Blood.Vol 43. No 2 (February). 1974 219 Familial Thrombosis Due to Antithrombin III Deficiency By Ewa Marciniak, Claude H. Farley, and Philip A. DeSimone A large kindred from eastern Kentucky, with extensive history of recurrent venous throm- basis and pulmonary embolism, was studied. Low antithrombin III titers, ranging from 26% to 49% of normal values, were found in plasma of nine members in three consecutive genera- tions; another five members, four of whom were not available for study, are suspected of having the biochemical defect. There was a good correlation between clinical symptoms and antithrombin Ill deficiency, although three of the younger members with the defect still remained free of thrombosis. In serum of the affected subjects antithrombin Ill was almost completely utilized, which indicates that stoich- iometric binding to coagulation enzymes domi- nates under biological conditions. Antithrombin and antifactor Xa activities residing in the macroglobulin region of plasma and serum re- mained unchanged. The responsiveness to hepa- rin in vitro and in vivo confirmed the evidence that antithrombin Ill is the sole blood com- ponent through which heparin exerts its anti- coagulant effect. In five affected members therapy with oral anticoagulants increased very significantly the level of antithrombin Ill in plasma and contributed to a remarkable in- crease of residual antithrombin Ill in serum. This objective improvement after warfarin ther- apy may create significant difficulties in the laboratory diagnosis of antithrombin III de- ficiency. T THE PRESENT time antithrombin III is recognized as an a2 globulin capable of inactivating both thrombin and factor Xa in blood.”2’3 This antiproteinase has been also found identical with so-called heparin cofactor.4’2 Reports on hereditary deficiency of antithrombin III have been restricted to a single Norwegian family studied by Egeberg and Abildgaard.5’6” A second large kindred from the Appalachian Mountains, unusually susceptible to thromboembolic disease in consequence of a bio- chemical defect, is the subject of the present study. The defect, inherited as an auto- somal dominant, was limited to a single protein fraction bearing the characteristics of antithrombin III. In the affected subjects we found a reduced neutralization of throm- bin and factor Xa both in the absence and in the presence of heparin. During the therapy with oral anticoagulants the level of antithrombin III in members with the defect has been significantly increased. These findings substantiate the outstanding biological role of antithrombin III in the support of blood fluidity and indicate that a decrease in vitamin-K-dependent coagulation factors abates the utilization of anti- thrombin III in vitro and probably also in vivo. MATERIALS AND METHODS Plasma was obtained by collecting 9 volumes of a fasting blood sample into 1 volume of citric acid-sodium citrate (0.1 M) applying a two-syringe technique. Immediately after drawing, blood From the Department of Medicine. Unii’ersitr of Kentucky Medical center, Lexington, Ky. 40506. Submitted May 7, 1973: revised July 5, 1973: accepted Juli’ 16, 1973. Supported in part by the A merican Heart Association with contribution from the Kentucky Heart Association, and in part bt’ the University of Kentucky Research Foundation. Ewa Marciniak, M.D.: Associate Professor of Medicine, University of Kentucky Medical center, Lexington. Ky. 40506. Claude H. Farley, M.D.: Assistant Professor of Medicine, University of Kentucky Medical center, Lexington, Kr. 40506. Philip A. DeSimone, M.D.: cluiical Fellow, Division of Hematology, Department of Medicine, Unii’ersit’i’ of Kentucky Medical center, Lexiizg- ton, Kr. 40506. ©1974 by Grune & Stratton, inc. For personal use only. on April 3, 2019. by guest www.bloodjournal.org From

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Blood.Vol 43. No 2 (February). 1974 219
Familial Thrombosis Due to
Antithrombin III Deficiency
By Ewa Marciniak, Claude H. Farley, and Philip A. DeSimone
A large kindred from eastern Kentucky, withextensive history of recurrent venous throm-basis and pulmonary embolism, was studied.Low antithrombin III titers, ranging from 26%to 49% of normal values, were found in plasmaof nine members in three consecutive genera-
tions; another five members, four of whomwere not available for study, are suspected ofhaving the biochemical defect. There was a
good correlation between clinical symptoms
and antithrombin Ill deficiency, although three
of the younger members with the defect stillremained free of thrombosis. In serum of the
affected subjects antithrombin Ill was almost
completely utilized, which indicates that stoich-iometric binding to coagulation enzymes domi-
nates under biological conditions. Antithrombinand antifactor Xa activities residing in themacroglobulin region of plasma and serum re-
mained unchanged. The responsiveness to hepa-
rin in vitro and in vivo confirmed the evidencethat antithrombin Ill is the sole blood com-ponent through which heparin exerts its anti-coagulant effect. In five affected memberstherapy with oral anticoagulants increased verysignificantly the level of antithrombin Ill in
plasma and contributed to a remarkable in-
crease of residual antithrombin Ill in serum.This objective improvement after warfarin ther-apy may create significant difficulties in thelaboratory diagnosis of antithrombin III de-ficiency.
T THE PRESENT time antithrombin III is recognized as an a2 globulin capable of
inactivating both thrombin and factor Xa in blood.”2’3 This antiproteinase has
been also found identical with so-called heparin cofactor.4’2 Reports on hereditary
deficiency of antithrombin III have been restricted to a single Norwegian family
studied by Egeberg and Abildgaard.5’6” A second large kindred from the Appalachian
Mountains, unusually susceptible to thromboembolic disease in consequence of a bio-
chemical defect, is the subject of the present study. The defect, inherited as an auto-
somal dominant, was limited to a single protein fraction bearing the characteristics of
antithrombin III. In the affected subjects we found a reduced neutralization of throm-
bin and factor Xa both in the absence and in the presence of heparin. During the
therapy with oral anticoagulants the level of antithrombin III in members with the
defect has been significantly increased. These findings substantiate the outstanding
biological role of antithrombin III in the support of blood fluidity and indicate that a
decrease in vitamin-K-dependent coagulation factors abates the utilization of anti-
thrombin III in vitro and probably also in vivo.
MATERIALS AND METHODS
Plasma was obtained by collecting 9 volumes of a fasting blood sample into 1 volume of citricacid-sodium citrate (0.1 M) applying a two-syringe technique. Immediately after drawing, blood
From the Department of Medicine. Unii’ersitr of Kentucky Medical center, Lexington, Ky.
40506.
Submitted May 7, 1973: revised July 5, 1973: accepted Juli’ 16, 1973.
Supported in part by the A merican Heart Association with contribution from the Kentucky
Heart Association, and in part bt’ the University of Kentucky Research Foundation.
Ewa Marciniak, M.D.: Associate Professor of Medicine, University of Kentucky Medical center,
Lexington. Ky. 40506. Claude H. Farley, M.D.: Assistant Professor of Medicine, University of
Kentucky Medical center, Lexington, Kr. 40506. Philip A. DeSimone, M.D.: cluiical Fellow,
Division of Hematology, Department of Medicine, Unii’ersit’i’ of Kentucky Medical center, Lexiizg-
ton, Kr. 40506.
©1974 by Grune & Stratton, inc.
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

220 MARCINIAK. FARLEY. AND DESIMONE
was centrifuged in a refrigerated centrifuge at 1 200 g for 20 mm. Plastic syringes, centrifuge tubes,
and storage containers were used. Serum was obtained from blood clotted in a glass tube and incu-
bated for 2 hr at 37CC prior to centrifugation. Ether extract of bovine brain, suspended in saline at
a concentration of 0.03%, was used as partial thromboplastin. This was mixed with an equal volume
of 4% (w/v) kaolin suspension for activated partial thromboptastin time (PTTa) determination.
Sodium heparin (Upjohn) was used. Purified bovine factor Xa,8 purified bovine thrombin,9 andpurified bovine antithrombin 10 were obtained as described before.
Prothrombin time was performed by the method of Quick.” Thrombin activity was standardized
in Iowa units.12 Two-stage prothrombin assay was performed according to the method of Ware and
3 Factors X and Xa were determined as described previously8’3 ; the activity in 1 ml of
normal human plasma was accepted for 100 U. Factor V. VIII, and IX assays were carried out by
one-stage technique on a substrate plasma deficient in the respective coagulation factor. Thrombin
time determination was performed by mixing equal volumes of plasma and purified thrombin
solution of varying activity, indicated in the text. Antitrypsin determination was according to
Homer Ct al.14
Gel Filiratioiz
A sampleof plasma or serum, exactly 5 ml in volume,was applied to the Sephadex G-150 column(Pharmacia) 45 x 2.5 cm, conditioned and eluted with 0.1 M NaCl in 0.04 M Tris-FIC1 buffer, pH
7.8. An up-flow adaptor was used giving the elution rate of 20-25 mI/hr. The efluent was collected
in fractions, exactly 3 ml in volume.
AiitiJ#{224}etor Xa Assay
One volume of the test fraction and 1 volume of saline containing 2 U of purified factor Xa perml and 0.2% of bovine albumin were mixed and incubated at 37#{176}Cfor 30 mm, unless stated other-wise. After the incubation the residual procoagulant activity of factor Xa was recorded as a
clotting time on the substrate bovine plasma3 and compared with a control value, ranging from 17
to 18 sec, and obtained by substituting buffer for the test fraction. The difference between thesetwo evaluations, expressed in seconds, represented the activity of antifactor Xa in the test fraction.
Applying this method of procedure to variable low concentrations of purified antithrombin III, a
rectilinear relationship between prolongations in clotting times and antithrombin III concentrations
was recorded. This did not, however, apply to higher concentrations of antithrombin III, rapidly
inactivating factor Xa, in which case the incubation time had to be considerably shortened.
Antithrombiii Assay
Purified thrombin, 0.1 ml of a 20 U/mI solution, was mixed with 0.1 ml of test fraction andincubated for 10 mm at 37#{176}C.In fractions obtained from plasma after heparin injection this incu-
bation was shortened to 5 mm. At the end of incubation 0.2 ml of acacia-calcium reagent’2 wasadded, immediately followed by addition of 0.1 ml of fibrinogen. The clotting time was recordedand compared with the control time (saline instead of the test fraction, usually 6.0-6.5 sec).Antithrombin activity in the test fraction was expressed as a difference in seconds between these
two clotting tunes.
Heparin �‘onceii tration
This was measured as based on the ability of heparin to potentiate the activity of purified anti-
thrombin Ill.’� Factor Xa was used as the substrate for the inhibition. One volume of the test
fraction was supplemented with 0.5 volume of purified factor Xa of high activity (20 U/mI) and
with 0.5 volume of purified antithrombin III (about 10% of the activity present in normal plasma).After 5 mm of incubation at 37#{176}Cthe residual activity of factor Xa was recorded. it was inversely
proportional to the heparin concentration in the test fraction. A reference curve was obtained with
known heparin concentrations by plotting heparin concentration versus the residual factor Xa
activity.
CASE REPORT
The propositus (ill-i 6) is a 24-yr-old white male who was in excellent health until June 3, 1972,
when waking from an afternoon nap he suffered a sudden onset of chest pain, dyspnca, and hemop-
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

FAMILIAL THROMBOSIS 221
Fig. 1. Pedigree of family H.
tysis. After admission to the University of Kentucky Medical Center pulmonary embolism wasdiagnosed. No signs of peripheral thrombophlebitis were noted on admission, but venograms per-
formed on the 3rd hospital day revealed the presence of thrombi in the left iliac and the right
femoral veins. Intravenous infusion of heparin was started on the 1st hospital day and continued
for 18 days. On the 8th hospital day the patient developed obvious signs of thrombophlebitis in
the left leg. Chest pain and hemoptysis reoccurred and lasted for a few hours. While continuingheparin, therapy with warfarin was initiated. Symptoms of thrombophlebitis resolved slowly and
disappeared completely by the 17th hospital day. Twenty-four hours after discontinuing heparin,
antithrombin III in patient’s plasma was evaluated and found markedly decreased . He was dis-
charged, continuing the medication with warfarin, and has been controlled periodically over 9 mo,
but no thrombotic episodes reoccurred. During the entire period of hospitalization the patient
demonstrated an unusual, apprehensive attitude. He stated repeatedly that symptoms similar tothese observed in him were seen previously in several members of his family causing sudden deathin two of his siblings.
History of Family H
The family has been known to inhabit an Appalachian region of Eastern Kentucky for at least acentury, and most of the members still reside there. A few of them moved to Ohio, Indiana, andMichigan. A history of consanguinity was denied. The four generations that we have examined are
presented in Fig. 1. Plasma level of antithrombin Ill for each investigated subject is shown in
Table 1.
The matriarch of the family is, at the age of 83, in considerably good health with normal anti-thrombin III level. Her husband died at age 70, of stroke. For many years he suffered recurrent
pain, swelling, and ulcerations of legs suggestive of thrombosis.
Subject 11-3, the 62-yr-old uncle of the propositus, with markedly decreased antithrombin III,
has a history of long-lasting swelling and pain in both legs with secondary crural ulcerations. Hewas hospitalized at the age of 58 with thrombophlebitis and suspicion of pulmonary embolism, and
treated briefly with oral anticoagulants. Thereafter he had at least one additional incident of
thrombophlebitis.
Subject 11-4, the 59-yr-old father of the propositus, suffered recurrent leg thrombosis since the
age of 26, and had two incidents of pulmonary embolism. When we initially evaluated his anti-
thrombin III and found it abnormally low, he had been irregularly treated with small dose ofhedulin for few years.
Subject 111-1 is a 34-yr-old woman, with decreased antithrombin III, who after the delivery of her
third child, at the age of 25, developed severe thrombophlebitis in left leg, which recurred several
times over the following few months. Treatment with oral anticoagulants lasted for 3 yr. Since
then she has remained free of thrombotic episodes, although for 3 yr she took oral contraceptives.
I �10ii -
‘U
� � r�56 7 S 9 0 II I��j�I4 1 9f 2Of 21 22 23 24
ASYMPTONATIC: HISTORY OF THROMBOSIS:
o normal A-� Q normal A-�
rA-nz<50S IA-Ill <50%
f�J not investigated � not investigated
�PROPOSITUS
f DEAD
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

222 MARCINIAK. FARLEY. AND DE SIMONE
Table 1. Antithrombin Ill Levels4 in Plasma from Members of Family H
Subject A�Ill (%) Subject A-Ill (%)
I-f 79 111-9
111-10
Ill-li
39
47
78
11-2 77 111-12 31
11-3 31 111-15 49
II.4t 32 III-16� 48
11-5 116 111-17 90
11-6 118 111-21
111-22
85
105
Ill-i 26 111-23 100
lll-4� 83
111-6 87 lV-1 91
111-7 89 IV-2 82
111-8 89 lV-3 32
Normal range 80%-117%.
tOn hedulin.
�On warfarin for 5 yr.
§ Propositus, on warfarin for a few days.
Subject 111-4 is a 26-yr-old man who had his first thrombosis and pulmonary embolism at the
age of 15 , after fracturing the left femur. Since then he has had 10 episodes of recurrent throm-bophlebitis and at least three additional incidents of pulmonary embolism. Continuous therapy
with warfarin was instituted at the age of 20, when multiple pulmonary embolization occurredafter a plastic surgery of the leg for crural ulcers. Since the age of 21 he has remained asympto-
matic but has continued the therapy with warfarin. Despite his dramatic clinical history the plasma
level of antithrombin III was now found within the normal range. After observing in the other
affected members of his family that a prolonged treatment with warfarin may considerably in-crease the biological activity of antithrombin III, we presume that this subject has the congenital
biochemical defect.
Subject IlI-lO, age 38, is the oldest brother of the propositus, with both legs amputated below
the hip. He lost his left leg at the age of 23, a few months after developing pain and progressive
numbness in this extremity.At that time he was told that he had Beurger’s disease. The right leg
was amputated at the age of 29 in consequence of severe circulatory disturbances indicative of
venous obstruction with secondary pretibial ulcerations, which lasted for 4 yr. He has had delayed
healing of the stump with recurrent ulcerations. We found that his antithrombin Ill is significantly
decreased.Subject 111-12 is a 33-yr-old brother of the propositus, with decreased antithrombin III. He had
a single incident of thrombophlebitis following appendectomy, at the age of 25.
Subject Ill-i 3, another brother of the propositus, is said to have had symptoms suggestive of
thrombophlebitis. He died suddenly at the age of 27, when in the military service in Korea. Hiscollegues were alarmed when they heard him breathing with an extreme difficulty, but found him
dead upon entering his room. On the autopsy a marked vascular congestion of the lungs, pulmon-ary edema, and right heart dilatation were noticed. This implies that pulmonary embolism was
most likely the cause of a sudden death.Subject 111-20, a sister of the propositus, died suddenly at the age of 18, with obvious signs of
pulmonary embolism. Shortly before death she was released from the local hospital where she
received treatment for bilateral pneumonia.Two individuals in the third generation (111-9, age 13, and 111-15, age 26) and one in the fourth
(IV-3, age 9) have the biochemical defect but have not shown any thromboembolic symptoms.They are of considerably young age. Since all of the older members of the family with the defecthave had symptoms, it can be predicted with a fair degree of probability that these three will also
in the future develop the clinical disease.
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

7
6
5
4
3
2
60
40
20 -�
U
In
w0�
I-
(9
60 Z
I-0-J
40 0
‘1
20
6
5
4
3
2
FAMILIAL THROMBOSIS 223
FRACTION NUMBER
Routine Laboratory Evaluations
RESULTS
The propositus and subjects 11-3, 11-4, and 111-1 were evaluated for evidence of
hemostatic abnormalities. The platelet count, fibrinogen level, PTTa, euglobulin lysis
time, and thrombin time with thrombin solutions ranging from 2 to 20 U of activity
per ml gave normal results. In addition, subjects 11-3 and 111-1 before the therapy with
oral anticoagulants had a norni�il prothrombmn time and two-stage prothrombmn level;
determinations of factOrs V, VIII, IX, and X were also within normal range. The
thromboplastin generation test with 11-3 plasma and serum, utilizing platelet substi-
tute, was normal. Cellulose acetate electrophoresis of serum from the propositus and
subject 111-1 showed no abnormalities. Serum levels of antitrypsin in subjects
11-3, 11-4, and 111-I were increased, assuming, respectively, values of 1.72, 2.22, and
1 .69 mg trypsin inactivated per ml of serum (normal range 1 - 19 + 0. 1 8).
Evaluation of Antithrombin III
Since in human blood �lt�tivities directed against thrombin’6”7 and against factor
)(.a3”8 are not limited to antithrombin III, but have been found also in connection
with macroglobulins, it was desirable to fractionate each specimen before analysis. For
this purpose plasma or serum was filtered on Sephadex G-1 50 and antiproteinases
were analyzed in isolated fractions.
Figure 2 compares the result obtaihed by measuring antithrombin and antifactor
Xa in normal plasma and serum with representative results from one of the affected
subjects (111-1). Antithrombin III, which is eluted from Sephadex with the last proiein
peak, was of significantly lower activity in 111-1 plasma than in normal plasma. In
Fig. 2� Antithrombin (trian-gles) and antifactor Xa (solid cir-cles) #{246}valuationsin plasmas andaera after gel filtration on Sepha-dex G-150.
C
0
4
NORMAL PLASMA
n�
Ill-I PLASMA
u�
NORMAL SERUM
�
ill-I SERUM
�30 40 50 6030 40 50 6O�
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

224 MARCINIAK, FARLEY. AND DE SIMONE
normal serum a partial utilization of antithrombin III during blood coagulation was
apparent. A total utilization took place in case of Ill-I serum from which antithrom-
bin III was virtually absent. This finding is ofparticular importance since it reflects an
extensive functional involvement of antithrombin III during the process of blood
coagdlatibn. The capacity of antithrombin in the macromolecular fraction from 111-1
serum was slightly greater than in control. In the macroglobulin fraction from plasma
aritithrombin was not analyzed since a considerable adsorption of thrombin on fibrin
that forms in these fractions interferes with the assay. Antifactor Xa in the macro-molecular region revealed activity in normal plasma and serum similar to that in ab-
normal plasma and serum.
The procedure of gel filtration was standardized and applied to plasma samples fromseveral normal subjects and to plasma from members of family i-i. Occasionally serum
samples were also analyzed. We limited the activity studies in filtered fractions to anti-
factor Xa assay because it gave in our hands steady results of a more reproducible
character than results obtained in the evaluation of antithrombin. The capacity of
antithrombin III in a given plasma sample was expressed as the sum of prolongations in
clotting time (during 30-nun incubation with factor Xa) in all fractions located within
the last protein peak. This value in the analysis of 14 normal plasmas ranged from 240to 350 sec with a mean of 299.6 ± 30.4 sec. Accepting antithrombin III activity in
normal plasma for 100% we thus obtained a normal range of 80%-l 17% and a standard
deviation of 10.1%. A normal plasma in which antithrombin III concentration was
evaluated as 92% was diluted with the buffer used in filtration and samples containing
80%, 50%, 40%, and 25% of plasma were subsequently analy±ed. Antithrombin III
titers of 73%, 43%, 35%, and 25% respectively, were obtained confirming the useful-
ness of the method for quantitative analysis.Table 1 shows the values obtained in plasma of family H members. Nine out of 24
analyzed subjects gave values that were significantly lower than those in the normal
group, ranging from 26%-49% of normal activity. Six of the biochemically abnormal
members had history of thrombosis. The seventh member with extensive history of
thrombosis (111-4) revealed normal antithrombin III level, bdt, as mentioned before,
he has been on long-term medication with warfarin. The effect of this medication on
antithrombin III in other members of the family H is documented below. Also the
values originally obtained in the propositus and in his father (11-4), although distinctlybelow normal, might have been to some extent altered by the theEapy with oral anti-
coagulants.
Effect of Heparin In Vitro and In Vivo
In vitro studies were performed on fractions from plasma and serum isolated by gel
filtration. Factor Xa was used as a substrate for inactivation. After addition of heparin
the inactivation of factor Xa was greatly accelerated, but limited to fractions located
in the antithrombin III region (Fig. 3). Plasma fractions from subject 11-4 showed a
diminished responsiveness to heparin. Fractions from 11-4 serum which contained
practically no antithrombin III were almost totally resistant to heparin. These results
are in agreement with the assumption that antithrombin III is the substance throughwhich heparin exerts its anticoagulant effect in blood.
The responsiveness in vivo was evaluated after intravenous injection of 100 U of
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

FRACTION NUMBER
60
40
Fig. 3. Effect of heparin in vi-tro on antifactor Xa activity (solidcircles) in fractions after gel fil- 20tration. Heparin at a concentra-tion of 0.25 �g/ml of fraction was
added; each fraction was then in-cubated with factor Xa (10 U/mI) 0for 5 mm and the loss of coagu-lant activity evaluated.
heparin/kg. In subjects 11-3 and 11-4 the hypocoagulable state, when evaluated by
thrombin time assay, was of much shorter duration and lower intensity than in normal
volunteers (Fig. 4). This was, however, less pronounced when we monitored the effect
of heparin by PTTa assay (Fig. 5). Particularly in the case of patient 111-1, the inhibi-
tion in PTTa after heparin was better expressed than in some of the controls and did
not correlate with her low antithrombin III level. Unfortunately, she was not followed
>6OQL CONTROL #{149}
CONTROL 0400 13-3 #{149}
fl-4 U
201
100
Fig. 4. Changes in thrombin time after heparin
injection in two normal volunteers and two sub-jects with antithrombin Ill deficiency.
I 2 3
HOURS AFTER HEPARIN
FAMILIAL THROMBOSIS 225
Ua,
U)
Lii
I.-
z
0cr
F-
EC
0
c’J4
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

15 60 120
MINUTES AFTER HEPARIN
up by thrombin time evaluations. However, we could demonstrate the insufficiency of
antithrombin III in her plasma even during the high heparin concentration in blood. As
shown in Fig. 6, the analysis of plasma obtained 15 mm after heparin injection re-
vealed a higher activity of heparin in subject 111-1 than in the normal volunteer. At the
same time, however, antithrombin III fraction of the affected subject remained in-
significant in its antithrombin activity, which was in sharp contrast to the eminent
elevation in the control. The discrepancy between this result and the marked hypo-
coagulability of whole plasma in subject III-! was apparently due to the fact that be-
fore the fractionation heparin at high concentration remained in contact with anti-
thrombin III compensating for its low level. During the fractionation on Sephadex
nuost of the heparin had been separated in association with other protein structures,’5
eliciting the defect.
Ua,10
Lii
I-
(9zF-F-0-JU
‘I
20 30 40 50 20 30 40 50
FRACTION NUMBER
226 MARCINIAK. FARLEY. AND DESIMONE
>10001 II � ft
GOOL
Ua,
(I)
0F-I-a.
o CONTROL
o CONTROL ()�o CONTROL Q#{225}�
D fl-3d’#{149}11-4 0’
0111-I �
Fig. 5. Changes in PTTa after heparin in-
jection in three volunteers and three subjectswith antithrombin III deficiency.
Fig. 6. Gel filtration ofplasma from blood taken 15mm after intravenous injection
of 100 U heparin/kg. For eval-uation of antithrombin ac-tivity (dotted line) each frac-tion was incubated withpurified thrombin (20 U/mI)for 5 mm. Heparin (solid cir-cles) filters presumably in as-sociation with beta lipo-proteins.1 �
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom
FAMILIAL THROMBOSIS 227
‘Patient postaortic valve replacement, on warfarin for 5 yr.tThis patient was taking hedulin irregularly at the time of analysis.
Table 2. The Effect of Therapy With Warfarin on Antithrombin Ill Level in Deficient Subjects
SubjectDuration of
TherapyProthrombin
Time (sect)
A-Ill Level
in Plasma (%)
11-3 Before4 days
4mo
12.9
18.3
17.3
31
41
56
11-4 Before’
5 days
3wk
2 mo
12.0
23.0
23.0
20.0
32
48
52
79
Ill-i Before
4 days1 mo
11.6
20.0
20.1
26
68
68
111-15 Before
6mo
11.8
18.5
48
76
111-16 14 days
20 days
4mo
6’/2 mo
9 mo
22.0
18.5
18.2
19.8
22.6
48
51
58
78
61
‘On hedulin.
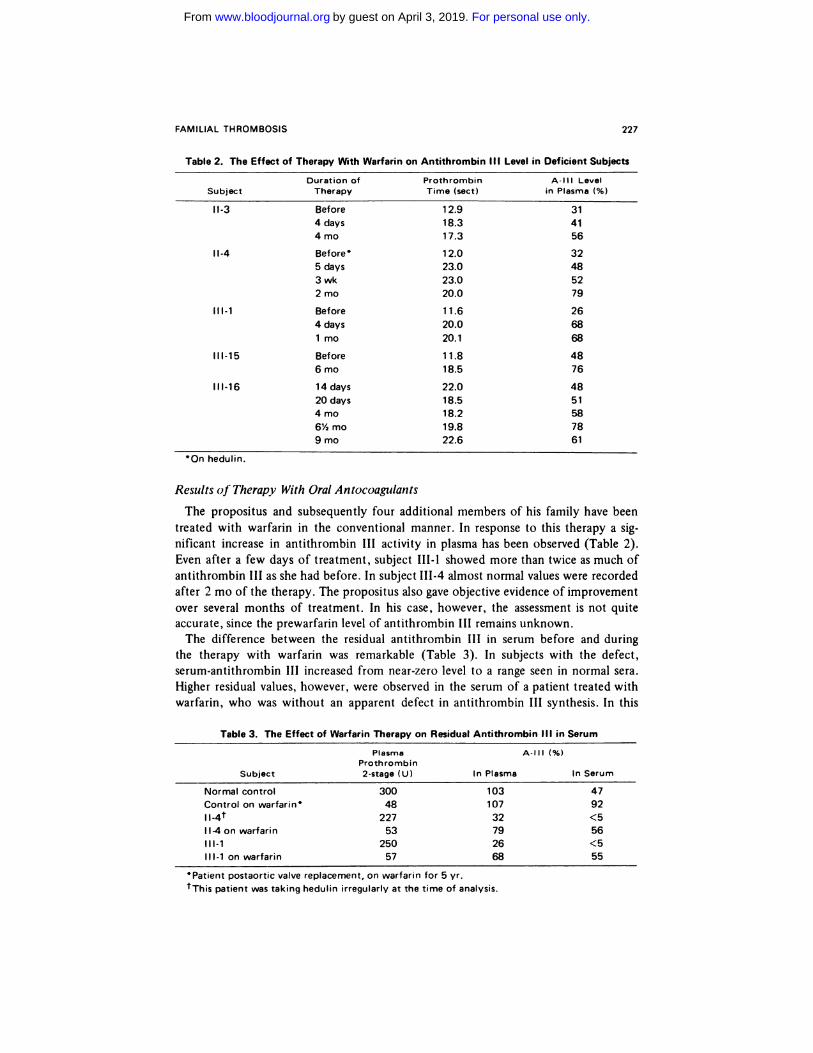
Results of Therapy With Oral Antocoagulants
The propositus and subsequently four additional members of his family have been
treated with warfarin in the conventional manner. In response to this therapy a sig-
nificant increase in antithrombin III activity in plasma has been observed (Table 2).
Even after a few days of treatment, subject 111-1 showed more than twice as much of
antithrombin III as she had before. In subject 111-4 almost normal values were recorded
after 2 mo of the therapy. The propositus also gave objective evidence of improvement
over several months of treatment. In his case, however, the assessment is not quite
accurate, since the prewarfarin level of antithrombin III remains unknown.
The difference between the residual antithrombin III in serum before and during
the therapy with warfarin was remarkable (Table 3). In subjects with the defect,
serum-antithrombin III increased from near-zero level to a range seen in normal sera.
Higher residual values, however, were observed in the serum of a patient treated with
warfarin, who was without an apparent defect in antithrombin III synthesis. In this
Table 3. The Effect of Warfarin Therapy on Res idual Antithrom bin I II in Serum
Plasma A-Ill (%)Prothrombin
Subject 2-stage (U) In Plasma In Serum
Normal control 300 103 47
Control on warfarin’ 48 107 92
lI.4� 227 32 <5ll-4onwarfarin 53 79 56
Ill-i 250 26 <5
Ill-i on warfarin 57 68 55
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

228 MARCINIAK. FARLEY. AND DESIMONE
latter case we could not account for a significant increase of plasma antithrombin III
above normal level. This leaves us with the impression that stern stochiometric propor-
tions are implicated in the neutralization ofcoagulation enzymes in blood.
DISCUSSION
The biochemical defect in family H is apparently transmitted by an autosomal gene
and has a dominant character with incomplete penetrance. Nine members are heter-
ozygotes with antithrombin III ranging approximately from 25% to 50% of normal
level, as evaluated by the anticoagulant properties. An additional five members, three
of whom died before we started the investigation, are suspected of having the de-
ficiency. Although there is a good correspondence between the presence of the bio-
chemical defect and the occurence of thrombosis, the clinical symptoms appear rather
late in life, frequently after the age of 20. A similar hereditary abnormality was re-
ported originally by Egeberg 8 yr ago.5 No other evidence in the literature indicates
that additional families are involved. Taking into consideration the dominant character
of this trait, one has to assume that the frequency of the abnormal gene must be
extremely low. On the other hand, the evaluation of antithrombin III, at the present
time, belongs to seldomly used laboratory procedures, and available methods are far
from being satisfactory. Thus, a number of cases may escape the evidence of the in-
vestigator, despite a remarkable family history. In studies conducted on sporadic cases
with thrombosis Abildgaard et al.’9 observed frequently a marked decrease in plasma
levels of antithrombin III, but attributed this to an enhanced consumption. Hensen
and Loeliger2#{176} recorded normal values in all their patients with thrombosis.
Antithrombin III has the distinction of being a protein with well-defined properties,
known to interact stoichiometrically with thrombin2’ and with factor Xa,’#{176}on ac-
count of which it can be visualized as an insurance agent against acute thrombotic
episodes. Nevertheless, the question which remains to be answered is, to what extent
normal persons benefit from these properties of antithrombin III. The existence of
individuals with incomplete antithrombin III synthesis due to a selective genetic de-
fect, many of whom develop deep vein thrombosis and pulmonary embolism without
any apparent cause, not only buttresses the biological significance of antithrombin III
but indicates that the tendency for intravascular coagulation has been generally under-estimated. The ratio of antithrombin III capacity to the potential capacity of thrombin
undoubtedly plays a very important role in the prevention of thrombosis. The liver
appears to be the only organ in which antithrombin III is produced. In addition to the
inborn defect, low levels are commonly observed in liver cirrhosis.’9’2#{176} The explana-
tion for the observation that thrombosis does not appear in the cirrhotic patient to the
same extent as in congenital deficiency of antithrombin III lies in the differential re-
quirements of the two abnormalities for antithrombin III. In liver cirrhosis the synthe-
sis of prothrombin and factor X is impaired, which lowers the requirement for the
inactivator. For members of family H with normal levels of vitamin-K-dependent
coagulants, higher levels of antithrombin III are required in order to support ade-
quately the fluidity of their blood. On this assumption one would expect a significant
improvement of the biologic equilibrium in patients with hereditary deficiency of
antithrombin III by lowering their level of circulating procoagulantsl The relatively
short time during which a systematical therapy with warfarin has been administered in
members of family H does not allow us yet to assess properly their clinical responsive-
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

FAMILIAL THROMBOSIS 229
ness. Nevertheless, as a result of the therapy, not only the residual antithrombin III in
serum appeared in quantities indicating a generous surplus over the capacity required
for thrombin inactivation, but a significant increase in plasma levels has been recorded.
The latter effect might be attributed to either the possibility that a catabolic pathway
of antithrombin III is also induced by its stochiometric binding to activated coagula-
tion enzymes, or that coumadin stimulates the synthesis. Of interest is the fact that,
although an increase in normal plasma levels of antithrombin III in patients on oral
anticoagulants has been noticed before,20’4 it was usually of a very moderate degree.
Similar therapy in some of the subjects with the defect whom we observed raised the
level of antithrombin III more than twice above the original value. At the present time
we are unable to offer an explanation for this discrepancy. The fact that must be taken
under consideration, however, is that a long-lasting therapy with oral anticoagulants
giv#{231}san objective improvement in patients with the hereditary antithrombin III de-
ficiency, which worsens the conditions for a laboratory diagnosis of this abnormality.
The responsiveness to heparin in vivo in nuembers of family H reflects a direct stimu-
lation of antithrombin III, which as a sole blood component in concert with heparin
provides the anticoagulant effect. Only in the event of a complete absence of anti-
thrombin III will this effect be abolished. Such a condition, however, in a human being
is unknown and probably incompatible with life. In heterozygotes, like the menubers
of family H, it is a question of supporting an adequate amount of heparin in order to
compensate for low antithrombin III level. This amount may not differ significantly
from a conventionally applied dose and is probably highly individual, since the distri-
bution of heparin in blood depends on other plasma components than antithrombin
111.15 When an abnormal type of gamma globulin appears in the circulation, the
therapy with heparin may be completely futile despite a normal antithrombin III
level.22 Partial neutralization of heparin by blood cell constituents23’24 found in
platelets, e�ythrocytes, and neutrophils also may contribute to a variable responsive-
ness. Furthermore, the rate of heparin decay or elimination from blood, the niecha-
nism of which remains unknown, will influence the duration and extent of the anti-
coagulant effect. Thus, variations in the responsiveness to heparin among persons with
an inborn error of antithrombin III metabolism, as unrelated to the profoundness of
the defect, are not surprising.
In the view of a high frequency of thrombosis in the family H, it seems unquestion-
able that antithrombin III represents the principal biochemical safeguard against fibrin
deposition inside the vessels. As documented previously,’0 under biological conditions
thrombin constitutes the main target for this antiproteinase, factor Xa being protected
by a complex formation with phospholipid and factor V. Of some concern, however,
is the specificity of other natural proteinase inhibitors. Despite elevated antitrypsin
activity in antithrombin Ill-deficient sera, we could not account for any thrombin
inhibition that might have corresponded to the alpha-i antitrypsin fraction. This con-
tradicts some of previously published suppositions25 in regard to the role of antitryp-
sin in binding and disposition of thrombin. In the case of this antiproteinase, however,
the time of interaction26 and species specificity of the reacting components21 may
contribute to outstanding discrepancies in experimental results. It is also difficult to
determine critically the biological implications of macroglobulin fraction for throm-
bosis and hemostasis. Although a bimolecular binding of thrombin’6 and factor Xa’8
by components of this fraction has been documented, the inhibitory capacity of
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

230 MARCINIAK. FARLEY, AND DESIMONE
macroglobulins for coagulation enzymes seems to remain unchanged after blood
clotting, even in subjects with antithrombin III deficiency. This may imply that the
biological role of macroglobulins is rather negligible. On the other hand, experimental
procedures may alter significantly the physiological environment in which macro-
globulins function as inactivators of coagulation enzymes.3”8
ACKNOWLEDGMENT
We would like to thank Dr. Douglas Rees for serum antitrypsin estimations. The technical
assistance of Mrs. Sharon Calhoun and the secretarial service of Mrs. Pat Schrils are gratefully
acknowledged.
REFERENCES
I. Seegers WH, Marciniak E: Inhibition of
autoprothrombin C activity with plasma. Nature
(Lond) 193:1188, 19622. Yin ET, Wessler 5, Stoll PJ: Identity of
plasma-activated factor X inhibitor with anti-
thrombin III and heparin co-factor. J Biol
Chem 246:37 12, 1971
3. Marciniak E, Tsukamura S: Two progres-
sive inhibitors of factor Xa in human blood. Br
J Haematol 22:34 1, 1972
4. Biggs R, Denson KWE, Akman N, Borrett
R. Hadden M: Antithrombin III, antifactor Xa
and heparin. Br J Haematol 19:283, 1970
5. Egeberg 0: Inherited antithrombin defi-
ciency causing thrombophilia. Thromb Diath
Haemorrh 13:5 16, 1965
6. Egeberg 0: On the natural blood coagula-
tion inhibitor system. Investigations of inhibitor
factors based on antithrombin deficient blood.
Thromb Diath Haemorrh 14:473, 19657. Abildgaard U, Egeberg 0: Thrombin in-
hibitory activity of fractions obtained by gel
filtration of antithrombin III deficient plasma.
Scand J Haematol 5:155, 1968
8. Marciniak E: Functional and steric charac-
teristics of modified thrombin zymogen.
Thromb Diath Haemorrh 24:361, 1970
9. Seegers WH, Levine WG, Shepard RS:
Further studies on the purification of throm-
bin. Can J Biochem Physiol 36:603, 1958
10. Marciniak E: Factor-Xa inactivation by
antithrombin III: evidence for biological stabili-
zation of factor Xa by factor V-phospholipid
complex. Br J Haematol 24:391, 1973
11. Quick A: On the quantitative estimation
of prothrombin. Am J Clin Pathol 15:560,
1945
12. Seegers WH, Smith, HP: Factors which
influence the activity of purified thrombin.
Am J Physiol 137:348, 1942
13. Ware AG, Seegers WH: Two-stage pro-
cedure for the quantitative determination of
prothrombin concentration. Am J Clin Pathol
19:47 1, 1949
14. Homer GM, Katchman BJ, Zipf RE: A
spectrophotometric method for measuring serum
trypsin inhibitor capacity. Clin Chem 9:428,
1963
15. Marciniak E: Binding and activity of
heparin in human plasma. Fed Proc 32:290,
1973
16. Lanchantin GF, Plesset ML, Friedman
JA, Hart DW: Dissociation of esterolytic and
clotting activities of thrombin by trypsin-bind-
ing macroglobulin. Proc Soc Exp Biol Med
121:444, 1966
17. Steinbuch M, Blatrix C, Josso F: Alpha2-
macroglobulin as progressive antithrombin. Na-
ture (Lond) 2 16:500, 1967
18. Marciniak E: Biological stability of factor
Xa. Thromb Diath Haemorrh (in press)19. Abildgaard U, Fagerhol MK, Egeberg 0:
Comparison of progressive antithrombin activ-
ity and the concentrations of three thrombin
inhibitors in human plasma. Scand J Clin Lab
Invest 26:349, 1970
20. Hensen A, Loeliger EA: Antithrombin
III: its metabolism and its function in blood
coagulation. Thromb Diath Haemorrh 9: 1(suppl
1), 1963
21. Abildgaard U: Binding of thrombin to
antithrombin III. Scand J Clin Lab Invest
24:23, 1969
22. Glueck HI, MacKenzie MR, Glueck CJ:
Crystalline IgG protein in multiple myeloma:
identification effects on coagulation and on
lipoprotein metabolism. J Lab Clin Med 79:73 1,
1972
23. Poplawski A, Niewiarowski S: Methodfor determining antiheparin activity of platelets
and erythrocytes. Thromb Diath Haemorrh
13: 149, 1965
24. Saba HI, Roberts HR. Herion JC: The
antiheparin activity of lysosomal cationic pro-
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

FAMILIAL THROMBOSIS 231
teins from polymorphonuclear leukocytes.
Blood 31:369, 1968
25. Gans H, Tan BH: Alpha I antitrypsin, an
inhibitor for thrombin and plasmin. Clin Chim
Acta 17:111, 1967
26. Rimon A, Shamash Y, Shapiro B: The
plasmin inhibitor of human plasma. IV: Its
action on plasmin, trypsin, chymotrypsin and
thrombin. J Biol Chem 241:5 102, 1966
27. Colman RW, Mitchell B: Specificity of
inhibitors lacking in alpha 1 antitrypsin defi-
ciency and hereditary angioedema toward hu-
man proteolytic enzymes. Clin Chim Acta 39:5,
1972
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

1974 43: 219-231
Ewa Marciniak, Claude H. Farley and Philip A. DeSimone Familial Thrombosis Due to Antithrombin III Deficiency
http://www.bloodjournal.org/content/43/2/219.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom
Related Documents