Deafness: Deafness: Providing a Providing a Pediatric Pediatric Medical Home Medical Home Rachel St. John, MD, CMHC Rachel St. John, MD, CMHC Director: Kids Clinic for the Deaf, Director: Kids Clinic for the Deaf, Georgetown University Hospital Georgetown University Hospital Visiting Professor: Gallaudet University, Visiting Professor: Gallaudet University, Dept. of Counseling Dept. of Counseling

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Families with Deafness: Families with Deafness: Providing a PediatricProviding a Pediatric
Medical HomeMedical Home
Rachel St. John, MD, CMHCRachel St. John, MD, CMHC
Director: Kids Clinic for the Deaf, Georgetown University Director: Kids Clinic for the Deaf, Georgetown University HospitalHospital
Visiting Professor: Gallaudet University, Dept. of Visiting Professor: Gallaudet University, Dept. of CounselingCounseling
General BackgroundGeneral Background
Incidence of congenital hearing loss is Incidence of congenital hearing loss is
0.5-3/1000 live births0.5-3/1000 live births
90% of deaf children born to hearing 90% of deaf children born to hearing parentsparents
90% of deaf parents have hearing children90% of deaf parents have hearing children

Why a Medical Home?Why a Medical Home?
Large cultural communities tend to Large cultural communities tend to congregate in urban areas, especiallycongregate in urban areas, especially
if residential school/university in areaif residential school/university in area
* Washington DC metropolitan area deaf * Washington DC metropolitan area deaf residents estimated in “hundreds of residents estimated in “hundreds of thousands”thousands”
Why a Medical Home?Why a Medical Home?
Legal Mandates:Legal Mandates:
-Americans with Disabilities Act (1990)-Americans with Disabilities Act (1990)
-DHHS Office for Civil rights policy -DHHS Office for Civil rights policy
statement regarding Low English statement regarding Low English
Proficiency patients (2000)Proficiency patients (2000)
Parents are primary historians for young Parents are primary historians for young children – good communication and children – good communication and cultural awareness criticalcultural awareness critical
Why a Medical Home?Why a Medical Home?
Parents often seek advice from health Parents often seek advice from health professionals related to areas outside professionals related to areas outside medical arena – familiarity with community medical arena – familiarity with community resources can be very helpfulresources can be very helpful
Areas of Decision-MakingAreas of Decision-Making
LANGUAGELANGUAGE
HEARING AMPLIFICATIONHEARING AMPLIFICATION
CULTURE & PSYCHOSOCIALCULTURE & PSYCHOSOCIAL
MEDICAL CONSIDERATIONSMEDICAL CONSIDERATIONS

LANGUAGELANGUAGE
Communication/Education ModesCommunication/Education Modes
SIGNED (ASL, SEE)SIGNED (ASL, SEE)
ORAL (cued speech, speech)ORAL (cued speech, speech)
TOTAL COMMUNICATIONTOTAL COMMUNICATION
BI-BIBI-BI
(No single “best-fit” answer – each family (No single “best-fit” answer – each family has unique set of circumstances)has unique set of circumstances)
HEARING AMPLIFICATIONHEARING AMPLIFICATION

Behind-The-Ear AidsBehind-The-Ear Aids

BAHABAHA(Bone-Anchored Hearing Aid)(Bone-Anchored Hearing Aid)
Conductive hearing Conductive hearing lossloss
Previous surgery or Previous surgery or malformation malformation prevents use of prevents use of conventional aidconventional aid
Screw implanted in Screw implanted in mastoid bone mastoid bone connects to external connects to external processorprocessor
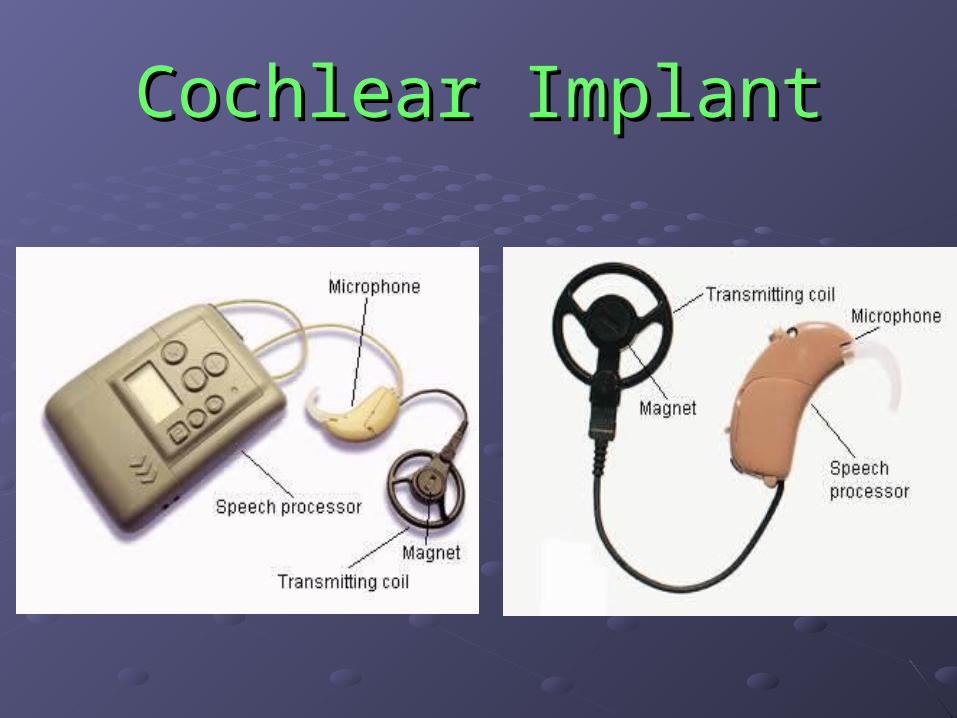
Cochlear ImplantCochlear Implant
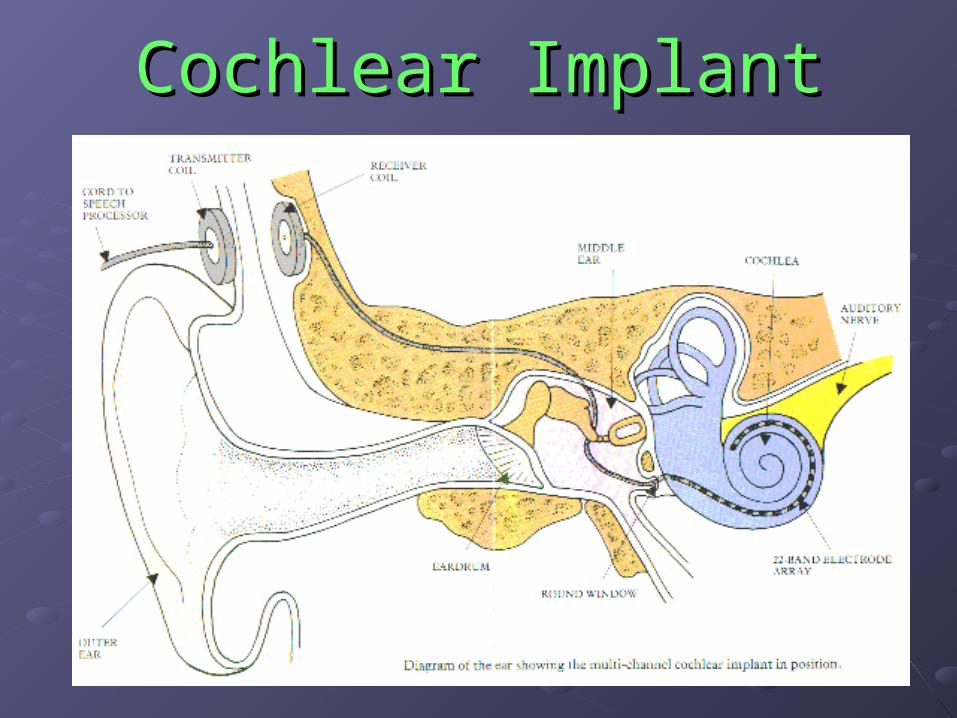
Cochlear ImplantCochlear Implant

FM SYSTEMFM SYSTEM
HEARING AMPLIFICATIONHEARING AMPLIFICATION
Again, no single “best-fit” option - Again, no single “best-fit” option - educated choices best made by evaluating educated choices best made by evaluating child’s form of deafness, family context, child’s form of deafness, family context, and social environmentand social environment

CULTURE & CULTURE & PSYCHOSOCIALPSYCHOSOCIAL
FACTORSFACTORS
Access to ResourcesAccess to Resources
Presence of Deaf communityPresence of Deaf community
Parental expectationParental expectation
Family MilieuFamily MilieuDeaf-of-Hearing:Deaf-of-Hearing:
*may have guilt, grief, sense of loss*may have guilt, grief, sense of loss
*potential unrealistic expectation/denial*potential unrealistic expectation/denial
*variable accessibility to resources*variable accessibility to resources
-geographic isolation-geographic isolation
-SES-SES
-education-education
Family MilieuFamily MilieuDeaf-of-Deaf:Deaf-of-Deaf:
*may be thrilled!!*may be thrilled!! *multi-generational: strong cultural*multi-generational: strong cultural heritageheritage *exposed to intact first language from*exposed to intact first language from birth – reduces sense of urgency forbirth – reduces sense of urgency for educational decision makingeducational decision making

MEDICAL CONSIDERATIONSMEDICAL CONSIDERATIONS
Medical ConsiderationsMedical ConsiderationsInitial considerations:Initial considerations: *PMH: TORCH *PMH: TORCH (CMV),(CMV), anoxia, ECMO, ototoxic anoxia, ECMO, ototoxic
drugs, hyperbili, etc.drugs, hyperbili, etc. *PE: dysmorphism, auricular or preauricular*PE: dysmorphism, auricular or preauricular distortiondistortion
Genetics referralGenetics referral *based on FH*based on FH *connexin 26*connexin 26
Audiology referralAudiology referral *report to state*report to state *sedated BAER*sedated BAER *recommendations for amplification*recommendations for amplification and follow-upand follow-up

Medical Considerations (cont)Medical Considerations (cont)
Coordinating SubspecialistsCoordinating Subspecialists
*syndrome-related deafness often requires multiple*syndrome-related deafness often requires multiple
subspecialist caresubspecialist care
Specific Medical ConsiderationsSpecific Medical Considerations
*often require increased ENT services*often require increased ENT services
*preventative care for cochlear implant patients*preventative care for cochlear implant patients

KIDS CLINIC FOR THE DEAFKIDS CLINIC FOR THE DEAF
KCD – The Medical HomeKCD – The Medical Home
ENVIRONMENTENVIRONMENT::
-pediatrician fluent in ASL: direct rapport-pediatrician fluent in ASL: direct rapport with families, preserves confidentialitywith families, preserves confidentiality -medical interpreter present for non--medical interpreter present for non- physician encounters (billing, check-in,physician encounters (billing, check-in, nursing screening)nursing screening) -dedicated TTY line-dedicated TTY line -staff exposure to Deaf culture via workshops-staff exposure to Deaf culture via workshops -HIPAA-compliant email communication system -HIPAA-compliant email communication system for non-medical issuesfor non-medical issues

KCD – The Medical HomeKCD – The Medical Home
CONSULTATIONCONSULTATION (often deaf children of (often deaf children of hearing parents): hearing parents):
*language choices*language choices
*E.I. Part C state coordinators*E.I. Part C state coordinators
*audiology support*audiology support
*school options*school options
*appropriate psychoeducational testing*appropriate psychoeducational testing
resources resources

KCD – The Medical HomeKCD – The Medical Home
SPECIFIC MEDICAL CARE SITUATIONSSPECIFIC MEDICAL CARE SITUATIONS:: -cochlear implants: appropriate vaccines,-cochlear implants: appropriate vaccines, coordinating with audiology/ENT,coordinating with audiology/ENT, monitoring language milestonesmonitoring language milestones -syndromic deafness: coordinating-syndromic deafness: coordinating subspecialty caresubspecialty care -normal development awareness for-normal development awareness for bilingual/trilingual householdsbilingual/trilingual households
KCD – The Medical HomeKCD – The Medical Home
EDUCATIONEDUCATION::
-Community workshops-Community workshops
-Involvement at local deaf-education -Involvement at local deaf-education
schools (i.e. Back-To-School night)schools (i.e. Back-To-School night)
-Grand Rounds lectures at area hospitals-Grand Rounds lectures at area hospitals
-Involvement of medical students and-Involvement of medical students and
residents fluent in ASL in clinicalresidents fluent in ASL in clinical
and educational activitiesand educational activities
KCD – The Medical HomeKCD – The Medical Home
RESOURCE COLLABORATIONRESOURCE COLLABORATION::
-Baby Watch-Baby Watch™™: continuity of care: continuity of care
-Georgetown Patient and Physician -Georgetown Patient and Physician
Advocacy department: interpreter Advocacy department: interpreter
services for hospitalservices for hospital
-Gallaudet Interpreting Service – medical-Gallaudet Interpreting Service – medical
interpreterinterpreter
-National Association of the Deaf-National Association of the Deaf
-Center for Families in Transition-Center for Families in Transition

REFERENCESREFERENCES
Acclaim Clipart : Acclaim Clipart : www.acclaimclipart.comwww.acclaimclipart.com
East Melbourne Hearing Research Group: East Melbourne Hearing Research Group: http://www.medoto.unimelb.edu.au/index.htmhttp://www.medoto.unimelb.edu.au/index.htm
Faulconbridge and Bowdler, Hearing Aids:Faulconbridge and Bowdler, Hearing Aids:
http://www.orl-baohns.org/public/hearingaids.htmhttp://www.orl-baohns.org/public/hearingaids.htm
Gallaudet University: Gallaudet University: www.gallaudet.eduwww.gallaudet.edu
““Genetics Evaluation Guidelines for the Etiologic Genetics Evaluation Guidelines for the Etiologic Diagnosis of CongenitalDiagnosis of Congenital
Hearing Loss”: ACMG statement, vol 4, no 3, Hearing Loss”: ACMG statement, vol 4, no 3, May/June 2002May/June 2002
““What Is A Cochlear Implant”: What Is A Cochlear Implant”: http://www.glanclwyd.demon.co.uk/audiology/cochinf.htmhttp://www.glanclwyd.demon.co.uk/audiology/cochinf.htm

Related Documents











