VOLUME 174 NUMBER 3 JULY, AUGUST, SEPTEMBER 2005 CONTENTS INCLUDE: CHD prescribing trends in Ireland Falls in an Acute Hospital Outcome of bone marrow transplantation The incidence of postoperative venous thrombosis Guidelines for the management of Hep C in general practice Schizophrenia in general practice Informed consent and patients’ understanding

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
VOLUME 174 NUMBER 3 JULY, AUGUST, SEPTEMBER 2005 CONTENTS INCLUDE:
CHD prescribing trends in IrelandFalls in an Acute HospitalOutcome of bone marrow transplantationThe incidence of postoperative venous thrombosisGuidelines for the management of Hep C in general practiceSchizophrenia in general practiceInformed consent and patients’ understanding
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 1
This journal is indexed by Current Contents, Embase and is included in the abstracting and indexing of the Bio Sciences Information Service of Biological Abstracts. It is available in microfilm from University Microfilms Ltd.
All communications to the Editor should be addressed to: 2nd Floor, International House, 20-22 Lower Hatch Street, Dublin 2 Tel: 00353-1-6623706 Fax: 00353-1-6611684 Email: [email protected] Website: www.rami.ie www.iformix.com
Annual Subscription: Ireland and EU Countries E 156 Non-EU E 192 Single Copy E 42
Published by The Royal Academy of Medicine in Ireland
ISSN 0021-1265
Designed by Austin Butler Email: [email protected]
EDIT
ORI
AL
BOA
RD
Editor-in-Chief David Bouchier-Hayes
Editor Brian Sheppard
Editorial Assistant Helen Moore
Editorial Consultant John Daly
Statistical Consultant Alan Kelly
Information Systems Consultant C Shields
JMS Doctor Awards Editor TN Walsh
Editorial Advisers OS Breathnach CF Donegan J Fenton ADK Hill F Howell H O’Connor S Sreenan S Tierney
EXECUTIVE OF THE ACADEMY President FD O’Kelly
General Secretary J O’Connor
Immediate Past President D Bouchier-Hayes
Members TN Walsh K O’Boyle E Kay D McCormack D Curtin
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 3
Original PaPers4. Changes in prevalence of and prescribing for Ischaemic heart disease in Ireland 1990-2002
K Bennett, H Johnson, P Dack, E Shelley, J Feely9. Efficacy of fibrinolysis in the emergency department for acute myocardial infarction
G Lane, J Cuddihy, P Wright, D Doherty, A McShane13. Outcome of bone marrow transplantation in acquired and inherited aplastic anaemia in the Republic of Ireland
A Piccin, A O’Marcaigh, O Smith, J O’ Riordan, M Crowley, E Vandenberg, N Gardiner, S Mc Cann20. The incidence of postoperative venous thrombosis among patients with ulcerative colitis
OJ O’Connor, RA Cahill, WO Kirwan, HP Redmond23. Impact of the informed consent process on patients’ understanding of varicose veins and their treatment
MF Dillon, CJ Carr, TMF Feeley, S Tierney28. Falls in an acute hospital and their relationship to restraint use
KM Tan, B Austin, M Shaughnassy, C Higgins, M McDonald, EC Mulkerrin, ST O’Keeffe32. Guidelines for the management of hepatitis C in general practice: a semi-qualitative interview survey of GPs’
views regarding content and implementationW Cullen, M O’Leary, D Langton, J Stanley, Y Kelly, G Bury
38. Schizophrenia in general practice: a national survey of general practitioners in IrelandB Gavin,W Cullen, B O’Donoghue, JC Ascencio-Lane, G Bury, E O’Callaghan
43. Attitudes to peer review as a competence assurance structure – results of a survey of Irish physiciansAC Moss, T Dugal, B Silke
47. General practice out-of-hours co-operatives in Ireland – emergency service or not?G Bury, D Janes, J Dowling
53. Elevated plasma concentrations of atrial and brain natriuretic peptide in type 1 diabetic subjectsK McKenna, D Smith, M Sherlock, K Moore, E O’Brien, W Tormey, CJ Thompson
58. The issue of Anti D: An integrated seamless approach from recognition of need to bedside administrationMJ Ryan, S Joyce, N O’Brien, E Lynch, G Burke, MR Cahill
64. Patient education in physiotherapy of low back pain: acute outcomes of group instructionSD Alston, TJ O’Sullivan
70. Differences between self-referred and physician-referred hospital admissionsJ Kellett, P McKeown, B Deane
reVieW79. The radial artery: an alternative access site for diagnostic and interventional coronary procedures
NT Mulvihill, PA Crean
Case rePOrTs84. A case of a gastrointestinal stromal tumour presenting as acute abdomen
SA Badger, M Yousaf, WJ Campbell86. Transient global amnesia after sexual intercourse
J Gallagher, MS Murphy, J Carroll88. Epidural abscess causing cauda equina syndrome
B Lenehan, P Sullivan, J Street, S Dudeney92. Gianotti-Crosti syndrome associated with HBV infection in an adult
V Turhan, N Ardic, B Besirbellioglu, T Dogru95. Macroglossia and carpal tunnel syndrome associated with multiple myeloma: a case report
M Kelly, J Moran97. CT Guided Radiofrequency ablation of intra-articular osteoid osteoma of the hip
CP Cantwell, T Scanlon, S Dudeney, J O’Byrne, S Eustace
COrresPOnDenCe100. Coincidental malignancy and abdominal aortic aneurysm: a clinical conundrum
N Ni Choileain, G Fulton101. Surgical treatment of pulmonary embolism
WS Soo, DG Healy, B Maurer¹, JF McCarthy
COnsensUs102. Conference on the living donor renal transplantation
BOOK reVieWs103. Case-based Haematology
PT Murphy104. Short answer questions for the MRCOpth Master Pass
L Cassidy
CON
TEN
TS
4 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 5
with respect to the general population. However, the GMS covers 1.2 million people and previous reports have estimated that it accounts for the majority of medicines prescribed in primary care in Ireland.11 In 2002, this amounted to a total cost of E538 million. The GMS database records basic demographic information on the patients (such as age and sex) and full details on all items dispensed in the scheme, including ingredient costs and pharmacist dispensing fees per item dispensed. Medicines are coded using the WHO Anatomical Therapeutic Chemical (ATC) classification system.12 It does not record data on diagnosis.
For the purpose of this study the GMS prescription database for the largest region in Ireland, the Eastern Regional Health Authority (ERHA), which includes Dublin and the surrounding counties of Kildare and Wicklow, from 1990 to 2002 was used. Patients with CHD were identified in two different ways: (a) prescription of any nitrate therapy in the year and (b) co-prescription of aspirin and nitrate therapy in any month during the year examined. Use of nitrate therapy alone has been shown to have low sensitivity (47%) but high positive predictive value (PPV=83%), whereas aspirin and nitrate has high sensitivity (82%), but low PPV (44%).13 For this reason both approaches were considered. In addition, trends in prescribing of secondary preventive therapies including statins, ACE-inhibitors and β blockers were examined in patients receiving both aspirin and nitrates, and the total number of therapies prescribed (including aspirin) in those receiving any nitrate therapy.
The following WHO ATC codes were used to identify patients on various cardiovascular therapies: nitrate therapy (C01DA), aspirin (B01AC06 and N02BA01), statins (C10AA), ACE inhibitors (C09A), β blockers (C07), and calcium channel blockers (C08).
Age-adjusted CHD rates were calculated per 1000 GMS population, based on the numbers of patients identified as being prescribed (a) aspirin and nitrate therapy, and (b) nitrate therapy alone, and the GMS population in that year. Rates of co-prescribing of secondary preventive therapies were calculated per 1000 GMS population with CHD (using aspirin and nitrate). Log linear (Poisson) regression was used to examine trends in prescribing rates over time, and rate ratios (ratio of two rates, adjusted for other covariates), are presented with 95% confidence intervals (95% CI). Analyses were performed using
K Bennett et al
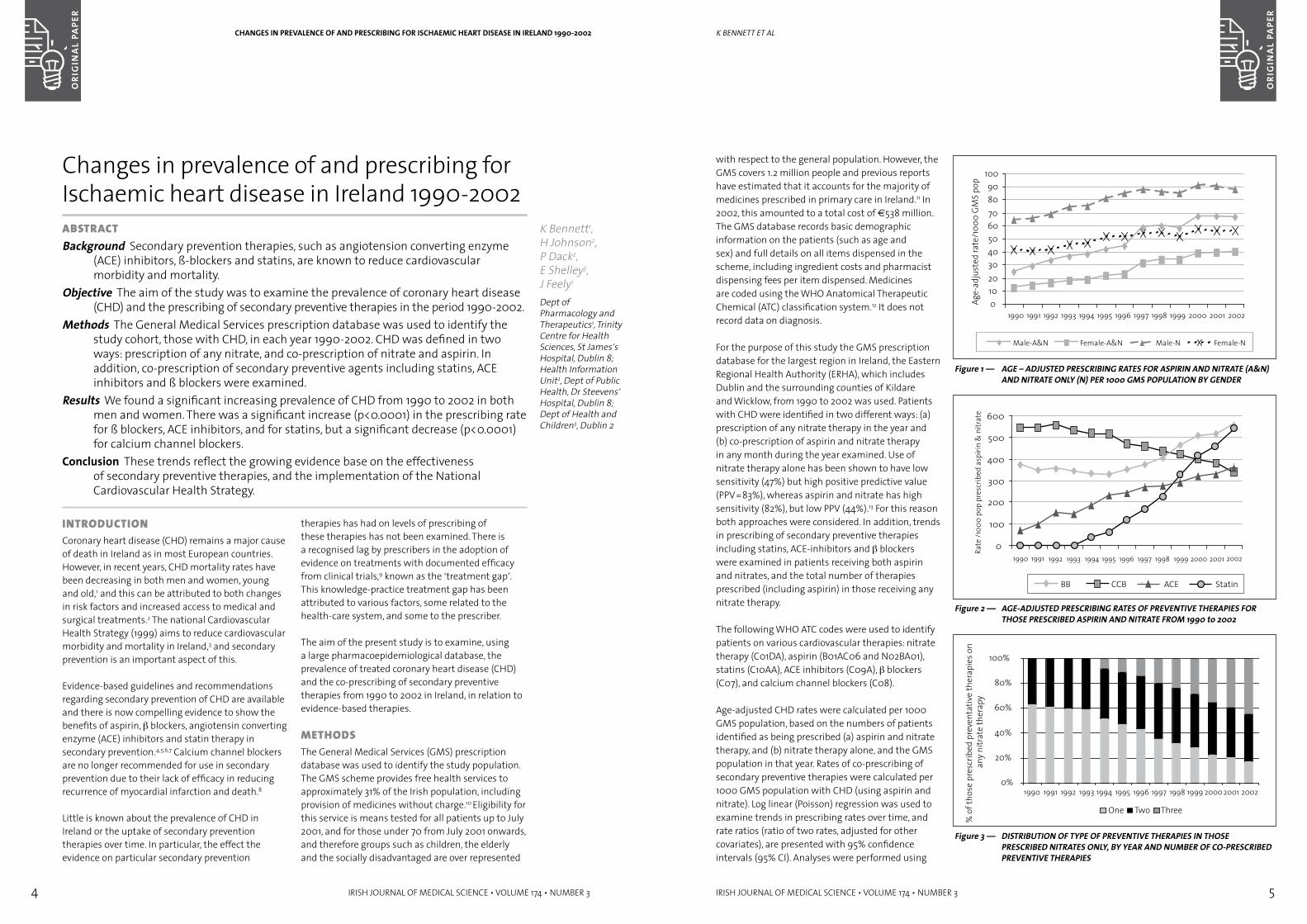
Figure 1 — AGE – ADJUSTED PRESCRIBING RATES FOR ASPIRIN AND NITRATE (A&N) AND NITRATE ONLY (N) PER 1000 GMS POPULATION BY GENDER
Figure 2 — AGE-ADJUSTED PRESCRIBING RATES OF PREVENTIVE THERAPIES FOR THOSE PRESCRIBED ASPIRIN AND NITRATE FROM 1990 to 2002
Figure 3 — DISTRIBUTION OF TYPE OF PREVENTIVE THERAPIES IN THOSE PRESCRIBED NITRATES ONLY, BY YEAR AND NUMBER OF CO-PRESCRIBED PREVENTIVE THERAPIES
inTrODUCTiOnCoronary heart disease (CHD) remains a major cause of death in Ireland as in most European countries. However, in recent years, CHD mortality rates have been decreasing in both men and women, young and old,1 and this can be attributed to both changes in risk factors and increased access to medical and surgical treatments.2 The national Cardiovascular Health Strategy (1999) aims to reduce cardiovascular morbidity and mortality in Ireland,3 and secondary prevention is an important aspect of this.
Evidence-based guidelines and recommendations regarding secondary prevention of CHD are available and there is now compelling evidence to show the benefits of aspirin, β blockers, angiotensin converting enzyme (ACE) inhibitors and statin therapy in secondary prevention.4,5,6,7 Calcium channel blockers are no longer recommended for use in secondary prevention due to their lack of efficacy in reducing recurrence of myocardial infarction and death.8
Little is known about the prevalence of CHD in Ireland or the uptake of secondary prevention therapies over time. In particular, the effect the evidence on particular secondary prevention
therapies has had on levels of prescribing of these therapies has not been examined. There is a recognised lag by prescribers in the adoption of evidence on treatments with documented efficacy from clinical trials,9 known as the ‘treatment gap’. This knowledge-practice treatment gap has been attributed to various factors, some related to the health-care system, and some to the prescriber.
The aim of the present study is to examine, using a large pharmacoepidemiological database, the prevalence of treated coronary heart disease (CHD) and the co-prescribing of secondary preventive therapies from 1990 to 2002 in Ireland, in relation to evidence-based therapies.
MeTHODsThe General Medical Services (GMS) prescription database was used to identify the study population. The GMS scheme provides free health services to approximately 31% of the Irish population, including provision of medicines without charge.10 Eligibility for this service is means tested for all patients up to July 2001, and for those under 70 from July 2001 onwards, and therefore groups such as children, the elderly and the socially disadvantaged are over represented
Changes in prevalence of and prescribing for Ischaemic heart disease in Ireland 1990-2002aBsTraCTBackground Secondary prevention therapies, such as angiotension converting enzyme
(ACE) inhibitors, ß-blockers and statins, are known to reduce cardiovascular morbidity and mortality.
Objective The aim of the study was to examine the prevalence of coronary heart disease (CHD) and the prescribing of secondary preventive therapies in the period 1990-2002.
Methods The General Medical Services prescription database was used to identify the study cohort, those with CHD, in each year 1990-2002. CHD was defined in two ways: prescription of any nitrate, and co-prescription of nitrate and aspirin. In addition, co-prescription of secondary preventive agents including statins, ACE inhibitors and ß blockers were examined.
Results We found a significant increasing prevalence of CHD from 1990 to 2002 in both men and women. There was a significant increase (p<0.0001) in the prescribing rate for ß blockers, ACE inhibitors, and for statins, but a significant decrease (p<0.0001) for calcium channel blockers.
Conclusion These trends reflect the growing evidence base on the effectiveness of secondary preventive therapies, and the implementation of the National Cardiovascular Health Strategy.
K Bennett1, H Johnson2, P Dack2, E Shelley3, J Feely1
Dept of Pharmacology and Therapeutics1, Trinity Centre for Health Sciences, St James’s Hospital, Dublin 8; Health Information Unit2, Dept of Public Health, Dr Steevens’ Hospital, Dublin 8; Dept of Health and Children3, Dublin 2
CHANGES IN PREVALENCE OF AND PRESCRIBING FOR ISCHAEMIC HEART DISEASE IN IRELAND 1990-2002
6 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 7
rate of aspirin and statin prescribing, but lower rates for β blockers and ACE inhibitors compared to other centres.21 The Irish rates now appear to be on the increase, but there still remains some under-prescribing in patients who would potentially benefit from such therapies.
Krumholz et al showed that prescribing of multiple secondary preventive therapies, such as aspirin and ACE inhibitors in confirmed MI cases, confers significantly greater benefit in lowering 1-year mortality.22 In the current analysis those on nitrate therapy alone were more likely to be on multiple preventive therapies over time. Nitrate therapy was used here as it has higher PPV, and it was of interest to examine all related cardiovascular therapies including aspirin. In particular aspirin was the most prescribed preventive therapy, with β blocker therapy closely followed by statin therapy in more recent times. This indicates a shifting emphasis towards increased numbers of evidence-based therapies being prescribed, particularly following the introduction of statins in 1994.
The implementation of the national Cardiovascular Health Strategy, ‘Building Healthier Hearts’3, is likely to have had additional influence on prescribing of secondary prevention therapies, particularly as its importance was highlighted in the recommendations. The HeartWatch programme, a structured approach to secondary prevention in those who have had a recent CHD event, has now been implemented in 20% of general practices.23 This is likely to lead to a further increase in the use of secondary therapies in primary care in the future.
Studies have shown improved adherence and reduced mortality in patients whose statin therapy was initiated in hospital, and hospital prescribing has been found to influence doctors’ prescribing behaviour.24,25 Prescriptions initiated by specialists are more likely to be continued. Central advice from health authorities on best practice prescribing is less likely to make an impact, whereas pharmaceutical company influence is more likely to impact on prescribing practices.24 Other influences on prescribing of new drugs are costs25 and whether the GP is based in a rural or urban area.26 Barriers to the implementation of preventive services include: patient factors including access to care or information, and social aspects; physician factors including the lack of incentives or training, and specialist communication; and barriers within
healthcare settings including acute care priority, resources, facilities and lack of policies.
COnClUsiOnsThe increased prescribing of statins, ACE inhibitors and β blockers are likely to explain some of the decline in cardiovascular mortality observed in recent times.
The trends we observe in our study are probably due to the growing awareness of the evidence base on the effectiveness or otherwise of secondary preventive therapies, the implementation of the national Cardiovascular Health Strategy, as well as the influence of pharmaceutical marketing.
Despite the increased prescribing of preventive therapies, there is still significant room for improvement with most of the therapies still only being prescribed to 40-50% of eligible patients. Closing the treatment gap further with additional use of appropriate therapies and with concurrent risk factor modification should have an additional impact on the decreasing CHD mortality rates in Ireland.
ACkNOwLEDGMENTS
We would like to thank the General Medical Services (Payments) Board for supplying us with the data on which this study is based, and the Health Research Board for funding.
REFERENCES1. 50 years of Heart Disease in Ireland. Mortality,
morbidity and health services implications. Dublin: Irish Heart Foundation, 2001.
2. Unal B, Critchley JA, Capewell, S. Explaining mortality trends from CHD in England and Wales, 1980-20o0.Circulation 2004: 109:1101-1107
3. The Cardiovascular Health Strategy Group. Building Healthier Hearts. Dublin: Stationery Office, 1999.
4. Antiplatelet Trialists’ Collaboration. Collaborative overview of randomised trials of antiplatelet therapy Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. Br Med J 1994;308:81-106.
5. Freemantle N, Cleland J, Young P, Mason J, Harrison J. β-Blockade after myocardial infarction: systematic review and meta regression analysis. Br Med J 1999; 318: 1730-7.
6. The Health Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high risk patients. New Engl J Med 2000; 342: 142-53.
K Bennett et al
SAS Version 8.0 (SAS Institute Inc.). Two-tailed significance at p <0.05 is assumed throughout.
resUlTsWe found a significant increasing prevalence of CHD (using aspirin and nitrate) from 1990 to 2002 in both men (p<0.0001) and women (p<0.0001), from 24.6 to 66.7 per 1000 GMS population in men and 12.2 to 40 per 1000 for women (Figure 1). Overall there was a significantly lower prevalence of CHD in women compared with men (rate ratio=0.52, 95% CI 0.51, 0.53), and in the under 65 compared with the over 65-year-olds (rate ratio= 0.249, 95% CI 0.236, 0.242 ).
There was a significant increase in the co-prescribing rate for β blockers (1.5 fold increase on 1990 rates, p<0.0001), ACE inhibitors (5 fold increase, p<0.0001), and for statins (12.9 fold increase on 1994 rates, p<0.0001) from 1990 to 2002 (Figure 2). However, we found a significant decrease in the co-prescribing rate for calcium channel blockers over the same time period (1.6 fold decrease, p<0.0001, Figure 2).
Figure 3 shows a steadily increasing use of a greater number of cardiovascular preventative therapies, over time, in those receiving nitrates alone. The most prescribed single therapy was aspirin (59% of individuals in 2002), followed by ACE inhibitors (16.5% in 2002). For dual prescribed preventive therapies, the most common was aspirin (41.7% of individuals in 2002), then β blockers (22%), statins (18.4%) and ACE inhibitors (17.9%). For triple preventive therapies, aspirin again was the most common (31.3% in 2002), then statins (26.8%), β blockers (24.8%) and ACE inhibitors (17.2%).
DISCUSSIONThe study shows that some major changes have occurred in the treatment of CHD in Ireland between 1990 and 2002. The prevalence of CHD, as defined by prescription of aspirin and nitrate therapy, has significantly increased over this time and the use of secondary preventive therapies, particularly ACE inhibitors, statins and β blockers has increased substantially, whereas prescribing of calcium channel blockers has decreased.
The increased prevalence of CHD we observe is probably due to an increase in the number of patients presenting and being diagnosed with CHD, as well as increased prescribing rates of nitrates and aspirin in these patients. Aspirin prescribing with nitrates was particularly evident from 1997 onwards,
after publication of a meta-analyses of trials.4 The hypothesis that population prevalence of CHD has increased is supported by the steady increase in hospital discharges for all ischaemic heart disease nationally, from 831 hospital discharges per 100,000 population in 1994 to 946 in 2001 for men and 346 per 100,000 population to 386 for women (age standardised).14
Lampe et al, in a study of British men, found that the prevalence of CHD, as defined by angina symptoms, decreased over time from 1978 to 1996.15 The authors concluded however that the need for secondary prevention among men with established CHD was as great as ever. Their findings contrast with the current study, which shows an increase in CHD, as defined by the prescription of both aspirin and nitrate therapy. A Canadian study found that in elderly patients attending outpatients after AMI, the use of β blockers, ACE inhibitors and statins increased from 1997 to 2000, but that calcium channel blockers and nitrates decreased.16 Martinez et al observed increased prescribing rates of β blockers in patients discharged with acute myocardial infarction in Spain from 1986/88 to 1989/91 (by 28%), but by 1994 these rates had reached a plateau.17 The rate of prescribing had increased in sub-groups, such as the elderly, where previously it had been low. Aspirin prescribing had increased (by 44%), but ACE inhibitors less so (9%), and the rate of calcium channel blockers had decreased by 19% indicating a move towards evidence-based prescribing.
An earlier study examining trends in statin prescribing, using the same GMS prescribing database between 1994 and 1998, found that although there was a rapid increase in the use of statins, the rates were below targets and were initially not directed at the population likely to benefit most or at the recommended dosage.18 The authors concluded that benefits projected from clinical trials may not be seen in clinical practice.
Systematic efforts to estimate the treatment gap, as in ASPIRE19 and EUROASPIRE I and II (European Action on Secondary Prevention through Intervention to Reduce Events),20 in patients hospitalised for coronary artery bypass grafts, percutaneous coronary interventions, acute myocardial infarction or acute myocardial ischaemia, demonstrated large gaps between recommended and implemented treatments for post-event care. The data from the Irish centres in EUROASPIRE II indicated a higher
CHANGES IN PREVALENCE OF AND PRESCRIBING FOR ISCHAEMIC HEART DISEASE IN IRELAND 1990-2002
8 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 9
inTrODUCTiOnCardiovascular disease is the single largest cause of death in Ireland, with over two in five (43%) of all deaths being attributed to this group of diseases.1 Within cardiovascular disease, Ischaemic Heart Disease (IHD) is by far the most common and it alone accounts for approximately 25% of all deaths. Three quarters of those who die from IHD have an Acute Myocardial Infarct (AMI) as their proximate cause of death.1
About 50% of AMI deaths occur within the first two hours from onset of symptoms.2, 3 This emphasises the importance of a rapid response after the onset of symptoms. It has been estimated that appropriate and timely administration of fibrinolysis prevents 20 – 30 deaths per 1000 patients in the first month after treatment.4 Clinical benefit may last a decade or more. The earlier fibrinolytic therapy is given the better for both immediate and long-term mortality and morbidity.5
The time interval between arriving at hospital and being administered fibrinolytic drugs, ‘ the door-to-needle time’, is a surrogate for ‘door to lytic state
time’ and has received much attention from service providers in an effort to reduce unnecessary delays.
Irish and UK targets for ‘door-to-needle time’ are shown in Table 1.
The European Society of Cardiology guidelines propose that patients with clear cut evidence of AMI should enter a ‘fast track’ system in which fibrinolysis is administered in the Emergency Department.6
In 1994 in Ireland, a national census of presentation and management of acute myocardial infarction showed substantial delays in time to treatment: (median time to treatment of 4 hours 30 minutes).7 A national cross-sectional survey of presentation and management of acute coronary syndromes carried out in 2003 showed that substantial improvements in time to thrombolysis had occurred since 1994.8
A similar study in England showed that 76% of patients achieved a 30-minute target door-to-needle time in the first three months of 2003.9 A systematic review of early thrombolysis for the treatment of acute
Efficacy of fibrinolysis in the emergency department for acute myocardial infarctionaBsTraCTBackground Patients with an acute myocardial infarction require a rapid response to
their symptoms and the earlier fibrinolysis is given (where indicated), the better the outcome.
Aims The aim of this study is to compare ‘door to needle times’ for fibrinolysis in Acute Myocardial Infarction (AMI) in three phases of one year each, at Letterkenny General Hospital.
Methods In the PREINTERVENTION year all fibrinolysis was performed in the Coronary Care Unit (CCU). In the INTERVENTION year Emergency Department (ED) fast track fibrinolysis was introduced and in the POST INTERVENTION year most fibrinolysis was performed on fast track in the ED.
Results The time saved by the introduction of ED fibrinolysis was significant, 41 minutes on average per patient. Elderly, female patients were more likely to bypass ED fast track fibrinolysis and to be brought to CCU for fibrinolysis, with attendant delays. This has educational implications in relation to the variation in clinical presentation of AMI with age and sex.
Conclusion The ED fast track fibrinolysis system is recommended as an effective, safe, achievable and worthwhile intervention towards improving ‘door to needle times’ for fibrinolysis in AMI.
G Lane,1 J Cuddihy,2 P Wright,2 D Doherty,2 A McShane1
Emergency Dept,1 Letterkenny General Hospital; Dept of Public Health,2 North Western Health Board2
EFFICACY OF FIBRINOLYSIS IN THE EMERGENCY DEPARTMENT FOR ACUTE MYOCARDIAL INFARCTION
7. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20 536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002;360:7-22.
8. Ryan TJ, Antman EM, Brooks NH et al. 1999 update: ACC/AHA Guidelines for the Management of Patients With Acute Myocardial Infarction: Executive Summary and Recommendations: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Acute Myocardial Infarction). Circulation 1999. 100; 1016-1030.
9. Pearson TA, Peters TD. The therapeutic gap in coronary artery disease and heart failure: Community Standards and Post-Discharge patient. Am J Cardiol. 1997; 80: 45H-52H.
10. Williams D, Feely J. Pharmacoepidemiology - an Irish perspective. Pharmacoepidemiol Drug Saf. 2001;10:641-5.
11. Feely J, Chan R, McManus J, O’Shea B. The influence of hospital-based prescribers on prescribing in general practice. Pharmacoeconomics 1999; 16:175-181.
12. ATC index with DDDs Oslo: WHO Collaborating Centre for Drug Statistics Methodology, 2003.
13. Gray J, Majeed A, Kerry S, Rowlands G. Identifying patients with ischaemic heart disease in general practice: cross sectional study of paper and computerised medical records. Br Med J 2000; 321: 548-550.
14. Public Health Information System (PHIS). Version 6. Information Management Unit, Department of Health and Children: Dublin, 2002.
15. Lampe FC, Morris RW, Whincup PH, Walker M, Ebrahim S, Shaper AG. Is the prevalence of coronary heart disease falling in British men? Heart 2001; 86: 499-505.
16. Pilote L, Beck CA, Karp I et al. Secondary prevention after acute myocardial infarction in four Canadian provinces, 1997-2000. Can J Cardiol 2004; 20: 61-7.
17. Martinez M, Agusti A, Arnau JM, Vidal X, Laporte JR. Trends of prescribing patterns for the secondary prevention of myocardial infarction over a 13-year period. Eur J Clin Pharmacol 1998; 54: 203-8.
18. Feely J, McGettigan P, Kelly A. Growth in use of statins after trials is not targeted to most appropriate patients. Clin Pharmacol Ther. 2000;67(4):438-41
19. Bowker TJ, Clayton TC, Ingham J et al. A British Cardiac Society survey of the potential for the secondary prevention of coronary disease: ASPIRE (Action on Secondary Prevention through Intervention to Reduce Events). Heart 1996 ;75(4):334-42.
20. EUROASPIRE II Study Group. Lifestyle and risk factor management and use of drug therapies in coronary patients from 15 countries; principal results from EUROASPIRE II Euro Heart Survey Programme. Eur Heart J 2001 ;22:554-72.
21. Hall M, McGettigan M, O’Callaghan P, Graham I, Shelley E, Feely J. Comparison of secondary prevention of heart disease in Europe: lifestyle getting worse, therapy getting better in Ireland. Ir Med J 2002; 95:272-4
22. Krumholz HM, Chen YT, Wang Y, Radford MJ. Aspirin and angiotensin-converting enzyme inhibitors among elderly survivors of hospitalisation for an acute myocardial infarction. Arch Intern Med 2001; 161: 538-44.
23. Heart Health Task Force. Ireland’s Changing Heart. Second report on implementation of the Cardiovascular Health Strategy. Dublin: Department of Health and Children, 2003.
24. Jones MI, Greenfield SM, Bradley CP. Prescribing new drugs: qualitative study of influences on consultants and general practitioners. Br Med J 2001; 18: 378-81
25. Jacoby A, Smith M, Eccles M. A qualitative study to explore influences on general practitioners’ decision to prescribe new drugs. Br J Gen Pract. 2003; 53: 120-5.
26. Cutts C, Tett SE. Doctors perceptions of the influences on their prescribing: a comparison of general practitioners based in rural and urban Australia. Eur J Clin Pharmacol 2003; 58: 761-6.
Correspondence to: Dr Kathleen Bennett, Dept of Pharmacology and Therapeutics, Trinity Centre for Health Sciences, St James’s Hospital, Dublin 8.Tel: +353 1 6081303 Fax: +353 1 4539033E-mail: [email protected]
CHANGES IN PREVALENCE OF AND PRESCRIBING FOR ISCHAEMIC HEART DISEASE IN IRELAND 1990-2002
10 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 11
ECGs are required to detect STEMI evolution and the need for subsequent fibrinolysis. These high-risk patients are referred to the Medical Team on-call and the Medical Doctor on duty must assess the patient immediately. If fibrinolysis becomes indicated it must be started as soon as possible.
The objectives of this study were:
(a) To compare door-to-needle time for patients in the ED fast track with door-to-needle times for patients who received fibrinolysis in CCU (i.e. BYPASS GROUP) in the PREINTERVENTION, INTERVENTION and POST INTERVENTION years.
(b) To describe the profile of patients in each of these groups.
(c) To compare mortality rates for patients fibrinolysed in the ED (Fast-Track) with rates for CCU patients (BYPASS GROUP).
resUlTsTable 2 shows the comparison of door-to-needle times in the ED with those in CCU in the PREINTERVENTION (2001), INTERVENTION (2002) and POST INTERVENTION (2003) years.
The time saved by the introduction of ED fibrinolysis was significant, 41 minutes on average per patient (P< 0.01, Wilcoxon two-sample rank sum test).
Of the 28 BYPASS patients in 2002 who were fibrinolysed in CCU, seven had door-to-needle times of greater than 100 minutes.
Table 3 shows the age and sex profile of patients fibrinolysed in the ED and of those who by-passed the ED and were fibrinolysed in CCU.
In the group who received CCU fibrinolysis, although there were more males than females, the median age of the females was 79 compared to 56 for the males. In the ED fibrinolysis group the median ages were 57 for females and 62 for males.The implication is that elderly female patients with AMI were brought to CCU for fibrinolysis with attendant delays.
The mortality rate in the ED group (Intervention) was 7.7% (3/39 patients) while in the CCU group (Pre-intervention) it was 6.3% (4/62 patients). The numbers are inadequately large to allow for testing of statistical significance and the data on mortality were not collected at a specific time interval from fibrinolysis.
Table 3AGE AND SEX OF FIBRINOLYSED PATIENTS
2002 eD CCU (BYPaSS GROUP)
Median age 61.5 72
Sex M 32 16
Sex F 7 12
Table 2COMPARISON OF MEDIAN ‘DOOR-TO-NEEDLE TIMES’
MEDIAN DOOR TO NEEDLE
(MINS)
25TH TO 75TH PERCENTILE
(MINS)
Pre intervention 2001 CCU (2001) (N=62) 62 39 - 93
Intervention 2002Emergency
Dept (N=39, 2002)
21 12.5 - 45.5
Intervention 2002 CCU * (N=28, 2002) 68.5 47.5 - 103
Post intervention 2003Emergency
Dept (N=53, 2003)
20 13.5 - 35
Post intervention 2003 CCU (n=5, 2003) 31 13 - 45
*BYPASS GROUP
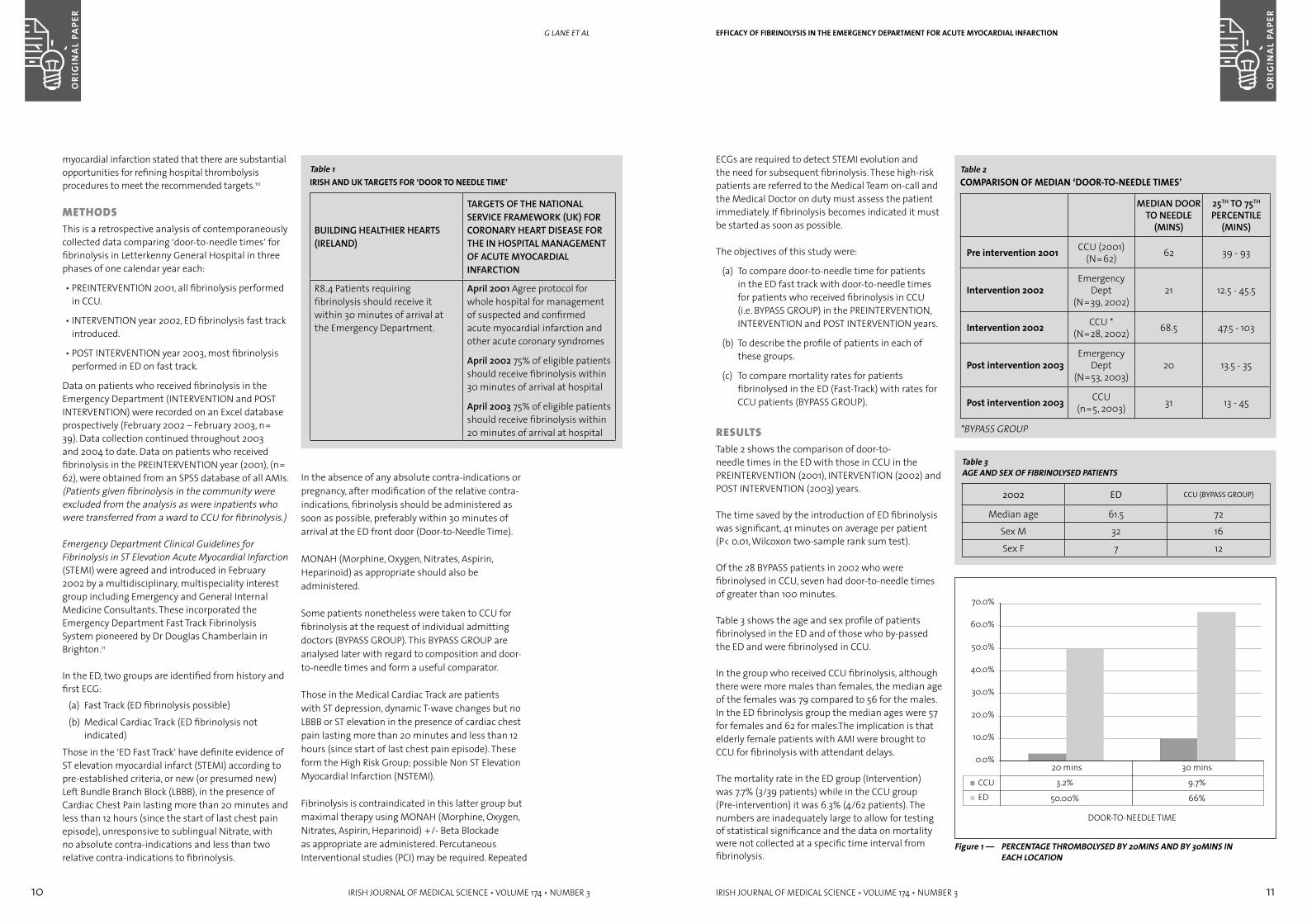
Figure 1 — PERCENTAGE THROMBOLYSED BY 20MINS AND BY 30MINS IN EACH LOCATION
EFFICACY OF FIBRINOLYSIS IN THE EMERGENCY DEPARTMENT FOR ACUTE MYOCARDIAL INFARCTION
myocardial infarction stated that there are substantial opportunities for refining hospital thrombolysis procedures to meet the recommended targets.10
MeTHODsThis is a retrospective analysis of contemporaneously collected data comparing ‘door-to-needle times’ for fibrinolysis in Letterkenny General Hospital in three phases of one calendar year each:
• PREINTERVENTION 2001, all fibrinolysis performed in CCU.
• INTERVENTION year 2002, ED fibrinolysis fast track introduced.
• POST INTERVENTION year 2003, most fibrinolysis performed in ED on fast track.
Data on patients who received fibrinolysis in the Emergency Department (INTERVENTION and POST INTERVENTION) were recorded on an Excel database prospectively (February 2002 – February 2003, n= 39). Data collection continued throughout 2003 and 2004 to date. Data on patients who received fibrinolysis in the PREINTERVENTION year (2001), (n= 62), were obtained from an SPSS database of all AMIs.(Patients given fibrinolysis in the community were excluded from the analysis as were inpatients who were transferred from a ward to CCU for fibrinolysis.)
Emergency Department Clinical Guidelines for Fibrinolysis in ST Elevation Acute Myocardial Infarction (STEMI) were agreed and introduced in February 2002 by a multidisciplinary, multispeciality interest group including Emergency and General Internal Medicine Consultants. These incorporated the Emergency Department Fast Track Fibrinolysis System pioneered by Dr Douglas Chamberlain in Brighton.11
In the ED, two groups are identified from history and first ECG:
(a) Fast Track (ED fibrinolysis possible)
(b) Medical Cardiac Track (ED fibrinolysis not indicated)
Those in the ‘ED Fast Track’ have definite evidence of ST elevation myocardial infarct (STEMI) according to pre-established criteria, or new (or presumed new) Left Bundle Branch Block (LBBB), in the presence of Cardiac Chest Pain lasting more than 20 minutes and less than 12 hours (since the start of last chest pain episode), unresponsive to sublingual Nitrate, with no absolute contra-indications and less than two relative contra-indications to fibrinolysis.
G lane et al
Table 1IRISH AND Uk TARGETS FOR ‘DOOR TO NEEDLE TIME’
BUILDING HEALTHIER HEARTS (IRELAND)
TARGETS OF THE NATIONAL SERVICE FRAMEWORK (UK) FOR CORONARY HEART DISEASE FOR THE IN HOSPITAL MANAGEMENT OF ACUTE MYOCARDIAL INFARCTION
R8.4 Patients requiring fibrinolysis should receive it within 30 minutes of arrival at the Emergency Department.
April 2001 Agree protocol for whole hospital for management of suspected and confirmed acute myocardial infarction and other acute coronary syndromes
April 2002 75% of eligible patients should receive fibrinolysis within 30 minutes of arrival at hospital
April 2003 75% of eligible patients should receive fibrinolysis within 20 minutes of arrival at hospital
In the absence of any absolute contra-indications or pregnancy, after modification of the relative contra-indications, fibrinolysis should be administered as soon as possible, preferably within 30 minutes of arrival at the ED front door (Door-to-Needle Time).
MONAH (Morphine, Oxygen, Nitrates, Aspirin, Heparinoid) as appropriate should also be administered.
Some patients nonetheless were taken to CCU for fibrinolysis at the request of individual admitting doctors (BYPASS GROUP). This BYPASS GROUP are analysed later with regard to composition and door-to-needle times and form a useful comparator.
Those in the Medical Cardiac Track are patients with ST depression, dynamic T-wave changes but no LBBB or ST elevation in the presence of cardiac chest pain lasting more than 20 minutes and less than 12 hours (since start of last chest pain episode). These form the High Risk Group; possible Non ST Elevation Myocardial Infarction (NSTEMI).
Fibrinolysis is contraindicated in this latter group but maximal therapy using MONAH (Morphine, Oxygen, Nitrates, Aspirin, Heparinoid) +/- Beta Blockade as appropriate are administered. Percutaneous Interventional studies (PCI) may be required. Repeated

12 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 13
inTrODUCTiOnThe term aplastic anaemia (AA) refers to a group of rare stem cells disorders characterised by pancytopenia and a hypocellular bone marrow in the absence of an abnormal infiltrate and with no increase in reticulin.1
Severe Aplastic Anaemia (SAA) is defined by a marrow cellularity of <25% and two of the following: neutrophil count <0.5 x 109/l; platelet count <20 x 109/l and a reticulocycte count <20 x 109/l (SAA EBMT Working Party consensus conference). The incidence of SAA varies worldwide between 1.5 - 7.8 per million per year. A higher incidence has been described in the elderly population and in Thailand.2 The aetiology of SAA is still poorly understood, however a large volume of evidence suggests an immune-mediated pathogenesis in the majority of patients.3 Acquired Aplastic Anemia, has occasionally been associated with exposure to drugs, environmental agents, industrial chemicals and viral infection. Chloramphenicol, other antibiotics, anticonvulsant drugs, anti-inflammatory, anti-arthritic, anti-
psychotic agents have been associated as causative agents in some patients. In the majority of cases no clear aetiology is evident and the disease is referred to as idiopathic acquired aplastic anaemia.
Congenital Aplastic Anaemia is a rare condition with an incidence of two per million per year worldwide. Different types of inherited Aplastic Anaemia have been described: Fanconi Anaemia, Blackfan Diamond and Dyskeratosis Congenita.4 Fanconi Anaemia (FA) is the most common of the inherited aplasias. It is associated with increased chromosomal fragility, in metaphase preparations (more evident following addition of clastogenic agents). Auerbach5 described at least eight genes responsible for this autosomal recessive condition. At least four distinct complementation groups have been recognised, each group representing distinct genes on the basis of their separate positions in the human genetic map. The disease becomes clinically evident in the majority of children between the ages of 5-10 years although occasionally the diagnosis may be made in adults. The first manifestation is thrombocytopenia, followed by anemia and
Outcome of bone marrow transplantation in acquired and inherited aplastic anaemia in the Republic of IrelandaBsTraCTBackground Severe Aplastic Anaemia (SAA) and Fanconi Anaemia (FA) are rare
haematological disorders characterised by pancytopenia and bone marrow hypoplasia.
Aims We performed a retrospective study of all patients who underwent BMT for SAA and FA at St James’s Hospital, Dublin, and at OLHSC, Crumlin, between 1985 and 2002.
Methods The medical records of 63 patients, 50 with acquired SAA and 13 with FA, were reviewed.
Results The median age at the time of transplant was 14 years (range 3-43 years). The actuarial survival (OS) (n=63) was 76% at 17 years. The transplant related mortality (TRM) was 22% (n=14). The most common cause of death was infection (46%). The survival was significantly better in patients receiving their transplant after 1995 (p=0.002). Outcome was superior in those receiving less than 20 red cell transfusions prior to transplant: OS 91% (<20 Units) versus 62% (≥20 Units).
Conclusions These national results are comparable to those of published international series and support the use of BMT in the treatment of SAA and FA. The known adverse effect of prior transfusion was confirmed.
A Piccin,1 A O’Marcaigh,2 O Smith,2 J O’ Riordan,1 M Crowley,1 E Vandenberg,1 N Gardiner,1 S Mc Cann1
St James’s Hospital1 and Our Lady’s Hospital for Sick Children,2 Dublin
OUTCOME OF BONE MARROw TRANSPLANTATION IN ACqUIRED AND INHERITED APLASTIC ANAEMIA IN THE REPUBLIC OF IRELAND
Figure 1 shows the percentage of patients fibrinolysed within 30 minutes and within 20 minutes in the CCU (2001) and ED (2002) respectively. In the ED in 2002, 66% of patients were fibrinolysed within 30 minutes of arrival, whereas only 9.7% of patients achieved this in CCU in 2001 prior to ED Fast-Track fibrinolysis (Intervention).
In the year 2003, 58 patients received fibrinolysis in the hospital, 53 within the Emergency Department and five within the Coronary Care Unit (most of these coming from Hospital Wards). For the 53 patients receiving this medication in the Emergency Department the median door-to-needle time was 20 minutes and 68% of patients received their medication within 30 minutes. This represents some further improvement on the median door-to-needle time and percentage receiving fibrinolysis within 30 minutes from the INTERVENTION year (21 minutes and 61% respectively).
DisCUssiOnThis is a sequential, observational study. The method of recording delay times differed in that it was retrospective for the pre-intervention year and prospective for the other two years of the study. This possible source of bias is not thought to be significant in view of the objective documentation of door-to-needle times across the duration of the study.
ED Fast-Track fibrinolysis is faster than admission to CCU for fibrinolysis, (41 minutes saved on average per patient, P<0.01).
Elderly female patients were disproportionately more likely to have by-passed ED fibrinolysis and to have received fibrinolysis in the CCU. This group is likely to benefit proportionately more from fibrinolysis – this has educational implications for doctors and nurses in terms of variation in clinical presentation of MI in relation to age and sex.
Effective from January 1, 2004, the Emergency Department Resuscitation Room became the primary site of fibrinolysis in Acute Myocardial Infarction with ST elevation/bundle branch block, supported by a written multidisciplinary protocol and a ‘Fast Track Tick Sheet’ to expedite drug delivery.
Dedicated teaching within the Emergency Department and on ward rounds continues to focus on the early, safe, rapid delivery of fibrinolysis, while Non-Consultant Hospital Doctors have a formal lecture thereon twice during each six months.
We recommend the Emergency Department Fast Track System as an effective, safe, achievable and worthwhile intervention to those hospitals not currently using ED fibrinolysis who seek to improve their door-to-needle times.
REFERENCES1. Building Healthier Hearts, The Report of the
Cardiovascular Health Strategy Group, Department of Health and Children, March 1999.
2. Gordon T and Kannel WB. Premature mortality from coronary heart disease. The Framingham Study. JAMA 1971; 125: 1617-25.
3. White NM, Parker WS, Binning RA et al. Mobile coronary care provided by ambulance personnel. BMJ 1973; 111: 618-22.
4. Fibrinolytic Therapy Trialists’ Collaborative Group. Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Lancet 1994; 343; 311-22.
5. Boersma E, Maas ACP, Simoons ML. Early thrombolytic treatment in acute myocardial infarction: reappraisal of the golden hour. Lancet 1996; 348: 771-5
6. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Acute Myocardial Infarction: pre-hospital and in-hospital management. Eur Heart J 1996; 17: 43-63.
7. McGee HM, Browne C, Horgan JH: Presentation and management of acute myocardial infarction in Irish hospitals: a national census. Dublin: The Council on Acute Coronary Care of the Irish Heart Foundation; 1996.
8. Doyle F, De La Harpe D, McGee H et al. CCU 2003 ; National Survey of the Presentation and Management of Acute Myocardial Infarction (AMI) and other Acute Coronary Syndromes (ACS) in Irish Hospitals. 2004. Royal College of Surgeons in Ireland, Dublin.
9. How Hospitals Manage Heart Attacks. Second Public Report of the Myocardial Infarction National Audit Project. June 2003. Clinical Effectiveness and Evaluation Unit, Royal College of Physicians, London.
10. Boland A, Dundar Y, Bagust A et al. Early thrombolysis for the treatment of acute myocardial infarction: a systemic review and economic evaluation. Health Technology Assessment 2003; 7 (15): 1-136.
11. Moore R, Moore K, Quinn E et al. Delay times in the administration of thrombolytic therapy: the Brighton experience. Int J Cardiol. 1995 Aug; 49 Suppl:S39-46.
Correspondence to: Dr. John Cuddihy, Dept of Public Health, North Western Health Board, Bishop Street, Ballyshannon, Co. Donegal
G lane et al
14 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 15
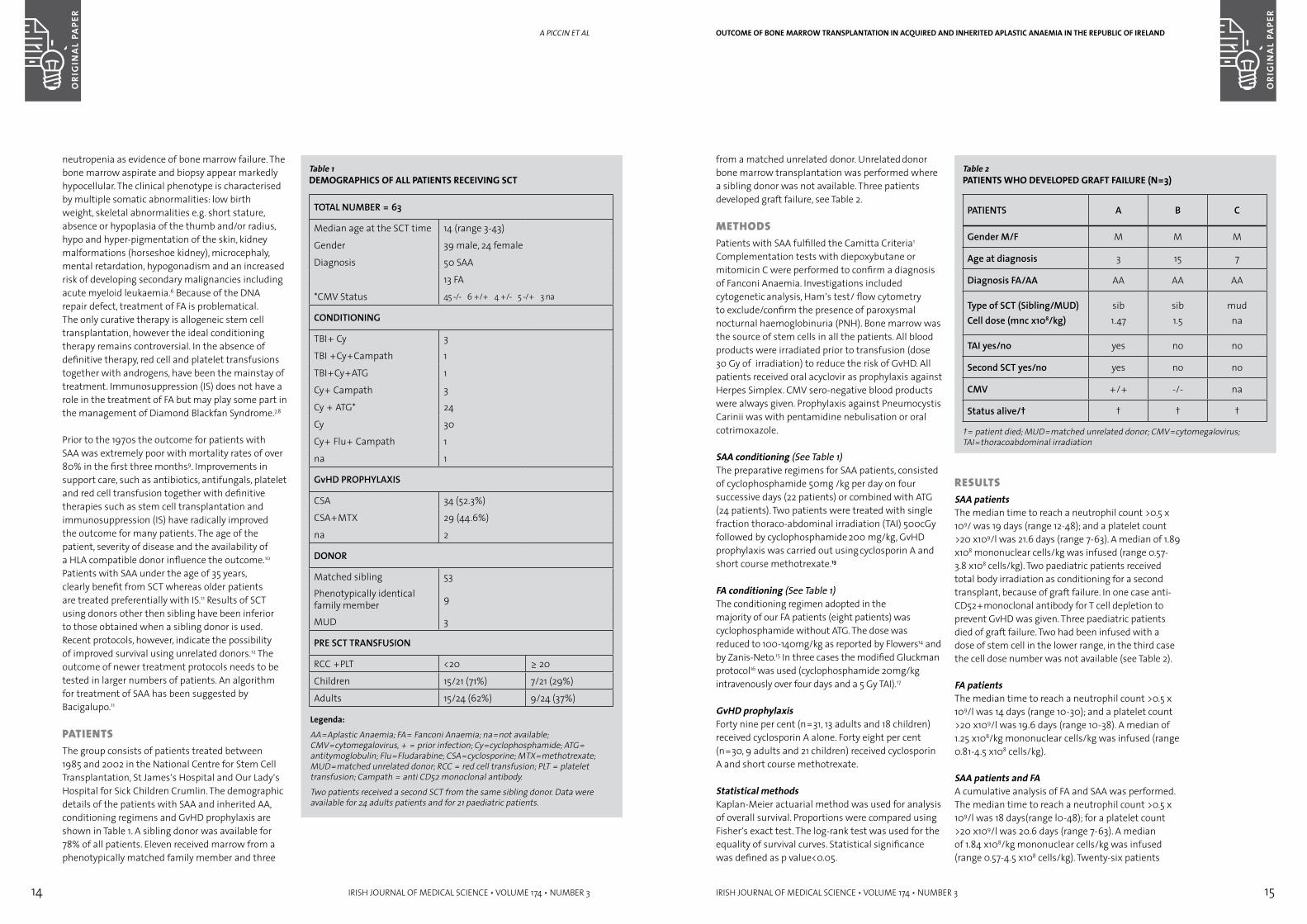
from a matched unrelated donor. Unrelated donor bone marrow transplantation was performed where a sibling donor was not available. Three patients developed graft failure, see Table 2.
MeTHODsPatients with SAA fulfilled the Camitta Criteria1
.
Complementation tests with diepoxybutane or mitomicin C were performed to confirm a diagnosis of Fanconi Anaemia. Investigations included cytogenetic analysis, Ham’s test/ flow cytometry to exclude/confirm the presence of paroxysmal
nocturnal haemoglobinuria (PNH). Bone marrow was the source of stem cells in all the patients. All blood products were irradiated prior to transfusion (dose 30 Gy of γ irradiation) to reduce the risk of GvHD. All patients received oral acyclovir as prophylaxis against Herpes Simplex. CMV sero-negative blood products were always given. Prophylaxis against Pneumocystis Carinii was with pentamidine nebulisation or oral cotrimoxazole.
SAA conditioning (See Table 1)The preparative regimens for SAA patients, consisted of cyclophosphamide 50mg /kg per day on four successive days (22 patients) or combined with ATG (24 patients). Two patients were treated with single
fraction thoraco-abdominal irradiation (TAI) 500cGy followed by cyclophosphamide 200 mg/kg, GvHD prophylaxis was carried out using cyclosporin A and short course methotrexate.13
FA conditioning (See Table 1)The conditioning regimen adopted in the majority of our FA patients (eight patients) was cyclophosphamide without ATG. The dose was reduced to 100-140mg/kg as reported by Flowers14 and by Zanis-Neto.15 In three cases the modified Gluckman protocol16 was used (cyclophosphamide 20mg/kg intravenously over four days and a 5 Gy TAI).17
GvHD prophylaxisForty nine per cent (n=31, 13 adults and 18 children) received cyclosporin A alone. Forty eight per cent (n=30, 9 adults and 21 children) received cyclosporin A and short course methotrexate.
Statistical methodsKaplan-Meier actuarial method was used for analysis of overall survival. Proportions were compared using Fisher’s exact test. The log-rank test was used for the equality of survival curves. Statistical significance was defined as p value<0.05.
OUTCOME OF BONE MARROw TRANSPLANTATION IN ACqUIRED AND INHERITED APLASTIC ANAEMIA IN THE REPUBLIC OF IRELAND
Table 2PATIENTS wHO DEVELOPED GRAFT FAILURE (N=3)
PATIENTS A B C
Gender M/F M M M
Age at diagnosis 3 15 7
Diagnosis FA/AA AA AA AA
Type of SCT (Sibling/MUD)Cell dose (mnc x108/kg)
sib1.47
sib1.5
mudna
TAI yes/no yes no no
Second SCT yes/no yes no no
CMV +/+ -/- na
Status alive/† † † †
†= patient died; MUD=matched unrelated donor; CMV=cytomegalovirus; TAI=thoracoabdominal irradiation
resUlTsSAA patientsThe median time to reach a neutrophil count >0.5 x 109/ was 19 days (range 12-48); and a platelet count >20 x109/l was 21.6 days (range 7-63). A median of 1.89 x108 mononuclear cells/kg was infused (range 0.57-3.8 x108 cells/kg). Two paediatric patients received total body irradiation as conditioning for a second transplant, because of graft failure. In one case anti-CD52+monoclonal antibody for T cell depletion to prevent GvHD was given. Three paediatric patients died of graft failure. Two had been infused with a dose of stem cell in the lower range, in the third case the cell dose number was not available (see Table 2).
FA patientsThe median time to reach a neutrophil count >0.5 x 109/l was 14 days (range 10-30); and a platelet count >20 x109/l was 19.6 days (range 10-38). A median of 1.25 x108/kg mononuclear cells/kg was infused (range 0.81-4.5 x108 cells/kg).
SAA patients and FAA cumulative analysis of FA and SAA was performed. The median time to reach a neutrophil count >0.5 x 109/l was 18 days(range l0-48); for a platelet count >20 x109/l was 20.6 days (range 7-63). A median of 1.84 x108/kg mononuclear cells/kg was infused (range 0.57-4.5 x108 cells/kg). Twenty-six patients
neutropenia as evidence of bone marrow failure. The bone marrow aspirate and biopsy appear markedly hypocellular. The clinical phenotype is characterised by multiple somatic abnormalities: low birth weight, skeletal abnormalities e.g. short stature, absence or hypoplasia of the thumb and/or radius, hypo and hyper-pigmentation of the skin, kidney malformations (horseshoe kidney), microcephaly, mental retardation, hypogonadism and an increased risk of developing secondary malignancies including acute myeloid leukaemia.6 Because of the DNA repair defect, treatment of FA is problematical. The only curative therapy is allogeneic stem cell transplantation, however the ideal conditioning therapy remains controversial. In the absence of definitive therapy, red cell and platelet transfusions together with androgens, have been the mainstay of treatment. Immunosuppression (IS) does not have a role in the treatment of FA but may play some part in the management of Diamond Blackfan Syndrome.7,8
Prior to the 1970s the outcome for patients with SAA was extremely poor with mortality rates of over 80% in the first three months9. Improvements in support care, such as antibiotics, antifungals, platelet and red cell transfusion together with definitive therapies such as stem cell transplantation and immunosuppression (IS) have radically improved the outcome for many patients. The age of the patient, severity of disease and the availability of a HLA compatible donor influence the outcome.10 Patients with SAA under the age of 35 years, clearly benefit from SCT whereas older patients are treated preferentially with IS.11 Results of SCT using donors other then sibling have been inferior to those obtained when a sibling donor is used. Recent protocols, however, indicate the possibility of improved survival using unrelated donors.12 The outcome of newer treatment protocols needs to be tested in larger numbers of patients. An algorithm for treatment of SAA has been suggested by Bacigalupo.11
PaTienTsThe group consists of patients treated between 1985 and 2002 in the National Centre for Stem Cell Transplantation, St James’s Hospital and Our Lady’s Hospital for Sick Children Crumlin. The demographic details of the patients with SAA and inherited AA, conditioning regimens and GvHD prophylaxis are shown in Table 1. A sibling donor was available for 78% of all patients. Eleven received marrow from a phenotypically matched family member and three
a PiCCin et al
Table 1DEMOGRAPHICS OF ALL PATIENTS RECEIVING SCT
TOTAL NUMBER = 63
Median age at the SCT time 14 (range 3-43)
Gender 39 male, 24 female
Diagnosis 50 SAA
13 FA
*CMV Status 45 -/- 6 +/+ 4 +/- 5 -/+ 3 na
CONDITIONING
TBI+ Cy 3
TBI +Cy+Campath 1
TBI+Cy+ATG 1
Cy+ Campath 3
Cy + ATG* 24
Cy 30
Cy+ Flu+ Campath 1
na 1
GvHD PROPHYLAXIS
CSA 34 (52.3%)
CSA+MTX 29 (44.6%)
na 2
DONOR
Matched sibling 53Phenotypically identical family member 9
MUD 3
PRE SCT TRANSFUSION
RCC +PLT <20 ≥ 20
Children 15/21 (71%) 7/21 (29%)
Adults 15/24 (62%) 9/24 (37%)
Legenda:
AA=Aplastic Anaemia; FA= Fanconi Anaemia; na=not available; CMV=cytomegalovirus, + = prior infection; Cy=cyclophosphamide; ATG= antitymoglobulin; Flu=Fludarabine; CSA=cyclosporine; MTX=methotrexate; MUD=matched unrelated donor; RCC = red cell transfusion; PLT = platelet transfusion; Campath = anti CD52 monoclonal antibody.
Two patients received a second SCT from the same sibling donor. Data were available for 24 adults patients and for 21 paediatric patients.
16 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 17
patients with FA were conditioned with low dose cyclophosphamide (100-140mg/kg) as reported by Flowers et al.14 The dose of cyclophosphamide was further reduced if there was concomitant use of TAI.20
Graft failure was not found in FA patients. It was not possible to establish if it was a significant difference in graft failure incidence between FA and AA group because of the small sample. FA patients are more sensitive to cytotoxic chemotherapy and low dose chemotherapy conditioning regimen without the use of total body irradiation (TBI) or TAI are recommended.21
SAA and FAAlthough radiation is useful in reducing the rejection rate, it should not be used because of the risk of secondary malignancies.22 Bone marrow cells rather than mobilised peripheral blood stem cells (PBSC) should be used as source material because of the increased risk of Graft versus Host Disease (GvHD) with PBSC, as reported by Schrezenmeier.23 The number of mononuclear cells infused has been shown to be inversely correlated with the incidence of graft failure. A dose of ≥ 3.0 x108 cells/kg has been shown to reduce this risk. A median of 1.84 x108/kg mononuclear marrow cells (range 0.57-4.5 x108 cells/kg) was given and the graft failure rate was 5%. Three paediatric patients experienced graft failure and in two the cell dose infused was low (Table 1). A large body of evidences exists indicating that the number of red cell and platelet transfusion prior to transplantation has a deleterious effect on the outcome.24 Graft rejection may be influenced by immunisation of the recipients following exposure to HLA antigens. Contaminating white cells in platelet transfusions may be more efficient at immunising recipients than those present in red cell transfusions because of their increased number. The early referral of patients for SCT and the use of universal leukodepletion for red cells may decrease the sensitisation to HLA antigens and may have contributed to improvements in survival in recent years.25,26 Dendritic cells contained in transfusion products may also contribute to sensitisation27.
A regression Cox model analysis carried out retrospectively by the EBMT working party for Severe Aplastic Anaemia in order to find differences in out-come over time clearly showed an improved survival after 1995.28 Similarly we found improved survival rates following SCT for SAA after 1995 (Figure 4).
OUTCOME OF BONE MARROw TRANSPLANTATION IN ACqUIRED AND INHERITED APLASTIC ANAEMIA IN THE REPUBLIC OF IRELAND
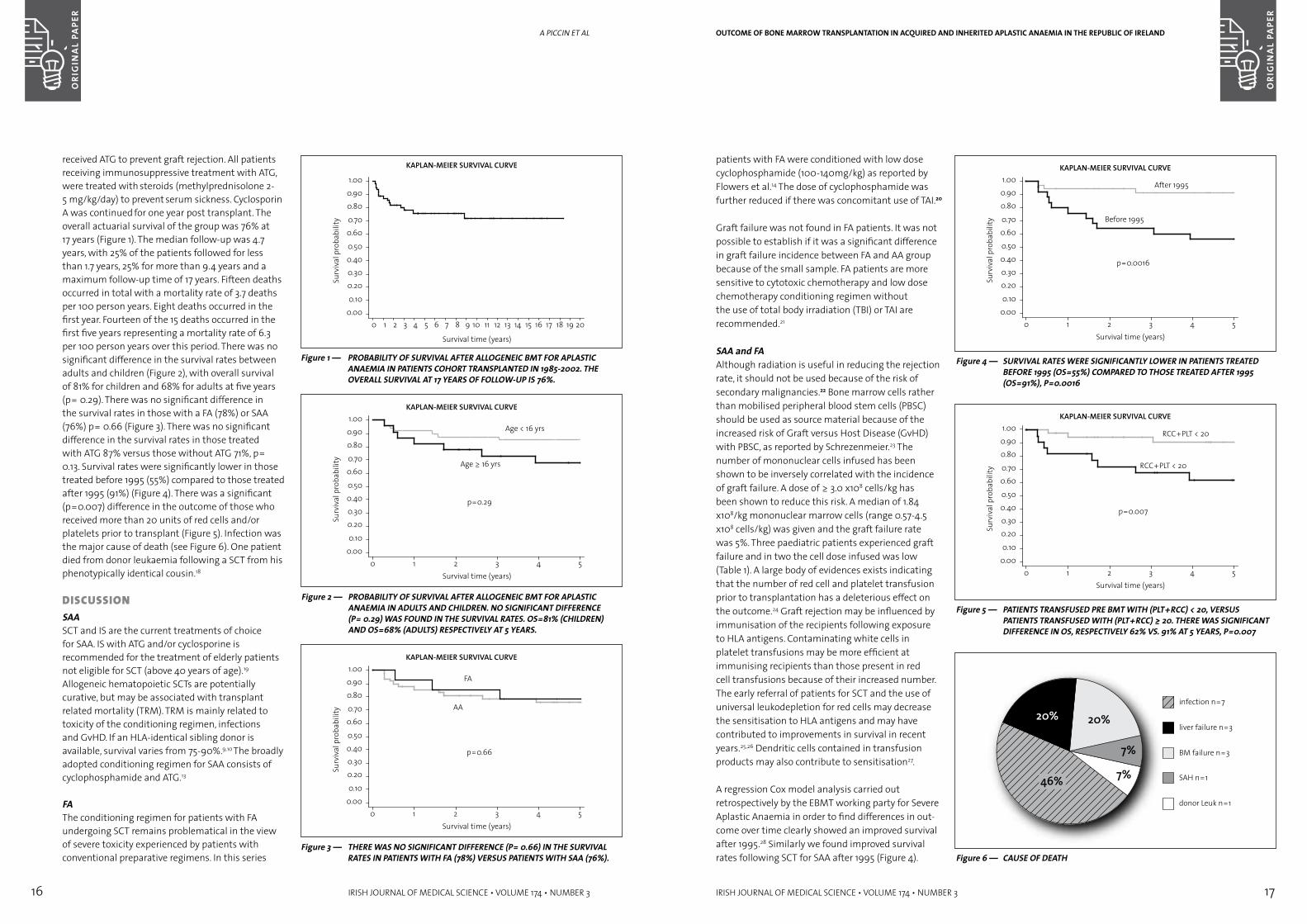
Figure 4 — SURVIVAL RATES wERE SIGNIFICANTLY LOwER IN PATIENTS TREATED BEFORE 1995 (OS=55%) COMPARED TO THOSE TREATED AFTER 1995 (OS=91%), P=0.0016
Figure 5 — PATIENTS TRANSFUSED PRE BMT wITH (PLT+RCC) < 20, VERSUS PATIENTS TRANSFUSED wITH (PLT+RCC) ≥ 20. THERE wAS SIGNIFICANT DIFFERENCE IN OS, RESPECTIVELY 62% VS. 91% AT 5 YEARS, P=0.007
Figure 6 — CAUSE OF DEATH
received ATG to prevent graft rejection. All patients receiving immunosuppressive treatment with ATG, were treated with steroids (methylprednisolone 2-5 mg/kg/day) to prevent serum sickness. Cyclosporin A was continued for one year post transplant. The overall actuarial survival of the group was 76% at 17 years (Figure 1). The median follow-up was 4.7 years, with 25% of the patients followed for less than 1.7 years, 25% for more than 9.4 years and a maximum follow-up time of 17 years. Fifteen deaths occurred in total with a mortality rate of 3.7 deaths per 100 person years. Eight deaths occurred in the first year. Fourteen of the 15 deaths occurred in the first five years representing a mortality rate of 6.3 per 100 person years over this period. There was no significant difference in the survival rates between adults and children (Figure 2), with overall survival of 81% for children and 68% for adults at five years (p= 0.29). There was no significant difference in the survival rates in those with a FA (78%) or SAA (76%) p= 0.66 (Figure 3). There was no significant difference in the survival rates in those treated with ATG 87% versus those without ATG 71%, p= 0.13. Survival rates were significantly lower in those treated before 1995 (55%) compared to those treated after 1995 (91%) (Figure 4). There was a significant (p=0.007) difference in the outcome of those who received more than 20 units of red cells and/or platelets prior to transplant (Figure 5). Infection was the major cause of death (see Figure 6). One patient died from donor leukaemia following a SCT from his phenotypically identical cousin.18
DisCUssiOnSAASCT and IS are the current treatments of choice for SAA. IS with ATG and/or cyclosporine is recommended for the treatment of elderly patients not eligible for SCT (above 40 years of age).19 Allogeneic hematopoietic SCTs are potentially curative, but may be associated with transplant related mortality (TRM). TRM is mainly related to toxicity of the conditioning regimen, infections and GvHD. If an HLA-identical sibling donor is available, survival varies from 75-90%.9,10 The broadly adopted conditioning regimen for SAA consists of cyclophosphamide and ATG.13
FA The conditioning regimen for patients with FA undergoing SCT remains problematical in the view of severe toxicity experienced by patients with conventional preparative regimens. In this series
Figure 1 — PROBABILITY OF SURVIVAL AFTER ALLOGENEIC BMT FOR APLASTIC ANAEMIA IN PATIENTS COHORT TRANSPLANTED IN 1985-2002. THE OVERALL SURVIVAL AT 17 YEARS OF FOLLOw-UP IS 76%.
Figure 2 — PROBABILITY OF SURVIVAL AFTER ALLOGENEIC BMT FOR APLASTIC ANAEMIA IN ADULTS AND CHILDREN. NO SIGNIFICANT DIFFERENCE (P= 0.29) wAS FOUND IN THE SURVIVAL RATES. OS=81% (CHILDREN) AND OS=68% (ADULTS) RESPECTIVELY AT 5 YEARS.
Figure 3 — THERE wAS NO SIGNIFICANT DIFFERENCE (P= 0.66) IN THE SURVIVAL RATES IN PATIENTS wITH FA (78%) VERSUS PATIENTS wITH SAA (76%).
a PiCCin et al
18 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 19
OUTCOME OF BONE MARROw TRANSPLANTATION IN ACqUIRED AND INHERITED APLASTIC ANAEMIA IN THE REPUBLIC OF IRELAND
12. Gupta V, Ball SE, Sage D et al. Marrow transplants from matched unrelated donors for aplastic anaemia using alemtuzumab, fludarabine and cyclophosphamide based conditioning. Bone Marrow Transplant 2005 Mar;35(5):467-71.
13. Storb R, Etzioni R, Anasetti C et al. Cyclophosphamide combined with antithymocyte globulin in preparation for allogeneic marrow transplants in patients with aplastic anaemia. Blood 1994 Aug; 84, (3): 941-949
14. Flowers ME, Doney KC, Storb R et al. Marrow transplantation for Fanconi anemia with or without leukemic transformation: an update of the Seattle experience. Bone Marrow Transplant 1992 Mar;9(3):167-73
15. Zanis-Neto, J, Ribeiro RC, Medeiros C et al. Bone marrow transplantation for patients with Fanconi anemia: a study of 24 cases from a single institution. Bone Marrow Transplant 1995 Feb;15(2):293-8.
16. Gluckman E, Devergie A, Schaison G et al. Bone marrow transplantation in Fanconi Anaemia. Br J Haematol 1980, 45, 557-64
17. Kohli-Kumar M, Morris C, De Laat C et al. Bone marrow transplantation in Fanconi anemia using matched sibling donors. Blood 1994 Sep 15;84(6):2050-4.
18. Browne PV, Lawler M, Humphries P, Mc Cann SR. Donor-cell Leukemia after bone marrow transplantation for severe aplastic anemia. New Engl J Med 1991, 325:710-713
19. Marsh JC, Ball SE, Darbyshire P et al. Guidelines for the diagnosis and management of acquired aplastic anaemia. Br J Haematol 2003 Dec;123(5):782-801.
20. Socie G, Gluckman E, Raynal B et al. Bone marrow transplantation for Fanconi anemia using low-dose cyclophosphamide/thoracoabdominal irradiation as conditioning regimen: chimerism study by the polymerase chain reaction. Blood 1993 Oct 1; 82(7):2249-56
21. De la Fuente J, Reiss S, McCloy M et al. Non-TBI stem cell transplantation protocol for Fanconi anaemia using HLA-compatible sibling and unrelated donors. Bone Marrow Transplant 2004 Jul;34(1):95
22. Deeg HJ, Socie G, Schoch G et al. Malignancies after marrow transplantation for aplastic anemia and fanconi anemia: a joint Seattle and Paris analysis of results in 700 patients. Blood 1996 Jan 1;87(1):386-92.
23. SchrezenmeierH, Bredeson C, Bruno B et al. Comparison of allogeneic bone marrow and peripheral stem cell transplantation for severe Aplastic anaemia: Collaborative study of the European Group for Blood and Marrow Transplantation (EBMT) and International Bone Marrow Transplantation Registry (IBMTR). [abstract]. Blood 2004; 102:#267
24. Doney K., Leisenring W, Storb R et al. Transplant Team (1997) Primary treatment of aquired aplastic anemia: outcomes with bone marrow transplantation and immunosuppressive therapy. Ann Int Med 126:107-115.
25. Weiden PL, Storb R, Slichter S, Warren RP, Sale GE. Effect of six weekly transfusions on canine marrow grafts: tests for sensitisation and abrogation of sensitisation by procarbazine and antithymocyte serum. J Immunol 1976 Jul;117(1):143-50
26. Bean MA, Graham T, Appelbaum FR et al. Gamma-irradiation of pretransplant blood transfusions from unrelated donors prevents sensitisation to minor histocompatibility antigens on dog leukocyte antigen-identical canine marrow grafts. Transplantation 1994 Feb;57(3):423-6.
27. Storb R, Deeg HJ. Failure of allogeneic canine marrow grafts after total body irradiation: allogeneic “resistance” vs transfusion induced sensitisation. Transplantation 42, 571
28. Passweg J. HLA-identical sibling bone marrow transplantation to treat severe aplastic anaemia.In: Schrezenmeier H. Bacigalupo A. Aplastic Anaemia, (1st edition) Cambridge: CambridgeUniversity Press. 2000: 230-25
29. Guardiola P, Socie G, Li X et al. Acute graft-versus-host disease in patients with Fanconi anemia or acquired aplastic anemia undergoing bone marrow transplantation from HLA-identical sibling donors: risk factors and influence on outcome. Blood 2004 Jan 1;103(1):73-77
30. Hows J, Veum Stone J, Camitta BM. In: Schrezenmeier H. Bacigalupo A. Aplastic Anaemia, (1st edition) Cambridge University Press 2000, pag 258-274
31. Niederwieser D, Pepe M, Storb R, Loughran TP Jr, Longton G. Related Improvement in rejection, engraftment rate and survival without increase in graft-versus-host disease by high marrow cell dose in patients transplanted for aplastic anaemia. Br J Haematol 1988 May;69(1):23-8.
32. Ljungman P, Deliliers GL, Platzbecker U et al. Cidofovir for cytomegalovirus infection and disease in allogeneic stem cell transplant recipients. The Infectious Diseases Working Party of the European Group for Blood and Marrow Transplantation. Blood 2001 Jan 15;97(2):388-92.
33. Ryan C. Nicholson S, O’Connell et al. The Hematology Journal 2004, (5), 548-55
Correspondence to: Dr Andrea Piccin, Trinity Centre, Durkan Building, St James’s Hospital, Dublin 8. e-mail: [email protected]
Larger series shows a relatively poor outcome for FA treated with SCT, as the FA patients are more sensitive to cytotoxic chemotherapy,29 therefore low dose conditioning without TBI is recommended.
In this retrospective study, patients with a diagnosis of FA did not show a significance difference in OS, when compared with patients with SAA probably because of the small numbers.
The relative use of SCT or IS in SAA patients, has been reported by Bacigalupo et al.10 They demonstrated that neutrophil count and patient age, at the time of treatment, are important predictors of outcome. SCT was shown to be advantageous in young patients (≤10 years of age) and in adults (≥50 years of age) with neutrophils of <0.1x109/l. In those with a neutrophil count of >0. 5x 109/l, IS was more efficient in those aged ≥50 years of age only. Patients aged 10 – 40 years with a neutrophil count ≤ 0.3x109/l, appeared to have the same outcome whether treated with either SCT or IS. In the absence of a matched sibling donor the use of unrelated matched donors has been evaluated. Results are significantly worse,30 than with sibling donors in part because of the late referral pattern to transplant units and the fact that patients are heavily pre-transfused at the time of SCT. Newer protocols using powerful immunosuppression with purine analogues may alter the outcome favorably.11
SCT for haematological malignancies is associated with the definitive risk of GvHD even in fully matched sibling pairs. In patients receiving SCT for leukaemia the so-called Graft versus Leukaemia (GvL) effect is closely associated with GvHD and a reduced risk of leukaemia relapse. The use of mobilised peripheral blood stem cells has been shown in randomised studies to increase the risk of chronic GvHD but reduce the relapse rate and therefore may be the stem cell sources of choice in patients with high-risk leukaemias. In SAA, however, the occurrence of GvHD offers no benefits and therefore the recommendation of the EBMT Working Party is that bone marrow should be the source of stem cell for patients undergoing SCT for SAA.31
Deaths from infections have decreased since the introduction of CMV antigen testing and pre-emptive treatment with ganciclovir.32 The introduction of antifungal prophylaxis and early treatment in conjunction with early diagnosis of invasive fungal pneumonia with CT scanning may have also contributed to reduced mortality post SCT.33
In the last 20 years the outcome for patients with SAA has improved significantly. Results obtained in the National Transplant Centre at St James’s and OLHSC Crumlin are in keeping with the international experience. The optimum treatment for FA remains problematical.
ACkNOwLEDGEMENTS
We would like to thank Dr Tony Fitzgerald for the supervision of the statistical analysis. We are grateful to Ms Fay Evans, Ms Eileen Nolan and Ms Hillary Kerrigan for helping in the data management. We acknowledge the support of the Bone Marrow for Leukaemia Trust.
REFERENCES1. Camitta BM. Criteria for severe aplastic anaemia. Lancet
1988 Feb 6;1(8580):303-4.
2. Heimpel H. Epidemiology and etiology of aplastic anaemia. In: Schrezenmeier H. Bacigalupo A. Aplastic Anaemia, (1st edition) Cambridge: Cambridge University Press. 2000: 97-116.
3. Nakao S. Role of T-lymphocytes in the pathophysiology of aplastic anemia. In: Schrezenmeier H. Bacigalupo A. Aplastic Anaemia, (1st edition) Cambridge: Cambridge University Press. 2000: 41-57.
4. Schroeder TM. Genetically determined chromosome instability syndromes. Cytogenet Cell Genet. 1982;33 (1-2):119-32.
5. Auerbach AD. Fanconi anaemia diagnosis and the diepoxybutane (DEB) test. Experimental Haematology 1993; 21, 731-733 Blood. 1996 Jan 1;87(1):386-92.
6. Butturini A, Gale RP, Verlander PC, Adler-Brecher B, Gillio AP, Auerbach AD. Hematologic abnormalities in Fanconi anemia: an International Fanconi Anemia Registry study. Blood 1994 Sep 1;84(5):1650-5.
7. Alessandri AJ, Rogers PC, Wadsworth LD, Davis JH. Diamond-blackfan anemia and cyclosporine therapy revisited. J Pediatr Hematol Oncol 2000 Mar-Apr;22(2):176-9.
8. Splain J, Berman BW. Cyclosporin A treatment for Diamond-Blackfan anemia. Am J Hematol 1993 Apr;42(4):406-7.
9. Passweg JR, Socie G, Hinterberger W et al. Bone marrow transplantation for severe aplastic anemia: has outcome improved? Blood 1997 Jul 15;90(2):858-64.
10. Bacigalupo A, Brand R., Oneto R et al. Treatment of acquired severe aplastic anaemia: Bone Marrow Transplantation Compared with immunosuppressive therapy-the European group for blood and marrow transplantation experience. Seminars in Hematology 2000 Jan, 37, (1), 69-80
11. Bacigalupo A. Third ESCT/AMGEN workshop on reduced-intensity conditioning allogeneic haemopoietic stem cell transplant (RIC-HISCT), and panel consensus. Bone Marrow Transplant 2004, 33: 691-696
a PiCCin et al
20 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 21
postoperative courses were examined for clinical or radiological evidence of DVT or PE within one month of major abdominal or pelvic surgery, the data being retrieved using radiological databases and the patients’ own medical records. Standard perioperative anti-thrombotic measures included thromboembolic deterent stockings (TEDS), early postoperative mobilisation and subcutaeneous low molecular weight heparin administration (enoxaparin 1991-1999, tinzaparin 1999-2001).
resUlTsSeventy-nine patients with UC undergoing major abdominal surgery were identified, 53 of whom were male and 26 female. The mean age was 38.2 yrs (range 2.5–72). In total, these patients underwent 180 operations: 70 had a subtotal colectomy, 51 had an proctectomy and ileoanal pouch formation and 41 had reversal of their defunctioning ileostomy performed. The remaining procedures included proctectomy alone (n=6), adhesiolysis for small bowel obstruction (n=3), repair of fistula (n=3), excision of J pouch (n=4) and revision of stoma (n=2).
Eighteen patients with FAP were identified, of whom 11 were male and 7 female. The mean age was 37.2 yrs (range 16.5–79). These patients had 35 operations performed with 13 having a restorative panproctocolectomy. Five patients had a subtotal colectomy with an ileorectal anastomosis, four a proctectomy with ileoanal pouch formation and a further 13 reversal of their ileostomy.
Postoperatively, nine UC patients were suspected clinically of having developed a postoperative venous thrombosis (two DVT andseven PE) and were administered therapeutic doses of heparin. Only three (3.8% of total) however were proven radiologically and therefore only these patients were anticoagulated with warfarin. One PE occurred after a subtotal colectomy (1.4%), one after a J pouch formation (2%) and one after a resection of a pouch for recurrent episodes of pelvic sepsis. Overall the postoperative venous thrombosis rate, on an intention to treat basis, was 1.7% (3/180) . No patient with FAP developed a venous thrombosis.
DisCUssiOnPatients with UC have inherent prothrombotic tendencies, the aetiology of which remains to be fully elucidated. The significance of such venous thromboses is considerable as these patients tend to be of a young age and the associated morbidity is
high. However, although the overall increase in clotting tendency remains of considerable concern to clinicians managing these patients in the perioperative setting, there are limited clinical data available to determine best practice. Furthermore, the experimental data that exist often appear contradictory.
While 33% of patients with UC who suffer thromboembolism may have at least one identifiable thrombophilia risk factor (most commonly Factor V Leiden), so too do many non-UC patients (Factor V Leiden is identifiable in 10-30% of the general population following thrombosis as well as in 3-7% of healthy controls8). Additionally, even though patients with inflammatory bowel disease have increased levels of anti-cardiolipin antibodies, elevated titres are not necessarily associated with thromboembolic events.9 Further studies have also failed to show an exact association between inflammatory bowel disease and hereditary prothrombotic conditions such as prothrombin gene mutations.10 Therefore, the value of routine thrombophilia assessment in patients with UC in order to stratify their risk (and therefore determine their antithrombosis prophylaxis requirements) is questionable.
This study, however, demonstrates that patients’ with UC undergoing major intra-abdominal and intra-pelvic procedures, and receiving appropriate prophylaxis, do not in fact manifest an increased clinical incidence of venous thrombosis in the first postoperative month. The incidence of 1.7% is comparable to the rate at which venous thrombosis occurs in our comparison group of FAP patients (although the numbers in this group are small) and, indeed, to its incidence after major abdominal surgery despite prophylaxis overall as determined by venographic screening (i.e. 6.3%).11
We thus conclude that standard prophylactic anti-thrombotic measures in patients with UC undergoing operation appear sufficient to deal with any potential increase in thrombotic risk and that additional measures are not necessary to ensure an acceptable incidence of postoperative venous thrombosis. These patients, therefore, need not be considered exceptionally ‘high-risk’ in issues regarding their consent for intervention and perioperative care.
REFERENCES1. Miehsler W, Reinisch W, Valic E et al. Is inflammatory
bowel disease an independent and disease specific risk factor for thromboembolism? Gut 2004; 53(4): 542-8
OJ O’COnnOR et al
inTrODUCTiOnPatients with inflammatory bowel disease have increased thrombotic tendencies.1 They have previously been shown to have a three-fold increase in the risk of developing both deep venous thrombosis (DVT) and pulmonary embolus (PE) compared to the average population.2 The exact mechanism by which this occurs is unclear although there are many potential contributing factors. These include alterations in the activity of the anticoagulant proteins C and S as well as the presence of the procoagulant Factor V Leiden.3,4 Furthermore, mucosal expression of endothelial protein C receptor and thrombomodulin is reduced5. This impairs protein C activation and so favours microthrombosis. Additionally, increased platelet concentration and activation may also contribute to the increased tendency towards thromboembolism in patients with UC.6,7 Lastly, patients with exacerbations of their disease have a tendency to dehydration and increased plasma viscosity (as a result of acute-phase protein release) which may compound each of the above prothrombotic tendencies.
As intra-abdominal surgery is a major risk factor for venous thrombosis, patients with UC should therefore be expected to have an increased risk of DVT and pulmonary PE, especially following emergency surgery. However, it is unclear whether this is actually so and therefore whether these patients should receive more anti-thrombotic precautions perioperatively than those routinely administered. To clarify these issues, we retrospectively studied our clinical experience of patients undergoing major abdominal surgery for UC using patients with FAP of similar age, demographics and operative histories as a control group. Postoperative courses were examined for evidence of suspected and proven venous thromboses in order to identify how best these patients should be managed in the perioperative period.
MeTHODsPatients with UC and FAP undergoing abdominal and pelvic surgical operation between 1991 and 2001 in a tertiary referral centre under a single consultant surgeon were identified using the Hospital Inpatient Enquiry (HIPE) system, our Inflammatory Bowel Disease database and theatre logbooks. Their
The incidence of postoperative venous thrombosis among patients with ulcerative colitisaBsTraCTBackground Patients with Ulcerative Colitis (UC) have inherent prothrombotic
tendencies. It is unknown whether this necessitates the use of additional perioperative anti-thrombotic prophylaxis when such patients require major surgery.
Methods The postoperative courses of 79 patients with UC undergoing 180 major abdominal and pelvic operations were examined for clinical and radiological evidence of venous thrombosis. Eighteen patients with Familial Adenomatous Polyposis (FAP) having surgery (35 operations) of similar magnitude were also studied. Standard anti-thrombosis prophylaxis was utilised in all patients.
Results Nine patients with UC were clinically suspected of developing postoperative venous thrombosis, but only three (3.8%) had their diagnosis confirmed radiologically (all had a pulmonary embolus). Therefore, the overall postoperative thrombosis rate, on an intention to treat basis, was 1.7% (3/180). No patient with FAP developed significant venous thrombosis.
Conclusion Standard perioperative antithrombotic modalities are sufficient to maintain any potential increase in postoperative thrombotic risk at an acceptable level in patients with UC undergoing operative intervention.
OJ O’Connor, RA Cahill, WO Kirwan, HP RedmondDept of Academic Surgery, Cork University Hospital, Wilton, Cork
THE INCIDENCE OF POSTOPERATIVE VENOUS THROMBOSIS AMONG PATIENTS wITH ULCERATIVE COLITIS
22 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 23
inTrODUCTiOnInformed consent is an essential component of good surgical practice, with the level of information transferred expected to be significantly higher in elective procedures. Conventional processes of obtaining informed consent may be inadequate to enable patients to understand important facts regarding their proposed surgery.1,2 This may affect patients’ ability to make reasoned decisions about potentially harmful interventions.
In addition, it is the responsibility of the surgeon not only to provide accurate information, but to address incorrect preconceptions that patients may have regarding their condition. Varicose veins, in particular, are often viewed by the public as contributing to a whole range of lower leg symptoms and as the precursor of serious medical conditions. There is no objective evidence to support this and varicose veins are considered by the medical community as a benign condition. The primary indication for varicose vein surgery is therefore for quality of life reasons.3
In this study, the level of incorrect preconceptions of patients seeking varicose vein surgery was
determined. The effectiveness of the outpatients’ visit and an educational leaflet in increasing patients’ knowledge of this procedure was analysed.
MeTHODsA questionnaire was administered at randomly selected vascular clinics to patients referred with varicose veins during the time period of January to December 2003. All new patients referred with this condition were eligible for the study. The initial questionnaire was completed by all patients who received it. Data collected included patient age, sex and educational level as well as previous sources of information on varicose veins. Their reasons for seeking treatment were assessed, as was their expectations of the outcome of surgery. Their perception of any serious threat to health due to varicose veins was also recorded.
At the outpatient consultation the patient was assessed by a vascular surgical trainee. They were then seen by one of two consultants who also assessed the patient. If suitable for surgery, the consultant discussed with them the nature and consequences of surgery. Following this, possible
Impact of the informed consent process on patients’ understanding of varicose veins and their treatmentaBsTraCTAim It is particularly important that patients have reasonable understanding of the
risks, benefits and nature of elective surgery. This study sought to analyse this level of understanding in patients undergoing varicose vein surgery.
Methods Eighty two patients completed a questionnaire in the vascular outpatient clinic and were asked to complete a telephone questionnaire following the clinic.
Results Pain (n=46) was the primary reason patients considered varicose vein surgery followed by appearance (n=32). Most patients felt that varicose veins placed them at high risk of leg ulcers (n=46) and DVT (n=41). A high level of expectation that surgery would significantly affect pain and flares was recorded. While the outpatient visit did not materially change these misconceptions, an educational leaflet significantly enhanced the recall of complications (p=0.028) in patients who remembered receiving a leaflet.
Conclusion Patients attending varicose vein clinics have an unrealistic expectation of the benefits of surgery and fail to understand the benign nature of their condition. The outpatient process has little effect on patient-held beliefs.
keywords varicose veins, informed consent, leaflet.
MF Dillon, CJ Carr, TMF Feeley, S Tierney Dept of General and Vascular Surgery, Adelaide & Meath Hospital & Trinity College Dublin, Tallaght, Dublin 24
IMPACT OF THE INFORMED CONSENT PROCESS ON PATIENTS’ UNDERSTANDING OF VARICOSE VEINS AND THEIR TREATMENT
2. Bernstein CN, Blanchard JF, Houstan DS, Wajda A. The incidence of deep venous thrombosis and pulmonary embolism among patients with inflammatory bowel disease: a population based cohort study. Thromb Haemost 2001; 85(3): 430-4
3. Liebman HA, Kashan N, Sutherland D, Mcgehee W, Kann AL. The factor V Leiden mutation increases the risk of venous thrombosis in patients with inflammatory bowel disease. Gastroenterol 1998; 115(4): 830-4
4. Jackson LM, O’Gorman PJ, O’Connell J, Cronin CC, Cotter KP, Shanahan F. Thrombosis in inflammatory bowel disease: clinical setting , procoagulant profile and Factor V Leiden. Q J Med 1997; 90: 183-188
5. Faioni EM, Ferrero S, Fontana G et al. Expression of endothelial protein C receptor and thrombomodulin in the intestinal tissue of patients with inflammatory bowel disease. Crit Care Med 2004; 32(5 Suppl): S266-70
6. Talbot RW, Heppell J, Dozois RR, Beart RW Jr. Vascular complications of inflammatory bowel disease. Mayo Clin Proc 1986; 61(2): 140-5
7. Danese S, Motte L, Fiocchi C. Platelets in inflammatory bowel disease: clinical, pathogenic, and therapeutic implications. Am J Gastroenterol 2004; 99(5): 938-45
8. Novacek G, Miehsler W, Kapiotis S, Katzenschlager R, Speiser W, Vogelsang H. Thromboembolism and resistance to activated protein C in patients with inflammatory bowel disease. Am J Gastroenterol 1999; 94(3): 685-90
9. Aichbichler BW, Petritsch W, Reicht GA et al. Anti-cardiolipin antibodies in patients with inflammatory bowel disease. Dig Dis Sci 1999; 44(4): 852-6
10. Vecchi M, Sacchi E, Saibeni S et al. Inflammatory bowel diseases are not associated with major hereditary conditions predisposing to thrombosis. Dig Dis Sci 2000; 45(7): 1465-9
11. Colditz G, Oster G, Tuden RL. Rates of venous thrombosis after general surgery: Combined results of randomised clinical trials. Lancet 1986; 19: 143-146
Correspondence to: Professor HP Redmond, Prof. of Surgery, Cork University Hospital and NUI Cork, Wilton, Cork. Fax: +353-21-4344370.Email: [email protected]
THE INCIDENCE OF POSTOPERATIVE VENOUS THROMBOSIS AMONG PATIENTS wITH ULCERATIVE COLITIS
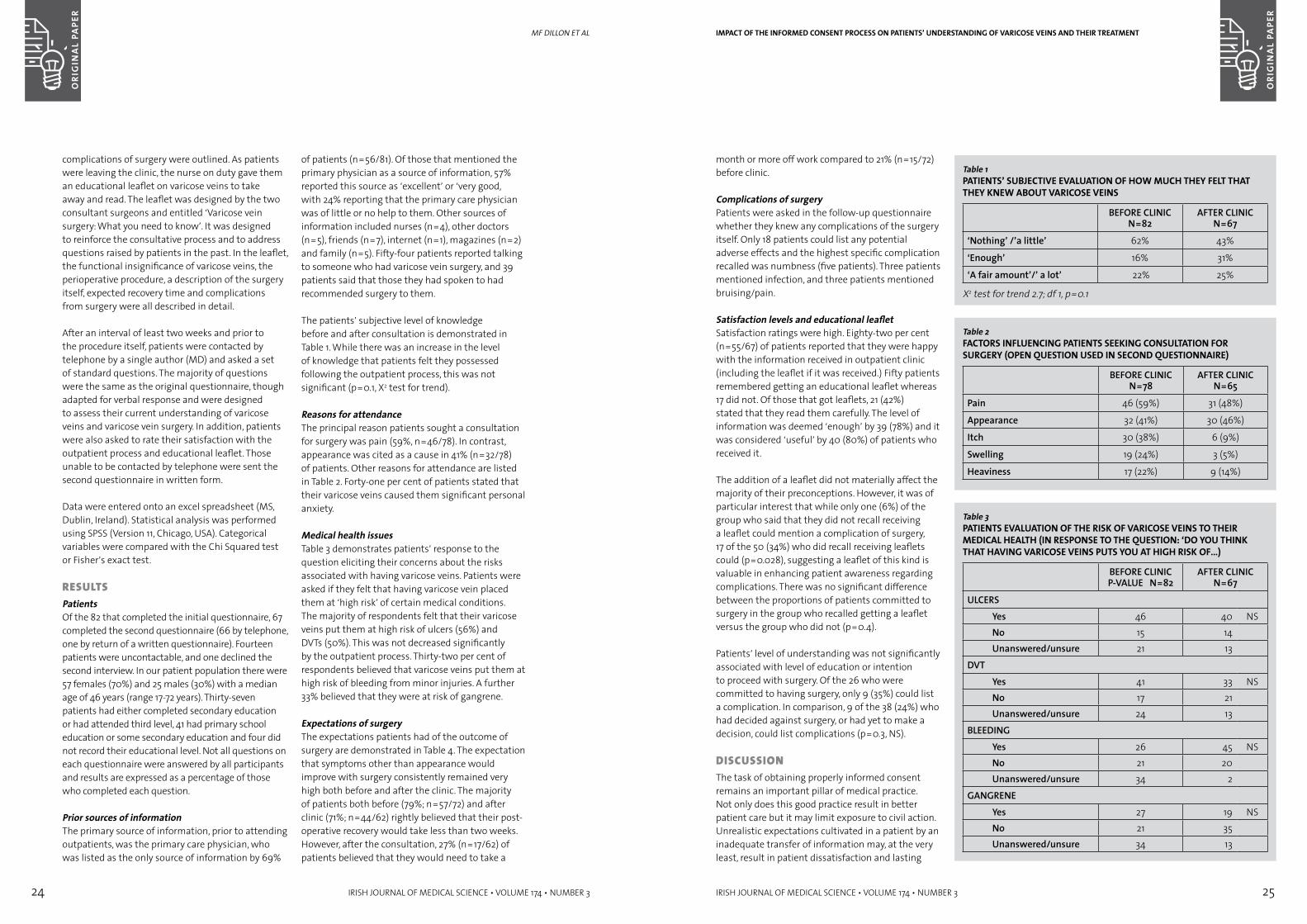
24 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 25
month or more off work compared to 21% (n=15/72) before clinic.
Complications of surgeryPatients were asked in the follow-up questionnaire whether they knew any complications of the surgery itself. Only 18 patients could list any potential adverse effects and the highest specific complication recalled was numbness (five patients). Three patients mentioned infection, and three patients mentioned bruising/pain.
Satisfaction levels and educational leafletSatisfaction ratings were high. Eighty-two per cent (n=55/67) of patients reported that they were happy with the information received in outpatient clinic (including the leaflet if it was received.) Fifty patients remembered getting an educational leaflet whereas 17 did not. Of those that got leaflets, 21 (42%) stated that they read them carefully. The level of information was deemed ‘enough’ by 39 (78%) and it was considered ‘useful’ by 40 (80%) of patients who received it.
The addition of a leaflet did not materially affect the majority of their preconceptions. However, it was of particular interest that while only one (6%) of the group who said that they did not recall receiving a leaflet could mention a complication of surgery, 17 of the 50 (34%) who did recall receiving leaflets could (p=0.028), suggesting a leaflet of this kind is valuable in enhancing patient awareness regarding complications. There was no significant difference between the proportions of patients committed to surgery in the group who recalled getting a leaflet versus the group who did not (p=0.4).
Patients’ level of understanding was not significantly associated with level of education or intention to proceed with surgery. Of the 26 who were committed to having surgery, only 9 (35%) could list a complication. In comparison, 9 of the 38 (24%) who had decided against surgery, or had yet to make a decision, could list complications (p=0.3, NS).
DisCUssiOnThe task of obtaining properly informed consent remains an important pillar of medical practice. Not only does this good practice result in better patient care but it may limit exposure to civil action. Unrealistic expectations cultivated in a patient by an inadequate transfer of information may, at the very least, result in patient dissatisfaction and lasting
IMPACT OF THE INFORMED CONSENT PROCESS ON PATIENTS’ UNDERSTANDING OF VARICOSE VEINS AND THEIR TREATMENT
Table 1PATIENTS’ SUBJECTIVE EVALUATION OF HOw MUCH THEY FELT THAT THEY kNEw ABOUT VARICOSE VEINS
BEFORE CLINICN=82
AFTER CLINICN=67
‘Nothing’ /’a little’ 62% 43%
‘Enough’ 16% 31%
‘A fair amount’/’ a lot’ 22% 25%
X2 test for trend 2.7; df 1, p=0.1
Table 2FACTORS INFLUENCING PATIENTS SEEkING CONSULTATION FOR SURGERY (OPEN qUESTION USED IN SECOND qUESTIONNAIRE)
BEFORE CLINICN=78
AFTER CLINICN=65
Pain 46 (59%) 31 (48%)
Appearance 32 (41%) 30 (46%)
Itch 30 (38%) 6 (9%)
Swelling 19 (24%) 3 (5%)
Heaviness 17 (22%) 9 (14%)
Table 3PATIENTS EVALUATION OF THE RISk OF VARICOSE VEINS TO THEIR MEDICAL HEALTH (IN RESPONSE TO THE qUESTION: ‘DO YOU THINk THAT HAVING VARICOSE VEINS PUTS YOU AT HIGH RISk OF…)
BEFORE CLINICP-VALUE N=82
AFTER CLINICN=67
ULCERSYes 46 40 NSNo 15 14Unanswered/unsure 21 13
DVTYes 41 33 NSNo 17 21Unanswered/unsure 24 13
BLEEDINGYes 26 45 NSNo 21 20Unanswered/unsure 34 2
GANGRENEYes 27 19 NSNo 21 35Unanswered/unsure 34 13
complications of surgery were outlined. As patients were leaving the clinic, the nurse on duty gave them an educational leaflet on varicose veins to take away and read. The leaflet was designed by the two consultant surgeons and entitled ‘Varicose vein surgery: What you need to know’. It was designed to reinforce the consultative process and to address questions raised by patients in the past. In the leaflet, the functional insignificance of varicose veins, the perioperative procedure, a description of the surgery itself, expected recovery time and complications from surgery were all described in detail.
After an interval of least two weeks and prior to the procedure itself, patients were contacted by telephone by a single author (MD) and asked a set of standard questions. The majority of questions were the same as the original questionnaire, though adapted for verbal response and were designed to assess their current understanding of varicose veins and varicose vein surgery. In addition, patients were also asked to rate their satisfaction with the outpatient process and educational leaflet. Those unable to be contacted by telephone were sent the second questionnaire in written form.
Data were entered onto an excel spreadsheet (MS, Dublin, Ireland). Statistical analysis was performed using SPSS (Version 11, Chicago, USA). Categorical variables were compared with the Chi Squared test or Fisher’s exact test.
resUlTsPatientsOf the 82 that completed the initial questionnaire, 67 completed the second questionnaire (66 by telephone, one by return of a written questionnaire). Fourteen patients were uncontactable, and one declined the second interview. In our patient population there were 57 females (70%) and 25 males (30%) with a median age of 46 years (range 17-72 years). Thirty-seven patients had either completed secondary education or had attended third level, 41 had primary school education or some secondary education and four did not record their educational level. Not all questions on each questionnaire were answered by all participants and results are expressed as a percentage of those who completed each question.
Prior sources of informationThe primary source of information, prior to attending outpatients, was the primary care physician, who was listed as the only source of information by 69%
of patients (n=56/81). Of those that mentioned the primary physician as a source of information, 57% reported this source as ‘excellent’ or ‘very good, with 24% reporting that the primary care physician was of little or no help to them. Other sources of information included nurses (n=4), other doctors (n=5), friends (n=7), internet (n=1), magazines (n=2) and family (n=5). Fifty-four patients reported talking to someone who had varicose vein surgery, and 39 patients said that those they had spoken to had recommended surgery to them.
The patients’ subjective level of knowledge before and after consultation is demonstrated in Table 1. While there was an increase in the level of knowledge that patients felt they possessed following the outpatient process, this was not significant (p=0.1, X2 test for trend).
Reasons for attendanceThe principal reason patients sought a consultation for surgery was pain (59%, n=46/78). In contrast, appearance was cited as a cause in 41% (n=32/78) of patients. Other reasons for attendance are listed in Table 2. Forty-one per cent of patients stated that their varicose veins caused them significant personal anxiety.
Medical health issuesTable 3 demonstrates patients’ response to the question eliciting their concerns about the risks associated with having varicose veins. Patients were asked if they felt that having varicose vein placed them at ‘high risk’ of certain medical conditions. The majority of respondents felt that their varicose veins put them at high risk of ulcers (56%) and DVTs (50%). This was not decreased significantly by the outpatient process. Thirty-two per cent of respondents believed that varicose veins put them at high risk of bleeding from minor injuries. A further 33% believed that they were at risk of gangrene.
Expectations of surgeryThe expectations patients had of the outcome of surgery are demonstrated in Table 4. The expectation that symptoms other than appearance would improve with surgery consistently remained very high both before and after the clinic. The majority of patients both before (79%; n=57/72) and after clinic (71%; n=44/62) rightly believed that their post-operative recovery would take less than two weeks. However, after the consultation, 27% (n=17/62) of patients believed that they would need to take a
MF DillOn et al
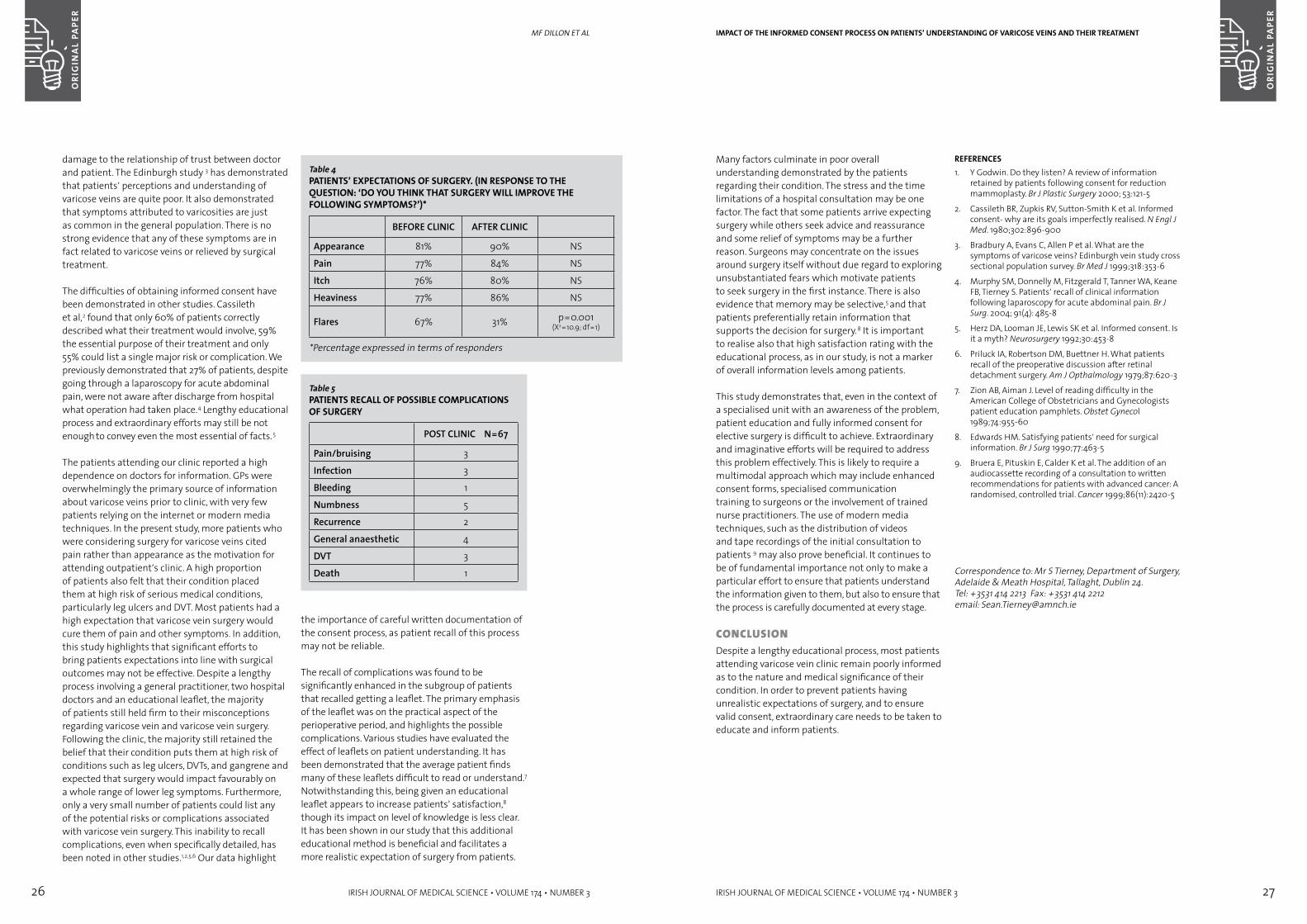
26 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 27
Many factors culminate in poor overall understanding demonstrated by the patients regarding their condition. The stress and the time limitations of a hospital consultation may be one factor. The fact that some patients arrive expecting surgery while others seek advice and reassurance and some relief of symptoms may be a further reason. Surgeons may concentrate on the issues around surgery itself without due regard to exploring unsubstantiated fears which motivate patients to seek surgery in the first instance. There is also evidence that memory may be selective,5 and that patients preferentially retain information that supports the decision for surgery. 8 It is important to realise also that high satisfaction rating with the educational process, as in our study, is not a marker of overall information levels among patients.
This study demonstrates that, even in the context of a specialised unit with an awareness of the problem, patient education and fully informed consent for elective surgery is difficult to achieve. Extraordinary and imaginative efforts will be required to address this problem effectively. This is likely to require a multimodal approach which may include enhanced consent forms, specialised communication training to surgeons or the involvement of trained nurse practitioners. The use of modern media techniques, such as the distribution of videos and tape recordings of the initial consultation to patients 9 may also prove beneficial. It continues to be of fundamental importance not only to make a particular effort to ensure that patients understand the information given to them, but also to ensure that the process is carefully documented at every stage.
COnClUsiOnDespite a lengthy educational process, most patients attending varicose vein clinic remain poorly informed as to the nature and medical significance of their condition. In order to prevent patients having unrealistic expectations of surgery, and to ensure valid consent, extraordinary care needs to be taken to educate and inform patients.
REFERENCES1. Y Godwin. Do they listen? A review of information
retained by patients following consent for reduction mammoplasty. Br J Plastic Surgery 2000; 53:121-5
2. Cassileth BR, Zupkis RV, Sutton-Smith K et al. Informed consent- why are its goals imperfectly realised. N Engl J Med. 1980;302:896-900
3. Bradbury A, Evans C, Allen P et al. What are the symptoms of varicose veins? Edinburgh vein study cross sectional population survey. Br Med J 1999;318:353-6
4. Murphy SM, Donnelly M, Fitzgerald T, Tanner WA, Keane FB, Tierney S. Patients’ recall of clinical information following laparoscopy for acute abdominal pain. Br J Surg. 2004; 91(4): 485-8
5. Herz DA, Looman JE, Lewis SK et al. Informed consent. Is it a myth? Neurosurgery 1992;30:453-8
6. Priluck IA, Robertson DM, Buettner H. What patients recall of the preoperative discussion after retinal detachment surgery. Am J Opthalmology 1979;87:620-3
7. Zion AB, Aiman J. Level of reading difficulty in the American College of Obstetricians and Gynecologists patient education pamphlets. Obstet Gynecol 1989;74:955-60
8. Edwards HM. Satisfying patients’ need for surgical information. Br J Surg 1990;77:463-5
9. Bruera E, Pituskin E, Calder K et al. The addition of an audiocassette recording of a consultation to written recommendations for patients with advanced cancer: A randomised, controlled trial. Cancer 1999;86(11):2420-5
Correspondence to: Mr S Tierney, Department of Surgery, Adelaide & Meath Hospital, Tallaght, Dublin 24.Tel: +3531 414 2213 Fax: +3531 414 2212email: [email protected]
IMPACT OF THE INFORMED CONSENT PROCESS ON PATIENTS’ UNDERSTANDING OF VARICOSE VEINS AND THEIR TREATMENT
damage to the relationship of trust between doctor and patient. The Edinburgh study 3 has demonstrated that patients’ perceptions and understanding of varicose veins are quite poor. It also demonstrated that symptoms attributed to varicosities are just as common in the general population. There is no strong evidence that any of these symptoms are in fact related to varicose veins or relieved by surgical treatment.
The difficulties of obtaining informed consent have been demonstrated in other studies. Cassileth et al,2 found that only 60% of patients correctly described what their treatment would involve, 59% the essential purpose of their treatment and only 55% could list a single major risk or complication. We previously demonstrated that 27% of patients, despite going through a laparoscopy for acute abdominal pain, were not aware after discharge from hospital what operation had taken place.4 Lengthy educational process and extraordinary efforts may still be not enough to convey even the most essential of facts. 5
The patients attending our clinic reported a high dependence on doctors for information. GPs were overwhelmingly the primary source of information about varicose veins prior to clinic, with very few patients relying on the internet or modern media techniques. In the present study, more patients who were considering surgery for varicose veins cited pain rather than appearance as the motivation for attending outpatient’s clinic. A high proportion of patients also felt that their condition placed them at high risk of serious medical conditions, particularly leg ulcers and DVT. Most patients had a high expectation that varicose vein surgery would cure them of pain and other symptoms. In addition, this study highlights that significant efforts to bring patients expectations into line with surgical outcomes may not be effective. Despite a lengthy process involving a general practitioner, two hospital doctors and an educational leaflet, the majority of patients still held firm to their misconceptions regarding varicose vein and varicose vein surgery. Following the clinic, the majority still retained the belief that their condition puts them at high risk of conditions such as leg ulcers, DVTs, and gangrene and expected that surgery would impact favourably on a whole range of lower leg symptoms. Furthermore, only a very small number of patients could list any of the potential risks or complications associated with varicose vein surgery. This inability to recall complications, even when specifically detailed, has been noted in other studies.1,2,5,6 Our data highlight
Table 4PATIENTS’ EXPECTATIONS OF SURGERY. (IN RESPONSE TO THE qUESTION: ‘DO YOU THINk THAT SURGERY wILL IMPROVE THE FOLLOwING SYMPTOMS?’)*
BEFORE CLINIC AFTER CLINIC
Appearance 81% 90% NS
Pain 77% 84% NS
Itch 76% 80% NS
Heaviness 77% 86% NS
Flares 67% 31% p=0.001 (X2=10.9; df=1)
*Percentage expressed in terms of responders
Table 5PATIENTS RECALL OF POSSIBLE COMPLICATIONS OF SURGERY
POST CLINIC N=67
Pain/bruising 3
Infection 3
Bleeding 1
Numbness 5
Recurrence 2
General anaesthetic 4
DVT 3
Death 1
the importance of careful written documentation of the consent process, as patient recall of this process may not be reliable.
The recall of complications was found to be significantly enhanced in the subgroup of patients that recalled getting a leaflet. The primary emphasis of the leaflet was on the practical aspect of the perioperative period, and highlights the possible complications. Various studies have evaluated the effect of leaflets on patient understanding. It has been demonstrated that the average patient finds many of these leaflets difficult to read or understand.7 Notwithstanding this, being given an educational leaflet appears to increase patients’ satisfaction,8 though its impact on level of knowledge is less clear. It has been shown in our study that this additional educational method is beneficial and facilitates a more realistic expectation of surgery from patients.
MF DillOn et al
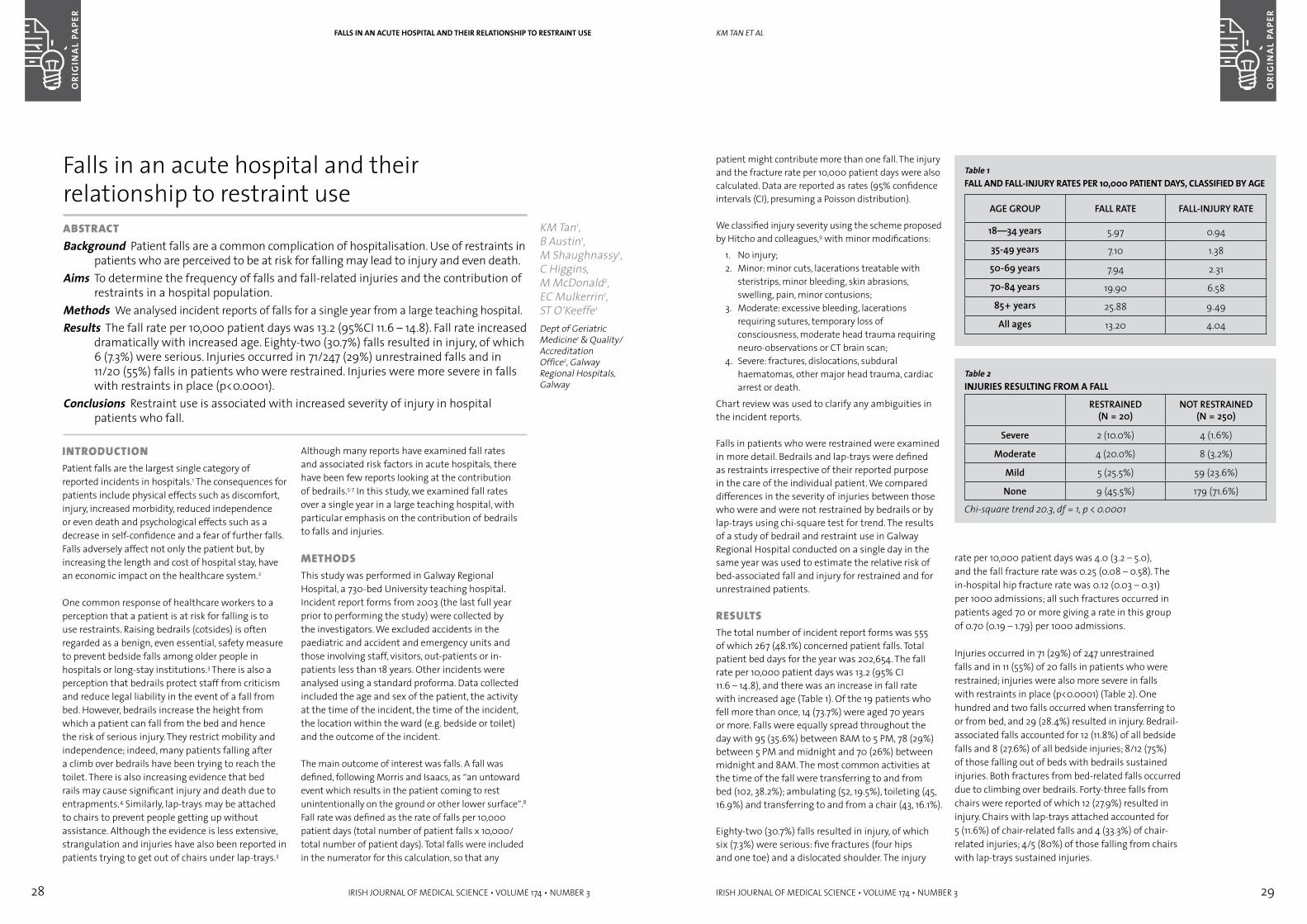
28 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 29
patient might contribute more than one fall. The injury and the fracture rate per 10,000 patient days were also calculated. Data are reported as rates (95% confidence intervals (CI), presuming a Poisson distribution).
We classified injury severity using the scheme proposed by Hitcho and colleagues,9 with minor modifications:
1. No injury;2. Minor: minor cuts, lacerations treatable with
steristrips, minor bleeding, skin abrasions, swelling, pain, minor contusions;
3. Moderate: excessive bleeding, lacerations requiring sutures, temporary loss of consciousness, moderate head trauma requiring neuro-observations or CT brain scan;
4. Severe: fractures, dislocations, subdural haematomas, other major head trauma, cardiac arrest or death.
Chart review was used to clarify any ambiguities in the incident reports.
Falls in patients who were restrained were examined in more detail. Bedrails and lap-trays were defined as restraints irrespective of their reported purpose in the care of the individual patient. We compared differences in the severity of injuries between those who were and were not restrained by bedrails or by lap-trays using chi-square test for trend. The results of a study of bedrail and restraint use in Galway Regional Hospital conducted on a single day in the same year was used to estimate the relative risk of bed-associated fall and injury for restrained and for unrestrained patients.
resUlTsThe total number of incident report forms was 555 of which 267 (48.1%) concerned patient falls. Total patient bed days for the year was 202,654. The fall rate per 10,000 patient days was 13.2 (95% CI 11.6 – 14.8), and there was an increase in fall rate with increased age (Table 1). Of the 19 patients who fell more than once, 14 (73.7%) were aged 70 years or more. Falls were equally spread throughout the day with 95 (35.6%) between 8AM to 5 PM, 78 (29%) between 5 PM and midnight and 70 (26%) between midnight and 8AM. The most common activities at the time of the fall were transferring to and from bed (102, 38.2%); ambulating (52, 19.5%), toileting (45, 16.9%) and transferring to and from a chair (43, 16.1%).
Eighty-two (30.7%) falls resulted in injury, of which six (7.3%) were serious: five fractures (four hips and one toe) and a dislocated shoulder. The injury
KM tan et al
Table 1FALL AND FALL-INJURY RATES PER 10,000 PATIENT DAYS, CLASSIFIED BY AGE
AGE GROUP FALL RATE FALL-INJURY RATE
18—34 years 5.97 0.94
35-49 years 7.10 1.38
50-69 years 7.94 2.31
70-84 years 19.90 6.58
85+ years 25.88 9.49
All ages 13.20 4.04
Table 2INJURIES RESULTING FROM A FALL
RESTRAINED (N = 20)
NOT RESTRAINED (N = 250)
Severe 2 (10.0%) 4 (1.6%)
Moderate 4 (20.0%) 8 (3.2%)
Mild 5 (25.5%) 59 (23.6%)
None 9 (45.5%) 179 (71.6%)
Chi-square trend 20.3, df = 1, p < 0.0001
rate per 10,000 patient days was 4.0 (3.2 – 5.0), and the fall fracture rate was 0.25 (0.08 – 0.58). The in-hospital hip fracture rate was 0.12 (0.03 – 0.31) per 1000 admissions; all such fractures occurred in patients aged 70 or more giving a rate in this group of 0.70 (0.19 – 1.79) per 1000 admissions.
Injuries occurred in 71 (29%) of 247 unrestrained falls and in 11 (55%) of 20 falls in patients who were restrained; injuries were also more severe in falls with restraints in place (p<0.0001) (Table 2). One hundred and two falls occurred when transferring to or from bed, and 29 (28.4%) resulted in injury. Bedrail-associated falls accounted for 12 (11.8%) of all bedside falls and 8 (27.6%) of all bedside injuries; 8/12 (75%) of those falling out of beds with bedrails sustained injuries. Both fractures from bed-related falls occurred due to climbing over bedrails. Forty-three falls from chairs were reported of which 12 (27.9%) resulted in injury. Chairs with lap-trays attached accounted for 5 (11.6%) of chair-related falls and 4 (33.3%) of chair-related injuries; 4/5 (80%) of those falling from chairs with lap-trays sustained injuries.
inTrODUCTiOnPatient falls are the largest single category of reported incidents in hospitals.1 The consequences for patients include physical effects such as discomfort, injury, increased morbidity, reduced independence or even death and psychological effects such as a decrease in self-confidence and a fear of further falls. Falls adversely affect not only the patient but, by increasing the length and cost of hospital stay, have an economic impact on the healthcare system.2
One common response of healthcare workers to a perception that a patient is at risk for falling is to use restraints. Raising bedrails (cotsides) is often regarded as a benign, even essential, safety measure to prevent bedside falls among older people in hospitals or long-stay institutions.3 There is also a perception that bedrails protect staff from criticism and reduce legal liability in the event of a fall from bed. However, bedrails increase the height from which a patient can fall from the bed and hence the risk of serious injury. They restrict mobility and independence; indeed, many patients falling after a climb over bedrails have been trying to reach the toilet. There is also increasing evidence that bed rails may cause significant injury and death due to entrapments.4 Similarly, lap-trays may be attached to chairs to prevent people getting up without assistance. Although the evidence is less extensive, strangulation and injuries have also been reported in patients trying to get out of chairs under lap-trays.3
Although many reports have examined fall rates and associated risk factors in acute hospitals, there have been few reports looking at the contribution of bedrails.5-7 In this study, we examined fall rates over a single year in a large teaching hospital, with particular emphasis on the contribution of bedrails to falls and injuries.
MeTHODsThis study was performed in Galway Regional Hospital, a 730-bed University teaching hospital. Incident report forms from 2003 (the last full year prior to performing the study) were collected by the investigators. We excluded accidents in the paediatric and accident and emergency units and those involving staff, visitors, out-patients or in-patients less than 18 years. Other incidents were analysed using a standard proforma. Data collected included the age and sex of the patient, the activity at the time of the incident, the time of the incident, the location within the ward (e.g. bedside or toilet) and the outcome of the incident.
The main outcome of interest was falls. A fall was defined, following Morris and Isaacs, as “an untoward event which results in the patient coming to rest unintentionally on the ground or other lower surface”.8 Fall rate was defined as the rate of falls per 10,000 patient days (total number of patient falls x 10,000/ total number of patient days). Total falls were included in the numerator for this calculation, so that any
Falls in an acute hospital and their relationship to restraint useaBsTraCTBackground Patient falls are a common complication of hospitalisation. Use of restraints in
patients who are perceived to be at risk for falling may lead to injury and even death. Aims To determine the frequency of falls and fall-related injuries and the contribution of
restraints in a hospital population.Methods We analysed incident reports of falls for a single year from a large teaching hospital. Results The fall rate per 10,000 patient days was 13.2 (95%CI 11.6 – 14.8). Fall rate increased
dramatically with increased age. Eighty-two (30.7%) falls resulted in injury, of which 6 (7.3%) were serious. Injuries occurred in 71/247 (29%) unrestrained falls and in 11/20 (55%) falls in patients who were restrained. Injuries were more severe in falls with restraints in place (p<0.0001).
Conclusions Restraint use is associated with increased severity of injury in hospital patients who fall.
KM Tan1, B Austin1, M Shaughnassy1, C Higgins, M McDonald2, EC Mulkerrin1, ST O’Keeffe1
Dept of Geriatric Medicine1 & Quality/Accreditation Office2, Galway Regional Hospitals, Galway
FALLS IN AN ACUTE HOSPITAL AND THEIR RELATIONSHIP TO RESTRAINT USE
30 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 31
risk of asphyxial death. While this is a particularly horrible complication, it is also rare. The present study adds to the very limited data supporting the importance of a more common consequence of restraint use – the increased severity of injury in restrained patients who fall. Our results further call into question the wisdom of using restraints to prevent falls in hospital patients.
REFERENCES1. Morse JM. Enhancing the safety of hospitalisation by
reducing patient falls. Am J Infect Control 2002; 30:376-380.
2. Bates DW, Pruess K, Souney P, Platt R. Serious falls in hospitalised patients: correlates and resource utilisation. Am J Med 1995;99:137-143.
3. Braun JA, Capezuti EA. The legal and medical aspects of physical restraints and bed siderails and their relationship to falls and fall-related injuries in nursing homes. DePaul J Healthcare 2000; 4:1-72.
4. O’Keeffe ST. Down with bedrails? Lancet 2004; 363:343-344.
5. Evans D, Hodgkinson B, Lambert L, Wood J, Kowanko I. Falls in Acute Hospitals. www.joannabriggs.edu.au/protocols/fallsinacute.pdf (accessed 22/11/04)
6. Capezuti E, Strumpf N, Evans L, Grisso J, Maislin G. The relationship between physical restraint removal and falls and injuries among nursing home residents. J Gerontol 1998; 53A: M47-M52.
7. Hanger HC, Ball MC, Wood LA. An analysis of falls in the hospital: can we do without bedrails?J Am Geriatr Soc 1999; 47:529-31.
8. Morris EV, Isaacs B. The prevention of falls in a geriatric hospital. Age Ageing 1980; 9: 181-185.
9. Hitcho EB, Krauss MJ, Birge S et al. Characteristics and circumstances of falls in a hospital setting: a prospective study. J Gen Intern Med 2004; 19:732-739.
10. Fall prevention. http://www.premierinc.com/all/safety/resources/falls/ (accessed 23/11/04)
11. Lane AJ. Evaluation of a fall prevention program in an acute care unit. Orthop Nurs 1999; 18:37-43.
12. Morgan VR, Mathison JH, Rice JC, Clemmer DI. Hospital falls: a persistent problem. Am J Public Health. 1985;75(7):775-7.
13. Brandis S. A collaborative occupational therapy and nursing approach to falls prevention in hospital inpatients. J Qual Clin Pract 1999; 19:215-220.
14. Pulcins I, Wan E. In-hospital hip fractures in Canada. http://www.longwoods.com/hq/HQ74-2004/HQ74Pulcins.pdf (accessed 23/11/04)
15. Isaacs B. The Challenge of Geriatric Medicine. Oxford University Press, Oxford, 1992.
16. Oliver D, Daly F, Martin FC, McMurdo ME. Risk factors and risk assessment tools for falls in hospital in-patients: a systematic review. Age Ageing 2004; 33:122-130.
17. Brush B, Capezuti E. Historical analysis of siderail use in American hospitals. J Nurs Scholar 2001; 33:381-385.
18. Myint S, Neufeld R, Dunbar J. Removal of bedrails on a short-term nursing home rehabilitation unit. Gerontologist 1999; 39:611-614.
19. Watson R, Brunton M. Restrain yourself. Nurs Elderly 1990; May, 20-21.
20. Noone I, Fleming H, Crowe M, O’Keeffe S. Use of cotsides in an Irish hospital. Ir Med J 1998; 91:134-135.
21. Raw J, Stacey S. Are the days of bedrails coming to an end? Age Ageing 2004; 33:641.
Correspondence to: Dr S O’Keeffe, Unit 4, Merlin Park Regional Hospital, Galway.Tel:091-775561 Fax:091-770515E-mail [email protected]
KM tan et alFALLS IN AN ACUTE HOSPITAL AND THEIR RELATIONSHIP TO RESTRAINT USE
A study in which all 642 patients in the study hospital were observed twice in a single 24-hour period in October 2003 (between 2 PM and 5 PM and between 11 PM and 2 AM) for use of bedrails or other restraints showed that 98 (22.4%) had bedrails raised and 53 (12.1%) had a lap-tray in place during at least one assessment; other restraints were not noted. Presuming that the same proportion of patients had bedrails raised throughout the year, the bed-associated fall rate was 3.72 per 10,000 bedrail-restrained patient days and 5.72 for non-restrained patient days (rate ratio (RR) 0.65, p = 0.52); injury rates in these groups were 2.48 and 0.25 respectively (RR 9.92, p = 0.18). A similar calculation with regard to lap-tray use gives a chair-associated fall rate of 2.04 per 10,000 lap-tray-restrained patient days and 2.13 for non-restrained patient days (RR 0.96, p = 0.97); chair-associated injury rates were 1.63 and 0.45 (RR 3.62, p = 0.41).
DisCUssiOnComparing falls data from different countries and different institutions is fraught with difficulties and potential biases. Nevertheless, the primary measure in this study, fall rate per 1,000 (increased to 10,000 for convenience) patient days has been recommended by the American Joint Commission for Accreditation of Health Organizations (JCAHO) for computing rates in facilities with varying case-mix, lengths of stay, and occupancy.10 American studies report fall rates in acute hospitals from 22 to 70 per 10,000 patient days,1,11,12 and the JCAHO has suggested 31.4 as an American national benchmark for patient falls.10 Similarly, the South East Australian Benchmarking Consortium suggested a benchmark standard of 40 falls per 10,000 patient days.13
The fall rate of 13.2 per 10,000 patient days in our institution seems to compare favourably with these benchmarks. However, case-mix may differ considerably between acute hospitals in different countries, and there is no agreed method for standardising fall rates. Also, our institution does not have on-site psychogeriatric or rehabilitation wards, both of which are associated with a particularly high fall risk.5 The hip fracture rate of 0.7 per 1000 admissions aged 70 or more in this study is similar to the unadjusted Canadian rate of 0.9 hip fractures per 1000 admissions in the same age group.14
Preventing hospital falls is seen as a major quality factor in many healthcare systems. However, a ‘zero tolerance’ approach to falls is not appropriate, especially in dealing with older people. As Isaacs
has noted, a unit where nobody falls is a unit where nobody moves.15 It is essential to balance the need to prevent avoidable falls with an acceptance that falls will inevitably occur if there is an active approach to rehabilitation and to promoting independence. These factors further complicate interpretation of fall data, and a low fall rate, as in our study, could reflect a failure to mobilise patients adequately.
The most striking feature of our results was the significantly higher proportion of severe injuries in patients who were restrained at the time they fell. Factors that predict restraint use such as agitation, cognitive impairment and gait disturbance also predict falls,16 and our data are insufficient to establish a causal relationship between falls, severity of injuries and restraint use. Nevertheless, it makes intuitive sense that patients who escape from restraints will fall more awkwardly or, if climbing over bedrails, will fall from a greater height, and be at greater risk of significant injury. This is contrary to the traditional belief that ‘out-of bed incidents’ with raised bedrails caused less severe injury because ‘patients had something to grasp when falling’.17 Moreover, our results are consistent with those from ‘before and after’ studies, where reduction in bedrail use has led to no change or a slight increase in fall risk but to a reduction in injury severity resulting from falls.7, 18, 19
A limitation of this study is that it was retrospective and relied on incident form reports. Underreporting is a potential problem with this approach, and it has been estimated that up to 15% of falls may not be reported.10 Injuries are much less likely to be underreported. A 30-40% risk of injury following a fall is a remarkably consistent result in studies from different countries.1,9,11 The injury rate of 31% in our study provides reassurance that underreporting of falls is not particularly common in our institution, since that would likely lead to a high injury rate. We extrapolated from the results of a single cross-sectional observational study of restraint use in our institution to estimate falls and fall-injury rates in restrained and unrestrained patients. It would be preferable to have prospective data of restraint use throughout the year. Nevertheless, the frequency of restraint use on the day we recorded is consistent with data from other Irish and British hospitals,20,21 and no initiatives were undertaken within the year of the study that might have influenced restraint use within our hospital.
Much of the concern regarding use of bedrails and other restraints in recent years has focussed on the
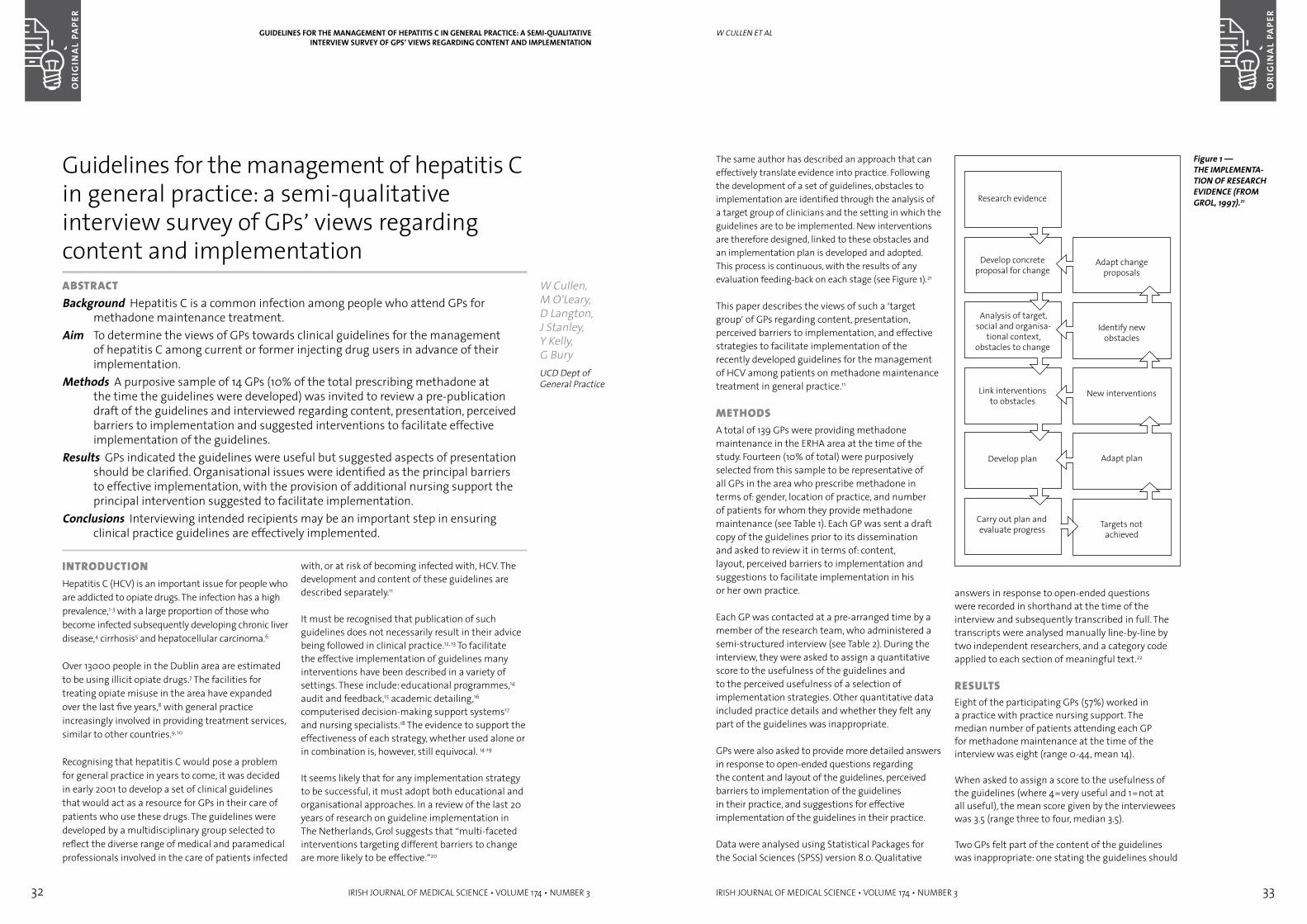
32 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 33
The same author has described an approach that can effectively translate evidence into practice. Following the development of a set of guidelines, obstacles to implementation are identified through the analysis of a target group of clinicians and the setting in which the guidelines are to be implemented. New interventions are therefore designed, linked to these obstacles and an implementation plan is developed and adopted. This process is continuous, with the results of any evaluation feeding-back on each stage (see Figure 1).21
This paper describes the views of such a ‘target group’ of GPs regarding content, presentation, perceived barriers to implementation, and effective strategies to facilitate implementation of the recently developed guidelines for the management of HCV among patients on methadone maintenance treatment in general practice.11
MeTHODs A total of 139 GPs were providing methadone maintenance in the ERHA area at the time of the study. Fourteen (10% of total) were purposively selected from this sample to be representative of all GPs in the area who prescribe methadone in terms of: gender, location of practice, and number of patients for whom they provide methadone maintenance (see Table 1). Each GP was sent a draft copy of the guidelines prior to its dissemination and asked to review it in terms of: content, layout, perceived barriers to implementation and suggestions to facilitate implementation in his or her own practice.
Each GP was contacted at a pre-arranged time by a member of the research team, who administered a semi-structured interview (see Table 2). During the interview, they were asked to assign a quantitative score to the usefulness of the guidelines and to the perceived usefulness of a selection of implementation strategies. Other quantitative data included practice details and whether they felt any part of the guidelines was inappropriate.
GPs were also asked to provide more detailed answers in response to open-ended questions regarding the content and layout of the guidelines, perceived barriers to implementation of the guidelines in their practice, and suggestions for effective implementation of the guidelines in their practice.
Data were analysed using Statistical Packages for the Social Sciences (SPSS) version 8.0. Qualitative
answers in response to open-ended questions were recorded in shorthand at the time of the interview and subsequently transcribed in full. The transcripts were analysed manually line-by-line by two independent researchers, and a category code applied to each section of meaningful text.22
resUlTs Eight of the participating GPs (57%) worked in a practice with practice nursing support. The median number of patients attending each GP for methadone maintenance at the time of the interview was eight (range 0-44, mean 14).
When asked to assign a score to the usefulness of the guidelines (where 4=very useful and 1=not at all useful), the mean score given by the interviewees was 3.5 (range three to four, median 3.5).
Two GPs felt part of the content of the guidelines was inappropriate: one stating the guidelines should
W CUllen et al
Figure 1 —THE IMPLEMENTA-TION OF RESEARCH EVIDENCE (FROM GROL, 1997).21
inTrODUCTiOn Hepatitis C (HCV) is an important issue for people who are addicted to opiate drugs. The infection has a high prevalence,1-3 with a large proportion of those who become infected subsequently developing chronic liver disease,4 cirrhosis5 and hepatocellular carcinoma.6
Over 13000 people in the Dublin area are estimated to be using illicit opiate drugs.7 The facilities for treating opiate misuse in the area have expanded over the last five years,8 with general practice increasingly involved in providing treatment services, similar to other countries.9, 10
Recognising that hepatitis C would pose a problem for general practice in years to come, it was decided in early 2001 to develop a set of clinical guidelines that would act as a resource for GPs in their care of patients who use these drugs. The guidelines were developed by a multidisciplinary group selected to reflect the diverse range of medical and paramedical professionals involved in the care of patients infected
with, or at risk of becoming infected with, HCV. The development and content of these guidelines are described separately.11
It must be recognised that publication of such guidelines does not necessarily result in their advice being followed in clinical practice.12, 13 To facilitate the effective implementation of guidelines many interventions have been described in a variety of settings. These include: educational programmes,14 audit and feedback,15 academic detailing,16 computerised decision-making support systems17 and nursing specialists.18 The evidence to support the effectiveness of each strategy, whether used alone or in combination is, however, still equivocal. 14-19
It seems likely that for any implementation strategy to be successful, it must adopt both educational and organisational approaches. In a review of the last 20 years of research on guideline implementation in The Netherlands, Grol suggests that “multi-faceted interventions targeting different barriers to change are more likely to be effective.”20
Guidelines for the management of hepatitis C in general practice: a semi-qualitative interview survey of GPs’ views regarding content and implementationaBsTraCTBackground Hepatitis C is a common infection among people who attend GPs for
methadone maintenance treatment. Aim To determine the views of GPs towards clinical guidelines for the management
of hepatitis C among current or former injecting drug users in advance of their implementation.
Methods A purposive sample of 14 GPs (10% of the total prescribing methadone at the time the guidelines were developed) was invited to review a pre-publication draft of the guidelines and interviewed regarding content, presentation, perceived barriers to implementation and suggested interventions to facilitate effective implementation of the guidelines.
Results GPs indicated the guidelines were useful but suggested aspects of presentation should be clarified. Organisational issues were identified as the principal barriers to effective implementation, with the provision of additional nursing support the principal intervention suggested to facilitate implementation.
Conclusions Interviewing intended recipients may be an important step in ensuring clinical practice guidelines are effectively implemented.
W Cullen, M O’Leary, D Langton, J Stanley, Y Kelly, G BuryUCD Dept of General Practice
GUIDELINES FOR THE MANAGEMENT OF HEPATITIS C IN GENERAL PRACTICE: A SEMI-qUALITATIVE INTERVIEw SURVEY OF GPS’ VIEwS REGARDING CONTENT AND IMPLEMENTATION
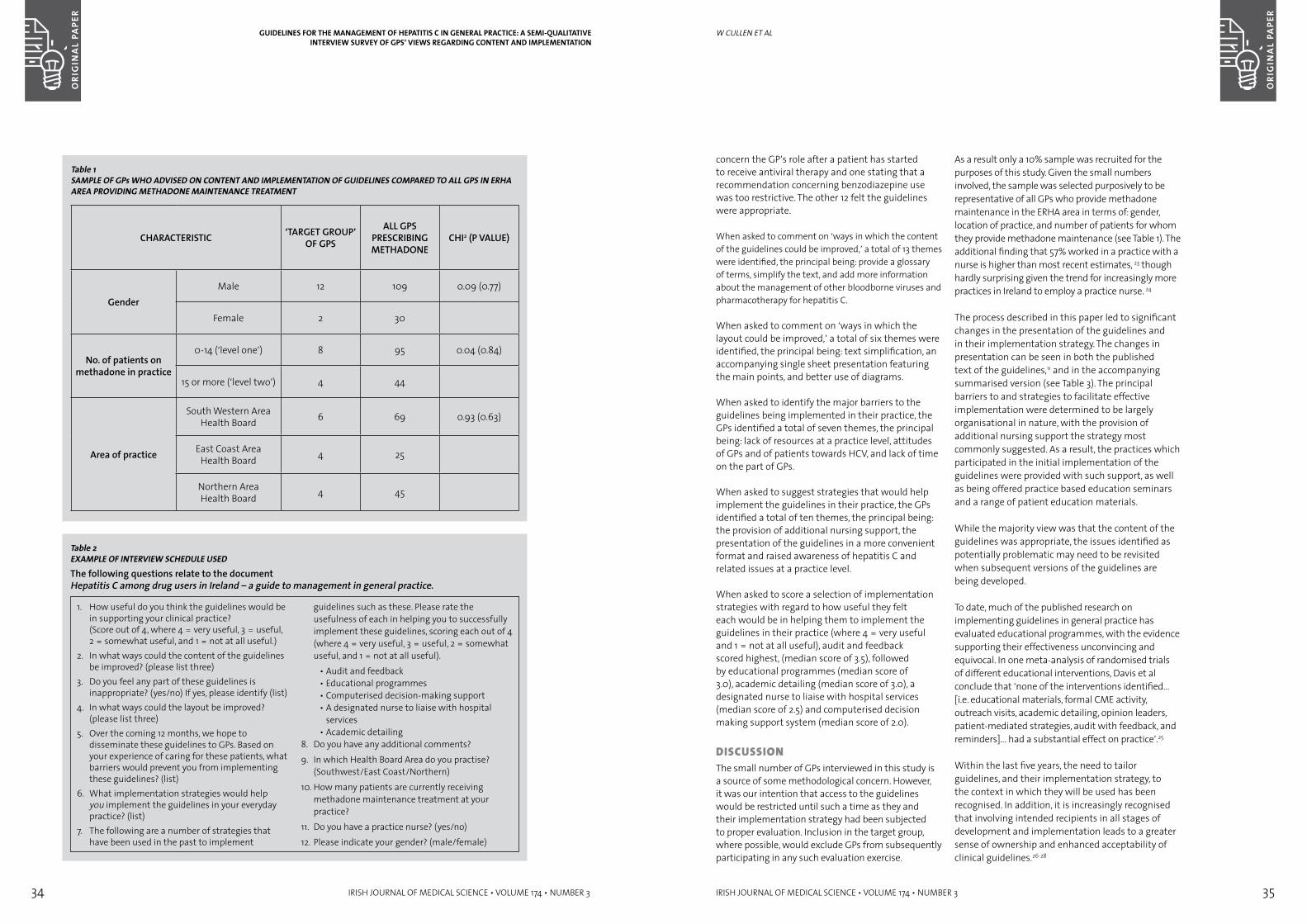
34 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 35
concern the GP’s role after a patient has started to receive antiviral therapy and one stating that a recommendation concerning benzodiazepine use was too restrictive. The other 12 felt the guidelines were appropriate.
When asked to comment on ‘ways in which the content of the guidelines could be improved,’ a total of 13 themes were identified, the principal being: provide a glossary of terms, simplify the text, and add more information about the management of other bloodborne viruses and pharmacotherapy for hepatitis C.
When asked to comment on ‘ways in which the layout could be improved,’ a total of six themes were identified, the principal being: text simplification, an accompanying single sheet presentation featuring the main points, and better use of diagrams.
When asked to identify the major barriers to the guidelines being implemented in their practice, the GPs identified a total of seven themes, the principal being: lack of resources at a practice level, attitudes of GPs and of patients towards HCV, and lack of time on the part of GPs.
When asked to suggest strategies that would help implement the guidelines in their practice, the GPs identified a total of ten themes, the principal being: the provision of additional nursing support, the presentation of the guidelines in a more convenient format and raised awareness of hepatitis C and related issues at a practice level.
When asked to score a selection of implementation strategies with regard to how useful they felt each would be in helping them to implement the guidelines in their practice (where 4 = very useful and 1 = not at all useful), audit and feedback scored highest, (median score of 3.5), followed by educational programmes (median score of 3.0), academic detailing (median score of 3.0), a designated nurse to liaise with hospital services (median score of 2.5) and computerised decision making support system (median score of 2.0).
DisCUssiOnThe small number of GPs interviewed in this study is a source of some methodological concern. However, it was our intention that access to the guidelines would be restricted until such a time as they and their implementation strategy had been subjected to proper evaluation. Inclusion in the target group, where possible, would exclude GPs from subsequently participating in any such evaluation exercise.
As a result only a 10% sample was recruited for the purposes of this study. Given the small numbers involved, the sample was selected purposively to be representative of all GPs who provide methadone maintenance in the ERHA area in terms of: gender, location of practice, and number of patients for whom they provide methadone maintenance (see Table 1). The additional finding that 57% worked in a practice with a nurse is higher than most recent estimates, 23 though hardly surprising given the trend for increasingly more practices in Ireland to employ a practice nurse. 24
The process described in this paper led to significant changes in the presentation of the guidelines and in their implementation strategy. The changes in presentation can be seen in both the published text of the guidelines,11 and in the accompanying summarised version (see Table 3). The principal barriers to and strategies to facilitate effective implementation were determined to be largely organisational in nature, with the provision of additional nursing support the strategy most commonly suggested. As a result, the practices which participated in the initial implementation of the guidelines were provided with such support, as well as being offered practice based education seminars and a range of patient education materials.
While the majority view was that the content of the guidelines was appropriate, the issues identified as potentially problematic may need to be revisited when subsequent versions of the guidelines are being developed.
To date, much of the published research on implementing guidelines in general practice has evaluated educational programmes, with the evidence supporting their effectiveness unconvincing and equivocal. In one meta-analysis of randomised trials of different educational interventions, Davis et al conclude that ‘none of the interventions identified… [i.e. educational materials, formal CME activity, outreach visits, academic detailing, opinion leaders, patient-mediated strategies, audit with feedback, and reminders]… had a substantial effect on practice’.25
Within the last five years, the need to tailor guidelines, and their implementation strategy, to the context in which they will be used has been recognised. In addition, it is increasingly recognised that involving intended recipients in all stages of development and implementation leads to a greater sense of ownership and enhanced acceptability of clinical guidelines.26-28
W CUllen et al
Table 1SAMPLE OF GPs wHO ADVISED ON CONTENT AND IMPLEMENTATION OF GUIDELINES COMPARED TO ALL GPS IN ERHA AREA PROVIDING METHADONE MAINTENANCE TREATMENT
CHARACTERISTIC ‘TARGET GROUP’ OF GPS
ALL GPS PRESCRIBING METHADONE
CHI2 (P VALUE)
GenderMale 12 109 0.09 (0.77)
Female 2 30
No. of patients on methadone in practice
0-14 (‘level one’) 8 95 0.04 (0.84)
15 or more (‘level two’) 4 44
Area of practice
South Western Area Health Board 6 69 0.93 (0.63)
East Coast Area Health Board 4 25
Northern Area Health Board 4 45
GUIDELINES FOR THE MANAGEMENT OF HEPATITIS C IN GENERAL PRACTICE: A SEMI-qUALITATIVE INTERVIEw SURVEY OF GPS’ VIEwS REGARDING CONTENT AND IMPLEMENTATION
Table 2EXAMPLE OF INTERVIEw SCHEDULE USEDThe following questions relate to the document Hepatitis C among drug users in Ireland – a guide to management in general practice.
1. How useful do you think the guidelines would be in supporting your clinical practice? (Score out of 4, where 4 = very useful, 3 = useful, 2 = somewhat useful, and 1 = not at all useful.)
2. In what ways could the content of the guidelines be improved? (please list three)
3. Do you feel any part of these guidelines is inappropriate? (yes/no) If yes, please identify (list)
4. In what ways could the layout be improved? (please list three)
5. Over the coming 12 months, we hope to disseminate these guidelines to GPs. Based on your experience of caring for these patients, what barriers would prevent you from implementing these guidelines? (list)
6. What implementation strategies would help you implement the guidelines in your everyday practice? (list)
7. The following are a number of strategies that have been used in the past to implement
guidelines such as these. Please rate the usefulness of each in helping you to successfully implement these guidelines, scoring each out of 4 (where 4 = very useful, 3 = useful, 2 = somewhat useful, and 1 = not at all useful).
• Audit and feedback• Educational programmes• Computerised decision-making support• A designated nurse to liaise with hospital
services • Academic detailing
8. Do you have any additional comments?9. In which Health Board Area do you practise?
(Southwest/East Coast/Northern)10. How many patients are currently receiving
methadone maintenance treatment at your practice?
11. Do you have a practice nurse? (yes/no)12. Please indicate your gender? (male/female)
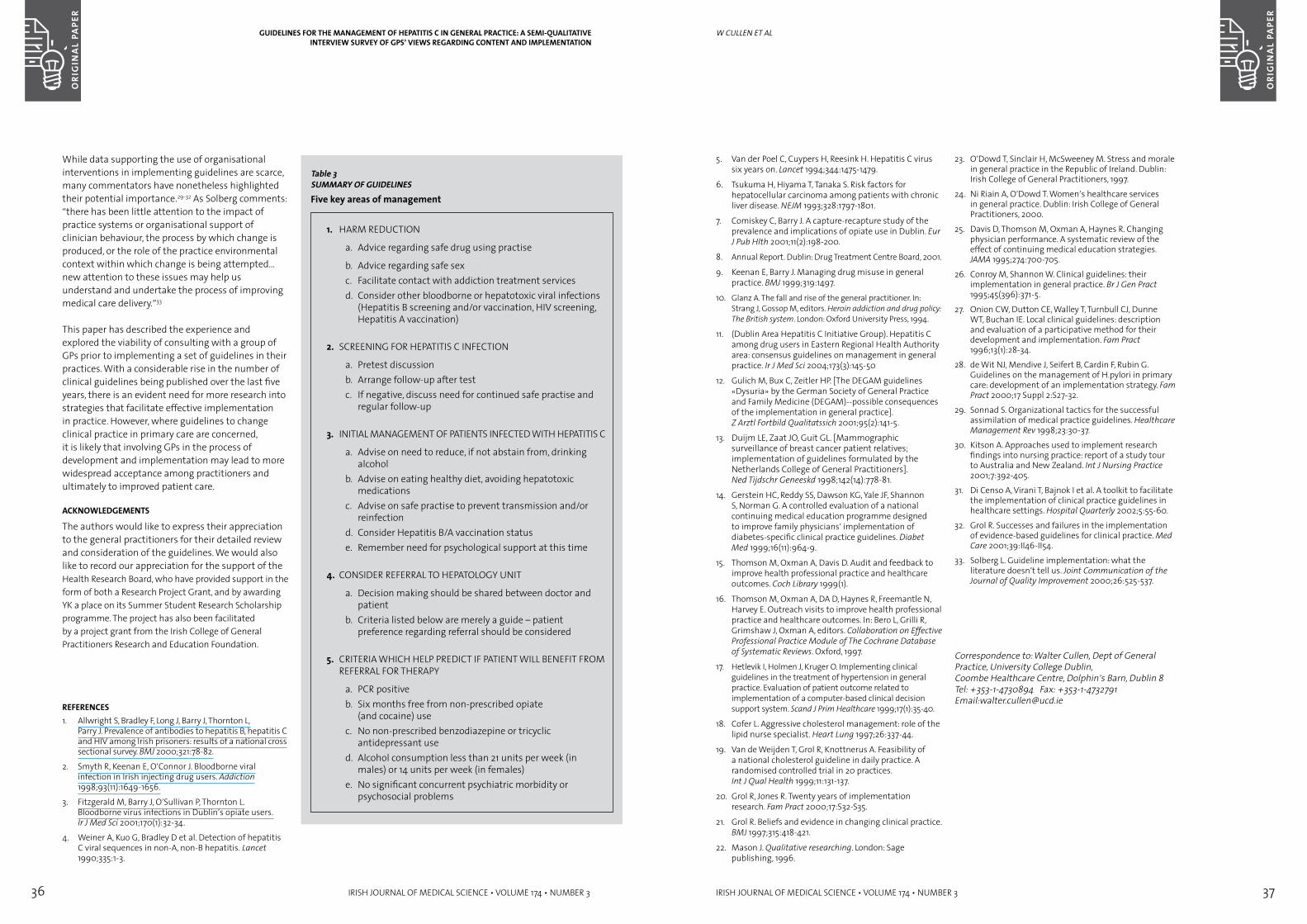
36 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 37
5. Van der Poel C, Cuypers H, Reesink H. Hepatitis C virus six years on. Lancet 1994;344:1475-1479.
6. Tsukuma H, Hiyama T, Tanaka S. Risk factors for hepatocellular carcinoma among patients with chronic liver disease. NEJM 1993;328:1797-1801.
7. Comiskey C, Barry J. A capture-recapture study of the prevalence and implications of opiate use in Dublin. Eur J Pub Hlth 2001;11(2):198-200.
8. Annual Report. Dublin: Drug Treatment Centre Board, 2001.
9. Keenan E, Barry J. Managing drug misuse in general practice. BMJ 1999;319:1497.
10. Glanz A. The fall and rise of the general practitioner. In: Strang J, Gossop M, editors. Heroin addiction and drug policy: The British system. London: Oxford University Press, 1994.
11. (Dublin Area Hepatitis C Initiative Group). Hepatitis C among drug users in Eastern Regional Health Authority area: consensus guidelines on management in general practice. Ir J Med Sci 2004;173(3):145-50
12. Gulich M, Bux C, Zeitler HP. [The DEGAM guidelines «Dysuria» by the German Society of General Practice and Family Medicine (DEGAM)--possible consequences of the implementation in general practice]. Z Arztl Fortbild Qualitatssich 2001;95(2):141-5.
13. Duijm LE, Zaat JO, Guit GL. [Mammographic surveillance of breast cancer patient relatives; implementation of guidelines formulated by the Netherlands College of General Practitioners]. Ned Tijdschr Geneeskd 1998;142(14):778-81.
14. Gerstein HC, Reddy SS, Dawson KG, Yale JF, Shannon S, Norman G. A controlled evaluation of a national continuing medical education programme designed to improve family physicians’ implementation of diabetes-specific clinical practice guidelines. Diabet Med 1999;16(11):964-9.
15. Thomson M, Oxman A, Davis D. Audit and feedback to improve health professional practice and healthcare outcomes. Coch Library 1999(1).
16. Thomson M, Oxman A, DA D, Haynes R, Freemantle N, Harvey E. Outreach visits to improve health professional practice and healthcare outcomes. In: Bero L, Grilli R, Grimshaw J, Oxman A, editors. Collaboration on Effective Professional Practice Module of The Cochrane Database of Systematic Reviews. Oxford, 1997.
17. Hetlevik I, Holmen J, Kruger O. Implementing clinical guidelines in the treatment of hypertension in general practice. Evaluation of patient outcome related to implementation of a computer-based clinical decision support system. Scand J Prim Healthcare 1999;17(1):35-40.
18. Cofer L. Aggressive cholesterol management: role of the lipid nurse specialist. Heart Lung 1997;26:337-44.
19. Van de Weijden T, Grol R, Knottnerus A. Feasibility of a national cholesterol guideline in daily practice. A randomised controlled trial in 20 practices. Int J Qual Health 1999;11:131-137.
20. Grol R, Jones R. Twenty years of implementation research. Fam Pract 2000;17:S32-S35.
21. Grol R. Beliefs and evidence in changing clinical practice. BMJ 1997;315:418-421.
22. Mason J. Qualitative researching. London: Sage publishing, 1996.
23. O’Dowd T, Sinclair H, McSweeney M. Stress and morale in general practice in the Republic of Ireland. Dublin: Irish College of General Practitioners, 1997.
24. Ni Riain A, O’Dowd T. Women’s healthcare services in general practice. Dublin: Irish College of General Practitioners, 2000.
25. Davis D, Thomson M, Oxman A, Haynes R. Changing physician performance. A systematic review of the effect of continuing medical education strategies. JAMA 1995;274:700-705.
26. Conroy M, Shannon W. Clinical guidelines: their implementation in general practice. Br J Gen Pract 1995;45(396):371-5.
27. Onion CW, Dutton CE, Walley T, Turnbull CJ, Dunne WT, Buchan IE. Local clinical guidelines: description and evaluation of a participative method for their development and implementation. Fam Pract 1996;13(1):28-34.
28. de Wit NJ, Mendive J, Seifert B, Cardin F, Rubin G. Guidelines on the management of H.pylori in primary care: development of an implementation strategy. Fam Pract 2000;17 Suppl 2:S27-32.
29. Sonnad S. Organizational tactics for the successful assimilation of medical practice guidelines. Healthcare Management Rev 1998;23:30-37.
30. Kitson A. Approaches used to implement research findings into nursing practice: report of a study tour to Australia and New Zealand. Int J Nursing Practice 2001;7:392-405.
31. Di Censo A, Virani T, Bajnok I et al. A toolkit to facilitate the implementation of clinical practice guidelines in healthcare settings. Hospital Quarterly 2002;5:55-60.
32. Grol R. Successes and failures in the implementation of evidence-based guidelines for clinical practice. Med Care 2001;39:II46-II54.
33. Solberg L. Guideline implementation: what the literature doesn’t tell us. Joint Communication of the Journal of Quality Improvement 2000;26:525-537.
Correspondence to: Walter Cullen, Dept of General Practice, University College Dublin, Coombe Healthcare Centre, Dolphin’s Barn, Dublin 8Tel: +353-1-4730894 Fax: +353-1-4732791Email:[email protected]
W CUllen et al
While data supporting the use of organisational interventions in implementing guidelines are scarce, many commentators have nonetheless highlighted their potential importance.29-32 As Solberg comments: “there has been little attention to the impact of practice systems or organisational support of clinician behaviour, the process by which change is produced, or the role of the practice environmental context within which change is being attempted…new attention to these issues may help us understand and undertake the process of improving medical care delivery.”33
This paper has described the experience and explored the viability of consulting with a group of GPs prior to implementing a set of guidelines in their practices. With a considerable rise in the number of clinical guidelines being published over the last five years, there is an evident need for more research into strategies that facilitate effective implementation in practice. However, where guidelines to change clinical practice in primary care are concerned, it is likely that involving GPs in the process of development and implementation may lead to more widespread acceptance among practitioners and ultimately to improved patient care.
ACkNOwLEDGEMENTS
The authors would like to express their appreciation to the general practitioners for their detailed review and consideration of the guidelines. We would also like to record our appreciation for the support of the Health Research Board, who have provided support in the form of both a Research Project Grant, and by awarding YK a place on its Summer Student Research Scholarship programme. The project has also been facilitated by a project grant from the Irish College of General Practitioners Research and Education Foundation.
REFERENCES1. Allwright S, Bradley F, Long J, Barry J, Thornton L,
Parry J. Prevalence of antibodies to hepatitis B, hepatitis C and HIV among Irish prisoners: results of a national cross sectional survey. BMJ 2000;321:78-82.
2. Smyth R, Keenan E, O’Connor J. Bloodborne viral infection in Irish injecting drug users. Addiction 1998;93(11):1649-1656.
3. Fitzgerald M, Barry J, O’Sullivan P, Thornton L. Bloodborne virus infections in Dublin’s opiate users. Ir J Med Sci 2001;170(1):32-34.
4. Weiner A, Kuo G, Bradley D et al. Detection of hepatitis C viral sequences in non-A, non-B hepatitis. Lancet 1990;335:1-3.
Table 3SUMMARY OF GUIDELINESFive key areas of management
1. HARM REDUCTION
a. Advice regarding safe drug using practise
b. Advice regarding safe sexc. Facilitate contact with addiction treatment servicesd. Consider other bloodborne or hepatotoxic viral infections
(Hepatitis B screening and/or vaccination, HIV screening, Hepatitis A vaccination)
2. SCREENING FOR HEPATITIS C INFECTION
a. Pretest discussionb. Arrange follow-up after testc. If negative, discuss need for continued safe practise and
regular follow-up
3. INITIAL MANAGEMENT OF PATIENTS INFECTED WITH HEPATITIS C
a. Advise on need to reduce, if not abstain from, drinking alcohol
b. Advise on eating healthy diet, avoiding hepatotoxic medications
c. Advise on safe practise to prevent transmission and/or reinfection
d. Consider Hepatitis B/A vaccination statuse. Remember need for psychological support at this time
4. CONSIDER REFERRAL TO HEPATOLOGY UNIT
a. Decision making should be shared between doctor and patient
b. Criteria listed below are merely a guide – patient preference regarding referral should be considered
5. CRITERIA WHICH HELP PREDICT IF PATIENT WILL BENEFIT FROM REFERRAL FOR THERAPY
a. PCR positiveb. Six months free from non-prescribed opiate
(and cocaine) usec. No non-prescribed benzodiazepine or tricyclic
antidepressant used. Alcohol consumption less than 21 units per week (in
males) or 14 units per week (in females) e. No significant concurrent psychiatric morbidity or
psychosocial problems
GUIDELINES FOR THE MANAGEMENT OF HEPATITIS C IN GENERAL PRACTICE: A SEMI-qUALITATIVE INTERVIEw SURVEY OF GPS’ VIEwS REGARDING CONTENT AND IMPLEMENTATION
38 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 39
They were asked to return the postcard separately to facilitate identification of non-responders. We repeated the exercise twice to minimise response bias. As confidentiality was assured the questionnaire did not contain any identifying (personal or practice) information. The questionnaires were coded numerically and entered by double entry data input to a Microsoft Excel Spreadsheet and later imported to the Statistical Packages for the Social Sciences (version 11.5) for analysis.
resUlTsThere were 421 questionnaires distributed, 261 were returned representing a response rate of 61.9%. Twelve of these questionnaires were not usable. The demographic characteristics of the doctors who participated were representative of previously reported surveys of GPs in Ireland (Table 1). 7, 8 The GPs gender, age, health board area or practice size did not have a significant influence on the assessment or management of patients. Post-graduate psychiatric training did not influence patient management significantly.
33.7% of respondents reported seeing 6-10 patients with chronic schizophrenia and 27.3% reported seeing more than 10 per year (Table 2). The management of patients with chronic schizophrenia most commonly entailed regular consultation with a specialist (44%). The next most common practice (22.2%) was referral to specialist services with subsequent treatment exclusively by the GP. Occasional consultation with a specialist was availed of by 17.3% with a further 13.1% passing over the care of patients with schizophrenia entirely to specialist services. A tiny minority (0.9%) manage patients with schizophrenia entirely in their own practice without ever referring them for a specialist opinion.
GPs were then asked about their preferred option for treating patients with schizophrenia. These responses largely mirrored the GPs actual management (Table 3). The largest difference was seen in the category of ‘complete handover of treatment to psychiatric services’. This was the preferred option of only 5.7% of GPs, but was the practice of 13.3%. In contrast more GPs (50.4%) would like to avail of regular consultation with psychiatry services than currently do (44%).
When asked about their prescribing practice in patients with chronic schizophrenia, a significant majority (88.7%) recommended that patients remain
on antipsychotics indefinitely, with only 4.8% recommending less than a year of treatment.
Respondents were asked to rate how often they experienced difficulties with schizophrenia in primary care to the extent of making the illness unmanageable. Thirty-four per cent reported that they ‘usually’ encounter such difficulties and 2.4% responded that they ‘always’ do so.
GPs were then asked, using free text, to expand on the problems they encountered. A significant number of GPs rated non-adherence with medication as the most significant problem in managing cases of established schizophrenia in general practice. Loss to follow-up with both psychiatric and primary care was also reported as a common problem among those that encountered difficulties. A significant number felt that the symptoms of the illness itself (i.e. relapse/acute psychosis/lack of insight) posed management difficulty in primary care. Factors associated with the illness such as substance misuse and aggression proved problematic for a very small number of GPs.
DisCUssiOnThe response rate of 62% is similar to that of other postal surveys of GPs.9 Non-response to postal questionnaires reduces the effective sample size and can introduce bias. However, the demographic characteristics of the doctors who participated are representative of previously reported surveys of GPs in Ireland.7, 8 We found that the management of patients with schizophrenia varied significantly between primary care settings. In particular the level of involvement of specialist services varied considerably with 23.1% of GPs managing cases of schizophrenia independent of psychiatric input. This variation was not associated with health board area and was thus unlikely to be explained by variable practices between mental health services in different areas. This is in accordance with a recent prospective study of psychiatric referrals made by GPs in London10 which found that subjective factors such as general practitioner attitudes were influential in the decision to involve psychiatric services in patient management. Furthermore when GPs in the present study were asked to give their ‘ideally preferred option’ in treating patients with schizophrenia, their responses essentially reflected their current practice (Table 3).
The commonest model of care for cases of established schizophrenia reported by respondents
B Gavin et al
inTrODUCTiOnSchizophrenia affects almost 1% of the population, typically disrupting a young person’s development at a critical stage. Drug and alcohol misuse is common among people with schizophrenia amplifying both their already high risk of suicide (20 fold) and their propensity to physical ill-health.1 Poor nutrition, heavy smoking and physical inactivity occur frequently among patients with chronic schizophrenia. 2 This may explain why patients with chronic schizophrenia are known to attend their GPs with physical problems up to three times more frequently than other attendees.3
Furthermore, a recent study in the UK found that one quarter of patients with a history of psychosis are disengaged from specialist psychiatry services and are looked after entirely in general practice. 4
GPs are thus charged with the task of managing a complex chronic psychiatric illness together with significant medical co-morbidity. However, it has been shown that regular structured assessments of mental state by GPs are not practical in routine appointments. 5
Despite their pivotal role in managing chronic schizophrenia, no management guidelines exist for primary care and the views of GPs on this issue have not been sought.
MeTHODThe study design was a cross-sectional, questionnaire survey. We randomly selected 20% (N=421) of GPs from the Irish Medical Directory and invited them to participate in the study. We estimated that a 50-60% participation rate would provide a sufficient size to inform us on the current practice and needs of general practitioners. We used a twenty seven-item questionnaire that assesses aspects of the detection and management of suspected and established schizophrenia in general practice. It contains fourteen questions about managing suspected first episode schizophrenia, six questions about managing patients with an established diagnosis of schizophrenia and seven questions regarding demographics. The questionnaire was translated from the original German version 6 and piloted among a cohort of GP tutors affiliated to the academic Department of General Practice (UCD). They suggested several modifications for use in an Irish setting. The questionnaire took 10 minutes to complete. We received ethical approval from the Research Ethics Committee of the ICGP Practitioners and the Provincial Ethics Committee of St. John of God Hospital. The sample was identified by computer generated random sampling. The questionnaire, explanatory letter, prepaid envelope and a postcard bearing the GP’s name was posted to each GP.
Schizophrenia in general practice: a national survey of general practitioners in IrelandaBsTraCTBackground Chronic schizophrenia is challenging to manage in primary care.Aims We sought to establish the views of General Practitioners about managing patients
with chronic schizophrenia in primary care. Methods A cross-sectional, postal survey questionnaire of a randomly selected sample of
20% of GPs was carried out. Results Most GPs (97.2%) have at least one person with schizophrenia attending their
practice. A substantial number of GPs (22.2%) treat cases of schizophrenia without specialist input following an initial referral to psychiatric services. Almost all (88.7%) advised patients who had experienced multiple relapses to remain on medication indefinitely. One third of GPs reported that they always experience difficulties managing patients with schizophrenia in their practice. Non-adherence with prescribed medication and loss to follow-up were the commonest impediments to treatment encountered.
Conclusion GPs require appropriate back up from specialist services to enable their management of chronic schizophrenia.
B Gavin,1 W Cullen,2 B O’Donoghue,2, 3 JC Ascencio-Lane,2, 3 G Bury,2 E O’Callaghan1, 3
St John of God Hospital, Dublin1, Dept of General Practice, UCD2, Dept of Psychiatry, UCD3
SCHIzOPHRENIA IN GENERAL PRACTICE: A NATIONAL SURVEY OF GENERAL PRACTITIONERS IN IRELAND

40 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 41
(44%) was regular consultation with specialist services. There is evidence that when specialist psychiatry services manage all patients with major mental illness, they are less able to respond adequately to urgent cases such as acute psychosis.11 This has led to the suggestion that it is more efficient for GPs to manage stable compliant cases with specialist resources focusing on more difficult acute cases, thus allowing more rapid response rates and potentially earlier detection of early psychosis. 4, 12
However, this is the preferred treatment model of less than one quarter of respondents.
There was significantly less variation in prescribing practice for this group of patients compared with those presenting with early symptoms of schizophrenia.13 Almost 90% of respondents indicated that they recommend to patients with multiple psychotic relapses to remain on medication indefinitely. It has previously been found that in established schizophrenia, GPs rarely make alterations in terms of type or dose of drug. 3 This is particularly relevant in the case of GPs managing schizophrenia without psychiatric input. However, teaching GPs to carry out structured assessments has been shown to have a direct input on patient management. It results in increased rates of medication changes and higher rates of referral to psychiatric services.
A significant minority (35.6%) of GPs reported that they frequently experienced difficulties in the management of patients with schizophrenia which they felt could not be managed in their practice. Non-adherence with medication was the commonest difficulty encountered. This mirrors the difficulty with compliance encountered within specialist services in Ireland and may, in some cases, be alleviated by minimising side-effects through use of atypical antipsychotics.15,16 In Ireland, as elsewhere, few practices have policies for the treatment of schizophrenia and the rates of ongoing use of typical antipsychotics are unknown.14
Failure to attend appointments impeded management of this group of patients in primary care leading to significant loss to follow-up. A substantial number of GPs reporting difficulties managing cases of schizophrenia felt that it was aspects of the illness itself that proved problematic in primary care settings. Acute psychotic symptoms were felt by a number of respondents to be unmanageable in their practice. Likewise, patients
without insight into their illness were felt by a number of GPs to be impractical to manage in their practice. Studies from the UK support the view that aspects of the illness may be difficult to manage in primary care settings. The impact on patient management of teaching GPs to carry out structured assessments of their chronically unwell psychiatric patients has been assessed.5 The results of this study demonstrated that regular structured assessments are not practical in routine appointments. However, regular assessments are considered to be essential to optimise management of psychosis and allow careful tapering of medication.
Factors that may be problematic even within acute inpatient settings, such as aggression and substance misuse, were not reported by a significant number of GPs to be an impediment to treatment in the primary care setting. This may simply reflect the fact that patients demonstrating these behaviour patterns may be more likely to be managed within specialist services.
This study indicates the wish of the majority of GPs to be closely involved with mental health services in managing cases of chronic schizophrenia. It highlights the need for adequate collaboration between the two disciplines to allow a more seamless provision of care and minimise loss to follow-up.
ACkNOwLEDGEMENTS
We thank our collaborators Andor Simon and Daniel Umbricht from Switzerland who designed the original German language questionnaire. The authors would like to express their gratitude to Mimi Copty, Director of the Mental Health in Primary Care Project at the Irish College of General Practitioners for initial guidance. We are grateful to the GPs who kindly assisted us with adapting the questionnaire for an Irish setting. We are especially appreciative of all the doctors from the ICGP who took the time to evaluate their practice. We would like to acknowledge with thanks, the funding received from the Research and Education Committee (General Practice) of the Department of Health and Children, which enabled us to complete this research.
B Gavin et alSCHIzOPHRENIA IN GENERAL PRACTICE: A NATIONAL SURVEY OF GENERAL PRACTITIONERS IN IRELAND
Table 1DEMOGRAPHIC CHARACTERISTICS OF PARTICIPATING GPs
VARIABLE CHARACTERISTICS SAMPLE GPS (N=249) NATIONAL POPULATION OF GPS1,2
GenderMale
Female69.1%30.5%
70%30%
Age
26-3536-4546-5556-65>66
11.4%32.5%38.8%15.3%2.0%
17%37%29%10%7%
Practice ClassificationUrban Rural
Combined urban/rural
34.9%22.0%43.1%
GMS ListYes No
93.4%6.6%
73%27%
Table 3PREFERRED VERSUS ACTUAL MANAGEMENT OF SCHIzOPHRENIA
PREFERRED ACTUAL
Treat exclusively by GP 0.8 0.9
Occasional consultation with specialist services 17.1 17.3
Regular consultation with psychiatric services 50.4 44.0
Exclusive treatment by GP following initial diagnosis 24.8 22.2
Complete handover to psychiatric services 5.7 13.3
Other 1.2 2.2
Table 2NUMBERS OF PATIENTS wITH SCHIzOPHRENIA ATTENDING GP
NUMBER PERCENTAGE
None 1-23-5
6-10>10
Total
2.812.423.733.727.3100
42 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 43
inTrODUCTiOnThe professional autonomy of physicians is based on the assumption that they will be deemed competent at graduation and remain competent as long as they practice. Although this retention of competence was previously left to the individual practitioner, formal assessment of physician competence has now been introduced in many countries to “protect the public from poor practice, and enhance doctors’ knowledge.”1 Such Competence Assurance Structures (CAS) have evolved in a number of different formats, ranging from voluntary educational activities and self-assessment, to mandatory performance assessments in the clinical setting.
The international experience has highlighted a number of potential challenges to the implementation, and success of, CAS, both in educating clinicians and improving patient care.
These range from physicians’ resistance to externally imposed change, to the financial and legal barriers that exist to detailed assessment.2,3 There is also limited evidence available to support the role of CAS in improving clinical outcomes, or changing physicians’ practice.4-7
The Irish Medical Council has introduced a system of Competence Assurance Structures to ‘ensure that doctors maintain the necessary knowledge and skills to function as effective practitioners throughout their working lives’.8 The initial programme of Continuing Medical Education (CME) started in January 2003. The second stage, involving Clinical Audit and Peer Review, was due to be introduced in January 2005.
We sought to survey physicians practising in Ireland to assess their attitudes to peer review as a method
Attitudes to peer review as a competence assurance structure – results of a survey of Irish physiciansaBsTraCTBackground The Medical Council in Ireland is currently implementing Competence
Assurance Structures (CAS). Peer review has been proposed as a tool to measure physician competence.
Aims To assess the attitudes of physicians working in the Irish healthcare system to a peer review programme of competence assurance prior to its implementation.
Methods A postal survey was sent to all physicians in the Irish Medical Directory in November 2003. Nine questions were asked to gauge attitudes to peer review as a CA tool. The returned questionnaires were collated and data extracted based on responses.
Results The response rate was 67%. The majority of respondents (92%) felt peer review would inform competence assurance in Ireland. Most physicians who were surveyed felt an on-site assessment (88%) every 5 years (87%) was the preferred method. Over 30% responded that there should be a financial incentive for completing a review, and 70% would pay to be assessed. The UK model of competence assurance was the model most physicians preferred for the Irish setting (42%).
Conclusion The majority of physicians practising in Ireland would favour a peer review system of competence assurance. The financial implications, and structure, of such a system would need to be explored prior to implementation.
keywords competence assurance, peer review
AC Moss, T Dugal, B SilkeDept of General Medicine, St James’s Hospital, Dublin
ATTITUDES TO PEER REVIEw AS A COMPETENCE ASSURANCE STRUCTURE – RESULTS OF A SURVEY OF IRISH PHYSICIANS
REFERENCES1. Kamali M, Kelly L, Gervin M, Browne S, Larkin C,
O'Callaghan E. The prevalence of comorbid substance misuse and its influence on suicidal ideation among in-patients with schizophrenia. Acta Psychiatr Scand 2000; 101(6):452-6.
2. Brugha ST, Wing JK, Smith BL. Physical health of the long term mentally ill in the community. Is there unmet need? Br J Psychiatry 1988; 155: 777-81.
3. King MB. Management of patients with schizophrenia in general practice. Br J Gen Practice, Aug 1992; 42: 310-1.
4. Kendrick T, Burns T. Mental health teams should concentrate on psychiatric patients with greatest needs. BMJ 1996; 313:884-5.
5. Kendrick T, Burns T, Freeling P. Randomised controlled trial of teaching general practitioners to carry out structured assessments of their long term mentally ill patients. BMJ 1995; 311: 93-97.
6. Simon A.E, Umbricht D, Merlo MCG. Swiss General Practitioners and first Episode Psychoses: Results of a National Survey. Schizophrenia Research 2002; 53 (3) suppl.15.
7. National General Practice Survey. Dublin: Irish College of General Practitioners, 1997.
8. O’Dowd T, Sinclair H, McSweeney M. Stress and morale in general practice in the Republic of Ireland. Dublin: Irish College of General Practitioners, 1997.
9. Edwards P, Roberts I, Clarke M, DiGuiseppi C et al. Increasing response rates to postal questionnaires: systematic review. BMJ. 2002 May 18; 324(7347): 1183.
10. Ashworth M, Clement S, Sandhu J, Farley N, Ramsay R, Davies T. Psychiatric referral rates and the influence of on-site mental health workers in general practice. Br J Gen Practitioners, Jan 2002; 52 (474): 39-41.
11. Wilkinson G, Piccinelli M, Falloon I, Krekorian H, McLees S. An evaluation of community based psychiatric care for people with treated long term mental illness. Br J Psychiatry, 1995; 167: 26-37.
12. Kendrick T, Burns T, Freeling P, Sibbald B. Provision of care to general practice patients with disabling long term mental illnesses: a survey of 16 practices. Br J Gen Practice 1994; 44: 301-5.
13. Gavin B, Cullen W, O’Donoghue B, Carlos J, Bury G, O’Callaghan E. First Episode Schizophrenia In General Practice: A National Survey of General Practitioners in Ireland. In Press.
14. Kendrick T, Sibbald B, Burns T, Freeling P. Role of general practitioners in care of long term mentally ill patients. BMJ 1991; 302: 508-10.
15. Kamali M, Kelly L, Gervin M, Browne S, Larkin C, O’Callaghan E. Psychopharmocology, insight and comorbid substance misuse and medication compliance among patients with schizophrenia. Psych Serv 2001, Feb 52(2) 161-3
16. O’Donnell C, Donohoe G, Sharkey L et al. Compliance Therapy: A Randomised Controlled Trial. BMJ 2003 Oct 11;327(7419):834.
Correspondence to: Prof. Eadbhard O’Callaghan, Hospitaller Order of St. John of God Hospital/Cluain Mhuire Service, Newtownpark Avenue, Blackrock, Co. Dublin. Tel: 01 2172100 Fax: 01 2833886E-mail: [email protected]
SCHIzOPHRENIA IN GENERAL PRACTICE: A NATIONAL SURVEY OF GENERAL PRACTITIONERS IN IRELAND
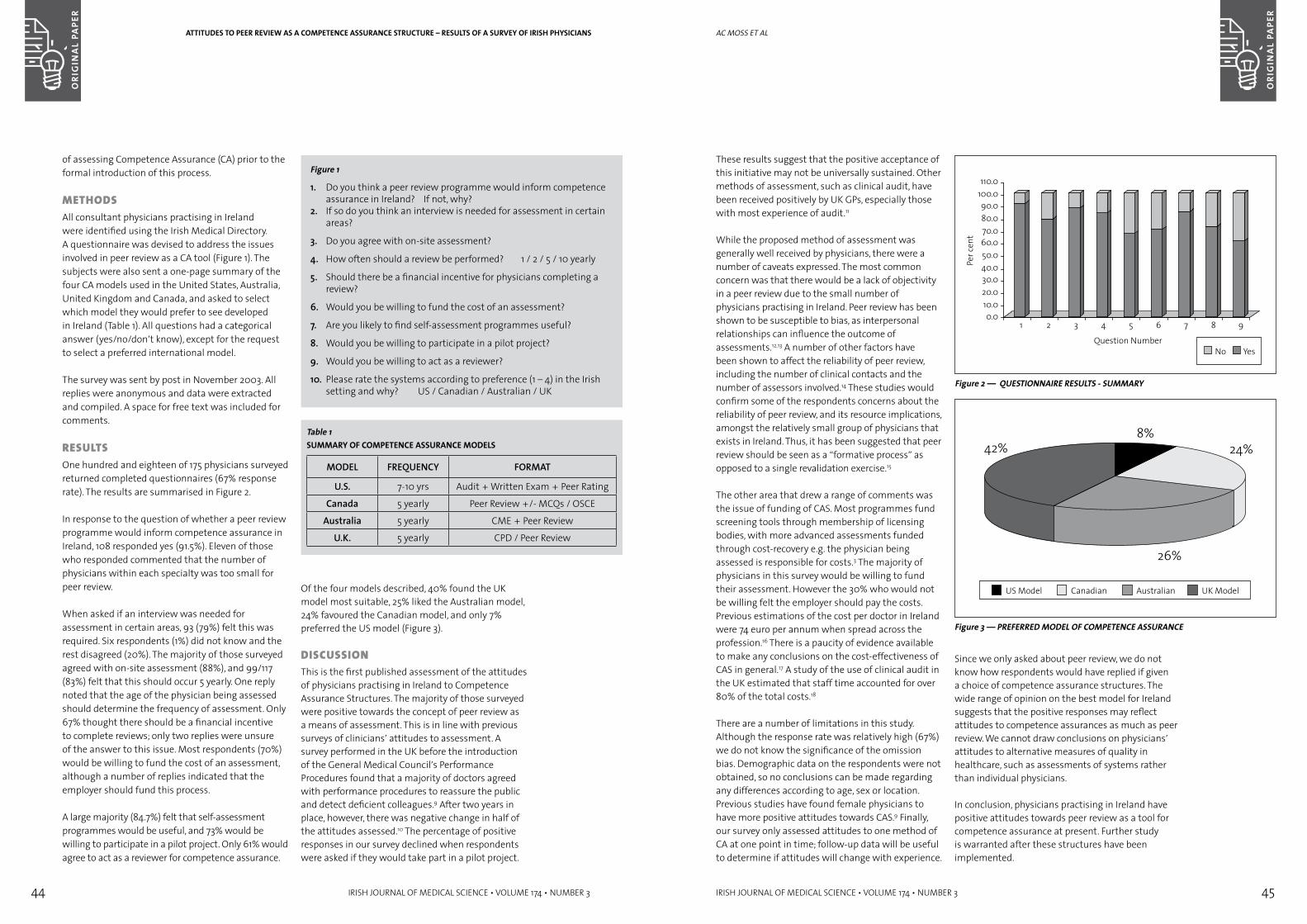
44 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 45
aC MOSS et al
These results suggest that the positive acceptance of this initiative may not be universally sustained. Other methods of assessment, such as clinical audit, have been received positively by UK GPs, especially those with most experience of audit.11
While the proposed method of assessment was generally well received by physicians, there were a number of caveats expressed. The most common concern was that there would be a lack of objectivity in a peer review due to the small number of physicians practising in Ireland. Peer review has been shown to be susceptible to bias, as interpersonal relationships can influence the outcome of assessments.12,13 A number of other factors have been shown to affect the reliability of peer review, including the number of clinical contacts and the number of assessors involved.14 These studies would confirm some of the respondents concerns about the reliability of peer review, and its resource implications, amongst the relatively small group of physicians that exists in Ireland. Thus, it has been suggested that peer review should be seen as a “formative process” as opposed to a single revalidation exercise.15
The other area that drew a range of comments was the issue of funding of CAS. Most programmes fund screening tools through membership of licensing bodies, with more advanced assessments funded through cost-recovery e.g. the physician being assessed is responsible for costs.3 The majority of physicians in this survey would be willing to fund their assessment. However the 30% who would not be willing felt the employer should pay the costs. Previous estimations of the cost per doctor in Ireland were 74 euro per annum when spread across the profession.16 There is a paucity of evidence available to make any conclusions on the cost-effectiveness of CAS in general.17 A study of the use of clinical audit in the UK estimated that staff time accounted for over 80% of the total costs.18
There are a number of limitations in this study. Although the response rate was relatively high (67%) we do not know the significance of the omission bias. Demographic data on the respondents were not obtained, so no conclusions can be made regarding any differences according to age, sex or location. Previous studies have found female physicians to have more positive attitudes towards CAS.9 Finally, our survey only assessed attitudes to one method of CA at one point in time; follow-up data will be useful to determine if attitudes will change with experience.
Figure 2 — qUESTIONNAIRE RESULTS - SUMMARY
Figure 3 — PREFERRED MODEL OF COMPETENCE ASSURANCE
Since we only asked about peer review, we do not know how respondents would have replied if given a choice of competence assurance structures. The wide range of opinion on the best model for Ireland suggests that the positive responses may reflect attitudes to competence assurances as much as peer review. We cannot draw conclusions on physicians’ attitudes to alternative measures of quality in healthcare, such as assessments of systems rather than individual physicians.
In conclusion, physicians practising in Ireland have positive attitudes towards peer review as a tool for competence assurance at present. Further study is warranted after these structures have been implemented.
of assessing Competence Assurance (CA) prior to the formal introduction of this process.
MeTHODsAll consultant physicians practising in Ireland were identified using the Irish Medical Directory. A questionnaire was devised to address the issues involved in peer review as a CA tool (Figure 1). The subjects were also sent a one-page summary of the four CA models used in the United States, Australia, United Kingdom and Canada, and asked to select which model they would prefer to see developed in Ireland (Table 1). All questions had a categorical answer (yes/no/don’t know), except for the request to select a preferred international model.
The survey was sent by post in November 2003. All replies were anonymous and data were extracted and compiled. A space for free text was included for comments.
resUlTsOne hundred and eighteen of 175 physicians surveyed returned completed questionnaires (67% response rate). The results are summarised in Figure 2.
In response to the question of whether a peer review programme would inform competence assurance in Ireland, 108 responded yes (91.5%). Eleven of those who responded commented that the number of physicians within each specialty was too small for peer review.
When asked if an interview was needed for assessment in certain areas, 93 (79%) felt this was required. Six respondents (1%) did not know and the rest disagreed (20%). The majority of those surveyed agreed with on-site assessment (88%), and 99/117 (83%) felt that this should occur 5 yearly. One reply noted that the age of the physician being assessed should determine the frequency of assessment. Only 67% thought there should be a financial incentive to complete reviews; only two replies were unsure of the answer to this issue. Most respondents (70%) would be willing to fund the cost of an assessment, although a number of replies indicated that the employer should fund this process.
A large majority (84.7%) felt that self-assessment programmes would be useful, and 73% would be willing to participate in a pilot project. Only 61% would agree to act as a reviewer for competence assurance.
Figure 1
1. Do you think a peer review programme would inform competence assurance in Ireland? If not, why?
2. If so do you think an interview is needed for assessment in certain areas?
3. Do you agree with on-site assessment?
4. How often should a review be performed? 1 / 2 / 5 / 10 yearly
5. Should there be a financial incentive for physicians completing a review?
6. Would you be willing to fund the cost of an assessment?
7. Are you likely to find self-assessment programmes useful?
8. Would you be willing to participate in a pilot project?
9. Would you be willing to act as a reviewer?
10. Please rate the systems according to preference (1 – 4) in the Irish setting and why? US / Canadian / Australian / UK
Table 1SUMMARY OF COMPETENCE ASSURANCE MODELS
MODEL FREQUENCY FORMAT
U.S. 7-10 yrs Audit + Written Exam + Peer Rating
Canada 5 yearly Peer Review +/- MCQs / OSCE
Australia 5 yearly CME + Peer Review
U.K. 5 yearly CPD / Peer Review
Of the four models described, 40% found the UK model most suitable, 25% liked the Australian model, 24% favoured the Canadian model, and only 7% preferred the US model (Figure 3).
DisCUssiOnThis is the first published assessment of the attitudes of physicians practising in Ireland to Competence Assurance Structures. The majority of those surveyed were positive towards the concept of peer review as a means of assessment. This is in line with previous surveys of clinicians’ attitudes to assessment. A survey performed in the UK before the introduction of the General Medical Council’s Performance Procedures found that a majority of doctors agreed with performance procedures to reassure the public and detect deficient colleagues.9 After two years in place, however, there was negative change in half of the attitudes assessed.10 The percentage of positive responses in our survey declined when respondents were asked if they would take part in a pilot project.
ATTITUDES TO PEER REVIEw AS A COMPETENCE ASSURANCE STRUCTURE – RESULTS OF A SURVEY OF IRISH PHYSICIANS
46 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 47
inTrODUCTiOnGeneral practice co-operatives have developed rapidly in Ireland and now represent a crucial component of out-of-hours services. The real or potential involvement of co-operatives with care of emergencies in the community has not been explored to date.
A wide range of strategic health policy initiatives in Ireland have in recent years emphasised the roles of primary care, general practice and GP co-operatives as key elements in the integrated healthcare structures planned for Ireland’s population.1,2,3 Out-of-hours GP co-operatives have been established in many parts of the country between 1998 and 2002. Activity levels and structures in these co-operatives have been reported separately.4
During 2002, the 11 co-operatives then functioning provided cover to approximately 1.5m people and had
340,000 contacts with patients.4 This study reports on the preparedness and contribution of co-operatives to the management of emergencies in the community during 2002, using both quantitative and qualitative elements.
MeTHODsDuring 2004, a questionnaire survey was carried out in all 11 co-operatives covering structures and staffing, training and policies and activity levels for 2002. All co-operatives responded to the survey. Information was requested on triage procedures to identify and deal with emergencies, on staffing and equipment levels and on the numbers of recorded emergencies dealt with during the 12-month period. The designation of emergencies within individual co-operatives is a clinical issue for that co-operative and its staff and the study records the numbers of calls designated as such without attempting to impose standardised definitions.
General practice out-of-hours co-operatives in Ireland – emergency service or not?aBsTraCTBackground Since 1998, Irish general practice has developed 11 out-of-hours co-operatives,
covering almost 40% of the population. The co-operatives vary in terms of triage mechanisms, treatment centres and domiciliary visits but no data exist on their role in the management of emergencies in the community.
Aims To describe the role of co-operatives in the management of emergencies, both in quantitative and qualitative terms.
Method A questionnaire survey for a 12-month period completed by all 11 co-operatives described structures and activity levels. Semi-structured interviews with senior management and GPs at five randomly selected co-operatives explored their understanding of the role of co-operatives.
Results The incidence of emergencies is very variable (10% of all contacts-virtually nil) with general reliance on the skills of triage staff rather than use of protocols to identify emergencies. Eight of 11 co-operatives provide a domiciliary service with some responding to calls from ambulance services and Gardai for medical assistance. There are very limited liaison structures with ambulance services at any level. Interviews with staff reveal concern with a perceived role as a service dealing with 999 type calls rather than with emergencies encountered in the course of normal general practice work.
Conclusions Clarification is urgently required of the extent to which GP co-operatives and ambulance services support each other. Examples include procedures for passing calls between services, mutual understanding of each others roles and development of common procedures.
G Bury, D Janes, J DowlingDept of General Practice, University College Dublin
GENERAL PRACTICE OUT-OF-HOURS CO-OPERATIVES IN IRELAND – EMERGENCY SERVICE OR NOT?
REFERENCES1. Competence Assurance Structures – An Agenda for
Implementation. Irish Medical Council, Dublin, March 2002.
2. Fox RD, Mazmanian PE, Putnam RW, eds. Change and learning in the lives of physicians. New York: Praegar, 1989.
3. Finucane PM, Bourgeois-Law GA, Ineson SL et al. A comparison of performance assessment programs for medical practitioners in Canada, Australia, New Zealand, and the United Kingdom. Acad Med. 2003;78(8):837-43. PMID: 12915380 [PubMed - indexed for MEDLINE]
4. Jamtvedt G, Young JM, Kristoffersen DT et al. Audit and feedback: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2003;(3):CD000259. Review. PMID: 12917891 [PubMed - indexed for MEDLINE]
5. Davis DA, Thomson MA, Oxman A et al. Changing physician performance. A systematic review of the effect of continuing medical education strategies. JAMA. 1995 6;274(9):700-5. PMID: 7650822 [PubMed - indexed for MEDLINE]
6. Olcott C IV, Mitchell RS, Steinberg GK, Zarins CK. Institutional peer review can reduce the risk and cost of carotid endarterectomy. Arch Surg. 2000 ;135(8):939-42. PMID: 10922256 [PubMed - indexed for MEDLINE]
7. Balla M, Knothe B, Lancaster J, Prager S, Beatson J. Group peer review in psychiatry: the relationship to quality improvement and quality care. Aust N Z J Psychiatry. 1996 Oct;30(5):653-9. PMID: 8902172 [PubMed - indexed for MEDLINE]
8. http://www.medicalcouncil.ie/assurance/default.asp
9. McManus IC, Gordon D, Winder BC. Duties of a doctor: UK doctors and good medical practice. Qual Healthcare. 2000 Mar;9(1):14-22. PMID: 10848365 [PubMed - indexed for MEDLINE]
10. McManus IC, Winder BC, Gordon D.UK doctors’ attitudes to the General Medical Council’s Performance Procedures, 1997-99. Med Educ. 2001 Dec;35 Suppl 1:60-9. PMID: 11895256 [PubMed - indexed for MEDLINE]
11. Chambers R, Bowyer S, Campbell I. Investigation into the attitudes of general practitioners in Staffordshire to medical audit. Qual Healthcare. 1996 Mar;5(1):13-9. PMID: 10157267 [PubMed - indexed for MEDLINE]
12. Norcini JJ. Peer assessment of competence. Med Educ. 2003 Jun;37(6):539-43. PMID: 12787377 [PubMed - indexed for MEDLINE]
13. Margo CE. Peer and expert opinion and the reliability of implicit case review. Ophthalmology. 2002 Mar;109(3):614-8. PMID: 11874771 [PubMed - indexed for MEDLINE]
14. Ramsey PG, Wenrich MD, Carline JD, Inui TS, Larson EB, LoGerfo JP. Use of peer ratings to evaluate physician performance. JAMA. 1993 Apr 7;269(13):1655-60. PMID: 8240483 [PubMed - indexed for MEDLINE]
15. Lewis M, Elwyn G, Wood F. Appraisal of family doctors: an evaluation study. Br J Gen Pract. 2003 Jun;53(491):454-60. PMID: 12939890 [PubMed - indexed for MEDLINE]
16. Hunter N. Actual CA cost 75 euro per doctor p.a., but real cost priceless, says Medical Council. Irish Medical News 2003; 20(33):1
17. C A Brown, C R Belfield, S J Field. Cost effectiveness of continuing professional development in healthcare: a critical review of the evidence. BMJ 2002;324:652-655 (16 March).
18. Lock P, McElroy B, Mackenzie M. The hidden cost of clinical audit: a questionnaire study of NHS staff. Health Policy. 2000 Apr;51(3):181-90. PMID: 10720687 [PubMed - indexed for MEDLINE]
Correspondence to: Bernard Silke, Consultant Cardiovascular Physician, St James’s Hospital, James Street, Dublin 8.Tel: 00 353 1 416 2149 Email: [email protected]
aC MOSS et al
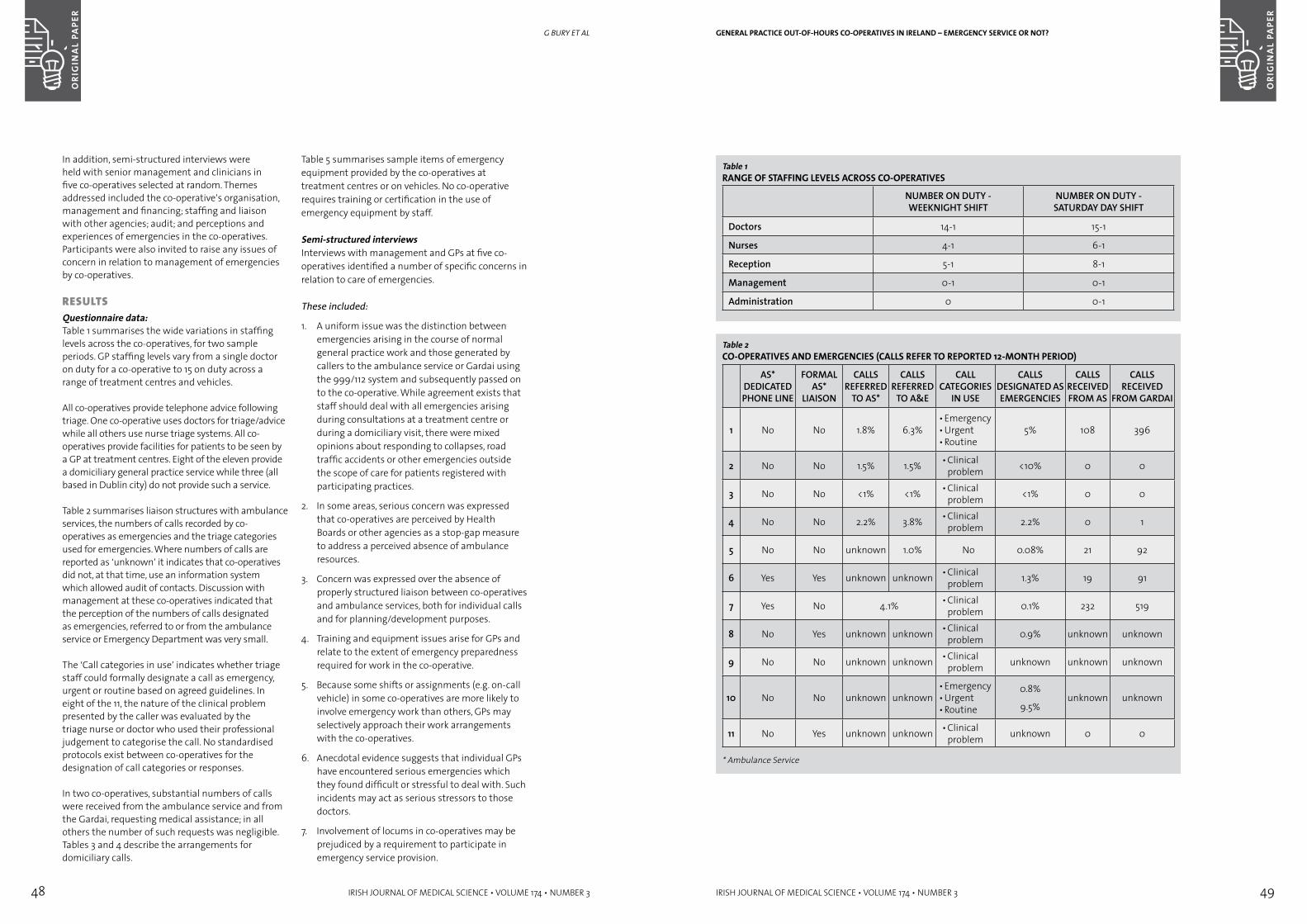
48 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 49
GENERAL PRACTICE OUT-OF-HOURS CO-OPERATIVES IN IRELAND – EMERGENCY SERVICE OR NOT?
Table 1RANGE OF STAFFING LEVELS ACROSS CO-OPERATIVES
NUMBER ON DUTY - WEEKNIGHT SHIFT
NUMBER ON DUTY - SATURDAY DAY SHIFT
Doctors 14-1 15-1
Nurses 4-1 6-1
Reception 5-1 8-1
Management 0-1 0-1
Administration 0 0-1
Table 2CO-OPERATIVES AND EMERGENCIES (CALLS REFER TO REPORTED 12-MONTH PERIOD)
AS* DEDICATED PHONE LINE
FORMAL AS*
LIAISON
CALLS REFERRED
TO AS*
CALLS REFERRED
TO A&E
CALL CATEGORIES
IN USE
CALLS DESIGNATED AS EMERGENCIES
CALLS RECEIVED FROM AS
CALLS RECEIVED
FROM GARDAI
1 No No 1.8% 6.3%• Emergency• Urgent• Routine
5% 108 396
2 No No 1.5% 1.5% • Clinical problem <10% 0 0
3 No No <1% <1% • Clinical problem <1% 0 0
4 No No 2.2% 3.8% • Clinical problem 2.2% 0 1
5 No No unknown 1.0% No 0.08% 21 92
6 Yes Yes unknown unknown • Clinical problem 1.3% 19 91
7 Yes No 4.1% • Clinical problem 0.1% 232 519
8 No Yes unknown unknown • Clinical problem 0.9% unknown unknown
9 No No unknown unknown • Clinical problem unknown unknown unknown
10 No No unknown unknown• Emergency• Urgent• Routine
0.8%
9.5%unknown unknown
11 No Yes unknown unknown • Clinical problem unknown 0 0
* Ambulance Service
In addition, semi-structured interviews were held with senior management and clinicians in five co-operatives selected at random. Themes addressed included the co-operative’s organisation, management and financing; staffing and liaison with other agencies; audit; and perceptions and experiences of emergencies in the co-operatives. Participants were also invited to raise any issues of concern in relation to management of emergencies by co-operatives.
resUlTsquestionnaire data: Table 1 summarises the wide variations in staffing levels across the co-operatives, for two sample periods. GP staffing levels vary from a single doctor on duty for a co-operative to 15 on duty across a range of treatment centres and vehicles.
All co-operatives provide telephone advice following triage. One co-operative uses doctors for triage/advice while all others use nurse triage systems. All co-operatives provide facilities for patients to be seen by a GP at treatment centres. Eight of the eleven provide a domiciliary general practice service while three (all based in Dublin city) do not provide such a service.
Table 2 summarises liaison structures with ambulance services, the numbers of calls recorded by co-operatives as emergencies and the triage categories used for emergencies. Where numbers of calls are reported as ‘unknown’ it indicates that co-operatives did not, at that time, use an information system which allowed audit of contacts. Discussion with management at these co-operatives indicated that the perception of the numbers of calls designated as emergencies, referred to or from the ambulance service or Emergency Department was very small.
The ‘Call categories in use’ indicates whether triage staff could formally designate a call as emergency, urgent or routine based on agreed guidelines. In eight of the 11, the nature of the clinical problem presented by the caller was evaluated by the triage nurse or doctor who used their professional judgement to categorise the call. No standardised protocols exist between co-operatives for the designation of call categories or responses.
In two co-operatives, substantial numbers of calls were received from the ambulance service and from the Gardai, requesting medical assistance; in all others the number of such requests was negligible. Tables 3 and 4 describe the arrangements for domiciliary calls.
Table 5 summarises sample items of emergency equipment provided by the co-operatives at treatment centres or on vehicles. No co-operative requires training or certification in the use of emergency equipment by staff.
Semi-structured interviewsInterviews with management and GPs at five co-operatives identified a number of specific concerns in relation to care of emergencies.
These included:
1. A uniform issue was the distinction between emergencies arising in the course of normal general practice work and those generated by callers to the ambulance service or Gardai using the 999/112 system and subsequently passed on to the co-operative. While agreement exists that staff should deal with all emergencies arising during consultations at a treatment centre or during a domiciliary visit, there were mixed opinions about responding to collapses, road traffic accidents or other emergencies outside the scope of care for patients registered with participating practices.
2. In some areas, serious concern was expressed that co-operatives are perceived by Health Boards or other agencies as a stop-gap measure to address a perceived absence of ambulance resources.
3. Concern was expressed over the absence of properly structured liaison between co-operatives and ambulance services, both for individual calls and for planning/development purposes.
4. Training and equipment issues arise for GPs and relate to the extent of emergency preparedness required for work in the co-operative.
5. Because some shifts or assignments (e.g. on-call vehicle) in some co-operatives are more likely to involve emergency work than others, GPs may selectively approach their work arrangements with the co-operatives.
6. Anecdotal evidence suggests that individual GPs have encountered serious emergencies which they found difficult or stressful to deal with. Such incidents may act as serious stressors to those doctors.
7. Involvement of locums in co-operatives may be prejudiced by a requirement to participate in emergency service provision.
G BURY et al
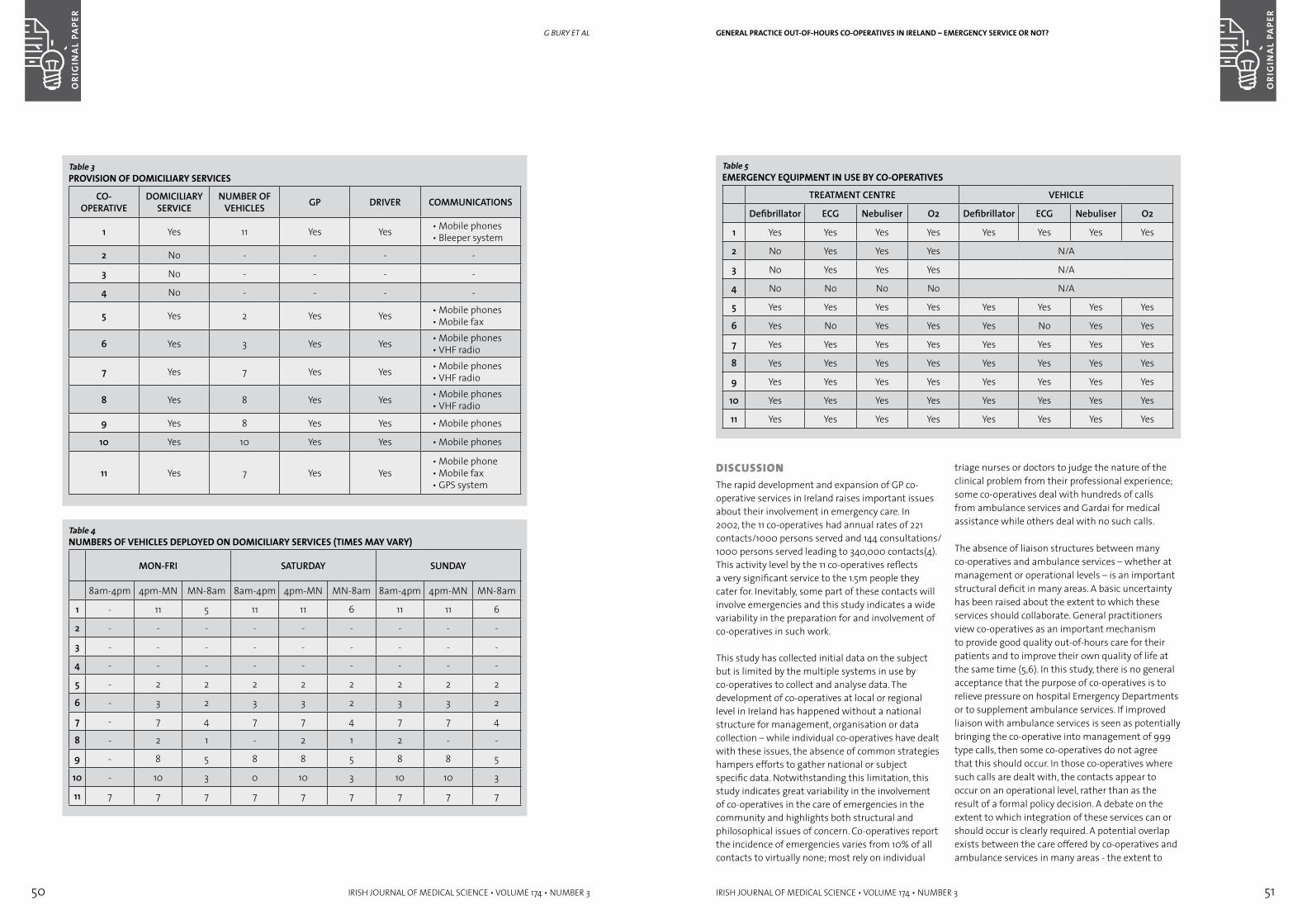
50 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 51
DisCUssiOnThe rapid development and expansion of GP co-operative services in Ireland raises important issues about their involvement in emergency care. In 2002, the 11 co-operatives had annual rates of 221 contacts/1000 persons served and 144 consultations/ 1000 persons served leading to 340,000 contacts(4). This activity level by the 11 co-operatives reflects a very significant service to the 1.5m people they cater for. Inevitably, some part of these contacts will involve emergencies and this study indicates a wide variability in the preparation for and involvement of co-operatives in such work.
This study has collected initial data on the subject but is limited by the multiple systems in use by co-operatives to collect and analyse data. The development of co-operatives at local or regional level in Ireland has happened without a national structure for management, organisation or data collection – while individual co-operatives have dealt with these issues, the absence of common strategies hampers efforts to gather national or subject specific data. Notwithstanding this limitation, this study indicates great variability in the involvement of co-operatives in the care of emergencies in the community and highlights both structural and philosophical issues of concern. Co-operatives report the incidence of emergencies varies from 10% of all contacts to virtually none; most rely on individual
triage nurses or doctors to judge the nature of the clinical problem from their professional experience; some co-operatives deal with hundreds of calls from ambulance services and Gardai for medical assistance while others deal with no such calls.
The absence of liaison structures between many co-operatives and ambulance services – whether at management or operational levels – is an important structural deficit in many areas. A basic uncertainty has been raised about the extent to which these services should collaborate. General practitioners view co-operatives as an important mechanism to provide good quality out-of-hours care for their patients and to improve their own quality of life at the same time (5,6). In this study, there is no general acceptance that the purpose of co-operatives is to relieve pressure on hospital Emergency Departments or to supplement ambulance services. If improved liaison with ambulance services is seen as potentially bringing the co-operative into management of 999 type calls, then some co-operatives do not agree that this should occur. In those co-operatives where such calls are dealt with, the contacts appear to occur on an operational level, rather than as the result of a formal policy decision. A debate on the extent to which integration of these services can or should occur is clearly required. A potential overlap exists between the care offered by co-operatives and ambulance services in many areas - the extent to
Table 5EMERGENCY EqUIPMENT IN USE BY CO-OPERATIVES
TREATMENT CENTRE VEHICLE
Defibrillator ECG Nebuliser O2 Defibrillator ECG Nebuliser O2
1 Yes Yes Yes Yes Yes Yes Yes Yes
2 No Yes Yes Yes N/A
3 No Yes Yes Yes N/A
4 No No No No N/A
5 Yes Yes Yes Yes Yes Yes Yes Yes
6 Yes No Yes Yes Yes No Yes Yes
7 Yes Yes Yes Yes Yes Yes Yes Yes
8 Yes Yes Yes Yes Yes Yes Yes Yes
9 Yes Yes Yes Yes Yes Yes Yes Yes
10 Yes Yes Yes Yes Yes Yes Yes Yes
11 Yes Yes Yes Yes Yes Yes Yes Yes
GENERAL PRACTICE OUT-OF-HOURS CO-OPERATIVES IN IRELAND – EMERGENCY SERVICE OR NOT?
Table 3PROVISION OF DOMICILIARY SERVICES
CO-OPERATIVE
DOMICILIARY SERVICE
NUMBER OF VEHICLES GP DRIVER COMMUNICATIONS
1 Yes 11 Yes Yes • Mobile phones• Bleeper system
2 No - - - -
3 No - - - -
4 No - - - -
5 Yes 2 Yes Yes • Mobile phones• Mobile fax
6 Yes 3 Yes Yes • Mobile phones• VHF radio
7 Yes 7 Yes Yes • Mobile phones• VHF radio
8 Yes 8 Yes Yes • Mobile phones• VHF radio
9 Yes 8 Yes Yes • Mobile phones
10 Yes 10 Yes Yes • Mobile phones
11 Yes 7 Yes Yes• Mobile phone• Mobile fax• GPS system
Table 4NUMBERS OF VEHICLES DEPLOYED ON DOMICILIARY SERVICES (TIMES MAY VARY)
MON-FRI SATURDAY SUNDAY
8am-4pm 4pm-MN MN-8am 8am-4pm 4pm-MN MN-8am 8am-4pm 4pm-MN MN-8am
1 - 11 5 11 11 6 11 11 6
2 - - - - - - - - -
3 - - - - - - - - -
4 - - - - - - - - -
5 - 2 2 2 2 2 2 2 2
6 - 3 2 3 3 2 3 3 2
7 - 7 4 7 7 4 7 7 4
8 - 2 1 - 2 1 2 - -
9 - 8 5 8 8 5 8 8 5
10 - 10 3 0 10 3 10 10 3
11 7 7 7 7 7 7 7 7 7
G BURY et al

52 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 53
inTrODUCTiOnThe pathophysiological significance of the albuminuric effect of atrial (ANP) and brain (BNP) natriuretic peptide, which has been extensively documented, in diabetes mellitus is not known. Animal and human studies have shown a close relationship between ANP and acute1 or chronic hyperglycaemia,2 and elevated plasma ANP concentrations have been reported in diabetic patients with systemic hypertension,3,4 glomerular hyperfiltration5 and microalbuminuria.6 In contrast, some studies show no association between plasma ANP and diabetic renal disease.7,8 The conflicting results may reflect differences in patient selection; one paper reported data from a small patient cohort7 while another study reported data from patients with both type 1 and 2 diabetes.8 The significance of plasma ANP concentrations in type 1 diabetes was emphasised by data from studies which showed that the intravenous infusion of ANP into diabetic subjects with either normal urine albumin excretion rate (UAER)8 or microalbuminuria has a profound albuminuric effect.9,10,11,12 These data suggest that ANP may play a role in the development and maintenance of albuminuria in diabetic subjects.
Brain natriuretic peptide concentrations (BNP) is structurally13 and functionally14 related to ANP, and plasma concentrations have been reported to be elevated in the non-diabetic population, in particular systemic arterial hypertension,15 congestive cardiac failure16,17 and chronic renal failure.18 However no previous studies have examined plasma BNP concentrations in diabetes. As the intravenous infusion of BNP increases urine albumin excretion rates in patients with type 1 diabetes,19 BNP may also modulate albumin excretion rate in type 1 diabetes.
In this study we report plasma ANP and BNP concentrations in a large cohort of patients with type 1 diabetes, and examine the relationship of the hormones to glycaemic control, arterial blood pressure, urine albumin excretion rate and left ventricular mass index.
MeTHODsFifty type 1 diabetic patients were recruited from the local diabetic out patient clinic (demographic data are summarised in Table 1). Subjects with valvular heart disease, overt congestive cardiac failure and
Elevated plasma concentrations of atrial and brain natriuretic peptide in type 1 diabetic subjectsaBsTraCTBackground The intravenous infusion of atrial (ANP) and brain (BNP) natriuretic peptides
have been shown to increase urinary albumin excretion in type 1 diabetes.Aims To measure plasma ANP and BNP concentrations in patients with type 1 diabetes
and to examine the parameters associated with elevated plasma concentrations.Methods We measured plasma ANP and BNP concentrations, UAER, HbA1C systolic blood
pressure, and left ventricular mass index. Plasma ANP and BNP were also measured in non-diabetic control subjects for comparison.
Results Using multivariate regression analysis plasma ANP correlated positively with HbA1C (1.9 + 0.47, p = 0.0002), UAER (0.37+ 0.05, p =0.00001), SBP (1.26 + 0.5, p=0.01) and LVMI (0.46 + 0.25, p = 0.07). BNP was positively related with LVMI (0.95 + 0.4, p=0.02), and UAER (0.56 + 0.08, p = 0.001).
Conclusions Plasma concentrations of ANP and BNP are elevated in some patients with type 1 diabetes. Plasma ANP concentrations are closely related to UAER and elevated plasma concentrations are associated with poor glycaemic control and systemic hypertension. Plasma BNP concentration is related to LVMI.
Abbreviations Atrial Natriuretic Peptide (ANP), Brain Natriuretic Peptide (BNP), Glycosylated haemoglobin (HBA1C), Urine albumin excretion rate (UAER), Systolic blood pressure (SBP), Left Ventricular Mass Index (LVMI).
K McKenna, D Smith, M Sherlock, K Moore, E O’Brien, W Tormey, CJ ThompsonDept of Diabetes, Beaumont Hospital, Dublin 9
ELEVATED PLASMA CONCENTRATIONS OF ATRIAL AND BRAIN NATRIURETIC PEPTIDE IN TYPE 1 DIABETIC SUBJECTS
which regional services collaborate requires explicit discussion and planning rather than an ad hoc operational norm.
It is also unclear to what extent the ambulance services have been prepared for the demands of working with a new GP service – co-operative staff perceive expectations among ambulance service staff ranging from no change to provision of a ‘paramedic’ type service to a possible threat to the role of the ambulance service. The perception that an ambulance can be ‘freed-up’ from an area because a co-operative vehicle is operating there is one example of a contentious issue. Others include procedures for passing calls between services and common protocols for clinical care of certain emergencies.
The possibility that co-operatives might routinely deal with serious emergencies in the community is an important one – earlier responses by a suitably equipped and supported doctor to incidents such as cardiac arrest, serious trauma or major medical emergencies could make a real difference to the patient’s survival or longer term care. However, such roles place new demands on the doctors and structures involved and cannot happen effectively without preparation and planning.
Training, equipment, protocols, indemnity, critical incident debriefing and skills maintenance are among the issues raised for doctors providing pre-hospital care in serious emergencies. In this study, concerns were expressed about issues such as these. Individual co-operatives are introducing triage protocols, standardising equipment, training drivers to provide CPR and other basic clinical skills and reviewing audit procedures. National structures to undertake tasks such as these or to share best practice and experience would be valuable in supporting the current work of the co-operatives.
New information handling systems within co-operatives may facilitate further research such as the use of standardised clinical audit of contacts and consultations, accurate identification of contacts with other agencies and validation of triage procedures. While co-operatives have made a major impact on ‘out-of-hours’ clinical care in the community in Ireland, the potential for co-operatives to enhance the care of serious emergencies has not yet been adequately explored.
GP co-operatives deal with very large numbers of patients and will continue to develop around the country. This study has identified a range of issues relating to the involvement of those services in the care of emergencies which require urgent clarification. While individual co-operatives, ambulance services and others are exploring these issues, a national framework would contribute significantly to their prompt, efficient and longer term resolution.
ACkNOwLEDGEMENTS
This work was supported by research grants from the Pre-Hospital Emergency Care Council and the Health Research Board.
REFERENCES1. Quality and Fairness. A Health System for You.
Department of Health and Children, Dublin, 2001.
2. Heart Health Task Force. Progress Report 1999-2001. Department of Health and Children, Dublin, 2001.
3. Primary Care. A New Direction. Department of Health and Children, Dublin, 2001.
4. Bury G, Dowling J, Janes D. General practice out-of-hours co-operatives in Ireland – population contact rates. Ir Med J (in press)
5. Hallam L, Henthorne K. Co-operatives and their primary care emergency centres: organisation and impact. Health Technology Assessment 1999;3:Number 7
6. Leibowitz R, Day S, Dunt D. A systematic review of the effect of different models of after-hours primary medical care services on clinical outcome, medical workload and patient and GP satisfaction. Family Practice 2003;20:311-317.
Correspondence to: G Bury, Department of General Practice, University College Dublin, E-mail:[email protected]
G BURY et al
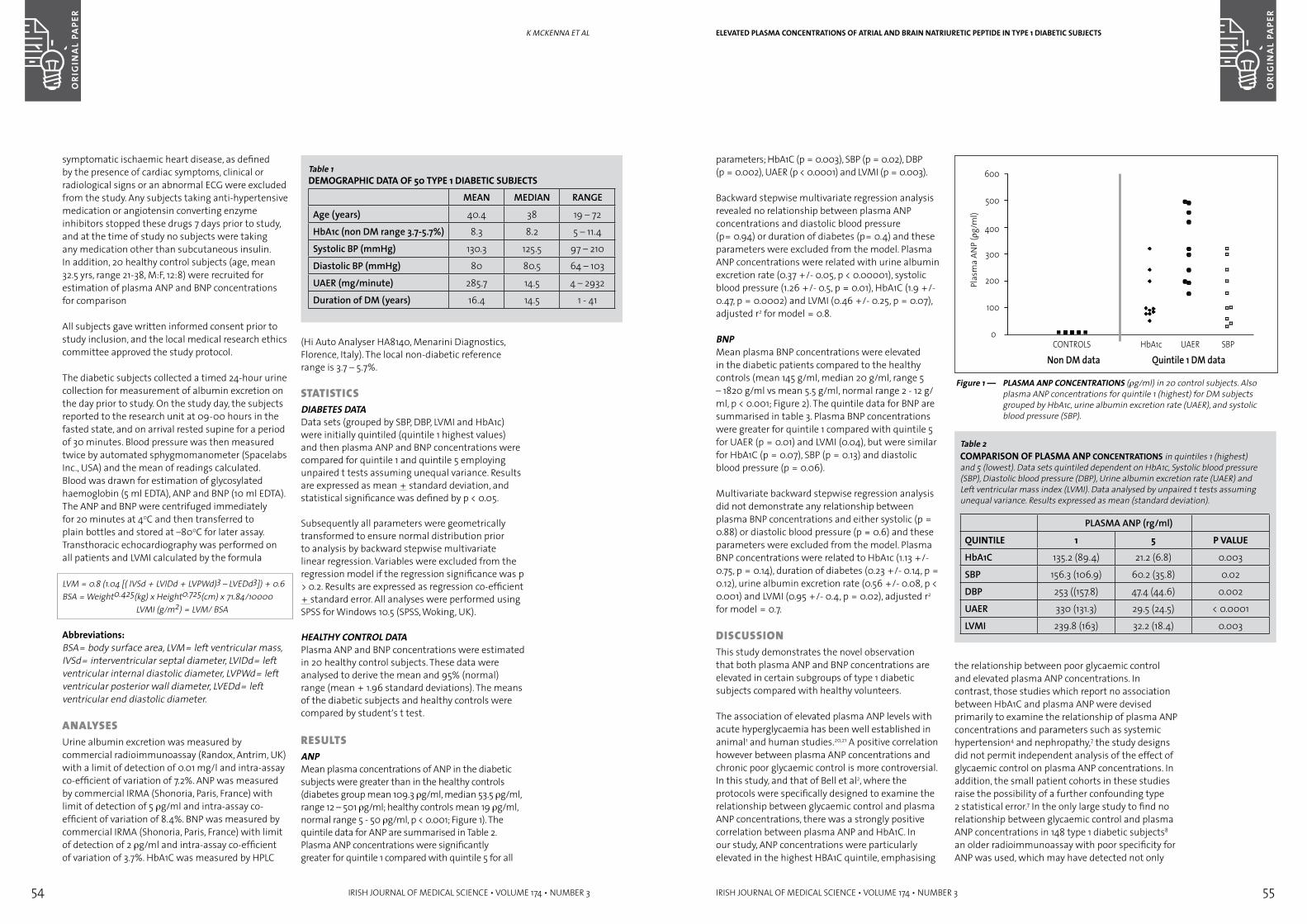
54 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 55
parameters; HbA1C (p = 0.003), SBP (p = 0.02), DBP (p = 0.002), UAER (p < 0.0001) and LVMI (p = 0.003).
Backward stepwise multivariate regression analysis revealed no relationship between plasma ANP concentrations and diastolic blood pressure (p= 0.94) or duration of diabetes (p= 0.4) and these parameters were excluded from the model. Plasma ANP concentrations were related with urine albumin excretion rate (0.37 +/- 0.05, p < 0.00001), systolic blood pressure (1.26 +/- 0.5, p = 0.01), HbA1C (1.9 +/- 0.47, p = 0.0002) and LVMI (0.46 +/- 0.25, p = 0.07), adjusted r2 for model = 0.8.
BNPMean plasma BNP concentrations were elevated in the diabetic patients compared to the healthy controls (mean 145 γg/ml, median 20 γg/ml, range 5 – 1820 γg/ml vs mean 5.5 γg/ml, normal range 2 - 12 γg/ml, p < 0.001; Figure 2). The quintile data for BNP are summarised in table 3. Plasma BNP concentrations were greater for quintile 1 compared with quintile 5 for UAER (p = 0.01) and LVMI (0.04), but were similar for HbA1C (p = 0.07), SBP (p = 0.13) and diastolic blood pressure (p = 0.06).
Multivariate backward stepwise regression analysis did not demonstrate any relationship between plasma BNP concentrations and either systolic (p = 0.88) or diastolic blood pressure (p = 0.6) and these parameters were excluded from the model. Plasma BNP concentrations were related to HbA1c (1.13 +/- 0.75, p = 0.14), duration of diabetes (0.23 +/- 0.14, p = 0.12), urine albumin excretion rate (0.56 +/- 0.08, p < 0.001) and LVMI (0.95 +/- 0.4, p = 0.02), adjusted r2 for model = 0.7.
DisCUssiOnThis study demonstrates the novel observation that both plasma ANP and BNP concentrations are elevated in certain subgroups of type 1 diabetic subjects compared with healthy volunteers.
The association of elevated plasma ANP levels with acute hyperglycaemia has been well established in animal1 and human studies.20,21 A positive correlation however between plasma ANP concentrations and chronic poor glycaemic control is more controversial. In this study, and that of Bell et al2, where the protocols were specifically designed to examine the relationship between glycaemic control and plasma ANP concentrations, there was a strongly positive correlation between plasma ANP and HbA1C. In our study, ANP concentrations were particularly elevated in the highest HBA1C quintile, emphasising
ELEVATED PLASMA CONCENTRATIONS OF ATRIAL AND BRAIN NATRIURETIC PEPTIDE IN TYPE 1 DIABETIC SUBJECTS
Figure 1 — PLASMA ANP CONCENTRATIONS (rg/ml) in 20 control subjects. Also plasma ANP concentrations for quintile 1 (highest) for DM subjects grouped by HbA1c, urine albumin excretion rate (UAER), and systolic blood pressure (SBP).
the relationship between poor glycaemic control and elevated plasma ANP concentrations. In contrast, those studies which report no association between HbA1C and plasma ANP were devised primarily to examine the relationship of plasma ANP concentrations and parameters such as systemic hypertension4 and nephropathy,7 the study designs did not permit independent analysis of the effect of glycaemic control on plasma ANP concentrations. In addition, the small patient cohorts in these studies raise the possibility of a further confounding type 2 statistical error.7 In the only large study to find no relationship between glycaemic control and plasma ANP concentrations in 148 type 1 diabetic subjects8
an older radioimmunoassay with poor specificity for ANP was used, which may have detected not only
Table 2COMPARISON OF PLASMA ANP CONCENTRATIONS in quintiles 1 (highest) and 5 (lowest). Data sets quintiled dependent on HbA1c, Systolic blood pressure (SBP), Diastolic blood pressure (DBP), Urine albumin excretion rate (UAER) and Left ventricular mass index (LVMI). Data analysed by unpaired t tests assuming unequal variance. Results expressed as mean (standard deviation).
PLASMA ANP (rg/ml)
qUINTILE 1 5 P VALUE
HbA1C 135.2 (89.4) 21.2 (6.8) 0.003
SBP 156.3 (106.9) 60.2 (35.8) 0.02
DBP 253 ((157.8) 47.4 (44.6) 0.002
UAER 330 (131.3) 29.5 (24.5) < 0.0001
LVMI 239.8 (163) 32.2 (18.4) 0.003
symptomatic ischaemic heart disease, as defined by the presence of cardiac symptoms, clinical or radiological signs or an abnormal ECG were excluded from the study. Any subjects taking anti-hypertensive medication or angiotensin converting enzyme inhibitors stopped these drugs 7 days prior to study, and at the time of study no subjects were taking any medication other than subcutaneous insulin. In addition, 20 healthy control subjects (age, mean 32.5 yrs, range 21-38, M:F, 12:8) were recruited for estimation of plasma ANP and BNP concentrations for comparison
All subjects gave written informed consent prior to study inclusion, and the local medical research ethics committee approved the study protocol.
The diabetic subjects collected a timed 24-hour urine collection for measurement of albumin excretion on the day prior to study. On the study day, the subjects reported to the research unit at 09-00 hours in the fasted state, and on arrival rested supine for a period of 30 minutes. Blood pressure was then measured twice by automated sphygmomanometer (Spacelabs Inc., USA) and the mean of readings calculated. Blood was drawn for estimation of glycosylated haemoglobin (5 ml EDTA), ANP and BNP (10 ml EDTA). The ANP and BNP were centrifuged immediately for 20 minutes at 40C and then transferred to plain bottles and stored at –800C for later assay. Transthoracic echocardiography was performed on all patients and LVMI calculated by the formula
LVM = 0.8 (1.04 [( IVSd + LVIDd + LVPWd)3 – LVEDd3]) + 0.6BSA = Weight0.425(kg) x Height0.725(cm) x 71.84/10000 LVMI (g/m2) = LVM/ BSA
Abbreviations:BSA= body surface area, LVM= left ventricular mass, IVSd= interventricular septal diameter, LVIDd= left ventricular internal diastolic diameter, LVPWd= left ventricular posterior wall diameter, LVEDd= left ventricular end diastolic diameter.
analYsesUrine albumin excretion was measured by commercial radioimmunoassay (Randox, Antrim, UK) with a limit of detection of 0.01 mg/l and intra-assay co-efficient of variation of 7.2%. ANP was measured by commercial IRMA (Shonoria, Paris, France) with limit of detection of 5 rg/ml and intra-assay co-efficient of variation of 8.4%. BNP was measured by commercial IRMA (Shonoria, Paris, France) with limit of detection of 2 rg/ml and intra-assay co-efficient of variation of 3.7%. HbA1C was measured by HPLC
K MCKenna et al
Table 1DEMOGRAPHIC DATA OF 50 TYPE 1 DIABETIC SUBJECTS
MEAN MEDIAN RANGE
Age (years) 40.4 38 19 – 72
HbA1c (non DM range 3.7-5.7%) 8.3 8.2 5 – 11.4
Systolic BP (mmHg) 130.3 125.5 97 – 210
Diastolic BP (mmHg) 80 80.5 64 – 103
UAER (mg/minute) 285.7 14.5 4 – 2932
Duration of DM (years) 16.4 14.5 1 - 41
(Hi Auto Analyser HA8140, Menarini Diagnostics, Florence, Italy). The local non-diabetic reference range is 3.7 – 5.7%.
sTaTisTiCsDIABETES DATAData sets (grouped by SBP, DBP, LVMI and HbA1c) were initially quintiled (quintile 1 highest values) and then plasma ANP and BNP concentrations were compared for quintile 1 and quintile 5 employing unpaired t tests assuming unequal variance. Results are expressed as mean + standard deviation, and statistical significance was defined by p < 0.05.
Subsequently all parameters were geometrically transformed to ensure normal distribution prior to analysis by backward stepwise multivariate linear regression. Variables were excluded from the regression model if the regression significance was p > 0.2. Results are expressed as regression co-efficient + standard error. All analyses were performed using SPSS for Windows 10.5 (SPSS, Woking, UK).
HEALTHY CONTROL DATAPlasma ANP and BNP concentrations were estimated in 20 healthy control subjects. These data were analysed to derive the mean and 95% (normal) range (mean + 1.96 standard deviations). The means of the diabetic subjects and healthy controls were compared by student’s t test.
resUlTsANPMean plasma concentrations of ANP in the diabetic subjects were greater than in the healthy controls (diabetes group mean 109.3 rg/ml, median 53.5 rg/ml, range 12 – 501 rg/ml; healthy controls mean 19 rg/ml, normal range 5 - 50 rg/ml, p < 0.001; Figure 1). The quintile data for ANP are summarised in Table 2. Plasma ANP concentrations were significantly greater for quintile 1 compared with quintile 5 for all
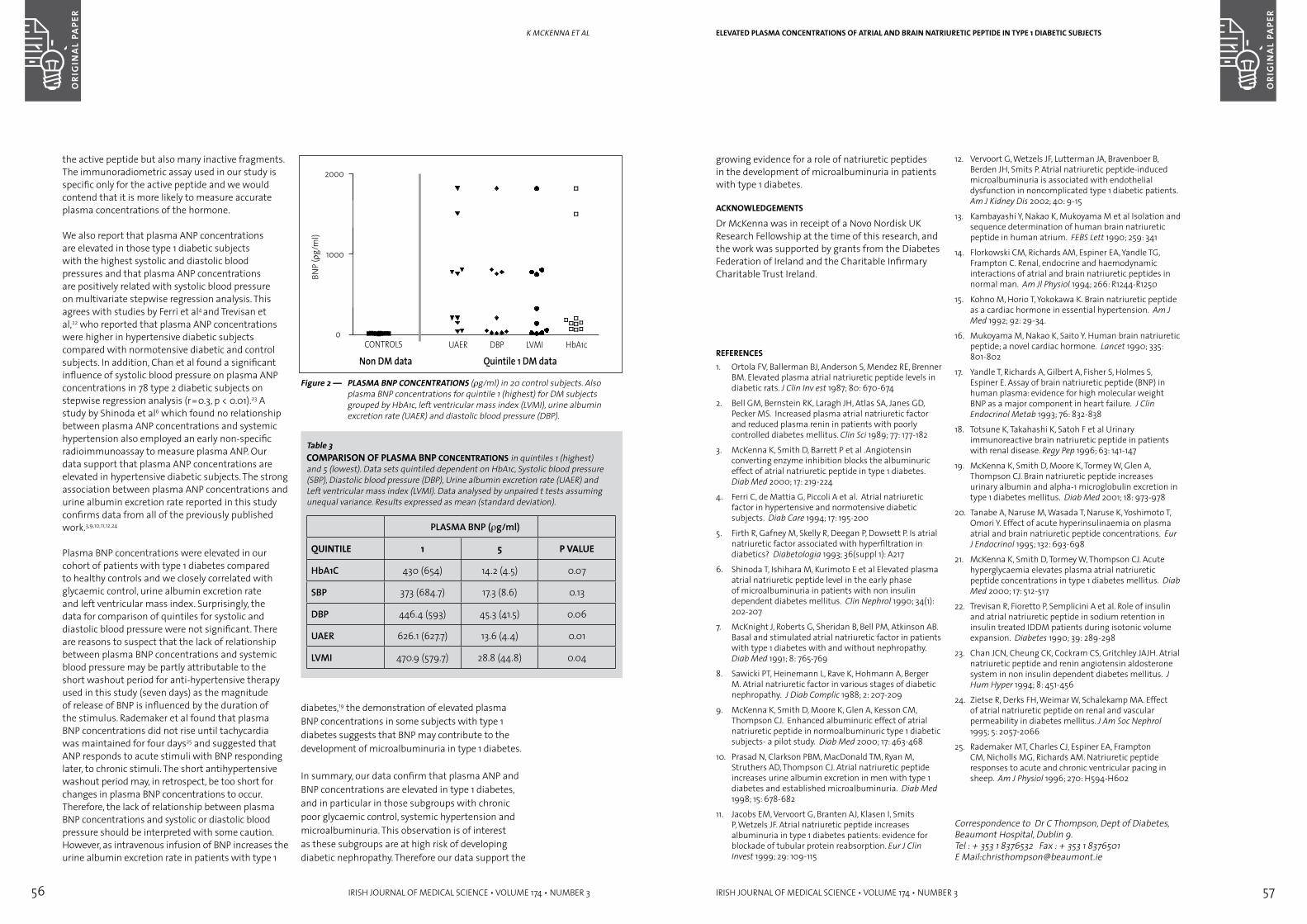
56 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 57
growing evidence for a role of natriuretic peptides in the development of microalbuminuria in patients with type 1 diabetes.
ACkNOwLEDGEMENTS
Dr McKenna was in receipt of a Novo Nordisk UK Research Fellowship at the time of this research, and the work was supported by grants from the Diabetes Federation of Ireland and the Charitable Infirmary Charitable Trust Ireland.
REFERENCES1. Ortola FV, Ballerman BJ, Anderson S, Mendez RE, Brenner
BM. Elevated plasma atrial natriuretic peptide levels in diabetic rats. J Clin Inv est 1987; 80: 670-674
2. Bell GM, Bernstein RK, Laragh JH, Atlas SA, Janes GD, Pecker MS. Increased plasma atrial natriuretic factor and reduced plasma renin in patients with poorly controlled diabetes mellitus. Clin Sci 1989; 77: 177-182
3. McKenna K, Smith D, Barrett P et al .Angiotensin converting enzyme inhibition blocks the albuminuric effect of atrial natriuretic peptide in type 1 diabetes. Diab Med 2000; 17: 219-224
4. Ferri C, de Mattia G, Piccoli A et al. Atrial natriuretic factor in hypertensive and normotensive diabetic subjects. Diab Care 1994; 17: 195-200
5. Firth R, Gafney M, Skelly R, Deegan P, Dowsett P. Is atrial natriuretic factor associated with hyperfiltration in diabetics? Diabetologia 1993; 36(suppl 1): A217
6. Shinoda T, Ishihara M, Kurimoto E et al Elevated plasma atrial natriuretic peptide level in the early phase of microalbuminuria in patients with non insulin dependent diabetes mellitus. Clin Nephrol 1990; 34(1): 202-207
7. McKnight J, Roberts G, Sheridan B, Bell PM, Atkinson AB. Basal and stimulated atrial natriuretic factor in patients with type 1 diabetes with and without nephropathy. Diab Med 1991; 8: 765-769
8. Sawicki PT, Heinemann L, Rave K, Hohmann A, Berger M. Atrial natriuretic factor in various stages of diabetic nephropathy. J Diab Complic 1988; 2: 207-209
9. McKenna K, Smith D, Moore K, Glen A, Kesson CM, Thompson CJ. Enhanced albuminuric effect of atrial natriuretic peptide in normoalbuminuric type 1 diabetic subjects- a pilot study. Diab Med 2000; 17: 463-468
10. Prasad N, Clarkson PBM, MacDonald TM, Ryan M, Struthers AD, Thompson CJ. Atrial natriuretic peptide increases urine albumin excretion in men with type 1 diabetes and established microalbuminuria. Diab Med 1998; 15: 678-682
11. Jacobs EM, Vervoort G, Branten AJ, Klasen I, Smits P, Wetzels JF. Atrial natriuretic peptide increases albuminuria in type 1 diabetes patients: evidence for blockade of tubular protein reabsorption. Eur J Clin Invest 1999; 29: 109-115
12. Vervoort G, Wetzels JF, Lutterman JA, Bravenboer B, Berden JH, Smits P. Atrial natriuretic peptide-induced microalbuminuria is associated with endothelial dysfunction in noncomplicated type 1 diabetic patients. Am J Kidney Dis 2002; 40: 9-15
13. Kambayashi Y, Nakao K, Mukoyama M et al Isolation and sequence determination of human brain natriuretic peptide in human atrium. FEBS Lett 1990; 259: 341
14. Florkowski CM, Richards AM, Espiner EA, Yandle TG, Frampton C. Renal, endocrine and haemodynamic interactions of atrial and brain natriuretic peptides in normal man. Am Jl Physiol 1994; 266: R1244-R1250
15. Kohno M, Horio T, Yokokawa K. Brain natriuretic peptide as a cardiac hormone in essential hypertension. Am J Med 1992; 92: 29-34.
16. Mukoyama M, Nakao K, Saito Y. Human brain natriuretic peptide; a novel cardiac hormone. Lancet 1990; 335: 801-802
17. Yandle T, Richards A, Gilbert A, Fisher S, Holmes S, Espiner E. Assay of brain natriuretic peptide (BNP) in human plasma: evidence for high molecular weight BNP as a major component in heart failure. J Clin Endocrinol Metab 1993; 76: 832-838
18. Totsune K, Takahashi K, Satoh F et al Urinary immunoreactive brain natriuretic peptide in patients with renal disease. Regy Pep 1996; 63: 141-147
19. McKenna K, Smith D, Moore K, Tormey W, Glen A, Thompson CJ. Brain natriuretic peptide increases urinary albumin and alpha-1 microglobulin excretion in type 1 diabetes mellitus. Diab Med 2001; 18: 973-978
20. Tanabe A, Naruse M, Wasada T, Naruse K, Yoshimoto T, Omori Y. Effect of acute hyperinsulinaemia on plasma atrial and brain natriuretic peptide concentrations. Eur J Endocrinol 1995; 132: 693-698
21. McKenna K, Smith D, Tormey W, Thompson CJ. Acute hyperglycaemia elevates plasma atrial natriuretic peptide concentrations in type 1 diabetes mellitus. Diab Med 2000; 17: 512-517
22. Trevisan R, Fioretto P, Semplicini A et al. Role of insulin and atrial natriuretic peptide in sodium retention in insulin treated IDDM patients during isotonic volume expansion. Diabetes 1990; 39: 289-298
23. Chan JCN, Cheung CK, Cockram CS, Gritchley JAJH. Atrial natriuretic peptide and renin angiotensin aldosterone system in non insulin dependent diabetes mellitus. J Hum Hyper 1994; 8: 451-456
24. Zietse R, Derks FH, Weimar W, Schalekamp MA. Effect of atrial natriuretic peptide on renal and vascular permeability in diabetes mellitus. J Am Soc Nephrol 1995; 5: 2057-2066
25. Rademaker MT, Charles CJ, Espiner EA, Frampton CM, Nicholls MG, Richards AM. Natriuretic peptide responses to acute and chronic ventricular pacing in sheep. Am J Physiol 1996; 270: H594-H602
Correspondence to Dr C Thompson, Dept of Diabetes, Beaumont Hospital, Dublin 9.Tel : + 353 1 8376532 Fax : + 353 1 8376501E Mail:[email protected]
ELEVATED PLASMA CONCENTRATIONS OF ATRIAL AND BRAIN NATRIURETIC PEPTIDE IN TYPE 1 DIABETIC SUBJECTS
the active peptide but also many inactive fragments. The immunoradiometric assay used in our study is specific only for the active peptide and we would contend that it is more likely to measure accurate plasma concentrations of the hormone.
We also report that plasma ANP concentrations are elevated in those type 1 diabetic subjects with the highest systolic and diastolic blood pressures and that plasma ANP concentrations are positively related with systolic blood pressure on multivariate stepwise regression analysis. This agrees with studies by Ferri et al4 and Trevisan et al,22 who reported that plasma ANP concentrations were higher in hypertensive diabetic subjects compared with normotensive diabetic and control subjects. In addition, Chan et al found a significant influence of systolic blood pressure on plasma ANP concentrations in 78 type 2 diabetic subjects on stepwise regression analysis (r=0.3, p < 0.01).23 A study by Shinoda et al6 which found no relationship between plasma ANP concentrations and systemic hypertension also employed an early non-specific radioimmunoassay to measure plasma ANP. Our data support that plasma ANP concentrations are elevated in hypertensive diabetic subjects. The strong association between plasma ANP concentrations and urine albumin excretion rate reported in this study confirms data from all of the previously published work.3,9,10,11,12,24
Plasma BNP concentrations were elevated in our cohort of patients with type 1 diabetes compared to healthy controls and we closely correlated with glycaemic control, urine albumin excretion rate and left ventricular mass index. Surprisingly, the data for comparison of quintiles for systolic and diastolic blood pressure were not significant. There are reasons to suspect that the lack of relationship between plasma BNP concentrations and systemic blood pressure may be partly attributable to the short washout period for anti-hypertensive therapy used in this study (seven days) as the magnitude of release of BNP is influenced by the duration of the stimulus. Rademaker et al found that plasma BNP concentrations did not rise until tachycardia was maintained for four days25 and suggested that ANP responds to acute stimuli with BNP responding later, to chronic stimuli. The short antihypertensive washout period may, in retrospect, be too short for changes in plasma BNP concentrations to occur. Therefore, the lack of relationship between plasma BNP concentrations and systolic or diastolic blood pressure should be interpreted with some caution. However, as intravenous infusion of BNP increases the urine albumin excretion rate in patients with type 1
K MCKenna et al
Figure 2 — PLASMA BNP CONCENTRATIONS (rg/ml) in 20 control subjects. Also plasma BNP concentrations for quintile 1 (highest) for DM subjects grouped by HbA1c, left ventricular mass index (LVMI), urine albumin excretion rate (UAER) and diastolic blood pressure (DBP).
diabetes,19 the demonstration of elevated plasma BNP concentrations in some subjects with type 1 diabetes suggests that BNP may contribute to the development of microalbuminuria in type 1 diabetes.
In summary, our data confirm that plasma ANP and BNP concentrations are elevated in type 1 diabetes, and in particular in those subgroups with chronic poor glycaemic control, systemic hypertension and microalbuminuria. This observation is of interest as these subgroups are at high risk of developing diabetic nephropathy. Therefore our data support the
Table 3COMPARISON OF PLASMA BNP CONCENTRATIONS in quintiles 1 (highest) and 5 (lowest). Data sets quintiled dependent on HbA1c, Systolic blood pressure (SBP), Diastolic blood pressure (DBP), Urine albumin excretion rate (UAER) and Left ventricular mass index (LVMI). Data analysed by unpaired t tests assuming unequal variance. Results expressed as mean (standard deviation).
PLASMA BNP (rg/ml)
qUINTILE 1 5 P VALUE
HbA1C 430 (654) 14.2 (4.5) 0.07
SBP 373 (684.7) 17.3 (8.6) 0.13
DBP 446.4 (593) 45.3 (41.5) 0.06
UAER 626.1 (627.7) 13.6 (4.4) 0.01
LVMI 470.9 (579.7) 28.8 (44.8) 0.04

58 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 59
high incidence of intrauterine foetal death due to hydrops foetalis or severe haemolytic anaemia of the new-born.
Estimation of the amount of foeto-maternal haemorrhage (FMH) is not universally carried out in Ireland. In many hospitals a standard dose of Anti-D is administered to Rhesus (D) negative women carrying Rhesus (D) positive babies after birth. FMH estimation is recommended by many authorities. 7-9
However, the use of IV Anti-D has been associated with the inadvertent transmission of the Hepatitis C Virus to recipients in Ireland1 and elsewhere.10 In Ireland, tragically, nearly 1000 women have been infected in this way.11-13 Unlike the IV product, intra muscular Anti-D Ig has never been associated with viral transmission. Both products are donor derived and carry a risk of viral or prion contamination. The IV product remains the product of choice where a large FMH requires a dose in excess of 2500 iu or the bleed is in excess of 16mls. Recombinant Anti-D is being developed but is not yet available.14
Therefore, although administration of Anti-D can prevent foetal and neonatal morbidity and mortality, judicious administration is mandatory. Systems should be in place in every hospital to ensure that Anti-D is given in compliance with published guidance in the appropriate dose and manner. 9
Much data exist on the additional efficacy of pre-natal prophylactic use of Anti-D6,15,16 This paper does not address this issue. However, the matter is being considered by Irish obstetricians currently and a consensus is expected soon. This is likely to lead to further changes in the way we use Anti-D. The authors recommend that each hospital has a robust system for issuing prenatal Anti-D for potentially sensitising events, post natal and emergency Anti-D, in advance of decisions on prophylactic ante- natal Anti-D.
An additional major influence on the use and surveillance of Anti-D in Ireland has been the introduction of a resourced haemovigilance system. In the Mid-West this has led to an overall reduction in transfusion with increasing documentation of appropriateness.17 The European Directive on blood transfusion, which become law in Ireland on February 5th 2005, is a further major imperative to audit and update transfusion practices for blood and blood products.18
Until recently most units in Ireland used a dose of 600 IU I.V (WinRhoTM), sufficient to antidote a haemorrhage of up to 4 mls of foetal red cells. Now, a licensed product (RhesonativTM) for IM injection has become available in 1250 IU vials (sufficient to antidote an 8 ml bleed). This new product is not manufactured in smaller vials. This has resulted in an increased routine dosage being given. Where larger amounts of Anti-D are needed, IV injection will be more comfortable than multiple IM injections. Because of variation of absorbtion from IM injection, IV injection is desirable to facilitate rapid clearance of potentially sensitising red cells. The IM product has never been associated with viral transmission and can be readily given by midwives making it the product of choice for routine use.
Review of the literature suggests that 99% of FMH is <4 ml.9 However, recent data from the UK show that 500 foetuses develop haemolytic disease of the newborn annually with 50 deaths.6 As noted in the consensus statement9, 1-2% of Rhesus negative women continue to be sensitised. There are two reasons for this; some women do not receive the benefit of standard post-natal Anti-D Ig while other women may be sensitised by small silent FMH, mainly in the last trimester. There is scope for the development and refinement of protocols and practice, initially rigorous, appropriate post natal and post event Anti-D and then prophylactic ante- natal Anti-D.
Rhesus D allo-immunisation can be reduced by ensuring adequate Anti-D prophylaxis, for which the estimation by volume of foeto- maternal haemorrhage is critical. Appropriate implementation of the current guidelines, will lead Irish doctors to consider the issue of prenatal prophylaxis as data16 and consensus6,15 already exist on the benefits of this approach.
Estimation of foeto-maternal haemorrhageIn some units estimation of FMH is not routinely carried out. These units rely on data confirming that 99% of bleeds are <4ml and therefore few women require more than standard doses of Anti-D. Confirmation of the actual haemorrhage allows administration of the appropriate dose of Anti-D immunoglobulin for every woman to prevent alloimmunisation.
Estimation of foeto-maternal haemorrhage may be carried out to diagnose larger bleeds and still
MJ RYan et al
inTrODUCTiOnHaemolytic disease of the newborn2 occurs when maternally derived red cell alloantibodies cause red cell destruction in the foetus. Severely affected babies may die in utero or after birth. Severe anaemia and cardiac failure with clinically obvious severe oedema characterise this condition (hydrops foetalis). Haemolytic disease of the newborn, worsened with each Rhesus positive pregnancy. Affected women
often lost more than one child. This condition is rarely seen since prophylactic measures to prevent sensitisation have been introduced in the late sixties.3-5 The use of anti-Rhesus D immunoglobulin has dramatically reduced the incidence of foetal death and severe haemolytic disease of the new-born. Perinatal deaths due to Rh D alloimmunisation have fallen a hundred fold since 1969.6 Rh D sensitised women carrying Rhesus (D) Positive babies for the second or subsequent pregnancies had a very
The issue of Anti-D: An integrated seamless approach from recognition of need to bedside administrationaBsTraCTBackground The appropriate and timely administration of Anti-D immunoglobulin to
Rhesus (D) negative women who have delivered Rhesus (D) positive babies is a vital part of obstetric care. Anti-D has an especially high profile in Ireland because of the tragic inadvertent transmission of Hepatitis C to Irish women in past decades.1
Audit We have reviewed our policy and procedures pertaining to the administration of Anti-D for sensitising events during pregnancy and postnatally, in the Mid-Western Health Board in 1999/2000. As a result, major changes were made in the storage, issue, recording and administration of Anti-D. New procedures in the transfusion laboratory and in the maternity hospital have been accepted by scientists and midwives and supported by haematology and obstetric medical staff. The pharmacy and haematology laboratory no longer have a role in this programme.
Implementation of multi-disciplinary change management As a result of these changes, the storage, issuing and tracking of Anti-D has become the responsibility of the hospital blood bank. Measurement of foeto-maternal haemorrhage (FMH) is now the responsibility of bio medical scientists in blood bank, utilising both flow cytometry (increasingly recognised as the gold standard method) and the Kleihauer method (Kleihauer-Betke). The programme has moved from a doctor-administered IV Anti-D Ig, to a midwife-administered IM preparation. Prescription remains the responsibility of the doctor. These changes are facilitated by the protocol guided issue of the appropriate dose of Anti-D Ig by bio medical scientists to midwives. The issue of the Anti-D Ig occurs simultaneously with issue of results of mother and baby’s serology testing and estimation of volume of FMH. These major changes have been guided by audit and needs assessment and require close liaison between medical, nursing and laboratory scientific staff in haematology, transfusion and obstetrics.
Critical incident audit-case report Before new procedures became official policy, a critical incident audit allowed us to pilot our protocol and to revise it using draft new procedures. In this critical incident we describe successful management of a patient with a large foeto-maternal haemorrhage. This incident supported the need for the procedural enhancements already underway. This critical incident re-emphasised the need for the planned systems improvements to be introduced quickly.
MJ Ryan, S Joyce, N O’Brien, E Lynch, G Burke, MR CahillDepts of Haematology and Obstetrics, Mid-Western Regional Hospital & Regional Maternity Hospital, Limerick
THE ISSUE OF ANTI-D: AN INTEGRATED SEAMLESS APPROACH FROM RECOGNITION OF NEED TO BEDSIDE ADMINISTRATION

60 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 61
hospitals. Concerns have been documented on the variability on lack of standardisation of Kleihauer testing19 but external quality control schemes have been developed since and are widely used. Quantitation of the disappearance of foetal cells from the maternal circulation can be most reliably estimated using flow cytometry. 20
In the Mid-Western Regional Hospital, in making the transition from traditional Kleihauer to flow cytometric estimation of foeto-maternal haemorrhage in the laboratory, we ensured that staff training, methodology and quality control were in place in accordance with international standards and standard operating procedures. The transfusion laboratory participates in the National External Quality Assessment Scheme run from the UK (NEQAS).21
Issuing Anti-D:Anti-D is a licensed medicine and a blood product. In most hospitals it is held in and issued by pharmacy or blood bank. The product must be prescribed by medical staff. However, women at risk of Anti-D alloimmunisation will be first identified by the midwives, medical and laboratory staff. Because Anti-D immunoglobulin is a blood derivative, inclusion of this product under haemovigilence surveillence is essential. The information on the mother’s and the baby’s blood groups and antibody screen, which determine the requirement for Anti-D Ig , is first available to transfusion scientists. Therefore a compelling argument can be made for Anti-D to be managed by blood bank scientific staff within a haemovigilance programme. With the implementation of the EU directive on blood and blood products18 in February 2005, Anti-D will be legally subject to identical traceability requirements as red cell concentrate. This will include procedures to ensure that batch numbers are identified for all women who receive the product and that each vial can be positively identified as given or wasted. This degree of traceability will facilitate recall and look back and is a legal requirement now that the EU directive has become law.
A new policyA new policy on feto-maternal haemorrhage and issuing Anti-D has been formulated and agreed by Consultant Obstetricians, Haematologist, Director of Midwifery, and Chief Medical Scientist in blood transfusion. This policy enhances the efficacy and safety of the Anti-D prophylaxis programme by introducing new procedures in respect of:
• FMH estimation by flow cytometry in blood transfusion laboratory
• changing the Anti-D product type and administration
• midwife administration instead of medical• issue and storage of Anti-D in hospital blood
transfusion by medical scientists• multidisciplinary patient focused approach.
The detailed changes are outlined in Table 1.
CriTiCal inCiDenT: Case HisTOrYSummaryA Rhesus (D) Negative mother sustained a large foetomaternal haemorrhage, which was accurately quantified flow cytometrically allowing accurate quantification of Anti-D Ig dose and the quantifiable disappearance of foetal cells from her circulation.
The 36-year-old patient presented with absent foetal movement 39 weeks into her fourth pregnancy. She had been fit and well with normal foetal growth measured by ultrasound and clinical criteria until then. Her antibody screening throughout pregnancy was negative.
She was Rhesus (D) Negative with no preformed Anti-D. Her first baby’s blood group was group A Rhesus D positive and 600iu of IV Anti-D (120ug) was administered post partum, her second baby was group B Rhesus D negative. Following this, she had a miscarriage at 14/40 and 600iu of Anti-D was administered also at that time.
At 39/40 in her fourth pregnancy decreased foetal movements persisted and foetal distress was detected. Emergency caesarean section was performed. Following delivery, baby’s Apgar score was initially 4 and resuscitation was required. Baby’s haemoglobin was 4 g/dl and emergency transfusion of red cells was undertaken.
A Kleihauer Acid elution test showed > 100 foetal cells per low power field. Additional Anti-D was advised and 3000 IU was immediately administered IV. (Figure 1) Flow cytometric estimation of the FMH indicated further Anti-D was needed. The clinical aim was to prevent sensitisation. Therefore a large volume of Anti-D (in divided doses) was administered to achieve free Anti-D and no foetal cells. Close flow cytometric monitoring assisted this and ensured accurate dosing of Anti-D. In the setting of a large FMH where more than 2500 IU are required, the IV preparation is preferred.
MJ RYan et alTHE ISSUE OF ANTI-D: AN INTEGRATED SEAMLESS APPROACH FROM RECOGNITION OF NEED TO BEDSIDE ADMINISTRATION
OLD SYSTEM NEW SYSTEM
Correctly identify patient on post natal ward.
Sample taken from all Rh(D) neg mother at variable time post delivery for Kleihauer –usually taken on post natal ward by phlebotomy staff the day after delivery*
Correctly identify patient in labour ward
Sample taken by midwives after delivery in labour ward and sent to transfusion laboratory with cord blood from baby.
Baby’s blood group determined in blood bank.
Results of baby’s blood group transmitted to maternity hospital*
Mother’s Kleihauer test assayed in haematology laboratory
Results of mother’s FMH from Kleihauer sent to maternity hospital*
Medical/midwife decision to administer Anti-D if necessary.
Dose of Anti-D calculated by medical staff.
Anti-D obtained from maternity or pharmacy stock with manual recording.
Discussion with consultant pathologist if necessary.
Baby’s blood group determined in blood bank. If Rhesus (D) positive and mother has no preformed Anti-D, transfusion scientists immediately issue standard dose of IM Anti-D and send it with the mother’s and baby’s blood group results to the midwife.
Mother’s blood group checked against historical laboratory record to detect misidentification and lab error.
Transfusion scientists carry out appropriate FMH testing on mother’s blood already available to them without the necessity for further samples or requests by clinical/staff. They calculate the FMH using an appropriate combination of flow cytometry and Kelihauer testing.
Discussion with consultant haematologist if necessary.
Anti-D administered IV by junior medical staff.* Anti-D administered IM by midwives following medical prescription.
Follow-up Kleihauer sent to haematology
Results transmitted to maternity*
Medical decision to request and administer more Anti-D based on repeated testing.
No follow-up on use or discard of Anti-D.
If further Anti-D is indicated, the appropriate amount is determined by transfusion scientists, issued with electronic traceability and sent to the midwives.
Follow-up samples for FMH estimation requested daily by blood bank staff until no foetal cells are detected with further appropriate automatic issue of Anti-D by transfusion scientists if required.
Haemovigilence follow-up on use (or discard) of each vial.
*potential sources of delay identified
Table 1COMPARISON OF OLD AND NEw SYSTEMS FOR THE ASSESSMENT OF FMH IN RHESUS D NEGATIVE wOMEN AND THE APPROPRIATE AND TIMELY ADMINISTRATION OF ANTI-D IN THE POST-NATAL SETTING.
represents best practice even with the adoption of 1250iu dose of Anti- D9. A significant minority of women (0.4%) have greater than 4ml and 0.3% suffer bleeds in excess of 15ml. Accurate estimation, allows administration of an adequate antidote of Anti-D.
Estimates of FMH can be made using two methodologies, the traditional Kleihauer (Betke) method and more recently introduced flow cytometry. At the current time, estimation of foeto maternal haemorrhage by flow cytometry is not standard practice in the majority of Irish or UK
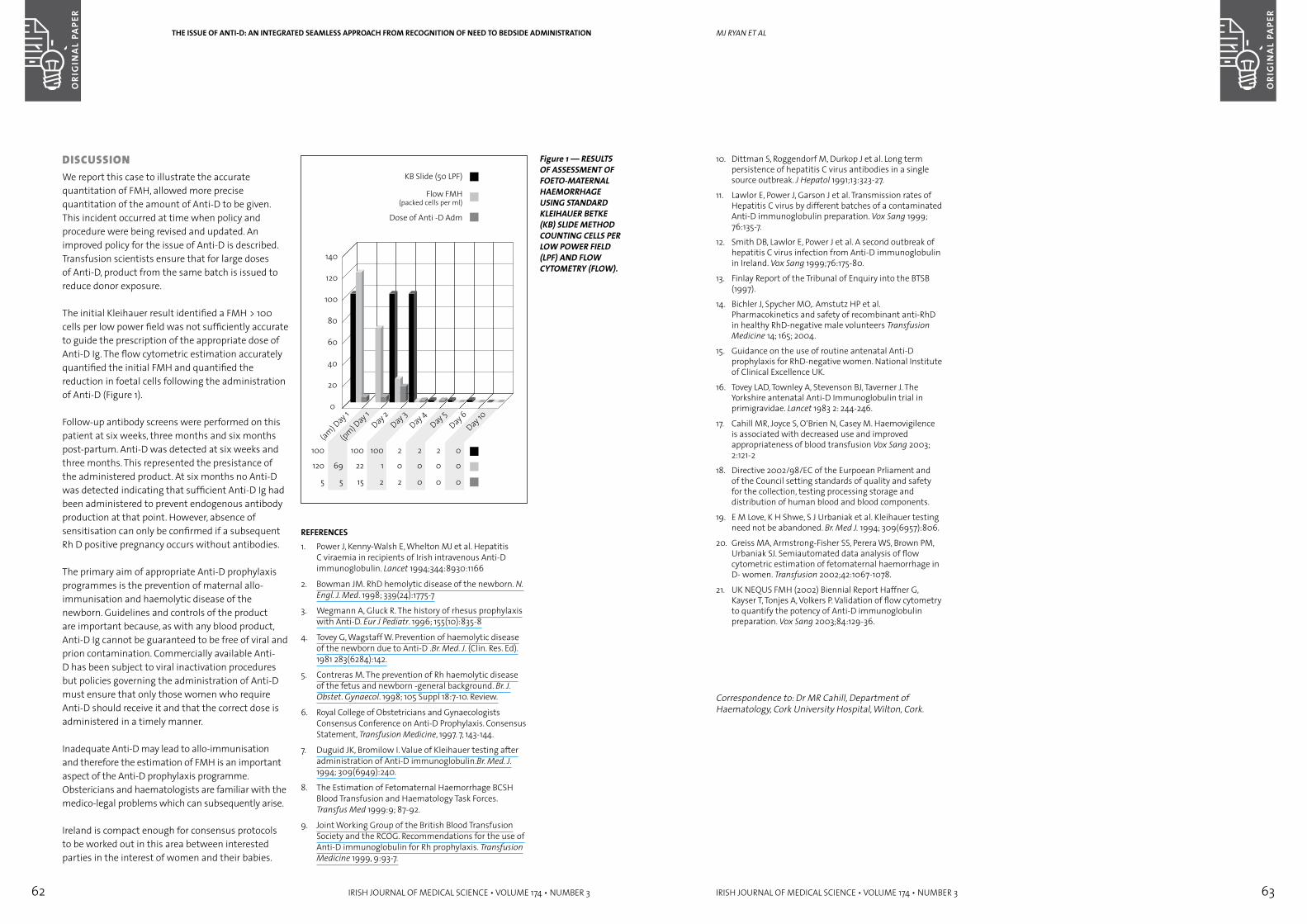
62 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 63
10. Dittman S, Roggendorf M, Durkop J et al. Long term persistence of hepatitis C virus antibodies in a single source outbreak. J Hepatol 1991;13:323-27.
11. Lawlor E, Power J, Garson J et al. Transmission rates of Hepatitis C virus by different batches of a contaminated Anti-D immunoglobulin preparation. Vox Sang 1999; 76:135-7.
12. Smith DB, Lawlor E, Power J et al. A second outbreak of hepatitis C virus infection from Anti-D immunoglobulin in Ireland. Vox Sang 1999;76:175-80.
13. Finlay Report of the Tribunal of Enquiry into the BTSB (1997).
14. Bichler J, Spycher MO,. Amstutz HP et al. Pharmacokinetics and safety of recombinant anti-RhD in healthy RhD-negative male volunteers Transfusion Medicine 14; 165; 2004.
15. Guidance on the use of routine antenatal Anti-D prophylaxis for RhD-negative women. National Institute of Clinical Excellence UK.
16. Tovey LAD, Townley A, Stevenson BJ, Taverner J. The Yorkshire antenatal Anti-D Immunoglobulin trial in primigravidae. Lancet 1983 2: 244-246.
17. Cahill MR, Joyce S, O’Brien N, Casey M. Haemovigilence is associated with decreased use and improved appropriateness of blood transfusion Vox Sang 2003; 2:121-2
18. Directive 2002/98/EC of the Eurpoean Prliament and of the Council setting standards of quality and safety for the collection, testing processing storage and distribution of human blood and blood components.
19. E M Love, K H Shwe, S J Urbaniak et al. Kleihauer testing need not be abandoned. Br. Med J. 1994; 309(6957):806.
20. Greiss MA, Armstrong-Fisher SS, Perera WS, Brown PM, Urbaniak SJ. Semiautomated data analysis of flow cytometric estimation of fetomaternal haemorrhage in D- women. Transfusion 2002;42:1067-1078.
21. UK NEQUS FMH (2002) Biennial Report Haffner G, Kayser T, Tonjes A, Volkers P. Validation of flow cytometry to quantify the potency of Anti-D immunoglobulin preparation. Vox Sang 2003;84:129-36.
Correspondence to: Dr MR Cahill, Department of Haematology, Cork University Hospital, Wilton, Cork.
MJ RYan et al
DisCUssiOnWe report this case to illustrate the accurate quantitation of FMH, allowed more precise quantitation of the amount of Anti-D to be given. This incident occurred at time when policy and procedure were being revised and updated. An improved policy for the issue of Anti-D is described. Transfusion scientists ensure that for large doses of Anti-D, product from the same batch is issued to reduce donor exposure.
The initial Kleihauer result identified a FMH > 100 cells per low power field was not sufficiently accurate to guide the prescription of the appropriate dose of Anti-D Ig. The flow cytometric estimation accurately quantified the initial FMH and quantified the reduction in foetal cells following the administration of Anti-D (Figure 1).
Follow-up antibody screens were performed on this patient at six weeks, three months and six months post-partum. Anti-D was detected at six weeks and three months. This represented the presistance of the administered product. At six months no Anti-D was detected indicating that sufficient Anti-D Ig had been administered to prevent endogenous antibody production at that point. However, absence of sensitisation can only be confirmed if a subsequent Rh D positive pregnancy occurs without antibodies.
The primary aim of appropriate Anti-D prophylaxis programmes is the prevention of maternal allo-immunisation and haemolytic disease of the newborn. Guidelines and controls of the product are important because, as with any blood product, Anti-D Ig cannot be guaranteed to be free of viral and prion contamination. Commercially available Anti-D has been subject to viral inactivation procedures but policies governing the administration of Anti-D must ensure that only those women who require Anti-D should receive it and that the correct dose is administered in a timely manner.
Inadequate Anti-D may lead to allo-immunisation and therefore the estimation of FMH is an important aspect of the Anti-D prophylaxis programme. Obstericians and haematologists are familiar with the medico-legal problems which can subsequently arise.
Ireland is compact enough for consensus protocols to be worked out in this area between interested parties in the interest of women and their babies.
Figure 1 — RESULTS OF ASSESSMENT OF FOETO-MATERNAL HAEMORRHAGE USING STANDARD kLEIHAUER BETkE (kB) SLIDE METHOD COUNTING CELLS PER LOw POwER FIELD (LPF) AND FLOw CYTOMETRY (FLOw).
REFERENCES1. Power J, Kenny-Walsh E, Whelton MJ et al. Hepatitis
C viraemia in recipients of Irish intravenous Anti-D immunoglobulin. Lancet 1994;344:8930:1166
2. Bowman JM. RhD hemolytic disease of the newborn. N. Engl. J. Med. 1998; 339(24):1775-7
3. Wegmann A, Gluck R. The history of rhesus prophylaxis with Anti-D. Eur J Pediatr. 1996; 155(10):835-8
4. Tovey G, Wagstaff W. Prevention of haemolytic disease of the newborn due to Anti-D .Br. Med. J. (Clin. Res. Ed). 1981 283(6284):142.
5. Contreras M. The prevention of Rh haemolytic disease of the fetus and newborn -general background. Br. J. Obstet. Gynaecol. 1998; 105 Suppl 18:7-10. Review.
6. Royal College of Obstetricians and Gynaecologists Consensus Conference on Anti-D Prophylaxis. Consensus Statement, Transfusion Medicine, 1997. 7, 143-144.
7. Duguid JK, Bromilow I. Value of Kleihauer testing after administration of Anti-D immunoglobulin.Br. Med. J. 1994; 309(6949):240.
8. The Estimation of Fetomaternal Haemorrhage BCSH Blood Transfusion and Haematology Task Forces. Transfus Med 1999:9; 87-92.
9. Joint Working Group of the British Blood Transfusion Society and the RCOG. Recommendations for the use of Anti-D immunoglobulin for Rh prophylaxis. Transfusion Medicine 1999, 9:93-7.
THE ISSUE OF ANTI-D: AN INTEGRATED SEAMLESS APPROACH FROM RECOGNITION OF NEED TO BEDSIDE ADMINISTRATION
64 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 65
inflammatory disorders of the spine. No patients received additional therapies, other than non-opioid analgesics, while participating in the programme.
Functional assessments and questionnaires before and after treatmentOn entry to the programme, and again 10 weeks after commencement of the programme, the following validated functional assays were performed15.
Lumbar flexionAfter three warm-up trunk forward bends, range was measured by inclinometry at T12 and S1.
Loaded reach with 2.25 kg for women and 3.6 kg for menThe subject reached forward while both heels remained on the ground. Distance was measured with a metre rule placed at shoulder level.
Repeated sit-to-standThe subject was instructed to rise to standing and return to sitting as quickly as possible five times. The average of two timed trials was recorded.
Fifty-foot (15.15-m) walkSubjects were timed as they walked 25 feet, turned around, and walked back to the starting position as fast as they could.
Sorensen fatigue testThis test measures time to fatigue for the back extensors. Until they reported fatigue, subjects lay prone with their spine in a neutral position on a Roman chair.
Self-report measuresSubjective questionnaires were administered prior to, and 10 weeks following, initiation of the programme. The questionnaires were mailed to each subject for completion at home. The Roland Disability Questionnaire is a 24-item questionnaire aimed at disability caused by LBP.16 The Modified Somatic Perception Questionnaire (MSPQ) and the Modified ZUNG Depression Questionnaire assess psychological components of pain.17 The Visual Analogue Scale requires the subject to place a mark on a 10-cm line at a point corresponding to the current level of pain. The Back Beliefs Questionnaire measures general views towards low back trouble.18
The programmeAfter patients were evaluated with respect to inclusion criteria, they were admitted to four 90-
min group sessions with one individual follow-up re-evaluation at ten weeks. There were six to 10 participants per group led by a physiotherapist. The group sessions provided education about back pain mechanisms, good posture and safe body mechanics, the role of stress on back pain, and self-management techniques for acute bouts of back pain.19 Subjects partook in an active muscle stretching and strengthening education programme.20-24 They were advised to spend 20 minutes, once or twice per day, repeating these exercises at home. Daily walking, biking, or swimming was also encouraged.25 Each subject received a manual containing instruction in each exercise. Participants were instructed in how to progress.23,26
Statistics Subjects were scored for each self-rated and objective assay before therapy and ten weeks after initiation of the therapy. Mean scores and standard deviations were calculated for the group as a whole, a medico-legal, and a non-medico-legal group. The medico-legal group included all subjects pursuing a medico-legal claim at the time of their therapy. Statistical significance was assessed by means of two-tailed z-tests or, for sample sizes of less than 30, two-tailed t-tests.
resUlTs Study SampleDuring seven months, 203 patients were evaluated (Table 1). Of these, 42 did not meet inclusion criteria, were already making satisfactory recovery, or required individual care. Table 1 depicts the numbers referred to other services, those who received individual follow-up care and the numbers scheduled for the back care programme. The attendance rates of those accepted for the programme are represented in Table 1.
The numbers seeking medico-legal claims and their attendance records are represented in Table 1.
Fifty of the patients originated from the orthopaedic waiting list. These were patients on the orthopaedic waiting list who did not meet criteria for surgery but met the inclusion criteria for the back care programme. These patients were then referred to the back care programme by their general practitioner. Patients from the waiting list were preferentially accommodated over new referrals. For new referrals, the average waiting time for an initial appointment was 16 business days. There was a non-attendance rate of 4% for the initial evaluation.
SD alStOn et al
inTrODUCTiOnMusculoskeletal disorders, with low back pain (LBP) accounting for more than half of the cases, are the most common cause of chronic incapacity in industrialised countries.1 The prevalence of disabling LBP for which benefits are paid has risen markedly during the past 20 years.2 Between 50% and 85% of adults will experience back pain.3 Most will have stopped consulting a physician within three months. However, only 25% of patients will have completely recovered one year after consultation with a physician.4 Previous LBP episodes are a strong predictor of future episodes.5 It therefore is desirable to define a management system for these patients in the Irish healthcare system. Although the causes of LBP are often elusive, empiric knowledge can be used to develop effective and efficient strategies for the care of chronic back pain.2 In particular, exercise is efficacious in the conservative treatment of LBP.6-11 Exercise can vary in expense and method of delivery. Group treatment may be as effective as individual treatment, and simple dynamic exercise
may be as effective as resistive exercise requiring expensive equipment.12 Moreover, programmes of modest duration may achieve high efficacy.13 Patients pursuing litigation are reported to achieve less desirable subjective outcomes, although levels of disability and impairment generally improve for all low back pain sufferers.14
In the South East of Ireland, adults with chronic and recurrent mechanical LBP could encounter unacceptable waiting periods of up to five years for specialised care. We therefore developed an expedited management system for patients with LBP of duration greater than six weeks.
PaTienTs & MeTHODsStudy populationPatients residing in the South East of Ireland, aged 20 to 60 years, with greater than six weeks of mechanical LBP, were accepted for evaluation. We excluded patients with non-mechanical back pain, pregnancy, neurological deficit, tumour, and
Patient education in physiotherapy of low back pain: acute outcomes of group instructionaBsTraCTBackground Adults with recalcitrant mechanical low back pain of more than six weeks
duration can encounter unacceptable waiting periods for specialised care.Aim To evaluate the effectiveness of rapid treatment by means of group sessions. Methods We instituted a rapidly accessed patient education programme in
physiotherapy for low back pain. Pain and disability were assessed before and after the programme. The programme included four sessions of group instruction for self-actuated physiotherapy. There were six to 10 patients per group.
Results In eight months, 160 patients were admitted to the programme. The average waiting time was 16 business days for the first appointment. Seventy-three per cent of the patients who attended some portion of the programme completed all sessions. At least 30% of the incompletions were ascribable to rapid improvement. Of patients completing the programme, 80% reported significant resolution of the pain and improvement in function. Twenty per cent reported no significant response, but no patients worsened during participation. Of the 20% with no subjective improvement, 50% were pursuing medico-legal claims. In comparison, 9% of those reporting a successful response were pursuing litigation.
Conclusions Group instruction in physiotherapy for low back pain is safe, generally successful, and highly acceptable to patients.
SD Alston, TJ O’SullivanBack Care Programme, Dept of Orthopaedic Surgery, Waterford Regional Hospital
PATIENT EDUCATION IN PHYSIOTHERAPY OF LOw BACk PAIN: ACUTE OUTCOMES OF GROUP INSTRUCTION
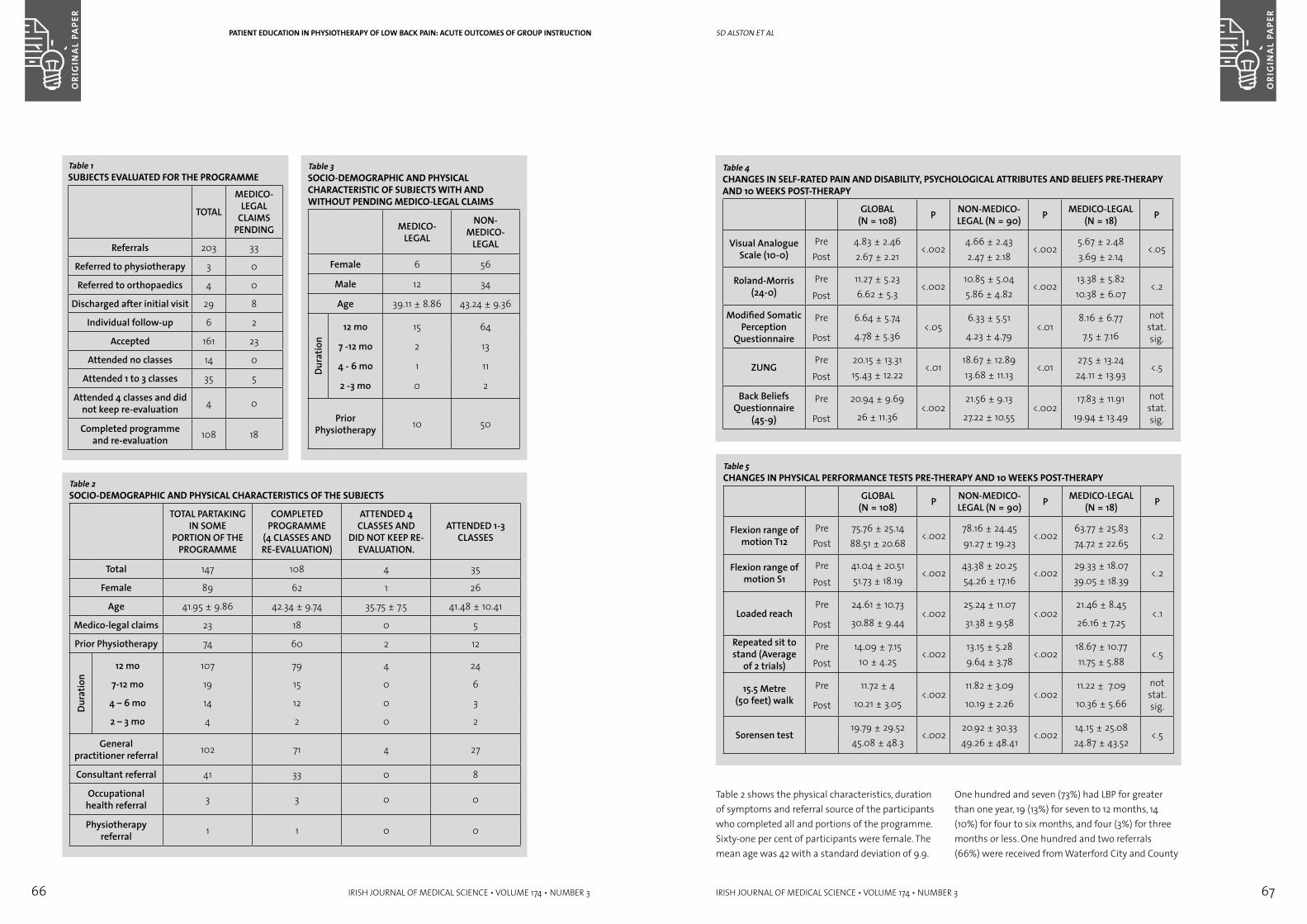
66 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 67
Table 2 shows the physical characteristics, duration of symptoms and referral source of the participants who completed all and portions of the programme. Sixty-one per cent of participants were female. The mean age was 42 with a standard deviation of 9.9.
One hundred and seven (73%) had LBP for greater than one year, 19 (13%) for seven to 12 months, 14 (10%) for four to six months, and four (3%) for three months or less. One hundred and two referrals (66%) were received from Waterford City and County
SD alStOn et al
Table 4CHANGES IN SELF-RATED PAIN AND DISABILITY, PSYCHOLOGICAL ATTRIBUTES AND BELIEFS PRE-THERAPY AND 10 wEEkS POST-THERAPY
GLOBAL (N = 108) P NON-MEDICO-
LEGAL (N = 90) P MEDICO-LEGAL (N = 18) P
Visual Analogue Scale (10-0)
Pre 4.83 ± 2.46<.002
4.66 ± 2.43<.002
5.67 ± 2.48<.05
Post 2.67 ± 2.21 2.47 ± 2.18 3.69 ± 2.14
Roland-Morris (24-0)
Pre 11.27 ± 5.23<.002
10.85 ± 5.04<.002
13.38 ± 5.82<.2
Post 6.62 ± 5.3 5.86 ± 4.82 10.38 ± 6.07
Modified Somatic Perception
Questionnaire
Pre 6.64 ± 5.74<.05
6.33 ± 5.51<.01
8.16 ± 6.77 not stat.sig.Post 4.78 ± 5.36 4.23 ± 4.79 7.5 ± 7.16
ZUNGPre 20.15 ± 13.31
<.0118.67 ± 12.89
<.0127.5 ± 13.24
<.5Post 15.43 ± 12.22 13.68 ± 11.13 24.11 ± 13.93
Back Beliefs Questionnaire
(45-9)
Pre 20.94 ± 9.69<.002
21.56 ± 9.13<.002
17.83 ± 11.91 not stat. sig.Post 26 ± 11.36 27.22 ± 10.55 19.94 ± 13.49
Table 5CHANGES IN PHYSICAL PERFORMANCE TESTS PRE-THERAPY AND 10 wEEkS POST-THERAPY
GLOBAL (N = 108) P NON-MEDICO-
LEGAL (N = 90) P MEDICO-LEGAL (N = 18) P
Flexion range of motion T12
Pre 75.76 ± 25.14<.002
78.16 ± 24.45<.002
63.77 ± 25.83<.2
Post 88.51 ± 20.68 91.27 ± 19.23 74.72 ± 22.65
Flexion range of motion S1
Pre 41.04 ± 20.51<.002
43.38 ± 20.25<.002
29.33 ± 18.07<.2
Post 51.73 ± 18.19 54.26 ± 17.16 39.05 ± 18.39
Loaded reachPre 24.61 ± 10.73
<.00225.24 ± 11.07
<.00221.46 ± 8.45
<.1Post 30.88 ± 9.44 31.38 ± 9.58 26.16 ± 7.25
Repeated sit to stand (Average
of 2 trials)
Pre 14.09 ± 7.15<.002
13.15 ± 5.28<.002
18.67 ± 10.77<.5
Post 10 ± 4.25 9.64 ± 3.78 11.75 ± 5.88
15.5 Metre (50 feet) walk
Pre 11.72 ± 4<.002
11.82 ± 3.09<.002
11.22 ± 7.09 not stat. sig.Post 10.21 ± 3.05 10.19 ± 2.26 10.36 ± 5.66
Sorensen test19.79 ± 29.52
<.00220.92 ± 30.33
<.00214.15 ± 25.08
<.545.08 ± 48.3 49.26 ± 48.41 24.87 ± 43.52
PATIENT EDUCATION IN PHYSIOTHERAPY OF LOw BACk PAIN: ACUTE OUTCOMES OF GROUP INSTRUCTION
Table 2SOCIO-DEMOGRAPHIC AND PHYSICAL CHARACTERISTICS OF THE SUBJECTS
TOTAL PARTAKING IN SOME
PORTION OF THE PROGRAMME
COMPLETED PROGRAMME
(4 CLASSES AND RE-EVALUATION)
ATTENDED 4 CLASSES AND
DID NOT KEEP RE-EVALUATION.
ATTENDED 1-3 CLASSES
Total 147 108 4 35
Female 89 62 1 26
Age 41.95 ± 9.86 42.34 ± 9.74 35.75 ± 7.5 41.48 ± 10.41
Medico-legal claims 23 18 0 5
Prior Physiotherapy 74 60 2 12
Dura
tion
12 mo 107 79 4 24
7-12 mo 19 15 0 6
4 – 6 mo 14 12 0 3
2 – 3 mo 4 2 0 2
General practitioner referral 102 71 4 27
Consultant referral 41 33 0 8
Occupational health referral 3 3 0 0
Physiotherapy referral 1 1 0 0
Table 1SUBJECTS EVALUATED FOR THE PROGRAMME
TOTAL
MEDICO-LEGAL
CLAIMS PENDING
Referrals 203 33
Referred to physiotherapy 3 0
Referred to orthopaedics 4 0
Discharged after initial visit 29 8
Individual follow-up 6 2
Accepted 161 23
Attended no classes 14 0
Attended 1 to 3 classes 35 5
Attended 4 classes and did not keep re-evaluation 4 0
Completed programme and re-evaluation 108 18
Table 3SOCIO-DEMOGRAPHIC AND PHYSICAL CHARACTERISTIC OF SUBJECTS wITH AND wITHOUT PENDING MEDICO-LEGAL CLAIMS
MEDICO-LEGAL
NON-MEDICO-
LEGAL
Female 6 56
Male 12 34
Age 39.11 ± 8.86 43.24 ± 9.36Du
ratio
n12 mo 15 64
7 -12 mo 2 13
4 - 6 mo 1 11
2 -3 mo 0 2
Prior Physiotherapy 10 50
68 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 69
greater than one year. In effect, subjects served as their own control group. All were referred by medical practitioners seeking assistance with management of the longstanding pain.
We find that group therapy, led by a specially dedicated physiotherapist, can efficiently provide an effective course of therapy that proves highly acceptable to most patients. Patients pursuing litigation because of LBP tend to do less well than other patients in group physiotherapy, but most do improve with our supervised exercise programme.
REFERENCES1. Clinical Standards Advisory Group. Back pain. Report of
a CSAG committee on back pain. London: HMSO,1994.
2. Waddell, G. The back pain revolution. Edinburgh: Churchill Livingstone, 1998.
3. Leboeuf-Yde C, Klougart N, Lauritzen T. How common is low back pain in the Nordic population? Data form a recent study on a middle-aged general Danish population and four surveys previously conducted in the Nordic countries. Spine 1996;13:1518-26.
4. Croft PR, Macfarlane GJ, Papageorgiou AC, Thomas E, Silma AJ. Outcome of low back pain in general practice: a prospective study. BMJ 1998;316:1356-9.
5. Biering-Sorensen F. A prospective study of low back pain in a general population. Scand J Rehabil Med 1983;15:71-9.
6. Kankaanpaa M, Taimela S, Airaksinen O, Hanninen O. The efficacy of active rehabilitation in chronic low back pain. Spine 1999 24(10);1034-1042.
7. Soukup MG, Glomsord B, Lonn JH, Bo K, Larsen S: The effect of a mensendieck exercise program as a secondary prophylaxis for recurrent low back pain: A randomised controlled trial with 12-month follow-up. Spine 1999;24(15):1585-1592.
8. Van Tudler M W, Koes BW, Bouter LM. Consevative treatment of acute and chronic non-specific low back pain. A systematic review of randomised controlled trials of the most common interventions. Spine 1997;22(18):2128-2156.
9. Lonn JH, Glomsrod B, Soukup MG, So K. Active Back School: Prophylactic management for low back pain. Spine 1999;24(9):865-871.
10. Bendix AF, Bendix T, Labriola M, Boekgaard P. Functional restoration of chronic low back pain. Spine 1998;23:717-725.
11. Klaber Moffett J, Torgenson D, Bell-Syer S et al. Randomised controlled trial of exercise for low back pain: clinical outcomes, cost and preferences. BMJ 1999;319:279-83.
12. Mannion, AF, Muntener M, Taimela S, Dvorak J. A randomised clinical trial of three active therapies for chronic low back pain. Spine 1999;24:2435-2448.
13. Rose MJ, Reilly JP, Pennie B, Bowen-Jones K, Stanley, IM, Slade PD. Chronic low back pain rehabilitation programs: A study of the optimum duration of treatment and a comparison of group and individual therapy. Spine 1997;22:2246-253.
14. Blake C, Garrett M. Impact of litigation on quality of life outcomes in patients with chronic low back pain. Ir J Med Sci 1997;166:124-6.
15. Simmonds M J, Olson SL, Jones S et al. Psychometric characteristics and clinical usefulness of physical performance tests in patients with low back pain. Spine 1998;23:2412-2421.
16. Roland M, Morris R. A study of the natural history of back pain: Part 1. Development of a reliable and sensitive measure of disability in low-back pain. Spine 1983;8:141-4.
17. Main CJ, Wood PLR, Hollis S, Spanswick CC, Waddell G: The distress and risk assessment method. A simple patient classification to identify distress and evaluate the risk of poor outcome. Spine;1992:17:42 –52.
18. Symonds TL, Burton AK, Tillotson KM, Main CJ. Do attitudes and beliefs influence work loss due to low back trouble? Occup Med 1996;46:25-32
19. Liebenson C (ed). Rehabilitation of the spine: a practitioner’s manual. Baltimore:Williams & Wilkins, 1996.
20. Madding S, Wong J, Hallum A, Medeiros J 1987 Effect of duration of passive stretch on hip abjuction range of motion. JOSPT 1987;8:409-16
21. O’Sullivan, Twomey L, Allison G 1998; Altered abdominal muscle recruitment in patients with chronic back pain following a specific exercise intervention. JOSPT 27:114-124.
22. Richardson CA, Jull GA. Muscle control- pain control. What exercises would you prescribe? Manual Therapy 1995;1:2-10
23. Richardson CA, Jull GZ, Hodges P, Hides J. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain- Scientific basis and clinical approach. Edinburgh: Churchill Livingston 1999: 145-155.
24. Hodges PW. Is there a role for transverses abdominis in lumbo-pelvic stability? Man Ther 1999;4:74-86.
25. Jette DU, Jette AM Physical therapy and health outcomes in patients with spinal impairments. Phys Ther 1996;76:930-41.
26. Hagins M, Adler K, Cash M, Daugherty J, Mitrani G Effects of practice on the ability to perform lumbar stabilization exercises. JOSPT 1999:29:546-555.
Correspondence to:Suzanne D. Alston, PT Associates, 76 Woodside Road, Winchester, MA 01890, USATel: 00 1 781 729 9705; Email: [email protected]
SD alStOn et al
general practitioners, 41 (31%) from Waterford Regional Hospital consultants, and four (3%) from occupational health clinicians or physiotherapists.
Table 3 contrasts the group seeking legal action from that not doing so. The group seeking legal action (n = 18) was predominantly (67%) male while the other group was larger (n = 90) and predominantly (62%) female. The mean age of the group seeking legal action was four years younger than the mean age of the larger group. In both groups, most of the patients had suffered from LBP for longer than a year. In both groups, about half of the patients had previously sought physiotherapy.
Outcome MeasurementsTen-week follow-up data were collected from those who attended all four classes and returned for the follow-up appointment. Data are presented separately for the group as a whole and for the non-medico-legal and the medico-legal groups (Tables 4 and 5).
Subjective Ratings (Table 4)Self-rated PainEach patient group demonstrated significant reduction in average pain after therapy. The changes were highly significant for the group as a whole and for the non-medico-legal group (p < .002). They were also statistically significant for the relatively small medico-legal group (p < .05).
DisabilitySelf-rated disability on the Roland-Morris scale (0-24) decreased significantly in the group as a whole and in the non-medico-legal group (p < .002). The change was less statistically significant for the small medico-legal group (p<.2)
Psychological ParametersMSPQ scores and ZUNG depression scores decreased significantly for the group as a whole and for the non-medico-legal group (p < .05 or better). The small medico-legal group exhibited a favorable trend, though statistical significance was not achieved.
Back Beliefs Questionnaire.Back beliefs improved significantly for the group as a whole and for the non-medico-legal groups (p<.002). Statistically significant improvement in beliefs was not achieved for the small medico-legal group, though a favorable trend is apparent. The scale runs from 45 to nine, and a decreased score indicates improvement.
Table 5 shows the performance before therapy and at 10 weeks following initial therapy with associated p values for each group.
Flexion range of motion improved for all groups of patients. This change was highly significant for the group as a whole and for the non-medico-legal groups (p<.002). The medico-legal group also improved (p<.2).
The distance patients could reach with a load increased significantly for the group as a whole and for the non-medico-legal group (p<.002). The medico-legal group also improved (p<.1).
The time required for participants to perform the repeated sit-to-stand test decreased significantly for all three groups after therapy (p<.002) for the whole group and the non-medico-legal group, and p<.05 for the medico-legal group).
The group as a whole and the non-medico-legal group improved their timed 50-foot walk test significantly (p<.002). The improvement of the small medico-legal group did not achieve statistical significance.
All groups demonstrated an improved ability to maintain the neutral position in the Sorensen test. The whole group and the non-medico-legal group achieved a statistically significance (p<.002), and a positive trend was seen in the medico-legal group (p<.5).
Having made both subjective and objective gains, 81% of the group as a whole was satisfied with their outcome. Of the non-medico-legal group, 89% were satisfied with their outcome while only 44% of the medico-legal group was satisfied. When medico-legal cases were combined with those on disability, only 25% were satisfied with their outcome. No patient worsened during participation.
DisCUssiOnLBP is a common cause of referral to orthopaedic and physiotherapy departments. It is second only to the common cold in the list of problems that trigger physician visits.4 In view of the high frequency of LBP; an efficient but compassionate system is required to deal with the problem. Few general practitioners have the temporal resources to personally guide individual patients out of prolonged back pain syndromes.
As it would be unethical to offer no treatment to patients applying for help with pain, our study did not include a group receiving no therapy. All but two of our 108 patients had pre-existing pain for at least four months, and the majority, 73%, had pain for
PATIENT EDUCATION IN PHYSIOTHERAPY OF LOw BACk PAIN: ACUTE OUTCOMES OF GROUP INSTRUCTION

70 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 71
Marquette MAC-PC computerised ECG interpretation program. Chest x-rays were examined and reported by a consultant radiologist to have either a normal or abnormal heart shadow, and/or normal or abnormal lung fields. Measures of association were determined using Epi-Info version 6.0, using the Student’s t test for comparison of means and Chi-square analysis for comparison of proportions.
resUlTsDuring the study period there were 3,076 admissions, the mean age was 67 +/- 15 years (median 60) and the mean length of stay was 5.3 +/- 4.7 days (median 4.0 days) – 842 patients (27%) were self-referred and 2234 (73%) referred by a physician. Self-referred patients were younger (50.6 +/- 21.9 vs. 63.7 +/- 19.5 years, p<.001), lived nearer the hospital (10.5 +/- 10.1 vs. 13.2 +/- 7.8 miles away, p<.001), and were more likely to be unmarried and current smokers and drinkers (Figure 1). Although patients referred by a doctor were more likely to have been in poor health prior to their current illness (23% vs. 12%, p<.001) they presented later for hospitalisation (7.7 +/- 19.9 vs. 3.6 +/- 12.4 days after symptom onset, p<.001) and were more likely to be ex-smokers, ex-drinkers and retired (Figure 1). Moreover, more of the patients referred by a doctor complained of breathlessness and suffered from heart and lung disease and were less likely to be drunk, have loss of mental competence or an alcohol-related illness (Figure 2). Both self- and physician-referred patients had the same rates of private health insurance (16.3% vs. 19.2%), prior stroke (2.6% vs. 3.0%), heart attack (4.6% vs. 5.6%) and diabetes (6.3% vs. 5.2%).
Parasuicide and/or alcohol were the cause of hospital admission for 27% of self-referred patients and only 4.5% of physician-referred patients (p<.001). Although self-referred patients had a shorter length of stay (3.8 +/- 4.3 vs. 6.0 +/- 4.8 days, p<.001), a lower death rate (1.4% vs. 3.8%, p<.001) and were more likely to be discharged home well and/or take their own discharge against medical advice, they had a significantly higher rate of readmission to hospital within 14 (7.9% vs. 4.8%, p<.001) and 30 days (14.6% vs. 8.5%, p<.001) of discharge (Figure 3). If alcohol and parasuicide related admissions were excluded and patients were corrected for age, self-referred patients still had a higher 30-day re-admission rate than those referred by a physician (13.8% vs. 6.0%, p<.001). Patients who were referred by a physician had an 87.4% chance of being referred again by a physician if they were readmitted to hospital within 30 days. On the other hand, self-
J Kellett et al
Figure 1 — SIGNIFICANT (P<.002) DIFFERENCES IN THE SOCIAL HISTORY OF PHYSICIAN AND SELF-REFERRED PATIENTS
* Statistical significance lost if parasuicides and illnesses related to alcohol excluded
Figure 2 — SIGNIFICANT (P<.001) DIFFERENCES IN THE PRESENTING COMPLAINTS AND PAST MEDICAL HISTORY OF PHYSICIAN- AND SELF- REFERRED PATIENTS
Figure 3 — SIGNIFICANT (P<.001) DIFFERENCES IN THE OUTCOMES OF PHYSICIAN- AND SELF- REFERRED PATIENTS
* Statistical significance lost if parasuicides and illnesses related to alcohol excluded
Figure 4 — SIGNIFICANT (P<.005) DIFFERENCES IN THE CLINICAL AND LABORATORY FINDINGS OF PHYSICIAN- AND SELF- REFERRED PATIENTS
* Statistical significance lost if parasuicides and admissions related to alcohol excluded
** Statistical significance lost if parasuicides and admissions related to alcohol excluded, and patients confined to those between 60 and 80 years of age
1
2
3
4
inTrODUCTiOnOver the last 30 years referral rates from general practice to hospital have increased steadily1 and acute medical emergency admissions to Irish hospitals having almost doubled over the last 20 years. In order to limit hospitalisation to those patients for whom it is appropriate, a considerable effort has been invested in accident and emergency (A&E) assessment prior to admission. The rationale for this policy is the large variation in hospital referral rates reported among general practitioners.2, 3
Despite a widespread assumption that high referring general practitioners tend to refer unnecessarily, studies comparing referrals from high and low referring doctors have not confirmed this.4, 5 Recent studies have shown, however, that general practitioner referral rates correlate strongly with hospital-doctor controlled admission rates.6
Most patients in Irish hospitals are now admitted as unplanned emergencies. In urban areas many patients refer themselves for admission directly through hospital accident and emergency (A&E) departments. In rural areas, however, it is still more common for patients to be referred for hospital admission by their family doctor after a house call or office consultation. Nenagh Hospital is a small hospital serving a widely dispersed rural population of 60,000. It has 35 medical beds, over 2,600 medical
admissions per year, 110% occupancy and an in-hospital mortality of 3.0%. Approximately two-thirds of medical patients are referred for admission by their family doctor and the rest present themselves for admission as emergencies.
The aim of this study was to determine if physician-referred and self-referred patients differed in any clinically significant ways. The study was based on data routinely collected on all medical admissions between August 1999 and October 2000.
MeTHODsOn August 13, 1999 a database of all medical admissions was established. Continuous variables (including age, vital signs, etc.) and categorical variables (including presenting complaint, demographic details, medical and social history, laboratory, ECG and x-ray findings, etc.) were collected. As of the October 31, 2000 data on 3,076 consecutive admissions have been entered into the database. Data were initially entered by the admitting house officer onto a standard data collection form, and then entered daily by a dedicated data collection officer (B.D.) into a computer database written in Epi-Info. Errors or omissions detected by the data collection officer were corrected after discussion with the admitting physician usually within 24 hours of the patient’s admission. ECGs were classified as normal or abnormal according to the interpretation of the
Differences between self-referred and physician-referred hospital admissionsaBsTraCTAim Compare self- and physician-referred hospital admissions. Methods Analysis of data prospectively collected on 3,076 consecutive acute medical
admissions to a small hospital.Results Self-referred patients were younger (50.6 vs. 63.7 years) and more likely to be
smokers and drinkers. Conversely, physician-referred patients were more likely to present later, be ex-smokers, ex-drinkers and have poor prior health. More self-referred admissions were related to parasuicide and/or alcohol (27% vs. 4.5%). The physical, x-ray and laboratory findings of both types of patient were similar. Although self-referred patients had a shorter length of stay (3.8 days vs. 6.0 days) and a lower death rate (1.5% vs. 3.8%), they had higher 30-day readmission rates (14.6% vs. 8.5%).
Conclusion Self-referred patients are less sick than those referred for hospital admission by a physician, have less psychosocial support, more alcohol-related illness and are nearly twice as likely to be readmitted within 30 days of discharge
J Kellett,1 P McKeown,2 B Deane1 Nenagh Hospital,1
Nenagh, Co. Tipperary; Mid-Western Health Board,2 Catherine St., Limerick
DIFFERENCES BETwEEN SELF-REFERRED AND PHYSICIAN-REFERRED HOSPITAL ADMISSIONS
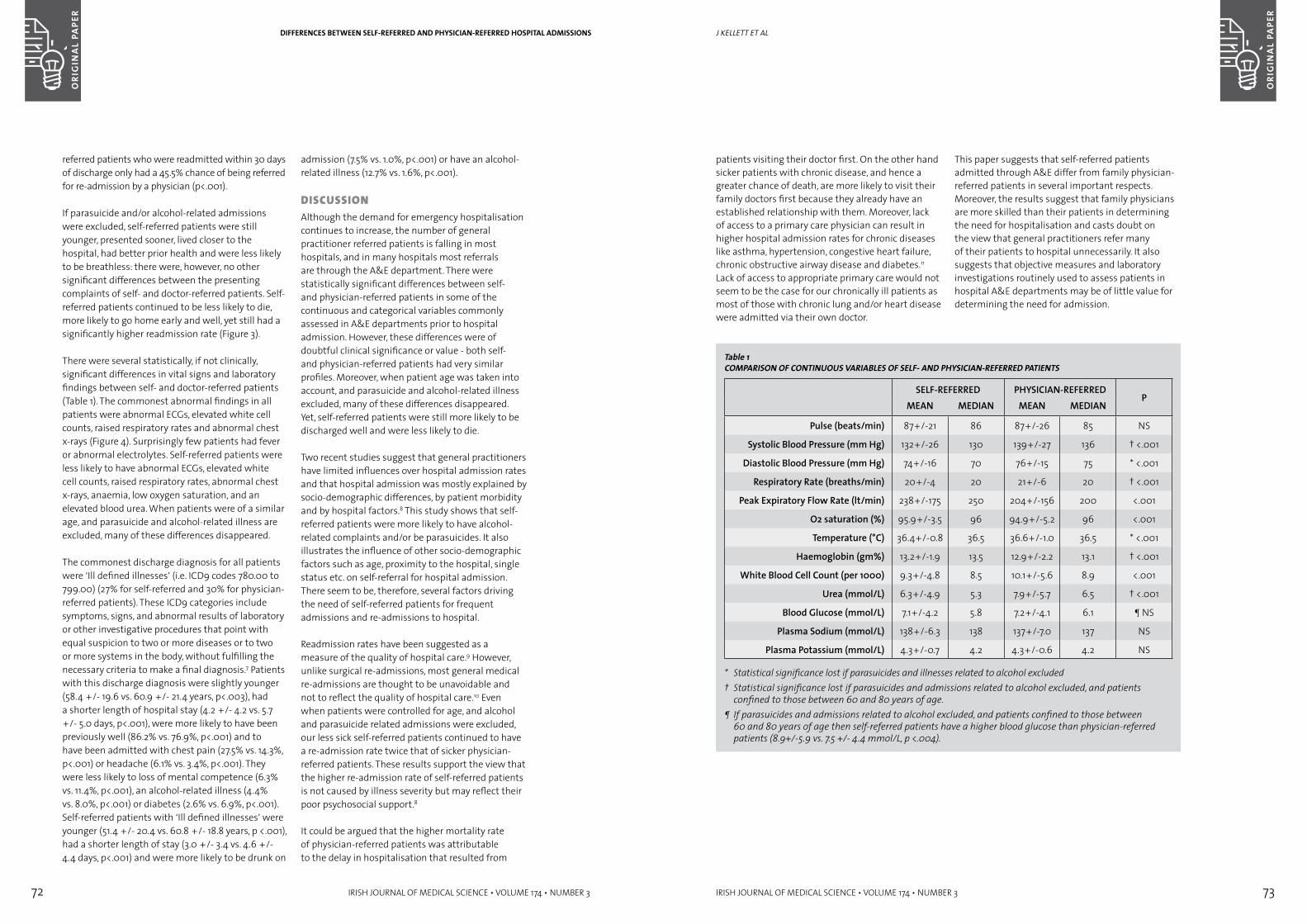
72 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 73
Table 1COMPARISON OF CONTINUOUS VARIABLES OF SELF- AND PHYSICIAN-REFERRED PATIENTS
SELF-REFERRED PHYSICIAN-REFERREDP
MEAN MEDIAN MEAN MEDIAN
Pulse (beats/min) 87+/-21 86 87+/-26 85 NS
Systolic Blood Pressure (mm Hg) 132+/-26 130 139+/-27 136 † <.001
Diastolic Blood Pressure (mm Hg) 74+/-16 70 76+/-15 75 * <.001
Respiratory Rate (breaths/min) 20+/-4 20 21+/-6 20 † <.001
Peak Expiratory Flow Rate (lt/min) 238+/-175 250 204+/-156 200 <.001
O2 saturation (%) 95.9+/-3.5 96 94.9+/-5.2 96 <.001
Temperature (°C) 36.4+/-0.8 36.5 36.6+/-1.0 36.5 * <.001
Haemoglobin (gm%) 13.2+/-1.9 13.5 12.9+/-2.2 13.1 † <.001
White Blood Cell Count (per 1000) 9.3+/-4.8 8.5 10.1+/-5.6 8.9 <.001
Urea (mmol/L) 6.3+/-4.9 5.3 7.9+/-5.7 6.5 † <.001
Blood Glucose (mmol/L) 7.1+/-4.2 5.8 7.2+/-4.1 6.1 ¶ NS
Plasma Sodium (mmol/L) 138+/-6.3 138 137+/-7.0 137 NS
Plasma Potassium (mmol/L) 4.3+/-0.7 4.2 4.3+/-0.6 4.2 NS
* Statistical significance lost if parasuicides and illnesses related to alcohol excluded† Statistical significance lost if parasuicides and admissions related to alcohol excluded, and patients
confined to those between 60 and 80 years of age.¶ If parasuicides and admissions related to alcohol excluded, and patients confined to those between
60 and 80 years of age then self-referred patients have a higher blood glucose than physician-referred patients (8.9+/-5.9 vs. 7.5 +/- 4.4 mmol/L, p <.004).
J Kellett et al
patients visiting their doctor first. On the other hand sicker patients with chronic disease, and hence a greater chance of death, are more likely to visit their family doctors first because they already have an established relationship with them. Moreover, lack of access to a primary care physician can result in higher hospital admission rates for chronic diseases like asthma, hypertension, congestive heart failure, chronic obstructive airway disease and diabetes.11 Lack of access to appropriate primary care would not seem to be the case for our chronically ill patients as most of those with chronic lung and/or heart disease were admitted via their own doctor.
This paper suggests that self-referred patients admitted through A&E differ from family physician-referred patients in several important respects. Moreover, the results suggest that family physicians are more skilled than their patients in determining the need for hospitalisation and casts doubt on the view that general practitioners refer many of their patients to hospital unnecessarily. It also suggests that objective measures and laboratory investigations routinely used to assess patients in hospital A&E departments may be of little value for determining the need for admission.
DIFFERENCES BETwEEN SELF-REFERRED AND PHYSICIAN-REFERRED HOSPITAL ADMISSIONS
referred patients who were readmitted within 30 days of discharge only had a 45.5% chance of being referred for re-admission by a physician (p<.001).
If parasuicide and/or alcohol-related admissions were excluded, self-referred patients were still younger, presented sooner, lived closer to the hospital, had better prior health and were less likely to be breathless: there were, however, no other significant differences between the presenting complaints of self- and doctor-referred patients. Self-referred patients continued to be less likely to die, more likely to go home early and well, yet still had a significantly higher readmission rate (Figure 3).
There were several statistically, if not clinically, significant differences in vital signs and laboratory findings between self- and doctor-referred patients (Table 1). The commonest abnormal findings in all patients were abnormal ECGs, elevated white cell counts, raised respiratory rates and abnormal chest x-rays (Figure 4). Surprisingly few patients had fever or abnormal electrolytes. Self-referred patients were less likely to have abnormal ECGs, elevated white cell counts, raised respiratory rates, abnormal chest x-rays, anaemia, low oxygen saturation, and an elevated blood urea. When patients were of a similar age, and parasuicide and alcohol-related illness are excluded, many of these differences disappeared.
The commonest discharge diagnosis for all patients were ‘Ill defined illnesses’ (i.e. ICD9 codes 780.00 to 799.00) (27% for self-referred and 30% for physician-referred patients). These ICD9 categories include symptoms, signs, and abnormal results of laboratory or other investigative procedures that point with equal suspicion to two or more diseases or to two or more systems in the body, without fulfilling the necessary criteria to make a final diagnosis.7 Patients with this discharge diagnosis were slightly younger (58.4 +/- 19.6 vs. 60.9 +/- 21.4 years, p<.003), had a shorter length of hospital stay (4.2 +/- 4.2 vs. 5.7 +/- 5.0 days, p<.001), were more likely to have been previously well (86.2% vs. 76.9%, p<.001) and to have been admitted with chest pain (27.5% vs. 14.3%, p<.001) or headache (6.1% vs. 3.4%, p<.001). They were less likely to loss of mental competence (6.3% vs. 11.4%, p<.001), an alcohol-related illness (4.4% vs. 8.0%, p<.001) or diabetes (2.6% vs. 6.9%, p<.001). Self-referred patients with ‘Ill defined illnesses’ were younger (51.4 +/- 20.4 vs. 60.8 +/- 18.8 years, p <.001), had a shorter length of stay (3.0 +/- 3.4 vs. 4.6 +/- 4.4 days, p<.001) and were more likely to be drunk on
admission (7.5% vs. 1.0%, p<.001) or have an alcohol-related illness (12.7% vs. 1.6%, p<.001).
DisCUssiOnAlthough the demand for emergency hospitalisation continues to increase, the number of general practitioner referred patients is falling in most hospitals, and in many hospitals most referrals are through the A&E department. There were statistically significant differences between self- and physician-referred patients in some of the continuous and categorical variables commonly assessed in A&E departments prior to hospital admission. However, these differences were of doubtful clinical significance or value - both self- and physician-referred patients had very similar profiles. Moreover, when patient age was taken into account, and parasuicide and alcohol-related illness excluded, many of these differences disappeared. Yet, self-referred patients were still more likely to be discharged well and were less likely to die.
Two recent studies suggest that general practitioners have limited influences over hospital admission rates and that hospital admission was mostly explained by socio-demographic differences, by patient morbidity and by hospital factors.8 This study shows that self-referred patients were more likely to have alcohol-related complaints and/or be parasuicides. It also illustrates the influence of other socio-demographic factors such as age, proximity to the hospital, single status etc. on self-referral for hospital admission. There seem to be, therefore, several factors driving the need of self-referred patients for frequent admissions and re-admissions to hospital.
Readmission rates have been suggested as a measure of the quality of hospital care.9 However, unlike surgical re-admissions, most general medical re-admissions are thought to be unavoidable and not to reflect the quality of hospital care.10 Even when patients were controlled for age, and alcohol and parasuicide related admissions were excluded, our less sick self-referred patients continued to have a re-admission rate twice that of sicker physician-referred patients. These results support the view that the higher re-admission rate of self-referred patients is not caused by illness severity but may reflect their poor psychosocial support.8
It could be argued that the higher mortality rate of physician-referred patients was attributable to the delay in hospitalisation that resulted from
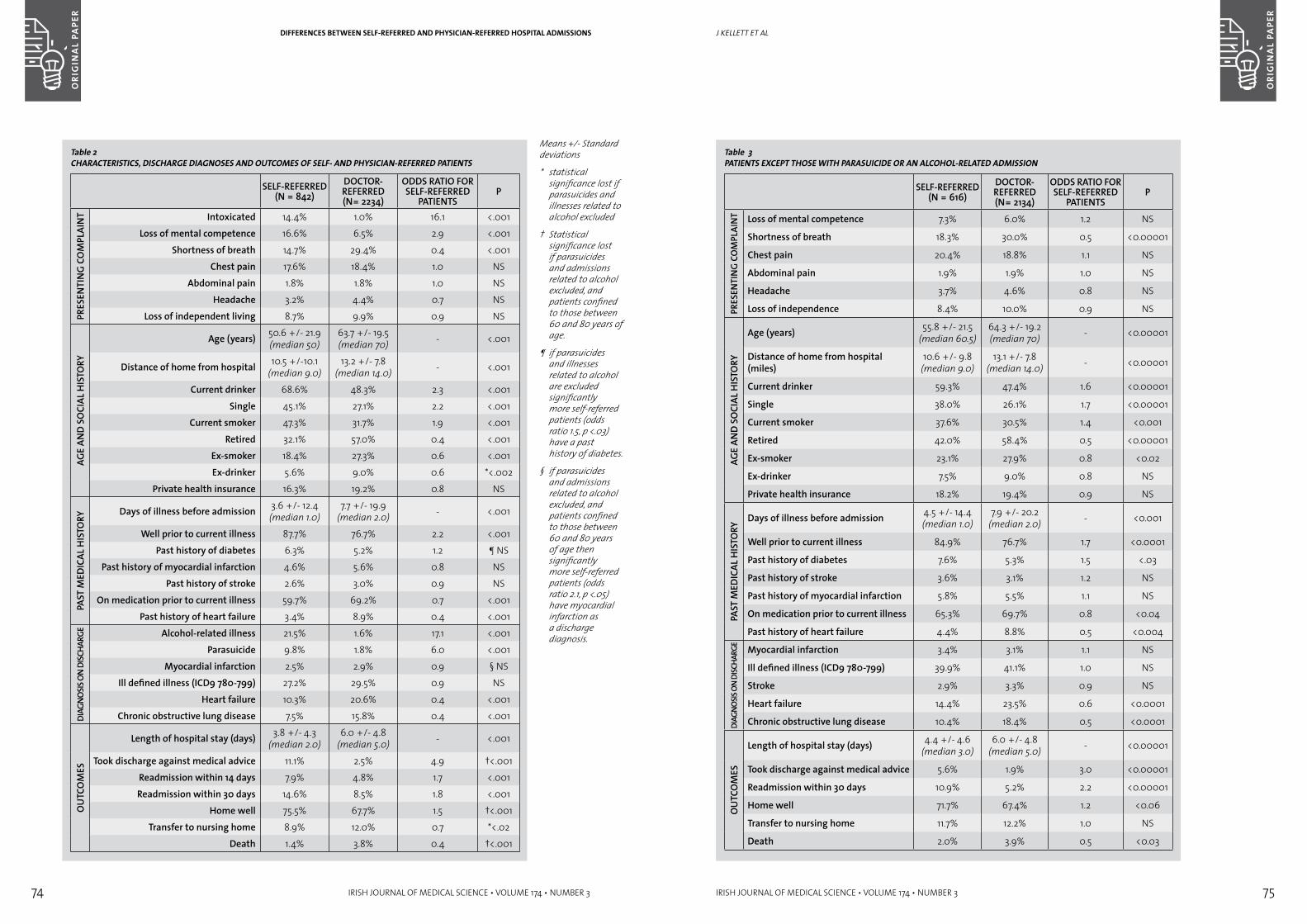
74 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 75
J Kellett et al
Table 3PATIENTS EXCEPT THOSE wITH PARASUICIDE OR AN ALCOHOL-RELATED ADMISSION
SELF-REFERRED (N = 616)
DOCTOR-REFERRED (N= 2134)
ODDS RATIO FOR SELF-REFERRED
PATIENTSP
PRES
ENTI
NG
COM
PLAI
NT Loss of mental competence 7.3% 6.0% 1.2 NS
Shortness of breath 18.3% 30.0% 0.5 <0.00001
Chest pain 20.4% 18.8% 1.1 NS
Abdominal pain 1.9% 1.9% 1.0 NS
Headache 3.7% 4.6% 0.8 NS
Loss of independence 8.4% 10.0% 0.9 NS
AGE
AND
SOCI
AL H
ISTO
RY
Age (years) 55.8 +/- 21.5 (median 60.5)
64.3 +/- 19.2 (median 70) - <0.00001
Distance of home from hospital (miles)
10.6 +/- 9.8 (median 9.0)
13.1 +/- 7.8 (median 14.0) - <0.00001
Current drinker 59.3% 47.4% 1.6 <0.00001
Single 38.0% 26.1% 1.7 <0.00001
Current smoker 37.6% 30.5% 1.4 <0.001
Retired 42.0% 58.4% 0.5 <0.00001
Ex-smoker 23.1% 27.9% 0.8 <0.02
Ex-drinker 7.5% 9.0% 0.8 NS
Private health insurance 18.2% 19.4% 0.9 NS
PAST
MED
ICAL
HIS
TORY
Days of illness before admission 4.5 +/- 14.4 (median 1.0)
7.9 +/- 20.2 (median 2.0) - <0.001
Well prior to current illness 84.9% 76.7% 1.7 <0.0001
Past history of diabetes 7.6% 5.3% 1.5 <.03
Past history of stroke 3.6% 3.1% 1.2 NS
Past history of myocardial infarction 5.8% 5.5% 1.1 NS
On medication prior to current illness 65.3% 69.7% 0.8 <0.04
Past history of heart failure 4.4% 8.8% 0.5 <0.004
DIAG
NOSIS
ON
DISC
HARG
E
Myocardial infarction 3.4% 3.1% 1.1 NS
Ill defined illness (ICD9 780-799) 39.9% 41.1% 1.0 NS
Stroke 2.9% 3.3% 0.9 NS
Heart failure 14.4% 23.5% 0.6 <0.0001
Chronic obstructive lung disease 10.4% 18.4% 0.5 <0.0001O
UTC
OM
ESLength of hospital stay (days) 4.4 +/- 4.6
(median 3.0)6.0 +/- 4.8
(median 5.0) - <0.00001
Took discharge against medical advice 5.6% 1.9% 3.0 <0.00001
Readmission within 30 days 10.9% 5.2% 2.2 <0.00001
Home well 71.7% 67.4% 1.2 <0.06
Transfer to nursing home 11.7% 12.2% 1.0 NS
Death 2.0% 3.9% 0.5 <0.03
DIFFERENCES BETwEEN SELF-REFERRED AND PHYSICIAN-REFERRED HOSPITAL ADMISSIONS
Table 2CHARACTERISTICS, DISCHARGE DIAGNOSES AND OUTCOMES OF SELF- AND PHYSICIAN-REFERRED PATIENTS
SELF-REFERRED (N = 842)
DOCTOR-REFERRED (N= 2234)
ODDS RATIO FOR SELF-REFERRED
PATIENTSP
PRES
ENTI
NG
CO
MPL
AIN
T Intoxicated 14.4% 1.0% 16.1 <.001Loss of mental competence 16.6% 6.5% 2.9 <.001
Shortness of breath 14.7% 29.4% 0.4 <.001Chest pain 17.6% 18.4% 1.0 NS
Abdominal pain 1.8% 1.8% 1.0 NSHeadache 3.2% 4.4% 0.7 NS
Loss of independent living 8.7% 9.9% 0.9 NS
AGE
AND
SOCI
AL H
ISTO
RY
Age (years) 50.6 +/- 21.9 (median 50)
63.7 +/- 19.5 (median 70) - <.001
Distance of home from hospital 10.5 +/-10.1 (median 9.0)
13.2 +/- 7.8 (median 14.0) - <.001
Current drinker 68.6% 48.3% 2.3 <.001Single 45.1% 27.1% 2.2 <.001
Current smoker 47.3% 31.7% 1.9 <.001Retired 32.1% 57.0% 0.4 <.001
Ex-smoker 18.4% 27.3% 0.6 <.001Ex-drinker 5.6% 9.0% 0.6 *<.002
Private health insurance 16.3% 19.2% 0.8 NS
PAST
MED
ICAL
HIS
TORY
Days of illness before admission 3.6 +/- 12.4 (median 1.0)
7.7 +/- 19.9 (median 2.0) - <.001
Well prior to current illness 87.7% 76.7% 2.2 <.001Past history of diabetes 6.3% 5.2% 1.2 ¶ NS
Past history of myocardial infarction 4.6% 5.6% 0.8 NSPast history of stroke 2.6% 3.0% 0.9 NS
On medication prior to current illness 59.7% 69.2% 0.7 <.001Past history of heart failure 3.4% 8.9% 0.4 <.001
DIAG
NOSIS
ON
DISC
HARG
E Alcohol-related illness 21.5% 1.6% 17.1 <.001Parasuicide 9.8% 1.8% 6.0 <.001
Myocardial infarction 2.5% 2.9% 0.9 § NSIll defined illness (ICD9 780-799) 27.2% 29.5% 0.9 NS
Heart failure 10.3% 20.6% 0.4 <.001Chronic obstructive lung disease 7.5% 15.8% 0.4 <.001
OU
TCO
MES
Length of hospital stay (days) 3.8 +/- 4.3 (median 2.0)
6.0 +/- 4.8 (median 5.0) - <.001
Took discharge against medical advice 11.1% 2.5% 4.9 †<.001Readmission within 14 days 7.9% 4.8% 1.7 <.001Readmission within 30 days 14.6% 8.5% 1.8 <.001
Home well 75.5% 67.7% 1.5 †<.001Transfer to nursing home 8.9% 12.0% 0.7 *<.02
Death 1.4% 3.8% 0.4 †<.001
Means +/- Standard deviations
* statistical significance lost if parasuicides and illnesses related to alcohol excluded
† Statistical significance lost if parasuicides and admissions related to alcohol excluded, and patients confined to those between 60 and 80 years of age.
¶ if parasuicides and illnesses related to alcohol are excluded significantly more self-referred patients (odds ratio 1.5, p <.03) have a past history of diabetes.
§ if parasuicides and admissions related to alcohol excluded, and patients confined to those between 60 and 80 years of age then significantly more self-referred patients (odds ratio 2.1, p <.05) have myocardial infarction as a discharge diagnosis.
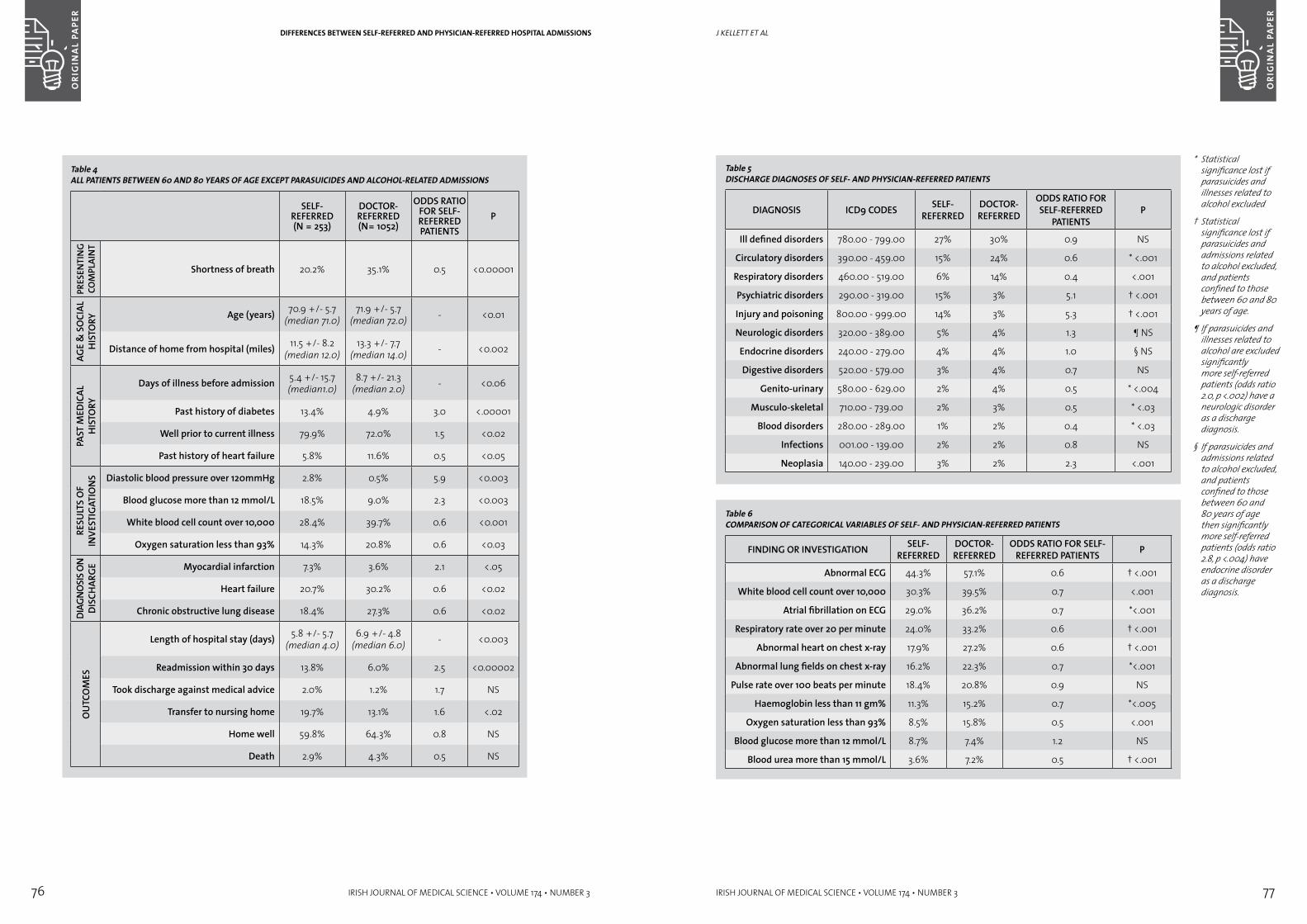
76 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 77
J Kellett et al
Table 5DISCHARGE DIAGNOSES OF SELF- AND PHYSICIAN-REFERRED PATIENTS
DIAGNOSIS ICD9 CODES SELF-REFERRED
DOCTOR-REFERRED
ODDS RATIO FOR SELF-REFERRED
PATIENTSP
Ill defined disorders 780.00 - 799.00 27% 30% 0.9 NS
Circulatory disorders 390.00 - 459.00 15% 24% 0.6 * <.001
Respiratory disorders 460.00 - 519.00 6% 14% 0.4 <.001
Psychiatric disorders 290.00 - 319.00 15% 3% 5.1 † <.001
Injury and poisoning 800.00 - 999.00 14% 3% 5.3 † <.001
Neurologic disorders 320.00 - 389.00 5% 4% 1.3 ¶ NS
Endocrine disorders 240.00 - 279.00 4% 4% 1.0 § NS
Digestive disorders 520.00 - 579.00 3% 4% 0.7 NS
Genito-urinary 580.00 - 629.00 2% 4% 0.5 * <.004
Musculo-skeletal 710.00 - 739.00 2% 3% 0.5 * <.03
Blood disorders 280.00 - 289.00 1% 2% 0.4 * <.03
Infections 001.00 - 139.00 2% 2% 0.8 NS
Neoplasia 140.00 - 239.00 3% 2% 2.3 <.001
Table 6COMPARISON OF CATEGORICAL VARIABLES OF SELF- AND PHYSICIAN-REFERRED PATIENTS
FINDING OR INVESTIGATION SELF-REFERRED
DOCTOR-REFERRED
ODDS RATIO FOR SELF-REFERRED PATIENTS P
Abnormal ECG 44.3% 57.1% 0.6 † <.001
White blood cell count over 10,000 30.3% 39.5% 0.7 <.001
Atrial fibrillation on ECG 29.0% 36.2% 0.7 *<.001
Respiratory rate over 20 per minute 24.0% 33.2% 0.6 † <.001
Abnormal heart on chest x-ray 17.9% 27.2% 0.6 † <.001
Abnormal lung fields on chest x-ray 16.2% 22.3% 0.7 *<.001
Pulse rate over 100 beats per minute 18.4% 20.8% 0.9 NS
Haemoglobin less than 11 gm% 11.3% 15.2% 0.7 *<.005
Oxygen saturation less than 93% 8.5% 15.8% 0.5 <.001
Blood glucose more than 12 mmol/L 8.7% 7.4% 1.2 NS
Blood urea more than 15 mmol/L 3.6% 7.2% 0.5 † <.001
* Statistical significance lost if parasuicides and illnesses related to alcohol excluded
† Statistical significance lost if parasuicides and admissions related to alcohol excluded, and patients confined to those between 60 and 80 years of age.
¶ If parasuicides and illnesses related to alcohol are excluded significantly more self-referred patients (odds ratio 2.0, p <.002) have a neurologic disorder as a discharge diagnosis.
§ If parasuicides and admissions related to alcohol excluded, and patients confined to those between 60 and 80 years of age then significantly more self-referred patients (odds ratio 2.8, p <.004) have endocrine disorder as a discharge diagnosis.
DIFFERENCES BETwEEN SELF-REFERRED AND PHYSICIAN-REFERRED HOSPITAL ADMISSIONS
Table 4ALL PATIENTS BETwEEN 60 AND 80 YEARS OF AGE EXCEPT PARASUICIDES AND ALCOHOL-RELATED ADMISSIONS
SELF-REFERRED (N = 253)
DOCTOR-REFERRED (N= 1052)
ODDS RATIO FOR SELF-REFERRED PATIENTS
P
PRES
ENTI
NG
COM
PLAI
NT
Shortness of breath 20.2% 35.1% 0.5 <0.00001
AGE
& S
OCI
AL
HIS
TORY Age (years) 70.9 +/- 5.7
(median 71.0)71.9 +/- 5.7
(median 72.0) - <0.01
Distance of home from hospital (miles) 11.5 +/- 8.2 (median 12.0)
13.3 +/- 7.7 (median 14.0) - <0.002
PAST
MED
ICAL
H
ISTO
RY
Days of illness before admission 5.4 +/- 15.7 (median1.0)
8.7 +/- 21.3 (median 2.0) - <0.06
Past history of diabetes 13.4% 4.9% 3.0 <.00001
Well prior to current illness 79.9% 72.0% 1.5 <0.02
Past history of heart failure 5.8% 11.6% 0.5 <0.05
RESU
LTS
OF
INVE
STIG
ATIO
NS Diastolic blood pressure over 120mmHg 2.8% 0.5% 5.9 <0.003
Blood glucose more than 12 mmol/L 18.5% 9.0% 2.3 <0.003
White blood cell count over 10,000 28.4% 39.7% 0.6 <0.001
Oxygen saturation less than 93% 14.3% 20.8% 0.6 <0.03
DIAG
NOSI
S ON
DI
SCH
ARGE Myocardial infarction 7.3% 3.6% 2.1 <.05
Heart failure 20.7% 30.2% 0.6 <0.02
Chronic obstructive lung disease 18.4% 27.3% 0.6 <0.02
OU
TCO
MES
Length of hospital stay (days) 5.8 +/- 5.7 (median 4.0)
6.9 +/- 4.8 (median 6.0) - <0.003
Readmission within 30 days 13.8% 6.0% 2.5 <0.00002
Took discharge against medical advice 2.0% 1.2% 1.7 NS
Transfer to nursing home 19.7% 13.1% 1.6 <.02
Home well 59.8% 64.3% 0.8 NS
Death 2.9% 4.3% 0.5 NS

78 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
ORI
GIN
AL
PAPE
R
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 79
REV
IEwDIFFERENCES BETwEEN SELF-REFERRED AND PHYSICIAN-REFERRED HOSPITAL ADMISSIONS
ACkNOwLEDGEMENTS
The authors would like to acknowledge the help of all the medical, nursing and administrative staff of Nenagh Hospital in the collection of the data that made this paper possible. In particular we would like to thank Dr Sean Darby, Consultant Radiologist, for his help. We would also like to thank Dr Kevin Kelleher, Director of Public Health of the Mid-Western Health Board.
REFERENCES1. Office of Population Censuses and Surveys. Living
in Britain: Results from the 1995 General Household Survey. London: Stationery Office, 1997.
2. Giuffrida A, Gravelle H, Roland M. Measuring quality of care: performance indicators should not be confused with health outcomes. BMJ. 1999;319:94-98.
3. Wilkin D. Patterns of referral: explaining variation. In: Roland M., Coulter A., eds. Hospital referrals. Oxford: Oxford University Press, 1992.
4. Knottnerus JA, Joosten J, Daams J. Comparing the quality of referrals of general practitioners with high and average referral rates: an independent panel review. Br. J. General Pract. 1990;40:178-181.
5. Fertig A, Roland M, King H, Moore T. Understanding variation in rates of referral among general practitioners: are inappropriate referrals important and would guidelines help to reduce rates? BMJ. 1993;307:1467-1470.
6. Coulter A, Seagroatt V, McPherson K. Relation between general practices’ outpatient referral rates and rates of elective admission to hospital. BMJ. 1990;301:273-276.
7. Puckett CD. Symptoms, signs, and ill-defined conditions. In: Puckett C.D. ed. The Educational Annotation of ICD-9-CM. 4th Edition. Nevada, Channel Publishing, 1998: 909.
8. Reid FDA, Cook D, Majeed FA. Variation in hospital admission rates between general practices: cross sectional study. BMJ. 1999;319:98-103.
9. Ashton CM, Kuykendall DH, Johnson ML, Wray NP, Wu L. The association between the quality of inpatient care and early readmission. Ann. Intern. Med. 1995;122:415-421.
10. Clarke A. Are readmissions avoidable? BMJ. 1990;301:1136-8.
11. Bindman AB, Grumbach K, Osmond D et al. Preventable hospitalisations and access to healthcare. JAMA. 1995;274:305-311.
Correspondence to: Dr John Kellett, Consultant Physician, Dept of Medicine, Nenagh Hospital, Nenagh, Co. Tipperary.Tel.: 353 67 31491. Fax.: 354 67 33440. E-mail: [email protected]
inTrODUCTiOnPercutaneous techniques are used to perform diagnostic and therapeutic procedures in many vascular territories. The commonest arterial access point for these procedures is the femoral artery. Over the past few years the complexity of the procedures performed has increased and we are more frequently dealing with significant co-morbidities as we treat older and sicker patients. The most frequently occurring complications are these involving the arterial access site which include local haematoma, haemorrhage and pesudoaneurysm formation. Operators are continually searching for better and safer ways to perform these procedures.
Transradial approach represents an alternative vascular access site to perform diagnostic and therapeutic coronary procedures. The local anatomy provides good bony support which allows for rapid hemostasis following removal of the arterial sheath. There is an extremely low rate of vascular access complications reported from centres that
use this technique regularly.1-3 In addition, this approach allows the immediate mobilisation of the patient, increasing patient comfort, reducing the duration of hospitalisation and resultant overall procedural costs.4,5 The establishing of a radial artery intervention service requires knowledge and appreciation of three specific aspects of the procedure performed form the radial artery which differentiate this from trans-femoral procedures: (i) pre-procedural assessment and preparation of the patient, (ii) peri-procedural technical issues and (iii) post procedural care.
1. Patient selection and preparationLeaning curveCompared to the transfemoral approach, transradial procedures are technically more demanding specifically in relation to greater difficulty of cannulating the smaller radial artery, potential anatomical difficulties (tortuosity of the subclavian or brachio-cephalic artery and anatomic variation of the radial artery), the occurrence of radial artery spasm (Figure 1) and technical difficulties in
The radial artery: an alternative access site for diagnostic and interventional coronary proceduresaBsTraCT Background Percutaneous techniques are routinely used in the diagnosis and treatment
of cardiovascular disease. The transfemoral route is the most frequently used arterial access site for performing these procedures
Aim To describe a technique to gain arterial access via the radial artery to perform diagnostic and invasive procedures.
Methods Patient selection is key to establishing a successful transradial service. Results There is a significant vascular complication rate when using the transfemoral
route. Transfemoral access can also be difficult in patients with peripheral vascular disease. Arterial access via the right radial artery represents a realistic alternative to the transfemoral route for performing diagnostic and therapeutic coronary procedures.
Conclusions The radial artery offers a safe and effective alternative access site for performing diagnostic and interventional coronary procedures. The need for alternatives to femoral artery access is critical in patients with severe peripheral vascular disease. The establishment and ongoing provision of radial artery intervention allows for a significant reduction in major vascular complication rates, earlier patient ambulation, increased patient comfort and the potential to establish day case coronary intervention.
NT Mulvihill, PA CreanDept of Cardiology, St. James’s Hospital, Dublin 8
THE RADIAL ARTERY: AN ALTERNATIVE ACCESS SITE FOR DIAGNOSTIC AND INTERVENTIONAL CORONARY PROCEDURES
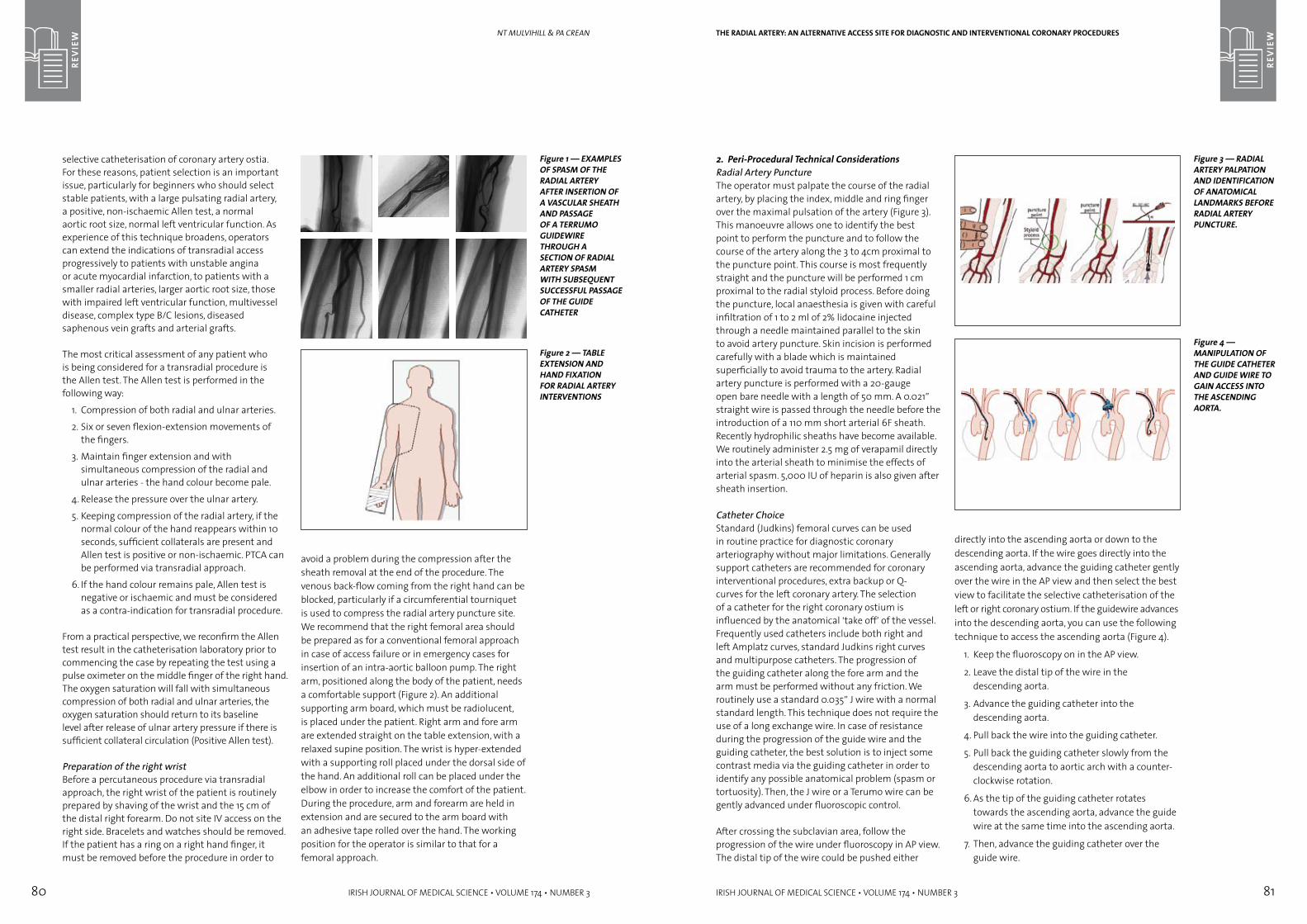
80 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
REV
IEw
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 81
REV
IEwnt MUlvihill & Pa CRean
selective catheterisation of coronary artery ostia. For these reasons, patient selection is an important issue, particularly for beginners who should select stable patients, with a large pulsating radial artery, a positive, non-ischaemic Allen test, a normal aortic root size, normal left ventricular function. As experience of this technique broadens, operators can extend the indications of transradial access progressively to patients with unstable angina or acute myocardial infarction, to patients with a smaller radial arteries, larger aortic root size, those with impaired left ventricular function, multivessel disease, complex type B/C lesions, diseased saphenous vein grafts and arterial grafts.
The most critical assessment of any patient who is being considered for a transradial procedure is the Allen test. The Allen test is performed in the following way:
1. Compression of both radial and ulnar arteries.
2. Six or seven flexion-extension movements of the fingers.
3. Maintain finger extension and with simultaneous compression of the radial and ulnar arteries - the hand colour become pale.
4. Release the pressure over the ulnar artery.
5. Keeping compression of the radial artery, if the normal colour of the hand reappears within 10 seconds, sufficient collaterals are present and Allen test is positive or non-ischaemic. PTCA can be performed via transradial approach.
6. If the hand colour remains pale, Allen test is negative or ischaemic and must be considered as a contra-indication for transradial procedure.
From a practical perspective, we reconfirm the Allen test result in the catheterisation laboratory prior to commencing the case by repeating the test using a pulse oximeter on the middle finger of the right hand. The oxygen saturation will fall with simultaneous compression of both radial and ulnar arteries, the oxygen saturation should return to its baseline level after release of ulnar artery pressure if there is sufficient collateral circulation (Positive Allen test).
Preparation of the right wristBefore a percutaneous procedure via transradial approach, the right wrist of the patient is routinely prepared by shaving of the wrist and the 15 cm of the distal right forearm. Do not site IV access on the right side. Bracelets and watches should be removed. If the patient has a ring on a right hand finger, it must be removed before the procedure in order to
Figure 1 — EXAMPLES OF SPASM OF THE RADIAL ARTERY AFTER INSERTION OF A VASCULAR SHEATH AND PASSAGE OF A TERRUMO GUIDEwIRE THROUGH A SECTION OF RADIAL ARTERY SPASM wITH SUBSEqUENT SUCCESSFUL PASSAGE OF THE GUIDE CATHETER
Figure 2 — TABLE EXTENSION AND HAND FIXATION FOR RADIAL ARTERY INTERVENTIONS
avoid a problem during the compression after the sheath removal at the end of the procedure. The venous back-flow coming from the right hand can be blocked, particularly if a circumferential tourniquet is used to compress the radial artery puncture site. We recommend that the right femoral area should be prepared as for a conventional femoral approach in case of access failure or in emergency cases for insertion of an intra-aortic balloon pump. The right arm, positioned along the body of the patient, needs a comfortable support (Figure 2). An additional supporting arm board, which must be radiolucent, is placed under the patient. Right arm and fore arm are extended straight on the table extension, with a relaxed supine position. The wrist is hyper-extended with a supporting roll placed under the dorsal side of the hand. An additional roll can be placed under the elbow in order to increase the comfort of the patient. During the procedure, arm and forearm are held in extension and are secured to the arm board with an adhesive tape rolled over the hand. The working position for the operator is similar to that for a femoral approach.
2. Peri-Procedural Technical ConsiderationsRadial Artery PunctureThe operator must palpate the course of the radial artery, by placing the index, middle and ring finger over the maximal pulsation of the artery (Figure 3). This manoeuvre allows one to identify the best point to perform the puncture and to follow the course of the artery along the 3 to 4cm proximal to the puncture point. This course is most frequently straight and the puncture will be performed 1 cm proximal to the radial styloid process. Before doing the puncture, local anaesthesia is given with careful infiltration of 1 to 2 ml of 2% lidocaine injected through a needle maintained parallel to the skin to avoid artery puncture. Skin incision is performed carefully with a blade which is maintained superficially to avoid trauma to the artery. Radial artery puncture is performed with a 20-gauge open bare needle with a length of 50 mm. A 0.021” straight wire is passed through the needle before the introduction of a 110 mm short arterial 6F sheath. Recently hydrophilic sheaths have become available. We routinely administer 2.5 mg of verapamil directly into the arterial sheath to minimise the effects of arterial spasm. 5,000 IU of heparin is also given after sheath insertion.
Catheter ChoiceStandard (Judkins) femoral curves can be used in routine practice for diagnostic coronary arteriography without major limitations. Generally support catheters are recommended for coronary interventional procedures, extra backup or Q-curves for the left coronary artery. The selection of a catheter for the right coronary ostium is influenced by the anatomical ‘take off’ of the vessel. Frequently used catheters include both right and left Amplatz curves, standard Judkins right curves and multipurpose catheters. The progression of the guiding catheter along the fore arm and the arm must be performed without any friction. We routinely use a standard 0.035” J wire with a normal standard length. This technique does not require the use of a long exchange wire. In case of resistance during the progression of the guide wire and the guiding catheter, the best solution is to inject some contrast media via the guiding catheter in order to identify any possible anatomical problem (spasm or tortuosity). Then, the J wire or a Terumo wire can be gently advanced under fluoroscopic control.
After crossing the subclavian area, follow the progression of the wire under fluoroscopy in AP view. The distal tip of the wire could be pushed either
THE RADIAL ARTERY: AN ALTERNATIVE ACCESS SITE FOR DIAGNOSTIC AND INTERVENTIONAL CORONARY PROCEDURES
Figure 3 — RADIAL ARTERY PALPATION AND IDENTIFICATION OF ANATOMICAL LANDMARkS BEFORE RADIAL ARTERY PUNCTURE.
Figure 4 — MANIPULATION OF THE GUIDE CATHETER AND GUIDE wIRE TO GAIN ACCESS INTO THE ASCENDING AORTA.
directly into the ascending aorta or down to the descending aorta. If the wire goes directly into the ascending aorta, advance the guiding catheter gently over the wire in the AP view and then select the best view to facilitate the selective catheterisation of the left or right coronary ostium. If the guidewire advances into the descending aorta, you can use the following technique to access the ascending aorta (Figure 4).
1. Keep the fluoroscopy on in the AP view.
2. Leave the distal tip of the wire in the descending aorta.
3. Advance the guiding catheter into the descending aorta.
4. Pull back the wire into the guiding catheter.
5. Pull back the guiding catheter slowly from the descending aorta to aortic arch with a counter-clockwise rotation.
6. As the tip of the guiding catheter rotates towards the ascending aorta, advance the guide wire at the same time into the ascending aorta.
7. Then, advance the guiding catheter over the guide wire.
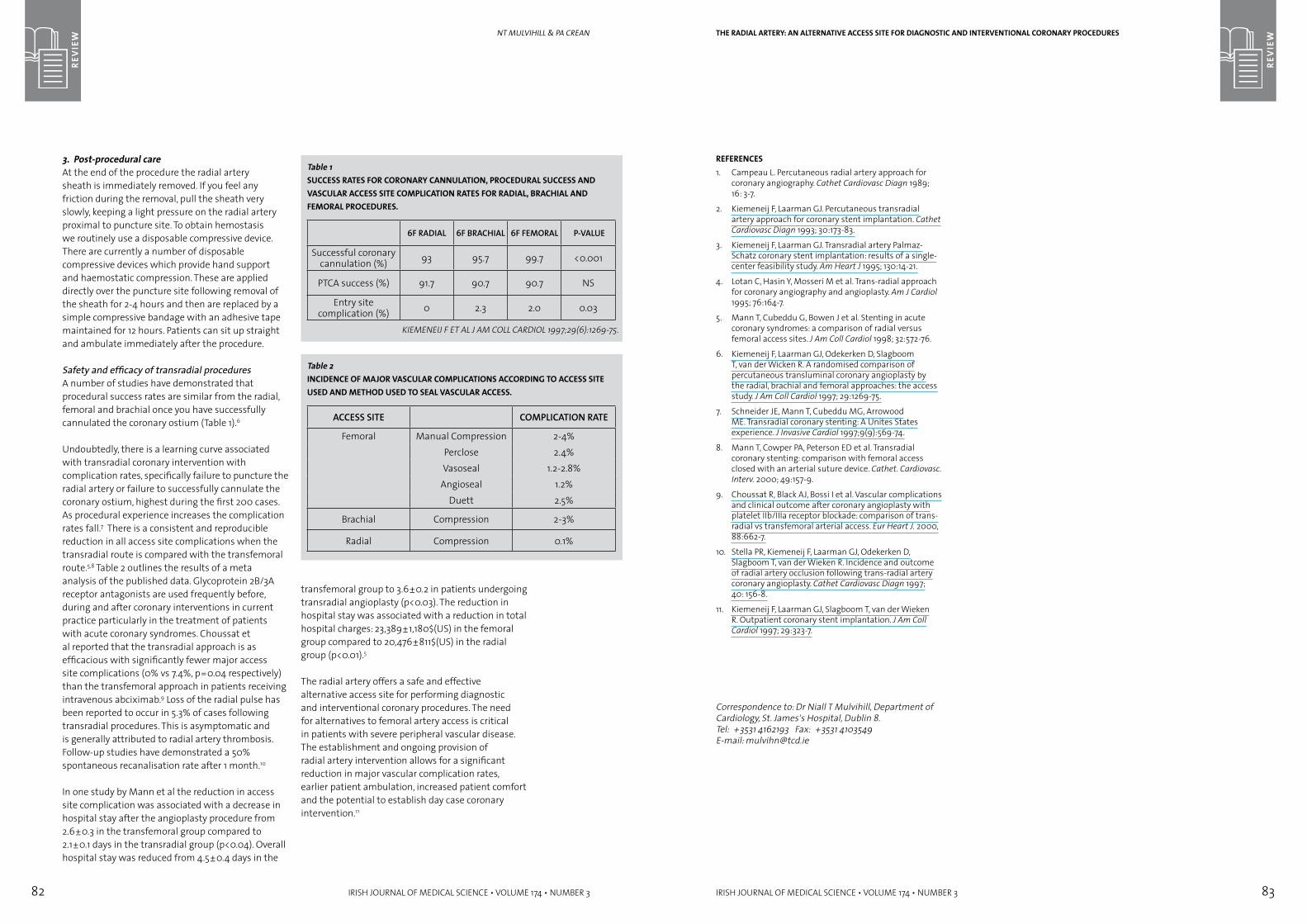
82 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
REV
IEw
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 83
REV
IEw
3. Post-procedural care At the end of the procedure the radial artery sheath is immediately removed. If you feel any friction during the removal, pull the sheath very slowly, keeping a light pressure on the radial artery proximal to puncture site. To obtain hemostasis we routinely use a disposable compressive device. There are currently a number of disposable compressive devices which provide hand support and haemostatic compression. These are applied directly over the puncture site following removal of the sheath for 2-4 hours and then are replaced by a simple compressive bandage with an adhesive tape maintained for 12 hours. Patients can sit up straight and ambulate immediately after the procedure.
Safety and efficacy of transradial proceduresA number of studies have demonstrated that procedural success rates are similar from the radial, femoral and brachial once you have successfully cannulated the coronary ostium (Table 1).6
Undoubtedly, there is a learning curve associated with transradial coronary intervention with complication rates, specifically failure to puncture the radial artery or failure to successfully cannulate the coronary ostium, highest during the first 200 cases. As procedural experience increases the complication rates fall.7 There is a consistent and reproducible reduction in all access site complications when the transradial route is compared with the transfemoral route.5,8 Table 2 outlines the results of a meta analysis of the published data. Glycoprotein 2B/3A receptor antagonists are used frequently before, during and after coronary interventions in current practice particularly in the treatment of patients with acute coronary syndromes. Choussat et al reported that the transradial approach is as efficacious with significantly fewer major access site complications (0% vs 7.4%, p=0.04 respectively) than the transfemoral approach in patients receiving intravenous abciximab.9 Loss of the radial pulse has been reported to occur in 5.3% of cases following transradial procedures. This is asymptomatic and is generally attributed to radial artery thrombosis. Follow-up studies have demonstrated a 50% spontaneous recanalisation rate after 1 month.10
In one study by Mann et al the reduction in access site complication was associated with a decrease in hospital stay after the angioplasty procedure from 2.6±0.3 in the transfemoral group compared to 2.1±0.1 days in the transradial group (p<0.04). Overall hospital stay was reduced from 4.5±0.4 days in the
nt MUlvihill & Pa CRean
Table 1SUCCESS RATES FOR CORONARY CANNULATION, PROCEDURAL SUCCESS AND VASCULAR ACCESS SITE COMPLICATION RATES FOR RADIAL, BRACHIAL AND FEMORAL PROCEDURES.
6F RADIAL 6F BRACHIAL 6F FEMORAL P-VALUE
Successful coronary cannulation (%) 93 95.7 99.7 <0.001
PTCA success (%) 91.7 90.7 90.7 NS
Entry site complication (%) 0 2.3 2.0 0.03
KIEMENEIJ F ET AL J AM COLL CARDIOL 1997;29(6):1269-75.
transfemoral group to 3.6±0.2 in patients undergoing transradial angioplasty (p<0.03). The reduction in hospital stay was associated with a reduction in total hospital charges: 23,389±1,180$(US) in the femoral group compared to 20,476±811$(US) in the radial group (p<0.01).5
The radial artery offers a safe and effective alternative access site for performing diagnostic and interventional coronary procedures. The need for alternatives to femoral artery access is critical in patients with severe peripheral vascular disease. The establishment and ongoing provision of radial artery intervention allows for a significant reduction in major vascular complication rates, earlier patient ambulation, increased patient comfort and the potential to establish day case coronary intervention.11
Table 2INCIDENCE OF MAJOR VASCULAR COMPLICATIONS ACCORDING TO ACCESS SITE USED AND METHOD USED TO SEAL VASCULAR ACCESS.
ACCESS SITE COMPLICATION RATE
Femoral Manual Compression 2-4%Perclose 2.4%Vasoseal 1.2-2.8%
Angioseal 1.2%Duett 2.5%
Brachial Compression 2-3%
Radial Compression 0.1%
REFERENCES 1. Campeau L. Percutaneous radial artery approach for
coronary angiography. Cathet Cardiovasc Diagn 1989; 16: 3-7.
2. Kiemeneij F, Laarman GJ. Percutaneous transradial artery approach for coronary stent implantation. Cathet Cardiovasc Diagn 1993; 30:173-83.
3. Kiemeneij F, Laarman GJ. Transradial artery Palmaz-Schatz coronary stent implantation: results of a single-center feasibility study. Am Heart J 1995; 130:14-21.
4. Lotan C, Hasin Y, Mosseri M et al. Trans-radial approach for coronary angiography and angioplasty. Am J Cardiol 1995; 76:164-7.
5. Mann T, Cubeddu G, Bowen J et al. Stenting in acute coronary syndromes: a comparison of radial versus femoral access sites. J Am Coll Cardiol 1998; 32:572-76.
6. Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wicken R. A randomised comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches: the access study. J Am Coll Cardiol 1997; 29:1269-75.
7. Schneider JE, Mann T, Cubeddu MG, Arrowood ME. Transradial coronary stenting: A Unites States experience. J Invasive Cardiol 1997;9(9):569-74.
8. Mann T, Cowper PA, Peterson ED et al. Transradial coronary stenting: comparison with femoral access closed with an arterial suture device. Cathet. Cardiovasc.Interv. 2000; 49:157-9.
9. Choussat R, Black AJ, Bossi I et al. Vascular complications and clinical outcome after coronary angioplasty with platelet IIb/IIIa receptor blockade: comparison of trans-radial vs transfemoral arterial access. Eur Heart J. 2000, 88:662-7.
10. Stella PR, Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wieken R. Incidence and outcome of radial artery occlusion following trans-radial artery coronary angioplasty. Cathet Cardiovasc Diagn 1997; 40: 156-8.
11. Kiemeneij F, Laarman GJ, Slagboom T, van der Wieken R. Outpatient coronary stent implantation. J Am Coll Cardiol 1997; 29:323-7.
Correspondence to: Dr Niall T Mulvihill, Department of Cardiology, St. James’s Hospital, Dublin 8.Tel: +3531 4162193 Fax: +3531 4103549E-mail: [email protected]
THE RADIAL ARTERY: AN ALTERNATIVE ACCESS SITE FOR DIAGNOSTIC AND INTERVENTIONAL CORONARY PROCEDURES
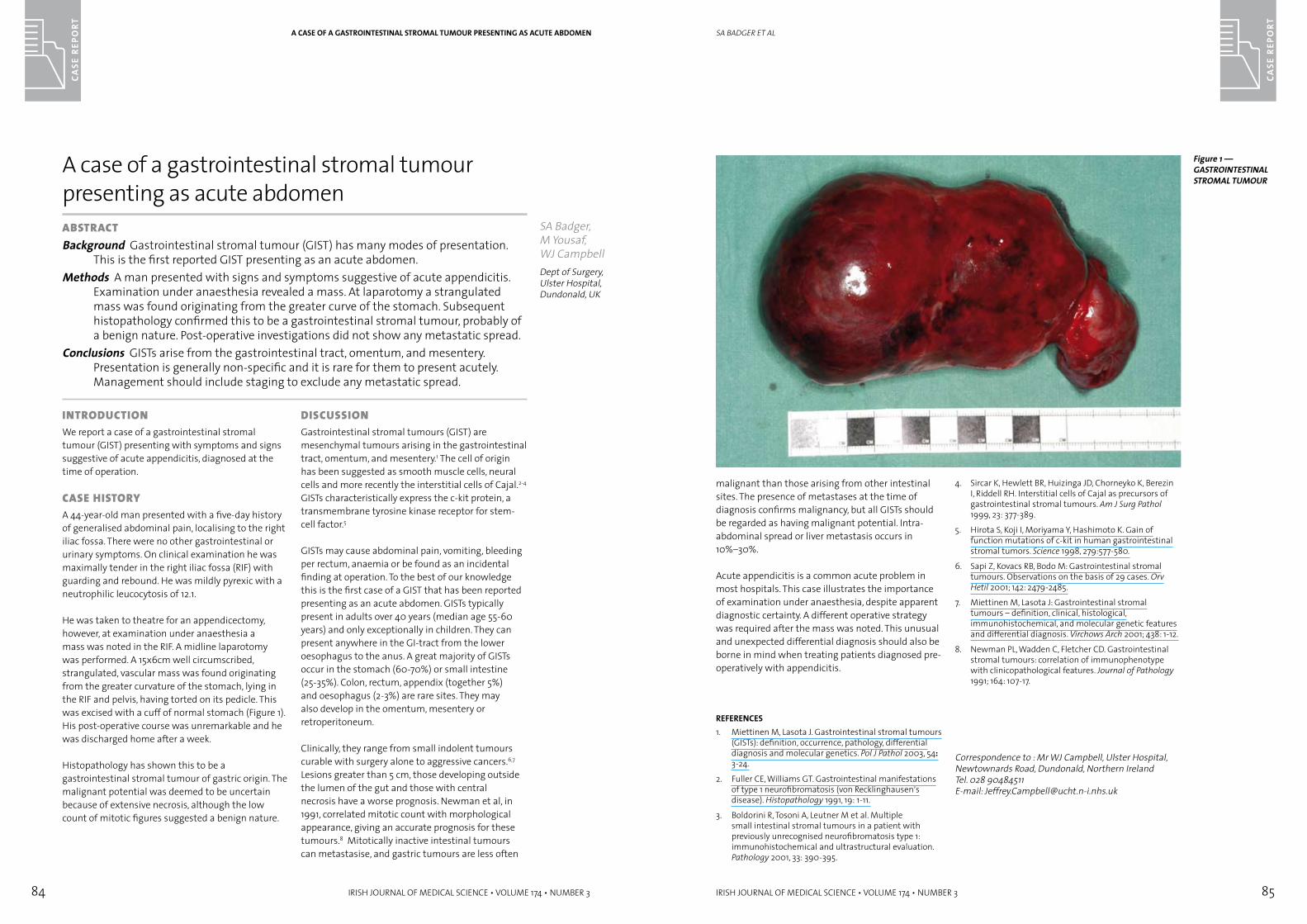
84 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CASE
REP
ORT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 85
CASE
REP
ORT
malignant than those arising from other intestinal sites. The presence of metastases at the time of diagnosis confirms malignancy, but all GISTs should be regarded as having malignant potential. Intra-abdominal spread or liver metastasis occurs in 10%–30%.
Acute appendicitis is a common acute problem in most hospitals. This case illustrates the importance of examination under anaesthesia, despite apparent diagnostic certainty. A different operative strategy was required after the mass was noted. This unusual and unexpected differential diagnosis should also be borne in mind when treating patients diagnosed pre-operatively with appendicitis.
REFERENCES1. Miettinen M, Lasota J. Gastrointestinal stromal tumours
(GISTs): definition, occurrence, pathology, differential diagnosis and molecular genetics. Pol J Pathol 2003, 54: 3-24.
2. Fuller CE, Williams GT. Gastrointestinal manifestations of type 1 neurofibromatosis (von Recklinghausen’s disease). Histopathology 1991, 19: 1-11.
3. Boldorini R, Tosoni A, Leutner M et al. Multiple small intestinal stromal tumours in a patient with previously unrecognised neurofibromatosis type 1: immunohistochemical and ultrastructural evaluation. Pathology 2001, 33: 390-395.
4. Sircar K, Hewlett BR, Huizinga JD, Chorneyko K, Berezin I, Riddell RH. Interstitial cells of Cajal as precursors of gastrointestinal stromal tumours. Am J Surg Pathol 1999, 23: 377-389.
5. Hirota S, Koji I, Moriyama Y, Hashimoto K. Gain of function mutations of c-kit in human gastrointestinal stromal tumors. Science 1998, 279:577-580.
6. Sapi Z, Kovacs RB, Bodo M: Gastrointestinal stromal tumours. Observations on the basis of 29 cases. Orv Hetil 2001; 142: 2479-2485.
7. Miettinen M, Lasota J: Gastrointestinal stromal tumours – definition, clinical, histological, immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch 2001; 438: 1-12.
8. Newman PL, Wadden C, Fletcher CD. Gastrointestinal stromal tumours: correlation of immunophenotype with clinicopathological features. Journal of Pathology 1991; 164: 107-17.
Correspondence to : Mr WJ Campbell, Ulster Hospital, Newtownards Road, Dundonald, Northern IrelandTel. 028 90484511E-mail: [email protected]
SA BADGER ET AL
inTrODUCTiOnWe report a case of a gastrointestinal stromal tumour (GIST) presenting with symptoms and signs suggestive of acute appendicitis, diagnosed at the time of operation.
Case HisTOrYA 44-year-old man presented with a five-day history of generalised abdominal pain, localising to the right iliac fossa. There were no other gastrointestinal or urinary symptoms. On clinical examination he was maximally tender in the right iliac fossa (RIF) with guarding and rebound. He was mildly pyrexic with a neutrophilic leucocytosis of 12.1.
He was taken to theatre for an appendicectomy, however, at examination under anaesthesia a mass was noted in the RIF. A midline laparotomy was performed. A 15x6cm well circumscribed, strangulated, vascular mass was found originating from the greater curvature of the stomach, lying in the RIF and pelvis, having torted on its pedicle. This was excised with a cuff of normal stomach (Figure 1). His post-operative course was unremarkable and he was discharged home after a week.
Histopathology has shown this to be a gastrointestinal stromal tumour of gastric origin. The malignant potential was deemed to be uncertain because of extensive necrosis, although the low count of mitotic figures suggested a benign nature.
DisCUssiOnGastrointestinal stromal tumours (GIST) are mesenchymal tumours arising in the gastrointestinal tract, omentum, and mesentery.1 The cell of origin has been suggested as smooth muscle cells, neural cells and more recently the interstitial cells of Cajal.2-4 GISTs characteristically express the c-kit protein, a transmembrane tyrosine kinase receptor for stem-cell factor.5
GISTs may cause abdominal pain, vomiting, bleeding per rectum, anaemia or be found as an incidental finding at operation. To the best of our knowledge this is the first case of a GIST that has been reported presenting as an acute abdomen. GISTs typically present in adults over 40 years (median age 55-60 years) and only exceptionally in children. They can present anywhere in the GI-tract from the lower oesophagus to the anus. A great majority of GISTs occur in the stomach (60-70%) or small intestine (25-35%). Colon, rectum, appendix (together 5%) and oesophagus (2-3%) are rare sites. They may also develop in the omentum, mesentery or retroperitoneum.
Clinically, they range from small indolent tumours curable with surgery alone to aggressive cancers.6,7 Lesions greater than 5 cm, those developing outside the lumen of the gut and those with central necrosis have a worse prognosis. Newman et al, in 1991, correlated mitotic count with morphological appearance, giving an accurate prognosis for these tumours.8 Mitotically inactive intestinal tumours can metastasise, and gastric tumours are less often
A case of a gastrointestinal stromal tumour presenting as acute abdomenaBsTraCTBackground Gastrointestinal stromal tumour (GIST) has many modes of presentation.
This is the first reported GIST presenting as an acute abdomen.Methods A man presented with signs and symptoms suggestive of acute appendicitis.
Examination under anaesthesia revealed a mass. At laparotomy a strangulated mass was found originating from the greater curve of the stomach. Subsequent histopathology confirmed this to be a gastrointestinal stromal tumour, probably of a benign nature. Post-operative investigations did not show any metastatic spread.
Conclusions GISTs arise from the gastrointestinal tract, omentum, and mesentery. Presentation is generally non-specific and it is rare for them to present acutely. Management should include staging to exclude any metastatic spread.
SA Badger, M Yousaf, WJ CampbellDept of Surgery, Ulster Hospital, Dundonald, UK
A CASE OF A GASTROINTESTINAL STROMAL TUMOUR PRESENTING AS ACUTE ABDOMEN
Figure 1 —GASTROINTESTINAL STROMAL TUMOUR

86 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CASE
REP
ORT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 87
CASE
REP
ORT
The abruptness of onset, brevity of attack, and reversal of symptoms has led to the proposition of an epileptic origin. However, EEG recordings during episodes of TGA are usually normal.2 Also the lack of impairment of cortical functions other than memory and the lack of stereotypical movements are against this as is the low rate of recurrence of TGA.3
Neuroimaging studies have shown that blood flow to specific brain areas that involve memory appears to be disrupted transiently during TGA. This includes the thalamus and/or mesial temporal structures.4,5 A recent study using serial MRI examination for three days showed focal hyperintense lesions of small size in the lateral aspect of the hippocampus on diffusion weighted imaging after 48 hours suggesting delayed ischaemia.6 Lesions were only noted in two patients in the hyperacute phase.
Thromboembolic disease does not appear to play a role in TGA. Studies have demonstrated that patients with TGA have fewer cerebrovascular risk factors than those with known cerebrovascular or coronary artery disease. Also, the prognosis for TGA is often better than for TIAs.3 Also platelet activation has been shown in blood samples from patients with TIA but not in patients with TGA.7
Migraine is significantly more common in those who suffer TGA.8 It has been proposed that a spreading depression of cerebral activity due to a migrainous disturbance of brain function is triggered by intense sensory or emotional experiences causing the release of glutamate in the hippocampus triggering both the spreading depression and transient hippocampal dysfunction.9 However, patients with TGA seldom report an associated headache, nausea, photophobia, or phonophobia and the recurrence of TGA attacks is low.10
TGA after sexual intercourse has been previously reported in the literature11 and TGA has also been reported during other intense emotional or painful experiences such as renal colic,12 trigeminal ganglion stimulation and contact with cold water.13 Triggers for TGA such as those above can increase sympathetic activity and/or intrathoracic pressure. The sympathetic activation and Valsalva manoeuvres during sexual intercourse and other highly emotional states may lead to retrograde transmission of high venous pressure to the cerebral venous system, resulting in venous ischaemia14 and has been proposed as a mechanism for TGA.
COnClUsiOnTransient Global Amnesia is a clinical diagnosis which has a benign prognosis. Its sudden onset and interference with memory while maintaining clear consciousness is very frightening for both the patient and relatives. The aetiology of TGA is still a matter of debate. An inciting event can often be identified and a targeted history should be used to help elicit such events.
REFERENCES
1. Fisher CM, Adams RD. Transient Global Amnesia. Trans Am Neurol Assoc 1958;83:143-146
2. Jacome DE. EEG features in transient global amnesia. Clin Electroencephalogr 1989;20:183-92
3. Zorzon M, Antonutti L, Mase G, Biasutti E, Vitrani B, Cazzoto G. Transient Global Amnesia and Transient Ischemic Attack. Stroke 1995;26:1536-1542
4. Takeuchi R, Matsuda H, Yoshioka K, Yonejura Y. Cerebral blood flow SPET in transient global amnesia with automated ROI analysis by 3DSRT Eur J Nucl Med Mol Imaging 2004;31(4):578-89
5. Tabunenca-Dopico O, Gutierrez-Mendigucia C, Lorenzo-Gonzalez JR, Cimas-Hernando I. Does brain blood flow HMPAO SPECT withhold the vascular etiopathogenic theory of transient global amnesia. Rev Neurol 2004;39(8):719-23
6. Sedlaczek O, Hirsch JG, Grips E et al. Detection of delayed focal MRI changes in he lateral hippocampus in transient global amnesia. Neurology 2004;62:2165-70
7. Hirabayashi H, Shimizu M, Kohara S, Shinohara Y. Activated platelets in transient global amnesia and TIA. Neurology 2004;63(4):736-8
8. Hodges JR, Warlow CP. The aetiology of transient global amnesia. A case-control study of 114 cases with prospective follow-up. Brain 1990;113(3):639-57
9. Olesen J, Jorgensen MB. Leao’s spreading depression in the hippocampus explains transient global amnesia: a hypothesis. Acta Neurol Scan 1986;73:219-20
10. Zorzon M, Antonutti L, Mase G, Biasutti E, Vitrani B, Cazzoto G. Transient Global Amnesia and Transient Ischemic Attack. Stroke 1995;26:1536-1542
11. Dang CV, Gardner LB. Transient Global Amnesia after sex. Lancet1998;352:1557-8
12. Kettaneh A, Gobron C, Fain O, Mohib S, Thomas M. Calculi and memory Eur J Neurol 2001;8(2):195-6
13. Fisher CM. Transient Global Amnesia. Precipitating activities and other observations. Arch Neurol 1982;39(10):605-8
14. Lewis SL Aetiology of transient global amnesia. Lancet 1998;352:397-99
Correspondence to: J Gallagher, St Lukes Hospital, Kilkenny. E-mail: [email protected]
J GALLAGHER ET AL
Case rePOrTA 58-year-old lady, on holiday in Ireland, presented to the Emergency Department with a two-hour history of memory loss for recent events. On questioning the patient exhibited marked anterograde amnesia, being unable to retain information for more than a few minutes.
She was slightly disinhibited and her Folstein mini mental state examination scored 24/30 with six marks lost in orientation. She also had variable retrograde amnesia not being able to remember where she was or the date of her wedding anniversary, but being able to identify family members and other personal details. She was quite distressed by this and repeatedly reminded medical staff that she had a penicillin allergy and asked questions regarding her diagnosis, believing she had had a stroke. She was unable to recall the day or date and was unable to remember the name of the town, hotel or previous town they had stayed in.
An infraclavicular malignant melanoma and a dermofibrosarcoma of the leg had been excised surgically 18 months ago and 12 years previously, respectively. Neither had required further treatment. She also had a history of pernicious anaemia and multiple allergies to antibiotics. She had no vascular risk factors and no focal neurological deficit was noted. Her white cell count was elevated at 13.2 x 109/L with a neutrophilia. She was commenced on acyclovir empirically pending the result of CSF analysis. This was discontinued following a full septic screen including lumbar puncture which revealed no infection. Her husband volunteered that the amnesia had occurred immediately following
sexual intercourse. All other laboratory investigations including toxicology screen were normal. MRI brain with MR angiogram and venogram were also normal.
Over the next 14 hours the patient’s ability to retain information and remember previous events improved until returning to normal. The following day the patient complained of a frontal headache but had no recollection of the events of the previous evening. She was discharged three days after the event having fully recovered although still having no recollection of the events occurring during the night of the episode. She was referred for follow-up by a neurologist and for EEG studies.
DisCUssiOnTransient global amnesia (TGA) has been a well-described phenomenon for more than 40 years.1 It presents as sudden memory loss lasting up to 24 hours and is characterised by an inability to retain new information and to recall previous events for a variable period of time. Immediate recall ability is preserved, as is remote memory. Since patients are aware of their memory impairment many patients are anxious and may repeatedly ask questions. Personal identity and consciousness are well preserved, as is the ability to perform tasks requiring even complex visual and spatial skills. As the syndrome resolves, the retrograde amnesia improves, but the patient may suffer permanent amnesia for events during the attack.
A variety of hypotheses have been reported for the pathogenesis of TGA. Transient cerebral ischaemia, epileptic discharge, migraine and transient venous hypertension have all been put forward as possible factors in the pathogenesis of TGA.
Transient global amnesia after sexual intercourseaBsTraCTBackground Transient global amnesia presents as paroxysmal, transient loss of memory
function and has been shown to have a number of inciting factors.Aims To report a case and its inciting factor in order to heighten awareness of the
condition.Methods A 56-year-old woman who presented with TGA after sexual intercourse is
reported.Results The episode of TGA resolved after 14 hours. Results of laboratory tests including
MRI brain and MR angiogram and venogram were normal.Conclusion An inciting event can often be identified for TGA and a targeted history
should be used to help elicit such events.
J Gallagher, MS Murphy, J CarrollDept of Geriatric Medicine, St. Luke’s Hospital, Kilkenny
TRANSIENT GLOBAL AMNESIA AFTER SEXUAL INTERCOURSE
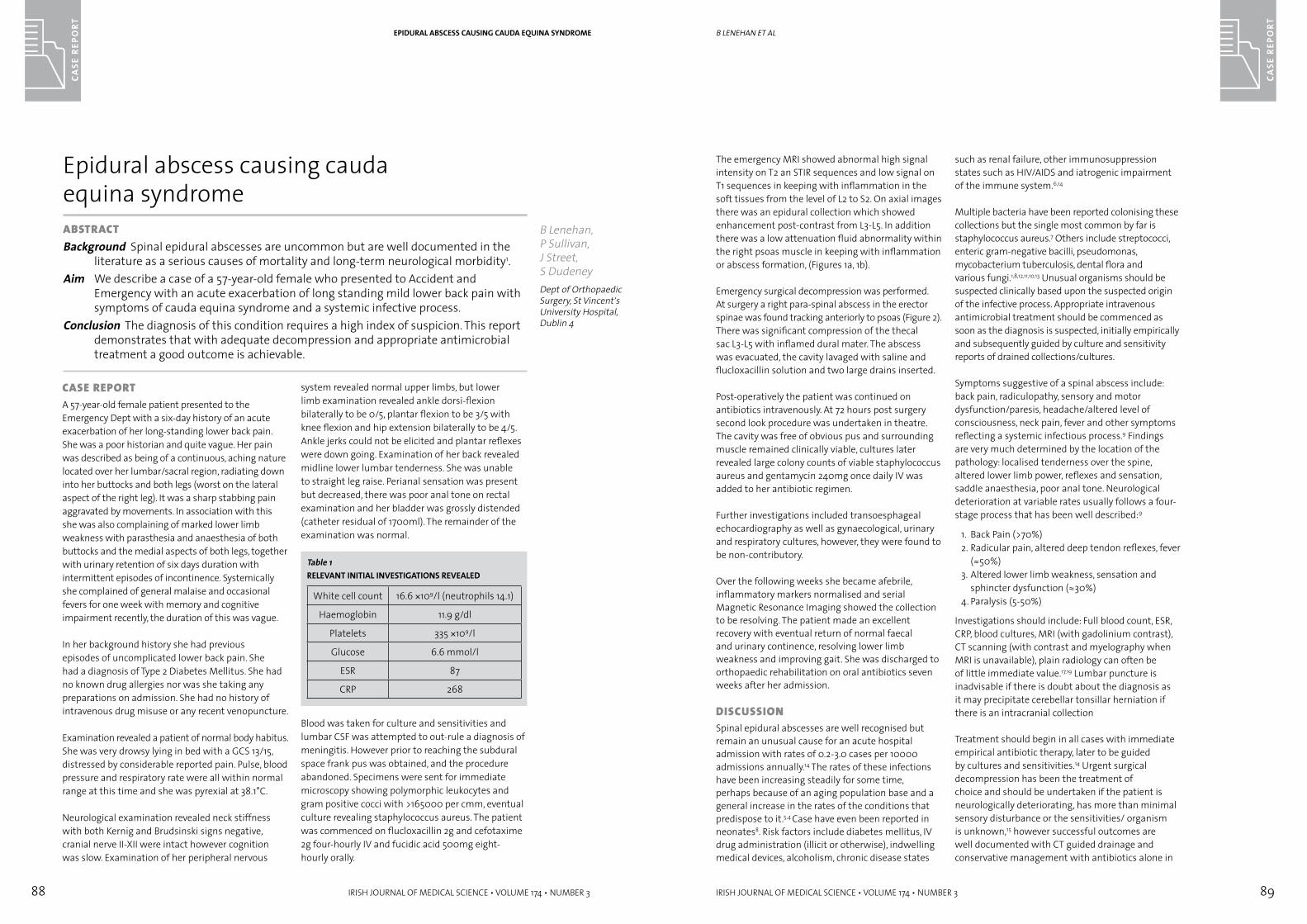
88 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CASE
REP
ORT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 89
CASE
REP
ORT
The emergency MRI showed abnormal high signal intensity on T2 an STIR sequences and low signal on T1 sequences in keeping with inflammation in the soft tissues from the level of L2 to S2. On axial images there was an epidural collection which showed enhancement post-contrast from L3-L5. In addition there was a low attenuation fluid abnormality within the right psoas muscle in keeping with inflammation or abscess formation, (Figures 1a, 1b).
Emergency surgical decompression was performed. At surgery a right para-spinal abscess in the erector spinae was found tracking anteriorly to psoas (Figure 2). There was significant compression of the thecal sac L3-L5 with inflamed dural mater. The abscess was evacuated, the cavity lavaged with saline and flucloxacillin solution and two large drains inserted.
Post-operatively the patient was continued on antibiotics intravenously. At 72 hours post surgery second look procedure was undertaken in theatre. The cavity was free of obvious pus and surrounding muscle remained clinically viable, cultures later revealed large colony counts of viable staphylococcus aureus and gentamycin 240mg once daily IV was added to her antibiotic regimen.
Further investigations included transoesphageal echocardiography as well as gynaecological, urinary and respiratory cultures, however, they were found to be non-contributory.
Over the following weeks she became afebrile, inflammatory markers normalised and serial Magnetic Resonance Imaging showed the collection to be resolving. The patient made an excellent recovery with eventual return of normal faecal and urinary continence, resolving lower limb weakness and improving gait. She was discharged to orthopaedic rehabilitation on oral antibiotics seven weeks after her admission.
DisCUssiOnSpinal epidural abscesses are well recognised but remain an unusual cause for an acute hospital admission with rates of 0.2-3.0 cases per 10000 admissions annually.14 The rates of these infections have been increasing steadily for some time, perhaps because of an aging population base and a general increase in the rates of the conditions that predispose to it.5,4 Case have even been reported in neonates8. Risk factors include diabetes mellitus, IV drug administration (illicit or otherwise), indwelling medical devices, alcoholism, chronic disease states
such as renal failure, other immunosuppression states such as HIV/AIDS and iatrogenic impairment of the immune system.6,14
Multiple bacteria have been reported colonising these collections but the single most common by far is staphylococcus aureus.7 Others include streptococci, enteric gram-negative bacilli, pseudomonas, mycobacterium tuberculosis, dental flora and various fungi.1,8,12,11,10,13 Unusual organisms should be suspected clinically based upon the suspected origin of the infective process. Appropriate intravenous antimicrobial treatment should be commenced as soon as the diagnosis is suspected, initially empirically and subsequently guided by culture and sensitivity reports of drained collections/cultures.
Symptoms suggestive of a spinal abscess include: back pain, radiculopathy, sensory and motor dysfunction/paresis, headache/altered level of consciousness, neck pain, fever and other symptoms reflecting a systemic infectious process.9 Findings are very much determined by the location of the pathology: localised tenderness over the spine, altered lower limb power, reflexes and sensation, saddle anaesthesia, poor anal tone. Neurological deterioration at variable rates usually follows a four-stage process that has been well described:9
1. Back Pain (>70%)2. Radicular pain, altered deep tendon reflexes, fever
(≈50%)3. Altered lower limb weakness, sensation and
sphincter dysfunction (≈30%)4. Paralysis (5-50%)
Investigations should include: Full blood count, ESR, CRP, blood cultures, MRI (with gadolinium contrast), CT scanning (with contrast and myelography when MRI is unavailable), plain radiology can often be of little immediate value.17,19 Lumbar puncture is inadvisable if there is doubt about the diagnosis as it may precipitate cerebellar tonsillar herniation if there is an intracranial collection
Treatment should begin in all cases with immediate empirical antibiotic therapy, later to be guided by cultures and sensitivities.14 Urgent surgical decompression has been the treatment of choice and should be undertaken if the patient is neurologically deteriorating, has more than minimal sensory disturbance or the sensitivities/ organism is unknown,15 however successful outcomes are well documented with CT guided drainage and conservative management with antibiotics alone in
B lenehan et al
Case rePOrTA 57-year-old female patient presented to the Emergency Dept with a six-day history of an acute exacerbation of her long-standing lower back pain. She was a poor historian and quite vague. Her pain was described as being of a continuous, aching nature located over her lumbar/sacral region, radiating down into her buttocks and both legs (worst on the lateral aspect of the right leg). It was a sharp stabbing pain aggravated by movements. In association with this she was also complaining of marked lower limb weakness with parasthesia and anaesthesia of both buttocks and the medial aspects of both legs, together with urinary retention of six days duration with intermittent episodes of incontinence. Systemically she complained of general malaise and occasional fevers for one week with memory and cognitive impairment recently, the duration of this was vague.
In her background history she had previous episodes of uncomplicated lower back pain. She had a diagnosis of Type 2 Diabetes Mellitus. She had no known drug allergies nor was she taking any preparations on admission. She had no history of intravenous drug misuse or any recent venopuncture.
Examination revealed a patient of normal body habitus. She was very drowsy lying in bed with a GCS 13/15, distressed by considerable reported pain. Pulse, blood pressure and respiratory rate were all within normal range at this time and she was pyrexial at 38.1°C.
Neurological examination revealed neck stiffness with both Kernig and Brudsinski signs negative, cranial nerve II-XII were intact however cognition was slow. Examination of her peripheral nervous
system revealed normal upper limbs, but lower limb examination revealed ankle dorsi-flexion bilaterally to be 0/5, plantar flexion to be 3/5 with knee flexion and hip extension bilaterally to be 4/5. Ankle jerks could not be elicited and plantar reflexes were down going. Examination of her back revealed midline lower lumbar tenderness. She was unable to straight leg raise. Perianal sensation was present but decreased, there was poor anal tone on rectal examination and her bladder was grossly distended (catheter residual of 1700ml). The remainder of the examination was normal.
Blood was taken for culture and sensitivities and lumbar CSF was attempted to out-rule a diagnosis of meningitis. However prior to reaching the subdural space frank pus was obtained, and the procedure abandoned. Specimens were sent for immediate microscopy showing polymorphic leukocytes and gram positive cocci with >165000 per cmm, eventual culture revealing staphylococcus aureus. The patient was commenced on flucloxacillin 2g and cefotaxime 2g four-hourly IV and fucidic acid 500mg eight-hourly orally.
Epidural abscess causing cauda equina syndromeaBsTraCTBackground Spinal epidural abscesses are uncommon but are well documented in the
literature as a serious causes of mortality and long-term neurological morbidity1.Aim We describe a case of a 57-year-old female who presented to Accident and
Emergency with an acute exacerbation of long standing mild lower back pain with symptoms of cauda equina syndrome and a systemic infective process.
Conclusion The diagnosis of this condition requires a high index of suspicion. This report demonstrates that with adequate decompression and appropriate antimicrobial treatment a good outcome is achievable.
B Lenehan, P Sullivan, J Street, S DudeneyDept of Orthopaedic Surgery, St Vincent’s University Hospital, Dublin 4
EPIDURAL ABSCESS CAUSING CAUDA EqUINA SYNDROME
Table 1RELEVANT INITIAL INVESTIGATIONS REVEALED
White cell count 16.6 ×109/l (neutrophils 14.1)
Haemoglobin 11.9 g/dl
Platelets 335 ×109/l
Glucose 6.6 mmol/l
ESR 87
CRP 268
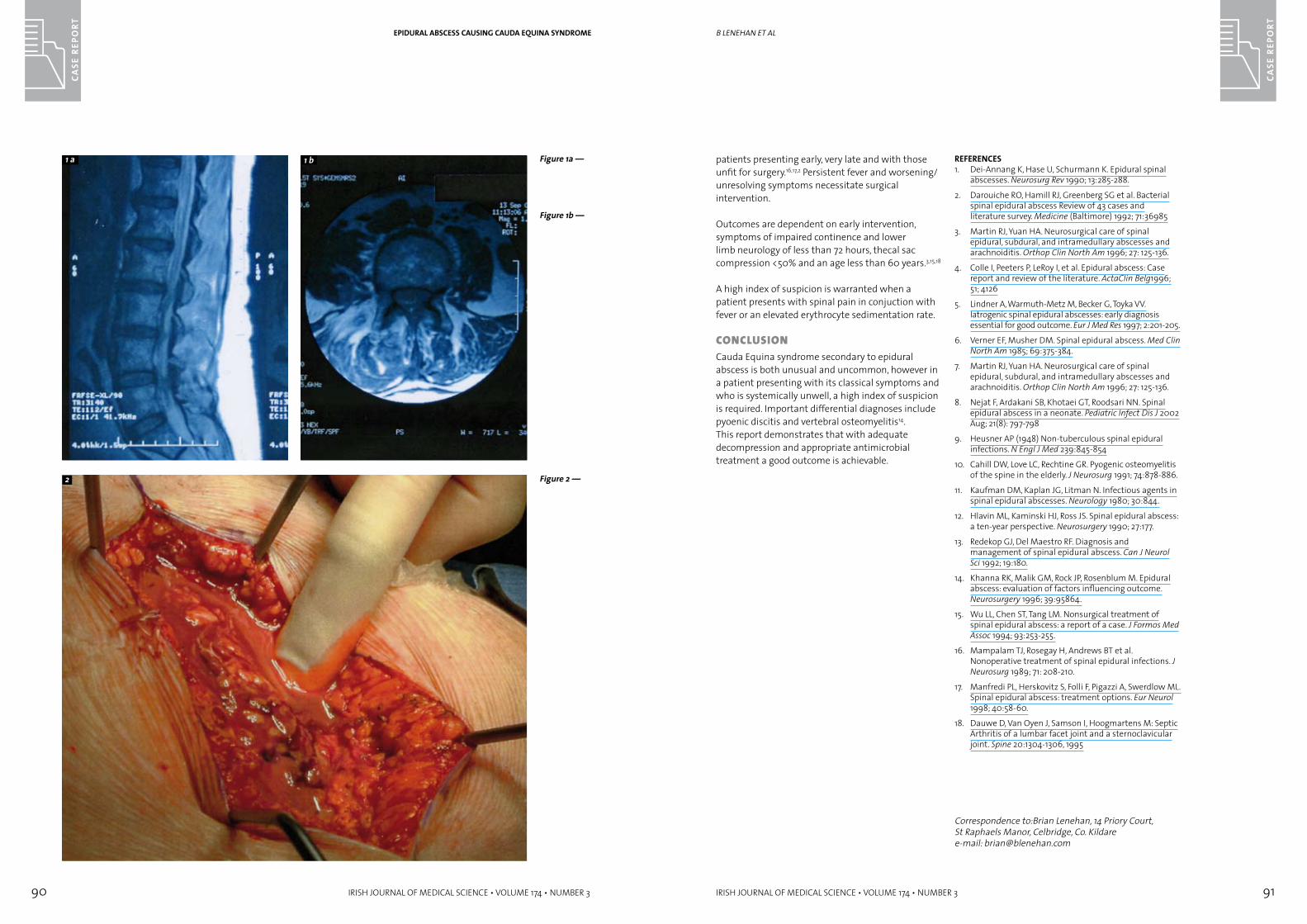
90 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CASE
REP
ORT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 91
CASE
REP
ORT
patients presenting early, very late and with those unfit for surgery.16,17,2 Persistent fever and worsening/unresolving symptoms necessitate surgical intervention.
Outcomes are dependent on early intervention, symptoms of impaired continence and lower limb neurology of less than 72 hours, thecal sac compression <50% and an age less than 60 years.3,15,18
A high index of suspicion is warranted when a patient presents with spinal pain in conjuction with fever or an elevated erythrocyte sedimentation rate.
COnClUsiOnCauda Equina syndrome secondary to epidural abscess is both unusual and uncommon, however in a patient presenting with its classical symptoms and who is systemically unwell, a high index of suspicion is required. Important differential diagnoses include pyoenic discitis and vertebral osteomyelitis14. This report demonstrates that with adequate decompression and appropriate antimicrobial treatment a good outcome is achievable.
REFERENCES1. Dei-Annang K, Hase U, Schurmann K. Epidural spinal
abscesses. Neurosurg Rev 1990; 13:285-288.
2. Darouiche RO, Hamill RJ, Greenberg SG et al. Bacterial spinal epidural abscess Review of 43 cases and literature survey. Medicine (Baltimore) 1992; 71:36985
3. Martin RJ, Yuan HA. Neurosurgical care of spinal epidural, subdural, and intramedullary abscesses and arachnoiditis. Orthop Clin North Am 1996; 27: 125-136.
4. Colle I, Peeters P, LeRoy I, et al. Epidural abscess: Case report and review of the literature. ActaClin Belg1996; 51; 4126
5. Lindner A, Warmuth-Metz M, Becker G, Toyka VV. Iatrogenic spinal epidural abscesses: early diagnosis essential for good outcome. Eur J Med Res 1997; 2:201-205.
6. Verner EF, Musher DM. Spinal epidural abscess. Med Clin North Am 1985; 69:375-384.
7. Martin RJ, Yuan HA. Neurosurgical care of spinal epidural, subdural, and intramedullary abscesses and arachnoiditis. Orthop Clin North Am 1996; 27: 125-136.
8. Nejat F, Ardakani SB, Khotaei GT, Roodsari NN. Spinal epidural abscess in a neonate. Pediatric Infect Dis J 2002 Aug; 21(8): 797-798
9. Heusner AP (1948) Non-tuberculous spinal epidural infections. N Engl J Med 239:845-854
10. Cahill DW, Love LC, Rechtine GR. Pyogenic osteomyelitis of the spine in the elderly. J Neurosurg 1991; 74:878-886.
11. Kaufman DM, Kaplan JG, Litman N. Infectious agents in spinal epidural abscesses. Neurology 1980; 30:844.
12. Hlavin ML, Kaminski HJ, Ross JS. Spinal epidural abscess: a ten-year perspective. Neurosurgery 1990; 27:177.
13. Redekop GJ, Del Maestro RF. Diagnosis and management of spinal epidural abscess. Can J Neurol Sci 1992; 19:180.
14. Khanna RK, Malik GM, Rock JP, Rosenblum M. Epidural abscess: evaluation of factors influencing outcome. Neurosurgery 1996; 39:95864.
15. Wu LL, Chen ST, Tang LM. Nonsurgical treatment of spinal epidural abscess: a report of a case. J Formos Med Assoc 1994; 93:253-255.
16. Mampalam TJ, Rosegay H, Andrews BT et al. Nonoperative treatment of spinal epidural infections. J Neurosurg 1989; 71: 208-210.
17. Manfredi PL, Herskovitz S, Folli F, Pigazzi A, Swerdlow ML. Spinal epidural abscess: treatment options. Eur Neurol 1998; 40:58-60.
18. Dauwe D, Van Oyen J, Samson I, Hoogmartens M: Septic Arthritis of a lumbar facet joint and a sternoclavicular joint. Spine 20:1304-1306, 1995
Correspondence to:Brian Lenehan, 14 Priory Court, St Raphaels Manor, Celbridge, Co. Kildaree-mail: [email protected]
B lenehan et alEPIDURAL ABSCESS CAUSING CAUDA EqUINA SYNDROME
Figure 1a —
Figure 2 —
1 a 1 b
2
Figure 1b —

92 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CASE
REP
ORT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 93
CASE
REP
ORT
considered to have acute hepatitis-B infection and supportive therapy was initiated.
On the second day of hospitalisation his temperature rose to 38.8ºC and pulse rate was recorded as 100/min. On the fourth day erythematous, papular, flat-topped, exanthematous lesions were noted symmetrically on the upper and lower extremities (Figures 1-2). These cutaneous lesions were also seen over the buttocks. The trunk was mostly spared. Because of the marked pruritus, cholestiramine at 16 g/day in divided doses and anti-pruritic lotion (oxy de zinc-diphenhydramine HCL-lidocaine HCL) were started.
Body temperature returned to normal level on the fourth day of hospitalisation. In this period, serologic markers for Cytomegalovirus, Ebstein-Barr virus, Herpes simplex virus (type 1-2), Human Immune Deficiency virus (HIV), Rubella virus and Brucella were negative. A skin biopsy was obtained and only intense perivascular infiltration caused by lymphocytes and histiocytes were seen. The biochemical tests were reanalysed: (WBC: 9400/mm3, hemoglobin: 16.5 g/dl, AST: 720 IU/L, ALT: 1780 IU/L, GGT: 154 IU/L, ALP: 365 IU/L, glucose: 82 mg/dl, creatinine: 0.82 mg/dl).
On the second week of hospitalisation, the patient felt better and the vital signs returned to normal levels.
During the third week of hospitalisation, laboratory findings were as follows: AST: 246 IU/L, ALT: 571 IU/L, total bilirubin: 4.4 g/dl, LDH: 590 IU/L, and normal PT. Complete blood count and urine test were normal.
The cutaneous lesions disappeared completely on the 61st day, and clearance for HBsAg and seroconversion of anti-HBs was also observed.
DisCUssiOn This case was evaluated as Gianotti-Crosti syndrome by reason of the characteristics of the rash. The lichenoid quality of the lesions (flat topped, distinct small papules), acral distribution, and long-standing duration of the rash led to us this diagnosis. The absence of any relevant history (like suspicious drug usage) and allergic diseases, and the nonspecific findings of cutaneous biopsy contributed to the diagnosis of this benign condition.
There are no specific clinical tests to confirm the diagnosis of GCS. Histopathological examination of the skin lesion usually shows nonspecific changes with mild hyperkeratosis, spongiosis and a lymphohistiocytic infiltrate in the upper dermis with a perivascular or lichenoid distribution.3
GCS is a self-limited cutaneous host response to different viruses. The clinical differences are probably due to the individual characteristics of each patient rather than to the causative infectious agent.2 The disease is generally benign and does not recur. The hepatitis usually resolves in 2-3 months but, rarely, may progress to chronic hepatitis with persistent antigenemia and elevated transaminase activity.5 In our patient, the cutaneous lesions disappeared completely and HBsAg clearance was also observed in two months. Gianotti found that Australia antigen (HBsAg) was always present in affected children. He also noted that, in many cases, HBsAg was also
v tURhan et al
inTrODUCTiOnGianotti-Crosti Syndrome (GCS) was first described with hepatitis B virus (HBV) infection in Italy by Ferdinando Gianotti in 1955.1 The syndrome is known as childhood papular acrodermatitis.2, 3 Three main characteristics of the syndrome were described: nonrelapsing erythematopapular dermatitis localised to the face and limbs, lasting about three weeks; paracortical hyperplasia of the lymph nodes; and acute hepatitis, usually anicteric, which lasts for at least two months and may progress to chronic liver disease. 4 Over the course of three or four days a profuse eruption of dull red spots develops first on the thighs and buttocks, then on the outer aspects of the arms, and finally on the face. 5 GCS is usually seen sporadically but epidemics have also been recorded. The incidence peaks in early childhood (typically between three months and seven years) and rarely occurs in adulthood.6
This report describes an adult with GCS associated with acute HBV infection and presenting icteric progress.
Case rePOrTA 21-year-old man was admitted to hospital complaining of fatigue, abdominal pain, generalised jaundice and dark urine. The patient had been well until 10 days earlier, when he began to experience the above symptoms.
On physical examination, the patient was pale. Significant jaundice was seen on the skin and scleras. His temperature was 37.9ºC, pulse 100/min. and blood pressure 120/70 mmHg. His consciousness level was normal and there were no signs of encephalopathy. Abdominal examination demonstrated painful hepatomegaly, estimated by palpation at 2-3 cm in size. There was diffused, mild tenderness in the abdomen without rebound tenderness or spasm. Examination of the other organ systems was unremarkable.
Laboratory tests were performed: WBC count was 4900/mm3 (56% polymorphonuclear leukocytes, 34% lymphocytes, 10% monocytes), hemoglobin: 14.2 g/dl, hematocrit: 43%, platelet count: 300,000/mm3, erythrocyte sedimentation rate: 26 mm/h, and prothrombin time (PT): 17 sec. Results of the biochemical tests included the following: aspartate aminotransaminase (AST): 1650 IU/L, alanine aminotransaminase (ALT): 2882 IU/L, direct bilirubin: 8.8 mg/dl, indirect bilirubin: 3.8 mg/dl, lactate dehydrogenase (LDH): 715 IU/L, alkaline phosphatase (ALP): 390 IU/L, gama glutamil transferase (GGT): 174 IU/L, glucose: 90 mg/dl, and creatinine: 0.86 mg/dl. Urine test results included proteinuria (+), bilirubinuria (+++), trace urobilinogen, and normal microscopic examination.
On serologic investigation, HBsAg and anti-HBc IgM were positive. Consequently, the patient was
Gianotti-Crosti syndrome associated with HBV infection in an adultaBsTraCTBackground Gianotti-Crosti Syndrome (GCS) is a characteristic cutaneous eruption
following a viral infection. Incidence peaks in early childhood and the syndrome rarely occurs in adulthood. Hepatitis associated with GCS is usually anicteric and acute form.
Aim To report an adult with GCS associated with HBV infection and presenting icteric progress.
Methods The clinical features of the GCS case associated with HBV infection were evaluated.
Result The cutaneous lesions disappeared completely on the 61st day and clearance for HBsAg was also observed.
Conclusion GCS may be seen in adults and may be associated with icteric HBV infection.
V Turhan,1 N Ardic,2 B Besirbellioglu,3 T Dogru4
Dept of Infectious Disease and Clinical Microbiology,1 Dept of Microbiology and Clinical Microbiology,2 Gulhane Military Medical Academy, Haydarpasa Training Hosp, Istanbul; Dept of Infectious Disease and Clinical Microbiology,3 Dept of Internal Medicine,4 Gulhane Military Medical Academy, School of Medicine, Ankara
GIANOTTI-CROSTI SYNDROME ASSOCIATED wITH HBV INFECTION IN AN ADULT
Figure 1 —COPPERY-RED PAPULES CAN BE SEEN ON THE UPPER EXTREMITIES
Figure 2 —DENSE EXANTHAMATOUS LESIONS ON THE LOwER EXTREMITIES
1 2
94 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CASE
REP
ORT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 95
CASE
REP
ORT
GIANOTTI-CROSTI SYNDROME ASSOCIATED wITH HBV INFECTION IN AN ADULT
present in the blood of the mother of the affected child. When evaluated, such cutaneous lesions were also noted in the siblings of the index case in the past. This suggests that the virus is transmitted by intrafamilial means, which is clearly the case with HBV1. It was also seen with infectious agents (Epstein-Barr virus, coxsackie virus, cytomegalovirus, parvovirus B19 etc.) other than HBV infection.7 Few cases were reported after immunisation with vaccines against such as measles, mumps, rubella, polio and influenza viruses.8, 9
GCS is seen equally in both sexes. Because of its generally benign and self-limited course, it is often undiagnosed and may be overlooked. It has a distinctive clinical picture because of the predominant location of the erythematous papules on the face and extremities. The rash chiefly involves the arms, legs, buttock and face. Trunk is strikingly spared. However, the face is rarely spared.7 This distinctive eruption is associated with malaise and low-grade fever. It is rarely associated with systemic findings except for generalised lymphadenopathy and hepatomegaly (in patients with hepatitis B viremia).6 There is generally no need to perform laboratory tests. A mild lymphocytosis and a relative monocytosis can be seen in blood counts. In cases associated with HBV infection, there is typically an anicteric acute hepatitis and elevations of hepatic transaminases and antiviral antibodies.
The majority of GCS cases are seen in paediatric patients, although occasional adult cases have been reported. The clinical features do not seem to differ significantly from those of paediatric cases.3 Our case was an adult and showed an icteric form of HBV infection.
We report the GCS case associated with HBV infection because of its icteric and pruritic manifestation and also because it represents an adult form of the syndrome.
REFERENCES1. Gianotti F. Papular acrodermatitis of childhood and
other papulo-vesicular acrolocated syndrome. Br J Dermatol 1979; 100: 49-59.
2. Caputo R, Gelmetti C, Ermacora E, Gianni E, Sivestri A. Gianotti-Crosti syndrome: a retrospective analysis of 308 cases. J Am Acad Dermatol 1992; 26: 207-10.
3. Gibbs S, Burrow N. Gianotti-Crosti syndrome in two unrelated adult. Clin Dermatol 2000; 25: 594-6.
4. Chuh A, Lee A, Zawar V. The diagnostic criteria of gianotti-crosti syndrome: are they applicable to children in India? Pediatr Dermatol. 2004; 21:542-7.
5. http://dermnetnz.org/viral/gianotti-crosti.html
6. Hurwitz S: Clinical Pediatric Dermatology, 2nd ed. W.B. Saunders. 1993; 128.
7. Lima DA, Rocha DM, Miranda MFR. Gianotti-Crosti syndrome: clinical, laboratorial features, and serologic profiles of 10 cases from Belém, State of Para, Brazil. An Bras Dermatol 2004; 79: 699-707.
8. Erkek E, Sentürk GB, Ozkaya O, Bukulmez G. Gianotti-Crosti syndrome preceded by oral polio vaccine and followed by varicella infection. Pediatr Dermatol 2001; 18: 516-8.
9. Andiran N, Senturk GB, Bukulmez G. Combined vaccination by measles and hepatitis B vaccines: a new cause of Gianotti-Crosti syndrome. Dermatology 2002; 204: 75-6.
Correspondence to: Nurittin Ardic, M.D., Department of Microbiology, Gulhane Military Medical Academy, Istanbul, Turkey.Tel: +90-216- 542 27 97 Fax: +90-216-348 78 80e-mail: [email protected]
inTrODUCTiOnOne of the challenges in primary care is to be able to manage unusual symptoms, which do not clearly ‘belong’ to a particular system, and to be able to effectively differentiate between what is serious and not so serious. Whereas carpal tunnel syndrome is common and its differential diagnosis may be reasonably well known, macroglossia is an unusual problem in primary care. The significance of their coexistence in a patient is probably not widely appreciated. We present the case of an elderly man who, following uneventful bilateral carpal tunnel syndrome surgery during the preceding twelve months, presented with gradual non-painful enlargement of his tongue, which was eventually diagnosed as amyloidosis, secondary to multiple myeloma.
This case is reported to inform primary care physicians of this link, as it is likely in our healthcare system, these patients will initially present in primary care. Plasma protein electrophoresis and Bence Jones protein testing can facilitate both early diagnosis and appropriate referral. These tests are readily available in general practice. In this context, we suggest that family doctors have a high degree of suspicion for multiple myeloma or plasma cell dyscrasia when they encounter elderly patients who present with macroglossia, particularly if associated with carpal tunnel syndrome.
Case rePOrTA 69-year-old man incidentally mentioned non-painful tongue enlargement during a routine cardiovascular check up. He had no other associated symptoms. On examination, his tongue looked
slightly enlarged, but was otherwise normal in appearance. The remainder of his head and neck examination was normal apart from poor dental hygiene. He was prescribed a course of metronidazole for his gingivitis. He returned two months later with the same symptom, which was now also associated with some difficulty in chewing his food. He also complained of associated tiredness, but was otherwise asymptomatic. On examination, at this stage, his tongue was obviously and smoothly enlarged. Again, the remainder of his head and neck examination was normal.
Past medical history included hypertension, myocardial infarction, hypercholesterolaemia, depression and bilateral carpel tunnel repair in the preceding year. Initial investigations consisted of a full blood count, renal, liver and thyroid function – all of which were normal, apart from a slightly elevated ESR of 38mm/hour.
The patient was referred for an urgent ENT consultation. The ENT Department prescribed a repeat course of antibiotics. At ENT OPD follow-up, a course of oral steroids was prescribed, no specific diagnosis was made. A CT scan of his head and neck confirmed macroglossia.
Two months after his initial presentation the patient reported increasing difficulty in eating solids and was unable to lie flat due to the size of his tongue. A dietary review revealed adequate nutritional intake and his weight was stable.
A second opinion was sought, this time with the local dental teaching hospital. A tongue biopsy
Macroglossia and carpal tunnel syndrome associated with multiple myeloma: a case reportaBsTraCTBackground Macroglossia is an unusual symptom in primary care. It may be an indicator
of an underlying plasma cell dyscrasia or multiple myeloma in the elderly.Aim To describe such a case of multiple myeloma.Results A 69-year-old man, with a recent history of bilateral carpal tunnel repair,
presented to his GP with progressive macroglossia. This was eventually diagnosed as being due to amyloidosis, secondary to multiple myeloma.
Conclusion Physicians should be aware of the association between macroglossia, carpal tunnel syndrome and multiple myeloma in this age group.
M Kelly, J MoranDept of General Practice, University College Cork, Distillery House, North Mall, Cork
MACROGLOSSIA AND CARPAL TUNNEL SYNDROME ASSOCIATED wITH MULTIPLE MYELOMA: A CASE REPORT
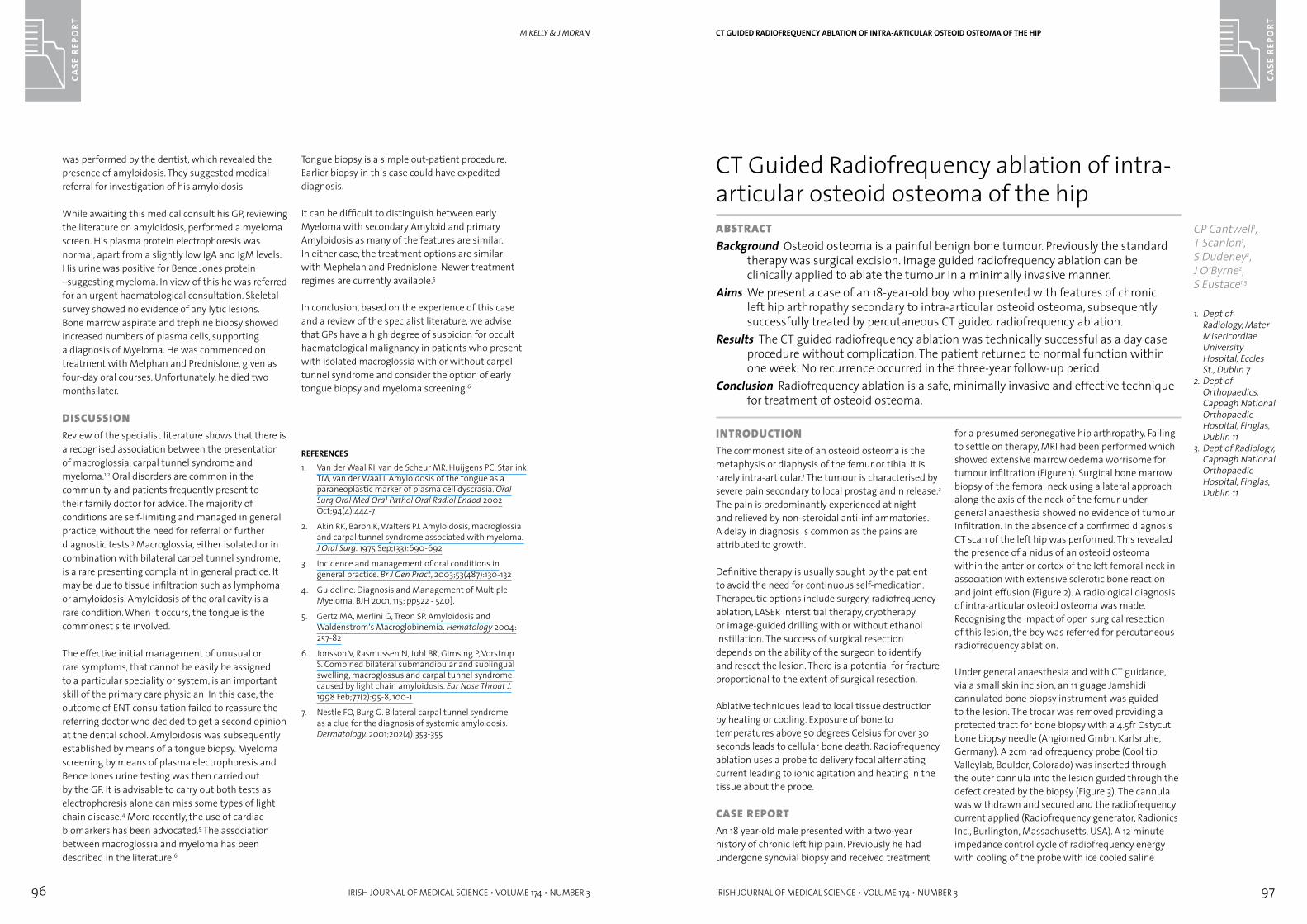
96 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CASE
REP
ORT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 97
CASE
REP
ORT
was performed by the dentist, which revealed the presence of amyloidosis. They suggested medical referral for investigation of his amyloidosis.
While awaiting this medical consult his GP, reviewing the literature on amyloidosis, performed a myeloma screen. His plasma protein electrophoresis was normal, apart from a slightly low IgA and IgM levels. His urine was positive for Bence Jones protein –suggesting myeloma. In view of this he was referred for an urgent haematological consultation. Skeletal survey showed no evidence of any lytic lesions. Bone marrow aspirate and trephine biopsy showed increased numbers of plasma cells, supporting a diagnosis of Myeloma. He was commenced on treatment with Melphan and Prednislone, given as four-day oral courses. Unfortunately, he died two months later.
DisCUssiOnReview of the specialist literature shows that there is a recognised association between the presentation of macroglossia, carpal tunnel syndrome and myeloma.1,2 Oral disorders are common in the community and patients frequently present to their family doctor for advice. The majority of conditions are self-limiting and managed in general practice, without the need for referral or further diagnostic tests.3 Macroglossia, either isolated or in combination with bilateral carpel tunnel syndrome, is a rare presenting complaint in general practice. It may be due to tissue infiltration such as lymphoma or amyloidosis. Amyloidosis of the oral cavity is a rare condition. When it occurs, the tongue is the commonest site involved.
The effective initial management of unusual or rare symptoms, that cannot be easily be assigned to a particular speciality or system, is an important skill of the primary care physician In this case, the outcome of ENT consultation failed to reassure the referring doctor who decided to get a second opinion at the dental school. Amyloidosis was subsequently established by means of a tongue biopsy. Myeloma screening by means of plasma electrophoresis and Bence Jones urine testing was then carried out by the GP. It is advisable to carry out both tests as electrophoresis alone can miss some types of light chain disease.4 More recently, the use of cardiac biomarkers has been advocated.5 The association between macroglossia and myeloma has been described in the literature.6
Tongue biopsy is a simple out-patient procedure. Earlier biopsy in this case could have expedited diagnosis.
It can be difficult to distinguish between early Myeloma with secondary Amyloid and primary Amyloidosis as many of the features are similar. In either case, the treatment options are similar with Mephelan and Prednislone. Newer treatment regimes are currently available.5
In conclusion, based on the experience of this case and a review of the specialist literature, we advise that GPs have a high degree of suspicion for occult haematological malignancy in patients who present with isolated macroglossia with or without carpel tunnel syndrome and consider the option of early tongue biopsy and myeloma screening.6
REFERENCES1. Van der Waal RI, van de Scheur MR, Huijgens PC, Starlink
TM, van der Waal I. Amyloidosis of the tongue as a paraneoplastic marker of plasma cell dyscrasia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002 Oct;94(4):444-7
2. Akin RK, Baron K, Walters PJ. Amyloidosis, macroglossia and carpal tunnel syndrome associated with myeloma. J Oral Surg. 1975 Sep;(33):690-692
3. Incidence and management of oral conditions in general practice. Br J Gen Pract, 2003;53(487):130-132
4. Guideline: Diagnosis and Management of Multiple Myeloma. BJH 2001, 115; pp522 - 540].
5. Gertz MA, Merlini G, Treon SP. Amyloidosis and Waldenstrom’s Macroglobinemia. Hematology 2004: 257-82
6. Jonsson V, Rasmussen N, Juhl BR, Gimsing P, Vorstrup S. Combined bilateral submandibular and sublingual swelling, macroglossus and carpal tunnel syndrome caused by light chain amyloidosis. Ear Nose Throat J. 1998 Feb;77(2):95-8, 100-1
7. Nestle FO, Burg G. Bilateral carpal tunnel syndrome as a clue for the diagnosis of systemic amyloidosis. Dermatology. 2001;202(4):353-355
M KellY & J MORan
inTrODUCTiOnThe commonest site of an osteoid osteoma is the metaphysis or diaphysis of the femur or tibia. It is rarely intra-articular.1 The tumour is characterised by severe pain secondary to local prostaglandin release.2 The pain is predominantly experienced at night and relieved by non-steroidal anti-inflammatories. A delay in diagnosis is common as the pains are attributed to growth.
Definitive therapy is usually sought by the patient to avoid the need for continuous self-medication. Therapeutic options include surgery, radiofrequency ablation, LASER interstitial therapy, cryotherapy or image-guided drilling with or without ethanol instillation. The success of surgical resection depends on the ability of the surgeon to identify and resect the lesion. There is a potential for fracture proportional to the extent of surgical resection.
Ablative techniques lead to local tissue destruction by heating or cooling. Exposure of bone to temperatures above 50 degrees Celsius for over 30 seconds leads to cellular bone death. Radiofrequency ablation uses a probe to delivery focal alternating current leading to ionic agitation and heating in the tissue about the probe.
Case rePOrTAn 18 year-old male presented with a two-year history of chronic left hip pain. Previously he had undergone synovial biopsy and received treatment
for a presumed seronegative hip arthropathy. Failing to settle on therapy, MRI had been performed which showed extensive marrow oedema worrisome for tumour infiltration (Figure 1). Surgical bone marrow biopsy of the femoral neck using a lateral approach along the axis of the neck of the femur under general anaesthesia showed no evidence of tumour infiltration. In the absence of a confirmed diagnosis CT scan of the left hip was performed. This revealed the presence of a nidus of an osteoid osteoma within the anterior cortex of the left femoral neck in association with extensive sclerotic bone reaction and joint effusion (Figure 2). A radiological diagnosis of intra-articular osteoid osteoma was made. Recognising the impact of open surgical resection of this lesion, the boy was referred for percutaneous radiofrequency ablation.
Under general anaesthesia and with CT guidance, via a small skin incision, an 11 guage Jamshidi cannulated bone biopsy instrument was guided to the lesion. The trocar was removed providing a protected tract for bone biopsy with a 4.5fr Ostycut bone biopsy needle (Angiomed Gmbh, Karlsruhe, Germany). A 2cm radiofrequency probe (Cool tip, Valleylab, Boulder, Colorado) was inserted through the outer cannula into the lesion guided through the defect created by the biopsy (Figure 3). The cannula was withdrawn and secured and the radiofrequency current applied (Radiofrequency generator, Radionics Inc., Burlington, Massachusetts, USA). A 12 minute impedance control cycle of radiofrequency energy with cooling of the probe with ice cooled saline
CT Guided Radiofrequency ablation of intra-articular osteoid osteoma of the hipaBsTraCTBackground Osteoid osteoma is a painful benign bone tumour. Previously the standard
therapy was surgical excision. Image guided radiofrequency ablation can be clinically applied to ablate the tumour in a minimally invasive manner.
Aims We present a case of an 18-year-old boy who presented with features of chronic left hip arthropathy secondary to intra-articular osteoid osteoma, subsequently successfully treated by percutaneous CT guided radiofrequency ablation.
Results The CT guided radiofrequency ablation was technically successful as a day case procedure without complication. The patient returned to normal function within one week. No recurrence occurred in the three-year follow-up period.
Conclusion Radiofrequency ablation is a safe, minimally invasive and effective technique for treatment of osteoid osteoma.
CP Cantwell1, T Scanlon1, S Dudeney2, J O’Byrne2, S Eustace1,3
1. Dept of Radiology, Mater Misericordiae University Hospital, Eccles St., Dublin 7
2. Dept of Orthopaedics, Cappagh National Orthopaedic Hospital, Finglas, Dublin 11
3. Dept of Radiology, Cappagh National Orthopaedic Hospital, Finglas, Dublin 11
CT GUIDED RADIOFREqUENCY ABLATION OF INTRA-ARTICULAR OSTEOID OSTEOMA OF THE HIP
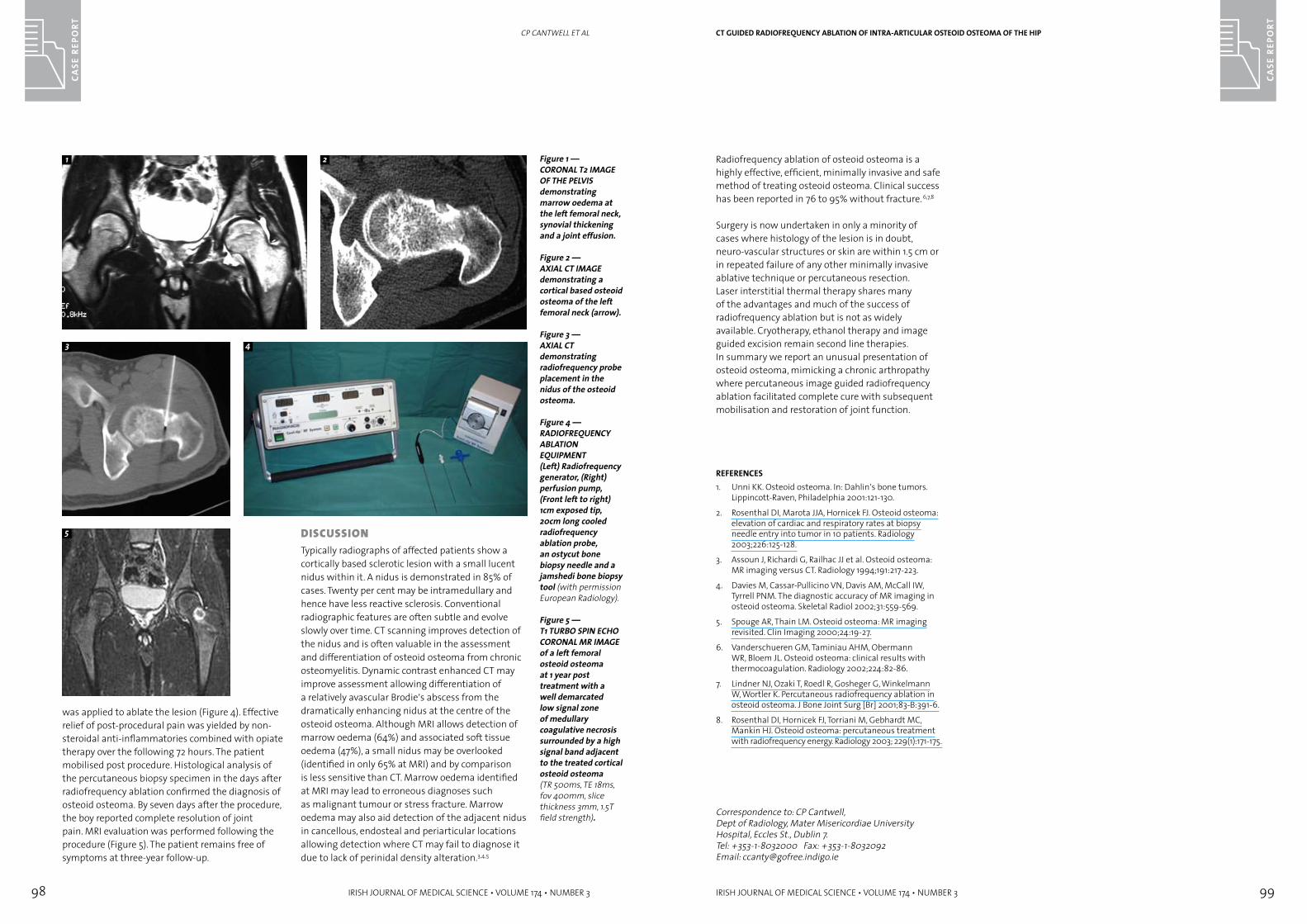
98 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CASE
REP
ORT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 99
CASE
REP
ORT
was applied to ablate the lesion (Figure 4). Effective relief of post-procedural pain was yielded by non-steroidal anti-inflammatories combined with opiate therapy over the following 72 hours. The patient mobilised post procedure. Histological analysis of the percutaneous biopsy specimen in the days after radiofrequency ablation confirmed the diagnosis of osteoid osteoma. By seven days after the procedure, the boy reported complete resolution of joint pain. MRI evaluation was performed following the procedure (Figure 5). The patient remains free of symptoms at three-year follow-up.
CP CANTWELL ET AL
Figure 1 —CORONAL T2 IMAGE OF THE PELVIS demonstrating marrow oedema at the left femoral neck, synovial thickening and a joint effusion.
Figure 2 —AXIAL CT IMAGE demonstrating a cortical based osteoid osteoma of the left femoral neck (arrow).
Figure 3 —AXIAL CT demonstrating radiofrequency probe placement in the nidus of the osteoid osteoma.
Figure 4 —RADIOFREqUENCY ABLATION EqUIPMENT(Left) Radiofrequency generator, (Right) perfusion pump, (Front left to right) 1cm exposed tip, 20cm long cooled radiofrequency ablation probe, an ostycut bone biopsy needle and a jamshedi bone biopsy tool (with permission European Radiology).
Figure 5 —T1 TURBO SPIN ECHO CORONAL MR IMAGE of a left femoral osteoid osteoma at 1 year post treatment with a well demarcated low signal zone of medullary coagulative necrosis surrounded by a high signal band adjacent to the treated cortical osteoid osteoma (TR 500ms, TE 18ms, fov 400mm, slice thickness 3mm, 1.5T field strength).
1 2
3 4
5 DisCUssiOnTypically radiographs of affected patients show a cortically based sclerotic lesion with a small lucent nidus within it. A nidus is demonstrated in 85% of cases. Twenty per cent may be intramedullary and hence have less reactive sclerosis. Conventional radiographic features are often subtle and evolve slowly over time. CT scanning improves detection of the nidus and is often valuable in the assessment and differentiation of osteoid osteoma from chronic osteomyelitis. Dynamic contrast enhanced CT may improve assessment allowing differentiation of a relatively avascular Brodie’s abscess from the dramatically enhancing nidus at the centre of the osteoid osteoma. Although MRI allows detection of marrow oedema (64%) and associated soft tissue oedema (47%), a small nidus may be overlooked (identified in only 65% at MRI) and by comparison is less sensitive than CT. Marrow oedema identified at MRI may lead to erroneous diagnoses such as malignant tumour or stress fracture. Marrow oedema may also aid detection of the adjacent nidus in cancellous, endosteal and periarticular locations allowing detection where CT may fail to diagnose it due to lack of perinidal density alteration.3,4,5
Radiofrequency ablation of osteoid osteoma is a highly effective, efficient, minimally invasive and safe method of treating osteoid osteoma. Clinical success has been reported in 76 to 95% without fracture. 6,7,8
Surgery is now undertaken in only a minority of cases where histology of the lesion is in doubt, neuro-vascular structures or skin are within 1.5 cm or in repeated failure of any other minimally invasive ablative technique or percutaneous resection.Laser interstitial thermal therapy shares many of the advantages and much of the success of radiofrequency ablation but is not as widely available. Cryotherapy, ethanol therapy and image guided excision remain second line therapies.In summary we report an unusual presentation of osteoid osteoma, mimicking a chronic arthropathy where percutaneous image guided radiofrequency ablation facilitated complete cure with subsequent mobilisation and restoration of joint function.
REFERENCES1. Unni KK. Osteoid osteoma. In: Dahlin’s bone tumors.
Lippincott-Raven, Philadelphia 2001:121-130.
2. Rosenthal DI, Marota JJA, Hornicek FJ. Osteoid osteoma: elevation of cardiac and respiratory rates at biopsy needle entry into tumor in 10 patients. Radiology 2003;226:125-128.
3. Assoun J, Richardi G, Railhac JJ et al. Osteoid osteoma: MR imaging versus CT. Radiology 1994;191:217-223.
4. Davies M, Cassar-Pullicino VN, Davis AM, McCall IW, Tyrrell PNM. The diagnostic accuracy of MR imaging in osteoid osteoma. Skeletal Radiol 2002;31:559-569.
5. Spouge AR, Thain LM. Osteoid osteoma: MR imaging revisited. Clin Imaging 2000;24:19-27.
6. Vanderschueren GM, Taminiau AHM, Obermann WR, Bloem JL. Osteoid osteoma: clinical results with thermocoagulation. Radiology 2002;224:82-86.
7. Lindner NJ, Ozaki T, Roedl R, Gosheger G, Winkelmann W, Wortler K. Percutaneous radiofrequency ablation in osteoid osteoma. J Bone Joint Surg [Br] 2001;83-B:391-6.
8. Rosenthal DI, Hornicek FJ, Torriani M, Gebhardt MC, Mankin HJ. Osteoid osteoma: percutaneous treatment with radiofrequency energy. Radiology 2003; 229(1):171-175.
Correspondence to: CP Cantwell, Dept of Radiology, Mater Misericordiae University Hospital, Eccles St., Dublin 7.Tel: +353-1-8032000 Fax: +353-1-8032092Email: [email protected]
CT GUIDED RADIOFREqUENCY ABLATION OF INTRA-ARTICULAR OSTEOID OSTEOMA OF THE HIP
100 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CORR
ESPO
ND
ENCE
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 101
LITE
RARY
& H
ISTO
RICA
LCO
RRES
PON
DEN
CE
Coincidental malignancy and abdominal aortic aneurysm: a clinical conundrumDear Editor
Incidental colorectal carcinoma, (CRC), discovered at the time of abdominal aortic aneurysm, (AAA), repair presents the surgeon with a significant therapeutic dilemma. The available literature provides little evidence that a staged or synchronous approach to treatment is preferable under such circumstances. Two patients with concomitant AAA and CRC were recently treated in our unit. The first was an 80-year-old man who was transferred from a peripheral hospital with lower abdominal pain. Physical examination revealed the presence of a pulsatile abdominal mass and subsequent ultrasound and CT of abdomen confirmed the presence of a 6cm infra-renal abdominal aortic aneurysm. Elective repair of AAA was undertaken and a non-obstructing caecal carcinoma was identified at laparotomy. A decision was made to perform a staged procedure of primary aneurysm repair with later tumour resection. The second patient was a 73-year-old man who was admitted with lower abdominal pain radiating to his back. CT of abdomen revealed the presence of a 9.5cm infrarenal abdominal aortic aneurysm. Open repair was performed, during which, the presence of a non-obstructing caecal carcinoma was noted. Both patients made a full recovery from their aneurysm surgery, and underwent subsequent right hemicolectomy six weeks later.
Synchronous colorectal cancer discovered at abdominal aortic aneurysm repair was first reported in 1967 by Szilagyi et al.1 yet the modern management of concomitant abdominal aortic aneurysm, (AAA), and colorectal carcinoma, (CRC), remains controversial. Treatment of the colorectal carcinoma first exposes the patient to the risk of aneurysm rupture in the post-operative period. This phenomenon was initially reported by Trueblood et al2 in 1976 and later by Swanson et al3 in 1980. Rupture was thought likely to be secondary to accelerated collagen lysis observed after surgery, aggravated by poor nutrition, pyrexia and the catabolic state of patients in the post-operative period. It is now known that the matrixmetalloproteinases, (MMPs), MMP inhibitors and vascular cell adhesion molecules, (VCAMs) also contribute to aortic collagen lysis after surgical
insult. Treatment of the aneurysm first, however, may disadvantage the patient by exposing him to the risk of tumour progression before resection. Concomitant treatment of both lesions, while sparing the patient two major procedures, also exposes him to the potential risk of aortic graft infection with its attendant high mortality. Several case studies reporting patients treated concomitantly for AAA and CRC have been published.4-6 Though there have been no reports of graft infection related to synchronous AAA and CRC resection in these studies, the total number of patients is small. While the optimal treatment of concomitant colorectal carcinoma and abdominal aortic aneurysm remains controversial and challenging, an individualised approach to the operative management of a patient discovered to have incidental colorectal cancer during aortic surgery remains essential. Although such combined pathology is at present uncommon, an increase in the frequency with which these conditions are observed together intraoperatively may result from the future introduction of screening programmes for abdominal aortic aneurysm and colorectal cancer.
REFERENCES 1. Szilagyi DE, Elliot JP, Berguer R. Coincidental malignancy
and abdominal aortic aneurysm: problems of management. Arch Surg 1967; 95: 402-12.
2. Trueblood HW, Williams DK, Gustafson JR. Aneurysmal rupture following resection of abdominal malignancy. Am Surg 1976; 42: 535-539.
3. Swanson RJ, Littooy FN, Hunt TK, Stoney RJ. Laparotomy as a precipitating factor in the rupture of intra-abdominal aneurysms. Arch Surg 1980; 115: 199-304.
4. Oshodi TO, Abraham JS, Brigg JK, Kelly JF. Management of co-existing intra-abdominal disease in aortic surgery. Eur J Vasc Endovasc Surg 2000; 19: 43-6
5. Bachoo P, Cooper G, Engeset J, Cross KS. Management of synchronous infrarenal aortic disease and large bowel cancer: a north-east of Scotland experience. Eur J Vasc Endovasc Surg 2000; 19: 614-8.
6. Gouny P, Leschi J, Nussaume O, Cheynel-Hocquet C, Decaix B, Vayssairat M. Single-stage management of abdominal aortic aneurysm and colon cancer. Ann Vasc Surg 1996; 10: 299-305.
Correspondence to: Niamh Ni Choileain, Dept of Surgery, Cork University Hospital, Wilton, Cork.Tel : (021) 4922371 Fax: (021) 4922811E-mail: [email protected]
N Ni Choileain, G FultonDept of Surgery, Cork University Hospital/N.U.I. Cork, Wilton, Cork
CORRESPONDENCE
Surgical treatment of pulmonary embolism Dear Editor
We present a 70-year-old female with atrial fibrillation and a lower limb deep venous thrombosis, with acute onset of dyspnoea. Investigations revealed a pulmonary embolism (PE) and a large mobile thrombus in the right atrium. She was haemodynamically stable but in light of embolic potential of the thrombus in the right atrium, surgical intervention was recommended. At surgery, performed with the aid of cardiopulmonary bypass, the atrial thrombus and PE were removed. Her subsequent recovery was uneventful and one year later, she is well.
Prior to the development of pharmacological anticoagulation, Trendelenburg had explored surgical pulmonary embolectomy with little success.1 However surgical results have greatly improved since of the development of cardiopulmonary bypass. Surgical pulmonary thromboembolectomy is indicated in three scenarios: 1] haemodynamic instability, 2] PE in the presence of an associated right heart chamber thrombus, 3] where therapeutic anticoagulation is contraindicated. It should only be considered for patients with a definite diagnosis of a PE with an otherwise reasonable life expectancy.
Comparisons between surgical and pharmacological treatments of massive PE show a higher mortality with pharmacological treatment alone (33% v 23% for surgery). Pharmacological treatment is also associated with a significant risk of major haemorrhage (25%) and a higher recurrence rate.2 Percutaneous catheter embolectomy is an alternative technique with a 80% success rate but with a risk of dispersal of the thrombus.3 Previous thrombolysis does not alter the surgical risks or outcome.4 The success of pharmacological therapies means that surgical intervention is rarely considered even though it may be the most appropriate in specific circumstances.
REFERENCES1. Fontana G., Sabiston D. Pulmonary embolism., in Surgery
of the Chest., D. Sabiston and F. Spencer, Editors. W.B. Saunders.: Philadelphia. 1995, p. 773-802.
2. Gulba D., Schmid C., Borst H., Lichtlen P., Dietz R., Luft F. Medical compared with surgical treatment for massive pulmonary embolism. Lancet 1994; 343:576-577.
3. Goldhaber S. Integration of catheter thrombectomy into our armementarium to treat acute pulmonary embolism. Chest 1998; 114:1237-1238.
4. Doerge H., Schoendube F., Loeser H., Walter M., Messmer B. Pulmonary embolectomy: review of a 15-year experience and role in the age of thrombolytic therapy. Eur J Cardiothorac Surg 1996; 10:952-957.
Correspondence to: WS Soo,Prof. Eoin O’Malley National Centre of Cardiothoracic Surgery, Mater Misericordiae University Hospital, Eccles St., Dublin 7.Tel: 00-353-1-8032163 Fax: 00-353-1-8034773e-mail: [email protected]
WS Soo, DG Healy, B Maurer¹1, JF McCarthyProf. Eoin O’Malley National Centre of Cardiothoracic Surgery, Mater Misericordiae University Hospital, Eccles St., Dublin 7; St. Vincent University Hospital1, Elm Park, Dublin 4
CORRESPONDENCE
102 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
CO
NSE
NSU
S ST
ATEM
ENT
IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3 103
LITE
RARY
& H
ISTO
RICA
LBO
Ok
REV
IEw
CONSENSUS STATEMENT
This meeting was held in the RCSI to discuss acceptable practices as to Living Donor Renal Transplantation in Ireland. The meeting was attended by Irish European and American experts in the field of renal transplantation, ethics and law. At the end of the meeting the following Consensus Statement was agreed by all parties:
1. Living Donor Transplantation should be available in Ireland as a form of treatment for patients with end stage renal failure.
2. All necessary protocols should be in place in order to minimise risk to the donor and recipient.
3. Living unrelated transplantation is a morally acceptable proceedure between emotionally related individuals.
4. A transplant committee should be established consisting of Transplant Surgeons, Nephrologist and Social Workers to sign off all Living Donor Transplants.
5. Appropriate resources should be provided by the Department of Health to ensure Living Donor Transplantation can be provided safely. The Department of Health should consider the issue of implementing legislation in the Republic of Ireland to govern transplantation and the use of human tissue generally.
Consensus conference on living donor renal transplantationRoyal College of Surgeons in IrelandFriday, 2 April 2004
P Conlon, D Cusack, P McClean, M Irvine, C Magee, B McGovern, L Plant, D Gill, D Smith, M Akyol, P Franklin, M Waldron, Dilly Little, J Douglas, D Hickey, D Murphy, M Donovan, A Mc Auley
Case-based HaematologyShaun McCann, Robin Foá, Owen Smith, Eibhlin ConneallyPublished by Blackwell Publishing ISBN 1-4051-1321-9Price Stg £16.95
PT MurphyBeaumont Hospital
The Haematology Department at St James’s Hospital, with its large number of high quality Consultant staff, is one of the top haematology centres in the Republic of Ireland. Case-based Haematology, whose co-authors include Professors McCann and Smith and Dr Conneally from St James’s Hospital, is, thus, to be warmly welcomed. This textbook, containing twenty real patient cases, is aimed at helping medical students and junior doctors to approach common haematology conditions in a logical and effective manner.
Each case history consists of history, physical examination, investigations and their interpretation, diagnosis and therapy, as well as including a helpful algorithm and good quality pathology and radiology photographs. The patient histories are often compelling, such as the football player dropped from the team or the elderly man no longer able to take his dog for a walk, and reflect the strong humanitarian ethos at St James’s Hospital Haematology Department. Each case covers an important area of haematology practice, although, when chapter topics are closely linked, such as those on haematinic deficiencies, there is inevitably a degree of repetition of information. There is also some useful information about the effects of alcohol in haematology practise, possibly reflecting one of the co-authors acclaimed expertise as a wine connoisseur.
I had a few minor disagreements with some parts of this book. For example, management of sickle cell crisis was inadequate and I did not think it helpful to describe the sickle cell patient as opiate dependent in case impressionable younger readers might become overly cautious in their future use of analgesia to treat this excruciatingly painful condition. In addition, treatment options for autoimmune haemolytic anaemia jumped, rather alarmingly, from corticosteroids to anti-B lymphocyte antibody therapy without mention of splenectomy or the vital need to exclude underlying lymphoma.
Overall, however, this text book conveys a great deal of useful and practical information. In particular, the chapter on blood transfusion was both succinct and highly informative. Published by Blackwell Publishing and with a retail price of £16.95, this textbook is good value for money and largely achieves the goals set out by Professor McCann in his preface. It should prove very useful to both medical undergraduates and to junior doctors. In particular, there will no longer be any excuses for junior doctors when the Haematology ‘boss’ comes calling.
BOOk REVIEw
104 IRISH JOURNAL OF MEDICAL SCIENCE • VOLUME 174 • NUMBER 3
BOO
k R
EVIE
w
Short Answer Questions for the MRCOpth Master PassNathaniel Knox Cartwright, Petros CarvounisPublished by Radcliffe Publishing Ltd.,ISBN 1-85775-884-6 Stg £21.95
L CassidyRoyal Victoria Eye and Ear Hospital
‘Short Answer Questions’ is a book written by a Senior House Officer and a Specialist Registrar who had recent experience of passing the MRCOphth examination.
They have produced an excellent text. Each subject is a question. Those questions which commonly come up in the MRCOphth, followed by the perfect answer.
This is the first book of its type, it is precise and to the point. I would highly recommend it for all candidates attempting the MRCOphth Examination.
BOOk REVIEw
The Irish Journal of Medical Science will consider for publication original research of relevance to clinical medicine. All material is assumed to be submitted exclusively to the Journal. Submitted material will be sent for peer review and for statistical assessment and may be styled and edited where appropriate. The evaluation of the editorial committee is final.
Manuscripts, with disc, should be posted to: The Editor, Irish Journal of Medical ScienceInternational House,20-22 Lower Hatch Street, Dublin 2.
Or by email to:[email protected]
laYOUT Of PaPerManuscriptsSubmit three copies, with disc, Word for Windows format, size 12 font, paginated and double-spaced.Scientific articles are set out under the headings: Abstract, Introduction, Methods, Results, Discussion, and References.The title page contains the title, authors, institution and name, contact number and e-mail address of the corresponding author.The Abstract of 150 words or less should be structured as Background, Aims, Methods, Results and Conclusions.Abbreviations should be kept to a minimum. Those listed may be used without definition (See overleaf). Measurements should be given in SI units. Blood pressure may be expressed in mmHg. Drugs should be given their approved name.Statistical Method used should be detailed in the Methods section and any not in common use should be referenced.Ethics Committee Approval by the relevant authority is needed for investigations on human subjects and animal studies must be in accordance with the appropriate laws.
Tables & IllustrationsTables should not duplicate text information. Illustrations should be professionally produced and may be photographic prints or computer generated. Top should be indicated on the back. Staining techniques should be stated for histological
material. An internal scale marker or the final print magnification of the photograph should be included on the photomicrograph. Patients shown in photographs should have their identity concealed or give written consent for publication. Provide Legends on a separate sheet. Get written consent from the authors and copyright holder to publish material published elsewhere.
References Number references consecutively in the Vancouver style (e.g. …style.1). In the references give the names and initials of all authors but if more than six authors only the first three followed by et al. Book titles should be followed by publisher, place of publication, year and pages.1. Allen JM, Keenan AK, McHale NG et al. Lymphatic
functions and cardiovascular disease. N Engl J Med 1999;123:10-14.
2. Davis GK, Mertt O. Transition metals in nutrition. In: Trace elements in nutrition (4th edition). Ed O Mertt. Academic Press, San Diego 1998:123-132.
PrOOfs & rePrinTs Proof corrections should be kept to a minimum and should conform to the conventions shown in Whitaker’s Almanack. A charge of E70 per page (600 words) will be levied on authors. Reprints are available; a scale of charges is included when a proof is sent.
leTTer Of releaseA covering letter must be included, signed by the Senior authors stating: ‘I have read this paper and the data and interpretation concurs with my views.’
CHeCKlisT fOr aUTHOrs We have checked that the submitted article follows the appropriate format:• Three hard copies plus disk; Use ‘Times New
Roman’; size 12 font; Normal typeface• Paginated and Double line spacing; Two spaces
after full stops; References super-script outside punctuation - Please follow reference style as detailed above;
• A structured abstract as detailed above;• Case reports must have a structured abstract;• Three copies of graphics;• A release letter by the senior author.
Submissions will not be processed if they are not presented in the correct format for the journal.
General instructions to authors

Related Documents











