F-IMNCI Case Study Southern Shan State MCSP Child Health Team 2016-2018

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

F-IMNCI Case Study
Southern Shan State
MCSP Child Health Team
2016-2018


Acknowledgements
The Maternal and Child Survival Program (MCSP) is a global United States Agency for
International Development (USAID) initiative to introduce and support high-impact health
interventions in 25 priority countries to help prevent child and maternal deaths. MCSP
supports programming in maternal, newborn and child health, immunization, family planning
and reproductive health, nutrition, health system strengthening, water/sanitation/ hygiene,
malaria control, prevention of mother to child transmission of HIV, and Pediatric HIV care
and treatment. MCSP tackles these issues through approaches that also focus on household
and community mobilization, gender integration and digital health, among others.
In Myanmar, under the leadership and direction of the Child Health Development Division
(CHD) and the support of pediatricians, neonatologists of Yangon Children's Hospital, Lashio
General Hospital and Taunggyi Women and Children Hospital (WCH), MCSP collaborated
with the MOHS in organizing F-IMNCI training to the health staff in hospitals of Southern
Shan State. With the support of the State Health Department and clinicians in Taunggyi
WCH, MCSP supported the post-training supervision and follow-up to the trained heath staff
and assessed the hospital infrastructure.
This report is made possible by the generous support of the American people through the
United States Agency for International Development (USAID) under the terms of the
Cooperative Agreement AID-OAA-A-14-00028. The contents of this report are the
responsibility of the Maternal and Child Survival Program and do not necessarily reflect the
views of USAID or the United States Government.
July 2018
Cover Photo: Dr Thein Thein Hnin, Professor Neonatologist of Taunggyi Women and
Children Hospital, demonstrating Intraosseous cannulation in the F-IMNCI training,
Taunggyi, Southern Shan State, November 2017


1
Contents Page
Figures........................................................................................................................................ 3
Abbreviations ............................................................................................................................. 4
1. Background ............................................................................................................................ 5
1.1 Global and Country situation ........................................................................................... 5
1.2 Goals and Objectives ........................................................................................................ 6
1.3 Overview of the intervention............................................................................................ 6
2. Methodology .......................................................................................................................... 8
2.1 Implementation Process ................................................................................................... 8
2.1.1 Coordination .............................................................................................................. 8
2.1.2 Training ..................................................................................................................... 8
2.1.3 Learning and Performance Improvement Center(L&PIC) ...................................... 12
2.1.4 Post-training supervision ......................................................................................... 13
2.1.5 End of Project .......................................................................................................... 14
3. Results .................................................................................................................................. 15
3.1 Quantitative and Qualitative findings ............................................................................ 15
3.1.1 Pre- and Post-test results in F-IMNCI training ........................................................ 15
3.1.2 Post-training supervision visits ................................................................................ 15
3.1.2.1 Knowledge assessment test findings ................................................................. 15
3.1.2.2 Case scenarios finding (6 OSCEs) .................................................................... 16
3.1.2.3 Supervision of hospital infrastructure .............................................................. 20
3.1.2.3.1 General assessment .................................................................................... 20
3.1.2.3.2 Emergency or Outpatient Department (OPD) ............................................ 21
3.1.2.3.3 Labor room and postnatal ward .................................................................. 21
3.1.2.3.4 Child Ward ................................................................................................. 22
3.1.2.3.5 Laboratory .................................................................................................. 23
3.1.2.3.6 Equipment .................................................................................................. 23
3.1.2.3.7 Human resources ........................................................................................ 24
3.1.2.3.8 Drug and Pharmacy .................................................................................... 24
3.1.2.3.9 Clinical practice and guidelines ................................................................. 24
4.Analysis................................................................................................................................. 25
4.1 Challenges ...................................................................................................................... 25
4.1.1 Training ................................................................................................................... 25

2
4.1.2 Post-training supervision ......................................................................................... 26
4.2 Lessons Learned ............................................................................................................. 27
4.3 Best Practices ................................................................................................................. 28
4.4 Recommendations .......................................................................................................... 28
4.4.1 Planning ................................................................................................................... 28
4.4.2 Training ................................................................................................................... 28
4.4.3 Post-training supervision ......................................................................................... 28
4.4.4 Hospital Infrastructure ............................................................................................ 28
4.4.5 Future planning ........................................................................................................ 29
5. References ............................................................................................................................ 29
6. Annexes................................................................................................................................ 31
Annex 1. Number and percentage of hospital staff reached through F-IMNCI training
and supervision ................................................................................................................30
Annex 2. Participants in training and supervision............................................................30
Annex 3. Hospital participation in training and supervision............................................31
Annex 4. Pre- and Post-test scores of participants during training...................................32
Annex 5. Achievement scores of 94 participants in six OSCEs in first supervision visit…..32
Annex 6. Average scores of supervised hospital staff during the post-training supervision
visits (6 OSCEs)................................................................................................................32
Annex 7. Multiple choice questions and answers used in Pre and post test of training and
during supervision (20 MCQs).........................................................................................33
Annex 8. Six OSCEs checklist used for skill assessment in supervision.........................37
Annex 9. Hospital assessment forms (3 groups)..............................................................47
Annex 10. Revised hospital assessment form recommended to use for future assessment
in township hospital..........................................................................................................72
Annex 11. F-IMNCI training materials............................................................................91
7. Success story........................................................................................................................93

3
Figures
Figure 1. Under 5, Infant and Neonatal mortality rates in Myanmar
Figure 2. Pre- and Post-test average scores of participants inF-IMNCI trainings
Figure 3. Number of health staff by achievement scores (6 OSCEs)
Figure 4. Number of medical doctors by achievement scores (6 OSCEs) N=17
Figure 5. Number of nurses by achievement scores (6 OSCEs) N=77
Figure 6. Percentage of medical doctors and nurses by achievement score groups (6 OSCEs)
Figure 7. Average scores of supervised hospital staff during the post-training supervision visits (6
OSCEs)
Figure 8. Difference between first and second post-training assessment scores (6 OSCEs) N= 9
Figure 9. Number of health staff by assessment status during second supervision visit (N=9)
Figure 10. Number of hospitals showing differences in general facilities before and after training
(N=19)
Figure 11. Number of hospitals showing differences in labor room and postnatal ward facilities before
and after training (N=19)
Figure 12. Number of hospitals showing differences in availability of equipment before and after
training (N=19)
Figure 13. Number of hospitals showing differences in clinical practice before and after training
(N=19)

4
Abbreviations
BHS Basic Health Staff
CME Continuing Medical Education
CSO Civil Society Organization
ETAT Emergency Triage Assessment and Treatment
F-IMNCI Facility-based Integrated Management of Neonatal and
Childhood Illness
KMC Kangaroo Mother Care
L&PIC Learning and Performance Improvement Center
LB Live births
MCQ Multiple Choice Questions
MDG Millennium Development Goals
MOHS Ministry of Health and Sports
MR Mortality Rate
OPD Outpatient Department
ORS Oral Rehydration Salt
ORT Oral Rehydration Therapy
OSCE Objective Structured Clinical Examination
PTFU Post-training Follow-up
SDG Sustainable Development Goal
SHD State Health Department
ToT Training of Trainers
TMO Township Medical Officer
WCH Women and Children Hospital

5
1. Background
1.1 Global and Country situation Substantial progress has been made globally in reducing under-5 mortality in the past several decades,
with the total number of under-five deaths declining from 12.6 million in 1990 to 5.6 million in 20161.
But this still represents 15,000 deaths every day globally and 46% of these deaths occur in the
neonatal period, the first 28 days of life. The global under-five mortality rate dropped to 41 deaths per
1,000 live births in 2016 from 93 in 19902.
In Myanmar’s National Demographic Health Survey (2015-16) the under-5 mortality rate was
reported as 50/1000 live births (LBs), infant mortality rate was 40/1000 LBs and neonatal mortality
rate was 25/1,000 live births3.
Although mortality gradually declined from 2011 to 2016 (Figure 1),
the Millennium Development Goals (MDG) target of U5MR of 38/1000 live births by 2015 was not
achieved and Myanmar’s rates are still higher than global mortality rates (Myanmar U5MR 50/1000
vs. Global 41/1000 live births and Myanmar IMR 40/1000 live births vs. Global 30.5/1000 live births)
4 (Figure 1).
Figure 1. Under 5, Infant and Neonatal mortality rates in Myanmar
By the end of the MDG period, most countries in the world had not reached the MDG 4 target of
reducing under-5 mortality by two-thirds, so a new global development agenda known as the
Sustainable Development Goals (2015-2030) were established. The child survival targets in the SDGs
are intended to reduce preventable deaths among children under 5. By 2030, the neonatal mortality
should be reduced to12 deaths per 1,000 live births and under-5 mortality rate to 25 deaths per 1,000
live births in all countries5.
Globally, in 2015, 46% of under-5 deaths occurred in the neonatal period and about half of all under-5
deaths were due to the infectious diseases, including pneumonia, diarrhea and malaria2. The majority
of these under-5 deaths are preventable through effective health care services and preventive
measures. From UNICEF’s review of under-five mortality in Myanmar in 2016, 49% of under-five
mortality occurred in the neonatal period. Among neonates, 31.8% of deaths were preterm babies,
26.8% died during the intrapartum period, and 14.6% of newborns died due to sepsis. Among the
0
10
20
30
40
50
60
70
2009 2010 2011 2012 2013 2014 2015 2016 2017
Under 5, Infant and Neonatal Mortality Rate Situation in Myanmar (per 1,00 live births)
Under 5 mortality rate Infant mortality rate Neonatal mortality rate

6
older children from 1- 59 months of age, 29.9% of children died with pneumonia, 15.7% with
diarrhea, and 13.5% died due to non-specified injuries4.
In order to achieve the targets of the SDGs, the Ministry of Health and Sports (MOHS) plans to
strengthen health care service facilities and upgrade the skill sets of service providers at all levels of
the health care system. Integrated Management of Childhood Illness (IMCI) has been implemented in
Myanmar since 1999, with the collaboration of WHO and UNICEF. The neonatal component was
incorporated in 2011 to complete the package of IMNCI. The updating of the IMNCI guidelines, the
approach and training roll-out are conducted regularly, under the leadership of the Child Health
Development Division, in close collaboration with national technical consultants.
In emergency situations and for severe illness, sick children are referred by the Basic Health Staff
(BHS) to the more advanced health care facilities for hospital-based management. The facility-based
integrated management of neonatal and childhood illness (F-IMNCI) approach was developed as the
standardized treatment protocol, procedures and treatment, by which the health service providers at
the township hospital level are to be trained for management of newborn and childhood illness at the
facility level.
1.2 Goals and Objectives The overall objectives of the F-IMNCI activity included utilizing and adapting existing training
materials to the county context, for improved management of newborn and childhood illnesses;
training hospital staff, including pediatricians, medical doctors and nurses to improve the clinical
management of sick newborns and children referred to the health facilities; and to inform future scale
up to expand the practice of F-IMNCI clinical care and management consistently in referral facilities
across the country. IMNCI is already being scaled up across the country, under MOHS leadership,
and utilization of the F-IMNCI approach will strengthen and improve the capacity of referral-level
facilities to correctly manage sick newborns and children further building the linkages across the
continuum of care, in order to save lives of newborns and children under five.
1.3 Overview of the intervention The F-IMNCI guideline package (2017) in Myanmar was developed based on the guideline package
utilized by the Ministry of Health and Family Welfare of the Government of India, in collaboration
with WHO and UNICEF. The F-IMNCI guideline package (2017) is composed of three books;
Participant Manual, Facilitator Guide and Chart Booklet, intended for hospital staff. These materials
were prepared in English because translation of medical terminology into Myanmar language was not
considered necessary. The participants of training and the users will be hospital staff, including
medical doctors and senior nurses, who are able to read and understand the medical terminology well
in English.
The F-IMNCI guideline package was used in the Central trainers/mentors training in Yangon Children
Hospital from 8th to 12
th May 2017. This was a five-day training on F-IMNCI care and management
led by the Child Health Development Division, in close collaboration with WHO. The training was
led by 4 international trainers from India and 9 resource persons as national trainers from the MOHS
in Myanmar. Twenty-nine participants, including pediatricians and child health team leaders from the
state and regional hospitals attended. The comments and recommendations from the Central TOT
training were used in the finalization of the guidelines by the national consultant. After the approval
of the Minister of MOHS, the F-IMNCI guidelines were used in the training for the hospital staff in
Southern Shan state, starting from November 2017.
7
The Child Health Development Division, MOHS requested support from the MCSP child health team
to introduce this revised package in one State, Southern Shan. MCSP participated in extensive
discussions and in 2017 it was agreed with the Director, CHD in Nay Pyi Taw, and the State Health
Department (SHD) in Southern Shan, that MCSP would support training and post-training supervision
activities for all township hospitals in Southern Shan state. MCSP’s child health team posted a
Program Officer, with the necessary experience and clinical skills in Taunggyi, where the SHD is
located, and coordinated the planning and implementation of the work closely with CHD and SHD.
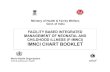
MCSP supported the conduct of the F-IMNCI implementation activity for 120 hospital staff in
Sothern Shan state, including pediatricians, neonatologists, assistant surgeons (AS), township medical
officers (TMO) and senior nurses from Taunggyi Women and Children Hospital, Loilen District
Hospital, Kho Lam 100-bedded hospital and 19 township hospitals. See map below for location of all
major hospitals in Southern Shan state.
Map 1. Location of major hospitals in Southern Shan state
Neonatologists and pediatricians who had received the F-IMNCI central training of trainers/mentors
in Yangon provided the dissemination training to the participants in six divided batches of
approximately 20 participants each. Every trainer and facilitator was provided with one set of three F-
IMNCI guideline books and each participant was provided with two guideline books.
Post-training supervision to the hospital level was conducted through joint-supervision visits by
trainers/supervisors from the Women and Children Hospital, Taunggyi along with the MCSP Program
Officer. Sometimes the MCSP Program Officer conducted supervision visits alone when others were
not able to join. The supervision visits were conducted at least once to each trained township hospital,

8
only three were inaccessible due to local security issues. The supervisors assessed the knowledge and
skills of the trained participants, gave guidance on how to further strengthen their performance, and
reviewed the hospital infrastructure questionnaire. The supervision records and data were recorded for
analysis, report preparation and inputs for the MOHS for future assessments and health system
strengthening.
2. Methodology
2.1 Implementation Process
2.1.1 Coordination
The MCSP child health team played an important role in coordination efforts to ensure that the F-
IMNCI introduction was well-aligned with the goals of the CHD and SHD/MOHS and other partners,
e.g. WHO, UNICEF. At the Central level MCSP facilitated the finalization of the materials for the
training. The MCSP child health team supported printing of the F-IMNCI guidelines. MCSP kept
WHO apprised of the progress as WHO is also planning support for rollout in some other
states/regions. MCSP provided regular feedback to CHD on the progress with implementation and
challenges in Southern Shan, through face-to-face meetings, phone calls and reports. At the State
Level, the MCSP Senior Child Health Advisor and the MCSP Program Officer coordinated closely
with the Deputy Director, SHD, to ensure that he was fully engaged in all decisions related to the
introduction, training and post-training follow-up. Feedback and planning for all fieldwork was done
through his office. Coordination with the leadership at WCH was also vital to establishing the training
venue, developing the tool for assessment of the infrastructure of the hospitals and for ensuring
quality training including links with the clinical sites on the wards. WCH provided some support for
Post-training follow-up (PTFU) as well. MCSP also procured the manikins used in trainings, other
materials needed for training (ie: guidelines and training posters), planned PTFU field visits and
reported out on progress and findings through quarterly reports and meetings. F-IMNCI materials
were also placed in the Learning and Performance Improvement Center (L&PIC) in Taunggyi for
continued access and learning opportunities.
2.1.2 Training
Before initiating each batch of training, a half-day meeting was organized by the trainers for general
preparation, including curriculum review and finalization, training design for groups of participants,
distribution of tasks and responsibilities among trainers and facilitators, and checking training
materials and guidelines.

9
Picture 1. Trainers meeting for general preparation on the day before starting the training
The Women and Child Hospital (WCH) of Taunggyi in Southern Shan state, was selected as the
training venue because of the availability of highly qualified pediatricians and neonatologists to serve
as trainers/facilitators and the ease of accessibility to clinical cases for practical sessions on the wards
of the hospital. They also had an appropriately sized training hall with adequate facilities.
The F-IMNCI training was of five days duration and all 6 batches were conducted in the training hall
of WCH for lectures and group discussion, between November 2017 and March 2018. A total of 131
participants were trained. For clinical skills training with real patients and for applying case scenarios,
participants learned about case management on the neonatal and child wards in the WCH (Annex 2).
The first batch was led by four trainers, 3 from Shan state and 1 from Yangon Children Hospital1. In
the next five batches, three trainers from Women and Children Hospital, Taunggyi (Prof. Thein Thein
Hnin, Dr. Nang Nweni Lynn and Dr. Nang Nilar Tun 2) led the trainings. The trained medical doctors
of Women and Children Hospital from the earlier batches supported the later trainings as facilitators.
__________________________________
1Professor Dr. Thein Thein Hnin, Professor Neonatologist of Taunggyi WCH
Dr. Naing Oo, Associate Professor /Pediatrician of Yangon Children's Hospital
Dr .Yan Naing Aung, Assistant Surgeon/Pediatrician of Lashio General Hospital
Dr. Nang Nweni Lynn, Consultant Pediatrician of Taunggyi WCH 2 Dr. Nang Nilar Tun, Consultant Pediatrician of Taunggyi WCH

10
There were 21 participants on average in each batch with the support of 3 trainers and 2-3 facilitators.
The trainer to participant ratio was 1:7 and the trainer/facilitator to participant ratio was closer to 1:
4.5. After 6 batches of training, 34 medical doctors and 97 nurses were trained from hospitals of
various levels throughout the state. Among the 131 participants, 34 persons were from Taunggyi
Women and Children Hospital (Annex 1,2).
Picture 2. Participants taking history from the mother of a low birth weight baby in neonatal ward, WCH
In addition to the participants from WCH in Taunggyi, nurses and doctors from Loilen District
hospital, a Kholam 100-bedded hospital, 19 township hospitals, 14 station hospitals and 1 dispensary,
all situated in Southern Shan state attended. The F-IMNCI training was targeted for the health care
service providers of township hospitals, but due to lack of availability of medical doctors in some
township hospitals, station medical officers were included in the trainings. The TMO made the final
selection of participants for training, as they were seen as best placed to understand the staffing
situation and reality in the hospital and township area.
In all trainings, pre- and post-tests with multiple choice questions (MCQs) were given on the first day
and the last day of the training, using the same question set. It was focused on assessing the
knowledge and clinical management skills of participants and the effectiveness of the training.
Additionally, participants could assess themselves by how much improvement they achieved.
The questions were designed to assess the essential health knowledge and clinical management skills
on newborn and childhood illness in the facility-based health care system. Participants circled or
ticked the correct answer on the individual answer sheet. There were a total of 20 questions covering

11
three modules of the F-MNCI training content; Emergency Triage Assessment and Treatment
(ETAT), care of the newborn and common diseases of young children. All questions were single
response, except one, which had two correct answers. If the answer was correct, it was recorded as
“1” and if the answer was not correct, it was recorded as zero. For the question with two correct
answers, if the participant got either one or two correct answers, it is recorded as “1” score (Annex 7).
The training curriculum covered both newborn and child health care services in the hospitals, with
time equally split, each age group covering about two and a half days. Training methodology included
lectures, power point presentations, group discussions, case scenarios, and clinical management
through the use of training aid materials, such as manikins and other medical supplies. Participants
attended the practical sessions with hospitalized patients in the neonatal and pediatric wards. The
standard protocols for patient management were shown through the use of flow charts.
In the morning sessions, lectures and group discussions were held in the training halls. In the
afternoon, participants were divided into three groups, with each group led by one trainer and one
facilitator for the practical sessions in the hospital wards. Dr. Ye Thwin, Program Officer of MCSP,
participated in all training batches and provided technical and logistic support as required.
Picture 3. Materials used in F-IMNCI trainings.
12
Picture 4. Additional materials used in F-IMNCI trainings.
At the end of the training, participants provided training evaluation and feedback to the training team.
Plans for joint post training supervision visit by MOHS and MCSP staff were drawn up. Dr. Naing
Oo, one of the trainers, suggested inclusion of clinical skills assessment questions in PTFU
questionnaires, in addition to the hospital infrastructure assessment forms. Feedback from participants
showed that knowledge and skills gained from F-IMNCI training were relevant and essential for their
daily practice. Some participants felt that 5 days of continuous training was too intense and training
should be divided into modules. (e.g. modularized trainings).
Each participant was provided with a Participant Manual and Chart Booklet. Each trainer and
facilitator was provided with a total of 3 books (the Participant Manual, the Chart Booklet and the
Facilitator Guide). According to the request of the Child Health Development Division, MOHS, office
copies of F-IMNCI guideline books were provided to the WCH of Taunggyi, the District hospital, all
Township hospitals and the Station hospitals in the Southern Shan state.
2.1.3 Learning and Performance Improvement Center (L&PIC)
An L&PIC was set up in the Taunggyi SHD with MCSP support, to provide participants an
opportunity to have more practice with the newly learned clinical skills. This was not established only
for F-IMNCI but for the broader range of MNCH trainings supported by MCSP. F-IMNCI training
aid materials such as manikins, other medical supplies and other training aid materials were displayed
in the L&PIC to be readily accessible to hospital staff. A register book was established to track those
BHS or hospital staff that used the materials post-trainings. The F-IMNCI guidelines and training aid
materials, including manikins were handed over to the LPIC after the training. One set of manikins
and materials was also given to the WCH in Taunggyi to facilitate clinical practice sessions for the
nurses, doctors and students posted there.

13
2.1.4 Post-training supervision
Post-training supervision visits for the trained health care service providers were planned to occur
about one month after the initial F-IMNCI training. The supervision team was composed of one
MOHS trainer/supervisor, in collaboration with Dr. Ye Thwin, Program Officer of MCSP’s child
health team. The WCH of Taunggyi, the District and Township hospitals were prioritized for
supervision visits. The supervision visit was scheduled according to the availability of the MOHS
supervisors and trained participants. There were 3 township hospitals that could not be reached due to
security issues.
The objectives of post-training supervision were:
1. To assess the knowledge and skills of F-IMNCI trained health care service providers in the
early post-training period (about one month after training)
2. To provide inputs to the CHD, MOHS for future analysis of the F-IMNCI training content,
methodology, and outcome of follow-up visits
3. To collect and analyze the achievement scores to contribute to the final report preparation to
inform the CHD-MOHS, SHD and MCSP about the overall implementation process
4. To assess the infrastructure of health facilities for effective child health care services
5. To share the follow-up findings with the SHD for further strengthening of the health system.
There were three sets of post-training supervision tools developed by Dr. Kyu Kyu Khin, retired
Professor/Pediatrician and Dr.Thein Thein Hnin, Professor/ Neonatologist at WCH: two questionnaire
sets for assessing the knowledge and clinical skills of trained participants and one checklist for
assessing the hospital infrastructure (Annex 7, 8 and 9).
For knowledge assessment, twenty single response questions were used, covering the three modules
of F-IMNCI training; ETAT, newborn care, and management of common diseases in children. A
correct answer was scored as “1” and an incorrect answer was scored as zero in the M&E system
(Annex 7).
There were 6 case scenarios (addressing anemia, jaundice, convulsions, diarrhea, newborn life support
and difficult breathing) used as Objective Structured Clinical Examination (OSCE) questions to assess
clinical skills. They mainly focused on assessing clinical skills, examination, diagnosis, management
procedure and practice of techniques that the participants learned during training (Annex 8).
Each participant was given 6 case scenarios and asked to describe a step-by-step case management
approach, according to the management protocols learned in the training, using teaching aids such as
manikins. One case scenario takes about 20 minutes to complete. Scores were recorded as “1” for a
correct answer and zero for an incorrect answer, for each step and procedure. At the end of the
assessment, the supervisor provided the correct answers and gave constructive feedback.
During data analysis, the achievement scores were calculated as percentages and divided into four
achievement groups: group 1 for those who achieved 0-20% scores; group 2 for 21 to 50 % scores;
group 3 for 51 to 80 % scores; and group 4 for 81 to 100 % scores.
The hospital facility infrastructure assessment tools package was based on the ETAT questions
developed by UNICEF and adapted to fit the country context. There were 3 components: Group 1-
Emergency Room, Outpatient and Laboratory assessment, Group 2 - Children's ward assessment and
Group 3 - Neonatal ward assessment at the township hospital level (Annex 9). Patient register books
were reviewed and assessed by the supervisors for patient documentation. Since the hospital

14
infrastructure assessment form used during the post- training supervision contained a lot of
information not relevant to the township level hospital and many duplicate questions, the MCSP team
and Dr. Kyu Kyu Khin developed a revised and shortened assessment form to be used in future
trainings and infrastructure assessments.
Lastly, one of the hospital administrative team members, such as the Medical Superintendent, senior
nurse or medical doctor took responsibility for completing the supervision checklist questions. After
completion, the MCSP Program Officer, Dr. Ye Thwin, reviewed the checklist. The assessment data
were recorded in Excel spread sheets and analyzed for supervision outputs and report preparation.
Picture 5. Follow-up supervision visit and skill assessment by Dr. Ye Thwin in Hsi Hseng township hospital
2.1.5 End of Project
All field activities for F-IMNCI follow-up supervision visits ended on 9 June 2018. The end of project
report and F-IMNCI case study documenting lessons learned are to be shared with the CHD of
MOHS, SHD, MCSP, USAID and other relevant key stakeholders.
15
3. Results
3.1 Quantitative and Qualitative findings
3.1.1 Pre- and Post-test results in F-IMNCI training
A total of 128 participants (31 medical doctors, 97 nurses) took part in both pre- and post-tests during
the training of 131 participants (98%). In the pre-test, the minimum score was 4, maximum score was
18 and the average score was 10.8. In the post-test, the minimum score was 6, maximum score was 19
and the average score was 14.1 out of total scores 20 (Annexes 1, 2, and 4).
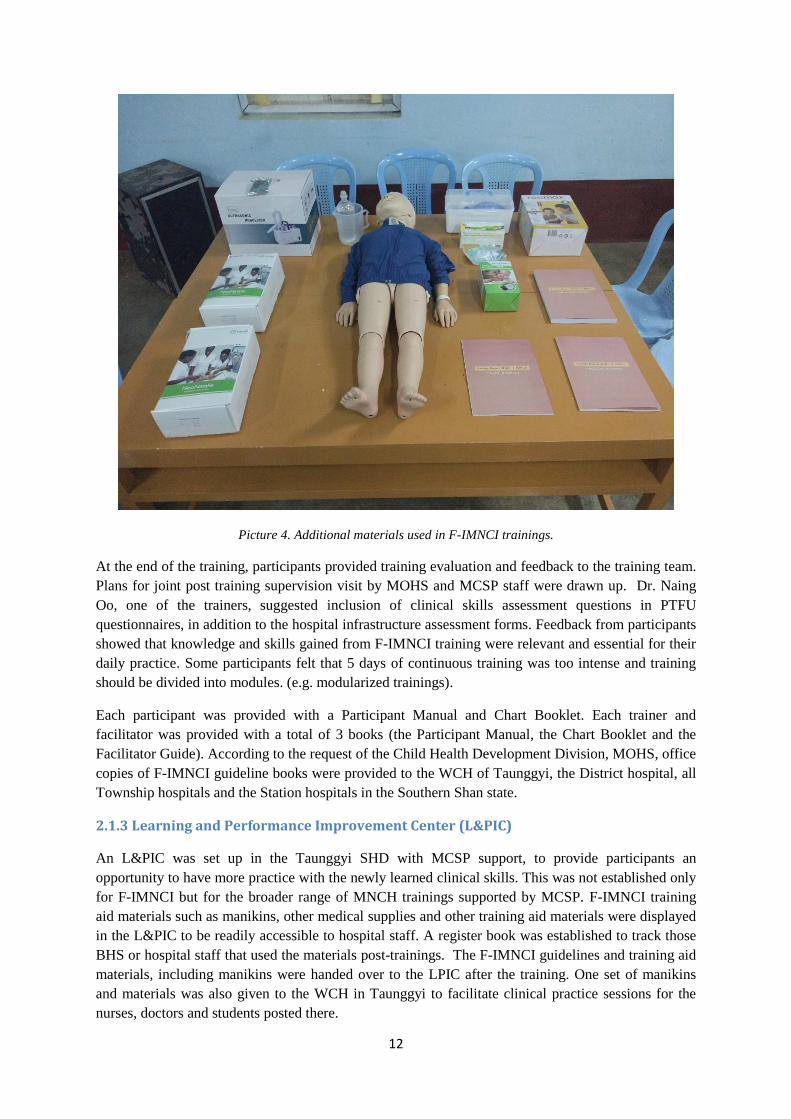
Among the medical doctors, the average scores increased from 13.5 to 16.2 between pre- and post-
test (a 20 % increase). There was an increase in average scores among nurses from 9.9 to 13.4 (35 %
increase) (see Figure 2 below).
Figure 2. Pre- and Post-test average scores of participants in F-IMNCI trainings
3.1.2 Post-training supervision visits
Ninety-four participants (17 medical doctors, 77 nurses) were included in the post-training
supervision visits, representing 72% (94/131) of all trained hospital staff. These staff were from the
WCH of Taunggyi, Loilem District hospital, Kho Lam 100-bedded hospital, 16 township hospitals
(Nyaung Shwe, Hopong, Pekon, Pindaya,Pin Laung, Hsi Hseng,Kalaw, Ywar Ngan, Nam Sang,
Mong Nai, Lang Kho, Mong Pan, Mauk Mai, Lai Kha, Kun Hing and Lawk Sawk) and 1 station
hospital Naung Ta Yar. Nine participants (2 medical doctors, 7 nurses) from Ho Pong, Pindaya and
Hsi Hseng township hospitals were supervised twice (Annex 1).
First supervision visits
3.1.2.1 Knowledge assessment test findings
Ninety-four health staff (17 medical doctors, 77 nurses) participated in the knowledge assessment test
as part of the post-training supervision assessment. The same 20 question MCQ was used. Among the
medical doctors, the minimal score was 12, the maximum score was 20, and the average was 15.8.
Among the nurses, the minimum score was 6, maximum score was 18, and the average score was
12.7.
13.5
9.9
16.2
13.4
MD Nurses
Pre- and Post-Test Average Scores of Medical Doctors and Nurses for F-IMNCI training (N=20)
Pre-test Post-test
16
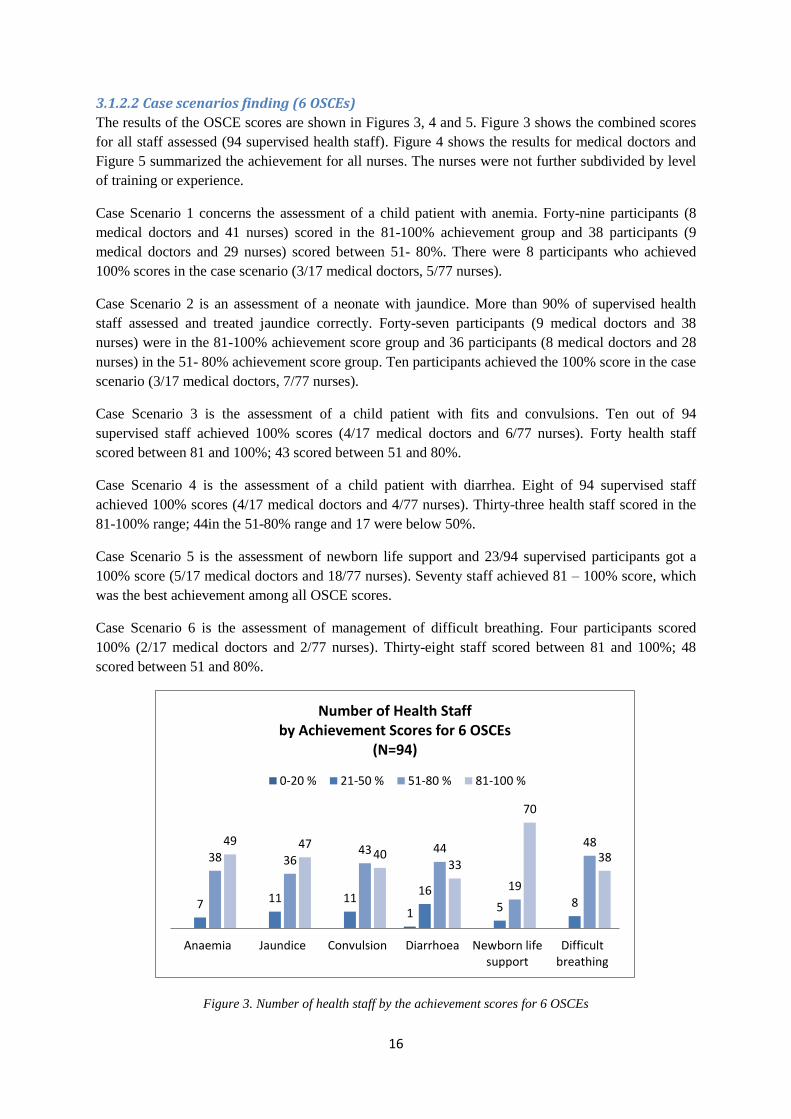
3.1.2.2 Case scenarios finding (6 OSCEs)
The results of the OSCE scores are shown in Figures 3, 4 and 5. Figure 3 shows the combined scores
for all staff assessed (94 supervised health staff). Figure 4 shows the results for medical doctors and
Figure 5 summarized the achievement for all nurses. The nurses were not further subdivided by level
of training or experience.
Case Scenario 1 concerns the assessment of a child patient with anemia. Forty-nine participants (8
medical doctors and 41 nurses) scored in the 81-100% achievement group and 38 participants (9
medical doctors and 29 nurses) scored between 51- 80%. There were 8 participants who achieved
100% scores in the case scenario (3/17 medical doctors, 5/77 nurses).
Case Scenario 2 is an assessment of a neonate with jaundice. More than 90% of supervised health
staff assessed and treated jaundice correctly. Forty-seven participants (9 medical doctors and 38
nurses) were in the 81-100% achievement score group and 36 participants (8 medical doctors and 28
nurses) in the 51- 80% achievement score group. Ten participants achieved the 100% score in the case
scenario (3/17 medical doctors, 7/77 nurses).
Case Scenario 3 is the assessment of a child patient with fits and convulsions. Ten out of 94
supervised staff achieved 100% scores (4/17 medical doctors and 6/77 nurses). Forty health staff
scored between 81 and 100%; 43 scored between 51 and 80%.
Case Scenario 4 is the assessment of a child patient with diarrhea. Eight of 94 supervised staff
achieved 100% scores (4/17 medical doctors and 4/77 nurses). Thirty-three health staff scored in the
81-100% range; 44in the 51-80% range and 17 were below 50%.
Case Scenario 5 is the assessment of newborn life support and 23/94 supervised participants got a
100% score (5/17 medical doctors and 18/77 nurses). Seventy staff achieved 81 – 100% score, which
was the best achievement among all OSCE scores.
Case Scenario 6 is the assessment of management of difficult breathing. Four participants scored
100% (2/17 medical doctors and 2/77 nurses). Thirty-eight staff scored between 81 and 100%; 48
scored between 51 and 80%.
Figure 3. Number of health staff by the achievement scores for 6 OSCEs
1 7 11 11
16
5 8
38 36 43 44
19
48 49 47 40
33
70
38
Anaemia Jaundice Convulsion Diarrhoea Newborn lifesupport
Difficultbreathing
Number of Health Staff by Achievement Scores for 6 OSCEs
(N=94)
0-20 % 21-50 % 51-80 % 81-100 %
17
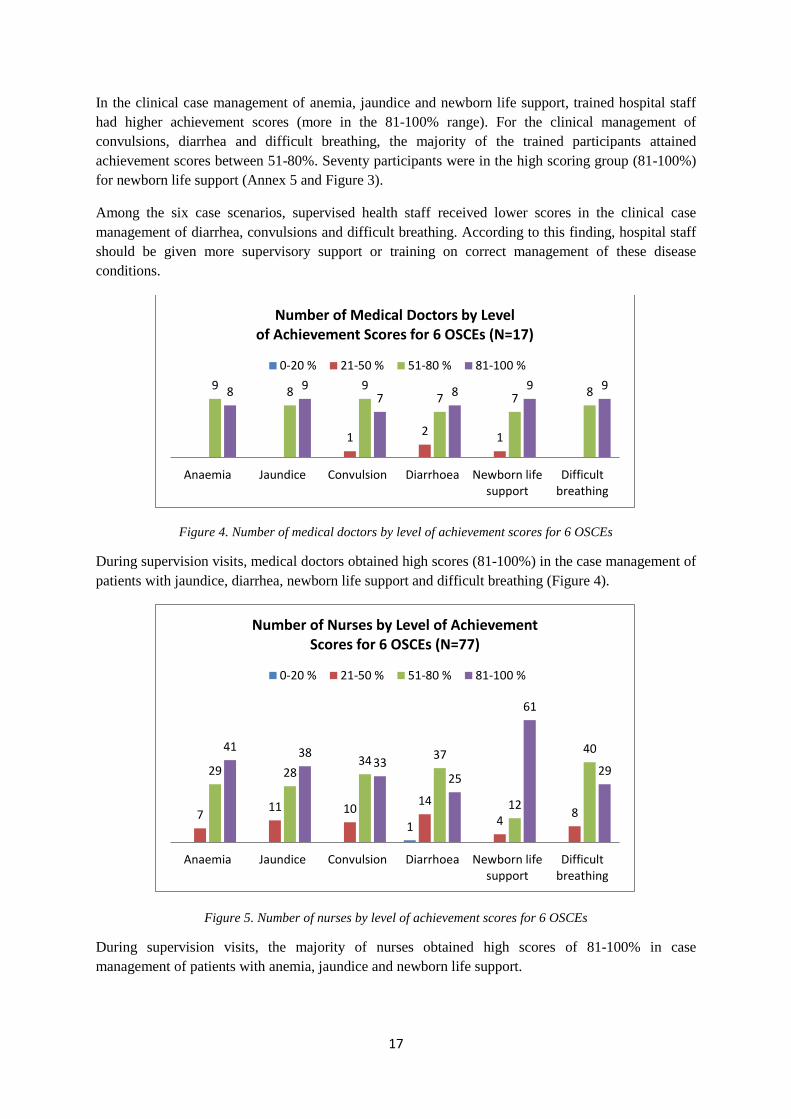
In the clinical case management of anemia, jaundice and newborn life support, trained hospital staff
had higher achievement scores (more in the 81-100% range). For the clinical management of
convulsions, diarrhea and difficult breathing, the majority of the trained participants attained
achievement scores between 51-80%. Seventy participants were in the high scoring group (81-100%)
for newborn life support (Annex 5 and Figure 3).
Among the six case scenarios, supervised health staff received lower scores in the clinical case
management of diarrhea, convulsions and difficult breathing. According to this finding, hospital staff
should be given more supervisory support or training on correct management of these disease
conditions.
Figure 4. Number of medical doctors by level of achievement scores for 6 OSCEs
During supervision visits, medical doctors obtained high scores (81-100%) in the case management of
patients with jaundice, diarrhea, newborn life support and difficult breathing (Figure 4).
Figure 5. Number of nurses by level of achievement scores for 6 OSCEs
During supervision visits, the majority of nurses obtained high scores of 81-100% in case
management of patients with anemia, jaundice and newborn life support.
1 2 1
9 8 9 7 7 8 8 9
7 8 9 9
Anaemia Jaundice Convulsion Diarrhoea Newborn lifesupport
Difficultbreathing
Number of Medical Doctors by Level of Achievement Scores for 6 OSCEs (N=17)
0-20 % 21-50 % 51-80 % 81-100 %
1 7
11 10 14
4 8
29 28 34 37
12
40 41 38 33
25
61
29
Anaemia Jaundice Convulsion Diarrhoea Newborn lifesupport
Difficultbreathing
Number of Nurses by Level of Achievement Scores for 6 OSCEs (N=77)
0-20 % 21-50 % 51-80 % 81-100 %

18
Both supervised medical doctors and nurses had stronger knowledge and clinical skills on
management of jaundice and newborn life support than for other case scenarios. Both groups of
participants needed to have more practice on the correct management of diarrhea. Nurses need to be
supported to strengthen their management of child with jaundice and convulsion. In hospitals, there is
limitation for nurses to prescribe controlled drugs, such as Diazepam, which is critical in the
management of convulsions.
Figure 6. Percentage of medical doctors and nurses by achievement score groups of 6 OSCEs
Among the supervised medical doctors, 47% had achievement scores of 51-80% and 49% attained 81-
100%. Among the supervised nurses, 39% achieved scores of 51-80% and 49% reached 81-100%.
Twelve percent of nurses achieved scores in the range from 21-50% (Figure 6).
Nearly half of supervised medical doctors and nurses (49% for each) showed high achievement scores
(81-100%). But 12% of nurses were still in the low scoring group of 21-50%. This difference may be
due to differences in basic medical knowledge, practical experience and decision-making skills and
opportunities (Figure 6).
The average achievement score among all supervised hospital staff obtained was 70% and above for
all six case scenarios (OSCEs) and the highest scores was in the newborn life support case scenario
(84.4%) (Figure 7 and Annex 6).
0 4%
47% 49%
0.2%
12%
39%
49%
0-20 % 21-50 % 51-80 % 81-100 %
Percentage of Medical Doctors and Nurses by Achievement Score Groups of 6 OSCEs (N=94)
% of MD % of Nurses

19
Figure 7. Average scores of supervised hospital staff during the post-training supervision visits of 6 OSCEs
Second supervision visit
Nine health staff (2 medical doctors, 7 nurses) from three township hospitals (Hopong, Hsi Hseng,
Pindaya) received a second supervisory visit by the MCSP Child Health Program Officer. The
participants and hospitals were randomly selected for the second supervision visit.
The average score in knowledge assessment of medical doctors increased from 15.8/20 to
18.5/20(representing a 17% increase) between the first and second assessment, while the score for
nurses increased from 12.7/20 to 14.1/20 (11% increase).
Figure 8. Difference between first and second post-training assessment scores (6 OSCEs)
Out of 94 supervised participants, 9 health staff (2 medical doctors, 7 nurses) were supervised twice.
Among the nine staff, in the first assessment, 2% were in the low score group (21-50%), but there
were none in the low score group in the second assessment. The high scores (81-100%) were
0%
20%
40%
60%
80%
100%Anaemia
Jaundice
Convulsion
Diarrhoea
Newborn life support
Difficulty breathing
Total given Average score
2%
44%
54%
46%
54%
0-20 % 21-50 % 51-80 % 81-100 %
Difference Between First and Second Post-Training Assessment of 6 OSCEs (N= 9)
First time assessment % Second time assessment %

20
maintained by 54% of supervised health staff in both assessments. The medium score group (51-80%)
was slightly improved from 44% to 46% of participants (Figure 8).
Figure 9. Number of health staff with assessment status in the second supervision
The overall training database allowed assessment of individual staff performance. During training,
7out of 9 participants (those who received a second post-training supervisory visit) had increased
scores in their post-test. In the Knowledge Assessment test during the supervision visit, 5 out of 9
participants had decreased scores, while 4 participants had increased scores on the second visit.
According to the OSCE case scenario results, more participants obtained higher scores in anaemia,
newborn life support and management of difficult breathing in the second supervision visit. However
more participants got lower scores in management of convulsions and diarrhea. (Fig 9)It is not
possible to reach any specific conclusions about the benefits of additional follow-up supervision visits
from these limited results.
3.1.2.3 Supervision of hospital infrastructure
Nineteen out of 22 hospitals (including the WCH of Taunggyi, the District and Township hospitals)
were supervised for assessment of hospital infrastructure1. Among these facilities, post training
supervision visits were conducted twice in Ho Pong, Pindaya and Hsi Hseng township hospitals
(Annex 3).
3.1.2.3.1 General assessment
All hospitals had running water at the emergency/OPD room at all times, both before and after the
training; 21 out of 22 hospitals have drinking water freely available for patients.
Three out of 19 hospitals (16%) had suitable washrooms/toilets for children. One hospital had added
this facility after the F-IMNCI training. All hospitals experienced frequent electricity cuts, but all had
backup generators to address this problem.
_____________________________________
1 Nyaung Shwe, Hopong, Pekon, Pindaya,Pin Laung, Hsi Hseng,Kalaw, Ywar Ngan, Nam Sang, Mong Nai, Lang Kho,
Mong Pan, Mauk Mai, Lai Kha, Kun Hing and Lawk Sawk township hospitals (16 township hospitals) , Taunggyi Women
and Children hospital, Kho Lam 100- bedded hospital and Loilem district hospital
7
4 4 3
2 3
5
7
2
5
3 3
6
4
2 1
0 0
2 3
1 2 2
1
No of health staff with assessment status in the second supervision (N=9)
Increased Decreased Same

21
Provision for sterilizing reusable equipment was adequate in 19 hospitals (100%). There was air
conditioning or a facility to provide warmth in 11 hospitals (58%) and among these 11 hospitals,
Pekon and Pindaya hospitals, installed this after F-IMNCI training. However, none of the hospitals
has an area for children to play with toys (Figure 10).
Figure 10. Number of hospitals showing differences in general facilities before and after training
3.1.2.3.2 Emergency or Outpatient Department (OPD)
Due to the limited space in all township hospitals, the emergency room and OPD were organized in
the same location. There was no separate waiting area for children before consultation. The
emergency/OPD was open for 24-hour service for hospital admission and there was no need for
mothers/caretakers to make appointments for consultation. Treatment was also given at the OPD in all
hospitals.
For follow-up visits, patients or mothers needed to come on the appointed date and time that was
scheduled by the assistant surgeon or township medical officer who had provided care for the case.
The WCH of Taunggyi already had a separate area to see children before training. In Pin Laung
township hospital, children are now being seen separately from adults and this was initiated after the
F-IMNCI training. Before the training, 11 out of 19 hospitals (58%) had a resuscitation area for
children. After the training, two more township hospitals established a pediatric resuscitation area,
resulting in 13 out of 19 township hospitals (68 %) having a resuscitation area.
3.1.2.3.3 Labor room and postnatal ward
Only in the WCH of Taunggyi and the Loilem District hospitals were newborns placed separately in
specific neonatal units, which were close to the labor room.
In other township hospitals, due to the limited available space, neonates were kept in cots beside their
mothers in the postnatal ward, which was close to the labor room. Delivery areas of all hospitals were
equipped with a newborn resuscitation table. Resuscitation for the newborn was done on the table or
next to the mother. Availability of resuscitation guidelines increased from 11 to 19 hospitals after
training. The number of township hospitals practicing immediate skin-to-skin contact increased from
7 to 12 hospitals (37% to 63%). The practice of using identification band for newborns was increased
from 4 to 6 hospitals after training (21% to 32%) (Figure 11).
2
9
12 14
17
3
11
17 19 19
WC for children Air conditionfacility
Resuscitationbox check list
Additionalsupport tomothers in
illness
Reusablesterilizing
equipments
Number of Hospitals Showing Differences in General Facilities Before and After Training (N=19)
Before training After training

22
Newborns were transferred from the labor room to the postnatal wards by nurses, along with required
equipment, such as oxygen and blankets. Oxygen was easily available in all resuscitation areas.
A toilet for women and warmers for babies were available in all supervised hospitals (100%) and 95%
had running water in the sink, plus provision of soap and towel. However, only half of them (42%)
had air-conditioned labor rooms.
Immediate skin-to-skin contact after delivery was practiced in 12 hospitals (63%). The majority of
supervised hospitals (90%) did not have any advertisements for formula milk and samples of formula
milk were not given to mothers. In 3 hospitals, (16%), all mothers and babies were kept in an area
which was visible from the nursing station. In all supervised hospitals (100%), mothers were provided
with additional support when they were ill. Only in 4 hospitals (21%), namely WCH in Taunggyi,
Loilem District hospital, Kalaw township hospital and Kho Lam 100-bedded hospital, was there a
specific area for pediatricians to conduct patient examination, although examination was done by
assistant surgeons or TMOs in the OPD or ward in the remainder of the hospitals.
There were 3 baby friendly hospitals (16%); WCH, Kalaw township hospital and Loi Lem district
hospital. Four out of 19 supervised hospitals (21%) had nurses who were specialized in supporting
breastfeeding; WCH of Taunggyi, Loilem district hospital, Lawksawk township hospital and Kho
Lam 100-bedded hospital.
Figure 11. Number of hospitals showing differences in labor room and postnatal ward facilities before and after
training
3.1.2.3.4 Child Ward
In all hospitals, the sickest children were placed where they could be observed best. There were no
mosquito nets available in all hospitals. There was a clearly identified resuscitation area, with all the
equipment needed for all ages of child, in 13 hospitals (68%). The emergency drug box was available
in the resuscitation areas and was regularly checked to ensure the equipment and drugs were up-to-
date in all hospitals, but only 89% of them had a proper check list for emergency drugs and
equipment.
4
7 7
11
6 8
12
19
Identification bandfor newborns
Air conditionedfacility in Labour
room
Immediate skin toskin contact
Newbornresuscitation
guidelines flowchart
Number of Hospitals Showing Differences in Labour Room and Postnatal Ward Facilities Before and After Training
(N=19)
Before training After training

23
3.1.2.3.5 Laboratory
HIV testing and malaria RDTs were available in all supervised hospitals (100%). None of the
hospitals, except WCH of Taunggyi, had a blood bank, obtained from donors such as CSOs and
monks, when needed. Emergency" O" negative blood was not available in any hospital. There was a
sink with running water, plus soap and towel available, in the working area of laboratories in all 19
hospitals (100%). The laboratories in all hospitals have full accreditation.
All hospitals, except one, had a lab technician for both daytime and nighttime laboratory services. In
that one hospital, the nurses performed the laboratory tests while waiting for the assigned laboratory
technician. Outside of office hours, laboratory technicians can be contacted by phone and will come in
for urgent cases. It was reported that it took about an hour to obtain results after blood samples were
sent. All specimens and results were labeled clearly in all hospitals. There was air conditioning to
protect machines from overheating in the laboratories of 6 hospitals (32%).
In all hospitals, the essential basic laboratory tests were available; Hemoglobin, Blood grouping and
matching, HIV testing, malaria RDT, TB microscopy and Dengue serology tests. About half of the
supervised hospitals had laboratory facilities for urea test (58%) and serum electrolytes (47%). About
one third of the supervised hospitals had the laboratory facility to test serum bilirubin (32%).
3.1.2.3.6 Equipment
For management of sick children in hospitals, there were 1 to 2 nebulizers accessible in all
township hospitals, which were used for both child and adult patients in OPD/emergency and in-
patient wards. However, spacers for children with difficult breathing were available only in 2
hospitals (11%). Three to 5 oxygen cylinders and concentrators were available in all township
hospitals. Pulse oximeters, with suitable probes for babies and children, were available in only 3
hospitals (16%).
For use in newborn babies, Vitamin K was available in all supervised hospitals (100%) with proper
documentation of administration. Identification bands for all newborn babies were used in 6 hospitals
(32%). Newborn resuscitation guidelines were available as flow charts in 18 supervised hospitals
(95%) (Figure 11). There were functioning phototherapy units for the newborns in need in all
hospitals (100%).
For emergency use, a glucometer with adequate sticks, functioning oxygen supply and Adrenaline/
Epinephrine of 1 in 1,000 solution were available in all supervised hospitals (100%). Clear
instructions for diluting Adrenaline were found in all hospitals.
For patient safety and infection control, all hospitals followed the universal precaution by using the
proper boxes for disposing of needles and sharp materials. All sharps were put in suitable boxes and
disposed of when ¾ full in all hospitals. In almost all hospitals, there was no practice of using
identification bands for children on admission. As infection control, 18 hospitals (95%) had hand-
washing gel available.
For the nutritional assessment of children, MUAC tapes were found in 5 hospitals (26%), and
weight-for-height charts were present in 15 hospitals (79%). All hospitals (100%) had weighing
machines and height measurement equipment. The majority of hospitals (90%) had newborn scales
and infantometres for weight and length measurement of newborns and infants (Figure 12).

24
Figure 12. Number of hospitals showing differences in availability of equipment before and after training
3.1.2.3.7 Human resources
On average, most of the hospitals have 3 to 6 nurses assigned in the daytime and 1 to 2 nurses at
night. In township hospitals, the assigned nurses take the responsibility for patients in all wards, with
no specific assignment for child wards. However, the WCH of Taunggyi and some hospitals with
higher workloads have separate nurses assigned for each specialty area. Medical doctors were
assigned for both day and night responsibility in the hospital. As clinical specialists, pediatricians
were assigned in three hospitals (WCH of Taunggyi, Loilem District hospital and Kalaw Township
hospital). The TMO was in the leading role for clinical management of all cases in the township
hospitals.
3.1.2.3.8 Drug and Pharmacy
Health education leaflets about ORS preparation and correct dosages of antimalarial drugs were
available in 16 hospitals (84 %). There was proper drug stock management (drugs were safely stored
and clearly labeled) in all hospitals (100%).
3.1.2.3.9 Clinical practice and guidelines
In 15 out of 19 supervised hospitals (78%), reference books, guidelines and formularies were
available. Visible treatment protocols and flow-charts were found on the wall in 17 hospitals (89%).
Twelve out of 19 hospitals (63%) were operating a triage system and 7 out of 12 hospitals had a well-
established triage system. Five hospitals (26%) had practiced KMC, but only 2 hospitals (11%) had an
ORT corner (Figure 13).
In all hospitals, sick children were transported from the emergency room/OPD to the ward by a nurse
or by parents or by wheel chair or trolley, with the necessary equipment such as oxygen cylinders and
blankets. Assistant surgeons in the emergency/OPD stabilized very sick children before transferring
them to the ward in all hospitals.
During the post-training supervision visits, some improvements in the clinical practice, due to
adherence to the F-IMNCI guidelines, were observed (Figure 13). There was significant improvement
in implementation of a triage system and displaying treatment guidelines and protocols on the walls of
hospitals, for easy reference of health staff while providing care.
1 1
3
11
2 3
5
15
Spacers Pulse Oximeter MUAC tape Weight for heightchart
Number of Hospitals Showing Difference in Availability of Equipments Before and After Training (N=19)
Before training After training

25
Figure 13. Number of hospitals showing differences in clinical practice before and after training
4. Analysis
4.1 Challenges
4.1.1 Training
Selection of Participants to receive training - It was originally planned that doctors and nurses from
22 hospitals (19 township hospitals, plus WCH of Taunggyi, one district hospital and one 100-bedded
hospital) would be included in this F-IMNCI introduction in S. Shan. However in the end, in addition
to these 22 facilities, some participants from 14 stations hospitals were also invited to attend by their
TMOs.
Delay in procurement of manikins (child, infant and newborn) and for training – The lack of
availability of the necessary manikins for the training, due to delays in procurement, meant that the
trainers had to borrow and try to make special arrangements to have the needed training materials
available for all batches. For example, the trainers/facilitators had to buy chicken bones for the
practical sessions for intraosseous cannulation and bring manikins from Yangon Children Hospital to
Taunggyi for the first training batch. Also, manikins were borrowed from the WCH of Taunggyi. It
also meant that during the early post-training supervision visits the Dr. Ye Thwin (MCSP PO) did not
have the manikins to take to the sites for practical assessments of the skills of the trained staff.
Difficult to impart newly learned knowledge and skills to untrained staff - Trained participants
were asked to return to their work sites and share what they had learned with their untrained
colleagues. However in reality, they had limited time available to disseminate the F-IMNCI training
content to the other hospital staff.
Limited availability of trainers - There was limited availability of trainers to lead the trainings. As
F-IMNCI training is facility-based and a highly technical training, the qualified trainers should be
pediatricians or neonatologists. Associate Professor Dr. Naing Oo, pediatrician from Yangon Children
Hospital, supported the first batch of the training. In Taunggyi, there were 2 pediatricians and 1
Neonatologist who had already attended the master ToT of the F-IMNCI training in Yangon and all
three trainers led the remaining five batches in Taunggyi. Facilitators supported them and assisted
0
4 5 5
12
2 5
12
17 15
ORT corner KMC Triage Visibletreatmentprotocol
Reference,guidelines,formularies
Number of Hospitals Showing Differences in Clinical Practice Before and After Training (N=19)
Before training After training

26
with the conduct of the training but ideally there would have been 4 trainers in each batch (plus the
facilitators).
Differing abilities among participants - Some nurses had certain levels of difficulty in
understanding the F-IMNCI training content in English language. Other nurses had excellent
comprehension and performed equally well with the medical doctors. There was some discussion
about whether or not doctors and nurses should be trained in different batches, as their skills and
experience put them at different levels. But overall it was considered desirable to have mixed batches,
with both doctors and nurses, working in small groups and as a team in the clinical sessions, as that
more closely resembles the reality at the hospital level. Since pre-tests are done before training it
should be possible, even during the initial training, to provide some additional support to the
participants/nurses who have more difficulty understanding the content and/or picking up the skills
and techniques needed. This is more difficult if the number of qualified trainers is not sufficient. After
training, there is another knowledge assessment and the trainers should be aware of which participants
need some additional support when they return to their posts. If this is conveyed to the post-training
supervisors, they could use a targeted approach to support those who need some more practice and
refresher on the job site.
4.1.2 Post-training supervision
Limited availability of supervisors - There was limited availability of the trainers or supervisors for
conducting the post-training supervision visits. Clinicians, who are the trainers and whose skills are
best suited for the post-training supervision, are also very busy with their clinical duties. At WHC
there is a huge clinical workload and teaching responsibility among the pediatricians and
Neonatologist. Prof/Neonatologist Dr. Thein Thein Hnin, retired at the end of March and there was
shortage of clinical staff for the hospital service facility. Dr. Ye Thwin, MCSP’s Program Officer, was
a medical doctor who had been working in a local NGO, which provided training to the local CSOs
about emergency health care services, in close collaboration with hospital staff in Taunggyi. He had
recently passed the MRCP Part 1 exam and was in the process of preparing for Part 2 exam, so very
well suited to provide the clinical type of support needed during post-training supervision. He
supported all 6 batches of F-IMNCI training as a facilitator and had already built up trust with the
WCH clinicians on his ability and capacity to conduct the post-training supervision alone to some
Township Hospitals. It was discussed and agreed by the SHD, Southern Shan state that when other
supervisors were not available he could proceed with the supervision visits, reporting back to the SHD
on the findings and future visit planning.
Infrastructure assessment – The MCSP inputs to strengthen F-IMNCI in Southern Shan were
limited to support for training, provision of training materials (including materials for the L&PIC) and
post-training follow-up supervision visits and guidance. There was no provision for providing any
equipment, supplies nor other essential materials to the hospitals. A tool was used in the assessments
to try to document the existing infrastructure constraints and any improvements that were made
through local management or through MOHS resources and findings are summarized in this report.
The tool will be revised (based on field experience) and shared with the MOHS for future expansion.
(Annex 10)
Limited time frame – The trainings were conducted from November 2017 to March 2018 and
follow-up visits were completed by June 9, 2018. Maintenance of skills and retention of knowledge
gained in the training was documented and any local infrastructure improvements noted and
encouraged. However, there was insufficient time to monitor any longer term changes in the

27
management of sick neonates and children in Southern Shan, but the SHD has been provided with all
the results and findings and can continue to monitor progress going forward.
4.2 Lessons Learned Different levels of the MOHS system will play vital roles for the successful scale up of F-IMNCI.
Township Hospital staff (nurses and doctors) appear eager to acquire updated knowledge and learn
new skills to save the lives of children and newborns. During the training their knowledge improved
(verified through pre and post training test scores) and back at their duty stations they showed
improvement in their management of anemia, jaundice, newborn life support. But they still need to
improve management of convulsions, diarrhea and difficult breathing. Skills were improved with
practice, on site, during the post-training supervision visits and with the guidance of a clinically
qualified supervisor, committed to the task of quality improvement after training. This model should
be considered for scale up – to have a qualified dedicated staff member (likely from a tertiary hospital
or state health department level) assigned and supported to conduct this task. Some infrastructure
changes were made in some hospitals to improve the readiness to manage sick children (triage plans,
visible newborn resuscitation guidelines flow chart, resuscitation boxes and updated checklists,
improved sterilization procedures, etc.) and further resources may be needed to support them to
improve further. While TMOs did not participate in the training they need to be involved in the
planning for infrastructure and procedural changes in their facilities to improve triage and
management of sick newborns and children under 5.
At the State level, the SHD was involved in all steps related to planning for training (venue, trainers,
dates, participants (also devolution of decision-making to the TMO) and plans for follow-up after
training. Although it was not possible for staff of the SHD to accompany the MCSP Program Officer
on some visits, their role is very important going forward in assuring the maintenance of program
quality in Southern Shan and in the scale up in additional states and regions.
The Central Level MOHS provided the overall guidance with policy setting and finalization of the
materials to be used for F-IMNCI scale up. Coordination with partners allowed selection of Southern
Shan as the site for MCSP support and other partners will support in other states/regions. Going
forward the MOHS will lead the coordination and planning for scale-up and should pursue adequate
resources for the township hospital level to improve the infrastructure as needed, and address any
shortages in essential equipment and supplies. The lessons learned from this “pilot” in Southern Shan
could be disseminated for learning in other states and regions.
In regard to the costs involved in supporting this F-IMNCI training and post-training follow-up in
Southern Shan, a summary of the expenses incurred by MCSP for printing and procurement of
training materials, for actual conduct of training for 6 batches and for supervision after training are
summarized below. These represent the level of resources that may be needed to further replicate and
support the F-IMNCI scale up in other states and regions.
Item Total cost (USD)
1 Staff cost (Qualified Clinical Officer for Supervision) for 9 month period* 2,200
2 F-IMNCI guideline books 8,735
3 Training materials (6 batches) 827
4 Manikins and accessories 3,985
5 Training cost 29,290
6 Supervision cost (Estimated) 1,852
Total cost 46,889 * 3 months for training and 6 months for post-training supervision and follow-up

28
4.3 Best Practices F-IMNCI training materials are very effective for management of the newborn and under-5 children
with severe illness. The F-IMNCI treatment and management protocols are appropriate topics for
discussion in the monthly CME sessions in the hospitals. In some township hospitals, trained medical
doctors led the CME sessions with key messages from the F-IMNCI for the training of doctors and
nurses in the hospitals who had not yet attended the training.
F-IMNCI flow-charts prepared in vinyl should be kept on the walls of the OPD, neonatal and child
wards in the hospital for easy reference by the hospital staff.
The newborn and under-5 in-patient registers, with progress notes maintained throughout the
hospitalized period, provide a good record for review of patient care and documentation for future
management of the patients by hospital staff.
At the end of the supervision visit in a hospital debriefing with the TMO about the findings of
infrastructure and capacity of the trained hospital staffs should be carried out.
4.4 Recommendations
4.4.1 Planning
More resources such as trainers, time and money should be made available to train more hospital staff
from all facility levels (e.g., township hospitals and station hospitals).
4.4.2 Training
To achieve consistent and correct management for pediatric patients, all hospital staff with
responsibility for the care of sick newborns and children under-5 should be provided with F-IMNCI
training.
There should be regular refresher courses on F-IMNCI training for both existing and new staff
assigned to the care of sick newborns and children under five.
4.4.3 Post-training supervision
Regular post-training supervision visits by clinically qualified supervisors and CME sessions should
be carried out. These can be targeted (to those who did not perform well during training or in previous
supervision visits) if resources (time, money, personnel) are limited. Manikins should be used for
refresher sessions whenever practical.
Register books for neonatal and under-5 children in-patients should be available in all facilities
providing pediatric care.
Following the F-IMNCI implementation, quality improvement activities to further strengthen
management of under-5 childhood illnesses are recommended, for future planning.
The learning models, like manikins, other medical supplies and materials, should be distributed to all
teaching hospitals in the States and Regions for easy accessibility for future trainings (initial and
refresher).
4.4.4 Hospital Infrastructure
Materials and equipment specific for children such as pulse oximeters, pediatric blood pressure cuffs,
resuscitation kits for children, intraosseous needles, spacers and baby-weighing scales should be
provided in all hospitals.

29
There should be a triage system in place in all hospitals.
There should be a separate space for OPD and emergency care of sick newborns and children in
township hospitals with a high patient load and adequate staffing.
Referral services such as vehicles, human resources and medical equipment should be provided in all
hospitals to provide proper and timely referral.
Health staff at various levels should be made aware of training materials and support that L&PICs
could provide them for the development and maintenance of their clinical skills.
4.4.5 Future planning
The F-IMNCI indicators should be integrated into the Health Management Information System
(HMIS) for better monitoring and statistical analysis.
Sufficient funding should be available for wider coverage and efficient trainings.
Training materials and manikins should be provided to all training units in the states and regions.

30
5. References 1. UNICEF Child Mortality Report. 2017.
https://www.unicef.org/publications/files/Child_Mortality_Report_2017.pdf
2. WHO, Global Health Observatory (GHO) Data, Under five mortality
http://www.who.int/gho/child_health/mortality/mortality_under_five_text/en/
3. MOHS, Nay Pyi Taw (2017) Myanmar Demographic Health Survey (2015-16). Available
at https://dhsprogram.com/pubs/pdf/FR324/FR324.pdf
4. UNICEF. Under 5 and Infant mortality rate. https://data.unicef.org/topic/child-
survival/under-five-mortality/
5. WHO. Health Targets for SDG3.www.who.int/sdg/targets/en
6. WHO, Myanmar, Training course on facility-based integrated management of neonatal
and childhood illness in Yangon, online documentation.
http://www.searo.who.int/myanmar/areas/rhtrainingonfbim/en/

31
6. Annexes
Annex 1. Number and percentage of hospital staff reached through F-IMNCI training
and supervision
Batch Participating hospitals and participants Total
trained
and
superv
ised
Types of
participants
Training
WCH
District
hospital
19
Township
hospitals
14 Station
hospitals,
1
Dispensar
y
Kholam
100
bedded
hospital
Medic
al
Doctor
s Nurses
1 7 4 8 2 5 26 6 20
2 7 0 13 3 0 23 6 17
3 6 4 9 4 0 23 5 18
4 6 0 11 3 0 20 6 14
5 6 0 9 6 0 21 5 16
6 2 0 11 2 3 18 6 12
No. of trained
health staff
Six
batch
es
34 8 61 20 8 131 34 97
No. of
supervised
health staff
26 5 46 10 7 94 17 77
% Supervised 76% 63% 75% 50% 88% 72% 50% 79%
Annex 2. Participants in training and supervision
No District Township Type of hospital
Batch of
training
Training
participants
Supervised
participants
First
time
Second
time
1 Taunggyi Taunggyi WCH
1,2,3,4,
5,6 34 26
2 Taunggyi
Nyaung
Shwe Township hospital 4
4 4
3 Taunggyi Ho Pong Township hospital 3 4 4 3
4 Taunggyi His Hseng Township hospital 6 3 3 3
5 Taunggyi Kalaw Township hospital 1,6 9 7
6 Taunggyi Pindaya Township hospital 2 3 3 3
7 Taunggyi Ywa Ngan Township hospital 6 1 1
8 Taunggyi Lawksawk Township hospital 5 1 0
9 Taunggyi Pin Laung Township hospital 5 1 1
10 Taunggyi Pekon Township hospital 1 3 3
11 Loilen Loilem District hospital 1,3 8 5
12 Loilen Lai Kha Township hospital 5 3 2
13 Loilen Nam Sang Township hospital 3 4 4
14 Loilen Kunhing Township hospital 3 1 1
15 Loilen Kyesi Township hospital 4 3 0
16 Loilen Mong Kai Township hospital 2 4 0

32
17 Loilen Mong Hsu Township hospital 2 3 0
18 Langkho Lang Kho Township hospital 2 3 3
19 Langkho Mong Nai Township hospital 4 4 4
20 Langkho Mawk Mai Township hospital 5 4 3
21 Langkho Mong Pan Township hospital 6 3 3
22 Loilen Nan Sang
Kho Lam 100
bedded hospital 1, 6
8 7
23 Pekon Moe Byae Station hospital 1 2 2
24 Mong Hsu
Loi Seng
Htout Station hospital 2
1
25 Pindaya Mai In Station hospital 2 1
26 Lang Kho Wan Hat Station hospital 2 1
27 Kunhing Karli Station hospital 3 3 2
28 Kunhing Ho Pan Dispensary 3 1 1
29 Nam Sang Keng Taung Station hospital 4 2
30 Kyesi Mong Naung Station hospital 4 1
31 Pin Laung Naung Ta yar Station hospital 5 1 1
32 Pin Laung Saung Pyaun Station hospital 5 1
33 Pin Laung Ti Kyit Station hospital 5 1
34 Lawksawk Kyine Kham Station hospital 5 1 1
35 Lawksawk Kyout Gu Station hospital 5 1 1
36 Lawksawk Pin Phyit Station hospital 5 1 1
37 Ywar Ngan Myo Gyi Station hospital 6 2 1
Total 131 94 9
Annex 3. Hospital participation in training and supervision
N
o District Township Type of hospital
Batch of
training
Training schedule Supervision
schedule
2017 2018
2018
1st
time
2nd
time
1 Taunggyi Taunggyi WCH 1,2,3,4, 5,6
Nov, Dec
Jan, Feb,
March May
2 Taunggyi Nyaung Shwe Township hospital 4 February April
3 Taunggyi Ho Pong Township hospital 3 January March May
4 Taunggyi His Hseng Township hospital 6 March April June
5 Taunggyi Kalaw Township hospital 1,6 November March May
6 Taunggyi Pindaya Township hospital 2 December March June
7 Taunggyi Ywa Ngan Township hospital 6 March May
8 Taunggyi Lawksawk Township hospital 5 March May *
9 Taunggyi Pin Laung Township hospital 5 March May
10 Taunggyi Pekon Township hospital 1 November May
11 Loilen Loilem District hospital 1,3 November January April
12 Loilen Lai Kha Township hospital 5 March June
13 Loilen Nam Sang Township hospital 3 January April
14 Loilen Kunhing Township hospital 3 January June
15 Loilen Kyesi Township hospital 4 February
16 Loilen Mong Kai Township hospital 2 December
17 Loilen Mong Hsu Township hospital 2 December
18 Langkho Lang Kho Township hospital 2 December May
19 Langkho Mong Nai Township hospital 4 February May
20 Langkho Mawk Mai Township hospital 5 March June
21 Langkho Mong Pan Township hospital 6 March May
22 Loilen Nan Sang Kho Lam 100 bedded 1, 6 November March April

33
hospital
23 Pekon Moe Byae Station hospital 1 November May
24 Mong Hsu Loi Seng Htout Station hospital 2 December
25 Pindaya Mai In Station hospital 2 December
26 Lang Kho Wan Hat Station hospital 2 December
27 Kunhing Karli Station hospital 3 January June
28 Kunhing Ho Pan Dispensary 3 January June
29 Nam Sang Keng Taung Station hospital 4 February
30 Kyesi Mong Naung Station hospital 4 February
31 Pin Laung Naung Ta yar Station hospital 5 March May
32 Pin Laung Saung Pyaun Station hospital 5 March
33 Pin Laung Ti Kyit Station hospital 5 March
34 Lawksawk Kyine Kham Station hospital 5 March May
35 Lawksawk Kyout Gu Station hospital 5 March May
36 Lawksawk Pin Phyit Station hospital 5 March May
37
Ywar
Ngan Myo Gyi Station hospital 6
March May
Station hospitals were not assessed for hospital infrastructures, only health staff assessment.
** Only hospital infrastructure
Annex 4. Pre- and Post-test scores of participants during training
Pre- Post- Increased
Percent
increase
Min 4 6 2 50
Max 18 19 1 6
Ave 10.8 14.1 3.3 27
Annex 5. Achievement scores of 94 participants in six OSCEs in first supervision visit
% of
achievement OSCE 1 OSCE 2 OSCE 3 OSCE 4 OSCE 5 OSCE 6
0-20 % 1
21-50 % 7 11 11 16 5 8
51-80 % 38 36 43 44 19 48
81-100 % 49 47 40 33 70 38
Annex 6. Average scores of supervised hospital staff during the post-training
supervision visits (6 OSCEs)
Total scores 100% Achievement scores in average %
Anemia 75.2%
Jaundice 73.4%
Convulsion 75.7%
Diarrhea 71.7%
Newborn life support 84.4%
Difficult breathing 73.0%

34
Annex 7. Multiple choice questions and answers used in Pre and post test of training
and during supervision (20 MCQs)
Pre/Post Test for FIMNCI
Name _______________________
Position _______________________
1. Which child should be triaged as an emergency?
a) 2 year old with cough and fever
b) 2 year old referred with pallor from another hospital
c) 6 week old baby with cough and fever
d) 1 year old who is floppy and responds to voice
e) 3 year old who had a convulsion one day ago and now responds only to pain
2. A 4-month old girl presents with fever after 2 convulsions earlier that day. Now she only
responds to pain (AVPU = P). Her pupils are equally reactive to light. What do you do first?
a) Give ceftriaxone 100mg/kg IV immediately
b) Perform a lumbar puncture then give Ceftriaxone 100mg/kg IV
c) Give phenobarbitone 20mg/kg IM
d) Check the blood glucose and a RDT (Rapid Diagnostic Test) for malaria
e) Give artesunate 2.4mg/kg intravenously
3. A 6-month old in the emergency department has blue lips. Which of the following is FALSE?
a) Cyanosis is difficult to assess if the child is anemic
b) Cyanotic children generally need oxygen
c) Cyanosis can occur in congenital heart disease
d) Peripheral cyanosis is a reliable sign of hypoxia
e) Cyanosis can occur in severe pneumonia
4. A four-year old male child was rushed in. He convulsed one hour ago. He is breathing fast but
there is no cyanosis and no respiratory distress. He feels very hot, but responds quickly to
questions. He has no diarrhea or vomiting. How do you triage this child?
a) Emergency due to high fever
b) Priority
c) Non urgent
d) Emergency due to shock
e) Emergency due to lethargy
5. Which answer is true of neonatal jaundice?
a) Jaundice of the eyes is classified as severe
b) Jaundice on day 1 is physiological
c) Neonatal jaundice always requires treatment
d) Jaundice can cause serious brain injury

35
e) Direct sunlight is as effective as phototherapy at reducing jaundice (bilirubin levels)
6. A 2-day old baby is seizing (convulsing). What is the best treatment?
a) Phenobarbitone 20mg/kg deep IM injection
b) Phenobarbitone 20mg/kg IV bolus
c) Diazepam 0.5mg/kg rectally
d) Phenobarbitone 15mg/kg IV
e) Diazepam 0.25mg/kg IV
7. A premature baby (weight 2kg) is 6 hours old. He is lethargic and has NOT breastfed. The
blood glucose is 22mg/dl (1.2mmol/L). Which treatment would you give?
a) Give 4mls IV 10% dextrose and offer breast feed
b) Breast feed immediately
c) Give expressed breast milk via nasogastric tube
d) Give 10mls IV 10% dextrose and offer breast feed
e) Offer breast feed then give expressed breast milk via nasogastric tube
8. Breast feeding: Which of the following is FALSE?
a) Expressed breast milk can be stored at room temperature safely for 8 hours.
b) Expressing milk maintains lactation for weeks for very low birth weight babies.
c) Signs of good attachment include a wide-open mouth, complete coverage of the lower nipple
and slow deep sucking.
d) If breast milk is inadequate, encourage more frequent suckling.
e) If breasts are engorged avoid expressing breast milk.
9. During newborn resuscitation, which of the following statements is FALSE?
a) The ratio of chest compressions to breaths is 3:1
b) If the baby is apneic (not breathing) give 2 effective breaths before chest compressions.
c) After 30 seconds of effective ventilation breaths, start chest compressions if the heart rate is <
60 beats per minute
d) Chest compressions should depress the chest by 1/3 its depth
e) After chest compressions, babies should to be admitted to the newborn unit for observation
10. Components of organization of neonatal transport include (single response)
a) Assess
b) Stabilize
c) Write a note
d) Encourage mother to accompany
e) All of the above
11. What is the normal temperature range for a healthy baby?
a) 36.5°C - 37.5°C
b) 34.0°C – 35.5°C
c) 35.5°C - 36.5°C
d) 37.5°C - 38.5°C

36
e) 35.5°C - 37.5°C
12. Which babies should be given vitamin K after birth?
a) Only babies with bleeding
b) Only babies with birth weight >2500 grams
c) All babies
d) Only sick babies
e) Only premature babies
13. Babies with what problem might benefit from cup feeding?
a) Vomiting with every feeding
b) Unable to awaken for feeding
c) Able to swallow but unable to suck effectively
d) Unable to swallow
e) Premature babies
14. When should a baby be treated with antibiotics?
a) If birth weight is less than 2000 grams
b) When a Danger Sign is present
c) If the baby cries often
d) If the baby appears to be in pain
e) If the baby is not sucking well
15. When should the first dose of an antibiotic be given?
a) After transfer for advanced care
b) As soon as possible after a Danger Sign has been identified
c) After all family members have been contacted
d) At a time that is convenient for the health care provider
e) When jaundice is present
16. After the first day following birth, jaundice is severe when it appears on what body area?
a) Back and abdomen
b) White part of the eye
c) Legs and arms
d) Palms and soles
e) Face
17. A 3-year old boy (weight 15kg) with diarrhea has a heart rate of 130 bpm, weak peripheral
pulses, cold hands and a capillary refill time of 4 seconds.
What is the best emergency treatment?
a) 300 ml IV Ringer lactate over 15 minutes
b) 150 ml IV normal saline over 30 minutes + oxygen
c) 450 ml IV Ringer lactate over 30 minutes + oxygen
d) 300 ml IV normal saline over 2 hours
e) 450 ml IV Ringer lactate over 4 hours

37
18. A 4-month old girl presents with fever after 2 convulsions earlier that day. Now she only
responds to pain (AVPU = P). Her pupils are equally reactive to light. What do you do first?
a) Give ceftriaxone 100mg/kg IV immediately
b) Perform a lumbar puncture then give Ceftriaxone 100mg/kg IV
c) Give phenobarbitone 20mg/kg IM
d) Check the blood glucose and a RDT (Rapid Diagnostic Test) for malaria
e) Give artesunate 2.4mg/kg intravenously
19. A child with severe wasting, oedema of both feet and a mid-upper arm circumference
(MUAC) of 10 cm presents with prolonged cough. After her ABCCD assessment, what do you
do first?
a) Check her sputum for TB
b) Check for electrolyte abnormalities and treat
c) Check for hypothermia and if temperature <35oC actively re-warm child
d) Give furosemide (Lasix)
e) Give F100 100mls/kg/day
20. In severe life threatening asthma, which of the following is FALSE?
a) Give continuous salbutamol nebulizers at a maximum rate of 0.5mg/kg/hr
b) Give oxygen to maintain saturations > 92%
c) Absence of wheeze is a sign the child is improving
d) If the child is vomiting, give IV hydrocortisone every 6 hours at 4mg/kg
e) If the child deteriorates acutely and air entry is significantly reduced on one side suspect
pneumothorax
FIMNCI Answer Key
1. C, E
2. D
3. D
4. B
5. D
6. B
7. A
8. E
9. B
10. E
11. A
12. C
13. C
14. B
15. B
16. D
17. C
18. D
19. C
20. C

38
Annex 8. Six OSCEs checklist used for skill assessment in supervision
No 1. Anemia (OSCE)
You are asked to see a 3-year old boy in the emergency room. He has been referred with fever and
extreme pallor. What will you do?
No. Action required Information / result Achieved? (1 or 0) ,
(yes or no)
1
SSSS
Observe the boy on his mother’s lap
Is the baby alert?
Ask the mother to call him by name
Place child on bed
Call for help
Any trauma or bleeding?
The boy is drowsy and looks very
pale. He feels very hot.
He wakes when called but closes
his eyes again immediately
No visible bleeding
1 if perform otherwise
0
2
A
Assess the airway
Watch look and listen to breathing
Breathing rapidly
No stridor, secretions
1 if perform otherwise
0
3
B
Assess breathing - rate, head
nodding, grunting, cyanosis, chest
in-drawing, acidotic breathing,
auscultation- air entry & added
sounds crackles and wheeze
You cannot judge cyanosis as he
is so pale
Breathing rate is deep and fast
(acidotic)
RR 45
Mild indrawing and nasal flaring
Chest sounds clear
1 if at least three of
them is performed
4
B
Pulse oximeter O2 sats air 85% in air 1 if perform otherwise
0
5
B
Oxygen - nasal prongs 2-4 L/min
May also suggest salbutamol
Sats increase to 93% in oxygen 1 if perform otherwise
0
6
C
Central pulse - pulse rate
Peripheral pulse (weak/strong)
Temperature gradient
Capillary refill
Pallor
Pulse fast 160
Peripheral pulses easy to feel.
Warm hands
Capillary refill time is 2 seconds.
There is severe palmar pallor.
Not in shock
1 if perform otherwise
0
7
C
AVPU
Confusion / Convulsions
Check glucose
The child responds to his name
but is not fully alert and cannot
sit up. AVPU=V
Not fitting
Blood glucose is 50mg/dl
1 if perform otherwise
0
8
D
Signs of severe dehydration No dehydration 1 if perform otherwise
0

39
9 Establish iv access, Take blood for
Hb, group and urgent Xmatch
Malaria rapid test
Hb is 2.8g/dl HCT 9%
RDT is positive
1 if perform otherwise
0
10 Admit to ward
Continue nasal prong oxygen
1 if perform otherwise
0
11 Complete full history and
examination
Investigations
1 if perform otherwise
0
Total marks /11
Name - Department
No 2. Jaundice (OSCE)
A 3-day old premature baby born at 35 weeks gestation (BW 2.2 kg) has become irritable and
jaundiced. He is not feeding. How would you assess him?
No. Action required Information / result Achieved? (1 or 0) ,
(yes or no)
1 Hand washing 1 if perform otherwise
0
2
A
Assess airway - secretions, stridor,
noisy breathing
No noisy breathing, no stridor 1 if perform otherwise
0
3
B
Assess breathing - rate, grunting,
cyanosis, chest in-drawing, acidotic
breathing, auscultation- air entry &
added
Breathing RR 70 fast and shallow
No cyanosis
No head bobbing or grunting
VBS no added sound
1 if at least three of
them is performed
4
B
Pulse oximeter O2 sats air 90% in air 1 if perform otherwise
0
5
B
Oxygen - nasal prongs 2-4 L/min Sats increase to 98% in oxygen 1 if perform otherwise
0
6
C
Central pulse - pulse rate
Peripheral pulse (weak/strong)
Temperature gradient
Capillary refill
Pallor
Central pulse fast 180bpm
Peripheral pulse normal
Hands warm
Capillary refill 1 seconds
Looks pale and jaundiced
1 if perform otherwise
0
7
CCC
Movement / tone
Convulsions
Check Blood sugar
Reduced movements, tone
increased
No convulsions
Blood sugar 4.2mmol/l (75mg/dl)
1 if perform otherwise
0
8
D
Check for signs of dehydration
Inability to feed
Sunken Eyes
Skin pinch ≥ 2 secs
Premature, not sucking
Skin pinch 2 secs
No sunken eyes
1 if perform otherwise
0

40
9 Start maintenance fluids straight
away
Day 3 -100ml/kg/day 10% dextrose
1 if perform otherwise
0
10 Reassess
ABCCD
Breathing RR 60
O2 sats in oxygen 94%
Central pulse fast 170bpm
No shock
Still irritable, increased tone, no
convulsions
Temperature 36.5
1 if perform otherwise
0
11 Consider infection screen
IV antibiotics (ampicillin with
gentamicin)
Assess and treat jaundice
Hb, Group mother and baby
1 if perform otherwise
0
Total marks /11
Name - Department
No 3. Convulsion (OSCE)
A 16-month old child presents to the emergency department with a 2 day history of reduced
feeding, lethargy, fever and fitting for approximately 10 minutes. Please show us how you would
manage this child.
No. Action required Information / result Achieved? (1 or 0) ,
(yes or no)
1 Open airway -
secretions, stridor, noisy breathing?
Support airway, put in recovery
position (if no cervical spine injury)
Breathing improved
No cyanosis, RR 40, no
indrawing.
1 if perform otherwise
0
2 Give anti-convulsant
Diazepam PR 0.5mg/kg ,
repeat PR Diazepam if still fitting
after 10 min
Weight 10kg
PR diazepam 5mg given
1 if at least three of
them is performed
3 Assess breathing - Rate, head
nodding, grunting, cyanosis, chest
in-drawing, acidotic breathing,
Breathing irregularly
Some noisy breathing
1 if perform otherwise
0
4 Pulse oximeter
Oxygen - nasal prongs 2-4 L/min
Sats 84% on air
Sats increase to 98% in oxygen
1 if perform otherwise
0
5 Auscultation- air entry & added
sounds crackles and wheeze
Fine inspiratory crackles and
expiratory wheeze bilaterally
1 if perform otherwise
0

41
6 Central pulse - pulse rate
Peripheral pulse (weak/strong)
Temperature gradient
Capillary refill
Pallor
Pulse fast 150
Normal peripheral pulses
Warm hands, CRT 2 seconds
1 if perform otherwise
0
7 Assess convulsions or coma
No more fitting 1 if perform otherwise
0
8 Measure blood sugar 100 mg/dl (5.5 mmol/L) 1 if perform otherwise
0
9 Obtain IV access 1 if perform otherwise
0
10 Reassess
Airway
Consider oropharyngeal airway
noisy breathing
Breathing RR 40
O2 sats 95% in oxygen
Pulse 150, capillary refill 2
1 if perform otherwise
0
11 Check for dehydration No dehydration 1 if perform otherwise
0
12 Admit to ward
Continue nasal prong oxygen
1 if perform otherwise
0
13 Complete full history and
examination
Investigations
1 if perform otherwise
0
Total marks /13
Name - Department
No 4. ABCCD/ Diarrhea (OSCE)
An 11-month old baby is seen as an emergency because she has very cold hands and a weak pulse.
She has a history of diarrhea for 3 days. What do you do?
You have help if you need it and the equipment is ready.
No. Action required Information / result Achieved? (1 or 0) ,
(yes or no)
1 SSSS
Hand washing, gloves
Observe the child -Is she alert?
Baby is limp in the mother’s arms
and is not alert
1 if perform otherwise
0
2 Place child on bed and call or
stimulate the child
The baby makes a weak cry but
does not open her eyes
1 if perform otherwise
0

42
3 Call for help Help is available 1 if perform otherwise
0
4 Look in the mouth
Open the airway (neutral position)
There is nothing in the mouth 1 if perform otherwise
0
5 Assess breathing No stridor or noisy breathing
The baby is breathing rapidly
1 if perform otherwise
0
6 Check for signs of respiratory
distress:
Cyanosis
Head nodding/nasal flaring
Chest Indrawing
Grunting
Auscultation - Crackles & wheeze
Acidotic breathing
Respiratory rate
Pulse oximeter
No head nodding/ nasal flaring
No grunting
No central cyanosis
Yes there is chest wall in-
drawing-
Yes there is acidotic breathing
Chest is clear
RR 60
No pulse oximeter machine
1 if perform otherwise
0
7 Give oxygen by nasal prongs 1-
2L/min
1 if perform otherwise
0
8 Assess large pulse- brachial,
femoral or carotid
HR fast 160 bpm 1 if perform otherwise
0
9 Assess warmth of hands and temp
gradient
The hands are cold up to the
elbow
1 if perform otherwise
0
10 Call for help if not before 1 if perform otherwise
0
11 Check peripheral pulses
Check capillary refill time
Recognizes shock
Peripheral pulse is hard to feel.
Capillary refill time is 5 sec
1 if perform otherwise
0
12 As in shock, check for
Pallor
Signs of malnutrition
Diarrhea/ signs of dehydration
There is no pallor
Yes – there is diarrhea & Skin
pinch >3 secs/ Sunken eyes/
lethargy
No signs of malnutrition
1 if perform otherwise
0

43
13 Attempt iv failed, attempt IO
access
IV unsuccessful
IO is successful
1 if perform otherwise
0
14 Give fluids for shock with diarrhea
Start plan C immediately
Ringers/ 0.9% saline
30ml/kg over 1 hour as she is
11months
Weight 10kg
(needs to be similar/safe if not
exactly correct treatment)
1 if perform otherwise
0
15 AVPU? P - Responds to pain only 1 if perform otherwise
0
16 Check blood sugar
Give 10% dextrose 5ml/kg bolus
There is no glucometer
1 if perform otherwise
0
17 Convulsions? No convulsions 1 if perform otherwise
0
18 Stop the scenario 1 if perform otherwise
0
Total marks /18
Name - Department
No 5. Newborn Life Support (OSCE)
A term baby is delivered after a prolonged labor. The baby makes no immediate cry as the cord is
being cut. There is no meconium. What do you do?
You have help if you would like it and the equipment has been checked and is working.
No. Action required Information / result Achieved? (1 or 0) ,
(yes or no)
1 Turn on warmer
Hand washing and gloves
Place baby on resuscitation table
Consider shouting for help
Start clock
1 if perform otherwise
0
2 Dry the baby, remove wet cloth and
wrap
in a dry cloth
Stimulate the baby by drying it
The baby does not cry when dried
1 if perform otherwise
0
3 Initial assessment while stimulating The baby is floppy and pale 1 if perform otherwise
0

44
Colour
Tone
Breathing: look listen and feel for 5
secs
Heart rate: listen with stethoscope
The baby is not breathing
Heart rate is very slow- much less
than 60bpm
4 Look in the mouth
(for meconium/blood)
Open the airway (‘neutral’ position;
face almost flat)
There is nothing in the mouth
No meconium, no blood
1 if perform otherwise
0
5 Call for help if not done before 1 if perform otherwise
0
6 Check mask and bag
Give effective BVM breaths for 30
secs rate ~40/min
Check for chest wall rising
Check bag, size mask
Correct grip for mask
Able to move the chest
effectively
1 if perform otherwise
0
7 If the chest wall does not move then
the candidate should reposition the
head and mask and try again.
(May mention double handed jaw
thrust suction or oropharyngeal
airway)
Provided the chest wall on the
mannequin moves then say ‘the
chest wall is rising’
If it is not then point that out to
them and ask them what else they
can do to improve the airway
1 if perform otherwise
0
8 Reassess breathing and heart rate The airway is clear
There is no breathing
HR is very slow- less than 60bpm
1 if perform otherwise
0
9 Give CPR 3:1 for 30 seconds Correct technique and timing
(Examiner to help with BVM,
candidate does compressions)
1 if perform otherwise
0
10 Re-assess breathing and heart rate Airway is clear
HR is slow: less than 60bpm
The baby is not breathing
1 if perform otherwise
0
11 Continue CPR 3: 1 for 30 secs 1 if perform otherwise
0

45
12 Re-assess breathing and heart rate The baby is gasping irregularly
HR over 100
1 if perform otherwise
0
13 Continue ventilation for 30 secs 1 if perform otherwise
0
14 Reassess Breathing well and starting to cry
HR over 100
1 if perform otherwise
0
15 Observe for 1-2 minutes, admit to
NICU, give oxygen by nasal prongs
if needed.
Close scenario. 1 if perform otherwise
0
Total marks /15
Name - Department
No 6. Difficult Breathing
A 6- month old infant in the Emergency Department with a 2-day history of cough and shortness
of breath. Please show us what you would do.
No. Action required Information / result Achieved? (1 or 0) ,
(yes or no)
1
SSSS
Observe
Safety hand-gel, Stimulation, Shout
for help, Setting
Child alert, sitting up on mother’s
lap.
1 if perform otherwise
0
2
A
Assess airway - secretions, stridor,
noisy breathing
Breathing rapidly
No stridor, secretions
1 if perform otherwise
0
3
B
Assess breathing - Rate, head
nodding, grunting, cyanosis, chest
in-drawing, acidotic breathing,
Breathing RR 70 1 if at least three of
them is performed
4
B
auscultation- air entry & added
sounds crackles and wheeze
Fine inspiratory crackles and
expiratory wheeze bilaterally
1 if perform otherwise
0
5
B
Pulse oximeter O2 sats air 87% in air 1 if perform otherwise
0
6
B
Oxygen - nasal prongs 1-2 L/min Sats increase to 92% in oxygen 1 if perform otherwise
0
7
C
Central pulse - pulse rate
Peripheral pulse (weak/strong)
Temperature gradient
Capillary refill
Pallor
Pulse rate 100 per minute
peripheral pulse strong
temperature 98.6 F
capillary refill time - 1 sec
no pallor
1 if perform otherwise
0

46
8
C
AVPU
Confusion / Convulsions
Alert , no convulsion 1 if perform otherwise
0
9
D
Signs of severe dehydration
Lethargy (AVPU < A) or
Unable to drink / drinks poorly
Sunken Eyes
Skin pinch ≥ 2 secs
No dehydration but breathless 1 if perform otherwise
0
10
ABCCD
Reassess Breathing RR 70
O2 sats 97% in nasal prong
oxygen
Chest indrawing and head
bobbing continues
Fine inspiratory crackles and
expiratory wheeze
Central pulse fast 140bpm
No signs of shock
1 if perform otherwise
0
11 Admit to ward
Continue nasal prong oxygen
1 if perform otherwise
0
12 Complete full history and
examination
Investigations
1 if perform otherwise
0
Total marks /12
Name - Department
47
Annex 9. Hospital assessment forms (3 groups)
Hospital Survey: Review group 1: A & E /Emergency Room , Out Patient Department ,
Laboratory
Name of hospital:___________________________ Date:___________________________
A & E or Emergency room
Category Question Comment Recommendations
Layout
Are children seen separately from adults?
Is triage up and running?
Who is doing it?
How is it documented?
Is there a guideline chart on the wall?
Is there an ORT corner?
Is there a resuscitation area for children clearly identified and
with all the necessary equipment?
What arrangements are made for transporting sick children to
the ward?
Is there enough space? Is it clean?
Are there formal clinics for out patients in this area or just
walk-in patients?
Other observations

48
Infrastructure
Is there running water in the sinks at all times?
Is drinking water freely available for patients?
Is there a sink with soap and towel in each area?
Are there suitable washrooms/WC for children?
Electricity: are there frequent power cuts? If so is there a
back up generator?
Is there adequate provision for sterilizing reusable
equipment?
Is there air conditioning or a facility to provide warmth when
needed?
Is there a play area with toys?
Other observations
Staffing numbers and
rotations
How many nurses on a shift on average?
By day?
By night?
How many junior doctors available on ward?
By day?
By night?
How many senior doctors available?
49
By day?
By night?
How do nurses call doctors when needed?
Other observations
Patient safety and
infection control
Do all children have an identification band if admitted to the
ward?
Are all sharps put in suitable boxes and disposed of when ¾
full?
Is hand washing gel available?
Are there any torn covers on couches?
Other observations
Investigations
Cotside
Is there a glucometer? Are there enough sticks?
Is there a pulse oximeter with suitable probes for babies and
children? How many?
Is HIV testing readily available?
Are RDTs for malaria available and in use?
Other observations
Drugs and pharmacy
Are the drugs dispensed here or elsewhere?
Are all the drugs safely stored and clearly labeled?

50
Are there any patient information leaflets about the common
treatments ORS, antimalarials, etc.?
Review 3 charts of children who have just been treated: is the
prescription clear, weight written and can you see how many
doses have been given?
Comment
Equipment
Are there nebulizers? How many?
Are there spacers available?
How many working oxygen cylinders are there?
How many working concentrators?
Resuscitation equipment: does it include bag and all sizes of
masks (0-4), wide bore cannulae and suction?
Is there any equipment which is not working
Are there baby-weighing scales?
Are there scales for weighing children?
Is there a height measure?
Are MUAC tapes available?
Comment?

51
Clinical practice and
guidelines
Are there guidelines or formularies available for staff to
check doses?
Are resuscitation guidelines visible as charts on the wall?
Are drug dose charts freely available or visible on the wall?
How are very sick children stabilized before transfer?
How are sick children transferred to the ward
Are weight/ height charts available?
How is follow up organized?
Comment
Outpatient clinics
Category Question Comment Recommendations
Layout
Are children seen separately from adults?
Is there a separate waiting area for children?
Is there an appointment system?
Is there enough space?

52
Comment
Infrastructure
Is there running water in the sinks at all times?
Is drinking water freely available for patients?
Is there a sink with soap and towel in every delivery area?
Are there adequate washrooms/WC for children?
Is the area child friendly?
Is the area clean?
Is there an area with toys suitable for play?
Comment
Staffing numbers and
rotations
How many nurses on a shift on average?
How many pediatric clinics are there each week?
Observations
Patient safety and
infection control
Are treatments given in OPD?
Are all sharps put in suitable boxes and disposed of when ¾
full?
Is hand washing gel available?
Comment?

53
Documentation and
patient records
Look at the notes available for 2-3 children in OPD. Any
comments?
Are they adequate?
Other observations
Investigations In Clinic
Is there a glucometer? Are there enough sticks?
Is there a pulse oximeter with suitable probes for babies and
children?
Is HIV testing readily available?
Are RDTs for malaria available and in use?
Comments?
Equipment
Are there nebulizers? How many?
Are there spacers available?
Are there baby-weighing scales?
Are there scales for weighing children?
Is there a height measure?
Are MUAC tapes available?
Comment?

54
Laboratory
Category Question Comment Recommendations
Layout
Is the laboratory on the same site as wards?
Which important tests are done elsewhere?
Is the room(s) spacious and well ventilated?
Is there a blood bank?
Where does the blood come from?
Other observations
Infrastructure
Is there running water in the sinks at all times?
Is there a sink with soap and towel in every working area?
Electricity: are there frequent power cuts? If so is there a
back up generator?
Is there adequate provision for sterilizing reusable
equipment?
Is there air conditioning to protect machines from
overheating?
Comment
Staffing numbers and
rotations How many senior technicians are in the laboratory?

55
In daytime?
At night?
How may other technicians are in the laboratory?
By day?
At night?
What arrangements are made for urgent on call work?
Other observations
Patient safety
Does the laboratory have full accreditation?
Comment?
Documentation and
patient records
Are all specimens and results labeled clearly?
Observations
Investigations
Which of these investigations are available by day and night?
Hb and CBC
Group and X match
Microscopy for malaria
TB microscopy

56
Dengue serology
Urea and electrolytes
Bilirubin: direct and indirect
Are there tests that cannot be done here?
Are RDTs for malaria easily available and in use?
Is HIV testing done in the laboratory or on the wards?
Comments?
Any comments from
staff

57
Hospital Survey: Review group 2: Children's Ward
Filled by: ...................
Children's Ward
Category Question Comment Recommendations
Layout
Are children nursed separately from adults?
Are surgical cases nursed in another ward?
Are breastfeeding mothers able to room in comfortably?
Is there a high dependency unit with a nursing station in it?
Are there nurses there at all times?
Are the sickest children placed where they can be observed best?
Describe the area where children are admitted. Is there enough space?
Are there nurses in all areas of the ward taking observations?

58
Is there a clearly identified resuscitation area with all the equipment
needed for all ages of child?
Other observations
Infrastructure
Is there running water in the sinks at all times?
Is drinking water freely available for patients?
Food: what are the arrangements for preparing food for the children?
Is there a sink with soap and towel in every delivery area?
Are there separate washrooms/WC for children?
What are the facilities for parents on the ward?
Washrooms/WC
Seating
Food preparation
Electricity: are there frequent power cuts? If so is there a back up
generator?

59
Is there adequate provision for sterilizing reusable equipment?
Is there air conditioning or facility to provide warmth when needed?
Other observations
Staffing numbers and
rotations
How many nurses on a shift - By day?
How many nurses on a shift - By night?
How many Junior doctors on a shift - By day?
How many Junior doctors on a shift - By night?
How many Senior doctors on a shift - By day?
How many Senior doctors on a shift - By night?
How do nurses call doctors when needed?
Patient safety and
infection control
Do all children have an identification band?
Are all sharps put in suitable boxes and disposed before they are
completely full?

60
Is hand washing gel available?
Do all beds have mosquito nets?
Are there any torn mattresses?
Other observations
Investigations cotside
Is there a glucometer on the ward? Are there enough sticks?
Are there pulse oximeters with suitable probes for babies and children?
How many?
Is HIV testing readily available on the ward?
Other observations
Drugs and pharmacy
Are there any essential drugs which are not available?
Are all the drugs safely stored and clearly labeled?
Is there an emergency drug box in the resuscitation area, checked and up
to date?

61
Equipment
Resuscitation equipment: does it include in each area a bag and all sizes
of mask (0,1,2,3,4) suction machine and wide bore cannulae, oxygen?
Is there a checklist for resuscitation equipment and a system for checking?
Oxygen: how many working cylinders?
How many oxygen concentrators?
Are there nebulizers? How many?
Is there any equipment on the ward that is not working?
Are there baby-weighing scales?
Are there scales for weighing children?
Is there a height measure?
Are MUAC tapes available?
Other observations
Clinical practice and
guidelines Are there guidelines or formularies available for staff to check doses?
62
Are resuscitation guidelines visible as charts on the wall?
Are weight/ height charts available?
Is there an ORT corner?
Other observations
Hospital Survey: Review group 3 Neonatal Care
Labor ward & Post natal ward
Filled by: .............................
Labor Ward
Category Question Comment Recommendations
Layout
Does each delivery area, including theatre,
have a resuscitation table or resuscitaire close to the mother?
Is the neonatal unit near the labor ward?
How are babies transferred to the neonatal unit?

63
Is oxygen available for newborn resuscitation in each area?
Infrastructure
Is there running water in the sinks at all times?
Is there a sink with soap and towel in every delivery area?
Are the washrooms/WCs for women nearby and satisfactory?
Electricity: are there frequent power cuts?
If so is there a back up generator?
Is there adequate provision for sterilizing reusable equipment?
Is there a warmer to provide warmth for a baby when needed?
Is the labor ward air-conditioned?
Staffing numbers and
rotations
How many nurses on a shift - By day?
How many nurses on a shift - By night?
Is a pediatric doctor available to come immediately to labor
ward - By day?

64
Is a pediatric doctor available to come immediately to labor
ward - By night?
How do nurses call pediatric doctors when needed?
Patient safety and
infection control
Do all newborn babies have an identification band in Labor
Ward?
Are all sharps put in suitable boxes and disposed of when ¾
full?
Is the area clean?
Investigations
cotside
Is there a glucometer on labor ward for IDDM babies? Are
there enough sticks?
Is there a pulse oximeter for use on babies?
Drugs and pharmacy
Is Vit K available on the Labor ward?
Is it given and documented in the patient file?
Are all the drugs safely stored and clearly labeled?
Is adrenaline/ epinephrine 1 in 10,000 available? If 1in 1000 is
available are there clear instructions on diluting it?

65
Is emergency O negative blood kept on the Labor ward?
Equipment
Resuscitation equipment:
Does it include in each area: a warmer, bag and 3 sizes of
mask 00,0,1, suction machine and wide bore cannulae, oxygen,
umbilical tape, umbilical catheters?
Is there a working clock?
Is there any equipment on the ward that is not working??
Are there baby-weighing scales?
Clinical practice and
guidelines
Is there a specified pediatric doctor on call for Labor ward?
Are resuscitation guidelines visible as charts on the wall?
Are well babies put skin to skin immediately after drying,
and put to the breast within 30 minutes?
How are babies transferred to the neonatal unit?

66
Are there any visible notices or advertisements for formula
milk?
Post Natal ward
Category Question Comment Recommendations
Layout
Are all mothers and babies visible from the nursing station?
Is there an area where mothers are given extra support - if
unwell or after C-section?
Are family carers able to help mothers who are unwell?
Is there an area for baby resuscitation with suitable equipment?
Is there an area set aside for pediatric doctors to do the baby
checks?

67
If not how/where are they done?
Infrastructure
Are there sinks for hand-washing in each area with running
water, soap and towels?
Is there drinking water freely available for mothers?
Are the washrooms for the mothers nearby and satisfactory?
Is oxygen available if needed?
Staffing numbers and
rotations
How many nurses on a shift - By day?
How many nurses on a shift - By night?
68
Is a pediatric doctor available to come immediately to labor
ward - By day??
Is a pediatric doctor available to come immediately to labor
ward - By night
How do nurses call pediatric doctors when needed?
Patient safety
and infection control
Is hand gel available in all areas?
Do all babies have identification bands?
Are the babies nursed in cots beside their mothers?
Are the cots and mattresses in good condition?

69
Are sharps boxes used and changed before they are completely
full?
Is the area clean?
Investigations cotside
Are there glucometers on the ward and are there enough
sticks?
Can bilirubin levels be measured on the ward?
If blood is sent to the lab how long does it take to get the
results
Drugs
Are drugs dispensed on the ward or from pharmacy?
Are all drugs safely stored?

70
Are all drugs in the store clearly labeled?
Equipment
Is phototherapy given on the postnatal ward? If so is the
equipment working well?
Are there baby scales and length boards?
Is there a pulse oximeter for babies on the ward?
Clinical practice
Is kangaroo care in use?
If not how are small babies kept warm?
Is this a Baby Friendly Hospital?
71
Is there any evidence of advertising for formula milk?
Are samples of formula milks ever given to mothers?
Is there a nurse who specializes in supporting breastfeeding?

72
Annex 10. Revised hospital assessment form recommended to use for future assessment in township hospital
Township Hospital Checklist to assess readiness to provide Child Health Services (F-IMNCI) - Myanmar
Form completed by (Name, Position): ……………………………………………………………………… Date .............................................
Category Question Comment Recommendations
Hospital Layout
Are children seen separately from adults?
Are the sickest children placed where they can be observed
best?
Is triage up and running?
Who is doing it?
How is it documented?
Is there a guideline chart on the wall?
Is there an ORT corner?
Is there a resuscitation area for children clearly identified
and with all the equipment needed for all ages of child?

73
What arrangements are made for transporting sick children
to the ward?
Is there enough space? Is it clean?
Are there formal clinics for out patients in this area or just
walk-in patients?
Other observations
Infrastructure
Is there running water in the sinks at all times?
Is drinking water freely available for patients?
Is there a sink with soap and towel in each area?
Are there suitable washrooms/WCs for children?
Electricity: are there frequent power cuts? If so is there a
back up generator?
74
Is there adequate provision for sterilizing reusable
equipment?
Is there air conditioning or a facility to provide warmth
when needed?
Is there a play area with toys?
Other observations?
Staffing numbers and rotations
How many nurses on a shift on average?
By day?
By night?
How many junior doctors are available on ward?
By day?
By night?
How many senior doctors available?
By day?
By night?

75
How do nurses call doctors when needed?
Other observations
Patient safety and infection
control
Do all children have an identification band if admitted to the
ward?
Are all sharps put in suitable boxes and disposed of when ¾
full?
Is hand washing gel available?
Are there any torn covers on couches/chairs?
Other observations
Investigations Cotside
Is there a glucometer? Are there enough sticks?
Is there a pulse oximeter with suitable probes for babies and
children? How many?
Is HIV testing readily available?

76
Are RDTs for malaria available and in use?
Other observations
Drugs and pharmacy
Are the drugs dispensed here or elsewhere?
Are all the drugs safely stored and clearly labeled?
Are there any patient information leaflets about the common
treatments ORS, antimalarials, etc.?
Are there any essential drugs that are not available?
Please list.
Are all the drugs safely stored and clearly labeled?
Is there an emergency drug box in the resuscitation area,
checked and up to date?
Comment
Equipment Are there nebulizers? How many?
Are there spacers available?

77
How many working oxygen cylinders are there?
How many working concentrators?
Resuscitation equipment: does it include an ambu bag and
all sizes of masks (0-4), wide bore cannulae and suction? If
not list what is missing.
Is there any equipment that is not working?
Are there baby-weighing scales?
Are there scales for weighing children?
Is there a height measure?
Comment?
Clinical practice and guidelines
Are there guidelines or formularies available for staff to
check doses?
Are resuscitation guidelines visible as charts on the wall?
Are drug dose charts freely available or visible on the wall?

78
How are very sick children stabilized before transfer to
ward?
How are sick children transferred to the ward?
Are weight/height charts available?
Who organizes follow-up and how?
Comment
Out patient clinics
Category Question Comment Recommendations
Layout
Are children seen separately from adults?
Is there a separate waiting area for children?
Is there an appointment system?
Is there enough space?
Comment
Infrastructure
Is there running water in the sinks at all times?
Is drinking water freely available for patients?

79
Is there a sink with soap and towel in every delivery area?
Are there adequate washrooms/WC for children?
Is the area child friendly?
Is the area clean?
Is there an area with toys suitable for play?
Comment
Staffing numbers and rotations
How many nurses on a shift on average?
How many pediatric clinics are there each week?
Observations
Patient safety and infection
control
Are treatments given in OPD?
Are all sharps put in suitable boxes and disposed of when ¾
full?
Is hand washing gel available?
Do all beds have mosquito nets?
Comment

80
Documentation and patient
records
Look at the notes available for 2-3 children in OPD. Any
comments?
Are they adequate?
Other observations
Investigations In Clinic
Is there a glucometer? Are there enough sticks?
Is there a pulse oximeter with suitable probes for babies and
children?
Is HIV testing readily available?
Are RDTs for malaria available and in use?
Comments?
Equipment
Are there nebulizers? How many?
Are there spacers available?
Are there baby-weighing scales?
Are there scales for weighing children?
Is there a height measure?
Comment

81
Laboratory
Category Question Comment Recommendations
Layout
Is the laboratory on the same site as the ward?
Which important tests are available?
Is the room(s) spacious and well ventilated?
Is there a blood bank?
Other observations
Infrastructure
Is there running water in the sinks at all times?
Is there a sink with soap and towel in every working area?
Electricity: are there frequent power cuts? If so is there a
back up generator?
Is there adequate provision for sterilizing reusable
equipment?
Is there air conditioning to protect machines from
overheating?
Comment

82
Staffing numbers and rotations
How many senior technicians are in the laboratory?
In daytime?
At night?
How may other technicians are in the laboratory?
· By day?
· At night?
What arrangements are made for urgent on-call work?
Other observations
Comment?
Documentation and patient
records
Are all specimens and results labeled clearly?
Observations
Investigations
Which of these investigations are available by day & night?
Hb and CBC
Group and X match
Microscopy for malaria
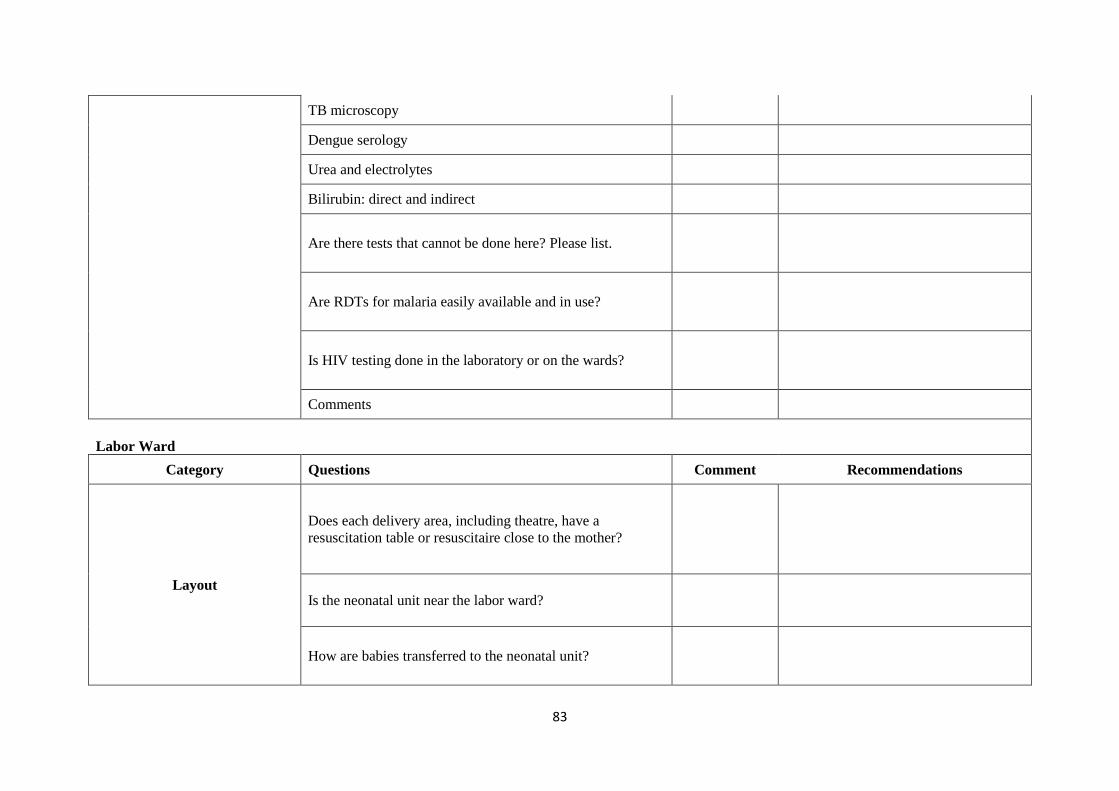
83
TB microscopy
Dengue serology
Urea and electrolytes
Bilirubin: direct and indirect
Are there tests that cannot be done here? Please list.
Are RDTs for malaria easily available and in use?
Is HIV testing done in the laboratory or on the wards?
Comments
Labor Ward
Category Questions Comment Recommendations
Layout
Does each delivery area, including theatre, have a
resuscitation table or resuscitaire close to the mother?
Is the neonatal unit near the labor ward?
How are babies transferred to the neonatal unit?

84
Is oxygen available for newborn resuscitation in each area?
Infrastructure
Is there running water in the sinks at all times?
Is there a sink with soap and towel in every delivery area?
Are the washrooms/WC for women nearby and satisfactory?
Is there adequate provision for sterilizing reusable
equipment?
Is there a warmer to provide warmth for a baby when
needed?
Is the labor ward air-conditioned?
Staffing numbers and
rotations
How many nurses on a shift - By day?
How many nurses on a shift -By night?
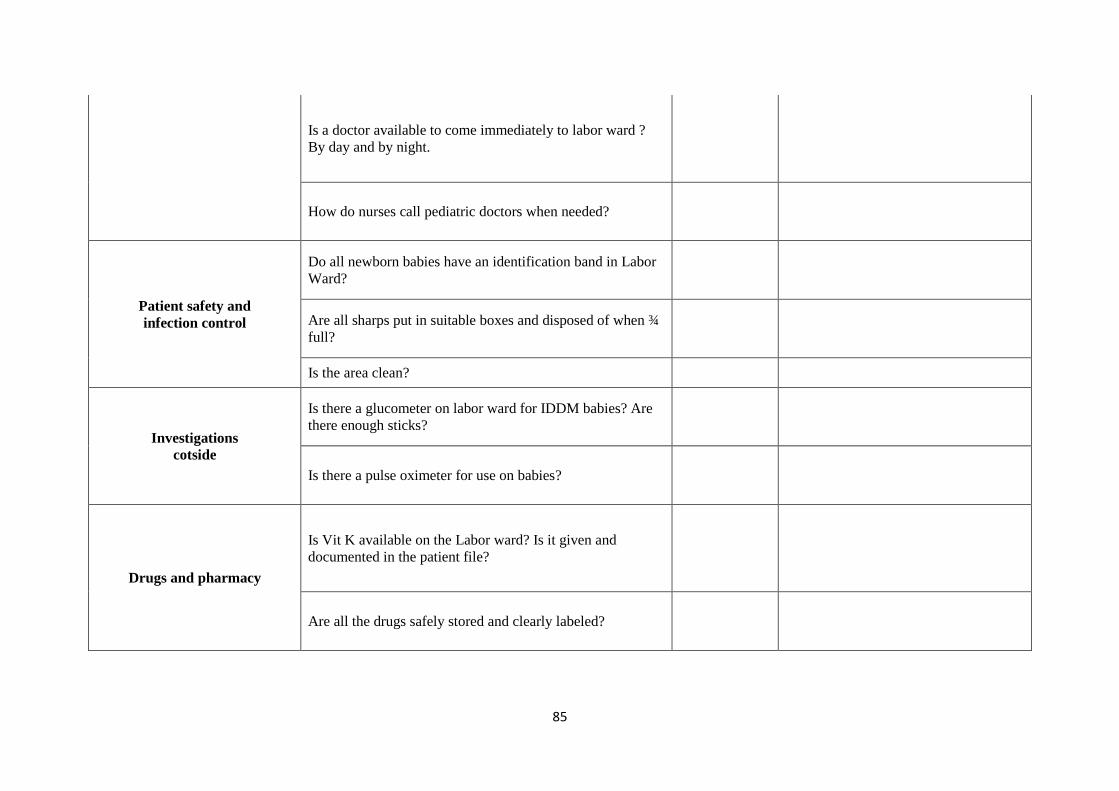
85
Is a doctor available to come immediately to labor ward ?
By day and by night.
How do nurses call pediatric doctors when needed?
Patient safety and
infection control
Do all newborn babies have an identification band in Labor
Ward?
Are all sharps put in suitable boxes and disposed of when ¾
full?
Is the area clean?
Investigations
cotside
Is there a glucometer on labor ward for IDDM babies? Are
there enough sticks?
Is there a pulse oximeter for use on babies?
Drugs and pharmacy
Is Vit K available on the Labor ward? Is it given and
documented in the patient file?
Are all the drugs safely stored and clearly labeled?
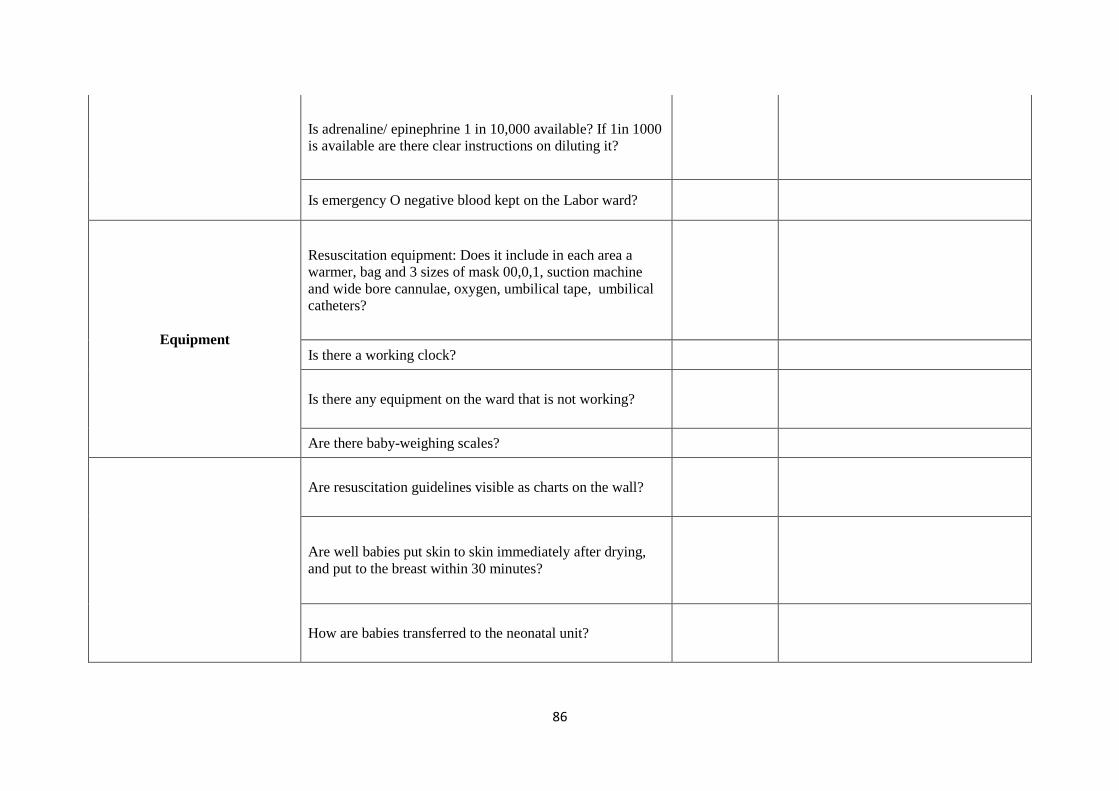
86
Is adrenaline/ epinephrine 1 in 10,000 available? If 1in 1000
is available are there clear instructions on diluting it?
Is emergency O negative blood kept on the Labor ward?
Equipment
Resuscitation equipment: Does it include in each area a
warmer, bag and 3 sizes of mask 00,0,1, suction machine
and wide bore cannulae, oxygen, umbilical tape, umbilical
catheters?
Is there a working clock?
Is there any equipment on the ward that is not working?
Are there baby-weighing scales?
Are resuscitation guidelines visible as charts on the wall?
Are well babies put skin to skin immediately after drying,
and put to the breast within 30 minutes?
How are babies transferred to the neonatal unit?

87
Are there any visible notices or advertisements for formula
milk?
Post Natal ward
Category Question
Layout
Are all mothers and babies visible from the nursing station?
Is there an area where mothers are given extra support - if
unwell or after C- section?
Are family carers able to help mothers who are unwell?
Is there an area for baby resuscitation with suitable
equipment?
Is there an area set aside for pediatric doctors to do the baby
checks?
If not how/where are they done?
Infra-structure Are there sinks for hand-washing in each area with running
water, soap and towels?

88
Is there drinking water freely available for mothers?
Is oxygen available if needed?
Staffing numbers and
rotations
How many nurses on a shift? By day?
How many nurses on a shift? By night?
Patient safety
and infection control
Is hand gel available in all areas?
Do all babies have identification bands?
Are the babies nursed in cots beside their mothers?
Are the cots and mattresses in good condition?
Are sharps boxes used and changed before they are
completely full?
Is the area clean?
Can bilirubin levels be measured on the ward?

89
If blood is sent to the lab how long does it take to get the
results?
Drugs
Are drugs dispensed on the ward or from pharmacy?
Are all drugs safely stored?
Are all drugs in the store clearly labeled?
Equipment
Is phototherapy given on the postnatal ward? If so is the
equipment working well?
Are there baby scales and length boards?
Is there a pulse oximeter for babies on the ward?
Clinical practice
Is Kangaroo Mother Care in use?
If not how are small babies kept warm?
Is this a Baby Friendly Hospital? A Baby Friendly Hospital
is an initiative and global effort to implement practices that
protect, promote and support breastfeeding?
Is there any evidence of advertising for formula milks?

90
Are samples of formula milks ever given to mothers?
Is there a nurse who specializes in supporting breastfeeding?
Is there a pediatric doctor available at this hospital? If no, this survey has ended. If yes please
answer the following additional questions:
Is a pediatric doctor available to come immediately to labor
ward -By day and by night?
How do nurses call pediatric doctors when needed?

91
Annex 11. F-IMNCI training materials
Guidelines
F-IMNCI Participants Manual
1 copy per participant &
facilitator
F-IMNCI Chart Booklet
1 copy per participant &
facilitator
F-IMNCI Facilitator guide 1 copy per facilitator
Training materials (international order)
1.NeoNatalie Manikin 3 pce
2.CPR Timmy (3-yr old) Manikin 3 pce
3.Infant IV arm Manikin 3 sets
4.Single Intraosseous Infusion Leg Manikin 3 sets
5.Infant Disposable Resuscitator with
Reservoir bag 3 sets
6.Pediatric Disposable Resuscitator with
Reservoir bag (<5 child) 3 sets
7. Laerdal Silicone Masks (4 different sizes,
preterm, term neonate,infant and under 5
children) 3 sets
8.Oropharyngeal air way (Infant and <5 child)
(Color-Coded Guedel Oral Airway Kit) 3 sets
Training materials (local order)
1.Pulse Oximeter 6 pce
2. Feeding Tube (Size 6) 10 pce
3. Feeding Tube (Size 8) 10 pce
4.Feeding Tube (Size 10) 10 pce
5. Feeding Tube (Size 12) 10 pce
6. IV Cannula or scalp vein (22g) 10 pce
7. IV Cannula or scalp vein (24g) 10 pce
8. Nasal Catheter (Neonate or infant size) 10 pce
9. Nasal Catheter (<5 size) 10 pce
10. Suction catheter (Size 10) 10 pce
11. Suction catheter (Size 12) 10 pce
12. Suction catheter (Size 14) 10 pce
13. Disposable syringes (10ml) 10 syringes
14. Disposable syringes (5ml) 10 syringes
15. Disposable syringes (3ml) 10 syringes
16. Disposable syringes (1ml) 10 syringes
17. Glucometer 6 pce
18. Glucometer test kits 25’s 3 box
19. Umbilical cord stump 10 lengths
20. Nebulizer with chamber 6 pce
21. MDI and Spacer 6 sets

92
22. IV Infusion: Dextrose (10%) 6 bottles
23. IV Infusion: Dextrose (25%) 6 bottles
24. Adrenaline injection (30mg/30ml) 6 bottles
25. Diazepam injection (10ml) 6 bottles
26.Salbutamol Respirator Solution (Ventolin
solution) 5mg/ml (10ml) 6 bottles
27. Bone marrow needle for Intraosseous line
or infusion (18 G) 10 pce
28. Graduated jar (500ml) & measuring spoons
2.5 ml-10ml 6 sets
29. Nasal Prongs (infant size) 6 pce
30. Nasal Prongs (child size) 6 pce

93
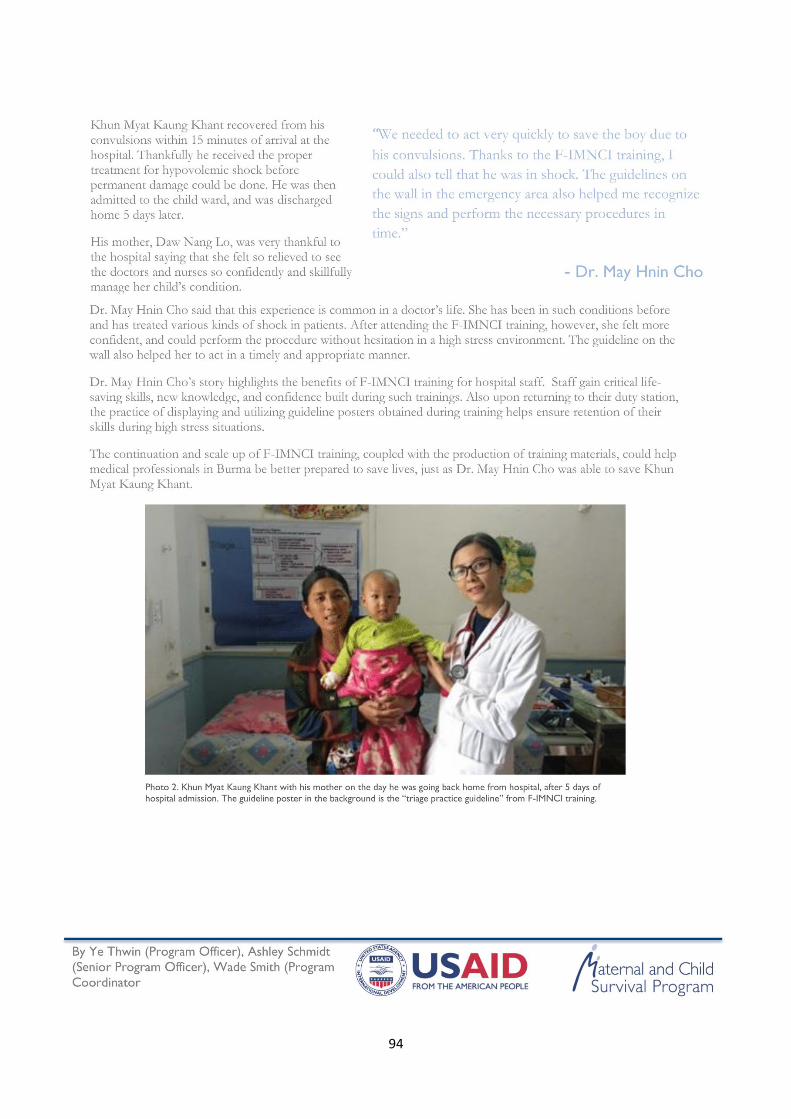
94
Related Documents