Fibroid Uterus

Fibroid Uterus. Fibroids are benign neoplasms of uterus arising from smooth muscle rests of vessel walls or uterine musculature Contain smooth muscle.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
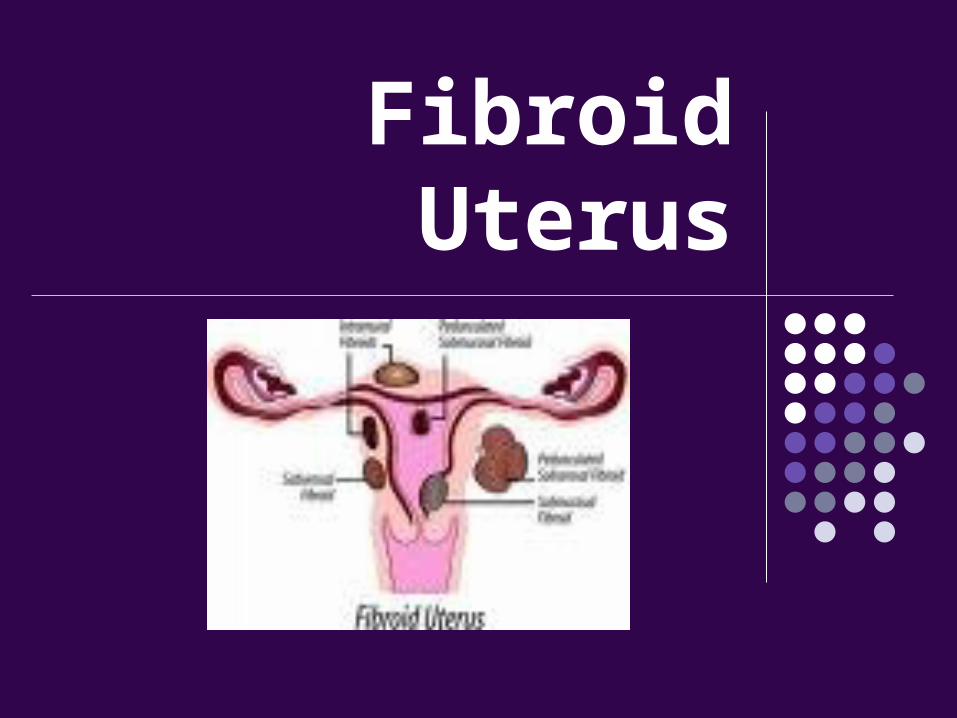
Fibroid Uterus
Fibroids are benign neoplasms of uterus arising from smooth muscle rests of vessel walls or uterine musculature
Contain smooth muscle cells and varying amounts of connective tissue.
Incidence - 5-20% Age -reprodutive age
more in forties
Etiology
Myomas are oestrogen dependent
-Rarely found before puberty
-Increase in size during pregnancy
-And during OC pill usage
-Regress after menopause Monoclonal in origin Chromosomal abnormalities 1,6,7,12,14,
del q 21-22 Seen more in black women
Classification
Based on uterine layer
interstitial 75%
(intramural)
submucous 15%
subserous 10% Various other cassifications based on
hysteroscopy and location of submucous fibroid
Classification
Based on location
- corporeal
- cervical
- isthmic Based on origin
-uterine
-Extrauterine –Ex: broad ligament
fibroid
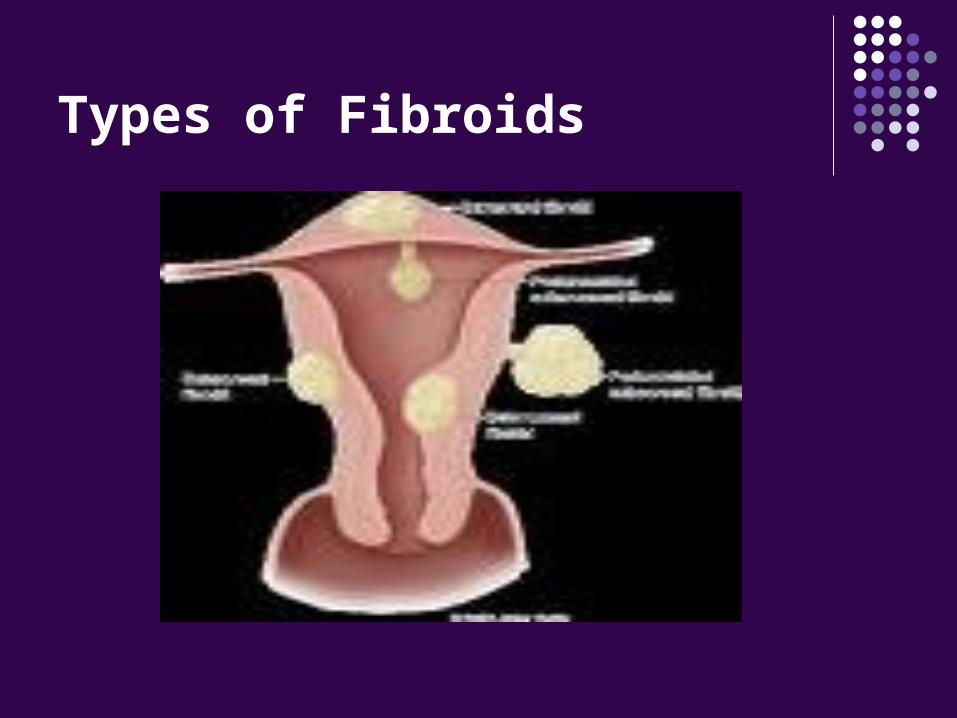
Types of Fibroids
Anatomy and histology
Well circumscribed Pseudoencapsulated Firm in consistency C/S - pinkish white,whorled in appearance Microscopically –bundles of plain muscle
cells,separated by varying amonts of fibrous strands
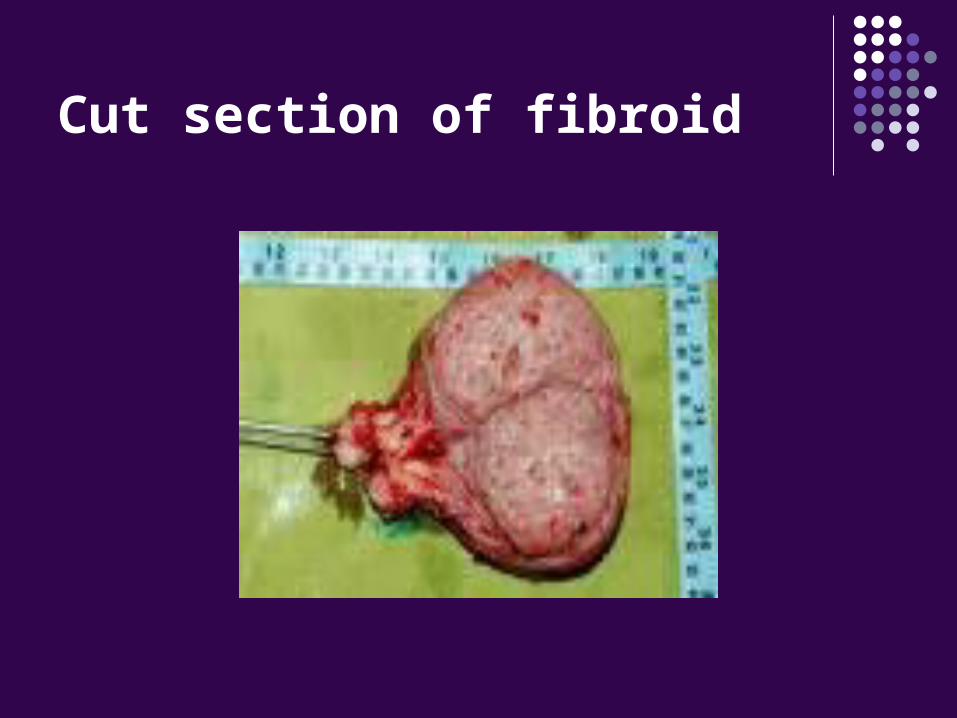
Cut section of fibroid
Secondary changes
Atrophic degeneration - seen after menopause Hyaline degeneration Cystic degeneration Calcareous degeneration Red degeneration - aseptic degeneration
seen in second trimester of
pregnancy Sarcomatous degeneration
Clinical features
Depend on size,site,reproductive status Asymptomatic 50% Menstrual symptoms 30-50% Pelvic pain 30% Subfertility Pressure symptoms Abdominal lump Pregnancy related complications
Menstrual symptoms Most common-menorrhagia Inter menstrual bleeding in submucous
myoma
Pelvic pain Dysmenorrhoea Dyspareunia Pelvic pressure Torsion of subserous pedunculated fibroid Red degeneration
Pressure symptoms
Urinary symptoms acute retention of urine Frequency urgency dysuriaRectal symptoms- constipation rectal pain difficult defaecationHydro ureteronephrosis due to pressure on ureter
Causes of menstrual symptoms
Increase in total surface area Mechanical distortion of uterine cavity Interference with contractility Dilatation and congestion of endometrial
venous plexuses Endometrial hyperplaia due to high estrogen Pelvic congestion Ulceration of endometrium over submucous
fibroids leading to intermenstrual bleeding
Causes of subfertility
Distortion and elongation of endometral cavity leading to difficult sperm ascent
Impaired contractility of uterus Congestion of endometrial venous plexuses Defective implantation Cornual blockdue to fibroid Elongation and streching of tube over a large
fibroid Associated anovulation

Pregnancy related symptoms
Effects on pregnancy Recurrent abortions Preterm labour Fetal malpresentations Obstructed labour Post partum haemorrhage Subinvolution Puerperal sepsisEffects on fibroid Increase in size Red degeneration
Physical signs
Woman may be anaemic
P/A -Suprapubic mass with well defined
margins
P/S –fibroid polyp may be seen
P/V –enlarged uterus-regular or irregular
cervical movements transmitted to the
mass
Associated conditions
Follicular cysts Theca lutein cysts Endometriotic cysts Pevic inflammatory disease Ovarian tumours Endometrial hyperplasia Endometrial carcinoma
Complications
Secondary changes Sarcomatous change <0.5% Torsion of pedunculated fibroid Inversion due to submucous fibroid Capsular haemorrhage Infection of myomatous polyp
Differential diagnosis
Full bladder Pregnancy Adenomyosis Bicornuate uterus Endometriosis-chocolate cyst Chronic PID Ovarian tumour Endometrial cancer Chronic inversion Pelvic kidney
Investigations
Hb% Blood grouping and typing Ultrasound abdomen to know site,size and
number Hysteroscopy HSG and sonosalpingogram for submucous
myoma MRI in case of sarcoma IVP in broad ligament fibroid
Ultasound picture
Management
Management
Asymptomatic Fibroids <12 weeksneed not be treated
surgical
Myomectomy Hysterectomy
medical
Indications for Medical management
To control menorrhagia To improve hemoglobin before surgery For preoperative shrinkage of large fibroid To reduce vascularity To postpone surgery if woman is not fit for surgery In elderly women until menopause is reached To convert abdominal hysterectomy to a vaginal
one by decreasing the size of uterus Iron therapy for anaemia
Medical management
Combined OC pills Progestogens like MPA, Norethisterone LNG – IUCD (MIRENA) NSAIDS Antifibrinolytics Mifepristone 10-25 mg daily for 3 months Danazol 400-800 daily for 3 to 6 months GnRH analogues for 3 months Gestrinone
Myomectomy
Indications Women with infertility where all other causes have been ruled out Women desirous of child bearing Women who wish to retain their menstrual functionRoutesAbdominal myomectomyVaginal - in submucous fibroid polypHysteroscopic –in submucous fibroid polypLaparoscopic myomectomy
Principals of myomectomy Preoperative Hb% restoration and to keep adequate
blood ready All other factors for infertility like azoospermia are
ruled out Consent for hysterectomy is taken Preoperative D&C and papsmear are taken Should be done in preovulatory phase of
menstruation to reduce blood loss Haemorrhage is controlled with myomectomy (Bonney’s) clamp,20 units of vasopressin in 60 ml
saline
Technique of myomectomy
Keep incision as anterior as possible A single incision is given As many fibroids as possible are removed
through multiple tunnelling incision Myoma cavity thoroughly obliterated with
several catgut sutures
Results Pregnancy rate of 40-50%

Laproscopic myomectomy
Complications of myomectomy
Primary ,reactionary and secondary haemorrhage
Trauma to the bladder,ureter and bowel during surgery
Adhesions and intestinal obstruction Recurrence of fibroids and persistence of
menorrhagia
Hysterectomy
Indications Woman over 40 yrs of age Multiparous women Associated pathology such as endometriosis,
PID, adenomyosis,endometrial hyperplasia Suspested malignancy
Hysterectomy
Routes Abdominal Vaginal Laparoscopic Laparoscopic assisted vaginal hysterectomy
Hysterectomy
Indications for vaginal hysterectomy When uterus is mobile Size<14 weeks No previous surgery No pelvic pathology
Other wise an abdominal hysterectomy is done
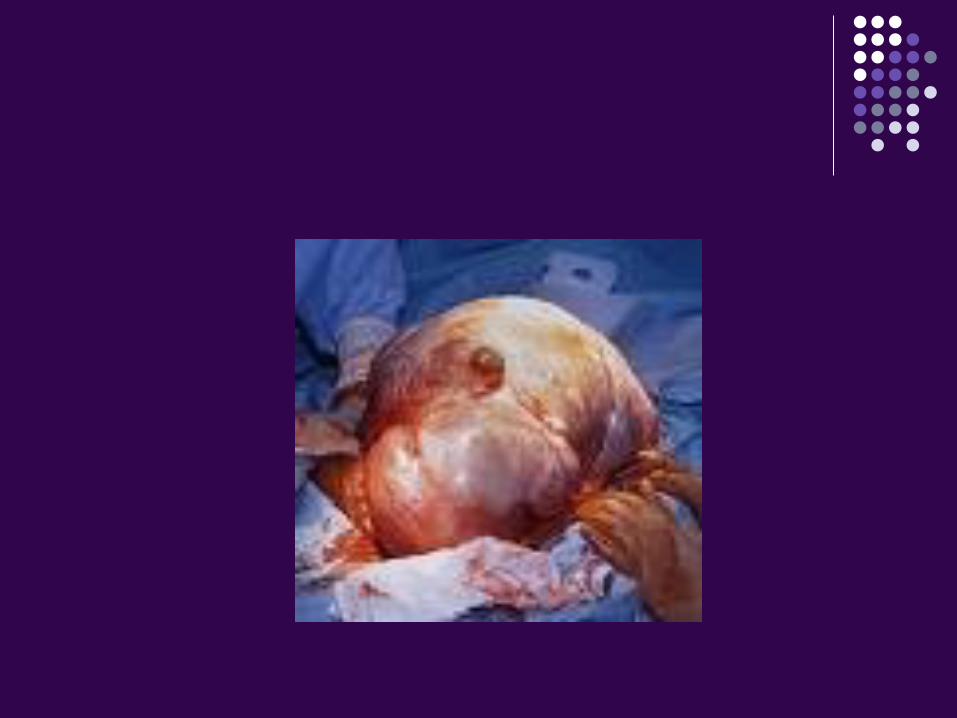

Multiple fibroids
Laparoscopic hysterectomy Avoids scar Minimizes pain Shortens hospital stay Early recovery
Contraindications to LAVH Uterus >14-16 weeks Broad ligament, cervical fibroid Extensive pelvic adhesions
Complications of hysterectomy
Anaesthetic complications Primary ,reactionary and secondary
haemorrhage Trauma to the bladder,ureter and bowel
during surgery Adhesions and intestinal obstruction Sepsis Burst abdomen Incisional hernia
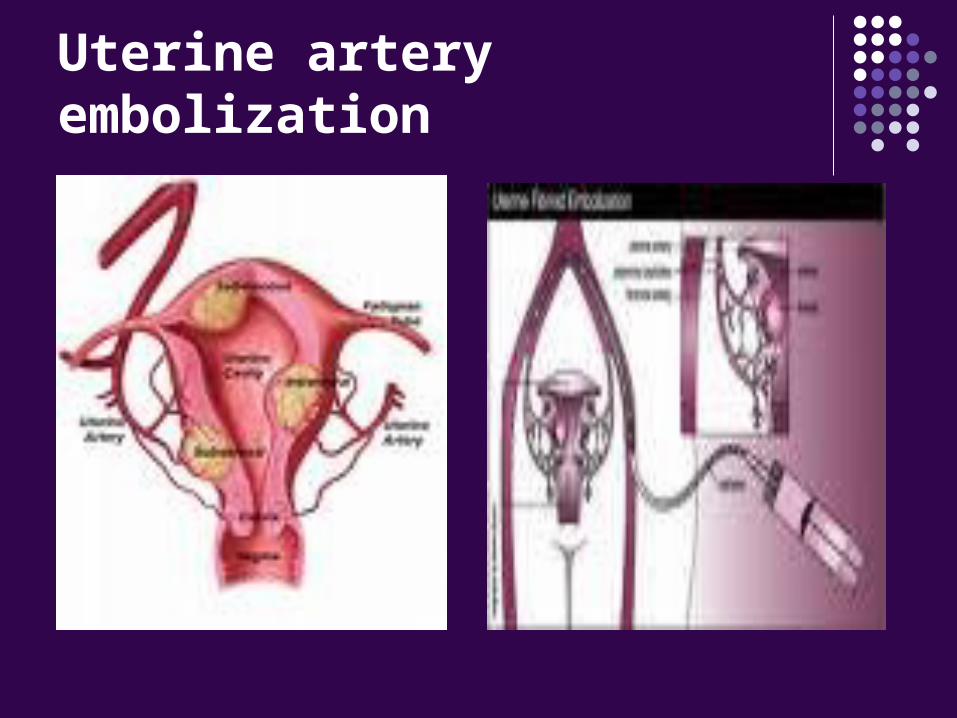
Uterine artery embolization
Improves symptoms in 70-80% of women Preoperative shrinkage Reduces vascularityTechnique Performed through percutaneous femoral
catheterization using polyvinyl alcohol,gel foam or metal coils
Contraindicated in subserous pedunculated fibroid and in women desirous of pregnancy
Uterine artery embolization

Thank you
Related Documents











