Family Engagement Quality Improvement Project: Learning Session June 3-4 2016 Hyatt Rosemont 6350 N River Road Rosemont, Illinois, 60018 Room: Coleman B Day 1, June 3, 2016 (Half Day), 1:30 – 7:00 pm TIME SESSION FACULTY/SPEAKER(S) 1:30 – 2:00 Registration NCMHI Staff 2:00 – 2:20 Welcome & Family Engagement Quality Improvement Project Overview Megan M. Tschudy, MD, MPH, FAAP 2:20- 2:30 Housekeeping Announcements Overview of Learning Session NCMHI Staff 2:30 – 3:10 Topical Session: Family Story and Introduction to Family Engagement Vicki Hunting, BA 3:10 – 3:30 Family Engagement: Team Time Practice Teams 3:30 – 4:00 Break 4:00 – 5:00 Breakout Session 1: Quality Improvement in the Real World Quality Improvement Science (continued) Project aims, measures, and goals Change package; sample tests of change; resources & tools Room: Coleman B Ruth Gubernick, MPH Breakout Session 2: Introduction to Quality Improvement with Parent/Caregiver Partners Room: Lindbergh A Vicki Hunting, BA 5:00 – 5:30 Topical Session: Sustainability Alan Weller, MD, FAAP 5:30 – 7:00 Working Dinner Storyboard presentations Beginning to plan Plan, Do, Study, Act (PDSA) cycles Collaborative learning time Project Teams Ruth Gubernick, MPH Alan Weller, MD, FAAP Julia Richerson, MD, FAAP Camille Graham, MD, FAAP Vicki Hunting, BA Brad Thompson, MA LPC 7:00 Closing Remarks, Adjourn for Day Camille Graham, MD, FAAP

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Family Engagement Quality Improvement Project: Learning Session
June 3-4 2016 Hyatt Rosemont
6350 N River Road Rosemont, Illinois, 60018
Room: Coleman B Day 1, June 3, 2016 (Half Day), 1:30 – 7:00 pm
TIME SESSION FACULTY/SPEAKER(S)
1:30 – 2:00 Registration
NCMHI Staff
2:00 – 2:20 Welcome & Family Engagement Quality Improvement Project Overview
Megan M. Tschudy, MD, MPH, FAAP
2:20- 2:30 Housekeeping Announcements Overview of Learning Session
NCMHI Staff
2:30 – 3:10 Topical Session: Family Story and Introduction to Family Engagement
Vicki Hunting, BA
3:10 – 3:30 Family Engagement: Team Time Practice Teams
3:30 – 4:00 Break
4:00 – 5:00 Breakout Session 1: Quality Improvement in the Real World
Quality Improvement Science (continued)
Project aims, measures, and goals
Change package; sample tests of change; resources & tools
Room: Coleman B
Ruth Gubernick, MPH
Breakout Session 2: Introduction to Quality Improvement with Parent/Caregiver Partners Room: Lindbergh A
Vicki Hunting, BA
5:00 – 5:30 Topical Session: Sustainability Alan Weller, MD, FAAP
5:30 – 7:00 Working Dinner
Storyboard presentations
Beginning to plan Plan, Do, Study, Act (PDSA) cycles
Collaborative learning time
Project Teams Ruth Gubernick, MPH Alan Weller, MD, FAAP Julia Richerson, MD, FAAP Camille Graham, MD, FAAP Vicki Hunting, BA Brad Thompson, MA LPC
7:00 Closing Remarks, Adjourn for Day Camille Graham, MD, FAAP

Family Engagement Quality Improvement Project: Learning Session
June 3-4, 2016 Hyatt Rosemont
6350 N River Road Rosemont, Illinois, 60018
Room: Coleman B Day 2, June 4, 2016 (Full Day), 7:30 am – 1:30 pm
TIME SESSION FACULTY/SPEAKER(S)
7:30 – 8:00 Breakfast/ Welcome Back & Overview of Day NCMHI Staff
8:00 – 8:30 Continuation of Storyboard Presentations Project Teams
8:30 – 9:10 Topical Session: Shared Decision Making
Brad Thompson, MA LPC Camille Graham, MD, FAAP
9:10 – 9:30 Shared Decision Making: Team Time Practice Teams
9:30 – 10:00 Breakout Session 3: Report on Baseline Data and Pre-Implementation Survey Room: Coleman B
Ruth Gubernick, MPH
Breakout Session 4: Helpful Tools for Your Role as a Parent/Caregiver Partner Room: Lindbergh A
Vicki Hunting, BA
10:00 – 10:30 Break
10:30 – 1:00 Lunch served at 12:00 (Noon)
Working Lunch:
Planning PDSA Cycles and Team Collaborative Learning Time (Continuation of Day 1 Session)
Practice Teams Report Back Drafted PDSA Cycles
Practice Teams Ruth Gubernick, MPH Julia Richerson, MD, FAAP Camille Graham, MD, FAAP Vicki Hunting, BA Brad Thompson, MA LPC
1:00 – 1:30 Wrap Up, Next Steps, Q&A, Learning Session Evaluation Ruth Gubernick, MPH NCMHI Staff
1:30 Closing Remarks, Adjourn Camille Graham, MD, FAAP

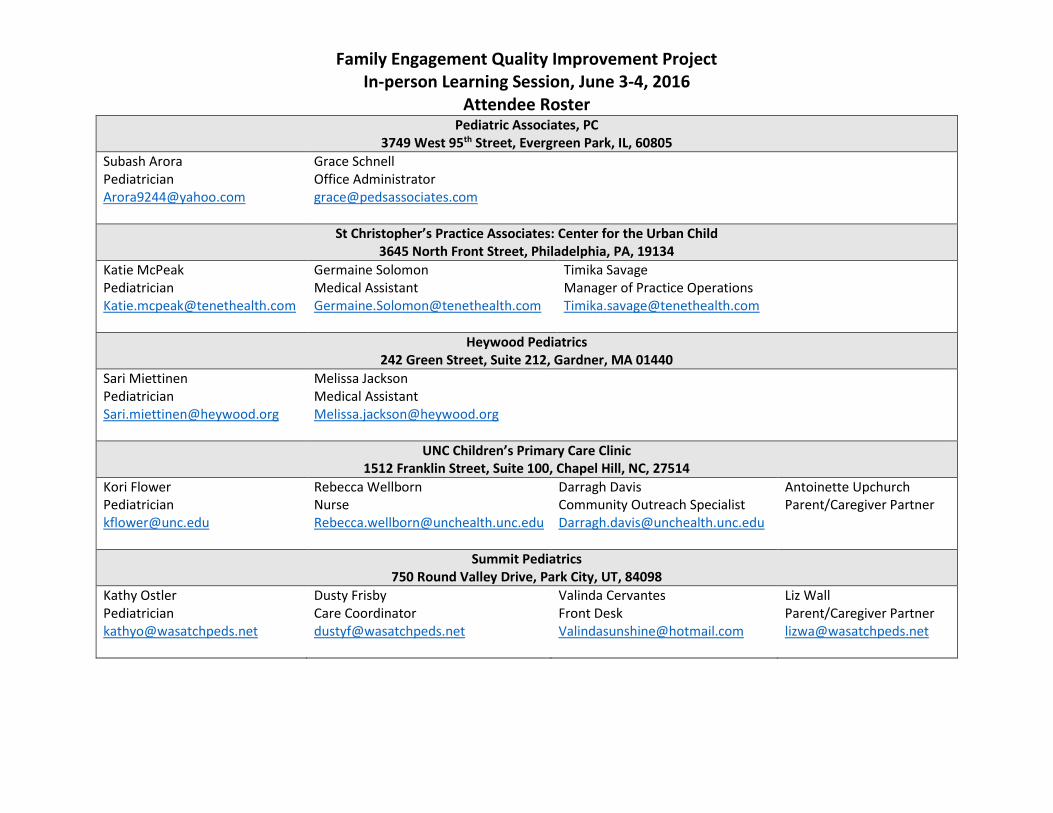
Family Engagement Quality Improvement Project In-person Learning Session, June 3-4, 2016
Attendee Roster
All About Children Pediatric Partners PC 655 Walnut Street, West Reading, PA, 19611
Anna Karasik Pediatrician [email protected]
Penny Porter Nurse Practitioner [email protected]
Eric Hamlette Intake Coordinator/Patient Advocate [email protected]
Elisa Cintron Parent/Caregiver Partner [email protected]
Southwest Montana Community Health Center 445 Centennial Ave, Butte, MT, 59701
Cathy White Pediatrician [email protected]
Betty Warren Nurse [email protected]
Shawna Holland Office Administrator [email protected]
Karla Ahlborn Parent/Caregiver Partner [email protected]
Doernbecher Pediatric and Adolescent Health 3181 SW Sam Jackson Park Road, Portland, OR, 97239
Melissa Weddle Pediatrician [email protected]
Nicole Ripsom Nurse [email protected]
Tyanne Conner Patient Access Services [email protected]
Kerri Derrevere Parent/Caregiver Partner [email protected]
Southeastern Pediatric Associates 364 Honeysuckle Road, Dothan, AL, 36305
Richa Gatlin Pediatrician [email protected]
Victoria Beverett Nurse [email protected]
Lindsey Hughes PCMH Patient Care Coordinator [email protected]
Tiffany Holloway Parent/Caregiver Partner [email protected]
Hamakua-Kohala Health 45-549 Plumeria Street, Honokaa, HI, 96727
Pamela McKenna Pediatrician [email protected]
Nellie Villena Nurse [email protected]
Dena Soares Front Desk Supervisor [email protected]
January Kauanoe [email protected] Parent/Caregiver Partner
Family Engagement Quality Improvement Project In-person Learning Session, June 3-4, 2016
Attendee Roster
Pediatric Associates, PC 3749 West 95th Street, Evergreen Park, IL, 60805
Subash Arora Pediatrician [email protected]
Grace Schnell Office Administrator [email protected]
St Christopher’s Practice Associates: Center for the Urban Child 3645 North Front Street, Philadelphia, PA, 19134
Katie McPeak Pediatrician [email protected]
Germaine Solomon Medical Assistant [email protected]
Timika Savage Manager of Practice Operations [email protected]
Heywood Pediatrics 242 Green Street, Suite 212, Gardner, MA 01440
Sari Miettinen Pediatrician [email protected]
Melissa Jackson Medical Assistant [email protected]
UNC Children’s Primary Care Clinic 1512 Franklin Street, Suite 100, Chapel Hill, NC, 27514
Kori Flower Pediatrician [email protected]
Rebecca Wellborn Nurse [email protected]
Darragh Davis Community Outreach Specialist [email protected]
Antoinette Upchurch Parent/Caregiver Partner
Summit Pediatrics 750 Round Valley Drive, Park City, UT, 84098
Kathy Ostler Pediatrician [email protected]
Dusty Frisby Care Coordinator [email protected]
Valinda Cervantes Front Desk [email protected]
Liz Wall Parent/Caregiver Partner [email protected]
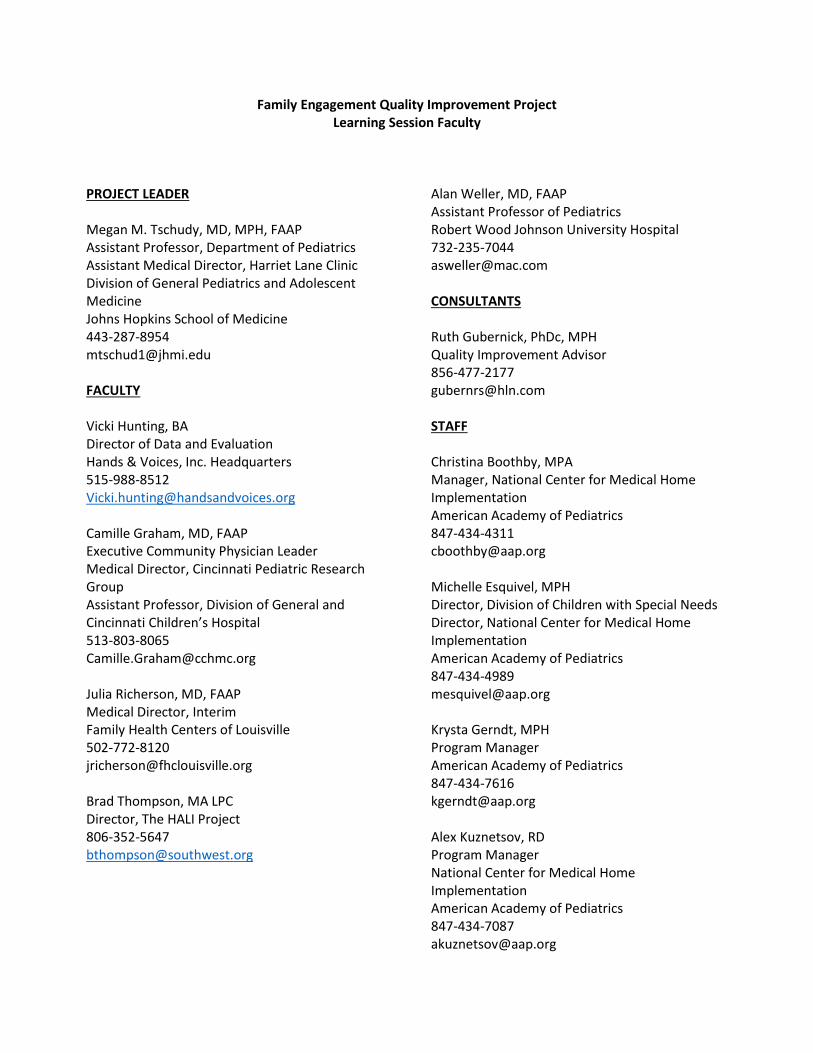
Family Engagement Quality Improvement Project Learning Session Faculty
PROJECT LEADER Megan M. Tschudy, MD, MPH, FAAP Assistant Professor, Department of Pediatrics Assistant Medical Director, Harriet Lane Clinic Division of General Pediatrics and Adolescent Medicine Johns Hopkins School of Medicine 443-287-8954 [email protected] FACULTY Vicki Hunting, BA Director of Data and Evaluation
Hands & Voices, Inc. Headquarters 515-988-8512 [email protected] Camille Graham, MD, FAAP Executive Community Physician Leader Medical Director, Cincinnati Pediatric Research Group Assistant Professor, Division of General and Cincinnati Children’s Hospital 513-803-8065 [email protected] Julia Richerson, MD, FAAP Medical Director, Interim Family Health Centers of Louisville 502-772-8120 [email protected] Brad Thompson, MA LPC
Director, The HALI Project 806-352-5647 [email protected]
Alan Weller, MD, FAAP Assistant Professor of Pediatrics Robert Wood Johnson University Hospital 732-235-7044 [email protected] CONSULTANTS Ruth Gubernick, PhDc, MPH Quality Improvement Advisor 856-477-2177 [email protected] STAFF Christina Boothby, MPA Manager, National Center for Medical Home Implementation American Academy of Pediatrics 847-434-4311 [email protected] Michelle Esquivel, MPH Director, Division of Children with Special Needs Director, National Center for Medical Home Implementation American Academy of Pediatrics 847-434-4989 [email protected] Krysta Gerndt, MPH Program Manager American Academy of Pediatrics 847-434-7616 [email protected] Alex Kuznetsov, RD Program Manager National Center for Medical Home Implementation American Academy of Pediatrics 847-434-7087 [email protected]

Family Engagement Quality Improvement Project Work Group Roster
PROJECT LEADER Megan M. Tschudy, MD, MPH, FAAP Assistant Professor, Department of Pediatrics Assistant Medical Director, Harriet Lane Clinic Division of General Pediatrics and Adolescent Medicine Johns Hopkins School of Medicine 443/287-8954 [email protected] MEMBERS Janet DesGeorges Executive Director, Hands and Voices, Inc. Parent Consultant, Colorado Home Intervention Program 303-492-6283 [email protected] Camille Graham, MD, FAAP Executive Community Physician Leader Medical Director, Cincinnati Pediatric Research Group Assistant Professor, Division of General and Cincinnati Children’s Hospital 513-803-8065 [email protected] Julia Richerson, MD, FAAP Medical Director, Interim Family Health Centers of Louisville 502-772-8120 [email protected] Alan Weller, MD, FAAP Assistant Professor of Pediatrics Robert Wood Johnson University Hospital 732/235-7044 [email protected]
CONSULTANTS Ruth Gubernick, PhDc, MPH Quality Improvement Advisor 856-477-2177 [email protected] Pam Kelley, PhD Research and Evaluation Consultant Kelley Analytics, LLC 732/742-8908 [email protected] STAFF Christina Boothby, MPA Manager, National Center for Medical Home Implementation American Academy of Pediatrics 847/434-4311 [email protected] Michelle Esquivel, MPH Director, Division of Children with Special Needs Director, National Center for Medical Home Implementation American Academy of Pediatrics 847/434-4989 [email protected] Krysta Gerndt, MPH Program Manager American Academy of Pediatrics 847/434-7616 [email protected] Alex Kuznetsov, RD Program Manager National Center for Medical Home Implementation American Academy of Pediatrics 847/434-7087 [email protected]

MODEL FOR IMPROVEMENT Team Name:
Plan a Test of Change Cycle #:___ Start Date: ____ End Date: ____
Objective for this PDSA Cycle (Aim):
PLAN: QUESTIONS PREDICTIONS
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE
Act Plan
Study Do

MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/12/16 End Date: 7//13
Objective for this PDSA Cycle (Aim): By September 30, 2016, our practice will be using the shared decision making (SDM) aid, “ADHD Medication Choice Cards,” with at least 95% of the parents/caregivers of our patients who are newly diagnosed with ADHD and are interested in medication as a treatment option.
PLAN: QUESTIONS Can our care coordinator send out this decision aid, as well as the Pre-encounter/visit cards and booklet on ADHD treatment modalities to the appropriate parents/caregivers via the patient portal at least 1 week prior to the scheduled visit? Will parents/caregivers read and complete the personal information and cost estimates prior to being seen by the physician? Will Dr. Gordon have time to review and discuss it with the family? Will this aid be helpful to parents/caregivers?
PREDICTIONS We predict that our care coordinator, Linda, will successfully send these resources/tools at least 1 week prior to the visit at least 95% of the time. We predict at least 90% of the parents/caregivers will complete the treatment goals and preferences card; 70% will add behavior treatments tried, currently trying or interested in trying; 75% will add personal information to the Medication Choice card; only 50% will complete the out-of-pocket cost estimates. Dr. Gordon predicts this will increase the visit time but will help the parent/caregiver be more knowledgeable and involved with the treatment plan.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Tasks: Linda will confirm that there is 1 or more patient(s), <11 yrs. old and newly diagnosed with ADHD scheduled for appointments on July 12th and/or 13th. She will also print out the Medication Choice cards, as instructed on the Cincinnati Children’s website (http://www.cincinnatichildrens.org/service/j/anderson-center/evidence-based-care/decision-aids/ ). Dr. Gordon will study the “Card Guide”( http://www.cincinnatichildrens.org/WorkArea/linkit.aspx?LinkIdentifier=id&ItemID=100745&libID=100440 ) for discussing medication treatment options with the parent/caregiver. On July 5th, Linda will send a message and the ADHD Pre-visit cards and Medication Choice cards via the patient portal to the parents/caregivers whose children meet the criteria, with instructions to complete the goals/preferences, behavior treatment(s) and personal information sections and out-of-pocket medication cost estimates, if appropriate. Parents will be asked to bring the completed information to their visit. Prior to entering the exam room, Dr. Gordon will be handed the parent-completed goal/preference card, behavioral treatment card and ADHD medication choice cards by the Joyce (MA).
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE At the end of each day, Linda will review the records of those newly diagnosed ADHD patients seen by Dr. Gordon. She will record total # of patients who brought with them the ADHD SDM aids and note what sections had been completed prior to the visit. Dr. Gordon will share parent/caregiver feedback and his own reflections about the process.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE
Act Plan
Study Do

MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/12/16 End Date: 7/1316
Objective for this PDSA Cycle (Aim): By September 30, 2016, our practice will be using the shared decision making (SDM) aid, “ADHD Medication Choice Cards,” with at least 95% of the parents/caregivers of our patients who are newly diagnosed with ADHD and are interested in medication as a treatment option.
PLAN: QUESTIONS Can our care coordinator send out this decision aid, as well as the Pre-encounter cards and booklet on ADHD treatment modalities to the appropriate parents/caregivers via the patient portal at least 1 week prior to the scheduled visit? Will parents/caregivers read and complete the personal information and cost estimates prior to being seen by the physician? Will Dr. Gordon have time to review and discuss it with the family? Will this aid be helpful to parents/caregivers?
PREDICTIONS We predict that our care coordinator, Linda, will successfully send these resources/tools at least 1 week prior to the
visit at least 95% of the time. We predict at least 90% of the parents/caregivers will complete the treatment goals and preferences card; 70% will add behavior treatments tried, currently trying or interested in trying; 75% will add personal information to the Medication Choice card; only 50% will complete the out-of-pocket cost estimates. Dr. Gordon predicts this will increase the visit time but will help the parent/caregiver be more knowledgeable and involved with the treatment planning.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Tasks: Linda will confirm that there is 1 or more patient(s), <11 yrs. old and newly diagnosed with ADHD scheduled for appointments on July 12th and/or 13th. She will also print out the Medication cards, as instructed on the Cincinnati Children’s website (http://www.cincinnatichildrens.org/service/j/anderson-center/evidence-based-care/decision-aids/ ). Dr. Gordon will study the “Card Guide” (http://www.cincinnatichildrens.org/WorkArea/linkit.aspx?LinkIdentifier=id&ItemID=100745&libID=100440) for discussing medication treatment options with the parent/caregiver. On July 5th, Linda will send a message and the ADHD Pre-visit cards and Medication cards via the patient portal to the parents/caregivers whose children meet the criteria, with instructions to complete the goals/preferences, behavior treatment(s) and personal information sections and out-of-pocket medication cost estimates, if appropriate. Parents will be asked to bring the completed information to their visit. Prior to entering the exam room, Dr. Gordon will be handed the parent-completed goal/preference card, behavioral treatment card and ADHD medication choice cards by the Joyce (MA).
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE At the end of each day, Linda will review the records of those newly diagnosed ADHD patients seen by Dr. Gordon. She will record total # of patients who brought with them the ADHD SDM aids and note what sections had been completed prior to the visit. Dr. Gordon will share parent/caregiver feedback and his own reflections about the process.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances. Linda sent messages and resources on July 5th to 3
parents/caregivers who children met the criteria and had appointments on July 13th. All 3 parents brought the cards with them but only one had completed all the requested information. All 3 parents wanted to discuss medication options. Dr. Gordon said the first discussion took a long time because he presented all of the medication choice issue cards but forgot to ask the parent which one she wanted to discuss first. Found he didn’t need to discuss all 5 cards when he remembered to do that (ask first) with the other 2 parents!
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED Only one parent completed the medication cost estimate. One parent was unable to get the info from her health plan and one forgot. Dr. Gordon reported that following the “card guide” was helpful for him but he feels he needs more practice! Parents reported that the aids increased their knowledge of ADHD treatment options, were easy to understand and helped them be involved in making the decision about their child’s treatment plan. Dr. Gordon reported parents more involved. They all liked the medication issue cards. One parent was surprised when Dr. Gordon asked her which medication issue she wanted to discuss first. One parent expressed appreciation for the booklet and for being referred to a parent support group.
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test? Plan for
next cycle: What happens when parent/caregiver has not completed or brought the cards with them? Can they be given
to the parent/caregiver to complete in the exam room or completed by Dr. Gordon, in discussion with the family? Note: We also need to learn what summer behavioral treatment programs are available in our community/county!
Act Plan
Study Do

MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/1/16 End Date: 7/2/16
Objective for this PDSA Cycle (Aim): By July 31, 2016, our practice will use the Teach Back Method as a strategy to actively Engage patients and their families with their Asthma Actions Plan so that at least 80% have documentation in their record of the use of this patient engagement tool at their most recent appropriate acute or well-care visit.
PLAN: QUESTIONS Do Dr. Green and the clinical staff know how to conduct Teach Back?
Can this strategy be incorporated into the visit? Can it be documented in the EHR? PREDICTIONS It will take some practice for Dr. Green to feel comfortable asking for patient/parent
to share in own words what she explained regarding when to use which asthma medications.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Task: Prior to 7/1, Dr. Green and clinical staff will review the Teach Back toolkit (http://www.nchealthliteracy.org/toolkit/tool5.pdf ) and the “Always Use Teach Back” resources (http://www.ihi.org/resources/Pages/Tools/AlwaysUseTeachBack!.aspx) Dr. Green will conduct teach-back with the last patient scheduled tomorrow who has a diagnosis of asthma and a newly created or updated asthma action plan. Dr. Green will review the plan with the patient and/or parent/caregiver and then will ask “I want to be sure that I explained the medications correctly. Can you tell me how and when you are going to take/give these medicines?” This process will be repeated until the patient/parent or caregiver can explain it properly in own words. At end of visit, Dr. Green will ask patient and/or parent/caregiver for their feedback about the usefulness of the technique.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE Documentation of feedback from patient and/or parent/caregiver about the usefulness of the method. Dr. Green will also give feedback and her reflections about using the teach-back method.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE
Act Plan
Study Do
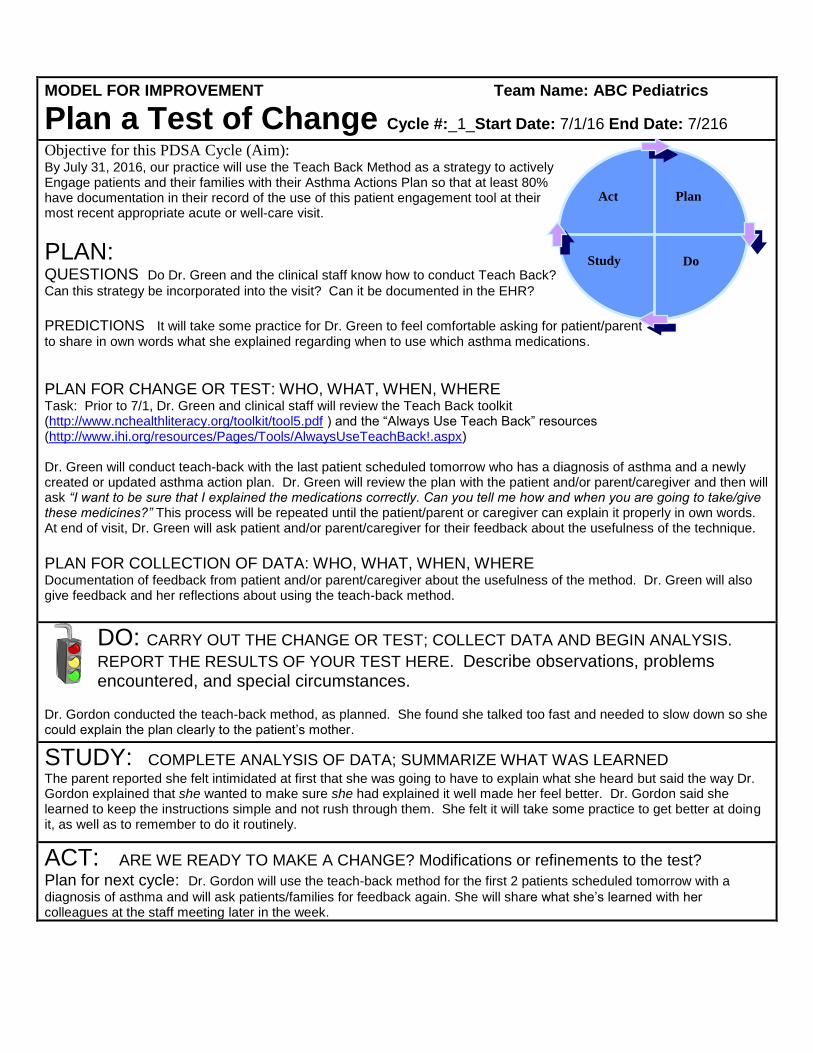
MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/1/16 End Date: 7/216
Objective for this PDSA Cycle (Aim): By July 31, 2016, our practice will use the Teach Back Method as a strategy to actively Engage patients and their families with their Asthma Actions Plan so that at least 80% have documentation in their record of the use of this patient engagement tool at their most recent appropriate acute or well-care visit.
PLAN: QUESTIONS Do Dr. Green and the clinical staff know how to conduct Teach Back?
Can this strategy be incorporated into the visit? Can it be documented in the EHR? PREDICTIONS It will take some practice for Dr. Green to feel comfortable asking for patient/parent to share in own words what she explained regarding when to use which asthma medications.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Task: Prior to 7/1, Dr. Green and clinical staff will review the Teach Back toolkit (http://www.nchealthliteracy.org/toolkit/tool5.pdf ) and the “Always Use Teach Back” resources (http://www.ihi.org/resources/Pages/Tools/AlwaysUseTeachBack!.aspx) Dr. Green will conduct teach-back with the last patient scheduled tomorrow who has a diagnosis of asthma and a newly created or updated asthma action plan. Dr. Green will review the plan with the patient and/or parent/caregiver and then will ask “I want to be sure that I explained the medications correctly. Can you tell me how and when you are going to take/give these medicines?” This process will be repeated until the patient/parent or caregiver can explain it properly in own words. At end of visit, Dr. Green will ask patient and/or parent/caregiver for their feedback about the usefulness of the technique. PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE Documentation of feedback from patient and/or parent/caregiver about the usefulness of the method. Dr. Green will also give feedback and her reflections about using the teach-back method.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
Dr. Gordon conducted the teach-back method, as planned. She found she talked too fast and needed to slow down so she could explain the plan clearly to the patient’s mother.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED The parent reported she felt intimidated at first that she was going to have to explain what she heard but said the way Dr. Gordon explained that she wanted to make sure she had explained it well made her feel better. Dr. Gordon said she learned to keep the instructions simple and not rush through them. She felt it will take some practice to get better at doing it, as well as to remember to do it routinely.
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
Plan for next cycle: Dr. Gordon will use the teach-back method for the first 2 patients scheduled tomorrow with a
diagnosis of asthma and will ask patients/families for feedback again. She will share what she’s learned with her colleagues at the staff meeting later in the week.
Act Plan
Study Do
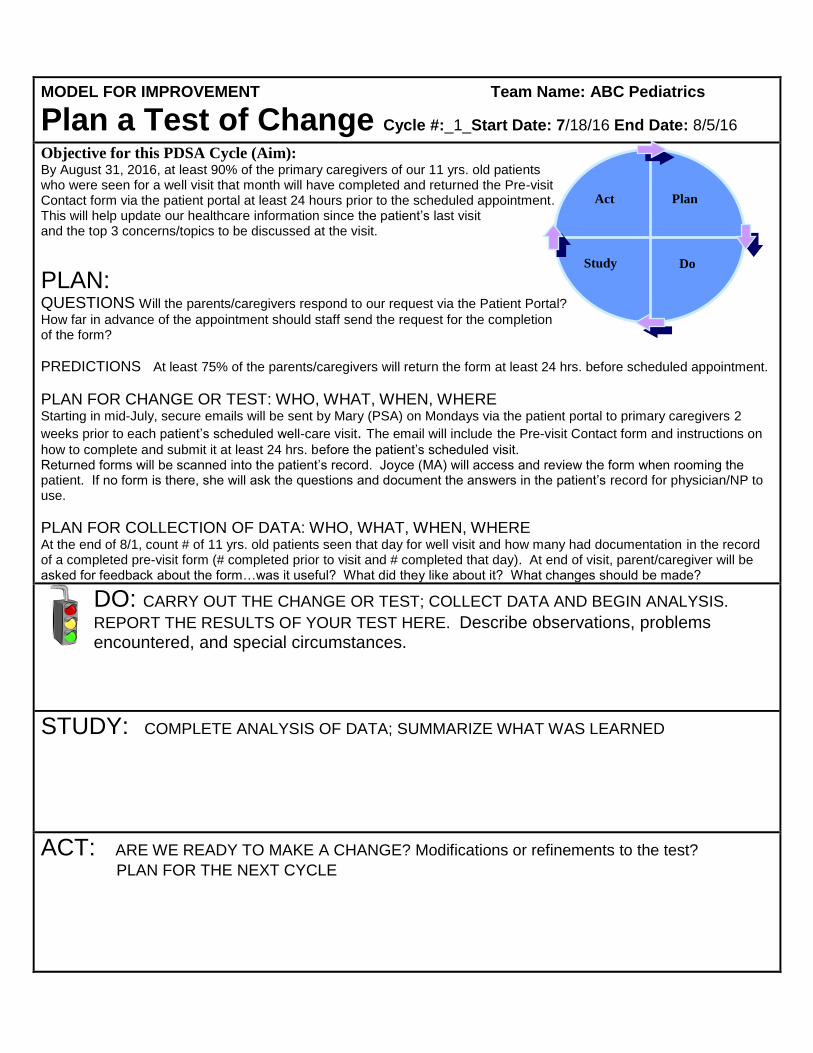
MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/18/16 End Date: 8/5/16
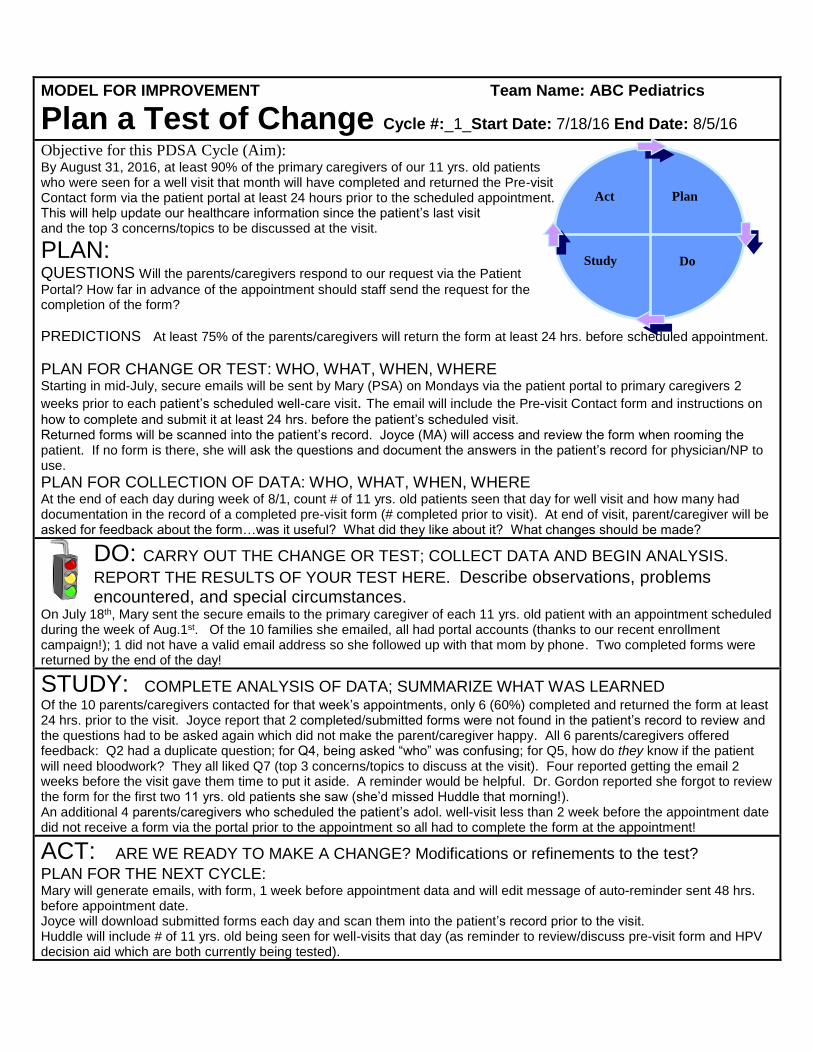
Objective for this PDSA Cycle (Aim): By August 31, 2016, at least 90% of the primary caregivers of our 11 yrs. old patients who were seen for a well visit that month will have completed and returned the Pre-visit Contact form via the patient portal at least 24 hours prior to the scheduled appointment. This will help update our healthcare information since the patient’s last visit and the top 3 concerns/topics to be discussed at the visit.
PLAN: QUESTIONS Will the parents/caregivers respond to our request via the Patient Portal?
How far in advance of the appointment should staff send the request for the completion of the form?
PREDICTIONS At least 75% of the parents/caregivers will return the form at least 24 hrs. before scheduled appointment.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Starting in mid-July, secure emails will be sent by Mary (PSA) on Mondays via the patient portal to primary caregivers 2
weeks prior to each patient’s scheduled well-care visit. The email will include the Pre-visit Contact form and instructions on
how to complete and submit it at least 24 hrs. before the patient’s scheduled visit. Returned forms will be scanned into the patient’s record. Joyce (MA) will access and review the form when rooming the patient. If no form is there, she will ask the questions and document the answers in the patient’s record for physician/NP to use.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE At the end of 8/1, count # of 11 yrs. old patients seen that day for well visit and how many had documentation in the record of a completed pre-visit form (# completed prior to visit and # completed that day). At end of visit, parent/caregiver will be asked for feedback about the form…was it useful? What did they like about it? What changes should be made?
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE
Act Plan
Study Do
MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/18/16 End Date: 8/5/16
Objective for this PDSA Cycle (Aim): By August 31, 2016, at least 90% of the primary caregivers of our 11 yrs. old patients who were seen for a well visit that month will have completed and returned the Pre-visit Contact form via the patient portal at least 24 hours prior to the scheduled appointment. This will help update our healthcare information since the patient’s last visit and the top 3 concerns/topics to be discussed at the visit.
PLAN: QUESTIONS Will the parents/caregivers respond to our request via the Patient
Portal? How far in advance of the appointment should staff send the request for the completion of the form?
PREDICTIONS At least 75% of the parents/caregivers will return the form at least 24 hrs. before scheduled appointment.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Starting in mid-July, secure emails will be sent by Mary (PSA) on Mondays via the patient portal to primary caregivers 2
weeks prior to each patient’s scheduled well-care visit. The email will include the Pre-visit Contact form and instructions on
how to complete and submit it at least 24 hrs. before the patient’s scheduled visit. Returned forms will be scanned into the patient’s record. Joyce (MA) will access and review the form when rooming the patient. If no form is there, she will ask the questions and document the answers in the patient’s record for physician/NP to use.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE At the end of each day during week of 8/1, count # of 11 yrs. old patients seen that day for well visit and how many had documentation in the record of a completed pre-visit form (# completed prior to visit). At end of visit, parent/caregiver will be asked for feedback about the form…was it useful? What did they like about it? What changes should be made?
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
On July 18th, Mary sent the secure emails to the primary caregiver of each 11 yrs. old patient with an appointment scheduled during the week of Aug.1st. Of the 10 families she emailed, all had portal accounts (thanks to our recent enrollment campaign!); 1 did not have a valid email address so she followed up with that mom by phone. Two completed forms were returned by the end of the day!
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED Of the 10 parents/caregivers contacted for that week’s appointments, only 6 (60%) completed and returned the form at least 24 hrs. prior to the visit. Joyce report that 2 completed/submitted forms were not found in the patient’s record to review and the questions had to be asked again which did not make the parent/caregiver happy. All 6 parents/caregivers offered feedback: Q2 had a duplicate question; for Q4, being asked “who” was confusing; for Q5, how do they know if the patient will need bloodwork? They all liked Q7 (top 3 concerns/topics to discuss at the visit). Four reported getting the email 2 weeks before the visit gave them time to put it aside. A reminder would be helpful. Dr. Gordon reported she forgot to review the form for the first two 11 yrs. old patients she saw (she’d missed Huddle that morning!). An additional 4 parents/caregivers who scheduled the patient’s adol. well-visit less than 2 week before the appointment date did not receive a form via the portal prior to the appointment so all had to complete the form at the appointment!
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE: Mary will generate emails, with form, 1 week before appointment data and will edit message of auto-reminder sent 48 hrs. before appointment date. Joyce will download submitted forms each day and scan them into the patient’s record prior to the visit. Huddle will include # of 11 yrs. old being seen for well-visits that day (as reminder to review/discuss pre-visit form and HPV decision aid which are both currently being tested).
Act Plan
Study Do
MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/15/16 End Date: 8/1/16
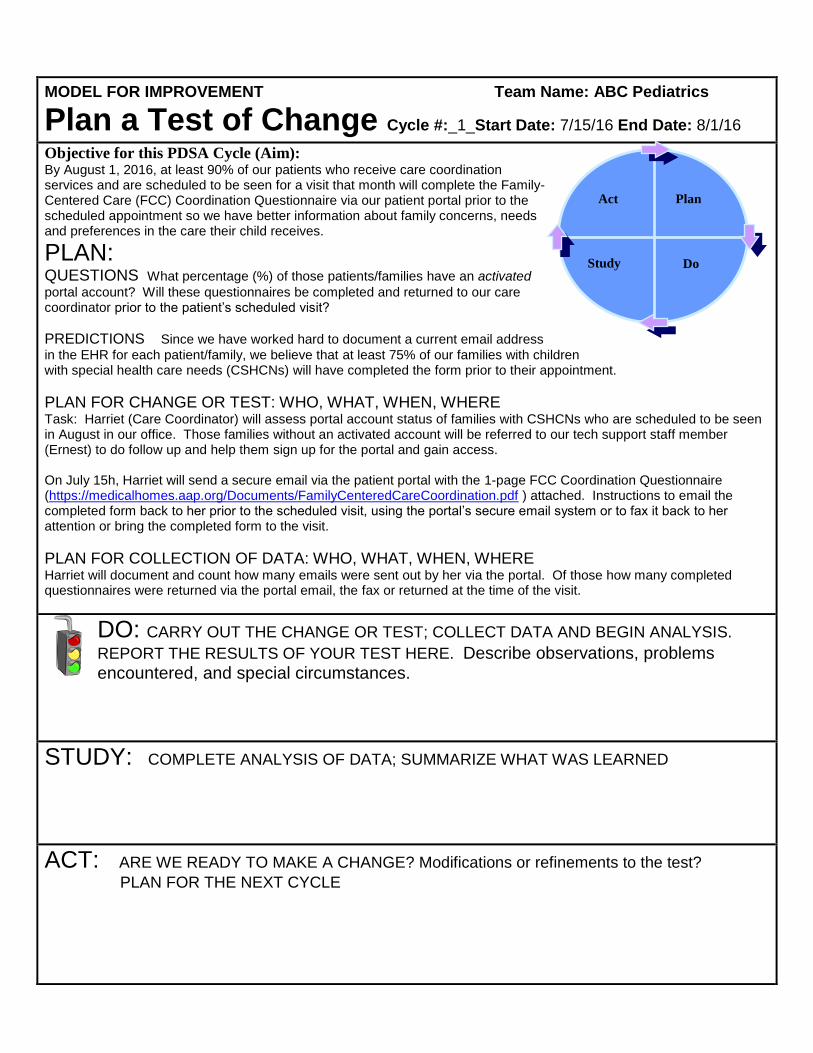
Objective for this PDSA Cycle (Aim): By August 1, 2016, at least 90% of our patients who receive care coordination services and are scheduled to be seen for a visit that month will complete the Family- Centered Care (FCC) Coordination Questionnaire via our patient portal prior to the scheduled appointment so we have better information about family concerns, needs and preferences in the care their child receives.
PLAN: QUESTIONS What percentage (%) of those patients/families have an activated
portal account? Will these questionnaires be completed and returned to our care coordinator prior to the patient’s scheduled visit?
PREDICTIONS Since we have worked hard to document a current email address in the EHR for each patient/family, we believe that at least 75% of our families with children with special health care needs (CSHCNs) will have completed the form prior to their appointment.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Task: Harriet (Care Coordinator) will assess portal account status of families with CSHCNs who are scheduled to be seen in August in our office. Those families without an activated account will be referred to our tech support staff member (Ernest) to do follow up and help them sign up for the portal and gain access. On July 15h, Harriet will send a secure email via the patient portal with the 1-page FCC Coordination Questionnaire (https://medicalhomes.aap.org/Documents/FamilyCenteredCareCoordination.pdf ) attached. Instructions to email the completed form back to her prior to the scheduled visit, using the portal’s secure email system or to fax it back to her attention or bring the completed form to the visit.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE Harriet will document and count how many emails were sent out by her via the portal. Of those how many completed questionnaires were returned via the portal email, the fax or returned at the time of the visit.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE
Act Plan
Study Do
MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/15/16 End Date: 8/1/16
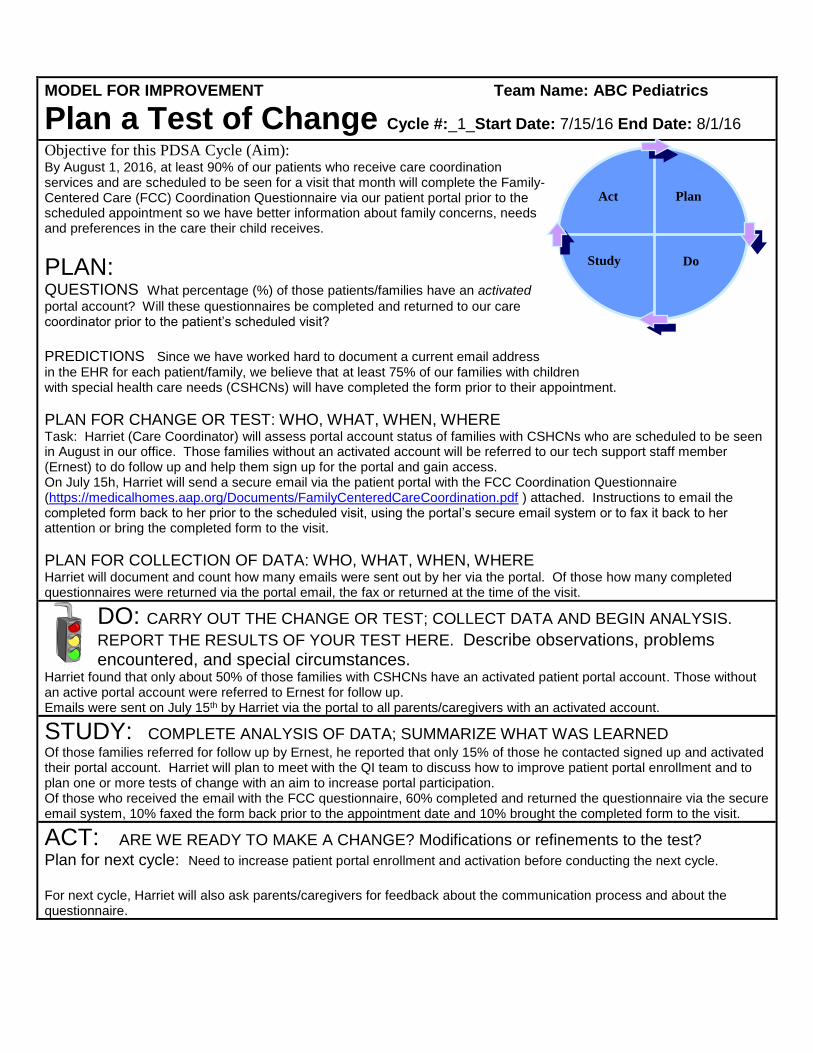
Objective for this PDSA Cycle (Aim): By August 1, 2016, at least 90% of our patients who receive care coordination services and are scheduled to be seen for a visit that month will complete the Family- Centered Care (FCC) Coordination Questionnaire via our patient portal prior to the scheduled appointment so we have better information about family concerns, needs and preferences in the care their child receives.
PLAN: QUESTIONS What percentage (%) of those patients/families have an activated
portal account? Will these questionnaires be completed and returned to our care coordinator prior to the patient’s scheduled visit?
PREDICTIONS Since we have worked hard to document a current email address in the EHR for each patient/family, we believe that at least 75% of our families with children with special health care needs (CSHCNs) will have completed the form prior to their appointment.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Task: Harriet (Care Coordinator) will assess portal account status of families with CSHCNs who are scheduled to be seen in August in our office. Those families without an activated account will be referred to our tech support staff member (Ernest) to do follow up and help them sign up for the portal and gain access. On July 15h, Harriet will send a secure email via the patient portal with the FCC Coordination Questionnaire (https://medicalhomes.aap.org/Documents/FamilyCenteredCareCoordination.pdf ) attached. Instructions to email the completed form back to her prior to the scheduled visit, using the portal’s secure email system or to fax it back to her attention or bring the completed form to the visit.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE Harriet will document and count how many emails were sent out by her via the portal. Of those how many completed questionnaires were returned via the portal email, the fax or returned at the time of the visit.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
Harriet found that only about 50% of those families with CSHCNs have an activated patient portal account. Those without an active portal account were referred to Ernest for follow up. Emails were sent on July 15th by Harriet via the portal to all parents/caregivers with an activated account.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED Of those families referred for follow up by Ernest, he reported that only 15% of those he contacted signed up and activated their portal account. Harriet will plan to meet with the QI team to discuss how to improve patient portal enrollment and to plan one or more tests of change with an aim to increase portal participation. Of those who received the email with the FCC questionnaire, 60% completed and returned the questionnaire via the secure email system, 10% faxed the form back prior to the appointment date and 10% brought the completed form to the visit.
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
Plan for next cycle: Need to increase patient portal enrollment and activation before conducting the next cycle.
For next cycle, Harriet will also ask parents/caregivers for feedback about the communication process and about the questionnaire.
Act Plan
Study Do

MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/1/16 End Date: 7/1/16
Objective for this PDSA Cycle (Aim): By July 31, 2016, our practice will routinely ask a set of questions to assess resilience of primary caregivers of our patients 0-3 yrs. old, as part of the well-child care (WCC) visit so we can better help them build their resilience and plan proactively how to respond to stressful parenting situations.
PLAN: QUESTIONS Can additional questions be integrated into the WCC visit?
How will they be documented in the patient’s record?
PREDICTIONS Questions will be verbally asked by Dr. Richards to at least 75% of the primary caregivers seen for a WCC visit tomorrow afternoon and documented in the patient records.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Completed Tasks: The 7 “Questions to ask” on the Strengthening Families’ “Parental Resilience: Action Sheet” (http://www.cssp.org/reform/strengtheningfamilies/about/body/ProtectiveFactorsActionSheets.pdf ) were reviewed by Parents/Caregivers who attended our June 15th Advisory Group meeting (PFAG). They reached consensus for Dr. Richards to test asking questions #4-6 at the initial visit. A smart set of those questions has been added to the EHR by Dr. Green. On Tuesday afternoon, Dr. Richards will test asking those questions to primary caregivers of patients 0-3 yrs. old being seen by him for a WCC visit.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE At the end of the afternoon, Joyce (MA) will tally the total # of patients 0-3 seen by Dr. Richards and the # of those with documentation that the “resilience” related questions were asked. The aggregate de-identified results also will be shared via email with the members of our PFAG.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE
Act Plan
Study Do

MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/1/16 End Date: 7/1/16
Objective for this PDSA Cycle (Aim): By July 31, 2016, our practice will routinely ask a set of questions to assess resilience of primary caregivers of our patients 0-3 yrs. old, as part of the well-child care (WCC) visit so we can better help them build their resilience and plan proactively how to respond to stressful parenting situations.
PLAN: QUESTIONS Can additional questions be integrated into the WCC visit?
How will they be documented in the patient’s record?
PREDICTIONS Questions will be verbally asked by Dr. Richards to at least 75% of the primary caregivers seen for a WCC visit tomorrow afternoon and documented in the patient records .
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Completed Tasks: The 7 “Questions to ask” on the Strengthening Families’ “Parental Resilience: Action Sheet” (http://www.cssp.org/reform/strengtheningfamilies/about/body/ProtectiveFactorsActionSheets.pdf ) were reviewed by Parents/Caregivers who attended our June 15th Advisory Group meeting (PFAG). They reached consensus for Dr. Richards to test asking questions #4-6 at the initial visit. A smart set of those questions has been added to the EHR by Dr. Green. On Tuesday afternoon, Dr. Richards will test asking those questions to primary caregivers of patients 0-3 yrs. old being seen by him for a WCC visit.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE At the end of the afternoon, Joyce (MA) will tally the total # of patients 0-3 seen by Dr. Richards and the # of those with documentation that the “resilience” related questions were asked. The aggregate de-identified results also will be shared via email with the members of our PFAG.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
Dr. Richards used the smart set questions as part of the appropriate WCC visits. He also took time to document the responses in the Notes section of the visit record. He felt it would be helpful information for future interactions with the family. He reported that the reaction from the parent of a 2-yrs. old was “why are you asking me these questions?” so he started prefacing his questions by saying that he is asking them to all parents/caregivers with a child 0-3 yrs. old.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED All 5 of the primary caregivers seen by Dr. Richards this afternoon were asked the resilience questions during the visit (except 1 grandmother who was not the primary caregiver) = 100%. Dr. Richards shared that the patients/families he saw this afternoon did not have any special needs so asking the questions did not blow his schedule out of the water but he expressed concern about taking the time when that is not the case. Can someone else ask those questions or should we consider sharing these questions with the family prior to the scheduled appointment and asking them to write down their answers?
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
Plan for next cycle: PFAG members would like to get informal feedback from the primary caregivers at the end of the
visit. For Cycle 2, Alice (N Manager) will ask those parents/caregivers (before check-out) for feedback about those
questions they were asked and what else they may want/need (e.g., would they like information or help developing a plan in advance for how they will keep themselves calm and centered in these stressful circumstances).
Act Plan
Study Do

MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/1/16 End Date: 7/25/16
Objective for this PDSA Cycle (Aim): By July 31, 2016, our practice will invite at least 1 community-based organization (CBO) or state agency on our referral/resource list, such as Early Intervention (EI) to attend our monthly physician and staff meeting to help us better connect our families with appropriate supports and services, based on their needs.
PLAN: QUESTIONS Who should we invite first? Will a rep from the organization/agency be
willing/able to attend our meeting? Can we allot a half hour of our agenda for this purpose? Will it be useful for everyone or just physicians?
PREDICTIONS We can schedule a rep to attend our next meeting but it may be difficult because it is summer and people are on vacation. This opportunity to meet with a CBO or state agency we currently refer patients to will be useful for both physicians and staff members.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Our core team decided that Mary Jo (Nurse Manager) will contact the EI program tomorrow and invite someone to attend our monthly meeting in our office and give a brief 15-20 minute presentation about services and eligibility and be prepared to take 10-15 minutes of questions from the group.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE An evaluation form will be completed by each participant at the end of the meeting: Was it helpful/useful? Why or why not? How can we improve it next time? What organization/agency should be invited to our next meeting?
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE
Act Plan
Study Do

MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/1/16 End Date: 7/25/16
Objective for this PDSA Cycle (Aim): By July 31, 2016, our practice will invite at least 1 community-based organization (CBO) or state agency on our referral/resource list, such as Early Intervention (EI) to attend our monthly physician and staff meeting to help us better connect our families with appropriate supports and services, based on their needs.
PLAN: QUESTIONS Who should we invite first? Will a rep from the organization/agency be
willing/able to attend our meeting? Can we allot a half hour of our agenda for this purpose? Will it be useful for everyone or just physicians?
PREDICTIONS We can schedule a rep to attend our next meeting but it may be difficult because it is summer and people are on vacation. This opportunity to meet with a CBO or state agency we currently refer patients to will be useful for both physicians and staff members.
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Our core team decided that Mary Jo (Nurse Manager) will contact the EI program tomorrow and invite someone to attend our monthly meeting in our office and give a brief 15-20 minute presentation about services and eligibility and be prepared to take 10-15 minutes of questions from the group.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE An evaluation form will be completed by each participant at the end of the meeting: Was it helpful/useful? Why or why not? How can we improve it next time? What organization/agency should be invited to our next meeting?
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
Two representatives from the EI program our staff meeting on July 25th. Good questions were asked. There was some confusion among the physicians about the referral process. A lengthy discussion followed about how communication and information sharing by EI with our practice needs to be improved. The program manager left her card and encouraged the physicians and staff to call her in the future with any questions or concerns related to these issues.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED All participants completed the evaluation form but it up took too much time. Overall, everyone thought the presentation and information shared was useful. The physicians especially liked the face-to-face interaction. Feedback included that next time 1 or more parents/caregivers who use or have used the services of the invited org/agency should be invited to attend that part of our meeting. Three physicians would like to learn more about the Family-to-Family Health Information Centers.
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
Plan for next cycle: There is no August meeting. Mary Jo will contact our state’s Family-to-Family Health Information
Center and invite them to attend our Sept. meeting. We will also identify 1 or more family(ies) who use the support and/or services that they offer and invite them to attend that portion of our meeting. Rather than collecting the evaluation/feedback on paper, we will test using Survey Monkey and send the URL via email to each meeting attendee after our next meeting.
Act Plan
Study Do
MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
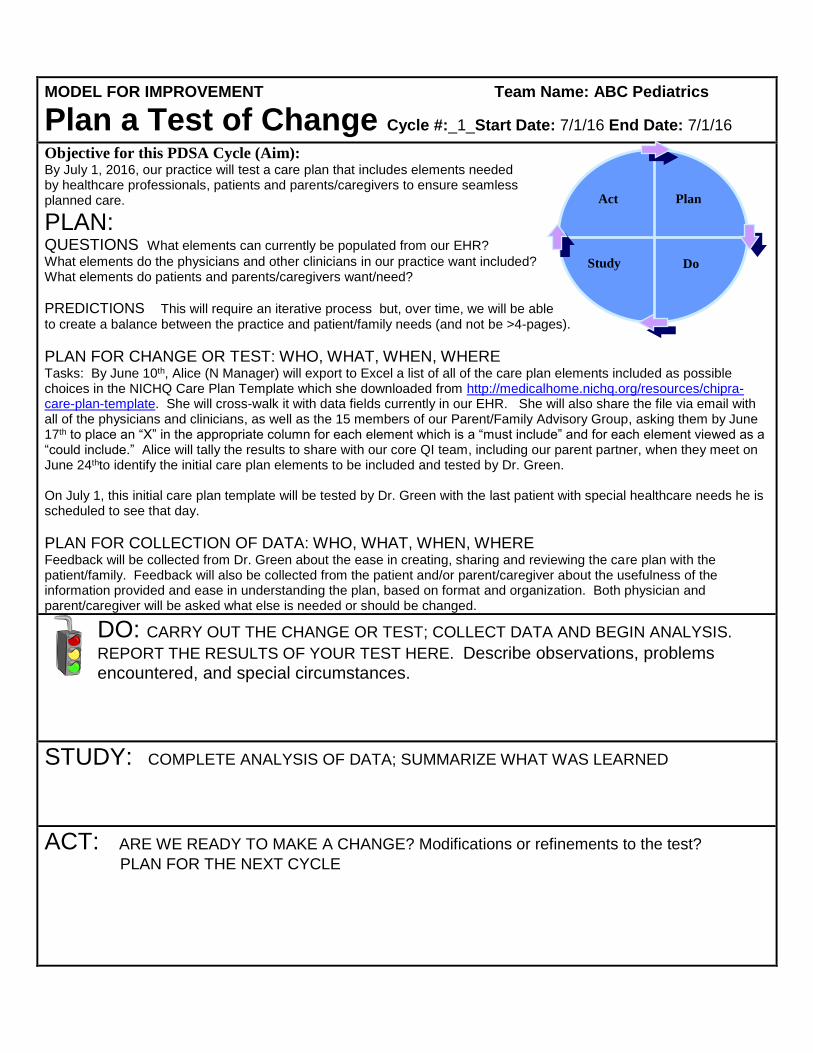
Plan a Test of Change Cycle #:_1_Start Date: 7/1/16 End Date: 7/1/16
Objective for this PDSA Cycle (Aim): By July 1, 2016, our practice will test a care plan that includes elements needed by healthcare professionals, patients and parents/caregivers to ensure seamless planned care.
PLAN: QUESTIONS What elements can currently be populated from our EHR?
What elements do the physicians and other clinicians in our practice want included? What elements do patients and parents/caregivers want/need?
PREDICTIONS This will require an iterative process but, over time, we will be able to create a balance between the practice and patient/family needs (and not be >4-pages).
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Tasks: By June 10th, Alice (N Manager) will export to Excel a list of all of the care plan elements included as possible choices in the NICHQ Care Plan Template which she downloaded from http://medicalhome.nichq.org/resources/chipra-care-plan-template. She will cross-walk it with data fields currently in our EHR. She will also share the file via email with all of the physicians and clinicians, as well as the 15 members of our Parent/Family Advisory Group, asking them by June 17th to place an “X” in the appropriate column for each element which is a “must include” and for each element viewed as a “could include.” Alice will tally the results to share with our core QI team, including our parent partner, when they meet on June 24thto identify the initial care plan elements to be included and tested by Dr. Green. On July 1, this initial care plan template will be tested by Dr. Green with the last patient with special healthcare needs he is scheduled to see that day.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE Feedback will be collected from Dr. Green about the ease in creating, sharing and reviewing the care plan with the patient/family. Feedback will also be collected from the patient and/or parent/caregiver about the usefulness of the information provided and ease in understanding the plan, based on format and organization. Both physician and parent/caregiver will be asked what else is needed or should be changed.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE
Act Plan
Study Do

MODEL FOR IMPROVEMENT Team Name: ABC Pediatrics
Plan a Test of Change Cycle #:_1_Start Date: 7/1/16 End Date: 7/1/16
Objective for this PDSA Cycle (Aim): By July 1, 2016, our practice will test a care plan that includes elements needed by healthcare professionals, patients and parents/caregivers to ensure seamless planned care.
PLAN: QUESTIONS What elements can currently be populated from our EHR?
What elements do the physicians and other clinicians in our practice want included? What elements do patients and parents/caregivers want/need?
PREDICTIONS This will require an iterative process but, over time, we will be able to create a balance between the practice and patient/family needs (and not be >4-pages).
PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Tasks: By June 10th, Alice (N Manager) will export to Excel a list of all of the care plan elements included as possible choices in the NICHQ Care Plan Template which she downloaded from http://medicalhome.nichq.org/resources/chipra-care-plan-template. She will cross-walk it with data fields currently in our EHR. She will also share the file via email with all of the physicians and clinicians, as well as the 15 members of our Parent/Family Advisory Group, asking them by June 17th to place an “X” in the appropriate column for each element which is a “must include” and for each element viewed as a “could include.” Alice will tally the results to share with our core QI team, including our parent partner, when they meet on June 24thto identify the initial care plan elements to be included and tested by Dr. Green. On July 1, this initial care plan template will be tested by Dr. Green with the last patient with special healthcare needs he is scheduled to see that day.
PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE Feedback will be collected from Dr. Green about the ease in creating, sharing and reviewing the care plan with the patient/family. Feedback will also be collected from the patient and/or parent/caregiver about the usefulness of the information provided and ease in understanding the plan, based on format and organization. Both physician and parent/caregiver will be asked what else is needed or should be changed.
DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS.
REPORT THE RESULTS OF YOUR TEST HERE. Describe observations, problems encountered, and special circumstances.
Tasks were completed as described in Plan. Dr. Green was able to create, print out, share and review the care plan with the last patient with special healthcare needs that he saw today. Many fields were populated with data from our EHR which was helpful but that did not include information recorded as a “Note.” It was “tested” with a 5 yrs. old child whose mom has been good advocate for her at her school. She reported that she likes the information about her child’s strengths and favorite activities but doesn’t like that it includes the fact that she has trouble paying for her daughter’s medications, since she shares this plan with the school nurse.
STUDY: COMPLETE ANALYSIS OF DATA; SUMMARIZE WHAT WAS LEARNED The feedback was shared with the QI team. Since the printed care plan was only 3 pages long, there is an opportunity to add some additional elements, preferably one or two “could include” that are already being collected in the EHR. The QI team is reconsidering including social risks which the physicians/clinicians wanted but not the parents/caregivers. Need to prioritize “must have” elements that currently require typing the information into the template, to see which could be created as data fields in the EHR that could then populate the care plan electronically.
ACT: ARE WE READY TO MAKE A CHANGE? Modifications or refinements to the test?
PLAN FOR THE NEXT CYCLE: Care plan template was tweaked, to remove social risks and add list of “primary”
school team members and community-based providers engaged with the child/youth (daycare, Early Intervention, Head Start, transportation providers, etc.), and contact information. Dr. Green will test the use, sharing and review of care plan with patients/families with CSHCNs seen tomorrow and will gather and give feedback to the QI team. Findings of these cycles will also be shared and discussed at the full staff meeting next week.
Act Plan
Study Do

ADHD Attention-Deficit Hyperactivity DisorderRead. Ask Questions. Think. Decide.
stuckere
Typewritten Text
©2011, Cincinnati Children's Hospital Medical Center. All Rights Reserved.
stuckere
Typewritten Text

2
USING THIS BOOKLET TO HELPIf a doctor is evaluating your child for ADHD,
this booklet is for you. It gives you the facts about
ADHD and your treatment choices if your child is
diagnosed with ADHD. It also describes the possible
results of those choices.
Learn all you can so you can make your choice.
Share this booklet with your doctor and loved ones.
Talk to people you trust. Many parents have
learned about ADHD and have been better able to help
their child. You can too.
ASKQUESTIONS
DECIDE
THINK
READ

3
WHAT IS ATTENTION-DEFICIT/HYPERACTIVITY DISORDER (ADHD)?
ADHD is a problem with paying attention and/or
being hyper and acting without thinking first. Most
children have trouble sitting still. Many kids don’t
finish their schoolwork. Few children sit through meals
without tapping, kicking, or drumming. For these
problems to be diagnosed as ADHD, they must be out
of the normal range for the child’s age and development.
So how do you know what is normal and what is ADHD?
Only a doctor can tell you for sure. ADHD behavior doesn’t
happen in only one place, like at school. It may happen
every day in the classroom, on the playground, and at
home. ADHD can lead to problems with learning,
friendships, and family life. Parents of children with ADHD
are often worn out and frustrated.

4
WHAT DOES ADHD LOOK LIKE?It is normal for all children to have problems paying attention, being
hyper or acting without thinking sometimes. But for children with ADHD,
these behaviors are more severe and occur more often. To be diagnosed
with ADHD, a child must have more symptoms than other children their
age for 6 or more months.
Children who have problems paying attention may:· Be distractible, miss details, and forget things
· Often switch from one activity to the next
· Have a hard time focusing on one thing
· Become bored with a task after only a few minutes,
unless they are doing something enjoyable
· Have a hard time planning and completing a task or
learning something new
· Have trouble completing or turning in homework
· Often lose things (e.g., pencils, toys, homework) needed
to complete tasks or activities
· Not seem to listen when spoken to
· Daydream, become easily confused, and move slowly
· Have a hard time thinking as quickly and precisely as others
· Struggle to follow instructions
Children who are hyper may:· Fidget and squirm in their seats
· Talk nonstop
· Dash around, touching or playing with everything in sight
· Have trouble sitting still during dinner, school, and story time
· Be constantly moving
· Have a hard time doing quiet tasks or activities
Children who act without thinking first may:· Be very impatient
· Blurt out inappropriate comments
· Show their emotions without restraint
· Act without regard for consequences
· Have difficulty waiting for things they want or waiting
their turns in games
· Often interrupt when other people are talking or
doing something else
5
HOW IS ADHD DIAGNOSED? Deciding if a child has ADHD is based on how they act. ADHD behavior
must be seen at home and at school. Children should be assessed if a
parent or teacher thinks the child has a problem. Assessment may include:
· Parent and teacher questionnaires (Vanderbilt, Conners)
· Psychological testing of the child AND family
(e.g., IQ testing and psychological testing)
· Doctors may ask about the child’s growth
and development
ARE THERE DIFFERENT TYPES OF ADHD?There are three different types of ADHD. Your child’s doctor will decide
which diagnosis fits your child’s symptoms.
· ADHD-Inattentive Type: Children who have trouble paying
attention, but are not very hyper and don’t have problems
acting without thinking first. This type of ADHD used to be
called ADD.
· ADHD-Hyperactive/Impulsive Type: Children who are very
hyper and have problems acting without thinking first, but
have few problems paying attention.
· ADHD-Combined Type: Children who have problems paying
attention, being hyper, and acting without thinking first.
DO CHILDREN ‘OUTGROW’ ADHD?Many people think of ADHD as a childhood problem. However, ADHD
can continue through the teen years and into adulthood. Symptoms
of ADHD do change over time.
Hyperactivity is often seen in very young children. The hyperactive
symptoms often decrease over time with or without treatment.
Children’s tendency to act without thinking because of ADHD gets
better over time. This problem is often replaced by a tendency to talk
without thinking.
Trouble paying attention may not get noticed until demands at school
increase. These problems often continue in the teen and adult years.
Using routines, study skills, and coping strategies can help people with
these problems.

6
HOW DO YOU KNOW FOR SURE IF ADHD IS THE PROBLEM?There are no tests for ADHD. Your child’s doctor may make a
diagnosis. Or sometimes the doctor may refer you to an expert
to assist with diagnosis.
Doctors need information from home and school to make the
diagnosis. They ask parents and children questions and examine
the children to make sure there aren’t other problems.
Doctors often ask parents and teachers to report the behaviors
that they have seen. Some doctors use the “Vanderbilt” form,
while other doctors use the “Conners” form. These forms are very
similar. The information that parents and teachers report on these
forms is very helpful. All children have trouble paying attention
sometimes. All children are hyper or act without thinking sometimes.
But when school-age children behave this way often or always, it
can cause problems at home and at school.
Doctors like to have parents and teachers fill out these forms
at least once a year. This can help determine if a child’s problems
are getting better or worse.

7
DO OTHER PROBLEMS OCCUR ALONG WITH ADHD?Some children will have more than just ADHD.
· Learning Disabilities: Many children with ADHD – up to 30 percent –
also have a specific learning disability. This can cause problems with reading,
writing, spelling, or math.
· Oppositional Defiant Disorder (ODD): As many as 33 percent of
children with ADHD will have this. These children are defiant and stubborn.
They have temper outbursts or become loud-mouthed. They argue with
adults and refuse to obey.
· Conduct Disorder: As many as 33 percent of children who have both
ADHD and ODD will develop conduct disorder. This is a more severe
pattern of antisocial actions. These children frequently lie or steal. They
fight or bully others. They are at risk of getting into trouble at school
or with the police. They are aggressive toward people and/or animals.
They destroy property. They break into people’s homes. They carry
or use weapons. As teens, they are at greater risk of substance abuse.
They need immediate help.
· Anxiety and Depression: About 25 percent of children with ADHD
also are anxious or depressed. These problems can be treated. Treating
ADHD may help these problems get better. Likewise, treating anxiety
or depression may help ADHD get better.
· Tic Disorders: Children may have eye blinks or facial twitches. They may
clear their throats frequently, snort, sniff, or bark out words. They cannot
control these behaviors. The most severe form of tics is Tourette’s disorder.
Very few children have this disorder.
The evaluation process helps find out whether something besides ADHD is
the problem. ADHD is very common and has the most established treatments.
If your child does not respond well to treatment, other evaluations may
be needed. Even if your child responds well to treatment, other problems may
develop over time.

8
SOME THINGS TO CONSIDER WHEN
DECIDING ON TREATMENTS:
· Every child is different. You know your child
better than anyone else. As a parent, trust your
thoughts and feelings.
· Balance possible benefits with side effects,
cost, and time.
· Discuss treatment options with your child’s doctor.
Gather as much information as you need to make a
decision that is right for you and your child.
· Track and monitor your child’s progress. Realize
that your decisions may change over time as your
child’s needs change.

9
WHAT ARE ADHD TREATMENT OPTIONS?Every effort should be made to manage symptoms and direct the
child to helpful paths. There are four treatment options to consider.
· Watchful Waiting
· Behavioral Treatment
· Medicine
· Combined Treatment (BOTH Behavioral Treatment AND
Medicine)
WHAT DOES THE BEST RESEARCH SAY TO DO?It is still not clear. Here’s why:
A study called “The Multimodal Treatment Study of Children with
ADHD” (MTA) showed that behavioral treatment, medicine, and
combined treatment all help some children with ADHD. The results
of this study will be shared with you throughout this booklet. Still,
it is impossible to predict how your child will respond because every
child is unique. The only way to find out if a treatment will
help your child for sure is by trying it.

10
WATCHFUL WAITING
Watchful waiting means that you do not start active treatment yet.
You and your child’s doctor watch your child to see how he or she
performs at home and school. If you become worried by your child’s
struggles, you can always start active treatment.
PROS & CONS How can this treatment help my child?
· You do not have to deal with the possible side effects from medicine.
· You can always change your mind and begin active treatment.
· It is low in cost (i.e. time, money).
What are possible problems with this treatment? · Your child’s struggles at home and school will likely continue or get worse.
HERE IS AN EXAMPLE OF HOW CHOICES ABOUT TREATMENT CAN CHANGE OVER TIME:Jane’s parents first met with the doctor to discuss treatment options.
Jane’s father did not think they needed to take action to help manage her
problems paying attention. He closely watched Jane’s behavior at home
and at school over the next month. Seeing that her struggles were continuing,
he decided to return to Jane’s doctor’s office to discuss treatment options.

11
Behavioral treatment is an active treatment where parents and teachers learn methods to
help children with ADHD.
TYPES OF ADHD BEHAVIORAL TREATMENTChildren with ADHD have different needs than other children. As a result,
different methods are needed to help them do their best. Parents and teachers
can learn methods to help children with ADHD.
Three types of methods have been proven to improve performance at school and at home:
· Methods for parents to use at home
· Methods for teachers and parents to use to improve classroom performance
· Methods to improve peer relations in classroom and play settings
It is possible to learn about these methods by: · Taking a class with a group of parents led by a counselor
· Working one-on-one with a clinical counselor
· Working with your child’s teacher and/or school counselor
· Reading about these approaches on your own
Learning these methods takes time and costs money. Therefore, it is important
to focus on the methods that are proven to work for children with ADHD. Proven
methods are described on the next few pages.
BEHAVIORAL TREATMENT
12
METHODS FOR PARENTS TO USE AT HOME How does this help? Parents learn how to manage their child’s problems caused by ADHD.
For example, parents can learn to give better commands, set small
goals, and use time-outs, reward systems, and point systems. This shows
parents how to help their child with ADHD to behave better. Because
the focus is on the child’s behavior, these methods are also called
“behavior therapy” or “behavior modification.” Unlike other therapies
you may have heard about, this does not mean talking with the child
about how they feel. Rather, counselors help parents learn practical
ways to help their child behave better.
What is usually involved? In studies where this helped, parents learned these methods in groups
with other parents. The groups met between 8 and 16 times. In addition
to learning new skills, parents often get support from being in a group
with other parents of children with ADHD.
What is available nearby? “Understanding and Managing ADHD: A Group Program for Parents
of Children Aged 6-12.” Cincinnati Children’s Hospital offers parent groups
at several places. The groups have 8 weekly sessions. Parents learn about
ADHD, how to manage child behavior, and how to work with teachers and
doctors to help their child. For more information, call (513) 636-4336 and
press the pound key (#) option or visit: http://www.cincinnatichildrens.org/
svc/alpha/b/behavioral-psych/clinical/group/default.htm
Also, your child’s doctor may be able to refer you to a local psychologist.
They are trained to help you learn ways to manage your child’s behavior.

13
What can I read to learn more about this on my own?· Taking Charge of ADHD: The Complete, Authoritative Guide for Parents
By Russell Barkley PhD
This is a book for parents of elementary-aged children with ADHD.
· ADHD in the Young Child
By Cathy Reimers, PhD, and Bruce A. Brunger
This is an excellent book for parents of children 5 and under.
· Teenagers with ADD and ADHD: A Guide for Parents and Professionals
By Chris A. Zeigler Dendy, MS
This is a book for parents of teenagers with ADHD.
What other things can I do now?Here are a few other resources that may be helpful:
· The website for Children and Adults with Attention-Deficit/
Hyperactivity Disorder (CHADD) offers advice and support for parents.
– www.chadd.org
· The series “Supernanny” has three shows that deal with children who
have ADHD. Families in these shows learn methods that help them
manage their child better. Watching these shows or reading the episode
guides (links shown) may provide helpful thoughts on how to work with
your ADHD child.
– Season 3, Episode 12: The Goins Family, originally aired 2/2/2007
http://www.Supernanny.com/tv-show/episodes/the-goins-family.aspx
– Season 4, Episode 9: The Prescott Family, originally aired 3/5/2008
http://www.Supernanny.com/tv-show/episodes/the-Prescott-family.aspx
– Season 6, Episode 6: The Beck Family, originally aired 12/11/2009
http://www.Supernanny.com/tv-show/episodes/the-beck-family.aspx
· The “Supernanny” website also provides advice on ADHD.
– http://www.supernanny.com/Advice/-/Your-child/-/Child-care/
Helping-your-ADHD-child-to-behave-.aspx

14
METHODS FOR TEACHERS AND PARENTS TO USE TO IMPROVE CLASSROOM PERFORMANCE How does this help?Teachers can use many of the same methods as parents to help children
behave in class (e.g. set small goals, use time-outs, reward systems, and point
systems). Daily Report Cards are often used to change behavior in class.
They provide a way for teachers and parents to better communicate about
progress toward goals. Classroom aides or tutors help children with
organization and study skills.
What is usually involved?In studies where this helped, teachers and classroom aides and tutors received
formal training on methods that are helpful for children with ADHD. This
was important because many teachers receive no formal education about ADHD
during their training. There are key differences in the types of methods that
work best for children with ADHD compared to those without ADHD.
What is available nearby?There are no programs nearby that will go to your child’s school and
work with your child’s teacher. The parent groups (described before) offered
by Cincinnati Children’s Hospital do include advice about how to work
better with your child’s teacher. This includes how to use a daily report card,
how to tailor classroom methods for children with ADHD, and how to
request aid for your child. For more information, call (513) 636-4336 and
press the pound key (#) or visit: http://www.cincinnatichildrens.org/
svc/alpha/b/behavioral-psych/clinical/group/default.htm

15
What can I read to learn more about this on my own?· Taking Charge of ADHD: The Complete, Authoritative Guide for Parents
By Russell Barkley PhD
· ADHD in the Young Child
By Cathy Reimers, PhD, and Bruce A. Brunger
· The ADD/ADHD Checklist: An Easy Reference for Parents and Teachers.
By Sandra Reif
· Teaching Teens with ADD and ADHD
By Chris A. Zeigler Dendy, MS
This is a resource for parents and teachers of students with ADHD
in the middle and high school years.
What other things can I do now?Here are a few other resources that may be helpful:
· The Center for Children & Families at the University of Buffalo
offers many online resources to parents and teachers of
children with ADHD.
– http://ccf.buffalo.edu/default.php
– Some that are of particular interest are:
· Creating a Daily Report Card for the Home
http://ccf.buffalo.edu/pdf/Home_Daily_Report_Card.pdf
· How to Establish a Daily Report Card (Home-School Note)
http://ccf.buffalo.edu/pdf/school_daily_report_card.pdf
· The website “Parents Helping Parents” offers a sample letter
to request further educational testing be done at school.
– http://www.php.com/specialed/story2

16
METHODS TO IMPROVE PEER RELATIONS IN CLASSROOM AND PLAY SETTINGS How does this help?Children learn how to more effectively interact with and relate to their peers
(e.g. social skills training). This helps children make and improve friendships
with their peers in classroom and play settings. Teachers and counselors use goal
setting, reward systems, point systems, and daily report cards. Children practice
social skills in the classroom, in team sports, and in other activities. The staff
works with parents to develop daily goals for each child. If the child achieves his
or her goal, the parent provides rewards at home.
What is usually involved?In studies where this helped, children typically attended a Summer Treatment
Program that lasted all day for 5 to 8 weeks. It is important to know that
social skills programs that meet once or twice a week at a clinic are not as helpful
as the summer programs that work with children in real world settings.
What is available nearby?There are no programs nearby that work with children in classroom and
play settings. The most well known summer treatment program is located in
Buffalo, New York (http://ccf.buffalo.edu/STP.php).
The two closest programs to Cincinnati are:
· Cleveland: www.clevelandclinic.org/STP.
· Chicago: www.jcys.org/campstar/
What can I read to learn more about this on my own?· Why Don’t They Like Me? Helping Your Child Make and Keep Friends
By Susan M. Sheridan, PhD
This is great book for parents of children with peer difficulties. The
methods Dr. Sheridan describes are similar to those taught in Summer
Treatment Programs for children with ADHD.

17
PROS & CONSHow can this treatment help my child?
· Behavioral treatment alone will help about one-third of children with ADHD. These
children will pay attention and control their impulses as well as the average child
their age that does not have ADHD. They also will be less hyper. Other children may
find behavioral treatment helpful without the same high level of success.
· You do not have to deal with the possible side effects from medicine.
· You can always change your mind and try medicine also.
Here is our best guess of what will happen to 100 children with ADHD if they
get behavioral treatment alone (with all 3 types described before) for 14 months.
What are possible problems with this treatment?
· Behavioral treatments take time for parents, teachers, and children to do.
· Formal programs may be limited nearby. There may be a wait list to access
the programs that are available.
· Behavioral treatments cost money (to you and/or your insurance plan).
IF YOU CHOOSE BEHAVIORAL TREATMENT:· Continuing behavioral treatment: The first step is learning methods to help
your child manage his or her behavior. Next, you need to use these methods
regularly. These methods will become part of your parenting skills. You may
need to refresh these skills through reading and/or meeting with professionals.
· Behavioral treatment changes: Certain methods may work for a while and
then stop working. You may need to learn different methods. It is very important
for you and your child’s teacher to keep a close eye on how things are going.
Contact your child’s doctor if any problems come up.
HERE IS AN EXAMPLE OF HOW CHOICES ABOUT TREATMENT CAN CHANGE OVER TIME:Erik’s mom used a reward system at home over the summer to help him complete tasks.
She noticed that he struggled with task completion when he started back to school. She
met with his teacher and they developed a daily behavioral report card.
34
66
Number who have self-control and focus as well as the average child their age who doesn’t have ADHD
Number who don’t improve to that level

18

19
Medication treatment is an active treatment that uses drug therapy to control ADHD
symptoms.
HOW DOES MEDICINE FOR ADHD WORK?These pictures show what the brain looks like when a child pays attention.
The yellow box shows the parts of the brain that are needed for attention.
Medicine for ADHD works by helping the brain send messages to these parts of the brain.
This helps children pay attention.
WHAT HAPPENS IF WE TRY MEDICINE?Unlike other medicines, the right amount of ADHD medicine is not based only on your
child’s weight. Instead, you must work with your child’s doctor to try a range of doses
(lower, medium, higher) and see how your child responds. You and your child’s teacher
will need to watch your child closely and complete evaluation forms. You will also need
to stay in close contact with the doctor’s office through follow-up calls and visits.
Here is our best guess of what will happen to 100 children with ADHD who try
3 different amounts of methylphenidate-based medicine.
77 CHILDREN FIND A DOSAGE THAT HELPS
MEDICATION
22 Children do best on the lower dosage
25 Children do best on the medium dosage
30 Children do best on the higher dosage
23 Children do NOT improve About half of these children will improve when they try an amphetamine-based medicine (e.g. Adderall, etc.)
77 CHILDREN FIND A DOSAGE
THAT HELPS
CHILDREN WITH ADHDNO MEDICATION
CHILDREN WITH ADHDWITH MEDICATIONWith medicine, children with ADHD have more activity in the parts of the brain that help them focus.
CHILDREN WITHOUT ADHDChildren without ADHD have more activity in the parts of the brain that help them focus.

20
TYPES OF ADHD MEDICATIONThere are two types of medicines that can be used. They are called stimulants and non-
stimulants.
Stimulant medicines are often tried first. In studies, more children benefit from stimulant
medicines than non-stimulant medicines. On average, stimulants reduce ADHD symptoms
better than non-stimulant medicines.
Among the different stimulant medicines available, some children do better on a
methylphenidate-based medicine. Others do better on an amphetamine-based medicine.
Some children do equally well on both. Others don’t respond to either.
Bottom-line: Each child is unique. At present, there is no way to predict which medicine
will work best for your child. Your child’s doctor can tell you about the differences
between medications. He or she can help you pick a medicine to try first, and work with
you to find a dose that is best for your child.
PROS & CONSHow can this treatment help my child?
· Medicine alone will help about half of children with ADHD. These children will pay
attention and control their impulses as well as the average child their age that does
not have ADHD. They also will be less hyper. Other children may find medicine
helpful without the same high level of success.· You can always change your mind
and try behavior therapy also.
Here is our best guess of what will happen to 100 children with ADHD if they get
medication treatment alone for 14 months.
What are possible problems with this treatment?
· Medicine must be taken, or it will not work.
· Medicine costs money (to you and/or your insurance plan).
· Your child may have side effects. These are usually minor. Side effects will
often decrease as a child gets used to the medicine. Other side effects
can persist. Taking less medicine often relieves these. Sometimes switching
to a different medicine is needed.
56
44
Number who have self-control and focus as well as the average child their age who doesn’t have ADHD
Number who don’t improve to that level

21
SIDE EFFECTS OF STIMULANT MEDICINESMost common side effects:
· Decreased appetite (this is usually worst at lunchtime)
· Trouble falling asleep
· Stomach aches
· Headaches
· Increased crabbiness
· Social withdrawal (i.e. they look like a ‘zombie,’ they are not interested
in normal activities): This is a sign that the child is taking too much medicine.
The amount needs to be lowered.
· Increased anxiety and/or crying over little things
· Rebound: Some children are more active or get in a bad mood when
the medicine is wearing off
Less common side effects: Tics (i.e. muscle twitches, movements, or unusual vocal sounds that a child can’t
control). Medicine does not cause tics, but may make them more likely to happen.
In general, tics are more likely in children with ADHD. In children who have tics
and start medicine for ADHD, tics may get better, worse, or stay about the same.
Rare side effects: · Increased heart rate and/or blood pressure
· Growth suppression/delay: On average, children with ADHD who take
medicine grow less than those children with ADHD who do not take medicine.
In the MTA study, some children took medicine for ADHD regularly for 3
years. Other children did not take medicine for 3 years. The children who took
medicine were 0.8 inches shorter. They were also about 0.9 pounds lighter.
This problem is more likely if the medicine makes your child feel less hungry.
Height and weight are checked at every doctor’s visit. We still do not know
if there is catch-up growth during adolescence.
· Hallucinations (i.e., seeing or hearing something that is not real): This
happens in about 3 out of 100 children who take medicine for a year. When
the medicine is stopped the hallucination goes away. Some children can
re-start a lower amount of medicine without a problem. Some children need
to try a different medicine.

22
36 Children have no side effects
50 Children have mild side effects: usually do not trouble the child or their parents enough to stop or change the medicine or dosage
11 Children have moderate side effects: troubling enough to adjust treatment
3 Children have severe side effects: troubling enough to adjust treatment
Children with pre-existing heart problems: Children who have heart problems may need to see a heart doctor before trying
medicine for ADHD. At present, there is no proof to suggest that taking medicine for
ADHD raises the risk of sudden death among children with a normal heart.
· Does your child have a history of heart disease, palpitations (feeling his
or her heart flutter), passing out, or seizures?
· Does anyone in your family have a history of sudden, unexplained death
in children or young adults? Hypertrophic cardiomyopathy? Heart rhythm
abnormality (e.g. Long QT syndrome)?
· If so, be sure to mention these things to your child’s doctor.
Here is our best guess of what will happen to 100 children with ADHD who take
medicine for 14 months:
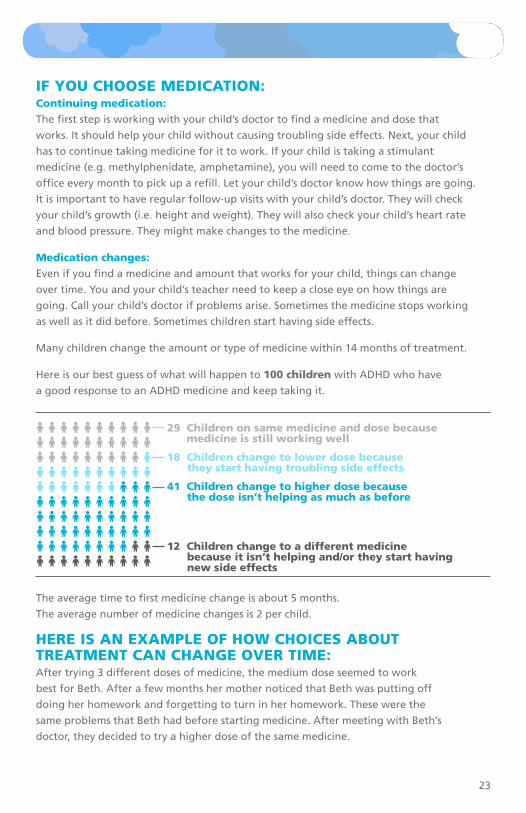
23
IF YOU CHOOSE MEDICATION:Continuing medication: The first step is working with your child’s doctor to find a medicine and dose that
works. It should help your child without causing troubling side effects. Next, your child
has to continue taking medicine for it to work. If your child is taking a stimulant
medicine (e.g. methylphenidate, amphetamine), you will need to come to the doctor’s
office every month to pick up a refill. Let your child’s doctor know how things are going.
It is important to have regular follow-up visits with your child’s doctor. They will check
your child’s growth (i.e. height and weight). They will also check your child’s heart rate
and blood pressure. They might make changes to the medicine.
Medication changes: Even if you find a medicine and amount that works for your child, things can change
over time. You and your child’s teacher need to keep a close eye on how things are
going. Call your child’s doctor if problems arise. Sometimes the medicine stops working
as well as it did before. Sometimes children start having side effects.
Many children change the amount or type of medicine within 14 months of treatment.
Here is our best guess of what will happen to 100 children with ADHD who have
a good response to an ADHD medicine and keep taking it.
The average time to first medicine change is about 5 months.
The average number of medicine changes is 2 per child.
HERE IS AN EXAMPLE OF HOW CHOICES ABOUT TREATMENT CAN CHANGE OVER TIME: After trying 3 different doses of medicine, the medium dose seemed to work
best for Beth. After a few months her mother noticed that Beth was putting off
doing her homework and forgetting to turn in her homework. These were the
same problems that Beth had before starting medicine. After meeting with Beth’s
doctor, they decided to try a higher dose of the same medicine.
29 Children on same medicine and dose because medicine is still working well
18 Children change to lower dose because they start having troubling side effects
41 Children change to higher dose because the dose isn’t helping as much as before
12 Children change to a different medicine because it isn’t helping and/or they start having new side effects

24

25
Combined treatment means the child gets both behavioral and medication treatments.
See prior sections which describe behavioral treatment and medicine.
PROS & CONS How can this treatment help my child?
· Combined treatment will help about two-thirds of children with ADHD. These
children will pay attention and control their impulses as well as the average child
their age that does not have ADHD. They also will be less hyper. Other children may
find combined treatment helpful without the same high level of success.
· Compared to children who only take medicine, children who get combined
treatment need 19% less medicine to improve the same amount. As a result,
side effects may be less severe on lower amounts of medicine.
Here is our best guess of what will happen to 100 children with ADHD if they get both
behavioral and medication treatments for 14 months.
What are possible problems with this treatment?· Behavioral treatments take time.
· Behavioral treatments and medicine cost money
(to you and/or your insurance plan).
· Your child may have side effects from medicine.
HERE IS AN EXAMPLE OF HOW CHOICES ABOUT TREATMENT CAN CHANGE OVER TIME:David was taking medicine for ADHD, but still had problems behaving at
home. David’s parents decided to try combined treatment. The doctor gave
them the phone number to a parenting class that was offered in their
town. The next month, David continued taking his medicine and his parents
went to their first parenting class.
COMBINED TREATMENT
68
32
Number who have self-control and focus as well as the average child their age who doesn’t have ADHD
Number who don’t improve to that level

26
Number who have self-control and focus as well as the average child their age who doesn’t have ADHD
Number who don’t improve to that level
COMPARING TREATMENT CHOICESHere is our best guess of what will happen to 100 children with ADHD
if they get the following treatments for 14 months.
BEHAVIOR THERAPY
34child their age who doesn’t have ADHD
66

27
BEHAVIOR THERAPY MEDICATION COMBINED TREATMENT
68
32
56
44

28
SOME CONSIDERATIONS REGARDING YOUR DECISION
Ongoing monitoring
· No matter what treatment you try, it is important
to keep a close eye on your child’s progress.
· You and your child’s teacher can fill out rating forms
(e.g. Vanderbilt, Conners, etc.) to see if symptoms are
getting better.
· Think about the goals that you, your child,
and your child’s teacher and doctor set.
· Meet with your child’s teacher and doctor to see
if your goals have been achieved.
· If a treatment goal is not achieved by a set
date, the treatment plan may need to be adjusted.
This may include adjusting a current treatment
(e.g. behavioral approach or medicine) or adding
a new approach that you haven’t tried yet (e.g.
behavioral approaches or medicine).

29
HERE ARE EXAMPLES OF HOW CHOICES ABOUT TREATMENT CAN CHANGE OVER TIME:Example 1: Johnny’s behavior improved after his mom started using
a reward system at home. He still had a very hard time paying attention
at school. As a result, she decided to give medicine a try.
Example 2: Vicky’s parents were pleased with the progress that she made
at school since starting medicine. They were still concerned about her
defiant behavior at home. As a result, they decided to attend a class designed
to help parents manage their child’s behavior.
Example 3: Albert was started on ADHD medicine when he was 7 years
of age. Albert also learned study skills that helped him. Each year, Albert and
his parents would meet with his doctor. They would plan a trial without
medicine to see if he still benefited from it. In the first year, Albert’s teacher
and parents knew that medicine was still needed to help Albert achieve
his goals. In later years, the trials off medicine lasted longer. Yet, Albert and
his parents still found that medicine was helpful for him. During a trial off
medicine when he was 15, using his study skills alone he was able to keep his
good grades. He remained off medicine. Since then, his parents and teachers have
continued to set goals and watch his progress closely.

30
FREQUENTLY ASKED QUESTIONS (1) Will my child outgrow ADHD?Many people think of ADHD as a childhood problem. However, ADHD can continue
through the teen years and into adulthood. Symptoms of ADHD do change over time.
(2) How do you know for sure if ADHD is the problem?There are no tests for ADHD. Your child’s doctor may make a diagnosis. Sometimes
the doctor may refer you to an expert to assist with diagnosis.
(3) What causes ADHD?No one knows for sure. ADHD probably comes from a combination of things.
Some possibilities are:
· Genes, because ADHD sometimes runs in families
· Lead in old paint and plumbing parts
· Smoking and drinking alcohol while pregnant
· Certain brain injuries
Food additives like artificial colors might make children more hyper, but they do not
cause ADHD.
Although the cause of ADHD is not certain, family stress, such as divorce,
does not cause ADHD.
(4) Who can develop ADHD?Children of all backgrounds can have ADHD. Teens and adults can have ADHD too.
(5) Will medication change my child’s personality? While your child may stop and think before talking or acting, his or her personality
should not change. If your child loses interest in the things he or she enjoys, he or she
may be on a dose that is too high.
(6) Will my child become addicted to the medication? Children do not crave the medicine when it is not given. Some children do notice
that it is harder to focus on days that they don’t take their medicine.
(7) Are there other resources to help me make the best choice for my child?See the Resources listed on the next page.
(8) Are there behavioral options nearby?Cincinnati Children’s Hospital Medical Center offers parent groups at several places.
The groups have 8 weekly meetings. Parents learn about ADHD, how to manage child
behavior, and how to work with teachers and doctors to help their child.
For more information, call (513) 636-4336 and press the pound key (#) option
or visit http://www.cincinnatichildrens.org/svc/alpha/b/behavioral-psych/
clinical/group/default.htm
31
RESOURCESThis list provides support groups and other resources for ADHD.
Check with your child’s doctor for other resources near you.
Organizations· Cincinnati Children’s Hospital Center for ADHD
513.636.4336 · www.cincinnatichildrens.org/svc/alpha/a/adhd/
· Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD)800.233.4050 · www.chadd.org
· National Resource Center for ADHD: A program of CHADDwww.help4adhd.org
· National Attention Deficit Disorder Association 856.439.9099 · www.add.org
· National Dissemination Center for Children with Disabilities 800.695.0285 · www.nichcy.org
· National Institute of Mental Health866.615.6464 · www.nimh.nih.gov
· The Center for Children & Families at the University of Buffalohttp://ccf.buffalo.edu/default.php
· Parents Helping Parentswww.php.com
Books· Taking Charge of ADHD: The Complete, Authoritative Guide for Parents
By: Russell Barkley, Ph.D.
· ADHD in the Young ChildBy: Cathy Reimers, Ph.D. & Bruce A. Brunger
· Teenagers with ADD and ADHD: A Guide for Parents and ProfessionalsBy: Chris A. Zeigler Dendy, MS
· The ADD/ADHD Checklist: An Easy Reference for Parents and TeachersBy: Sandra Reif
· Teaching Teens with ADD & ADHDBy: Chris A. Zeigler Dendy, MS
· Why Don’t They Like Me? Helping Your Child Make and Keep Friends
By: Susan M. Sheridan, Ph.D.
Technical Documentation· For complete list of citations to scientific evidence referenced in this booklet, please email [email protected]

ADHD Attention-Deficit Hyperactivity DisorderRead. Ask Questions. Think. Decide.
Updated: 04/20/2011

These cards will help you and your child set goals for treatment. It provides an overview of treatment options available to you.
The booklet lists more information on treatment options. The booklet also lists resources available to you. The booklet will help you to determine if your child reaches the goals you set in these cards.
Share these cards with your child’s doctor. Talk with the doctor about your goals and work together to make a treatment plan.
Even if you choose to let the doctor decide what treatment(s) to give your child for ADHD, you need to be well informed and monitor progress toward your goals.
If a doctor is evaluating your child for ADHD, these cards are for you.
ADHD Attention-Deficit Hyperactivity DisorderRead. Ask Questions. Think. Decide.
Updated: 04/19/2011
stuckere
Typewritten Text
©2011, Cincinnati Children's Hospital Medical Center. All Rights Reserved.

· Your child’s struggles at home and school will likely continue or get worse.
DOWNSIDES
You do not have to deal with the possible side effects from medicine. You can always change your mind and begin active treatment.
It is low in cost (i.e. time, money).
BENEFIT
Watchful waiting means that you do not start active treatment yet.
INTRODUCTION
You and your child’s doctor watch your child to see how he or she performs at home and school.
If you become worried by your child’s struggles, you can start active treatment at any time.
1. WATCHFUL WAITING
Updated: 04/19/2011
stuckere
Typewritten Text
©2011, Cincinnati Children's Hospital Medical Center. All Rights Reserved.

Behavioral treatment is an active treatment where parents and teachers can learn methods to help children with ADHD. Three types of methods have been proven to improve performance at school and at home:
Methods for parents to use at homeIn studies where this helped, parents met in groups with other parents. Parents learn how to manage their child’s problems caused by ADHD. They learn how to give better commands, set small goals, and use time-outs, reward systems, and point systems. The groups meet between 8 and 16 times. Parents often get support from being in a group with other parents of children with ADHD.
Methods for teachers and parents to use to improve classroom performanceTeachers can use many of the same methods as parents to help children behave in class (e.g. setting small goals, using time-outs, reward systems, and point systems). In studies where this helped, teachers, classroom aides, and
tutors received formal training on methods that are helpful for children with ADHD. This was important because many teachers receive no formal education about ADHD during their training. There are key differences in the types of methods that work best for children with ADHD compared to those without ADHD.
Methods to improve peer relations in classroom and play settingsChildren learn how to more effectively interact with and relate to their peers (e.g. social skills training). This helps children make and improve friendships with their peers in classroom and play settings. In studies where this helped, children attended a Summer Treatment Program that lasted all day for 5 to 8 weeks. It is important to know that social skills programs that meet once or twice a week at a clinic or hospital are not as helpful as the summer programs that work with children in real world settings.
INTRODUCTION
· Behavioral treatments take time for parents, teachers, and children to do. · Formal programs may be limited nearby. There may be a wait list to access the
programs that are available.
· Behavioral treatments cost money (to you and/or your insurance plan).
DOWNSIDES
34
66
Here is our best guess of what will happen to 100 children with ADHD if they get behavioral treatment alone for 14 months.
BENEFIT
2.BEHAVIORAL TREATMENT
Number who have self-control and focus as well as the average child their age who doesn’t have ADHD
Number who don’t improve to that level
Updated: 04/19/2011
stuckere
Typewritten Text
©2011, Cincinnati Children's Hospital Medical Center. All Rights Reserved.

· Medicine costs money. · Your child may have side effects. These are usually minor and decrease as a child gets used to the medicine. Side effects of stimulant medicines include:
· Most common: Decreased appetite, trouble falling asleep, stomach aches, headaches, increased crabbiness, social withdrawal, anxiety and/or
crying. Some children are more active or get in a bad mood when the medicine is wearing off.
· Less common: Tics (i.e. muscle twitches, movements, or unusual vocal sounds that a child can’t control).
· Rare: Increased heart rate and/or blood pressure, growth delay, hallucinations.
Talk with your doctor to discuss these side effects in more detail.
DOWNSIDES
Medication treatment is an active treatment that uses drug therapy to control ADHD symptoms.
Parts of the brain help children pay attention. Medicine for ADHD works by helping the brain send messages to these parts of the brain. This helps children to pay attention.
There are two types of medicines that can be used. One type is called stimulants and the second is called non-stimulants. Stimulant medicines are often tried first. In studies, more children benefit from
stimulant medicines than non-stimulant medicines.
Unlike other medicines, the right amount of ADHD medicine is not based only on your child’s weight. Instead, you must work with your child’s doctor to try a range of doses (lower, medium, higher) and see how your child responds. You and your child’s teacher will need to watch your child closely and complete evaluation forms. You will also need to stay in close contact with the doctor’s office through follow-up calls and visits.
INTRODUCTION
Here is our best guess of what will happen to 100 children with ADHD if they get medication treatment alone for 14 months.
56
44
BENEFIT
3. MEDICATION TREATMENT
Number who have self-control and focus as well as the average child their age who doesn’t have ADHD
Number who don’t improve to that level
Updated: 04/19/2011
stuckere
Typewritten Text
©2011, Cincinnati Children's Hospital Medical Center. All Rights Reserved.

68
32
INTRODUCTION
Combined treatment means the child gets both behavioral and medication treatments. See prior sections which describe behavioral and medication treatments.
Compared to children who only take medicine, children who get combined treatment need 19% less medicine to improve the same amount. As a result, side effects may be less severe on lower amounts of medicine.
DOWNSIDES
Here is our best guess of what will happen to 100 children with ADHD if they get both behavioral and medication treatments for 14 months.
BENEFIT
· Behavioral treatments take time.· Behavioral treatments and medicine cost · money.· Your child may have side effects from · medicine.
4. COMBINED TREATMENT
Number who have self-control and focus as well as the average child their age who doesn’t have ADHD
Number who don’t improve to that level
Updated: 04/19/2011
stuckere
Typewritten Text
©2011, Cincinnati Children's Hospital Medical Center. All Rights Reserved.

IF YOU ARE INTERESTED IN TRYING WATCHFUL WAITING…
What would you like to see change? __________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________
What would your child like to see change? ___________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________
To get started, please complete the following sentences regarding you and your child’s treatment goals.
You do not have to deal with the possible side effects from medicine. You can always change your mind and begin active treatment.
What problems or behaviors will you watch for? _______________________________________
____________________________________________________________________________________
How do you know when to try an active treatment? ___________________________________
____________________________________________________________________________________
Please answer the following questions about pre-existing heart problems.
What do you like most and least about each treatment option?
Does your child have a history of…
Heart disease?................... Yes No
Palpitations or feeling
his/her heart flutter?..
Passing out?...................... Yes No
Seizures?........................... Yes No
Does anyone in your family have a history of...
Sudden death in children
or young adults?........... Yes No
Hypertrophic
Cardiomyopathy?..........
Long QT syndrome?............ Yes No
Please fill out the box below
Please fill out the orange card (behavioral treatment)
Please fill out the blue card (medication treatment)
Please check all the options you want to discuss with your child’s doctor.
WATCHFUL WAITING
Watchful waiting
Try a behavioral treatment
Try a medication treatment
Most Least
Watchful Waiting ___________________________ ______________________________
Behavioral Treatment ___________________________ ______________________________
Medication Treatment ___________________________ ______________________________
Combined Treatment ___________________________ ______________________________
Yes No
Yes No
PLEASE REMEMBER TO FILL OUT THIS WORKSHEET AND BRING IT TO YOUR CHILD’S NEXT APPOINTMENT.
GOALS / PREFERENCES
Updated: 04/19/2011
stuckere
Typewritten Text
©2011, Cincinnati Children's Hospital Medical Center. All Rights Reserved.

IF YOU ARE INTERESTED IN TRYING BEHAVIORAL TREATMENT…
In order to decide which behavioral options to try, it may help your child’s doctor to know what you’ve done in the past and what you are doing now. Please think about methods you’ve done and answer these questions.
What behavioral methods…... have you
tried in the past
... are you currently trying
… are you interested in trying next
Methods for teachers & parents to use to improve classroom performance:
Seat child in front of class near the board.
Utilize a daily report card for teacher to communicate with parents.
Meet with your child’s teacher to set goals and develop a plan.
Request in writing that child’s school tests for learning disabilities.
Other: _________________________________
What behavioral methods…... have you
tried in the past
... are you currently trying
… are you interested in trying next
Methods for parents:
Watch an episode of “Supernanny” that deals with children who have ADHD.
Read a book about managing behaviors for ADHD children.
Visit a website about ADHD.
Call a psychologist recommended by your doctor to ask about services offered for ADHD.
Call Cincinnati Children’s to ask about “Understanding & Managing ADHD” groups.
Attend a support group for parents to learn about managing ADHD.
Other: _________________________________
BEHAVIORAL TREATMENT
Updated: 04/19/2011
stuckere
Typewritten Text
©2011, Cincinnati Children's Hospital Medical Center. All Rights Reserved.

Copyright © 2012 Cincinnati Children's Hospital Medical Center; all rights reserved. Evidence-Based Decision Making (EBDM) – http://www.cincinnatichildrens.org/evidence James M. Anderson Center for Health Systems Excellence
Shared Decision Making Decision Aid
Bone Infection
1. What are the options for treating children with a bone infection? (also called osteomyelitis) After getting medicine through an intravenous line (IV) while in the hospital (i.e. <7 days), your child could…..
A. Go home and take medicine by mouth for a
total of 4–6 weeks
OR
B. Get a peripherally inserted central catheter (PICC), you would learn how to use and care for it, then go home and give IV medicine by PICC line for a total of 4–6 weeks
2. Issues you and your doctor may discuss:
• How your child is responding to medicine (e.g. fever, symptoms)
• The bacteria causing the infection, if known • What is involved in giving your child medicine
by mouth at home? (e.g. liquid vs. pill, how often)
• What is involved in getting a PICC line? • What is involved in caring for a PICC line at
home? • What is involved in giving medicine through a
PICC line at home? • Your preferences for treatment
3. What is known about the risk of a bone infection that fails to get better after 4–6 weeks? (also called chronic osteomyelitis)
Medicine by mouth • Less than 5% risk*
Medicine by PICC line • Less than 5% risk*
*No significant risk difference between these treatment options 4. What are the potential risks and complications?
Medicine by mouth • Allergic reaction • Child spits it up
Medicine by PICC line • Allergic reaction • Line stops working (e.g. it comes out or clogs) • Bacteria gets into blood through the line and
causes another infection • Skin gets infected where the line enters skin • At CCHMC, 15-20% of PICC lines for bone
infections had one of these problems last year
5. Assessment A. Do you know enough about the benefits and
side effects of each option? Y / N B. Do you have enough support and advice from
others to make a choice? Y / N C. Do you feel relatively sure about the best
choice for your son/daughter? Y / N 6. What do you want to do now?
Go home and take medicine by mouth for a total of 4-6 weeks
Get a peripherally inserted central catheter (PICC), learn how to use and care for it, then go home and give medicine for a total of 4-6 weeks
Not sure, prefer to decide later or need more help choosing
7. How could we have engaged you and your family in the decision more successfully?

Sustainability Planner INSTRUCTION SHEET & TOOL
Why use a Sustainability Planner? An important part of the improvement journey is planning how you are going to sustain your improvement efforts. The beneficial results of an improvement project have been sustained when the new ways of working have become the norm, or when things have not returned to the old way of doing things after a year. In order to ensure that an improvement is sustained, the changes made need continuously improve, evolve and adapt to both internal and external pressures. The Sustainability Planner encourages quality improvement teams to think about the seven key factors that will help practices sustain the improvements that they have made. These seven factors are:
1. Clarify what you are sustaining 2. Engage leaders 3. Involve and support front-line staff 4. Communicate the benefits of the improved process 5. Ensure the change is ready to be implemented and sustained 6. Embed the improved process 7. Build in ongoing measurement
The seven key factors for success are discussed below. For each factor, a set of ideas to consider has been provided, as has a small area for your team to plan your next steps. Although not all of the ideas provided will be applicable to your practice, the more ideas that are considered, the higher the chances of successful sustainability. How do I consider the key factors for success? 1. Clarifying what you are sustaining It is necessary that the entire team agrees upon what is being sustained. Is your team planning on sustaining a specific change idea, such as max packing patient visits to do as much as possible with the patient at each visit? Or is the team trying to sustain a change concept, such as reducing demand for visits through a number of different change ideas.
We are planning to sustain:

2. Engage leaders Research and experience demonstrate that the support of organizational leadership is essential to successful quality improvement work. Clinical and administrative leaders who work directly on, or indirectly support, the improvement project must ensure that all barriers to success are removed and project priorities are clearly identified and communicated.
Think about who needs to be on-side for changes to happen. Think about who ultimately influences whether or not something happens - these are the leaders within your practice/clinic. For small offices, the leaders may be everyone who works in the office (e.g., physicians/NPs, RN and receptionist).
Ideas to Consider Next Steps ☐ A provider champion (physician and/or NP), has been identified and has
agreed to participate in the improvement efforts.
☐ The provider champion has devoted time to dialogue with and participate as a member of the improvement team.
☐ If applicable, your business manager or executive director has agreed to support the improvement efforts.
☐ Leaders have the skills/knowledge required to support successful implementation.
☐ Leaders have removed barriers or threats to facilitate process improvement.
☐ Leaders are able to clearly articulate the benefits of the improvement project such as: improved access to care, patient safety, improved patient experience and/or increased staff skills.
☐ Leaders have provided the required resources to ensure the changes are sustained (e.g., time for staff to incorporate the changes into day to day operations).
To strengthen leadership engagement, we will:
3. Involve and support front-line staff Front-line staff members play an important role throughout every quality improvement initiative. In the early phases of a project, they may be involved in identifying problem areas and solutions to test. Later, they may be involved in identifying training needs and delivering / receiving training themselves. Continual support and evaluation of the needs of those working within changed processes is necessary to ensure that changes are sustained.
Ideas to Consider Next Steps ☐ Staff members were provided with information about the purpose and
significance of the improvement initiative.
☐ Front-line staff helped to identify issues from their perspective.
☐ Front-line staff members have been involved in developing solutions.
☐ The ‘right’ (most appropriate or qualified) staff are involved in the improvement project.
☐ Methods to regularly communicate with staff other than those directly working on the improvement team have been identified and used.
☐ A plan to address future skills and training needs has been created.
To strengthen the involvement of front-line staff, we will:

4. Communicate the benefits of the improved process Changes should address the root causes of problems and produce measurable benefits that meet the needs of all stakeholders (i.e., patients, front-line staff, providers, and leaders). Each stakeholder should be able to determine what benefits the changes bring to him or her.
Ideas to Consider Next Steps ☐ Unique and targeted ‘what’s in it for me’ characteristics have been
communicated to different stakeholders.
☐ Baseline data and ongoing real-time data for the measures is being collected regularly, tracked on a run chart and shared.
☐ Stories, updates at staff meetings and a visual display of data have been shared.
☐ Information about the improvement (i.e., patient outcomes, improved efficiencies, how the improvement efforts have been able to reduce or eliminate duplication of effort, unnecessary or repetitive work, unreliable processes, or excessive waits or delays) have been shared with stakeholders as the new way of work.
To communicate the benefits of change, we will:
5. Ensure the change is ready to be implemented and sustained If your improvement team has not finished testing their change ideas through PDSA cycles, then it is too early to consider full implementation and sustainability. Similarly, if the change is perceived as an additional duty or task, then the improvement is unlikely to be integrated into the clinic’s culture or become ‘the way things are done’. It is important to ensure that the change idea is effective and beneficial before moving to the implementation/sustainability phase. Many practices have expended a great deal of energy and time on the implementation of change ideas that did not improve quality or streamline processes.
Ideas to Consider Next steps ☐ There is clear evidence that solutions address the root causes of real
issues.
☐ The change has been successfully tested in a variety of conditions.
☐ The change will not benefit from any further testing or modification.
☐ The project measures are demonstrating real improvement.
☐ Improvement targets or goals have been achieved or are close to being achieved.
☐ The changes have improved efficiency or made jobs easier (reduced waste, avoided duplication, made things run smoother).
To ensure the change is ready to be implemented and sustained, we will:
6. Embed the improved process A common barrier to sustainability is not linking the goal of the improvement project to the strategy or vision of the organization. Without this link, it is often difficult for people to determine why valuable resources are being allocated to the improvement project. An improvement is much more likely to be sustained if it is well integrated into the culture and core processes of a practice/clinic and if it is flexible and able to respond to changes in the environment. In order to do so, the systems supporting the improvement need to be adapted so that they are compatible with the change.

Ideas to Consider Next Steps ☐ The improvement project is important to the continued success of the
practice/clinic.
☐ The necessary facilities, supplies, and equipment are in place to support the new process.
☐ Training has been provided to staff and providers about the improved processes and changes so they know what is expected of them.
☐ Job descriptions have been updated to reflect the altered roles.
☐ Policies and procedures have been updated or created to reflect the new processes.
☐ The new processes are now “standard work” and supported with medical directives, forms, checklists, reminders (visual cues), and technology.
☐ The team has a mechanism for discussing, examining and adapting the improved processes in response to internal and external changes.
To embed the improved process and make it the new standard, we will:
7. Build in ongoing measurement Establishing an ongoing measurement system and a standardized way of communicating results reinforces that the change is important to the practice. A mechanism for looking at a few key and relatively easy to extract measures allows teams to see if there is slippage and to take action to resolve any issues. It also allows teams to celebrate when an indicator has stayed at an improved level over time.
Ideas to Consider Next Steps ☐ There are internal skills and a culture for continuous improvement.
☐ A refined set of measures to track on an ongoing basis is identified. (If the team is sustaining improvements in access, track future open capacity and third next available appointment.)
☐ A group or person has been assigned responsibility to extract the data for this refined set of measures.
☐ There is a structure or mechanism in place for reviewing the measures on a regular basis.
☐ There is a plan for communicating performance to front-line staff, providers, and leaders within the practice.
☐ There is a plan to outline what we will do to reflect on our progress – to celebrate continued success and to respond if our measures start to slip.
☐ Celebrate accomplishments and aspire to take performance to a new level.
To strengthen our capacity for ongoing measurement, we will:
Helpful Sources
x Centre for Healthcare Quality Improvement (2010). Sustainability Planning: A Guide for ED-PIP Coaches &Team Leads. CHQI: Toronto, Ontario.
x NHS Modernization Agency (2002). Improvement leader’s guide to sustainability and spread. Ancient House Printing Group: Ipswich, England.
x Maher, Lynn, Gustafson, D. and Evans, A. (2007). NHS Sustainability: Model and Guide. NHS Institute for Innovation and Improvement: England.
ISBN 978-1-4606-3780-7 (PDF)
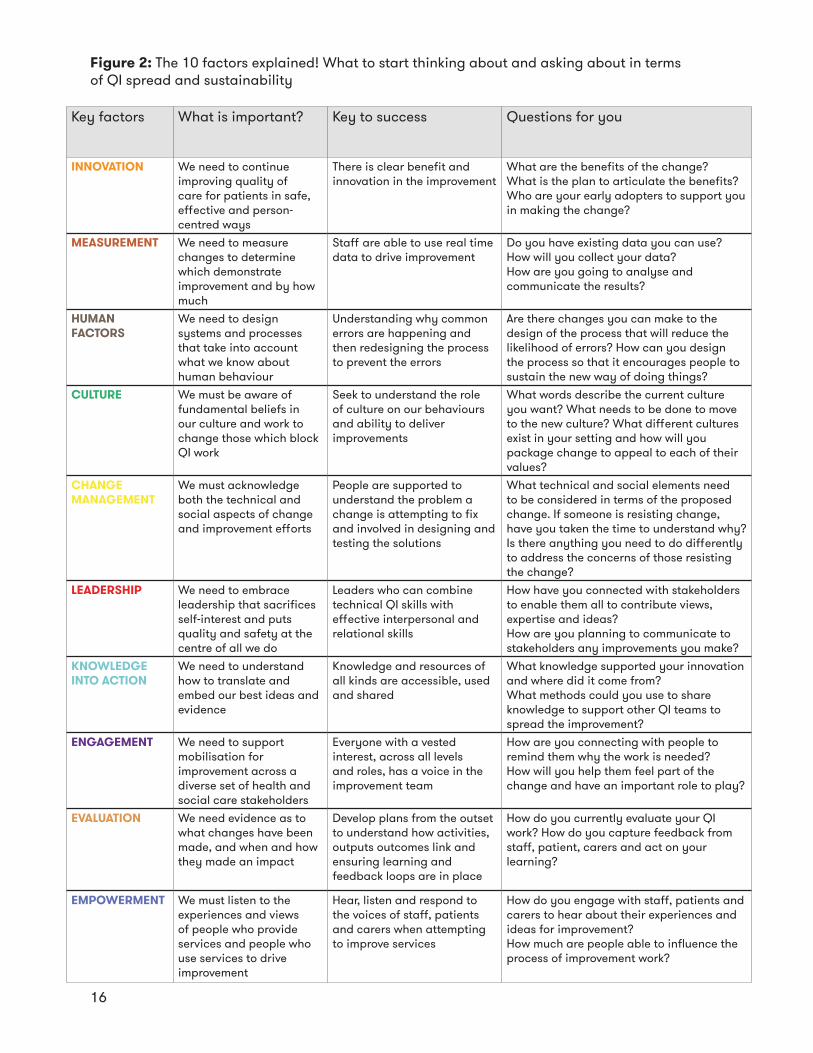
Key factors What is important? Key to success Questions for you
INNOVATION We need to continue improving quality of care for patients in safe, effective and person-centred ways
There is clear benefit and innovation in the improvement
What are the benefits of the change?What is the plan to articulate the benefits? Who are your early adopters to support you in making the change?
MEASUREMENT We need to measure changes to determine which demonstrate improvement and by how much
Staff are able to use real time data to drive improvement
Do you have existing data you can use?How will you collect your data?How are you going to analyse and communicate the results?
HUMAN FACTORS
We need to design systems and processes that take into account what we know about human behaviour
Understanding why common errors are happening and then redesigning the process to prevent the errors
Are there changes you can make to the design of the process that will reduce the likelihood of errors? How can you design the process so that it encourages people to sustain the new way of doing things?
CULTURE We must be aware of fundamental beliefs in our culture and work to change those which block QI work
Seek to understand the role of culture on our behaviours and ability to deliver improvements
What words describe the current culture you want? What needs to be done to move to the new culture? What different cultures exist in your setting and how will you package change to appeal to each of their values?
CHANGE MANAGEMENT
We must acknowledge both the technical and social aspects of change and improvement efforts
People are supported to understand the problem a change is attempting to fix and involved in designing and testing the solutions
What technical and social elements need to be considered in terms of the proposed change. If someone is resisting change, have you taken the time to understand why? Is there anything you need to do differently to address the concerns of those resisting the change?
LEADERSHIP We need to embrace leadership that sacrifices self-interest and puts quality and safety at the centre of all we do
Leaders who can combine technical QI skills with effective interpersonal and relational skills
How have you connected with stakeholders to enable them all to contribute views, expertise and ideas?How are you planning to communicate to stakeholders any improvements you make?
KNOWLEDGE INTO ACTION
We need to understand how to translate and embed our best ideas and evidence
Knowledge and resources of all kinds are accessible, used and shared
What knowledge supported your innovation and where did it come from?What methods could you use to share knowledge to support other QI teams to spread the improvement?
ENGAGEMENT We need to support mobilisation for improvement across a diverse set of health and social care stakeholders
Everyone with a vested interest, across all levels and roles, has a voice in the improvement team
How are you connecting with people to remind them why the work is needed?How will you help them feel part of the change and have an important role to play?
EVALUATION We need evidence as to what changes have been made, and when and how they made an impact
Develop plans from the outset to understand how activities, outputs outcomes link and ensuring learning and feedback loops are in place
How do you currently evaluate your QI work? How do you capture feedback from staff, patient, carers and act on your learning?
EMPOWERMENT We must listen to the experiences and views of people who provide services and people who use services to drive improvement
Hear, listen and respond to the voices of staff, patients and carers when attempting to improve services
How do you engage with staff, patients and carers to hear about their experiences and ideas for improvement?How much are people able to influence the process of improvement work?
Figure 2: The 10 factors explained! What to start thinking about and asking about in terms of QI spread and sustainability
16
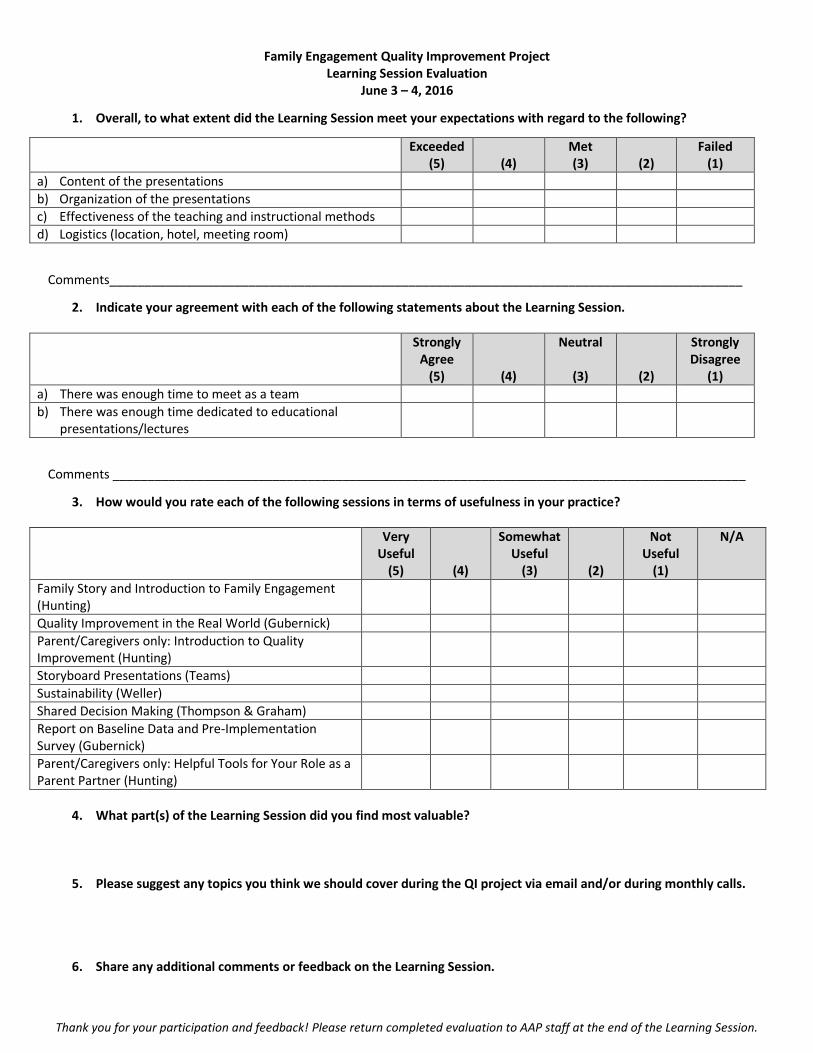
Thank you for your participation and feedback! Please return completed evaluation to AAP staff at the end of the Learning Session.
Family Engagement Quality Improvement Project Learning Session Evaluation
June 3 – 4, 2016
1. Overall, to what extent did the Learning Session meet your expectations with regard to the following?
Exceeded (5)
(4)
Met (3)
(2)
Failed (1)
a) Content of the presentations
b) Organization of the presentations
c) Effectiveness of the teaching and instructional methods
d) Logistics (location, hotel, meeting room)
Comments___________________________________________________________________________________________
2. Indicate your agreement with each of the following statements about the Learning Session.
Strongly Agree
(5)
(4)
Neutral
(3)
(2)
Strongly Disagree
(1)
a) There was enough time to meet as a team
b) There was enough time dedicated to educational presentations/lectures
Comments ___________________________________________________________________________________________
3. How would you rate each of the following sessions in terms of usefulness in your practice?
Very Useful
(5)
(4)
Somewhat Useful
(3)
(2)
Not Useful
(1)
N/A
Family Story and Introduction to Family Engagement (Hunting)
Quality Improvement in the Real World (Gubernick)
Parent/Caregivers only: Introduction to Quality Improvement (Hunting)
Storyboard Presentations (Teams)
Sustainability (Weller)
Shared Decision Making (Thompson & Graham)
Report on Baseline Data and Pre-Implementation Survey (Gubernick)
Parent/Caregivers only: Helpful Tools for Your Role as a Parent Partner (Hunting)
4. What part(s) of the Learning Session did you find most valuable?
5. Please suggest any topics you think we should cover during the QI project via email and/or during monthly calls.
6. Share any additional comments or feedback on the Learning Session.
Related Documents











