Brief report Factor structure of the Brief Psychiatric Rating Scale in unipolar depression Bruno Biancosino a,b , Angelo Picardi c , Luciana Marmai a,b , Massimo Biondi d , Luigi Grassi a,b, ⁎ a Section of Psychiatry, Department of Medical Sciences of Communication and Behaviour, University of Ferrara, Ferrara, Italy b Department of Mental Health, Ferrara, Italy c Center of Epidemiology, Surveillance and Health Promotion, Mental Health Unit, Italian National Institute of Health, Mental Health Unit, Rome, Italy d Section of Clinical Psychiatry III, Department of Psychiatric Sciences and Psychological Medicine, University “La Sapienza” of Rome, Rome, Italy article info abstract Article history: Received 6 October 2009 Received in revised form 23 November 2009 Accepted 23 November 2009 Available online 6 January 2010 Background: In clinical practice patients with unipolar depression present with a variety of symptom clusters that may combine together in many different ways. However, only few factor analytic studies used general psychopathology scales to investigate the symptom structure of unipolar depression. Methods: The study included 163 consecutive inpatients with an ICD-10 diagnosis of depressive disorder (ICD-10 codes F32 to F33). All patients were assessed with the 18-item version of the Brief Psychiatric Rating Scale (BPRS) within 3 days from admission. Exploratory factor analysis with Varimax rotation was performed on BPRS items. Results: Four factors were extracted, explaining 52% of total variance. They were interpreted as Apathy, Dysphoria, Depression and Psychoticism. The distribution of factor scores was approximately normal for Apathy, while it displayed a slight negative skewness for Depression, a slight positive skewness for Dysphoria, and a marked positive skewness for Psychoticism. Patient sex, family history of depression, lifetime history of suicide attempt, and recent serious family conflict were not associated with any factor. Occupational status, age, and age at onset displayed a positive correlation with Apathy. Duration of illness and number of previous admissions were positively correlated with Dysphoria. Limitations: Patients were not administered a structured diagnostic interview, and no detailed assessment of personality disorders was performed; also, patients were recruited only at a single site, which reduces the generalizability of the results. Conclusions: Our findings suggest that in depressive disorders there are psychopathological dimensions other than depressed mood that are worthy of greater clinical attention and research. Dimensions such as apathy and dysphoria may play an important part in the clinical phenomenology of unipolar depression and deserve systematic and careful assessment in order to provide patients with the best possible treatment and improve clinical outcomes. © 2009 Elsevier B.V. All rights reserved. Keywords: Depression Dysphoria Apathy Dimensional psychopathology Factor analysis 1. Introduction Most studies of the symptom structure of unipolar depression used depression-specific assessment instruments. The use of disease-specific scales is consistent with a view of mental disorders as independent entities. However, there is increasing support for a multidimensional view according to which each clinical picture usually results from a mixture of symptom dimensions (Goldberg, 2000; Van Praag et al., 1990). Indeed, factor studies using broad-based assessment instruments detected a variety of symptom clusters in depression (Pasquini et al., 2004; Biondi et al., 2005; Cassano et al., 2009). Journal of Affective Disorders 124 (2010) 329–334 ⁎ Corresponding author. Clinica Psichiatrica, Università di Ferrara, Corso Giovecca 203, 44100 Ferrara, Italy. Tel.: +39 0532 236 409; fax: +39 0532 212 240. E-mail address: [email protected] (L. Grassi). 0165-0327/$ – see front matter © 2009 Elsevier B.V. All rights reserved. doi:10.1016/j.jad.2009.11.019 Contents lists available at ScienceDirect Journal of Affective Disorders journal homepage: www.elsevier.com/locate/jad

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Affective Disorders 124 (2010) 329–334
Contents lists available at ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r.com/ locate / j ad
Brief report
Factor structure of the Brief Psychiatric Rating Scale in unipolar depression
Bruno Biancosino a,b, Angelo Picardi c, Luciana Marmai a,b, Massimo Biondi d, Luigi Grassi a,b,⁎a Section of Psychiatry, Department of Medical Sciences of Communication and Behaviour, University of Ferrara, Ferrara, Italyb Department of Mental Health, Ferrara, Italyc Center of Epidemiology, Surveillance and Health Promotion, Mental Health Unit, Italian National Institute of Health, Mental Health Unit, Rome, Italyd Section of Clinical Psychiatry III, Department of Psychiatric Sciences and Psychological Medicine, University “La Sapienza” of Rome, Rome, Italy
a r t i c l e i n f o
⁎ Corresponding author. Clinica Psichiatrica, UniveGiovecca 203, 44100 Ferrara, Italy. Tel.: +39 0532 23212 240.
E-mail address: [email protected] (L. Grassi).
0165-0327/$ – see front matter © 2009 Elsevier B.V.doi:10.1016/j.jad.2009.11.019
a b s t r a c t
Article history:Received 6 October 2009Received in revised form 23 November 2009Accepted 23 November 2009Available online 6 January 2010
Background: In clinical practice patients with unipolar depression present with a variety ofsymptom clusters that may combine together inmany different ways. However, only few factoranalytic studies used general psychopathology scales to investigate the symptom structure ofunipolar depression.
Methods:The study included 163 consecutive inpatients with an ICD-10 diagnosis of depressivedisorder (ICD-10 codes F32 to F33). All patients were assessed with the 18-item version of theBrief Psychiatric Rating Scale (BPRS) within 3 days from admission. Exploratory factor analysiswith Varimax rotation was performed on BPRS items.
Results: Four factors were extracted, explaining 52% of total variance. They were interpreted asApathy, Dysphoria, Depression and Psychoticism. The distribution of factor scores wasapproximately normal for Apathy, while it displayed a slight negative skewness for Depression,a slight positive skewness for Dysphoria, and a marked positive skewness for Psychoticism.Patient sex, family history of depression, lifetime history of suicide attempt, and recent seriousfamily conflict were not associated with any factor. Occupational status, age, and age at onsetdisplayed a positive correlation with Apathy. Duration of illness and number of previousadmissions were positively correlated with Dysphoria.
Limitations: Patients were not administered a structured diagnostic interview, and no detailedassessment of personality disorders was performed; also, patients were recruited only at asingle site, which reduces the generalizability of the results.
Conclusions: Our findings suggest that in depressive disorders there are psychopathologicaldimensions other than depressed mood that are worthy of greater clinical attention andresearch. Dimensions such as apathy and dysphoria may play an important part in the clinicalphenomenology of unipolar depression and deserve systematic and careful assessment in orderto provide patients with the best possible treatment and improve clinical outcomes.
© 2009 Elsevier B.V. All rights reserved.
Keywords:DepressionDysphoriaApathyDimensional psychopathologyFactor analysis
1. Introduction
Most studies of the symptom structure of unipolardepression used depression-specific assessment instruments.
rsità di Ferrara, Corso6 409; fax: +39 0532
All rights reserved.
The use of disease-specific scales is consistent with a view ofmental disorders as independent entities. However, there isincreasing support for a multidimensional view according towhich each clinical picture usually results from a mixture ofsymptom dimensions (Goldberg, 2000; Van Praag et al.,1990). Indeed, factor studies using broad-based assessmentinstruments detected a variety of symptom clusters indepression (Pasquini et al., 2004; Biondi et al., 2005; Cassanoet al., 2009).
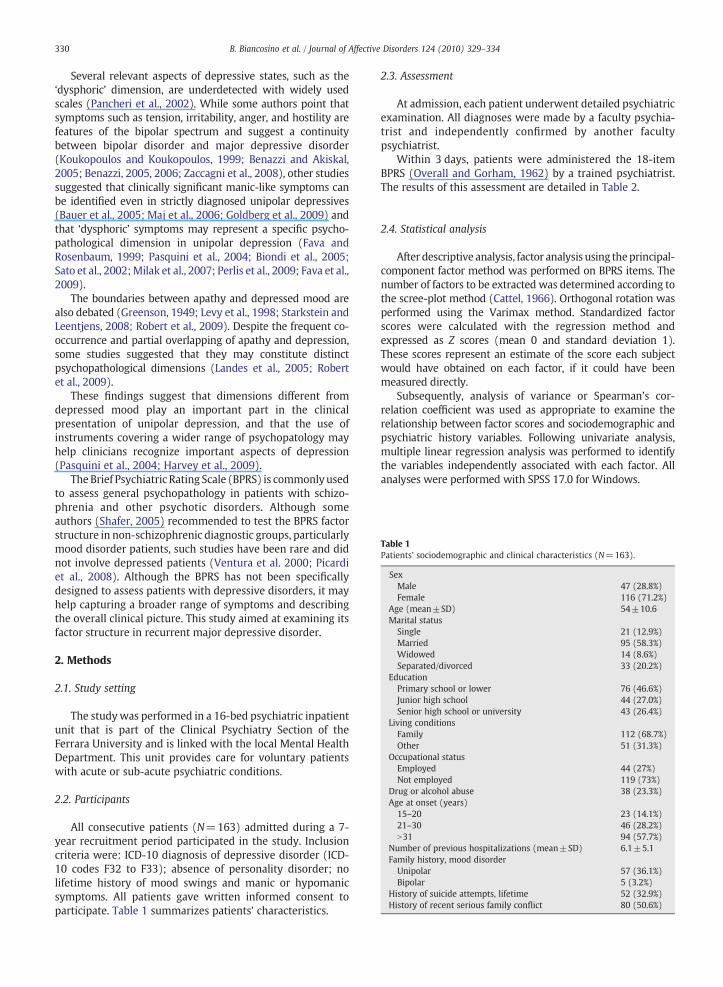
Table 1Patients' sociodemographic and clinical characteristics (N=163).
SexMale 47 (28.8%)Female 116 (71.2%)
Age (mean±SD) 54±10.6Marital status
Single 21 (12.9%)Married 95 (58.3%)Widowed 14 (8.6%)Separated/divorced 33 (20.2%)
EducationPrimary school or lower 76 (46.6%)Junior high school 44 (27.0%)Senior high school or university 43 (26.4%)
Living conditionsFamily 112 (68.7%)Other 51 (31.3%)
Occupational statusEmployed 44 (27%)Not employed 119 (73%)
Drug or alcohol abuse 38 (23.3%)Age at onset (years)
15–20 23 (14.1%)21–30 46 (28.2%)N31 94 (57.7%)
Number of previous hospitalizations (mean±SD) 6.1±5.1Family history, mood disorder
Unipolar 57 (36.1%)Bipolar 5 (3.2%)
History of suicide attempts, lifetime 52 (32.9%)History of recent serious family conflict 80 (50.6%)
330 B. Biancosino et al. / Journal of Affective Disorders 124 (2010) 329–334
Several relevant aspects of depressive states, such as the‘dysphoric’ dimension, are underdetected with widely usedscales (Pancheri et al., 2002). While some authors point thatsymptoms such as tension, irritability, anger, and hostility arefeatures of the bipolar spectrum and suggest a continuitybetween bipolar disorder and major depressive disorder(Koukopoulos and Koukopoulos, 1999; Benazzi and Akiskal,2005; Benazzi, 2005, 2006; Zaccagni et al., 2008), other studiessuggested that clinically significant manic-like symptoms canbe identified even in strictly diagnosed unipolar depressives(Bauer et al., 2005; Maj et al., 2006; Goldberg et al., 2009) andthat ‘dysphoric’ symptoms may represent a specific psycho-pathological dimension in unipolar depression (Fava andRosenbaum, 1999; Pasquini et al., 2004; Biondi et al., 2005;Sato et al., 2002;Milak et al., 2007; Perlis et al., 2009; Fava et al.,2009).
The boundaries between apathy and depressed mood arealso debated (Greenson, 1949; Levy et al., 1998; Starkstein andLeentjens, 2008; Robert et al., 2009). Despite the frequent co-occurrence and partial overlapping of apathy and depression,some studies suggested that they may constitute distinctpsychopathological dimensions (Landes et al., 2005; Robertet al., 2009).
These findings suggest that dimensions different fromdepressed mood play an important part in the clinicalpresentation of unipolar depression, and that the use ofinstruments covering a wider range of psychopatology mayhelp clinicians recognize important aspects of depression(Pasquini et al., 2004; Harvey et al., 2009).
The Brief Psychiatric Rating Scale (BPRS) is commonlyusedto assess general psychopathology in patients with schizo-phrenia and other psychotic disorders. Although someauthors (Shafer, 2005) recommended to test the BPRS factorstructure in non-schizophrenic diagnostic groups, particularlymood disorder patients, such studies have been rare and didnot involve depressed patients (Ventura et al. 2000; Picardiet al., 2008). Although the BPRS has not been specificallydesigned to assess patients with depressive disorders, it mayhelp capturing a broader range of symptoms and describingthe overall clinical picture. This study aimed at examining itsfactor structure in recurrent major depressive disorder.
2. Methods
2.1. Study setting
The studywas performed in a 16-bed psychiatric inpatientunit that is part of the Clinical Psychiatry Section of theFerrara University and is linked with the local Mental HealthDepartment. This unit provides care for voluntary patientswith acute or sub-acute psychiatric conditions.
2.2. Participants
All consecutive patients (N=163) admitted during a 7-year recruitment period participated in the study. Inclusioncriteria were: ICD-10 diagnosis of depressive disorder (ICD-10 codes F32 to F33); absence of personality disorder; nolifetime history of mood swings and manic or hypomanicsymptoms. All patients gave written informed consent toparticipate. Table 1 summarizes patients' characteristics.
2.3. Assessment
At admission, each patient underwent detailed psychiatricexamination. All diagnoses were made by a faculty psychia-trist and independently confirmed by another facultypsychiatrist.
Within 3 days, patients were administered the 18-itemBPRS (Overall and Gorham, 1962) by a trained psychiatrist.The results of this assessment are detailed in Table 2.
2.4. Statistical analysis
After descriptive analysis, factor analysis using theprincipal-component factor method was performed on BPRS items. Thenumber of factors to be extracted was determined according tothe scree-plot method (Cattel, 1966). Orthogonal rotation wasperformed using the Varimax method. Standardized factorscores were calculated with the regression method andexpressed as Z scores (mean 0 and standard deviation 1).These scores represent an estimate of the score each subjectwould have obtained on each factor, if it could have beenmeasured directly.
Subsequently, analysis of variance or Spearman's cor-relation coefficient was used as appropriate to examine therelationship between factor scores and sociodemographic andpsychiatric history variables. Following univariate analysis,multiple linear regression analysis was performed to identifythe variables independently associated with each factor. Allanalyses were performed with SPSS 17.0 for Windows.
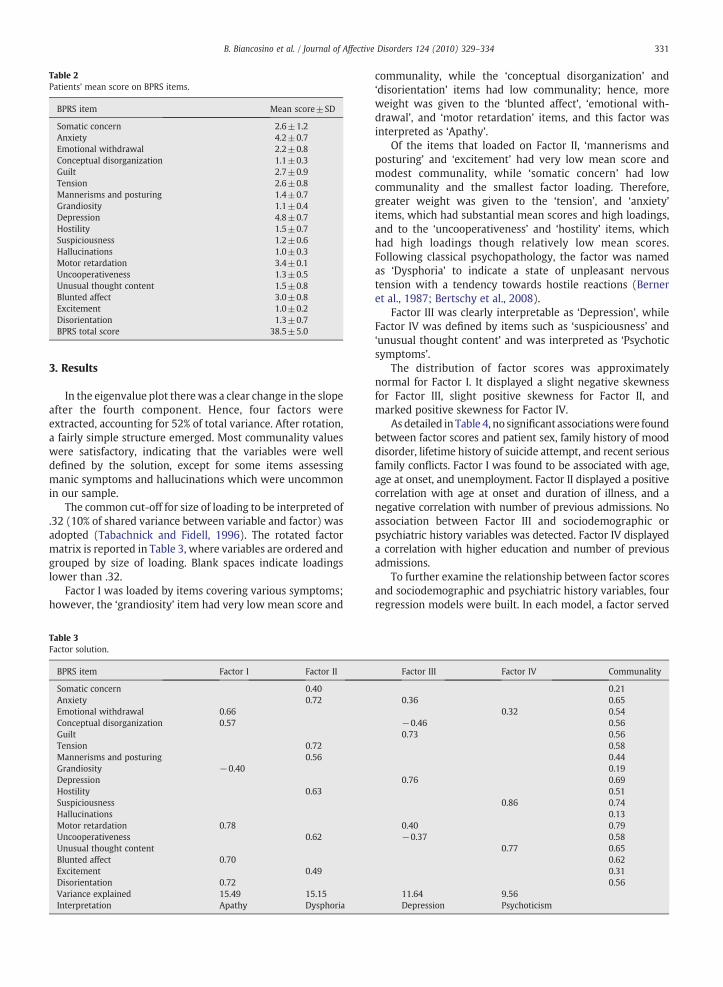
Table 2Patients' mean score on BPRS items.
BPRS item Mean score±SD
Somatic concern 2.6±1.2Anxiety 4.2±0.7Emotional withdrawal 2.2±0.8Conceptual disorganization 1.1±0.3Guilt 2.7±0.9Tension 2.6±0.8Mannerisms and posturing 1.4±0.7Grandiosity 1.1±0.4Depression 4.8±0.7Hostility 1.5±0.7Suspiciousness 1.2±0.6Hallucinations 1.0±0.3Motor retardation 3.4±0.1Uncooperativeness 1.3±0.5Unusual thought content 1.5±0.8Blunted affect 3.0±0.8Excitement 1.0±0.2Disorientation 1.3±0.7BPRS total score 38.5±5.0
331B. Biancosino et al. / Journal of Affective Disorders 124 (2010) 329–334
3. Results
In the eigenvalue plot therewas a clear change in the slopeafter the fourth component. Hence, four factors wereextracted, accounting for 52% of total variance. After rotation,a fairly simple structure emerged. Most communality valueswere satisfactory, indicating that the variables were welldefined by the solution, except for some items assessingmanic symptoms and hallucinations which were uncommonin our sample.
The common cut-off for size of loading to be interpreted of.32 (10% of shared variance between variable and factor) wasadopted (Tabachnick and Fidell, 1996). The rotated factormatrix is reported in Table 3, where variables are ordered andgrouped by size of loading. Blank spaces indicate loadingslower than .32.
Factor I was loaded by items covering various symptoms;however, the ‘grandiosity’ item had very low mean score and
Table 3Factor solution.
BPRS item Factor I Factor II
Somatic concern 0.40Anxiety 0.72Emotional withdrawal 0.66Conceptual disorganization 0.57GuiltTension 0.72Mannerisms and posturing 0.56Grandiosity −0.40DepressionHostility 0.63SuspiciousnessHallucinationsMotor retardation 0.78Uncooperativeness 0.62Unusual thought contentBlunted affect 0.70Excitement 0.49Disorientation 0.72Variance explained 15.49 15.15Interpretation Apathy Dysphoria
communality, while the ‘conceptual disorganization’ and‘disorientation’ items had low communality; hence, moreweight was given to the ‘blunted affect’, ‘emotional with-drawal’, and ‘motor retardation’ items, and this factor wasinterpreted as ‘Apathy’.
Of the items that loaded on Factor II, ‘mannerisms andposturing’ and ‘excitement’ had very low mean score andmodest communality, while ‘somatic concern’ had lowcommunality and the smallest factor loading. Therefore,greater weight was given to the ‘tension’, and ‘anxiety’items, which had substantial mean scores and high loadings,and to the ‘uncooperativeness’ and ‘hostility’ items, whichhad high loadings though relatively low mean scores.Following classical psychopathology, the factor was namedas ‘Dysphoria’ to indicate a state of unpleasant nervoustension with a tendency towards hostile reactions (Berneret al., 1987; Bertschy et al., 2008).
Factor III was clearly interpretable as ‘Depression’, whileFactor IV was defined by items such as ‘suspiciousness’ and‘unusual thought content’ and was interpreted as ‘Psychoticsymptoms’.
The distribution of factor scores was approximatelynormal for Factor I. It displayed a slight negative skewnessfor Factor III, slight positive skewness for Factor II, andmarked positive skewness for Factor IV.
As detailed in Table 4, no significant associationswere foundbetween factor scores and patient sex, family history of mooddisorder, lifetime history of suicide attempt, and recent seriousfamily conflicts. Factor I was found to be associated with age,age at onset, and unemployment. Factor II displayed a positivecorrelation with age at onset and duration of illness, and anegative correlation with number of previous admissions. Noassociation between Factor III and sociodemographic orpsychiatric history variables was detected. Factor IV displayeda correlation with higher education and number of previousadmissions.
To further examine the relationship between factor scoresand sociodemographic and psychiatric history variables, fourregression models were built. In each model, a factor served
Factor III Factor IV Communality
0.210.36 0.65
0.32 0.54−0.46 0.560.73 0.56
0.580.440.19
0.76 0.690.51
0.86 0.740.13
0.40 0.79−0.37 0.58
0.77 0.650.620.310.56
11.64 9.56Depression Psychoticism
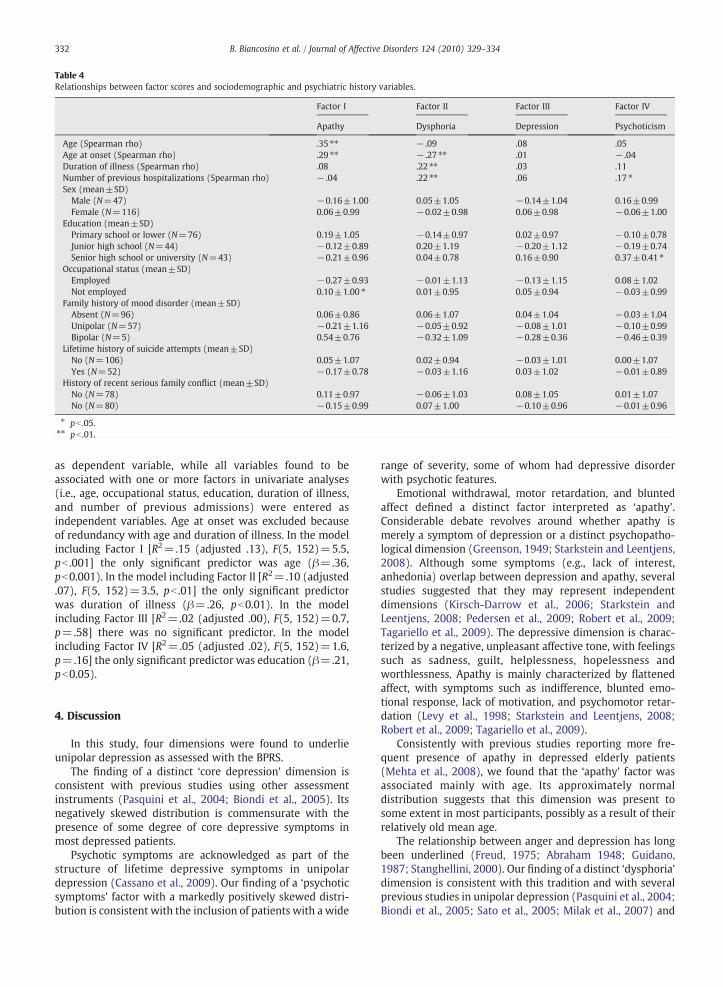
Table 4Relationships between factor scores and sociodemographic and psychiatric history variables.
Factor I Factor II Factor III Factor IV
Apathy Dysphoria Depression Psychoticism
Age (Spearman rho) .35 ⁎⁎ − .09 .08 .05Age at onset (Spearman rho) .29 ⁎⁎ − .27 ⁎⁎ .01 − .04Duration of illness (Spearman rho) .08 .22 ⁎⁎ .03 .11Number of previous hospitalizations (Spearman rho) − .04 .22 ⁎⁎ .06 .17 ⁎Sex (mean±SD)
Male (N=47) −0.16±1.00 0.05±1.05 −0.14±1.04 0.16±0.99Female (N=116) 0.06±0.99 −0.02±0.98 0.06±0.98 −0.06±1.00
Education (mean±SD)Primary school or lower (N=76) 0.19±1.05 −0.14±0.97 0.02±0.97 −0.10±0.78Junior high school (N=44) −0.12±0.89 0.20±1.19 −0.20±1.12 −0.19±0.74Senior high school or university (N=43) −0.21±0.96 0.04±0.78 0.16±0.90 0.37±0.41 ⁎
Occupational status (mean±SD)Employed −0.27±0.93 −0.01±1.13 −0.13±1.15 0.08±1.02Not employed 0.10±1.00 ⁎ 0.01±0.95 0.05±0.94 −0.03±0.99
Family history of mood disorder (mean±SD)Absent (N=96) 0.06±0.86 0.06±1.07 0.04±1.04 −0.03±1.04Unipolar (N=57) −0.21±1.16 −0.05±0.92 −0.08±1.01 −0.10±0.99Bipolar (N=5) 0.54±0.76 −0.32±1.09 −0.28±0.36 −0.46±0.39
Lifetime history of suicide attempts (mean±SD)No (N=106) 0.05±1.07 0.02±0.94 −0.03±1.01 0.00±1.07Yes (N=52) −0.17±0.78 −0.03±1.16 0.03±1.02 −0.01±0.89
History of recent serious family conflict (mean±SD)No (N=78) 0.11±0.97 −0.06±1.03 0.08±1.05 0.01±1.07No (N=80) −0.15±0.99 0.07±1.00 −0.10±0.96 −0.01±0.96
⁎ pb .05.⁎⁎ pb .01.
332 B. Biancosino et al. / Journal of Affective Disorders 124 (2010) 329–334
as dependent variable, while all variables found to beassociated with one or more factors in univariate analyses(i.e., age, occupational status, education, duration of illness,and number of previous admissions) were entered asindependent variables. Age at onset was excluded becauseof redundancy with age and duration of illness. In the modelincluding Factor I [R2=.15 (adjusted .13), F(5, 152)=5.5,pb .001] the only significant predictor was age (β=.36,pb0.001). In the model including Factor II [R2=.10 (adjusted.07), F(5, 152)=3.5, pb .01] the only significant predictorwas duration of illness (β=.26, pb0.01). In the modelincluding Factor III [R2=.02 (adjusted .00), F(5, 152)=0.7,p=.58] there was no significant predictor. In the modelincluding Factor IV [R2=.05 (adjusted .02), F(5, 152)=1.6,p=.16] the only significant predictor was education (β=.21,pb0.05).
4. Discussion
In this study, four dimensions were found to underlieunipolar depression as assessed with the BPRS.
The finding of a distinct ‘core depression’ dimension isconsistent with previous studies using other assessmentinstruments (Pasquini et al., 2004; Biondi et al., 2005). Itsnegatively skewed distribution is commensurate with thepresence of some degree of core depressive symptoms inmost depressed patients.
Psychotic symptoms are acknowledged as part of thestructure of lifetime depressive symptoms in unipolardepression (Cassano et al., 2009). Our finding of a ‘psychoticsymptoms’ factor with a markedly positively skewed distri-bution is consistent with the inclusion of patients with a wide
range of severity, some of whom had depressive disorderwith psychotic features.
Emotional withdrawal, motor retardation, and bluntedaffect defined a distinct factor interpreted as ‘apathy’.Considerable debate revolves around whether apathy ismerely a symptom of depression or a distinct psychopatho-logical dimension (Greenson, 1949; Starkstein and Leentjens,2008). Although some symptoms (e.g., lack of interest,anhedonia) overlap between depression and apathy, severalstudies suggested that they may represent independentdimensions (Kirsch-Darrow et al., 2006; Starkstein andLeentjens, 2008; Pedersen et al., 2009; Robert et al., 2009;Tagariello et al., 2009). The depressive dimension is charac-terized by a negative, unpleasant affective tone, with feelingssuch as sadness, guilt, helplessness, hopelessness andworthlessness. Apathy is mainly characterized by flattenedaffect, with symptoms such as indifference, blunted emo-tional response, lack of motivation, and psychomotor retar-dation (Levy et al., 1998; Starkstein and Leentjens, 2008;Robert et al., 2009; Tagariello et al., 2009).
Consistently with previous studies reporting more fre-quent presence of apathy in depressed elderly patients(Mehta et al., 2008), we found that the ‘apathy’ factor wasassociated mainly with age. Its approximately normaldistribution suggests that this dimension was present tosome extent in most participants, possibly as a result of theirrelatively old mean age.
The relationship between anger and depression has longbeen underlined (Freud, 1975; Abraham 1948; Guidano,1987; Stanghellini, 2000). Our finding of a distinct ‘dysphoria’dimension is consistent with this tradition and with severalprevious studies in unipolar depression (Pasquini et al., 2004;Biondi et al., 2005; Sato et al., 2005; Milak et al., 2007) and

333B. Biancosino et al. / Journal of Affective Disorders 124 (2010) 329–334
may support the proposal of a separate affective ‘dysphoric’dimension in mood disorders (Berner et al., 1987; Bertschyet al., 2008).
The ‘dysphoria’ dimension correlated mainly with dura-tion of illness, which corroborates the notion that dysphoricsymptoms may characterize more severe forms of depression(Perlis et al., 2009). Interestingly, this factor displayed apositively skewed distribution, which suggests that patientsmay be divided into two groups, one relatively free from andone with varying severity of dysphoric symptoms. Anaccurate assessment of anger-related symptoms in depressedpatients is important (Posternak and Zimmerman, 2002) toprovide optimal treatment as patients with prominentdysphoria may require modifications of standard pharmaco-logical (Koukopoulos et al., 2005; Koukopoulos et al., 2007;Pasquini et al., 2007) and psychotherapeutic (Enright andFitzgibbons, 2000) interventions.
Our study has several limitations. First, patients were notassessed with a structured diagnostic interview. However, alldiagnoses were made independently by two psychiatrists.Also, patients were systematically asked about lifetimehistory of mood swings and manic or hypomanic symptoms.This precaution should have minimised the risk of misdiag-nosing bipolar patients as unipolar.
Second, the 18-item BPRS does not adequately assesssymptoms of hypomania or mania, as it contains no specificitem and only few items partially tapping such symptoms.This may have prevented us from detecting a mania-likedimension.
Third, no standardized assessment of personality wasperformed. Although personality may have a pathoplasticeffect on the presentation of depression (Stanghellini et al.,2006), the exclusion of patients with a clinically diagnosedpersonality disorder should have reduced the influence ofpersonality on the results.
Another issue is the possible confounding by antidepres-sant medication. However, the BPRS was administered beforestarting antidepressant treatment, and only very few patientsreceived antidepressants before admission.
Finally, participants were recruited only at a singleinpatient unit. This may reduce the generalizability of ourresults to milder forms of depression, outpatient settings, andother countries.
In conclusion, although our findings are preliminary andneed confirmation, they suggest that in unipolar depressionthere are psychopathological dimensions other than de-pressed mood, such as apathy and dysphoria, that are worthyof greater clinical attention and research in order to optimizetreatment and improve outcome.
Role of funding sourceThe funding source (FAR Porject 2008 — University of Ferrara, Italy) has
been used to conduct statistical analysis of the data.
Conflict of interestAll the authors do not report any conflict of interest for the submitted
study.
Acknowledgements
The study has been partially funded by the University ofFerrara, Italy — FAR Project 2008.
References
Abraham, K., 1948. Notes on the Psychoanalytical Investigation of Manic–Depressive Insanity and Allied Conditions. Selected Papers of KarlAbraham. Hogarth Press, London.
Bauer, M.S., Simon, G.E., Ludman, E., Unutzer, J., 2005. Bipolarity in bipolardisorder: distribution of manic and depressive symptoms in a treatedpopulation. Br. J. Psychiatry 187, 87–88.
Benazzi, F., 2005. The relationship of major depressive disorder to bipolardisorder: continuous or discontinuous? Curr. Psychiatry Rep. 7, 462–470.
Benazzi, F., 2006. Symptoms of depression as possible markers of bipolar IIdisorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 30, 471–477.
Benazzi, F., Akiskal, H.S., 2005. Irritable–hostile depression: further valida-tion as a bipolar depressive mixed state. J. Affect. Disord. 84, 197–207.
Berner, P., Musalek, M., Walter, H., 1987. Psychopathological concepts ofdysphoria. Psychopathology 20, 93–100.
Bertschy, G., Gervasoni, N., Favre, S., Liberek, C., Ragama-pardos, E., Aubry, J.M.,Gex-Fabry, M., Dayer, A., 2008. Frequency of dysphoria and mixed states.Psychopathology 41, 187–193.
Biondi, M., Picardi, A., Pasquini, M., Gaetano, P., Pancheri, P., 2005. Dimensionalpsychopathology of depression: detection of an ‘activation’ dimension inunipolar depressed outpatients. J. Affect. Disord. 84, 133–139.
Cassano, G.B., Benvenuti, A., Miniati, M., Calugi, S., Mula, M., Maggi, L., Rucci, P.,Perris, F., Frank, E., 2009. The factor structure of lifetime depressivesprctrum in patientswith unipolar depression. J. Affect. Disord. 115, 87–99.
Cattel, R.B., 1966. The scree test for the number of factor. Multivariate Behav.Res. 1, 245–276.
Enright, R.D., Fitzgibbons, R.P., 2000. Helping Clients Forgive: An EmpiricalGuide for Resolving Anger and Restoring Hope. American PsychologicalAssociation Books, Washington D.C.
Fava, M., Rosenbaum, J.F., 1999. Anger attacks in patients with depression.J. Clin. Psychiatry 60 (Suppl 15), 21–24.
Fava, M., Hwang, I., Rush, A.J., Sampson, N., Walters, E.E., Kessler, R.C., 2009.The importance of irritability as a symptom of major depressivedisorder: results from the National Comorbidity Survey Replication.Mol. Psychiatry Mar. 10 Electronic publication ahead of print.
Freud, S., 1975. Mourning andmelancholia. Standard Edition of the CompletePsychological Works of Sigmund Freud, vol 4. Hogarth Press, London.
Goldberg, D., 2000. Plato versus Aristotle: categorical and dimensional modelsfor common mental disorders. Compr. Psychiatry 41 (Suppl. 1), 8–13.
Goldberg, J.F., Perlis, R.H., Bowden, C.L., Thase,M.E., Miklowitz, D.J., Marangell,L.B., Calabrese, J.R., Nierenberg, A.A., Sachs, G.S., 2009. Manic symptomsduring depressive episodes in 1,380 patients with bipolar disorder:findings from the STEP-BD. Am. J. Psychiatry 166, 173–181.
Greenson, R.R., 1949. The psychology of apathy. Psychoanal. Q. 18, 290–302.Guidano, V.F., 1987. Complexity of the Self. Guilford Press, New York.Harvey, P.D., Young, K.P., Reichenberg, A., Pogge, D.L., 2009. The factor
structure of clinical symptoms in depressed inpatients with unipolar orbipolar spectrum disorders. J. Nerv. Ment. Dis. 197, 161–165.
Kirsch-Darrow, L., Fernandez, H.H., Marsiske, M., Okun, M.S., Bowers, D.,2006. Dissociatine apathy and depression in Parkinson disease. Neurol-ogy 67, 33–38.
Koukopoulos, A., Koukopoulos, A., 1999. Agitated depression as a mixedstate and the problem of melancholia. Psychiatr. Clin. North Am. 22,547–564.
Koukopoulos, A., Albert, M.J., Sani, G., Koukopoulos, A.E., Girardi, P., 2005.Mixed depressive states: nosologic and therapeutic issues. Int. Rev.Psychiatry 17, 21–37.
Koukopoulos, A., Sani, G., Koukopoulos, A.E., Manfredi, G., Pacchiarotti, I.,Girardi, P., 2007. Melancholia agitata and mixed depression. Acta.Psychiatr. Scand. Suppl 433, 50–57.
Landes, A.M., Sperry, S.D., Strass, M.E., 2005. Prevalence of apathy, dysphoria,and depression in relation to dementia severity in Alzheimer's disease.J. Neuropsychiatry Clin. Neurosci. 17, 342–349.
Levy, M.L., Cummings, J.L., Fairbanks, L.A., Masterman, D., Miller, B.L., Craig,A.H., Paulsen, J.S., Litvan, I., 1998. Apathy is not depression. J. Neuro-psychiatry Clin. Neurosci. 10, 314–319.
Maj, M., Pirozzi, R., Magliano, L., Fiorillo, A., Batoli, L., 2006. Agitated“unipolar”major depression: prevalence, phenomenology, and outcome.J. Clin. Psychiatry 67, 712–719.
Mehta,M.,Whyte, E., Lenze, E., Hardy, S., Roumani, Y., Subashan, P., Huang,W.,Studenski, S., 2008. Depressive symptoms in late life: associations withapathy, resilience and disability vary between young-old and old-old.Int. J. Geriatr. Psychiatry 23, 238–243.
Milak, M.S., Aniskin, D.B., Eisenberg, D.P., Prikhojan, A., Cohen, L.J., Yard, S.S.,Galynker, I.I., 2007. The negative syndrome as a dimension: factor analysesof PANSS inmajor depressive disorder and organic brain disease comparedwith negative syndrome structures found in the schizophrenia literature.Cogn. Behav. Neurol. 20 (2), 113–120.

334 B. Biancosino et al. / Journal of Affective Disorders 124 (2010) 329–334
Overall, J.E., Gorham, D.R., 1962. The Brief Psychiatric Rating Scale. Psychol.Rep. 10, 799–812.
Pancheri, P., Picardi, A., Pasquini, M., Gaetano, P., Biondi, M., 2002.Psychopathological dimensions of depression: a factor study of the 17-item Hamilton Depression Rating Scale in unipolar depressed out-patients. J. Affect. Disord. 68, 41–47.
Pasquini, M., Picardi, A., Biondi, M., Gaetano, P., Morosini, P., 2004. Relevanceof anger and irritability in outpatients with major depressive disorder.Psychopathology 37, 155–160.
Pasquini, M., Picardi, A., Speca, A., Orlandi, V., Tarsitani, L., Morosini, P.,Cascavilla, I., Biondi, M., 2007. Combining an SSRI with an anticonvulsantin depressed patients with dysphoric mood: an open study. Clin. Pract.Epidemiol. Ment. Health. 3, 3.
Pedersen, K.F., Larsen, J.P., Alves, G., Aarsland, D., 2009. Prevalence andclinical correlates of apathy in Parkinson's disease: a community-basedstudy. Parkinsonism Relat. Disord. 15, 295–299.
Perlis, R.H., Fava, M., Trivedi, M.H., Alpert, J., Luther, J.F., Wisniewski, S.R.,Rush, J.A., 2009. Irritability is associated with anxiety and greaterseverity, but not bipolar spectrum features, in major depressive disorder.Acta Psychiatr. Scand. 119, 282–289.
Picardi, A., Battisti, F., De Girolamo, G., Morosini, P., Norcio, B., Bracco, R.,Biondi, M., 2008. Symptom structure of acute mania: a factor study of the24-item Brief Psychiatric Rating Scale in a national sample of patientshospitalized for a manic episode. J. Affect. Disord. 108, 183–189.
Posternak, M.A., Zimmerman, M., 2002. Anger and aggression in psychiatricoutpatients. J. Clin. Psychiatry 63, 665–672.
Robert, P., Onyike, C.U., Leentjens, A.F.G., Dujardin, K., Aalten, P., Starkstein, S.,Verhey, F.R.J., Yessavage, J., Clement, J.P., Drapier, D., Bayle, F., Benoit, M.,Boyer, P., Lorca, P.M., Thibaut, F., Gauthier, S., Grossberg, G., Vellas, B.,Byrne, J., 2009. Proposed diagnostic criteria for apathy in Alzheimer'sdisease and other neuropsychiatric disorders. Eur. Psychiatry 24, 98–104.
Sato, T., Bottlender, R., Kleindienst, N., Moller, H.J., 2002. Syndromes andphenomenological subtypes underlying acute mania: a factor analyticstudy of 576 manic patients. Am. J. Psychiatry 159, 968–974.
Sato, T., Bottlender, R., Kleindienst, N., Moller, H.J., 2005. Irritable psycho-motor elation in depressed inpatients: a factor validation of mixeddepression. J. Affect. Disord. 84, 187–196.
Shafer, A., 2005. Meta-analysis of the Brief Psychiatric Rating Scale factorstructure. Psychol. Assess. 17, 324–335.
Stanghellini, G., 2000. Dysphoria, vulnerability and identity. An eulogy foranger. Psychopathology 33, 198–203.
Stanghellini, G., Bertelli, M., Raballo, A., 2006. Typus melancholicus:personality structure and the characteristics of major unipolar depres-sive episode. J. Affect. Disord. 93, 159–167.
Starkstein, S.E., Leentjens, A.F.G., 2008. The nosological position of apathy inclinical practice. J. Neurol. Neurosurg. Psychiatry 79, 1088–1092.
Tabachnick, B., Fidell, L., 1996. Using Multivariate Statistics. HarperCollinsCollege Publishers, New York.
Tagariello, P., Girardi, P., Amore, M., 2009. Depression and apathy indementia: same syndrome or different construct? A critical review.Arch. Gerontol. Geriatr. 21, 1–8.
Van Praag, H.M., Asnis, G.M., Kahn, R.S., Brown, S.L., Korn, M., Harkavy-Friedman, J.M., Wetzler, S., 1990. Nosological tunnel vision in biologicalpsychiatry. A plea for a functional psychopathology. Ann. N. Y. Acad. Sci.600, 501–510.
Ventura, J., Nuechterlein, K.H., Subotnik, K.L., Gultkind, D., Gilbert, E.A., 2000.Symptom dimensions in recent-onset schizophrenia and mania: aprincipal component analysis of the 24-item Brief Psychiatric RatingScale. Psychiatry Res. 97, 129–135.
Zaccagni, M., Colombo, P.P., Aceti, F., 2008. Storia del disturbo bipolare: daAreteo di Cappadocia al DSM-IV e Bipolar Spectrum. Riv. Psichiatr. 43,348–360.
Related Documents











