This article was downloaded by: [christie zunker] On: 17 October 2011, At: 14:44 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Qualitative Research in Sport, Exercise and Health Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rqrs21 Fear of physical response to exercise among overweight and obese adults Brooks C. Wingo a , Retta R. Evans b , Jamy D. Ard a , Diane M. Grimley c , Jane Roy b , Scott W. Snyder b , Christie Zunker d , Alison Acton a & Monica L. Baskin e a Department of Nutrition Sciences, University of Alabama, Birmingham, AL, USA b Department of Human Studies, University of Alabama, Birmingham, AL, USA c Department of Health Behavior, University of Alabama, Birmingham, AL, USA d North Dakota and Department of Clinical Neuroscience, University of North Dakota School of Medicine & Health Sciences, Grand Forks, ND, USA e Department of Preventive Medicine, University of Alabama, Birmingham, AL, USA Available online: 11 Oct 2011 To cite this article: Brooks C. Wingo, Retta R. Evans, Jamy D. Ard, Diane M. Grimley, Jane Roy, Scott W. Snyder, Christie Zunker, Alison Acton & Monica L. Baskin (2011): Fear of physical response to exercise among overweight and obese adults, Qualitative Research in Sport, Exercise and Health, 3:2, 174-192 To link to this article: http://dx.doi.org/10.1080/2159676X.2011.572994 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and- conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

This article was downloaded by: [christie zunker]On: 17 October 2011, At: 14:44Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Qualitative Research in Sport, Exerciseand HealthPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rqrs21
Fear of physical response to exerciseamong overweight and obese adultsBrooks C. Wingo a , Retta R. Evans b , Jamy D. Ard a , Diane M.Grimley c , Jane Roy b , Scott W. Snyder b , Christie Zunker d ,Alison Acton a & Monica L. Baskin ea Department of Nutrition Sciences, University of Alabama,Birmingham, AL, USAb Department of Human Studies, University of Alabama,Birmingham, AL, USAc Department of Health Behavior, University of Alabama,Birmingham, AL, USAd North Dakota and Department of Clinical Neuroscience,University of North Dakota School of Medicine & Health Sciences,Grand Forks, ND, USAe Department of Preventive Medicine, University of Alabama,Birmingham, AL, USA
Available online: 11 Oct 2011
To cite this article: Brooks C. Wingo, Retta R. Evans, Jamy D. Ard, Diane M. Grimley, Jane Roy,Scott W. Snyder, Christie Zunker, Alison Acton & Monica L. Baskin (2011): Fear of physical responseto exercise among overweight and obese adults, Qualitative Research in Sport, Exercise and Health,3:2, 174-192
To link to this article: http://dx.doi.org/10.1080/2159676X.2011.572994
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representationthat the contents will be complete or accurate or up to date. The accuracy of anyinstructions, formulae, and drug doses should be independently verified with primarysources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand, or costs or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

Fear of physical response to exercise among overweight and obeseadults
Brooks C. Wingoa*, Retta R. Evansb, Jamy D. Arda, Diane M. Grimleyc, JaneRoyb, Scott W. Snyderb, Christie Zunkerd, Alison Actona and Monica L. Baskine
aDepartment of Nutrition Sciences, University of Alabama, Birmingham, AL, USAbDepartment of Human Studies, University of Alabama, Birmingham, AL, USAcDepartment of Health Behavior, University of Alabama, Birmingham, AL, USA; dNorthDakota and Department of Clinical Neuroscience, University of North Dakota School ofMedicine & Health Sciences, Grand Forks, ND, USA; eDepartment of PreventiveMedicine, University of Alabama, Birmingham, AL, USA
(Received 3 January 2011; final version received 3 January 2011)
Regular physical activity has been shown to have significant impact on bothphysical and mental health; however, over half of adults in the US do not meetcurrent recommendations for physical activity. Pain is one of the most com-monly cited barriers to physical activity among adults. Fear of pain has beenshown to have a significant correlation with pain-related disorders includingback pain and arthritis, but no studies have examined the role that weight playson these fears. We conducted three focus groups (n = 21) to explore the role offear-avoidance beliefs related to exercise among a group of overweight andobese adults. Focus group members discussed their beliefs that overweight andobese adults have more exaggerated physical responses to exercises than normalweight adults. They also endorsed a belief that overweight and obese individualsinterpret similar physical responses differently than normal weight individuals,and that these interpretations lead to fear that may result in exercise avoidance.Further exploration of the role of fear in exercise avoidance will be useful indesigning tailored exercise prescriptions and physical activity interventions thatmay increase adherence among overweight and obese adults.
Keywords: fear-avoidance beliefs; exercise avoidance; weight loss; obesity; sed-entary lifestyle
Introduction
Physical activity is associated with multiple health benefits, including decreasedrisks for heart disease, diabetes, and colon and breast cancers, as well as enhancedpsychological well-being through reduced anxiety and depression (Paluskai andSchwenk 2000, US Department of Health and Human Services (USDHHS) 2008).Regular activity is also a key factor in maintaining a healthy body weight and pre-venting loss of muscle mass during weight loss (USDHHS 1996, National HeartLung and Blood Institute (NHLBI) 2000, USDHHS 2008).
Despite the multiple benefits of exercise, physical activity levels have declinedover the last 40 years, due in part to environmental changes such as occupational
*Corresponding author. Email: [email protected]
Qualitative Research in Sport, Exercise and HealthAquatic InsectsVol. 3, No. 2, July 2011, 174–192
ISSN 2159-676X print/ISSN 2159-6778 online� 2011 Taylor & Francishttp://dx.doi.org/10.1080/2159676X.2011.572994http://www.tandfonline.com
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
activity and a heavy reliance on motorised transportation (French et al. 2001, Hillet al. 2003). Physical inactivity, along with poor diet was found to be the secondleading actual cause of death in 2000, with 400,000 (16.6%) deaths attributed tothese modifiable behaviours (Mokdad et al. 2004).
According to results from the 2007 Behavioral Risk Factor Surveillance System(BRFSS), 51.2% of adults in the US did not meet the recommendations for physicalactivity (CDC 2008). Physical inactivity appears to be disproportionally high amongsome demographic groups. Discrepancies can be seen among racial groups andbetween genders. African-Americans or Hispanic adults are more likely to be inac-tive than Caucasian adults (59.6%, 57.9% and 48.3%, respectively). Additionally,53% of females do not meet recommendations compared to 49.3% of men (CDC2008).
Another population that is particularly at-risk for sedentary lifestyle is individu-als who are overweight and obese. Data from the Weight Loss Maintenance Trialsuggested that physical activity declined as weight increased (Young et al. 2009).This large-scale, multi-site trial recorded physical activity using accelerometry for1648 overweight and obese adults. Authors found that on average participants accu-mulated less than 16 minutes per day of moderate to vigorous physical activity.When minutes of activity were analysed by weight class, 19.6% of overweight par-ticipants met recommendations to accumulate 30 minutes or more of moderate tovigorous physical activity whereas only 14.8% of obese participants met this recom-mendation. Davis et al. (2006) found similar differences between overweight andnormal weight participants. While 26% of normal weight participants met IOMexercise recommendations of 60 minutes of moderate-level activity per day,only13% of overweight participants met this recommendation.
Qualitative studies have used focus groups and semi-structured interviews toexplore barriers to exercise among overweight adult populations. Young et al.(2001) conducted a series of four focus groups with African-American women theyclassified as active or inactive and with successful or unsuccessful weight loss.When discussing barriers that led women to stop a routine exercise pattern, partici-pants noted pain from arthritis and health concerns caused them to stop physicalactivities they once participated in regularly. Pain or disability was also noted as abarrier to exercise in other qualitative studies focusing on African-American adults(Eyler et al. 1998, Carter-Nolan et al. 1996). None of these studies explored howthe inactive groups differed on pain levels compared to active groups, so one cannotinfer if the active group did not experience similar pain, or if they differed in theirreaction to the pain.
While physical inactivity is often cited as a cause of obesity, it may be thatobesity is also a cause of physical inactivity. In a study conducted from across-sectional population survey of 2298 Australian adults, 9.3% of respondentswith a BMI over 25kg/m2 reported that they were ‘too fat to exercise’, and 13.8%reported that ‘my health is not good enough’ to exercise (Ball et al. 2000). A com-monly cited deterrent to physical activity is physical pain (Clark 1999, Grubbs andCarter 2002). Sedentary individuals who begin to increase physical activity willoften experience pain as a result of increased movements. Pain can be worse inpeople who are overweight or obese since extra body weight can induce joint paindue to the extra force exerted on the joints (Nevitt and Lane 1999, Melissas et al.2005, Tukker et al. 2009). Overweight and obese individuals have also been foundto experience increased symptoms of exertion as compared to sedentary individuals
Qualitative Research in Sport, Exercise and Health 175
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

of normal weight. These symptoms include a higher heart rate and percentage ofcardiovascular capacity used compared to a normal weight person when performingan equal amount of work. This may result in a higher rate of perceived exertion(RPE) and decreased enjoyment of activity (Ekkekakis and Lind 2006). More workis needed to explore how overweight and obese individuals interpret pain, and howthose who succeed in developing regular exercise routines differ from those whoavoid exercise based on their interpretation of pain.
Fear-avoidance beliefs
As an individual initiates a new exercise programme, he or she will commonlyexperience some form of exercise-induced pain or discomfort. This pain may takethe form of joint pain or cardiovascular discomfort from increased heart rate andincreased respiratory rate. After exercise, the pain experienced may be from soremuscles or joint stiffness. ACSM encourages health care providers and fitness pro-fessionals to describe muscle soreness and pain after exercise as the body adaptingto new movements. An ACSM statement on this topic stated, ‘Some people thinkthey have no business exercising because exercise is ‘painful’. That’s not the case.The soreness is there simply because your muscle is learning something new, andthe benefits of exercise far outweigh any initial discomfort’ (ACSM 2003). Individ-uals who are new to exercise should be prepared to experience some pain, andunderstand that pain is not always a sign of injury or harm.
The fear-avoidance model proposes that individuals can interpret pain in twoways (Lethem et al. 1983). If pain is perceived as a normal part of the activityprocess, the individual will find ways to cope with the pain and continue with theactivity. If the individual perceives pain as a warning sign of harm, he or she maybegin a process of activity avoidance that will lead to continued sedentarybehaviour.
Avoidance of movement may also be a predictive behaviour in addition to apurely responsive one. Some individuals will avoid a movement based on theassumption that the movement will cause pain, even if they have never experiencedthe pain first hand. This may result in the individual avoiding interactions withmovements that are perceived to cause pain, which in turn leads to fewer opportuni-ties for the individual to perform activities and learn that they do not always causepain. When this level of avoidance is reached, a loss of daily function often occurs.Loss of functioning, along with the preoccupation of pain-related fear, often resultsin psychological impairments such as depression.
The process of avoiding fear-inducing activity has been referred to as the disusesyndrome (Kori et al. 1990). This term is used to characterise two facets of disuse:physical deconditioning due to reduced muscle use, and impairments in musclecoordination which can lead to guarded movements. Physical deconditioning refersto general decline in physical fitness due to avoiding activity that is thought tocause pain. Impairments in muscle coordination refer to problems that can be seenin activities such as walking. In the case of chronic pain such as back pain, an indi-vidual may overcompensate some movements to protect against pain, which canlead to gait impairments or other losses in physical function. Disability and the lossof physical function have been the primary focus of much of the research infear-avoidance beliefs to date.
176 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

High fear-avoidance beliefs have been found to be correlated with the level ofpain an individual reports, as well as the level of physical disability reported. Fear-avoidance beliefs have also been shown to be negatively correlated with results ofphysical function tests (Crombez et al. 1999, Geisser et al. 2000, Swinkels-Meewiseet al. 2006, George et al. 2007).
Despite the number of studies that have examined the role of pain-related fear indisability and physical function, very few have examined the role of pain-related fearin leisure time physical activity. Physical activity is often prescribed as treatment forchronic pain conditions, however, little is known about the effect of pain-related fearon moderate or vigorous levels of physical activity. In the only study found on thistopic, Elfving et al. (2007) studied the relationship of fear-avoidance and physicalactivity in individuals suffering from low back pain. Odds ratios for low physicalactivity ranged from 4 to 8.5 for medium to high pain-related fear scores (p < 0.05).
Only one study was found that addressed the role of pain-related fear in exer-cise-induced pain in a generally healthy sample. George et al. (2007) examined therelationship between fear-avoidance beliefs and pain in a sample of 42 healthy par-ticipants who had no history of neck or back pain. Twenty-four hours after partici-pating in a shoulder fatigue procedure intended to induce delayed-onset musclesoreness (DOMS), fear of pain accounted for 16% (p = 0.008) of the variance inclinical pain, and 10% (p = 0.047) of variance in evoked pain tests. Fear of painand clinical pain scores accounted for 50% (p = 0.001) of the variance in disability.While these results indicate a significant relationship between fear-avoidance beliefsand exercise-induced pain, this study did not report findings for predictability ofdisability based on fear of pain while controlling for pain intensity. Together thefindings of these studies lend initial support for the idea that individuals may avoidphysical activity due to pain-related fear, but more research is needed on the role ofpain-related fear in physical activity levels and exercise avoidance among individu-als with exercise-induced pain.
Existing literature has primarily examined the role of fear-avoidance beliefs indisease-specific population, such as arthritis or back pain (Crombez et al. 1999,Cai et al. 2007, Coudeyre et al. 2007, Elfving and Grooten 2007). No studieshave examined the role of weight in fear-avoidance beliefs. Overweight and obes-ity often compound pain symptoms in conditions such as arthritis, and pain hasbeen found to be more prevalent in some overweight populations, such as olderadults the (Andersen et al. 2003, Patterson et al. 2004, Heim et al. 2008). Theclose relationship between physical pain and weight suggests the need for addi-tional research in the area of fear-avoidance beliefs among overweight and obesepopulations.
The purpose of this study was to explore fear-avoidance beliefs related to exer-cise among a group of overweight and obese adults seeking treatment in a medicalweight loss programme. Specifically, we designed this study to qualitatively explorefears related to physical responses to exercise, and the role that weight plays ininterpretation of physical responses and the development of fear.
Methods
Participants
Participants were recruited from medically-supervised weight management pro-grammes at the University of Alabama at Birmingham (UAB). These programmes
Qualitative Research in Sport, Exercise and Health 177
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

focus on behavioural adaptations of ineffective diet and exercise habits and manyof the participants are at high risk for, or already diagnosed with, medical condi-tions associated with a high BMI including diabetes, hypertension, hyperlipidemia,polycystic ovarian syndrome and arthritis. A physician, registered dietician, exercisetrainer and psychologist monitor patients. Treatment plans for patients in the pro-grammes may include individualised nutrition and exercise plans, referral to physi-cal therapy or other rehabilitative services and prescription medication. Treatmentgoals may include weight loss, improved health indicators or preparation for otherweight loss programmes including surgical options. This study was approved by theUAB Institutional Review Board and informed consent was obtained from eachparticipant.
Participant recruitment
A query of electronic patient records was conducted to find patients who metpreliminary eligibility. The query used the following variables to determine preli-minary eligibility: patient last name, patient first name, patient status, patientage, current BMI, and patient gender. Patient age was filtered to include onlythose patients aged 20–65 years. Current BMI, which gives patients’ BMI at themost recent visit, was filtered to include only those patients with BMI measure-ments of 25–60 kg/m2. Because an extreme BMI could skew results as outliers,an upper limit of 60 kg/m2 was set for BMI. The mean age of potentially eligi-ble participants was 47.18 years, and the mean BMI was 36.91kg/m2. Addition-ally, individuals who were under instructions to avoid physical activity or limitexercise due to a medical condition were excluded. These instructions may influ-ence participants’ perception of the safety of exercise and therefore skewresponses.
Patients were selected using maximum variation purposive sampling, which isintended to increase group diversity and encourage discussion of differing view-points. Maximum variation is a sampling strategy determined during the planningphase of a qualitative study that identifies a wide range of individuals with mul-tiple perspectives to contribute to the meaning of the given phenomenon(Creswell 2007). It allows the researchers to purposefully choose cases to getvariation on dimensions of interest (Patton 2002). We selected participants thatwould create groups that offered diversity in characteristics including race, age,gender, educational level, physical activity level and length of time in the pro-gramme (Krueger 1988). Participants were called or emailed to introduce thestudy and assess interest in participation. If the patient agreed to participate,screening questions were asked to validate eligibility criteria. Thirty-three patientswere invited to participate; 23 agreed to participate and 21 attended the focusgroups.
Measures
Body mass index
Participants’ weight was taken at the time they participated in the study. Patientswere weighed in light clothing without shoes, using a Tanita digital scale (Model#BWB500A). Height was measured using a wall-mounted stadiometer. BMI wascalculated using the formula kilograms/meters2.
178 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

Body composition
Body composition was measured to ensure that all participants met criterion foroverweight/obesity based on body fat, as well as BMI. Because individuals with aBMI in the lower range of overweight can sometimes have an increased BMI dueto muscle mass, they can have health characteristics that are more representative ofa normal weight individual than an overweight individual. BIA cut points were32% for females and 24% for males (ACSM 2006).
Body composition was measured using bioelectrical impedance (BIA). For thisstudy, BIA was measured using the Tanita digital scale (Model #BWB500A). Toensure the most accurate measure of body composition participants were instructednot to eat or drink four hours prior to measurement and to avoid strenuous activitiesincluding exercise the day of participation.
Physical activity
Physical activity was estimated using the physical activity questions from theBehavioral Risk Factor Surveillance System (CDC 2008). This set of questionsasked participants if they engaged in moderate-level activity during a normal week.If they responded yes, they were asked how many days per week they participatedin these activities and the length of time the sessions lasted. This series of questionswas then repeated for vigorous level activity. Responses were divided into four cat-egories: (1) inactivity, (2) low activity, (3) medium activity, and (4) high activity,based on the current CDC recommendations. Inactivity was defined as engaging inno activity above baseline activities. Low activity was defined as engaging in moreactivity than baseline, but less than 150 minutes each week. Medium activity wasdefined as engaging in 150 to 299 minutes of activity each week. High activity wasdefined as engaging in 300 minutes or more of activity each week (USDHHS2008).
Effect of pain on daily function
The effect of pain on daily function was measured because being overweight orobese can worsen pain-related conditions such as chronic back pain, arthritis andfibromyalgia, and many times pain from these conditions is made worse with theinitiation of a new exercise routine. It is difficult to quantify pain because it is asubjective experience that will be interpreted and measured differently by each indi-vidual (Carr et al. 2005). Therefore, we chose a measure that did not attempt toquantify pain, but instead dealt with the outcome of pain, as measured by interfer-ence with daily function.
The effect of pain on daily function was measured using the Pain DisabilityIndex (PDI; Pollard 1984). This scale asked participants to measure the level towhich pain interfered with various aspects of life including family and homeresponsibilities, recreation, social activities, occupation, sexual behaviour and life-support activities. Participants were asked to rate the effect of pain on a scale of0 to 10, with 0 indicating no disability at all, and 10 indicating total disability.The scale was scored by adding the responses to the seven categories. Scoresrange from 0–70, with higher scores indicating greater disability. This scale waschosen due to its focus on impairment from pain, and because it relates to general
Qualitative Research in Sport, Exercise and Health 179
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
daily impairment rather than pain level at a specific point in time or associatedwith a specific action. It should be noted that while this scale refers to disabilityfrom pain, the term disability, in this case, refers to the extent to which a partici-pant perceives pain interferes with daily activity, not a diagnosed disability orfunctional status.
Data collection
We chose to conduct focus groups for this study due to the exploratory nature ofthe topic. Focus groups are particularly beneficial when the topic is broad, or whenparticipants may not be familiar enough with the topic to successfully participate inan individual interview (Bogdan and Biklen 2003). The idea of fear-avoidancebeliefs has never been studied in relation to weight. Although our hypothesis wasthat overweight and obese individuals would express this fear, we did not haveenough evidence to begin with a fully developed individual interview script. Focusgroups allowed us to frame the ideas we wanted to explore in broad questions.Additionally, the group setting allowed participants to generate discussion and buildideas that may not have been expressed in individual interviews.
The primary goals of the focus groups were to discuss fear related to physicalresponses to exercise, explore how overweight and obese adults interpret thesephysical responses, and how fear leads to avoidance of exercise. Focus groupsbegan with broad questions such as identifying common physical responses to exer-cise. These were followed by more specific questions of perceptions and interpreta-tions of these responses (Krueger 1988, Stewart and Shamdasani 1990). A total ofsix questions were used for the focus group discussions (Table 1).
Groups were conducted until responses were repetitive and no new informationwas gained. A total of three focus groups were held before saturation was reached.Groups were audio taped and the moderator and an assistant took notes. Audiotapeswere transcribed and checked with notes taken during the groups. MaxQDA(VERBI Software, Berlin 2008) was used to code transcriptions. The group
Table 1. Focus group discussion guide.
1. When thinking about exercise such as brisk walking, jogging, aerobic classes, orswimming, what are some typical physical responses you experience during or afterexercise? These can be things you have experienced in the past, or things that youexpect to experience from exercise.
2. What are some factors that would make you think responses to exercises are safe? Whatare some factors that would make you think responses are signaling some form ofdanger?
3. How are physical responses to exercise different between overweight and normal weightindividuals?
4. How might a physical response be interpreted differently for an overweight person and anormal weight person? For example, would an increased heart rate mean the same thingfor an overweight person as it would for a normal weight person?
5. Is exercise safe for people who are overweight?a. For those who have lost weight: Do you feel safer exercising since losing weight?Why?b. For those who have not lost weight yet: Do you think you will feel safer exercising ifyou lost weight? Why?
6. Tell me about any circumstances or situations that make you feel safer exercising? Tellme about any circumstances or situations that make you feel less safe exercising?
180 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
moderator reviewed each transcription multiple times and identified primary themes.The moderator and group assistants reviewed the themes individually and as agroup and then further reviewed the transcriptions to identify subthemes within eachtheme. This process was completed with each focus group, and then themes andsubthemes from each group were compared and merged. The moderator, groupassistants and other members of the research team reviewed merged themes andsubthemes for clarification.
Results
Focus group participants
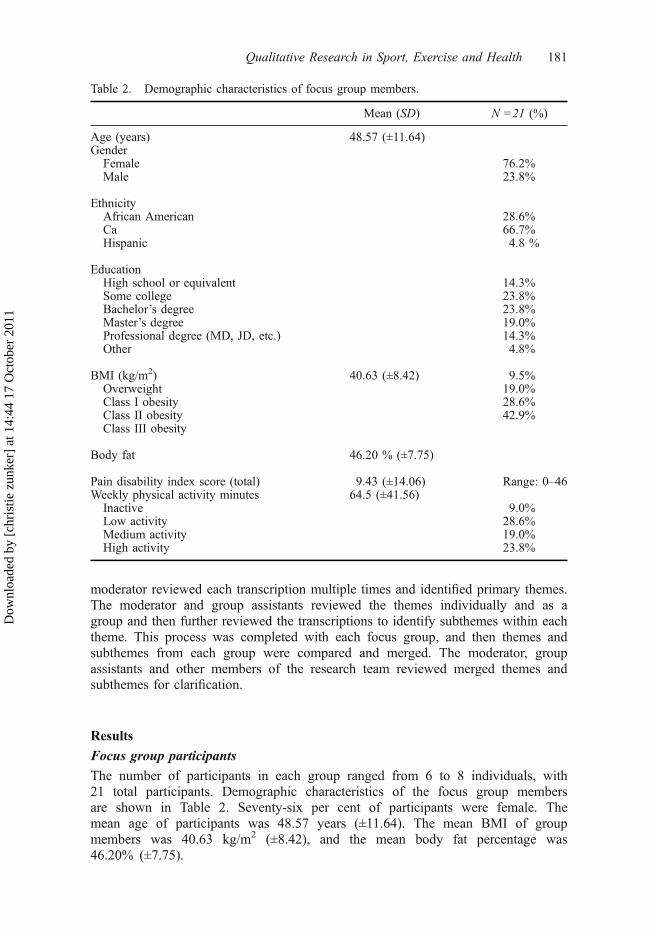
The number of participants in each group ranged from 6 to 8 individuals, with21 total participants. Demographic characteristics of the focus group membersare shown in Table 2. Seventy-six per cent of participants were female. Themean age of participants was 48.57 years (±11.64). The mean BMI of groupmembers was 40.63 kg/m2 (±8.42), and the mean body fat percentage was46.20% (±7.75).
Table 2. Demographic characteristics of focus group members.
Mean (SD) N =21 (%)
Age (years) 48.57 (±11.64)Gender
Female 76.2%Male 23.8%
EthnicityAfrican American 28.6%Ca 66.7%Hispanic 4.8 %
EducationHigh school or equivalent 14.3%Some college 23.8%Bachelor’s degree 23.8%Master’s degree 19.0%Professional degree (MD, JD, etc.) 14.3%Other 4.8%
BMI (kg/m2) 40.63 (±8.42) 9.5%Overweight 19.0%Class I obesity 28.6%Class II obesity 42.9%Class III obesity
Body fat 46.20 % (±7.75)
Pain disability index score (total) 9.43 (±14.06) Range: 0–46Weekly physical activity minutes 64.5 (±41.56)
Inactive 9.0%Low activity 28.6%Medium activity 19.0%High activity 23.8%
Qualitative Research in Sport, Exercise and Health 181
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
Focus group themes
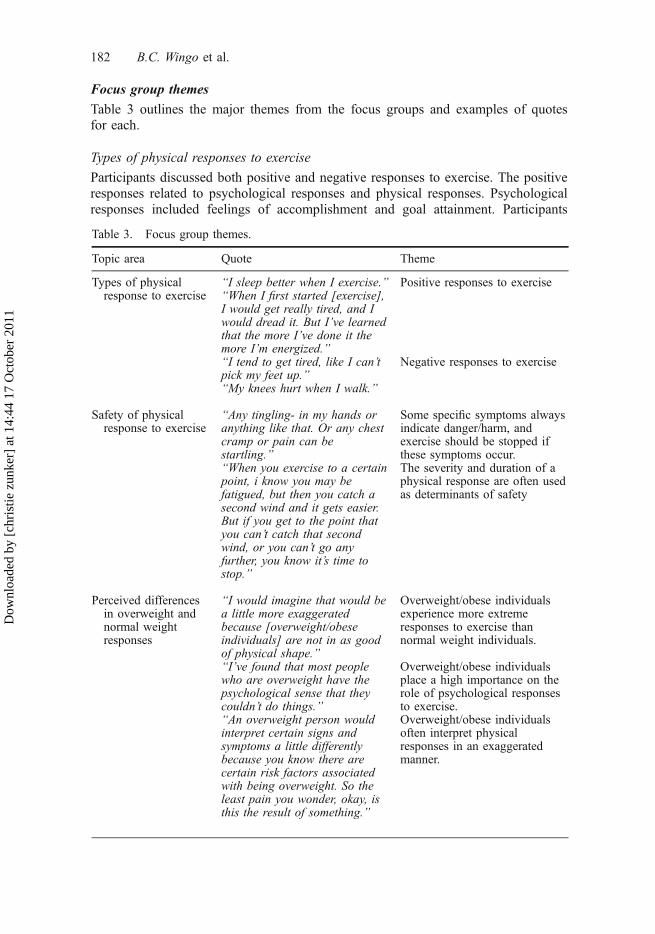
Table 3 outlines the major themes from the focus groups and examples of quotesfor each.
Types of physical responses to exercise
Participants discussed both positive and negative responses to exercise. The positiveresponses related to psychological responses and physical responses. Psychologicalresponses included feelings of accomplishment and goal attainment. Participants
Table 3. Focus group themes.
Topic area Quote Theme
Types of physicalresponse to exercise
“I sleep better when I exercise.” Positive responses to exercise“When I first started [exercise],I would get really tired, and Iwould dread it. But I’ve learnedthat the more I’ve done it themore I’m energized.”“I tend to get tired, like I can’tpick my feet up.”
Negative responses to exercise
“My knees hurt when I walk.”
Safety of physicalresponse to exercise
“Any tingling- in my hands oranything like that. Or any chestcramp or pain can bestartling.”
Some specific symptoms alwaysindicate danger/harm, andexercise should be stopped ifthese symptoms occur.
“When you exercise to a certainpoint, i know you may befatigued, but then you catch asecond wind and it gets easier.But if you get to the point thatyou can’t catch that secondwind, or you can’t go anyfurther, you know it’s time tostop.”
The severity and duration of aphysical response are often usedas determinants of safety
Perceived differencesin overweight andnormal weightresponses
“I would imagine that would bea little more exaggeratedbecause [overweight/obeseindividuals] are not in as goodof physical shape.”
Overweight/obese individualsexperience more extremeresponses to exercise thannormal weight individuals.
“I’ve found that most peoplewho are overweight have thepsychological sense that theycouldn’t do things.”
Overweight/obese individualsplace a high importance on therole of psychological responsesto exercise.
“An overweight person wouldinterpret certain signs andsymptoms a little differentlybecause you know there arecertain risk factors associatedwith being overweight. So theleast pain you wonder, okay, isthis the result of something.”
Overweight/obese individualsoften interpret physicalresponses in an exaggeratedmanner.
182 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

endorsed that these responses were particularly related to exercising despite a lackof motivation to do so, or completing a particularly difficult workout. Physicalresponses included improved sleep patterns and increased energy. Several partici-pants conveyed feelings of fatigue during and immediately after exercise, followedby an increase in overall energy level after a consistent exercise routine has beenestablished.
Participant A: “When I first started I felt tired and I was actually out of breath. Now Iwalk 3miles a day, and I have a lot more energy, and I look forward to it. I actuallyenrolled in a water aerobics class and I start next week.”
Participant B: “Yeah, before starting [this program] exercise was out of the question.And when I first started I did the elliptical because that was low impact and didn’thurt my back, because walking just hurts my back. But now I look forward to goingafter work and I do 45 minutes on the elliptical, and I feel really good during andafterward.”
Interestingly, energy level was also viewed as a negative response by somegroup members. Members all related to the feelings of fatigue during and immedi-ately following exercise. However, some group members stated they were so tiredafter exercise that it discouraged them from continuing to the point of developing aconsistent routine.
In addition to energy level, two other types of negative physical responses werediscussed: cardio-respiratory responses and pain responses. Cardio-respiratoryresponses included increased heart rate, laboured breathing or shortness of breath,and clammy hands or numbness in extremities. Pain responses included joint painor stiffness and muscle pain including soreness and strained muscles.
Safety of physical responses to exercise
Specific Symptoms. When asked to identify differences between safe and unsafephysical responses to exercise, some participants named specific responses which
Table 3. (Continued).
Topic area Quote Theme
Factors influencingphysical safety
“I had a physical and had allthree of my doctors tell me ‘yes’that should be [exercising].”
Medical clearance to check forhealth concerns is needed priorto starting exercise.
“In the beginning, it should bealmost like a rehab setting.Where we’re monitored whileyou’re exercising.”
Supervised exercise helps toreduce anxiety by offeringinstruction and continualmonitoring.
“I do strength training twice aweek with a trainer. It’s stuff Icould doon my own, but justhaving her there. . .it makes mefeel better. You know, 150pounds from now I may notneed her, but right now it makesme feel a lot better.”
Qualitative Research in Sport, Exercise and Health 183
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

they categorised as always indicating danger. These included numbness in handsand/or feet, clammy hands, dizziness and blurred vision.
Severity/duration of symptoms. Many members reported that they based interpre-tations of responses such as joint pain or chest pain on the degree or severity of theresponse.
Group members discussed that some level of pain or discomfort is to beexpected with exercise; however, pain or discomfort that does not go away after aperiod of time, or is worse than what has been experienced during past exercise ses-sions, could be a sign of injury. Participants noted that there is a ‘different kind ofpain’ that signals injury or unsafe conditions.
Participant A: “I do strength training twice a week with a trainer and she will pushme to the point where it hurts, but you know. . .”
Participant B: “It’s a good hurt.”
Participant A: “Right. And she’s never pushed me past the point of that. But yeah, sowhen it hurts but it’s a good hurt you know it’s okay. That’s how I know – if I work-out and I can’t sit down the next day – I know I’ve worked out.
Other participants noted that the expectation of pain prevented them from work-ing hard enough to experience pain.
Participant A: “I don’t want to hurt.”
Participant B: “But it’s good because you know your muscles are tearing apart andthen healing themselves. It’s a great feeling!”
Participant A: “I’ve never felt any of that – I don’t push myself that far.”
Similar ideas were voiced in relation to cardiovascular responses. Participantsstated that exercise will often cause deep breathing, but that there is a differencebetween breathing heavy and shortness of breath. One participant noted, “I feelokay if I am tired, but I usually catch a second wind. It’s when I can’t catch thatsecond wind that I know I’ve gone too far.”
Differences in overweight and normal weight responses
Two primary themes emerged when participants were asked about differences inthe way the bodies of normal weight and overweight individuals react to exercise.First, most groups members agreed that overweight and obese individuals experi-enced more extreme responses to exercise than normal weight individuals. Groupmembers reported that they believed normal weight individuals were more tolerantto pain, and had more stamina, which made exercise easier for them. Words suchas ‘heightened’ and ‘exaggerated’ were commonly used when describing theresponses of overweight and obese individuals. Group members noted that thesemore intense responses may be due to deconditioning, poor circulation ordecreased muscle tone, but all noted that these responses decreased as weightdecreased.
184 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

The second theme that emerged was the importance of the role of psychologi-cal responses to exercise. One member, who reported being active when she wasyounger and at a healthy weight, stated that she felt resentful and frustrated thatshe could not do the same activities she could do previously. Many membersreported getting frustrated with exercise because they felt that they could not keepup in a group setting, or they felt they had to exercise at a level that was notintense enough for weight loss. Others noted that safety concerns dampened moti-vation to exercise. One participant noted that he felt he was ‘too heavy to walk’,but also noted that he thought that this was ‘just an excuse because I’m tooheavy because I don’t walk’. Many members felt that these psychological con-cerns about exercise were concerns that an individual of normal weight would notexperience.
Participants were also asked to discuss possible differences in the way normalweight individuals and overweight individuals may interpret physical responses toexercise. The primary theme that emerged from this discussion related to an overre-action to pain or cardio-respiratory responses.
Participant A: “I’ll tell you – the overweight person thinks he’s dying because he’sdoing things physically that he’s never done. Like the pain in the side when you runtoo fast. Runners know it happens normally – I remember from gym class, when theymade you run, your side hurt. But you think something’s wrong.”
Participant B: “And you want to quit.”
Participant A: “Exactly. And also because you don’t have the experience to know thatit’s part of the process to develop a little pain so you get stronger. But initially you’rerecognizing pain you don’t know, your mind doesn’t know. Psychologically you’rehaving a difficult time with it because your first reaction is to stop.”
Participants in each group stated that this overreaction to physical responsesstems, in part, from a fear of weight-related risk factors. Many participantsreported that knowing they were at an increased risk for heart attack and strokedue to their weight made them more aware of physical responses during and afterexercise. One participant described one of her first experiences with walking on atreadmill:
Participant A: “I think you’re so programmed by everyone like all your doctors thatyou’re at such risk because you’re overweight that you think this pain is like, ‘oh mygosh, I’m having the heart attack that [my doctor] said I was going to have.”
Participant B: “You’re scared.”
Participant A: “And the normal weight person, they know that it’s okay.”
A participant in a different focus group noted similar fear:
“I think that for me, heredity factors into it. My mother had a heart attack early on –in her early 40s. And although I don’t have – I’m overweight, but I don’t have highblood pressure, all those other things, but I’m always afraid. I’m afraid that somethinglike that will happen to me. Just (snap) something out the blue. And it makes me a lit-tle bit paranoid.”
Qualitative Research in Sport, Exercise and Health 185
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

This fear of risk factors tended to be especially relevant to trying new activities.Participants noted that while they may feel comfortable doing a routine exercisesuch as walking, they would not feel safe trying new exercises such as higher inten-sity aerobic exercises or weight training.
Some group members noted that this fear is often used as an excuse to avoidexercise. One participant discussed thoughts that overweight and obese individualsare ‘always thinking about pain’. She pointed to this as the reason that some over-weight or obese individuals may overlook a potentially dangerous reaction, thinkingthat it is a result of weight rather than a medical condition. But she also noted thatthis is a reason many overweight individuals avoid exercise, explaining that theyare in a constant state of pain, so they avoid intentionally increasing this painthrough exercise. Other group members discussed thinking that exercise was unsafedue to their weight and found that they would talk themselves out of exercising bysaying they needed to lose weight before they could exercise safely.
Factors influencing physical safety
When asked to discuss factors that influenced feelings of comfort or safety withexercise, two primary themes emerged: medical clearance and supervised exer-cise. Group members reported feeling safer after receiving medical clearance toexercise. This clearance ranged from having a physician tell the individual whatexercises were physically safe or unsafe, to undergoing an exercise stress test.
The second theme, supervised exercise, ranged from working with a personaltrainer to having frequent interactions with a physician or other medical staff whileinitiating an exercise programme. Many participants noted that while they felt safedoing familiar exercise such as walking, they were not comfortable trying new exer-cises such as resistance training or increasing their exercise intensity without super-vision from a trainer. While some participants felt safe in a gym setting that wasstaffed with personal trainers, others noted they felt more comfortable in a medicalsetting or a setting where personnel specialised in working with individuals who areoverweight and obese. One difference of opinion was related to group-based exer-cise classes. While some participants felt safer in a group setting than exercisingalone, others felt that the group setting fostered a feeling of needing to ‘keep up’,which they felt was not physically safe for individuals who are overweight orobese. While all agreed that working with a trainer individually was the ideal situa-tion, some participants noted that they felt safer to determine their own intensitywhile exercising alone than follow directions of an instructor in the context of agroup setting.
“At one point I was working with a personal trainer and I felt safer. I felt like if some-thing happened to me the trainer was there and she could see about it. And I haverecently tried attending classes, just with a friend, like at the Y. And although I’veenjoyed the classes, there is something in me that feels like if something happened tome it’s just, I don’t know, like something terrible could happen while I’m in the class.Like no one would– I don’t know it’s paranoia.”
Discussion
Three focus groups with a total of 21 participants were conducted to explore fear-avoidance beliefs related to exercise among a group of overweight and obese adults
186 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
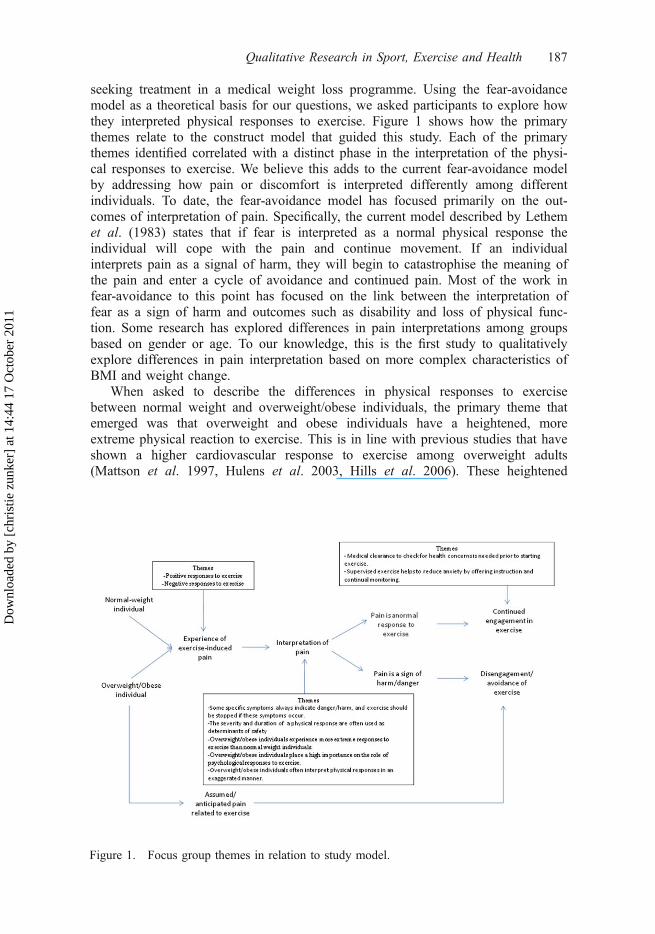
seeking treatment in a medical weight loss programme. Using the fear-avoidancemodel as a theoretical basis for our questions, we asked participants to explore howthey interpreted physical responses to exercise. Figure 1 shows how the primarythemes relate to the construct model that guided this study. Each of the primarythemes identified correlated with a distinct phase in the interpretation of the physi-cal responses to exercise. We believe this adds to the current fear-avoidance modelby addressing how pain or discomfort is interpreted differently among differentindividuals. To date, the fear-avoidance model has focused primarily on the out-comes of interpretation of pain. Specifically, the current model described by Lethemet al. (1983) states that if fear is interpreted as a normal physical response theindividual will cope with the pain and continue movement. If an individualinterprets pain as a signal of harm, they will begin to catastrophise the meaning ofthe pain and enter a cycle of avoidance and continued pain. Most of the work infear-avoidance to this point has focused on the link between the interpretation offear as a sign of harm and outcomes such as disability and loss of physical func-tion. Some research has explored differences in pain interpretations among groupsbased on gender or age. To our knowledge, this is the first study to qualitativelyexplore differences in pain interpretation based on more complex characteristics ofBMI and weight change.
When asked to describe the differences in physical responses to exercisebetween normal weight and overweight/obese individuals, the primary theme thatemerged was that overweight and obese individuals have a heightened, moreextreme physical reaction to exercise. This is in line with previous studies that haveshown a higher cardiovascular response to exercise among overweight adults(Mattson et al. 1997, Hulens et al. 2003, Hills et al. 2006). These heightened
Figure 1. Focus group themes in relation to study model.
Qualitative Research in Sport, Exercise and Health 187
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

reactions, may lead to more focus on the response, which could influence the inter-pretation of the response as a harmful event.
In addition to describing the differences in terms of what physical responseswere experienced, participants were also asked to explore how these responses areinterpreted differently between normal weight and overweight/obese individuals.Participants described exaggerated interpretations of fear and increased focus onthe responses than would be expected from normal weight individuals. Whilemultiple studies have found a difference in affective response to exercise betweenweight groups, the researchers are unaware of any that have explored the sourceof these differences. Existing studies used quantitative scales of pleasure/displea-sure (Ekkekakis and Lind 2006; Ekkekakis et al. 2009), or mood state batteries(Carels et al. 2006) to measure affective state. While the latter often includesscreening for tension or anxiety, it does not specify whether or not the anxiety iscaused by the exercise. Rather, most have evaluated the effect of exercise inimproving or changing general mood state, and have not addressed exercise-induced anxiety. While participants of these focus groups did endorse similarmood improvements related to exercise, they also expressed a separate fear thatoccurred as a direct result of exercise. Identifying exercise-induced fears and dif-ferentiating these from other psychological barriers to exercise such as social phy-sique anxiety may lead to more ailored treatments and better adherence toexercise prescription.
This study has limitations that should be addressed. The first relates to the levelof experience that focus group members had with the topic of the study. Not allgroup members were able to relate to the concept of fear-avoidance, because theydid not personally endorse fear of physical response to exercise. While participantswere recruited in such a way as to increase group diversity on many levels, theirfear-avoidance beliefs related to exercise were unknown. Some participants did notfeel they had much to offer the discussion once it focused specifically on fear sincethey did not personally experience this. However, due to the exploratory nature ofthis study, it was important to have these participants in the focus group discus-sions. In order to fully understand the complexity and range of fears associated withexercise in this population, it was necessary to explore the interpretation of physicalresponses both in individuals who experience fear and those who do not.
The second limitation of note is that of selection bias. Participants wererecruited from a population of patients in a weight loss programme. These partici-pants may have experiences and motivations that are inherently different from over-weight or obese individuals who are not actively engaged in a weight loss attempt,or who may be attempting weight loss outside of a formal or structured programme.The results of this study may have limited generalisability beyond participantsenrolled in medically-supervised weight loss programmes. Future research shouldfocus on exploring the concept of fear-avoidance beliefs in a more heterogeneoussample including individuals not currently engaged in weight loss efforts.
Additionally, these groups consisted only of individuals with BMIs in the over-weight or obese categories. We asked participants to describe differences in exerciseexperiences between overweight/obese individuals and normal weight individuals.One goal of this comparison was to explore how the participants who had alreadylost weight felt differently about exercise after weight loss, and to ask those who hadnot yet lost weight to hypothesise how exercise would be different if they weighedless. No comparison can be made from these groups as to the real perceptional dif-
188 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1

ferences between normal weight and overweight/obese adults. Future research plansinclude expanding these questions to individuals who are normal weight and to com-pare the responses of these individuals to the current group of participants.
Exercise is recommended as a primary course of treatment for overweight andobesity (NHLBI 2000), but developing an exercise prescription that patients feelconfident in carrying out is often difficult due to barriers related to pain and cardio-vascular conditions. The discussions of these focus group members indicated thatfear of pain is often as much of a barrier as pain itself for adults who are over-weight or obese. Because fear-avoidance beliefs may be predictive as well as reac-tive, it is important that these beliefs be identified early in the exercise prescriptionprocess to provide an exercise environment that increases self-efficacy. These fearsmay be difficult for patients to articulate however, and addressing fear-avoidancebeliefs may prove difficult for some healthcare providers and fitness professionals.Standardised screening tools to assess fear-avoidance beliefs may prove to be avaluable source of information in both preventive care and secondary treatment ofoverweight and obesity, especially when compared to the proposition of quantifyingan individual’s subjective experience of pain. Previous qualitative work in painmeasurement indicates that attempting to measure pain in a quantitative way can bedifficult and may discount the perceptions of the individual in pain (Carr et al.2005; Sparks and Smith 2008). For this reason, it may be more productive to focuson assessing the interpretation of pain, and fear related to these interpretations,rather than attempting to quantify the pain itself.
Assessing fear-avoidance beliefs in individuals who are at risk for hypoki-netic diseases can assist healthcare providers and fitness professionals in creatingtailored interventions designed to increase activity levels prior to the onset ofdisease. Assessment tools will also be useful in the secondary and tertiary treat-ments of overweight and obesity, as these are settings in which patients oftenpresent for treatment with habits that have been developing over a long periodof time. By the time an individual seeks medical attention for weight-relatedhealth issues, he or she may have already reached the point of avoiding move-ment and exercise due to fear of pain. For this reason, early recognition of fear-avoidance beliefs in overweight and obese individuals is important for prescrip-tion of an exercise routine that is tailored to their specific needs, which, in turn,may lead to increased self-efficacy and improvements in programme retentionand adherence.
Notes on contributorsBrooks C. Wingo is a postdoctoral fellow in the UAB Department of Nutrition Sciences.Her research interests focus on psychosocial barriers to physical activity and dietary changein overweight and obese adults.
Retta Evans is an associate professor and programme coordinator in Health Education at theUniversity of Alabama at Birmingham. Dr Evans has published widely on various topicsrelated to youth health, body image of adult females and health behaviour change. She hasan interest in using technology to enhance health education and physical activity in thepublic schools.
Jamy Ard is an associate professor in the UAB Department of Nutrition Sciences. Hiscurrent research interests include behavioural therapies that are focused on cardiovascularrisk reduction. He has a special interest in the African-American population and developingstrategies for behaviour modification that are culturally appropriate for this group.
Qualitative Research in Sport, Exercise and Health 189
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
Diane M. Grimley is a psychologist and a professor of public health at the University ofAlabama at Birmingham. Her research interests include the development of theory-based,tailored, Internet– and cell phone-delivered behavioural interventions, measurementdevelopment and model testing, sexual risk behaviours and the non-medical use ofprescription drugs.
Jane Roy is an associate professor of exercise science in the UAB Department of HumanStudies. Her research interests focus on body image, barriers to exercise and obesity.
Scott Snyder is an associate professor and associate dean at the University of Alabama atBirmingham. His research interests include psychometric theory and programme evaluation.
Christie Zunker was a Research Assistant at UAB. She has a doctoral degree from theDepartment of Health Behavior in the School of Public Health at the University of Alabamaat Birmingham. She recently moved to Fargo for a postdoctoral fellowship position to focuson obesity and eating disorders research. Her research interests include weight management,eating disorders and physical activity.
Alison Acton is a fitness specialist in the UAB Department of Nutrition Sciences. Herinterests lie in the obesity, and physical activity in older adults.Monica Baskin is anassociate professor at the University of Alabama at Birmingham. Her research interests arebehavioural weight management, minority health and health disparities, and community-based participatory research.
ReferencesAmerican College of Sports Medicine, 2006. ACSM’s guidelines for exercise testing and pre-
scription. 7th ed. Baltimore, MA: Lippincott Williams and Wilkins.American College of Sports Medicine, 2003. Tips address exercise-induced muscle pain and
soreness. http://www.acsm.org. [Accessed 29 August 2008].Andersen, R.E., et al., 2003. Relationship between body weight gain and significant knee,
hip, and back pain in older Americans. Obesity research, 11, 1159–1162.Ball, K., Crawford, D, and Owen, N., 2000. Too fat to exercise? Obesity as a barrier to
physical activity. Australian and New Zealand journal of public health, 24 (3), 331–333.Bogdan, R.C. and Biklen, S.K., 2003. Qualitative research for education: an introduction to
theories and methods. 4th ed. Boston: Pearson Education Group.Cai, C., Pua, Y., and Lim, K., 2007. Correlates of self-reported disability in patients with
low back pain: the role of fear-avoidance beliefs. Annals of academy of medicine, 36,1013–1020.
Carels, R.A., Berger, B., and Darby, L., 2006. The association between mood states andphysical activity in postmenopausal, obese, sedentary women. Journal of aging andphysical activity, 14, 12–28.
Carr, D., Loeser, J., and Morris, D., 2005. Narrative, pain, and suffering, Vol. 34. Seattle:IASP Press.
Carter-Nolan, P.L., Adams-Campbell, L.L., and Williams, J., 1996. Recruitment strategiesfor black women at risk for noninsulin-dependent diabetes mellitus into exercise proto-cols: a qualitative assessment. Journal of the national medical association, 88, 558–562.
Centers for Disease Control and Prevention, 2008. Behavioral risk factor surveillance systemsurvey data. Atlanta, Georgia: US Department of Health and Human Services, Centersfor Disease Control and Prevention, 2008.
Clark, D., 1999. Identifying psychological, physiological and environmental barriers andfacilitators to exercise among older low income adults. Journal of clinical geropsycholo-gy, 5 (1), 51–62.
Coudeyre, E., et al., 2007. Fear-avoidance beliefs about back pain in patients with acuteLBP. Clinical journal of pain, 23 (8), 720–725.
Creswell, J.W., 2007. Qualitative inquiry & research design: choosing among the fiveapproaches. 2nd ed. Thousand Oaks, CA: Sage.
190 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
Crombez, G., et al., 1999. Pain-related fear is more disabling than pain itself: evidence onthe role of pain-related fear in chronic back pain disability. Pain, 80, 329–229.
Davis, J.N., Hodges, V.A., and Gillham, M.B., 2006. Physical activity compliance: differ-ences between overweight/obese and normal-weight adults. Obesity, 14, 2259–2265.
Ekkekakis, P. and Lind, E., 2006. Exercise does not feel the same when you are overweight:the impact of self-selected and imposed intensity on affect and exertion. Internationaljournal of obesity, 30, 652–660.
Ekkekakis, P., Lind, E., and Vazou, S., 2009. Affective response to increasing levels of exer-cise intensity in normal-weight, overweight, and obese middle-aged women. Obesity, 18,79–85.
Elfving, B.T. and Grooten, W., 2007. Low levels of physical activity in back pain patientsare associated with high levels of fear-avoidance beliefs and pain catastrophizing. Phys-iotherapy research international, 12 (1), 14–24.
Eyler, A.A., et al., 1998. Physical activity and minority women: a qualitative study. Healtheducation and behavior, 25, 640–652.
French, S., Story, M., and Jeffery, R., 2001. Environmental influences on eating and physicalactivity. Annual review of public health, 22, 309–335.
Geisser, M.E., Haig, A.J., and Theisen, M.E., 2000. Activity avoidance and function in per-sons with chronic back pain. Journal of occupational rehabilitation, 10 (3), 215–227.
George, S.Z., Dover, G.C., and Fillingim, R.B., 2007. Fear of pain influences outcomes afterexercise-induced delayed-onset muscle soreness at the shoulder. The clinical journal ofpain, 23 (1), 76–84.
Grubbs, L. and Carter, J., 2002. The relationship of perceived barriers to reported exercisebehaviors in college undergraduates. Family community health, 25 (2), 76–84.
Heim, N., et al., 2008. Obesity in older adults is associated with an increased prevalenceand incidence of pain. Obesity, 16 (11), 2510–2517.
Hill, J., et al., 2003. Obesity and the environment: where do we go from here? Science, 299,853–855.
Hills, A.P., et al., 2006. Validation of the intensity of walking for pleasure in obese adults.Preventive medicine, 42, 47–50.
Hulens, M., et al., 2003. Predictors of 6-minute walk test results in lean, obese and morbidlyobese women. Scandinavian journal of medicine and science in sports, 13, 98–105.
Kori, S., Miller, R., and Todd, D., 1990. Kinesiophobia: a new view of chronic pain behav-ior. Pain management, (Jan/Feb), 35–43.
Krueger, R., 1988. Focus groups: a practical guide for applied research. London: Sage.Lethem, J., et al., 1983. Outline of a fear-avoidance model of exaggerated pain perceptions.
Behavior research and therapy, 21, 401–408.Mattsson, E., Larsson, U.E., and Rossner, S., 1997. Is walking for exercise too exhausting
for obese women? International journal of obesity, 21, 380–386.Melissas, J., et al., 2005. The effect of surgical weight reduction on functional status in mor-
bidly obese patients with low back pain. Obesity surgery, 15 (3), 378–381.Mokdad, A.H., et al., 2004. Actual causes of death in the United States, 2000. Journal of
the American medical association, 291 (10), 1238–1245.National Heart Lung and Blood Institute, 2000. The practical guide: identification evaluation
and treatment of overweight and obesity in adults (NIH Publication No. 00- 4084).Bethesda MD.
Nevitt, M.C. and Lane, N., 1999. Body weight and osteoarthritis. American journal of medi-cine, 107, 632–633.
Paluskai, S. and Schwenk, T., 2000. Physical activity and mental health: current concepts.Sports medicine, 29 (3), 167–180.
Patterson, R.E., et al., 2004. A comprehensive examination of health conditions associatedwith obesity in older adults. American journal of preventive medicine, 27 (5), 385–390.
Patton, M., 2002. Qualitative research and evaluation methods. 3rd ed. Thousand Oaks, CA:Sage.
Pollard, C., 1984. Preliminary validity study of the pain disability index. Perceptual andmotor skills, 59, 974.
Sparks, A.C. and Smith, B., 2008. Men, spinal cord injury, memories and the narrative per-formance of pain. Disability and society, 23 (7), 679–690.
Qualitative Research in Sport, Exercise and Health 191
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
Stewart, D. and Shamdasani, P., 1990. Focus groups: theory and practice. London: Sage.Swinkels-Meewise, E., et al., 2006. Psychometric properties of the Tampa scale for Kinesio-
phobia and the fear-avoidance beliefs questionnaire in acute low back pain. Manual ther-apy, 8 (1), 29–36.
Tukker, A., Visscher, T.L., and Picavet, H.S., 2009. Overweight and health problems of thelower extremities: osteoarthritis, pain and disability. Public health nutrition, 12 (3), 359–368.
United States Department of Health and Human Services, 1996. Physical activity and health:a Report of the surgeon general. Atlanta, GA: US Department of Health and Human Ser-vices, Centers for Disease Control and Prevention, National Center for Chronic DiseasePrevention and Health Promotion, 1996.
United States Department of Health and Human Services, 2008. 2008 physical activityguidelines for Americans. ODPHP Publication No. U0036.
Young, D.R., et al., 2001. Motivations for exercise and weight loss among African Americanwomen: focus group results and their contribution towards program development. Ethnic-ity & health, 6 (3/4), 227–245.
Young, D.R., et al., (2009). Patterns of physical activity among overweight and obese adults.Preventing Chronic Disease, 6 (3). http://www.cdc.gov/pcd/issues/2009/jul/08_0186.htm.
192 B.C. Wingo et al.
Dow
nloa
ded
by [
chri
stie
zun
ker]
at 1
4:44
17
Oct
ober
201
1
Related Documents











