ACID BASE DISORDERS F. Rashid Farokhi Nephrologist Masih Daneshvari Hospital

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ACID BASE DISORDERS
F. Rashid FarokhiNephrologist
Masih Daneshvari Hospital

Extra cellular fluid H+ concentration
[H +] = 40 10 meq/lit = 40 10 Eq/litPH = - log [H+]PH = 7.35 - 7.45
- 9- 9- 6- 6
- 7- 7
meq

7.47.35 7.456.8 7.8
Arterial PH

How can the body regulate H+ concentration in such a low concentration despite of
Daily production of 15000 meq CO2 Daily production of 50-100 meq nonviolate acids Entrance of exogenous acids
?

CO2 +H2O H+ + HCO3-
circulation

Buffering systemsBuffering systems
H2CO3 H+ + HCO3- H2PO4 - H+ +H PO4 2- HAlb H+ + Alb- HHgb H+ + Hgb - HProt H+ + Prot – HPhosphate- H+ + phosphate -
H2CO3 H+ + HCO3- H2PO4 - H+ +H PO4 2- HAlb H+ + Alb- HHgb H+ + Hgb - HProt H+ + Prot – HPhosphate- H+ + phosphate -

H2CO3 H+ + HCO3 –V1 [H2CO3]
H+ + HCO3- H2CO3 V2 [H+] [HCO3-]
V1 =V2[H2CO3] [H+] [HCO3-]
[H+] [HCO3-][H2CO3]
K1[CO2] K2[Halb] K3[H2PO4-] Kn[HA] [HCO3-] [alb-] [HPO4-2] [A-]
H2CO3 H+ + HCO3 –V1 [H2CO3]
H+ + HCO3- H2CO3 V2 [H+] [HCO3-]
V1 =V2[H2CO3] [H+] [HCO3-]
[H+] [HCO3-][H2CO3]
K1[CO2] K2[Halb] K3[H2PO4-] Kn[HA] [HCO3-] [alb-] [HPO4-2] [A-]
= = =
= K= K
[H+] =[H+] =

BB=
12.2 × PCO2/(10 ) + [Albumin] ×(0.123×PH-0.0631) + [PO4]}×(0.309× PH-0.469)
BB=
12.2 × PCO2/(10 ) + [Albumin] ×(0.123×PH-0.0631) + [PO4]}×(0.309× PH-0.469)-PH

H20 + CO2 H2CO3 H+ + HCO3-
[CO2] [H+] = K ×
[HCO3-]
PCO2 × 0.03[H+] = 800 ×
[HCO3-]
PCO2= 24 ×
[HCO3-]

Example 1:Example 1:
PH=7.50 , HCO3 =28 , PCO2=40PH=7.50 , HCO3 =28 , PCO2=40
PCO2[H+] = 24 ×
[HCO3-]
40? = 24 ×
[HCO3-]

PCO2 [ HCO3-]
[H+] PH 40 1.25 1.25 1.25 = 80 7.1 40 1.25 1.25 = 63 7.2 40 1.25 = 50 7.3 40 7.4 40 0.8 = 32 7.5 40 0.8 0.8 = 26 7.6 40 0.8 0.8 0.8 = 20 7.7
PCO2 [ HCO3-]
[H+] PH 40 1.25 1.25 1.25 = 80 7.1 40 1.25 1.25 = 63 7.2 40 1.25 = 50 7.3 40 7.4 40 0.8 = 32 7.5 40 0.8 0.8 = 26 7.6 40 0.8 0.8 0.8 = 20 7.7
[H+] =24× [H+] =24×
PH=7.50 , HCO3 = 30 , PCO2=40PH=7.50 , HCO3 = 30 , PCO2=40
PCO2[H+] = 24 ×
[HCO3-]
4032 = 24 ×
30

The effect of respiratory system on acid base balance
The effect of respiratory system on acid base balance
C6H12O6 + 602 6CO2 +6H2O
CO2 + H2O H2CO3 H+ + HCO3-
C6H12O6 + 602 6CO2 +6H2O
CO2 + H2O H2CO3 H+ + HCO3-

Proximal tube
H+
HCO3
OH-
H+Na+
+ H20CO2 +
NaHCO3
Proxoimal tubuleProxoimal tubule

Distal tubules
H+H++A-
HA
OH-
H+
CO2
HCO3-
H+ + HCO3- H2O + CO2 + A-
HA


Acid base disordersAcid base disorders

What is the difference between acidemia and acidosis, alkalemia and
alkalosis?
What is the difference between acidemia and acidosis, alkalemia and
alkalosis?

PH = 6.1+ log {HCO3- / [0.03 x PCO2]}
AcidemiaPH
Metabolic acidosis
HCO3
Respiratory Acidosis
PCO2

PH = 6.1+ log {HCO3- / [0.03 x PCO2]}
AlkalemiaPH
Metabolic alkalosis
HCO3
Respiratory Alkalosis
PCO2

Respiratory compensation in metabolic acidosis
PH = 6.1+ log {HCO3- / [0.03 x PCO2]}
AcidemiaPH
Metabolic acidosis
HCO3
PCO2 = (1.5×Hco3) + 8 ± 2Or
1.25 mmHg fall in the PCO2 for every 1 meq/lit reduction in the bicarbonate
PCO2 = (1.5×Hco3) + 8 ± 2Or
1.25 mmHg fall in the PCO2 for every 1 meq/lit reduction in the bicarbonate

Respiratory compensation in metabolic alkalosis
PH = 6.1+ log {HCO3- / [0.03 x PCO2]}
AlkalemiaPH Metabolic
alkalosis HCO3
PCO2 = HCO3 + 15Or
0.75 mmHg rise in the PCO2 for every 1 meq/lit elevation in the bicarbonate
PCO2 = HCO3 + 15Or
0.75 mmHg rise in the PCO2 for every 1 meq/lit elevation in the bicarbonate

PH = 6.1+ log {HCO3- / [0.03 x PCO2]}Acidemia
PH
Respiratory Acidosis
PCO2
Acute: HCO3 rises 1 meq/lit for every 10 mmHg elevation in PCO2Chronic: HCO3 rises 4 meq/lit for every 10 mmHg elevation in PCO2Acute: HCO3 rises 1 meq/lit for every 10 mmHg elevation in PCO2
Chronic: HCO3 rises 4 meq/lit for every 10 mmHg elevation in PCO2

PH = 6.1+ log {HCO3- / [0.03 x PCO2]}Alkalemia
PH
Respiratory Alkaloosis
PCO2
Acute: HCO3 falls by 2 meq/lit for every 10 mmHg decline in PCO2Chronic: HCO3 falls by 4 meq/lit for every 10 mmHg decline in PCO2Acute: HCO3 falls by 2 meq/lit for every 10 mmHg decline in PCO2
Chronic: HCO3 falls by 4 meq/lit for every 10 mmHg decline in PCO2

Example 1:Example 1:
PH=7.50 , HCO3 = 30 , PCO2=40
Mixed metabolic and respiratory alkalosis
PH=7.50 , HCO3 = 30 , PCO2=40
Mixed metabolic and respiratory alkalosis
Examples 2:Examples 2:
1- PH =7.25 ,HCO3=12 , PCO2=25 compensated metabolic acidosis
2-PH=7.1 , HCO3 =12 , PCO2=30 mixed metabolic and respiratory acidosis
1- PH =7.25 ,HCO3=12 , PCO2=25 compensated metabolic acidosis
2-PH=7.1 , HCO3 =12 , PCO2=30 mixed metabolic and respiratory acidosis

Example 3:Example 3:
PH=7.35 , HCO3= 28 , PCO2=60
Acute respiratory acidosis + metabolic alkaosisChronic respiratory acidosis +metabolic acidosis
PH=7.35 , HCO3= 28 , PCO2=60
Acute respiratory acidosis + metabolic alkaosisChronic respiratory acidosis +metabolic acidosis

In a patient there is following arterial blood values:
In a patient there is following arterial blood values:
PH=7.22 , PCO2 =70 , HCO3= 31 What is the acid base disorder?
PH=7.22 , PCO2 =70 , HCO3= 31 What is the acid base disorder?

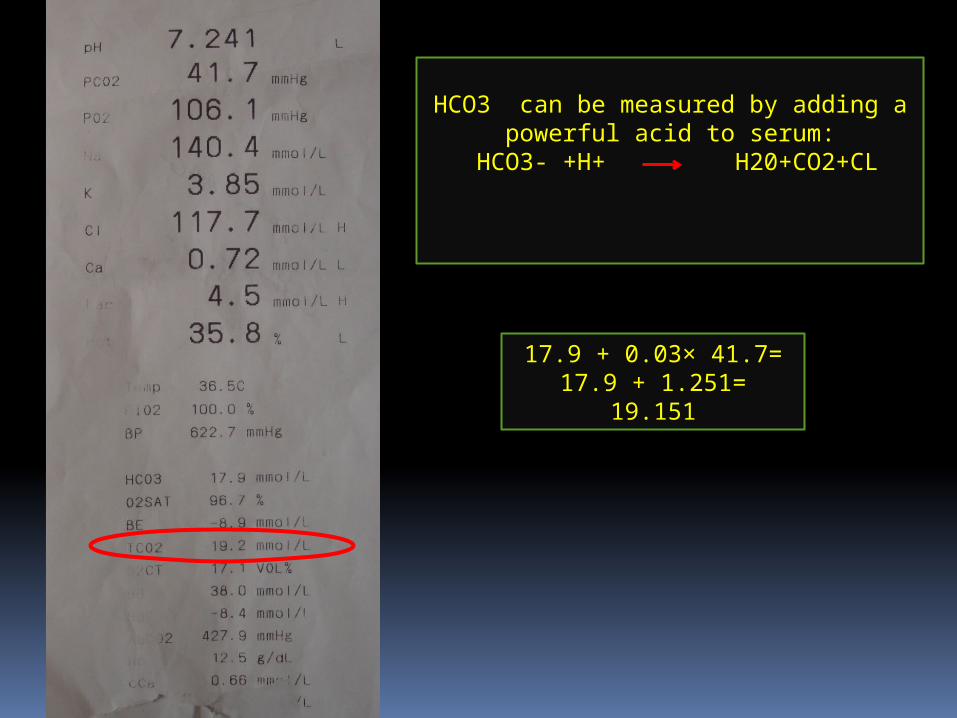
HCO3 can be measured by adding a powerful acid to serum:
HCO3- +H+ H20+CO2+CL
17.9 + 0.03× 41.7=17.9 + 1.251=
19.151

What are the problems with PCO2/HCO3 in evaluation of acid base condition
What are the problems with PCO2/HCO3 in evaluation of acid base condition
It can not determine the: Severity of metabolic disturbance can not be
determined The etiology of acid base disorder
It can not determine the: Severity of metabolic disturbance can not be
determined The etiology of acid base disorder

anion gap in approach of metabolic acidosis

All Anions = All cations
Measured Anions +Unmeasured Anions= Measured Cation +Unmeasured Cations
M C – MA = UA - UC[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
Anion gap should be corrected with albumin
All Anions = All cations
Measured Anions +Unmeasured Anions= Measured Cation +Unmeasured Cations
M C – MA = UA - UC[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
Anion gap should be corrected with albumin

Example 4:A previously well 55 year old woman is admitted with a complaint of severe vomiting for 5 days.
Physical examination reveals postural hypotension, tachycardia and diminished skin
turgor. The laboratory findings include:
Example 4:A previously well 55 year old woman is admitted with a complaint of severe vomiting for 5 days.
Physical examination reveals postural hypotension, tachycardia and diminished skin
turgor. The laboratory findings include: PH=7.23 , PCO2 =22 , HCO3= 9
Na: 140, K: 3.4, Cl: 77, Cr: 2.1, Ketone: trace what is the metabolic disturbances?
PH=7.23 , PCO2 =22 , HCO3= 9
Na: 140, K: 3.4, Cl: 77, Cr: 2.1, Ketone: trace what is the metabolic disturbances?

High anion gap metabolic acidosisHigh anion gap metabolic acidosis
H+ + HCO3- H2O + CO2 + A-
H+ + HCO3- H2O + CO2 + A-
HA

Hyperchloremic metabolic acidosisHyperchloremic metabolic acidosis
H+ + HCO3- H2O + CO2 + Cl-
H+ + HCO3- H2O + CO2 + Cl-
HCl

[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
HCL + NaHCO3 NaCl +H2O+CO2HA + NaHCO3 NaA +H2O+CO2
[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
HCL + NaHCO3 NaCl +H2O+CO2HA + NaHCO3 NaA +H2O+CO2
∆ AG
∆ HCO3

[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
HCL + NaHCO3 NaCl +H2O+CO2HA + NaHCO3 NaA +H2O+CO2
[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
HCL + NaHCO3 NaCl +H2O+CO2HA + NaHCO3 NaA +H2O+CO2
∆ AG
∆ HCO3

[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
HCL + NaHCO3 NaCl +H2O+CO2HA + NaHCO3 NaA +H2O+CO2
[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
HCL + NaHCO3 NaCl +H2O+CO2HA + NaHCO3 NaA +H2O+CO2
∆ AG
∆ HCO3 AG / HCO3 > 2 : metabolic alkalosis + high anion gap metabolic acidosis

[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
HCL + NaHCO3 NaCl +H2O+CO2HA + NaHCO3 NaA +H2O+CO2
[Na+] – { [CL-] +[HCO3-] } = UA-UC = AG
HCL + NaHCO3 NaCl +H2O+CO2HA + NaHCO3 NaA +H2O+CO2
∆ AG
∆ HCO3 AG / HCO3 <1 : hyperchloremic metabolic acidosis + high anion gap metabolic acidosis or urine loss of organic anions

Example 4:A previously well 55 year old woman is admitted with a complaint of severe vomiting for 5 days.
Physical examination reveals postural hypotension, tachycardia and diminished skin
turgor. The laboratory findings include:
Example 4:A previously well 55 year old woman is admitted with a complaint of severe vomiting for 5 days.
Physical examination reveals postural hypotension, tachycardia and diminished skin
turgor. The laboratory findings include: PH=7.23 , PCO2 =22 , HCO3= 9
Na: 140, K: 3.4, Cl: 77, Cr: 2.1, Ketone: trace what is the metabolic disturbances?
PH=7.23 , PCO2 =22 , HCO3= 9
Na: 140, K: 3.4, Cl: 77, Cr: 2.1, Ketone: trace what is the metabolic disturbances?
∆ AG
∆ HCO3
AG=140-86=54 ∆ AG = 54-10=44
∆ HCO3 = 24-9= 15
44/15=3

Example 5: A 58 year old man with a history of chronic bronchitis develop severe diarrhea. The
volume of diarrheal fluid is approximately 1 lit/hour.
Results of the initial laboratory test is:
Example 5: A 58 year old man with a history of chronic bronchitis develop severe diarrhea. The
volume of diarrheal fluid is approximately 1 lit/hour.
Results of the initial laboratory test is:
PH=6.97 , PCO2 =40 , HCO3= 9
Na: 138, K: 3.8, Cl: 115, aibumin: 2 What is the acid base disorder?
PH=6.97 , PCO2 =40 , HCO3= 9
Na: 138, K: 3.8, Cl: 115, aibumin: 2 What is the acid base disorder?
∆ AG
∆ HCO3
AG=138-124=1414+5+=19
∆ AG = 19-10= 9
∆ HCO3 = 24-9= 15
9/15 <1

Example 6: A 25 years woman complains of easy fatigability and weakness. She has no other complains. The physical examination is unremarkable, with the blood pressure being normal. The following laboratory data are obtained:
plasma [Na+]: 141 meq/lit [K=]: 2.1 meq/lit [Cl-]:85meq/lit [HCo3]: 45 meq/lit urine [Na+]: 80 meq/lit urine [K+]: 170 meq/lit
what are your differential diagnosis? What test would you order next?

What is base excess?What is base excess?
the amount of base that should be removed from whole blood invitro to restore PH of it
to 7.4, while pco2 is held at 40 mmHgthis calculation is accurate invitro but not
invivo, so SBE is calculated
the amount of base that should be removed from whole blood invitro to restore PH of it
to 7.4, while pco2 is held at 40 mmHgthis calculation is accurate invitro but not
invivo, so SBE is calculated

Base excess in acid base disordersBase excess in acid base disorders
Metabolic acidosis: SBE<-5 PCO2 = 40 + SBEMetabolic alkalosis: SBE>+5 PCO2= 40+ 0.6 SBEAcute respiratory acidosis: SBE=0Chronic respiratory acidosis: SBE=0.4(PCO2-40)Acute respiratory alkalosis: SBE=0 Chronic respiratory alkalosis: SBE=0.4(PCO2-40)
Metabolic acidosis: SBE<-5 PCO2 = 40 + SBEMetabolic alkalosis: SBE>+5 PCO2= 40+ 0.6 SBEAcute respiratory acidosis: SBE=0Chronic respiratory acidosis: SBE=0.4(PCO2-40)Acute respiratory alkalosis: SBE=0 Chronic respiratory alkalosis: SBE=0.4(PCO2-40)

Example 7:In a patient there is following arterial
blood values:
Example 7:In a patient there is following arterial
blood values:
PH=7.22 , PCO2 =70 , HCO3= 31 BE: 5.7 What is the acid base disorder?
PH=7.22 , PCO2 =70 , HCO3= 31 BE: 5.7 What is the acid base disorder?

Pitfalls of ABG resultsPitfalls of ABG results
1- air bubbles in the syringe Decreased PCO2 and increased PO2 due to
existence of bubbles in the sample
1- air bubbles in the syringe Decreased PCO2 and increased PO2 due to
existence of bubbles in the sample
Prevention: gentle removal of bubbles, rapid sample anaysis
Prevention: gentle removal of bubbles, rapid sample anaysis

Pitfalls of ABG resultsPitfalls of ABG results
2- the effect of heparin Dilution of blood parameters , CO2
2- the effect of heparin Dilution of blood parameters , CO2
Prevention: Use of minimum amount of heparin, no less than 2 cc of blood should be obtained
Prevention: Use of minimum amount of heparin, no less than 2 cc of blood should be obtained

Pitfalls of ABG resultsPitfalls of ABG results
3- Specimen transport without ice Decreased PO2 due to oxygen consumption of
leukocytes Decreased PH and HCO3 due to anaerobic metabolism
3- Specimen transport without ice Decreased PO2 due to oxygen consumption of
leukocytes Decreased PH and HCO3 due to anaerobic metabolism
Prevention: Rapid cooling of specimen, rapid sample anaysis
Prevention: Rapid cooling of specimen, rapid sample anaysis

Comparison of normal arterial and venous blood gas parameters
Comparison of normal arterial and venous blood gas parameters
ABG mmHg VBG mmHg Pco2 35-45 42-50 HCO3 22-26 23-27 PH 7.35-7.45 7.32-7.38
ABG mmHg VBG mmHg Pco2 35-45 42-50 HCO3 22-26 23-27 PH 7.35-7.45 7.32-7.38


STRONG ION DIFFERENCES

What are the problems with PCO2/HCO3 in evaluation of acid base condition
What are the problems with PCO2/HCO3 in evaluation of acid base condition
It can not determine the: Severity of metabolic disturbance can not be
determined The etiology of acid base disorder
It can not determine the: Severity of metabolic disturbance can not be
determined The etiology of acid base disorder

STRONG ION DIFFERENCES APPROACH TO ACID BASE DISORDERS
Most internists traditional approach to acid base disorders considering : H+ = K× PCO2/HCO3 popularized by Relman and Schwartz in 1960s
Many surgeons, critical care specialists and anesthesiologists are interested in an alternative approach, termed strong ion differerences introduced by Stewart in 1981

Acid is a proton donor Base is a proton acceptor
DEFINITION OF ACIDS AND BASES BASED ON TRADITIONAL APPROACH

DEFINITION OF ACIDS AND BASES IN STEWART APPROACH:
Acid is as ion that shift the dissociation equilibrium of water to: higher concentration of H+ and lower concentration of OH- Base is as ion that shift the dissociation equilibrium of water to: lower concentration of H+ and higher concentration of OH-

Pure Water
H20 H+ + OH-
Body
H20 H+ + OH-
Pure Water
H20 H+ + OH-
Body
H20 H+ + OH-
H+ = 10
H+ = 4 ×10
-7
-8

Strong cations : Na, Ca, Mg, KWeak cations: H
Strong Anions: Cl, Lactate, Weak Anions: Albumin, Phosphate, HCO3
Strong cations : Na, Ca, Mg, KWeak cations: H
Strong Anions: Cl, Lactate, Weak Anions: Albumin, Phosphate, HCO3

[ Na + Ca + Mg + K] - [Cl + lactate] = SID( apparent) SID>40 : metabolic alkalosis
[ Na + Ca + Mg + K] - [Cl + lactate] = SID( apparent) SID>40 : metabolic alkalosis
H2O
OH- H+ H20 H+ + OH-
[ Na + Ca + Mg + K] > [Cl + lactate]

[ Na + Ca + Mg + K] - [Cl + lactate] = SID( apparent) SID<40 : metabolic acidosis [ Na + Ca + Mg + K] - [Cl + lactate] = SID( apparent) SID<40 : metabolic acidosis
H2O
OH- H+ H20 H+ + OH-
[ Na + Ca + Mg + K] < [Cl + lactate]

[ Na + Ca + Mg + K] - [Cl + lactate] = SID( apparent) SID<40 : metabolic acidosis [ Na + Ca + Mg + K] - [Cl + lactate] = SID( apparent) SID<40 : metabolic acidosis
H2O
OH- H+ H20 H+ + OH-
[ Na + Ca + Mg + K] < [Cl + lactate]

According to modified SID theory variables responsible for change in acid
base balance are :
According to modified SID theory variables responsible for change in acid
base balance are :
PCO2 Nonvolatile weak acids Strong Ions
PCO2 Nonvolatile weak acids Strong Ions

Strong Cations + weak cations = Strong Anions + Weak Anions Strong Cations - Strong Anions= Weak Anions - Weak Cations
[ Na + Ca + Mg + K] - [Cl + lactate] = Weak anions
Strong Cations + weak cations = Strong Anions + Weak Anions Strong Cations - Strong Anions= Weak Anions - Weak Cations
[ Na + Ca + Mg + K] - [Cl + lactate] = Weak anions

H2CO3 H+ + HCO3 –V1 [H2CO3]
H+ + HCO3- H2CO3 V2 [H+] [HCO3-]
V1 =V2[H2CO3] [H+] [HCO3-]
[H+] [HCO3-][H2CO3]
K1[CO2] K2[Halb] K3[H2PO4-] Kn[HA] [HCO3-] [alb-] [HPO4-2] [A-]
H2CO3 H+ + HCO3 –V1 [H2CO3]
H+ + HCO3- H2CO3 V2 [H+] [HCO3-]
V1 =V2[H2CO3] [H+] [HCO3-]
[H+] [HCO3-][H2CO3]
K1[CO2] K2[Halb] K3[H2PO4-] Kn[HA] [HCO3-] [alb-] [HPO4-2] [A-]
= = =
= K= K
[H+] = [H+] =

[ Na + Ca + Mg + K] - [Cl + lactate] = SID( apparent)[ Na + Ca + Mg + K] - [Cl + lactate] = SID( apparent)
SID app – SID eff = SID gap

If we consider anion gap and serum albumin
in traditional approach stewart approach does not appear a
clinically significant advantage
Related Documents











