New Conditions: Overall Condition: Better Worse Same Other Describe How Better: Describe How Worse: What Aggravates: What Improves: On the drawing, place a number on the areas of injury and describe it using the letters A = Achy Pain B = Burning Pain N = Numbness S = Stabbing Pain P = Pins & Needles M = Musc. Spasm 1. 1 5 10 2. 5. 1 5 10 1 5 10 3. 6. 1 5 10 1 5 10 4. 1 5 10 Please fill out all the information requested below - leave no blanks Initials_______ Pain Spasm ROM C-Sp T-Sp L-Sp Pelvis U/L Ext [ ] [ ] L [ ] R [ ] [ [ [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] L [ ] R [ ] [ ] [ ] [ ] [ [ ] [ ] [ ] [ ] [ ] [ ] L [ ] R [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ [ [ BedSd IC XF EFF TP P-A A-P Rib FlMalPos ExMalPos FD Scol ] Kyph IC XF EFF TP SidePost Fd Scol Disc IC XF EFF TP SidePost Block Cat3 PI-L PI-R AS-L AS-R IC XF EFF TP IC ] XF ] EFF ] TP Supine ] L ] R Spasm Pain C T L P C T L P SERVICES RENDERED [ ] New Patient Exam [ ] Est. Patient Exam [ ] Re-Exam [ ] Report of Findings [ ] Consultation-Short [ ] Consultation-Long [ ] Emergency Service [ ] Adjustment [ ] Flexion Distraction [ ] Massage 1st Region [ ] Massage 2 Regions [ ] Massage 3 Regions [ ] Massage 1 Region Short [ ] Hot Packs [ ] UltraSound [ ] E-Stimulation [ ] US/E-Stim Combo [ ] Staff Office Visit [ ] Ltr 1 2 3 4 [ ] Other ______ ( ) Improving ( ) Sltly Wrs ( ) Mch Wrs ( ) Flare Sx ( ) Imprved ( ) Slt Imprv ( ) No Chng ( ) Sltly Wrs ( ) Mch Wrs ( ) Stable ( ) Improving ( ) Refer ( ) New Sx ( ) Slt Imprv ( ) Same ( ) Deteriorating ( ) No Imprvmnt ( ) Cont Estab Tx Plan ( ) Change Plan Since Last Visit: After Today’s TX: Case Impression: Name _________________________ Date ____________________

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
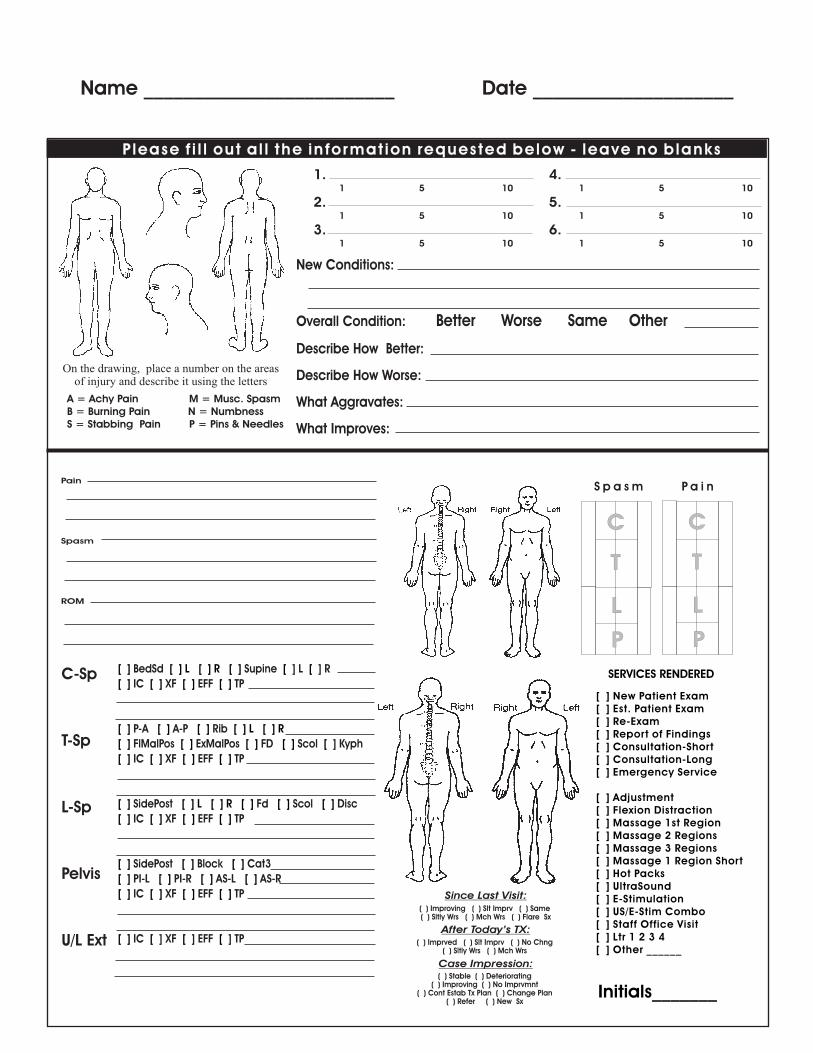
New Conditions:
Overall Condition: Better Worse Same Other
Describe How Better:
Describe How Worse:
What Aggravates:
What Improves:
On the drawing, place a number on the areas of injury and describe it using the letters
A = Achy Pain B = Burning Pain N = NumbnessS = Stabbing Pain P = Pins & Needles
M = Musc. Spasm
1. 1 5 10
2. 5. 1 5 10 1 5 10
3. 6. 1 5 10 1 5 10
4. 1 5 10
P lease f i l l out a l l the in fo rmat ion requested below - leave no b lanks
Initials_______
Pain
Spasm
ROM
C-Sp
T-Sp
L-Sp
Pelvis
U/L Ext
[ ] [ ] L [ ] R [ ] [ [
[ ] [ ] [ ] [ ]
[ ] [ ] [ ] [ ] L [ ] R
[ ] [ ] [ ] [ ] [
[ ] [ ] [ ] [ ]
[ ] [ ] L [ ] R [ ] [ ] [ ]
[ ] [ ] [ ] [ ]
[ ] [ ] [ ]
[ ] [ ] [ ] [ ]
[ ] [ ] [ ] [ ]
[ ] [ [ [
BedSd
IC XF EFF TP
P-A A-P Rib
FlMalPos ExMalPos FD Scol ] Kyph
IC XF EFF TP
SidePost Fd Scol Disc
IC XF EFF TP
SidePost Block Cat3
PI-L PI-R AS-L AS-R
IC XF EFF TP
IC ] XF ] EFF ] TP
Supine ] L ] R
S p a s m P a i n
C
T
L
P
C
T
L
P
SERVICES RENDERED
[ ] New Patient Exam[ ] Est. Patient Exam[ ] Re-Exam[ ] Report of Findings[ ] Consultation-Short[ ] Consultation-Long[ ] Emergency Service [ ] Adjustment[ ] Flexion Distraction[ ] Massage 1st Region[ ] Massage 2 Regions[ ] Massage 3 Regions[ ] Massage 1 Region Short[ ] Hot Packs[ ] UltraSound [ ] E-Stimulation[ ] US/E-Stim Combo[ ] Staff Office Visit[ ] Ltr 1 2 3 4[ ] Other ______
( ) Improving ( ) Sltly Wrs ( ) Mch Wrs ( ) Flare Sx
( ) Imprved ( ) Slt Imprv ( ) No Chng ( ) Sltly Wrs ( ) Mch Wrs
( ) Stable ( ) Improving
( ) Refer ( ) New Sx
( ) Slt Imprv ( ) Same
( ) Deteriorating ( ) No Imprvmnt
( ) Cont Estab Tx Plan ( ) Change Plan
Since Last Visit:
After Today’s TX:
Case Impression:
Name _________________________ Date ____________________
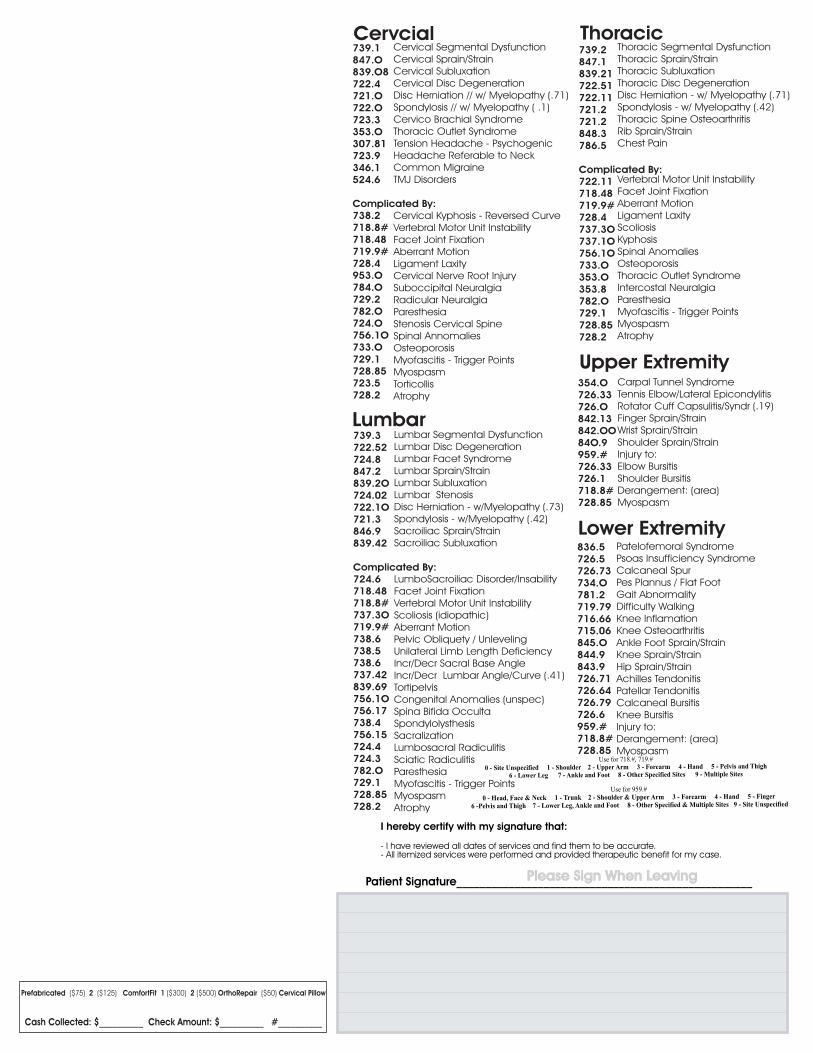
Thoracic Segmental DysfunctionThoracic Sprain/Strain
Thoracic Disc DegenerationDisc Herniation - w/ Myelopathy (.71)Spondylosis - w/ Myelopathy (.42)
Rib Sprain/Strain
Vertebral Motor Unit Instability
Aberrant Motion
Intercostal NeuralgiaParesthesia
MyospasmAtrophy
Thoracic Subluxation
Thoracic Spine Osteoarthritis
Chest Pain
Facet Joint Fixation
Ligament LaxityScoliosisKyphosisSpinal Anomalies OsteoporosisThoracic Outlet Syndrome
Myofascitis - Trigger Points
739.3
847.2
722.1O721.3
724.6718.48718.8#
719.9#
839.69
782.O
728.85728.2
722.52724.8
839.2O724.02
846.9839.42
Complicated By:
737.3O
738.6738.5738.6737.42
756.1O756.17738.4756.15724.4724.3
729.1
Lumbar Segmental Dysfunction
Lumbar Sprain/Strain
Disc Herniation - w/Myelopathy (.73)Spondylosis - w/Myelopathy (.42)
LumboSacroiliac Disorder/InsabilityFacet Joint FixationVertebral Motor Unit Instability
Aberrant Motion
Tortipelvis
Lumbosacral RadiculitisSciatic RadiculitisParesthesia
MyospasmAtrophy
Lumbar Disc DegenerationLumbar Facet Syndrome
Lumbar SubluxationLumbar Stenosis
Sacroiliac Sprain/StrainSacroiliac Subluxation
Scoliosis (idiopathic)
Pelvic Obliquety / UnlevelingUnilateral Limb Length DeficiencyIncr/Decr Sacral Base AngleIncr/Decr Lumbar Angle/Curve (.41)
Congenital Anomalies (unspec)Spina Bifida OccultaSpondylolysthesisSacralization
Myofascitis - Trigger Points
Cervical Segmental DysfunctionCervical Sprain/Strain
Cervical Disc DegenerationDisc Herniation // w/ Myelopathy (.71)Spondylosis // w/ Myelopathy ( .1)
Vertebral Motor Unit Instability
Suboccipital Neuralgia
Paresthesia
MyospasmTorticollis
Cervical Subluxation
Cervico Brachial SyndromeThoracic Outlet SyndromeTension Headache - PsychogenicHeadache Referable to NeckCommon MigraineTMJ Disorders
Cervical Kyphosis - Reversed Curve
Facet Joint FixationAberrant MotionLigament LaxityCervical Nerve Root Injury
Radicular Neuralgia
Stenosis Cervical SpineSpinal AnnomaliesOsteoporosisMyofascitis - Trigger Points
Atrophy
739.2847.1
722.51722.11721.2
848.3
718.48719.9#
353.O
782.O
728.85728.2
839.21
721.2
786.5
Complicated By:722.11
728.4737.3O737.1O756.1O733.O
353.8
729.1
739.1847.O
722.4
722.O723.3
718.8#
719.9#
729.2782.O
728.85723.5
839.O8
721.O
353.O307.81723.9346.1524.6
Complicated By:738.2
718.48
728.4953.O784.O
724.O756.1O733.O729.1
728.2
Cervcial Thoracic
Lumbar
Carpal Tunnel SyndromeTennis Elbow/Lateral EpicondylitisRotator Cuff Capsulitis/Syndr (.19)Finger Sprain/StrainWrist Sprain/StrainShoulder Sprain/StrainInjury to:Elbow BursitisShoulder BursitisDerangement: (area)Myospasm
Patelofemoral SyndromePsoas Insufficiency SyndromeCalcaneal SpurPes Plannus / Flat FootGait AbnormalityDifficulty WalkingKnee InflamationKnee OsteoarthritisAnkle Foot Sprain/StrainKnee Sprain/StrainHip Sprain/StrainAchilles TendonitisPatellar TendonitisCalcaneal BursitisKnee BursitisInjury to:Derangement: (area) Myospasm
836.5726.5726.73734.O781.2719.79716.66715.06845.O844.9843.9726.71726.64726.79726.6959.#718.8#728.85
Upper Extremity
Lower Extremity
Use for 718.#, 719.#
0 - Site Unspecified 1 - Shoulder 2 - Upper Arm 3 - Forearm 4 - Hand 5 - Pelvis and Thigh
6 - Lower Leg 7 - Ankle and Foot 8 - Other Specified Sites 9 - Multiple Sites
Use for 959.#
0 - Head, Face & Neck 1 - Trunk 2 - Shoulder & Upper Arm 3 - Forearm 4 - Hand 5 - Finger
6 -Pelvis and Thigh 7 - Lower Leg, Ankle and Foot 8 - Other Specified & Multiple Sites 9 - Site Unspecified
354.O726.33726.O842.13842.OO84O.9959.#726.33726.1718.8#728.85
Prefabricated ($75) 2 ($125) ComfortFit 1 ($300) 2 ($500) OrthoRepair ($50) Cervical Pillow
Cash Collected: $__________ Check Amount: $__________ #__________
Please Sign When LeavingPatient Signature___________________________________________________
I hereby certify with my signature that:
- I have reviewed all dates of services and find them to be accurate.- All itemized services were performed and provided therapeutic benefit for my case.
Related Documents











