Feedback to SANAC Plenary Thami Mseleku DG of National Department of Health and Chair of PIC Helen Rees PIC Co-Chair Executive director, Wits Reproductive Health and HIV Research Unit Honorary Professor, London School of Hygiene and Tropical Medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Feedback to SANAC Plenary
Thami MselekuDG of National Department of Health and Chair of PIC
Helen ReesPIC Co-Chair
Executive director, Wits Reproductive Health and HIV Research UnitHonorary Professor, London School of Hygiene and Tropical Medicine

Structure of presentation• Governance matters
– Provincial, District and Local AIDS Councils
• Monitoring the NSP– Mid term review– Know your Epidemic
• Brief summaries of work in progress
• Major topics for discussion– Male circumcision– Treatment guidelines– Task shifting

SANAC Governance matters • Getting PIC to work better:
– Regular communication between PIC co-chairs and TTT chairs between meetings
• New sectors of SANAC– Sex workers, MSM– Government: Dept Science and Technology
Plenary to request:• PIC through Law & Human Rights TTT to develop guidelines for recognition of new sectors• DP’s office to discuss with Minister of Science and Technology about SANAC membership
SANAC Governance matters
• SANAC action required around Provincial, District and Local AIDS Councils– AIDS Councils not integrated into SANAC structures and
activities– Sectors reporting that Provincial and Local AIDS Councils
are dysfunctional for reasons including lack of resources – PIC’s attempts since 2007 to understand AIDS Council
problems and to intervene have been unsuccessfulRecommendations for SANAC Plenary: Office of DP, SANAC Deputy Chair, PIC Chair and Co-Chair work together:• To develop and implement a strategy to address this problem and report back to next plenary• Office of the DP to engage the Offices of the Premiers so that support for intervention comes from highest political level in provinces

Evaluating progress of the National Strategic Plan
Know Your epidemicMid term review

How will ‘Knowing our Epidemic’ help us intervene?
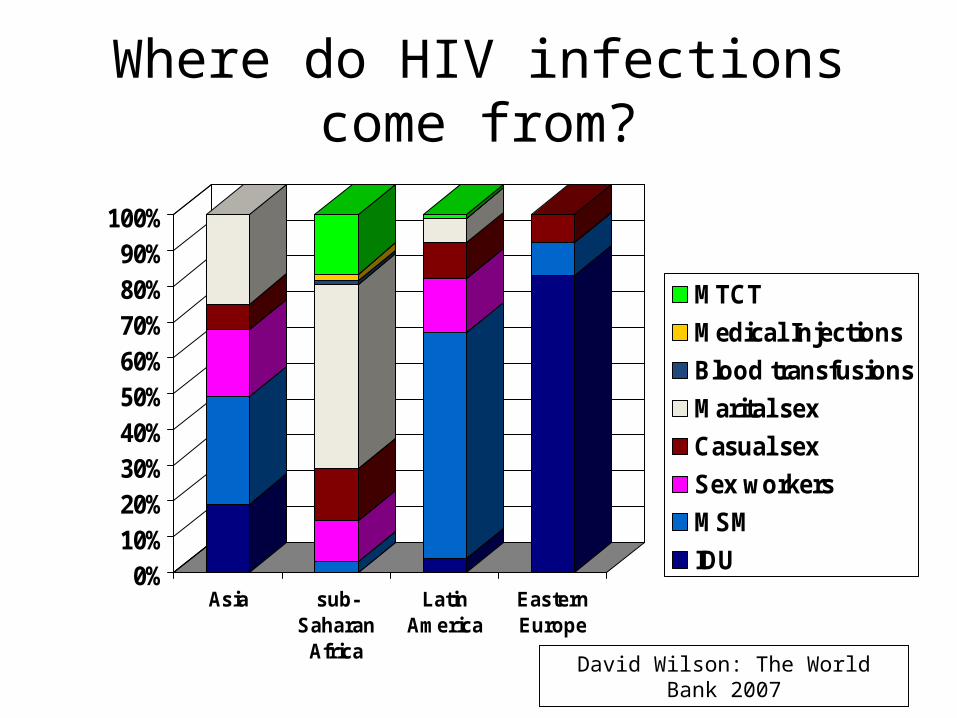
Where do HIV infections come from?
0%10%20%30%40%50%60%70%80%90%
100%
Asia sub-Saharan
Africa
LatinAmerica
EasternEurope
MTCT
Medical Injections
Blood transfusions
Marital sex
Casual sex
Sex workers
MSM
IDU
David Wilson: The World Bank 2007

If I ‘Know My Epidemic’ I can ask the key questions-
Where did my last 1000 infections come from?
And how can I prevent them?
David Wilson: The World Bank 2007

Products from the ‘Know your Epidemic’ activity
1. The evidence base for national HIV prevention policies
2. An understanding of whether existing HIV prevention policies are likely to impact on the risk factors and drivers of the epidemic
3. Provides data that will further inform the new Prevention Strategy being developed by the NDoH and the Prevention TTT
4. Outlines funding for National HIV prevention programme
5. Presents recommendations:– Policy level– Programmatic level– Capacity building– M&E

Epidemiological review Incidence data
(modelled or otherwise)
Prevention policies, response and strategic info
review
Review of resources for
prevention
SYNTHESIS
ANALYSIS OF EPIDEMIC
ANALYSIS OF RESPONSE
Four components of Know Your Epidemic methodology
Draft Strategy by November 2009

Rationale for Mid Term Review of National Strategic Plan
• Take stock of achievements and document status of collective efforts to-date
• Undertake a SWOT analysis of the National, Provincial, District, Sectoral and Community Responses
• Document best practices to be scaled up
• Document emerging issues
MTR generates strategic information to guide policy and programmes

Focus areas for NSP Mid Term Review • Review coordinating structures of NSP
– SANAC structures– National, Provincial, District and Sectoral
• Assessment of implementation of the NSP across all levels, sectors and role-players
• Monitoring and Evaluation processes of Government & Civil society
• Cross cutting issues: Gender, Harmonisation & Alignment, Mainstreaming, TB, SRH etc
Plenary requested to support:• Know your Epidemic Activities• Mid term review process

Key areas for review
Decriminalisation of Sex work NSP recommends decriminalisation of sex work Human Rights TTT made submission to South African Law Reform
Commission (SALRC)Harmonised Assessment Tool and a Chronic Illness Grant
Plenary to endorse PIC recommendation that : no HAT without strategy to address those who'll fall of Disability Grant.
SANAC Plenary to consider PIC recommendation: That SANAC endorses the decriminalisaton of sex work
SANAC plenary to recommend: Not to introduce HAT without considering those who will fall of Disability Grant.

Preparations for 2010 World Cup
Sports sector is convening a summit of all SANAC Sectors on 2010 world cup. Summit to consider:
Potential opportunity of 2010 to support NSP Potential risks of 2010
Impact on children of school closure (potential or abuse, impact on school nutrition)
Potential for sex trafficking
NDOH to convene multi-sector meeting of SANAC role-players and FIFA organising coommittee.
Progress with Female condoms NDOH tender for new prototype, cheaper female condom is pending 4.5million female condoms on order UNFPA and USAID might increase female condom number through donation Civil society sector including women's sector and research sector need to assist with social mobilsation around uptake of FC.Communication TTT will consider Communications strategy in supportMC distribution condom distribution: 450million

PMTCT rollout Dual ARV therapy (AZT and NVP) now
available in most public sector ANCs. Accelerated PMTCT programme in 18 most
deprived and poorly performing districts. Social mobilisation remains inadequate
Communications TTT to address this. All sectors to develop relevant strategies
to
PMTCT must include ARV treatment for mothers to address transmission to infants and maternal mortality.

Male Circumcision

Recommendations from SANAC plenary to PIC November 2008
• Request that the next step is to take information sharing sessions into communities through SANAC sectors eg men, women, labour– Sector workshops: Men, Women PLWHAs, NGOs, Youth
• Implement provincial consultations with traditional practitioners– Work in progress
• Arrange consultations with Houses of Traditional Leaders – PIC Chair and Co-Chair have addressed National House of
traditional leaders and Traditional leaders in Kwazulu-Natal. Work ongoing
Background to recommendations about a male circumcision (MC) policy
• Strong epidemiological evidence and evidence from 3 randomised controlled trials undertaken in South Africa, Tanzania and Uganda that medical MC to be highly efficacious (50-60%) in protecting men against HIV, sustained for 42 months (Tanzania), without behavioural disinhibition being shown
Background to recommendations about a male circumcision (MC) policy

Background to recommendations about a male circumcision policy
• MC offers other health benefits for men and women:– Men: Reduces other anogenital cancers in men and reduces some STIs– Women: reduced HPV, reduced Cancer of cervix
• WHO recommends MC ‘as a new additional prevention strategy for HIV prevention in men’.
• Other high HIV prevalence African countries are developing and implementing MC policies
• Communities aware of MC data and some men already seeking safe, and unsafe, access to MC
• Impact of MC on HIV takes years but the faster the rollout the quicker the impact

Importance of a sexual health package
• MC should be introduced to adolescents and young men as part of a comprehensive sexual health package for men including VCT :
• Messages must be clear– Partial efficacy– Sustaining safer Sexual practices including Delay sexual debut, avoiding
concurrent partnerships– Alcohol abuse– Changing gender norms including gender based violence – ‘Male Morality’ e.g. respect of women
• Messaging must also inform women who are partners and mothers of sons
• Appropriate media for the disabled

MC rollout in health servicesPIC Recommendations: • Design and cost programmes for public health sector
introduction of MC which provide an integrated sexual health package and which will consider who will be offered Medical male circumcision (adolescents, older men, infants)
• Communications TTT to develop comprehensive communication policy
• Continue all other community discussion strategies with communities and selected sectors including traditional leaders and traditional practitioners
• Consideration on whether MC should be a policy itself or part of a National Prevention Policy
Plenary to consider endorsement PIC’s recommendations

Task shifting

Task-shifting/sharing Defined• Re-allocation of clinical and non-clinical support
tasks across the health care team, in order to better utilize existing capacity to increase access and maintain quality of services
• Task-shifting is not new to global north or south

Task-Shifting/Sharing Recommendations
• Nurses – Professional nurses: initiation and management of ART,
including midwives’ initiation of ART during pregnancy– Staff nurses: management of stable patients on ART
• Pharmacist’s assistants– Dispense pre-packed, pre-labeled ARVs
• Lay counsellors – Administer HIV testing: finger and heel-prick to for rapid
testing and collecting dried blood spots for early infant diagnosis via HIV DNA PCR
– Facility-based adherence counselling– Community-based defaulter tracking

Task-shifting improves quality
• Improves patient adherence• Integration of services at primary care level• Provides continuity of HIV care • Decentralized services can improved PMTCT
outcomes

Task-shifting improves access and is effective
• Additional points of care and brings services closer to where patients live
• Decreases cost to patients• Increasing data about safety and effectiveness
of strategy in South Africa and the region
SANAC plenary to support PIC’s recommendation that the NDoH urgently considers this strategy as part of its broader task shifting review

Treatment Guidelines
Progress on HIV Treatment guidelines
SANAC Plenary November 2008 was presented with Treatment TTT’s recommendations on Treatment Guidelines
• Adult • Paediatric, • PMTCT • TB/HIV
Growing body of evidence – presented at IAS in Capetown 18-23 July 2009

Adult ARV guidelines
• Increase ART eligibility to CD4 of < 350 for ALL persons, based on:– Reduced prevalence of TB– Fewer hospitalizations– Fewer babies born HIV+– Reduced infant and maternal mortality – Possible large HIV prevention impact
Major savings in LIFE and reduced hospitalizations.Significant economic impact of workforce kept healthy
Paediatric ARV guidelines• ALL infants (< 1yr olds) to be started on ARVS
upon diagnosis based on the CHER study (South African study – Soweto and Capetown)

CHER Study Findings
Major Findings• Early HIV diagnosis (from 4 - 6 weeks) and early
ARVs reduced death by 76%• Early ARVs reduced progression of disease by
75 %• Current ARV guidelines for children are
outdated and in urgent need of revision

PMTC Recommendations
• Pregnant women be started on ARVs if CD4 <350
• For those CD4 >350 to have Dual Therapy (AZT + Nevirapine in labour)
• Mother to have one week of AZT/3TC to reduce Nevirapine resistance
• Baby gets single dose Nevirapine and 28 days of AZT

Treatment Guidelines Adoption Proposals
• First prize – adopt all TTT recommendations and ensure treasury/donors allocate sufficient funding
• Second prize – where funding unavailable either :– Phased Approach – with selected groups starting
with CD4 < 350 e.g Pregnant women or TB– Pragmatic Approach – where 200 is the minimum
point to start, but clinicians have flexibility to start < 350 where capacity allows this.
Minister of Health will be presenting to NHCSANAC Plenary to note implement options proposed by PIC
Thank you
Related Documents











