and Kathleen Bennett Marta Pereira, Ana Azevedo, Nuno Lunet, Helena Carreira, Martin O'Flaherty, Simon Capewell 2008 Explaining the Decline in Coronary Heart Disease Mortality in Portugal Between 1995 and Print ISSN: 1941-7705. Online ISSN: 1941-7713 Copyright © 2013 American Heart Association, Inc. All rights reserved. Greenville Avenue, Dallas, TX 75231 is published by the American Heart Association, 7272 Circulation: Cardiovascular Quality and Outcomes published online November 5, 2013; Circ Cardiovasc Qual Outcomes. http://circoutcomes.ahajournals.org/content/early/2013/11/05/CIRCOUTCOMES.113.000264 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circoutcomes.ahajournals.org/content/suppl/2013/11/05/CIRCOUTCOMES.113.000264.DC1.html Data Supplement (unedited) at: http://circoutcomes.ahajournals.org//subscriptions/ at: is online Circulation: Cardiovascular Quality and Outcomes Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Question and Answer Permissions and Rights page under Services. Further information about this process is available in the which permission is being requested is located, click Request Permissions in the middle column of the Web Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for can be obtained via RightsLink, a service of the Circulation: Cardiovascular Quality and Outcomes in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from by guest on November 6, 2013 http://circoutcomes.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
and Kathleen BennettMarta Pereira, Ana Azevedo, Nuno Lunet, Helena Carreira, Martin O'Flaherty, Simon Capewell
2008Explaining the Decline in Coronary Heart Disease Mortality in Portugal Between 1995 and
Print ISSN: 1941-7705. Online ISSN: 1941-7713 Copyright © 2013 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Circulation: Cardiovascular Quality and Outcomes
published online November 5, 2013;Circ Cardiovasc Qual Outcomes.
http://circoutcomes.ahajournals.org/content/early/2013/11/05/CIRCOUTCOMES.113.000264World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circoutcomes.ahajournals.org/content/suppl/2013/11/05/CIRCOUTCOMES.113.000264.DC1.htmlData Supplement (unedited) at:
http://circoutcomes.ahajournals.org//subscriptions/
at: is onlineCirculation: Cardiovascular Quality and Outcomes Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theCirculation: Cardiovascular Quality and Outcomesin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from by guest on November 6, 2013http://circoutcomes.ahajournals.org/Downloaded from
1
The trends in coronary heart disease (CHD) mortality rates differ widely across countries.1 In Europe, there is a north-
east to southwest gradient in age-standardized CHD mortal-ity,2 and Portugal has been a low-risk country for decades.3 Although the CHD mortality rates have been declining since the 1980s, more steeply after the mid-1990s, particularly among women,1,3 CHD remains the second most common cause of death in Portugal.4
A high prevalence of hypertension and high stroke mortality are distinguishing features of the cardiovascular disease epi-demiology in Portugal.5 However, the risk factor distributions changed in the past several decades, with steep decreases in blood pressure levels since the 1970s,6 a decrease in the preva-lence of smoking among men but increase among women,7 and an increase in the frequency of obesity in the younger age groups.8 In addition, there were several improvements in the management of CHD, namely, in the availability of drug treatments, in the access to reperfusion and revascularization interventions, with the development of a hospital referral net-work for interventional cardiology, and the implementation of a coronary fast track system.9
It is important to assess the relative contribution of these underlying factors to the observed decline in CHD mortality in different settings, plan future health policy, and prioritize strategies for primary and secondary prevention. The IMPACT model, a cell-based policy model, uses epidemiological infor-mation to estimate the contributions of population-level risk factor changes (impacting mainly on incidence) and changes in the uptake of evidence-based treatments (impacting mainly on case fatality) on mortality decline between 2 points in time (the start year and the end year). In the present investigation, we aimed to model the decline in CHD mortality between 1995 and 2008 in Portugal, quantifying the contribution of changes in the use of evidence-based treatments and in the levels of major cardiovascular risk factors using IMPACT.
MethodsIMPACT CHD Mortality ModelWe used an updated version of the IMPACT CHD mortality model to investigate how changes in risk factors and treatments have affected the substantially decreasing mortality rates in CHD among men and women 25 to 84 years of age in Portugal. The IMPACT model has
Background—We aimed to quantify the contribution of treatments and risk factors to the decline in coronary heart disease (CHD) mortality in Portugal, 1995 to 2008.
Methods and Results—The IMPACT mortality model was used to integrate data on trends in uptake of treatments and exposure to risk factors to explain the CHD mortality variation. Between 1995 and 2008, CHD mortality rates in Portugal decreased by 29% in men and 21% in women aged 25 to 84 years, corresponding to 3760 fewer deaths in 2008 than expected if 1995 mortality rates had persisted. Approximately 92% of the estimated decrease in number of deaths could be explained by the model; the remaining 8% were attributed to changes in unmeasured factors. Approximately 50% of the decrease explained by the model was attributable to an increased uptake of treatments, mainly antihypertensive medication (12%) and initial treatments after an acute myocardial infarction (10%), and 42% to population risk factor reductions, mainly blood pressure (27% in men and 60% in women), total cholesterol (14% in men and 5% in women), and smoking (11% in men). However, these reductions were partially offset by adverse trends in diabetes mellitus (18% in men and 2% in women) and obesity (6% in men and 5% in women) and smoking (2% in women).
Conclusions—In this low CHD risk population, modern treatments explained approximately half of the overall decline in CHD deaths. The biggest contributions to the CHD mortality decline came from secular decreases in blood pressure and increases in hypertension treatment. (Circ Cardiovasc Qual Outcomes. 2013;6:00-00.)
Key Words: coronary artery disease ◼ decision modeling ◼ mortality ◼ risk factors ◼ therapeutics
© 2013 American Heart Association, Inc.
Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org DOI: 10.1161/CIRCOUTCOMES.113.000264
Received March 28, 2013; accepted September 13, 2013.From the Department of Clinical Epidemiology, Predictive Medicine and Public Health, University of Porto Medical School, Porto, Portugal (M.P.,
A.A., N.L., H.C.); Institute of Public Health, University of Porto (ISPUP), Porto, Portugal (M.P., A.A., N.L., H.C.); Department of Public Health and Policy, University of Liverpool, Liverpool, United Kingdom (M.O.’F., S.C.); and Department of Pharmacology and Therapeutics, Trinity Centre for Health Sciences, St. James’s Hospital, Dublin, Ireland (K.B.).
The online-only Data Supplement is available at http://circoutcomes.ahajournals.org/lookup/suppl/doi:10.1161/CIRCOUTCOMES.113.000264/-/DC1.Correspondence to Marta Pereira, PhD, Department of Clinical Epidemiology, Predictive Medicine and Public Health, University of Porto Medical
School, Al. Prof. Hernâni Monteiro, 4200-319 Porto, Portugal. E-mail [email protected]
Explaining the Decline in Coronary Heart Disease Mortality in Portugal Between 1995 and 2008
Marta Pereira, PhD; Ana Azevedo, MD, PhD; Nuno Lunet, MPH, PhD; Helena Carreira, MSc; Martin O’Flaherty, MD, PhD; Simon Capewell, MD, PhD; Kathleen Bennett, PhD
Original Article

2 Circ Cardiovasc Qual Outcomes November 2013
been used previously in diverse populations, namely, in the United States,10 New Zealand,11 China,12 and Europe,13 including other Southern European populations, namely, Italy14 and Spain.15
The IMPACT model incorporates data on trends in the distribu-tion of the main cardiovascular risk factors: high systolic blood pres-sure (SBP), smoking, high total cholesterol, high body mass index (BMI), diabetes mellitus, and physical inactivity. It also includes ≈50 evidence-based treatments for all CHD patient groups: acute myo-cardial infarction (AMI), cardiac arrest, unstable and chronic angina, and mild and acute heart failure (Appendix in the online-only Data Supplement). The model compares data from a baseline year (1995) against data observed in a more recent year (2008). The main out-come of the model is the relative contributions of cardiovascular risk factors and treatment groups to CHD mortality decline, measured as deaths prevented or postponed (DPPs). The calculation of the relative contributions is based on the well-studied relationships between each risk factor change and the relative reduction in CHD mortality and between treatment uptake and reductions in case-fatality in patients with a specific form of CHD.
Number of DPPsThe starting point for the model is to calculate the target number of deaths the model needs to explain. Data on the total population and the number of CHD deaths for Portugal, according to the International Classification of Diseases (ICD), in 1995 and 2008, were obtained from the Portuguese official statistics, by 10-year age bands.4
We calculated the number of CHD deaths expected in 2008 if the CHD mortality rates in 1995 had persisted by multiplying the age-specific mortality rates for 1995 by the population for each 10-year age stratum in the year 2008 (ie, simple direct standardization). Subtracting the number of observed deaths in 2008 from the number of expected deaths generates the reduction in the number of CHD deaths in 2008, which the model aims to explain. We will refer to them as DPPs.
Identification and Assessment of Relevant DataTo build the Portuguese IMPACT model, we used specific data from the Portuguese population whenever possible. When >1 data source was available, we chose the most representative and least biased source. A detailed description of all the sources of data used is found in the Appendix in the online-only Data Supplement.
Data on number of patients admitted to a hospital with myocardial infarction, unstable angina, and heart failure were obtained from the National Hospital Discharge Registry, centrally held in the Central Administration of the Health System for Portugal.16 The proportion of patients treated for myocardial infarction, unstable angina, or heart failure during hospitalization were obtained from clinical epi-demiological studies on samples of patients consecutively admitted to Portuguese hospitals.17,18 The number of patients in the community eligible for treatments for chronic angina and heart failure and for statin therapy to reduce cholesterol and antihypertensive medications to control blood pressure was obtained from epidemiological studies on representative samples of the general Portuguese population; the proportion of patients treated for those conditions were taken from the same studies.19,20
Data on the effectiveness of therapeutic interventions, on the association between cardiovascular risk factors and CHD mortality and case-fatality rates, were obtained from published meta-analyses, randomized controlled trials, and international cohort studies (see Appendix in the online-only Data Supplement).
In 1995, data on mean total cholesterol, mean SBP, mean BMI, and prevalence of diabetes mellitus were obtained from a systematic review that summarizes the evidence from studies providing data on the distribution of risk factors in Portuguese adults.6,21,22 Data on the prevalence of smoking and physical inactivity were obtained from the National Health Survey conducted from 1995 to 1996.23 Data of risk factors in 2008 were obtained from 2 cross-sectional studies in random samples of the general population.20,24
Mortality Reductions Attributable to TreatmentsThe analysis of the contribution of treatments is reported for men and women together after confirming that in this population, no important sex heterogeneity was found in these results. Therefore, the propor-tional contribution of each treatment presented in the Results section and Figure 2 was computed using all DPPs as the denominator.
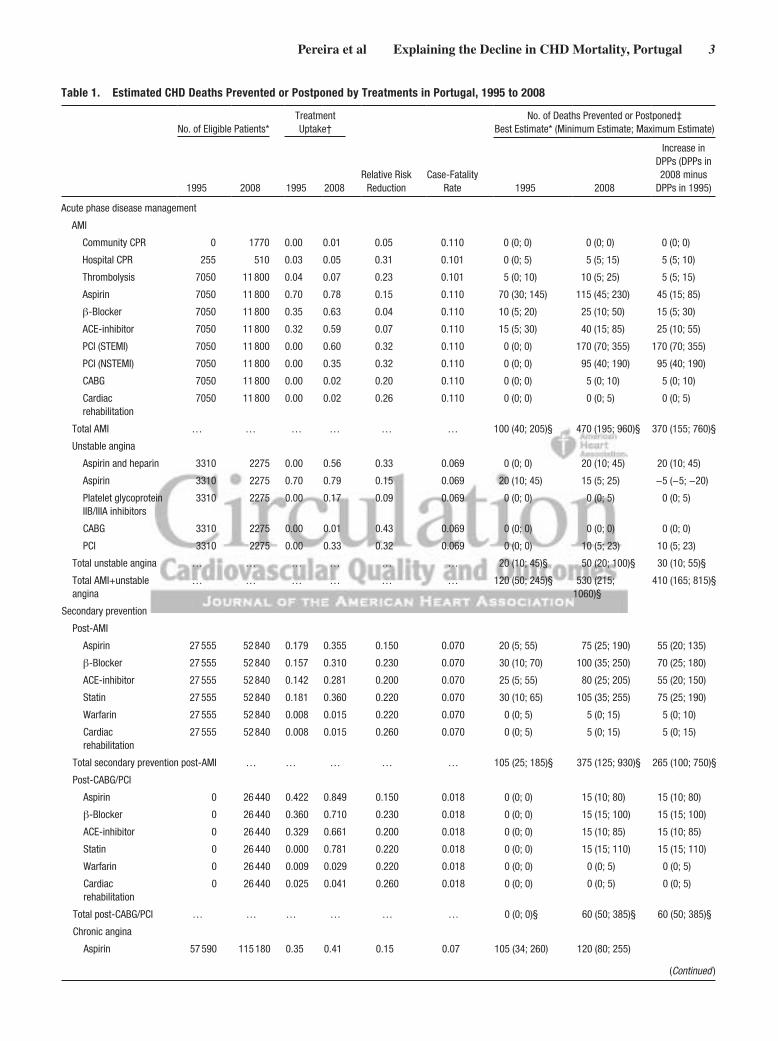
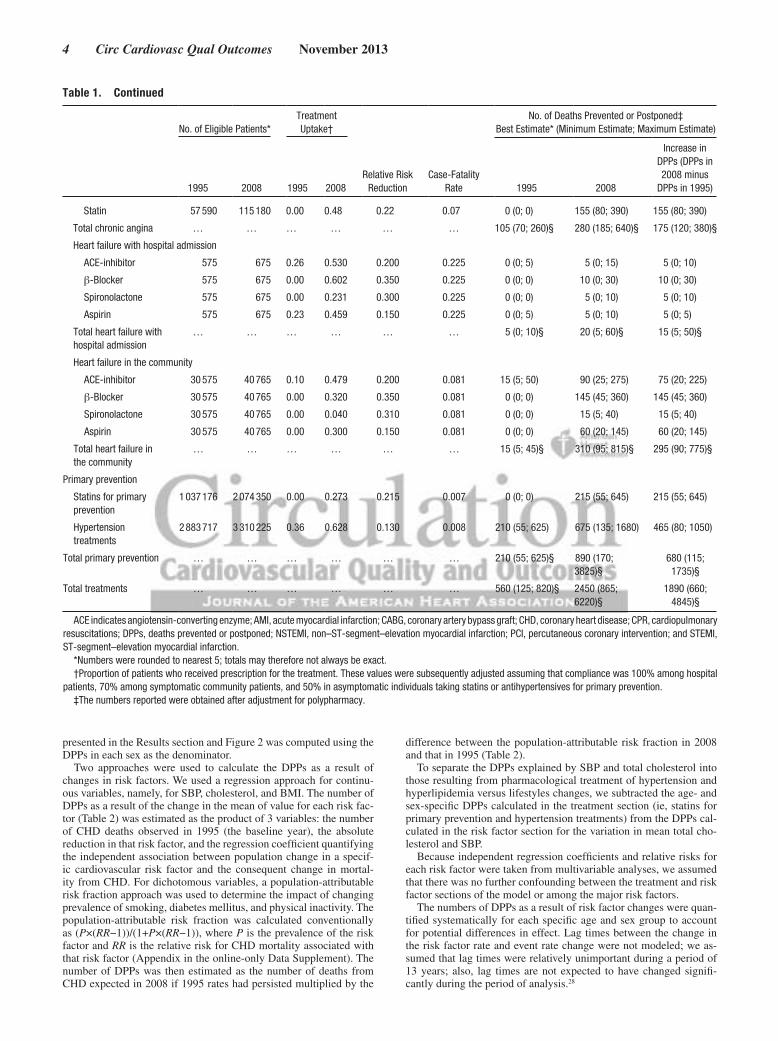
The DPPs associated with a specific CHD treatment within a dis-ease subgroup at a specific time point (in either 2008 or 1995 for treatments available at that time) was estimated by taking the product of the number of people in the subgroup by the proportion of those patients who received the particular treatment at that time, 1-year case-fatality rates, and the relative risk reduction attributed to that specific treatment based on the published literature (Table 1).
We assumed that the compliance (proportion of treated patients actually taking therapeutically effective levels of medication) was 100% among hospital patients, 70% among symptomatic commu-nity patients, and 50% among asymptomatic community patients
.25,26
To avoid double counting of patients treated, we identified potential overlaps between different groups of patients and made appropriate adjustments (Appendix in the online-only Data Supplement). To ad-dress the potential effect of multiple treatments in the same patient on the relative reduction in case-fatality rate, we used the Mant and Hicks cumulative relative benefit approach27 (Appendix in the online-only Data Supplement).
.The effect of the increase in the use of treatments from 1995 to
2008 was assessed by subtracting the DPPs attributable to each treat-ment in 1995 from those in 2008.
Mortality Reductions Attributable to Changes in Risk FactorsThe time trends in risk factors followed different patterns in men and women, resulting in heterogeneous contribution to the CHD mortality decline. The results of the analysis of the contribution of risk fac-tors are therefore presented by sex, and the proportional contribution
WHAT IS KNOWN
• Trends in coronary heart disease mortality rates dif-fer widely across countries; Portugal has been a low-risk country for decades.
• Coronary heart disease mortality rates in Portugal have been declining since the 1980s, more steeply after the mid-1990s, particularly among women.
• A relatively high prevalence of hypertension and high stroke mortality are distinguishing features of the cardiovascular disease epidemiology in Portugal.
WHAT THE STUDY ADDS
• Approximately half of the coronary heart disease deaths prevented or postponed between 1995 and 2008 were attributed to increasing use of evidence-based therapies.
• Approximately 42% of the decline was attributable to the trends in major risk factors, mainly systolic blood pressure, although the rise in the prevalence of diabetes mellitus and mean body mass index in both sexes and in smoking prevalence among women generated additional deaths.
• The proportional contribution of treatments and risk factors for coronary heart disease mortality trends in Portugal differs from other countries mainly because of a higher contribution of treatments.
Pereira et al Explaining the Decline in CHD Mortality, Portugal 3
Table 1. Estimated CHD Deaths Prevented or Postponed by Treatments in Portugal, 1995 to 2008
No. of Eligible Patients*Treatment Uptake†
Relative Risk Reduction
Case-Fatality Rate
No. of Deaths Prevented or Postponed‡Best Estimate* (Minimum Estimate; Maximum Estimate)
1995 2008 1995 2008 1995 2008
Increase in DPPs (DPPs in 2008 minus
DPPs in 1995)
Acute phase disease management
AMI
Community CPR 0 1770 0.00 0.01 0.05 0.110 0 (0; 0) 0 (0; 0) 0 (0; 0)
Hospital CPR 255 510 0.03 0.05 0.31 0.101 0 (0; 5) 5 (5; 15) 5 (5; 10)
Thrombolysis 7050 11 800 0.04 0.07 0.23 0.101 5 (0; 10) 10 (5; 25) 5 (5; 15)
Aspirin 7050 11 800 0.70 0.78 0.15 0.110 70 (30; 145) 115 (45; 230) 45 (15; 85)
β-Blocker 7050 11 800 0.35 0.63 0.04 0.110 10 (5; 20) 25 (10; 50) 15 (5; 30)
ACE-inhibitor 7050 11 800 0.32 0.59 0.07 0.110 15 (5; 30) 40 (15; 85) 25 (10; 55)
PCI (STEMI) 7050 11 800 0.00 0.60 0.32 0.110 0 (0; 0) 170 (70; 355) 170 (70; 355)
PCI (NSTEMI) 7050 11 800 0.00 0.35 0.32 0.110 0 (0; 0) 95 (40; 190) 95 (40; 190)
CABG 7050 11 800 0.00 0.02 0.20 0.110 0 (0; 0) 5 (0; 10) 5 (0; 10)
Cardiac rehabilitation
7050 11 800 0.00 0.02 0.26 0.110 0 (0; 0) 0 (0; 5) 0 (0; 5)
Total AMI … … … … … … 100 (40; 205)§ 470 (195; 960)§ 370 (155; 760)§
Unstable angina
Aspirin and heparin 3310 2275 0.00 0.56 0.33 0.069 0 (0; 0) 20 (10; 45) 20 (10; 45)
Aspirin 3310 2275 0.70 0.79 0.15 0.069 20 (10; 45) 15 (5; 25) −5 (−5; −20)
Platelet glycoprotein IIB/IIIA inhibitors
3310 2275 0.00 0.17 0.09 0.069 0 (0; 0) 0 (0; 5) 0 (0; 5)
CABG 3310 2275 0.00 0.01 0.43 0.069 0 (0; 0) 0 (0; 0) 0 (0; 0)
PCI 3310 2275 0.00 0.33 0.32 0.069 0 (0; 0) 10 (5; 23) 10 (5; 23)
Total unstable angina … … … … … … 20 (10; 45)§ 50 (20; 100)§ 30 (10; 55)§
Total AMI+unstable angina
… … … … … … 120 (50; 245)§ 530 (215; 1060)§
410 (165; 815)§
Secondary prevention
Post-AMI
Aspirin 27 555 52 840 0.179 0.355 0.150 0.070 20 (5; 55) 75 (25; 190) 55 (20; 135)
β-Blocker 27 555 52 840 0.157 0.310 0.230 0.070 30 (10; 70) 100 (35; 250) 70 (25; 180)
ACE-inhibitor 27 555 52 840 0.142 0.281 0.200 0.070 25 (5; 55) 80 (25; 205) 55 (20; 150)
Statin 27 555 52 840 0.181 0.360 0.220 0.070 30 (10; 65) 105 (35; 255) 75 (25; 190)
Warfarin 27 555 52 840 0.008 0.015 0.220 0.070 0 (0; 5) 5 (0; 15) 5 (0; 10)
Cardiac rehabilitation
27 555 52 840 0.008 0.015 0.260 0.070 0 (0; 5) 5 (0; 15) 5 (0; 15)
Total secondary prevention post-AMI … … … … … 105 (25; 185)§ 375 (125; 930)§ 265 (100; 750)§
Post-CABG/PCI
Aspirin 0 26 440 0.422 0.849 0.150 0.018 0 (0; 0) 15 (10; 80) 15 (10; 80)
β-Blocker 0 26 440 0.360 0.710 0.230 0.018 0 (0; 0) 15 (15; 100) 15 (15; 100)
ACE-inhibitor 0 26 440 0.329 0.661 0.200 0.018 0 (0; 0) 15 (10; 85) 15 (10; 85)
Statin 0 26 440 0.000 0.781 0.220 0.018 0 (0; 0) 15 (15; 110) 15 (15; 110)
Warfarin 0 26 440 0.009 0.029 0.220 0.018 0 (0; 0) 0 (0; 5) 0 (0; 5)
Cardiac rehabilitation
0 26 440 0.025 0.041 0.260 0.018 0 (0; 0) 0 (0; 5) 0 (0; 5)
Total post-CABG/PCI … … … … … … 0 (0; 0)§ 60 (50; 385)§ 60 (50; 385)§
Chronic angina
Aspirin 57 590 115 180 0.35 0.41 0.15 0.07 105 (34; 260) 120 (80; 255)
(Continued )
4 Circ Cardiovasc Qual Outcomes November 2013
presented in the Results section and Figure 2 was computed using the DPPs in each sex as the denominator.
Two approaches were used to calculate the DPPs as a result of changes in risk factors. We used a regression approach for continu-ous variables, namely, for SBP, cholesterol, and BMI. The number of DPPs as a result of the change in the mean of value for each risk fac-tor (Table 2) was estimated as the product of 3 variables: the number of CHD deaths observed in 1995 (the baseline year), the absolute reduction in that risk factor, and the regression coefficient quantifying the independent association between population change in a specif-ic cardiovascular risk factor and the consequent change in mortal-ity from CHD. For dichotomous variables, a population-attributable risk fraction approach was used to determine the impact of changing prevalence of smoking, diabetes mellitus, and physical inactivity. The population-attributable risk fraction was calculated conventionally as (P×(RR−1))/(1+P×(RR−1)), where P is the prevalence of the risk factor and RR is the relative risk for CHD mortality associated with that risk factor (Appendix in the online-only Data Supplement). The number of DPPs was then estimated as the number of deaths from CHD expected in 2008 if 1995 rates had persisted multiplied by the
difference between the population-attributable risk fraction in 2008 and that in 1995 (Table 2).
To separate the DPPs explained by SBP and total cholesterol into those resulting from pharmacological treatment of hypertension and hyperlipidemia versus lifestyles changes, we subtracted the age- and sex-specific DPPs calculated in the treatment section (ie, statins for primary prevention and hypertension treatments) from the DPPs cal-culated in the risk factor section for the variation in mean total cho-lesterol and SBP.
Because independent regression coefficients and relative risks for each risk factor were taken from multivariable analyses, we assumed that there was no further confounding between the treatment and risk factor sections of the model or among the major risk factors.
The numbers of DPPs as a result of risk factor changes were quan-tified systematically for each specific age and sex group to account for potential differences in effect. Lag times between the change in the risk factor rate and event rate change were not modeled; we as-sumed that lag times were relatively unimportant during a period of 13 years; also, lag times are not expected to have changed signifi-cantly during the period of analysis.28
Statin 57 590 115 180 0.00 0.48 0.22 0.07 0 (0; 0) 155 (80; 390) 155 (80; 390)
Total chronic angina … … … … … … 105 (70; 260)§ 280 (185; 640)§ 175 (120; 380)§
Heart failure with hospital admission
ACE-inhibitor 575 675 0.26 0.530 0.200 0.225 0 (0; 5) 5 (0; 15) 5 (0; 10)
β-Blocker 575 675 0.00 0.602 0.350 0.225 0 (0; 0) 10 (0; 30) 10 (0; 30)
Spironolactone 575 675 0.00 0.231 0.300 0.225 0 (0; 0) 5 (0; 10) 5 (0; 10)
Aspirin 575 675 0.23 0.459 0.150 0.225 0 (0; 5) 5 (0; 10) 5 (0; 5)
Total heart failure with hospital admission
… … … … … … 5 (0; 10)§ 20 (5; 60)§ 15 (5; 50)§
Heart failure in the community
ACE-inhibitor 30 575 40 765 0.10 0.479 0.200 0.081 15 (5; 50) 90 (25; 275) 75 (20; 225)
β-Blocker 30 575 40 765 0.00 0.320 0.350 0.081 0 (0; 0) 145 (45; 360) 145 (45; 360)
Spironolactone 30 575 40 765 0.00 0.040 0.310 0.081 0 (0; 0) 15 (5; 40) 15 (5; 40)
Aspirin 30 575 40 765 0.00 0.300 0.150 0.081 0 (0; 0) 60 (20; 145) 60 (20; 145)
Total heart failure in the community
… … … … … … 15 (5; 45)§ 310 (95; 815)§ 295 (90; 775)§
Primary prevention
Statins for primary prevention
1 037 176 2 074 350 0.00 0.273 0.215 0.007 0 (0; 0) 215 (55; 645) 215 (55; 645)
Hypertension treatments
2 883 717 3 310 225 0.36 0.628 0.130 0.008 210 (55; 625) 675 (135; 1680) 465 (80; 1050)
Total primary prevention … … … … … … 210 (55; 625)§ 890 (170; 3825)§
680 (115; 1735)§
Total treatments … … … … … … 560 (125; 820)§ 2450 (865; 6220)§
1890 (660; 4845)§
ACE indicates angiotensin-converting enzyme; AMI, acute myocardial infarction; CABG, coronary artery bypass graft; CHD, coronary heart disease; CPR, cardiopulmonary resuscitations; DPPs, deaths prevented or postponed; NSTEMI, non–ST-segment–elevation myocardial infarction; PCI, percutaneous coronary intervention; and STEMI, ST-segment–elevation myocardial infarction.
*Numbers were rounded to nearest 5; totals may therefore not always be exact.†Proportion of patients who received prescription for the treatment. These values were subsequently adjusted assuming that compliance was 100% among hospital
patients, 70% among symptomatic community patients, and 50% in asymptomatic individuals taking statins or antihypertensives for primary prevention.‡The numbers reported were obtained after adjustment for polypharmacy.
Table 1. Continued
No. of Eligible Patients*Treatment Uptake†
Relative Risk Reduction
Case-Fatality Rate
No. of Deaths Prevented or Postponed‡Best Estimate* (Minimum Estimate; Maximum Estimate)
1995 2008 1995 2008 1995 2008
Increase in DPPs (DPPs in 2008 minus
DPPs in 1995)
Pereira et al Explaining the Decline in CHD Mortality, Portugal 5
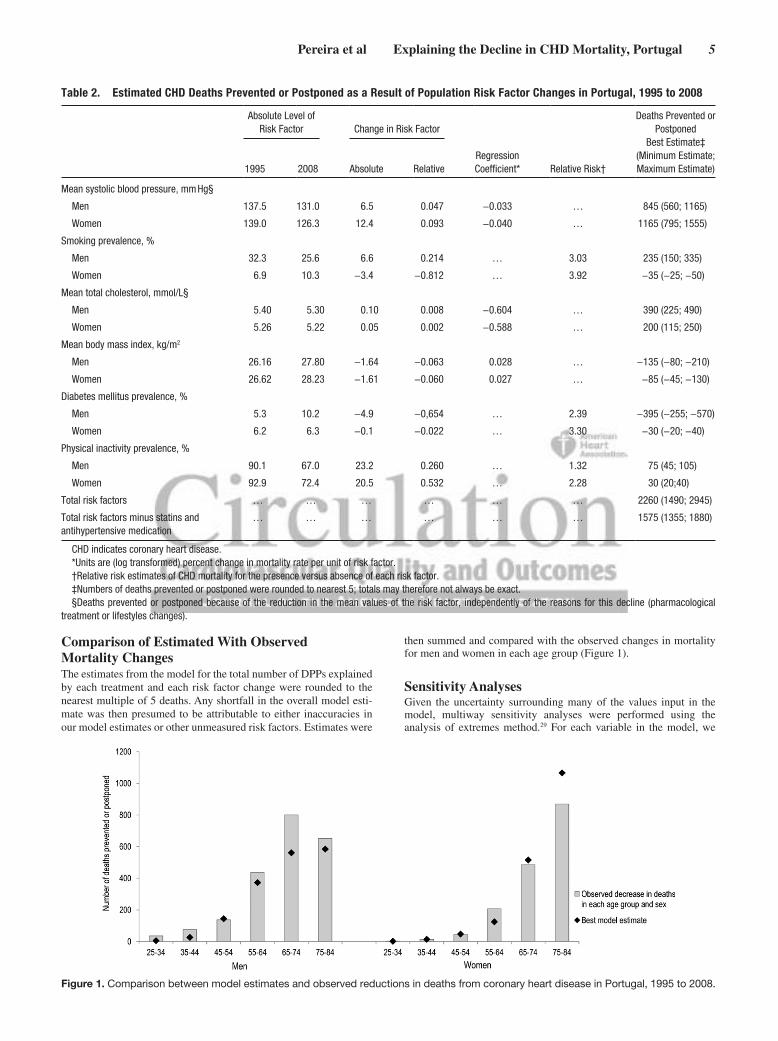
Comparison of Estimated With Observed Mortality ChangesThe estimates from the model for the total number of DPPs explained by each treatment and each risk factor change were rounded to the nearest multiple of 5 deaths. Any shortfall in the overall model esti-mate was then presumed to be attributable to either inaccuracies in our model estimates or other unmeasured risk factors. Estimates were
then summed and compared with the observed changes in mortality for men and women in each age group (Figure 1).
Sensitivity AnalysesGiven the uncertainty surrounding many of the values input in the model, multiway sensitivity analyses were performed using the analysis of extremes method.29 For each variable in the model, we
Table 2. Estimated CHD Deaths Prevented or Postponed as a Result of Population Risk Factor Changes in Portugal, 1995 to 2008
Absolute Level of Risk Factor Change in Risk Factor
Regression Coefficient* Relative Risk†
Deaths Prevented or Postponed
Best Estimate‡(Minimum Estimate; Maximum Estimate)1995 2008 Absolute Relative
Mean systolic blood pressure, mm Hg§
Men 137.5 131.0 6.5 0.047 −0.033 … 845 (560; 1165)
Women 139.0 126.3 12.4 0.093 −0.040 … 1165 (795; 1555)
Smoking prevalence, %
Men 32.3 25.6 6.6 0.214 … 3.03 235 (150; 335)
Women 6.9 10.3 −3.4 −0.812 … 3.92 −35 (−25; −50)
Mean total cholesterol, mmol/L§
Men 5.40 5.30 0.10 0.008 −0.604 … 390 (225; 490)
Women 5.26 5.22 0.05 0.002 −0.588 … 200 (115; 250)
Mean body mass index, kg/m2
Men 26.16 27.80 −1.64 −0.063 0.028 … −135 (−80; −210)
Women 26.62 28.23 −1.61 −0.060 0.027 … −85 (−45; −130)
Diabetes mellitus prevalence, %
Men 5.3 10.2 −4.9 −0,654 … 2.39 −395 (−255; −570)
Women 6.2 6.3 −0.1 −0.022 … 3.30 −30 (−20; −40)
Physical inactivity prevalence, %
Men 90.1 67.0 23.2 0.260 … 1.32 75 (45; 105)
Women 92.9 72.4 20.5 0.532 … 2.28 30 (20;40)
Total risk factors … … … … … … 2260 (1490; 2945)
Total risk factors minus statins and antihypertensive medication
… … … … … … 1575 (1355; 1880)
CHD indicates coronary heart disease.*Units are (log transformed) percent change in mortality rate per unit of risk factor.†Relative risk estimates of CHD mortality for the presence versus absence of each risk factor.‡Numbers of deaths prevented or postponed were rounded to nearest 5; totals may therefore not always be exact.§Deaths prevented or postponed because of the reduction in the mean values of the risk factor, independently of the reasons for this decline (pharmacological
treatment or lifestyles changes).
Figure 1. Comparison between model estimates and observed reductions in deaths from coronary heart disease in Portugal, 1995 to 2008.
6 Circ Cardiovasc Qual Outcomes November 2013
assigned a lower value and an upper value, using 95% confidence in-tervals when available and otherwise using ±20% (for the number of patients, use of treatment, and compliance). For treatments assumed as 0, no uncertainty analysis was performed.
Detailed information on all methods is shown in the Appendix in the online-only Data Supplement.
ResultsFrom 1995 to 2008, the age-adjusted mortality rate of CHD fell from 157.7 to 112.3 cases per 100 000 population among men aged 25 to 84 years and from 113.3 to 89.1 among women of the same age range. This resulted in 3760 fewer deaths in 2008, 2136 in men and 1624 in women, compared with the expected number if the rates in 1995 had persisted.
Approximately 3465 (92%) of the estimated decrease in number of deaths between 1995 and 2008 could be explained using the Portugal IMPACT model. The remaining 8% were attributed to changes in other unmeasured factors. Under the assumptions of the sensitivity analysis, the extreme minimum and the maximum number of deaths from CHD that were explained were 2015 (54%) and 6725 (180%). The agree-ment between the estimated and observed mortality decreases for men and women in each age group was generally good, except for men aged 65 to 74 years of age, where the model explained less than the observed DPPs, and women aged 75 to 84 years, where the model predicted more DPPs than observed (Figure 1).
TreatmentsTreatments together prevented or postponed ≈1890 deaths (minimum estimate, 660; maximum estimate, 4845) related to CHD (Table 1). These treatment effects together explained ≈50% of the mortality reduction. The largest reductions came from the use of antihypertensive medication (12%) and initial treatments for AMI or unstable angina (11%). Within initial AMI treatments, the largest contributions came from percuta-neous coronary intervention and aspirin.
The mortality decreases attributable to secondary preven-tion after AMI and heart failure treatments were 7% and 8%, respectively. Smaller proportions were explained by primary prevention using statins (6%) and treatment of chronic angina (5%). Secondary prevention after coronary artery bypass sur-gery and percutaneous coronary intervention accounted for <2% of deaths DPPs (Table 1).
Risk FactorsChanges in the major cardiovascular risk factors together accounted for ≈1575 fewer deaths (42%; minimum estimate: 1225; maximum: 2310; Table 2), 630 (29%) among men and 945 (58%) among women, after subtracting the effect of statins and antihypertensive treatment for primary prevention.
Decreases in mean population SBP, by 6.5 mm Hg in men and 12.4 mm Hg in women, were estimated to have contrib-uted to 40% of the decrease in deaths in men and 72% in women. This difference was mainly attributable to lifestyle changes because the effect of antihypertensive treatment was smaller in men and women (13% and 12%, respectively). Mean population total cholesterol levels decreased by 0.10 mmol/L in men and 0.05 mmol/L in women, contributing to
18% of the estimated decrease in DPPs in men and 12% in women, approximately half attributable to lifestyle changes and half to the use of statins. Physical inactivity prevalence decreased by 23.2% in men and 20.5% in women, contribut-ing to a decrease of 4% in DPPs in men and 2% in women (Table 2). Adverse trends were observed in diabetes mellitus and BMI, with the prevalence of diabetes mellitus increasing from 5.3% to 10.2% in men and 6.2% to 6.3% in women and mean BMI increasing from 26.2 to 27.8 kg/m2 in men and 26.6 to 28.2 kg/m2 in women between 1995 and 2008. These 2 risk factors together generated a 25% increase in DPPs in men and 7% in women. In men, the prevalence of smoking decreased, contributing to a 11% decrease in DPPs, whereas it increased in women, resulting in 2% extra deaths.
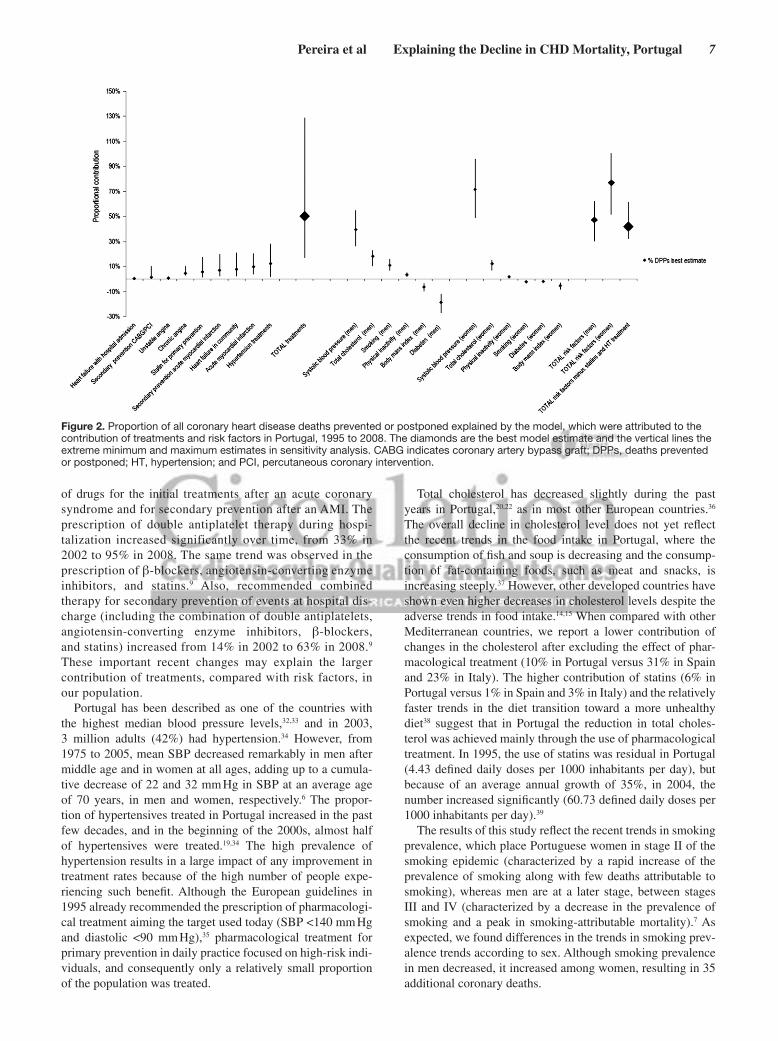
Sensitivity AnalysesThe proportional contributions of specific treatments and risk factor changes to the overall decrease in CHD mortality in Portugal between 1995 and 2008 remained relatively consis-tent in the sensitivity analysis (Figure 2).
DiscussionWe quantified the contribution of risk factors and treatments to the decline in CHD mortality in Portugal, a country in South-ern Europe where the CHD mortality rates are much lower than in Northern Europe or the United States.1,10 CHD mortal-ity rates in Portugal fell by >25% between 1995 and 2008. The reductions attributable to evidence-based therapies accounted for approximately half of the DPPs. Approximately 42% of the fall was because of the trends in major risk factors, mainly SBP, although the rise in the prevalence of diabetes melli-tus and mean BMI in both sexes and in smoking prevalence among women generated additional deaths.
The observed decrease in the mortality in the period con-sidered was noteworthy,1 despite the lower rates in the base-line year, even when compared with other Southern European countries with low baseline CHD mortality rates where this model was applied, namely, Spain (1988–2005)15 and Italy (1980–2000).14 The proportional contribution of treatments and risk factors for CHD mortality trends in Portugal is to some extent different from the aforementioned countries mainly because of a higher contribution of treatments. Most of the previous studies have consistently shown either a simi-lar or slightly higher contribution of reduction in population risk factor levels compared with treatments,10,14,15 but in the Icelandic population, the proportional contribution of risk fac-tors was much higher than in Portugal.30 However, compari-sons with previous models must be interpreted with caution because of different time periods being assessed and the pace of evolution in treatments in the past 15 years.31
Advances in CHD diagnosis and treatment allowed the earlier identification of cases, the diagnoses of milder cases of disease, and consequently the decrease in the proportion of fatal acute events. The increasing number of centers with catheterization laboratory and the implementation of the coro-nary fast track system in the early 2000s in Portugal allowed for a more effective use of percutaneous coronary intervention and other invasive treatments.9 Also, the period of analysis covers a time of steep changes in the availability and uptake
Pereira et al Explaining the Decline in CHD Mortality, Portugal 7
of drugs for the initial treatments after an acute coronary syndrome and for secondary prevention after an AMI. The prescription of double antiplatelet therapy during hospi-talization increased significantly over time, from 33% in 2002 to 95% in 2008. The same trend was observed in the prescription of β-blockers, angiotensin-converting enzyme inhibitors, and statins.9 Also, recommended combined therapy for secondary prevention of events at hospital dis-charge (including the combination of double antiplatelets, angiotensin-converting enzyme inhibitors, β-blockers, and statins) increased from 14% in 2002 to 63% in 2008.9 These important recent changes may explain the larger contribution of treatments, compared with risk factors, in our population.
Portugal has been described as one of the countries with the highest median blood pressure levels,32,33 and in 2003, 3 million adults (42%) had hypertension.34 However, from 1975 to 2005, mean SBP decreased remarkably in men after middle age and in women at all ages, adding up to a cumula-tive decrease of 22 and 32 mm Hg in SBP at an average age of 70 years, in men and women, respectively.6 The propor-tion of hypertensives treated in Portugal increased in the past few decades, and in the beginning of the 2000s, almost half of hypertensives were treated.19,34 The high prevalence of hypertension results in a large impact of any improvement in treatment rates because of the high number of people expe-riencing such benefit. Although the European guidelines in 1995 already recommended the prescription of pharmacologi-cal treatment aiming the target used today (SBP <140 mm Hg and diastolic <90 mm Hg),35 pharmacological treatment for primary prevention in daily practice focused on high-risk indi-viduals, and consequently only a relatively small proportion of the population was treated.
Total cholesterol has decreased slightly during the past years in Portugal,20,22 as in most other European countries.36 The overall decline in cholesterol level does not yet reflect the recent trends in the food intake in Portugal, where the consumption of fish and soup is decreasing and the consump-tion of fat-containing foods, such as meat and snacks, is increasing steeply.37 However, other developed countries have shown even higher decreases in cholesterol levels despite the adverse trends in food intake.14,15 When compared with other Mediterranean countries, we report a lower contribution of changes in the cholesterol after excluding the effect of phar-macological treatment (10% in Portugal versus 31% in Spain and 23% in Italy). The higher contribution of statins (6% in Portugal versus 1% in Spain and 3% in Italy) and the relatively faster trends in the diet transition toward a more unhealthy diet38 suggest that in Portugal the reduction in total choles-terol was achieved mainly through the use of pharmacological treatment. In 1995, the use of statins was residual in Portugal (4.43 defined daily doses per 1000 inhabitants per day), but because of an average annual growth of 35%, in 2004, the number increased significantly (60.73 defined daily doses per 1000 inhabitants per day).39
The results of this study reflect the recent trends in smoking prevalence, which place Portuguese women in stage II of the smoking epidemic (characterized by a rapid increase of the prevalence of smoking along with few deaths attributable to smoking), whereas men are at a later stage, between stages III and IV (characterized by a decrease in the prevalence of smoking and a peak in smoking-attributable mortality).7 As expected, we found differences in the trends in smoking prev-alence trends according to sex. Although smoking prevalence in men decreased, it increased among women, resulting in 35 additional coronary deaths.
Figure 2. Proportion of all coronary heart disease deaths prevented or postponed explained by the model, which were attributed to the contribution of treatments and risk factors in Portugal, 1995 to 2008. The diamonds are the best model estimate and the vertical lines the extreme minimum and maximum estimates in sensitivity analysis. CABG indicates coronary artery bypass graft; DPPs, deaths prevented or postponed; HT, hypertension; and PCI, percutaneous coronary intervention.

8 Circ Cardiovasc Qual Outcomes November 2013
Apart from smoking among women, 2 other major risk fac-tors led to increases in CHD deaths. The contribution of BMI to the increase in the total number of CHD deaths was impor-tant, as well as the dramatic increase in diabetes mellitus prev-alence. These trends are consistent with recent studies in other industrialized countries.14,15 Efforts to address obesity and diabetes mellitus should therefore receive particular attention in future policies to improve the public’s health, especially because the prevalence of overweight/obesity in younger age groups of the Portuguese population is increasing.8,21
Modeling studies have several potential strengths, includ-ing the ability to transparently integrate and simultaneously consider huge amounts of data from many sources and test-ing the uncertainty inherent to such complexity by sensitivity analyses. However, models are highly dependent on the qual-ity of data available. We made all the efforts to include in this model the most representative and unbiased data available in Portugal. We performed a systematic review that aimed to crit-ically summarize the evidence from studies that quantified the distribution and frequency of all risk factors included in this model.6,7,21,22 It was not possible to obtain representative data of treatment uptake in Portugal in 1995 because most of the existing studies reflected the usual care in higher quality spe-cialized centers, which limits their generalizability. Therefore, we included estimates that represented a general consensus of a group of experts who critically evaluated the evidence avail-able. The majority of the treatment data for 2008 were from EURHOBOP, a study that reported data from 3009 patients with acute coronary syndrome consecutively recruited in 10 Portuguese hospitals.17 Even so, in some cases, the data used were obtained from studies possibly constrained by geographic or selection bias. In addition, because we used data from dif-ferent studies for the first and last years, the variations in the study designs and study populations can potentially influence the results of the model. The majority of treatment uptake and case-fatality rates were based on data from the United Kingdom and the United States because little or no specific Portuguese data were available. Although major efforts were made to address overlaps, residual double counting of some individual patients remains possible. We also assumed that, after adjustments for imperfect compliance,25 the efficacy of treatments in randomized controlled trials could be general-ized to population effectiveness in usual clinical practice. All the assumptions that we made are presented in the Appendix in the online-only Data Supplement (Tables 1 and 2). Finally, we did not consider the direct effect of trends in socioeco-nomic status, compliance, or access to care. Although the trends in socioeconomic status and access to care are some-how indirectly measured because of their effect on the varia-tion of risk factors and treatments, the variation in compliance was not assessed, and we do not have data in the Portuguese population to be able to estimate in which direction and to which extent this may have affected the results.
In conclusion, CHD mortality in Portugal decreased 25% between 1995 and 2008. Overall, treatments explained half of the overall decline in CHD deaths, and risk factor changes were more important among women than men. The decrease in mean SBP and increase in hypertension treatment contributed most to the CHD mortality decline. These results encourage
the use of comprehensive efforts to actively promote primary prevention, particularly a healthy diet and tobacco control, as well as maximizing the population coverage of effective treatments.
AcknowledgmentsWe gratefully acknowledge the contribution of the authors Ana Cristina Santos, Henrique Barros, Jaume Marrugat, João Morais, Luís Gardete Correia, Luís Raposo, Paulo Bettencourt, and Salvador Massano Cardoso; scientific societ-ies Sociedade Portuguesa de Cardiologia, Sociedade Portuguesa de Endocrinologia, Diabetes e Metabolismo, and Sociedade Portuguesa de Diabetologia, who provided data in different for-mats than presented in their original reports, which were impor-tant for decisions of selection and presentation of data in our analysis; and Maria Júlia Maciel and Paula Dias, who gave their expert opinion about the treatment uptake.
Sources of FundingThis work was supported by 2 grants from Fundação para a Ciência e a Tecnologia (PIC/IC/83006/2007 and SFRH/BD/46703/2008).
DisclosuresNone.
References 1. Levi F, Chatenoud L, Bertuccio P, Lucchini F, Negri E, La Vecchia C.
Mortality from cardiovascular and cerebrovascular diseases in Europe and other areas of the world: an update. Eur J Cardiovasc Prev Rehabil. 2009;16:333–350.
2. EUROCISS Working Group. Coronary and cerebrovascular popu-lation-based registers in Europe: are morbidity indicators compa-rable? Results from the EUROCISS Project. Eur J Public Health. 2003;13:55–60.
3. Levi F, Lucchini F, Negri E, La Vecchia C. Trends in mortality from car-diovascular and cerebrovascular diseases in Europe and other areas of the world. Heart. 2002;88:119–124.
4. Óbitos (N.º) por Sexo e Causa de morte. Anual [database on the Internet]. Instituto Nacional de Estatística. http://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_main. 2010.
5. Nichols M, Townsend N, Luengo-Fernandez R, Leal J, Gray A, Scarborough P, Rayner M. European Cardiovascular Disease Statistics 2012. Brussels: European Society of Cardiology, Sophia Antipolis; 2012.
6. Pereira M, Carreira H, Vales C, Rocha V, Azevedo A, Lunet N. Trends in hypertension prevalence (1990-2005) and mean blood pressure (1975-2005) in Portugal: a systematic review. Blood Press. 2012;21:220–226.
7. Carreira H, Pereira M, Azevedo A, Lunet N. Trends in the prevalence of smoking in Portugal: a systematic review. BMC Public Health. 2012;12:958.
8. Ferreira RJ, Marques-Vidal PM. Prevalence and determinants of obesity in children in public schools of Sintra, Portugal. Obesity (Silver Spring). 2008;16:497–500.
9. Santos JF, Aguiar C, Gavina C, Azevedo P, Morais J; Registo Nacional de Síndromes Coronárias Agudas da Sociedade Portuguesa de Cardiologia. Portuguese Registry of Acute Coronary Syndromes: seven years of activ-ity. Rev Port Cardiol. 2009;28:1465–1500.
10. Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, Giles WH, Capewell S. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356:2388–2398.
11. Capewell S, Beaglehole R, Seddon M, McMurray J. Explanation for the decline in coronary heart disease mortality rates in Auckland, New Zealand, between 1982 and 1993. Circulation. 2000;102:1511–1516.
12. Critchley J, Liu J, Zhao D, Wei W, Capewell S. Explaining the increase in coronary heart disease mortality in Beijing between 1984 and 1999. Circulation. 2004;110:1236–1244.
13. Unal B, Critchley JA, Capewell S. Explaining the decline in coronary heart disease mortality in England and Wales between 1981 and 2000. Circulation. 2004;109:1101–1107.

Pereira et al Explaining the Decline in CHD Mortality, Portugal 9
14. Palmieri L, Bennett K, Giampaoli S, Capewell S. Explaining the decrease in coronary heart disease mortality in Italy between 1980 and 2000. Am J Public Health. 2010;100:684–692.
15. Flores-Mateo G, Grau M, O’Flaherty M, Ramos R, Elosua R, Violan-Fors C, Quesada M, Martí R, Sala J, Marrugat J, Capewell S. Analyzing the coronary heart disease mortality decline in a Mediterranean population: Spain 1988-2005. Rev Esp Cardiol. 2011;64:988–996.
16. Correia R. Geographic and Temporal Variation of the Procedures Used in Myocardial Infarction. Porto: University of Porto, Medical School; 2011.
17. Kirchberger I, Azevedo A, Davoli M, Farmakis D, Ferrieres J, Garel P, Haekkinen U, Marrugat J, Torre M, Meisinger C. European Hospital Benchmarking in Acute Coronary Syndrome: the EURHOBOP project. Congress of the European Society of Cardiology (ESC). 2012;22:297.
18. Almeida P, Rodrigues J, Lourenço P, Maciel MJ, Bettencourt P. Prognostic significance of applying the European Society of Cardiology consensus algorithm for heart failure with preserved systolic function diagnosis. Clin Cardiol. 2012;35:770–776.
19. Pereira M, Azevedo A, Barros H. Determinants of awareness, treatment and control of hypertension in a Portuguese population. Rev Port Cardiol. 2010;29:1779–1792.
20. Gray LJ, Barros H, Raposo L, Khunti K, Davies MJ, Santos AC. The de-velopment and validation of the Portuguese risk score for detecting type 2 diabetes and impaired fasting glucose. Prim Care Diabetes. 2013;7:11–18.
21. Carreira H, Pereira M, Azevedo A, Lunet N. Trends of BMI and preva-lence of overweight and obesity in Portugal (1995-2005): a systematic review. Public Health Nutr. 2012;15:972–981.
22. Carreira H, Pereira M, Alves L, Lunet N, Azevedo A. Dyslipidaemia, and mean blood cholesterol and triglycerides levels in the Portuguese popula-tion: a systematic review. Arq Med. 2012;26:112–123.
23. Instituto Nacional de Estatística. Inquérito Nacional de Saúde 1995–1996. Lisbon: Instituto Nacional de Saúde Doutor Ricardo Jorge; 1997.
24. Gardete-Correia L, Boavida JM, Raposo JF, Mesquita AC, Fona C, Carvalho R, Massano-Cardoso S. First diabetes prevalence study in Portugal: PREVADIAB study. Diabet Med. 2010;27:879–881.
25. Nichol MB, Venturini F, Sung JC. A critical evaluation of the method-ology of the literature on medication compliance. Ann Pharmacother. 1999;33:531–540.
26. Butler J, Arbogast PG, BeLue R, Daugherty J, Jain MK, Ray WA, Griffin MR. Outpatient adherence to beta-blocker therapy after acute myocardial infarction. J Am Coll Cardiol. 2002;40:1589–1595.
27. Mant J, Hicks N. Detecting differences in quality of care: the sensitivity of measures of process and outcome in treating acute myocardial infarction. BMJ. 1995;311:793–796.
28. McAlister FA. Commentary: relative treatment effects are consistent across the spectrum of underlying risks usually. Int J Epidemiol. 2002;31:76–77.
29. Briggs A, Sculpher M, Buxton M. Uncertainty in the economic evaluation of health care technologies: the role of sensitivity analysis. Health Econ. 1994;3:95–104.
30. Aspelund T, Gudnason V, Magnusdottir BT, Andersen K, Sigurdsson G, Thorsson B, Steingrimsdottir L, Critchley J, Bennett K, O’Flaherty M, Capewell S. Analysing the large decline in coronary heart disease mortal-ity in the Icelandic population aged 25-74 between the years 1981 and 2006. PLoS One. 2010;5:e13957.
31. Nabel EG, Braunwald E. A tale of coronary artery disease and myocardial infarction. N Engl J Med. 2012;366:54–63.
32. Danaei G, Finucane MM, Lin JK, Singh GM, Paciorek CJ, Cowan MJ, Farzadfar F, Stevens GA, Lim SS, Riley LM, Ezzati M; Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Pressure). National, regional, and global trends in systolic blood pressure since 1980: systematic analysis of health examination surveys and epide-miological studies with 786 country-years and 5·4 million participants. Lancet. 2011;377:568–577.
33. The INTERSALT Co-operative Research Group. Appendix tables. Centre-specific results by age and sex. J Hum Hypertens. 1989;3:331–407.
34. Macedo ME, Lima MJ, Silva AO, Alcantara P, Ramalhinho V, Carmona J. Prevalence, awareness, treatment and control of hypertension in Portugal: the PAP study. J Hypertens. 2005;23:1661–1666.
35. WHO. 1993 guidelines for the management of mild hypertension: memorandum from a WHO/ISH meeting. Bull World Health Organ. 1993;71:503–517.
36. Farzadfar F, Finucane MM, Danaei G, Pelizzari PM, Cowan MJ, Paciorek CJ, Singh GM, Lin JK, Stevens GA, Riley LM, Ezzati M; Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Cholesterol). National, regional, and global trends in serum total choles-terol since 1980: systematic analysis of health examination surveys and epidemiological studies with 321 country-years and 3·0 million partici-pants. Lancet. 2011;377:578–586.
37. Marques-Vidal P, Ravasco P, Dias CM, Camilo ME. Trends of food intake in Portugal, 1987-1999: results from the National Health Surveys. Eur J Clin Nutr. 2006;60:1414–1422.
38. Chen Q, Marques-Vidal P. Trends in food availability in Portugal in 1966-2003: comparison with other Mediterranean countries. Eur J Nutr. 2007;46:418–427.
39. Teixeira IJ, Escoval A, Schiappa M. Lipid-lowering drugs: use and expen-diture in Portugal (1995-2004). Rev Port Cardiol. 2007;26:475–493.
CIRCCQO/2013/000264R1
1
Supplemental Material
eAppendix. The Portuguese IMPACT model
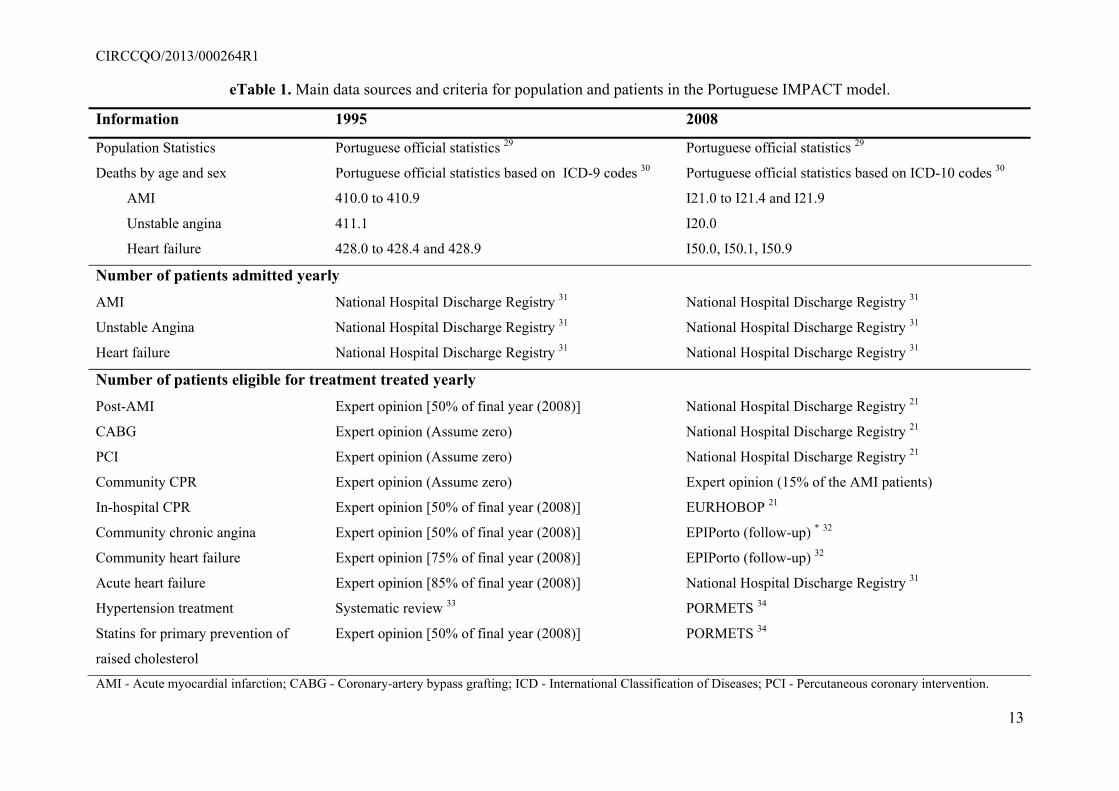
eTable 1. Main data sources for population and patients in the Portuguese IMPACT model
eTable 2. Estimates of the treatment uptake and data sources
eTable 3. Age-specific case fatality rates for each patient group
eTable 4. Clinical efficacy of interventions: relative risk reductions obtained from meta-analyses and randomized controlled trials
eTable 5. Estimates of the risk factor values and data sources
eTable 6. Regression coefficients for the effect of risk factors (continuous: cholesterol, blood pressure, body mass index) on coronary heart
disease mortality
eTable 7. Odds ratios for the effect of risk factors (dichotomous: smoking, exercise, diabetes) on coronary heart disease mortality
eTable 8. Description of the studies that provided data for the Portuguese IMPACT model
eReferences
CIRCCQO/2013/000264R1
2
eAppendix. The Portuguese IMPACT model
We evaluated the Portuguese population aged from 25 to 84 years using an updated version of the IMPACT model. This is a cell-based model,
constructed using Microsoft Excel, which integrates available country-specific epidemiological data to explain an observed change in coronary
heart disease (CHD) mortality. The main outcome of the model is the relative contributions of treatments and cardiovascular risk factors to the
CHD mortality change. The tables included in this supplementary material provide details about these methods. This model has been validated in
several European countries 1-11, Syria 12, West Bank 13, New Zealand 14, China 15, Canada 16 and the United States 17.
Changes in mortality rates from CHD in Portugal from 1995 to 2008
Mortality rates from CHD were calculated using the underlying cause of death according to the International Classification of Diseases (ICD)
codes. Myocardial infarction was defined by the codes 410.0 to 410.9 from ICD 9 or I21.0 to I21.4 and I21.9 from ICD 10, unstable angina by
the codes 411.1 from ICD 9 or I20.0 from ICD 10, and heart failure by the codes 428.0 to 428.4 and 428.9 from ICD 9 or I50.0, I50.1, I50.9
from ICD 10. The data sources used are shown in eTable 1.
CHD deaths prevented or postponed in 2008
The primary output of the IMPACT model is the number of deaths prevented or postponed (DPPs) in 2008 due to the reduction in CHD
mortality rates since 1995. This was calculated as the difference between the observed 2008 CHD deaths and the expected CHD deaths in 2008
CIRCCQO/2013/000264R1
3
if 1995 mortality rates had remained constant. The expected number of CHD deaths was calculated by multiplying age- and sex- specific
mortality rates in 1995 by the population size for each 10-year age- and sex- stratum in 2008.
Patient groups
The treatment arm of the model includes the following target groups of patients:
• hospitalized patients with an acute myocardial infarction (AMI) within the last year;
• hospitalized patients with unstable angina within the last year;
• community-dwelling patients who have survived an AMI in the past 10 years;
• community-dwelling patients with chronic angina who have undergone a revascularisation procedure (coronary artery bypass grafting
(CABG) or a percutaneous coronary intervention (PCI)), within the last year, for chronic angina;
• community-dwelling patients with chronic angina (no revascularisation and/or previous AMI);
• hospitalized patients with heart failure within the last year;
• community-dwelling patients with heart failure;
• hypertensive patients eligible for pharmacological therapy and who have not suffered any of the above events;
• hypercholesterolemic patients eligible for cholesterol lowering therapy (statin) and who have not suffered any of the above events.
CIRCCQO/2013/000264R1
4
Data sources for patient groups (eTable 1)
Hospital patient groups: numbers of hospitalized patients in all public hospitals, obtained from the National Hospital Discharge Register
(eTable8, for study details), separately for AMI, unstable angina and acute heart failure.
Patients with chronic angina: follow-up assessment of the EPIPorto cohort study (eTable 8, for study details). Estimates included in the model
were reduced by 50% to account for patients with chronic angina who also contributed as hospital CHD cases, CABG, AMI survivals and
community heart failure.
Patients with heart failure in the community: follow-up assessment of the EPIPorto study (eTable 8, for study details). Estimates included in
the model were reduced by 50%, assuming that only half of heart failure cases had CHD as etiology of heart failure.
Patients eligible for treatment with a statin for primary prevention: PORMETS study (eTable 8, for study details), which provided estimates
of the number of hypercholesterolemia patients (defined as total cholesterol ≥250 mg/dl or receiving lipid lowering drugs).
CIRCCQO/2013/000264R1
5
Patients eligible for antihypertensive medication: PORMETS study (eTable 8, for study details), which provided estimates of the number of
hypertensive patients (defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg and/or receiving drugs for
hypertension).
Patients eligible for secondary prevention post AMI: calculated based on the number of hospitalised AMI in 2008. We assumed 10% fewer in
each preceding year and 10% case fatality rate every year.
Patients eligible for secondary prevention following CABG/PCI: calculated based on the number of patients submitted to CABG, defined
using the ICD 9 code for procedures 36.1, and PCI, defined using the ICD 9 codes 36.01 to 36.07, in all public hospitals, obtained from the
National Hospital Discharge Registry (eTable 8, for study details). We adjusted these numbers assuming that 50% the patients were AMI
survivals and 33% later developed heart failure.
Treatments uptake
Treatment uptake during hospitalization for AMI, unstable angina and CABG or PCI patients was obtained from the EURHOBOP study (eTable
8, for study details). Treatment uptake during hospitalization for acute heart failure patients was obtained from the EDIFICA study (eTable 8, for
CIRCCQO/2013/000264R1
6
study details). According to local expert opinion, all treatment data for acute heart failure were adjusted by a factor of 0.9, since the quality of
treatment in this hospital is expected to be higher than in a representative sample of the country.
Treatment uptake for patient groups in the community was collected using two different sources of data: the PORMETS study (eTable8, for
study details) was used to estimate the proportion of patients treated with statins and anti-hypertensive medication (plain ACE-inhibitors and/or
beta-blocking agents and/or calcium channel blockers and/or diuretics); the EPIPorto study (eTable8, for study details) was used to estimate the
proportion of treatment in patients with a diagnosis of chronic angina and heart failure.
For each of the groups, we estimated the number of DPPs that were attributable to various treatments. All treatments of interest are listed in
eTable 2.
The DPPs associated with a specific CHD treatment at a specific time point within a disease subgroup, in comparison with no such treatment,
was estimated by taking the product of the number of people in the subgroup (eTable 1) and the proportion of those patients who received a
particular treatment (eTable 2) at that time, 1-year case-fatality rates (eTable 3), and the relative risk reduction attributed to that specific
treatment based on the published literature (eTable 4). We assumed that compliance, defined as the proportion of patients actually on therapeutic
doses of medication among those who received prescriptions, was 100% among hospital patients, 70% among symptomatic community patients
and 50% in asymptomatic individuals taking statins or anti-hypertensives for primary prevention 18-20.
CIRCCQO/2013/000264R1
7
The effect of the increase in use of treatments from 1995 to 2008 was assessed by subtracting the DPPs attributable to each treatment in 1995
from those in 2008.
EXAMPLE 1: estimation of DPPs from a specific treatment
In Portugal in 2008, 1759 men aged 55-64 were hospitalized with AMI, utilization of aspirin in this age group in men was 84% 21, 1-year case-
fatality rate was 0.054. The relative risk reduction in CHD mortality associated with the use of aspirin is 15% 22.
The number of DPPs in 2008 due to aspirin use for AMI was calculated as:
Patient number * treatment uptake * one-year case fatality * relative mortality reduction
= 1759 * 0.84 * 0.054 * 0.15 = 12 DPPs in 2008
In 1995, 1106 men aged 55-64 were hospitalized with AMI, utilization of aspirin in this age group in men was 70% (expert opinion), 1-year
case-fatality rate was 0.054 (Medicare). The relative risk reduction in CHD mortality associated with the use of aspirin is 15% 22.
The number of DPPs in 1995 due to aspirin use for AMI was calculated as:
= 1106 * 0.70 * 0.054 * 0.15 = 6 DPPs in 1995
The effect of the increase in use of treatments from 1995 to 2008 was calculated as:
DPPs in 2008 - DPPs in 1995 = 12 - 6 = 6 DPPs
Risk factors
CIRCCQO/2013/000264R1
8
The IMPACT model calculates the DPPs associated with changes in CHD risk factors, including smoking, total cholesterol, systolic blood
pressure, body mass index, diabetes mellitus, and physical inactivity. Data sources are shown in eTable 5.
In 1995, data for mean total cholesterol, mean systolic blood pressure, mean body mass index and prevalence of diabetes were obtained from
systematic reviews that summarize the evidence from studies providing data on the distribution of risk factors in Portuguese adults (eTable 8, for
study details); while data on prevalence of smoking and physical inactivity were obtained using data from the National Health Survey (eTable 8,
for study details). In 2008, data on mean total cholesterol, mean systolic blood pressure, prevalence of smoking and prevalence of physical
inactivity were obtained from the PORMETS study (eTable 8, for study details); while data on mean body mass index and prevalence of diabetes
were obtained from PREVADIAB study (eTable 8, for study details).
Two approaches were used to calculate DPPs, the regression approach and the population-attributable risk factor (PARF) approach. The
regression approach was used for continuous variables (systolic blood pressure, total cholesterol, and body mass index). The number of expected
deaths from CHD occurring in 2008 was multiplied by the absolute change in risk factor prevalence, and by a regression coefficient quantifying
the change in CHD mortality that would result from the change in risk factor level (eTable 6). Natural logarithms of the mean risk factor values
were used, assuming a log-linear relationship between changes in risk factor levels and mortality.
Data sources for the number of CHD deaths and risk factors are shown in eTable 5, and sources for the coefficients in eTable 6.
CIRCCQO/2013/000264R1
9
EXAMPLE 2: estimation of DPPs from risk factor change using the regression method:
Mortality fall due to reduction in systolic blood pressure in women aged 55-64
In 2008, there were 342 CHD expected deaths (had 1995 mortality rates remained constant) among 657 309 women aged 55-64 years. Mean
systolic blood pressure decreased by 11.2 mmHg (from 145.3 in 1995 to 134.1 mmHg in 2008). For every 20 mmHg reduction in systolic blood
pressure, we estimated an age- and sex-specific reduction in mortality of 50%, which corresponds to a logarithmic coefficient of –0.035 23.
The number of DPPs:
= (1-(EXP(coefficient*change))*expected deaths in 2008)
= (1-(EXP(-0.035*11.2))* 342)
= 111 DPPs
The PARF approach was used for categorical variables (smoking, diabetes, and physical inactivity). PARF was calculated as:
(P * (RR-1)) / (P * (RR-1)) +1
where P is the prevalence of the risk factor and RR is the relative risk for CHD mortality associated with that risk factor. DPPs were then
estimated as the expected CHD deaths in 2008 multiplied by the difference in the PARF between 2008 and 1995.
CIRCCQO/2013/000264R1
10
Data sources for the prevalence of risk factors and for the number of CHD deaths are shown in eTable 1. The relative risks used in these PARF
analyses were obtained from the INTERHEART study (eTable 6), which provides independent OR values, adjusted for other major risk factors.
EXAMPLE 3: estimation of DPPs from risk factor change using the PARF method
In 2008, there were 1702 CHD expected deaths (had 1995 mortality rates remained constant) among 449 870 men aged 65-74 years. The
prevalence of diabetes was 20.6% in 1995 and 28.5% in 2008. Assuming a relative risk of 1.93 24, the PARF was 0.16 in 1995 and 0.21 in 2008.
The number of deaths attributable to the increase in diabetes prevalence from 1995 to 2008 was therefore:
(1702) * (0.21-0.16) = 83 DPPs
Other methodological considerations
Systolic blood pressure and hyperlipidemia
In order to separate the DPPs from pharmacological versus non-pharmacological primary prevention of hypertension and hyperlipidemia, we
subtracted the age- and sex-specific DPPs calculated in the treatment section (i.e. for primary hyperlipidemia and hypertension patient groups),
from the DPPs calculated in the risk factor section.
Polypharmacy issues
CIRCCQO/2013/000264R1
11
There is a paucity of data on the efficacy of treatment combinations. Simply assuming that the efficacy of multiple treatments was additive
would lead to overestimate the treatment effect; we therefore we used the Mant and Hicks method to estimate case-fatality reduction by
polypharmacy for all treatments evaluated 25. This approach was subsequently endorsed by Yusuf 26 and Law and Wald 27.This approach
estimates a cumulative relative benefit as follows:
Relative Benefit = 1 - ((1-relative reduction in case-fatality rate for treatment A) * (1- relative reduction in case-fatality rate for treatment B) *
...* (1- relative reduction in case-fatality rate for treatment N)
EXAMPLE 4: estimation of reduced benefit in patients taking multiple medications
For AMI survivors, applying relative risk reductions (RRR) for aspirin, beta-blockers, ACE-inhibitors, statins and rehabilitation gives:
Relative Benefit = 1 - [(1 –aspirin RRR) * (1 - beta-blockers RRR) * (1 – ACE-inhibitors RRR) * (1- statins RRR) * (1- rehabilitation RRR)]
= 1 - [(1- 0.15) * (1-0.23) * (1-0.20) * (1- 0.22) * (1- 0.26)]
= 1 - [(0.85) * (0.77) * (0.80) * (0.78) * (0.74)]
= 0.70 i.e. a 70% lower case fatality
Potential overlaps between patient groups
There are potential overlaps between patient groups (meaning that one person may belong to more than one patient group). In this
model, each individual was considered only one time in hospital data and community data.
CIRCCQO/2013/000264R1
12
For instance, to avoid double counting of patients treated for two or more conditions within the year (e.g. heart failure develops within 1
year after myocardial infarction in approximately 30% of survivors) we quantified overlaps between different groups and made
appropriate adjustments, by subtracting one group from another. Following the basic logic of the natural history of coronary disease,
patients recorded as having two or more conditions were allocated to the condition that was further along the disease pathway.
The assumptions made to adjust for overlaps between groups were based on the literature and expert opinion.
Sensitivity analyses
Because of the uncertainty surrounding the values, multi-way sensitivity analyses were performed 28. For each model variable, a
maximum and minimum plausible values were assigned using the 95% confidence intervals from the source documentation or 99%
confidence intervals in the case of the odds ratios for the effect of risk factors; if these were unavailable, we defined these limits as 20%
above and below the best estimate. For treatments assumed as 0, no uncertainty analysis was performed. The maximum and minimum
plausible values were fed in to the model generating maximum and minimum estimates for DPPs.
CIRCCQO/2013/000264R1
13
eTable 1. Main data sources and criteria for population and patients in the Portuguese IMPACT model.
Information 1995 2008
Population Statistics Portuguese official statistics 29 Portuguese official statistics 29
Deaths by age and sex
AMI
Unstable angina
Heart failure
Portuguese official statistics based on ICD-9 codes 30
410.0 to 410.9
411.1
428.0 to 428.4 and 428.9
Portuguese official statistics based on ICD-10 codes 30
I21.0 to I21.4 and I21.9
I20.0
I50.0, I50.1, I50.9
Number of patients admitted yearly
AMI National Hospital Discharge Registry 31 National Hospital Discharge Registry 31
Unstable Angina National Hospital Discharge Registry 31 National Hospital Discharge Registry 31
Heart failure National Hospital Discharge Registry 31 National Hospital Discharge Registry 31
Number of patients eligible for treatment treated yearly
Post-AMI Expert opinion [50% of final year (2008)] National Hospital Discharge Registry 21
CABG Expert opinion (Assume zero) National Hospital Discharge Registry 21
PCI Expert opinion (Assume zero) National Hospital Discharge Registry 21
Community CPR Expert opinion (Assume zero) Expert opinion (15% of the AMI patients)
In-hospital CPR Expert opinion [50% of final year (2008)] EURHOBOP 21
Community chronic angina Expert opinion [50% of final year (2008)] EPIPorto (follow-up) * 32
Community heart failure Expert opinion [75% of final year (2008)] EPIPorto (follow-up) 32
Acute heart failure Expert opinion [85% of final year (2008)] National Hospital Discharge Registry 31
Hypertension treatment Systematic review 33 PORMETS 34
Statins for primary prevention of
raised cholesterol
Expert opinion [50% of final year (2008)] PORMETS 34
AMI - Acute myocardial infarction; CABG - Coronary-artery bypass grafting; ICD - International Classification of Diseases; PCI - Percutaneous coronary intervention.
CIRCCQO/2013/000264R1
14
* Since these data were self-reported, we adjusted by a factor of 1.3 in men, to take into account the lack of awareness; in women, we did not apply any correction assuming
that any potential lack of awareness counterbalances with the proportion of women with false positives.
CIRCCQO/2013/000264R1
15
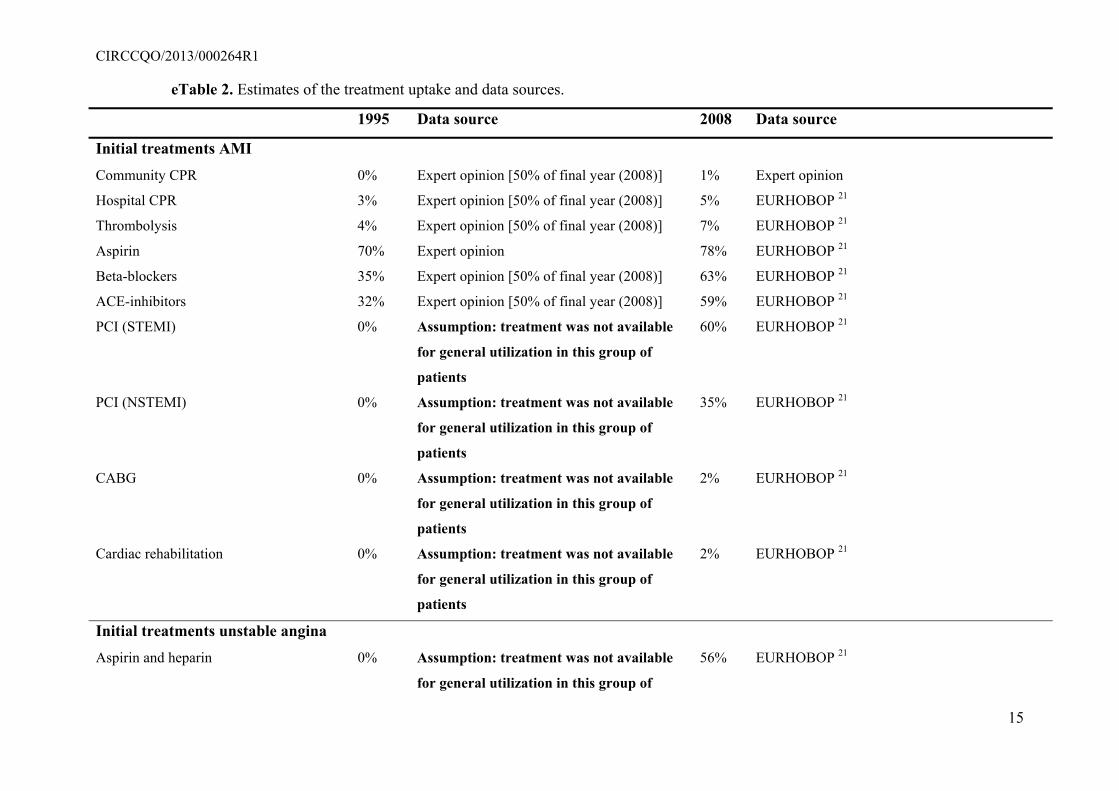
eTable 2. Estimates of the treatment uptake and data sources.
1995 Data source 2008 Data source
Initial treatments AMI
Community CPR 0% Expert opinion [50% of final year (2008)] 1% Expert opinion
Hospital CPR 3% Expert opinion [50% of final year (2008)] 5% EURHOBOP 21
Thrombolysis 4% Expert opinion [50% of final year (2008)] 7% EURHOBOP 21
Aspirin 70% Expert opinion 78% EURHOBOP 21
Beta-blockers 35% Expert opinion [50% of final year (2008)] 63% EURHOBOP 21
ACE-inhibitors 32% Expert opinion [50% of final year (2008)] 59% EURHOBOP 21
PCI (STEMI) 0% Assumption: treatment was not available
for general utilization in this group of
patients
60% EURHOBOP 21
PCI (NSTEMI) 0% Assumption: treatment was not available
for general utilization in this group of
patients
35% EURHOBOP 21
CABG 0% Assumption: treatment was not available
for general utilization in this group of
patients
2% EURHOBOP 21
Cardiac rehabilitation 0% Assumption: treatment was not available
for general utilization in this group of
patients
2% EURHOBOP 21
Initial treatments unstable angina
Aspirin and heparin 0% Assumption: treatment was not available
for general utilization in this group of
56% EURHOBOP 21
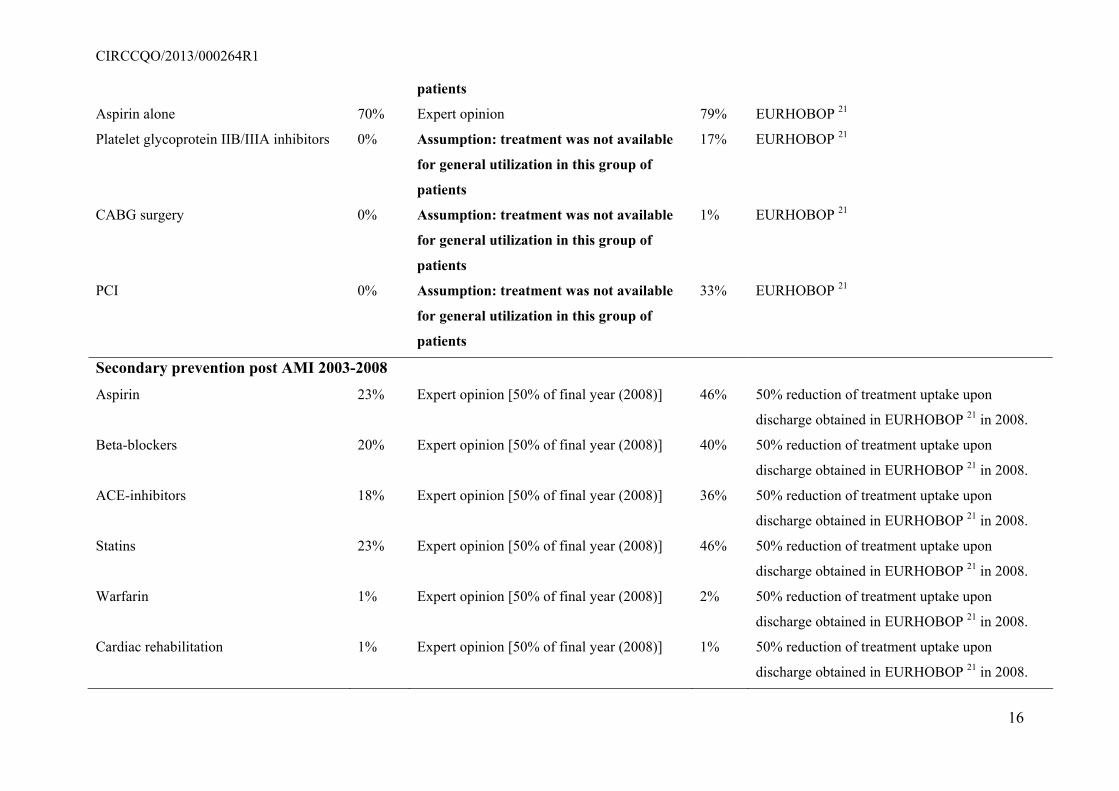
CIRCCQO/2013/000264R1
16
patients
Aspirin alone 70% Expert opinion 79% EURHOBOP 21
Platelet glycoprotein IIB/IIIA inhibitors 0% Assumption: treatment was not available
for general utilization in this group of
patients
17% EURHOBOP 21
CABG surgery 0% Assumption: treatment was not available
for general utilization in this group of
patients
1% EURHOBOP 21
PCI 0% Assumption: treatment was not available
for general utilization in this group of
patients
33% EURHOBOP 21
Secondary prevention post AMI 2003-2008
Aspirin 23% Expert opinion [50% of final year (2008)] 46% 50% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
Beta-blockers 20% Expert opinion [50% of final year (2008)] 40% 50% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
ACE-inhibitors 18% Expert opinion [50% of final year (2008)] 36% 50% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
Statins 23% Expert opinion [50% of final year (2008)] 46% 50% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
Warfarin 1% Expert opinion [50% of final year (2008)] 2% 50% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
Cardiac rehabilitation 1% Expert opinion [50% of final year (2008)] 1% 50% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
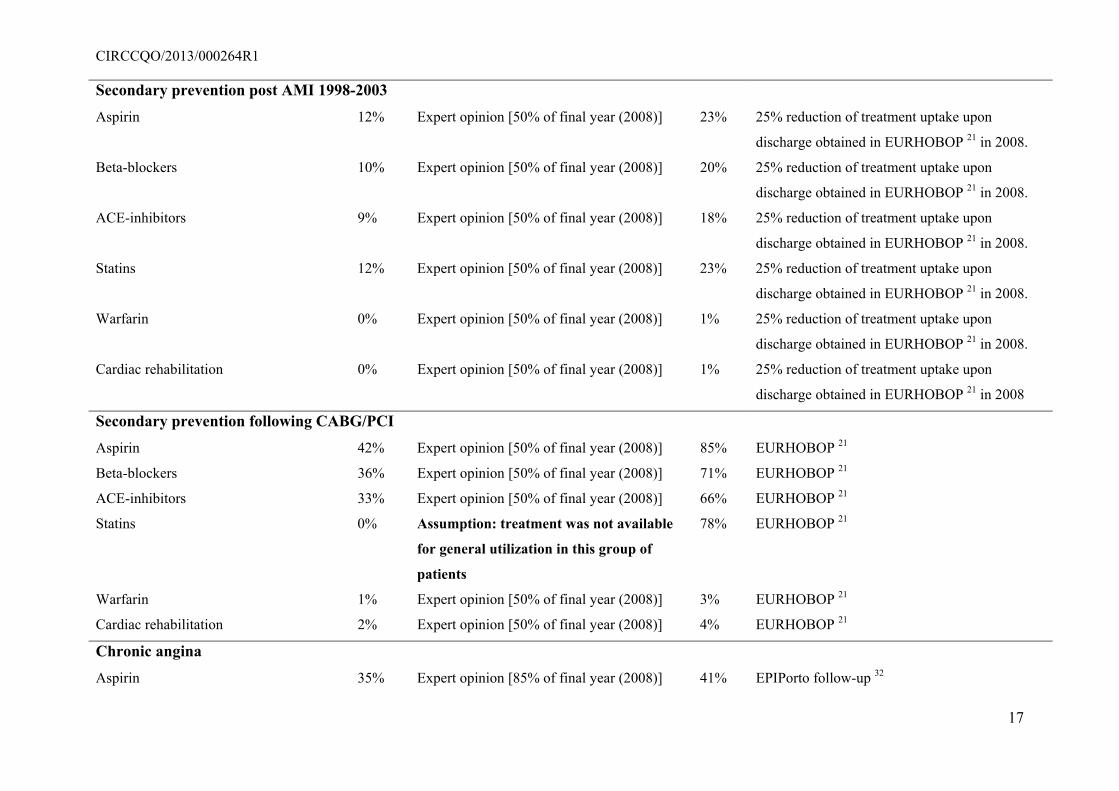
CIRCCQO/2013/000264R1
17
Secondary prevention post AMI 1998-2003
Aspirin 12% Expert opinion [50% of final year (2008)] 23% 25% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
Beta-blockers 10% Expert opinion [50% of final year (2008)] 20% 25% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
ACE-inhibitors 9% Expert opinion [50% of final year (2008)] 18% 25% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
Statins 12% Expert opinion [50% of final year (2008)] 23% 25% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
Warfarin 0% Expert opinion [50% of final year (2008)] 1% 25% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008.
Cardiac rehabilitation 0% Expert opinion [50% of final year (2008)] 1% 25% reduction of treatment uptake upon
discharge obtained in EURHOBOP 21 in 2008
Secondary prevention following CABG/PCI
Aspirin 42% Expert opinion [50% of final year (2008)] 85% EURHOBOP 21
Beta-blockers 36% Expert opinion [50% of final year (2008)] 71% EURHOBOP 21
ACE-inhibitors 33% Expert opinion [50% of final year (2008)] 66% EURHOBOP 21
Statins 0% Assumption: treatment was not available
for general utilization in this group of
patients
78% EURHOBOP 21
Warfarin 1% Expert opinion [50% of final year (2008)] 3% EURHOBOP 21
Cardiac rehabilitation 2% Expert opinion [50% of final year (2008)] 4% EURHOBOP 21
Chronic angina
Aspirin 35% Expert opinion [85% of final year (2008)] 41% EPIPorto follow-up 32
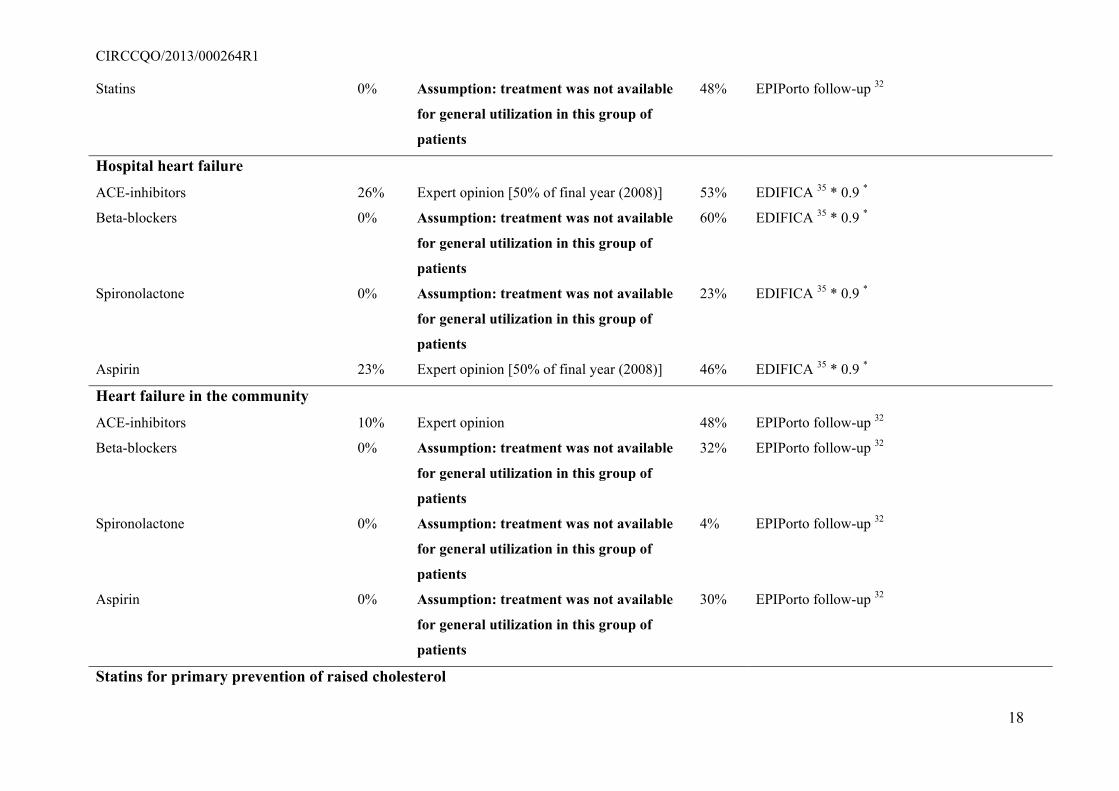
CIRCCQO/2013/000264R1
18
Statins 0% Assumption: treatment was not available
for general utilization in this group of
patients
48% EPIPorto follow-up 32
Hospital heart failure
ACE-inhibitors 26% Expert opinion [50% of final year (2008)] 53% EDIFICA 35 * 0.9 *
Beta-blockers 0% Assumption: treatment was not available
for general utilization in this group of
patients
60% EDIFICA 35 * 0.9 *
Spironolactone 0% Assumption: treatment was not available
for general utilization in this group of
patients
23% EDIFICA 35 * 0.9 *
Aspirin 23% Expert opinion [50% of final year (2008)] 46% EDIFICA 35 * 0.9 *
Heart failure in the community
ACE-inhibitors 10% Expert opinion 48% EPIPorto follow-up 32
Beta-blockers 0% Assumption: treatment was not available
for general utilization in this group of
patients
32% EPIPorto follow-up 32
Spironolactone 0% Assumption: treatment was not available
for general utilization in this group of
patients
4% EPIPorto follow-up 32
Aspirin 0% Assumption: treatment was not available
for general utilization in this group of
patients
30% EPIPorto follow-up 32
Statins for primary prevention of raised cholesterol
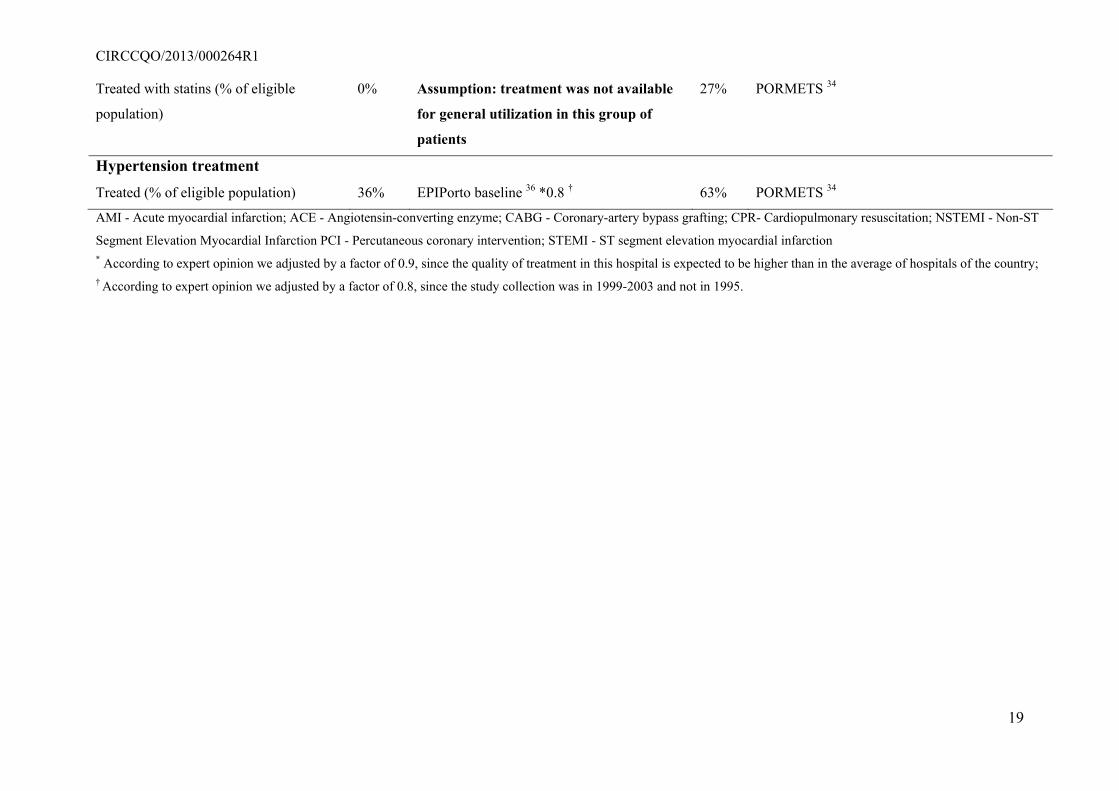
CIRCCQO/2013/000264R1
19
Treated with statins (% of eligible
population)
0% Assumption: treatment was not available
for general utilization in this group of
patients
27% PORMETS 34
Hypertension treatment
Treated (% of eligible population) 36% EPIPorto baseline 36 *0.8 † 63% PORMETS 34
AMI - Acute myocardial infarction; ACE - Angiotensin-converting enzyme; CABG - Coronary-artery bypass grafting; CPR- Cardiopulmonary resuscitation; NSTEMI - Non-ST
Segment Elevation Myocardial Infarction PCI - Percutaneous coronary intervention; STEMI - ST segment elevation myocardial infarction * According to expert opinion we adjusted by a factor of 0.9, since the quality of treatment in this hospital is expected to be higher than in the average of hospitals of the country; † According to expert opinion we adjusted by a factor of 0.8, since the study collection was in 1999-2003 and not in 1995.
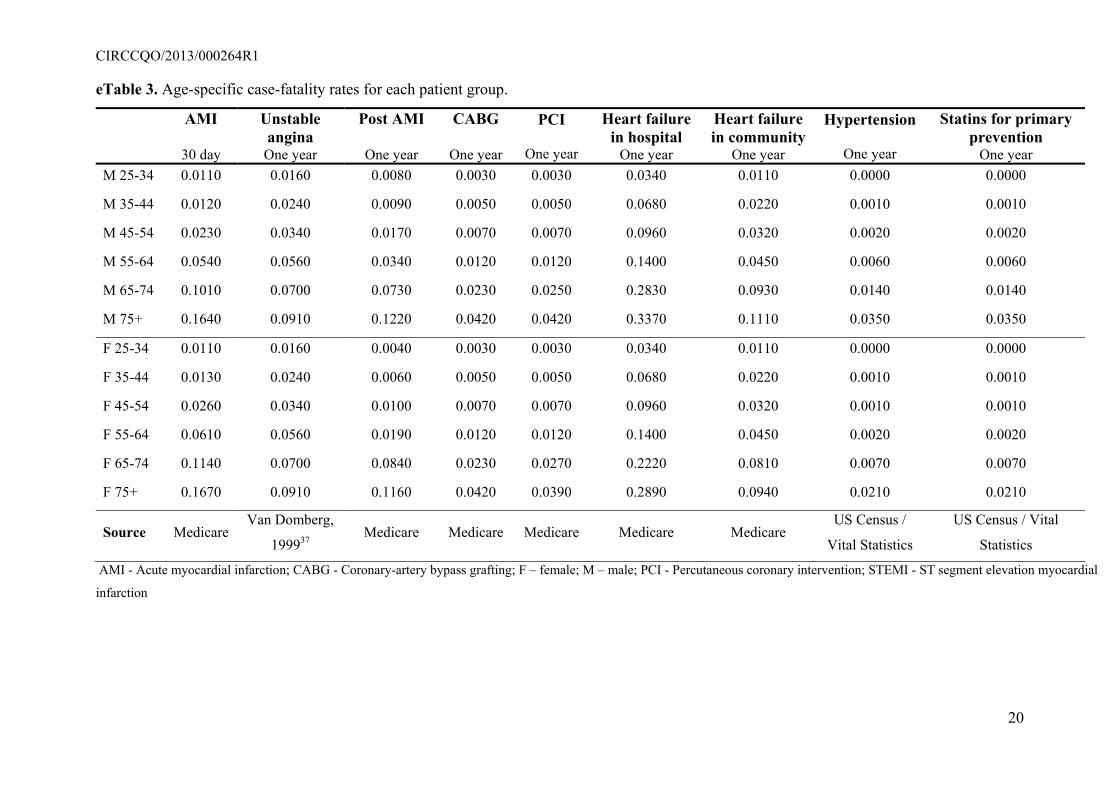
CIRCCQO/2013/000264R1
20
eTable 3. Age-specific case-fatality rates for each patient group.
AMI
30 day
Unstable angina One year
Post AMI
One year
CABG
One year
PCI
One year
Heart failure in hospital
One year
Heart failure in community
One year
Hypertension
One year
Statins for primary prevention
One year M 25-34 0.0110 0.0160 0.0080 0.0030 0.0030 0.0340 0.0110 0.0000 0.0000
M 35-44 0.0120 0.0240 0.0090 0.0050 0.0050 0.0680 0.0220 0.0010 0.0010
M 45-54 0.0230 0.0340 0.0170 0.0070 0.0070 0.0960 0.0320 0.0020 0.0020
M 55-64 0.0540 0.0560 0.0340 0.0120 0.0120 0.1400 0.0450 0.0060 0.0060
M 65-74 0.1010 0.0700 0.0730 0.0230 0.0250 0.2830 0.0930 0.0140 0.0140
M 75+ 0.1640 0.0910 0.1220 0.0420 0.0420 0.3370 0.1110 0.0350 0.0350
F 25-34 0.0110 0.0160 0.0040 0.0030 0.0030 0.0340 0.0110 0.0000 0.0000
F 35-44 0.0130 0.0240 0.0060 0.0050 0.0050 0.0680 0.0220 0.0010 0.0010
F 45-54 0.0260 0.0340 0.0100 0.0070 0.0070 0.0960 0.0320 0.0010 0.0010
F 55-64 0.0610 0.0560 0.0190 0.0120 0.0120 0.1400 0.0450 0.0020 0.0020
F 65-74 0.1140 0.0700 0.0840 0.0230 0.0270 0.2220 0.0810 0.0070 0.0070
F 75+ 0.1670 0.0910 0.1160 0.0420 0.0390 0.2890 0.0940 0.0210 0.0210
Source MedicareVan Domberg,
199937 Medicare Medicare Medicare Medicare Medicare
US Census /
Vital Statistics
US Census / Vital
Statistics
AMI - Acute myocardial infarction; CABG - Coronary-artery bypass grafting; F – female; M – male; PCI - Percutaneous coronary intervention; STEMI - ST segment elevation myocardial
infarction
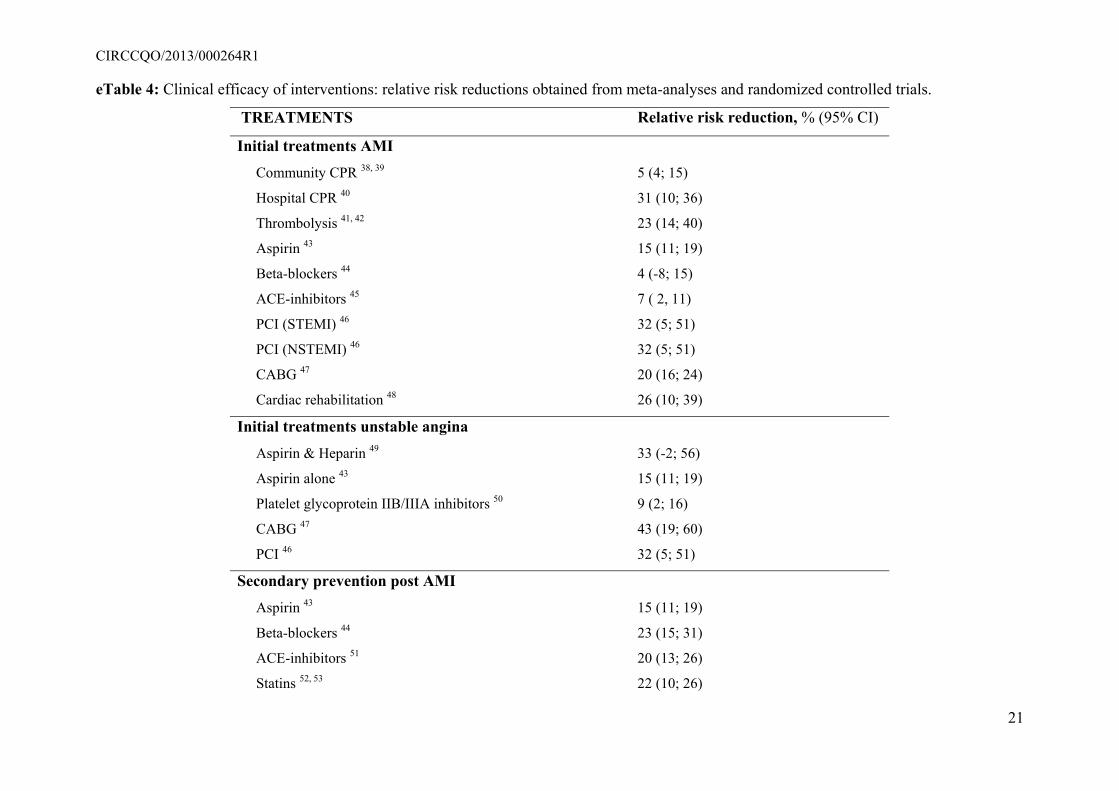
CIRCCQO/2013/000264R1
21
eTable 4: Clinical efficacy of interventions: relative risk reductions obtained from meta-analyses and randomized controlled trials.
TREATMENTS Relative risk reduction, % (95% CI)
Initial treatments AMI
Community CPR 38, 39 5 (4; 15)
Hospital CPR 40 31 (10; 36)
Thrombolysis 41, 42 23 (14; 40)
Aspirin 43 15 (11; 19)
Beta-blockers 44 4 (-8; 15)
ACE-inhibitors 45 7 ( 2, 11)
PCI (STEMI) 46 32 (5; 51)
PCI (NSTEMI) 46 32 (5; 51)
CABG 47 20 (16; 24)
Cardiac rehabilitation 48 26 (10; 39)
Initial treatments unstable angina
Aspirin & Heparin 49 33 (-2; 56)
Aspirin alone 43 15 (11; 19)
Platelet glycoprotein IIB/IIIA inhibitors 50 9 (2; 16)
CABG 47 43 (19; 60)
PCI 46 32 (5; 51)
Secondary prevention post AMI
Aspirin 43 15 (11; 19)
Beta-blockers 44 23 (15; 31)
ACE-inhibitors 51 20 (13; 26)
Statins 52, 53 22 (10; 26)
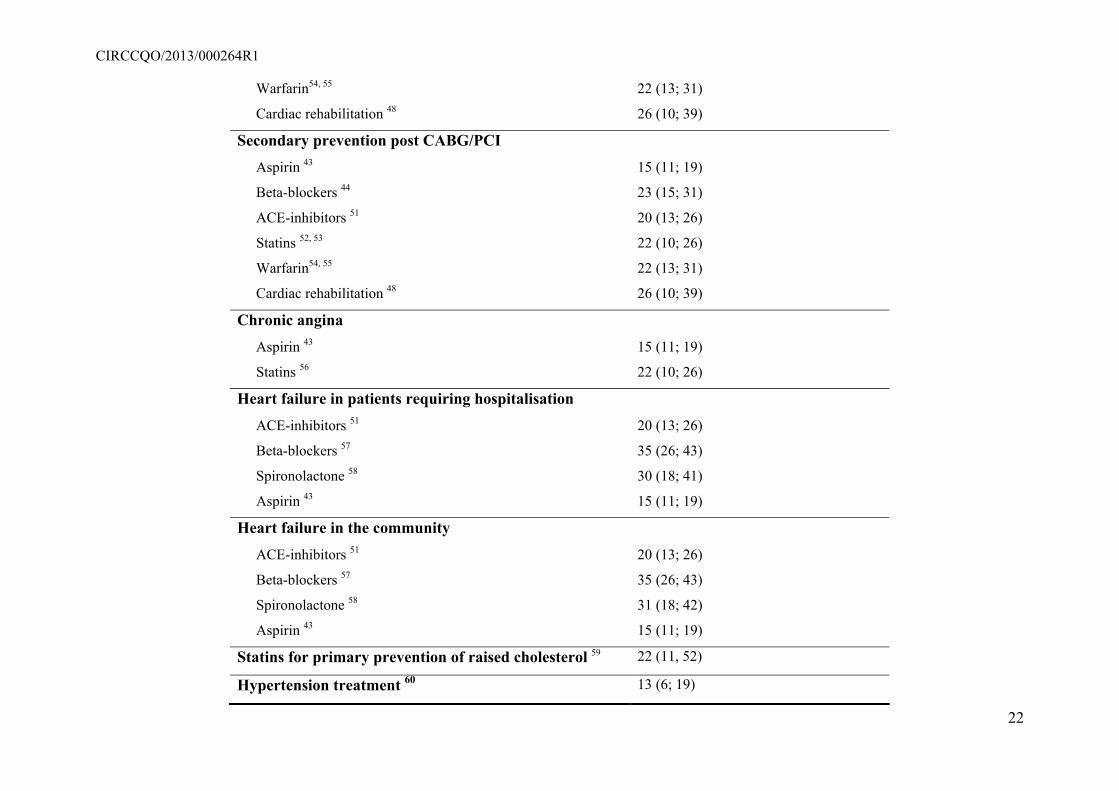
CIRCCQO/2013/000264R1
22
Warfarin54, 55 22 (13; 31)
Cardiac rehabilitation 48 26 (10; 39)
Secondary prevention post CABG/PCI
Aspirin 43 15 (11; 19)
Beta-blockers 44 23 (15; 31)
ACE-inhibitors 51 20 (13; 26)
Statins 52, 53 22 (10; 26)
Warfarin54, 55 22 (13; 31)
Cardiac rehabilitation 48 26 (10; 39)
Chronic angina
Aspirin 43 15 (11; 19)
Statins 56 22 (10; 26)
Heart failure in patients requiring hospitalisation
ACE-inhibitors 51 20 (13; 26)
Beta-blockers 57 35 (26; 43)
Spironolactone 58 30 (18; 41)
Aspirin 43 15 (11; 19)
Heart failure in the community
ACE-inhibitors 51 20 (13; 26)
Beta-blockers 57 35 (26; 43)
Spironolactone 58 31 (18; 42)
Aspirin 43 15 (11; 19)
Statins for primary prevention of raised cholesterol 59 22 (11, 52)
Hypertension treatment 60 13 (6; 19)
CIRCCQO/2013/000264R1
23
95% CI – 95% Confidence interval; AMI - Acute myocardial infarction; ACE - Angiotensin-converting enzyme; CABG - Coronary-artery bypass
grafting; CPR- cardiopulmonary resuscitation; PCI - Percutaneous coronary intervention; STEMI - ST segment elevation myocardial infarction.
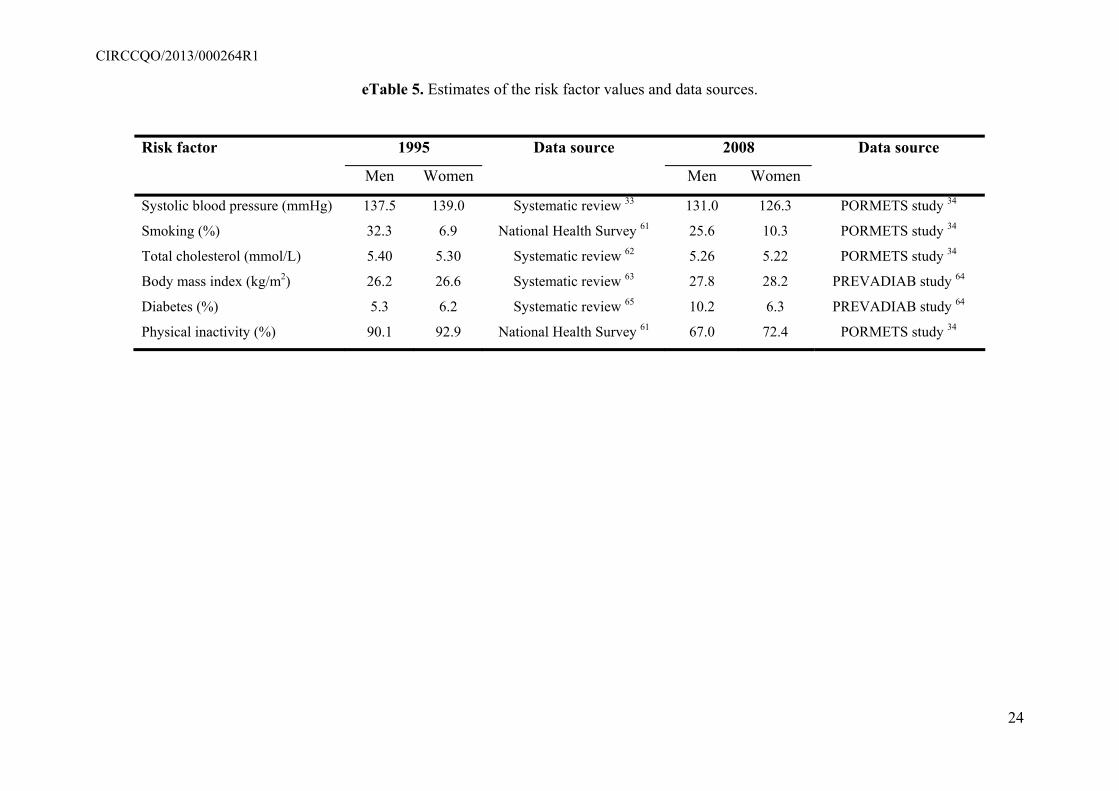
CIRCCQO/2013/000264R1
24
eTable 5. Estimates of the risk factor values and data sources.
Risk factor 1995 Data source 2008 Data source
Men Women Men Women
Systolic blood pressure (mmHg) 137.5 139.0 Systematic review 33 131.0 126.3 PORMETS study 34
Smoking (%) 32.3 6.9 National Health Survey 61 25.6 10.3 PORMETS study 34
Total cholesterol (mmol/L) 5.40 5.30 Systematic review 62 5.26 5.22 PORMETS study 34
Body mass index (kg/m2) 26.2 26.6 Systematic review 63 27.8 28.2 PREVADIAB study 64
Diabetes (%) 5.3 6.2 Systematic review 65 10.2 6.3 PREVADIAB study 64
Physical inactivity (%) 90.1 92.9 National Health Survey 61 67.0 72.4 PORMETS study 34
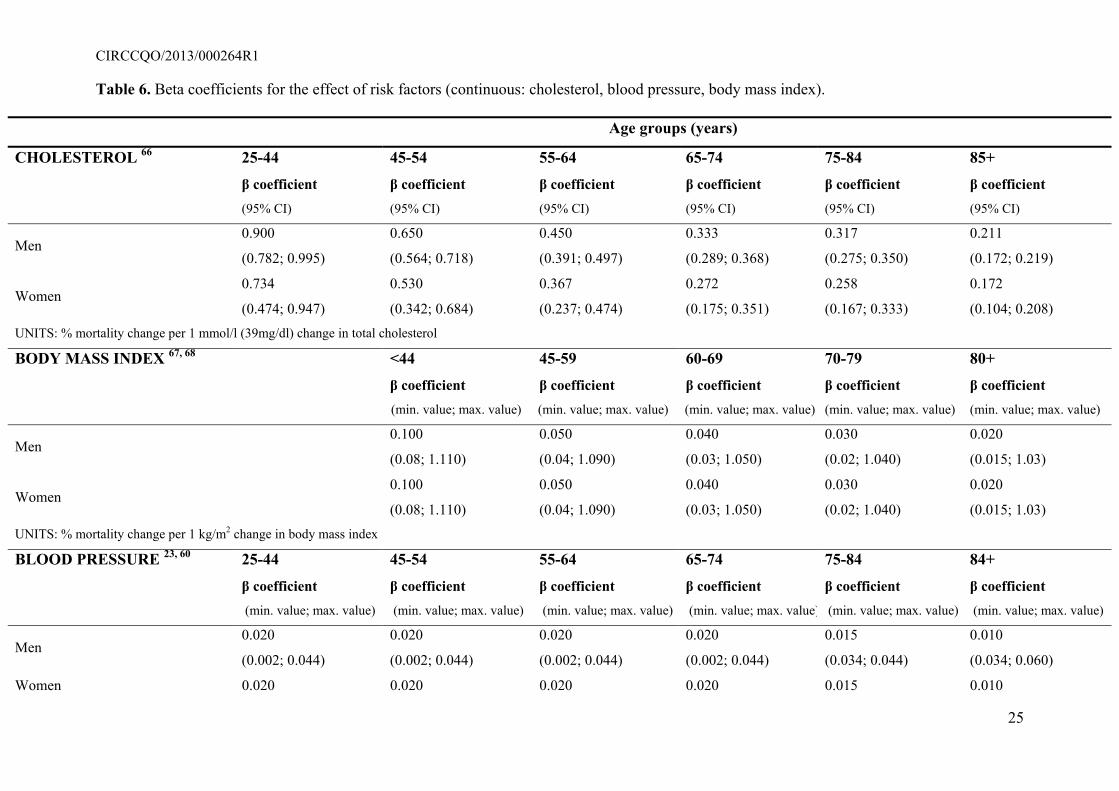
CIRCCQO/2013/000264R1
25
Table 6. Beta coefficients for the effect of risk factors (continuous: cholesterol, blood pressure, body mass index).
Age groups (years)
CHOLESTEROL 66 25-44 45-54 55-64 65-74 75-84 85+
β coefficient (95% CI)
β coefficient (95% CI)
β coefficient (95% CI)
β coefficient (95% CI)
β coefficient (95% CI)
β coefficient (95% CI)
Men 0.900
(0.782; 0.995)
0.650
(0.564; 0.718)
0.450
(0.391; 0.497)
0.333
(0.289; 0.368)
0.317
(0.275; 0.350)
0.211
(0.172; 0.219)
Women 0.734
(0.474; 0.947)
0.530
(0.342; 0.684)
0.367
(0.237; 0.474)
0.272
(0.175; 0.351)
0.258
(0.167; 0.333)
0.172
(0.104; 0.208) UNITS: % mortality change per 1 mmol/l (39mg/dl) change in total cholesterol
BODY MASS INDEX 67, 68 <44 45-59 60-69 70-79 80+
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
Men 0.100
(0.08; 1.110)
0.050
(0.04; 1.090)
0.040
(0.03; 1.050)
0.030
(0.02; 1.040)
0.020
(0.015; 1.03)
Women 0.100
(0.08; 1.110)
0.050
(0.04; 1.090)
0.040
(0.03; 1.050)
0.030
(0.02; 1.040)
0.020
(0.015; 1.03) UNITS: % mortality change per 1 kg/m2 change in body mass index
BLOOD PRESSURE 23, 60 25-44 45-54 55-64 65-74 75-84 84+
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
β coefficient (min. value; max. value)
Men 0.020
(0.002; 0.044)
0.020
(0.002; 0.044)
0.020
(0.002; 0.044)
0.020
(0.002; 0.044)
0.015
(0.034; 0.044)
0.010
(0.034; 0.060)
Women 0.020 0.020 0.020 0.020 0.015 0.010
CIRCCQO/2013/000264R1
26
(0.002; 0.044) (0.002; 0.044) (0.002; 0.044) (0.002; 0.044) (0.034; 0.044) (0.034; 0.060) UNITS: % mortality change per 20 mmHg change in systolic blood pressure.
95% CI – 95% Confidence interval; min. – minimum; max. – maximum.
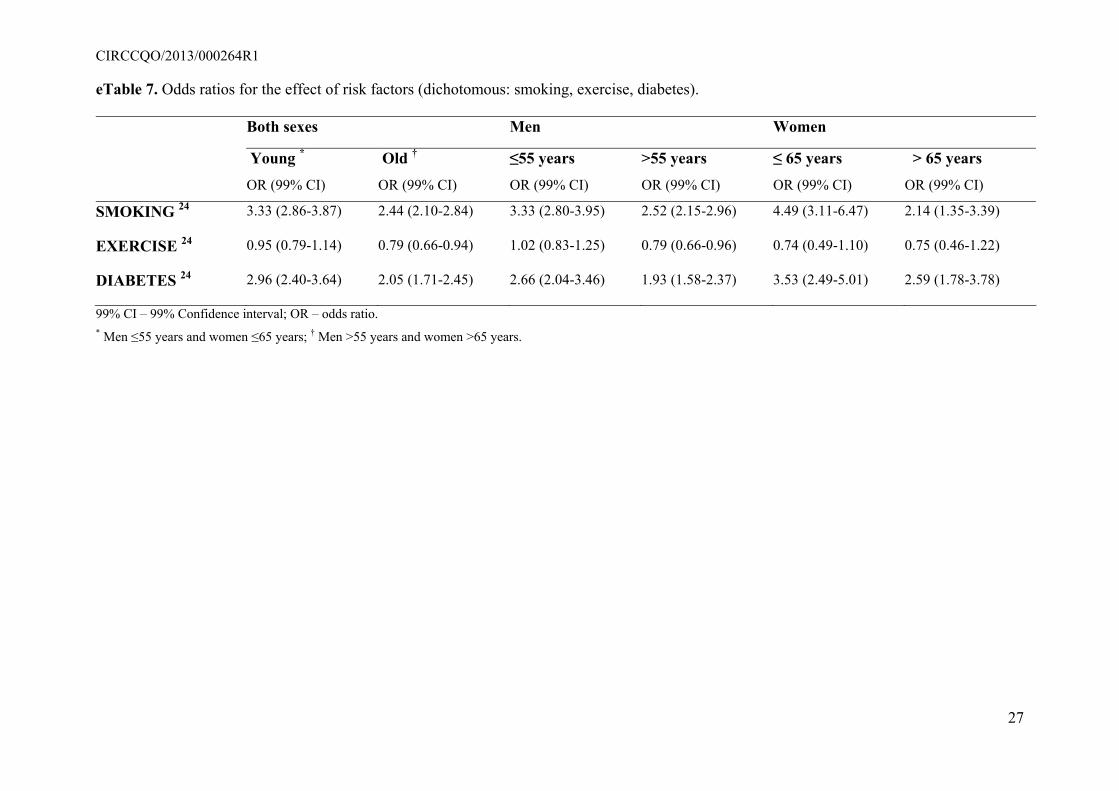
CIRCCQO/2013/000264R1
27
eTable 7. Odds ratios for the effect of risk factors (dichotomous: smoking, exercise, diabetes).
Both sexes Men Women
Young *
OR (99% CI)
Old †
OR (99% CI)
≤55 years
OR (99% CI)
>55 years
OR (99% CI)
≤ 65 years
OR (99% CI)
> 65 years
OR (99% CI)
SMOKING 24 3.33 (2.86-3.87) 2.44 (2.10-2.84) 3.33 (2.80-3.95) 2.52 (2.15-2.96) 4.49 (3.11-6.47) 2.14 (1.35-3.39)
EXERCISE 24 0.95 (0.79-1.14) 0.79 (0.66-0.94) 1.02 (0.83-1.25) 0.79 (0.66-0.96) 0.74 (0.49-1.10) 0.75 (0.46-1.22)
DIABETES 24 2.96 (2.40-3.64) 2.05 (1.71-2.45) 2.66 (2.04-3.46) 1.93 (1.58-2.37) 3.53 (2.49-5.01) 2.59 (1.78-3.78)
99% CI – 99% Confidence interval; OR – odds ratio. * Men ≤55 years and women ≤65 years; † Men >55 years and women >65 years.
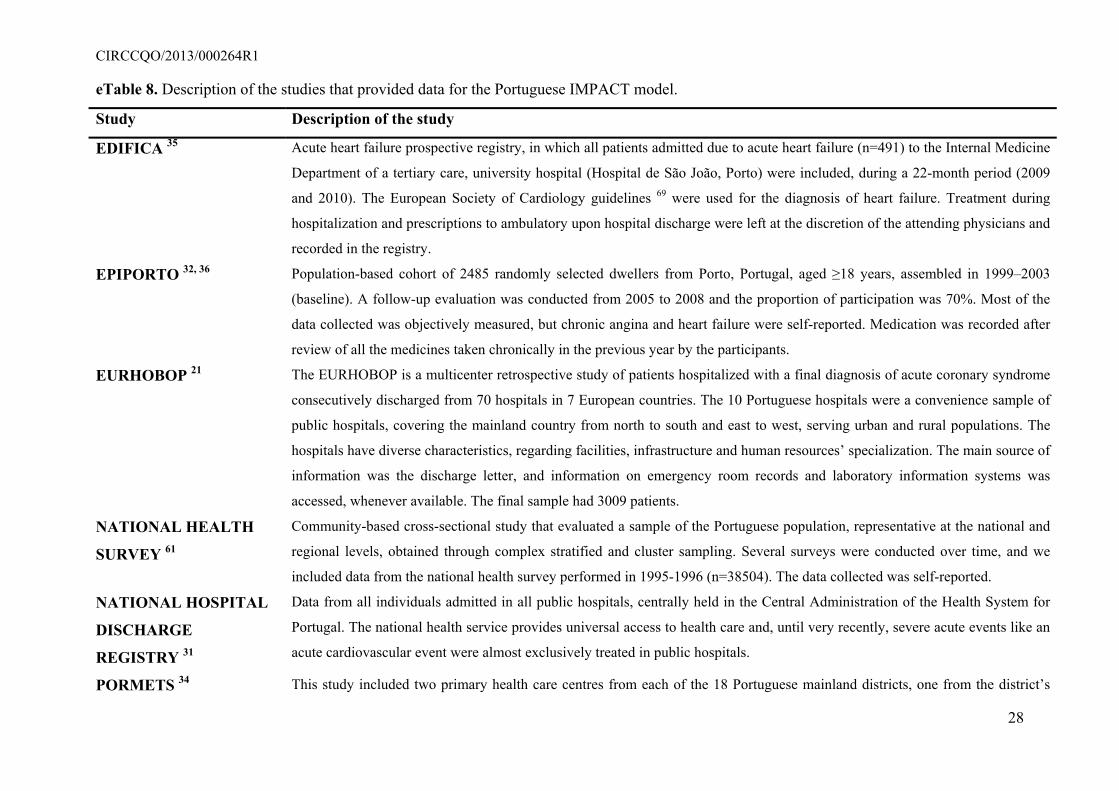
CIRCCQO/2013/000264R1
28
eTable 8. Description of the studies that provided data for the Portuguese IMPACT model.
Study Description of the study
EDIFICA 35 Acute heart failure prospective registry, in which all patients admitted due to acute heart failure (n=491) to the Internal Medicine
Department of a tertiary care, university hospital (Hospital de São João, Porto) were included, during a 22-month period (2009
and 2010). The European Society of Cardiology guidelines 69 were used for the diagnosis of heart failure. Treatment during
hospitalization and prescriptions to ambulatory upon hospital discharge were left at the discretion of the attending physicians and
recorded in the registry.
EPIPORTO 32, 36 Population-based cohort of 2485 randomly selected dwellers from Porto, Portugal, aged ≥18 years, assembled in 1999–2003
(baseline). A follow-up evaluation was conducted from 2005 to 2008 and the proportion of participation was 70%. Most of the
data collected was objectively measured, but chronic angina and heart failure were self-reported. Medication was recorded after
review of all the medicines taken chronically in the previous year by the participants.
EURHOBOP 21 The EURHOBOP is a multicenter retrospective study of patients hospitalized with a final diagnosis of acute coronary syndrome
consecutively discharged from 70 hospitals in 7 European countries. The 10 Portuguese hospitals were a convenience sample of
public hospitals, covering the mainland country from north to south and east to west, serving urban and rural populations. The
hospitals have diverse characteristics, regarding facilities, infrastructure and human resources’ specialization. The main source of
information was the discharge letter, and information on emergency room records and laboratory information systems was
accessed, whenever available. The final sample had 3009 patients.
NATIONAL HEALTH
SURVEY 61
Community-based cross-sectional study that evaluated a sample of the Portuguese population, representative at the national and
regional levels, obtained through complex stratified and cluster sampling. Several surveys were conducted over time, and we
included data from the national health survey performed in 1995-1996 (n=38504). The data collected was self-reported.
NATIONAL HOSPITAL
DISCHARGE
REGISTRY 31
Data from all individuals admitted in all public hospitals, centrally held in the Central Administration of the Health System for
Portugal. The national health service provides universal access to health care and, until very recently, severe acute events like an
acute cardiovascular event were almost exclusively treated in public hospitals.
PORMETS 34 This study included two primary health care centres from each of the 18 Portuguese mainland districts, one from the district’s
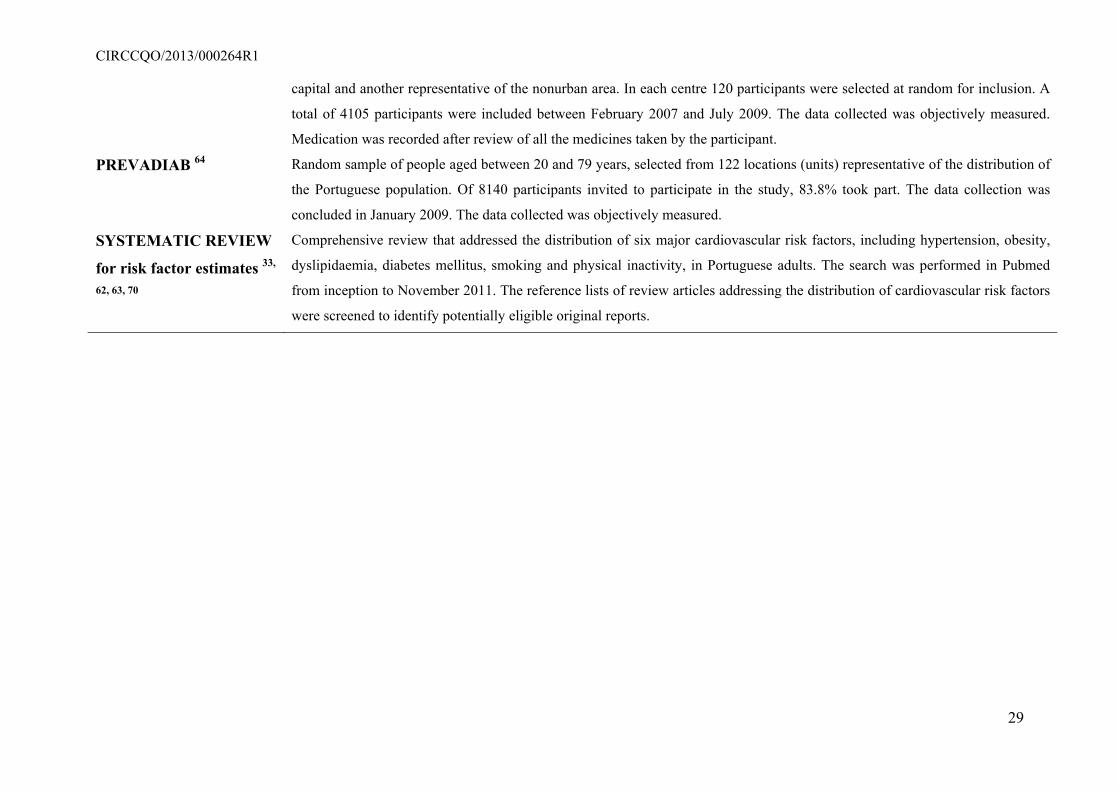
CIRCCQO/2013/000264R1
29
capital and another representative of the nonurban area. In each centre 120 participants were selected at random for inclusion. A
total of 4105 participants were included between February 2007 and July 2009. The data collected was objectively measured.
Medication was recorded after review of all the medicines taken by the participant.
PREVADIAB 64 Random sample of people aged between 20 and 79 years, selected from 122 locations (units) representative of the distribution of
the Portuguese population. Of 8140 participants invited to participate in the study, 83.8% took part. The data collection was
concluded in January 2009. The data collected was objectively measured.
SYSTEMATIC REVIEW
for risk factor estimates 33,
62, 63, 70
Comprehensive review that addressed the distribution of six major cardiovascular risk factors, including hypertension, obesity,
dyslipidaemia, diabetes mellitus, smoking and physical inactivity, in Portuguese adults. The search was performed in Pubmed
from inception to November 2011. The reference lists of review articles addressing the distribution of cardiovascular risk factors
were screened to identify potentially eligible original reports.
CIRCCQO/2013/000264R1
eReferences
1. Flores-Mateo G, Grau M, O'Flaherty M, Ramos R, Elosua R, Violan-Fors Cn,
Quesada M, Marta R, Sala J, Marrugat J, Capewell S. Analyzing the coronary heart
disease mortality decline in a mediterranean population: Spain 1988-2005. Rev Esp
Cardiol.64:988-996
2. Palmieri L, Bennett K, Giampaoli S, Capewell S. Explaining the decrease in coronary
heart disease mortality in italy between 1980 and 2000. Am J Public Health.
2010;100:684-692
3. Unal B, Critchley JA, Capewell S. Explaining the decline in coronary heart disease
mortality in england and wales between 1981 and 2000. Circulation. 2004;109:1101-
1107
4. Laatikainen T, Critchley J, Vartiainen E, Salomaa V, Ketonen M, Capewell S.
Explaining the decline in coronary heart disease mortality in finland between 1982
and 1997. Am J Epidemiol. 2005;162:764-773
5. Aspelund T, Gudnason V, Magnusdottir BT, Andersen K, Sigurdsson G, Thorsson B,
Steingrimsdottir L, Critchley J, Bennett K, O'Flaherty M, Capewell S. Analysing the
large decline in coronary heart disease mortality in the icelandic population aged 25-
74 between the years 1981 and 2006. PLoS One. 2010;5:e13957
6. Bennett K, Kabir Z, Unal B, Shelley E, Critchley J, Perry I, Feely J, Capewell S.
Explaining the recent decrease in coronary heart disease mortality rates in ireland,
1985-2000. J Epidemiol Community Health. 2006;60:322-327
7. Bandosz P, O'Flaherty M, Drygas W, Rutkowski M, Koziarek J, Wyrzykowski B,
Bennett K, Zdrojewski T, Capewell S. Decline in mortality from coronary heart
disease in poland after socioeconomic transformation: Modelling study. BMJ.
2012;344:d8136
30
CIRCCQO/2013/000264R1
8. Capewell S, Morrison CE, McMurray JJ. Contribution of modern cardiovascular
treatment and risk factor changes to the decline in coronary heart disease mortality in
scotland between 1975 and 1994. Heart. 1999;81:380-386
9. Bjorck L, Rosengren A, Bennett K, Lappas G, Capewell S. Modelling the decreasing
coronary heart disease mortality in sweden between 1986 and 2002. Eur Heart J.
2009;30:1046-1056
10. Hughes J, Kee F, O'Flaherty M, Critchley J, Cupples M, Capewell S, Bennett K.
Modelling coronary heart disease mortality in northern ireland between 1987 and
2007: Broader lessons for prevention. Eur J Prev Cardiol. 2012;[Epub ahead of print]
11. Bruthans J, Cifkova R, Lanska V, O'Flaherty M, Critchley JA, Holub J, Jansky P,
Zvarova J, Capewell S. Explaining the decline in coronary heart disease mortality in
the czech republic between 1985 and 2007. Eur J Prev Cardiol. 2012;[Epub ahead of
print]
12. Rastam S, Al Ali R, Maziak W, Mzayek F, Fouad FM, O'Flaherty M, Capewell S.
Explaining the increase in coronary heart disease mortality in syria between 1996 and
2006. BMC Public Health. 2012;12:754
13. Abu-Rmeileh NM, Shoaibi A, O'Flaherty M, Capewell S, Husseini A. Analysing falls
in coronary heart disease mortality in the west bank between 1998 and 2009. BMJ
Open. 2012;2
14. Capewell S, Beaglehole R, Seddon M, McMurray J. Explanation for the decline in
coronary heart disease mortality rates in auckland, new zealand, between 1982 and
1993. Circulation. 2000;102:1511-1516
15. Critchley J, Liu J, Zhao D, Wei W, Capewell S. Explaining the increase in coronary
heart disease mortality in beijing between 1984 and 1999. Circulation.
2004;110:1236-1244
31
CIRCCQO/2013/000264R1
16. Wijeysundera HC, Machado M, Farahati F, Wang X, Witteman W, van der Velde G,
Tu JV, Lee DS, Goodman SG, Petrella R, O'Flaherty M, Krahn M, Capewell S.
Association of temporal trends in risk factors and treatment uptake with coronary
heart disease mortality, 1994-2005. JAMA. 2010;303:1841-1847
17. Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, Giles WH,
Capewell S. Explaining the decrease in u.S. Deaths from coronary disease, 1980-
2000. N Engl J Med. 2007;356:2388-2398
18. Butler J, Arbogast PG, BeLue R, Daugherty J, Jain MK, Ray WA, Griffin MR.
Outpatient adherence to beta-blocker therapy after acute myocardial infarction. J Am
Coll Cardiol. 2002;40:1589-1595
19. Unal B, Critchley J, Capewell S. Impact, a validated, comprehensive coronary heart
disease model. 2006
20. Nichol M, Venturini F, Sung J. A critical evaluation of the methodology of the
literature on medication compliance. Ann Pharmacother. 1999;33:531-540
21. Kirchberger I, Azevedo A, Davoli M, Farmakis D, Ferrieres J, Garel P, Haekkinen U,
Marrugat J, Torre M, Meisinger C. European hospital benchmarking in acute coronary
syndrome: The eurhobop project. Congress of the European Society of Cardiology
(ESC) 2012; 22(1):297
22. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention
of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324:71-86
23. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies
Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A
meta-analysis of individual data for one million adults in 61 prospective studies.
Lancet. 2002;360:1903-1913
32
CIRCCQO/2013/000264R1
24. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A,
Pais P, Varigos J, Lisheng L. Effect of potentially modifiable risk factors associated
with myocardial infarction in 52 countries (the interheart study): Case-control study.
Lancet. 2004;364:937-952
25. Mant J, Hicks N. Detecting differences in quality of care: The sensitivity of measures
of process and outcome in treating acute myocardial infarction. BMJ. 1995;311:793-
796
26. Yusuf S. Two decades of progress in preventing vascular disease. Lancet. 2002;360:2-
3
27. Wald NJ, Law MR. A strategy to reduce cardiovascular disease by more than 80%.
BMJ. 2003;326:1419
28. Briggs A, Sculpher M, Buxton M. Uncertainty in the economic evaluation of health
care technologies: The role of sensitivity analysis. Health Econ. 1994;3:95-104
29. Estimativas anuais da população residente. 2010;2011
30. Óbitos (n.º) por sexo e causa de morte; anual. 2010;2011
31. Correia R. Geographic and temporal variation of the procedures used in myocardial
infarction. 2011;Master in Medicine
32. Pereira M, Lunet N, Paulo C, Severo M, Azevedo A, Barros H. Incidence of
hypertension in a prospective cohort study of adults from porto, portugal. BMC
Cardiovascular Disorders. 2012;28:114
33. Pereira M, Carreira H, Vales C, Rocha V, Azevedo A, Lunet N. Trends in
hypertension prevalence (1990-2005) and mean blood pressure (1975-2005) in
portugal: A systematic review. Blood Press. 2012;21:220-226
33
CIRCCQO/2013/000264R1
34. Gray LJ, Barros H, Raposo L, Khunti K, Davies MJ, Santos AC. The development
and validation of the portuguese risk score for detecting type 2 diabetes and impaired
fasting glucose. Prim Care Diabetes. 2013;[Epub ahead of print]
35. Almeida P, Rodrigues J, Lourenço P, Julia Maciel M, Bettencourt P. Prognostic
significance of applying the european society of cardiology consensus algorithm for
heart failure with preserved systolic function diagnosis. Clin Cardiol. 2012;35:770-
778
36. Pereira M, Azevedo A, Barros H. Determinants of awareness, treatment and control of
hypertension in a portuguese population. Rev Port Cardiol. 2010;29:1779-1792
37. van Domburg RT, van Miltenburg-van Zijl AJ, Veerhoek RJ, Simoons ML. Unstable
angina: Good long-term outcome after a complicated early course. J Am Coll Cardiol.
1998;31:1534-1539
38. Nichol G, Stiell IG, Hebert P, Wells GA, Vandemheen K, Laupacis A. What is the
quality of life for survivors of cardiac arrest? A prospective study. Acad Emerg Med.
1999;6:95-102
39. Rea TD, Eisenberg MS, Culley LL, Becker L. Dispatcher-assisted cardiopulmonary
resuscitation and survival in cardiac arrest. Circulation. 2001;104:2513-2516
40. Tunstall-Pedoe H, Bailey L, Chamberlain D, Marsden A, Ward M, Zideman D.
Survey of 3765 cardiopulmonary resuscitations in british hospitals (the bresus study):
Methods and overall results. BMJ. 1992;304:1347-1351
41. Estess JM, Topol EJ. Fibrinolytic treatment for elderly patients with acute myocardial
infarction. Heart. 2002;87:308-311
42. Collins R, MacMahon S, Flather M, Baigent C, Remvig L, Mortensen S, Appleby P,
Godwin J, Yusuf S, Peto R. Clinical effects of anticoagulant therapy in suspected
34
CIRCCQO/2013/000264R1
acute myocardial infarction: Systematic overview of randomised trials. BMJ.
1996;313:652-659
43. Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised
trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke
in high risk patients. BMJ. 2002;324:71-86
44. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after
myocardial infarction: Systematic review and meta regression analysis. BMJ.
1999;318:1730-1737
45. Latini R, Maggioni AP, Flather M, Sleight P, Tognoni G, participants ftm. Ace
inhibitor use in patients with myocardial infarction: Summary of evidence from
clinical trials. Circulation. 1995;92:3132-3137
46. Fox KAA, Poole-Wilson P, Clayton TC, Henderson RA, Shaw TRD, Wheatley DJ,
Knight R, Pocock SJ. 5-year outcome of an interventional strategy in non-st-elevation
acute coronary syndrome: The british heart foundation rita 3 randomised trial. Lancet.
2005;366:914-920
47. Yusuf S, Zucker D, Passamani E, Peduzzi P, Takaro T, Fisher LD, Kennedy JW,
Davis K, Killip T, Norris R, Morris C, Mathur V, Varnauskas E, Chalmers TC. Effect
of coronary artery bypass graft surgery on survival: Overview of 10-year results from
randomised trials by the coronary artery bypass graft surgery trialists collaboration.
Lancet. 1994;344:563-570
48. Taylor RS, Brown A, Ebrahim S, Jolliffe J, Noorani H, Rees K, Skidmore B, Stone
JA, Thompson DR, Oldridge N. Exercise-based rehabilitation for patients with
coronary heart disease: Systematic review and meta-analysis of randomized
controlled trials. Am J Med. 2004;116:682-692
35
CIRCCQO/2013/000264R1
49. Oler A, Whooley MA, Oler J, Grady D. Adding heparin to aspirin reduces the
incidence of myocardial infarction and death in patients with unstable angina: A meta-
analysis. JAMA. 1996;276:811-815
50. Boersma E, Harrington RA, Moliterno DJ, White H, Théroux P, Van de Werf F, de
Torbal A, Armstrong PW, Wallentin LC, Wilcox RG, Simes J, Califf RM, Topol EJ,
Simoons ML. Platelet glycoprotein iib/iiia inhibitors in acute coronary syndromes: A
meta-analysis of all major randomised clinical trials. Lancet. 2002;359:189-198
51. Flather MD, Yusuf S, Kober L, Pfeffer M, Hall A, Murray G, Torp-Pedersen C, Ball
S, Pogue J, Moyé L, Braunwald E. Long-term ace-inhibitor therapy in patients with
heart failure or left-ventricular dysfunction: A systematic overview of data from
individual patients. Lancet. 2000;355:1575-1581
52. Cholesterol Treatment Trialists' (CTT) Collaborators, Kearney P, Blackwell L,
Collins R, Keech A, Simes J, Peto R, Armitage J, Baigent C. Efficacy of cholesterol-
lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: A
meta-analysis. Lancet. 2008;371:117-125
53. Wilt T, Bloomfield HE, MacDonald R, Nelson D, Rutks I, Ho M, Larsen G, McCall
A, Pineros S, Sales A. Effectiveness of statin therapy in adults with coronary heart
disease. Arch Intern Med. 2004;164:1427-1436
54. Anand S, Yusuf S. Oral anticoagulant therapy in patients with coronary artery disease:
A meta-analysis. JAMA. 1999;282:2058-2067
55. Lau J, Antman EM, Jimenez-Silva J, Kupelnick B, Mosteller F, Chalmers TC.
Cumulative meta-analysis of therapeutic trials for myocardial infarction. N Engl J
Med. 1992;327:248-254
56. Baigent C, Keech A, Kearney P, Blackwell L, Buck G, Pollicino C, Kirby A, Sourjina
T, Peto R, Collins R, Simes R, Cholesterol Treatment Trialists' (CTT) Collaborators.
36
CIRCCQO/2013/000264R1
Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of
data from 90,056 participants in 14 randomised trials of statins. Lancet.
2005;366:1267-1278
57. Shibata MC, Flather MD, Wang D. Systematic review of the impact of beta blockers
on mortality and hospital admissions in heart failure. Eur J Heart Fail. 2001;3:351-357
58. Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, Palensky J, Wittes J.
The effect of spironolactone on morbidity and mortality in patients with severe heart
failure. N Engl J Med. 1999;341:709-717
59. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention
of coronary heart disease: Meta-analysis of randomised trials. BMJ. 2000;321:983
60. Law M, Wald N, Morris J. Lowering blood pressure to prevent myocardial infarction
and stroke: A new preventive strategy. Health Technol Assess. 2003;7:1-94
61. Instituto Nacional de Estatística. Inquérito nacional de saúde 1995-1996. 1997
62. Carreira H, Pereira M, Alves L, Lunet N, Azevedo A. Dyslipidaemia, and mean blood
cholesterol and triglycerides levels in the portuguese population: A systematic review.
Arq Med 2012;26:112-123
63. Carreira H, Pereira M, Azevedo A, Lunet N. Trends of bmi and prevalence of
overweight and obesity in portugal (1995-2005): A systematic review. Public Health
Nutr. 2012;15:972-981
64. Gardete-Correia L, Boavida JM, Raposo JF, Mesquita AC, Fona C, Carvalho R,
Massano-Cardoso S. First diabetes prevalence study in portugal: Prevadiab study.
Diabet Med. 2010;27:879-881
65. Pereira M, Carreira H, Lunet N, Azevedo A. Trends in prevalence of diabetes mellitus
and mean fasting glucose levels in portugal (1987-2009): Systematic review.
European Congress of Epidemiology. 2012;27:S14
37
CIRCCQO/2013/000264R1
38
66. Law MR, Wald NJ, Thompson SG. By how much and how quickly does reduction in
serum cholesterol concentration lower risk of ischaemic heart disease? BMJ.
1994;308:367-372
67. Whitlock G, Lewington S, Mhurchu C. Coronary heart disease and body mass index:
A systematic review of the evidence from larger prospective cohort studies. Semin
Vasc Med. 2002;2:369-381
68. James W, Jackson-Leach R, Mhurchu C. Overweight and obesity (high body mass
index). In: Ezzati M, Lopez A, Rodgers A, Murray C, eds. Comparative
quantification of risk. Global and regional burden of disease attributable to selected
major risk factors. Geneva: World Health Organization; 2004:497-596.
69. McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, Falk
V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Kober L, Lip GY,
Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Ronnevik PK, Rutten FH,
Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A.
Esc guidelines for the diagnosis and treatment of acute and chronic heart failure 2012:
The task force for the diagnosis and treatment of acute and chronic heart failure 2012
of the european society of cardiology. Developed in collaboration with the heart
failure association (hfa) of the esc. Eur Heart J. 2012;33:1787-1847
70. Carreira H, Pereira M, Azevedo A, Lunet N. Trends in the prevalence of smoking in
portugal: A systematic review. BMC Public Health. 2012;12:958
Related Documents











