..................................................................................................................................................................................... ..................................................................................................................................................................................... CLINICAL RESEARCH Heart failure/cardiomyopathy Exercise oscillatory breathing in diastolic heart failure: prevalence and prognostic insights † Marco Guazzi 1 * , Jonathan Myers 2 , Mary Ann Peberdy 3 , Daniel Bensimhon 4 , Paul Chase 4 , and Ross Arena 3 1 Cardiopulmonary Unit, University of Milano, San Paolo Hospital, Via A. di Rudinı `, 8, 20142 Milano, Italy; 2 VA Palo Alto Health Care System, Palo Alto, CA, USA; 3 Virginia Commonwealth University, Richmond, VA, USA; and 4 LeBauer Cardiovascular Research Foundation, Greensboro, NC, USA Received 24 April 2008; revised 22 August 2008; accepted 12 September 2008; online publish-ahead-of-print 4 October 2008 Aims Exercise intolerance occurs in both systolic and diastolic heart failure (HF). Exercise oscillatory breathing (EOB) is a powerful predictor of survival in patients with systolic HF. In diastolic HF, EOB prevalence and prognostic impact are unknown. Methods and results A total of 556 HF patients (405 with systolic HF and 151 with diastolic HF) underwent cardiopulmonary exercise testing (CPET). Diastolic HF was defined as signs and symptoms of HF, a left ventricular ejection fraction 50%, and a Doppler early (E) mitral to early mitral annulus ratio (E 0 ) 8. CPET responses, EOB prevalence and its ability to predict cardiac-related events were examined. EOB prevalence in systolic and diastolic HF was similar (35 vs. 31%). Compared with the patients without EOB, patients with EOB and either systolic or diastolic HF had a higher New York Heart Association class, lower peak VO 2 and higher E/E 0 ratio (all P , 0.01). Univariate Cox regression analysis demonstrated that peak VO 2 , VE/VCO 2 slope and EOB all were significant predictors of cardiac events in both systolic and diastolic HF. Multivariable analysis revealed that EOB was retained as a prognostic marker in systolic HF and was the strongest predictor of cardiac events in diastolic HF. Conclusion EOB occurrence is similar in diastolic and systolic HF and provides relevant clues for the identification of diastolic HF patients at increased risk of adverse events. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Diastolic heart failure † Exercise oscillatory breathing Introduction The occurrence of symptoms and signs of heart failure (HF) with normal ejection fraction (EF) and predominant anomalies of active relaxation and passive stiffness (i.e. diastolic HF) is increas- ingly recognized. 1 This diagnosis carries a mortality risk that is cur- rently estimated to be similar to that seen in systolic HF, 15% per year in older patients. 2,3 Remarkably, in recent year’s survival rate of systolic HF has improved, whereas the prognosis for diastolic HF remains unchanged. 2 This is at least in part attributable to the fact that the definition, diagnosis, and natural history of diastolic HF are less well characterized. 4–6 Limitation to physical activity occurs in conjunction with both systolic and diastolic HF and cardinal manifestations of exercise intolerance are a reduction in peak oxygen consumption (VO 2 ), 7 an excessive ventilation to CO 2 output rate (VE/VCO 2 ), 8–11 and the occurrence of exercise oscillatory breathing (EOB). 12 – 14 These variables are established markers in the clinical and prognos- tic assessment of systolic HF, but their significance in diastolic HF has not been fully explored. There has been a recent appreciation for the clinical relevance of EOB, a complex and intriguing pathophysiological phenomenon characterized by waxing and waning of tidal volume that leads to an oscillatory kinetics in measured VO 2 and VCO 2 , reflecting an instability in central and peripheral controllers of ventilation. Clinically, interest in EOB has arisen because of its strong prognostic power; in fact, recent reports have demonstrated that EOB is actually superior to both peak VO 2 and the VE/VCO 2 slope 15 – 17 and may be valuable in the prediction of arrhythmic cardiac death. 18 EOB has been substantially characterized in patients with sys- tolic HF, but no information is available on its prevalence or * Corresponding author. Tel: þ39 02 5032 3144, Fax: þ39 02 5032 3144, Email: [email protected] † Presented in part at the 80th American Heart Association Scientific Session, Orlando, Florida, November 3 –7, 2007. Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected]. European Heart Journal (2008) 29, 2751–2759 doi:10.1093/eurheartj/ehn437 by guest on May 27, 2016 http://eurheartj.oxfordjournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CLINICAL RESEARCHHeart failure/cardiomyopathy
Exercise oscillatory breathing in diastolic heartfailure: prevalence and prognostic insights†
Marco Guazzi1*, Jonathan Myers2, Mary Ann Peberdy3, Daniel Bensimhon4,Paul Chase4, and Ross Arena3
1Cardiopulmonary Unit, University of Milano, San Paolo Hospital, Via A. di Rudinı, 8, 20142 Milano, Italy; 2VA Palo Alto Health Care System, Palo Alto, CA, USA;3Virginia Commonwealth University, Richmond, VA, USA; and 4LeBauer Cardiovascular Research Foundation, Greensboro, NC, USA
Received 24 April 2008; revised 22 August 2008; accepted 12 September 2008; online publish-ahead-of-print 4 October 2008
Aims Exercise intolerance occurs in both systolic and diastolic heart failure (HF). Exercise oscillatory breathing (EOB) is apowerful predictor of survival in patients with systolic HF. In diastolic HF, EOB prevalence and prognostic impact areunknown.
Methodsand results
A total of 556 HF patients (405 with systolic HF and 151 with diastolic HF) underwent cardiopulmonary exercisetesting (CPET). Diastolic HF was defined as signs and symptoms of HF, a left ventricular ejection fraction �50%,and a Doppler early (E) mitral to early mitral annulus ratio (E0) �8. CPET responses, EOB prevalence and itsability to predict cardiac-related events were examined. EOB prevalence in systolic and diastolic HF was similar(35 vs. 31%). Compared with the patients without EOB, patients with EOB and either systolic or diastolic HF hada higher New York Heart Association class, lower peak VO2 and higher E/E0 ratio (all P , 0.01). Univariate Coxregression analysis demonstrated that peak VO2, VE/VCO2 slope and EOB all were significant predictors ofcardiac events in both systolic and diastolic HF. Multivariable analysis revealed that EOB was retained as a prognosticmarker in systolic HF and was the strongest predictor of cardiac events in diastolic HF.
Conclusion EOB occurrence is similar in diastolic and systolic HF and provides relevant clues for the identification of diastolic HFpatients at increased risk of adverse events.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Diastolic heart failure † Exercise oscillatory breathing
IntroductionThe occurrence of symptoms and signs of heart failure (HF) withnormal ejection fraction (EF) and predominant anomalies ofactive relaxation and passive stiffness (i.e. diastolic HF) is increas-ingly recognized.1 This diagnosis carries a mortality risk that is cur-rently estimated to be similar to that seen in systolic HF, �15% peryear in older patients.2,3 Remarkably, in recent year’s survival rateof systolic HF has improved, whereas the prognosis for diastolic HFremains unchanged.2 This is at least in part attributable to the factthat the definition, diagnosis, and natural history of diastolic HF areless well characterized.4– 6
Limitation to physical activity occurs in conjunction with bothsystolic and diastolic HF and cardinal manifestations of exerciseintolerance are a reduction in peak oxygen consumption (VO2),
7
an excessive ventilation to CO2 output rate (VE/VCO2),8 – 11 and
the occurrence of exercise oscillatory breathing (EOB).12 –14
These variables are established markers in the clinical and prognos-tic assessment of systolic HF, but their significance in diastolic HFhas not been fully explored.
There has been a recent appreciation for the clinical relevanceof EOB, a complex and intriguing pathophysiological phenomenoncharacterized by waxing and waning of tidal volume that leads toan oscillatory kinetics in measured VO2 and VCO2, reflecting aninstability in central and peripheral controllers of ventilation.Clinically, interest in EOB has arisen because of its strongprognostic power; in fact, recent reports have demonstrated thatEOB is actually superior to both peak VO2 and the VE/VCO2
slope15– 17 and may be valuable in the prediction of arrhythmiccardiac death.18
EOB has been substantially characterized in patients with sys-tolic HF, but no information is available on its prevalence or
* Corresponding author. Tel: þ39 02 5032 3144, Fax: þ39 02 5032 3144, Email: [email protected]† Presented in part at the 80th American Heart Association Scientific Session, Orlando, Florida, November 3–7, 2007.
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected].
European Heart Journal (2008) 29, 2751–2759doi:10.1093/eurheartj/ehn437
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

prognostic utility in diastolic HF. Such information would be helpfulin order to better stratify diastolic HF patients at increased risk.Therefore, the present study was aimed at elucidating the pre-valence and the prognostic relevance of EOB in diastolic HF com-pared with systolic HF.
MethodsThis was a multicentre study consisting of HF patients referred to thecardiopulmonary exercise laboratories at San Paolo Hospital, Milan,Italy, Virginia Commonwealth University, Richmond, Virginia, USA,VA Palo Alto Health Care System, Palo Alto, California, USA andLeBauer Cardiovascular Research Foundation, Greensboro, NC,USA. A total of 556 consecutive subjects diagnosed with HF whounderwent a symptom-limited cardiopulmonary exercise testing(CPET) between June 1998 and June 2007 were included. Subjectswith significant obstructive lung disease, evidenced by a forced expira-tory volume in 1 s �70%, or who were unable to perform a maximalexercise test, were excluded from the study.
Smokers were 15–20% of the population and were similarly distri-buted across different subgroups. All patients were in New York HeartAssociation (NYHA) functional classes II– III and 40 had been alreadyhospitalized for acute HF.
Inclusion criteria for systolic HF were signs and symptoms of HFwith a left ventricular (LV) EF � 40%.
Inclusion criteria for diastolic HF consisted of a diagnosis based on(i) signs and symptoms of HF (ii) presence of preserved LV systolicfunction (EF � 50%) as assessed by two-dimensional echocardio-graphy, and (iii) documentation of a mitral inflow early (E) velocityto mitral annulus early velocity (E0) �8.19,20 Approval of the Insti-tutional Review Board at each institution was obtained.
Cardiopulmonary exercise testing procedureand data collectionSymptom-limited CPET was performed in all patients after writteninformed consent had been obtained. Each centre used individualizedramp protocols and maximal tests were designed to obtain exerciseduration between 8 and 10 min. USA centres utilized a treadmill andthe Italian centre used a cycle ergometer. Potential bias related todifferent exercise modes can reasonably be excluded given that a pre-vious study has shown that comparing these two modes of exerciseyields identical predictive cut-off values for both peak VO2 and theVE/VCO2 slope.21 Ventilatory expired gas analysis was performedusing a metabolic cart at all four centres (Medgraphics CPX-D,Minneapolis, MN or Sensormedics Vmax, Yorba Linda, CA, USA).
Standard 12-lead electrocardiograms were obtained at rest, eachminute during exercise and for at least 5 min during the recoveryphase; blood pressure was measured using a standard cuff sphygmo-manometer. Minute ventilation (VE, BTPS), oxygen uptake (VO2,STPD), carbon-dioxide output (VCO2, STPD), and other cardiopul-monary variables were acquired breath-by-breath, averaged over30 s, and printed using rolling averages every 10 s. The V-slopemethod was used to measure the anaerobic threshold (AT).22 Differ-ent methods for calculating the VE/VCO2 slope have been proposed.We measured this variable by including all data points from the begin-ning to the end of exercise, in agreement with previous studies by ourgroup23 and others.24 Measurement of VE/VCO2 slope by using theentire data points may offer some advantages over the calculation ofthe first slope of VE/VCO2 relationship (from rest to the isocapnic buf-fering at ventilatory threshold). Specifically, in patients with EOB, cal-culation of first VE/VCO2 slope linear relationship may represent an
issue, because of the scattered distribution of breath-by-breathvalues, making it impossible to detect the ventilatory threshold. Itfollows that the use of the whole VE/VCO2 relationship for bothEOB and no-EOB patients allows a comparable measurementbetween groups. In addition, we deemed this calculation useful toprevent variability among laboratories.
Ten-second averaged VE and VCO2 data, from the initiation to peakexercise, were input into spreadsheet software (Microsoft Excel,Microsoft Corp., Bellevue, WA, USA) to calculate the VE/VCO2
slope through least squares linear regression (y ¼ mx þ b,m ¼ slope). Ten-second averaged VE data were also analysed todetermine if a subject demonstrated EOB during testing.
EOB was defined accordingly to the following criteria: (i) oscillationsof �60% of exercise data at an amplitude of .15%; (ii) minimalaverage amplitude of ventilatory oscillation of 5 L (peak value minusthe average of two in-between consecutive nadirs); (iii) a regular oscil-lation as defined by a SD of three consecutive cycle lengths (timebetween two consecutive nadirs) within 20% of the average.17,18
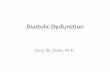
Different patters of oscillations may be encountered across the widespectrum of HF populations. As depicted in Figure 1, some noisy oscil-lations (A) may occur at early exercise that are considered as no-EOB(absence of criteria above-reported); an EOB pattern that may last forthe initial and intermediate phases of exercise and disappears after.60% of whole exercise (B) or EOB with cycles of very wide ampli-tude that last for the entire exercise duration (C). In patients withEOB that persisted for the whole exercise duration VO2 at peak exer-cise was calculated as average of the last 60 s of exercise.
Test termination criteria consisted of symptoms (i.e. dyspnoea and/or fatigue), ventricular tachycardia, �2 mm of horizontal or downsloping ST segment depression, drop of systolic blood pressure�20 mmHg during progressive exercise. A qualified exercise physio-logist with physician supervision conducted each exercise test.
EchocardiographyLV chamber dimensions were evaluated using standard procedures.LVEF was calculated from two-dimensional apical images accordingto the Simpson method. LV mass was calculated with the formula pro-posed by Devereux et al.25
Conventional Doppler and tissue Dopplerimaging measurementsMitral inflow measurements included peak early (E) and peak late (A)flow velocities, the deceleration time (DT) of early mitral flow velocity,the E/A ratio and the isovolumic relaxation time (IVRT). The tissueDoppler imaging of the mitral annulus was obtained from the apicalfour-chamber view. A 1.5 sample was placed sequentially at thelateral and septal annular sites. Analysis was performed for the early(E0) and late (A0) diastolic peak velocities. The ratio of early transmitralflow velocity to annular mitral velocity of the lateral LV wall (E/E0) wastaken as an estimate of LV filling pressure.26
EndpointsSubjects were followed for cardiac-related death after CPET throughhospital and outpatient medical chart review at the respectivecentres. Cardiac-related mortality was defined as death directly result-ing from failure of the cardiac system. An example fitting this definitionis myocardial infarction followed by cardiac arrest. Subjects were fol-lowed by the institution where CPET was conducted providing forthe high likelihood that all major events were captured. Clinicalfollow-up to ascertain predefined outcome was obtained every6 months. The last follow-up assessment was obtained at 4 years.
M. Guazzi et al.2752
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

Any death with a cardiac-related discharge diagnosis was considered anevent. Clinicians conducting the CPET were not involved in decisionsregarding the cause of death or heart transplant/LVAD implantation.
Statistical analysisIn an earlier study,11 the incidence of cardiac mortality at 1 year inpatients with EOB vs. no-EOB was 30 vs. 12%, respectively; thus, ifwe hypothesized a similar association in this study, a population of
126 patients would be needed to detect this difference witha ¼ 0.05 and a power of 0.90.
All continuous data are reported as means+SD. Categorical dataare reported as percentages or frequencies. Unpaired t-testing wasused to compare continuous data between subjects with no-EOBand that with EOB. Differences between no-EOB and EOB patientsfor systolic vs. diastolic HF were tested by two-way analysis of variance(ANOVA). Both main (no-EOB vs. EOB and systolic vs. diastolic HF)and interaction (EOB*HF type) effects were assessed. All tests weretwo-sided.
Variables included in the Cox regression model were only exercisevariables (peak VO2, VE/VCO2 slope and EOB). Peak VO2 andVE/VCO2 slope are the most established prognostic exercise indi-cators as suggested by several consistent studies. EOB is the new vari-able we are assessing, which has recently shown a strong prognosticvalue primarily in systolic HF.16– 18
Univariate Cox regression analysis was used to assess the prognosticability of EOB in the overall group. Multivariable Cox regression analy-sis was performed by using the forward stepwise method with entryand removal of P-value for multivariate analyses set at 0.05 and 0.10,respectively.
For variables included in the Cox regression analysis, proportionalhazards assumption was assessed by plotting log–log survival curves.These plots revealed all variables included in the analysis were parallel,satisfying the proportional hazards assumption. Kaplan–Meier analysisassessed the differences in survival between subjects with and withoutEOB in the overall group. The log-rank test determined statistical sig-nificance between groups in the Kaplan–Meier analysis. Statisticaldifferences with a P, 0.05 were considered significant.
Results
Follow-up on survivalAmong the 630 patients initially assessed, 48 did not fulfil the eli-gibility criteria; 15 patients did not provide their consent to beincluded in the study follow-up and 11 patients were excludedbecause lost at follow-up. The median follow-up duration was13 months with an interquartile range of 8 (25%) and 34 (75%)months for diastolic HF and of 6 (25%) and 31.3 (75%) monthsfor systolic HF. During this period, there were 99 major events(78 deaths, 5 LVADs, 16 transplants), with an overall annual mor-tality rate of 12.4% for the systolic HF group, and 17 major events(16 deaths, 1 transplant) with an annual mortality rate of 5.7% fordiastolic HF group. For diastolic HF group, the mean follow-up forsurvivors was 22.4+19.5 months and that for non-survivors was19.0+ 18.4 months. For systolic HF group, the mean follow-up forsurvivors was 17.6+15.4 months and that for non-survivors was17.6+ 17.5 months.
Baseline characteristicsThe EOB prevalence in patients with systolic vs. diastolic HF was35 and 31%, respectively. A total of 251 patients were tested ona bike and 305 on a treadmill. Interestingly, EOB prevalence was25% among those tested on a bike vs. 41.3% among those testedon a treadmill. Nonetheless, the prognostic characteristics ofEOB was the same for bike (hazard ratio: 3.6, 95% CI: 2.1–6.3,P , 0.001) and treadmill (hazard ratio: 3.2, 95% CI: 1.9–5.2,P , 0.001) tests.
Figure 1 Examples of different patterns of oscillatory venti-lation. (A) Some noisy oscillations may occur at early exercisethat are considered as no-exercise oscillatory breathing. (B) Anexercise oscillatory breathing pattern that may last for theinitial and intermediate phases of exercise and disappearingafter 60% of whole exercise. (C) Exercise oscillatory breathingwith very wide amplitude of cycles that persist for the entireexercise.
Oscillatory breathing in diastolic heart failure 2753
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

Comparisons of key variables between no-EOB and EOB amongsubjects with systolic and diastolic HF are listed in Tables 1 and 2,respectively. For patients with systolic HF, no significant differenceswere detected between those with and without EOB in terms ofage, gender distribution, aetiology of cardiomyopathy, and EF.Conversely, EOB patients exhibited a higher NYHA functionalclass and fewer were taking beta-blockers. ACE-inhibitors anddiuretics were prescribed similarly between the subgroups.Among patients with diastolic HF, there were fewer females withEOB and NYHA functional class was higher. In addition, patientswith EOB were more frequently prescribed RAS inhibitors anddiuretics.
Echocardiographic characteristicsTable 3 reports the echocardiographic data. The two-way ANOVAanalysis documented a significant EOB main effect for both leftventricular end-diastolic volume (LVEDV) and left ventricular end-systolic volume (LVESV) (P ¼ 0.04) with a significant main effectfor systolic vs. diastolic HF (P , 0.001). Diastolic HF patients hada significantly lower LVEDV and LVESV (P , 0.01) vs. systolic HF.An EOB and HF type interaction was detected for diastolic HFpatients with EOB who presented significantly lower LVEDV andLVESV compared with no-EOB systolic HF patients (P ¼ 0.001).As to left ventricular mass (LVM), there was a main effect forEOB and patients with no-EOB had a significantly lower LVM com-pared with EOB patients (P ¼ 0.02). The main effect for systolic vs.diastolic HF was also significant (P , 0.001). Systolic HF patientshad a significantly higher LVM. A significant interaction effect
between EOB and HF type was observed and diastolic HF patientswith EOB had a significantly lower LVM vs. systolic HF patients andEOB (P ¼ 0.003). A significant main effect for EOB was observed forLVM/LVEDV just in diastolic HF patients (P ¼ 0.002). A significantinteraction effect emerged between EOB and HF type with diastolicHF patients and EOB showing a higher LVM/LVEDV compared withsystolic HF patients and EOB. No main or interaction effectsemerged for IVRT, DT, and E/A ratio (P . 0.05). As to E/E’ lateral,there was a main effect for EOB. No-EOB vs. EOB patients hada significantly lower E/E’ lateral (P , 0.001). The main effect forsystolic vs. diastolic HF was also significant (P ¼ 0.001) in thatpatients with diastolic HF and no-EOB had a significantly lowerE/E0 lateral vs. systolic HF with EOB. There was, however, no inter-action effect between EOB and HF type (P ¼ 0.61).
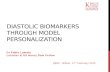
Cardiopulmonary dataTwo representative cases of systolic and diastolic HF eithershowing a similar EOB pattern are reported in Figure 2.
Exercise gas exchange data are summarized in Table 4. Allpatients exercised above their AT and the mean peak respiratoryexchange ratio (RER) was �1.05 in all groups, suggesting thatthey developed significant metabolic acidosis and exercised closeto maximal intensity. At the two-way ANOVA analysis, therewas no main or interaction effect for peak RER. As to peak VO2
and VO2 at AT, there was a main effect for EOB. Patients withno-EOB had significantly higher values compared with the subjectswith EOB (P , 0.001). The main effect for systolic vs. diastolic HFwas not significant (P ¼ 0.07). There was, however, an interaction
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Demographic and clinical characteristics according to presence or absence of exercise oscillatory breathing insystolic heart failure
Overall group (n 5 405) No-EOB (n 5 263) EOB (n 5 142) P-value (EOB vs. no-EOB)
Age, years 56.0+13.4 55.3+13.2 57.1+13.8 0.34
Gender (male/female), % 71/29 75/25 69/31 0.26
LV ejection fraction, % 25.3+7.9 25.5+8.0 25.2+7.7 0.88
NYHA (average) 2.4+ .76 2.3+0.76 2.6+ .72 ,0.001
Heart rate at rest, beats/min 74+24 72+28 74+30 0.47
Blood pressure at rest, mmHg
Systolic 118+25 120+26 117+26 0.43
Diastolic 72+24 74+25 70+27 0.81
Aetiology
Ischaemic (%) 203 (50) 123 (47) 80 (56) 0.12
Hypertensive (%) 122 (30) 82 (31) 40 (28) 0.35
Post-myocarditis (%) 40 (10) 28 (11) 12 (8) 0.44
Idiopathic (%) 40 (10) 30 (11) 10 (7) 0.31
Drug therapy distribution
Prescribed ACE-inhibitor (%) 312 (77) 200 (76) 111 (78) 0.60
Prescribed diuretic (%) 311 (76) 184 (70) 99 (70) 0.98
Prescribed beta-blocker (%) 296 (73) 200 (76) 95 (67) 0.007
Prescribed antialdosterone agents (%) 202 (50) 131 (50) 71 (50) 0.95
Prescribed inotropic agents (%) 162 (40) 121 (46) 77 (54) 0.55
NYHA, New York Heart Association.
M. Guazzi et al.2754
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

effect between EOB and HF type. Patients with diastolic HF andno-EOB had a significantly higher peak VO2 compared with thesubjects with systolic HF and no-EOB (P ¼ 0.005).
As to VE/VCO2 slope, there was a main effect for EOB; patientswith no-EOB had a significantly lower VE/VCO2 slope comparedwith EOB patients (P , 0.001). The main effect for systolic vs. dia-stolic HF was also significant (P ¼ 0.009). Patients with diastolic HFand EOB had a significantly lower VE/VCO2 slope compared with
the subjects with systolic HF. There was, however, no interactioneffect between EOB and HF type (P ¼ 0.90).
Cox regression analysesUnivariate Cox regression analysis demonstrated that EOB was asignificant predictor of cardiac mortality in both populations(Table 5A and B). At multivariable analyses, EOB was retained asprognostic indicator in systolic HF and emerged as the most
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Demographic and clinical characteristics according to presence or absence of exercise oscillatory breathing indiastolic heart failure
Overall group (n 5 151) No-EOB (n 5 103) EOB (n 5 48) P-value (EOB vs. no-EOB)
Age, years 58.5+13.4 57.0+12.6 61.8+14.4 0.04
Gender (male/female), % 67/33 63/37 75/25 0.005
Left ventricular ejection fraction, % 47.8+7.8 47.8+7.9 47.6+7.8 0.83
NYHA (average) 2.0+0.85 1.8+0.78 2.6+0.0 ,0.001
Heart rate at rest, beats/min 78+28 77+30 78+29 0.06
Blood pressure at rest, mmHg
Systolic 125+26 126+26 124+26 0.67
Diastolic 84+25 83+24 84+26 0.62
Aetiology
Ischaemic (%) 75 (50) 50 (48) 25 (52) 0.73
Hypertensive (%) 45 (30) 34 (33) 11 (23) 0.24
Post-myocarditis (%) 8 (5) 6 (6) 2 (4) 0.1
Idiopathic (%) 23 (15) 13 (13) 10 (21) 0.08
Therapy distribution
Prescribed ACE-inhibitor (%) 108 (72) 46 (45) 26 (55) 0.015
Prescribed diuretics (%) 92 (61) 52 (51) 23 (49) 0.12
Prescribed beta-blockers (%) 84 (56) 46 (45) 26 (55) 0.018
Prescribed antialdosterone agents (%) 60 (40) 49 (48) 25 (52) 0.52
Prescribed inotropic agents (%) 27 (18) 51 (50) 24 (50) 0.64
NYHA, New York Heart Association.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Echocardiographic data characteristics of systolic and diastolic heart failure
Systolic HF Diastolic HF
No-EOB EOB No-EOB EOB
LVESV, mL 107.0+29.0 122.0+30.0* 100.3+32.0# 88.6+28.6*,§,#
LVEDV, mL 185.0+29.0 200.0+30.0* 160.0+31.0# 140+29.0*,§,#
LVM, g 221.0+21.0 237.0+20.0* 219.0+23.0§,# 215.0+22.7*,§,#
LVM/LVEDV, g/mL 1.19+2.0 1.20+1.0 1.37+1.5 1.53+1.2*,§,#
Mitral inflow pattern and tissue Doppler
IVRT, ms 99.0+7.0 92.0+6.0 92.0+4.0 90.0+3.0
E/A ratio 1.13+0.9 1.30+0.8 1.22+0.4 1.13+0.3
DT, ms 220+30 170+28 200+27 190+27
E/E0 lateral 9.0+1.0 12.0+3.0* 9.0+1.0§ 14.0+2.0@,#
*P , 0.05 vs. no-EOB; @P , 0.01 vs. no-EOB; §P , 0.01 vs. EOB systolic HF; #P , 0.01 vs. no-EOB systolic HF. Abbreviations: LVESV, left ventricular end-systolic volume;LVEDV, left ventricular end-diastolic volume; LVM, left ventricular mass; IVRT, isovolumic relaxation time; E, early mitral flow velocity; A, late mitral flow velocity; DT, decelerationtime; E0 , early annular mitral velocity.
Oscillatory breathing in diastolic heart failure 2755
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

powerful indicator in diastolic HF (Table 6A and B). Thecardiac-related event rate was higher in systolic than diastolic HF.Specifically, 99 (24%) major cardiac-related events were observedamong patients with systolic HF (78 deaths, five LVADs, 16 trans-plants) and 17 (11%) major events were observed for those withdiastolic HF (16 deaths, one transplant).
When Cox regression analysis was performed looking at cardiacmortality without LVADs and transplants, EOB was prognostic inboth diastolic (x2 ¼ 12.0, hazard ratio: 5.4, 95% CI: 1.9–15.7,P ¼ 0.001) and systolic (x2 ¼ 21.3, hazard ratio: 3.0, 95% CI:1.9–4.8, P , 0.001) HF groups.
Looking also at predictive differences according to a peak RERcut-off of 1.05, it emerged that in the diastolic HF group, 44% ofpatients had RER �1.05. EOB was prognostic in this group(x2 ¼ 12.3, hazard ratio: 9.7, 95% CI: 2.1–45.7, P , 0.001) butnot in those with a RER , 1.05 (x2 ¼ 1.2, hazard ratio: 2.4, 95%CI: 0.48–12.5, P ¼ 0.27). The latter finding may be due to theless number of events in the latter group (only six).
In the systolic HF group, 53% had RER �1.05 and EOBwas prognostic in both patients with EOB and peak RER�1.05(x2 ¼ 7.6, hazard ratio: 2.1, 95% CI: 1.2–3.7, P ¼ 0.007), andbelow (x2 ¼ 11.7, hazard ratio: 2.8, 95% CI: 1.5–5.2, P ¼ 0.001).
Kaplan–Meier analysesKaplan–Meier analysis results for the four subgroups are illustrated inFigure 3. Survival rate was significantly lower in those with EOB andeither systolic or diastolic dysfunction. Patients with diastolic HF andEOB had a lower survival rate than systolic HF patients without EOB.
DiscussionResults of the present study define, for the first time, the preva-lence and the prognostic significance of exercise oscillatory gasexchange kinetics in patients with diastolic HF. EOB, a pheno-menon that has been traditionally linked to advanced systolicHF,12,27 is also part of the syndrome of diastolic HF and its recog-nition may help to identify a subset of diastolic HF patients atincreased risk of cardiac mortality.
Notably, as in systolic HF, EOB in diastolic HF showed aprognostic power superior to peak VO2 and the VE/VCO2
slope, parameters that have become standards regarding hearttransplantation urgency in advanced HF patients (peak VO2), andrisk stratification across HF populations with varying diseaseseverity (VE/VCO2 slope).8– 11
Figure 2 Representative cases of exercise oscillatory breathing patterns in systolic (A) and diastolic (B) heart failure.
M. Guazzi et al.2756
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

Diastolic heart failure, exercise gasexchange and ventilationThe natural history of diastolic HF is less well characterized thanthat of systolic HF; thus, precise management guidelines andoptimal therapeutic approaches can present a challenge for thesepatients. In particular, information on diastolic HF and CPET per-formance are limited. Six studies have investigated exercise
pathophysiology by gas exchange analysis,28– 33 although just onehas addressed prognosis.29 In these studies, disparate criteriawere used for diastolic HF definition, and there was a wide hetero-geneity among populations concerning age and gender distribution.However, although exercise performance and peak VO2 variedwidely across these studies, the cardiopulmonary exercisepattern common to all studies but one33 was an increasedVE/VCO2 slope and an excessive dyspnoea sensation. The presentobservations further support this evidence given that multivariableanalysis demonstrated that the VE/VCO2 slope outperformed peakVO2 in predicting cardiac events. In addition, these findings under-score the importance of addressing abnormalities in the exerciseventilatory pattern to better characterize symptomatic diastolicHF. Interestingly, patients with diastolic HF and a high VE/VCO2
Figure 3 Kaplan–Meier analysis for patients with no-exerciseoscillatory breathing and exercise oscillatory breathing for sys-tolic vs. diastolic heart failure subgroups.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 Cardiopulmonary exercise testing data of systolic and diastolic heart failure
Systolic HF Diastolic HF
No-EOB EOB No-EOB EOB
Peak RER 1.06+0.13 1.06+0.12 1.06+0.11 1.05+0.12
Peak VO2, mL O2 . kg21 . min21 15.5+5.0 12.1+3.8@ 17.8+5.5§,# 11.9+3.9@,#
VO2 at anaerobic threshold, mL O2 . kg21 . min21 10.6+5.0 9.2+4.0* 14.5+5.5§,# 9.6+3.9@
VE/VCO2 slope 35.3+10.1 39.7+9.1@ 32.8+7.9§,# 36.9+6.7@,#
*P , 0.05 vs. no-EOB; @P , 0.01 vs. no-EOB; §P , 0.01 vs. EOB systolic HF; #P , 0.01 vs. no-EOB systolic HF. RER, respiratory exchange ratio; VE, ventilation; VCO2, CO2
output.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 6 Multivariable Cox regression analysis forsystolic and diastolic heart failure
x2b Hazard ratio (95% CI) P-value
Systolic heart failure
VE/VCO2 slope 38.4 1.05 (1.03–1.07) ,0.001
EOBa 13.0 2.0 (1.3–3.1) ,0.001
Peak VO2 3.0 — 0.08
Diastolic heart failure
EOB 14.1 5.9 (2.1–16.9) ,0.001
VE/VCO2 slopea 6.5 1.09 (1.03–1.16) 0.01
Peak VO2 0.23 — 0.63
RER, respiratory exchange ratio; VE, ventilation; VCO2, CO2 output. aRetained inthe regression. bResidual x2.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 5 Univariate Cox regression analysis for systolicand diastolic heart failure
x2 Hazard ratio (95% CI) P-value
Systolic heart failure
VE/VCO2 slope 38.4 1.05 (1.03–1.07) ,0.001
Peak VO2 16.3 0.91 (0.86–0.95) ,0.001
EOB 22.8 2.5 (1.6–3.7) ,0.001
Diastolic heart failure
VE/VCO2 slope 11.9 1.10 (1.04–1.16) 0.001
Peak VO2 6.1 0.87 (0.77–0.97) 0.01
EOB 14.1 5.9 (2.1–16.9) ,0.001
RER, respiratory exchange ratio; VE, ventilation; VCO2, CO2 output.
Oscillatory breathing in diastolic heart failure 2757
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

slope were more commonly observed in the EOB subgroup. Indeed,this population presented with an average VE/VCO2 slope of 37that, although a little lower than the average value of 40 observedin systolic EOB patients, is strongly predictive of worse prognosis.11
Exercise oscillatory breathing: clinicaland prognostic characteristicsBased on our numbers, the prevalence of abnormal ventilatoryoscillation in patients with diastolic HF approximates 30%, and issimilar to that observed in systolic HF in both the present and pre-vious reports.17,18 Likewise, as in systolic HF, a close link betweenEOB and clinical severity exists. Aside from the above-reporteddifferences in VE/VCO2 slope, the clinical picture of patientswith diastolic HF and EOB overlaps that observed among systolicHF patients with EOB; overall exercise performance and peakVO2 were similar and LV end-diastolic pressure (E/E0) was similarlyincreased. EOB diastolic HF patients exhibited normal LV chambersize, increased LV mass and a higher LV mass to volume ratio, pro-viding evidence of a remodelling pattern at high risk. The 1-yearmortality rate for diastolic HF is reported to be �15% in patients�65 years.3 The average age of present diastolic HF populationwas 62 years and this may explain the observed 1-year mortalityrate of 5.7%. Almost all cardiac events occurred in the EOB sub-group, with a 1-year event rate of 10%. It is also interesting tonote that in diastolic HF, presence of gas exchange oscillatory kin-etics during exercise yielded an event-free survival rate worse thanthat in systolic HF patients without EOB (83 vs. 75%; P , 0.001).
In a recent study by our group, primarily involving systolic HFpatients, we found EOB to be a potent predictor of suddencardiac death.18 In this study, we were unable to define whetherthis may also be the case in diastolic HF patients. Consideringthe unquestionable impact of sudden death on the naturalhistory of HF, further investigation in this area would be desirable.
Study limitationsDefinition of the mechanisms underlying EOB in diastolic HF wasbeyond the purposes of the study. Although our findings suggestsimilar EOB prognostic characteristics in diastolic as systolic HF,the pathogenetic mechanisms of the phenomenon in diastolic HFare unclear. However, it is tempting to speculate that an increasedfiling pressure at rest would lead to a further increase during exer-cise, leading to pulmonary interstitial fluid accumulation and stimu-lation of the J-receptors beyond normal reflexogenic control.34
A potential selection bias is represented by the fact that onlypatients who were referred to CPET were included. Thus, in astudy of prevalence, one may argue that, in most clinical settings,physician may favour referral of patients with systolic dysfunctionto CPET and even more, that populations of diastolic HF patientsreferred to a CPET evaluation may not be entirely representativeof the whole spectrum of diastolic HF patients.
Gender distribution was predominantly male for both systolicand diastolic HF, although EOB appeared to be independent ofgender. In addition, the average age of our diastolic HF patientswas somewhat lower compared with previous reports. This maybe unusual because of the well recognized higher diastolic HFrate in female and older populations. However, the lower
propensity of primary care providers to exercise older or femalepatients to exhaustion must be considered. These considerationsall together may offer a conceivable explanation on the differencesbetween our sample of diastolic HF study population and thebroader unselected samples of diastolic HF followed-up in largerepidemiological studies.
Conclusions and perspectivesThe current findings suggest that (i) in diastolic HF, EOB occur-rence and prevalence is similar to systolic HF; (ii) EOB recognitionimplements the ability to identify diastolic HF patients at increasedrisk; and (iii) confirmatory data and definitive strategies to treatoscillatory breathing patterns are warranted.
FundingThis work was supported by a grant provided by the Monzino Foun-dation, Milano, Italy.
Conflict of interest: none declared.
References1. Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure: abnormalities in active
relaxation and passive stiffness of the left ventricle. N Engl J Med 2004;350:1953–1959.
2. Owan TE, Hodge DO, Herges RM, Jacobson SJ, Roger VL, Redfield MM. Trend inprevalence and outcome of heart failure with preserved ejection fraction. N EnglJ Med 2006;355:251–259.
3. Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haduzi A, Gang Y, Liu PP. Outcome ofheart failure with preserved ejection fraction in a population-based study. N EnglJ Med 2006;355:260–269.
4. Vasan RS, Levy D. Defining diastolic heart failure: a call for standardized diagnosticcriteria. Circulation 2000;101:2118–2121.
5. Zile MR, Gaasch WH, Carroll JD, Feldman MD, Aurigemma GP, Schaer GL,Ghali JK, Liebson PR. Heart failure with a normal ejection fraction: is measure-ment of diastolic function necessary to make the diagnosis of diastolic heartfailure? Circulation 2001;104:779–782.
6. Zile MR, Brutsaert DL. New concept in diastolic dysfunction and diastolic heartfailure: part I. Diagnosis, prognosis and measurements of diastolic function. Circula-tion 2002;105:1387–1393.
7. Myers J, Gullestad L, Vagelos R, Do D, Bellin D, Ross H, Fowler MB. Cardiopul-monary exercise testing and prognosis in severe heart failure: 14 mL/kg/minrevisited. Am Heart J 2000;139:78–84.
8. Chua TP, Ponikowski P, Harrington D, Anker SD, Webb-People K, Clark AL,Poole-Wilson PA, Coats AJ. Clinical correlates and prognostic significance ofthe ventilatory response to exercise in chronic heart failure. J Am Coll Cardiol1997;29:1585–1590.
9. Arena R, Myers J, Aslam SS, Varughese EB, Peberdy MA. Peak VO2 and VE/VCO2slope in patients with heart failure: a prognostic comparison. Am Heart J 2004;147:354–360.
10. Guazzi M, Reina G, Tumminello G, Guazzi MD. Exercise ventilation inefficiencyand cardiovascular mortality in heart failure: the critical independent prognosticvalue of the arterial CO2 partial pressure. Eur Heart J 2005;26:472–480.
11. Arena R, Myers J, Abella J, Peberdy MA, Bensimhon D, Chase P, Guazzi M.Development of a ventilatory classification system in patients with heart failure.Circulation 2007;115:2410–2417.
12. Ben-Dov I, Sietsema KE, Casaburi R, Wasserman K. Evidence that circulatoryoscillations accompany ventilatory oscillations during exercise in patients withheart failure. Am Rev Resp Dis 1992;145:776–781.
13. Francis DP, Davies LC, Piepoli M, Rauchhaus M, Ponikowski P, Coats AJ. Origin ofoscillatory kinetics of respiratory gas exchange in chronic heart failure. Circulation1999;100:1065–1070.
14. Francis DP, Willson K, Davies LC, Coats AJ, Piepoli M. Quantitative generaltheory for periodic breathing in chronic heart failure and its clinical implications.Circulation 2000;102:2214–2221.
15. Leite JJ, Mansur AJ, de Freitas HF, Chizola PR, Bocchi EA, Terra-Filho M, Neder JA,Lorenzi-Filho G. Periodic breathing during incremental exercise predicts mortalityin patients with chronic heart failure evaluated for cardiac transplantation. J AmColl Cardiol 2003;41:2175–2181.
M. Guazzi et al.2758
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

16. Corra U, Pistono M, Mezzani A, Braghiroli A, Giordano A, Lanfranchi P, Bosimini E,Gnemmi M, Giannuzzi P. Sleep and exertional periodic breathing in chronic heartfailure: prognostic importance and interdependence. Circulation 2006;113:44–50.
17. Guazzi M, Arena R, Ascione A, Piepoli M, Guazzi MD. Exercise oscillatory breathingand increased ventilation to carbon dioxide production slope in heart failure: anunfavorable combination with high prognostic value. Am Heart J 2007;153:859–867.
18. Guazzi M, Raimondo R, Vicenzi M, Arena R, Proserpio C, Sarzi Braga S, Pedretti R.Exercise oscillatory ventilation may predict sudden cardiac death in heart failurepatients. J Am Coll Cardiol 2007;50:299–308.
19. Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE,Marino P, Smiseth OA, De Keulenaer G, Leite-Moreira AF, Borbely A, Edes I,Handoko ML, Heymans S, Pezzali N, Pieske B, Dickstein K, Fraser AG,Brutsaert DL. How to diagnose diastolic heart failure: a consensus statementon the diagnosis of heart failure with normal left ventricular ejection fractionby the Heart Failure and Echocardiography Associations of the EuropeanSociety of Cardiology. Eur Heart J 2007;28:2539–2550.
20. Kasner M, Westermann D, Steendijk P, Gaub R, Wilkenshoff U, Weitmann K,Hoffmann W, Poller W, Schultheiss HP, Pauschinger M, Tschope C. Utility ofDoppler echocardiography and tissue Doppler imaging in the estimation ofdiastolic function in heart failure with normal ejection fraction: a comparativeDoppler-conductance catheterization study. Circulation 2007;116:637–647.
21. Arena R, Guazzi M, Myers J, Peberdy A. Prognostic characteristics of cardio-pulmonary exercise testing in heart failure: comparing american and europeanmodels. Eur J Cardiov Prev 2005;12:562–567.
22. Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobicthreshold by gas exchange. J Appl Physiol 1986;60:2020–2027.
23. Arena R, Myers J, Aslam SS, Varughese EB, Peberdy MA. Technical considerationsrelated to the minute ventilation/carbon dioxide output slope in patients withheart failure. Chest 2003;124:720–727.
24. Tabet JY, Beauvais F, Thabut G, Tartiere JM, Logeart D, Cohen-Solal A. A criticalappraisal of the prognostic value of the VE/VCO2 slope in chronic heart failure.Eur J Cardiovasc Prev Rehabil 2003;10:267–272.
25. Devereux RB, Casale PN, Kligfield P, Eisenberg RR, Miller D, Campo E,Alonso DR. Echocardiographic assessment of left ventricular hypertrophy:comparison to necroscopy findings. Am J Cardiol 1986;57:450–458.
26. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA. Dopplertissue imaging: a noninvasive technique for evaluation of left ventricular relaxationand estimation of filling pressures. J Am Coll Cardiol 1997;30:1527–1533.
27. Ribeiro JP, Knutzen A, Rocco MB, Hartley LH, Colucci WS. Periodic breathingduring exercise in severe heart failure. Reversal with milrinone or cardiac trans-plantation. Chest 1987;92:555–556.
28. Kitzman DW, Little WC, Brubaker PH, Anderson RT, Hundley WG,Marburger CT, Brosnihan B, Morgan TM, Stewart KP. Pathophysiological charac-terization of isolated diastolic heart failure in comparison to systolic heart failure.J Am Med Assoc 2002;288:2144–2150.
29. Guazzi M, Myers J, Arena R. Cardiopulmonary exercise testing in the clinical andprognostic assessment of diastolic heart failure. J Am Coll Cardiol 2005;46:1883–1890.
30. Witte KK, Nikitin NP, Cleland JG, Clark AL. Excessive breathlessness in patientswith diastolic heart failure. Heart 2006;92:1425–1429.
31. Borlaug BA, Melenovsky V, Russell SD, Kessler K, Pacak K, Becker LC, Kass DA.Impaired chronotropic and vasodilator reserves limit exercise capacity in patientswith heart failure and a preserved ejection fraction. Circulation 2006;114:2138–2147.
32. Arruda AL, Pellikka PA, Olson TP, Johnson BD. Exercise capacity, breathingpattern, and gas exchange during exercise for patients with isolated diastolicdysfunction. J Am Soc Echocardiogr 2007;20:838–846.
33. Moore B, Brubaker PH, Stewart KP, Kitzman DW. VE/VCO2 slope in older heartfailure patients with normal versus reduced ejection fraction compared withage-matched healthy controls. J Card Fail 2007;13:259–262.
34. Olson TP, Frantz RP, Snyder EM, O’Malley KA, Beck KC, Johnson BD. Effects ofacute changes in pulmonary wedge pressure on periodic breathing at rest in heartfailure patients. Am Heart J 2007;153:104e1–107.
Oscillatory breathing in diastolic heart failure 2759
by guest on May 27, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
Related Documents