Pamela E. Knapp, Ph.D. Dept. of Anatomy & Neurobiology Embryology DEVELOPMENT OF THE FACE, PALATE & SKULL READING: Larsen, 4 th Edition, Chapter 16; or Langman, 8 th Edition, pp. 366-380; pp. 161-166 OBJECTIVES: Following lecture and assigned reading, students should be able to: • Explain the development of the face from the unpaired frontonasal prominence and paired maxillary and mandibular processes. Be able to trace the derivation of major parts of the face. -Define the facial primordia in terms of the underlying mesenchyme that elevates them. -Discuss the role of nasal placodes in the formation of medial and lateral nasal processes. -Explain how facial processes merge. -Discuss the significance of the nasolacrimal groove. -Describe the fate of the various facial primordia. • Distinguish between the developmental processes of merging and fusion. • Give an account of the formation of primary and secondary palates and discuss the embryological basis of facial clefts, cleft lip and primary and secondary cleft palates. • Describe the separation of oral and nasal cavities and the specialization of certain cells of the nasal sac that become olfactory receptor cells. • Understand the basis of macrostomia and microstomia. • Distinguish between the neurocranium and the viscerocranium. • Distinguish between bones that first form as cartilage models (undergoing subsequent endochondral ossification) and those “membrane bones” that form directly into bone by differentiation of primitive connective tissue (mesenchyme) cells. • Describe the formation and fusion of occipital, parachordal and prechordal cartilages that make up the median cartilaginous plate of the chondrocranium. • Understand the structures that fuse to form the cartilaginous median plate, thus completing the chondrocranial “floor” of the neurocranium. • Label simple sketches of the fetal skull that show bones of the membranous neurocranium, its sutures and fontanelles. • Identify components of the membranous viscerocranium that form the skeletal components of the face. • Review the pharyngeal arch cartilages that comprise the cartilaginous viscerocranium and the structures that they form.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pamela E. Knapp, Ph.D. Dept. of Anatomy & Neurobiology Embryology
DEVELOPMENT OF THE FACE, PALATE & SKULL
READING: Larsen, 4th Edition, Chapter 16; or Langman, 8th Edition, pp. 366-380; pp. 161-166 OBJECTIVES: Following lecture and assigned reading, students should be able to: • Explain the development of the face from the unpaired frontonasal prominence and
paired maxillary and mandibular processes. Be able to trace the derivation of major parts of the face.
-Define the facial primordia in terms of the underlying mesenchyme that elevates them.
-Discuss the role of nasal placodes in the formation of medial and lateral nasal processes.
-Explain how facial processes merge. -Discuss the significance of the nasolacrimal groove. -Describe the fate of the various facial primordia.
• Distinguish between the developmental processes of merging and fusion. • Give an account of the formation of primary and secondary palates and discuss the
embryological basis of facial clefts, cleft lip and primary and secondary cleft palates.
• Describe the separation of oral and nasal cavities and the specialization of certain cells of the nasal sac that become olfactory receptor cells.
• Understand the basis of macrostomia and microstomia. • Distinguish between the neurocranium and the viscerocranium. • Distinguish between bones that first form as cartilage models (undergoing subsequent
endochondral ossification) and those “membrane bones” that form directly into bone by differentiation of primitive connective tissue (mesenchyme) cells.
• Describe the formation and fusion of occipital, parachordal and prechordal cartilages that make up the median cartilaginous plate of the chondrocranium.
• Understand the structures that fuse to form the cartilaginous median plate, thus completing the chondrocranial “floor” of the neurocranium.
• Label simple sketches of the fetal skull that show bones of the membranous neurocranium, its sutures and fontanelles.
• Identify components of the membranous viscerocranium that form the skeletal components of the face.
• Review the pharyngeal arch cartilages that comprise the cartilaginous viscerocranium and the structures that they form.
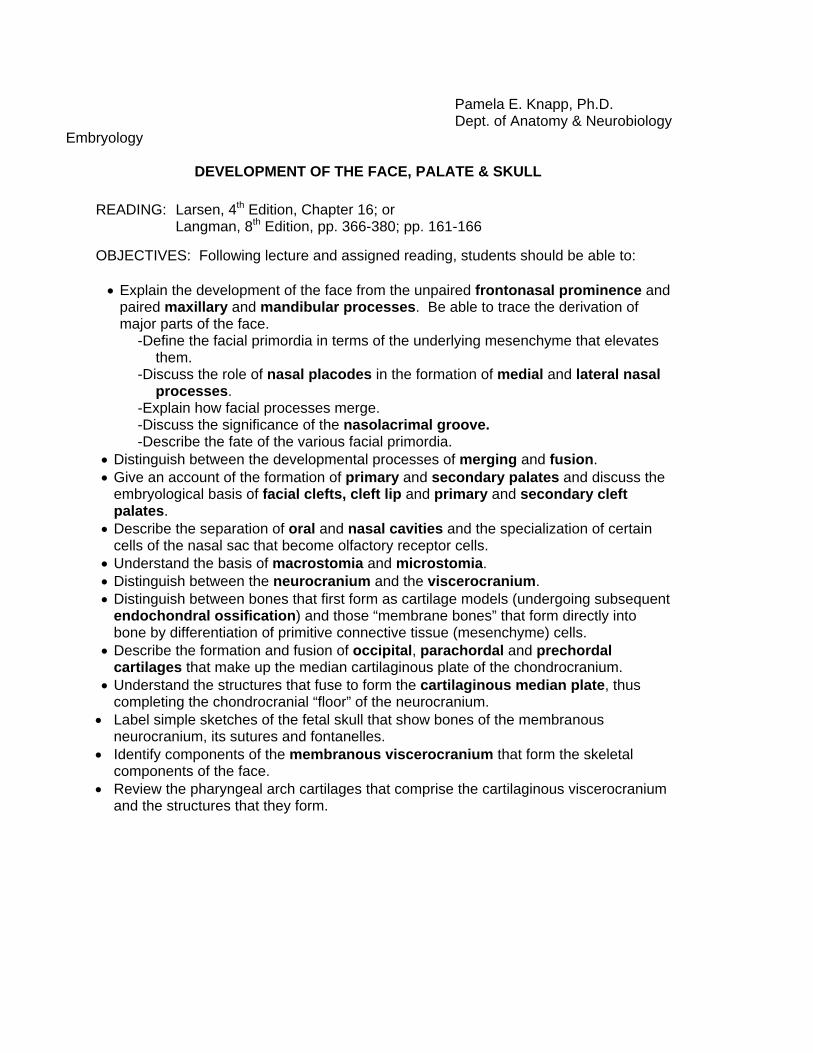
01. The facial primordia appear in the 4th week as a series of 5 ventral swellings
The frontonasal prominence is a single swelling located anterior to the stomodeum. It is not derived from pharyngeal arch tissue, but from mesenchyme proliferating ventral to the developing brain vesicles.
• The maxillary prominences are paired swellings which are components of the pharyngeal arches. They lie lateral to the stomodeum and below the frontonasal prominence.
• The mandibular prominences are paired swellings which are the posterior components of the 1st pharyngeal arches. They are located at the posterior border of the stomodeum
• On the lateral sides of the frontonasal prominence are the nasal placodes, bilateral ectodermal thickenings. They will invaginate to form at first a nasal sac, and later a deeper nasal pit.
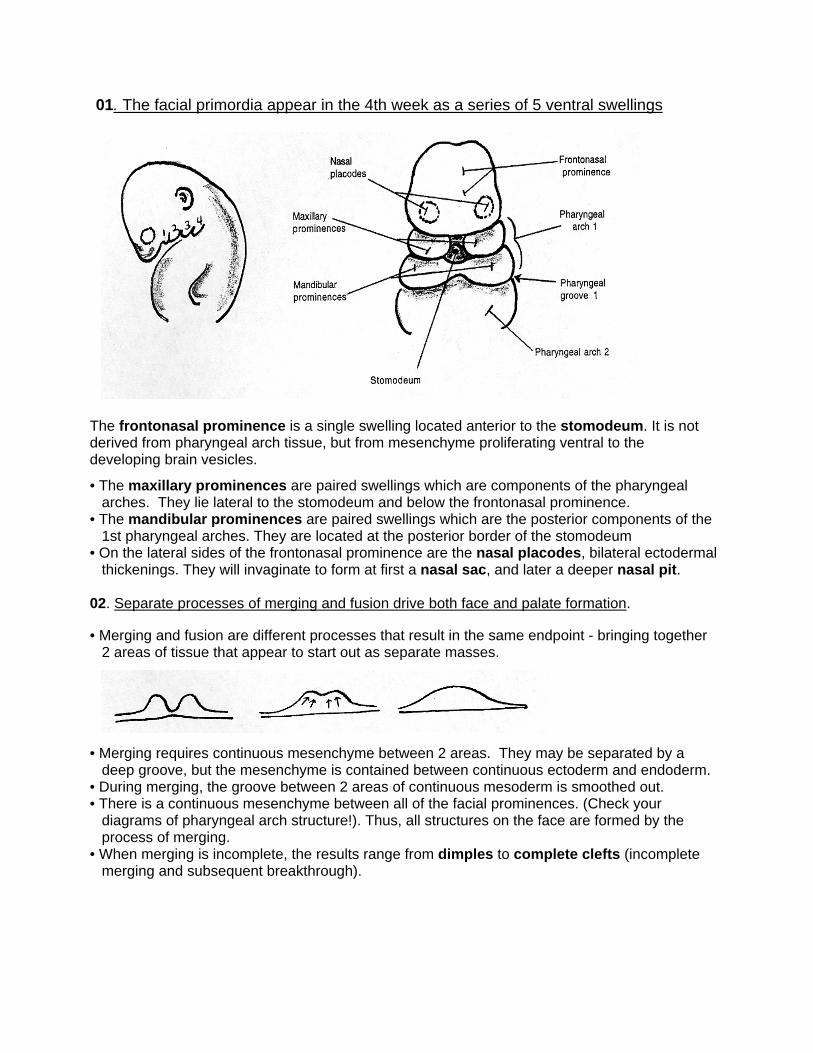
02. Separate processes of merging and fusion drive both face and palate formation. • Merging and fusion are different processes that result in the same endpoint - bringing together
2 areas of tissue that appear to start out as separate masses.
• Merging requires continuous mesenchyme between 2 areas. They may be separated by a deep groove, but the mesenchyme is contained between continuous ectoderm and endoderm.
• During merging, the groove between 2 areas of continuous mesoderm is smoothed out. • There is a continuous mesenchyme between all of the facial prominences. (Check your
diagrams of pharyngeal arch structure!). Thus, all structures on the face are formed by the process of merging.
• When merging is incomplete, the results range from dimples to complete clefts (incomplete merging and subsequent breakthrough).
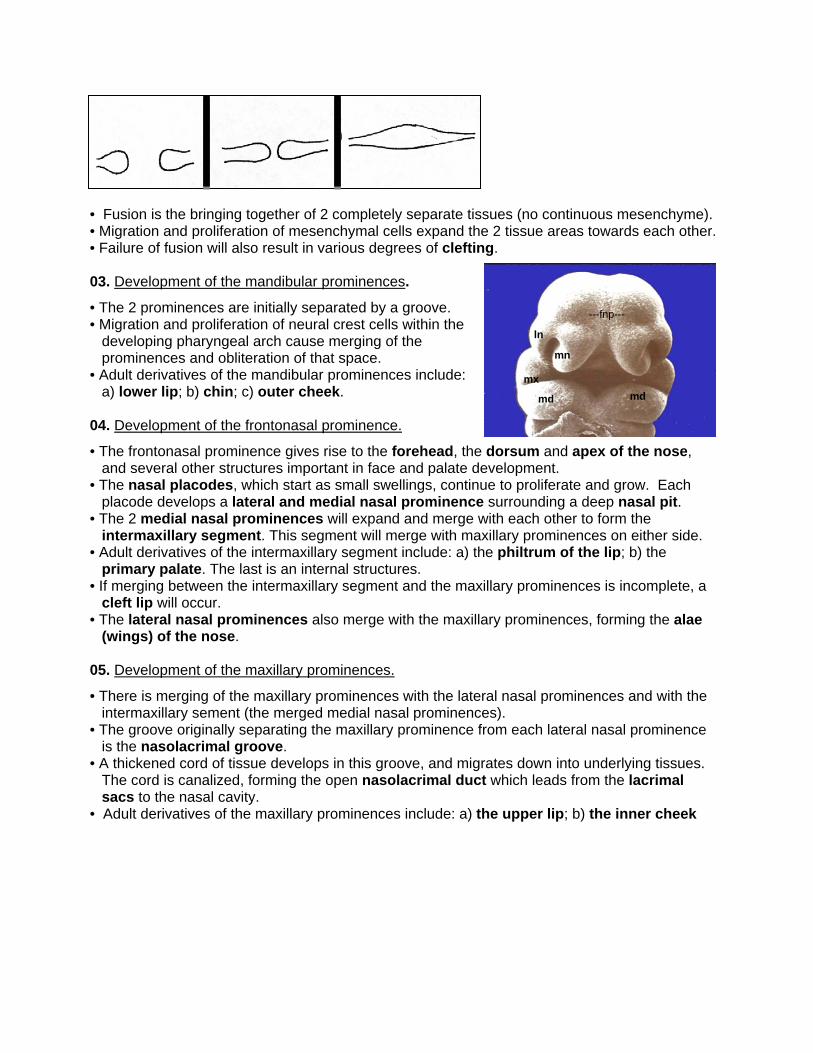
• Fusion is the bringing together of 2 completely separate tissues (no continuous mesenchyme). • Migration and proliferation of mesenchymal cells expand the 2 tissue areas towards each other. • Failure of fusion will also result in various degrees of clefting.
mn
mx
md
ln
md
---fnp---
03. Development of the mandibular prominences.
• The 2 prominences are initially separated by a groove. • Migration and proliferation of neural crest cells within the
developing pharyngeal arch cause merging of the prominences and obliteration of that space.
• Adult derivatives of the mandibular prominences include: a) lower lip; b) chin; c) outer cheek.
04. Development of the frontonasal prominence.
• The frontonasal prominence gives rise to the forehead, the dorsum and apex of the nose, and several other structures important in face and palate development.
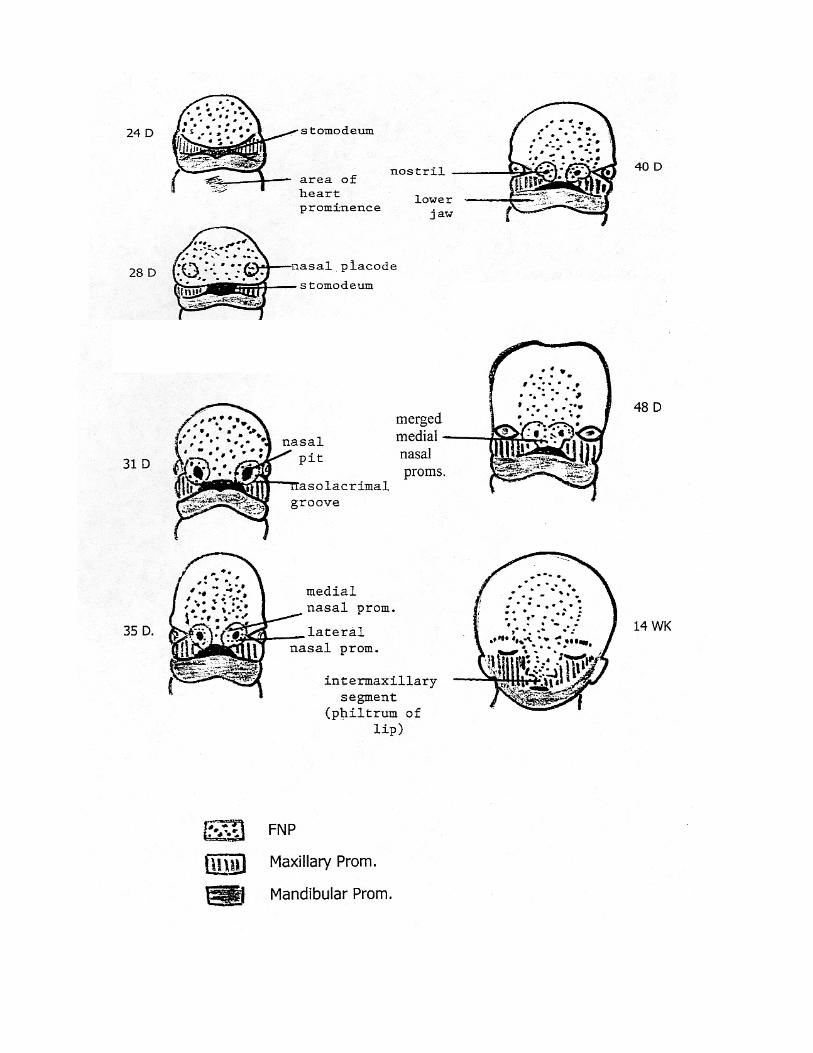
• The nasal placodes, which start as small swellings, continue to proliferate and grow. Each placode develops a lateral and medial nasal prominence surrounding a deep nasal pit.
• The 2 medial nasal prominences will expand and merge with each other to form the intermaxillary segment. This segment will merge with maxillary prominences on either side.
• Adult derivatives of the intermaxillary segment include: a) the philtrum of the lip; b) the primary palate. The last is an internal structures.
• If merging between the intermaxillary segment and the maxillary prominences is incomplete, a cleft lip will occur.
• The lateral nasal prominences also merge with the maxillary prominences, forming the alae (wings) of the nose.
05. Development of the maxillary prominences.
• There is merging of the maxillary prominences with the lateral nasal prominences and with the intermaxillary sement (the merged medial nasal prominences).
• The groove originally separating the maxillary prominence from each lateral nasal prominence is the nasolacrimal groove.
• A thickened cord of tissue develops in this groove, and migrates down into underlying tissues. The cord is canalized, forming the open nasolacrimal duct which leads from the lacrimal sacs to the nasal cavity.
• Adult derivatives of the maxillary prominences include: a) the upper lip; b) the inner cheek
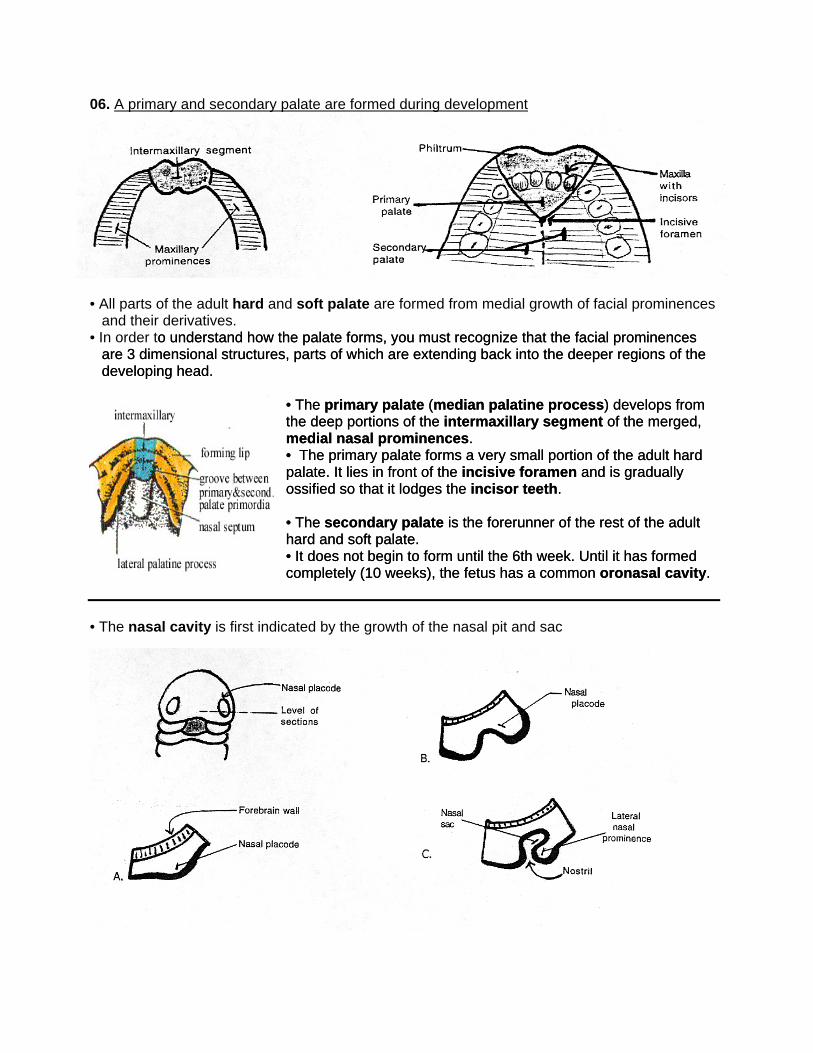
06. A primary and secondary palate are formed during development
All parts of the adult hard and soft palate are formed from medial growth of facial prominences
• he facial prominences
The primary palate (median palatine process) develops from
ery small portion of the adult hard
The secondary palate is the forerunner of the rest of the adult
rm until the 6th week. Until it has formed .
he facial prominences
The primary palate (median palatine process) develops from
ery small portion of the adult hard
The secondary palate is the forerunner of the rest of the adult
rm until the 6th week. Until it has formed .
•
and their derivatives. In order to understand how the palate forms, you must recognize that to understand how the palate forms, you must recognize that tare 3 dimensional structures, parts of which are extending back into the deeper regions of thedeveloping head. are 3 dimensional structures, parts of which are extending back into the deeper regions of thedeveloping head.
• • the deep portions of the intermaxillary segment of the merged, medial nasal prominences. • The primary palate forms a v
the deep portions of the intermaxillary segment of the merged, medial nasal prominences. • The primary palate forms a vpalate. It lies in front of the incisive foramen and is gradually ossified so that it lodges the incisor teeth.
palate. It lies in front of the incisive foramen and is gradually ossified so that it lodges the incisor teeth. • • hard and soft palate. • It does not begin to fohard and soft palate. • It does not begin to focompletely (10 weeks), the fetus has a common oronasal cavitycompletely (10 weeks), the fetus has a common oronasal cavity
• The nasal cavity is first indicated by the growth of the nasal pit and sac
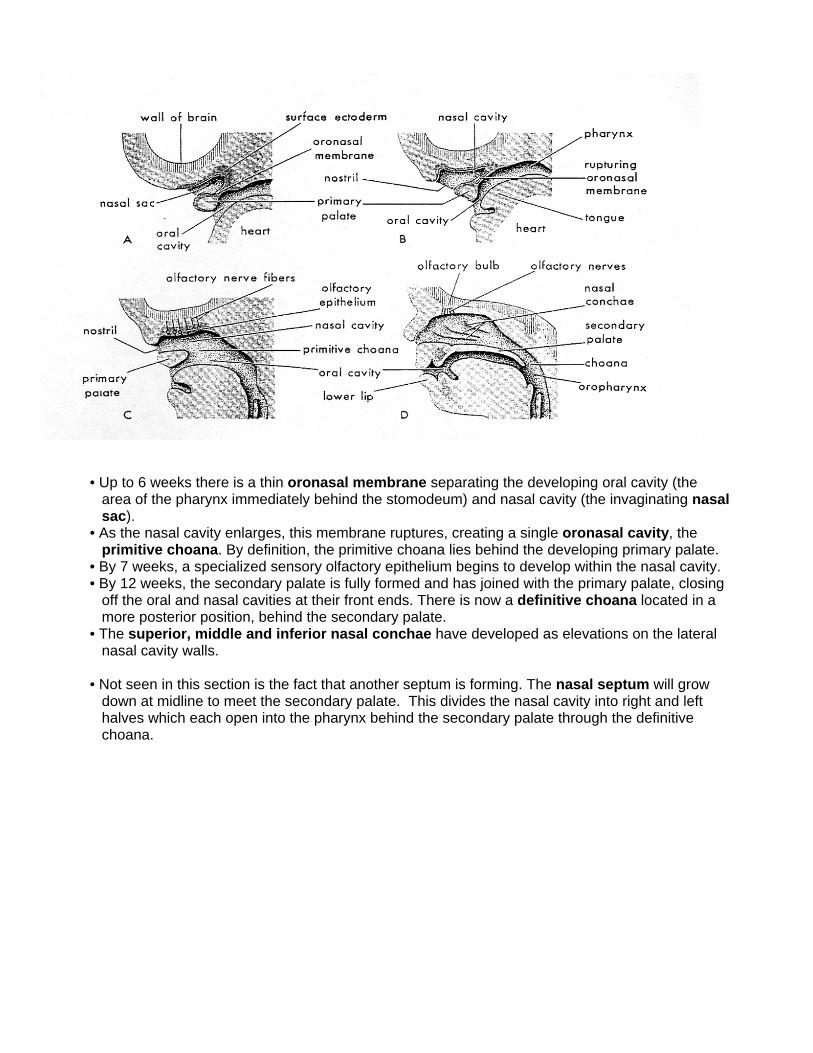
• Up to 6 weeks there is a thin oronasal membrane separating the developing oral cavity (the
area of the pharynx immediately behind the stomodeum) and nasal cavity (the invaginating nasal sac).
• As the nasal cavity enlarges, this membrane ruptures, creating a single oronasal cavity, the primitive choana. By definition, the primitive choana lies behind the developing primary palate.
• By 7 weeks, a specialized sensory olfactory epithelium begins to develop within the nasal cavity. • By 12 weeks, the secondary palate is fully formed and has joined with the primary palate, closing
off the oral and nasal cavities at their front ends. There is now a definitive choana located in a more posterior position, behind the secondary palate.
• The superior, middle and inferior nasal conchae have developed as elevations on the lateral nasal cavity walls.
• Not seen in this section is the fact that another septum is forming. The nasal septum will grow
down at midline to meet the secondary palate. This divides the nasal cavity into right and left halves which each open into the pharynx behind the secondary palate through the definitive choana.
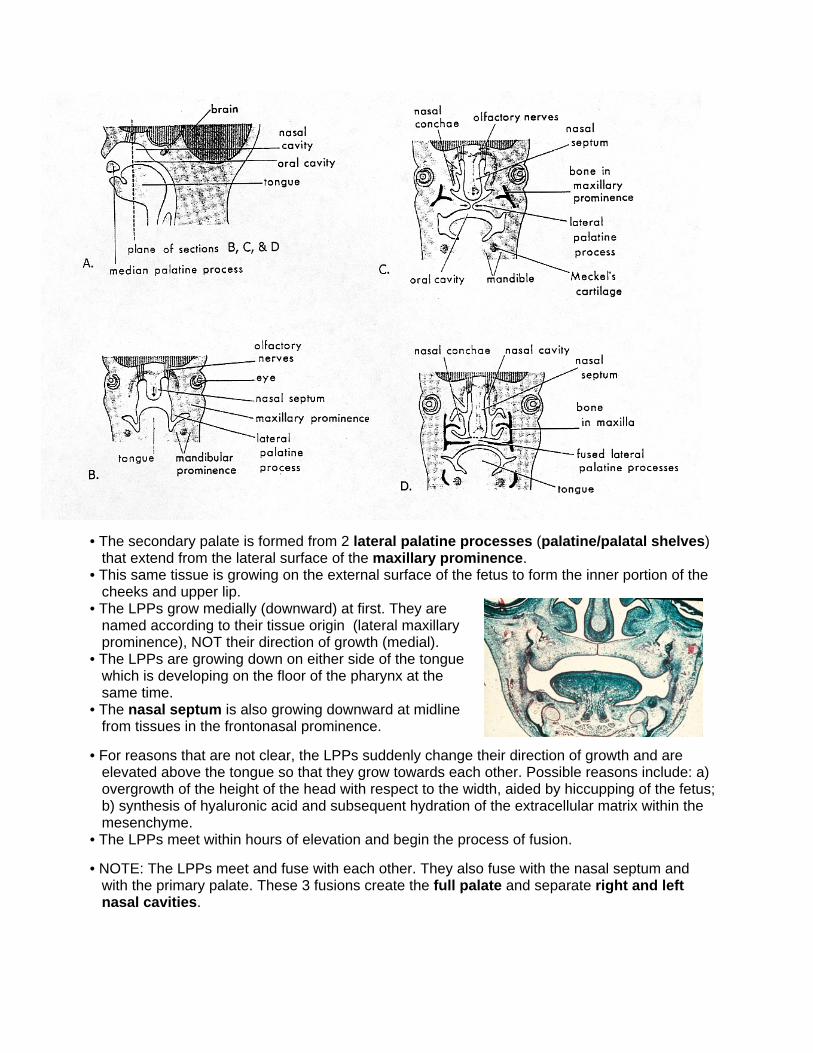
• The secondary palate is formed from 2 lateral palatine processes (palatine/palatal shelves)
that extend from the lateral surface of the maxillary prominence. • This same tissue is growing on the external surface of the fetus to form the inner portion of the
cheeks and upper lip. • The LPPs grow medially (downward) at first. They are
named according to their tissue origin (lateral maxillary prominence), NOT their direction of growth (medial).
• The LPPs are growing down on either side of the tongue which is developing on the floor of the pharynx at the same time.
• The nasal septum is also growing downward at midline from tissues in the frontonasal prominence.
• For reasons that are not clear, the LPPs suddenly change their direction of growth and are
elevated above the tongue so that they grow towards each other. Possible reasons include: a) overgrowth of the height of the head with respect to the width, aided by hiccupping of the fetus; b) synthesis of hyaluronic acid and subsequent hydration of the extracellular matrix within the mesenchyme.
• The LPPs meet within hours of elevation and begin the process of fusion. • NOTE: The LPPs meet and fuse with each other. They also fuse with the nasal septum and
with the primary palate. These 3 fusions create the full palate and separate right and left nasal cavities.
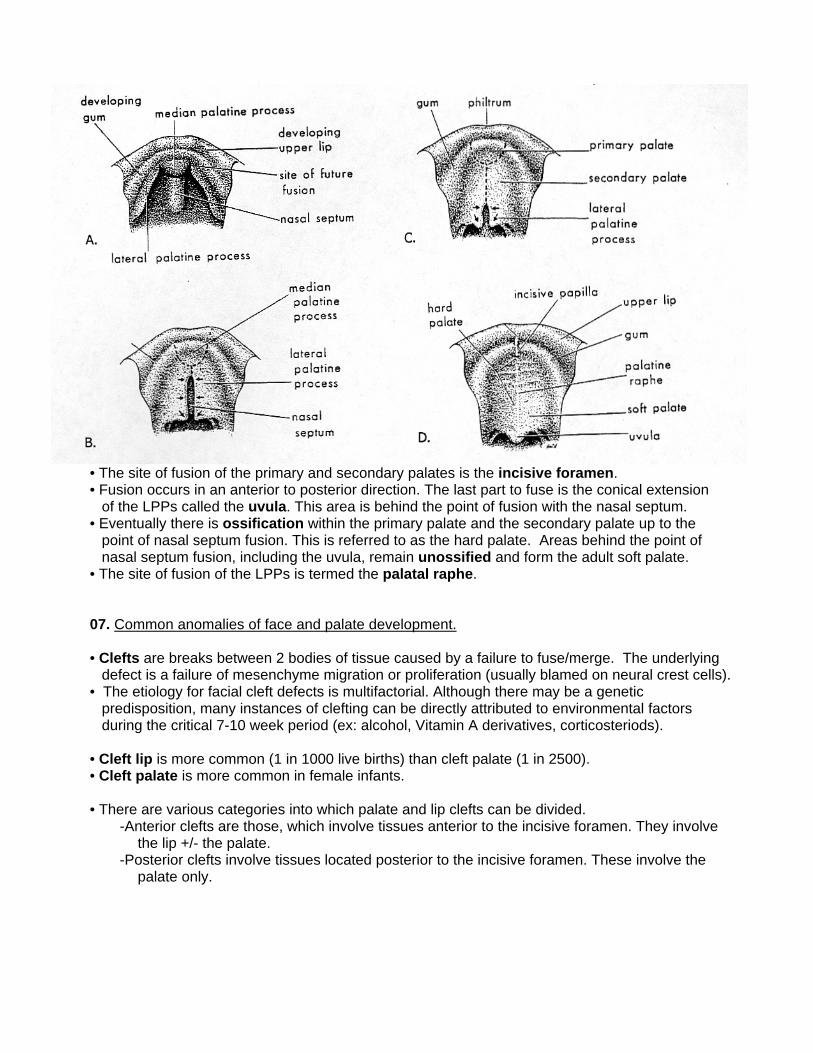
• The site of fusion of the primary and secondary palates is the incisive foramen. • Fusion occurs in an anterior to posterior direction. The last part to fuse is the conical extension
of the LPPs called the uvula. This area is behind the point of fusion with the nasal septum. • Eventually there is ossification within the primary palate and the secondary palate up to the
point of nasal septum fusion. This is referred to as the hard palate. Areas behind the point of nasal septum fusion, including the uvula, remain unossified and form the adult soft palate.
• The site of fusion of the LPPs is termed the palatal raphe. 07. Common anomalies of face and palate development. • Clefts are breaks between 2 bodies of tissue caused by a failure to fuse/merge. The underlying
defect is a failure of mesenchyme migration or proliferation (usually blamed on neural crest cells). • The etiology for facial cleft defects is multifactorial. Although there may be a genetic
predisposition, many instances of clefting can be directly attributed to environmental factors during the critical 7-10 week period (ex: alcohol, Vitamin A derivatives, corticosteriods).
• Cleft lip is more common (1 in 1000 live births) than cleft palate (1 in 2500). • Cleft palate is more common in female infants. • There are various categories into which palate and lip clefts can be divided.
-Anterior clefts are those, which involve tissues anterior to the incisive foramen. They involve the lip +/- the palate.
-Posterior clefts involve tissues located posterior to the incisive foramen. These involve the palate only.
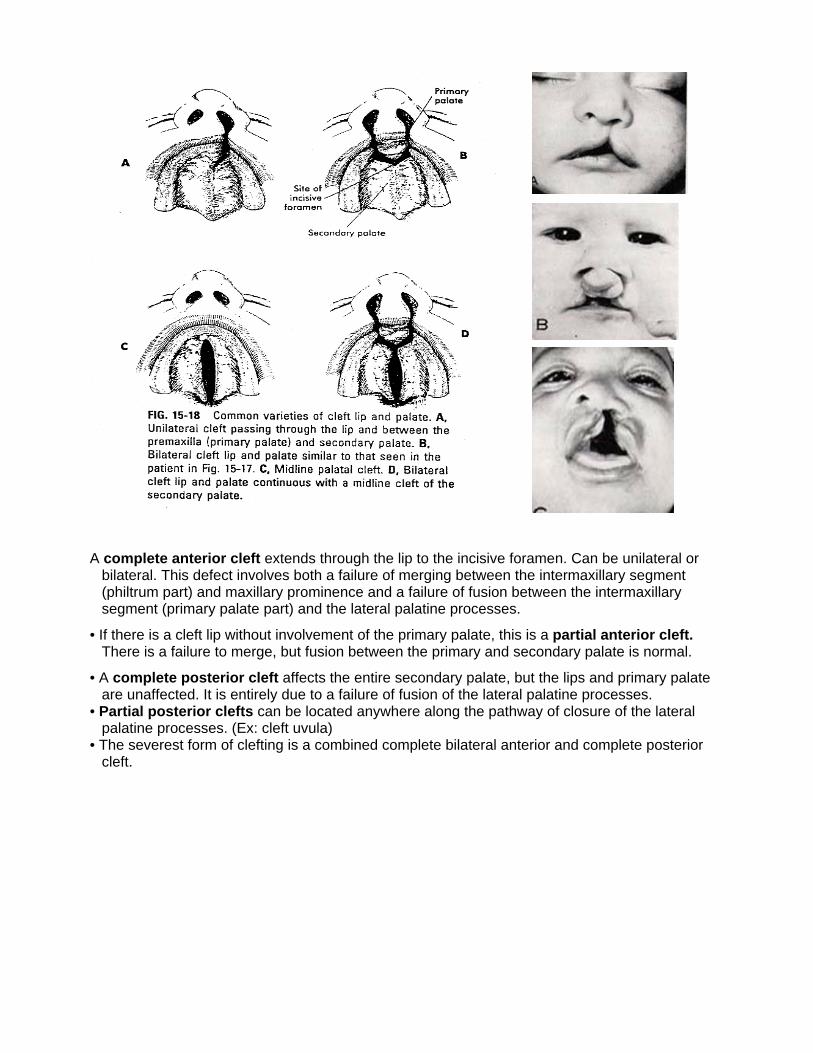
A complete anterior cleft extends through the lip to the incisive foramen. Can be unilateral or
bilateral. This defect involves both a failure of merging between the intermaxillary segment (philtrum part) and maxillary prominence and a failure of fusion between the intermaxillary segment (primary palate part) and the lateral palatine processes.
• If there is a cleft lip without involvement of the primary palate, this is a partial anterior cleft. There is a failure to merge, but fusion between the primary and secondary palate is normal.
• A complete posterior cleft affects the entire secondary palate, but the lips and primary palate are unaffected. It is entirely due to a failure of fusion of the lateral palatine processes.
• Partial posterior clefts can be located anywhere along the pathway of closure of the lateral palatine processes. (Ex: cleft uvula)
• The severest form of clefting is a combined complete bilateral anterior and complete posterior cleft.
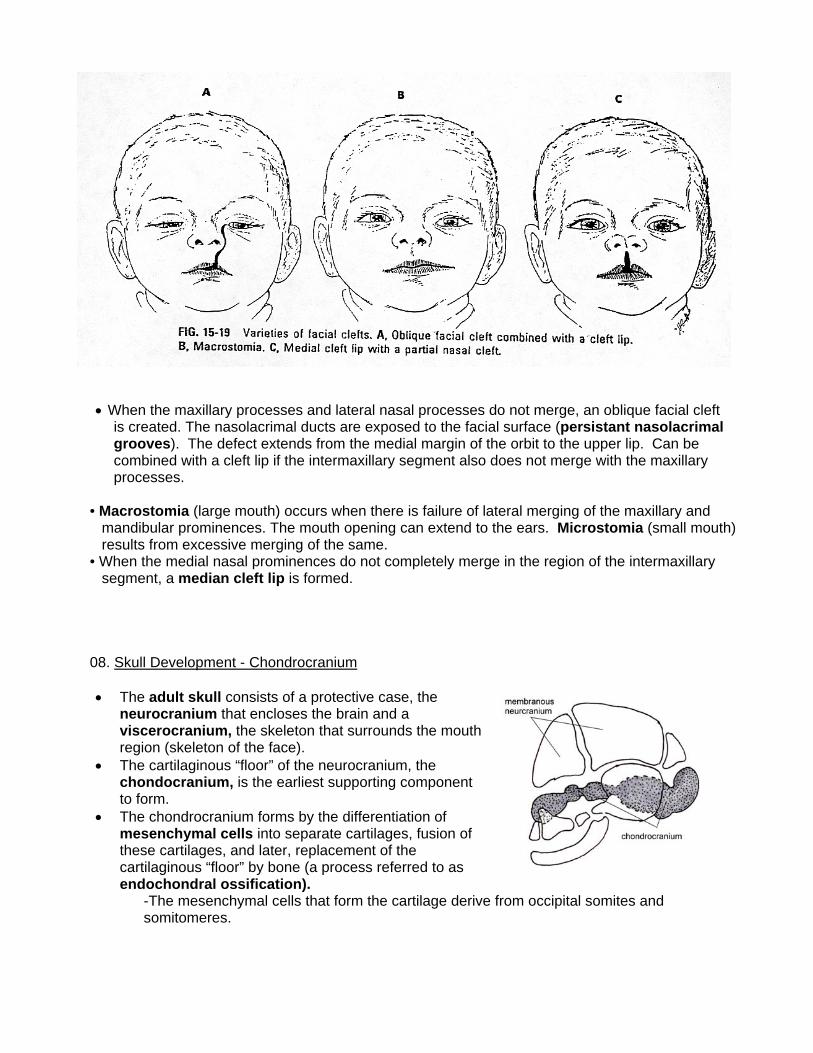
• When the maxillary processes and lateral nasal processes do not merge, an oblique facial cleft
is created. The nasolacrimal ducts are exposed to the facial surface (persistant nasolacrimal grooves). The defect extends from the medial margin of the orbit to the upper lip. Can be combined with a cleft lip if the intermaxillary segment also does not merge with the maxillary processes.
• Macrostomia (large mouth) occurs when there is failure of lateral merging of the maxillary and
mandibular prominences. The mouth opening can extend to the ears. Microstomia (small mouth) results from excessive merging of the same.
• When the medial nasal prominences do not completely merge in the region of the intermaxillary segment, a median cleft lip is formed.
08. Skull Development - Chondrocranium • The adult skull consists of a protective case, the
neurocranium that encloses the brain and a viscerocranium, the skeleton that surrounds the mouth region (skeleton of the face).
• The cartilaginous “floor” of the neurocranium, the chondocranium, is the earliest supporting component to form.
• The chondrocranium forms by the differentiation of mesenchymal cells into separate cartilages, fusion of these cartilages, and later, replacement of the cartilaginous “floor” by bone (a process referred to as endochondral ossification).
-The mesenchymal cells that form the cartilage derive from occipital somites and somitomeres.
• An occipital cartilage forms by differentiation of
(scleratomal) mesenchymal cells from several pairs of occipital somites. The precartilaginous components unite and form a single cartilage that entends laterally and dorsally to surround the neural tube and form the foramen magnum.
• Paired parachordal cartilages develop from mesenchyme of somitomeres around the cranial tip of the notochord and fuse with the occipital cartilage.
• Both the parachordal and occipital cartilages make up the cartilaginous model that ultimately is replaced by endochondral ossification to form the base and superior portion of the occipital bone.
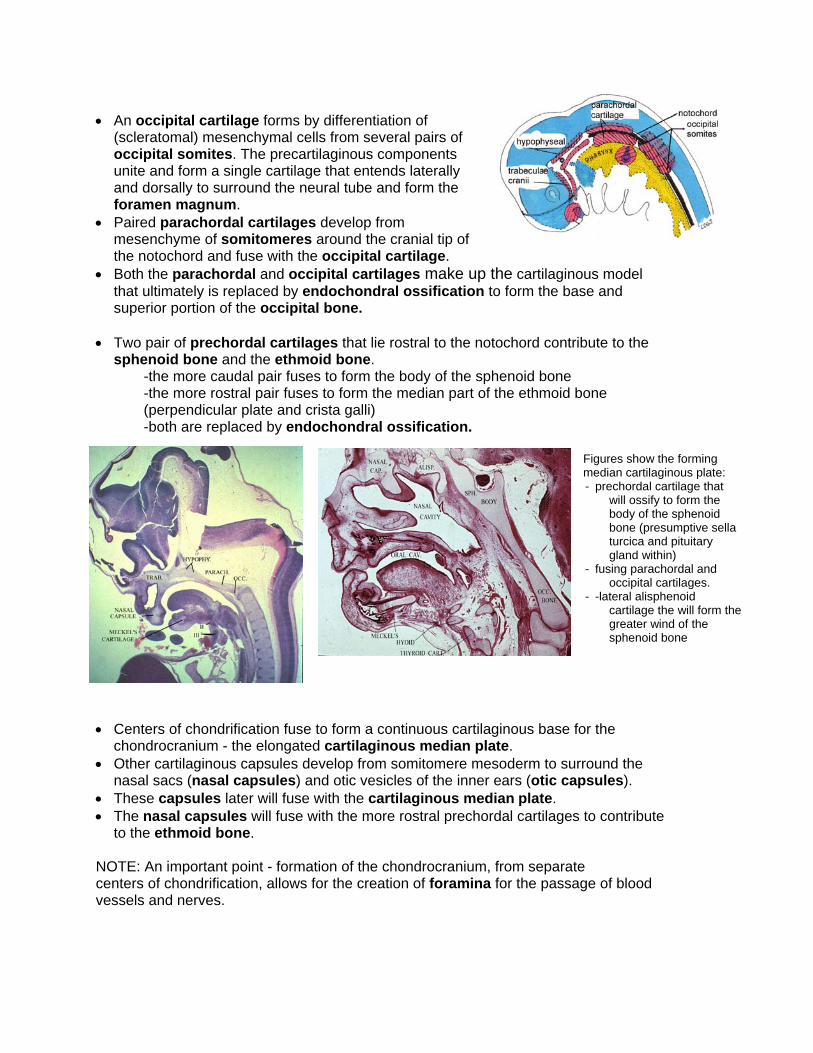
• Two pair of prechordal cartilages that lie rostral to the notochord contribute to the sphenoid bone and the ethmoid bone.
-the more caudal pair fuses to form the body of the sphenoid bone -the more rostral pair fuses to form the median part of the ethmoid bone (perpendicular plate and crista galli) -both are replaced by endochondral ossification.
Figures show the forming median cartilaginous plate: - prechordal cartilage that
will ossify to form the body of the sphenoid bone (presumptive sella turcica and pituitary gland within)
- fusing parachordal and occipital cartilages.
- -lateral alisphenoid cartilage the will form the greater wind of the sphenoid bone
• Centers of chondrification fuse to form a continuous cartilaginous base for the
chondrocranium - the elongated cartilaginous median plate. • Other cartilaginous capsules develop from somitomere mesoderm to surround the
nasal sacs (nasal capsules) and otic vesicles of the inner ears (otic capsules). • These capsules later will fuse with the cartilaginous median plate. • The nasal capsules will fuse with the more rostral prechordal cartilages to contribute
to the ethmoid bone. NOTE: An important point - formation of the chondrocranium, from separate centers of chondrification, allows for the creation of foramina for the passage of blood vessels and nerves.
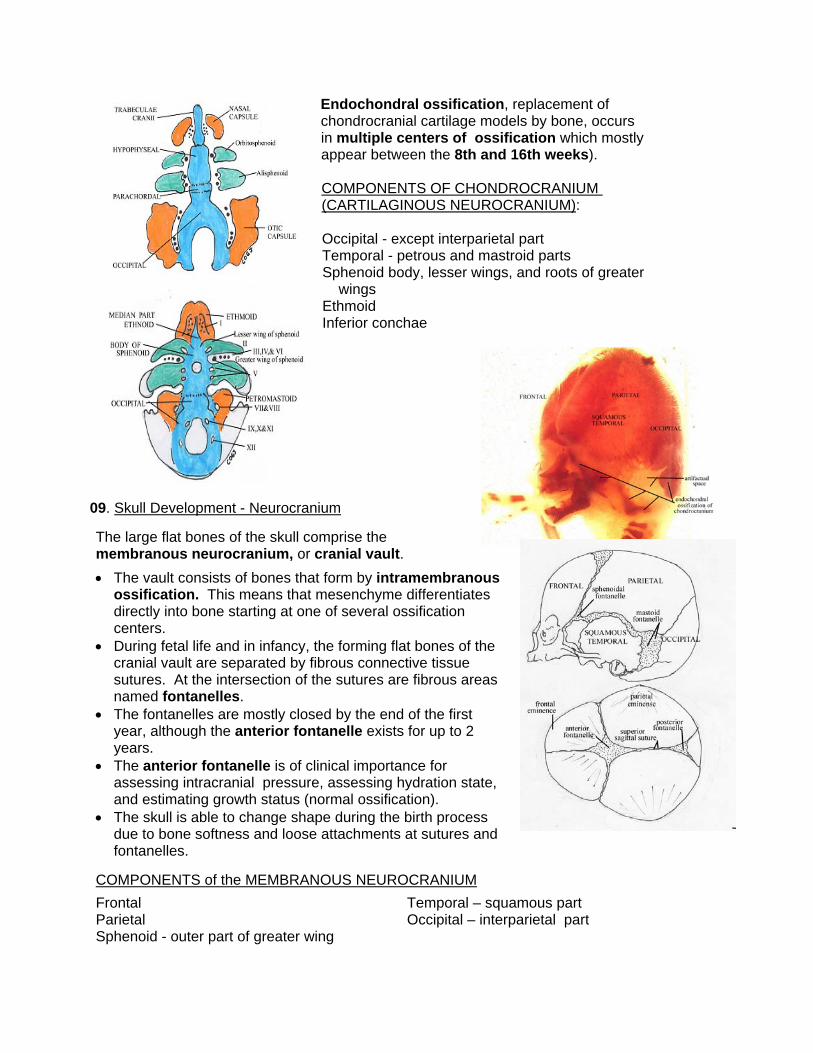
Endochondral ossification, replacement of chondrocranial cartilage models by bone, occurs in multiple centers of ossification which mostly appear between the 8th and 16th weeks). COMPONENTS OF CHONDROCRANIUM (CARTILAGINOUS NEUROCRANIUM): Occipital - except interparietal part Temporal - petrous and mastroid parts Sphenoid body, lesser wings, and roots of greater wings Ethmoid Inferior conchae
09. Skull Development - Neurocranium The large flat bones of the skull comprise the membranous neurocranium, or cranial vault.
• The vault consists of bones that form by intramembranous ossification. This means that mesenchyme differentiates directly into bone starting at one of several ossification centers.
• During fetal life and in infancy, the forming flat bones of the cranial vault are separated by fibrous connective tissue sutures. At the intersection of the sutures are fibrous areas named fontanelles.
• The fontanelles are mostly closed by the end of the first year, although the anterior fontanelle exists for up to 2 years.
• The anterior fontanelle is of clinical importance for assessing intracranial pressure, assessing hydration state, and estimating growth status (normal ossification).
• The skull is able to change shape during the birth process due to bone softness and loose attachments at sutures and fontanelles.
COMPONENTS of the MEMBRANOUS NEUROCRANIUM
Frontal Parietal Sphenoid - outer part of greater wing
Temporal – squamous part Occipital – interparietal part
10. Skull Development – Viscerocranium
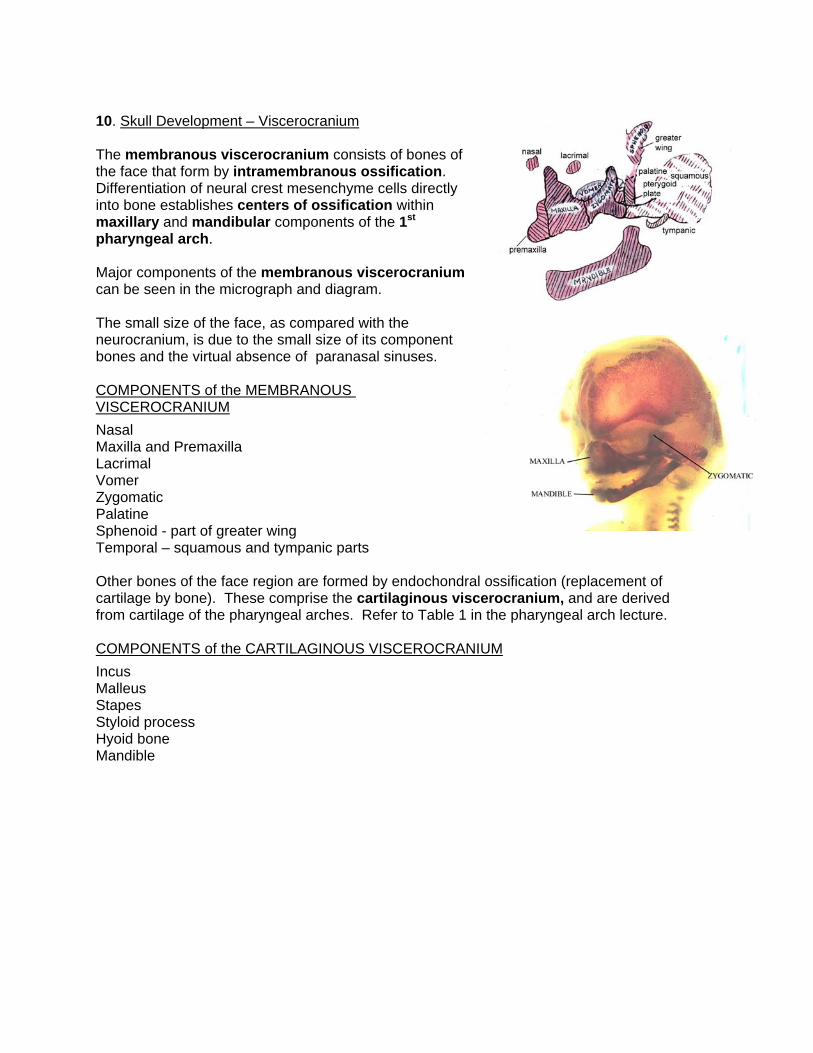
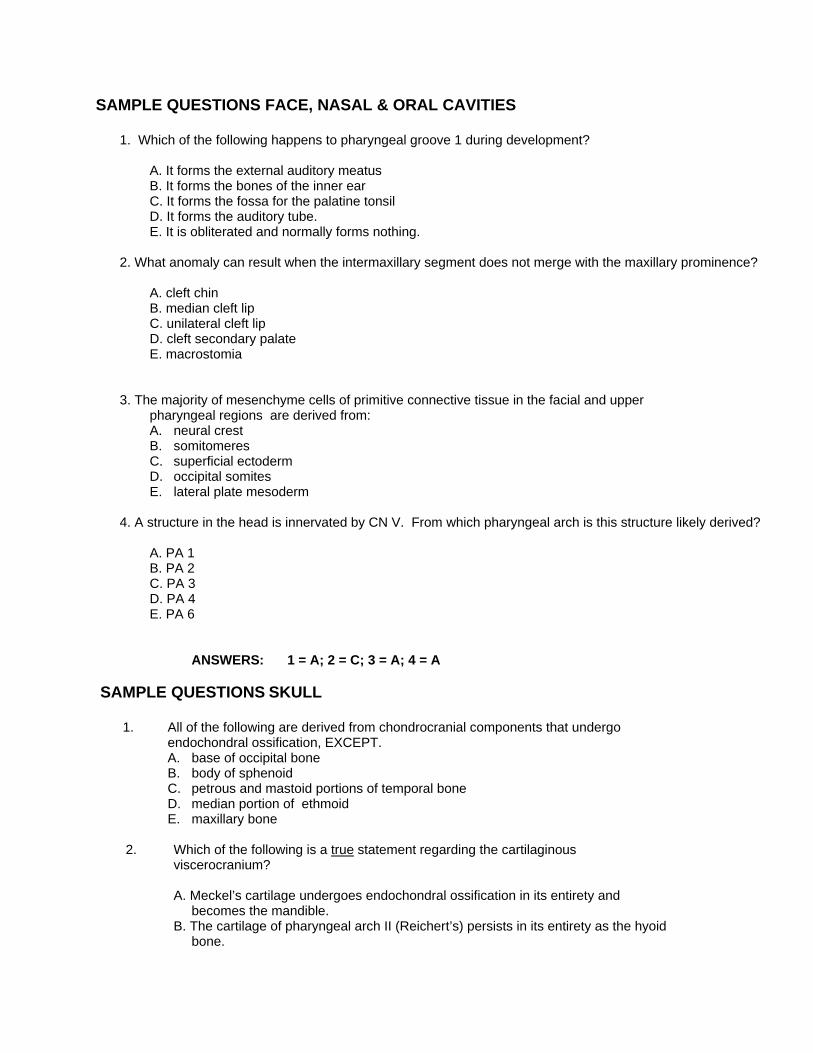
The membranous viscerocranium consists of bones of the face that form by intramembranous ossification. Differentiation of neural crest mesenchyme cells directly into bone establishes centers of ossification within maxillary and mandibular components of the 1st pharyngeal arch. Major components of the membranous viscerocranium can be seen in the micrograph and diagram. The small size of the face, as compared with the neurocranium, is due to the small size of its component bones and the virtual absence of paranasal sinuses.
COMPONENTS of the MEMBRANOUS VISCEROCRANIUM
Nasal Maxilla and Premaxilla Lacrimal Vomer Zygomatic Palatine Sphenoid - part of greater wing Temporal – squamous and tympanic parts Other bones of the face region are formed by endochondral ossification (replacement of cartilage by bone). These comprise the cartilaginous viscerocranium, and are derived from cartilage of the pharyngeal arches. Refer to Table 1 in the pharyngeal arch lecture. COMPONENTS of the CARTILAGINOUS VISCEROCRANIUM
Incus Malleus Stapes Styloid process Hyoid bone Mandible
SAMPLE QUESTIONS FACE, NASAL & ORAL CAVITIES
1. Which of the following happens to pharyngeal groove 1 during development?
A. It forms the external auditory meatus B. It forms the bones of the inner ear C. It forms the fossa for the palatine tonsil D. It forms the auditory tube. E. It is obliterated and normally forms nothing.
2. What anomaly can result when the intermaxillary segment does not merge with the maxillary prominence?
A. cleft chin B. median cleft lip C. unilateral cleft lip D. cleft secondary palate E. macrostomia
3. The majority of mesenchyme cells of primitive connective tissue in the facial and upper pharyngeal regions are derived from: A. neural crest B. somitomeres C. superficial ectoderm D. occipital somites E. lateral plate mesoderm
4. A structure in the head is innervated by CN V. From which pharyngeal arch is this structure likely derived?
A. PA 1 B. PA 2 C. PA 3 D. PA 4 E. PA 6
ANSWERS: 1 = A; 2 = C; 3 = A; 4 = A
SAMPLE QUESTIONS SKULL
1. All of the following are derived from chondrocranial components that undergo endochondral ossification, EXCEPT. A. base of occipital bone B. body of sphenoid C. petrous and mastoid portions of temporal bone D. median portion of ethmoid E. maxillary bone
2. Which of the following is a true statement regarding the cartilaginous
viscerocranium?
A. Meckel’s cartilage undergoes endochondral ossification in its entirety and becomes the mandible.
B. The cartilage of pharyngeal arch II (Reichert’s) persists in its entirety as the hyoid bone.
C. A portion of the cartilage of pharyngeal arch III undergoes endochondral ossification and forms the stapes.
D. Cartilages of pharyngeal arch IV and VI persist as cartilages of the larynx. E. All pharyngeal arch cartilages differentiate from mesodermal mesenchyme.
3. All of the following are components of the membranous viscerocranium EXCEPT:
A. maxilla B. zygomatic C. mandible D. palatine E. malleus
ANSWERS: 1 = E; 2 = D; 3 = E
Related Documents











