1.396% 0.952% 0.713%
$450,000 800 3.114% 1.929% 1.229% 0.846% 0.652%
$450,000 900 2.913% 1.776% 1.127% 0.784% 0.615%
$450,000 1,000 2.662% 1.580% 0.992% 0.696% 0.562%
$450,000 1,500 1.948% 1.113% 0.726% 0.569% 0.511%
* Applied to total projected claims49

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$450,000 2,000 1.533% 0.865% 0.603% 0.517% 0.493%
$450,000 3,000 1.011% 0.615% 0.512% 0.492% 0.489%
$450,000 4,000 0.817% 0.549% 0.498% 0.490% 0.488%
$450,000 5,000 0.709% 0.520% 0.492% 0.489% 0.488%
$450,000 10,000 0.517% 0.492% 0.490% 0.489% 0.488%
$450,000 20,000 0.395% 0.394% 0.393% 0.392% 0.391%
$450,000 30,000 0.395% 0.394% 0.393% 0.392% 0.391%
$450,000 40,000 0.395% 0.394% 0.393% 0.392% 0.391%
$455,000 25 26.971% 24.977% 23.164% 21.517% 20.007%
$455,000 50 18.923% 16.939% 15.184% 13.630% 12.250%
$455,000 100 12.647% 10.694% 9.025% 7.611% 6.412%
$455,000 150 10.080% 8.176% 6.609% 5.329% 4.297%
$455,000 200 8.397% 6.560% 5.092% 3.947% 3.069%
$455,000 300 6.369% 4.691% 3.435% 2.513% 1.860%
$455,000 400 5.000% 3.518% 2.483% 1.776% 1.304%
$455,000 500 4.652% 3.166% 2.144% 1.477% 1.060%
$455,000 600 3.873% 2.513% 1.639% 1.111% 0.811%
$455,000 700 3.408% 2.164% 1.400% 0.956% 0.715%
$455,000 800 3.122% 1.935% 1.233% 0.849% 0.653%
$455,000 900 2.920% 1.781% 1.131% 0.786% 0.617%
$455,000 1,000 2.669% 1.584% 0.995% 0.698% 0.563%
$455,000 1,500 1.949% 1.112% 0.725% 0.568% 0.510%
$455,000 2,000 1.537% 0.867% 0.604% 0.518% 0.494%
$455,000 3,000 1.014% 0.616% 0.513% 0.492% 0.489%
$455,000 4,000 0.819% 0.550% 0.498% 0.490% 0.489%
$455,000 5,000 0.711% 0.521% 0.493% 0.490% 0.489%
$455,000 10,000 0.518% 0.492% 0.491% 0.490% 0.489%
$455,000 20,000 0.396% 0.394% 0.393% 0.392% 0.391%
$455,000 30,000 0.395% 0.394% 0.393% 0.392% 0.391%
$455,000 40,000 0.395% 0.394% 0.393% 0.392% 0.391%
$460,000 25 26.997% 25.003% 23.190% 21.543% 20.033%
$460,000 50 18.949% 16.965% 15.210% 13.657% 12.277%
$460,000 100 12.668% 10.715% 9.047% 7.633% 6.434%
$460,000 150 10.103% 8.198% 6.631% 5.350% 4.317%
$460,000 200 8.417% 6.578% 5.110% 3.962% 3.083%
$460,000 300 6.384% 4.704% 3.446% 2.523% 1.868%
$460,000 400 5.013% 3.530% 2.492% 1.784% 1.310%
$460,000 500 4.664% 3.176% 2.151% 1.483% 1.065%
* Applied to total projected claims50

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$460,000 600 3.883% 2.521% 1.645% 1.115% 0.813%
$460,000 700 3.416% 2.171% 1.405% 0.959% 0.718%
$460,000 800 3.130% 1.941% 1.237% 0.852% 0.655%
$460,000 900 2.928% 1.787% 1.135% 0.789% 0.618%
$460,000 1,000 2.675% 1.589% 0.998% 0.699% 0.564%
$460,000 1,500 1.954% 1.116% 0.727% 0.569% 0.511%
$460,000 2,000 1.541% 0.869% 0.605% 0.519% 0.494%
$460,000 3,000 1.016% 0.617% 0.513% 0.493% 0.489%
$460,000 4,000 0.821% 0.551% 0.498% 0.490% 0.489%
$460,000 5,000 0.712% 0.521% 0.493% 0.490% 0.489%
$460,000 10,000 0.518% 0.492% 0.491% 0.490% 0.489%
$460,000 20,000 0.396% 0.394% 0.393% 0.392% 0.391%
$460,000 30,000 0.395% 0.394% 0.393% 0.392% 0.391%
$460,000 40,000 0.395% 0.394% 0.393% 0.392% 0.391%
$465,000 25 27.024% 25.029% 23.217% 21.569% 20.060%
$465,000 50 18.975% 16.991% 15.236% 13.684% 12.304%
$465,000 100 12.689% 10.737% 9.068% 7.655% 6.455%
$465,000 150 10.125% 8.221% 6.653% 5.371% 4.337%
$465,000 200 8.436% 6.596% 5.127% 3.978% 3.098%
$465,000 300 6.399% 4.717% 3.459% 2.533% 1.877%
$465,000 400 5.027% 3.541% 2.501% 1.791% 1.316%
$465,000 500 4.675% 3.186% 2.160% 1.490% 1.069%
$465,000 600 3.893% 2.529% 1.651% 1.120% 0.816%
$465,000 700 3.424% 2.177% 1.410% 0.962% 0.720%
$465,000 800 3.138% 1.947% 1.241% 0.854% 0.657%
$465,000 900 2.936% 1.793% 1.139% 0.791% 0.620%
$465,000 1,000 2.681% 1.593% 1.001% 0.701% 0.566%
$465,000 1,500 1.959% 1.119% 0.729% 0.570% 0.511%
$465,000 2,000 1.544% 0.871% 0.606% 0.519% 0.494%
$465,000 3,000 1.019% 0.619% 0.514% 0.493% 0.489%
$465,000 4,000 0.823% 0.552% 0.499% 0.491% 0.489%
$465,000 5,000 0.714% 0.522% 0.493% 0.490% 0.489%
$465,000 10,000 0.519% 0.493% 0.491% 0.490% 0.489%
$465,000 20,000 0.396% 0.394% 0.393% 0.392% 0.391%
$465,000 30,000 0.395% 0.394% 0.393% 0.392% 0.391%
$465,000 40,000 0.395% 0.394% 0.393% 0.392% 0.391%
$470,000 25 27.049% 25.054% 23.242% 21.594% 20.085%
$470,000 50 19.000% 17.016% 15.262% 13.709% 12.329%
* Applied to total projected claims51

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$470,000 100 12.710% 10.758% 9.089% 7.676% 6.476%
$470,000 150 10.147% 8.243% 6.674% 5.392% 4.357%
$470,000 200 8.455% 6.614% 5.144% 3.994% 3.112%
$470,000 300 6.414% 4.731% 3.471% 2.544% 1.885%
$470,000 400 5.040% 3.553% 2.511% 1.799% 1.321%
$470,000 500 4.687% 3.196% 2.168% 1.496% 1.074%
$470,000 600 3.902% 2.537% 1.657% 1.124% 0.819%
$470,000 700 3.432% 2.184% 1.415% 0.966% 0.722%
$470,000 800 3.146% 1.953% 1.245% 0.857% 0.658%
$470,000 900 2.943% 1.799% 1.143% 0.794% 0.622%
$470,000 1,000 2.688% 1.598% 1.003% 0.703% 0.567%
$470,000 1,500 1.964% 1.122% 0.731% 0.571% 0.512%
$470,000 2,000 1.548% 0.873% 0.607% 0.520% 0.494%
$470,000 3,000 1.021% 0.620% 0.514% 0.493% 0.489%
$470,000 4,000 0.826% 0.553% 0.499% 0.491% 0.489%
$470,000 5,000 0.715% 0.522% 0.494% 0.490% 0.489%
$470,000 10,000 0.519% 0.493% 0.491% 0.490% 0.489%
$470,000 20,000 0.396% 0.395% 0.394% 0.393% 0.392%
$470,000 30,000 0.396% 0.395% 0.394% 0.393% 0.392%
$470,000 40,000 0.396% 0.395% 0.394% 0.393% 0.392%
$475,000 25 27.073% 25.078% 23.265% 21.618% 20.108%
$475,000 50 19.024% 17.040% 15.286% 13.733% 12.354%
$475,000 100 12.729% 10.777% 9.109% 7.695% 6.496%
$475,000 150 10.168% 8.264% 6.695% 5.412% 4.375%
$475,000 200 8.473% 6.631% 5.160% 4.009% 3.125%
$475,000 300 6.428% 4.744% 3.482% 2.554% 1.894%
$475,000 400 5.053% 3.564% 2.520% 1.807% 1.327%
$475,000 500 4.698% 3.206% 2.175% 1.502% 1.078%
$475,000 600 3.912% 2.544% 1.663% 1.128% 0.822%
$475,000 700 3.439% 2.190% 1.419% 0.969% 0.724%
$475,000 800 3.153% 1.959% 1.250% 0.860% 0.660%
$475,000 900 2.951% 1.804% 1.147% 0.796% 0.623%
$475,000 1,000 2.694% 1.602% 1.006% 0.705% 0.568%
$475,000 1,500 1.969% 1.126% 0.733% 0.572% 0.513%
$475,000 2,000 1.552% 0.876% 0.608% 0.520% 0.495%
$475,000 3,000 1.024% 0.621% 0.515% 0.493% 0.490%
$475,000 4,000 0.828% 0.553% 0.499% 0.491% 0.489%
$475,000 5,000 0.717% 0.523% 0.494% 0.490% 0.489%
* Applied to total projected claims52

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$475,000 10,000 0.520% 0.493% 0.491% 0.490% 0.489%
$475,000 20,000 0.396% 0.395% 0.394% 0.393% 0.392%
$475,000 30,000 0.396% 0.395% 0.394% 0.393% 0.392%
$475,000 40,000 0.396% 0.395% 0.394% 0.393% 0.392%
$480,000 25 27.097% 25.102% 23.289% 21.641% 20.132%
$480,000 50 19.048% 17.064% 15.310% 13.757% 12.378%
$480,000 100 12.748% 10.797% 9.129% 7.715% 6.515%
$480,000 150 10.190% 8.285% 6.716% 5.433% 4.394%
$480,000 200 8.490% 6.648% 5.176% 4.024% 3.138%
$480,000 300 6.443% 4.757% 3.494% 2.564% 1.902%
$480,000 400 5.066% 3.575% 2.529% 1.814% 1.333%
$480,000 500 4.709% 3.215% 2.183% 1.508% 1.083%
$480,000 600 3.922% 2.552% 1.669% 1.132% 0.825%
$480,000 700 3.447% 2.196% 1.424% 0.972% 0.726%
$480,000 800 3.161% 1.965% 1.254% 0.862% 0.662%
$480,000 900 2.958% 1.810% 1.151% 0.799% 0.625%
$480,000 1,000 2.700% 1.607% 1.009% 0.707% 0.569%
$480,000 1,500 1.975% 1.129% 0.735% 0.573% 0.513%
$480,000 2,000 1.555% 0.878% 0.609% 0.521% 0.495%
$480,000 3,000 1.027% 0.622% 0.515% 0.494% 0.490%
$480,000 4,000 0.830% 0.554% 0.500% 0.491% 0.490%
$480,000 5,000 0.718% 0.523% 0.494% 0.491% 0.490%
$480,000 10,000 0.520% 0.493% 0.492% 0.491% 0.490%
$480,000 20,000 0.397% 0.395% 0.394% 0.393% 0.392%
$480,000 30,000 0.396% 0.395% 0.394% 0.393% 0.392%
$480,000 40,000 0.396% 0.395% 0.394% 0.393% 0.392%
$485,000 25 27.121% 25.126% 23.313% 21.665% 20.156%
$485,000 50 19.070% 17.086% 15.332% 13.780% 12.401%
$485,000 100 12.767% 10.816% 9.148% 7.734% 6.534%
$485,000 150 10.210% 8.305% 6.736% 5.452% 4.412%
$485,000 200 8.507% 6.664% 5.191% 4.038% 3.151%
$485,000 300 6.456% 4.770% 3.506% 2.574% 1.910%
$485,000 400 5.078% 3.586% 2.539% 1.822% 1.339%
$485,000 500 4.720% 3.225% 2.191% 1.514% 1.087%
$485,000 600 3.931% 2.560% 1.675% 1.137% 0.828%
$485,000 700 3.454% 2.202% 1.428% 0.975% 0.729%
$485,000 800 3.168% 1.971% 1.258% 0.865% 0.664%
$485,000 900 2.966% 1.816% 1.155% 0.801% 0.626%
* Applied to total projected claims53

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$485,000 1,000 2.706% 1.611% 1.012% 0.709% 0.570%
$485,000 1,500 1.979% 1.132% 0.736% 0.574% 0.514%
$485,000 2,000 1.559% 0.880% 0.611% 0.521% 0.495%
$485,000 3,000 1.029% 0.623% 0.516% 0.494% 0.490%
$485,000 4,000 0.832% 0.555% 0.500% 0.492% 0.490%
$485,000 5,000 0.720% 0.524% 0.494% 0.491% 0.490%
$485,000 10,000 0.521% 0.494% 0.492% 0.491% 0.490%
$485,000 20,000 0.397% 0.395% 0.394% 0.393% 0.392%
$485,000 30,000 0.396% 0.395% 0.394% 0.393% 0.392%
$485,000 40,000 0.396% 0.395% 0.394% 0.393% 0.392%
$490,000 25 27.143% 25.148% 23.335% 21.687% 20.178%
$490,000 50 19.091% 17.107% 15.353% 13.801% 12.422%
$490,000 100 12.784% 10.833% 9.166% 7.752% 6.552%
$490,000 150 10.229% 8.324% 6.755% 5.471% 4.430%
$490,000 200 8.523% 6.679% 5.206% 4.052% 3.163%
$490,000 300 6.469% 4.781% 3.516% 2.583% 1.917%
$490,000 400 5.090% 3.596% 2.547% 1.829% 1.344%
$490,000 500 4.730% 3.233% 2.198% 1.519% 1.091%
$490,000 600 3.940% 2.567% 1.680% 1.141% 0.830%
$490,000 700 3.460% 2.207% 1.432% 0.978% 0.731%
$490,000 800 3.175% 1.976% 1.262% 0.868% 0.665%
$490,000 900 2.973% 1.821% 1.158% 0.804% 0.628%
$490,000 1,000 2.712% 1.615% 1.015% 0.710% 0.571%
$490,000 1,500 1.984% 1.135% 0.738% 0.575% 0.514%
$490,000 2,000 1.562% 0.882% 0.612% 0.522% 0.496%
$490,000 3,000 1.031% 0.624% 0.516% 0.494% 0.490%
$490,000 4,000 0.834% 0.556% 0.500% 0.492% 0.490%
$490,000 5,000 0.721% 0.524% 0.495% 0.491% 0.490%
$490,000 10,000 0.521% 0.494% 0.492% 0.491% 0.490%
$490,000 20,000 0.397% 0.395% 0.394% 0.393% 0.392%
$490,000 30,000 0.396% 0.395% 0.394% 0.393% 0.392%
$490,000 40,000 0.396% 0.395% 0.394% 0.393% 0.392%
$495,000 25 27.164% 25.168% 23.356% 21.708% 20.199%
$495,000 50 19.109% 17.126% 15.372% 13.820% 12.441%
$495,000 100 12.800% 10.850% 9.182% 7.769% 6.569%
$495,000 150 10.246% 8.343% 6.773% 5.488% 4.446%
$495,000 200 8.539% 6.694% 5.220% 4.065% 3.175%
$495,000 300 6.481% 4.792% 3.526% 2.592% 1.925%
* Applied to total projected claims54

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Aggregate Stop Loss Rate Factors *
Exhibit 8A
ISL limit members 110% 115% 120% 125% 130%
$495,000 400 5.101% 3.606% 2.555% 1.836% 1.350%
$495,000 500 4.740% 3.242% 2.205% 1.524% 1.095%
$495,000 600 3.949% 2.574% 1.685% 1.144% 0.833%
$495,000 700 3.467% 2.212% 1.436% 0.981% 0.733%
$495,000 800 3.182% 1.981% 1.265% 0.870% 0.667%
$495,000 900 2.979% 1.826% 1.162% 0.806% 0.629%
$495,000 1,000 2.717% 1.619% 1.017% 0.712% 0.572%
$495,000 1,500 1.988% 1.137% 0.739% 0.575% 0.515%
$495,000 2,000 1.565% 0.884% 0.613% 0.522% 0.496%
$495,000 3,000 1.034% 0.625% 0.516% 0.494% 0.491%
$495,000 4,000 0.836% 0.556% 0.500% 0.492% 0.490%
$495,000 5,000 0.722% 0.525% 0.495% 0.491% 0.490%
$495,000 10,000 0.521% 0.494% 0.492% 0.491% 0.490%
$495,000 20,000 0.397% 0.395% 0.394% 0.393% 0.392%
$495,000 30,000 0.396% 0.395% 0.394% 0.393% 0.392%
$495,000 40,000 0.396% 0.395% 0.394% 0.393% 0.392%
$500,000 25 27.185% 25.189% 23.377% 21.729% 20.219%
$500,000 50 19.128% 17.145% 15.391% 13.840% 12.461%
$500,000 100 12.816% 10.866% 9.199% 7.786% 6.586%
$500,000 150 10.264% 8.361% 6.791% 5.506% 4.463%
$500,000 200 8.554% 6.709% 5.234% 4.078% 3.187%
$500,000 300 6.493% 4.804% 3.536% 2.600% 1.932%
$500,000 400 5.112% 3.616% 2.564% 1.843% 1.355%
$500,000 500 4.749% 3.250% 2.212% 1.529% 1.099%
$500,000 600 3.957% 2.581% 1.690% 1.148% 0.835%
$500,000 700 3.473% 2.217% 1.440% 0.984% 0.735%
$500,000 800 3.188% 1.986% 1.269% 0.872% 0.668%
$500,000 900 2.985% 1.831% 1.165% 0.808% 0.631%
$500,000 1,000 2.723% 1.623% 1.020% 0.714% 0.573%
$500,000 1,500 1.992% 1.140% 0.741% 0.576% 0.515%
$500,000 2,000 1.569% 0.886% 0.613% 0.523% 0.496%
$500,000 3,000 1.036% 0.626% 0.517% 0.495% 0.491%
$500,000 4,000 0.838% 0.557% 0.501% 0.492% 0.490%
$500,000 5,000 0.724% 0.525% 0.495% 0.491% 0.490%
$500,000 10,000 0.522% 0.494% 0.492% 0.491% 0.490%
$500,000 20,000 0.397% 0.396% 0.395% 0.394% 0.393%
$500,000 30,000 0.397% 0.396% 0.395% 0.394% 0.393%
$500,000 40,000 0.397% 0.396% 0.395% 0.394% 0.393%
* Applied to total projected claims55

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$30,000 25 7.403% 6.144%
$30,000 50 4.960% 3.797%
$30,000 100 3.318% 2.251%
$30,000 150 2.697% 1.715%
$30,000 200 2.204% 1.289%
$30,000 300 1.785% 0.933%
$30,000 400 1.385% 0.632%
$30,000 500 1.248% 0.523%
$30,000 600 1.072% 0.409%
$30,000 700 0.928% 0.323%
$30,000 800 0.829% 0.264%
$30,000 900 0.741% 0.217%
$30,000 1,000 0.696% 0.192%
$30,000 1,500 0.445% 0.085%
$30,000 2,000 0.330% 0.045%
$30,000 3,000 0.170% 0.011%
$30,000 4,000 0.114% 0.004%
$30,000 5,000 0.084% 0.003%
$30,000 10,000 0.022% 0.001%
$30,000 20,000 0.003% 0.001%
$30,000 30,000 0.002% 0.001%
$30,000 40,000 0.002% 0.001%
$35,000 25 8.196% 6.881%
$35,000 50 5.480% 4.255%
$35,000 100 3.671% 2.539%
$35,000 150 2.989% 1.944%
$35,000 200 2.450% 1.471%
$35,000 300 1.983% 1.069%
$35,000 400 1.544% 0.734%
$35,000 500 1.404% 0.617%
$35,000 600 1.215% 0.490%
$35,000 700 1.056% 0.390%
$35,000 800 0.947% 0.322%
$35,000 900 0.851% 0.267%
$35,000 1,000 0.797% 0.236%
$35,000 1,500 0.519% 0.110%
$35,000 2,000 0.392% 0.061%
* Applied to total projected claims1

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$35,000 3,000 0.204% 0.016%
$35,000 4,000 0.138% 0.006%
$35,000 5,000 0.102% 0.003%
$35,000 10,000 0.028% 0.001%
$35,000 20,000 0.004% 0.001%
$35,000 30,000 0.002% 0.001%
$35,000 40,000 0.002% 0.001%
$40,000 25 8.882% 7.520%
$40,000 50 5.928% 4.656%
$40,000 100 3.975% 2.794%
$40,000 150 3.240% 2.146%
$40,000 200 2.662% 1.633%
$40,000 300 2.151% 1.188%
$40,000 400 1.683% 0.827%
$40,000 500 1.538% 0.701%
$40,000 600 1.336% 0.562%
$40,000 700 1.166% 0.451%
$40,000 800 1.052% 0.377%
$40,000 900 0.950% 0.316%
$40,000 1,000 0.887% 0.278%
$40,000 1,500 0.584% 0.133%
$40,000 2,000 0.448% 0.077%
$40,000 3,000 0.236% 0.021%
$40,000 4,000 0.161% 0.008%
$40,000 5,000 0.119% 0.004%
$40,000 10,000 0.034% 0.001%
$40,000 20,000 0.004% 0.001%
$40,000 30,000 0.002% 0.001%
$40,000 40,000 0.002% 0.001%
$45,000 25 9.508% 8.108%
$45,000 50 6.341% 5.029%
$45,000 100 4.258% 3.034%
$45,000 150 3.471% 2.334%
$45,000 200 2.857% 1.785%
$45,000 300 2.308% 1.302%
$45,000 400 1.813% 0.917%
$45,000 500 1.663% 0.782%
* Applied to total projected claims2

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$45,000 600 1.446% 0.629%
$45,000 700 1.268% 0.510%
$45,000 800 1.150% 0.432%
$45,000 900 1.041% 0.363%
$45,000 1,000 0.969% 0.319%
$45,000 1,500 0.645% 0.156%
$45,000 2,000 0.501% 0.094%
$45,000 3,000 0.266% 0.026%
$45,000 4,000 0.183% 0.010%
$45,000 5,000 0.135% 0.006%
$45,000 10,000 0.039% 0.001%
$45,000 20,000 0.005% 0.001%
$45,000 30,000 0.002% 0.001%
$45,000 40,000 0.002% 0.001%
$50,000 25 10.079% 8.645%
$50,000 50 6.719% 5.372%
$50,000 100 4.520% 3.259%
$50,000 150 3.684% 2.508%
$50,000 200 3.040% 1.930%
$50,000 300 2.452% 1.407%
$50,000 400 1.933% 1.001%
$50,000 500 1.780% 0.860%
$50,000 600 1.547% 0.692%
$50,000 700 1.364% 0.567%
$50,000 800 1.240% 0.483%
$50,000 900 1.126% 0.409%
$50,000 1,000 1.046% 0.359%
$50,000 1,500 0.704% 0.180%
$50,000 2,000 0.551% 0.111%
$50,000 3,000 0.296% 0.032%
$50,000 4,000 0.204% 0.013%
$50,000 5,000 0.152% 0.007%
$50,000 10,000 0.045% 0.001%
$50,000 20,000 0.006% 0.001%
$50,000 30,000 0.002% 0.001%
$50,000 40,000 0.002% 0.001%
$55,000 25 10.603% 9.141%
* Applied to total projected claims3

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$55,000 50 7.073% 5.694%
$55,000 100 4.765% 3.470%
$55,000 150 3.880% 2.670%
$55,000 200 3.212% 2.067%
$55,000 300 2.585% 1.506%
$55,000 400 2.044% 1.080%
$55,000 500 1.889% 0.934%
$55,000 600 1.641% 0.752%
$55,000 700 1.452% 0.621%
$55,000 800 1.324% 0.533%
$55,000 900 1.207% 0.454%
$55,000 1,000 1.118% 0.397%
$55,000 1,500 0.759% 0.204%
$55,000 2,000 0.599% 0.128%
$55,000 3,000 0.325% 0.038%
$55,000 4,000 0.224% 0.016%
$55,000 5,000 0.168% 0.009%
$55,000 10,000 0.051% 0.001%
$55,000 20,000 0.007% 0.001%
$55,000 30,000 0.002% 0.001%
$55,000 40,000 0.002% 0.001%
$60,000 25 11.080% 9.595%
$60,000 50 7.401% 5.992%
$60,000 100 4.988% 3.662%
$60,000 150 4.062% 2.822%
$60,000 200 3.372% 2.196%
$60,000 300 2.707% 1.598%
$60,000 400 2.144% 1.153%
$60,000 500 1.988% 1.002%
$60,000 600 1.729% 0.810%
$60,000 700 1.534% 0.673%
$60,000 800 1.402% 0.579%
$60,000 900 1.282% 0.497%
$60,000 1,000 1.186% 0.434%
$60,000 1,500 0.812% 0.227%
$60,000 2,000 0.644% 0.144%
$60,000 3,000 0.353% 0.045%
* Applied to total projected claims4

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$60,000 4,000 0.244% 0.019%
$60,000 5,000 0.182% 0.010%
$60,000 10,000 0.057% 0.001%
$60,000 20,000 0.008% 0.001%
$60,000 30,000 0.002% 0.001%
$60,000 40,000 0.002% 0.001%
$65,000 25 11.518% 10.013%
$65,000 50 7.707% 6.271%
$65,000 100 5.195% 3.844%
$65,000 150 4.231% 2.965%
$65,000 200 3.525% 2.320%
$65,000 300 2.821% 1.685%
$65,000 400 2.238% 1.222%
$65,000 500 2.082% 1.067%
$65,000 600 1.811% 0.864%
$65,000 700 1.610% 0.721%
$65,000 800 1.474% 0.624%
$65,000 900 1.352% 0.538%
$65,000 1,000 1.250% 0.469%
$65,000 1,500 0.863% 0.250%
$65,000 2,000 0.687% 0.161%
$65,000 3,000 0.380% 0.051%
$65,000 4,000 0.264% 0.022%
$65,000 5,000 0.197% 0.012%
$65,000 10,000 0.062% 0.001%
$65,000 20,000 0.009% 0.001%
$65,000 30,000 0.003% 0.001%
$65,000 40,000 0.002% 0.001%
$70,000 25 11.929% 10.406%
$70,000 50 7.993% 6.534%
$70,000 100 5.390% 4.014%
$70,000 150 4.390% 3.099%
$70,000 200 3.668% 2.436%
$70,000 300 2.931% 1.770%
$70,000 400 2.327% 1.288%
$70,000 500 2.170% 1.129%
$70,000 600 1.887% 0.915%
* Applied to total projected claims5

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$70,000 700 1.684% 0.769%
$70,000 800 1.542% 0.665%
$70,000 900 1.417% 0.577%
$70,000 1,000 1.310% 0.503%
$70,000 1,500 0.911% 0.273%
$70,000 2,000 0.727% 0.177%
$70,000 3,000 0.407% 0.059%
$70,000 4,000 0.284% 0.025%
$70,000 5,000 0.211% 0.014%
$70,000 10,000 0.067% 0.001%
$70,000 20,000 0.010% 0.001%
$70,000 30,000 0.003% 0.001%
$70,000 40,000 0.002% 0.001%
$75,000 25 12.314% 10.775%
$75,000 50 8.265% 6.788%
$75,000 100 5.575% 4.179%
$75,000 150 4.540% 3.229%
$75,000 200 3.800% 2.544%
$75,000 300 3.035% 1.852%
$75,000 400 2.410% 1.351%
$75,000 500 2.252% 1.187%
$75,000 600 1.958% 0.963%
$75,000 700 1.752% 0.814%
$75,000 800 1.605% 0.705%
$75,000 900 1.477% 0.613%
$75,000 1,000 1.367% 0.536%
$75,000 1,500 0.956% 0.294%
$75,000 2,000 0.764% 0.193%
$75,000 3,000 0.433% 0.066%
$75,000 4,000 0.303% 0.029%
$75,000 5,000 0.225% 0.016%
$75,000 10,000 0.072% 0.001%
$75,000 20,000 0.011% 0.001%
$75,000 30,000 0.003% 0.001%
$75,000 40,000 0.002% 0.001%
$80,000 25 12.678% 11.127%
$80,000 50 8.524% 7.029%
* Applied to total projected claims6

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$80,000 100 5.751% 4.337%
$80,000 150 4.684% 3.351%
$80,000 200 3.924% 2.648%
$80,000 300 3.133% 1.930%
$80,000 400 2.488% 1.410%
$80,000 500 2.331% 1.244%
$80,000 600 2.027% 1.010%
$80,000 700 1.818% 0.858%
$80,000 800 1.664% 0.742%
$80,000 900 1.534% 0.648%
$80,000 1,000 1.421% 0.568%
$80,000 1,500 0.998% 0.315%
$80,000 2,000 0.801% 0.208%
$80,000 3,000 0.457% 0.073%
$80,000 4,000 0.321% 0.032%
$80,000 5,000 0.239% 0.018%
$80,000 10,000 0.077% 0.002%
$80,000 20,000 0.013% 0.001%
$80,000 30,000 0.003% 0.001%
$80,000 40,000 0.002% 0.001%
$85,000 25 13.018% 11.456%
$85,000 50 8.763% 7.254%
$85,000 100 5.914% 4.487%
$85,000 150 4.815% 3.464%
$85,000 200 4.038% 2.744%
$85,000 300 3.224% 2.002%
$85,000 400 2.560% 1.465%
$85,000 500 2.404% 1.298%
$85,000 600 2.090% 1.054%
$85,000 700 1.877% 0.898%
$85,000 800 1.716% 0.776%
$85,000 900 1.587% 0.681%
$85,000 1,000 1.471% 0.598%
$85,000 1,500 1.037% 0.335%
$85,000 2,000 0.834% 0.223%
$85,000 3,000 0.480% 0.080%
$85,000 4,000 0.338% 0.036%
* Applied to total projected claims7

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$85,000 5,000 0.253% 0.020%
$85,000 10,000 0.082% 0.002%
$85,000 20,000 0.014% 0.001%
$85,000 30,000 0.003% 0.001%
$85,000 40,000 0.002% 0.001%
$90,000 25 13.345% 11.774%
$90,000 50 8.987% 7.464%
$90,000 100 6.073% 4.633%
$90,000 150 4.943% 3.574%
$90,000 200 4.148% 2.835%
$90,000 300 3.311% 2.071%
$90,000 400 2.629% 1.518%
$90,000 500 2.475% 1.350%
$90,000 600 2.152% 1.097%
$90,000 700 1.934% 0.936%
$90,000 800 1.766% 0.808%
$90,000 900 1.637% 0.713%
$90,000 1,000 1.519% 0.627%
$90,000 1,500 1.075% 0.354%
$90,000 2,000 0.866% 0.237%
$90,000 3,000 0.502% 0.086%
$90,000 4,000 0.355% 0.040%
$90,000 5,000 0.265% 0.022%
$90,000 10,000 0.087% 0.002%
$90,000 20,000 0.015% 0.001%
$90,000 30,000 0.003% 0.001%
$90,000 40,000 0.002% 0.001%
$95,000 25 13.652% 12.076%
$95,000 50 9.197% 7.662%
$95,000 100 6.222% 4.770%
$95,000 150 5.064% 3.679%
$95,000 200 4.251% 2.922%
$95,000 300 3.392% 2.136%
$95,000 400 2.695% 1.568%
$95,000 500 2.542% 1.399%
$95,000 600 2.210% 1.138%
$95,000 700 1.989% 0.973%
* Applied to total projected claims8

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$95,000 800 1.813% 0.838%
$95,000 900 1.685% 0.743%
$95,000 1,000 1.564% 0.655%
$95,000 1,500 1.111% 0.373%
$95,000 2,000 0.897% 0.251%
$95,000 3,000 0.523% 0.093%
$95,000 4,000 0.372% 0.043%
$95,000 5,000 0.278% 0.024%
$95,000 10,000 0.091% 0.002%
$95,000 20,000 0.016% 0.001%
$95,000 30,000 0.004% 0.001%
$95,000 40,000 0.002% 0.001%
$100,000 25 13.939% 12.359%
$100,000 50 9.398% 7.851%
$100,000 100 6.362% 4.898%
$100,000 150 5.175% 3.776%
$100,000 200 4.348% 3.005%
$100,000 300 3.469% 2.198%
$100,000 400 2.755% 1.615%
$100,000 500 2.605% 1.446%
$100,000 600 2.264% 1.177%
$100,000 700 2.038% 1.008%
$100,000 800 1.856% 0.867%
$100,000 900 1.730% 0.772%
$100,000 1,000 1.606% 0.681%
$100,000 1,500 1.145% 0.391%
$100,000 2,000 0.925% 0.265%
$100,000 3,000 0.543% 0.099%
$100,000 4,000 0.388% 0.047%
$100,000 5,000 0.290% 0.026%
$100,000 10,000 0.096% 0.002%
$100,000 20,000 0.017% 0.001%
$100,000 30,000 0.004% 0.001%
$100,000 40,000 0.002% 0.001%
$105,000 25 14.220% 12.638%
$105,000 50 9.597% 8.039%
$105,000 100 6.502% 5.026%
* Applied to total projected claims9

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$105,000 150 5.283% 3.870%
$105,000 200 4.445% 3.087%
$105,000 300 3.545% 2.260%
$105,000 400 2.814% 1.662%
$105,000 500 2.667% 1.493%
$105,000 600 2.317% 1.215%
$105,000 700 2.088% 1.042%
$105,000 800 1.899% 0.896%
$105,000 900 1.775% 0.801%
$105,000 1,000 1.648% 0.708%
$105,000 1,500 1.179% 0.409%
$105,000 2,000 0.953% 0.278%
$105,000 3,000 0.563% 0.106%
$105,000 4,000 0.403% 0.051%
$105,000 5,000 0.302% 0.028%
$105,000 10,000 0.100% 0.002%
$105,000 20,000 0.018% 0.001%
$105,000 30,000 0.004% 0.001%
$105,000 40,000 0.002% 0.001%
$110,000 25 14.490% 12.908%
$110,000 50 9.786% 8.218%
$110,000 100 6.635% 5.148%
$110,000 150 5.389% 3.962%
$110,000 200 4.538% 3.166%
$110,000 300 3.620% 2.320%
$110,000 400 2.871% 1.707%
$110,000 500 2.726% 1.537%
$110,000 600 2.368% 1.252%
$110,000 700 2.135% 1.075%
$110,000 800 1.941% 0.925%
$110,000 900 1.817% 0.829%
$110,000 1,000 1.689% 0.734%
$110,000 1,500 1.211% 0.427%
$110,000 2,000 0.980% 0.290%
$110,000 3,000 0.582% 0.112%
$110,000 4,000 0.418% 0.055%
$110,000 5,000 0.314% 0.030%
* Applied to total projected claims10

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$110,000 10,000 0.105% 0.002%
$110,000 20,000 0.019% 0.001%
$110,000 30,000 0.004% 0.001%
$110,000 40,000 0.002% 0.001%
$115,000 25 14.739% 13.157%
$115,000 50 9.962% 8.387%
$115,000 100 6.756% 5.261%
$115,000 150 5.487% 4.048%
$115,000 200 4.625% 3.242%
$115,000 300 3.689% 2.377%
$115,000 400 2.924% 1.749%
$115,000 500 2.779% 1.578%
$115,000 600 2.415% 1.287%
$115,000 700 2.178% 1.106%
$115,000 800 1.980% 0.951%
$115,000 900 1.857% 0.855%
$115,000 1,000 1.727% 0.759%
$115,000 1,500 1.240% 0.444%
$115,000 2,000 1.006% 0.303%
$115,000 3,000 0.600% 0.118%
$115,000 4,000 0.432% 0.058%
$115,000 5,000 0.326% 0.033%
$115,000 10,000 0.109% 0.003%
$115,000 20,000 0.020% 0.001%
$115,000 30,000 0.004% 0.001%
$115,000 40,000 0.002% 0.001%
$120,000 25 14.980% 13.398%
$120,000 50 10.138% 8.555%
$120,000 100 6.877% 5.373%
$120,000 150 5.582% 4.133%
$120,000 200 4.711% 3.316%
$120,000 300 3.756% 2.432%
$120,000 400 2.977% 1.792%
$120,000 500 2.831% 1.618%
$120,000 600 2.461% 1.322%
$120,000 700 2.221% 1.136%
$120,000 800 2.017% 0.977%
* Applied to total projected claims11

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$120,000 900 1.897% 0.882%
$120,000 1,000 1.763% 0.783%
$120,000 1,500 1.269% 0.460%
$120,000 2,000 1.030% 0.315%
$120,000 3,000 0.618% 0.125%
$120,000 4,000 0.445% 0.062%
$120,000 5,000 0.337% 0.035%
$120,000 10,000 0.113% 0.003%
$120,000 20,000 0.022% 0.001%
$120,000 30,000 0.005% 0.001%
$120,000 40,000 0.002% 0.001%
$125,000 25 15.215% 13.633%
$125,000 50 10.311% 8.721%
$125,000 100 6.995% 5.482%
$125,000 150 5.675% 4.215%
$125,000 200 4.796% 3.390%
$125,000 300 3.822% 2.487%
$125,000 400 3.030% 1.833%
$125,000 500 2.882% 1.657%
$125,000 600 2.507% 1.355%
$125,000 700 2.261% 1.165%
$125,000 800 2.054% 1.002%
$125,000 900 1.935% 0.908%
$125,000 1,000 1.799% 0.807%
$125,000 1,500 1.297% 0.476%
$125,000 2,000 1.055% 0.327%
$125,000 3,000 0.635% 0.131%
$125,000 4,000 0.458% 0.066%
$125,000 5,000 0.348% 0.037%
$125,000 10,000 0.117% 0.003%
$125,000 20,000 0.023% 0.001%
$125,000 30,000 0.005% 0.001%
$125,000 40,000 0.002% 0.001%
$130,000 25 15.433% 13.853%
$130,000 50 10.474% 8.879%
$130,000 100 7.104% 5.583%
$130,000 150 5.762% 4.292%
* Applied to total projected claims12

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$130,000 200 4.878% 3.461%
$130,000 300 3.885% 2.539%
$130,000 400 3.079% 1.873%
$130,000 500 2.931% 1.695%
$130,000 600 2.550% 1.388%
$130,000 700 2.300% 1.193%
$130,000 800 2.089% 1.026%
$130,000 900 1.971% 0.933%
$130,000 1,000 1.834% 0.829%
$130,000 1,500 1.324% 0.492%
$130,000 2,000 1.078% 0.339%
$130,000 3,000 0.652% 0.137%
$130,000 4,000 0.471% 0.069%
$130,000 5,000 0.359% 0.040%
$130,000 10,000 0.121% 0.003%
$130,000 20,000 0.024% 0.001%
$130,000 30,000 0.005% 0.001%
$130,000 40,000 0.002% 0.001%
$135,000 25 15.640% 14.063%
$135,000 50 10.630% 9.031%
$135,000 100 7.210% 5.680%
$135,000 150 5.843% 4.365%
$135,000 200 4.958% 3.531%
$135,000 300 3.944% 2.589%
$135,000 400 3.126% 1.911%
$135,000 500 2.977% 1.732%
$135,000 600 2.590% 1.418%
$135,000 700 2.336% 1.219%
$135,000 800 2.122% 1.050%
$135,000 900 2.005% 0.956%
$135,000 1,000 1.866% 0.851%
$135,000 1,500 1.349% 0.507%
$135,000 2,000 1.100% 0.350%
$135,000 3,000 0.668% 0.143%
$135,000 4,000 0.484% 0.073%
$135,000 5,000 0.369% 0.042%
$135,000 10,000 0.125% 0.004%
* Applied to total projected claims13

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$135,000 20,000 0.025% 0.001%
$135,000 30,000 0.005% 0.001%
$135,000 40,000 0.002% 0.001%
$140,000 25 15.845% 14.271%
$140,000 50 10.784% 9.180%
$140,000 100 7.314% 5.777%
$140,000 150 5.923% 4.436%
$140,000 200 5.037% 3.600%
$140,000 300 4.003% 2.638%
$140,000 400 3.172% 1.948%
$140,000 500 3.023% 1.768%
$140,000 600 2.631% 1.448%
$140,000 700 2.372% 1.245%
$140,000 800 2.155% 1.073%
$140,000 900 2.039% 0.980%
$140,000 1,000 1.898% 0.872%
$140,000 1,500 1.375% 0.521%
$140,000 2,000 1.122% 0.362%
$140,000 3,000 0.684% 0.149%
$140,000 4,000 0.496% 0.076%
$140,000 5,000 0.380% 0.044%
$140,000 10,000 0.129% 0.004%
$140,000 20,000 0.026% 0.001%
$140,000 30,000 0.006% 0.001%
$140,000 40,000 0.002% 0.001%
$145,000 25 16.039% 14.467%
$145,000 50 10.931% 9.324%
$145,000 100 7.414% 5.870%
$145,000 150 5.999% 4.505%
$145,000 200 5.113% 3.666%
$145,000 300 4.060% 2.686%
$145,000 400 3.216% 1.983%
$145,000 500 3.067% 1.803%
$145,000 600 2.669% 1.477%
$145,000 700 2.406% 1.270%
$145,000 800 2.187% 1.096%
$145,000 900 2.072% 1.003%
* Applied to total projected claims14

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$145,000 1,000 1.928% 0.893%
$145,000 1,500 1.399% 0.536%
$145,000 2,000 1.143% 0.373%
$145,000 3,000 0.699% 0.155%
$145,000 4,000 0.508% 0.080%
$145,000 5,000 0.389% 0.047%
$145,000 10,000 0.133% 0.004%
$145,000 20,000 0.027% 0.001%
$145,000 30,000 0.006% 0.001%
$145,000 40,000 0.002% 0.001%
$150,000 25 16.216% 14.648%
$150,000 50 11.071% 9.461%
$150,000 100 7.509% 5.958%
$150,000 150 6.072% 4.570%
$150,000 200 5.183% 3.729%
$150,000 300 4.113% 2.731%
$150,000 400 3.258% 2.018%
$150,000 500 3.109% 1.836%
$150,000 600 2.705% 1.504%
$150,000 700 2.439% 1.294%
$150,000 800 2.218% 1.118%
$150,000 900 2.103% 1.025%
$150,000 1,000 1.957% 0.913%
$150,000 1,500 1.422% 0.550%
$150,000 2,000 1.163% 0.384%
$150,000 3,000 0.714% 0.161%
$150,000 4,000 0.519% 0.083%
$150,000 5,000 0.399% 0.049%
$150,000 10,000 0.137% 0.004%
$150,000 20,000 0.028% 0.001%
$150,000 30,000 0.006% 0.001%
$150,000 40,000 0.002% 0.001%
$155,000 25 16.385% 14.819%
$155,000 50 11.204% 9.594%
$155,000 100 7.601% 6.044%
$155,000 150 6.143% 4.634%
$155,000 200 5.251% 3.789%
* Applied to total projected claims15

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$155,000 300 4.164% 2.775%
$155,000 400 3.299% 2.051%
$155,000 500 3.150% 1.869%
$155,000 600 2.740% 1.531%
$155,000 700 2.470% 1.317%
$155,000 800 2.248% 1.139%
$155,000 900 2.133% 1.047%
$155,000 1,000 1.985% 0.933%
$155,000 1,500 1.444% 0.563%
$155,000 2,000 1.183% 0.395%
$155,000 3,000 0.728% 0.166%
$155,000 4,000 0.530% 0.087%
$155,000 5,000 0.408% 0.051%
$155,000 10,000 0.140% 0.004%
$155,000 20,000 0.029% 0.001%
$155,000 30,000 0.006% 0.001%
$155,000 40,000 0.002% 0.001%
$160,000 25 16.546% 14.982%
$160,000 50 11.334% 9.724%
$160,000 100 7.690% 6.126%
$160,000 150 6.213% 4.697%
$160,000 200 5.315% 3.847%
$160,000 300 4.214% 2.818%
$160,000 400 3.339% 2.084%
$160,000 500 3.190% 1.901%
$160,000 600 2.774% 1.557%
$160,000 700 2.499% 1.339%
$160,000 800 2.277% 1.160%
$160,000 900 2.163% 1.068%
$160,000 1,000 2.012% 0.951%
$160,000 1,500 1.466% 0.576%
$160,000 2,000 1.202% 0.405%
$160,000 3,000 0.742% 0.171%
$160,000 4,000 0.541% 0.090%
$160,000 5,000 0.418% 0.053%
$160,000 10,000 0.144% 0.005%
$160,000 20,000 0.030% 0.001%
* Applied to total projected claims16

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$160,000 30,000 0.007% 0.001%
$160,000 40,000 0.002% 0.001%
$165,000 25 16.696% 15.134%
$165,000 50 11.457% 9.846%
$165,000 100 7.774% 6.205%
$165,000 150 6.280% 4.758%
$165,000 200 5.376% 3.901%
$165,000 300 4.261% 2.858%
$165,000 400 3.377% 2.115%
$165,000 500 3.229% 1.932%
$165,000 600 2.806% 1.582%
$165,000 700 2.527% 1.360%
$165,000 800 2.305% 1.180%
$165,000 900 2.191% 1.088%
$165,000 1,000 2.038% 0.969%
$165,000 1,500 1.487% 0.589%
$165,000 2,000 1.220% 0.415%
$165,000 3,000 0.755% 0.177%
$165,000 4,000 0.552% 0.094%
$165,000 5,000 0.427% 0.055%
$165,000 10,000 0.148% 0.005%
$165,000 20,000 0.032% 0.001%
$165,000 30,000 0.007% 0.001%
$165,000 40,000 0.002% 0.001%
$170,000 25 16.837% 15.278%
$170,000 50 11.576% 9.965%
$170,000 100 7.855% 6.282%
$170,000 150 6.345% 4.817%
$170,000 200 5.435% 3.954%
$170,000 300 4.307% 2.898%
$170,000 400 3.414% 2.146%
$170,000 500 3.266% 1.962%
$170,000 600 2.838% 1.606%
$170,000 700 2.555% 1.380%
$170,000 800 2.333% 1.200%
$170,000 900 2.218% 1.107%
$170,000 1,000 2.062% 0.986%
* Applied to total projected claims17

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$170,000 1,500 1.508% 0.602%
$170,000 2,000 1.238% 0.425%
$170,000 3,000 0.768% 0.182%
$170,000 4,000 0.562% 0.097%
$170,000 5,000 0.435% 0.058%
$170,000 10,000 0.151% 0.005%
$170,000 20,000 0.033% 0.001%
$170,000 30,000 0.007% 0.001%
$170,000 40,000 0.002% 0.001%
$175,000 25 16.976% 15.418%
$175,000 50 11.694% 10.081%
$175,000 100 7.936% 6.357%
$175,000 150 6.411% 4.877%
$175,000 200 5.492% 4.005%
$175,000 300 4.353% 2.937%
$175,000 400 3.450% 2.176%
$175,000 500 3.302% 1.991%
$175,000 600 2.869% 1.630%
$175,000 700 2.583% 1.401%
$175,000 800 2.360% 1.220%
$175,000 900 2.244% 1.126%
$175,000 1,000 2.086% 1.002%
$175,000 1,500 1.528% 0.615%
$175,000 2,000 1.255% 0.434%
$175,000 3,000 0.780% 0.187%
$175,000 4,000 0.572% 0.100%
$175,000 5,000 0.444% 0.060%
$175,000 10,000 0.154% 0.005%
$175,000 20,000 0.034% 0.001%
$175,000 30,000 0.007% 0.001%
$175,000 40,000 0.002% 0.001%
$180,000 25 17.105% 15.549%
$180,000 50 11.805% 10.193%
$180,000 100 8.009% 6.426%
$180,000 150 6.474% 4.935%
$180,000 200 5.546% 4.053%
$180,000 300 4.396% 2.974%
* Applied to total projected claims18

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$180,000 400 3.485% 2.205%
$180,000 500 3.337% 2.019%
$180,000 600 2.898% 1.653%
$180,000 700 2.609% 1.421%
$180,000 800 2.386% 1.239%
$180,000 900 2.269% 1.145%
$180,000 1,000 2.109% 1.018%
$180,000 1,500 1.548% 0.627%
$180,000 2,000 1.271% 0.444%
$180,000 3,000 0.793% 0.192%
$180,000 4,000 0.581% 0.103%
$180,000 5,000 0.452% 0.062%
$180,000 10,000 0.158% 0.006%
$180,000 20,000 0.034% 0.001%
$180,000 30,000 0.008% 0.001%
$180,000 40,000 0.002% 0.001%
$185,000 25 17.232% 15.678%
$185,000 50 11.915% 10.303%
$185,000 100 8.081% 6.494%
$185,000 150 6.536% 4.992%
$185,000 200 5.598% 4.100%
$185,000 300 4.438% 3.011%
$185,000 400 3.520% 2.235%
$185,000 500 3.371% 2.046%
$185,000 600 2.927% 1.675%
$185,000 700 2.635% 1.440%
$185,000 800 2.411% 1.258%
$185,000 900 2.294% 1.163%
$185,000 1,000 2.131% 1.034%
$185,000 1,500 1.567% 0.639%
$185,000 2,000 1.288% 0.453%
$185,000 3,000 0.804% 0.197%
$185,000 4,000 0.591% 0.107%
$185,000 5,000 0.461% 0.064%
$185,000 10,000 0.161% 0.006%
$185,000 20,000 0.035% 0.001%
$185,000 30,000 0.008% 0.001%
* Applied to total projected claims19

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$185,000 40,000 0.002% 0.001%
$190,000 25 17.357% 15.804%
$190,000 50 12.021% 10.410%
$190,000 100 8.151% 6.561%
$190,000 150 6.596% 5.048%
$190,000 200 5.650% 4.146%
$190,000 300 4.480% 3.046%
$190,000 400 3.554% 2.263%
$190,000 500 3.405% 2.074%
$190,000 600 2.956% 1.698%
$190,000 700 2.660% 1.460%
$190,000 800 2.436% 1.277%
$190,000 900 2.319% 1.181%
$190,000 1,000 2.153% 1.050%
$190,000 1,500 1.586% 0.651%
$190,000 2,000 1.304% 0.462%
$190,000 3,000 0.816% 0.202%
$190,000 4,000 0.600% 0.110%
$190,000 5,000 0.469% 0.066%
$190,000 10,000 0.164% 0.006%
$190,000 20,000 0.036% 0.001%
$190,000 30,000 0.008% 0.001%
$190,000 40,000 0.002% 0.001%
$195,000 25 17.475% 15.924%
$195,000 50 12.122% 10.511%
$195,000 100 8.219% 6.626%
$195,000 150 6.655% 5.102%
$195,000 200 5.699% 4.190%
$195,000 300 4.519% 3.081%
$195,000 400 3.587% 2.291%
$195,000 500 3.438% 2.101%
$195,000 600 2.983% 1.719%
$195,000 700 2.685% 1.479%
$195,000 800 2.460% 1.295%
$195,000 900 2.343% 1.198%
$195,000 1,000 2.175% 1.065%
$195,000 1,500 1.605% 0.663%
* Applied to total projected claims20

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$195,000 2,000 1.319% 0.471%
$195,000 3,000 0.827% 0.207%
$195,000 4,000 0.609% 0.113%
$195,000 5,000 0.477% 0.068%
$195,000 10,000 0.167% 0.006%
$195,000 20,000 0.037% 0.001%
$195,000 30,000 0.008% 0.001%
$195,000 40,000 0.002% 0.001%
$200,000 25 17.586% 16.037%
$200,000 50 12.220% 10.610%
$200,000 100 8.286% 6.690%
$200,000 150 6.711% 5.154%
$200,000 200 5.747% 4.233%
$200,000 300 4.557% 3.114%
$200,000 400 3.619% 2.318%
$200,000 500 3.470% 2.127%
$200,000 600 3.010% 1.741%
$200,000 700 2.709% 1.498%
$200,000 800 2.484% 1.313%
$200,000 900 2.366% 1.215%
$200,000 1,000 2.196% 1.080%
$200,000 1,500 1.623% 0.674%
$200,000 2,000 1.334% 0.479%
$200,000 3,000 0.839% 0.212%
$200,000 4,000 0.618% 0.116%
$200,000 5,000 0.485% 0.071%
$200,000 10,000 0.170% 0.007%
$200,000 20,000 0.038% 0.001%
$200,000 30,000 0.008% 0.001%
$200,000 40,000 0.002% 0.001%
$205,000 25 17.694% 16.147%
$205,000 50 12.315% 10.706%
$205,000 100 8.352% 6.754%
$205,000 150 6.767% 5.207%
$205,000 200 5.795% 4.277%
$205,000 300 4.595% 3.147%
$205,000 400 3.651% 2.345%
* Applied to total projected claims21

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$205,000 500 3.503% 2.154%
$205,000 600 3.037% 1.762%
$205,000 700 2.734% 1.517%
$205,000 800 2.508% 1.331%
$205,000 900 2.388% 1.232%
$205,000 1,000 2.217% 1.095%
$205,000 1,500 1.641% 0.686%
$205,000 2,000 1.349% 0.488%
$205,000 3,000 0.850% 0.217%
$205,000 4,000 0.627% 0.119%
$205,000 5,000 0.493% 0.073%
$205,000 10,000 0.173% 0.007%
$205,000 20,000 0.039% 0.001%
$205,000 30,000 0.009% 0.001%
$205,000 40,000 0.002% 0.001%
$210,000 25 17.799% 16.253%
$210,000 50 12.409% 10.801%
$210,000 100 8.417% 6.816%
$210,000 150 6.822% 5.258%
$210,000 200 5.842% 4.319%
$210,000 300 4.632% 3.179%
$210,000 400 3.683% 2.372%
$210,000 500 3.534% 2.180%
$210,000 600 3.064% 1.784%
$210,000 700 2.758% 1.537%
$210,000 800 2.531% 1.348%
$210,000 900 2.410% 1.248%
$210,000 1,000 2.237% 1.109%
$210,000 1,500 1.658% 0.697%
$210,000 2,000 1.364% 0.497%
$210,000 3,000 0.860% 0.221%
$210,000 4,000 0.636% 0.122%
$210,000 5,000 0.501% 0.075%
$210,000 10,000 0.177% 0.007%
$210,000 20,000 0.040% 0.001%
$210,000 30,000 0.009% 0.001%
$210,000 40,000 0.003% 0.001%
* Applied to total projected claims22

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$215,000 25 17.899% 16.354%
$215,000 50 12.498% 10.891%
$215,000 100 8.479% 6.875%
$215,000 150 6.875% 5.308%
$215,000 200 5.887% 4.359%
$215,000 300 4.667% 3.210%
$215,000 400 3.714% 2.398%
$215,000 500 3.565% 2.205%
$215,000 600 3.089% 1.804%
$215,000 700 2.782% 1.555%
$215,000 800 2.553% 1.365%
$215,000 900 2.432% 1.264%
$215,000 1,000 2.256% 1.123%
$215,000 1,500 1.675% 0.708%
$215,000 2,000 1.378% 0.505%
$215,000 3,000 0.871% 0.226%
$215,000 4,000 0.645% 0.125%
$215,000 5,000 0.509% 0.077%
$215,000 10,000 0.180% 0.007%
$215,000 20,000 0.041% 0.001%
$215,000 30,000 0.009% 0.001%
$215,000 40,000 0.003% 0.001%
$220,000 25 17.994% 16.451%
$220,000 50 12.582% 10.977%
$220,000 100 8.536% 6.931%
$220,000 150 6.926% 5.356%
$220,000 200 5.929% 4.397%
$220,000 300 4.701% 3.240%
$220,000 400 3.743% 2.422%
$220,000 500 3.593% 2.229%
$220,000 600 3.114% 1.823%
$220,000 700 2.804% 1.572%
$220,000 800 2.574% 1.382%
$220,000 900 2.452% 1.279%
$220,000 1,000 2.275% 1.137%
$220,000 1,500 1.691% 0.718%
$220,000 2,000 1.391% 0.513%
* Applied to total projected claims23

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$220,000 3,000 0.881% 0.230%
$220,000 4,000 0.653% 0.128%
$220,000 5,000 0.517% 0.080%
$220,000 10,000 0.183% 0.008%
$220,000 20,000 0.042% 0.001%
$220,000 30,000 0.009% 0.001%
$220,000 40,000 0.003% 0.001%
$225,000 25 18.087% 16.545%
$225,000 50 12.664% 11.061%
$225,000 100 8.591% 6.984%
$225,000 150 6.974% 5.401%
$225,000 200 5.969% 4.434%
$225,000 300 4.733% 3.269%
$225,000 400 3.771% 2.446%
$225,000 500 3.621% 2.253%
$225,000 600 3.137% 1.842%
$225,000 700 2.825% 1.590%
$225,000 800 2.595% 1.397%
$225,000 900 2.472% 1.294%
$225,000 1,000 2.293% 1.150%
$225,000 1,500 1.707% 0.728%
$225,000 2,000 1.404% 0.520%
$225,000 3,000 0.891% 0.235%
$225,000 4,000 0.661% 0.131%
$225,000 5,000 0.524% 0.082%
$225,000 10,000 0.185% 0.008%
$225,000 20,000 0.043% 0.001%
$225,000 30,000 0.010% 0.001%
$225,000 40,000 0.003% 0.001%
$230,000 25 18.177% 16.636%
$230,000 50 12.743% 11.142%
$230,000 100 8.646% 7.038%
$230,000 150 7.021% 5.445%
$230,000 200 6.008% 4.469%
$230,000 300 4.765% 3.297%
$230,000 400 3.798% 2.469%
$230,000 500 3.648% 2.275%
* Applied to total projected claims24

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$230,000 600 3.159% 1.860%
$230,000 700 2.846% 1.606%
$230,000 800 2.615% 1.413%
$230,000 900 2.491% 1.308%
$230,000 1,000 2.310% 1.162%
$230,000 1,500 1.722% 0.738%
$230,000 2,000 1.416% 0.528%
$230,000 3,000 0.901% 0.239%
$230,000 4,000 0.669% 0.134%
$230,000 5,000 0.531% 0.084%
$230,000 10,000 0.188% 0.008%
$230,000 20,000 0.044% 0.001%
$230,000 30,000 0.010% 0.001%
$230,000 40,000 0.003% 0.001%
$235,000 25 18.263% 16.723%
$235,000 50 12.819% 11.220%
$235,000 100 8.701% 7.090%
$235,000 150 7.067% 5.489%
$235,000 200 6.047% 4.505%
$235,000 300 4.796% 3.325%
$235,000 400 3.824% 2.491%
$235,000 500 3.674% 2.297%
$235,000 600 3.182% 1.878%
$235,000 700 2.867% 1.623%
$235,000 800 2.634% 1.428%
$235,000 900 2.509% 1.322%
$235,000 1,000 2.327% 1.175%
$235,000 1,500 1.737% 0.748%
$235,000 2,000 1.428% 0.535%
$235,000 3,000 0.910% 0.243%
$235,000 4,000 0.676% 0.137%
$235,000 5,000 0.538% 0.086%
$235,000 10,000 0.191% 0.009%
$235,000 20,000 0.045% 0.001%
$235,000 30,000 0.010% 0.001%
$235,000 40,000 0.003% 0.001%
$240,000 25 18.347% 16.808%
* Applied to total projected claims25

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$240,000 50 12.894% 11.296%
$240,000 100 8.754% 7.142%
$240,000 150 7.112% 5.532%
$240,000 200 6.086% 4.540%
$240,000 300 4.827% 3.353%
$240,000 400 3.850% 2.513%
$240,000 500 3.700% 2.319%
$240,000 600 3.204% 1.896%
$240,000 700 2.887% 1.638%
$240,000 800 2.653% 1.443%
$240,000 900 2.527% 1.335%
$240,000 1,000 2.344% 1.187%
$240,000 1,500 1.752% 0.758%
$240,000 2,000 1.440% 0.542%
$240,000 3,000 0.919% 0.247%
$240,000 4,000 0.684% 0.139%
$240,000 5,000 0.545% 0.088%
$240,000 10,000 0.193% 0.009%
$240,000 20,000 0.046% 0.001%
$240,000 30,000 0.010% 0.001%
$240,000 40,000 0.003% 0.001%
$245,000 25 18.427% 16.888%
$245,000 50 12.966% 11.369%
$245,000 100 8.806% 7.193%
$245,000 150 7.158% 5.575%
$245,000 200 6.124% 4.574%
$245,000 300 4.858% 3.380%
$245,000 400 3.876% 2.535%
$245,000 500 3.724% 2.339%
$245,000 600 3.225% 1.913%
$245,000 700 2.905% 1.653%
$245,000 800 2.671% 1.457%
$245,000 900 2.545% 1.349%
$245,000 1,000 2.360% 1.199%
$245,000 1,500 1.766% 0.767%
$245,000 2,000 1.451% 0.549%
$245,000 3,000 0.927% 0.251%
* Applied to total projected claims26

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$245,000 4,000 0.691% 0.142%
$245,000 5,000 0.552% 0.090%
$245,000 10,000 0.196% 0.009%
$245,000 20,000 0.047% 0.001%
$245,000 30,000 0.011% 0.001%
$245,000 40,000 0.003% 0.001%
$250,000 25 18.500% 16.962%
$250,000 50 13.030% 11.435%
$250,000 100 8.856% 7.241%
$250,000 150 7.200% 5.615%
$250,000 200 6.160% 4.607%
$250,000 300 4.887% 3.407%
$250,000 400 3.900% 2.555%
$250,000 500 3.748% 2.359%
$250,000 600 3.245% 1.929%
$250,000 700 2.923% 1.668%
$250,000 800 2.689% 1.471%
$250,000 900 2.562% 1.361%
$250,000 1,000 2.376% 1.210%
$250,000 1,500 1.780% 0.776%
$250,000 2,000 1.462% 0.555%
$250,000 3,000 0.935% 0.255%
$250,000 4,000 0.698% 0.145%
$250,000 5,000 0.558% 0.092%
$250,000 10,000 0.198% 0.009%
$250,000 20,000 0.047% 0.001%
$250,000 30,000 0.011% 0.001%
$250,000 40,000 0.003% 0.001%
$255,000 25 18.569% 17.032%
$255,000 50 13.091% 11.498%
$255,000 100 8.903% 7.288%
$255,000 150 7.241% 5.653%
$255,000 200 6.194% 4.638%
$255,000 300 4.915% 3.432%
$255,000 400 3.923% 2.575%
$255,000 500 3.770% 2.378%
$255,000 600 3.264% 1.945%
* Applied to total projected claims27

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$255,000 700 2.940% 1.681%
$255,000 800 2.706% 1.484%
$255,000 900 2.578% 1.373%
$255,000 1,000 2.391% 1.221%
$255,000 1,500 1.793% 0.785%
$255,000 2,000 1.472% 0.561%
$255,000 3,000 0.943% 0.258%
$255,000 4,000 0.705% 0.147%
$255,000 5,000 0.564% 0.094%
$255,000 10,000 0.201% 0.010%
$255,000 20,000 0.048% 0.001%
$255,000 30,000 0.011% 0.001%
$255,000 40,000 0.003% 0.001%
$260,000 25 18.637% 17.101%
$260,000 50 13.151% 11.559%
$260,000 100 8.951% 7.335%
$260,000 150 7.282% 5.692%
$260,000 200 6.229% 4.670%
$260,000 300 4.943% 3.457%
$260,000 400 3.947% 2.595%
$260,000 500 3.793% 2.397%
$260,000 600 3.283% 1.960%
$260,000 700 2.957% 1.695%
$260,000 800 2.723% 1.497%
$260,000 900 2.593% 1.385%
$260,000 1,000 2.406% 1.232%
$260,000 1,500 1.806% 0.793%
$260,000 2,000 1.482% 0.568%
$260,000 3,000 0.950% 0.262%
$260,000 4,000 0.712% 0.150%
$260,000 5,000 0.570% 0.096%
$260,000 10,000 0.203% 0.010%
$260,000 20,000 0.049% 0.001%
$260,000 30,000 0.011% 0.001%
$260,000 40,000 0.003% 0.001%
$265,000 25 18.705% 17.169%
$265,000 50 13.210% 11.620%
* Applied to total projected claims28

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$265,000 100 8.998% 7.381%
$265,000 150 7.322% 5.730%
$265,000 200 6.263% 4.702%
$265,000 300 4.971% 3.483%
$265,000 400 3.970% 2.615%
$265,000 500 3.815% 2.416%
$265,000 600 3.302% 1.975%
$265,000 700 2.973% 1.709%
$265,000 800 2.740% 1.511%
$265,000 900 2.609% 1.397%
$265,000 1,000 2.421% 1.243%
$265,000 1,500 1.819% 0.802%
$265,000 2,000 1.492% 0.574%
$265,000 3,000 0.958% 0.265%
$265,000 4,000 0.718% 0.152%
$265,000 5,000 0.576% 0.098%
$265,000 10,000 0.206% 0.010%
$265,000 20,000 0.050% 0.001%
$265,000 30,000 0.012% 0.001%
$265,000 40,000 0.003% 0.001%
$270,000 25 18.772% 17.238%
$270,000 50 13.268% 11.680%
$270,000 100 9.045% 7.428%
$270,000 150 7.363% 5.768%
$270,000 200 6.298% 4.734%
$270,000 300 4.999% 3.508%
$270,000 400 3.993% 2.635%
$270,000 500 3.837% 2.435%
$270,000 600 3.321% 1.991%
$270,000 700 2.990% 1.722%
$270,000 800 2.757% 1.524%
$270,000 900 2.624% 1.409%
$270,000 1,000 2.436% 1.255%
$270,000 1,500 1.832% 0.811%
$270,000 2,000 1.502% 0.580%
$270,000 3,000 0.966% 0.269%
$270,000 4,000 0.725% 0.155%
* Applied to total projected claims29

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$270,000 5,000 0.583% 0.100%
$270,000 10,000 0.208% 0.010%
$270,000 20,000 0.051% 0.001%
$270,000 30,000 0.012% 0.001%
$270,000 40,000 0.003% 0.001%
$275,000 25 18.838% 17.304%
$275,000 50 13.326% 11.739%
$275,000 100 9.091% 7.473%
$275,000 150 7.403% 5.806%
$275,000 200 6.332% 4.766%
$275,000 300 5.026% 3.533%
$275,000 400 4.017% 2.655%
$275,000 500 3.859% 2.454%
$275,000 600 3.339% 2.006%
$275,000 700 3.007% 1.736%
$275,000 800 2.774% 1.538%
$275,000 900 2.640% 1.421%
$275,000 1,000 2.451% 1.266%
$275,000 1,500 1.845% 0.820%
$275,000 2,000 1.512% 0.586%
$275,000 3,000 0.974% 0.273%
$275,000 4,000 0.732% 0.158%
$275,000 5,000 0.589% 0.102%
$275,000 10,000 0.210% 0.011%
$275,000 20,000 0.051% 0.001%
$275,000 30,000 0.012% 0.001%
$275,000 40,000 0.003% 0.001%
$280,000 25 18.901% 17.367%
$280,000 50 13.383% 11.797%
$280,000 100 9.136% 7.517%
$280,000 150 7.442% 5.843%
$280,000 200 6.366% 4.797%
$280,000 300 5.053% 3.558%
$280,000 400 4.040% 2.674%
$280,000 500 3.881% 2.472%
$280,000 600 3.358% 2.021%
$280,000 700 3.023% 1.749%
* Applied to total projected claims30

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$280,000 800 2.791% 1.551%
$280,000 900 2.655% 1.432%
$280,000 1,000 2.466% 1.277%
$280,000 1,500 1.858% 0.829%
$280,000 2,000 1.522% 0.593%
$280,000 3,000 0.981% 0.276%
$280,000 4,000 0.739% 0.160%
$280,000 5,000 0.594% 0.104%
$280,000 10,000 0.213% 0.011%
$280,000 20,000 0.052% 0.001%
$280,000 30,000 0.012% 0.001%
$280,000 40,000 0.003% 0.001%
$285,000 25 18.963% 17.430%
$285,000 50 13.439% 11.855%
$285,000 100 9.181% 7.560%
$285,000 150 7.481% 5.880%
$285,000 200 6.399% 4.828%
$285,000 300 5.080% 3.582%
$285,000 400 4.063% 2.694%
$285,000 500 3.903% 2.491%
$285,000 600 3.376% 2.036%
$285,000 700 3.039% 1.762%
$285,000 800 2.807% 1.564%
$285,000 900 2.670% 1.444%
$285,000 1,000 2.481% 1.288%
$285,000 1,500 1.871% 0.837%
$285,000 2,000 1.532% 0.599%
$285,000 3,000 0.989% 0.280%
$285,000 4,000 0.746% 0.163%
$285,000 5,000 0.600% 0.106%
$285,000 10,000 0.215% 0.011%
$285,000 20,000 0.053% 0.001%
$285,000 30,000 0.012% 0.001%
$285,000 40,000 0.003% 0.001%
$290,000 25 19.021% 17.489%
$290,000 50 13.492% 11.909%
$290,000 100 9.223% 7.603%
* Applied to total projected claims31

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$290,000 150 7.518% 5.916%
$290,000 200 6.430% 4.858%
$290,000 300 5.105% 3.605%
$290,000 400 4.085% 2.713%
$290,000 500 3.924% 2.509%
$290,000 600 3.393% 2.050%
$290,000 700 3.054% 1.774%
$290,000 800 2.823% 1.577%
$290,000 900 2.684% 1.455%
$290,000 1,000 2.495% 1.299%
$290,000 1,500 1.883% 0.845%
$290,000 2,000 1.541% 0.605%
$290,000 3,000 0.996% 0.283%
$290,000 4,000 0.752% 0.166%
$290,000 5,000 0.606% 0.108%
$290,000 10,000 0.217% 0.011%
$290,000 20,000 0.054% 0.001%
$290,000 30,000 0.013% 0.001%
$290,000 40,000 0.003% 0.001%
$295,000 25 19.076% 17.544%
$295,000 50 13.541% 11.959%
$295,000 100 9.264% 7.643%
$295,000 150 7.553% 5.950%
$295,000 200 6.461% 4.886%
$295,000 300 5.129% 3.627%
$295,000 400 4.107% 2.732%
$295,000 500 3.944% 2.526%
$295,000 600 3.410% 2.064%
$295,000 700 3.069% 1.787%
$295,000 800 2.838% 1.589%
$295,000 900 2.698% 1.466%
$295,000 1,000 2.508% 1.309%
$295,000 1,500 1.894% 0.853%
$295,000 2,000 1.550% 0.610%
$295,000 3,000 1.003% 0.287%
$295,000 4,000 0.759% 0.168%
$295,000 5,000 0.611% 0.110%
* Applied to total projected claims32

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$295,000 10,000 0.220% 0.012%
$295,000 20,000 0.054% 0.001%
$295,000 30,000 0.013% 0.001%
$295,000 40,000 0.003% 0.001%
$300,000 25 19.128% 17.597%
$300,000 50 13.589% 12.008%
$300,000 100 9.305% 7.684%
$300,000 150 7.587% 5.983%
$300,000 200 6.491% 4.915%
$300,000 300 5.153% 3.649%
$300,000 400 4.129% 2.750%
$300,000 500 3.963% 2.544%
$300,000 600 3.426% 2.077%
$300,000 700 3.083% 1.799%
$300,000 800 2.853% 1.601%
$300,000 900 2.712% 1.477%
$300,000 1,000 2.521% 1.319%
$300,000 1,500 1.905% 0.861%
$300,000 2,000 1.559% 0.616%
$300,000 3,000 1.010% 0.290%
$300,000 4,000 0.765% 0.171%
$300,000 5,000 0.616% 0.112%
$300,000 10,000 0.222% 0.012%
$300,000 20,000 0.055% 0.001%
$300,000 30,000 0.013% 0.001%
$300,000 40,000 0.003% 0.001%
$305,000 25 19.178% 17.648%
$305,000 50 13.636% 12.057%
$305,000 100 9.345% 7.724%
$305,000 150 7.620% 6.016%
$305,000 200 6.520% 4.943%
$305,000 300 5.176% 3.670%
$305,000 400 4.150% 2.769%
$305,000 500 3.983% 2.560%
$305,000 600 3.442% 2.091%
$305,000 700 3.097% 1.810%
$305,000 800 2.868% 1.612%
* Applied to total projected claims33

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$305,000 900 2.726% 1.487%
$305,000 1,000 2.534% 1.329%
$305,000 1,500 1.916% 0.868%
$305,000 2,000 1.568% 0.621%
$305,000 3,000 1.017% 0.294%
$305,000 4,000 0.771% 0.173%
$305,000 5,000 0.621% 0.114%
$305,000 10,000 0.224% 0.012%
$305,000 20,000 0.056% 0.001%
$305,000 30,000 0.013% 0.001%
$305,000 40,000 0.003% 0.001%
$310,000 25 19.226% 17.696%
$310,000 50 13.682% 12.104%
$310,000 100 9.384% 7.763%
$310,000 150 7.653% 6.048%
$310,000 200 6.550% 4.970%
$310,000 300 5.199% 3.690%
$310,000 400 4.171% 2.786%
$310,000 500 4.002% 2.577%
$310,000 600 3.458% 2.104%
$310,000 700 3.111% 1.822%
$310,000 800 2.882% 1.624%
$310,000 900 2.739% 1.498%
$310,000 1,000 2.547% 1.338%
$310,000 1,500 1.927% 0.876%
$310,000 2,000 1.576% 0.627%
$310,000 3,000 1.024% 0.297%
$310,000 4,000 0.777% 0.175%
$310,000 5,000 0.626% 0.115%
$310,000 10,000 0.226% 0.012%
$310,000 20,000 0.057% 0.001%
$310,000 30,000 0.014% 0.001%
$310,000 40,000 0.003% 0.001%
$315,000 25 19.273% 17.743%
$315,000 50 13.728% 12.151%
$315,000 100 9.422% 7.801%
$315,000 150 7.685% 6.080%
* Applied to total projected claims34

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$315,000 200 6.578% 4.998%
$315,000 300 5.221% 3.711%
$315,000 400 4.192% 2.804%
$315,000 500 4.020% 2.593%
$315,000 600 3.473% 2.117%
$315,000 700 3.125% 1.833%
$315,000 800 2.895% 1.634%
$315,000 900 2.752% 1.508%
$315,000 1,000 2.559% 1.348%
$315,000 1,500 1.937% 0.883%
$315,000 2,000 1.584% 0.632%
$315,000 3,000 1.030% 0.300%
$315,000 4,000 0.783% 0.178%
$315,000 5,000 0.631% 0.117%
$315,000 10,000 0.228% 0.013%
$315,000 20,000 0.057% 0.001%
$315,000 30,000 0.014% 0.001%
$315,000 40,000 0.003% 0.001%
$320,000 25 19.319% 17.790%
$320,000 50 13.771% 12.195%
$320,000 100 9.459% 7.839%
$320,000 150 7.717% 6.111%
$320,000 200 6.607% 5.025%
$320,000 300 5.243% 3.731%
$320,000 400 4.212% 2.821%
$320,000 500 4.039% 2.609%
$320,000 600 3.489% 2.129%
$320,000 700 3.139% 1.844%
$320,000 800 2.909% 1.645%
$320,000 900 2.764% 1.518%
$320,000 1,000 2.571% 1.357%
$320,000 1,500 1.948% 0.890%
$320,000 2,000 1.592% 0.637%
$320,000 3,000 1.037% 0.303%
$320,000 4,000 0.789% 0.180%
$320,000 5,000 0.636% 0.119%
$320,000 10,000 0.230% 0.013%
* Applied to total projected claims35

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$320,000 20,000 0.058% 0.001%
$320,000 30,000 0.014% 0.001%
$320,000 40,000 0.003% 0.001%
$325,000 25 19.364% 17.835%
$325,000 50 13.812% 12.237%
$325,000 100 9.496% 7.876%
$325,000 150 7.749% 6.143%
$325,000 200 6.635% 5.051%
$325,000 300 5.266% 3.752%
$325,000 400 4.232% 2.839%
$325,000 500 4.057% 2.625%
$325,000 600 3.504% 2.142%
$325,000 700 3.152% 1.855%
$325,000 800 2.922% 1.656%
$325,000 900 2.777% 1.527%
$325,000 1,000 2.583% 1.366%
$325,000 1,500 1.958% 0.897%
$325,000 2,000 1.600% 0.642%
$325,000 3,000 1.044% 0.307%
$325,000 4,000 0.795% 0.183%
$325,000 5,000 0.641% 0.120%
$325,000 10,000 0.232% 0.013%
$325,000 20,000 0.059% 0.001%
$325,000 30,000 0.014% 0.001%
$325,000 40,000 0.003% 0.001%
$330,000 25 19.404% 17.876%
$330,000 50 13.850% 12.276%
$330,000 100 9.530% 7.911%
$330,000 150 7.778% 6.172%
$330,000 200 6.662% 5.077%
$330,000 300 5.286% 3.770%
$330,000 400 4.250% 2.854%
$330,000 500 4.074% 2.639%
$330,000 600 3.517% 2.153%
$330,000 700 3.164% 1.865%
$330,000 800 2.934% 1.665%
$330,000 900 2.788% 1.536%
* Applied to total projected claims36

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$330,000 1,000 2.594% 1.375%
$330,000 1,500 1.967% 0.904%
$330,000 2,000 1.607% 0.647%
$330,000 3,000 1.049% 0.310%
$330,000 4,000 0.801% 0.185%
$330,000 5,000 0.645% 0.122%
$330,000 10,000 0.234% 0.014%
$330,000 20,000 0.059% 0.001%
$330,000 30,000 0.014% 0.001%
$330,000 40,000 0.003% 0.001%
$335,000 25 19.441% 17.913%
$335,000 50 13.885% 12.311%
$335,000 100 9.563% 7.944%
$335,000 150 7.806% 6.199%
$335,000 200 6.687% 5.101%
$335,000 300 5.304% 3.788%
$335,000 400 4.268% 2.870%
$335,000 500 4.089% 2.653%
$335,000 600 3.529% 2.163%
$335,000 700 3.176% 1.875%
$335,000 800 2.946% 1.674%
$335,000 900 2.799% 1.545%
$335,000 1,000 2.605% 1.383%
$335,000 1,500 1.977% 0.910%
$335,000 2,000 1.614% 0.651%
$335,000 3,000 1.055% 0.312%
$335,000 4,000 0.806% 0.187%
$335,000 5,000 0.649% 0.123%
$335,000 10,000 0.236% 0.014%
$335,000 20,000 0.060% 0.001%
$335,000 30,000 0.015% 0.001%
$335,000 40,000 0.003% 0.001%
$340,000 25 19.477% 17.949%
$340,000 50 13.918% 12.345%
$340,000 100 9.596% 7.978%
$340,000 150 7.833% 6.226%
$340,000 200 6.711% 5.124%
* Applied to total projected claims37

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$340,000 300 5.322% 3.804%
$340,000 400 4.284% 2.884%
$340,000 500 4.105% 2.667%
$340,000 600 3.542% 2.174%
$340,000 700 3.187% 1.884%
$340,000 800 2.957% 1.683%
$340,000 900 2.809% 1.553%
$340,000 1,000 2.615% 1.390%
$340,000 1,500 1.985% 0.916%
$340,000 2,000 1.621% 0.656%
$340,000 3,000 1.061% 0.315%
$340,000 4,000 0.811% 0.189%
$340,000 5,000 0.653% 0.125%
$340,000 10,000 0.238% 0.014%
$340,000 20,000 0.061% 0.001%
$340,000 30,000 0.015% 0.001%
$340,000 40,000 0.003% 0.001%
$345,000 25 19.510% 17.982%
$345,000 50 13.949% 12.376%
$345,000 100 9.627% 8.010%
$345,000 150 7.859% 6.251%
$345,000 200 6.735% 5.146%
$345,000 300 5.340% 3.820%
$345,000 400 4.301% 2.898%
$345,000 500 4.120% 2.680%
$345,000 600 3.554% 2.184%
$345,000 700 3.197% 1.893%
$345,000 800 2.968% 1.692%
$345,000 900 2.819% 1.561%
$345,000 1,000 2.624% 1.398%
$345,000 1,500 1.993% 0.922%
$345,000 2,000 1.627% 0.660%
$345,000 3,000 1.066% 0.318%
$345,000 4,000 0.816% 0.191%
$345,000 5,000 0.657% 0.126%
$345,000 10,000 0.239% 0.014%
$345,000 20,000 0.061% 0.001%
* Applied to total projected claims38

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$345,000 30,000 0.015% 0.001%
$345,000 40,000 0.003% 0.001%
$350,000 25 19.543% 18.015%
$350,000 50 13.979% 12.407%
$350,000 100 9.658% 8.041%
$350,000 150 7.886% 6.277%
$350,000 200 6.758% 5.168%
$350,000 300 5.357% 3.836%
$350,000 400 4.317% 2.912%
$350,000 500 4.134% 2.693%
$350,000 600 3.566% 2.194%
$350,000 700 3.208% 1.902%
$350,000 800 2.979% 1.701%
$350,000 900 2.829% 1.568%
$350,000 1,000 2.634% 1.405%
$350,000 1,500 2.001% 0.928%
$350,000 2,000 1.633% 0.664%
$350,000 3,000 1.071% 0.320%
$350,000 4,000 0.821% 0.193%
$350,000 5,000 0.661% 0.128%
$350,000 10,000 0.241% 0.014%
$350,000 20,000 0.062% 0.001%
$350,000 30,000 0.015% 0.001%
$350,000 40,000 0.003% 0.001%
$355,000 25 19.576% 18.048%
$355,000 50 14.009% 12.438%
$355,000 100 9.688% 8.071%
$355,000 150 7.912% 6.302%
$355,000 200 6.781% 5.191%
$355,000 300 5.374% 3.852%
$355,000 400 4.333% 2.926%
$355,000 500 4.149% 2.706%
$355,000 600 3.578% 2.204%
$355,000 700 3.219% 1.911%
$355,000 800 2.990% 1.709%
$355,000 900 2.838% 1.576%
$355,000 1,000 2.644% 1.413%
* Applied to total projected claims39

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$355,000 1,500 2.009% 0.933%
$355,000 2,000 1.640% 0.668%
$355,000 3,000 1.076% 0.323%
$355,000 4,000 0.826% 0.195%
$355,000 5,000 0.665% 0.129%
$355,000 10,000 0.243% 0.015%
$355,000 20,000 0.062% 0.001%
$355,000 30,000 0.015% 0.001%
$355,000 40,000 0.003% 0.001%
$360,000 25 19.609% 18.081%
$360,000 50 14.039% 12.468%
$360,000 100 9.719% 8.102%
$360,000 150 7.938% 6.328%
$360,000 200 6.804% 5.213%
$360,000 300 5.391% 3.868%
$360,000 400 4.349% 2.941%
$360,000 500 4.165% 2.720%
$360,000 600 3.590% 2.214%
$360,000 700 3.229% 1.919%
$360,000 800 3.001% 1.718%
$360,000 900 2.848% 1.584%
$360,000 1,000 2.653% 1.420%
$360,000 1,500 2.017% 0.939%
$360,000 2,000 1.646% 0.672%
$360,000 3,000 1.082% 0.326%
$360,000 4,000 0.831% 0.197%
$360,000 5,000 0.669% 0.131%
$360,000 10,000 0.244% 0.015%
$360,000 20,000 0.063% 0.001%
$360,000 30,000 0.015% 0.001%
$360,000 40,000 0.003% 0.001%
$365,000 25 19.643% 18.115%
$365,000 50 14.068% 12.498%
$365,000 100 9.749% 8.133%
$365,000 150 7.964% 6.353%
$365,000 200 6.828% 5.235%
$365,000 300 5.409% 3.884%
* Applied to total projected claims40

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$365,000 400 4.365% 2.955%
$365,000 500 4.180% 2.733%
$365,000 600 3.602% 2.224%
$365,000 700 3.240% 1.928%
$365,000 800 3.011% 1.726%
$365,000 900 2.858% 1.592%
$365,000 1,000 2.663% 1.428%
$365,000 1,500 2.025% 0.945%
$365,000 2,000 1.653% 0.676%
$365,000 3,000 1.087% 0.328%
$365,000 4,000 0.836% 0.199%
$365,000 5,000 0.673% 0.132%
$365,000 10,000 0.246% 0.015%
$365,000 20,000 0.064% 0.001%
$365,000 30,000 0.016% 0.001%
$365,000 40,000 0.003% 0.001%
$370,000 25 19.674% 18.147%
$370,000 50 14.096% 12.526%
$370,000 100 9.778% 8.163%
$370,000 150 7.990% 6.378%
$370,000 200 6.850% 5.257%
$370,000 300 5.426% 3.900%
$370,000 400 4.381% 2.969%
$370,000 500 4.194% 2.746%
$370,000 600 3.614% 2.234%
$370,000 700 3.250% 1.937%
$370,000 800 3.022% 1.735%
$370,000 900 2.868% 1.600%
$370,000 1,000 2.673% 1.435%
$370,000 1,500 2.033% 0.950%
$370,000 2,000 1.659% 0.680%
$370,000 3,000 1.092% 0.331%
$370,000 4,000 0.840% 0.201%
$370,000 5,000 0.677% 0.134%
$370,000 10,000 0.248% 0.015%
$370,000 20,000 0.064% 0.001%
$370,000 30,000 0.016% 0.001%
* Applied to total projected claims41

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$370,000 40,000 0.004% 0.001%
$375,000 25 19.702% 18.175%
$375,000 50 14.121% 12.552%
$375,000 100 9.805% 8.190%
$375,000 150 8.013% 6.402%
$375,000 200 6.870% 5.276%
$375,000 300 5.442% 3.915%
$375,000 400 4.396% 2.982%
$375,000 500 4.208% 2.758%
$375,000 600 3.625% 2.244%
$375,000 700 3.259% 1.945%
$375,000 800 3.032% 1.743%
$375,000 900 2.877% 1.607%
$375,000 1,000 2.681% 1.442%
$375,000 1,500 2.040% 0.955%
$375,000 2,000 1.664% 0.684%
$375,000 3,000 1.097% 0.333%
$375,000 4,000 0.845% 0.203%
$375,000 5,000 0.681% 0.135%
$375,000 10,000 0.249% 0.016%
$375,000 20,000 0.065% 0.001%
$375,000 30,000 0.016% 0.001%
$375,000 40,000 0.004% 0.001%
$380,000 25 19.730% 18.202%
$380,000 50 14.147% 12.578%
$380,000 100 9.831% 8.217%
$380,000 150 8.037% 6.425%
$380,000 200 6.891% 5.296%
$380,000 300 5.458% 3.930%
$380,000 400 4.410% 2.995%
$380,000 500 4.221% 2.770%
$380,000 600 3.637% 2.253%
$380,000 700 3.269% 1.953%
$380,000 800 3.042% 1.750%
$380,000 900 2.885% 1.614%
$380,000 1,000 2.690% 1.449%
$380,000 1,500 2.047% 0.960%
* Applied to total projected claims42

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$380,000 2,000 1.670% 0.688%
$380,000 3,000 1.102% 0.336%
$380,000 4,000 0.849% 0.205%
$380,000 5,000 0.685% 0.136%
$380,000 10,000 0.251% 0.016%
$380,000 20,000 0.065% 0.001%
$380,000 30,000 0.016% 0.001%
$380,000 40,000 0.004% 0.001%
$385,000 25 19.757% 18.229%
$385,000 50 14.173% 12.605%
$385,000 100 9.857% 8.244%
$385,000 150 8.059% 6.447%
$385,000 200 6.911% 5.315%
$385,000 300 5.474% 3.945%
$385,000 400 4.425% 3.008%
$385,000 500 4.234% 2.781%
$385,000 600 3.648% 2.263%
$385,000 700 3.278% 1.960%
$385,000 800 3.051% 1.758%
$385,000 900 2.894% 1.621%
$385,000 1,000 2.698% 1.455%
$385,000 1,500 2.054% 0.965%
$385,000 2,000 1.675% 0.691%
$385,000 3,000 1.106% 0.338%
$385,000 4,000 0.854% 0.207%
$385,000 5,000 0.688% 0.138%
$385,000 10,000 0.252% 0.016%
$385,000 20,000 0.066% 0.001%
$385,000 30,000 0.016% 0.001%
$385,000 40,000 0.004% 0.001%
$390,000 25 19.783% 18.256%
$390,000 50 14.198% 12.631%
$390,000 100 9.881% 8.269%
$390,000 150 8.081% 6.470%
$390,000 200 6.930% 5.334%
$390,000 300 5.489% 3.959%
$390,000 400 4.439% 3.021%
* Applied to total projected claims43

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$390,000 500 4.247% 2.793%
$390,000 600 3.659% 2.272%
$390,000 700 3.286% 1.967%
$390,000 800 3.060% 1.765%
$390,000 900 2.902% 1.628%
$390,000 1,000 2.706% 1.462%
$390,000 1,500 2.061% 0.970%
$390,000 2,000 1.681% 0.695%
$390,000 3,000 1.111% 0.340%
$390,000 4,000 0.858% 0.209%
$390,000 5,000 0.692% 0.139%
$390,000 10,000 0.254% 0.016%
$390,000 20,000 0.066% 0.001%
$390,000 30,000 0.016% 0.001%
$390,000 40,000 0.004% 0.001%
$395,000 25 19.808% 18.280%
$395,000 50 14.224% 12.657%
$395,000 100 9.905% 8.293%
$395,000 150 8.103% 6.491%
$395,000 200 6.949% 5.352%
$395,000 300 5.504% 3.973%
$395,000 400 4.452% 3.033%
$395,000 500 4.259% 2.804%
$395,000 600 3.669% 2.281%
$395,000 700 3.294% 1.974%
$395,000 800 3.069% 1.772%
$395,000 900 2.911% 1.634%
$395,000 1,000 2.714% 1.468%
$395,000 1,500 2.068% 0.975%
$395,000 2,000 1.686% 0.698%
$395,000 3,000 1.115% 0.343%
$395,000 4,000 0.862% 0.211%
$395,000 5,000 0.695% 0.140%
$395,000 10,000 0.255% 0.016%
$395,000 20,000 0.067% 0.001%
$395,000 30,000 0.017% 0.001%
$395,000 40,000 0.004% 0.001%
* Applied to total projected claims44

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$400,000 25 19.832% 18.305%
$400,000 50 14.249% 12.682%
$400,000 100 9.927% 8.316%
$400,000 150 8.124% 6.512%
$400,000 200 6.967% 5.370%
$400,000 300 5.519% 3.987%
$400,000 400 4.465% 3.045%
$400,000 500 4.271% 2.814%
$400,000 600 3.679% 2.289%
$400,000 700 3.302% 1.981%
$400,000 800 3.078% 1.779%
$400,000 900 2.918% 1.641%
$400,000 1,000 2.721% 1.473%
$400,000 1,500 2.074% 0.980%
$400,000 2,000 1.691% 0.701%
$400,000 3,000 1.119% 0.345%
$400,000 4,000 0.866% 0.213%
$400,000 5,000 0.698% 0.142%
$400,000 10,000 0.257% 0.017%
$400,000 20,000 0.067% 0.001%
$400,000 30,000 0.017% 0.001%
$400,000 40,000 0.004% 0.001%
$405,000 25 19.857% 18.329%
$405,000 50 14.272% 12.706%
$405,000 100 9.949% 8.337%
$405,000 150 8.144% 6.532%
$405,000 200 6.985% 5.387%
$405,000 300 5.533% 4.000%
$405,000 400 4.478% 3.056%
$405,000 500 4.282% 2.824%
$405,000 600 3.689% 2.297%
$405,000 700 3.310% 1.988%
$405,000 800 3.086% 1.786%
$405,000 900 2.926% 1.647%
$405,000 1,000 2.729% 1.479%
$405,000 1,500 2.080% 0.984%
$405,000 2,000 1.696% 0.705%
* Applied to total projected claims45

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$405,000 3,000 1.123% 0.347%
$405,000 4,000 0.870% 0.214%
$405,000 5,000 0.701% 0.143%
$405,000 10,000 0.258% 0.017%
$405,000 20,000 0.068% 0.001%
$405,000 30,000 0.017% 0.001%
$405,000 40,000 0.004% 0.001%
$410,000 25 19.882% 18.354%
$410,000 50 14.296% 12.729%
$410,000 100 9.969% 8.358%
$410,000 150 8.165% 6.553%
$410,000 200 7.003% 5.404%
$410,000 300 5.548% 4.014%
$410,000 400 4.490% 3.068%
$410,000 500 4.294% 2.835%
$410,000 600 3.698% 2.305%
$410,000 700 3.318% 1.994%
$410,000 800 3.094% 1.793%
$410,000 900 2.934% 1.653%
$410,000 1,000 2.736% 1.485%
$410,000 1,500 2.087% 0.989%
$410,000 2,000 1.700% 0.708%
$410,000 3,000 1.127% 0.349%
$410,000 4,000 0.874% 0.216%
$410,000 5,000 0.705% 0.144%
$410,000 10,000 0.260% 0.017%
$410,000 20,000 0.068% 0.001%
$410,000 30,000 0.017% 0.001%
$410,000 40,000 0.004% 0.001%
$415,000 25 19.908% 18.380%
$415,000 50 14.319% 12.752%
$415,000 100 9.989% 8.379%
$415,000 150 8.185% 6.574%
$415,000 200 7.020% 5.420%
$415,000 300 5.562% 4.027%
$415,000 400 4.503% 3.079%
$415,000 500 4.306% 2.845%
* Applied to total projected claims46

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$415,000 600 3.708% 2.313%
$415,000 700 3.325% 2.001%
$415,000 800 3.102% 1.799%
$415,000 900 2.941% 1.660%
$415,000 1,000 2.743% 1.490%
$415,000 1,500 2.093% 0.993%
$415,000 2,000 1.705% 0.711%
$415,000 3,000 1.131% 0.351%
$415,000 4,000 0.877% 0.217%
$415,000 5,000 0.708% 0.145%
$415,000 10,000 0.261% 0.017%
$415,000 20,000 0.069% 0.001%
$415,000 30,000 0.017% 0.001%
$415,000 40,000 0.004% 0.001%
$420,000 25 19.931% 18.402%
$420,000 50 14.340% 12.774%
$420,000 100 10.008% 8.398%
$420,000 150 8.205% 6.593%
$420,000 200 7.036% 5.436%
$420,000 300 5.575% 4.040%
$420,000 400 4.515% 3.090%
$420,000 500 4.317% 2.855%
$420,000 600 3.717% 2.321%
$420,000 700 3.333% 2.007%
$420,000 800 3.110% 1.805%
$420,000 900 2.949% 1.665%
$420,000 1,000 2.750% 1.496%
$420,000 1,500 2.099% 0.997%
$420,000 2,000 1.710% 0.714%
$420,000 3,000 1.135% 0.353%
$420,000 4,000 0.881% 0.219%
$420,000 5,000 0.711% 0.146%
$420,000 10,000 0.262% 0.017%
$420,000 20,000 0.069% 0.001%
$420,000 30,000 0.017% 0.001%
$420,000 40,000 0.004% 0.001%
$425,000 25 19.952% 18.424%
* Applied to total projected claims47

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$425,000 50 14.359% 12.794%
$425,000 100 10.026% 8.416%
$425,000 150 8.224% 6.613%
$425,000 200 7.052% 5.452%
$425,000 300 5.589% 4.052%
$425,000 400 4.527% 3.101%
$425,000 500 4.328% 2.865%
$425,000 600 3.725% 2.329%
$425,000 700 3.340% 2.013%
$425,000 800 3.117% 1.812%
$425,000 900 2.956% 1.671%
$425,000 1,000 2.757% 1.501%
$425,000 1,500 2.105% 1.001%
$425,000 2,000 1.714% 0.717%
$425,000 3,000 1.139% 0.355%
$425,000 4,000 0.885% 0.221%
$425,000 5,000 0.714% 0.148%
$425,000 10,000 0.264% 0.018%
$425,000 20,000 0.069% 0.001%
$425,000 30,000 0.017% 0.001%
$425,000 40,000 0.004% 0.001%
$430,000 25 19.973% 18.444%
$430,000 50 14.379% 12.813%
$430,000 100 10.043% 8.434%
$430,000 150 8.242% 6.631%
$430,000 200 7.067% 5.467%
$430,000 300 5.601% 4.064%
$430,000 400 4.538% 3.112%
$430,000 500 4.338% 2.874%
$430,000 600 3.734% 2.336%
$430,000 700 3.346% 2.019%
$430,000 800 3.125% 1.817%
$430,000 900 2.962% 1.677%
$430,000 1,000 2.763% 1.506%
$430,000 1,500 2.110% 1.005%
$430,000 2,000 1.718% 0.719%
$430,000 3,000 1.143% 0.357%
* Applied to total projected claims48

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$430,000 4,000 0.888% 0.222%
$430,000 5,000 0.716% 0.149%
$430,000 10,000 0.265% 0.018%
$430,000 20,000 0.070% 0.001%
$430,000 30,000 0.018% 0.001%
$430,000 40,000 0.004% 0.001%
$435,000 25 19.992% 18.464%
$435,000 50 14.397% 12.832%
$435,000 100 10.058% 8.450%
$435,000 150 8.259% 6.648%
$435,000 200 7.081% 5.481%
$435,000 300 5.613% 4.075%
$435,000 400 4.548% 3.121%
$435,000 500 4.347% 2.882%
$435,000 600 3.742% 2.343%
$435,000 700 3.353% 2.024%
$435,000 800 3.131% 1.823%
$435,000 900 2.969% 1.683%
$435,000 1,000 2.769% 1.510%
$435,000 1,500 2.115% 1.009%
$435,000 2,000 1.722% 0.722%
$435,000 3,000 1.146% 0.359%
$435,000 4,000 0.891% 0.224%
$435,000 5,000 0.719% 0.150%
$435,000 10,000 0.266% 0.018%
$435,000 20,000 0.070% 0.001%
$435,000 30,000 0.018% 0.001%
$435,000 40,000 0.004% 0.001%
$440,000 25 20.012% 18.483%
$440,000 50 14.415% 12.850%
$440,000 100 10.074% 8.466%
$440,000 150 8.276% 6.666%
$440,000 200 7.096% 5.495%
$440,000 300 5.624% 4.086%
$440,000 400 4.559% 3.131%
$440,000 500 4.357% 2.891%
$440,000 600 3.750% 2.350%
* Applied to total projected claims49

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$440,000 700 3.359% 2.030%
$440,000 800 3.138% 1.829%
$440,000 900 2.976% 1.688%
$440,000 1,000 2.775% 1.515%
$440,000 1,500 2.121% 1.013%
$440,000 2,000 1.726% 0.724%
$440,000 3,000 1.150% 0.360%
$440,000 4,000 0.894% 0.225%
$440,000 5,000 0.721% 0.151%
$440,000 10,000 0.267% 0.018%
$440,000 20,000 0.070% 0.001%
$440,000 30,000 0.018% 0.001%
$440,000 40,000 0.004% 0.001%
$445,000 25 20.031% 18.503%
$445,000 50 14.434% 12.869%
$445,000 100 10.089% 8.482%
$445,000 150 8.293% 6.683%
$445,000 200 7.111% 5.510%
$445,000 300 5.636% 4.097%
$445,000 400 4.570% 3.141%
$445,000 500 4.366% 2.900%
$445,000 600 3.758% 2.357%
$445,000 700 3.365% 2.035%
$445,000 800 3.145% 1.834%
$445,000 900 2.982% 1.693%
$445,000 1,000 2.780% 1.519%
$445,000 1,500 2.126% 1.017%
$445,000 2,000 1.730% 0.727%
$445,000 3,000 1.153% 0.362%
$445,000 4,000 0.898% 0.227%
$445,000 5,000 0.724% 0.152%
$445,000 10,000 0.268% 0.018%
$445,000 20,000 0.071% 0.001%
$445,000 30,000 0.018% 0.001%
$445,000 40,000 0.004% 0.001%
$450,000 25 20.050% 18.521%
$450,000 50 14.452% 12.888%
* Applied to total projected claims50

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$450,000 100 10.104% 8.497%
$450,000 150 8.309% 6.700%
$450,000 200 7.125% 5.524%
$450,000 300 5.648% 4.108%
$450,000 400 4.580% 3.150%
$450,000 500 4.376% 2.908%
$450,000 600 3.766% 2.364%
$450,000 700 3.371% 2.040%
$450,000 800 3.152% 1.840%
$450,000 900 2.989% 1.699%
$450,000 1,000 2.786% 1.524%
$450,000 1,500 2.131% 1.020%
$450,000 2,000 1.734% 0.730%
$450,000 3,000 1.156% 0.364%
$450,000 4,000 0.901% 0.228%
$450,000 5,000 0.726% 0.153%
$450,000 10,000 0.269% 0.019%
$450,000 20,000 0.071% 0.001%
$450,000 30,000 0.018% 0.001%
$450,000 40,000 0.004% 0.001%
$455,000 25 20.068% 18.539%
$455,000 50 14.470% 12.906%
$455,000 100 10.119% 8.513%
$455,000 150 8.325% 6.716%
$455,000 200 7.139% 5.538%
$455,000 300 5.659% 4.118%
$455,000 400 4.590% 3.160%
$455,000 500 4.385% 2.916%
$455,000 600 3.774% 2.371%
$455,000 700 3.377% 2.046%
$455,000 800 3.159% 1.845%
$455,000 900 2.995% 1.704%
$455,000 1,000 2.791% 1.528%
$455,000 1,500 2.136% 1.024%
$455,000 2,000 1.737% 0.732%
$455,000 3,000 1.160% 0.366%
$455,000 4,000 0.904% 0.229%
* Applied to total projected claims51

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$455,000 5,000 0.729% 0.154%
$455,000 10,000 0.270% 0.019%
$455,000 20,000 0.072% 0.001%
$455,000 30,000 0.018% 0.001%
$455,000 40,000 0.004% 0.001%
$460,000 25 20.087% 18.558%
$460,000 50 14.488% 12.924%
$460,000 100 10.134% 8.527%
$460,000 150 8.340% 6.731%
$460,000 200 7.153% 5.551%
$460,000 300 5.670% 4.128%
$460,000 400 4.600% 3.169%
$460,000 500 4.394% 2.924%
$460,000 600 3.782% 2.377%
$460,000 700 3.383% 2.051%
$460,000 800 3.165% 1.850%
$460,000 900 3.001% 1.709%
$460,000 1,000 2.797% 1.532%
$460,000 1,500 2.141% 1.027%
$460,000 2,000 1.741% 0.735%
$460,000 3,000 1.163% 0.367%
$460,000 4,000 0.907% 0.231%
$460,000 5,000 0.731% 0.155%
$460,000 10,000 0.271% 0.019%
$460,000 20,000 0.072% 0.001%
$460,000 30,000 0.018% 0.001%
$460,000 40,000 0.004% 0.001%
$465,000 25 20.105% 18.576%
$465,000 50 14.506% 12.942%
$465,000 100 10.148% 8.542%
$465,000 150 8.356% 6.747%
$465,000 200 7.166% 5.565%
$465,000 300 5.681% 4.139%
$465,000 400 4.610% 3.178%
$465,000 500 4.403% 2.932%
$465,000 600 3.790% 2.384%
$465,000 700 3.390% 2.056%
* Applied to total projected claims52

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$465,000 800 3.172% 1.856%
$465,000 900 3.008% 1.714%
$465,000 1,000 2.802% 1.536%
$465,000 1,500 2.146% 1.031%
$465,000 2,000 1.745% 0.737%
$465,000 3,000 1.166% 0.369%
$465,000 4,000 0.910% 0.232%
$465,000 5,000 0.734% 0.156%
$465,000 10,000 0.273% 0.019%
$465,000 20,000 0.072% 0.001%
$465,000 30,000 0.018% 0.001%
$465,000 40,000 0.004% 0.001%
$470,000 25 20.123% 18.594%
$470,000 50 14.524% 12.959%
$470,000 100 10.162% 8.556%
$470,000 150 8.371% 6.762%
$470,000 200 7.179% 5.578%
$470,000 300 5.691% 4.149%
$470,000 400 4.620% 3.187%
$470,000 500 4.411% 2.940%
$470,000 600 3.798% 2.391%
$470,000 700 3.396% 2.061%
$470,000 800 3.178% 1.861%
$470,000 900 3.014% 1.720%
$470,000 1,000 2.808% 1.541%
$470,000 1,500 2.150% 1.034%
$470,000 2,000 1.748% 0.739%
$470,000 3,000 1.169% 0.371%
$470,000 4,000 0.913% 0.234%
$470,000 5,000 0.736% 0.156%
$470,000 10,000 0.274% 0.019%
$470,000 20,000 0.073% 0.001%
$470,000 30,000 0.018% 0.001%
$470,000 40,000 0.004% 0.001%
$475,000 25 20.140% 18.610%
$475,000 50 14.540% 12.976%
$475,000 100 10.175% 8.569%
* Applied to total projected claims53

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$475,000 150 8.385% 6.777%
$475,000 200 7.192% 5.590%
$475,000 300 5.702% 4.159%
$475,000 400 4.630% 3.196%
$475,000 500 4.420% 2.948%
$475,000 600 3.806% 2.398%
$475,000 700 3.402% 2.066%
$475,000 800 3.185% 1.866%
$475,000 900 3.020% 1.725%
$475,000 1,000 2.813% 1.545%
$475,000 1,500 2.155% 1.038%
$475,000 2,000 1.752% 0.742%
$475,000 3,000 1.172% 0.372%
$475,000 4,000 0.916% 0.235%
$475,000 5,000 0.738% 0.157%
$475,000 10,000 0.275% 0.019%
$475,000 20,000 0.073% 0.001%
$475,000 30,000 0.019% 0.001%
$475,000 40,000 0.004% 0.001%
$480,000 25 20.156% 18.627%
$480,000 50 14.557% 12.992%
$480,000 100 10.188% 8.583%
$480,000 150 8.400% 6.792%
$480,000 200 7.204% 5.602%
$480,000 300 5.713% 4.169%
$480,000 400 4.639% 3.205%
$480,000 500 4.429% 2.955%
$480,000 600 3.814% 2.404%
$480,000 700 3.408% 2.072%
$480,000 800 3.191% 1.872%
$480,000 900 3.026% 1.730%
$480,000 1,000 2.818% 1.549%
$480,000 1,500 2.160% 1.041%
$480,000 2,000 1.756% 0.744%
$480,000 3,000 1.176% 0.374%
$480,000 4,000 0.919% 0.236%
$480,000 5,000 0.741% 0.158%
* Applied to total projected claims54

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$480,000 10,000 0.276% 0.020%
$480,000 20,000 0.073% 0.001%
$480,000 30,000 0.019% 0.001%
$480,000 40,000 0.004% 0.001%
$485,000 25 20.174% 18.644%
$485,000 50 14.572% 13.008%
$485,000 100 10.201% 8.596%
$485,000 150 8.413% 6.806%
$485,000 200 7.216% 5.614%
$485,000 300 5.723% 4.178%
$485,000 400 4.649% 3.213%
$485,000 500 4.437% 2.963%
$485,000 600 3.822% 2.411%
$485,000 700 3.413% 2.076%
$485,000 800 3.197% 1.877%
$485,000 900 3.032% 1.735%
$485,000 1,000 2.823% 1.553%
$485,000 1,500 2.164% 1.044%
$485,000 2,000 1.759% 0.747%
$485,000 3,000 1.179% 0.376%
$485,000 4,000 0.922% 0.238%
$485,000 5,000 0.743% 0.159%
$485,000 10,000 0.277% 0.020%
$485,000 20,000 0.074% 0.001%
$485,000 30,000 0.019% 0.001%
$485,000 40,000 0.004% 0.001%
$490,000 25 20.189% 18.659%
$490,000 50 14.586% 13.022%
$490,000 100 10.212% 8.607%
$490,000 150 8.426% 6.819%
$490,000 200 7.227% 5.625%
$490,000 300 5.732% 4.187%
$490,000 400 4.657% 3.221%
$490,000 500 4.444% 2.970%
$490,000 600 3.829% 2.417%
$490,000 700 3.418% 2.081%
$490,000 800 3.203% 1.881%
* Applied to total projected claims55

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$490,000 900 3.038% 1.739%
$490,000 1,000 2.828% 1.557%
$490,000 1,500 2.168% 1.047%
$490,000 2,000 1.762% 0.749%
$490,000 3,000 1.181% 0.377%
$490,000 4,000 0.925% 0.239%
$490,000 5,000 0.745% 0.160%
$490,000 10,000 0.278% 0.020%
$490,000 20,000 0.074% 0.001%
$490,000 30,000 0.019% 0.001%
$490,000 40,000 0.004% 0.001%
$495,000 25 20.203% 18.673%
$495,000 50 14.599% 13.035%
$495,000 100 10.223% 8.618%
$495,000 150 8.438% 6.831%
$495,000 200 7.238% 5.636%
$495,000 300 5.741% 4.195%
$495,000 400 4.665% 3.229%
$495,000 500 4.451% 2.976%
$495,000 600 3.835% 2.423%
$495,000 700 3.423% 2.085%
$495,000 800 3.208% 1.886%
$495,000 900 3.043% 1.744%
$495,000 1,000 2.833% 1.561%
$495,000 1,500 2.172% 1.050%
$495,000 2,000 1.766% 0.751%
$495,000 3,000 1.184% 0.379%
$495,000 4,000 0.927% 0.240%
$495,000 5,000 0.747% 0.161%
$495,000 10,000 0.279% 0.020%
$495,000 20,000 0.074% 0.001%
$495,000 30,000 0.019% 0.001%
$495,000 40,000 0.004% 0.001%
$500,000 25 20.218% 18.688%
$500,000 50 14.612% 13.048%
$500,000 100 10.234% 8.630%
$500,000 150 8.450% 6.844%
* Applied to total projected claims56

Blue Cross and Blue Shield of Vermont
Q3 2017 Large Group Rating Program Filing
Experience Refund Risk Charge Factors*
Exhibit 9A
Pooling
Limitmembers 5% Margin 10% Margin
$500,000 200 7.249% 5.646%
$500,000 300 5.750% 4.204%
$500,000 400 4.673% 3.237%
$500,000 500 4.459% 2.983%
$500,000 600 3.842% 2.428%
$500,000 700 3.428% 2.089%
$500,000 800 3.213% 1.890%
$500,000 900 3.048% 1.748%
$500,000 1,000 2.838% 1.564%
$500,000 1,500 2.176% 1.053%
$500,000 2,000 1.769% 0.753%
$500,000 3,000 1.187% 0.380%
$500,000 4,000 0.930% 0.241%
$500,000 5,000 0.749% 0.162%
$500,000 10,000 0.279% 0.020%
$500,000 20,000 0.074% 0.001%
$500,000 30,000 0.019% 0.001%
$500,000 40,000 0.004% 0.001%
* Applied to total projected claims57
Related Documents











