1 Fever Fever

Fever
Jan 01, 2016
Fever. Fever in the elderly adult be defined as persistent elevation of body temperature of at least (1.1 C) over baseline values or oral temperatures of (37.2 C) or greater on repeated measures or rectal temperatures of (37.5 C) or greater on repeated measures. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

11
FeverFever

22
Fever in the elderly adult be defined as Fever in the elderly adult be defined as persistent elevation of body persistent elevation of body temperature of at least (1.1 C) over temperature of at least (1.1 C) over baseline values or oral temperatures of baseline values or oral temperatures of (37.2 C) or greater on repeated (37.2 C) or greater on repeated measures or rectal temperatures of measures or rectal temperatures of (37.5 C) or greater on repeated (37.5 C) or greater on repeated measures. measures.

33
The most common sign that triggers The most common sign that triggers the clinician to look for infection, fever, the clinician to look for infection, fever, is often absent in the elderly patient. is often absent in the elderly patient. Animal models of aging demonstrate Animal models of aging demonstrate that temperature elevations in response that temperature elevations in response to endogenous pyrogens (IL-1, IL-6, to endogenous pyrogens (IL-1, IL-6, Tumor Necrosis Factor) are diminished Tumor Necrosis Factor) are diminished with advanced age. with advanced age.
44
הקשיש עם מחלת חום 78מ"ד קשיש בן
מובא לחדר מיון עם חום גבוה ועירפול
הכרה. אישתו מספרתכי הוא סובל מבעיות
של "פרוסטטה" ושבימים האחרונים
. סבל משעול קשהפרט לכך מ"ד הוא
…איש בריא

55

66
Presentation of illnessPresentation of illnessInfectious diseases frequently present with Infectious diseases frequently present with atypical features in older adults. Serious atypical features in older adults. Serious infections may be heralded by nonspecific infections may be heralded by nonspecific declines in functional or mental status, or declines in functional or mental status, or anorexia with decreased oral intake. anorexia with decreased oral intake. Underlying illness (e.,g. congestive heart Underlying illness (e.,g. congestive heart failure or diabetes) may be exacerbated. failure or diabetes) may be exacerbated.
77
Presentation of illnessPresentation of illness
Cognitive impairment heavily Cognitive impairment heavily contributes to the difficulty in contributes to the difficulty in diagnosing infection in the elderly. diagnosing infection in the elderly.

88
ComorbiditiesComorbiditiesIn the elderly individual, the increased In the elderly individual, the increased incidence of infection and mortality for incidence of infection and mortality for many infectious diseases is likely a many infectious diseases is likely a direct result of the comorbid direct result of the comorbid conditions:conditions:DiabetesDiabetesRenal failureRenal failureChronic pulmonary diseaseChronic pulmonary disease

99
NutritionNutrition
Protein-energy malnutrition is present Protein-energy malnutrition is present in 30 to 60 percent of subjects older in 30 to 60 percent of subjects older than 65 years of age who are admitted than 65 years of age who are admitted to the hospital and is linked to delayed to the hospital and is linked to delayed wound healing, decubitus ulcer wound healing, decubitus ulcer formation, CAP, increased risk of formation, CAP, increased risk of nosocomial infection, extended lengths nosocomial infection, extended lengths of stay and increased mortality.of stay and increased mortality.
1010
Clinical Syndromes in The Clinical Syndromes in The ElderlyElderly
Urinary Tract Infections Urinary Tract Infections in the Elderlyin the Elderly
1111
UTI.UTI.
Urinary infection in the elderly person Urinary infection in the elderly person is usually asymptomatic. is usually asymptomatic. Recurrent urinary infection, which may Recurrent urinary infection, which may be either be either reinfectionreinfection or or relapserelapse, is , is frequent. frequent. ReinfectionReinfection is recurrent is recurrent urinary infection with an organism urinary infection with an organism isolated following antimocrobial isolated following antimocrobial therapy which differs from the therapy which differs from the pretherapy isolatepretherapy isolate . .

1212
UTI.UTI.
RelapseRelapse is recurrent urinary is recurrent urinary infection with the organism infection with the organism isolated posttherapy similar to isolated posttherapy similar to that which was present prior to that which was present prior to therapy. therapy.

1313
UTI.UTI.
The prevalence of bacteriuria is 2 to 3 The prevalence of bacteriuria is 2 to 3 percent in young women, and increases to percent in young women, and increases to more than 10 percent for women older than more than 10 percent for women older than age 65 years. Bacteriuria is uncommon in age 65 years. Bacteriuria is uncommon in younger men. With aging, particularly younger men. With aging, particularly coincident with the development of prostatic coincident with the development of prostatic hypertrophy, the prevalence of bacteriuria hypertrophy, the prevalence of bacteriuria increases substantially, and approximately 5 increases substantially, and approximately 5 percent of men older than age 70 years living percent of men older than age 70 years living in the community have bacteriuria.in the community have bacteriuria.

1414
UTI.UTI.
The prevalence of asymptomatic The prevalence of asymptomatic bacteriuria in institutionalized elderly bacteriuria in institutionalized elderly populations is remarkably high. Women populations is remarkably high. Women have a higher frequency than men, with have a higher frequency than men, with 25 to 50 percent of women being 25 to 50 percent of women being bacteriuric, as compared to 15 to 40 bacteriuric, as compared to 15 to 40 percent of men.percent of men.
1515
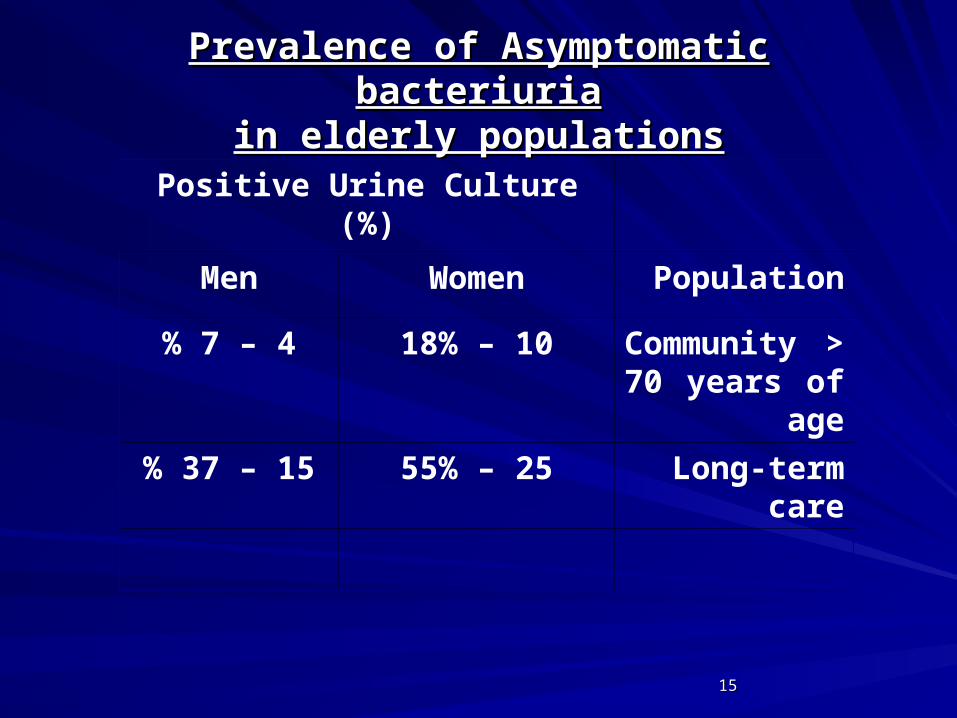
Prevalence of Asymptomatic bacteriuriaPrevalence of Asymptomatic bacteriuriain elderly populationsin elderly populations
Positive Urine Culture)%(
PopulationWomenMen
Community > 70 years of age
10 – 18%4 – 7%
Long-term care25 – 55%15 – 37%

1616
Infecting bacteria Infecting bacteria
CommunityCommunity vs.vs. InstitutionInstitution
WomenWomen:: Escherichia coli 68% - 47%Escherichia coli 68% - 47%
Proteus mirab.Proteus mirab. 1% 1% - 27%- 27%
Klebsiella Klebsiella 7% - 10%7% - 10%
Enterococcus spp. 5%- 6%Enterococcus spp. 5%- 6%
Coagulas- neg.Coagulas- neg. staph. 7% -1%staph. 7% -1%
Pseudomonas aeruginosa 0-5%Pseudomonas aeruginosa 0-5%
Providencia spp. 0-7% Providencia spp. 0-7%

1717
Infecting bacteria Infecting bacteria
CommunityCommunity vs.vs. InstitutionInstitution
MenMen:: Escherichia coli 20% - 11%Escherichia coli 20% - 11%
Proteus mirab.Proteus mirab. 5%-5%- 30% 30%
Klebsiella Klebsiella 6% - 5%6% - 5%
Enterococcus spp. 25%- 5%Enterococcus spp. 25%- 5%
Coagulas- neg.Coagulas- neg. staph.39% -2%staph.39% -2%
Pseudomonas Pseudomonas 5% 5% -19%-19%
Providencia 0-16%Providencia 0-16%

1818
Factors contributing to the high prevalence of Factors contributing to the high prevalence of bacteriuria in elderly populationsbacteriuria in elderly populations
Women : Loss of estrogen effect on Women : Loss of estrogen effect on
genitourinary mucosagenitourinary mucosa
Changes in colonizing floraChanges in colonizing flora
Increased residual Increased residual
volumevolume

1919
Factors contributing to the high prevalence of Factors contributing to the high prevalence of bacteriuria in elderly populationsbacteriuria in elderly populations
Men:Men:
Prostatic hypertrophyProstatic hypertrophy
Bacterial prostatitisBacterial prostatitis
Prostatic calculiProstatic calculi
Urethral stricturesUrethral strictures
External urine collecting devicesExternal urine collecting devices
2020
Factors contributing to the high prevalence of Factors contributing to the high prevalence of bacteriuria in elderly populationsbacteriuria in elderly populations
Both:Both:
Genitourinary abnormalitiesGenitourinary abnormalities
Bladder diverticulae Bladder diverticulae
Urinary catheters (intermittent, indwelling)Urinary catheters (intermittent, indwelling)
Associated illnessesAssociated illnesses
Neurologic disease with neurogenic bladder Neurologic disease with neurogenic bladder dysfunction dysfunction
Diabetes Mellitus.Diabetes Mellitus.

2121
Symptomatic Urinary InfectionSymptomatic Urinary Infection
From 8 to 30 percent of transfers to an From 8 to 30 percent of transfers to an acute care facility from long-term care acute care facility from long-term care are necessitated by acute urinary are necessitated by acute urinary infection. infection.

2222
Symptomatic Urinary InfectionSymptomatic Urinary InfectionMorbidity and MortalityMorbidity and Mortality
Urinary infection occurs by the Urinary infection occurs by the ascending route. Organism that ascending route. Organism that colonize the periurethral area ascend colonize the periurethral area ascend the urethra into the bladder, kidney, the urethra into the bladder, kidney, with renal infection. For men, with renal infection. For men, ascending infection may also lead to ascending infection may also lead to prostatic infection. Renal localization is prostatic infection. Renal localization is more frequent with increasing age, and more frequent with increasing age, and in residents of nursing homes.in residents of nursing homes.
2323
Clinical presentations of symptomatic urinary Clinical presentations of symptomatic urinary
tract infection in elderly populationstract infection in elderly populations Probable urinary infection:Probable urinary infection:Acute lower tract irritative symptoms: Acute lower tract irritative symptoms: frequency, dysuria, urgency, increased frequency, dysuria, urgency, increased incontinence .incontinence .Acute pyelonephritis (fever, flank pain, and Acute pyelonephritis (fever, flank pain, and tenderness).tenderness).Fever with urinary retention or obstruction of Fever with urinary retention or obstruction of the urinary tract .the urinary tract .Fever with chronic indwelling urethral Fever with chronic indwelling urethral catheter.catheter.
2424
Unlikely caused by urinary infection:Unlikely caused by urinary infection:
Gross hematuriaGross hematuria
Not caused by urinary infection:Not caused by urinary infection:
Chronic incontinenceChronic incontinenceOther chronic genitourinary symptomsOther chronic genitourinary symptoms
2525
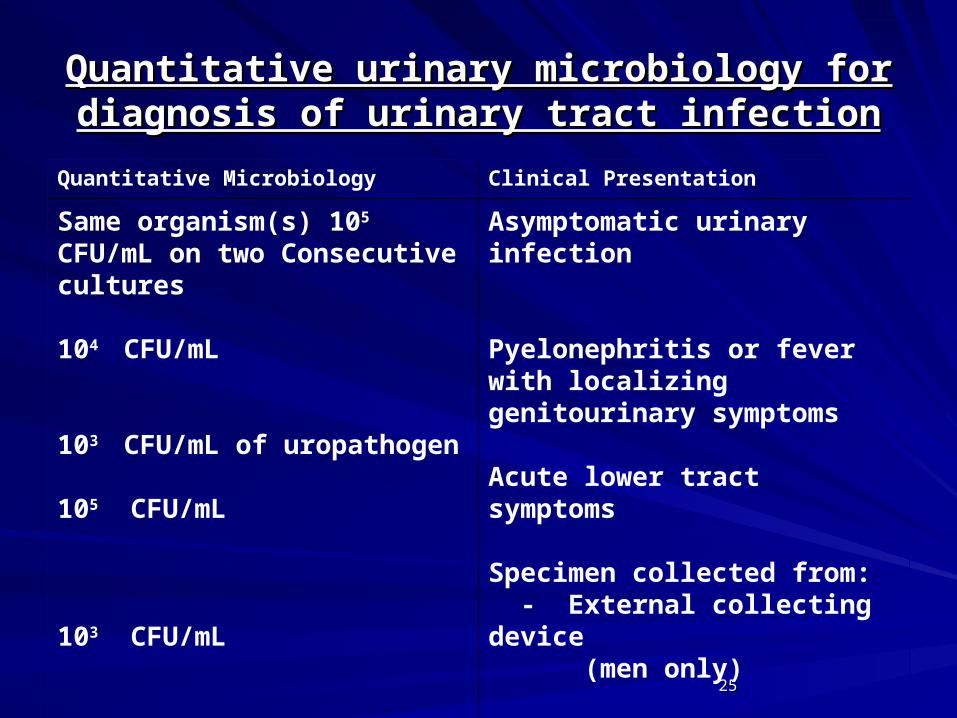
Quantitative urinary microbiology for diagnosis Quantitative urinary microbiology for diagnosis of urinary tract infectionof urinary tract infection
Clinical PresentationQuantitative Microbiology
Asymptomatic urinary infection
Pyelonephritis or fever with localizing genitourinary symptoms
Acute lower tract symptoms
Specimen collected from: - External collecting device (men only)
- Aspirated indwelling catheter
Same organism(s) 105
CFU/mL on two Consecutive cultures
104 CFU/mL
103 CFU/mL of uropathogen
105 CFU/mL
103 CFU/mL

2626
Symptomatic Urinary InfectionSymptomatic Urinary Infection
Treatment of symptomatic urinary Treatment of symptomatic urinary infection requires optimal use of urine infection requires optimal use of urine culture for diagnosis, appropriate culture for diagnosis, appropriate antimicrobial selection, and an antimicrobial selection, and an appropriate duration of therapy. A urine appropriate duration of therapy. A urine specimen for culture should be specimen for culture should be obtained prior to antimicrobial therapy. obtained prior to antimicrobial therapy.

2727
Symptomatic Urinary Infection (cont.)Symptomatic Urinary Infection (cont.)
Antimicrobial selection for treatment of Antimicrobial selection for treatment of urinary infection is similar for elderly urinary infection is similar for elderly and younger populations. Therapy may and younger populations. Therapy may be given either orally or, when oral be given either orally or, when oral administration cannot be tolerated or administration cannot be tolerated or absorption is uncertain, by parenteral absorption is uncertain, by parenteral therapy. Antimicrobial cost will also therapy. Antimicrobial cost will also usually be a factor, especially for usually be a factor, especially for institutionalized populations.institutionalized populations.

2828
Oral antimicrobial regimens for treatment of Oral antimicrobial regimens for treatment of acute urinary tract infectionacute urinary tract infection
AgentDose*
First line
Nitrofurantoin50 – 100 mg qid
Trimethoprim/sulfamethoxazole
160/800 mg bid
Trimethoprim100 mg bid
Amoxicillin500 mg tid

2929
Oral antimicrobial regimens for treatment of Oral antimicrobial regimens for treatment of acute urinary tract infection (cont.)acute urinary tract infection (cont.)
AgentDose*Other
Amoxicillin/clavulanic acid500 mg tid
Norfloxacin400 mg bid
Ciprofloxacin250 – 500 mg bid
Ofloxacin200 – 400 mg bid
Cephalexin500 mg qid
Cefaclor500 mg qid
Cefixime400 mg od

3030
Parenteral antimicrobial regiments for the Parenteral antimicrobial regiments for the treatmenttreatment
of urinary tract infection of urinary tract infection
AgentDose
Preferred
Gentamicin1-1.5mg/kg q8h or 4-5 mg/kg q24h
Tobramycin1-1.5 mg/kg q8h or 4-9 mg/kg q24h
Ampicillin1 g q4-6h
Cefazolin1-2 g q8h

3131
AgentDose
Other
Trimethoprim- sulfamethoxazole
160/800 mg q12h
Amikacin5 mg/kg q8h or 15 mg/kg q24h
Piperacillin3 g q4h
Piperacillin/tazobactam4 g/500mg q8h
Cefotaxime1-2 g q8h
Ceftriaxone1-2 g q24h
Cefepime2 g q12h
Ceftazidime0.5-2 g q8h
Aztreonam1-2 g q6h
Imipenem/cilastatin500 mg q6h
Vancomycin500mg q6h or 1 g q12h
Ciprofloxacin200-400 mg q12h
Ofloxacin400 mg q12h
3232
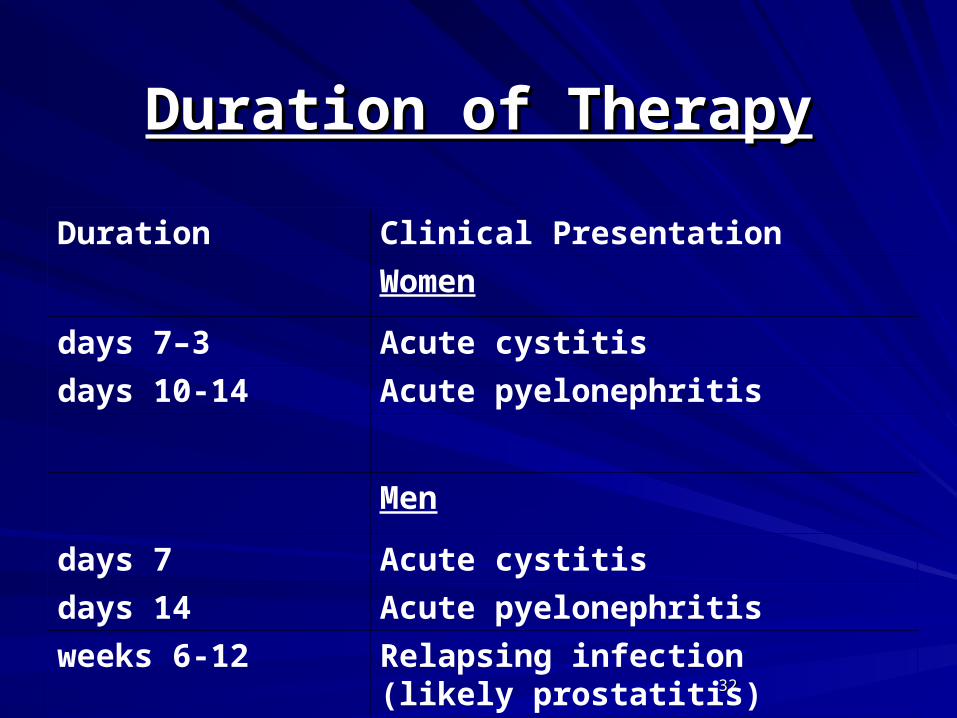
Duration of TherapyDuration of Therapy
Clinical PresentationDuration
Women
Acute cystitis3–7 days
Acute pyelonephritis10-14 days
Men
Acute cystitis7 days
Acute pyelonephritis14 days
Relapsing infection (likely prostatitis)
6-12 weeks
3333
Long Term Indwelling CathetersLong Term Indwelling Catheters
Between 5 and 10 percent of elderly Between 5 and 10 percent of elderly residents of institutions have urinary residents of institutions have urinary voiding managed with long-term voiding managed with long-term indwelling catheters. The major indwelling catheters. The major indications for catheterization are indications for catheterization are retention and continence control. retention and continence control. Subjects with long-term indwelling Subjects with long-term indwelling catheters are always bacteriuric, catheters are always bacteriuric, usually with two to five organisms at usually with two to five organisms at any time.any time.
3434
Long Term Indwelling CathetersLong Term Indwelling Catheters
Morbidity from urinary infection is Morbidity from urinary infection is increased in the presence of a long-increased in the presence of a long-term indwelling catheter. Symptomatic term indwelling catheter. Symptomatic presentations include febrile urinary presentations include febrile urinary infection and complications such as infection and complications such as stone formation and urethral stone formation and urethral abscesses. Catheter obstruction abscesses. Catheter obstruction occurs frequently in some patients. occurs frequently in some patients. Obstruction is usually secondary to Obstruction is usually secondary to struvite formation.struvite formation.

3535
Long Term Indwelling CathetersLong Term Indwelling Catheters
Mucosal trauma may occur with Mucosal trauma may occur with catheter change, and in the presence of catheter change, and in the presence of infected urine may lead to fever. infected urine may lead to fever. However, this occurs in less than 10 However, this occurs in less than 10 percent of episodes of catheter change. percent of episodes of catheter change. Residents with an indwelling urinary Residents with an indwelling urinary catheter also have an increased catheter also have an increased mortality compared to noncatheterized mortality compared to noncatheterized residents.residents.
3636
PneumoniaPneumonia
3737
The clinician defines pneumonia as a The clinician defines pneumonia as a combination of combination of symptoms:symptoms:
feverfever
chillschills
cough cough
pleuritic chest painpleuritic chest pain
sputumsputum
3838
PneumoniaPneumonia
SingsSings: : hyperthermiahyperthermia hypothermiahypothermia increased respiratory rateincreased respiratory rate dullness to percussiondullness to percussion bronchial breathingbronchial breathing cracklescrackles wheezeswheezes pleural friction rubpleural friction rub opacity on a chest radiographopacity on a chest radiograph

3939
PneumoniaPneumonia
In addition, laboratory findings, such In addition, laboratory findings, such as increased white blood cell count and as increased white blood cell count and decreased level of oxygen saturation, decreased level of oxygen saturation, may also be part of the definition.may also be part of the definition.
4040
PneumoniaPneumonia
The epidemiologist or clinical trialist The epidemiologist or clinical trialist defines pneumonia as two or more of defines pneumonia as two or more of the symptoms listed above, one or the symptoms listed above, one or more of the physical findings listed more of the physical findings listed above, and a new opacity on chest above, and a new opacity on chest radiograph that is not cause by a radiograph that is not cause by a condition other than pneumonia (such condition other than pneumonia (such as congestive heart failure, vasculitis, as congestive heart failure, vasculitis, pulmonary infarction, atelectasis, or pulmonary infarction, atelectasis, or drug reaction).drug reaction).

4141
PneumoniaPneumonia
Pneumonia may be also be categorized Pneumonia may be also be categorized according to the place of acquisition: according to the place of acquisition: communitycommunity, , hospitalhospital (nosocomial) or (nosocomial) or nursing home.nursing home.
4242
PneumoniaPneumonia
Approximately 80 percent of adults with Approximately 80 percent of adults with CAP are treated on an ambulatory CAP are treated on an ambulatory basis. The mortality rate for those who basis. The mortality rate for those who are 65 years of age is approximately 5 are 65 years of age is approximately 5 percent. The 20 percent of patients with percent. The 20 percent of patients with CAP who require admission to hospital, CAP who require admission to hospital, the mean age of patients with CAP the mean age of patients with CAP requiring admission to hospital was 55 requiring admission to hospital was 55 years in 1955, by year 2001, it was 71 years in 1955, by year 2001, it was 71 years.years.

4343
Risk factor for community Risk factor for community acquired pneumonia:acquired pneumonia:
AlcoholismAlcoholism AsthmaAsthma Immunosuppression Immunosuppression Age > 70Age > 70 AspirationAspiration Low serum albuminLow serum albumin Swallowing disorderSwallowing disorder Poor quality of lifePoor quality of life

4444
Risk factors for pneumococcal Risk factors for pneumococcal pneumonia:pneumonia:
DementiaDementia
SeizuresSeizures
Congestive heart failureCongestive heart failure
Cerebrovascular diseaseCerebrovascular disease
Tobacco smoking Tobacco smoking
Chronic obstructive lung diseaseChronic obstructive lung disease
4545
Risk factors for legionnaires Risk factors for legionnaires disease include:disease include:
Male genderMale gender
Tobacco smokingTobacco smoking
DiabetesDiabetes
Hematologic malignancyHematologic malignancy
Cancer Cancer
End-stage renal diseaseEnd-stage renal disease
HIV infection.HIV infection.

4646
PneumoniaPneumonia
Significant predictors of a fatal outcome: Significant predictors of a fatal outcome: bedridden state prior to onset of pneumonia; bedridden state prior to onset of pneumonia; temperature, (39 C), respiratory rate 30 temperature, (39 C), respiratory rate 30 breaths per minute; shock; creatinine greater breaths per minute; shock; creatinine greater than 1.4 mg/dL; and three or more lobes than 1.4 mg/dL; and three or more lobes involved on chest radiograph.involved on chest radiograph.
Pneumonia is the leading cause for transfer Pneumonia is the leading cause for transfer of nursing home patients to hospital.of nursing home patients to hospital.

4747
Most common causes of community – acquired Most common causes of community – acquired pneumonia in the pneumonia in the elderly populationelderly population
Streptococcus pneumoniaeStreptococcus pneumoniaeChlamydia pneumoniaeChlamydia pneumoniaeEnterobacteriaceaeEnterobacteriaceaeLegionella pneumophilaLegionella pneumophilaHaemophilus influenzaeHaemophilus influenzaeMoraxella catarrhalisMoraxella catarrhalisStaphylococcus aureusStaphylococcus aureusInfluenza A and B virusInfluenza A and B virus

4848
PneumoniaPneumonia
PresentationPresentation
Pneumonia can be one of the causes of Pneumonia can be one of the causes of insidious or nonspecific deterioration insidious or nonspecific deterioration in general health and/or activities, for in general health and/or activities, for example, confusion or falls in the example, confusion or falls in the elderly.elderly.
4949
Frequency of various signs and symptoms in adults Frequency of various signs and symptoms in adults with community – acquired pneumoniawith community – acquired pneumonia
Symptoms and Signs%
Respiratory symptoms
Cough85
Dyspnea75
Sputum production73
Pleuritic chest pain57
Hemoptysis20

5050
Frequency of various signs and symptoms in adults Frequency of various signs and symptoms in adults with community – acquired pneumonia (cont.)with community – acquired pneumonia (cont.)
Nonrespiratory symptoms
Fatigue90 Fever82
Anorexia73 Chills72 Sweats70
Headache50 Myalgia45
Nausea40 Sore throat29
Confusion38 Vomiting32 Diarrhea30
Abdominal pain29
5151
Antibiotic therapy (first and second choices) Antibiotic therapy (first and second choices) for community acquired pneumonia when for community acquired pneumonia when
etiology is unknownetiology is unknown A. A. Patient to be treated on an Patient to be treated on an ambulatory basis.ambulatory basis.
1. Macrolide1. Macrolide
2. Doxycycline2. Doxycycline
5252
Antibiotic therapy (first and second choices) Antibiotic therapy (first and second choices) for community acquired pneumonia when for community acquired pneumonia when
etiology is unknownetiology is unknown B. B. Patient to be treated in hospital Patient to be treated in hospital wardward
Fluoroquinolone.Fluoroquinolone.
CefuroximeCefuroxime
C. C. Patient to be treated in an intensive Patient to be treated in an intensive care unitcare unit
AzithromycinAzithromycin

5353
Antibiotic therapy (first and second choices) Antibiotic therapy (first and second choices) for community acquired pneumonia when for community acquired pneumonia when
etiology is unknownetiology is unknown D. D. Patient to be treated in a nursing Patient to be treated in a nursing home.home.
Fluoroquinolone .Fluoroquinolone .
Ceftriaxone.Ceftriaxone.
E. E. Aspiration pneumonitis/pneumoniaAspiration pneumonitis/pneumonia
Poor dental hygiene and anaerobic Poor dental hygiene and anaerobic infection suspected: Metronidazole.infection suspected: Metronidazole.
Related Documents




![1. fever [`fiv2] n. [U][C] 狂熱;發燒 Many Taiwanese like to watch baseball games. They have fever baseball fever. I had a cold and got a high fever fever.](https://static.cupdf.com/doc/110x72/56649e255503460f94b148e4/1-fever-fiv2-n-uc-many-taiwanese-like-to-watch-baseball.jpg)